Coffee: The world's favourite cuppa' caffeine - Khazanah ...

EXPERIMENTAL STUDIES
CAFFEINE IMPAIRS SHORT-TERM NEUROLOGICAL
OUTCOME AFTER CONCUSSIVE HEAD INJURY IN RATS
Khalaf Al Moutaery,F.R.C.S.Neuroscience Research Group,Armed Forces Hospital, Riyadh,Saudi Arabia
Saleh Al Deeb, F.R.C.P.Neuroscience Research Group,Armed Forces Hospital, Riyadh,Saudi Arabia
Haseeb Ahmad Khan,Ph.D.Neuroscience Research Group,Armed Forces Hospital, Riyadh,Saudi Arabia
Mohammad Tariq,F.R.C.Path., F.R.S.C.Neuroscience Research Group,Armed Forces Hospital, Riyadh,Saudi Arabia
Reprint requests:Mohammad Tariq, Ph.D.,F.R.C.Path., F.R.S.C., NeuroscienceResearch Group, Armed ForcesHospital, P.O. Box 7897 (W-912),Riyadh 11159, Saudi Arabia.
Received, July 10, 2002.
Accepted, May 14, 2003.
OBJECTIVE: Adenosine is an endogenous neuroprotective agent that is released duringischemia, hypoxia, epilepsy, and ischemic brain injury. Caffeine is a receptor antag-onist for adenosine that might interfere with the neuroprotective effect of adenosine inischemic-hypoxic conditions. An investigation was undertaken to study the effect ofcaffeine on neurological function, edema formation, and blood-brain barrier perme-ability after experimental head injury in rats.METHODS: Adult female Wistar rats classified into different groups received caffeine intra-peritoneally at doses of 0, 50, 100, and 150 mg/kg body weight. Thirty minutes after thecaffeine treatment, the animals were subjected to concussive head injury (CHI) administered bya controlled cortical impact device. Neurological severity score was recorded in each rat at 2hours after CHI. Specific gravity, water content (as an indicator of edema), and blood-brainbarrier impairment were analyzed in the cortical tissue surrounding the injury site. The levelsof myeloperoxidase and malondialdehyde in the cortical region were measured as indicatorsof neutrophil infiltration and lipid peroxidation, respectively.RESULTS: A significant increase in righting latency and neurological deficiency afterCHI was observed in caffeine-treated rats as compared with untreated animals. Al-though no deaths occurred in the rats exposed to CHI after pretreatment with saline,pretreatment with caffeine caused significant mortality of animals after trauma in adose-dependent manner. Caffeine also exacerbated neutrophil infiltration, edema, anddisruption of blood-brain barrier in the traumatic cortex. Light microscopy of brainrevealed more severe hemorrhage and neuronal degeneration in the injured hemi-sphere of caffeine-treated rats as compared with rats in the injury-alone group. Asignificant increase in malondialdehyde in the brain of injured rats treated withcaffeine before CHI clearly indicated the role of oxidative stress.CONCLUSION: Caffeine adversely affects outcome after CHI, possibly as a result ofblockade of adenosine receptors. The findings also point toward the involvement of freeradical-mediated neuronal damage in caffeine-induced exacerbation of neurotrauma.
KEY WORDS: Adenosine, Caffeine, Free radicals, Head injury, Neurotrauma, Secondary injury
Neurosurgery 53:704-712, 2003 DOI: 10.1227/01.NEU.0000079487.66013.6F www.neurosurgery-online.com
Posttraumatic neuronal injury is considered to be a con-sequence of the combination of the initial physical insultand the subsequent secondary injury, which may be
more hazardous than the primary source of injury (82). Thesecondary phase consists of loss of autoregulation, elevatedintracranial pressure, systemic hypotension, hemorrhage,thrombosis, edema, inflammation, and vasospasm leading tohypoperfusion and ischemia (55, 57). Any interference withthe body’s defense or natural protective mechanism is likely toalter the course of recovery and outcome after head injury.Adenosine, an endogenous neuromodulator, is released afterischemic-hypoxic insult (9, 62) and provides neuroprotection
by its action on neuronal and glial cells in the still viableborder zone of the ischemic focus (53, 62). Adenosine stimu-lates several processes to alleviate ischemic brain damage byincreasing blood flow, reducing trauma-induced excitatoryamino acid release, preventing neuronal influx of calciumions, and degenerating oxygen-derived free radicals (ODFR).It has also been demonstrated repeatedly that adenosine re-ceptor agonists reduce and antagonists aggravate ischemicbrain injury when provided at the time of insult (24, 79).
Caffeine (1,3,7-trimethylxanthine) is a broad-spectrumadenosine receptor antagonist, and most of its pharmacologi-cal actions are attributed to its ability to block adenosine A1
704 | VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 www.neurosurgery-online.com

and A2 receptors (16, 26). Today, caffeine is the world’s mostwidely consumed and socially acceptable mind-altering drug.It is used by 80% of the adult population of the world in itsvarious forms. Approximately 70% of the hot and cold bever-ages consumed in United States contain caffeine (35–120 mgper serving) as an ingredient (30). Coffee usually contains 80to 120 mg of caffeine per cup; tea contains 30 to 100 mg percup (12). On average, Americans consume approximately 3 to10 mg/kg caffeine daily. In addition to being a commoningredient in soft drinks, caffeine has also been used for thetreatment of a variety of diseases, including apnea (22), fatigue(63), obesity (51), asthma (8), and allergies (75), and it has beenused as an enhancer of alertness and intellectual performance(39, 46). It is also used as an adjuvant with analgesics (44, 66)and anticancer drugs (1). Caffeine (200–400 mg) has beendemonstrated to improve alertness and counteract alcohol-related driving impairment and accidents (47). In the presentstudy, we sought to investigate the effect of acute caffeineadministration on neurological outcome after experimentalhead injury in rats.
MATERIALS AND METHODS
Animals and Drugs
Six groups (n � 10) of adult female Wistar rats weighing 220� 20 g were housed in a temperature-controlled room andmaintained on a 12-hour light-dark cycle, with free access tofood and water. Caffeine (BDH Laboratory Supplies, Poole,England) was administered at doses of 0, 50, 100, and 150mg/kg intraperitoneally to four different groups of rats, 30minutes before head injury. The animals in the fifth groupserved as controls (sham, without head injury), whereas theanimals in the sixth group received caffeine (150 mg/kg) plussham treatment. The use of 50 to 150 mg/kg of caffeine in thisstudy was intended to block most of the adenosine receptors.Studies from our laboratory (3) that used 50 to 150 mg/kg ofcaffeine, as well as data from other centers (19, 40, 43), havedemonstrated that this dose range is well tolerated in rats. Theanimal study protocol was approved by the Research andEthics Committee of Armed Forces Hospital, Riyadh, SaudiArabia.
Head Injury Method
The head injury was produced by means of a previouslyreported method (31, 72) with minor modifications. Beforeinjury, the rat was provided light ether anesthesia for ease inhandling and for proper positioning of the animal on theinjury apparatus. The animal was held by the dorsal skin ofthe neck, and the head was carefully positioned under theinjury apparatus with the chin resting firmly on the base of theapparatus. A weight (200 g) was then released from a height of30 cm; the weight fell freely to strike a Teflon impounderresting on a prefixed point (1–2 mm lateral from the midline).Two hours after injury, the neurological severity score wasanalyzed. The selection of time for the neurological severity
score was based on our pilot studies and reports from variousother laboratories (70, 73, 74) that clearly suggested that themaximum neurological severity score and mortality occurwithin the first 2 hours, with a subsequent gradual recovery.Immediately after behavioral studies, the rats were decapi-tated and their brains were rapidly removed. Tissue samplesof cortex surrounding the traumatic impact (5 mm anteriorand 5 mm posterior to the center of impact) were collected forfurther studies, as described below.
Neurological Severity Score
The assessment of neurological status of the rats was per-formed according to the method described by Shapira et al.(71, 72). The scoring criteria are summarized in Table 1. Thelatency to the righting reflex and survival time were alsorecorded.
Measurement of Tissue Specific Gravity
The specific gravity of cortical tissue was analyzed accord-ing to previously described procedures (49). The timings ofmeasurement were followed as earlier suggested by Shapira etal. (72). A density gradient column was prepared that usedsolutions of kerosene and bromobenzene. After stabilizationfor 15 minutes, the column was calibrated with standard so-lutions of anhydrous potassium sulfate of known specificgravity. The cortical tissue (approximately 2–3 mm3 in size)was placed on the top of a linear gradient, and the specificgravity was analyzed on the basis of its equilibrium position inthe column.
Measurement of Tissue Water Content
Change in cortical tissue water content was measured bythe procedure of Marmarou et al. (49). The specific gravity ofwet (sp grw) and dried tissue (sp grd), heated at 100°C until theweight became constant, were measured by a gradient col-umn, and the water content was calculated by the followingequation:
% water content � (m/sp grw � b) � 100
where m � [(sp grd)/(sp grd � 1)] and b � [1/(sp grd � 1)].
Measurement of Blood-Brain Barrier Permeability
The integrity of the blood-brain barrier was evaluated bythe method described by Uyama et al. (85). Evans blue dye(2% wt/vol in saline), in a volume of 5 ml/kg, was injectedintravenously and allowed to circulate for 60 to 70 minutesbefore the animal was killed. For removal of the intravascu-larly localized dye, the animals were perfused with heparin-free saline through the left ventricle until a colorless perfusionfluid was obtained from the right atrium. After the animalswere decapitated, the brains were removed and the ipsilateraland contralateral cortical tissues were dissected (5 mm ante-rior and 5 mm posterior to the center of impact), as previouslydescribed (18). Each tissue sample was weighed, homogenizedin 2 ml of 50% trichloroacetic acid (wt/vol), and centrifuged at
CAFFEINE AND HEAD INJURY
NEUROSURGERY VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 | 705
10,000 � g for 20 minutes. The supernatant was diluted four-fold with ethanol, and fluorescence was measured at an exci-
tation wavelength of 620 nm and emission wavelength of 680nm with a Shimadzu spectrofluorometer (Model 610; Shi-madzu, Kyoto, Japan).
Determination of Myeloperoxidase
Myeloperoxidase (MPO) activity in the cortical regions sur-rounding the injury site was measured according to the meth-ods described earlier (7, 10). Preweighed tissue was homoge-nized (1:20 wt/vol) in 5 mmol/L potassium phosphate buffer(pH 6.0) with an Ultraturrax homogenizer (Janke & Kunkel,Staufen, Germany) and then centrifuged at 17,000 � g (15 min,4°C). The supernatant was discarded, and the pellet was ex-tracted by 0.5% hexadecyltrimethylammonium bromide (Sig-ma Chemical Co., St. Louis, MO) in 50 mmol potassium phos-phate buffer (pH 6.0). Three freeze-thaw cycles wereperformed, with sonication (10 s, 25°C) between cycles. Afterthe last sonication, the samples were incubated at 4°C for 2minutes and centrifuged at 12,500 � g (15 min, 4°C). MPO inthe supernatant was assayed by mixing 0.1 ml of supernatantwith 2.9 ml of 50 mmol/L potassium phosphate buffer (pH6.0) containing 0.167 mg/ml o-dianasidine dihydrochloride(Sigma Chemical Co.) and 0.0005% hydrogen peroxide (ICNPharmaceuticals, Irvine, CA). The change in absorbance at 460nm was measured for 3 minutes with an ultraviolet-visiblespectrophotometer (Shimadzu).
Determination of Lipid Peroxidation
Lipid peroxidation in the cortical tissue was assessed bymeasuring malondialdehyde (MDA) (56). The cortical tissue(approximately 0.5 g) from the area adjacent to the traumaticlesion was homogenized in 1.15% cold KCl with an Ultratur-rax homogenizer. After centrifugation at 3000 � g for 5 min-utes, an aliquot of supernatant was mixed with 2 ml of reac-tion mixture (containing 15% trichloroacetic acid and 0.375%thiobarbituric acid solution in 0.25 N HCl) and heated for 5minutes in a boiling water bath. The tubes were cooled atroom temperature and centrifuged at 1000 � g for 10 minutes.The absorbance of supernatant was read at 535 nm against ablank that contained all reagents except homogenate. Tissuelipid peroxide levels were calculated as nanomoles of MDA;tetramethoxy propane was used as standard.
Histopathology of Brain
While under ether anesthesia, the rat underwent intracar-diac perfusion with 10% neutral buffered formalin. After fix-ation, the rat was decapitated, and the whole cerebrum wasremoved and stored in a formalin solution. The samples wereprocessed with an automated processor (2L MKII; ShandonSouthern, Cheshire, England) for dehydration and clearingsteps. The specimens were embedded in paraffin blocks, and4-�m-thick coronal sections were stained with hematoxylinand eosin for light microscopy observations. For macroscopicmorphology, a coronal view of the sample block was digitizedwith a scanner, and the image was captured.
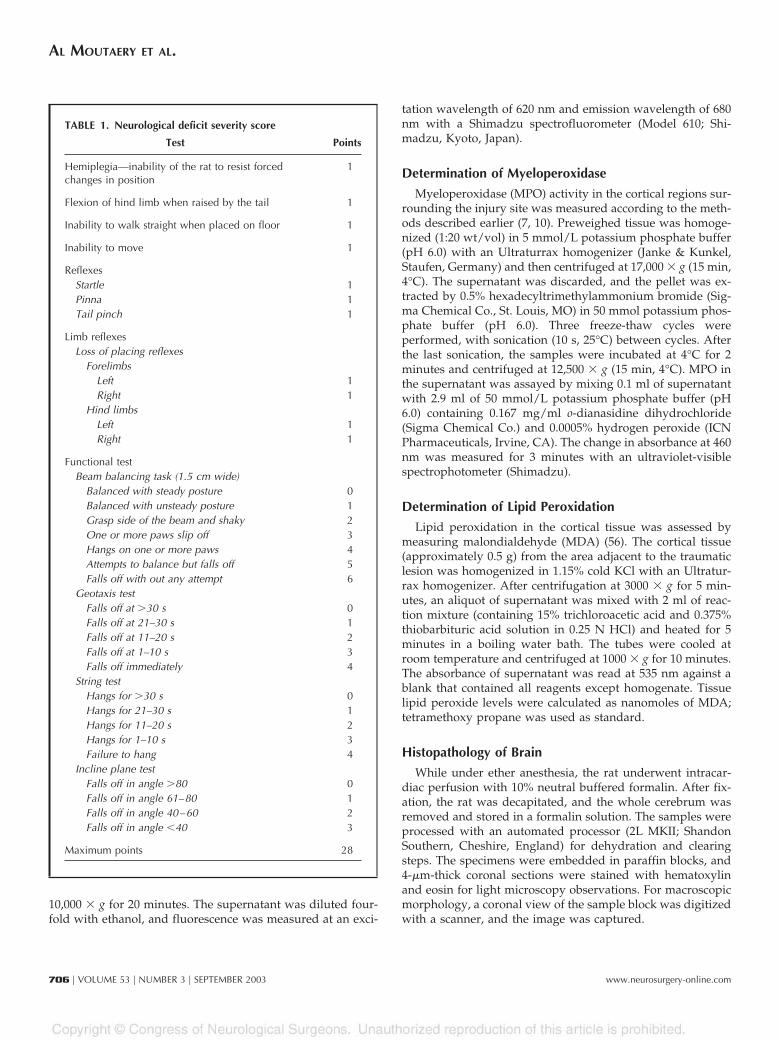
TABLE 1. Neurological deficit severity score
Test Points
Hemiplegia—inability of the rat to resist forcedchanges in position
1
Flexion of hind limb when raised by the tail 1
Inability to walk straight when placed on floor 1
Inability to move 1
ReflexesStartle 1Pinna 1Tail pinch 1
Limb reflexesLoss of placing reflexes
ForelimbsLeft 1Right 1
Hind limbsLeft 1Right 1
Functional testBeam balancing task (1.5 cm wide)
Balanced with steady posture 0Balanced with unsteady posture 1Grasp side of the beam and shaky 2One or more paws slip off 3Hangs on one or more paws 4Attempts to balance but falls off 5Falls off with out any attempt 6
Geotaxis testFalls off at �30 s 0Falls off at 21–30 s 1Falls off at 11–20 s 2Falls off at 1–10 s 3Falls off immediately 4
String testHangs for �30 s 0Hangs for 21–30 s 1Hangs for 11–20 s 2Hangs for 1–10 s 3Failure to hang 4
Incline plane testFalls off in angle �80 0Falls off in angle 61–80 1Falls off in angle 40–60 2Falls off in angle �40 3
Maximum points 28
AL MOUTAERY ET AL.
706 | VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 www.neurosurgery-online.com
Statistical Analysis
The statistical significance was evaluated by Student’s t test.Log-rank �2 test was used to analyze survival data.
RESULTS
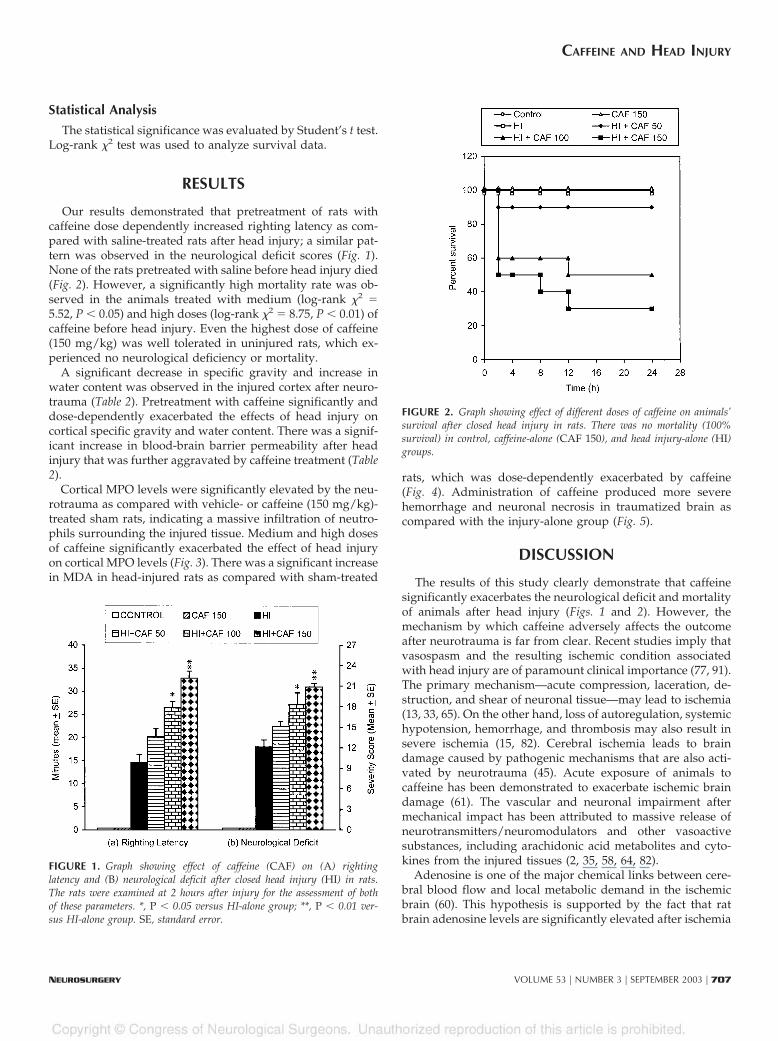
Our results demonstrated that pretreatment of rats withcaffeine dose dependently increased righting latency as com-pared with saline-treated rats after head injury; a similar pat-tern was observed in the neurological deficit scores (Fig. 1).None of the rats pretreated with saline before head injury died(Fig. 2). However, a significantly high mortality rate was ob-served in the animals treated with medium (log-rank �2 �5.52, P � 0.05) and high doses (log-rank �2 � 8.75, P � 0.01) ofcaffeine before head injury. Even the highest dose of caffeine(150 mg/kg) was well tolerated in uninjured rats, which ex-perienced no neurological deficiency or mortality.
A significant decrease in specific gravity and increase inwater content was observed in the injured cortex after neuro-trauma (Table 2). Pretreatment with caffeine significantly anddose-dependently exacerbated the effects of head injury oncortical specific gravity and water content. There was a signif-icant increase in blood-brain barrier permeability after headinjury that was further aggravated by caffeine treatment (Table2).
Cortical MPO levels were significantly elevated by the neu-rotrauma as compared with vehicle- or caffeine (150 mg/kg)-treated sham rats, indicating a massive infiltration of neutro-phils surrounding the injured tissue. Medium and high dosesof caffeine significantly exacerbated the effect of head injuryon cortical MPO levels (Fig. 3). There was a significant increasein MDA in head-injured rats as compared with sham-treated
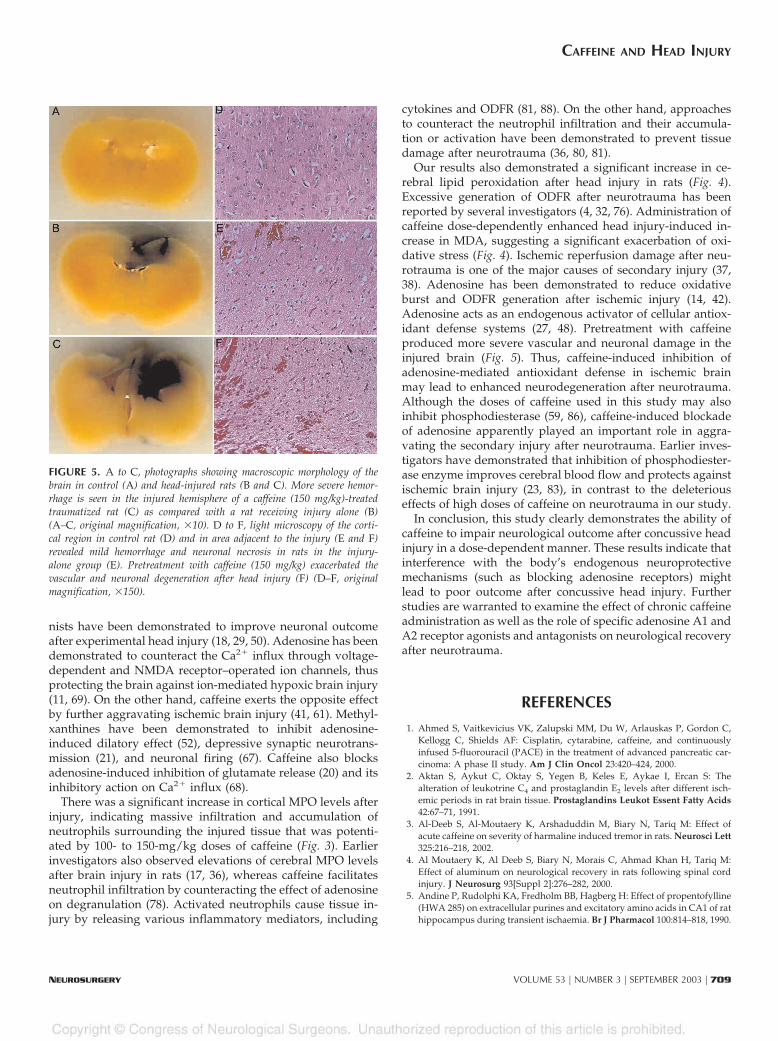
rats, which was dose-dependently exacerbated by caffeine(Fig. 4). Administration of caffeine produced more severehemorrhage and neuronal necrosis in traumatized brain ascompared with the injury-alone group (Fig. 5).
DISCUSSION
The results of this study clearly demonstrate that caffeinesignificantly exacerbates the neurological deficit and mortalityof animals after head injury (Figs. 1 and 2). However, themechanism by which caffeine adversely affects the outcomeafter neurotrauma is far from clear. Recent studies imply thatvasospasm and the resulting ischemic condition associatedwith head injury are of paramount clinical importance (77, 91).The primary mechanism—acute compression, laceration, de-struction, and shear of neuronal tissue—may lead to ischemia(13, 33, 65). On the other hand, loss of autoregulation, systemichypotension, hemorrhage, and thrombosis may also result insevere ischemia (15, 82). Cerebral ischemia leads to braindamage caused by pathogenic mechanisms that are also acti-vated by neurotrauma (45). Acute exposure of animals tocaffeine has been demonstrated to exacerbate ischemic braindamage (61). The vascular and neuronal impairment aftermechanical impact has been attributed to massive release ofneurotransmitters/neuromodulators and other vasoactivesubstances, including arachidonic acid metabolites and cyto-kines from the injured tissues (2, 35, 58, 64, 82).
Adenosine is one of the major chemical links between cere-bral blood flow and local metabolic demand in the ischemicbrain (60). This hypothesis is supported by the fact that ratbrain adenosine levels are significantly elevated after ischemia
FIGURE 1. Graph showing effect of caffeine (CAF) on (A) rightinglatency and (B) neurological deficit after closed head injury (HI) in rats.The rats were examined at 2 hours after injury for the assessment of bothof these parameters. *, P � 0.05 versus HI-alone group; **, P � 0.01 ver-sus HI-alone group. SE, standard error.
FIGURE 2. Graph showing effect of different doses of caffeine on animals’survival after closed head injury in rats. There was no mortality (100%survival) in control, caffeine-alone (CAF 150), and head injury-alone (HI)groups.
CAFFEINE AND HEAD INJURY
NEUROSURGERY VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 | 707

(89), hypoxia (87), and sustained hypotension (90). Adenosineenhances blood flow, decreases excitatory amino acid, reducestransmembrane Ca2� influx, and inhibits ODFR formation,leading to attenuation of ischemic brain damage (27). It hasalso been demonstrated that adenosine receptor agonists re-duce and antagonists aggravate (34) ischemic brain damagewhen provided at the time of insult. Elevation of brain aden-osine levels by dipyridamole (60) or propentofylline (5) hasbeen demonstrated to reduce ischemic neuronal damage,whereas blockade of adenosine receptor by caffeine totallysuppresses the systemic and cerebrovascular effects of aden-osine, leading to cerebral vasoconstriction, brain hypoperfu-sion, and aggravation of ischemic neurodegeneration (54, 61).Moreover, massive sympathetic discharge and catecholaminesurge during the initial phase (first 10 min) are crucial fordetermining the mortality and morbidity associated with headinjury (6). Caffeine has been demonstrated to stimulate
catecholamine-containing neurons in brain (54). Hence, thesynergistic effect of caffeine in a catecholamine surge attrib-utable to neurotrauma may contribute to the exacerbation ofconcussive head injury.
Significant increases in edema formation and disruption ofblood-brain barrier were observed in the traumatic cortex ofrats pretreated with caffeine (Table 2). Excessive release ofglutamate and overactivation of N-methyl-d-aspartate(NMDA) receptors is considered to be one of the most impor-tant pathophysiological mechanisms in head injury (18, 25).Ion pump failure attributable to adenosine triphosphate de-pletion, intracellular accumulation of Ca2�, and disruption ofblood-brain barrier lead to cell death through neuronal edemaand excessive activation of Ca2�-dependent lytic enzymes(lipases, proteases), causing mitochondrial lysis (28, 84). Com-petitive as well as noncompetitive NMDA receptor antago-
TABLE 2. Effect of caffeine on cortical tissue specific gravity, water content, and extravasation of Evans blue dye after closed head injuryin ratsa
Group Specific gravity Water content (%) Evans blue (ng/g)
Control 1.0448 � 0.0004 79.26 � 0.24 224 � 7.5
Caffeine, 150 mg/kg 1.0445 � 0.0005 79.61 � 0.23 214 � 10.4
HI 1.0355 � 0.0003b 83.57 � 0.16b 424 � 12.0b
HI � caffeine, 50 mg/kg 1.0348 � 0.0012 83.90 � 0.55 473 � 12.9c
HI � caffeine, 100 mg/kg 1.0324 � 0.0004d 84.99 � 0.20c 500 � 4.20d
HI � caffeine, 150 mg/kg 1.0316 � 0.0010d 85.33 � 0.47c 606 � 16.0d
a Values are mean � Standard error. HI, head injury.b P � 0.001 versus control.c P � 0.01 versus HI group.d P � 0.001 versus HI group.
FIGURE 3. Graph showing effect of caffeine (CAF) on cortical MPO lev-els after experimental head injury (HI) in rats. #, P � 0.01 versus con-trol; *, P � 0.05 versus head injury group.
FIGURE 4. Graph showing effect of caffeine on cortical MDA levels afterexperimental head injury in rats. *, P � 0.05 versus control group; **, P� 0.01 versus control group.
AL MOUTAERY ET AL.
708 | VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 www.neurosurgery-online.com
nists have been demonstrated to improve neuronal outcomeafter experimental head injury (18, 29, 50). Adenosine has beendemonstrated to counteract the Ca2� influx through voltage-dependent and NMDA receptor–operated ion channels, thusprotecting the brain against ion-mediated hypoxic brain injury(11, 69). On the other hand, caffeine exerts the opposite effectby further aggravating ischemic brain injury (41, 61). Methyl-xanthines have been demonstrated to inhibit adenosine-induced dilatory effect (52), depressive synaptic neurotrans-mission (21), and neuronal firing (67). Caffeine also blocksadenosine-induced inhibition of glutamate release (20) and itsinhibitory action on Ca2� influx (68).
There was a significant increase in cortical MPO levels afterinjury, indicating massive infiltration and accumulation ofneutrophils surrounding the injured tissue that was potenti-ated by 100- to 150-mg/kg doses of caffeine (Fig. 3). Earlierinvestigators also observed elevations of cerebral MPO levelsafter brain injury in rats (17, 36), whereas caffeine facilitatesneutrophil infiltration by counteracting the effect of adenosineon degranulation (78). Activated neutrophils cause tissue in-jury by releasing various inflammatory mediators, including
cytokines and ODFR (81, 88). On the other hand, approachesto counteract the neutrophil infiltration and their accumula-tion or activation have been demonstrated to prevent tissuedamage after neurotrauma (36, 80, 81).
Our results also demonstrated a significant increase in ce-rebral lipid peroxidation after head injury in rats (Fig. 4).Excessive generation of ODFR after neurotrauma has beenreported by several investigators (4, 32, 76). Administration ofcaffeine dose-dependently enhanced head injury-induced in-crease in MDA, suggesting a significant exacerbation of oxi-dative stress (Fig. 4). Ischemic reperfusion damage after neu-rotrauma is one of the major causes of secondary injury (37,38). Adenosine has been demonstrated to reduce oxidativeburst and ODFR generation after ischemic injury (14, 42).Adenosine acts as an endogenous activator of cellular antiox-idant defense systems (27, 48). Pretreatment with caffeineproduced more severe vascular and neuronal damage in theinjured brain (Fig. 5). Thus, caffeine-induced inhibition ofadenosine-mediated antioxidant defense in ischemic brainmay lead to enhanced neurodegeneration after neurotrauma.Although the doses of caffeine used in this study may alsoinhibit phosphodiesterase (59, 86), caffeine-induced blockadeof adenosine apparently played an important role in aggra-vating the secondary injury after neurotrauma. Earlier inves-tigators have demonstrated that inhibition of phosphodiester-ase enzyme improves cerebral blood flow and protects againstischemic brain injury (23, 83), in contrast to the deleteriouseffects of high doses of caffeine on neurotrauma in our study.
In conclusion, this study clearly demonstrates the ability ofcaffeine to impair neurological outcome after concussive headinjury in a dose-dependent manner. These results indicate thatinterference with the body’s endogenous neuroprotectivemechanisms (such as blocking adenosine receptors) mightlead to poor outcome after concussive head injury. Furtherstudies are warranted to examine the effect of chronic caffeineadministration as well as the role of specific adenosine A1 andA2 receptor agonists and antagonists on neurological recoveryafter neurotrauma.
REFERENCES
1. Ahmed S, Vaitkevicius VK, Zalupski MM, Du W, Arlauskas P, Gordon C,Kellogg C, Shields AF: Cisplatin, cytarabine, caffeine, and continuouslyinfused 5-fluorouracil (PACE) in the treatment of advanced pancreatic car-cinoma: A phase II study. Am J Clin Oncol 23:420–424, 2000.
2. Aktan S, Aykut C, Oktay S, Yegen B, Keles E, Aykae I, Ercan S: Thealteration of leukotrine C4 and prostaglandin E2 levels after different isch-emic periods in rat brain tissue. Prostaglandins Leukot Essent Fatty Acids42:67–71, 1991.
3. Al-Deeb S, Al-Moutaery K, Arshaduddin M, Biary N, Tariq M: Effect ofacute caffeine on severity of harmaline induced tremor in rats. Neurosci Lett325:216–218, 2002.
4. Al Moutaery K, Al Deeb S, Biary N, Morais C, Ahmad Khan H, Tariq M:Effect of aluminum on neurological recovery in rats following spinal cordinjury. J Neurosurg 93[Suppl 2]:276–282, 2000.
5. Andine P, Rudolphi KA, Fredholm BB, Hagberg H: Effect of propentofylline(HWA 285) on extracellular purines and excitatory amino acids in CA1 of rathippocampus during transient ischaemia. Br J Pharmacol 100:814–818, 1990.
FIGURE 5. A to C, photographs showing macroscopic morphology of thebrain in control (A) and head-injured rats (B and C). More severe hemor-rhage is seen in the injured hemisphere of a caffeine (150 mg/kg)-treatedtraumatized rat (C) as compared with a rat receiving injury alone (B)(A–C, original magnification, �10). D to F, light microscopy of the corti-cal region in control rat (D) and in area adjacent to the injury (E and F)revealed mild hemorrhage and neuronal necrosis in rats in the injury-alone group (E). Pretreatment with caffeine (150 mg/kg) exacerbated thevascular and neuronal degeneration after head injury (F) (D–F, originalmagnification, �150).
CAFFEINE AND HEAD INJURY
NEUROSURGERY VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 | 709

6. Atkinson JLD: The neglected prehospital phase of head injury: Apnea andcatecholamine surge. Mayo Clin Proc 75:37–47, 2000.
7. Barone FC, Hillegass LM, Price WJ, White RF, Feuerstein GZ, Saran HM,Clark RK, Griswold DE: Polymorphonuclear leukocyte infiltration into ce-rebral focal ischemic tissue: Myeloperoxide activity assay and histologicverification. J Neurosci Res 29:336–348, 1991.
8. Becker AB, Simons KJ, Gillespie CA, Simons FE: The bronchodilator effectsand pharmacokinetics of caffeine in asthma. N Engl J Med 310:743–746,1984.
9. Berne RN, Rubio R, Curnish RR: Release of adenosine from ischemic brain.Circ Res 35:262–271, 1974.
10. Bradley PP, Priebat DA, Christensen RD, Rothstein G: Measurement ofcutaneous inflammation: Estimation of neutrophil content with an enzymemarker. J Invest Dermatol 78:206–209, 1982.
11. Buck LT, Bickler PE: Adenosine and anoxia reduce N-methyl-d-aspartatereceptor open probability in turtle cerebrocortex. J Exp Biol 201:289–297,1998.
12. Burg AW: Effects of caffeine on the human system. Tea Coffee Trade J147:40–42, 1975.
13. Collins WF: A review and update of experimental and clinical studies ofspinal cord injury. Paraplegia 21:204–219, 1983.
14. Cronstein BN: Adenosine, an endogenous anti-inflammatory agent. J ApplPhysiol 76:5–13, 1994.
15. Czosnyka M, Smielewski P, Piechnik S, Steiner L, Pickard J: Cerebral auto-regulation following head injury. J Neurosurg 95:756–763, 2001.
16. Daly : Mechanism of action of caffeine, in Garattini S (ed): Caffeine, Coffee andHealth. New York, Raven Press, 1993, pp 97–150.
17. Darakchiev BJ, Itkis M, Agajanova T, Itkis A, Hariri RJ: Changes of MPOactivity and brain water accumulation in traumatic brain injury experi-ments. Acta Neurochir (Wien) 70:98–101, 1997.
18. Dempsey RJ, Baskaya MK, Dogan A: Attenuation of brain edema, blood-brain barrier breakdown, and injury volume by ifenprodil, a polyamine-siteN-methyl-d-aspartate receptor antagonist, after experimental traumaticbrain injury in rats. Neurosurgery 47:399–406, 2000.
19. Derlett RW, Tseng JC, Albertson TE: Potentiation of cocaine andd-amphetamine toxicity with caffeine. Am J Emerg Med 10:211–216, 1992.
20. Dolphin AC, Archer ER: An adenosine agonist inhibits and a cyclic AMPanalogue enhances the release of glutamate but not GABA from slices of ratdentate gyrus. Neurosci Lett 43:49–54, 1983.
21. Dunwiddie TV, Hoffer BJ: Adenosine nucleotides and synaptic transmissionin the in vitro rat hippocampus. Br J Pharmacol 69:59–68, 1980.
22. Erenberg A, Leff RD, Haack DG, Mosdell KW, Hicks GM, Wynne BA:Caffeine citrate for the treatment of apnea of prematurity: A double-blind,placebo-controlled study. Pharmacotherapy 20:644–652, 2000.
23. Eun BL, Liu XL, Barks JD: Pentoxifylline attenuates hypoxic-ischemic braininjury in immature rats. Pediatr Res 47:73–78, 2000.
24. Evans MC, Swan JH, Meldrum BS: An adenosine analogue,2-chloroadenosine, protects against long term development of ischaemic cellloss in the rat hippocampus. Neurosci Lett 83:287–292, 1987.
25. Faden AI, Demediuk P, Panter SS, Vink R: The role of excitatory amino acidsand NMDA receptors in traumatic head injury. Science 244:798–800, 1989.
26. Fredholm BB: Adenosine, adenosine receptors and the action of caffeine.Pharmacol Toxicol 76:93–101, 1995.
27. Fredholm BB: Adenosine and neuroprotection. Int Rev Neurobiol 40:259–280, 1997.
28. Garthwaite G, Hajos F, Garthwaite J: Ionic requirements for neurotoxiceffects of excitatory amino acid analogues in rat cerebellar slices. Neuro-science 18:437–447, 1986.
29. Golding EM, Vink R: Efficacy of competitive vs noncompetitive blockade ofthe NMDA channel following traumatic brain injury. Mol ChemNeuropathol 24:137–150, 1995.
30. Griffiths RR, Vernotica EM: Is caffeine a flavoring agent in cola soft drinks?Arch Family Med 9:727–734, 2000.
31. Hall ED: High dose of glucocorticoid treatment improves neurological re-covery in head-injured mice. J Neurosurg 62:882–887, 1985.
32. Hall ED, Andrus PK, Yonkers PA, Smith SL, Zhang JR, Taylor BM, Sun FF:Generation and detection of hydroxyl radical following experimental headinjury. Ann N Y Acad Sci 738:15–24, 1994.
33. Hall ED, Yonkers PA, Horan KL: Correlation between attenuation of post-traumatic spinal cord ischemia and preservation of tissue vitamin E by the21-aminosteroid U74006 F: Evidence for an in vivo antioxidant mechanism.J Neurotrauma 6:169–176, 1989.
34. Heron A, Larbennes F, Seylaz J: Adenosine modulation of amino acidrelease in rat hippocampus during ischemia and veratridine depolarization.Brain Res 608:27–32, 1993.
35. Hsu CY, Halushka PV, Hogan EL, Banik NL, Lee WA, Perot PL: Alterationof thromboxane and prostacyclin levels in experimental spinal cord injury.Neurology 35:1003–1009, 1985.
36. Hudone S, Palmer C, Roberts RL, Manger D, Housman C, Towfighi J: Therole of neutrophils in the production of hypoxic-ischemic brain injury in theneonatal rat. Pediatr Res 41:607–616, 1997.
37. Ikeda Y, Long DM: Comparative effects of direct and indirect hydroxylradical scavengers on traumatic brain edema. Acta Neurochir Suppl (Wien)51:74–76, 1990.
38. Inci S, Ozcan OE, Kilinc K: Time-level relationship for lipid peroxidationand the protective effect of �-tocopherol in experimental mild and severebrain injury. Neurosurgery 43:330–336, 1998.
39. Kamimori GH, Penetar DM, Headley DB, Thorne DR, Otterstetter R,Belenky G: Effect of three caffeine doses on plasma catecholamines andalertness during prolonged wakefulness. Eur J Clin Pharmacol 56:537–544,2000.
40. Karas M, Chakrabarti SK: Influence of caffeine on allyl alcohol-inducedhepatotoxicity in rats: Part I—In vivo study. J Environ Pathol Toxicol Oncol20:141–154, 2001.
41. Karhapaa L, Tornquist K: Effects of caffeine on the influx of extracellularcalcium in GH4C1 pituitary cells. J Cell Physiol 171:52–60, 1997.
42. Kochanek PM, Hallenbeck JM: Polymorphonuclear leukocytes andmonocytes/macrophages in the pathogenesis of cerebral ischaemia andstroke. Stroke 23:1367–1379, 1992.
43. Kulkarni C, Joseph T, David J: Inhibition of anticonvulsant action ofcarbamazepine by aminophylline and caffeine in rats. Indian J Exp Biol27:1048–1051, 1989.
44. Laska EM, Sunshine A, Mueller F, Elvers WB, Siegel C, Rubin A: Caffeine asan analgesic adjuvant. J Am Med Assoc 251:1711–1718, 1984.
45. Leker RR, Shohami E: Cerebral ischemia and trauma-different etiologies yetsimilar mechanisms: Neuroprotective opportunities. Brain Res Brain ResRev 39:55–73, 2002.
46. Lieberman HR, Wurtman RJ, Emde GG, Roberts C, Coviella ILG: The effectsof low doses of caffeine on human performance and mood. Psychopharma-cology 92:308–312, 1987.
47. Ligouri A, Robinson JH: Caffeine antagonism of alcohol-induced drivingimpairment. Drug Alcohol Depend 63:123–129, 2001.
48. Maggirwar SB, Dhanraj DN, Somani SM, Ramkumar V: Adenosine acts asan endogenous activator of the cellular antioxidant defense system.Biochem Biophys Res Commun 201:508–515, 1994.
49. Marmarou A, Poll W, Shulman K: A simple gravimetric technique formeasurement of cerebral edema. J Neurosurg 49:530–537, 1978.
50. McIntosh TK, Vink R, Soares H, Hayes R, Simon R: Effects of noncompeti-tive blockade of N-methyl-d-aspartate receptors on the neurochemical se-quelae of experimental brain injury. J Neurochem 55:1170–1179, 1990.
51. Molnar D, Torok K, Erhardt E, Jages S: Safety and efficacy of treatment withan ephedrine/caffeine mixture: The first in adolescents. Int J Obes RelatMetab Disord 24:1573–1578, 2000.
52. Morii S, Winn HR, Berne RM: Effect of theophylline, an adenosine receptorblocker on cerebral blood flow (CBF) during rest and transient hypoxia.J Cereb Blood Flow Metab 3[Suppl 1]:S480–S481, 1983.
53. Nakamichi T: Glutamate neurotoxicity during spinal cord ischemia: Theneuroprotective effects of adenosine [in Japanese]. Jpn J Thorac CardiovascSurg 46:354–360, 1998.
54. Nehlig A, Daval JL, Debry G: Caffeine and the central nervous system:Mechanism of action, biochemical, metabolic and psychostimulant effects.Brain Res Rev 17:139–170, 1992.
55. Nilsson B, Ponten U: Experimental head injury in the rat: Part 2—Regionalbrain energy metabolism in concussive trauma. J Neurosurg 47:252–261,1977.
AL MOUTAERY ET AL.
710 | VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 www.neurosurgery-online.com

56. Ohkawa H, Ohishi N, Yagi K: Assay for lipid peroxides in animal tissues bythiobarbituric acid reaction. Anal Biochem 95:351–358, 1979.
57. Okiyama K, Smith DH, Gennarelli TA, Simon RP, Leach M, McIntosh TK:The sodium channel blocker and glutamate release inhibitor BW1003C87and magnesium attenuate regional cerebral edema following experimentalbrain injury in the rat. J Neurochem 64:802–809, 1995.
58. Osterholm JL, Mathews GJ: Altered norepinephrine metabolism followingexperimental spinal cord injury: Part I—Relationship to hemorrhagic necro-sis and post-wounding neurological deficits. J Neurosurg 36:386–394, 1972.
59. Petkov VV, Rousseva S: Effects of caffeine on aggressive behavior andavoidance learning of rats with isolation syndrome. Methods Find Exp ClinPharmacol 6:433–436, 1984.
60. Puiroud S, Pinard E, Seylaz J: Dynamic cerebral and systemic circulatoryeffects of adenosine, theophylline and dipyridamole. Brain Res 453:287–298,1988.
61. Rudolphi KA, Keil M, Grome JJ: Adenosine: A pharmacological concept forthe treatment of cerebral ischemia? in Krieglstein J, Oberpichler H (eds):Pharmacology of Cerebral Ischemia. Stuttgart, WissenschaftlicheVerlagsgesellschraft mbH, 1990, pp 439–448.
62. Rudolphi KA, Schubert P, Parkinson FE, Fredholm BB: Neuroprotective roleof adenosine in cerebral ischemia. Trends Pharmacol Sci 13:439–445, 1992.
63. Ruijter J, Lorist MM, Snel J, De Ruiter MB: The influence of caffeine onsustained attention: An ERP study. Pharmacol Biochem Behav 66:29–37,2000.
64. Salzman SK, Hirofuji E, Llados-Eckman C, MacEwen GD, Beckman AL:Monoaminergic responses to spinal trauma: Participation of serotonin inposttraumatic progression of neural damage. J Neurosurg 66:431–439, 1987.
65. Sandler AN, Tator CH: Review of the effect of spinal cord trauma on thevessels and blood flow in the spinal cord. J Neurosurg 45:638–646, 1976.
66. Sawynok J, Yaksh TL: Caffeine as an analgesic adjuvant: A review ofpharmacology and mechanisms of action. Pharmacol Rev 45:43–85, 1993.
67. Schubert P, Mitzdorf U: Analysis and quantitative evaluation of the depres-sive effect of adenosine on evoked potentials in hippocampal slices. BrainRes 172:186–190, 1979.
68. Schubert P, Heinemann U, Kolb R: Differential effects on adenosine on pre-and postsynaptic Ca2� influxes. Brain Res 376:382–386, 1986.
69. Schubert P, Ogata T, Marchini C, Ferroni S, Rudolphi K: Protective mecha-nisms of adenosine in neurons and glial cells. Ann N Y Acad Sci 825:1–10,1997.
70. Shapira Y, Artru AA, Cotev S, Muggia-Sulam M, Freund HR: Brain edemaand neurologic status following head trauma in the rat. Anesthesiology77:79–85, 1992.
71. Shapira Y, Artru AA, Yadid G, Shohami E: Methylprednisolone does notdecrease eicosanoid concentrations or edema in brain tissue or improveneurologic outcome after head trauma in rats. Anesth Analg 75:238–244,1992.
72. Shapira Y, Setton D, Artru AA, Shohami E: Blood-brain barrier permeability,cerebral edema, and neurologic function after closed head injury in rats.Anesth Analg 7:141–148, 1993.
73. Shapira Y, Shohami E, Sidi A, Soffer D, Freeman S, Cotev S: Experimentalclosed head injury in rats: Mechanical, pathophysiologic, and neurologicproperties. Crit Care Med 16:258–265, 1988.
74. Shapira Y, Yadid G, Cotev S, Niska A, Shohami E: Protective effect ofMK-801 in experimental brain injury. J Neurotrauma 3:131–139, 1990.
75. Shapiro P: Caffeine for allergic rhinitis. Lancet 1:793, 1982.76. Smith SL, Andrus PK, Zhang JR, Hall ED: Direct measurement of hydroxyl
radicals, lipid peroxidation and blood-brain barrier disruption followingunilateral cortical impact head injury in the rat. J Neurotrauma 11:393–404,1994.
77. Soustiel JF, Shik V, Feinsod M: Basilar vasospasm following spontaneousand traumatic subarachnoid haemorrhage: Clinical implications. ActaNeurochir (Wien) 144:137–144, 2002.
78. Sullivan GW, Luong LS, Carper HT, Barnes RC, Mandell GL:Methylxanthines with adenosine alter TNF �-primed PMN activation. Im-munopharmacology 31:19–29, 1995.
79. Sutherland GR, Peeling J, Lesiuk HJ, Brownstone RM, Rydzy M, SaundersJK, Geiger JD: The effects of caffeine on ischemic neuronal injury as deter-mined by magnetic resonance imaging and histopathology. Neuroscience42:171–182, 1991.
80. Taoka Y, Okajima K, Uchiba M, Murakami K, Harada N, Johno M, Naruo M,Okabe H, Takatsuki K: Reduction of spinal cord injury by administration ofiloprost, a stable prostacyclin analog. J Neurosurg 86:1007–1011, 1997.
81. Taoka Y, Okajima K, Uchiba M, Murakami K, Kushimoto S, Johno M, NaruoM, Okabe H, Takatsuki K: Gabexate mesilate, a synthetic protease inhibitor,prevents compression-induced spinal cord injury by inhibiting activation ofleukocytes in rats. Crit Care Med 25:874–879, 1997.
82. Tator CH, Fehlings MG: Review of the secondary injury theory of acutespinal cord trauma with emphasis on vascular mechanisms. J Neurosurg75:15–26, 1991.
83. Turcani P, Tureani M: Effect of propentofylline on cerebral blood flow in agerbil focal cerebral ischemia. J Neurol Sci 183:57–60, 2001.
84. Ustun ME, Gurbilek M, Ak A, Vatansev H, Duman A: Effects of magnesiumsulfate on tissue lactate and malondialdehyde levels in experimental headtrauma. Intensive Care Med 27:264–268, 2001.
85. Uyama O, Okamura N, Yanase M, Narita M, Kawabata K, Sujita M: Quan-titative evaluation of vascular permeability in the gerbil brain after transientischemia using Evans blue fluorescence. J Cereb Blood Flow Metab 8:282–284, 1988.
86. Watanabe H, Ikeda M, Watanabe K: Properties of rotational behavior pro-duced by methylxanthine derivatives in mice with unilateral6-hydroxydopamine-induced lesions. J Pharmacobiodyn 4:301–307, 1981.
87. Wei EP, Kontos HA: Role of adenosine in cerebral arteriolar dilation fromarterial hypoxia. J Cereb Blood Flow Metab 1[Suppl 1]:S395–S396, 1981.
88. Wilson JT, Gross CE, Bednar MM, Schackford SR: U83836E reduces second-ary brain injury in a rabbit model of cryogenic trauma. J Trauma 39:473–477,1995.
89. Winn HR, Rubio R, Berne RM: Brain adenosine production during 60seconds of ischemia. Circ Res 45:486–492, 1979.
90. Winn HR, Welsh JE, Rubio R, Bern M: Brain adenosine production in ratduring sustained alteration in systemic blood pressure. Am J Physiol 239:H639–H641, 1980.
91. Zubkov AY, Pilkington AS, Parent AD, Zhang J: Morphological presentationof posttraumatic vasospasm. Acta Neurochir Suppl (Wien) 76:223–226,2000.
AcknowledgmentsThis study was financially supported by Research and Ethical Committee,
Riyadh Armed Forces Hospital, Saudi Arabia. We thank Deivekadatcham Nay-agam, Jesuraja Rajakanna, and Khalid Elfaki Abdalla for technical assistance andTess Jaime for secretarial assistance.
COMMENTS
Al Moutaery et al. present a detailed description of theeffects of high doses of caffeine in rats undergoing exper-
imental brain injury. Using measures such as cortical tissuespecific gravity and water content, amount of Evans blue dyeextravasation, level of myeloperoxidase activity, neurologicalseverity score, and righting latency at two hours postinjury,they demonstrate that gradually increasing the dose of caf-feine causes progressive worsening of these markers. Addi-tional outcome studies would be of interest to see whetherhigh-dose caffeine affects long-term behavioral recovery afterexperimental brain injury.
A word of caution is necessary to put this study into per-spective. Note that the lowest dose of caffeine administered inthis study was 50 mg/kg. This is roughly equivalent to theamount of caffeine in a cup of brewed coffee, which generally
CAFFEINE AND HEAD INJURY
NEUROSURGERY VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 | 711
varies between 40 and 180 mg/cup. Although different spe-cies metabolize caffeine differently, even a crude extrapolationof the doses used in this study to the clinical situation wouldrequire that a human drink gallons of coffee. Thus, the pop-ular media should not interpret this study as indicating thatcoffee and caffeine-containing soft drinks worsen brain injury.Instead, it would be best to view this study as one in whichinvestigators used massive doses of caffeine to demonstratethat blocking adenosine receptors has detrimental effects afterexperimental traumatic brain injury.
Alex B. ValadkaHouston, Texas
Al Moutaery et al. have investigated the effects of caffeineon the neurological recovery of rats with closed head
injuries. In their study, 50 rats were divided into 5 groups andadministered 0, 50, 100, and 150 mg/kg of caffeine through theperitoneum. Thirty minutes later, head injuries were inducedin the rats (200 g weight released from 30 cm height). The rats
were tested for neurological function, and their cortical tissueswere analyzed for water content, blood-brain barrier perme-ability, myeloperoxidase and lipid peroxidase activity, andhistopathology. The authors show not only that caffeine ad-versely affected neurological recovery but also, on the basis ofbrain tissue analysis, that water content, the permeability ofthe cerebral vasculature, and tissue damage increased in adose-dependent manner. They postulate that the adenosine-blocking effects of caffeine interfered with adenosine-mediated neuroprotective mechanisms. The relevance of thesedata to humans is unclear. In this study, the authors admin-istered high doses of caffeine; thus, some of the findings maybe related to severe hypertensive surges rather than to subtleadenosine-related mechanisms. Nevertheless, the findings areintriguing. We wonder in which direction the authors willtake this line of investigation in the future.
Raj K. NarayanDavid YehCincinnati, Ohio
Pioneer Arctic and Antarctic aviator Richard E. Byrd. He is shown here in his naval aviator’sattire. His aviation exploits included being the first person to fly over the North Pole, for which he wasawarded the Congressional Medal of Honor, and he was also the third person to fly solo across theAtlantic. He spent the last 3 decades of his life exploring Antarctica. (Also see pp. 695, 722, and 742.)
AL MOUTAERY ET AL.
712 | VOLUME 53 | NUMBER 3 | SEPTEMBER 2003 www.neurosurgery-online.com
Copyright © 2022 FDOKUMEN




















