By Dissertation Submitted to the Rajiv Gandhi University Of ...
109
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE) WITH LAKSHA KSHEERA AND MANJISTADI LEPA By Dr. VIJITH V. NANGELIL Dissertation Submitted to the Rajiv Gandhi University Of Health Sciences,Bangalore,Karnataka In partial fulfilment of the requirements for the degree of Ayurveda Vachaspathi M.S. (AYURVEDA) in Shalya Tantra Under the guidance of Dr.MANONMANI L M.D (Shalya), H.O.D, Shalya Tantra T.M.A.E’S AMC, Hospet & Under the Co-guidance of Dr.RADHA B.K M.S (Ayu) Asst.proffessor, Shalya Tantra T.M.A.E’S AMC, Hospet DEPARTMENT OF POST GRADUATE STUDIES IN SHALYA TANTRA T.M.A.E. SOCIETY’S AYURVEDIC MEDICAL COLLEGE& HOSPITAL HOSPET – 583 201 2014
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of By Dissertation Submitted to the Rajiv Gandhi University Of ...
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE)
WITH LAKSHA KSHEERA AND MANJISTADI LEPA
By
Dr. VIJITH V. NANGELIL
Dissertation Submitted to the
Rajiv Gandhi University Of Health Sciences,Bangalore,Karnataka
In partial fulfilment of the requirements for the degree of
Ayurveda Vachaspathi
M.S. (AYURVEDA)
in
Shalya Tantra
Under the guidance of
Dr.MANONMANI L M.D (Shalya),
H.O.D, Shalya Tantra
T.M.A.E’S AMC, Hospet
&
Under the Co-guidance of
Dr.RADHA B.K M.S (Ayu)
Asst.proffessor, Shalya Tantra
T.M.A.E’S AMC, Hospet
DEPARTMENT OF POST GRADUATE STUDIES IN SHALYA TANTRA
T.M.A.E. SOCIETY’S AYURVEDIC MEDICAL COLLEGE& HOSPITAL
HOSPET – 583 201
2014
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE)
WITH LAKSHA KSHEERA AND MANJISTADI LEPA
T.M.A.E. SOCIETY’S AYURVEDIC MEDICAL COLLEGE& HOSPITAL
HOSPET – 583 201
(Affiliated to Rajiv Gandhi University Of Health Sciences,Bangalore,Karnataka)
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “ Management Of Bahir
Prakoshtasthi Bhagna (Colle’s Fracture) with Laksha Ksheera And Manjistadi
Lepa” is a bonafide research work done by “Dr. Vijith V. Nangelil ” in partial
fulfilment for the degree of Ayurveda Vachaspathi (Master of Surgery) in Shalya
Tantra.
Date:
Place: Hosepet Dr.MANONMANI L M.D(Shalya)
Professor and H.O.D
P G Studies in Shalya Tantra,
T.M.A.E. Society’s Ayurvedic Medical
College, Hosepet.
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE)
WITH LAKSHA KSHEERA AND MANJISTADI LEPA
T.M.A.E. SOCIETY’S AYURVEDIC MEDICAL COLLEGE& HOSPITAL
HOSPET – 583 201
(Affiliated to Rajiv Gandhi University Of Health Sciences,Bangalore,Karnataka)
CERTIFICATE BY THE CO-GUIDE
This is to certify that the dissertation entitled “ Management Of Bahir
Prakoshtasthi Bhagna (Colle’s Fracture) with Laksha Ksheera And Manjistadi
Lepa” is a bonafide research work done by “Dr. Vijith V. Nangelil ” in partial
fulfilment for the degree of Ayurveda Vachaspathi (Master of Surgery) in Shalya
Tantra.
Date:
Place: Hosepet Dr Radha B.K M.S(Ayu)
Asst. Professor and P.G Guide
P G Studies in Shalya Tantra,
T.M.A.E. Society’s Ayurvedic Medical
College, Hosepet.
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
BANGALORE,KARNATAKA
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation / thesis entitled “ Management Of Bahir
Prakoshtasthi Bhagna (Colle’s Fracture) with Laksha Ksheera And Manjistadi Lepa”
is a bonafide and genuine research work carried out by me under the guidance of
Dr.MANONMANI M.D(Ayu), Professor & HOD, and Dr Radha B.K M.S(Ayu) Asst
Professor & Co Guide, Department Of Post Graduate Studies In Shalya Tantra,T.M.A.E.
Society’s Ayurvedic Medical College,Hosepet.
Date: Dr. VIJITH V. NANGELIL
Place: Hosepet

DEPARTMENT OF POST GRADUATE STUDIES IN
SHALYA TANTRA
T.M.A.E. SOCIETY’S AYURVEDIC MEDICAL COLLEGE& HOSPITAL
HOSPET – 583 201
(Affiliated to Rajiv Gandhi University Of Health Sciences,Bangalore,Karnataka)
ENDORSEMENT BY THE H O D, PRINCIPAL / HEAD OF THE
INSTITUTION
This is to certify that the dissertation entitled “ Management Of Bahir
Prakoshtasthi Bhagna (Colle’s Fracture) with Laksha Ksheera And Manjistadi
Lepa” is a bonafide research work done by “Dr. Vijith V. Nangelil ” under the
guidance of Dr.MANONMANI Professor and HOD, Department Of Post Graduate
Studies In Shalya Tantra,T.M.A.E. Society’s Ayurvedic Medical College,Hosepet.
Seal & signature of the H.O.D Seal & signature of the Principal
Guide Principal
Dr. MANONMANI L M.D(Ayu) Dr. Dr. MANONMANI L M.D(Ayu)
Professor and HOD Principal
Dept. of P G Studies in Shalya Tantra, T.M.A.E. Society’s Ayurvedic Medical
T.M.A.E. Society’s Ayurvedic Medical College, Hosepet.
College, Hosepet.

COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that this dessetation / thesis entitled “ A clinical study in Rajiv
Gandhi University of Health Sciences, Karnataka shall have the rights to preserve, use
and disseminate this dissertation / thesis in print or electronic format for academic /
research purpose.
Hosepet Dr. Vijith V. Nangelil
© Rajiv Gandhi University of Health Sciences, Karnataka.
OM NAMAMI DHANVANTHARI

ACKNOWLEDGEMENT
I offer my sincere devotion to LORD DHANWANTHARI for showering his
blessings and who gave me strength.
I record my indebtedness to my beloved parents Shri Dr.Vijayan nangelil,
Smt Dr.Jaya Vijayan for their untiring support and out lasting affection.
I feel very fortune enough to work under the guidance of Dr.ManonmaniL
M.D (Shalya) my Guide & Head of the department Shalyatantra,. for her functional
freedom, encouragement, support and sharpening my professional skills. I offer my
extreme thanks and deep sense of gratitude to my teacher.
I express my deep sense of gratitude to Dr Radha B.K M.S, Asst Professor &
Co-Guide,Department of ShalyaTantra,for her support for her untiring help and
constant attention and affection.
I convey my sincere gratitude to my beloved incharge Principal, my teacher
Dr. Chandra Shekar Rogi M.D (Ayu) & Asst. Professer Dr.B.B Bhatt M.S(Ayu) ,
Dr. Shariffuddin M.S(Ayu) department of P.G studies in Shalya Tantra T.M.A.E
Society’s Ayurveda Medical College and Hospital whose valuable timely suggestions,
untiring encouragement and unforgettable parental affection.
I am grateful thanks to my classmates, my junior friends of my department for
their good co-operation and support.
I express my sincere gratitude to all the faculty members of the institution, and
offer my sincere thanks to all my patients and who have rendered their wholehearted
support.
Date :
Hosepet Dr.Vijith V.Nangelil

CONTENTS
Page No.
I. Introduction 1 – 4
II. Objectives 5
III. Review of Literature
(a) On Ayurveda 6 – 34
(b) On Modern 35 – 46
(c) On Drugs 47 – 57
IV. Methodology 58 – 63
V. Observations &Results 64 - 71
VI. Discussion 72 – 86
VII. Conclusion 87
VIII. Summary 88
IX. Bibliography 89 – 91
X. Annexure (case proforma) 92 – 95
i
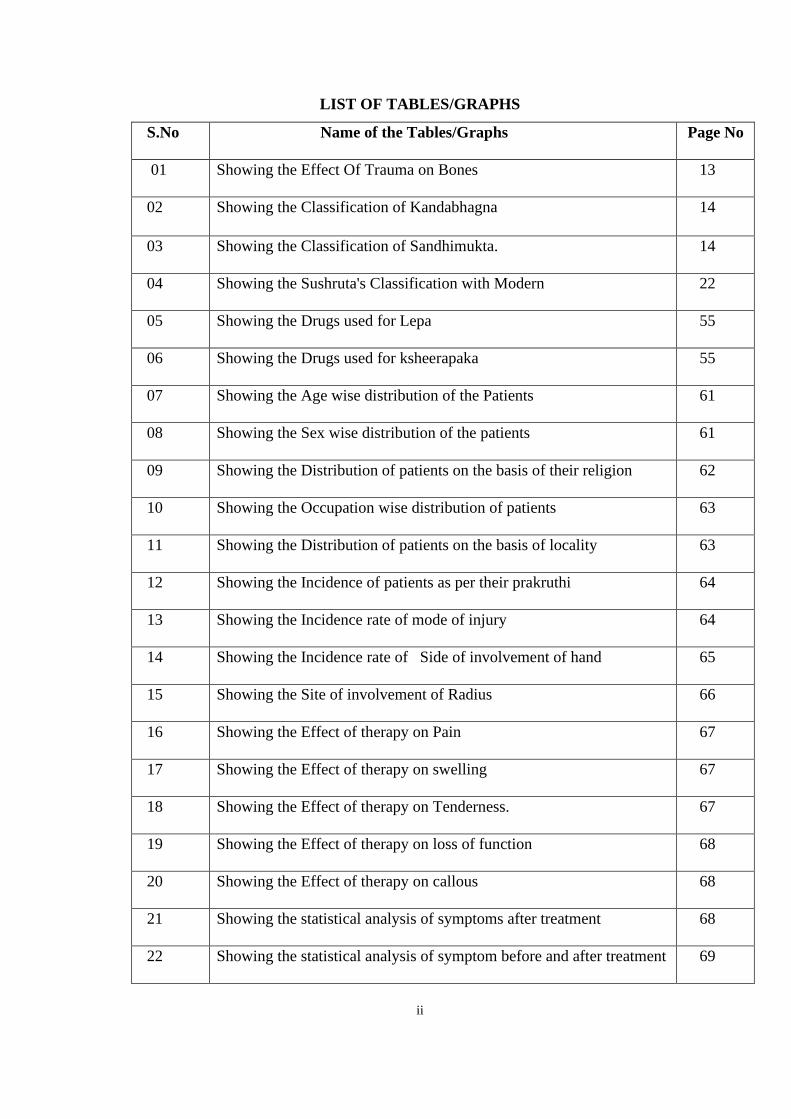
LIST OF TABLES/GRAPHS
S.No Name of the Tables/Graphs Page No
01 Showing the Effect Of Trauma on Bones 13
02 Showing the Classification of Kandabhagna 14
03 Showing the Classification of Sandhimukta. 14
04 Showing the Sushruta's Classification with Modern 22
05 Showing the Drugs used for Lepa 55
06 Showing the Drugs used for ksheerapaka 55
07 Showing the Age wise distribution of the Patients 61
08 Showing the Sex wise distribution of the patients 61
09 Showing the Distribution of patients on the basis of their religion 62
10 Showing the Occupation wise distribution of patients 63
11 Showing the Distribution of patients on the basis of locality 63
12 Showing the Incidence of patients as per their prakruthi 64
13 Showing the Incidence rate of mode of injury 64
14 Showing the Incidence rate of Side of involvement of hand 65
15 Showing the Site of involvement of Radius 66
16 Showing the Effect of therapy on Pain 67
17 Showing the Effect of therapy on swelling 67
18 Showing the Effect of therapy on Tenderness. 67
19 Showing the Effect of therapy on loss of function 68
20 Showing the Effect of therapy on callous 68
21 Showing the statistical analysis of symptoms after treatment 68
22 Showing the statistical analysis of symptom before and after treatment 69
ii

FIGURES
1. Karkata Bhagna
2. Ashwkarna Bhagna
3. Churnita Bhagna
4. Pichhit Bhagna
5. Asthichalitha Bhagna
6. Kanda Bhagna
7. Majjanugata Bhagna
8. Atipatita Bhagna
9. Vakara Bhagna
10. Chinna Bhagna
11. Patita Bhagna
12. Sphutia Bhagna
13. Anchana
14. Pidana
15. Sankshepana
16. Bandhana
17. Mritpinda Dharana
18. Lavana Dharana
19. Pashana Dharana
20. Bone cells
21. Compact and Spongy bone
22. Compact bone structure
23. Spongy bone structure
24. Classification of the bones
25. Structure of the long bone
26. Structure of the short bone
27. Structure of the flat bone
28. Structure of the irregular bone
29. Mechanism of fracture by compression
30. Mechanism of fracture by angulation
31. Mechanism of fracture by tension
iii

32. Mechanism of fracture by rotation
33. Mechanism of fracture by shearing
34. Transverse fracture
35. Spiral fracture
36. Oblique fracture
37. Comminuted fracture
38. Compression fracture
39. Simple or Closed fracture
40. Open or Compound fracture
41. Traumatic fracture
42. Pathological fracture
43. Stress fracture
44. Single fracture
45. Multiple fracture
46. Undisplaced fracture
47. Displaced fracture
48. Infarction fracture
49. Greenstick fracture
50. Torus or Buckle fracture
51. Bending mechanism of fracture
52. Three point bending mechanism of fracture
53. Four point bending mechanism of fracture
54. Compression and bending of fracture
55. Bone healing
56. Manjishata- a) Plant, b) Stem, c) Powder
57. Yashtimadhu - a) Plant, b) Stem, c) Powder
58. Shali a) Plant b) Grains
59. a ) Gritha, b) Shathadhauta gritha
60. Raktachandana a) Plant, b) Stem
61. Grshata Ksheera
62. Laksha Powder
63. Udumbara
iv

64. Ashwatha
65. Palasha
66. Drugs used for Lepa
67. Application of a) Lepa, , b) Splints, c) bandha
68. Ksheera paka
69. Follow up x- rays
v

OBJECTIVES
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
5
AIMS AND OBJECTIVES OF THE STUDY
“To evaluate the efficacy of Ayurvedic management on Colle’s fracture”
The objectives of the study includes:
1. Restoration of anatomy of wrist and forearm.
2. Early reduction of pain and swelling by external application.
3. Effectiveness in allowing early mobilization and rehabilitation.
4. Reduction of immobilization period by giving Laksha Ksheerapaka internally and
Manjistadhi Lepa externally.
INTRODUCTION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
1
INTRODUCTION
The practical knowledge along with the theoretical knowledge is very much
essential. Whatever is seen while doing practical study and going through concerned
literature , adds the knowledge when both are applied together. Keeping these golden
words of Sushruta the following study is carried out.
The population based incidence of work-related fractures and associated risk
factors have not been well documented. It is identified that incidence rate of fracture was
highest in the agricultural sector (194.5 per 10,000 workers), followed by mining (168.8
per 10,000 workers), construction (111.7 per 10,000 workers) and manufacturing (87.5
per 10,000 workers). In each industrial sector, males had significantly higher incidence
rate than females except for the educational sector. (Ref: Incidence and Risk of Work-
related Fracture Injuries: Experience of a State Managed Workers Compensation
System—Islam SS, Biswas RS, Nambiar AM, Syamlal G, Velilla AM, Doyle EJ,
Ducatman AM). So the problem faced by the medical practitioner regarding fractures and
dislocations provide much scope for systematic study.
Ayurveda is the upaveda of Atharvanaveda which deals with science of life. This
science is valuable heritage of India. Almost all types of therapies are described
comprehensively in Ayurvedic texts. The art of healing of the ailments has been known
from the time immemorial. Many indigenous ways and methods have been followed for
the relief of suffering of man kind since Veda's. The reference of trauma is as old as the
beginning of human being.
Traumatic surgery has been in practice since Vedic period. Ashwini Kumaras
used to perform surgeries like limb replacement, fixation of severed head, transplantation
of eyes and teeth etc. The same science is developed, practiced, and well documented by
'Famous Indian surgeon Acharya Sushruta'. He deserves the credit of classifying skeletal
injuries into various groups. This classification has been done on the basis of anatomical
variations and prognostic values for ensuring proper management. Elaborate description

INTRODUCTION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
2
of this branch of surgery is available in his treatise-"Sushruta Samhita". After going
through the chapters of bone injuries in this book one cannot resist in forming a positive
opinion about the most systematic and extensive study of these cases made by him. Now
the methods of management of fractures have been modified greatly. But the principles of
diagnosis of fractures and treatment laid down by Sushruta still hold good and deserve
appreciation. The Sushruta Samhita is considered as a treasure of time-tested surgical
knowledge which has been proved to be valuable resource for treatment and guiding the
research in present surgical era. The present status of Modern surgery has reached the
summit of progress in all aspects. In spite of this there are many challenges to be taken
up. The world of medical scientists is anxiously scanning the Ayurvedic surgery as an
alternative.
Bhagna it is an epitome were bone or bones get interrupted. This is classified on
the basis of its clinical importance in to Avrana (Simple fracture) and Savrana
(Compound fracture).In modern literature, a fracture is defined as a break or loss of
continuity in the substance of the bone.
Acharya Sushruta has advocated the principles of reducing the fracture. They are
Anchana (Traction), Peedana (Manipulation), Sankeshpana (Opposition), and Bandhana
(Immobilization) which is practiced regularly even today. In modern orthopedics the
simple fractures are managed by closed reduction followed by application of POP. The
hazards of POP are Pain, Pressure sore, Compartmental syndrome, Nerve compression,
Plaster blisters, etc.Considering the above problems, we are justified to find out a binding
material to attain immobilization without much complications the Lepa is selected in the
present study.
All this has been the inspiration for undertaking the study pertaining to traumatic
surgery of Ayurveda. Throughout India till now 212 P.G. dissertations and 48 Ph.D.
works are carried out in post graduate department of Shalyatantra at various institutes
from 1966 to 1996,out of which 27 P.G. dissertations and 1 Ph.D. work is related to the
traumatic orthopedic surgery. In Rajiv Gandhi University of health sciences from 1996 to
INTRODUCTION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
3
1999, 25 dissertations in postgraduate department of Shalyatantra are submitted out of
which 1work is related to Bhagna Chikitsa.
Everyday 40-50% cases of surgical OPD are suffering from such types of
ailments. Few traditional practitioners specifically dealing with fractures, called 'Bone
setters', have been effectively using herbo-mineral drugs over many centuries. Many of
these drugs are simple, easily available, cost effective and potent.
The scientific evaluation of such drugs along with their fundamental principles is
essential for their universal acceptance. Hence in this study an attempt is made to put
forth such principles of Sushruta and the preparations like Lepa and Ksheerapaka for the
clinical trial. In the present study the comparison between contemporary management of
simple fractures with that of Sushruta's technique is made. It has been also tried to assess
the efficacy of these Ayurvedic drugs in bone healing and in providing symptomatic
relief.
The thesis is discussed under these headings.
Ayurvedic literature review: In this chapter Asthi shareera,Bhagna nirukti,
Classification of Bhagna,Bhagna Chikitsa is discussed in detail. A special effort has made
to assess Bhagna types radiolgically.
Modern literature review: In this chapter Bone anatomy, types of bones, fracture
classification, and its management is discussed in detail.
Drug-review: The drugs used for trial are reviewed in detail.
Materials and Methods: under this heading the materials used in the clinical trial and
methods adopted are explained in detail.
Results: The statistical analysis of the signs and symptoms before and after treatment of
both the groups is done in detail manner.
Discussion: It includes the discussion on the literature review, on materials and methods,
observations and on results.

INTRODUCTION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
4
Summary and conclusions: Total work with its results are summarized under this
heading.
However the idea of the present work is to find out Management Of Bahir
Prakoshtasthi Bhagna (Colles’ Fracture) with Lakshaksheera And Manjistadi Lepa
and to open new way of treatment which is easily available, economical, as well as
minimize the problems of POP.

OBJECTIVES
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
5
AIMS AND OBJECTIVES OF THE STUDY
“To evaluate the efficacy of Ayurvedic management on Colle’s fracture”
The objectives of the study includes:
1. Restoration of anatomy of wrist and forearm.
2. Early reduction of pain and swelling by external application.
3. Effectiveness in allowing early mobilization and rehabilitation.
4. Reduction of immobilization period by giving Laksha Ksheerapaka internally and
Manjistadhi Lepa externally.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
6
LITERATURE REVIEW
An approach to human ailments is as old as the evolution of human being. The
most ancient practiced medical science is Ayurveda. It is the fore runner of all the
therapies of the world, since man has thought of providing an effective remedy to the
diseases suffered by him.
Ayurveda or science of life describes prophylaxis, prevention, and therapeutic
principles for the diseases. This being the branch of Veda's it relates with knowledge of
philosophy, medicine, and art of surgery. Fore most surgeon of the world, Acharya
Sushruta, most revered physician Acharya Charaka and acharya Vagbhata are the
foundation tripods of Ayurveda. The texts conceived and devised by the honoured trio
have over the ages proved to be the baseline of reference for the knowledge of diseases
suffered by mankind.
The Ayurvedic philosophy is specific pertaining to the body constitution. The
human body (Shareera) is described as a combination of external factors the Atma1
(soul), Manas (mind) and Pancha maha bhoota (five mega elements). In all the living
beings the matter and energy is existing in the form of Dosha Dhatu & Mala . The most
important supportive framework of the body among these is Asthi (Bone tissue).
The branch of surgery that deals with deformities of the bones is known as
orthopedics. Orthopedic surgery has its aim the '' maintenance of normal mechanical
function of the deformed bones''. This part of the treatment in Ayurveda is called bhagna
Chikitsa. It was at its peak optimum level during the period of ancient famous Indian
surgeon Sushruta acharya. He has given clear and elaborate ideas about this branch.
The subject of this clinical reaserch is to evaluate Management Of Bahir Prakoshtasthi
Bhagna (Colles’ Fracture) with Lakshaksheera And Manjistadi Lepa. Hence it is must
to describe the literature about bhagna-Fractures, in this topic of literature review.
6

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
7
In this chapter first of all Ayurvedic literature is described and then the Modern
part of the literature are reviewed. In Ayurvedic literature about Asthi dhatu will be
described briefly.
The Nidana Panchaka part Patho physiology of bhagna will be discussed. Which
contains definition of bhagna, its etiology , classification, general features, special
features, and prognosis. The treatment of the fracture includes treatment principles then
specific treatment for different bones, clinical criteria's to assess bone healing, followed
by pathyaa pathya (Prophylactic do's and don'ts).
ASTHI SHAREERA
Asthi is one among seven dhatu- specific body constituents. It is more stable and
strong among seven dhatu.
Nirukti : The word Asthi is derived from Asthi-dhatu and Katina - pratyaya it means
stable and strong.
Paryaya : Keekasa, Kulyam, and Medoja
Utpattij : According to Sushruta Asthi starts developing during third month of
intrauterine life and totally organizes with complete manifestation in the seventh month
of gestation.
Embryology of bones : The embryo is formed by some important factors known as
bhava's. There are six bhava's namely matruja, pitruja, satwaja, satmyaja, Rasaja, Atmaja.
Amongst these Bhava's, Pitrujabhava is especially responsible for the formation of Asthi
in the embryo. According to Charaka, the bone formation in the embryological stage
takes place out of Panchamahabhoota having the dominance of Prithvi and Agni
[Chakrapani]. But Dalhana opines that there will be predominance of Prithvi , Agni and
vayu.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
8
According to the sequence of dhatu in the body, Asthi is the fifth dhatu. It is
formed from the Sukshmabhaga of Medodhatu, by the action of Asthidhatwagni. Here
Medodhatu is acted upon by Agni which results in to a hard and dry substance having the
dominance of Prithvi, it is made porous and spongy by vayu. These pores are filled up by
sneha called Majja. One can appreciate the role of all Mahabhoota in Asthi. Like shallow
places are because of Akasha which is filled up by Jala Mahabhoota' in the form of
Majja. Ghanatwa is because of Prithvi, Laghutva by Vayu. and paka during the formation
is by the influence of Tejomahabhoota. Asthi posses the qualities like Guru, Katina,
Sthoola, Sthira, and predominantly constituted of Prithvimahabhoota.
Different analogies are there about the formation of dhatu, namely, Ksheera-
Dadhi Nyaya, Kedara-Kulya Nyaya. Asthi is the dhatu which does the Dharana of the
body. Medodhatu nourishes the Asthidhatu and in turn Asthidhatu nourishes Majjadhatu.
The strength of the Dhatvagni decides the formation of any dhatu. The formation of
Asthidhatu takes place from Medodhatu acted upon by Medodhatwagni. On the other
hand if the formation of Asthi is not proper or if it is not at all formed ,then it may be due
to improper state of Medodhatwagni. In the same way when Asthidhatwagni works,
Majjadhatu is formed . and when this Dhatvagni is not proper ,then Majjadhatu may not
form and may retard the formation of other Dhatu's.
Medas and Jaghana are the Moola of Asthivaha srotas. It is the channel through
which the nutrients are being circulated within the Asthidhatu.
Ativyayama, Abhighata, Vatala Ahara etc, are Nidanas, which vitiate these srotas
and results into Asthibheda, Adyasthi, Asthishoola etc. Bhagna is the one of the Vikaras
of Asthivahasrotodusthi, because of Abhighata depending on force of impact, the bones
of the particular part of the body will break in one or two, if subjected to sudden violent
injury.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
9
ASTHI SANKHYA
Regarding the number of bones in the body, we find difference of opinions in the
classics.
Name of the Acharya's No. of bones
1. Sushruta 300
2. Vagbhata 360
3. Charaka 360
4. Bhavamishra 300
5. Sharangadhara 300
According to modern science the total numbers of bones in the body are 206.
These numerical difference in the bone is due to the different ideology such as counting
methods, inclusive of Teeth, Tubercles and facets etc.
ASTHI PRAKARA
Based on structures and shapes, different types are identified in the body.
Sushruta has classified Asthi into 5 varieties.
1. Kapalasthi (Flat Bones) e.g.- Scapula, Hipbone.
2. Ruchakasthi (Lustrous Bones) e.g.- Teeth
3. Tarunasthi (Cartilage) e.g.- Cartilage's of Ear
4. Vayalasthi (Curved Bones) e.g.- Ribs
5. Nalkasthi (LongBones) e.g.- Humerus, Femur.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
10
ASTHI KARYA
Sushruta says that the body of the living beings stands by the support of the
bones, just as trees stand by support of their Sara. In the same manner the Asthi sustains
the human body.
According to Charaka the bones give a framework to the body and provide
nutrition to the majjadhatu. The shape, position, support and body performance basically
depends on the asthidhatu. Katina, sthira, and khara Guna protect the marma and at the
same time help the attachment of Mamsa Sira & Kandara etc .
Formation of the asthidhatu occurs in Asthivahastrotas. Asthidharakala and
Maladharakala are considered as same, as in the disorders of colon,the bony tissue gets
affected and the salts like calcium,Phosphorous etc , which build bony tissue are more
over getting absorbed in the colon. Some of the e.g.'s which tells the relation between
Asthidharakala and maladharakala in Ayurvedic texts like, Diarrhoea is the main
symptom in Asthikshaya. All these factors are to say that , the site of Asthidharakala has
an identical relation ship with the maladharakala.
HISTORICAL ASPECTS OF BHAGNA
Pre-samhita Period: The mechanism of repair following an injury to any tissue had
been known to man kind from time immemorial. To make injured tissue heal many
measures had been employed according to their knowledge and facilities available. The
trauma and its management, history goes back to earliest time of Rigveda (3500-1800
BC).More details of medicinal herbs and there usage in fracture healing are available in
Athaervaveda, here the precise reference of bone healing is first seen. Whitney (1962) in
his English translation of Athaervaveda quotes as '' Grower art though, grower; grower of
severed bone; make this grow, O Arundhati'', Let thy marrow come together with
marrow, and thy joint together with joint, together let what of thy flesh has fallen apart ,
together let thy bone grow over'', ''let marrow be put together with marrow, let skin grow
with skin; let thy blood , bone grow let flesh grow with flesh''.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
11
The other reference of Koushika Sutra states about sprinkling of fractured part
with Laksha Quatha and healing enhancement of fracture is done by the intake of Laksha
Shruta Dugdha etc. Instantaneously Vishala's leg was replaced by Ayas (copper or iron),
when in the war she lost her leg and was able to fight the next day in war field. The
surgical science was much advanced with specialization subjects in various fields
including Orthopedics the same concept can also be ascertained with reference available
today for scientific approach of splints for bone setting.
Samhita Period: A vivid description of Aetiology, Classification, Symptomatology,
Prognosis, Complications and Management of fractures, are available in the ancient
surgical treatise like that of Sushruta Samhita (600BC) written by Acharya Sushruta. The
history of modern orthopedic surgery did not start before Hippocrates. He is believed to
have been born about 460BC. in the Island of COS. and died about 370 BC. At much
later period than Sushruta.
In Charaka Samhita Charakacharya has mentioned the setting of bone in 'Vrana
Context' only, but not as separate topic like Sushruta . But regarding the treatment of
fractures he has insisted to compare the fracture part with normal part. Charaka has not
classified the fractures like Sushruta. Vagbhata Acharya follows Sushruta's classification
of fractures mainly two types i.e. Sandhimuktha and Asandhibhagna. Vagbhata has the
significance of identifying the place of fractures and dislocations at the given differences
like sandhi and asandhi. However there is no much contradiction between both the
authors. Thus Vagbhata relates the terminology of Kandabhagna of Sushruta with the
possible name as Asandhibhagna.In addition to above Vagbhata contributes certain
variety of Yoga's like Lasunadi Taila & Gandha Taila etc.
Nighantu period: The Nigantu's like Yogaratnakara, Madhavakara and Bhavapraksha
etc. have followed Sushruta in relation with fracture classification. The additions they
have made in relation with therapeutics, like Lakshagodhumadi Yoga, Rasonadi Gugglu,
Lakshadi Gugglu, Shali saindhva yoga etc. While Bhavapraksha & Yogaratnakara have

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
12
mentioned different yoga's as well as suggested to use 'Panka' in Avaranabhagna in the
place of cotton before a splint as a buffer but no where it can be traced in Sushruta or
Charaka samhita. Other Nighantus like Kaiyadeva or Shodala, Madanapala etc. have not
mentioned about 'Bhagna' but mentioned about the drugs that are used to treat fractures,
under the name of Sandhaniya dravyas e.g. Arjuna. All this indicates the Nighantukaras
have accepted Sushruta's classification of bhagna with minimal alterations and in its
management they have added certain formulations and drugs .
BHAGNA - REVIEW
Shabdhotpatti : The Word Bhagna is derived from the word bhanj-dhatu and Katu-
pratyaya meaning to break Bhanj means motion, which once again means to break.
Vyakhyana: Bhanjayatithi bhagna || (Shabdasthoma nidhi).
Bhagna, can be defined as a phenomenon in which a bone or bones gets
interrupted. The word bhagna, in Ayurvedic texts refers to for both fractures and
dislocations. Bhagna is mainly classified in to two groups as Kandabhagna which is of
twelve (12) types. And sandhimukta is of six (6) types.
Paryaya: Bhagna, Bheda, Bhedana, Bhanjana, Vibhaga.
Nidana:
• Patana : Fall from height.
• Peedana : Violent pressure or compression.
• Prahara : Direct or indirect blow.
• Akshepana : Violent jerks.
• Vyalamrugadashana : Animal bites, Attacks of wild beasts.
• Balavadnigraha : Strong block from strong persons.
• Abhighatavishesha : Trauma caused by different causes.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
13
Great attention has been given by Acharya Sushruta towards aetiology, which is
still seen now a days. Vagbhata has also given the fracture causes in detail. While others
like Acharya Charaka, Bhavamishra, Madhavakara, Sharangdhra are silent. The
pathological fractures will occur due to the conditions like asthikshaya, majjakshaya,
asthividrudi, pakshaghata, phiranga, asthimajjagatakushta, asthimajjagatavata etc.
EFFECT OF TRAUMA ON BONES :
The bones sustain trauma in different ways. Acharya Sushruta has paid due
attention to this fact and observed that all the bones do not show similar type of effect to
the trauma. He has then classified these effects in different groups and correlated with the
types involved the same is mentioned below.
(TABLE-01)
1) Cartilages - Bend
2) Long bones -Break
3) Flat bones - Crack
4) Teeth - Fragmented
5) Curved bones - Crack or Break.
CLASSIFICATION OF BHAGNA
The classification of Bhagna given by Sushruta, Madhavakara, Chakradatta,
Bhavaprakash and Gadanigraha resembles each other. Vagbhata's opinion differs in this
regard. Charaka has not given any classification.
Sushruta's classification: The skeletal injuries have been divided on the basis of
structure involved as, 1) Sandhimukta 2) Kandabhagna.
Vagbhata's classification : Vagbhata has mentioned same classification in different
words as, 1) Sandhibhagna 2) Asandhibhagna.Apart from this classification Sushruta
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
14
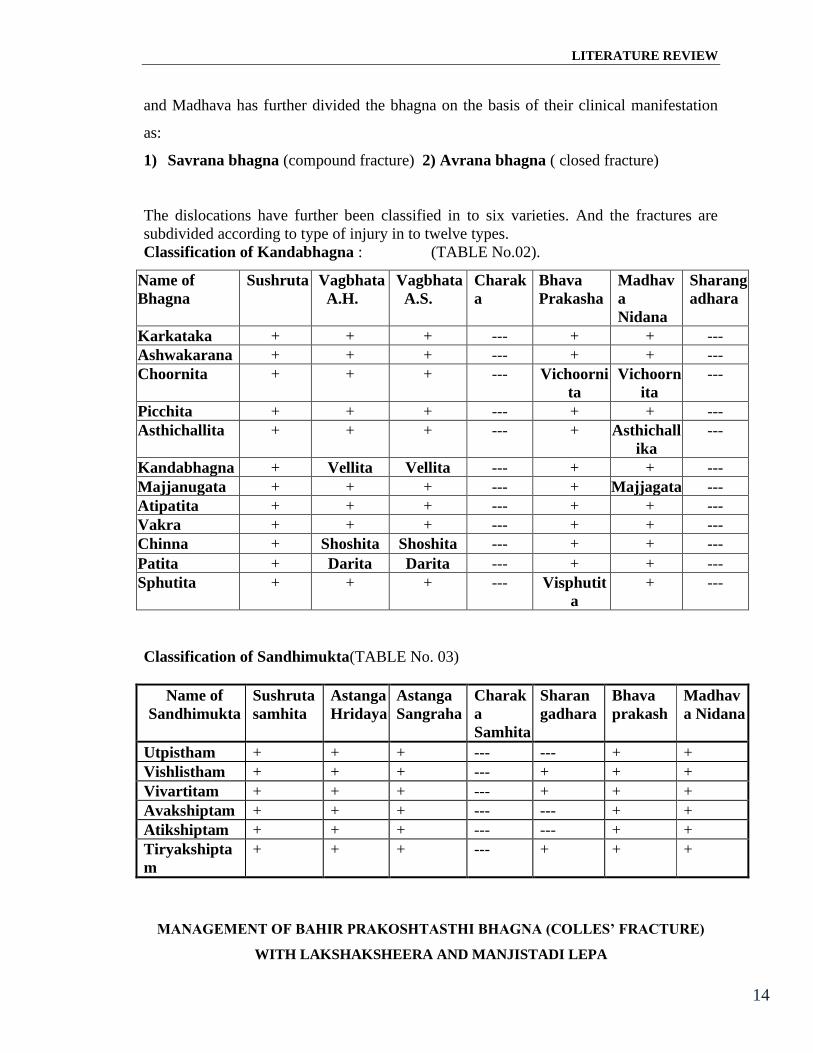
and Madhava has further divided the bhagna on the basis of their clinical manifestation
as:
1) Savrana bhagna (compound fracture) 2) Avrana bhagna ( closed fracture)
The dislocations have further been classified in to six varieties. And the fractures are
subdivided according to type of injury in to twelve types.
Classification of Kandabhagna : (TABLE No.02).
Name of
Bhagna
Sushruta Vagbhata
A.H.
Vagbhata
A.S.
Charak
a
Bhava
Prakasha
Madhav
a
Nidana
Sharang
adhara
Karkataka + + + --- + + ---
Ashwakarana + + + --- + + ---
Choornita + + + --- Vichoorni
ta
Vichoorn
ita
---
Picchita + + + --- + + ---
Asthichallita + + + --- + Asthichall
ika
---
Kandabhagna + Vellita Vellita --- + + ---
Majjanugata + + + --- + Majjagata ---
Atipatita + + + --- + + ---
Vakra + + + --- + + ---
Chinna + Shoshita Shoshita --- + + ---
Patita + Darita Darita --- + + ---
Sphutita + + + --- Visphutit
a
+ ---
Classification of Sandhimukta(TABLE No. 03)
Name of
Sandhimukta
Sushruta
samhita
Astanga
Hridaya
Astanga
Sangraha
Charak
a
Samhita
Sharan
gadhara
Bhava
prakash
Madhav
a Nidana
Utpistham + + + --- --- + +
Vishlistham + + + --- + + +
Vivartitam + + + --- + + +
Avakshiptam + + + --- --- + +
Atikshiptam + + + --- --- + +
Tiryakshipta
m
+ + + --- + + +
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
15
The Sushruta's classification is followed by every one. Vagabhata has given
different terminology's for some varieties. He has mentioned Vellita in place of
Kandabhagna. Darita in the place of Patita and Shoshita at the place of Chinna. Acharya
Madhavakara has also used some other terminology like vichurnita at the place churnita.
Asthichallita at the place of Asthichallita and Majjagata at the place Majjanugata. He has
described Chinna is of two types: 1) Ekamanuvidaritam 2) Bahunuvidaritam.
Acharya Sharangadhara has not followed Sushruta's classification but he has
described the eight varieties of bhagna. These are similar to Sushruta's classification.
1) Bhagna prista 5) Adhogata
2) Vidarita 6) Urdhvagata and
3) Vivartita 7) Sanghibhagna.
4) Vishlishat 9) Tiryaka kshipata
CLINICAL FEATURES
The presence of fracture can be made out by history and clinical findings. The
clinical signs described in Ayurvedic texts stand the same as mentioned in any modern
surgical text book. The Sushruta's contribution in this aspect is so perfect that it has
hardly any room for alteration even today. He has mentioned signs and symptoms both
in general and specific.
GENERAL FEATURES OF 'KANDABHAGNA'
Shvayathubahulyam (Marked swelling) : Generally fracture, whether it is hair line
or comminuted, it will be associated with moderate to severe swelling.
Sparshasahisnutvam (Tenderness) : Tenderness is such a sign that it is invariably
present in all types of fractures.
Avapidyamane shabda (Crepitus) : Presence of the crepitus is a definite indicative
of fracture, can confirm diagnosis clinically.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
16
Vividhavedanapradurbhavah (Different types of pain ) : The fractured bone
before its reduction and immobilization produces variety of pain. This depends on
nature of trauma, bone fractured, displacements of the fragments, and nature of soft
tissue injury.
SarvasuAvasthasu Na Sharmalabha (Inability to get comfort in any position):
Fracture gives to pain and discomfort to the patient till immobilizing it. The
discomfort is such that patient remains restless in any posture of fractured part.
SPECIFIC FEATURES OF INDIVUDAL 'KANDABHAGNA'
(1) Karkataka (FIG -01)
The fracture which has a shape similar to 'crab' is named as Karkataka. The case
where the fractured bone is depressed at its two articular extremities and bulges out at the
middle, resemble the shape of gland is called as Karkataka.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
17
(2)Ashwakarana: (FIG -02)
Here fractured bone projects upwards like the ear of horse is called as Ashwakarana
(3)Churnitam : (FIG -03)
The fractured bone is found to be shattered into fragments or the powder form. This
Bhagna can be detected clinically by presence of crepitus.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
18
(4) Pichhitam : (FIG -04)
In this type of fractures, the bone is compressed between the two opposite forces, it gets
expanded transversely and marked swelling occurs.
(5) Asthichallita: (FIG -05)
In this type of fracture, the periosteum is splintered off, where the fracture fragment
slightly elevates into one side, as the bark gets away from the main stem.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
19
(6) Kanda bhagna : (FIG -06)
In this type of fracture the shaft of the bone is fractured. The fractured part shows
abnormal movement.
(7) Majjanugatam: (FIG -07)
In a fracture one fragment gets impacted into another causing displacement of bone
marrow, then it is said to be Majjanugatam. It may be resulted due to force of violence.
This type of fracture is very difficult to diagnose because the signs and symptoms like
transmitted movements crepitus etc. are absent due to impaction.
(8) Atipatitam : (FIG -08)

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
20
A case where the fracture occurs throughout the plane of the bone is named as Atipatita.
Here the fragments are completely separated and the separated fragments hang or
angulated.
(9) Vakra : (FIG -09)
The bones get bent, but not broken, especially in tarunasthi's in children
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
21
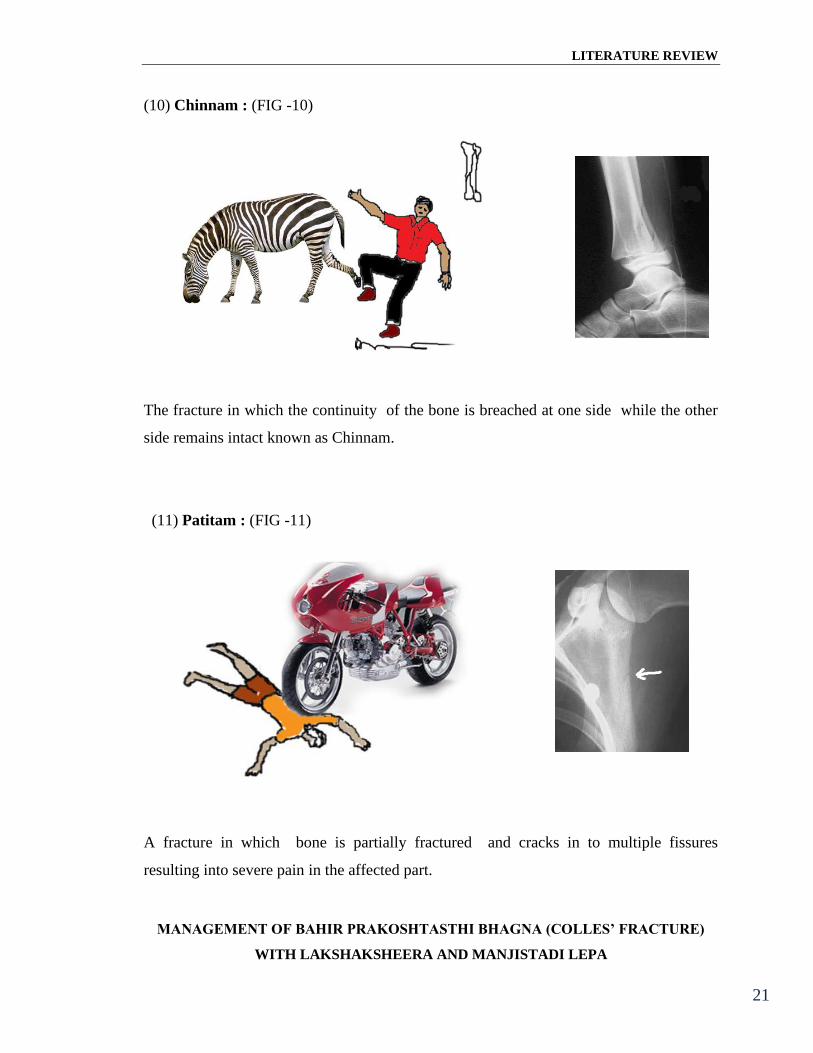
(10) Chinnam : (FIG -10)
The fracture in which the continuity of the bone is breached at one side while the other
side remains intact known as Chinnam.
(11) Patitam : (FIG -11)
A fracture in which bone is partially fractured and cracks in to multiple fissures
resulting into severe pain in the affected part.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
22
(12) Sputita : (Fig. 12)
will be pricking pain due to sharp points of bristles. Such type mostly occurs in small
bones and teeth etc.
SUSHRUTA'S CLASSIFICATION WITH NEAREST MODERN COMPARISON
TABLE No. 04
Karkataka : Depressed fracture.
Ashwakarana: Complete oblique fracture.
Churnitam : Comminuted fracture
Pichhitam : Fracture by compression.
Asthichallita : Sub periosteal avulsion.
Kanda bhagna : Complete spiral fracture.
Majjanugatam : Impacted fracture.
Atipatitam : Complete compound fracture.
Vakra : Green stick fracture.
Chinnam : Incomplete fracture.
Patitam : Comminuted fracture flat bones.
Sputita : Fissured fracture.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
23
The above mentioned classification of fractures is described by Sushruta Acharya
. This indicates his accuracy in clinical diagnosis. He has classified those varieties
merely on clinical assessment, such as according to position of broken fragments, site of
fracture, direction of force, and from the deformity caused by broken fragments. While
classifying the types of fractures he did not include only the varieties of fracture known
and compared today but also added even his minute observations like periosteal avulsion.
In fact Sushruta has viewed fractures as " Bone Injuries" in the true sense and not merely
as the discontinuity in the surface of the bone.
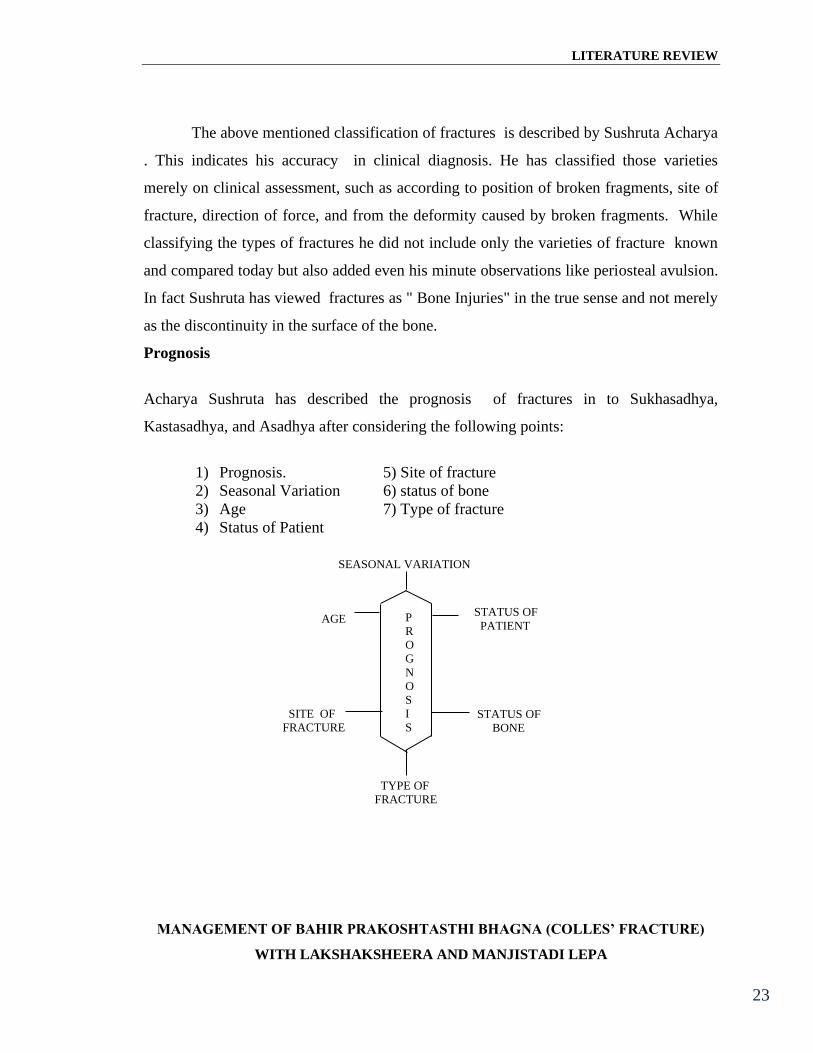
Prognosis
Acharya Sushruta has described the prognosis of fractures in to Sukhasadhya,
Kastasadhya, and Asadhya after considering the following points:
1) Prognosis. 5) Site of fracture
2) Seasonal Variation 6) status of bone
3) Age 7) Type of fracture
4) Status of Patient
SEASONAL VARIATION
AGE P
R
O
G
N
O
S
I
S
STATUS OF
PATIENT
SITE OF
FRACTURE STATUS OF
BONE
TYPE OF
FRACTURE
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
24
Aacharya Sushruta has described that cures are effected with extreme difficulty in
Churnita Bhagna (Comminuted#),ChinnaBhagna (Incomplete#), Atipatita Bhagna
(Complete #), Majjanugata Bhagna (Impacted #) and in Intraarticular Fractures.
The fractures occurring in (1) Paediatric age group (2) Frail and emaciated
persons (3)Individuals suffering with Dermatological , Asthmatic anomalies and other
supervening disorders (4) A person with intemperate habits or Vatika temperament or
who is sparing in his diet have also poor prognosis.
The Following Fractures have Guarded Prognosis (Asadhya):
(1)Complete fracture and dislocation of Pelvic bone with displacement.
(2) Comminuted (Churnita) fractures of Iliac bone and Frontal bone.
(3)Dislocations of the cranial bones.
(4)Fracture of sternum, temporal bone, vertebral column and cranium.
The bone or joint having congenital anomaly, diseased bone, fracture of bones
which was reduced properly but displaced due to improper immobilization or improper
bandaging, or if the fractured part is disturbed, all these circumstances leads to failure of
treatment.
The fractures treated by an expert surgeon get properly united if the- it occurs at
the first three stages of life (childhood, adolescence, adult).
The management of fractures is difficulty in the patients who consumes excessive
Lavan, Katu, Kshara, Amala dravyas etc. Also one who is performing Vyayama,
Maithuna, etc.
Complications
Acharya Dalhana has mentioned, the complications22 of the bone injury may be
(1) Local or (2) Systemic.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
25
(1) Local complications are Malunion and Fragmented Fracture. The variety of
complication which could occur due to tight bandaging is swelling, pain, avascularization
and gangrene
(2) Systemic complications are Fever, Abdominal distension, and Cessation of passages
of excreta like urine and feces .
BHAGNA CHIKITSA
The ancient Ayurvedic texts have described ' Asthibhagna Chikitsa' thoroughly. This
includes :
(1) Principles of Bhagna Chikitsa.
(2) General Management of Bhagna.
(3) Specific Management for different types of fractures.
(4) Medicinal preparations for different kinds of fractures.
(5) Pathyaa-Pathya.
(6) Clinical criteria of fracture healing.
(1) Principles of Bhagna Chikitsa
The management of the case will be always changing. What is accepted as the
best type today is found to be modified tomorrow. It is always devised to suit the needs of
the day. Therefore, to expect that whatever means Sushruta adopted in the treatment of a
case of skeletal injury nearly 3,000 years age would be as effective even today is
certainly not justifiable. The tremendous developments in all the fields of science and
technology have changed the entire picture of the situation. However, there are certain
principles behind every line of management, if correctly laid down, would universly
remain unchanged whatever be the means that may be adopted to achieve them. The
efficiency of Sushruta's skill regarding the management of a fracture case can be very
well put to test on this base.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
26
(2) Four Principles of Treatment
1) Anchana (Fig.- 13) 2) Peedana (Fig. 14)
3) Sankshepa (Fig .15) 4)Bandhana (Fig. 16)
(1) Anchana- Traction
(2) Peedana- Manipulation by local pressure.
(3) Sankshepa- Opposition and stabilization.
(4) Bandhana- Immobilization.
Sushruta has mentioned the principles of reducing a fracture, which is still
adopted today. According to him, surgeon should apply first traction from either side of
the fragments (Anchana), then elevate depressed fragments or depress the elevated
fragments (Peedana). The far displaced or overlapping fragments should be brought in
close contact with each other by manipulating them separately (Samkshepana). The fore

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
27
going principles devote the efforts to achieve proper alignment of fractured fragments
before final immobilization (Bandhana).
Immobilization: An adequate immobilization of the fractured limb is one of the most
essential methods in the management, for this step usage of splints has been adequately
described by Sushruta. He has selected some important tree barks24 for this purpose. The
tree barks he has recommended are Ashwatha, (Ficus religiosa), Vamsha (Bambusa),
Kakubha (Terminalia Arjuna), Madhuka (Madhuka indica) Palasha (Butea monosperma),
Sala (Shovera robusta Gaertn.) Udumbara (Ficus Racemosa Linn.), Vata (Ficus
bengalensis),. Such splints were applied due to their availability without much difficulty.
Other aims of selecting these specific barks are
1) Barks were fit into the limb due to their concave inner surface.
2) Rigid and firm outer surface.
3) Inner surface being soft would act as the cushion to the limb there by avoiding
pressure sore.
(3) General treatment of Bhagna.
Sushruta instructs the surgeons before going to above steps he should follow the general
line of treatment i.e. 1) Pariseka 2) Lepana.
1) Pariseka : This means continuos sprinkling of the medicine in the liquid form e.g.
decoction, oil, ghee, etc. over the affected part for certain period of time. This
procedure induces analgesia and also causes dosha shamana. Different kinds of
Pariseka dravyas are described on the basis of Prakruti of the patient and season.
These are:
a) Nyagrodhadi decocation.: It is used in the patient of Pittika Prakruti and during
summer.

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
28
b) Pancha mula Siddha dughda.: When fracture is in Vata pradhana Prakruti and
mainly suffering from pain, then Panchamula Siddha dugdha is preferred for Pariseka.
This preparation is also Pitta shamaka.
c) Chakra Taila: This is used in mainly vata and kapha prakruti persons and when
fracture has occurred in winter season and associated with severe pain. This
preparation is Ushna viryatmaka and reduces the pain and swelling at the fracture site.
2) Lepa: The local application at the affected part with medicinal paste or ointment is
called as the Lepa. Sushruta has described the Manjisthadi Lepa. It contains
Manjistha, Yastimadhu, Shalipisti, Raktachandana, and Shatadhautagritha. This lepa
reduces local pain and swelling. The ingredients get absorbed per cutenously and
helps bone healing.
After this the Anchana like procedures is to be followed. After completing the
general measures Aacharya has described the treatment part of various kinds of fractures
occurring in the each bone of the body.
(4) Specific Management for different types of fractures
In case of fracture associated with the wound or a compound fracture locally a
mixture of 'Nyagrodhadi gana dravyas' in paste form, Honey and Ghee should be
applied. Rest of management is as in case of general management.
In case of the phalanx fracture or dislocation, it should be first set in its natural
position and bandaged with pieces of thin linen and should be then sprinkled with ghee.
This ancient method resembles with modern management, in which the affected part is
supported by bandaging it along with a splint or neighbor finger.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
29
In case of Foot bone fracture the foot should be gently massaged with Ghee,
then duly splinted up, and then bandaged with linen. Such patient should forego all kinds
of movements.
In case of a fracture of Tibia - Fibula or Femur, the affected part should be
massaged with ghee and traction is carefully applied along the direction of the bone
carefully. after which it should be splinted with the barks and bandaged with the help of
linen. A case of fractured arm should be treated in the same manner.
In case of Hip joint dislocation reduction should be done by traction and
rotational movements then splint should be applied and bandaged in an appropriate
manner. In case of cracked or bruised femur fracture, the part should be bandaged in a
foresaid manner.
In case of Iliac fracture it should be reduced by manipulative procedures
including elevation of depressed fracture followed by bandaging the patient should be
treated with a sneha basthi.
Ancient Acharays in order to describe the poor prognosis of Katibhagna. They
have advised surgeons not to treat the same. Hence patients should be treated and
followed up very carefully by surgeon till the complete union of fractured bone .
In case of dislocation of Amasandhi (Shoulder joint.) the region of Kaksa
(Axilla) should be raised with an iron / wooden rod (Musala) then the surgeon should
bandage the part by Swastika Bandha ( Figure of Eight Bandage).
A dislocated Elbow joint first should be massaged with thumb, after which it
should be pressed with a view to set in its normal position alternating with flexion or
extension of the same. Then it should be sprinkled with any oleaginous substance. The
same measures should be adopted in case of dislocation of knee joint, wrist joint and
ankle joint.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
30
The fractured Metacarpal bones of the palm, the two palms should be made
even and opposed and bandaged together for support. In case of metacarpal bone fracture
of both the hands the splint should be applied to each palm for support. Then the affected
part is sprinkled with Taila.
In case of fracture of the Cervical spine causing lateral flexion or shortening of
the neck, a traction is applied in upward direction. Then around neck an appropriate
splint should be applied and tied with the help of linen. Then the patient is advised
complete bed rest in supine position for next seven days.
The Mandibular dislocation the region is fomented thoroughly then the
mandible is duly reduced its appropriate position and Panchangi Bandha is applied for
support. Gritha medicated with Madhura (Kakolyadi Gana) and Vataghana (Cavyadi
Gana) should be used for Nasya.
A Depressed Nose should be elevated with the help of the thin capillary rod
(Salaka) while it should be straightened in case of lateral displacement. Then two
hollow tubes should be inserted in to each nostril (to facilitate breathing) then nose is
bandaged and sprinkled with Gritha.
In case of Tered Ear Cartilage, Ghritha should be applied locally, then it
should be brought in to its natural position and bandage measures and remedial agents as
in the case of Sadhyo Vrana are adopted in the present instance.
In case of Frontal Bone Fracture which is not associated with any oozing out of
brain matter, it should be bandaged with local application of Honey and Gritha the patient
is advised to take only Gritha for further one week. In case of traumatic contusions the
surgeon should appliy the medicated pastes or ointments locally.
The Malunited Fractures to be re-fractured then it should be reduced properly
and treated in an appropriate manner.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
31
The Fractures occurring at the upper part of the body should be treated with
Sirobasthi, Karnapurana, Grithpana, and Nasya. The Fractures occurring at the
extremities should be treated with the Anuvasana Basthi.
In Old Dislocations the affected part is relaxed first by local lubrication of
oleaginous substances and hot fomentation. After achieving relaxation it should be
reduced with appropriate manipulative procedure.
Warning against Infection, A surgeon should exert his guard against the advent
of any Pyogenic infection setting in a fractured bone because of suppuration of local
muscles, vessels, and ligaments lead to poor prognosis of the fracture.
In case of Tibia, Fibula or Femur fracture Acharya have described the special
immobilization method, known as 'Kapata ShayanaVidhi'. In this method the patient
should be laid down on a plank or aboard and bound to five pegs or stakes in five
different places for the purpose of immobilization of affected limb. The distribution of
the pegs in each case should be as follows, in femur fracture a fair of peg should be
placed at either side of the hip joint and another pair should be placed at either side of the
knee joint and a peg should be placed at the sole. Thus it will cause immobilization of the
affected limb. In case of Tibia Fibula instead of putting pegs at the hip joint they should
be placed at the either side of the ankle joint. Rest of the pegs should be placed as
previous manner. The same procedure should be followed in case of fractures and
dislocations of pelvic joint , vertebral column, chest and shoulder joint.
The principle behind this procedure is the immobilization of the affected part
which is reduced properly. Acharays have the idea that the major fractures can not be
immobilized properly with the help of splints, also these bones require the
immobilization for longer period, hence they may have mentioned this procedure.
Rehabilitation: The importance of Physiotherapy in a limb injury was also appreciated
by Sushruta. He has prescribed the exercises starting in small doses, which may be
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
32
gradually increased at any rate, and exercises should not be prescribed all at once in the
beginning. E.g. For rehabilitation of upper limb, in the beginning mud ball is held and
then a heavier substance like a lump of rock-salt and finally harder object like stones.
1) Mritapinda Dharana(Fig.17) 2) Lavana Dharana(Fig.18) 3)
PashanaDharana(Fig.19)
Along with all these measures ancient Acharya's have described numerous
medicinal preparations for the faster union of the fractured bone. These are chiefly
described as general tonics to provide liberal amount of proteins, fats, calcium and other
minerals. These Asthi Sandhaniya Dravyas not only hasten the bony union but also make
it strong they are also good for general health Some of the AsthiSandhniya Yogas
described in ancient texts are mentioned below.
THE LIST OF DRUGS IN THE MANAGEMENT OF FRACTURES
1. Gandha Taila 2. Gandhaprasarini Taila
3. Chakra Taila 4. BhagnasandhanaTaila
5. BhagnasandhanaVati 6. Laksha Guggulu
7. Lashunadi Vati 8. Ashwagandha Chaturbhadra choorna
9. Madhuyasthi Ksheerapaka 10. Pravala Panchamruta
11. Agarvadi Taila 12. Dhataki Lepa
13. Yastimadhu Taila 14. Sudha Bhasma
15. Rajata Bhasma

LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
33
Rejuvenators
1. Haritaki 2. Yastimadhu
3. Amalaki 4. Lashuna
5. Pippali 6. Kakoli, Ksheera Kakoli etc.
7. Shilajitu 8. Godhooma
9. Priyangu 10. Kapitha Phala Majja.
In addition to all these Acharya Sushruta advises to take the milk of Primiparous
Cow processed with gritha, drugs of Madhuragana. And Laksha daily during the morning
hours.
Pathypathya: A fracture patient must forego the use of Lavana, Katu Rasa, Kshara and
Alma articles of food and should live on strictest continence, avoid over exposure to sun
and forego physical exercises.
A diet consisting of Shali rice, meat soup, milk, ghee, soup of satina pulse and all
other nutritive and constructive food and drink, should be descriminately given to the
patient. As a general rule milk should not be prescribed to a patient suffering from Vrana
(Wound) in general, but a case of fracture forms an exception. There to some authorities
hold that the lukewarm milk may be given to the fracture patient, if there be no ulcer.
A case of fracture occurring in a youth or a person slightly deranged dosha or
(Alpadosa) or in winter season, is hailed to be easily curable with a help of aforesaid
methods. A fracture in youth gets healed in course of a month. In two months in a case of
middle aged man, and three months in the old aged man.
LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
34
CLINICAL SIGNS OF IDEALLY UNITED BONE
1) No swelling or hardness on palpation.
2) Absence of shortening and deformity.
3) Painless and easy movements
In such a detailed, scientific manner, ancient Acharays have described the condition of
Asthi Bhagna.
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
35
MODERN LITERATURE REVIEW
The living thing is described by the general term as 'PROTOPLASM'. These
have many microscopic and submicroscopic structures. The smallest unit of protoplasm is
CELL, which has capacity of carrying out an independent existence. The Cell is the
structural and functional unit of living things. It is always seen in multicellular animals
that many cells of one kind constitute one kind of TISSUE. This tissue performs one
particular function. The human body composed of following elementary tissues:
1) Epithelial tissue.2) Connective tissue.3) Muscular tissue.4) Nervous tissue.
Osseous tissue or Bone: The framework of bones and cartilage that provides support,
protects our organs and allows us to move is called the skeletal system. Structurally, the
skeletal system consists of several types of connective tissue: cartilage, bone, red and
yellow bone marrow, the periosteum, and the endosteum. Bone tissues are connective
tissues that means that bone cells are scattered in the matrix, far apart from each others.
Bone cells lying in the matrix are enclosed in individual little chambers called lacunae.
Other types of bones cells are found on the bone membranes lining up the outer surface
of the bones as well as the bone cavities containing blood vessels and bone marrow.
Bone tissue is the one of the connective tissues. It is made up of the bone cells and
intercellular ground substance. The organic part of an Intercellular tissue is about 40%
and is composed of collagen fibers, bounded by mucopolysaccharide cementing material
called Ossein. The remaining 60% which are deposited as a dense substance are inorganic
mainly as calcium salt. Inorganic components that set it apart structurally and
functionally from all other tissues. Roughly, the matrix is about 20% water, 20% protein
and 60% mineral salts.
Inorganic Components: 1) They are mineral salts, mainly Hydroxyapatite (a
crystallized form of tricalcium phosphate), some calcium carbonate, and small amount
of magnesium hydroxide, flouride and sulfate. They give the bone its characteristic that
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
36
makes it unique among all the other tissues: an exceptional hardness which allows it to
resist compression. 2) Mineral salts are abundance: they make 65% of the bone mass and
nearly 2/3 of the matrix.
Organic Components: The organic component of the bone matrix is called osteoid.It
contains proteoglycans, glycoproteins and collagen fibers
Without the organic components of the matrix, the bone would be very brittle and it
would break if twisted or stretched. These organic molecules, especially the collagen
fibers act like reinforcing metal rods in concrete (the concrete here being the mineral
salts). They provide bone with great flexibility and tensile strength (resistance to being
stretch or torn apart).
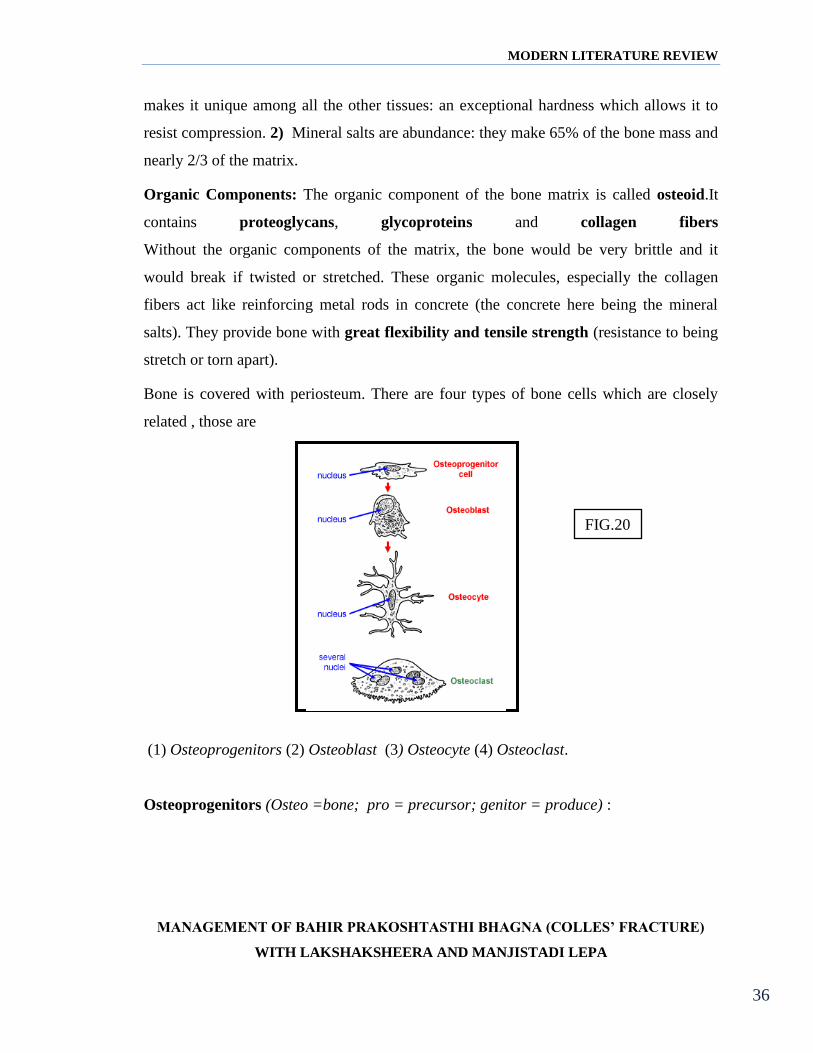
Bone is covered with periosteum. There are four types of bone cells which are closely
related , those are
(1) Osteoprogenitors (2) Osteoblast (3) Osteocyte (4) Osteoclast.
Osteoprogenitors (Osteo =bone; pro = precursor; genitor = produce) :
FIG.20
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
37
They are in differentiated cells that will undergo mitosis and develop into
osteoblasts. They are found on the surfaces of bones and bone cavities containing blood
vessels and bone marrow.
Osteoblasts (Osteo =bone; blast = germ) :
These are found in growing surface where bony matrix is deposited. This cell
secretes the bone matrix and helps calcification. Because of its function of calcification,
bone forming possesses a rich enzyme, alkaline phosphate in the cytoplasm. They are
derived from Osteoprogenitor cells. Osteoblasts build bones: they are also found on the
surfaces of bones and bone cavities containing blood vessels and bone marrow. There,
they secrete the matrix. This is found in growing surface where bony matrix is
deposited.
Osteocytes (Osteo =bone; cyte = cell) :
These types of cells are trapped within the lacuna. These cells have got no active
synthesizing properties. They make the majority of the bone cells and are found
embedded in the bone matrix. Osteocytes derive from osteoblasts. Osteoblasts secrete
matrix, they surround themselves with the material and become "walled up" in the matrix
then, and they stop secreting matrix and become osteocytes. Osteocytes do not secrete
bone matrix: they only maintain the matrix surrounding them in good condition.
Osteoclasts (Osteo =bone; clast = destroy) :
This is a large bone cell found in the area where active reabsorption of bone takes
place. The cell is associated with the process of growth and remodeling bone. Probably it
secretes a proteolytic enzyme to dissolve bony tissue and its function is to reabsorb or
destroy the bone.
Classification of the bone : (I) Depending on the size, shape and distribution of the
cavities, the bone tissues will be categorized

MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
38
(a) Compact or Ivory bone. (b) Cancelled or spongy bone.
By looking at the figures the two bony tissues can be identified
One that looks like Swiss cheese or like a sponge (the cheese stuff and sponge stuff being
the bone stuff): this is the spongy bone tissue. It is located inside bones. one that looks
denser, more compact: the compact bone. It makes the outer part of bones.
Compact bone tissue: (FIG.22)
C) Endosteum, D) Periosteum, E) Haversian canal,
I) Osteocytes J) Concentric lamellae, K) Interstitial lamellae,
L) Circumferential lamellae H)Osteon
The compact bone tissue made up of bone matrix deposited in layers 3-7 micrometers
thick.These layers of bone matrix are called lamellae (J, K, L).
The lamellae of compact bone are disposed in three different patterns:
FIG.21

MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
39
1. The concentric lamellae (J) are arranged concentrically around longitudinal vascular
channels to form the osteons (cylindrical units of the compact bone tissue H) they
have been coloured to differentiate them easily from the two other types of lamellae.
2. The interstitial lamellae (K) fill the spaces between osteons
3. The Circumferential lamellae (L) run around the circumference of the bone. The
inner circumferential lamellae are located on the inner side of the compact bone tissue
and the outer circumferential lamellae are located on the outside.
The bulk of the compact bone tissue is made of cylindrical units: the osteons (H). The
osteons are made of osteocytes (I) arranged in circles and concentric layers of bone
matrix (concentric lamellae J). The concentric lamellae are like tubes of different size.
Fitting inside each other to make an osteon. Running through the core of an osteons and
along its axis is the central canal (Haversian canal E) that contains blood vessels and
nerves.
Spongy bone tissue: This tissue does not contain osteons. It consists of layers of bone
matrix (lamellae) and thin plates of bone called trabeculae. The spaces within the
trabeculae are filled with red bone marrow and blood vessels connected to vessels of
haversian canal .
Periosteum: The periosteum (D) is lining of the outer surface of bones. It is made of a
tough outer fibrous layer (in black) and a thin inner osteogenic layer (in orange). The
fibrous layer (superficial layer) is made up of dense connective tissue fibers and
fibroblast with rich supply of blood vessels and lymphatic from which a good part of the
FIG.23
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
40
nutrition of the bone is supplied. This later has got no osteogenic function and thus limits
bone growth.
Functions of Periosteum:
(1) It serves as tough fibrous covering and checks excessive bony growth. Normal bone
formation is controlled primarily by the periosteum. When due to injury or surgical
operation, it is torn off from the underlying bone, the liberated Osteoblasts start from
new bone at the site of injury and thus gives abnormal bone formation.
(2) Carries blood vessels.
(3) Affords attachment to the muscles and tendons.
Endosteum: It is lining the outside of the trabeculae and the wall of the Haversian and
Volkmann'canals. It is formed by condensation of the stroma of bone marrow. It contains
reticular cells.
Functions:
It possesses osteogenic and haemopoietic functions. Its activity takes part in the healing
of the fractures.
Bone marrow : The central marrow cavities of long bones and between the spicules of
latticework of spongy bones are filled with bone marrow. When the Osteoblasts invade
the cartilage model, marrow begins to form it. Yellow marrow is composed of mainly fat
cells or adipose tissue and is found in the marrow of cavity of long bones. Where as red
marrow is associated with the spongy bones, and contains certain amount of adipose
tissue and mostly blood forming tissue.
Functions:
(1) Production of blood cells and there release to circulation.
(2) Ethroclasia.
(3) Reticulo-endothelial functions.
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
41
(4) Osteogenic functions.
(5) Immunologic functions.
(6) General connective tissue functions.
Composition of Bone : 1) Water -25% 2) Solids- 75%
(A) Organic ( Mainly proteins) - 30%
Three proteins (a) Ossein- Asclero protein is the chief constituent.
(b) Osseomucoid- amucoprtein. (c) Osseo-albuminoid- a Keratin
(B) Inorganic-70%
The chief elements. calcium(Ca), Phosphorus (P), and Magnesium(Mg).
Potassium(K), Sodium(Na), and Chlorine (Cl),in small amounts, Iron(Fe),
Fluorine(F), Lithium (Li), and Strontium (Sr)- in traces.
Ca- remains mainly as phosphates and carbonates and slightly as chlorides and
fluorides Mg- is found mainly as phosphate.
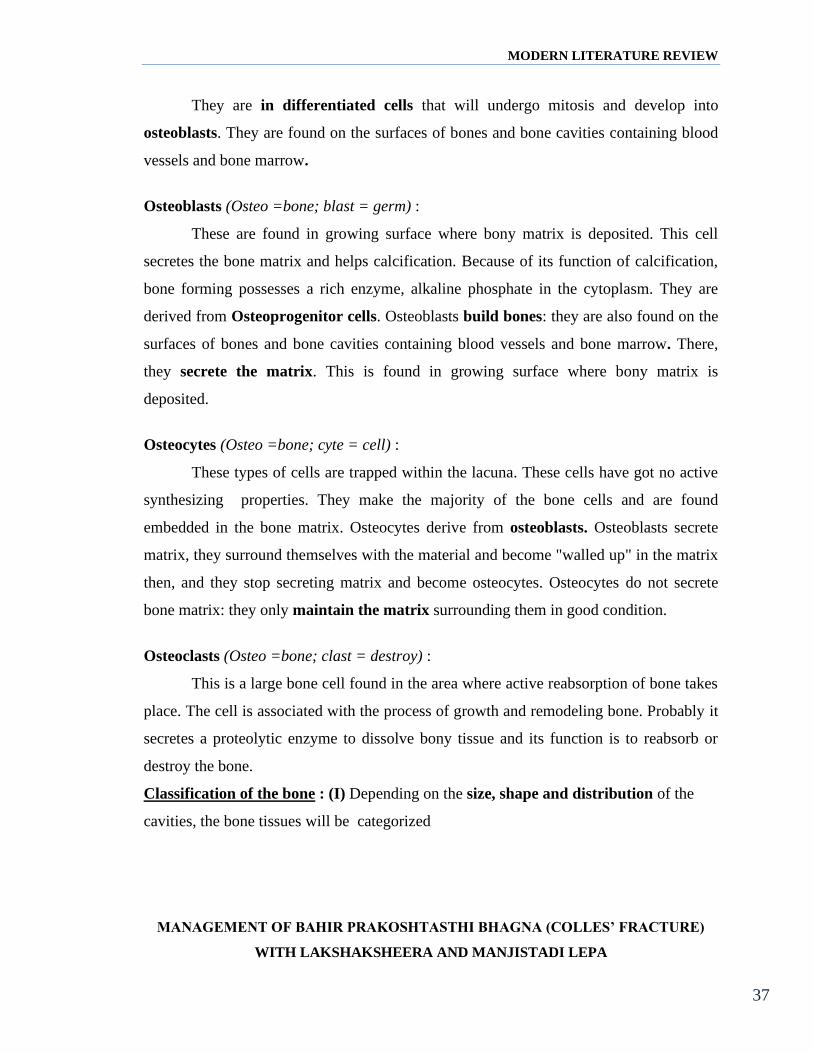
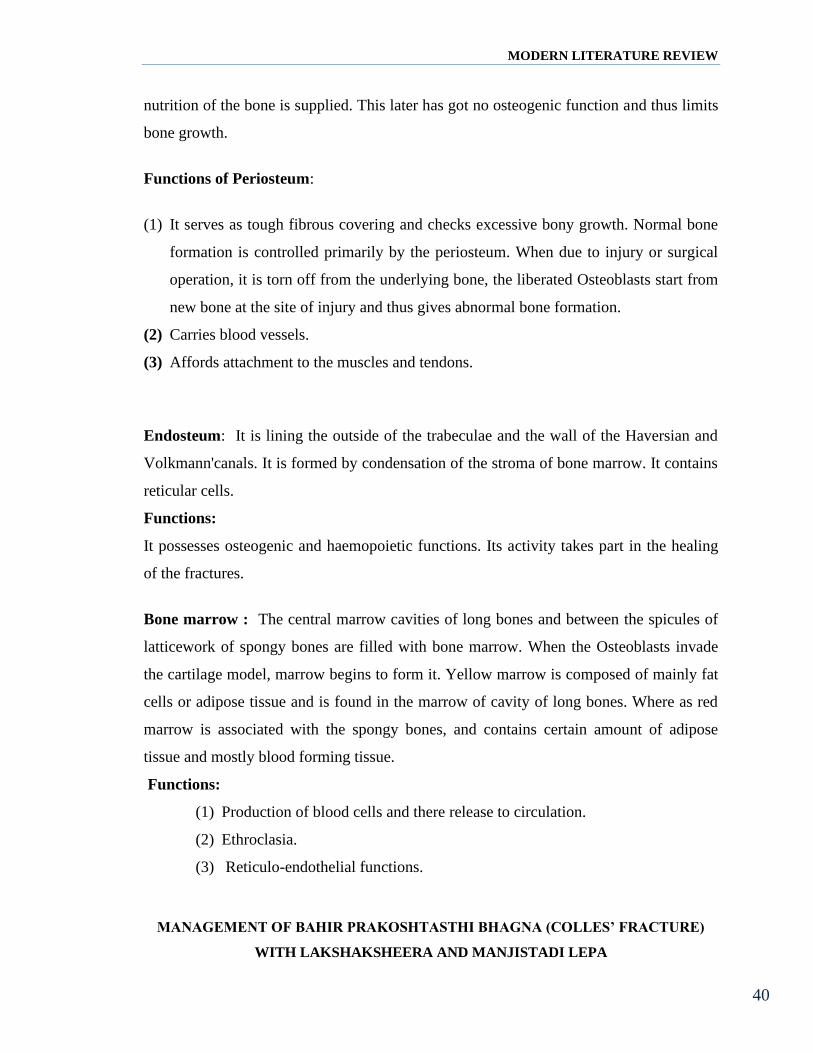
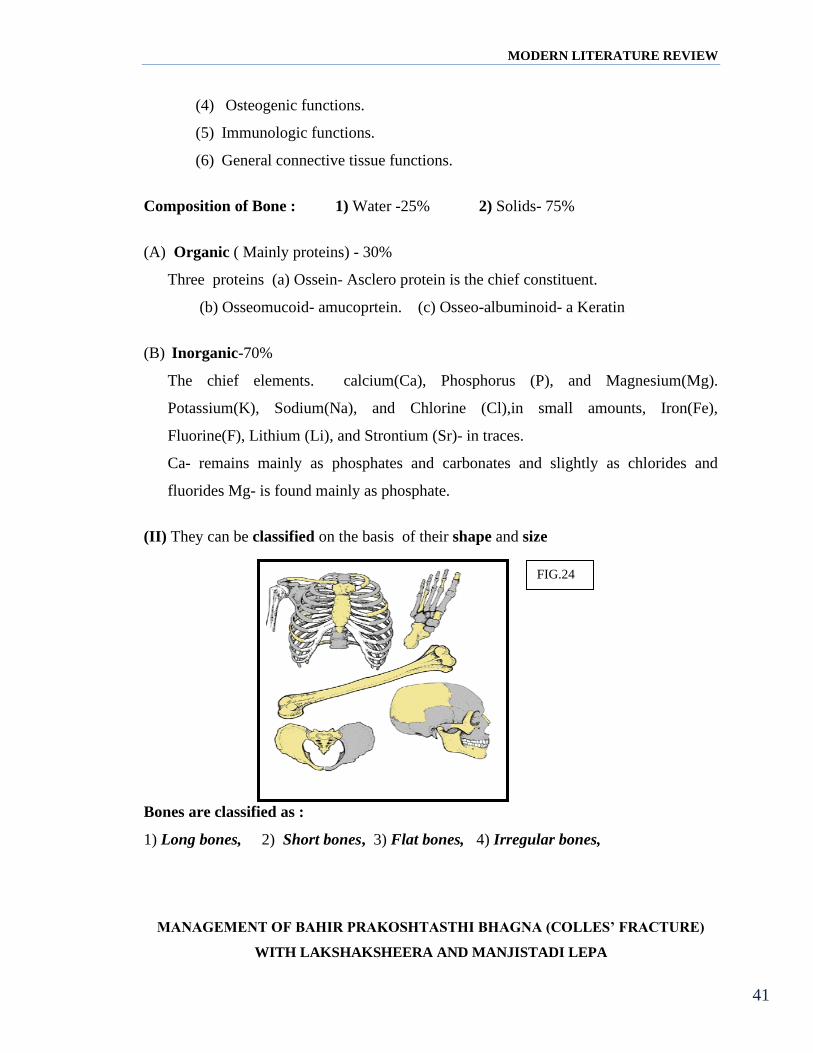
(II) They can be classified on the basis of their shape and size
Bones are classified as :
1) Long bones, 2) Short bones, 3) Flat bones, 4) Irregular bones,
FIG.24
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
42
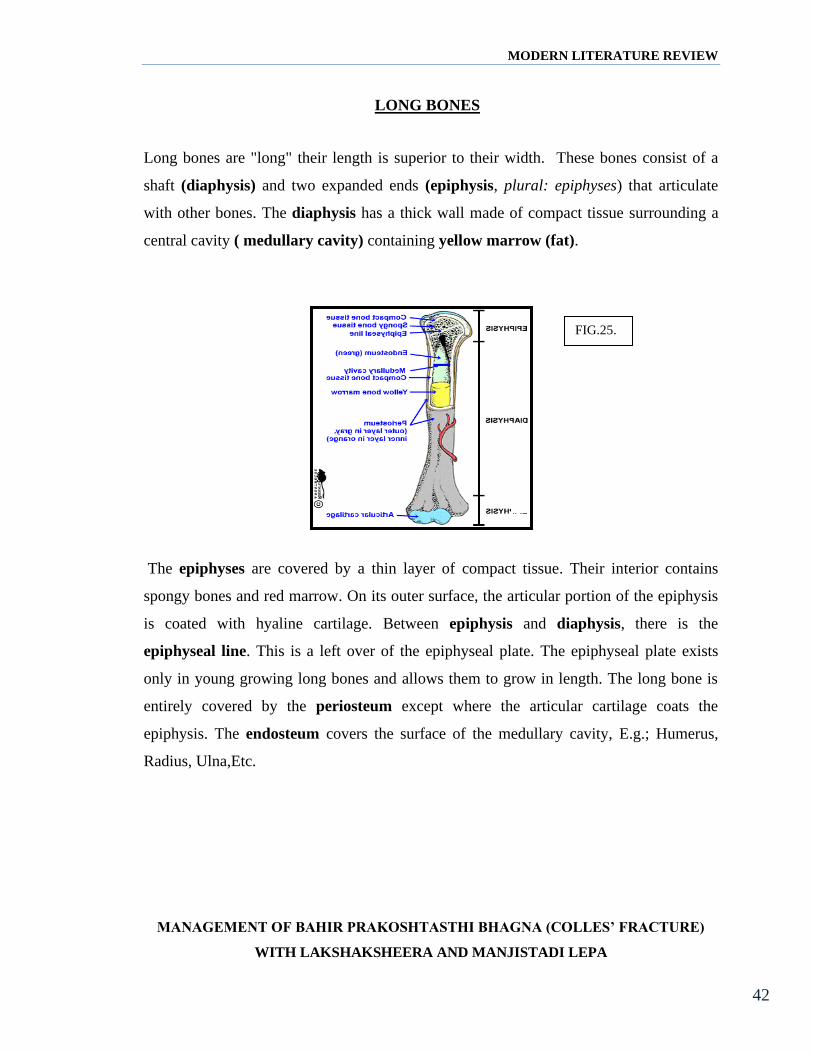
LONG BONES
Long bones are "long" their length is superior to their width. These bones consist of a
shaft (diaphysis) and two expanded ends (epiphysis, plural: epiphyses) that articulate
with other bones. The diaphysis has a thick wall made of compact tissue surrounding a
central cavity ( medullary cavity) containing yellow marrow (fat).
The epiphyses are covered by a thin layer of compact tissue. Their interior contains
spongy bones and red marrow. On its outer surface, the articular portion of the epiphysis
is coated with hyaline cartilage. Between epiphysis and diaphysis, there is the
epiphyseal line. This is a left over of the epiphyseal plate. The epiphyseal plate exists
only in young growing long bones and allows them to grow in length. The long bone is
entirely covered by the periosteum except where the articular cartilage coats the
epiphysis. The endosteum covers the surface of the medullary cavity, E.g.; Humerus,
Radius, Ulna,Etc.
FIG.25.
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
43
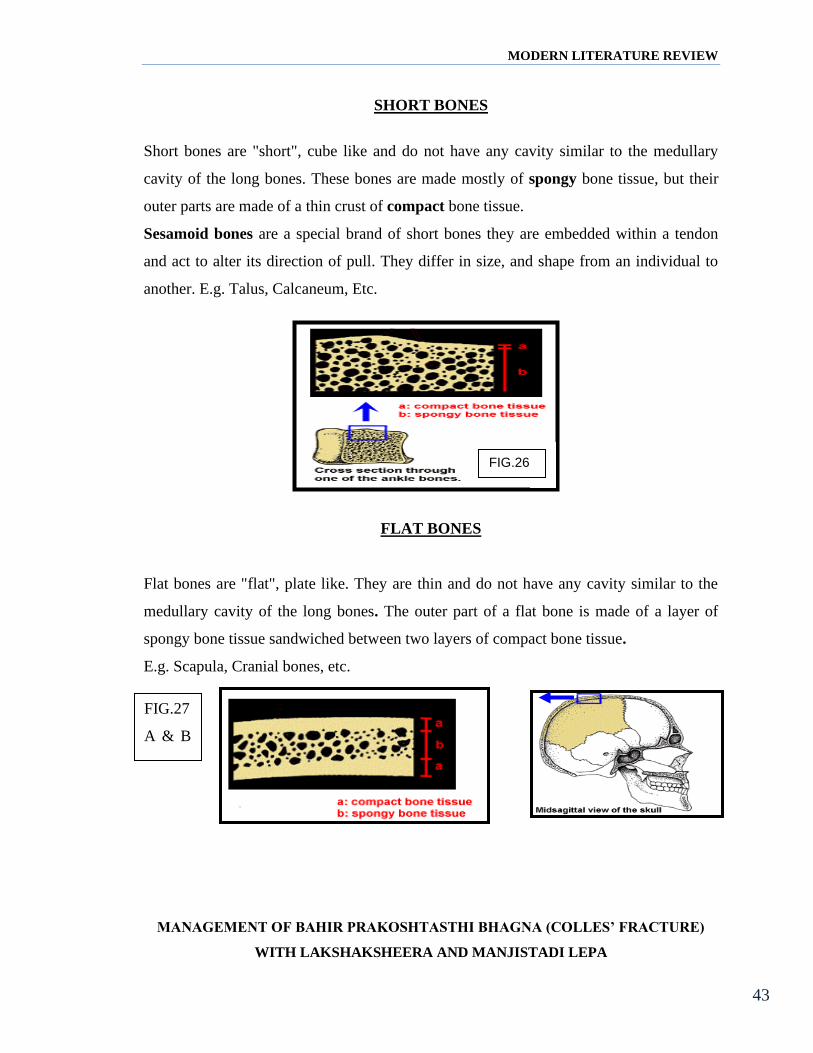
SHORT BONES
Short bones are "short", cube like and do not have any cavity similar to the medullary
cavity of the long bones. These bones are made mostly of spongy bone tissue, but their
outer parts are made of a thin crust of compact bone tissue.
Sesamoid bones are a special brand of short bones they are embedded within a tendon
and act to alter its direction of pull. They differ in size, and shape from an individual to
another. E.g. Talus, Calcaneum, Etc.
FLAT BONES
Flat bones are "flat", plate like. They are thin and do not have any cavity similar to the
medullary cavity of the long bones. The outer part of a flat bone is made of a layer of
spongy bone tissue sandwiched between two layers of compact bone tissue.
E.g. Scapula, Cranial bones, etc.
FIG.26
FIG.27
A & B
FIG.27
. B
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
44
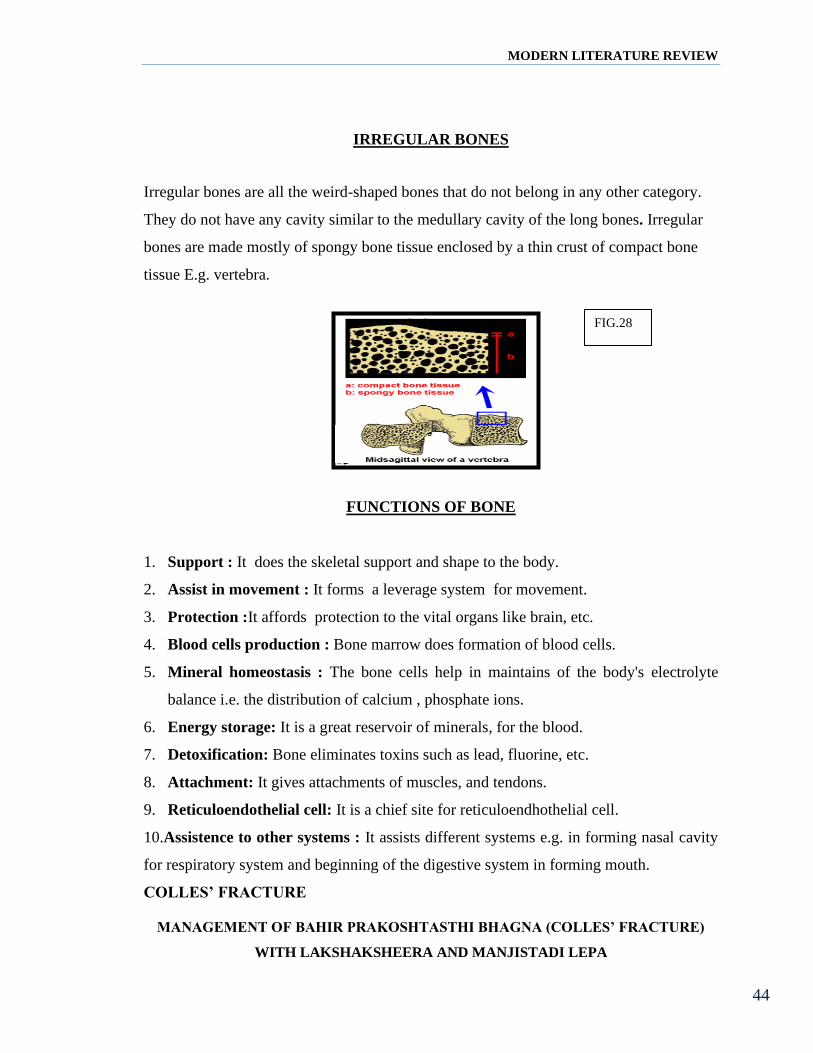
IRREGULAR BONES
Irregular bones are all the weird-shaped bones that do not belong in any other category.
They do not have any cavity similar to the medullary cavity of the long bones. Irregular
bones are made mostly of spongy bone tissue enclosed by a thin crust of compact bone
tissue E.g. vertebra.
FUNCTIONS OF BONE
1. Support : It does the skeletal support and shape to the body.
2. Assist in movement : It forms a leverage system for movement.
3. Protection :It affords protection to the vital organs like brain, etc.
4. Blood cells production : Bone marrow does formation of blood cells.
5. Mineral homeostasis : The bone cells help in maintains of the body's electrolyte
balance i.e. the distribution of calcium , phosphate ions.
6. Energy storage: It is a great reservoir of minerals, for the blood.
7. Detoxification: Bone eliminates toxins such as lead, fluorine, etc.
8. Attachment: It gives attachments of muscles, and tendons.
9. Reticuloendothelial cell: It is a chief site for reticuloendhothelial cell.
10.Assistence to other systems : It assists different systems e.g. in forming nasal cavity
for respiratory system and beginning of the digestive system in forming mouth.
COLLES’ FRACTURE
FIG.28
MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
45
Colles’ fractures are very common extra-articular fractures of the distal radius
that occur as the result of a fall onto an out stretched hand. They consist of a fracture of
the distal radial metaphyseal region with dorsal angulation and impaction, but without
involvement of the articular surface.
Etymology
Originally named by Abraham Colles (1773-1843) Irish surgeon, Dublin.
Epidemiology
Colles’ fractures are the most common type of distal radial fracture and are seen in all
adult age groups and demographics. They are particularly common in patients with
osteoporosis and as such, they are most frequently seen in elderly women. The
relationship between Colles’ fractures and osteoporosis is strong enough that when an
older male patient presents with a Colles’ fracture, he should be investigated
for osteoporosis because his risk of a hip fracture is also elevated.
Younger patients who sustain Colles’ fractures have usually been involved in high impact
trauma or have fallen, e.g. contact sports, skiing, horse riding.
Mechanism
Most Colles’ fractures are secondary to a fall on an outstretched hand with a pronated
forearm in dorsiflexion (the position one adopts when trying to break a forward fall). The
proximal row of the carpus (particularly the lunate and scaphoid) transfer energy to the
distal radius, both in the dorsal direction and along the long axis of the radius. Most
fractures are therefore dorsally angulated and impacted.
Radiographic features
A number of classification systems exist for distal forearm fractures. One of the more
popular is the Frykman classification system, although it fails to distinguish between
Smith and Colles’ fractures as it is based on AP radiographs. As such, in clinical practice,
the use of the term Colles’ fracture with an appropriate description of any associated
injuries is sufficient in most instances.

MODERN LITERATURE REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
46
Plain films usually suffice, although if there is concern of intra-articular extension then
CT may be beneficial.
Plain film
AP and lateral wrist x-rays usually suffice. The fracture appears extra articular, and
usually proximal to the radioulnar joint. Dorsal angulation of the distal fracture fragment
is present to a variable degree (as opposed to volar angulation of a Smith fracture). There
is also usually impaction with resultant shortening of the radius. An associated ulnar
styloid fracture is present in up to 50% of cases.
Treatment and prognosis
The vast majority of Colles’ fractures can be treated with closed reduction and
cast immobilisation. The cast extends from below the elbow to the metacarpal heads and
holds the wrist somewhat flexed and in ulnar deviation. Open reduction and internal
fixation should be considered when the fracture is unstable, and/or unsatisfactory closed
reduction is achieved (e.g. >10 degrees dorsal angulation; >5 mm shortening; significant
comminution).
Complications include :
• malunion resulting in dinner fork deformity
• median nerve palsy and post traumatic carpal tunnel syndrome
• reflex sympathetic dystrophy
• secondary osteoarthritis, more frequently seen in patients with intra-articular
involvement
• EPL tendon tear

DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
47
DRUG REVIEW
''……. I often say that when you can measure what you are speaking about and
express it in numbers. You know some thing about it' but when you cannot measure it ,
when you cannot express it in numbers. Your knowledge is of a meager and
unsatisfactory kind; it may be the beginning of the knowledge, but you have scarily, in
your thoughts, advanced to the stage of science what ever the matter may be…….."
-------------- LORD KELVIN
There are large numbers of medicinal preparations mentioned by acharya
Sushruta in for the management of bone injuries. In the present study the medicaments
mentioned by Sushruta in his treatise Sushruta Samhita Chikitsa Sthana 3rd chapter is
evaluated. Where he mentions the Lepa, for external application over fracture site
followed by bandhana for immobilization with plant barks. For internal administration he
indicates Ksheerapaka. The ingredients of these preparations are as follows.
1) Lepa : Manjishta (Rubia cordfolia), Yashtimadhu (Glycyrhzia glabra),
Raktachandana (Santalum rubrum), ShaliPishti (Oryza sativa), Shatadhauta Gritha
(hundred times processed Ghee).
2) Ksheerapaka : Grishta Ksheera (Primy cow's milk), Sarpi (Ghee), Laksha (Lacciferus
lecca), Madhura gana Dravya's( Kakolyadi gana Dravya's).

DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
48
DRUGS USED FOR LEPA
MANJISTHA
(FIG.56)
Lat. Name : Rubia cordifolia, Linn, R.manjista, R. secunda.
Sans,Mah.& Kan - Manjista, Chitravalli. Eng Indian Madder, Dyer's Madder.
Morphology - This is a climbing plant growing in the north- Himalayas, Pushpakala -
Sharata Rutu. Phala kala - Shishir Rutu. Useful part - Root.
Guna & Karma :
Rasa: Madhura, Tikata, Kashya. Guna : Guru , Ruksha.
Veerya: Ushana. Vipaka: Katu. Doshagnata - Kapha-Pitta shamaka.
Karmas : Varnya, Swarya, Vishghna, Raktashodaka, Mootra visarjaniya,
Bahaya Karma: Shotahara, Vrana Ropana, & Kushtagna,
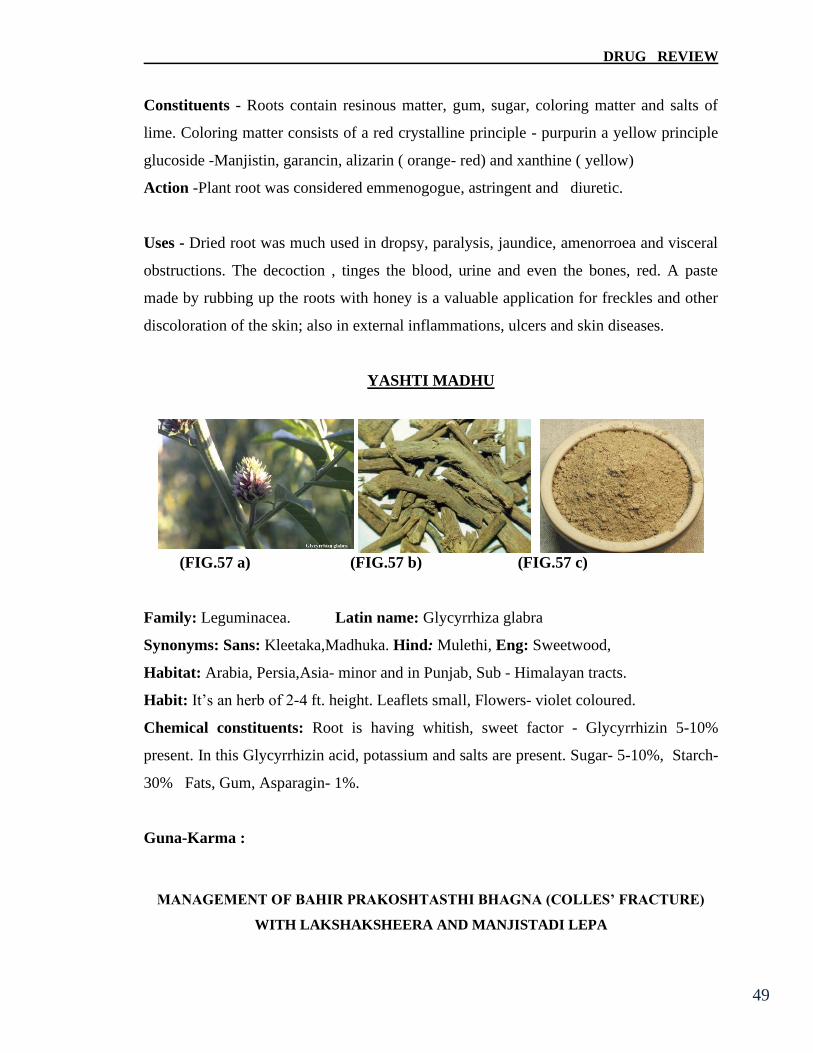
DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
49
Constituents - Roots contain resinous matter, gum, sugar, coloring matter and salts of
lime. Coloring matter consists of a red crystalline principle - purpurin a yellow principle
glucoside -Manjistin, garancin, alizarin ( orange- red) and xanthine ( yellow)
Action -Plant root was considered emmenogogue, astringent and diuretic.
Uses - Dried root was much used in dropsy, paralysis, jaundice, amenorroea and visceral
obstructions. The decoction , tinges the blood, urine and even the bones, red. A paste
made by rubbing up the roots with honey is a valuable application for freckles and other
discoloration of the skin; also in external inflammations, ulcers and skin diseases.
YASHTI MADHU
(FIG.57 a) (FIG.57 b) (FIG.57 c)
Family: Leguminacea. Latin name: Glycyrrhiza glabra
Synonyms: Sans: Kleetaka,Madhuka. Hind: Mulethi, Eng: Sweetwood,
Habitat: Arabia, Persia,Asia- minor and in Punjab, Sub - Himalayan tracts.
Habit: It’s an herb of 2-4 ft. height. Leaflets small, Flowers- violet coloured.
Chemical constituents: Root is having whitish, sweet factor - Glycyrrhizin 5-10%
present. In this Glycyrrhizin acid, potassium and salts are present. Sugar- 5-10%, Starch-
30% Fats, Gum, Asparagin- 1%.
Guna-Karma :
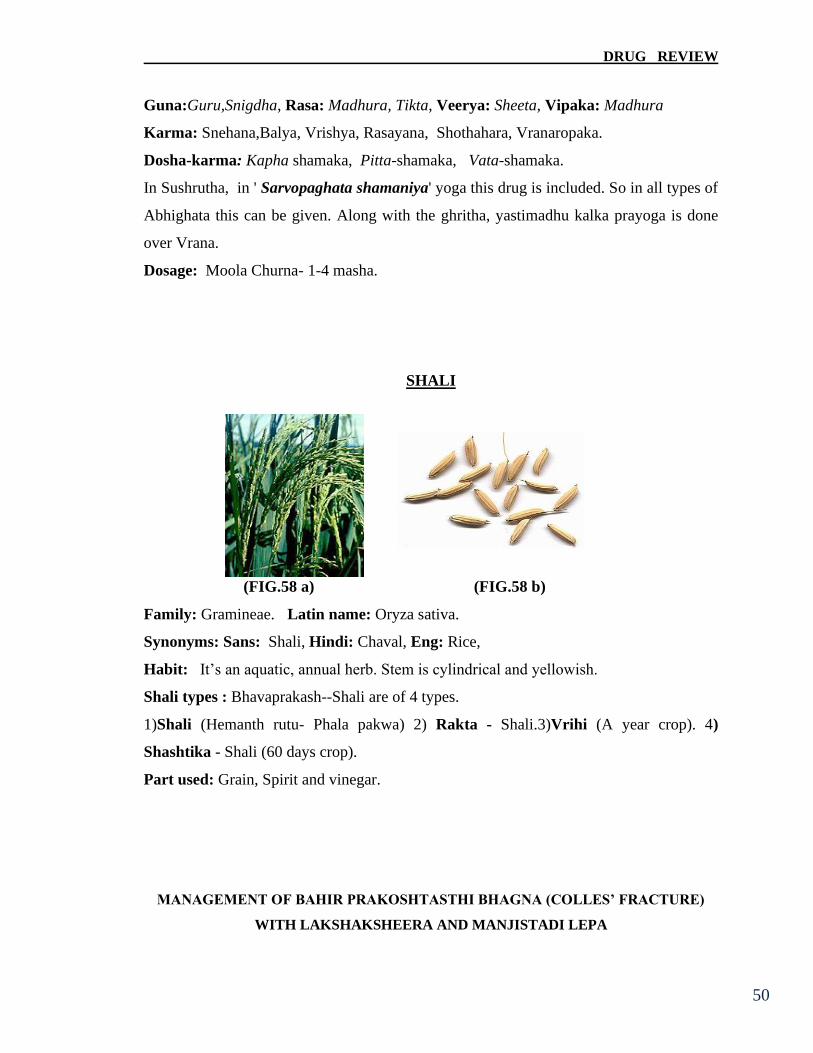
DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
50
Guna:Guru,Snigdha, Rasa: Madhura, Tikta, Veerya: Sheeta, Vipaka: Madhura
Karma: Snehana,Balya, Vrishya, Rasayana, Shothahara, Vranaropaka.
Dosha-karma: Kapha shamaka, Pitta-shamaka, Vata-shamaka.
In Sushrutha, in ' Sarvopaghata shamaniya' yoga this drug is included. So in all types of
Abhighata this can be given. Along with the ghritha, yastimadhu kalka prayoga is done
over Vrana.
Dosage: Moola Churna- 1-4 masha.
SHALI
(FIG.58 a) (FIG.58 b)
Family: Gramineae. Latin name: Oryza sativa.
Synonyms: Sans: Shali, Hindi: Chaval, Eng: Rice,
Habit: It’s an aquatic, annual herb. Stem is cylindrical and yellowish.
Shali types : Bhavaprakash--Shali are of 4 types.
1)Shali (Hemanth rutu- Phala pakwa) 2) Rakta - Shali.3)Vrihi (A year crop). 4)
Shashtika - Shali (60 days crop).
Part used: Grain, Spirit and vinegar.

DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
51
Chemical constituents: Rice contains more starch, small amount of fat, proteins and a
trace of mineral matter. Of the total protein 5 p.c. present in rice globulin is 0.14,
Albumin 0.04 and the remainder is just like a protein Glutenin.
Guna-Karma: Guna: Laghu ,Snigdha. Rasa: Madhura, Kashaya.
Veerya: Sheeta Vipaka: Madhura.
Dosha karma: Vata - Pitta Prashamana. Alpa kaphakara.
Action: Balya, Ruchya, Swarya, Vrishya, Brimhana, Mootrala,
Uses: Poultice of the rice with curd from which excess of water is removed applied
comfortably hot, four times a day gives ample relief in abscesses, by diminishing its pain
and burning sensation; by diminishing the thickness of the base. The rice poultice
requires changing twice or even thrice daily. It is an excellent application to abscesses,
boils, ulcers and other local inflammatory affections.
SHATADHOUTA-GRITHA
(FIG.59 a) (FIG.59 b)
Ingredients: Goghrita.
Method of preparation: Pure cows ghee taken in big bronze plate, and cold water
should be poured above the level of ghee. It should be rubbed vigorously for a few
minutes. When the water becomes slightly warm, it is replaced by a fresh cold water.

DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
52
This method is repeated for 100 times. Such a processed ghee is called "Shatadhouta
ghritha".
Water pouring will modify the properties & effects of the ghritha. However ghritha is
laghu, but in a short amount of time, it is disintegrated & assimilated by virtue of 100
times washing, at certain height 3 feet a sterile cool water poured over ghee. Because of
this ghritha attains readily the absorbability, either by internal or by external application.
Both these aggreability presumed both at the mucosa of G.I.T. & at the cellular level. So
this preparation is introduced into the text mostly for an acute conditions where tissue
repairs is needed. So it can be indicated in Bhagna, Urahakshata, Dagdha Vrana,
Netrabhishyanda, Arbuda etc…
Guna-Karma: Guna: Laghu, Snigdha. Rasa: Shadrasa.
Veerya: Sheeta. Vipaka: Madhura.
Doshakarma: Pitta-Vata hara
Karma: Deepana, Rasayana, Deerghamayusyakaram.
RAKTA CHANDANA
(FIG.60 a) (FIG.60 b)
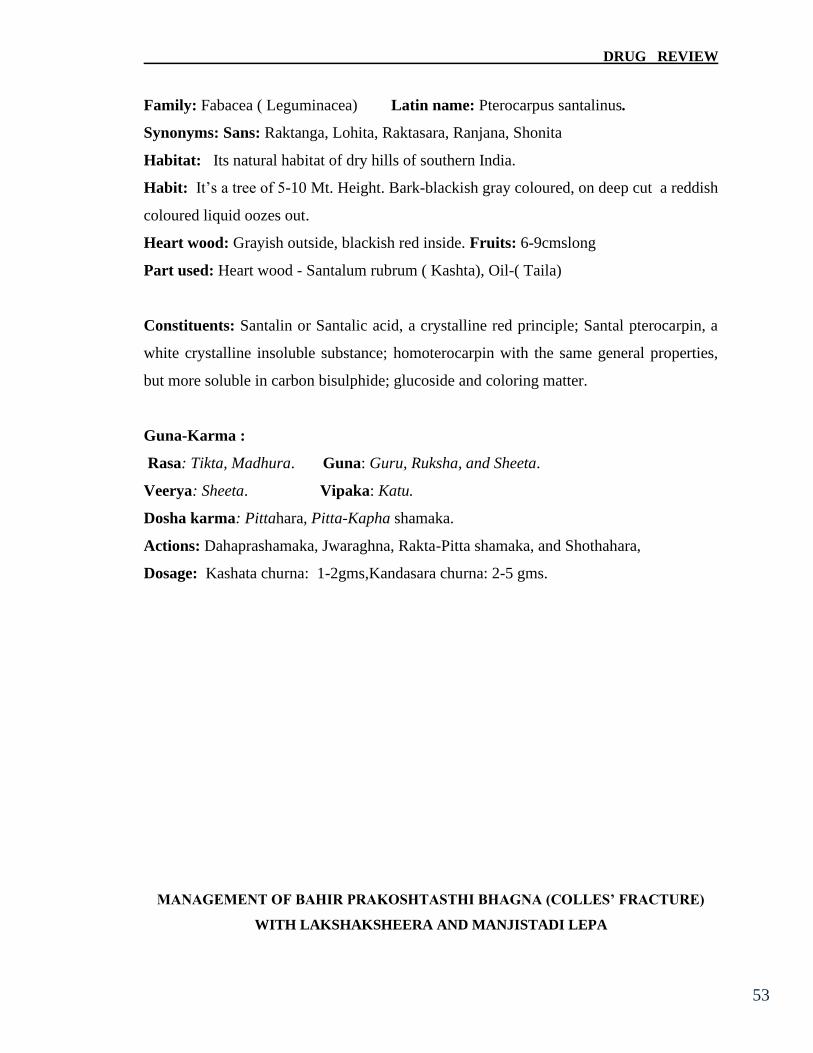
DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
53
Family: Fabacea ( Leguminacea) Latin name: Pterocarpus santalinus.
Synonyms: Sans: Raktanga, Lohita, Raktasara, Ranjana, Shonita
Habitat: Its natural habitat of dry hills of southern India.
Habit: It’s a tree of 5-10 Mt. Height. Bark-blackish gray coloured, on deep cut a reddish
coloured liquid oozes out.
Heart wood: Grayish outside, blackish red inside. Fruits: 6-9cmslong
Part used: Heart wood - Santalum rubrum ( Kashta), Oil-( Taila)
Constituents: Santalin or Santalic acid, a crystalline red principle; Santal pterocarpin, a
white crystalline insoluble substance; homoterocarpin with the same general properties,
but more soluble in carbon bisulphide; glucoside and coloring matter.
Guna-Karma :
Rasa: Tikta, Madhura. Guna: Guru, Ruksha, and Sheeta.
Veerya: Sheeta. Vipaka: Katu.
Dosha karma: Pittahara, Pitta-Kapha shamaka.
Actions: Dahaprashamaka, Jwaraghna, Rakta-Pitta shamaka, and Shothahara,
Dosage: Kashata churna: 1-2gms,Kandasara churna: 2-5 gms.

DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
54
DRUGS USED FOR KSHEERAPAKA
GHRISHTA-KSHEERA
(FIG.61)
Sans -Dugdha,Ksheera. Eng -Milk. Arab-Halib.Pers-Sher. Kan- Haalu.
Sources-Mammary glands of females, cows, she-goats,ewes, etc.
Characters - It’s a collagein type of milk, in each milk collagein occurs either an alkali
or acid. When joins with the natural milk collagein out of milk is exposed or time lapsed
milk also gets fermented and which epicts the collagein part of the milk is said otherwise
as grishta-ksheera. Collagein is a calcium in structure. It supports in making any layer or
wet substances may be in the form of lepam or paste, induces hardness this property of
grishta-ksheera helps in the ossification of injured bone internally and when applied
externally supports the casting material to get hardness.
As in this study due to rare availability of collagein milk (grishta-ksheera) the
cows milk is used for the purpose. Hence its characters are mentioned as below:
Constituents.- Milk contains all the elements necessary for the growth and nutrition of
bones, nerves, muscles and other tissue. Milk contains also vitamins which are Nature's
antidotes to rickets, scurvy. It contains a large proportion of calcium phosphates an
important salt required for the formation of bone and also for the proper
coagulibility of the blood.
DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55
LAKSHA
(FIG. 62a) (FIG. 62b)
San.- Laksha Eng.- Lac, Shellac, Hind., Mah. & Kon. - Lakh, Ben - Gala.
Mal. - Lakasha. Kan.- Aragu ; Laksha Tam - Kombarakku ; Araku.
Source:- Lac is resinous substance usually reddish or dark brown in colour. Deposited
on the twigs of the trees such as Banyan, acacia and peepu, by small insect called
''Carteria Lacca''.
Regarding the formation of Lacca there are different opinions. Some state that insects
attack the young branches of the trees above mentioned and fix themselves to the
branches; the female insect after oviposition dies, giving out her body a reddish liquid
which solidifies and forms a crust about an inch thick round the branch attacked; others
again affirm that the sting of the insect affects the sap or gum of the trees, which forms
the lac. Another opines that the deposit is an excreta of the insect Tacchicardia lacca.
Guna Karma: Rasa- Kashaya Veerya - Sheeta Vipaka- Katu
Doshaghnata- Pitta- Kaphaharam Guna- Snigdha,
This is a drug of choice in bone healing. Lac is a specific application in dental caries and
diseased teeth. Lakshadi taila is used as an in unction in several diseases. The fine
powder of Laksha is mixed with honey and given in haematemesis. Lac is specific
DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
56
application for caries and disease teeth. Madhura gana dravya's: Sushruta has
mentioned Kakolyadi gana Dravya's and few other drugs under this heading.
Kakolyadi gana dravyas: Kakoli, Ksheera kakoli, Jeevaka, Rishabhaka, Mudgaparni,
Mashaparni, Meda, Mahameda, Chinnaruha, Karkatakashringi, Tugaksheeri, Padmaka,
Prapundarika, Riddhi, Ruddhi, Mrudwika, Jivanti, Madhuka.
Milk, Ghee, Vasa (Muscle fat), Majja (marrow), Shashitika Shali,Yava (Barely),
Godhuma, Masha, Shringataka (Trapa bispinosa),Kasheruka (Scirpus kysoor), Trapusha
(Cucumis sativus), Ervaruka (Cucumis utilissimus), Karkaruka (Cucumis melo), Alabu
(Lagenaria vulgaris), Kalinda (water melon), Kataka (Strychnous potatorum),
Gilodya, Piyaala (Buchananialanzan.spreng),Pushakara bija, Kashmari, Madhuka,
Draksha,Kharjura, Rajaadana, Taala(Barassus flabelliformis), Narikela( Cocus nucifera),
Ikshu vikara(Products of sugarcane), Bala (Sida cordifolia), Atibala, Vidari,
Payasya(Vidari bheda), Goksuraka, Ksheeramorata, Madhulika (Glycyrhizza glabra),
Kushmanda.
Madhura Rasa Guna:
Veerya: Sheetha. Vipaka: Madhura.
Dosha-Karmata: Pitta-Vata shamaka & Kapha vardhaka.
Madhura Rasa gives the happiness, Does the Dharana of Sharira, rasadi all
Dhatu's are increased with Upadhatu's. Good for eyes, hairs, complexion, strength, Which
does the union of two break ends, Rakta and Rasa prasadaka, Gives comfort in Baala,
Vriddha, Injured/weak- debilitated persons, reduces thirst, Moorcha, Burning sensation.
All the indrias including Manas are nourished.
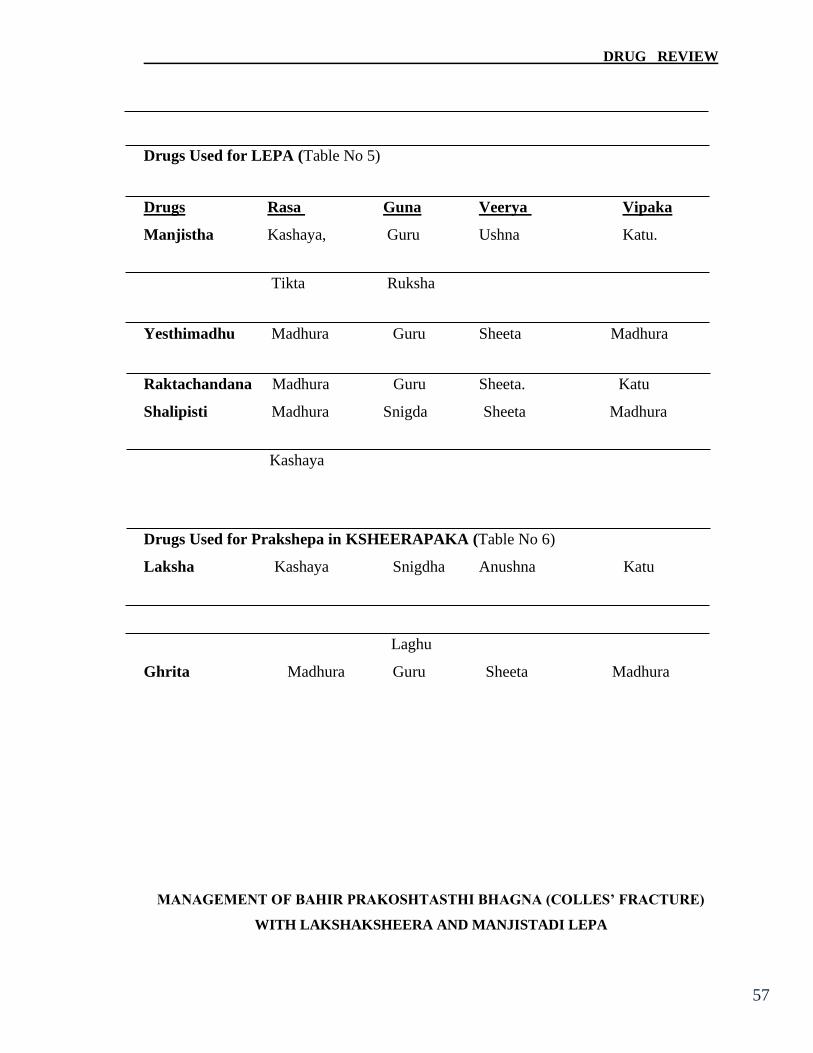
DRUG REVIEW
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
57
Drugs Used for LEPA (Table No 5)
Drugs Rasa Guna Veerya Vipaka
Manjistha Kashaya, Guru Ushna Katu.
Tikta Ruksha
Yesthimadhu Madhura Guru Sheeta Madhura
Raktachandana Madhura Guru Sheeta. Katu
Shalipisti Madhura Snigda Sheeta Madhura
Kashaya
Drugs Used for Prakshepa in KSHEERAPAKA (Table No 6)
Laksha Kashaya Snigdha Anushna Katu
Laghu
Ghrita Madhura Guru Sheeta Madhura

MATERIALS & METHODS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 55 58
MATERIALS AND METHODS
The present clinical study was aimed to assess the efficacy of the Laksha
ksheera and Manjistadi Lepa on management of Bahir Prokoshtasth bhagna (Colles’
Fracture).
Study design- An open clinical trial was undertaken on 30 patients.
Source of data:
30 Patients of Colles’ Fracture were selected randomly from the Surgical out patient and
in patient Dept. of Shalya Tantra, T.M.A.E. Society’s Ayurvedic Medical
College,Hosepet.
Inclusion criteria
1. Stable Colles’ fractures
2. Both Male and Female patients
3. Patients with simple (closed) Colles’ fracture)
4. Patient’s age group between 15 to 60 years.
Exclusion criteria
1. Open radius fractures
2. Patients with nerve and vessel injury
3. Patient suffering with any other debilitating diseases
4. Infective diseases of the bone like osteomyelitis
5. Patients of deficiency diseases.
Diagnostic criteria
1. The clinical features like History of trauma, Pain and swelling in the affected
forearm.
2. Positive findings of Colles’ fracture radiographically.
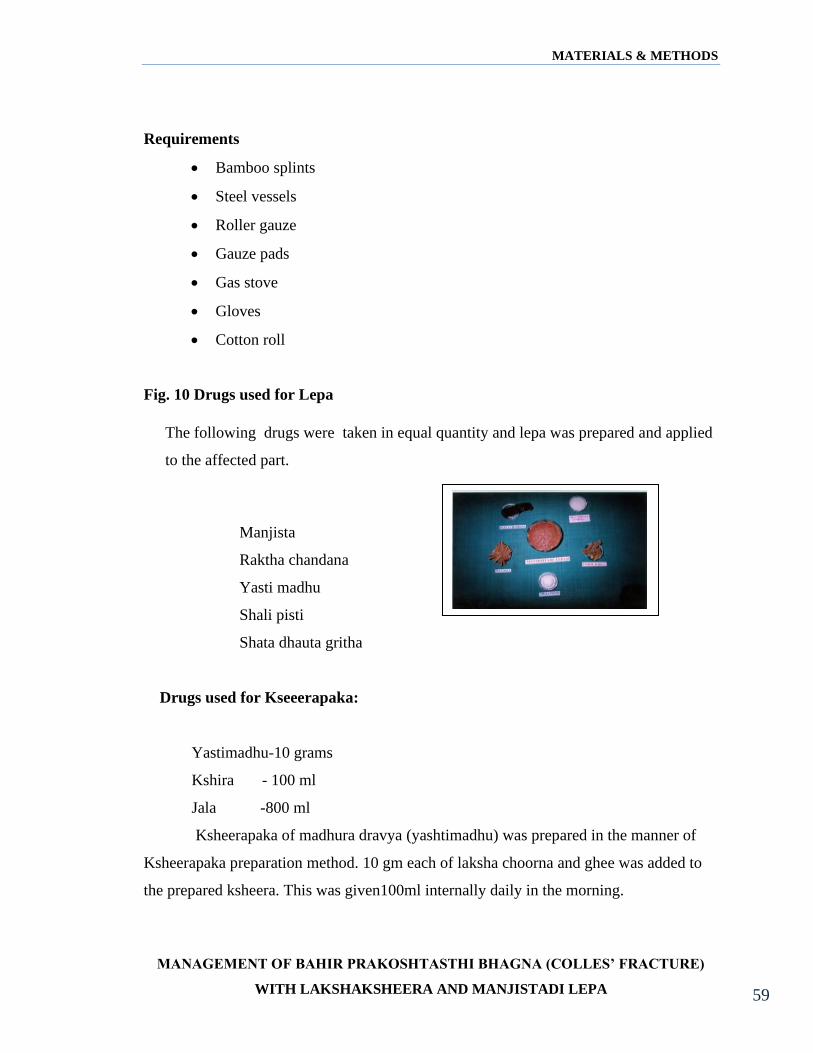
MATERIALS & METHODS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 55 59
Requirements
• Bamboo splints
• Steel vessels
• Roller gauze
• Gauze pads
• Gas stove
• Gloves
• Cotton roll
Fig. 10 Drugs used for Lepa
Manjista
Raktha chandana
Yasti madhu
Shali pisti
Shata dhauta gritha
Drugs used for Kseeerapaka:
Yastimadhu-10 grams
Kshira - 100 ml
Jala -800 ml
Ksheerapaka of madhura dravya (yashtimadhu) was prepared in the manner of
Ksheerapaka preparation method. 10 gm each of laksha choorna and ghee was added to
the prepared ksheera. This was given100ml internally daily in the morning.
The following drugs were taken in equal quantity and lepa was prepared and applied
to the affected part.

MATERIALS & METHODS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 55 60
Intervention:
Selected patients were examined as per the clinical proforma prepared for
the study and subjected to routine blood and urine examinations to rule out other systemic
disorders.
The selected patients were subjected to parisheka of laghupanchamoola
ksheera paka. This was followed by Realignment of the fractured ends by reduction
techniques of conventional closed methods by shake hand method as in Colle’s fracture.
After reduction, Manjistadi lepa was applied. To maintain this reduced
position, splints prepared out of bamboo sticks covered with cotton roll were placed in
position with roller gauge kept in collar sling. Laksha ksheera was given internally.
The bandha was changed once in week without disturbing the fracture alignments.
This treatment was continued for 6 weeks.
After confirming the bony union clinically, active physiotherapy like
initially mrtpinda dharana, lavana pinda dharana and pashana dharana was followed in
successive days. The patients were advised to take with restrictions of lavana, katu and
amla rasa, kshara and ruksha dravyas. Advised to avoid atyadhika maithuna, atapa sevana
and vyayama.

MATERIALS & METHODS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 55 61
Fig. 12: Sushruta’s Procedure
Follow up study –
Patients were examined on initial day zero and further followed up weekly and
the changes of signs and symptoms in the patients were recorded weekly once based on
the research proforma like
1. Subjective improvements
2. Objective improvements
Subjective improvements: The improvement in the clinical symptoms of the disease
was assessed based on the gradation of each symptom as follows.
The Clinical gradations of symptoms are as follows
1) Pain: No pain-00
Tolerable pain - 01
Intolerable pain - 02
Parisheka Alepa
Bandhana Kusha Bandhana
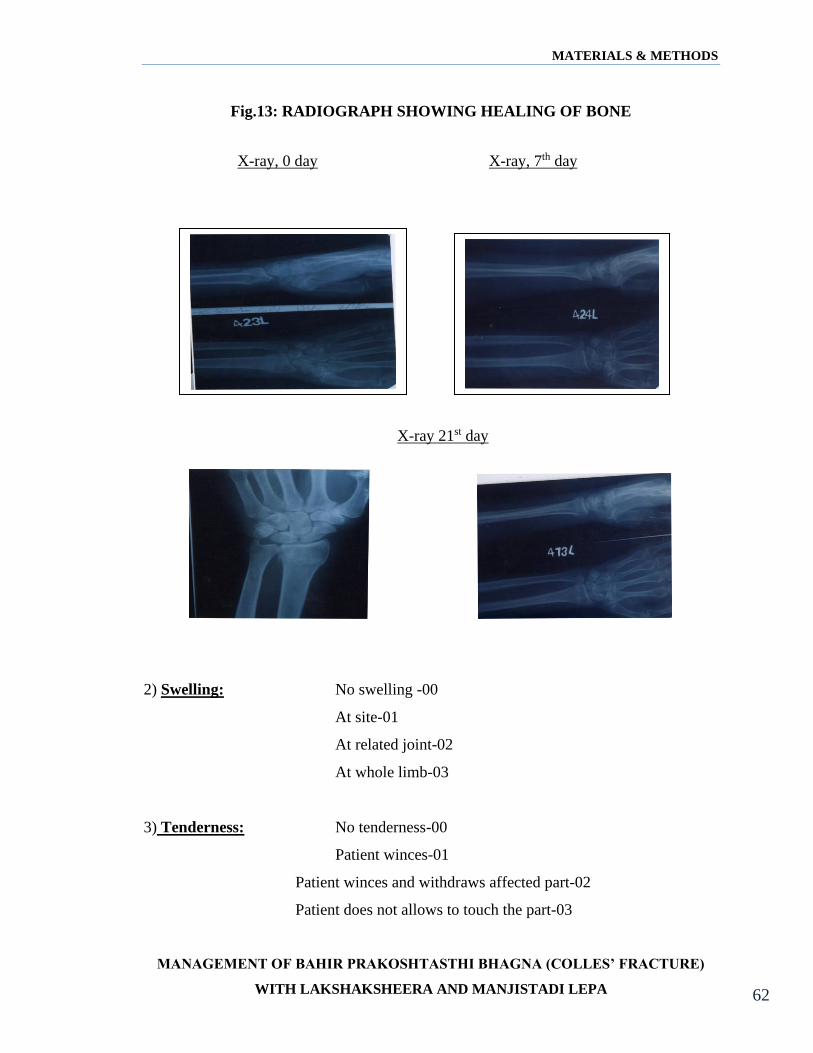
MATERIALS & METHODS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 55 62
Fig.13: RADIOGRAPH SHOWING HEALING OF BONE
2) Swelling: No swelling -00
At site-01
At related joint-02
At whole limb-03
3) Tenderness: No tenderness-00
Patient winces-01
Patient winces and withdraws affected part-02
Patient does not allows to touch the part-03
X-ray, 0 day X-ray, 7th day
X-ray 21st day
MATERIALS & METHODS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 55 63
4) Loss of function: Normal function-00
Able to perform with difficulty-01
Unable to perform-02
5) Callus assessment: Good callus - 00
Mild callus - 01
No callus - 02
Objective improvement – To assess the objective improvements, radiographic
examination carried out before the initiations of treatment then weekly till the clinical
union of the fracture.
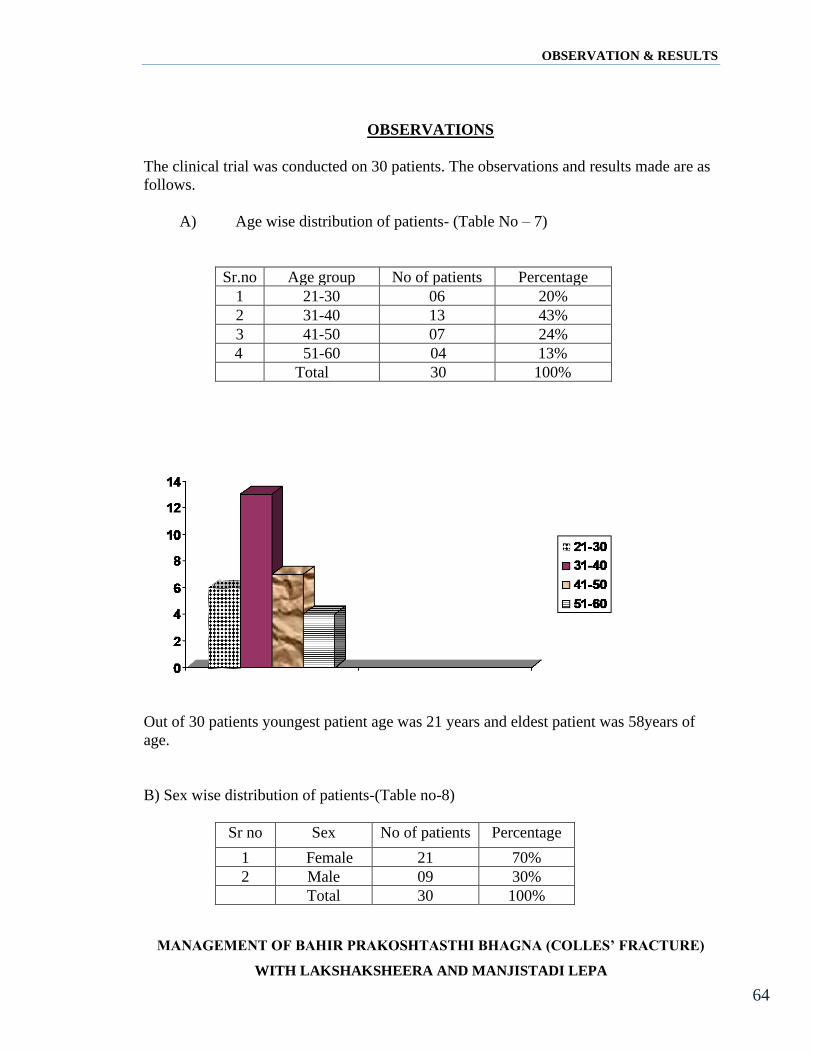
OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 64
OBSERVATIONS
The clinical trial was conducted on 30 patients. The observations and results made are as
follows.
A) Age wise distribution of patients- (Table No – 7)
Sr.no Age group No of patients Percentage
1 21-30 06 20%
2 31-40 13 43%
3 41-50 07 24%
4 51-60 04 13%
Total 30 100%
Out of 30 patients youngest patient age was 21 years and eldest patient was 58years of
age.
B) Sex wise distribution of patients-(Table no-8)
Sr no Sex No of patients Percentage
1 Female 21 70%
2 Male 09 30%
Total 30 100%

OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 65
After analyzing the data related to sex 21 patients were female and 09 patients are male.
C) Distribution of patients on the basis of their Economical status- (Table no-9)
Sr. no Socioeconomic
status
No of patients Percentage
1. Lower class 15 50%
2. Middle class 12 40%
3. Upper class 03 10%
Total 30 100%
0
2
4
6
8
10
12
14
16
Lower class
Middle class
Upper class
After analysis the socioeconomic status of 30 patients found that 15 patients were from
low socioeconomic status, 12 patients of middle class and only 03 patients of upper class.
0
5
10
15
20
25
Female
Male

OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 66
D) Occupation wise distribution of patients- (Table no-10)
Sr no Occupation No of patients Percentage
1 House worker 12 40%
2 Labour 09 30%
3 Job holder 06 20%
4 Students 03 10%
Total 30 100%
0
2
4
6
8
10
12
House Worker
Labour
Job holder
Stuents
After analyzing the occupation data it was found that maximum patients were house
worker.
E) Distribution of patients on the basis of locality. (Table no-11)
Sr no Locality No of patients Percentage
1 Rural 18 60%
2 Urban 12 40%
Total 30 100%
0
5
10
15
20
Rural
Urban

OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 67
Cases were analyzed in view of their habitat, out of 30 patients 18 patients were reported
from rural area and 12 patients from urban area.
F) Incidence of patients as per their prakruthi. (Table no-12)
Sr no Prakruthi No of patients Percentage
1. Vata-pitta 15 50%
2. Pitta-kapha 9 30%
3. Vata-kapha 6 20%
0
2
4
6
8
10
12
14
16
Vata-pitta
Pitta-kapha
Vata-kapha
After analyzing the data related to prakruthi it was found that maximum i.e. 9 patients
were reported as vata-pitta prakruthi.
G) Incidence rate of mode of injury: (Table no-13)
Sr no Type of injury No of patients Percentage
1 Road traffic
accidents
09 30%
2 Domestic fall 15 50%
3 Hit 03 10%
4 Fighting 03 10%
Total 30 100%

OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 68
Incidence rate of mode of injury Among 20 patients was about 50% by domestic fall.
H) Incidence rate of Side of involvement of (dominant or non dominant) hand.
(Table no-14)
Sr no Involved Side No of patients Percentage
1 Right side 24 80%
2 Left side 06 20%
Total 30 100%
In 80% of patient’s right side hand was found to be involved more dominant.
0
5
10
15
20
25
Right
Left
0
5
10
15
R TA
Domestic fall
Hit
Fighting
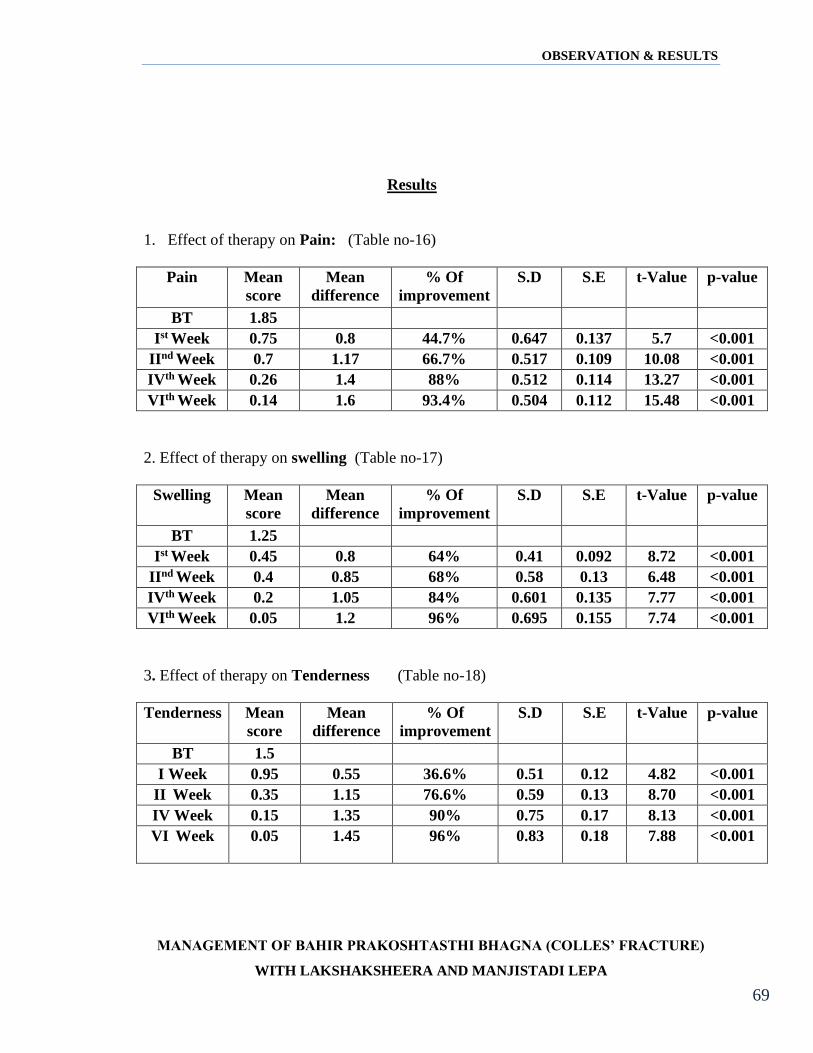
OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 69
Results
1. Effect of therapy on Pain: (Table no-16)
Pain Mean
score
Mean
difference
% Of
improvement
S.D S.E t-Value p-value
BT 1.85
Ist Week 0.75 0.8 44.7% 0.647 0.137 5.7 <0.001
IInd Week 0.7 1.17 66.7% 0.517 0.109 10.08 <0.001
IVth Week 0.26 1.4 88% 0.512 0.114 13.27 <0.001
VIth Week 0.14 1.6 93.4% 0.504 0.112 15.48 <0.001
2. Effect of therapy on swelling (Table no-17)
Swelling Mean
score
Mean
difference
% Of
improvement
S.D S.E t-Value p-value
BT 1.25
Ist Week 0.45 0.8 64% 0.41 0.092 8.72 <0.001
IInd Week 0.4 0.85 68% 0.58 0.13 6.48 <0.001
IVth Week 0.2 1.05 84% 0.601 0.135 7.77 <0.001
VIth Week 0.05 1.2 96% 0.695 0.155 7.74 <0.001
3. Effect of therapy on Tenderness (Table no-18)
Tenderness Mean
score
Mean
difference
% Of
improvement
S.D S.E t-Value p-value
BT 1.5
I Week 0.95 0.55 36.6% 0.51 0.12 4.82 <0.001
II Week 0.35 1.15 76.6% 0.59 0.13 8.70 <0.001
IV Week 0.15 1.35 90% 0.75 0.17 8.13 <0.001
VI Week 0.05 1.45
96% 0.83 0.18 7.88 <0.001

OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 70
4. Effect of therapy on loss of function (Table no-19)
Lossof
function
Mean
score
Mean
difference
% Of
improvement
S.D S.E t-Value p-value
BT 1.1
I Week 0.75 0.35 31.8% 0.49 0.11 3.21 <0.001
II Week 0.35 0.75 68% 0.44 0.09 7.58 <0.001
IV Week 0.20 0.9 81% 0.45 0.10 9.0 <0.001
VI Week 0.1 1.0 90% 0.46 0.10 9.8 <0.001
5. Effect of therapy on callus (Table no-20)
Callus Mean
score
Mean
difference
% Of
improvement
S.D S.E t-
Value
p-
value
BT 2
I Week 2 0 0 0 0 0
II Week 1.8 0.25 12.5% 0.44 0.09 2.52 <0.05
IV Week 0.8 1.20 60% 0.52 0.13 10.34 <0.001
VI Week 0.45 1.65 82.50% 0.49 0.11 15.08 <0.001
Table No - 21 Showing the statistical analysis of symptoms after treatment.
Sr.no Symptoms Mean
score
% Of
improvement
S.D S.E t-Value p value
1 Pain 0.15 91.4% 0.502 0.112 14.28 <0.001
2 Swelling 0.05 96% 0.695 0.155 7.74 <0.001
3 Tender ness 0.05 96% 0.83 0.18 7.88 <0.001
4 Loss of
function
0.10 90% 0.46 0.10 9.8 <0.001
5 Callus 0.45 82.50% 0.49 0.11 15.08 <0.001
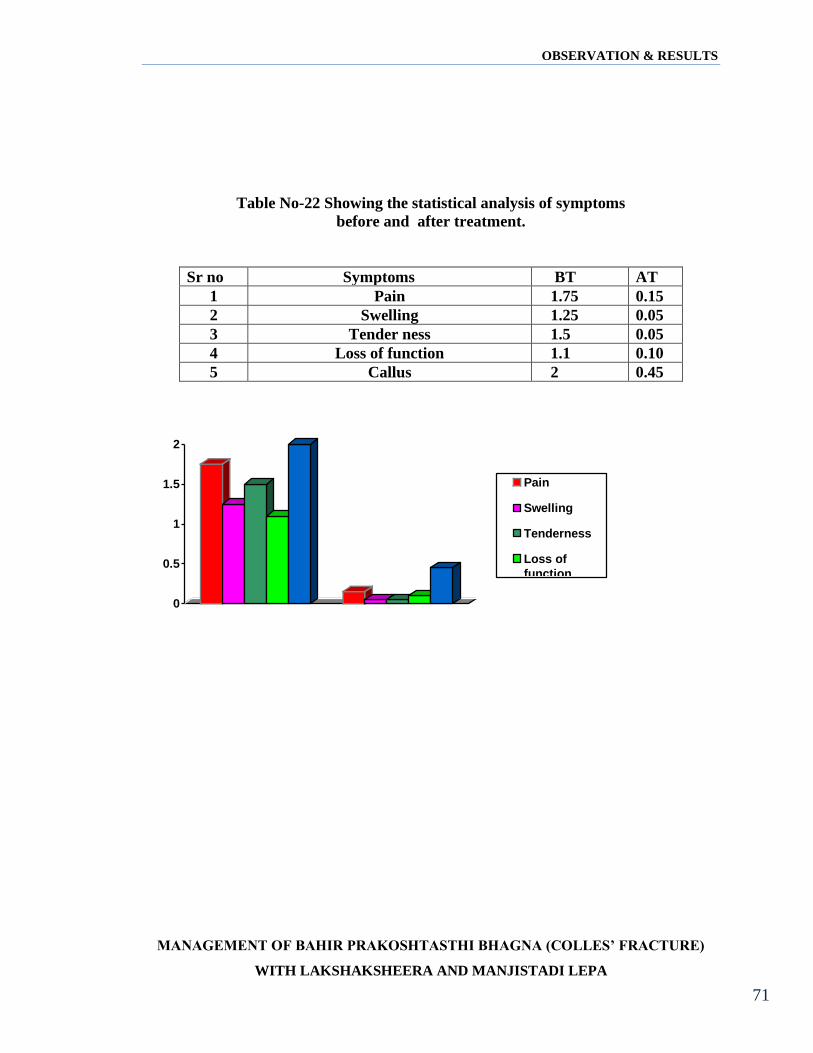
OBSERVATION & RESULTS
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
55 71
Table No-22 Showing the statistical analysis of symptoms
before and after treatment.
Sr no Symptoms BT AT
1 Pain 1.75 0.15
2 Swelling 1.25 0.05
3 Tender ness 1.5 0.05
4 Loss of function 1.1 0.10
5 Callus 2 0.45
0
0.5
1
1.5
2
Pain
Swelling
Tenderness
Loss of
functionCallus
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
72
DISCUSSION
"It is too bad that we cannot cut the patient in half in order to compare two régimes of
treatment" --- Bela Shick.
01) Bahir Prakoshtasthi Bhagna is a troublesome disease.
Bahir Prakoshtasthi Bhagna is a condition where the suffering patients are generally
immobilised for a period of one month up to six months, which naturally affects their
physical, social, economical as well as psychological status of life. Due to increasing
faster competitive lifestyle, the incidence of trauma is increasing day by day.
02) Focus on modern management.
There is an established modern line of treatment for fracture, though showing
good results in the management and prognosis, it is time consuming. The orthopedic
branch of modern science has grown very well since last few decades. New methods of
fracture treatments are being introduced day by day. The main intention of these new
modern techniques is to make affected bone in to normal bone both by structurally as
well as functionally. Also the intention is to reduce the time consumption for
immobilisation. The modern science has succeeded in this part after invention of modern
techniques like open reduction along with internal fixation. This type of treatment has
given good results in major, compound, comminuted and complicated fractures. But the
management of fracture patient with a help of open reduction and internal fixation carries
a great amount of risk of infection. Modern science has not found out any oral
preparation those which will enhance bone healing. For simple fractures the management
recommended is application of POP as a cast and a splint for achievement of total
immobilisation of fractured bone. This application of Plaster Of Paris has got many
hazards like, nerve compression, compartmental syndrome and muscle wasting etc. and
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
73
the Plaster of Paris has no role in bone healing. Hence in these conditions to check the
efficacy of Sushruta's technique, certain Ayurvedic preparation being tried.
What so ever the advanced means and methods attained so far, the basic
principles are similar to Ayurvedic methods. The body physiology and pathology are
primly considered in fracture management apart from fracture treatment by ancient
scholars. The modern science upholds the fact that only the approximation is not the sole
treatment in the fractures but there are certain other factors which are responsible for
union of fractures such as hormones, vitamins, minerals, etc. Acharya Sushruta has
primly mentioned about such facts and his Technique of management of Asthibhagna.
03) Sushruta's technique of management
Acharya Sushruta has described different steps for fracture management, for early
healing of fracture and strengthening it. The same being tried in the present study.
Sushruta has indicated a LEPA for application over fracture site and administration of
Ksheerapaka internally for proper union of fractured bone. The LEPA consists of
Manjistha, Yastimadhu, Shatadouta gritha, Raktachandana and Shalipishiti. The
ingredients of Ksheerapaka are Yastimadhu, Ksheera, and Laksha. These are available in
all parts of India and they are harmless and cheapest preparation, even for low
economical groups. These preparations can be administered on OPD basis does not
require any hospitalization.
04) Theoretical co-relation of Ayurveda and Modern literature.
a) Aetiology: The main cause for fracture is trauma which is mentioned in both
Ayurveda and Modern literature. In olden days the common causes for fractures were
Fall, Compression, blow, etc. such types of Trauma's will usually exerts much force
which usually results with fracture bone. Hence even today these etiological factors will
cause the fracture.

DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
74
b) Symptomatology: The signs and symptoms which are mentioned by Sushruta are
Swelling, Tenderness, Crepitus, Loss of function, Different types of pain and Inability
to find comfort in any position. These general features mentioned by him are just the
same as are written in any standard modern orthopedic surgical text book. In other
words what Sushruta wrote several centuries ago with a meager facilities of carrying
clinical investigations is as a principle so thorough and perfect that it hardly had room
to permit any alteration.
c) Prognosis: Sushruta has mentioned prognosis of fractured patient depends on
1) General condition, health and age of the patient.
2) The type of fracture and the bone involved.
These detailed descriptions of prognosis are so specific and fundamental inspire of
tremendous progress in Orthopedic branch of surgery most of its parts has remained
unchanged. The prognosis of fracture mentioned by Sushruta is yet identical with
that mentioned in Modern Orthopedic text.
d) Management: It is true that the methods of management of fractures have now been
modified greatly over a period of nearly 3000 years but the fact cannot be denied that
the principles of fracture management laid down by Sushruta still hold good and
deserve appreciation. The fundamental principles which Sushruta mentioned are
Anchana, Pidana, Sankshepana, and Bandhana which are identical with the
fundamental treatment of fracture described by Modern Orthopedic science. These
principles of orthopedic surgery speak for the perfection achieved in those days.
Acharya Sushruta has described treatment part of fracture in such a detailed manner
that most of its basic parts are yet to be used with a great success and its use will be
continued in future also.
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
75
e) Warning against infection: Whatever be the management of bone injury the
primary duty of a surgeon is to see no infection takes place at the injured site. He
should make every possible effort to avoid contamination and infection. Once the
bone infection sets in, it is a difficult job to manage the case and life of the patient
becomes miserable. Sushruta had known this fact and therefore he has strongly
recommended the adaptation of measures that would avoid suppuration.
f) Rehabilitation: The importance of physiotherapy in a limb injury was practiced by
Acharya Sushruta. Sushruta has prescribed the exercises in this regard like, lifting of
lighter objects in beginning e.g.: mud-ball, and then heavier substances like a lump of
rock-salt, and finally still harder objects like stones. This would avoid sudden jerking
at freshly healed region and would permit better union by improving circulation.
Sushruta's contribution also includes indication of special devices like fracture
bed, treatment of protruding bone fragments, treatment of malunited bones, treatment
of injured tooth and finally he gives certain criteria of ideally united bone and what a
surgeon is to expect in a case of ideally healed fracture. Those are:
i) Absence of gap between broken fragments ii) Absence of shortening iii) Absence
of deformity iv) Return of painless and easy movements.
All these signs are exactly similar to those signs described in Modern Orthopedic
texts to assess clinical bony union. In short ancient acharya have described the disease
fracture in such a detailed specific and cautious manner that it is referred successfully
in these days of modernization.
05) Role of trauma as nidana:
The etiology of fracture in this trial it is observed is due to trauma, which is
commonest etiological factor for fracture. Trauma caused due to vehicular accidents, due
to fall, assault injuries reported more in this study.
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
76
06) Role of X-ray :
After clinical diagnosis of fracture, X-ray investigation was performed to confirm
it. The X-ray enables a surgeon to know about type of fracture, Plain of fracture,
Displacements of fracture in terms of shift, Angulation, Shortening, Rotation and
distraction.
Acharya Sushruta has given elaborate idea about such types of diagnosis that is,
he has mentioned the effect of trauma on bones involved and particular type of fracture at
particular site. E.g.: Cartilage's bend, The long bones break, Flat bones cracks, Small
bones fragmented. Today we are able to examine an injured bone directly under
radiological examination, but in the absence of these methods, Sushruta evolved this
useful and most logical method of determining the type of fracture.
07) Classification of Bhagna.
Sushruta has classified the skeletal injuries in to two groups according to their
therapeutical importance that is Savrana and Avrana Bhagna. This is a broad type of
classification of skeletal injuries but in the management it plays an important role. Even
in Modern orthopedic text books we find this type of classification that is simple and
compound fractures.
Sushruta had very clear idea about difference between fracture and dislocation,
Hence in the beginning only he has classified the skeletal injuries into two broad groups
namely (a) Injuries of skeletal origin involving joints (b) Skeletal injuries proper. The
same he has further classified in to six types of dislocations and twelve types of fractures.
Such type of classification covers the classification seen in modern orthopedic text books.
The twelve varieties of fracture classification and their nearest modern synonyms are
mentioned in literature review.

DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
77
The very fact that he was able to diagnose the particular variety without the help of
Roentgen rays (which were not discovered in those days ) Only from the direction of a
force causing fracture and the deformity at the site caused by muscular components is
suggestive of his keen clinical sense and the power of logical imagination. The important
point to note in this classification is that, it not only includes the varieties of fractures
known today, but it also carries some minute observations like periosteal avulsion and is
therefore more complete and superior to modern classification of fractures. In fact
Sushruta has viewed fractures as "bone injuries" in the true sense and not merely as
discontinuity of bony surface. This speaks for his deep understanding and capacity of
recognizing the facts without altering their originality.
8) Chikitsa: Sushruta’s principles of fracture management still holds good, it is true that
the methods of management of fractures have now been modified greatly over a period of
nearly 3000 years but the fact cannot be denied and deserves appreciation. The
fundamental principles laid down by Sushruta are Anchana, Pidana, Sankshepana, and
Bandana, which are identical with the fundamental treatment of fractures in
Orthopaedics. These principles of orthopaedic surgery speak for the perfection achieved
in those days. Acharya Sushruta has described treatment part of fracture in such a
detailed manner that most of its basic parts are yet to be used with a great success.
Whatever is the management of bone injury the primary duty of a surgeon is to see no
infection takes place at the injured site, he should make every possible effort to avoid
contamination and infection. Once the bone infection sets in, it is a difficult job to
manage the case and life of the patient becomes miserable. Sushruta was known this fact
and hence he has strongly recommended the adaptation of measures that would avoid
suppuration.
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
78
9) Rehabilitation: Acharya substrata advised the patients to perform different exercises
in a limb injury. like, lifting of lighter objects in beginning e.g. mud-ball, and then
heavier substances like a lump of rock salt, and finally still harder objects like stones.
This would avoid sudden jerking at freshly healed region and would permit better union
by improving circulation.
Sushruta's contribution also includes indication of special devices like fracture
bed, treatment of protruding bone fragments, treatment of malunited bones, treatment of
injured tooth and finally he gives certain criteria of ideally united bone and what a
surgeon is to expect in a case of ideally healed fracture. Those are:
i) Absence of gap between broken fragments
ii) Absence of shortening
iii) Absence of deformity
iv) Return of painless and easy movements.
All these signs are exactly similar to those signs described in Modern Orthopedic
texts to assess clinical bony union. In short ancient acharya have described the disease
fracture in such a detailed specific and cautious manner that it is referred successfully
in these days of modernization.
10) Discussion on materials and methods
In present days the bhagna Chikitsa is not widely in use though it was practiced and used
more than 3000 years with great success. But there are some problems in adopting this
line of treatment. May be due to lack of qualified persons, lack of exposure, fear to
manage, the advanced management techniques of modern science etc. But being all this
Ayurvedic line of management for fractures is still alive in rural areas; certain folklore
practitioners are using these skills and managing the cases successfully. Considering
these facts and also to assess the efficacy of Sushruta's technique scientifically taking
radius as an individual bone this present study was carried out. Before this there were few
works carried out ingenerally, But most of them tried partially, to check the efficacy of
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
79
different Ayurvedic formulations, which are recommended for fracture healing. But in
present study it is taken in total, the principles and drugs been put on for research to
check their efficacy. In this study 30 patients of Colle’s fractures were taken and they
were managed with Ayurvedic management i.e. after Parisheka, Anchana, Peedana,
Sankshepanadi kriyas, the fractured limb was immobilized with application of Lepa and
by using bomboo splints. Internally the patient was given Laksha Ksheerapaka.
11) Discussion on observations and results
A) The study revealed that the incidence of Bhagna was commonly seen in the
age group of 31-40 years i.e. 43%. Mostly this may be due to this age group patients are
young adults and are more labour group by which, they happen to be sustain more
trauma.
B) The sex incidence shows there was 70% of patient’s females also do the hard works
like men. This May be the reason why female patients were more in number the fractures
are limited to a particular community or more prevalent in one aspect as they generally
distribute among the people and the community plays no part in it.
C) The economical status wise incidence shows that, there was more number of patients
reported from lower class i.e 50%. Here it may be due to strenuous work, poor and
vitamin deficient food of lower class people are reported more. May be they drive more
or they are more in number but these all facts do not have to play any role in fracture
incidence.
D) The locality wise incidence shows that more number of patients from rural area i.e.
60%. This may be due to the rural people do more laborious works otherwise there is no
special cause why the rural patients are reported more.
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
80
E) The Prakruti wise incidence indicates, there were more patients from Vata-Pitta
Prakruti i.e. 50%. This may be because Vata Prakruti people are more active also may be
because these people may have more fragile bones. This may be the reason why these
group patients were reported more.
12) Signs and symptoms
The most commonly observed signs in fractured patients were swelling and pain.
To assess these signs and symptoms they are graded as per their characters. As the aim of
clinical study is to assess the efficacy of Ayurvedic management of Radius as individual
bone. Pain and swelling are important symptoms of this fracture. In this study neither a
single anti inflammatory nor analgesic drug was used. The initial mean value of pain was
1.75, and then it was reduced to 0.15,Usually this pain was relieved to the patients
immediately after parisheka But in most of the patients after one week of observation it
came down drastically. Hence these observations indicate the parisheka with
laghupanchamoola ksheerapaka has got analgesic action.
The observations towards swelling also show that there was drastic reduction of swelling
after application of lepa for 2 or 3 sittings. The initial mean value was 1.25, which was
reduced to 0.05 after the application of Lepa. The same indicates the efficacy of lepa in
reducing the swelling. That means this lepa has got definite role to play with anti-
inflammatory action.
As callus formation is the part of fracture healing, the patient, tissue, and treatment
variables influence it. Subsequently, these factors can influence the time of appearance of
callus in the radiograph. The age is one of the important variables that influence fracture
healing. This may be related to the increased vascularity and ability of the cells of
periosteum to differentiate in younger individuals. Certain tissue variables can also affect
the development of callus formation. Radiographic evidence of callus is dependent on
site of bone involved, as well as the nature of fracture. Fractures, particularly in the

DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
81
diaphyseal region develop more callus than metaphyseal fractures. The difference is
related to the amount of periosteum enveloping the bone. In these cases, clinical
parameters, such as lack of pain with movement or tenderness on palpation, are used to
assess fracture healing. This is also true for impacted fractures. As in this study the age
group 20-60 patients are taken, the number of patients with radius lower end fractures are
more, hence callus assessment was difficult. But in these cases direct diaphysis involved,
in these cases the same is assessed properly and callus formation was early in these cases.
The P value is < 0.001 this statistical analysis shows that the treatment is effective in
reliving the symptoms like pain, swelling, tenderness and loss of function.
In few patients early callus formation was observed that this might be due to the
effect of Ksheerapaka. Still more researches need to be carried out to assess the same.
13) Discussion on probable mode of Action of Drugs
Parisheka: In this study the action of trial preparation like parisheka, lepa and
ksheerapaka of the drugs explained on the basis of their Rasa, Guna, Veerya and Vipaka.
In kandabhagna, vedana and shotha are the two dominant features, so for parisheka, laghu
pancha mula ksheerapaka is the right choice.
The vedana / arthi/ruja are because of vata this can be known through a quotation
by sushruta ‘Na arthi aniladhrugam’. When all dravys of laghu pancha moolas are
evaluated for its properties it can explained that out of five drugs three are having
vatahara gunas (snigdha), three are having vata hara rasa (madhura), four are having
vatahara virya(unsha) and three are having vatahara vipaka(madhura) and also these
drugs mainly indicated in ‘vatoottara shula’ condition as these drugs processed with
ksheera which is again vatahara . So totally this combination is vatagna in nature

DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
82
In charaka samhita sutrastana 4th chapter mahakashaya vargas are mentioned. Among that
shotagna mahakashaya includes laghupancha moola dravys , so shotagna action of this
laghupancha moola dravys can be considerd without any question . Totally with pariseka
of laghupancha moola dravys, kandabhagna with vedhana and shotha can be managed
effectively.
Sushurta in chikista 3rd chapter mentioned the laghupancha moola’s in the bhagna
condition when shula and shota are present in pitta prakruthi, and ushna kala for
sandhanaartha, pakapariharatha and vedhana pariharatha. In case of vatoottara shula also
the same combination mentioned works better.
Sushruta in shareera 9th chapter explained tiryagatha dhaminis functions like
‘gavakshi’, the tiryagatha dhaminis sira mukha’s present in roma kupas, so the
parishrka stimulates Brajaka pitta, and absorbes, there by paka occurs, thus shota and
shula are reduced. The samprapti shows the involvement of raktha and vata, where rakta
causing avaraana to vata. Thus the parisheka relives the avaraana and subsides the pain
and swelling.
For each patient this procedure was done for five minutes in one sitting about four angula
in height (Ref-Takradhara atsangahrudaya sutra.)
Lepa: Almost in all the patients the swelling was reduced within 24-36 hours after
application of the lepa. This may be because; the lepa consists of following drugs,
Manjistha
Manjistha by its action it is raktaprasadaka and as it is having Ushna Veerya due
to which it will dilate the peripheral vessels, especially there will be venous dilatation
followed by increased peripheral arterial blood flow. This may be the reason for the
reduction of the swelling around fracture area. As it is having kapha-pitta-shamaka
property by which it will reduce the local edematous residue and its ushna veerya
property helps to penetrate in to local tissue. The chemical composition is calcium salts,
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
83
gum, resinous matter may be absorbed, by these properties it initiates for early callus
formation.
The swelling is the one of the reason for pain at fracture site due to pressure on peripheral
sensory nerves. Where in here the reduction of the swelling and pain may be due to its
ushna property and madhura rasa by which local vata shamana action takes place and
pain is reduced.
Yashtimadhu
This drug is told in Sandhaneeya gana by charaka, and with madhura and kashaya
rasas, it definitely enhances the bone healing. As this drug is having Madhura and
Snigdha properties due to which it reduces the Pitta i.e. it does anti-inflammatory action
locally. And also this drug, which is having the property of Madhura Vipaka and guru
guna due to which it, does vata shamana i.e. responsible for shoolahara. As it is having
anti-microbial properties by which it doesn't allow to grow any microbes in the lepa and
its chemical composition includes salts and potassium, these may also help for bone
growth when it is absorbed internally.
Shatadouta ghritha The Laghu Guna of gritha enhances, after it has been washed
hundred times. Means it attains much Laghutva by its sanskara and becomes readily
permeable in to skin by body temperature. As the molecules of ghrita and further
reducedwhich is now rendered easily into the skin. The Snigdha and Madhura property
of the same reduces swelling and pain. The Snigdha guna may also enhance the bone
formation at fractured site. The fatty lobules of the absorbed ghritha may help for tissue
repair as in case of fractures.
Raktachandana Due to its Madhura Rasa and Sheeta Veerya it reduces Sthanika daha
by which it helps to reduce pain. By shotahara property of this drug it will take out the
edematous fluid of fractured site.

DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
84
Shalipisti The Laghu Guna makes the drug penetrate through skin very easily. The pisti
prepared out of it will be having Pichhila guna, at the time the Sheeta Veerya and
Snigdha property of the drug creates stickiness on the skin by which it puts a local
pressure which makes the collected tissue fluid to escape out. The same drug may again
absorb this. The starch content of the Shali gives strong support to fractured bone. Hence
this may be very important drug in reducing swelling, pain and for immobilisation.
Ksheerapaka It consists of highly active principles of drugs like Yashtimadhu, Laksha,
and ghritha. As Yashtimadhu is balya and dhatuvardhaka, raktastambaka, pittashamaka,
by these properties, administered internally, initially it may act as anti-inflammatory.
Then due to its other properties like madhura rasa,madhura vipaka and sandhaneeya guna
definitely it plays a major role in early callus formation.
The study, which was carried out at Banaras Hindu University by Dr. P. J.
Deshpande on "effect of Shell-lac in healing of fracture." Where they did an animal
experiment and it was a chemical and histological study. The results says that the Laksha
when administered orally in milk basis acts beneficial in fracture healing by influencing
cellular organization and activity in the repair phenomena. The mucopolysacchride
contents sharply raised in the first week, soon followed by study rise in the collagen
content of the treated bones. This suggests the collagenization phase starts much earlier
than the control series. The good amount of proteins supplied through the milk could also
contribute to better healing of fracture of the treated animals. There is fibroblastic
proliferation mainly in the first and second week and Osteoblastic proliferation in the
third and fourth week. Although the cellular activities continue throughout the period of
healing, the maximum activities seen in the period mentioned above. Apart from the
histological evidence the bio-chemical observations suggest increased collagen content of
the treated bone tissue in the first and subsequent weeks.
In the third and fourth week the histological studies are also well supported by the bio-
chemical observations. During this period chondroblasts, which are rapidly multiplying,
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
85
penetrate in the region of collagen fibers and are followed by proliferating Osteoblasts.
All this phenomena especially Osteoblastic proliferation and Osteochondral ossification
seems to be stimulated in the animals receiving this drug. However, the stimulation is not
as pronounced as other known anabolic hormones like dianabol, testosterone etc.
Similarly in the fourth and fifth week the remodeling process also takes place more
rapidly than the control animals. This all indicates that the drug may probably be having
some anabolic activity, which produces general retention of nitrogen and minerals
leading to the positive nitrogen balance.
Thus the researches have proven that the Laksha has got definite role in forming
Osteoblastic cells at fractured bone. The Grishtaksheera (collestrum milk) that has got
rich proteins, calcium and other minerals. Hence by virtue of these properties it helps in
early bone healing by nourishing the injured bone.
Splints
The barks of several trees were advised for splintage. But in present study the splints
prepared out of bamboo were used due to its easy availability. These splints can be made
as per the size required; the limbs can exactly fit in to the inner concave surface of the
bark. The outer surface of the bark being rigid gives adequate support for broken limbs,
but the disadvantage observed that, if it is not properly rolled by cloth it may rub against
the skin and create wounds. As Sushruta has named few drugs for ideal splintage and the
drugs are having similar properties like Ruksha, Kashaya, Sheeta, Mrudu these may have
definitely to do something with fracture healing. A further study is required in this regard.
14) Discussion on Results
From this study it was found that pain,swelling,tenderness and loss of function
was very effectively reduced within one week of treatment,which is stastically proved
with p-value <0.001.This may be attributed to the treatment modalityadopted.The callus
DISCUSSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
86
formation in the present study was started early by the end of 2nd week.This shows that,
the present treatment stimulated the callus formation at an earlystage to fascilitate early
bone healing.
CONCLUSION
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 87
CONCLUSION
Based on the analysis and observations made in this clinical study the following conclusions
can be drawn.
1. This is an open clinical trial done on 30 patients.
2. Colle’s Fractures continue to most common skeletal injuries treated by Orthopaedic
Surgeons.
3. Acharya Sushruta’s principles confidently implemented in this study.
4. The fractures were reported more from labour class and female patients.
5. Most of the cases were reported due to domestic fall, vehicle accident, are chief cause of
fracture was reported.
6. The two important factors like pain and swelling before and after treatment are with mean
value of 1.75 to 0.15, 1.25 to 0.05respictively with statistically highly significant.
7. Administration of Laksha Ksheerapaka is effective in early bone healing
8. In this study bamboo splints were used to maintain reduction in position.
9. This procedure is safe, easily available, less complications, and better acceptability.
10. Thus management with manjishtadi lepam and laksha ksheeram is found effective in the
management of Bahir prakoshtasthi bhagna
11. The null hypothesis is rejected and alternate hypothesis is accepted.
SCOPE FOR FURTHER STUDY
1. Further wide range of study is to be needed to say authoritatively whether the lepa and
parisheka have any added advantages, separately with the help of bio-chemical analysis.
2. Ksheerapaka may be administered along with internal fixations in compound fractures, its
efficacy can be made out.
3. The same technique can be tried in the cases like delayed union or non-union.
The bio-chemical, Histological studies to be carried out to assess the efficacyof
ksheerpaka in enhancing bone healing.
SUMMARY
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 88
SUMMARY
The title of the dissertation is
“Management of Bahir Prakoshtasthi Bhagna (Colle’s Fracture) with Lakshaksheera and
Manjistadhi Lepa.
The study confined only to Colle’s fractures.Described the fracture from the
therotical, practical and clinical point of view in a systematic way.
Acharya Sushruta than Charaka extensively deals the concept of fractures and its
management. And the later authors like Vagbhata, Bhavapraksha, Yogaratnakara etc.
have followed Sushruta’s aspects of classification and nomenclature of fractures.
The introduction consists of incidences of fractures and the importance of
Ayurvedic management of fractures and need of current study.
Then the next chapter deals with Ayurvedic literature review. This includes
Rachana and kriya shareera of Asthi, Asthi dhatu karma, classifications of Bhagna, its
management, possible complications and post healed fracture maintainance.In this the
photo clips of four principles of Sushruta’stechniques are shown.
A chapter follows this on Modern literature review where bone anatomy is dealt
in detail with Radius and its applied aspects then followed by the causes for fractures,
mechanism of fractures, different types of fractures, management, and concept of fracture
healing.
Then the next chapter deals with Drug review, where in the drugs, which are used
for fracture management as per Sushruta Samhita is discussed in detail. Then the
materials and methods followed in the present study were mentioned in detail with
evidence of Radiographs of callus formation are shown.
Under the chapter observations and results, the observations made out during the
study were explained with the help of graphs and tables.
The next part includes discussion and conclusion where the observations made
out during the study, the literature review and about materials and methods adopted and
results discussed in detail.
BIBILIOGRAPHY
BIBLIOGRAPHY
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 89
1. A.D. Shastri, Susruta Samhita, Part I-II, Chaukhambha Samskrita Sansthana, Varanasi, 11th edn,
1997
2. Amarasimha, Amarakosha, Chaukhambha Sanskrit Sansthan, 3rd edn, 1968
3. B.G. Ghanekar, Susruta Samhita, Meharchand Lachmandas Pub.,New Delhi, Reprint-2006
4. Dale M Daniel, Wayne H Akeson, John Joseph O’Connor, Knee ligaments : Structure, function,
injury and repair, Raven Press, New York, 1990
5. Dr. J.L.N. Sastry, Dravyaguna vijnana, Chaukhambha Orientalia, Varanasi, 3rd edn, 2008
6. Dr. K. M. Nadkarni, Indian Materia Medica,volume one, Popular Prakashan Private Limited,
Mumbai, 3rd edition,2009
7. H.P. Vaidya, Ashtanga Hrdaya with Sarvangasundari and Ayurvedarasayana treaty, Chaukhambha
Orientalia, Varanasi, 9th edn, 2005
8. Hariprasad Pandey, Bhavaprakash vidyotini tika, Chaukhambha Sanskrit Samsthan, 6th edn, 1997
9. Harsh Mohan, Textbook of pathology, Jaypee brothers, New Delhi, 5th edn, 2006
10. http://wikipedia.org
11. http://www.biosearch.in
12. http://www.ncbi.nlm.nih.gov
13. John Ebnezar, Textbook of orthopaedics, JAYPEE Brothers Medical Publishers (P)Ltd, New Delhi,
4th edition,2010.
14. K. Ramachandran Reddy, Bhaishajya kalpana vijnanam, Chaukhambha Sanskrit Bhavan, Varanasi,
1st edn, 1998
15. K.D. Tripathi, Essentials of medical pharmacology, Jaypee Brothers Medical Publishers (P) Ltd, 6th
edn, 2010
16. K.L. Bhishagratna, Susruta Samhita, Part II, Chaukhambha Sanskrit Series Office, Varanasi, 4th
edition, 1991
BIBILIOGRAPHY
BIBLIOGRAPHY
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 90
17. K.M. Nadkarni, Indian Materia Medica, Bombay Popular Prakashan, Mumbai, 3rd edn, 1994
18. K.N.Shastri, G.N.Chaturvedi, Caraka Samhita, Part I-II, Chaukhambha Bharati Academy, Varanasi,
2002
19. K.R. Kirtikar, B.D. Basu, Indian Medicinal Plants, Int. Book distributors, Dehradun, 3rd edn, 1991
20. K.R. Srikantha Murthy, Astanga Sangraha, Chaukhambha Orientalia, Varanasi, 9th edn, 2005
21. K.R. Srikantha Murthy, Bhavaprakasa of Bhavamisra, Chaukhambha Krishnadas Academy,
Varanasi, 2008
22. N.S. Williams, C.J.K. Bulstrode, P.R. O’Connell, Bailey & Love’s Short Practice of Surgery,
Edward Arnold Publishers Ltd, 25th edn, 2008
23. P.K. Warrier, V.P.K. Nambiar, P.K.C. Ramankutty, Indian Medicinal Plants, Aryavaidyasala, Orient
Longman Pvt. Ltd., Chennai, 1994
24. P.V. Sharma, Dravyaguna vijnana, 2nd volume, Chaukhambha Bharati Academy, Varanasi, 2001
25. P.V. Sharma, Susruta Samhita, Part I-II, Chaukhambha Viswabharati, Varanasi, 2005
26. R. Remadevi, Bhaishajyakalpana, Perfect Publications, Kottakkal, 2004
27. Raja Radhakantadev Bahadur, Shabdakalpadruma, Chaukhambha Ayurveda Pratisthana, 2006
28. Robert Hannon Fitzgerald, Herbert Kaufer, Arthur L Malkani, Orthopaedics, Elsevier Health
Sciences, 2002
29. Ronald McRae, Clinical Orthopaedic Examination, Elsevier Limited, 6th edn, 2010
30. S. Das, A concise textbook of surgery, Calcutta, 3rd edn, 2006
31. S. Das, A manual on clinical surgery, Calcutta, 6th edn, 2004
32. S. Poddar, Handbook of osteology, Scientific book company, Ashok Rajpath, 11th edn, 2003
33. Sabiston, Textbook of Surgery, Elsevier Saunders, Philadelphia, 17th edn, 2004
34. Sailaja Srivastav, Sarngadhara Samhita, Chaukhambha Orientalia, Varanasi, 2nd edn, 1998
BIBILIOGRAPHY
BIBLIOGRAPHY
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLES’ FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA 91
35. Vd. Yadavji Trivikramji Acharya, Susruta Samhita with Nibandha Sangraha, Chaukhambha
Orientalia, Varanasi, 1997
36. Watson-Jones Fractures and Joint Injuries, edited by J.N. Wilson, B.I. Churchill Livingstone Pvt.
Ltd, New Delhi, 1st edn, 1992
37. William C Whiting, Ronald F Zernicke, Biomechanics of musculoskeletal injury, Human Kinetics,
2nd edition, 2008

ANNEXURE
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
92
T.M.A.E. Society’s Ayurvedic Medical College
Department of P.G.Studies in ShalyaTantra
Case sheet
Title: “Management of BahirPrakoshtasthiBhagna (Colles’Fracture) with
Lakshaksheera and ManjistadiLepa”
Name of scholar: Dr Vijith V Nangelil
Guide: Dr Manonmani L M.D (Shalya)
Co- Guide Dr Radha B.K M.S (Ayu)
Reg. No. Hospital No.
Age : Sex :
Name :
Religion : D.O.A :
Address : D.O.D :
1. HISTORY OF PRESENT ILLNESS &DURATION :
Mechanism of injury ;
Patana / Peedana / Praharana / Akshepana / VyalamrugadaSana
2. SITE OF INJURY :
Upper limb - a) Fore Arm Radius
Ulna
Radius & Ulna
3. TYPE OF FRACTURE :
1. Displaced 2.Undisplaced
ANNEXURE
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
92
2. FRACTURE LINE :
1. Transverse 3.Oblique
2. Spiral 4. Hair line
5. HISTORY OF PAST ILLNESS:
6. H/O PREVIOUS BONE DISORDERS & TREATMENT IF ANY:
7. ADDITIONAL DATA:
1. Occupation
2. Socioeconomic status – lower / middle / upper
3. Inhabitance – Rural / Urban
4. Habit- Alcohol / Tobacco / Drugs / Any other
5. Diet – Veg / Non veg
8. DATA RELATING TO FRACTURE:
1. Extension of swelling: only at the fracture site / related
joint / whole limb
2. Presence of Crepitus
3. Loss of function
4. Pain
5. Tenderness
6.In ability to find comfort in any position
9. GENERAL EXAMINATION:
Pulse: BP: Temp: Wt:
Prakruti: V / P / K, VP / PK / KV, & VPK
Sara: Rasa / Rakta / Mamsa / Meda / Asthi / Majja / Shukra / Satva
Samhanana: Pravara / Madhyama / Avara
Satva: Pravara / Madhyama / Avara
ANNEXURE
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
92
Satmya: Pravara / Madhyama / Aavra
Vyayama :Pravra / Madhyma / Avara
Pramana :Pravara / Madhyama / Avara
10. SYSTEMIC EXAMINATIONS:
CVS:
CNS:
RS:
PA:
11. INVESTIGATIONS:
Blood; Hb% TC ESR DC
Urine:
Rdiological findings:
12. VYADHI VINISCHAYA:
13. MANAGEMENT: PARISHEKA - Lagupanchamoolaksheerapaka.
BHAGNA-STHAPANA
ALEPA - Manjistadilepa
BANDHANA
INTERNALLY -Lakshadiksheerapaka.
14. FOLLOW UP: (in days)

ANNEXURE
MANAGEMENT OF BAHIR PRAKOSHTASTHI BHAGNA (COLLE’S FRACTURE)
WITH LAKSHAKSHEERA AND MANJISTADI LEPA
92
PERFOMANCE
STATUS
1st 7th 14th 21st 28th 42nd 56th
Swelling
Tenderness
Loss of function
Pain
Radiological findings
15. RESULT:
Signature of the Scholar Signature of the Co-Guide Signature of the Guide