
REVIEW: Vitamin transport and homeostasis in mammalian brain: focus on Vitamins B and E
Upload
independentCategory
view
5download
0
Calcium Homeostasis in Children and
Adolescents with Vitamin D deficiency
Effects of Intramuscular Injection of a
Megadose of Cholecalciferol.
Ashraf Soliman , Rania Elalaily , Ashraf Adel , Magda Wagdy , Maryam AlAli
The Department of Pediatrics, Hamad Medical Center, Doha, Qatar
In humans the main source of vitamin D
Solar ultraviolet light B radiation acting on 7- dehydrocholesterol in skin.
Small amounts are also derived from dietary sources:
oily fish and eggs, and
fortified foods, such as margarine and breakfast cereals.

In The Arab Gulf States
Rickets cases are still being reported in all the Arab gulf area and worldwide.
Osteomalacia also still occurs, but its symptoms are much less specific and are easily missed

Normal metabolism
Vit D
25-HCC (Liver)
PTH
1,25-DHCC 24,25-DHCC
(Kidney) (Kidney)

GH / IGF-I axis
Both systemic and local (growth plate) production of IGF-I
exerts direct actions in the growth plate.
Growth Plate Hormones
PTHrP acts on PTHrP receptors (PTHrPR) that are expressed in uncommitted chondrocytes to delay differentiation and maintain cell proliferation.
Vitamin D deficiency
Tendency to hypocalcaemia, secondary hyperparathyroidism and increased bone turnover.
This may be associated with osteoporosis and fractures

The clinical spectrum
Ranges from :
subclinical (more common) to
Frank deficiency ( with serum 25- OH D levels less than 5ng/dl).

The clinical severity of the disease does not correlate with vitamin D level ???
Although in small children vitamin D insufficiency often manifests as clinical rickets this occur infrequently in adolescence .
Subtle effects of vitamin D inadequacy may occur, which include the failure to achieve peak bone mass or the development of hyperparathyroidism with bone loss and fractures
Marjo KM Lehtonen-Veromaa, Am J Clin Nutr 2002;76:1446–53.
Pubertal girls with hypovitaminosis D seem to be at risk of not reaching maximum peak bone mass, particularly at the lumbar spine.
Dietary enrichment or supplementation with vitamin D should be considered to ensure an adequate vit-D
In prolonged and severe cases
Progressive bone pains ( back, large joints and long bones)
Chvostek’s sign, Carpopedal spasms, tetany.
Myopathy and progressive weakness- difficulty climbing stairs, inability to stand up from squatting position.
Waddling gait and deformity (genu-valgum and coxa vara, knock-knee, )
Fractures

The aim of this study
1. Investigate the magnitude of VDD in random adolescent sample
2. Correlaate the clinical picture with the degree of severity
3. Monitor the effects of treating with a mega dose of IM cholecalciferol versus oral vitamin D.
Inclusion criteria included
Low serum 25-hydroxyvitamin D (25OHD) +/-
Elevated serum alkaline phosphatase (ALP)
Investigations done prior to treatment included:
X-ray of the wrist or knee joints.
All patients with VDD 40 adolescents and 40 children
History taking including nutritional intake and exposure to sun
Physical exam including clinical manifestations of vitamin D deficiency.
Anthropometric measurements including weight, height, and head circumference.

Lab Investigations
Serum creatinine,
Ca, PO4, albumin,
ALP,
(PTH) (intact molecule)
25OHD concentrations
IGF-I.
Patients with plasma 25-OHD levels less than 25 nmol/l (10 ng/ml) were considered to have vitamin D deficiency

Treatment
All participants with VVD were treated with a therapeutic intramuscular injection of cholecalciferol (10,000 U/kg , max 600000IU (15mg).
Patients who refused IM injection received oral Vit D ( 50,000 IU/ week for 12 weeks)

F/U
During each clinic visit every 2-3 months for 1 year
1. Anthropometric and
2. Biochemical and
3. Radiological parameters were reassessed and recorded and the laboratory tests repeated.
High Incidence of VDD (Epidemic)
In the 100 adolescents randomly selected from schools 65% of them have VDD ( 25OHD < 10 ng/ml)

Bener A, Al-Ali M, Hoffmann GF.
Minerva Pediatr. 2009 Feb;61(1):15-22.
The total number of 458 children surveyed, 228 (49.8%) were males and 230 (50.2%) females.
The prevalence of vitamin D deficiency among the studied Qatari children was (68.8%), mostly in the age group (11-16) years (61.6%).
Bener A, Al-Ali M, Hoffmann GF. Minerva Pediatr. 2009 Feb;61(1):15-22.
Exposure to sunlight was limited
Low duration of time spent outdoors, and low physical activity were significant predictors for vitamin D deficiency
Limitations in sunlight exposure and a low oral intake of vitamin D

Table 1: Lab data before vs after vitamin D injection Infants with vit D deficiency Adolescents with Vit D Deficiency
Before After Before After
Ca mmol/L Mean 2.1 2.3* 2.1 2.3 *
SD 0.3 0.1 0.3 0.1
PO4 mmol/L Mean 1.4 1.65* 1.4 1.7 *
SD 0.5 0.4 0.5 0.4
ALP U/L Mean 769.5 # 404.4* 404.0 196 *
SD 316.7 162.9 212.0 69*
25 OH D ng/ml Mean 6.7 28.2 * 9.3 27.7*
SD 4.5 12.1 4.6 9.2
PTH pg/ml Mean 249.5 # 35.5* 122.9 34.8*
SD 87.0 15.3 55.5 9.5
* P < 0.01 after vs before treatment
# P < 0.05 infants vs adolescents

Before treatment
25 OH D and Ca concentrations did not differ among the 2 groups.
Serum PO4 concentration was significantly lower and PTH and ALP concentrations higher in children compared to adolescents with VDD
This reflects slower rate of growth and/or better adaptation (larger bone mass) in
adolescents.
25OHD and PTH in VDD adolescents
Inverse relationship between serum 25-OHD levels and PTH levels in adolescents with VDD
symptoms related to vitamin D deficiency in adolescents
Pain in weight bearing joints, back, thighs, and calves ( 32/40)
Difficulty walking and/or climbing stairs and/or running (9/40)
Muscle cramps and/or facial twitches and/or carpopedal spasms (16/40)
Genu valgus ( 2/40)
Disappearance or improvement of these symptoms were achieved in the majority (37/40) of these patients 3 months after the injection.

Three months after injecting vitamin D
Serum 25 OH D, Ca and PO4 concentrations increased significantly in the 2 groups and ALP and PTH concentrations significantly decreased.
ALP concentrations were still significantly higher in infants vs adolescents (reflecting rapid growth ( IGF-I)
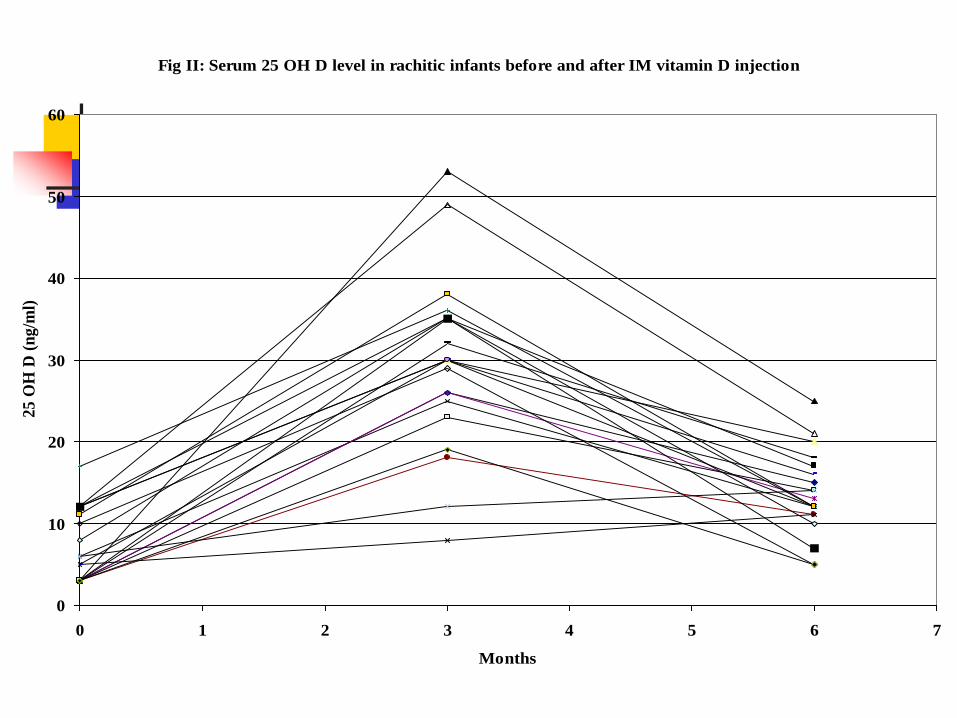
Fig II: Serum 25 OH D level in rachitic infants before and after IM vitamin D injection
0
10
20
30
40
50
60
0 1 2 3 4 5 6 7
Months
25 O
H D
(n
g/m
l)
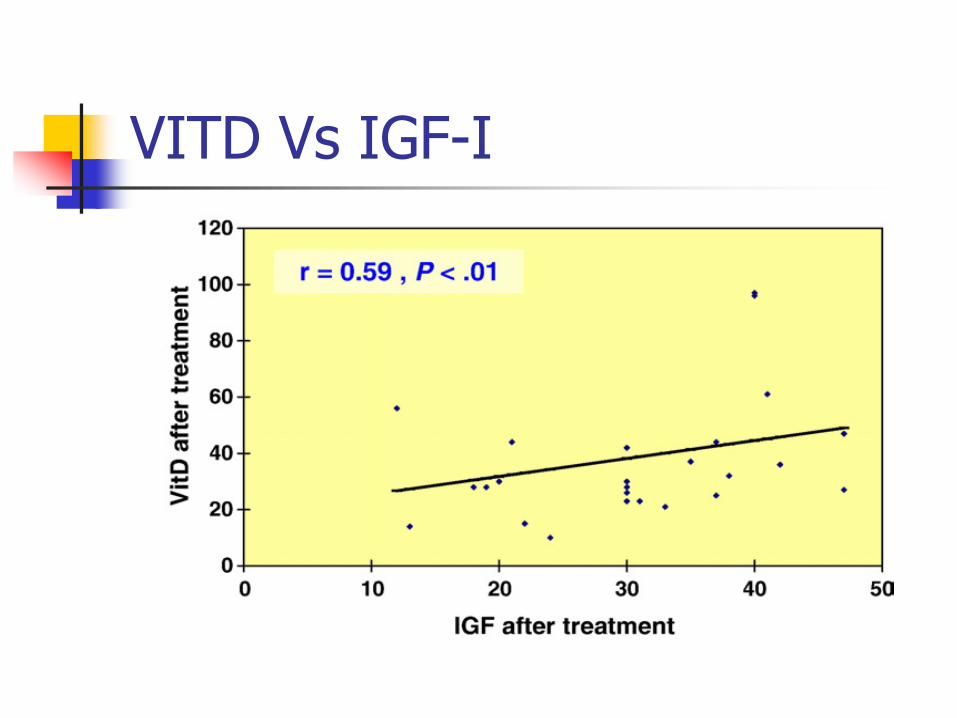
VITD Vs IGF-I
Duration of Mega-dose Effect
3 months after injecting vitamin D the mean 25 OH D level (28.2 +/-12.1 and 27.7 +/- 9.2 ng/ml)
6 months after injecting vitamin D the mean 25 OH D level ( 11.9 +/- 4.3 ng/ml and 12.8 +/- 5.2 ng/ml).
6 months after injecting mega dose of vitamin D only 1 adolescent and 3 children had 25 OH D = or above 20 ng/dl

In adolescents with VDD
An IM megadose of vitamin D increased serum 25OHD levels to normal level ( > 20 ng/ml) in the majority (37/40) for 3 months.
This was associated with a corresponding decrease in
serum PTH and ALP and significant increase of serum PO4 and Ca concentrations.
Symptoms related to VDD in adolescents disappeared in the majority of patients after 4 weeks of the injection
Serum creatinine levels remained normal in all participants throughout the study, while increases in 2-hour urine calcium/creatinine excretion index were seen in 2 adolescents (5%) at 3 months.
6 months after IM Vit D megadose
39/40 adolescents had 25OHD level < 20 ng/ml)
An IM mega dose of cholecalciferol is an effective therapy for treatment of hypovitaminosis D in children and adolescents for 3 months but not for 6 months.

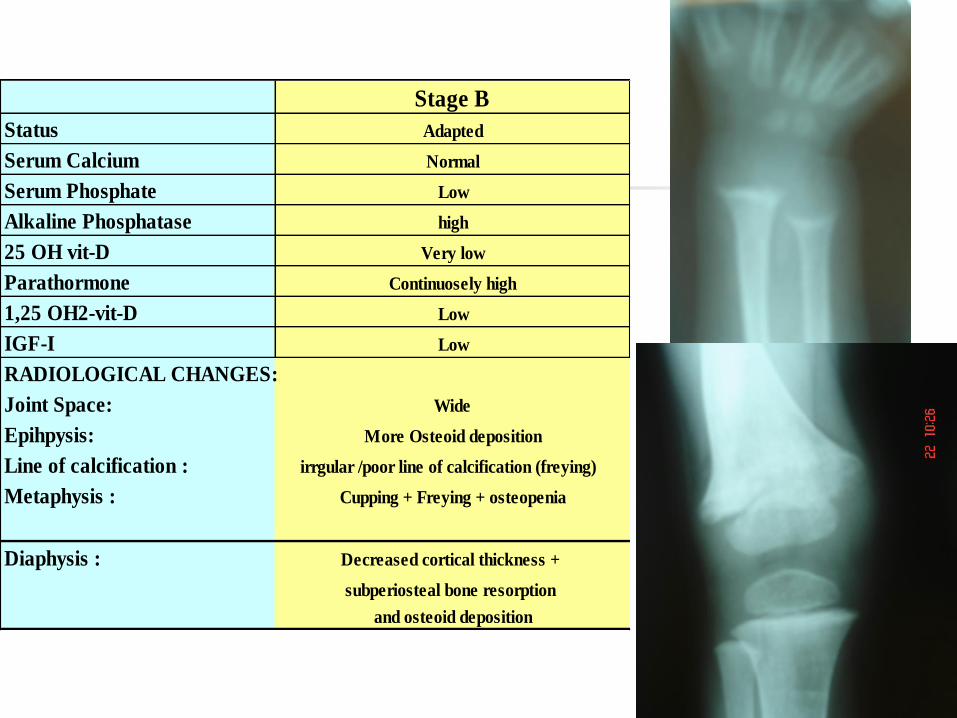
Stage B
Status Adapted
Serum Calcium Normal
Serum Phosphate Low
Alkaline Phosphatase high
25 OH vit-D Very low
Parathormone Continuosely high
1,25 OH2-vit-D Low
IGF-I Low
RADIOLOGICAL CHANGES:
Joint Space: Wide
Epihpysis: More Osteoid deposition
Line of calcification : irrgular /poor line of calcification (freying)
Metaphysis : Cupping + Freying + osteopenia
Diaphysis : Decreased cortical thickness +
subperiosteal bone resorption
and osteoid deposition
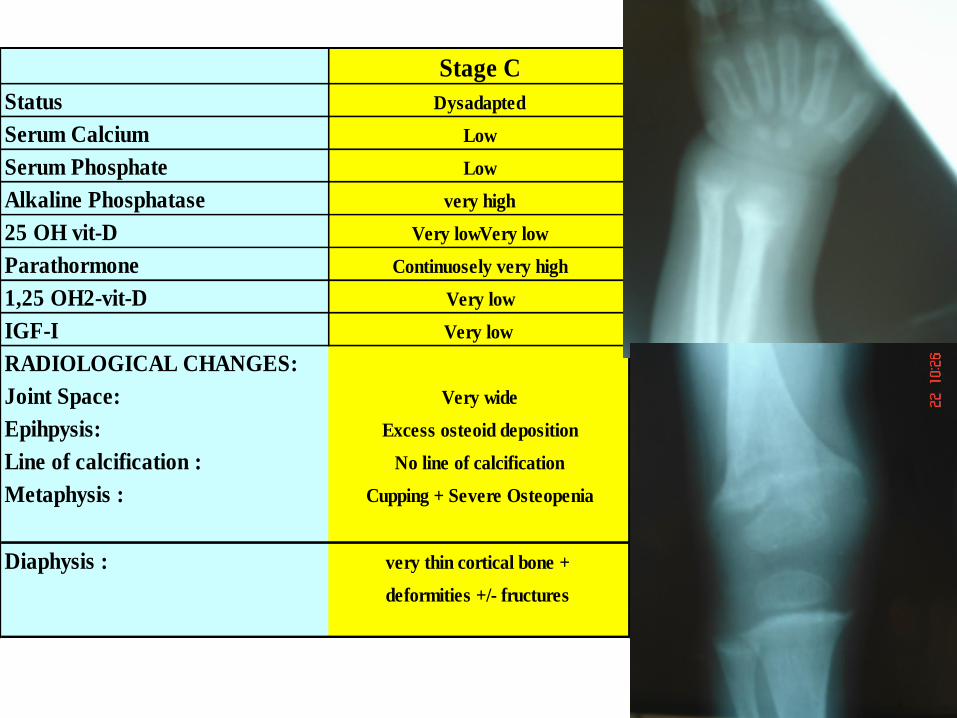
Stage C
Status Dysadapted
Serum Calcium Low
Serum Phosphate Low
Alkaline Phosphatase very high
25 OH vit-D Very lowVery low
Parathormone Continuosely very high
1,25 OH2-vit-D Very low
IGF-I Very low
RADIOLOGICAL CHANGES:
Joint Space: Very wide
Epihpysis: Excess osteoid deposition
Line of calcification : No line of calcification
Metaphysis : Cupping + Severe Osteopenia
Diaphysis : very thin cortical bone +
deformities +/- fructures

Stage C Stage B Stage A

Stage C Stage B Stage A

Lab data
before Vs after treatment
Ca PO4 ALP Vit D PTH IGF-I
mmol/l mmol/l U/l ng/dl pg/ml ng/ml
Before 2.07 1.23 1083 4.5 294 22.7
After 2.44 1.94 341 44.5 35.2 52.2
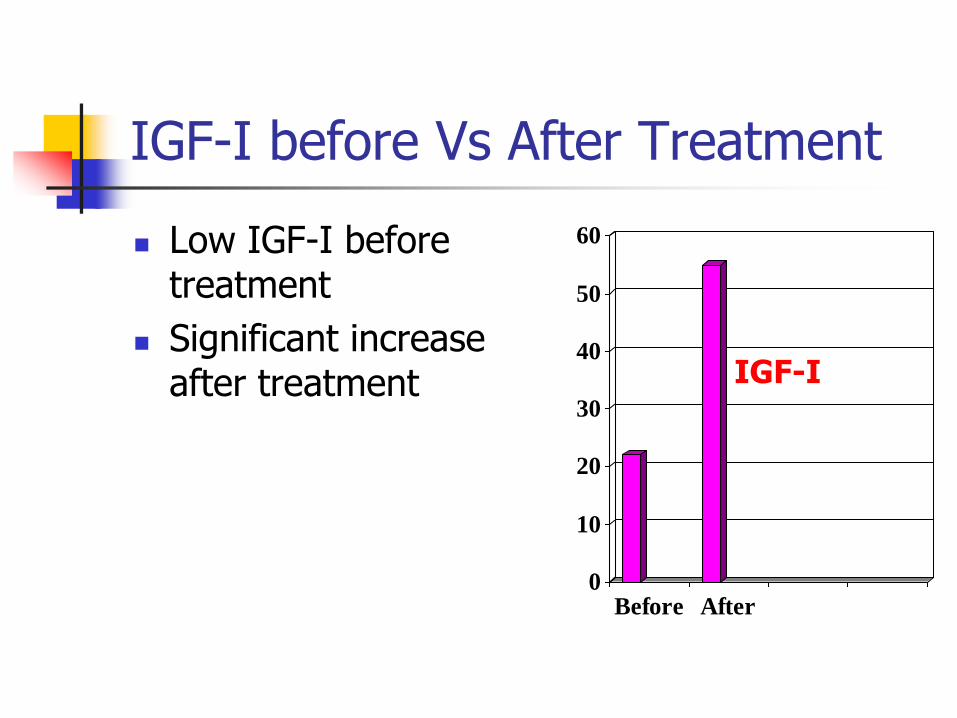
IGF-I before Vs After Treatment
Low IGF-I before treatment
Significant increase after treatment
0
10
20
30
40
50
60
Before After
IGF-I
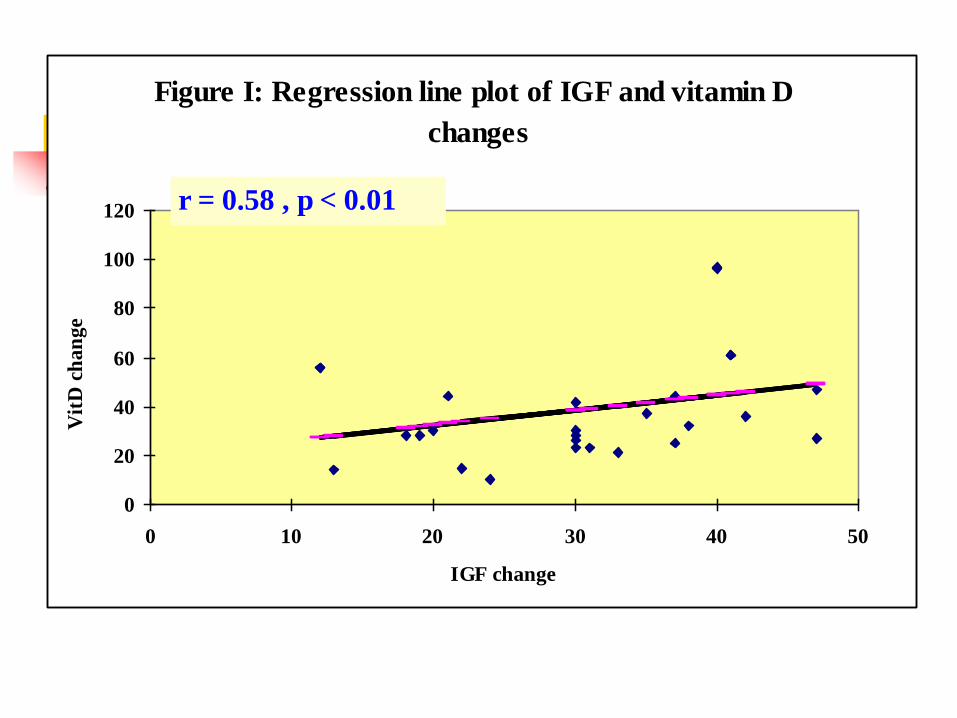
Figure I: Regression line plot of IGF and vitamin D
changes
0
20
40
60
80
100
120
0 10 20 30 40 50
IGF change
Vit
D c
ha
ng
e
r = 0.58 , p < 0.01

Vit D effect on IGF-I WHY AND HOW
1. Central effect 2. Peripheral effect
1. Vit D on Pituitary
There are some good evidence that vitamin D may regulate pituitary function.
Vitamin D receptor (VDR) mRNA expression has been demonstrated in the human pituitary gland suggesting the possibility that VDR may regulate the human pituitary gene expression and hormone secretion.

A permissive or regulatory role of vitamin D in the normal pituitary gland
This suggest that 1,25-(OH) 2D3 may act to increase GH secretion in our rachitic patients with subsequent increase in IGF-I synthesis and secretion after treatment with vitamin D
In our study
Significant correlation between:
IGF-I and vitamin D levels
GVSDS and IGF-I
Catch-up Growth during treatment of Vit-
D Deficiency rickets is IGF-I dependent
Adaptation to vitamin D deficincy
1. low IGF-I decelerates linear growth and decreases Calcium use in bones.
2. Increased PTH stimulates 1 alpha hydroxylation of vit D---- more calcium absorption from the gut.
3. Low IGF-I permits the catabolic action of PTH on the bone to maintain serum calcium level
Adaptation Theory
Decreased circulating and locally produced IGF-I in rachitic children appears to be an adaptive process to inhibit linear growth (in growth plate) and bone mineral accretion (diaphysis) during vitamin D deficiency.
This process conserves bone minerals and proteins to maintain normal serum calcium concentration and slows down the breakdown of the already formed bones instead of using them in forming new bones.
Conclusion
The accelerated linear growth after treatment of nutritional vitamin D deficiency is mediated through activation of the GH/IGF-I system
This suggests an important role of vitamin D as a link between the proliferating cartilage cells of the growth plate and GH/IGF-I secretion.
Three different sequential stages of vitamin D deficiency can be recognized according to clinical/radiological, biochemical and hormonal data.
Adolescents Vs Children with VDD


Fig 1: Pattern (I) Adolescent Vitamin DD Rickets : AP & Lat. Views of three different patients with VDDR having the same skeletal manifestation at different locations ; upper tibia, lower femur and lower tibia : the lesions appear as multilocular bone cystic lesion with sclerotic margins , exocentric subcortical location with no cortical erosions, no periosteal reaction , no osteoporosis , no other metaphyseal manifestations of the well known VDDR, the lesions simulate 1ry bone tumors (giant cell variant) mainly non-ossifying fibroma but mostly it represent
brown tumor of 2ry hyperparathyroidism 2ry to adolescent rickets.

Fig 2 : Pattern (II) Adolescent Vitamin DD Rickets ; Plain X rays knee, ankle, shoulder as well hips & hand demonstrating Mild generalized diminished bone density with prominent primary and 2ry bone trabiculation and there is well identified wide metaphyseal zone of relatively more lucency with rather loss of bone trabiculation representing wide metaphyseal zone of poor ossification of bone matrix 2ry to rachitic changes , no cupping or fraying of metaphyses identified
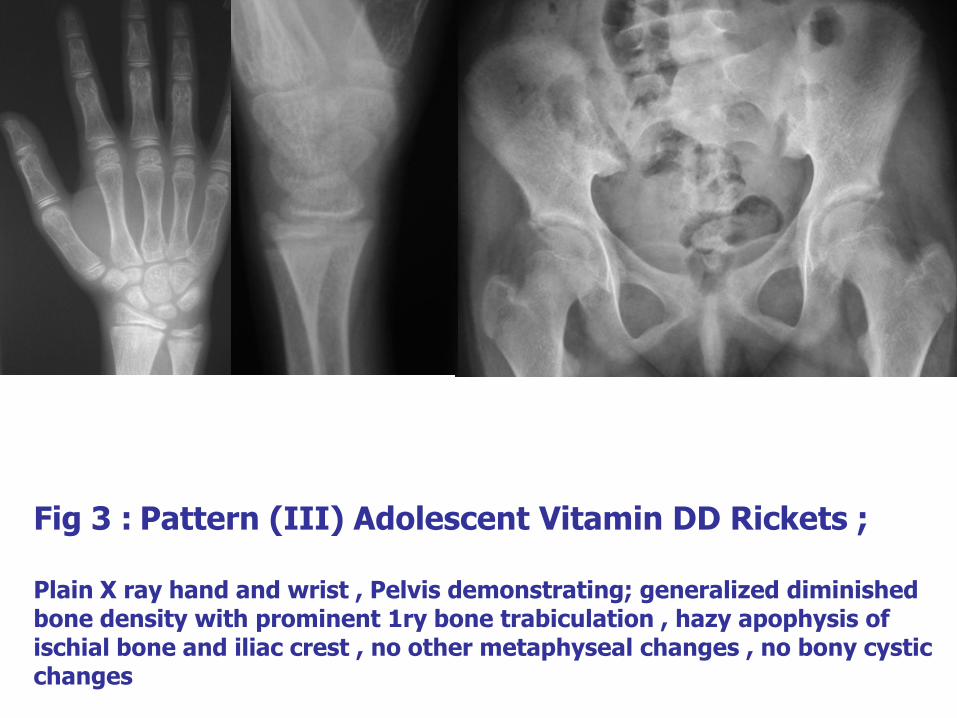
Fig 3 : Pattern (III) Adolescent Vitamin DD Rickets ; Plain X ray hand and wrist , Pelvis demonstrating; generalized diminished bone density with prominent 1ry bone trabiculation , hazy apophysis of ischial bone and iliac crest , no other metaphyseal changes , no bony cystic changes
A&B
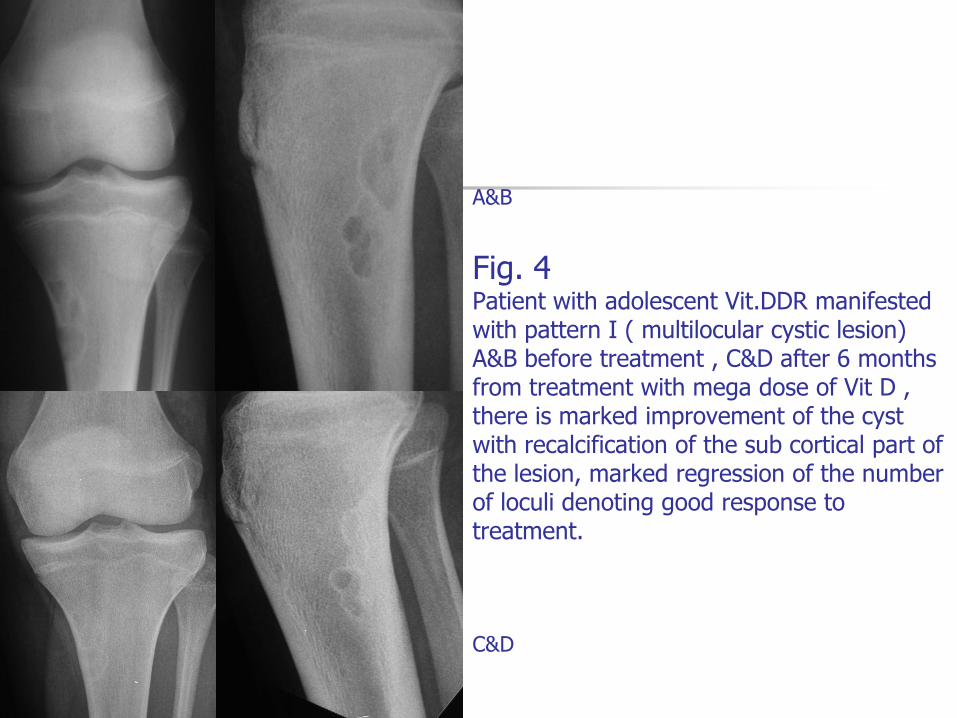
Fig. 4 Patient with adolescent Vit.DDR manifested with pattern I ( multilocular cystic lesion) A&B before treatment , C&D after 6 months from treatment with mega dose of Vit D , there is marked improvement of the cyst with recalcification of the sub cortical part of the lesion, marked regression of the number of loculi denoting good response to treatment. C&D

Plain Films at Presentation
Metaphyseal osteoporosis
Prom. Primary striations
2ry Hypo PO4

Before Vs after 2 injections of Vit D 3 600,000IU (4month) Before After
Metaphyseal osteoporosis
Prom. Primary striations
2ry Hypo PO4

Before Vs after Vit D (6 mon)
Metaphyseal osteoporosis
Prom. Primary striations

12 Months after Vit D
Marked resolution of the cyst with mild persistence of
the linear trabecular pattern of the metaphysis
Even in sunny climates
Adolescents, especially females, can be at risk of rickets.
Limb and joint (knee, ankle, hip) pains and myopathy were the most common presenting symptoms.
Radiological evidence was present in some cases.
Risk In Adolescents
Adolescence is a critical period of skeletal mineralisation, when over 35% of the peak bone mass (PBM) of a mature adult is accrued during the four years surrounding the peak pubertal growth spurt.
It is widely accepted that subjects who attain a lower PBM at maturity have a higher risk of sustaining osteoporotic fractures in later life.
Thus, inadequate skeletal mineralisation secondary to vitamin D deficiency during this period might compromise the acquisition of PBM and thus potentially increase the risk of osteoporosis in later life.
We therefore recommend that a prospective study is needed to determine the prevalence of vitamin D deficiency among adolescents whose exposure to sunshine is limited for cultural and religious reasons.
Copyright © 2022 FDOKUMEN




















