Capa N2 2015 X3 - Sociedade Portuguesa de Oftalmologia
88
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Capa N2 2015 X3 - Sociedade Portuguesa de Oftalmologia



Vol. 39 - Nº 2 - Abril-Junho 2015 | I
Oftalmologia - Vol. 39
Comissão CentralPresidenteMaria João Capelo Quadrado
Vice-PresidenteAntónio Mário Chéu Limão Oliveira
TesoureiroJoão Paulo Castro Sousa
VogaisÂngela Maria Veloso Guimarães CarneiroPedro Miguel Alves Moreira Menéres
Secretário-Geral AdjuntoAntónio Manuel Santos de Melo
Secretário-GeralRita Maria Rio Pedro Flores
Mesa da Assembleia GeralPresidenteJoaquim Carlos Neto Murta
Vice-PresidenteGil Machado Resendes
1º SecretárioFernando Albino Santos Rebelo Vaz
2° SecretárioAntónio José Elias Rodrigues
Conselho FiscalJoaquim Manuel Estrada Lopes Luis Manuel de Sousa Pinto Agrelos Maria Sandra Ferreira da Silva Moniz
Coordenadores das Secções da S.P.O.Grupo Português de Retina-VítreoJoão Pereira Figueira
Grupo Português de Inflamação OcularMaria João Capelo Quadrado
Grupo Português de Oftalmologia Pediátrica e EstrabismoMaria Catarina dos Santos Isabel Rodrigues de Paiva
Cirurgia Implanto-Refractiva de PortugalMaria da Conceição Lopes Lobo da Fonseca
Grupo de Superfície Ocular Córnea e Contactologia de PortugalAna Esmeralda Oliveira Guedes Costa
Grupo Português de GlaucomaJosé António Alves de Moura Pereira
Grupo Português de NeuroftalmologiaPedro Luis Martins da Fonseca
Grupo Português de Patologia, Oncologia e Genética OcularMaria João Capelo Quadrado
Grupo Português de Órbita e OculoplásticaRui Guilherme Pereira Leite Castela
Grupo Português de ErgoftalmologiaJosé Miguel Quaresma Nolasco
Coordenador SPO JovemRicardo Miguel Bastos Amorim
Editor da página da SPO na InternetHelena Maria Prior Santos Costa Filipe
EditorAmândio António Rocha Dias de [email protected]
OftalmologiaPublicação Trimestral | Vol. 39 | Abril - Junho 2015
REVISTA DA SOCIEDADE PORTUGUESA DE OFTALMOLOGIA
Composição e ImpressãoSUBLINHADO Publicações e Publicidade Unipessoal - R. Prof. Vieira de Almeida, 38 - Lj. A - Bloco B - Piso 0 - 1600-371 LISBOA - Tel.: 21 757 81 35 | Depósito Legal 93 889/95 - ISSN 1646-6950
Conselho RedactorialAugusto Manuel Chambel Candeias David da Fonseca Martins Fernanda Maria Fernandes Vaz Helena Sofia Ferrão Mesquita Proença João Carlos Marques Chibante Pedro João Paulo Pedrosa Branco da Cunha Manuel Alberto de Almeida e Sousa Falcão Manuel Santos Mariano Maria Angelina da Costa Meireles SilvaPaula Alexandra Ribeiro Tenedório
Sociedade Portuguesa de Oftalmologia


Vol. 39 - Nº 2 - Abril-Junho 2015 | III
Índice
EditorialManuel Alberto Falcão, Amândio Rocha Sousa
Artigo de RevisãoIntravitreal injection of pharmacological agents: from clinical trial to clinical practice
Rufino Silva, João Pedro Marques
Artigos OriginaisInternal limiting membrane inverted flap technique: a new paradigm in large macular hole surgery
Carlos Menezes, José Alberto Lemos, Rui Carvalho, Josefina Serino, Rita Gonçalves, Bruna Cardoso Vieira, Pedro Coelho, Tiago Maio, Paula Tenedório
10 anos de experiência no tratamento de retinoblastoma
Cristina Santos, Inês Coutinho, Ana Rita Azevedo, Cláudia Constantino, Ana Berta Sousa, Filomena Pereira, José Laranjeira, João Cabral, Susana Teixeira
Neovascularização coroideia de causa inflamatória: Opções terapêuticas
Bárbara Borges, Ana Cabugueira, Isabel Domingues, Miguel Marques, Pinto Ferreira, João Lisboa, Rita Flores
Flash LookOCT angiography: redefining standards
João Pedro Marques, Rufino Silva
Paracentral Acute Middle Maculopathy: a novel clinical finding
Sara Vaz-Pereira
V
75
91
97
103
111
115
Miopia patológica - novos conceitos e achados OCT
Francisco Trincão
Paracentese diagnóstica da câmara anterior – como e quando?
Sofia Fonseca
Comunicações Curtas e Casos ClínicosAcidúria metilmalónica com homocistinúria, tipo cobalamina c: fenótipo oftalmológico
Ana Figueiredo, Mafalda Macedo, Vasco Miranda, Ricardo Parreira, Salomé Gonçalves, Pedro Menéres
Retinal angiogenesis arrest in a full term infant with congenital toxoplasmosis
Cristina Santos, Mário Ramalho, Catarina Pedrosa, Inês Coutinho, Marta Ferreira, Maria João Brito, Susana Teixeira.
Chorioretinal atrophy in a patient with Buerger’s disease
André Marques, Joana Portelinha, Ana Almeida, Marta Guedes
Melanoma da íris em idade pediátricaInês Coutinho, Peter Pêgo, Mário Ramalho, Catarina Pedrosa,Cristina Santos,Mafalda Mota, Isabel Prieto, João Cabral
Indicações aos Autores e Normas de Publicação
119
127
129
137
139
145
151
Oftalmologia - Vol. 39


Vol. 39 - Nº 2 - Abril-Junho 2015 | V
Oftalmologia - Vol. 39
A prática médica relacionada com as doenças da retina encontra-se num período fértil de inovação quer a nível do diagnós-tico quer a nível das opções de tratamento.
A utilização maciça de tratamentos intravítreos para as doenças retinianas mais frequentes (retinopatia diabética, dege-nerescência macular da idade, oclusões venosas, ...) com fármacos anti-VEGF e corticoides começou há cerca de 10 anos. Ainda não está completamente definida a melhor forma de atingir os resultados dos ensaios clínicos na nossa prática clínica. Neste número fazemos a revisão dos últimos anos desta prática bem como as fórmulas que podemos utilizar para melhorar os resultados visuais dos nossos doentes.
O desenvolvimento dos meios auxiliares de diagnóstico tem vindo a modificar e a melhorar a medicina ao longo dos últi-mos anos. Em oftalmologia, graças as características do globo ocular que permite a passagem de luz até às estruturas mais internas do olho, esse desenvolvimento tem vindo a ser excepcional.
O OCT de domínio espectral (SD-OCT) que surgiu no início do século XXI revolucionou a prática da medicina na área da retina. Devido à sua rapidez de execução, pelo facto de ser inócuo, este exame passou rapidamente a ser o meio auxiliar de diagnóstico mais realizado nesta prática e hoje em dia assume um papel praticamente indispensável nesta área. Este exame em algumas plataformas é acompanhado de outras modalidades de imagem que também contribuem para um melhor diagnóstico e acompanhamento dos nossos doentes (autofluorescência, infravermelho).
Para além de permitir estudar melhor e acompanhar melhor processos patológicos já sobejamente conhecidos como o edema macular diabético ou os buracos maculares, estes exames permitiram esclarecer melhor a morfologia “histológica” de algumas doenças. Por outro lado, outras patologias que eram desconhecidas passaram a ser identificadas e descritas demonstrando que ainda não temos a capacidade de identificar e estudar tudo o que se passa a nível retiniano. Neste número revemos como o SD-OCT permitiu estudar e identificar diferentes formas de maculopatia miópica e perceber quais as opções de tratamento para esta patologia. Debruçamo-nos sobre uma entidade recentemente descrita, a maculopatia paracentral aguda - paracentral acute middle maculopathy (PAMM) e como os novos meios auxiliares de diagnóstico permitem o diagnóstico desta patologia.
Recentemente surgiu um novo meio auxiliar de diagnóstico que recorre à tecnologia de OCT para efetuar angiografia retiniana sem o uso de contraste. É um método de imagem inovador que também promete revolucionar a nossa prática clínica. Aproveitamos este número para compreendermos melhor as vantagens, limitações e possibilidades deste novo método de ima-gem que esperamos que brevemente também possa fazer parte do nosso quotidiano na clínica.
Finalmente, neste número apresentamos alguns casos clínicos raros e interessantes e revemos a prática clínica da cirurgia retiniana na retinopatia diabética proliferativa.
Manuel Alberto Falcão Amândio Rocha Sousa (Adjunto do editor para este número)
Editorial
Manuel Alberto FalcãoAmândio Rocha Sousa


Vol. 39 - Nº 2 - Abril-Junho 2015 | 75
Intravitreal injection of pharmacological agents: From clinical trial to clinical practice
Rufino Silva1, 2, 3, João Pedro Marques1,3 1Ophthalmology Department, Centro Hospitalar e Universitário de Coimbra (CHUC) - Coimbra, Portugal
2Faculty of Medicine, University of Coimbra (FMUC) – Coimbra, Portugal 3Association for Innovation and Biomedical Research on Light and Image (AIBILI) – Coimbra, Portugal
INTRODUCTION
Intravitreal delivery bypasses the blood-retinal barrier, leading to a higher intraocular drug con-centration for a longer period of time, while lessening the systemic toxicity. A wide variety of intravitreal pharmacological agents has been used: anti-infective (antibiotic, antifungal, and an-tiviral), anti-inflammatory (nonsteroidal anti-inflammatory agents, steroids and immunomodu-lators), anticancer agents, gas, anti-vascular endothelium growth factor (VEGF), among others1. Over the last decade, intravitreal corticosteroids and/or anti-VEGF have become the therapeu-tic backbone of several retinal disorders, including age-related macular degeneration (AMD), diabetic retinopathy (DR), retinal vein occlusions (RVO) and myopic neovascularization. In-dustry supported clinical research has helped propelling several drugs with encouraging visual and anatomic outcomes. With numerous novel therapies currently being investigated in clinical trials, the number of available drugs will likely continue to rise. High-quality imaging and the application of pharmacogenomic principles are probably guiding future therapies that through a comprehensive approach will hopefully meet the patients’ needs and expectations.We should keep in mind that everyday clinical practice differs greatly from a clinical trial set-ting and this inevitably affects the treatment results. The dependence on the center’s resources (public or private) and agenda may delay the beginning of treatment, the interval between in-jections, between evaluations and injections (when performed separately), and even follow-up appointments. This usually leads to poorer than expected visual outcomes, patient dissatisfaction and physician frustration. Lack of patient motivation directly disturbs compliance and a vicious circle ensues. In order to provide the best possible treatment to our patients in a clinical setting, a balance between cost, effectiveness, compliance and agenda needs to be found. The purpose of this paper is (1) to review the available drugs for intravitreal use, (2) to explore their approved indications and off-label use in the management of retinal diseases and (3) to present the treatment protocols currently being used at the Retinal Department of the Centro Hospitalar e Universitário de Coimbra (CHUC), Coimbra, Portugal.
Artigo de Revisão
Oftalmologia - Vol. 39: pp.75-89
1. AVAILABLE DRUGS FOR INTRAVITREOUS USE
1.1. ANTI-VASCULAR ENDOTHELIAL GROWTH FACTOR
BevacizumabBevacizumab (Avastin®, Genentech, South San Fran-
cisco, CA) is a full-length antibody against VEGF isoforms
that prevents binding of VEGF to its receptors2,3. The intrave-nous administration of Bevacizumab is approved by the Uni-ted States (U.S.) Food and drug Administration (FDA) for the treatment of metastatic colorectal cancer2. Despite its inclu-sion in several clinical trials for the treatment of exudative AMD, diabetic macular edema (DME) and RVO, the drug has not received approval for intravitreous use. Its first use in exudative AMD dates back to 20054. Because of similar

76 | Revista da Sociedade Portuguesa de Oftalmologia
clinical effects at a remarkably lower cost5,6, bevacizumab is still a commonly used off-label drug throughout the world.
RanibizumabRanibizumab (Lucentis®, Genentech, Inc., South San
Francisco, CA, USA) is a much smaller anti-VEGF anti-gen-binding antibody fragment that was found to achieve better retinal penetration than the full-length antibody1. Ranibizumab binds all VEGF isoforms with an affinity that is 5- to 10-fold higher than that of bevacizumab7. The drug was specifically developed for intraocular use and has been approved by the FDA, EMA and Infarmed for the mana-gement of exudative AMD, DME (European Medicines Agency) and macular edema secondary to RVO. Ranibizu-mab has been extensively studied and compared with other anti-VEGF agents since it was the first to receive approval for intravitreous injection (IVI).
AfliberceptPreviously known as VEGF trap-eye8, aflibercept (Eylea®,
Regeneron Pharmaceuticals, Tarrytown, NY, USA) is a solu-ble decoy receptor fusion protein specifically purified and formulated for intraocular injection9. Aflibercept is a chime-ric molecule composed of an Fc fragment linked to the extra-cellular portions of the VEGFR1 and VEGFR2 receptors. It binds to all isoforms of VEGF and prevents activation of VEGF receptors1. The drug binds to VEGF with substantially greater affinity than bevacizumab or ranibizumab. The idea that this would translate into less frequent dosing through a substantially longer duration of action was later confirmed by several clinical trials9-11 and led to its approval by the FDA, EMA and Infarmed for the management of exudative AMD, DME and macular edema secondary to CRVO in 2014.
1.2. CORTICOSTEROIDS
Corticosteroids have a wide range of functions and different action mechanisms. Besides reducing local inflammatory mediators, they act by diminishing VEGF levels, intraocular cell proliferation and stabilizing the blood-retinal barrier function while simultaneously increa-sing the activity and density of the gap junctions in the reti-nal capillary endothelium and improving oxygenation of ischemic areas12. Delivery of steroids to the vitreous cavity has been accomplished via direct injection through the pars plana, introduction of sustained-release or biodegradable implants, and injection of conjugate compounds13.
Triamcinolone AcetonideIntravitreal triamcinolone acetonide (IVTA) is a synthetic
glucocorticoid corticosteroid that has been used in several intraocular diseases. One of its most common applications is macular edema (ME), a condition most frequently seen following intraocular surgery, RVO, DR and posterior seg-ment inflammatory disease14. ME treatment varies depending on the underlying etiology, with uneven degrees of success. Due to its low cost and relative effectiveness, IVTA has been used in an off-label basis in refractory ME. However, this is frequently limited by its well-established side effects such as elevated intraocular pressure and cataract formation12,13,15,16.
DexamethasoneThe dexamethasone drug delivery system (Ozurdex®,
Allergan, Irvine, CA, USA) is a biodegradable, sustained--release device approved by the U.S. FDA and EMA for DME, macular edema secondary to RVO and non-infec-tious posterior uveitis. Ozurdex® is preloaded into a sin-gle-use applicator to facilitate injection of the rod-shaped implant directly into the vitreous. It provides 0.7 mg of dexamethasone in sustained release, administered via pars plana using the 22-gauge injecting applicator. Given the increased risk of cataract formation/progression, the U.S. FDA approved the drug only for pseudophakic patients or those that are phakic but with a scheduled cataract surgery. In Europe, Ozurdex® is indicated for pseudophakic patients or those who are considered insufficiently responsive to, or unsuitable for a corticosteroid sparing therapy.
When this delivery system is used, peak dexamethasone concentration is reached in the retina and vitreous at 2 mon-ths and is detectable for 6 months with minimal systemic absorption17. The pharmacokinetic profile of Ozurdex is thought to be similar between vitrectomized and nonvitrec-tomized eyes18,19.
Fluocinolone AcetonideThe fluocinolone acetonide sustained delivery device
(Iluvien®, Alimera Sciences, Alpharetta, GA, USA) is a small (3.5 x 0.37 mm), non-biodegradable cylindrical tube with a central drug–polymer matrix that releases 0.19 mg of fluocinolone acetonide in submicrogram doses into the vitreous cavity over a 3-year period with no systemic absorption20. The device is inserted into the vitreous cavity through a 25-gauge needle. Iluvien® received approval from the U.S. FDA to treat refractory macular edema in patients who have been previously treated with a course of corti-costeroids and did not have a clinically significant rise in intraocular pressure. Even though the drug is not approved by the EMA, several european countries have approved it, including Portugal. Cataract formation/progression is one of the most significant side effects21.
Rufino Silva, João Pedro Marques

Vol. 39 - Nº 2 - Abril-Junho 2015 | 77
2. INJECTION TECHNIQUE
After topical anesthesia and 5% povidone-iodine solu-tion are applied in the conjunctival fornix, the 30-gauge injection needle is inserted via pars plana, 3.5-4.0 mm pos-terior to the limbus into the vitreous cavity, aiming towards the centre of the globe. Preferably, a different scleral site is used for subsequent injections. Although not an ubiquitous practice pattern since it has been postulated to paradoxi-cally increase the risk of endophthalmitis22,23, our treatment protocol involves, until a consensus document is approved, antibiotic prophylaxis with a topical quinolone 4id 4 days before and 4 days after the IVI.
3. INTRAVITREAL INJECTIONS IN THE MANA-GEMENT OF RETINAL DISEASES
3.1. AGE-RELATED MACULAR DEGENERATION
3.1.1. BACKGROUNDAMD is a progressive, degenerative disease of the retina
that occurs with increasing frequency with age24. Its neovas-cular form is the leading cause of irreversible vision loss in subjects >65 years of age living in economically developed countries25,26, thus constituting a significant public health problem in regions where life expectancy is highest24. In the Coimbra Eye Study27, the first AMD epidemiological
study in a Portuguese population, the prevalence of early- (11.22%) and late-AMD (0.98%) were comparable to what has been described in other Western and Asian countries. As birthrates drop and life expectancy rises, the social bur-den of age-related conditions increases and a higher preva-lence of AMD is expected in the future.
3.1.2. AVAILABLE TREATMENTS AND TREAT-MENT REGIMENSUntil the advent of anti-VEGF agents, the most fre-
quently used treatments for neovascular AMD were ther-mal laser photocoagulation28 and verteporfin photodynamic therapy (PDT)29. Despite initially promising results, neither of these treatment modalities proved to offer any signifi-cant chance for visual improvement24. Treatments targeting VEGF have revolutionized the management of neovascular AMD and are now considered the mainstay of therapy24,30. Three commonly used intravitreous VEGF inhibitors — bevacizumab, ranibizumab and aflibercept — have proved safe and effective for the treatment of exudative AMD, but only ranibizumab and aflibercept are approved by the U.S. FDA, EMA and Infarmed for this indication (Table 1).
Several non-inferiority trials have been conducted to compare the efficacy of bevacizumab vs. ranibizumab. The results of these trials (CATT31,32, IVAN33, MANTA34, GEFAL35 and LUCAS5 studies) have shown that bevacizu-mab is comparable to ranibizumab and hence an effective treatment option for neovascular AMD. Stein et al6 found
Intravitreal injection of pharmacological agents: from clinical trial to clinical practice
Table 1 | Currently available intravitreous anti-VEGF agents used in the clinical practice for the management of neovascular age-related macular degeneration.
FDA approval EMA approval Infarmed approval Relevant studies and level of evidence
Bevacizumab No No No
• CATT Study31,32 [1b]• IVAN Study33 [1b]• MANTA Study34 [1b]• GEFAL Study35 [1b]• LUCAS Study5 [1b]
Ranibizumab Yes, at a dose of 0.5 mg
Yes, at a dose of 0.5 mg
Yes, at a dose of 0.5 mg
• ANCHOR Study36,37 [1b]• MARINA Study38,39 [1b]• PIER Study49,50 [1b]• PrONTO Study40 [1b]• EXCITE Study51 [1b]• HORIZON Study52 [1b]• SUSTAIN Study42 [1b]• SAILOR Study43 [1b]
Aflibercept Yes, at a dose of 2.0 mg
Yes, at a dose of 2.0 mg
Yes, at a dose of 2.0 mg • VIEW Studies9 [1b]
Notes: The provided levels of evidence are based on the Centre for Evidence Based Medicine, Oxford (March 2009). Last assessed on 27th June 2015 at http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/Abbreviations: FDA, US Food and Drug Administration; EMA, European Medicines Agency; Infarmed, Autoridade Nacional do Medicamento e Produtos de Saúde, I.P

78 | Revista da Sociedade Portuguesa de Oftalmologia
that bevacizumab confers considerably greater value than ranibizumab for the treatment of neovascular AMD when the costs of a 20-year treatment of a hypothetical patient were compared between the two drugs. In spite of the strong body of evidence favoring the use of bevacizumab, the drug has not received approval for intravitreal use from FDA, EMA or Infarmed and has been used as an off label therapy for wet AMD since 2005.
The treatment protocols using IVI of anti-VEGF drugs for neovascular AMD have evolved from a monthly dosing (ANCHOR36,37 and MARINA38,39) to a less rigorous, as-nee-ded approach (PrONTO40, HORIZON41, SUSTAIN42 and SAILOR43), in order to decrease treatment burden (Table 2). Despite minimizing the hazards associated with frequent dosing (potential increase in geographic atrophy44,45 and an alleged higher risk of stroke, endophthalmitis, retinal tears and retinal detachment24), a trend toward worsening outco-mes with less frequent dosing has been noted30.
While most of the AMD clinical trials have evaluated monthly, quarterly, bimonthly, treat and extend (TAE) or pro re nata (PRN) treatment strategies, most retina spe-cialists use different dosing regimens in their daily clini-cal practice30. According to the 2014 American Society of Retina Specialists (ASRS) Preferences and Trends (PAT) Survey, 78% of US retinal specialists (and 56% of interna-tional retinal specialists) treat neovascular AMD using the TAE regimen) employed in the LUCAS trial5. Freund et al46 recently published a consensus article to consider the best-practice approach to the use of TAE with anti-VEGF agents, based on available scientific and clinical experience. A level 1 evidence for TAE is still lacking.
3.1.3. FROM TRIAL TO PRACTICEThe ophthalmologic community faces a huge dilemma
in the management of neovascular AMD, with substantial controversies over the efficacy of substances, choice of
Rufino Silva, João Pedro Marques
Table 2 | Treatment regimens for the management of exudative AMD with anti-VEGF compounds.
Monthly or bimonthly dosing Treat and Extend Regimens Pro re nata (PRN)
Treatment Schedule - Continuous monthly or bimonthly dosing
- Initial monthly dosing until the macula is dry; than treatment is continued with gradual extension of the intervals between doses
- Initial 3 months loading dose, followed by as-needed dosing based on retreatment criteria
Advantages - Maximum visual improvement and reduction of CRT
- Visual improvement and reduction of CRT- Decreased burden of frequent assessments and dosing- Decreased risks of frequent dosing
- Visual improvement and reduction of CRT- Decreased burden and risks of frequent dosing
Disadvantages
- High costs of frequent assessment and frequent dosing- Risks of frequent dosing (e.g. GA, stroke, etc)
- Few clinical trials have provided evidence for use of this regimen
- Despite less frequent injections, the number of clinical visits remains high
Mean number of visits in the 1st year 12 8 12
Mean number of injections in the 1st year
12 8 6
Clinical Trials Providing Evidence
• MARINA38
• ANCHOR36,37
• VIEW 1 and 29
• LUCAS5
• SALUTE54
• PrONTO40
• HORIZON52
• SAILOR43
• SUSTAIN42
• CATT31
• GEFAL35
• MANTA34
Notes: This table was adapted from Agarwal et al30
Abbreviations: CRT, central retinal thickness

Vol. 39 - Nº 2 - Abril-Junho 2015 | 79
therapeutic regimens, exponentially growing costs from highly priced drugs, increasing patient numbers and disease chronicity with inherent monitoring needs47.
A recent retrospective, interventional case series of 212 eyes treated in a clinical practice setting has shown that visual and anatomic improvements are maintained after 3 years using the treat-and-extend regimen with ranibizumab and bevacizumab48.
The Seven Year Update of Macular Degeneration Patients (SEVEN-UP) study53 was a multicenter, non--interventional cohort study to examine the 7-year results after entering the original ANCHOR36,37/MARINA38 trials. This group had received 2 years of monthly ranibizumab, followed by an additional 2 years of as-needed ranibizu-mab treatment in the HORIZON protocol52. Compared with baseline, almost half of the eyes were stable, whe-reas one third declined by 15 letters or more53. Despite the small sample size (n=65), this study helped elucidate the challenges associated with the long-term management of wet AMD by showing that these patients remain at risk of vision loss many years after treatment. The best treatment regimen is yet to be determined. The best results were shown in clinical trials with a monthly regimen. However, due to extremely high costs and burden this is clinically unfeasible. During the last years our treatment protocol for newly diagnosed patients with typical neovascular AMD or retinal angiomatous proliferation involved a 3-month loading dose of IVI ranibizumab 0.5 mg/0.05 ml. Clinical and tomographic examination were performed after the 3rd injection and a PRN regimen was followed thereafter.
Retreatment criteria included visual acuity loss (≥5 ETDRS letters) and/or the presence of hemorrhage, fluid (intraretinal and/or subretinal) and/or pigment epithe-lial detachment (PED) in spectral domain optical cohe-rence tomography (SD-OCT). When using Aflibercept 2.0 mg/0.05 ml, a bimonthly regimen was implemented in the first year after the 3-month loading dose, followed by PRN in the second year. Molecule switch was implemented whe-never clinical response to the first drug subsided and always after a minimum of 3 injections.
More recently, a change to a treat and extend (TAE) regimen was implemented in our clinic, in agreement with the recent trends around the world46. Either ranibizumab or aflibercept are injected monthly until the retina is dry and a TAE regimen with a maximum interval of 3 mon-ths is then applied. In polypoid choroidal vasculopathy (PCV), PDT in association with intravitreal ranibizumab or aflibercept is used as a first line approach, provided that polyps are identified in indocyanine green angiography (ICGA).
The efficacy of any treatment regimen depends on its correct application. Economical and logistic restrictions and constrictions are responsible, all over the world, for an inadequate application of the chosen treatment regimen, with a great impact on the final efficacy.
Aflibercept 2q8 has shown to be as effective as mon-thly Ranibizumab. The implementation of this regimen can be applied with reduced burden (less number of injections and visits) and great efficacy, only in the first year. Afli-bercept, with the 2q8 regimen in the first year and a ‘treat and observe’ strategy with a 3-month cap (that required injection)9; ranibizumab and bevacizumab with monthly regimens36-39 or a PRN regimen with zero tolerance32, are all able, like the TAE regimen46, to improve vision in the first year and to preserve the VA gain in the second year.
When it is not possible to apply one of these treatment regimens in the first or following years, due to logistical or economical restrictions, then, a different strategy should be implemented in order to avoid unnecessary loss of vision. This adjustment in the treatment regimen, when necessary, should reflect the recent evidences coming from clinical trials and clinical practice, which include:
a. a better baseline VA is associated with a better final VA
b. a higher number of injections is associated with a better final VA (better results associated with 7 to 8 injections in the first year, 4 or more in the second year)
c. a retreatment before a VA drop occurs is associated with a better final VA
d. a long-term evaluation and treatment of AMD patients is associated with a better final VA (rarely a patient is discharged)
The chosen strategy should assure an early treatment, a minimum of seven to eight injections in the first year and four or more in the following years (in addition of allowing a reduction in the number of visits), and must include:
a) a green line for patients with exudative AMD assu-ring an earlier diagnosis and treatment
b) First year treatment scheduling: a. With Aflibercept: a loading dose of 3 injections
followed by 2q8 in the first year. b. With Ranibizumab or Bevacizumab: a loading
dose of 3 injections, followed by: i. two injections with a 6-weeks interval, and 3
bimonthly injections (total of 8 injections) or ii. a bimonthly regimen (total of 7 injections)
Intravitreal injection of pharmacological agents: from clinical trial to clinical practice

80 | Revista da Sociedade Portuguesa de Oftalmologia
c) Treatment scheduling for the second and following years:
a. quarterly treatment regimen that can be adjusted according to the evaluation visits.
d) Evaluation visits: a variable number of evaluation visits, after the loading dose, for adjusting the inter-val between injections, in the first and following years.
Whenever this strategy is implemented, at least 7 to 8 injections are assured in the first year (and four in the following years) and the number of visits can be decrea-sed. The evaluation visits may allow for any correction in the prescheduled treatments. The results of this proposed regimen, although potentially inferior, for some patients, to those described for the treatment regimens with the best known results, are able to prevent vision loss in the majority of patients, while the burden is reduced.
3.2. DIABETIC RETINOPATHY
3.2.1 BACKGROUNDAccording to the PREVADIAB study55, the preva-
lence of type 2 diabetes in the Portuguese population aged between 20 and 79 years old is 11.7% (95% confidence interval 10.8–12.6%). When pre-diabetic patients are taken together, this number rises to 34.9%, about 1/3 of the Portuguese population. Recently, the RETINODIAB study56 found a prevalence of DR of 16.3% in a cohort of 52,739 Portuguese patients from a DR screening program in Lisbon and Tagus Valley region. Of these, 5484 patients (10.4%) had mild non-proliferative (NP) DR, 1457 patients (2.8%) had moderate NPDR, 672 (1.3%) had severe NPDR and 971 patients (1.8%) had proliferative DR requiring urgent referral to an ophthalmologist.
There is growing evidence that DR is the leading cause of visual impairment in working-age patients of indus-trialized countries57. Vision loss may arise from diabe-tic macular edema (DME), macular ischemia or vitreous hemorrhage58.
A meta-analysis from the META-EYE Study group59 involving individual participant data from population--based studies around the world found that 28 million of people suffer from vision-threatening DR. DME is the most frequent cause of visual impairment in patients with DR, occurring most often in patients with high levels of hemoglobin A1C and longer diabetes duration59.
The increasing prevalence of diabetes worldwide emphasizes the importance of DME as a global public health issue.
3.2.2. AVAILABLE TREATMENTS AND TREAT-MENT REGIMENSWith the introduction of intravitreal anti-VEGF agents
and corticosteroids, the therapeutic perspective for DME has undergone a seismic change58. These drugs are asso-ciated with favorable anatomical and functional outcomes in a large proportion of treated patients, with results repli-cated in multiple randomized controlled trials.
The IVI of anti-VEGF agents has been shown to be superior to focal and grid LASER photocoagulation60-62, the gold standard treatment for DME since the Early Treatment Diabetic Retinopathy Study (ETDRS) in 198563. Three commonly used intravitreous VEGF inhi-bitors - bevacizumab, ranibizumab and aflibercept, - have proved safe and effective for the treatment of DME10,64,65, but only aflibercept and ranibizumab are approved by the FDA and EMA for this indication.
A recently published comparative-effectiveness rando-mized clinical trial from the Diabetic Retinopathy Clinical Research Network (DRCR.net), was conducted to com-pare intravitreous aflibercept (2.0 mg), bevacizumab (1.25 mg) and ranibizumab (0.3 mg) for the treatment of visually impairing DME66. The authors concluded that intravi-treous aflibercept, bevacizumab and ranibizumab improve vision in eyes with center-involved DME, even though the relative effect depends on baseline visual acuity (VA). For mild baseline visual loss there were no apparent differen-ces, on average, among study groups. However, for worse levels of baseline VA, aflibercept proved more effective than bevacizumab or ranibizumab66.
In addition to anti-inflammatory properties, corticoste-roids reduce the activity of VEGF by inhibiting the expres-sion of VEGF and the VEGF gene58. The dexamethasone drug delivery system (Ozurdex®, Allergan, Irvine, CA, USA) is a biodegradable, sustained-release device appro-ved by the U.S. FDA and EMA for DME. After promising results from the BOZURDEX study (a phase II randomized clinical trial that compared bevacizumab with the dexame-thasone implant), the MEAD study67 ultimately led to the FDA approval of the Ozurdex®. In this phase III, three-year, randomized, sham-controlled clinical trial in patients with DME, the dexamethasone implant proved safe and met the primary efficacy endpoint for improvement in BCVA. Sig-nificant cataracts requiring cataract surgery were found in 59% of the phakic eyes. Two patients (0.3%) developed uncontrolled elevated intraocular pressure that required trabeculectomy. In the FAME studies21,68, Campochiaro et al found that the fluocinolone implant could provide subs-tantial visual benefit for up to 3 years in the treatment of DME. In the 15 European countries (including Portugal)
Rufino Silva, João Pedro Marques

Vol. 39 - Nº 2 - Abril-Junho 2015 | 81
where it is currently approved, its use is limited for the treatment of vision impairment associated with chronic DME considered insufficiently responsive to available therapies. In the U.S., the FDA approved Iluvien® for the treatment of DME in patients previously treated with a course of corticosteroids that did not develop a significant rise in intraocular pressure.
3.2.3. FROM TRIAL TO PRACTICEMost likely, distinctive pathophysiological features
exist between recent-onset and chronic DME. The deci-sion on the adequate therapeutic approach should take in consideration the chronicity of DME as well as the num-ber of and response to previous treatment modalities.
As DME initially develops, VEGF-associated hyper-permeability, acute inflammation, and vascular dysfunc-tion likely dominate58. In this setting, using an anti-VEGF drug seems to be the best possible strategy. On the other hand, chronic DME is likely associated with a higher non--VEGF cytokine milieu, chronic inflammation, and neuro-nal damage. This is probably a situation where corticoste-roids may be more effective58.
Regardless of the local ocular treatment chosen, evi-dence indicates that optimal systemic control of blood glucose, blood pressure, lipid parameters and physical
exercise reduce complications related to diabetic retinopa-thy in the long term75.
Our current treatment protocol (Fig 1) for newly diag-nosed patients with focal DME is focal LASER photo-coagulation of leaking microaneurysms. In cases of no clinical response or whenever diffuse DME is present, a 3-month loading dose with ranibizumab 0.5 mg/0.05 ml or aflibercept 2.0 mg/0.05 ml is started. Patients are observed after the loading dose. If a clinical response is achieved, regular clinical and OCT observation followed by an as needed treatment regimen is usually employed. More than one intravitreal injection may be prescribed between eva-luation visits. In patients with persistent DME despite the use of anti-VEGF and a switch to a different anti-VEGF agent, the use of a steroid implant is the preferred treat-ment modality.
The implant of Dexametasone is our first option for non-responders to anti-VEGF, i.e. DME persistence with a tomographic reduction <20% in the central subfield thick-ness and/or VA improvement < 5 ETDRS letters. Patients need to be evaluated every 2 months after the implant and 2 to 3 implants may be needed in the first year. Some patients may respond to anti-VEGF again after a treatment period with costicosteroids.
The implant of Fluocinolone is indicated in chronic
Intravitreal injection of pharmacological agents: from clinical trial to clinical practice
Table 3 | Currently available intravitreous anti-VEGF agents and steroid implants used in the clinical practice for the manage-ment of diabetic macular edema.
FDA approval EMA approval Infarmed approval Relevant studies and level of evidence
Bevacizumab No No No • BOLT study65,69 [1b]• Protocol T from DRCR.net66 [1b]
Ranibizumab Yes, at a monthly dose of 0.3 mg
Yes, at a monthly dose of 0.5 mg
Yes, at a monthly dose of 0.5 mg
• RESOLVE study70• RISE and RIDE studies60,64 [1b]• READ-2 Study62 [1b]• Protocol I from DRCR.net71,72 [1b]• Protocol T from DRCR.net66 [1b]
Aflibercept
Yes, at a dose of 2.0 mg (every 8w after 5 initialmonthly injections)
Yes, at a dose of 2.0 mg (every 8w after 5 initialmonthly injections)
Yes, at a dose of 2.0 mg (every 8w after 5 initialmonthly injections)
• VIVID and VISTA studies10 [1b]• Protocol T from DRCR.net66 [1b]
Dexamethasone implant
Yes, at a dose of 0.7 mg
Yes, at a dose of 0.7 mg
Yes, at a dose of 0.7 mg
• CHAMPLAIN study73 [1b]• BEVORDEX study74 [1b]• MEAD study67 [1b]
FluocinoloneAcetonide Delivery Device
Yes, at a dose of 0.19 mg No Yes, at a dose of
0.19 mg• FAMOUS study20 [1b]• FAME A and B studies21,68 [1b]
Notes: The provided levels of evidence are based on the Centre for Evidence Based Medicine, Oxford (March 2009). Last assessed on 17th July 2015 at http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/Abbreviations: FDA, US Food and Drug Administration; EMA, European Medicines Agency; Infarmed, Autoridade Nacional do Medicamento e Produtos de Saúde, I.P

82 | Revista da Sociedade Portuguesa de Oftalmologia
DME with no response to anti-VEGF. According to our protocol, it is proposed in:
1 - Chronic DME diagnosed at least one year before and with:
a. Non-response to anti-VEGF and b. At least 6 months of treatment and 3 or more
anti-VEGF injections and c. Pseudophakic patients or with a programmed
cataract surgery 2 - Chronic DME diagnosed at least one year before and
with: a. Recent (less than six months) myocardial
infarction or stroke and/or b. Absolute incapacity for monthly or less fre-
quent visits to the Clinical centre and c. Pseudophakic patients or with a programmed
cataract surgery
Patients are evaluated 1 month after the treatment and every 3 months after that.
3.3. RETINAL VEIN OCCLUSIONS
3.3.1. BACKGROUNDRVO is the second leading cause of retinal vascular
disease after DR, with an estimated prevalence of 16.4 million adults worldwide76. When left untreated, visual impairment frequently develops, as well as other significant ocular complications77. Macular edema can be found in the vast majority of cases with central retinal vein occlusion (CRVO) and develops in 5-15% of eyes with branch reti-nal vein occlusion (BRVO)78,79. Both BRVO and CRVO are associated with a significant impairment in vision-related quality of life (as measured by the National Eye Institute visual function questionnaire, NEI- VFQ)80.
3.3.2. AVAILABLE TREATMENTS AND TREAT-MENT REGIMENSFollowing the recommendations of the CRVO and
BRVO study groups81,82, for many years the treatment of macular edema due to CRVO was based on clinical obser-vation, while in BRVO grid laser photocoagulation was
Rufino Silva, João Pedro Marques
Fig. 1 | Diabetic macular edema treatment flowchart.

Vol. 39 - Nº 2 - Abril-Junho 2015 | 83
applied. Over the last decade, significant innovations have reshaped the management of macular edema due to RVO. These include the FDA, EMA and Infarmed approval of anti--VEGF agents (ranibizumab and aflibercept) and dexametha-sone implant for the treatment of visual impairing macular edema caused by either CRVO or BRVO (Table 4). Both compounds provided valuable anatomical and functional out-comes that have been reported in multiple randomized con-trolled trials83-87. However, head-to-head comparison studies sponsored by Novartis (COMRADE-B and COMRADE-C studies for BRVO and CRVO, respectively) have shown that ranibizumab is superior to the dexamethasone implant80.
The use of steroids had already been investigated with intravitreal triamcinolone. In the SCORE study88,89, intra-vitreal triamcinolone showed to be superior to observation for treating vision loss associated with macular edema secondary to CRVO88 and BRVO89. Despite the promising results, the important adverse effects commonly associated with triamcinolone prevented its approval for the manage-ment of macular edema due to RVO.
Although not developed or licensed for intravitreal use, bevacizumab has long been used as an off-label therapy for macular edema due to RVO. Several studies have proven that the drug is safe and effective both for CRVO90 and BRVO91.
Like in exudative AMD and DME, the first clinical trials tested monthly regimens. However, a shift towards PRN or treat-and-extend approaches is being noted, accompanying the needs of a clinical practice approach.
3.2.3. FROM TRIAL TO PRACTICEOur current treatment protocol for newly diagnosed
patients with visually impairing macular edema due to
CRVO or BRVO involves a 3-month loading dose with bevacizumab 1.5 mg/0.05 mL, ranibizumab 0.5 mg/0.05 mL or aflibercept 2.0 mg/0.05 mL, followed by a PRN regi-men. More than one intravitreal injection may be prescri-bed between evaluation visits. In patients with persistent macular edema despite the use of anti-VEGF, switch to a different anti-VEGF agent or the use of the dexamethasone implant is our preferred approach.
3.4. MYOPIC NEOVASCULARIZATION
3.4.1. BACKGROUNDEven though myopia is already the most common eye
condition worldwide, recent epidemiologic studies have shown that its prevalence is significantly increasing96. This increase is especially observed in Southeast Asia but Euro-pean countries and the U.S. are also being affected by this global epidemic. Although education levels are associa-ted with myopia, higher education seems to be an addi-tive rather than explanatory factor97. Increasing levels of myopia carry a significant clinical and economic burden, by conveying an increased risk of the sight-threatening complications of high myopia98. The most fearsome con-sequence of pathologic myopia is choroidal neovasculari-zation, which occurs in approximately 5%-10% of patients with pathological myopia99.
3.4.2. AVAILABLE TREATMENTS AND TREAT-MENT REGIMENSFor a long time, LASER photocoagulation was the
only treatment for extrafoveal myopic neovasculariza-tion. LASER scar expansion and recurrence of CNV were
Intravitreal injection of pharmacological agents: from clinical trial to clinical practice
Table 4 | Currently available intravitreous agents used in the clinical practice for the management of macular edema secondary to retinal vein occlusion.
FDA approval EMA approval Infarmed approval Relevant studies and level of evidence
Bevacizumab No No No • Epstein et al90 [2b] (CRVO)• Russo et al91 [2b] (BRVO)
Ranibizumab Yes, at a monthly dose of 0.5 mg
Yes, at a monthly dose of 0.5 mg
Yes, at a monthly dose of 0.5 mg
• CRUISE study84,92 [1b] (CRVO)• BRAVO study93 [1b] (BRVO)• HORIZON study83 [1b] (CRVO and BRVO)• RABAMES study94 [1b] (BRVO)
Aflibercept Yes, at a monthly dose of 2.0 mg
Yes, at a monthly dose of 2.0 mg
Yes, at a monthly dose of 2.0 mg
• COPERNICUS study85,95 [1b] (CRVO)• VIBRANT study86 [1b] (BRVO)
Dexamethasone implant
Yes, at a dose of 0.7 mg
Yes, at a dose of 0.7 mg
Yes, at a dose of 0.7 mg • GENEVA study87 [1b] (CRVO and BRVO)
Notes: The provided levels of evidence are based on the Centre for Evidence Based Medicine, Oxford (March 2009). Last assessed on 17th July 2015 at http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/Abbreviations: FDA, US Food and Drug Administration; EMA, European Medicines Agency; Infarmed, Autoridade Nacional do Medicamento e Produtos de Saúde, I.P; CRVO, central retinal vein occlu-sion; BRVO, branch retinal vein occlusion

84 | Revista da Sociedade Portuguesa de Oftalmologia
frequently observed complications and led to the disconti-nuation of this treatment modality99.
In cases of subfoveal CNV, photodynamic therapy (PDT) with verteporfin has proven safe and effective with stabilization of VA in 72% of the eyes with at 12 months100. Unfortunately, no significant benefit in visual outcome was found at 24 months101. Nowadays, the use of PDT remains a viable option, especially for patients with juxtafoveal CNV and whenever anti-VEGF therapy is unsuitable102.
Anti-VEGF drugs are currently the gold standard for the management of myopic CNV98,103 but only ranibizu-mab has received FDA, EMA and Infarmed approval for this indication. After the MYRROR study104, aflibercept received approval for myopic CNV but only in Japan.
3.4.3. FROM TRIAL TO PRACTICELong-term results with ranibizumab and bevacizumab
(used off label) for myopic CNV in clinical practice are similar. A recent study from Ruiz-Moreno et al105 reported statistically significant improvements in visual acuity at 3 years but loss of statistical significance at 4, 5 and 6 years of follow-up.
In our department, myopic CNV is treated with a loa-ding dose of 2 IVI of ranibizumab or Bevcizumab followed by an as needed approach. Retreatment is based on loss of visual acuity (≥5 ETDRS letters) and/or the presence of fluid on OCT and/or significant metamorphopsia.
3.5. MISCELLANEOUS CAUSES OF CNV
Miscellaneous causes of CNV include central serous chorioretinopathy, angioid streaks, choroidal rupture after blunt trauma, birdshot retinopathy, presumed ocular hito-plasmosis syndrome, white-dot syndromes or idiopathic forms. Due to its rare nature, clinical guidelines are not available for the management of these conditions. We usually employ an individualized approach based on the clinical findings and complemented by multimodal reti-nal imaging. We usually start with an IVI of ranibizumab or Aflibercept 0.5 mg/0.05 mL followed by an as needed treatment regimen.
4. CONCLUSION
Because of their chronic nature and poor visual outco-mes when left untreated, neovascular AMD, DME, macu-lar edema due to RVO and myopic neovascularization are important examples of retinal diseases that require IVI of
therapeutic agents. The advent of intravitreal anti-VEGF drugs and corticosteroids has restyled the management of these conditions, allowing for better anatomical and func-tional results without significant side effects. However, monthly injections and monthly clinic visits may reduce long-term compliance and increase costs46. To optimize the benefit/risk ratio and cost- effectiveness of intravitreal treatment, flexible dosing strategies are increasingly being used in clinical practice (PRN and treat-and-extend regi-mens). These approaches are a lot easier to implement in a daily basis with acceptable results and patient compliance.
New agents are currently being developed, aimed at improving the patient’s quality of life by minimizing visual impairment and treatment burden in these highly consequential and burdensome diseases.
REFERENCES
1. Peyman GA, Lad EM, Moshfeghi DM. Intravitreal injection of therapeutic agents. Retina 2009;29:875-912.
2. Ferrara N, Hillan KJ, Novotny W. Bevacizumab (Avas-tin), a humanized anti-VEGF monoclonal antibody for cancer therapy. Biochemical and biophysical research communications 2005;333:328-35.
3. Ferrara N, Gerber HP, LeCouter J. The biology of VEGF and its receptors. Nature medicine 2003;9:669-76.
4. Rosenfeld PJ, Moshfeghi AA, Puliafito CA. Optical coherence tomography findings after an intravitreal injection of bevacizumab (avastin) for neovascular age-related macular degeneration. Ophthalmic surgery, lasers & imaging : the official journal of the Internatio-nal Society for Imaging in the Eye 2005;36:331-5.
5. Berg K, Pedersen TR, Sandvik L, Bragadottir R. Com-parison of ranibizumab and bevacizumab for neovas-cular age-related macular degeneration according to LUCAS treat-and-extend protocol. Ophthalmology 2015;122:146-52.
6. Stein JD, Newman-Casey PA, Mrinalini T, Lee PP, Hutton DW. Cost-effectiveness of bevacizumab and ranibizumab for newly diagnosed neovascular macular degeneration. Ophthalmology 2014;121:936-45.
7. Mordenti J, Cuthbertson RA, Ferrara N, et al. Compari-sons of the intraocular tissue distribution, pharmacoki-netics, and safety of 125I-labeled full-length and Fab antibodies in rhesus monkeys following intravitreal administration. Toxicologic pathology 1999;27:536-44.
8. Holash J, Davis S, Papadopoulos N, et al. VEGF-Trap: a VEGF blocker with potent antitumor effects. Pro-ceedings of the National Academy of Sciences of the
Rufino Silva, João Pedro Marques

Vol. 39 - Nº 2 - Abril-Junho 2015 | 85
United States of America 2002;99:11393-8.9. Heier JS, Brown DM, Chong V, et al. Intravitreal afli-
bercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012;119:2537-48.
10. Korobelnik JF, Do DV, Schmidt-Erfurth U, et al. Intra-vitreal aflibercept for diabetic macular edema. Ophthal-mology 2014;121:2247-54.
11. Heier JS, Boyer D, Nguyen QD, et al. The 1-year results of CLEAR-IT 2, a phase 2 study of vascular endothelial growth factor trap-eye dosed as-needed after 12-week fixed dosing. Ophthalmology 2011;118:1098-106.
12. Gomez-Ulla F, Marticorena J, Alfaro DV, 3rd, Fernan-dez M, Mendez ER, Rothen M. Intravitreal triamcino-lone for the treatment of diabetic macular edema. Cur-rent diabetes reviews 2006;2:99-112.
13. Cunningham MA, Edelman JL, Kaushal S. Intravitreal steroids for macular edema: the past, the present, and the future. Survey of ophthalmology 2008;53:139-49.
14. Tranos PG, Wickremasinghe SS, Stangos NT, Topou-zis F, Tsinopoulos I, Pavesio CE. Macular edema. Sur-vey of ophthalmology 2004;49:470-90.
15. Stewart MW. Corticosteroid use for diabetic macular edema: old fad or new trend? Current diabetes reports 2012;12:364-75.
16. Abraldes MJ, Fernandez M, Gomez-Ulla F. Intravitreal triamcinolone in diabetic retinopathy. Current diabetes reviews 2009;5:18-25.
17. Chang-Lin JE, Attar M, Acheampong AA, et al. Phar-macokinetics and pharmacodynamics of a sustained--release dexamethasone intravitreal implant. Investiga-tive ophthalmology & visual science 2011;52:80-6.
18. Chang-Lin JE, Burke JA, Peng Q, et al. Pharmacoki-netics of a sustained-release dexamethasone intravi-treal implant in vitrectomized and nonvitrectomized eyes. Investigative ophthalmology & visual science 2011;52:4605-9.
19. Medeiros MD, Alkabes M, Navarro R, Garcia-Arumi J, Mateo C, Corcostegui B. Dexamethasone intravitreal implant in vitrectomized versus nonvitrectomized eyes for treatment of patients with persistent diabetic macu-lar edema. Journal of ocular pharmacology and thera-peutics : the official journal of the Association for Ocu-lar Pharmacology and Therapeutics 2014;30:709-16.
20. Campochiaro PA, Hafiz G, Shah SM, et al. Sustained ocular delivery of fluocinolone acetonide by an intravi-treal insert. Ophthalmology 2010;117:1393-9 e3.
21. Campochiaro PA, Brown DM, Pearson A, et al. Long--term benefit of sustained-delivery fluocinolone ace-tonide vitreous inserts for diabetic macular edema. Ophthalmology 2011;118:626-35 e2.
22. Storey P, Dollin M, Rayess N, et al. The effect of pro-phylactic topical antibiotics on bacterial resistance pat-terns in endophthalmitis following intravitreal injec-tion. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur kli-nische und experimentelle Ophthalmologie 2015.
23. Meredith TA, McCannel CA, Barr C, et al. Postinjec-tion endophthalmitis in the comparison of age-rela-ted macular degeneration treatments trials (CATT). Ophthalmology 2015;122:817-21.
24. Solomon SD, Lindsley K, Vedula SS, Krzystolik MG, Hawkins BS. Anti-vascular endothelial growth factor for neovascular age-related macular degene-ration. The Cochrane database of systematic reviews 2014;8:CD005139.
25. Pascolini D, Mariotti SP, Pokharel GP, et al. 2002 global update of available data on visual impairment: a compilation of population-based prevalence studies. Ophthalmic epidemiology 2004;11:67-115.
26. Tomany SC, Wang JJ, Van Leeuwen R, et al. Risk factors for incident age-related macular degeneration: pooled findings from 3 continents. Ophthalmology 2004;111:1280-7.
27. Cachulo Mda L, Lobo C, Figueira J, et al. Prevalence of Age-Related Macular Degeneration in Portugal: The Coimbra Eye Study - Report 1. Ophthalmologica Jour-nal international d’ophtalmologie International jour-nal of ophthalmology Zeitschrift fur Augenheilkunde 2015;233:119-27.
28. Virgili G, Bini A. Laser photocoagulation for neovas-cular age-related macular degeneration. The Cochrane database of systematic reviews 2007:CD004763.
29. Wormald R, Evans J, Smeeth L, Henshaw K. Photo-dynamic therapy for neovascular age-related macular degeneration. The Cochrane database of systematic reviews 2007:CD002030.
30. Agarwal A, Rhoades WR, Hanout M, et al. Manage-ment of neovascular age-related macular degeneration: current state-of-the-art care for optimizing visual out-comes and therapies in development. Clinical ophthal-mology 2015;9:1001-15.
31. Group CR, Martin DF, Maguire MG, et al. Ranibi-zumab and bevacizumab for neovascular age-related macular degeneration. The New England journal of medicine 2011;364:1897-908.
32. Comparison of Age-related Macular Degeneration Treatments Trials Research G, Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two--year results. Ophthalmology 2012;119:1388-98.
Intravitreal injection of pharmacological agents: from clinical trial to clinical practice

86 | Revista da Sociedade Portuguesa de Oftalmologia
33. Chakravarthy U, Harding SP, Rogers CA, et al. Alter-native treatments to inhibit VEGF in age-related cho-roidal neovascularisation: 2-year findings of the IVAN randomised controlled trial. Lancet 2013;382:1258-67.
34. Krebs I, Schmetterer L, Boltz A, et al. A randomised double-masked trial comparing the visual outcome after treatment with ranibizumab or bevacizumab in patients with neovascular age-related macular degeneration. The British journal of ophthalmology 2013;97:266-71.
35. Kodjikian L, Souied EH, Mimoun G, et al. Ranibizu-mab versus Bevacizumab for Neovascular Age-rela-ted Macular Degeneration: Results from the GEFAL Noninferiority Randomized Trial. Ophthalmology 2013;120:2300-9.
36. Sadda SR, Stoller G, Boyer DS, Blodi BA, Shapiro H, Ianchulev T. Anatomical benefit from ranibizumab treatment of predominantly classic neovascular age--related macular degeneration in the 2-year anchor study. Retina 2010;30:1390-9.
37. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascu-lar age-related macular degeneration: Two-year results of the ANCHOR study. Ophthalmology 2009;116:57-65 e5.
38. Kaiser PK, Blodi BA, Shapiro H, Acharya NR, Group MS. Angiographic and optical coherence tomographic results of the MARINA study of ranibizumab in neo-vascular age-related macular degeneration. Ophthal-mology 2007;114:1868-75.
39. Boyer DS, Antoszyk AN, Awh CC, et al. Subgroup analysis of the MARINA study of ranibizumab in neo-vascular age-related macular degeneration. Ophthal-mology 2007;114:246-52.
40. Lalwani GA, Rosenfeld PJ, Fung AE, et al. A varia-ble-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. American journal of ophthalmo-logy 2009;148:43-58 e1.
41. Regnier SA, Malcolm W, Haig J, Xue W. Cost-effec-tiveness of ranibizumab versus aflibercept in the treat-ment of visual impairment due to diabetic macular edema: a UK healthcare perspective. ClinicoEcono-mics and outcomes research : CEOR 2015;7:235-47.
42. Holz FG, Amoaku W, Donate J, et al. Safety and effi-cacy of a flexible dosing regimen of ranibizumab in neovascular age-related macular degeneration: the SUSTAIN study. Ophthalmology 2011;118:663-71.
43. Boyer DS, Heier JS, Brown DM, Francom SF, Ian-chulev T, Rubio RG. A Phase IIIb study to evaluate the safety of ranibizumab in subjects with neovascular
age-related macular degeneration. Ophthalmology 2009;116:1731-9.
44. Grunwald JE, Pistilli M, Ying GS, et al. Growth of geographic atrophy in the comparison of age-related macular degeneration treatments trials. Ophthalmology 2015;122:809-16.
45. Grunwald JE, Daniel E, Huang J, et al. Risk of geogra-phic atrophy in the comparison of age-related macu-lar degeneration treatments trials. Ophthalmology 2014;121:150-61.
46. Freund KB, Korobelnik JF, Devenyi R, et al. Treat an extend regimens with anti-VEGF agents in rretinal diseases. A Literature Review and Consensus Recom-mendations. Retina 2015.
47. Schmidt-Erfurth U, Chong V, Loewenstein A, et al. Guidelines for the management of neovascular age--related macular degeneration by the European Society of Retina Specialists (EURETINA). The British journal of ophthalmology 2014;98:1144-67.
48. Rayess N, Houston SK, 3rd, Gupta OP, Ho AC, Regillo CD. Treatment outcomes after 3 years in neovascular age-related macular degeneration using a treat-and--extend regimen. American journal of ophthalmology 2015;159:3-8 e1.
49. Regillo CD, Brown DM, Abraham P, et al. Randomi-zed, double-masked, sham-controlled trial of ranibizu-mab for neovascular age-related macular degeneration: PIER Study year 1. American journal of ophthalmo-logy 2008;145:239-48.
50. Abraham P, Yue H, Wilson L. Randomized, double--masked, sham-controlled trial of ranibizumab for neovascular age-related macular degeneration: PIER study year 2. American journal of ophthalmology 2010;150:315-24 e1.
51. Schmidt-Erfurth U, Eldem B, Guymer R, et al. Effi-cacy and safety of monthly versus quarterly ranibi-zumab treatment in neovascular age-related macular degeneration: the EXCITE study. Ophthalmology 2011;118:831-9.
52. Singer MA, Awh CC, Sadda S, et al. HORIZON: an open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology 2012;119:1175-83.
53. Rofagha S, Bhisitkul RB, Boyer DS, Sadda SR, Zhang K, Group S-US. Seven-year outcomes in ranibizu-mab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology 2013;120:2292-9.
54. Eldem BM, Muftuoglu G, Topbas S, et al. A rando-mized trial to compare the safety and efficacy of two
Rufino Silva, João Pedro Marques
Vol. 39 - Nº 2 - Abril-Junho 2015 | 87
ranibizumab dosing regimens in a Turkish cohort of patients with choroidal neovascularization secondary to AMD. Acta ophthalmologica 2014.
55. Gardete-Correia L, Boavida JM, Raposo JF, et al. First diabetes prevalence study in Portugal: PREVADIAB study. Diabetic medicine : a journal of the British Dia-betic Association 2010;27:879-81.
56. Dutra Medeiros M, Mesquita E, Papoila AL, Genro V, Raposo JF. First diabetic retinopathy prevalence study in Portugal: RETINODIAB Study-Evaluation of the screening programme for Lisbon and Tagus Valley region. The British journal of ophthalmology 2015.
57. Adelman R, Parnes A, Michalewska Z, Parolini B, Bos-cher C, Ducournau D. Strategy for the management of diabetic macular edema: the European vitreo-retinal society macular edema study. BioMed research inter-national 2015;2015:352487.
58. Colucciello M. Current intravitreal pharmacologic the-rapies for diabetic macular edema. Postgraduate medi-cine 2015:1-14.
59. Yau JW, Rogers SL, Kawasaki R, et al. Global preva-lence and major risk factors of diabetic retinopathy. Diabetes care 2012;35:556-64.
60. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizu-mab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology 2012;119:789-801.
61. Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTORE study: ranibizumab monotherapy or com-bined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology 2011;118:615-25.
62. Nguyen QD, Shah SM, Khwaja AA, et al. Two--year outcomes of the ranibizumab for edema of the mAcula in diabetes (READ-2) study. Ophthalmology 2010;117:2146-51.
63. Group ETDRSR. Photocoagulation for diabetic macu-lar edema. Early Treatment Diabetic Retinopathy Study report number 1. Archives of ophthalmology 1985;103:1796-806.
64. Brown DM, Nguyen QD, Marcus DM, et al. Long-term outcomes of ranibizumab therapy for diabetic macular edema: the 36-month results from two phase III trials: RISE and RIDE. Ophthalmology 2013;120:2013-22.
65. Rajendram R, Fraser-Bell S, Kaines A, et al. A 2-year prospective randomized controlled trial of intravitreal bevacizumab or laser therapy (BOLT) in the manage-ment of diabetic macular edema: 24-month data: report 3. Archives of ophthalmology 2012;130:972-9.
66. Diabetic Retinopathy Clinical Research N, Wells JA, Glassman AR, et al. Aflibercept, bevacizumab, or
ranibizumab for diabetic macular edema. The New England journal of medicine 2015;372:1193-203.
67. Boyer DS, Yoon YH, Belfort R, Jr., et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology 2014;121:1904-14.
68. Campochiaro PA, Brown DM, Pearson A, et al. Sus-tained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabe-tic macular edema. Ophthalmology 2012;119:2125-32.
69. Michaelides M, Kaines A, Hamilton RD, et al. A pros-pective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (BOLT study) 12-month data: report 2. Ophthal-mology 2010;117:1078-86 e2.
70. Massin P, Bandello F, Garweg JG, et al. Safety and efficacy of ranibizumab in diabetic macular edema (RESOLVE Study): a 12-month, randomized, control-led, double-masked, multicenter phase II study. Diabe-tes care 2010;33:2399-405.
71. Elman MJ, Ayala A, Bressler NM, et al. Intravitreal Ranibizumab for diabetic macular edema with prompt versus deferred laser treatment: 5-year randomized trial results. Ophthalmology 2015;122:375-81.
72. Diabetic Retinopathy Clinical Research N, Elman MJ, Qin H, et al. Intravitreal ranibizumab for diabetic macular edema with prompt versus deferred laser treat-ment: three-year randomized trial results. Ophthalmo-logy 2012;119:2312-8.
73. Boyer DS, Faber D, Gupta S, et al. Dexamethasone intra-vitreal implant for treatment of diabetic macular edema in vitrectomized patients. Retina 2011;31:915-23.
74. Gillies MC, Lim LL, Campain A, et al. A randomi-zed clinical trial of intravitreal bevacizumab ver-sus intravitreal dexamethasone for diabetic macu-lar edema: the BEVORDEX study. Ophthalmology 2014;121:2473-81.
75. Colucciello M. Diabetic retinopathy. Control of sys-temic factors preserves vision. Postgraduate medicine 2004;116:57-64.
76. Rogers S, McIntosh RL, Cheung N, et al. The preva-lence of retinal vein occlusion: pooled data from popu-lation studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010;117:313-9 e1.
77. Adelman RA, Parnes AJ, Bopp S, Saad Othman I, Ducournau D. Strategy for the management of macular edema in retinal vein occlusion: the European Vitreo-Retinal Society macular edema study. BioMed research international 2015;2015:870987.
78. Rogers SL, McIntosh RL, Lim L, et al. Natural history
Intravitreal injection of pharmacological agents: from clinical trial to clinical practice

88 | Revista da Sociedade Portuguesa de Oftalmologia
of branch retinal vein occlusion: an evidence-based systematic review. Ophthalmology 2010;117:1094-101 e5.
79. McIntosh RL, Rogers SL, Lim L, et al. Natural history of central retinal vein occlusion: an evidence-based systematic review. Ophthalmology 2010;117:1113-23 e15.
80. Glanville J, Patterson J, McCool R, Ferreira A, Gairy K, Pearce I. Efficacy and safety of widely used treat-ments for macular oedema secondary to retinal vein occlusion: a systematic review. BMC ophthalmology 2014;14:7.
81. Group TCVOS. Evaluation of grid pattern photocoa-gulation for macular edema in central vein occlusion. The Central Vein Occlusion Study Group M report. Ophthalmology 1995;102:1425-33.
82. Group TBVOS. Argon laser photocoagulation for macular edema in branch vein occlusion. The Branch Vein Occlusion Study Group. American journal of ophthalmology 1984;98:271-82.
83. Heier JS, Campochiaro PA, Yau L, et al. Ranibizumab for macular edema due to retinal vein occlusions: long--term follow-up in the HORIZON trial. Ophthalmology 2012;119:802-9.
84. Brown DM, Campochiaro PA, Singh RP, et al. Rani-bizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology 2010;117:1124-33 e1.
85. Brown DM, Heier JS, Clark WL, et al. Intravitreal afli-bercept injection for macular edema secondary to cen-tral retinal vein occlusion: 1-year results from the phase 3 COPERNICUS study. American journal of ophthal-mology 2013;155:429-37 e7.
86. Campochiaro PA, Clark WL, Boyer DS, et al. Intravi-treal aflibercept for macular edema following branch retinal vein occlusion: the 24-week results of the VIBRANT study. Ophthalmology 2015;122:538-44.
87. Haller JA, Bandello F, Belfort R, Jr., et al. Dexame-thasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlu-sion twelve-month study results. Ophthalmology 2011;118:2453-60.
88. Ip MS, Scott IU, VanVeldhuisen PC, et al. A randomi-zed trial comparing the efficacy and safety of intravi-treal triamcinolone with observation to treat vision loss associated with macular edema secondary to central retinal vein occlusion: the Standard Care vs Corticoste-roid for Retinal Vein Occlusion (SCORE) study report 5. Archives of ophthalmology 2009;127:1101-14.
89. Scott IU, Ip MS, VanVeldhuisen PC, et al. A randomi-zed trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular Edema secondary to branch retinal vein occlusion: the Standard Care vs Corticoste-roid for Retinal Vein Occlusion (SCORE) study report 6. Archives of ophthalmology 2009;127:1115-28.
90. Epstein DL, Algvere PV, von Wendt G, Seregard S, Kvanta A. Benefit from bevacizumab for macular edema in central retinal vein occlusion: twelve-month results of a prospective, randomized study. Ophthalmo-logy 2012;119:2587-91.
91. Russo V, Barone A, Conte E, Prascina F, Stella A, Noci ND. Bevacizumab compared with macular laser grid photocoagulation for cystoid macular edema in branch retinal vein occlusion. Retina 2009;29:511-5.
92. Campochiaro PA, Brown DM, Awh CC, et al. Sus-tained benefits from ranibizumab for macular edema following central retinal vein occlusion: twelve--month outcomes of a phase III study. Ophthalmology 2011;118:2041-9.
93. Brown DM, Campochiaro PA, Bhisitkul RB, et al. Sus-tained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophthalmology 2011;118:1594-602.
94. Pielen A, Mirshahi A, Feltgen N, et al. Ranibizumab for Branch Retinal Vein Occlusion Associated Macu-lar Edema Study (RABAMES): six-month results of a prospective randomized clinical trial. Acta ophthalmo-logica 2015;93:e29-37.
95. Boyer D, Heier J, Brown DM, et al. Vascular endothe-lial growth factor Trap-Eye for macular edema secon-dary to central retinal vein occlusion: six-month results of the phase 3 COPERNICUS study. Ophthalmology 2012;119:1024-32.
96. Dolgin E. The myopia boom. Nature 2015;519:276-8.97. Williams KM, Bertelsen G, Cumberland P, et al. Increa-
sing Prevalence of Myopia in Europe and the Impact of Education. Ophthalmology 2015;122:1489-97.
98. Silva R. Myopic maculopathy: a review. Ophthalmolo-gica 2012;228:197-213.
99. El Matri L, Chebil A, Kort F. Current and emerging treatment options for myopic choroidal neovasculari-zation. Clinical ophthalmology 2015;9:733-44.
100. Verteporfin in Photodynamic Therapy Study G. Pho-todynamic therapy of subfoveal choroidal neovascula-rization in pathologic myopia with verteporfin. 1-year results of a randomized clinical trial--VIP report no. 1. Ophthalmology 2001;108:841-52.
Rufino Silva, João Pedro Marques

Vol. 39 - Nº 2 - Abril-Junho 2015 | 89
Intravitreal injection of pharmacological agents: from clinical trial to clinical practice
101. Blinder KJ, Blumenkranz MS, Bressler NM, et al. Verteporfin therapy of subfoveal choroidal neovas-cularization in pathologic myopia: 2-year results of a randomized clinical trial--VIP report no. 3. Ophthalmo-logy 2003;110:667-73.
102. Chew MC, Tan CS. Treatment options for myopic CNV--is photodynamic therapy still relevant? Indian journal of ophthalmology 2014;62:834-5.
103. Silva RM, Ruiz-Moreno JM, Nascimento J, et al. Short-term efficacy and safety of intravitreal
ranibizumab for myopic choroidal neovascularization. Retina 2008;28:1117-23.
104. Ikuno Y, Ohno-Matsui K, Wong TY, et al. Intravi-treal Aflibercept Injection in Patients with Myopic Choroidal Neovascularization: The MYRROR Study. Ophthalmology 2015;122:1220-7.
105. Ruiz-Moreno JM, Montero JA, Araiz J, et al. Intravi-treal anti-vascular endothelial growth factor therapy for choroidal neovasculrization secobndary to pathological myopia: Six Years Outcome. Retina 2015.


Vol. 39 - Nº 2 - Abril-Junho 2015 | 91
Internal limiting membrane inverted flap technique: a new paradigm in large
macular hole surgery
Carlos Menezes1, José Alberto Lemos1, Rui Carvalho2, Josefina Serino2, Rita Gonçalves1, Bruna Cardoso Vieira2, Pedro Coelho1, Tiago Maio1, Paula Tenedório3
1Interno Complementar de Oftalmologia no Hospital Pedro Hispano2Assistente Hospitalar de Oftalmologia no Hospital Pedro Hispano
3Diretora do Serviço de Oftalmologia no Hospital Pedro Hispano
RESUMO
Objetivo: Avaliar e eficácia e a segurança da pelagem da membrana limitante interna (MLI) com a técnica dos flaps invertidos (TFI) na cirurgia do buraco macular (BM) grande.Material e Métodos: Análise retrospetiva dos pacientes com BMs grandes submetidos a vi-trectomia com pelagem da MLI com a TFI entre Janeiro de 2013 e Dezembro de 2014, com um seguimento mínimo de 6 meses. Compararam-se os valores de MAVC pré e pós-operatórios e avaliou-se o encerramento documentado por OCT e a ocorrência de complicações. O teste de Wilcoxon foi usado para comparar a melhor acuidade visual corrigida, MAVC (p<0,05).Resultados: Estudaram-se 17 olhos de 17 pacientes. 76,5% tinham BMs primários, 11,8% pós--vitrectomia e 11,8% traumáticos. O diâmetro mínimo médio foi de 578,5 ± 147μm e a dura-ção média da sintomatologia foi de 35,9 meses. 47,1% dos olhos eram fáquicos, 11,8% tinham catarata e 41,2% eram pseudofáquicos. A cirurgia de catarata concomitante foi realizada em 47,1% dos casos. Para o seguimento médio de 7,76 meses a taxa de encerramento foi de 100%. A MAVC melhorou de 1,20 ± 0,48 para 0,68 ± 0,36 unidades logMar. A MAVC melhorou em todos os olhos, com 64,7% a ganhar duas ou mais linhas de Snellen. A taxa de complicações foi de 5,6%.Conclusões: A pelagem da MLI com a TFI é eficaz e segura. Neste estudo, com BMs grandes, o sucesso anatómico foi 100% e a MAVC melhorou de forma estatisticamente significativa.
Palavras-chaveMembrana limitante interna, técnica dos flaps invertidos, buraco macular, cirurgia.
ABSTRACT
Purpose: To evaluate the efficacy and safety of the internal limiting membrane (ILM) inverted flap technique (IFT) in large macular hole (MH) surgery.Material and Methods: Retrospective analysis of eyes of patients with large MHs who un-derwent vitrectomy with ILM IFT between January 2013 and December 2014, with a minimum follow-up of 6 months. Myopic macular holes were excluded. We evaluated best-corrected vi-sual acuity (BCVA), hole closure documented by OCT and complications.We compared preoperative and postoperative values.
Artigo Original
Oftalmologia - Vol. 39: pp.91-96

92 | Revista da Sociedade Portuguesa de Oftalmologia
INTRODUCTION
Macular hole (MH) was until twenty-five years ago an incurable disease and a main cause of legal blindness. And so it was until Kelly and Wendel12 in 1991 proposed pars plana vitrectomy with posterior hyaloid peeling and air--fluid exchange to treat MH. With this approach, the main source of anterior-posterior traction on the retina was eli-minated and the borders of the MH were dehydrated and approximated to facilitate glial proliferation and cellular migration. The first results claimed a closure rate of 58%1.
In 1997, Eckhart et al.5, in the light of knowledge of the importance of tangential traction exerted by the contraction of myofibroblasts over the internal limiting membrane (ILM) in the aetiology of MH8, introduced the ILM peeling as part of MH surgery. ILM peeling relie-ves tangential traction, but also seems to stimulate glial cells to proliferate, increases retina elasticity and ensu-res the complete removal of an epiretinal membrane22. This meticulous procedure was later aided, in 2000, with the introduction of indocianine green by Brooks et al.3 to stain the ILM, which made the peeling safer and more effective. Independently of the questions related to indo-cianine green retinal toxicity or the use of other more recent vital dyes such as infracianine blue, trypan blue, brilliant blue or lutein-based dyes, staining is mandatory6 and closure rates around 90% can be found in most of the case-series published in the literature1, 2, 6, 20.
Although conventional ILM peeling has an undenia-ble anatomical effect in relation to closure rate, its func-tional advantages are controversial and a recent systema-tic review found no differences in best-corrected visual acuity (BCVA)20.
Apart from this issue, it is consensual that not all MHs close with conventional ILM peeling and that anatomic success is dependent on MH size, chronicity, pre-operative BCVA and aetiology6, 18, 19, 21. Particularly large MHs with a minimum diameter of 400μm, MHs with more than 1 year duration and all secondary MHs in general are associated with both a worse anatomic and functional outcome19. Moreover, in these cases, a “flat--open” outcome was considered a success, despite being associated with a poor visual outcome19.
In 2010 Michalewska et al. presented the ILM inver-ted flap technique (IFT) for the treatment of large MHs15. It consists of an incomplete ILM peeling till the bounda-ries of the MH with inversion of its borders upside-down into the MH. The first results claimed a closure rate of 100% (when a free-flap did not occur), no “flat-open” appearance and a significant improvement in VA in rela-tion to the conventional peeling15.
In this article we proposed to evaluate the efficacy and safety of the ILM IFT in the management of large MH. To do it, we evaluated MH closure rate documented by spectral domain optical coherence tomography (SD--OCT), BCVA and complications.
MATERIAL E METHODS
A longitudinal, retrospective, descriptive and obser-vational study was performed.
We analysed the medical records of patients with large MHs undergoing surgery with the ILM IFT between January 2013 and December 2014. Only eyes with a minimum follow-up of 6 months were included.
Carlos Menezes, José Alberto Lemos, Rui Carvalho, Josefina Serino, Rita Gonçalves, Bruna Cardoso Vieira, Pedro Coelho, Tiago Maio, Paula Tenedório
The Wilcoxon test was used for comparing BCVA (p <0.05).Results: 17 eyes of 17 patients with a mean age of 63.24 years were studied. 76.5% of eyes had primary MHs, 11,8% post-vitrectomy and 11,8% post-traumatic. Mean minimum MH diameter was 578,5 ± 147μm and the mean MH duration was 35,9 months. According to lens status, 47,1% were phakic, 11,8% had cataract and 41,2% were pseudophakic. Concomitant cataract surgery was performed in 47,1% of cases. At the mean follow-up of 7,76 months, closure rate was 100%, with BCVA improving from 1,20 ± 0,48 to 0,68 ± 0,36 logMar units. All patients improved BCVA, with 64,7% gaining two or more Snellen lines of BCVA. Complication rate was 5.6%. Conclusions: ILM IFT is an effective and safe technique in MH surgery. In this study, with large MH, the anatomic success rate was 100% and BCVA improvement was significant.
Key-wordsInternal limiting membrane, inverted flap technique, macular hole surgery.

Vol. 39 - Nº 2 - Abril-Junho 2015 | 93
We defined large MHs according to the new classifica-tion of the International Vitreomacular Traction Classifica-tion System4, namely a full-thickness MH with a minimum diameter of 400 μm. Minimum diameter was calculated with the calliper function of our SD-OCT devices and was defi-ned as the shortest distance, parallel to the retinal pigment epithelium, between the borders of the MH (Fig.1). We used Corpernicus SD-OCT (OPTOPOL Technology SA, Poland) or Cirrus SD-OCT (Carl Zeiss, Meditec, Dublin, CA).
We collected, in addition to the demographic data (age and sex), eye laterality and the post-operative follow-up, closure rate evaluated by SD-OCT, BCVA and complica-tions. MH closure was defined as the absence of neurosen-sory defect over the fovea11. We compared the preoperative and postoperative values, for the average time of follow-up. For the study purposes, in order to homogenize the posto-perative results, the last postoperative consultation between 6 and 12 months after surgery was considered.
All surgeries were performed by a single surgeon (RC). All patients underwent a 23G three –port pars plana vitrec-tomy, as a single procedure or combined with cataract sur-gery. Posterior hyaloid detachment was aided by triamci-nolone acetonide and the vitreous base was vitrectomized with identation. Membrane blue-dual (tripan-blue 0,15% + brilliant blue 0,025%) was used to stain an eventual epi-retinal membrane and the ILM. If an epiretinal membrane was present, it was peeled. An incomplete ILM peeling was performed, in a circular fashion, from a distance of at least 2 disc diameters until the MH edges where the ILM was left attached. After cutting the peripheral edges of the ILM with the vitrectome with low aspiration until a one and a half hole diameter size, its central remnants hanging in the vitreous cavity were inverted over the hole. The peeling
was then enlarged up to the vascular arcades. After a low--pressure fluid-air exchange (around 15-20mmHg), the air was replaced with 20% SF6. The patient was kept in face--down position for 3 days.
Statistical analysis was performed using the software IBM Statistical Package for Social Sciences (SPSS) version 20.0®. BCVA was evaluated in Snellen charts and conver-ted into the logarithm of the minimal angle of resolution (logMar) for statistical analysis. “Counting fingers” (CF) visual acuity was globally considered as 0,01 in decimal Snellen scale and later converted into logMar units. The normality of the variables was checked using the Kolmogo-rov-Smirnov test. Due to absence of normality, the Wilco-xon test was used to compare BCVA. A p value <0,05 was considered statistical significant.
RESULTS
A total of 17 eyes (70,6% right eyes, 12 eyes) of 17 patients with large MHs who underwent ILM IFT were studied.
The mean age of the 17 patients was 63.24 ± 15.09 years, with a predominance of males (9 eyes, 52.9%). The mean follow-up was 7.76 ± 2.22 months, ranging between 6 and 12 months.
All eyes had large MHs with complete posterior vitreous detachment (old stage 4 MHs). The majority of cases were primary MHs (76,5%, 13 eyes) with the exception of 2 trau-matic and post-vitrectomy MHs (both 11,8%). Relatively to MHs dimensions, the mean minimum and maximum dia-meters were, respectively, 578,5 ± 147,1μm and 1004,1 ± 254,6μm. Mean MH duration (82,35%, 14 eyes), evaluated
Internal limiting membrane inverted flap technique: a new paradigm in large macular holes surgery
Fig. 1 | SD-OCT scans (A,B and C – Copernicus, Optopol; D- Cirrus, Carl Zeiss) showing the preoperative (at left) and the post--operative (at right) images of some of the MH submitted to the ILM inverted flap technique. Four examples are shown (A-D). All cases were primary MH, which duration was, respectively, 48 and 72 months in examples A and B and unknown in examples C and D. MH dimensions are shown with the calliper function of the OCT device (minimum diameters were, res-pectively, 701, 565, 568 and 963μm), BCVA is shown in the right-inferior corner of the image in Snellen decimal scale and the postoperative period is shown in the top-superior corner of the postoperative image.

94 | Revista da Sociedade Portuguesa de Oftalmologia
by the duration of the patient’s complaints, was 35,86 ± 40,33 months, being superior to 1 year in 47,1% (8 eyes). MH duration was unknown in 17,65% (3 eyes).
According to lens status, 47,1% (8 eyes) were phakic and with clear media, 11,8% (2 eyes) had cataract and 41,2% (7 eyes) were already pseudophakic. Combined surgery with cataract phacoemulsification was performed in 47,1% of cases (8 eyes), with the exception of 2 of the phakic eyes without cataract.
All surgeries were uneventful with the exception of one case of an iatrogenic peripheral retinal tear that was successfully treated with endolaser. No cases of free flap occurred, namely during the cutting of the ILM flap with the vitrectome, during its inversion into the MH or during the fluid-air exchange.
After a mean follow-up period of 7,76 months, closure rate was of 100% and all MH closed with a “U-shape” foveal morphology (Fig. 1). No cases of flat-open MH occurred. BCVA improved from 1,20 ± 0,48 to 0,68 ± 0,36 logMar units (approximately from 1/10 to 3/10 in Snellen decimal scale), which was statistically significant (p<0,05). All eyes improved their BCVA and 64,7% (11 eyes) gained two or more Snellen lines of BCVA. The per-centage of eyes having at least BCVA of 2/10 was 23,5% (4 eyes) and 71,4% (10 eyes), respectively, in the preopera-tive (range CF-2/10) and in the postoperative period (range 1/20-8/10).
DISCUSSION
We proposed to evaluate retrospectively the efficacy and safety of the ILM IFT in the treatment of large MHs. Large MHs represent a true surgical challenge, since both
anatomic6, 18, 19, 21 and functional6, 10, 19 successes are more difficult to achieve.
Conventional ILM peeling aided by vital dyes was an important landmark in MH surgery and its usage in asso-ciation with gas tamponade is widespread. Although clo-sure rates superior to 90% can be found in the literature case-series1, 2, 3, not only some MHs don´t close with this technique19, but also the functional gains in BCVA in rela-tion to vitrectomy without ILM peeling are controversial20. In fact, a “flat-open” outcome was commonly considered a surgical success, despite being associated with a poor visual outcome19. With the exclusion of “flat-open” MHs, a global closure rate of 85,7% was found in the EVRS MH Study, and of 78,2% in complete MHs with complete posterior vitreous detachment (old stage 4 MHs), inde-pendently of its size6. Minimum MH diameter seems to be particularly important in both anatomic and functional outcomes, with the closure rate (excluding flat-open outco-mes) around 75% between 400 and 500μm and inferior to 50% above 500μm19.
Our sample included only large MHs. The mean mini-mum diameter was 578,5 ± 147,1μm, being bigger than 500μm and 600μm in 71,6% and 41,2% of the cases, res-pectively. Other important features that contribute to the bad prognosis of this sample are the long duration of symp-toms, with a mean value of almost 3 years, the presence of 4 cases of secondary MH (23,5%) and the low mean BCVA preoperative value (Table 1). Although concomitant cata-ract surgery, a predictor of a better postoperative BCVA, was performed in 47,1% of cases (8 eyes), only 11,8% (2 eyes) had cataract.
In this study, anatomic success was of 100%. Not only all MHs closed with absence of “flat-open” outcomes, but also all MHs closed in a “U-shaped” foveal configuration, associated with best visual outcome (Fig. 1). A moderate to evident restoration of both the ellipsoid band and the cone outer segment tips (COST) line was observed (Fig.1), as previously reported9. In fact, BCVA improvement from 1,20 ± 0,48 preoperatively to 0,68 ± 0,36 logMar units pos-toperatively was statistical significant. All eyes improved BCVA and 64,7% gained at least two Snellen lines. The ILM IFT, not only stimulates Muller cells, but also seems to act as a scaffold for tissue proliferation, resulting in an increased gliosis which seems to promote the centripetal migration of the perifoveal photoreceptors, improving both anatomic and functional success16. As BCVA seems to keep improving during the first year after surgery with the ILM IFT7, 9, our results may also even improve.
These results, with closure rates around 100% and significant improvement in BCVA, are common in recent
Fig. 2 | BCVA variation (Snellen lines) at the mean follow-up time after the ILM IFT. The percentage of eyes gai-ning one, two, three, four and six lines of BCVA were, respectively, 35,3%, 35,3%, 17,9%, 5,9% and 5,9%. Im-provement from CF to 0,05 was considered as an impro-vement of one line.
Carlos Menezes, José Alberto Lemos, Rui Carvalho, Josefina Serino, Rita Gonçalves, Bruna Cardoso Vieira, Pedro Coelho, Tiago Maio, Paula Tenedório

Vol. 39 - Nº 2 - Abril-Junho 2015 | 95
case-series reports with the ILM IFT, even in extremely large MHs, where a free-flap did not occur and a com-plete peeling was not done inadvertently14, 17. Almost all eyes improve BCVA and even eyes that don’t improve BCVA may have visual gains in visual field evaluated by microperimetry.
ILM IFT is a safe procedure. As a complication, we had a single case of a peripheral iatrogenic tear success-fully treated with endolaser. ILM IFT most common com-plication is the occurrence of a “free-flap” which most often occurs during fluid-air exchange and that, in practice, results in a conventional complete ILM peeling15. No cases of free-flaps occurred in the eyes studied. In order to peel the ILM without losing it, apart from stopping ILM peeling before the hole edges and cutting the ILM flap with low aspiration to avoid detaching it, it is fundamental to mini-mize intraocular pressure variations. This can be achieved by the usage of valved trocars and low pressures during fluid-air exchange. Retinal nerve fiber layer damage cau-sing paracentral scotomas as a consequence of the ILM pee-ling were not evaluated by multifocal electroretinography or microperimetry. However, in our opinion, its occurrence is not increased by the ILM IFT in relation to the complete conventional ILM peeling.
ILM IFT is until now a short history of success. Although we did exclude myopic MHs, ILM IFT has been used successfully, with a similar closure rate, in myopic MH in the absence of a concomitant foveoschisis or reti-nal detachment17. In its presence, in cases of extreme axial lengths, ILM IFT also seems to improve both anatomic and functional outcomes13, being possible to associate it with macular indentation.
As a conclusion, we can say that ILM IVT is an effec-tive and safe technique, which, in our opinion, represents
a paradigm shift in large MHs surgery. In this study, with large MH with bad prognosis, the anatomic success rate was 100% and the gain in terms of functional BCVA was significant.
BIBLIOGRAPHY
1. Ando F, Sasano K, Ohba N, Hirose H, Yasui O. Anato-mic and visual outcomes after indocyanine green-assis-ted peeling of the retinal internal limiting membrane in idiopathic macular hole surgery. Am J Ophthalmol. 2004 Apr; 137(4):609-14.
2. Beutel J, Dahmen G, Ziegler A, Hoerauf H. Internal limiting membrane peeling with indocyanine green or trypan blue in macular hole surgery: a randomized trial. Arch Ophthalmol. 2007 Mar; 125(3):326-32.
3. Brooks HL Jr. Macular hole surgery with and without internal limiting membrane peeling. Ophthalmology. 2000 Oct; 107(10):1939-48.
4. Duker JS, Kaiser PK, Binder S, de Smet MD, Gaudric A, Reichel E, et al. The International Vitreomacular Trac-tion Study Group classification of vitreomacular adhe-sion, traction, and macular hole. Ophthalmology. 2013 Dec; 120(12):2611-9.
5. Eckardt C, Eckardt U, Groos S, Luciano L, Reale E. Removal of the internal limiting membrane in macular holes. Clinical and morphological findings. Ophthalmo-loge. 1997 Aug; 94(8):545-51.
6. Nawrocki J, Othman IS. EVRS Macular Hole Study. Multi-center study presented at : EVRS 2013; September 2013, Rhodes, Greece (available in: http://www.evrs.eu/mh-study-connect/)
Table 1 | Preoperative characterization of the MH submitted to ILM inverted flap technique.
Parameter (unit) Mean ± SD Range (min/max) Percentage / number of eyes
Minimum diameter (μm) 578,5 ± 147,1 405/ 963 ---≥ 500 μm --- --- 71,6% / 12≥ 600 μm --- --- 41,2% / 7
Maximum diameter (μm) 1004,1 ± 254,6 479/ 1113 ---Duration (months)
Known 35,9 ± 40,3 1/ 132 82,4%/ 14< 12 months --- --- 35,3% / 6≥ 12 months --- --- 47,1% / 8Unknown --- --- 17,6% / 3
BCVA (logMar) 1,20 ± 4,85 0,52 / 2,00 ---
Abbreviators: SD- standard deviation; min- minimum; max-maximum.
Internal limiting membrane inverted flap technique: a new paradigm in large macular holes surgery

96 | Revista da Sociedade Portuguesa de Oftalmologia
7. Ferreira N, Meireles A. O que é um buraco macular grande. In: Quintão T, Brandão E, Martins N, Neves CM, Silva R. A interface vitre-retiniana – Adesão vítreo--macular, tração vítreo-macular e buraco macular – 25 perguntas e respostas. Lisboa: Euromedice; 2014. p. 43-49.
8. Gass JD. Idiopathic senile macular hole: its early stages and pathogenesis. Arch Ophthalmol. 1988 May; 106(5): 629-39.
9. Michalewska Z, Michalewski J, Nawrocki J. Continuous changes in macular morphology after macular hole clo-sure visualized with spectral optical coherence tomo-graphy. Graefes Arch Clin Exp Ophthalmol 2010 Sep; 248(9):1249-55.
10. Gupta B, Laidlaw DA, Williamson TH, Shah SP, Wong R, Wren S. Predicting visual success in macular hole sur-gery. Br J Ophthalmol. 2009 Nov; 93(11):1488-91.
11. Kang SW, Ahn K, Ham DI. Types of macular hole clo-sure and their clinical implications. Br J Ophthalmol. 2003 Aug; 87(8):1015-9.
12. Kelly NE, Wendel RT. Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthal-mol. 1991 May; 109(5):654-9.
13. Kuriyama S, Hayashi H, Jingami Y, Naofumi K, Akita J, Matsumoto M. Efficacy of inverted internal limiting membrane flap technique for the treatment of macu-lar hole in high myopia. Am J Ophthalomol. 2013 Jul; 156(1):125-131.
14. Mahalingam P, Sambhav K. Surgical ouctomes of inverted internal limiting membrane flap technique for large macular hole. Indian J Ophthalmol. 2013 Oct; 61(10):601-3.
15. Michalewska Z, Michalewski J, Adelman RA, Nawro-cki J. Inverted internal limiting membrane flap tech-nique for large macular holes. Ophthalmology.2010Oct;117(10):2018–25.
16. Michalewska Z, Michalewski J, Nawrocki J. Long-term decrease of retinal pigment epithelium defects in large
stage IV macular holes with borders mechanically joi-ned during surgery. Case Rep Ophthalmol 2011 May; 2(2):215-21.
17. Michalewska Z, Michalewski J, Dulczewska-Cichecka K, Nawrocki J. Inverted internal limiting membrane flap technique for surgical repair of myopic macular holes. Retina 2014 Apr; 34(4):664-9.
18. Salter AB, Folgar FA, Weissbrot J, Wald KJ. Macular hole surgery prognostic success rates based on macular hole size. Ophthalmic Surg Lasers Imaging. 2012 May--Jun; 43(3):184-9.
19. Susini A, Gastaud P. Ces trous maculaires qu’il vaut mieux ne pas opérer. J Fr Ophthalmol. 2008 Feb; 31(2):214-20.
20. Spiteri Cornish K, Lois N, Scott N, Burr J, Cook J, Boa-chie C, et al. Vitrectomy with internal limiting mem-brane (ILM) peeling versus vitrectomy with no peeling for idiopathic full-thickness macular hole (FTMH). Cochrane Database Syst Rev. 2013 Jun 5; 6: CD009306.
21. Wakely L, Rahman R, Stephenson J. A comparison of several methods of macular hole measurement using optical coherence tomography, and their value in predi-citing anatomical and visual outcomes. Br J Ophthalm. 2012 Jul; 96(7):1003-7.
22. Yooh HS, Brooks HL Jr, Capone A Jr, et al. Ultrastructu-ral features of tissue removed during idiopathic macular hole surgery. Am J Ophthalmol 1996 Jul; 122(1):67-75.
Os autores não têm nenhum interesse financeiro a declarar com este tra-balho.Este artigo é original, não tendo sido publicado ou apresentado previamente. Os autores cedem os direitos de autor à SPO.
CONTACTOCarlos MenezesRua Arménio Reis, lote B4, 4700-267 Real, [email protected]
Carlos Menezes, José Alberto Lemos, Rui Carvalho, Josefina Serino, Rita Gonçalves, Bruna Cardoso Vieira, Pedro Coelho, Tiago Maio, Paula Tenedório

Vol. 39 - Nº 2 - Abril-Junho 2015 | 97
10 anos de experiência no tratamento de retinoblastoma
Cristina Santos1, Inês Coutinho1, Ana Rita Azevedo2, Cláudia Constantino3, Ana Berta Sousa4, Filomena Pereira3, José Laranjeira5, João Cabral6, Susana Teixeira1
1Serviço de Oftalmologia, Hospital Prof. Doutor Fernando da Fonseca, E.P.E. 2Serviço de Oftalmologia, Hospital Beatriz Ângelo
3Serviço de Pediatria, Instituto Português de Oncologia de Lisboa, Francisco Gentil, E.P.E.4Serviço de Genética Médica, Hospital de Santa Maria, Centro Hospitalar de Lisboa Norte, E.P.E.
5Unidade de Oftalmologia, Instituto Português de Oncologia de Lisboa, Francisco Gentil, E.P.E.6Oftalmologia, Hospital da Luz
RESUMO
Objectivo: Descrever a experiência do Serviço de Oftalmologia do Hospital Prof. Doutor Fer-nando Fonseca no diagnóstico e tratamento de retinoblastoma entre Janeiro de 2004 e Dezembro de 2014. Métodos: Revisão retrospectiva dos processos clínicos e exames complementares de diagnóstico. Resultados: Foram tratados dezasseis doentes no período em estudo, sendo cinco casos bilate-rais. O diagnóstico foi estabelecido em média aos 27 meses de idade e a forma de apresentação mais frequente foi leucocória. Dois casos apresentavam história familiar. O tempo médio de seguimento foi de 51,6 meses. Um dos doentes desenvolveu um pineoblastoma, tendo acabado por falecer de complicações relacionadas com a quimioterapia sistémica. De entre as 16 crianças, 11 realizaram quimioterapia sistémica. Nove olhos foram submetidos a enucleação, dois deles após falência da terapêutica conservadora. Os restantes doze olhos foram sujeitos a tratamento conservador, cinco dos quais exclusivamente em Portugal, recorrendo a quimioterapia sistémica, crioterapia e fotocoagulação com LASER. Oito doentes (nove olhos) foram encaminhados para o Hôpital Ophtalmique Jules Gonin na Suíça, para complementar a terapêutica realizada. Conclusões: O tratamento do retinoblastoma tem evoluído nos últimos anos. As novas opções para tratamento local, mais eficazes e seguras, têm tornado possível cada vez mais preservar a vida, o órgão e a função. No entanto, para o sucesso terapêutico é fundamental o diagnóstico precoce.
Palavras-chaveRetinoblastoma, quimioterapia, tratamento conservador.
ABSTRACT
Purpose: To describe the experience of the Ophthalmology Department at Hospital Prof. Dou-tor Fernando Fonseca in diagnosis and treatment of retinoblastoma between January 2004 and December 2014. Methods: Retrospective review of clinical records and complementary exams. Results: Sixteen patients were treated during the study period, of whom five had bilateral disease. Mean age at diagnosis was 27 months and the most common presenting sign was leukocoria. Two cases had a positive family history. Mean follow-up time was 51.6 months. One of the patients developed pineoblastoma, and died as a consequence of systemic chemotherapy treatment. Eleven
Artigo Original
Oftalmologia - Vol. 39: pp.97-102

98 | Revista da Sociedade Portuguesa de Oftalmologia
patients received systemic chemotherapy. Nine eyes were enucleated, two of them after local treatment failure. Twelve eyes were subject to conservative treatment, five of them exclusively in Portugal, with systemic chemotherapy, cryotherapy and LASER photocoagulation. Eight patients (nine eyes) were referred to Hôpital Ophtalmique Jules Gonin in Switzerland for complementary conservative treatment. Conclusions: Treatment options for retinoblastoma have evolved in recent years. New options for safer and more effective local treatment have increased the chances of preserving life, organ and vision. Early diagnosis however, is fundamental for treatment success.
Key-wordsRetinoblastoma, chemotherapy, conservative treatment.
INTRODUÇÃO
O retinoblastoma é uma doença rara, sendo no entanto a neoplasia maligna intraocular mais comum da infância com uma incidência estimada de 1 para 15.000 nascimentos1. Um diagnóstico tardio relaciona-se com a perda de função visual, do globo ocular e potencialmente da vida.
É causado por uma mutação de ambos os alelos do gene RB1, um supressor tumoral2. A mutação do primeiro alelo pode ocorrer numa célula de linhagem germinativa (forma hereditária) ou numa célula somática progenitora de retina (forma esporádica). A segunda mutação ocorre na célula somática que origina o tumor. Existindo mutação na linha-gem germinativa, a doença é geralmente bilateral multifocal com vários tumores primários em ambos os olhos. Apesar de poder ser uma doença hereditária, 95% dos doentes não tem história familiar, pelo que se compreende a importância da pesquisa do reflexo vermelho em todas as crianças pelo seu médico assistente.
O estudo genético é útil para determinar a frequência e tipo de monitorização, assim como o risco de tumores extra-oculares (com destaque para osteossarcomas, sarco-mas dos tecidos moles e melanomas). Além disso, é essen-cial para o aconselhamento genético do próprio e familia-res. Os doentes sem mutações na linhagem germinativa não estão em maior risco de desenvolver tumores adicionais do que o resto da população.
A idade média aquando do diagnóstico é de 12 meses nas crianças com predisposição genética3. Nos casos espo-rádicos apresenta-se geralmente como doença unilateral, em média aos 24 meses3.
Os diagnósticos diferenciais mais importantes são a per-sistência da vascularização fetal, doença de Coats, toxoca-ríase e retinopatia da prematuridade.
Actualmente, a classificação mais utilizada no estadia-mento das formas localizadas deste tumor é o Sistema de
Classificação Internacional do Retinoblastoma Intraocular4 (Quadro I). Esta classificação baseia-se essencialmente na dimensão da lesão, distância em relação à fóvea e disco óptico, e presença de disseminação vítrea ou subretiniana.
O tratamento do retinoblastoma tem sofrido grandes alterações nas últimas décadas, com o advento de tratamen-tos cada vez mais selectivos, que têm permitido uma maior sobrevida e, principalmente, maior capacidade de preservar visão útil. Hoje em dia, podemos oferecer, além da enu-cleação e radioterapia externa nos casos mais avançados, várias estratégias conservadoras: crioterapia, braquitera-pia, quimioterapia (sistémica, intra-arterial, subtenoniana ou intravítrea), fotocoagulação e termoterapia transpupilar. A quimioterapia (QT) sistémica apresenta toxicidade sisté-mica mínima, sendo o efeito adverso mais frequente a pan-citopénia transitória, tem a vantagem de além de reduzir o volume tumoral, diminuir a incidência de pineoblastoma5. Este é um tumor primitivo da neuroectoderme descrito pela primeira vez em 19776 - “retinoblastoma trilateral” - cuja incidência está aumentada em sobreviventes de retinoblas-toma. De acordo com uma meta-análise, a probabilidade de vir a desenvolver pineoblastoma foi inferior a 0,5% em crianças com retinoblastoma unilateral mas entre 5 a 15% nos casos de retinoblastoma bilateral7.
OBjECTIVO
Relatar a experiência do serviço de Oftalmologia do Hos-pital Prof. Doutor Fernando Fonseca (HFF) em colaboração com o Instituto Português de Oncologia de Lisboa Francisco Gentil (IPO), Serviço de Genética Médica do Hospital Santa Maria do Centro Hospitalar Lisboa Norte (HSM) e o Hôpi-tal Ophthalmique Jules Gonin (HOJG) em Lausanne (Suíça) no diagnóstico e tratamento de crianças com retinoblastoma entre Janeiro 2004 e Dezembro de 2014.
Cristina Santos, Inês Coutinho, Ana Rita Azevedo, Cláudia Constantino, Ana Berta Sousa, Filomena Pereira, José Laranjeira, João Cabral, Susana Teixeira

Vol. 39 - Nº 2 - Abril-Junho 2015 | 99
MéTODOS
Revisão retrospectiva dos processos clínicos e exames complementares de diagnóstico dos doentes com retino-blastoma. Descrição de um caso seleccionado da série.
RESULTADOS
Foram tratadas no total dezasseis crianças com diag-nóstico de retinoblastoma, sendo cinco casos bilaterais. No Quadro II estão representadas características dos doentes, bem como as modalidades terapêuticas utilizadas. A média da idade de diagnóstico foi de 27 meses, sendo de 8,6 meses para os casos bilaterais e de 35,5 meses para os casos uni-laterais, (um deles diagnosticado aos nove anos de idade (Caso 13)).
Dois casos apresentavam história familiar da doença: o Caso 5 um irmão e o Caso 7 dois tios paternos.
A forma de apresentação mais frequente foi leucocória. Um caso foi detectado aos 4 meses de idade por rastreio devido a história familiar de retinoblastoma e outro foi um achado ao exame oftalmológico na sequência de rastreio de retinopatia da prematuridade. De destacar o Caso 3, com doença unilateral e anomalia congénita do disco óptico do tipo morning glory do olho adelfo.
O estudo genético não foi realizado em 3 dos primei-ros casos da série. Em 6 doentes não foi detectada mutação genética com os testes realizados, 5 casos foram positivos e num caso foi detectada uma mutação de significado incerto.
O tempo médio de seguimento foi de 51,6 meses. Nenhum caso apresentava sinais de invasão extra-ocular do tumor primário no momento do diagnóstico ou durante o tempo de seguimento.
Um dos casos, uma menina com doença unilateral e estudo genético negativo, desenvolveu pineoblastoma, detectado três anos após o diagnóstico (aos 44 meses de vida). Foi submetida a ressecção cirúrgica do tumor e qua-tro ciclos de quimioterapia sistémica com ciclofosfamida, vincristina, cisplatina e etoposido. Por resposta incom-pleta optou-se pela realização de QT de altas doses (car-boplatina, etoposido e tiotepa), seguida de auto-transplante medular. Infelizmente a doente faleceu de complicações do tratamento.
Actualmente, todas as crianças sobreviventes se man-têm em seguimento excepto três. Os Casos 1 e 2 por motivo de emigração para o estrangeiro e o Caso 3 por abandono.
De entre as 16 crianças, 11 (82%) realizaram ciclos de quimioterapia sistémica de acordo com o protocolo do Hos-pital St. Bartholomew, de Londres, com vincristina, etopo-sido e carboplatina a cada 3-4 semanas
Nove olhos foram submetidos a enucleação (43%), sete
10 anos de experiência no tratamento de retinoblastoma
Quadro I | Sistema de Classificação Internacional do Retinoblastoma Intraocular.
Sistema de Classificação Internacional do Retinoblastoma Intraocular4 Taxa de preservação do globo na literatura4
Grupo A - Risco muito pequenoPequenos tumores que não ameaçam a visão
Tumores ≤3mm, 3mm da fóvea, >1,5mm do disco ópticoSem invasão do vítreo ou subretiniana 100%
Grupo B – Risco pequenoTumores sem disseminação do vítreo ou subretiniana
Qualquer dimensão ou que não entre no Grupo ALíquido subretiniano <5mm da margem do tumor
Sem invasão do vítreo ou subretiniana93%
Grupo C – Risco moderadoDisseminação focal do vítreo ou subretiniana
Seeding do vítreo ou subretiniano a <6mm da margem do tumor 90%
Grupo D – Risco elevadoDisseminação do vítreo ou subretiniana
Seeding do vítreo ou subretiniano a ≥ 6mm da margem do tumor
Líquido subretiniano a >6mm da margem do tumor47%
Grupo E – Risco muito elevadoPresença de uma ou mais das características seguintes
Tumor no segmento anteriorTumor no corpo ciliarGlaucoma neovascular
HemovítreoPhtisis
Apresentação tipo celulite
0%*
* Nesta série, todos os tumores Estádio E foram tratados com enucleação.

100 | Revista da Sociedade Portuguesa de Oftalmologia
como tratamento primário e dois secundário, após falência da terapêutica conservadora. Entre os olhos enucleados, a análise anatomo-patológica não revelou em nenhum dos casos invasão do nervo óptico além da lâmina crivosa, linfo-vascular, da esclerótica ou extra-escleral.
Os restantes doze olhos (57%) foram tratados de forma conservadora, cinco dos quais exclusivamente em Portugal, resultado da colaboração entre o IPO de Lisboa e o HFF. As modalidades terapêuticas conservadoras disponíveis no HFF são o LASER fotocoagulador e a crioterapia. A foto-coagulação foi realizada com LASER Nd:YAG de dupla frequência de 532nm (Iris Medical Oculight GL®, Iridex)
com oftalmoscópio binocular indirecto. A potência utili-zada foi geralmente de 100mW, suficiente para produzir um spot branco nas margens do tumor e tempo de exposição prolongado (0,6 segundos). Realizou-se tratamento con-fluente, sobreposto no tumor e periferia. Quando necessário o procedimento foi repetido com intervalos de 4 semanas até à regressão completa do tumor.
A crioterapia (CryoStar®, DORC) foi preferencialmente utilizada nos casos de tumores de pequenas dimensões (<4mm de diâmetro basal e <3mm de espessura), acessíveis por via transescleral. Realizaram-se três ciclos de congela-ção/ descongelação em cada localização.
Quadro II | Resumo das características dos doentes com diagnóstico de retinoblastoma e modalidades terapêuticas utilizadas.
Nº d
o do
ente
Sexo
/ ida
de d
o di
agnó
stic
o em
mes
es
Form
a de
ap
rese
ntaç
ão
Dat
a 1ª
Obs
Lat
eral
idad
e
Cla
ssifi
caçã
o In
tern
acio
nal
Est
udo
gené
tico
Tem
po d
e se
guim
ento
(mes
es)
QT
sist
émic
a
RT
exte
rna
Bra
quite
rapi
a
LA
SER
Cri
o
TT
T
IVT
Sub-
Teno
nian
o
QT
IA
Stat
us
1 F/51 Leucocória 15/10/2004 Unilateral D Ø 74 Ø Ø Ø Ø Ø Ø Ø Ø Ø Enucleação
2 M/8 Leucocória 16/12/2004 Bilateral DD Ø 19 sim sim Ø sim
Øsim Ø
ØØ
ØØ
ØØ
ØØ
EnucleaçãoEnucleação
3 M/26 Estrabismo 5/7/2005 Unilateral E “-” 112 sim sim Ø sim sim Ø Ø Ø Ø Enucleação
4 M/38 Leucocória 3/10/2005 Unilateral D Ø 57 Ø Ø Ø Ø Ø Ø Ø Ø Ø Enucleação
5 F/4 Rastreio 23-3-2006 Bilateral AA “-” 107 Ø Ø Ø sim
simsim Ø
ØØ
ØØ
ØØ
ØØ
10/10 10/10
6 F/11 Leucocória 13-3-2007 Unilateral D “-” 95 sim Ø sim sim sim sim Ø Ø Ø 0.8
7 F/11 Estrabismo 26-10-2007 Unilateral B VSI 87 sim Ø Ø sim Ø sim Ø Ø Ø PL
8 F/7 Achado 1-6-2009 Unilateral B “-” 48 sim Ø sim sim sim sim sim Ø Ø Faleceu
9 F/66 Leucocória 27-4-2010 Unilateral C + 62 sim Ø Ø sim sim sim Ø Ø Ø 0.8
10 M/9 Tipo celulite 27-9-2011 Bilateral EB + 45 sim Ø Ø Ø
simØ
simØØ
ØØ
ØØ
ØØ
?Enucleação
11 M/13 Leucocória 22-8-2012 Bilateral BD + 34 sim Ø Ø Ø
Øsimsim
simsim
ØØ
ØØ
ØØ
??
12 M/30 Leucocória 9-4-2013 Unilateral D “-” 26 sim Ø Ø Ø sim sim sim sim sim 0.3
13 F/118 Leucocória 3-5-2013 Unilateral D “-” 25 Ø Ø Ø Ø sim Ø sim Ø sim 0.6
14 F/9 Leucocória 24-3-2014 Bilateral BD + 14 sim Ø Ø sim
Øsim Ø
ØØ
ØØ
ØØ
ØØ
?Enucleação
15 M/9 Estrabismo 3-7-2014 Unilateral D + 11 Ø Ø Ø Ø Ø Ø Ø Ø Ø Enucleação
16 M/24 Leucocória 18-10-2014 Unilateral E Em curso 8 Ø Ø Ø Ø Ø Ø Ø Ø Ø Enucleação
F: feminino; M: masculino; Obs: observação; Ø: não realizado; “-”: não foi detectada mutação; VSI: variante de significado incerto; QT: quimioterapia; RT: radioterapia; Crio: crioterapia; TTT: termoterapia transpupilar; IVT: injecção intravítrea de melfalana; QTIA: quimioterapia intra-arterial com melfalana± topotecano; PL: percepção luminosaNota: nos tumores bilaterais, a linha superior refere-se ao olho direito e a linha inferior ao olho esquerdo.
Cristina Santos, Inês Coutinho, Ana Rita Azevedo, Cláudia Constantino, Ana Berta Sousa, Filomena Pereira, José Laranjeira, João Cabral, Susana Teixeira

Vol. 39 - Nº 2 - Abril-Junho 2015 | 101
Não se verificaram complicações com nenhuma das modalidades terapêuticas (rasgaduras da retina, hemoví-treo, tracção ou descolamento da retina).
Seis doentes (sete olhos) após tratamento local inicial em Portugal, foram encaminhados para o HOJG para comple-mentar a terapêutica com termoterapia transpupilar (TTT), braquiterapia, radioterapia externa, QT intra arterial, QT
sub-tenoniana e/ou QT intra-vítrea. Duas crianças (2 olhos) foram directamente encaminhadas para o HOJG, dado apre-sentarem doença avançada mas com possibilidade de con-servação do globo ocular com terapêutica local agressiva. No Quadro III discriminam-se as modalidades terapêuticas conservadoras utilizadas.
A título de exemplo são apresentadas imagens do Caso clínico 5, criança de 4 meses de idade observada por histó-ria familiar de retinoblastoma. Apresentava lesão estádio A, nasal ao disco óptico em ambos os olhos mas maior no olho direito (Fig.1A e E). Realizou-se tratamento com crioterapia e LASER na lesão de maiores dimensões, no olho direito e apenas com LASER no olho esquerdo (Fig.1B e F). Observou-se regressão inicial das lesões mas recidiva aos seis meses no olho direito, tendo-se realizado nova sessão de laserterapia sobre a recidiva (Fig.1C). Na Figura 1D e H podem ver-se as cicatrizes planas (padrão de regressão tipo 4) sete anos após o tratamento inicial. Aos nove anos de idade a criança apresenta acuidade visual de 10/10, sem sinais de recidiva local. Os controlos com ressonância magnética crânio-encefálica foram até à data negativos.
Na Figura 2 são apresentadas fotografias do Caso 13, criança de 9 anos de idade com retinoblastoma unilateral com mais de 9 mm de espessura e disseminação extensa do vítreo, referenciada para o HOJG para realização de quimioterapia intra-arterial. Actualmente com dois anos de seguimento, apresenta acuidade visual de 0.6 no olho tratado.
Quadro III | Modalidades terapêuticas locais utilizadas.
Modalidade Terapêutica Nº de olhos (HFF/HOJG)
Fotocoagulação 12/2
Termoterapia transpupilar 0/7
Crioterapia 11/8
Braquiterapia 0/2
Topotecano subtenoniano 0/1
Melfalana intravítreo 0/4
Melfalana intra-arterial 0/2
Radioterapia externa 1/1
Enucleação primária 7/0
Enucleação secundária 1/1
Fig. 1 | Imagens do fundo ocular Caso Clínico 5, obtidas com oftalmoscopia indirecta. Em cima, imagens correspondentes ao olho direito (A, B, C e D) e em baixo, correspondentes ao olho esquerdo (E, F, G e H). A tumor nasal ao disco óptico OD. E tumor nasal ao disco óptico OE. B e F imediatamente após tratamento C imediatamente após LASER por recidiva 6 meses após o tratamento inicial. G cicatrização plana OE 6 meses após tratamento inicial. D e H 4 anos após o tratamento, cicatrização plana ODE (padrão de regressão tipo 4).
10 anos de experiência no tratamento de retinoblastoma

102 | Revista da Sociedade Portuguesa de Oftalmologia
DISCUSSÃO
O tratamento do retinoblastoma sofreu grandes avanços nas últimas décadas, utilizando-se cada vez mais vias de administração locais com o objectivo de controlar a doença com menos efeitos sistémicos. A escolha da modalidade terapêutica depende da idade da criança, do tamanho do tumor e do potencial de preservar a visão. O objectivo pri-mordial é preservar a vida. Quanto mais precoces forem o diagnóstico e o tratamento, maior o número de doentes que fica livre de doença e em que é possível preservar a visão8. É portanto, essencial implementar o diagnóstico precoce que pode ser levado a cabo pelo médico assistente não oftalmo-logista com recurso à pesquisa do reflexo vermelho9.
O tratamento destes doentes requer uma equipa multidis-ciplinar com observações frequentes para detectar recorrên-cia, envolvimento do sistema nervoso central, complicações relacionadas com a terapêutica e diagnóstico de segundos tumores. O aconselhamento genético ao doente e aos pais tem também um lugar muito importante, nomeadamente no esclarecimento do risco de recorrência da doença na fratria.
Dada a raridade e especificidade desta patologia, cujo tra-tamento é cada vez mais especializado, o encaminhamento destas crianças para centros de referência torna-se essencial e é cada vez mais uma realidade. Deste modo podem ser aproveitadas sinergias, rentabilizados meios e coordenados os exames complementares de diagnóstico com os actos terapêuticos e observações periódicas.
Agradecimentos – Ao Dr. Francis Munier e restante
equipa do Hôpital Ophthalmique Jules Gonin pelo trabalho e dedicação ao tratamento desta doença.
BIBLIOGRAFIA
1. Seregard S, Lundelli G, Svedberg H, Kivela T. Inci-dence of retinoblastoma from 1958 to 1998 in Northern Europe: advantages of birth cohort analysis. Ophthal-mology, 2004;111(6):1228-1232.
2. Friend SH, Bernards R, Rogelj S, Weinber RA et al. A
human DNA segment with properties of the gene that predisposes to retinoblastoma and osteosarcoma. Nature 1986; 323(6089):643
3. Abramson DH, Frank CM, Susman M, Whalen MP, Dunkel IJ, Boyd NW. Presenting signs of retinoblas-toma. J Pediatr. 1998;132(3 Pt 1):505.
4. Shields CL, Mashayekhi A, Au AK, Czyz C., et al. The International Classification of Retinoblastoma Pre-dicts Chemoreduction Success. Ophthalmology 2006; 113:2276-2280.
5. Shields CL, Meadows AT, Shields JA, Carvalho C, Smith AF. Chemoreduction for retinoblastoma may prevent intracranial neuroblastic malignancy (trilateral retinoblastoma). Arch Ophthalmology 2011; 119(9): 1269-72.
6. Jakobiec FA, Tso MO, Zimmerman LE, Danis P. Reti-noblastoma and intracranial malignancy. Cancer 1977; 39(5):2048-58.
7. Gündüz K, Shields CL. Retinoblastoma Update. Focal points: Clinical Modules for Ophthalmologists. Volume XXIII (7) American Academy of Ophthalmology. Sep-tember 2005.
8. Goddard AG, Kingston JE, Hungerford JL. Delay in diagnosis of retinoblastoma: risk factors and treatment outcome. Br J Ophthalmol. 1999;83(12):1320-1323.
9. Boas Práticas em Oftalmologia – Elementos Clínicos de Avaliação e Referenciação. Direcção Geral de Saúde, 2008.
Os autores não têm qualquer interesse financeiro neste trabalho. Este artigo é original não tendo sido previamente publicado. Os autores cedem os direitos de autor à Sociedade Portuguesa de Oftalmo-logia.
CONTACTOCristina Santos Serviço de Oftalmologia Hospital Prof. Doutor Fernando da Fonseca Hospital Prof. Doutor Fernando Fonseca E.P.E., IC 192720-276 [email protected]
Fig. 2 | Fotografias do Caso Clínico 5. A) massa retro-lenticular volumosa do olho direito. B) vasos da arcada temporal superior tortuo-sos e engurgitados. C) massa subretiniana com vasos tortuosos e disseminação do vítreo.
Cristina Santos, Inês Coutinho, Ana Rita Azevedo, Cláudia Constantino, Ana Berta Sousa, Filomena Pereira, José Laranjeira, João Cabral, Susana Teixeira

Vol. 39 - Nº 2 - Abril-Junho 2015 | 103
Artigo Original
Neovascularização coroideia de causa inflamatória: Opções terapêuticas
Bárbara Borges1, Ana Cabugueira1, Isabel Domingues2, Miguel Marques3, Pinto Ferreira3, João Lisboa3, Rita Flores3
Serviço de oftalmologia - Centro Hospitalar de Lisboa Central, Lisboa, Portugal 1Médico Interno de oftalmologia - Centro Hospitalar Lisboa Central, Lisboa, Portugal
2Assistente Hospitalar de Oftalmologia - Centro Hospitalar Lisboa Central, Lisboa, Portugal3Assistente Hospitalar Graduado de oftalmologia - Centro Hospitalar Lisboa Central, Lisboa, Portugal
RESUMO
Introdução: Uma complicação das doenças oculares inflamatórias é a neovascularização coroi-deia (NVC). Apesar de ser rara, é uma causa importante de perda de visão nestes doentes. As opções terapêuticas incluem, além do tratamento dirigido à doença inflamatória, a fotocoagulação a LASER, terapia fotodinâmina com verteporfina (TFD) e, mais recentemente, agentes farmaco-lógicos anti-VEGF.Objectivo: Analisar uma série de 10 casos de NVC de etiologia inflamatória.Métodos: Os autores descrevem uma série de 10 casos (10 olhos) de NVC de causa inflamatória. Os parâmetros analisados incluem: etiologia da uveíte, localização da NVC, evolução das acui-dades visuais e da espessura macular central (EMC) após TFD ou injecção intravítrea (IV) de fármacos anti-VEGF (bevacizumab ou ranibizumab).Resultados: Na série apresentada, a coroidite multifocal surge como a etiologia mais frequente. Apenas um doente apresentava NVC extrafoveal (justapapilar), sendo que 5 apresentavam NVC justafoveal e 4 NVC subfoveal. Seis doentes foram tratados com IV anti-VEGF, com uma mé-dia de 3 IV e quatro doentes foram submetidos a TFD, com uma média de 2 sessões. No grupo tratado com IV, assistiu-se a melhoria das acuidades visuais em 5 casos. No grupo tratado com TFD verificou-se melhoria da AV em 2 doentes e a manutenção da mesma acuidade visual em 2 doentes. Observou-se uma diminuição da EMC em todos os doentes, sendo esta mais marcada no grupo tratado com IV anti-VEGF.Discussão / Conclusão: A NVC é uma complicação grave das doenças inflamatórias, para a qual não existem guidelines de tratamento. Apesar de a nossa amostra ser pequena, os resultados pare-cem mostrar um bom outcome nos doentes tratados com IV anti-VEGF, sugerindo assim que esta é uma opção terapêutica importante para estes doentes. Enfatizamos a importância da realização de estudos multicêntricos, randomizados e controlados para validar esta opção terapêutica.
Palavras chave Neovascularização inflamatória, terapia fotodinâmica, injecção intravítrea de agente anti-VEGF.
ABSTRACT
Introduction: Choroidal neovascularization (CNV) is a documented complication of uveitis. Despite being rare, it is an important cause of loss of vision in these patients. Therapeutic options include, in addition to treatment directed to inflammatory disease, LASER photocoagulation, pho-todynamic therapy with verteporfin (PDT) and, more recently, antivascular endothelial growth factor (VEGF) drugs.
Oftalmologia - Vol. 39: pp.103-110

104 | Revista da Sociedade Portuguesa de Oftalmologia
INTRODUÇÃO
A neovascularização coroideia (NVC) é uma compli-cação reconhecida da doença inflamatória ocular. Apesar de ser rara, é uma das causas mais importantes de diminui-ção grave da acuidade visual nestes doentes1.
Tanto as uveítes infecciosas como as não infecciosas podem complicar-se de NVC. Apesar de os mecanismos de formação de neovasos nestes doentes não serem ainda completamente compreendidos, acredita-se que nas uveí-tes infecciosas o mecanismo resulte de uma acção directa dos microorganismos no espaço sub-retiniano, enquanto nas uveítes não-infecciosas a NVC se deva a um processo auto-inflamatório2.
A NVC inflamatória é tipicamente uma NVC tipo 2, isto é, os neovasos atingem o espaço sub-retiniano, atra-vessando o epitélio pigmentar da retina (EPR). Ocorre a deposição de antigénios na membrana de Bruch, que desencadeiam uma resposta inflamatória local, levando à formação de rupturas na membrana de Bruch; ocorre então uma proliferação de tecido de granulação para o espaço sub-retiniano. Observou-se também uma expres-são aumentada de factor de crescimento endotelial vascu-lar nos doentes com NVC2, 3, 4.
O curso natural na NVC inflamatória extrafoveal e justafoveal é variado. Alguns autores descrevem casos selecionados que apresentaram bom prognóstico sem
tratamento ou quando tratados com fotocoagulação a LASER5, 6. Durante alguns anos, as opções terapêuticas nestes casos incluíam a fotocoagulação a LASER, a admi-nistração de corticoides locais e sistémicos ou a excisão cirúrgica. No entanto, grande parte destes procedimentos apresentavam limitações e uma taxa muita alta de recor-rências5. Até recentemente, a TFD com verteporfina era a única opção que permitia o tratamento de lesões subfo-veais com algum sucesso7. Actualmente, com o apare-cimento de agentes inibidores do factor de crescimento endotelial vascular (anti-VEGF) surge uma nova alterna-tiva terapêutica para estes doentes1.
OBjECTIVO
Analisar uma série de 10 casos de NVC de etiologia inflamatória e seu outcome após terapêutica.
MATERIAL E MéTODOS
Os autores descrevem uma série de 10 casos (10 olhos) de NVC de causa inflamatória.
Nesta revisão, foram incluídos doentes com diagnóstico de doença inflamatória ocular não-activa, com NVC, que foram submetidos a TFD com verteporfina ou IV anti-VEGF.
Purpose: To evaluate a series of 10 cases of inflammatory CNV. Methods: The authors describe a series of 10 cases (10 eyes) of inflammatory CNV. The following parameters were evaluated: uveitis etiology, CNV location, visual acuity changes and central macular thickness (CMT) after PDT with verteporfin or intravitreal injeccion (IV) of anti-VEGF drugs (bevacizumab or ranibizumab). Results: In our series, multifocal coroiditis emerges as the most frequent etiology. Only 1 patient presented with extrafoveal CNV (justapapilar), 5 presented with justafoveal CNV and 4 with subfoveal CNV. Six patients were treated with anti-VEGF IV, with an average of 3 IV, and four patients underwent PDT, with an average of 2 sessions. In the group treated with anti-VEGF IV, visual acuity improved in 5 cases. In the group treated with PDT, visual acuity improved in 2 patients and remained the same in 2 patients. There was a decrease of CMT in all patients, wich was more evident in the group treated with anti-VEGF IV.Discussion / Conclusion: CNV is a serious complication of inflammatory diseases, for which there are no treatment guidelines. Although our sample is small, the results seem to show a good outcome in patients treated with anti-VEGF IV, suggesting that this is an important therapeutic option for these patients. We emphasize the importance of multicenter, randomized and controlled studies to validate this therapeutic option.
Key-wordsInflammatory choroidal neovascularization, photodynamic therapy, ani-VEGF intravitreal in-jeccion.
Bárbara Borges, Ana Cabugueira, Isabel Domingues, Miguel Marques, Pinto Ferreira, João Lisboa, Rita Flores

Vol. 39 - Nº 2 - Abril-Junho 2015 | 105
O tratamento foi realizado na evidência de NVC activa. O diagnóstico de NCV activa foi baseado nos resultados da observação do fundo ocular por biomicroscopia (presença de descolamento seroso com ou sem hemorragias retinia-nas), angiografia fluoresceínica (presença de uma fase pre-coce de hiperfluorescência com difusão numa fase tardia), e tomografia de coerência óptica (OCT; presença de fluido intra-retiniano ou subretiniano).
Foi analisada a etiologia da doença inflamatória e a loca-lização da NVC.
As acuidades visuais foram avaliadas pela escala ETDRS (Early Treatment Diabetic Retinopathy Study) em logMAR à data do diagnóstico de NVC, um mês após terapêutica e no momento actual. Nas mesmas datas foi também avaliada a espessura macular central (EMC) por OCT.
Os doentes submetidos a TFD foram tratados de acordo com o protocolo standart (injecção de verteporfina na dose de 6 mg/m² de superfície corporal e irradiação com laser de diodo de 689 nm na dose de 50 J/cm², com irradiância de 600 mW/cm², 15 minutos após o início da injecção). Os doentes tratados com IV foram injectados com bevacizumab ou ranibizumab.
RESULTADOS
A coroidite multifocal surge como a etiologia mais fre-quente nos 10 casos apresentados (n = 5), seguida de coroi-dopatia ponteada interna (n = 2), toxoplasmose (n=2) e sín-drome Vogt-Koyanagi-Harada (n = 1). (Tabela 1)
Apenas um doente apresentava NVC de localização extra-foveal (justapapilar-Coroidite Multifocal), sendo que 5 apre-sentavam NVC justafoveal e 4 NVC subfoveal. (Tabela 2)
Em relação à terapêutica instituída, 6 doentes foram tra-tados com IV anti-VEGF e 4 doentes foram submetidos a TFD com verteporfina.
No grupo tratado com IV, os doentes foram subme-tidos em média a 3 IV. Três doentes foram tratados com ranibizumab e 3 doentes foram tratados com bevacizumab.
Neovascularização coroideia de causa inflamatória: Opções terapêuticas
Assistiu-se a melhoria das acuidades visuais em 5 casos e a manutenção da acuidade visual num dos casos; em todos os casos observou-se uma redução da ECM. (Tabelas 3 e 4)
No grupo tratado com TFD, os doentes foram submeti-dos a uma média de 2 sessões. Verificou-se melhoria da AV em 2 doentes e a manutenção da mesma acuidade visual em
Tabela 1 | Etiologia da doença inflamatória.
Etiologia da doença inflamatória
Coroidite Multifocal 5
Coroidopatia Ponteada Interna 2
Toxoplamose 2
Síndrome VKH 1
Tabela 2 | Localização da NVC.
Localização da NVC
Extrafoveal 1
Subfoveal 4
Justafoveal 5
Tabela 3 | Evolução da AV (logMAR) no grupo tratado com IV anti-VEGF.
Evolução da AV (logMAR) IV anti-VEGF
AV Baseline AV 1 mês após IV AV final Ganho
linhas AV
1 0,30 0,15 0,00 4
2 0,30 0,10 0,00 4
3 0,70 0,70 0,70 0
4 1,30 1,00 0,52 11
5 0,20 0,17 0,10 2
6 1,30 0,89 0,80 7
Tabela 4 | Evolução da EMC (μm) no grupo tratado com IV anti-VEGF.
Evolução EMC (μm) IV anti-VEGF
EMC Baseline
EMC 1 mês após IV EMC final Δ EMC
1 414 366 298 -116
2 628 476 266 -362
3 499 412 363 -136
4 451 395 312 -139
5 457 400 302 -155
6 518 432 338 -180

106 | Revista da Sociedade Portuguesa de Oftalmologia
2 doentes; observou-se também uma diminuição da EMC em todos os doentes. (Tabelas 5 e 6)
Quando comparados os grupos em relação a melhoria da AV, verifica-se um maior ganho de linhas de acuidade visual no grupo tratado com IV anti-VEGF.(Tabelas 3 e 5)
Observa-se também uma redução da EMC maior no grupo tratado com IV anti-VEGF quando comparada com a redução da EMC no grupo submetido a TFD com vertepor-fina. (Tabelas 4 e 6)
Não foram registadas complicações da TFD ou da IV anti-VEGF.
DISCUSSÃO
Não existem actualmente guidelines específicas para o tratamento de NVC resultante de doenças inflamatórias.
Até recentemente, as opções terapêuticas para a CNV inflamatória limitavam-se à observação, fotocoagulação a LASER, corticoterapia e TFD8-44.
A fotocoagulação a LASER é utilizada em casos de CNV extrafoveais; no entanto está associada a uma taxa
de recidiva considerável e não está indicada para lesões justafoveais ou subfoveais devido ao risco de expansão da cicatriz coriorretiniana e consequência diminuição da AV45.
A administração de corticoides por via sistémica ou sub-tenoniana visa controlar a inflamação e reduzir os estí-mulos pró-angiogénicos; ainda assim, em muitos assiste-se a uma progressão da NVC mesmo com controlo adequado da inflamação33.
A TFD com verteporfina surgiu como uma opção tera-pêutica para os doentes com lesões subfoveais e justafo-veais. O valor desta terapêutica é ainda incerto, sendo que a sua maior limitação diz respeito ao desenvolvimento de atrofia subfoveal significativa. Apesar de na maior parte das séries descritas verificar-se uma estabilização da lesão, a melhoria da acuidade visual não é tão consistente. Sapers-tein et al reportou uma série de 26 doentes em que 14 apre-sentaram melhoria da AV, 7 mantiveram a mesma AV e 4 apresentaram deterioração da AV ao fim de 12 meses.43 Já na série descrita por Leslie e seus associados, é rela-tada uma melhoria da AV em todos os doentes após TFD com verteporfina. Estes autores defendem que em alguns doentes a redução da resposta inflamatória, responsável pela neoangiogénese, pode não ser suficiente para induzir a regressão da NVC após a sua formação; assim a TFD tem um papel importante nestes casos uma vez que actua atra-vés de um mecanismo distinto. Segundo Leslie et al lesões iniciais poderão regredir quando tratadas com agentes imu-nossupressores em altas doses mas o tratamento de NVC instalada requer TFD46.
A identificação de factores estimulantes envolvidos no mecanismo de formação dos neovasos permite-nos desen-volver e utilizar fármacos que inibam o processo, com efei-tos adversos mínimos. Na NVC inflamatória, em particular, o VEGF parece desempenhar um papel crucial na angiogé-nese. Os leucócitos e os macrófagos são capazes de produ-zir VEGF e este, por sua vez, é capaz de estimular a sua pro-dução por parte das células inflamatórias. Assim, é criado um circuito fechado que leva a uma formação contínua de neovasos e manutenção da neovascularização47. Tendo por base esta premissa, parece-nos que a utilização de agentes anti-VEGF, que interfiram e inibam o processo seja uma opção terapêutica importante nestes doentes. Mansour e os seus associados descreveram os resultados de uma série em que 81 olhos com diagnóstico de NVC inflamatória foram tratados com IV de bevacizumab; os resultados foram posi-tivos, verificando-se não só uma melhoria da AV na maior parte dos doentes como uma redução da EMC significativa1. Também Rouvas et al descreve resultados semelhantes quando os doentes são submetidos a IV de ranibizumab48.
Na série apresentada neste trabalho, os resultados
Tabela 5 | Evolução da AV (logMAR) no grupo tratado com TFD.
Evolução da AV (logMAR) TFD
AV Baseline AV 1 mês após TFD AV final Ganho
linhas AV
1 0,40 0,40 0,40 0
2 0,15 0,10 0,00 1
3 0,40 0,40 0,40 0
4 0,30 0,18 0,00 4
Tabela 6 | Evolução da EMC (μm) no grupo tratado com TFD.
Evolução EMC (μm) PDT
EMC Baseline
EMC 1 mês após TFD EMC final Δ EMC
1 430 410 404 -26
2 484 421 306 -178
3 470 399 352 -118
4 482 358 291 -191
Bárbara Borges, Ana Cabugueira, Isabel Domingues, Miguel Marques, Pinto Ferreira, João Lisboa, Rita Flores

Vol. 39 - Nº 2 - Abril-Junho 2015 | 107
trata-se de um doente com uma lesão extensa de localização subfoveal, com diagnóstico de síndrome de Vogt-Koya-nagi-Harada; a NVC como complicação desta doença é um factor de pior prognóstico23. (Fig.4)
O outcome visual final relacionou-se de uma forma mais significativa com a localização da lesão do que com a sua etiologia, apresentando as lesões justafoveais e a lesão jus-tapapilar melhores resultados do que as lesões subfoveais. Os resultados obtidos com as IV de bevacizumab foram similares aos resultados obtidos com as IV de ranibizumab.
Poder-se-á discutir que os doentes com doenças infla-matórias podem manter inflamação crónica, indolente, mesmo após o tratamento da uveíte, o que poderá predis-por ao desenvolvimento de NVC, sendo por isso aconse-lhável a terapia imunomoduladora sistémica. No entanto, Arevalo e seus colaboradores defendem que a IV anti--VEGF é menos prejudicial em termos de efeitos adversos
são coincidentes com os resultados de outros trabalhos publicados.
Trata-se de um estudo retrospectivo com um recuo de 10 anos; assim, 4 doentes foram tratados com TFD na era pré-anti-VEGF.
Nos doentes tratados com TFD, observou-se redução da EMC em todos os doentes, melhoria da AV em 2 doentes e manutenção da AV em 2 doentes. Os dois doentes em que não se verificou melhoria da AV apresentavam doença subfoveal e uma AV na altura do diagnóstico pior que os doentes que melhoraram.
Os resultados obtidos nos doentes tratados com IV anti--VEGF são globalmente melhores. (Fig. 1)
Em todos estes doentes observou-se uma redução da EMC significativa. (Fig. 2 e Fig. 3)
Apenas um doente não apresentou melhoria da AV;
Fig. 1 | Doente do sexo feminino, 42 anos, com diagnóstico de toxoplasmose. As imagens superiores mostram a angio-grafia fluoresceínica à data de diagnóstico de NVC. As imagens inferiores mostram a EMC antes e depois de terapêutica com anti-VEGF. As acuidades visuais evo-luíram de 0.30 para 0.00 (logMAR).
Fig. 3 | Doente do sexo feminino, 50 anos, com diagnóstico de coroidopatia ponteada interna. As imagens superiores mostram a angiografia fluoresceínica à data de diagnós-tico de NVC. As imagens inferiores mostram a EMC antes e depois de terapêutica com anti-VEGF.
Fig. 2 | Doente do sexo feminino, 45 anos, com diagnóstico de coroidite multifocal. As imagens superiores mostram a angiografia fluoresceínica à data de diagnóstico de NVC. As imagens inferiores mostram a EMC antes e depois de terapêutica com anti-VEGF.
Fig. 4 | Doente do sexo feminino, 32 anos, com diagnóstico de síndrome Vogt-Kyonagi-Harada. As imagens superiores mostram a angiografia fluoresceínica à data de diagnós-tico de NVC. As imagens inferiores mostram a EMC antes e depois de terapêutica com anti-VEGF.
Neovascularização coroideia de causa inflamatória: Opções terapêuticas

108 | Revista da Sociedade Portuguesa de Oftalmologia
sistémicos e que permite a obtenção de níveis terapêuticos na coróide de forma rápida e eficaz3.
CONCLUSÃO
A NVC é uma complicação grave das doenças inflama-tórias, para a qual não existem guidelines de tratamento. Apesar do pequeno número de doentes da nossa série e da inexistência de controlos, a terapêutica com IV anti-VEGF mostra resultados promissores na melhoria da AV e redu-ção da EMC que sugerem assim que esta é uma opção importante no tratamento destes doentes. Enfatizamos a importância da realização de estudos multicêntricos, rando-mizados e controlados para validar esta opção terapêutica.
BIBLIOGRAFIA
1. Mansour AM, Arevalo JF, Fardeau C, Hrisomalos EN, Chan WM, Lai TY, Ziemssen F, Ness T, Sibai AM, Mackensen F, Wolf A, Hrisomalos N, Heiligenhaus A,Spital G, Jo Y, Gomi F, Ikuno Y, Akesbi J, LeHoang P, Adan A, Mahendradas P, Khairallah M, Guthoff R, Ghandour B, Küçükerdönmez C, Kurup SK. Three-year visual and anatomic results of administrating intravi-treal bevacizumab in inflammatory ocular neovascula-rization.Can J Ophthalmol. 2012 Jun;47(3):269-74.
2. Grossniklaus HE, Green WR. Choroidal neovasculari-zation. Am J Ophthalmol. 2004 Mar;137(3):496-503.
3. Arevalo JF, Adan A, Berrocal MH, Espinoza JV, Maia M, Wu L, Roca JA, Quiroz-Mercado H, Ruiz-Moreno JM, Serrano MA; Pan-American Collaborative Retina Study Group. Intravitreal bevacizumab for inflam-matory choroidal neovascularization: results from the Pan-American Collaborative Retina Study Group at 24 months. Retina. 2011 Feb;31(2):353-63.
4. B Lafaut, S Aisenbrey, B Vanden, R Krott, C Jonescu--Cuypers, S Reynders, and K Bartz-Schmidt. Clinico-pathological correlation of retinal pigment epithelial tears in exudative age related macular degeneration: pretear, tear, and scarred tear. Br J Ophthalmol. Apr 2001; 85(4): 454–460.
5. Adán A, Mateo C, Navarro R, Bitrian E, Casaroli--Marano RP. Intravitreal bevacizumab (avastin) injec-tion as primary treatment of inflammatory choroidal neo-vascularization. Retina. 2007 Nov-Dec;27(9):1180-6.
6. Watzke RC, Packer AJ, Folk JC, Benson WE, Bur-gess D, Ober RR. Punctate inner choroidopathy. Am J Ophthalmol. 1984 Nov;98(5):572-84.
7. Spaide RF, Sorenson J, Maranan L. Combined photo-dynamic therapy with verteporfin and intravitreal tria-mcinolone acetonide for choroidal neovascularization. Ophthalmology. 2003 Aug;110(8):1517-25.
8. Watzke RC, Packer AJ, Folk JC, et al. Punctate inner choroidopathy. Am J Ophthalmol 1984;98:572–84.
9. Krause AC, Hopkins WG. Ocular manifestation of his-toplasmosis. Am J Ophthalmol 1951;34:564–6.
10. Brown J Jr, Folk JC, Reddy CV, et al. Visual prognosis of multifocal choroiditis,punctate inner choroidopathy and the diffuse retinal fibrosis syndrome. Ophthalmo-logy 1996;103:1100–5.
11. Kleiner RC, Ratner CM, Enger MS, et al. Subfoveal neovascularization in the ocular histoplasmosis syn-drome: a natural history study. Retina 1988;8:225–9.
12. Olk JR, Burgess DB, McCormick PA. Subfoveal and Juxtafoveal Subretinal Neovascularisation in the Pre-sumed Ocular Histoplasmosis syndrome: visual prog-nosis. Ophthalmology 1984;91:1592–602.
13. Flaxel CJ, Owens SL, Mulholland B, et al. The use of corticosteroids for choroidal neovascularisation in young patients. Eye 1998;12:266–72.
14. Fine SL, Wood WJ, Isernhagen RD, et al. Laser treat-ment for subfoveal neovascular membranes in ocular histoplasmosis syndrome: results of a pilot randomized clinical trial. Arch Ophthalmol 1993;111:19–20.
15. Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neo-vascularization in age-related macular degeneration with verteporfin. One year results of two randomi-zed clinical trials—TAP report 1. Arch Ophthalmol 1999;117:1329–45.
16. Motero JA, Ruiz-Moreno JM. Verteporfin photodyna-mic therapy in highly myopic subfoveal choroidal neo-vascularisation. Br J Ophthalmol 2003;87:173–6.
17. Spaide RF, Martin ML, Slakter J, et al. Treatment of idiopathic subfoveal choroidal neovascular lesions using photodynamic therapy with verteporfin. Am J Ophthalmol 2002;134:62–8.
18. Karacorlu M, Karacorlu S, Ozdemir H, et al. Photo-dynamic therapy with verteporfin for choroidal neo-vascularization in patients with angioid streaks. Am J Ophthalmol 2002;134:360.
19. Shaikh S, Ruby AJ, Williams GA. Photodynamic the-rapy using verteporfin for choroidal neovascularization in angioid streaks. Am J Ophthalmol 2003;135:1–6.
20. Wang LK, Kansal S, Pulido JS. Photodynamic the-rapy for the treatment of choroidal neovascularization secondary to rubella retinopathy. Am J Ophthalmol
Bárbara Borges, Ana Cabugueira, Isabel Domingues, Miguel Marques, Pinto Ferreira, João Lisboa, Rita Flores

Vol. 39 - Nº 2 - Abril-Junho 2015 | 109
2002;134:790–2.21. Spaide RF, Freund KB, Slakter J, et al. Treatment of
subfoveal choroidal neovascularization associated with multifocal choroiditis and panuveitis with photodyna-mic therapy. Retina 2002;22:545–9.
22. Coquelet P, Postelmans L, Snyers B, et al. Successful photodynamic therapy combined with laser photocoa-gulation in three eyes with classic subfoveal choroidal neovascularisation affecting two patients with multi-focal choroiditis: case reports. Bulletin de la Societe Belge d Ophtalmologie 2002;283:69–73.
23. Farah ME, Costa RA, Muccioli C, et al. Photodynamic therapy with verteporfin for subfoveal choroidal neo-vascularization in Vogt-Koyanagi-Harada syndrome. Am J Ophthalmol 2002;134:137–9.
24. Dantas MA, Slakter JS, Negrao S, et al. Photodyna-mic therapy with verteporfin in mallatia leventinese. Ophthalmology 2002;109:296–301.
25. Valmaggia C, Niederberger H, Helbig H. Photodyna-mic therapy for choroidal neovascularization in fundus flavimaculatus. Retina 2002;22:111–13.
26. Battaglia Parodi M, Da Pozzo S, Toto L, et al. Photo-dynamic therapy for choroidal neovascularization asso-ciated with choroidal osteoma. Retina 2001;21:660–1.
27. Battaglia Parodi M, Da Pozzo S, Ravalico G. Photo-dynamic therapy for choroidal neovascularization asso-ciated with pattern dystrophy. Retina 2003;23:171–6.
28. Potter MJ, Szabo SM, Chan EY, et al. Photodynamic therapy of a subretinal neovascular membrane in type 2A idiopathic juxtafoveolar retinal telangiectasis. Am J Ophthalmol 2002;133:144–51.
29. Rogers AH, Greenberg PB, Martidis A, et al. Photo-dynamic therapy of polypoidal choroidal vasculopathy. Ophthalmic Surg Lasers Imaging 2003;34:60–3.
30. Battaglia Parodi M, Da Pozzo S, Ravalico G. Photo-dynamic therapy in chronic serous chorioretinopathy. Retina 2003;23:235–7.
31. Macular Photocoagulation Study Group. Argon laser photocoagulation for neovascular maculopathy. Five year results from randomized clinical trials. Arch Ophthalmol 1991;109:1109–14.
32. Macular Photocoagulation Study Group. Laser pho-tocoagulation for juxtafoveal choroidal neovasculari-zation. Five year results from randomized trials. Arch Ophthalmol 1994;112:500–9.
33. Martidis A, Miller DG, Ciulla TA, et al. Corticoste-roids as an antiangiogenic agent for histoplamosis--related subfoveal choroidal neovascularization. J Ocul harmacol Ther 1999;15:425–8.
34. Dees C, Arnold JJ, Forrester JV, et al.
Immunosuppressive treatment of choroidal neovascu-larization associated with endogenous posterior uveitis. Arch Ophthalmol 1998;116:1456–61.
35. Olsen TW, Capone A Jr, Sternberg P Jr, et al. Subfo-veal choroidal neovascularization in punctate inner choroidopathy. Surgical management and pathologic findings. Ophthalmology 1996;103:2061–9.
36. Thomas MA, Dickinson JD, Melberg NS, et al. Visual results after surgical removal of subfoveal choroidal neovascular membranes. Ophthalmology 1994;101:1384–96.
37. Berger AS, Conway M, Del Priore LV, et al. Submacu-lar surgery for subfoveal choroidal neovascular mem-branes in patients with presumed ocular histoplasmo-sis. Arch Ophthalmol 1997;115:991–6.
38. Holekamp NM, Thomas MA, Dickinson JD, et al. Sur-gical removal of subfoveal choroidal neovasculariza-tion in presumed ocular histoplasmosis: stability of early visual results. Ophthalmology 1997;104:22–6.
39. Stone TW, Sternberg P Jr. Submacular surgery trials update. Ophthalmol Clin North Am 2002;15:479–88.
40. Chatterjee S, Gibson JM. Photodynamic therapy: a treatment option in choroidal neovascularisation secon-dary to punctate inner choroidopathy. Br J Ophthalmol 2003;87:925–7.
41. Rogers AH, Duker JS, Nichols N, et al. Photodyna-mic therapy of idiopathic and inflammatory choroidal neovascularization in young adults. Ophthalmology 2003;110:1315–20.
42. Sickenberg M, Schmidt-Erfurth U, Miller JW, et al. A preliminary study of photodynamic therapy using ver-teporfin for choroidal neovascularization in patholo-gic myopia, ocular histoplasmosis syndrome, angioid streaks and idiopathic causes. Arch Ophthalmol 2000;118:327–36.
43. Saperstein DA, Rosenfeld PJ, Bressler NM, et al. Pho-todynamic therapy of subfoveal choroidal neovascula-rization with verteporfin in the ocular histoplasmosis syndrome: one-year results of an uncontrolled, prospec-tive case series. Ophthalmology 2002;109:1499–505.
44. Busquets MA, Shah GK, Wickens J, et al. Ocular photodynamic therapy with verteporfin for choroidal neovascularization secondary to ocular histoplasmosis syndrome. Retina 2003;23:299–306.
45. Macular Photocoagulation Study Group.Argon laser photocoagulation for neovascular maculopathy. Five--year results from randomized clinical trials. Arch Ophthalmol. 1991 Aug;109(8):1109-14.
46. Leslie T, Lois N, Christopoulou D, Olson JA, Forrester JV. Photodynamic therapy for inflammatory choroidal
Neovascularização coroideia de causa inflamatória: Opções terapêuticas

110 | Revista da Sociedade Portuguesa de Oftalmologia
neovascularisation unresponsive to immunosuppres-sion. Br J Ophthalmol. 2005 Feb;89(2):147-50.
47. Tatar O, Yoeruek E, Szurman P, Bartz-Schmidt KU; Tübingen Bevacizumab Study Group, Adam A, Shinoda K, Eckardt C, Boeyden V, Claes C, Pertile G,Scharioth GB, Grisanti S. Effect of bevacizumab on inflammation
and proliferation in human choroidal neovasculariza-tion. Arch Ophthalmol. 2008 Jun;126(6):782-90.
48. Rouvas A1, Petrou P, Douvali M, Ntouraki A, Ver-gados I, Georgalas I, Markomichelakis N. Intravitreal ranibizumab for the treatment of inflammatory choroi-dal neovascularization. Retina. 2011 May;31(5):871-9.
Bárbara Borges, Ana Cabugueira, Isabel Domingues, Miguel Marques, Pinto Ferreira, João Lisboa, Rita Flores

Vol. 39 - Nº 2 - Abril-Junho 2015 | 111
OCT angiography: redefining standards
João Pedro Marques1, 2, Rufino Silva1, 2, 3 1Centro de Responsabilidade Integrado em Oftalmologia do Centro Hospitalar
e Universitário de Coimbra (CRIO-CHUC), Coimbra, Portugal2Associação para Investigação Biomédica em Luz e Imagem (AIBILI), Coimbra, Portugal
3Faculdade de Medicina da Universidade de Coimbra (FMUC), Coimbra, Portugal
Flash Look
Oftalmologia - Vol. 39: pp.111-114
BACKGROUND
The advent of optical coherence tomography (OCT) revolutionized retinal imaging by providing a fast, sim-ple, and noninvasive method to assess retinal structure at a microscopic level1,2. Since its debut more than two decades ago, the technology behind OCT has evolved drastically, with profound improvements in speed, resolution and ima-ging depth. The explosive growth of OCT in clinical prac-tice was noted after the commercial introduction of the Stra-tus OCT by Carl Zeiss Meditec (Jena, Germany). With the emergence of spectral-domain (SD) OCT systems, higher scanning speeds and eye tracking have led to higher-resolu-tion cross-sectional images of the retina that cannot be obtai-ned by any other noninvasive diagnostic technique3. SD--OCT has improved the quality of clinical decision making4, hence becoming an invaluable tool for any retinal specialist.
With enhance depth imaging (EDI) and swept-source (SS) OCT systems, better penetration and improved signal strength in the choroid have facilitated a qualitative and quantitative assessment of this structure5. However, even the most advanced structural OCTs do not provide an adequate visualization of the choriocapillaries, rendering it necessary to call upon angiography systems - fluorescein angiography (FA) and indocyanine green angiography (ICGA).
Both FA and ICGA are invasive imaging techniques that require intravenous injection of a dye – fluorescein or indo-cyanine green, respectively. Although generally safe, side effects like nausea, vomiting or even severe allergic reac-tions may develop in a minority of patients, thus limiting its repeated use6,7. Furthermore, given its dynamic nature, ICGA and FA are time-dependent, with an initial, interme-diate and late phase8. FA has been adopted as the gold stan-dard for in vivo evaluation of the retinal circulation because the architecture of the blood vessels, the blood flow and leakage from damaged/diseased retinal capillaries can be evaluated easily9. However, not all the capillary networks can be appraised with FA9,10. Fluorescein spreads through the fenestrations of the choriocapillaries, rendering it difficult
to accurately assess this vascular layer8. To overcome this issue, ICGA is usually performed whenever a good visua-lization of the choroidal anatomy is needed (e.g. exudative age-related macular degeneration, namely in polypoidal choroidal vasculopathy or occult choroidal neovasculariza-tion)11. Nevertheless, ICGA is neither available nor routi-nely performed in many institutions throughout the world.
OPTICAL COHERENCE TOMOGRAPHY AN-GIOGRAPHY
OCT angiography (OCTA) is a revolutionary imaging technique that allows noninvasive, three-dimensional visua-lization of the retinal and choroidal vasculature via motion contrast imaging12,13. Angio-OCT is capable of detecting endoluminal flow by mapping erythrocyte movement over time and comparing sequential OCT B-scans at a given crosssection12. The split-spectrum amplitude-decorrelation angiography (SSADA) algorithm and the motion correc-tion tool are two patented primary technologies developed to improve the signal-to-noise ratio of flow detection and to remove unavoidable saccadic artifacts, respectively14,15. These technologies have significantly improved the quality of the vascular images, thus enabling the in vivo acquisition of high-speed, dyeless, microvascular angiograms, repre-senting a true extension of capabilities from SD-OCT4,13. The inherent advantages of OCTA appear to be the ability to optically dissect and visualize flow in various layers of the retina, the high obtainable resolution and the freedom and safety of frequent examinations because of not having to use an injected dye9.
By using the en face OCT technology, layer segmenta-tion is automatically generated to identify areas of interest, such as the superficial and deep retinal vascular plexuses or the choriocapillaries (Fig 1). The superficial vascular plexus, located in the ganglion cell layer (GCL) and nerve fiber layer (NFL) is exposed at a thickness of 60 μm from the internal limiting membrane (ILM). Although anatomically distinct,

112 | Revista da Sociedade Portuguesa de Oftalmologia
the two deep plexuses, located in the inner nuclear layer (INL) and outer plexiform layer (OPL), cannot be individua-lized and are thus seen as one single vascular plexus (Fig 1B).
The parameters for the deep plexuses are defined with reference to the inner plexiform layer (IPL) in a 30 μm thick scan8. To evaluate the choriocapillaries, segmentation is per-formed at the level of Bruch’s membrane.
CLINICAL APPLICATIONS
Recently, the 70 kHz Avanti RTVue XR equipped with the AngioVue software (Optovue, Fremont, CA, USA) has become commercially available, facilitating a wider--spread clinical access to OCTA. While still in a germinal stage, descriptive studies on the clinical applications of OCTA are beginning to materialize12,13,16-21. Exudative age--related macular degeneration and other causes of choroidal
neovascularization (CNV); diabetic retinopathy (DR); reti-nal vein occlusions (RVO) and glaucoma are some of the finest examples.
An unrivaled visualization of the CNV net is now pos-sible with OCTA. The morphology (tree-like, glomerular, fragmented), the presence of a fibrovascular capsule, affe-rent feeder trunk and peripheral anastomosis can be clearly assessed. Furthermore, the non-invasive nature of the tech-nique allows for a convenient lesion monitoring through sequential examinations during and after treatment (Fig 2).
In RVO, OCTA may show capillary dropout and focal non-perfusion as dark areas (similar to FA), foveal ring dis-ruption, increased foveal avascular zone (FAZ) and collate-rals, both in the superficial and in the deep vascular plexuses (Fig 3).
In patients with DR, OCTA shows a foveal avascular zone (FAZ) larger than in healthy subjects (normal FAZ ~500 μm) and according to Lumbroso et al8 this is an early
João Pedro Marques, Rufino Silva
Fig. 1 | Optical coherence tomography angiography (OCTA) of a healthy subject showing the superficial vasculae plexus (A), deep vascular plexus (B) and choriocapillaris (C). The clear individualization of the superficial and deep vascular plexuses is a re-markable novelty in retinal imaging brought by OCTA.
A B C
Fig. 2 | A tree-like choroidal neovascularization net of a patient with exudative age-related macular degeneration before (A) and 1 week after (B) an intravitreal injection of afli-bercept. Note the afferent feeder trunk (yellow arrow), the peripheral anastomosis and the loss of peripheral ca-pillaries, vessel fragmentation and decreased vessel den-sity after treatment (right).
Fig. 3 | Superficial (A) and deep (B) retinal vascular plexuses in a patient with superior temporal branch retinal vein occlusion (BRVO). Note the areas of capillary dropout and nonperfusion (dark areas), the disruption of the fo-veal ring, increased foveal avascular zone (FAZ) and collaterals. All the changes are evident in both vascular networks.
A B A B

Vol. 39 - Nº 2 - Abril-Junho 2015 | 113
sign of DR that appears before the inception of microaneu-rysms. As clearly depicted in Figure 4, a loose network with large and sparse meshes can be easily appreciated, even in patients with mild nonproliferative DR. Microaneurysms appear as focally dilated saccular or fusiform capillaries on OCT angiograms of the superficial and/or deep capillary ple-xus (Fig 4). Retinal non-perfused areas are seen as lesions with no or sparse capillaries on OCT angiograms (Fig 4). Ishibazawa et al17 have concluded from a pilot study with OCTA in diabetic retinopathy that this new imaging techni-que may be clinically useful to evaluate the microvascular status and therapeutic effect of treatments for DR. Neovas-cularization at the optic disc or posterior pole can also be imaged and clearly discernible with OCTA8,17.
OCTA of the optic nerve head of healthy subjects shows a very dense vascular network around the disc that cannot be detected in FA (Fig 5). Jia et al18 have found that this network is greatly attenuated in glaucomatous discs. Further studies are needed to determine its correlation with the rate of progression and whether disc perfusion can be used as a prognostic indicator.
CONCLUSION
This path-breaking imaging modality is redefining our understanding of several vascular disorders by conveying detailed, depth-resolved information on the retinal and cho-roidal vascular networks, both at a structural and functio-nal level. Although far from perfect, the technology behind OCTA may very well be the future gold standard of retinal and choroidal imaging.
REFERENCES
1. Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science 1991;254:1178-81.
2. Swanson EA, Izatt JA, Hee MR, et al. In vivo retinal imaging by optical coherence tomography. Optics Let-ters 1993;18:1864-6.
3. Drexler W, Fujimoto JG. State-of-the-art retinal opti-cal coherence tomography. Progress in Retinal and Eye Research 2008;27:45-88.
4. Puliafito CA. OCT angiography: the next era of OCT technology emerges. Ophthalmic Surgery, Lasers & Imaging retina 2014;45:360.
5. Alasil T, Ferrara D, Adhi M, et al. En face imaging of the choroid in polypoidal choroidal vasculopathy using swept-source optical coherence tomography. American Journal of Ophthalmology 2015;159:634-43 e2.
6. Su Z, Ye P, Teng Y, Zhang L, Shu X. Adverse reac-tion in patients with drug allergy history after simulta-neous intravenous fundus fluorescein angiography and indocyanine green angiography. Journal of ocular phar-macology and therapeutics : the official journal of the Association for Ocular Pharmacology and Therapeutics 2012;28:410-3.
7. Lipson BK, Yannuzzi LA. Complications of intravenous fluorescein injections. International Ophthalmology Cli-nics 1989;29:200-5.
8. Lumbroso BH, D.; Jia, Y; Fujimoto, J.G.; Rispoli, M. Clinical Guide to Angio-OCT: Non Invasive, Dyeless OCT Angiography. First ed: Jaypee Brothers Medical Publishers; 2015.
9. Spaide RF, Klancnik JM, Jr., Cooney MJ. Retinal vascu-lar layers imaged by fluorescein angiography and optical coherence tomography angiography. JAMA Ophthal-mology 2015;133:45-50.
10. Matsunaga D, Yi J, Puliafito CA, Kashani AH. OCT
OCT angiography: redefining standards
Fig. 4 | Superficial (A) and deep (B) retinal vascular plexuses in a patient with long.standing type 2 diabetes mellitus and mild nonproliferative diabetic retinopathy. Note the mi-croaneurysms both in the superficial and deep plexuses (yellow circles), areas of capillary dropout and nonperfu-sion (dark areas) and a large and irregular foveal avascu-lar zone (FAZ) with loss of the usual centripetal arrange-ment of the bordering vascular network.
A B
Fig. 5 | Optical coherence tomography angiography (OCTA) of a healthy subject showing a dense vascular network inside and around the optic disc.

114 | Revista da Sociedade Portuguesa de Oftalmologia
angiography in healthy human subjects. Ophthalmic Surgery, Lasers & Imaging Retina 2014;45:510-5.
11. Stanga PE, Lim JI, Hamilton P. Indocyanine green angiography in chorioretinal diseases: indications and interpretation: an evidence-based update. Ophthalmo-logy 2003;110:15-21; quiz 2-3.
12. de Carlo TE, Bonini Filho MA, Chin AT, et al. Spectral--Domain Optical Coherence Tomography Angiogra-phy of Choroidal Neovascularization. Ophthalmology 2015;122:1228-38.
13. Moult E, Choi W, Waheed NK, et al. Ultrahigh--speed swept-source OCT angiography in exudative AMD. Ophthalmic Surgery, Lasers & Imaging Retina 2014;45:496-505.
14. Jia Y, Tan O, Tokayer J, et al. Split-spectrum ampli-tude-decorrelation angiography with optical coherence tomography. Optics Express 2012;20:4710-25.
15. Tokayer J, Jia Y, Dhalla AH, Huang D. Blood flow velocity quantification using split-spectrum amplitude--decorrelation angiography with optical coherence tomo-graphy. Biomedical Optics Express 2013;4:1909-24.
16. Dansingani KK, Naysan J, Freund KB. En face OCT
angiography demonstrates flow in early type 3 neovas-cularization (retinal angiomatous proliferation). Eye 2015;29:703-6.
17. Ishibazawa A, Nagaoka T, Takahashi A, et al. Optical Coherence Tomography Angiography in Diabetic Reti-nopathy: A Prospective Pilot Study. American Journal of Ophthalmology 2015 [Epub ahead of print].
18. Jia Y, Wei E, Wang X, et al. Optical coherence tomo-graphy angiography of optic disc perfusion in glaucoma. Ophthalmology 2014;121:1322-32.
19. Jia Y, Bailey ST, Wilson DJ, et al. Quantitative optical coherence tomography angiography of choroidal neo-vascularization in age-related macular degeneration. Ophthalmology 2014;121:1435-44.
20. Jia Y, Bailey ST, Hwang TS, et al. Quantitative optical coherence tomography angiography of vascular abnor-malities in the living human eye. Proceedings of the National Academy of Sciences of the United States of America 2015;112:E2395-402.
21. Thorell MR, Zhang Q, Huang Y, et al. Swept-source OCT angiography of macular telangiectasia type 2. Ophthal-mic Surgery, Lasers & Imaging Retina 2014;45:369-80.
João Pedro Marques, Rufino Silva

Vol. 39 - Nº 2 - Abril-Junho 2015 | 115
Paracentral Acute Middle Maculopathy: a novel clinical finding
Sara Vaz-Pereira1,2 1Department of Ophthalmology, Hospital de Santa Maria, Lisbon, Portugal
2Department of Ophthalmology, Faculty of Medicine, University of Lisbon, Portugal
Flash Look
Oftalmologia - Vol. 39: pp.115-117
The advent of retinal multimodal imaging and the rapid advances in high-resolution imaging systems have not only improved the understanding of the health and diseased retina, but also allowed for the recognition of new clini-cal findings, such as paracentral acute middle maculopathy (PAMM)1-3.
PAMM was first described in 2013 by Sarraf et al2 as a new variant of acute macular neuroretinopathy (AMN) associated with retinal capillary ischemia. In the original report, all patients presented with the typical findings of AMN such as an acute paracentral scotoma associated with a gray wedge-shaped paracentral lesion in near--infrared imaging (NIR). The differentiating features were the spectral-domain optical coherence tomography (SD-OCT) findings. While some patients showed hyper- reflective bands in the outer plexiform layer (OPL)/ inner nuclear layer (INL) region with subsequent INL thinning and sparring of the outer retina - a novel finding - and were classified as having type 1 AMN, also referred as PAMM, others had hyperreflective bands in the OPL/ outer nuclear layer (ONL) region with subsequent ONL thinning and ellipsoid disruption, and thus were termed type 2 AMN (classic AMN). These two different tomographic presen-tations (above or below the ONL), were hypothesized to be related to the occlusion of the superficial capillary ple-xus in type 1 AMN/ PAMM or deep capillary plexus in type 2 AMN2. The PAMM variant was also noted to occur more frequently in older male patients with vasculopathic risk factors2,3.
However, after the recent description of PAMM as a subtype of AMN characterized by a hyperreflective band--like SD-OCT lesion affecting the middle layers of the retina at the level of the INL because of superficial capil -lary plexus ischemia,2,4 it has now been recognized that the lesion instead relates to ischemia of the intermediate and deep retinal capillary plexuses (deep capillary ische-mia), anatomically located at the inner and outer zones of the INL, respectively, and represents a nonspecific finding of retinal ischemia5-8.
Indeed, it has been shown that PAMM can also occur in the setting of various retinal vascular diseases, such as diabetic retinopathy, retinal vein occlusion, retinal artery occlusion, sickle cell retinopathy and Purtscher’s retinopathy3,5,7-11.
In this context, SD-OCT is an invaluable tool as it improves the in vivo visualization of the retinal microcir-culation and allows for a more precise location of the reti-nal ischemia5,6. It also permits the differentiation between the “cotton-wool spot”, a lesion of superficial capillary plexus ischemia,3,7 and PAMM, consequence of interme-diate and deep retinal capillary plexuses ischemia3,5-7. This latter assumption has been recently confirmed by Sarraf and associates using OCT angiography11. Neverthess, the exact physiopathological mechanism underlying PAMM lesions is still not completely understood. It could be that the deep capillary plexus is located in an oxygen supply watershed zone and therefore more vulnerable to ischemia or that the paucity of superficial capillaries in the perifovea is responsible3,5,7.
As the clinical manifestations of PAMM can be sub-tle, the diagnosis should be made by NIR reflectance and SD-OCT5,6. Fundus autofluorescence can also be helpful (Fig.1A, D and G)2. NIR allows for the visualization of a sharply demarcated dark wedge-shaped lesion, that fades with serial follow-up imaging (Fig. 1B, E and H). SD-OCT demonstrates the typical hyperreflective lesion in the acute phase that resolves with thinning of the INL (Fig.1 C, F and I). This thinning is usually accompanied by persistent scotomas. It should be noted that conventional fluorescein angiography is usually unremarkable, as it cannot properly assess the intermediate and deep capillary plexus5. There is no current treatment for PAMM, except for the recog-nition and treatment of possible associated vasculopathic risk factors5.
In conclusion, although just recently described, PAMM is now widely accepted to be a novel SD-OCT sign of retinal deep capillary plexus ischemia, which may occur in isolation (?novel variant of AMN) or complicating an

116 | Revista da Sociedade Portuguesa de Oftalmologia
underlying retinal vascular disorder. Ophthalmologists should be aware of PAMM as it is more common than previously believed and may be responsible for non-spe-cific visual complaints, especially when the examination is unremarkable.
REFERÊNCIAS
1. Kiernan DF, Mieler WF, Hariprasad SM. Spectral--domain optical coherence tomography: a comparison of modern high-resolution retinal imaging systems. Am J Ophthalmol. 2010;149:18-31.
2. Sarraf D, Rahimy E, Fawzi AA, et al. Paracentral acute middle maculopathy: a new variant of acute macular neuroretinopathy associated with retinal capillary
ischemia. JAMA Ophthalmol. 2013;131:1275–1287.3. Dansingani KK, Freund KB. Paracentral Acute Middle
Maculopathy and Acute Macular Neuroretinopa-thy: Related and Distinct Entities. Am J Ophthalmol. 2015;160:1-3.e2.
4. Tsui I, Sarraf D. Paracentral acute middle maculopathy and acute macular neuroretinopathy. Ophthalmic Surg Lasers Imaging Retina. 2013;44:S33–35.
5. Rahimy E, Sarraf D. Paracentral acute middle maculo-pathy spectral-domain optical coherence tomography feature of deep capillary ischemia. Curr Opin Ophthal-mol. 2014;25:207–212.
6. Yu S, Wang F, Pang CE, Yannuzzi LA, Freund KB. Multimodal imaging findings in retinal deep capillary ischemia. Retina. 2014;34:636-46.
7. Yu S, Pang CE, Gong Y, et al. The spectrum of
Sara Vaz-Pereira
Fig. 1 | Patient with an isolated paracentral acute middle maculopathy (PAMM) lesion in the right eye. Baseline autofluorescence (AF) and near infra-red (NIR) reflectance images showed a paracentral dark wedge-shaped lesion (arrowhead), respectively (A) and (B). Same visit spectral-domain optical coherence tomography (SD-OCT) revealed a characteristic hyperreflective lesion (arrowhead) at the level of the inner nuclear layer (C), consistent with PAMM. Follow-up imaging at 1 month demonstrated attenuation of the lesion in both AF and NIR, respectively (D) and (E), with subsequent resolution at 3 months, (G) and (H). SD-OCT at 1 and 3 months, showed gradual resolution of the PAMM lesion (F) with following severe INL thinning (I) (between arrowheads).

Vol. 39 - Nº 2 - Abril-Junho 2015 | 117
superficial and deep capillary ischemia in retinal artery occlusion. Am J Ophthalmol. 2015;159:53-63.e1-2.
8. Rahimy E, Sarraf D, Dollin ML, Pitcher JD, Ho AC. Paracentral acute middle maculopathy in nonische-mic central retinal vein occlusion. Am J Ophthalmol. 2014;158:372-380.e1.
9. Chen X, Rahimy E, Sergott RC, et al. Spectrum of retinal vascular diseases associated with paracen-tral acute middle maculopathy. Am J Ophthalmol. 2015;160:26–34.
10. Ilginis T, Keane PA, Tufail A. Paracentral acute middle maculopathy in sickle cell disease. JAMA Ophthal-mol. 2015;133:614-6.
11. Christenbury JG, Klufas MA, Sauer TC, Sarraf D. OCT Angiography of Paracentral Acute Middle
Maculopathy Associated With Central Retinal Artery Occlusion and Deep Capillary Ischemia. Ophthalmic Surg Lasers Imaging Retina. 2015;46:579-81.
The author received no financial support and has no proprietary inte-rest in the subject or materials discussed in this manuscript.
CONTACTOSara Vaz-PereiraDepartment of Ophthalmology, Hosp. de Santa Maria,Av. Prof. Egas Moniz, 1649-035 Lisbon, PortugalEmail: [email protected]: (+351) 217 805 252Fax: (+351) 217 805 610
Paracentral Acute Middle Maculopathy: a novel clinical finding


Vol. 39 - Nº 2 - Abril-Junho 2015 | 119
Miopia patológica - novos conceitos e achados OCT
Francisco TrincãoCentro Hospitalar de Lisboa Central; Departamento de Retina Cirúrgica
Flash Look
Oftalmologia - Vol. 39: pp.119-126
RESUMO
A miopia patológica é uma causa importante de cegueira, com prevalência crescente nos paí-ses desenvolvidos e em idades progressivamente mais jovens. É-lhe tradicionalmente atribuída uma forte componente genética, reconhecendo-se hoje fatores ambientais que podem limitar a sua progressão. Embora em muitos casos o agravamento da acuidade visual fosse atribuído à presença de neovascularização coroideia, descolamento de retina ou desenvolvimento de bura-co macular, noutros esta progressão permanece por explicar. Novas técnicas de tomografia por coerência óptica permitiram recentemente a descoberta de entidades patológicas relacionadas com a maculopatia miópica, que abrem portas ao avanço na compreensão fisiopatológica da doença e na sua abordagem terapêutica, particularmente cirúrgica. Salientam-se os fenómenos de foveosquisis miópica, cavitação intracoroideia, tração vítrea paravascular (com formação de quistos, micropregas e defeitos lamelares) e fenómenos de distorção macular que revemos neste trabalho.
Palavras-chaveMiopia patológica; OCT; Foveosquisis; Cavitação; Distorção Macular.
ABSTRACT
Pathological myopia is a major cause of blindness, with growing prevalence in developed coun-tries and at increasingly younger ages. It is traditionally believed to have a strong genetic com-ponent, but environmental factors that may limit its progression have been identified. Although the deterioration of visual acuity is usually attributed to the presence of choroidal neovascula-rization, retinal detachment or the development of a macular hole, it remains to be explained in numerous cases. Recently, optical coherence tomography techniques led to the discovery of pathologies related to myopic maculopathy. These represented a breakthrough in pathophysio-logical understanding of the disease and identification of promising therapeutic approaches. In this paper we review myopic foveoschisis, intrachoroidal cavitation, paravascular vitreous traction (with the development of cysts, microfolds and lamellar defects) and macular distortion phenomena.
Keywords Pathologic myopia; OCT; Foveoschisis; Cavitation; Macular bending

120 | Revista da Sociedade Portuguesa de Oftalmologia
INTRODUÇÃO
A miopia patológica (MP) é uma causa importante de cegueira, afetando até cerca de 3% da população mundial1 e emergindo como um verdadeiro problema de saúde em áreas urbanas dos países asiáticos, onde atinge 10-20% dos jovens que completam o ensino secundário2. Desde o início dos anos 90, estudos populacionais3,4,5 têm demonstrado este aumento de prevalência em idades mais precoces e também noutras regiões do planeta, em populações caucasianas6,7,8,9.
Indivíduos com MP sofrem alongamento e distorção oculares com alterações degenerativas, particularmente do polo posterior e peripapilares, muitas vezes subtis e difíceis de observar na fundoscopia. Com o advento da tomografia de coerência óptica (OCT), grande parte destas lesões passaram a ser melhor caracterizadas, assim como novas lesões foram identificadas, resultando numa melhor compreensão da sua fisiopatologia.
ETIOLOGIA MULTIFATORIAL
A MP resulta de fatores não exclusivamente genéticos, cuja contribuição permanece pouco evidente10,11. Enquanto nos casos sindrómicos (ex: Marfan, Stickler), é comum a participação de genes envolvidos na matriz extracelular escleral (ECM), na miopia patológica não sindrómica são várias as localizações cromossómicas reportadas (MYP1--MYP17) mas poucos genes específicos identificados.
Nesse sentido, é cada vez mais dada relevância a fato-res ambientais, apoiados por modelos animais e estudos epidemiológicos12. É consistente a associação da miopia à urbanização, elevada exigência escolar e modificações do estilo de vida que promovem o excessivo trabalho para perto13,14. Pelo contrário, a promoção de hábitos de vida no exterior e a maior exposição solar minimizam a progressão da miopia15,16.
CLASSIFICAÇÃO
A MP foi originalmente descrita como uma miopia ele-vada acompanhada por alterações degenerativas caracterís-ticas na esclera, coróide e epitélio pigmentar da retina com compromisso da visão17. Nem todos os olhos com miopia elevada desenvolvem miopia patológica, mas a prevalên-cia de lesões ocorre predominantemente em idades menos jovens e em olhos com comprimentos axiais superiores a 3 desvios padrão da média da emetropia, correspondendo grosseiramente a 26mm ou -6D18,19.
Achados imagiológicos permitem verificar que os olhos dos grandes míopes não são só olhos mais compridos mas também gravemente deformados20 com lesões retinianas, coroideias, esclerais, visuais e campimétricas correspon-dentes21 e relacionados com os vários sinais anatómicos que lhes são classicamente identificados: estafiloma posterior, lacquer cracks, atrofia corioretiniana, mancha de Fuchs e neovascularização coroideia miópica. Várias classificações da maculopatia miópica (MM) foram propostas de acordo com estas anomalias22,23, e relacionando a presença dum estafiloma posterior com a progressão da doença (que nem sempre acontece nem é linear). Estas classificações ana-tómicas identificam em estádios iniciais alterações fun-doscópicas mínimas com fundo de aspeto quadriculado (tesselated fundus), passando por um estádio de atrofia corioretiniana difusa e depois em padrão com áreas de palidez marcada bem delimitadas, cuja coalescência e a proximidade foveal se acompanham dum agravamento da acuidade visual24. À semelhança do que se passa na dege-nerescência macular da idade, constitui uma forma parti-cularmente grave da doença o desenvolvimento duma neo-vascularização coroideia (NVC miópica). Efetivamente, a MM representa a principal causa de NVC na população em idade ativa e particularmente abaixo dos 50 anos25. O seu curso passa por uma fase ativa com a presença em angio-grafia duma membrana do tipo clássico, uma fase cicatri-cial fibrovascular que frequentemente reduz o tamanho da lesão e lhe confere uma coloração acinzentada (man-cha de Fuchs) e uma fase atrófica, e que se acompanha duma baixa da acuidade visual pronunciada26. A atrofia em padrão e especialmente as lacquer cracks são consideradas precursoras desta forma húmida da MM, particularmente se ocorrerem próximo (menos de 1 diâmetro de disco) do nervo óptico27 e podendo surgir em formas menos avança-das da doença.
São contudo apontadas várias limitações a estas classi-ficações clínicas, como a subjetividade na caracterização de lesões, a baixa correlação destas lesões com dados bio-métricos e a sua variabilidade de apresentação no mesmo olho. O OCT veio indubitavelmente revolucionar a forma como observamos a patologia. A melhor caracterização imagiológica tem fornecido dados valiosos que permitem a criação de modelos de classificação com valor preditivo mais fiável do que os tradicionais modelos clínicos anató-micos e refrativos. Neste sentido, é proposto que a medição da espessura coroideia macular permite prever melhor a baixa da acuidade visual, a gravidade da MM e a formação de lacquer cracks do que o erro refractivo, aspecto fundos-cópico, presença de estafiloma ou comprimento axial nas formas secas (não neovasculares) da doença28. O grau de
Francisco Trincão

Vol. 39 - Nº 2 - Abril-Junho 2015 | 121
afilamento coroideu, invariavelmente presente na miopia patológica, é tanto maior quanto a gravidade da doença e é especialmente marcado em olhos com lacquer cracks e NVC29 (Figura 1).
NOVAS ENTIDADES OCT
Na última década fomos testemunhas de avanços tre-mendos nas técnicas de observação do segmento posterior. O time-domain OCT (TD-OCT; com resolução axial de 10µm) revolucionou o diagnóstico na patologia retiniana e foi rapidamente substituído pelo spectral-domain OCT (SD-OCT) que proporciona uma resolução axial substan-cialmente superior (3µm) e a capacidade de formar ima-gens tridimensionais. Com as novas técnicas de OCT de domínio espectral (SD-OCT) conseguimos hoje avaliar em detalhe a anatomia da interface vítreo-retiniana e da estru-tura da retina neurosensorial, identificando muitas vezes lesões que não eram detetadas na fundoscopia e técnicas de imagem convencionais, particularmente nos estádios iniciais da MP.
O “OCT en face” (ou OCT-C scan) permite a reali-zação de planos transversais bidimensionais em qualquer profundidade da retina, com localização determinada pelo operador numa imagem confocal simultânea, visualizando em extensão lateral as diferentes lesões30 (Figura 2). É especialmente útil nestes doentes em que na presença dum estafiloma posterior, a imagem B-scan se encontra dema-siado distorcida e muitas vezes alterada por artefactos de espelho31 (Figura 3).
Aproximando a coróide da linha de zero-delay, tornou--se também possível a visualização e medição da coroide pela inversão da imagem, técnica conhecida como “enhan-ced depth imaging OCT” (EDI-OCT)32. Mais recentemente,
adotando um maior comprimento de onda (1050nm em vez de 840nm no SD-OCT) e fotodetetores (em vez de câmaras CCD) o swept-source OCT (SS-OCT) conseguiu ultrapas-sar a dispersão de sinal provocada pelo epitélio pigmentado da retina (EPR) que impedia a visualização de estruturas mais profundas (particularmente as camadas coroideias) e aumentar a resolução da imagem obtida (1µm). O aumento em 4 vezes da velocidade de aquisição (100.000 scans A/segundo), permitiu ainda obter imagens de maior campo e visualizar simultâneamente o vítreo, retina e coroide a nível macular e papilar.
Esta melhor resolução e capacidades acrescidas trazi-das por novas técnicas OCT tornaram possível a descrição de entidades que nos permitem uma melhor compreensão da doença e das suas complicações, das quais se salien-tam a deiscência das camadas retinianas (retinosquisis), fenómenos de tracção vítrea e formação de quistos para-vasculares na retina interna, formação de buracos lame-lares e maculares completos, cavitações intracoroideias peripapilares e maculares, e distorções da arquitectura macular como a mácula em cúpula e o estafiloma asso-ciado a tilt-disc.
Miopia patológica – novos conceitos e achados OCT
Fig. 1 | Imagens de verde de indocinanina e comparação de es-pessura coroideia (seta branca) em doente com (cima) e sem (baixo) lacquer cracks.*
Fig. 2 | OCT C-scan: vasos retiniano rígidos e em tenda (setas vermelhas), que podem contribuir para a formação duma esquísis retiniana.**
Fig. 3 | OCT B-scan convencional: artefacto de espelho num olho grande míope. Quanto maior o estafiloma, maior a distorção causada na imagem B-scan.**
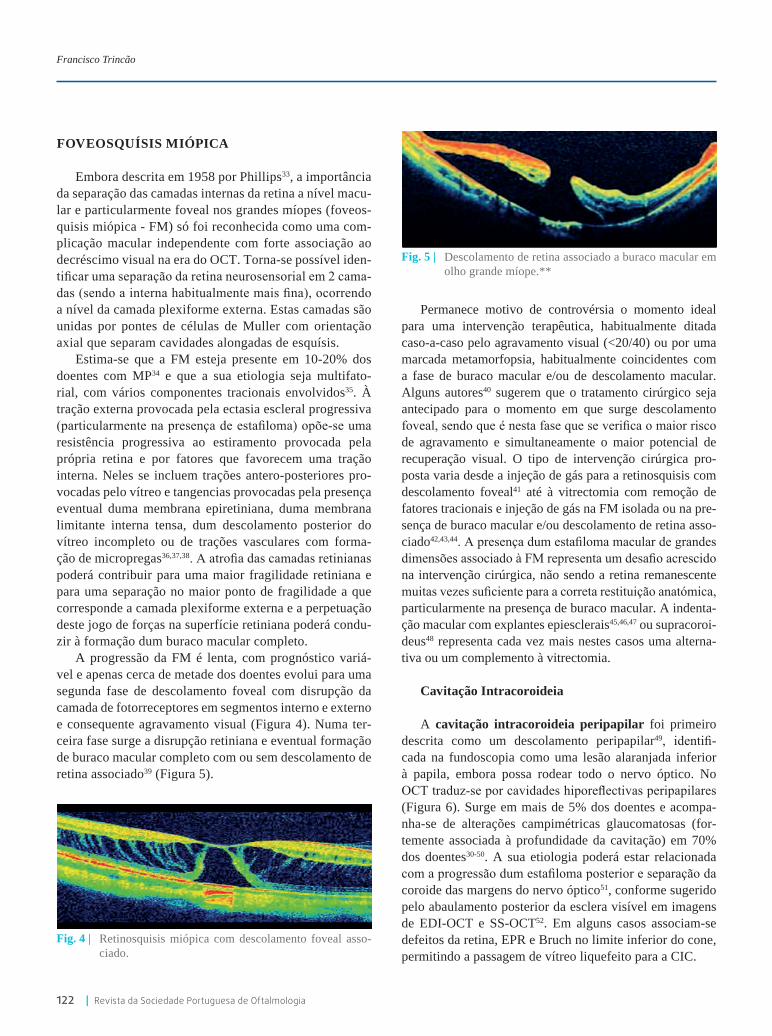
122 | Revista da Sociedade Portuguesa de Oftalmologia
FOVEOSQUíSIS MIÓPICA
Embora descrita em 1958 por Phillips33, a importância da separação das camadas internas da retina a nível macu-lar e particularmente foveal nos grandes míopes (foveos-quisis miópica - FM) só foi reconhecida como uma com-plicação macular independente com forte associação ao decréscimo visual na era do OCT. Torna-se possível iden-tificar uma separação da retina neurosensorial em 2 cama-das (sendo a interna habitualmente mais fina), ocorrendo a nível da camada plexiforme externa. Estas camadas são unidas por pontes de células de Muller com orientação axial que separam cavidades alongadas de esquísis.
Estima-se que a FM esteja presente em 10-20% dos doentes com MP34 e que a sua etiologia seja multifato-rial, com vários componentes tracionais envolvidos35. À tração externa provocada pela ectasia escleral progressiva (particularmente na presença de estafiloma) opõe-se uma resistência progressiva ao estiramento provocada pela própria retina e por fatores que favorecem uma tração interna. Neles se incluem trações antero-posteriores pro-vocadas pelo vítreo e tangencias provocadas pela presença eventual duma membrana epiretiniana, duma membrana limitante interna tensa, dum descolamento posterior do vítreo incompleto ou de trações vasculares com forma-ção de micropregas36,37,38. A atrofia das camadas retinianas poderá contribuir para uma maior fragilidade retiniana e para uma separação no maior ponto de fragilidade a que corresponde a camada plexiforme externa e a perpetuação deste jogo de forças na superfície retiniana poderá condu-zir à formação dum buraco macular completo.
A progressão da FM é lenta, com prognóstico variá-vel e apenas cerca de metade dos doentes evolui para uma segunda fase de descolamento foveal com disrupção da camada de fotorreceptores em segmentos interno e externo e consequente agravamento visual (Figura 4). Numa ter-ceira fase surge a disrupção retiniana e eventual formação de buraco macular completo com ou sem descolamento de retina associado39 (Figura 5).
Permanece motivo de controvérsia o momento ideal para uma intervenção terapêutica, habitualmente ditada caso-a-caso pelo agravamento visual (<20/40) ou por uma marcada metamorfopsia, habitualmente coincidentes com a fase de buraco macular e/ou de descolamento macular. Alguns autores40 sugerem que o tratamento cirúrgico seja antecipado para o momento em que surge descolamento foveal, sendo que é nesta fase que se verifica o maior risco de agravamento e simultaneamente o maior potencial de recuperação visual. O tipo de intervenção cirúrgica pro-posta varia desde a injeção de gás para a retinosquisis com descolamento foveal41 até à vitrectomia com remoção de fatores tracionais e injeção de gás na FM isolada ou na pre-sença de buraco macular e/ou descolamento de retina asso-ciado42,43,44. A presença dum estafiloma macular de grandes dimensões associado à FM representa um desafio acrescido na intervenção cirúrgica, não sendo a retina remanescente muitas vezes suficiente para a correta restituição anatómica, particularmente na presença de buraco macular. A indenta-ção macular com explantes epiesclerais45,46,47 ou supracoroi-deus48 representa cada vez mais nestes casos uma alterna-tiva ou um complemento à vitrectomia.
Cavitação Intracoroideia
A cavitação intracoroideia peripapilar foi primeiro descrita como um descolamento peripapilar49, identifi-cada na fundoscopia como uma lesão alaranjada inferior à papila, embora possa rodear todo o nervo óptico. No OCT traduz-se por cavidades hiporeflectivas peripapilares (Figura 6). Surge em mais de 5% dos doentes e acompa-nha-se de alterações campimétricas glaucomatosas (for-temente associada à profundidade da cavitação) em 70% dos doentes30-50. A sua etiologia poderá estar relacionada com a progressão dum estafiloma posterior e separação da coroide das margens do nervo óptico51, conforme sugerido pelo abaulamento posterior da esclera visível em imagens de EDI-OCT e SS-OCT52. Em alguns casos associam-se defeitos da retina, EPR e Bruch no limite inferior do cone, permitindo a passagem de vítreo liquefeito para a CIC.
Fig. 4 | Retinosquisis miópica com descolamento foveal asso-ciado.
Fig. 5 | Descolamento de retina associado a buraco macular em olho grande míope.**
Francisco Trincão

Vol. 39 - Nº 2 - Abril-Junho 2015 | 123
À semelhança do que se passa a nível papilar, podemos também encontrar uma forma de CIC macular e extra-macular no interior e áreas limítrofes de atrofia coriore-tiniana em padrão53. O abaulamento posterior da esclera ultrapassa nestes casos os limites observáveis fundosco-picamente da área de atrofia, facilitando fenómenos de retinosquisis local.
Tração Vítrea Paravascular
Fenómenos de tração vítrea paravascular têm tam-bém permitido explicar lesões adjacentes aos vasos de 1ª ordem de doentes grandes míopes, particularmente nos doentes mais idosos e com maior comprimento axial54. Traduzem-se na formação de quistos retinianos paravas-culares visíveis no OCT de cerca de metade dos doentes com MP (Figura 7), como espaços sem sinal em torno de
vasos retinianos. Associadas a estes quistos podem sur-gir micropregas vasculares30,54 (Figura 8), resultantes da tração vítrea sobre vasos especialmente rígidos e pouco flexíveis, que ao perpetuar-se poderá conduzir à extensão dos quistos e originar uma retinosquisis paravascular ou a uma decapitação do quisto formando um buraco lamelar paravascular (Figura 9).
Distorção macular
Vários são os fenómenos identificados por OCT rela-cionados com a distorção da arquitetura macular do olho grande míope. Nestas alterações de torção macular (macu-lar bending) salienta-se a presença não rara duma protusão convexa da mácula no interior dum estafiloma posterior, conhecida como mácula em cúpula (dome-shaped macula). Foi originalmente descrita como um achado inesperado num olho que sofre alongamento e estiramento das suas estruturas e que se espera com uma parede uniformemente fina55. Associa-se frequentemente a alterações atróficas do EPR e descolamento seroso da retina (Figura 10). As técni-cas de EDI-OCT e SS-OCT demonstraram que resulta dum espessamento localizado da esclera e afilamento da coroide
Fig. 6 | Cavitações intracoroideias peripapilares, frequentemen-te relacionadas com defeitos campimétricos glaucoma-tosos.**
Fig. 7 | Quistos paravasculares múltiplos adjacentes aos vasos de 1ª ordem da retina.**
Fig. 8 | Pregas microvasculares adjacentes a estafiloma poste-rior.**
Fig. 9 | Buraco lamelar paravascular (possivelmente resultante da decapitação dum quisto paravascular) com retinos-quisis paravascular associada.**
Fig. 10 | Mácula em cúpula associada a descolamento seroso.***
Miopia patológica – novos conceitos e achados OCT

124 | Revista da Sociedade Portuguesa de Oftalmologia
a nível macular e que nem sempre surge na presença de estafiloma. A acumulação de líquido sub-retiniano poderá dever-se ao constrangimento coroideu provocado por este espessamento escleral subjacente56,57, que não é exclusivo da mácula em cúpula, ocorrendo também fora da mácula e em regiões extrapapilares de doentes com MP57. Tal reforça os achados MRI que sugerem que a esclera do pólo posterior se deforma de forma não homogénea.
Outros achados identificados no OCT relacionam alte-rações maculares com o tilted-disc (TD). Embora esta incidência oblíqua do nervo óptico no olho não se reverta isoladamente de pior prognóstico, são várias as complica-ções maculares associadas que o agravam, como alterações coroideias degenerativas, neovasculares e descolamento seroso. Tem sido recentemente proposto que o estafiloma relacionado com o TD possa ser responsável por estas alterações. Surge habitualmente abaixo da mácula, com o seu limite superior atravessando-a no centro, traduzindo-se nesse local com defeito de janela na angiografia fluoresceí-nica (por atrofia do EPR), e por uma hiperfluorescência na angiografia por verde de indocianina (por oclusão corioca-pilar associada)58. Adicionalmente, estudos por EDI-OCT e SS-OCT demonstraram que a coroide subfoveal é mais fina e que a esclera subfoveal correspondente é mais espessa dentro da área do estafiloma59, o que à semelhança do que se passa com a mácula em cúpula poderia explicar a restrição ao fluxo coriocapilar local e a formação dum descolamento seroso.
CONCLUSÃO
A miopia patológica e suas complicações (neovascu-larização coroideia, desenvolvimento de buraco macular e de descolamento de retina) são uma causa crescente de cegueira nos países desenvolvidos. A par da identificação de fatores preventivos, a descoberta recente de novas enti-dades patológicas por OCT (foveosquisis miópica, cavita-ção intracoroideia, tração vítrea paravascular e fenómenos de distorção macular) abre portas ao avanço na compreen-são fisiopatológica da doença e na abordagem médica e cirúrgica que temos assistido, não só com novas técnicas como melhores indicações.
* imagem reproduzida de Wang NK et al. Choroidal thickness and bio-metric markers for the screening of lacquer cracks in patients with high myopia. PLoS One. 2013;8(1) Epub 2013 Jan 22; open access
** imagem reproduzida de Faghihi H. et al. Optical Coherence Tomo-graphic Findings in Highly Myopic Eyes. J Ophthalmic Vis Res. 2010 Apr; 5(2): 110–121; open-access.
*** imagem reproduzida de Dirani A. Et al. Resolution of foveal deta-chment in dome-shaped macula after treatment by spironolactone: report of two cases and mini-review of the literature. Clin Ophthal-mol. 2014 May 20;8:999-1002, com autorização não-comercial.
BIBLIOGRAFIA
1. Curtin BJ. The Myopias: basic science and clinical management. In. Philadelphia: Harper&Row; 1985.
2. Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;(33): p. 27–33.
3. Wang Q, Klein BE, Klein R, Moss SE. Refractive status in the Beaver Dam Eye Study. Invest Ophthalmol Vis Sci. 1994;(35): p. 4344–4347.
4. Attebo K, Ivers RQ, Mitchell P. Refractive errors in an older population: the Blue Mountains Eye Study. Ophthalmology. 1999;(106): p. 1066–1072.
5. Klein R, Klein BEK, Lee KE, Cruickshanks KJ, Cha-ppell RJ. Changes in visual acuity in a population over a 10-year period: The Beaver Dam Eye Study. Ophthal-mology. 2001;(108): p. 1757–1766.
6. Wong TY, Foster PJ, Hee J, et al. Prevalence and risk fac-tors for refractive errors in adult Chinese in Singapore. Invest Ophthalmol Vis Sci. 2000; 41: p. 2486–2494.
7. Wensor M, McCarty CA, Taylor HR. Prevalence and risk factors of myopia in Victoria. Aust Arch Ophthal-mol. 1999;(117): p. 658–663.
8. Wu SY, Nemesure B, Leske MC. Refractive errors in a black adult population: The Barbados Eye Study. Invest Ophthalmol Vis Sci. 1999;(40): p. 2179–2184.
9. I M, et al. Myopia. Lancet. 2012;(379(9827)): p. 1739–1748.
10. Wojciechowski R. Nature and nurture: the complex genetics of myopia and refractive error. Clin Genet. 2011;(79): p. 301–20.
11. Hornbeak DM, Young TL. Myopia genetics: a review of current research and emerging trends. Curr Opin Ophthalmol. 2009;(20): p. 356–62.
12. Morgan I RK. How genetic is school myopia? Prog Retin Eye Res. 2005;(24): p. 1–38.
13. A R, J. B. Refraction, near work and education: a population study in Newfoundland. Acta Ophthalmol (Copenh). 1980;(58): p. 468–478.
14. Katz J, Tielsch JM, Sommer A. Prevalence and risk fac-tors for refractive errors in an adult inner city population. Invest Ophthalmol Vis Sci. 1997;(38): p. 334-340.
15. Rose KA, et al. Outdoor activity reduces the prevalence
Francisco Trincão

Vol. 39 - Nº 2 - Abril-Junho 2015 | 125
of myopia in children. Ophthalmology. 2008;(115(8)): p. 1279–1285.
16. Smith ELI, et al. Protective effects of high ambient lighting on the development of form-deprivation myo-pia inrhesus monkeys. Invest Ophthalmol Vis Sci. 2012;(53(1)): p. 421–428.
17. Duke-Elder S, Abrams D. Pathological refractive errors. In Duke-Elder S e. Systems of ophthalmology. St Louis: CV Mosby; 1970. p. 297–374.
18. Gao LQ, Liu W, Liang YB, et al. Prevalence and charac-teristics of myopic retinopathy in a rural Chinese adult population: the Handan Eye Study. Arch Ophthalmol. 2011;(129): p. 1199–204.
19. Vongphanit J, Mitchell P, Wang JJ. Prevalence and pro-gression of myopic retinopathy in an older population. Ophthalmology. 2002;(109): p. 704-11.
20. Moriyama M, Ohno-Matsui K, Hayashi K, et al. Topo-graphic analyses of shape of eyes with pathologic myo-pia by high-resolution three-dimensional magnetic reso-nance imaging. Ophthalmology. 2011;(118): p. 1626-37.
21. Ohno-Matsui K, Shimada N, Yasuzumi K, et al. Long--term development of signifi cant visual fi eld defects in highly myopic eyes. Am J Ophthalmol. 2011;(152): p. 256–65.e1.
22. Avila MP, Weiter JJ, Jalkh AE, et al. Natural history of choroidal neovascularization in degenerative myopia. Ophthalmology. 1984; 91(12): p. 1573-81.
23. Vongphanit J, Mitchell P, Wang JJ. Prevalence and pro-gression of myopic retinopathy in an older population. Ophthalmology. 2002; 4(109): p. 704-711.
24. Hayashi K, Ohno-Matsui K, Shimada N, et al. Long--term pattern of progression of myopic maculopathy: a natural history study. Ophthalmology. 2010; 8(117): p. 1595-1611.
25. Cohen SY, Laroche A, Leguen Y, Soubrane G, Coscas GJ. Etiology of choroidal neovascularization in young patients. Ophthalmology. 1996 Aug; 8(103): p. 1241-4.
26. Neelam K, Cheung CM, Ohno-Matsui K, Lai TY, Wong TY. Choroidal neovascularization in pathological myo-pia. Prog Retin Eye Res. 2012; 5(31): p. 495-525.
27. Ohno-Matsui K, Yoshida T, Futagami S, Yasuzumi K, Shimada N, Kojima A, et al. Patchy atrophy and lacquer cracks predispose to the development of choroidal neo-vascularisation in pathological myopia. Br J Ophthal-mol. 2003 May; 5(87): p. 570-3.
28. Wang NK, Lai CC, Chu HY, Chen YP, Chen KJ, Wu WC, et al. Classification of early dry-type myopic maculopathy with macular choroidal thickness. Am J Ophthalmol. 2012 Apr; 4(153): p. 669-77.
29. Ikuno Y, Jo Y, Hamasaki T, Tano Y. Ocular risk factors
for choroidal neovascularization in pathologic myopia. Invest Ophthalmol Vis Sci. 2010;(51): p. 3721-3725.
30. Forte R, Cennamo G, Pascotto F, deCrecchio G. En face optical coherence tomography of the posterior pole in high myopia. Am J Ophthalmol. 2008;(145): p. 281-288.
31. Wang K, Ding Z, Zeng Y, Meng J, Chen M. Sinusoidal B-M method based spectral domain optical coherence tomography for the elimination of complex-conjugate artifacts. Opt Express. 2009;(17): p. 16820-16833.
32. Spaide RF, Koizumi H, Pozzoni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2008;(146): p. 496-500.
33. Philips CI. Retinal detachment at the posterior pole. Br J Ophthalmol. 1958; 12(42): p. 749-753.
34. Henaine-Berra A, Zand-Hadas IM, Fromow-Guerra J, Garcia-Aguirre G. Prevalence of macular anatomic abnormalities in high myopia. Ophthalmic Surg Lasers Imaging Retina. 2013; 2(44): p. 140-144.
35. Wu PC, Chen YJ, Chen YH, Chen CH, Shin SJ, Tsai CL, et al. Factors associated with foveoschisis and foveal detachment without macular hole in high myopia. Eye. 2009; 2(23): p. 356-361.
36. Ikuno Y, Gomi F, Tano Y. Potent retinal arteriolar trac-tion as a possible cause of myopic foveoschisis. Am J Ophthalmol. 2005; 3(139): p. 462-467.
37. Bando H, Ikuno Y, Choi JS, Tano Y, Yamanaka I, Ishi-bashi T. Ultrastructure of internal limiting membrane. Am J Ophthalmol. 2005; 1(139): p. 197-199.
38. Sebag J. Anomalous posterior vitreous detachment: a unifying concept in vitreo-retinal disease. Graefes Arch Clin Exp Ophthalmol. 2004; 8(242): p. 690-698.
39. Shimada N, Ohno-Matsui K, Yoshida T, Sugamoto Y, Tokoro T, Mochizuki M. Progression from macular reti-noschisis to retinal detachment in highly myopic eyes is associated with outer lamellar hole formation. Br J Ophthalmol. 2008; 6(92): p. 762-4.
40. Ikuno Y, Sayanagi K, Soga K, Oshima Y, Ohj iM, Tano Y. Foveal anatomical status and surgical results in vitrec-tomy for myopic foveoschisis. Jpn J Ophthalmol. 2008; 4(52): p. 269-76.
41. Wu TY, Yang CH, Yang CM. Gas tamponade for myo-pic foveoschisis with foveal detachment. Graefes Arch Clin Exp Ophthalmol. 2013 May; 5(251): p. 1319-24.
42. Gaucher D, Haouchine B, Tadayoni R, Massin P, Ergi-nay A, Benhamou N, et al. Long-term follow-up of high myopic foveoschisis: natural course and surgical out-come. Am J Ophthalmol. 2007; 3(143): p. 455-462.
43. Ikuno Y, Sayanagi K, Ohji M, Kamei M, Gomi F, Harino S, et al. Vitrectomy and internal limiting membrane pee-ling for myopic foveoschisis. Am J Ophthalmol. 2004;
Miopia patológica – novos conceitos e achados OCT

126 | Revista da Sociedade Portuguesa de Oftalmologia
4(137): p. 719-724.44. Kim KS, Lee SB, Lee WK. Vitrectomy and internal
limiting membrane peeling with and without gas tampo-nade for myopic foveoschisis. Am J Ophthalmol. 2012; 2(153): p. 320-6.
45. Ando F. Use of special macular explant in surgery for retinal detachment with macular hole. Jpn J Ophthalmol. 1980;(24): p. 29-34.
46. Theodossiadis GP, Theodossiadis PG. The macular buckling procedure in the treatment of retinal detach-ment in highly myopic eyes with macular hole and pos-terior staphyloma: mean follow-up of 15 years. Retina. 2005; 3(25): p. 285-9.
47. Ripandelli G, Coppé AM, Fedeli R, Parisi V, D’Amico DJ, Stirpe M. Evaluation of primary surgical procedures for retinal detachment with macular hole in highly myo-pic eyes: a comparison [corrected] of vitrectomy versus posterior episcleral buckling surgery. Ophthalmology. 2001; 108(12): p. 2258-65.
48. Rayes E, Elborgy E. Suprachoroidal Buckling: Techni-que and Indications. J Ophthalmic Vis Res. 2013; 4(8): p. 393-399.
49. Freund KB, Ciardella AP, Yannuzzi LA, Pece A, Gol-dbaum M, Kokame GT, et al. Peripapillary detachment in pathologic myopia. Arch Ophthalmol. 2003;(121): p. 197-204.
50. Shimada N, Ohno-Matsui K, Yoshida T, Yasuzumi K, Kojima A, Kobayashi K, et al. Characteristics of peripa-pillary detachment in pathologic myopia. Arch Ophthal-mol. 2006;(124): p. 46-52.
51. Toranzo J, Cohen SY, Erginay A, Gaudric A. Peri-papillary intrachoroidal cavitation in myopia. Am J
Ophthalmol. 2005;(140): p. 731-732.52. Spaide RF, Akiba M, et al. Evaluation of Peripapillary
Intrachoroidal Cavitation with Swept Source and Enhan-ced Depth Imaging Optical Coherence Tomography. Retina. 2012;(32): p. 1037-1044.
53. Ohno-Matsui K, Akiba M, et al. Intrachoroidal cavita-tion in macular area of eyes with pathologic myopia. Am J Ophthalmol. 2012;(154): p. 382-393.
54. Shimada N, Ohno-Matsui K, Nishimuta A, Moriyama M, Yoshida T, Tokoro T, et al. Detection of paravascular lamellar holes and other paravascular abnormalities by optical coherence tomography in eyes with high myopia. Ophthalmology. 2008;115;(115): p. 708-717.
55. Gaucher D, Erginay A, Lecleire-Collet A, et al. Dome--shaped macula in eyes with myopic posterior sta-phyloma. Am J Ophthalmol. 2008; 5(145): p. 909–914.
56. Imamura Y, Iida T, Maruko I, Zweifel SA, Spaide RF. Enhanced depth imaging optical coherence tomography of the sclera in dome-shaped macula. Am J Ophthalmol. 2011; 2(151): p. 297-302.
57. Maruko I, Iida T, Sugano Y, Oyamada H, Akiba M, Seki-ryu T. Morphologic analysis in pathologic myopia using high-penetration optical coherence tomography. Invest Ophthalmol Vis Sci. 2012 Jun 20; 7(53): p. 3834-8.
58. Nakanishi H, Tsujikawa A, et al. Macular complica-tions on the border of an inferior staphyloma associa-ted with tilted disc syndrome. Retina. 2008; 10(28): p. 1493-1501.
59. Maruko I, Iida T, et al. Morphologic choroidal and scle-ral changes at the macula in tilted disc syndrome with staphyloma using optical coherence tomography. Invest Ophthalmol Vis Sci. 2011; 12(52): p. 8763-8768.
Francisco Trincão

Vol. 39 - Nº 2 - Abril-Junho 2015 | 127
Paracentese diagnóstica da câmara anterior – como e quando?
Sofia Fonseca Assistente hospitalar de oftalmologia do Centro Hospitalar de Vila Nova de Gaia/Espinho
Flash Look
A análise do humor aquoso pode ser uma arma valiosa no estudo do doente com inflamação ocular, podendo dife-renciar uveítes infeciosas e não infeciosas , assim como identificar doença neoplásica. Trata-se de um procedi-mento simples e seguro, que poderá ser a chave de diag-nóstico quer em uveítes anteriores, quer em uveítes poste-riores. Contudo, o volume de humor aquoso que é possível colher é escasso (entre 100 a 200µl) e as análises são dis-pendiosas. Como tal, é necessário ser criterioso na seleção dos doentes e dos exames a realizar.
No âmbito da investigação científica, a análise do humor aquoso pode ser feita para muitos aspetos. No con-texto clínico, é de realçar que a análise do humor aquoso nos permite:
1. Diagnóstico de uveítes infeciosas – através da dete-ção de anticorpos e pesquisa de pequenas quanti-dade de DNA através de polymerase chain reaction (PCR). O material é escasso para cultura.
2. Diagnóstico de doença neoplásica, através da análise de células por citometria de fluxo.
MétodoAntes da recolha do humor aquoso, devem contactar-se
os laboratórios para onde se vai enviar a amostra. Em cada hospital, deve definir-se o método de colheita, a forma de preservação e o modo de transporte da amostra.
A colheita de humor aquoso pode ser feita no bloco operatório, utilizando os meios de desinfeção de uma cirur-gia intra-ocular (povidona iodada a 5%) e recorrendo ao uso de microscópio. O doente ficará deitado, realiza-se anestesia tópica (instilação de colírio de oxibuprocaína) e coloca-se blefarostato. Realiza-se incisão corneana, com lâmina 15, paralela à íris, junto ao limbo. A incisão deve parar imediatamente após a membrana de Descemet, sem perda de humor aquoso. Recolhe-se cerca de 100 a 200 µl de humor aquoso, aspirando com cânula 27 gauge para uma seringa sem heparina. Fecha-se com tampa de acesso arterial. Não é necessária dilatação pupilar1.
É possível realizar a colheita de humor aquoso na
lâmpada de fenda, fazendo a punção diretamente com uma agulha de 27 ou 30 gauge e aspirando. No entanto, os ris-cos de infeção e de tocar com a agulha no cristalino pode-rão ser superiores. Existe ainda disponível no mercado um dispositivo que poderá facilitar a técnica na lâmpada de fenda e que consiste na aspiração do humor aquoso com uma pipeta de aquoso desenhada por O’Rourke, após rea-lização da paracentese. No entanto, é necessário ter esse material disponível e continua a colocar-se a questão do maior risco infecioso.
Os riscos do procedimento incluem infeção, trauma-tismo da íris e do cristalino, embora os casos de complica-ções sérias sejam raros1, 2.
Não existem estudos que comparem a eficácia e a segu-rança dos diferentes métodos.
PCRA polymerase chain reaction (PCR) é uma análise de
biologia molecular que permite a deteção de DNA a partir de pequenas quantidades de material biológico. Trata-se de um exame simples, com elevada sensibilidade e especifi-cidade3,4. É útil em dilemas diagnósticos, com suspeita de toxoplasmose ou uveítes víricas.
Indicações:1. Uveítes posteriores – revelou-se útil em casos de
retinite, sobretudo em casos atípicos ou com opaci-dade de meios. Deverão ser pesquisados os vírus do grupo herpes, nomeadamente vírus herpes simples (HSV) 1 e 2, citomegalovírus (CMV), vírus vari-cela zóster (VZV) e o parasita Toxoplasma gondii. No entanto, também pode ser utilizado para outros microorganismos5,6,7.
2. Uveítes anteriores – nestes casos a utilidade parece ser inferior, uma vez que os casos positivos são escassos6. Sendo assim, a seleção dos casos é ainda mais crucial, devendo-se reservar a análise para casos atípicos e com suspeita de uveíte vírica, geral-mente herpes (uveíte hipertensiva, associada a atrofia da íris e com precipitados queráticos pigmentados).
Oftalmologia - Vol. 39: pp.127-128

128 | Revista da Sociedade Portuguesa de Oftalmologia
CitologiaNa suspeita de neoplasia intra-ocular, nomeadamente
de doenças linfoproliferativas, é possível fazer análise celular do humor aquoso9. Devem selecionar-se casos com células suspeitas na câmara anterior. A análise celu-lar deverá ser célere e a colheita e o transporte devem ser discutidos no próprio dia com o laboratório que vai reali-zar a análise, uma vez que as células são frágeis e escas-sas. No caso de o hospital não dispor de análise de cito-metria de fluxo, deve equacionar-se transferir o doente para realizar a paracentese diagnóstico no hospital onde se dispõe desta técnica.
Deve fazer-se a contagem diferencial de leucócitos e a quantificação e caracterização de linfócitos e plasmó-citos. A análise de citoquinas ainda não é realizada por rotina, em contexto clínico.
Em conclusão, a análise de humor aquoso pode ser muito valiosa e ser a chave do diagnóstico em algumas situações difíceis. Para otimizarmos resultados, devemos selecionar bem os doentes e a análise que devemos fazer, para cada caso. É também fundamental uma boa articula-ção entre o serviço de oftalmologia e os laboratórios de análises.
No futuro, poderão estar disponíveis na prática clínica outras análises com impacto no diagnóstico. A pesquisa de sequências específicas de DNA de bactérias por PCR poderá confirmar a presença de endoftalmite bacteriana em escassas horas e a determinação das citoquinas pre-sentes no humor aquoso, poderá indicar-nos não só o diagnóstico como até o alvo terapêutico.
REFERÊNCIAS
1. Van der Lelij A, Rothova A. Diagnostic anterior cham-ber paracentesis in uveitis: a safe procedure? Br J Ophthalmol. 1997 Nov;81(11):976-9.
2. Cheung CM, Durrani OM, Murray PI. The safety of anterior chamber paracentesis in patients with uveitis. Br J Ophthalmol. 2004 Apr;88(4):582-3.
3. Nandi K1, Ranjan P, Therese L, Biswas J. Polyme-rase chain reaction in intraocular inflammation. Open Ophthalmol J. 2008 Oct 22;2:141-5.
4. Van Gelder RN. Applications of the polymerase chain reaction to diagnosis of ophthalmic disease. Surv Ophthalmol. 2001 Nov-Dec;46(3):248-58.
5. Tran TH1, Rozenberg F, Cassoux N, Rao NA, LeHoang P, Bodaghi B. Polymerase chain reaction analysis of aqueous humour samples in necrotising retinitis. Br J Ophthalmol. 2003 Jan;87(1):79-83.
6. Rothova A, de Boer JH, Ten Dam-van Loon NH, et al. Usefulness of aqueous humor analysis for the diagnosis of posterior uveitis. Ophthalmology. 2008 Feb;115(2):306-11.
7. Van Gelder. Polymerase chain reaction diagnos-tics for posterior segment disease. Retina. 2003 Aug;23(4):445-52.
8. Anwar Z, Galor A, Albini TA, Miller D, Perez V, Davis JL. The diagnostic utility of anterior chamber paracen-tesis with polymerase chain reaction in anterior uveitis. Am J Ophthalmol. 2013 May;155(5):781-6.
9. Finger PT, Papp C, Latkany P, Kurli M, Iacob CE. Anterior chamber paracentesis cytology (cytospin tech-nique) for the diagnosis of intraocular lymphoma. Br J Ophthalmol. 2006 Jun;90(6):690-2.
Sofia Fonseca

Vol. 39 - Nº 2 - Abril-Junho 2015 | 129
Acidúria metilmalónica com homocistinúria, tipo cobalamina c: fenótipo oftalmológico
Ana Figueiredo1, Mafalda Macedo2,7, Vasco Miranda3, Ricardo Parreira4, Salomé Gonçalves5, Pedro Menéres6,7
1Interna de Formação Específica em Oftalmologia do Centro Hospitalar do Porto, EPE (CHP)2Assistente Hospitalar do Centro Hospitalar do Porto, EPE3Assistente Hospitalar do Centro Hospitalar do Porto, EPE4Assistente Hospitalar do Centro Hospitalar do Porto, EPE
5Ex-Chefe de Serviço de Oftalmologia do Hospital Central Especializado de Crianças Maria Pia6Assistente Hospitalar Sénior do Centro Hospitalar do Porto, EPE
7Instituto de Ciências Biomédicas de Abel Salazar da Universidade do Porto (ICBAS- UP)Hospital de Santo António - Centro Hospitalar do Porto, EPE
Director de Serviço: Dr. Pedro Menéres
RESUMO
Introdução: A acidúria metilmalónica com homocistinúria constitui um distúrbio genético raro resultando da conversão deficiente da vitamina B12 proveniente da dieta nas suas formas me-tabolicamente activas. Caracteriza-se por atraso de desenvolvimento, alterações hematológicas, disfunção neurológica, maculopatia progressiva e, por vezes, atrofia do nervo óptico. Caso clínico: Os autores apresentam o caso clínico de uma criança de sexo masculino, internada aos 27 dias de vida em estado comatoso, tendo sido feito o diagnóstico de acidúria metilmaló-nica com homocistinúria, tipo cobalamina C. Desde então, mantém-se medicado com vitamina B12, suplementos de betaína, carnitina e cumpre restrições dietéticas rigorosas. Aos 7 meses de idade identificou-se um nistagmo manifesto pendular horizontal de baixa amplitude e frequência rápida. No primeiro ano de vida era capaz de seguir e fixar objectos, não havendo alterações fundoscópicas. Durante o segundo ano de vida desenvolveu uma lesão arredondada e amarela-da circunscrita à fóvea bilateralmente. A lesão aumentou progressivamente adquirindo um tom acinzentado, com áreas periféricas de pigmentação em formato de espículas ósseas. Com a pro-gressão da maculopatia a criança desenvolveu uma fixação extrafoveal, bem definida por volta dos seis anos, com aparente preservação do campo visual periférico. Os autores apresentam as fotografias, retinografias e o estudo electrofisiológico ocular na documentação do caso. Conclusão: A acidúria metilmalónica com homocistinúria de início precoce surge quase sem-pre associada a manifestações oftalmológicas. O tratamento preconizado visa aumentar os níveis de metionina, e muito embora se acredite que este possa restabelecer a sensibilidade normal dos fotorreceptores, não reverte a maculopatia ou a resposta retiniana anómala. Com efeito, a observação oftalmológica assume-se mandatória a fim de tentar assegurar que o me-lhor potencial visual seja atingido. Por outro lado, muito embora seja uma entidade de ocorrên-cia rara torna-se crucial que o Oftalmologista tenha presente esta patologia nos diagnósticos diferenciais das maculopatias infantis.
Palavras-chaveAcidúria metilmalónica, homocistinúria, maculopatia infantil, fenótipo ocular.
Comunicações Curtas e Casos Clínicos
Oftalmologia - Vol. 39: pp.129-136
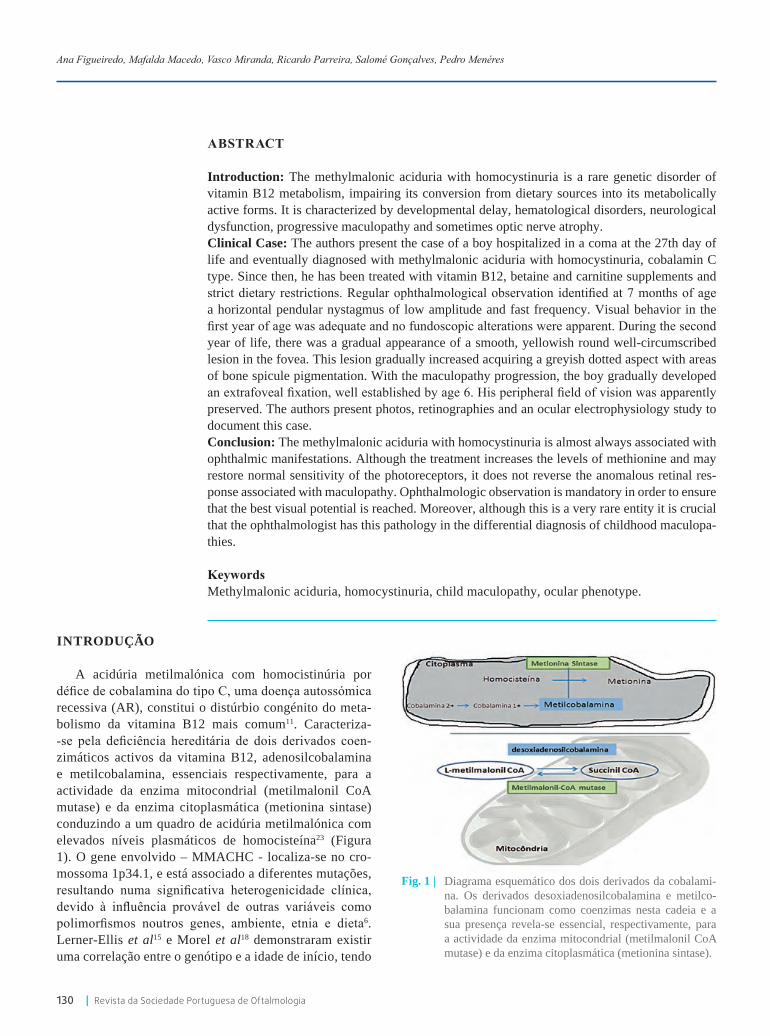
130 | Revista da Sociedade Portuguesa de Oftalmologia
ABSTRACT
Introduction: The methylmalonic aciduria with homocystinuria is a rare genetic disorder of vitamin B12 metabolism, impairing its conversion from dietary sources into its metabolically active forms. It is characterized by developmental delay, hematological disorders, neurological dysfunction, progressive maculopathy and sometimes optic nerve atrophy.Clinical Case: The authors present the case of a boy hospitalized in a coma at the 27th day of life and eventually diagnosed with methylmalonic aciduria with homocystinuria, cobalamin C type. Since then, he has been treated with vitamin B12, betaine and carnitine supplements and strict dietary restrictions. Regular ophthalmological observation identified at 7 months of age a horizontal pendular nystagmus of low amplitude and fast frequency. Visual behavior in the first year of age was adequate and no fundoscopic alterations were apparent. During the second year of life, there was a gradual appearance of a smooth, yellowish round well-circumscribed lesion in the fovea. This lesion gradually increased acquiring a greyish dotted aspect with areas of bone spicule pigmentation. With the maculopathy progression, the boy gradually developed an extrafoveal fixation, well established by age 6. His peripheral field of vision was apparently preserved. The authors present photos, retinographies and an ocular electrophysiology study to document this case. Conclusion: The methylmalonic aciduria with homocystinuria is almost always associated with ophthalmic manifestations. Although the treatment increases the levels of methionine and may restore normal sensitivity of the photoreceptors, it does not reverse the anomalous retinal res-ponse associated with maculopathy. Ophthalmologic observation is mandatory in order to ensure that the best visual potential is reached. Moreover, although this is a very rare entity it is crucial that the ophthalmologist has this pathology in the differential diagnosis of childhood maculopa-thies.
Keywords Methylmalonic aciduria, homocystinuria, child maculopathy, ocular phenotype.
INTRODUÇÃO
A acidúria metilmalónica com homocistinúria por défice de cobalamina do tipo C, uma doença autossómica recessiva (AR), constitui o distúrbio congénito do meta-bolismo da vitamina B12 mais comum11. Caracteriza--se pela deficiência hereditária de dois derivados coen-zimáticos activos da vitamina B12, adenosilcobalamina e metilcobalamina, essenciais respectivamente, para a actividade da enzima mitocondrial (metilmalonil CoA mutase) e da enzima citoplasmática (metionina sintase) conduzindo a um quadro de acidúria metilmalónica com elevados níveis plasmáticos de homocisteína23 (Figura 1). O gene envolvido – MMACHC - localiza-se no cro-mossoma 1p34.1, e está associado a diferentes mutações, resultando numa significativa heterogenicidade clínica, devido à influência provável de outras variáveis como polimorfismos noutros genes, ambiente, etnia e dieta6. Lerner-Ellis et al15 e Morel et al18 demonstraram existir uma correlação entre o genótipo e a idade de início, tendo
Ana Figueiredo, Mafalda Macedo, Vasco Miranda, Ricardo Parreira, Salomé Gonçalves, Pedro Menéres
Fig. 1 | Diagrama esquemático dos dois derivados da cobalami-na. Os derivados desoxiadenosilcobalamina e metilco-balamina funcionam como coenzimas nesta cadeia e a sua presença revela-se essencial, respectivamente, para a actividade da enzima mitocondrial (metilmalonil CoA mutase) e da enzima citoplasmática (metionina sintase).

Vol. 39 - Nº 2 - Abril-Junho 2015 | 131
ainda identificado um efeito fundador das mutações entre determinadas etnias. A doença tem sido classificada em duas formas com base na idade de início: de início pre-coce (infantil) e de início tardio (não infantil). A forma de início precoce caracteriza-se pelo aparecimento dos sintomas antes do primeiro ano de idade, por atingimento sistémico grave cujo espectro clínico inclui dificuldade na alimentação, défices de crescimento, atraso de desen-volvimento, hipotonia, crises convulsivas, anemia mega-loblástica, trombocitopenia, neutropenia e microangio-patia11,12,23. A doença de início tardio manifesta-se após o primeiro ano de vida caracterizando-se por disfunções neurológicas como défice cognitivo, anomalias da mar-cha, sintomas extrapiramidais, distúrbios psiquiátricos e degenerescência subaguda da espinal medula, mas sem expressão em termos retinianos3,11,12,28. O rastreio precoce dos recém-nascidos permite a detecção de casos muitas vezes antes do início dos sintomas e a instituição ime-diata de tratamento. O tratamento sistémico da doença inclui tipicamente compostos como a hidroxicobalamina, betaína, suplementação vitamínica e carnitina11.
O atingimento oftalmológico pode ser significativo e inclui redução da acuidade visual (AV), estrabismo, nis-tagmo e doença retiniana progressiva (que varia desde uma diminuição ligeira da espessura da camada de fibras nervosas até situações de atrofia macular e óptica com pig-mentação em padrão de “espículas ósseas”9. Estas altera-ções ocorrem habitualmente na forma de doença de início precoce e raramente naqueles com doença de início tardio.
Um número limitado de relato de casos ou estudos longitudinais incidindo no envolvimento oftalmológico associado a esta doença foi publicado até à actualidade1,8,
10,13,17,19,21,22,24,27, 29.
CASO CLíNICO
Menino nascido às 40 semanas de gestação por parto eutócico sem complicações, Apgar de 9 ao primeiro minuto e 10 ao quinto minuto (9/10) e peso ao nascer de 2700g. À data da gravidez a mãe tinha 28 anos e o pai 32 anos, eram ambos saudáveis e sem relação de consangui-nidade. Tinham um filho mais velho saudável.
Aos 27 dias de vida é admitido no serviço de urgên-cia por insuficiência respiratória, hipotonia, encefalo-patia, hipotermia, desnutrição, desidratação e ausência de resposta a estímulos. Os exames complementares de diagnóstico efetuados revelaram acidose metabólica, anemia megaloblástica, neutropenia, trombocitopenia e disfunção hepática. Analiticamente apresentava também
um aumento dos níveis plasmáticos de homocisteína e presença de ácido metilmalónico na urina. A Tomogra-fia computorizada (TC) cerebral, a ressonância magnética (RM) e a ecografia transfontanelar após o nascimento não revelaram alterações de relevo. O exame oftalmológico efectuado nesta altura não apresentava alterações. Diver-sos exames foram realizados para investigação etiológica sendo de destacar o estudo genético, o qual permitiu con-cluir tratar-se de um caso de acidúria metilmalónica com homocistinúria do tipo cobalamina C – homozigotia para a mutação.271dupA (p.R91Kfs*14) no gene MMACHC.
Foi iniciado um esquema terapêutico específico que incluiu injecções intramusculares de hidroxicobalamina, suplementação com carnitina, betaína e folato oral bem como implementado um rigoroso plano de restrição pro-teica. Os marcadores bioquímicos são desde então monito-rizados semestralmente o que permite um ajuste concertado destas diferentes variáveis. Em termos de crescimento o rapaz cruzou percentis de forma descendente, mantendo-se actualmente estável, apresentando ainda défice intelectual e microcefalia. Mantém seguimento multidisciplinar em consultas de Pediatria, Cirurgia Pediátrica, Oftalmologia, Neurologia e Cardiologia Pediátrica.
Aos 3 anos foi-lhe diagnosticada epilepsia, estando actualmente medicado com valproato de sódio, mantendo--se sem crises convulsivas desde 2009. Foi-lhe ainda docu-mentada uma dilatação ligeira e não progressiva da raiz da aorta, pelo que está medicado com atenolol; o último eco-cardiograma realizado evidenciava um coração estrutural e funcionalmente sem alterações relevantes. Aos 8 anos foi detectada criptorquidia, motivo pelo qual foi cirurgica-mente intervencionado e mantém seguimento em consulta de Cirurgia Pediátrica.
Em termos oftalmológicos o exame efectuado ao nas-cimento e aos 2 meses de vida não revelou alterações de relevo. Contudo, aos 7 meses foi identificado nistagmo manifesto pendular horizontal rápido e de baixa amplitude. Aos 2 anos, o nistagmo mantinha as mesmas características, fixava e seguia os objectos, os reflexos pupilares estavam presentes e eram simétricos, com retinoscopia cicloplégica (sob atropina) de +1.00 D. Bilateralmente, o exame fundos-cópico revelava a presença de uma área de atrofia do epitélio pigmentado da retina (EPR) envolvendo a fóvea e ocupando a parte inferior da mácula com restante retina e papila sem alterações. Aos 5 anos foi pela primeira vez observada uma exotropia alternante com preferência de fixação do olho esquerdo e ângulo variável. A retinoscopia cicloplégica (atropiníca) era nessa altura de +2.75 D bilateralmente. Aos 6 anos a exotropia mantinha características semelhantes mas tornou-se evidente um padrão de fixação extrafoveal. A
Acidúria metilmalónica com homocistinúria, tipo cobalamina c: fenótipo oftalmológico

132 | Revista da Sociedade Portuguesa de Oftalmologia
retinoscopia cicloplégica (atropínica) bilateralmente era de +3.00+1.00x180º; a melhor acuidade visual para longe obtida em binocularidade foi de 3/10 (Snellen). Na fun-doscopia era de destacar a ausência de alterações do disco óptico, com presença de alterações pigmentares da retina que compreendiam a área papilomacular e as arcadas que a limitam; a lesão era amarela, ovalada com dimen-são próxima de metade do disco óptico; a restante retina tinha coloração ligeiramente acinzentada. Aos 8 anos
era evidente um défice visual central grave; no entanto apesar deste défice central a orientação espacial era boa: caminhava, subia e descia escadas com facilidade. Não apresentava queixas de nictalopia, fotofobia ou hemera-lopia. Aos 13 anos a acuidade visual mantém-se difícil de obter e pouco fiável dado o atraso em termos de desen-volvimento cognitivo. As características do nistagmo e o comportamento visual permaneciam inalterados (Figura 2 A-D). O fundo ocular apresenta as características já
Fig. 2 | A: Padrão de fixação extrafoveal; B: boa orientação espacial na caminhada; C-D: baixa visão central.
A
B
C D
Fig. 3 | Retinografia do olho direito evidenciando palidez do disco óptico, atrofia macular exibindo um aspecto de aglomeração pigmen-tar placóide central e retina periférica em padrão de espículas ósseas.
Fig. 4 | Retinografia do olho esquerdo evidenciando palidez do disco óptico, atrofia macular exibindo um aspecto de aglomeração pig-mentar placóide central e retina periférica em padrão de espículas ósseas.
Ana Figueiredo, Mafalda Macedo, Vasco Miranda, Ricardo Parreira, Salomé Gonçalves, Pedro Menéres

Vol. 39 - Nº 2 - Abril-Junho 2015 | 133
descritas, acrescentando ainda a presença de vasos reti-nianos maculares atenuados e pigmentação em padrão de espículas ósseas na média periferia (Figura 3 e 4). Foi efectuada eletrorretinografia de campo total com elé-trodos cutâneos segundo as recomendações do ISCEV (International Society for Clinical Electrophysiology of Vision), após midríase farmacológica com tropicamida e fenilefrina (diâmetro pupilar 9 mm) que evidenciou uma diminuição moderadamente grave de amplitude das ondas a e b e atraso da sua latência, quer em condições escotópicas, quer em condições fotópicas, o que é com-patível com uma disfunção generalizada moderadamente grave da retina a nível dos fotorreceptores. Estas altera-ções deverão posteriormente ser confirmadas através da realização de ERG de campo total com eléctrodos de folha de ouro, quando a colaboração do doente assim o permitir (Figura 5).
DISCUSSÃO
A acidúria metilmalónica com homocistinúria de tipo cobalamina C constitui um distúrbio AR do metabolismo da vitamina B12 que afecta múltiplos sistemas de órgãos, incluindo o sistema visual, mesmo com a instituição de um tratamento precoce.
Há que referir que um pequeno volume de casos está reportado em todo o mundo, havendo poucos dados publi-cados no que se refere à evolução oftalmológica a longo prazo. Um total de 22 casos com alterações oftalmológi-cas documentadas foi descrito na literatura11,19, 21 22, 24, 27, 29.
O fenótipo ocular relacionado com esta doença é extre-mamente variado, parecendo estar intimamente relacionado com a idade de início. A sua avaliação é particularmente desafiante face aos défices cognitivos que alguns destes casos podem apresentar. No que respeita à acuidade visual,
Fig. 5 | Electroretinograma (EGG) de campo total.
Acidúria metilmalónica com homocistinúria, tipo cobalamina c: fenótipo oftalmológico

134 | Revista da Sociedade Portuguesa de Oftalmologia
esta é extremamente variável, variando de percepção lumi-nosa até aos 10/1011,12. Em termos de erros refractivos, o espectro é igualmente amplo, contemplando casos de hiper-metropia entre hipermetropia (+1.25 a +5.0 D) e miopia elevada (-10.0 D)11.
As características morfológicas da maculopatia são tam-bém heterogéneas: desde maculopatia em alvo até diferen-tes padrões de alterações pigmentares e atróficas da retina, vários foram já descritos11, constituindo elementos úteis e muitas vezes cruciais para o diagnóstico definitivo da doença. Quando ocorre maculopatia esta geralmente surge muito precocemente e é provável que se desenvolva antes do nascimento, ao invés do que sucede com outras maculo-patias hereditárias cujo aparecimento se faz em idades mais tardias9. A mutação identificada neste doente aparece asso-ciada a AV muito reduzida em casos idênticos publicados na literatura, estando ainda relacionada com situações de maculopatia grave e atrofia óptica1,11,17.
No caso descrito coexistem além da maculopatia, alte-rações pigmentares periféricas. Foi ainda identificado nis-tagmo e palidez papilar moderada (referidos mais rara-mente na literatura)20,30. Segundo alguns autores, a palidez do disco pode ser explicada pela presença simultânea de algum grau de retinopatia pigmentar12. Outros sugerem que a anormal formação ou perda de mielina que caracteri-zam esta entidade possa contribuir para a palidez do nervo óptico5,12. A Deficiência de S-adenosilmetionina (SAM), o principal substrato em muitas reacções de metilação, tem sido apontado como contribuindo para a desmielinização em pacientes com defeitos de metilação26.
Foi ainda identificada no nosso caso a presença de estrabismo, como já descrito anteriormente em algumas séries de casos12.
O ERG de campo total que revelou disfunção gene-ralizada do tipo cones-bastonetes tanto na resposta fotó-pica quanto escotópica. Segundo vários autores a dete-rioração do ERG ocorre precocemente e vai evoluindo de forma progressiva afectando cones e bastonetes10,11,22,24. Ao mesmo tempo, no que se remete à sua história natural estudos apontam para uma degenerescência progressiva da retina que se inicia nos primeiros meses de vida e pro-gride rapidamente ao longo dos primeiros anos de vida24. Num estudo conduzido por Gaillard e colaboradores10 não se estabeleceu qualquer correlação entre a aparência do fundo de olho e o tipo de disfunção de fotorrecepto-res. Já a microscopia electrónica evidenciou inclusões granulares finas nas células ganglionares da retina e do epitélio pigmentar bem como mitocôndrias de tamanho aumentado compondo os fotorreceptores27. Assim sendo, acredita-se mais que esta doença seja responsável por uma
degenerescência retiniana progressiva ao invés da hipótese da existência de base de um desenvolvimento retiniano deficitário24. Contudo, a patogénese da doença retiniana permanece mal esclarecida. É possível que a proteína MMACHC possa desempenhar um papel específico nos tecidos oculares5. No entanto, a ausência de uma forma característica de retinopatia e maculopatia em pacientes com outras formas de acidúria metilmalónica e na maioria dos defeitos da metilação sugere um mecanismo fisiopa-tológico distinto. Por oposição, uma das teorias existentes aponta para que esta degenerescência retiniana progressiva possa resultar dos baixos níveis de metionina associados à acidúria metilmalónica com homocistinúria24,29. A metio-nina condiciona a produção de baixos níveis de glutationa, um importante protector de stress oxidativo do EPR25. Todavia, apesar do tratamento utilizado restabelecer a sen-sibilidade normal dos fotorreceptores (principalmente dos bastonetes), este não reverte a maculopatia ou as respostas retinianas anómalas já estabelecidas29. O tratamento pré ou pós-natal desta entidade também parece não prevenir o desenvolvimento de nistagmo ou retinopatia14.
Apesar dos níveis de homocisteína elevados serem uma importante característica desta doença, casos de ectopia lentis não foram até agora descritos, contrastando com a homocistinúria clássica (défice enzimático da cistatiotina β sintase) na qual a luxação do cristalino se assume como um achado típico12.
A acidúria metilmalónica com homocistinúria associada a défice de cobalamina tipo C é apenas diagnosticada atra-vés de rastreio em alguns países2. A referenciação de doen-tes com lesões oftalmológicas suspeitas permitirá a rápida intervenção dietética e farmacológica6. Uma intervenção precoce possibilita obter melhorias a nível do crescimento, status neurológico e hematológico, muito embora não tenha sido documentado até ao presente qualquer efeito no curso da doença oftalmológica5. Na verdade, alguns doen-tes parecem apresentar alguma resposta ao tratamento16 muito embora, em termos de saúde global, este pareça não oferecer benefícios significativos5. Por outro lado, a even-tual descoberta dos verdadeiros factores responsáveis pela degenerescência retiniana poderá abrir portas ao desenvol-vimento de uma terapêutica eficaz.
Com efeito, a acidúria metilmalónica com homocisti-núria representa uma entidade menos conhecida no seio da Oftalmologia correspondendo a uma das possíveis causas de maculopatia na infância.
O fenótipo ocular assume-se extremamente variável, estando a sua gravidade correlacionada com a idade de iní-cio da doença e com um importante envolvimento oftalmo-lógico descrito nas formas de início precoce11. No entanto,
Ana Figueiredo, Mafalda Macedo, Vasco Miranda, Ricardo Parreira, Salomé Gonçalves, Pedro Menéres

Vol. 39 - Nº 2 - Abril-Junho 2015 | 135
o escasso número de casos na literatura contemplando uma descrição detalhada da função visual não permitem ainda estabelecer uma correlação genótipo-fenótipo11,12.
Neste contexto, a monitorização oftalmológica destes doentes é fundamental para garantir que o melhor potencial visual seja atingido. É também muito importante a integra-ção destas crianças em programas de intervenção precoce a fim de compensar o défice visual na sua aprendizagem e desenvolvimento psicomotor.
Apesar de ser uma entidade de ocorrência rara é impor-tante que o Oftalmologista tenha presente esta patologia no seio do leque de diagnósticos diferenciais das maculopatias infantis.
REFERÊNCIAS
1. Andersson HC, Shapira E. Biochemical and clinical response tohydroxocobalamin versus cyanocobalamin treatment in patients with methylmalonic acidemia and homocystinuria (cblC). J Pediatr 1998; 132:121-4.
2. Auray-Blais C, Cyr D, Drouin R. Quebec neonatal mass urinary screening programme: from micromole-cules to macromolecules. J Inherit Metab Dis 2007;30: 515–21.
3. Ben-Omran TI, Wong H, Blaser S, Feigenbaum A. Late-onset cobalamin-C disorder: A challenging diag-nosis. Am J Med Genet 2007; 143A:979-84.
4. Bodamer OA, Sahoo T, Beaudet AL, O’Brien WE, Bot-tiglieri T, Stockler-Ipsiroglu S, Wagner C, Scaglia F. Creatine metabolism in combined methylmalonic acidu-ria and homocystinuria. Ann Neurol. 2005;57:557–560
5. Carrillo-Carrasco N, Charles P. Venditti C P .Combi-ned methylmalonic acidemia and homocystinuria, cblC type. II. Complications, pathophysiology, and outco-mes. J Inherit Metab Dis. 2012 Jan; 35(1): 103–114.
6. Carrillo-Carrasco N, Chandler RJ, Venditti CP. Combi-ned methylmalonic acidemia and homocystinuria, cblC type. I. Clinical presentations, diagnosis and manage-ment. J Inherit Metab Dis 2012; 35:91–102.
7. Debray FG, Boulanger Y, Khiat A, Decarie JC, Orquin J, Roy MS, Lortie A, Ramos F, Verhoeven NM, Struys E, Blom HJ, Jakobs C, Levy E, Mitchell GA, Lambert M. Reduced brain choline in homocystinuria due to remethylation defects. Neurology. 2008;71:44–49
8. Francis J H, Rao L, Rosen R B; Methylmalonic acidu-ria and homocystinuria-associated maculopathy. Eye (2010) 24, 1731–1732;
9. Fuchs LR, Robert M, Ingster-Moati I, et al.
Ocular manifestations of cobalamin C type methylma-lonic aciduria with homocystinuria. J AAPOS. 2012 Aug;16(4):370-5
10. Gaillard MC, Matthieu JM, Borruat FX. Retinal dys-function in combined methylmalonic aciduria and homocystinuria (Cblc) disease: a spectrum of disorders. Klin Monbl Augenheilkd. 2008;225:491–494
11. Gerth C, Morel CF, Feigenbaum A, Levin AV. Ocu-lar phenotype in patients with methylmalonic aciduria and homocystinuria, cobalamin C type. J AAPOS. 2008 Dec;12(6):591-6
12. Gizicki R, Robert MC, Gómez-López L, et al. Long--term visual outcome of methylmalonic aciduria and homocystinuria, cobalamin C type. Ophthalmology. 2014 Jan;121(1):381-6
13. Grant LW, McCandless SE, Traboulsi EI. Maculopathy due to cobalamin C (cblC) disease in an Amish child. J Pediatr Ophthalmol Strabismus 2009; Oct 2:1–3.
14. Huemer M, Simma B, Fowler B, Suormala T, Bodamer OA, Sass JO.Prenatal and postnatal treatment in cobala-min C defect. J Pediatr. 2005;147:469-72.
15. Lerner-Ellis JP, Tirone JC, Pawelek PD, Dore C, Atkin-son JL, Watkins D, et al. Identification of the gene res-ponsible for methylmalonic aciduria and homocystinu-ria, cblC type. Nat Genet 2006; 38:93-100.
16. Lin HJ, Neidich JA, Salazar D, et al. Asymptomatic maternal combined homocystinuria and methylmalonic aciduria (cblC) detected through low carnitine levels on newborn screening. J Pediatr 2009; 155:924–7.
17. Mitchell GA, Watkins D, Melancon SB, Rosenblatt DS, Geoffroy G, Orquin J, et al. Clinical heterogeneity in cobalamin C variant of combined homocystinuria and methylmalonic aciduria. J Pediatr 1986;108: 410-5.
18. Morel CF, Lerner-Ellis JP, Rosenblatt DS. Combined methylmalonic aciduria and homocystinuria (cblC): Phenotype-genotype correlationsand ethnic-specific observations. Mol Genet Metab 2006; 88:315-21.
19. Patton N, Beatty S, Lloyd IC, Wraith JE. Optic atro-phy in association with cobalamin C (cblC) disease. Ophthalmic Genet 2000; 21:151-4.
20. Pinar-Sueiro S, Martinez-Fernandez R, Lage-Medina S, Aldamiz-Echevarria L, Vecino E. Optic neuropathy in methylmalonic acidemia: the role of neuroprotection. J Inherit Metab Dis. 2010
21. Ricci D, Pane M, Deodato F, Vasco G, Rando T, Cavi-glia S, et al. Assessment of visual function in children with methylmalonic aciduria and homocystinuria. Neu-ropediatrics 2005; 36:181-5.
22. Robb RM, Dowton SB, Fulton AB, Levy HL. Retinal degeneration in vitamin B12 disorder associated with
Acidúria metilmalónica com homocistinúria, tipo cobalamina c: fenótipo oftalmológico

136 | Revista da Sociedade Portuguesa de Oftalmologia
methylmalonic aciduria and sulfur amino acid abnor-malities. Am J Ophthalmol 1984; 97:691-6.
23. Rosenblatt DS, Fenton WA. Inherited disorders of folate and cobalamin transport and metabolism. In: Scriver CR, Beaudet AF, Sly WS, Valle D, editors. The Meta-bolic and Molecular Bases of Inherited Disease. New York: McGraw-Hill; 2001. p. 3897-933.
24. Schimel AM, Mets MB. The natural history of retinal degeneration in association with cobalamin C (cbl C) disease. Ophthalmic Genet 2006;27:9-14.
25. Sternberg P Jr, Davidson P, Jones DP, et al. Protection of retinal pigment epithelium from oxidative injury by glutathione and precursors. Invest Ophthalmol Vis Sci 1993; 34:3361–8.
26. Surtees R. Demyelination and inborn errors of the sin-gle carbon transfer pathway. Eur J Pediatr. 1998; 157 (Suppl 2):S118–S121.
27. Traboulsi EI, Silva JC, Geraghty MT, Maumenee IH, Valle D,Green WR. Ocular histopathologic charac-teristics of cobalamin C type vitamin B12 defect with methylmalonic aciduria and homocystinuria. Am J Ophthalmol 1992; 113:269-80.
28. Tsai AC, Morel CF, Scharer G, Yang M, Lerner-Ellis JP, Rosenblatt DS, et al. Late-onset combined homocystinuria
and methylmalonic aciduria (cblC) and neuropsychiatric disturbance. Am J Med Genet 2007;143 A:2430-4
29. Tsina EK, Marsden DL, Hansen RM, Fulton AB. Maculopathy and retinal degeneration in cobalamin C methylmalonic aciduria and homocystinuria. Arch Ophthalmol. 2005 Aug;123(8):1143-6.
30. Williams ZR, Hurley PE, Altiparmak UE, Feldon SE, Arnold GL, Eggenberger E, Mejico LJ. Late onset optic neuropathy in methylmalonic and propionic acidemia. Am J Ophthalmol. 2009;147:929– 933.
Todos os autores declaram não haver qualquer conflito de interesse, assumem que este trabalho científico nunca foi publicado e cedem os direitos de autor à Sociedade Portuguesa de Oftalmologia
CONTACTOAna FigueiredoHospital de Santo António - Centro Hospitalar do Porto, EPEServiço de OftalmologiaLargo Professor Abel Salazar – Edifício Neoclássico4099-001 PortoE-mail: [email protected]
Ana Figueiredo, Mafalda Macedo, Vasco Miranda, Ricardo Parreira, Salomé Gonçalves, Pedro Menéres

Vol. 39 - Nº 2 - Abril-Junho 2015 | 137
Retinal angiogenesis arrest in a full term infant with congenital toxoplasmosis
Cristina Santos1, Mário Ramalho1, Catarina Pedrosa1, Inês Coutinho1, Marta Ferreira2, Maria João Brito2, Susana Teixeira1
1Ophthalmology Department Hospital Prof. Doutor Fernando Fonseca, EPE2Pediatrics Department Hospital Prof. Doutor Fernando Fonseca, EPE
RESUMO
Apresentamos um caso de toxoplasmose congénita, numa criança de termo, com área de retina avascular na vizinhança de lesões de retinocoroidite. Admitimos que um estímulo antiangio-génico in utero possa ter interrompido o desenvolvimento normal dos vasos retinianos.
Palavras-chaveToxoplasmose congénita, retinocoroidite, angiogénese, neovascularização.
ABSTRACT
We report the finding of avascular retina in the vicinity of toxoplasmosis retinochoroiditis le-sions in a full term infant. We postulate that an antiangiogenic stimulus in utero might have interrupted normal retinal vessel growth.
Keywords Congenital toxoplasmosis, retinochoroiditis, angiogenesis, neovascularization.
Comunicações Curtas e Casos Clínicos
Oftalmologia - Vol. 39: pp.137-138
INTRODUCTION
Congenital toxoplasmosis results from transplacental passage of the parasite Toxoplasma gondii from an infected mother to the foetus. These children are often assymptoma-tic at birth1 but the majority of them will develop severe complications such as chorioretinitis, blindness, hydroce-phalus, microcephaly, psychomotor or mental retardation, epilepsy or deafness months to years later2.
CASE DESCRIPTION
A full term infant born from non-consanguinous parents was referred to our hospital with the diagnosis of severe congenital toxoplasmosis. Pre-natal care revealed maternal seroconversion for toxoplasmosis at 18 weeks gestational age (GA) (IgM > 40 IU/mL, IgG > 7000 IU/mL). Treatment
was delayed, and spiramycin was started at 28 weeks GA. Fetal ultrasound revealed moderate bilateral ventriculo-megalia and brain calcifications, confirmed by fetal brain--Magnetic Ressonance Imaging (MRI) at 30 weeks gesta-cional age.
Birth at 39 weeks GA from an uneventfull vaginal delivery, with birthweight of 2122g (percentile <5) and head circumference of 33 cm (percentile 10). Follow up was made in another center and anti-toxoplasma medica-tion was not started at birth. The diagnosis of congenital toxoplasmosis was made at 10 months of age. He presen-ted microcephaly (head circumference <5th percentile), inferior member hypertonia and left hemiparesis. Serology for toxoplasmosis IgG 240 IU/mL and negative IgM. Brain MRI showed multiple parenchymal nodular calcifications and mild ventricular dilation. No organomegalia on abdo-minal ultrasound. Specific toxoplasmosis treatment was started with pyrimethamine, sulfadiazine and folinic acid.
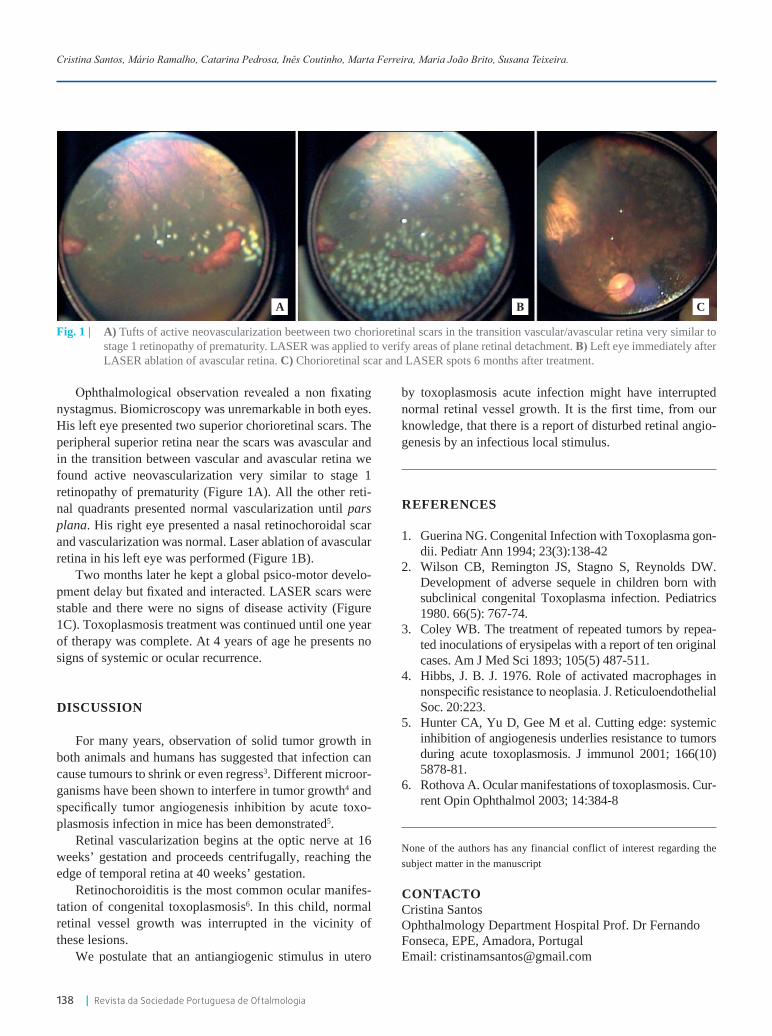
138 | Revista da Sociedade Portuguesa de Oftalmologia
Ophthalmological observation revealed a non fixating nystagmus. Biomicroscopy was unremarkable in both eyes. His left eye presented two superior chorioretinal scars. The peripheral superior retina near the scars was avascular and in the transition between vascular and avascular retina we found active neovascularization very similar to stage 1 retinopathy of prematurity (Figure 1A). All the other reti-nal quadrants presented normal vascularization until pars plana. His right eye presented a nasal retinochoroidal scar and vascularization was normal. Laser ablation of avascular retina in his left eye was performed (Figure 1B).
Two months later he kept a global psico-motor develo-pment delay but fixated and interacted. LASER scars were stable and there were no signs of disease activity (Figure 1C). Toxoplasmosis treatment was continued until one year of therapy was complete. At 4 years of age he presents no signs of systemic or ocular recurrence.
DISCUSSION
For many years, observation of solid tumor growth in both animals and humans has suggested that infection can cause tumours to shrink or even regress3. Different microor-ganisms have been shown to interfere in tumor growth4 and specifically tumor angiogenesis inhibition by acute toxo-plasmosis infection in mice has been demonstrated5.
Retinal vascularization begins at the optic nerve at 16 weeks’ gestation and proceeds centrifugally, reaching the edge of temporal retina at 40 weeks’ gestation.
Retinochoroiditis is the most common ocular manifes-tation of congenital toxoplasmosis6. In this child, normal retinal vessel growth was interrupted in the vicinity of these lesions.
We postulate that an antiangiogenic stimulus in utero
by toxoplasmosis acute infection might have interrupted normal retinal vessel growth. It is the first time, from our knowledge, that there is a report of disturbed retinal angio-genesis by an infectious local stimulus.
REFERENCES
1. Guerina NG. Congenital Infection with Toxoplasma gon-dii. Pediatr Ann 1994; 23(3):138-42
2. Wilson CB, Remington JS, Stagno S, Reynolds DW. Development of adverse sequele in children born with subclinical congenital Toxoplasma infection. Pediatrics 1980. 66(5): 767-74.
3. Coley WB. The treatment of repeated tumors by repea-ted inoculations of erysipelas with a report of ten original cases. Am J Med Sci 1893; 105(5) 487-511.
4. Hibbs, J. B. J. 1976. Role of activated macrophages in nonspecific resistance to neoplasia. J. Reticuloendothelial Soc. 20:223.
5. Hunter CA, Yu D, Gee M et al. Cutting edge: systemic inhibition of angiogenesis underlies resistance to tumors during acute toxoplasmosis. J immunol 2001; 166(10) 5878-81.
6. Rothova A. Ocular manifestations of toxoplasmosis. Cur-rent Opin Ophthalmol 2003; 14:384-8
None of the authors has any financial conflict of interest regarding the subject matter in the manuscript
CONTACTOCristina SantosOphthalmology Department Hospital Prof. Dr Fernando Fonseca, EPE, Amadora, Portugal Email: [email protected]
Cristina Santos, Mário Ramalho, Catarina Pedrosa, Inês Coutinho, Marta Ferreira, Maria João Brito, Susana Teixeira.
Fig. 1 | A) Tufts of active neovascularization beetween two chorioretinal scars in the transition vascular/avascular retina very similar to stage 1 retinopathy of prematurity. LASER was applied to verify areas of plane retinal detachment. B) Left eye immediately after LASER ablation of avascular retina. C) Chorioretinal scar and LASER spots 6 months after treatment.
A B C

Vol. 39 - Nº 2 - Abril-Junho 2015 | 139
Chorioretinal atrophy in a patient with Buerger’s disease
André Marques1, Joana Portelinha1, Ana Almeida1, Marta Guedes1,2
1Egas Moniz Hospital (Lisbon, Portugal)2Head of the Uveitis Department, Egas Moniz Hospital (Lisbon, Portugal)
RESUMO
A doença de Buerger é uma vasculopatia inflamatória oclusiva que afecta os vasos de pequeno e médio calibre, sobretudo arteriais, das extremidades e que está associada ao tabagismo. O envolvimento visceral é pouco frequente e as complicações oculares são ainda mais raras, even-tualmente caracterizadas por oclusões vasculares retinianas.Reportamos o caso de um doente com doença de Buerger com diversas complicações sistémicas associadas que se apresentou com diminuição progressiva e bilateral da acuidade visual. À ob-servação oftalmológica, registou-se uma atrofia coriorretiniana difusa em ambos os olhos com marcado prolongamento do tempo braço-retina na angiografia fluoresceínica. O doente negou quaisquer antecedentes familiares compatíveis com distrofias coriorretinianas.Para o nosso conhecimento, este é o primeiro caso publicado de doença de Buerger com compli-cações oculares graves associadas.
Palavras-chaveBuerger, coriorretiniana, atrofia, vasculopatia, oclusão.
ABSTRACT
Buerger’s disease is an occlusive inflammatory vasculopathy of the small and medium-sized vessels, predominantly arterial, of the extremities largely associated with smoking. Visceral involvement is uncommon and ocular complications are even rarer, possibly characterized by retinal vascular occlusions.We report a case of a patient diagnosed with Buerger’s disease with important systemic vascular involvement who presented with progressive bilateral visual acuity decrease. Careful ophthalmo-logical examination revealed a diffuse chorioretinal atrophy in both eyes and markedly delayed arm-to-retina time in fluorescein angiography. There was no family history of retinal dystrophies.To our knowledge, this is the first reported case of Buerger’s disease with such dramatic ocular manifestations.
KeywordsBuerger, chorioretinal, atrophy, vasculopathy, occlusion.
Oftalmologia - Vol. 38: pp.139-143
Comunicações Curtas e Casos Clínicos
INTRODUCTION
Buerger’s disease (BD), or thromboangiitis obliterans, is an inflammatory occlusive vasculopathy characterized
by the development of segmental occlusions of small and medium-sized vessels, particularly arterial. Its physio-pathology is not completely understood but the immune system seems to have a major role, having been already

140 | Revista da Sociedade Portuguesa de Oftalmologia
detected antiendothelial antibodies in patients with BD. An hypersensitivity response to cigarettes’ constituents, especially nicotine, is possibly responsible for the endo-thelial damage. Histopathologic studies revealed an initial polymorphonuclear infiltrate on the vascular walls and the development of an immune cellular thrombus on the lumen; later, there is a replacement of the neutrophils by mononuclear cells, fibroblasts and giant cells, with peri-vascular fibrosis in the more advanced cases1,2. The esti-mated prevalence is 12.6-20:100 000, higher in the Indian, Korean and Ashkenazi populations. Its incidence is also higher in men younger than forty, although it has been noted an increase in its prevalence between female patients by the also increasing number of women who smoke3.
Clinically, BD tends to manifest by signs of arterial insufficiency or a migratory thrombophlebitis, accompa-nied by intense pain, even at rest, possibly related to nerve involvement and release of inflammatory mediators. The involvement of the vessels of the extremities is the rule, especially of the radial and tibial arteries, leading to necro-sis which may require amputation of the distal segments. Other frequent associations include Raynaud’s phenome-non and claudication of the affected extremity (usually confined to the calves and feet or the forearms and hands). Patients seem to be otherwise healthy, with no other syste-mic symptoms. Visceral involvement is rare and available published cases with ocular complications are even fewer, possibly characterized by retinal vascular occlusions4 – predominantly of the arterial branches – and secondary neovascularization with its consequences; normotensional glaucoma5 and changes in the anterior segment vessels6 are also mentioned, although less frequently.
We report, to our knowledge, the first case of BD with extensive chorioretinal atrophy, with no positive family history of retinal dystrophies, which we believe to be secondary to an important compromise of the retinal and choroidal vasculature.
CASE REPORT
M.P.A., male Caucasian patient, sixty-four years old, driver, previous smoker (15 pack-year), was seen in our ophthalmology department for progressive bilateral visual acuity decrease and nyctalopia, which he started to note 10 years ago. He was diagnosed with BD in his thirties and had already been submitted to several procedures over the years, including amputation of some of his hands’ and feet’s fingers as well as to endovascular treatments due to significant carotid and iliac compromise. He denied any
other relevant conditions, such as hypertension, diabetes, coagulation disorders or autoimmune diseases. He also denied any past or current chronic medication, including other treatments for BD targeting his vascular compro-mise. Trips abroad were also excluded, having never left his country, Portugal. His family history was also negative to any relevant systemic or ocular diseases, namely retinal or choroidal dystrophies.
On careful examination, his best corrected visual acuity was of counting fingers on his right eye and 0.7 (Snellen chart) on his left eye, with a refraction of +1.5D in both eyes. Pupil examination and ocular motility were both unre-markable. The anterior segment was normal on slit-lamp observation, with only phacosclerosis. Intraocular pres-sure was 12mmHg bilaterally. Fundus examination revea-led extensive confluent areas of chorioretinal atrophy with involvement of the posterior pole except in the perifoveal area of the left eye, where it remained some normal shar-ply demarcated retinal tissue. The atrophy extended to the
André Marques, Joana Portelinha, Ana Almeida, Marta Guedes
Fig. 1 |
Fig. 2 |
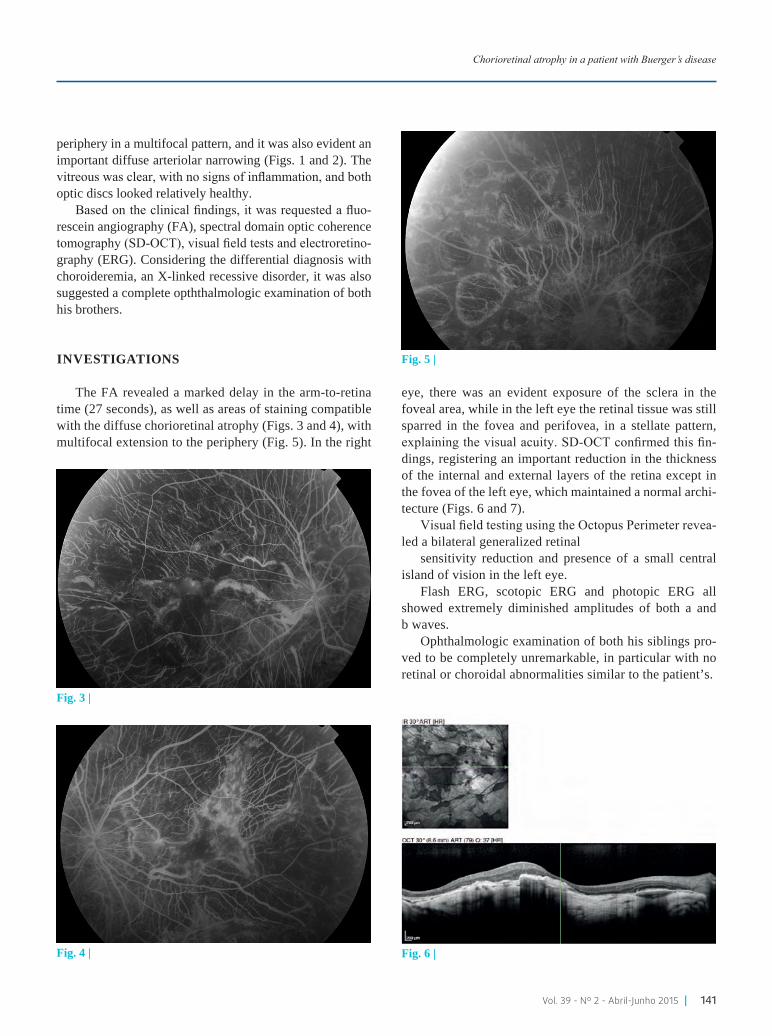
Vol. 39 - Nº 2 - Abril-Junho 2015 | 141
periphery in a multifocal pattern, and it was also evident an important diffuse arteriolar narrowing (Figs. 1 and 2). The vitreous was clear, with no signs of inflammation, and both optic discs looked relatively healthy.
Based on the clinical findings, it was requested a fluo-rescein angiography (FA), spectral domain optic coherence tomography (SD-OCT), visual field tests and electroretino-graphy (ERG). Considering the differential diagnosis with choroideremia, an X-linked recessive disorder, it was also suggested a complete opththalmologic examination of both his brothers.
INVESTIGATIONS
The FA revealed a marked delay in the arm-to-retina time (27 seconds), as well as areas of staining compatible with the diffuse chorioretinal atrophy (Figs. 3 and 4), with multifocal extension to the periphery (Fig. 5). In the right
eye, there was an evident exposure of the sclera in the foveal area, while in the left eye the retinal tissue was still sparred in the fovea and perifovea, in a stellate pattern, explaining the visual acuity. SD-OCT confirmed this fin-dings, registering an important reduction in the thickness of the internal and external layers of the retina except in the fovea of the left eye, which maintained a normal archi-tecture (Figs. 6 and 7).
Visual field testing using the Octopus Perimeter revea-led a bilateral generalized retinal
sensitivity reduction and presence of a small central island of vision in the left eye.
Flash ERG, scotopic ERG and photopic ERG all showed extremely diminished amplitudes of both a and b waves.
Ophthalmologic examination of both his siblings pro-ved to be completely unremarkable, in particular with no retinal or choroidal abnormalities similar to the patient’s.
Chorioretinal atrophy in a patient with Buerger’s disease
Fig. 3 |
Fig. 4 |
Fig. 5 |
Fig. 6 |

142 | Revista da Sociedade Portuguesa de Oftalmologia
DIFFERENTIAL DIAGNOSIS
Even though a number of other causes could explain the chorioretinal atrophy seen in our patient - high myopia, hypertensive choroidopathy or chronic therapy with thiori-dazine or deferoxamine, for example - his medical history was relevant only to BD with associated distal, iliac and carotid involvement. The most important differential in this case, therefore, is a generalized choroidal and retinal dystrophy, namely choroideremia. This dystrophy could justify the clinical and fundoscopic findings in our patient, such as the bilaterally diminished visual acuity, nyctalo-pia and corresponding visual field changes, as well as the arteriolar narrowing and relatively sparred optic discs and foveal area of the left eye, which is possible even in advan-ced cases7,8.
An immunoblot analysis with anti-REP-1 antibody9 (which would show absence of immunohistochemical staining of REP-1 protein in cells from peripheral tissues, with a predictive value of 100% in male patients, since all known mutations in the choroideremia gene CHM result in truncated or completely absent REP-1 protein) and genetic testing for CHM mutations10 (with sensitivity and specifi-city values > 98%) could confirm this dystrophy, but we were unable to conduct those. However, various aspects are against this diagnosis. Choroideremia typically manifests in an earlier age, usually in the first decade of life, and is frequently associated with other ocular findings, such as posterior subcapsular lens changes and fine fibrillar dege-neration of the vitreous, both absent in our case. The lack of a positive family history and its low prevalence11, esti-mated to be around 1:50-100 000), also make this diagnosis very unlikely. In addition, our patient presented with other
changes which are not found in choroideremia such as a marked arm-to-retina delay. Considering the already men-tioned diffuse systemic vascular involvement in our patient, we think it’s possible and even likely this delay and secon-dary chorioretinal atrophy could be caused by BD.
TREATMENT
We decided to give an antiplatelet agent (acetylsali-cylic acid 150mg/day), although the only proven therapeu-tic measure is smoking cessation12, which our patient had already successfully accomplished.
Other measures have been tried to deal with the ische-mia of the extremities, such as the use of calcium-channel blockers, systemic prostaglandin analogues or revasculari-zation procedures, but with limited success and their effects on retinal vasculature compromise have yet to be studied.
OUTCOME AND FOLLOW-UP
Although an improvement in his right eye’s vision is impossible due to the macular lesions, the patient main-tains a relatively good visual acuity in his left eye, at a one year follow-up. Every effort should be therefore made to preserve the remaining vision with close monitoring and screening of other ocular comorbidities. We also decided to prescribe a platelet aggregator inhibitor as a prophylac-tic measure (with systemic effects), although no published data supports this measure.
DISCUSSION
BD, or thromboangiitis obliterans, is an uncommon vascular disease with which not many ophthalmologists are particularly familiar. Its rarity also means that reports of atypical manifestations and involvement of other organs and systems not usually affected are not frequent, making it sometimes difficult to correctly interpret such cases.
Some authors described cases of retinal vascular occlusions in patients with BD who showed vascular nar-rowing, retinal atrophy and secondary pigmentary chan-ges, thought to be related to the involvement of the central artery and vein of the retina4,5 by the systemic vasculo-pathy. This same vascular compromise, characterized not only by segmental occlusions of the small and medium--sized vessels but also by a disturbance of the vasodilation process with vasospasm could also lead in certain patients
Fig. 7 |
André Marques, Joana Portelinha, Ana Almeida, Marta Guedes

Vol. 39 - Nº 2 - Abril-Junho 2015 | 143
to normotensional glaucoma5, in which vascular factors seem to have a substantial role in its development and progression.
On par with the previously described changes, the anterior segment can also be affected in some of these patients, as depicted in an article in which its authors men-tion a reduction in the arteriolar caliber and an increase in the venular tortuosity due to flow redistribution in the conjunctival vessels of nine patients with BD6.
In fact, being a systemic disease, it seems unlikely there is no associated compromise of the ocular circula-tion, even though most patients present with more peri-pheral changes. It is then possible that ophthalmic compli-cations are underdiagnosed in BD.
In conclusion, while it is not completely possible to exclude the presence of a dystrophy such as choroidere-mia as cause of the extensive chorioretinal atrophy veri-fied, the late presentation, lack of other frequently asso-ciated findings and presence of angiographically proven arm-to-retina delay, negative family history with normal examination of his siblings and rarity of both diseases makes this diagnosis unlikely. Therefore, we believe that the ocular findings reported are secondary to a significant compromise of the retinal and choroidal vasculature, in accordance to the important distal, carotid and iliac arte-rial insufficiency already present in our patient, a compli-cation of Buerger’s disease never published before.
REFERENCES
1. Fauci AS, Braunwald E, Kasper DL et al. Harrison’s Principles of Internal Medicine 17th edition: Chap-ter 243 - Vascular diseases of the extremities. USA: McGraw Hill Medical;2008.
2. Joviliano EE, Dellalibera-Joviliano R, Dalio M et al. Etiopathogenesis, clinical diagnosis and treatment of thromboangiitis obliterans - current practices. Int J Angiol 2009;18(3):119-125.
3. Mary Kugler, R.N.. Buerger Disease. About.com rare
diseases. [http://rarediseases.about.com/od/rarediseases b/ a/022605.htm]
4. Puttanna ST. Thromboangeitis associated with retinal vasculititis. Indian J Ophthalmol 1966;14:209-213.
5. Ohguro I, Ohguro H, Ohta T et al. A case of normal tension glaucoma associated with Buerger’s disease. Tohoku J Exp Med 2006 May;209(1):49-52.
6. Homma S, Tsushima N, Minamiyama M et al. Microvas-cular blood is distributed more to venules than to arte-rioles in patients with Buerger’s disease. Observation of bulbar conjunctiva by intravital microscope system. In Angiol 2000;19(2):135-41.
7. Hereditary Retinal and Choroidal Dystrophies, in Ame-rican Academy of Ophthalmology - Basic and Clini-cal Science Course Section 12 Retina and Vitreous 2011-2012:247-48.
8. Sandeep G, Gerald AF: Choroidal dystrophies, in Yanoff Ophthalmology 3rd edition 2009:569-74.
9. MacDonald IM, Mah DY, Lewis RA, et al. A practi-cal diagnostic test for choroideremia. Ophthalmology 1998;105:1637-1640.
10. Moosajee M, Ramsden SC, Black GCM, et alt. Clinical utility gene card for: Choroideremia. European Journal of Human Genetics (2014):22.
11. How common is choroideremia? Choroideremia, Gene-tics Home Reference Jul 2013. http://ghr.nlm.nih.gov/condition/choroideremia.
12. Stvrtinova V, Ambrozy E, Stvrtina S et al. 90 years of Buerger’s disease - what has changed? Bratisl Lek Listy 1999;100(3):123-8.
Presented as a poster in the 56th Congress of the Portugue-se Ophthalmology Society (SPO).No commercial interests to report.
CONTACTOAndré Marques Rua Marquês de Pombal nº287A 3º andar 2775-265 ParedeE-mail: [email protected]
Chorioretinal atrophy in a patient with Buerger’s disease


Vol. 39 - Nº 2 - Abril-Junho 2015 | 145
Melanoma da íris em idade pediátrica
Inês Coutinho1, Peter Pêgo2, Mário Ramalho1, Catarina Pedrosa1,Cristina Santos1,Mafalda Mota1, Isabel Prieto2, João Cabral3
Serviço de Oftalmologia do Hospital Prof. Doutor Fernando da Fonseca, EPE 1Interna de Formação Especifica de Oftalmologia
2Chefe de Serviço de Oftalmologia3Assistente Hospitalar Graduado de Oftalmologia
RESUMO
Objectivos: Relato de um caso clínico referente a um melanoma da íris em idade pediátrica, tratado com feixe de protões externo, seus resultados e complicações associadas.Métodos: Criança de 8 anos de idade, com lesão pigmentada inferotemporal da íris do olho esquerdo. A lesão foi interpretada como um nevus da íris e documentada através de fotografias seriadas do segmento anterior e biomicroscopia ultra-sónica. Verificou-se crescimento da lesão e perante esta evolução, assumiu-se a hipótese de melanoma difuso da íris. Foi realizada radio-terapia com feixe de protões externo.Resultados: Após 18 meses de radioterapia, desenvolveu catarata subcapsular posterior no olho esquerdo, tendo sido submetido a cirurgia de facoemulsificação. Com 5 meses de seguimento, a acuidade visual é de 10/10, sem complicações a relatar. Três anos após a radioterapia, não se observa qualquer recorrência do tumor nem evidência de doença metastática.Conclusões: A radioterapia com feixe de protões foi uma opção terapêutica com boa resposta e bem tolerada. A principal complicação foi o desenvolvimento de catarata, que, embora consti-tuísse um desafio cirúrgico, foi resolvida com sucesso. O uso de micro-incisão, capsulorexis pos-terior e triamcinolona intracamerular asseguram mais rápida recuperação visual e transparência do eixo visual, com menor inflamação. Palavras-chaveNevus da íris, Melanoma da íris, Radioterapia com feixe de protões, Catarata, Idade pediátrica.
ABSTRACT
Purpose: Case report of a child with iris melanoma treated with proton beam, results and related complications. Methods: A 8-year-old child presented with a pigmented lesion in the inferotemporal iris of the left eye. It was interpreted as a nevus and documented by photography of the anterior segment and ultrasonic biomicroscopy in serial reassessments. The lesion had grown and was assumed the diagnosis of a diffuse iris melanoma. It was performed proton beam therapy (PBT).Results: After 18 months of radiotherapy, developed a posterior subcapsular cataract on his left eye being submitted to phacoemulsification. Five months later, visual acuity was 20/20, without complications. Three years post PBT, we did not report any recurrence of the tumor neither evi-dence of metastatic disease.Conclusion: Primary PBT was a good option and well tolerated. The main complication was cata-ract, which was successfully treated, although in pediatric age is always a surgical challenge. The use of micro-incision with posterior capsulorhexis and intracameral triamcinolone seems to allow faster visual recovery, no visual axis obscuration and providing significantly less inflammation.
Oftalmologia - Vol. 38: pp.145-149
Comunicações Curtas e Casos Clínicos

146 | Revista da Sociedade Portuguesa de Oftalmologia
KeywordsIris nevi, Iris melanoma, Proton beam therapy, Cataract, Pediatric age.
INTRODUÇÃO
O melanoma da íris é uma neoplasia maligna melanocí-tica, com origem no estroma da íris. É a neoplasia primária da íris mais comum, apesar de corresponder apenas a 2-5% dos melanomas da úvea. Face ao melanoma da coroideia e do corpo ciliar o diagnóstico é feito por volta dos 50 anos, cerca de 10 anos antes, tem melhor prognóstico e menor potencial metastático (cerca de 5% após 10 anos de tratamento).
A maioria dos melanomas da íris são assintomáticos e o primeiro sinal de alarme pode ser o aumento progressivo das dimensões de um nevus pré-existente.
Podem apresentar pigmentação variável, serem circuns-critos, difusos, em tapioca ou em anel (trabeculares) e, em 80% dos casos, localizam-se na porção inferior da íris.
O diagnóstico diferencial entre melanoma da íris e nevus nem sempre é fácil e alguns dos factores preditivos de evo-lução para melanoma são: tamanho >3mm em diâmetro e espessura >2mm, vascularização intrínseca que pode causar episódios de hifema espontâneo e envolvimento das estru-turas adjacentes, condicionando ectrópio uveal, anisocória, células no humor aquoso, catarata sectorial ou glaucoma. A sigla ABCDEF, pode ajudar a lembrar alguns dos facto-res preditivos:
A= age <40 years, B=blood/hyfema, C=clock hour infe-rior (4- 9h), D=diffuse tumor, E=ectropion uvea and F= feathery margin.
Quanto aos factores de risco que predispõem para mela-noma, podem referir-se: pele e íris clara, nevus cutâneos múltiplos, melanocitose ocular congénita, nevus de Ota,
melanocitoma uveal, nevus cutâneo displásico, melanoma cutâneo familiar e neurofibromatose tipo 1. Não há evidên-cia consistente quanto ao papel da radiação ultravioleta.
O melhor tratamento para o melanoma da íris perma-nece controverso.
As opções terapêuticas incluem a iridectomia, iridoci-clectomia, braquiterapia, radioterapia com feixe de protões externo ou enucleação. A escolha depende, entre outros fac-tores, do tamanho e extensão do tumor, idade, estado geral do doente e do olho adelfo, assim como, dos recursos tera-pêuticos disponíveis.
No melanoma localizado da íris a iridectomia ou a iri-dociclectomia, se invasão do ângulo, são uma opção com baixa mortalidade e bom prognóstico visual.
Actualmente, a radioterapia é uma opção terapêutica cada vez mais consensual no melanoma da íris.
A radioterapia com feixe de protões, face à braquitera-pia, tem a vantagem de possibilitar uma libertação homogé-nea da radiação e apenas na área definida, o que minimiza o dano nos tecidos adjacentes; contudo, encontra-se dispo-nível em poucos centros e exige a colaboração do doente.
A enucleação reserva-se para situações particulares, como nos tumores de grandes dimensões (>20mm em diâ-metro, espessura >10mm, envolvimento extraescleral) ou na presença de glaucoma secundário grave.
Foi demostrado que a enucleação não apresenta benefí-cio em termos de sobrevida, nem diminui o risco de metas-tização sistémica, face à terapêutica conservadora.
CASO CLíNICO
Rapaz, 8 anos de idade, pele e olhos claros, sem antece-dentes pessoais ou familiares relevantes.
Ao exame oftalmológico apresentava lesão pigmentada inferotemporal da íris do olho esquerdo (OE), sem outras alterações. Negava sintomas oftalmológicos.
A lesão foi interpretada como nevus da íris e documen-tada através de fotografia do segmento anterior (Fig.1) e biomicroscopia ultra-sónica em reavaliações seriadas.
Após 6 meses, verificou-se crescimento da lesão, em diâ-metro e espessura, com corectopia e ectrópio uveal (Fig.2).
Apresentava acuidade visual (AV) de 10/10 e pressão intra-ocular (PIO) de 10mmHg em ambos os olhos, sem outras alterações no segmento anterior ou à fundoscopia. Fig. 1 | Lesão pigmentada inferior da íris do OE.
Inês Coutinho, Peter Pêgo, Mário Ramalho, Catarina Pedrosa,Cristina Santos,Mafalda Mota, Isabel Prieto, João Cabral

Vol. 39 - Nº 2 - Abril-Junho 2015 | 147
A biomicroscopia ultra-sónica (UBM) confirmou aumento da espessura tumoral (1,6mm para 2,3mm) com ausência de invasão do corpo ciliar ou ângulo irido-corneano (Fig.3).
Sob a suspeita clínica de evolução para melanoma, refe-renciou-se ao Hôpital Ophtalmique Jules-Gonin, em Lau-sanne, onde se estabeleceu o diagnóstico provável de mela-noma difuso da íris. Fez radioterapia com feixe acelerado de protões, com excisão e recolocação de células limbares (Fig.4), para prevenir a insuficiência limbar e a epitelização corneana secundária.
RESULTADOS
Após 18 meses de radioterapia constatou-se desen-volvimento de catarata subcapsular posterior no OE, com
evolução rápida para catarata branca, contribuindo para a diminuição progressiva da AV até percepção luminosa (Fig.5).
A microscopia especular revelou boa densidade de célu-las endoteliais com 2667células/mm2 no OE e 3040 célu-las/mm2 no OD.
Fig. 2 | Crescimento tumoral com corectopia.
Fig. 3 | UBM: confirmação do crescimento tumoral.
Fig. 4 | Auto-transplante das células limbares superiores após radioterapia.
Fig. 5 | Catarata no OE.
Fig. 6 | Capsulorexis posterior.
Melanoma da íris em idade pediátrica

148 | Revista da Sociedade Portuguesa de Oftalmologia
Aos 11 anos, foi submetido a cirurgia de facoemulsifica-ção micro-incisional do OE, combinada com capsulorexis posterior primária, injecção intracamerular de triamcino-lona e implante de lente monobloco intra-ocular (Fig.6).
Não se registaram complicações intra-operatórias.Com 5 meses de seguimento, a AV do OE é de 10/10,
sem complicações a registar.Três anos após a radioterapia, não se observa qualquer
recorrência do tumor (Fig.7) nem evidência de doença metastática ou outras complicações associadas à radiotera-pia, tais como, pressão intra-ocular elevada e retinopatia.
Mantém-se em reavaliações periódicas.
CONCLUSÃO
Apesar da grande maioria das lesões pigmentadas da íris serem benignas, estas devem ser vigiadas periodicamente pelo seu potencial de malignidade. A vigilância deve incluir fotografias do segmento anterior (com e sem midríase) e UBM seriadas para documentar o crescimento da lesão, permitindo um diagnóstico precoce.
O melanoma da íris é raro na faixa etária pediátrica e per-manece ainda controverso qual a melhor opção terapêutica.
Vários estudos têm mostrado que a radioterapia com feixe de protões externo é uma excelente opção para o tratamento primário e não só no tratamento de resgate em casos de recidiva ou em associação com outras modalidades terapêuticas.
Actualmente, a radioterapia com feixe de protões externo é uma das melhores opções de tratamento, contudo, a baixa disponibilidade a nível mundial limita a sua maior utilização e difusão.
O protocolo consiste na irradiação com 60GyRBE, em fracções de 15GyRBE por 4 sessões, com duração de apro-ximadamente 30 segundos cada. O tratamento é realizado com o doente em posição sentada, sob anestesia tópica, com pupila em midríase e com retractores palpebrais para protecção dessa estrutura. É fundamental assegurar a imo-bilização da cabeça, conseguida através do uso de máscara facial de acrílico termoplástico e peça bucal, individuali-zada para cada doente. É também importante garantir a fixa-ção do alvo definido para correcta irradiação.
Este tratamento é bem tolerado, apresenta boa sobrevida e baixa taxa de recidiva local, sendo que a maioria ocorre nos primeiros 3 anos.
A principal complicação é o desenvolvimento de cata-rata, geralmente subcapsular posterior, uma vez que, o cris-talino é a estrutura ocular mais radiosensível.
O glaucoma, o olho seco e raramente a irite, a querato-patia e a retinopatia são outras das possíveis complicações.
A cirurgia de catarata pós-radiação deve ser realizada 2 anos após o tratamento e, apesar dos bons resultados, é uma cirurgia desafiante podendo haver marcada opacificação da cápsula posterior, assim como, exuberante reacção inflama-tória no pós-operatório.
Aliado a isto, a catarata em idade pediátrica constitui também, um desafio cirúrgico importante.
O uso de micro-incisão, capsulorexis posterior primária e a aplicação de triamcinolona intracamerular asseguram maior segurança no procedimento, uma mais rápida recu-peração visual com transparência duradoura do eixo visual e redução da inflamação no pós-operatório.
Agradecimentos - Ao Professor Doutor L.Zografos e à Dra. Ann Schalenbourg pela sua disponibilidade e ajuda.
BIBLIOGRAFIA
1. Damato B, Kacperek A, Errington D, Heimann H. Proton beam radiotherapy of uveal melanoma. Saudi J Ophthalmol. 2013 Jul;27(3):151-7.
Fig. 7 | Fotografia do segmento anterior e UBM após 3 anos de radioterapia.
Inês Coutinho, Peter Pêgo, Mário Ramalho, Catarina Pedrosa,Cristina Santos,Mafalda Mota, Isabel Prieto, João Cabral

Vol. 39 - Nº 2 - Abril-Junho 2015 | 149
2. Henderson E, Margo CE. Iris melanoma. Arch Pathol Lab Med. 2008. Feb;132(2):268-72.
3. Jager MJ, Desjardins L, Kivela T, Damato BE (eds): Current Concepts in Uveal Melanoma. Dev Ophthal-mol. Basel, Karger, 2012, vol 49, pp 16-26; 41-57.
4. Lloyd IC, Ashworth J, Biswas S, Abadi RV. Advances in the management of congenital and infantile cataract. Eye (Lond). 2007 Oct;21(10):1301-9.
5. Lumbroso-Le Rouic L, Delacroix S, Dendale R, Levy--Gabriel C, Feuvret L, Noel G, Plancher C, Nauraye C, Garcia P, Calugaru V, Asselain B, Desjardins L. Pro-ton beam therapy for iris melanomas. Eye (Lond). 2006 Nov;20(11):1300-5.
6. McLaughlin JP, Fung AT, Shields JA, Shields CL. Iris melanoma in children: Current approach to manage-ment. Oman J Ophthalmol. 2013 Jan;6(1):53-5.
7. Rundle P, Singh AD, Rennie I. Proton beam therapy for iris melanoma: a review of 15 cases. Eye (Lond). 2007 Jan;21(1):79-82.
8. Shields CL, Kaliki S, Shah SU, Luo W, Furuta M, Shields JA. Iris melanoma: features and prognosis in 317
children and adults. J AAPOS. 2012 Feb;16(1):10-6.9. Shields CL, Kaliki S, Hutchinson A, Nickerson S, Patel
J, Kancherla S, Peshtani A, Nakhoda S, Kocher K, Kol-bus E, Jacobs E, Garoon R, Walker B, Rogers B, Shields JA. Iris nevus growth into melanoma: analysis of 1611 consecutive eyes: the ABCDEF guide. Ophthalmology. 2013 Apr;120(4):766-72.
10. Singh AD, Rennie IG, Seregard S, Giblin M, McKenzie J. Sunlight exposure and pathogenesis of uveal mela-noma. Surv Ophthalmol. 2004 Jul-Aug;49(4):419-28.Review.
11. Zetterström C, Lundvall A, Kugelberg M. Cata-racts in children. J Cataract Refract Surg. 2005 Apr;31(4):824-40.
Apresentado como Poster no 57º Congresso Português de Oftal-mologia - Algarve, Portugal, Dezembro 2014
Os autores negam qualquer interesse comercial e cedem os seus direitos de autor à SPO
Melanoma da íris em idade pediátrica


Vol. 39 - Nº 2 - Abril-Junho 2015 | 151
Indicações aos Autores e Normas de Publicação
“Oftalmologia” é a revista oficial da Sociedade Portuguesa de Oftalmologia (SPO) e publica de forma prioritária traba-lhos de investigação básica e clínica, sob a forma de artigos de revisão, “guidelines”, artigos originais, casos clínicos relacionados com oftalmologia, bem como artigos que ver-sem áreas de conhecimento fronteira com interesse para a prática oftalmológica.
PROCESSO EDITORIAL
1. Condições gerais - Os artigos devem ser preferencial-mente redigidos em Português ou Inglês, sendo desejável que progressivamente sejam em Inglês. Será dada sempre preferência de publicação aos artigos submetidos simulta-neamente em Português e Inglês. Poderão ser publicados artigos numa outra língua (espanhol ou francês), sendo que estes tem de ser obrigatoriamente submetidos também em Inglês. Os manuscritos depois de rececionados são encaminhados para o editor da revista, que fará uma primeira avaliação editorial com o fim de comprovar a sua adequação (no âmbito temático e de interesse para a revista) e o cumpri-mento dos requisitos de apresentação formal exigidos nas normas de publicação. Desta apreciação resulta a aceitação para revisão por pares ou a sua devolução ao autor para cor-reção e nova submissão.Os manuscritos devem ser submetidos em ficheiros de texto em formato Word (.DOC ou .DOCX), com texto seguido e sempre com o mesmo tipo de letra. Os textos devem ser for-matados em letra “Arial”, tamanho 11 com espaçamento de 1,5 linhas. Os títulos e sub-títulos deverão estar assinalados a negrito e em tamanho 12. A primeira página (página de rosto) deve conter somente os elementos descritos adiante na rubrica “Organização do Artigo”.Os documentos submetidos para publicação serão pro-priedade da revista Oftalmologia da SPO transferindo os seus autores o direito de propriedade (copyright) a partir do momento que são aceites para publicação. Não serão aceites artigos simultaneamente submetidos noutras publi-cações científicas. Os trabalhos devem ser submetidos em formato electrónico, na plataforma da revista da SPO, acessível a partir do site
da SPO: http://www.spoftalmologia.pt ou da plataforma da revista “Oftalmologia” no serviço de alojamento de revis-tas científicas do Repositório Científico de Acesso Aberto de Portugal (RCAAP): https://revistas.rcaap.pt/index.php/oftalmologia.2. - Uma vez aprovado pelo editor o manuscrito será enviado para revisão por parte de dois ou mais revisores, de forma confidencial e anónima. Os autores receberão a infor-mação da avaliação dos revisores através do editor, sendo--lhes solicitadas as correções oportunas e consequente re--submissão. A seleção dos revisores realiza-se através do conselho redatorial da revista, tendo em conta os méritos académicos, científicos e experiência profissional, em cada uma das subespecialidades oftalmológicas, incluindo inves-tigadores nacionais ou internacionais. Cada artigo será obri-gatoriamente revisto por um membro do conselho redato-rial e por um revisor externo ao mesmo.3. Política editorial - a decisão do editor, após consultados os revisores, para aceitação-rejeição de um trabalho subme-tido baseia-se nos seguintes fatores:I. Originalidade - assunto e/ou método original, com infor-mação valiosa e apresentação de resultados novos ou con-firmação de resultados já anteriormente verificados.II. Atualidade e/ou novidade - tema que está na agenda das reuniões ou comunicações científicas ou é novo.III. Relevância - aplicabilidade dos resultados para a reso-lução de problemas concretos da prática oftalmológica.IV. Inovação e significância - avanço do conhecimento científico, técnico e/ou prática clínica.V. Fiabilidade e validade científica - boa qualidade meto-dológica evidenciada.VI. Apresentação - boa redação e organização do texto (boa coerência lógica e apresentação do material).
SECÇÕES
1. Editoriais e notas - Os editoriais e notas editoriais serão ou encomendados pelo editor da revista a quem considere oportuno ou da sua responsabilidade.2. Cartas ao editor - Esta secção pode incluir comentários sobre artigos previamente publicados ou comentários sobre outras matérias de interesse científico para oftalmologia.
152 | Revista da Sociedade Portuguesa de Oftalmologia
Esta correspondência estará sujeita ao processo de revisão pelos pares e será publicada na medida em que o espaço, as prioridades e interesse o permitam. Estas não devem ultra-passar as 500 palavras. As cartas ao editor que versem sobre artigos previamente publicados terão direito de resposta, preferencialmente no mesmo número.3. Artigos de revisão e “guidelines” - O objetivo da sec-ção é atualizar determinados temas de oftalmologia, dis-cutir novos conceitos ou rever conceitos clássicos tendo em vista os novos avanços de diagnóstico e tratamento e a divulgação das boas práticas em oftalmologia. Serão soli-citados pelo Editor / Conselho Redatorial a personalidades reconhecidas e ou grupos de trabalho. Para além das revi-sões por convite, os artigos de revisão podem ainda ser sub-metidos por autores com elevada experiência numa área de estudo da oftalmologia para serem submetidos ao processo editorial. 4. Artigos originais - Podem incluir-se tanto trabalhos experimentais como clínicos, sempre que se trate de traba-lhos de investigação. Os trabalhos de investigação devem ser inéditos e não podem ter sido submetidos para publica-ção em outra revista estrangeira indexada. Incluem-se nesta rubrica os prémios atribuídos no âmbito da SPO.5. Comunicações curtas e casos clínicos - Deverão ser manuscritos resumidos descrevendo inovações técnicas e tecnológicas, manobras cirúrgicas inovadoras, aspectos de outras áreas do conhecimento relacionados com a prática oftalmológica, bem como casos clínicos com informação de prática clínica relevante. 6. Histórias da História da Oftalmologia Portuguesa - Será uma rubrica curta realçando aspectos relacionados com personalidades ou acontecimentos da oftalmologia portuguesa.7. Flash-look - Nesta rúbrica agrupam-se artigos curtos de atualização em conceitos básicos da prática clínica de oftal-mologia, como classificação, opções terapêuticas, manuais de procedimentos de determinadas patologias.
ORGANIZAÇÃO DO ARTIGO
Os artigos devem ser submetidos em formato bilingue (sendo que a segunda língua do manuscrito deve ser o Inglês), ou somente em Inglês.1. Pagina do título/identificação - (página separada) Con-tendo título do artigo, nome (s) dos (s) autor (es), serviço (s) hospitalar (es) e departamentos ou organismos onde foi realizada a investigação, títulos académicos e/ou hospitala-res dos autores. Nesta página deve ainda figurar o endereço postal completo para envio de correspondência e o endereço
eletrónico do autor correspondente. Se o trabalho já tiver sido apresentado, indicar onde e em que data, bem como a referência a prémio obtido. Os autores deverão manifestar a existência de conflito de interesse (nomeadamente comer-cial no produto, equipamento ou processo), certificar que o trabalho não foi publicado previamente e que cedem os direitos de autor à SPO.2. Resumo - Em Português e em Inglês com o máximo 250 palavras. O resumo deve ser subdividido em: Objetivos, Material e Métodos, Resultados, Conclusões.3. Palavras chave - Duas listas de cinco palavras chave, em Português e Inglês, que resumam e classifiquem os princi-pais assuntos focados no texto :estas destinam-se a codifi-cação no índex.4. Texto - Recomenda-se que o texto tenha as seguintes sec-ções separadas: Introdução, Material e Métodos, Resultados, Discussão; poderá ser necessário fazer adaptações a circuns-tâncias particulares, como no caso dos casos clínicos ou dos artigos de “flash look”. O autor deverá indicar no texto, em local apropriado, em numeração árabe e em “superscript”, as citações bibliográficas que fizer. É da exclusiva respon-sabilidade do autor a verificação da exatidão das referências bibliográficas e da sua colocação no texto.5. Agradecimentos - Tanto a pessoas, como a entidades, quando tal for justificado.6. Declaração de interesses financeiros7. Bibliografia - De modo geral segue-se o sistema de Van-couver, com a diferença principal de que a lista das referen-cias bibliográficas deve ser alfabetada e subsequentemente numerada. Se houver mais de uma referencia do mesmo autor, serão indicadas em primeiro lugar aquelas em que o autor aparece isolado e só depois aquelas em que há mais que um autor.8. Quadros, tabelas e figuras - são enviados em formato eletrónico, em ficheiros separados do texto. Os quadros e tabelas podem ser feitos num processador de texto ou numa folha de calculo (em Excel). As figuras devem ser feitos formato editável tipo “TIF”, um ficheiro para cada imagem com qualidade de impressão (≥ 300 dpi). As figuras qua-dros e tabelas devem ser referenciadas no texto e deve ser indicado a zona do texto às quais ficarão adstritas após for-matação do artigo.9. Legendas das figuras - As figuras devem ser obrigato-riamente legendadas e as legendas enviadas nesta secção. Os quadros e tabelas não devem ter legendas.10. Abreviaturas e símbolos - Só devem ser usadas abre-viaturas de uso corrente. Se for imprescindível recorrer a abreviaturas menos usuais, na primeira vez em que o termo aparece no texto ele deve figurar por extenso, logo seguido pela abreviatura entre parêntesis.