
Cancer patient preferences for quality and length of life
15
Cancer Patient Preferences for Quality and Length of Life Neal J. Meropol, MD 1 , Brian L. Egleston, MPP, Ph.D. 1 , Joanne S. Buzaglo, Ph.D. 1 , Al B. Benson III, MD 2 , Donald J. Cegala, Ph.D. 3,4 , Michael A. Diefenbach, Ph.D. 5 , Linda Fleisher, MPH 1 , Suzanne M. Miller, Ph.D. 1 , Daniel P. Sulmasy, O.F.M., M.D., Ph.D. 7 , Kevin P. Weinfurt, Ph.D 6 , and the CONNECT Study Research Group * 1Fox Chase Cancer Center, Philadelphia, PA 2Robert H. Lurie Comprehensive Cancer Center, Northwestern University, Chicago, IL 3Department of Communication, Ohio State University, Columbus, OH 4Department of Family Medicine, College of Medicine, Ohio State University, Columbus, OH 5Department of Urology, Mount Sinai Medical Center, New York, NY 6Duke University School of Medicine, Duke University, Durham, NC 7Bioethics Institute, New York Medical College, Valhalla, NY Abstract Background—Optimal patient decision making requires integration of patient values, goals, and preferences with information received from the physician. In the case of life-threatening illness such as cancer, the weights placed on quality of life (QOL) and length of life (LOL) represent critical values. The objective of this study is to describe cancer patient values regarding QOL and LOL, and explore associations with communication preferences. Methods—Patients with advanced cancer completed a computer-based survey prior to the initial consultation with a medical oncologist. Assessments included sociodemographics, physical and mental health state, values regarding quality and length of life, communication preferences and cancer-related distress. Results—Seven hundred forty three advanced cancer patients were enrolled. Among 459 advanced cancer patients, fifty-five percent of patients equally valued QOL and LOL, 27% preferred QOL, and 18% preferred LOL. Patients with a QOL preference had lower levels of cancer-related distress (p < 0.001). QOL preference was associated with older age (p = 0.001), male gender (p = 0.003), and higher education (p = 0.062). Patients who preferred LOL over QOL desired a more supportive and less pessimistic communication style from their oncologists. Conclusions—These data indicate that a values preference for length vs. quality of life may be simply measured, and is associated with wishes regarding the nature of oncologist communication. Awareness of these values during the clinical encounter could improve decision making by influencing the style and content of the communication between oncologists and their patients. Address correspondence to: Neal J. Meropol, M.D., Fox Chase Cancer Center, 333 Cottman Avenue, Philadelphia, PA 19111, Phone: 215-728-2450, Fax: 215-728-3639. * The CONNECT Study Research Group includes: Andrew Balshem, BA 1 ; Ellyn Micco, MS 1 ; Jennifer L. Millard, BS 1 ; Eric A. Ross, Ph.D. 1 ; Kevin A. Schulman, M.D. 6 ; Elyse Slater, MS 1 ; Nicholas Solarino, MS 1 ; Jonathan Trinastic, BS 1 , all of whom contributed to the authorship of this paper. NIH Public Access Author Manuscript Cancer. Author manuscript; available in PMC 2009 December 15. Published in final edited form as: Cancer. 2008 December 15; 113(12): 3459–3466. doi:10.1002/cncr.23968. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Cancer patient preferences for quality and length of life

Cancer Patient Preferences for Quality and Length of Life
Neal J. Meropol, MD1, Brian L. Egleston, MPP, Ph.D.1, Joanne S. Buzaglo, Ph.D.1, Al B.Benson III, MD2, Donald J. Cegala, Ph.D.3,4, Michael A. Diefenbach, Ph.D.5, Linda Fleisher,MPH1, Suzanne M. Miller, Ph.D.1, Daniel P. Sulmasy, O.F.M., M.D., Ph.D.7, Kevin P. Weinfurt,Ph.D6, and the CONNECT Study Research Group*
1Fox Chase Cancer Center, Philadelphia, PA
2Robert H. Lurie Comprehensive Cancer Center, Northwestern University, Chicago, IL
3Department of Communication, Ohio State University, Columbus, OH
4Department of Family Medicine, College of Medicine, Ohio State University, Columbus, OH
5Department of Urology, Mount Sinai Medical Center, New York, NY
6Duke University School of Medicine, Duke University, Durham, NC
7Bioethics Institute, New York Medical College, Valhalla, NY
AbstractBackground—Optimal patient decision making requires integration of patient values, goals, andpreferences with information received from the physician. In the case of life-threatening illness suchas cancer, the weights placed on quality of life (QOL) and length of life (LOL) represent criticalvalues. The objective of this study is to describe cancer patient values regarding QOL and LOL, andexplore associations with communication preferences.
Methods—Patients with advanced cancer completed a computer-based survey prior to the initialconsultation with a medical oncologist. Assessments included sociodemographics, physical andmental health state, values regarding quality and length of life, communication preferences andcancer-related distress.
Results—Seven hundred forty three advanced cancer patients were enrolled. Among 459 advancedcancer patients, fifty-five percent of patients equally valued QOL and LOL, 27% preferred QOL,and 18% preferred LOL. Patients with a QOL preference had lower levels of cancer-related distress(p < 0.001). QOL preference was associated with older age (p = 0.001), male gender (p = 0.003),and higher education (p = 0.062). Patients who preferred LOL over QOL desired a more supportiveand less pessimistic communication style from their oncologists.
Conclusions—These data indicate that a values preference for length vs. quality of life may besimply measured, and is associated with wishes regarding the nature of oncologist communication.Awareness of these values during the clinical encounter could improve decision making byinfluencing the style and content of the communication between oncologists and their patients.
Address correspondence to: Neal J. Meropol, M.D., Fox Chase Cancer Center, 333 Cottman Avenue, Philadelphia, PA 19111, Phone:215-728-2450, Fax: 215-728-3639.*The CONNECT Study Research Group includes: Andrew Balshem, BA1; Ellyn Micco, MS1; Jennifer L. Millard, BS1; Eric A. Ross,Ph.D. 1; Kevin A. Schulman, M.D.6; Elyse Slater, MS1; Nicholas Solarino, MS1; Jonathan Trinastic, BS1, all of whom contributed tothe authorship of this paper.
NIH Public AccessAuthor ManuscriptCancer. Author manuscript; available in PMC 2009 December 15.
Published in final edited form as:Cancer. 2008 December 15; 113(12): 3459–3466. doi:10.1002/cncr.23968.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

KeywordsQuality of Life; Cancer Communication; Doctor-Patient Communication; Patient Preferences;Communication Preferences; Cancer-Related Distress; Length of Life Preferences; Patient DecisionMaking; Cancer Communication Aid; Patient Values
IntroductionPatients with advanced cancer exist in a unique medical context in which they are facingmortality and may be considering treatment options that have significant potential for toxicity.In addition, therapeutic choices are characterized by uncertain outcomes, and may be variedand complex, including supportive care alone, standard treatments (e.g. chemotherapy,radiation, biologic), and investigational approaches. Quality patient decision making requiresan adequate patient understanding of treatment options, including potential benefit and harm.The physician serves as the primary source of medical information for cancer patients;1, 2 assuch, the communication between doctor and patient is of critical importance to quality decisionmaking.3-5
In a survey of cancer patients who were considering participation in phase I trials, we observeddiscordance between patient and oncologist perceptions about the content of theirconsultations6. In particular, patients were far less likely to report discussion of quality of lifeissues than their physicians. This lack of agreement is a potential source of concern insofar asnearly all of the patients taking part in the survey valued quality of life at least as highly aslength of life.
Adequate communication about the impact of treatment on quality of life is of particularimportance given that patient preference for either quality of life or length of life can influencepatient treatment decision making. For example, among cancer patients with advanced disease,an individual's preference for length of life over quality of life is associated with treatmentpreference for chemotherapy over watchful waiting7. Further, a number of sociodemographicfactors are associated with preference for quality or length of life. Preference for quality of lifeis associated with older age8-9, and having no children7,8. In contrast, preference for lengthof life is associated with being young, having children, and good functional health status8,10. Despite its importance for cancer patient treatment decision making, few studies haveexplored how individual preference for quality or length of life influences the way in whichpatients wish their doctors to present prognostic and treatment-related information.
To approach the understanding of how patient preferences impact decision making, we haveapplied the Cognitive-Social Health Information Processing (C-SHIP) model11,12. This is acomprehensive framework which delineates the cognitive and affective factors involved inhealth information processing11,12. These factors include the individual's self-construals (e.g.perceived vulnerability to disease), affect (e.g. anxious preoccupation with cancer), values andgoals (e.g. about the doctor-patient encounter and importance of quality of life), as well asgoals related to achieving desired treatment outcomes (e.g. expressing one's concerns andvalues)11. The C-SHIP model emphasizes the role of distress in information processing anddecision-making13. Since distress can impact a patient's ability to process critical prognosticand treatment-related information relevant to treatment choice14, examination of itsrelationship to an individual's values (e.g. importance of quality of life and length of life) andcommunication preferences is essential.
In an effort to improve the matching of consultation content with individual patient values, wedeveloped a computer-based communication aid. We are conducting a randomized clinical
Meropol et al. Page 2
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

trial to assess the impact of this intervention on the content of oncology consultations andpatient satisfaction with physician communication. In this manuscript we describe the baselinecharacteristics of the study population in an effort to define the cognitive-affective profiles andcommunication preferences among those cancer patients who prefer quality of life and thosethat prefer length of life.
MethodsPatient Selection
This report describes baseline survey data obtained as part of an intervention study to evaluatethe efficacy of a computer-based communication aid on treatment decision making in advancedcancer patients. The parent study is a three-arm randomized clinical trial. Two of the armsinclude the survey items that form the basis for this report.
Participants were advanced cancer patients at three United States academic cancer centers.Eligibility criteria included: 1) first outpatient consultation with a medical oncologist; 2)documented metastatic malignancy; 3) 18 years of age or older; 4) able to read and verballycommunicate in English; 5) ability to provide written informed consent to participate. Potentialstudy participants were ascertained between January 2005 and January 2007 by review of newpatient schedules and medical information forwarded at the time of scheduling, before theinitial medical oncologist consultation.
ProcedureFollowing ascertainment, consent to contact potential participants was obtained from thephysician with whom the patient was scheduled. A research assistant then contacted patientsby phone to explain the study. After providing verbal consent, participants were given theoption to complete the computer-based survey at home, using a secure web-interface15, orarrive one hour before their appointment to complete at the clinical site. Participants using thesecure website to complete the survey signed informed consent documents electronically.Participants were given a toll-free number for technical support and to ask any questionsregarding the study. All participants provided written consent upon arrival for their physicianappointments. The study was approved by the Institutional Review Boards at the participatingcenters.
MeasuresPatient Characteristics included gender, age, marital status, education, employment status,race, ethnicity, cancer diagnosis, and treatment history.
Physical and Emotional Health State was assessed using the Short-Form (SF)-12 and theRevised Impact of Events Scale (RIES). The SF-1216 is a highly reliable shortened version ofthe SF-36,17 and is intended to provide indices of quality of life similar to the longer instrumentwhile reducing participant burden. Subscales include a Physical Component Scale (PCS) andMental Component Scale (MCS). Cancer-Related Distress was measured using the RIES, awell-validated 15-item questionnaire measuring event-related intrusion and avoidance.18
Quality of Life and Length of Life Preferences were assessed with three items to determine therelative value that an individual assigns to quality of life (QOL) and quantity of life (LOL).This instrument, designed and refined based on prior research6, 19 with the target population,asked participants to select from among 4 choices about whether QOL or LOL was moreimportant (QOL is all that matters, QOL is more important but LOL matters, LOL is moreimportant but QOL matters, LOL is all that matters). Participants were also asked to rate the
Meropol et al. Page 3
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

importance of QOL and LOL as independent domains on 5-point scales (not at all, somewhat,moderately, quite a bit, very important).
Communication Preferences were assessed using an eight-item survey developed based on areview of relevant literature and existing doctor-communication assessments.20-24Participants were asked to rank their agreement with each of these eight preferences regardingphysician communication about prognostic and probabilistic information on a 5-point scalefrom “Strongly Agree” to “Strongly Disagree.”
Statistical ConsiderationsWe defined QOL and LOL preferences in two ways. We initially defined QOL vs. LOLpreference based upon the single 4-point survey item that required patients to prioritize QOLand LOL. In an effort to discriminate patient preferences further given infrequent selection ofthe extreme values of this single-item measure, we defined three preference groups based uponindependent rating of QOL and LOL on the two 5 point scales. For this composite analysis,we categorized patients with regard to whether they selected equal ratings for QOL and LOLon the independent measures, or whether they rated one of these preferences higher on one ofthe measures. The analyses described below utilize the composite measure.
For unadjusted analyses comparing the quality of life preference groups with potentialconfounders, we used multiple linear regressions with robust standard errors of the continuousconfounders to assess statistically significant differences among groups. We used robuststandard errors to weaken the ANOVA assumption of normally distributed errors. We usedWald tests of the regression parameters to test the null hypothesis that there were no differencesin mean responses among the three quality of life preference groups. For categoricalconfounders, we used Fisher's Exact tests. We used correlations to assess the relationship ofthe communication preference variables with the RIES distress score.
To adjust for age, education, sex, race, SF-12 PCS, and MCS scores in analyses relating qualityof life preferences with communication preferences and distress, we used propensity scoreadjustment through propensity score-based weighting with doubly robust estimation25. Wecalculated robust standard errors using the sandwich estimator of Huber26; our standard errorsaccount for the uncertainty associated with the estimation of the propensity scores. Propensityscore-based weighting is an effective means of adjusting for potential confounders because itallows for the creation of an adjusted population in which the balance of confounders betweenquality of life preference groups can be assessed directly. If the average covariatecharacteristics between quality of life preference groups in the adjusted population are similar,then it is unlikely that the covariates are confounding the adjusted inferences. The adjustedmean communication preference scores presented in Table 4 and adjusted mean distress scorespresented in Figure 1 represent estimates of mean responses in the adjusted population.
To develop the propensity score model, we used a multinomial logistic regression of thenominal three-category quality of life variable. The age, SF-12, education, sex, and race termswere entered into the model using restricted cubic splines for age, SF-12 PCS, and SF-12MCS27 and interactions of sex with age and education. The appropriateness of the model wasmeasured by it ability to balance the covariates among the three groups, as demonstrated inTable 3.
ResultsParticipant Characteristics
1932 patients were contacted and 1101 (57%) agreed to be assigned a password to considerparticipation in this three-arm study; 743 patients (68%) provided informed consent and
Meropol et al. Page 4
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

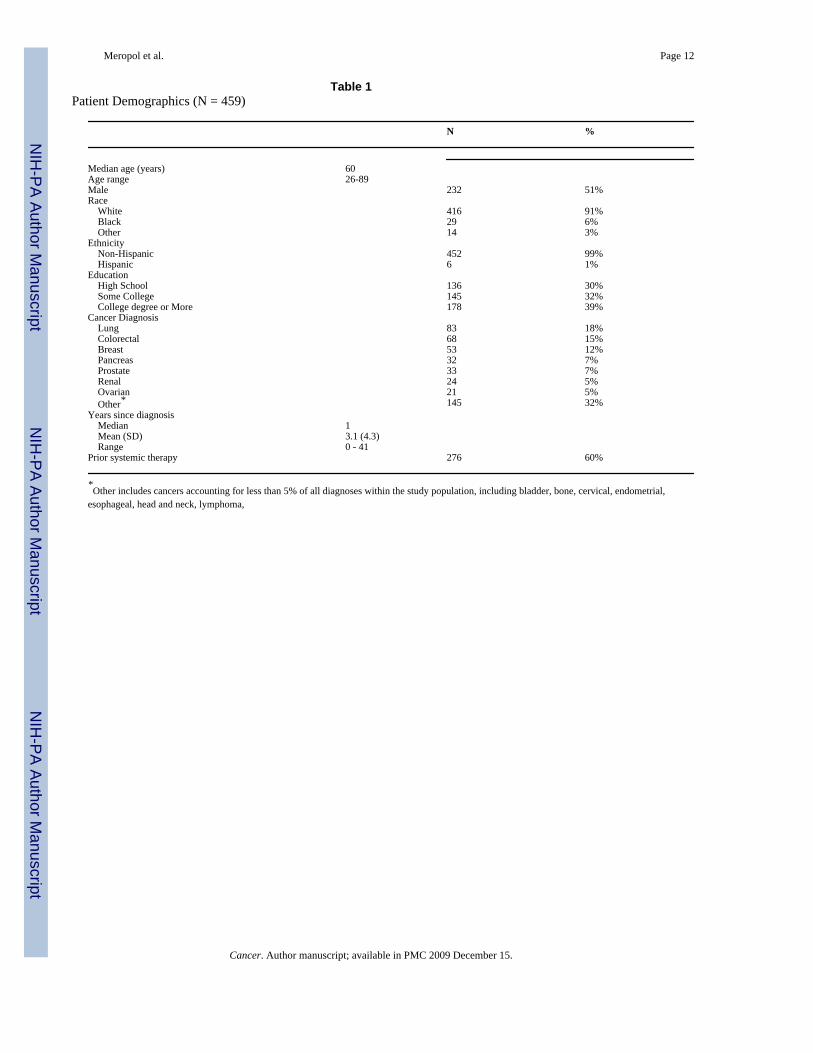
completed baseline surveys. 471 patients were randomized to the two intervention arms, and12 patients with missing data are not included in these analyses. Therefore, 459 patients formthe basis of this report. While all 459 patients were used to derive propensity scores, eachcommunication preference response had an additional one or two missing values. Patientdemographics are shown in Table 1. The sample was primarily White (91%), 51% male, andwell-educated (70% some college or more).
Preferences regarding quality and length of life are summarized in Table 2. Approximatelyhalf of the patient participants (55%) equally valued QOL and LOL based upon the compositemeasure. Of those patients with a preference, quality of life was selected more commonly thanlength of life, 27% vs. 18%. This finding is consistent with the selection of QOL as moreimportant on the single-item scale (80% of patients) where patients were required to committo a preference. Older age (p<.001) and male gender (p<.004) were positively associated witha preference for QOL. To remove possible confounding by these variables in the subsequentcommunication preference analyses, we used propensity score adjustment. In the propensityweighted population, older age and male gender were no longer associated with a preferencefor QOL, indicating successful adjustment. In the adjusted population, all p-values were greaterthan 0.32. Compared to patients with other diseases, those with prostate cancer preferred QOL(p=0.021).
Given a potential relationship between affect and values, an association between patientdistress and QOL vs. LOL preferences was investigated. As shown in Figure 2, those patientswith a preference for quality of life had lower levels of cancer-related distress than thosepatients with a length of life preference or no preference. There was a significant associationbetween the mental health component summary score of the SF12 (p=0.031) and a marginalassociation between the physical health component summary score of the SF12 (p=0.075), andpreferences for quality or length of life, with inferior quality of life on these measures associatedwith a preference for length of life. There was no association between length of time sincediagnosis or previous receipt of systemic therapy, and QOL vs. LOL preferences.
We next explored whether QOL/LOL preferences are associated with preferences forcommunication with the physician. As shown in Table 4, after propensity score-weightedadjustment, regression analyses indicate significant differences in preferences for style ofcommunication between those patients preferring QOL and those preferring LOL. Specifically,compared to the other groups, individuals who indicated that they prefer LOL over QOL(testing for the equality of three means) were more likely to indicate that they would like thedoctor to speak more positively (p<.001), to want the doctor to use general terms (p<.004), towant doctor to soften bad news (p<.001), and to want the doctor to speak in an emotionallysupportive way (p<.001). In contrast, they were less likely to indicate that they wanted thedoctor to give the worst possible results (p<.044).
DiscussionThere is great variability in cancer patients' preferences regarding the content and format ofcommunication from their physicians28,29-31. Matching communication to patientpreferences contributes to quality patient decision making and satisfaction32, 33. Thus toolsto assist physicians in identifying relevant patient preferences and guiding communicationaccordingly could improve clinical outcomes. The data we present indicate that a valuespreference for length vs. quality of life may be simply measured, and is associated with a desirefor more supportive and less pessimistic communication from the oncologist.
Communication skill in the cancer context is particularly critical given that patients arecommonly facing mortality and “bad news,” treatment outcomes are characterized by
Meropol et al. Page 5
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

uncertainty, and treatment is associated with significant potential for morbidity. Previousreports have identified a variety of patient characteristics that bear on their wishes regardingphysician communication. For example, women and patients with higher levels of educationalattainment have been shown to want more detailed information about their prognosis.31, 34,35 Female gender is also associated with desire for a supportive communication style over ablunter approach, while patients with more education31 and older patients36; have been shownto prefer a more fact-oriented style of communication). The data we present support thehypothesis that preference regarding quality and length of life is a key value that impactstreatment goals and desires regarding physician communication. We also observed that olderage (p=0.001), male gender (p=0.004), and higher education (p=0.068) were associated witha preference for quality of life. Even after propensity score adjustment, the QOL/LOLpreference was predictive of patient communication preferences.
It is notable that patients with less cancer-related distress were more likely to favor quality oflife over length of life. The direction of causation in this relationship cannot be inferred fromthese data. It is possible that increased distress is associated with greater difficulty in processingquality of life issues when faced with a life-threatening illness, and therefore a focus on lengthof life is preferred. It is also plausible that a greater concern for one's length of life leads togreater anxiety in the context of an immediate threat to longevity. In either case, high levelsof distress can negatively impact risk information processing and communication, andultimately decision making. The fact that those patients who favor length of life seek a moresupportive communication style and content is consistent with a desire to minimize additionaldistress in this patient subgroup. Further, an alternate explanation exists; patients who relymore heavily on blunting or denial as a way to manage their distress may be more inclined toavoid thinking about end of life and report a preference for length of life without fullyconsidering the range of options, namely, shorter but enhanced quality of life. This subgroupof individuals may be more inclined to prefer provider communications that “soften the blow”and avoid discussion of a difficult reality, and experience heightened distress when providedtoo much threat-relevant information37. Further research is required to more finely delineatethe relationship between these cognitive and affective influences on downstream events.
Although patients who value length of life over quality of life prefer a more supportivecommunication style, this does not imply that communication of “bad news” should be avoided.Withholding of negative prognostic information may result in loss of trust in the physician,decreased compliance, communication barriers between partners, patient isolation and loss ofcontrol, and a lost opportunity to adapt to new circumstances38-40. Furthermore, recent datasuggest that prognostic disclosure may be associated with increased hope, even in the face ofpoor prognosis41. Our data support the recommendation that communication must be tailoredsuch that medical information is conveyed in a manner that serves the cognitive and affectiveneeds of individual patients28, 38-40.
Our findings also show that patients who value LOL over QOL have lower scores on indicatorsof mental health with a trend for these patients to score lower on indicators of physical health.We previously reported that the decision to take part in an experimental therapy program(perhaps indicative of a length of life focus) was related to a patient's reference point regardingthe threat that their cancer posed to their quality adjusted survival.42 Further exploration ofthe relationship between health state and preferences regarding quality and length of life iswarranted.
Because the study population in this report is racially homogenous and relatively well educated,it is difficult to generalize these results to a more diverse population. It is possible that therelationships we observed between distress, QOL and LOL preferences, and communicationpreferences may differ in various socioeconomic or racial groups. Furthermore, this study is
Meropol et al. Page 6
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

limited in that the assessment was conducted at a single time point, and does not capturepotential variations in values and goals over the course of illness. Finally, the method we usedto classify patients' preferences for length vs. quality of life assumed that a 1-point differenceon a 5-point scale represents a precise, meaningful difference. If such differences were notmeaningful, there would be greater noise in our classification of patients' preference, thusleading to an underestimation of the relationships reported here. It is important to note thatbefore this classification method is adopted as a component of routine care, further work toestablish its discriminant ability is appropriate. Nevertheless, this study represents one of thelargest surveys of cancer patient preferences reported to date, and patient ascertainmentprocedures sought to identify and enroll all eligible subjects.
In summary, this study provides evidence that patient differences in the value placed on qualityand length of life can be easily assessed, and these values are associated with preferences forthe content and format of physician communication. We are conducting a prospectiverandomized clinical trial (NCT00244868) to assess whether reporting patient values andpreferences to the oncologist before the initial consultation will impact communication contentand format, and improve patient satisfaction with the consultation.
AcknowledgementsWe also acknowledge the contributions of the Fox Chase Cancer Center Behavioral Research Core Facility,Biostatistics Department and the Population Studies Facility.
Supported by R01CA082085 and Fox Chase Cancer Center Population Studies Facility and Behavioral Research CoreFacility (P30CA06927) from the National Cancer Institute.
We thank the following clinical sites and individuals for enrolling patients to this study: Fox Chase Cancer Center(PI: Neal J. Meropol, MD; Research Assistants: Nicholas Solarino and Jonathan Trinastic); Robert H. LurieComprehensive Cancer Center, Northwestern University (PI: Al B. Benson; Research Assistants: Sheano Gold andLisa Stucky-Marshall), Meharry Medical College (PI: Steven N. Wolff, MD; Research Assistants: Kim Burlison andRoslyn Hatchett-Pope)
References1. Engelman KK, Perpich DL, Peterson SL, Hall MA, Ellerbeck EF, Stanton AL. Cancer information
needs in rural areas. J Health Commun 2005;10(3):199–208. [PubMed: 16036728]2. Liang, W.; Burnett, CB.; Rowland, JH.; Meropol, NJ.; Eggert, L.; Hwang, YT., et al. Communication
between physicians and older women with localized breast cancer: implications for treatment andpatient satisfaction; J Clin Oncol. 2002. p. 1008-16.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=11844824
3. Sepucha KR, Belkora JK, Tripathy D, Esserman LJ. Building bridges between physicians and patients:results of a pilot study examining new tools for collaborative decision making in breast cancer. J ClinOncol 2000;18(6):1230–8. [PubMed: 10715292]
4. Fallowfield L, Jenkins V. Effective communication skills are the key to good cancer care. Eur J Cancer1999;35(11):1592–97. [PubMed: 10673967]
5. Fallowfield L, Jenkins V, Farewell V, Solis-Trapala I. Enduring impact of communication skillstraining: results of a 12-month follow-up. Br J Cancer 2003;89(8):1445–9. [PubMed: 14562015]
6. Meropol, NJ.; Weinfurt, KP.; Burnett, CB.; Balshem, A.; Benson, AB., 3rd; Castel, L., et al. Perceptionsof patients and physicians regarding phase I cancer clinical trials: implications for physician-patientcommunication; J Clin Oncol. 2003. p. 2589-96.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12829680
7. Koedoot, CG.; de Haan, RJ.; Stiggelbout, AM.; Stalmeier, PF.; de Graeff, A.; Bakker, PJ., et al.Palliative chemotherapy or best supportive care? A prospective study explaining patients' treatmentpreference and choice; Br J Cancer. 2003. p. 2219-26.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=14676798
Meropol et al. Page 7
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

8. Stiggelbout, AM.; de Haes, JC.; Kiebert, GM.; Kievit, J.; Leer, JW. Tradeoffs between quality andquantity of life: development of the QQ Questionnaire for Cancer Patient Attitudes; Med DecisMaking. 1996. p. 184-92.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8778537
9. Voogt, E.; van der Heide, A.; Rietjens, JA.; van Leeuwen, AF.; Visser, AP.; van der Rijt, CC., et al.Attitudes of patients with incurable cancer toward medical treatment in the last phase of life; J ClinOncol. 2005. p. 2012-9.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15774792
10. Rietjens, JA.; van der Heide, A.; Voogt, E.; Onwuteaka-Philipsen, BD.; van der Maas, PJ.; van derWal, G. Striving for quality or length at the end-of-life: attitudes of the Dutch general public; PatientEduc Couns. 2005. p. 158-63.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=16257620
11. Miller, SM.; Shoda, Y.; Hurley, K. Applying cognitive-social theory to health-protective behavior:breast self-examination in cancer screening; Psychol Bull. 1996. p. 70-94.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8559860
12. Miller, SM.; Diefenbach, MA. The Cognitive-Social Health Information Processing (C-SHIP) model:A theoretical framework for research in behavioral oncology. In: Krantz, D., editor. Perspectives inBehavioral Medicine. Mahwah, NJ: Lawrence Erlbaum; 1998. p. 219-44.
13. Diefenbach, MA.; Miller, SM.; Daly, MB. Specific worry about breast cancer predicts mammographyuse in women at risk for breast and ovarian cancer; Health Psychol. 1999. p. 532-6.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=10519469
14. Erblich J, Montgomery GH, Valdimarsdottir HB. Biased cognitive processing of cancer-relatedinformation among women with family histories of breast cancer: evidence from a cancer stroop task.Health Psychology 2003;22(3):235–44. [PubMed: 12790250]
15. Buzaglo, JS.; Millard, JL.; Ridgway, CG.; Ross, EA.; Antaramian, SP.; Miller, SM., et al. An internetmethod to assess cancer patient information needs and enhance doctor-patient communication: a pilotstudy; J Cancer Educ. 2007. p. 233-40.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18067435
16. Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales andpreliminary tests of reliability and validity. Medical Care 1996;34(3):220–33. [PubMed: 8628042]
17. Ware, JE.; Snow, KK.; Kosinski, M.; Gandek, B. SF-36 health survey: Manual and interpretationguide. Boston: 1993.
18. Horowitz M, Wilner N, Alvarez W. Impact of Event Scale: a measure of subjective stress. PsychosomMed 1979;41(3):209–18. [PubMed: 472086]
19. Weinfurt KP, Castel LD, Li Y, Sulmasy DP, Balshem AM, Benson AB III, et al. The correlationbetween patient characteristics and expectations of benefit from phase I clinical trials. Cancer 2003;98(1):166–75. [PubMed: 12833469]
20. Bilodeau BA, Degner LF. Information needs, sources of information, and decisional roles in womenwith breast cancer. Oncol Nurs Forum 1996;23(4):691–96. [PubMed: 8735327]
21. Hack TF, Degner LF, Dyck G. Relationship between preferences for decisional control and illnessinformation among women with breast cancer. Soc Sci Med 1994;39(2):279–89. [PubMed: 8066506]
22. Detmar SB, Aaronson NK, Wever LDV, Muller M, Schornagel JH. How are you feeling? Who wantsto know? Patients' and oncologists' preferences for discussing health-related quality-of-life issues. JClin Oncol 2000;18(18):3295–301. [PubMed: 10986063]
23. Dowsett SM, Saul JL, Butow PN, Dunn SM, Boyer MJ, Findlow R. Communication styles in thecancer consultation: preferences for a patient-centered approach. Psychooncology 2000;9(2):147–56. [PubMed: 10767752]
24. Leighl NB, Gattellari M, Butow PN, Brown R, Tattersall MHN. Discussing adjuvant cancer therapy.J Clin Oncol 2001;19(6):1768–78. [PubMed: 11251008]
25. Lunceford, JK.; Davidian, M. Stratification and weighting via the propensity score in estimation ofcausal treatment effects: a comparative study; Stat Med. 2004. p. 2937-60.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15351954
26. Huber P. Robust estimation of a location parameter. The Annals of Mathematical Statistics 1964;35(1):73–101.
Meropol et al. Page 8
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8778537

27. Harrell, F. Regression modeling strategies. New York: Springer; 2001.28. Helft, PR. Necessary collusion: prognostic communication with advanced cancer patients; J Clin
Oncol. 2005. p. 3146-50.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15860876
29. Elkin, EB.; Kim, SH.; Casper, ES.; Kissane, DW.; Schrag, D. Desire for information and involvementin treatment decisions: elderly cancer patients' preferences and their physicians' perceptions; J ClinOncol. 2007. p. 5275-80.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18024875
30. Kutner, JS.; Steiner, JF.; Corbett, KK.; Jahnigen, DW.; Barton, PL. Information needs in terminalillness; Soc Sci Med. 1999. p. 1341-52.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=10369435
31. Butow, PN.; Maclean, M.; Dunn, SM.; Tattersall, MH.; Boyer, MJ. The dynamics of change: cancerpatients' preferences for information, involvement and support; Ann Oncol. 1997. p.857-63.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=9358935
32. Schofield, PE.; Butow, PN.; Thompson, JF.; Tattersall, MH.; Beeney, LJ.; Dunn, SM. Psychologicalresponses of patients receiving a diagnosis of cancer; Ann Oncol. 2003. p. 48-56.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12488292
33. Dowsett, SM.; Saul, JL.; Butow, PN.; Dunn, SM.; Boyer, MJ.; Findlow, R., et al. Communicationstyles in the cancer consultation: preferences for a patient-centred approach; Psychooncology. 2000.p. 147-56.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=10767752
34. Parker, PA.; Baile, WF.; de Moor, C.; Lenzi, R.; Kudelka, AP.; Cohen, L. Breaking bad news aboutcancer: patients' preferences for communication; J Clin Oncol. 2001. p. 2049-56.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=11283138
35. Butow, PN.; Kazemi, JN.; Beeney, LJ.; Griffin, AM.; Dunn, SM.; Tattersall, MH. When the diagnosisis cancer: patient communication experiences and preferences; Cancer. 1996. p. 2630-7.Availablefromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8640715
36. Fujimori, M.; Akechi, T.; Morita, T.; Inagaki, M.; Akizuki, N.; Sakano, Y., et al. Preferences of cancerpatients regarding the disclosure of bad news; Psychooncology. 2007. p. 573-81.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=16998948
37. Miller, SM. Monitoring versus blunting styles of coping with cancer influence the information patientswant and need about their disease. Implications for cancer screening and management; Cancer. 1995.p. 167-77.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8625088
38. Girgis, A.; Sanson-Fisher, RW. Breaking bad news: consensus guidelines for medical practitioners;J Clin Oncol. 1995. p. 2449-56.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=7666105
39. Fallowfield, LJ.; Jenkins, VA.; Beveridge, HA. Truth may hurt but deceit hurts more: communicationin palliative care; Palliat Med. 2002. p. 297-303.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12132542
40. Baile, WF.; Beale, EA. Giving bad news to cancer patients: matching process and content; J ClinOncol. 2003. p. 49s-51s.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12743192
41. Mack, JW.; Wolfe, J.; Cook, EF.; Grier, HE.; Cleary, PD.; Weeks, JC. Hope and prognostic disclosure;J Clin Oncol. 2007. p. 5636-42.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18065734
42. Gaskin, DJ.; Weinfurt, KP.; Castel, LD.; DePuy, V.; Li, Y.; Balshem, A., et al. An exploration ofrelative health stock in advanced cancer patients; Med Decis Making. 2004. p. 614-24.Available fromhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15534342
Meropol et al. Page 9
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=9358935
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8640715
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8625088

Figure 1.QOL-LOL preferences among patients with different cancer types.
Meropol et al. Page 10
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Cancer related distress and quality of life versus length of life preferences.The center bars represent the means of the propensity score adjusted Total RIES measurements,while the whiskers represent the 95% confidence intervals. P<0.001 for a hypothesis test ofthe equality of the three means.
Meropol et al. Page 11
Cancer. Author manuscript; available in PMC 2009 December 15.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Meropol et al. Page 12
Table 1Patient Demographics (N = 459)
N %
Median age (years) 60Age range 26-89Male 232 51%Race White 416 91% Black 29 6% Other 14 3%Ethnicity Non-Hispanic 452 99% Hispanic 6 1%Education High School 136 30% Some College 145 32% College degree or More 178 39%Cancer Diagnosis Lung 83 18% Colorectal 68 15% Breast 53 12% Pancreas 32 7% Prostate 33 7% Renal 24 5% Ovarian 21 5% Other* 145 32%Years since diagnosis Median 1 Mean (SD) 3.1 (4.3) Range 0 - 41Prior systemic therapy 276 60%
*Other includes cancers accounting for less than 5% of all diagnoses within the study population, including bladder, bone, cervical, endometrial,
esophageal, head and neck, lymphoma,
Cancer. Author manuscript; available in PMC 2009 December 15.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Meropol et al. Page 13
Table 2Preferences for Quality and Length of Life
Single-Item measure N %
Quality of life is all that matters 67 15%Quality of life is more important, but length of life matters 299 65%Length of life is more important, but quality of life matters 89 19%Length of life is all that matters 4 1%Composite Measure Mean S.D.
How important is quality of life to you? 4.4 0.8How important is length of life to you? 4.2 1.0
N %
Quality of life more important 123 27%Equally important 252 55%Length of life more important 84 18%
Cancer. Author manuscript; available in PMC 2009 December 15.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Meropol et al. Page 14
Table 3Relationship between patient characteristics and values preferences.
Values PreferenceQOL Equal LOL p
N 123 252 84Agemean (SD)
62.6(10.5)
59.2(11.9)
57.3(11.9) .001
PCS -12 43.5(10.6)
44.6(11.0)
41.6(10.4) .075
MCS-12 44.5(5.4)
42.9(6.3)
43.0(7.9) .031
Male 34% 49% 17% .003Female 20% 61% 19%Race .67 Black 17% 59% 24% White 27% 55% 18% Other 35% 50% 14%Education .062 High School or Less 18% 62% 19% Some College 28% 51% 21% College or more 32% 52% 16%QOL, quality of life preferred; LOL, length of life preferred
Cancer. Author manuscript; available in PMC 2009 December 15.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Meropol et al. Page 15Ta
ble
4R
elat
ions
hip
betw
een
com
mun
icat
ion
pref
eren
ces,
dist
ress
, and
LO
L/Q
OL
pref
eren
ce
Tot
al R
IES
Adj
uste
dM
ean
(SE
)p-
valu
e
Cor
rela
tion
pQ
OL
Equ
alL
OL
p
I wan
t the
doc
tor t
o sp
eak
in a
pos
itive
man
ner
0.09
6p=
0.04
03.
65(.0
9)4.
03(.0
5)4.
19(.0
9)<.
001
I wan
t to
hear
gen
eral
term
s (fo
r exa
mpl
e, “t
he tr
eatm
ent i
s lik
ely
to w
ork”
)ra
ther
than
stat
istic
s (fo
r exa
mpl
e, “
the
treat
men
t has
a 7
5% li
kelih
ood
ofw
orki
ng”)
.
0.03
4p=
0.46
83.
22(.1
2)3.
63(.0
7)3.
76(.1
2).0
02
I wan
t the
doc
tor t
o so
ften
the
blow
whe
n gi
ving
me
bad
new
s0.
321
p<0.
001
2.17
(.10)
2.74
(.08)
2.93
(.16)
<.00
1
I wan
t the
doc
tor t
o sp
eak
to m
e in
an
emot
iona
lly su
ppor
tive
way
0.28
9p<
0.00
13.
83(.0
8)4.
15(.0
4)4.
24(.0
7)<.
001
I wan
t to
hear
det
aile
d st
atis
tics
0.07
4p=
0.11
23.
87(.1
0)3.
96(.0
6)3.
81(.1
0).3
58I w
ant t
he d
octo
r to
spea
k m
atte
r-of
-fac
tly (f
or e
xam
ple,
giv
e m
e th
e co
ldha
rd fa
cts)
-0.2
17p<
0.00
13.
92(.1
0)3.
82(.0
7)3.
88(.1
0).7
21
I wan
t to
hear
ave
rage
s abo
ut p
eopl
e lik
e m
e0.
034
p=0.
463
4.05
(.07)
4.01
(.05)
4.01
(.10)
.910
I wan
t to
hear
the
doct
or's
opin
ion
abou
t my
case
in p
artic
ular
-0.0
87p=
0.06
44.
70(.0
5)4.
66(.0
4)4.
64(.0
7).7
88
QO
L, q
ualit
y of
life
pre
ferr
ed; L
OL,
leng
th o
f life
pre
ferr
ed; S
core
s rep
rese
nt a
vera
ge re
spon
ses,
1 =
Stro
ngly
Dis
agre
e, 5
= S
trong
ly A
gree
(sta
ndar
d de
viat
ion)
Cancer. Author manuscript; available in PMC 2009 December 15.




















