
CARE-2 MANUAL: Child and Adolescent Risk and Needs Evaluation
58
1 © 2003-2012 by Kathryn Seifert CARE-2 Manual manua L CARE-2 DR. KATHRYN SEIFERT assessment CHILD AND ADOLESCENT RISK/NEEDS EVALUATION
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of CARE-2 MANUAL: Child and Adolescent Risk and Needs Evaluation

© 2003-2012 by Kathryn Seifert 1 © 2003-2012 by Kathryn SeifertCARE-2 Manual
manuaL
CARE-2
DR. KATHRYN SEIFERT
assessmentCHILD AND ADOLESCENT RISK/NEEDS EVALUATION
2 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
CARE-2 Rev: Child and adolescent Risk/Needs Evaluation Revised Edition is the product of a collaborative effort of the Eastern Shore Psychological Services (ESPS) Research and Consultation Team, led by Dr. Kathryn Seifert. Their efforts and hard work are gratefully acknowledged.
Published by Acanthus Publishinga division of The Ictus Group, LLC343 Commercial StUnit 214, Union WharfBoston, MA 02109
Copyright © 2003-2012 by Dr. Kathryn SeifertAll rights reserved in all media. Printed in the United States of America.10 9 8 7 6 5 4 3 2 1
All rights reserved. No part of this book may be reproduced or transmitted in any form or by any means, electronic or mechani-cal, including photocopying, recording, or by any information storage and retrieval system, without written permission from the author, except for the inclusion of brief quotations in a review. Excerpts may be printed in connection with published reviews in periodicals without express permission. No other part of this manual may be reproduced by any means without the written per-mission of the publisher.
ISBN 978-1-933631-95-0
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 3 © 2003-2012 by Kathryn SeifertCARE-2 Manual
TABLE OF CONTENTS
PREFACE ....................................................................................................... 5
CHAPTER 1: AN OVERVIEW OF RISK AND PROTECTIVE FACTORS ..... 8YOUTH VIOLENCE: RISK AND RESILIENCY .................................................................................... 10
THE CASE FOR RISK AND PROTECTIVE FACTORS ASSOCIATED WITH YOUTH VIOLENCE .... 11
YOUTH CHARACTERISTICS .............................................................................................................. 11
PEERS .................................................................................................................................................. 12
SCHOOL AND EDUCATION ............................................................................................................... 13
FAMILY CHARACTERISTICS AND ENVIRONMENT FACTORS ....................................................... 13
PROTECTIVE FACTORS AND RESILIENCY .................................................................................... 14
CHAPTER 2: ADMINISTRATION AND SCORING OF THE CARE-2 .......... 15GENERAL INSTRUCTIONS FOR COMPLETING THE CARE-2 ASSESSMENT FORM ................. 15
ITEM SPECIFIC INSTRUCTIONS FOR COMPLETING THE CARE-2 ............................................. 16
BACKGROUND INFORMATION .................................................................................................. 16
RISK FACTORS ............................................................................................................................ 16
INSTRUCTIONS FOR SCORING THE CARE-2 ........................................................................... 24
DEFINITIONS ................................................................................................................................ 25
INTERAGENCY COORDINATION ................................................................................................ 26
SERVICES NEEDED, BUT NOT IN PLACE ................................................................................. 26
POSSIBLE RESOURCES AND BARRIERS ................................................................................. 26

4 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
OTHER COMMENTS .................................................................................................................... 26
READING THE SCORING TABLE ................................................................................................ 26
PLACEMENT ................................................................................................................................ 27
INTERVENTIONS .......................................................................................................................... 27
CASE STUDY ....................................................................................................................................... 31
ITEMS THAT WOULD BE SCORED FOR JENNIFER .................................................................. 31
CHAPTER 3: TECHNICAL SUMMARY......................................................... 33SCALE DEVELOPMENT PROCESS ................................................................................................... 33
DISCRIMINANT FUNCTION ANALYSIS ............................................................................................. 34
THE SAMPLE....................................................................................................................................... 35
RELIABILITY ........................................................................................................................................ 37
VALIDITY .............................................................................................................................................. 38
RISK BY GENDER AND AGE ............................................................................................................. 38
I. PRE-ADOLESCENT MALES ..................................................................................................... 38
II. ADOLESCENT MALES ............................................................................................................. 41
III. PRE-ADOLESCENT FEMALES .............................................................................................. 44
IV. TEEN FEMALES ...................................................................................................................... 47
ITEM SELECTION ............................................................................................................................... 51
REFERENCES AND RESOURCES ............................................................... 52

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 5 © 2003-2012 by Kathryn SeifertCARE-2 Manual
As I describe in my books, How Children Become Violent (Acanthus Publishing, 2006), my interest in risk assess-ment began with my work in the adult prison system. I was assaulted by an inmate that another professional had de-clared to be “not an imminent danger to self or others.” This inmate went on to kill several teenagers when he was released from prison. I decided then that we needed better ways to determine future risk of violence than we had been using. As with most violent offenders, he had a history of childhood trauma. The model upon which this instru-ment is built is based on a holistic evaluation of strengths and problems. Evidence based practices are connected to each problem area to guide treatment planning. I have made it my life’s mission to participate in the research and development of more accurate risk tools that inform risk management and treatment.
Over the years I have assessed or supervised the assess-ment of hundreds of children and adolescents. During that process, I began to organize information for those psycho-logical evaluations in a list of commonalities I found among youth with severe behavior problems. Through a literature review of risk and resiliency factors, I triangulated my ob-servations with the existing literature on risk. I added scor-ing based on correlations of the item with actual acts of violence, and then began to collect a database. As I pro-gressed, I refined the list of items multiple times in order to advance the accuracy of the CARE-2. The criterion vari-able for this instrument is more than 3 assaults on others.
Those with more than 3 assaults on others are more likely to use assaultive behavior to solve their problems and dis-putes in the future.
The CARE-2 is a combination risk and treatment needs as-sessment, delineating the estimated short term risk for vio-lence and the treatment and structure needs of the client. The sample includes 1031 youth from the East Coast and Mid-West. It can be used for youth ages 6 to 19. There are rural, suburban, and urban youth in the sample. Addition-ally, the youth have a full range of behavioral problems. The psychometrics on the CARE-2 are included in this manual. One unique feature of the CARE-2 is that interventions are listed with each item of the instrument. The risk score states that the “youth is (not, mildly, moderately, highly, or very highly) similar to youth with chronic (a history of more than three) assaults on others.” The scaling was made us-ing means and standard deviations and scatter plots of the particular group being evaluated. Youth who are highly similar to young people with chronic (more than three) as-saults are two standard deviations above the mean for the total group. The mean for the low risk group is two standard deviations below the mean for the total group. The “not similar group” was determined by the score be-low which there were no cases for which there were as-sault histories. The moderate group contained both youth with and without histories of assaults. The “highly and very highly similar” groups contained only youth with histories of chronic (more than 3) assaults.
PREFACE

6 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
Several researchers have determined that unaided clini-cal judgment in the assessment of future risk of violence is little better than chance (a 50% error rate). Guided clini-cal judgment tools have error rates from 30% to 40%. The CARE-2 has an error rate of less than 20%. There is a school of thought that supports the use of guided clinical judgment without a formal scoring system (SAVRY). The CARE-2 was developed with the idea that to improve risk tools, we must constantly measure their ability to assess the criterion variable, A HISTORY OF MORE THAN 3 AS-SAULTS, and adjust the tools accordingly. More than 3 assaults was used as the criterion variable because youth with more than 3 past assaults were more likely to com-mit a future assault within 12 months ( n = 14; r = .75). The CARE-2 has a scoring system, and research is ongoing.
Chronic past assaults is the strongest predictor of future assaults. So why not just have one item: “Chronic Past As-saults”? The importance of this assessment is in the provi-sion of treatment modalities that are supported by research or are considered evidence-based practice. The CARE-2 is a way to assess risk and resiliency factors and develop a treatment plan to reduce the risk of future violence. It is to be used as a prevention and treatment tool. It is not to be used to label youth and should be re-administered at least yearly. This is because youth change rapidly and the CARE-2 is designed to have a lower score when the youth improves skills and functioning. The greater the number and severity of behavior problems, the higher the level of external structure is needed for interventions to be suc-cessful. Therefore, instead of a youth having to “fail” an intervention before being considered for a higher level of care, a professional can estimate the need for intensive or
residential services that provide increased levels of struc-ture. This helps the system use limited resources more ef-ficiently and effectively. It also does not force professionals to wait until a youth “fails” before they can give him/her the appropriate services.
While there is still a long way to go in developing risk as-sessment tools, the CARE-2 is a huge improvement over the incorrect clinical judgment that resulted in my assault many years ago. I am sure that in a few years there will be other improvements, as well.
The next assessment you can expect to see is the CARE-2 for youth with sexual behavior problems. Visit my website at http://www.drkathyseifert.com/ to look for this and other assessment tools. The RME is a similar risk assessment tool for adult violence and sexual offending. It is very simi-lar to the CARE-2. Watch the website for the release of the RME, as well. My book, Youth Violence: Theory, Preven-tion and Intervention (Springer Publishers) describes the prevention, assessment, and treatment of violence among youth.
The CARE-2 was developed with two purposes in mind. One was to identify youth who were at risk for violence and aggression and to determine the interventions needed to prevent any future risk of aggression. We must be very careful to be aware of the problem of labeling and how that can become a self-fulfilling prophecy. However, noth-ing in the literature supports labeling as a risk factor for future violence. Most violent and aggressive youth have been raised in chaotic, violent, neglectful, and abusive en-vironments. We must look at this process as a preventive

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 7 © 2003-2012 by Kathryn SeifertCARE-2 Manual
one and these children as youth in need of services. In developing an intervention plan, it is not sufficient to look at only the child’s needs, but also the family and envi-ronmental needs, such as school, agency, and commu-nity. With all the pieces of the puzzle in place, a youth has a chance to become a positively pro-social functioning member of society. Another perspective to keep in mind is that many of these youth have developmentally delayed skills. Identifying where skills need to be strengthened is
very important to the entire process. The CARE-2 can be a communication tool to allow various agencies to coor-dinate their efforts, reduce duplication, and increase ef-fectiveness. And finally, risk and needs in children and teens changes quickly. This means that youth should be re-assessed every six months to one year to see if there is progress and if the efforts of the agencies are on target.

8 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
Assessing risk and protective factors associated with dif-ferent personal and psychological characteristics and home, school, and community environments has proven to be a useful way for clinicians to gain insights into the personal functioning of individuals. Within this model, the level of personal functioning is seen as a weighted balance between risk and protective factors. In cases where an individual is exposed to or experiences a pre-ponderance of risk factors rather than protective factors, the scales tip away from positive personal functioning. In cases where an individual is exposed to or experiences a preponderance of protective factors, personal function-ing is enhanced. Understanding the risk and protective factors associated with particular behaviors provides an index of the stressors and supports that exist for an indi-vidual and can allow clinicians to help children and teens make changes that enhance future functioning.
The CARE-2 is based on this type of model. Specifically, it uses research on the risk and protective factors associated with youth violence to provide insights into the functioning of youth at risk for violent and other problematic behaviors. It was developed as a prevention tool, so that youth who are at risk could be identified as early as possible. In this way, appropriate interventions could be started early in a child’s life. This approach is consistent with studies that have demonstrated that early severe problems indicate a lifelong problem with violence (Moffit, 2001). Additionally, earlier interventions have a higher probability of success
(Olds, 2002; Thornton, Craft, Dahlberg, Lynch, and Baer, 2000, Hahn, 2005).
In addition to its demonstrated ability to identify youth at risk for violent behavior, the CARE-2 also provides infor-mation that can be used as a case management planning tool, which assists the clinician in developing treatment plans to meet youth needs (Seifert, Phillips, and Parker, 2002). Because youth at risk for violent behavior often have an array of problems, the CARE-2 is designed to provide the clinician with data that gives a broader view of such youth and allows the clinician to plan a more com-plete intervention. The scores derived from the CARE-2 help the clinician to gauge the intensity of the interven-tions needed.
Juveniles accounted for 16% of all violent crime arrests in 2008. From 199 to 2008, aggravated assault declined 21% among juveniles (Puzzanchera, 2009).
Problem behaviors often began before the age of 13. Some juveniles committed serious violent acts as early as age 10 (Browning, Huizinga, Loeber, and Thornberry, 1999; US Department of Justice, 2009). Based on this data, the CARE-2 sample included youth of all ages.
Twenty-five percent of all arrests in the US in 2009 were of females and 17% of that number were under the age of 18 (Seifert, 2012). Therefore, despite the fact that fe-males commit fewer violent offenses than males, there is
CHAPTER 1: AN OVERVIEW OF RISK AND PROTECTIVE FACTORS

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 9 © 2003-2012 by Kathryn SeifertCARE-2 Manual
a substantial population of violent girls with aggressive behaviors. Consequently, both males and females were included in the CARE-2 sample with separate norms.
Violence is a problem that transverses settings, includ-ing outpatient services, hospitals, and prisons. Arboleda-Flórez, Holley, and Crisanti (1996) found a significant relationship between mental illness and violence, while Meloy (2000) and Monahan, Steadman, Robbins, Ap-pelbaum, Banks, Grisso, Heilbrun, Mulvey, and Silver (2005) report that substance abuse increases the risk of violence among adult mentally ill persons. For that rea-son, the sample includes those with and without identi-fied mental illness and substance abuse, as well as those with juvenile justice involvement.
Clinical judgment alone has not been found to be effec-tive in predicting violence among adults. Actuarial tools based on statistical analyses have been found to be more effective than clinical judgment when assessing adults (Quinsey, Harris, Rice, and Cormier, 1998). The existing tools and many studies have identified risk factors, such as past violent acts that are positively associated, and resiliency factors, such as a supportive adult and school success, that are negatively associated with violence (Christle, Jolivette, and Nelson, 2000) among juveniles.
The CARE-2 was developed using the various factors that have been identified in the literature and statistical analyses as predictors of youth violence. It is not merely an interview guide, but a reliable and valid measurement tool that provides additional data to the clinician charged with making an important judgment. Data should be col-lected from as many sources as possible.
The question becomes, “How much error is acceptable? In which direction are errors acceptable in making deci-sions about which youth are to be placed in a structured setting and which ones will remain in the community?” Some of the guided clinical interview assessments for ju-veniles have not been tested for criterion validity (DVI-J, RSTI, EARL-20B and 21G). So there is no way to know what the error rate is. ROC is a statistic that can be used to evaluate the relationship of an assessment score and the criterion variable and compensate for the low base rate of the behavior. From this we can estimate the cor-rect classification rate and the incorrect classification or error rate. ROC’s of .51 to .75 still have a substantial er-ror rate (49% to 25% of the time your risk classification will be wrong). If we assume, as in adults that the ROC for unaided clinical judgment is around .51, then any im-provement over that is progress. ROC’s above .76 should be the preferred standard (CARE-2, SAVRY).
10 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
Although the rates of juvenile crime declined from 1993 through 2008, there is still a significant problem with ju-venile violence and sex offending (Puzzanchera, 2009). Research in this area has identified five broad categories of risk and protective factors (Howell, 1995; Browning et al., 1999, Hahn, et. al., 2007, Milder, et. al., 2011, Seifert, 2012).
These broad categories are labeled differently by vari-ous researchers. For our purpose of creating the CARE-2 items are divided into historical items (happened any time in the youth’s lifetime) and recent descriptors (oc-curred in the last six months). Additionally, there are static (items that are historical and cannot change) and dynamic factors (items, such as skill proficiency and resiliency factors that can change over time). Categori-cally, there are items related to:
(1) behavior
(2) family characteristics
(3) neurological and substance abuse
(4) mental health
(5) skill and educational factors
(6) resiliency factors
(Seifert, 2007; Werner, 1996).
The CARE-2 is designed to collect data on specific be-haviors or individual characteristics associated with each of the categories. Each specific behavior or individual characteristic is further categorized as either a risk or protective factor.
Once the form is completed, the scoring system pro-vides the clinician with an effective and research-based approach to summarizing the collected ratings. Simply put, the greater the number of risk factors and the fewer the protective factors, the more likely it is that a child or adolescent will be violent. It is important not to label chil-dren or teens, but to provide them with services as soon as possible. Across from each item are suggested inter-ventions for each problem area. These are general sug-gestions that need to be adjusted to the specific needs of the youth and his family. The CARE-2 is intended to be used as a prevention and treatment planning tool.
YOUTH VIOLENCE: RISK AND RESILIENCY

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 11 © 2003-2012 by Kathryn SeifertCARE-2 Manual
Over time, a number of behaviors and individual char-acteristics have been hypothesized to either increase or decrease the likelihood that youths will engage in vio-lent behaviors. The Office of Juvenile Justice and Delin-quency Prevention (OJJDP) has identified five categories of risk and protective factors for youth violence. These factors include individual characteristics, peer relation-
ships, school, family, and environment. Children with more than five risk factors and less than six protective factors have an 80% chance of committing future violent acts (Howell, 1995). The following sections outline re-search findings related to these variables and detail how these variables are assessed by the CARE-2.
THE CASE FOR RISK AND PROTECTIVE FACTORS ASSOCIATED WITH YOUTH VIOLENCE
YOUTH CHARACTERISTICS
Individual youth characteristics encompass tempera-ment, skills, history, and behavior. Aggressive youth have serious and chronic behavior problems that often begin before the age of 12 (Thornton et al., 2000). Ad-ditionally, past aggression is the best predictor of future aggression (Quinsey, et al., 1998, Borum, 2000, Mulder et al., 2011, Seifert, 2012). In an extensive review of the literature, Leschied et al. (1993) found that escape from custody, re setting, and harming animals were signifi-cant risk factors in predicting youth violence. They also reported that chronic delinquencies, favorable attitudes toward antisocial acts, and other behavior problems are significantly associated with violence.
Additionally, Dr. Dorothy Otnow Lewis (1998) in her book,
Guilty by Reason of Insanity, stated that many such chil-dren have brain damage and/or a psychiatric disorder, in-cluding psychosis. She also found that paranoia and the over-attribution of hostile intent fueled much of teen and preteen aggression. Epidemiological studies have esti-mated the overlap between violence and mental illness to be 8% to 50% (Leschied, et al., 1993). Often, violent children have a combination of symptoms including hy-peractivity, impulsivity, depression, anxiety, obsessive/compulsive or bipolar symptoms, and frank psychosis. According to Fago (1999), ADHD is a strong predictor of delinquency and conduct disorders in adolescence. Shamsie, Lawrence, and Hood (2002) discuss the role of enuresis and encopresis, especially as it relates to ADHD, in the history of aggressive children. Violent chil-

12 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
dren are often also substance abusers (Arboleda-Florez, Holley, and Crisanti, 1996).
Several skill deficits are associated with aggression as well. Children with these deficits have difficulty manag-ing their emotions, solving problems, monitoring their behavior, and having empathy for others. They do not learn from their mistakes and they are not able to delay gratification (Braaten, 1998, Seifert, 2012). Youth who perform violent acts often do not understand how to use means-ends relationships, generating alternative solu-tions, looking at consequences before action, evaluating outcomes, and planning (Christle et al., 2000). They do not cope well with the stressors of everyday living. They often experience little emotion, but when they do, it can be explosive. They are frequently unable to self-soothe or self-calm. Another very important aspect appears to be attachment issues. “Attachment is the deep and
enduring connection established between a child and caregiver in the first several years of life. It profoundly influences every component of the human condition— mind, body, emotions, relationships, and values” (Levy and Orlans, 1998, p.1). Problems in the development of these primary attachment bonds because of early ne-glect, abuse, or exposure to violence can result in chil-dren who do not know how to participate in appropriate relationships with others. These youth can be violent, without empathy, and out of control. Boys who experi-ence attachment problems early in life are three times more likely to be violent (Levy and Orlans, 1998). Eighty percent of maltreated children show disorganized-dis-oriented attachment patterns resulting in children who are impulsive, rageful, out of control, and violent (Van der Kolk, 2003). They do not trust and they do not have empathy for others (Levy and Orlans, 1998).
Success, relationships, and positive self-worth are uni-versal needs. When children with disruptive attachment patterns fail to find them, they seek out others with simi-lar problems and views. In this deviant peer culture, they can become successful in their own eyes and the eyes of peers. Violent children often seek out younger and
weaker children and bully them (Leschied et al., 1993). They are rejected by pro-social peers and consequently, they befriend deviant youth who reinforce their negative behaviors (Thornton et al., 2000). Sometimes they be-come angry “loners.”
PEERS

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 13 © 2003-2012 by Kathryn SeifertCARE-2 Manual
Violent teens often have academic failure beginning in elementary school. Consequently, they lack a commit-ment to school, which holds no success or positive re-wards for them. Many of these children have learning disabilities or have low IQ. This makes school success difficult, if not impossible, especially if they do not re-
ceive needed services. Lacking success, they soon drop out of school or are truant, preferring to find high-risk activities in the community to sedentary days at school (Andrews, Hoge, and Leschied, 1992, Surgeon General’s Report on Youth Violence, 2001).
The families of violent children are often aggressive, vio-lent (Youth Violence: A Report of the Surgeon General, 2001), abusive, and neglectful, with problem behaviors, weak family bonding, and little warmth and nurturing (Crespi and Rigazio-DiGilio, 1996). Lewis (1998), as well, identified horrific abuse and violent family background as factors leading to youth violence.
When children are not nurtured or protected, they fail to thrive emotionally, behaviorally, and cognitively. There is now some evidence that childhood abuse and neglect can affect brain development and chemistry. Research at the Baylor University Medical School found that mal-treated children react to anger more strongly than non-abused children due to chronic elevation of stress and alarm neurotransmitters (Pollack, Cicchetti, Klorman, and
Brumaghine, 1997). Perry and Pollard (1997) found small-er brains among maltreated children when compared to non-maltreated children. This might explain the faulty per-ceiving and processing among maltreated children.
Environmental risk factors include communities where there is easy availability of and community standards that favor the use of drugs and rearms. If there is an ac-ceptance of crime as a way of life, the children of that neighborhood are more likely to use violent means to ac-complish their goals and to see violence as acceptable (Elliott, D.S. 1997). When extreme economic deprivation and other factors cause the path of pro-social success to be blocked or unavailable, youth may seek out other, of-ten antisocial, means to have money, “things,” and power (Andrews et al., 1992).
SCHOOL AND EDUCATION
FAMILY CHARACTERISTICS AND ENVIRONMENT FACTORS

14 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
If we look at the reverse of the above risk factors, we will find the conditions that have the potential to protect youth from a violent lifestyle. It gives us hints as to where to proceed with treatment. Children need consistent, positive, and nurturing caregivers that set rules, respect a child’s individuality, and provide secure attachment in order for them to grow up emotionally healthy. School success and pro-social peers can be a protective fac-tor. A positive social orientation is also helpful. Higher IQ and resilient temperament can help a child heal from environmental insults and learn to cope more effectively. When there are bonds to a supportive and pro-social
family, teachers, counselors, or other adults, youth have a chance to make choices other than violence. Clearly stated family and community rules and expectations and monitoring of child behavior can be effective in helping children learn to follow social norms (Andrews et al., 1992). A child who has good social and problem solv-ing skills, moral maturity, and an ability to manage emo-tions, particularly anger, will have fewer problems with violence. Children who are curious, enthusiastic, alert, set goals for themselves, and have high self-esteem and internal locus of control will be more resilient (Levy and Orlans, 1998).
PROTECTIVE FACTORS AND RESILIENCY
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 15 © 2003-2012 by Kathryn SeifertCARE-2 Manual
GENERAL INSTRUCTIONS FOR COMPLETING THE CARE-2 ASSESSMENT FORM
As I describe in my books, How Children Become Violent (Acanthus Publishing 2006), my interest in risk assessment began with my work in the adult prison system. I was as-saulted by an inmate that another professional had de-clared to be “not an imminent danger to self or others.” This inmate went on to kill several teenagers when he was released from prison. I decided then that we needed better ways to determine future risk of violence than we had been using. As with most violent offenders, he had a history of childhood trauma. The model upon which this instru-ment is built is based on a holistic evaluation of strengths and problems. Evidence based practices are connected to each problem area to guide treatment planning. I have made it my life’s mission to participate in the research and development of more accurate risk tools that inform risk management and treatment.
Over the years I have assessed or supervised the assess-ment of hundreds of children and adolescents. During that process, I began to organize information for those psycho-logical evaluations in a list of commonalities I found among youth with severe behavior problems. Through a literature review of risk and resiliency factors, I triangulated my ob-servations with the existing literature on risk. I added scor-
ing based on correlations of the item with actual acts of violence, and then began to collect a database. As I pro-gressed, I refined the list of items multiple times in order to advance the accuracy of the CARE-2. The criterion vari-able for this instrument is more than 3 assaults on others. Those with more than 3 assaults on others are more likely to use assaultive behavior to solve their problems and dis-putes in the future.
The CARE-2 is a combination risk and treatment needs as-sessment, delineating the estimated short term risk for vio-lence and the treatment and structure needs of the client. The sample includes 1031 youth from the East Coast and Mid-West. It can be used for youth ages 6 to 19. There are rural, suburban, and urban youth in the sample. Addition-ally, the youth have a full range of behavioral problems. The psychometrics on the CARE-2 are included in this manual. One unique feature of the CARE-2 is that interventions are listed with each item of the instrument. The risk score states that the “youth is (not, mildly, moderately, highly, or very highly) similar to youth with chronic (a history of more than three) assaults on others.” The scaling was made us-ing means and standard deviations and scatter plots of the particular group being evaluated. Youth who are highly
CHAPTER 2: ADMINISTRATION AND SCORING OF THE CARE-2

16 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
similar to young people with chronic (more than three) as-saults are two standard deviations above the mean for the total group. The mean for the low risk group is two stan-dard deviations below the mean for the total group. The “not similar group” was determined by the score below which there were no cases for which there were assault
histories. The moderate group contained both youth with and without histories of assaults. The “highly and very highly similar” groups contained only youth with histories of chronic (more than 3) assaults.
This section lists all items on the CARE-2 form. Some items are self-explanatory and require little or no ad-ditional information to guide you in filling out the form. Other items include explanation of the intent of the item to increase consistency across evaluators.
BACKGROUND INFORMATION
• Evaluator – Person completing the evaluation• Agency – Agency for which the evaluator is preparing
the report• Date – Date form completed
• Youth’s Name • Birth date • Age • Gender • Grade• Ethnicity• Problem behaviors - List all behaviors that are of concern
• Present placement – Where is the youth housed? At home or in a facility? Where is the youth’s present placement? If it is a temporary placement, state both the temporary and permanent placements.
Now you will see that there are four columns of scores across from the items. The CARE-2 is now normed for pre-teen (6 to 12) males, teen (13 to 19) males, preteen females (6 to 12), and teen females (13 to 19). Choose the column that is appropriate for the youth being evalu-ated. You will only use that column. Circle every number and “*” in that column for which that item is “True.” His-torical items are on pages 2 through 7 and present (last six months) items are on pages 8 through 11.
RISK FACTORS
Historical Behavior Factors. Score if this item occurred any time in the youth’s history.
ITEM SPECIFIC INSTRUCTIONS FOR COMPLETING THE CARE-2

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 17 © 2003-2012 by Kathryn SeifertCARE-2 Manual
1. SEVERITY OF BEHAVIORAL PROBLEMS. CHOOSE ONE.
• No history of behavior problems
• History of primarily mild and incidental behavior prob-lems (such as coming half-hour late for a curfew) or other psychiatric problems, such as depression. Can-not get one in trouble with the law.
• History of primarily moderate behavior problems (such as verbally bullies other children, minor theft. Can get one in trouble with the law.)
• History of chronic or severe behavior problems (such as assaults other children or adults). Has harmed another person in a way that can get one in trouble with the law.
2. SEVERITY AND CHRONICITY OF ASSAULTIVE BEHAVIOR. CHOOSE ALL THAT APPLY.
Use known physical assaults whether prosecuted or not.
a. One minor, isolated assault, minor fights with peers or siblings
b. Two or three intentional assaults
c. Assaults that causes harm, injury (required medical attention), or death to another (Severe assaultive be-havior that causes injury or death is also coded as a severe behavior problem on item 1d.)
d. Chronic assaults (more than three) (Chronic assaul-tive behavior is also coded as a severe behavior problem on item 1d)
e. Assault involving use of a weapon (such as gun, knife, baseball bat. Also check 1d).
3. SEXUAL ASSAULT OR VIOLATION OF ANOTHER
Any sexual assault is counted. Penetration is not nec-essary. It can be a touching or non-touching offense. Behaviors include offensive touching, exhibitionism, obscene phone calls, child abuse, incest, or rape.
4. ASSAULT OF AN AUTHORITY FIGURE (ALSO CHECK 1D)
Authority figures include teachers, policemen, and caregivers.
5. ESCAPE FROM CUSTODY
Youth escaped or has run away from a residential place-ment, detention center, group home, or other facility.
Note: Running away from home or a foster home is cod-ed below as runaway behavior.
6. HISTORY OF FIRE SETTING
Youth has set at least one fire, large or small, for no ap-parent utilitarian reason, or youth is fascinated with fires. Camp fires or rubbish fires that serve a purpose do not count for this item.

18 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
7. HISTORY OF HARMING ANIMALS
Youth has intentionally harmed, injured, tortured, or killed a pet or other animal. This includes wild or domestic an-imals, but does not include organized and supervised hunting or fishing.
8. MODERATE TO SEVERE BEHAVIOR PROBLEMS BEGINNING BEFORE THE AGE OF 13
Examples include theft, aggression, bullying, fighting, severe or chronic classroom disruption, vandalism, or substance abuse.
9. ENURESIS OR ENCOPRESIS
Bed-wetting or soiling occurs, day or night, after the age of 4 or 5. While some children have this prob-lem and it is a physical problem, it is still scored. Many youth with behavior disorders and attachment problems have wetting and soiling problems well into adolescence. This is related to immature brain de-velopment.
10. DELINQUENCY
Examples include theft, vandalism, destruction of prop-erty, threats of harm to others, disorderly conduct, or un-authorized use of a motor vehicle.
11. ATTACHMENT PROBLEMS OR REACTIVE ATTACHMENT DISORDER
a. Attachment problems, but no diagnosis of Reactive Attachment Disorder
Youth with attachment problems have some mild to moderate symptoms as listed below, but the disorder is not severe. There has been some early abuse or neglect, but it was not severe.
b. Diagnosis of Severe Attachment Disorder
For diagnosis of Reactive Attachment Disorder, youth must have had pathological caregiving, such as abuse, neglect, or exposure to domestic violence in the first four years of life.
Additionally, youth will display several of the following: aggression, lack of remorse, cold and calculating manner, manipulative behavior, poor eye contact, not following the rules, hyperactivity, food issues, roaming the house at night, anger management problems, and enuresis.
12. ABUSE IN THE FIRST THREE YEARS OF LIFE
This information can be from official reports and investiga-tions or reports by the youth, family, or caregiver. It may also be part of a case record. Any abuse by a family mem-ber or primary caregiver is recorded. If a parent or caregiver was severely depressed, psychotic, a victim of domestic violence, or a substance abuser, careful and complete in-quiry should be made to ascertain if abuse occurred.
13. NEGLECT IN THE FIRST FOUR YEARS OF LIFE
This information can be from official reports and inves-

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 19 © 2003-2012 by Kathryn SeifertCARE-2 Manual
tigations or reports by the youth, family, or caregiver. It may also be part of a case record. Any neglect by a family member or caregiver is recorded. If a parent or caregiver was severely depressed, psychotic, a victim of domestic violence, or a substance abuser, careful and complete inquiry should be made to ascertain if neglect occurred. Neglect can be emotional or physical and includes not providing the necessities of life, such as food, a safe and healthy environment, nurturing, and opportunities for growth and development.
14. ABUSE OR NEGLECT AT AGE 4 AND ABOVE
Score this item regardless of whether you have scored 2 points for abuse and neglect before the age of 4 in Items 34 and 35. If there is a history of family or caregiver violence, serious inquiry is needed. If there is chronic substance abuse by the family or caregiver, inquire about neglect of physical and emotional needs of the youth.
15. HISTORY OF VIOLENCE, ABUSE OR NEGLECT, OR CRIMINALITY IN THE FAMILY OR CAREGIVER
Score this item if any family member in the household (including aunts, uncles, and grandparents) or a care-giver who had significant interaction with the youth had a history of any of these problems.
16. INAPPROPRIATE DISCIPLINARY PRACTICES BY PARENTS. DISCIPLINE OR SUPERVISION THAT IS TOO LAX, TOO SEVERE, OR INCONSISTENT
Score for any caregiver, past or present. Parent or care-giver enables the youth to display or use poor limits, boundaries, or choices. Parent or caregiver does not monitor youth’s behavior. OR parent or caregiver uses discipline that is harsher than the infraction calls for. OR parent or caregiver vacillates between discipline that is too lax and too harsh. There is little or no consistency. If a youth is in placement, answer this item according to the behavior of the previous caregivers.
17. IF ANY ITEMS, 14 – 16, ARE CHECKED, CIRCLE THE “*” OR SCORE OF THIS ITEM.
18. FAMILY HAS LOW WARMTH AND/OR HIGH CONFLICT
Score for any caregiver, past or present. This item in-cludes significant conflict or fighting within the home and little warmth and nurturing between family or care-giver and the youth.
19. CAREGIVER HISTORY OF INSUFFICIENTLY TREATED SUBSTANCE ABUSE OR PSYCHIATRIC DISORDERS
Score for parent or any caregiver with whom the child has lived for more than six months.
20. ONE OR BOTH PARENTS ADDICTED, DEAD, OR UNINVOLVED IN YOUTH’S LIFE.
Score for any caregiver, past or present.

20 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
21. HAS BEEN BULLIED BY PEERS OR OTHERS AT ANY TIME IN HIS OR HER LIFE.
Youth has been intimidated, mistreated, harassed, ostra-cized, or otherwise abused by peers or others.
HISTORICAL SUBSTANCE ABUSE AND NEUROLOGICAL PROBLEMS
22. SUBSTANCE ABUSE
Youth uses alcohol or drugs of any kind, including abuse of prescription medications. Substance abuse before the age of 12 is a strong predictor of life-long problems with substance abuse.
23. NEUROLOGICAL IMPAIRMENT
Circle or specify the cause of neurological impairment. It may be due to a head injury, fetal alcohol syndrome, being born crack addicted, lead poisoning, or substance abuse.
24. PSYCHIATRIC SYMPTOMATOLOGY
Circle or specify psychiatric symptoms, such as anxiety, panic attacks, depression, mood swings, hyperactivity, poor concentration, obsessions, compulsions, halluci-nations, delusions, Bipolar disorder, PTSD.
RECENT MENTAL HEALTH, BEHAVIOR/SKILL/ EDUCATION ITEMS. SCORE IF ITEM IS
PROMINENTLY PRESENT ANY TIME DURING THE LAST SIX MONTHS.
25. ANGER MANAGEMENT PROBLEMS
Include over-controlled and out-of-control anger. Youth has a “hot” temper or is easily angered without sufficient provocation. When provoked, anger is often out of con-trol and may lead to yelling, pushing, hitting, punching walls, or throwing things. Over-controlled anger is dem-onstrated by having no demonstrable anger most of the time, even when justified. However, at some point, sometimes over trivial matters, over-controlled youth ex-plode with out-of-control anger or rage.
26. RUNAWAY BEHAVIOR
Youth has run away from home, a foster home, or other caregiver.
27. LACKS REMORSE FOR OFFENSES OR EMPATHY FOR OTHERS
Youth is sad that he/she was caught, but does not ex-press sorrow for harm caused to another. He/she does not express sadness in response to someone who has been harmed or is sad.
28. PROBLEM SOLVING
a. Problem solving includes generating several possi-ble solutions, weighing pros and cons, making good

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 21 © 2003-2012 by Kathryn SeifertCARE-2 Manual
choices, and making another choice if the first choice does not work.
b. Good problem solving skill most of the time
c. Deficient problem solving skills most of the time Can-not follow the above steps more than 30% of the time.
The youth can be asked, “If you lost your favorite ___ _____, what would you do?” and/or “If you were lost in a strange city, what would you do?” The youth must be able to generate at least two possible solutions and pro-pose that he/she would try one and if it did not work, he/she would try another possible solution.
If a youth breaks societal norms or is in conflict with oth-ers more than 50% of the time, it is likely he/she uses aggression to solve problems and does not have alter-native strategies for day-to-day problem solving.
29. BELIEF IN THE LEGITIMACY OF AGGRESSION AS A MEANS TO AN END
Youth believes that it is acceptable to use aggression to get what one wants.
30. FAVORABLE ATTITUDE TOWARD ANTISOCIAL BEHAVIOR
Youth favors antisocial activities, such as theft, vandal-ism, or selling drugs. Peers who are engaged in antiso-cial acts influence him/her. Example: Stealing is OK if you get away with it.
31. POOR SOCIAL SKILLS
Youth has difficulty sharing and communicating feelings and needs to others appropriately. He/she fights with or bullies peers, is overly shy or aggressive, and is rejected by peers. Youth does not often participate well in social activities with peers.
32. BULLYING BEHAVIOR
Youth bullies, intimidates, harasses, ostracizes, or ex-torts money from other youth.
33. DEVIANT PEER GROUP
Peer group is not prosocial and is antisocial or sexually deviant. Youth prefers to spend time with other youth who also have behavior problems, get into trouble, and are delinquent, substance abusing, and truant.
34. LIMITED ASSOCIATION WITH PRO-SOCIAL PEERS
Youth does not associate with or have close friends who follow the rules and don’t get into trouble or have behav-ior problems.
35. PARANOIA OR INTERPRETATION OF BENIGN EVENTS AS HOSTILE
Youth believes that many or most people are against, angry with, or intend to harm him/her. Youth is constantly on guard against harm from others. Small or accidental slights or bumps are interpreted as intentional harm.

22 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
36. TRUANT
Youth has missed more than 20 days of school in a school year without a valid excuse or has dropped out of school and has not attempted to get a GED. If the youth is work-ing, rather than attending school, he/she has missed work regularly (more than five days) without a valid excuse or has been dismissed from a job for absenteeism.
37. IQ BELOW 80
Full scale IQ can be estimated from what is known or IQ tests can be used. Youth has developmental disabili-ties, receives special education, or does not do well in school due to IQ.
38. LEARNING PROBLEMS WITH POOR SCHOOL PERFORMANCE AND FRUSTRATION
Youth is working two or more years below grade level. Grades are less than average. Youth is frustrated with school due to lack of success. Tests indicate skills are two years below expected age level.
39. CHRONIC SCHOOL BEHAVIOR PROBLEMS
Youth has more than three suspensions, expulsion, reg-ular fights with peers or assaults on staff, or frequent classroom disruptions.
40. LACKS COMMITMENT TO EDUCATION
Youth does not expect to graduate or get a GED and
does not think that it is important to do so.
41. AT RISK FOR INCARCERATION OR SECURE PLACEMENT
Youth has failed outpatient treatment and presents a danger to the community. Consideration is being given to higher level of care.
42. IMPULSIVITY
Youth regularly acts quickly without thinking about the consequences of the actions. A past diagnosis of ADHD may include a history of impulsivity.
43. EMOTIONS POORLY REGULATED.
Youth has flat or blunted affect or emotions are out of control. Youth displays no emotions and/or emotions are explosive and out of proportion or inappropriate to the situation. Youth with flat affect do not demonstrate laughing, crying, anger, even when the situation would warrant it.
44. PSYCHOSIS, SELF-HARM, SUICIDE ATTEMPT
Some youth have strange, odd, or unusual behav-iors, ideas, speech, or mannerisms. They may have nonfunctional rituals that they repeat over and over again in order to feel OK. They have no friends or only one friend and are unable to relate to others in a posi-tive way. Other youth reject them. They have strange behaviors or hallucinations, and their appearance is
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 23 © 2003-2012 by Kathryn SeifertCARE-2 Manual
odd. This category includes self-harm and suicide at-tempts. Check those that apply.
RESILIENCY FACTORS – CHECK IF THESE APPLY FOR ANY TIME IN THE LAST SIX MONTHS
45. AVERAGE IQ AND ABOVE
Full Scale IQ can be estimated from what is known or results of IQ tests can be used.
46. SUPPORTIVE, NURTURING CAREGIVER, OR OTHER ADULT WHO PROVIDES APPROPRIATE BOUNDARIES AND LIMITS
Score for parent or present caregiver. If the youth is in residential placement, score for a staff member who has a relationship with the youth or a relative or community member, such as a minister or mentor, who visits regu-larly and has a positive relationship with the youth.
47. APPROPRIATE PARENTAL OR CAREGIVER DISCIPLINE AT THE PRESENT TIME
Parental or caregiver discipline is neither punitive nor harsh. There is appropriate reinforcement of positive be-haviors and discipline is consistent and effective.
48. POSITIVE SCHOOL EXPERIENCE
Child achieves at least average grades, expresses posi-tive feelings about school and his/her progress in school, and has good school behavior.
49. LACK OF OR INSUFFICIENTLY TREATED PSYCHIATRIC OR SUBSTANCE ABUSE PROBLEMS IN YOUTH OR FAMILY OF ORIGIN
Neither youth nor any family member has a history of psychiatric problems (anxiety, depression, OCD, ADHD, panic attacks, or “nervous breakdown”) or substance abuse problems without sufficient treatment.
50. APPROPRIATE AND ACHIEVABLE FUTURE GOALS
Youth plans to finish high school or to complete GED and plans for appropriate, achievable career, or job based on ability and motivation. Being a basketball star with no back-up career is not a realistic goal. Joining the military is not realistic if the youth has poor disci-pline habits and does not finish high school.
51. REGULARLY PARTICIPATES IN POSITIVE ACTIVITY
Positive activities include sports, civic activities, church, or clubs.
52. SIX MONTHS EFFECTIVE TREATMENT
The total amount of time in any effective treatment can be used. If behaviors are improving, treatment is effective.
24 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
53. RELATES POSITIVELY TO PRO-SOCIAL PEERS
Socializes with persons who attend school, work, and do not break the law.
54. MODULATES EMOTIONS WELL
Is able to calm down when upset in a reasonable period of time. Has a full range of emotions and displays them appropriately when the situation calls for it.
55. TAKES MEDICATION AS PRESCRIBED
Does not miss doses or stop medication without con-sulting physician.
56. PARENTS/CAREGIVERS SUPPORTIVE OF TREATMENT AND RECOVERY
Parents or caregivers facilitate and/or attend treatment sessions and make sure medication is available and is taken as prescribed.
57. MINIMAL CONFLICT WITH PARENTS, SIBLINGS, CAREGIVERS, PEERS, TEACHERS
Gets along well with others most of the time. When there is conflict, it is not out of control and good problem solv-ing is used.
INSTRUCTIONS FOR SCORING THE CARE-2
Add all of the Risk Factors and record the total as the Risk Score. Add all of the Protective Factors and record the total as the Resiliency Score. Subtract the Resilien-cy Score from the Risk Score. This is the Total CARE-2 Score. Circle the range that contains the youth’s score on the chart on page 14. The categories are “ Not, Mild-ly, Moderately, and Highly Similar” to youth with a his-tory of chronic (more than 3) assaults on others. This chart is based on the placement of scores on a normal bell curve using group means and standard deviation of the sample group. Highly similar youth are more than 2 standard deviations above the mean for Chronic As-saults and Mildly similar youth are less than 2 standard deviations below the mean for chronic assaults in the sample. Use the column that represents the gender and age of the youth being evaluated. As the Total CARE-2 Score increases, the need for structure and intensity of services also increases. There is always a degree of error in any test score. Consequently, the categories should be seen as a continuum. If a score is within 2 or 3 points of the next highest or lowest category, clinical judgment should be used to determine the appropriate classifica-tion. Those in the Highly similar category are often in an “out of home” placement.
INTENSITY OF SERVICES
If a youth has a Low CARE-2 score, weekly services are probably sufficient. Those in the moderate category
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 25 © 2003-2012 by Kathryn SeifertCARE-2 Manual
need services more than once per week. Those in the “Highly Similar Category” need daily in home services, often in an “out of home placement.” As the similarity to chronically assaultive youth increases, the level of struc-ture needed for the youth to be successful also increas-es. Those needing more structure often need help with the activities of daily living and may have developmental delays in basic life skills. A developmental assessment such as the Behavioral Objective Sequence by Dr. Braat-en is needed in these cases.
IN COMMUNITY VS. OUT OF COMMUNITY PLACEMENT
Youth need a developmentally healthy environment in or-der to grow up in a healthy manner. The lower the simi-larity to youth at risk for chronic violence, the healthier the present home environment and the supportiveness of parents or caregivers can help determine the appro-priateness of placement in the community. Check those items that apply on Page 16 to assist in determining like-ly success in a community placement.
IN HOME VS. OUT OF HOME PLACEMENT
Check all items that apply. Healthy home environments, supportive families, and low similarity to youth with chronic assaults can assist in determining the likelihood of success when a youth receives treatment while re-maining in the home. If all items are answered “yes,” it is likely that the youth can be treated in the home. If there
are “no” responses to more than 3 items, the likelihood of successful treatment is lower.
LENGTH OF TREATMENT NEEDED
Check all boxes that apply. When developmental skills are delayed (measured by the Behavioral Objective Se-quence by Dr. Sheldon Braaten), developmental inter-ventions are needed until high school level of skills is reached and environmental problems are reduced to a minimum.
DEFINITIONS
Assault — Intentionally striking another person more than once with sufficient force to inflict moderate to se-vere pain or any level of injury. The striking is not done in play or in the course of an organized game. It includes physical fighting with peers or physical bullying of other youth.
Attachment — The deep, enduring emotional relation-ship between a child and a caregiver established in the first three years of life.
Authority figures — Those persons in a capacity of power, such as judges, police, teachers, and caregivers.
Caregiver — The person responsible for the youth’s care, preferably the person with whom the youth lives. If the youth is in residential care, the “present” caregiver is the primary therapist, nurse, or counselor.

26 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
Neglect — Not adequately providing the necessities of life, i.e., insufficient food, shelter, emotional nurturing, stimulation, opportunity to play and learn, and caregiv-ing. It includes leaving a small child or infant alone for long periods of time.
Severe Attachment Disorder (e.g., Developmental or Complex Trauma Disorder – Van der Kolk) — Can be the result of the disruption of the normal attachment bonds by pathological caregiving, such as abuse, se-vere neglect, separation from caregiver, or exposure to violence. Pathological caregiving is essential to the diagnosis. Youth with Severe/Disorganized Attachment Disorder are aggressive, violent, out of control, hyperac-tive, may harm animals, and frequently have enuresis. Youth with attachment disorders may also have poor eye contact. Attachment can be anxious, ambivalent, disor-ganized, or absent. Youth with disorganized type of at-tachment bonds are emotionally cold and lack empathy for others. They are manipulative and self-centered.
Serious Injury — An injury that requires medical attention.
Sexual Offense — Any behavior of a sexual nature com-mitted against a child or teen who is more than three years younger than the offender or an offense that is against the victim’s will or without consent. It can include rape, molestation, exhibitionism, peeping, and fetishes.
Weapon — Any instrument that is used to cause harm, such as a gun, knife, or baseball bat, or common objects used to cause harm, such as a hammer, wrench, lamp, bottle, or vase.
INTERAGENCY COORDINATION
Youth with multiple problems will need a greater variety of services that target the youth’s problem areas. When multiple agencies are involved, interagency coordination is essential. In this section, list the agencies involved with the youth and family or caregiver.
SERVICES NEEDED, BUT NOT IN PLACE
List the services that are indicated by this case manage-ment planning form, but are not yet provided.
POSSIBLE RESOURCES AND BARRIERS
List the resources in the community that could help the youth as well as the barriers that need to be addressed in order to optimize success.
OTHER COMMENTS
List any other information that would be helpful in plan-ning treatment for the youth.

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 27 © 2003-2012 by Kathryn SeifertCARE-2 Manual
CHART 2.1. SCORING CHART
Male, ages less than 13, Chronic As-saults.Circle the box that applies. The high-er the score, the greater the external level of structure needed to ensure good boundaries.
Male, ages greater than 12, Chronic Assaults.Circle the box that applies. The higher the score, the greater the external lev-el of structure needed to ensure good boundaries.
Preteen Female Chronic Assaults.Circle the box that applies. The higher the score, the greater the external lev-el of structure needed to ensure good boundaries.
Adolescent Female Chronic As-saults.Circle the box that applies.
The higher the score, the greater the external level of structure needed to ensure good boundaries.
Negative numbers to 20
Youth is not similar to youth with chronic assaultive behavior.
Negative numbers to 20
Youth is not similar to youth with chronic assaultive behavior.
Negative Numbers to 39
Youth is not similar to youth with chronic assaultive behavior.
Negative Numbers to 29
Youth is not similar to youth with chronic assaultive behavior.
21 to 57
Youth is mildy similar to youth with chronic assaultive behavior. Outpa-tient services that are specific to as-saultive behavior problems plus any other intervention needed.
21 to 51
Youth is mildly similar to youth with chronic assaultive behavior. Outpa-tient services that are specific to as-saultive behavior problems plus any other intervention needed.
40 to 62
Youth is mildly similar to youth with chronic assaultive behavior. Out-patient services that are specific to problems of aggression plus any oth-er intervention needed.
30 to 61
Youth is mildly similar to youth with chronic assaultive behavior. Out-patient services that are specific to problems of aggression plus any oth-er intervention needed.
58 to 65
Youth is moderately similar to youth with chronic assaultive behavior. Mul-tiple services and supports are needed. Therapy related to chronic assaultive behavior. Family therapy, skill building, anger management. Therapy that coor-dinates the efforts of the various agen-cies involved with the family. Rules for supervised contact with children of same age and gender as victim.
52 to 63
Youth is moderately similar to youth with chronic assaultive behavior. Mul-tiple services and supports are needed. Therapy related to chronic assaultive behavior. Family therapy, skill build-ing, anger management. Therapy that coordinates the efforts of the various agencies involved with the family. Rules for supervised contact with children of same age and gender as victim.
63 to 100
Youth Is moderately similar to youth with chronic assaultive behavior. Mul-tiple services and supports are needed. Therapy related to chronic assaultive behavior. Family therapy, skill building, anger management. Therapy that coor-dinates the efforts of the various agen-cies involved with the family. Rules for supervised contact with children of same age and gender as victim.
62 to 84
Youth Is moderately similar to youth with chronic assaultive behavior. Mul-tiple services and supports are needed. Therapy related to chronic assaultive behavior. Family therapy, skill build-ing, anger management. Therapy that coordinates the efforts of the various agencies involved with the family. Rules for supervised contact with children of same age and gender as victim.
66+
Youth is highly similar to youth with chronic assaultive behaviors. Highly structured living environment such as Wrap Around in the home or treat-ment foster care with no other chil-dren in the home and a high level of services. Rules for supervised con-tact with children of same age and gender as victim.
64+
Youth is highly similar to youth with chronic assaultive behaviors. Highly structured living environment such as Residential Placement. Rules for supervised contact with children of same age and gender as victim.
101+
Youth is highly similar to youth with chronic assaultive behaviors. Highly structured living environment such as Wrap Around in the home or treat-ment foster care with no other chil-dren in the home and a high level of services. Rules for supervised contact with children of same age and gender as victim.
85+
Youth is highly similar to youth with chronic assaultive behaviors. Highly structured living environment such as Residential Placement. Rules for supervised contact with children of same age and gender as victim.

28 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
READING THE SCORING TABLE
The scoring table gives four sets of norms: pre-teen male, adolescent male, pre-teen female, and adolescent female. Use the column that applies to the youth being assessed. Circle the youth’s score in that column. The cell will give you suggestions that indicate how this youth may be simi-lar to others his/her own age and what interventions may be needed. Remember, this is only a guide; always take individual circumstances into account.
PLACEMENT
It is appropriate to place children below the age of 13 in a home-type setting. The more prone to aggression a youth is, however, the greater the level of monitoring, services, consistency, structure, natural consequences, and positive reinforcement is needed. Older youth can be considered for out-of-home placements. This in-crease in structure is indicated in the scoring chart at the end of the assessment for each age group.
INTERVENTIONS
Assess family functioning. Youth live within the con-text of a family. Their recovery and ability to gain skills and improve functioning depends on the skill level and support of parents and siblings. Interview the family to determine if there are other family needs to be met that might improve the youths’ chances for success.
Assess for neurological disorders. If there is evidence
of past head injury, lead paint ingestion, loss of con-sciousness, seizure activity, refer to primary care physi-cian or neurologist.
Assess for psychiatric disorders. If any symptoms of sadness, anxiety, hypomania, phobias, night terrors, mood swings, impulsivity, inattention, lack of concentra-tion, refer to mental health provider.
Assess for trauma history or early problems with pathological caregiving. Ask about past traumatic events, caregiving, and losses. If present, refer to mental health provider. Assess for developmental delays related to early trauma.
Attachment-informed therapy. When there has been pathological caregiving resulting in persistent devel-opmental delays in interpersonal functioning, the pro-fessional must strengthen the skills in the appropriate developmental sequence. The Behavior Objective Se-quence is helpful for this (Sheldon Braaten, http://Re-searchPress.com).
Behavioral health services or mental health services. Look for social worker, licensed counselor, or psycholo-gist in your area. Many will be listed in the phone book. Ask your insurance company.
Behavior modification, positive reinforcement. Posi-tive reinforcement should outnumber punishments by a ratio of 4 to 1. Find reinforcers that the youth desires enough to work for him. Use privileges he may already have, but make him earn them. Use a chart to count compliance. Gear the whole process for success. Start

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 29 © 2003-2012 by Kathryn SeifertCARE-2 Manual
with goals that are easily accomplishable. What you re-inforce will increase.
Behavior Objective Sequence (Sheldon Braaten). De-velopmental Sequencing of behavioral assessment and training. (www.researchpress.com)
Build anger management skills. There are many CBT anger management groups and individual workbooks on the market.
Build drug resistance skills. Life Skills Training – www.lifeskillstraining.com.
Build problem solving skills. There are many CBT Problem-solving groups and individual workbooks on the market, such as PSST (Problem Solving Skills Train-ing).
Build self soothing skills, increase ability to man-age emotions well. There are many CBT “manage your emotions” group and individual workbooks on the mar-ket. (PATHS - www.prevention.psu.edu)
Build social skills. There are many CBT social skill group and individual workbooks on the market. (PATHS – www.prevention.psu.edu)
Cognitive Behavioral Therapy (CBT). Cognitive Behav-ioral Therapy involves changing how you think to change how you feel and behave. A type of CBT is Dilectical Be-havioral Therapy or DBT (www.behavioraltech.org).
Contracting. It helps a youth and family plan and orga-nize if they participate in developing and writing down
a contract of responsibilities and reciprocal meeting of needs. Everyone participates in making the contract for “buy-in,” and everyone agrees to follow it, and everyone signs it. It is re-evaluated periodically for changes.
Coordinate the efforts of the various agencies in-volved with the family. When there are multiple agen-cies involved with a family, arrangements for coordina-tion is essential.
Criminogenic factors. Criminogenic factors include be-liefs that: 1) other people’s needs don’t need to be taken into consideration; 2) the rules don’t apply to me; 3) if I get away with something, it is OK; 4) Stealing doesn’t hurt anyone. These errors in thinking can be examined using programs like Thinking For a Change (http://www.nicic.org/T4C).
Education on substance abuse and psychiatric is-sues. Education on the basic issues of symptoms, treat-ment, medication, and aftercare.
Educational services, educational testing, IEP. Schools can be contacted for additional services for children who are below the age of 18.
End abuse, neglect, and domestic violence. Call au-thorities, such as police or department of Social Servic-es to intervene.
End the source of bullying. School or classroom pro-gram such as Olweus Bullying Program ([email protected]).
Family Therapy. A youth functions within the context of

30 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
a family. Family therapy involves all members of the fam-ily. Examples include Functional Family Therapy (www.fftinc.com).
Fire setting specific treatment. There are a few re set-ting treatment programs involving education and CBT for errors in thinking. Family therapy may also be ap-propriate.
Grief therapy. When there is a loss, a therapist can help a person recover from the loss by being supportive and empathetic.
Highly structured living environment. When a youth does not have the internal structure (motivation) to con-trol his own actions, the environment must control his actions for him. This usually means some form of a level system, strict rules, ample staff, youth monitoring of be-havior, and sometimes locked doors.
Intensive outpatient services. For youth with multiple problems and a high level of treatment needs, more than one service per week will be needed. Intensive outpa-tient services is usually several hours per day and sever-al days per week. It includes skill building and individual and family therapy.
Interactive journaling – The Change Companies. The Change Companies make a variety of interactive jour-nals on many topics. They are CBT oriented. (http://www.changecompanies.net/)
Mentoring. Mentoring such as Big Brothers and Big Sis-ters of America (http://www.bbbsa.org)
Motivational interviewing. Motivational interviewing developed out of the substance abuse field. It is very effective with youth who have forensic issues, as well. (http://www.motivationalinterview.org/)
Multisystemic Therapy (MST). This therapy involves CBT, parent training, and family therapy (www.mstser-vices.com).
Multimodal Therapy. Where there are problems in mul-tiple aspects of youth and family’s life, address these problems in an organized way, directly or through refer-ral to an appropriate agency.
Parent education. Parent management training has been found to be effective (http://www.apa.org/divi-sions/div12/rev_est/pmt_child.html).
Pro-social peers. Increase association with pro-social peers and activities
Psychiatric Rehabilitation (PRP). PRP is used to assist the therapist in providing skill building for clients in their everyday life and support treatment goals.
Stages of change. A good resource is Changing for Good: A Revolutionary Six-Stage Program for Overcom-ing Bad Habits and Moving Your Life Positively Forward by James O. Prochaska, John C. Norcross, Carlo C. Di-clemente
Substance abuse assessment and treatment for youth and family. If you suspect substance abuse prob-lems, refer to an assessment by a substance abuse pro-fessional.

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 31 © 2003-2012 by Kathryn SeifertCARE-2 Manual
Supervised contact with other children. The youth should be supervised when interacting with children who are of the same approximate age and gender of the youth’s victim(s). If there have been victims of multiple ages and both genders, supervision should include all younger or more vulnerable children.
Therapy specific to assaultive behavior. Assaultive children have learned to solve their problems with anger and assault. These issues can be addressed with CBT. If it is a home that has violence, this must be addressed and stopped. If there has been trauma in the past, this must be addressed in therapy. Family therapy may be needed. Assess the level of problem solving skill and emotional regulation.
Thinking for a Change (http://www.nicic.org/T4C). CBT program for juvenile corrections available for free down-load.
Trauma therapy. When a youth has experienced a trau-ma, it can affect his behavior and ability to regulate emo-tions. A therapist trained in addressing trauma issues should be consulted.
Treatment specific to sexual behavior problems. Youth with sexual behavior problems have confusion and lack of understanding about sexual issues and be-
haviors. These issues can be addressed with educa-tion. Errors in thinking can be addressed with CBT. If it is a home that has inappropriate sexual boundaries, this must be addressed and stopped. If there has been trauma in the past, this must be addressed in therapy. Family therapy may be needed.
Vocational services, career planning. Positive future goals and the ability to reach them is a resiliency factor. Schools and vocational rehabilitation centers and devel-opmental disability centers can help with these tasks.
Wrap around services or intensive home services. In order to keep a child with a very high level of treatment needs in the home, a high level of services can be pro-vided in the home to the entire family.
Possible barriers. Barriers are things that might prevent the youth or family from being successful. Strategize how to remove barriers.
Youth and family strengths to build upon. List the youth and family strength. Consistently praise their strengths and use them to build toward other success where skills may not be so strong. Use it as an example and encouragement.
32 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
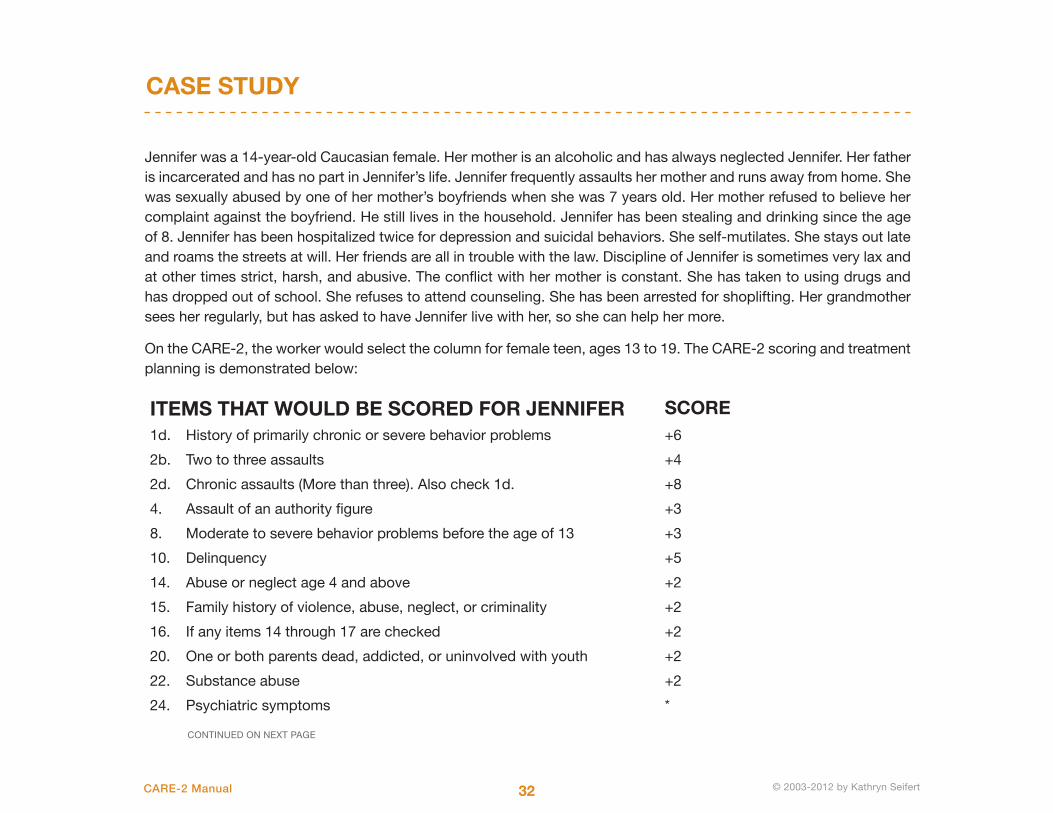
CASE STUDY
Jennifer was a 14-year-old Caucasian female. Her mother is an alcoholic and has always neglected Jennifer. Her father is incarcerated and has no part in Jennifer’s life. Jennifer frequently assaults her mother and runs away from home. She was sexually abused by one of her mother’s boyfriends when she was 7 years old. Her mother refused to believe her complaint against the boyfriend. He still lives in the household. Jennifer has been stealing and drinking since the age of 8. Jennifer has been hospitalized twice for depression and suicidal behaviors. She self-mutilates. She stays out late and roams the streets at will. Her friends are all in trouble with the law. Discipline of Jennifer is sometimes very lax and at other times strict, harsh, and abusive. The conflict with her mother is constant. She has taken to using drugs and has dropped out of school. She refuses to attend counseling. She has been arrested for shoplifting. Her grandmother sees her regularly, but has asked to have Jennifer live with her, so she can help her more.
On the CARE-2, the worker would select the column for female teen, ages 13 to 19. The CARE-2 scoring and treatment planning is demonstrated below:
ITEMS THAT WOULD BE SCORED FOR JENNIFER SCORE1d. History of primarily chronic or severe behavior problems +6
2b. Two to three assaults +4
2d. Chronic assaults (More than three). Also check 1d. +8
4. Assault of an authority figure +3
8. Moderate to severe behavior problems before the age of 13 +3
10. Delinquency +5
14. Abuse or neglect age 4 and above +2
15. Family history of violence, abuse, neglect, or criminality +2
16. If any items 14 through 17 are checked +2
20. One or both parents dead, addicted, or uninvolved with youth +2
22. Substance abuse +2
24. Psychiatric symptoms *
CONTINUED ON NEXT PAGE
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 33 © 2003-2012 by Kathryn SeifertCARE-2 Manual
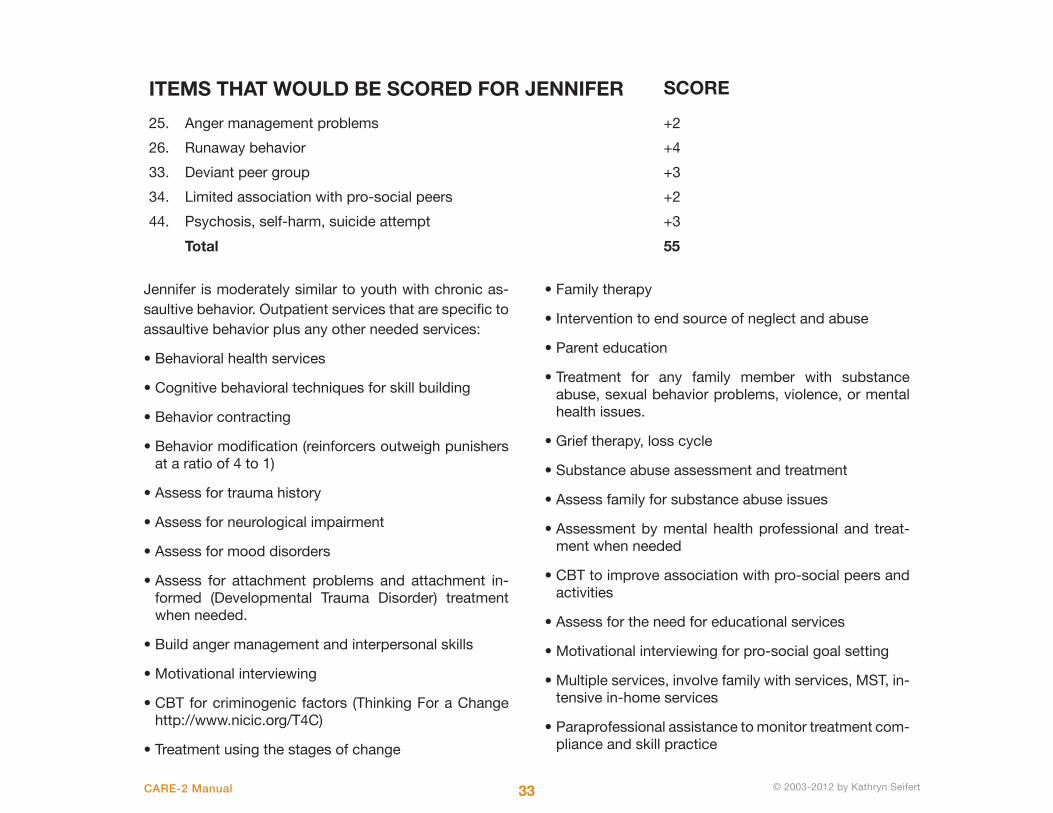
Jennifer is moderately similar to youth with chronic as-saultive behavior. Outpatient services that are specific to assaultive behavior plus any other needed services:
• Behavioral health services
• Cognitive behavioral techniques for skill building
• Behavior contracting
• Behavior modification (reinforcers outweigh punishers at a ratio of 4 to 1)
• Assess for trauma history
• Assess for neurological impairment
• Assess for mood disorders
• Assess for attachment problems and attachment in-formed (Developmental Trauma Disorder) treatment when needed.
• Build anger management and interpersonal skills
• Motivational interviewing
• CBT for criminogenic factors (Thinking For a Change http://www.nicic.org/T4C)
• Treatment using the stages of change
• Family therapy
• Intervention to end source of neglect and abuse
• Parent education
• Treatment for any family member with substance abuse, sexual behavior problems, violence, or mental health issues.
• Grief therapy, loss cycle
• Substance abuse assessment and treatment
• Assess family for substance abuse issues
• Assessment by mental health professional and treat-ment when needed
• CBT to improve association with pro-social peers and activities
• Assess for the need for educational services
• Motivational interviewing for pro-social goal setting
• Multiple services, involve family with services, MST, in-tensive in-home services
• Paraprofessional assistance to monitor treatment com-pliance and skill practice
25. Anger management problems +2
26. Runaway behavior +4
33. Deviant peer group +3
34. Limited association with pro-social peers +2
44. Psychosis, self-harm, suicide attempt +3
Total 55
ITEMS THAT WOULD BE SCORED FOR JENNIFER SCORE
34 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
SCALE DEVELOPMENT PROCESS
CHAPTER 3: TECHNICAL SUMMARY
The original CARE was developed from a list of perceived common characteristics Dr. Kathryn Seifert observed among behaviorally disturbed youth when administering approximately 30 to 60 psychological evaluations per year in the 1990s. Items were added to the list by per-forming a literature review of identified risk and resiliency factors for violence among youth, including existing risk tools. Once the list was developed, the author created a checklist and began collecting data by administering the checklist to youth (with signed consents) in three public mental health clinics (two of which were school based programs working closely with school personnel), sev-eral juvenile detention centers, youth hospitalized for a mental illness, youth incarcerated for a violent crime and sentenced as adults, several residential treatment cen-ters in the Mid-Atlantic region and the Midwestern re-gion, youth in a foster care/adoption agency, youth with no observable behavior problems, and those referred by courts for psychological evaluations.
Raters varied, depending on the data gathering setting. The majority of raters were mental health providers with advanced degrees who were therapists for the youth’s case, a psychologist providing a psychological evaluation for the therapist, or an independent rater in an institution
for which they had no connection with the clients or staff.
The hypothesis included:
• Youth with violent behaviors have a unique set of riskand resiliency factors.
• The more risk factors a youth had and the fewer resil-iency factors, the more likely he/she was to engage inviolent and other inappropriate interpersonal behaviors.
• Factors carry different salience based on their correla-tions to actual violent behavior problems. Thus, CARE-2 items were weighted based on the strength of theircorrelation with chronic violent behaviors (more than 3)committed by the youth.
• Maltreatment and exposure to violence in childhoodcan be related to delays in the development of skills,such as interpersonal relatedness, moral development,social skills, problem solving, and affect and behav-ior self-regulation. Dynamic risk factors, although lessreliable to measure, are essential factors to measurebecause of the theoretical underpinnings of the tool.
• Each problem area should be paired with an evi-dence-based intervention in a suggested case man-agement plan.
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 35 © 2003-2012 by Kathryn SeifertCARE-2 Manual
• Youth change over time and therefore their risk can change over time as well. Risk estimates should be ap-plied for a period of six months, and then a youth should be re-evaluated. This is especially true since dynamic factors, subject to change, are used in the tool.
The original CARE has one scale. The sample was not sufficiently large to justify separate age and gender norms, however, they were planned from the beginning. Nor did the statistics indicate that gender or age had significant correlations with the original CARE score.
The CARE-2 has four norms: Males 6 to 12, Males 13 to 19, Females 6 to 12, and Females 13 to 19. It was decided that interventions for very small children should be developed separately and that the sample was too
small to include children under the age of 6. The entire CARE sample was re-analyzed according to the gender and age groups above. Correlations were used to weight the items in each group. Numerical weights were used only to calculate risk scores. Those that did not enter the equation for the risk score were marked with an “*”. All items (numerical or “*”) remained in the scale because of the need to address interventions for that item if it was a problem for that particular youth. Items with and “*” that did not enter the risk score were retained because of their clinical importance in generating a treatment plan.
Various analyses were performed on the CARE and CARE-2. The CARE score correlated with the BASC Ag-gression Scale (r = .92), the PCL-YV (r = .71), and the SAVRY (r = .72).
DISCRIMINANT FUNCTION ANALYSIS
The items with numerical scores were subjected to dis-criminant function analysis. For males ages 6 to 12, there were four functions, listed below:
I. DELINQUENCY, AGGRESSION, LACKS REMORSE
• Assaults: not chronic, chronic, severe, using a weapon, and against an authority figure
• Believing in the legitimacy of aggression as a means to an end
• Delinquency
• Lacking remorse for one’s misdeeds or victims
II. BEHAVIOR PROBLEMS AND SKILL DELAYS
• A history of behavior problems
• Behavior problems before the age of 12
• Poor anger management
36 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
THE SAMPLE
• Impulsivity
• Poor problem solving skills
• Poor social skills
• Few pro-social peers
• Chronic school behavior problems
III. DEVELOPMENTAL TRAUMA DISORDER
• Childhood trauma
• Lacks commitment to school
• Harms animals
• Exhibits bullying behavior
IV. DISORGANIZED ATTACHMENT TYPE
• Attachment problems
• Fire setting
• Enuresis or encopresis
• Favorable attitudes toward anti-social behavior
Function I accounts for 97% of the variance, while all four functions combined account for 98% of the vari-ance. Other discriminant function analyses will be issued in an addendum to this manual.
To establish the statistical characteristics of the revised CARE-2 Assessment, it was administered to 1,026 in-dividuals. Of that number, 369 were children (ages 2 to 12), 636 were adolescent (ages 13 to 19), and 21 with missing data. From the sample, 677 were male and 328 were female, and 21 of the profiles were missing data. In terms of estimated intelligence, 72% of the sample (739) had average intelligence, 19% (195) had above average intelligence, 5% (51) had below average intelligence and 4% had missing data.
Data was collected from youth in outpatient treatment programs, residential settings, juvenile detention set-tings, group home facilities, and school settings. Of the outpatient group, approximately one third were Court involved. For comparison purposes data was also col-lected from a subset of youth with no reported behav-ioral problems. The main locations for data collection were the Mid-Atlantic and the Midwestern regions of the United States.

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 37 © 2003-2012 by Kathryn SeifertCARE-2 Manual
Youth placement varied as well, with 72% (739) living at home, 6% (62) in detention, 7% (72) in residential treatment placement, 4% (41) split between all other placement locations (e.g., foster care, independent liv-ing, group home placement, hospital, or prison), and 5% (51) had data missing. A variety of settings were used because it is likely that this instrument will be used in multiple settings.
The sample was assessed for other characteristics in-cluding trauma and abuse history, family history, assault and delinquency history, school background informa-tion, mental health and substance abuse history, and presenting social and psychological traits. Of the 1,026 individuals, 57% (759) did not report a history of early abuse, 25% (256) reported a history of early abuse, and 1% (11) had no data. Fifty-four percent (554) of the youth
200 –
150 –
100 –
50 –
0 –
Adolescents13-19 years of age
Pre-adolescents2-12 years of age
Num
ber
of In
divi
dual
s
CHART 3.1 HISTORY OF BEHAVIOR PROBLEMS BY AGE GROUP
History of Behavior Problems
NoneMildModerate
SevereAssaultiveBehavior Causes Harm or Injury
50 –
40 –
30 –
20 –
10 –
0 –
No History of Violence History of Violence
Num
ber
of In
divi
dual
s
Mild Post CARE-2 Behavior ProblemsModerate Post CARE-2 Behavior ProblemsSevere Post CARE-2 Behavior ProblemsAssaultive Post CARE-2 Behavior Problems
CHART 3.2 RELATIONSHIP BETWEEN HISTORY OF FAMILY VIOLENCE AND POST CARE-2 BEHAVIOR PROBLEMS

38 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
sampled reported that they had experienced a childhood trauma. Forty five percent (462) did not report a child-hood trauma, and one percent (10) had no data entered.
Assessment of family history traits indicated that 60% (616) of the youth sampled have a family history of vio-lence, 39% (400) did not report a family history of vio-lence, and 1% (10) had missing data. In comparison, of the 1,026 individuals sampled, 61% (400) did not report a history of low warmth in their families, 59% (605) did report a history of low warmth in their families, and 2% (21) had data missing.
History of violence, behavioral problems, and aggres-sive personality traits of the sample characteristics were also assessed. Of those sampled, 81% (831) reported moderate to severe behavior problems and 19% (195) reported mild behavior problems. Specifi-cally, 52% (534) have a chronic history of behavioral problems in school compared to 46% (472) who do not have a history of behavioral problems in school; 2% (20) had missing data. Eighty-one percent (831) of the sample reported a history of anger manage-ment problems compared to 18% (185) who did not report a history of anger management problems; 10
100 –
80 –
60 –
40 –
20 –
0 –
Positive Attitude Toward Antisocial
Behavior
Denied Positive Attitude Toward
Antisocial Behavior
Num
ber
of In
divi
dual
s
No Post CARE-2 AssaultsPost CARE-2 Assaults
CHART 3.3 RELATIONSHIP BETWEEN POSITIVE ATTITUDES TOWARD ANTISOCIAL BEHAVIOR AND POST CARE-2 ASSAULTS
CHART 3.4 SAMPLE CHARACTERISTICS BY PSYCHIATRIC PROBLEMS
No Psychiatric ProblemsPsychiatric ProblemsMissing Data
Frequency
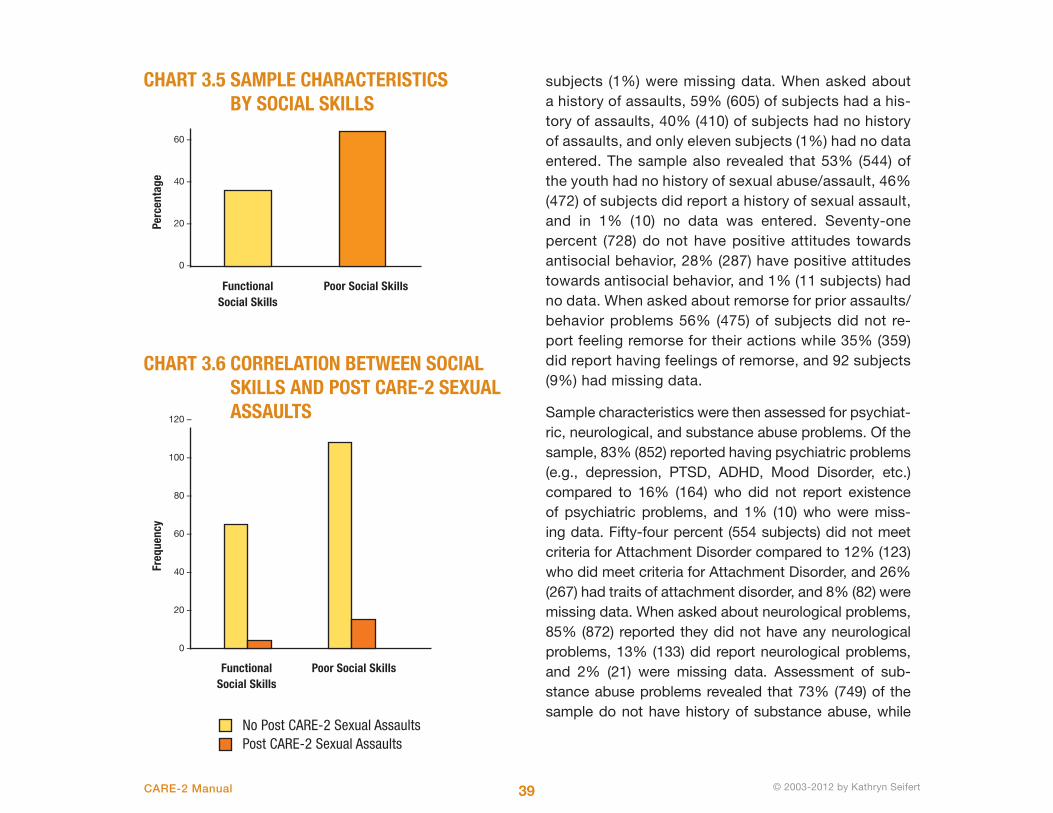
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 39 © 2003-2012 by Kathryn SeifertCARE-2 Manual
subjects (1%) were missing data. When asked about a history of assaults, 59% (605) of subjects had a his-tory of assaults, 40% (410) of subjects had no history of assaults, and only eleven subjects (1%) had no data entered. The sample also revealed that 53% (544) of the youth had no history of sexual abuse/assault, 46% (472) of subjects did report a history of sexual assault, and in 1% (10) no data was entered. Seventy-one percent (728) do not have positive attitudes towards antisocial behavior, 28% (287) have positive attitudes towards antisocial behavior, and 1% (11 subjects) had no data. When asked about remorse for prior assaults/ behavior problems 56% (475) of subjects did not re-port feeling remorse for their actions while 35% (359) did report having feelings of remorse, and 92 subjects (9%) had missing data.
Sample characteristics were then assessed for psychiat-ric, neurological, and substance abuse problems. Of the sample, 83% (852) reported having psychiatric problems (e.g., depression, PTSD, ADHD, Mood Disorder, etc.) compared to 16% (164) who did not report existence of psychiatric problems, and 1% (10) who were miss-ing data. Fifty-four percent (554 subjects) did not meet criteria for Attachment Disorder compared to 12% (123) who did meet criteria for Attachment Disorder, and 26% (267) had traits of attachment disorder, and 8% (82) were missing data. When asked about neurological problems, 85% (872) reported they did not have any neurological problems, 13% (133) did report neurological problems, and 2% (21) were missing data. Assessment of sub-stance abuse problems revealed that 73% (749) of the sample do not have history of substance abuse, while
60 –
40 –
20 –
0 –
Functional Social Skills
Poor Social Skills
Perc
enta
ge
CHART 3.5 SAMPLE CHARACTERISTICS BY SOCIAL SKILLS
120 –
100 –
80 –
60 –
40 –
20 –
0 –
Functional Social Skills
Poor Social Skills
Freq
uenc
y
No Post CARE-2 Sexual AssaultsPost CARE-2 Sexual Assaults
CHART 3.6 CORRELATION BETWEEN SOCIAL SKILLS AND POST CARE-2 SEXUAL ASSAULTS

40 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
RELIABILITY
Reliability was assessed for the CARE-2. Chronbach’s Alpha for internal reliability is .82. Other reliability statis-tics include correlation between forms = .54, Guttman Spit-Half = .70, Alpha for Part 1 = .84, Alpha for Part 2 = .76, Equal Length Spearman Brown = .70. Test-Retest
correlations were .70 and .72. There are items on the CARE that are very difficult to measure reliably, such as anger management, social skills, and problem solving ability. This reduces the reliability of the scale, but these items are essential for the development of a treatment plan. Making these items more precise would increase reliability, but reduce its practicality, by increasing its length. Additionally, youth change rapidly and often and it is important to have a scale that can show change and progress in skill development.
26% (267) do have a history of substance abuse, and 1% (10) were missing data. Seventy-seven percent (790) report symptoms of impulsivity, 22% (226) are not impul-sive, and 1% (10) was missing data.
Assessment of traits related to social skills and social functioning revealed that revealed that 63% (646) of the sample have poor social skills, 36% (369) have some
functional social skills, and 1% (11) was missing data. Of that sample, 66% (677) did not report having deviant peer group, while 33% (330) did report a deviant peer group, and 1% (10) was missing data.
A cross validation study by Salisbury University (2014) found test-retest reliability of .99.
drkathy2
Typewritten Text
drkathy2
Cross-Out
drkathy2
Cross-Out
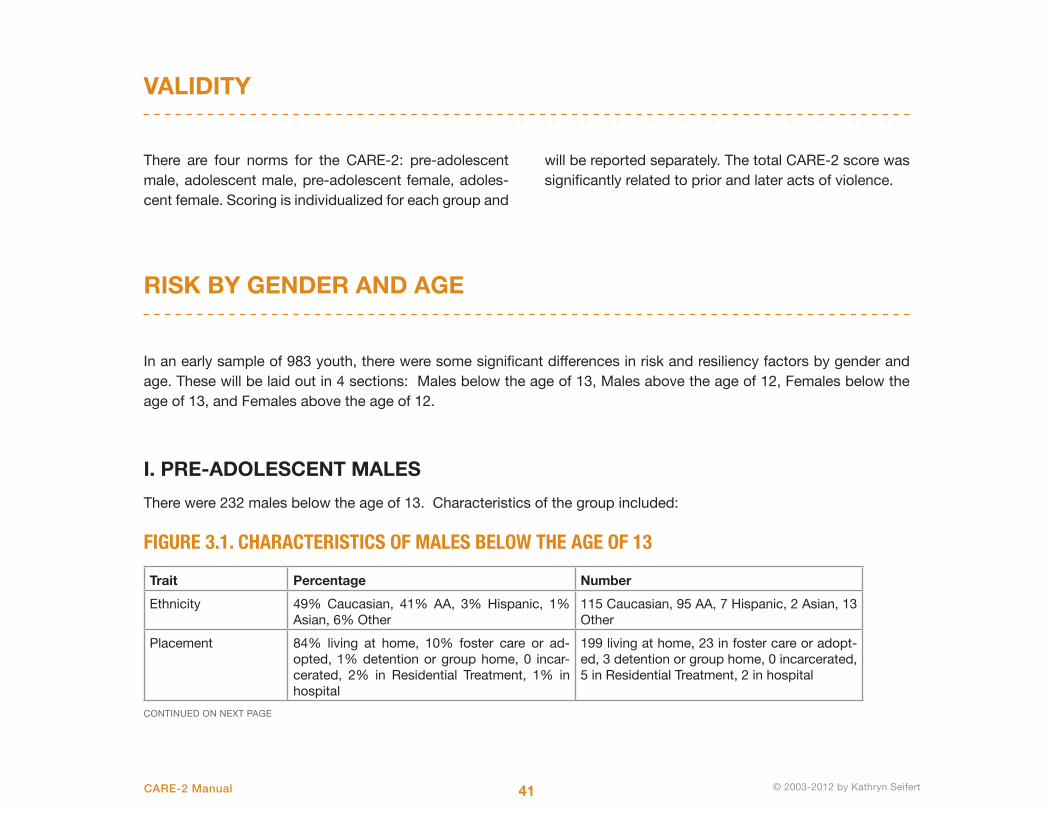
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 41 © 2003-2012 by Kathryn SeifertCARE-2 Manual
VALIDITY
RISK BY GENDER AND AGE
There are four norms for the CARE-2: pre-adolescent male, adolescent male, pre-adolescent female, adoles-cent female. Scoring is individualized for each group and
will be reported separately. The total CARE-2 score was significantly related to prior and later acts of violence.
I. PRE-ADOLESCENT MALES
There were 232 males below the age of 13. Characteristics of the group included:
FIGURE 3.1. CHARACTERISTICS OF MALES BELOW THE AGE OF 13
Trait Percentage Number
Ethnicity 49% Caucasian, 41% AA, 3% Hispanic, 1% Asian, 6% Other
115 Caucasian, 95 AA, 7 Hispanic, 2 Asian, 13 Other
Placement 84% living at home, 10% foster care or ad-opted, 1% detention or group home, 0 incar-cerated, 2% in Residential Treatment, 1% in hospital
199 living at home, 23 in foster care or adopt-ed, 3 detention or group home, 0 incarcerated, 5 in Residential Treatment, 2 in hospital
CONTINUED ON NEXT PAGE
In an early sample of 983 youth, there were some significant differences in risk and resiliency factors by gender and age. These will be laid out in 4 sections: Males below the age of 13, Males above the age of 12, Females below the age of 13, and Females above the age of 12.
drkathy2
Text Box
The CARE2 is also significantly correlated with the SAVRY (r = .71), the PCL-YV (r = .71) and the Forceful subscale of the MACI (r = .29).
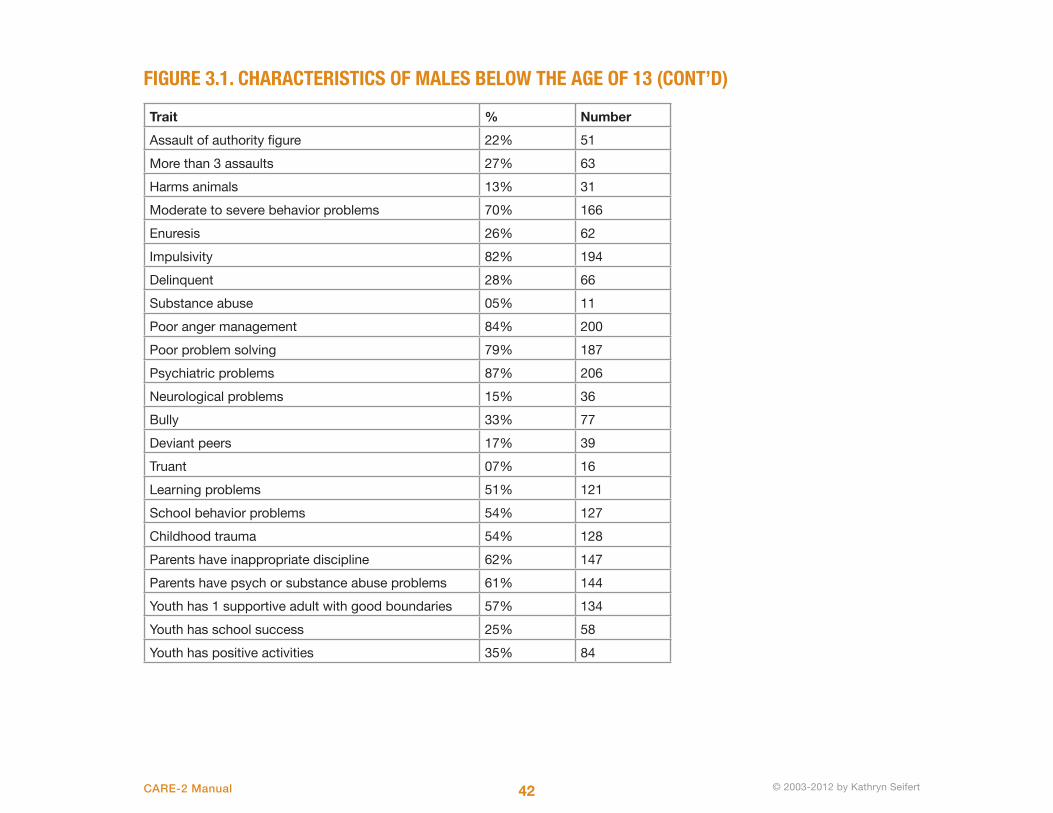
42 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
FIGURE 3.1. CHARACTERISTICS OF MALES BELOW THE AGE OF 13 (CONT’D)
Trait % Number
Assault of authority figure 22% 51
More than 3 assaults 27% 63
Harms animals 13% 31
Moderate to severe behavior problems 70% 166
Enuresis 26% 62
Impulsivity 82% 194
Delinquent 28% 66
Substance abuse 05% 11
Poor anger management 84% 200
Poor problem solving 79% 187
Psychiatric problems 87% 206
Neurological problems 15% 36
Bully 33% 77
Deviant peers 17% 39
Truant 07% 16
Learning problems 51% 121
School behavior problems 54% 127
Childhood trauma 54% 128
Parents have inappropriate discipline 62% 147
Parents have psych or substance abuse problems 61% 144
Youth has 1 supportive adult with good boundaries 57% 134
Youth has school success 25% 58
Youth has positive activities 35% 84
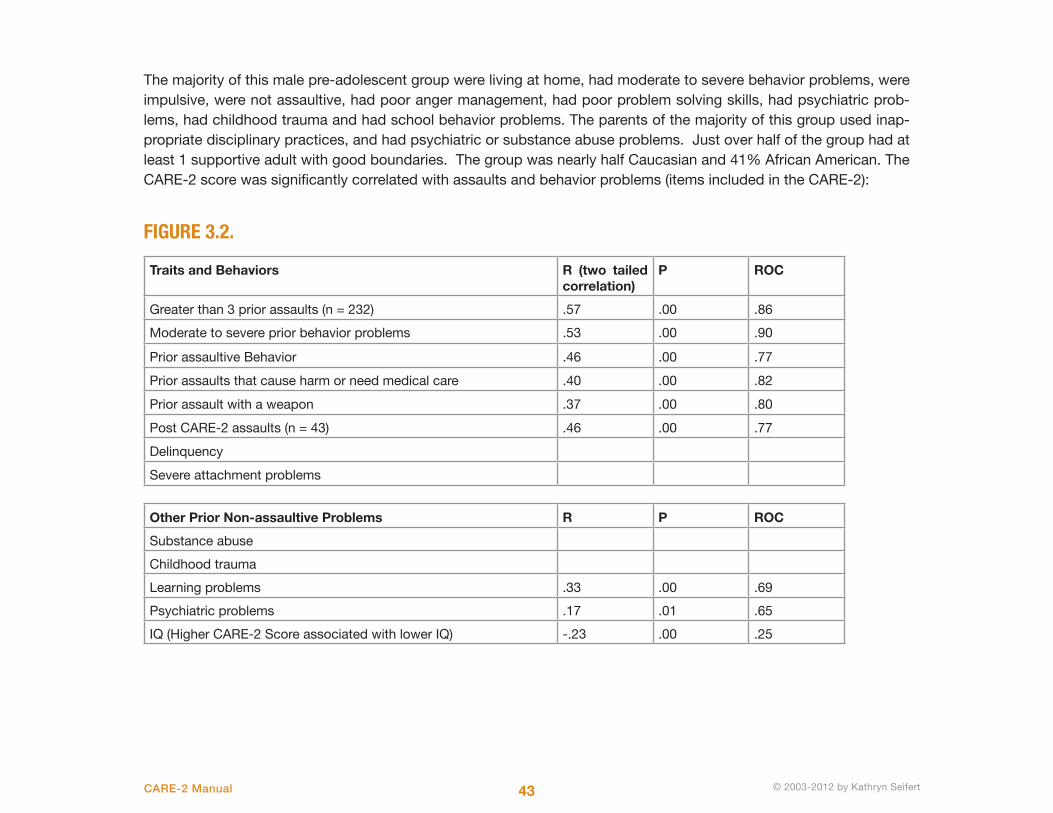
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 43 © 2003-2012 by Kathryn SeifertCARE-2 Manual
The majority of this male pre-adolescent group were living at home, had moderate to severe behavior problems, were impulsive, were not assaultive, had poor anger management, had poor problem solving skills, had psychiatric prob-lems, had childhood trauma and had school behavior problems. The parents of the majority of this group used inap-propriate disciplinary practices, and had psychiatric or substance abuse problems. Just over half of the group had at least 1 supportive adult with good boundaries. The group was nearly half Caucasian and 41% African American. The CARE-2 score was significantly correlated with assaults and behavior problems (items included in the CARE-2):
FIGURE 3.2.
Traits and Behaviors R (two tailed correlation)
P ROC
Greater than 3 prior assaults (n = 232) .57 .00 .86
Moderate to severe prior behavior problems .53 .00 .90
Prior assaultive Behavior .46 .00 .77
Prior assaults that cause harm or need medical care .40 .00 .82
Prior assault with a weapon .37 .00 .80
Post CARE-2 assaults (n = 43) .46 .00 .77
Delinquency
Severe attachment problems
Other Prior Non-assaultive Problems R P ROC
Substance abuse
Childhood trauma
Learning problems .33 .00 .69
Psychiatric problems .17 .01 .65
IQ (Higher CARE-2 Score associated with lower IQ) -.23 .00 .25

44 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
FIGURE 3.3. MEAN CARE-2 SCORES WITH ASSAULTS, DELINQUENCY, AND SEVERE ATTACHMENT PROBLEMS
Mean CARE-2 Score
Mean +1 SD Mean + 2SD CARE-2 Score Range
ROC
No Assaults 13 14 15 0-14
1 Assault 24 36 48 15-30 .77
Delinquency 30 41 52 30+
Chronic Assaults 31 42 53 31+ .86
Severe Attachment Problems 31 42 53 31+
II. ADOLESCENT MALES
There were 424 males above the age of 13. The CARE-2 score was significantly correlated with a history of severe behavior problems and assaultive behaviors.
Characteristics of the group included:
FIGURE 3.4. CHARACTERISTICS OF MALES ABOVE THE AGE OF 13
Trait Percentage Number
Ethnicity 53% Caucasian, 38% AA, 4% Hispanic, .5% Asian, 3% Other, 2% missing
228 Caucasian, 163 AA, 17 Hispanic, 2 Asian, 14 Other, 10 missing
Placement 61% living at home, 4% foster care or adopt-ed, 12% detention or group home, 4% incar-cerated, 14% in Residential Treatment, 1% in hospital, 1% in Independent living.
264 living at home, 18 in foster care or adopt-ed, 51 detention or group home, 18 incarcer-ated, 62 in Residential Treatment, 3 in hospital, 3 in Independent living
CONTINUED ON NEXT PAGE

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 45 © 2003-2012 by Kathryn SeifertCARE-2 Manual
FIGURE 3.4. CHARACTERISTICS OF MALES ABOVE THE AGE OF 13 (CONT’D)
Trait % Number
Assault of authority figure 25% 108
More than 3 assaults 36% 158
Harms animals 17% 72
Moderate to severe behavior problems 71% 307
Enuresis 20% 88
Impulsivity 82% 357
Delinquent 60% 259
Substance abuse 43% 186
Poor anger management 83% 358
Poor problem solving 83% 358
Psychiatric problems 78% 338
Neurological problems 14% 61
Bully 23% 101
Deviant peers 45% 194
Truant 37% 161
Learning problems 59% 256
School behavior problems 61% 262
Childhood trauma 58% 251
Parents have inappropriate discipline 64% 279
Parents have psych or substance abuse problems 65% 280
Youth has 1 supportive adult with good boundaries 46% 199
Youth has school success 12% 53
Youth has positive activities 26% 112
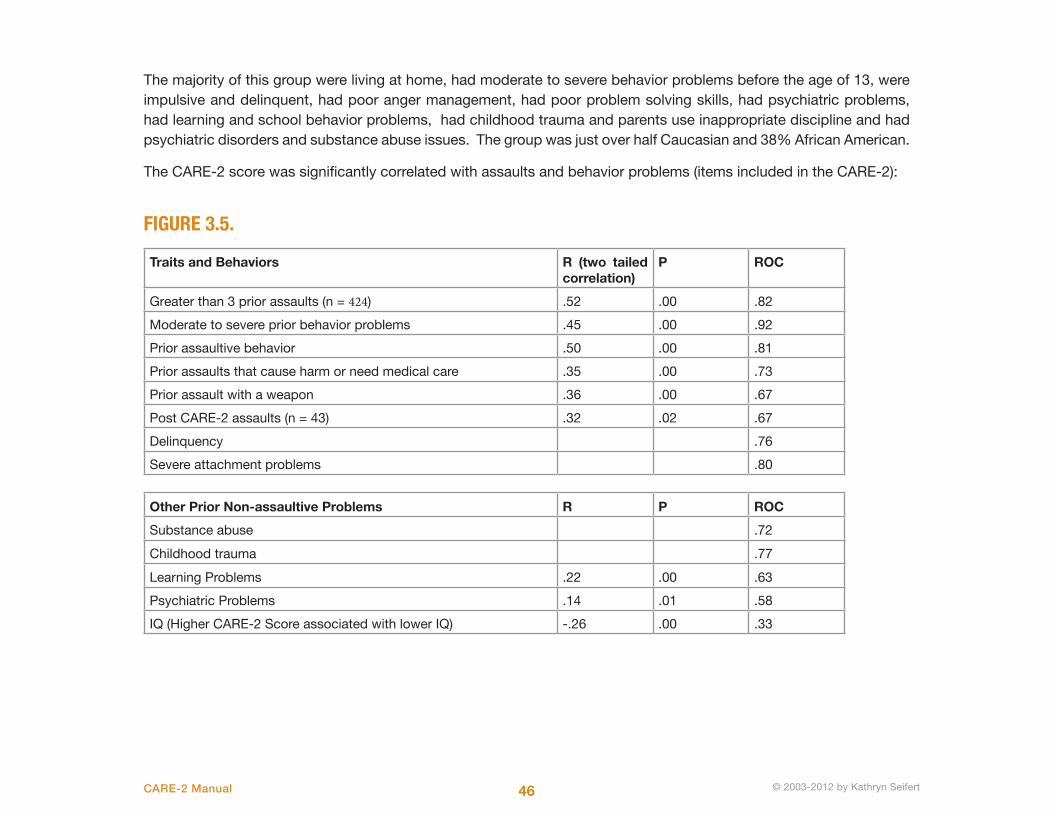
46 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
The majority of this group were living at home, had moderate to severe behavior problems before the age of 13, were impulsive and delinquent, had poor anger management, had poor problem solving skills, had psychiatric problems, had learning and school behavior problems, had childhood trauma and parents use inappropriate discipline and had psychiatric disorders and substance abuse issues. The group was just over half Caucasian and 38% African American.
The CARE-2 score was significantly correlated with assaults and behavior problems (items included in the CARE-2):
FIGURE 3.5.
Traits and Behaviors R (two tailed correlation)
P ROC
Greater than 3 prior assaults (n = 424) .52 .00 .82
Moderate to severe prior behavior problems .45 .00 .92
Prior assaultive behavior .50 .00 .81
Prior assaults that cause harm or need medical care .35 .00 .73
Prior assault with a weapon .36 .00 .67
Post CARE-2 assaults (n = 43) .32 .02 .67
Delinquency .76
Severe attachment problems .80
Other Prior Non-assaultive Problems R P ROC
Substance abuse .72
Childhood trauma .77
Learning Problems .22 .00 .63
Psychiatric Problems .14 .01 .58
IQ (Higher CARE-2 Score associated with lower IQ) -.26 .00 .33

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 47 © 2003-2012 by Kathryn SeifertCARE-2 Manual
For teen males the association with prior moderate to severe behavior problems, more than 3 prior assaults and severe attachment problems was strong; The association with prior assaults causing harm was moderate; The association with assaults with a weapon and post CARE-2 assaults were weak; associations of the CARE-2 score with learn-ing problems was weak or non-existent for psychiatric problems or average or better IQ. The CARE-2 score is more strongly associated with assaults and behavior problems than learning or psychiatric problems. It appears to distin-guish chronic assaultive behaviors more than single assaults.
FIGURE 3.6.
Mean CARE-2 Score
Mean +1 SD Mean + 2SD CARE-2 Score Range
ROC
No Assaults 12 23 34
1 Assault 27 38 49 .67-.81
Delinquency 27 38 49 .76
Chronic Assaults 31 41 51 .82
Severe Attachment Problems .80
III. PRE-ADOLESCENT FEMALES
The CARE-2 score was significantly correlated with a history of more than 3 prior assaults among pre-teen females.
There were 124 females below the age of 13. Characteristics of the group included:
FIGURE 3.7. CHARACTERISTICS OF FEMALES BELOW THE AGE OF 13
Trait Percentage Number
Ethnicity 46% Caucasian, 40% AA, 2% Hispanic, 1% Asian, 11% Other
57 Caucasian, 50 AA, 2 Hispanic, 1 Asian, 13 Other
Placement 87% living at home, 7% foster care or adopted, 1% detention or group home, 0 incarcerated, 0% in Residential Treatment, 0% in hospital
108 living at home, 9 in foster care or adopted, 1 detention or group home, 0 incarcerated, 0 in Residential Treatment, 0 in hospital
CONTINUED ON NEXT PAGE
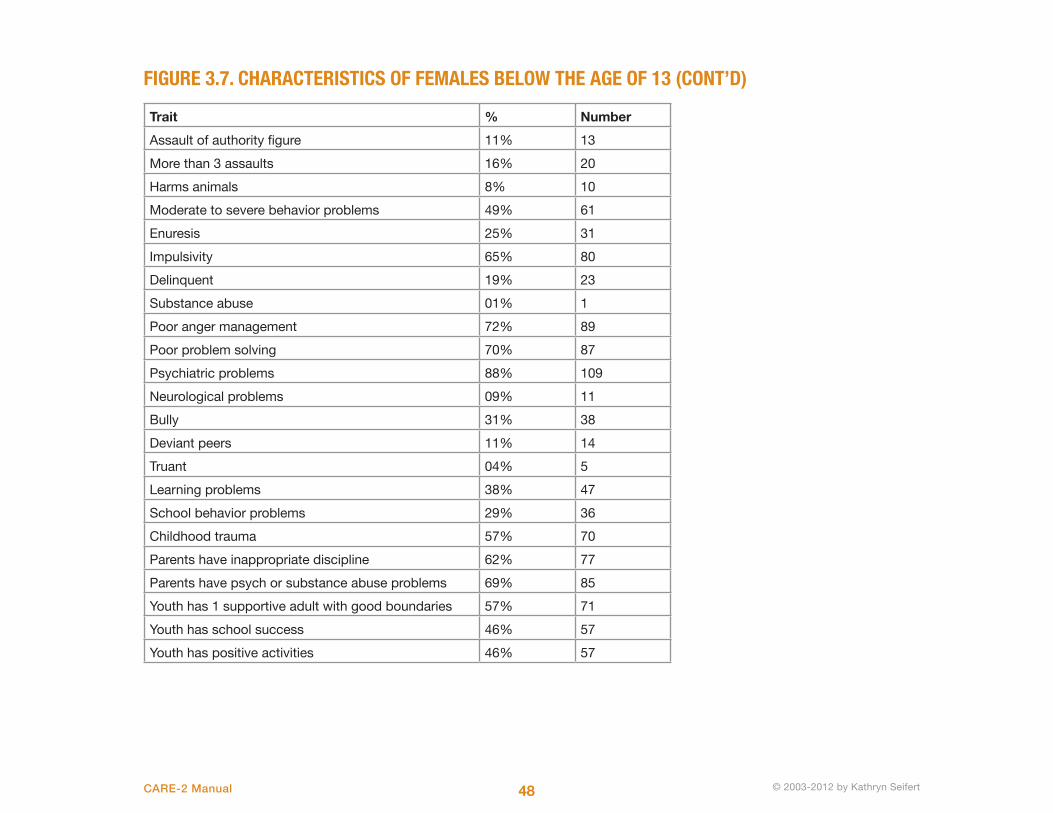
48 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
FIGURE 3.7. CHARACTERISTICS OF FEMALES BELOW THE AGE OF 13 (CONT’D)
Trait % Number
Assault of authority figure 11% 13
More than 3 assaults 16% 20
Harms animals 8% 10
Moderate to severe behavior problems 49% 61
Enuresis 25% 31
Impulsivity 65% 80
Delinquent 19% 23
Substance abuse 01% 1
Poor anger management 72% 89
Poor problem solving 70% 87
Psychiatric problems 88% 109
Neurological problems 09% 11
Bully 31% 38
Deviant peers 11% 14
Truant 04% 5
Learning problems 38% 47
School behavior problems 29% 36
Childhood trauma 57% 70
Parents have inappropriate discipline 62% 77
Parents have psych or substance abuse problems 69% 85
Youth has 1 supportive adult with good boundaries 57% 71
Youth has school success 46% 57
Youth has positive activities 46% 57

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 49 © 2003-2012 by Kathryn SeifertCARE-2 Manual
The majority of this pre-adolescent female group were living at home, were impulsive, had poor anger management, had poor problem solving skills, had psychiatric problems, and had childhood trauma. The parents of the majority of this group used inappropriate disciplinary practices, and had psychiatric or substance abuse problems. Just over half of the group had at least 1 supportive adult with good boundaries. The group was nearly half Caucasian and 41% African American.
The CARE-2 score was significantly correlated with assaults and behavior problems (items included in the CARE-2):
FIGURE 3.8. ASSOCIATIONS OF CARE-2 SCORES AND GROUP TRAITS AND BEHAVIORS
Traits and Behaviors R (two tailed correlation)
P ROC
Greater than 3 prior assaults (n = 232) .57 .00 .91
Moderate to severe prior behavior problems .62 .00 .90
Prior assaultive Behavior .51 .00 .80
Prior assaults that cause harm or need medical care .39 .00 .87
Prior assault with a weapon .31 .00 .82
Post CARE-2 assaults (n = 43) .52 .00 .80
Delinquency .87
Severe attachment problems .87
Other Prior Non-assaultive Problems R P ROC
Substance abuse
Childhood trauma .68
Learning problems .35 .00 .71
Psychiatric problems .31 .00 .79
IQ (Higher CARE-2 Score associated with lower IQ) -.21 .02 .25

50 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
ROC’s for CARE-2 scores and pre-adolescent female assaults, behavior problems, delinquency and severe attachment problems are strong. The associations are moderate to weak for other non-assaultive problems. The CARE-2 appears to discriminate between pre-teen females with and without assaultive behaviors.
FIGURE 3.9.
Mean CARE-2 Score
Mean +1 SD Mean + 2SD CARE-2 Score Range
ROC
No Assaults 8 18 28 0-18
1 Assault 21 33 45 19-33 .80
Delinquency 30 40 50 34-50 .91
Chronic Assaults 28 42 56 28+ .87
Severe Attachment Problems 30 42 54 30+ .87
IV. TEEN FEMALES
The CARE-2 score was significantly correlated with a history of severe behavior problems and assaultive behaviors.
There were 203 females above the age of 13.
Characteristics of the group included:
FIGURE 3.10. CHARACTERISTICS OF FEMALES ABOVE THE AGE OF 13:
Trait Percentage Number
Ethnicity 64% Caucasian, 32% AA, 1% Hispanic, 1% Asian, 1% Other, .5% missing
131 Caucasian, 65 AA, 2 Hispanic, 2 Asian, 3 Other, 1 missing
Placement 77% living at home, 7% foster care or adopt-ed, 4% detention or group home, 0% incarcer-ated, 3% in Residential Treatment, 0% in hos-pital, 2% in Independent living.
156 living at home, 14 in foster care or adopt-ed, 8 detention or group home, 0 incarcerated, 6 in Residential Treatment, 3 in hospital, 4 in Independent living
CONTINUED ON NEXT PAGE

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 51 © 2003-2012 by Kathryn SeifertCARE-2 Manual
FIGURE 3.10. CHARACTERISTICS OF FEMALES ABOVE THE AGE OF 13 (CONT’D)
Trait % Number
Assault of authority figure 21% 42
More than 3 assaults 22% 45
Harms animals 3% 5
Moderate to severe behavior problems 54% 110
Enuresis 7% 14
Impulsivity 70% 142
Delinquent 37% 76
Substance abuse 30% 62
Poor anger management 83% 81
Poor problem solving 71% 145
Psychiatric problems 90% 183
Neurological problems 10% 21
Bully 14% 28
Deviant peers 40% 81
Truant 33% 67
Learning problems 39% 79
School behavior problems 47% 95
Childhood trauma 47% 96
Parents have inappropriate discipline 63% 128
Parents have psych or substance abuse problems 69% 140
Youth has 1 supportive adult with good boundaries 48% 97
Youth has school success 25% 50
Youth has positive activities 25% 51
The majority of this group were living at home, had moderate to severe behavior problems before the age of 13, were impulsive, had poor anger management and poor problem solving skills, had psychiatric problems, and parents use
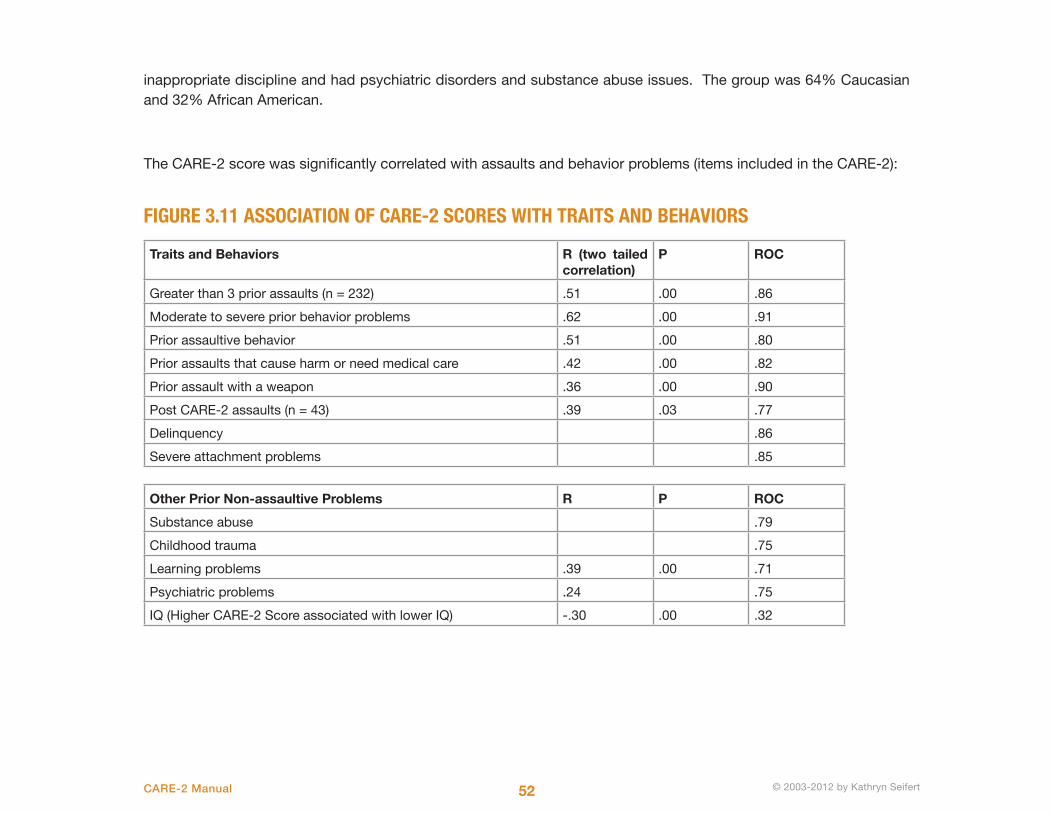
52 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
inappropriate discipline and had psychiatric disorders and substance abuse issues. The group was 64% Caucasian and 32% African American.
The CARE-2 score was significantly correlated with assaults and behavior problems (items included in the CARE-2):
FIGURE 3.11 ASSOCIATION OF CARE-2 SCORES WITH TRAITS AND BEHAVIORS
Traits and Behaviors R (two tailed correlation)
P ROC
Greater than 3 prior assaults (n = 232) .51 .00 .86
Moderate to severe prior behavior problems .62 .00 .91
Prior assaultive behavior .51 .00 .80
Prior assaults that cause harm or need medical care .42 .00 .82
Prior assault with a weapon .36 .00 .90
Post CARE-2 assaults (n = 43) .39 .03 .77
Delinquency .86
Severe attachment problems .85
Other Prior Non-assaultive Problems R P ROC
Substance abuse .79
Childhood trauma .75
Learning problems .39 .00 .71
Psychiatric problems .24 .75
IQ (Higher CARE-2 Score associated with lower IQ) -.30 .00 .32

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 53 © 2003-2012 by Kathryn SeifertCARE-2 Manual
For teen females the association with assaultive behaviors, moderate to severe behavior problems, severe attachment problems and delinquency was strong; The association with learning, substance abuse, psychiatric, and trauma prob-lems was moderate. The CARE-2 score is more strongly associated with assaults and behavior problems than learning or psychiatric problems.
FIGURE 3.12.
Mean CARE-2 Score
Mean +1 SD Mean + 2SD CARE-2 Score Range
ROC
No Assaults 11 22 33 0-22
1 Assault 24 36 42 23-29 .77-80
Delinquency 27 37 47 27+ .86
Chronic Assaults 30 40 50 30+ .86
Severe Attachment Problems 33 44 55 33+ .85

54 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
In the original CARE, all items were used in the calcula-tion of the CARE score because it was thought it was im-portant to include all items that would inform treatment planning. In the CARE-2, all items which have numeri-cal scores correlate with the total score at a significant level that is less than .01. Items which have a correla-
tion significance that is greater than .01 were not given a numerical score, but were kept for use in the treatment plan by using a non-numerical marker, “*”. The numeri-cal score of items was derived from the correlation of the item with the total score.
ITEM SELECTION
© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 55 © 2003-2012 by Kathryn SeifertCARE-2 Manual
REFERENCES AND RESOURCES
Andrews, D. A. (1992, November). Review of the parole, classificaion and treatment literature with young offenders: A social-psychological approach. Ottawa: Ministry of Communty Social Services.
Arboleda-Florez, J. H. (1996). Mental illness and violence: Proof or stereotype. Ottawa: Health Canada.
Big Brothers Big Sisters. (n.d.). Retrieved on 2/12/12 from http://www.bbbs.org/site/c.9iILI3NGKhK6F/b.5962335/k.BE16/Home.htm
Borum, R. B. (2002). Structured assessment of violence risk in youth (SAVRY). Tampa, FL: University of South Florida.
Braaten, S. (1998). Behavioral objective sequence. Champaign, IL: Research Press.
Browning, K., Huizinga, D., Loeber, R., and Thornberry, T. P. (1999). Causes and Correlates of Delinquency Program.Fact Sheet #100. Ofce of Justice Programs. Ofce of Juvenile Justice and Delinquency Prevention. Washington, DC: U.S. Department of Justice.
CBT. (n.d.). Retrieved on 02/05/12 from http://behavioraltech.org
Christle, C. A., Jolivette, K., Nelson, C. M. (2000). Youth aggression and violence: Risk, resilience, and prevention. ERIC Identier: ED449632. ERIC Digest #E602. Arlington, VA: ERIC Clearinghouse on Disabilities and Gifted Education.
Crespi, T. D., and Rigazio-DiGilio, S. A. (1996, Summer). Adolescent homicide and family pathology: Implication for research and treatment with adolescents. Adolescence, 31, 122, 353(15).
Elliott, D.S. Blueprints for Violence Prevention (Vols. 1–11). Boulder: Center for the Study and Prevention of Violence, Institute of Behavioral Science, University of Colorado, 1997.
Fago, D. P. (1999). Co-morbidity of Attention Decit Hyperactivity Disorder (ADHD) in sexually aggressive children and adolescents. The Forum, Vol. 6, 3-4.
Functional Family Therapy. (n.d.). Retrieved on 02/01/12 from http://fftinc.com
Hahn, R. F.-W. (2007, August 10). The effectiveness of universal school-based programs for the prevention of violent
56 © 2003-2012 by Kathryn SeifertCARE-2 Manual © 2003-2012 by Kathryn Seifert
and aggressive behavior. Retrieved February 26, 2011, from Center for Disease Control: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5607a1.htm
Howell, A J. and Enns, R. A. (1995). A high risk recognition program for adolescents in conflict with the law. Journal of Canadian Psychology, Vol. 36.
Kolk, B. (2003). The neurobiology of childhood trauama and abuse. Child and Adolescent Psychiatric Clinics, 12, 293-317.
Leschied, A.W., Andrews, D. A., and Hoge, R. (1993, August). Youth at risk: A review of Ontario young offenders, pro-grams and literature that supports effective intervention. Ontario: Ministry of Community and Social Services.
Levy, T. &. (1998). Attachment, trauma, and healing: Understanding and treating attachment disorder in children and families. Washington, DC: Child Welfare League of America.
Lewis, D. O. (1998). Guilty by reason of insanity: A psychiatrist explores the minds of killers. New York: Fawcett Columbine.
Life Skills Training. (n.d.). Retrieved on 2/12/12 from http://lifeskillstraining.com.
Meloy, R., C. Gacono, and M. Bridges. (2000) A Rorschach comparison of psychopaths, sexual homicide perpetrators, and nonviolent pedophiles. Journal of Clinical Psychology, 56:757-777.
Moffit, T. and Caspi, A. (2001). Childhood predictors differentiate life-course persistent and adolescence-limited anti-social pathways among males and females. Development and Psychopathology 13:355-375.
Monahan, J, Steadman, H., Robbins, P., Appelbaum, P., Banks, S., Grisso, T., Heilbrun, K., Mulvey, E., Roth, L., and Sil-ver, E. (2005). An actuarial model of violence risk assessment for persons with mental disorders. Psychiatric Services, 56, 810-815.
Motivational Interviewing. (n.d.). Retrieved on 2/12/12 from http://www.motivationalinterview.org
MST. (n.d.). Retrieved on 02/02/2012 from http://mstservices.com
Nunnally, J. C. (1994). Psychometric theory (3rd ed.). New York: McGraw-Hill.
Olds, D. (2002). Home Visiting by paraprofessionals and by nurses: A randomized, controlled trial. Pediactrics, 100, 486-496.
Olweus, D. L. (1999, 2006). Bullying prevention program: Blueprints for violence prevention, book nine. In D. S. Elliott, Blueprints for Violence Prevention Series. Boulder, CO: Center for the Study and Prevention of Violence, Institute of

© 2003-2012 by Kathryn Seifert© 2003-2012 by Kathryn Seifert 57 © 2003-2012 by Kathryn SeifertCARE-2 Manual
Behavioral Science, University of Colorado.
Parent Management Training. (n.d.). Retrieved on 2/12/12 from http://www.apa.org/div12/rev_est/pmt_child.html
PATHS. (n.d.). Retrieved on 2/12/12 from http://www.prevention.psu.edu
Perry, B. D., and Pollard, R. (1997). Altered brain development following global neglect in early childhood. Proceedings from annual meeting. New Orleans: Society for Neuroscience.
Pollack, S., Cicchetti, D., Klorman, R., Brumaghine, J. (1997). Cognitive brain event-related potentials and emotion processing in maltreated children. Child Development, 68, 773-787.
Prochaska, J. O. (1995). Changing for good: A revolutionary six-stage program for overcoming bad habits and moving your life positively forward. William Morrow Paperbacks.
Puzzanchera C. Juvenile Arrests 2008. Juvenile Justice Bulletin. Washington, DC: Office of Juvenile Justice and Delin-quency Prevention; 2009. [2010 Jun 14]. Available from URL: www.ncjrs.gov.
Quinsey, V. L., Harris, G. T., Rice, M. E., and Cormier, C. A. (1998). Violent offenders: Appraising and managing risk. Washington, DC: American Psychological Association.
Seifert, K. (2006). How children become violent. Boston, MA: Acanthus.
Seifert, K. (2007). CARE2 Manual. Boston, MA: Acanthus.
Seifert, K. (2012). Youth Violence: Theory, Prevention, and Intervention. New York: Springer.
Shamsie, J., Lawrence, J., and Hood, C. (Eds.). (2002). Antisocial and violent youth, Vol. 2. Toronto: The Institute for the Study of Antisocial Behavior in Youth.
The Change Companies. (n.d.). Retrieved on 2/12/12 from http://changecompanies.net
Thinking For a Change. (n.d.). Retrieved on 2/12/12 from http://www.nicic.org/T4
Thornton, T. N. (2000). Best practices of youth violence prevention: A sourcebook for community action. Atlanta, GA: Division of Violence Prevention, National Center for Injury Prevention and Control.
Werner, E. (1996). How kids become resilient: Observations and cautions. Resiliency in Action, 1(1), 18-28.

Dr. Seifert is a psychotherapist, author, speaker, and researcher who specializes in family violence and trauma and has over 30 years of experience in mental health, addictions, and criminal justice work. She is Founder and CEO of Eastern Shore Psychological Services (www.ESPSMD.com), a private practice that focuses on serving children, adolescents, and at-risk youth and their families.
Dr. Seifert’s articles on violence, trauma, and risk have appeared in The Journal of Psychiatry and Law, Paradigm Magazine, Reaching Today’s Youth, Forensic Focus, Self-Help and Psychology Magazine, The Maryland Psychologist, Hot Psychology Magazine, and the Forensic Examiner
Besides the CARE-2, Dr. Seifert has authored and published a training DVD on disrupted attachment patterns and two guided imagery CD and journal sets. Her book, How Children Become Violent: How to Keep Your Kids out of Gangs, Terrorist Organizations and Cults, (Acanthus 2006) won an Independent Publisher Book Award, and another book on women and violence will be available next year.
Dr. Seifert is a member of the International Association of Forensic Mental Health Services, the American and Maryland Psychological Associations, the Association for the Treatment of Sexual Abusers, the Maryland Mental Health Association, and The American College of Forensic Examiners International.
For more information about Dr. Seifert please visit her website at www.DrKathySeifert.com, or her company’s website at www.ESPSMD.com
ABOUT DR. KATHRYN SEIFERT
OTHER PRODUCTS FROM DR. SEIFERT
How Children Become Violent: Keeping Your Kids out of Gangs,Terrorist Organizations, and Cults$19.95 (Paperback)Acanthus Publishing, 2006ISBN: 978-1-933631-48-6
How Children Become Violent: For Parents$17.95 (40-page downloadable PDF eBook) Acanthus Publishing, 2007ISBN: 978-1-933631-74-5
Managing Stress and Trauma: A Dance of Life$12.95 (24-page downloadable PDF eBook)Acanthus Publishing, 2007ISBN: 978-1-933631-71-4
Youth Violence: Theory, Prevention, and Intervention
$45.00 (Paperback)Springer Publishing Company, 2011ISBN: 978-0826107-40-4
Boston, Massachusettswww.AcanthusPublishing.com




















