
Cambodia closes in on IDD elimination - Iodine Global Network
20
IDD NEWSLETTER In this Issue: VOLUME 32 NUMBER 2 MAY 2009 INTERNATIONAL COUNCIL FOR CONTROL OF IODINE DEFICIENCY DISORDERS THE INTERNATIONAL COUNCIL FOR CONTROL OF IODINE DEFICIENCY DISORDERS (ICCIDD) is a nonprofit, nongovernmental organization dedicated to sustained optimal iodine nutrition and the elimination of iodine deficiency throughout the world. Its activities have been supported by the international aid programs of Australia, Canada, Netherlands, USA, and also by funds from UNICEF, the World Bank and others. ICCIDD Iodine Safety Declaration 10 Thailand 11 Kosovo 14 Biofortification 16 Meetings and Announcements 18 Abstracts 18 IDD has long been a significant public health problem in Cambodia. The Royal Government of Cambodia initiated a National Sub-Committee for Control of Iodine Deficiency Disorders in 1996 to fight this problem, focusing on Universal Salt Iodization (USI) as the primary strategy to improve iodine status. Cambodia closes in on IDD elimination Pollin Prize 5 Nigeria 6 Pakistan 8 History of Iodine Research 12 Ping Sivlay, Mam Borath and Chan Puong Vatnana Cambodian National Sub-Committee for Control of IDD; Un Sam Oeurn UNICEF Cambodia; Gregory Gerasimov and Cres Eastman ICCIDD Although production of iodized salt start- ed in 1999, there had been only limited success in producing it in large quantities. In 2000 the household consumption of iodized salt was only 12%.This was due to the existence of many small to medium- sized salt producers in Kampot and Kep provinces which were hard to bring under control and the lack of legislation requi- ring them to iodize all their salt.The situation changed dramatically after the Sub-Decree No. 69 on “The Management of Iodized Salt Exploitation” was signed by the Prime Minister on 20 October 2003 and put into effect in October 2004.The Salt Producers Community of Kampot and Kep (SPCKK) was formed with participation of 167 salt producers. The SPCKK is overseeing most of pro- duction and distribution of iodized salt in the country. Some salt is also supplied (often illegally) from neighboring coun- tries (Fig. 1). Cambodian iodized salt ensures optimal infant development Cambodia 1
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Cambodia closes in on IDD elimination - Iodine Global Network
IDDNEWSLETTERIn this Issue:
VOLUME 32 NUMBER 2 MAY 2009
INTERNATIONAL COUNCIL FOR CONTROL OF IODINE DEFICIENCY DISORDERS
THE INTERNATIONAL COUNCIL FOR CONTROL OF IODINE DEFICIENCY DISORDERS (ICCIDD) is a nonprofit, nongovernmental organizationdedicated to sustained optimal iodine nutrition and the elimination of iodine deficiency throughout the world. Its activities have been supported bythe international aid programs of Australia, Canada, Netherlands, USA, and also by funds from UNICEF, the World Bank and others.
ICCIDD
Iodine SafetyDeclaration 10Thailand 11
Kosovo 14Biofortification 16Meetings and Announcements 18Abstracts 18
IDD has long been a significant public health problem in Cambodia. The RoyalGovernment of Cambodia initiated a National Sub-Committee for Control of IodineDeficiency Disorders in 1996 to fight this problem, focusing on Universal SaltIodization (USI) as the primary strategy to improve iodine status.
Cambodia closes inon IDD elimination
Pollin Prize 5Nigeria 6Pakistan 8
History ofIodine Research 12
Ping Sivlay, Mam Borath andChan Puong Vatnana CambodianNational Sub-Committee for Control of IDD; Un Sam Oeurn UNICEF Cambodia;Gregory Gerasimov andCres Eastman ICCIDD
Although production of iodized salt start-ed in 1999, there had been only limitedsuccess in producing it in large quantities.In 2000 the household consumption ofiodized salt was only 12%.This was due tothe existence of many small to medium-sized salt producers in Kampot and Kepprovinces which were hard to bring undercontrol and the lack of legislation requi-
ring them to iodize all their salt.Thesituation changed dramatically after theSub-Decree No. 69 on “The Managementof Iodized Salt Exploitation” was signedby the Prime Minister on 20 October2003 and put into effect in October 2004.The Salt Producers Community ofKampot and Kep (SPCKK) was formedwith participation of 167 salt producers.The SPCKK is overseeing most of pro-duction and distribution of iodized salt in the country. Some salt is also supplied(often illegally) from neighboring coun-tries (Fig. 1).
Cambodian iodized salt ensures optimal infant development
Cambodia 1
IDD NL may09 27.5.2009 9:39 Uhr Seite 1

The basis for production and supply ofiodized salt in Cambodia is the producti-on and harvesting of solar salt in Kampotand Kep provinces. Annual production ofiodized salt ranges from 72,000 to106,000 MT depending on weather con-ditions and the duration of the overcastperiod during the production season.
A first national school-based survey ofiodized salt use was conducted inCambodia in 2005. A total of 2,878 saltsamples were tested with rapid test kits(RTK) of which 2,121 samples (73.7%)tested positive.The salt producing Kampotand Kep provinces had the lowest iodizedsalt consumption, at 19.3% and 27.7%,respectively, due to non-iodized saltcoming from salt fields and storage barns.A lower use of iodized salt was also regi-stered in some border provinces due tothe illegal importation of non-iodizedsalt.Thus, despite significant progress,Cambodia had not reached the goal ofIDD elimination by 2005.
To track further country progress, in 2008 the NSCIDD with UNICEF andICCIDD support conducted a nationalschool-based survey to assess iodized saltuse and the iodine nutrition. In total,2,329 school-children (8 to 10 years) wereassessed. Household salt samples wereidentified as either “coarse” or “refined”salt and were tested for iodine withRTKs. Every third sample of salt wastaken to a laboratory for quantitative iodine determination by titration.Urinary iodine (UI) determinations (a total of 1072 samples) were performed
in the laboratory of Mahidol University(Bangkok,Thailand).
Coverage and quality of iodizedsalt in Cambodia
The performance of the salt iodizationprogram in Cambodia has remainedessentially unchanged over the last 3years. Results of the 2008 survey shownearly the same proportion of householdsusing iodized salt 73.7% as in 2005.Thesame provinces were identified as havingan insufficient proportion of iodized saltat the household level.Thus, only 7.9% ofhouseholds in Kep were using iodized salt(27.7% in 2005) and 27.8% in Kampot
(19.3% in 2005). Six provinces out of 24had household coverage rates of 90% orbetter, and 13 were between 70 and 90%(Fig 2).
Importantly, coarse salt was reported as63% iodized, and refined salt as 91% iodi-zed. The “coarse” salt is produced fromsea water by solar evaporation almostexclusively in the southern provincesKampot and Kep. The “refined” salt isproduced in Kampot province and bysmall producers of boiled salt in manyprovinces of Cambodia. Although thedefinition of “refined salt” may besomewhat subjective, it appears the salt ofhigher quality complies much better with
the iodization requirement, both in termsof proportion iodized as well as in theiodine amount of the salt that was iodi-zed, the median iodine content was 25mg/kg for the coarse salt and 32 mg/kgfor the “refined” salt. Also, while 73.7%salt samples collected in households acrossCambodia were iodized, only 61.7% ofsalt samples were adequately iodized (defined as an iodine level of 15 ppm or more).
These data suggest that with the excepti-on of the salt producing provinces of theSouth, the salt iodization program ofCambodia is providing sufficient iodine to almost the entire population.
Iodine nutrition of the Cambodiapopulation
In the 2008 national survey, UI levels weredetermined in 1072 schoolchildren.Themedian UI level (221.5 µg/L) indicatesiodine intake at the national level is slightlyabove the recommended range of 100-199µg/L.While this level of iodine intake islikely to provide an adequate intake forpregnant and lactating women, it may alsopose a slight risk of more than adequateiodine intake in the population. Only 2.9%of urinary samples had iodine concentrati-on <20 µg/L; 8.9% of samples were <50µg/L and more than 88% of urine sampleshad iodine concentration >100 µg/L.
2 IDD NEWSLETTER MAY 2009 CAMBODIA
Figure 1: Main sources of iodized salt in Cambodia
IDD NL may09 27.5.2009 9:27 Uhr Seite 2

IDD NEWSLETTER MAY 2009 CAMBODIA 3
These UI data suggest the IDD controlprogram in Cambodia is performing bet-ter than indicated by data on coverage ofthe population with iodized salt, based onsalt testing with RTK. In only 3 provinces(Kep and Kampot in the South andMondul Kiri in the East), the median UIwas lower than 100 µg/L, indicating ina-dequate intake of iodine (Fig. 3).
The low median UIs in schoolchildren inKep and Kampot is clearly associated withthe lack of well iodized salt in these pro-vinces. However, it is more difficult toexplain the low UI in Mondul Kiri,because the proportion of householdsusing iodized salt and the iodine concen-trations in salt were identified as accepta-ble. At the same time, the median UIs inSvay Rieng, Kampong Chhnang, SiemReap, Kandal and several other provinceswere surprising in that a high UI is asso-ciated with a relatively short supply ofiodized salt in the homes.The IDD situa-tion in these provinces is more difficult to explain, and it may be attributable tofailure of the RTK to detect the presence of iodine in the coarse salt common inCambodia. Alternately, the contributionfrom other sources rich in iodine, e.g. fishsauce made with iodized salt, may play arole.
The results of the present survey indicateonly 4.9% of the Cambodian population,specifically in Kampot and Kep provinces,have inadequate iodine nutrition whilethe rest of population (more than 95%)have a normal or more than sufficientsupply of iodine.The UI results suggestthe iodine intake of most of the Cambodiapopulation is sufficient. In some regions itis likely at the high end of recommendedintake, because for 10 provinces more than40% of the urine samples had iodine levels>300 µg/L, the cut-off point to identifyexcessive intake of iodine.
Figure 2: Percentage of households using iodized salt in different provinces ofCambodia (red color indicates <50% coverage; blue – 50-89%; green - > 90%).
Figure 3: Median UI in the provinces of Cambodia
IDD NL may09 27.5.2009 9:27 Uhr Seite 3

4 IDD NEWSLETTER MAY 2009 CAMBODIA
One of the reasons for normal or slightlyelevated median UI in regions with arelatively low proportion of adequatelyiodized salt may be the overall high percapita salt consumption of the Cambodiapopulation (directly and through condi-ments such as fish sauce). Also, the lack ofa direct relationship between median UIand household consumption of iodized
salt may be explained by the contributionof other food sources rich in iodine, suchas fish sauce. However, the 2008 surveywas designed and powered to provide datarepresentative for entire population ofCambodia, not for separate provinces orgroups of provinces, so it is difficult todraw conclusions on regional differences.
The similarity between the results of the2008 survey and the data from the previo-us (2005) assessment implies the salt iodi-zation program in Cambodia may have
reached a plateau of performance fromthe activities that have so far been imple-mented. Improvement of the coverage andquality of iodized salt in the provincesthat fail to reach adequate coverage(Kampot and Kep) likely will require spe-cial targeted approaches and strategies.These provinces are major salt productionregions, where non-iodized salt from eva-
poration ponds or storage barns likelyenters the market. These limitations arenot going to be solved by paying moreattention to the iodization process, butcan only be rectified by working with saltproducers and the local communities toteach them the health risks of consumingnon-iodized salt.While the iodine nutriti-on of the entire population of Cambodiais optimal, additional efforts are needed toimprove the quality of production andiodization of domestically produced salt,especially in Kampot and Kep provinces.
Acknowledgements
The authors wish to extend their thanksto field and laboratory personnel whoparticipated in this survey, to UNICEFCambodia (V. Berdaga), to Dr. O. Dary(AED,Washington, USA) and to Dr. K.Caldwell and Dr. A. Makhmudov (CDC,Atlanta, USA).
Iodized salt increases productivity of Cambodian workers Many small salt producers in Cambodia are still producing noniodized salt
IDD NL may09 27.5.2009 9:27 Uhr Seite 4

IDD NEWSLETTER MAY 2009 POLLIN PRIZE 5
The 2009 Pollin Prize for Researchin Pediatrics has been awarded toBasil S. Hetzel, M.D. for his disco-very that maternal iodine deficien-cy can cause brain damage in newborns. It is estimated that Dr. Hetzel’s work has protectednearly 80 million newborns frombrain damage, and saved over onebillion intelligence quotient points.
Basil S. Hetzel, M. D. was born inLondon in 1922 and was educatedat King’s College and St. Peter’sCollege in Adelaide,Australia.Afterreceiving his medical degree fromthe University of Adelaide, he pur-sued his postgraduate educationand research in Adelaide (1945-51),New York (Fulbright ResearchScholar 1951-54), and London(1954-55). He returned to theUniversity of Adelaide to serve asProfessor of Medicine (1956-68)and later spent seven years in thepost of Foundation Professor ofSocial and Preventive Medicine atMonash University in Melbourne.In 1975, Dr. Hetzel joined theCommonwealth Scientific andIndustrial Research Organization(CSIRO) as their first Chief of theDivision of Human Nutrition.
From 1964 to 1972, he, along with a team of researchers in Papua NewGuinea, established that severe braindamage could be prevented by correc-ting iodine deficiencies before pregnan-cy. Subsequent studies in animal models
confirmed the effect of severe maternaliodine deficiency on fetal brain develop-ment. Because of Dr. Hetzel’s importantresearch, the World Health Organization(WHO) now recognizes iodine deficien-cy as the most common preventablecause of brain damage in the world.Despite this understanding, it is believed
that each year nearly 41 millionnewborns from 130 countries arestill at risk for brain damage causedby iodine deficiency. Dr. Hetzel has devoted his life to preventingneedless brain damage in newborns.In 1985 he played a key role inestablishing and then leading theICCIDD, which has since growninto a multidisciplinary global network of 700 professionals frommore than 100 countries. In 1995,he became Chairman of theICCIDD and still serves as a senioradvisor to the organization today.
In addition to his ground breakingwork in iodine deficiency, Dr.Hetzel has published articles inmore than 200 scientific publicati-ons and has worked as the author,editor, or co-editor of 18 books.His book,“The Story of IodineDeficiency:A Challenge inInternational Nutrition” (1989) has been translated into French,Spanish, Chinese, Japanese, andRussian. Dr. Hetzel has been therecipient of numerous awards,including the Award for Disting-uished Research Achievement fromthe International Association for the
Scientific Study of Intellectual Disability;the Living National Treasure Award,National Trust of Australia; ProfessorKazue McLaren Leadership AchievementAward, from the Asia Pacific AcademicConsortium in Public Health; andCentenary Medal, Federation ofAustralia.
Pollin Prize awarded to BasilHetzel for his pioneering workon IDD
IDD NL may09 27.5.2009 9:27 Uhr Seite 5

6 IDD NEWSLETTER MAY 2009 NIGERIA
Did universal salt iodization helpreduce the infant mortality ratein Nigeria?
Nigeria is the most populous country inAfrica. Between 1995 and 2006, the infantmortality rate in Nigeria decreased from114‰ to 99‰.Although many factorscontributed to the reduction in the infantmortality rate during this period, it is likelythat IDD elimination played a role, as seve-re iodine deficiency may increase infantmortality (1).
At the 2007 Micronutrient ForumMeeting in Istanbul,Turkey, Nigeria washonored with the Universal Salt Iodization(USI) certification award, in recognition ofthe nation’s pragmatic approach in comba-ting endemic IDD through an aggressivesalt iodization program (2).The WHORegional Committee for Africa in its 58thsession at Yaounde, Cameroon in 2008recognized that “currently, only Nigeriahas been certified as having achieved thegoals of sustained elimination of IDD inthe African Region.This achievement waspossible because of a decentralized monito-ring system, an efficient ultra-modern ana-
lytical laboratory, sensitized salt market,strict inspection and enforcement of uni-versal salt iodization laws, intensive masscommunication, social marketing, public-private partnership, collaboration withinternational organizations, and high-leveladvocacy” (3).The Nigerian action was anorganized response to a major publichealth challenge.
Goiter was known to be endemic in partsof Nigeria, particularly in the Eastern,Western and Northern Regions.Oyenekwe et al. (4) comprehensivelyreviewed the pioneering studies of goiterprevalence in Nigeria. It was then widelybelieved goiter was due to low iodine con-tent in the soil and foods, aggravated bygoitrogens such as excessive cassava con-sumption.
With UNICEF support , in 1993 Egbutaconducted the National Baseline Survey ofIDD in Nigeria and found a mean goiterrate of 20%, indicating moderate endemici-ty (5). Urinary iodine excretion (UI) wasnot measured in this survey.This was follo-wed by a Federal Government Act stipula-ting that all food grade salt (both forhuman and animal consumption) shouldbe iodized at 50 ppm. Compliance by themany Nigerian salt producers was excellentand they were monitored by the StandardsBoard of Nigeria (SON).
In 1995 (6), a Seven Africa Country Studyon the impact of USI included Nigeria.Dan Lantum from ICCIDD led a nationaland international team, including SON,that studied iodization practices in indu-stries and retailers. It also randomly selec-ted two states with sentinel sites that hadparticipated in the 1993 survey to assess
USI impact. One was Igarra Communityin the Local Government Area of Edo, andthe other was Enugu State, OmolopaCommunity. School children 5-12 years-old were studied.The team found USI wasalready well established and goiter rateswere falling. Urine was collected for iodinemeasurement in Belgium and in parallel atthe Federal Government Laboratory inYaba.
In 1998, Unicef supported a SecondNational Impact Survey, done under theleadership of Prof. Onyenekwe at theUniversity of Nigeria Teaching Hospital(UNTH) Enugu (4).This included elevenStates of Nigeria covering the four PublicHealth Ecologic Zones. It measured household availability of iodized salt,retail salt iodine levels with rapid test kits, the goiter rate and UI. It set up anIodine Analysis Laboratory at the UNTH
Daniel N. Lantum ICCIDD Regional Coordinator for Africa
This article is a summary of a presentation given at the Nigerian Academy of Sciences Workshop:“Reducing maternal and infant mortality inNigeria, bridging the gap from knowledge to action” at the Peiz Continental Hotel,Abuja-Nigeria, 24–26 March, 2009.
Iodized salt provides ample iodine for thisNigerian girl
IDD NL may09 27.5.2009 9:27 Uhr Seite 6

IDD NEWSLETTER MAY 2009 NIGERIA 7
Hospital.The results showed persistent progress in USI with decreasing goiterrates and rising UI.All salt samples wereiodized,TGR was 11.8% and the medianUI was 146.8µg/L (Table 1).
Maxiya Dixon (7), a Food Technologistworking at International Institute forTropical Agriculture (IITA) Ibandan wascommissioned by the Federal Governmentwith support of USAID to lead a nationalsurvey including children, mothers andpregnant women in 2001. Urine sampleswere anlyzed in Cape Town at the MedicalResearch Council Laboratory.The resultsindicated IDD was virtually eliminated inNigeria (Table 1).
In December 2002 (8), an IDD task forceconsisting of SON, the National Agencyfor Food and Drug Administration Control(NAFDAC) and the National PrimaryHealth Care Development Agency(NPHCDA) carried out an assessment ofproduction, marketing and consumption of iodized salt in Nigeria.The study concluded:“Overall, the findings of thesurvey indicated that in any given place in Nigeria, consumers can be more than97.5% confident that when they buy bran-ded salt, it is iodized. Furthermore, 98.3%of salt consumed at the household level isiodized, although 9.7% had lost sufficientiodine to drop below the 15ppm thres-hold.At the factory level, all the salt sam-ples analyzed contained iodine at >15ppm.
The retail level contained iodine at>15ppm in all but 2 States (Taraba andEbonyi States) where 4%, and 25% respec-tively of the samples assayed contained<15ppm iodine.”Thus the survey sugge-sted USI had been generally sustained inNigeria (9,10).
To further improve the situation, it wasrecommended:
1.The capacity of health and regulatoryagencies is to be strengthened throughtraining on quality control and monito-ring, for institutionalized compliancemonitoring.
2.The salt survey should be incorporatedinto NAFDAC’s Annual Work Plan justlike other inspectorate activities, andshould be performed quarterly at thedistribution level and annually at theretail level to ensure sustainability ofmonitoring.3.As a routine activity, monitoring ofthe micronutrient deficiency controlprogram should be integrated into otherHealth Service deliveries, eg. primaryhealth care.4. NAFDAC should conduct quantitativeanalysis of salt samples.
In 2004, another National Survey wasdone, to assess USI impact and progress ingeneral and in endemic zones. UI wasmeasured in the new Iodine Laboratory atthe University College HospitalLaboratory, Department of ChemicalPathology.The median UI again suggestedvirtual IDD elimination.The GlobalNetwork for Sustainable Elimination ofIDD sent a team of external assessors toreview the Nigerian USI/IDD situationand confirmed sustained elimination ofIDD, a remarkable achievement for thislarge African country.
Current recommendations (2009):1. Sustain the USI Program as it is2. Intensify proper case clerking in hospitals, especially by obstetrics,neonatology and pediatrics3. Intensify operational research in healthcare delivery4. Increase diagnostic capacity of healthinstitutions including laboratory infra-structure and scope of those laboratories5. Intensify clinical research and repor-ting of hospital and health center stati-stics.6.Assess improvements in IQ in childrendue to iodine malnutrition.7. Investigate the possibility of goitroge-nesis at Ekiti.8. Endocrinologists and cardiologistsshould study the likelihood of iodineinduced hyperthyroidism.
References1. Cobra C et al. Infant survival is improved by oral iodine sup-plementation. J Nutr 1997;127(4):574-8.2. Accolades to NAFDAC as Nigeria bags universal salt iodizati-on award.Vanguard, Friday April 27, 2007.3. WHO AFRO. 2008 Director’s Report of RC 58 on IDD(citing SCN News 35, 43-47, 2007).4. Oyenekwe B et al. Consultancy Report on ImpactEvaluation of USI Programme in Nigeria. Unicef Nigeria, 1999.5. Egbuta JO. Consultancy Report on Iodine DeficiencyDisorders in Nigeria, Unicef, 1993.6. Lantum DN. Multicentre Study to Assess the Impact of SaltIodization on Iodine Status of the Population of Nigeria,ICCIDD, 1995.7. Bussie Maxiya-Dixon. National Assessment of IodineConsumption by Children under-5, Mothers, and PregnantWomen, IITA, Ibadan, 2004.8. IDD Task Force. Report on Situation Assessment ofProduction, Marketing, and Consumption of Iodized Salt inNigeria, 2002.9. Egbuta JO, et al. Sustaining control of IDD in Nigeria and theWest African Sub-Region. IDD Newsletter 1998;August:42-43.10. Egbuta JO, et al. Impact evaluation of efforts to eliminateIDD in Nigeria, Public Health Nutrition 2002;6(2):169-173.
The Nigerian IDD control program is a model for all Africa
Table 1: Urinary iodine in Nigeria in 2003, by age/population group
Group No Observations Median µg/L Mean µg/L Std Error
Children under 5 2428 183.7 249.5 4.8
Mothers 3104 151.9 197.4 3.2
Pregnant Women 660 167.1 210.0 6.5
IDD NL may09 27.5.2009 9:27 Uhr Seite 7

8 IDD NEWSLETTER MAY 2009 PAKISTAN
According to the WHO Global Databaseon Iodine Deficiency, Pakistan is a countrystruggling with severe iodine deficiency(1). In 1993-1994, a national survey ofiodine status found a median urinary iodi-ne concentration (UI) of 16 µg/L and90.4% of the population had a UI <100µg/L.The total goiter prevalence was esti-mated to be 85% (1).About 17% of house-holds were using iodized salt and 128 mil-lion people in Pakistan were at risk ofiodine deficiency (2).
In 2005, Pakistan’s Ministry of Health fina-lized the National Plan for Action withtechnical and financial assistance from theMicronutrient Initiative (MI). One of itshighest priorities is to increase access toand use of adequately iodized salt inPakistan (2). In 2008, the Nutritional Wingof the Ministry launched a project in 65districts of Pakistan to enhance productionof iodized salt in the country. Iodized saltproduction has increased from 17% to 70%in the districts where incidence of iodinedeficiency is high (3).
In the Northern Areas of Pakistan, severeiodine deficiency has been recognized for a
century, particularly in Gilgit and Chitral(4). Baltistan, in the northeast of Pakistan,lies within the belt of IDD spreading fromBukhara and Samarkand in southern SovietUnion along the Himalayas and downthrough South East Asia to Papua NewGuinea and New Britain (5).
From 1981-1986, Dr.Alex Stewart studiedthe prevalence of goiter and water iodinecontent in Baltistan. His studies demonstra-ted the prevalence of goiter in males was34% and in females was 49%. Iodine con-tent in water was low, with a mean valueof 11.8 nmol/l, compared to mean waterconcentrations of iodine in other non-iodine deficient regions of 40 nmol/l (5).A Northern Areas Health Survey 1999reported the goiter prevalence amongvarious districts of the Northern Areas.Theprevalence of grade 2 (visible) goiter wasparticularly high in the District ofGhanche Baltistan(Table 1) (6).
Because data on UIand thyroid functionwere not available forthe Balti population, asentinel study wasconducted in four vil-lages of Baltistan inthe District ofGhanche in 2005.Blood and urine sam-ples from 120 indivi-duals were collected.Samples were collec-ted from pregnantwomen (n=19), non-pregnant women aged 13-60 yrs (n=48),
males aged 13-60 yrs (n=45) and children6-12 yrs (n=8).
Urinary Iodine. The results of the surveyof urinary iodine are shown in Table 2. Ofgreat concern, the data suggest pregnantwomen and children are severely iodinedeficient. Males and females aged 13-60years are moderately iodine deficient.Three quarters of the population has a UI<100µg/L.
Thyroid Function Tests. The results ofthe analysis of total and free triiodothyro-nine (T3), total and free thyroxine (T4)and thyrotropin (TSH) are shown in Table2. Pregnant women with severe iodinedeficiency have abnormally high TSH andlow FT4 concentrations.Thyroid hormoa-ne concentrations are within the normalrange in females and males aged 13-60years and in children.
Severe IDD in pregnancy in Northern Pakistan: a sentinel studyHamida Ali and Peerzada Qasim Raza Siddiqui (Department of Physiology, University of Karachi), Junaid Mahmood Alam andTehseen H Kazmi (Liaquat National Hospital Karachi) and Ghulam Mehdi (District Health Office, Khaplu Ghanche, Baltistan)
Rugged mountains in northern Pakistan: a region of severe IDD
IDD NL may09 27.5.2009 9:27 Uhr Seite 8
IDD NEWSLETTER MAY 2009 PAKISTAN 9
This small sentinel study clearly demon-strates Baltistan remains severely iodinedeficient. It also suggests thyroid functionis impaired in pregnant women puttingthem at high risk of delivering an infantwho may be brain damaged due to iodinedeficiency.This highlights the urgent needto strengthen the national IDD controlprogram in the region.
References1. World Health Organization. Iodine statusworldwide WHO Global Database on IodineDeficiency. Department of Nutrition for Healthand Development. Geneva:World HealthOrganization 2004.2. MicroNutrient Initiative. Pakistan.http://www.micronutrient.org (accessed Mar27, 2009).3. Associated Press of Pakistan. Project launchedin 65 districts to produce iodized salt.http://www.app.com.pk (accessed April 25,2009).4. Azizi F.IDD in the Middle East. ICCIDDNewsletter 2001; 17:3.5. Stewart AG.Drifting continents and endemicgoiter in northern Pakistan.BMJ 1990;300:1507-1512.6. Agha Khan Health Service. Northern Areasand Chitral,Annual Report 2000.
Goiter Ghizar Gilgit Diamir Skardu Ghanche All
Grade 0 97.1 89.8 87.8 60.0 37.7 77.8
Grade 1 2.9 8.7 12.2 29.5 39.8 16.4
Grade 2 0.0 1.5 0.0 10.5 22.5 5.8
Table 1: Prevalence of goiter (%) among children 6-11 years in various districtsof Northern Areas of Pakistan in 1999 (4).
Table 2: Urinary iodine concentrations and thyroid function tests in Balti in 2005.
Median T3 T4 TSH FT3 FT4UI (µg/L) (ng/mL) (µg/dL) (mU/L) (pg/mL) (ng/mL)
Pregnant 15 1.5 8.3 14.5 2.8 0.84women
Non–pregnant 37 1.3 6.6 2.6 3.2 1.01 women 13-60 years
Males 13-60 23 1.4 7.4 2.4 3.1 1.2years
Children 6-12 18 1.4 8.5 2.4 3.9 1.3years
Balti infants urgently need more iodine
Most Pakistani children are iodine deficient increasing risk for poor development
IDD NL may09 27.5.2009 9:27 Uhr Seite 9
10 IDD NEWSLETTER MAY 2009 IODINE SAFETY DECLARATION
Iodine deficiency is still prevalent world-wide. It can lead to goiter, thyroid dysfunction and is the main preventablecause of mental retardation globally.
Optimizing iodine intake is widely recog-nized as the most cost effective solutionfor achieving optimal intellectual develop-ment in addition to normalized thyroidfunction in iodine deficient areas.
The issue of the safety of increasing iodine intake has recently been raisedbased on occasional regional reports ofdetrimental side effects due to excessiveamounts of iodine.
The current WHO recommended dailyintake of iodine for adults is between 150 µg and 300 µg per day. The EuropeanCommission and the US Institute ofMedicine have discussed tolerable upper
iodine intake for adults and have indicatedintakes of 600 µg and 1100 µg per day,respectively.
Mild thyroid hyperfunction may occur following an increase of iodine intake within the recommended range as a consequence of pre-existing autonomousnodular goitre due to long standing iodine deficiency. This is a transienteffect.The single relevant adverse effect is iodine induced overt hyperthyroidism(IIH), only observed in severely iodinedeficient populations after a rapid intro-duction of excessive iodine supplementa-tion which should and can be avoided.
Excessive iodine intake may lead to atransient small increase in the prevalenceand incidence of subclinical hypothyroi-dism and thyroid autoimmunity, especiallyin older individuals.
Insufficient monitoring of salt iodine content and iodine intakes in populationsincreases the risk of iodine inducedhyperthyroidism and other side effects.With sustained quality assurance andmonitoring these can be almost entirelyavoided.
While the overall incidence of thyroidcancer in populations does not appear tobe influenced by iodine intake, a shift toless malignant types of thyroid cancer iswidely recognized as a consequence ofintroducing iodine prophylaxis.
In conclusion, optimal iodine intake supported by adequate monitoring hasbeen widely shown to improve the qualityof various health aspects.The benefits ofiodine supplementation far outweigh therelatively small risks of iodine excess.
ICCIDD DECLARATION
Importance and Safetyof Optimizing IodineNutrition
ICCIDDINTERNATIONAL COUNCIL FOR CONTROL
OF IODINE DEFICIENCY DISORDERS
IDD NL may09 27.5.2009 9:27 Uhr Seite 10

IDD NEWSLETTER MAY 2009 THAILAND 11
The median urinary iodine concentration(UI) in school-aged children is recommen-ded for assessment of iodine nutrition inpopulations. If the median UI is adequate inschool-aged children, it is usually assumediodine intakes are also adequate in theremaining population, including pregnantwomen. But iodine requirements are sharplyincreased during pregnancy. Recommendediodine intakes during pregnancy are 250µg/d compared to 150 µg/d for nonpreg-nant women.The corresponding medianurinary iodine concentration (UI) that indi-cates optimal iodine nutrition increases from100-199 µg/L in nonpregnant women to150-250 µg/L during pregnancy.
To clarify this issue, measuring UI frompairs of pregnant women and their school-aged children from the same family wouldbe valuable.The value of matched pairs wit-hin a family is that both groups are sharingmost meals from the same household foodbasket.Thus, a study of pairs can directlyassess whether a diet that supplies adequateiodine to school-aged children also coversthe needs of pregnant women in the house-hold. In Thailand, although about 66% of
households use iodized salt, recent surveyshave suggested iodine status in pregnancymay not be optimal.Therefore, the studyquestion was: if the median UI is adequatein school-aged children, can one assume themedian UI is also adequate in pregnantwomen? If so, then the median UI inschool-aged children could continue to beused as a surrogate for monitoring iodinestatus in pregnancy; if not, then pregnantwomen would need to be directly monito-red.
UI was measured in spot urine samples frompairs (n=302) of healthy pregnant mothersand their school-aged children in metropo-litan Bangkok,Thailand.A dietary question-naire was filled out.The median UI (range)in the pregnant women was 108 (11-558)µg/L and was lower than that of theirschool-aged children [200 (25-835) µg/L]
(p<0.001), indicating optimal iodine statusin the children but mild-to-moderate iodinedeficiency in their pregnant mothers.Estimated iodine intakes in the two groupswere in the range of 130-170 µg/d.Therewas a modest positive correlation betweenUI in the pairs (r= 0.253, p<0.01).A higherfrequency of seafood meals was a significantpredictor of UI in both groups, but house-hold use of iodized salt was not.
The findings indicate that in this region of Thailand the median UI in school-agedchildren may not be an adequate surrogatefor monitoring iodine nutrition in pregnantwomen.These data need to be confirmed in other populations with varying dietaryhabits and iodine intake, but suggest ade-quate monitoring of IDD in populationsshould include specific monitoring of pregnant women.
Urinary iodine concentrations indicate iodinedeficiency in pregnant Thai women but iodinesufficiency in their school-aged childrenSueppong Gowachirapant Mahidol University, Thailand
Figure 1: Frequency distribution of spot urinary iodine concentrations (µmol/L) inmatched pairs of Thai pregnant women and their school-aged children (n=302).The recommended ranges for the median urinary iodine concentration for preg-nant women (—) and children (---) are shown. Conversion from SI to conventio-nal units, 0.0079 µmol/L=1 µg/L.
35
30
25
20
15
10
5
0
Freq
uenc
y, %
<0.39
0.39
- <0.
79
0.79
- <1.
19
1.19
- <1.
58
1.58
- <1.
98
1.98
- <2.
37
>2.37
Pregnant women School-age children
Urinary iodine concentration, µmol/L
Pregnant Thai women are iodine deficientwhile their children have enough iodine
IDD NL may09 27.5.2009 9:27 Uhr Seite 11

12 IDD NEWSLETTER MAY 2009 HISTORY OF IODINE RESEARCH
IntroductionIn 1811, France was at war, and BernardCourtois was producing saltpeter for gun-powder for Napoleon’s army. He was bur-ning seaweed to isolate sodium bicarbona-te, and when he added sulfuric acid to theash he produced an intense violet vaporthat crystallized on cold surfaces. He sentthe crystals to Gay-Lussac, who subse-quently identified it as a new element,and named it iodine, from the Greek for‘violet’.
The ancient Greeks, including Galen, usedthe marine sponge to treat swollen glands.The sponge and dried seaweed remained a'goiter cure' in the medical armamentari-um through the Middle Ages. In 1813,learning of the discovery of iodine in sea-weed, Coindet, a physician in Geneva,Switzerland, hypothesized the traditionaltreatment of goiter with seaweed or spon-ges was effective because of their iodinecontent. He began giving oral iodinetincture to goitrous patients at an initialdaily dose at 165 mg.This provoked strongopposition among the medical profession;opponents claimed it was poisonous, and itwas suggested “…Coindet would not leavehis house for fear of being stoned in thestreet by his poisoned patients…”AlthoughCoindet insisted his treatment was safe, theoften acrimonious debate on the safety ofiodine would continue into the early 20thcentury.
First proposals to use iodized salt The French chemist Boussingault, was thefirst to advocate prophylaxis with iodine-rich salt to prevent goiter. He measurediodine levels in rock and in salt deposits ofthe Andean region, and, in 1825, he repor-ted villages in the province of Antioquiatreated goiter with 'aceyte de sal', an acrid,‘marine smelling’ fluid from the salt depo-sits. He demonstrated in 1835 that salt sentfrom goiter-free Antioquia to neighboringregions reduced goiter endemia.Boussingault was the first to recommendgoiter prophylaxis with iodized salt; itwould be nearly 100 years before theirvision was realized!
Chatin and goiter prophylaxis in FranceThe French chemist Chatin was the first topublish, in 1851, the hypothesis that iodinedeficiency was the cause of goiter. Chatin,the director of the School of Pharmacy inParis concluded: "Too low a concentrationof iodine in the drinking waters of certainareas appears to be the principal cause ofgoiter.” However, his estimates of foodiodine content were about 10-fold toohigh and Chatin's work was greeted withgreat skepticism by the French Academy of Science.
Despite this, French authorities, in threeDepartments where goiter was severe –Bas-Rhin, Seine-Inferieure and Haute-Savoie), began distributing iodine tabletsand salt together with other prophylacticmeasures. In the prefect of Haute-Savoie,the cause of goiter was attributed by localphysicians to drunkenness, dampness, poorhygiene and contaminated drinking water.Various measures were taken: large treesthat prevented the entry of fresh air to vil-lages were felled, wet streets were drained,the water tested for potability and schoolhygiene improved. In addition, iodized saltwas distributed and schoolchildren weregiven iodine tablets daily.The program was clearly effective: in a survey of 5000goitrous children, 80% were cured orimproved by the iodine treament.
Research on iodine deficiencyand goiter in the 19th andearly 20th centuryMichael B. Zimmermann ICCIDD Deputy Regional Coordinator for Western and Central Europe
I am satisfied. I have seen the principal features of Swiss scenery – Mount Blancand the goiter – and now for home. Mark Twain, 1880
Figure 2. In 1915, the ruralSwiss general prac-titioner Bayard didthe first dose-response trial ofiodized salt to treatgoiter in schoolchil-dren
Figure 1. Theodor Kocher,Swiss surgeon, wonthe Nobel Prize inmedicine for hiswork on the physio-logy and pathologyof the thyroid gland
IDD NL may09 27.5.2009 9:27 Uhr Seite 12

IDD NEWSLETTER MAY 2009 HISTORY OF IODINE RESEARCH 13
However, because goiter exemptedyoung men from unpopular mili-tary service in the French army,many parents, fearing their sonswould be enlisted, were againstiodine prophylaxis.Also, the dosesof iodine administered both intable salt and tablets were toohigh: a concentration of 100-500mg/kg was chosen for salt iodiza-tion, and the tablets, which wereto be taken daily, contained 100mg KI.This high dose of iodinewas consistent with the enormousdoses of iodine used to treat manydiseases at the time (scrofula,syphilis, arthritis).While manypeople tolerated the high doses ofiodine well, it likely precipitatediodine-induced hyperthyroidism insome individuals, and as a result,the program was discredited anddiscontinued.
Myxedema and cretinismMedical authorities recognized cretinism only occurred in areas of ende-mic goiter, but were puzzled by the factthat many cretins had an atrophic or absentthyroid gland, the opposite of goiter. Aclue to this apparent paradox appearedwhen a related disease, myxedema, thatresembled cretinism, was described by Ordin 1877 in London. In 1883, Semon sugge-sted myxedema was due to a lack of activi-ty of the thyroid after reading a report bythe Swiss surgeon Kocher (Figure 1) des-cribing myxedemic symptoms in patientsafter total thyroidectomy. British physici-ans began successfully treating myxedemawith injections and/or oral doses of animalthyroid extracts; a 1893 review exclaimed"it was one of the greatest therapeutic triumphs of the age".
The link between goiter, myxedema andiodine was established when, in 1896,Baumann and Roos, working in Freiburg,Germany, digested animal thyroid glandsand were surprised to isolate a residualinsoluble fraction that was ca. 10% iodine.They found this substance, termed "thy-roiodine", to be effective in the treatmentof both myxedema and goiter.They cor-rectly surmised iodine itself was not thera-peutically active, but had to be first incor-porated into an organic molecule.
The Swiss introduce iodized salt Switzerland’s iodized salt program has beenoperating uninterrupted since 1922. Beforeits introduction, Switzerland was severelyiodine deficient. For example, in 1800, acensus ordered by Napoleon reported 4000cretins among the 70,000 inhabitants ofthe Canton Valais, in the Swiss Alps. In1918, the Swiss physician Bayard (Figure 2)did the first dose-response trial of iodine totreat goiter. He did this in Grachen, an iso-lated village at the base of the famousMatterhorn mountain in the Zermatt valley, reachable only by mule track. Hegave iodized salt for six months to familiesin the village with 3 different iodine con-tents (3, 6 and 15 mg/kg). Bayard establis-hed that as little as 30 µg of iodine dailyhad a clear beneficial effect on goiter, andnoted 'soft' diffuse goiters in children weremore responsive than the nodular forms.
The Swiss Goiter Committee was formedin 1922. Initially, the committee cautiouslyadvised the introduction of salt iodized at1.9 to 3.75 mg/kg nationwide on a volun-tary basis, a compromise between the pro-ponents and opponents of iodized salt.The first canton in which iodized salt wasintroduced was Appenzell AR, in 1922,where salt was iodized at 7.5 mg/kg withspectacular results: newborn goiter disap-
peared, no new cretins wereborn, and goiters in childrenwere reduced in size or disap-peared.
Iodine supplementation studies in the USAAt about the same time as thefirst Swiss iodine studies in1915-1919, Marine and Kimballwere introducing iodine pro-phylaxis in the Midwest regionof the U.S. David Marine(Figure 3) trained at JohnsHopkins was appointed to a residency in pathology atLakeside Hospital in Cleveland,Ohio.According to legend, hewas surprised when asked on hisfirst day what research problemhe would like to work on. Hehad noticed several dogs withlarge goiters in the neighbor-hood and replied without muchreflection he would like to workon thyroid disease. Marine sub-
sequently confirmed Baumann’s findingthat large goiters contained less total iodinethan in healthy glands.The American sur-geon Halsted had reported when part ofthe thyroid was resected, the remaining tis-sue increased in size. Marine extended thisobservation and suggested goiter was "acompensatory reaction to some deficiency"and it appeared “…iodine is the mostimportant single factor...".
Marine realized goiter was a serious publichealth problem and in 1916 he planned todo an intervention with iodine in school-children in Cleveland. However, the schoolboard refused, concerned iodine could bepoisonous.With the help of Kimball hereceived permission to do the study inneighboring Akron, Ohio.The treatmentgroup of girls received 200-400 mg NaIper school day for 10 d.The treatment wasclearly effective and Marine and Kimballconcluded goiter: "…is as easily preventedin man as in fish or in domestic animals".
Figure 3. In 1916-17, the American physician David Marine conducted the first large-scale trials of iodine supplementation to prevent goiter in children in Akron, Ohio
IDD NL may09 27.5.2009 9:27 Uhr Seite 13

14 IDD NEWSLETTER MAY 2009 KOSOVO
Kosovo is a small landlocked territory of10,908 km2 in the center of the BalkanPeninsula with a population of ≈2.1million.Kosovo is divided into six regions and 30municipalities.The capital city is Prishtina.Iodine deficiency has been historically
present, with especially high goitre rates inWestern Kosovo (Deçan, Peja, Gjakova andPrizren), ranging from 30 to 60%. All salt is imported in Kosovo.
A representative Micronutrient StatusSurvey conducted in 2001 in Kosovo revea-led that 84% of households were using iodi-zed salt and thyroid was palpable in 3% ofwomen of which 0.2% had visible goitre.Half (51%) of the women and school-agechildren studied had low values (below 100µg/l) of urinary iodine concentration. Basedon these results, Kosovo institutions decidedto step up the strategic approaches toaddress IDD and more vigorously monitorthe imports of salt for adequate iodine con-tent.
The main means of coordination of thenational IDD programme is the workinggroup for IDD and other micronutrientdeficiencies, a multi-sector group consisting
of health officials, public health experts,clinicians, sanitary inspectors, laboratorytechnicians, media, salt importers, flour millers, veterinary inspectors,WHO andUNICEF.The Ministry of Health hasrecently endorsed an AdministrativeInstruction for mandatory quality of salt,stipulating the requirement of 30 - 40 mgKIO3 per kg salt at import.
All salt shipments that enter in Kosovo arechecked at the border points prior to therelease of the shipment.Testing of salt isperformed periodically at wholesale andretail points.The National Institute ofPublic Health in Prishtina and the Instituteof Agriculture in Peja have established labo-ratories for salt quality monitoring.The dis-tribution of iodine content (routinely repor-ted in mg KIO3/kg salt) for the 210 saltshipments inspected during 2006, 2007 andJanuary-April 2008 is shown in Figure 1.
Based on these studies, general prophylaxiswith iodized salt was introduced in thestate of Michigan in 1924.There were pro-tests, and at first the Bureau of Chemistryof the Department of Agriculture deman-ded the iodized salt packages be markedwith the skull and crossbones used to indi-cate a poison, but then backed down. In1948, the U.S. Endemic Goiter Committeetried to introduce iodized salt to all thestates by federal law, but the bill failed.
The modern era: 1930 to the presentIn 1980, the first global estimate fromWHO on the prevalence of goiter wasreported: it estimated 20-60% of theworld’s population was iodine deficientand/or goitrous, with most of the burden
in developing countries. But although itwas recognized many countries were affec-ted by goiter, little attention was paid toiodine deficiency in public health pro-grams. Goiter was considered a lump inthe neck primarily of cosmetic concern; itgenerated little political attention or actionand few resources were allocated for itscontrol.
This changed during the period of 1970-90. Controlled studies in iodine-deficientregions showed that iodine supplementati-on not only eliminated the incidence ofcretinism but also improved cognitivefunction in the remaining population.Iodine deficiency was thus shown to havesocial and economic consequences fargreater than previously appreciated, that
could slow country development.Thischanging view allowed iodine deficiencyand goiter to be repositioned in the deve-lopment perspective.The term ‘the iodinedeficiency disorders (IDD)’ was coined, andIDD was repositioned as a spectrum ofrelated disorders affecting 1.5 billion indi-viduals. Programs against IDD had obviouspolitical appeal because its human, econo-mic and social consequences could beaverted by a low-cost intervention, univer-sal salt iodization. Since 1990, eliminationof IDD has been an integral part of manynational nutrition strategies.
Progress towards eliminationof IDD in KosovoTahire Maloku–Gjergji National Institute of Public Health, Prishtina, Kosovo; Ilirjana Zymberaj Chief Sanitary Inspector of Kosovo,Prishtina, Kosovo; Agron Gashi UNICEF, Prishtina, Kosovo; and Frits van der Haar ICCIDD
IDD NL may09 27.5.2009 9:27 Uhr Seite 14
IDD NEWSLETTER MAY 2009 KOSOVO 15
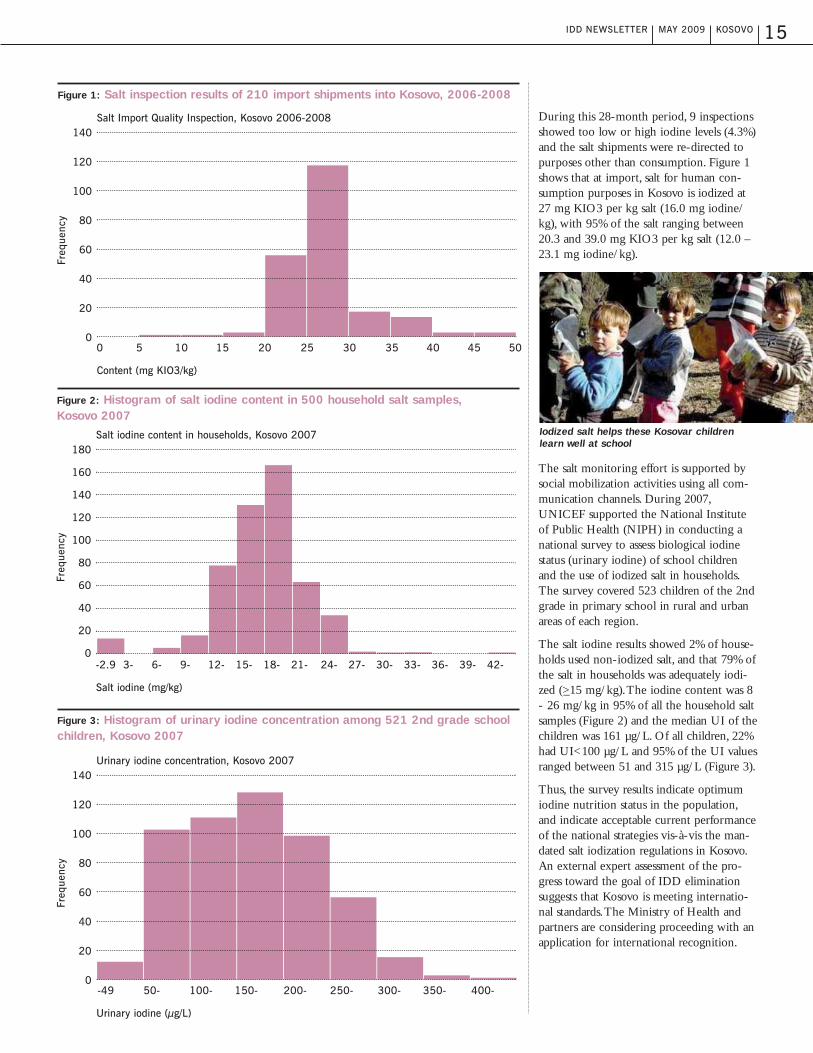
During this 28-month period, 9 inspectionsshowed too low or high iodine levels (4.3%)and the salt shipments were re-directed topurposes other than consumption. Figure 1shows that at import, salt for human con-sumption purposes in Kosovo is iodized at27 mg KIO3 per kg salt (16.0 mg iodine/kg), with 95% of the salt ranging between20.3 and 39.0 mg KIO3 per kg salt (12.0 –23.1 mg iodine/kg).
The salt monitoring effort is supported bysocial mobilization activities using all com-munication channels. During 2007,UNICEF supported the National Instituteof Public Health (NIPH) in conducting anational survey to assess biological iodinestatus (urinary iodine) of school childrenand the use of iodized salt in households.The survey covered 523 children of the 2ndgrade in primary school in rural and urbanareas of each region.
The salt iodine results showed 2% of house-holds used non-iodized salt, and that 79% ofthe salt in households was adequately iodi-zed (>_15 mg/kg).The iodine content was 8- 26 mg/kg in 95% of all the household saltsamples (Figure 2) and the median UI of thechildren was 161 µg/L. Of all children, 22%had UI<100 µg/L and 95% of the UI valuesranged between 51 and 315 µg/L (Figure 3).
Thus, the survey results indicate optimumiodine nutrition status in the population,and indicate acceptable current performanceof the national strategies vis-à-vis the man-dated salt iodization regulations in Kosovo.An external expert assessment of the pro-gress toward the goal of IDD eliminationsuggests that Kosovo is meeting internatio-nal standards.The Ministry of Health andpartners are considering proceeding with anapplication for international recognition.
Iodized salt helps these Kosovar childrenlearn well at school
Figure 1: Salt inspection results of 210 import shipments into Kosovo, 2006-2008
140
120
100
80
60
40
20
0
Freq
uenc
y
Salt Import Quality Inspection, Kosovo 2006-2008
Content (mg KIO3/kg)
0 5 10 15 20 25 30 35 40 45 50
Figure 3: Histogram of urinary iodine concentration among 521 2nd grade schoolchildren, Kosovo 2007
140
120
100
80
60
40
20
0
Freq
uenc
y
Urinary iodine concentration, Kosovo 2007
Urinary iodine (µg/L)
-49 50- 100- 150- 200- 250- 300- 350- 400-
Figure 2: Histogram of salt iodine content in 500 household salt samples, Kosovo 2007
180
160
140
120
100
80
60
40
20
0
Freq
uenc
y
Salt iodine content in households, Kosovo 2007
Salt iodine (mg/kg)
-2.9 3- 6- 9- 12- 15- 18- 21- 24- 27- 30- 33- 36- 39- 42-
IDD NL may09 27.5.2009 9:27 Uhr Seite 15
16 IDD NEWSLETTER MAY 2009 BIOFORTIFICATION
Iodine stimulates crop growth.A smalldose of this nutrient improves the assimila-tion of nitrogen from fertilizers. In thisway, iodine nutrition increases crop yields,fertilizer specialist Kari Jokinen fromKemira GrowHow in Finland concludesfrom experiments with oilseed rape, rye-grass and wheat. Jokinen discloses this fin-ding in a recently published patent applica-tion. If nitrogen stays for a shorter time inthe soil, the nutrient is less prone to lea-ching, volatilization or denitrification.Theaddition of iodine is especially beneficial tofertilizers high in nitrogen, the Finnish fer-tilizer specialist says. In his field experi-ments with arable crops and grass he testedgranular fertilizer compositions containing50 ppm iodine. Besides iodine, the experi-mental fertilizer compositions of Jokinenalso contain traces of selenium. From theexperiments with oilseed rape, ryegrass andwheat, he concludes that iodine and seleni-um enhance crop growth in a synergisticway.At the moment nothing is knownabout an eventually commercialization ofthese experimental fertilizer formulations.
Iodine too may stimulate the plants’ antio-xidant defense system. Proof of an iodine-induced enhancement of the antioxidantlevel in plants comes from the Spanishplant nutrition specialist Begoña Blasco.
Recently she examined the effects of iodi-ne nutrition on hydroponically grown let-tuce in an experimental greenhouse of theLaboratory of Plant Nutrition, at theUniversity of Granada.The treated plantsshowed a significant increase in antioxidantcompounds after the application of iodine.This research however doesn’t give insightin the possible growth or yield effects ofthe enhanced antioxidant level.Examination of the antioxidant status ofiodine-fed lettuce was a part of the iodinebiofortification project.The most appro-priate application rate in hydroponic lettu-ce cultivation was 40 µM, Begoña Blascoconcludes. In spite of a significant iodineaccumulation in the leaves, this concentra-tion didn’t reduce the biomass of the trea-ted plants.
Although iodine nutrition is also the sub-ject of other patent applications, up untilnow, iodine has not been recognized as anessential plant nutrient. Even a possiblybeneficial status of this element is contro-versial to many plant nutrition specialists.Some studies show stimulating effects ofiodine as plant nutrient, while many otherexperiments demonstrate harmful effects,illustrated by the herbicidal and defoliantproperties of iodide. Iodine too is used asbiocide. According to Japanese researchers
an iodine-releasing resin is highly effectivein the control of a bacterial disease.Thisiodinated anion exchange resin is also con-sidered to be suitable for iodine fortificati-on of crops.
Nearly two dozen Chinese patent applica-tions from scientists at Zhejiang Universityrelate to the culture or planting methods of iodine-rich crops and the production of iodine-rich food.The boost in iodinenutrition-related patent publicationsreflects the increasing interest in iodinebiofortification. Huanxin Weng ofZhejiang University primarily examinesiodine nutrition for the sake of biofortifi-cation of arable and vegetable crops. In themost remote regions of China, he suggeststhat salt fortification with iodine may notbe enough to eliminate iodine deficiencydisorders.Weng’s work has lead to a seriesof Chinese and international publicationson topics ranging from iodine-enrichedamaranth to iodine-fortified vigna.At theResearch Center for EcoenvironmentalSciences,Yongguan Zhu studies the pro-spects of iodine fortification of edible partsof plants. He argues that spinach is particu-larly suited for iodine fortification.
Iodine biofortification of plants:an ‘alternative’ to iodized salt?A low dose of iodine can stimulate the growth of plants. Small doses may also enhance the ant-oxidant content – a favorable effect for both crops and consumers. But there is another reason for the growing interest in plant iodine nutrition: food biofortification to control iodine deficiency.Biofortification of staple food crops with micronutrients by either breeding for higher uptake efficiency or fertilization can be an effective strategy to address widespread dietary deficiency inhuman populations. But is iodine biofortification realistic? Expert views on this potential ‘alterna-tive’ to iodized salt differ greatly. The following article summarizes recent discussion in this area.
The pros and cons of iodine in plant nutrition.
G.C. van den Berg Beneficial Nutrients News 4;3:August 2008
IDD NL may09 27.5.2009 9:27 Uhr Seite 16
IDD NEWSLETTER MAY 2009 BIOFORTIFICATION 17
These plant biologists from universities inthe United Kingdom discuss the potentialof iodine fortification of plants throughseveral means, including iodine-containingfertilizers. In most soils, iodine is present insolution as iodide, although iodate can alsobe present under strongly oxidizing condi-tions. Fertilization with soluble iodideand/or iodate salts has been practised in
agriculture, and the iodinization of irrigati-on water has successfully increased thedelivery of iodine to humans through edi-ble crops.The iodine concentrations inroot crops and leafy vegetables can beincreased greatly by the application ofiodine fertilizers, and, although iodine isnot readily mobile in the phloem, iodineconcentrations in tubers, fruits and seeds
can also be increased by iodine fertilizationto nutritionally significant concentrations.It has been even been suggested that,because human dietary iodine require-ments are quite low, iodine fertilizers mightbe added to large areas of agricultural pro-duction from aeroplanes.
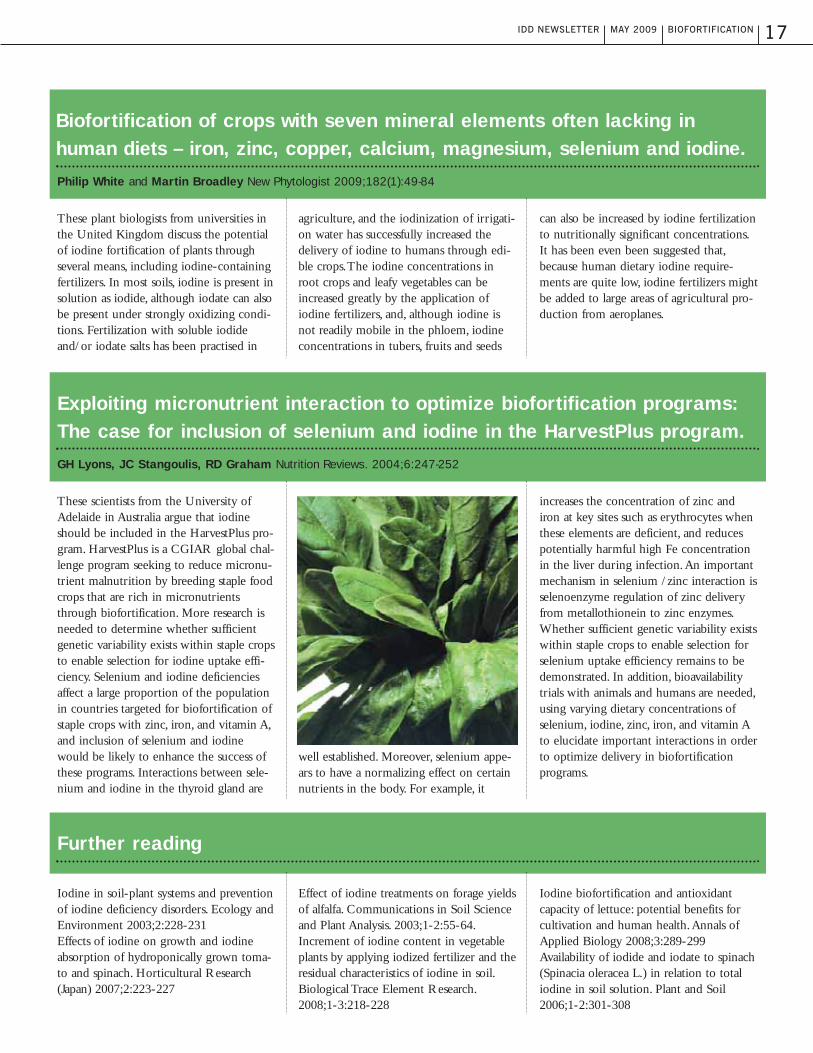
These scientists from the University ofAdelaide in Australia argue that iodineshould be included in the HarvestPlus pro-gram. HarvestPlus is a CGIAR global chal-lenge program seeking to reduce micronu-trient malnutrition by breeding staple foodcrops that are rich in micronutrientsthrough biofortification. More research isneeded to determine whether sufficientgenetic variability exists within staple cropsto enable selection for iodine uptake effi-ciency. Selenium and iodine deficienciesaffect a large proportion of the populationin countries targeted for biofortification ofstaple crops with zinc, iron, and vitamin A,and inclusion of selenium and iodinewould be likely to enhance the success ofthese programs. Interactions between sele-nium and iodine in the thyroid gland are
well established. Moreover, selenium appe-ars to have a normalizing effect on certainnutrients in the body. For example, it
increases the concentration of zinc andiron at key sites such as erythrocytes whenthese elements are deficient, and reducespotentially harmful high Fe concentrationin the liver during infection.An importantmechanism in selenium /zinc interaction isselenoenzyme regulation of zinc deliveryfrom metallothionein to zinc enzymes.Whether sufficient genetic variability existswithin staple crops to enable selection forselenium uptake efficiency remains to bedemonstrated. In addition, bioavailabilitytrials with animals and humans are needed,using varying dietary concentrations ofselenium, iodine, zinc, iron, and vitamin Ato elucidate important interactions in orderto optimize delivery in biofortificationprograms.
Iodine in soil-plant systems and preventionof iodine deficiency disorders. Ecology andEnvironment 2003;2:228-231Effects of iodine on growth and iodineabsorption of hydroponically grown toma-to and spinach. Horticultural Research(Japan) 2007;2:223-227
Effect of iodine treatments on forage yieldsof alfalfa. Communications in Soil Scienceand Plant Analysis. 2003;1-2:55-64.Increment of iodine content in vegetableplants by applying iodized fertilizer and theresidual characteristics of iodine in soil.Biological Trace Element Research.2008;1-3:218-228
Iodine biofortification and antioxidantcapacity of lettuce: potential benefits forcultivation and human health.Annals ofApplied Biology 2008;3:289-299Availability of iodide and iodate to spinach(Spinacia oleracea L.) in relation to totaliodine in soil solution. Plant and Soil2006;1-2:301-308
Biofortification of crops with seven mineral elements often lacking in human diets – iron, zinc, copper, calcium, magnesium, selenium and iodine.Philip White and Martin Broadley New Phytologist 2009;182(1):49-84
Exploiting micronutrient interaction to optimize biofortification programs: The case for inclusion of selenium and iodine in the HarvestPlus program.GH Lyons, JC Stangoulis, RD Graham Nutrition Reviews. 2004;6:247-252
Further reading
IDD NL may09 27.5.2009 9:27 Uhr Seite 17

18 IDD NEWSLETTER MAY 2009 MEETINGS AND ANNOUNCEMENTS
Meetings and AnnouncementsAnnual Meeting of the Institute ofFood Technologists, June 8, 2009,Anaheim, CA, USADavid Haxton, ICCIDD ExecutiveDirector and Dick Hanneman, ICCIDDBoard Member, are co-chairing a sessionon June 8, 2009 at the Annual Meeting ofthe Institute of Food Technologists inAnaheim, CA, USA.There will be a paneldiscussing use of iodized salt in processedfoods; the five-person panel includes threeICCIDD board members (VenkateshMannar, Gregory Gerasimov and KevinSullivan); the other two are from the saltindustry (Wally Becky of Morton Salt andYang Haiyan of China Salt).
Salt Symposium, September 4-6,2009, Beijing, ChinaThe 2009 Salt Symposium will take placeSeptember 4-6, 2009 in Beijing, China.The Symposium is held every eight ornine years.The last one took place in TheHague,The Netherlands in 2000, and gavebirth to the Global Network for theSustained Elimination of IDD. China Salt,a Network board member, is the organizerof the Symposium. IDD elimination is oneof the main themes of the Symposium andthere will also be a Round Table whichaims to reinvigorate the salt industry andto mobilize a new generation of salt lead-ers for universal salt iodization (USI).
ICCIDD, the Network and UNICEF planto make the Beijing Symposium a majoradvocacy event on USI/IDD elimination.High level participation from the Chinesegovernment, UNICEF and various IDDstakeholders is expected.
AbstractsMethods of assessment of iodinestatus in humans: a systematicreview. The authors performed a structured searchfor iodine intervention studies and a ran-dom-effects meta-analysis was performed.Twenty-one intervention studies wereincluded. Urinary iodine (in children andadolescents and in those with low andmoderate baseline iodine status), thyroglo-bulin (in children and adolescents but notin pregnant and lactating women), serumthyroxine (in children and adolescents,adults, women, and those with moderatebaseline thyroxine status but not in preg-nant and lactating women), and serumthyroid-stimulating hormone (in pregnantand lactating women but not in children
and adolescents or those at moderate baseline status), but not triiodothyronine,proved to be useful biomarkers of iodinestatus.Ristic-Medic D et al. Am J Clin Nutr.2009 May 6. [Epub]
Thyroid volume changes duringpregnancy and after delivery in an iodine-sufficient Republic ofSlovenia. The authors prospectively studied healthypregnant women living in an iodine-suffi-cient area. 118 pregnant women were stu-died in the first trimester, in the third tri-mester and 4 and 14 months after delivery.All women were negative for thyroidautoantibodies. Median UIC in the third
trimester (176 µg/g creatinine) was signifi-cantly higher than 4 and 14 months afterdelivery. Mean thyroid volume in the thirdtrimester (11.3 mL) was significantlygreater than in the first trimester (8.7 mL),4 months after delivery (8.6 mL) and 14months after delivery (7.8 mL).TSH con-centration was significantly higher in thethird trimester than in the first trimesterand 4 months after delivery. In an iodine-sufficient area, thyroid volume increasesduring pregnancy but then decreases backto prepregnancy size after delivery.Fister P et al. Eur J Obstet GynecolReprod Biol. 2009 Apr 28. [Epub]
IDD NL may09 27.5.2009 9:27 Uhr Seite 18

IDD NEWSLETTER MAY 2009 ABSTRACTS 19
Iodine concentration of milk in adose-response study with dairycows and implications for consumeriodine intake.Most feed is poor in iodine and iodinesupplementation of cow's diets must gua-rantee milk iodine concentrations forhumans that contribute to prevention ofthe deficiency and minimize the risk ofexceeding an upper limit of iodine intake.Holstein cows were fed four iodine dosesin four sequential 14-d periods, doses of0.2 (basal diet), 1.3, 5.1, and 10.1 mg iodi-ne/kg diet dry matter (DM) were admini-stered. Samples of milk were collectedduring each period.The mean levels forthe four doses tested in milk were 101,343, 1215, and 2762 µg/kg.The iodinesupplementation of 0.5-1.5 mg/kg dietDM represents the requirement of thecow, resulting in 100-300 µg/L milk,which optimally contributes to humansupply.The maximum dietary levels of for-mer and present EU legislations (10 and 5mg iodine/kg cow feed) increase the riskof iodine excess in humans.Schöne F et al. J Trace Elem Med Biol.2009;23(2):84-92.
Association of iodine fortificationwith incident use of anti-thyroidmedication - A Danish nationwidestudy.The objective of this study was to monitorthe effect of the Danish iodine fortificati-on program on incidence of hyperthyroi-dism as measured by the incident use ofanti-thyroid medication. In the regionwith previous moderate iodine deficiencythe number of incident users of anti-thy-roid medication increased 46% in the firstfour years of iodine fortification. In thepreviously mildly iodine-deficient regionthe number of incident users increasedonly 18%.After four years of fortificationthe incidence rates started to fall and rea-ched baseline, for most groups, six yearsafter onset of fortification.This study
shows that iodine fortification induced atemporary, modest increase in the inci-dence of hyperthyroidism as measured byuse of anti-thyroid medication.Cerqueira C et al. J Clin EndocrinolMetab. 2009 Apr 14. [Epub]
Delayed neurobehavioral develop-ment in children born to pregnantwomen with mild hypothyroxinemiaduring the first month of gestation:the importance of early iodine sup-plementation.The authors evaluated the neurocognitiveperformance at 18 months of age in threegroups of children: group 1 included chil-dren of women with free thyroxine >20thpercentile at 4-6 gestational weeks and atfull-term. Group 2 included children ofmildly hypothyroxinemic women diagno-sed during the first 12-14 weeks and withFT(4) >20th percentile at full-term.Women were iodine supplemented fromthe day of enrollment until the end of lac-tation. Group 3 included children born tomildly hypothyroxinemic women at full-term, without iodine supplementationduring gestation.The data suggested adelay of 6-10 weeks in iodine supplemen-tation (200 µg KI/d) of hypothyroxinemicmothers at the beginning of gestationincreases the risk of neurodevelopmentaldelay in the progeny.Berbel P et al.Thyroid. 2009;19(5):511-9.
Using bread as a vehicle to improvethe iodine status of New Zealandchildren.The authors determined the iodine statusin 93 New Zealand school children, andestimated how the addition of iodized saltto bread will improve their iodine status.Iodine status was assessed by urinary iodi-ne concentration (UIC), serum thyroglo-bulin (Tg), and dietary iodine intake wasestimated using an iodine-specific foodfrequency questionnaire. It was estimatedthat the addition of iodized salt to bread
would increase the average iodine intakeof these children to 75-104 µg/day, de-crease the number of children who havean iodine intake less than the EAR to 4-46% and increase the median UIC of these children to 95-151 µg/L.Thus,the introduction of iodized salt to bread,which is currently scheduled to becomemandatory in September 2009, shouldimprove the iodine status of New Zealandchildren.Rose M et al. N Z Med J.2009;122(1290):14-23.
Requesting iodine supplementationin children on parenteral nutrition.Iodine supplementation of parenterally fedinfants is recommended at 1 µg/kg/day.Children (1-17 yrs; n=15), undergoingparenteral nutrition (PN) and receiving aniodine supply of 1 µg/kg/day, were enrol-led. They were on PN from 14 to 84weeks; nine had short bowel syndrome(SBS) and six had other intestinal diseasesrequiring PN.The authors found an inver-se correlation between duration of PN inmonths and urinary iodine concentration(UIC).After 12 weeks, 53% of patientshad UIC<50 µg/L, but thyroxine,TSHand thyroid volume remained unchanged.Thus, a PN iodine supply of 1µg/kg/daymay be suboptimal in PN.Cicalese MP et al. Clin Nutr. 2009 Mar 6.[Epub]
IDD NL may09 27.5.2009 9:27 Uhr Seite 19

Thyroid function in early pregnancyin Japanese healthy women: relati-on to urinary iodine excretion, eme-sis, and fetal and child develop-ment.The objective of the study was to examineurinary iodine excretion and thyroidfunction in early pregnancy in Japanesehealthy women (n=662), and fetal matura-tion and child development in thesewomen.The distribution of urinary iodineconcentrations was large, and the averagewas extremely high.There were significantpositive correlations between urinary iodi-ne and serum TSH (r = 0.1326; P <0.005), but iodine excess during earlypregnancy had no measurable adverseeffects on the fetus.Orito Y et al. J Clin Endocrinol Metab.2009;94(5):1683-8.
Association of high iodine intakewith the T1799A BRAF mutation inpapillary thyroid cancer.Epidemiological studies have indicatedthat high iodine intake might be a riskfactor for papillary thyroid cancer (PTC),which commonly harbors the oncogenicT1799A BRAF mutation.The objective ofthe study was to investigate the relations-hip between BRAF mutation in PTC andiodine intake in patients (n=1032) fromfive regions in China that harbor differentiodine contents in natural drinking water,ranging from normal (10-21 µg/L) to high(104-287 µg/L).The prevalence of BRAFmutation was significantly higher in theregions with high iodine content than anyof the regions with normal iodine con-tent.Guan H et al. J Clin Endocrinol Metab.2009;94(5):1612-7.
Iodine levels and thyroid hormonesin healthy pregnant women and birthweight of their offspring.The study assessed the association betweenthyroid hormones (TH)s and urinary iodi-ne concentration (UIC) in healthy preg-nant women (n=657) and the birth weightof their children. Six percent of newbornswere classified as small for gestational age(SGA).Women with the third trimesterUICs between 100 and 149 µg/L hadlower risk of having an SGA newbornthan women with UICs below 50 µg/L(adjusted OR (95%CI): 0.15 (0.03-0.76).There was no significant reduction in SGAamong mothers with higher UICs.Thus,iodine status during pregnancy may berelated to prenatal growth in healthywomen.Alvarez-Pedrerol M et al. Eur J Endocrinol.2009 Mar;160(3):423-9.
THE IDD NEWSLETTER is published quarterly by ICCIDD and distributed free of charge in bulk by international agencies and by individual mailing.The Newsletter is also distributed to email subscribers and appears on ICCIDD’s website (www.iccidd.org). The Newsletter welcomes comments, newinformation, and relevant manuscripts on all aspects of iodine nutrition, as well as human interest stories on IDD elimination in countries.
For further details about the IDD Newsletter, please contact:Michael B. Zimmermann, M.D., the editor of the Newsletter, at the Human Nutrition Laboratory, Swiss Federal Institute of Technology Zürich, ETHZentrum, Schmelzbergstrasse 7, LFW E19, CH-8092 Zürich, Switzerland, phone: +41 44 632 8657, fax: +41 44 632 1470,[email protected].
ICCIDD gratefully acknowledges the support of the Swiss Federal Institute of Technology Zürich for the IDD Newsletter.
© Copyright 2009 by International Council for Control of Iodine Deficiency Disorders
Des
ign:
ww
w.im
holz
desi
gn.c
hPr
int:
Spä
lti
Dru
ck A
GC
H-8
750
Gla
rus
20 IDD NEWSLETTER MAY 2009
IDD NL may09 27.5.2009 9:27 Uhr Seite 20


















![[•] ISSUE CLOSES ON - Farmico Cold Chain & Logistics](https://static.fdokumen.com/doc/165x107/633355ac3108fad7760f0033/-issue-closes-on-farmico-cold-chain-logistics.jpg)

