
Canine visceral leishmaniosis: a remarkable histopathological picture of one case reported from...
10
Veterinary Parasitology 96 (2001) 203–212 Canine visceral leishmaniosis: a remarkable histopathological picture of one case reported from Brazil Wagner L. Tafuri a,* , Marcia Rosa de Oliveira b , Maria N. Melo c , Washington L. Tafuri a a Departamento de Patologia Geral, Instituto de Ciencias Biológicas (ICB), Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil b Departamento de Biologia, Molecular do Centro de Ciências Exatas e da Natureza da Universidade Federal da Para´ ıba (UFPB), João Pessoa, PB, Brazil c Departamento de Parasitologia, ICB/UFMG, Belo Horizonte, MG, Brazil Received 22 June 2000; received in revised form 14 November 2000; accepted 15 November 2000 Abstract This report describes a remarkable histopathological presentation of a symptomatic dog naturally infected with Leishmania (Leishmania) chagasi from Brazil. An intense inflammatory granuloma- tous reaction was observed in the liver and spleen associated with hypertrophy and hyperplasia of the mononuclear system (the classical histopathological picture of the disease). In addition, a spectrum of vascular lesions was observed in many organs. However, we did not find parasites (amastigotes of Leishmania) in any skin fragments of the ear, nose and or abdominal tissue. In fact, this animal had severe clinical signs, showed parasites in many organs, but no parasites in the skin. It appears that the presence or absence of parasites in the skin is not a good indicator of parasites in other organs or vice versa. © 2001 Elsevier Science B.V. All rights reserved. Keywords: Dog; Visceral leishmaniosis; Histopathology; Brazil Northeast 1. Introduction Human and canine visceral leishmaniosis in the New World are caused by Leishmania (Leishmania) chagasi which is transmitted by the phlebotomine Lutzomyia (Lutzomyia) longipalpis. Leishmania is an intracellular protozoan parasite that is delivered to its verte- brate host by the bite of an infected sandfly. Following injection into the skin, the extra- cellular promastigote form of the parasite must rapidly enter its host cell, the macrophage, * Corresponding author. Fax: +55-31-499-2889. E-mail address: [email protected] (W.L. Tafuri). 0304-4017/01/$ – see front matter © 2001 Elsevier Science B.V. All rights reserved. PII:S0304-4017(00)00436-2
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Canine visceral leishmaniosis: a remarkable histopathological picture of one case reported from...

Veterinary Parasitology 96 (2001) 203–212
Canine visceral leishmaniosis: a remarkablehistopathological picture of one case
reported from Brazil
Wagner L. Tafuria,∗, Marcia Rosa de Oliveirab,Maria N. Meloc, Washington L. Tafuria
a Departamento de Patologia Geral, Instituto de Ciencias Biológicas (ICB), Universidade Federal de MinasGerais (UFMG), Belo Horizonte, MG, Brazil
b Departamento de Biologia, Molecular do Centro de Ciências Exatas e da Natureza da Universidade Federalda Paraıba (UFPB), João Pessoa, PB, Brazil
c Departamento de Parasitologia, ICB/UFMG, Belo Horizonte, MG, Brazil
Received 22 June 2000; received in revised form 14 November 2000; accepted 15 November 2000
Abstract
This report describes a remarkable histopathological presentation of a symptomatic dog naturallyinfected withLeishmania(Leishmania) chagasifrom Brazil. An intense inflammatory granuloma-tous reaction was observed in the liver and spleen associated with hypertrophy and hyperplasiaof the mononuclear system (the classical histopathological picture of the disease). In addition, aspectrum of vascular lesions was observed in many organs. However, we did not find parasites(amastigotes ofLeishmania) in any skin fragments of the ear, nose and or abdominal tissue. In fact,this animal had severe clinical signs, showed parasites in many organs, but no parasites in the skin.It appears that the presence or absence of parasites in the skin is not a good indicator of parasitesin other organs or vice versa. © 2001 Elsevier Science B.V. All rights reserved.
Keywords:Dog; Visceral leishmaniosis; Histopathology; Brazil Northeast
1. Introduction
Human and canine visceral leishmaniosis in the New World are caused byLeishmania(Leishmania) chagasiwhich is transmitted by the phlebotomineLutzomyia(Lutzomyia)longipalpis. Leishmaniais an intracellular protozoan parasite that is delivered to its verte-brate host by the bite of an infected sandfly. Following injection into the skin, the extra-cellular promastigote form of the parasite must rapidly enter its host cell, the macrophage,
∗ Corresponding author. Fax:+55-31-499-2889.E-mail address:[email protected] (W.L. Tafuri).
0304-4017/01/$ – see front matter © 2001 Elsevier Science B.V. All rights reserved.PII: S0304-4017(00)00436-2

204 W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212
and later transform into the intracellular amastigote form. Visceral leishmaniosis remains aserious public health problem in the world and dogs (Canis familaris) are the peridomesticreservoir host (Anderson et al., 1980; Grimaldi et al., 1989; Tesh, 1995).
In Brazil, the studies by Deane and Deane (1995) and Deane and Deane (1962) haveshown that canine visceral leishmaniosis is an important zoonotic endemic disease. Theprevalence of the disease was described in many regions of the country, especially in thenortheast (Chagas et al., 1937, 1938). According to these authors, parasites can be frequentlyfound in the skin of infected animals and this appears to play an important role in the trans-mission of the disease. Additionally, some authors believe that the parasites (amastigotesof Leishmania) are always present in the skin of dogs even when they begin to disappearfrom the viscera (Ciaramella et al., 1997).
The most common clinical aspects of the canine disease are the chronic wasting diseasewith anemia, pale mucous membranes, generalized lymphadenomegaly and cutaneous le-sions characterized by a dry exfoliative dermatitis, alopecia and scars (Chagas et al., 1938;Deane and Deane, 1995; Anosa and Idowu, 1983; Keenan et al., 1984; Marzochi et al.,1985; Ciaramella et al., 1997).
The principal histopathological lesions observed in dogs are the hypertrophy and hyper-plasia of cells of the mononuclear phagocyte system (spleen, lymph nodes, liver and bonemarrow mainly), a chronic inflammation in the skin (Keenan et al., 1984), granulomatousinflammatory reactions in livers and spleens (Tafuri et al., 1996), interstitial pneumoni-tis (Tryphomas et al., 1977; Duarte et al., 1986) and glomerulonephritis with or withoutnephrotic syndrome (Marcussen et al., 1989; Tafuri et al., 1989; Nieto et al., 1992; Fontand Closa, 1997).
In this work, we report a remarkable histopathological picture of one symptomatic dogfrom Brazil. All of the organs showed an intense parasitism associated with a severe patho-logical picture and a spectrum of alterations of blood vessels. However, fragments of ear,nose and abdominal skin showed only a discrete chronic inflammatory reaction. Amastigoteforms ofLeishmaniacould not be found in any of these tissues.
2. Materials and methods
2.1. Animals
A symptomatic mongrel dog was identified by an epidemiological survey of caninevisceral leishmaniosis from the City Hall (Zoonosis Department) of João Pessoa, ParaıbaCity, Brazil Northeast. This inquiry is based on the serological survey of the canine popula-tion using anti-antigen (leishmania) indirect immunofluorescence (IFAT) and complementfixation reaction (CFR) (Pellegrino and Brener, 1958).
Clinical signs of the animal were a chronic wasting disease with anemic mucous mem-branes, generalized lymphadenomegaly and cutaneous lesions (dry exfoliative dermatitis,alopecia and scars).
The parasites present in the liver were identified to a genetic level by PCR using conservedregions of kinetoplastidae and by hybridization with kDNA probes asLeishmania chagasi(Wilson, 1991; Laskay et al., 1995).

W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212 205
2.2. Histopathology
The naturally infected dog was sacrificed with an overdose of thiopental sodium (33%,5 ml/kg dose, iv.). After the necropsy, small samples of liver, spleen and lymph nodeswere obtained for slides “imprint smears”. Then, Giemsa staining was carried out to deter-mine the presence of amastigotes ofLeishmaniaby light microscopy using oil immersionat 100x.
Fragments of liver, lungs, kidneys, skin and lymphoid organs (abdominal lymph nodes,spleen and bone marrow) were collected and fixed in 10% buffered formalin solution. Alltissues samples were dehydrated, cleared, embedded in paraffin, cut (4–5mm thickness)and stained with hematoxylin and eosin (HE). Gomori’s Trichrome stain and the periodicacid shift (PAS) stain were carried out to identify collagen fibers and basal membranes,respectively.
3. Results
3.1. Liver
Fragments of liver showed a remarkable leishmaniotic chronic granulomatous inflam-matory reaction. There were many intralobular hepatic granuloma formations of variablesize constituted by macrophages (parasitized or not with amastigotes ofL. chagasi), someepitheloid cells, small numbers of lymphocytes, plasmocytes and rare neutrophils. The gran-ulomas were rarely confluent and were localized in the sinusoid lumen, partially occludingit or not, and around the portal vessels. Pigments were detected microscopically as browncrystals (hemosiderin) and were detected chiefly in kupffer cells and in macrophages withingranulomas (Fig. 1).
Other lesions observed were hypertrophy and hyperplasia of kupffer cells loaded withamastigotes, an intense congestion of the sinusoid vessels and moderate mononuclear in-flammatory cell foci around portal spaces with hyaline thrombosis of the vessels.
Leishmaniaamastigote forms were observed in macrophages in granulomas, kupffer cellsand hepatocytes. In general the hepatic lobules were preserved, but the hepatocytes aroundthe granulomas were atrophic because of the compression.
3.2. Spleen
A diffuse chronic inflammatory reaction was observed in the capsule, subcapsular region,trabecular system and red pulp. The capsule and the trabecular system were thickened and thetrabecular vessels were dilated and congested. The red pulp showed profound modificationsdue to the marginal macrophage proliferation and the granulomatous inflammatory reaction.Macrophages were organized in granulomas and loaded with parasites and brown crystals(hemosiderin) (Fig. 2). The white pulps were formed by only some lymphocytes aroundthe central arteriole. An intense parasitism was observed in the thickness of the capsule,subcapsular and perifollicular region (marginal zone). Thrombus formation was observedin some blood vessels of the red pulp.
206 W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212
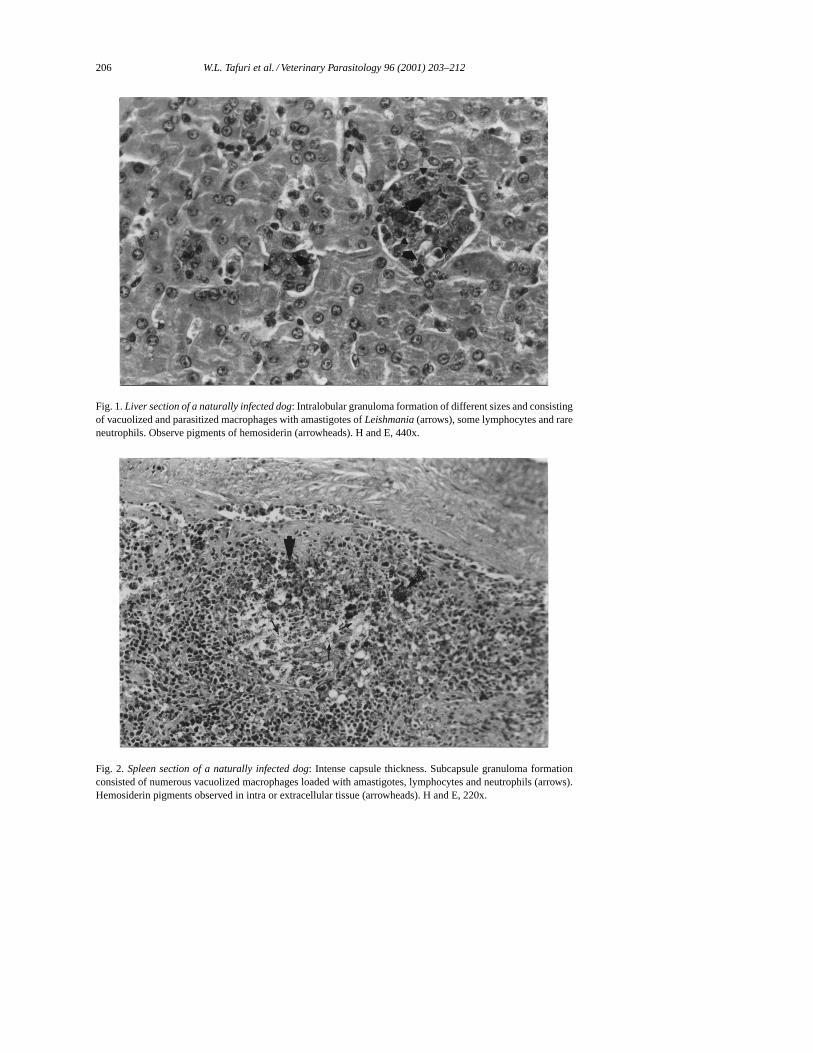
Fig. 1.Liver section of a naturally infected dog: Intralobular granuloma formation of different sizes and consistingof vacuolized and parasitized macrophages with amastigotes ofLeishmania(arrows), some lymphocytes and rareneutrophils. Observe pigments of hemosiderin (arrowheads). H and E, 440x.
Fig. 2. Spleen section of a naturally infected dog: Intense capsule thickness. Subcapsule granuloma formationconsisted of numerous vacuolized macrophages loaded with amastigotes, lymphocytes and neutrophils (arrows).Hemosiderin pigments observed in intra or extracellular tissue (arrowheads). H and E, 220x.

W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212 207
3.3. Lungs
The central feature observed in the samples from the lungs was the chronic and diffuse in-terstitial pneumonia. The lesions had an intraalveolar accumulation of various macrophagesand interstitial thickening due to accumulations of lymphoid cells and fibrous tissue. How-ever, interstitial pneumonia was observed in different phases: the exudative phase and theproliferative phase. Histologically, the intralobular septal thickening was made up of leuko-cytes, fibroblasts, and collagen, respectively. A chronic peripheric bronchopneumonia wascharacterized by a cellular exudate of lymphocytes, plasmocytes and macrophages. Hyper-plasia of smooth muscle was observed in all intralobular septal walls.
Arteries and arterioles showed a spectrum of pathological alterations. The endothelial andthe medial vessel layers were deeply damaged and associated with hyaline thrombosis orprogressive fibroblastic proliferation. These alterations could be seen to occlude the lumenof the vessels (Fig. 3a and b).
Inflammatory foci in the subpleural region were characterized by focal accumulations offoamy macrophages. Areas of emphysema were recognized as abnormal enlargements ofair spaces distal to terminal bronchioles with evidence of destruction of their walls.
3.4. Kidneys
The glomeruli showed a diffuse membranoproliferative glomerulonephritis. Cellularityof the glomerular tufts was increased by proliferation of endothelial, epithelial, or mesangialcells. Intravascular accumulations of neutrophils and monocytes accompanied the cellularproliferation. The glomerular capillary walls were thickened due to the thickening of thebasement membrane and the parietal and visceral endothelial and epithelial swelling. Accu-mulation of hyaline material (homogeneous, eosinophilic, PAS-positive), was observed inthe mesangial areas (Fig. 4a and b). Thickening of Bowman’s capsule occurred due to the hy-perplasia of parietal epithelial cells, thickening of the basement membrane and periglomeru-lar fibrosis. We observed some glomeruli with tuft atrophy due to scarring. Non-glomerularalterations included tubular proteinuria and an intense and diffuse chronic interstitial in-flammation. This inflammation was made up of a cellular exudate of mononucleated cells(lymphocytes, plasmocytes and macrophages) accompanied by a tubulointerstitial damageand initial thickening of the interlobular arteries and arterioles (hyperplastic arteriolitis).
3.5. Lymph nodes
The main lesion observed in lymph nodes was the hypertrophy of the cortical and medularregions. Amastigotes were observed inside of the medular macrophages.
3.6. Bone marrow
In the bone marrow, hypoplasia of the cells, mainly white cells, was the principal patho-logical alteration. Mielocytic blood cells were not observed. Red cells predominated overother cell types in all tissue sections examined. Amastigotes were observed inside of mono-cytes.

208 W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212
Fig. 3. (a) and (b)Lung section of naturally infected dog: (a) Chronic interstitial pneumonia and vascular throm-bositosis. The intralobular septal thickening consisted of leukocytes (mononuclear cells). Observe two arteriolarocclusive thrombus with different morphological aspects. One appeared as a hyaline thrombosis and the otherwas characterized by a progressive fibroblastic proliferation. Gomori’s Trichrome stain, 110x. (b) Detail of thearteriolar organized thrombus. Gomori’s Trichrome stain, 440x.

W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212 209
Fig. 4. (a) and (b)Kidney section of naturally infected dog: (a) Membranoproliferative glomerulonephritis withcellularity of the glomerular tuft increasing by proliferation of endothelial, epithelial, or mesangial cells. Noteinflammatory exudate of mononuclear cells and a tubular proteinuria, PAS, 110x. (b) Detail of one glomerularcapillary presented thickening of Bowman’s capsule due to the thickening of the basement membrane and the pari-etal and visceral endothelial and epithelial swelling. An intense accumulation of hyaline material (homogeneous,eosinophilic, PAS-positive) in the mesangial areas are observed, PAS, 440x.

210 W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212
3.7. Skin
Various skin samples from the ears, nose and abdominal tissue showed discrete areasof chronic inflammation. An exudate of mononuclear cells was observed around the smallvessels and glands of the skin. Amastigotes ofLeishmaniawere not observed in any of theskin tissue sections.
4. Discussion
American visceral leishmaniosis (AVL), a common endemic disease in Brazil, is one ofthe most important emerging parasitic diseases. AVL is endemic in rural areas and, recently,has occurred in suburban areas of major Brazilian cities, such as Belo Horizonte, Fortaleza,Natal, Terezina, São Luis, Santarem and Rio de Janeiro. In these cities, dogs alone seemto be the major reservoir of the parasite (Deane and Deane, 1962; Iversson et al., 1983;Michalick, 1993; Marzochi et al., 1985; Tesh, 1995). We have known that the etiologicalagent of the disease in this area isLeishmania(Leishmania) chagasi. In the present case fromJoão Pessoa City, we have identified parasites asL. chagasiby serological and moleculartechniques.
The anatomical and pathological alterations observed in human and canine visceral leish-maniosis are very similar and are related to the immune status of the host (Carvalho andBacellar, 1983; Bacellar et al., 1991; Carvalho et al., 1992; Martinez-Moreno et al., 1993;Pinelli et al., 1994). Both of these diseases show a histopathological picture characterized byhypertrophy and hyperplasia of cells of the mononuclear phagocyte system; hepatitis withintralobular granulomas; interstitial pneumonitis, glomerulonephritis and chronic inflam-mation of the skin.Leishmaniaamastigote forms are detected in many organs, but mainlyin the mononuclear cells of spleen, liver, lymph nodes and bone marrow (Keenan et al.,1984; Tafuri et al., 1996; Ciaramella et al., 1997). In the present case, we also observedamastigotes ofLeishmaniainside hepatocytes. This has also been shown in human visceralleishmaniosis (Bambirra et al., 1980).
Thrombotic manifestations in dogs have been associated with idiopathic, infectious orparasitic diseases, pancreatitis, hyperadrenocorticism, immune-mediated hemolytic anemia,diabetes mellitus, nephrotic syndrome and tumor metastasis. Glomerulonephritis and renalfailure is a frequent diagnosis in areas where leishmaniosis is endemic. Font and Closa(1997) reported thrombosis in one dog with leishmaniosis as a result of a glomerular diseasecomplicated by a state of hypercoagulability created by a nephrotic syndrome. In this casereport the authors showed a hypercoagulable state by demonstrating abnormal values foranti-thrombin III, fibrinogen, platelet count and other parameters. In this case we havedescribed remarkable glomerular lesions with a chronic and intense interstitial nephritis.Based on the severe lesions observed, we conclude that this histopathological picture iscompatible with a nephrotic syndrome in this dog.
Most importantly we did not find parasites in the skin. In fact, this animal with severeclinical signs had parasites in all of the tissues described, but not in the skin. It could beconsidered that presence or absence of the parasites in the skin does not depend on theparasitism of the other organs or vice versa.

W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212 211
References
Anderson, D.C., Buckner, R.G., Glenn, B.L., MacVean, D.W., 1980. Endemic canine leishmaniasis. Vet. Pathol.17, 94–96.
Anosa, V.O., Idowu, A.L., 1983. The clinico-haematological features and pathology of leishmaniasis in a dog inNigeria. Zbl. Vet. Med. B 30, 600–608.
Bacellar, O., Barral-Neto, M., Badaró, R., Carvalho, E.M., 1991. Gamma interferon production by lymphocytesfrom children infected withL. chagasi. Brazilian Med. Biol. Res. 24, 791–795.
Bambirra, E.A., Tafuri, W.L., Raso, P., 1980. Alterações ultra-estruturais do fıgado na leishmaniose visceral(Calazar). Estudo de três casos. Rev. Goiana Med. 26, 47–54.
Carvalho, E.M., Bacellar, D.A., 1983. Lymphocytes reactivity to mitogens in American visceral leishmaniasis.Brazilian J. Med. Biol. Res. 16, 35–41.
Carvalho, E.M., Barral, A., Pedral-Sampaio, D., Barral-Neto, M., Badaró, R., Rocha, H., Johnson, W.D., 1992.Immunologic markers of clinical evolution in children recently infected withLeishmania donovani chagasi.JID 165, 535–540.
Chagas, E., Cunha, A.M., Castro, G.O., Ferreira, L.C., Romana, C., 1937. Leishmaniose visceral americana.Relatório dos trabalhos da Comissão encarregada dos estudos da Leishmaniose Visceral Americana em 1936.Mem. Inst. Oswaldo Cruz Rio J. 32, 321–385.
Chagas, E., Cunha, A.M., Ferreira, L.C., Deane, G., Guimarães, F.N., Paugarten, M.J., von e Sá, B., 1938.Leishamniose visceral americana. Relatório dos trabalhos da Comissão encarregada dos estudos da leishmaniosevisceral Americana em 1937. Mem. Inst. Oswaldo Cruz Rio J. 33, 89–229.
Ciaramella, P., Oliva, G., Lura, P.D., Gradoni, L., Ambrosio, R., Cortese, L., Scalone, A., Persechino, 1997. Aretrospective clinical study of canine leishmaniasis in 150 dogs naturally infected byLeishmania infantumA.Vet. Rec. 141, 539–543.
Deane, L.M., Deane, M.P., 1962. Visceral leishmaniasis in Brazil. Geographical distribution and transmission.Rev. Inst. Med. Trop. São Paulo 4, 149–212.
Deane, L.M., Deane, M.P., 1995. Leishmaniose visceral urbana (no cão e no homem) em Sobral Ceará, 1955. OHospital 47, 75–87.
Duarte, M.I.S., Laurenti, M.D., Brandão Nunes, V.L., Rego Jr., A.F., Oshiro, E.T., Corbett, C.E.P., 1986. Intersticialpneumonitis in canine visceral leishmaniasis. Rev. Inst. Med. Trop. São Paulo 28, 431–436.
Font, A., Closa, J.M., 1997. Ultrasonographic localization of a caudal vena cava thrombus in a dog withleishmaniasis. Vet. Radiol. Ultrasound 38, 394–396.
Grimaldi, G., Tesh, R.B., Mc Mathon-Pratt, D.A., 1989. A review of the geographic distribution and epidemiologyof leishmaniasis in the New World. Am. J. Trop. Med. Hyg. 41, 687–725.
Iversson, L.B., Camargo, M.E., Villa Nova, A., Reichmann, M.L.A.B., Andrade, E.A., Tolelano, J.E., 1983.Inquérito sorológico para pesquisa de leishmaniose visceral em população canina-urbana do municıpio de SãoPaulo, Brasil (1979–1982). Rev. Inst. Med. Trop. São Paulo 25, 310–317.
Keenan, C.N., Hendricks, L.D., Lightner, L., Johnson, A.J., 1984. Visceral leishmaniasis in the German ShepherdDog. II. Pathology. Vet. Pathol. 21, 80–86.
Laskay, T., Diefenbach, A., Rollinghoff, M., Solbach, W., 1995. Early parasite containment is decisive for resistanceto Leishmania majorinfection, 1995. Eur. J. Immunol. 25, 2220–2227.
Marcussen, N., Vetner, M., Kristensensen, H.M., 1989. Interstiscial nephritis and glomerulonephritis in visceralleishmaniasis in a dog. APMIS 97, 1137–1140.
Martinez-Moreno, A., Martinez-Cruz, M.S., Hernández-Rodriguez, S., 1993. Immunological and histologicalstudy of T- and B-lymphocyte activity in canine visceral leishmaniosis. Vet. Parasitol. 51, 49–59.
Marzochi, M.C.A., Coutinho, S.G., Souza, W.J.S., Toledo, L.M., Grimaldi, J.R., Momen, H., Pacheco, R.S.,Sabroza, P.C., Souza, M.A., Rangel, J.R., Tramontano, N., 1985. Canine visceral leishmaniasis in Rio deJaneiro, Brazil. Clinical, parasitological, therapeutical and epidemiological findings (1977–1983). Mem. Inst.Oswaldo Cruz Rio J. 80, 349–357.
Michalick, M.S.M., 1993. Spreading of visceral leishmaniasis in urban area of Belo Horizonte, MG, Brazil. Mem.Inst. Oswaldo Cruz, Rio de Janeiro 88 (Suppl. I), 53.
Nieto, C.G., Navarrete, I., Habela, M.A., Serrano, F., Redondo, E., 1992. Pathological changes in kidneys of dogswith naturalLeishmaniainfection. Vet. Parasitol. 45, 33–47.

212 W.L. Tafuri et al. / Veterinary Parasitology 96 (2001) 203–212
Pellegrino, J., Brener, Z., 1958. Reação de fixação de complemento com sangue dessecado no diagnóstico docalazar canino. Rev. Bras. Malariol. Doenças Trop. Publ. Avulsas 10, 39–44.
Pinelli, E., Killick-Kendrick, R., Wagenaar, J., Bernadina, W., Real, G., Ruittenberg, J., 1994. Cellular and humoralimmune responses in dogs experimentally and naturally infected withLeishmania infantum. Infect. Immun.62, 229–235.
Tafuri, Wg.L., Tafuri, W.L., Barbosa, A.J.A., Michalick, M.S.M., Genaro, O., Franca-Silva, J.C., Mayrink, W.,Nascimento, E., 1996. Histopathology and immunocytochemical study of type 3 and type 4 complementreceptors in the liver and spleen of dogs naturally and experimentally infected withLeishmania(Leishmania)chagasi. Rev. Inst. Med. Trop. São Paulo 38, 81–89.
Tafuri, W.L., Michalick, M.S.M., Dias, M., Leite, V.H.R., Barbosa, A.J.A., Bambirra, E.A., da Costa, C.A., Melo,M.N., Mayrink, W., 1989. Estudo ao microscópio óptico e eletrônico, do rim de cães natural e experimentalmenteinfectados comLeishmania(Leishmania) chagasi. Rev. Inst. Med. Trop. São Paulo 31, 139–145.
Tesh, R.B., 1995. Control of zoonotic visceral leishmaniasis: is it time to change strategies? Am. J. Trop. Hyg.52, 287–292.
Tryphomas, L., Zawdzka, Z., Bernard, M.A., Janzen, E.A., 1977. Visceral leishmaniasis in a dog: clinicalhematological and pathological observations. Can. J. Comp. Med. 41, 1–12.
Wilson, S.M., 1991. Nuclei acid techniques and detection of parasitic diseases. Parasitol. Today 7, 255–259.




















