Bullet Points in ENT Postgraduate and Exit Exam ... - 1 File Download
316
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Bullet Points in ENT Postgraduate and Exit Exam ... - 1 File Download



Thiem e
Philpott_9783131662316_FM.indd i 5/27/14 10:53 AM

Philpott_9783131662316_FM.indd ii 5/27/14 10:53 AM

Bullet Points in ENT
Postgraduate and Exit Exam Preparation
Carl Philpott, MB ChB, DLO, FRCS (ORL-HNS), MD, PGCME
Anthony Long Senior Lecturer in OtorhinolaryngologyDivision of Medicine, Norw ich Medical School Universit y of East Anglia, Norw ichUnited Kingdom
Peter Tassone, MB ChB, FRCSGlasg(ORL-HNS)
Consultant ENT, Thyroid, and Head and Neck SurgeonJam es Paget , Norfolk and Norw ich Universit y Hospitals, NorfolkUnited Kingdom
Matthew Clark, BSc, MBBS, FRCS (ORL-HNS)
Consultant Otologist and ENT SurgeonGloucestershire Royal Hospital, GloucesterUnited Kingdom
Thiem eStut tgart • New York • Delhi • Rio
105 illust rat ions
Philpott_9783131662316_FM.indd iii 5/27/14 10:53 AM

Library of Congress Cataloging-in-Publicat ion Data
Philpot t , Carl, author. Bullet poin ts in ENT : postgraduate and exit exam preparat ion / Carl Philpot t , Peter Tassone, Mat thew Clark. p . ; cm . Includes bibliographical references and index. Sum m ary: "Concise and to-the-point, this book provides a highly e ective review and study aid for postgraduate and exit exam candidates in otolaryngology-head and neck surgery. It covers the full breadth of the eld in m anageable nuggets of inform ation that are easily learned and retained, and ensures that trainees are prepared for all frequently asked exam questions. Special Features: Distills key facts into bullet points for rapid access to essential inform ation, w ithout the need to wade through lengthy, extraneous m aterial, Covers the full range of topics in the m odern ENT syllabus, as well as other important areas (e.g., im aging techniques, pharm acology, m edical stat ist ics) that are encountered in todays exam s, Organized by subspecialty for quick, convenient review of selected topics, Serves equally well as a compact reference and refresher in the clinic, hospital or operating theatre, O ers a valuable overview of otolaryngology for trainees in allied specialt ies, such as m axillofacial and plastic surgery, audiology and speech-language pathology. Prim arily geared to the Diplom a of Otolaryngology-Head Neck Surgery (DOHNS) and Fellowship Intercollegiate (FRCS-ORL HNS) exam s in the UK, Bullet points in ENT is also an excellent learning resource for sim ilar tests in Europe, India, Canada, Australia, New Zealand, South Africa and other countries. It is ideal as a current, comprehensive, study and revision aid in this rapidly expanding specialty"—Provided by publisher. ISBN 978-3-13-166221-7 (alk. paper) — ISBN 978-3-13-166231-6 (eISBN) I. Tassone, Peter, author. II. Clark, Mat thew (Mat thew P. A.), author. III. Tit le. [DNLM: 1. Otorhinolaryngologic Diseases—Outlines. 2. Otorhinolaryngologic Surgical Procedures—Outlines. W V 18.2]
RF56 617.5'1—dc23
2014018597
Im portant note: Medical knowledge is ever-changing. As new research and clin ical experience broaden our knowledge, changes in t reatm ent and drug therapy m ay be required. The authors and editors of the m ater ial herein have consulted sources believed to be reliable in their e or ts to provide inform at ion that is com plete and in accord w ith the standards accepted at the t im e of publicat ion . However, in view of the possibilit y of hum an error by the authors, editors, or publisher of the work herein or changes in m edical knowledge, neither the authors, editors, nor publisher, nor any other party w ho has been involved in the preparat ion of th is work, warrants that the inform ation contained herein is in every respect accurate or complete, and they are not responsible for any errors or om issions or for the results obtained from use of such inform at ion . Readers are encouraged to con rm the inform at ion contained herein w ith other sources. For exam ple, readers are advised to check the product inform at ion sheet included in the package of each drug they plan to adm inister to be cer tain that the inform at ion contained in th is publicat ion is accurate and that changes have not been m ade in the recom m ended dose or in the contraindicat ions for adm inist rat ion . This recom m endat ion is of part icular im por tance in connect ion w ith new or infrequently used drugs.
Som e of the product nam es, patents, and registered designs referred to in this book are in fact registered t radem arks or proprietary nam es even though speci c reference to th is fact is not always m ade in the text . Therefore, the appearance of a nam e w ithout designat ion as proprietary is not to be const rued as a representat ion by the publisher that it is in the public dom ain .
This book, including all parts thereof, is legally protected by copyright . Any use, exploitat ion , or com m ercializat ion outside the narrow lim its set by copyright legislat ion , w ithout the publisher’s consent , is illegal and liable to prosecut ion . This applies in part icular to photostat reproduct ion, copying, m im eographing or duplicat ion of any kind, t ranslat ing, preparat ion of m icro lm s, and elect ronic data processing and storage.
© 2014 Georg Thiem e Verlag KG
Thiem e Publishers Stut tgar tRüdigerst rasse 14, 70469 Stut tgart , Germ any+49 [0]711 8931 421, custom erservice@thiem e.de
Thiem e Publishers New York333 Seventh Avenue, New York, NY 10001 USA+1 800 782 3488, custom erservice@thiem e.com
Thiem e Publishers Delh iA-12, Second Floor, Sector-2, Noida-201301Uttar Pradesh , India+91 120 45 566 00, custom erservice@thiem e.in
Thiem e Publishers Rio, Thiem e Publicações Ltda. Argent ina Building 16th oor, Ala A, 228 Praia do BotafogoRio de Janeiro 22250-040 Brazil+55 21 3736 3631
Cover design: Thiem e Publish ing Group
Typeset t ing by Thom son Digital, India
Prin ted in India by Replika Press Pvt . Ltd. 5 4 3 2 1
ISBN 978-3-13-166221-7
Also available as an e-book:eISBN 978-3-13-166231-6
Philpott_9783131662316_FM.indd iv 5/27/14 10:53 AM

v
Contents
Section I Otology and Audiology ................................................................. 1
Foreword ..................................................................................................... viii
Preface ........................................................................................................... ix
Acknowledgements ......................................................................................... x
Figure Acknowledgements ............................................................................. xi
Contributors .................................................................................................. xii
About the Authors ........................................................................................ xiii
Abbreviations ............................................................................................... xiv
1 Em bryology and Anatomy of the Ear .................................................. 3
2 Physiology of the Ear ............................ 8
3 External Ear Disease ...........................10
4 Ot it is Media ...........................................13
5 Middle Ear Surgery .............................16
6 Otosclerosis ...........................................20
7 Sensorineural Hearing Loss ..............23
8 Other Hearing Disorders ...................25
9 Tinnitus ...................................................27
10 Vest ibular Schwannom a ....................30
11 Tum ours of the Ear and Skin ............33
12 Ear and Tem poral Bone Traum a ......38
13 Otalgia .....................................................41
14 Audiology—Term inology and Tests .................................................42
15 Hearing Aids ..........................................48
16 Cochlear Im plantat ion .......................51
17 Vest ibular Disorders ...........................54
18 Vest ibular Exam inat ion and Invest igat ion .................................60
19 Facial Nerve ...........................................64
20 Im aging of the Ear ...............................68
Section II Rhinology ................................................................................... 71
21 Sinonasal Anatomy and Physiology .....................................73
22 Acute and Chronic Nasal Disorders ................................................78
23 Granulom atosis w ith Polyangiit is and Other Vasculit ides in the ENT Region ................................83
24 European Posit ion Paper on Rhinosinusit is and Nasal Polyps .....87
25 Com plicat ions of Sinusit is.................93
26 Fungal Sinus Disease ...........................96
27 Endoscopic Sinus Surgery and Com plicat ions ............................ 101
Philpott_9783131662316_FM.indd v 5/27/14 10:53 AM
vi
Contents
28 Ciliary Mot ilit y Disorders .............. 105
29 Epistaxis .............................................. 107
30 Headache and Facial Pain ............... 109
31 Tum ours of the Nose and Paranasal Sinuses ..................... 113
32 Snoring and Sleep Apnoea ............. 118
33 Anatomy and Physiology of the Olfactory and Gustatory System s ............................ 120
34 Olfactory and Gustatory Disorders ............................................. 125
35 Nasolacrim al Disorders .................. 128
36 Cerebrospinal Fluid Rhinorrhoea ....................................... 133
37 Rhinoplasty and Nasal Cosm esis .............................................. 135
38 Facial Fractures and Swelling ........ 138
39 Facial Flaps, Scars, and Keloids ..... 140
Section III Laryngology, Head and Neck .................................................... 145
40 Laryngeal Anatomy and Physiology .................................. 147
41 Non-neoplast ic Laryngeal Pathology ............................................ 150
42 Benign Laryngeal Tum ours ............ 156
43 Malignant Laryngeal Tum ours ...... 158
44 Vocal Fold Palsy ................................. 162
45 Non-neoplast ic Salivary Gland Disease .................................... 165
46 Major Salivary Gland Tum ours ..... 168
47 Diseases of the Oral Cavity and Oropharynx ................................ 170
48 Tum ours of the Lip and Oral Cavity .................................. 174
49 Benign Thyroid Disease .................. 180
50 Thyroid Nodule.................................. 183
51 Tum ours of the Thyroid and Parathyroid Glands .................. 185
52 Mult iple Endocrine Neoplasia ...... 191
53 Tracheostomy ..................................... 192
54 Neck, Laryngeal, and Tracheal Traum a and Stenosis ........................ 193
55 Deep Neck Space Infect ion ............ 197
56 Benign Neck Disease ........................ 200
57 Tum ours of the Pharynx ................. 207
58 Tum ours of the Parapharyngeal Space ..................... 210
59 Metastat ic Neck Disease ................. 213
60 Chem otherapy and Radiotherapy in Head and Neck Cancer ............... 218
61 Robot ic Surgery and Transoral Laser Surgery in Head and Neck .. 222
Section IV Paediatric Otorhinolaryngology ................................................ 225
62 Congenital Malform at ions of the Ear ............................................. 227
63 Deafness in Children ........................ 229
64 Paediat ric Hearing Assessm ent .... 231
65 Congenital Abnorm alit ies of the Head and Neck ...................... 233
Philpott_9783131662316_FM.indd vi 5/27/14 10:53 AM

vii
Contents
Section V Miscellaneous ........................................................................... 259
73 Microbiology of ENT ........................ 261
74 Pharm acology and Anaesthet ics .. 264
75 Medical Stat ist ics .............................. 267
76 Clin ical Governance and Audit ..... 271
77 Classi cat ions .................................... 272
66 Paediat ric Laryngeal Pathology .... 238
67 Paediat ric Tracheal and Oesophageal Pathology ................... 242
68 Paediat ric Neck Masses ................... 245
69 Paediat ric Airway Assessm ent and Managem ent .............................. 248
70 Developm ent and the Drooling Child .................................... 253
71 Tonsils and Adenoids ....................... 255
72 Haem angiom as and Other Vascular Malform at ions ................. 258
Bibliography ................................................................................................ 281
Index ........................................................................................................... 287
Philpott_9783131662316_FM.indd vii 5/27/14 10:53 AM

viii
Foreword
The w ise doctor is a d iscern ing doctor. Arr iving at sound professional decisions in com plex clin ical sit uat ions is a key and unavoidable responsibil-it y of the professional, and the exercise of such du t y usually separates professionals from lay-persons. Clearly, doctors in t rain ing m ust acquire th is abilit y as a p r ior it y, and the beginn ing of th is com plex process is the acquisit ion of factual know ledge.
A doctor w ith increasing expert ise and m atu-rit y is also in terested in the w ider m edical com -m unity. The m ark of such senior professionals is their grasp of the signi cance of contr ibut ing to the professional developm ent of colleagues and the progress of their profession. The co-authors are such doctors—they have produced a textbook
that w ill undoubtedly guide ENT t rainees on their road to becom ing w ise doctors.
A basic textbook should be simple, clear and didact ic. It is m uch harder to w rite a book w here m uch in terest ing detail m ust be excluded; and the m anner in w hich th is has been at tained re ects the thought and care exercised by these authors. It w ill undoubtedly be a useful revision aid for those sit t ing exam s and as a quick reference source in their everyday pract ice (especially as the e-book w ill be available to th is new generat ion of t rainees on their sm art phones! ).
Chris Milford FRCS (ORL-HNS)Consultant ENT Surgeon
John Radcliffe Hospital, Oxford
Philpott_9783131662316_FM.indd viii 5/27/14 10:53 AM

ix
Preface
This book is designed to provide up-to-date and comprehensive coverage of all the topics w ith in the specialt y of Otolaryngology–Head and Neck Surgery and its allied specialt ies. It is the ult i-m ate t rainee com panion, providing the pert inent aspects of th is ourishing specialt y.
Designed w ith the Diplom a in Otolaryngology–Head & Neck Surgery (DOHNS) and Fellowship In tercollegiate (FRCS-ORL HNS) exam inat ions in m ind, it is equally suitable for sim ilar exam s in countr ies outside of the United Kingdom .
The reader should be able to delve deep in to th is book easily and nd the relevant key facts on a part icular topic w ith ease, w ithout being m ired
by lengthy prose. The compact nature of the book lends it self to being carried w ith the t rainee doctor as a revision aid and inform at ion source in clin ic or in the operat ing theater.
We hope th is book, born of an unm et need we ourselves had as t rainees, p rovides a fram e-w ork on w h ich to base your know ledge of the specialt y as w ell as gu idance in your p reparat ion for exam s.
Carl Philpot tPeter Tassone
Matthew Clark
Philpott_9783131662316_FM.indd ix 5/27/14 10:53 AM

x
Acknow ledgements
We would like to thank all those w ho have contr ibuted to the w rit ing of th is book, their m entors w ho provided cont inued guidance, and their fam ilies for helping to keep work in perspect ive.
Carl Philpot tPeter Tassone
Matthew Clark
Philpott_9783131662316_FM.indd x 5/27/14 10:53 AM

xi
Figure Acknowledgements
• Figs. 1.1–1.4, 2.1–2.3, 3.1, 4.1, 4.2, 5.1, 5.3, 10.1, 10.2, 11.1–11.4, 14.1–14.5, 15.1, 16.1, 18.1, 18.2, 19.1, 19.2, 20.1, 21.1, 21.3, 21.4, 29.1, 33.1, 38.1, 39.1–39.8, 41.1–41.16, 42.1, 43.1, 44.1, 45.1, 45.2, 47.1–47.3, 48.1, 48.2, 54.1, 55.1, 55.2, 56.1–56.5, 57.1–57.3, 59.1, 59.2, 61.1, 62.1 from Behrbohm H, Kaschke O, Naw ka T, Sw ift A. Ear, Nose, and Throat Diseases With Head and Neck Surgery, 3rd ed. Stut tgart , New York: Thiem e Medical Publishers.
• Figs. 24.1–24.3 from Fokkens WJ, Lund VJ, Mullol J, et al. The European Posit ion . Paper on rh inosinus-it is and nasal polyps 2012. Rhinology 2012;(Suppl. 23):1–299 w ith perm ission.
• Fig. 33.2a from Yarm olinsky DA, Zuker CS, Ryba NJP. Com m on sense about taste: from m am m als to insects. Cell 2009;139:234-244. (Reproduced w ith perm ission of Cell Press.)
• Fig. 49.1 from Gem senjaeger. Atlas of Thyroid Surgery. Stu t tgar t , New York: Thiem e Medical Publishers; 2009.
• Fig. 65.1 from Stewart MG, Selesnick SH. Di erent ial Diagnosis in Otolaryngology. Stut tgar t , New York: Thiem e Medical Publishers; 2010.
• Fig. 66.1 from Bull TR, Alm eyda JS. Color Atlas of ENT Diagnosis, 5th ed. Stut tgart , New York: Thiem e Medical Publishers; 2009.
• Fig. 66.2 from Pensak ML. Otolaryngology Cases. Stut tgart , New York: Thiem e Medical Publishers; 2010.
Philpott_9783131662316_FM.indd xi 5/27/14 10:53 AM

xii
Contributors
David M. Baguley, PhD, MBAHead of Audiology Departm ent , Cam bridge Universit y HospitalCam bridgeUnited Kingdom
Allan B. Clark, BSc (Hons), PhDSenior Lecturer in Medical Stat ist icsNorw ich Medical School, Universit y of East Anglia Norw ichUnited Kingdom
Matthew Clark, BSc, MBBS, FRCS (ORL-HNS)Consultant Otologist and ENT SurgeonGloucestershire Royal HospitalGloucester United Kingdom
Junaid Hanif, FRCS, FRCS (ORL-HNS), MPhilConsultant ENT SurgeonJam es Paget , Norfolk and Norw ich Universit y HospitalsNorfolkUnited Kingdom
Honorary Senior LecturerNorw ich Medical School, Universit y of East AngliaNorw ichUnited Kingdom
Iain F. Hathorn, MBChB, BSc, DOHNS, PGCME, FRCSEd (ORL-HNS)Consultant ENT Surgeon, Honorary Clin ical Senior LecturerUniversit y of Edinburgh, Royal In rm ary Edinburgh, ENT Depar tm ent EdinburghUnited Kingdom
Am in R. Javer, MD, FRCSC, FARSAssociate Clin ical ProfessorENT Departm ent , St Paul’s Sinus Centre, St . Paul’s HospitalUniversit y of Brit ish Colum biaBrit ish Colum biaCanada
John Phillips, BSc (Hons) MBBS MRCS (Eng), FRCS (ORL-HNS)Norfolk and Norw ich Universit y Hospitals NHS Foundat ion TrustNorw ichUnited Kingdom
Carl Philpott, MB ChB, DLO, FRCS (ORL-HNS), MD, PGCMEAnthony Long Senior Lecturer in OtorhinolaryngologyDivision of Medicine, Norw ich Medical School Universit y of East Anglia, Norw ichHonorary Consultant ENT Surgeon & Rhinologist Jam es Paget , Norfolk and Norw ich Universit y HospitalsNorfolkUnited Kingdom
Silke Schelenz, MD, PhD, FRCPath, DipHICClinical Senior LecturerMedical MicrobiologyNorw ich Medical School, Universit y of East Anglia Norw ichUnited Kingdom
Ibrahim Albert Srouji, FRCSConsultant ENT SurgeonPeterborough City HospitalPeterboroughUnited Kingdom
Vishnu Sankalp Sunkaraneni, BSc (Hons), MBBS, MRCS, DOHNS, LLM, FRCS (ORL-HNS) Royal Surrey County HospitalSurreyUnited Kingdom
Peter Tassone, MB ChB, FRCSGlasg (ORL-HNS)Consultant ENT, Thyroid, and Head and Neck SurgeonJam es Paget , Norfolk and Norw ich Universit y HospitalsNorfolkUnited Kingdom
Brian David Westerberg, MDENT Departm ent , St . Paul’s Rotary Hearing Clin icVancouverCanada
Matthew W. Yung, MS (Lond), PhD (Liver), FRCS DLOConsultant Otolaryngologist - Head and Neck SurgeonDept . of Otolaryngology & Head and Neck SurgeryThe Ipsw ich Hospital NHS TrustSu olkUnited Kingdom
Philpott_9783131662316_FM.indd xii 5/27/14 10:53 AM

xiii
About the Authors
Carl Philpott, MB ChB, DLO, FRCS (ORL-HNS), MD, PGCME, is a senior lecturer/honorary consultant ENT surgeon and rh inologist at the Universit y of East Anglia (UEA). His m ain clin ical and research in terests comprise the m edical and surgical t reat-m ent of chronic rh inosinusit is, allergic fungal rh i-nosinusit is, and other sinonasal disorders as well as establish ing a dedicated sm ell and taste clin ic. He has been t rained under Dr. Am in Javer in the Rhinology and Anterior Skull Base fellowship in Vancouver, Brit ish Colum bia, and now regu-larly teaches rh inology courses and works w ith colleagues in Uganda to help develop endoscopic surgery.
Peter Tassone , MB ChB, FRCSGlasg(ORL-HNS), is an ENT consultant and head and neck/thyroid surgeon at the Jam es Paget , Norfolk and Norw ich Univer-sity Hospitals, Norfolk, United Kingdom . He has a
special interest in thyroid/parathyroid and salivary gland surgery. He was t rained as a registrar in the Eastern Deanery, including Cam bridge and Nor-w ich, and completed a fellowship in head and neck surgery at the Western Hospital and Peter MacCal-lum Cancer Centre, Melbourne, Australia. He is also a part of the m odule team for delivery of under-graduate educat ion at Norw ich Medical School.
Matthew Clark, BSc, MBBS, FRCS (ORL-HNS), was t rained in ENT on the Oxford rotat ion before un-dertaking a year’s otology and neurotology fellow-ship through the Universit y of Brit ish Colum bia, Vancouver. He is now a consultant in Cheltenham and Gloucester w ith a specialt y in adult and paedi-at ric otology. He is passionate about t rain ing, w ith a grow ing in terest in surgical sim ulat ion . He also undertakes hum anitarian surgery and t rain ing in Uganda, Nepal, and Cam bodia.
Philpott_9783131662316_FM.indd xiii 5/27/14 10:53 AM

xiv
Abbreviations
# fracture ” inches−ve negat ive+ve posit ive5-HT serotonina ar teryaa ar teriesAB ant ibiot icABG air–bone gapABR auditory brainstem responseABx ant ibiot icsAC air conduct ionACE angiotensin-convert ing enzym eACE-Is angiotensin-conver t ing enzym e
inhibitorsAERD aspir in-exacerbated respiratory
diseaseAFRS allergic fungal rh inosinusit isAIDS acquired im m unodeficiency
syndrom eant anter iorAOM acute ot it is m ediaAP act ion potent ialARIA allergic rh in it is in asthm aARS acute rh inosinusit isAV ar teriovenousAXR abdom inal X-rayBa bariumBAHA bone-anchored hearing aidBC (audiology bone conduct ioncontext) BC (m icrobio- blood culturelogy context) BCC basal cell carcinom aBM basem ent m em braneBPD bipolar diathermyBPPV benign paroxysm al posit ional
vert igoBSER brainstem evoked responseca carcinom ac/o com plain ing ofcAMP cyclic adenosine m onophosphateCF cyst ic fibrosiscGMP cyclic guanosine m onophosphateCHL conduct ive hearing lossCI cochlear implantCMV cytom egalovirusCN cranial nerve
CNS central nervous systemCO carbon m onoxideCO2 carbon dioxideCOM chronic ot it is m ediaCOPD chronic obst ruct ive pulm onary
airways diseaseCPA cerebellopont ine angleCPAP cont inuous posit ive airway
pressureCRF chronic renal failureCRS chronic rh inosinusit isCRSsNPs CRS w ithout polypsCRSw NPs CRS w ith polypsCSA central sleep apneaCSF cerebrospinal fluidCT com puted tom ographyCVA cerebrovascular accidentCXR chest X-raydB decibeldB A decibel A-weight ingDCIA deep circum flex iliac ar teryDDx different ial diagnosisDM diabetes m ellitusDNS deviated nasal septumDTC different iated thyroid cancerDx diagnosisEAC external auditory canalEAM external auditory m eatusEB external beamEBV Epstein–Barr virusECA external carot id ar teryECG elect rocardiogramECoG elect rocochleographyEFRS eosinophilic fungal rh inosinusit isELISA enzym e-linked im m unosorbent
assayEMRS eosinophilic m ucinous
rh inosinusit isENoG elect roneuronographyESR erythrocyte sedim entat ion rateESS endoscopic sinus surgeryET eustachian tubeETT endotracheal tubeF fem aleFB foreign bodyFBC (CT/ frontal bullar cellanatomy context)
Philpott_9783131662316_FM.indd xiv 5/27/14 10:53 AM

xv
Abbreviat ions
FBC full blood count(invest igat ioncontext) (F)ESS (funct ional) endoscopic sinus
surgeryFFP fresh frozen plasm aFH fam ily h istory(f)MRI (funct ional) m agnet ic resonance
im agingFNA fine needle aspirat ionft feetFU follow upGA general anesthet icGABHS group A β-hem olyt ic st reptococcusGG gast rograffinGORD gast ro-eosophageal reflux diseaseGy gray (unit of absorbed radiat ion)h hourHA hearing aidH&N head and neckHDU high dependency unitHHT hereditary hem orrhagic
telangiectasiaHI hearing im pairm entHIV hum an im m unodeficiency virusHL hearing lossHPV hum an papillom avirusHx historyHz her tzI&D incision and drainageIAC/M internal auditory canal/m eatusIBS irr itable bowel syndrom eICA internal carot id ar teryICP in t racranial pressureIg A/E/G/M im m unoglobulin A/E/G/MIJV in ternal jugular veinIL in terleukinIM infect ious m ononucleosisISJ incudostapedial join tISSC in tersinus septal cellIT inferior turbinateITU/ ICU in tensive care unitIV in t ravenousIx invest igat ionskHz kilohertzKOL potassium hydroxideKTP potassium t itanyl phosphateL leftLA local anesthet icLDH lactate dehydrogenaseLFT liver funct ion testsLLC lower lateral car t ilage
LN lymph nodeLPR laryngopharyngeal refluxLRTI lower respiratory t ract infect ionm m uscleM m aleMALT m ucosa-associated lym phoid t issuem Ci m illicurieMDT m ult idisciplinary teamME m iddle earMEN m ult iple endocrine neoplasiam et m etastasisMIBG m etaiodobenzylguanidineMLB m icrolaryngoscopy and
bronchoscopym m m usclesMNG m ult inodular goiterMR m agnet ic resonanceMRI m agnet ic resonance im agingMRND m odified radical neck dissect ionMT m iddle turbinaten nerveN&V nausea and vom it ingNaOH sodium hydroxideNd:YAG neodym ium -doped yt t r ium
alum inum garnetNF neurofibrom atosisNG nasogast r icNHL non-Hodgkin’s lym phom aNM neurom uscularnn nervesNO nit rous oxideNP nasal polypNPC nasopharyngeal carcinom aNSAID non-steroidal ant i-inflam m atory
drugOA esophageal at resiaOAE otoacoust ic em issionOCP oral contracept ive pillOME ot it is m edia w ith effusionOPA outpat ient appointm entOPG orthopantogramOSA obst ruct ive sleep apneaOSAS obst ruct ive sleep apnea syndrom ePCD prim ary ciliary dyskinesiaPCR polym erase chain react ionPEG percutaneous endoscopic
gast rostomyPET posit ron em ission tom ographyPHP prim ary hyperparathyroidismPICU pediat ric in tensive care unitPND postnasal dr ipPNS postnasal space
Philpott_9783131662316_FM.indd xv 5/27/14 10:53 AM

xvi
Abbreviat ions
PORT postoperat ive radiotherapyPPI proton pum p inhibitorPTA pure tone audiogramPTH parathyroid horm onePx prognosisQoL qualit y of lifeR rightRAST radioallergosorbent testRBC red blood cellRCT random ized cont rolled t r ialRET rearranged during t ransfect ionRFFF radial forearm free flapRLN recurrent laryngeal nerveRND radical neck dissect ionRT radiotherapyRTA road t raffic acciden tRx t reatm entSCBU special care baby unitScc sem icircular canalSCC squam ous cell carcinom aSCM sternocleidom astoidSER sphenoethm oidal recessSLE system ic lupus erythem atosusSLN superior laryngeal nerveSMAS superficial m uscular aponeurot ic
systemSMG subm andibular glandSNHL sensorineural hearing lossSNOT sinonasal outcom e testSOE supraorbital ethm oid cellSPA sphenopalat ine ar terySPT skin prick testSSRI select ive serotonin reuptake
inhibitorST superior turbinateSx sym ptom sTB tuberculosis
TCA tricyclic ant idepressantTFT thyroid funct ion testTg thyroglobulinTGF t issue grow th factorTH T helper cellTIVA total in t ravenous anesthesiaTM tym panic m em braneTMJ temporom andibular join tTNF tum or necrosis factorTOF t racheoesophageal fistulaTORCH toxoplasm osis, other (hepat it is B,
syphilis, herpes zoster), rubella, CMV, herpes simplex
TPN total parenteral nutrit ionTSH thyroid st im ulat ing horm oneULC upper lateral car t ilageURTI upper respiratory t ract infect ionUS ult rasoundUSS ult rasound scanUTC undifferent iated thyroid cancerv veinVAS visual analogue scoreVC vocal cordsVF vocal foldsVII n facial nerve (CN VIII)VPI velopharyngeal insufficiencyvv veinsVZV varicella zoster virusWCC w hite cell countw k weekx/12 num ber of m onthsx/40 num ber of weeks gestat ionx/52 num ber of weeksx/7 num ber of daysXR X-rayYAG yt t r ium alum inum garnet (laser)yr year
Philpott_9783131662316_FM.indd xvi 5/27/14 10:53 AM

Sect ion I
Otology and Audiology
Philpott_9783131662316_Ch01.indd 1 02/05/14 8:01 AM

Philpott_9783131662316_Ch01.indd 2 02/05/14 8:01 AM

3
1.1 External Ear1.1.1 Embryology (Fig. 1.1)• External auditory m eatus from 1st pharyngeal
cleft; at 3/12 cells at bot tom of cleft form m eatal plug of proliferat ing cells, that by 7/12 dissolves; epithelium form s outer part of t ym panic m em -brane (TM)
• TM has ectoderm al outer, endoderm al inner lin ing, and m esoderm al m iddle layer
• Auricle develops from six h illocks of His from 1st (m andibular) and 2nd (hyoid) pharyngeal arches, around the 1st pharyngeal groove during 5th week; rudim entary pinna by ~8/40
• Bulk of auricle derived from the m esenchym e of 2nd arch that extends around the top of the groove to becom e w hat w ill be the helix
• As the face develops the auricle gradually t rans-locates from its original locat ion low on the side of the neck to a m ore lateral and cranial site
1.1.2 Anatomy• Auricle projects at ~30° angle from the side
of the head; angle of inclinat ion is 20 to 30° (generally parallel to nasal pro le); norm al angle between concha and scapha is ~90°
• Pinna has a skeleton of th in elast ic brocart ilage ◦ Curved r im is the helix, w hich at it s postero-superior aspect a sm all tubercle (Darw in) m ay be found (hom ologous w ith the t ip of the m am m alian ear)
◦ Parallel to the helix is the ant ihelix that divides superiorly in to two crura, between w hich is the t r iangular fossa; scaphoid fossa lies above the superior of the two crura
◦ Anterior to ant ihelix is the concha; in it s anterosuperior aspect the crus of the helix form s a divide, such that the cym ba conchae lies superiorly (direct lateral relat ion to the supram eatal t r iangle of the tem poral bone)
◦ Tragus part ly covers the m eatus ◦ At the inferior aspect of the ant ihelix is the ant it ragus, w hich has the in ter t ragic notch between it and the t ragus
◦ Medial (cranial) aspect of auricle has eleva-t ions that correspond to depressions on lateral
1 Embryology and Anatomy of the Ear
surface, and have corresponding nam es, e.g., the em inent ia conchae
◦ Caudal aspect of the pinna is cart ilage free, and is know n as the lobule; contains brofat ty t issue
• Car t ilage covered by th in skin to w hich it is closely adherent to perichondrium ; sebaceous glands m ost num erous in the scaphoid fossa and concha; th icker hairs m ay develop in the inter t ragic notch in older m en
• Car t ilage cont inues inwards in a tubular fashion to becom e the car t ilaginous part of the exter-nal auditory m eatus; at taches to bone and so stabilizes the auricle in posit ion; fur ther xat ion from ligam ents
• Muscles: auricularis anterior and superior supplied by tem poral branch of VII nerve (n); auricularis posterior by posterior auricular branch
• Blood supply of pinna is derived from branches of the external carot id; poster ior auricular supplies cranial aspect , an ter ior auricular branches of super cial tem poral ar tery supply m ost of lateral surface; sm all auricular branch of occipital helps supply m edial aspect; ar teries have corresponding veins
• Car t ilage relies on it s overlying perichon-drium for supply of nut rients and rem oval of by-products
• Lym phat ic drainage from the posterior par t is to nodes at the m astoid t ip , from the t ragus and upper anter ior part of the auricle is to the pre-auricular nodes, and from the rest of the pinna to upper cervical nodes
• Cutaneous nerve supply is variable and w ith overlap ◦ Greater auricular n (from cervical plexus C2, 3) supplies cranial surface of auricle and lower part of lateral surface
◦ Auriculotem poral (from m andibular division of V n) supplies upper par t of lateral surface and m ost of m eatal skin and t ragus
◦ Auricular branch (from vagus) supplies sm all areas of skin in cranial auricular surface, poste-rior wall of the concha and oor of m eatus and adjoin ing part of TM
◦ Lesser occipital n (from cervical plexus C2, 3) supplies sm all area of m edial aspect at top of pinna
Philpott_9783131662316_Ch01.indd 3 02/05/14 8:01 AM

4
1 Embryology and Anatomy of the Ear
m astoid ant rum ; the lower aspect of the additus corresponds to line going between pars tensa and accida, and on to eustachian tube
• Medial wall of additus corresponds to the lateral Scc prom inence w ith fallopian canal housing VII n below
• Lower part of poster ior wall is bony w ith the pyram id; fossa incudis (w here ligam ent from short process incus at taches to but t ress) above and sinus t ym pani below
• Fossa incudis is sm all depression in lower/post part epitympanic recess that houses short pro-cess incus
• Lateral to the pyram id is the facial recess: col-lect ion of air cells im m ediately lateral to VII n at 2nd genu; relat ionships are: ◦ Medial: facial n ◦ Superior: fossa incudis/pont iculus ◦ Inferior: subiculum / then round w indow below th is
◦ Lateral: chorda t ym pani ◦ Anterior (and lateral): TM
• Opening in to facial recess from m astoid cavity = posterior tympanotomy; allows addit ional aerat ion route for m astoid vent ilat ion, bet ter visualizat ion of horizontal part VII n , round w indow (i.e., for cochlear implant insert ion), ac-cess to otherw ise hidden cholesteatom a, lent icu-lar process of incus going to ISJ, stapedial tendon
• Sinus t ym pani: m edial (deep) to VII n• Processus cochleariform is: bony process anter ior
to oval w indow to w hich the tensor t ym pani at taches via a pulley; rarely dest royed by disease
◦ VII n m ay supply a sm all region in root of concha• External auditory canal ~2.5 cm ; hair and ce-
rum inous glands (m odi ed apocrine glands) in outer 1/3
• TM 3-layered: outer squam ous, m iddle lam ina propria ( brous), inner m ucosal; pars accida has less m arked brous layer w ith m ore ran-dom ly arranged bres
1.2 Middle Ear1.2.1 Embryology (Fig. 1.1)• Tym panic cavity endoderm al in origin from 1st
pharyngeal pouch; pouch grows laterally, so lateral par t form s m iddle ear (ME) and m edial sect ion form s eustachian tube
• Malleus and incus from Meckel cart ilage of 1st pharyngeal arch (dorsal end); stapes (suprast ruc-ture) from 2nd (Reichert cart ilage); from 4/40; rem ain em bedded in m esenchym e t ill 8/12, w hen dissolves save for support ing ligam ents
• Tensor t ym pani (to m alleus) supplied by m an-dibular branch V n; stapedius by VII n
• Tym panic ant rum form ed by bir th ; subsequent pneum at izat ion of m astoid after bir th
1.2.2 Anatomy• Epitym panum (at t ic; above level of m alleolar
folds); m esotym panum ; hypotym panum (below level of inferior part of t ympanic sulcus)
• The poster ior wall of ME has open upper part—the additus, going from epit ym panum to
Fig. 1.1a, b Developmental stages of the external auditory canal, middle ear, and labyrinth.a Approx. 8th week. 1, Otic vesicle; 2, primary auditory
canal; 3, tubotympanic recess; 4, mesenchymal con-densation; 5, acousticofacial ganglion.
b Approx. 7th month. 2, Primary auditory canal; 6, primordium of the auditory ossicles; 7, t ympanic cavity; 8, primordium for the labyrinth.
ba
1
42
35
2 6
8
7
Philpott_9783131662316_Ch01.indd 4 02/05/14 8:01 AM

5
Inner Ear
and cochlear duct (vent ral) and ut ricle, Sccs and endolym phat ic duct: i.e., the m em branous labyrin th
• As vesicle form s, som e cells break o to form statoacoust ic ganglion (also gets cells from neural crest) that supplies sensory cells to cochlear and vest ibular par ts
• By 8/40 cochlear duct has grow n and com pleted 2.5 turns; connect ion to saccule rem ains as ductus reuniens
• Mesenchym e around cochlear duct form s cart ilage; by 10/40 vacuolizes in to scala vest ibuli and t ym pani
• Epithelial cells of cochlear duct develop in to two ridges on the basilar m em brane; inner r idge form s spiral lim bus w ith at tached tectorial m em brane; outer form s hair cells (all together = organ of Cort i) by ~25/40
• By 6/40 Sccs are at tened outpockets of ut ricular part of ot ic vesicle, at r ight angles to each other; central parts disappear to give canals, and one end of each dilates to ampulla
• Cells of am pulla form crest (crista am pullar is) of sensory cells; sim ilar in saccule and ut r icle
1.3.2 Anatomy (Figs. 1.2, 1.3, and 1.4)• Inner ear or labyrin th has bony and m em bra-
nous com ponents
• Macewen t r iangle: tem poral line (cont inu-ous w ith superior aspect of zygom at ic arch); perpendicular drop from th is dow n through m astoid t ip; diagonal through spine of Henle; t r iangle corresponds to cribriform area of tem -poral bone (through w hich infect ion can spread from antrum to subperiosteum ); deep relat ion-ship corresponds to m astoid ant rum
• Trautm ann t r iangle: tegm en (superior base); sigm oid sinus (posterior); bony labyrin th (anterior); th is t r iangular area is broadly w here posterior fossa dura is found
• Donaldson line passes along the lateral Scc to divide Trautm ann t r iangle; below the line, in the t r iangle, is the endolymphat ic sac
• Prussak space is an area behind the pars accida, lateral to the neck of m alleus and lateral m al-leolar fold; site of at t ic ret ract ions
• Cog divides at t ic from anterior epitym panum ; com es dow n from tegm en (disease can h ide behind it )
1.3 Inner Ear1.3.1 Embryology (Fig. 1.1)• 3/40 ot ic placode form s a th ickening on the
surface ectoderm• Invaginates to form ot ic vesicles or otocyst (via
ot ic pit ) by 4/40, that divides later in to saccule
Fig. 1.2a, ba The inner ear. 1, Oval window with stapes; 2, saccule;
3, utricle; 4, ampulla of the semicircular canals, with cupula; 5, membranous semicircular canals (hori-zontal, superior, and posterior); 6, ductus reuniens; 7, cochlear duct; 8, helicotrema; 9, the perilymphatic duct, which passes through the cochlear aqueduct;
10, round window; 11, endolymphatic sac on the posterior surface of the pyramid.
b The vestibular apparatus. 1, Lateral semicircular canal; 2, vertical semicircular canal; 3, posterior semicircular canal; 4, utricle; 5, saccule; 6, endolymphatic duct; 7, endolymphatic sac; 8, ductus reuniens; 9, cochlea. Arrows mark the direction of movement.
11
7
2 3 4
4
5
9
10
1
8
6
1
3
4
5
6
8
7
9
2
a b
Philpott_9783131662316_Ch01.indd 5 02/05/14 8:01 AM

6
1 Embryology and Anatomy of the Ear
• Each canal has a dilated anter ior end—am pulla, w ith in w hich are the neuroepithelial cr ista cells; hairs from these em bed in the overlying gelat i-nous cupula; angular accelerat ion (or conven-t ion currents from hot and cold st im uli) m oves endolym ph and displaces the cupula, leading to sensat ion of m ovem ent
• The anterior ends of Sccs, com m on crus and posterior end of lateral Scc, all open in to ut r icle; th is and the saccule lie w ith in bony vest ibule; both contain neuroepithelial m acula cells (like the ampullary crista) that have a surface of stereocilia (and a kinocilium ); the overlying otoconial m em brane contains par t icles of calcium carbonate called otoconia
• Macula st im ulated by gravitat ional pull and linear accelerat ion; has cent ral st r iola that m arks point at w hich polarit y of cells changes
• Endolym phat ic duct from sac joins in to ut ricle/saccule (duct passes through, and e ect ively plugs, the vest ibular aqueduct from posterior cranial fossa; perilym ph can escape only if abnorm ally w idened); sac lies outside the dura
• Saccule detects ver t ical accelerat ion , ut r icle horizontal
• Superior vest ibular nerve supplies superior Scc, lateral Scc, and ut ricle
• Bony “ot ic” capsule w ith in pet rous tem poral bone; cochlea, vest ibule, ×3 Sccs; hollow and contain perilymph
• Perilym ph: sim ilar to extracellular uid, low K+ h igh Na+; possible ult ra lt rate of CSF or blood; com m unicates w ith subarachnoid space via cochlear aqueduct
• Suspended w ith in perilym ph is m em branous labyrin th, a ser ies of sacs and tubes contain ing endolymph
• Endolym ph: sim ilar to in t racellular uid, h igh K+ low Na+; produced by st r ia vascular is from perilymph, absorbed by endolym phat ic sac; m aintained by st r ia vascularis
• 3 m em branous Sccs (lateral, an terior, posterior), set at r ight angles to each other, each represent-ing a plane in space; anterior and poster ior canals unite to form a com m on crus
Fig. 1.3a, b Axial cross section through the cochlea (a) and cochlear canal (b). Central modiolus (1); spiral ganglion of the cochlear nerve (2); its nerve bres (3) join to form the cochlear nerve (4). Spiral plate (5) runs from the base to the apex (7). Cochlear duct (scala media) (8) lies between scala vestibuli (9) above and scala tympani (10) below, both of which contain perilymph (6). Reissner membrane (11) separates the scala vestibuli and the cochlear duct. Tectorial membrane (12) covers the sensory cells of the organ of Corti. Stria vascularis (14) forms the lateral wall of the cochlear duct. Laterally, it borders on the spiral ligament of the cochlea (13).
a
b
1
2
3
9
10
8
7
5
6
9
10
8
2
5
3
11 12
13
14
4
Fig. 1.4a, b The cochlear duct (a) and spiral organ of Corti (b). The organ of Corti (b) rests on the basilar membrane (1, 2) in the cochlear duct. Limbus of the spiral lamina (4), internal spiral sulcus (5), stria vascularis (3). Inner hair cells (6) and outer hair cells (7) supported by pillar cells (8, 9), perilymph (11, 14), external phalangeal cells of Deiters (10), outer tunnel (12), external spiral sulcus (15), tectorial membrane (13), a gelatinous mass extending from the limbus of the spiral lamina (4).
b
a
45
6
8 9
21
14
11 12
10
7
13
3
15
Philpott_9783131662316_Ch01.indd 6 02/05/14 8:01 AM

7
Skull Foramina
• Infer ior vest ibular nerve supplies posterior Scc and saccule
• Am pullary, ut ricular, and saccular nerves unite to form vest ibular nerve
• Mem branous cochlear duct: 2½ turns• Cochlear duct has SV on superior aspect , ST on
inferior side, both of w hich contain perilym ph (as are spaces between ot ic capsule and m em -branous part)
• At basal turn of cochlea SV opens at oval w in-dow, ST at round w indow ; at apex of cochlea SV and ST are cont inuous w ith each other around end of cochlear duct (at the helicot rem a); ST connects w ith subarachnoid space in posterior cranial fossa (via cochlear aqueduct or perilym -phat ic duct)
• Cochlear duct t r iangular in sect ion; three sides: Reissener m em brane, basilar m em brane, st r ia vascularis
• Neuroepithelium arranged along basilar m em -brane: organ of Cort i, w hich contains the hair cells
• High-frequency sounds st im ulate at base of cochlea, low -frequency at apex; cilia of basal hair cells are short and num erous, w hereas at the apex they are long and m ore sparse
• Nerve bres pass cent rally via cochlear nerve; spiral ganglion of cochlear nerve in m odiolus in centre of cochlea
• Neural pathway: cochlear n → cochlear nuclei → superior olivary com plex → lateral lem -niscus → inferior colliculi → m edial geniculate bodies → auditory cortex
• Blood supply to labyrin th : anterior inferior cerebellar ar tery (AICA)
1.4 Internal Auditory Canal and Cerebellopontine Angle1.4.1 Anatomy• In ternal auditory canal relat ionships:
◦ Anterior: pet rous apex, cochlea ◦ Posterior: com m on crus, vest ibular aqueduct
◦ Inferior: cochlear aqueduct , jugular foram en, jugular bulb
◦ Lateral (to fundus): cochlea, vest ibule, ME ◦ Medial: opens in to cerebellopont ine angle (CPA)
• CPA relat ionships: ◦ Posterior: cerebellum , occulus ◦ Medial: pons, m edulla ◦ Anterolateral: pet rous temporal bone ◦ Superior: tentorium ◦ Inferior: basal cisterns, foram en m agnum
1.5 Skull Foramina• Opt ic canal: opt ic n , ophthalm ic a• Superior orbital ssure: lacr im al n , frontal v,
t rochlear n , superior ophthalm ic v, nasociliary n , inferior ophthalm ic v, abducent n , oculom otor n , ophthalm ic n (Vi n); [lazy French tar ts sit naked in ant icipat ion of orgasm ]
• Infer ior orbital ssure: m axillary n (VII n)• Foram en rotundum : m axillary n (VII n)• Foram en ovale: m andibular n (VIII n)• Foram en spinosum : m iddle m eningeal vessels• Carot id canal: in ternal carot id a, sym pathet ic
plexus• Foram en lacerum : carot id a passes over brous
plug• Jugular foram en: pars nervosa is anterom edial,
contain ing infer ior pet rosal sinus glossopha-ryngeal n ; pars vascularis is posterolateral, contain ing vagus, accessory (cranial part) n’s, IJV (em erging below as cont inuat ion of sigm oid sinus)
• In ternal acoust ic m eatus: facial, vest ibuloco-chlear nerves (VII n anterosuperior, cochlear anteroinferior, superior vest ibular posterosupe-rior, inferior vest ibular posteroinferior), labyrin-th ine a
• Hypoglossal canal: hypoglossal n• Stylom astoid foram en: facial n• Foram en m agnum : m edulla oblongata and m e-
ninges; ver tebral, anterior, and posterior spinal a; accessory n (spinal parts)
Philpott_9783131662316_Ch01.indd 7 02/05/14 8:01 AM

8
2 Physiology of the Ear
2.1 External Ear• The tym panic m em brane (TM) outer layer is
kerat in izing squam ous epithelium• Super cial cells are shed and cleared from
the cent re of the TM by an “escalator” e ect; ret ract ion pockets m ay a ect th is process leading to kerat in accum ulat ion and potent ial cholesteatom a form at ion
2.2 Middle Ear• The m iddle ear (ME) is a sound–pressure
t ransform er• The resistance to the passage of sound through
a m edium is it s acoust ic im pedance—if sm all, m ost sound is t ransm it ted; from m iddle to inner ear, sound passes from air to uid, result ing in im pedance m ism atch
• The acoust ic role of the TM is to t ransform sound pressure over it s outer surface to m alleus vibrat ion (the um bo m oves m ost)
• The lever e ects of the ossicles (m echanical advantage of incudom alleolar join t is 1:1.3) and the area rat io of TM to stapes footplate (1:17) allows for sound–pressure t ransform at ion (and ~25 dB gain of energy to cochlea)
• The total pressure on the stapes footplate is therefore enhanced by a factor of 22 (17 × 1.3)
• Sound is t ransm it ted from ear canal to cochlea via t ym pano-ossicular system and direct acoust ic st im ulat ion of oval and round w indows (acoust ic coupling)
• The ME loses gases to the t issues constant ly; th is is com pensated for by in ux from the nasopharynx via the eustachian tube; w hen gas input < output , negat ive ME pressure is created, w hich is a factor in TM ret ract ion
2.3 Inner Ear2.3.1 Cochlear Mechanism (Figs. 2.1 and 2.2)• Vibrat ion at oval w indow results in wave that
t ravels up basilar m em brane, increases to a m axim um am plitude, then dies away; point of m axim um am plitude depends on frequency
in t roduced (h igh frequency = apical, low frequency = basal)
• Each hair cell has an opt im al frequency that it responds to, but responds to other frequencies to lesser extent
• Hum ans can discr im inate between sounds di ering by 0.75 Hz frequency, and we can hear over the range 20 to 20,000 Hz
• Vibrat ion of basilar m em brane boosted by act ive m echanical am pli er m echanism ; as basilar m em brane m oves, get shearing forces between it and overlying tectorial m em brane, result ing in de ect ion of stereocilia of hair cells
• Ion channels open in cell m em brane, and neurotransm it ter is released at base of cell
• Most a erent auditory nerve bres are st im ulated in th is way by inner hair cells (95% a erents); they convert the m echanical energy to bioelect r ical energy
• De ect ion of hair cell cilia towards the cells’ longest cilia leads to depolarizat ion , w hereas de ect ion away leads to hyperpolarizat ion
• Outer hair cells (OHCs) have role in act ive m echanical am pli er m echanism ; they m ay am plify the e ect of the sound st im ulus and increase the sensit ivit y and frequency select ivit y of the cochlear output (in presbyacusis, lose OHCs and therefore lack of am pli cat ion so thresholds rise and discrim inat ion falls)
2.3.2 Vestibular Mechanism (Fig. 2.3)• Utricle has receptor cells orientated horizontally,
saccule vert ically• The m aculae of the saccule and ut r icle have hair
cells w ith stereocilia em bedded in overlying brogelat inous m ass (otoconial m em brane); on it s surface are otoconia (calcium carbonate) that m ake it denser than the endolym ph
• Linear accelerat ion (and gravity) m oves the otolith ic m em brane relat ive to the hair cells, bends stereocilia, thus st im ulat ing the sensory cell by alterat ion of the rest ing potent ial
• If accelerated, the inert ia of the otoconia causes them to lag behind the m aculae (w hich m ove w ith skull), hence stereocilia de ected; w hen
Philpott_9783131662316_Ch02.indd 8 02/05/14 8:20 AM

9
Inner Ear
accelerat ion is over, elast ic recoil restores steady state
• Likew ise the crista/cupula of the Scc am pulla relies on the sam e type of m echanism ; the cupula is of sam e density as endolym ph
• Angular m ovem ent m oves endolym ph and cupula, bends stereocilia, and st im ulates hair cells; a m ovem ent m oves the crista (as at tached to head) w hile the endolym ph in it ially rem ains
stat ic due to inert ia; therefore there is relat ive m ovem ent between the two
• Neural bres of each canal re at a basal rate• In the lateral Scc, displacem ent of stereocilia
towards vest ibule (ampullopetal) increases r ing rate, displacem ent away (am pullofugal) decreases rate
• Opposite situation for posterior and superior Sccs• Each hair cell has a kinocilium that gives the cell
it s polar it y; m ovem ent of stereocilia towards kinocilium increases r ing rate and vice versa
• For exam ple, in R lateral Scc: if accelerate head to L, endolym ph ows to R due to iner t ia, therefore displacem ent of cilia is away from the ut ricle (ampullofugal) and r ing rate reduces; if then decelerate to L, opposite w ill occur
• Vest ibulo-ocular, vest ibulospinal, and cerebellovest ibular re exes link the system s and allow vest ibular system to help m aintain posture and m uscle tone and eye stability w hen m oving
• Vest ibulo-ocular re ex speci cally stabilizes the ret inal im age, allow ing visual cont rol of the environm ent during m ovem ent of the head; it is responsible for the fast com ponent of vest ibular nystagm us
Fig. 2.3 Oscillation of the cupula. When the head is rotated (arrow), the semicircular canals rotate as well. Owing to its viscosity, the endolymph initially remains motionless and directs the cupula in the opposite direction. This causes the cilia to bend. 1, Labyrinth; 2, membranous canal; 3, cupula; 4, vestibular nerve.
3
2
4
1
Fig. 2.1 Three-dimensional representation of the vibration of the basilar membrane. The travelling wave runs from the stapes along the basilar membrane, the tectorial membrane, and the Reissner membrane to the apex of the cochlea. 1, Stapes in the oval window; 2, round window; 3, scala vestibuli; 4, scala tympani, 5, basilar membrane with spiral organ of Corti; 6, maximum amplitude of the travelling wave.
3
46
5
2
1
Fig. 2.2 Depolarization (excitation) of the sensory hair cells by de ection of the cilia (2) and opening of stretch-sensitive K+ channels. Stretching of the channels is induced by tension to the tip links (1). K+ ions escape the hair cell at the base through stretch-sensitive channels, leading to repolarization of the cells.
K+K+
K+K+
K+
K+
Excitation Inhibition
2
1
Philpott_9783131662316_Ch02.indd 9 02/05/14 8:20 AM

10
3.1 In ammatory Disorders of the Auricle• Cellulit is of auricle: regional neck nodes m ay
be in am ed; usually gram +ve cocci (not Pseudom onas)
• Allergic derm at it is: no h istory of t raum a, peau d’orange/shiny appearances m ay occur; c/o itching; sensit izat ion m ay occur w ith repeated exposure
• Auricular erysipelas: super cial cellulit is caused by group A Streptococcus; often preceded by t raum a; m ay lead to system ic toxicit y, contagious
• Infect ious (peri)chondrit is (Fig. 3.1): Pseudom onas, Staphylococcus aureus, and Streptococcus; aggressive Rx required; clin ically sparing of lobule
• Relapsing polychondrit is: recurring in am m ation of cart ilage throughout body (e.g., nose, larynx); autoim m une response to t ype II collagen; 85 to 90% of these pat ients get auricular car t ilage involvem ent; recurrent episodes m ay cause “cauli ower” ear; system ic cor t icosteroids for acute episodes
• Eczem a, psoriasis
3.2 In ammatory Disorders of the External Auditory Meatus• Furuncle: sm all abscess in a hair follicle; if ready
to rupture, gently open w ith t ip of ster ile needle• Acute ot it is externa:
◦ Pseudom onas infect ion m ost com m on; also S. aureus, Candida, Aspergillus
◦ Risk factors: prolonged water exposure, repeated t raum a (e.g., cot ton buds), eczem a/psoriasis, m iddle ear discharge
◦ Painful (especially on t ragal m ovem ent): narcot ic painkillers m ay be required
◦ Rx: aural toilet , Pope w ick and ant ibiot ic/steroid drops, water exclusion
◦ May spread to cause facial cellulit is, requiring system ic ant ibiot ics
◦ Otom ycosis: fungal infect ion often follows prolonged t reatm ent w ith topical an t ibiot ics
• Malignant (necrot izing) ot it is externa: ◦ Otit is externa becom ing an invasive infect ion , leading to osteomyelit is (t ym panic plate to skull base)
◦ Pseudom onas aeruginosa usual infect ing organism
◦ Diabet ic pat ients and im m unocom prom ised m ost a ected, often elderly
◦ Unresolving infect ion w ith deep otalgia and granulat ions noted at car t ilage/bone junct ion of external ear canal—here the clefts of Santorin i provide the pathway for the spread of infect ion
◦ Cranial nerve (CN) palsies (7–12) and death (in t racranial infect ion) can occur in severe cases
◦ Rx: r igorous diabet ic control, long-term in t ravenous (IV) ant ibiot ic, topical cipro oxacin drops; possible role for hyperbaric oxygen
• Chronic ot it is externa: chronic itching w ith skin often shiny, scaling and devoid of wax; cultures can be non-speci c or m isleading; t reat secondary infect ion and use topical steroids
• Post-in am m atory stenosis of EAM (external auditory m eatus) subepithelial brosis w ith progressive narrow ing of EAM; early m anagem ent includes local steroids; once scar is m ature, consider t issue excision and split-th ickness graft ing but r isk of recurrence
3.3 In ammatory Disorders of the Tympanic Membrane• Myringit is bullosa hem orrhagica:
◦ Painful infect ion of t ym panic m em brane (TM), uncertain causat ive organism
◦ Mostly in autum n, benign and self-lim it ing ◦ Blisters of varying size on TM/EAM— lled w ith serous/hem orrhagic uid
◦ Analgesia (± ant ibiot ic/steroid drops)• Granular myringit is:
◦ Separate or con uent granulat ions on surface of TM
◦ Topical drops and super cial curet tage ◦ Som e progress to in am m atory obliterat ion of deep EAM
3 External Ear Disease
Philpott_9783131662316_Ch03.indd 10 02/05/14 8:34 AM

11
Non-in ammatory Lesions of the External Ear
3.4 Non-in ammatory Lesions of the External EarChondroderm at it is nodularis chronica helicis (Winkler nodule)• Benign, usually on r im of helix/ant ihelix• Red, raised, and tender nodule w ith central
depression/crater• Tenderness a ects sleeping posit ion• Full-th ickness excision; topical steroids m ay
help w hile wait ing for surgery
3.4.1 Other Pinna Lesions• Gout y tophi: yellow /pink nodules on helix;
control of gout required• Keratoacanthom a: benign tum our of hair
follicles m ost com m on anterior to t ragus; rapidly grow ing and painless—biopsy to dist inguish from neoplast ic lesions
• Hypert rophic scars rem ain con ned to site of injury
• Keloid scars invade adjacent norm al t issue, com m only lobule from earr ings; topical inject ion of steroids (± excision)
3.4.2 Carcinoma of the Auricle• Risk factors:
◦ Older m en, light-haired, fair-skinned individuals
◦ End stage of act in ic-induced epiderm al dysplasia
• Basal cell carcinom a: ◦ Gradual pushing deep invasive m argin ◦ Local excision
• Squam ous cell carcinom a (SCC): ◦ Aet iology sun exposure, arsenic, radiat ion , previous scarr ing
◦ Usually progress from solar keratosis through dysplasia and carcinom a in situ
◦ Protuberant areas like helix m ost a ected ◦ Local excision w ith aps for early lesions, ± radiotherapy
3.4.3 Wax• Produced from cerum inous glands in outer 1/3
of ear canal• Usually natural clearance aided by epithelial
m igrat ion
• “Wet wax” is determ ined by a dom inant gene (seen com m only in Europeans and Africans); dry t ype is recessive (seen com m only in people of eastern Asian descent)
3.4.4 Keratosis Obturans• Kerat in form at ion disorder involving deep
external auditory canal (EAC)• Pat ients present w ith kerat in plug, pressure
from w hich m ay cause bony rem odelling over t im e and canal w idening
• c/o pain and conduct ive hearing loss• Periodic debridem ent required
3.4.5 Canal Cholesteatoma• Cholesteatom a can form secondary to t raum a to
EAC skin• Focal osteit is w ith granulat ion t issue and a
secondary hyperkeratot ic skin react ion in adjacent canal
• Obst ruct ion , pain , and otorrhea• Debridem ent of accum ulated kerat in and
in am ed/devitalized bone; topical ant ibiot ics bene cial
Fig. 3.1 Perichondrit is of the auricle.
Philpott_9783131662316_Ch03.indd 11 02/05/14 8:34 AM

12
3 External Ear Disease
3.4.6 Exostosis• Hyperostosis of t ym panic r ing, usually m ult iple,
broad-based, and bilateral• St rat i ed lam ellar grow th; periost it is• Com plete obliterat ion m ay occur• Direct relat ionship to cold water exposure
3.4.7 Osteomas• True neoplasm s, solitary, often unilateral,
benign• Arise spontaneously; som et im es pedunculated;
no lam ellar grow th• Cancellous bone w ith brovascular channels• Rem ove if obst ruct ive
3.4.8 Soft Tissue Tumours of the EAM• EAM polyps are rare• Pyogenic granulom a after m inor t raum a• Kerat in im plantat ion granulom as• Cerum inom as; adenoid cyst ic carcinom a m ost
com m on type, but adenocarcinom a m ore aggressive
• Squam ous carcinom as m ost com m on m alignancy of ear canal; usually present as a change in sym ptom s in a chronically infected ear; bleeding, pain , and VII n palsy are aler t ing signs to SCC; lateral tem poral bone resect ion required—5-yr survival rate <25%
Philpott_9783131662316_Ch03.indd 12 02/05/14 8:34 AM

13
4.1 Acute, Chronic, and Secretory Acute Otitis Media (AOM)• Com m only children in between 3 to 7 years of
age• Viral (rh inovirus, RSV, adenovirus)—m ost
resolve w ith in 24 hours; or bacterial (Streptococcus pneum oniae, Haem ophilus in uenzae, Moraxella catarrhalis)
• C/o: fever, rubbing ear, pain , hearing loss (HL); sym ptom s m ay improve w hen tympanic m em brane (TM) ruptures/discharge
• Predisposing factors include: age (<7 years), non-breastfeeding, day care at tendance, race, anatomy (e.g., cleft palate), im m unode ciency
• Rx: analgesia; consider ant ibiot ics if failure to resolve after 24 to 48 hours or im m ediately if age <2 years or system ically unwell
4.1.1 Recurrent AOM• Consider if 3 episodes in 6 m onths or ≥4 in a year• Treatm ent opt ions include watchful wait , long-
term low -dose ant ibiot ics (e.g., t r im ethoprim ) or grom m et insert ion
4.2 Chronic Otitis Media4.2.1 Various classi cations; consider:• Healed chronic ot it is m edia (COM): healed
perforat ion , t ympanosclerosis• Inact ive m ucosal COM: dry TM perforat ion , non-
in am ed m iddle ear (ME) m ucosa• Inact ive squam ous COM: TM ret ract ion , not
retain ing debris or infected• Act ive m ucosal COM: TM perforat ion w ith
m ucopus, in am ed ME m ucosa• Act ive squam ous COM: cholesteatom a
4.2.2 Tympanosclerosis• Term ed myringosclerosis w hen con ned to TM• May arise from abnorm al healing in response
to in am m atory episodes or t raum a (e.g., post-myringotomy)
• See changes to lam ina propria connect ive t issue com ponent of TM and ME m ucosa
• In am m ation dam ages collagen bres, broblasts invade in reparat ive phase causing excess collagen synthesis and hyalin izat ion; bres fuse as indist inct m ass
• Usually asym ptom at ic; large plaques in TM m ay cause conduct ive HL; m ay cause ossicular xat ion in ME
4.2.3 TM Perforations• Surgery indicated to prevent discharge/
waterproo ng; w hile repair m ay improve hearing (closure of air–bone gap) it also risks m aking hearing worse
• HL w ith perforat ion related to: ◦ Size ◦ Loss of ba ing e ect on round w indow ◦ Reduced rat io of TM: footplate to overcom e air: uid impedance m ism atch
◦ Associated ossicular chain dam age, e.g., if over incudostapedial join t
◦ Posit ion (um bo involvem ent = worse hearing)• Success of surgery m ay relate to surgeon,
eustachian tube (ET) funct ion , sm oking, discharging at t im e of surgery
• Traum at ic perforat ions: water exclusion, m ost heal by 6 weeks
4.2.4 TM Retractions• Classi cat ion at t ic ret ract ions (pars
accida)—Tos ◦ I: d im ple ◦ II: onto m alleus neck ◦ III: bony erosion (of scutum ) ◦ IV: kerat in accum ulat ion/cholesteatom a
• Sadé’s Classi cat ion of pars tensa ret ract ions ◦ I: annular ret ract ion ◦ II: onto long process of incus ◦ III: onto stapes/prom ontory ◦ IV: adhesive to m edial wall
• Rx: m ost asym ptom at ic and do not lead to cholesteatom a; watchful wait often best; consider vent ilat ion tube insert ion , t reatm ent of sinonasal disease to im prove ET funct ion,
4 Otitis Media
Philpott_9783131662316_Ch04.indd 13 02/05/14 8:36 AM

14
4 Otit is Media
excision of pocket w ith graft ing (e.g., car t ilage) and cor t ical m astoidectomy to increase air reservoir; lit t le good evidence to support in tervent ion
4.2.5 Cholesteatoma (Figs. 4.1 and 4.2)• A 3D epiderm al st ructure exhibit ing
independent grow th, replacing ME m ucosa, resorbing underlying bone, and tending to recur after rem oval—bad skin in the ME cleft
• Epithelial sac lls w ith desquam ated kerat in that becom es infected (e.g., Pseudom onas) and purulent; sac surrounded by granulat ion t issue
• Classi cat ion: congenital or acquired• Congenital cholesteatom a: seen in children ,
em erging from behind in tact TM. Uncertain aet iology but m ay be related to em bryonic ectoderm al rests or a m etaplast ic process
• Acquired (prim ary and secondary): ◦ Prim ary: ET dysfunct ion causing ret ract ion pocket , w hich subsequently develops disordered epithelial m igrat ion and retains kerat in
◦ Secondary (four theories): - Im plantat ion: after surgery or t raum a - Metaplasia: to kerat in izing squam ous epithelium follow ing chronic infect ion
- Papillary ingrow th: of squam ous epithelium through intact pars accida follow ing infection
- Migrat ion: of squam ous epithelium inwards through exist ing perforat ion
4.3 Complications of Otitis Media• AOM thought to be m ore com m on cause of
com plicat ions than COM: ◦ Deafness ◦ Dizziness (labyrinth ine stula) ◦ Discharge (m ucopurulent from ME infect ion , seropurulent from cholesteatom a)
◦ Facial palsy: m ore com m on w ith AOM, especially w ith dehiscent nerve
◦ Mastoidit is and subperiosteal abscess: - Spread to digast r ic fossa: Citelli abscess - Spread inferiorly to anter ior border of sternocleidom astoid sheath : Bezold abscess
- Spread anter ior to subtem poral region: Luc abscess
◦ Acute pet rosit is (Gradenigo syndrom e: AOM, diplopia due to ipsilateral VI palsy, pain in t r igem inal dist r ibut ion)
◦ In t racerebral or ext radural abscess ◦ Meningit is: AOM is the m ost com m on cause of bacterial m eningit is
Fig. 4.1a, b Development of an at tic cholesteatoma.a Retraction and invagination of the pars accida into the epitympanum; the keratinized squamous epithelium is thus
displaced into the middle ear. 1, Invaginated pars accida; 2, at tic.b Chronic in ammation causes hyperplasia of the mucosa of the at t ic and prevents adequate aeration of the region.
3, Cholesteatoma sac; 4, hyperplastic mucosa.
4321
ba
Philpott_9783131662316_Ch04.indd 14 02/05/14 8:36 AM

15
Otit is Media with E usion
◦ Lateral (sigm oid and t ransverse) sinus throm bosis
◦ Otit ic hydrocephalus: im paired cerebrospinal u id resorpt ion secondary to superior sagit tal sinus throm bosis follow ing lateral sinus throm bosis
4.4 Otitis Media w ith E usion• Ot it is m edia w ith e usion (OME) (aka secretory
OM, glue ear) is the presence of uid w ith in the ME (w ithout infect ion and w ith an in tact TM), associated w ith chronic in am m atory changes in the ME and ET m ucosa ◦ Aetiology unclear but consider:
- ET dysfunct ion: oxygen is constant ly absorbed by ME m ucosa; if ET blocked get
negat ive ME pressure and retent ion of m ucus and possible uid t ransduct ion in to ME; a m ore sclerot ic (rather than pneum at ized) m astoid m ight help bu er th is e ect . Upper respiratory t ract infect ions m ay in it iate m ucosal oedem a in ET and a ect ciliary funct ion
- In a poorly aerated ME, the m ucosa m ay undergo m etaplast ic change such that m ore goblet cells now produce m ore secret ions
- The adenoids m ay provide a reservoir of m icro-organism s that secrete ciliotoxins such that the ME cleft no longer clears uid well; chronic in am m at ion w ith m ucosal hypert rophy m ay lead to secondary ET occlusion, negat ive ME pressure, subsequent raised ME carbon dioxide, and hence a reduced cilial funct ion
- Bio lm s m ay be involved in the pathogenesis; raising the oxygen concent rat ion in the ME (via vent ilat ion tubes) m ay help deter bio lm form at ion
- Other r isk factors include craniofacial abnorm alit ies (e.g., Dow n, cleft palate) and ciliary dysfunct ion; parental sm oking, gast ro-oesophageal re ux, allergy, day care at tendance, and bot t le-feeding m ay also be signi cant
◦ Present w ith HL and speech and language developm ental delay, clum siness
◦ Peak incidence 2.5 and 5 years; greater in w inter m onths
◦ >90% children have at least one episode before 8 years old
◦ Indicat ion for surgical in tervent ion considered w hen sym ptom at ic on two occasions, three m onths apar t , w ith conduct ive loss (25–30 dB or worse in bet ter ear) indicated by audiological tests and at t ym panom etry t race; w ith in these three m onths ~50% children w ill resolve spontaneously
◦ Adjuvant adenoidectom y (in children) doubles the bene t from vent ilat ion tube insert ion by extending bet ter hearing through the second year after insert ion , and reduces eligibilit y for revision surgery (TARGET)
Fig. 4.2 Pathways of cholesteatoma extension: from the epitympanum into the at tic (1); posteriorly, towards the mastoid and the sigmoid sinus (2) and the posterior (3) and middle cranial fossa (4); or medially, towards the internal meatus (5); and anteriorly towards the labyrinth (6) or the facial canal (7).
3
21
4 5
6
7
Philpott_9783131662316_Ch04.indd 15 02/05/14 8:36 AM

16
5.1 General Considerations for Ear Surgery• Consider the hearing in the other ear, co-
m orbidit y, and pat ient’s w ishes; great caut ion in operat ing on the bet ter-hearing ear
• When considering the risks of ear surgery, weigh up against the r isks of leaving the condit ion untreated; e.g., lifet im e r isk of developing an otogenic in t racranial abscess ~1:200 but poor evidence that surgery lessens th is r isk
5.2 Cholesteatoma Surgery• Modi ed radical m astoidectom y (MRM) or canal
wall dow n m astoidectom y: ◦ Preserves rem nants of t ympanic m em brane (TM) and ossicular chain , keeping eustachian tube ori ce covered (as dist inct from radical procedure)
◦ Leaves open m astoid cavity ◦ Cavity problem s m inim ized by creat ing well-saucerized sm all cavity, covering m iddle ear (ME) m ucosa w ith TM rem nant , keeping facial r idge low, and creat ing adequate m eatoplasty for vent ilat ion and access
◦ Often necessitates long-term aural toilet and water exclusion; m ay be m ore di cult to create well- t t ing hearing aid (HA) m old or reconst ruct hearing by ossiculoplasty
• Com bined approach tym panoplasty or canal wall up m astoidectomy: ◦ Preservat ion of ear canal wall w ith poster ior t ym panotomy to allow for access to facial recess
◦ Requires second-look surgery to exclude residual disease (found in up to 20% of cases), so need to be m edically t for at least two general anaesthet ics and have reliable follow -up
◦ Use of potassium t itanyl phosphate laser can help reduce residual disease rate and allow for ossicular chain preservat ion to preserve hearing
◦ Di usion-weighted m agnet ic resonance im aging techniques m ay allow for detect ion of
residual disease and so prevent unnecessary second-look procedures
◦ In the long term , no need for con t inued au ral toilet or w ater exclusion ; m ay allow for bet ter ossicu lop last y resu lt s and easier HA t t ing
• At t icoant rostomy or front-to-back surgery: ◦ For m ore lim ited at t ic disease can allow for disease rem oval w ith a sm all cavity
◦ Can be extended to an MRM• Revision m astoidectom y:
◦ A problem cavity m ay be im proved by lowering facial r idge, obliterat ing cavity, closing TM perforat ion , or creat ing larger m eatus
◦ If no hearing, consider subtotal pet rosectom y and blind sac closure
• Com plicat ions: ◦ Much the sam e as for untreated disease: deafness, dizziness, facial palsy
◦ Taste disturbance, sigm oid sinus bleed, sem icircular canal stu la
5.3 Tympanoplasty• Operat ion to eradicate disease in the ME w ith or
w ithout TM reconst ruct ion• Myringoplasty: operat ion to repair TM w ithout
rem oval of disease from the ME ◦ In children , generally consider after ~8 years of age, once grow n out of childhood ear condit ions
• Modi ed Wullstein classi cat ion (Fig. 5.1): ◦ Type 1: reconst ruct ion TM w ith in tact and m obile ossicular chain (myringoplasty)
◦ Type 2: absent m alleus handle; TM reconst ructed over m alleus rem nant and long process incus
◦ Type 3: no incus/m alleus; TM reconst ructed to lie on stapes head (myringostapediopexy)
◦ Type 4: stapes footplate present; exteriorized, exposed in m astoid cavity; TM reconst ructed over round w indow to create ba e
◦ Type 5: xed footplate; fenest rate lateral Scc ◦ Type 6: sono-inversion; TM reconst ructed over oval w indow (ba e) w ith round w indow uncovered
5 Middle Ear Surgery
Philpott_9783131662316_Ch05.indd 16 02/05/14 8:46 AM

17
Ossiculoplast y
5.4 Ossiculoplasty• Operat ion to repair or reconst ruct the ossicular
chain• Ossicles form part of ME sound pressure
t ransform er designed to overcom e the im pedance m ism atching that occurs between the ME air and inner ear uid
• Ossicular discont inuity generally gives pure tone average ~55 to 70 dB
a b
c d
e
Fig. 5.1a–e Types of tympanoplasty as de ned by Wullstein. a Type I: simple myringo-
plasty. b Type II: reconstruction
of the defective ossicular chain.
c Type III: direct transmission of sound waves from the t ympanic membrane to the stapes by the columella e ect.
d Type IV: the ossicular chain is absent; sound is transmit ted directly to the oval window, and sound protection is provided for the round window.
e Type V. The oval window is completely closed by bony xation of the footplate. A window is made in the horizontal semicircular canal so that sound is transmit ted directly to this fenestration.
• Surgical outcom es: ◦ Belfast rule of thum b: for a pat ient to appreciate im proved hearing, operated ear should reach AC 30 dB or bet ter or AC w ith in 15 dB of contralateral ear
◦ Glasgow bene t plot (Fig. 5.2): m ean AC thresholds of non-operated ear plot ted (horizontal axis) against operated ear; 30 dB taken as norm al hearing. Preoperat ively m ost
Philpott_9783131662316_Ch05.indd 17 02/05/14 8:46 AM

18
5 Middle Ear Surgery
pat ients w ill fall in to areas 2, 5, or 6. Procedure should m ove them to a di erent area
◦ Pat ients w ith bilateral asym m etric hearing loss (HL) repor t greater bene t than those w ith sym m etric im pairm ent , w ho in turn repor t greater bene t than those w ith unilateral impairm ent; proviso here is those w ith bilateral hearing loss (HL), the operat ion m akes the operated ear the bet ter-hearing ear
◦ It is the m agnitude of the change in hearing that m easures bene t , rather than achieving a certain hearing level (i.e., 30 dB); it is the am ount of reduct ion of the disabilit y rather than the residual disabilit y that m at ters
◦ Reported results vary, but consider closing ABG to <20 dB in 40 to 70% par t ial ossicular replacem ent prosthesis procedures (PORPs) and 30 to 60% total (TORPs)
5.5 ME Implants (Fig. 5.3)• May be applied to incus or in to round w indow
niche
• Avoid occlusion e ects and feedback problem s of convent ional aids, and m ay be useful for pat ients unable to wear m olds (e.g., derm at it is, chronic OE)
• Both piezoelect ric and elect rom agnet ic devices exist
• Devices m ay be part ially or totally im plantable
• May help rehabilitate pat ients in the ‘grey area’ between convent ional HA usage and the need for cochlear im plantat ion
5.6 Temporal Bone Dissection Questions• You have dam aged the VII n—w hat now ?
◦ Consider cable graft if >50% division—e.g., sural or greater auricular n
◦ Call another colleague to do it• Pat ient develops VII n palsy in recovery or
im m ediate post-operat ive period: ◦ Give steroids and rem ove any packs
Fig. 5.2a, b Glasgow bene t plot. a The mean AC thresholds in the non-operated ear
( horizontal axis) are plot ted against the ear to be operated on (vertical axis). 30 dB is considered normal. Areas: 1, (bilateral normal hearing); 2 and 3 (one normal hearing ear); 4 and 6 (bilateral hearing loss, asymmetric); 5 (bilateral symmetric hearing loss). Most preoperative patients usually fall into areas 2, 5, or 6.
b Pre-/post-operative audiometric changes in plot. If surgery improves the AC thresholds the patient can change area on the plot. Patients with bilateral asym-metric preoperative impairment report greater bene t than those with bilateral symmetric impairment, who report greater bene t than those with unilateral impairment (provided those with bilateral hearing loss have an operation that makes the operated ear the bet ter-hearing ear).
100Operated ear
Non-operated ear (dB)a b
80
60
40
20
00 20 40 60 80 100
2
6
5
4
31
100Operated ear
Non-operated ear (dB)
80
60
40
20
00 20 40 60 80 100
26
6 6
5
5
5
4
4
331
Philpott_9783131662316_Ch05.indd 18 7/7/14 3:18 PM

19
Temporal Bone Dissect ion Quest ions
◦ Consider return to theat re next day or later that day—but rst allow t im e for any local anaesthet ic to wear o
• You expose a lateral Scc stula—w hat now ? ◦ Avoid using suct ion near defect
◦ Try to n ish procedure and cholesteatom a rem oval, leaving th is area to last
◦ Can carefully peel cholesteatom a sac from m em branous Scc
◦ May need to convert canal wall up procedure to canal wall dow n, thus exter iorizing any disease that cannot be rem oved
• You have breached the sigm oid sinus: ◦ Apply digital pressure ◦ Ask for haem ostat ic agent (e.g., Surgicel, Eth icon, Som erville, NJ, United States) and insert in to the hole in a dum b-bell fashion
◦ Apply bone wax over the site ◦ If large hole, uncap the bone from the sigm oid sinus ~1 cm above and below the hole and com press the sinus by packing under the exposed bony edges w ith Surgicel proxim ally and distally
◦ Consider put t ing the pat ient in a head dow n posit ion
• You have caused a dural tear: ◦ Insert som e tem poralis m uscle/fascia through the hole to plug it
◦ Tissue glue m ay aid repair ◦ Consider Silast ic sheet cut to size, inserted inside the hole in the bone, and laid over the dura
◦ Lum bar drain can be inserted for 72 h if large tear w ith considerable cerebrospinal u id leak (10–15 m L/h)
Fig. 5.3 The principle of an implantable hearing aid. An externally worn microphone and speech processor (1) transmits sound through the skin to an implanted receiver (2). A cable (3) connected to a t iny transducer (4) directly vibrates the ossicles, sending an enhanced signal to the cochlea.
1
2
3
4
Philpott_9783131662316_Ch05.indd 19 02/05/14 8:46 AM

20
6.1 De nition• An autosom al dom inant disease of incom plete
penet rance a ect ing bone derived from the ot ic capsule in w hich m ature lam ellar bone is replaced by woven bone of greater cellularit y and vascularit y
6.2 Pathology• Aet iology
◦ Genet ics: autosom al dom inant w ith incomplete penet rance
◦ Autoim m une: there m ay be an autoim m une com ponent to the aet iology (autoim m unity to t ype II collagen)
◦ Horm onal: oest rogens st im ulate osteoclast ic act ivit y; disease noted to progress w ith pregnancy/m enopause
◦ Viral: m easles infect ion in part icular m ay have a secondary role in those w ith a genet ic predisposit ion
• Con ned to hum an tem poral bone derived from ot ic capsule; the new woven bone has increased cellularit y and vascularit y alongside brous replacem ent and sclerosis; alternat ing phases of bone resorpt ion and form at ion
• During em bryonic ossi cat ion of cochlea the area anterior to oval w indow rem ains cart ilaginous before degenerat ing to simple brous t issue and form ing ssula ante fenestram , w hich becom es the m ost com m on site for otosclerot ic focus
• Vascular connect ive t issue replaced by neo-osteogenesis
6.3 Clinical Presentation6.3.1 History• M:F 1:2, m iddle-aged; posit ive fam ily h istory in
50%; e ect• Gradual onset of conduct ive hearing loss (CHL);
in t im e ~10% develop sensorineural hearing loss (SNHL)
• Act ive progression during pregnancy• Paracusis of Willis—speech perceived bet ter in a
noisy background because bet ter discrim inat ion
w hen st im ulus is raised above norm al conversat ional level
• Bilateral in ~80%• Tinnitus com m on• Vert igo can occur w ith an otosclerot ic focus in
labyrin th• May coexist w ith Ménière disease (relat ive
cont raindicat ion to stapedectomy)
6.3.2 Examination• t ym panic m em brane (TM) usually unrem arkable• Schwartze sign—vascular or “ am ingo” ush
over the prom ontory• CHL ± SNHL• Tuning forks: usually Rinne –ve (256 Hz ips
at ~15–20 dB air–bone gap (ABG), 512 Hz at ~25 dB, 1024 Hz at ~30–35 dB)
6.3.3 Audiometry• pure tone audiogram :
◦ Progressive conduct ive hearing loss (HL) ◦ When cochlea involved, SNHL added com ponent
◦ Carhart notch (Fig. 6.1) is an elevat ion of bone conduct ion (BC) threshold of ≥10 dB at one or m ore frequencies (usually centred at 3 kHz); m ay disappear after stapes surgery or show apparent overclosure of the ABG (Carhar t e ect)
• Speech audiom etry: ◦ Want opt im al discrim inat ion score >70% w hen considering surgery
• Tym panom etry—usually norm al (reduced m obilit y unreliably show n)
• Stapedial re ex (as m easured by changes in compliance): ◦ Loss of re ex m ay help dist inguish otosclerosis from superior sem icircular canal dehiscence
◦ In earlier stages of disease m ay show overcom pliance, followed by undercom pliance (“on–o ” e ect)—m ay precede ABG
• Vest ibulom etry ◦ Caloric st im ulat ion can show evidence of reduced labyrin th ine funct ion , especially after stapedectomy; indicated prior to operat ing on
6 Otosclerosis
Philpott_9783131662316_Ch06.indd 20 02/05/14 8:55 AM

21
Management
second ear if signi cant dizziness after the rst procedure
6.3.4 Radiology: CT• Otosclerosis at oval w indow m ay be seen• Post-operat ively m ay be used to ident ify
dislodged or too deeply placed prosthesis• Otospongiot ic foci in cochlear capsule m ay be
delineated• Not rout inely warranted pre-operat ively unless
congenital CHL or onset at early age• Halo around cochlea in far advanced
otosclerosis
6.4 Management6.4.1 Options• No t reatm ent is necessary• Hearing aids• Bisphosphonates:
◦ May prevent further SNHL and/or resolve vest ibular sym ptom s by inhibit ing bone resorpt ion
• Sodium uoride: ◦ For exam ple, 20 m g three t im es/day (avoid in pregnancy, renal disease)
◦ May prevent fur ther SNHL and/or resolve vest ibular sym ptom s by stabilizing otospongiot ic lesions
• Stapedotomy
6.4.2 Stapedotomy (Fig. 6.2)• Indicat ions:
◦ CHL of 30 dB or m ore, associated w ith otosclerot ic xat ion of footplate; consider if m ixed loss to allow for hearing aid usage
◦ Disabilit y associated w ith HL ◦ Tympanogram type A and stapedial re exes absent
◦ BC>air conduct ion (AC) w ith Rinne using 512-Hz tuning fork
◦ Belfast rule of thum b?• Contraindicat ions:
◦ Active ear infect ion ◦ Poor eustachian tube funct ion and/or TM perforat ion
1.25 mm1 mm
1
5
47
2 636
Fig. 6.2 The principle of stapedectomy. A piston (1) is placed in the opening in the footplate (2) and xed to the crura of the incus. Loose connective and fat tissue (3) is placed around the piston and the footplate to close o the perforation. The small distances between the stapedial footplate and the saccule (4) and utricle (5) are surgically important. 6, Otosclerotic focus on the footplate; 7, vestibule.
-10
0
10
20
30
40
50
60
70
80
90
100
110
120125 250 500 1000 2000 4000 8000
Hearing level (dB)
-20
Frequency (Hz)
Fig. 6.1 Audiogram of the right ear demonstrating a Carhart notch.
Philpott_9783131662316_Ch06.indd 21 02/05/14 8:55 AM

22
6 Otosclerosis
◦ Sense of im balance not uncom m on im m ediately post-operat ively; consider vest ibular sedat ives
◦ If ver t igo/dysequilibrium star ts 3–7 days post-operat ively consider labyrin th it is; t reat w ith cor t icosteroids
◦ Perilym phat ic leak—dysequilibrium and uctuat ing HL; “otologic em ergency,” plug w ith fat /vein graft if possible
◦ If uctuat ions in hearing follow an in it ial im m ediate closure of ABG, prosthesis m ay have displaced or be associated w ith necrosis of the long process of incus (LPI)
• Outcom es and com plicat ions: ◦ Closure of ABG to <10 dB in >90% ◦ SNHL: 5% have >15 dB loss at 4 kHz ◦ Dead ear in <1% ◦ TM perforat ion , taste disturbance, im balance ◦ Tinnitus m ay get bet ter (especially if successful hearing im provem ent), stay sam e, or get worse
◦ VII n palsy ~1:1000, m ay be delayed in onset
◦ Active otosclerosis w ith Schwartze sign ◦ Absent hearing on opposite side ◦ Ménière disease ◦ Inadequate exposure at t im e of surgery (e.g., overhanging facial nerve)
◦ Occupat ions w here balance loss unacceptable (e.g., p ilot , professional diver)
• Operat ive technique: ◦ Sm all fenest ra—“stapedotom y” ◦ Large fenest ra—port ion of footplate rem oved, “stapedectom y”
◦ Can use argon, potassium t itanyl phosphate or CO2 laser; m icro-drill; or hand t rephine
◦ Prosthesis inserted between long/lent icular process incus and fenest ra
◦ Consider bene ts of vein graft or fat packing around fenest rat ion
• Post-operat ive m anagem ent: ◦ Avoid blow ing nose and sneezing for 2 weeks ◦ Resum e norm al act ivit ies after 2 weeks (including ying)
Philpott_9783131662316_Ch06.indd 22 02/05/14 8:55 AM

23
7 Sensorineural Hearing Loss
7.1 Traumatic Sensorineural Hearing Loss• For noise-induced hearing loss (HL) and that
related to tem poral bone fractures, see Chapter 12: Ear and Tem poral Bone Traum a
7.2 Sudden Sensorineural Hearing Loss• Loss of >30 dB in three cont iguous frequencies
over 3 days• Usually unilateral and idiopathic (~60%)• Ident i able causes include:
◦ Head injury, barotraum a, blast injuries ◦ Ototoxic drugs ◦ Bacterial infect ions—suppurat ive labyrin th it is, m eningit is, syphilis
◦ Viral infect ions—m um ps, m easles, rubella, varicella zoster virus
◦ Vest ibular schwannom a ◦ Iat rogenic, after ear surgery ◦ Cardiovascular accident (CVA) ◦ Mult iple sclerosis (MS)
• Ix: pure tone audiogram , m agnet ic resonance im aging; consider FBC, erythrocyte sedim enta-t ion rate (ESR), autoim m unity screen, syphilis serology, Lym e disease
• Poor prognost ic factors: raised ESR, severe vert igo, age >60 years, degree of sensorineu-ral hearing loss (SNHL) (greater loss = worse prognosis)
• Rx: ◦ 60% of idiopathic group recover spontaneously ◦ Steroids: oral prednisolone 40 m g once daily for 1/52 (or up to 1 m g/kg per day); earlier star ted, bet ter the prognosis
◦ In t ratym panic steroids m ay be of bene t ◦ Acyclovir of dubious bene t ◦ Peripheral vasodilator, e.g., carbogen (5% CO2, 95% O2) dubious bene t
◦ Possible role for hyperbaric oxygen (problem is availabilit y)
◦ Psychological help and rehabilitat ion , hearing aid
• Som e evidence that sudden SNHL is an early warning sign of im pending st roke
7.3 Presbyacusis• The lessening of the acuteness of hearing that
characterizes old age• 40 to 50% >75-year-olds have HL that can im pair
com m unicat ion; ~80% of 80-year-olds• Cause probably m ult ifactorial; an accum ulation
of m etabolic and physiological changes associated w ith increased susceptibility to disease
• Accum ulat ive oxidat ive dam age and m itochon-drial DNA m utat ions leading to cellular dysfunc-t ion and a decrease in auditory sensit ivit y
7.4 Asymmetric Sensorineural Hearing Loss• What di erence is signi cant?
◦ Consider >15 dB at 4 kHz, for example, or for two consecut ive frequencies
• Causes ◦ 85% unknow n ◦ Vest ibular schwannom a ◦ Vest ibular syndrom es (e.g., Ménière, labyrin-th it is) m ay have associated asym m etric SNHL
◦ Congenital and childhood infect ions (e.g., m easles, m um ps, bacterial m eningit is)
◦ ~1% of noise-induced HL show asym m etry of >15 dB (for average of 0.5, 1, 2, 4 kHz)
◦ Temporal bone fracture ◦ Drugs: only one ear a ected in 60% cases of am inoglycoside ototoxicit y
7.5 Ototoxicity• Can cause SNHL, t innitus, and ver t igo.
◦ Am inoglycosides: - May be predom inantly cochleotoxic (e.g., neomycin) or vest ibulotoxic (e.g., gentam icin)
- Cause m itochondrial dysfunct ion in suscept ible pat ien ts that leads to toxic accum ulat ion of in t racellu lar ions and ult im ate cell death
- Apparent cum ulat ive e ect because 6-m onth half-life in outer hair cells
- Suscept ibilit y m aternally t ransm it ted; there appears to be a genet ic suscept ibilit y (e.g.,
Philpott_9783131662316_Ch07.indd 23 02/05/14 9:01 AM

24
7 Sensorineural Hearing Loss
• Bilateral SNHL, progressive, uctuat ing• Progression usually over weeks to m onths
(too slow for sudden SNHL, too quick for presbyacusis)
• Vest ibular sym ptom s m ay be severe and episodic
• System ic autoim m une disease in 15 to 30% (often poorer prognosis)
• Ix: ESR, autoant ibody screen (none are speci c); Western blot shows 68-kDa (heat shock?) protein—probably not speci c or helpful in diagnosis
• +ve response to steroids or im m unosuppres-sants helps con rm diagnosis (consider 1 m g/kg per day prednisolone for 1/12 then slowly reduce to a m aintenance dose)
• Cogan syndrom e: system ic autoim m une disorder preferent ially a ect ing ear and eye; sym ptom s closely follow or precede ocular in am m ation; possible cardiac abnorm alit ies
• Behçet syndrom e: autoim m une t r iad of oral and genital ulcers, ir it is or uveit is, and progressive SNHL, ± vert igo; probable vasculit is
7.7 Other Causes of Sensorineural Hearing Loss• Other causes include:
◦ General disease: diabetes, syphilis, Paget disease, hum an im m unode ciency virus
◦ Cardiovascular disease: m yocardial infarct , CVA
◦ Genet ic: connexin 26 m utat ion responsible for m ost cases of nonsyndrom ic SNHL (30–40% of all childhood genet ic deafness in w hite Western Europeans)
◦ Retrocochlear lesions (e.g., vest ibular schwannom a, m eningiom a, MS)
A1555G m utat ion seen m ore in Asians/those of Spanish descent)
- Dam age enhanced by synchronous use of loop diuret ic
- Ant ioxidants m ay have protect ive e ect , as m ay aspirin
- Renal failure and advanced age increase chance ototoxicit y
- C/o: t innitus, HL (high-frequency SNHL), vert igo
- Am inoglycosides cause dam age to the dark cells of the st r ia vascularis, therefore reducing endolym ph product ion and thus helping in the control of Ménière disease
◦ Loop diuret ics: - May produce reversible h igh-tone SNHL
◦ Cisplat in : - Cochleotoxic; can cause perm anent h igh-tone SNHL
- E ect sim ilar to am inoglycosides ◦ Salicylates:
- High-frequency t innitus preceding SNHL - Usually reversible on w ithdrawal of aspir in
◦ Quinine: - E ects sim ilar to aspir in - Potent ially huge im plicat ions in developing world as inexpensive t reatm ent for m alaria
7.6 Autoimmune Sensorineural Hearing Loss• Rare, m iddle-aged wom en• The labyrin th m ay be involved in an autoim -
m une process as par t of a system ic or non-organ-speci c disease (e.g., polyarterit is nodosa, Cogan syndrom e, relapsing polychondrit is, system ic lupus erythem atosus) or as an isolated organ-speci c autoim m unit y ( rst described by McCabe in 1979)
Philpott_9783131662316_Ch07.indd 24 02/05/14 9:01 AM
25
8 Other Hearing Disorders
8.1 Non-organic Hearing Loss• Presentat ion:
◦ Consistent display of auditory de cit w hen none exists or exaggerat ion of a real hearing loss
◦ Need high index of clin ical suspicion for diagnosis
◦ May be m ore com m on in those seeking com pensat ion claim s and adolescent girls w ith underlying psychological concerns
• Invest igat ions: ◦ Tuning forks: e.g., Stenger test ◦ Pure tone audiogram : m ay show errat ic or hesitan t perform ance; look for den ial of crossover e ect (w hen st im ulus >70 dB played to “deaf” ear it should be heard by the nontest ear)
◦ Tym panom etry: norm ally stapedial re ex 70–95 dB greater than the pure-tone thresh-old; if thresholds are w ith in 20 dB or less—NOHL likely
◦ Otoacoust ic em ission (OAE), evoked response audiom etry (especially cort ical responses): provide object ive assessm ent
◦ Speech audiom et ry: harder to “fake” ◦ Delayed auditory feedback test
• Managem ent: ◦ Main aim is recognit ion of NOHL and ascer tain ing the t rue auditory thresholds
◦ In child pat ient w ith psychological issues, norm ally disappears w ith in a few weeks or m onths, but up to 20% m ay require referral to psychiat ry
8.2 Auditory Processing Disorder• De nit ion
◦ Also know n as: select ive dysacusis, King–Kopetzky syndrom e, obscure auditory dysfunct ion
◦ An um brella term for a variet y of disorders that a ect the way the brain processes auditory inform at ion; relates to the di erence between hearing and listening
◦ NB: not = m alingering!
• Presentat ion ◦ Convincing self-repor t of auditory disabilit y accom panied by norm al pure-tone thresholds
◦ Results from impaired neural funct ion and is character ized by poor recognit ion , discrim i-nat ion , separat ion , grouping, localizat ion , or ordering of non-speech sounds; does not result from a de cit in general at tent ion , language, or other cognit ive processes; auditory process-ing disorder should not cause problem s w ith language and literacy
◦ Norm al functioning ear does not guarantee nor-m al hearing; di cult ies w ith personal, social, and professional environm ents; features are non-speci c (overlap w ith dyslexia, ADHD, etc.)
◦ Pat ients have a genuine perform ance de cit for understanding speech in noise, accom pa-nied by personalit y-related factors
◦ Incidence unknow n; F:M = 2:1; in telligent (42% have universit y degrees); “listening” jobs (teachers, telephonists, air-t ra c controllers)
• Di erent categories recognized: ◦ Developm ental: present in childhood, m ay lead to learning di cult ies and poor school perform ance, m ay be retained in to adulthood
◦ Acquired: associated w ith know n postnatal event (e.g., neurological t raum a, infect ion)
◦ Secondary: occurs in presence of (or as result of) peripheral hearing impairm ent
• Aet iology: various theories: ◦ Cochlea—very high frequency loss ◦ Psychoacoust ic ◦ Cognit ive ◦ Psychological—perceive that they do worse than they actually do in perform ance; APD pat ients are signi cant ly m ore obsessive and depressed
• Assessm ent: ◦ Mult idisciplinary and requires pat ient’s full at tent ion
• Ix: ◦ Includes baseline audiom etry, speech in noise assessm ent , OAE, auditory brainstem response (ABR); to diagnose need abnorm al results in at least two tests, one of w hich is non-speech
• Rx: ◦ Counselling, hearing therapy, m odi ed educat ional environm ent (m any classroom s
Philpott_9783131662316_Ch08.indd 25 02/05/14 9:10 AM

26
8 Other Hearing Disorders
have poor acoust ics), auditory t rain ing, com pensatory linguist ic/other st rategies
8.3 Auditory Neuropathy• De nit ion:
◦ A condit ion characterized by norm al cochlear outer hair cell (OHC) funct ion (hence norm al OAE and a present cochlear m icrophonic) but abnorm al VIII n funct ion (as assessed by ABR)
◦ Blanket term encom passing di erent situat ions/range of potent ial pathologies: - Auditory dyssynchrony: these pat ients have OAE present; prim ary problem is loss of inner hair cells (IHC) w ith survival of OHCs, so IHC output is dyssynchronized and basilar m em brane inappropriately tuned (75% cases); m ay get abnorm al ABR
- Those w ith absent ABRs: t rue auditory neuropathy w here OHC survival associated w ith dysfunct ion of VIII n and/or brainstem /central pathways
• Clin ical features: ◦ In both , elect rocochleography shows large cochlear m icrophonic; di erent sum m ation potent ial m ay fur ther help di erent iate those that do or do not bene t from cochlear implant (CI)
◦ ABR can dist inguish the t ype depending upon presence or absence of wave V (absent in t rue neuropathy versus dyssynchrony); if
dyssynchrony, get bet ter speech percept ion outcom es from CI
◦ Funct ional e ect ranges from total deafness to impaired hearing in background noise; level of HL does not correspond to ABR results (so behavioural test ing required)
• Epidem iology: ◦ Incidence unknow n ◦ Risk factors include hyperbilirubinem ia, anoxia, hypoxia/prolonged assisted vent ilat ion , prem aturit y (<28 w k), presence of other con-genital abnorm alit ies, demyelinat ing condi-t ions, genet ic factors, syndrom es associated w ith other peripheral neuropathies
• Managem ent and prognosis: ◦ Natural h istory variable, w ith som e children show ing im provem ent and possible norm al m orphology to ABR
◦ Those due to prem aturity (± hyperbilirubi-nem ia) tend to recover by 18 m onths of age; di culty detecting these children as newborn screening w ill m iss them (norm al OAE); if they are identi ed, early intervention w ith CI m ay not be good, as m ight show subsequent recovery
◦ In children w ith auditory neuropathy, preoperat ive m agnet ic resonance im aging before CI can show that those w ith a de cient cochlear nerve (size compared w ith VII n) do less well on speech percept ion
◦ Som e children do as well w ith a convent ional hearing aid (HA) as a CI; failure to get bene t from an HA m ay be a good indicator for a CI
Philpott_9783131662316_Ch08.indd 26 02/05/14 9:10 AM
27
9.1 De nition• Tinnitus is a sym ptom , not a disease• It is the sensat ion of sound not brought about
by sim ultaneously externally applied m echano-acoust ic or elect rical signals—the percept ion of sound generated involuntar ily w ith in the head of an individual
• Suggests problem between cochlea and auditory cor tex
• Central auditory system plays vital and cr it ical role in experience of t innitus
9.2 Classi cation• Som atosounds:
◦ Cochlear—spontaneous otoacoust ic em issions ◦ Extracochlear
- Muscular [eustachian tube (ET) funct ion , sta-pedial, tensor t ympani or palatal myoclonus]
- Vascular (in ternal carot id ar tery or ICA)—pulsat ile
- Crepitus (tem porom andibular join t) - Respiratory (patulous eustachian tube)
• Subject ive t innitus: ◦ May arise from a source/t r igger = t innitus-related neural act ivit y (TRNA) in cochlea, brainstem or h igher centres (neurophysiological)
◦ Usually unable to determ ine the source clin ically
◦ May be facilitated and sustained by hearing loss (HL)—reduced percept ion of external environm ental sounds leading to increased central gain
• Non-organic t innitus: lit t le know n, and no de n it ive test
9.3 Incidence and Epidemiology• 94% of norm al-hearing subjects placed in a
soundproof room for up to 5 m in have t innitus-like experiences
• 10% of adults have experienced t innitus for >5 m in
• 4% have t innitus causing sleep disturbance• 0.5% severely disabled by t innitus
• Som e pat ients m ay have norm al audiom etry—but there m ay be subt le auditory dysfunct ion not ident i ed by pure tone audiogram
• 27% of cochlear im plant pat ients experience no t innitus, so t innitus not ubiquitous in profound sensorineural hearing loss
• Risk factors: ◦ Noise exposure ◦ Hearing loss ◦ Increasing age ◦ Pre-exist ing anxiet y/depression ◦ Associat ion w ith ear pathology (e.g., otosclero-sis, Ménière, t ym panic m em brane perforat ion , vest ibular schwannom a)
◦ Ototoxic m edicat ion (e.g., salicylates, am ino-glycosides, loop diuret ics)
9.4 Impact• Em otional dist ress, insom nia, concentrat ion ,
depression, potent ial self-harm
9.5 Jastrebo Neurophysiologi-cal Model of Tinnitus (Fig. 9.1)• When silence is present there is random neural
act ivit y—if th is is altered it m ay result in TRNA• Discordant dam age between OHCs and IHCs
can produce abnorm alit ies of auditory nerve pat terning result ing in fur ther TRNA
• TRNA detected at brainstem level, and perceived as int rusive/threat
• Inst igates sym pathet ic autonom ic nervous system arousal—agitat ion , irr itabilit y, and lim bic system (em ot ional) response—fear, anxiety
• TRNA undergoes considerable processing in subcor t ical auditory pathways to nally be perceived at a conscious level as sound
• Em otional dist ress inst igated by condit ioned response to TRNA
• Problem s w ith Jast rebo neurophysiological m odel (JNM): simplist ic (but th is helps w ith dist ressed pat ients); insists that condit ioned responses involved—but no empirical evidence, and hum ans m ore com plex than that im plies; thus m inim izes role of personalit y, experience, social context
9 Tinnitus
Philpott_9783131662316_Ch09.indd 27 02/05/14 9:27 AM

28
9 Tinnitus
9.6 Psychological Model• Hum ans usually habituate to cont inuous
background st im uli• Troublesom e t innitus represents a failure of
habituat ion , w hich is m ore likely if person is st ressed; signal is em ot ionally m eaningful (e.g., result of assault , failed surgery); signal is especially unpleasant/aversive
• Vicious circle of awareness and st ress set up• Em otional react ion to t innitus a m ajor factor in
dist ress• Problem s w ith psychological m odel: potent ially
overem phasizes em ot ion, underem phasizes m echanism s of t innitus
9.7 British Tinnitus Association Information• Although the ear is probably the m ost com m on
source of disorder that generates the abnorm al t rain of neuronal signals that underlie m ost form s of t innitus, it is usually unim portant w ith respect to the “severit y” of the t innitus, i.e., the extent and nature of its adverse e ects on the pat ient
• Degree of dist ress depends on the way in w hich the neuronal signal is processed in the brain , including par ts of it outside the auditory system
• Process involves neuronal networks and lters responsible for select ive hearing
• These networks and lters have plast icit y: ◦ This m eans they can react , som et im es as a form of condit ioned response, to the apparent potent ial threat of any new or st range sound
◦ This enhances the detect ion of such new pat terns of auditory neuronal signal
◦ In turn , the links between the central auditory pathways and the lim bic and autonom ic nervous system s m ay lead to a variet y of unpleasant and physical responses to the new sound
• These processes can be reversed by appropriate counselling to reduce or rem ove the anxiet ies and fears caused by t innitus: ◦ As people com e to term s w ith their t innitus, lose m uch of their fear of it , and learn to reduce the at tent ion they give to their t innitus, so the neuronal pathways and lter set t ings change, leading to the gradual habituat ion to t innitus, w hich is the general rule
◦ Counselling aim s to speed up and enhance the habituat ion process.
◦ Counselling m ust be encouraged, giving con dence, hope, and expectat ion of worthw hile im provem ent at least and possibly even vir tual elim inat ion
• Habituat ion can be further assisted by decreasing the t innitus-to-noise rat io: ◦ This m ay be done by increasing the acoust ic input to the pat ient , either by enriching the pat ient’s acoust ic environm ent or by reinforcing it by m eans of wearable sound- generat ing or amplifying instrum ents or both
◦ Such sound therapy m akes it easier for the person to disregard (or lter out) the t innitus signal
• Sound therapy also counteracts the big enemy of the person w ith t innitus—quietness ◦ In the quiet , and par t icularly if there is hearing loss, the central auditory system increases it s sensit ivit y to detect any fain t sounds
◦ This increases the apparent loudness of the t innitus, and also that of external sounds—thus causing the oversensit ivit y to sounds, hyperacusis
◦ If the added sound is loud enough to render the t innitus sound inaudible, to completely “m ask” it , th is m ay, however, delay habitua-t ion; you cannot habituate to som ething you cannot perceive
Fig. 9.1 Jastrebo neurophysiological model of tinnitus.
Percept ion andEvaluat ionAuditory and
other cortical areas
EmotionalassociationsLimbic system
Detect ionSubcortical
Source
Body react ionAutonomic
nervous system
Philpott_9783131662316_Ch09.indd 28 02/05/14 9:27 AM

29
Somatosounds
◦ hearing aids (HAs)—10% w ill experience total suppression of t innitus, m any experience part ial inhibit ion
◦ White noise generator and HA com bined som et im es useful
• Direct ive counseling, e.g., inform at ion and explanat ion
• Relaxat ion therapy• Cognit ive-behavioural therapy: explanat ion ,
relaxat ion , change of beliefs about t innitus• Sound therapy for hyperacusis• Transcranial m agnet ic st im ulat ion under
invest igat ion
9.11 Somatosounds• Pulsat ile:
◦ Venous hum s: turbulent ow through jugular bulb, unilateral and pulse synchronous, m ay be altered by neck m ovem ent and posture, possible to hear w ith a stethoscope
◦ Arterial loops: IAM compression , pulsat ile t innitus w ith uctuat ing HL, consider MRI (often incidental nding)
◦ Carot id t ransm issions: carot id bruits, systolic hear t m urm urs
• Non-pulsat ile: ◦ Patulous ET:
- Aural fu llness, autophony - May occur after weight loss - Surgery to ET ori ce possible (but m ay lead to obst ruct ion)
◦ Palatal myoclonus: - Irregular clicking sound—one/both ears - Myoclonic contract ions in tensor/levator palate
- May be underlying brainstem lesion - Rx: m asking techniques or botox inject ions
◦ Tensor t ympani syndrom e: - Flut tering low -frequency sound - Increased tension in m uscle - Rx: m uscle sect ion or relaxat ion/reassurance
◦ Nevertheless, som e pat ients nd such m asking very helpful, and in others it m ay be all they want
9.8 Hyperacusis• Decreased sound tolerance or em ot ional dislike
of noise• 40% of t innitus pat ients• Can be dem onst rated by loudness discom for t
test ing (but unpleasant for pat ient and of lit t le value)
• Mechanism usually increased central gain• Treat w ith inform at ion , relaxat ion , w ide band
sound generators
9.9 Management Algorithm• Pulsat ile—if yes, unilateral, and no conduct ive
HL or negat ive m iddle ear pressure, consider glom us tum our (Ix by m agnet ic resonance im ag-ing or MRI, then CT scan if nothing show n on MRI): w hen have conduct ive HL, body sounds are heard m ore easily (as environm ental sounds at tenuated) so often hearing a norm al pulsat ion
• Non-pulsat ile w ith norm al hearing: refer; consider hearing therapy
• Non-pulsat ile w ith deafness: if sym m etrical loss, for hearing therapy; if unilateral consider MRI for acoust ic neurom a
• Clicking noises m ay im ply m uscle tw itches of the palate, stapedius, and tensor t ympani (rare)
9.10 Treatment• Most habituate naturally• Tinnitus ret rain ing therapy: object ive is to
e ect perm anent changes in auditory lters and pat tern recognit ion involved in the detect ion and enhancem ent of TRNA
• Inst rum entat ion: ◦ Masking devices (w hite noise generators); change at tent ional focus
Philpott_9783131662316_Ch09.indd 29 02/05/14 9:27 AM

30
10.1 Terminology• Som et im es called acoust ic neurom a, but is
not on the cochlear (acoust ic) nerve, nor is it a neurom a
10.2 Epidemiology• Male = fem ale dist r ibut ion; t ypically present
40 to 60 years (younger if neuro brom atosis 2 [NF2])
• Incidence 1/100,000 per year (autopsy studies show up to 0.7% populat ion m ay have vest ibular schwannom a at death)
• 95% unilateral, sporadic• 5% bilateral—associated w ith NF2• Account for 80% of cerebellopont ine angle (CPA)
tum ours and 6% of all in t racranial tum ours
10.3 Pathology• May originate from junct ion of glial and
Schwann cells of vest ibular nerve, w ith in in ter-nal auditory m eatus (Obersteiner–Redlich zone)
• Haem orrhage can occur in ret icular t ype leading to sudden increase in size
• Cyst ic degenerat ion possible• NF2—autosom al dom inant; aberrat ion on
long arm of chrom osom e 22 leading to defect in tum our suppressor protein m erlin (aka schwannom in, neuro brom in 2)
• Quest ioned link w ith cellphone usage, but evidence not conclusive
10.4 Clinical Features (Fig. 10.1)• Otological phase: sm all tum our com presses
st ructures in the m eatus ◦ Gradual and progressive unilateral deafness (90%)—degree of hearing loss (HL) not related to size of tum our
◦ Sudden-onset HL (10%) ◦ Norm al hearing (5%) ◦ Associated w ith unilateral t innitus (70%)—can be the only symptom
◦ Im balance unusual unless acutely due to bleed inside tum our (slow compression allows for
10 Vestibular Schwannoma
gradual com pensat ion); dysequilibrium often present w ith rapid head m ovem ents
◦ Hitzelberger sign: anaesthesia of m edial, poster ior, or superior areas of the external auditory canal
• Neurological phase: expansion in to CPA: ◦ Trigem inal nerve symptom s: facial pain , num bness, loss of corneal re ex
◦ Headache—posterior fossa dura irr itat ion leading to dull aching around ear
◦ Late sym ptom s - Facial weakness—uncom m on (gradual com -pression allows for com pensat ion as norm al num ber of end plates are innervated by fewer neurons)
- Ataxia/unsteadiness—brainstem /cerebellar involvem ent
- Diplopia (VI n)—rare - Hoarseness and dysphagia (IX n , X n)—rare
◦ Term inal symptom s (raised cerebrospinal u id or CSF): failing vision (papilloedem a), head-ache, reduced Glasgow com a score; com a
10.5 Investigations• Magnet ic resonance im aging (MRI) scan:
non-cont rast screening protocols; usually iso/hypointense to brain , hyperin tense to CSF on T1 and isoin tense to slight ly hyperin tense on T2; best show n w ith T1 cont rast (gadolin ium ) or FIESTA or CISS (T2-weighted) sequences
• (CT w ith contrast if MRI cont raindicated)• Pure tone audiogram : 65% have h igh-frequency
loss• Brainstem evoked response (in teraural latency
of wave V)—accuracy bet ter for larger tum ours (>1.5 cm )
• Speech discrim inat ion: “roll-over” seen as in tensit y increase and opt im um discrim inat ion score reduces
10.6 Di erential Diagnosis of CPA Tumours• Meningiom a• VII n neurom a• Cochlear nerve neurom a—rare
Philpott_9783131662316_Ch10.indd 30 02/05/14 11:52 AM

31
Management : Mult idisciplinary Team Approach
• Congenital epiderm oid• Aneurysm of basilar/vertebral ar teries• Cholesterol granulom a of pet rous apex• Cerebellar tum our
10.7 Management: Multidisci-plinary Team Approach10.7.1 Conservative• ~65% do not show any signs of grow th, so
watchful wait w ith ser ial scanning, especially in elderly or m edically un t
• Has best rates of hearing preservat ion com pared w ith surgery or radiotherapy
• If grow, usually <2 m m /year• If no grow th over 5 years, unlikely to ever grow
10.7.2 Radiosurgery or Radiotherapy• Considered for tum ours <3 cm diam eter at CPA• Hyperfract ionated stereotact ic radiotherapy• Gam m a knife/CyberKnife—uses an alternat ive
radiat ion source• Bene ts
◦ Som e studies suggest bet ter hearing preservat ion compared w ith surgery
◦ Risks are delayed, versus upfront r isks of surgery
◦ Outpat ient procedure ◦ Avoids r isks of craniotomy
• Risks ◦ Future surgery m ore di cu lt—greater r isk facial nerve paresis/paralysis
Fig. 10.1a–c The three stages of a vestibular schwannoma.a Intrameatal tumour.b Intrameatal and extrameatal tumour.c A mainly extrameatal medial tumour compressing the brainstem and cerebellum.
ba c
Fig. 10.2a–c Otological and neurosurgical routes of access to the internal meatus.a The transtemporal
approach through the middle cranial fossa.
b, c The translabyrinthine and retrosigmoid approaches, respectively.
a cb
Philpott_9783131662316_Ch10.indd 31 02/05/14 11:52 AM

32
10 Vest ibular Schwannoma
◦ Facial weakness/tw itching ◦ Risk of inducing m alignancy in eld (1:1000)
◦ Failure of tum our control in 5 to 10% ◦ Does not m ake tum our disappear, just stop grow ing, so requires long-term follow -up to ensure no further grow th
◦ Brainstem radiat ion e ects ◦ Trigem inal involvem ent
10.7.3 Microsurgery• General
◦ The larger the tum our the greater the risks (e.g., to facial nerve)
◦ If tum our >1.5 cm at CPA, r isks to hearing and facial nerve increase
◦ If tum our >2.5 cm , generally requires surgery
• Approaches (Fig. 10.2) ◦ Translabyrin th ine
- Hearing sacri ced therefore useful for pat ients w ith no serviceable hearing
- Excellent CPA exposure w ith m inim al cerebellar ret ract ion
- Drilling bone done before opening dura—fewer headaches
◦ Middle fossa route - Lim ited access to CPA so suitable for sm all in t ram eatal tum ours
- VII n and hearing can be preserved, although need to work around VII n , w hich usually runs along top of IAC
◦ Retrosigm oid approach - Direct approach to tum our in CPA w ith w ide exposure
- Possible VII n and hearing preservat ion
Philpott_9783131662316_Ch10.indd 32 02/05/14 11:52 AM

33
11.1 Incidence and Site• Tum ours of the ear are rare: ~70% pinna, 20%
external auditory canal (EAC), 10% m iddle ear (ME)
11.2 Pinna• Squam ous cell carcinom a (SCC) and basal cell
carcinom a (BCC) m ost com m on (respect ive incidences vary country to count ry) (Figs. 11.1 and 11.2a)
• Rx: prim ary resect ion w ith appropriate m argins; m inor super cial lesions w ith no cart ilage invasion or xat ion m ay have radiotherapy (RT) alone
• Benign include nevus, epitheliom a adenoides cyst icum , m olluscum contagiosum
11.3 EAC• SCC (Fig. 11.2b)
◦ 90% of m alignant tum ours, slow -grow ing, spread via cart ilage port ion and later in to ME, parot id, sternocleidom astoid m uscle
◦ 20% lym ph node (LN) spread (poster iorly to m astoid nodes, inferiorly to level III, an teriorly to preauricular)
◦ Associated w ith chronic in am m ation, RT ◦ Rx: consider lateral tem poral bone resect ion , ± neck dissect ion; post-operat ive RT
◦ Prognosis very poor if node posit ive• Adenocarcinom a: very aggressive (usually fatal
w ithin 4 years), often present ing w ith VII n palsy• Adenoid cyst ic: m ost com m on “cerum inous”
tum our; long natural h istory, painful• Also adenom a, m ucoepiderm oid carcinom a;
m alignant m elanom a very rare, as is BCC of EAC
11.4 Middle Ear• Choristom a = norm al t issue in abnorm al
site (e.g., salivary gland in ME): rare; m ay be at tached to VII n
• Adenom a (benign): cause unilateral progressive conduct ive hearing loss (HL), TM intact in 75% cases; 2nd m ost com m on after glom us tum ours, but st ill rare
11 Tumours of the Ear and Skin
• Adenocarcinom a: very rare; cause deafness, pain , VII n palsy
• SCC: ◦ Most com m on epithelial ME m alignancy, but rare
◦ Associat ion w ith chronic ot it is m edia in 85%, irradiat ion
◦ Extensive bony dest ruct ion , m ost easily through tegm en to m iddle cranial fossa (dura is a relat ively st rong barrier); in t racranial invasion along VII n and VIII n in in ternal auditory canal; IX n and XII n involvem ent shows skull base involved; can also extend to tem porom andibular join t , parot id , via eustachian tube to nasopharynx
◦ LN involvem ent in 10 to 15% at presentat ion , rare distant m etastasis; death by cachexia secondary to pain because cranial nerve (CN) involvem ent , though som et im es invasion of m eninges leads to in t racranial com plicat ions and erosion of jugular bulb or carot id is possible
◦ Rx: surgery (pet rosectomy) + RT; palliat ive ◦ 5-year survival ~35% (bet ter for EAC than ME); prognosis very poor if node posit ive
• Other benign tum ours: ◦ Osteom a ◦ VII n schwannom a (usually at geniculate ganglion)
◦ Hem angiom a, neurogenic
Fig.11.1a, ba Senile keratosis of the auricle.b Basal cell carcinoma.
Philpott_9783131662316_Ch11.indd 33 02/05/14 2:26 PM

34
11 Tumours of the Ear and Skin
• Other m alignant tum ours: ◦ Sarcom a ◦ Mult iple myelom a ◦ Malignant xanthom a ◦ Rhabdomyosarcom a m ost com m on in children; m ay require surgery ± chem oradiotherapy
◦ Also direct extension (e.g., from nasopharynx, external ear, parot id, m eningiom a) and distant m etastases (kidney, lung, prostate, thyroid, breast)
11.5 Glomus Tumours• Pathology:
◦ Correct (WHO) term is paragangliom as; aka chem odectom as; arise from paraganglionic t issue (chem oreceptor cells)
◦ Com m on em bryological or igin (neural crest) and associat ion w ith neural st ructures
◦ 90% adrenal (phaeochrom ocytom as); 10% nonadrenal (85% of w hich are abdom inal, only 3% H&N); subdivided in to abdom inal and extra-abdom inal
◦ H&N paragangliom as associated w ith parasympathet ic system
• Epidem iology: ◦ Relat ive incidence: carot id > jugulotympanic > vagal
◦ 5th decade, F>M, m ay be m ult iple (show m ult icentr icit y); ~10%, autosom al dom inant; usually benign and slow -grow ing but ~5% m alignant; rarely (<1%) secrete neuropept ides (e.g., serotonin , vasoact ive in test inal pept ide)
• Tem poral bone paragangliom a classi cat ion (Fisch): ◦ A: ar ise along t ympanic plexus on prom ontory; blood supply from tym panic a (from ascending pharyngeal a)
◦ B: originate in canalis t ym panicum of hypotym panum and invade ME/m astoid; invade bone, but that over jugular bulb in tact
◦ C: arise in dom e of jugular bulb and dest roy overlying bone; spread inferiorly along jugular vein and lower CNs, posteriorly to sigm oid sinus, superiorly towards ot ic capsule and in ternal auditory m eatus, laterally to hypotym panum and ME, m edially to jugular foram en and cerebellopont ine angle; subclassi ed according to degree of erosion of carot id canal - C1: erode carot id foram en, not invade carot id a
- C2: dest roy vert ical carot id canal between foram en and bend
- C3: grow along horizontal por t ion carot id a, not reach foram en lacerum
- C4: grow to lacerum and along carot id a to cavernous sinus
◦ D: in t racranial extension; De: in t racranial, ext radural, De1 < 2 cm , De2 >2 cm ; Di: in t racranial, in t radural extension, Di1 < 2 cm , Di2 >2 cm , Di3 unresectable
• Ix: ◦ Magnet ic resonance im aging ± angiogram (salt and pepper appearance on T1,2)
◦ Computed tom ography (CT) temporal bone (m ay show “m otheaten” bony dest ruct ion)
◦ 24-h urinary VMA, norm etanephrine if sym ptom at ic (headaches, palpitat ions, ushing, perspirat ion)
◦ Consider genet ic test ing for SDH m utat ions• General Rx:
◦ May be slow-grow ing and present late in life, so conservat ive t reatm ent appropriate
◦ Possible role for som atostat in therapy ◦ Focused RT m ay stop fur ther grow th (but r isks osteoredionecrosis and m ay m ake subsequent surgery m ore challenging)
11.5.1 Carotid Body and Glomus Vagale Tumours• See Chapter 58: Tum ours of the Parapharyngeal
Space
Fig. 11.2a, b Squamous cell carcinoma.a A small erosive carcinoma invading the helix.b Carcinoma growing out of the external meatus.
Philpott_9783131662316_Ch11.indd 34 02/05/14 2:26 PM

35
Skin Cancer
11.5.2 Glomus Jugulare (Fig. 11.3)• From paraganglionic cells around jugular bulb• Com m only as m uch above skull base as below it;
m ay involve ME, m astoid, neck• Palsies IX n , X n , XI n , XII n possible• Rx: consider preoperat ive em bolizat ion (usually
fed by ascending pharyngeal a); surgery (via m astoid or infratem poral approach depending upon size)
11.5.3 Glomus Tympanicum (Fig. 11.4)• On prom ontory of ME along course of Jacobson
n and Arnold n• Most com m on neoplasm of ME
• May extend to m astoid but jugular bulb not involved
• Sym ptom s include deafness (conduct ive HL), pulsat ile t innitus (80%), vert igo, pain in ear, VII n palsy
• Di erent ial of vascular ME m ass: h igh jugular bulb, VII n neurom a, aberrant in ternal carot id ar tery
• CT best to di erent iate t ym panicum from jugulare
• Rx: surgery, t ranscanal if all visible on otoscopy, or else via m astoid
11.6 Skin Cancer• BCC and SCC com prise >80% of skin cancers;
basal: squam ous: m elanom a rat io = 30:4:1
Fig. 11.3a, b Glomus jugulare tumour.a The arrows mark the pos-
sible direction of tumour growth into the epitym-panum, the hypotym-panum and through the tympanic membrane.
b There is a blue-coloured tumour shining through the tympanic membrane.
ba
Fig. 11.4a, b Glomus tympanicum tumour.a The arrows mark the
possible direction of tumour growth.
b A small red tumour becomes visible.
a b
Philpott_9783131662316_Ch11.indd 35 02/05/14 2:26 PM

36
11 Tumours of the Ear and Skin
• Risk factors ◦ Ult raviolet radiat ion (UVB m ost dangerous); sunburn m ay relate to BCC, prolonged exposure to SCC
◦ Red/fair hair, pale eyes, long-term im m unosuppression; NB: Fitzpat rick skin t ypes I (v. pale)–VI (v. dark)
◦ Associat ions: solar (act in ic) keratosis has cancer r isk ~0.1%; Bowen disease (squam ous carcinom a in situ) has h igher rate m alignant t ransform at ion (~30%); xeroderm a pigm entosum (autosom al recessive) causes skin cancers by 8 years; albin ism
◦ Non-m alignant (or prem alignant) lesions included in di erent ials (e.g., seborrhoeic keratosis, keratoacanthom a)
11.7 Non-Melanomas11.7.1 Basal Cell Carcinoma• Most com m on; 90% on H&N; 60 to 65 years of age• May be solid, cyst ic and pigm ented; 75%
nodular, 10% super cial, in lt rat ive 5%• Higher recurrence rates at m edial canthus and
nasolabial fold (H-zone of face), and in lt rat ive subtype
11.7.2 Squamous Cell Carcinoma—Cutaneous• Malignant proliferat ion of epiderm al
kerat inocytes• 70% on H&N; increasing incidence over 70 years• Possible h igher m etastat ic potent ial on ear/
upper lip• TNM staging:
◦ T1: ≤2 cm ◦ T2: >2 cm ≤ 5 cm ◦ T3: >5 cm ◦ T4: invades deep extraderm al st ructures (cart ilage, skeletal m uscle, bone)
◦ N0: no nodes; N1: regional nodes
11.7.3 Management (Non-melanoma)• Low risk, sm all lesions, can be t reated by
curet tage (e.g., <4 m m well-de ned BCC)• Consider liquid n it rogen cryotherapy, CO2 laser
and RT in ~10% BCCs
• Biopsy: ellipt ical excision m ay be therapeut ic; need to exclude benign lesions m im icking cancer (e.g., derm at it is ar t ifacta secondary to eczem a)
• BCC excision m argins: if lesion <1 cm , m argin 2–3 m m gives 95% clearance; if >1 cm , m argin 5 m m
• SCC m argins at least 1 cm (5 m m m argins give 85% clearance)
• Mohs m icrographic surgery helps ensure complete excision—gold standard for h istological accuracy; especially helpful for t reat ing recurrence; excises under frozen sect ion control, using horizontal sect ions (rather than t radit ional ver t ical ones that sample ~1% of surgical m argin) that allows in t ra-operat ive exam inat ion of the ent ire surgical m argin
• Neck im aging considered if h igh risk site or T4; m ay require neck dissect ion (m ore com m on for SCC than BCC); h igh r isk if >2 cm diam eter, >6 m m thick, perineural/vascular invasion, local recurrence, poorly di erent iated
• 5-year cure rate is h igh (>90%)
11.8 Melanoma (Cutaneous) of H&N• Relat ionship to sun exposure less clear; genet ic
factors im plicated• While only 5% skin cancers, account for 65% skin
cancer-related deaths• ~70% arising on H&N do so from pre-exist ing
pigm ented lesion• 20% of total in H&N; M>F• Types:
◦ Super cial spreading (m ost com m on) ◦ Lent igo m aligna ◦ Acral lent iginous ◦ Mucosal lent iginous ◦ Nodular
• Histological prognost ic factors: th ickness m ost im portant; as increases, so does r isk of nodal m etastases
• Clin ical diagnosis (ABCDE): ◦ A: asym m etry ◦ B: borders (sharp, irregularly serrated) ◦ C: colour (brow n, black, blue, uneven) ◦ D: diam eter (>7–9 m m ) ◦ E: elevat ion (raised, so palpable)
• Rx: excisional biopsy w ith 1–2 m m m argin, and m ore radical de n it ive surgery w ith in 4/52;
Philpott_9783131662316_Ch11.indd 36 02/05/14 2:26 PM

37
Melanoma (Cutaneous) of H&N
◦ T3a: >1.5 m m ≤3.0 m m (Clark IV) ◦ T3b: >3.0 m m ≤4.0 m m (Clark V) ◦ T4a: >4.0 m m and/or invades subcutaneous t issue
◦ T4b: satellite(s) w ith in 2 cm of prim ary ◦ N1: m etastases ≤3 cm ◦ N2: m etastases >3 cm or in-t ransit m etastases (>2 cm from prim ary but not beyond regional lym ph nodes)
prim ary excised w ith 1 cm m argin for every 1 m m thickness
• If node posit ive and prim ary in upper face/temporal region, radical neck dissect ion
• TNM: done post-excision , so pT (NB: Clark levels and Breslow m icrostages) ◦ Tis: m elanom a in situ (Clark level I) ◦ T1: ≤0.75 m m thick (Clark II) ◦ T2: >0.75 m m ≤1.5 m m (Clark III)
Philpott_9783131662316_Ch11.indd 37 02/05/14 2:26 PM

38
12 Ear and Temporal Bone Trauma
12.1 Pinna• Auricular haem atom a: r isk of “cauli ower ear”
if inadequately aspirated/drained• Earr ing “pull-outs”: repair under local
anaesthet ic (LA)• Bites/lacerat ions: washout , debridem ent ,
closure under LA ± ant ibiot ics• Am putat ions: place ear in saline gauze, in plast ic
bag, on ice; consider referral to plast ics for replantat ion if feasible
12.2 Tympanic Membrane• Traum at ic t ym panic m em brane (TM)
perforat ions: ~95% heal by 6 weeks after injury• Water exclusion and t reat concurrent infect ion
if present• Consider possibilit y of ossicular injury—pure
tone audiogram
12.3 Blast Injuries• TM injuries com m on• Im plantat ion cholesteatom a possible• Conduct ive hearing loss (HL) (from TM or
ossicular chain dam age) or sensorineural hearing loss (SNHL) (from im pulse noise)
• Vert igo usually tem porary
12.4 Barotrauma• Tissue injury caused by a change in pressure
that compresses or expands gas contained in body st ructures
• Middle ear (ME) is a noncom pressible gas- lled space
• In diving, failure of eustachian tube (ET) to open causes squeeze e ect in ME: ◦ As descend, gas compresses, TM ret racts, Valsalva to open ET and equalize—pain com m on
◦ As ascend, increased gas volum e aids equalizat ion through ET (if pressure di erent ial >15 m m Hg)
◦ Rapid change in relat ive pressure of ME can cause implosive or explosive forces on TM, round w indow (RW), or oval w indow: - Explosive injury: on descent if inadequate ET funct ion, negat ive ME pressure relat ive to in t ra-labyrin th ine uid pressure; increasing cerebrospinal u id (CSF) uid pressure then t ransm it ted to inner ear via cochlear aqueduct , w hich fur ther increases pressure di erent ial between labyrin th ine uid and ME space and causes outward bulging and rupture of RW
- Im plosive injury: on descent relat ive negat ive pressure develops in ME and TM ret racts; if ET funct ioning norm ally sudden force-ful Valsalva to equilibrate; TM approaches neut ral posit ion; relat ive posit ive pressure of ME com pared w ith in t ralabyrin th ine u ids so RW pushes inwards and can rupture
◦ Both im plosive and explosive barot raum a to inner ear can cause sudden SNHL; t innitus and ver t igo possible; large pressure di erences can also cause TM rupture
◦ Increased risks w ith ET dysfunct ion , rh inosinusit is/allergy
• Other: canal “squeeze” from im pacted wax; vest ibular sym ptom s (perilym phat ic stula, caloric e ect through perforat ion , labyrin th ine decompression sickness w here bubbles causing ischem ia to labyrin th via AICA)
12.5 Temporal Bone Fractures• Half a m illion head injuries each year; up to a
quar ter include sym ptom s related to injury of the tem poral bone
• Various classi cat ions, e.g., longitudinal or t ransverse fractures (# s) relat ing to orientat ion of fracture line; however, >80% m ixed; ot ic capsule involvem ent m ay be a m ore relevant way to classify
• Longitudinal (Fig. 12.1): ◦ Dom inant in 80%; usually blow to side of head ◦ Symptom s m ainly related to ME ◦ # runs from squam ous tem poral bone in roof of external auditory canal to TM and roof of ME, then anter ior towards labyrin th
Philpott_9783131662316_Ch12.indd 38 02/05/14 2:36 PM

39
Noise-Induced HL
◦ Findings: bleeding from ear canal, TM rupture (or haem otym panum ), SNHL usually due to concussion so temporary, CSF otorrhoea via disrupted tegm en, Bat t le sign (post-auricular bruising from # d m astoid cor tex)
◦ May dislocate incudom alleolar join t; consider if conduct ive hearing loss persists to 6 m onths post injury, w hen ossiculoplast y m ay be warranted
◦ VII n injury in ~20% (neuropraxia or axonotm esis) a ect ing perigeniculate ganglion/tym panic region
• Transverse (Fig. 12.1): ◦ Less com m on; usually from blow to front or back of skull
◦ Symptom s m ainly related to inner ear ◦ # runs across axis of pet rous bone through the labyrin th ine capsule
◦ Findings: hem otympanum (in tact TM usually), ir reversible SNHL, dead ear, vert igo (nystagm us to opposite ear), IX n–XII n cranial n injury, CSF rhinorrhea (as in tact TM directs it dow n ET)
◦ VII n palsy in up to 50% (m ore severe: axonotm esis or neurotm esis—up to 50% im m ediately), a ect ing distal labyrin th ine segm ent
• Rx: ABC/resuscitat ion; general head injury m anagem ent
• Ix: com puted tom ography (CT) scan, audiom etry• Generally no operat ive in tervent ion , unless clear
h istory of im m ediate total VII n lower m otor neuron injury w hen decom pression of VII n m ay be considered
• If VII n paresis or delayed palsy generally w ill recover w ith conservat ive m anagem ent
12.6 CSF Otorrhoea• Aet iology: post-head injury, spontaneous,
iat rogenic• Have ~ 1% risk each year of m eningit is w ith a
CSF leak, the risk being cum ulat ive (so longer left unt reated, greater the risk)
• Ix: β 2 t ransferrin (protein speci c to CSF, aka tau protein); halo test on lter paper (less speci c); h igh-resolut ion CT scan; T2-weighted MRI m ay dem onstrate leak; consider cisternogram or in t rathecal uorescein
• Conservat ive Rx: m ost resolve spontaneously; bed rest , head elevat ion , avoid raised in t racranial pressure (st rain ing and stooping), consider uid rest rict ion , laxat ives, and lum bar drain ; ant ibiot ics generally reserved unless any signs of m eningit is
• Surgical Rx: consider if leakage persists >2 weeks after t raum a (or if recurrent m eningit is or persistent pneum ocephalus)
12.7 Noise-Induced HL• Excessive noise can dam age cochlear by both
m etabolic and m echanical m echanism s: ◦ Metabolic: oxidat ive st ress, synapt ic hyperact ivit y, altered blood ow im plicated; outer hair cell in t racellu lar calcium levels r ise causing cell injury
◦ Mechanical: large-am plitude m ot ion m ay disrupt cochlear st ructures and even cause cell m em brane rupture
• After exposure, hearing threshold m ay return to norm al—tem porary threshold shift
• Greater cellular dam age leads to a perm anent threshold shift; ~125 dB is the crit ical level at w hich tem porary becom es perm anent
• Loss t ypically seen as notch at 3, 4, and 6 kHz• Hazards: occupat ional, m ilitary, social (m usic),
reworks
Fig. 12.1 Temporal bone fractures. 1, Longitudinal fractures; 2, transverse fracture.
21
Philpott_9783131662316_Ch12.indd 39 02/05/14 2:36 PM

40
12 Ear and Temporal Bone Trauma
• Equal energy hypothesis: h igh-in tensit y sound for shor ter period of t im e leads to sim ilar dam age as less in tense st im ulus for longer exposure
• European direct ives dictate acceptable occupat ional noise levels, e.g., 85 dB for 8 h , 88 dB for 4 h , 91 dB for 2 h—rem em ber log scale; applies to cont inuous noise rather than im pulse noise
• Individual suscept ibilit y: relates to genet ics, drug exposure, age, etc.
• Forensic audiom etry to assess HL for pension policies and compensat ion claim s; considers w hat loss expected at any part icular age
• Prevent ion: r isk ident i cat ion , hearing screening, educat ion , hearing protectors
• Hearing protectors: passive or act ive; for every 3 dB at tenuat ion of sound exposure, the potent ial dam age is halved (or exposure t im e can be doubled)
12.8 Perilymphatic Fistula• Perilymph leak into ME from defect in oval or RW• Aet iology: barot raum a; head injury; iat rogenic
(e.g., stapedectomy) congenital m alform at ions (e.g., Mondini dysplasia); increased CSF pressure (coughing, sneezing)
• Findings: constant , uctuat ing, or progressive SNHL, vert igo (50%), t innitus
• Ix: stula test , audiom etry, CT scan• Rx: m ay resolve spontaneously (bed rest ,
avoid st rain ing, sit-up); consider surgery w ith exploratory t ympanotomy and plugging of defect
12.9 Vestibular System• Associat ion of benign paroxysm al posit ional
vert igo w ith head injury; t reat in usual m anner (e.g., Epley)
Philpott_9783131662316_Ch12.indd 40 02/05/14 2:36 PM

41
13 Otalgia
13.1 Otalgic Neuralgia• Anatomy:
◦ Medial surface of t ym panic m em brane, m iddle ear (ME), m astoid air cells, and ET get sensat ion/autonom ics from the t ym panic plexus
◦ Tympanic plexus lies on prom ontory, anterior to round w indow niche
◦ Parasym pathet ic input from glossopharyngeal via Jacobson n (preganglionic secretom otor from inferior salivatory nucleus: supply dest ined for parot id via lesser super cial pet rosal n and thence auriculotem poral nn)
◦ Jacobson n also supplies sensory elem ent to ME and bony ET
◦ Tym panic plexus also gets a parasympathet ic input from nervus in term edius (w hich unites w ith VII n at geniculate ganglion); VII n (nervus in term edius) gives sensory bres to posterosuperior aspect of deep external auditory canal (EAC)
◦ Sympathet ic (vasoconst rictor, carot ico-t ym panic) bres to plexus from sym pathet ic bres that accompany in ternal carot id ar tery (from superior cervical ganglion)
• Characterist ics: ◦ Pain m ay result from direct st im ulat ion of sensory nn in ME/EAC or be referred from areas these nerves supply; various neuralgias described, but m ust rst exclude disease in distant territories and ear disease
◦ Glossopharyngeal neuralgia: lancing pain star t ing in tonsillar fossa/tongue base, radiat ing to deep in ear, w ith salivat ion and induced by swallow ing, talking or other m ovem ents of throat or tongue
◦ Geniculate ganglion neuralgia: m ay be considered a par t ial glossopharyngeal neuralgia, w ith sam e pain in and around EAC but not induced by tongue m ovem ents or accom panied by salivat ion
◦ Chorda tympani neuralgia: episodic, severe pain in and around ear, som et im es associated w ith bit ter taste; can sect ion nerve
◦ Nervus in term edius neuralgia: episodic unilateral otalgia like lightning, deep in ear som et im es radiat ing to eye (not throat), reproduced by st im ulat ing post-sup skin of deep EAC; consider sect ion at cerebellopont ine angle - To di erent iate the above w ith certain ty m ay need to do tym panotomy or craniotom y under local anaesthet ic w ith direct elect rical st im ulat ion to reproduce the otalgia; as all the t ym panic branches of these nn are accessible via the ME, t ym panotomy is preferable; also consider lidocaine test described below
◦ Tym pan ic neuralgia: st abbing deep -seated pain , one ear, u sually ou t of blue, fairly in tense, can last for 2 to 4 h ; m any pat ien t s have 2 to 4/w eek; exam inat ion usually norm al
• Rx: ◦ Consider neurom odulator (e.g., carbam azepine, gabapent in); can sect ion Jacobson n ± chorda tympani; best to see pat ient w hen they have the pain ; as if inject plain 1% lidocaine (in t ratym panic) and pain goes, m akes diagnosis
13.2 Referred Otalgia• 2nd/3rd cervical nerves: osteoar thrit is,
rheum atoid ar thrit is, prolapsed in tervertebral join t , facet join t subluxat ion , soft t issue injury
• Tr igem inal n : nasal/paranasal sinus d isease, nasopharyngeal d isease (adenoidectom y, upper resp iratory t ract in fect ion , u lcerat ion , t um our), den tal/jaw disease (car ies, abscess, m olar im pact ion , tem porom andibular join t ), salivary gland/duct d isease (calcu lus, sialaden it is, neoplasm )
• Glossopharyngeal n : oropharyngeal disease (tonsillectomy, pharyngit is, tonsillit is, neoplasm ); hypopharyngeal disease (neoplasm , tuberculosis); tongue disease (u lcer, benign or m alignant); st ylohyoid (Eagle) syndrom e
Philpott_9783131662316_Ch13.indd 41 02/05/14 2:39 PM

42
14.1 Decibels and Decibel Scales• Subject ive loudness is proport ional to equal
m ult iples of sound in tensit y• Bel = log10 (sound in tensit y/in tensit y reference
(10–12 W/m 2); 10 × rat io = dB• Sound in tensit y � sound pressure2; sound
in tensit y (dB) = 20 log10 sound pressure level• Doubling sound in tensit y = 3 dB increase; each
10 dB increase = 3.3 increase in sound pressure• Sound pressure level scale (dB SPL)—produces
curved audiogram in norm al circum stances because the auditory system is less e cient at detect ing sounds at certain frequencies
• Hearing level scale (dB HL/ISO)—designed so that 0 dB = expected threshold for every frequency—reference zero = group of otologically norm al young adults; 0 dB HL is the in tensit y needed for a norm al ear to perceive sound 50% of the t im e
• A-weighted scale (dB A)—reduced contribut ion of the lowest and highest frequencies; used in indust rial and noise-exposure set t ings
14.2 Clinical Hearing Testing• Free- eld thresholds equate to the voice and
distance level the subject gets >50% correct• Use num ber and let ter com binat ions• Mask nontest ear w ith t ragal rub (at tenuate
by ~50 dB) for w hispered and conversat ional speech, Barany box (at tenuates by ~90 dB w hen held at r ight-angle to ear) for loud voice
• Test order: w hisper 2 ft (60 cm ) then 6″ (15 cm ), conversat ion 2 ft then 6″, loud voice 2 ft then 6″
• If cannot hear w hisper at 2 ft , subject is hearing im paired (norm ally can hear th is at 12 ft [3.5 m ]); if can hear th is pure tone thresholds w ill be bet ter than 30 dB
• If hear w hisper at 6″ or conversat ion at 2 ft 6″, threshold in range 30 to 70 dB HL
• If only hear loud voice, thresholds >70 dB HL
14.3 Tuning Fork Tests• Usually use 512-Hz tuning fork as tone does not
decay too quickly or produce too m uch vibrat ion
• Activat ion by nger compression produces sound level ~70 dB; on knee (w ithout pain) ~90 dB
• Weber test (Fig. 14.1): ◦ Tuning fork placed in m idline ◦ With unilateral or asym m etric HL if conduct ive localizes to a ected ear, if sensorineural localizes to nona ected ear
◦ Can detect as lit t le as a 5 dB loss, but error rate up to 25%
• Rinne test (Fig. 14.2): ◦ Hold tuning fork next to ear, then onto m astoid process—w hich sound is heard loudest? ( Originally described as fork held next to ear unt il no longer heard, then see if heard via bone)
◦ Posit ive w hen air conduct ion (AC) > bone conduct ion (BC); i.e., norm al ears or SNHL in test ear
◦ Negat ive w hen BC > AC (conduct ive loss in test ear)
◦ In dead ear get false negat ive due to t ranscranial st im ulat ion of nontest ear; hence need to m ask (e.g., w ith Barany box)
◦ Test less sensit ive than Weber; for ABG 20 dB, sensit ivit y 50 to 70%, speci cit y ~95%; for ABG 40 dB, sensit ivit y and speci cit y ~95%
• Stenger test: ◦ Can help detect pat ient w ith a nonorganic unilateral HL
◦ Relies on fact that if pure tones of sam e frequency but di erent in tensit ies are presented sim ultaneously to each ear, pat ient w ill only be aware of the louder st im ulus
◦ Present two tuning forks, but one to “deaf” ear closer; if genuine w ill hear fork in good ear, if “fake” w ill only be aware of sound in “deaf” ear so w ill deny hearing anything
◦ Equivalent test can be perform ed w ith audiom eter
14.4 Pure-Tone Audiometry (Fig. 14.3)• A subject ive test of a pat ient’s hearing com pared
w ith an established “norm al”• Test perform ed according to standard protocols
(Brit ish Society of Audiology)
14 Audiology—Terminology and Tests
Philpott_9783131662316_Ch14.indd 42 02/05/14 2:42 PM

43
Loudness Recruitment
• BC at 250 Hz causes m ore vibrat ion than sound, so test 0.5 to 4 kHz range (test–retest variabilit y >10 dB, so di erences only considered signi cant if at least th is)
14.5 Loudness Recruitment• Subject ive loudness sensat ion greater
than expected w ith an increase in sound in tensit y
• Soundproofed facilit ies needed for de n it ive/diagnost ic test ing
• Test order of frequencies 1, 2, 4, 8 kHz then 500 and 250 Hz; repeat 1 kHz again to check w ith in 5 dB of rst result
• Subject ively bet ter-hearing ear tested rst• Test to w ith in 5 dB (to account for test–retest
variabilit y)• Test ing involves ascending in 5-dB increm ents
unt il pat ient gets 50% responses correct , then descending 10 dB and ascending in 5 dB again
Fig. 14.1a–d The Weber test . A vibrating tuning fork is placed on the midline of the skull.a Equal loudness
perceived in both ears means symmetrical hearing.
b Lateralization of sound to the a ected ear (right) is present in the case of conduc-tive hearing loss.
c In cases of sensori-neural hearing loss, the sound is lateral-ized to the bet ter ear (left).
d Correct orientation of the tuning fork.ba
c
lr lr
lr
d
Philpott_9783131662316_Ch14.indd 43 02/05/14 2:42 PM

44
14 Audiology—Terminology and Tests
a b c
Fig. 14.2a–c The Rinne test. Air and bone conduction are compared in the same ear.a Rinne positive, normally hearing ear. Air conduction is perceived louder than bone conduction in the test ear.b Rinne negative, conductive hearing loss. Bone conduction is perceived louder than air conduction.c Rinne posit ive, sensorineural hearing loss. Air conduction is perceived louder or longer than bone conduction (but
the duration is shorter than in normal hearing).
Fig. 14.3 A normal pure-tone audiogram.
0-10
102030405060708090
100110120130
.125 .250 .5 21 43 86 10
Air conductionBone conduction
Right ear
Frequency in kHz
H
e
a
r
i
n
g
t
h
r
e
s
h
o
l
d
(
d
B
)
0-10
102030405060708090
100110120130
.125 .250 .5 21 43 86 10
Air conductionBone conduction
Left ear
Frequency in kHz
H
e
a
r
i
n
g
t
h
r
e
s
h
o
l
d
(
d
B
)
• Norm al-hearing pat ients nd sound unpleasant above a level between 90 and 105 dB above threshold
• If recruitm ent present in a pat ient w ith cochlear HL, loudness discom for t level m ay be sim ilar to norm al-hearing people
• If no recruitm ent present , discom fort m ay not be experienced even at the m axim um output of the audiom eter
• The di erence between the hearing level and the loudest com fortable level reduces—a reduced dynam ic range
• Associated w ith disorders a ect ing hair cells of cochlea—absent in VIII n disorders
14.6 Acoustic Re ex Measurements• The quietest sound that elicits a re ex
cont ract ion of the stapedius m uscle is the acoust ic re ex threshold; the m uscle cont ract ion changes m iddle ear im m it tance, w hich can be recorded via t ympanom etry
Philpott_9783131662316_Ch14.indd 44 02/05/14 2:42 PM

45
Tympanometry (Fig. 14.4)
• The half-peak level (HPL) is w here half of the words are ident i ed correctly (norm al ~15 dB)
• CHL: ODS 100%, HPL raised (e.g., 35 dB)• SNHL: recruitm ent reduces speech
discrim inat ion so ODS ~60%, HPL ~30 dB• “Roll-over”: in ret rocochlear lesions as in tensit y
increase, ODS m ay reduce• Clin ical applicat ions:
◦ Predict ion of bene t from hearing aid ◦ Di cult to “fake,” so useful if suspect nonorganic HL
◦ Cochlear im plant candidacy ◦ May aid decisions about under taking procedures dest ruct ive to hearing (e.g., in Ménière disease)
14.8 Tympanometry (Fig. 14.4)• An object ive m easure of com pliance of the
t ym panic m em brane using re ected sound• Middle ear pressure inferred from point at
w hich TM is m ost accid: ◦ Type A: norm al response, apex w ith norm al range
◦ Type B: apex reduced to at line (e.g., w ith glue ear)
◦ Type C: apex shifted to negat ive pressures (im plies ET dysfunct ion)
• Perforated TM indicated by anom alously h igh ear canal volum e
• High-frequency st im uli used in young paediat ric test ing
• The re ex pathway has both ipsilateral and cont ralateral project ions
• A erent lim b of stapedial re ex arc: ◦ Middle ear ◦ Cochlea ◦ Cochlear n ◦ Cochlear nucleus and superior olive
• E erent lim b of stapedial re ex arc: ◦ VII n ◦ Stapedial m uscle/tendon ◦ Stapes
• Norm al m inim um sound in tensit y required to elicit re ex is 75 to 95 dB above norm al threshold
• No response seen in either ear w hen: ◦ A conduct ive loss in test ear ◦ Severe cochlear im pairm ent (60–70 dB) in test ear
◦ Mild VIII n auditory im pairm ent (0–40 dB) in test ear
◦ VII n gross dysfunct ion proxim al to stapedius nerve branch
14.7 Speech Audiometry• Uses standardized test m aterial to determ ine
auditory discr im inat ion abilit ies of pat ients—the abilit y to understand speech rather than pure tones
• It is norm al to hear 100% of the words ( opt im al discrim inat ion score, ODS), but som e pat ients need the sound to be presented m ore loudly
Loudspeaker
Microphone
Air pump
Reflextone
“ipsi”
Probetone
220 Hz
Fig. 14.4 Tympanometry. Tubes passing through an airtight plug transmit the test tone and the re ected tone. The exibility of the tympanic membrane, com-pliance, is calculated from the measured sound level. Pressure-dependent dis-placement of the tympanic membrane is regulated by an air pump.
Philpott_9783131662316_Ch14.indd 45 02/05/14 2:42 PM

46
14 Audiology—Terminology and Tests
14.10.2 Brainstem Evoked Responses (Fig. 14.5)• Aka: ABRs• Act ive elect rode on vertex, reference elect rode
on ipsilateral (test ear) m astoid process• Wideband clicks and h igh-frequency tone bursts• Air- and bone-conducted st im uli can be used• Pat ient required to stay st ill and relaxed
throughout• Looks at I–V latency of waves produced:
◦ I—VIII n ◦ II—cochlear nuclei ◦ III—superior olive ◦ IV—lateral lem niscus ◦ V—inferior colliculus (m idbrain) ◦ Beyond wave V is the h igher CNS
• Indicat ions: ◦ Threshold test ing in children (lim ited frequency speci cit y)
◦ Brainstem lesions ◦ In t raoperat ive test ing
14.9 Otoacoustic Emissions• An object ive test , detect ing outer hair cell
vibrat ions in the external auditory canal• Act ive outer hair cell processes in the cochlea
can em it sound: ◦ Spontaneous (SOAE): in the absence of any st im ulus
◦ Transient (TEOAE): em it ted follow ing an abrupt click st im ulus
◦ Distort ion product (DPOAE): sounds em it ted in response to two sim ultaneous tones of di erent frequencies
• Only a healthy cochlea w ith well-funct ioning OHC produces TEOAE/DPOAE
• Clin ical applicat ions: ◦ New born hearing screening ◦ Suspected nonorganic HL
14.10 Auditory Evoked Potentials• Works on principle that an auditory st im ulus
evokes elect r ical potent ials that can be recorded w ith elect rodes placed on the subject
14.10.1 Electrocochleography• Measurem ent of elect rical output of cochlea and
VIII n in response to acoust ic st im ulat ion• Avoids the need for m asking• Transtym panic placem ent of th in needle
elect rode on prom ontory (requires LA/sedat ion); ext rat ym panic m easurem ent w hen elect rode onto TM (less robust results)
• Response: ◦ Cochlear m icrophonic—hair cell signal (basem ent m em brane vibrat ion)
◦ Sum m at ing potent ial—alterat ion of elect r ical potent ial baseline in response to sound st im ulus
◦ Compound cochlear n act ion potent ial—cochlear n depolarizat ion
• Wideband clicks and h igh-frequency tone burst s
• Indicat ions: ◦ Threshold test ing in very young children or neurological disorders
◦ Ménière disease—increase in sum m ating potent ial in a ected ear, but lacks sensit ivit y
◦ In t raoperat ive m onitoring
0.5
0
-0.5
Amplitude (mV)
Time after acoustic st imulus (ms)0 987654321 10 11
I
II
III
IVV
VI VII
Fig. 14.5 Auditory brainstem response (ABR). The typical waveform consists of 5 or 7 waves (I–VII), which re ect the acoustically induced activity of the anatomi-cal structures of the auditory system.
Philpott_9783131662316_Ch14.indd 46 02/05/14 2:42 PM

47
Masking
• Rule 2: BC audiom etry: ◦ Masking is needed at any frequency w here the nonm asked BC threshold is lower (i.e., bet ter) than the AC threshold of either ear by 10 dB or m ore
◦ The worse ear (by AC) would then be the test ear and the bet ter ear would be the nontest ear to be m asked
◦ Note: If the BC th reshold w ith m asking rem ains the sam e or on ly increases by 5 or 10 dB, it is possible that the not -m asked BC resu lt w as from the ear w ith the w orse AC th reshold , and it m ay be necessary to test the bet ter ear w h ile app lying m asking to the w orse ear; th is w ill est ablish the t rue BC th reshold of the ear w ith the bet ter AC.
• Rule 3: AC audiom etry: ◦ Masking w ill be needed addit ionally w here Rule 1 has not been applied , bu t w here the BC th reshold of the bet ter ear is m ore acu te by 40 dB (if supra- or circum aural earphones have been used) or 55 dB (if in ser t earphones have been used) or m ore than the nonm asked AC th reshold at t r ibu ted to the w orse ear
◦ The worse ear would then be the test ear and the bet ter ear would be the nontest ear, to be m asked
◦ Note: Rule 3 is necessary because an AC frequency that does not require m asking under Rule 1 m ay need to be m asked if the BC results show that the nontest ear has a conduct ive elem ent
◦ Note that it is the sensit ivit y of the nontest cochlea (as indicated by the BC threshold) that is the im portant factor in cross-hearing
14.10.3 Cortical Electrical Response Audiometry• Late phenom enon—bi/t r iphasic wave star t ing
after 50 m s and last ing >200 m s• Secondary cor t ical perceptual phenom enon• Indicat ions:
◦ Threshold test ing (m edicolegal) ◦ Central deafness ◦ Nonorganic HL
14.10.4 Auditory Steady-State Responses• Evoked by cont inuous am plitude m odulated
st im uli• Frequency speci c, and several frequencies can
be assessed sim ultaneously• Not yet in w idespread clin ical use
14.11 Masking• When tones are applied to one ear, they
cause vibrat ion that passes to the opposite cochlea w here it w ill be detected (albeit at an at tenuated level of ~40 dB)
• Therefore the nontest ear som et im es requires “m asking” to ensure that it is not receiving the test signal
14.11.1 Rules for Masking• Rule 1: AC audiom et ry:
◦ Masking is needed at any frequency w here the di erence between the ears’ unm asked AC thresholds is ≥40 dB w hen using supra- or circum aural earphones or ≥55 dB if inser t earphones are used
Philpott_9783131662316_Ch14.indd 47 02/05/14 2:42 PM

48
15.1 Principles• A hearing aid (HA) is any device that
am pli es sound or assists the hearing-im paired individual (generally considered elect roacoust ic devices)
• Consider w hen hearing loss (HL) ~≥30 dB, though m ay be suitable for m inim al losses w ith t innitus, or for listening in speci c circum stances
• For asym m etric HL generally t poorer-hearing ear, although binaural t t ing usually preferable
• Glasgow bene t scale and Belfast rule of thum b can be considered for HA applicat ion as well as surgery
15.2 Components• Microphone: converts acoust ic energy to
elect r ical energy• Am pli er: boosts the elect rical signal• Receiver: t ransform s elect rical signal back to
acoust ic signal and broadcasts it in to the ear
15.3 Types of HAs• Behind the ear (Fig. 15.1): m ost com m only
available on NHS; best for m ore severe losses as less issues of feedback com pared w ith in-the-ear aids ◦ Open t: avoids problem s of occlusion caused by convent ional aids, helping w ith low -frequency noise appreciat ion , quick t t ing (no m old required), and allows bet ter ear canal vent ilat ion; generally good for h igh-tone losses (>1 kHz); bet ter cosm et ically
• In the ear (Fig. 15.1): lls concha; su itable for m ild, severe loss
• In the canal: m ore di cu lt to inser t (relevant if pat ient has ar th rit is, for exam ple)
• Com pletely in the canal• Bone conductor: suitable w hen no ear canal
or pinna, or chronic discharge; body-worn and bone-anchored types
• CROS: contralateral rout ing of signal• Im plantable devices: m iddle ear t ransducers,
cochlear im plants, and auditory brainstem implants
15.4 Principles• Gain: am pli cat ion of sound su cient for it to
be heard, though not uncom fortable (acoust ic gain = input–output dB)
• Frequency response: can be varied in m ost aids to have low - or h igh-frequency emphasis
• Com pression: so that the output does not exceed the com fortable listening levels of the individual
• Telecoil: allows aid to pick up sound by elect rom agnet ic induct ion (e.g., telephones, cinem a), excluding environm ental sounds
• Molds: ◦ Looser, m ore com fortable, and prevents occlusion e ect , w hich m akes pat ient’s voice sound louder because of the conduct ive loss a t ight m old gives; however, greater potent ial for feedback; vent ing m ay help t ighter m olds - Feedback occurs w hen am pli ed sound leaks from receiver back in to m icrophone
◦ A m old blocks the external auditory canal, w hich t raps low-frequency energy, m aking low-frequency internal sound (speaking, chew ing) unpleasantly loud, especially if the HL is not >40 dB; vented m olds help reduce this; even m ore if pat ient has “open t” aid
• Binaural am pli cat ion: bene ts include: ◦ Im proved word ident i cat ion and sound localizat ion
◦ Sense of balanced hearing and elim inat ion of head shadow e ect
◦ Need for less gain• Acclim at izat ion: it takes several weeks for
central auditory compensat ion to allow pat ient to acclim at ize to the new am pli cat ion of an HA; adjustm ents are often required after in it ial t t ing, but can be autom at ically program m ed
• Data logging: som e aids can be set to record t im ing and context of use
15.5 Bone-Anchored HAs15.5.1 Indications• Suitable for pat ients w ho are hearing im paired
but cannot wear convent ional aids, w ith conduct ive or m ixed loss:
15 Hearing Aids
Philpott_9783131662316_Ch15.indd 48 02/05/14 2:45 PM

49
Bone-Anchored HAs
• Children: earliest age of im plantat ion determ ined by skull th ickness and potent ial dam age to implant (by boisterous behaviour! ); 3 years probably m inim um , m ore usually ~ 5 years; younger children can use BAHA w ith “softband” unt il of suitable age for implantat ion
• “Softband” or bite-bar can help user appreciate potent ial bene t of BAHA before surgery
15.5.3 Principles• Osseointegrat ion: act ive bond form ed between
bone and t itanium ; irrigat ion during procedure helps preserve bone vitalit y
• Fixture and inst rum ents are t itan ium ; w hen in air, p icks up an oxide covering that is thought to be osteogenic
• First realized by Brånem ark t rying to nd suitable im plant m aterial for jaw /teeth
• Also observed that reindeer antlers (a form of osseointegrat ion) get no skin react ion because skin direct ly and t ightly applied: hence principle of rem oving subcutaneous t issue during procedure
15.5.4 Considerations• Staged procedure (im plant then abutm ent)
m ay be suitable in children to ensure adequate osseointegrat ion has occurred
• In children w ith congenital abnorm alit ies, need to consider r isk endocardit is from implant infect ion , if have concurrent cardiac abnorm alit ies—a relat ive contraindicat ion
• Consider sit ing of im plant if pat ient w ill require fu ture reconst ruct ion for m icrot ia
• Pat ient’s occupat ion: if they have to wear a hat , for exam ple, th is m ay be a cont raindicat ion
• “Sleeper” im plant in young to use if rst im plant fails
• Bilateral BAHAs can help provide binaural hearing e ect , im proving sound localizat ion and speech recognit ion in noise
• MRI not contraindicated (in norm al-st rength m achines)
15.5.5 Outcomes• >90% wear aid for w hole of waking day• Outcom e m easures show good stabilit y,
audiological bene t , and reduct ion in discharge w ith increased com for t
◦ Congenital (bilateral, conduct ive) ear abnorm alit ies
◦ Discharge, irr itat ion, or feedback prevents use of convent ional aid: bilateral chronic ot it is m edia w ith discharge is m ost com m on reason for bone-anchored hearing aids (BAHAs)
◦ Pat ients w ith m astoid cavity and unm anageable feedback, w here m old- t t ing is a challenge
◦ Children w ith Dow n syndrom e ◦ Otosclerosis if cannot or w ill not wear convent ional aid or contem plate stapedectomy
◦ If unilateral conduct ive or m ixed loss and other ear dead, so otosurgery considered too h igh a r isk to the residual hearing
• Unilateral severe to profound sensorineural HL: ◦ Fit t ing BAHA to deaf side allows t ranscranial st im ulat ion of other ear; th is helps lose head shadow and speech discr im inat ion in noise, but m inim al help w ith sound localizat ion; bene t is less cer tain and extended pre-operat ive t r ial w ith headband indicated to nd those w ho w ill nd it bene cial
15.5.2 Criteria• Bone conduction thresholds bet ter than ~40 dB for
head-level devices; bet ter than ~ 65 dB for body-level devices (which can provide better gain)
• With unilateral sensorineural hearing loss, profound-severe HL on a ected side (air conduct ion threshold worse than ~ 90 dB) w ith poor speech discrim inat ion and norm al hearing on contralateral side: h ighly m ot ivated and realist ic candidate
Fig. 15.1a, b Di erent types of HAs.a A behind-the-ear device.b An in-the-ear device with an ear mold t ted.
Philpott_9783131662316_Ch15.indd 49 02/05/14 2:45 PM

50
15 Hearing Aids
• Skin react ions around abutm ent in ~25% but only ~1% prevent BAHA being worn
• Failure to use BAHA long term is 2%, usually due to further deter iorat ion in hearing rendering aid inadequate
15.5.6 Complications• No operat ive risks to exist ing hearing, balance,
or facial nerve• Loss of xture from the bone ~1% (higher
in syndrom ic children because tend to have th inner cortex)
Philpott_9783131662316_Ch15.indd 50 02/05/14 2:45 PM

51
16.1 Principles• A CI is a device im planted in to the cochlea that
direct ly st im ulates nerve bres w ith in the auditory system , allow ing the percept ion of sound (Fig. 16.1) ◦ Stim ulates cochlear n bres (spiral ganglion cells) w ith acoust ic sounds that have been processed into elect rical energy
◦ Prim ary aim is to provide user w ith greater speech recognit ion abilit y than is possible w ith convent ional ampli cat ion
◦ Microphone (worn like an HA) conver ts sound in to elect r ical signals; speech processor analyzes and digit izes th is inform at ion in to coded signals (split t ing in to frequency bands); t ransm it ter is held over receiver by a m agnet and sends the code across the skin as radiofrequency waves; coded signal is conver ted to elect r ical signals that pass to the elect rode to allow for st im ulat ion of the nerve bres (tonotopic arrangem ent)
◦ Goal in children: to achieve age-appropriate speech, language, and listening skills; to reduce in tervent ion over t im e; to have m ainst ream educat ion; to be fully in tegrated in to hearing world
◦ Goal in adults: to support lip -reading; to improve com m unicat ion abilit y and develop telephone and open-set speech; to reduce e or t of com m unicat ion; to be in touch w ith surroundings
16.2 Indications• Paediat ric: children w ith pre-lingual deafness
have a cr it ical period in w hich they can be usefully im planted (<2 years) for greatest ben-e t; those children (or adults) w ho lost hear-ing after language acquisit ion have established cent ral auditory pathways so can be im planted up to 10 years after the onset of deafness: ◦ Profound sensorineural hearing loss in both ears (e.g., unaided >90 dB across speech frequencies)
◦ Lack of progress in the developm ent of auditory skills
◦ No m edical contraindicat ions
◦ High m ot ivat ion and appropriate expectat ions from fam ily
◦ Precise audiom etric inclusion criteria vary from centre to centre and as experience in CI grows
◦ Assess speech, language, and listening skills appropriate for age, developm ental stage, and cognit ive abilit y
• Adult >18 years: ◦ Pre-linguist ic or post-linguist ic onset of severe-to-profound hearing loss
◦ Audiom etric criter ia and exact test used to m ake assessm ent vary between centres
◦ Consider w hen hearing worse than 90 dB HL at 2 and 4 Hz; adequate bene t from a convent ional HA considered w hen >50% score on BKB (Bam ford-Kowal-Bench) sentence test-ing at sound in tensit y of 70 dB SPL, so needs to be worse to just ify CI
◦ No m edical cont raindicat ions ◦ A desire to be part of the hearing world
16.3 Contraindications• Audiom etr ic:
◦ Presence of signi cant residual hearing• Medical:
◦ Active infect ion (acute or chronic OM) ◦ Ossi ed cochlea ◦ Cochlea non-developm ent ◦ Unrealist ic expectat ions
16.4 Surgery• Procedure:
◦ General anaesthesia, m astoidectomy w ith posterior t ympanotomy
◦ Cochleostomy anteroinferior to round w indow m em brane
• Device: ◦ Mult i-channel elect rodes generally used, w ith variable num ber of speci c elect rodes depending upon device used
◦ In t ra-operat ive test ing w ith neural response telem etry, checks that im plant is working and in contact w ith auditory n endings
◦ Post-operat ive sw itch-on usually after ~4 to 6 weeks w ith cont inued “rem apping” over next few years
16 Cochlear Implantation
Philpott_9783131662316_Ch16.indd 51 5/20/14 11:45 AM

52
16 Cochlear Implantat ion
• Risks of surgery: ◦ Facial paresis/paralysis (tem porary or perm anent): 1:500 to 1:1000
◦ Taste disturbance (tem porary): 10% ◦ Loss of residual hearing: dependent on surgical technique and implant used
◦ Balance dysfunct ion/vert igo—tem porary: m ost pat ients; long-term balance dysfunct ion rare
◦ Infect ion: <1% but m ay/usually necessitate rem oval of im plant
◦ Meningit is—perioperat ive: 1:5000 (vaccinate vs. pneum oncoccus, Hib); long-term risk sim ilar to general populat ion
16.5 Expected Outcomes• Does not provide norm al hearing• Gradual im provem ent in perform ance especially
in rst 6 m onths, but for up to 2 years• 95% adults have im proved lip -reading, 50% have
acquired open-set speech discrim inat ion , 35% can use telephone
• 90% children aided <2 years enter m ainst ream educat ion
• Reliabilit y: 97 to 99% funct ioning at 10 years
16.6 Special Considerations• Which ear?
◦ Bet ter-hearing or worse-hearing ear, depending if plan for bim odal st im ulat ion
◦ HA use in im planted ear usually predict ive of bet ter perform ance than non-aided ear
◦ Vest ibular funct ion• Bim odal st im ulat ion; HA one ear, CI in the other
◦ Helps in background noise, for sound localizat ion , and allows for bet ter m usic appreciat ion
• Bilateral CIs ◦ Im proved sound localizat ion , speech understanding in quiet and noise
◦ Guaranteed to im plant bet ter ear ◦ Im proved speech, language, and auditory developm ent in children
◦ If one fails, not com pletely isolated ◦ Sim ultaneous bilateral CI recom m ended in adults and children , especially w hen codisabilit y (e.g., blindness)
• Hybrid im plants, “elect roacoust ic st im ulat ion” ◦ Shorter elect rodes used for h igh tone loss w ith convent ional HA for lower frequencies
◦ Helps w ith pitch percept ion , speech discrim inat ion in quiet
• MRI scanning in CI recipients ◦ Usually requires rem oval of m agnet prior to MRI scan; depends upon tesla st rength of MRI m achine and speci c implant inst ruct ions
◦ Causes ar tefact (shadow ing) surrounding im plant
◦ Must rem ove speech processor and headset before entering MRI room
16.7 Auditory Brainstem Implants• Auditory brainstem im plants (ABIs) bypass
auditory n to directly st im ulate the cochlear nucleus com plex, exploit ing it s tonotopic organizat ion (although th is is a com plex arrangem ent in the nucleus, so results less sat isfying than for CI)
• Indicat ions: ◦ Neuro brom atosis t ype 2 (NF2): develop bilateral vest ibular schwannom as; if undergoing tum our rem oval w ith predicted loss of hearing consider insert ing ABI at t im e of surgery (som et im es as sleeper if cont ralat-eral ear st ill has useful hearing—cont roversial)
1
2 3
4
6
5
Fig. 16.1 Cochlear implant. Microphone (1), external speech processor (2), electronic receiver (3), electrode array (4), cochlea (5), vestibulocochlear n (6).
Philpott_9783131662316_Ch16.indd 52 5/20/14 11:45 AM

53
Auditory Brainstem Implants
◦ Non-tum our ABI inser t ion: considered in children w ith congenital bilateral HL that precludes CI (inner ear m alform at ions, cochlear n hypoplasia); also in post-m eningit is ossi cat ion , t raum a, severe cochlear otosclerosis
• Speech percept ion results not as good as CI; bet ter in non-tum our pat ients
• In com binat ion w ith lip -reading m ay aid oral com m unicat ion
• Results from non-tum our group seem to be bet ter than for NF2
Philpott_9783131662316_Ch16.indd 53 5/20/14 11:45 AM

54
17.1 Principles and De nitions• Postural control required to m aintain stable
im age on the ret ina despite head m ovem ents and to prevent falling and possible injury
• Balance is dependent upon visual input (~70%), propriocept ion (~15%), and vest ibular input (~15%)
• Dizziness encom passes various sym ptom s, including vert igo, w hich tends to be associated w ith peripheral vest ibular disorders
• However, ver t igo can be seen w ith m igraine, m ult iple sclerosis (MS), cerebrovascular ac-cident (CVA), vest ibular schwannom a, epilepsy, m edicat ion
• Vert igo is the sensat ion of rotat ion or m ovem ent of one’s self or of one’s surroundings in any plane; it is disabling
• Dysequilibr ium is w hen the brain gets inad-equate inform at ion from som atosensory, visual, or vest ibular system s and pat ient feels unsteady
• An individual w ith vert igo or dizziness that im pairs their driving has an obligat ion to inform the relevant authorit y to assess their tness to m aintain a license; at tacks com ing on w ithout enough warning to be able to safely get to the side of the road w ill be signi cant , as w ill re-sponse to t reatm ent; speci c guidance is usually available (such as from the DVLA in the United Kingdom )
• Mult i-level vest ibulopathy: in elderly people w here reduced qualit y and quant it y of sensory inform at ion arise from m ult iple sensory path-ways, all of w hich m ay be opt im ized to aid the pat ient
• Anxiety can lead to hypervent ilat ion w ith light-headedness and dizziness rather than t rue vert igo; the anxiety m ay result from a previous vest ibular insult that has been com pensated for
17.2 Benign Paroxysmal Positional Vertigo17.2.1 Assessment and Management• The Brit ish Society of Otology has a select ion of
videos relat ing to benign paroxysm al posit ional
vert igo (BPPV) assessm ent and m anagem ent , and clin ical balance funct ion test ing (h t tps://entuk.org/bso/videos). These include: ◦ Test ing for posterior and anterior canal BPPV: h t tp://w w w.youtube.com /watch?v=Ew 14aZqiUrw
◦ Treatm ent for canalith iasis of posterior and anterior canal: h t tp://w w w.youtube.com /watch?v=o4CKy3R1SPA
◦ Stapedectomy: h t tp://w w w.youtube.com /watch?v=h2G2xuB0kOo
◦ Rinne and Weber tuning fork tests: h t tp://w w w.youtube.com /watch?v=RVH4K4EcsiA
◦ Hearing m echanism : h t tp://w w w.youtube.com /watch?v=GGqfRvCkt-w
17.2.2 Posterior Scc BPPV• Pathology:
◦ Usually in posterior Scc ◦ Canalolith iasis or free- oat ing debris ( otoconia) in endolym ph causes cont inuing st im ulat ion after m ovem ent of head has ceased
◦ Cupulolith iasis: debris from otolith organ becom es at tached to cupula
• Aet iology: ◦ Usually idiopathic; ~20% associated w ith m inor head t raum a
• Epidem iology: ◦ Any age (peak 6th–7th decades); m ost com m on cause of ver t igo
◦ Associated w ith preceding inner ear disease (e.g., Ménière, vest ibular neurit is)
• Sym ptom s: ◦ Vert igo of seconds to m inutes durat ion associated w ith rapid changes in head posit ion (e.g., rolling over in bed, turning to reach objects on h igh shelves)
◦ Attacks often in clusters, m ay recur after period of rem ission
• Ix: ◦ Dix–Hallpike m anoeuvre: provokes ver t igo and nystagm us (a ected ear dow nwards) - Nystagm us rotatory w ith latency of a few seconds, fat igues after 30 to 40 s
- Torsional, beats towards oor (geotropic), direct ion reverses on sit t ing up
17 Vestibular Disorders
Philpott_9783131662316_Ch17.indd 54 02/05/14 2:51 PM

55
Ménière Disease
- Rinne and Weber tuning fork tests: h t tp://w w w.youtube.com /watch?v=RVH4K4EcsiA
- Hearing m echanism : h t tp://w w w.youtube.com /watch?v=GGqfRvCkt-w
17.2.3 Lateral Canal or Horizontal BPPV• Less com m on; can be tested for by sit t ing
pat ient at 30° head-up on couch and laterally rotat ing head to either side
• Will give geotropic nystagm us (horizontal) w hen head turned to either side
• Epley equivalent involves “barbecue-spit” rotation• Potent ial to surgically occlude a ected canal
17.2.4 Superior Scc BPPV• Dow nbeat nystagm us w ith torsional com ponent
17.3 Ménière Disease• Disease described below; syndrom e associated
w ith other diagnoses (e.g., syphilis, otosclerosis)• Pathology: uncertain and all theories have aws:
◦ Disease of the m em branous inner ear, w ith excess endolym ph (endolym phat ic hydrops) product ion (st r ia vascularis), or reduced absorpt ion (endolym phat ic sac)
• Rx: ◦ Spontaneous rem ission rate h igh ◦ Epley m anoeuvre (Fig. 17.1) to disperse canal debris in to ut ricle (w here it is inact ive); e ect ive in ~85% cases
◦ Sem ont m anoeuvre is alternat ive: head rotated 45° away from a ected ear; lie quickly on side of a ected ear; stay 1 m in then quickly over onto opposite side (i.e., for R side, go from R ear dow n to L eye dow n)
◦ Brandt–Daro head exercises ◦ Avoid vest ibular sedat ives (e.g., prochlorperazine)
◦ Poster ior Scc occlusion in severe recurrent cases; singular neurectomy possible
• Assessm ent and m anagem ent ◦ The Brit ish Society of Otology has a select ion of videos relat ing to BPPV assessm ent and m anagem ent , and clin ical balance funct ion test ing (h t tps://entuk.org/bso/videos). These include: - Test ing for posterior and anterior canal BPPV: ht tp://w w w.youtube.com /watch?v=Ew 14aZqiUrw
- Treatm ent for canalith iasis of posterior and anterior canal: h t tp://w w w.youtube.com /watch?v=o4CKy3R1SPA
- Stapedectomy: h t tp://w w w.youtube.com /watch?v=h2G2xuB0kOo
Fig. 17.1a–e The Epley manoeuvre (shown testing the right ear).a The patient is seated upright with the head turned 45° to the right.b The patient is moved rapidly into the supine position with the head extending just beyond the examining table and
the right ear downward. The posit ion is held until nystagmus fatigues, usually ~ 30 s.c The head is rotated 90° to the opposite side, stopping with the right ear upward. The position is held for ~ 30 s.d The patient rolls onto the left side while the examiner maintains the head position looking over the left shoulder
such that the nose is now angled to the oor. The position is held for ~ 30 s.e The patient is lifted to a sit ting position, swinging their legs over the left side of the bed.
a b c d e
Philpott_9783131662316_Ch17.indd 55 7/7/14 3:24 PM

56
17 Vest ibular Disorders
◦ De nite: two or m ore de n ite episodes vert igo ≥20 m in, audiom etrically docum ented HL at least once, t innitus or aural fullness
◦ Certain : de n ite w ith h istopathological con rm at ion
• Prognosis: recognized stages: ◦ I: episodic disabling ver t igo; norm al caloric funct ion; HL norm al between at tacks; 50% progress to
◦ II: vert igo peaks and abates; 20 to 50% canal paresis; HL established (low -frequency SNHL); ~5% progress to
◦ III: burnt-out vert igo; 50% vest ibular funct ion can rem ain; severe HL (SNHL at ~60 dB)
◦ Spontaneous resolut ion in 70% (com pare w ith success of t reatm ent opt ions)
• Ix: ◦ Diagnosis m ade m ainly on h istory:
- Exclude vest ibular schwannom a w hen unilateral inner ear sym ptom s (MRI)
- PTA - Calorics: develop canal paresis on side of lesion, direct ional preponderance towards norm al ear
- ECoG: broadening of sum m ating potent ial/ act ion potent ial
- Glycerol dehydrat ion test: m easures audiom etric reponse to oral dose of glycerol; works on basis that dehydrates cochlea, so should im prove sym ptom s; lowers plasm a osm olalit y and im proves PTA thresholds and speech discrim inat ion exclusively in Ménière disease
• Nonsurgical Rx: ◦ Spontaneous resolut ion ~70% ◦ Vest ibular sedat ives during at tacks (m ay be counterproduct ive if used regularly for prevent ion)
◦ Betahist ine up to 16 m g three t im es a day; lit t le evidence of bene t (but lit t le harm )
◦ Salt-rest ricted diet (and possibly alcohol, ca eine)
◦ Thiazide diuret ics have lit t le proven bene t ◦ In t rat ym pan ic gen tam icin : con t rol of at tacks in up to 90%; hear ing preserved or im proved in ~75% (gentam icin is m ore vest ibu lotoxic than coch leotoxic); am inoglycosides cause dam age to the dark cells of the st r ia vascu lar is, therefore reducing endolym ph product ion
◦ In t ratym panic steroid inject ion has been show n to be bet ter than placebo
◦ Vasospasm theory: basis of using betahist ine (vasodilator)
◦ Rupture theory: increased uid ruptures Reissner m em brane, so potassium leaks, get perilym ph and endolym ph m ixing, and paralysis of nerves
◦ Chem ical theory: potassium in toxicat ion of perilymph (from endolym ph) because leakage at m echanically st ressed t ight junct ions
◦ Drainage theory (Gibson m odel of hydrops): loss of norm al m echanism that detects increased endolymph volum e unt il cr it ical pressure in it iates ow to endolym phat ic sac; the narrow aqueduct lim its ow to sac, so som e goes ret rograde to ut r icle, a ect ing ut ricular valve and producing ver t igo
◦ Im m unological theory: circulat ing im m une complexes m ay produce in am m ation and in terfere w ith funct ion of sac
• Epidem iology: ◦ Middle-aged F>M, 10% fam ilial, usually unilateral; at 2 years 15% bilateral, at 20 years 40%
◦ Incidence ~1:1000• Sym ptom s:
◦ Episodic t r iads of in term it tent disabling vert igo, uctuat ing HL, t innitus and associated pressure sensat ion; at tacks tend to occur in clusters over several weeks - Vert igo: recurrent episodes last ing 20 m in to 24 h , associated nystagm us, nausea and vom it ing, no neurological sym ptom s
- Deafness: low -frequency uctuat ing SNHL, progressive
- Tinnitus: variable, louder during at tacks, unilateral on a ected side
- Drop at tacks possible: acute at tack of ver t igo causing pat ient to drop to the oor as if st ruck by a sledgeham m er (w ith nausea and vom it ing)
- “Otolith ic crisis of Tum arkin”: a drop at-tack w ithout Ménière symptom s, followed by im m ediate recovery upon standing up; no warning or loss of consciousness; m ay be due to disturbance in otolith ic organs; seen in 1 to 2% pat ients w ith Ménière disease
• Diagnost ic categories: ◦ Possible: episodic vert igo w ithout HL, or SNHL w ith dysequilibr ium but not de n ite episodes
◦ Probable: one de n ite episode vert igo, audiom etr ically docum ented HL at least once, t innitus or aural fullness
Philpott_9783131662316_Ch17.indd 56 02/05/14 2:51 PM

57
Migrainous Vert igo
◦ Decom pensat ion episodes w ith disequilibrium com m on over next two years, but generally gradually reduce in in tensit y, durat ion , and frequency
• Rx: ◦ Com pensat ion prom oted by vest ibular rehabilitat ion (often physiotherapy led)
◦ Those w ith visual vert igo (overreliance on visual input) require physiotherapy exercises in visually st im ulat ing environm ents
◦ Vest ibular sedat ive helpful in acute period but counterproduct ive in long term
• Sequelae: ◦ Increased incidence of BPPV
17.5 Migrainous Vertigo• De nit ion:
◦ Various term s include m igraine-associated dizziness, vest ibular m igraine, and m igrainous ver t igo (MV)
• Pathology: ◦ Pathogenesis unclear, but m ay be due to vasoconst rict ion of in ternal auditory ar tery or asym m etric release of neuropept ides that have an excitatory e ect on the vest ibular nuclei
• Epidem iology: ◦ Migraine is com m on (up to 30% F, 20% M at som e point in life)
◦ Vert igo m ay be due to m igraine, or sim ply co-exist w ith it (3–4% populat ion likely to have both by coincidence alone)
◦ Associat ion w ith m enstruat ion , older pat ients have past h istory of m igraine, FH com m on
17.5.1 ICHD-II Criteria for Migraine:• Migraine w ithout aura: ≥ 5 at tacks w ith
◦ Headache 4 to 72 h ◦ Headache w ith 2 of: unilateral locat ion , pulsat-ing qualit y, m oderate–severe pain , aggravat ion by or causing avoidance of rout ine physical act ivit y (e.g., walking)
◦ During headache, nausea and vom it ing and/or photophobia/phonophobia
◦ Not at t r ibuted to another disorder• Migraine w ith aura: ≥2 at tacks w ith :
◦ Aura w ith one of follow ing, but no m otor weakness: - Fully reversible visual sym ptom s ( ickering lights, spots, lines, loss of vision)
◦ Cognit ive-behavioural therapy (CBT): a severe Ménière at tack is st ressfu l, scoring to a com parable level as those su ering from a heart at tack or bypass surgery—so m ay experience post t raum at ic st ress disorder as a result; CBT can help som e people deal w ith the uncer tain ty of the disease that leads to the anxiety and dist ress
• Surgical Rx: ◦ Consider in 30% of pat ients w ho do not spontaneously resolve or fail to be helped by m edical therapy
◦ Choice depends on w hether or not hearing is serviceable: - Hearing-preserving procedures: grom m et (vent ilat ion tube) inser t ion , endolym phat ic sac decom pression, vest ibular n sect ion
- Meniet t device—m icropressure to inner ear via grom m et; m ay work by allow ing in term it tent low -pressure waves to pass through grom m et to round w indow m em brane, t ransm it to perilym ph, com press endolym phat ic labyrin th to redist r ibute endolym ph pressure to sac and blood vessels; alternat ively m ay a ect oxygenat ion , horm ones (at r ial nat riuret ic pept ide), or dow nregulate uid product ion
- Hearing-dest ruct ive (so m ainly indicated w hen hearing has already gone): osseous labyrin thectomy is the gold standard t reatm ent w ith 98% vert igo control; m ain concern is if subsequently develop bilateral disease
- Bilateral end-stage Ménière disease is indica-t ion for cochlear implantat ion
17.4 Acute Vestibular Failure• De nit ions:
◦ Labyrin th it is suggests coexistent HL ± t innitus ◦ Neuronit is im plies just vest ibular sym ptom s
• Aet iology: ◦ Possible viral role (HSV) ◦ Vascular, t raum a, iat rogenic (e.g., post gentam icin), bacterial infect ion , local disease (cholesteatom a, vest ibular schwannom a), autoim m une (e.g., Cogan syndrom e)
• Sym ptom s and natural h istory: ◦ Vert igo last ing > 24 h ; often bed-bound for a few days
◦ Recovery usually spontaneous over ~1 week as cent ral compensat ion occurs
Philpott_9783131662316_Ch17.indd 57 02/05/14 2:51 PM
58
17 Vest ibular Disorders
• Nausea and im balance• May not occur at sam e t im e as headache• Phonophobia, photophobia (so rest in darkened
room ), other sym ptom s of aura• HL, t innitus unusual (but presence not exclude
diagnosis)
17.5.3 Rx:• Vert igo associated w ith m igraine should re-
spond to sam e t reatm ent as m igraine• Diet: rest r ict ca eine, chocolate, red w ine,
cheese, processed m eat• Reduce st ress• Com bined OCP m ay help• Migraine prophylact ics:
◦ β-Blockers (e.g., m etoprolol, propanolol) ◦ Tricyclic ant idepressants (e.g., low-dose am it r iptyline)
◦ Pizot ifen (ant ih istam ine, serotonin antagonist)• Acute m igraine m edicat ions m ay help (e.g.,
sum atriptan , ergotam ine)
17.6 Superior Semicircular Canal Dehiscence• Theory:
◦ When bone is m issing over the superior Scc, th is acts as an addit ional w indow for the vest ibular system , allow ing pressure and noise changes to induce vest ibular act ivit y
• Features: ◦ Tullio sign: vest ibular sym ptom s due to loud sound
◦ Hennebert sign: vest ibular sym ptom s due to changes in EAC pressure
◦ Gaze-evoked t innitus (25% pat ients): sw ishing noise w hen m ove eyes
◦ Hyperacusis ◦ Chronic im balance ◦ Autophony ◦ May detect ver t ical torsional nystagm us, slow waves directed away from labyrin th suspected of being dehiscent if st im ulated by stula test (pressure on t ragus), opposite if done w ith Valsalva; if st im ulate w ith noise (e.g., Baranay box), nystagm us away from side of lesion
• Ix: ◦ PTA: although AC thresholds m ay be norm al, need to do BC thresholds (m asked) as m ay nd hyperacusis to BC w ith an ar t i cial ABG
- Fully reversible sensory sym ptom s (pins and needles, num bness)
- Fully reversible dysphasic speech disturbance ◦ Two of follow ing:
- Hom onym ous visual sym ptom s and/or unilateral sensory sym ptom s
- At least one aura sym ptom develops gradually over ≥5 m in and/or di aura sym ptom s occur in succession over ≥5 m in
- Each sym ptom lasts ≥5 m in and ≤ 60 m in ◦ Headache (as for m igraine w ithout aura) begins during aura or follows aura w ith in 60 m in
◦ Not at t r ibuted to another disorder• De nit ive MV: each of follow ing cr iter ia m ust
be m et: ◦ Migraine (as per above) ◦ Moderate–severe episodic sym ptom s of vest ibular involvem ent including: - Spontaneous or posit ional vert igo - Other spontaneous or posit ional sym ptom s of self or object , not rotat ional
- Head m ovem ent-provoked sym ptom s of in tolerance, im balance, rotat ional, or non-rotat ional ver t igo
◦ At least one m igraine sym ptom occurring during a m inim um of two of pat ient’s repor ted episodes of “dizziness”
◦ Rule out other causes of dizziness• Probable MV: each of follow ing:
◦ Moderate–severe episodic sym ptom s of vest ibular involvem ent including: - Spontaneous or posit ional vert igo - Other spontaneous or posit ional sym ptom s of self or object , not rotat ional
- Head-m ovem ent-provoked sym ptom s of in tolerance, im balance, rotat ional, or non-rotat ional ver t igo
◦ One of: - Migraine (as per above) - Migraine sym ptom s during at least two dizzy spells
- Two or m ore dizzy spells responded to use of ant im igraine m eds, or two or m ore spells pro-voked by m igraine-speci c t riggers ( including foods, beverages, horm onal changes, sleep disrupt ions, sudden exposure to bright light)
17.5.2 Symptoms:• Spontaneous or posit ional vert igo (variable
durat ion seconds–days)
Philpott_9783131662316_Ch17.indd 58 02/05/14 2:51 PM

59
Superior Semicircular Canal Dehiscence
e ect; a low-threshold VEMP raises suspicion rather than con rm s diagnosis (VEMPs have ~80% sensit ivit y and speci cit y for condit ion)
• Rx: ◦ Surgical correct ion (by plugging or resurfacing) for pat ients w ith severe disabling sym ptom s (e.g., via m iddle cranial fossa or t ransm astoid approach)
◦ CT: h igh-resolut ion , reconst ructed in the plane of the superior Scc; low speci cit y w ith overdiagnosis of condit ion
◦ Vest ibular evoked myogenic potent ials (VEMPs): response at low thresholds (<65 dB) produces a VEMP on a ected side; m ay be because of hypercom pliance of vest ibular system on a ected side due to the 3rd-w indow
Philpott_9783131662316_Ch17.indd 59 02/05/14 2:51 PM

60
18.1 Diagnosis• Most vest ibular disorders are diagnosed from
the h istory, but exam inat ion and som et im es invest igat ion m ay be helpful
18.2 Examination• Need to assess various aspects that contr ibute
to balance
18.2.1 Ear• EAC, TM (for COM), PTA (asym m etrical SNHL
consider vest ibular schwannom a), tuning fork test ing
• Fistula test: if bone over lateral Scc eroded by COM, exposes m em branous canal: in term it tent pressure on t ragus induces ver t igo/t ransient nystagm us; a stula m ay also cause a Tullio phenom enon: ver t igo w ith loud sounds (sound energy via m obile footplate to labyrin th)
18.2.2 Vestibulo-Ocular• Vest ibulo-ocular re ex (VOR) m aintains gaze
stabilit y during head m ovem ents (detected by labyrin th)
• Ocular palsies (III n , IV n , VI n) suggest in t racranial pathology
• Nystagm us: a rhythm ic, oscillat ing, involuntary m ovem ent of the eyes that m ay be horizontal, vert ical, rotatory, or m ixed; m ay be physiologi-cal or pathological (congenital, spontaneous, posit ional): ◦ Slow phase beats to a ected side, due to impulses from vest ibule (or visually induced) if paralyt ic problem (m ost com m on)
◦ Fast phase is w hat is described, the recovery m ovem ent , a central correct ing (saccadic) re ex
◦ Nystagm us m ay be in par t a failure of the VOR, due to peripheral (labyrin th ine) or cent ral pathology
◦ If ir r itat ive vest ibular problem (e.g., acute Ménière at tack) nystagm us (fast phase) beats towards bad ear
◦ 75% norm al people get physiological nystagm us if eye deviates fur ther horizontally than canaliculi, or w hen looking out of w in-dow of m oving t rain (optokinet ic nystagm us— indicates in tact visual pathways)
◦ Congenital nystagm us is present from bir th ◦ Spontaneous nystagm us present w hen pat ient sit t ing st ill, no external st im ulus; increasing degrees of severit y (Alexander law: in pat ient w ith vest ibular lesion the nystagm us becom es m ore pronounced w hen pat ient looks in direct ion of the quick-phase): - 1st degree: present w hen eyes deviated in direct ion of fast component
- 2nd degree: present on central gaze - 3rd degree: w hen eyes deviated in direct ion of slow phase
◦ If spontaneous nystagm us + dysequilibr ium at the t im e = peripheral (otological) cause; usually fat igues
◦ If spontaneous nystagm us + no dysequilibrium at the t im e = central cause
◦ Spontaneous nystagm us m ay be due to current drug therapy (e.g., benzodiazepines, phenyto-in , barbiturates, w hich m ay be being taken for dysequilibrium )
◦ Posit ional nystagm us: e.g., w hen head in a speci c posit ion or m oved quickly to a speci c posit ion
Note: When test ing eye m ovem ent in horizontal plane, failure of conjugate gaze (hence inability to m ove both eyes in the sam e direction) = internu-clear ophthalm oplegia, a sign of m ultiple sclerosis ◦ Nystagm us (spontaneous) assessm ent; pat ient sit s up, looking ahead and then 30° to either side; Frenzel glasses prevent visual xat ion and m ake easier observat ion (enhance periph-eral induced nystagm us, suppress central)
◦ Dix–Hallpike test for posit ional nystagm us: +ve for BPPV if delayed rotatory nystagm us w ith dist ress that resolves; if central cause get sudden onset nystagm us w ithout dist ress and no resolut ion
◦ Optokinet ic re ex m aintains visual xat ion on a m oving object w hen the head is stat ionary: - Sm ooth pursuit: the response for slowly m oving objects that keeps the target on
18 Vestibular Examination and Investigation
Philpott_9783131662316_Ch18.indd 60 02/05/14 2:53 PM

61
Invest igat ion
plane, w ith pat ient’s eyes closed); if nystag-m us, pathology in vest ibular input in plane of rotat ion (odd nystagm us if cent ral problem )
◦ Dynam ic visual acuity: (reading during headshake); reduced acuit y probable vest ibular problem ; get oscillopsia, a visual blurring on head m ovem ent
◦ VOR suppression test: (follow object that rotates w ith head, e.g., tongue depressor held in teeth , w hich has a pin stuck vert ically in it); should be able to visually suppress vest ibular signal, but if CNS pathology get nystagm us due to incom plete visual xat ion
18.2.3 Vestibulospinal• Vest ibulospinal response preserves appropriate
m uscle tone to avoid falling w hen environm ent is m oving
• Unterberger test (Fig. 18.1): m ark t im e stepping on spot w ith arm s outst retched, palm s faced up, eyes closed; reduces input from propriocept ion and eyes; rotate to side of paralyt ic labyrin th ine lesion (in the acute set t ing)
• Rom berg test: stand w ith feet together, arm s by side, eyes shut; +ve if im balanced (visual sup-pression); sway to side of lesion if labyrinth ine problem ; central cerebellar lesion gives sym -m etrical sway less a ected by eye closure; can m ake test m ore sensit ive to vest ibular de cits by standing pat ient on 3″ (8 cm ) foam or assessing them in tandem gait (rem oves propriocept ive input)
• Heel/toe gait; failure im plies central ( cerebellar) component (if not during acute vest ibular epi-sode); gait w ith eyes closed—veers towards side of vest ibular lesion (but non-speci c)
• General gait observat ion as pat ient walks
18.2.4 Other• Hypervent ilat ion: m ight reproduce sym ptom s• Cerebellar function ( nger–nose, dysdiadokokinesis)• Other CNS• Consider cardiovascular exam inat ion (e.g., for
postural drop in blood pressure, arrhythm ias)
18.3 Investigation• Vest ibular funct ion test ing is rarely diagnost ic,
but m ay help to determ ine w hether a condit ion is cent ral or peripheral, uni- or bilateral
the fovea; pat ient t racks a target m oving sinusoidally (e.g., follows sw inging pendu-lum ); unilateral im pairm ent im plies CNS pathology, m aybe cerebellar (bilateral m ore non-speci c, m ay be drug-induced)
- Saccadic eye m ovem ents: the response to objects that m ove out of the visual eld requiring a restorat ive m ovem ent of the eyes (a saccade) to bring back to the fovea; pat ient looks back and for th between exam iner’s ngers, separated horizontally or ver t i-cally; abnorm alit ies imply central pathology ( assum ing norm al ocular m uscles)
◦ Head thrust /Halm agyi test: (pat ient xes on target , e.g., your nose, as you turn head rapidly to each side); if re xat ion saccade back to target im plies reduced vest ibular funct ion in plane of rotat ion for ear ipsilateral to thrust , because reduced input to VOR
◦ Post-headshake nystagm us: (t ilt head 30° forward and shake in horizontal or vert ical
Fig. 18.1 The Unterberger stepping test. The patient is asked to walk on the spot with eyes closed.
Philpott_9783131662316_Ch18.indd 61 02/05/14 2:53 PM

62
18 Vest ibular Examinat ion and Invest igation
• In terpretat ion: cold causes nystagm us to opposite side, warm to sam e (COWS) ◦ Warm water causes endolym ph to rise in later-al Scc, so de ect ing kinocilium towards u t ricle and hence increasing r ing rate; consider test on R ear—this response, via VOR, causes eyes to m ove to L, so the correct ive response is a saccade to the R (so R-beat ing nystagm us)
• Form ulas based on recorded t im es predict degree of vest ibular act ivit y
• Unilateral canal paresis denotes response of one side is reduced or absent compared w ith other side; usually im plies lesion of peripheral vest ibular system ; signi cant canal paresis is >20–25%
• A direct ional preponderance (DP) denotes non-speci c enhancem ent of nystagm us in one part icular direct ion; suggests pathology but is usually non-localising (i.e., peripheral or central); signi cant if ~>20%; m ay be localizing w ith som e peripheral lesions w hen DP is usually directed away from diseased ear
• This test ing relies on com paring the two ears, so if both im paired ident ically, w ill fail to dem onstrate th is
18.3.2 Electronystagmography• Elect ronystagm ography (ENG) evaluates the
VOR object ively• Best done w ith Frenzel lenses to prevent visual
xat ion that can inhibit nystagm us• Uses norm al elect r ical potent ial between cornea
and ret ina; eye m ovem ents alter th is potent ial relat ive to surface elect rodes placed around the eye
18.3.1 Calorics• Physiology:
◦ Sccs detect angular accelerat ion ◦ Within am pulla of each canal have the crista on w hich sit s the cupula
◦ Endolymph lls the m em branous canal and has inert ia, so there is a relat ive di erence in velocity of canal and the uid w ith head m ove-m ents; so uid forced through gap between crista and cupula causing de ect ion of stereo-cilia, increasing or decreasing the rest ing tonic discharge depending on direct ion of de ect ion
◦ The two labyrin ths work in conjunct ion, so increase in neural signals from one is associated w ith decrease in other
◦ The three Sccs are at r ight angles so 3D infor-m at ion provided
• Caloric test ing alters the tem perature of endo-lym ph to set up therm ally induced convect ion currents that st im ulates stereocilia and causes nystagm us and vert igo (Fig. 18.2a)
• St im ulat ing tem ps are equally above and below body temp (30° and 44°C)
• Only the lateral Scc is st im ulated• Pat ient at 30° recline, thus put t ing the lateral
Scc in the vert ical plane• Cold water rst , t im ing unt il nystagm us stops,
then other ear, then warm water• Can use air to supply therm al st im ulus w hen
TM perforat ion• Can record nystagm us elect rically (elect ronys-
tagm ography) or simply observe (Fig. 18.2b, c)• Tests in part the in tegrit y of the VOR; the
response should be sym m etrical w hen both lateral Sccs are in tact
Fig. 18.2a–c Principle of caloric labyrinthine tests.a Temperature changes at the lateral labyrinthine cause a change in the density of the perilymph, leading either to an
in ux away from the ampulla (cold stimulus) or to an in ux towards the ampulla (warm stimulus). The oscillation of the cupula produces a neural st imulus that is transmit ted by the vestibular nerve (3) to the vestibular nucleus (1) and ocular muscle nucleus (2).
b Examination with electrode de ection.c Examination with videonystagmography.
Nystagmus
30 C
44 C
1
22
3a
Philpott_9783131662316_Ch18.indd 62 02/05/14 2:53 PM

63
Invest igat ion
18.3.4 Vestibular Evoked Myogenic Potentials• Infer ior vest ibular n innervates the saccule,
w hich has som e sound sensit ivit y• Has its m ain input to the lateral vest ibular
nucleus w here the two m ain postural t racts originate: ◦ The m edial vest ibulospinal t ract m aintains posture in the neck
◦ The lateral vest ibulospinal t ract is for lower t runk and lim bs
• Vest ibular evoked m yogenic potent ials (VEMPs) test for re ex that begins as sound presented to ear and ends as inhibitory response of ipsilateral sternocleidom astoid (SCM) m
• Loud clicks or tone bursts (95–100 dB) are repeatedly presented to each ear; elect rodes on SCM; pat ient holds head up unsupported using anterior neck m ’s and tenses SCM during acoust ic st im ulat ion , then relaxes once st im ulat ion stops
• If neck m ’s are inact ivated (i.e., inhibitory re ex), VEMP is produced
• Findings ◦ In patients w ith superior Scc dehiscence, a re-sponse at very low thresholds (<65 dB) or of high amplitude produces a VEMP on a ected side
◦ VEMPs m ay be of use in Ménière disease to look at side not currently a ected and predict if it w ill becom e sym ptom at ic
• St ill largely experim ental; other t ypes of VEMPs also being developed, e.g., ocular
• Used to record: ◦ Spontaneous nystagm us ◦ Saccades ◦ Sm ooth pursuit ◦ Optokinet ic nystagm us ◦ Rotat ion tests ◦ Bitherm al caloric test
• ENG helps localize pathology, i.e., central versus peripheral, unilateral versus bilateral
18.3.3 Posturography• Posturography tests system by rem oving
or altering input from the visual and propriocept ive system s
• Uses force plate to detect how cent re of gravity changes in t im e, giving a m easure of postural sway
• Helps assess the vest ibulospinal re ex• Main use in devising m anagem ent plan rather
than m aking diagnosis• Stat ic posturography: pat ient stands w ith eyes
open/closed, feet together/apart , heel to toe; foam surface can be used to reduce propriocep-t ive input; visual eld can also be m anipulated; results com pared w ith age- and height-m atched norm als
• Dynam ic posturography: force plate and visual eld m anipulat ion to confuse propriocept ive and visual senses; six test condit ions: plate xed (norm al propriocept ion) w ith eyes open/closed/m isled; plate un xed w ith eyes open/closed/ m isled; com pare results w ith norm als
Philpott_9783131662316_Ch18.indd 63 02/05/14 2:53 PM

64
19 Facial Nerve
foram en; posterior belly of digast ric at taches to digast r ic groove, w hich leads forward to the foram en
◦ Nerve turns forward to enter parot id, w ith in w hich it branches to upper and lower divisions in it ially (at the pes anserinus)
◦ Note: n not protected by m astoid t ip unt il 18/12 age
19.1.2 Branches• Greater (super cial) pet rosal: from geniculate
ganglion , gets branch from tym panic plexus, enters m iddle cranial fossa, joined by deep pet rosal (from sym pathet ic plexus of in ternal carot id); now term ed vidian n (n of the pterygoid canal), passes through pterygoid canal to pterygopalat ine ganglion; taste bres pass on through to palate; secretom otor bres synapse and pass on to lacrim al, nasal, and palat ine glands
• Nerve to stapedius• Chorda t ym pani: across m iddle ear between
m alleus and incus; leaves via pet rotym panic ssure; joins w ith lingual nerve (of V n); parasym pathet ic bres leave lingual to pass to subm andibular ganglion , synapse, and supply subm andibular and sublingual glands; m ajorit y of other bres are for taste; projects to nucleus t ractus solitarius
• Post-auricular branch: to post-auricular m , post-in t r insic m m , and occipital m
• Digast ric branch: to posterior belly of digast r ic m
• Stylohyoid branch: to stylohyoid m• Tem poral: to frontalis, orbicularis oculi• Zygom at ic: to orbicularis oris• Buccal: to buccinator• Marginal m andibular: to lower lip , chin• Cervical: to plat ysm a
19.2 Surgical Anatomy: Facial N Identi cation during Surgery• 1 cm inferior and deep to cart ilaginous t ragal
pointer• Proxim ity to t ym panom astoid ssure (sulcus)
(~5 m m below ssure)
19.1 Anatomy (Fig. 19.1)• Mixed cranial n :
◦ E erent m otor bres to m uscles of facial expression, buccinator, stapedius, digast ric (poster ior belly), and st ylohyoid
◦ A erent taste bres to anterior two-th ird tongue and palate (chorda tym pani)
◦ E erent secretom otor (preganglionic parasympathet ics from superior salivary nucleus) bres to lacr im al and nasal glands (via sphenopalat ine ganglion), subm andibular and sublingual salivary glands (via subm andibular ganglion)
◦ A erent sensory bres to par t of concha ± area behind ear (passing w ith auricular branches of vagus: Arnold n)
◦ Motor bres from facial nucleus in pons, having received pyram idal bres from m otor cortex; m ost from cont ralateral side but those for forehead have bilateral cor t ical representa-t ion (hence forehead spared in upper m otor neuron lesions)
◦ Sensory root enters brainstem as nervus in term edius
19.1.1 Course• Meatal, labyrin th ine, t ym panic, m astoid,
ext ratem poral parts (Fig. 19.1) ◦ At in ternal auditory m eatal fundus, m otor root of VII n and nervus in term edius join ; in cross-sect ion , facial anterosuperior, cochlear n anteroinferior, vest ibular nn post; Bill bar separates facial from superior vest ibular, crista falciform is separates both of these from cochlear and inferior vest ibular nn
◦ Enters facial (fallopian) canal, narrowest segm ent of n course (labyrin th ine)
◦ At m edial wall of m iddle ear, turns at geniculate ganglion (1st genu) (processus cochleariform is is landm ark); runs poster iorly w ith prom ontory below, lateral Scc above (nerve dehiscent in ~10% here)
◦ After oval w indow turns inferiorly in to descending m astoid part (2nd genu); shor t process of incus is lateral at th is turn
◦ Descends posterior and deep to t ym panic annulus, to em erge from stylom astoid
Philpott_9783131662316_Ch19.indd 64 02/05/14 2:57 PM

65
Facial Nerve Palsy
• Nerve injury t ypes: ◦ Neuropraxia: no axonal or connect ive t issue disrupt ion
◦ Axonotm esis: distal waller ian degenerat ion ◦ Neurotm esis: disrupted endoneurium
• Causes: ext racranial, in t ratem poral, in t racranial ◦ Bell palsy (55%): diagnosis of exclusion, idiopathic: - “Rule of 3’s”: pain <3/7, onset over 3/52, resolut ion w ith in 3/12
- May have viral aet iology w ith herpes sim plex type 1 virus react ivat ion in the geniculate ganglion
- May be due to m icrocirculatory failure - Usually aged 15 to 60 years; sudden onset often follow ing viral prodrom e
- 85% show som e recovery w ithin 3/52; 85% w ill go to HB I or II (70% by 6/12), 5% left w ith HB IV or worse
◦ Traum a (19%): including iat rogenic, temporal bone # , forceps delivery
◦ Ram say–Hunt (7%): - Herpes zoster (dorm ant chickenpox virus react ivates to a ect m otor axons of VII n ,
• Anterosuperior to angle between poster ior belly digast r ic and anterior border m astoid (SCM), just deep to digast r ic; st ylom astoid foram en is deep to styloid process found by t racing back posterior belly of digast ric
• Marginal m andibular branch 1 cm inferior to angle of m andible; exits gland w ith ret rom andibular v
• Zygom at ic branch crosses zygom at ic arch• Buccal branch 1 cm superior to parot id duct• Tem poral branch bisects line from t ragus to
lateral canthus
19.3 Facial Nerve Palsy• House–Brackm ann (HB) grading (has
considerable in terobserver variabilit y): ◦ I—norm al ◦ II—slight weakness ◦ III—obvious weakness; com plete eye closure ◦ IV—obvious dis guring weakness; incom plete eye closure; sym m etric at rest
◦ V—m otion barely perceptible; asym m etric at rest ◦ VI—total paralysis; loss of tone
Fig. 19.1 Anatomy of the course of the facial nerve. Intratemporal section: 1, meatal segment; 2, laby-rinthine segment; 3, t ym-panic segment; 4, mastoid segment. Extratemporal section: 5, temporal rami; 6, zygomatic rami; 7, tem-porofacial portion; 8, buccal rami; 9, cervical rami; 10, marginal mandibular ramus; 11, cervical part; 14, extratemporal part. Other structures: 12, parotid duct; 13, parotid gland.
1
10
6 5
4
9 13 11 14
3
2
12
8
7
Philpott_9783131662316_Ch19.indd 65 02/05/14 2:57 PM

66
19 Facial Nerve
◦ Bell palsy: - Scot t ish Bell palsy study: early t reatm ent w ith prednisolone signi cantly improves com plete recovery at 3/12 (64–83%) and 9/12 (82–94%); no evidence acyclovir m akes any di erence alone or in com binat ion w ith prednisolone
- Prednisolone: 30 to 60 m g 5 to 7 days once daily; (1–2 m g/kg per day) helps to reduce oedem a that compresses n and it s blood supply at m eatal foram en (narrowest point)
- Consider surgical decom pression (Fig. 19.2) - If ENoG >10%, 95%+ go on to HB I–II; if <10% funct ion , 50% go on to HB III or worse; in th is group consider m iddle fossa decom pression w ith in 10 to 14 days
- If palsy progresses after 3/52 or not recover by 6/52, Ix for neoplasm
◦ Ram say–Hunt syndrom e: acyclovir (e.g., 800 m g ×5/day for 1 week), analgesia, steroids m ay reduce pain
◦ Traum a: - Consider anastom osis ± graft (e.g., sural, great auricular); hypoglossal to facial
possibly as result of system ic disease or im m unocomprom ise)
- C/o severe pain , vesicles present , viral prodrom e
- Worse sym ptom s and recovery than Bell ◦ Tum our (6%): in t rinsic (VII schwannom a), compression (VIII schwannom a), invasion (parot id)
◦ Infect ion (4%): acute suppurat ive OM (m aybe in those w ith dehiscent t ympanic por t ion of nerve), COM/cholesteatom a, m alignant ot it is externa
◦ Central: m ult iple sclerosis, CVAs ◦ Congenital:
- Möbius syndrom e (w ith VI n palsy, club foot) - Melkersson–Rosenthal syndrom e (recurrent palsies, unknow n cause, associated oedem a of face)
- Myotonic dyst rophy - Goldenhar syndrom e (hem ifacial m icrosom ia—defect ive developm ent of 1st and 2nd branchial arches)
• Ix: ◦ Audiogram ◦ Consider CT, MRI if any suspicious features ◦ If features of system ic disease consider FBC, ESR, CRP, ACE, cANCA, glucose
◦ Serial ENoG is a good predictor of poor outcom e; can determ ine % bres that have degenerated; <25% degenerat ion at 2/52 post onset m ay indicate sat isfactory restorat ion of facial funct ion in 98% Bell palsy (probably less reliable for Ram say–Hunt)
◦ EMG considered by som e to give bet ter inform at ion on all branches, and be bet ter predictor for w hen surgery indicated
◦ Consider n excitabilit y tests, m axim um st im ulat ion test
◦ Schirm er test: for degree tearing (if reduced, lesion is proxim al to geniculate ganglion w here greater pet rosal n leaves)
◦ Stapedius contract ion on im pedance audiom etry (st im uli 70–100 dB > hearing threshold); lost if lesion proxim al to stapedius n
◦ Taste (elect rogustom etry) assesses chorda tympani funct ion
◦ Salivary ow unreliable to m easure• Rx
◦ Eye protect ion (drops, taping at n ight , tarsorrhaphy, gold weights) to prevent exposure kerat it is
Fig. 19.2 Facial nerve decompression and reconstruc-tion. Decompression and reconstruction in the internal auditory canal can be performed using the translaby-rinthine approach. The greater petrosal nerve (1) is cut and the facial nerve (2) is rerouted and anastomosed in the mastoid. 3, stapes; 4, malleus handle.
1
4
3
2
2
Philpott_9783131662316_Ch19.indd 66 02/05/14 2:57 PM

67
Facial Nerve Palsy
som et im es used w hen proxim al stum p cannot be ident i ed
- If paresis, no surgery - If delayed paralysis also tend to get good recovery, so no surgery
- If im m ediate-onset paralysis surgery generally indicated; supported by CT ndings of a bony step and >90% degeneration on ENoG
- Middle fossa approach (m ost com m only aim ing for 1st genu region) w ith in 1 week of t raum a
◦ Iat rogenic: if unexpected and not iced soon after surgery, release t ight dressings, let local anaesthet ic wear o (lidocaine half-life is 2 h); consider surgical explorat ion and decompression (w ith colleague; Fig. 19.2)
◦ Ear infect ion: surgical drainage (e.g., grom m et), an t ibiot ics
◦ Reanim at ion - In older pat ients: consider stat ic posit ion w ith use of fascial slings (e.g., fascia lata)
- Younger people: consider dynam ic repair to create anim ated sm ile (w ith nerve graft ing and m uscle t ransfer)
• Prognosis: ◦ Recovery can take up to 1 year ◦ Postrecovery m ay have synkinesis (abnorm al synchronizat ion), m ass m ovem ent , crocodile tears (gustatory tearing due to bres that norm ally innervate salivary glands, innervat ing lacrim al glands), facial myokym ia (bag of worm s); consider use of botox
Philpott_9783131662316_Ch19.indd 67 02/05/14 2:57 PM

68
20 Imaging of the Ear
steady-state acquisit ion), w hich allows fast acquisit ion of th in slice inform at ion that is good for spat ial resolut ion at expense of contrast resolut ion
◦ DWI (di usion-weighted im aging): looks at how water m oves through cells; “dead” cells (e.g., post-CVA) t rap water (so rest rict di usion) show ing up as h igh in tensit y, as does kerat in , so useful for epiderm oid cysts and cholesteatom a; echo-planar (EPI) and non-echo-planar im aging types
20.2 Imaging of Ear Pathology20.2.1 External Ear• Congenital at resia of EAC: CT scan can help w ith
surgical planning• Osteomyelit is (m alignant ot it is externa):
◦ CT w ith contrast yields bony detail; coronal CT m ay show e acem ent of the t ym panic ring
◦ MRI (± gadolin ium ) can de ne m edial extent of soft t issue disease at the skull base, dural enhancem ent and cerebral involvem ent
◦ Technet ium -99 m bone scanning and gallium -67 scanning helpful; their sensit ivit y for the presence of infect ion is far greater than their speci cit y for the cause
◦ Tc-99 m gives excellent inform at ion about bone funct ion (but poor for bone st ructure); +ve scan thought to represent osteoblast ic act ivit y as lit t le as 10% above norm al; +ve in acute and chronic osteomyelit is and in areas of act ive bone repair w ithout infect ion (e.g., t raum a); increases in Tc-99 m uptake between 4 and 24 h post-inject ion is the m ost sensit ive indicator of temporal bone osteomyelit is
◦ Ga-67 w ill highlight an acute infect ive focus but not the full extent of an osteomyelit ic process; as t reatm ent progresses the scan w ill revert to norm al (Tc-99 m w ill lag behind for m onths)
◦ Baseline studies of both thus considered, and sequent ial im aging is used to m onitor the response to therapy
◦ Indium -111 labeled leucocyte planar scin t igra-phy can yield even bet ter results for detect ion of osteomyelit is and m ay replace above
20.1 Imaging Modalities20.1.1 Computed Tomography (CT)• Describe areas of h igh or low at tenuat ion• Uses convent ional X-rays (ionizing radiat ion)
w ith com puter processing of digital inform at ion obtained from layer or spiral tom ographs
• For im aging of the tem poral bone use h igh-resolut ion algorithm , bone w indows, th in slices (0.5–1 m m ); spiral scanning allows for m ult iplanar reform at t ing
• Problem s of part ial volum e averaging can apply to th in bony divisions, especially w hen slice th ickness is h igher
20.1.2 Magnetic Resonance Imaging (MRI)• Describes areas as h igh or low signal in tensit y• Uses the m agnet ic proper t ies of biological
m aterials and generates im ages w ithout the use of ionizing radiat ion
• Tissues contain protons; apply st rong m agnet ic eld and these align, then impart energy (radio wave) to excite photons, w hich resonate; turn o radio wave and protons relax and in doing so give o a radio wave that is detected as the MR signal
• Excellent for contrast ing soft t issues: ◦ T1: good for anatomy; uid (water, CSF, vit reous, m ucus) black; fat w hite; hyperin tense st ructures m ost likely fat , protein , m ethem oglobin , or contrast
◦ T2: good for pathology; uid (water, vit reous, CSF) w hite; pathological t issue usually bright; fat , m uscle in term ediate; blood variable; air, bone, rapid vascular ow black
◦ STIR: (short tau inversion recovery) suppresses fat to help show tum our; applied to T2 im ages; water w hite, fat black
◦ Can fat suppress either T1 or T2; lat ter fat-suppressed vir tually indist inguishable from T2 STIR sequence
◦ Gadolin ium can be used as cont rast ◦ Various other sequences can help m anipulate im age, e.g., FIESTA (fast im aging employing
Philpott_9783131662316_Ch20.indd 68 02/05/14 2:59 PM

69
Imaging of Ear Pathology
• Neoplasia: CT shows irregular bony erosion for m eningiom a, glom us, chordom a, chondrosarcom a; sm ooth erosion for schwannom a, chondrom a; m etastases vary
20.2.3 Inner Ear• To assess cochlear anom alies associated w ith
SNHL, both CT and MRI help• Superior Scc dehiscence: both CT and T2 MRI
can be reconst ructed in plane and at r ight angles to plane of superior Scc to dem onstrate defect
• Precochlear im plantat ion need to con rm a patent cochlea—both CRT and MRI helpful; MRI also provides inform at ion on the presence of VIII n
• Halo sign m ay be seen around ot ic capsule in otosclerosis, w ith CT
20.2.4 Temporal Bone (Fig. 20.1)• CT for t raum a• CT also best for bony dysplasias, e.g., brous
dysplasia w ith ground glass appearance yet sparing of the ot ic capsule
• Glom us tum ours: CT and MRI helpful; CT gives bony anatomy and extent of bony ero-sion; rapid ow in in t ratum oural vessels m ay appear as black ow voids result ing in a “salt and pepper” appearance; hypo/isoin tense on T1, hyperin tense on T2, enhances dram at ically on postcont rast T1 (because of h igh vascularit y)
• Pulsat ile t innitus m ay prom pt im aging to ident ify vascular anom alies; in addit ion to MRI, MR angiography m ay help de ne anom alous vasculature, and MR venography m ay ident ify venous throm bosis; object ive t innitus should prompt catheter angiography w hen suspicion is h igh for a vascular lesion such as dural ar ter iovenous stulas
20.2.5 Internal Auditory Canal, Skull Base• MRI is the gold standard for evaluat ing the IAC
and CPA• Vest ibular schwannom a: usually isoin tense to
hypointense to brain , hyperin tense to CSF on T1 and isoin tense to slight ly hyperin tense on T2; best show n w ith T1 contrast (Gd); enhanced T1 im ages usually show a hom ogeneously enhanc-ing m ass centred near the porus acoust icus
20.2.2 Middle Ear/Mastoid, Petrous Apex• ME e usion w ill often be an incidental nd-
ing on MRIs of brain ; especially com m on in in tubated pat ients; norm ally hyperin tense on T2, hypointense on T1, non-enhancing w ith contrast
• Rout ine assessm ent of COM best w ith CT, but in t racranial complicat ions (dural venous sinus throm bosis, abscesses, m eningit is) best evaluated by MRI
• Sigm oid sinus throm bosis: cont rast-enhanced CT, acute throm bus hyperdense w ith contrast enhancing dura around throm bus (but not throm bus)—w hen chronic it revascular izes so enhances; hypo/isoin tense w ith ow voids on T1 and T2 MRI
• Petrosit is: CT—opaci ed cells and lysis of septat ions; MRI—m eningeal enhancem ent w here dura a ected w ith hyperin tensit y on T2 (not T1)
• Cholesterol granulom a: expansile cyst w ith in pneum at ized apex, so sm ooth expansion of cort ical m argins on CT; h igh signal on both T1 and T2 MRI (because h igh on T1, probably due to m ethem oglobin , dist inguished from sim ple u id, apicit is, cholesteatom a); can have hypointensit y patches on both T1 and T2
• Cholesteatom a: ◦ CT m ost helpful to see pat tern of bony dest ruc-t ion , but cannot di erent iate cholesteatom a from other soft t issue; key features: scutum , lateral Scc, ossicular chain (e.g., long process of incus) erosion
◦ May be helpful in surgical planning, e.g., a sm all m astoid or low tegm en m ight m ean canal wall up surgery is di cu lt and at t icoant rostomy is bet ter indicated
◦ MRI late T1 Gd get r im enhancem ent w ith non-enhancing cholesteatom a (kerat in)—in am m atory t issue, granulat ion enhances; sequence takes 45 m in but can show lesions dow n to 3 m m
◦ T2 m oderately hyperin tense and can di erent iate cholesteatom a from brain herniat ion if dehiscent tegm en
◦ DWI EPI: detects lesions ≥5 m m , high signal; but temporal lobe ar t ifact
◦ DWI non-EPI: lesions 2 m m +, less ar tefact , poor bony anatomy; m ay be suitable to screen before 2nd-look canal wall up surgery
Philpott_9783131662316_Ch20.indd 69 02/05/14 2:59 PM

70
20 Imaging of the Ear
◦ Epiderm oids, in cont rast , contain st rat i ed squam ous epithelium , and certain MRI sequences (DWI, FIESTA) m ay reveal signal that does not follow that of CSF, hence dist inguishing these lesions
◦ Hyperin tensit y on DWI and hypointensit y on fast im aging em ploying steady-state acquisit ion di erent iates epiderm oid from arachnoid cysts (w hich are low in tensit y on DWI)
◦ Epiderm oids tend to insinuate in to clefts and dissect in to natural t issue planes; vessels tend to be encased in epiderm oids and draped in arachnoid cysts; epiderm oids hypodense and non-enhancing on CT
• VII n neurom a enhance w ith Gd on MRI• Lipom a: hyperin tense fat signal on T1, so can
easily be m isin terpreted as an enhancing lesion (e.g., vest ibular schwannom a) if the pre-contrast T1 im age is not inspected; suppression of MR by applying fat saturat ion w ill con rm diagnosis
• Hem angiom a at CPA: can appear sin ister, w ith bony dest ruct ion on CT, hypodense, non-enhancing (possible late peripheral enhancem ent w ith cont rast , though rarely done); variable in tensity on MRI w ith possible ow voids
• Meningit is: enhancem ent on T1 MRI
w ith IAC extension; both h igh-resolut ion T2 and cont rast-enhanced T1 can detect ext rem ely sm all lesions (2 m m ); both cyst ic and haem orrhagic areas m ay be seen associated w ith larger tum ours, but calci cat ion is rare; w hen MRI contraindicated, >90% w ill enhance hom ogeneously w ith CT w ith contrast; CT m ay also show dilat ion of IAC
• Meningiom a: characterist ics sim ilar to schwannom as; isoin tense to brain on T1 and T2 and both hom ogeneously enhanced; m eningiom a tends to have T1 signals m ore sim ilar to brain parenchym a than schwannom a; other dist inguishing characterist ics include presence of in ternal cysts in large vest ibular schwannom a, the broad-based dural at tachm ent and tail of m eningiom a, and site of origin (IAC vs. poster ior pet rous bone), presence of pial vessel ow voids; dense calci cat ion (hypointense on T2) m ay be seen in the m eningiom a (CT m uch m ore sensit ive than MRI for detect ion of calci cat ion)
• Epiderm oid and arachnoid cysts: both show m ass e ect and distort ion of neural st ructures; signal ident ical to CSF on T1 and T2 (neither enhances) ◦ Arachnoid cyst content t ruly m atches that of CSF
Fig. 20.1 Axial (a) and coronal (b) CT scans of the temporal bone. 1, t ympanic cavity with ossicles; 2, antrum; 3, internal acoustic canal; 4, cochlea; 5, labyrinth; 6, external acoustic canal; 7, pneumatized mastoid cells.
Philpott_9783131662316_Ch20.indd 70 02/05/14 2:59 PM

Sect ion II
Rhinology
Philpott_9783131662316_Ch21.indd 71 02/05/14 3:17 PM

Philpott_9783131662316_Ch21.indd 72 02/05/14 3:17 PM

73
21.1 Nasal Septum21.1.1 Structure• Quadrilateral car t ilage• Perpendicular plate of the ethm oid• Vom er• Maxillary crest
21.1.2 Blood Supply• Facial ar tery—labial branch• Palat ine ar tery• Anterior ethm oid ar tery• Posterior ethm oid ar tery• Sphenopalat ine ar tery—posterior septal
branch
21.1.3 Innervation• Anterior ethm oidal nerve
• Medial superior poster ior nasal (inc. nasopalat ine n)
21.1.4 Adjacent Structures• Maxilla• Nasal bones• Upper and lower lateral car t ilages• Sphenoid sinuses• Cribriform plate
21.2 Nasal Conchae (Turbinates) (Fig. 21.1)21.2.1 Superior• In cont inuity w ith MT• Overlie the superior m eatus• Variable at tachm ents posteriorly to the
sphenoid face or lam ina papyracea• Medial surface contains olfactory epithelium
21 Sinonasal Anatomy and Physiology
Fig. 21.1 Lateral nasal wall. I, superior meatus; ii middle meatus; iii, inferior meatus.1, nasal vestibule; 2, open-ing of the nasolacrimal duct; 3, origin of the infe-rior turbinate; 4, semilunar hiatus; 5, insertion of the middle turbinate; 6, sphe-noid sinus; 7, insertion of the superior turbinate; 8, frontal sinus; a, drain-age of the antral cavity; b, drainage of the frontal sinus; c, drainage of the anterior ethmoid cells; d, drainage of the posterior ethmoid cells; e , drainage of the sphenoid sinus; f, area of infundibulum (dot ted area).
6 7 5 8
I
II
III
e
d
c b
f
a3
2
4
1
Philpott_9783131662316_Ch21.indd 73 02/05/14 3:17 PM

74
21 Sinonasal Anatomy and Physiology
◦ H. sem ilunaris superior: crescent-shaped cleft between ethm oid bulla and m iddle turbinate
• Ost iom eatal com plex: ◦ Final com m on drain pathway for anterior sinuses—a funct ional unit
◦ Includes: - Uncinate process - Ethm oid infundibulum - Anterior ethm oid cells - Ost ia of anterior ethm oid, m axillary, and frontal sinuses
21.3.4 Potential Spaces• Sinus lateralis = suprabullar and ret robullar
recesses• Suprabullar recess: space between roof of
ethm oid bulla and skull base• Ret robullar recess: space between posterior wall
of ethm oid bulla and m iddle turbinate basal lam ella
21.3.5 Uncinate Process• Crescenteric bone that form s part of the
ethm oid bone
21.2.2 Middle• Has four par ts—anterior and posterior
but t resses, vert ical at tachm ent , and basal lam ella (horizontal at tachm ent)
• Separates ethm oidal cells in to anter ior and posterior
• Various anom alies include pneum at izat ion ( concha bullosa) and paradoxical con gurat ions
• Overlies the m iddle m eatus
21.2.3 Inferior• Largest turbinate• Overlies infer ior m eatus (valve of Hassner)
21.2.4 Supreme• May also exist in som e people
21.3 Paranasal Sinuses, Ostia, and Ostiomeatal Complex21.3.1 Embryology• Weeks 9–10: Form at ion of six r idges.• Ridges form ethm oturbinals:
◦ Pars ascendens and pars descendens ◦ Middle turbinate: th ird ethm oturbinal ◦ Superior turbinate: fourth ethm oturbinal ◦ Suprem e turbinate: fth ethm oturbinal ◦ Inferior turbinate: m axilloturbinal
21.3.2 Messerklinger Landmarks (Fig. 21.2)• Four consistent/constant landm arks:
◦ Uncinate process ◦ Ethm oid bulla: anterior wall ◦ Middle turbinate basal lam ella ◦ Sphenoid face
• Three inconsistent landm arks: ◦ Ethm oid bulla: poster ior wall ◦ Superior turbinate basal lam ella ◦ Suprem e turbinate basal lam ella
21.3.3 Middle Meatus• Hiatus sem ilunaris:
◦ H. sem ilunaris inferior: shor test distance between free posterior m argin of uncinate process and anterior face of ethm oid bulla
Fig. 21.2 Four Messerklinger landmarks. Sph, sphenoid sinus; SEC(OC), spheno-ethmoidal recess (olfactory cleft); SpM, supreme meatus; SM, superior meatus; RBR, retrobullar recess; FS, frontal sinus; ANC, agger nasi cell; EB, ethmoid bulla; Max O, maxillary ostium. 1, uncinate process; 2a, anterior wall of EB; 2b, posterior wall of EB; 3, basal lamella of middle turbinate; 3a, superior turbinate; 3b, supreme turbi-nate; 4, anterior face of sphenoid sinus.
Sph
IT
FS
EB
122a
3 3a 3b
SEC(OC)
SpM RBRSM
4
MAX O
ANC
P
Philpott_9783131662316_Ch21.indd 74 02/05/14 3:17 PM

75
Paranasal Sinuses, Ost ia, and Ost iomeatal Complex
• Anterior cells—drain in to m iddle m eatus ◦ Agger nasi:
- Most anterior of the ethm oid cells - De nes the anter ior aspect of the frontal recess
◦ Ethm oid bulla: - Lies posterior to the uncinate process and anterior to the basal lam ella
- At tached to the skull base superiorly de n ing the poster ior end of the frontal recess and dem arcat ing the anterior ethm oidal a
- Drains posteriorly in to the ret robullar space
- Sm all w hen a pneum at ized MT present ◦ Infra-orbital (Haller) ethm oidal cells:
- Pneum at izat ion along the orbital wall opposite the uncinate process—m ay narrow the infundibulum
◦ Supraorbital ethm oid cells - Pneum at izat ion along the anterior skull base posterior to the frontal sinus
• Posterior cells—drain in to superior m eatus: ◦ Between one and nine in num ber ◦ No m iddle cells ◦ A variant m ay pneum at ize superior and lateral to the sphenoid sinus (sphenoethm oidal [Onodi] cell)
21.3.8 Sphenoid Sinus• Occupies sphenoid bone• In tersinus septum not usually m idline• Post-ethm oid a and n give vascular and sensory
supplies, respect ively• Ost ium ~1 cm above choana• Main developm ent occurs after puberty• Relat ions:
◦ Pituitary fossa and m iddle cranial fossa superiorly
◦ Cavernous sinus and ICA laterally ◦ Pons and posterior cranial fossa posteriorly ◦ Form s roof of nasopharynx ◦ Optic nerve lies next to or even w ith in the sinus
◦ Pterygoid canal w ith nerve inferiorly
21.3.9 Frontal Sinus• Frontal recess:
◦ Nasofrontal duct—incorrect ◦ Inverted funnel shape ◦ Anterior skull base is poster ior boundary
• Free m edial edge, being at tached to the lateral wall of the nose—upper two-th ird lies in a ver t ical plane, lower one-th ird lies in a horizontal plane
• Three t ypes of superior at tachm ent: ◦ To lam ina papyracea (A) form ing a recessus term inalis
◦ To the skull base (B) ◦ To the m iddle turbinate (C)
• With t ype A at tachm ents, m ucociliary out ow from the frontal sinus is direct ly in to the m iddle m eatus, in t ype B/C at tachm ents, that m ucociliary ow is in to the ethm oid infundibulum
• “Doorway to the sinuses”
21.3.6 Maxillary Sinus• Present at bir th• Located beneath the orbit• Anterior to the infratem poral and
pterygopalat ine fossae• Natural m axillary ost ium lies at the lateral
end of the ethm oid infundibulum , behind the uncinate process; accessory ost ia are often seen and m istaken for the natural ost ium and can lie w ith in the lower uncinate process or poster ior to the free edge of the uncinate process
• Blood supply—facial, m axillary, infra-orbital, and greater palat ine ar ter ies
• Nerve supply—infra-orbital and superior alveolar branches of m axillary nerve
21.3.7 Ethmoidal Cells• Ethm oid bone:
◦ Paired bony sca olds, connected by cribriform plate
• Boundaries: ◦ Lam ina papyracea of orbit ◦ Orbital process of the frontal bone ◦ (Fovea ethm oidalis 1 orbital plate of the frontal bone)
◦ Middle and superior turbinates m edially ◦ Lateral cribriform plate lam ella (also m edially)
◦ Sphenoid sinus• Nerve supply—anterior and poster ior
ethm oidal nn• Blood supply—anterior and poster ior ethm oidal
ar teries from the ophthalm ic a
Philpott_9783131662316_Ch21.indd 75 02/05/14 3:17 PM

76
21 Sinonasal Anatomy and Physiology
• Phonet ic: ◦ Voice resonance ◦ Reduces bone conduct ion of ow n speech
• Im m unological—hum oral and cellular:• Olfactory• Mechanical:
◦ Reduce skull weight ◦ Heat insulat ion
21.4.2 Mucociliary Clearance (Fig. 21.3)• Speech of par t icle m ovem ent = 3 to 25 m m /m in
at ~12 Hz• Low levels of n it r ic oxide related to ciliary
dysfunct ion• Mucous secret ions (from goblet cells) t rap
part iculate m at ter, w hich is then propelled to nasopharynx
• Watery secret ions from serous glands evaporate to m oisten the inspired air
• Sinus cilial t rain beats towards natural ost ium
• Ost ial patency required for adequate m ucociliary clearance and gas exchange (n it r ic oxide)
• Frontal sinus out ow along m edial wall and in to either infundibulum or m iddle m eatus direct—depending on uncinate at tachm ent
◦ Agger nasi cell and frontal cells m ay occupy space in funnel—m ake ident i cat ion and drainage di cult
◦ Anterior ethm oid ar tery close• Frontal recess cells:
◦ Agger nasi cell ◦ Frontal cells (t ypes I–III/IV) ◦ Supraorbital ethm oid cell ◦ Frontal bullar cell ◦ Suprabullar cell ◦ Frontal in tersinus septal cell
• Occasionally absent; underdeveloped in CF pat ients
• Variable in size• Bounded by anterior cranial fossa and orbits• Star t to form after age 2 years• Blood supply = supraorbital and anterior
ethm oid ar teries• Nerve supply = supraorbital nn
21.4 Sinonasal Physiology21.4.1 True or Perceived Sinonasal Physiological Functions• Vent ilatory:
◦ Hum idi cat ion ◦ Filt rat ion ◦ Airway ◦ Bu er pressure changes
Fig. 21.3a–b a The mucociliary apparatus is the most important defence mechanism in the respiratory epithelium. Goblet cells
and seromucous glands produce a two-layered lm consisting of a low-viscosity sol phase and a higher- viscosit y gel phase. The cilia beat in the sol phase to transport the gel along distinct pathways across the mucosa of the nose and paranasal sinuses towards the choana. The mucociliary apparatus simultaneously facilitates secretion and absorption, and it is the region where initial non-speci c and speci c immunological responses to antigens and allergens occur. 1, gel layer; 2, sol layer; 3, cilia (beating); 4, cilia (recovering); 5, ciliated epithelial cell; 6, goblet cell; 7, seromucous gland.
b Mucociliary transportation of secretions in the frontal sinus (adapted by Messerklinger).
1
a
23
5
6
7
4
b
Philpott_9783131662316_Ch21.indd 76 02/05/14 3:17 PM

77
Sinonasal Physiology
21.4.3 Autonomic Regulation• Mucous m em brane very vascular—large venous
sinusoids and AV shunts—esp. IT• Vidian nerve (pterygoid canal)—form ed by union
of greater pet rosal nerve ( parasympathet ic) and deep pet rosal nerve (sym pathet ic)—runs forward to pterygopalat ine ganglion (Fig. 21.4)
• Branches from ganglion carry sensory, secretom otor and sym pathet ic bres
• Ganglion connects w ith m axillary nerve to pass sensory bres
• Branches: ◦ Medial posterior superior nasal nn (inc. nasopalat ine)—septum
◦ Lateral posterior superior nasal nn—via sphenopalat ine foram en to posterior superior lateral wall of nose
◦ Greater palatine n—via greater palatine canal to hard palate; also supplies posterior inferior part of lateral wall and m edial wall of m axillary sinus
◦ Lesser palat ine nn—via lesser palat ine foram ina to soft palate—taste bres included
Fig. 21.4 Pterygopalatine ganglion.
1
7
5
8
4
3
9
6
TrigeminalParasympatheticSympathetic
2
◦ Pharyngeal nerve—via palatovaginal canal to nasopharynx; orbital branches supply ethm oid and sphenoid sinuses and orbital oor
Philpott_9783131662316_Ch21.indd 77 02/05/14 3:17 PM

78
For acute and chronic disease also involving sinuses—see related chapters 24–26
22.1 Bacterial Infections22.1.1 Folliculitis and Vestibulitis• Invasion of pilosebaceous follicle by
Staphylococcus aureus• Risk of cavernous sinus throm bosis—m ortalit y
of 10 to 27%
22.1.2 Erysipelas• Acute β-haem olyt ic st reptococcal infect ion• Follows a cut or incision• But ter y pat tern on face• Responds well to penicillin /erythromycin
22.1.3 Rhinoscleroma• Large deform ing m asses distending the nasal
cavit y• Klebsiella rhinosclerom at is• Disease found in developing countr ies• Three phases: rh in it ic, in lt rat ive, and nodular• Finally result ing in adhesions, stenosis, and atresia• Large red tum our-like m asses of the nodular
phase are character ized by: ◦ Mikulicz cells (large cells w ith clear cytoplasm contain ing the bacilli)
◦ Russell bodies (w hich are plasm a cells w ith eosinophilic-stain ing cytoplasm and prom inent nuclei)
• Large doses of st reptomycin and tet racycline over 4 to 6 weeks are needed unt il two consecut ive biopsies are negat ive
• Topical acri avine solut ion has also been used
22.1.4 Leprosy• Fingernail t ransm ission in to nose• Incubat ion can take 10 years• Tuberculous or leprom atous form s• Sm all anesthet ic patches (tuberculoid) or
nodular th ickening around ant IT (leprom atous)• Perforat ion and nasal deform ity follow• Dapsone ± rifam picin /clofazim ine to t reat
22 Acute and Chronic Nasal Disorders
22.1.5 Tuberculosis• Nasal involvem ent secondary to chest• Nodular/ulcerat ive lesions on ant septum or ITs
or choanae• Caseat ing epithelioid granulom as w ith acid-fast
bacilli• Responds to standard Rx w ith saline douching• Lupus vulgaris = variant—nodules at vest ibule
22.1.6 Syphilis• Congenital/pr im ary/secondary/ter t iary• Prim ary chancre on external nose or vest ibule
at 3–4 weeks after contact; disappears spontaneously after 6 to 10 weeks
• Serology m ay be negat ive in early stages, 90% +ve in ter t iary stage
• Secondary stage m ay appear as sim ple rh in it is
• Tert iary gum m as produce tenderness over bridge of nose, posterior septal perforat ions, and nasal collapse
• Congenital form m ay present at puber ty: ◦ Nasal saddling ◦ Dental abnorm alit ies ◦ SNHL
• Penicillin Rx required
22.2 Allergic Rhinitis22.2.1 De nition of Rhinitis• An in am m atory disorder of the nasal m ucosa
characterized by 2 or m ore of the follow ing sym ptom s: ◦ Rhinorrhea (anterior and/or poster ior) ◦ Blockage ◦ Itching/sneezing
22.2.2 Facts about Rhinitis• Com m onest im m unological disorder in hum ans:
10 to 25% of individuals globally• Signi cant e ects on qualit y of life for
su erers—m ay account for 30 to 40% of reduced product ivit y in the workplace
• Most asthm at ics also su er from rhin it is
Philpott_9783131662316_Ch22.indd 78 02/05/14 3:20 PM

79
Non-allergic, Non-infect ious Rhinit is
• Paternal atopy (h igher if both parents a ected)• Drug history—e.g., use of nasal sprays, β-blockers
22.3.4 Assessment of the Rhinitic Patient—Examination and Investigations• Endoscopic exam inat ion of nose• Skin prick allergy tests or radioallergosorbent
test (RAST)• Other rh inological assessm ent:
◦ Spatula m ist ing ◦ Peak inspiratory nasal ow rate ◦ Acoust ic rh inom etry ◦ Rhinom anom etry ◦ Mucociliary clearance
22.3.5 Management Options (Fig. 22.2)• Allergen avoidance• Topical steroids• Topical decongestants• Oral/(topical) ant ih istam ines• System ic steroids• Crom olyn sodium• Leukotriene receptor antagonists• Iprat ropium brom ide• Im m unotherapy• Surgical turbinate opt ions
22.3.6 Summary• Rhinit is is a com m on problem w ith signi cant
socio-econom ic e ects• A careful h istory and exam inat ion w ith skin
prick test (SPT) can determ ine the appropriate level of m edical m anagem ent
• Rem em ber to m anage the com bined airway
22.4 Non-allergic, Non-infectious Rhinitis22.4.1 Non-allergic, Non-eosinophilic Rhinitis (NENAR)Also know n as idiopath ic or vasom otor rh in it is• Diagnosis of exclusion• Non-speci c t r iggers: temperature, hum idity,
irr itants (e.g., cigaret te sm oke)
• Allergic rh in it is and asthm a share m any com m on in am m atory processes
22.2.3 Rhinitis and Asthma• Both allergic and non-allergic rh in it is are r isk
factors for asthm a• Most exacerbat ions of asthm a are com m enced
by upper respiratory t ract infect ion (URTI)• Rhinit is causes bronchial hyperreact ivit y• Allergic rh in it is increases the risk of asthm a
about threefold
22.2.4 Allergic Rhinitis Classi cation (ARIA)• In term it tent—<4 days/week or <4 weeks/year• Persistent—opposite of in term it tent• Mild—norm al sleep, daily act ivit ies, work/
school; no t roublesom e sym ptom s• Moderate/severe—one or m ore of item s not
found in m ild rh in it is
22.3 Pathophysiology of Rhinitis (Fig. 22.1)22.3.1 Early Stage• Allergen contact w ith IgE on m ast cell surface• Mast cell degranulat ion releasing m ediators and
cytokines leads to in it ial sym ptom s of: ◦ Sneezing ◦ Running ◦ Itching ◦ Blockage after 15 to 20 m in
22.3.2 Late Phase• Leukotrienes, cytokines, and chem okines cause
in ux of in am m atory cells (eosinophils)• Cells secrete fur ther m ediators and cytokines• In am m atory response perpetuated for days/
weeks
22.3.3 History• Dist inguish from other t ypes of rh in it is or
rh inosinusit is• Allergen contact—pets, dam p hom e, etc.• Seasonal vs. perennial• Concurrent asthm a
Philpott_9783131662316_Ch22.indd 79 02/05/14 3:20 PM

80
22 Acute and Chronic Nasal Disorders
Fig. 22.1 Pathophysiology of allergic rhinitis. CNS, central nervous system; ICAM, intercel-lular adhesion molecule; IL, interleukin; LT, leukotriene; PG, prostaglandin.
Rhinorrhoea mucosaloedema
Chronic nasalobstruct ion
HistamineLTsPGs
Tryptase
ExudationVasodilatation
Cellular infiltration:Eosinophils
BasophilsT-LymphocytesMacrophages
IL-4IL-3
Adhesionmolecules (ICAM-1)
IL-5EotaxinsRANTES
Sneeze/itch
CNS/Peripheralnerves
Nasal epithelium
Mast cell
Bone marrow
Eosinophils
Basophils+
+
Late-phaseresponse
Early-phaseresponse
RANTESEndothelium
Fig. 22.2 ARIA algorithm for the treatment of allergic rhinitis.
ImmunotherapyIntranasal steroid
Local CromoneOral or local non-sedative H1-blocker
Intranasal decongestant (<10 days)/oral decongestant
Allergen and irritant avoidance
MildIntermit tent
Mild,Persistent
ModerateSevere
Persistent
ModerateSevere
Intermit tent
• Sm okers > non-sm okers• Main sym ptom s:
◦ Nasal blockage ◦ Anterior rh inorrhea ◦ Postnasal drip ◦ ± Sneezing
• No st igm a of allergy or seasonal variat ion• Cort icosteroids ± iprat ropium brom ide
22.4.2 Non-allergic Rhinitis w ith Eosinophilia Syndrome (NARES)• Subgroup of idiopathic rh in it is• Perennial sym ptom s• Absence of allergy as proven w ith SPT/RAST
Philpott_9783131662316_Ch22.indd 80 02/05/14 3:20 PM

81
Granulomatosis with Polyangiit is
• Alcohol causes physiological vasodilat ion ± react ion to ingredients of drinks
• Gustatory rh in it is (probably capsaicin induced)
22.4.7 Atrophic Rhinitis• Prim ary cases secondary to Klebsiella ozaenae
infect ion• Occurs after puber ty• Fem ale > m ale• Environm ental and general health factors also
have a role• Progressive m ucosal at rophy w ith loss of
turbinate bone• Cavernous, crusty, and sm elly nose; epistaxis
and subject ive blockage• Secondary causes:
◦ Excessive surgery ◦ Traum a ◦ Radiotherapy ◦ Chronic granulom atous disease
• Saline/alkaline douching• Em ollients• Lubricants—25% glucose in glycerin drops• Regular decrust ing• Lim ited role for ABx (cipro oxacin/
m etronidazole)• Young procedure for in t ractable cases
22.5 Sarcoidosis• Non-caseat ing epithelioid granulom as• Certain geographic areas and ethnic groups
(e.g., West Indians)• Fem ale > m ale• Nasal obst ruct ion , m ucopurulent bloodstained
discharge, and crust ing• Associated features m ay include: sinus infect ion ,
saddling, lupus pernio on external nose• Bloods—erythrocyte sedim entat ion rate (ESR),
Ca2+, ACE• CXR—hilar adenopathy• Saline douching and in t ranasal steroids but oral
cort icosteroids usually required
22.6 Granulomatosis w ith Polyangiitis• Granulom atous disease of unknow n origin• URT and LRT + focal glom erulonephrit is
• May represent an early stage of aspirin sensit ivity and be associated w ith asthm a and NPs
• In t ranasal cor t icosteroids
22.4.3 Occupational/Environmen-tal Rhinitis• Allergic or hyperresponsive• Com m on chem ical irr itants:
◦ Acid anhydrides ◦ Plat inum salts ◦ Glues ◦ Solvents ◦ Grain/wood dust
• O3/SO2/NO2/other pollu tants—possible culprits• Rem oval of pat ient from exposure, but m ay take
up to a week or m ore to disappear• Asthm a, conjunct ivit is, and derm at it is m ay also
be present• Speci c nasal challenge w ith object ive nasal
m easurem ents m ay be required
22.4.4 Hormonal/Endocrine Rhinitis• Fem ale physiological and non-physiological
states—e ects largely seen during pregnancy and not in response to exogenous horm ones
• Nasal stu ness and discharge in acrom egaly and hypothyroidism
22.4.5 Drug-Induced Rhinitis• Aspir in /non-steroidal ant i-in am m atory drugs
possible role for desensit izat ion• Ant ihypertensives e.g., ACE-Is, α -blockers,
m ethyldopa, reserpine, phentolam ine• Topical ophthalm ic β-blockers• Chlorprom azine• Oral contracept ive pills—not supported by
recent evidence• Recreat ional cocaine• Decongestant overuse—rhinit is m edicam entosa
22.4.6 Food-Induced Rhinitis• Food allergy rarely causes isolated rh in it is• Oral allergy syndrom e—irritat ion of oral cavit y
and nose—associat ion of groups of food allergies w ith seasonal allergic rh in it is
• May be hypersensit ivit y to colourants or preservat ives
Philpott_9783131662316_Ch22.indd 81 02/05/14 3:20 PM

82
22 Acute and Chronic Nasal Disorders
◦ Whistling noise w ith breathing (sm all perforat ions)
◦ Cacosm ia ◦ Asymptom at ic—possible w ith m ore posterior perforat ions
• Diagnost ic work-up: ◦ Blood tests for above condit ions (ANCA, ACE, VRDL, ESR)
◦ Biopsy m ay be required w here doubt rem ains, especially w here pain is a feature
• Managem ent: ◦ Conservat ive/m edical:
- Topical em ollients e.g., saline (NasoGel), Vaseline, etc.
- Nasal douching - 5% glucose in glycerin drops w here crust ing is resistant
◦ Surgical: - Inser t ion of septal but ton - Reconst ruct ion—num erous techniques described
- Widening procedure—for larger perforat ions—allows a fresh m ucosal fold to dress the posterior edge of the perforat ion , reducing crust ing and bleeding
22.9 Rhinophyma• Overgrow th of sebaceous t issue• Begins at t ip and progresses to involve ala nasi
and colum ella• Reduct ion of a ected t issue possible w ith
knife/elect rodissect ion/laser
• Variable rate of onset• Progressive m alaise, pyrexia, weight loss• Blockage and bloodstained crust ing• Septal collapse and saddling• Other par ts of ENT system m ay be involved• c-ANCA and biopsy m ay be helpful but are not
diagnost ic• Cort icosteroids and cytotoxics and m ainstay of
t reatm ent• Nasal Rx as for sarcoid
22.7 Hereditary Haemorrhagic Telangiectasia• Autosom al dom inant• Non-m uscular/elast ic t issue a ected
22.8 Septal Perforation• Causes:
◦ Traum a ◦ Nasal surgery ◦ Finger picking ◦ Rhinit is sicca anter ior ◦ Cocaine snor t ing ◦ Infect ion (TB, syphilis, leprosy, lupus) ◦ Granulom atous disease (sarcoid, granulom atosis w ith polyangiit is, etc.)
◦ Rarely tum ours (lym phom a, SCC, etc.)• Clin ical features:
◦ Crust ing ◦ Bleeding (usually spot t ing)
Philpott_9783131662316_Ch22.indd 82 02/05/14 3:20 PM

83
23.1 General Description• Vasculit is consists of a heterogeneous group of
system ic condit ions involving the in am m ation of blood vessels
• Tissue dam age occurs either due to vessel wall dam age and haem orrhage in to adjacent t issue (e.g., vasculit ic rash), or secondary to endothelial t issue, im pairm ent of blood ow, and ischaem ia of dependent st ructures (e.g., septal perforat ion)
• In each type of vasculit is the disease generally follows a cer tain organ dist r ibut ion pat tern but can nevertheless a ect a variable com binat ion of organs in any given pat ient
• There can be a signi cant overlap between each form of vasculit is as well as w ith other im m une-m ediated condit ions. Although classi cat ions are essent ial for designing the best t reatm ent , com m unicat ion , and research , always consider that these are “m an-m ade” boundaries w hen assessing ENT pat ients w ith suspected vasculit is
• These condit ions are specialty exam inat ion favorites. When suspect ing vasculit is as the pat ient’s diagnosis, rem em ber to seek the opinion of a rheum atologist or other physician w ith a special interest in vasculit is as part of the answer
23.2 Vasculitis in ENT• Fig. 23.1 dem onstrates t ypes of vasculit is m ore
com m only a ect ing the ENT region (shaded), w ith in the w ider vasculit is disease group
• Recent pathophysiological and eth ical developm ents have led to new nom enclature for the ANCA-associated vasculit ides: ◦ Granulom atosis w ith polyangiit is (GPA, form erly Wegener granulom atosis or WG)
◦ Eosinophilic granulom atosis w ith polyangiitis (EGPA, form erly Churg–Strauss syndrom e or CSS)
23.3 Granulomatosis w ith Polyangiitis or Wegener Granulomatosis• Mult isystem granulom atous vasculit is of sm all/
m edium arter ies, m ost com m only a ect ing the paranasal sinuses, lungs, and kidneys
• System ic sym ptom s: m alaise, unexplained pyrexia, weight loss
• ENT involvem ent: resistan t sinusit is, puru len t rh inorrhoea, epistaxis, septal perforat ion , saddlenose deform it y, secondary at rophic rh in it is w ith nasal crust ing that con t inues after rem ission of d isease act ivit y, m iddle ear disease, laryngeal in am m at ion , subglot t ic stenosis
• Over 60% of all GPA pat ients in it ially present w ith ENT symptom s, h ighlight ing the role of otolaryngologists in it s diagnosis
• Delay in diagnosis and t reatm ent can lead to irreversible t issue dam age in vital organs (e.g., kidneys), h ighlight ing the im portance of early diagnosis
• Over 80% of pat ients w ith classic m ult isystem involvem ent have raised ant i-neutrophil cytoplasm ic ant ibody (ANCA) t iters, m ost ly of the cytoplasm ic pat tern (c-ANCA) and against the proteinase 3 ant igen (c-ANCA-PR3)
• ANCA posit ivit y occasionally occurs in other non-vasculit ic condit ions such as in am m atory bowel disease, rheum atoid ar thrit is, and other autoim m une diseases, HIV, and other chronic infect ions
• In the lim ited form of GPA (ENT ± lungs) over 50% of pat ients are ANCA negat ive, posing a diagnost ic challenge for the ENT surgeon
• Always consider CXR (cavitat ing pulm onary nodules) and urinalysis (blood cells, proteins) in addit ion to ANCA if suspect ing GPA
• Nasal biopsies have a m axim um diagnost ic yield of 25% and only w hen large samples are taken from m acroscopically abnorm al areas
• Sam ples from clin ically norm al nasal m ucosa or quiescent subglot t ic lesions (stenoses) are nondiagnost ic
• Paranasal sinus CT ndings m ay include bony dest ruct ion , new bony form at ion, and orbital pseudotum ours
• Associat ion w ith relapsing polychondrit is, present ing w ith lobule-sparing pinna chondrit is, nasal pain , subglot t ic stenosis, and vest ibulocochlear involvem ent
• Treatm ent requires im m unosuppressant agents in addit ion to cor t icosteroids in the m ajorit y of pat ients (compare w ith CSS)
23 Granulomatosis w ith Polyangiitis and Other Vasculitides in the ENT Region
Philpott_9783131662316_Ch23.indd 83 02/05/14 3:25 PM

84
23 Granulomatosis with Polyangiit is and Other Vasculit ides in the ENT Region
• Main cause of m orbidity and m ortalit y: cardiac involvem ent (up to 50% of pat ients)
• Three stages of the disease are seen in m ost but not in all pat ients, and w ith h ighly variable lengths and pat terns: ◦ Allergic phase: adult-onset asthm a, rh in it is, and severely recurrent nasal polyps m ay be present for several years
◦ Eosinophilic phase: pneum onia and gast roenter it is
◦ Vasculit ic phase: all other m anifestat ions m ent ioned above
• Although ENT diagnosis is not achieved through nasal polyp h istology, it m ay be reached through H&N skin lesion biopsy coupled w ith a suggest ive clin ical picture (cranial nerve palsy, abnorm al CXR, etc.)
• Associated w ith raised ANCA t iters, m ost ly of the perinuclear pat tern (p -ANCA) and against the myeloperoxidase ant igen (p -ANCA-MPO), but m ore than 50% of EGPA pat ients are ANCA negat ive, posing a diagnost ic challenge
23.4 Eosinophilic Granulomato-sis w ith Polyangiitis (Formerly Churg–Strauss Syndrome or CSS)• Eosinophilic granulom atous necrot ising
in am m ation of the sm all/m edium blood vessels, half as com m on as GPA but com m oner in the United Kingdom than in other count ries
• ENT involvem ent: h ighly recurrent nasal polyps (75%), CN palsy, facial skin lesions, occasional m iddle ear disease (e.g., chronic m astoidit is)
• Nasal polyps respond to system ic steroids, frequently require surgery but are h istologically nondiagnost ic of vasculit is
• Other im portant features: late-onset asthm a (>55%), eosinophilia of >10% of leucocyte count (in >95% of pat ients, but m ay be m asked by system ic steroid t reatm ent), m ononeurit is m ult iplex (70%), vasculit ic skin lesions (50%), GI involvem ent (30%), renal impairm ent (20%)
Fig. 23.1 Types of vasculitis more commonly a ecting the ENT region (shaded), within the wider vasculitis disease group.
Giant CellArterit is
TakayasuArterit is
Vasculit is
Large vessel Medium vessel Medium/small vessel Small vessel
KawazakiDisease
Others
ANCA-associated
BehçetDisease
Others
Henoch-SchönleinPurpura
GPA (WegnerGranulomatosis),granulomatosiswith polyangiits
EGPA(Churg-Strauss
syndrome),eosinophilic
granulomatosiswith polyangiit is
Microscopicpolyangiitis
Others
Philpott_9783131662316_Ch23.indd 84 02/05/14 3:25 PM

85
Behçet Syndrome
nerve. The super cial tem poral branch of the external carot id ar tery divides ~5 cm above the poster ior root of the zygom at ic process in to parietal and frontal branches. The lat ter runs tor tuously upward and forward to the forehead and is the biopsy target . Lesions m ay be patchy or segm ental so take at least 3 to 6 cm of for h istologic analysis
• Biopsy is recom m ended w ith in 7 days of star t ing cort icosteroid therapy (sensit ivit y 85%), but can st ill be diagnost ic later even in pat ients on long-term steroids. A contralateral biopsy m ay be just i ed in di cult cases (increases overall sensit ivit y to 95%)
23.6 Behçet Syndrome• Vasculit is of both ar teries and veins (com pare
w ith GPA, EGPA, and giant cell ar ter it is or GCA)• Com m onest in Middle Eastern , Mediterranean,
and Japanese pat ients (old silk t rade route), half as com m on in western Europe
• Associated w ith HLA-B51 and tum our necrosis factor (TNF)-β2 alleles M:F, m ean age 40 years
• Clin ical t r iad of oropharyngeal ulcerat ion , genital ulcerat ion , and uveiit is
• ENT: m ult iple (>5) painful aphthous u lcers at di erent stages w ith scarring, vest ibulocochlear involvem ent
• Aphthous ulcerat ion preferent ially occurs in the lips, buccal m ucosa, gingiva, and tongue. Tonsillar, palatal, and pharyngeal u lcerat ion are less frequent but can rarely lead to laryngopharyngeal stenosis. Consider infect ion and in am m atory bowel disease as part of the di erent ial diagnosis
• Other features: skin lesions, CNS involvem ent (raised CSF protein), and ar thrit is
• Raised ESR, CRP, IgG, IgM, and IgA occur during acute exacerbat ions only and are non-speci c
• Pathergy test (react ive pustule 1–2 days after sterile needle skin prick) is speci c, but only 60% sensit ive in Middle Eastern pat ients, even less so in European pat ients w here it is not w idely used
• Topical t reatm ent: t r iam cinolone-tet racycline m outhwash, m ucosal steroid applicat ion via inhaler, local anaesthet ics
• Shor t-term system ic steroids, colchicine, and thalidom ide
• Im m unosuppressants and ant i-TNFα agents are uncom m on th ird-line t reatm ents and only for vital organ involvem ent
• For th is reason, if request ing ANCA, always consider urinalysis (blood cells, proteins) and CXR (non-cavitat ing pulm onary nodules (compare w ith GPA), patchy in lt rates, and pleural e usions, w hich are h ighly eosinophilic if sam pled)
• Delay in diagnosis and t reatm ent can lead to irreversible t issue dam age in vital organs (e.g., cardiomyopathy), h ighlight ing the im portance of early diagnosis
• Treatm ent w ith system ic cor t icosteroids alone is su cient for m any pat ients (com pare w ith GPA)
• Addit ional im m unosuppression (e.g., cyclophospham ide) only required in relapsing cases, h igh levels of proteinuria, cardiac or CNS involvem ent , or if peripheral nervous system involvem ent is m ult iple and disabling
23.5 Giant Cell (Temporal) Arteritis• Large-vessel vasculit is m ore com m only
occurring in nor thern Europeans age >50, 10 t im es as com m on in age >80 and tw ice as com m on in wom en
• Preponderance for the ext racranial carot id circulat ion (branches of external carot id and ophthalm ic branches of in ternal carot id ar teries), st roke from involvem ent of the in t racranial circulat ion is m uch less com m on
• ENT features: headaches, facial pain , tender pulseless super cial temporal ar teries, tongue and jaw claudicat ion , unexplained cough, sudden SNHL, ver t igo, rarely scalp or tongue necrosis m im icking H&N m alignancy
• Other features: erythrocyte sedim entat ion rate (ESR) >80 to 100 m m /h, visual disturbance (blindness in 15% if unt reated, 1% in t reated pat ients), polymyalgia rheum at ica (20–50%), unexplained pyrexia (15%), anem ia
• Oral cort icosteroid is the m ainstay of t reatm ent (60 m g prednisolone daily unt il norm alizat ion of sym ptom s and ESR, then tapering dose over 6 m onths w ith long-term low-dose m aintenance in som e pat ients)
• A tem poral ar tery biopsy m ay be requested from the ENT surgeon for diagnosis. ◦ Technique: ident ify ar tery by Doppler ult rasound, LA or GA incision of overlying skin staying above super cial temporal fascia avoiding the temporal branch of the facial
Philpott_9783131662316_Ch23.indd 85 02/05/14 3:25 PM
86
23 Granulomatosis with Polyangiit is and Other Vasculit ides in the ENT Region
• Most serious com plicat ion is coronary ar tery aneurysm (CAA) (4% of pat ients, 25% if untreated)
• CAA is associated w ith both an acute m ortalit y rate (1–2%) and long-term cardiovascular r isk in to adult life, em phasizing the im portance of early diagnosis and referral by the ENT specialist
• Aspirin and im m unoglobulins are the m ainstay of t reatm ent
• Cort icosteroids are not rst-line t reatm ents and should not be com m enced by the non-specialist as they m ay adversely a ect the outcom e of som e pat ients
23.7 Kawasaki Disease• Self-lim it ing m edium -vessel vasculit is of children• UK incidence 8.1/106 (16 t im es m ore com m on
in Japan)• Uncom m on in age <3 m onths or >5 years. If
a ected, both these age groups have a h igher r isk of ser ious com plicat ions
• ENT: oral, pharyngeal, and lip in am m ation, st raw berry tongue, cervical lym phadenopathy
• Other clin ical features: unexplained pyrexia >4 to 5 days, non-infect ive lim bic-sparing conjunct ivit is, delayed peripheral oedem a, and desquam at ion of ext rem it y skin
Philpott_9783131662316_Ch23.indd 86 02/05/14 3:25 PM

87
24.1 De nitions• Rhinosinusit is:
◦ Nasal blockage/obst ruct ion/congest ion or nasal discharge + at least one of: - Facial pain /pressure - Hyposm ia/anosm ia
◦ In addit ion, endoscopic and/or CT changes required to con rm symptom s above of acute rhinosinusit is (ARS)/chronic rhinosinusit is (CRS)
◦ <12 weeks = acute ◦ >12 weeks = chronic ◦ Symptom -free in tervals (com plete resolut ion) but >12 weeks in total = recurrent acute
◦ <10 days = com m on cold (viral upper respiratory t ract infect ion , i.e., URTI)
◦ Increase in Sx after 5 days OR persistence of Sx after 10 days = non-viral ARS
◦ Severit y de ned by VAS (0–10)—“How troublesom e are your Sx of ARS/CRS?”: - Mild = 0 to 3 - Moderate = >3 to 7 - Severe = >7 to 10
• Epidem iology: ◦ ARS:
- 8.4% of Dutch populat ion su er w ith ≥ 1 episode of ARS/year
- Fifth m ost com m on reason for ABx prescript ion in the United States
◦ CRS: - 11% of populat ion su er w ith CRS (prevalence)
- ≥15% of outpat ient consultat ions in ENT - 10,000 sinus procedures per year in the United Kingdom (1999–2010)
- Cost of $500 per year to pat ients w ith CRS in the United States
- Increasing incidence of CRS w ith increasing age—m ean age of 53
- Slight m ale preponderance - AFRS accounts for ~10% of CRS w ith nasal polyps (CRSw NPs)
24.2 Aetiology24.2.1 Acute Rhinosinusitis• Bacterial superinfect ion of virally dam aged
m ucosa:
◦ Bacteria - Streptococcus pneum oniae - Haem ophilus in uenzae - Moraxella catarrhalis (esp. children)
• Ciliary im pairm ent—im paired by viral infect ion• Allergy—m ay be a factor but evidence lim ited• Helicobacter pylori and laryngopharyngeal re ux
(LPR)—lit t le evidence• Presence of NG tube
24.2.2 Chronic Rhinosinusitis w ithout Polyps• Ciliary im pairm ent—secondary ciliary
dyskinesia• Allergy—m ay be presen t in 50 to 90% of
pat ien ts• Asthm a—m any asthm at ics w ill show abnorm al
m ucosal CT ndings (approxim ately 88%)• Im m unocom prom ised state—low IgA, IgG,
IgM; HIV• Genet ics—CF (m utat ions of CFTR gene) and
prim ary ciliary dyskinesia• Pregnancy—11 to 32% of wom en su er
pregnancy rh in it is• Local host factors—con ict ing evidence for
DNS, conchae bullosae, etc. Beware of dental infect ions
• Micro-organism s: ◦ Bacteria—pathogens or colonizers?
- S. aureus (36%) - Coagulase –ve staphylococcus (20%) - Streptococcus pneum oniae (17%)
◦ Fungi—colonize only or prom oters of allergic/eosinophilic response?
• Osteit is—anim al studies only—m ay explain resistance to ABx
• Environm ental: ◦ Sm oking ◦ Low incom e ◦ Atm ospheric pollutants—no convincing evidence
• Iat rogenic: ◦ Mucoceles associated w ith previous ESS ◦ Recirculat ion of m ucus from natural to surgical ost ia
• Helicobacter pylori and LPR—DNA detected in 11 to 33% of CRS pat ients—causal?
24 European Position Paper on Rhinosinusitis and Nasal Polyps
Philpott_9783131662316_Ch24.indd 87 02/05/14 3:31 PM

88
24 European Posit ion Paper on Rhinosinusit is and Nasal Polyps
• CD4+ TH cells—init iate and regulate in am m ation
• Macrophages (CD68+ cells) increase• Mast cell num bers raised• Cytokine m ediators: IL-1, 3, 6 and 8; tum our
necrosis factor-α (TNF-α ), GM-CSF, ICAM-1, MPO, and eosinophil cat ionic protein (ECP)—the lat ter is the m ain di erence from ARS
• IFN-γ and TGF-β = TH1 pathway; TGF-β expression h igher than CRS w ith NPs
• Chem okines, e.g., CCR4+• Eicosanoids—COX-2 m RNA and PGE2 higher
than CRS w ith NPs• Metalloproteinases—low MMP-9 act ivit y• Nasal n it r ic oxide (nNO) shows increase
the correlates w ith subject ive and object ive m easures of im provem ent
• Neuropept ides such as VIP m ay play a role• Mucins—MUC5AC and MUC5B increased in
CRS• Increased vascular endothelial grow th factor
(VEGF)• Bio lm s—structured specialized com m unit ies of
adherent m icro-organism s encased in a com plex ext racellular polym eric substance (EPS)
24.4.3 CRS w ith NPs• Eosinophils present in 80% = m arker of
in am m ation in CRSw NPs• Increased num bers of T cells and plasm a cells• S. aureus superant igens in teract w ith T cells
in 35%• Macrophages increased w ith an increase in
m acrophage m annose receptors in polyps• Mast cells—m ore often IgE+• Increased neutrophils• Overexpression of MUC8 m RNA and
dow nregulat ion of MUC5AC m RNA expression—alters m ucus com posit ion
• Cytokines and chem okines—di erences from CRSsNPs: ◦ IL-5 and IgE = CRS w ith NPs (TH2) ◦ Exaggerated hum oral and cellu lar response to airborne fungi
• Adhesion m olecules—ICAM-1 am ong others expressed on polyp surface
• Leukot rienes and their receptors unregulated in NP t issue
• S. aureus en terotoxins induce a m ore severe eosinophilic in am m ation and cause m ult iclonal IgE synthesis
24.2.3 Chronic Rhinosinusitis w ith Nasal Polyps• Polyps present in 0.5 to 4.3% of the populat ion;
only two-th ird seek m edical advice• Allergy—varying reports between 10 and 81%• Asthm a—31 to 42% of pat ients w ith NPs (7% of
asthm at ics have NPs)• Aspirin sensit ivit y—36 to 96% have CRS w ith NPs• Genet ics:
◦ 14 to 52% have +ve fam ily h istory ◦ Tw in studies do not show that both develop NPs
◦ HLA associat ions, e.g., A74, DR7 ◦ Gene polym orphism s ◦ Mult iple gene expressions for im m une m odulat ion
◦ Cyst ic brosis• Environm ental factors—unclear
24.3 Children• Day care• Nasal obst ruct ion• Passive sm oking• Bot t le-feeding• Urban atm ospheric pollut ion• Tonsillit is (im m unological de ciency)• OME (im m unological de ciency)• Ciliary dyskinesia, e.g., CF, prim ary ciliary
dyskinesia
24.4 In ammatory Mechanisms24.4.1 Acute Rhinosinusitis• Elevat ion of IL-1, IL-6, IL-8• Neut rophils—source of IL-8 and TNF-α• Expression of in t racellular adhesion m olecule 1
(ICAM-1)• T lym phocytes—st im ulated by IL-1 and 6, TNF-α
24.4.2 CRS w ithout NPs• Neut rophils predom inate• Sm all num bers of eosinophils, m ast cells,
basophils• Mucosal changes:
◦ BM thickening ◦ Goblet cell hyperplasia ◦ Subepithelial oedem a ◦ Mononuclear cell in lt rat ion
Philpott_9783131662316_Ch24.indd 88 02/05/14 3:31 PM

89
Future Research Needs and Priorit ies
24.6.3 Adults w ith CRS without NPs (Fig. 24.1)• Long-term ABx (>12/52)—low-dose m acrolide,
e.g., clar ithrom ycin (if IgE not elevated)• Topical steroids• Saline douching
24.6.4 Adults w ith CRS without NPs Postop(There is a paucity of data to suppor t post- operat ive m anagem ent)• Oral ant ibiot ics for 1 to 2 weeks if pus seen, but
long-term ABx also recom m ended• Topical steroids• Shor t-term oral steroids• Nasal douching
24.6.5 Adults w ith CRS with NPs (Fig. 24.2)• Oral ABx >12/52 for late relapse—consider
doxycycline• Topical/oral steroids—as guided by VAS• Nasal douche• Oral ant ih istam ine—if atopic
24.6.6 Adults w ith CRS With NPs Postop• As for CRSsNPs postop
24.6.7 Children with CRS (Fig. 24.3)• Oral ABx• Topical steroids• Saline douching• PPI
24.7 Future Research Needs and Priorities• Consider the role of:
◦ Socio-econom ic status ◦ Severit y staging w ith respect to QoL ◦ Prognost ic Sx in prim ary care ◦ Endotyping and phenotyping—including how to assess th is and the im pact upon m anagem ent and outcom es
• In CF—very prom inent neutrophilic in am m at ion
• Aspirin sensit ivit y—inhibit ion of cyclooxygenase-1 causing release of lipid and non-lipid m ediators
• IgE+ cell num bers raised in pat ients w ith allergic, fungal, and eosinophilic CRS
• Fungal-speci c IgG and IgA higher in CRS w ith eosinophilic m ucus
24.5 Investigations• Endoscopy• Endoscopic-guided nasal swabs—87% accurate• CT scan (± MRI w here neoplasia suspected)• Lund–Mackay scoring system for CT:
◦ 0 to 2 score for each of m axillary, ant . ethm oid, post . ethm oid, sphenoid, frontal
◦ Score of 0 or 2 for OMCs ◦ Max. score = 24 (12 each side)
• Saccharin test for m ucociliary clearance—useful if norm al (<35 m inutes)
• Ciliary beat frequency (>8 Hz for IT = norm al) and elect ron m icroscopy for PCD
• Nit r ic oxide: ◦ LRT = <20 ppb ◦ Nose = 400 to 900 ppb ◦ Sinuses = 20 to 25 ppm
• Nasal airway—PIFR/acoust ic rh inom etry/rh inom anom etry/nasal spirom etry
• Olfactory test ing—see Chapter 34• Aspir in challenge• QoL quest ionnaires—SF-36, RSOM, SNOT-22,
RSDI, RQLQ, et al.
24.6 Recommended Treatment Regimes24.6.1 Adults w ith ARS• Oral ABx—after 5/7• Topical cort icosteroid• Oral cort icosteroid—if severe to reduce pain• Oral ant ih istam ine—if atopic• Decongestant
24.6.2 Children with ARS• Oral ant ibiot ics—after 5/7• Topical cort icosteroids• Saline douching
Philpott_9783131662316_Ch24.indd 89 02/05/14 3:31 PM

90
24 European Posit ion Paper on Rhinosinusit is and Nasal Polyps
◦ Understand the pathogenesis of “allergic” fungal rh inosinusit is and AERD.
◦ Understand the link between CRSw NP and lower airway disease
• Im prove professional educat ion and e cient dissem inat ion of evidence-based guidelines to opt im ize outcom es and reduce referral rates to secondary care
• Conduct a large prospect ive placebo-controlled study of long-term ant ibiot ic t reatm ent in a well-de ned CRS populat ion, exploring e ects on the
◦ Osteit is ◦ Purulence in assessing response to Rx ◦ Childhood events, smoking, and AR as risk factors ◦ Psychological, neurological, GORD risk factors
• To fur ther invest igate: ◦ Olfactory disorders, headache, facial pain ◦ To develop new classi cat ions based on endotypes and phenotypes
◦ To bet ter understand in am m atory pathways including TGF-β, T cells, dendrit ic cells, m icrobiom es
Fig. 24.1 Management scheme for ENT specialists treating CRS without NPs in adults.From Fokkens WJ, Lund VJ, Mullol J, et al. The European Position Paper on rhinosinusitis and nasal polyps 2012. Rhinology 2012;Suppl. 23:1–299, with permission.
2 symptoms: one of which should be nasal obstructionor discoloured discharge± frontal pain, headache± smell disturbanceENT examination including endoscopyConsider CT scanCheck for allergyConsider diagnosis and treatment of co-morbidities eg. asthma
MildVAS 0-3
No serious mucosal disease at endoscopy
Follow-up +nasal saline irrigation
Topical steroidsConsider long-term
antibiotics
Topical steroidsNasal saline irrigation
No improvementafter 3 month
Improvement
Moderate/severeVAS >3-10Mucosal
disease at endoscopy
Topical steroidsNasal saline irrigation
CultureConsider long-termantibiotics (if IgE is
not elevated)
Follow-up +topical steroids
Nasal saline irrigationCulture
Consider long-termantibiotics
CT scan
CT scanif not done before
No Improvement
Consider surgery
Consider surgery
Consider other diagnosis: unilateral symptoms bleeding crusting cacosmia
Orbital symptoms: peri-orbital oedema/erythema displaced globe double or reduced vision opthalmoplegia
Severe frontal headacheFrontal swellingSigns of meningitisNeurological signs
Urgent investigationand intervention
Philpott_9783131662316_Ch24.indd 90 02/05/14 3:31 PM

91
Future Research Needs and Priorit ies
• Conduct m ult icent re RCTs on surgery vs. no t reatm ent for pat ients w ith CRSw NP to establish the natural course of disease
• Conduct RCTs on m inim al vs. m ore extensive endoscopic sinus surgery
• Invest igate the e ect of early surgical in tervent ion on CRSw NP to see if it alters the course of the disease
pat ients’ QoL, im m une system , m icrobiota of the airway, as well as the health econom ic im pact
• Seek bet ter local therapies for im m unom odulat ion
• Conduct an RCT on oral steroids vs. surgery on the long-term outcom es of CRSw NP
• Conduct an RCT studying the e ects of oral cort icosteroids on olfactory funct ion in CRSw NP
Fig. 24.2 Management scheme for ENT specialists treating CRS with NPs in adults.From Fokkens WJ, Lund VJ, Mullol J, et al. The European Position Paper on rhinosinusitis and nasal polyps 2012. Rhinology 2012;Suppl. 23:1–299, with permission.
2 symptoms: One of which should be nasal obstructionor discoloured discharge± Frontal pain, headache± Smell disturbanceENT examination, including endoscopyConsider CT scanCheck for allergyConsider diagnosis and treatment of co-morbidities, e.g., asthma
MildVAS 0–3
No serious mucosal disease at endoscopy
Continue withtopical steroids
Nasal saline irrigation
Topical steroidsNasal saline irrigation
Topical steroid sprayNasal saline irrigationConsider increase dose
Consider dropsConsider doxycycline
Improvement No improvement Improvement
Review after 3 month Review after 1 month
Review every 6 month
SevereVAS >7–10Mucosal
disease at endoscopy
Follow-up+ nasal irrigation
+ topical ± orals steroids± long-term antibiotics
Moderate/severeVAS >3–7Mucosal
disease at endoscopy
Topical steroidsNasal saline irrigation
Oral steroids(short course)
CT scan
No improvement
Surgery
Consider other diagnosis: Unilateral symptoms Bleeding Crusting Cacosmia
Orbital symptoms: Peri-orbital oedema/erythema Displaced globe Double or reduced vision Opthalmoplegia
Severe frontal headacheFrontal swellingSigns of meningitisNeurological signs
Urgent investigationand intervention
Philpott_9783131662316_Ch24.indd 91 02/05/14 3:31 PM

92
24 European Posit ion Paper on Rhinosinusit is and Nasal Polyps
Fig. 24.3 Management scheme for ENT specialists treating chronic rhinosinusitis without NPs in children.From Fokkens WJ, Lund VJ, Mullol J, et al. The European Position Paper on rhinosinusitis and nasal polyps 2012. Rhinology 2012;Suppl. 23:1–299, with permission.
2 symptoms: One of which should be nasal obstructionor discoloured discharge± Frontal pain, headache± Smell disturbanceENT examination including endoscopyConsider CT scanCheck for allergyConsider diagnosis and treatment of co-morbidities, e.g., asthma
MildVAS 0–3
Follow-up +nasal irrigationTopical steroids
Follow-up +nasal irrigationTopical steroids
Consider long-termantibiotics
Nasal irrigationNasal steroids Failure after 3 month
CT scan
Consider FESS
Moderate/severeVAS >3–10
+ Consider culture+ Consider long-term
antibiotics
Consider adenoi-dectomy and
sinus irrigation
Consider other diagnosis: Unilateral symptoms Bleeding Crusting Cacosmia
Orbital symptoms: Peri-orbital oedema/erythema Displaced globe Double or reduced vision Opthalmoplegia
Severe frontal headacheFrontal swellingSigns of meningitisNeurological signs
Urgent investigationand intervention
Philpott_9783131662316_Ch24.indd 92 02/05/14 3:31 PM

93
25.1 Complications of Acute Sinusitis• Divided in to orbital (60–75%), in t racranial
(15–20%), and osseous (5–10%) complicat ions• Sinus disease accounts for:
◦ 10% of in t racranial suppurat ion ◦ 10% of pre-septal orbital infect ion ◦ 90% of post-septal orbital infect ion
• Incidence of com plicat ions: ◦ 2.7 to 4.3 per m illion (in t racranial com plicat ions)
◦ 2.5 per m illion adults (all acute rh inosinusit is (ARS) com plicat ions)
◦ 1 per 12,000 ARS episodes (children) ◦ 1 per 36,000 ARS episodes (adults)
• More com m on during w inter m onths• Males > fem ales• Ant ibiot ics for ARS do not change the incidence
of complicat ions
25.1.1 Orbital Complications• Most com m on type of com plicat ion• Associated w ith ethm oid, m axillary, frontal,
sphenoid in reducing frequency• Chandler classi cat ion (Fig. 25.1)
◦ I—pre-septal cellulit is (st r ict ly speaking, outside the orbit)
◦ II—orbital cellulit is ◦ III—subperiosteal abscess ◦ IV—orbital abscess ◦ V—cavernous sinus throm bosis (again , not “orbital,” and not necessarily the end stage of orbital infect ion)
• An ophthalm ology review is m andatory• IV ant ibiot ics covering aerobic and anaerobic
organism s• Presence of ophthalm oplegia, loss of red–green
vision/visual acuity—CT w ith contrast required → surgical drainage
• No im provem ent/deteriorat ion after 48 h IV ant ibiot ics → surgical drainage
• CT appearance: ◦ Subperiosteal abscess:
- Medial rectus oedem a - Lateralizat ion of m edial rectus/periorbita - Globe displacem ent inferolaterally
◦ Orbital abscess: - Loss of detail of ext raocular m uscles/opt ic nerve
- Possible orbital air• Surgical drainage should also include addressing
the adjacent sinuses• Som e evidence to suggest in sm all children
w ith subperiosteal abscesses IV ant ibiot ics su cient if: ◦ Im proving over 48 h ◦ Norm al visual acuity ◦ <1 m L volum e, m edial locat ion ◦ <4 years of age ◦ System ically well
25.1.2 Intracranial Complications• Spread from sinuses through diploic veins or
direct ly through bone erosion• Often involve anaerobic or m ixed aerobic/
anaerobic organism s• These include:
◦ Epidural, subdural, cerebral abscesses ◦ Meningit is, encephalit is ◦ Superior sagit tal, cavernous sinus throm bosis
• Sym ptom s: ◦ Nausea and vom it ing ◦ Neck st i ness ◦ Altered m ental state ◦ Focal neurological de cits ◦ Headache
• Invest igat ions ◦ CT scan w ith cont rast—bone erosion ◦ MRI—soft t issue involvem ent , cavernous sinus throm bosis
◦ Consider lum bar puncture• Treatm ent
◦ Long-term , h igh-dose IV ant ibiot ics ◦ Craniotomy and abscess drainage ◦ Endoscopic drainage of sinuses ◦ MC&S of pus, biopsy of abnorm al t issue
25.1.3 Cavernous Sinus Thrombosis• Venous drainage of paranasal sinuses to
cavernous sinus—allows haem atogenous spread of infect ion
25 Complications of Sinusitis
Philpott_9783131662316_Ch25.indd 93 02/05/14 3:34 PM

94
25 Complications of Sinusit is
◦ Anterior table—oedem a of skin producing a m ass (Pot t pu y tum our)
◦ Posterior table—leads to in t racranial sepsis• Treatm ent
◦ High-dose IV ant ibiot ics ◦ Drainage of adjacent sinuses ◦ Surgical debridem ent of infected bone
25.2 Complications of Chronic Sinusitis• Rare• Usually due to bone erosion/expansion/
rem odelling
• Can lead to CN palsies: ◦ Bilateral ptosis ◦ Proptosis ◦ Retro-ocular pain ◦ Ophthalm oplegia ◦ Papilloedem a ◦ Spiking fevers
• Invest igat ions (as above), plus MR venogram to show lling defects
25.1.4 Bone Complications• Usually osteom yelit is of the frontal or m axillary
(infants) bones• Frontal
Fig. 25.1 Chandler classi cation.
VIVIII
III
Philpott_9783131662316_Ch25.indd 94 02/05/14 3:34 PM

95
Complicat ions of Chronic Sinusit is
◦ MRI—low T1, h igh T2 signal• Treatm ent
◦ Surgery—endoscopic m arsupializat ion; occasionally com bined endoscopic/external approach required
25.2.2 Osseous Metaplasia• New bone form at ion , e.g., in lum en of sinuses
25.2.3 Others• Osteit is• Opt ic neuropathy
25.2.1 Mucocoeles• Epithelial-lined, m ucus-contain ing sac
completely lling the sinus• May lead to expansion or bone erosion• Can cause displacem ent of adjacent st ructures,
e.g., eye• Often associated w ith sinus out ow
obst ruct ion• Can becom e acutely infected• Most com m only in frontoethm oid region (86%)• Invest igat ion
◦ CT—expansile lesion , w ith bony e acem ent or erosion
Philpott_9783131662316_Ch25.indd 95 02/05/14 3:34 PM

96
26 Fungal Sinus Disease26 Fungal Sinus Disease
26.3 Chronic Invasive Fungal Sinusitis• Aspergillus fum igatus, dem at iaceous m olds
(Bipolaris, Curvularia, Alternaria)• Locally invasive disease >3 m onths durat ion ,
usually have DM or on cort icosteroids• Orbit and CNS invasion less com m on than in
acute t ype• Presents w ith chronic sinusit is ± sym ptom s of
local invasion (eye swelling, decrease in vision and eye m ovem ent—orbital apex syndrom e)
• CT of paranasal sinuses—hyperdense soft t issue, dem onst rates bony involvem ent
• MRI—hypointense on T1 and very hypointense on T2, in t racranial extension
• Diagnosis con rm ed on biopsy revealing invasion in to the surrounding t issues
• Histology—bone necrosis w ith lym phocytes, neutrophils, eosinophils, Langhans cells
• Treatm ent involves urgent surgery (FESS/surgical debridem ent), system ic ant ifungals (am photeracin B—change to it raconazole once controlled, cont inue for up to 1 year)
• Long-term follow -up required as th is condit ion tends to recur
26.4 Granulomatous Invasive Fungal Sinusitis• Aspergillus avus• North Africa, India, Pakistan• Locally invasive disease over at least 3 m onths
durat ion , im m unocompetent• Present w ith chronic sinusit is and proptosis or
enlarging m ass in a ected sinus• Histology—non-caseat ing granulom a, foreign
body/Langhans giant cells w ith necrosis• Surgical debridem ent is required followed by
system ic ant ifungal m edicat ion• Recurrence is less com m on and prognosis good
• Inhaled fungi can cause both acute and chronic rh inosinusit is
• Fungal colonizat ion of the sinuses is com m on and is rarely of clin ical consequence
26.1 Types of Fungal Sinusitis26.1.1 Invasive• Acute invasive (fu lm inant) fungal sinusit is• Chronic invasive fungal sinusit is• Granulom atous invasive fungal sinusit is
26.1.2 Non-invasive (Majority)• Fungal balls (mycelium m ass)• Allergic fungal rh inosinusit is
26.2 Acute Invasive (Fulminant) Fungal Sinusitis• Saprophyt ic fungi of the m ucoracious m olds
(Mucor, Rhizopus, Absidia)• <4 weeks durat ion in im m unocom prom ised
pat ients (DM, HIV, neutropenia, chem otherapy)• Rare, h igh m ortalit y rate—50% w ith CNS or
cavernous sinus involvem ent• Invades soft t issue and vessels causing local
throm bosis, infarct ion , and necrosis• Pat ients very unwell w ith fever, nasal discharge,
headache, m ental state changes• Necrot ic black areas on septum , turbinates, or
palate, CN involvem ent and proptosis• CT—to assess extent and bony involvem ent
(Fig. 26.1), MRI—vascular/in t racranial involvem ent
• Requires urgent t reatm ent w ith surgery (FESS and surgical debridem ent unt il norm al t issue ident i ed) and h igh-dose system ic ant ifungal t reatm ent (amphotericin B or posaconazole, w hich is the drug of choice)
• Treat underlying im m une de ciency if possible
Philpott_9783131662316_Ch26.indd 96 02/05/14 4:16 PM

97
Allergic Fungal Rhinosinusit is (AFRS)
• No predom inance of eosinophils or granulom a or allergic m ucin , and no histopathologic evidence of fungal invasion of m ucosa
• Treatm ent is surgical (FESS, rem ove fungal ball and open a ected sinus)
• Sinus full of m ucopurulent cheesy m aterial at surgery (Fig. 26.2)
• Follow ing rem oval of the fungal ball no ant ifungal t reatm ent is required
• No long-term follow-up required once patency and healing of sinus con rm ed
26.6 Allergic Fungal Rhinosinus-itis (AFRS)• Eosinophilic fungal rh inosinusit is (EFRS) and
eosinophilic m ucinous rh inosinusit is (EMRS) are poorly di erent iated from AFRS and it is unclear
26.5 Fungal Balls (Mycelia Mass)• Mainly Aspergillus species, e.g., Aspergillus
fum igatus in im m unocom petent• More com m on in m iddle-aged and elderly
wom en, in cont rast to all form s of invasive and chronic aspergillosis, w hich are m ore com m on in m ales
• Chronic sinusit is of one sinus, usually m axillary (then sphenoid)
• Chronic nasal discharge, nasal obst ruct ion , headache, facial pain , cacosm ia
• Can be associated w ith unilateral proptosis and facial hypoesthesia
• CT—unilateral, single sinus disease, heterogeneous opaci cat ion (Fig. 26.2)
• Cultures are posit ive in less than one-th ird of pat ients despite fungal elem ents on h istopathology in >90% of those a ected
Fig. 26.1 Acute invasive fungal sinusitis of the sphe-noid sinus, bony erosion shown on CT.
Philpott_9783131662316_Ch26.indd 97 02/05/14 4:16 PM

98
26 Fungal Sinus Disease
• Allergic m ucin is produced—thick, tenacious, peanut but ter-like (Fig. 26.3)
• The term eosinophilic m ucin is now preferred to allergic m ucin
• Present w ith chronic sinusit is—nasal obst ruct ion, congest ion , purulent rh inorrhoea, post-nasal drainage, facial pain and headaches
• Elevated IgE, eosinophilia• Histology of allergic m ucin con rm s presence of
Charcot–Leyden crystals (non-invasive, fungal hyphae w ith in sheets of eosinophils)
• CT—“double densit y” (presence of heavy m etals, e.g., m anganese in allergic m ucin)
• MRI—allergic m ucin hyperin tense on T1 and signal void on T2
• Diagnost ic criter ia: allergic m ucin (eosinophilic w ithout t issue invasion), characterist ic ndings on CT (heterogeneous opaci cat ion), posit ive fungal stain /culture, nasal polyps, t ype I hypersensit ivit y
• Fungi m ay elicit eosinophilic in am m at ion in the absence of t ype 1 hypersensit ivit y, therefore im m unocom petence m ay replace t ype I response in the diagnost ic criter ia
current ly w hether these are di erent clin ical and pathological ent it ies
• All p resen t w ith ch ron ic rh inosinusit is (CRS) >12 w eeks, sinus opaci cat ion , and th ick m ucin
• AFRS—allergic m ucin w ith m any eosinoph ils, non-invasive fungi and raised fungal speci c IgE
• EFRS and EMRS do not have speci c IgE and di er depending on w hether fungus can be ident i ed or not
• EMRS is bilateral, w ith a h igher frequency of asthm a and increased incidence of aspirin sensit ivit y (com pared w ith AFRS), and often an im m unoglobulin G1 de ciency
• ~10% of CRS is AFRS• A ects ~1% of the populat ion• Dem at iaceous m olds (e.g., Alternaria,
Cladosporium , Bipolaris, Curvularia) and Aspergillus fum igatus in im m unocom petent
• The m ajorit y of AFRS causes unilateral or asym m etric involvem ent of sinuses
• In am m atory (IgE m ediated) response to inhaled fungi results in oedem a and polyps
Fig. 26.2 Fungal ball in right maxillary sinus.
Philpott_9783131662316_Ch26.indd 98 02/05/14 4:16 PM

99
Allergic Fungal Rhinosinusit is (AFRS)
• Requires regular and close follow-up because of the r isk of relapse and recurrence
• Philpot t–Javer post-operat ive endoscopic staging system (Table 26.1) allows accurate m onitoring and recording of disease severit y during follow -up
• Surgery (FESS) w ith rem oval of all allergic m ucin and fungal debris, and opening all a ected sinuses to allow post-operat ive access
• Post-operat ive oral and topical steroids
Table 26.1 Philpot t–Javer endoscopic staging system for AFRS
Grading State of mucosa
0 No oedema
1–3 Mucosal oedema (mild/moderate/severe)
4–6 Polypoid oedema (mild/moderate/severe)
7–9 Frank polyps (mild/moderate/severe)
Sinus cavity Right Mucin Left Mucin
Frontal 0–9 1 0–9 1
Ethmoid 0–9 1 0–9 1
Maxillary 0–9 1 0–9 1
Sphenoid 0–9 1 0–9 1
Total 40 40 40
Bilateral total 80
Fig. 26.3 Allergic fungal sinusitis—“double density” on CT and allergic mucin.
Philpott_9783131662316_Ch26.indd 99 02/05/14 4:16 PM

100
26 Fungal Sinus Disease
• System ic steroids are useful shor t-term for relapses and post-operat ively but because of adverse e ects are not ideal for long-term use
• Am photericin B sinus washes• Manuka honey irr igat ions
• System ic ant ifungals—oral it raconazole, m ust m onitor LFTs
• Im m unotherapy—fungal desensit izat ion m ay reduce pat ient symptom s, relapse rates, and cor t icosteroid dependence after surgery in som e pat ients
Philpott_9783131662316_Ch26.indd 100 02/05/14 4:16 PM

101
27.1 Nasal Preparation27.1.1 Options for Pre-operative Preparation and Perioperative Control• Pre-operat ive steroids/ant ibiot ics• Xylom etazoline (Otrivine)/other decongestants• Mo at solut ion• Cocaine paste• Topical adrenaline• Hypotensive anaesthesia (TIVA)• Careful t issue handling
27.1.2 Multisystemic E ects of Cocaine• Altered m ental status• New -onset seizures• Hypertension• Chest pain• Myocardial ischem ia or infarct ion• Shortness of breath• In t racranial hem orrhage• Epistaxis• Hypertherm ia
27.1.3 Treatment of Cocaine Toxicity• β-blockers (propranolol)—depress CO• GTN and sodium bicarbonate m ay be required• Benzodiazepines (lorazepam ) for seizures
27.2 Pre-operative CT Checklist• Nasal cavity roof—slope, height , th in and th ick
areas, Keros classi cat ion of cribriform plate• Medial orbital wall—shape and in tegrit y, opt ic
nerve, infundibulum• Maxillary sinus—Haller cells, retent ion cysts,
dent igerous cysts• Ethm oids—vert ical height , an terior (and
posterior) ethm oid ar ter ies, basal lam ella, size of bulla
• Sphenoid sinus—pneum at izat ion , in tersinus septum , carot ids, Onodi cells
• Frontal recess—size, posit ion of cells (Kuhn, ISSC, SOE, FBC), agger nasi
• Middle turbinates—paradoxical, resected, conchae bullosae
• Can you m anage all the eventualit ies?
27.3 Four Constant Landmarks in Sinus Surgery• Uncinate process• Face of the bulla• Basal lam ella• Face of the sphenoid sinus
27.4 A Stepwise Approach to Sinus Surgery• Total uncinectomy—upper uncinate (0° scope)
and lower uncinate (30° scope)• Visualizat ion of the natural m axillary sinus
ost ium w ith preservat ion of the out ow t ract (infundibulum ) (30° scope)
• Debridem ent or lavage of m axillary sinus contents (30° scope)
• Resect ion of bulla (0° scope)• Penetrat ion of basal lam ella (0° scope)• Posterior ethm oidectomy to sphenoid face
(0° scope)• Sphenoidotomy via Bolger/Lanza/t ransnasal
approach ± lavage/debridem ent of contents (0° (± 30°) scope)
• Clearance of the skull base from sphenoid face to frontal recess (0° and 30° scope)
• Rem oval of the agger nasi cap (30° scope)• Frontal sinusotomy including rem oval/opening
of any frontal cells (Kuhn, etc.) (30° and 70° scope)
• Lavage/debridem ent of frontal sinus contents (70° scope)
27.5 Exceptions to the Rule• Wide ant rostomy perform ed w hen:
◦ Tum our ◦ AFRS ◦ Cyst ic brosis
27 Endoscopic Sinus Surgery and Complications
Philpott_9783131662316_Ch27.indd 101 02/05/14 4:19 PM

102
27 Endoscopic Sinus Surgery and Complicat ions
• Middle turbinate resect ion perform ed w hen: ◦ Conchae bullosa ◦ Polypoid port ions ◦ Tum our
27.6 Sphenoid Approaches• Superior turbinate at tachm ent to sphenoid face
(Parson r idge) cr it ical in determ ining ent ry to sphenoid: ◦ Type A: sup turbinate at tachm ent in m edial 1/3: 40%
◦ Type B: sup turbinate at tachm ent in m iddle 1/3: 40%
◦ Type C: sup turbinate at tachm ent in lateral 1/3: 19%
◦ Type D: sup turbinate at tachm ent to orbit: 1%• 3 endoscopic approaches:
◦ Transnasal (via sphenoethm oidal recess) ◦ Bolger—parallelogram m ethod (natural ost ium not used)
◦ Lanza—resect ion of inferior por t ion of Parson ridge to allow t ransethm oidal access to ost ium
27.7 Frontal Recess (Kuhn) Cells• Type I—one ethm oid cell in associat ion w ith
agger nasi• Type II—stacked ethm oid cells in frontal recess• Type III—single large ethm oid cell extending in to
frontal sinus• Type IV—isolated ethm oid cell w ith in frontal
sinus w ithout connect ion to frontal recess (probably an ar t ifact of older CT im aging protocols)
27.8 Skull Base Con guration—Keros• (A) Type I—olfactory fossa 1 to 3 m m deep• (B) Type II—olfactory fossa 4 to 7 m m deep• (C) Type III—olfactory fossa 8 to 16 m m deep• (D) Asym m etric fossae
27.9 Frontal Sinus Surgery27.9.1 Techniques—Endoscopic• Balloon sinuplasty• Draf t ype 1—dissect ion of frontal
recess (uncapping the egg—Stam m berger)
• Draf t ype 2a—frontal sinusotomy—frontal sinus oor between MT insert ion and orbit
• Draf t ype 2b—m iddle turbinate rem oved and sinusotomy extended to m idline
• Draf t ype 3—rem oval of nasal and in tersinus septae (m odi ed Lothrop)
27.9.2 External Approaches• Trephinat ion (± endoscopic approach)• Lynch procedure w ith Sewall-Boyden ap• Osteoplast ic ap ± obliterat ion—avoid lat ter
w here tum our present• Cranializat ion• Ridel procedure
27.9.3 Indications for External Approach• Mucocoeles• Know n/suspected neoplasia• Failure of endoscopic approach• Access to lateral or superior aspects of frontal
sinuses
27.10 Image-Guided Surgery• The use of pre-operat ive CT and/or MR im ages
to dynam ically t rack the posit ion of surgical inst rum ents relat ive to the scan im ages in 3 planes (axial/coronal/sagit tal)
• Allows m apping of com plex 3D anatomy throughout the operat ion
• What it does not do: ◦ Update the pre-operat ive im ages ◦ Warn of impending danger ◦ Avoid the need for thorough anatom ical know ledge and experience
• Principles for IGS use: ◦ The surgeon should spend t im e studying the pre-operative CT scans on the computer to develop a 3D m ap of the patient’s sinus anatomy
◦ Precise surgical dissect ion is of pr im e im portance
◦ The navigat ion system should not be an excuse to “point and hunt” for a st ructure but to help the surgeon con rm the posit ion of the inst rum ent
• Applicat ions for use: ◦ Revision sinus surgery ◦ Distorted sinus anatomy of developm ent , pathological, post-operat ive, or t raum atic origin
Philpott_9783131662316_Ch27.indd 102 02/05/14 4:19 PM

103
Complications
◦ Extensive sinonasal polyposis ◦ Pathology involving the frontal, posterior ethm oid, and sphenoid sinuses
◦ Disease abut t ing the skull base, orbit , opt ic n , or carot id a
◦ CSF rhinorrhea or condit ions w here there is a skull base defect
◦ Benign and m alignant sinonasal neoplasm s ◦ Training
• Accuracy factors: ◦ CT scan and its reconst ruct ion ◦ Tolerances of the sensor device ◦ Abilit y of the surgeon to place the probe on an exact point
◦ Mathem at ical round-o errors ◦ Pat ient m ot ion ◦ In terference by surrounding ferrom agnet ic st ructures (EM system s)
◦ In terference w ith line of sight (IR system s)• Accuracy in pract ice:
◦ Range 0.5 to 3 m m , m ean ~1 m m ◦ Check at regist rat ion—external and in ternal ◦ Cont inue to check at key landm arks ◦ Always rely on endoscopic view and anatom ical knowledge + inst incts rst
◦ Do not be afraid to reregister the scan if unhappy
◦ Rem em ber to register di erent probes/suct ions if required
27.11 Complications27.11.1 Minor• Hem orrhage• Orbital ecchym osis• Dehiscence of lam ina papyracea• Local infect ion (postop nose/sinus/abscess/
cellulit is)• Synechiae (requir ing division)• Sym ptom at ic septal perforat ion as a result
of surgery
27.11.2 Major• Epiphora• Orbital com plicat ions:
◦ Medial orbital wall penetrat ion ◦ Orbital fat herniat ion ◦ In t raorbital bleeding ◦ Medial rectus injury ◦ Lacrim al duct injury
◦ Optic nerve injury ◦ Loss/disturbance of vision
• CSF leak• External nasal deform ity (saddle/deviat ion/
colum ellar ret ract ion)• Distant com plicat ion (DVT, etc.)• Death
27.11.3 Managing Complications• The “m ajor” com plicat ions (orbital injuries and
CSF leaks)—incidence est im ated at 0.5%• Medial orbital wall penetrat ion—prevent ion:
◦ Very careful preop evaluat ion of CT ◦ Relat ion of uncinate to m edial orbital wall ◦ Sickle knife rem oval of uncinate discouraged ◦ Be aware of anatom ical variat ions ◦ Uncinate process adherent to lam ina papyracea ◦ Maxillary sinus hypoplasia
- Com m on after previous Caldwell–Lucs - Silent sinus syndrom e
◦ Orbital dehiscence from previous surgical m ishap—need to be extra careful
◦ Lam ina m edial to m axillary sinus ost ium (ethm oid hypoplasia)
• In t raorbital bleeding m anagem ent: ◦ Average orbital volum e = 26 m L (con ned cavit y)
◦ ↑ in volum e of 4 m L =16% (6 m m proptosis) ◦ Arterial:
- Fast - Ant ethm oidal ar tery - Rem ove packing + suct ion - Canthotom y—cantholysis - Orbital decom pression - No need to search for ar tery
◦ Venous: - Slow - Venule w ith in fat - Mannitol—1 gm /kg IV over 30 m in - Acetazolam ide (sulfa drug)—500 m g IV - Ophthalm ology consultat ion - Vision m onitoring - Canthotom y—cantholysis - Orbital decom pression
• Opt ic nerve injury ◦ Risk m uch lower w ith appropriate anatom ical know ledge and availabilit y of IGS
◦ Look out for sphenoethm oidal cell/Onodi cell ◦ Avoid superior-lateral dissect ion in the sphenoid and poster ior ethm oids
◦ Dehiscent opt ic nerve in sphenoid
Philpott_9783131662316_Ch27.indd 103 02/05/14 4:19 PM

104
27 Endoscopic Sinus Surgery and Complicat ions
• CSF leak repair ◦ Must recognize in t raoperat ively (wash-out e ect) or early post-operat ively: - Meningit is, pneum ocephalus, severe headaches, psychological signs/sym ptom s
◦ Treat /repair int raoperat ively if recognized ◦ Options:
- In t racranial approach - Extracranial external approach (e.g., via Lynch incision)
- Endoscopic approaches: - (a) sim ple plugging w ith turbinate ap m ay be feasible if spot ted in t raoperat ively, and
- (b) delayed detect ion m ay need evaluat ion and m ore form al repair (see Chapter 36)
◦ Most com m on locat ion during FESS: lateral cr ibriform plate lam ella (LCPL) at level of anterior ethm oid ar tery (bone th ickness <1 m m )
◦ Always work from m edial to lateral and posterior to anter ior
◦ Work “away” from sloping skull base• Surgical afterm ath:
◦ Incom plete uncinectom y ± inferior ant ral w indows
◦ Overresect ion of turbinates ◦ Agger nasi in tact ◦ Bony fragm ents deposited in sinus cavit ies ◦ Synechiae ◦ Lateralized MT ◦ Chronic infect ion post-operat ively
- Assess in context of pat ient - Acquire sinus aspirate/swab endoscopically - Treat on m erit of culture and sensit ivit y, not via a generic prescript ion
- Topical ant ibiot ics good for persistent infect ions such as (a) direct inoculat ion in to sinus cavit ies and (b) sinus lavages w ith saline/sham poo/ant ibiot ics
◦ Managem ent of scar t issue: - Can rem ove using through-cut inst rum entat ion
- Can do it in the clin ic if technically able - Reduce recirculat ion - Need excellent clin ic inst rum entat ion and endoscopy skills—esp. frontal recess
Philpott_9783131662316_Ch27.indd 104 02/05/14 4:19 PM

105
28.1 Types of Ciliary Motility Disorders28.1.1 Cystic Fibrosis• Autosom al recessive• Defect ive m ucosal chloride t ranspor t gene• Malabsorpt ion and progressive obst ruct ive
pulm onary disease• One-th ird children su er w ith bilateral NPs• Most pat ients have chronic pansinusit is• Histology of NPs in CF di ers—fewer eosinophils
and m ore lym phocytes• Pseudom onas aeruginosa com m only found in the
sinus disease• Sweat test to detect abnorm al chloride levels:
>60 m Eq/L = diagnost ic• Other diagnost ic tests:
◦ CT scans of sinuses ◦ Genotyping—PCR ◦ Sem en analysis ◦ Nasal PD m easurem ent
28.1.2 Primary Ciliary Dyskinesia• Prim arily a dysfunct ion of the cilial m ot ilit y
rather than a loss of their funct ion outr ight• Usually a recessive condit ion , but there can be
genet ic heterogeneity
28.1.3 Kartagener Syndrome• Prim ary ciliary dyskinesia (PCD) w ith situs
inversus• Chronic rh inosinusit is, bronchiectasis, and situs
inversus• Ciliary m ot ilit y lacking or possibly severely
impaired
28.2 Pathophysiology• B m icrotubules are incom plete w ith respect to
the A tubules: only 2 rather than 13 parallel proto lam ents
• The A m icrotubules’ dynein arm s and radial spokes contain abnorm alit ies and also lack a
cent ral pair of doublets, hence have an 8 + 1 con gurat ion (i.e., not 9 + 2)
• Occasionally pat ients m ay have an abnorm al cilial beat frequency in the presence of a norm al st ructural con gurat ion
• Another aberrat ion can be a disordered orientat ion of the cilia (w hen beat ing)
• 3 genet ic defects have been discovered w hich a ect the dynein of the axonem e
• Som e PCD pat ients have a h igh incidence of ciliary disorientat ion
• Abnorm al m ucus could also have a role to play in the process w ith prolonged m ucociliary clearance t im es in 57% of pat ients w ith chronic rh inosinusit is and bronchiectasis
28.3 Clinical Presentation• Sym ptom s of rh inorrhea and/or m ucopus
discharge from bir th• >⅓ of pat ients w ith th is syndrom e are found
to have NPs• If polyps present—sweat test could be
perform ed; if absent , nasal brushings are m ore useful
• All pat ients fail the saccharin clearance test• Haem ophilus in uenzae is the m ost com m on
organism found in nasal cultures• OME is also a com m on m anifestat ion• PCD m ay be m issed in children thought
to be atopic w ith rh in it is and asthm a—dist inguished by m icrobiological analysis of nasal discharge
• Pat ients can also su er infer t ilit y and cases have been reported w here th is occurs in the absence of any respiratory disease
28.4 Investigation• Mucociliary (saccharin) clearance test• Fur ther con rm at ion can be achieved using
nasal biopsies or bronchial brush biopsies for elect ron m icroscopy—diagnost ic feature = dynein de ciency
• Ciliary funct ion analysis follow ing ciliogenesis (h igh speci cit y and sensit ivit y)
28 Ciliary Motility Disorders
Philpott_9783131662316_Ch28.indd 105 02/05/14 4:22 PM

106
28 Ciliary Motilit y Disorders
• UK Cent res w ith a diagnost ic service perform ing nasal brushing for PCD: ◦ Royal Brompton Hospital, London ◦ Leicester Royal In rm ary ◦ Southam pton General Hospital
28.5 Management• Genet ic counselling should be o ered
(predom inantly autosom al recessive t rait)
• Regular chest physiotherapy to ensure drainage of dependent areas of the lungs
• ABx ± surgical in tervent ion for problem at ic cases or to alleviate symptom s w here NPs are present
• Surgery m ay also be necessary in cases w ithout NPs to facilitate drainage and local applicat ion of topical ABx
Philpott_9783131662316_Ch28.indd 106 02/05/14 4:22 PM
107
29.1 Aetiology29.1.1 Common Conditions• Atherosclerosis, i.e., hypertensive pat ients• Ant icoagulants, e.g., warfarin• Ant iplatelet agents, i.e., aspirin• Traum a (inc. nger picking)• Iat rogenic (i.e., postop, inc. septal perforat ion)
29.1.2 Uncommon Conditions• Congenital: haem ophilia, HHT• Infect ive: rh inosinusit is, TB, syphilis, leprosy• In am m atory: at roph ic rh in it is, granu lo-
m atous d isease (e.g., granulom atosis w ith polyangiit is)
• Metabolic: vitam in de ciency, alcohol abuse• Endocrine: pregnancy, (m enstruat ion)• Traum a: foreign bodies• Idiopathic• Iat rogenic: chem otherapy, non-steroidal
ant i-in am m atory drugs, ABx• Neoplast ic: any sinonasal tum our, especially
lym phom a, leukaem ia, w idespread m ets, angio brom a, others
• Bleeding dyscrasias: hepat ic/renal failure, m assive t ransfusion
29.1.3 Assessment• In all pat ients:
◦ Check ABC, cardiovascular status• History:
◦ Site, frequency, and durat ion of epistaxis. ◦ Aspirin /warfarin /bleeding disorders ◦ Possibilit y of t raum a ◦ Hypertension, alcohol consum ption
29.2 Management/Examination29.2.1 General Measures• Rem em ber ABCDE• Ensure FBC, coag, G&S for all pat ients adm it ted
w ith epistaxis• IV uids and O2 m ay well be required• Control BP• Stop ant icoagulants if possible
• Ant ibiot ics if indicated (should be given w hen packs in place for m ore than 24 h)
• Blood t ransfusion• Haem atology advice
29.2.2 Speci c Measures• Local pressure and ice• Suct ion clearance• Co-phenylcaine (lidocaine + phenylephrine)/
cocaine paste/other com binat ions of decongestant and anaesthet ic
• Anterior rh inoscopy ± nasendoscopy (ideally w ith rigid scope to allow for t reatm ent)
• Silver n it rate cautery• Packing if required—various packs available• Check oropharynx• Gold standard pack rem ains as BIPP gauze and
Foley catheter secured w ith gate/um bilical clamp
29.2.3 Surgical Measures• Opt ions w ill depend on local resources and
skills available• Gold standard is now endoscopic SPA ligat ion
(clips/diathermy) (Fig. 29.1)• Other opt ions:
◦ EUA, cautery w ith BPD/silver n it rate and repacking (± PNS pack)
◦ Septoplasty ◦ Em bolizat ion ◦ Ligat ion of other ar teries (Fig. 29.3)
- Anterior ethm oid—m edial orbital incision (Lynch–Howarth); ar tery found 24 m m deep to orbital r im
- Maxillary—via Caldwell–Luc approach or even endoscopically
- Ext . carot id—ligated in the neck
29.3 Sphenopalatine Artery Ligation• Perform ed endoscopically• Can be under LA or GA; in lt rat ion of the
sphenopalat ine foram en should be perform ed regardless of anaesthesia given
29 Epistaxis
Philpott_9783131662316_Ch29.indd 107 02/05/14 4:25 PM

108
29 Epistaxis
• Will need an appropriate bipolar diatherm y or ligaclip applicator
• Elevate a shor t m ucosal ap underneath the poster ior but t ress of the m iddle turbinate and ident ify the crista ethm oidalis (w hich can be resected)
• Suct ion elevators are very useful for th is technique
• Typically 2 to 3 branches can be ident i ed• If done e ect ively should not require
repacking afterwards
29.4 Hereditary Haemorrhagic Telangiectasia (Osler– Rendu–Weber Disease)• Hom ozygot ic carriers a ected by recurrent
haem orrhage
• Traum a to m ucosa should be avoided• Barrier oin tm ents to protect m ucosa help
avoid bleeds• Various t reatm ent opt ions are described:
◦ Laser therapy to telangiectasia ◦ Derm oplasty (rem oval of anterior septal skin and replacem ent w ith a split skin graft)
◦ Young procedure (occlusion of nasal cavity)
Fig. 29.1a–d Sites for liga-tion in severe epistaxis.a Overview. 1, Internal
maxillary artery; 2, liga-tion of the external ca-rotid artery; 3, external carotid artery; 4, internal carotid artery; 5, com-mon carotid artery.
b Ligation or emboliza-tion of the ethmoidal arteries.
c Ligation or embolization of the internal maxillary artery or sphenopalatine artery in the pterygo-palatine fossa.
d Embolization with a coil.
1
234
5
a
c
d
b
Philpott_9783131662316_Ch29.indd 108 02/05/14 4:25 PM

109
30 Headache and Facial Pain
• Severe unilateral throbbing; 40% bilateral• Sudden onset; last 4 to 72 h• Often after waking in the m orning; or due
to st ress• Rout ine act ivit ies exacerbate sym ptom s• Coexist ing sym ptom s:
◦ N&V ◦ Photophobia ◦ Phonophobia
• Com m on fam ily h istory
30.4 Types of Migraine30.4.1 Migraine w ithout Aura• At least 5 at tacks fu l lling follow ing criter ia and
not at t r ibuted to another disorder: ◦ Headache at tacks last ing 4 to 72 h (unt reated or unsuccessfully t reated)
◦ Headache has at least 2 of the follow ing characterist ics: - Unilateral locat ion - Pulsat ing qualit y - Moderate or severe pain in tensit y - Aggravat ion by or causing avoidance of rout ine physical act ivit y (e.g., walking or clim bing stairs)
◦ During headache at least 1 of the follow ing: - Nausea and/or vom it ing - Photophobia and phonophobia
30.5 Migraine w ith Aura• Aura lasts <1 h and im m ediately precedes
cephalalgia• May be precipitated by changes in fem ale sex
horm ones, certain foods, or bright lights• At least two at tacks• Typical aura w ith m igraine headache
◦ Aura consist ing of at least 1 of the follow ing, but no m otor weakness: - Fully reversible visual sym ptom s including posit ive features (e.g., ickering lights, spots or lines) and/or negat ive features (i.e., loss of vision)
- Fully reversible sensory sym ptom s including posit ive features (i.e., pins and needles) and/or negat ive features (i.e., num bness)
30.1 Pathophysiology• Sustained m uscle contract ion (tension headache)• NO product ion or ischem ia—causat ive of m uscle
contract ion?• Vasodilat ion of in t racranial ar teries—st im ulates
V n pathways → release vasoact ive pept ides that increase pain response
• 5-HT receptor subtypes in vascular walls responsible for vasodilat ion
• If neuropept ides released (e.g., substance P) → m ucosal in am m ation
• Direct nerve pressure m ay induce nociceptor act ivit y
• Agents that can t r igger vasodilat ion: ◦ Hypoxia ◦ CO ◦ Ca eine w ithdrawal ◦ Acute alcohol w ithdrawal ◦ Oral cont racept ive pill ◦ Hypoglycem ia ◦ Antihypertensives ◦ Chinese food ingredients, e.g., n it roglycerin , m onosodium glutam ate
• Defect ive release of endogenous opiates (m igraine)
• Lowered cor t ical pain thresholds (chronic tension headaches)
30.2 Epidemiology• Headache a ects ~40% of the populat ion at som e
point in their life• Migraine occurs in 15% of adult populat ion;
3 fem ale: 1 m ale rat io• 100,000 absentees from work due to m igraine• Tension headache a ects up to 80% of people at
som e t im e• 3% have chronic tension headache for
>15 days/m onth• Medicat ion overuse headache a ects 2% of adults
30.3 Primary Headaches30.3.1 Migraine-Type Headaches• Prevalence = 18% wom en, 6% m en• Peak age of onset = 2nd to 3rd decades
Philpott_9783131662316_Ch30.indd 109 02/05/14 4:40 PM

110
30 Headache and Facial Pain
- Fully reversible dysphasic speech disturbance
◦ At least two of the follow ings: - Hom onym ous visual sym ptom s and/or unilateral sensory symptom s
- At least one aura sym ptom develops gradually over ≥5 m in and/or di erent aura sym ptom s occur in succession over ≥5 m in
- Each sym ptom lasts ≥5 and ≤60 m in ◦ Headache ful lling sam e criteria m igraine w ithout aura begins during the aura or follows aura w ith in 60 m in
• Typical aura w ith non-m igraine headache• Typical aura w ithout headache
◦ Headache does not occur during aura nor follow aura w ith in 60 m in
◦ Aura otherw ise as above w ith /w ithout speech disturbance
• Fam ilial hem iplegic m igraine• Sporadic hem iplegic m igraine• Basilar-t ype m igraine
30.6 Ophthalmic and Retinal Migraine• Paresis of ipsi- or cont ralateral oculom otor
nerves or m onocular blindness secondary to ret inal ischem ia
30.6.1 Treatment• Analgesics• 5-HT1 agonists (t r iptans)• Ant iem et ics
30.6.2 Prophylaxis• Relaxat ion and lifestyle changes including diet• Ant idepressants, e.g., am it r ipt yline• Ergotam ine• β-Blockers, e.g., propranolol• Non-steroidal ant i-in am m atory drugs• Calcium channel blockers, e.g., verapam il• Ant iconvulsants, e.g., valproate• Others, inc. pizot ifen
30.6.3 Tension-Type Headache• A ict ~80% of adults• Fem ale > m ale• Bilateral
• Tightening or band-like sensat ion around forehead and tem ples—m ay spread to occiput
• Sim ple analgesia• Am itr iptyline et al. for refractory cases
30.6.4 Infrequent Episodic Tension-Type Headache• At least 10 episodes occurring on <1 day/
m onth on average (<12 days/year) and ful lling follow ing criteria: ◦ Headache last ing from 30 m in to 7 days ◦ Headache has at least 2 of the follow ing characterist ics: - Bilateral locat ion - Pressing/t ighten ing (non-pulsat ing) qualit y - Mild or m oderate in tensit y - Not aggravated by rout ine physical act ivit y such as walking or clim bing stairs
◦ Both of the follow ings: - No nausea or vom it ing (anorexia m ay occur) - No m ore than one of photophobia or phonophobia
30.6.5 Frequent Episodic Tension-Type Headache• As above except at least 10 episodes occurring
on ≥1 but <15 days/m onth for ≥3 m onths (≥12 and <180 days/year)
30.6.6 Cluster Headaches• At least ve at tacks ful lling follow ing criteria:
◦ Severe or very severe unilateral orbital, supraorbital, and/or tem poral pain last ing 15 to 180 m in if untreated
◦ Headache is accom panied by at least 1 of the follow ings: - Ipsilateral conjunct ival inject ion and/or lacr im at ion
- Ipsilateral nasal congest ion and/or rh inorrhea - Ipsilateral eyelid oedem a - Ipsilateral forehead and facial sweat ing - Ipsilateral m iosis and/or ptosis - A sense of restlessness or agitat ion
◦ Attacks have a frequency from 1 every other day to 8/day
• Middle-aged pat ients• Several t im es per day for several weeks and then
have sym ptom -free periods
Philpott_9783131662316_Ch30.indd 110 02/05/14 4:40 PM

111
Ophthalmic and Ret inal Migraine
• Alcohol can precipitate at tacks• In t racranial lesions/condit ions can m im ic these
sym ptom s, e.g., cavernous sinus lesion , viral m eningit is, NPC
• Hypothalam ic dysfunct ion and excitat ion of carot id sheath nerve plexus?
• Ergotam ine sublingually can arrest at tack• Calcium channel blockers usefu l for
prophylaxis
30.6.7 Episodic Cluster Headache• At tacks ful lling criteria cluster headache w ith
at least 2 cluster periods last ing 7 to 365 days and separated by pain-free rem ission periods of ≥1 m onth
30.6.8 Chronic Cluster Headache• At tacks fu l lling cr iter ia cluster headache w ith
recurrence over >1 year w ithout rem ission per iods or w ith rem ission periods last ing <1 m onth
30.6.9 Secondary HeadachesPost-traum at ic headache at tributed to m oderate or severe head injury• Headache, no t ypical characterist ics know n,
fu l lling follow ing criteria: ◦ Head t raum a w ith at least 1 of the follow ings:
- Loss of consciousness for >30 m in - Glasgow Com a Scale (GCS) <13 - Post t raum at ic am nesia for >48 h - Im aging dem onstrat ion of a t raum at ic brain lesion (cerebral haem atom a, in t racerebral/subarachnoid hem orrhage, brain contusion, skull fracture)
◦ Develops w ith in 7 days after head t raum a or after regaining consciousness follow ing head t raum a
◦ Persists for >3 m onths after head t raum a
30.6.10 Headache Associated w ith Vascular Disorders• In t racranial haem atom a (in t racerebral/subdural/
ext radural)• Subarachnoid hem orrhage• Tem poral (giant cell) ar terit is—raised eryth-
rocyte sedim entat ion rate/biopsy/60 m g prednisolone
• Carot id ar tery pain—dissect ion or in am m at ion of carot id fascia/advent it ia
• Arterial hypertension—suspect secondary cause such as pheochrom ocytom a
30.6.11 Headache Associated with Non-vascular Intracranial Disorders• Raised in t ra-cranial pressure (ICP) caused by
neoplasm ◦ Di use non-pulsat ing headache w ith at least 1 of the follow ing character ist ics: - Associated w ith nausea and/or vom it ing - Worsened by physical act ivit y and/or m aneuvers know n to increase ICP (such as Valsalva m aneuver, coughing, or sneezing)
- Occurring in at tacklike episodes• Benign in t racranial hyper tension (IIH—see
Chapter 36) ◦ Progressive headache w ith at least 1 of the follow ing character ist ics: - Daily occurrence - Di use and/or constant (non-pulsat ing) pain - Aggravated by coughing or st rain ing
• Low CSF pressure• In t racranial infect ion• In t racranial neoplasm s:
◦ Progressive ◦ Localized ◦ Worse in the m orning ◦ Aggravated by coughing or bending forward
30.6.12 Headache Associated w ith Substances or Their Withdrawal• CO poisoning:
◦ Bilateral and/or cont inuous headache for up to 72 h
◦ Com es on w ith in 12 h of exposure• Alcohol:
◦ Overuse headache• Overt reatm ent of other form s of headache
( m igraine), e.g., aspir in , paracetam ol,
30.6.13 NSAIDs, Barbiturates ◦ Headache present on ≥15 days/m onth ful lling criter ia: - Regular overuse for >3 m onths of one or m ore drugs that can be taken for acute and/or symptom at ic t reatm ent of headache
Philpott_9783131662316_Ch30.indd 111 02/05/14 4:40 PM

112
30 Headache and Facial Pain
• Occipital neuralgia• Trigem inal neuralgia
◦ Usually age >50 ◦ Fem ale > m ale ◦ Ipsilateral tw itching m ay occur ◦ Paroxysm al at tacks of pain last ing from a fract ion of a second to 2 m in , a ect ing one or m ore divisions of the t r igem inal n (usually V⅔) and ful lling follow ing criter ia: - Pain has at least one of the follow ing characterist ics: (a) in tense, sharp, super cial, or stabbing and (b) precipitated from t r igger areas or by t r igger factors
- At tacks are stereot yped in the individual pat ient
- There is no clin ically evident neurological de cit; MRI m ay be warranted to ru le out other causes
◦ Tricyclic ant idepressants useful
30.6.17 Atypical Facial Pain/ Persistent Idiopathic Facial Pain• Diagnosis of exclusion• Non-localizing• No sensory loss or other physical signs• Pain is con ned at onset to a lim ited area on one
side of the face• Invest igat ions norm al• Pat ients have other non-speci c complain ts such
as irr itable bowel syndrom e, chronic fat igue• Depression com m on• De cient t yram ine m etabolism causing
disinhibit ion of pain neuroregulat ion cent rally
- Headache has developed or m arkedly worsened during m edicat ion overuse
- Headache resolves or reverts to it s previous pat tern w ith in 2 m onths after discont inuat ion of overused m edicat ion
• Ca eine
30.6.14 Metabolic Disorders• Hypoxia—alt itude• Obstruct ive sleep apnoea
30.6.15 Craniofacial or Cervical Disorders• Cervicogenic headache:
◦ C-spine origin ◦ Often after t raum a ◦ Clin ical, laboratory, and/or im aging evidence of a d isorder or lesion w ith in the cervical sp ine or soft t issues of the neck know n
• Sinonasal disorders inc. septal spurs• Elongated styloid process (Eagle syndrom e)• Tem porom andibular join t dysfunct ion
30.6.16 Cranial Neuralgias• Acute herpes zoster• Chronic post-herpet ic neuralgia• Tolosa–Hunt syndrom e• Gradenigo syndrom e• Raeder parat r igem inal neuralgia• Glossopharyngeal neuralgia• Superior laryngeal neuralgia
Philpott_9783131662316_Ch30.indd 112 02/05/14 4:40 PM

113
31 Tumours of the Nose and Paranasal Sinuses
• Pain less, sw elling of m axilla or m andible, facial asym m et r y ground glass appearance on CT
• Ossifying brom a = variant , peak age = 3rd to 4th decades, 75% m andible >~15% m axilla
31.2.4 Inverted (Transitional Cell) Papilloma• 0.5 to 4% of all rem oved sinonasal tum ours,
~1/1,000,000/y, M 2 to 5:1 F, peak 5th to 6th decade
• Presents—unilateral polyp, epistaxis, rhinorrhoea, nasal obstruction, proptosis (Fig. 31.1)
• CT—focal hyperostosis or osteit ic changes indicate origin of lesion (Fig. 31.2)
• Origin—m axillary (49%), frontal (18%), ethm oid (14%), sphenoid (12%), septum (5%), lateral wall (1%) (Table 31.1)
• Histology—epithelium invert ing in to the st rom a, in tact basem ent m em brane
• Malignant t ransform at ion ~10%, t reatm ent requires thorough rem oval of diseased m ucosa
• Endoscopic resect ion w ith m edial m axillectomy (recurrence rate or rr: 12%) vs. open approaches (rr 20%)
31.1 Surgical Pathology31.1.1 Epidemiology• Sinonasal neoplasm s account for ~1% of all
m alignancies, 3 to 5% of head and neck (H&N) m alignancies
• 1/100,000/y incidence (UK/USA), M 2:1 F, 75% of m alignant tum ours in those >50 years
31.1.2 Risk Factors• Hardwood dust (adenocarcinom a)• Toxin exposure (n ickel, chrom ium ,
hydrocarbons, radium )• Snu • Hum an papillom avirus (HPV) (cofactor)
31.1.3 Site of Origin• Sinonasal tum ours:
◦ Nose 25% ◦ Sinuses 75%
• Sinus tum ours: ◦ 60 to 80% arise from m axillary sinus
31.2 Benign Tumours31.2.1 Exophytic Papilloma• Arise from nasal septum and nasal vest ibule• Usually single• Associated w ith HPV types 6 and 11
31.2.2 Osteomas• Most com m on benign sinonasal tum our (~1%),
M2:1F, 2nd to 6th decade (m ost ly 5th–6th)• Frontal m ost com m on (57%), frontal lesions
often silent and discovered incidentally• Ethm oid lesions m ay cause proptosis and
usually invade the orbit• Gardner syndrom e (AD)—m ult iple osteom as,
soft-t issue tum ours, and polyposis of colon
31.2.3 Fibrous Dysplasia• F>M, usually diagnosed in childhood (<20), 80%
m onostot ic (1 bone involved) Fig. 31.1 Inverted papilloma.
Philpott_9783131662316_Ch31.indd 113 02/05/14 4:44 PM

114
31 Tumours of the Nose and Paranasal Sinuses
Table 31.1 Krouse staging system for inverting papilloma
I Tumour con ned to nasal cavity
IITumour involving osteomeatal complex and eth-moids and/or medial wall of maxillary sinus (with or without nasal cavity involvement)
IIITumour involving any wall of maxillary sinus (but medial wall), sphenoid or frontal sinus, with or without stage II criteria
IVTumours with extranasal and extrasinus extension
Tumours associated with malignancy
31.2.5 Juvenile Nasopharyngeal Angio broma• 0.5% of all H&N tum ours, exclusively m ales,
usually 7 to 19, rare >25, horm onal aet iology• Originates at sphenopalat ine foram en, slow
grow ing, locally invasive (Fig. 31.3)• Presents unilateral nasal obst ruct ion (90%),
epistaxis (50%), headache (25%)
Table 31.2 Fisch classi cation system for JNA
Stage
I Limited to nasal cavity, nasopharynx with no bony destruction
II Invading pterygomaxillary fossa, paranasal sinuses with bony destruction
III Invading infratemporal fossa, orbit , and/or para-sellar region
IV Invading cavernous sinus, optic chiasmal region, and/or pituitary fossa
Fig. 31.3 Juvenile nasopharyngeal angio broma.
Fig. 31.2 CT scan of inverted papilloma showing osteit ic change at the site of origin.
• Nasal m ass (80%), orbital m ass (15%), proptosis (10–15%)
• CT—extent of tum our, bow ing of poster ior m axillary wall
• MRI—extent/in t racranial involvem ent• Histology—encapsulated, vascular t issue, and
brous st rom a (avoid preop biopsy)• Staged according to Sessions or Fisch
classi cat ion system s (Table 31.2)• Preoperat ive angiogram and em bolizat ion
(24 h preop)• Treatm ent—horm onal ( utam ide—testosterone
receptor blocker), surgery, radiotherapy for in t racranial/recurrent disease
• Surgery—endoscopic resect ion (Fisch I/II), open approach if m ore extensive
• Open—lateral rh inotomy, t ranspalatal, t ransm axillary, m idfacial degloving
31.2.6 Haemangioma• Usually on nasal septum , also frontal bone, nasal
bones, m axilla• F>M, 20 to 50 years, presents w ith epistaxis,
soap -bubble appearance radiologically
Philpott_9783131662316_Ch31.indd 114 02/05/14 4:44 PM

115
Malignant Tumours
• Mucoepiderm oid carcinom a: ◦ Very rare ◦ Maxillary ant rum > nasal cavity > nasopharynx > ethm oid
31.3.3 Adenocarcinoma• Hardwood indust ry/propyl alcohol/
chrom e inhalat ion• 8 to 15% of sinonasal m alignancies, M>F, m ost
com m on in the ethm oid sinuses• Sam e bone-erosive propert ies and nodal
m etastasis as SCC• High-grade—80% die of disease, presents w ith
pain and deform ity• Low -grade—90% cure rate, 6th decade, presents
w ith nasal obst ruct ion
31.3.4 Malignant Melanoma• 4% of sinonasal neoplasm s, M>F, 5th to 8th
decades, 0% 10-year survival• Arise from nasal septum /lateral wall > sinuses• Grey/blue/black polypoidal swellings• 5% are deposits from cutaneous lesions, regional
satellites frequent , ~⅓ have posit ive neck nodes• Wide local excision—endoscopic vs. open-
lateral rh inotomy, part ial/total m axillectomy ± orbital exenterat ion
• 85% relapse locally, radiotherapy helps local-regional control
31.3.5 Esthesioneuroblastoma (Olfactory Neuroblastoma)• Bim odal frequency (2nd and 6th decade), M=F,
~5% of nasal m alignant tum ours• Presents w ith nasal obst ruct ion (70%), epistaxis,
unilateral polyp, anosm ia• Slow grow ing but can becom e large
and dest ruct ive• Surgical excision (endoscopic/craniofacial
resect ion), postoperat ive radiotherapy (radiosensit ive)
31.3.6 Sarcomas• Osteogenic sarcom a presents as an enlarging
rm m ass (rock hard), m andible > m axilla• Aggressive, poor prognosis (part icularly w ith skull
base involvem ent), 5-year survival = 10 to 20%
• Pyogenic granulom a (lobular capillary haem angiom a), F>M, peak 3rd decade
31.2.7 Pleomorphic Adenoma• F>M• Peak incidence 5th decade• Nasal septum >m axillary sinus
31.2.8 Schwannoma• Most arise in 2nd to 5th decades• M=F• Mainly nasoethm oid• Posit ive S-100 protein stain ing
31.2.9 Other Benign Tumours• Leiomyom a• Paragangliom a• Myoepitheliom a• Oncocytom a• Occur sporadically
31.3 Malignant Tumours31.3.1 Squamous Carcinoma• Most com m on sinonasal m alignancy, M 2:1 F,
peak incidence 60–70 years of age• Maxillary sinus (60–70%) > nasal cavity
(20–30%) > ethm oid (10–15%) > frontal/sphenoid (1%)
• Maxillary tum ours poster ior or superior to Ohngren line have poorer prognosis
• Male preponderance, ver t ical grow th, and m etastat ic potent ial (1–4%)
• Squam ous cell carcinom a (SCC) of vest ibule t ypical in elderly m en, colum ella form very aggressive
• Treatm ent is excision ± radiotherapy
31.3.2 Tumours of Minor Salivary Glands• Adenoid cyst ic carcinom a:
◦ Aggressive ◦ Local recurrence and distant m ets com m on ◦ Perineural spread occurs w ith bony invasion ◦ Maxillary sinus > nasal cavit y m ost com m on sites
Philpott_9783131662316_Ch31.indd 115 02/05/14 4:44 PM

116
31 Tumours of the Nose and Paranasal Sinuses
◦ Toothache ◦ Facial swelling/pain ◦ Trism us
• Ethm oid: ◦ Nasal obst ruct ion ◦ Epistaxis ◦ Proptosis/diplopia
31.4.2 Examination• Fullness/num bness of cheek• Ptosis, proptosis/ophthalm oplegia• Evidence of tum our in nose/postnasal space/
m outh• Loose teeth or ill- t t ing dentures• Persistent oroant ral stula• Num bness of hard palate• Trism us• IX n and X n palsies in laryngopahrynx• Palpable disease on hard palate, buccal sulcus,
or anterior antrum• Cerebrospinal u id (CSF) leak• Lym ph nodes
31.4.3 Investigations• CT sinuses ± neck/chest
◦ May overest im ate spread by 30%• MRI scan (+ Gd enhancem ent)
◦ Depicts soft-t issue extension deep in face, in t racranially, in orbit , d ist inguishes tum ours from sinusit is
◦ Correlate T1, T2, and postcont rast T1• B2-t ransferrin /tau protein for CSF leak• Urine for catecholam ines• Biopsy
31.4.4 Staging for Paranasal Sinus Carcinomas• See Table 31.3
31.5 Treatment31.5.1 Benign Tumours• If asym ptom at ic consider observat ion (e.g.,
osteom a)• Endoscopic vs. external vs. com bined
resect ion
• Others: chondrosarcom a, rhabdom yosarcom a (aggressive), leiomyosarcom a
31.3.7 Haemangiopericytoma• Vascular tum our occurs rarely in ethm oid, nasal
cavit y, sphenoid sinus• Mean age 55, M=F, h igh recurrence rate, 2.5%
m etastasize, 3% die of disease• Presents w ith epistaxis, nasal obst ruct ion , facial
swelling, proptosis• Pain less grey to tan coloured polypoidal spongy
haem orrhagic m ass• Occasionally causes rare paraneoplast ic
syndrom es• Preoperat ive em bolizat ion prior to w ide
local excision
31.3.8 Lymphomas• Non-Hodgkin lym phom a (NHL) typically, M>F,
m edian age 50• Western countries—sinonasal involvem ent in
~1% of NHL, predom inantly B cell• Asia/South Am erica—higher sinonasal
involvem ent ~5% of NHL, T or NK cell predom inant
• Poor prognost ic factors—Asian ethnicit y, age > 60, advanced stage, B symptom s
• Epstein–Barr virus (EBV) associated w ith Burkit t lym phom a and nasal NK-T lymphom a
• <60% 5-year survival w ith radio(chem o)therapy
31.3.9 Metastasis• Most sinonasal m alignancies are prim ary,
m etastasis is uncom m on• >50% from renal cell carcinom a, lung (12%),
breast (9%), GI (6%)• Most com m only m axillary sinus (50%), ethm oid
(18%), nasal cavity (15%)
31.4 Clinical Features of Sinonasal Malignancy31.4.1 History• Maxillary:
◦ Obstruct ion ◦ Epistaxis ◦ Infra-orbital anaesthesia
Philpott_9783131662316_Ch31.indd 116 02/05/14 4:44 PM

117
Treatment
• Endoscopic rem oval of inverted papillom a (IP) gives as good, if not bet ter, results w hen compared w ith external approaches
31.5.2 Malignant Tumours• Surgery (endoscopic or open) ± radiotherapy
required for m ost SCC cases• Concurrent chem oradiotherapy can im prove
survival by 4%
• Neck m etastases present in 5% at presentat ion—treated by neck dissect ion or radiotherapy
• Approaches—endoscopic, t ransfacial, t ranspalatal, t ranscranial
• Resect ions—m edial m axillectomy, total m axillectomy, craniofacial resect ion (CFR)
• Endoscopic surgery is replacing CFR and oncological control is not sacri ced
• Lym phom a <60% 5-year survival w ith radio(chem o)therapy
Table 31.3 T Staging for nasal and paranasal sinus tumours
Maxillary Nasal cavity/ethmoid
T1 Limited to maxillary sinus mucosa Limited to one subsite (± bony invasion)
T2 Bone erosion except posterior wall of maxillary sinus/pterygoid plates
Invading two subsites in a single region, or extending to adjacent region within nasoethmoidal complex
T3 Invades posterior wall, subcutaneous tissues, oor/medial wall of orbit, ethmoid
Invades medial wall or oor of orbit , maxillary sinus, palate, or cribriform plate
T4a Invades anterior orbit , skin of cheek, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid/frontal sinuses
Invades anterior orbit , skin, anterior cranial fossa, pterygoid plates, or sphenoid or frontal sinuses
T4b Invades orbital apex, dura, brain, middle cra-nial fossa, cranial nerves (except V2), naso-pharynx, or clivus
Invades orbital apex, dura, brain, middle cranial fossa, cranial nerves (except V2) nasopharynx, or clivus
Philpott_9783131662316_Ch31.indd 117 02/05/14 4:44 PM

118
32 Snoring and Sleep Apnoea
32.1 Introduction• Snoring, obst ruct ive sleep apnoea (OSA), and
upper airway resistance syndrom e (UARS) are condit ions w ith in the sam e spect rum of sleep -related breath ing disorders (SRBDs)
• Prevalence of OSA is 1 to 4% (adults)• SRBD is caused by u t ter and collapse of t issues
in the pharynx, predom inantly the palate/uvula and tongue base/epiglot t is
32.2 De nitions• Apnoea = cessat ion of respiratory air ow for at
least 10 s w ith respiratory e or t• Hypopnoea = reduced respiratory ow by at
least 50% for at least 10 s and a drop of SaO2 by at least 4%, w ith respiratory e or t
• Apnoea/hypopnoea index (AHI) = (apnoea + hypopnoea)/hour of sleep
• OSA = AHI ≥5; subdivided in to: ◦ Mild: AHI = 5 to 15 ◦ Moderate: AHI = 15 to 30 ◦ Severe: AHI > 30
• Obst ruct ive sleep apnoea syndrom e (OSAS) = OSA w ith symptom s
• UARS = sym ptom s of OSA and som nographic evidence of sleep fragm entat ion but AHI ≤5
• Cent ral sleep apnoea = apnoea w ithout respira-tory e or t . This has neurological aet iology and there is no upper airway obst ruct ion
• Arousal = abrupt change from sleep to wakefulness
• Microarousal = par t ial awakening, from a “deep” to a “light” sleep; pat ient is not aware of wakefulness
32.3 Pathophysiology• Inward collapse of loose and oppy t issues
in pharynx secondary to Bernoulli pr inciple (reduced in t ralum inal pressure w ith increased air ow ) w ith increased respiratory e or t , leading to airway obst ruct ion or ut ter
• Mult ilevel areas of obst ruct ion w hen consider-ing snoring and OSA w ith involvem ent of: soft palate, lateral pharyngeal wall, palat ine tonsils, tongue base/lingual tonsils, epiglot t is
• Apnoea/hypopnoea → hypoxia →increased respiratory e or t →increased venous return →risk of r ight heart failure and cor pulm onale in the long term
• Arousals/m icro-arousals → sleep fragm entat ion → physiological st ress (catecholam ines and other chem ical release) →ιncreased risk of other com plicat ions, e.g., arrhythm ias
• Sleep fragm entat ion results in poor qualit y sleep leading to excessive dayt im e sleepiness
• OSA leads to increased risk of arrhythm ias, cerebrovascular accidents, cardiovascular disease, insulin resistance, lower life expectancy
• Sleep fragm entation also causes excessive daytim e sleepiness, w hich has been show n to increase risk of road tra c accidents. It also causes poor concentration and m ood changes
32.4 Clinical Evaluation• Risk factors:
◦ Raised body m ass index (BMI) ◦ Increased neck circum ference ◦ Retrognathia/m icrognathia ◦ Macroglossia ◦ Increasing age ◦ Tonsillar hyper t rophy ◦ Large soft palate/uvula in relat ion to oropharyngeal cross sect ion
◦ Sedat ive and alcohol use ◦ Floppy eyelid syndrom e ◦ Uncom m on in prem enopausal wom en
• Sym ptom s: ◦ Snoring (up to 95%) ◦ Witnessed apnoeas ◦ Nocturnal arousals or arousals w ith sensat ion of “choking”
◦ Excessive dayt im e sleepiness ◦ Morning headaches ◦ Reduced libido ◦ Mood changes ◦ Poor concent rat ion ◦ Reduced qualit y of life ◦ Im pact on daily act ivit ies, e.g., dr iving
• Epworth Sleepiness Score (ESS): ◦ Excessive dayt im e sleepiness is w idely evaluated by th is
◦ Not a very good predictor of OSA
Philpott_9783131662316_Ch32.indd 118 02/05/14 4:48 PM

119
Treatment
◦ Berlin sleep disorders quest ionnaire has bet ter sensit ivit y but would not rule out OSA
• Important to docum ent h istory of cardiovascular disease and diabetes
• Exam inat ion: ◦ BMI ◦ Neck circum ference ◦ Retrognathia/m icrognathia ◦ Tonsil grade (grades 1–4) ◦ Friedm an tongue posit ion (1–4) ◦ Size and redundancy of palate/uvula ◦ Flut ter of uvula on sim ple respirat ion (snoring) ◦ Nasal patency ◦ Correlat ion between clin ical signs and OSA diagnosis is not of good sensit ivit y, although neck circum ference and BMI have reasonably good speci cit y (~90%).
◦ Exclude features of hypothyroidism and acrom egaly
◦ Although uncom m on, OSA can exist in pat ients w ithout any of these clin ical features
32.5 Investigations• Bloods:
◦ Hem oglobin ◦ TFTs ◦ Blood glucose
• Sleep nasendoscopy: ◦ Evaluat ion of upper airway during pharm aco-logically induced sleep w ith target cont rolled induct ion pump using propofol
◦ Good for evaluating the levels of obstruction by directly visualizing the collapse of involved tissues
◦ Also good for seeing if collapse occurs in an antero-poster ior plane, side-to-side (lateral) plane, or if it is concentric collapse
◦ May help w ith direct ing any t reatm ent to the level involved
◦ Does not induce natural sleep, and EEG brain act ivit y is com pletely di erent to that of natural sleep
◦ Correlat ion w ith snoring sym ptom s is excellent and it is probably a good m ethod of evaluat ing OSA from a surgical point of view
• Polysom nography: ◦ Conducted in sleep centres w ith in hospitals and requires hospital bed
◦ Measures EEG, elect rooculography (to ident ify sleep stage), nasal/oral air ow, chest and abdom inal m ovem ents, heart rate, oxygen saturat ion , expired CO2, EMG, body posit ion
◦ Problem s w ith full polysom nography: - Expensive - Hospital adm ission - No inform at ion on the level of obst ruct ion - Cannot be perform ed on everyone suspected of OSA
• Por table dom iciliary sleep study: ◦ Various di erent devices available ◦ Attached to pat ient and program m ed to star t recording various param eters w hen asleep, at hom e
◦ Most cannot m easure EEG, EOG, expired CO2 or EMG to show sleep stage
◦ Newer devices recent ly in t roduced in the m arket that w ill m easure the stage of sleep and a device that w ill m easure air ow and pressures in the di erent levels of upper airway and in t rathoracic pressure
◦ Most studies show good correlat ion between fu ll polysom nography and a hom e sleep study w hen com paring AHI
◦ For m ost pat ients suspected of OSA the dom iciliary sleep study is adequate
32.6 Treatment• Weight loss• Reduct ion in alcohol and sedat ive use• Sleep posit ion t rain ing• Correct ion of nasal obst ruct ion , usually to
improve cont inuous posit ive airway pressure (CPAP) com pliance. Nasal abnorm alit ies are not contributory to OSA/snoring in m ost cases
• Mandibular advancem ent oral appliances (poorly tolerated but e ect ive)
• CPAP; autom ated posit ive airway pressure (APAP). With good counseling and m ot ivat ion the com pliance w ith CPAP/APAP is good. But there are always som e w ho cannot tolerate it
• Surgery: ◦ Procedures aim ed at:
- Reduct ion in size of palate - Palatal st i en ing - Tonsillectomy, lateral pharyngoplast ies to st i en lateral walls
- Reduct ion/st i ening of tongue base bulk - Hyoid suspension (pulling tongue base anteriorly and inferiorly)
◦ Good for prim ary snoring and cases of m ild/m oderate OSA
◦ Som e success in t reat ing severe OSA w ith fairly m ajor throat and jaw surgery
Philpott_9783131662316_Ch32.indd 119 02/05/14 4:48 PM

120
33 Anatomy and Physiology of the Olfactory and Gustatory Systems
• Receptor cells give rise to basal axons that form roughly 20 bundles of ~50 axons each know n as “ la”
• Glial cells provide sheath ing to axons• Sustentacular cells provide insulat ion between
receptor cells
33.2 Layers of the Olfactory Bulb33.2.1 Structure• Olfactory nerve• Glom erular• External plexiform• Mit ral cell• In ternal plexiform• Granule cell
33.2.2 Function• Receptor cell axons synapse w ith the second-
order neurons (m it ral and tufted cells) inside the glom eruli, w hich are the second layer of the bulbs
• Negat ive and posit ive feedback is provided by m eans of parallel circuits in the periglom erular and external plexiform layers
• Olfactory epithelium undergoes ret ract ion w ith increasing age, and the num bers of glom eruli decrease in conjunct ion w ith the decline in olfactory receptor cell num bers w ith in the epithelium ; they are alm ost non-existent by the age of 80 years
33.3 Olfactory Projections33.3.1 Structure• Olfactory receptor cells are prim ary
a erent neurons that synapse directly w ith telencephalonic neurons rather than proceeding through other levels of synapses
• Axons of these prim ary-order neurons are unmyelinated and hence the propagat ion of elect r ical impulses along them occurs at low velocit ies
33.1 Olfactory Epithelium• Neuroepithelium is prim arily located
underneath the cribriform plate ◦ May also be found on parts of the superior and m iddle turbinates and the nasal septum
◦ May contain islands of respiratory epithelium at the peripheries
• Prim ary area is know n as the olfactory cleft• 1–2 m m w ide w ith ~200 to 400 m m 2 of
olfactory epithelium• Propor t ionally, hum ans derive less from
olfact ion in the con text of nasal surface area; on ly 15% of hum an nasal m ucosa is designated to olfactory funct ion com pared w ith 40% in rat s
33.1.1 Cell Types• Bipolar sensory receptor• Sustentacular• Microvillar cells• Globose basal• Horizontal basal• Bow m an gland and duct cells
33.1.2 Function (Fig. 33.1)• Sensory receptor cells have cilia• Cilia contain receptors that enable olfactory
detect ion (as discussed below )• Receptors project in to the m ucus layer• Derive from the ectoderm al epithelium
(olfactory placode)• Axons of receptor cells grow upwards
in to the bulbs• Basal layer provides cont inuous neurogenesis
despite the longevity of m any receptor cells (unless dam aged)
• Regulated biochem ically at various stages of cell developm ent using apoptosis to elim inate surplus cells under the in uence of endogenous and exogenous factors
• Funct ional at bir th w ith neonates responding preferent ially to m aternal odours
• Transm em brane receptors on cilia have 7 dom ains
Philpott_9783131662316_Ch33.indd 120 7/7/14 3:28 PM

121
Physiological Mechanisms
• Second-order neurons project posteriorly as the olfactory t racts to: ◦ Thalam us ◦ Lim bic system ◦ Orbitofrontal neocortex (secondary olfactory cortex)
33.3.2 Function• Odour discrim inat ion takes place in secondary
cor tex• A ective responses controlled by the limbic system• Projections of the second-order neurons to the
prim ary olfactory cortex are direct connections w ith som e neurons connecting in turn directly to the secondary olfactory cortex and som e relaying via the thalam us between these two cortical areas
33.4 Primary Olfactory Cortex• Anterior olfactory nucleus (AON)• Olfactory tubercle• Entorhinal area• Piriform cor tex• Periam ygdaloid cortex• Cort icom edial am ygdala• Anterior com m issure m ay also carry decussat ing
bres from pyram idal cells of the AON to contralateral elem ents of the prim ary olfactory cor tex
33.5 Vomeronasal Organ• Present in 75 to 100% of the populat ion• Innervated by n term inalis (CN 0)• In other species CN 0 would connect the VNO to
the accessory olfactory bulbs (AOBs), amygdala, and hypothalam us
• Hum ans do not appear to possess AOBs and lack the septal organ of Masera
• Blind-ending pit of VNO contains pseudost rat i ed colum nar epithelium
• On elect ron m icroscopy: dark support ing cells and light sensory cells w ith neuro lam ents
• Em bryologically VNO is form ed w hen the nasal m ucosal epithelium invaginates to form bilateral tubular st ructures, w hich appear to be at their greatest size during the 25th week of developm ent
33.6 Physiological Mechanisms33.6.1 Odour Classi cation• Floral• Pungent• Putrid• Ethereal• Pepperm int• Musk• Cam phoraceous
Fig. 33.1a–c Olfactory detection. a 1, Scent molecules dock on to receptors; 2, bipolar nerve cells; 3, olfactory bulb with 4, glomerulus (microcentre)
and 5, mitral cells. b 1, Scent molecules; 2, scent receptors. Each olfactory cell bears only a single type of receptor. There are 350 types of
receptor in humans. A receptor can recognize up to 100 structurally similar molecules in a scent category. c Scent molecules t only one speci c receptor. They trigger a biochemical reaction and a subsequent electrical signal,
which is transmit ted to the olfactory function in the brain.
b c
1
22
1
1
2
3 54
a
Philpott_9783131662316_Ch33.indd 121 7/7/14 3:28 PM

122
33 Anatomy and Physiology of the Olfactory and Gustatory Systems
gustatory cells are m ore sensit ive to certain tastes and any par t icular taste percept ion is the result of act ivit y of a group of gustatory cells in a group fashion
• Funct ional units exist because each olfactory neuron expresses a speci c receptor gene, of w hich there are thousands, and all neurons w ith the sam e expression project to the sam e glom eruli of the olfactory bulb
• In teract ion between odour m olecules and receptor is debated to be either due to shape theory or due to elect ron tunnelling (vibrat ional) theory
33.6.4 Cellular Mechanism in Receptor Cells• Guanine nucleot ide-binding protein (Golf)
act ivates the enzym e adenyl cyclase to induce product ion of the second m essenger cAMP or w ith som e odourants cGMP
• These products enable cellu lar depolarizat ion by opening cyclic nucleot ide-gated ionic channels and Ca2+-dependent Cl– or K+ channels having di used through the cytoplasm
• Golf is one of 13 G proteins present in receptor cells
• Cellular m echanism s allow the hum an nose to detect ~10,000 odours (a bloodhound can detect 40,000)
33.6.5 Cortical Activity• Concentrat ion dependency in odour detect ion
has been dem onstrated as being relevant to cerebellar act ivat ion w hereby postero-lateral areas of the cerebellum have been show n to be st im ulated w ith funct ional im aging studies
• Anterior cerebellar act ivat ion evident w ith sn i ng alone
• Probably because the size of sn i ng is m odi ed via the cerebellum in proport ion to the odour in tensit y
33.7 Vomeronasal Organ Physiology• Serous glands present suggest a gustatory
feature innervated autonom ically• Blood vessels w ith autonom ic innervat ion run
alongside the VNO suggest ing a vasom otor
33.6.2 Olfactory Transduction• Relies on in teract ion between m olecules
dissolved in the m ucus layer and the t ransm em brane receptors of the cilia
• Cilia are im m otile and do not funct ion to m ove nasal m ucus; rather they aid t ransduct ion of m olecules
• Process is aided by the shunt ing of up to 15% of the incom ing air stream towards the olfactory cleft during inhalat ion enabling odourant m olecules to m ove from the de ected air st ream to the largely aqueous phase of the olfactory m ucus
• Turbulence provided by the turbinates m ixes odours during inspirat ion
• Turbulent air ow during exhalat ion also provides odour presentat ion to olfactory cleft
• Orthonasal olfact ion = sm ell odours from the outside
• Retronasal olfact ion = passage of food odours from the oral cavit y w hile eat ing
• 80% of food avor is due to ret ronasal olfact ion , not taste
• Sni ng im proves the processes of increasing air ow and m ixing
• Nasal m ucus is produced by the Bow m an glands and to a lesser degree by the sustentacular cells
• Odourant m olecules reach the olfactory receptors by di using through the m ucus, or alterat ively are act ively t ransported via odourant binding proteins
• Sustentacular cells m ay also deact ivate som e odourants and xenobiot ic agents
• Funct ion of m icrovilli of m icrovillar and sustentacular cells is not at present understood
33.6.3 Receptor Mechanism• Odourant arrival at a G-protein coupled seven-
dom ain receptor st im ulates AP in the prim ary a erent bre
• AP is increased in proport ion to the odourant concentrat ion
• Receptors appear to be located in speci c groups according to the class of odours that they are sensit ive to
• Arrangem ent of groups in di erent areas of the m ucosa enables the CNS to receive a spat ially coded signal that conveys in part the qualit y of the odours
• “Labelled-line” system is not dissim ilar to that used in taste percept ion w here individual
Philpott_9783131662316_Ch33.indd 122 7/7/14 3:28 PM

123
Vomeronasal Organ Physiology
• II—Possible secretory funct ion• III—Gustatory sensory cells• IV—Undi erent iated stem cells• V—Marginal cells
Gustatory Innervation• Gustatory (chorda t ym pani) and som atosensory
bres run in the lingual nerve to fungiform (± foliate) papillae on anter ior two-th ird of tongue
• Greater pet rosal nerve supplies taste buds on soft palate
• Glossopharyngeal nerve supplies vallate and foliate papillae and pharyngeal taste buds
• Super ior lar yngeal branch of the vagus supplies t aste buds on ep iglot t is, larynx, and oesophagus
Central Processing• St ructures involved include:
◦ Nucleus of the solitary t ract ◦ Thalam ic taste area ◦ Insular-opercular (prim ary) taste cortex ◦ Caudolateral orbitofrontal secondary cort ical taste area
◦ Am ygdala ◦ Hypothalam us ◦ Basal ganglia
33.7.2 Gustatory System PhysiologyTaste Detection• Taste m odalit ies detected by receptors for:
◦ Um am i—L-glutam ate and nucleot ide enhancers
◦ Sweet—sugars, ar t i cial sweeteners, D-am ino acids, glycine, sweet proteins
◦ Bit ter—cyclohexam ide, denatonium , salicin , PTC, saccharin , quinine, st rychnine, atropine
◦ Salt—NaCl and sodium salts ◦ Sour—acids ◦ Carbonated drinks
Receptor Cell Distribution (Fig. 33.2)• No topographic m ap of taste qualit ies on the
tongue (Fig. 33.2b)
pum p to act ively enhance st im ulant uptake by the organ (“ ehm en”)
• 7-Transm em brane proteins in receptors suggest ing a response to non-volat ile cues
• In anim als th is leads to act ivat ion of the hypothalam us via the AOBs and amygdala
• How ever, the use of a vom eropher in has been show n to cause changes of au tonom ic funct ion : ◦ Pulsat ile release of lutein izing and follicle-st im ulat ing horm ones (in m ales)
◦ Decreased respiratory frequency ◦ Increased cardiac frequency ◦ Event-related changes of elect roderm al act ivit y and EEG pat tern
• Anim al studies suggest that the VNO enables ham sters to di erent iate di erent sm ells
33.7.1 Gustatory System AnatomyLingual Papillae• Taste buds are located in papillae in the
follow ing locat ions: ◦ Tongue ◦ Palate ◦ Oropharynx ◦ Larynx (epiglot t is) ◦ Upper oesophagus
• Bulb-shaped st ructures com prising 50 to 120 bipolar cells
• Microvilli prot rude from the cells in to a m ucus- lled taste pit
• Vallate papillae (48%) ◦ Lie anter ior to sulcus term inalis and extend in a V-shaped line across the tongue root
◦ CN IX innervat ion• Foliate papillae (28%)
◦ Located along posterolateral m argins of the tongue surface
◦ CNs IX and VII (chorda tympani) innervat ion• Fungiform papillae (24%)
◦ Seen easily as the pink elevat ions on the anterior tongue
◦ 3½ taste buds per papilla—1120 fungiform taste buds
• Filiform papillae—do not contain taste buds
Taste Bud Cell Types• I—Insulat ing cells to envelop axons
Philpott_9783131662316_Ch33.indd 123 7/7/14 3:28 PM

124
33 Anatomy and Physiology of the Olfactory and Gustatory Systems
Other Functions• Other tongue sensory funct ions via t r igem inal n :
◦ Texture
◦ Tem perature ◦ Piquancy
• Eat ing food is a com plex in teract ion centrally between inputs from 6 CNs: I, II, V, VII, IX, X
Fig. 33.2a, b a Gustatory receptor cell distribution. Labelled lines mediate taste sensation. Sweet (red), bit ter (blue), sour (green),
umami (yellow), and sodium (purple) are mediated by separate populations of selectively tuned taste recep-tor cells. From Yarmolinsky DA, Zuker CS, Ryba NJP. Common sense about taste: from mammals to insects. Cell 2009;139:234–44. Cell by Cell Press. Reproduced with permission.
b Taste buds from all regions of the oral cavity contain cells that respond to the 5 basic modalit ies.
ba
Umami
Umami
HO
O O HO OH OH
OO OH
HOHO
OHO
O
OHOH
OHO
OH
HO
Sweet
Bit ter
Bit terO HO
H HN
H
Sweet
OSour
Sour
SaltyNa+ Cl–
Salty
H2N O–
Bit ter Sour
Salty
Umami
Sweet
Philpott_9783131662316_Ch33.indd 124 7/7/14 3:28 PM

125
34.1 A Stepwise Assessment• History
◦ Onset , t im ing, durat ion , associated sym ptom s ◦ Listen carefully to details of actual com plain t—sm ell, “taste,” t rue taste, distort ion
◦ If distort ions present , do they coincide w ith a st im ulus?
◦ Original precipitat ing factor? ◦ Other speci c nasal or oral sym ptom s?
• Exam inat ion ◦ Rigid endoscopy of the nose w ith a 30° scope to visualize olfactory clefts
◦ Exam inat ion of the tongue, oral cavity and oropharynx ± hypopharynx
• Psychophysical test ing—consider birh inal test ing• Further invest igat ions:
◦ Blood tests—LFTs, TFTs, 9 AM cort isol, U&Es, ESR, ANCA, TPHA/VRDL, HbA1C
◦ For taste consider B12, folate, Mg/Ca/Zn levels ◦ MRI—if norm al endoscopy or in unilateral olfactory/taste dysfunct ion
◦ CT—if posit ive endoscopic ndings or h istory suggest ive of possible in am m atory sinonasal disease
34.2 Psychophysical Testing34.2.1 Olfactory Testing• Should be considered rst unless clear h istory of
speci c taste m odalit y losses• Sni n’ Sticks—threshold, discrim ination and iden-
ti cation (international validation including UK)• Com bined olfactory test—threshold and
ident i cat ion (United Kingdom /New Zealand validated)
• UPSIT—ident i cat ion only (in ternat ional validat ion , especially North Am erica)
• CCCRT—threshold and ident i cat ion• Sm ell disket tes—ident i cat ion• BAST-24• Others include: Leicester olfactom eter (thresh-
old), Japanese odour pens, European Sm ell Test• Ret ronasal test ing—for avor percept ion via the
ret ronasal route• Malingering not ru led out by am m onia test due
to olfactory/t r igem inal in teract ions centrally;
should be suspected w ith very low scores on test ing (i.e., forcing a low score)
34.2.2 Gustatory Testing• Taste test st r ips/sprays
34.2.3 Specialist Investigations• Olfactory event-related potent ials (OERPs)
◦ EEG of olfact ion t ypically w ith a pleasant and unpleasant odour
◦ Durat ion of test = 30 to 40 m in ◦ If absent , suggest anosm ia w ith bad prognosis but not absolute
◦ If present , suggest pat ient can sm ell and has a good prognosis
• Gustatory event-related potent ials—as for OERPs• Funct ional MRI—w ith odour/taste st im ulus• Olfactory bulb volum e m easurem ent—derived
from MRI• Trigem inal test ing—chem osensory event-related
potent ials—using CO2 direct in to the nose• Olfactory/gustatory elect rogram (research tool)
34.2.4 Olfactory Loss—TerminologyQuantitative Loss• Norm osm ia• Hyposm ia• Anosm ia• Funct ional anosm ia—abilit y to occasionally
detect spurious olfactory sensat ions• Presbyosm ia—age-related decline (especially
after 70 years)• Olfactory agnosia—inabilit y to detect and
specify one odour• Hyper/superosm ia
Qualitative Loss• Dysosm ia—any distort ion of the sense of sm ell
◦ Parosm ia: - Perceived distort ion w hen the st im ulus is present
- Overall prevalence 4%
34 Olfactory and Gustatory Disorders
Philpott_9783131662316_Ch34.indd 125 02/05/14 4:54 PM

126
34 Olfactory and Gustatory Disorders
- Mostly follows post-viral upper respiratory t ract infect ion (URTI) loss and t raum a
- Olfactory bulb volum e decreased - Reduced orbitofrontal cortex, cingulate and thalam us act ivat ion on fMRI
- Disappears in 29% - Troposm ia—perceived unpleasant odour in the presence of a pleasant st im ulus
- Cacosm ia—unpleasant odour sensat ion—stim ulus m ay or m ay not be present
◦ Phantosm ia - Olfactory sensat ion in the absence of a st im ulus
- Usually unpleasant sensat ion - Disappears in 53%
34.2.5 Olfactory Loss—AetiologyCommon Causes• Conduct ive:
◦ Sinonasal pathology (15–20%) ◦ Nasal obst ruct ion (foreign body, deviated nasal septum , turbinate hyper t rophy— especially of MT/STs causing obliterat ion of olfactory clefts)
• Sensorineural: ◦ URTIs (15–20%) ◦ Traum a (10%)
• Iat rogenic (10%) ◦ Inadequate/incom plete sinus surgery ◦ Synechiae from previous sinonasal surgery ◦ Drugs:
- Allopurinol - Am it riptylline - Am phetam ines - Am photericin B - Azathioprine - Carbim azole - Cocaine - Codeine - Colchicine - Dilt iazem - Gold - Methotrexate - Metron idazole - Morphine - Nifedipine - St reptom ycin - Thiouracil
• Idiopathic (20%)
Uncommon Causes• Cerebrovascular disease• Epilepsy (tem poral lobe), Parkinson disease• In t racranial neoplasia (e.g., m eningiom a)• Toxic exposure• Medical co-m orbidity (e.g., hypothyroidism , DM,
hepat ic or renal failure)• Chronic alcoholism (Wernicke–Korsako )• Recreat ional drug use (e.g., cocaine)• Psychogenic (e.g., schizophrenia)
34.2.6 Management of Olfactory LossMedical• Trial of prednisolone for 2–3/52• If responsive to oral prednisolone, fur ther use of
steroid drops/spray to olfactory clefts• Caroverine 120 m g for 4/52 (not available in
United Kingdom )• Pentoxifylline 400 m g 3 t im es daily for 3/52
Surgical• Appropriate t reatm ent of any conduct ive causes,
e.g., CRS/DNS (if m edicat ion has failed)
Conservative• Alternat ive therapies:
◦ α -Lipoic acid ◦ Gingko biloba ◦ Acupuncture
• Sm ell t rain ing• Labelling of food• Gas detectors• Other dom est ic safety m easures• Good personal hygiene• Appropriate m anagem ent of psychosocial
factors including depression
34.2.7 Management of Dysosmia• Reduct ion in perceived olfact ion:
◦ Nose clip ◦ Hypertonic saline drops or decongestants to induce rh in it is m edicam entosa
◦ Cocaine to olfactory m ucosa—if bene cial consider surgical st r ipping of olfactory m ucosa
• Gabapent in and other ant i-epilept ics and ant idepressants can be ut ilised along w ith m ethods above
Philpott_9783131662316_Ch34.indd 126 02/05/14 4:54 PM

127
Psychophysical Test ing
34.2.8 Prognosis in Olfactory Loss• 30 to 70% spontaneous recovery depending on
the cause• Highest chance if loss present for less t im e and
hyposm ia rather than anosm ia
34.2.9 Gustatory Disorders• Com plete ageusia very rare due to m ult iple
innervat ions of taste• Hypogeusia and dysgeusia m ore likely but st ill
uncom m on
34.2.10 AetiologyDisorders of the Oral Cavity• Mucosal/lingual
◦ Autoim m une—e.g., Behçet syndrom e, granulom atosis w ith polyangiit is
◦ Discoloured lesions—e.g., chronic ulcerat ive stom at it is, leukoplakia
◦ Metabolic—prim ary amyloidosis ◦ Infect ion—e.g., candida, viral (HSV) ◦ Injury—therm al/chem ical/radiotherapy/t raum a ◦ Neoplasia—SCC, m elanom a
• Burning m outh syndrom e• Gingival/dental
◦ Acute necrot izing ulcerat ive gingivit is (ANUG) ◦ AIDS-related periodont it is ◦ Dental caries ◦ Gingivit is
• Salivary glands ◦ Acute/chronic sialadenit is—of various causes
• gast ro-eosophageal re ux disease/ laryngopharyngeal re ux
• PND from acute/chronic sinonasal disease
34.2.11 Disorders of Peripheral Gustatory Nerves—CNs VII, IX, and X• Infect ive—e.g., herpes, AOM, Bell palsy• Neoplast ic—glom us, schwannom a, parot id,
neuro brom a, skull-based m ets• Traum a—bir th , barotraum a, tem poral bone # ,
penetrat ing neck t raum a, SB#• Neurological—CVA, MS, sarcoid, carot id a
aneurysm• Iat rogenic—m iddle ear surgery, tonsillectomy,
laryngoscopy
34.2.12 CNS Disorders• St roke—brainstem , insula, thalam us• Epilepsy—am ygdala, h ippocam pus, operculum ,
r ight T1/2 gyrus• Neoplasia—brainstem , parietal/tem poral lobes• Encephalit is• MS
34.2.13 Systemic Disorders• Renal failure• Cirrhosis• Malnutrit ion• Trace m etal and vitam in de ciencies (Zn, Cu,
Mg, B3, B12, C)• Wast ing syndrom e—cancer/HIV• Endocrine—adrenocor t ical insu ciency, con-
genital adrenal hyperplasia, Cushing, cret in ism , DM, hypothyroidism , panhypopituitarism
34.2.14 Iatrogenic• Ant ibiot ics/ant ifungals• Ant iconvulsants• Ant idepressants• Ant ih istam ines• Ant ihypertensives• Ant iparkinsonian drugs• Ant ipsychot ics• Carbim azole• Decongestants• Lith ium• Muscle relaxants• NSAIDs• Stat ins
34.2.15 Psychiatric• Bulim ia• Depression• Malingering• Schizophrenia• Conversion disorder
34.2.16 Genetic• For exam ple, Fam ilial dysautonom ia
34.2.17 Management• This is largely directed at the cause of the
gustatory disorder w here possible
Philpott_9783131662316_Ch34.indd 127 02/05/14 4:54 PM

128
35 Nasolacrimal Disorders
• The t ransfer of tears through the lacrim al drainage system is predom inately through act ive pum ps in the eyelids, punct i, canaliculi, and sac
• The valves w ith in the lacrim al out ow system allow the unidirect ional ow of tears from the canaliculi to the inferior m eatus
• The valve of Rosenm uller is situated at the in ternal opening of the com m on canaliculus w ith in the lacrim al sac
• The valve of Hasner lies at the distal opening of the lacr im al duct at the infer ior m eatus
35.2 Classi cation of Lacrimal Obstruction• Proxim al:
◦ Punctal stenosis/absence ◦ Single canalicular ◦ Com m on canalicular (lateral or m edial)—m edial com m on canalicular blockage could be regarded as a distal blockage as it is usually caused by a m em brane w ith in the lacrim al sac closing o the in ternal opening of the com m on canaliculus w ith in a brot ic lacrim al sac
• Distal: sac and duct• Funct ional: related to poor lacrim al pum p
funct ion , w hich m ay be due to a displaced punctum , eyelid laxity, weak orbicular is, or facial nerve palsy
35.3 Symptoms and Signs of Lacrimal Blockage• Signs and sym ptom s of lacrim al blockage can be
ow -related or volum e-related. ◦ Flow -related sym ptom s are due to low conductance w ith in the canaliculi or nasolacrim al duct . This leads to excessive aqueous tears building up in the tear lake causing blurred vision - The blurr ing is worse on dow n-gaze w hen the visual axis passes near the enlarged tear m eniscus in the lower lid . Spillage of tear can lead to skin soreness
35.1 Anatomy and Physiology of the Lacrimal System• The anatomy of the lacrim al system can be
divided in to the secretory, dist r ibutory, and drainage com ponents: ◦ Secretory system = lacrim al glands ◦ Dist r ibutory system = eyelids ◦ Lacrim al drainage system = lacrim al puncta, canaliculi, sac, and nasolacrim al duct (Fig. 35.1)
• Lacrim al sac sits in the lacrim al fossa that com prises the frontal process of the m axilla anteriorly and the lacrim al bone posteriorly
• Frontal process of the m axilla is the dom inant bone encountered during lacrim al surgery
• The upper punctum lies slight ly m edial to the lower punctum
• During blinking, the puncta com e together• In it ial por t ion of the canaliculi underneath the
puncta is vert ical and 2 m m in length• Canaliculi term inate in a saccular dilatat ion
called “am pulla” surrounded by m uscle, w hich can expand and contract w ith blinking, and m ay play a role in the drainage of tear through the canaliculus
• The upper and lower canaliculi m eet m edially to form the com m on canaliculus
• Average length of the com m on canaliculus is 1.2 m m (range 1–5 m m )
• Enters lacrim al sac at an acute angle rather than at r ight angle (believed to prevent re ux of u id back to the canaliculus w hen the sac is full)
• The lacrim al sac varies in size, being 12 to 15 m m long and 4 to 8 m m deep
• The anterior to posterior dim ension of the lacrim al sac often lim its the size of the lacrim al w indow in dacryocystorhinostomy (DCR)
• The lacrim al sac courses poster iorly and inferiorly to becom e the nasolacrim al duct that term inates in the infer ior m eatus beneath the inferior turbinates
• With blinking, closure of the palpebral aper ture occurs from lateral to m edial, thus propelling the tears toward the punct i—the compressive act ion of one lid against the other is im portant in the drainage of ears through the canaliculi
Philpott_9783131662316_Ch35.indd 128 7/7/14 3:32 PM

129
Proximal Lacrimal Obstruction
◦ Volum e-related sym ptom s are due to accum ulat ion of uid in the lacrim al sac and the backwash of the debris in to the tear lake - The in term it tent back ow of the sac content causes blurred vision by st rings of m ucus m aking the lids stay closed in the m orning
- The dead space w ith in the lacrim al sac causes bacterial overgrow th and predisposes the eye to recurrent conjunct ivit is
- Som et im es, a m ass can appear at the inner canthus, from w hich debris can be expressed in to the tear lake
- If unt reated, the lum p can develop in to a m ucocele or pyocele, perhaps even result ing in a stu la
• A well-perform ed dacryocystorhinostom y procedure w ith a com plete m arsupializat ion of the lacrim al sac w ith in the nose should theoret ically overcom e 100% of volum e-related sym ptom s. However, it m ay not elim inate all ow -related sym ptom s as they are lim ited by the conductance of the canaliculi
35.4 Diseases of the Lacrimal Sac and Duct• Congenital obst ruct ion of the nasolacrim al duct:
◦ Thought to be due to an imperforate valve of Hasner w ith in the infer ior m eatus
◦ Com m on in children during their rst year of life
◦ High rate of spontaneous resolu t ion ◦ Persistent epiphora beyond the age of 1 year m ay require lacrim al probing to ident ify the level of the blockage
• Acquired obst ruct ion of the lacrim al sac/duct can be non-speci c or speci c: ◦ Non-speci c acquired nasolacrim al blockage is by far the com m onest - Most com m on in the elderly and fem ale populat ions
◦ Speci c acquired nasolacrim al blockage includes: - Sarcoidosis - Wegener granulom atosis
◦ Once the sarcoidosis and Wegener granulom atosis are controlled by steroids, the residual epiphora can be t reated by dacryocystorhinostomy - Traum a—nasal fractures or injury from surgery on the m axilla or sinuses
- Neoplasm s involving the nasolacrim al sac/duct can ar ise:
◦ From t issues w ith in the sac/duct: - Squam ous cell papillom a - Transit ional cell papillom a - Squam ous cell carcinom a - Adenocarcinom a
◦ Grow th invading the sac/duct from the outside: - Maxillary and ethm oid sinus tum our - Lym phom a
35.5 Proximal Lacrimal Obstruction• Approxim ately 1 in 3 cases of epiphora• Proxim al lacrim al apparatus includes the
canaliculi and their puncta w ith the caruncle separat ing the puncta
• Aet iology: ◦ Congenital causes (10%): Absence or im perfect ion of lacrim al puncta and/or canaliculi (± obliterat ion of m ore distal parts of the lacrim al apparatus)
◦ Ciactrical conjunct ival disorders (~2%)—subepithelial brosis of the conjunct iva - Ocular pem phigoid - Stevens–Johnson syndrom e
◦ Drug-induced canalicular stenosis (2%) - Phospholine iodide
Fig. 35.1 The lacrimal drainage system.
5mm8mm
10mm
2mm
Philpott_9783131662316_Ch35.indd 129 7/7/14 3:32 PM

130
35 Nasolacrimal Disorders
◦ Gross nasal septal deviat ion m ay hinder the in t ranasal access to the lacrim al sac, and the pat ient should be counselled for septal surgery together w ith the DCR
35.6.2 Jones Dye Tests• Fluorescein dye disappearance test
◦ A drop of 2% uorescein dye is placed in the inferior fornix
◦ Disappearance of the dye from the eyes is assessed after 10 to 15 m in
◦ Retent ion of dye indicates blockage in the lacrim al drainage system
• Jones I test ◦ Dye is inst illed in pat ient’s eye, and a cot ton bud is placed in the inferior m eatus
◦ If dye is present after 5 m in th is indicates a patent system
◦ Absence of dye indicates the anatom ical obst ruct ion between the punctum and valve of Hasner
◦ False-negat ive rate of up to 20%
35.6.3 Regurgitation Test• Finger pressure is applied on the lacrim al sac
area; look for m ucous or purulent discharge from the punct i
• A posit ive test indicates patent canaliculus and the presence of dacryocyst it is
35.6.4 Ophthalmology Tests• The ophthalm ologist m ay perform other tests
to locate the level of lacrim al blockage, such as lacrim al irr igat ion , Jones II dye test , and lacrim al probing ◦ Jones II dye test
- Perform ed after a negat ive Jones I test - Lacrim al system is ushed by syringing and washing of excess uorescein from the conjunct ival sac
- Test is posit ive if dye is detected on the cot ton bud and th is suggests funct ional obst ruct ion of the nasolacrim al duct
- Negat ive test indicates punctal or canalicular stenosis
- Regurgitat ion indicates com plete nasolacri-m al duct obst ruct ion or com plete com m on canaliculus block
- Penicillin - Fluorouracil
◦ Infect ive causes (30%) - HSV or iat rogenic e ect of ant ivirals - Herpes zoster (and vaccine)—canalicular obst ruct ion
- Chlam ydial infect ions ◦ Therm al and t raum at ic injuries and radiotherapy-induced injury (34%) - Radiotherapy—especially w ith dosing to basal cell carcinom as in the inner canthal area and for sinonasal tum ours
- Surgical rem oval of adjacent skin lesions ◦ Canalicular neoplasm s (2%)
- Papillom as - Basal cell carcinom as
◦ The causes cited above can cause lateral com m on canalicular obst ruct ions in the sam e m anner as they a ect the individual canaliculi
◦ Other m iscellaneous causes - Failed lacrim al surgery (10%) - Facial nerve palsy (2%) - Maxillary sinusit is (0.3%) - Lid abscess (0.3%) - Sarcoidosis (nasal) (0.3%) - Idiopathic (9%)
35.6 Investigation of Lacrimal Obstruction• In the UK, pat ients w ith epiphora are in it ially
referred to an ophthalm ologist• However, there are certain lacrim al assessm ents
that otolaryngologists should be fam iliar w ith
35.6.1 Examination• Inspect ion of the lid
◦ Look for signs of punctual involvem ent , including posit ion of puncta
◦ Any sign of weakness in opening and closing the eyelid should be noted
◦ If sclera show is evident on exam ining the relat ionship of the lower lid to the inferior lim bus, a lacrim al pump problem m ay be present
• Nasal exam inat ion ◦ The role of the otolaryngologist is to pick up other nasal pathologies that m ay be of importance
Philpott_9783131662316_Ch35.indd 130 7/7/14 3:32 PM

131
Current Management Strategies
• If the stenosis is long, one of the best m ethods of obtain ing lacrim al drainage is conjunct ivoDCR and the use of a bypass tube, e.g., Jones bypass tube.
• The m ain problem of Jones’ tube is m igrat ion of the tube and the need for life-long care of the tube.
• If the tube stays in place, the success rate of reducing epiphora could be h igh.
35.7.2 Distal: Endoscopic Dacryocystorhinostomy• The principles involve creat ing a large
osteotomy to m arsupialize the w hole sac w ith in the nose, and creat ing an epithelial-lined lacrim al w indow to facilitate healing by rst in tent ion (Fig. 35.2)
• Large lacrim al w indow allows rem oval of calculus w ith in the sac or any m em branous covering of the com m on canaliculus (m em branectomy)
• Im portant to note that a m ajor port ion of the lacrim al sac is located above the insert ion of the anterior end of the m iddle turbinate
- If no saline appears in the nose then there is a source of com plete obst ruct ion som ew here in the lacrim al drainage system
◦ Lacrim al probing/irrigat ion - May be par t diagnost ic and par t therapeut ic, e.g., dislodging a stone
- May be used in an at tem pt to palpate or localize the site of obst ruct ion
- Can m easure the length of canalicular patency distal to the punctum , and from that est im ate the length of the canalicular blockage
35.6.5 Dacryocystography• Contrast m aterial is injected in to the canaliculi• Enables visualizat ion of the anatom ical details
of the lacrim al drainage system• De nit ive test for assessing the nasolacrim al
system• Digital subtract ion techniques are now usually
em ployed
35.6.6 Dacryoscintigraphy• Physiological assessm ent in w hich a drop of
technet ium is placed in the conjunct ival cul-de-sac and followed through the lacrim al system using a gam m a cam era
• 10-µL drop of technet ium -99 pertechnetate is placed on the m arginal tear st r ip
• Useful for assessing funct ional lacrim al duct obst ruct ion—indicated by a delay or absence of t ransit of technet ium in to the nose
• May be used as com plem entary invest igat ion to ophthalm ology tests
35.6.7 CT Scan• This m ay be indicated if t raum a or neoplasm s
are suspected, or in certain cases w here DCR is perform ed
35.7 Current Management Strategies35.7.1 Proximal Stenosis• If the stenosis is part ial, or if the stenot ic
segm ent is lim ited, t rephenat ion and bicanicular in tubat ion is the t reatm ent of choice.
Fig. 35.2a–f A diagrammatic illustration showing the surgical steps in dacryocystorhinostomy—the whole lacrimal sac and the upper portion of the lacrimal duct are marsupialized into the nasal cavity.
d e f
a b c
Philpott_9783131662316_Ch35.indd 131 7/7/14 3:32 PM

132
35 Nasolacrimal Disorders
• Bone rem oval can be done by using bony rongeurs, chisels, or a drill ◦ The drill is par t icularly useful in rem oving the th ick bone above the insert ion of the m iddle turbinate to expose the fundus of the sac
• One should be able to see the in ternal opening of the com m on canaliculus at the n ish of the operat ion . Care should be taken during
probing or stent ing to avoid false passages w hen inst rum ents are in t roduced from the canaliculi in to the sac
• Debate st ill rages on w hether silicone stent ing of the lacrim al system is necessary follow ing a DCR procedure or how long the stent should be left in . The success rate in relieving the symptom of epiphora from endoscopic DCR has been reported to be in the region of 90%
Philpott_9783131662316_Ch35.indd 132 7/7/14 3:32 PM

133
36 Cerebrospinal Fluid Rhinorrhoea
36.1 Aetiology of Cerebrospinal Fluid Rhinorrhoea• Spontaneous—m ay be associated w ith benign
in t racranial hyper tension• Iat rogenic (see Chapter 27)• Traum a• Infect ious/in am m atory—erosive sinonasal
disease (see Chapters 25 and 26)• Neoplast ic
36.2 Benign (Idiopathic) Intracranial Hypertension• Unknow n aet iology that predom inantly a ects
obese wom en of childbearing age• Incidence of 0.9 to 1.0 per 100,000 in the general
populat ion ◦ 1.6 to 3.5 per 100,000 in wom en ◦ 7.9 to 20 per 100,000 in wom en w ho are overweight
• Key features: ◦ Chronically elevated ICP ◦ Papilledem a present , w hich m ay lead to progressive opt ic at rophy and blindness
• The diagnost ic criteria: ◦ Symptom s and signs of increased ICP ◦ No localizing neurological signs (w ith the except ion of a unilateral or bilateral CN VI paresis)
◦ Cerebrospinal u id (CSF) m ay show increased pressure, but there are no cytologic or chem ical abnorm alit ies
◦ Norm al to sm all sym m etric vent ricles m ust be dem onst rated
• Diagnost ic steps: ◦ Lum bar puncture (LP) should be done w ith the pat ient in the lateral decubitus posit ion . Lum bar puncture is perform ed to m easure the opening pressure, as well as to obtain CSF to exclude alternat ive diagnoses
◦ MRI or venography should be included to rule out in t racranial venous sinus throm boses
◦ Other causes of in t racranial hypertension should be ruled out
• If not overweight , ru le out associated risk factors: ◦ Exposure to or w ithdrawal from cer tain exogenous substances (e.g., drugs)
◦ System ic diseases - Anem ia - Chronic respiratory insu ciency - Fam ilial Mediterranean fever - Hyper tension - MS - Polyangiit is overlap syndrom e - Psit tacosis - Chronic renal disease - Reye syndrom e - Sarcoidosis - System ic lupus erythem atosus - Throm bocytopenic purpura
◦ Disrupt ion of cerebral venous ow ◦ Endocrine or m etabolic disorders:
- Adrenal insu ciency - Cushing disease - Hypoparathyroidism - Hypothyroidism - Excessive thyroxine replacem ent in children
• Treatm ent m ay be m edical and/or surgical involving neurologists, neurosurgeons, and ophthalm ologists
36.3 Diagnostic Tests• Diagnost ic endoscopy• CT: Thin cut coronal, axial w ith sagit tal
reconst ruct ion (1.0-m m intervals)• Clear rh inorrhoea—collect and send for β2-t ransferrin assay
• Glucose d ipst ick—high false posit ive (not done)
• MR cisternography (MRC): ◦ Non-invasive technique (no LP) ◦ Active or recently leaking ◦ Ident i cat ion of leak predicted w ith signi cant cer tain ty
• Best to consult w ith local radiologists as to im aging techniques available/preferred and in accordance w ith ter t iary referral centre w ho w ill conduct any repair required
Philpott_9783131662316_Ch36.indd 133 02/05/14 5:00 PM

134
36 Cerebrospinal Fluid Rhinorrhoea
36.4 Operative Repair• In t raoperat ive in t rathecal uorescein:
◦ Lum bar drain placed preoperat ively ◦ 0.1 m L of 10% IV uorescein m ixed w ith 10 m L CSF
◦ Slowly infused in t rathecally ◦ Not approved by MHRA in the United Kingdom , so special consent from pat ient (seizures at h igh concentrat ions)
• Underlay repair technique: ◦ Once leak posit ively ident i ed, m ucosal m em brane around leak rem oved
◦ Dural layer elevated o bone in t racranially ◦ Tem poralis fascia graft between dura and bone ◦ Defect >5 m m : bone or cart ilage piece between fascia and bone (in t racranial/ext radural)
◦ Another piece of temporalis fascia on ent ire defect on nasal side
◦ Free m ucosal graft over repair site ( nal t issue layer)
• Onlay repair technique: ◦ Simpler ◦ Mucosa around leak rem oved ◦ Mult ilayer onlay repair w ith bone/car t ilage, fascia, free m ucosa, and brin glue
◦ No di erence between onlay and underlay• Packing/postop
◦ Fibr in glue/sealan t (Tisseel, Baxter, Deer eld , IL, Un ited States) over repair site w ith gelfoam
◦ Sterile absorbable lm (Gel lm , P zer, New York, NY, United States) m oistened in tobramycin against repair site in inverted U posit ion
◦ PVA sponge (Merocel, Medt ronic, Inc., Minneapolis, MN, United States) packing layered under Gel lm to oor of nose
◦ Lum bar drain opened to drain 10 m L/h for 1–2 days
◦ 24-h bed rest and then m obilized
Philpott_9783131662316_Ch36.indd 134 02/05/14 5:00 PM

135
37.1 Cosmetic Assessment of the Nose (Fig. 37.1)• Divide in to 1/5s• Brow–t ip aesthet ic line• Length of nasal bones• Asym m etry• Width/height rat io of nose (6:8)—nasion
to t ip• Infrat ip lobule• Overall facial contour
◦ Glabella ◦ Radix—depth and project ion ◦ Dorsal pro le and suprat ip ◦ Tip project ion ◦ Colum ella show ◦ Nasiolabal angle 90 to 120°
37.2 Radix Deformities• Radix = 4 to 6 m m posterior to glabella• Tem poralis fascia can be used to augm ent
radix• Spreader grafts used to w iden lower por t ion of
nose and correct car t ilaginous deform ity
37.3 Indications for Open Rhinoplasty• Highly asym m etric t ip• Markedly overprojected t ip• Severely underprojected t ip• Secondary revision cases
37.4 Indications for Good Prognosis• Obvious dis gurem ent• Occupat ional reason to im prove appearance• Realist ic w ish to appear younger• Long-standing desire to have surgery
perform ed
37.5 Causes for Caution in Rhinoplasty Patient Selection (Schulman)• Unrealist ic m ot ive• Sudden w him to have surgery• Expectat ion of surgery being solut ion for all
problem s (e.g., save m arriage)• History of hospitalizat ion or recurrent
psychiat ric illness• Relentless “surgeon shopping”• Repeated surgery w ith consistent dissat isfact ion• Unable or unw illing to follow im portant
inst ruct ions provided by surgeon or sta • OCD tendencies• Poor in teract ion w ith m edical sta
37.6 Classic Rhinoplasty Steps• Septoplasty• Tip rem odelling, project ion , and cephalic
rotat ion• Hum p rem oval (pro le line)• Narrow ing of nose (osteotom ies)• Final correct ion of subt le deform it ies
37.7 Tip Support Mechanisms• Major:
◦ Medial and lateral crura (size/shape/resilience) ◦ Medial crural footplate at tachm ent to caudal border of quad. car t ilage
◦ Attachm ent of ULCs to lower lateral car t ilages (LLCs) (scroll area)
• Minor: ◦ Ligam entous sling spanning paired dom es of LLCs
◦ Cart ilaginous septal dorsum ◦ Sesam oid com plex extending support of lateral crura to piriform aperture
◦ Attachm ent of LLCs to overlying skin and m usculature
◦ Nasal spine ◦ Mem branous septum
37 Rhinoplasty and Nasal Cosmesis
Philpott_9783131662316_Ch37.indd 135 02/05/14 5:02 PM

136
37 Rhinoplasty and Nasal Cosmesis
• Delivery approaches—abnorm al t ip anatomy ◦ In tercart ilaginous and m arginal incisions ◦ Indicat ions:
- Alar car t ilages are unpleasant ly - Tip t r iangularit y unsat isfactory - Am orphous/bulbous t ip - Dom al angles too w ide - In terdom al distance excessive
• Open (external) approach—see above
37.8 Surgical Approaches to the Nasal Tip—Favourable Tip Anatomy or Radical Re nement• Non-delivery approaches
◦ Transcar t ilaginous ◦ Retrograde approach ◦ Cephalic t r im ◦ Enhancem ent of t ip project ion
Fig. 37.1a–d Important surface landmarks of the nose.1. Glabella; 2. Nasion; 3. Tip-de ning points; 4. Alar sidewall; 5. Supra-alar crease; 6. Philtrum; 7. Infratip lobule; 8. Columella; 9. Facet, or soft-t issue triangle; 10. Nostril sill; 11. Columella-labial angle or junction; 12. Alar-facial groove or junction; 13. Nasofrontal angle; 14. Rhinion (osseocartilaginous junction); 15. Supratip.a Frontal view. 1, glabella; 2, nasion; 3, t ip-de ning points; 4, alar sidewall; 5, supra-alar crease; 6, philtrum.b View from base. 3, t ip-de ning points; 4, alar sidewall; 7, Infratip lobule; 8, columella; 9, facet, or soft-t issue triangle;
10, nostril sill; 11, columella-labial angle or junction; 12, alar-facial groove or junction.c Lateral view. 1, glabella; 2, nasion; 3, t ip-de ning points; 7, infratip lobule; 8, columella; 11, columella-labial angle or
junction; 12, alar-facial groove or junction; 14, rhinion (osseocartilaginous junction); 15, supratip.d Oblique view. 1, glabella; 2, nasion; 3, t ip-de ning point; 4, alar sidewall; 6, philtrum; 12, alar-facial groove or
junction; 14, rhinion (osseocartilaginous junction); 15, supratip.
10
11
84
712
6
35
4 45
3
12144
3 6
1512
9
3 3
12
ba
dc
1214
15 8
1112
73
Philpott_9783131662316_Ch37.indd 136 02/05/14 5:02 PM

137
Pro le Alignment
• Excision of caudal m argins of overlong ULCs• Septal shor tening w ith a h igh t rans xion
incision• In terrupted st r ip technique if signi cant
overrotat ion present—caut ion w ith th in skin and delicate car t ilages
37.12 Causes of Overprojection of the Nasal Tip• Alar cart ilage overdevelopm ent• Nasal spine overdevelopm ent• Caudal or dorsal septum overdevelopm ent• Elongated colum ella and m edial crura• Com bined anatom ical abnorm alit ies• Iat rogenic overproject ion
37.13 Pro le Alignment• Anatom ical com ponents responsible for
preop pro le: ◦ Nasal bones ◦ Cart ilaginous septum ◦ LLCs
• Landm arks: ◦ Nasofrontal angle ◦ Tip-de n ing point
• Access to nasal dorsum : ◦ Transcar t ilaginous approach ◦ In tercar t ilaginous approach ◦ Transcolum ellar incision
• Techniques: ◦ Increm ental—increm ental shaving of car t ilaginous dorsum followed by osteotom e rem oval of dorsal hum p
◦ En bloc• Correct rem aining irregularit ies w ith knife/rasp• Mucoperichondrium at taching ULCs to septum
should not be divided unless nose large or severely tw isted
37.9 Nasal Tip Sculpturing Procedures• Volum e reduct ion w ith residual com plete st r ip
(4–8 m m rem ains) ◦ Preferent ial approach
• Volum e reduct ion w ith suture reorientat ion of residual com plete st r ip ◦ Reorientat ion of breadth of dom al angle ◦ Project ion m odi cat ion ◦ Narrow ing re nem ent
• Volum e reduct ion w ith in terrupted st r ip—tip support adjuncts usually required: ◦ Colum ella st ru ts ◦ Infrat ip lobule car t ilage grafts ◦ Transdom al suturing
37.10 Tip Projection and Cartilage Tip Grafts• Ensure t ip support is preserved or corrected• Harvest from septal or auricular car t ilage• Inser t in to sm all pockets ± sutures to alar
car t ilages (depending on approach)• Marginal incisions below anatom ical dom e
facilitate careful pocket creat ion• Bevel edges of grafts• Autogenous car t ilage st ru ts posit ioned below
and/or between m edial crura aid t ip stabilit y
37.11 Tip Rotation• Planned degree of t ip rotat ion depends on:
◦ Length of nose ◦ Length of face ◦ Length of upper lip ◦ Facial balance and propor t ions ◦ Pat ient’s aesthet ic desires ◦ Surgeon’s aesthet ic judgem ent
• Shor tening of caudal edge of septum
Philpott_9783131662316_Ch37.indd 137 02/05/14 5:02 PM

138
38 Facial Fractures and Swelling
38.1 Mandibular Fractures• Condyle 36%• Body 21%• Angle 20%• Sym physis 14%• Alveolar process 3%• Ram us 3%• Coronoid process 2%
38.2 Maxillary (Le Fort) Fractures (Fig. 38.1)• Bones involved:
◦ Maxilla ◦ Sphenoid ◦ Vom er ◦ Ethm oid ◦ Palat ine bones ◦ Zygom a ◦ Nasal bones
• Le Fort I ◦ Floor of nose ◦ Lower one-th ird of m axilla ◦ Palate ◦ Pterygoid plates
• Le For t II ◦ Across nasal bony superst ructure and frontal process of m axilla
◦ Across face of anterior m axilla ◦ Across orbital oor (inc. infra-orbital foram en) ◦ Lateral wall of m axilla extending to pterygoid plates
• Le Fort III ◦ Lateral fracture extending across orbital oor in to lateral orbit through zygom a
◦ Zygom a w ill m ove during palpat ion of palate
38.3 Frontal Sinus Fractures• Usually due to road t ra c accidents• Fracture/dam age involving frontonasal recess
likely to cause stenosis• Dam aged frontal sinus m ucosa has a propensity
for subepithelial brosis w ith a tendency to cyst form at ion
• Mucoceles and m ucopyoceles can result—bone erosion possible
• Classi cat ions: ◦ Structures involved:
- Anterior wall - Posterior wall - Nasofrontal recess - “Through and through”
◦ Type: - Linear—no operat ive in tervent ion required - Displaced - Com pound - “Missing bone”
◦ Depressed fractures require elevat ion of fragm ents and excision of m ucosa t rapped between fragm ents—bicoronal or but ter y ap
◦ Displaced posterior wall fractures—osteoplast ic ap and fat obliterat ion
◦ Through and through fractures usually require a cranializat ion procedure at the t im e of anterior craniotomy—all m ucosa is rem oved
Fig. 38.1 Types of middle-third fracture. Le Fort classes I, II, III; 1, naso-orbito-ethmoid complex; 2, nasomaxil-lary complex; 3, orbital oor; 4, zygomatic bone.
I
II
III
1
2
3
4
Philpott_9783131662316_Ch38.indd 138 02/05/14 5:05 PM

139
Facial Swelling
and frontonasal recesses plugged w ith tem po-ralis fascia
38.4 Facial Swelling• Infect ive and in am m atory:
◦ Sinusit is—including acute and chronic; com -plicat ions such as subperiosteal abscess, (pyo)m ucocele are m ore likely
◦ Osteomyelit is—sinugenic, dental, radiotherapy ◦ Zygom at ic abscess—due to ot it is m edia
◦ Sialadenit is of parot id/SM glands ◦ Sialadenosis ◦ Dacrocyst it is ◦ Odontogenic cysts
• Neoplast ic: ◦ Sinugenic ◦ Salivary glands
• Traum a—see above• Angioedem a—sudden onset , especially a ect ing
lip and eyelid and associated w ith prurit is
Philpott_9783131662316_Ch38.indd 139 02/05/14 5:05 PM

140
39 Facial Flaps, Scars, and Keloids39 Facial Flaps, Scars, and Keloids
39.1 Advancement Flaps (Fig. 39.1)• Lesions in nasolabial fold, infraciliary area, and
junct ion of nose to face• Advanced along sam e axis as defect• Exam ples:
- Cheek advancem ent ap
39.2 Rotation Flaps (Figs. 39.2 and 39.3)• Flap in di erent plane from defect• Exam ples:
◦ Nasolabial rotat ion ap ◦ Glabellar rotat ion ap ◦ Regional island rotat ion ap
39.3 Transposition Flaps (Figs. 39.4, 39.5, 39.6)• Most versat ile of adjacent aps• Exam ples:
◦ Classic t ransposit ion ap ◦ Bilobed ap (inc. glabellar and m elolabial)Fig. 39.1 Advancement ap. Tissue elongation or
release of tension with a VY-plasty.
Fig. 39.3a–c Regional island ap transplantation.
ba
Fig. 39.2a, b Rotation aps.a Random-pat tern ap
(with random blood supply from area).
b Axial-pat tern ap (with blood supply from a single longitudinal artery).
ba
Philpott_9783131662316_Ch39.indd 140 02/05/14 5:07 PM

141
Fig. 39.4a, b Transposition aps.a Tissue transposition with a Z-plasty.b Coverage plasty using a bilobed
ap.
b
a
1
2
1
2
1
2
2
1
Fig. 39.5a, b Coverage of a defect with a bilobed ap.
a
L1
L2
b
Transposit ion Flaps
Philpott_9783131662316_Ch39.indd 141 02/05/14 5:07 PM

142
39 Facial Flaps, Scars, and Keloids
◦ Rhom boid ap ◦ Z-plasty
39.4 Midline Forehead Flap (Fig. 39.7)• Midline ver t ical ap• Width of 2.5 to 4 cm• Suprat rochlear and dorsal nasal vessels• 2-stage procedure— ap bridge tested then
divided at 14 to 18 days after rst procedure
39.5 Keloids• Keloid = an abnorm al scar that grow s beyond
the boundar ies of the or iginal site of skin inju ry
• Keloids appear clin ically like a raised am orphous grow th
• Frequently associated w ith pruritus and pain• Microscopy: random ly organized collagen bers
in a dense connect ive t issue m at rix• Com m on sites:
◦ Earlobes (posterom edial surface)
Fig. 39.6a–d Reconstruction of a large defect with a bilobed ap following resection of a malignant skin tumour.a Defect.b Dermoplasty with allopastic material (after histologic control of wound margins).c Three days postoperatively.d Six months later.
Fig. 39.7a–d Reconstruction of the t ip of the nose using a forehead ap.a Elevation of the ap.b Temporary wound closure.c Four weeks later, before severing the pedicle.d Six months after the operation.
Philpott_9783131662316_Ch39.indd 142 02/05/14 5:07 PM
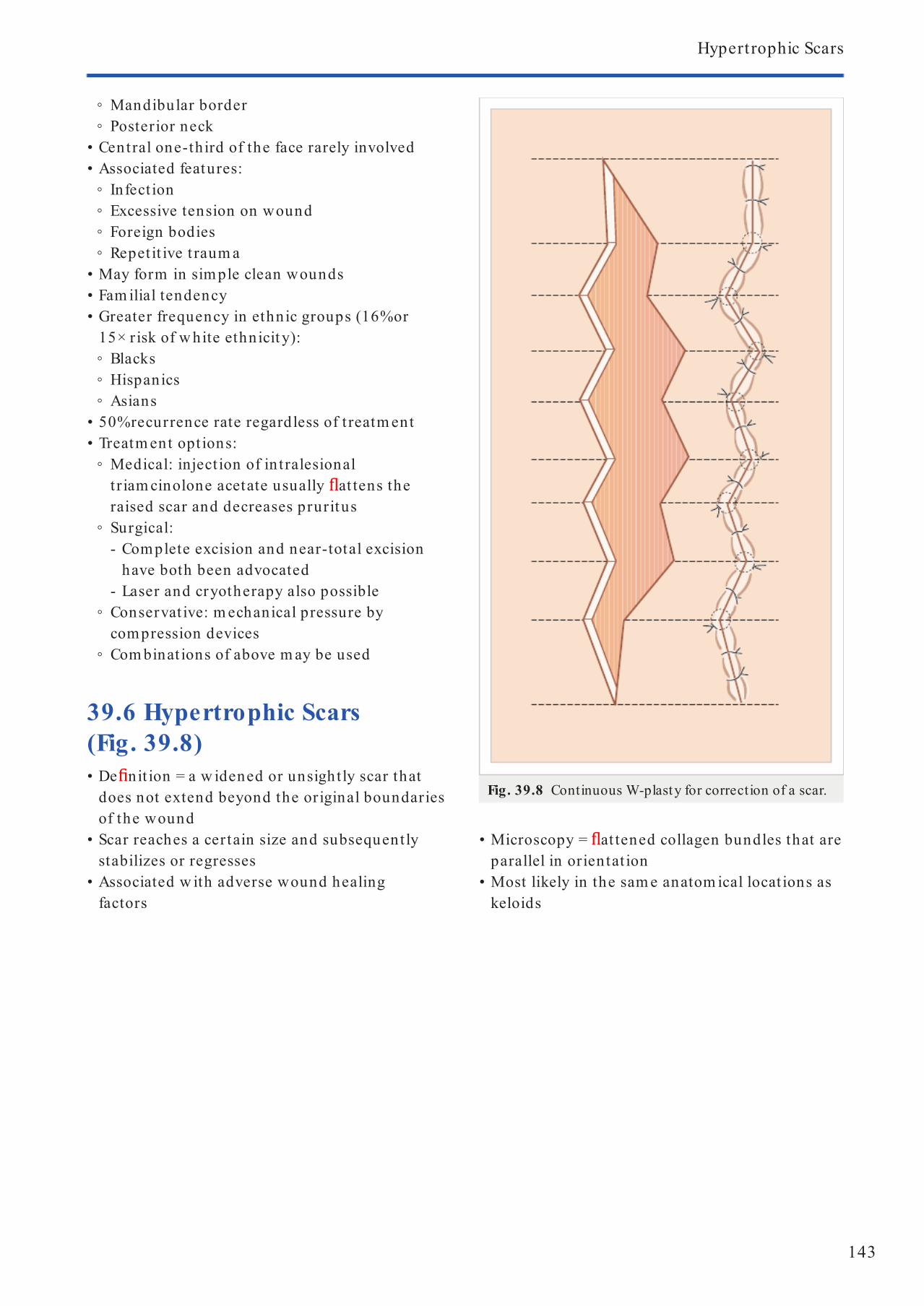
143
Hypertrophic Scars
• Microscopy = at tened collagen bundles that are parallel in orientat ion
• Most likely in the sam e anatom ical locat ions as keloids
◦ Mandibular border ◦ Posterior neck
• Central one-third of the face rarely involved• Associated features:
◦ Infect ion ◦ Excessive tension on wound ◦ Foreign bodies ◦ Repet it ive t raum a
• May form in sim ple clean wounds• Fam ilial tendency• Greater frequency in ethnic groups (16% or
15× r isk of w hite ethnicit y): ◦ Blacks ◦ Hispanics ◦ Asians
• 50% recurrence rate regardless of t reatm ent• Treatm ent opt ions:
◦ Medical: inject ion of in t ralesional t r iam cinolone acetate usually at tens the raised scar and decreases pruritus
◦ Surgical: - Com plete excision and near-total excision have both been advocated
- Laser and cryotherapy also possible ◦ Conservat ive: m echanical pressure by compression devices
◦ Com binat ions of above m ay be used
39.6 Hypertrophic Scars (Fig. 39.8)• De nit ion = a w idened or unsightly scar that
does not extend beyond the original boundaries of the wound
• Scar reaches a certain size and subsequently stabilizes or regresses
• Associated w ith adverse wound healing factors
Fig. 39.8 Continuous W-plasty for correction of a scar.
Philpott_9783131662316_Ch39.indd 143 02/05/14 5:08 PM

Philpott_9783131662316_Ch39.indd 144 02/05/14 5:08 PM

Sect ion III
Laryngology, Head and Neck
Philpott_9783131662316_Ch40.indd 145 02/05/14 5:16 PM

Philpott_9783131662316_Ch40.indd 146 02/05/14 5:16 PM

147
40.1 Anatomy40.1.1 Cartilages• Thyroid
◦ Two lam inae fused in m idline anter ior ◦ Superior cornu ar t iculates w ith greater horn of hyoid
◦ Inferior cornu form s synovial join t w ith cricoid ◦ An oblique line along lateral surface of lam ina allows for at tachm ent of sternothyroid and thyrohyoid m uscles
◦ Inferior pharyngeal const r ictor at taches to poster ior border of lam ina
• Cricoid ◦ Complete solid ring cart ilage ◦ Superior ar t iculat ion w ith the inferior cornu of thyroid cart ilage
◦ Inferior a m em brane at taches to rst t racheal r ing
◦ Anterior the r ing is narrow com pared w ith poster ior
◦ The cricothyroid m em brane is form ed between these aspects of the ring
• Arytenoid ◦ Two pyram id-shaped car t ilages ◦ They ar t iculate w ith posterior par t of cr icoid (cr icoarytenoid join t).
◦ Muscular process is lateral w here the in t rinsic laryngeal m uscles at tach
◦ Vocal process m edial w here the vocal ligam ent at taches
• Accessory: Cuneiform and corniculate car t ilages ◦ Both in t im ately related to arytenoids providing support to aryepiglot t ic folds
• Epiglot t is ◦ Superior is free edge ◦ Inferiorly it at taches to the inner surface of the thyroid car t ilage superior to anterior com m issure
40.1.2 Muscles• Extr insic
◦ Infrahyoid and suprahyoid m uscles• In t rinsic
◦ Adductors - Cricothryoid*
- Lateral cricoarytenoid* - Thyroarytenoid* - In terarytenoid
◦ Unpaired w ith bilateral nerve innervat ion , hence unilateral RLN palsy can st ill result in som e adduct ion
• Abductor ◦ Posterior cricoarytenoid
*Control vocal length, tension and frequency
40.1.3 Joints• Cricothyroid
◦ Synovial join t ◦ 2 act ions: antero-posterior sliding and rotat ion inferior cornu on cricoid
◦ Contract ion pulls thyroid ala anterior result ing in lengthening and tension of vocal cords (VCs)
• Cricoarytenoid ◦ Each join t is placed 45° to the horizontal on the cr icoid
◦ Allows for arytenoid rocking, sliding w hich alters the vocal process posit ion w hich a ects the VCs
40.1.4 Fibroelastic Tissue• Quadrangular m em brane
◦ Accessory elast ic support ◦ Superiorly is a free edge form ing the aryepiglot t ic fold
◦ Inferiorly form s the m edial wall of the piriform fossa
◦ Form s the vest ibular ligam ent inferiorly ◦ Anteriorly at taches to lateral edges of epiglot t is
◦ Posteriorly at taches to arytenoids• Conus elast icus
◦ Fibroelast ic m ain support of supraglot t is and glot t is
◦ Superiorly at taches to anterior com m issure and vocal processes
◦ Inferior at taches to superior border cricoid car t ilage
◦ Medially becom es vocal ligam ent ◦ Anteriorly is cont inuous w ith cr icothyroid m em brane
40 Laryngeal Anatomy and Physiology
Philpott_9783131662316_Ch40.indd 147 02/05/14 5:16 PM

148
40 Laryngeal Anatomy and Physiology
40.1.5 Vocal Fold• Layers from super cial to deep:
◦ Mucosa: st rat i ed squam ous epithelium ◦ Lam ina propria
- Super cial layer: gelat inous layer w ith loose brous components, aka Reinke space
- In term ediate layer*: elast in bres - Deep layer*: collagen bres
◦ Muscle: vocalis
*Form vocal ligam ent
40.1.6 Blood Supply• Superior laryngeal ar tery
◦ Branch of the superior thyroid ar tery (level of hyoid), w hich arises from the external carot id ar tery
◦ Enters larynx via thyrohyoid m em brane w ith in ternal branch of superior laryngeal nerve
◦ Main branch is cr icothyroid ar tery, w hich runs along inferior surface of thyroid cart ilage
• Infer ior laryngeal ar tery ◦ Branch of inferior thyroid ar tery ◦ Enters larynx between infer ior const rictor bres
40.1.7 Nerve Supply• Anatom y
◦ Brainstem (m edulla) at nucleus am biguus ◦ Rootlets leave between olive and pyram id ◦ These m erge to form vagus ◦ Exit skull base at jugular foram en ◦ Descend in carot id sheath ◦ Three branches:
- Pharyngeal n - Superior laryngeal n - Recurrent laryngeal n
• Superior laryngeal n arises from the inferior as-pect of the inferior ganglion of the vagus passing m edial to in ternal and external carot id ar teries giving o 2 branches: ◦ External laryngeal—m otor branch to cricothyroid
◦ In ternal laryngeal—sensat ion to supraglot t is• External branch is close to superior thyroid ar-
tery and runs anteroinferiorly on lateral aspect of inferior const rictor
• In ternal branch passes between the thyrohyoid m uscle and m em brane w ith the superior laryn-geal ar tery piercing the m em brane
• The RLN arises from the vagus in the upper chest w here it loops around arch of aor ta on the left and subclavian ar tery on the right and ascends w ith in the t racheoesophageal groove to enter the posterior larynx at the cricothyroid join t
• Recurrent laryngeal n supplies sensat ion to glot-t is and subglot t is and provides m otor funct ion to all the in t r insic m uscles of the larynx except the cr icothyroid
40.1.8 Lymphatics• Paucity over the t rue VCs• Supraglot t ic and infraglot t ic system s• Supraglot t ic has a cross drainage system and
em pt ies in to superior and m iddle deep cervical nodal basins
• Infraglot t ic system em pties in to infer ior deep cervical and parat racheal nodal basins
40.1.9 Physiology• Funct ions
◦ Airway protect ion ◦ Respiratory funct ion ◦ Swallow ing ◦ Phonat ion
40.1.10 Airway Protection• Prevents saliva and food/drink aspirat ion• Acts as a three-t iered valve: aryepiglot t ic fold,
false and t rue VC star t ing w ith adduct ion of the lat ter
40.1.11 Respiratory Function• Medulla and h igher CNS drive synchronous
opening of the glot t is and diaphragm at ic descent during inspirat ion
• Glot t is opening = prim arily posterior cricoarytenoid (PCA)
• In hyperpnea—cricothyroid contracts rhythm i-cally w ith PCA—increases glot t is aperture
• In bilateral RLN palsy cricothyroid further adducts paralysed VCs—eased by SLN sect ion
• In hypocapnia phrenic nerve and PCA rhythm icity reduced
• When vent ilatory load elim inated, re ex abduc-tor act ivit y of PCA also elim inated—the longer it is lost the longer it takes to re-establish—hence
Philpott_9783131662316_Ch40.indd 148 02/05/14 5:16 PM

149
Anatomy
need to gradually dow nsize t rachy tube prior to decannulat ion
• Tim e of expirat ion dependent on vent ilatory resistance produced by glot t is
• Cr icothyroid con t ract ion du r ing exp irat ion occurs w h en subglot t ic p ressu re ch ange of 30 cm H2O is exceeded an d con t in -ues w h ile posit ive subglot t ic p ressu re is m ain t ain ed—th is th reshold is reduced in hypercapn ia
40.1.12 Swallowing• 3 sphincters rem ain closed on deglut it ion• Larynx elevates on swallow ing to open
cricopharyngeus allow ing t ransit of food in to the oesophagus
• Hyoid bone m oves causing the epiglot t is to t ilt towards the posterior pharyngeal wall closing o the laryngeal in let
40.1.13 Phonation• Motor cortex (precentral gyrus) ® m otor nuclei
in brainstem and spinal cord ® respiratory, laryngeal, and ar t iculatory m uscles
• Fine control exerted by: ◦ Cerebral cor tex ◦ Cerebellum ◦ Basal ganglia
• Laryngeal m uscles star t to contract ~100 to 200 m s prior to onset of phonat ion
• Thyroarytenoid m uscle = m ost im portant in varying phonat ion style
• Thyroarytenoid and lateral cricoarytenoid m uscles show burst-like activity at the start of phonation and weaken during prolonged phonation
• In terarytenoid m uscle has an increased latency of contract ion and regular tone during pro-longed phonat ion
• Frequency of vibrat ion depends on: ◦ Vibratory m ass of both VCs ◦ Anterior to posterior tension ◦ Funct ional damping at h igh pitch ◦ Subglot t ic pressure
• Vibratory cycle has 3 phases: ◦ Opening ◦ Closing ◦ Closed
• Other contributory factors include: ◦ Lung capacity ◦ Pharyngeal, nasal, and oral anatom y
Philpott_9783131662316_Ch40.indd 149 02/05/14 5:16 PM

150
41 Non-neoplastic Laryngeal Pathology
41.1 Conditions Associated w ith Laryngopharyngeal Re ux• Paroxysm al laryngospasm• Laryngeal stenosis• Laryngeal carcinom a• Vocal cord nodules• Globus pharyngeus• Laryngom alacia
41.1.1 Extraesophageal Re ux Scoring Systems• Re ux sym ptom index
◦ Validated and highly reproducible ◦ 9-item quest ionnaire ◦ Scores per item vary from 0 (no problem ) to 5 (severe problem )
◦ Max score 45 ◦ Score > 15 about 90% chance of supra-oesophageal re ux
◦ Item s: - Hoarseness or problem w ith your voice - Clearing your throat - Excessive m ucous or postnasal drip - Di culty swallow ing food, liquid, or pills - Coughing after you ate or lying dow n - Breath ing di cult ies or choking episodes - Troublesom e or annoying cough - Sensat ion of som ething st icking in your throat or a lump in your throat
- Hear tburn , chest pain , indigest ion , or stom ach acid com ing up
• Re ux nding score ◦ Validated ◦ 8-item scale ◦ Based on beropt ic laryngoscopic ndings ◦ Max score 26 ◦ Score m ore >5 is abnorm al ◦ Item s:
- Infraglot t ic oedem a: 0, absent; 2, present - Vent ricular obliterat ion: 0, absent; 2, present; 4, com plete
- Erythem a: 0, none; 2, arytenoids; 4, di use - Laryngeal oedem a: 0, none; 1, m ild; 2, m oderate; 3, severe; 4, polypoid
- Post-com m issure hypert rophy: 1, m ild; 2, m oderate; 3, severe; 4, obst ruct ing
- Granulom a/granulat ion t issue: 0, absent; 2, present
- VF oedem a: 0, none; 1, m ild; 2, m oderate; 3, severe; 4, polypoid
- Thick m ucus: 0, absent; 2, present
41.2 Laryngitis• Acute <3 weeks• Self-lim it ing• Erythem a and oedem a of vocal cord• Typically a ects 18- to 40-year-olds• Aet iology includes vocal m isuse, infect ion
typically viral• Treatm en t: hum idi cat ion , voice rest ,
Cochrane database show ed no evidence for an t ibiot ics
• Chronic >3 weeks• Fluctuat ing dysphonia, chronic cough
(n ight>day), laryngospasm secondary to m ucous st rands
• Consider occupat ional h istory including exposure to toxic substances
• Consider drug h istory: e.g., diuret ics m ay dry m ucosa, calcium channel blockers/n it rates m ay predispose to gast ro-eosophageal re ux disease (GORD) secondary to reduct ion in tone of lower oesophageal sphincter
• Autoim m une causes include: ◦ Granulom atosis w ith polyangiit is (GPA)
- Hem optysis - St ridor - Upper airway narrow ing
◦ Amyloidosis ◦ Relapsing polychondrit is
- May have tender larynx and develop t racheom alacia
• System ic cutaneous causes include: ◦ SLE—nodules, u lcerat ion ◦ Pem phigus ◦ Stevens–Johnson syndrom e ◦ Rheum atoid ar thrit is—paralysis of cricothyroid/arytenoids join t
• Treatm ent: ◦ Conservat ive:
- Avoid st im ulat ing/irr itat ing factors, e.g., cigaret te sm oke
- Treat underlying m edical cause
Philpott_9783131662316_Ch41.indd 150 02/05/14 12:48 PM

151
Funct ional Voice Disorders
- Support ive m easures include good oral hydrat ion , steam inhalat ions
◦ Surgery: - Biopsy to con rm diagnosis
41.3 Chronic Granulomatous Laryngeal Conditions• Tuberculosis: posterior one-th ird larynx m ay
m im ic carcinom a• Sarcoidosis: granulom as, nodules, supraglot t ic
swelling, vocal cord palsy• GPA: subglot t is ± renal involvem ent
41.4 Angioedema• With or w ithout anaphylaxis• Acute allergic h istam ine-m ediated
in am m atory react ion• Acute vascular dilat ion and capillary
perm eabilit y• Oral and laryngopharyngeal st ructures
frequently a ected• Precipitat ing factors:
◦ Medicat ions: - Penicillin - Aspir in - Other non-steroidal ant i-in am m atory drugs
- Angiotensin-convert ing enzym e inhibitors ◦ Food addit ives and preservat ives ◦ Blood t ransfusions ◦ Infect ions ◦ Insect bites
• Hereditary form : ◦ De ciency of C1 esterase inhibitor ◦ Recurrent at tacks of m ucocutaneous oedem a
• Occult lym phom a leading to C1 esterase inhibitor de ciency can occur
• Associated w ith pruritus• Hoarseness present w hen larynx involved• Treatm ent involves:
◦ Adrenaline ◦ Cort icosteroids ◦ Antih istam ines ◦ Am inophylline ◦ Airway m anagem ent as required
• Treatm ent of hereditary form : ◦ Prophylact ic danazol ◦ Fresh frozen plasm a acutely
41.5 Neurological Disorders Causing Laryngeal Dysfunction• Upper m otor neuron disorders:
◦ Cerebrovascular accident (bilateral vocal cord involvem ent)
◦ Parkinson disease (soft voice + other features of Parkinson disease)
◦ Progressive supranuclear palsy ◦ Pseudobulbar palsy—vascular and degenerative disease a ecting cort icobulbar tracts—bilaterally
◦ Mult iple sclerosis ◦ Myoclonus
• Lower m otor neuron disorders: ◦ Amyotrophic lateral sclerosis ◦ Myasthenia gravis—m ay have hypernasal speech/nasal regurgitat ion and dysphagia
◦ Wallenberg syndrom e (posterior ICA occlusion) ◦ Postpolio syndrom e
41.6 Functional Voice Disorders41.6.1 Spasmodic Dysphonias (SD)• Aka laryngeal dystonia• Categories:
◦ Adductor SD—uncontrolled closing of VFs ◦ Abductor SD—prolonged VF opening for voiceless sounds extending in to vowels
◦ VF t rem or—m odulat ions in pitch and loudness m ost evident during prolonged vowels
• Characterist ic features: ◦ Onset between 30 to 50 years of age ◦ 60% fem ale ◦ Aetiology unknow n but believed to be part of a neurological problem w ith other dystonic features, e.g., blepharospasm , dyskinesias, orom andibular dystonia, or t rem or
◦ Re exive and em ot ional aspects of voice funct ion una ected, e.g., coughing, shout ing, laughter
◦ Diagnosed by listening to voice, w hich sounds like pat ient is st rain ing on the toilet
◦ Consider neurology referral to exclude other dystonias
• Treatm ent: ◦ Medicat ion—ant icholinergics e ect ive in 50% cases
◦ Voice therapy ◦ Surgery—Botox, though often requires m ult iple procedures
◦ Surgery on recurrent laryngeal nerve including avulsion procedure
Philpott_9783131662316_Ch41.indd 151 02/05/14 12:48 PM

152
41 Non-neoplast ic Laryngeal Pathology
41.6.2 Paradoxical Vocal Fold Movement• Adduct ion of VFs during inspiratory phase of
respirat ion leading to total obst ruct ion or st r idor• Categories:
◦ Idiopathic focal dystonia ◦ Part of Meige syndrom e ◦ Associated w ith or m asquerading as asthm a ◦ Exercise-induced st r idor ◦ Psychogenic ◦ Associated w ith GORD
41.6.3 Disorders of Vocal Misuse• Muscular tension dysphonia• Voice fat igue syndrom e• Abnorm al loudness—e.g., w ith poor hearing• Abnorm al pitch• False-cord phonat ion
41.6.4 Psychogenic Voice Disorders• Conversion react ion dysphonia—stressor related
to onset of dysphonia• Malingering dysphonia• Pyschogenic dysphonia—stressor is in
in term ediate or distant past• Elect ive m ut ism• Psychogenic overlay
41.7 Laryngocele (Fig. 41.1)• Air- lled dilatat ion of the saccule of the
laryngeal ventr icle• 80% m ale• Mean age 55 years• 30/year in the United Kingdom• Associated w ith vent ricular cancer in 5 to 54%• Aet iology is unknow n• Characterist ic features:
◦ Neck swelling that increases w ith increased in t ralaryngeal pressure
◦ In ternal laryngocele presents hoarseness and dyspnea and st ridor
◦ Sm ooth dilat ion at false-cord level ◦ Acute infect ion w ith pus form at ion (laryngopyocele): pain ± airway obst ruct ion
◦ May expand in ternally through vallecula or externally (m ore com m on) through thyrohyoid m em brane to neck or in com binat ion
◦ May increase w ith increased in t ralaryngeal pressure, e.g., coughing, sneezing
• Invest igat ions ◦ Plain AP/lat soft t issue neck—air- lled sac ◦ CT/MRI fur ther invest igat ion
• Managem ent ◦ Laryngoscopic decom pression if sm all ◦ Lateral external approach larger lesions including excision of upper half thyroid cart ilage
◦ Laser endoscopy (CO2) m arsupializat ion ◦ Direct laryngoscopy + biopsy suspicious lesions
◦ Surgical steps: - Incision in skin crease at or just below hyoid - Incise dow n through platysm a and raise subplat ysm al aps
- Cyst encountered anterior to carot id sheath - Retract st raps, soft t issues excised o cyst then t raced to thyrohyoid m em brane
- Ident ify and preserve superior laryngeal nerve
- If no in ternal par t then do not enter larynx and ligate stum p
- If com bined laryngocele can perform lateral thyrotomy having incised sternohyoid at upper border and ret racted and divide thyrohyoid
41.8 Vocal Cord Nodule (Fig. 41.2)• Aet iology phonotraum a: repet it ive excessive
vibrat ion m ucosa
Fig. 41.1 An internal laryngocele protruding into the right vocal fold.
Philpott_9783131662316_Ch41.indd 152 02/05/14 12:48 PM

153
Laryngeal Cysts
• BM torn at area of m ax am plitude (anterior m iddle ⅓)
• Histologically th ickened basem ent m em brane w ith bronect in w ith in lam ina propria
• Most com m on cause of dysphonia in children• Treatm ent:
◦ Nonsurgical: speech therapy ◦ Surgical:
- CO2 laser (1–3 W, 0.1 s pulse) ▪ Do not go deep to Reinke space, m ucosal preservat ion is key ▪ Risk of webbing at anterior com m issure—consider staged procedure
41.9 Reinke Oedema (Fig. 41.3)• Associat ion w ith sm oking + vocal abuse• Di use polypoidal changes to VFs• Typically bilateral• No de n ite m echanism of injury has been
ident i ed• Accum ulat ion of uid in the super cial layer of
the lam ina propria along length of VF• Treatm ent:
◦ Nonsurgical: speech therapy ◦ Surgical (Fig. 41.4)
- Lateral incision on superior aspect of vocal fold
- Ext ravasat ion of uid before replacing m ucosa
- Avoid dam age to underlying vocal ligam ent
41.10 Laryngeal Cysts• In t racordal cysts are often found w ith in m iddle ⅓ vocal fold
• Can occur throughout larynx including supraglot t is
• Single or m ult iple• Mucus-contain ing• Video uoroscopy to di erent iate• Treatm ent: m arsupialize or enucleate
Fig. 41.2a, ba Vocal fold nodules during respiration. They are bilateral but often of di erent sizes, located in the middle of the
membranous part of the vocal fold.b Vocal fold nodules during phonation. The glot tis has a t ypical hourglass shape. The narrowing is caused by the vocal
fold nodules touching.
ba
Fig. 41.3 Reinke oedema.
Philpott_9783131662316_Ch41.indd 153 02/05/14 12:48 PM

154
41 Non-neoplast ic Laryngeal Pathology
41.11 Vocal Process Granulomas (Fig. 41.5)• M>F• Associated w ith re ux• Arise posteriorly adjacent to vocal process• History of t raum a to larynx, e.g., in tubat ion• May be bilateral• Treatment: cold steel or laser via microlaryngoscopy
41.12 Vocal Fold Polyps (Fig. 41.6)• Typically unilateral• Variable appearance from hem orrhagic to
oedem atous• Felt to arise from phonot raum a w ith a
subm ucosal bleed form ing a haem atom a resolving w ith in am m ation and brosis
Fig. 41.4a–g The principle of surgery for Reinke oedema.a The epithelium over the oedematous area is not sharply demarcated from the surrounding epithelium.b, c An incision or very small excision is made into the epithelium as far laterally as possible on the upper surface of the
bulging vocal fold (b, c).d, e The liquid or gelatinous intercellular material is suctioned (d) or extruded (e) from the lamina propria.f, g Finally, the redundant, stretched epithelium is resected (f) until the wound margins are smoothly apposed (g).
a b
c d
fe
g
Philpott_9783131662316_Ch41.indd 154 02/05/14 12:48 PM

155
Other Laryngeal Lesions
• Histologically norm al basem ent m em brane and bronect in deposits around new vessels
• Polyps usually involve free edge of vocal cord in terrupt ing the m ucosal wave and im peding glot t ic closure result ing in dysphonia
• Can involve superior and inferior aspects of the cord
• Surgical rem oval if h istology doubtfu l or airway comprom ise
41.13 Other Laryngeal Lesions• Chondrom as• Schwannom as*—solitary + encapsulated• Neuro brom as*—m ult iple + unencapsulated• Am yloidosis—larynx m ost com m on site in
respiratory t ract• Sarcoidosis: epiglot t is m ost com m on
*Typically occur on aryepiglot t ic fold
Fig. 41.5 Bilateral intubation granulomas in the carti-laginous part of the glot tis.
Fig. 41.6 A large polyp on the left vocal fold.
Philpott_9783131662316_Ch41.indd 155 02/05/14 12:48 PM

156
42.1 Recurrent Respiratory Papillomas (Fig. 42.1)42.1.1 Epidemiology• Most com m on benign tum our of the larynx• HPV types 6, 11• Bim odal dist r ibut ion: 2 to 3 years; 20 to
30 years; M:F• Incidence 4.5 per 100,000 children and 2 per
100,000 adults• Occurs anyw here from lips to lungs• Ext ralaryngeal spread 30%• VFs, anter ior com m issure, and false cords are
the m ost com m on sites• Aim s of t reatm ent include m aintenance of a safe
airway and laryngeal funct ion , w hile wait ing for resolut ion
• Mechanism of t ransm ission unknow n, possible link to cervical papillom as and vaginal delivery
• Rem ission rate is h igh necessitat ing m ult iple surgeries if presents at ages 6–10 years and con ned to larynx
• Typically presents w ith dysphonia m ay have st r idor and airway obst ruct ion
• Risk of m alignant change 2 to 3%• Seeding risk if t racheostom y perform ed
42.1.2 Treatments• Medical
◦ α -In terferon - Subcutaneous inject ion alternate days for 6 m onths
- Adverse e ects com m on including neurologi-cal im pairm ent , decreased renal funct ion , and hepatocellular dam age
- Cessat ion results in regenerat ion ◦ Cidofovir
- Cytosine nucleot ide analogue - Mechanism of act ion: select ive inhibit ion of viral DNA polym erase and therefore preven-t ion of viral replicat ion and t ranscript ion
- Independent of phosphorylat ion by viral enzym es, unlike acyclovir
- First licensed for use in cytom egalovirus-related ret in it is in AIDS
42 Benign Laryngeal Tumours
Table 42.1 Pros and cons of di erent surgical ap-proaches to recurrent respiratory papillomatosis
Pros Cons
CO2 laserPrecise Plume
Hemostatis Fire risk
Cold steelNo plume
Lack hemostasisNo re risk
Microdebrider Quick Lack hemostasis
- Risk of dysplasia is sam e as spontaneous risk: 2 to 3%
- Risk of renal im pairm ent reduced w ith coadm inist rat ion of probenecid
• Surgery ◦ Anterior com m issure lesions should be staged to avoid r isk of webbing
◦ See Table 42.1
42.1.3 Haemangiomas• Sm all cavernous haem angiom as—supraglot t is
m ost com m on site• Usually seen in adults• Neodym ium -doped yt t r ium alum inum garnet
laser m ay be helpful to lim it bleeding• Capillary haem angiom as congenital and rare in
adults—present w ith dyspnoea in weeks 3–16 of life
Fig. 42.1 Laryngeal papilloma.
Philpott_9783131662316_Ch42.indd 156 02/05/14 12:51 PM

157
Recurrent Respiratory Papillomas
• CO2 laser useful for lat ter variant; som e regress after age 12 years
42.1.4 Other Laryngeal Tumours• Chondrom a• Schwannom a
• Neuro brom a• Adenom a• Granular cell m yoblastom a• Paragangliom a• Leiomyom a• Rhabdom yom a• Fibrom a• Lipom a
Philpott_9783131662316_Ch42.indd 157 02/05/14 12:51 PM

158
43.1 Squamous Carcinoma (Fig. 43.1)• 1% of all m alignancies in Brit ish m en• 85% of all laryngeal m alignancies• 3 to 4 m ale: 1 fem ale• Age 55–65 peak• High incidence = Brazil, United States, India, France• Low incidence = Japan, Scandinavia• Lower social class• African-Caribbean origin• Aet iological factors:
◦ Sm oking ◦ Dark spirit consumption ◦ Asbestos exposure ◦ Form aldehyde exposure ◦ Radiat ion (therapeut ic for thyroid) ◦ Keratosis and leukoplakia
43.2 Squamous Intraepithelial Neoplasia• Keratosis—kerat in form at ion by super cial
layer only• Parakeratosis—nucleus retained abnorm alit y in
super cial layer of kerat in-producing cells• Dyskeratosis—kerat in izat ion w ith in prickle
cell layer• Dysplasia—nuclear variat ion , m itosis, loss of
norm al epithelial layering ◦ Grade I—squam ous cell hyperplasia w ith m ild dysplasia and keratosis
◦ Grade II—keratosis and squam ous cell dysplasia w ith occasional nuclear atypia
◦ Grade III—squam ous cell hyperplasia• Ca in situ—m alignant cells con ned super cially
to basem ent m em brane• Ca in situ shows course abnorm alit ies of
di erent iat ion and nuclear atypia in alm ost all areas of epithelium w ith basal cell proliferat ion and m itoses regards as prem alignant
43.3 Supraglottic Carcinoma (40%)• Classi cat ion
◦ T1—lim ited to 1 subsite of supraglot t is; VF m ovem ent norm al
43 Malignant Laryngeal Tumours
◦ T2—>1 subsite of supraglot t is/glot t is/hypopharynx w ithout xat ion of larynx
◦ T3—lim ited to larynx w ith vocal folds (VF) xat ion and/or invades: postcr icoid/pre-epiglot t ic/tongue base t issues
◦ T4—invades through thyroid cart ilage and/or invades in to soft t issues of neck/thyroid/oesophagus
• Suprahyoid and infrahyoid epiglot t is ◦ Arytenoid ◦ Aryepiglot t ic folds ◦ False cords
• Chance of occult nodal m ets ◦ T1/T2: 16% ◦ T3/4 up to 62%
43.4 Glottic Carcinoma (50%)• Classi cat ion
◦ T1—lim ited to VF (± ant ./post . com m issures) w ith norm al m obilit y - A—one VF - B—both VFs
◦ T2—extends to supraglot t is and/or subglot t is and/or w ith im paired VF m obilit y
◦ T3—lim ited to larynx w ith VF xat ion ◦ T4—invades through thyroid cart ilage and/or extends to other t issues beyond the larynx
• Causes of VF xat ion ◦ Deep invasion w ith involvem ent of at least the thyroarytenoid m uscle
◦ If poster ior part of VF involved, xat ion due to involvem ent of cr icoarytenoid join t /cricoid car t ilage/arytenoid
◦ Perineural invasion of recurrent laryngeal nerve
• Incidence of lym ph node m etastases ◦ <10% T1/2 ◦ 10–37% T3/4
43.5 Subglottic Carcinoma (5%)• Classi cat ion
◦ T1—lim ited to subglot t is ◦ T2—extends to VF(s) w ith norm al or impaired m obilit y
◦ T3—lim ited to larynx w ith VF xat ion ◦ T4—invades through thyroid/cr icoid cart ilage and/or extends to other t issues beyond larynx
Philpott_9783131662316_Ch43.indd 158 02/05/14 12:54 PM

159
Treatment of Laryngeal Carcinoma
• Follow -up reliabilit y• Physician’s preference• Availabilit y of h igh-qualit y im aging• Skilled pathology• Skilled surgeon• Treatm ents
◦ Stage I–II - Surgical resect ion including cold steel or laser.
- Radiotherapy typically 66–74 Gy in 2 Gy fract ions (Prognost ic variables related to favourable outcom e include low tum our volum e <3 cm , m obile vocal folds, lack of subglot t ic spread)
◦ Stage III–IV - Surgery ± post-operat ive radiotherapy ( w ith in 6 weeks of surgery up to 66 Gy) ± chem otherapy dependent on in it ial
Table 43.1 Overall staging grouping for laryngeal carcinomas
Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage II T2 N0 M0
Stage IIIT1–2 N1 M0
T3 N0/1 M0
Stage IVAT4 N0/1 M0
T1–3 N2 M0
Stage IVB T1–3 N2 M0?
Stage IVC T1–4 N0–3 M1
43.6 Overall Staging Grouping for Laryngeal Cancer• See Table 43.1
43.7 Unusual Tumours• Verrucous carcinom a
◦ Consists of unusually well-di erent iated kerat in izing squam ous epithelium arranged in com pressed invaginat ing folds
◦ Warty papillary surface ◦ Clefts between adjacent capillary folds can be t raced to depths of the tum our
◦ In lt rat ion is on a broad base w ith pushing m argins against a st rom a contain ing a prom inent in am m atory react ion
◦ Usual cytological and in lt rat ing grow th pat tern of squam ous carcinom a is absent
◦ Non-aggressive; seldom m etastasizes• Kaposi sarcom a
43.8 Treatment of Laryngeal Carcinoma43.8.1 Factors to ConsiderAll pat ients w ith m alignancy should be discussed in a m ult idisciplinary m eet ing• Perform ance status• Pat ient preference• Previous t reatm ent• Pat ient’s distance from t reatm ent facilit y
Fig. 43.1a, ba Carcinoma of the right vocal fold (T1N0M0). b Carcinoma of the left vocal fold comprising the anterior commissure (T3N2M0).
a b
Philpott_9783131662316_Ch43.indd 159 02/05/14 12:54 PM
160
43 Malignant Laryngeal Tumours
presentat ion/de n it ive pathology and m ult idisciplinary m eet ing opinion
- Concurrent chem o*-radiotherapy - Induct ion chem otherapy† (to shrink dow n tum our bulk) prior to surgery or radiotherapy
*cisplat in/cetuxim ab/5- uorouracil†paclitaxel
◦ Reasons for surgery in T1/2 (endoscopic laser excision) - Severe radiotherapy react ion - Chronic laryngit is - Nasal sepsis - Chronic bronchit is - Industrial area - Lack of adequate local radiotherapy facilit ies
◦ Prognost ic variables related to favorable outcom e w ith radiotherapy - Low tum our volum e (<3 cm 3) - Mobile VF - No involvem ent of ventricle - No deep ulcerat ion - No xat ion of anterior VF - Lack of subglot t ic spread - Only one site involved - Cessat ion of sm oking
43.8.2 Surgical Treatment Options• Microendolaryngeal and laser surgery• Vert ical hem ilaryngectom y, e.g., cordectomy• Horizontal par t ial laryngectomy, e.g.,
epiglot tectomy• Supracricoid (subtotal) laryngectomy• Near-total laryngectomy• Total/extended total laryngectomy
43.8.3 Indications for Partial Supraglottic Laryngectomy• No VF involvem ent• Norm al VF m obilit y• No cart ilage dest ruct ion• No paraglot t ic space involvem ent• No signi cant pre-epiglot t ic space involvem ent• Absence of tongue base involvem ent• No prior radiotherapy• Age <70 years• Good cardiopulm onary reserve• Experienced surgeon
43.8.4 Complications of Surgery• Fistulas• Pharyngeal stenosis• Stom al stenosis• Pharyngeal/stom al recurrence
◦ Stom al recurrence—incidence = 5 to 15% ◦ Anterior stom al recurrence has poor prognosis as it is often w rapped around great vessels in m ediast inum
◦ Stom al recurrence—incidence = 5 to 15% ◦ Causes of stom al recurrence
- Inadequate resect ion w ith +ve m argins - Residual disease in parat racheal nodes - Subglot t ic extension - Tracheostomy perform ed close to tum our prior to resect ion
◦ Classi cat ion—Sisson t ypes - Discrete nodule in superior aspect of stom a—good Px if detected early
- Involvem ent of oesophagus (no infer ior involvem ent)—fair-good Px
- Originates inferior to stom a and has direct extension in to m ediast inum
- Extension laterally under either side of clavicles
◦ Prognosis - Types I and II = 45% 5-year survival - Types III and IV = 9% 5-year survival - 6 m onths survival if no surgical in tervent ion
43.9 Indications for Postoperative Radiotherapy
◦ T4 tum our ◦ Microscopically +ve m argins ◦ Extensive in t ravascular/perineural invasion ◦ T3 tum ours t reated by supraglot t ic laryngectomy
◦ Mutiple +ve nodes in 1st-echelon drainage areas
◦ Extracapsular spread ◦ When both sides of neck have not been t reated surgically
43.10 Radiotherapy Techniques• Supraglot t ic carcinom a
◦ Pat ient supine w ith neck im m obilized in neutral posit ion
◦ Typical eld 8 × 6 cm
Philpott_9783131662316_Ch43.indd 160 02/05/14 12:54 PM

161
Indications for Postoperat ive Radiotherapy
◦ Treatm ent volum e includes: - Whole supraglot t is - Pre-epiglot t ic space - Level II and III nodes
◦ 4 to 6 MV X-rays from linear accelerator ◦ Com m on dose fract ionat ion schedule = 66 Gy in 33 fract ions over 6.5 weeks
◦ Alternat ives = 50–55 Gy in 15 to 20 fract ions over 3 to 4 weeks for 5 days/week
◦ When palpable LNs = 40 Gy in 20 fract ions w ith shielding to m idline
◦ Lower neck t reated w ith 50 Gy in 25 fract ions ◦ 2nd phase of t reatm ent = 26 Gy in 13 fract ions to prim ary tum our and LNs
• Glot t ic carcinom a ◦ Very sm all elds for T1/2 ◦ Fields cent red on VFs (thyroid cart ilage to cricoid)
• Subglot t ic cancer ◦ Volum e includes larynx, upper t rachea, LNs level VI and VII
◦ Wedges used to even out dose dist r ibut ion ◦ Lower corners blocked to shield lung apices
• Postoperat ive radiotherapy ◦ Extralaryngeal tum our extension ◦ Posit ive resect ion m argins ◦ Lymph node (LN) involvem ent (especially if m ult iple nodes or ext racapsular spread)
• Cont inuous, hyperfract ionated, accelerated radiotherapy (CHART) t r ial
◦ Dose of 54 Gy was given in 36 fract ions over 12 days
◦ 3:2 random isat ion either to CHART or to convent ional therapy
◦ Greater response to CHART in younger pat ients (p = 0.041)
◦ Poorly di erent iated tum ours bet ter w ith convent ional radiotherapy (p = 0.030)
◦ Trend towards increasing bene t w ith m ore advanced T stage (p = 0.002)
◦ Evidence of reduced severit y in several late m orbidit ies in favor of CHART
◦ Sim ilar local tum our control was achieved by CHART as com pared w ith convent ional radiotherapy despite the reduct ion in total dose from 66 to 54 Gy support ing the importance of repopulat ion as a cause of radiat ion failure
• Veterans A airs Cancer Study Group: ◦ Random ised cont rolled t r ial (RCT) ◦ 332 pat ients ◦ Stage III/IV disease ◦ Random ised in to: total laryngectomy followed by RT, or chem o (×3 cycles cisplat in + 5FU) + RT
◦ No di erence in survival ◦ 64% chem o-RT preserved laryngeal funct ion
◦ All pat ients w ith advanced laryngeal cancer should be o ered both t reatm ents
Philpott_9783131662316_Ch43.indd 161 02/05/14 12:54 PM
162
44 Vocal Fold Palsy
44.1 Anatomy of Vagus/Recurrent Laryngeal Nerve• Brainstem —m edulla nucleus am biguus• Carot id sheath—between in ternal jugular vein
and in ternal carot id ar tery• Left vagus crossing arch of aorta gives r ise to left
recurrent laryngeal nerve (RLN), w hich ascends in t racheoesophageal groove and then enters larynx at cricothyroid join t
• Right vagus loops around subclavian ar tery to ascend to the larynx
• RLN supplies m otor bres to all the m uscles of the larynx except the cricothyroid m uscle (w hich adducts the vocal cords) and sensat ion to the glot t is/subglot t is and t rachea
• The in terarytenoid m uscle (cont ract ion causes approxim at ion of the arytenoid m uscles closing the posterior por t ion of the glot t is) is the only m uscle w ith bilateral innervat ion
• A paralysed vocal fold (VF) m ay assum e three posit ions: ◦ Adducted ◦ Abducted ◦ Param edian
• Theories that at tem pt to explain th is: ◦ Sem on law: recurrent laryngeal nerve palsy the abductors are a ected before the adductors
◦ Wagner and Grossm an hypothesis relates to cricothyroid act ivit y
◦ Movem ent m ay be present of arytenoids despite VF palsy due to bilateral innervat ion of in terarytenoid m uscles
44.2 Unilateral Vocal Fold Palsy44.2.1 Clinical Features (Fig. 44.1)• Presentat ion
◦ Hoarse voice ◦ Breathy voice ◦ Weak cough ◦ Di cult y in breath ing ◦ Pain ◦ Choking w ith liquids—aspirat ion
• Aet iology ◦ Congenital: hydrocephalus
• Acquired: ◦ Iat rogenic surgery
- Head and neck including thyroid - Vascular: carot id, cardiothoracic - Cervical spine and m ediast inal operat ions
• In tubat ion ◦ Malignancy: thyroid, laryngeal, lung, skull base or oesophageal cancers
◦ Traum a ◦ Idiopathic
44.2.2 Diagnosis• Invest igat ions
◦ Unknow n aet iology: - Chest X-ray - CT skull base to m ediast inum
• Prognosis on recovery: ◦ Elect romyelography—percutaneous placem ent of needle
44.2.3 Treatment• Medical
◦ Bet ter outcom es if VF is m edialized• Surgical
◦ VF inject ion ◦ Laryngeal fram ework surgery
44.2.4 Surgical Treatment Options• Inject ion laryngoplasty
◦ One-way procedure ◦ Can consider inject ion for pat ients w ith lung m alignancy prior to t reatm ent of cancer
◦ Local anaesthet ic inject ion dependent on m aterial t ype and respiratory status
◦ Present injectables: - Collagen: bovine extract decreasing use, check allergy status w ith in t raderm al inject ion before use
- Hyaluronic acid: can inject percutaneously w ith 24/25-G needle; m ay last 4 m onths
- Fat: requires abdom inal fat harvest ± centrifuging, variable survival
Philpott_9783131662316_Ch44.indd 162 02/05/14 12:59 PM

163
Unilateral Vocal Fold Palsy
• Laryngeal fram ework surgery ◦ Isshiki t ype 1 m edializat ion procedure ◦ Materials:
- Silast ic - Gore-Tex - Hydroxyapat ite - Titanium
◦ Surgery bet ter under local anaesthet ic ◦ Assistant perform s nasendoscopy to assess the airway and approxim at ion of glot t is
◦ Window is cut in thyroid car t ilage ◦ Posit ion is dependent on sex:
- In m ales vocal fold is longer and thyroid alae form m ore acute angle, therefore w indow is cut m ore posterior in m ales
◦ Distance from m idline m ay vary dependent on im plant used
◦ Inner perichondrium should be preserved to help prevent im plant ext rusion
44.2.5 Voice Outcome Measures• Voice Handicap Index (VHI):
◦ 30-item quest ionnaire that targets pat ients’ percept ion of their voice
◦ Can be used before or after t reatm ent ◦ Three par ts: funct ional, physical, em ot ional
◦ 10 quest ions in each part ◦ Scored 0–4 (0, never; 1, alm ost never; 2, som et im es; 3, alm ost always; 4, always)
- Calcium hydroxyapat ite: bene t lasts from 3 m onths to 2 years
- Silicone-based im plants: need a gun to inject the im plant via endolaryngeal inject ion , perm anent
- Gel foam : lasts 2 to 3 m onths ◦ Approaches for inject ion:
- Cricothyroid inject upper border of cr icoid to avoid vessels
- Thyrohyoid (needle m ay be too h igh) - Transthyroid - Endolaryngeal: t ransoral (advance bent needle through m outh)
- Microlaryngoscopy: general anaesthet ic ◦ Use local anaesthet ic spray in nose and oropharynx
◦ Consider nebulized lidocaine 10 m L 4% undiluted via u lt rasonic nebulizer
◦ Do not inject anterior par t of larynx as w ill get st rained voice qualit y
◦ Stack system and distal chip endoscopic cam era gives bet ter de n it ion of cricothyroid m em brane w here needle pierces
◦ Di cult situat ions: - Wom en - Obese - Previous t raum a, neck surgery - Atrophic VFs - Com orbidit ies: Parkinson, other m ovem ent disorders
- Supraglot t ic const r ict ion
Fig. 44.1a, ba Palsy of the left vocal fold during respiration, with atrophy of the muscle in the intermediate posit ion. The arytenoid
cartilage is t ilted anteriorly, as there is no pull from the posterior cricoarytenoid muscle.b The same patient during phonation. There is a considerable gap between the vocal folds, causing phonatory
dyspnea.
a b
Philpott_9783131662316_Ch44.indd 163 02/05/14 12:59 PM

164
44 Vocal Fold Palsy
◦ 8 points on any subscale is considered stat ist ically signi cant or a change of 18 points in total score
◦ Shortened version adapted is the VHI-10• Voice Sym ptom Scale (VoiSS):
◦ Most extensively validated self-reported voice m easure available
◦ In it ially a 43-item quest ionnaire reduced to 30 item s
◦ 3 areas: impairm ent (15 quest ions), em ot ion (8 quest ions), and physical sym ptom s (7 quest ions)
◦ Scored 0 to 4 (0, never; 1, occasionally; 2, som e of the t im e; 3, m ost of the t im e; 4, always)
◦ Total score: 120 (impairm ent m ax, 60; em ot ion m ax, 32; physical m ax, 28)
44.3 Bilateral Vocal Fold Palsy44.3.1 Aetiology• Idiopathic• Traum a—arytenoid dislocat ion
◦ Bilateral RLN dam age, e.g., total thyroidectom y ◦ Excessive cu pressures on endotracheal tube
• In am m ation ◦ Cricoarytenoid join t
- Rheum atoid ar thrit is - Gout - System ic lupus erythem atosus
◦ Larynx - Wegener - Amyloidosis - Sarcoidosis - Tuberculosis - Syphilis
• Malignancy ◦ Squam ous cell carcinom a ◦ Verrucous carcinom a
• Radiat ion
• Neurological ◦ Myasthenia gravis ◦ Charcot–Marie–Tooth ◦ Creutzfeldt–Jacob ◦ Mobius syndrom e ◦ Lym e disease ◦ Arnold–Chiari m alform at ion—hydrocephalus/m eningomyelocele
• Metabolic ◦ Diabetes m ellitus ◦ Hypokalem ia ◦ Hypocalcaem ia
44.3.2 Treatment• Treat underlying m edical cause• If from nerve injury consider
elect romyelography• Can m anage airway expectant ly, although any
addit ional insult to airway (e.g., respiratory t ract infect ion) m ay t rigger a m ore severe episode of airway com prom ise, e.g., st r idor
• Consider earlier in tervent ion if poor respiratory reserve
44.3.3 Surgery• Tracheostom y• Posterior cordectomy• Par t ial/ total arytenoidectomy• Suture lateralizat ion• Laryngo ssure w ith posterior
cricoidotomy + stent / graft
44.3.4 Future• Experim ental
◦ Posterior cr icoaryetnoid st im ulat ion ◦ Electr ical st im ulat ion through laryngeal pacing
Philpott_9783131662316_Ch44.indd 164 02/05/14 12:59 PM
165
45.1 Viral Infections (Mumps)• Mostly children• Usually param yxovirus (Rubulavirus)• Infect ion is system ic• 2- to 3-week incubat ion period• 3- to 5-day period of virem ia—localizes in parot id,
germ inal t issues, and central nervous system• Fever, m alaise, headaches• Trism us and dysphagia• Bilateral involvem ent; m ay involve other m ajor
salivary glands• Com plicat ions:
◦ Orchit is—20 to 30% of m ales ◦ Oophorit is—5% of fem ales ◦ Sterilit y rare ◦ Asept ic m eningit is 10% ◦ Pancreat it is 5% ◦ Sensorineural hearing loss 0.5 to 4% (rapid onset , profound, perm anent , and unilateral)
• Con rm diagnosis w ith viral serology• Frontal bullar cell shows raised w hite cell count
(lym phocytes)• Support ive t reatm ent
45.2 Sjögren Syndrome (Fig. 45.1)• Chronic autoim m une disorder• 44× r isk of developing lym phom a• Schirm er test—docum ents lacr im at ion• Slit lam p exam inat ion—corneal ulcerat ions• SS-A (ant i-Ro) 38 to 60%; ELISA—95%• SS-B (ant i-La) 25 to 40%; ELISA—87%• Autoant ibodies not speci c• Minor salivary gland biopsy used to
diagnose—95% speci cit y
45.3 Acute and Chronic Bacterial Infections• Bacterial sialadenit is m ost com m on in parot id• Chronic picture w ith acute exacerbat ions
possible• Ret rograde t ransm ission from oral cavity or
stasis of salivary ow• Stone form at ion m ay be causat ive
• Elderly pat ients at r isk due to m edicat ions that reduce salivary ow: ◦ Diuret ics ◦ Antidepressants ◦ β-blockers ◦ Ant icholinergics ◦ Ant ih istam ines
• Staphylococcus aureus m ost com m on organism ; others: ◦ β-haem olyt ic st rep ◦ H. in uenzae ◦ Pneum ococcus ◦ Gram –negat ive organism s
• May progress to abscess form at ion• If failure to respond to ABx, consider:
◦ Lymphom a ◦ Cat-scratch disease ◦ Sjögren syndrom e ◦ Granulom atosis w ith polyangiit is (form erly know n as Wegener granulom atosis).
• Ant ibiot ics for gram -negat ive and anaerobes• Sepsis and m ult iorgan failure possible in
debilitated pat ients
45.4 Chronic Sialadenitis (Fig. 45.1)• Recurrent low -grade in am m ation and oedm ea
of the gland• Strep. viridans = o ending organism• Need to encourage salivary ow• Benign lym phoepithelial lesions m ay arise• Ident ify any stones/st r ictures• May have sym ptom -free periods• Surgical excision for refractory cases (Fig. 45.2)• Sialoendoscopy (see end of chapter)
45.5 Sialolithiasis (Fig. 45.1)• 80% a ect subm andibular gland• 1.2% general populat ion• Subm andibular predisposing factors include:
◦ More viscous consistency ◦ Wharton duct has a superior course ◦ Gland is dependent
• Im aging: ◦ Most im aging m odalit ies can detect calculi: p lain radiograph (80–95% subm andibular and
45 Non-neoplastic Salivary Gland Disease
Philpott_9783131662316_Ch45.indd 165 02/05/14 1:02 PM

166
45 Non-neoplast ic Salivary Gland Disease
70% parot id stones); US (90% if >2 m m ); CT—noncontrast (as vessels m ay m im ic stones) is good for detect ing m ult iple sm all stones
◦ MRI is good at evaluat ing ductal system , e.g., st r ictures but m ay m iss sm all stones
◦ In noncalculi disease then MRI m ay be considered
◦ Autoim m une condit ions have dist inct ive picture w ith pruned, t runcated m ain ducts, and globular collect ions peripherally
◦ Sialography - Contrast injected in to the duct m ay show stones, st r ictures, and help “ ush” the system
- Cont raindicated in acute infect ion ( recom m end US)
- May cause t raum a to duct and subsequent st r icturing
- MRI sialography m ay replace the convent ional technique
• Treatm ent: ◦ Transoral rem oval if in distal duct system ◦ Subm andibular gland excision for m ore proxim al stones
◦ Be aware of retained stone in distal par t of duct w hen rem oving gland, w hich can result in cont inuing infect ions - Sialoendoscopy
45.6 Non-parotid Swellings in Parotid Region• Mandibular tum our• Enlarged m asseter m uscle
Fig. 45.1a–e Typical sialograms.a A normal submandibular gland.b Chronic recurrent obstructive parotitis with ectasia of
the acini and terminal ducts, showing a “tree in leaf” appearance. The excretory duct shows a “string of beads” pat tern.
c A stone in the submandibular duct. There is ectasia due to retention of secretions and extensive paren-chymatous atrophy.
d Chronic nonobstructive parotit is, showing an “apple tree in bloom” appearance.
e The “ripe tree,” “bare tree,” and “frosted tree” pat-terns seen in di erent stages of ductal rarefaction and parenchymal atrophy, such as that occurring in Sjögren syndrome.
a
b
ed
c
Fig. 45.2 Removal of the submandibular gland. 1, submandibular gland; 1a ligated submandibular duct; 2, anterior belly of the digastric muscle; 3, stylohyoid muscle, covered by the posterior belly of the digastric muscle; 4, horizontal ramus of the mandible; 5, facial artery and vein ligated; 6, marginal mandibular branch of the facial nerve (must be preserved, as it innervates the muscles of the lower lip); 7, lingual nerve; 8, hypo-glossal nerve.
75
5
8
4
1
6
3
2
1a
Philpott_9783131662316_Ch45.indd 166 02/05/14 1:02 PM

167
Sialoendoscopy
• Non-parot id cysts• Schwannom a facial nerve
45.7 Sialoendoscopy• Indicat ions:
◦ Stones <6 m m ◦ Strictures (m ore com m on in parot id)
• Cont ra indicat ions: ◦ Acute sialadenit is
• Technique: ◦ Incise/dilate duct opening ◦ Saline then used to dilate ducts ◦ Stones: grasping, w ire basket (stones <4 m m in subm andibular and <3 m m in parot id gland) and fragm entat ion w ith lithot ripter or laser and subsequent rem oval (3–6 m m stones)
◦ Stent insert ion after stone rem oval ◦ Strictures can be dilated w ith a 3-m m balloon or dilator
Philpott_9783131662316_Ch45.indd 167 02/05/14 1:02 PM

168
46 Major Salivary Gland Tumours
46.1 Benign Tumours• Pleom orphic adenom a—m ost com m on in
parot id, 1% risk of m alignant change per year after 10 years
• Warth in (papillary cystadenom a lym phom atosum )—sm oking risk factor, 10% bilateral, M:F 5:1
• Monom orphic adenom a—m ost com m on is basal cell adenom a
• Oncocytom as—m ore com m on in elderly
46.2 Parotid Tumours• 80% benign• Most com m on pleom orphic adenom a• Invest igat ions
◦ Fine needle aspirat ion (FNA) ± US guided - Pros—preop planning and pat ient counselling - Cons—m ost likely t reatm ent is surgical so result does not change plans
◦ CT/MRI - Pros—deep lobe com ponent can be ident i ed, good for preop planning and counseling; lymph nodes not detected clin ically m ay be ident i ed therefore a ect ing t reatm ent plan; in lt rat ive m argins m ay raise possibilit y of m alignancy
- Cons—if no nodes palpable, unlikely to change t reatm ent
46.3 Submandibular Tumours• 50% benign• Invest igat ions
◦ FNA ± US guided - Pros—treatm ent planning - Cons—m anagem ent of non-diagnost ic sam -ples; som e laboratories require larger cellular volum es to diagnose lym phom as
46.4 Minor Salivary Gland Tumours• 25% benign• Can occur w ith in sinuses, nasal cavity, and
larynx
• Invest igat ions ◦ Biopsy under local anaesthet ic or general anaesthet ic
◦ CT/MRI to evaluate the extent of tum our and nodal status
46.5 General Notes on Salivary Gland Malignancy• Epidem iology
◦ 1 to 2/100,000 ◦ 3 to 4% total head and neck m alignancy ◦ 25% parot id, 50% SM glands, 75% m inor salivary glands
◦ Risk factors include: RT exposure and occupat ional silica dust (blast furnaces, cem ent , glass, ceram ic, and clay indust ries) and n it rosam ine (rubber and t ire indust ries)
◦ Mucoepiderm oid m ost com m on (inc. children) ◦ In children 65% tum ours are benign, w ith haem angiom as being the m ost com m on
• Presentat ion ◦ Typically pain less neck swelling ◦ CN VII n weakness indicat ive of m alignancy ◦ Malignancy norm ally >6th decade ◦ Benign tum ours norm ally >4th decade
46.6 Malignant Tumours• Mucoepiderm oid carcinom a—m ost com m on
m alignant tum our, graded: low, m edium , h igh• Adenoid cyst ic carcinom a—m ost com m on
subm andibular gland m alignancy, increased risk perineural invasion, lung m etastases m ore com m on than nodal
• Acinic cell carcinom a—low -grade neoplasm , late recurrences even after 30 years
• Adenocarcinom a—classi ed in to low - and high-grade types
• Squam ous cell carcinom a—consider lym ph node m etastases from m elanom a, skin
• Carcinom a ex-pleom orphic adenom a—long-standing h istory of parot id swelling w ith rapid increase in size, aggressive, 5-year survival 40%
• Salivary duct carcinom a—poor prognosis, 50% present w ith nodal m etastases
• Lymphom a—m ay require trucut biopsy to diagnose
Philpott_9783131662316_Ch46.indd 168 02/05/14 1:07 PM

169
Malignant Tumours
46.6.1 Staging of Salivary Gland Malignancies• See Table 46.1• T1—≤2 cm• T2—2 to 4 cm• T3—extraparenchym al extension w ithout VII n
involvem ent and <6 cm• T4—invades skull base, VII n and/or >6 cm
46.6.2 Presentation of Facial Nerve Paralysis in Malignant Tumours• Poorly di erent iated carcinom a—23 to 26%• Adenoid cyst ic carcinom a—23 to 26%• Carcinom a ex-pleom orphic adenom a—9 to 14%• Acinic cell carcinom a 3%
46.6.3 Treatment for Parotid Malignancy• Most com m on is surgery ± postoperat ive
radiotherapy (PORT)• Operat ions include:
◦ Super cial parot idectomy + VII n preservat ion ◦ Total parot idectomy ± excision of VII n + graft ing
- ± Excision skin w ith free ap or keystone repair
- ± Neck dissect ion - ± Pinnectomy - ± Petrosectomy - ± Tem porom andibular join t excision
46.6.4 Treatment for Submandibular Malignancy• Most com m on is surgery ± PORT
◦ Subm andibular gland excision ± neck dissect ion
46.6.5 Treatment for Minor Salivary Gland Malignancy• Dependent on site of tum our m ay require
jaw split
46.6.6 Complications of Parotidectomy• VII n injury• Frey syndrom e
◦ 10% complain; dem onstrable in 90% ◦ Only 10 to 15% require further t reatm ent ◦ Most resolve spontaneously in t im e ◦ Best t reated w ith ant iperspirant (alum inum chloride hexahydrate)
◦ Alternat ives are topical ant icholinergics and Botox
◦ Surgical intervent ions include: - Tym panic neurectomy - Sect ion of auriculotem poral nerve - In terposit ion of fascia lata/fat - Stellate ganglion blockade - In t racranial neurolysis of IX n - Elevat ion of SMAS ap at t im e of parot idectomy
• Num bness of the ear• Salivary stula• Xerostom ia
46.6.7 Complications of Submandibular Gland Removal• Marginal m andibular branch of VII n
(perm anent in 7%)• Lingual nerve• Hypoglossal nerve• Recurrent swelling if excision for calculi and
stone retained in distal duct
Table 46.1 Staging of salivary gland tumours
Stage I T1–2 N0 M0
Stage II T3 N0 M0
Stage III T1–2 N1 M0
Stage IV
T4 N0/1 M0
T3 N1 M0
T1–4 N2/3 M0
T1–4 N0–3 M1
Philpott_9783131662316_Ch46.indd 169 02/05/14 1:07 PM

170
47.1 Oral Manifestations of Systemic Diseases47.1.1 Infections• Measles—Koplik spots• Varicella zoster virus (VZV) (chickenpox)—vesicles
47.1.2 In ammatory Disorders• Behçet syndrom e
◦ Rare ◦ Recurrent oral and genital u lcers ◦ Ocular in am m ation
• Reiter syndrom e ◦ Uncom m on ◦ Urethrit is ◦ Uveit is ◦ Conjunct ivit is ◦ Arthrit is ◦ Tongue ulcers m ay be m istaken for geographic tongue
• Granulom atosis w ith polyangiit is ◦ Gingival hyperplasia ◦ Lingual, palatal, and buccal ulcers also com m on
• Erythem a m ult iform e ◦ Mult iple erosions of lip and tongue
• Pem phigus/pem phigoid (Fig. 47.1) ◦ Autoim m une vesicobullous disorders ◦ 90% of pemphigus pat ients w ill have oral cavity involvem ent
• Kawasaki disease (m ucocutaneous lym ph node syndrom e) ◦ Straw berry tongue ◦ Dry ssured lips ◦ Pharyngeal inject ion ◦ Necrot izing pharyngit is
• Sjögren syndrom e ◦ Keratoconjunct ivit is ◦ Xerostom ia—ulcers of tongue, lips, and buccal m ucosa
◦ Arthrit is• SLE
◦ Xerostom ia ◦ Petechiae, haem orrhagic bullae, and w hite keratot ic plaques on tongue and oral m ucosa
47.1.3 Miscellaneous Disorders• Vitam in C de ciency (scurvy)
◦ Swollen red gingival u lcerat ive oral petechiae ± haem orrhage
◦ Stom at it is• Vitam in B2 de ciency
◦ Glossit is ◦ Angular chelit is ◦ Oral burning
• Vitam in B12/folate de ciency ◦ Recurrent oral u lcers ◦ Painful at rophy of oral m ucosa and tongue ◦ Necrot izing ulcerat ive gingivit is ◦ Angular chelit is
• Throm bocytopaenia ◦ Petechiae ecchym oses and haem orrhages
• Polycythem ia ◦ Purple-blue discolourat ion of tongue and gum s
• Leukaem ia ◦ Gingival hyper t rophy
47.2 Infections47.2.1 Viral Infections• Herpangia
◦ Coxsackie viruses ◦ Mult iple sm all vesicles and super cial u lcers—posterior oropharynx
• Hand-foot-and-m outh disease ◦ Coxsackie A virus ◦ Anterior oral cavit y
• Herpes sim plex ◦ Either prim ary or recurrent secondary ◦ Com m on in preschool children ◦ Di use bilateral lymphadenopathy com m on ◦ Painful ulcerat ion ◦ Precipitat ing factors for recurrent t ype:
- Sunlight - Fever - Bacterial infect ions - Stress - Im m unode ciency - Other system ic illness
• Herpes zoster (VZV) ◦ Lesions along V2 and V3
◦ Uncom m on in infants and children
47 Diseases of the Oral Cavity and Oropharynx
Philpott_9783131662316_Ch47.indd 170 02/05/14 1:10 PM

171
Infect ions
• Cytom egalovirus infect ion ◦ Large ulcers ◦ Exudat ive pharyngotonsillit is ◦ Cervical lym phadenopathy
• Infect ious m ononucleosis• HIV
◦ Oral candidiasis ◦ Recurrent herpet ic and aphthous ulcers ◦ Angular cheilit is ◦ Hairy leukoplakia ◦ Periodont it is and gingivit is ◦ Papillom as ◦ Di use parot it is ◦ Kaposi sarcom a (Fig. 47.2)
• Recurrent respiratory papillom atosis ◦ Recurrences in oral cavity uncom m on after com plete excision
47.2.2 Bacterial Infections• St reptococcus (scarlet fever)
◦ Group A β-haem olyt ic st rep m ay cause severe pharyngit is
◦ Sym ptom s sim ilar to tonsillit is ◦ Straw berry tongue ◦ Cervical lym phadenopathy ◦ Penicillin /am oxicillin Rx
• Diphtheria ◦ Necrot izing pharyngit is
◦ Severe erythem a and th ick pseudom em brane ◦ May spread to larynx and t rachea
• Syphilis (and gonorrhoea) ◦ Hypoplast ic teeth w ith notching of central incisors in congenital syphilis
◦ Chancre = prim ary lesions ◦ Secondary super cial ulcers m ay occur ◦ Tert iary lesions = gum m as of palate
47.2.3 Fungal Infections—Candidiasis• Predisposing condit ions:
◦ Long-term ABx ◦ Diabetes m ellitus ◦ Steroid therapy ◦ Im m unosuppression
• Pseudom em branous candidiasis (thrush) ◦ Com m on in infants ◦ Fine w hite lacey plaques w ith raw surface if rem oved
◦ Burning, dryness, and oral pain• Acute at rophic candidiasis
◦ Long-term im m unosuppression w ith ABx/steroids/other
◦ Foul taste ◦ Ulcerated red m ucosa
• Angular cheilit is
Fig. 47.1 Pemphigus. Two large, isolated serous bullae on the soft palate. The bullous stage is very short, so that this stage is rarely observed. Usually, the ruptured shreds of the blister membrane are all that can be seen.
Fig. 47.2 Kaposi sarcoma. The gingiva is the second most common location for oral Kaposi sarcomas. Proceeding from uncharacteristic swelling of the gums, blue-black changes with bleeding develop.
Philpott_9783131662316_Ch47.indd 171 02/05/14 1:10 PM

172
47 Diseases of the Oral Cavit y and Oropharynx
47.3 Miscellaneous Conditions47.3.1 Leukoplakia• Prevalence of 0.1 to 5%• Malignant t ransform at ion in 2 to 6%• If keratosis present r isk of m alignancy increases• Hairy leukoplakia suggests AIDS
47.3.2 Aphthous Stomatitis• Possibly altered cellular im m une response• Older children and adolescents—init ial
presentat ion• Fem ale > m ale• Prodrom e of t ingling/burning 24 to 48 h before
they appear
Minor Aphthous Ulcers• 80% of cases• Painful, shallow• <0.6 cm in size• Resolve w ith in 2 weeks• Recur in 1- to 5-m onth in tervals
Major Aphthous Ulcers• 1 to 5 ulcers >0.6 cm and m ore painful• May also occur on soft palate, oor of m outh ,
and peritonsillar area• Persist for 3 to 6 weeks and m ay leave a scar
Herpetiform Ulcers• Crops of m ult iple painful pinpoint ulcers• May coalesce leaving large irregular ulcers• Persist for 1 to 2 weeks• Recur at 1- to 3-year in tervals
Treatment• Topical cor t icosteroids/lidocaine• Mouthwashes• In t ralesional/system ic cor t icosteroids and
acyclovir m ay help severe cases
47.3.3 Lichen Planus (Fig. 47.3)• Prim arily m iddle-aged adults• Unknow n cause—possible cell-m ediated im -
m une response disorder• Usually found on tongue, buccal m ucosa, and
gingival• May follow course of exacerbat ions and
rem issions• Ret icular form = m ost com m on—sm all w hite
papules (± Wickham st riae)• Erosive form = painful ulcers• Treat as for aphthous ulcers if sym ptom at ic
47.3.4 Burning Mouth Syndrome• Peri- and postm enopausal wom en• Burning on t ip and lateral border of tongue• Norm al appearance clin ically• Neuropathic t reatm ent w ith am it r ipt yline,
clonazepam , etc.
47.3.5 Median Rhomboid Glossitis• Congenital disorder due to persistence of
tuberculum impar• Rhom boid area free of papillae on dorsum of
tongue• Som e cases associated w ith candida infect ion
Fig. 47.3 Lichen planus (lichen ruber). Bluish-white papules with a mother-of-pearl shimmer, small and sharply bordered, posteriorly connected by ne lines forming a network. Delicate shapes are seen, usually with a symmetrical distribution. Leukoplakia and mucous plaques need to be included in the di erential diagnosis.
Philpott_9783131662316_Ch47.indd 172 02/05/14 1:10 PM

173
Miscellaneous Condit ions
47.3.6 Geographic Tongue (Benign Migratory Glossitis)• All age groups• Prevalence of 1 to 2%• May be inherited• Loss of liform papillae• W hite m argin of desquam at ing ep ithelium
of var ious shapes and sizes on dorsum of tongue su r rounding a cen t ral red at roph ic area
• Lesions disappear and m igrate to other areas of tongue
• May persist for years• No t reatm ent required
47.3.7 Fissured Tongue• Mult iple ssures or grooves on dorsum
of tongue• Usually asym ptom at ic• May becom e sym ptom at ic if food/bacteria/
fungi get t rapped in ssures• Associated w ith genet ic disorders, e.g., Dow n
syndrom e• No t reatm ent required
47.3.8 Hairy Tongue• Hypert rophy and grow th of liform papillae• May becom e colonized w ith pigm ented
bacteria—com m only black• Predisposing factors:
◦ Tobacco abuse ◦ Oral ABx ◦ Poor oral hygiene ◦ Radiat ion therapy
• Benign and usually asym ptom at ic• Long papillae m ay be t reated w ith brushing
47.3.9 Macroglossia• Relat ive m acroglossia
◦ Pierre–Robin syndrom e ◦ Dow n syndrom e, etc.
• Prim ary m acroglossia ◦ Hypothyroidism ◦ Acrom egaly ◦ Beckw ith–Wiedem ann syndrom e
47.3.10 Ranulas• See Chapter 56: Benign Neck Disease
Philpott_9783131662316_Ch47.indd 173 02/05/14 1:10 PM

174
48 Tumours of the Lip and Oral Cavity
m axillary sinus, tooth socket (super cial erosion alone is insu cient)
• T4b—invades m ast icator space, pterygoid plates, or skull base or encases the carot id a
48.1.5 Repair of Defects• Verm ilion
◦ Mucosal advancem ent• Lower lip
◦ <1/3—prim ary closure ◦ 1/3 to 2/3—Abbe*, Abbe Estlander, or Karapan-dzic aps
◦ >2/3—bilateral Gillies fan aps, axial scalp ap, or free t issue t ransfer
• Upper lip ◦ <1/3—prim ary closure or Abbe ap ◦ 1/3 to 2/3—reverse Karapandzic or perialar advancem ent
◦ >2/3—com binat ion periala advancem ent or above techniques
• Com m issure ◦ Abbe Est lander, double rhom boid aps, or free t issue t ransfer
* Full-thickness com posite ap involving transfer of skin, m uscle, and m ucosa from central part of low er lip to up-per lip, aka a cross ap. Flap is based on labial vessels
48.1.6 Aftercare follow ing Lip Lesion Excision• No sucking• Keep wound clean by rem oving crusts tw ice a
day• Bactroban or fucidin m ay be applied• Half of external sutures m ay be rem oved at 3 to
4 days; rest rem oved at 1 week as appropriate• Soft diet• Abbe lip sw itch:
◦ Feed pat ient w ith feeding cup or st raw ◦ Transect pedicle after 3 weeks as second stage and com plete suturing
48.1.7 Other Treatment Modalities• 300 kV orthovoltage X-ray therapy: 50 Gy in 15
fract ions over 3 weeks
48.1 The Lip48.1.1 Surgical Pathology• 6/1,000,000• 93% lower lip, 5% upper, 2% angle• 2:1 m ale to fem ale• 6th decade
48.1.2 Risk Factors• White European ethnicit y (×10) especially Celt ic
descent• Cigaret te/pipe sm oking• Poor dental hygiene• Chronic alcoholism (com bined w ith sm oking is
15× increased risk)• Chron ic erosive skin d iseases, e.g., lichen
planus• Im m unosuppression• Outdoor occupat ion
48.1.3 Tumour Type• Squam ous cell carcinom a (SCC) (98%)
◦ Exophyt ic (com m onest) ◦ Verrucous ◦ Ulcerat ive
• Rare lesions ◦ Melanom a ◦ Sarcom a ◦ Salivary gland tum ours (m ucoepiderm oid/
adenoid cyst ic ca) ◦ Myoblastom as ◦ Pyogenic granulom as ◦ Keratocanthom a ◦ Granulom atous cheilit is, e.g., syphilis, sarcoid
• Upper lip and angular lesions m etastasize sooner
• <10% of lower lip lesions present w ith LN m ets
48.1.4 Staging• T1—≤2 cm greatest dim ension• T2—2 ≤4 cm• T3—>4 cm• T4a—invades adjacent st ructures e.g., cort ical
bone, inf. alveolar nerve, deep m uscle of tongue,
Philpott_9783131662316_Ch48.indd 174 29/04/14 3:35 PM

175
Oral Cavit y
Channels of Spread of Tumours• Sm all bony canals in hard palate• Greater and lesser palat ine foram ina• Lateral incisive foram ina
48.2.2 Surgical PathologyMalignant Tumour Types• SCC (85%) 3 t ypes—exophyt ic, ulcerat ive,
in lt rat ive• Malignant salivary (5%)—adenoid cyst ic,
m ucoepiderm oid• Melanom a (1%)• Hodgkin lym phom a (0.1%)• Fibrosarcom a (0.5%)• Metastases to tongue—breast , lung, kidney m ost
com m on
Sites of Squamous Carcinoma• Tongue (lateral border; Fig. 48.1) (35%)• Floor of m outh (30%)• Lower alveolus (15%)• Upper alveolus (5%)• Buccal m ucosa (10%)• Hard palate (3%)• Retrom olar (2%)• Synchronous prim ary 10–15% larynx,
oesophagus, lungs
Risk Factors• Sm oking-nit rosam ines• High alcohol in take• Dental caries• Betel nut /tobacco chew ing
• In terst it ial therapy—rigid needles contain ing cesium
48.2 Oral Cavity• Variable worldw ide incidence but accounts for
50% of all cancers in India• Male:fem ale rat io 3–4:1• More frequent after 5th decade of life
48.2.1 Anatomical RegionsSubsites• Buccal m ucosa
◦ Mucosal surfaces of upper and lower lips ◦ Mucosal surfaces of cheeks ◦ Retrom olar areas ◦ Buccoalveolar su lci, upper and lower
• Upper alveolus and gingiva• Lower alveolus and gingiva• Hard palate• Tongue—anterior 2/3• Floor of m outh
Sites of Minor Salivary Glands• Subm ucosa of inner surface of lips• Ret rom olar (parot id duct vicin it y)• Mucous m em brane of cheek• Floor of m outh• Lesser sublinguals (near m ajor sublingual)• Glossopalat ine (poster ior to lesser sublinguals)• Palat ine—hard and soft palate and uvula (not
m idline)• Lingual—inferior surface of tongue on each side
of frenulum and at base and lateral borders of tongue
Fig. 48.1a, b Carcinoma of the lateral tongue.
a b
Philpott_9783131662316_Ch48.indd 175 29/04/14 3:35 PM

176
48 Tumours of the Lip and Oral Cavity
Hard Palate Tumours• Minor salivary gland m alignancy (m ucoepider-
m oid, adenoid cyst ic carcinom a) followed by SCC m ost com m on aet iology
• Rarer pathology includes sarcom a, m elanom a, or lymphom a
• Presentat ion ◦ Swelling roof m outh ◦ Ill- t t ing dentures ◦ Nasal obst ruct ion w ith extension in to nose and m axillary sinus
◦ Trism us w ith poster ior extension involving pterygoids
◦ Middle ear e usion w ith extension in to the nasopharynx, eustachian tube
◦ Absent corneal re ex or palatal hypesthesia from invasion of m axillary division of t r igem i-nal n in the sphenopalat ine fossa
◦ Masseter or tem poralis wast ing from invasion of m andibular division of t r igem inal n
◦ Gingiva involvem ent w ith extension to upper or lower alveolus via dental sockets w ith loosening of teeth
◦ Lymph node involvem ent (levels I and II) in up to 30% of SCC ± ret ropharyngeal nodes
48.2.5 Overall Staging for Oral and Lip Tumours• See Table 48.1
48.2.6 Prognostic Factors• Site• Depth• Histology type
• Hum an papillom avirus• Chronic glossit is• Malnutr it ion• Syphilis• Cirrhosis• Plum m er–Vinson syndrom e*• Lichen planus• Chronic hyperplast ic candidiasis• HIV• Xeroderm a pigm entosa• Congenital dyskeratosis• Subm ucosal brosis• Discoid lupus• Reverse sm oking (Chut ta, pract iced in India) in
hard palate cancer
* Achlorhydria; iron de ciency anaem ia; and m ucosal atrophy of the m outh, pharynx, and oesophagus
48.2.3 Premalignant Conditions• Leukoplakia* (average ~5%)• Erythroplakia (75–90% show ca, ca in situ , or
severe dysplasia)• Speckled leukoplakia (m ixed w hite and red
patches) increased risk of m alignancy com pared w ith leukoplakia alone
* DDx-pem phigus, pem phigoid, lichen planus, candida, ill- t t ing dentures, oral hairy leukoplakia
48.2.4 Biopsy Oral Lesions• Incisional recom m ended• Biopsy red part if speckled leukoplakia• Stain ing w ith tolu id ine blue and Lugol’s
iodine m ay help locate best biopsy site if m ult ip le areas
Aggressive Features of Posterior Tongue Tumours• Increased incidence of LN m ets• Tum our can spread to tonsillar pillars, ret rom o-
lar area, and oor of m outh• Large invasive carcinom as can extend beneath
in tact m ucosa in to m uscles of posterior th ird of tongue and thence pre-epiglot t ic space
• Tum our extends w ith in m usculature of tongue part icularly in posterior direct ion beneath in tact m ucosa
Table 48.1 Overall staging for oral and lip tumours
Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage II T2 N0 M0
Stage III T1/2 N1 M0
T3 N0/1 M0
Stage IVA T4 N0/1 M0
T1–3 N2 M0
Stage IVB T1–3 N3 M0
Stage IVC T1–4 N0–3 M1
Philpott_9783131662316_Ch48.indd 176 29/04/14 3:35 PM

177
Oral Cavit y
• Lateral border of tongue ◦ In terst it ial irradiat ion ◦ Part ial glossectomy ◦ (External beam radiotherapy)
• Anterior oor of m outh ◦ No bony invasion—soft -t issue reconst ruct ion w ith pec m ajor ap or rad ial free forearm ap
◦ Bony invasion—rim resect ion of m andible and reconst ruct ion as above
◦ ± in terst it ial radiotherapy• Lateral oor of m outh and lower alveolus
◦ Rim resect ion for early invasion ◦ Rem ove oor of m outh w ith part ial m andibulectomy if m ore extensive bony involvem ent
◦ If m odi ed radical neck dissect ion/radical neck dissect ion perform ed at sam e t im e = com m ando procedure
◦ Reconstruct w ith pec m ajor or radial forearm free ap
• Di erent iat ion• Perineural spread• Level and size of LN m ets• Mandibular invasion
48.2.7 Radiology in Oral/Lip Tumours• Orthopantogram
◦ Show state of dent it ion and posit ion of m ental foram en
◦ Assess m andibular invasion• Chest X-ray—chest m ets• CT/MRI*
◦ Site/size/extent of prim ary ◦ Depth of tum our ◦ Mandibular invasion ◦ Assess neck ◦ Assess chest/abdom en
• Posit ron em ission tom ography ◦ Com bined w ith CT ◦ Good di erent iat ing between brous t issue and recurrence
* MRI advantage T2-w eighted im ages show ed increased t issue contrast betw een norm al m uscle and tum our. No dental artefact.
48.2.8 Surgical Treatment of Oral Cavity Tumours• Access to oral cavity (Fig. 48.2):
◦ Peroral ◦ Lip split w ith sym physeal or param edian m andibulotomy
◦ Lateral m andibulotomy ◦ Mandibulectomy ◦ Pull-through procedure ◦ Upper lip split
• Leukoplakia—cold steel/ laser excision• Buccal carcinom a
◦ Sm all tum ours—local excision only ◦ Sm all tum our w ith surrounding leukoplakia—skin graft
◦ Larger tum ours—radiotherapy ◦ Bone erosion (upper alveolus only)—bipaddled deepithelialized m iddle segm ent radial free forearm ap
• Tip of tongue—V-shaped excision• Dorsum of tongue
◦ <2 cm —excise w ith ellipse ◦ >2 cm —radiotherapy ± in terst it ial im plant
Fig. 48.2 Routes of access for tumours of the mouth and pharynx. 1, transoral; 2, temporary mandibulotomy; 3, suprahyoid median pharyngotomy; 4, subhyoid median pharyngotomy; 5, lateral pharyngotomy.
1
2
3
4
5
Philpott_9783131662316_Ch48.indd 177 29/04/14 3:35 PM

178
48 Tumours of the Lip and Oral Cavity
Mandibulotomy• Aftercare
◦ Trachy kept in for 1 week ◦ (Pre-op percutaneous endoscopic gast rostomy or PEG)—star t soft diet after 10 days; star t to chew after 6 weeks
◦ No dentures worn for 2 to 3 m onths; then insert epithelial in lay
◦ Consider for osseointegrated im plants ◦ Cont inued dental care
• Com plicat ions ◦ Bleeding from tongue ◦ Non-union of m andible ◦ Poor speech ◦ Recurrence in prim ary site ◦ Recurrence in nodes
Radiotherapy• Prim ary t reatm ent sm all tongue tum ours
(brachytherapy) w ho refuse surgery or poor surgical candidates
• Increased side e ects including m ucosit is, xerostom ia, osteoradionecrosis (ORN)
• Adjuvant t reatm ent after surgery in m ore advanced stage tum ours w ith poor pathological factors, i.e., lym phovascular and perineural invasion
• Com bined w ith chem otherapy w ill im prove radiosensit ivit y, possible im proved locoregional control and survival
• The associated endar terit is m ay com plicate healing if salvage surgery is being contemplated
• May need to supplem ent feeding enterally, e.g., nasogast ric (shor t-term : days) or PEG (long term : weeks to m onths)
Risk of Osteoradionecrosis• <60 Gy—~0%• 60–70 Gy—1.8%• >70 Gy—9%• ×3 higher in dentate pat ients• Dental ext ract ions should be perform ed
m et iculously and 2 to 3 weeks prior to star t ing radiotherapy to reduce the risk of ORN
Risk of Nodal Metastases• T1—20%• T2—43%• T3—77%
• Hard palate ◦ T1–T2: t ransoral excision including periosteum w ith 1 cm m argin w ith healing by secondary in tent ion and granulat ion or local m ucosal ap - Use of a prem olded palatal acrylic prosthesis m ay help
◦ T3–T4: m axillectomy (par t ial or total) w ith access via a t ransoral gingivobuccal incision ± m odi ed lateral rhinotomy inci-sion or lateral rh inotomy w ith extension to philt rum
◦ Ident ify and consider frozen sect ion of greater palat ine n ; closure w ith prosthesis (postop support on ipsilateral central and lateral incisors if oncologically possible) or vascularized free ap
• Tips on excising tongue lesions: ◦ Regular palpat ion of tum our to en-sure cont inual correct 3D orientat ion m aintain ing good surgical m argin resect ion m argins
◦ Electrocautery to reduce bleeding ◦ Frozen sect ions of surgical bed to ensure clearance
◦ Resect ions con ned to tongue m ay heal best w ith secondary in tent ion
◦ Early t racheostomy in large tongue tum ours requiring free ap im proves oral access for tum our resect ion
• Closure of oral cavity defects ◦ Prim ary ◦ Split skin grafts ◦ Flaps:
- Buccal - Lingual - Nasolabial - Distant
• Myocutaneous aps include: ◦ Pec m ajor ◦ Lat dorsi ◦ Sternocleidom astoid or myocutaneous ap ◦ Trapezius myocutaneous ap ◦ Platysm a ap
• Free t issue t ransfer opt ions: ◦ Radial free forearm ap ◦ Lateral arm ap ◦ Lat dorsi ap ◦ Rectus abdom inis ◦ Deep circum ex iliac ar tery ap ◦ Scapular ap ◦ Fibula
Philpott_9783131662316_Ch48.indd 178 29/04/14 3:35 PM

179
Oral Cavit y
Consider Treatment of the Neck if:• N+ neck• N0 neck if >20% chance m etastases• Adverse pathological features of prim ary:
◦ Lymphovascular/perineural invasion ◦ Depth of tum our invasion >7 m m ◦ Resect ion m argins <5 m m
Prognosis• 5-year survival rate
◦ Stage I—75–95% ◦ Stage II—65–85% ◦ Stage III—45–65% ◦ Stage IV—10–35%
Philpott_9783131662316_Ch48.indd 179 29/04/14 3:35 PM

180
49.1 Clinical Features• Mult inodular, sim ple (sm oothly enlarged),
ret rosternal goit res• Increased w here iodine is de cient• Long-standing m ay develop clin ical or
subclin ical thyrotoxicosis• Sym ptom s
◦ Neck swelling ◦ Dyspnea ◦ Dysphagia ◦ Choking ◦ Stridor
49.2 Epidemiology• Ethnicit y
◦ No racial predilect ion exists• Incidence
◦ Mult inodular goit res is one of the com m on endocrine condit ions, a ect ing 500 m illion people worldw ide
• Sex ◦ F:M 5:1 ◦ In the Wickham study, 26% of wom en had a goit re com pared w ith 7% of m en
◦ Thyroid nodules are less frequent in m en than in wom en, but w hen found, they are m ore likely to be m alignant
• Age ◦ The frequency of goit res decreases w ith advancing age
◦ The decrease in frequency di ers from the incidence of thyroid nodules, w hich increases w ith advancing age
• Aet iology ◦ Iodine de ciency ◦ Autoim m une thyroidit is—Hashim oto or postpar tum thyroidit is
◦ Excess iodine (Wol –Chaiko e ect) or lith ium ingest ion , w hich decrease release of thyroid horm one
◦ Goitrogens, e.g., propylth iouracil, lith ium , carbam azepine
◦ St im ulat ion of thyroid st im ulat ing horm one (TSH) receptors by TSH from pituitary tu-m ours, pituitary thyroid horm one resistance,
49 Benign Thyroid Disease
gonadotropins, and/or thyroid-st im ulat ing im m unoglobulins
◦ Inborn errors of m etabolism causing defects in biosynthesis of thyroid horm ones
◦ Exposure to radiat ion ◦ Deposit ion diseases ◦ Thyroid horm one resistance ◦ Subacute thyroidit is (de Quervain thyroidit is) ◦ Silent thyroidit is ◦ Riedel thyroidit is ◦ Infect ious agents
- Acute suppurat ive—bacterial - Chronic—mycobacteria, fungal, and parasit ic
◦ Granulom atous disease ◦ Thyroid m alignancy
49.3 Simple Goitres (Fig. 49.1)• Physiological
◦ Puber ty ◦ Pregnancy ◦ oral contracept ive pill (OCP)
• Pathological—iodine de ciency• Medical t reatm ents
◦ Radioact ive iodine: - Up to 50% reduct ion in goit re volum e - Risks include: hypothyroidism , Graves - Contraindicated in pregnant wom en or wom en want ing to get pregnant w ith in 1 year of t reatm ent
◦ Suppression therapy: - Thyroxine adm inist rat ion decreases TSH leading to a reduct ion in volum e
- Risks include: thyrotoxicosis, cardiac arrythm ias, thyroid increases to pret reatm ent size on cessat ion of thyroxine, osteopenia in long-term thyroxine use
◦ Ant ithyroid m edicat ion: - Indicated for thyrotoxic pat ients, e.g., propylth iouracil (side e ects: rash and agranulocytosis)
- 50% relapse rate• Retrosternal goit re
◦ May present w ith dyspnea, st r idor that is posit ional/nocturnal, or coincidentally on chest X-ray w ith shadow ing in upper m ediast inum
Philpott_9783131662316_Ch49.indd 180 02/05/14 11:55 AM

181
In ammatory Goitres
◦ Clinically: - Inabilit y to palpate below it - Dullness to percussion over sternum - May only be a sm all cervical com ponent - Pem berton sign: facial ushing after raising both arm s in the air due to com pression of jugular veins by thyroid
◦ Invest igat ions: - CT scan good for dem onst rat ing ret rosternal extent ± t racheal com pression
- Spirom etry ◦ Treatm ent:
- Conservat ive (if m edically un t) - Surgery: m ost can be rem oved via cervical route (unless below aor t ic arch) m ay need cardiothoracic input ± sternotomy
- Increasing role of radioact ive iodine in euthyroid ret rosternal goit re safe to use dow n to a t racheal diam eter of 1 cm
49.3.1 Toxic Goitres49.3.2 Clinical Features• Graves disease
◦ Most com m on ◦ One or m ore:
- Thyrotoxicosis - Goit re - Eye signs: lid lag, exophthalm os, chem osis - Skin signs: acropachy, pret ibial myxedem a
◦ Autoim m une w ith thyroid ant ibodies ◦ 15% fam ily h istory ◦ F>M 5:1; m iddle ages ◦ Treatm ents:
- Radioact ive iodine - Ant ithyroid drugs, e.g., carbim azole or propylth iouracil
- Block and replace: ant ithyroid drugs full dose + thyroxine to replace thyroid funct ion
- Surgery• Solitary toxic nodule• Long-standing MNGs (Plum m er disease)
49.3.3 Treatment• 50% of pat ients relapse on carbim azole/
propylth iouracil—m ay request thyroidectomy• When considering surgery need to achieve
euthyroid state preop w ith ant ithyroid m edicat ion , β-blockade and Lugol iodine (up to 2 weeks preop)
• Mult idisciplinary approach w ith endocrinology and anaesthet ics
49.3.4 Thyroid Storm• Features
◦ Life threatening ◦ Hyperpyrexia (>40°C) ◦ Palpitat ions ◦ Shortness of breath and sweat ing ◦ Confusion and disorientat ion
• Treatm ent includes: ant ipyret ics, hydrocort isone, ant ithyroid drugs, β-blockers, ICU m onitoring
49.4 In ammatory Goitres• Hashim oto:
◦ Autoim m une ◦ Chronic lymphocyt ic thyroidit is ◦ Late m iddle-aged wom en (15:1 F:M) ◦ Dx: increased ant ithyroid peroxidase ant ibodies
◦ Often +ve fam ily h istory of thyroid problem s ◦ Hard, pain less goit re ◦ In it ially hyper thyroid, later hypothyroid ◦ Rx = Hypothyroidism w ith levothyroxine ◦ Indicat ions for surgery:
- Obst ruct ive Sx - Abnorm al FNA
◦ Risk of lym phom a• De Quervain:
◦ Subacute granulom atous thyroidit is ◦ Due to acute viral infect ion (adenovirus, m um ps)
◦ Tenderness of gland ◦ Transient hyperthyroidism (sim ilar to Graves) plus neck pain and fever
◦ Hypothyroidism follows ◦ Painful dysphagia m ay be present
Fig. 49.1 Goitre. (a) Lateral view. (b) Anterior view.
a b
Philpott_9783131662316_Ch49.indd 181 02/05/14 11:55 AM

182
49 Benign Thyroid Disease
◦ Autoant ibodies produced ◦ Self-lim it ing condit ion m ay require β-blockers and NSAIDs
◦ Low uptake on radionuclide scan (di erent iat-ing from Graves, w hich has increased uptake)
• Riedel ◦ Rare
◦ Marked brosis that invades adjacent neck st ructures
◦ 30% hypothyroid ◦ Possible react ion to underlying ca/lym phom a or par t of m ult ifocal brosclerosis
◦ Treatm ent: steroids, surgery (isthm usectomy) for com pression, and tam oxifen
Philpott_9783131662316_Ch49.indd 182 02/05/14 11:55 AM

183
50.1 Epidemiology• Incidence
◦ 4 to 7% populat ion (autopsies suggest prevalence as h igh as 40 to 70% of populat ion)
◦ 5 to 10% m alignant• Incidentalom as
◦ A nonpalpable nodule detected on im aging ◦ Sam e r isk of m alignancy as palpable ◦ 1 to 2% incidence of “PETom as” (33% risk m alignancy)
◦ Di use posit ron em ission tom ography uptake: thyroidit is
• Malignant r isk factors ◦ History irradiat ion or exposure to radioact ive m aterial
◦ Fam ily h istory thyroid cancer ◦ Age <20 or >70 years ◦ Fam ilial adenom atous polyposis ◦ Cow den syndrom e (m acrocephaly, m ild learning di cult ies, carpet-pile tongue, benign or m alignant breast disease)
◦ Sex: m ale ◦ Vocal cord palsy ◦ Fixat ion to surrounding st ructures ◦ Cervical lym ph nodes
50.2 Investigations• Serum thyroid st im ulat ing horm one (thyro-
globulin and calcitonin levels are not rout inely invest igated)
• Radionuclide scan* if TSH raised-hyperfunct ioning (hot nodule) less likely m alignant
• Ult rasound scan ◦ Benign or suspicious features
• Suspicious features ◦ Microcalci cat ion ◦ Hypoechoic ◦ In lt rat ive m argins ◦ Taller than w ide on t ransverse view ◦ Absent halo ◦ Correspond to clin ical ndings ◦ Detect lym ph nodes ◦ Pure cyst ic nodule (<2% of nodules) is h ighly unlikely to be m alignant
50 Thyroid Nodule
◦ Mult ip le m icrocyst ic com ponen t (spongiform ) >50% nodule is 99% speci c for ben ign nodule
• Microcalci cat ion• Hypoechoic• In lt rat ive m argins• Taller than w ide on t ransverse view• Absent halo• Fine needle aspirat ion (FNA): invest igat ion of
choice (overall sensit ivit y of 83% speci cit y of 92% though gures can vary w ith operator experience, concom itant use of u lt rasound (US), presence of cytologist in clin ic) ◦ Consider US-directed FNA if:
- Nodule nonpalpable - Predom inantly cyst ic - Within posterior thyroid - In it ial nondiagnost ic result
◦ Thy FNA classi cat ion - Thy 1: inadequate (no cells) - Thy 2: benign colloid - Thy 3: follicular cells (10–30% chance m alignancy)
- Thy 4: suspicious m alignancy - Thy 5: m alignant (papillary/m edullary/anaplast ic/lym phom a/m etastat ic tum our)
• MRI or CT scan (non-contrast , as contrast m ay reduce subsequent radioiodine uptake) indicated if: ◦ Haem optysis
- Posit ive nodes in neck for thyroid cancer to determ ine extent including m ediast inum
◦ Lim its of goit re cannot be determ ined ◦ Mass xed ◦ Haem optysis
*Either technet ium -99 or iodine-123
50.3 Clinical Features and Management• Part ially cyst ic nodules that are repeatedly
nondiagnost ic need close m onitoring or excision; consider m ult idisciplinary team review
• Mult iple nodular goit res have sam e r isk for m alignancy as solitary nodules
Philpott_9783131662316_Ch50.indd 183 02/05/14 11:57 AM

184
50 Thyroid Nodule
• FNA any suspicious or the largest nodule• Nodule grow th is not pathognom onic for
m alignancy but warrants repeat FNA• 60 to 90% recurrence rate of cyst ic nodules
w here sym ptom at ic (com pression or cosm esis) nodules can be t reated w ith surgical excision
• Medical suppression of thyroid nodules w ith thyroxine is not indicated
• During pregnancy if nodule is determ ined to be m alignant surgery can be delayed un t il after delivery un less there is substan t ial grow th , then consider surgery at earliest in the 2nd t r im ester
• For m anagem ent of proven m alignancy see Chapter 51: Tum ours of the Thyroid and Parathyroid Glands
Philpott_9783131662316_Ch50.indd 184 02/05/14 11:57 AM

185
51 Tumours of the Thyroid and Parathyroid Glands
51.1 Benign Tumours• Usually present as solitary nodule or dom inant
nodule in MNG• Middle-aged wom en• Not prem alignant• Rarely becom e toxic• Encapsulated• Microscopic pat terns:
◦ Follicular ◦ Microfollicular ◦ Hürthle cell ◦ Em bryonal
• Malignancy excluded by ruling out capsular or vascular invasion on histology
51.2 Malignancy Risk Factors • Fam ily h istory of thyroid cancer• Exposure to ionizing radiat ion
51.3 Malignant Tumours51.3.1 Papillary Adenocarcinoma• 80% of thyroid m alignancy• “Only” thyroid cancer in children• 5th decade• Presents as thyroid nodule• Microcarcinom a <1 cm diam eter• Histological subtypes:
◦ Pure papillary ◦ Mixed papillary–follicular (m ost com m on) ◦ Follicular
• Psam m om a bodies in brous stalk• Ground-glass “orphan Annie” nuclei• High incidence of LNs in levels III to VII (60%)• Prim ary tum our m ay be im palpable—therefore
often presents w ith LNs• 20% have pulm onary m ets at presentat ion• Bony m ets less com m on• More aggressive in older age groups—m ay
invade larynx/t rachea• 10-year survival >90%
51.3.2 Follicular Adenocarcinoma• 6th decade• 20% of all thyroid m alignancies• Decreasing incidence in endem ic goit re areas• Com m only presents as solitary thyroid nodule• May present w ith m ets—bone/lung in 20 to 30%• Non-vesicular nuclei• Histology required follow ing surgical resect ion
to determ ine diagnosis
51.3.3 Hürthle Cell Tumours• Aka eosinophilic/oncocyt ic/oxyphilic cell• More aggressive variant of follicular ca (2% total)• Is possibly a degenerat ive/m etaplast ic
phenom enon• Found in :
◦ Nodular goit res ◦ Chronic lymphocyt ic thyroidit is ◦ Di use toxic goit re ◦ Post-radiat ion ◦ Post-chem otherapy ◦ Aging thyroids
• Malignant tum ours display capsular and vascu-lar invasion
• May invade surrounding t issue and extrathyroid st ructures
• LN m ets com m on
51.3.4 Medullary Thyroid Carcinoma• 5% of all thyroid m alignancies• May occur as part of MEN syndrom e:
◦ MEN IIA ◦ MEN IIB ◦ Fam ilial non-MEN ◦ Sporadic
• Bilateral in 90% of cases w ith MEN• LN m ets in 25 to 30%• Arise from parafollicular/C cells• Calcitonin = tum our m arker• Uniform spindle-shaped cells w ith variable
brous st rom a on histology
Philpott_9783131662316_Ch51.indd 185 02/05/14 9:51 AM

186
51 Tumours of the Thyroid and Parathyroid Glands
51.3.5 Lymphoma• Account for <5% of all lym phom a• Classically rapidly increasing swelling in neck
of an elderly wom an• Im m unocytochem ist ry needed to dist inguish
from anaplast ic carcinom a• Usually ar ises on background of chronic
autoim m une thyroidit is• Most are h igh-grade B-cell NHL• Mostly stage I or II• Occasionally thyroid involved in w idespread
system ic lym phom a
51.3.6 Anaplastic Cancers• Elderly wom en• Often long-standing enlargem ent of thyroid• Rapid increase in size associated w ith pain
referred to ear and hoarseness ± airway obst ruct ion
• Aggressively m alignant w ith h igh m etastat ic potent ial
• Com m only invade surrounding st ructures• Most pat ients dead w ith in 1 year of presentat ion
51.3.7 Metastatic Deposits• Kidney and breast
51.4 Radiology• CXR
◦ Tracheal deviat ion ◦ Mediast inal extension/LNs ◦ Pulm onary m ets ◦ Co-m orbidity
• USS ◦ Tum our size ◦ Diagnosing MNGs ◦ Excludes contralateral disease ◦ Evaluate com plex cysts ◦ Fine calci cat ion 85 to 95% speci c for papillary thyroid ca
◦ Com bined w ith FNA for in it ial diagnosis ◦ Evaluate m etastat ic neck disease if suspected com bined w ith FNA and thyroglobulin washout
• CT scan ◦ Avoid the use of iodinated contrast m edia w hen perform ing CT scans. This m ay reduce the subsequent radioiodine uptake by thyroid t issue and therefore delay its use
◦ Assess extent of larger tum ours including larynx/t rachea/oesophagus/m ajor vessels
◦ Dem onst rates nodal deposits in neck/m ediast inum
◦ Direct ret rosternal extension ◦ Pulm onary m ets
• MRI scan ◦ Assess possible vessel involvem ent (MR angiography)
◦ No contrast required• Scin t igraphy
◦ Poorly speci c and sensit ive ◦ Technet ium -99m m ostly used due to cost and availabilit y
◦ 90% of nodules are cold ◦ 20% risk of m alignancy in a cold nodule (50% if cyst excluded on USS)
◦ Hot nodules unlikely to be m alignant ◦ 123I-MIBG used for suspected MEN ◦ 131I radioiodine used for post-operat ive abla-t ion and to search for m ets
51.5 Laboratory Investigations• TFTs—m andatory• Thyroid autoant ibodies
◦ May assist diagnosis of chronic lym phocyt ic thyroidit is
◦ Predict post-operat ive hypothyroidism ◦ Helps in terpretat ion of thyroid funct ion and thyroglobulin
◦ Preop thyroglobulin not helpful ◦ Serum calcium and calcitonin—if m edullary ca suspected
51.5.1 Prognostic Factors • The Brit ish Thyroid Associat ion (Guidelines
2007) recom m end either use of TNM staging or MACIS system s to determ ine w hen a pat ient is low r isk or h igh r isk for recurrence.
• TNM: Tum our size, node m etastases, and distant m etastases
• MACIS: Metastases, age at presentat ion , com -pleteness of surgical resect ion , invasion (extra thyroidal), size
51.6 Poor Prognostic Factors for DTC• Age > 45 years• Male
Philpott_9783131662316_Ch51.indd 186 02/05/14 9:51 AM

187
Referral Guidelines from General Pract ice
• Larger tum our size and h igher grade• LN m ets in elderly pat ients• Local invasion• Extent of surgery (large)• Poor surgeon experience• Absence of post-operat ive radioiodine t reatm ent• Delay in therapy• Distant m ets
51.7 Staging for DTC• pT1—intrathyroidal tum our, ≤1 cm in greatest
dim ension• pT2—intrathyroidal tum our, >1 to 4 cm in great-
est dim ension• pT3—intra-thyroidal tum our, >4 cm in greatest
dim ension• pT4—extending beyond thyroid capsule• N0—no nodes involved• N1—regional nodes involved
◦ N1a—ipsilateral cervical nodes ◦ N1b—bilateral, m idline, or contralateral cervical nodes or m ediast inal nodes
• Stage grouping for papillary or follicular is show n in Table 51.1
• Stage grouping for m edullary is show n in Table 51.2
• Undi erent iated TC = all stage IV
51.8 Referral Guidelines from General Practice• Thyroid nodules and goit re are com m on
and often noted coincidentally w hen pat ients are being im aged for other reasons
• The vast m ajorit y (95%) of cases have benign disease
• Prim ary care physicians m ust exercise com m on sense in select ing w hich cases should be referred and w ith w hat degree of urgency
51.8.1 Patients w ith Thyroid Nodules Who May Be Managed in Primary Care (IV, C)• Pat ients w ith a h istory of a nodule or goit re that
has not changed for years and in the absence of other worrying features: ◦ Adult pat ient ◦ No history of neck irradiat ion ◦ No fam ily history of thyroid cancer ◦ No palpable cervical lym phadenopathy
• Pat ients w ith a non-palpable asym ptom at ic nodule discovered coincidentally by im aging of the neck w ithout other worrying features
51.8.2 Patients Who Should Be Referred Nonurgently• Nodules w ith abnorm al TFTs (cancer is very
rare) should be referred to an endocrinologist• Sudden onset of pain in a thyroid lum p (bleed
in to a benign thyroid cyst)• Thyroid lum p—new ly present ing or increasing
in size over m onths
Table 51.1 Stage grouping for papillary or follicular adenocarcinoma of the thyroid
10-Year survival rate
Stage I(<45 y) T1–4 N0/1 M0 98.3%
(>45 y) T1 N0 M0
Stage II(<45 y) T1–4 N0/1 M1 84.2%
(>45 y) T2 N0 M0
Stage IIIT3 N0 M0 70%
T1–4 N1 M0
Stage IV T1–4 N0/1 M1 39.1%
Table 51.2 Stage grouping for medullary thyroid carcinoma
Stage I T1 N0 M0
Stage II T2–4 N0 M0
Stage III T1–4 N1 M0
Stage IV T1–4 N0/1 M1
Philpott_9783131662316_Ch51.indd 187 02/05/14 9:51 AM

188
51 Tumours of the Thyroid and Parathyroid Glands
51.8.3 Symptoms Needing Urgent Referral (2-Week Rule)• Unexplained hoarseness or voice changes
associated w ith a goit re• Thyroid nodule in a child• LNs associated w ith a thyroid lum p (usually
deep cervical or supraclavicular region)• Rapidly enlarging pain less thyroid m ass over a
period of weeks
51.8.4 Symptoms Needing Immediate (Same Day) Referral (IV, C)• St ridor associated w ith a thyroid lum p
51.9 Paediatric Thyroid Mass• Increased r isk of m alignancy• USS FNA for invest igat ion if felt clin ically
appropriate• May require hem ithyroidectomy to con rm
diagnosis
51.10 Treatment51.10.1 Papillary Adenocarcinoma• Surgical t reatm ent
◦ Low-risk pat ient + low-risk tum our = lobectomy ◦ Low -risk pat ient + h igh-risk tum our or vice versa = lobectom y/total thyroidectom y
◦ High-risk pat ient + h igh-risk tum our = total thyroidectomy
◦ Top r isk also need: - Select ive neck dissect ion (levels IIb, III, IV, Va, VI)
- Radioiodine ablat ion - TSH suppression w ith thyroxine - Measurem ent of serum Tg
◦ Thyroglossal cyst lesion w ith no LNs (having undergone Sist runk procedure) - TSH suppression w ith thyroxine - Measurem ent of serum Tg
• Radioiodine ◦ T3 4/52 then stop ◦ Increase in TSH leads to increased uptake in 131I, w hich dest roys m icrom ets and rem aining thyroid and allows for thyroglobulin m onitoring as m arker
◦ Pat ient scanned 24–72 h later and if any increase in uptake t reatm ent dose of 131I given
◦ Pat ient rescanned after 1/52 to see if there is any fur ther rem aining uptake - Test dose: 2–5 m Ci - Treatm ent dose in it ial: 30 to 50 m Ci - Metastat ic/recurrent: 100 to 200 m Ci
◦ Note cum ulat ive doses >800 m Ci causes perm anent sterilit y (60% M/80% F)
◦ Afterwards pat ient is placed on suppressive T4 keeping TSH norm al or undetectable
◦ Regular m onitoring of neck, serum thyroglobulin , T4, and TSH
◦ Recom binant TSH allows pat ient to avoid discom fort of hypothyroidosm given as IM inject ion
◦ External beam RT for bony m ets ◦ Radioact ive iodine should be avoided if pat ient is pregnant and should use cont racept ion during t reatm ent and up unt il 6 m onths after com plet ion
◦ Breastfeeding should be stopped up to 8 weeks before t reatm ent and should not star t again afterwards
◦ Males should not t ry for children for 4 m onths after com plet ion of t reatm ent and sure no further t reatm ent is required
◦ Risk of osteoporosis on pat ients on long-term thyroxine and role of in terval bone densitom et ry scans
51.10.2 Follicular Adenocarcinoma• Generally m anaged as per papillary (above)• Haem atogenous spread m ore com m on—lung
and bone• 50% receiving radioiodine for pulm onary
deposits survive for 10 to 15 years• Bony m ets have poorer prognosis
51.10.3 Hürthle Cell Tumours• Should be m anaged as follicular
51.10.4 Medullary Carcinoma• Total thyroidectom y and radical neck dissect ion• Post-operat ive radiotherapy m ay be required if
residual disease suspected and/or large nodal m ets w ith extracapsular extension
Philpott_9783131662316_Ch51.indd 188 02/05/14 9:51 AM

189
Parathyroid Glands
• Radiotherapy m ay also be considered as the prim e t reatm ent m odalit y for advanced stage disease or pat ient co-m orbidity
• Lim ited role of I131-MIBG m ore useful in the di-agnost ic work-up and bet ter sensit ivit y for MEN 2 disease detect ing adrenal lesions
• Genet ic studies and screening (RET proto-oncogene)
51.10.5 Thyroid Lymphoma• Fully stage pat ient prior to t reatm ent w here
possible ◦ Stage I—con ned to thyroid ◦ Stage II—nodal disease in neck/m ediast inum ◦ Stage III—subdiaphragm at ic disease ◦ Stage IV—extranodal involvem ent , e.g., liver, gut , bone m arrow
• Thyroidectomy if feasible appears to im prove local cont rol
• Main Rx = radiotherapy ± chem otherapy• Invest igat ions required during Rx phase:
◦ TFTs ◦ Thyroid autoant ibodies ◦ FNAC and open biopsy/Tru-cut ◦ Whole-body CT ◦ Bone m arrow and t rephine ◦ LDH ◦ ESR
51.10.6 Anaplastic Tumours• Biopsy m andatory to exclude lym phom a• Tracheostomy if required m ay result in seeding
and fungat ion• Regression m ay be achieved by radical
radiotherapy but usually recurrence leading to death w ith in 6 to 12 m onths
51.11 Parathyroid Glands51.11.1 Parathyroid Hormone—Actions• Increases:
◦ Osteolyt ic act ivit y of osteocytes and osteoclasts
◦ Bone rem odelling ◦ Tubular resorpt ion of calcium ◦ Phosphate excret ion ◦ Product ion of vitam in D
◦ Facilitates uptake of calcium from kidney, bone, and in test ine
51.11.2 Primary Hyperparathyroidism• Epidem iology
◦ Sporadic disease, cause unknow n ◦ May be fam ilial inheritance ◦ Can occur as part of MEN syndrom e ◦ Most com m on cause of hypercalcaem ia ◦ 1/1000 populat ion ◦ Fem ales > m ales
• Clin ical m anifestat ions ◦ Renal stones in 25% ◦ Urinary frequency, nocturia and polyuria; pro-gressive CRF can occur from nephrocalcinosis and calculi
◦ General m alaise and painful bones ◦ Chondrocalcinosis and join t e usions ◦ Gout and pseudogout ◦ Psychiat ric symptom s
• Pathology ◦ 80% due to single adenom a ◦ 15% due to m ult iple gland hyperplasia ◦ Double adenom as in 2 to 5% ◦ Parathyroid carcinom a 1%
• Diagnost ic assessm ent and evaluat ion ◦ Elevated Ca2+ and PTH w ith norm al renal funct ion
◦ Di erent ial diagnosis includes m alignancy, sarcoidosis, thyrotoxicosis
• Surgical indicat ions ◦ Sym ptom at ic disease + Ca2+ > 2.6 m m ol/L ◦ Query role of surgery in pat ients under 50 and sym ptom at ic. In these cases the pat ient’s current co-m orbid status and opinion from the endocrinology team are key factors to take in to considerat ion
◦ 90 to 95% can be cured by init ial neck explorat ion
◦ Ectopically located adenom as account for m ost failed ops
• Preoperat ive localizat ion ◦ 99mTc sestam ibi radionuclide im aging ◦ USS ◦ CT/MRI scan ◦ Select ive venous sam pling m ay be required if these Ix are unyielding
◦ In travenous m ethylene blue 3 to 3.5 m g/kg diluted in 500 m L norm al saline infused
Philpott_9783131662316_Ch51.indd 189 02/05/14 9:51 AM
190
51 Tumours of the Thyroid and Parathyroid Glands
over 1 h ; repor ts of tem porary neurological sequelae at doses of ≥5 m g/kg w ith pat ients taking SSRIs
◦ In t raop gam m a probe; if no uptake on nuclear scan pre-operat ively the sensit ivit y is poor
• Sites of ectopic glands ◦ Retro-oesophageal and ret ropharyngeal area ◦ Superior m ediast inum (thym us) ◦ Thyroid gland ◦ Carot id sheath (inferior to bifurcat ion of carot id)
51.11.3 Secondary Hyperparathyroidism• Mostly in pat ients w ith CRF• Most m anaged m edically w ith phosphate
binders and alfacalcidol• 5% of CRF pat ients require parathyroidectom y• Som e pat ients w ith long-standing CRF
develop persistent symptom at ic ter t iary hyperparathyroidism even after successful t ransplantat ion
• Serum calcium usually norm al
51.11.4 Tertiary Hyperparathyroidism• Glands becom e autonom ous and serum calcium
rises• PTH produced w ithout st im ulat ion
51.11.5 Quaternary Hyperparathyroidism• Further adenom a form at ion secondary to
ter t iary hyperparathyroidism
51.11.6 Parathyroid Carcinoma• 1% of pat ients w ith PHP• Ca2+ > 3.0• PTH = 4× norm al• LN m ets in 30%• Wide local excision and ipsilateral thyroid
lobectomy ± SND• Post-op radiotherapy if +ve m argins• 5-year survival = 50%• Distant m ets possible in liver, lung, and bone• Death usually due to hypercalcaem ia
Philpott_9783131662316_Ch51.indd 190 02/05/14 9:51 AM

191
52.1 Type 1 MEN• Hyperplasia of all four parathyroid glands• Pancreat ic islet tum ours (including gast r inom a,
insulinom a, glucagonom a, vasoact ive in test inal pept ide (VIP) tum our (VIPom a), or pancreat ic polypept ide–producing tum our [PPom a])
• Anterior pituitary tum ours (including prolact inom a, som atotropinom a, cort icot ropinom a, or non-funct ioning tum ours)
• Other associated cutaneous tum ours, including lipom as, angio brom as, hypopigm ented collagenom as
• 1 in 30,000 incidence• Typically present in 2nd decade but diagnosis
m ay be delayed for m any years• Cutaneous tum ours m ay present rst• May be fam ily h istory of skin lesions• Angio brom as are telangiectat ic papules 1 to
4 m m m ainly involving central face and upper lip• Tuberous sclerosis m ay present w ith sim ilar
lesions but are m ore num erous and spare the upper lip and present in 1st decade
52.2 Type 2 MEN• Autosom al dom inant• Mutat ion of RET proto-oncogene, if +ve consider
prophylact ic thyroidectomy by age 5• Role of screening fam ily m em bers for the
m utat ion - Medullary thyroid cancer: pentagast rin st im ulat ion test m easuring serum calcitonin at 2, 5, and 10 m in
- Phaeochrom ocytom as: urinary catecholam ines and m etanephrines
- Prim ary hyperparathyroidism : serum calcium and parathyroid horm one levels
• Monitoring for recurrence w ith repeated calcitonin and carcinoem bryonic ant igen levels
• Mult idisciplinary team including surgeons (H&N, paediat r ic, GI); endocrinologists; oncologists; genet icists
52.2.1 Type 2A MEN• Medullary thyroid carcinom a (MTC) less
invasive compared w ith t ype 2B, bilateral and m ult icentric
• Pheochrom ocytom a (~50% of cases and 60–80% bilateral) ◦ May present w ith a hypertensive crisis and tachycardia
◦ Consider adrenalectomy• Parathyroid hyperplasia 20 to 30%; m ay present
w ith hypercalcaem ia• Main t reatm ent is surgery• Total thyroidectom y recom m ended for
ch ild ren w ith RET genet ic m utat ion as young as 3 years
52.2.2 Type 2B MEN• Medullary thyroid tum our• Pheochrom ocytom a• Associated abnorm alit ies include m ucosal
neurom as, m edullated corneal nerve bres, and m arfanoid habitus
52 Multiple Endocrine Neoplasia
Philpot_9783131662316_Ch52.indd 191 02/05/14 10:17 AM

192
53 Tracheostomy
53.1 Indications• Respiratory obst ruct ion• Respiratory failure• Respiratory paralysis• Rem oval of retained secret ions• Reduct ion of dead space
53.2 Cricothyroidotomy• Indicat ions
◦ Suspicion of acute upper airway problem ◦ Worsening st ridor ◦ Reducing self-vent ilat ion
• Procedure ◦ Extend neck and palpate cr icothyroid m em brane
◦ Midline incision or IV cannula ◦ Conver t to form al t racheostomy asap
53.3 Tubes• Inner tube• Cu ed/uncu ed• Fenest rated/unfenest rated• Speaking valve• Suct ion port below cu
53.4 Tracheostomy Care• Fixat ion of tube• Rem oval of secret ions• Hum idi cat ion—“Swedish nose”• Changing of t racheostomy tube• Care of in atable cu • Breath ing exercises• Dressings
53.5 Principles of Decannulation• In it ial indicat ions for t racheostomy are
im proving, resolved
• Pat ient m ust be able to dem onstrate a stable respiratory status breath ing around tube before rem oval, w hich m ay require dow nsizing if too large
• No further need for t racheal suct ion• Rem ove tube and plug t racheostom y site
(ECG elect rode w ith self-adhesive is a good dressing; pat ient places nger over elect rode to prom ote speech and prevent dressing com ing away)
53.6 Advantages of Tracheostomy when in ITU• Lower doses of sedat ion• Preservat ion of cough re ex• More e cient pulm onary toilet• Reduced durat ion of vent ilat ion• Less laryngeal t raum a
53.7 Percutaneous Tracheostomy• Advantages
◦ ICU bedside procedure ◦ Can be perform ed by nonsurgical team ◦ Seldinger technique w ith t racheal puncture, guidew ire placem ent followed by sequent ial dilatat ion allow ing for t racheostomy tube inser t ion
◦ Comparable complicat ion rates to open technique
• Contraindicat ions ◦ Children ◦ Bleeding diathesis ◦ Previous surgery ◦ Infect ion ◦ Enlarged thyroid
Philpott_9783131662316_Ch53.indd 192 02/05/14 10:27 AM

193
54 Neck, Laryngeal, and Tracheal Trauma and Stenosis
54.1 Classi cation of Laryngeal Trauma• Type:
◦ Penetrat ing ◦ Blunt ◦ High velocity ◦ Low velocit y
• Site: ◦ Supraglot t is ◦ Glot t is ◦ Subglot t is ◦ Hyoid ◦ Cricoarytenoid ◦ Cricothyroid
54.2 Soft Tissue Injury• Oedem a• Haem atom a (Fig. 54.1)
◦ Supraglot t ic ◦ Paraglot t ic ◦ Reinke space
• Web: abrasions at anter ior com m issure• Glot t ic incom petence
◦ Arytenoid xat ion ◦ Resorpt ion of the thyroarytenoid m uscle ◦ Atrophy of the cord ◦ Recurrent laryngeal nerve palsies
54.3 Injuries to Skeletal Frame-work (High-Velocity Blunt)• Loss of U-shaped r ings—exert ional dyspnea• Granulom a form at ion• Hyoid # (± bursa form at ion)• Thyroid cart ilage and arytenoids—depends on
calci cat ion: ◦ # Line dow n thyroid prom inence ◦ Elast ic car t ilage—pre-epiglot t ic space bleeding w ith posterior displacem ent of epiglot t is
◦ Calci ed cart ilage—detachm ent of tendon of ant . com m issure and pet iole of epiglot t is
◦ Compressed calci ed thyroid car t ilage has to be reconst ituted and stented
• Cricotracheal separation—usually results in fatality
54.4 Clinical Features of Upper Airway Injury• Sym ptom s of upper airway injury
◦ Dysphonia ◦ Dyspnea ◦ Odynophagia ◦ Neck pain
• Signs of upper airway injury ◦ Stridor ◦ Cervical ecchym osis ◦ Surgical em physem a in the neck ◦ Loss of thyroid prom inence ◦ VC xat ion ◦ Gast ric dilatat ion ◦ Associated dam age:
- Great vessels - Cervical spine - Chest—hem othorax/pneum othorax/em physem a/distant oesophageal tears
54.5 CXR Signs• Incom plete bronchial t ransact ion—apex of
collapsed lung sits at level of h ilum• Deep cervical em physem a—radiolucent line
along prever tebral fascia• Peribronchial air• Sudden obst ruct ion along course of air- lled
bronchus• Fracture of 1st r ib/scapula/sternum suggests
severe injury w ith airway t raum a
54.6 ManagementRem em ber airway, breath ing and circulat ion and also C-spine!• Oedem a only—bed rest• No m ajor m ucosal lacerat ion w ith visualizat ion
of t racheal lum en—ETT• Im m ediate threat of loss of
airway—tracheostomy• Associated bronchial injury—intubate uninjured
bronchus before thoracotomy• Em ergency thoracotom y for great vessel
dam age
Philpott_9783131662316_Ch54.indd 193 02/05/14 10:30 AM

194
54 Neck, Laryngeal, and Tracheal Trauma and Stenosis
54.6.1 Laryngeal Framework Damage• General suppor t ive m easures:
◦ Bed rest and voice rest ◦ High hum idity ◦ O2
◦ Antibiot ics if compound fracture ◦ Max dose parenteral steroid therapy ◦ PPI to reduce risk of granulat ion and stenosis
• Penetrat ing injuries ◦ If bleeding in to supraglot t is—open larynx to drain and quilt
◦ Bullet wounds—débridem ent ◦ Total laryngectomy m ay follow a bullet wound
• Low-velocity blunt injuries ◦ Overnight observat ion ◦ ETT m ay be required
• High-velocity blunt injuries ◦ 50% of those result ing from RTA require laryngeal explorat ion and reconst ruct ion
◦ Stent ing for laryngeal fram ework ◦ Drain bleeding in to potent ial spaces and quilt ◦ Attem pt prim ary repair of any cricoid injury ◦ If cr icothyroid m em brane separated—m obilize larynx and t rachea for reanastom osis
• Speci c injuries: ◦ Fractured hyoid
- Conservat ive for m inim ally displaced fractures
- Sm all pharyngeal lacerat ions w ith displaced fractures—endoscopic reduct ion
- Com m inuted or grossly displaced fractures—external explorat ion
• Thyroid car t ilage ◦ Reduce fractures if >15 to 20° angulat ion between fragm ents
◦ Perform a laryngo ssure through fracture line ◦ Vocal cords resutured to vocal processes or ant . com m issure
◦ Suture m ucosal lacerat ions ◦ Anchor epiglot t is to hyoid bone ◦ Steel w ires or t itanium m iniplates m ay be used to x cart ilage fragm ents
◦ Sm all pieces of car t ilage w ith no in tact peri-chondrium are rem oved to reduce chondrit is
• Laryngeal stents ◦ Indicat ions:
- Maintain shape of cart ilaginous fram ework ◦ Poster ior displacem ent of base of epiglot t is ◦ Dislocat ion of arytenoids ◦ Depressed # cricoid ◦ Markedly displaced thyroid ◦ To separate m ucosal lacerat ions ◦ Applicat ion
- May be used up to 3 m onths after injury - No ideal stent available - Stents are xed w ith w ires - Rem ain in place for at least 3 m onths
54.6.2 Tracheal Injuries• Sim ple—repair lacerat ion greater than one-th ird
t rachea or a m ajor bronchus• Major—adequate débridem ent and m ucosal
apposit ion• Avulsion—im m ediate t racheostomy and
explorat ion of larynx
54.7 Laryngeal Stenosis54.7.1 Aetiology• Traum a
◦ External (blunt , penetrat ing) ◦ In ternal (in tubat ion , radiat ion , burn) ◦ Iat rogenic (laser)
• Failed t reatm ent on nonrecognit ion of acute t raum a
• Infect ion ◦ Diphtheria ◦ Syphilis ◦ Mycobacterium
• In am m ation ◦ Granulom atosis w ith polyangit is ◦ Sarcoid
Fig. 54.1 Laryngeal trauma, with a haematoma on the inner larynx.
Philpott_9783131662316_Ch54.indd 194 02/05/14 10:30 AM
195
Neck Trauma Zones
◦ Relapsing polychondrit is ◦ Autoim m une thyroidit is
• As a com plicat ion of: ◦ Tracheostomy ◦ In tubat ion ◦ Part ial laryngectomy
• Soft t issue dam age due to: ◦ Mucosal loss ◦ Mucosal adhesions ◦ Haem atom a organizat ion in spaces
• Glot t ic com petence a ected by: ◦ Web form at ion anteriorly ◦ Arthrodesis of arytenoid posteriorly ◦ RLN injury
54.7.2 Investigations• Do not at tem pt to increase laryngeal lum en
unt il 18 m onths have passed• Assess length of neck and cervical t rachea
available for m obilizat ion• CT (± MRI) scan• Laryngoscopy/bronchoscopy—assess
t racheom alacia and arytenoids• Oesophagoscopy
54.7.3 Treatment• Warn pat ient that t racheostom y m ay be
perm anent if already in place• Postop nasogast ric tube w ill be required• Avoid surgical t reatm ent of system ic condit ions,
e.g., Granulom atosis w ith polyangit is
54.8 Supraglottic Stenosis• Laryngeal w idening procedure—rem oval of
subm ucosal scar t issue• Laser excision is an alternat ive
54.9 Glottic Stenosis• Anterior glot t is
◦ <5 m m height CO2 laser excision ◦ >5 m m laryngo ssure and keel insert ion
• Posterior glot t is ◦ Posterior glot t ic stenosis classi cat ion:
- Type I: in terarytenoid adhesion - Type II: posterior com m issure - Type III: poster ior com m issure and cricoarytenoid ankylosis (unilateral)
- Type IV: posterior com m issure and cricoarytenoid ankylosis (bilateral)
- Treatm ent poster ior glot t ic stenosis: - Type I: divide web and splin t inser t ion - Type II
◦ If <3 m m incision cold steel/laser ± keel. ◦ If >4 m m laryngo ssure + scar resect ion ◦ Type III: laryngo ssure + scar resect ion ◦ Type IV: arytenoidectomy
• Com plete glot t ic stenosis—free m ucosal graft (buccal) com bined w ith local m ucosal aps
54.10 Cricoid Stenosis• Graft m ust keep area open perm anently• Free bone/cart ilage from ribs gives unsat isfac-
tory result• Allografts have no place• Body of hyoid can be sw ung dow n on m uscle
pedicle of sternohyoid• For m arked stenosis, cricoid is rem oved leaving
part of posterior lam ina support ing arytenoids
54.11 Tracheal Stenosis• Dilatat ion for m inor stenosis• Tracheal resect ion if severe enough to warrant
t racheostomy• Grillo procedure for extensive stenosis• Laser excision for distal stenosis• Controversies
◦ 40% bet ter chance of good voice and 3× less chance of perm anent t rachy if severe injuries recognized and t reated early
◦ If pat ient has no t rachy—advise against surgery ◦ Persistent and increasing scarring—best to avoid fur ther surgery
54.12 Neck Trauma Zones• Zone I: Super ior cr icoid to in fer ior thoracic
in let• Zone 2: Superior angle of m andible to inferior
cr icoid• Zone 3: Superior skull base to inferior angle of
m andible ◦ Zone 2: Most com m on site for carot id injury ◦ Zone 1: Most com m on site for thoracic injury; m inim ally needs CXR
◦ Angiography indicated in zone I and III + XII nerve dam age
Philpott_9783131662316_Ch54.indd 195 02/05/14 10:30 AM

196
54 Neck, Laryngeal, and Tracheal Trauma and Stenosis
◦ Em bolizat ion m ay be required in zone III; thoracotomy in zone I
◦ Zone II injuries seldom occult and physical exam inat ion is a good indicator of severit y - If platysm a is breached suspect serious injury
- Subclavian vein injury has increased m ortalit y com pared w ith ar ter ial injury because of the risk or air em bolism
- Median sternotomy is usually indicated for repair
Philpott_9783131662316_Ch54.indd 196 02/05/14 10:30 AM
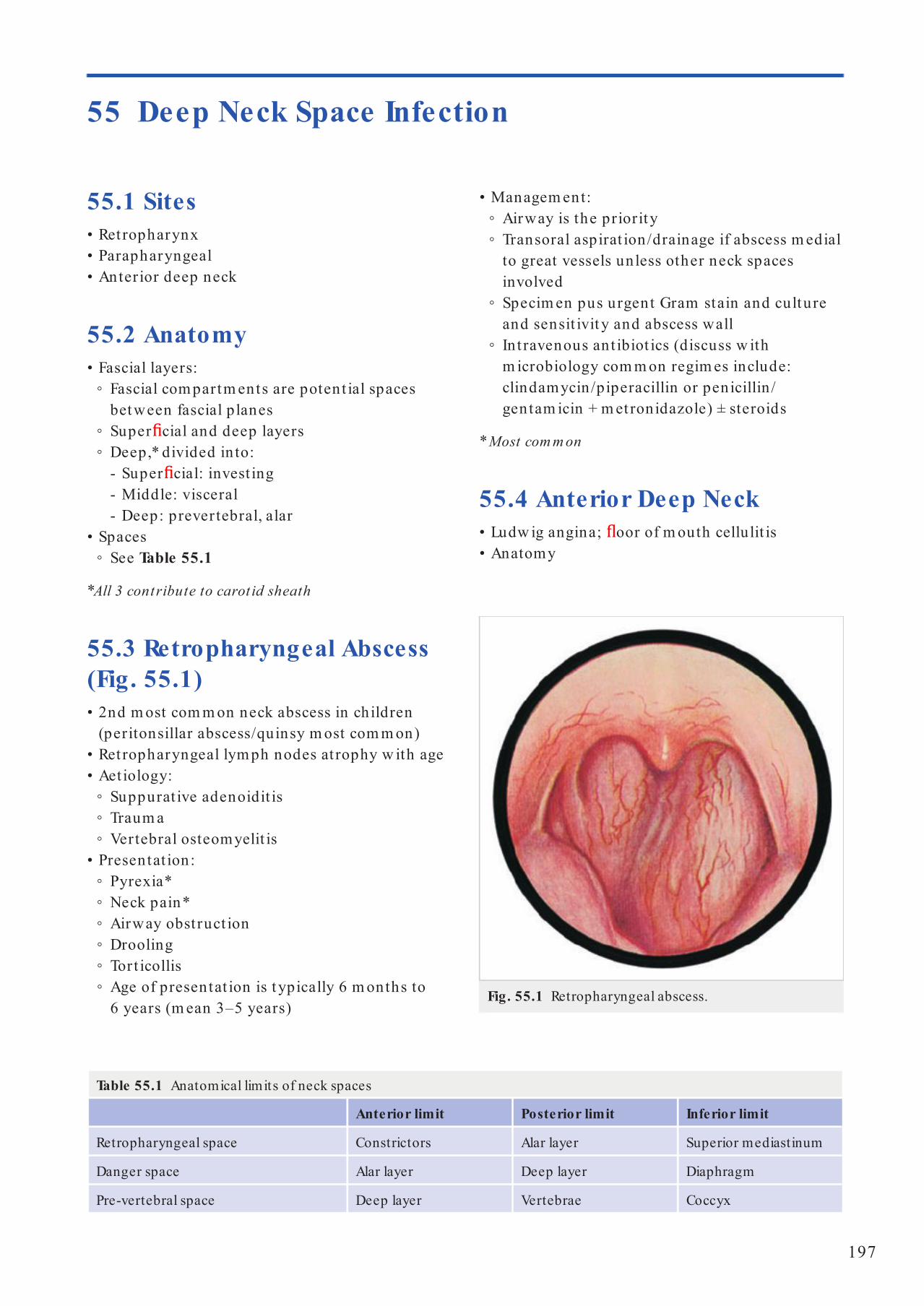
197
55 Deep Neck Space Infection
55.1 Sites• Ret ropharynx• Parapharyngeal• Anterior deep neck
55.2 Anatomy• Fascial layers:
◦ Fascial com partm ents are potent ial spaces between fascial planes
◦ Super cial and deep layers ◦ Deep,* divided in to:
- Super cial: invest ing - Middle: visceral - Deep: prevertebral, alar
• Spaces ◦ See Table 55.1
*All 3 contribute to carot id sheath
55.3 Retropharyngeal Abscess (Fig. 55.1)• 2nd m ost com m on neck abscess in children
(peritonsillar abscess/quinsy m ost com m on)• Ret ropharyngeal lym ph nodes at rophy w ith age• Aet iology:
◦ Suppurat ive adenoidit is ◦ Traum a ◦ Vertebral osteomyelit is
• Presentat ion: ◦ Pyrexia* ◦ Neck pain* ◦ Airway obst ruct ion ◦ Drooling ◦ Tort icollis ◦ Age of presentat ion is t ypically 6 m onths to 6 years (m ean 3–5 years)
• Managem ent: ◦ Airway is the priorit y ◦ Transoral aspirat ion/drainage if abscess m edial to great vessels unless other neck spaces involved
◦ Specim en pus urgent Gram stain and culture and sensit ivit y and abscess wall
◦ In t ravenous ant ibiot ics (discuss w ith m icrobiology com m on regim es include: clindamycin/piperacillin or penicillin /gentam icin + m et ronidazole) ± steroids
* Most com m on
55.4 Anterior Deep Neck• Ludw ig angina; oor of m outh cellulit is• Anatomy
Table 55.1 Anatomical limits of neck spaces
Anterior limit Posterior limit Inferior limit
Retropharyngeal space Constrictors Alar layer Superior mediastinum
Danger space Alar layer Deep layer Diaphragm
Pre-vertebral space Deep layer Vertebrae Coccyx
Fig. 55.1 Retropharyngeal abscess.
Philpott_9783131662316_Ch55.indd 197 02/05/14 10:39 AM

198
55 Deep Neck Space Infect ion
• Presentat ion ◦ Airway obst ruct ion—stridor/ster tor ◦ Pain ◦ Dysphagia/dysphonia ◦ Trism us (20%) ◦ Snoring/OSA ◦ Neck swelling/fu llness/increasing erythem a
• Aet iology ◦ Tonsillit is (part icularly im m unocomprom ised) (Fig. 55.2)
◦ Dental ◦ IV drug abusers ◦ Epiglot t it is ◦ Parot it is ◦ Foreign body ◦ Branchial cleft cysts (if recur) ◦ Extension from petrous apex/m astoid t ip (Citelli abscess)
• Treatm ent ◦ Ensure airway stable, m ay need t racheostomy
◦ May require ICU adm ission ◦ Preop CT scan for surgical planning (if airway stable), and cardiothoracic referral if m ediast inum involved
◦ Incision guided by im aging and clin ical exam inat ion
◦ Urgent m icrobiology inc. Gram stain and culture
◦ Mult iple neck spaces m ay need opening, nger dissect ion useful at breaking dow n loculat ions and entering planes
◦ Subm andibular space extends from hyoid to m andible divided by mylohyoid m uscle
◦ Sublingual space superior to m uscle ◦ Subm axillary space inferior
• Features ◦ Mouth pain ◦ Drooling ◦ Dysphagia ◦ Neck pain ◦ Swelling in oor of m outh ◦ Superior tongue displacem ent
• Aet iology ◦ 80% dental—typically lower 3rd m olar ◦ 20% soft t issue/tonsil infect ion
• Managem ent ◦ Airway is priority consider HDU for observat ion ◦ Tim ely surgical in tervent ion w ith appropriate IV ABx
◦ Surgical drainage - Sublingual space only—int ra-oral - Subm axillary space—external
55.5 Parapharyngeal Abscess• Anatom y
◦ Parapharyngeal space 2 com partm ents: pre- (anterior) and post-styloid
◦ Com m unicates anterior w ith subm axillary space via buccopharyngeal gap created by styloglossus
◦ Com m unicates posteriorly w ith the ret ropharyngeal and danger spaces
Fig. 55.2a, b Tonsillo-genic complications. a Extension to the
immediately surrounding tissues. 1, internal jugular vein; 2, vagus nerve; 3, internal carotid artery.
b Further possible directions of spread of a tonsillogenic infection.
1
ba
CSF
Orbit
Cavernoussinus
Parotid Cervicalsoft t issue
Carotidartery
From tonsil
Thrombosisof jugular vein
Para-pharyngeal
space
23
Philpott_9783131662316_Ch55.indd 198 02/05/14 10:39 AM

199
Parapharyngeal Abscess
◦ May need repeated Ix + Dx procedures dependent on clin ical response + results of repeated CT scans and haem atological tests
◦ IV Abs guided by m icrobiology and m onitored use of steroids (unless de nite contraindications) dependent on the patient's clinical response
• Radiology ◦ Lateral soft t issue neck X-ray has 33% false-negat ive rate
◦ CT w ith contrast is im aging m odalit y of choice ◦ Features:
- Radio-opacity - Rim enhancem ent - Air
◦ Increasing posit ive predict ive value if m ore features present
◦ Orthopantogram (OPG) of the m andible m ay show radiolucency around the base of tooth socket suggest ive of a dental abscess
• Microbiology ◦ Staph. aureus, H. in uenzae ◦ Group A β-hem olyt ic st rep, e.g., Strep. pyogenes
◦ Anaerobes: Bacteroides, Fusobacterium , and Peptostreptococci
• Com plicat ions ◦ Rupture: aspirat ion , pneum onia ◦ Overw helm ing sepsis ◦ IJV throm bosis (Lem ierre syndrom e) ◦ Carot id blowout ◦ Mediast in it is ◦ Empyem a ◦ Pericardial e usions ◦ Epidural abscess ◦ Atlanto-axial dislocat ion
• Since the use of ABx com plicat ions have signi cant ly decreased
• Be wary of the im m unocom prom ised pat ient
Philpott_9783131662316_Ch55.indd 199 02/05/14 10:39 AM

200
56.1 Congenital Neck Masses56.1.1 Lymphangiomas• Pathophysiology
◦ Norm ally 2 jugular sacs, 2 posterior sciat ic sacs, and 1 ret roperitoneal sac develop endothelial outbuddings and extend centrifugally to form lymphat ic system
◦ Endothelial brillar m em branes sprout from walls of sacs, penetrate surrounding t issue, canalize it , and produce m ore cysts
◦ Pressure of cysts forces tum our along lines of least resistance in to planes or spaces between large m uscles or vessels
• Types ◦ Simple—thin-walled capillary sized (40%) ◦ Cavernous—dilated spaces (35%) ◦ Cyst ic hygrom a—various sizes (25%)
• Locat ions ◦ Oral 35% ◦ Cervical 50 to 75% ◦ Axillary 15%
• Clin ical features ◦ Equal sex dist r ibut ion ◦ No preponderance to one side ◦ Age at presentat ion:
- 60% bir th - 75% by 1 year - 90% by 2 years
◦ Stridor w ith t racheal displacem ent ◦ Brachial plexus com pression w ith pain and hyperesthesia
◦ Sudden increase in size due to haem orrhage m ay be fatal
• Managem ent ◦ Cryotherapy and sclerosant inject ion m et w ith lim ited success
◦ Excision required ◦ Preop CT to exclude m ediast inal involvem ent ◦ Use nerve st im ulator to avoid CNs VII, XI, and XII
◦ Excise excess skin ◦ Mult iple excisions m ay be needed ◦ External approach for in t raoral lesions ◦ Recurrence rate is 10 to 15%; cavernous t ype m ost likely to recur
56 Benign Neck Disease
56.1.2 Midline Dermoids• Characterist ic features
◦ Always m idline in neck ◦ Equal sex dist r ibut ion
• Epiderm oid cyst ◦ Most com m on ◦ No adnexal st ructures ◦ Contains cheesy kerat inous m aterial
• True derm oid cyst ◦ Contains skin appendages—hair follicles, etc. ◦ Can be acquired through im plantat ion of epiderm is in a puncture wound
◦ Most occur in the oor of m outh w ith ¼ involving neck
◦ Present as slow-grow ing lesions ◦ Managem ent is surgical excision
• Teratoid cyst ◦ Rare ◦ May be lined by respiratory epithelium ◦ Contains elem ents from ectoderm , endoderm , and m esoderm
56.1.3 Thyroglossal Cysts• Em bryology
◦ Thyroid arises from oor of pr im it ive pharynx between 1st and 2nd pouches
◦ Median thyroid anlage loses lum en at 5 weeks and breaks in to fragm ents—lower end divides in to 2 por t ions that becom e lobes
◦ Stalk should at rophy at 6 weeks; if not , it becom es a duct
◦ Cysts form w hen epithelial cells cease to rem ain inact ive
◦ Duct runs through hyoid to foram en cecum
◦ Fistula results from inadequate t reatm ent• Presentat ion
◦ Equal sex dist r ibut ion ◦ Mean age 5 (range 4 m onths–70 years) ◦ Midline (90%), lateral (left ) 10% ◦ 3× m ore com m on than branchial cysts ◦ 65% infrahyoid, 20% suprahyoid, 15% juxtahyoid
◦ Also described in t ralingual, suprasternal, and in t ralaryngeal
Philpott_9783131662316_Ch56.indd 200 7/2/14 4:03 PM
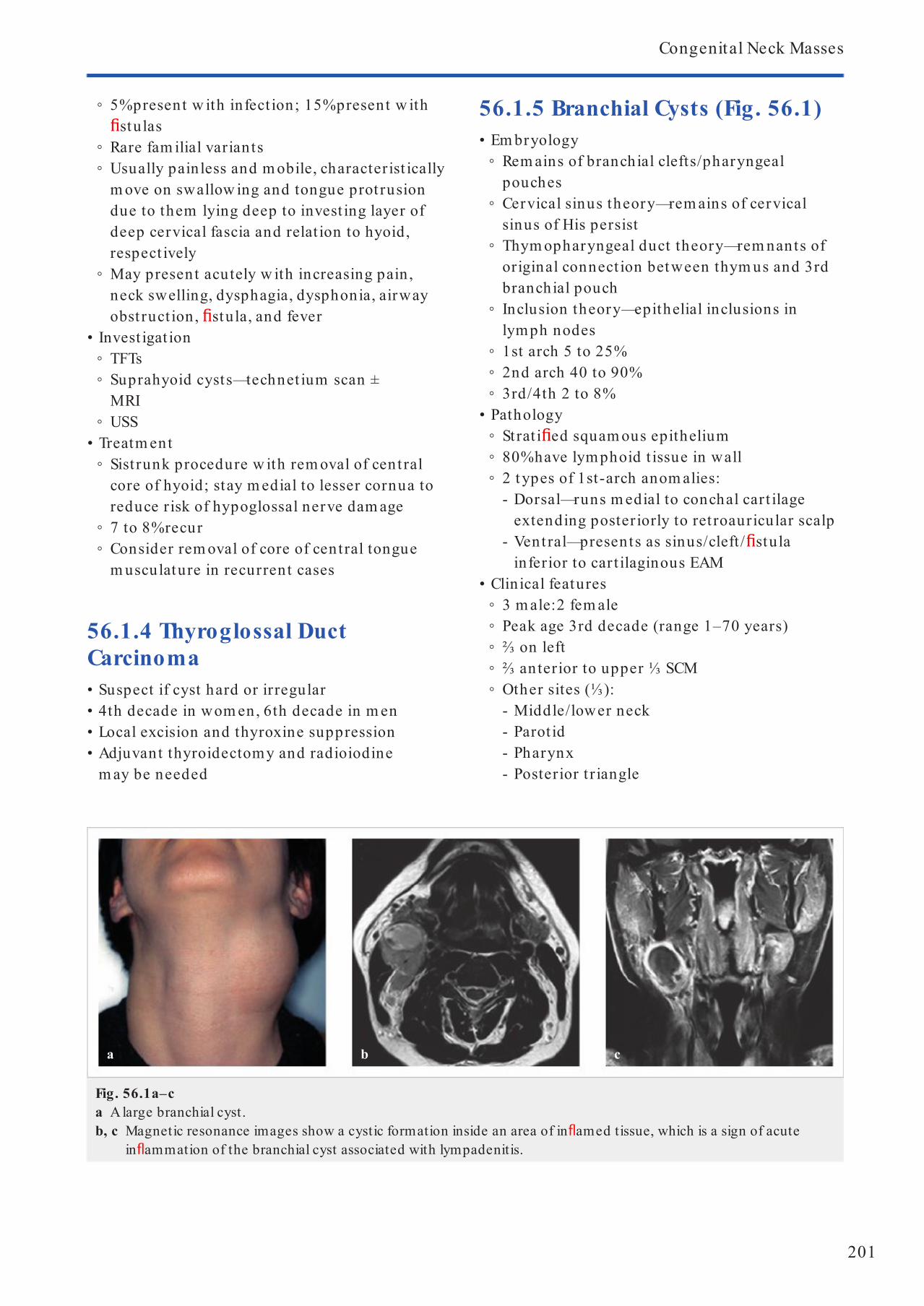
201
Congenital Neck Masses
◦ 5% present w ith infect ion; 15% present w ith stulas
◦ Rare fam ilial variants ◦ Usually pain less and m obile, character ist ically m ove on swallow ing and tongue prot rusion due to them lying deep to invest ing layer of deep cervical fascia and relat ion to hyoid, respect ively
◦ May present acutely w ith increasing pain , neck swelling, dysphagia, dysphonia, airway obst ruct ion , stula, and fever
• Invest igat ion ◦ TFTs ◦ Suprahyoid cysts—technet ium scan ± MRI
◦ USS• Treatm ent
◦ Sist runk procedure w ith rem oval of cent ral core of hyoid; stay m edial to lesser cornua to reduce risk of hypoglossal nerve dam age
◦ 7 to 8% recur ◦ Consider rem oval of core of central tongue m usculature in recurrent cases
56.1.4 Thyroglossal Duct Carcinoma• Suspect if cyst hard or irregular• 4th decade in wom en, 6th decade in m en• Local excision and thyroxine suppression• Adjuvant thyroidectomy and radioiodine
m ay be needed
56.1.5 Branchial Cysts (Fig. 56.1)• Em bryology
◦ Rem ains of branchial clefts/pharyngeal pouches
◦ Cervical sinus theory—rem ains of cervical sinus of His persist
◦ Thym opharyngeal duct theory—rem nants of original connect ion between thym us and 3rd branchial pouch
◦ Inclusion theory—epithelial inclusions in lymph nodes
◦ 1st arch 5 to 25% ◦ 2nd arch 40 to 90% ◦ 3rd/4th 2 to 8%
• Pathology ◦ Strat i ed squam ous epithelium ◦ 80% have lym phoid t issue in wall ◦ 2 t ypes of 1st-arch anom alies:
- Dorsal—runs m edial to conchal cart ilage extending poster iorly to ret roauricular scalp
- Vent ral—presents as sinus/cleft / stula inferior to car t ilaginous EAM
• Clin ical features ◦ 3 m ale:2 fem ale ◦ Peak age 3rd decade (range 1–70 years) ◦ ⅔ on left ◦ ⅔ an terior to upper ⅓ SCM ◦ Other sites (⅓):
- Middle/lower neck - Parot id - Pharynx - Posterior t r iangle
Fig. 56.1a–ca A large branchial cyst.b, c Magnetic resonance images show a cystic formation inside an area of in amed tissue, which is a sign of acute
in ammation of the branchial cyst associated with lympadenitis.
a b c
Philpott_9783131662316_Ch56.indd 201 7/2/14 4:03 PM

202
56 Benign Neck Disease
◦ Persistent swelling in 80% ◦ Pain 30% ◦ Infect ion 15% ◦ Clinically cyst ic 70% ◦ ≤ 20% recurrence after excision
56.1.6 Branchial Fistulas• 1st-arch stu las open at junct ion of
car t ilaginous and bony EAM• 2nd-arch origin :
◦ Skin-lined t ract opening on anterior aspect of tonsillar fossa
◦ Opens externally at anterior border of SCM (junct ion of m iddle and lower ⅓)
◦ Invariably presents as discharging sinus in young infants
• 3rd/4th-arch stulas open at piriform sinus or below
• Excise in stepladder fashion• Tract t ravels below stylohyoid and post . belly
of digast ric, above XII n , between ECA and ICA• If t ract goes up towards ear, need to rem ove
super cial lobe of parot id gland
56.1.7 Branchiogenic Carcinoma• Arises from wall of branchial cyst• Should occur in a line running from just anterior
to t ragus along anter ior border of SCM• Histology should be com pat ible w ith t issue
origin from branchial vest iges• No other prim ary should becom e evident in
5-year follow-up• Often actually cyst ic nodal secondary from
tonsillar prim ary• Wide local excision , radical neck dissect ion ,
and radiotherapy
56.1.8 Thymic Cysts• Thym us develops from 3rd pouch at 6/40
and rests in superior m ediast inum at 12/40• Typically boys aged 3 to 8 years• Pain less swelling• 50% com m unicate w ith m ediast inum
56.1.9 Haemangiomas• Most com m on benign tum our of infancy• 14 to 21% in H&N
• Within m asseter and t rapezius• Typically appear short ly after bir th and
proliferate for 6 to 12 m onths• Up to 50% involute spontaneously• Propranolol speeds up regression• 3 fem ale:1 m ale
56.2 Acquired Neck Masses56.2.1 Ranulas• Overview
◦ From Lat in word “rana” m eaning frog ◦ Cyst ic m ass in oor of m outh or tongue ◦ Due to obst ruct ion of m inor salivary glands or sublingual gland or t raum a or ductal abnorm alit y
◦ The sublingual gland secretes cont inuously unlike the other m ajor salivary glands
◦ Simple ranulas are con ned to sublingual space present ing as pain less bluish cyst under the tongue (and raising it )
◦ Plunging ranulas result from extravasat ion of m ucus below mylohyoid or ectopic t issue or a duct com m unicat ing w ith the subm andibulaar gland—present ing as pain less im m obile neck swellings
◦ Present in 2nd and 3rd decade ◦ Reports of SCC w ith in cyst wall and cystadenocarcinom a present ing as ranula so h istology is recom m ended
• Treatm ents: ◦ Marsupializat ion (sm aller cysts<1.5 cm ) ± packing of cyst
◦ Seton suture ◦ Sclerosant inject ion , e.g., OK-432, bleomycin
◦ CO2 laser ◦ Radiotherapy ◦ Sublingual gland + ranula excision ◦ Transoral vs. t ranscervical (di cult to excise the sublingual gland) approach for plunging ranulas
• Com plicat ions of surgery: ◦ Recurrence—50% if sublingual gland is not excised, 2% if it is
◦ Lingual nerve injury—paresthesia tongue
◦ Wharton duct injury—obstruct ive sialadenit is
◦ Marginal m andibular branch facial nerve in plunging ranula
Philpott_9783131662316_Ch56.indd 202 7/2/14 4:03 PM

203
Acquired Neck Masses
Fig. 56.2a, ba Genesis of a hypopharyn-
geal pulsion diverticulum. The red area indicates the inferior part of the cricopharyngeus muscle.
b Principle of endoscopic spur division. 1, Oesopha-gus; 2, spur; 3, diverticu-lum.
ba
1
2
3
◦ May result from rest rict ive defect of upper sphincter leading to increased pressure in hypopharynx
56.2.2 Laryngoceles (see Fig. 41.1)• Overview
◦ Arise w ith in saccule of laryngeal ventr icle ◦ Bryce sign—m anual compression causes escape of uid and gas in to airway
◦ 5 m ale:1 fem ale ◦ Peak age—6th decade ◦ 80% unilateral ◦ 30% external (expand through thyrohyoid m em brane)
◦ 20% internal and present in valleculae ◦ 50% com bined ◦ 1% contain carcinom a ◦ Possibly rem nant of air sacs found in other anim al species
• Clin ical features ◦ Hoarseness ◦ Neck swelling ◦ Stridor/sore throat , snoring, pain on cough ◦ Air- lled sac on plain XR
• Treatm ent ◦ Excision via incision over thyroid car t ilage ◦ Rem ove upper half of thyroid car t ilage ◦ Sac is divided at neck and st itched as in hernia repair
◦ Perichondrium placed over defect and wound closed
56.2.3 Pharyngeal Pouches (Figs. 56.2 and 56.3)• Pathology
◦ Most com m on type is acquired pulsion divert iculum of m edian posterior wall (Killian dehiscence)
Fig. 56.3 The typical topographical situation in a Zenker diverticulum. It develops in the Killian triangle between the inferior constrictor and the cricopharyngeus muscle.
Philpott_9783131662316_Ch56.indd 203 7/2/14 4:03 PM

204
56 Benign Neck Disease
◦ Biopsies of cricopharyngeus show brot ic changes, hypert rophy, necrosis, and in am m at ion
◦ Possibly autoim m une origin to som e in am m atory change
• Clin ical features ◦ 2 m ale:1 fem ale ◦ 7th to 8th decades ◦ 98% have dysphagia ◦ Halitosis, regurgitat ion , and weight loss ◦ Cough/recurrent LRTI in 30% ◦ Occasional hoarseness, neck m ass ◦ Barium swallow diagnost ic ◦ Pharyngoesophagoscopy m ay be required to exclude a carcinom a
• Treatm ent ◦ Endoscopic stapling (Fig. 56.4)—cure rate of 90%
◦ Alternat ive endoscopic techniques include: - Diathermy (Dohlm an procedure) - Laser
◦ Open procedures - Divericulectomy—collar incision at level of cricoid cart ilage
- Cricopharyngeal myotomy—reduces incidence of recurrence if perform ed at the sam e t im e
• Com plicat ions ◦ ⅓ pat ients su er these w ith open procedures ◦ Infect ion ◦ Fistulas ◦ Stenosis
◦ VF paralysis ◦ Object ive recurrence in 44%, but th is does not re ect sym ptom s
• Carcinom a in a pharyngeal pouch ◦ 0.5% of pouches ◦ 5 m ale:1 fem ale ◦ Long-standing divert iculae (>7 years) ◦ Due to chronic irr itat ion from food retent ion ◦ Increased dysphagia ◦ Weight loss ◦ Occasionally blood in regurgitated food ◦ Mass in neck ◦ Constant lling defect on barium swallow ◦ Treatm ent is as for postcricoid carcinom a
56.2.4 Tuberculous Cervical Adenitis (Fig. 56.5)• Long-standing lym phadenopathy• Pain indicates m ore recent onset• Sinus form at ion or cold abscess• 90% single nodal group• Diagnose w ith Heaf test and presence of
acid-fast bacilli in biopsy/swab• Typical t reatm ent course long-term t riple
or quadruple therapy: ◦ Etham butol/st reptomycin
Fig. 56.4 The Weerda diverticuloscope.
Fig. 56.5 An in amed cutaneous reaction and lymph-node swelling due to a tuberculous infection.
Philpott_9783131662316_Ch56.indd 204 7/2/14 4:03 PM

205
Acquired Neck Masses
◦ Ison iazid ◦ Rifam picin ◦ Pyrazinam ide
56.2.5 Head and Neck Manifestations of AIDS• Mult icentric sim ple parot id cysts• Benign lym phoid follicular hyperplasia• Cutaneous/oropharyngeal lesions of
Kaposi sarcom a• Hairy leukoplakia• Upper aerodigest ive t ract candidiasis• Massive cervical lym phadenopathy• Invasive fungal sinusit is
56.2.6 Toxoplasmosis• Toxoplasm a gondii = protozoon• Transm it ted by ingest ion of cysts from :
◦ Faeces of infected cats ◦ Undercooked beef/lam b
• Sym ptom s ◦ Generalized aches and pains ◦ Pyrexia ◦ Cough ◦ Malaise ◦ Maculopapular rash
• May be asym ptom at ic or present in an isolated LN
• Lym phocytosis on FBC (atypical m ononuclear cells)
• Con rm diagnosis w ith : ◦ Serum ant ibodies ◦ LN biopsy ◦ CSF analysis (if encephalit is)
• Treatm ent for infants and im m unocomprom ised: ◦ Sulphadim idine ◦ Pyrim etham ine ◦ Folic acid ◦ Weekly FBC
56.2.7 Actinomycosis• Presents w ith swelling around m andible/
subm andibular area w ith sinus form at ion , discharge and red/bluish discolourat ion to skin .
• Typically secondary to dental problem s.
• Diagnosed from histology-sinus t racts w ith su lphur granules and not serology.
• Treatm ent is w ith penicillin • Surgery lim ited role for drainage of
abscess
56.2.8 Infectious Mononucleosis• Clin ical form s of EBV infect ion
◦ Frequent subclin ical infect ion in early childhood
◦ 2nd wave seroconversion associated IM ◦ NPC ◦ African Burkit t lym phom a
• Pathophysiology ◦ Virus accesses B-lym phocytes via C3d receptor
◦ Virus persists in oropharynx of pat ients for up to 18 m onths after clin ical recovery
◦ Found in throat washings of 50% of renal t ransplant pat ients
◦ Spread by t ransfer of saliva (kissing) ◦ 1–2 m onth incubat ion period ◦ Mononuclear lym phocytosis seen in rst few weeks of clin ical illness
◦ 10% atypical lymphocytes on WCC• Clin ical features
◦ Pyrexia, sore throat , lym phadenopathy ◦ Rash in 5% (100% if am picillin given) ◦ Palatal petechiae or splenom egaly in up to 50%
◦ Raised LFTs ◦ Usually subsides over 2 to 3 weeks
• Com plicat ions ◦ Autoim m une haem olyt ic anaem ia ◦ Throm bocytopenia ◦ Splenic rupture ◦ Encephalit is ◦ CN palsies ◦ Acute upper airway obst ruct ion
• Treatm ent ◦ Support ive ◦ Avoid contact spor ts or heavy lift ing during rst 2 to 3 weeks
◦ Avoid alcohol for a few m onths ◦ Cort icosteroids m ay be required if above complicat ions ensue
Philpott_9783131662316_Ch56.indd 205 7/2/14 4:03 PM

206
56 Benign Neck Disease
56.2.9 Castleman Disease• Benign grow th of lym phoid t issue through B cell
proliferat ion w ith cytokine hypersecret ion (in terleukin 6)
• Can a ect any lym phoid t issue in the body• Unicentric vs. m ult icent ric t ypes
• Can m im ic lym phom a• Associat ion w ith HIV• May be t reated system ically in m ult icent ric
cases, including thalidom ide, chem otherapy, and cor t icosteroids
Philpott_9783131662316_Ch56.indd 206 7/2/14 4:03 PM

207
57.1 Oropharynx• Subsites
◦ Soft palate—anterior pillar lateral, posterior hard palate, free m argin inferior including uvular
◦ Base of tongue—anterior m argin is circumvallate papilla, poster ior is vallecular
◦ Tonsil—m ost com m on
57.1.1 Soft Palate• 2% of all H&N m alignancy• 80% SCC• Minor salivary gland tum ours (present
subm ucosal) w ith adenoid cyst ic m ost com m on• Uvular involvem ent or disease involving m idline
consider bilateral neck t reatm ent• High rate of occult m etastases (20–30%)
including ret ropharyngeal nodes• Velopharyngeal insu ciency w ith nasal regurgi-
tat ion can occur follow ing surgical resect ion• Radiotherapy ± chem otherapy is t reatm ent of
choice for m ost lesions• Post-radiotherapy recurrence and larger
tum ours surgical t reatm ent includes lip -split , m andibulotom y w ith preincision plat ing, oor of m outh incision extending poster iorly, includ-ing division of mylohyoid, to gain m axim um exposure
• Tum our resect ion w ith radial forearm free ap reconst ruct ion and covering t racheostomy
57.1.2 Tonsil• Aet iology
◦ HPV (bet ter prognosis P16 posit ive) ◦ Sm oking
• SCC m ost com m on (Fig. 57.1) followed by lym phom a
• Presents w ith ulcerat ion or asym m etrical tonsil enlargem ent or lym phadenopathy ± previous presentat ions
• Metastases to neck nodes levels 2 and 3 m ost com m on and often cyst ic (m isdiagnosed as branchial cysts)
• Trism us indicates pterygoid m uscle involvem ent
57 Tumours of the Pharynx
57.1.3 Tongue Base• Features
◦ May present late due to sym ptom s m isin terpreted as infect ion
◦ Subm ucosal disease m ay m ake prim ary easily m issed on exam inat ion
◦ Palpat ion of tongue base is vital part of exam inat ion and consider general anaesthe-sia ± biopsy if the gag re ex is too st rong but clin ically suspicious
◦ Can present as m etastat ic neck disease of unknow n prim ary
◦ Need to assess relat ion to m idline and hence w hether ipsilateral or bilateral neck requires t reatm ent
• Treatm ent ◦ Surgery, radiotherapy, or chem oradiotherapy ◦ There is a signi cant impact on speech and swallow ing funct ion w ith all t reatm ent opt ions, part icularly w ith large disease
◦ Mandibulotomy for access m ay be required ◦ Consider supplem entary feeding via gast rostomy before or after t reatm ent
• Staging ◦ T0: no evidence of prim ary tum our ◦ T1: tum our ≤ 2 cm ◦ T2: tum our 2–4 cm ◦ T3: tum our >4 cm ◦ T4a: tum our invades adjacent st ructures, e.g., cor t ical bone m andible, hard palate, larynx, and deep m uscles of tongue
◦ T4b: tum our invades lateral pterygoid m uscle, pterygoid plates, lateral nasopharynx, skull base, or encases carot id ar tery
57.2 Hypopharynx57.2.1 Subsites• Posterior pharyngeal wall—superior level of
hyoid bone to inferior border of cricoid• Piriform fossa (Fig. 57.2)—pharyngoepiglot t ic
fold to upper oesophagus• Postcricoid space (Fig. 57.3)—arytenoid
cart ilages to infer ior border of cricoid cart ilage
Philpott_9783131662316_Ch57.indd 207 02/05/14 10:47 AM

208
57 Tumours of the Pharynx
57.2.2 Surgical Pathology (SCC)• Piriform sinus = site in 50 to 66% of cases• Incidence of LN m ets:
◦ Piriform fossa 65%
◦ Postcr icoid 30% ◦ Posterior pharyngeal wall 40% ◦ Overall 45%
• T staging—based on oropharynx 2/4/larger m odel except also: ◦ T2—m ay invade m ore than 1 subsite w ithout xat ion of hem ilarynx
◦ T3—w ith xat ion of hem ilarynx ◦ Overall staging as for oropharynx
• Poor prognost ic factors ◦ Tum our >5 cm ◦ Postcr icoid area ◦ Vocal cord paresis ◦ LN m ets (h igher N stage) ◦ Distant m ets ◦ Perineural spread
57.2.3 Treatment• Treatm ent opt ions
◦ ~25% of pat ients untreatable at presentat ion ◦ Stage I to II usually require prim ary radiotherapy or a com binat ion of par t ial/total pharyngectomy and laryngectomy (± oesophagectomy) depending on site
◦ Stage II to IV usually require surgery (as above) and postop RT
◦ No established role for chem otherapy ◦ Neck dissect ion = select ive—levels II–IV + ret ropharyngeal space
• Inclusion criter ia for pr im ary radical radiotherapy ◦ Vert ical length of tum our <5 cm ◦ VCs m obile ◦ N0 neck
• 5-year survival rates ◦ Stage I—40 to 90% ◦ Stage II—28 to 82% ◦ Stage III—20 to 58% ◦ Stage IV—15 to 18% ◦ Overall—28 to 56% ◦ Piriform fossa—31 to 55% ◦ Pharyngeal wall—44% ◦ Postcricoid—29%
• Com plicat ions of total pharyngectomy ◦ Fistula form at ion ◦ Stricture form at ion (30–50% of cases w ith skin ap repair, uncom m on w ith free jejunal t ransfer)
◦ Flap necrosis (5–10%)• Com plicat ions of pharyngolaryngoesophagec-
tomy and gast ric t ransposit ion
Fig. 57.1 Carcinoma of the right tonsil.
Fig. 57.2 Carcinoma of the left piriform recess.
Fig. 57.3 Carcinoma of the postcricoid region at the oesophageal inlet .
Philpott_9783131662316_Ch57.indd 208 02/05/14 10:47 AM

209
Nasopharynx
◦ Pneum othorax ◦ Fistula form at ion ◦ Regurgitat ion
• Post-operat ive care ◦ CXR ◦ Feeding jejunostom y/TPN ◦ Start NG feeding w hen bowel sounds return; peroral feeding by day 7
◦ Chest and neck drains as appropriate ◦ Thyroid/parathyroid replacem ent ◦ Insert ion of speech valve
• Radiotherapy regim es ◦ Localized disease = 4–6 MV X-rays @ 55 Gy in 20 daily fract ions
◦ Advanced disease = 40 Gy in 20 fract ions over 4 weeks followed by 2nd phase of 26 Gy in 13 fract ions over 2.5 weeks
◦ Residual palpable nodes after phase 2 = 4 Gy in 2 fract ions over ½ week
57.3 Nasopharynx57.3.1 Surgical Pathology• Epidem iology
◦ NPC = 18% of all m alignancies in Cantonese ◦ Highest rates in Hong Kong ◦ Risk factors
- Genet ic—+ve FH - EBV infect ion—ant ibody response to viral capsid ant igen, early ant igen, and nuclear ant igen years after peak incidence of EBV infect ion
- Dietary habits—salted preserved sh + vitam in C de ciency
• Tum our t ypes ◦ SCC (85%)
- Kerat in izing - Non-kerat in izing - Undi erent iated
◦ Lymphom a—NHL = 95% ◦ Angio brom a—rare
• TNM classi cat ion ◦ T1—con ned to nasopharynx ◦ T2—extends to soft t issue of oropharynx and/or nasal fossa - a/b—w ithout/w ith parapharyngeal extension
◦ T3—invades bony st ructures and/or sinuses
◦ T4—intracranial extension and/or CNs/infratemporal fossa/hypopharynx/orbit )
◦ N1—unilateral ≤6 cm above supraclavicular fossa
◦ N2—bilateral ≤6 cm above supraclavicular fossa
◦ N3—>6 cm or in supraclavicular fossa
57.3.2 Common Presenting Symptoms• Nasal obst ruct ion• Cervical LNs• Unilateral ot it is m edia w ith e usion• CN palsies
57.3.3 Investigations• FBC• ESR• PTA + tym panom etry• Visual eld tests• EBV-related ant igen t iters• CT scan (± MRI)• Biopsy
57.3.4 Treatment• Radiotherapy
◦ Phase I—en bloc t reatm ent of nasopharynx and upper neck w ith parallel opposed lateral elds; lower neck and supraclavicular fossa t reated w ith anter ior eld
◦ Phase II—reduced elds using elect rons over posterior neck to reduce spinal cord dose
• Chem otherapy—plat inum -based com binat ions• Surgery
◦ Lim ited role: - In it ial diagnost ic biopsy - Sm all prim ary or recurrence locally—nasopharyngectomy via palate/m idfacial degloving or endoscopic resect ion dependent on tum our size
- Com plicat ions include: osteomyelit is of clivus, nasopharyngeal stenosis, oronasal stula, and glue ear
- Recurrence or non-responsive neck m etastases—neck dissect ion
• 5-year survival rates ◦ Stage I—90% ◦ Stage II—70% ◦ Stage III—60% ◦ Stage IV(A/B)—40% ◦ Stage IVC—0%
Philpott_9783131662316_Ch57.indd 209 02/05/14 10:47 AM

210
• Characterist ics ◦ Arise from deep lobe of parot id or cranial nerves posterior to carot id sheath
◦ Usually cause displacem ent of ret rom andibular port ion of parot id regardless of in t ra- or ext raparot id origin
◦ Masses m ay grow silent ly to 4 to 5 cm• Anatomy
◦ Inverted pyram id bounded by layers of deep cervical fascia
◦ Base is skull base ◦ Apex is greater cornu hyoid ◦ Lateral is fascia over m andible and m edial pterygoids
◦ Medial is fascia over superior const r ictor ◦ Divided in to pre- and postst yloid spaces (Table 58.1)
• Present ing sym ptom s ◦ Painless m ass ◦ Sore throat ◦ Dysphonia ◦ Dysphagia ◦ Trism us ◦ Nasal obst ruct ion ◦ Oral fullness
• Pathology ◦ React ive LNs ◦ Metastases—lym phom a, NPC ◦ Salivary (45%)—parot id/prestyloid salivary rests/m inor salivary glands
◦ Neurogenic (25%)—schwannom a, neuro brom a, neurosarcom a
◦ Paragangliom as (chem odectom as)—glom us vagale, carot id body, glom us jugulare
• Diagnosis ◦ CT scan ◦ FNAC ◦ Avoid open biopsy
• Surgical approaches to parapharyngeal space ◦ Cervical
- Poor exposure superior - Transverse incision level of hyoid - SM gland re ected upwards - Styloglossus and stylohyoid ligam ents divided - Parapharyngeal space is entered - Indicat ions: sm all ext raparot id tum our, neural sheath tum ours, carot id body tum ours
◦ Transparot id - Perform super cial parot idectomy w ith full exposure of CN VII
- Indicat ions: deep lobe parot id tum ours ◦ Cervicotranspharyngeal w ith m idline m andibulotom y - Maxim um exposure - Covering t racheostom y - Lip -split - ECA ligated - Indicat ions: large tum ours, h igh tum ours of vascular origin
58.1 Neuro bromas58.1.1 Pathology• Usually part of von Recklinghausen syndrom e
(NF1)—autosom al dom inant• NF2 less com m on• Tend to undergo fat t y degenerat ion• Malignant change can occur
58.1.2 Clinical Features• Slowly enlarging pain less neck m ass over several
years• Angiography to dist inguish from paragangliom as
58.1.3 Treatment• Excise sim ple tum ours and at tem pt to rejoin or
graft nerve• Som et im es vagus nerve has to be resected w ith
tum our
58.2 Glomus Tumours58.2.1 Features• They are paragangliom as (85% in abdom en,
12% chest , 3% H&N), w hich are neuroendocrine neoplasm s
• 1 per 1.3 m illion people• F:M 4:1• Most com m on benign tum ours in m iddle
ear and 2nd m ost com m on in tem poral bone (vest ibular schwannom a is m ost com m on)
58 Tumours of the Parapharyngeal Space
Philpott_9783131662316_Ch58.indd 210 02/05/14 11:13 AM

211
Glomus Tumours
• They are h ighly vascular tum ours that grow slowly w ith m arked bone erosion (can spare the ossicular chain) and expansion
• 5% grow rapidly w ith shor t survival periods• Potent ial to secrete catecholam ines result ing in
hypertension and tachycardia• 75% sporadic 25% fam ilial (autosom al dom inant
w ith incomplete penet rance)• 10% par t of MEN syndrom e• Rarer head and neck sites include larynx and
t rachea• In t racran ial involvem ent m ay lead to raised
ICP, hydrocephalus, ataxia, and brainstem sym ptom s
• 4% m etastasize• Histologically the cells are clustered together in
“Zellballen”• Im m unohistochem ist ry: + ve for chrom ogranin ,
neuron-speci c enolase, and serotonin• Main blood supply: ascending pharyngeal
ar tery from ECA and branches from pet rous par t of ICA
58.2.2 Investigation• Caut ious FNAC• Carot id ± ver tebral angiography (larger tum ours
involving the ICA and in t racranial extension, respect ively)
• CT/MRI (T1/T2 weighted—im ages w ith signal voids (pepperpot appearance) ◦ ± MIBG scin t igraphy
58.2.3 Treatment• Observat ion w ith ser ial scans• Medical
◦ β-Blockers for catecholam ine-secreting tum ours ◦ Chem otherapy for m ets
• Surgery ◦ Indicat ions
- Extending into palate/pharynx and interfering w ith swallow ing/speaking/breathing
- Aggressive grow th pat tern - Pat ient co-m orbidit ies do not cont raindicate
◦ Approaches - Type A—transm eatal approach - Type B—extended poster ior t ym panotomy - Type C—transm astoid/t ranstem poral + infratem poral approach + EEG m onitoring ± inject ion of cyanoacrylate glue for hem ostasis
- Type D—as above poster ior fossa explorat ion• Radiotherapy or [131I]MIBG therapy m ay be used
in non-surgical candidates or w here m ets• Gam m a knife radiosurgery• Em bolizat ion
58.2.4 Tumour Types• Glom us vagale tum ours
◦ Arise from nests of paraganglionic t issue w ithin perineurium of vagus (just below skull base)
◦ Most com m only present as slowly grow ing painless m ass
Table 58.1 Tumours of the parapharyngeal spaces
Prestyloid space Post-styloid space
Frequency 45% 55%
Contents Deep lobe parotid CN IX–XII
Maxillary artery IJV, ICA
Vii Cervical symp
Fat LNs
Loose areolar t issue
Pathology Salivary gland tumours:• Pleomorphic adenoma• Mucoepidermoid• Acinic cell
Paragangliomas
Neuro bromas
Lymphomas
SCC mets (oropharynx)
Lipomas (liposarcomas)
Philpott_9783131662316_Ch58.indd 211 02/05/14 11:13 AM

212
58 Tumours of the Parapharyngeal Space
◦ Other sym ptom s: - Pulsat ing t innitus - Deafness (conduct ive ± sensorineural) - Syncope - Vert igo - Pharyngeal pain = late sign
◦ Diagnosis con rm ed by angiography ◦ Excision required due to tendency to spread in t racranially
• Carot id body tum our (chem odectom as) ◦ Features
- High incidence in South Am erica at h igh alt itude
- Most com m on in 5th decade - Equal sex dist r ibut ion - Arises from chem oreceptor cells on m edial side of carot id bulb
◦ Presentat ion - Long history of slow ly enlarging pain less lump (years)
- 30% present w ith displacem ent of tonsil in oropharynx
- Firm , rubbery, and pulsat ile on palpat ion - Bruit m ay be present
• Glom us jugulare and tym panicum ◦ Usually present w ith pulsat ile t innitus, possible hearing loss
◦ Glom us tym panicum is con ned to m iddle ear space
◦ May involve cranial nerves around jugular foram en result ing in di culty in swallow ing, hoarseness, and weakness of shoulder
◦ Glom us jugulare tum ours norm ally a ect wom en in their 5th /6th decade
◦ Arise from non-chrom a n paraganglionic cells around jugular ganglion in jugular bulb
• Fisch classi cat ion of glom us tum ours ◦ Type A: localized to m iddle ear cleft ◦ Type B: t ym panom astoid tum ours w ith no dest ruct ion of bone in the infralabyrin th ine compartm ent of tem poral bone
◦ Type C: invading bone of infralabyrin th ine ◦ Type D: in t racranial extension
Philpott_9783131662316_Ch58.indd 212 02/05/14 11:13 AM

213
59.1 Triangles of the Neck• Anterior
◦ Subm ental ◦ Subm andibular ◦ Carot id ◦ Muscular
• Poster ior ◦ Occipital ◦ Subclavian
59.2 Head and Neck Lymphatics59.2.1 Waldeyer Internal Ring• Circular collect ion of lym phoid t issue aggregates
w ith in pharynx at skull base ◦ Adenoids ◦ Tubal and lingual tonsils ◦ Palat ine tonsils ◦ Aggregates of lym phoid t issue on posterior pharyngeal wall
59.2.2 Waldeyer External Ring• Super cial nodal system
◦ Occipital ◦ Postauricular ◦ Parot id ◦ Preauricular ◦ Buccal/facial ◦ Super cial cervical ◦ Subm andibular ◦ Subm ental ◦ Anterior cervical
• Drains ◦ Skin ◦ Scalp ◦ Eyelids ◦ Face ◦ Waldeyer in ternal r ing ◦ Sinuses ◦ Oral cavity
59.2.3 Deep System (Cervical Lymph Nodes)• Deep st ructures drain directly or through
super cial system ◦ Junct ional ◦ Upper cervical ◦ Middle cervical ◦ Lower cervical ◦ Spinal accessory group ◦ Nuchal ◦ Visceral ◦ Upper m ediast inal
• Jugular t runks form from con uence of deep lym phat ics ◦ On right ends at junct ion of IJV and brachiocephalic vein or joins right lym phat ic duct
◦ On left joins thoracic duct
59.2.4 Drainage by Level• I
◦ Subm ental = lower lip , oor of m outh , lower gum
◦ Subm andibular = face, nose, sinuses, oral cavit y, SMG
• II = oral cavity, pharynx, supraglot t ic larynx• III = thyroid, larynx, hypopharynx, cervical
oesophagus• IV = in t ra-abdom inal organs, breast , lung,
oesophagus, thyroid• V = nasopharynx, thyroid, oesophagus, lung, breast• VI = anter ior com partm ent (visceral) group, e.g.,
para- and preotracheal LNs• VII = upper anterior m ediast inum
59.2.5 Nodal Classi cation in Malignancy• N1—m ets in single ipsilateral node £3 cm
diam eter
59 Metastatic Neck Disease
Philpott_9783131662316_Ch59.indd 213 02/05/14 11:40 AM

214
59 Metastat ic Neck Disease
• N2—3 to 6 cm ◦ N2a—single ipsilateral node ◦ N2b—m ult iple ipsilateral nodes ◦ N2c—bilateral/cont ralateral nodes
• N3—>6 cm diam eter
59.2.6 Suspicious Imaging Features• >1 cm diam• Rim enhancem ent follow ing IV contrast• Central necrosis
◦ Spherical shape
59.3 Features of Metastatic Neck Disease• See Figs. 59.1 and 59.2
59.4 The N0 Neck• Argum ents for elect ive surgery
◦ High incidence of occult m etastat ic disease (Table 59.1)
◦ Lim ited neck dissect ion has low m orbidity and m ortalit y
◦ If prim ary lesion has to be rem oved from the neck, en-bloc resect ion is preferable
◦ No clin ical abilit y to detect conversion of N0 to N1
◦ Allow ing neck m ets to develop increases incidence of distant m ets
◦ Cure rate for neck dissect ion decreased if gland enlargem ent occurs or m ult iple nodes appear
• Argum ents against elect ive surgery ◦ Cure rates are no lower in the N1 neck ◦ Careful clin ical follow -up w ill allow detect ion at earliest conversion from N0 to N1
◦ Radiat ion is as e ect ive as neck dissect ion for non-palpable disease
◦ Elect ive neck dissect ion results in a large num ber of unnecessary surgical procedures
◦ Rem oves barrier to spread of disease and m ay have det r im ental im m unological e ect
• Indicat ions for elect ive neck t reatm ent ◦ > 20 to 25% chance of subclin ical disease ◦ Vigilant follow-up is not possible ◦ Clinical evaluat ion of neck is di cult ◦ Surgery is being perform ed for access or reconst ruct ion
◦ Im aging suggests possible occult nodal spread
• Contraindicat ions to neck dissect ion: ◦ Prim ary tum our unt reatable ◦ Un t for m ajor surgery ◦ Inoperable neck disease inc. carot id encasem ent and skull base/in t racranial involvem ent
59.5 Radiotherapy for Metastatic Neck Disease• Clin ically negat ive neck (N0)• Clin ically posit ive neck• Elect ively after surgery
◦ Node-posit ive disease ◦ Other r isk factor for local recurrence inc. ext racapsular spread
• Neck disease developing or recurring after in it ial t reatm ent: ◦ Nodal m ets developing in untreated neck after in it ial t reatm ent of prim ary tum our alone
◦ Recurrence after previous surgery to neck ◦ Nodal recurrence after com bined t reatm ent
Table 59.1 Incidence of neck metastases
Subsite % Risk of neck metastases
Oral cavity >20%
Glot tis 0–15%
Supraglot tis 8–30%
Oropharynx >50%
Hypopharynx >50%
Fig. 59.1a,ba Lymph-node metastases are solid, indolent, and xed
to the surrounding tissue.b Exulceration of the metastases produces
haemorrhagic secretion and often an in amed reaction in the surrounding skin.
Philpott_9783131662316_Ch59.indd 214 02/05/14 11:40 AM

215
Management of Locoregional Recurrence
59.6 Management of Locoregional Recurrence• Need histological con rm at ion and fu ll restaging
(clin ical + radiological) w ith discussion at MDT• Opt ions:
◦ Surgery (salvage)
◦ RT (reirradiat ion but dose m ust exceed 50 Gy) ◦ Palliat ion
• Meta-analysis of ret rospect ive case ser ies shows a 39% 5-year survival follow ing salvage surgery for recurrent previously irradiated laryngeal, pharyngeal, and oral cavit y tum our; th is is not in uenced by original m odalit y of t reatm ent
Fig. 59.2a–h a Typical sites for
regional lymph-node metastases. 1, sub-mental lymph nodes; 2, submandibular lymph nodes; 3, pa-rotid and preauricular lymph nodes; 4, retro-auricular lymph nodes; 5, lymph nodes in the jugulofacial venous angle; 6, deep cervical lymph nodes; 7, lymph nodes in the juguloclavicular venous angle: lower deep cervical lymph nodes and supracla-vicular lymph nodes; 8, pretracheal and peritracheal lymph nodes; 9, prelaryngeal lymph nodes.
b Laryngeal carcinoma.c Carcinoma of di erent
parts of the tongue.d Tonsillar carcinoma.e Lower lip carcinoma.f Carcinoma of the
external ear. Note the segmental lymphatic e erent from the auricle.
g Parotid carcinoma (the intraglandular lymph-node metasta-ses should be noted).
h Submandibular gland carcinoma.
ba
dc
fe
hg
4
3
12
6
5
7
9
8
Philpott_9783131662316_Ch59.indd 215 02/05/14 11:40 AM

216
59 Metastat ic Neck Disease
59.7 Incisions for Neck Dissection• See Fig. 59.3
◦ Schobinger ◦ Horizontal-T (Het ter) ◦ McFee ◦ Lateral ut ilit y ◦ Utilit y ◦ Visor ◦ Extended thyroid ◦ H-incision
59.8 Corners of Consternation• Lower end of IJV• Junct ion of lateral border of clavicle w ith lower
edge of t rapezius
• Upper end of IJV• Subm andibular t r iangle
59.9 Modi ed Radical Neck Dissection• Type 1
◦ Removal of all LNs (I–IV) with preservation of XI n ◦ For operable palpable neck disease (N1, N2a/b); occasionally N0
• Type 2 ◦ As for t ype 1 w ith preservat ion of IJV ◦ For sam e indicat ions as t ype 1 w hen:
- Second side operat ion - Microvascular anastom osis required - Histology dictates that IJV need not be resected (DTC)
Fig. 59.3 Incisions for neck dissection.
a b c
Horizontal-T (Het ter) McFee
Visor
Schobinger
d e f
Extended thyroid
g
H-Incision
h
Utilit yLateral utility
Philpott_9783131662316_Ch59.indd 216 02/05/14 11:40 AM
217
The Occult Primary
• Type 3 ◦ As for t ype 2 w ith preservat ion of SCM ◦ Indicat ions:
- N0 neck - DTC - Skin tum ours (m elanom a, SCC, Merkel cell ca)
59.10 Selective Neck Dissection• Indicat ions
◦ For the previously untreated N0 neck ◦ Preservat ion of SCM, IJV, and XIn
• Supraom ohyoid ◦ Levels I to III ◦ T1–T4 N0 SCC oral cavit y
• Extended supraom ohyoid ◦ Levels I to IV ◦ Skin cancer anterior to line of t ragus ◦ Perform ed in conjunct ion w ith super cial parot idectomy
• Lateral ◦ Levels II to IV ◦ T2 to T4 N0 SCC larynx/oropharynx/hypopharynx
• Posterolateral ◦ Levels II to V plus postauricular and suboccipital nodes
◦ SCC/m elanom a posterior to line of t ragus• Anterior/cent ral
◦ Level VI ◦ DTC, subglot t ic, and hypopharyngeal SCC
• Superior m ediast inum ◦ Level VII ◦ DTC and m edullary thyroid ca ◦ Subglot t ic and hypopharyngeal SCC ◦ Cervical oesophageal ca
59.11 The Occult Primary59.11.1 Features• Solitary LN m et in neck—90% from H&N• Vigilant search w ill nd source in 50% of cases
• Post-t r iangle nodes = PNS com m only (esp. if young)
• Supraclavicular fossa (r ising sun) nodes = lung/stom ach/breast /other
• 4 m ale: 1 fem ale• Tum our t ype
◦ SCC = 33 to 50% ◦ UTC/anaplast ic = 25% ◦ Adenocarcinom a = 25%
• Prim ary sites in order of frequency ◦ Nasopharynx ◦ Tonsil ◦ Retrom olar t r igone ◦ Tongue base ◦ Piriform sinus ◦ Other m isc. H&N sites ◦ Bronchus/breast/stom ach
• 50% 5-year survival rate
59.11.2 Stepwise Investigation• History—other aerodigest ive t ract Sx?• Exam inat ion
◦ LN or direct extension of prim ary tum our ◦ Full H&N exam inat ion
• FNAC ◦ Suspicious—repeat FNAC/incisional Bx/frozen sect ion
◦ Malignant—re-exam ine “co n corners” ◦ Ret iculoendothelial—incisional biopsy ◦ Benign/react ive/thyroid—as appropriate
• Radiology ◦ MRI ◦ PET scan
• Endoscopy ◦ Panendoscopy and PNS exam inat ion and tongue base palpat ion
◦ If no obvious lesion-blind biopsy tongue base, unilateral tonsillectomy and post-nasal space
• Treatm ent ◦ Neck dissect ion and postop radiotherapy ◦ Role for frozen sect ion before proceeding to neck dissect ion
◦ 33% of cases—prim ary is revealed during 5-year follow -up
Philpott_9783131662316_Ch59.indd 217 02/05/14 11:40 AM

218
60.1 Chemotherapy60.1.1 General Principles• Role of neoadjuvant (before de n it ive
t reatm ent) aim s to decrease tum our size, object ive response rates range from 30 to 90%
• No increase in survival but m ay decrease m ass, painful in lt rat ion + regression of lung m ets w ith increase in QoL
• No regim en has been able to induce com plete responses, i.e., disappearance of all detectable evidence of cancer
• Adjuvant chem o is adm inistered after prim ary t reatm ent if pat ient has h igh risk of recurrence
• Chem o RT increases response rates and survival for unresectable stage III/IV disease. Relat ive r isk of death decreases m ore for oropharynx and larynx if <60 years (compared w ith oral cavity and hypopharynx)
60.1.2 Agents• Cisplat in :
◦ In terferes w ith t ranscript ion , result ing in new m utat ions
◦ Plat inum -based drug “alkylat ing-like” agent ◦ Cyclophospham ide is t rue alkylat ing agent ◦ 28% response rate ◦ Side e ects: nausea and vom it ing, renal failure, peripheral neuropathy, alopecia, elect rolyte loss (Na, K, Mg)
• 5-Fluorouracil/m ethot rexate: ◦ Antim etabolite, im pairs norm al product ion of nucleot ides
◦ 15% response rate ◦ Side e ects: nausea and vom it ing, m ucosit is, photosensit ivit y, myelosuppression
• Paclitaxel: ◦ Mitot ic inhibitor ◦ In terferes w ith m icrotubules disrupt ing cell division
◦ 38% response rate ◦ Side e ects: peripheral neuropathy, alopecia, nausea and vom it ing, myelosuppression
60 Chemotherapy and Radiotherapy in Head and Neck Cancer
• Vincrist ine/vinblast ine: ◦ Plant derivat ives ◦ Prevent spindle form at ion during m itosis by binding to tubulin , leading to m etaphase arrest
◦ Side e ects: neuropathy• Act inomycin D, bleom ycin , doxorubicin :
◦ Ant itum our ant ibiot ics ◦ In tercalate between DNA base pairs, prevent ing cell division
◦ Side e ects: m yelosuppression, cardiotoxicit y, alopecia
• Cetuxim ab: ◦ Monoclonal ant ibody directed against epiderm al grow th factor receptor, w hich is a grow th-prom ot ing protein that is overexpressed in the m ajorit y of SCC in H&N
◦ Com bined w ith RT in locoregional advanced H&N cancer provides 10% increased overall survival com pared w ith RT alone
◦ No RCTs looking at chem o RT ± concurrent cetuxim ab
◦ Indicated in pat ients not t enough for concurrent chem o + RT
60.1.3 Complications of Chemotherapy• Acute:
◦ Myelosuppression—anaem ia, throm bocytopenia, neutropenia
◦ Nausea and vom it ing ◦ Diarrhoea ◦ Soft t issue necrosis w ith ext ravasat ion ◦ Alopecia
• Late: ◦ Renal failure ◦ Haem orrhagic cyst it is ◦ Neurotoxicit y (peripheral neuropathy) ◦ Cardiotoxicit y—acute arrhythm ias ◦ Pulm onary toxicit y— brosis ◦ Infer t ilit y ◦ Second m alignant neoplasm s, e.g., leukaem ia
Philpott_9783131662316_Ch60.indd 218 02/05/14 12:44 PM

219
Radiotherapy
60.2 Radiotherapy60.2.1 General Principles• Dam ages cells that are rapidly dividing, t ypically
through delivery of h igh-energy photons or elect rons (via linear accelerator); norm al cells m ay be dam aged but w ith a slower regenerat ion allow ing for repair to occur
• Unit of absorbed dose is the gray (Gy)• Pre-t reatm ent CT scan is necessary before any
t reatm ent can begin• Sim ulat ion w here t reatm ent posit ion is at tained
and blocks can be m ade for t reatm ent process (now com bined w ith CT in m any units)
• Tat toos help guide placem ent of t reatm ent elds
• Styrofoam casts that conform to the pat ient’s body allow the sam e posit ion to be adopted for each daily t reatm ent
• Opt im al dose dist r ibut ion is determ ined by dosim et rist and several plans are generated
60.2.2 Conventional: Single Daily Fractions• 1.8 to 2.0 Gy ×5/w k• Total ~60 Gy
60.2.3 Modi ed• Hypofract ionat ion:
◦ >2 Gy/fract ion ◦ Indicat ions: glot t icca
• Hyperfract ionat ion ◦ <1.8 Gy/fract ion ◦ Increased num ber of t reatm ents ◦ Increase acute toxicit y, not late e ects ◦ RCT data shows increased locoregional control in locally advanced ca
• Accelerated ◦ >10 Gy/w k ◦ Decrease in fract ion t im e ◦ 72 Gy in 5/52 ◦ 3 fract ions/day ◦ Increase grade III/IV and late e ects ◦ Increase locoregional cont rol
• CHART ◦ Cont inuous hyperfract ionated accelerated radiotherapy
◦ 54 Gy in 36 fract ions over 12/7
◦ Addit ion of chem o leads to increase locoregional cont rol + survival but also increased m ucosal toxicit y
• IMRT ◦ In tensit y-m odulated RT ◦ Minim izes exposure to spinal cord, opt ic nerve, and salivary glands
60.2.4 Indications for Adjuvant RT after Surgery• T3–T4 tum our• Invasion bone or beyond prim ary site• Mult iple +ve LNs• +ve level IV/V nodes• Perineural invasion• Extracapsular nodal invasion• Lym phovascular invasion• +ve m argins of resect ion of either prim ary
tum our/neck disease• Recurrent disease• Oral cavity prim ary
60.2.5 Indications for RT Alone• T1/T2 tongue, tonsil, larynx, and hypopharynx• N0/N1• Except ions are nasopharynx w here RT is
standard t reatm ent regardless of T or N stage• Tum ours of salivary glands + oor of m outh are
norm ally m anaged by surgery prim arily
60.2.6 Other Notes on Radiotherapy• A clin ically –ve undissected neck w ill be
controlled w ith a probabilit y of >90% if a total of 54 Gy delivered in daily fract ions of 1.8 Gy
• Postop doses are h igher because of brosis and scar t issue w ith reduced blood ow ◦ Minim um dosage of 57.6 Gy up to 63 Gy if neck dissect ion dem onstrates ext racapsular spread or other h igh-risk features
• RT should be com pleted 10–11/52 after surgery w ith delays a ect ing survival and locoregional control
• If RT is being used as the single m odalit y, a m odi ed fract ionat ion schem e should be used
• Salvage surgery should be available if organ preservat ion is being pursued
Philpott_9783131662316_Ch60.indd 219 02/05/14 12:44 PM

220
60 Chemotherapy and Radiotherapy in Head and Neck Cancer
• In a node +ve neck there is insu cient evidence to suppor t use of select ive neck dissect ion (indicated in node N0 neck)
• Tum ours encroaching on the m idline need to have considerat ion for the contralateral as well as ipsilateral neck
• Brachytherapy is another m odalit y of t reatm ent in oral cavit y ca
• If surgery is to be considered reconst ruct ion of defect should be thought of w ith the aim s of achieving good funct ional and cosm et ic outcom e
• Oral cavity N0 neck—consider select ive neck dissect ion/RT levels I to III
• Oropharyngeal N0 neck—consider levels II–IV unless tongue base levels II to V
60.2.7 Complications of Radiotherapy• Acute:
◦ Skin react ion ◦ Mucosal react ion ◦ First 2–3/52 ◦ Resolve w ith in 4–6/52 ◦ Skin erythem a, dryness, pruritus, hoarseness, serous OM, m ucosit is, xerostom ia + odynophagia
◦ Xerostom ia m ay be perm anent if m ajor salivary glands (>20 Gy) are w ithin the RT eld
◦ Pilocarpine 5 to 10 m g 3× daily during and after t reatm ent m ay reduce th is (cont raindicated in uncontrolled asthm at ics/COPD)
◦ Benzydam ine oral r inse m ay also help but can cause st inging
• Late ◦ Xerostom ia ◦ Osteoradionecrosis
- Osteoradionecrosis is greatly decreased by m et iculous dental care before, during, and after RT
- Any teeth requiring extract ion should be perform ed before RT, allow ing 2–4/52 healing t im e
◦ Telangectasia ◦ Skin at rophy ◦ Hypopigm entat ion ◦ Fibrosis ◦ L’Herm it te syndrom e, aka barber chair syndrom e (shoot ing pains dow n arm s and legs on neck exion due to dem yelinat ion at 12 weeks)
◦ Hypothyroidism ◦ Visual problem s ◦ Subm ental oedm ea (dewlap) ◦ Laryngeal oedm ea ◦ Induct ion of 2nd cancers
60.3 Clinical Evidence60.3.1 Department of Veterans A airs Laryngeal Cancer Study• The Departm ent of Veterans A airs Laryngeal
Cancer Study Group. Induct ion chem otherapy plus radiat ion com pared w ith surgery plus radiat ion in pat ients w ith advance laryngeal cancer. N Engl J Med 1991;324:1685–90 ◦ Random assignm ent: Stage III and IV laryngeal SCC
◦ Arm s: - Total laryngectomy and adjuvant RT - Induct ion chem otherapy w ith cisplat in and uorouracil, followed by RT
- If no response to chem otherapy or residual/recurrent disease after chem o RT then salvage surgery indicated
◦ Results: - 2-year survival rate in non-salvage groups was 68%
- Laryngeal preservat ion: possible in 64% of induct ion chem otherapy (41% overall)
◦ Conclusions: - The study showed the e cacy of chem otherapy followed by radiotherapy was sim ilar to that of surgery followed by radiotherapy and w ith the addit ional advantage of laryngeal preservat ion in two-th irds of the pat ients
60.3.2 RTOG (Radiation Therapy Oncology Group) Study• Forast iere AA, Goepfert H, Maor M, et al.
Concurrent chem otherapy and radiotherapy for organ preservat ion in advanced laryngeal cancer. N Engl J Med 2003;349:2091–8 ◦ Stage III and IV laryngeal SCC ◦ Does radiotherapy alone have sim ilar survival and laryngeal preservat ion to chem o RT?
◦ Arm s: - Induct ion chem otherapy followed by RT - Concurrent chem o RT
Philpott_9783131662316_Ch60.indd 220 02/05/14 12:44 PM

221
Clinical Evidence
- RT alone - Pat ients w ith large, T4 lesions (tum ours extending through the thyroid cart ilage or in to the base of the tongue) were excluded
◦ Results: - 2-year and 5-year survival rates were sim ilar am ong the three groups
- Concurrent chem otherapy: h igher rates of laryngeal preservat ion and local control
- Acute toxic e ects were h igher in both chem otherapy groups than in the RT group
- Late toxic e ects, including swallow ing dysfunct ion, were sim ilar
◦ Conclusions: - In it ial t reatm ent aim ed at laryngeal preservat ion is an opt ion for m ost pat ients w ith in term ediate- or late-stage laryngeal cancer
- Chem otherapy tolerated best as concurrent w ith radiotherapy
- Induct ion chem otherapy followed by radiotherapy is not supported by these results
- Pat ients unable to tolerate concom itant chem otherapy and radiotherapy should receive radiotherapy alone
Philpott_9783131662316_Ch60.indd 221 02/05/14 12:44 PM

222
61.1 Robotic Surgery in Head and Neck• History
◦ Da Vinci Robot ◦ 1st ever robot ic operat ion was a hear t bypass in Leipzig, Germ any, in 1998
◦ 1st t ransoral resect ion by Weinstein /O’Malley at Universit y of Pennsylvania, USA, 2004
• Indicat ions ◦ Oropharyngeal, laryngeal, hypopharyngeal m alignancy
◦ Parapharyngeal tum ours ◦ Thyroid and parathyroid surgery ◦ (In it ial cadaveric studies show tongue base hyper t rophy contr ibut ing to obst ruct ive apnea m ay be an applicat ion for the robot)
• Advantages ◦ Increased visualizat ion and precision through lim ited access
◦ Transoral approach ◦ Reduced surgical t im e ◦ Shorter hospital stay ◦ Avoidance/dose reduct ion in chem o/RT
• Disadvantages ◦ Expense ◦ Learning curve for surgeons and theat re sta ◦ Lim ited software to run the robot ◦ No tact ile feedback
• Setup ◦ Surgeon’s console (in room w ith pat ient) ◦ Inst rum ent car t w ith robot w ith 4 in teract ive robot ic arm s adjacent to pat ient
◦ 3 arm s are holders for inst rum ents such as scalpel, scissor, and cautery
◦ 1 arm is a cam era (0° or 30°) w ith 2 lenses a ording stereoscopic vision
◦ Surgeon looks via the w ired vision cart at a h igh-de n it ion 3D im age on the console w hile using 2 foot- and 2 hand-cont rolled pedals that m ove the arm s
◦ Movem ents by the surgeon are converted in to m icroscopic m ovem ents by the robot’s computer system
◦ The range of m ovem ent is 540° of rotat ion
◦ Com puterized m ot ion scaling elim inates t rem ors and fat igue
◦ Process relies on hum an operator for all input ◦ Future developm ents include rem ote operat ing, i.e., the pat ient and robot are in a di erent place to the surgeon; role in m etastat ic SCC in the neck; and developm ent of hapt ic feedback system s
61.2 Transoral Laser Surgery in Head and Neck• History
◦ 1985 Steiner, Am brosch: Universit y of Göt t ingen, Germ any
◦ See Table 61.1• Advantages
◦ Less local recurrence ◦ Less salvage laryngectomy ◦ Organ sparing ◦ Morbidity/com plicat ion rate lower
• Disadvantages ◦ Laser injury ◦ Learning curve
• European Laryngological Society classi cat ion of endoscopic resect ion (Fig. 61.1) ◦ Type I—subepithelial cordectomy
- Resect ion VF epithelium passing through the super cial layer of lam ina propria
◦ Type II—subligam ental cordectomy - Resect ion of epithelium , Reinke space, and the vocal ligam ent
◦ Type III—transm uscular cordectomy - Resect ion of the VF dow n through vocalis m uscle
◦ Type IV—total cordectomy - Resect ion of the cord that extends from the vocal process to the anterior com m isure ± in ternal perichondrium of the thyroid ala
◦ Type V—Extended cordectomy - Va: + cont ralateral vocal fold and anterior com m issure
- Vb: + arytenoids - Vc: + subglot t is - Vd: + vent ricle and false cords
61 Robotic Surgery and Transoral Laser Surgery in Head and Neck
Philpott_9783131662316_Ch61.indd 222 02/05/14 1:14 PM

223
Transoral Laser Surgery in Head and Neck
◦ Type VI—resect ion of the anterior com m issure w ith bilateral anterior cordectomy ± subglot t ic m ucosa and cricothyroid m em brane
• CO2 laser resect ion principles ◦ Should be o ered as another t reatm ent opt ion to all pat ients w ith early stage tum ours
◦ Typical set t ings include 5 W cont inuous (alternat ives m ay vary dependent on local policy)
◦ The laser beam is re ected by opt ical aim ing m irrors w ith a spot size of 250 µm
◦ Placem ent of wet swabs including eyes, face, and neurosurgical pat t ies w ithin the t rachea a ording increased protect ion of surrounding t issues against laser de ect ion dam age
◦ All theat re sta m ust wear glass or plast ic goggles for eye protect ion
◦ Matt- n ish scopes reduce light re ect ion w ith integrated sm oke evacuat ion pipes to rem ove laser plum e via disposable suct ion tubing
◦ Distending “Steiner” laryngopharyngoscope is good for supraglot t ic/hypopharyngeal tum ours
◦ Consider false cord resect ion to gain exposure to lateral tum our m argin of larynx
◦ Specim en orientat ion ◦ Standard head and neck m argins are not applicable, so 1 m m or m ore is acceptable in larynx
◦ Biopsy resect ion m argins and consider second-look procedure if posit ive or close
◦ In t raoperat ive photo docum entat ion ◦ Larger tum ours can be t ransected w ithout r isk of seeding as lym ph vessels are sim ultaneously sealed
◦ Di erent iat ion can be seen between healthy t issue and tum our under the m icroscope; if in doubt consider frozen sect ion
◦ Failure before 12 m onths is considered residual disease
◦ Failure after 12 m onths is recurrent ◦ Use of voice outcom es including Voice Sym ptom Scale (VoiSS) pret reatm ent , 3, 6, and 12 m onths post-op
Table 61.1 Steiner’s results
Tonsil Tongue base
Supraglottis Hypopharynx Advanced larynx
Early larynx± anterior commissure
Number 102 82 277 172 117 444
Overall local control 76.5% 84% 81% 71.5% 74% 84%/72%
5-yr overall survival 57.5% 59% 67.5% 58%
5-yr recurrence-free survival
Stage I–II 64% 70% 81% 73% 71% 95%
Stage III 60% 44% 65% 59% 47% 69%
Stage IV 60% 58% 65% 47% 47% 69%
Chemotherapy 66% 55% 22% 52% 38% 0%
Sources:1. Hinni ML, Salassa JR, Grant DG, et al. Transoral laser microsurgery for advanced laryngeal cancer. Arch Otolaryngol Head
Neck Surg 2007;133(12):1198–2042. Canis M, Ihler F, Wol HA, Christiansen H, Mat thias C, Steiner W. Oncologic and functional results after transoral laser
microsurgery of tongue base carcinoma. Eur Arch Otorhinolaryngol 2013;270(3):1075–833. Rödel RM, Steiner W, Müller RM, Kron M, Mat thias C. Endoscopic laser surgery of early glot tic cancer: involvement of
the anterior commissure. Head Neck 2009;31(5):583–924. Martin A, Jäckel MC, Christiansen H, Mahmoodzada M, Kron M, Steiner W. Organ preserving transoral laser microsur-
gery for cancer of the hypopharynx. Laryngoscope 2008;118(3):398–4025. Canis M, Martin A, Ihler F, et al. Results of transoral laser microsurgery for supraglot tic carcinoma in 277 patients. Eur
Arch Otorhinolaryngol 2013;270(8):2315–266. Canis M, Martin A, Kron M, et al. Results of transoral laser microsurgery in 102 patients with squamous cell carcinoma
of the tonsil. Eur Arch Otorhinolaryngol 2013;270(8):2299–306
Philpott_9783131662316_Ch61.indd 223 02/05/14 1:14 PM

224
61 Robotic Surgery and Transoral Laser Surgery in Head and Neck
Fig. 61.1a–f The classi cation of cordectomies.a Subepithelial cordectomy (type I): resection of the vocal fold epithelium, passing through the super cial layer of the
lamina propria.b Subligamental cordectomy (type II): resection of the epithelium, Reinke space, and vocal ligament.c Transmuscular cordectomy (type III): through the vocalis muscle.d Total cordectomy (type IV) extends from the vocal process to the anterior commissure. The depth of the surgical
margins reaches the internal perichondrium of the thyroid ala, and sometimes the perichondrium is included in the resection.
e Extended cordectomy: type Va encompasses the contralateral vocal fold and the anterior commissure; t ype Vb includes the arytenoids; type Vc encompasses the subglot tis; and type Vd includes the ventricle.
f Anterior commissurectomy (type VI): a bilateral anterior cordectomy for cancer originating in the anterior commis-sure without in ltration into the thyroid cartilage, either extending or not extending to one or both vocal folds.
a
b
c
d
e
f
Philpott_9783131662316_Ch61.indd 224 02/05/14 1:14 PM

Sect ion IV
Paediatric Otorhinolaryngology
Philpott_9783131662316_Ch62.indd 225 02/05/14 1:17 PM

Philpott_9783131662316_Ch62.indd 226 02/05/14 1:17 PM

227
62.1 Inner Ear• Com m on in those w ith SNHL; m ay involve
m em branous, bony, or both par ts of labyrin th (form er probably m ost com m on but do not show on im aging)
• Various classi cat ion system s—Jackler et al (1987) based on their occurrence in em bryogenesis; m ost likely to arise between 4–8/40
• Michel aplasia: arrest of inner ear developm ent before 4/40—complete aplasia of all inner ear st ructures; associated w ith thalidom ide exposure, anencephaly, Klippel–Feil syndrom e; total SNHL, not candidate for CI
62.1.1 Cochlear Anomalies• Com m on cavit y: failure at 4/40, w ith
m em branous labyrin th poorly di erent iated in a large com m on cavit y; severe to profound HL; can t ry CI (risk CSF gusher)
• Cochlear aplasia: failure at 5/40; rare; norm al vest ibular developm ent; profound SNHL, unlikely candidate for CI
• Cochlear hypoplasia: failure at 6/40 w ith variable HL
• Mondini dysplasia; failure at 7/40, w ith incomplete part it ion of cochlea so only basal turn cochlea present (m ost com m on cochlear m alform ation seen on im aging) w ith variable HL (som e high-tone residual hearing possible); m ay be associated w ith w idened vest ibular aqueduct , som e associated w ith stapes footplate anom alies, Waardenburg, DiGeorge, Pendred syndrom es
• Widened vest ibular aqueduct: de n it ion varies, e.g., ≥1.5 m m ; m ay be associated w ith Pendred and branchio-otorenal syndrom e, coch lear dysplasias, or stapes xat ion; often norm al hearing at bir th w ith progressive SNHL, som et im es sudden after m ild HI; avoid HI/pressure changes ( ights, diving); 30% have vest ibular disturbance; autosom al recessive
62.1.2 Vestibular Anomalies• Aplasia or dysplasia of lateral Scc m ost com m on
(because develops later than other Sccs); m ay
62 Congenital Malformations of the Ear
be associated w ith CHARGE (colobom a, heart defects, at resia of nasal choanae, retardat ion of grow th, genital and/or urinary abnorm alit ies, ear abnorm alit ies and deafness) syndrom e (w hich also has stenot ic cochlear aperture, underdeveloped vest ibule, incom plete part it ion of cochlea)
62.1.3 Membranous Anomalies• Occur in isolat ion or w ith bony labyrin th ine
anom alies (because do not show on im aging, only determ ined histologically) ◦ Bing–Siebenm ann m alform at ion: isolated m em branous m alform at ion w ith in well-form ed bony capsule; profound SNHL; associated w ith Usher and Jervell–Lange-Nielsen syndrom es
◦ Scheibe m alform at ion : m ost com m on m em branous inner ear m alform at ion—m alform ed organ of Cor t i and saccu le; severe to p rofound SNHL; associated w ith Usher, Jer vell–Lange-Nielsen , Refsum , Waardenbu rg, t r isom y 18; au tosom al recessive inher it ance
◦ Alexander m alform at ion: least severe—dysplast ic basal turn of cochlea; h igh-frequency SNHL
62.2 Middle Ear• Num erous ossicular abnorm alit ies; m alleus
head xat ion m ost com m on (due to incom plete pneum at izat ion of epitympanum )
• Persistent stapedial ar tery: 2nd arch rem nant , should regress at 10/40; if it does not , passes over stapes footplate; m ay be associated w ith aberrant course of ICA
• High jugular bulb• Facial nerve: aberrant course m ost likely in
presence of other congenital abnorm alit ies
62.3 External Ear• Microt ia
◦ 1:10,000, M>F, R>L-hand side; 4:1 unilateral: bilateral
Philpott_9783131662316_Ch62.indd 227 02/05/14 1:17 PM

228
62 Congenital Malformations of the Ear
◦ Associat ion w ith other congenital abnorm alit ies in ~50% cases (e.g., Treacher–Collins, Goldenhar, hem ifacial m icrosom ia) and teratogens (e.g., thalidom ide)
◦ Weerda classi cat ion: - 1st degree dysplasia: m ost st ructures of norm al auricle recognizable
- 2nd degree: som e recognizable st ructures but addit ional skin /cart ilage required for reconst ruct ion
- 3rd degree: no norm al st ructures seen so total reconst ruct ion required
◦ Rx: do nothing; m inor m alform at ions can be excised/repaired w ith aps; consider autogenous reconst ruct ion (e.g., using rib car t ilage) or prosthesis; bone conduct ion hearing aid
◦ Associat ion w ith canal at resia (especially 3rd degree cases)
• Pre-auricular tags and accessory auricles ◦ Usually anterior to t ragus ◦ If cart ilage present = accessory auricle ◦ Often bilateral; m ay be part of a syndrom e (e.g., Goldenhar)
◦ Beware excision in children as VII n m ay be involved in root of accessory auricle
• Pre-auricular pits and sinuses (Fig. 62.1) ◦ Related to incom plete fusion of the h illocks of His and 1st branchial arch form at ion
◦ Anterior to anterior crus of helix ◦ Pits m ay extend dow n to cart ilage; sinuses extend to t ym panic ring; possible relat ionship to facial nerve
◦ Autosom al inheritance w ith incom plete penet rance
◦ Usually asym ptom at ic but recurrent infect ion possible
◦ Com plete excision usually requires rem oval of a sm all oval of helical car t ilage at base of t ract
• Prom inent ears ◦ Pinna stops grow ing by ~5 years of age and children becom e “body aware” by ~7 years
◦ 5% populat ion have prot ruding ears ◦ Usually a failure of folding of the ant ihelix or hyperplasia of the conchal bow l
◦ Norm al auriculotemporal angle ~30°; >40° is prot ruding
◦ In new borns m ay be corrected by taping
◦ Surgical repair: various techniques used to create an ant ihelical fold - Marking of desired site for ant ihelical fold w ith m ethylene blue dye
- Car t ilage weakening, e.g., by anter ior scoring (Converse technique); as lateral surface of auricle involved in procedure, r isk of poor cosm esis
- Stay sutures techniques (e.g., Mustardé) - Diam ond burr drilling of groove on m edial surface
- Conchom astoid sutures and cart ilage excision m ay help reduce deep conchal bowl appearance
- Can also excise m edial par t of conchal bowl ± soft t issue over m astoid
• Canal at resia ◦ Altm an classi cat ion:
- I: TM present - II: at ret ic plate, norm al t ym panic cavity - III: hypoplast ic t ym panic cavity
◦ Jahrsdorfer grading system assesses CT ndings to determ ine suitabilit y for surgery
◦ BAHA often best opt ion rather than canal reconst ruct ion
Fig. 62.1 Pre-auricular stula.
Philpott_9783131662316_Ch62.indd 228 02/05/14 1:17 PM

229
63 Deafness in Children
63.1 Classi cation• Only 5 to 10% deaf children have deaf parents• Congenital: sensorineural, conduct ive, or m ixed;
isolated or part of syndrom e; 1:1000 children born w ith SNHL (50% of these profound) ◦ Genet ic: usually SNHL, usually from single gene disorders - Single gene disorders - Syndrom ic
◦ Perinatal/in t rauterine causes ◦ Congenital disorders causing deafness to develop in childhood
• Acquired: hearing norm al at bir th ◦ Meningit is (bacterial): com m onest cause of acquired SNHL seen in ~10% children infected; fast t rack for CI due to risk of cochlear ossi cat ion
◦ Mum ps, m easles ◦ Traum a ◦ OME
63.2 Genetic Nonsyndromic Sensorineural Hearing Loss• Autosom al or X-linked; 1:8 people carry a
recessive gene for deafness; of hereditary deafness (1:4000 live bir ths) 80% autosom al recessive, 15% auto dom inant , 4% X-linked, 1% m itochondrial
• Connexin 26 m ost com m on type (50% non-syndrom ic autosom al recessive HL) ◦ Mutat ion in GJB2 gene alter funct ion of connexin-26 gap junct ion protein causing potassium in toxicat ion of organ of Cor t i
◦ Hom ozygous m utat ions usually cause non-progressive HL, heterozygous ones cause progressive HL
◦ Genet ic test ing available
63.3 Syndromal• Many are associated w ith congenital deafness
and include: ◦ Autosom al recessive:
- Pendred syndrom e: SNHL and thyroid goit re ±vest ibular disturbance; usually euthyroid,
m ay be hypothyroid; associated w ith w idened vest ibular aqueduct and Mondini; m ost com m on cause of syndrom ic deafness (10% cases)
- Usher syndrom e: SNHL and ret in it is pigm entosa; som e types have absent vest ibular responses
- Jervell–Lange-Nielsen syndrom e: SNHL and prolonged ECG QT in terval that disturbs cardiac conduct ion and leads to fain t ing and sudden death ; gene m apped to short arm chrom osom e 11; h igh incidence of consanguinity in parents
- Refsum disease: SNHL and ret in it is pigm entosa, cerebellar ataxia, and peripheral neuropathy
- Branchio-otorenal syndrom e; branchial arch anom alies (abnorm al external ear, preauricular pits), renal dysplasia, and m ixed HL; gene m apped to long arm chrom osom e 8
◦ Autosom al dom inant: - Waardenburg syndrom e: SNHL and hy-pertelorism , pigm ent disorder (e.g., w hite forelock, heterochrom ia ir idis); various genes and t ypes ident i ed
- Treacher–Collins syndrom e: hypoplasia of zygom a, m axilla, m andible ± m icrot ia, dow n-slant ing palpebral ssures, external and inner ear deform it ies; deafness—CHL, m ixed, or SNHL
- Pierre Robin syndrom e: hypoplast ic m an-dible, cleft palate, glossoptosis ± external, m iddle, and inner ear deform it ies, club foot
- Crouzon disease: hypoplast ic m andible and m axilla, parrot beak nose, craniostenosis, proptosis, external and m iddle ear abnorm alit ies (CHL)
- Apert syndrom e: xed stapes footplate (CHL), OME, acrocephaly, syndact yly, cleft palate, saddle nose, m axillary hypoplasia, m entally retarded
- Leopard syndrom e: lent igines (brow n spots), ECG abnorm alit ies, hyper telorism , pulm onary stenosis, abnorm al genitalia, retarded grow th, SNHL
- St ickler syndrom e: SNHL, cleft palate (m ay be w ith Pierre Robin sequence), ret inal degenerat ion , early ar thrit is
Philpott_9783131662316_Ch63.indd 229 02/05/14 1:20 PM
230
63 Deafness in Children
◦ X-linked: - Alport syndrom e: X-linked recessive, defect in collagen gene; chronic renal failure, progressive SNHL, ophthalm ic signs, m ilder in F; som e pedigrees exist that are autosom al dom inant
◦ Dow n syndrom e: - Trisomy 21, 1:600 live bir ths (1:100 for m others >40 years old)
- Prone to OME, recurrent URTIs, narrow EACs, increased rate of ossicular abnorm alit ies (hence CHL) and cochlear abnorm alit ies (hence SNHL)
63.4 Perinatal/Intrauterine• Potent ially preventable• Maternal infect ion: TORCH
◦ Rubella: a com m on ident i able cause of congenital SNHL (cookie bite pat tern on PTA) that is progressive in ¼; deafness a ects ~1/3 rubella children; infect ion can cause deafness at any stage of pregnancy; m aternal infect ion of-ten subclinical—m others often not im m unized
◦ CMV: infect ion can be congenital, perinatal, or acquired; m ost infect ions subclin ical at bir th ; get dest ruct ion of cochlear and labyrin th ine st ructures, usually severe bilateral SNHL; com m onest in t rauterine infect ion causing deafness (0.5% bir ths, 4% of w hich w ill be deaf, r ising to 8% by 5 years, i.e., can be progressive); t reatm ent can arrest progressive HL
◦ Toxoplasm osis: often subclin ical at bir th ; progressive blindness, SNHL (in ~15% infected children)
◦ Congenital syphilis: onset deafness usually early adulthood; m iddle ear problem s + SNHL
◦ Herpes sim plex: ver t ical t ransm ission possible; incidence rising (Rx: acyclovir)
• Ototoxic m edicat ion: e ect on fetal cochlea, e.g., loop diuret ics, am inoglycoside ant ibiot ics (r isk from lat ter less in children than adults), cisplat in chem otherapy, quinine
• Metabolic: e.g., m aternal diabetes, fetal alcohol syndrom e
• Perinatal: prem aturit y associated w ith hypoxia, hyperbilirubinem ia, low bir thweight , suscept ibilit y to infect ion—m ay act synergist ically to a ect hearing
63.5 Disorders Causing Deafness to Develop in Childhood• Congenital cholesteatom a: develops behind
in tact TM, no Hx ear infect ions, m ay occur from EAC to pet rous apex and CPA
• Fibrous dysplasia: m ay a ect tem poral bone giving progressive CHL; ground-glass appearance on CT
• Goldenhar syndrom e: faulty developm ent of 1st and 2nd branchial arches; hem ifacial m icrosom ia, vertebral problem s, derm oids, CHL (external ear abnorm alit ies, e.g., tags); m ult ifactorial causat ion w ith genet ic com ponent
• Osteogenesis im perfect: t ype I collagen synthesis disorder; various t ypes, both autosom al recessive and dom inant; t ype II usually fatal in early life; m ay be associated w ith blue sclera, Schwartze sign , scoliosis; deafness from ~6 years
• Congenital disorders that predispose to OME: cyst ic brosis, cleft palate, Dow n, im m une de -ciency, Kartagener
63.6 Investigations• Consider the follow ing in those w ith severe-
profound SNHL: ◦ Im aging: CT petrous tem poral bones (dysplasias, w idened vest ibular aqueduct); MRI can also be helpful
◦ Genet ic test ing: - Various relevant genet ic m alform at ions can be detected (e.g., connexin-26 and -30, A1555G); counselling required
- Chrom osom al abnorm alit ies only if developm ental delay or dysm orphic features
◦ Infect ion screen (i.e., TORCH) ◦ Ophthalm ology: 40% of children w ith SNHL have ophthalm ic condit ions
◦ ECG: screen for Jervell–Lange-Nielsen syndrom e
◦ Serological test ing, im m unologic screening, renal tests—only if otherw ise directed
Philpott_9783131662316_Ch63.indd 230 02/05/14 1:20 PM

231
64 Paediatric Hearing Assessment
64.1 Reaction to Sounds• After bir th : star t les to sudden loud noise• 1/12: not ices prolonged noise (e.g., vacuum
cleaner) and m ay turn to it• 4/12: quietens or sm iles to fam iliar voice and
turns to it w hen cannot see speaker• 7/12: turns im m ediately to fam iliar voice across
room or to quiet noises m ade on each side• 9/12: listens to everyday sounds and searches
for quiet sounds m ade out of sight• 12/12: som e response to ow n nam e• >18/12: reluctant to turn to sound that is not
m eaningful• From 3.5 years earphones m ay be used for
test ing
64.2 Making Sounds• 4/12: soft sounds w hen awake; gurgles and coos• 6/12: laughter-like sounds; sing-song vowel
sounds (aa, m u, goo)• 9/12: sounds to com m unicate in fr iendliness or
annoyance; babbles (da da da); star ts to im itate sounds
• 12/12: babbles loudly, conversat ional-t ype rhythm ; use one or two recognizable words
• 15/12: lots of speech-like sounds; 2 to 6 recognizable words m eaningfully
• 18/12: up to 20 words; t r ies to join in nursery songs
• 24/12: 50+ words appropriately; sim ple sentences (e.g., m ore m ilk)
• 30/12: 200+ words; pronouns (I, m e, you); asks quest ions; few nursery rhym es
• 36/12: large vocabulary in telligible to everyone
64.3 Neonatal Screening• Problem w ith target ing “at r isk” babies: 50% of
hearing-im paired babies have no “risk” factors• Late diagnosis has im plicat ions for language
developm ent and com m unicat ion—earlier in tervent ion leads to bet ter outcom e—therefore screening in t roduced
• Requires object ive test that can (for exam ple) be perform ed on all babies prior to discharge from m aternit y unit
• Various protocols, but consider OAE, if fail repeat OAE, if fail again , then autom ated ABR, if fail that refer for form al assessm ent
• Visit the NHS New born Hearing Screening Program m e website for fur ther inform at ion: h t tp://hearing.screening.nhs.uk/publicat ions
64.4 Distraction Testing• Behavioural orientat ion audiom etry;
free- eld test• For 8–20/12 age group• Child on parent’s lap, assistant plays in front ,
tester dist racts child w ith sounds of various in tensit y to one side of child; +ve if child turns to sound
64.5 Visual Reinforcement Audiometry• Free- eld audiom etry• Child plays w ith toy, sounds produced from
speaker at 30° on either side, if child turns to correct side gets visual (reinforcing) st im ulus; tester outside observing
• Can obtain frequency- and ear-speci c inform at ion
• For age group 8/12–3 years; pass 25–30 dB A
64.6 Speech Discrimination Testing• Child points to or handles toys, nam es of w hich
are selected to cover a range of speech pat terns• McCorm ick toy test: 7 pairs toys w ith
acoust ically sim ilar nam es (cup, duck; key, t ree; shoe, spoon; house, cow; horse, fork; plate, plane; lam b, m an); assess speech level that gives 80% correct response rate (at 40–45 dB A)
• Various t ypes, test ing age range 2 years onwards
Philpott_9783131662316_Ch64.indd 231 02/05/14 1:23 PM

232
64 Paediatric Hearing Assessment
64.7 Audiometry• Play audiom etry w hen child carr ies out task
(e.g., put peg in hole) in response to hearing a tone, from age 2.5 years
• From ~3.5 years can perform PTA in free- eld• From ~ 5 years can perform PTA w ith
headphone, unm asked• From ~ 8 years can perform PTA m ore reliably
w ith m asking
64.8 Tympanometry, OAEs, ABRs• Object ive tests, can be perform ed at any age
(detailed in other notes)• Tym panom etry in those <4/12 need h igher
test frequency (1 kHz) due to problem s of com pliance in nonrigid EAC
Philpott_9783131662316_Ch64.indd 232 02/05/14 1:23 PM

233
65.1 Choanal Atresia65.1.1 Epidemiology• 1/7000 to 8000 live bir ths• Com m on cause of neonatal respiratory dist ress• 50 to 60% unilateral• 29% pure bony, 71% m ixed bony and
m em branous• Fem ale > m ale (2:1)• Autosom al recessive inheritance• Gene chrom odom ain 7
65.1.2 Aetiology• Failure of breakdow n of buccopharyngeal
m em brane on day 45 of gestat ion• Neural crest m igrat ion failure = another theory• Com m on associat ion w ith other anom alies:
◦ CHARGE: - C—colobom a (eye defects) - H—heart defects - A—choanal at resia (nasal blockage) - R—retardat ion of grow th and developm ental delay
- G—genitalia (sm all penis, undescended test icles)
- E—ear anom alies—m alform ed pinnae, hypo-plast ic incus, cochlear anom alies, absent Sccs
◦ Branchial abnorm alit ies ◦ Hum eroradial synostosis ◦ Mandibular facial synostosis ◦ Microcephaly ◦ Micrognathia ◦ Nasopharyngeal abnorm alit ies ◦ Palatal defects
65.1.3 Symptoms• Respiratory dist ress at bir th• Infant crying relieves obst ruct ion• When neonate closes m outh pat tern of cyclic
obst ruct ion develops leading to respiratory failure
• Unilateral cases present later in life w ith unilateral rh inorrhoea
• Obligate nose breathers unt il 6 to 9 m onths age
65.1.4 Investigations• Con rm ed by inabilit y to pass � Fr gauge
feeding tube• Endoscopic exam inat ion• CT scan determ ines t ype of obst ruct ion and
th ickness• ECHO
65.1.5 Treatment• Transnasal correct ion in 1st week of life• Unilateral can be corrected at 1 year
Transnasal Approach• Curet te par t it ion• Use 3.5 m m ETT as stent• Use posterior m em branous aps to cover bone• Com plicat ions:
◦ Meningit is ◦ CSF leak ◦ Brain injuries ◦ Gradenigo syndrom e ◦ Cervical ver tebral subluxat ion ◦ Restenosis
• CO2 laser, endoscopically guided, Nd:YAG laser = alternat ives
Transpalatal Approach• Superior visualizat ion• Im paired palatal grow th a potent ial problem
in neonate—suitable only for >5 years old
65.2 Thornwaldt Cyst and Rathke Pouch Cyst65.2.1 Embryology/Pathology• Pharyngeal segm ents of prim it ive notochord
rem ain connected to endoderm in nasopharynx• Bursa located in m idline of nasopharynx• If bursa occluded by in am m at ion →
Thornwaldt cyst—can becom e infected• Anterior to invaginat ion and above bursa is
a sm all pharyngeal hypophysis developed
65 Congenital Abnormalities of the Head and Neck
Philpott_9783131662316_Ch65.indd 233 02/05/14 1:26 PM

234
65 Congenital Abnormalit ies of the Head and Neck
from Rathke pouch—som et im es persists as craniopharyngeal canal running from sella turcica through body of sphenoid
65.2.2 Thornwaldt Cysts• Appear clin ically in 2nd to 3rd decades• Male = fem ale• In term it tent /persistent postnasal discharge
(tenacious m ucus/purulent m aterial)• Associated w ith odynophagia, halitosis,
dysgeusia, dull occipital headache• Midline cyst ic m ass superior to adenoids seen
on endoscopy• Cyst lined by respiratory epithelium• CT/MRI—well de ned• Excision or w ide m arsupializat ion
65.2.3 Rathke Pouch Cysts• Lined by colum nar or cuboidal ciliated
epithelium• May becom e infected or rupture in t racranially• Com m only associated w ith galactorrhea, visual
eld loss, and hypopituitarism• Transsphenoidal cyst drainage and biopsy of the
wall required
65.3 Chordomas• Rare m alignant neoplasm s ar ising from
notochordal rem nants• 5th to 6th decade of life• 50% in spheno-occipital area• Male = fem ale• Expanding nasopharyngeal m ass• Frontal headaches• CN palsies (VI n in 60%)• Pituitary abnorm alit ies• Children <5 years have w ider range of
present ing symptom s• CT/MRI to invest igate and plan surgery• Surgical resect ion via skull base approach• 5-year survival = 50%• Radiotherapy increases survival rates• Chem otherapy indicated if m ets occur
65.3.1 Craniopharyngiomas• Arise from Rathke pouch• Located in sellar, parasellar, and III vent ricle
regions
• Com posed of well-di erent iated epithelial elem ents, e.g., cysts, am eloblasts
• 10 to 15% of all childhood int racranial neoplasm s• Visual eld defects, sudden blindness, ext raocu-
lar m otor paralysis, and hypopituitarism• Median age = 7.5 years• Male = fem ale• Surgical resect ion followed by radiotherapy• 10-year survival = 90%• Surgical rem oval has h igh risk of death
endocrinologic com plicat ions, and behavioural dysfunct ion
• Those located in an enlarged sella can be rem oved t ranssphenoidally
65.4 Cleft Lip and Palate65.4.1 Epidemiology• 1/700 bir ths• Increased r isk if older sibling a ected• Teratogens: ethanol, ret inoids, folate antagonists• Maternal sm oking also causat ive• Syndrom ic or nonsyndrom ic
◦ Over 20 syndrom es associated, e.g., Aper t , Treacher–Collins, Pierre Robin , and DiGeorge
65.4.2 Aetiology• Cleft lip is due to failure of fusion between
m edial nasal, m axillary, and lateral nasal prom inences
• Cleft lip either com plete (m uscular diastasis [separat ion] of orbicularis or is) or incomplete
• Cleft palate form at ion is hypothesized to result from : ◦ Defects in palatal shelf grow th ◦ Delayed shelf elevat ion ◦ Failed shelf elevat ion ◦ Defect ive shelf fusion
• Prim ary palate: lip , alveolar arch , palate anterior to incisive foram en (prem axilla)
• Secondary palate: soft palate and hard palate posterior to incisive foram en
65.4.3 Features and SymptomsCleft Lip• See Fig. 65.1• Alone, feeding is not norm ally a problem• Norm ally repaired at 2–6/12 of age
Philpott_9783131662316_Ch65.indd 234 02/05/14 1:26 PM
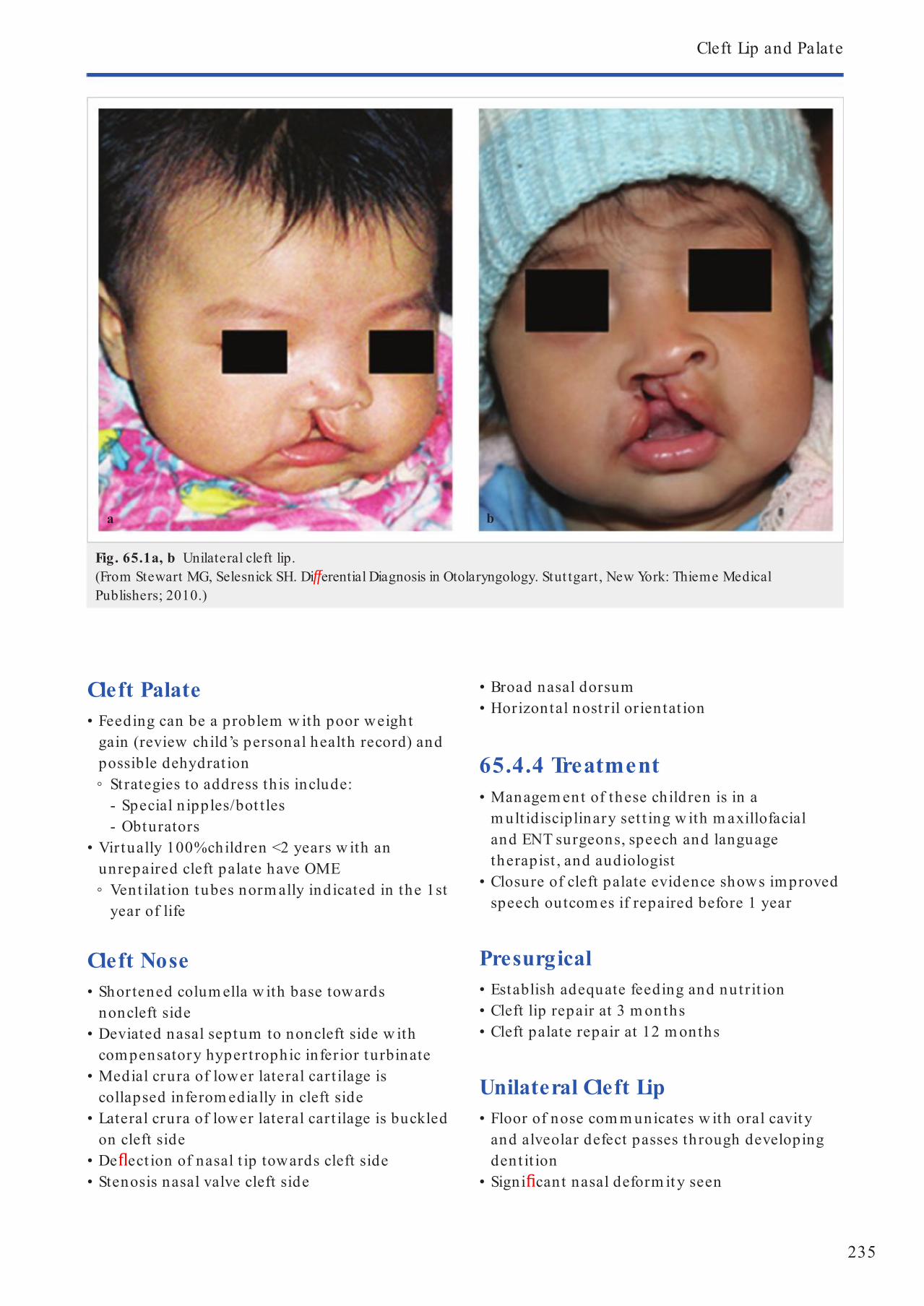
235
Cleft Lip and Palate
Cleft Palate• Feeding can be a problem w ith poor weight
gain (review child’s personal health record) and possible dehydrat ion ◦ Strategies to address th is include:
- Special n ipples/bot t les - Obturators
• Vir tually 100% children <2 years w ith an unrepaired cleft palate have OME ◦ Vent ilat ion tubes norm ally indicated in the 1st year of life
Cleft Nose• Shor tened colum ella w ith base towards
noncleft side• Deviated nasal septum to noncleft side w ith
compensatory hypert rophic inferior turbinate• Medial crura of lower lateral car t ilage is
collapsed inferom edially in cleft side• Lateral crura of lower lateral car t ilage is buckled
on cleft side• De ect ion of nasal t ip towards cleft side• Stenosis nasal valve cleft side
• Broad nasal dorsum• Horizontal nost ril or ientat ion
65.4.4 Treatment• Managem ent of these children is in a
m ult idisciplinary set t ing w ith m axillofacial and ENT surgeons, speech and language therapist , and audiologist
• Closure of cleft palate evidence shows im proved speech outcom es if repaired before 1 year
Presurgical• Establish adequate feeding and nutrit ion• Cleft lip repair at 3 m onths• Cleft palate repair at 12 m onths
Unilateral Cleft Lip• Floor of nose com m unicates w ith oral cavity
and alveolar defect passes through developing dent it ion
• Signi cant nasal deform it y seen
Fig. 65.1a, b Unilateral cleft lip. (From Stewart MG, Selesnick SH. Di erential Diagnosis in Otolaryngology. Stut tgart, New York: Thieme Medical Publishers; 2010.)
a b
Philpott_9783131662316_Ch65.indd 235 02/05/14 1:26 PM

236
65 Congenital Abnormalit ies of the Head and Neck
• Goals of surgery: ◦ Restorat ion of orbicularis m uscle funct ion ◦ Alar base and colum ellar height restorat ion ◦ Creat ion of sym m etry of philt ral colum ns, t ip height , Cupid’s bow, and verm illion
• Millard rotation advancem ent procedure w ith pre-operative orthodontic appliances or lip adhesion
Bilateral Cleft Lip• Absent oor of nose• Central alveolar arch is displaced forward and
superiorly• Goals are as for unilateral• Bilateral lip adhesion perform ed at 2 to 4 weeks
old w ith de n it ive lip repair at 4 to 6 m onths
Cleft Palate• Goals for repair:
◦ Close defect w ithout inhibit ing m axillary arch grow th
◦ Achieve adequate velopharyngeal funct ion ◦ Norm alize oronasal resonance and speech pat terns
• Perform ed at 10 to 18 m onths• May require preoperat ive or thopaedic devices
to m ove prem axilla posteriorly and to extend lateral m axillary segm ents
• 2- ap Bardach palatoplasty• Secondary problem s that require fur ther
t reatm ent: ◦ Correct ion of nasal airway impairm ent ◦ Cosm et ic nasal defects ◦ Velopharyngeal insu ciency ◦ Recurrent AOM and OME
65.5 Pierre Robin Sequence• Autosom al dom inant• Micrognathia + cleft palate• May arise from hypoplast ic m andible before
9/52 in utero allow ing tongue to be m ore posteriorly located and thereby im pair ing the closure of the posterior palatal shelves that m ust grow over tongue and m eet in m idline
• Feeding problem s com m on and m ay need NG tube• May have low -set ears, hypoplast ic, and
dehiscent VII n• Managem ent of airway in order of invasiveness:
◦ Prone posit ion ◦ Nasopharyngeal airway
◦ Mandibular dist ract ion ◦ Glossopexy (suture tongue t ip to verm illion lower lip)
◦ Tracheostomy
65.6 Congenital Midline Nasal Swellings• Nasal derm oid cysts (61%) 40% associated w ith
other craniofacial abnorm alit ies• Nasal encephaloceles• Nasal gliom as
65.6.1 Nasal Dermoid Cysts• Slow grow ing nasal m ass/m idline pit• Do not com press or t ransillum inate• Contains skin and derm al elem ents including
hair follicles and sebaceous glands• MRI m ay reveal in t racranial extension• Furstenberg –ve: no increase w hen crying
65.6.2 Nasal Encephalocoeles/ Gliomas• Norm ally present at bir th : m ass, blockage, or
CSF leak• Mass is com pressible• 60% extranasal• 30% in t ranasal• 10% m ixed• Gliom a: Furstenberg –ve• Encephalocele: Furstenberg +ve
65.6.3 Investigation• MRI in sagit tal plane: check for int racranial
extension
65.6.4 Surgery• Lateral rh inotomy• Endoscopic excision• Com bined approach w ith craniotomy
65.7 Dow n Syndrome• Narrow EAC• OME• Stapes xat ion• Short cochlea
Philpott_9783131662316_Ch65.indd 236 02/05/14 1:26 PM

237
Crouzon
• OSA ◦ Macroglossia ◦ Narrow nasopharynx
• Sinusit is• Midfacial hypoplasia• Atlantoaxial instabilit y—need lat soft t issue
neck X-ray• Subglot t ic stenosis
65.8 Treacher Collins Syndrome65.8.1 Aetiology• Aka m andibulofacial dysostosis*• Autosom al dom inant• Gene on long arm chrom osom e 5• Failure of neural crest cells through early
dest ruct ion of facial and auditory prim ordial, w hich m igrate to 1st and 2nd branchial arches
• 1 in 10,000• Overall hypoplasia of m any derivat ives of 1st
and 2nd branchial arches
*Disorder of developm ent of bone
65.8.2 Features• Malar hypoplasia• Dow nslant ing palpebral ssures• Malform at ions of external ear
• Micrognathia• Early respiratory problem s m ay develop as a
result of having a narrow airway; m ay need temporary t racheostomy
• Majorit y have norm al in telligence
65.9 Crouzon65.9.1 Aetiology• Aka craniofacial dysostosis• Autosom al dom inant• Locus on long arm chrom osom e 10• Mutat ion in broblast grow th factor receptor
2 gene• 1 in 25,000
65.9.2 Features• Shallow orbits• Prem ature craniosynostosis (coronal and sagit tal
sutures)• Maxillary hypoplasia• Conduct ive hearing loss: ossicular chain
problem (50%), at ret ic canals (15%)• May have raised ICP• Lack of syndactyly di erent iates it from Apert
(tower skull: turribrachycephaly: fusion of frontoparietal suture)
Philpott_9783131662316_Ch65.indd 237 02/05/14 1:26 PM

238
66 Paediatric Laryngeal Pathology
66.1 Laryngomalacia66.1.1 Incidence and Aetiology• Most com m on cause of st r idor in new born• May be autosom al dom inant• 68% have other respiratory disorders (as seen
on exible bronchoscopy)
66.1.2 Clinical Features• Inspiratory st r idor• Feeding problem s• Gast ric re ux (80%), regurgitat ion (40%)• Worsens w ith increased respiratory e or t• Begins short ly after bir th get t ing worse unt il
6 to 8 m onths• Plateau at 9 m onths and steadily im prove after• Flaccid epiglot t is w ith short and redundant
aryepiglot t ic folds• OSA (23%), CSA (10%)• Aspirat ion pneum onit is in 7%• May be concurrent laryngeal congenital lesions
(18–60%)
66.1.3 Investigations• Direct laryngobronchoscopy if failure to thr ive
66.1.4 Treatment• Observat ion su cient in m ost cases• 10 to 15% (failure to thrive/>1 lesion) m ay
need in tervent ion• Supraglot toplasty and anter ior epiglot toplexy
66.2 Absent/Rudimentary Epiglottis• Rare bi d epiglot t is can be associated w ith
st r idor and aspirat ion• Mult iple congenital anom alies com m on• Direct laryngoscopy ± t racheostomy
66.3 Laryngeal Atresia• Rarest laryngeal lesion• Child m akes st rong respiratory e or ts at bir th
but no air m ovem ent , cry, or st r idor
• Marked cyanosis w hen cord clam ped• Most die w ithout em ergency t racheostomy• If large TOF present they m ay survive
66.3.1 Laryngeal Webs• Mostly occur in glot t is• Most located anter iorly and extend towards
arytenoids• Vary in th ickness• 5% of all congenital laryngeal lesions• Acquired lesions m ore com m on• Sym ptom s present at bir th in 75% and all at
1 year• Many asym ptom at ic unt il st ressed, have an
infect ion , or are in tubated• Vocal dysfunct ion and airway obst ruct ion
(inspiratory st r idor)• Needs direct laryngoscopy• 60% require surgical in tervent ion• 30 to 40% require t racheostomy• 4 t ypes of lesions
66.4 Saccular Cysts• Most arise in infancy• Str idor in 90%—inspiratory (occ. biphasic)• Respiratory di culty in 55%• Failure to thrive due to feeding di cult ies• Direct laryngoscopy required• May require em ergency t racheostomy• De nit ive t reatm ent is endoscopic I&D
(laryngo ssure if required)
66.5 Laryngoceles• See Chapter 56: Benign Neck Disease
66.6 Laryngeal Clefts• Characterized by a de ciency in
separat ion between oesophagus and larynx/t rachea
• Posterior glot t ic (laryngeal/t racheal) wall• Associated w ith h igh m ortalit y• Autosom al dom inant inheritance
Philpott_9783131662316_Ch66.indd 238 02/05/14 1:28 PM

239
Subglot t ic Stenosis
66.6.1 Embryology• 4/52 gestat ion prim ordium of respiratory
system appears as outgrow th from the foregut
• The outgrow th expands in a caudal direct ion and becom es separated from the foregut by the developm ent of 2 longitudinal r idges (oesophagot racheal r idges), w hich fuse to form the septum
• Failure of fusion results in a cleft
66.6.2 Types• I: in terarytenoid• II: in to cr icoid• III: through poster ior cricoid• IV: m em branous t rachea
66.6.3 Clinical Features• Aspirat ion and cyanosis—53%• Postpar tum asphyxia—33%• Increased m ucus product ion—23%• Recurrent pneum onia—16%• Voiceless crying—16%• Str idor—10%• Im paired swallow ing—5%
66.6.4 Investigations• Contrast swallow• MRI• Laryngoscopy
66.6.5 Treatment• Poor prognosis—due to other congenital
anom alies• 50% need a t racheostomy• Surgical repair opt ions include anterior
laryngo ssure (w ith rib graft)
66.7 Vocal Fold Paralysis• Congenital (10% of all congenital) or acquired• Bilateral m ore frequent• Com m on associat ion w ith :
◦ Hydrocephalus ◦ Meningomyelocoele ◦ Arnold–Chiari m alform at ion ◦ Other CNS lesions
66.7.1 Incidence and Aetiology• 1.5 to 23% = frequency• Congenital lesions m ore com m on
Acquired Causes• Traum at ic
◦ Vaginal delivery ◦ Surgery for congenital m alform at ion, e.g., TOF
• Infect ious ◦ Whooping cough ◦ Encephalit is ◦ Poliomyelit is ◦ Syphilis
• Neoplast ic—tum ours of brain and spinal colum n
Congenital Causes• Probably due to com pression of vagus
through foram en m agnum —im proves w hen hydrocephalus of Arnold–Chiari m alform at ion decompressed
• Brainstem dysgenesis and t ract ion of vagal nerve roots are other theories
66.7.2 Treatment• Secure airway (ETT/t racheostomy) if bilateral• Relieve com pression—if w ith in 24 h—nerve w ill
regain funct ion in 2 weeks; otherw ise m ay take 1.5 years
• Periodic exam inat ions to assess VF funct ion
66.8 Subglottic Stenosis66.8.1 Incidence and Aetiology• Figs. 66.1 and 66.2• Congenital—cricoid car t ilage deform ity• Acquired:
◦ External injury (including t rachy too h igh) ◦ In ternal injury, e.g., prolonged in tubat ion (90%) - ETT that allows a leak at pressure <20 cm H2O should be chosen to avoid problem
- Predisposing factors include repeat in tubat ion, local/system ic infect ion , GORD, other system ic factors such as anaem ia, dehydrat ion , etc.
Philpott_9783131662316_Ch66.indd 239 02/05/14 1:28 PM
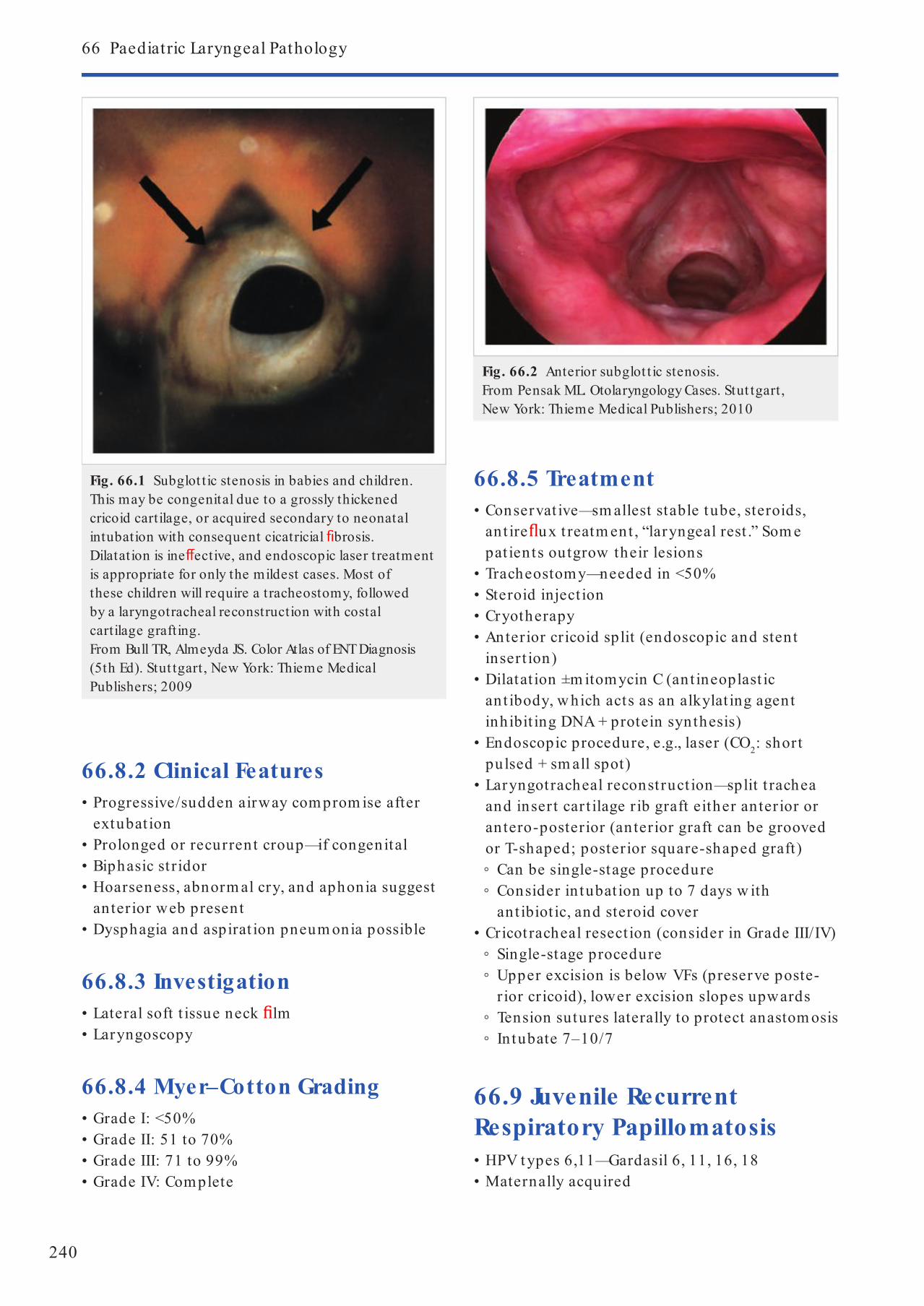
240
66 Paediatric Laryngeal Pathology
66.8.2 Clinical Features• Progressive/sudden airway com prom ise after
extubat ion• Prolonged or recurrent croup—if congenital• Biphasic st r idor• Hoarseness, abnorm al cry, and aphonia suggest
anter ior web present• Dysphagia and aspirat ion pneum onia possible
66.8.3 Investigation• Lateral soft t issue neck lm• Laryngoscopy
66.8.4 Myer–Cotton Grading• Grade I: <50%• Grade II: 51 to 70%• Grade III: 71 to 99%• Grade IV: Com plete
66.8.5 Treatment• Conservat ive—sm allest stable tube, steroids,
ant ire ux t reatm ent , “laryngeal rest .” Som e pat ients outgrow their lesions
• Tracheostom y—needed in <50%• Steroid inject ion• Cryotherapy• Anterior cricoid split (endoscopic and stent
insert ion)• Dilatat ion ±m itomycin C (ant ineoplast ic
ant ibody, w hich acts as an alkylat ing agent inhibit ing DNA + protein synthesis)
• Endoscopic procedure, e.g., laser (CO2: short pulsed + sm all spot)
• Laryngotracheal reconst ruct ion—split t rachea and insert car t ilage r ib graft either anter ior or antero-posterior (anterior graft can be grooved or T-shaped; posterior square-shaped graft) ◦ Can be single-stage procedure ◦ Consider in tubat ion up to 7 days w ith ant ibiot ic, and steroid cover
• Cricot racheal resect ion (consider in Grade III/IV) ◦ Single-stage procedure ◦ Upper excision is below VFs (preserve poste-r ior cricoid), lower excision slopes upwards
◦ Tension sutures laterally to protect anastom osis ◦ In tubate 7–10/7
66.9 Juvenile Recurrent Respiratory Papillomatosis• HPV types 6,11—Gardasil 6, 11, 16, 18• Maternally acquired
Fig. 66.1 Subglot tic stenosis in babies and children. This may be congenital due to a grossly thickened cricoid cartilage, or acquired secondary to neonatal intubation with consequent cicatricial brosis. Dilatation is ine ective, and endoscopic laser treatment is appropriate for only the mildest cases. Most of these children will require a tracheostomy, followed by a laryngotracheal reconstruction with costal cartilage grafting. From Bull TR, Almeyda JS. Color Atlas of ENT Diagnosis (5th Ed). Stut tgart , New York: Thieme Medical Publishers; 2009
Fig. 66.2 Anterior subglot tic stenosis.From Pensak ML. Otolaryngology Cases. Stut tgart, New York: Thieme Medical Publishers; 2010
Philpott_9783131662316_Ch66.indd 240 02/05/14 1:28 PM

241
Juvenile Recurrent Respiratory Papillomatosis
• Viral DNA m ay be present in clin ically norm al respiratory t ract
• 7/m illion/year• Early—hoarseness, abnorm al cry, dyspnoea,
st r idor• Late—acute respiratory obst ruct ion , pulm onary
sequelae• Laser now superseded by m icrodebrider• Cidofovir—cytosine nucleoside analogue—
response variable
• Side e ects: nephrotoxicit y, neutropenia, fever, asthenia, alopecia, nausea, vom it ing, hypotony, decreased in t raocular pressure, ir it is, uveit is
• In infected cells, nucleot ide analogues such as cidofovir inhibit viral DNA polym erase, w hich is responsible for replicat ion of new viral RNA and DNA
• Other m edical Rx = α -interferon, indol-3-carbinol, m ethotrexate
Philpott_9783131662316_Ch66.indd 241 02/05/14 1:28 PM

242
67.1 Tracheobronchomalacia• Car t ilage to m uscle rat io should be 2:1• Secondary condit ion m ay occur secondary to
external com pression—vascular/m ediast inal m ass/vent ilat ion , e.g., double aort ic arch
• Usually im proves by 18 m onths• Larsen syndrom e• TOF• Sym ptom s/signs:
◦ Cyanot ic episodes ◦ Cough ◦ Aspirat ion ◦ Tim ing of st r idor—prolonged expiratory phase seen on Ba swallow
◦ MLB required—avoid airway splin t ing—underdiagnosis
67.2 Tracheoesophageal Fistula (TOF)67.2.1 Epidemiology and Aetiology• Majorit y associated w ith oesophageal at resia
(96–97%)• 1 in 3000/4000 bir ths• Failure of com plete separat ion of foregut from
respiratory t ract• 40% have other m alform at ions
◦ OA + distal TOF 87% ◦ OA alone 6–7% ◦ OA + prox TOF 2% ◦ OA + prox + distal TOF <1% ◦ TOF alone 3–4%
• Infants often prem ature and have polyhydram nios
• Associated m alform at ions: ◦ V: ver tebral ◦ A: anal ◦ C: cardiac ◦ T: t rachea ◦ E: oesophageal ◦ R: renal ◦ L: lim b
67.2.2 Symptoms• Often asym ptom at ic at bir th• Respiratory:
◦ Cough; choke; cyanosis (w hen feeding); aspirat ion (leading to respiratory dist ress, atelectasis, pneum onia)
• GI: ◦ Excessive drooling, gast ric distension—respiratory com prom ise
67.2.3 Investigation• Oesophageal catheter, i.e., NG tube, and check
posit ion on plain CXR• AXR: air stom ach/sm all bowel suggests distal
stula. Lack of air in stom ach suggests oesopha-geal at resia
• Bronchoscopy + oesophagoscopy• ECHO diagnoses any cardiac abnorm alit ies +
posit ion of aort ic arch• GG swallow (r isk of aspirat ion)
67.2.4 Waterson Classi cation• Pret reatm ent r isk evaluat ion
◦ Category A - Bir th w t >5.5 lb (2.5 kg) - Receive prom pt surgery
◦ Category B - Bir th w t 4–5.5 lb (1.8–2.5 kg) or - Pneum onia or congenital anom aly - Short-term delay in t reatm ent - Preop gast rostom y
◦ Category C - Bir th w t <4 lb (1.8 kg) or - Severe pneum onia or congenital anom aly - Stage repair - TPN
67.2.5 Surgery• Preop care
- Keep pat ient in head-up posit ion - Oroesophageal tube on cont inuous suct ion - Frequent pharyngeal aspirat ion
67 Paediatric Tracheal and Oesophageal Pathology
Philpott_9783131662316_Ch 67.indd 242 02/05/14 1:31 PM

243
Caust ic Ingest ion
- Broad-spect rum ABx - Rule out VACTERL anom alies - Gast rostomy tube for feeding and decompression of abdom en if respiratory comprom ise
• Procedure - Right posteriolateral thoracotom y at 4th in tercostal space, unless anom alous right-sided aor t ic arch , then incision on left
- Procedure is usually ext rapleural w ith dissect ion posterior and lung re ected anter ior
- Divide stula, close w ith su tures - Direct approxim at ion of 2 ends of esophagus - May require st retching of proxim al segm ent w ith bougies
67.2.6 Prognosis• Spitz classi cat ion:
◦ Group 1: bir th w t >1.5 kg, no m ajor cardiac anom aly, 98.5% survival
◦ Group 2: bir th w t <1.5 kg or m ajor cardiac abnorm alit y, 82% survival
◦ Group 3: bir th w t <1.5 kg + m ajor cardiac abnorm alit y, 50% survival
67.2.7 Complications• Early
◦ Tracheom alacia ◦ Repeated chest infect ions ◦ Anastom otic leak occurs in 11 to 21% ◦ Oesophageal st r icture in 50% of leak pat ients ◦ Major disrupt ion (rare) ◦ GOR occurs in 35 to 58% (in t rinsic oesophageal dysfunct ion)
• Late ◦ Respiratory com plicat ions occur in up to 46% of pat ients - 19% have recurrent pneum onia - 23% have repeated episodes of aspirat ion - These respiratory com plicat ions are secondary to:
▪ GOR (74%) ▪ Tracheom alacia (13%) ▪ Recurrent TOF (13%) ▪ Oesophageal st r icture (10%)
◦ Anastom otic st r icture ◦ TOF recurs in ~9% of cases
67.3 Paediatric GORD + Aspiration• Infants are m ore prone to aspirat ion than adults
because of: ◦ Relat ively lax epiglot t is ◦ Large arytenoids ◦ Wide aryepiglot t ic folds
• Most com m on cause of GORD in children is t ran-sient lower oesophageal sphincter relaxat ion ◦ Other factors predisposing to aspiration include: ◦ CNS disease ◦ Prem aturit y ◦ Mechanical barr iers, e.g., NG or ET tube, t racheostomy tube
◦ Anatom ical barriers, e.g., oesophageal at resia, st r icture, vascular r ings, TOF, scoliosis
• Most com m on sign of GORD is regurgitat ion• Sensit ivit y of 24-h pH probe is 92 to 94%• 85% recover spontaneously
67.3.1 Treatment• Conservat ive: reassure, reverse Trendelenburg,
prone posit ion after feed• Surgery: fundoplicat ion , endolaryngeal stent ,
laryngeal closure or laryngot racheal separat ion
67.4 Caustic Ingestion• Caust ic agent: a substance that can burn m ucosa
of the aerodigest ive t ract• Alkaline agents: liquefact ion necrosis → rapid
+ deep burn , e.g., alkaline bat ter ies contain ing NaOH + KOH
• Bleach: norm ally <4%, need to ingest large am ounts
• Acid agents: coagulat ion necrosis → coagulum form s in terface → reduced penetrat ion of m ucosa → less likely to cause severe burns
67.4.1 Management• Secure airway + cardiovascular support• Determ ine agent and volum e ingested• Contact poisons unit• In terview any w itnesses• Skin/oral burns: wash w ith copious am ounts
of water
Philpott_9783131662316_Ch 67.indd 243 02/05/14 1:31 PM

244
67 Paediatric Tracheal and Oesophageal Pathology
• Flexible nasoendoscope determ ines upper airway injury
• CXR• In children , drooling and refusal to take liquids
by m outh usually indicates som e degree of m ucosal injury
• 10 to 20% oesophageal burns occur w ithout any evidence in oropharynx
• Dysphonia and st r idor are signs of possible dam age to pharynx/larynx or t rachea requiring urgent evaluat ion ± t rachy
• Chest or abdom inal pain indicates possible perforated viscus
67.4.2 Classi cation• 1st degree—erythem a and oedem a m ucosa• 2nd degree—full-th ickness injury to m ucosa
including sloughing/ulcerat ion
• 3rd degree—full-th ickness oesophageal injury including perforat ion → scar + st r icture
67.4.3 Treatment• Steroids if suspect 1st degree to reduce local
in am m ation• ABx reduce local bacterial colonizat ion• Acid suppressant , e.g., PPI• Oesophagoscopy indicated for all st rong acid/
base ingest ion• Flexi safer; allows visualizat ion of the stom ach• Consider NG tube inser t ion in theat re• Consider barium swallow 3/52 after discharge to
exclude st r icture form at ion• Str ictures can be m anaged w ith serial
dilatat ions though if com plete m ay require oesophagectomy + pull-up
• Note: long-term risk of developing an SCC
Philpott_9783131662316_Ch 67.indd 244 02/05/14 1:31 PM

245
68.1 Thyroglossal Cyst• If USS shows no thyroid gland—refer to paediatric
endocrinologist for further assessm ent• First described by Sist runk in 1920• Recurrence rate 10 to 30%• Thyroglossal t ract is a m ult iple branching
st ructure—ensuring th is is rem oved m eans perform ing a cent ral neck dissect ion—this m ay be reserved for recurrent cases
68.2 Branchial Anomalies68.2.1 Preauricular Sinuses• 1/100 incidence• Rem ove only if sym ptom at ic• Recurrence of 32% after sinusectomy• Avoid recurrence by taking w ide m argin of
norm al t issue around the sinuses
68.2.2 Branchial Cysts/Sinuses/Fistulas• Sinogram m ay be useful to con rm pathway of
stula• Tonsillectom y probably unnecessary
68.2.3 First Branchial Cleft Anomalies• Type I—super cial to VII n• Type II—m ay lie deep to VII n
68.2.4 Fourth Pouch Sinus• Opening in piriform fossa• Causes cervical abscesses• Endoscopic diatherm y to in ternal opening can
be e ect ive
68.3 Vascular Abnormalities68.3.1 Haemangiomas• Flat /absent at bir th• Proliferate and then regress
68 Paediatric Neck Masses
• Involute spontaneously• In tervent ion only for funct ional problem s• Cort icosteroids or in terferon m ay be used• Vincrist ine m ay also be used
68.3.2 Vascular Malformations• Low ow lesions—lym phat ic/venous/capillary• High ow lesions—AV m alform at ions (m ostly
in t racranial)• Cyst ic hygrom as—excision is rst choice w hen
below digast ric but inject ion sclerotherapy also e ect ive
• If tongue involved—laser m ay be needed• Sclerotherapy—OK 432/sodium am idot rizoate
(Ethibloc)/bleomycin—intracyst ic inject ion under US
• Com plicat ions: acute in am m atory response, abscess, scarr ing, surgery follow ing sclerotherapy has h igher m orbidit y
68.4 Acute In ammatory Problems• Suppurat ive LNs—I&D and pack/drain overnight
68.4.1 Lymphadenopathy in Children (Algorithm for Management)• Be suspicious for neoplasia + consider
excision if: ◦ History of m alignancy ◦ Node >2 cm ◦ Supraclavicular node (61–89% m alignant) ◦ Parents’ dem ands
• FNA not useful as w ill be done under GA• Durat ion of h istory not useful predictor of
m alignancy• Fever, w t loss, organom egaly, num ber of nodes,
and consistency of nodes useful but published evidence is inadequate as a predictor
• 1st visit ◦ CXR:
- ¾ neoplasia w ill have abnorm al CXR - If abnorm al consider excision
Philpott_9783131662316_Ch68.indd 245 02/05/14 1:36 PM

246
68 Paediatric Neck Masses
◦ USS: - If abnorm al (round, loss fat t y h ilum , disorganized vascularit y w ith new blood vessels from periphery, >1 cm ) consider excision
◦ Blood FBC: - Hb <10 or pancytopenia consider excision (note m ost lymphom as have norm al FBCs)
◦ Blood serology: - EBV, toxo, CMV, brucella - If abnorm al (9% +ve) consider discharge
68.4.2 Atypical Mycobacterial Infection• Mycobacterium bovis and Avium intracellulare
present in soil• Enter via oral ingest ion and pass to regional LNs
(typically parot id and SM nodes)• Presents as neck lum p, w hich develops violet-
red skin discolorat ion + eventual breakdow n• Sinus discharges for m onths before healing w ith
a puckered scar• Whole process can take years• Child is t ypically well and apyrexial• Mainly a clin ical diagnosis• Avoid aspirat ion/I&D because risk of discharging
sinus• Get CXR• Tuberculin test ing if h igh risk of TB• Early surgery is t reatm ent of choice to prevent
skin loss and opt im ize cosm et ic outcom e• Surgery:
◦ Node excision ◦ Parot idectomy ◦ Select ive neck dissect ion ◦ Specim ens for h isto + m icro ◦ Consider postop clarithromycin for 3/12
• Medical: ◦ 6/12 com bined t reatm ent:
- Clarithromycin or cipro oxacin + isoniazid or r ifam but in + etham butol
68.5 Malignancy• Lym phom a 60%• Rhabdom yosarcom a 30%• Others 10% inc
◦ thyroid ◦ nasopharyngeal carcinom a ◦ neuroblastom a
◦ salivary gland m alignancies ◦ teratom as
• Lym phom as—NHL occur in younger children , HL in older
• Rhabdomyosarcom as—can occur in m any H&N sites and are e ect ively t reated w ith chem otherapy
• Thyroid carcinom a—m ainly papillary ◦ 14 to 40% of nodules reported as m alignant
• Teratom as 7 to 9% in H&N—can be successfully rem oved by surgical excision
68.5.1 Paediatric LymphomaHodgkin Lymphoma• Malignancy of lym phoret icular system a ect ing
adolescents and young adults• Rarely occurs in children <5 years• F:M 1:2• Arises in LNs 90%• Extranodal involvem ent usually associated w ith
progression of disease, spleen m ost com m on ext ranodal site
• Cervical and supraclavicular nodes m ost com m on
• Waldeyer r ing rarely involved• Dx: LN biopsy posit ive Reed–Sternberg cells
(m ult inucleate giant cells)• 4 subtypes:
◦ Lymphocyte-predom inant ◦ Nodular sclerosis (m ost com m on)
Table 68.1 Ann Arbor classi cation of lymphoma
Stage I• Single nodal region• Localized single extralymphatic
organ/site
Stage II
• 2 or more nodal regions same side of diaphragm
• Localized single extralymphatic organ/ site + LNs (regional) or other LNs same side diaphragm
Stage III
• Nodal regions both sides diaphragm ± localized single extralymphatic organ/site
• Spleen or both
Stage IV
• Di use/multifocal extralymphatic organ ± regional nodes
• Isolated extralymphatic organ + nonregional nodes
B symptoms: unexplained wt loss ≥10% body wt in 6/12, unexplained fever>38°, night sweats
Philpott_9783131662316_Ch68.indd 246 02/05/14 1:36 PM
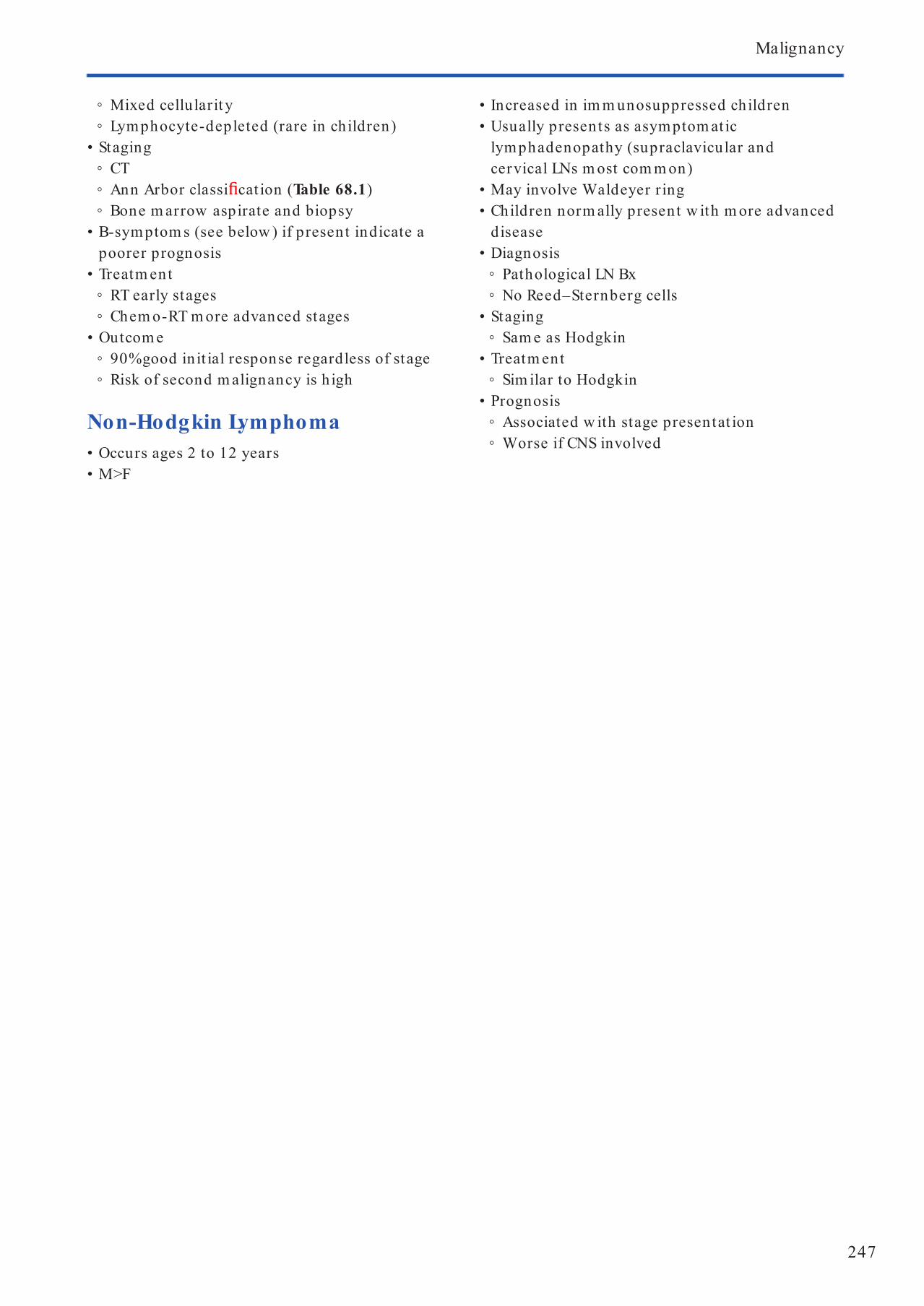
247
Malignancy
◦ Mixed cellularit y ◦ Lymphocyte-depleted (rare in children)
• Staging ◦ CT ◦ Ann Arbor classi cat ion (Table 68.1) ◦ Bone m arrow aspirate and biopsy
• B-sym ptom s (see below ) if present indicate a poorer prognosis
• Treatm ent ◦ RT early stages ◦ Chem o-RT m ore advanced stages
• Outcom e ◦ 90% good in it ial response regardless of stage ◦ Risk of second m alignancy is h igh
Non-Hodgkin Lymphoma• Occurs ages 2 to 12 years• M>F
• Increased in im m unosuppressed children• Usually presents as asym ptom at ic
lymphadenopathy (supraclavicular and cervical LNs m ost com m on)
• May involve Waldeyer r ing• Children norm ally present w ith m ore advanced
disease• Diagnosis
◦ Pathological LN Bx ◦ No Reed–Sternberg cells
• Staging ◦ Sam e as Hodgkin
• Treatm ent ◦ Sim ilar to Hodgkin
• Prognosis ◦ Associated w ith stage presentat ion ◦ Worse if CNS involved
Philpott_9783131662316_Ch68.indd 247 02/05/14 1:36 PM
248
69.1 Paediatric Larynx• Funct ions:
◦ Protect ion of t racheobronchial t ree on swallow ing
◦ Coughing ◦ Phonat ion ◦ Strain ing
• Di erences from adult larynx: ◦ More anterior ◦ Higher: C3 to C4 (C6 in adults) ◦ Larger epiglot t is+ om ega-shaped ◦ Cricoid cart ilage narrowest par t of airway 4 to 5 m m (adult is glot t is 7 × 4 m m )
69.1.1 Child w ith StridorFeatures• Biphasic (h igh in t rachea)
◦ Subglot t ic stenosis ◦ Subglot t ic haem angiom a ◦ Croup
• Expiratory ◦ Asthm a ◦ FB
• Inspiratory (level of larynx) ◦ Web ◦ VF palsy ◦ Papillom a ◦ Haem angiom a ◦ In am m atory, e.g., epiglot t it is
• Ster tor ◦ Choanal at resia ◦ Ads ◦ Macroglossia, e.g., Dow n syndrom e ◦ Micrognathia, e.g., Pierre Robin sequence ◦ Muscular incoordinat ion , e.g., cerebral palsy
Timing of Onset• Bir th
◦ Subglot t ic stenosis ◦ Web ◦ VF palsy (hydrocephalus—Arnold–Chiari)
• 1st few weeks ◦ Laryngom alacia
• 2–6/12 ◦ Subglot t ic haem angiom a ◦ Vascular r ing
69 Paediatric Airway Assessment and Management
• 1 year ◦ Papillom a
• Iat rogenic ◦ Subglot t ic stenosis
Speci c Points from History• Di culty feeding• Poor w t gain (grow th curves), i.e., failure to
thrive• Any cyanosis: lung/cardiac problem s• Voice/cry norm al: papillom as• Worse supine: laryngom alacia• Previous in tubat ions, PICU, SCBU,
prem —subglot t ic stenosis• Cardiac surgery—VF palsy, subglot t ic stenosis• Respiratory sym ptom s—lung disease• GORD
Examination• Respiratory—tracheal tug, in tercostal recession ,
respiratory rate, cyanosis• Cutaneous haem angiom a—50% w ith subglot t ic
haem angiom a have a cutaneous one• Nasal airway• Micrognathia• Syndrom al• Oropharynx—tonsil size
All children w ith st ridor need direct laryngoscopy!
Di erentiating between Epiglottitis and Croup• See Table 69.1
69.1.2 How to Examine Paediatric Larynx• See Table 69.2
Order of Frequency of Endoscopies for Airway Problem1. Subglot t ic stenosis2. Laryngom alacia3. VF palsy4. Tracheom alacia
Philpott_9783131662316_Ch69.indd 248 02/05/14 1:39 PM

249
Paediatric Tracheostomy
• Op ◦ Rem ove fat pad to expose st raps ◦ Separate st raps and stay in m idline checking all t im e
◦ Divide isthm us w ith elect rocautery ◦ Check cricoid by running pair of forceps dow n from thyroid cart ilage
◦ Do not dam age 1st t racheal r ing ◦ Place ×2 3.0 Prolene stay sutures across 2 t racheal r ings (2nd–4th)
◦ Incision is m ade between 2nd and 4th rings ◦ ET tube is w ithdraw n and an appropriately sized t rachy tube is inserted, tube is secured w ith tapes
◦ Stay sutures are taped to chest and m arked “do not rem ove” and “right” and “left”
5. Foreign body6. Subglot t ic haem angiom a7. Recurrent respiratory papillom atosis
69.2 Paediatric Tracheostomy69.2.1 Procedure• Posit ioning
◦ Supine, sandbag shoulders, head r ing, pat ient st raight , sleek
◦ Tower cover head and split drape, m ark m idline chin—sternal notch
• Incision ◦ Horizontal 1 nger breadth above suprasternal notch
Table 69.1 Di erentiating between epiglot titis and croup
Epiglottitis Croup
Cause Haemophilus type B Parain uenza
Age 2–5 yrs 6/12–2 yrs
Onset Fast (hours) Slow
Fever High Low grade
Dysphagia Marked None
Drooling Yes Minimal
Cough No Barking
Voice Mu ed Hoarse
Stridor Inspiratory Initially inspiratory then biphasic
Treatment
• Do not distress child• Secure airway in theatre with senior
anaesthesiologist• IV access• Swab• BCs• ABx 3rd-generation cephalosporin
(Ceftriaxone) or chloramphenicol
• Humidi cation• Oxygen• Nebulized adrenaline (1 mL of 1 in 1000 over
30 min)• ABx (cephalosporin)• Dex (0.25 mg/kg)
Table 69.2 How to examine a paediatric larynx
Pros Cons
1. Awake exi-nasendoscopy<18/12—child that tolerates
• Laryngomalacia• VF palsy
• View trachea• View subglot tis
2. Flexi bronchoscopy*• Laryngomalacia• VF palsy• Tracheomalacia
• Check laryngeal cleft• Doing anything
3. Rigid bronchoscopy/* laryngoscopy• Gd image• Check clefts• Can instrument airway
• Distorts dynamics• Traumatic, may make bad airway worse
* Tubeless inhalational anaesthetic with halothane/sevo uorane + oxygen
Philpott_9783131662316_Ch69.indd 249 02/05/14 1:39 PM

250
69 Paediatric Airway Assessment and Management
• Day 4 ◦ Child can leave ward but m ust stay w ith in local area/hospital
• Day 5 ◦ Discharge after lunch ◦ If older child m ay need m ore stages to dow nsize, w hich m ay take m ore days
◦ If child is <1 year or sm all consider decannulat ion to a size 2.5 before rem oval
◦ If it is post MLB there should be a rest day before decannulat ion
◦ FU OPA 8–10/52, cont inue school career unt il review
69.3.2 Failed Paediatric Tracheostomy Decannulation• Stom al granulat ion
◦ Part icularly upper m argin ◦ Cold steel/CO2 laser ◦ ± Auricular cart ilage/r ib
• Laryngom alacia ◦ Assessed during dynam ic airway w ith spontaneous vent ilat ion
◦ May need supraglot toplasty if severe• Tracheo/bronchom alacia
◦ May occur if been on vent ilatory support w ith h igh pressures
◦ Either t racheostomy itself or in am m atory process causing severe t racheobronchit is, often at tening of the car t ilaginous anterior arch , w hich m ay extend below the t racheostomy tube to involve m ainstem bronchi
◦ Treatm ent opt ions: - Aortopexy and suspension of the anterior t racheal wall
- Resect ion t rachea and reconstruct ion/anastom osis
- Endoscopic placem ent stent• Vascular com pression
◦ Most com m on is late takeo of innom inate ar tery w here m ay see a pulsat ile m ass com pressing anter ior t racheal wall
◦ Others include double aor t ic arch , r ight at r ial dilat ion
• Vocal cord dislocat ion/ xat ion ◦ Cricoarytenoid join t if prolonged dislocat ion ◦ May need laser arytenoidectomy + part ial cordectomy this m ay a ect voice
• Subglot t ic anom alies ◦ Cysts, haem angiom as
◦ Tube is not secured to chest as th is causes scarring
◦ Som e recom m end m aturat ion sutures and here the t racheostomy is approxim ated to the skin edge w ith 4.0 and 5.0 Monocryl (Johnson & Johnson Medical, Livingston, Scot land) - There is not an increased incidence of t racheocutaneous stu la
69.3 Paediatric Tracheostomy Tube Sizes• See Table 69.3
69.3.1 Paediatric Tracheostomy Decannulation (Great Ormond Street Protocol)• Need to ensure underlying pathology has set t led
and no need for ext rapulm onary support or fur ther surgery. Norm ally have MLB prior to decannulat ion
• Day 1 ◦ Adm it ward ◦ Decrease tube to size 3 ID ◦ Can leave ward area
• Day 2 ◦ Block tube 24 h ◦ Can leave ward area ◦ Encourage to cough ◦ Do not suct ion unless necessary
• Day 3 ◦ Rem ove tube ◦ Child m ust rem ain on ward ◦ Review BLS w ith parents
Table 69.3 Paediatric tracheostomy tube sizes
Age or weight Inner diameter (mm)
Prem
<1 kg 2.5
1–2.5 kg 3.0
Neonate
6/12 3.0–3.5
6/12–1 y 3.5–4.0
1–2 y 4.0–5.0
>2 y (Age + 16)/4
Philpott_9783131662316_Ch69.indd 250 02/05/14 1:39 PM

251
Paediatric FBs Airway/Oesophagus
69.4.3 Operative Technique• GA• Pulse oxim et ry• Cooperat ion between surgeon and
anaesthesiologist• ET in tubat ion for oesophageal FBs• Spontaneous respirat ion for airway FBs
(safer than apneic technique w here pat ient is completely paralyzed + cannot m ove air should the airway be tem porarily lost
• +ve pressure vent ilat ion is avoided as drives the FB deeper in to airway
• Inhalat ional anaesthet ic (e.g., halothane) is delivered through a closed system or a r igid bronchoscope
• Forceps are pract iced in advance on duplicate FB• Have spare pair in case of problem• Before grabbing FB determ ine size, shape,
posit ion , and probable locat ion of unseen par ts and relat ionship to surrounding st ructures
• Forceps advanced unt il light ly touches FB• Endoscope is w ithdraw n a short distance to
perm it the blades of the forceps to be opened• Forceps blades are advanced so that the t ips pass
the equator of the object• Tip of endoscope is advanced against the FB,
w hich is held against the tube m outh• Extract and w ithdraw forceps and scope as one• Pointed objects pose a special problem . First
priorit y is to ident ify the point . It is then released and sheathed w ith in the endoscope. May need to m ove object distally to disim pact it
• “St ripping o ” m ay occur: as the FB is brought through the larynx the lateral pressure of the VFs m ay st r ip the FB from the grip of the forceps
• Airway should be re-established im m ediately by either rem oving the object or pushing it dow n in to bronchus from w hich it has been ext racted, allow ing vent ilat ion of the good lung
69.4.4 ComplicationsComplications of Laryngeal, Tracheal, and Bronchial FBs• Im m ediate
◦ Pneum om ediast inum ◦ Im pact ion ◦ Com plete obst ruct ion ◦ Failure to recover—thoracotomy/t racheostomy ◦ Obst ruct ive em physem a
• Adhesions, webs, st r ictures• Neurological/ neurom uscular problem s possibly
result ing in aspirat ion• Obst ruct ive Sleep Apnoea
69.4 Paediatric FBs Airway/Oesophagus• Organic m at ter in bronchus requires urgent
rem oval because swelling/irritat ion leads to asphyxia and airway occlusion
• Disc bat tery in oesophagus requires urgent rem oval ◦ Bat teries contain NaOH, KOH, and m ercury ◦ Mucosal dam age occurs w ith in 1 h w ith erosion of m ucosal layers w ith in 2 to 4 h and perforat ion in 8 to 12 h
• If in stom ach allow to progress w ith repeat X-ray after 4/7 if not found in stool
69.4.1 History• Choking• Cough• Wheeze• May adm it to it• Often a period after in it ial event w here there is
an absence of sym ptom s• 3rd stage: obst ruct ion , erosion, infect ion
◦ Fever, m alaise, cough, haem atem esis, pneum onia, atelectasis, lung abscess, m assive exsanguinat ion
• Right m ain bronchus is m ore com m on because w ider and less acute angle from t rachea
• Laryngeal foreign bodies ◦ Com plete obst ruct ion leading to arrest ◦ Croup ◦ Hoarseness ◦ Cough ◦ Stridor ◦ Dyspnoea
69.4.2 Radiology• CXR—PA + lat• During expiration bronchial FB obstructs exit of
air leading to obstructive emphysem a leading to air trapping + persistent in at ion of obstructed lung result ing in m ediastinal shift to opposite side
• Atelectasis is a late nding
Philpott_9783131662316_Ch69.indd 251 02/05/14 1:39 PM

252
69 Paediatric Airway Assessment and Management
• Mild—self-lim it ing• Severe—surgical in tervent ion challenging and
m ay be fatal• DDx = stenosis or external m ass com pression
• Late ◦ Atelectasis ◦ Granulom a ◦ Stricture ◦ Pneum onia
Complications of Oesophageal FBs• Perforat ion• Abscess• St ricture
69.4.5 Paediatric Bronchoscopy• See Table 69.4 for bronchoscopies by age• Bronchography gives com plem entary info• Long t rachy tube ± CPAP• Aortopexy, bronchopexy, stents
Table 69.4 Bronchoscopies by age
Bronchoscope size/external diameter (mm)
Age Length (cm)
2.5–30 Preterm 20
3.5 0–18/12 20–30
4 18/12–3 y 30
5 3–12 y 30
6 >12 y 30
Philpott_9783131662316_Ch69.indd 252 02/05/14 1:39 PM

253
70 Development and the Drooling Child
70.1 Speech Development• 4/12 m akes vowel sounds• 6/12 uses consonants m onosyllables like “da”
or “ba”• 7–8/12 acquires bisyllabic babble like “dada” or
“m am a” non-speci cally• 13/12 uses sim ple words like “m am a” or “dada”
appropriately, understands sim ple com m ands like “no” or “yes,” and responds to their nam e
• 18/12 has acquired 10-word vocabulary• 20/12 can com bine 2 words• 24/12 has acquired 50-word vocabulary
70.2 Paediatric Development• Walking unsupported
◦ 25% by 11/12 ◦ 50% by 12/12 ◦ 90% by 15/12 ◦ 97.5% by 18/12
• Vision ◦ 6/52 w ill turn head to follow object
• Fine m otor skills ◦ New born w ill grasp object placed across palm of hand-grasp re ex
◦ At 6/12 reach + grasp + t ransfer objects ◦ At 10/12 have pincer grip w ith thum b and 2nd nger
• Feeding ◦ 6/12 put solid food in m outh ◦ 12/12 drink from cup ◦ 18/12 spoon and feed them selves
70.3 Drooling70.3.1 Features• Norm al phenom enon prior to developm ent of
oral neurom uscular control (18–24/12)• Anterior or posterior t ypes w ith increased risk
of aspirat ion w ith the lat ter• After 4 years consider abnorm al• Children w ith neurom uscular im pairm ent m ay
show im provem ent unt il 6 years
• 10 to 37% children w ith cerebral palsy drool• May be hypersecret ion—prim ary
sialorrhoea• Im paired neurom uscular cont rol and
dysfunct ional voluntary oral m otor act ivit y—secondary sialorrhoea
• This is com pounded by ine cient and infrequent swallow /poor head control/neck weakness/dental m alocclusion/large tongue and tongue thrust ing
• Subm andibular gland produces 70% rest ing secret ions
• Address num ber of bib changes and state of perioral skin (m acerat ion and infect ion)
70.3.2 Assessment• Teacher Drool Scale:
1. No drooling2. Infrequent drooling, sm all am ount3. Occasional drooling, on and o all day4. Frequent drooling, but not profuse5. Constant ly wet saliva leaking on clothes and
furniture• Salivary ow rate (m L/m in): dental rolls at the
ori ces of large salivary glands ◦ Unst im ulated norm al is 0.3 to 0.4 m L/m in
• Drooling quot ient: num ber of drooling episodes/40 observat ions (every 15 s) in 10 m in × 100%
• Radiology: ◦ Barium swallow: exclude oesophageal pathology
◦ Radiosialography: m ore for research evaluat ing secretory funct ion
70.3.3 Treatment• Conservat ive
◦ Oral m otor t rain ing - Behavioural therapy - Appliances, e.g., Palatal Train ing Appliance, Cast illo-Morales plate
- Drugs: ant icholinergics, Botox - RT: risk of m alignancy
Philpott_9783131662316_Ch70.indd 253 02/05/14 1:43 PM

254
70 Development and the Drooling Child
• Surgery ◦ Adenotonsillectomy if adenoidal sym ptom s and tonsil hyper t rophy
◦ Decrease saliva ow - Excision glands - Ligat ion ducts
- Tym panic neurectomy - Reroute saliva ow - Transposit ion duct to behind ant tonsillar pillar (r isk of ranula if sublingual glands not excised)
Philpott_9783131662316_Ch70.indd 254 02/05/14 1:43 PM

255
71 Tonsils and Adenoids
71.1 Anatomy71.1.1 Waldeyer Ring• Lym phoid t issue encircling the pharynx• Consists of palat ine tonsils (the tonsils),
pharyngeal tonsils (the adenoids), lingual tonsils, and tubal tonsils
• Constant ly exposed to new ant igens• Par t of the MALT, w hich processes ant igens and
presents them to TH cells and B cells• Secretes IgA and IgG
71.1.2 Palatine Tonsils• Boundaries:
◦ Anterior: palatoglossus ◦ Posterior: palatoglossus ◦ Lateral: superior const rictor
• Vascular supply: ◦ Tonsillar a ◦ Ascending pharyngeal a ◦ Tonsil branch of facial a ◦ Dorsal lingual branch of lingual a ◦ Ascending palat ine branches of facial a
• Venous drainage: ◦ Peritonsillar plexus to lingual and pharyngeal vv to in ternal jugular v
• Nerve supply: ◦ Tonsillar branches of m axillary n and glossopharyngeal n
• Lym phat ic drainage: ◦ Direct ly to jugulodigast r ic nodes and upper deep cervical LNs and indirect ly through ret ropharyngeal LNs
71.1.3 Adenoids• Boundaries:
◦ Posterosuperior: poster ior pharyngeal wall and base of skull
• Vascular supply: ◦ Ascending pharyngeal a ◦ Ascending palat ine a ◦ Tonsillar branch of facial a ◦ Pharyngeal branch of m axillary a ◦ A of pterygoid canal ◦ Basisphenoid a
• Venous drainage: ◦ Peritonsillar plexus in conjunction w ith pterygoid plexus to internal jugular and facial vv
• Nerve supply: ◦ Pharyngeal plexus
• Lym phat ic drainage: ◦ Retropharyngeal and pharyngom axillary space LNs
71.2 Histology• Tonsils: lym phoid t issue covered w ith
nonkerat in izing st rat i ed squam ous epithelium• Adenoids: lym phoid t issue covered w ith
pseudost rat i ed ciliated colum nar epithelium• Only the tonsils lie in a capsule, th is is
form ed from a specialized condensat ion of pharyngobasilar fascia
71.3 Tonsil Pathology71.3.1 Tonsillitis• Viral tonsillit is: adenovirus, rh inovirus, reovirus,
RSV, in uenza, parain uenza, CMV• Bacterial tonsillit is is usually due to group A β-haem olyt ic st reptococcus (GABHS) but m ay also be due to staphylococcus, nonhaem olyt ic st reptococci, Lactobacillus, Bacteroides, and Act inom yces
• Other form s of tonsillit is include fungal tonsillit is (due to candidiasis, usually in im m unocomprom ised pat ients), mycoplasm al tonsillit is, parasit ic tonsillit is (toxoplasm a), and tonsillit is due to chlamydia
• Rare form s of tonsillit is include Vincent angina, caused by Treponem a vincent ii and Spirochaeta dent iculata
Types• Acute parenchym atous: the w hole tonsil is
infected but no exudat ive pus• Acute follicular: the crypts are lled w ith
infected brin• Chronic form s: chronic parenchym atous
and chronic follicular; these are som et im es associated w ith tonsillolith form at ion
Philpott_9783131662316_Ch71.indd 255 5/20/14 11:50 AM

256
71 Tonsils and Adenoids
Complications• Suppurat ive
◦ Peritonsillar abscess (quinsy) ◦ Deep neck infect ions: parapharyngeal and ret ropharyngeal esses
◦ Throm bophlebit is: Lem ierre disease (Fusobacterium necrophorum )
◦ Chronic adenotonsillar hypert rophy• Nonsuppurat ive
◦ Scarlet fever ◦ Acute rheum at ic fever ◦ Postst reptococcal glom erulonephrit is
71.3.2 Glandular Fever• Infect ious m ononucleosis• Usually due to EBV, 10% of cases due to CMV• Transm it ted by oral contact• Fever, generalized m alaise, lym phadenopathy,
hepatosplenom egaly, and pharyngit is• 10% becom e jaundiced• Blood count: lym phocytosis w ith atypical
lym phocytes (act ivated T cells)• Sheep RBC agglut inat ion in the presence of
heterophile ant ibodies is the basis for the Paul–Bunnell test
• Horse RBC agglut inat ion in the presence of heterophile ant ibodies is the basis for the Monospot test ◦ This test is 100% speci c and 85% sensit ive, but m ore sensit ive than the Paul–Bunnell test
◦ This test m ay be negat ive early in the course of EBV infect ious m ononucleosis
Complications• Airway obst ruct ion• Myocardit is• Splenic rupture• Haem olyt ic anaem ia• Acute in terst it ial nephrit is, glom erulonephrit is• Fat igue, depression• Neurological: opt ic neur it is, t ransverse
myelit is, asept ic m en ingit is, encephalit is, m en ingoencephalit is, CN palsy or Guillain–Barré syndrom e
• Maculopapular rash develops w ith am oxicillin• Pat ients to avoid st renuous exercise for the rst
3 weeks of illness• Prevent spread by avoiding close contact w ith
body uid secret ions
71.3.3 Obstructive Sleep Apnoea Syndrome• Due to adenotonsillar hypert rophy• Associat ion between OSAS and households
w here adults sm oke• Com plicat ions: pulm onary hypertension, cor
pulm onale, alveolar hypovent ilat ion causing chronic CO2 retent ion
• May result in craniofacial abnorm alit ies over t im e
71.3.4 Neoplasms• Benign: lipom as, brom as, schwannom as• Malignant: lym phom a, SCC
71.3.5 Post-transplant Lymphoproliferative Disorder• Not a t rue neoplasm• Life-threatening com plicat ion of
im m unosuppression• Proliferat ive B-cell disorder associated w ith EBV
in an im m unocomprom ised host• Tonsillectomy is required to restore an airway
and to provide t issue for diagnosis
71.4 Adenoid Pathology• Adenoidit is• OSAS as a consequence of their hypert rophy in
conjunct ion w ith enlarged tonsils• Nasal obst ruct ion• Cont ribut ion to recurrent or persistent ot it is
m edia• Cont ribut ion to recurrent acute sinusit is or
chronic sinusit is
71.5 Tonsillectomy71.5.1 Indications• Enlarged tonsils result ing in upper airway
obst ruct ion/OSAS• Recurrent acute tonsillit is
◦ 7 or m ore episodes in the preceding year ◦ 5 or m ore episodes in each of the 2 preceding years
◦ 3 or m ore episodes in each of the 3 preceding years
Philpott_9783131662316_Ch71.indd 256 5/20/14 11:50 AM

257
Adenoidectomy
• Tonsillectomy to provide t issue for diagnosis ◦ Other reported indicat ions:
- Swallow ing di cult ies - Tonsillar crypt debris (tonsilloliths) - Enlarged cervical LNs - Gut tate psoriasis
71.5.2 Brodsky Tonsil Classi cation• See Fig. 71.1
◦ Tonsil 0: Tonsils t w ith in the tonsillar fossa ◦ Tonsil 1+: Tonsils <25% of space between pillars ◦ Tonsil 2+: Tonsils <50% of space between pillars ◦ Tonsil 3+: Tonsils <75% of space between pillars ◦ Tonsil 4+: Tonsils >75% of space between pillars
71.5.3 Contraindications• Bleeding diathesis• Anaem ia• Acute infect ion• Poor anaesthet ic candidate
71.5.4 Techniques• Cold steel dissect ion• Diathermy• Laser—CO2, KTP, diode• Coblat ion• Radiofrequency• Ult rasonic scalpel• Ligasure
71.5.5 Complications • Post-operat ive haem orrhage• Dam age to teeth
• UK Nat ional Tonsillectom y Audit: “hot techniques” associated w ith 3-fold risk in post-operat ive haem orrhage
71.6 Adenoidectomy71.6.1 Indications• Enlargem ent resulting in upper airway obstruction• Recurrent or persistent ot it is m edia• Recurrent acute sinusit is or chronic sinusit is• Dysphagia w ith failure to thrive• Signi cant speech problem s
71.6.2 Contraindications• Bleeding diathesis• Risk of velopharyngeal insu ciency (VPI),
especially in pat ients w ith short palate, subm ucous cleft palate (be suspicious if bi d uvula present), t rue cleft palate, palatal hypotonia
• Risk of at lantoaxial join t laxity, especially in pat ients w ith Dow n syndrom e (observed in 10% of pat ients)
71.6.3 Techniques• Curet tage• Suct ion diathermy• Microdebrider
71.6.4 Complications• Post-operat ive haem orrhage• Dam age to teeth• VPI• Atlantoaxial subluxat ion in cer tain pat ients• Nasopharyngeal stenosis• Eustachian tube injury
Fig. 71.1 Brodsky Tonsil Classi cation .
Grade 3: Tonsil >50% crossing midpoint between
uvular and pillar
Grade1: Tonsil withinthe pillars
Grade 2: Tonsil <50% from midpoint between
uvular and pillar
Grade 4: Tonsils meetin midline
Philpott_9783131662316_Ch71.indd 257 5/20/14 11:50 AM

258
72.1 Haemangioma• Benign endothelial tum our• Develops after bir th• Histologically, cell proliferat ion• 60% involve head and neck w ith other sites
including t runk and extrem it ies• First 6–8/12 rapid grow th (proliferat ive
phase)• Begins to involute (slow phase)• By 9 years of age m ost have involuted• Majorit y do not require t reatm ent• Indicat ions for t reatm ent
◦ Size ◦ Ulcerat ion ◦ Dis gurem ent ◦ Haem atological com prom ise, e.g., Kasabach–Merrit t syndrom e
◦ Cardiovascular com prom ise, e.g., h igh-output cardiac failure
◦ Aerodigest ive com prom ise ◦ Large periorbital lesions—visual im pairm ent
• Treatm ent opt ions ◦ Laser-pulsed-dye m ost com m on, consider repeat ing m onthly unt il response
◦ Surgical excision ◦ Pharm acology-steroids (oral, in t ralesional), propranolol, α -in terferon
◦ Tracheostomy and wait for regression
72.1.1 Subglottic Haemangioma• Usually asym ptom at ic at bir th• Develop increasing biphasic st r idor often
m im icking croup and failure to thrive• 1% of children w ith cutaneous haem angiom a
have subglot t ic haem angiom a• 50% of children w ith subglot t ic haem angiom a
have cutaneous haem angiom a• Subglot t ic haem angiom a best diagnosed by
laryngoscopy• Most are posterolateral and subm ucosal• Biopsy is often not required—risk of
haem orrhage
72 Haemangiomas and Other Vascular Malformations
• Tracheostom y w ill secure the airway w hile allow ing for spontaneous involut ion
• Other t reatm ent opt ions are h ighlighted above
72.2 Vascular Malformation• Congenital anom aly of vessels• Present at bir th• Grows w ith child and does not involute• Histologically, vessel dilatat ion• Related to vessel of origin
◦ AV m alform at ion ◦ Lymphangiom a ◦ Capillary (port w ine stain)
72.2.1 Lymphangioma• Sim ple—thin walled• Cavernous—dilated lym phat ic spaces• Cyst ic hygrom a—cysts, varying sizes• Slow ow vessel• Typically a ects lips, cheeks, oor m outh• Aim s Rx: relief sym ptom s, good cosm et ic
results, preservat ion funct ion• If involves in t r insic m uscles of tongue, m ay be
very di cult to resect• Ix: USS (low ow ) + MRI (no enhancem ent w ith
cont rast)• Rx cyst ic hygrom a:
◦ Inject ion of sclerosant (OK 432) ◦ Surgical excision easier (m acrocyst ic) if below hyoid
72.2.2 AV Malformation• Fast ow w ith absence of capillary bed• Red hue and warm• May bleed• May cause cardiac failure• Seen in hereditary haem orrhagic telangectasia• Ix: USS (high ow ) + MRI (no m ass seen on scan,
unlike a haem angiom a) + angiography• Treatm ent opt ions: em bolizat ion , surgery, or
sclerotherapy
Philpott_9783131662316_Ch72.indd 258 02/05/14 2:01 PM

Sect ion V
Miscellaneous
Philpott_9783131662316_Ch73.indd 259 02/05/14 2:04 PM

Philpott_9783131662316_Ch73.indd 260 02/05/14 2:04 PM

261
73 Microbiology of ENT
73.1 Ear Infections(See also chapters in Sect ion I)
73.1.1 Otitis Externa• Acute infect ion
◦ This is an in am m at ion of the ear canal, com m only caused by bacterial infect ion
◦ Sym ptom s can include itchiness, discharge, and pain
◦ Com m on bacterial causes: Staphylococcus aureus (yellow crusted discharge), Streptococcus pyogenes are the m ost com m on pathogens
◦ Treatm ent should be w ith ear drops if m ild or system ic in severe cases
• Chronic (sw im m er’s ear) infect ion ◦ Ongoing m ild infect ion— m ay be due to underlying seborrhoeic derm at it is or frequent sw im m ing or diving leaving the ear canal wet
◦ Typical pathogens are Pseudom onas species (they are water loving), S. aureus, Enterobacteriaceae, and Aspergillus species
◦ Treatm ent includes aural toilet by ENT specialist and ear drops (e.g., o oxacin 0.3% or polymyxin B + neomycin + hydrocor t isone)
◦ If S. aureus and associated pinna cellulit is, system ic t reatm ent w ith ant istaphylococcal agent (e.g., oxacillin) m ay be appropriate
• Malignant/necrot izing infect ion ◦ This is a very severe form of acute ot it is externa
◦ It presents acutely w ith a system ic in am m atory response and fever
◦ High-risk groups are pat ients w ith diabetes, AIDS, and those on chem otherapy; usually seen in elderly pat ients
◦ The infect ion is m ainly bacterial and includes Pseudom onas aeruginosa (90%) and S. aureus
◦ Bony involvem ent is not uncom m on ◦ Ear swab and t issue should be cultured for pathogens prior to ant ibiot ic t reatm ent
◦ Treatm ent m ust be in it iated rapidly and includes system ic ant ibiot ics w ith ant ipseudom onal act ivit y, e.g., m eropenem ,
ceftazidim e, tazobactam , gentam icin , or cipro oxacin
◦ In osteomyelit is t reatm ent should be for 4 to 6 weeks (CT or MRI m ay aid diagnosis); m onitoring of in am m atory m arkers (e.g., C-react ive protein) can help indicate response to t reatm ent
73.1.2 Otitis Media• Acute infect ion
◦ This is an infect ion of the m iddle ear caused by viruses and/or bacter ia (S. pneum oniae, Haem ophilus in uenzae, occasionally Moraxella catarrhalis)
◦ Tym panic m em brane m ay be perforated w ith purulent yellow m ucus and pain
◦ Children should not rout inely be prescribed em pirical ant ibiot ics im m ediately
◦ Symptom at ic children (fever, pain) and adults m ay be given em pirical t reatm ent in severe cases or if sym ptom s persist for m ore than 48 to 72 h
◦ Ant ibiot ics (am oxicillin or am oxicillin /clavulanate or another cephalosporin) and analgesic (paracetam ol) m ay be prescribed for 5 to 10 days
◦ Com plicat ion: m astoidit is• Chronic infect ion
◦ Chronic m iddle ear infect ion w ith in term it tent purulent discharge (>2 weeks) but often no pain or fever. Mastoid cavity m ay also be a ected. Im paired hearing is com m on.
◦ Risk factors: recurrent episodes of acute ot it is m edia, crow ded living condit ions, craniofacial anom alies (e.g., cleft lip)
◦ Cases should be assessed by ENT specialist . Rem oval of debris and topical ant ibiot ics are advisable
◦ Avoid sw im m ing; keep ear dry ◦ Complicat ions: facial paralysis, labyrin th it is, lateral sinus throm bophlebit is, in t racranial abscess, m eningit is, hearing loss
• Mastoidit is ◦ Causat ive pathogens: S. pneum oniae, S. aureus, S. pyogenes, H. in uenzae, P. aeruginosa, and others
Philpott_9783131662316_Ch73.indd 261 02/05/14 2:04 PM

262
73 Microbiology of ENT
◦ Sym ptom s are ear pain , ear discharge, fever, hearing loss, headache, redness, and swelling behind the ear
◦ Invest igat ions: CT im aging and culture of discharge
◦ Treatm ent should include system ic ant ibiot ics (as per acute ot it is m edia) and surgical drainage and debridem ent if ant ibiot ics are unsuccessful
◦ In chronic m astoidit is, osteomyelit is should be excluded (CT and MRI)
◦ There is a r isk of CNS spread (epidural abscess, suppurat ive phlebit is, brain abscess)
73.2 Infections of the Sinuses73.2.1 Acute Rhinosinusitis• This is usually due to an obst ruct ion of the sinus
ost ia as a result of a viral infect ion or allergies and subsequent bacter ial infect ion
• Pathogens involved are: viruses, S. pneum oniae, H. in uenzae, M. catarrhalis, S. pyogenes, S. aureus, and anaerobic bacteria
• Antibiotic treatm ent (e.g., am oxicillin/clavulanate, cephalosporins) is indicated if patient presents w ith fever, pain, purulent discharge
• Adjunct ive therapy: topical decongest ions and irrigat ions
73.2.2 Chronic Sinusitis• Chronic sinusit is in adults m ay be due
to anaerobes (Prevotella sp. st reptococci, Fusobacterium spp.) and H. in uenzae, P. aeruginosa, S. aureus, M. catarrhalis, or fungi
• Ant ibiot ics are usually not very e ect ive• Pathogenesis is unclear; polyps, allergy, occult
im m unode ciency m ay play a role
73.2.3 Fungal SinusitisSee Chapter 26: Fungal Sinus Disease
73.3 Pharyngeal/Throat Infections/Tonsillitis73.3.1 Bacterial Pharyngitis• Caused m ainly by S. pyogenes or st reptococcus
group C• Clin ical sym ptom s: fever, sore throat
• Treatm ent: 1st line penicillin , 2nd line clarythromycin
• Com plicat ion: peritonsillar abscess (quinsy) ◦ This m ust be surgically drained ◦ Im m unological com plicat ion of S. pyogenes: rheum at ic fever, glom erulonephrit is
73.3.2 Lemmier Disease• This is a speci c form of bacter ial pharyngit is
followed by jugular vein throm bosis• Very severe sore throat in young adults or
adolescence followed by suppurat ive phlebit is of the in ternal jugular vein
• Sept ic pulm onary and system ic em boli are com m on
• Cause: Fusibacterium necrophorum or F. fusiform is• Diagnosis: bacter ial throat swab, blood culture,
Doppler echo• Treatm ent: penicillin , carbapenem , or
clindamycin (m acrolides are not e ect ive)
73.3.3 Diphtheria• Mem branous pharyngit is caused by toxin-
producing Corynebacterium diphtheria• Local in am m ation of nasopharynx, “bull neck”
appearance due to enlarged lym ph nodes. Toxin acts system ically causing mycocardit is, polyneurit is
• Diagnosis m ade by throat swab, serology• Therapy: passive im m unizat ion (ant i-diphtheria
ant ibody-rich im m unoglobulins)• Ant ibiot ics m ay reduce toxin product ion
(penicillin or erythrom ycin)• Not i able disease
73.3.4 Trench Mouth• Painful bacterial infect ion of the m outh
w ith swelling and ulcers of the gum (acute necrot izing ulcerat ive gingivit is)
• Com m on in World War I due to poor oral hygiene• Main sym ptom s are foul breath , fever, painful
gum s (gingivit is)• Causat ive pathogens: polym icrobial infect ion
w ith m ainly anaerobic bacteria• Risk factor: poor oral hygiene and nut rit ion ,
AIDS, im m unode ciency• Treatm ent: pain relief, im proved oral
hygiene, and ant ibiot ics (e.g., m etronidazole, clindamycin , or am oxicillin /clavulanate)
Philpott_9783131662316_Ch73.indd 262 02/05/14 2:04 PM

263
Pharyngeal/Throat Infect ions/Tonsillit is
73.3.5 Viral Pharyngitis (Common Cold, In uenza)• Sym ptom s: sore throat , runny nose,
conjunct ivit is, headache• Diagnosis: throat swab, serology• Treatm ent: sym ptom at ic (for in uenza,
neuram inidase inhibitor in severe infect ion)
73.3.6 Epiglottitis• ENT em ergency• Often a ects children• Caused by H. in uenzae, S. pyogenes
• Clin ically st r idor, fever, respiratory dist ress• Treatm ent: system ic ant ibiot ics (3rd-generat ion
cephalosporin), steroids if severe oedem a, t racheostomy if respiratory dist ress
73.3.7 Laryngitis/Tracheitis• Clin ically presents w ith hoarse voice,
ret rosternal discom fort• Caused m ainly by viruses (e.g.,
parain uenza)• Mucosal m em brane swelling is cause of
st r idor on inspirat ion (croup)• Diagnosis: throat swab, serology
Philpott_9783131662316_Ch73.indd 263 02/05/14 2:04 PM

264
74.1 Local Anaesthetics• Am ides, e.g., lidocaine, bupivacaine• Esters, e.g., cocaine, benzocaine• Most LAs are weak bases and exist as protonated
form at body pH• Block Na+ channels in axons →prevent
generat ion of APs• Sm all-diam eter nerve bres m ore sensit ive to
LAs ◦ Therefore coarse touch and m ovem ent usually spared
• At h igh concentrat ions can depress other excitable t issues e.g., m yocardium
• Main system ic e ects are on CNS—sedat ion and light-headed; som et im es anxiety and rest lessness
• High toxic doses cause tw itching and visual disturbances
• Severe toxicit y causes convulsions, com a, cardiorespiratory depression
• Lidocaine—rapid act ing and m ost stable; durat ion of act ion 90 m in
• Bupivacaine—slow onset (30 m in) but durat ion 8 h
• Cocaine used for surface Anaesthesia w here int rinsic vasoconst rictor act ion desirable
• Hypersensit ivit y react ions m ay occur w ith LAs, especially w ith atopic pat ients
• Opening of Na+ channels leads to Na+ entry exceeding K+ exit , fur ther depolarizing m em brane opening m ore Na+ channels, etc.—leads to AP
• LAs block Na+ channels by prevent ing opening of h-gates
• LAs are use dependent , i.e., degree of block proport ional to rate of nerve st im ulat ion
• More drug m olecules (in protonated form ) enter Na+ channels w hen they are open and cause m ore inact ivat ion
• Cocaine causes vasoconstrict ion by blocking norepinephrine reuptake and potent iates sym pathet ic act ivit y
• Most am ides cause vasoconstr ict ion at low doses and vasodilatat ion at h igher concentrat ions
• Durat ion and potency related to lipid solubilit y
• Parallel use of vasoconstrictor prolongs e ect• Am ides m etabolized in liver• Esters (not cocaine) hydrolyzed by plasm a
pseudocholinesterase• Max. dose of lidocaine = 200 m g (500 m g w ith
adrenaline), e.g., 5 m L of 2% lidocaine w ith adrenaline = 100 m g
• Bupivacaine = m ax. 60 m L using a 2.5 m g/m L (0.25%) solut ion
74.1.1 Mo at Solution• Cocaine 10% 1 m L or 5% 2 m L @ 50 m g/m L =
100 m g (1.5 m g/kg m ax); adrenaline 1 m L 1:1000 (m ax. 100 m g/10 m in); NaHCO3 2 m L 8.4%
• Risk of arrhythm ias—especially halothane• Risk of hypercapnia and hyper tension
74.1.2 Laryngopharyngeal Local Anaesthesia• Krause m ethod—swab soaked in 4% lidocaine
held by Krause forceps in each pir iform fossa for 1 m in
• Percutaneous inject ion of LA at greater cornu of hyoid also anaesthet izes superior laryngeal n
• Sprayed/nebulized lidocaine• Benzocaine lozenge
74.1.3 Ear Anaesthesia• Auriculotem poral block—2 m L of lidocaine
injected anterior to m eatus• Greater auricular n block—inject anter ior and
posterior to m astoid t ip
74.2 Neuromuscular Blocking Drugs• Com pet it ive, e.g., at racurium —lasts 15 to 30 m in• Depolarizing—suxam ethonium —rapid onset and
durat ion of 3 to 7 m in ◦ Drug does not dissociate rapidly from receptors at cholinergic nerve term inals
◦ Prolonged receptor act ivat ion is produced
74 Pharmacology and Anaesthetics
Philpott_9783131662316_Ch74.indd 264 02/05/14 2:06 PM

265
General Anaesthet ics
◦ Endplate depolar izat ion in it ially causes brief t rain of m uscle APs
◦ NM block then occurs because: - Inact ivat ion of voltage-sensit ive Na+ channels in surrounding m uscle bre m em brane—APs no longer generated
- Transform at ion of act ivated receptors to desensit ized state—unresponsive to ACh
◦ In it ial m uscle tw itch can cause m uscle pain the next day
74.3 Autonomic Nervous System• Sym pathet ic system = norepinephrine at α and β
receptors• Parasym pathet ic system = acetylcholine (ACh) at
m uscarin ic receptors• All ANS preganglionic bres are myelinated
and release ACh from nerve term inals—act ivate n icot in ic receptors at ganglionic synapse
• Postganglionic bres = short in parasym pathet ic nerves
• Sym pathet ic nerves synapse in paravertebral/prevertebral ganglia or abdom inal plexuses
• Act ion of ACh is greater at m uscarin ic receptors—parasympathet ic predom inates
• Muscarin ic agonists, e.g., p ilocarpine—reduce in t raocular pressure in glaucom a
• Muscarin ic antagonists, e.g., at ropine, hyoscine, iprat ropium —reduce secret ions of SGs, bronchi, and sweat glands
• Sym pathom im et ics: ◦ Indirect ly act ing, e.g., ephedrine, cocaine ◦ Directly act ing
- α -agonists, e.g., adrenaline, noradrenaline - β-agonists, e.g., adrenaline (β1 and β2 receptors), noradrenaline (β1 receptors), salbutam ol (β2 receptors)
• Adrenoceptor antagonists: ◦ α -blockers, e.g., prazosin ◦ β-blockers, e.g., atenolol, propranolol
74.4 Bronchodilators• β-agonists—SEs include ne t rem or, nervous
tension, and tachycardia• Iprat ropium —reduces re ex vagal
bronchoconst rict ion• Xanthines, e.g., theophylline—antagonist at
adenosine receptors
74.5 Cromoglycate• Most e ect ive in atopic pat ients, especially
children w ith m ult iple sensit ivit y• Needs to be given regularly and for several
weeks before bene t obtained• Reduces in ux of calcium in to ant igen-
sensit ized m ast cells and prevents degranulat ion (h istam ine release)
74.6 Antihistamines• Block H1 receptors• Older versions have ant im uscarin ic act ions
and pass BBB leading to drowsiness and psychom otor impairm ent
• Newer versions do not cross blood–brain barrier
74.7 General Anaesthetics74.7.1 Premedication• Benzodiazepines—relief from anxiet y• Atropine/hyoscine—prevent salivat ion and
bronchial secret ions• Morphine—m ay be given; fentanyl often used to
supplem ent NO during op• Ant iem et ics occasionally given w ith prem ed
74.7.2 IV Agents• Barbiturates e.g., th iopentone—induces in <30 s
because lipid soluble; m ay occasionally cause anaphylaxis
• Propofol—avoids barbiturate SEs: less myocardial depression, m ore rapid elim inat ion , no nausea/hangover; rare occurrences of convulsions and anaphylaxis
• Ketam ine—m ay cause n ightm ares
74.7.3 Inhalational Agents• Nit rous oxide
◦ Com m only used as a carrier gas for volat ile agents and reducing their concentrat ion
◦ Lit t le e ect on CVS or respiratory system ◦ Low solubilit y—therefore ar terial tension if it r ises quickly (com pared w ith halothane)
• Halothane ◦ Sm ooth induct ion ◦ Nonirritant vapour
Philpott_9783131662316_Ch74.indd 265 02/05/14 2:06 PM

266
74 Pharmacology and Anaesthet ics
◦ Concent rat ion-dependent hypotension ◦ Can cause arrhythm ias ◦ Depresses respiratory centre ◦ Toxic e ect = m assive hepat ic necrosis ◦ Used for inhalat ion-only induct ion (paediat ric)
• En urane ◦ Concent rat ion-dependent hypotension ◦ Depresses myocardial contract ilit y ◦ Less sensit izat ion of myocardium (inc. arrhythm ias)
◦ May occasionally cause seizure act ivit y in EEG
• Iso uorane ◦ Less cardiodepressant than halothane and does not sensit ize heart to adrenaline
◦ Concent rat ion-dependent hypotension• Sevo urane
◦ Low solubilit y ◦ Less cardiodepressant than halothane, and sensit izat ion of heart to adrenaline is equal to iso urane
◦ Preferred for inhalat ion induct ion (paediat r ic)• Des urane—sim ilar to sevo urane
74.7.4 Complications• Death < 1:10,000• Frequency of sym ptom s during the rst 24 h
follow ing am bulatory surgery is as follows: ◦ Bleeding, vom it ing, nausea—<5% ◦ Fever—5 to 15% ◦ Dizziness, headache, drowsiness, hoarseness—>15%
◦ Sore throat—25% ◦ Incisional pain—30%
74.7.5 Induced Hypotension• Techniques:
◦ Prevent anxiety-related tachycardia—good prem ed
◦ Avoidance of hypertension during laryngoscopy and in tubat ion
◦ Volat ile agent-induced vasodilatat ion ◦ Head-up posit ioning
• Speci c drugs used: ◦ Sodium nit roprusside—dilates ar terioles and venules
◦ GTN—dilates capacitance vessels ◦ Trim etaphan—release h istam ine, blocks ganglia, and reduces PVR
◦ Labetolol—reduces ar terial tone and HR
74.7.6 Shared Airway• Heliox m ay provide som e relief to dist ress• Beware anxiolyt ics in respiratory dist ress• Long-standing airway obst ruct ion allows
adaptat ion , and narrow ing can be very pronounced w ith a “solid” process, e.g., brosis
• Fibre-opt ic laryngoscopy m ay be considered in awake pat ient
74.8 Antiepileptic Drugs• Carbam azepine
◦ SEs include nausea, headache, drowsiness, diplopia, ataxia
◦ Reduces presynapt ic Na+ uptake• Gabapent in
◦ Possible enhanced neuronal GABA synthesis ◦ Diarrhoea, dry m outh , dyspepsia, nausea, vom it ing
74.9 Tricyclic Antidepressants• Inhibit uptake of 5HT and norepinephrine at
postsynapt ic receptors (cholinergic m uscarin ic, α -adrenoceptors, and h istam ine)
• Cause at ropine-like e ects: dry m outh , blurred vision, const ipat ion , urinary retent ion , tachycardia, postural hypotension
Philpott_9783131662316_Ch74.indd 266 02/05/14 2:06 PM

267
75.1 Data Display and Summary• Categorical data—nom inal (sex), grade of
tum our (ordinal)• Quant itat ive data—m easured or counted, e.g.,
age, blood pressure• Measure of variat ion—interquart ile range and
m edian• Histogram s—display grouped frequency
(dist r ibut ion of a cont inuous variable)—should generally have 5 to 15 groups
• Bar char ts—dist ribut ion of a discrete variable or a categorical one (spaces between bars)
75.2 Summary Statistics for Quantitative and Binary Data• Mean w ill be a ected by outlying data, m edian
w ill not• Standard deviat ion (SD) gives an indicat ion of
the spread about the m ean—relies on the data being sym m etrically dist r ibuted
• If norm al dist r ibut ion occurs: ◦ Mean ± 1 SD = 68% of data ◦ Mean ± 2 SD = 95% of data ◦ Mean ± 3 SD = 99.7% of data
• SD in ungrouped data uses degrees of freedom = division by total num ber of observat ions m inus 1
• Skewed data are often best presented via a log t ransform at ion
• Measurem ent error—SD for repeated m easurem ents
• Coe cient of variat ion = in t rasubject SD/m ean expressed as a percentage
• Absolute r isk reduct ion (ARR) = di erence between 2 risks for 2 t reatm ents (%age)
• If new therapy bene cial = num ber needed to t reat—ARR w ill be +ve (1/(P1 − P2))
• Risk rat io or relat ive r isk (RR)—if <1 = lower risk in control group
• RR reduct ion = (cont rol r isk—experim ental r isk)/control r isk
• Odds (event) = probabilit y of event happening (P)/(1 − P)
• Odds rat io (OR) = odds of event 1/odds of event 2
• Use of m edian or m ean does not depend necessarily on dist r ibut ion of data; if there is a sm all group at one ext rem e of the dist r ibut ion then the m edian w ill be m ore useful, otherw ise the m ean is generally preferred
• Data not norm ally dist r ibuted m ay well derive useful inform at ion from both m edian and m ean
• SD is only in terpretable for variables that have approxim ately sym m etrical dist r ibut ion
• SD should not be used for data that are not plausibly norm al e.g., age—interquart ile range (IQR) bet ter
• Case-control studies—quote OR• Cross-sect ional studies—either OR or RR
75.3 Populations and Samples• Standard error (SE) used to study signi cance
of di erence between 2 m eans = SD/√n; m easure of precision of a populat ion param eter
• Random sam pling allows a populat ion to be studied m ore convenient ly—m ay be st rat i ed to allow for age/sex dist r ibut ion
• Unbiased m easurem ent = average of a large set w ill be close to the t rue value
• Precise m easurem ent = repeatable• Non-random sam ples, e.g., hospital pat ients vs.
com m unity, volunteers vs. non; reduce biases by providing dem ographic data
• Acceptable response rate from a survey = 65 to 70%; useful to present data on non-responders; sm aller responses valid if no biases
• Sam ple SD = est im ate of populat ion param eter (variabilit y of observat ions)
• SE of an est im ate w ill decrease w ith increasing sam ple size
• SD is used to describe data, i.e., norm al dist r ibut ion
• SE is used to describe the outcom e of a study, e.g., est im ate the prevalence of disease
75 Medical Statistics
Philpott_9783131662316_Ch75.indd 267 02/05/14 2:11 PM

268
75 Medical Stat ist ics
75.4 Statements of Probability and Con dence Intervals• 95% lim its = reference range = m ean ± 1.96 SD
(~ 2 SD)• p-value = probabilit y of get t ing the observed
value (or m ore extrem e) if the null hypothesis were correct (e.g., p < 0.05)
• 95% CI = m ean ± 1.96 SE (~ 2 SE)—this indicates that only 5% chance that th is range excludes the m ean
• Reference range refers to individuals; con dence in terval (CI) refers to est im ates
75.5 Di erences between Means: Type I and Type II Errors and Power• Null hypothesis = no di erence between
populat ions compared• Type I error = reject ion of null hypothesis w hen
in fact it is t rue—using m ean ± 1.96 SE = 1/20 chance of being w rong
• A non-signi cant di erence does not m ake the null hypothesis likely; th is is just absence of evidence
• If CI excludes 0, the chance of sam ples being from sam e populat ion is less than 5%
• p-value signi cant if less than speci ed value (usually 5%)—probabilit y of get t ing the observed value (or m ore extrem e) if null hypothesis were correct
• Type II error = not reject ing the null hypothesis w hen there is a di erence between the 2 groups (alternat ive hypothesis—w hat di erence would be clin ically useful)
• Type I error rate = α• Type II error rate = β• Power of a study = 1 − β = probabilit y of
reject ing the null hypothesis w hen it is false• 1-sided test = considers that m ean of a group is
> than the other (expectat ion of result to show di erence in one direct ion)
• 2-sided test = considers that m ean of group is either > or < than the other
75.6 Con dence Intervals for Summary Statistics of Binary Data• If 95% CI for OR excludes 1 = signi cant
di erence between groups• If 95% CI is large = uncertain ty about t rue
di erence between groups
75.7 The t Tests• Preferable test w hen num ber of observat ions
<60 (especially <30)• One sam ple t test—data m ust be:
◦ Representat ive of sam ple populat ion ◦ Quant itat ive and norm ally dist r ibuted ◦ Independent of each other (any repeated m easurem ents on one individual = not independent e.g., 18 results on 15 subjects—only 15 results are independent)
• Two sam ple t test—data m ust: ◦ Have sam ples that com e from dist r ibut ions that m ay di er in their m ean value but not their SD
◦ Be from independent sam ples ◦ Be quant itat ive and norm ally dist r ibuted
• If SDs in 2 groups m arkedly di erent—Welsh test required
• Paired t tests used w hen the follow ing criteria m et: ◦ Data quant itat ive ◦ Dist r ibut ion of di erences (not or iginal data) is norm al
◦ Di erences independent of each other• If m ore than 2 t reatm ents being studied—not
valid to com pare each t reatm ent w ith the other t reatm ents using t test—leads to h igher t ype I error rate; use 1-way ANOVA
75.8 The Chi-Squared Test• Used to com pare dist r ibut ion of categorical
variables in 2 separate sam ples• Null hypothesis = no di erence in dist r ibut ion
between 2 groups
Philpott_9783131662316_Ch75.indd 268 02/05/14 2:11 PM

269
Statist ical Tests in Study Design
• In 2 × 2 tables, chi-squared test inappropriate if total of table < 20; needs Yates correct ion
• Observed values for one sam ple can be compared w ith theoret ical samples for the sam e sam ple
75.9 Exact Probability Test• If frequency of observat ions in a 2 × 2 table are
too sm all, use Fisher exact test• Can be 1- or 2-tailed
75.10 Rank Score Tests• Wilcoxon test: for paired non-norm ally
dist ributed data ◦ Assumptions for Wilcoxon:
- Paired di erences are independent - Di erences com e from a sym m etrical dist r ibut ion
• Mann–Whitney U test (MW UT): ◦ For unpaired non-norm ally dist r ibuted data ◦ For a di erence in dist r ibut ion
• Im portant to report 95% CIs for rank score tests
75.11 Correlation and Regression• Correlat ion = associat ion between 2 quant itat ive
variables• Assum es linear associat ion• Regression involves est im at ing best st raight line
to sum m arize the associat ion• Degree of associat ion m easured by a correlat ion
coe cient—scale = −1 to +1• Pearson correlat ion coe cient = r; perfect
correlat ion = +1 or −1• Posit ive correlat ion = one variable increases as
the other increases• Need to create scat ter plot and decide w hich
variable is the “dependent” variable• Arrange observat ions in serial order of
independent variables• Correlat ion ≠causat ion; any connect ion m ay be
indirect
• Signi cance of correlat ion assessed by m odi ed t test w ith follow ing assum pt ions: ◦ Both variables norm ally dist r ibuted ◦ Linear relat ionship between variables ◦ Null hypothesis = no relat ionship between them
◦ Do not use for com paring 2 m ethods of m easuring the sam e quant it y
• Spearm an rank correlat ion useful w hen: ◦ Outlying data points on scat ter plot , i.e., “non-param etric”
◦ Quant itat ive discrete data, e.g., m ole count ◦ Ordered categorical data, e.g., pain score ◦ Non-linear, but ordinal, associat ion
• Regression equat ion = average value of y is a funct ion of x (i.e., it changes w ith x)—slope created (y = m x + c)
• Generally bet ter to use regression if there is a clear causal pathway
75.12 Survival Analysis• Can be used for m ore than just m ortalit y
est im at ion , e.g., dose of m edicat ion required to create a m easured e ect
• Kaplan–Meier survival curve• Log rank test com pares 2 survival curves w ith
follow ing assum ptions: ◦ Survival t im es are ordinal or cont inuous ◦ Risk of an event in one group relat ive to the other does not change w ith t im e (propor t ional hazards assum pt ion)
• If there are no censored observat ions (knowledge only that pat ient was alive at last FU)—reasonable to use MW UT; however, survival m ethod yields an est im ate of r isk
75.13 Statistical Tests in Study Design• Most powerful studies = prospect ive (RCT)• Crossover study = w here ≥2 t reatm ents are
applied sequent ially to the sam e subject• Cluster t r ials = w here groups of pat ients rather
than individuals are random ized
Philpott_9783131662316_Ch75.indd 269 02/05/14 2:11 PM
270
75 Medical Stat ist ics
• Com pliance issues tackled w ith “in tent ion to t reat”: analyze data by t reatm ent the subject was assigned to, not the one they actually took
• Dropouts should be reported by t reatm ent group• Quasi-experim ental design = non-random ized
t reatm ent• Cohort study = w here subjects in it ially free of
disease are followed up over a period of t im e• Case-control studies look at data ret rospect ively,
som et im es w ith a view to a prospect ive study; problem w ith recall bias
• Cross-sect ional studies include surveys, laboratory experim ents, and studies to exam ine prevalence of a disease
• For calculat ing sam ple size α (t ype I error) and β (t ype II error) are usually xed at 5% and 20%, respect ively
• Sam ple size for a cont inuous outcom e depends on α and α , variabilit y of data (σ2), and the e ect size (d): n (for each Rx group) = 16 x σ2/d2 for 2-sided α of 5% and β of 20%
• Stat ist ical test used depends on hypothesis; som e studies (e.g., prevalence) m ay have no hypothesis
• If test ing >1 hypothesis use Bonferroni correct ion = signi cance level of 0.05/n , w here n = num ber of hypotheses
• Choice of stat ist ical test from paired or m atched observat ions: ◦ Nom inal = McNem ar test ◦ Ordinal = Wilcoxon ◦ Quant itat ive (discrete or skewed) = Wilcoxon ◦ Quant itat ive (norm al dist r ibut ion) = paired t test
• Choice of test for independent variables ◦ Nom inal: Chi-squared test or exact probabilit y test
◦ Ordinal: Mann-Whitney ◦ Quant itat ive (discrete or skewed) = Mann-Whitney
◦ Quant itat ive (norm al dist r ibut ion) = independent samples t test
Philpott_9783131662316_Ch75.indd 270 02/05/14 2:11 PM

271
76.1 Clinical Governance (CG)• De nit ion: “A fram ework that helps
organizat ions provide safe and high-qualit y care”
• Based on three key at t r ibutes: ◦ High standards of care ◦ Transparent responsibilit y and accountabilit y ◦ Constant dynam ic of improvem ent
• There are seven pillars of CG: ◦ Educat ion and t rain ing ◦ Clinical audit ◦ Clinical e ect iveness ◦ Risk m anagem ent ◦ Research and developm ent ◦ Openness ◦ Pat ient and public involvem ent
76.2 Audit• De nit ion: “A process encapsulat ing
im provem ents in pat ient care”• Com parison of current standards of pract ice
w ith that of the gold standard• Recom m ended change in pract ice is then
reviewed after a designated t im e period thereby closing the audit loop
• Audit cycle is therefore broken dow n in to the follow ing stages: ◦ Ident ify the problem ◦ De ne cr iteria/standards ◦ Data collect ion ◦ Comparison w ith criteria and standards ◦ Im plem ent ing change ◦ Sustain ing im provem ent through reaudit ing
76.2.1 Completed ENT AuditsNational Prospective Tonsillectomy Audit• ENT UK in collaborat ion w ith Royal College of
Surgeons of England• 33,000 tonsillectom ies
76 Clinical Governance and Audit
• July 2003–Septem ber 2004• 95% pat ients uneventful recovery• 3.6% had either pr im ary (0.6%) or secondary
(3%) haem orrhage• 0.9% required return to theat re w ith in 28 days
(0.4% during in it ial adm ission and 0.5% after readm ission)
• “Hot” technique (bipolar diathermy) for both dissect ion and haem ostasis had 3× increased r isk of secondary haem orrhage
• “Cold” dissect ion and “hot” haem ostasis had 1.5× increased risk secondary haem orrhage
• Slight lower r isk of prim ary haem orrhage w ith diathermy if used for dissect ion and haem ostasis or haem ostasis alone
• No st rong stat ist ical signi cance for return to theat re rate and technique used except for coblat ion
• No associat ion between com plicat ions and surgeon’s experience
National Comparative Audit of Surgery for Nasal Polyposis and Chronic Rhinosinusitis• ENT UK in collaborat ion w ith Royal College of
Surgeons of England• 57% NHS Trusts part icipated• 3,128 pat ients• 6-m onth period in 2000• Quest ionnaires (SNOT22) com pleted preop,
3 and 12 m onths postop• Signi cant reduct ion in scores post-op w ith
slight deteriorat ion from 3 to 12 m onths• Major it y of pat ien t s were sat is ed w ith
surgery• Major com plicat ions low (0.26%)• 8.6% await ing or had reoperat ion• Pat ients having either prim ary surgery or
polypectomy derived the m ost bene t• Polyp or asthm at ic pat ients are m ost likely to
have second procedure
Philpott_9783131662316_Ch76.indd 271 02/05/14 2:14 PM
272
77.1 Otology77.1.1 Chronic Otitis Media• Healed COM: healed perforat ion ,
t ym panosclerosis• Inact ive m ucosal COM: dry TM perforat ion ,
unin am ed ME m ucosa• Inact ive squam ous COM: TM ret ract ion , not
retaining debris or infected• Act ive m ucosal COM: TM perforat ion w ith
m ucopus, in am ed ME m ucosa• Act ive squam ous COM: cholesteatom a
77.1.2 Retraction Pockets• TOS classi cat ion: pars accida/at t ic ret ract ions
◦ Type I: dimple/visible air space ◦ Type II: ret ract ion to neck of m alleus + no visible air space
◦ Type III: bony erosion (scutum ); ret ract ion beyond osseous m alleus w ith fu ll extent seen
◦ Type IV: kerat in accum ulat ion/cholesteatom a• SADE classi cat ion: pars tensa ret ract ions
◦ Type I: annular ret ract ion ◦ Type II: ret ract ion onto long process of incus/ISJ
◦ Type III: ret ract ion onto prom ontory (nonadhesive)
◦ Type IV: adhesion onto m edial wall
77.1.3 Petrous Apex Cholesteatoma• Mo et t–Sm ith classi cat ion
◦ Supralabyrin th ine: above the labyrin th ◦ Supralabyrin th ine–apical: above the labyrin th extending to pet rous apex
◦ Infralabyrin th ine: below the labyrin th ◦ Infralabyrin th ine–apical: below labyrin th extending to pet rous apex
◦ Massive labyrin th ine: extensive dest ruct ion of inner ear
◦ Massive labyrin th ine apical: extensive dest ruct ion of inner ear extending to pet rous apex
◦ Apical: con ned to pet rous apex
77.1.4 Glomus Tumours• Fisch
◦ Type A: lim ited to m iddle ear ◦ Type B: lim ited to t ympanom astoid area w ith no infralabyrin th ine extension
◦ Type C: infralabyrin th ine involvem ent to pet rous apex - C1: lim ited involvem ent of vert ical por t ion of carot id canal
- C2: invasion of ver t ical por t ion of carot id canal
- C3: invasion of horizontal carot id canal ◦ Type D1: in t racranial ext <2 cm ◦ Type D2: in t racranial ext >2 cm
77.1.5 Facial Nerve Palsy• House–Brackm ann
◦ See Table 77.1 ◦ Clinically im portant to di erent iate grade III from IV as th is relates to pat ients' abilit y to be able to fully close and therefore protect their eye
77.2 Rhinology77.2.1 Nasal Fracture• Class I (Chevallet): fronto/frontolateral blow
w ith ver t ical fracture septum + depressed/displaced nasal bone
• Class II (Jarjavay): lateral blow w ith horizontal C-shaped fracture septum + perpendicular plate of ethm oid and frontal process m axilla
• Class III: fracture extends to ethm oid labyrin th, septum collapses in to face, nasal bones pushed under frontal bone leading to telecanthus
77.2.2 Olfactory Neuroblastoma• Kadisch staging
◦ Type A: lim ited to nasal cavity ◦ Type B: + paranasal sinuses ◦ Type C: extension beyond
77 Classi cations
Philpott_9783131662316_Ch77.indd 272 02/05/14 2:16 PM

273
Rhinology
77.2.3 Oroantral Fistulas• Type 1: from m olar ext ract ion and healthy
m axillary sinus (1–5 m m )• Type 2: from m olar ext ract ion and m axillary
sinus acute/chronic disease (6–19 m m )• Type 3: secondary to surgical rem oval (>20 m m )
77.2.4 Frontal Sinus Surgery• Draf I—frontal recess is de ned + opened + agger
nasi cell roof is “uncapped”• Draf IIA—frontal sinus opened between lam ina
papyracea and insert ion of m iddle turbinate• Draf IIB—frontal sinus opened m edial to m iddle
turbinate by rem oval of m ost of anterior at tachm ent of m iddle turbinate to skull base
• Draf III ◦ Aka endoscopic Lothrop ◦ Transseptal frontal sinusotomy w ith superior par t of nasal septum and oor of frontal sinuses and in tersinus septum rem oved to create one large cavity
77.2.5 Juvenile Angio broma• Andrews staging
◦ Stage I: lim ited to nasopharynx/sphenopalat ine foram en w ith m inim al bone dest ruct ion
◦ Stage II: invading pterygopalat ine fossa or m axillary, ethm oid, sphenoid sinus, and bone dest ruct ion
◦ Stage III: invading infratem poral fossa or orbit
- A: w ithout in t racranial involvem ent - B: in t racranial/ext radural involvem ent
◦ Stage IV: in t racranial in t radural involvem ent - A: no cavernous sinus, pituitary fossa, or opt ic chiasm involvem ent
- B: all areas above involved
77.2.6 Lund–Mackay Staging Sinus Disease on CT Scans• Scores
◦ 0 (norm al) ◦ 1 (par t ial opaci cat ion) ◦ 2 (complete opaci cat ion) ◦ Osteom eatal com plex:
- 0 (not occluded) - 2 (occluded)
• Areas scored ◦ Maxillary ◦ Frontal ◦ Anterior ethm oid ◦ Posterior ethm oid ◦ Sphenoid ◦ Osteom eatal com plex
• Score range ◦ 0 to 24 (m ax. 12 each side) ◦ Score ≥4 for FESS or 2 w ith unilateral disease
77.2.7 Kuhn Cells• Anterior ethm oidal cells im pinging on frontal
recess or frontal sinus ◦ Type 1: single frontal recess cell above agger nasi
Table 77.1 House–Brackmann classi cation of facial nerve palsy
Grade Tone at rest/symmetry Weakness Forehead Eye closure Mouth
I Normal
II Normal Slight Good–moderate Y Slight asymmetry with
movement
III Normal Obvious Slight–moderate Y Slight weakness + max. e ort
IV Normal (+ synkinesis + hemifacial spasm) Dis guring None N Asymmetry + max. e ort
V Asymmetrical Barely any movement None N Slight movement with e ort
VI No function at all
Philpott_9783131662316_Ch77.indd 273 02/05/14 2:16 PM

274
77 Classi cat ions
◦ Type 2: t ier of cells in frontal recess above the agger nasi
◦ Type 3: single large cell extending beyond frontal os
◦ Type 4: isolated cell w ith in frontal recess—probably an ar t ifact of older im aging protocols
77.2.8 Nasal Polyp Grading• Lindholt
◦ 0: no visible polyps ◦ 1: polyps con ned to m iddle m eatus ◦ 2: polyps below the m iddle turbinate ◦ 3: m assive polyps completely obst ruct ing the nasal cavity
• (Alternat ive = grade I–IV w here III is to nasal oor and IV is to anterior nares)
77.2.9 Frontal Sinus Mucocele• Type I: lim ited to the frontal sinus only w ith or
w ithout orbital extension• Type II: frontal and ethm oidal sinuses w ith or
w ithout orbital extension• Type IIIa: erosion of the posterior wall
frontal sinus w ith m inim al or no in t racranial involvem ent
• Type IIIb: erosion of the posterior wall w ith m ajor in t racranial extension
• Type IV: erosion of the anter ior wall of the frontal sinus
• Type Va: erosion of both anter ior and posterior walls of frontal sinus w ithout or m inim al in t racranial extension
• Type Vb: erosion of both anterior and poster ior walls of frontal sinus a m ajor in t racranial extension
77.2.10 Saddle Nose Deformity• Tardy
◦ Minim al: suprat ip depression greater than the ideal 1–2 m m t ip–suprat ip di erent ial
◦ Moderate: m oderate degrees of saddling due to loss of height of the quadrangular car t ilage, usually w ith septal dam age
◦ Major: m ore severe degree of saddling w ith m ajor car t ilage loss and m ajor st igm ata of a saddlenose deform ity
77.2.11 Orbital Cellulitis Complicating Sinusitis• Chandler
◦ Group 1: preseptal cellulit is ◦ Group 2: orbital cellulit is ◦ Group 3: subperiosteal abscess ◦ Group 4: orbital abscess ◦ Group 5: cavernous sinus throm bosis
77.2.12 Olfactory Fossa Depth• Keros
◦ Type I: 1 to 3 m m ◦ Type II: 4 to 7 m m ◦ Type III: 8 to 16 m m ◦ Type IV: asym m etrical
77.2.13 Inverting Papilloma• Krouse
◦ Type I: tum our con ned to nasal cavity ◦ Type II: tum our involving osteom eatal com plex and ethm oids and/m edial wall of m axillary sinus (w ith or w ithout nasal cavity involvem ent)
◦ Type III: tum our involving any wall of m axillary sinus (but m edial wall), sphenoid or frontal sinus, w ith or w ithout stage II criteria
◦ Type IV: - Tum our w ith ext ranasal and extrasinus extension
- Tum ours associated w ith m alignancy• Modi ed Krouse
◦ Type A: lim ited to w ith in the nasal cavity, ethm oid sinus, or m edial m axillary wall
◦ Type B - Involvem ent of any m axillary wall (other than m edial wall), or
- Frontal sinus or sphenoid sinus ◦ Type C: extension beyond the paranasal sinus
77.2.14 Sinonasal Sarcoidosis• Krespi
◦ Stage 1: lim ited reversible involvem ent ◦ Stage 2: m oderate disease involvem ent or lim ited single sinus involvem ent
◦ Stage 3: irreversible disease causing synechiae, stenosis, and car t ilage dest ruct ion
Philpott_9783131662316_Ch77.indd 274 02/05/14 2:16 PM

275
Head and Neck
Table 77.2 Grading system for sinus cavities in post-op AFRS patients
Grading State of mucosa
0 No oedema
1–3 Mucosal oedema (mild/moderate/severe)
4–6 Polypoid oedema (mild/moderate/severe)
7–9 Frank polyps (mild/moderate/severe)
77.2.15 Staging System for Sinus Cavities in Post-op AFRS Patients• See Tables 77.2 and 77.3
77.3 Head and Neck77.3.1 Neck Trauma• Zone I: superior cricoid to inferior thoracic in let• Zone II: superior angle of m andible to infer ior
cricoid• Zone III: superior skull base to inferior angle of
m andible
77.3.2 Apnoea/Hypopnea Index• 5 to 20: m ild• 20 to 40: m oderate• >40: severe
77.3.3 Posterior Glottic Stenosis• Type I: in terarytenoid adhesion• Type II: posterior com m issure
• Type III: posterior com m issure + cr icoarytenoid ankylosis (unilateral)
• Type IV: posterior com m issure + cr icoarytenoid ankylosis (bilateral)
77.3.4 Stomal Recurrence• Sisson
◦ I: discrete nodule superior aspect stom a ◦ II: involvem ent oesophagus superior (no inferior involvem ent)
◦ III: originates inferior to stom a and has direct extension in to m ediast inum
◦ IV: extension laterally under either side of clavicles
77.3.5 Graves Ophthalmopathy1. Spasm under eyelids2. Soft t issue involvem ent and periorbital oedem a
and chem osis3. Proptosis4. Muscle involvem ent and gaze lim itat ion5. Corneal involvem ent (keratosis)6. Visual loss secondary to opt ic nerve
involvem ent
77.3.6 AJCC (American Joint Committee on Cancer) Staging System• See Table 77.4
Table 77.3 Scoring system for sinus cavities in post-op AFRS patients
Sinus cavity Right Mucin Left Mucin
Olfactory cleft 0–9 1 0–9 1
Frontal 0–9 1 0–9 1
Ethmoid 0–9 1 0–9 1
Maxillary 0–9 1 0–9 1
Sphenoid 0–9 1 0–9 1
Total 50 50
Bilateral total 100
Table 77.4 AJCC (American Joint Commit tee on Cancer) staging system
Stage 0 Tis N0 M0
Stage 1 T1 N0 M0
Stage 2 T2 N0 M0
Stage 3 T1T2T3
N1N0/N1
M0M0
Stage 4a T4 N0/N1 M0
Stage 4b Any T N2 M0
Stage 4c Any T Any N M1
Philpott_9783131662316_Ch77.indd 275 02/05/14 2:16 PM

276
77 Classi cat ions
77.3.7 Nasopharyngeal Carcinoma• WHO
◦ Type I: kerat in izing SCC ◦ Type II: non-kerat inzing SCC ◦ Type III: undi erent iated
77.3.8 Lymphoma• Ann Arbor
◦ Stage I - Single nodal region - Localized single extralym phat ic organ/site
◦ Stage II - 2 or m ore nodal regions sam e side of diaphragm
- Localized single ext ralym phat ic organ/site + LNs (regional) or other LNs sam e side diaphragm
◦ Stage III - Nodal regions both sides diaphragm ± localized single extralym phat ic organ/site
- Spleen or both ◦ Stage IV
- Di use/m ult ifocal ext ralymphat ic organ ± regional nodes
- Isolated extralym phat ic organ + nonregional nodes
77.3.9 Midfacial Fractures• Le Fort
◦ Type I: palate–face disjunct ion - Fracture through piriform aper ture above alveolar r idge and oor of m axillary sinus extending posterior through pterygoid plates
- Lower m axilla and palate m ove separate from face
◦ Type II: pyram idal disjunct ion - Risk of CSF leak - Fracture through nasal bones, lacr im al bones, and lam ina papyracea across orbital oor and m edial and inferior orbital r im and across pterygoid plates
- Maxilla and nasal regions are m obile relat ive to the rest of the m idface and skull
◦ Type III: craniofacial disjunct ion - Risk of CSF leak - Fracture t raverses all but t resses linking m axilla to skull, inc. nasal bones, frontoethm oid suture, superior orbit , frontozygom at ic suture, root zygom a, and
temporal fossa including pterygom axillary space
- Pterygoid plates are # free from skull base - The ent ire upper face (nasal, m axillary, and zygom at ic bones) is m obile
- Key features ▪ Mobile palate ▪ Facial oedem a ▪ Ecchym osis ▪ Epistaxis ▪ CSF rhinorrhoea ▪ Airway obst ruct ion ▪ Blindness
77.3.10 Malocclusion• Class I: norm al• Class II: m andibular ret rognathia• Class III: m andibular prognathia
77.3.11 ECOG (Eastern Coopera-tive Performance Group) Perfor-mance Status• ECOG 0: Asymptom atic (fully active, able to carry
on all pre-disease act ivit ies w ithout restrict ion)• ECOG 1: Sym ptom at ic but com pletely
am bulatory (rest ricted in physically st renuous act ivit y but am bulatory and able to carry out work of a light or sedentary nature, e.g., light housework, o ce work)
• ECOG 2: Sym ptom at ic, <50% in bed during the day (am bulatory and capable of all self-care but unable to carry out any work act ivit ies; up and about >50% of waking hours)
• ECOG 3: Sym ptom at ic, >50% in bed, but not bedbound (capable of only lim ited self-care, con ned to bed or chair ≥50% of waking hours)
• ECOG 4: Bedbound (com pletely disabled, cannot carry out any self-care; totally con ned to bed or chair)
• ECOG 5: Death
77.3.12 Cytology Thyroid Classi cation• Thy 1: acellular• Thy 2: colloid• Thy 3: follicular cells• Thy 4: suspicious carcinom a• Thy 5: carcinom a
Philpott_9783131662316_Ch77.indd 276 02/05/14 2:16 PM

277
Head and Neck
77.3.13 Epworth Sleepiness Score• Situat ions: sit t ing + reading, watching TV, sit t ing
inact ive in public place, as a car passenger for an hour w ithout a break, lying dow n to rest in the afternoon, sit t ing and talking to som eone, sit t ing quiet ly after lunch w ithout alcohol, in a car w hile stopped for a few m inutes in t ra c ◦ 0: no chance of dozing ◦ 1: slight chance of dozing ◦ 2: m oderate chance of dozing ◦ 3: h igh chance of dozing
• Norm al: 0 to 10• Borderline: 10 to 12• Abnorm al: 12 to 24
77.3.14 Tonsil Grade• Brodsky
◦ Grade 0: tonsils w ith in fossa ◦ Grade I: just outside tonsillar fossa <25% oropharyngeal w idth
◦ Grade II: 25 to 50% oropharyngeal w idth ◦ Grade III: 51 to 75% oropharyngeal w idth ◦ Grade IV: >75% oropharyngeal w idth
77.3.15 Mallampati Score• Class 1: full visibilit y of tonsils, uvula, and soft
palate• Class 2: visibilit y of hard and soft palate, upper
port ion of tonsils, and uvula• Class 3: soft and hard palate and base of the
uvula are visible• Class 4: only hard palate visible
77.3.16 Laryngeal Dysplasia• WHO
◦ Mild dysplasia: m inim al nuclear changes in basal layer of epithelium and parabasal m itoses
◦ Moderate dysplasia: m ore m arked nuclear changes w ith prom inent nucleoli; in term ediate and parabasal m itoses
◦ Severe dysplasia: m arked nuclear change, m itoses in m ore super cial epithelium preserving m ost super cial cells
◦ Carcinom a in situ: fu ll-th ickness involvem ent w ith no st rom al invasion
• Ljubljana ◦ Sim ple hyperplasia: m aintenance of norm al epithelium w ith absence of cellular atypia
◦ Abnorm al hyperplasia: t ypical m itoses seen in basal layer
◦ Atypical hyperplasia: enlarged nuclei w ith variable stain ing, increased nucleoli, increased nuclear:cytoplasm ic rat io
◦ Carcinom a in situ: features of carcinom a w ithout invasion
77.3.17 European Laryngological Society Classi cation of Endoscopic Cordectomies• Type 1: subepithelial resect ion• Type 2: subligam ental resect ion between vocal
ligam ent and vocalis• Type 3: transm uscular resection through vocalis
m uscle from vocal process to anterior com m issure• Type 4: total cordectom y• Type 5: extended cordectom y
◦ 5a: anter ior com m issure and part of contralateral VF and Broyle ligam ent
◦ 5b: includes par t or all of arytenoids ◦ 5c: includes ventricle and ventricular fold ◦ 5d: 1 cm below VFs to expose cricoid
• Type 6: anter ior com m issurectom y and bilateral anterior VF resect ion
77.3.18 2nd Branchial Arch Anomalies• Type I: located along the anterior m argin of
sternocleidom astoid m uscle at the junct ion of the m iddle and lower ⅓ , deep to the platysm a and cervical fascia
• Type II: anom alies lie in contact w ith the great vessels
• Type III: anom alies pass m edially between the in ternal and external carot id aa, extending towards the lateral pharyngeal wall and lying above the glossopharyngeal and hypoglossal nn and below the stylohyoid ligam ent
• Type IV anom alies are very rare and are located next to the pharyngeal wall, m edial to the great vessels at the level of the tonsillar fossa
77.3.19 Thyroid Eye Signs• Am erican Thyroid Associat ion
◦ Class 1: spasm of upper eyelids w ith thyrotoxicosis
◦ Class 2: soft t issue involvem ent w ith periorbital oedem a and chem osis
Philpott_9783131662316_Ch77.indd 277 02/05/14 2:16 PM

278
77 Classi cat ions
Table 77.5 Flaps in head and neck reconstruction
Type Use BS Pros Cons
Pectoralis major
Regional MC/MF Most H&N Pec branch thoraco-acrom ± lat thoracic
Post RT Bulky donor site
Quick Insensate
Radial forearm
Fascio-cutComplex intraoral Rad art/ceph v
Thin, pliable, sensate
Hand ischaemia
Tendon expPharynx defects Lat/med branch n SSG 2 donor
Fibular
Osteocutaneous Oromandibular defects Peroneal a/vLong bone 24 cm Min. soft t issue
Support implants Donor site
Gracilis
Free ap Facial reanimation (obturator nerve)
Adductor art/deep fem vein
Min. donor site prob 6 cm long vas ped
Jejunum
Sup mesenteric a/v Secretory nature Donor site
Anterola tera l thigh
Free ap Total laryngopharynx defect repair
Desc lat fem circum ex a/v
Easy harvest
Lengthy pedicle
Sensate
Multiple comps*
Primary closure
Donor site
*Adipofascial, muscle, skin ± bula graft.
◦ Class 3: proptosis ◦ Class 4: ext raocular m uscle involvem ent (inferior rectus m ost com m on w ith lim ited upward gaze)
◦ Class 5: corneal involvem ent ◦ Class 6: loss of vision due to opt ic nerve involvem ent
77.3.20 Flaps in Head and Neck Reconstruction• See Table 77.5
77.3.21 Hard Palate Defect after Resection• Mount Sinai
◦ Class Ia: hard palate but tooth-bearing alveolus preserved
◦ Class Ib: hard palate and extension to prem axilla or any por t ion of m axillary alveolus posterior to canines
◦ Class II: hard palate and one canine ◦ Class III: hard palate and both canines
77.4 Paediatric Otolaryngology77.4.1 Paediatric Tracheostomy Tube Sizes• <1 kg—2.5• 1–2.5 kg—3.0• Neonate–6/12—3.0 to 3.5• 6/12–1 yr—3.5 to 4.0
Philpott_9783131662316_Ch77.indd 278 02/05/14 2:16 PM

279
Paediatric Otolaryngology
• 1–2 yrs—4.0 to 5.0• >2 yrs—(age + 16)/4
77.4.2 Myer–Cotton Classi cation Subglottic Stenosis• Grade I: <50%• Grade II: 51 to 70%• Grade III: 71 to 99%• Grade IV: com plete
77.4.3 Laryngotracheal Clefts• I: in terarytenoid• II: in to cr icoid• III: through poster ior cricoid• IV: m em branous t rachea
77.4.4 Paediatric Bronchoscopy Sizes• See Table 77.6
77.4.5 Microtia• Marx
◦ Grade 1: abnorm al auricle w ith all ident i able landm arks
◦ Grade 2: abnorm al auricle w ithout som e ident i able landm arks
◦ Grade 3: very sm all auricular tag ◦ Grade 4: anot ia
• Weerda ◦ Grade 1:
- Mild deform ity w ith slight ly dysm orphic helix and anithelix
- All m ajor st ructures are present , e.g., cup or lop ear
◦ Grade 2: - All m ajor st ructures present to som e degree, external auditory m eatus is present but w ith stenosis
- Repair requires car t ilage or skin , e.g., severe lop ear
◦ Grade 3: - Few if any landm arks present - The lobule is t ypically placed anterior, e.g., peanut deform ity and anot ic ear
77.4.6 Canal Atresia• Altm an classi cat ion
◦ Type I: TM present ◦ Type II: at ret ic plate, norm al t ym panic cavity
◦ Type III: hypoplast ic t ym panic cavit y
77.4.7 Tracheoesophageal Fistula• Waterson classi cat ion• Pret reatm ent r isk evaluat ion
◦ Category A - Bir th w t>5.5 lb (2.5 kg) - Receive prom pt surgery
◦ Category B - Bir th w t 4–5.5 lbs (1.8–2.5 kg), or pneum onia or congenital anom aly
- Short-term delay in t reatm ent - Preop gast rostomy
◦ Category C - Bir th w t <4lb (1.8 kg), or severe pneum onia or congenital anom aly
- Stage repair - TPN
77.4.8 Lymphovascular Malformation• De Serres
◦ Stage I: unilateral infrahyoid ◦ Stage II: unilateral suprahyoid ◦ Stage III: unilateral supra- and infrahyoid ◦ Stage IV: bilateral suprahyoid ◦ Stage V: bilateral supra- and infrahyoid
77.4.9 Arteriovenous Malformation• See Table 77.7
Table 77.6 Paediatric bronchoscopy sizes
Bronchoscope size/external diameter (mm)
Age Length (cm)
2.5–30 Preterm 20
3.5 0–18/12 20–30
4 18/12–3 y 30
5 3–12 y 30
6 >12 y 30
Philpott_9783131662316_Ch77.indd 279 02/05/14 2:16 PM

280
77 Classi cat ions
77.4.10 Drooling• Teacher scale
1. No drooling2. Infrequent drooling, sm all am ount3. Occasional drooling, on and o all day4. Frequent drooling, but not profuse5. Constant ly wet saliva leaking on clothes and
furniture
Table 77.7 Schobinger staging of arteriovenous malformation
Stage Description Hallmark
I Quiescent Skin discolouration
II Expansion Pulsation
III Destruction Overlying skin change
IV Decompensation Heart failure
Philpott_9783131662316_Ch77.indd 280 02/05/14 2:16 PM

281
The follow ing list of key references is a useful select ion of som e research papers on the topic. It is by no m eans exhaust ive, but instead a good star t ing point for som e further reading.
OtologyConlin AE, Parnes LS. Treatm ent of sudden sen-
sorineural hearing loss: I. A system at ic re-view. Arch Otolaryngol Head Neck Surg 2007;133(6):573–581
Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG. Surgical m anagem ent of Bell’s palsy. Laryngo-scope 1999;109(8):1177–1188
Jast rebo PJ, Hazell JW. A neurophysiological ap -proach to t innitus: clin ical im plicat ions. Br J Audiol 1993;27(1):7–17
Maw R, Baw den R. Spontaneous resolut ion of se-vere chronic glue ear in children and the ef-fect of adenoidectomy, tonsillectomy, and in-sert ion of vent ilat ion tubes (grom m ets). BMJ 1993;306(6880):756–760
MRC Mult icentre Ot it is Media Study Group. Ad-juvant adenoidectomy in persistent bilateral ot it is m edia w ith e usion: hearing and revi-sion surgery outcom es through 2 years in the TARGET random ised t r ial. Clin Otolaryngol 2012;37(2):107–116
Medical Research Council Mult icentre Ot it is Me-dia Study Group. Surgery for persistent ot it is m edia w ith e usion: generalizabilit y of results from the UK t rial (TARGET). Trial of Alternat ive Regim ens in Glue Ear Treatm ent . Clin Otolaryn-gol Allied Sci 2001;26(5):417–424
Nat ional Inst itute for Health and Clin ical Excel-lence. NICE technology appraisal guidance 166: Cochlear implants for severe to pro-found deafness in children and adults, 2009. w w w.nice.org.uk/TA166
Nunez DA, Brow ning GG. Risks of developing an otogenic in t racranial abscess. J Laryngol Otol 1990;104(6):468–472
Prasad S, Janecka IP. E cacy of surgical t reatm ents for squam ous cell carcinom a of the tem poral bone: a literature review. Otolaryngol Head Neck Surg 1994;110(3):270–280
Stangerup SE, Caye-Thom asen P, Tos M, Thom sen J. Change in hearing during ‘wait and scan’ m an-agem ent of pat ients w ith vest ibular schwanno-m a. J Laryngol Otol 2008;122(7):673–681
Sullivan FM, Swan IR, Donnan PT, et al. Early t reat-m ent w ith prednisolone or acyclovir in Bell’s palsy. N Engl J Med 2007;357(16):1598–1607
Thom sen J, Bret lau P, Tos M, Johnsen NJ. Ménière’s disease: endolym phat ic sac decom pression compared w ith sham (placebo) decom pression. Ann N Y Acad Sci 1981;374:820–830
RhinologyBaiardini I, Braido F, Tarant in i F, et al; GA2LEN.
ARIA-suggested drugs for allergic rh in it is: w hat im pact on qualit y of life? A GA2LEN review. Al-lergy 2008;63(6):660–669
Bedwell J, Baum an NM. Managem ent of pediat r ic orbital cellulit is and abscess. Curr Opin Otolar-yngol Head Neck Surg 2011;19(6):467–473
Bent JP III, Kuhn FA. Diagnosis of allergic fun-gal sinusit is. Otolaryngol Head Neck Surg 1994;111(5):580–588
Berden A, Göçeroglu A, Jayne D, et al. Diagnosis and m anagem ent of ANCA associated vasculit is. BMJ 2012;344:e26
Berm an B, Flores F. The t reatm ent of hyper-t rophic scars and keloids. Eur J Derm atol 1998;8(8):591–595
Bhargava D, Bhargava K, Al-Abri A, Al-Bassam W, Al-Abri R. Non allergic rh in it is: prevalence, clin ical pro le and knowledge gaps in litera-ture. Om an Med J 2011;26(6):416–420
Brit ish Associat ion for the Study of Headache. w w w.bash.org.uk
Brozek JL, Bousquet J, Baena-Cagnani CE, et al; Global Allergy and Asthm a European Network; Grading of Recom m endat ions Assessm ent , De-velopm ent and Evaluat ion Working Group. Al-lergic Rhinit is and it s Impact on Asthm a (ARIA) guidelines: 2010 revision . J Allergy Clin Im m u-nol 2010;126(3):466–476
Buck L, Axel R. A novel m ult igene fam ily m ay en-code odorant receptors: a m olecular basis for odor recognit ion . Cell 1991;65(1):175–187
Bibliography
Philpott_9783131662316_BM.indd 281 02/05/14 3:55 PM

282
Bibliography
Carta F, Verillaud B, Herm an P. Role of endoscopic approach in the m anagem ent of inver ted pap-illom a. Curr Opin Otolaryngol Head Neck Surg 2011;19(1):21–24
Chakrabart i A, Denning DW, Ferguson BJ, et al. Fun-gal rhinosinusit is: a categorization and de ni-t ional schem a addressing current controversies. Laryngoscope 2009;119(9):1809–1818
Chatsis V, Spry C. Diagnosis of snoring and sleep apnea: A review of the accuracy. (Health Tech-nology Inquiry Service). Ot tawa: Canadian Agency for Drugs and Technologies in Health ; 2009
Croy I, Negoias S, Novakova L, Landis BN, Hum m el T. Learning about the funct ions of the olfactory system from people w ithout a sense of sm ell. PLoS ONE 2012;7(3):e33365
Devars du Mayne M, Moya-Plana A, Malinvaud D, Laccourreye O, Bon ls P. Sinus m ucocele: natural h istory and long-term recurrence rate. Eur Ann Otorhinolaryngol Head Neck Dis 2012;129(3):125–130
Dische S, Saunders M, Barret t A, Harvey A, Gib-son D, Parm ar M. A random ised m ult icent re t r ial of CHART versus convent ional radiother-apy in head and neck cancer. Radiother Oncol 1997;44(2):123–136
Feuillet-Fieux MN, Lenoir G, Serm et I, et al. Nasal polyposis and cyst ic brosis(CF): review of the literature. Rhinology 2011;49(3):347–355
Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European posit ion paper on rh inosinusit is and nasal polyps 2012. A sum m ary for oto-rh inolaryngologists. Rhinology 2012;50(1):1–12
Hopkins C, Brow ne JP, Slack R, et al. The nat ional com parat ive audit of surgery for nasal polypo-sis and chronic rh inosinusit is. Clin Otolaryngol 2006;31(5):390–398
Hudson DA. Achieving an opt im al cosm et ic result w ith excision of lesions on the face. Ann Plast Surg 2012;68(3):320–325
Kalish LH, Arendts G, Sacks R, Craig JC. Topical ste-roids in chronic rh inosinusit is w ithout polyps: a system at ic review and m eta-analysis. Otolar-yngol Head Neck Surg 2009;141(6):674–683
Kastner J, Taudy M, Lisy J, Grabec P, Betka J. Orbital and in t racranial com plicat ions after acute rh i-nosinusit is. Rhinology 2010;48(4):457–461
Landis BN, Konnerth CG, Hum m el T. A study on the frequency of olfactory dysfunction. Laryngo-scope 2004;114(10):1764–1769
Lund VJ, Stam m berger H, Nicolai P, et al; European Rhinologic Society Advisory Board on Endo-scopic Techniques in the Managem ent of Nose, Paranasal Sinus and Skull Base Tum ours. Euro-pean posit ion paper on endoscopic m anage-m ent of tum ours of the nose, paranasal sinuses and skull base. Rhinol Suppl 2010;22(22):1–143
McNeill E, Ram akrishnan Y, Carrie S. Diagnosis and m anagem ent of olfactory disorders: survey of UK-based consultants and literature review. J Laryngol Otol 2007;121(8):713–720
Melia L, McGarry G. Epistaxis in adults: a clini-cal review. Br J Hosp Med (Lond) 2008;69(7):404–407
Melis M, Zawaw i K, al-Badaw i E, Lobo Lobo S, Mehta N. Com plex regional pain syndrom e in the head and neck: a review of the literature. J Orofac Pain 2002;16(2):93–104
Motam edi MH. An assessm ent of m axillofacial fractures: a 5-year study of 237 pat ients. J Oral Maxillofac Surg 2003;61(1):61–64
Nicolai P, Castelnuovo P, Bolzoni Villaret A. En-doscopic resect ion of sinonasal m alignancies. Curr Oncol Rep 2011;13(2):138–144
Oberm ann M, Holle D, Katsarava Z. Trigem inal neuralgia and persistent idiopathic facial pain . Expert Rev Neurother 2011;11(11):1619–1629
Olesen J. The in ternat ional classi cat ion of head-ache disorders. Headache 2008;48(5):691–693
Oo KK, Park SS. The m idline forehead ap in nasal reconst ruct ion . Facial Plast Surg Clin North Am 2011;19(1):141–155
Papadopoulos H, Salib NK. Managem ent of naso-orbital-ethm oidal fractures. Oral Maxillofac Surg Clin North Am 2009;21(2):221–225, vi
Payne KF, Tahim A, Goodson AM, Colbert S, Bren-nan PA. A review of t raum a and t raum a-related papers published in the Brit ish Journal of Oral and Maxillofacial Surgery in 2010-2011. Br J Oral Maxillofac Surg 2012;50(8):769–773
Philpot t CM, Javer AR, Clark A. Allergic fungal rh -inosinusit is—a new staging system . Rhinology 2011;49(3):318–323
Philpot t CM, McKiernan DC. Bronchiectasis and sino-nasal disease: a review. J Laryngol Otol 2008;122(1):11–15
Philpot t CM, Rim al D, Tassone P, Prinsley PR, Prem -achandra DJ. A study of olfactory test ing in pa-t ients w ith rh inological pathology in the ENT clin ic. Rhinology 2008;46(1):34–39
Pino Rivero V, González Palom ino A, Trin idad Ruiz G, et al. Risk factors and clin ical variables in
Philpott_9783131662316_BM.indd 282 02/05/14 3:55 PM

283
Bibliography
pat ients hospitalized for epistaxis. Review of 200 pat ients [in spanish]. An Otorrinolaringol Ibero Am 2005;32(3):229–237
Pirom chai P, Thanaviratananich S, Laopaiboon M. System ic antibiotics for chronic rhinosinusitis w ithout nasal polyps in adults. Cochrane Data-base Syst Rev 2011;11(5):CD008233
Robinson GV, Pepperell JC, Segal HC, Davies RJ, St radling JR. Circulat ing cardiovascular r isk factors in obst ruct ive sleep apnoea: data from random ised controlled t r ials. Thorax 2004;59(9):777–782
Rockey JG, Anand R. A crit ical audit of the surgi-cal m anagem ent of intractable epistaxis using sphenopalatine artery ligation/diathermy. Rhi-nology 2002;40(3):147–149
Rohr AS, Spector SL. Paranasal sinus anato-my and pathophysiology. Clin Rev Allergy 1984;2(4):387–395
Rose G. The apparent paradox of “success” in lac-rim al drainage surgery. In : Gutho R, Katow itz J, eds. Oculoplast ics and Orbit . Berlin : Springer; 2006:51–59
Sillers MJ, Morgan CE, el Gam m al TE. Magnet ic resonance cisternography and th in coronal com puterized tom ography in the evaluat ion of cerebrospinal u id rh inorrhea. Am J Rhinol 1997;11(5):387–392
Srouji I, Lund V, Andrews P, Edwards C. Rhinologic sym ptom s and qualit y-of-life in pat ients w ith Churg-Strauss syndrom e vasculit is. Am J Rhinol 2008;22(4):406–409
Srouji IA, Andrews P, Edwards C, Lund VJ. Pat terns of presentat ion and diagnosis of pat ients w ith Wegener’s granulom atosis: ENT aspects. J Lar-yngol Otol 2007;121(7):653–658
Stam m berger H, Hosem ann W, Draf W. Anatom ic term inology and nom enclature for paranasal sinus surgery [in Germ an]. Laryngorhinootolo-gie 1997;76(7):435–449
Stam m berger H, Posawetz W. Funct ional endo-scopic sinus surgery. Concept , indicat ions and results of the Messerklinger technique. Eur Arch Otorhinolaryngol 1990;247(2):63–76
Stankiew icz JA, Lal D, Connor M, Welch K. Complica-tions in endoscopic sinus surgery for chronic rhi-nosinusitis: a 25-year experience. Laryngoscope 2011;121(12):2684–2701
Stannard WA, Chilvers MA, Rutm an AR, William s CD, O’Callaghan C. Diagnost ic test ing of pa-t ients suspected of prim ary ciliary dyskinesia. Am J Respir Crit Care Med 2010;181(4):307–314
Terán-Santos J, Jim énez-Góm ez A, Cordero-Gue-vara J; Cooperat ive Group Burgos-Santander. The associat ion between sleep apnea and the risk of t ra c accidents. N Engl J Med 1999;340(11):847–851
Weber R, Keerl R, Draf W, Schick B, Mosler P, Saha A. Managem ent of dural lesions occurr ing dur-ing endonasal sinus surgery. Arch Otolaryngol Head Neck Surg 1996;122(7):732–736
Worm ald PJ, Kew J, Van Hasselt A. In t ranasal anatomy of the nasolacrim al sac in endoscopic dacryocystorhinostomy. Otolaryngol Head Neck Surg 2000;123(3):307–310
Yarm olinsky DA, Zuker CS, Ryba NJP. Com m on sense about taste: from m am m als to insects. Cell 2009;139(2):234–244
Yung MW, Hardm an-Lea S. Endoscopic inferior dacryocystorhinostomy. Clin Otolaryngol Allied Sci 1998;23(2):152–157
Zweig JL, Carrau RL, Celin SE, et al. Endoscopic re-pair of cerebrospinal u id leaks to the sinonasal t ract: predictors of success. Otolaryngol Head Neck Surg 2000;123(3):195–201
Laryngology, Head and NeckAbdurehim Y, Hua Z, Yasin Y, Xukurhan A, Im am
I, Yuqin F. Transoral laser surgery versus radio-therapy: system at ic review and m eta-analysis for t reatm ent opt ions of T1a glot t ic cancer. Head Neck 2012;34(1):23–33
Aspinall SR, Ong SG, Wilson MS, Lennard TW. How shall we m anage the incidentally found thyroid nodule? Surgeon 2013;11(2):96–104
Au J, Patel D, Cam pbell JH. Oral lichen planus. Oral Maxillofac Surg Clin North Am 2013;25(1):93–100, vii
Balaker AE, Abem ayor E, Elasho D, St John MA. Cancer of unknow n prim ary: does t reatm ent m odalit y m ake a di erence? Laryngoscope 2012;122(6):1279–1282
Bianchi B, Ferri A, Ferrari S, Copelli C, Magri AS, Sesenna E. Single, subcondylar m andibular osteotomy: a new access route for extensive, benign parapharyngeal neoplasm s. J Laryngol Otol 2010;124(8):909–912
Bjørndal K, Krogdahl A, Therkildsen MH, et al. Sali-vary gland carcinom a in Denm ark 1990-2005: outcom e and prognost ic factors. Results of the Danish Head and Neck Cancer Group (DAHAN-CA). Oral Oncol 2012;48(2):179–185
Philpott_9783131662316_BM.indd 283 02/05/14 3:55 PM

284
Bibliography
Bradley PJ, Bradley PT, Olsen KD. Update on the m anagem ent of parapharyngeal tu-m ours. Curr Opin Otolaryngol Head Neck Surg 2011;19(2):92–98
Brennan S, Corry J, Kleid S, et al. Prospect ive t r ial to evaluate staged neck dissect ion or elect ive neck radiotherapy in pat ients w ith CT-staged T1-2 N0 squam ous cell carcinom a of the oral tongue. Head Neck 2010;32(2):191–198
Canis M, Ihler F, Wol HA, Christ iansen H, Mat-th ias C, Steiner W. Oncologic and funct ional results after t ransoral laser m icrosurgery of tongue base carcinom a. Eur Arch Otorhinolar-yngol 2013;270(3):1075–1083
Canis M, Mart in A, Ih ler F, et al. Results of t ransoral laser m icrosurgery for supraglot t ic carcinom a in 277 pat ients. Eur Arch Otorhinolaryngol 2013;270(8):2315–2326
Canis M, Mart in A, Kron M, et al. Results of t ran-soral laser m icrosurgery in 102 pat ients w ith squam ous cell carcinom a of the tonsil. Eur Arch Otorhinolaryngol 2013;270(8):2299–2306
Chang JI, Bevans SE, Schwartz SR. Otolaryngol-ogy clin ic of North Am erica: evidence-based pract ice: m anagem ent of hoarseness/dyspho-nia. Otolaryngol Clin North Am 2012;45(5):1109–1126
Cheng J, Elden L. Children w ith deep space neck infect ions: our experience w ith 178 children . Otolaryngol Head Neck Surg 2013;148(6):1037–1042 [Epub ahead of prin t]
Compilato D, Cirillo N, Term ine N, et al. Long-standing oral ulcers: proposal for a new ‘S-C-D classi cat ion system ’. J Oral Pathol Med 2009;38(3):241–253
Cools-Lar t igue J, Aboalsaud A, Gill H, Ferri L. Evo-lut ion of percutaneous dilatat ional t racheos-tomy-a review of current techniques and their pit falls. World J Surg 2013;37(7):1633–1646
Cooper DS, Dohert y GM, Haugen BR, et al; Am eri-can Thyroid Associat ion (ATA) Guidelines Task-force on Thyroid Nodules and Di erent iated Thyroid Cancer. Revised Am erican Thyroid As-sociat ion m anagem ent guidelines for pat ients w ith thyroid nodules and di erent iated thyroid cancer. Thyroid 2009;19(11):1167–1214
Cooper DS, Tufano RP. Prophylact ic central neck dissect ion in di erent iated thyroid cancer: a procedure in search of an indicat ion . Thyroid 2012;22(4):341–343
Corry J, Rischin D, Cot ton S, et al. Larynx preserva-t ion w ith prim ary non-surgical t reatm ent for
loco-regionally advanced larynx cancer. J Med Im aging Radiat Oncol 2011;55(2):229–235
Departm ent of Veterans A airs Laryngeal Cancer Study Group. Induct ion chem otherapy plus ra-diat ion com pared w ith surgery plus radiat ion in pat ients w ith advanced laryngeal cancer. N Engl J Med 1991;324(24):1685–1690
Ellington CL, Goodm an M, Kono SA, et al. Adenoid cyst ic carcinom a of the head and neck: Inci-dence and survival t rends based on 1973-2007 Surveillance, Epidem iology, and End Results data. Cancer 2012;118(18):4444–4451
Eskander A, Merdad M, Freem an JL, Wit terick IJ. Pat tern of spread to the lateral neck in m eta-stat ic well-di erent iated thyroid cancer: a system at ic review and m eta-analysis. Thyroid 2013;23(5):583–592
Et t l T, Schwarz-Furlan S, Gosau M, Reichert TE. Salivary gland carcinom as. Oral Maxillofac Surg 2012;16(3):267–283
Feng Y, Wang B, Wen S. Laser surgery versus radiotherapy for T1-T2N0 glot t ic cancer: a m eta-analysis. ORL J Otorhinolaryngol Relat Spec 2011;73(6):336–342
Forast iere AA, Zhang Q, Weber RS, et al. Long-term resu lt s of RTOG 91-11: a com parison of th ree nonsurgical t reatm en t st rategies to pre-serve the larynx in pat ien ts w ith locally ad-vanced larynx cancer. J Clin Oncol 2013;31(7):845–852
Freling N, Roele E, Schaefer-Prokop C, Fokkens W. Predict ion of deep neck abscesses by contrast-enhanced com puterized tom ography in 76 clin ically suspect consecut ive pat ients. Laryn-goscope 2009;119(9):1745–1752
Gaztam bide S, Vazquez F, Castaño L. Diagnosis and t reatm ent of m ult iple endocrine neo-plasia t ype 1 (MEN1). Minerva Endocrinol 2013;38(1):17–28
Goon P, Sonnex C, Jani P, Stanley M, Sudho H. Re-current respiratory papillom atosis: an overview of current th inking and t reatm ent . Eur Arch Otorhinolaryngol 2008;265(2):147–151
Harris L, Higgins K, Enepekides D. Local ap recon-st ruct ion of acquired lip defects. Curr Opin Oto-laryngol Head Neck Surg 2012;20(4):254–261
Hinni ML, Salassa JR, Grant DG, et al. Transoral laser m icrosurgery for advanced larynge-al cancer. Arch Otolaryngol Head Neck Surg 2007;133(12):1198–1204
Hoang JK, Branstet ter BF IV, Gafton AR, Lee WK, Glastonbury CM. Im aging of thyroid carcinom a
Philpott_9783131662316_BM.indd 284 02/05/14 3:55 PM

285
Bibliography
w ith CT and MRI: approaches to com m on sce-narios. Cancer Im aging 2013;13:128–139
Joseph J, Lim K, Ram sden J. Invest igat ion prior to thyroglossal duct cyst excision. Ann R Coll Surg Engl 2012;94(3):181–184
Lakhani R, Fishm an JM, Bleach N, Costello D, Birchall M. Alternat ive injectable m aterials for vocal fold m edialisat ion in unilateral vo-cal fold paralysis. Cochrane Database Syst Rev 2012;10:CD009239
Lam L, Sam m an N. Speech and swallow ing fol-low ing tongue cancer surgery and free ap re-const ruct ion—a system at ic review. Oral Oncol 2013;49(6):507–524
Lee AW, Lin JC, Ng W T. Current m anagem ent of nasopharyngeal cancer. Sem in Radiat Oncol 2012;22(3):233–244
Lippert BM, Eggers S, Schlü ter E, Ruder t H, Wer-ner JA. Lipom a of the larynx. Report of 2 cases and review of the literature. Otolaryngol Pol 2002;56(6):669–674
Maan ZN, Gibbins N, Al-Jabri T, D’Souza AR. The use of robot ics in otolaryngology-head and neck surgery: a system at ic review. Am J Otolar-yngol 2012;33(1):137–146
Magdy EA, Ashram YA. First branchial cleft anom a-lies: presentat ion , variabilit y and safe surgi-cal m anagem ent . Eur Arch Otorhinolaryngol 2013;270(6):1917–1925
Marsh DJ, Gim m O. Mult iple endocrine neo-plasia: t ypes 1 and 2. Adv Otorhinolaryngol 2011;70:84–90
Mart in A, Jäckel MC, Christ iansen H, Mahm oodza-da M, Kron M, Steiner W. Organ preserving t ran-soral laser m icrosurgery for cancer of the hypo-pharynx. Laryngoscope 2008;118(3):398–402
Mays JW, Sarm adi M, Moutsopoulos NM. Oral m anifestat ions of system ic autoim m une and in am m atory diseases: diagnosis and clin ical m anagem ent . J Evid Based Dent Pract 2012; 12(3, Suppl):265–282
McGrath BA, Thom as AN. Pat ient safety incidents associated w ith t racheostom ies occurring in hospital wards: a review of reports to the UK Nat ional Pat ient Safety Agency. Postgrad Med J 2010;86(1019):522–525
Mendelsohn AH, Sidell DR, Berke GS, John MS. Opt im al t im ing of surgical in tervent ion fol-low ing adult laryngeal t raum a. Laryngoscope 2011;121(10):2122–2127
Misono S, Merat i AL. Evidence-based pract ice: evaluat ion and m anagem ent of unilateral
vocal fold paralysis. Otolaryngol Clin North Am 2012;45(5):1083–1108
Mitchell RB, Hussey HM, Setzen G, et al. Clin ical consensus statem ent: t racheostomy care. Oto-laryngol Head Neck Surg 2013;148(1):6–20
Moline J, Eng C. Mult iple endocrine neoplasia t ype 2: an overview. Genet Med 2011;13(9):755–764
Monroe MM, Gross ND. Evidence-based pract ice: m anagem ent of the clin ical node-negat ive neck in early-stage oral cavit y squam ous cell carcinom a. Otolaryngol Clin North Am 2012;45(5):1181–1193
Moorthy R, Balfour A, Jeannon JP, Sim o R. Recur-rent laryngeal nerve palsy in benign thyroid disease: can surgery m ake a di erence? Eur Arch Otorhinolaryngol 2012;269(3):983–987
Nikiforov YE, Yip L, Nikiforova MN. New st rate-gies in diagnosing cancer in thyroid nodules: im pact of m olecular m arkers. Clin Cancer Res 2013;19(9):2283–2288
Özdem ir S, Tuncer U, Tarkan O, Kara K, Sürm elioğlu O. Carbon dioxide laser endoscopic posterior cordotomy technique for bilateral abductor vocal cord paralysis: a 15-year experience. JAMA Otolaryngol Head Neck Surg 2013;139(4):401–404
Paler i V, Thom as L, Basavaiah N, Drinnan M, Me-hanna H, Jones T. Oncologic outcom es of open conservat ion laryngectomy for radiorecurrent laryngeal carcinom a: a system at ic review and m eta-analysis of English-language literature. Cancer 2011;117(12):2668–2676
Parker NP, Bandyopadhyay D, Misono S, Goding GS Jr. Endoscopic cold incision , balloon dilat ion , m itom ycin C applicat ion , and steroid inject ion for adult laryngotracheal stenosis. Laryngo-scope 2013;123(1):220–225
Pedersen M, McGlash an J. Surgical versus non -su rgical in ter ven t ion s for vocal cord nod-u les. Cochrane Database Syst Rev 2012;6:CD001934
Ri at F, Del Pero MM, Fish B, Jani P. Radiologically predict ing w hen a sternotomy m ay be required in the m anagem ent of ret rosternal goiters. Ann Otol Rhinol Laryngol 2013;122(1):15–19
Rödel RM, Steiner W, Müller RM, Kron M, Mat thias C. Endoscopic laser surgery of early glot t ic can-cer: involvem ent of the anterior com m issure. Head Neck 2009;31(5):583–592
Royal College of Physicians. Radioiodine in the m anagem ent of benign thyroid disease. Clin ical
Philpott_9783131662316_BM.indd 285 02/05/14 3:55 PM

286
Bibliography
guidelines. June 2007. h t tp://w w w.rcplondon.ac.uk/publicat ions/rad ioiod ine-m anagem ent -benign-thyroid-disease.
Sam an DM. A review of the epidem iology of oral and pharyngeal carcinom a: update. Head Neck Oncol 2012;4:1
Shiro AM, Gale SC, Mart in ND, et al. Penetrat ing neck t raum a: a review of m anagem ent st rate-gies and discussion of the ‘No Zone’ approach. Am Surg 2013;79(1):23–29
Shum an AG, Shaha AR, Tut t le RM, Fins JJ, Mor-ris LG. Medullary thyroid carcinom a: eth i-cal issues for the surgeon. Ann Surg Oncol 2012;19(7):2102–2107
Singh M, Gupta SC, Singla A. Our experiences w ith parapharyngeal space tum ors and system at ic review of the literature. Indian J Otolaryngol Head Neck Surg 2009;61(2):112–119
Sobrino-Guijarro B, Cascarin i L, Lingam RK. Ad-vances in im aging of obst ructed salivary glands can im prove diagnost ic outcom es. Oral Maxil-lofac Surg 2013;17(1):11–19
Stoeckli SJ, Broglie MA. Recent innovat ions in head and neck oncology: a repor t from the ICHNO. Expert Rev Ant icancer Ther 2013;13(5):535–539
Takes RP, St rojan P, Silver CE, et al; In ternat ional Head and Neck Scient i c Group. Current t rends in in it ial m anagem ent of hypopharyngeal can-cer: the declin ing use of open surgery. Head Neck 2012;34(2):270–281
Thom as BL, Brow n JE, McGurk M. Salivary gland disease. Front Oral Biol 2010;14:129–146
Veivers D, Dent J. Lateral cervical cysts: an Australian perspect ive. ANZ J Surg 2012;82(11):799–802
Vilaseca I, Blanch JL, Bernal-Sprekelsen M. Tran-soral laser surgery for hypopharyngeal carci-nom as. Curr Opin Otolaryngol Head Neck Surg 2012;20(2):97–102
Wierzbicka M, Jackowska J, Bartochowska A, Józe- ak A, Szyfter W, Kędzia W. E ect iveness of cidofovir intralesional t reatm ent in recurrent respiratory papillom atosis. Eur Arch Otorhino-laryngol 2011;268(9):1305–1311
Wong DK, Brow n C, Mills N, Spielm ann P, Nee M. To drain or not to drain—m anagem ent of pediat ric deep neck abscesses: a case-control study. Int J Pediatr Otorhinolaryngol 2012;76(12):1810–1813
Zenk J, Koch M, Klin tworth N, et al. Sialendoscopy in the diagnosis and t reatm ent of sialolith iasis: a study on m ore than 1000 pat ients. Otolaryn-gol Head Neck Surg 2012;147(5):858–863
Paediatric ENTBajaj Y, Cochrane LA, Jephson CG, et al. Laryn-
got racheal reconst ruct ion and cricot racheal resect ion in children: recent experience at Great Orm ond Street Hospital. Int J Pediatr Otorhinolaryngol 2012;76(4):507–511
Bjornson C, Russell KF, Vanderm eer B, Durec T, Klassen TP, Johnson DW. Nebulized epineph-rine for croup in children . Cochrane Database Syst Rev 2011; (2):CD006619
Drolet BA, From m elt PC, Cham lin SL, et al. In it ia-t ion and use of propranolol for infant ile hem -angiom a: report of a consensus conference. Pediatrics 2013;131(1):128–140
Jayachandra S, Eslick GD. A system at ic review of paediat ric foreign body ingest ion: presentat ion , complicat ions, and m anagem ent . Int J Pediatr Otorhinolaryngol 2013;77(3):311–317
Lowe D, van der Meulen J; Nat ional Prospect ive Tonsillectomy Audit . Tonsillectomy technique as a r isk factor for postoperat ive haem orrhage. Lancet 2004;364(9435):697–702
Luu TM, Chevalier I, Gauthier M, Carceller AM, Bensoussan A, Tapiero B. Acute adenit is in children: clin ical course and factors predic-t ive of surgical drainage. J Paediatr Child Health 2005;41(5-6):273–277
Mallam pat i SR, Gat t SP, Gugino LD, et al. A clin i-cal sign to predict di cult t racheal in tuba-t ion: a prospect ive study. Can Anaesth Soc J 1985;32(4):429–434
Paradise JL, Bluestone CD, Bachm an RZ, et al. E cacy of tonsillectomy for recurrent throat in-fect ion in severely a ected children . Results of parallel random ized and nonrandom ized clin i-cal t r ials. N Engl J Med 1984;310(11):674–683
Reed J, Mans CK, Brietzke SE. Surgical m anagem ent of drooling: a m eta-analysis. Arch Otolaryngol Head Neck Surg 2009;135(9):924–931
Singh A, Georgalas C, Patel N, Papesch M. ENT pre-sentat ions in children w ith HIV infect ion . Clin Otolaryngol Allied Sci 2003;28(3):240–243
Spyridis P, Maltezou HC, Hantzakos A, Scondras C, Kafetzis DA. Mycobacterial cervical lym phade-nit is in children: clin ical and laboratory factors of im portance for di erent ial diagnosis. Scand J Infect Dis 2001;33(5):362–366
Tweedie DJ, Skilbeck CJ, Cochrane LA, Cooke J, Wyat t ME. Choosing a paediat r ic t racheostomy tube: an update on current pract ice. J Laryngol Otol 2008;122(2):161–169
Philpott_9783131662316_BM.indd 286 02/05/14 3:55 PM

287
Page num bers in italics refer to illust rat ions.
Aacinic cell carcinom a 168, 169acoust ic re ex m easurem ents 44–45act inomycin D 218act inomycosis 205acute ot it is m edia (AOM) 13, 261acute rh inosinusit is (ARS) 87, 88, 89, 262
complicat ions 93–94, 94fungal 96, 97
adenocarcinom a 33, 115, 168adenoid cyst ic carcinom a
external auditory canal 33salivary glands 115, 168, 169
adenoidectomy 257adenoids 255, 256adrenoceptor antagonists 265advancem ent aps 140, 140ageusia 127airway
paediat ric, assessm ent and m anagem ent 248–252
shared 266AJCC (Am erican Join t Com m it tee on Cancer)
staging system 275alcohol-related headache 111Alexander law 60Alexander m alform at ion 227allergic derm at it is 10allergic fungal rh inosinusit is (AFRS) 97–100,
99, 275allergic rh init is 78–79, 80Alport syndrom e 230am inoglycosides 23–24, 56anaesthet ics 264–266anaplast ic thyroid carcinom a 186, 189angioedem a 151anosm ia 125–127anterior deep neck space infect ion 197–198ant iepilept ic drugs 266ant ih istam ines 265ant i-neutrophil cytoplasm ic ant ibodies
(ANCA) 83, 84–85ant ithyroid drugs 180, 181Apert syndrom e 229
aphthous stom at it is 172apnoea/hypopnoea index (AHI) 118, 275arachnoid cyst 70Arnold nerve 64ar teriovenous (AV) m alform at ion 258, 279–280arytenoid cart ilages 147, 193aspirat ion , paediat r ic 243asthm a 79, 88atropine 266at t icoantrostomy 16atypical facial pain 112audiology 42–47audiom etry
cort ical elect rical response 47paediat ric pat ients 232pure-tone 42–43, 44speech 45visual reinforcem ent 231
audit 271auditory brainstem im plants (ABIs) 52–53auditory brainstem responses (ABR) 46, 46, 232auditory evoked potent ials 46–47auditory neuropathy 26auditory processing disorder 25–26auditory steady-state responses 47auricle (pinna)
benign tum ours 33, 33carcinom a 11, 33, 33, 34in am m atory disorders 10, 11t raum a 38
autonom ic nervous system 77, 265axonotm esis 65
Bbacterial infect ions
deep neck spaces 197–199ear 10, 13, 23, 261–262oral cavit y/pharynx 171, 255, 262salivary glands 165sinonasal 78, 87
barbiturates 111–112, 265barot raum a 38basal cell carcinom a 11, 33, 33, 36basilar m em brane 5, 6, 8, 9Behçet syndrom e 24, 85, 170Belfast rule of thum b 17
Index
Philpott_9783131662316_BM.indd 287 02/05/14 3:55 PM

288
Index
Bell palsy 65, 66benign (idiopathic) in t racranial hypertension 111,
133benign paroxysm al posit ional vert igo (BPPV) 40,
54–55betahist ine 56Bezold abscess 14Bing–Siebenm ann m alform at ion 227blast injuries 38bleomycin 218branchial cleft /arch anom alies 201–202, 245, 277branchial cysts 201, 201–202, 245branchial stulas 202, 245branchial sinuses 245branchiogenic carcinom a 202branchio-otorenal syndrom e 229bronchodilators 265bronchoscopy, paediat ric 252, 279burning m outh syndrom e 172
Ccaloric test ing 62, 62candidiasis, oral 171carbam azepine 266carbon m onoxide (CO) poisoning 111carcinom a ex-pleom orphic adenom a 168, 169Carhart notch 20, 21carot id body tum ours 212Cast lem an disease 206caust ic ingest ion 243–244cavernous sinus throm bosis 93–94cellu lit is 10, 93, 274cerebellopont ine angle (CPA) 7
tum ours 30–31cerebrospinal u id (CSF) leaks 39, 133–134
iat rogenic 103, 104cerum inom as 12cervical adenit is, tuberculous 204, 204–205cervical lymphadenopathy, paediat ric 245–246cervical lymph node m etastases 213–217,
214, 215classi cat ion 213–214locoregional recurrence 215occult prim ary 217radiotherapy 214see also neck dissect ion
cervical lymph nodes 213cervicogenic headache 112cetuxim ab 218Chandler classi cat ion 93, 94, 274CHARGE associat ion 227, 233
chem otherapy 218, 220–221chi-squared test 268–269choanal at resia 233cholesteatom a 14, 14, 15
canal 11congenital 14, 230im aging 69Mo et t–Sm ith classi cat ion 272surgery 16, 19
cholesterol granulom a 69chondroderm at it is nodularis chronica helicis 11chorda tym pani 64, 123chorda tym pani neuralgia 41chordom as 234choristom a 33chronic ot it is m edia (COM) 13–14, 69, 261, 272chronic rh inosinusit is (CRS) 87–91, 262
complicat ions 94–95fungal 96Lund–Mackay scoring 89, 273w ith nasal polyps 88–89, 91, 271w ithout polyps 87, 88, 89, 90, 92
Churg–Strauss syndrom e 84–85cidofovir 156, 241ciliary m ot ilit y disorders 105–106cisplat in 24, 218Citelli abscess 14, 198classi cat ions 272–280cleft lip and palate 234–236, 235clin ical governance 271cluster headache 110–111cocaine 101, 264cochlea 6, 8, 9
congenital anom alies 227cochlear duct (scala m edia) 5, 6, 7cochlear implants (CI) 51–52, 52Cogan syndrom e 24cognit ive-behavioural therapy (CBT) 57com m on cold 263com puted tom ography (CT), ear 68, 69, 70con dence in tervals 268connexin 26 m utat ions 24, 229conus elast icus 147correlat ion 269Cort i, spiral organ of 6, 7cor t ical elect rical response audiom etry 47cosm esis, nasal 135–137Cow den syndrom e 183cranial neuralgias 112craniopharyngiom as 234cricoarytenoid join t 147
Philpott_9783131662316_BM.indd 288 02/05/14 3:55 PM

289
Index
cricoid car t ilage 147cricoid stenosis 195cricothyroid join t 147cricothyroid m uscle 147, 148, 149, 162cricothyroidotomy 192crom oglycate 265croup 249Crouzon disease 229, 237cyclophospham ide 85, 218cyst ic brosis (CF) 105cyst ic hygrom a 245, 258cytom egalovirus (CMV) 171, 230
Ddacryocystography 131dacryocystorhinostomy 131, 131–132dacryoscint igraphy 131danger space 197deafness see hearing lossdecibels 42deep neck space infect ion 197–199De Quervain thyroidit is 181–182derm oids, m idline 200, 236developm ent , paediat ric 253diphtheria 171, 262dist ract ion test ing 231divers, barot raum a 38Dix–Hallpike m anoeuvre 54, 60dizziness 54Donaldson line 5Dow n syndrom e 230, 236–237doxorubicin 218drooling, paediat r ic 253–254, 280drop at tacks 56dural tears 19dysequilibrium 54dysgeusia 127dysosm ia 125–126dysphonia 151–152
Eear
anaesthesia 264congenital m alform at ions 227–228em bryology and anatom y 3–7im aging 68–70infect ions 261–262physiology 8–9t raum a 38–40tum ours 33–37
ECOG (Eastern Cooperat ive Perform ance Group) perform ance status 276
elect rocochleography 46elect ronystagm ography (ENG) 62–63encephalocoele, nasal 236endolym ph 6, 9, 62endoscopic dacryocystorhinostomy 131–132endoscopic sinus surgery 101–104en urane 266eosinophilic fungal rh inosinusit is (EFRS) 97–98eosinophilic granulom atosis w ith polyangiit is
(EGPA) 84–85eosinophilic m ucinous rh inosinusit is
(EMRS) 97–98epiderm oid cyst 70, 200epiglot t is 147
absent /rudim entary 238epiglot t it is 249, 263epistaxis 107–108, 108Epley m anoeuvre 55, 55Epstein–Barr virus (EBV) 116, 205, 209, 256Epworth Sleepiness Score 277erysipelas 10, 78erythem a m ult iform e 170erythroplakia 176esthesioneuroblastom a 115ethm oidal ar tery ligat ion 107, 108ethm oidal cells 73, 75ethm oid bulla (EB) 74, 75European Laryngological Society classi cat ion of
endoscopic resect ion 222–223, 224, 277exophyt ic papillom a, nasal 113exostosis 12external auditory canal (or m eatus) (EAC or
EAM) 4at resia 68, 228, 279in am m atory disorders 10tum ours 12, 33, 34
external carot id ar tery ligat ion 107, 108external ear 3–4, 4, 8
congenital m alform at ions 227–228disease 10–12im aging 68prom inent 228tum ours 33, 215see also auricle
extraesophageal re ux scoring system s 150
Ffacial aps 140–142facial fractures 138–139, 276
Philpott_9783131662316_BM.indd 289 02/05/14 3:55 PM

290
Index
facial nerve (VII) 64–67, 65aberrant 227surgical dam age 18–19, 66, 67
facial nerve palsy 65–67complicat ing ot it is m edia 14House–Brackm ann grading 65, 272, 273treatm ent 66, 66–67tum our-related 169
facial pain , persistent idiopathic 112facial swelling 139 brous dysplasia 113, 230Fisher exact probabilit y test 269 stula test 60 aps, reconst ruct ive 140–142, 278 uorescein dye disappearance test 1305- uorouracil (5-FU) 218folate de ciency 170follicular thyroid adenocarcinom a 185,
187, 188folliculit is 78food allergy 81foram ina, skull 7forehead ap 142, 142foreign bodies (FBs), paediat ric 251–252fourth pouch sinus 245Frey syndrom e 169frontal sinus 73, 74, 75–76
fractures 138–139m ucocoele 274surgery 102, 273
fungal balls, paranasal sinuses 97, 98fungal infect ions, oral cavity/oropharynx 171fungal sinus disease 96–100furuncle 10
Ggabapent in 266gallium -67 scanning 68Gardner syndrom e 113gast roesophageal re ux disease (GORD),
paediat ric 243general anaesthet ics 265–266geniculate ganglion neuralgia 41geographic tongue 173giant cell ar terit is 85, 111glandular fever 205, 256Glasgow bene t scale 17–18, 18gliom a, nasal 236glom us tum ours 34–35, 69, 210–212
Fisch classi cat ion 34, 212, 272jugulare 35, 35, 212
tym panicum 35, 35, 212vagale 211–212
glossit isbenign m igratory 173m edian rhom boid 172
glossopharyngeal neuralgia 41glot t ic carcinom a 158, 161glot t ic incom petence 193glot t ic stenosis 195, 275glue ear 15glycerol dehydrat ion test 56goit re
in am m atory 181–182sim ple 180–181, 181toxic 181
Goldenhar syndrom e 66, 230gouty tophi 11Gradenigo syndrom e 14granulom atosis w ith polyangiit is (GPA) 83
larynx 150, 151oral cavity 170sinonasal 81–82
granulom atous invasive fungal sinusit is 96Graves disease 181Graves ophthalm opathy 275greater pet rosal nerve 64, 123gustatory disorders 125, 127gustatory event-related potent ials 125gustatory system 123–124, 124
Hhaem angiom as 258
cerebellopont ine angle 70larynx 156–157nasal region 114–115neck 202, 245subglot t ic 258
haem angiopericytom a 116hair cells 6, 7, 8–9, 9Halm agyi test 61halothane 265–266hand-foot-and-m outh disease 170hard palate
defects after resect ion 278tum ours 176, 178
Hashim oto thyroidit is 181headache 109–112head and neck
congenital abnorm alit ies 233–237lym phat ics 213reconst ruct ive aps 140–142, 278
Philpott_9783131662316_BM.indd 290 02/05/14 3:55 PM

291
Index
robot ic surgery 222t ransoral laser surgery 222–223
head and neck cancerchem otherapy 218neck m etastases 213–217radiotherapy 219–221
head injury, headache after 111head thrust test 61hearing, m echanism of 8, 9hearing aids (HAs) 48–50
bone-anchored (BAHA) 48–50implantable 18, 19, 48t ypes 48, 49
hearing assessm ent 42–44clin ical 42paediat ric 231–232tuning fork 42, 43, 44see also audiom etry
hearing loss (HL)children 229–230noise-induced 39–40non-organic 25sensorineural (SNHL) 23–24, 229–230
heel/toe gait test 61Hennebert sign 58hereditary haem orrhagic telangiectasia
82, 108herpangina 170herpes sim plex virus (HSV) infect ions 65,
170, 230herpes zoster 65–66, 170herpet iform ulcers 172Hitzelberger sign 30HIV infect ion/AIDS 171, 205Hodgkin lym phom a 246–247hum an papillom aviruses (HPV) 113, 156Hürth le cell tum ours 185, 188hydrocephalus, ot it ic 15hyoid fractures 194hyoscine 266hyperacusis 29hyperparathyroidism
prim ary 189–190, 191quaternary 190secondary 190ter t iary 190
hypert rophic scars 11, 143, 143hypervent ilat ion 54, 61hypogeusia 127hypopharyngeal tum ours 207–209, 208hypotension, induced 266
Iidiopathic (benign) in t racranial
hypertension 111, 133im aging, ear 68–70indium -111 labelled leucocyte planar
scin t igraphy 68infect ious m ononucleosis 205, 256inferior laryngeal ar tery 148in uenza 263inner ear 4, 5, 5–7, 6
congenital m alform at ions 227im aging 69physiology 8–9
interarytenoid m uscle 147, 149, 162α -in terferon 156internal auditory canal 7, 69–70internuclear ophthalm oplegia 60int racranial hyper tension, benign
(idiopathic) 111, 133int racranial pressure, raised 111inver ted papillom a, sinonasal 113, 114
staging 114, 274iso urane 266
JJast rebo neurophysiological m odel, t innitus
27, 28Jervell–Lange–Nielsen syndrom e 229Jones dye tests 130–131jugular foram en 7juvenile nasopharyngeal angio brom a 113–114,
114, 273
KKaposi sarcom a 171Kartagener syndrom e 105Kawasaki disease 86, 170keloids 11, 142–143keratoacanthom a 11keratosis, larynx 158keratosis obturans 11Kuhn cells 102, 273–274
Llabyrin th it is 57lacrim al obst ruct ion 128–132
causes 129–130invest igat ions 130–131m anagem ent 131–132
Philpott_9783131662316_BM.indd 291 02/05/14 3:55 PM

292
Index
sym ptom s and signs 128–129lacrim al sac 128
diseases 129lacrim al system 128, 129laryngeal carcinom a 158–161, 159
classi cat ion of cordectom ies 222–223, 224, 277
nodal m etastases 158, 215staging 159stom al recurrence 160, 275treatm ent 159–161, 220–221
laryngit is 150–151, 263laryngocele 152, 152, 203laryngom alacia 238, 250laryngopharyngeal re ux 150laryngoplasty, inject ion 162–163laryngotracheal clefts 238–239, 279larynx 147–149
anatomy 147–148atresia 238benign tum ours 156–157clefts 238–239, 279cysts 153dysplasia 158, 277foreign bodies 251–252fram ework surgery 163non-neoplast ic pathology 150–155paediat r ic, assessm ent 248–249paediat r ic pathology 238–241physiology 148–149saccular cysts 238stenosis 194–195traum a 193–194, 194webs 238
laser surgery, t ransoral 222–223lateral cr icoarytenoid m uscle 147, 149Le Fort fractures 138, 138, 276Lem m ier disease 262Leopard syndrom e 229leprosy 78leukoplakia, oral 172, 176lichen planus 172, 172lingual papillae 123lipom a 70lip tum ours 174–175, 176, 177, 215local anaesthet ics (LAs) 264loudness recruitm ent 43–44Luc abscess 14Ludw ig angina 197–198lymphangiom a 200, 258lymphom a 116
Ann Arbor classi cat ion 246, 276
paediat r ic 246–247salivary gland 168thyroid 186, 189
lym phovascular m alform at ion 279
MMacewen t riangle 5m acroglossia 173m agnet ic resonance im aging (MRI), ear 68, 69–70Mallam pat i score 277m alocclusion 276m andibular fractures 138m andibulotomy 178Mann–Whitney U test 269m asking 47m astoid, im aging 69m astoidectomy 16, 18–19m astoidit is 14, 261–262m axillary ar tery ligat ion 107, 108m axillary fractures 138, 138m axillary sinus 75McCorm ick toy test 231m easles 170m edian rhom boid glossit is 172m edicat ion overuse headache 111–112m edullary thyroid carcinom a 185, 187,
188–189, 191m elanom a 36–37, 115Melkersson–Rosenthal syndrom e 66Ménière disease 55–57Meniet t device 57m eningiom a 70m eningit is 14, 39, 229Messerklinger landm arks 74, 74m etastat ic disease 116, 213–217m ethot rexate 218Michel aplasia 227m icrobiology 261–263m icrot ia 227–228, 279m iddle ear (ME) 4, 4–5, 8
congenital m alform at ions 227im aging 69implants 18, 19surgery 16–19tum ours 33–35
m idfacial fractures 138, 138, 276m idline forehead ap 142, 142m igraine 57–58, 109–110m igrainous vert igo 57–58m inor salivary glands 175
tum ours 115, 168, 169
Philpott_9783131662316_BM.indd 292 02/05/14 3:55 PM

293
Index
Möbius syndrom e 66Mo at solut ion 264Mondini dysplasia 227m onom orphic adenom a, salivary gland 168m orphine 266m outh ulcers 172m ucociliary clearance, sinonasal 76, 76m ucocoeles, paranasal sinus 95, 274m ucoepiderm oid carcinom a 115, 168m ult iple endocrine neoplasia (MEN)
syndrom e 185, 191m um ps 165m uscarin ic agents 265mycelia m ass, paranasal sinuses 97, 98mycobacterial infect ion , atypical 246myringit is, granular 10myringit is bullosa haem orrhagica 10myringoplasty 16myringosclerosis 13
Nnasal conchae (turbinates) 73, 73–74nasal polyps (NPs) 88–89
eosinophilic granulom atosis w ith polyangiit is 84
grading 274m anagem ent 89, 91, 271
nasal septum 73perforat ion 82
nasolacrim al disorders 128–132nasolacrim al duct 128
diseases 129nasopharyngeal carcinom a (NPC) 209, 276nasopharynx
juvenile angio brom a 113–114, 114, 273tum ours 209
Nat ional Com parat ive Audit of Surgery for Nasal Polyposis and Chronic Rhinosinusit is 271
Nat ional Prospect ive Tonsillectom y Audit 271neck
benign disease 200–206clin ically negat ive (N0) 214deep space infect ions 197–199lymphat ic drainage 213m etastat ic disease 213–217spaces 197t raum a 193–196t raum a zones 195–196, 275t riangles 213
neck dissect ion 216–217
corners of consternat ion 216incisions 216, 216m odi ed radical 216–217N0 neck 214select ive 217
neck m assesacquired 202–206congenital 200–202m alignant 246–247paediat ric 245–247
neonatal screening 231nervus in term edius neuralgia 41neuro brom as, parapharyngeal space 210neuro brom atosis
type 1 (NF1) 210type 2 (NF2) 30, 52
neurological disorders 151neurom uscular blocking drugs 264–265neuropraxia 65neurotm esis 65nit rous oxide 265noise-induced hearing loss 39–40non-allergic, non-eosinophilic rh in it is
(NENAR) 79–80non-allergic rhin it is w ith eosinophilia syndrom e
(NARES) 80–81non-Hodgkin lym phom a (NHL) 116, 247non-steroidal ant i-in am m atory drugs (NSAIDs),
overuse headache 111–112nose
acute and chronic disorders 78–82anatom y 73, 73–74cleft 235congenital m idline swellings 236cosm esis 135–137, 136fractures, classi cat ion 272physiology 76, 76–77tum ours 113–117
nystagm us 60, 61, 62
Oobstruct ive sleep apnoea (OSA) 118–119, 256odds rat io 267odour
classi cat ion 121detect ion 120, 121, 122
oesophagusat resia (OA) 242foreign bodies 251, 252paediat ric pathology 242–244
olfact ion 120, 121, 121–122
Philpott_9783131662316_BM.indd 293 02/05/14 3:55 PM
294
Index
disorders 125–127test ing 125
olfactory bulb 120olfactory cor tex, pr im ary 121olfactory epithelium 120olfactory event-related potent ials (OERPs) 125olfactory fossa depth 274olfactory loss 125–127olfactory neuroblastom a 115, 272olfactory system 120–123, 121oncocytom a 168optic nerve, surgical injury 103optokinet ic re ex 60–61oral allergy syndrom e 81oral cavity
anatom ical regions 175biopsy 176diseases 170–173tum ours 175–179, 177
orbital abscess 93orbital cellulit is 93, 274orbital com plicat ions, acute sinusit is 93,
94, 274oroantral stulas 273oropharynx
diseases 170–173tum ours 207, 208
osseous m etaplasia 95ossicles, auditory 8ossiculoplasty 17–18, 18osteogenesis imperfecta 230osteogenic sarcom a 115–116osteom as 12, 113osteomyelit is 10, 68, 94, 261osteoradionecrosis 178, 220ost iom eatal com plex 74, 74otalgia, referred 41otalgic neuralgia 41ot it is externa 261
acute 10, 261chronic 10, 261m alignant (necrot izing) 10, 68, 261
ot it is m edia 13–15, 261–262acute (AOM) 13, 261chronic (COM) 13–14, 69, 261, 272complicat ions 14–15w ith e usion (OME) 15
otoacoust ic em issions (OAE) 46, 232otolith ic crisis of Tum arkin 56otomycosis 10otosclerosis 20–22ototoxicit y 23–24
Ppaclitaxel 218paediat r ic pat ients 225–258
classi cat ion system s 278–280deafness 229–230rhinosinusit is 88, 89, 92thyroid m ass 188
palatal myoclonus 29papillary cystadenom a lym phom atosum 168, 188papillary thyroid adenocarcinom a 185, 187paracusis of Willis 20paragangliom as see glom us tum oursparakeratosis, larynx 158parapharyngeal abscess 198–199parapharyngeal space, tum ours 210–212parathyroid carcinom a 190parathyroid disorders 189–190parathyroid horm one (PTH) 189parot idectomy 169parot id region, non-parot id swellings 166–167parot id tum ours 168, 169, 215parot it is, chronic 166Pem berton sign 181pem phigus/pemphigoid 170, 171Pendred syndrom e 229perichondrit is, infect ious 10, 11perilym ph 6, 7perilym phat ic stula 40peritonsillar abscess 262pet rosit is 14, 69pet rous apex, im aging 69phaeochrom ocytom a 191phantosm ia 126pharm acology 264–266pharyngeal pouches 203, 203–204, 204pharynx
infect ions (pharyngit is) 171, 262–263tum ours 207–209
Philpot t–Javer staging system 99phonat ion 149Pierre Robin sequence 229, 236pinna see auriclepiriform fossa tum ours 207, 208, 208pleom orphic adenom a 115, 168polysom nography 119postcr icoid space tum ours 207, 208, 208posterior cr icoarytenoid (PCA) m uscle 147,
148–149posterior pharyngeal wall tum ours 207, 208post-styloid space, tum ours 211post-t ransplant lymphoproliferat ive disorder 256
Philpott_9783131662316_BM.indd 294 02/05/14 3:55 PM

295
Index
post-t raum at ic headache 111posturography 63power, study 268preauricular pits and sinuses 228, 228, 245prem edicat ion 265presbyacusis 23presbyosm ia 125pre-septal cellulit is 93prestyloid space, tum ours 211prim ary ciliary dyskinesia (PCD) 105–106propofol 265Prussak space 5psychogenic voice disorders 152pterygopalat ine ganglion 77, 77pure-tone audiom etry 42–43, 44p-value 268
Qquadrangular m em brane 147quinsy 262
RRadiat ion Therapy Oncology Group (RTOG)
study 220–221radioact ive iodine 180, 188radiotherapy 219–221
complicat ions 130, 220laryngeal carcinom a 160–161m etastat ic neck disease 214oral tum ours 178pharyngeal carcinom a 209thyroid cancer 188–189vest ibular schwannom a 31–32
Ram say–Hunt syndrom e 65–66ranulas 202Rathke pouch cysts 233–234recurrent laryngeal nerve (RLN) 148, 162Refsum disease 229regression 269Reinke oedem a 153, 153, 154Reissner m em brane 6, 9Reiter syndrom e 170relapsing polychondrit is 10, 150respiratory papillom atosis, recurrent 156,
156, 171juvenile 240–241
ret ropharyngeal abscess 197, 197rhabdomyosarcom a 246rhinit is
allergic 78–79, 80
at rophic 81drug-induced 81food-induced 81horm onal/endocrine 81non-allergic, non-infect ious 79–81occupat ional/environm ental 81
rhinophym a 82rhinoplasty 135–137rhinosclerom a 78rhinosinusit is (sinusit is) 87–91
acute see acute rh inosinusit ischildren 88, 89, 92chronic see chronic rh inosinusit iscom plicat ions 93–95, 274European Posit ion Paper 87–92fungal 96–100
Riedel thyroidit is 182Rinne test 42, 44r isk rat io (relat ive r isk) 267robot ic surgery 222Rom berg test 61rotat ion aps 140, 140rubella, congenital 230
Ssaccadic eye m ovem ents 61saddle nose deform ity 274salicylates 24salivary duct carcinom a 168salivary gland disease, non-neoplast ic
165–167salivary gland tum ours 168–169
m alignant 168–169, 175m inor 115, 168, 169
sam ple size, calculat ion 270sarcoidosis 81, 151, 274sarcom as 115–116Scheibe m alform at ion 227Schirm er test 66schwannom a
sinonasal 115vest ibular 30–32, 31, 69–70
Schwartze sign 20scurvy 170sem icircular canals (Scc) 5, 6
congenital anom alies 227dehiscence, superior 58–59, 69 stu la 19, 60funct ion 9, 9, 62unilateral paresis 62
Sem ont m anoeuvre 55
Philpott_9783131662316_BM.indd 295 02/05/14 3:55 PM

296
Index
sensorineural hearing loss (SNHL) 23–24, 229–230
sevo urane 266sialadenit is
bacterial 165chronic 165, 166
sialoendoscopy 167sialography 166, 166sialolith iasis 165–166, 166sigm oid sinus
surgical breach 19throm bosis 69
sinonasal regionanatomy 73–76physiology 76–77tum ours 113–117
sinuses, paranasalanatomy 73, 74–76endoscopic surgery 101–104infect ions 262physiology 76, 76–77tum ours 113–117
sinusit is see rh inosinusit isSjögren syndrom e 165, 166, 170skin cancer 35–37skull base, im aging 69–70sleep apnoea 118–119sleep nasendoscopy 119sleep -related breath ing disorders 118–119sleep study, por table dom iciliary 119sm ell, sense of see olfact ionsm ooth pursuit eye m ovem ents 60–61snoring 118–119soft palate tum ours 207som atosounds 27, 29sound, pressure t ransform at ion 8spasm odic dysphonias (SD) 151Spearm an rank correlat ion 269speech audiom etry 45speech developm ent 253speech discrim inat ion test ing 231sphenoid sinus
anatomy 73, 74, 75surgical approach 102
sphenopalat ine ar tery (SPA) ligat ion 107–108, 108
squam ous cell carcinom a (SCC)cutaneous 36external ear 11, 12, 33, 34larynx 158, 159lip 174m iddle ear 33
oral cavit y 175–176pharynx 207, 208, 209salivary gland 168sinonasal 115
squam ous in t raepithelial neoplasia, larynx 158standard deviat ion (SD) 267standard error (SE) 267stapedial ar tery, persistent 227stapedial re ex 20, 44–45stapedotom y 21, 21–22stat ist ics, m edical 267–270Stenger test 42ster tor, ch ildhood 248St ickler syndrom e 229streptococcal pharyngit is 171, 262st r idor 248study design 269–270subglot t ic carcinom a 158, 161subglot t ic haem angiom a 258subglot t ic stenosis 239–240, 240
Myer–Cot ton grading 240, 279subm andibular gland
surgical excision 166, 166, 169tum ours 168, 169, 215
subperiosteal abscess 14, 93superior laryngeal ar tery 148superior laryngeal nerve 148superior orbital ssure 7superior sem icircular canal dehiscence 58–59, 69supraglot t ic carcinom a 158, 160–161supraglot t ic laryngectom y, par t ial 160supraglot t ic stenosis 195survival analysis 269suxam ethonium 264–265swallow ing 149sw im m er’s ear 261sym pathom im et ics 265syphilis 78, 171
congenital 230system ic lupus erythem atosus (SLE) 170
Ttaste
detect ion 123–124, 124disorders 125, 127test ing 125
taste buds 123Teacher Drool Scale 253, 280technet ium -99 m bone scanning 68temporal ar terit is 85, 111temporal bone
Philpott_9783131662316_BM.indd 296 02/05/14 3:55 PM

297
Index
dissect ion , complicat ions 18–19fractures 38–39, 39im aging 69, 70paragangliom a 34
tension-type headache 109, 110tensor t ym pani syndrom e 29Thornwaldt cysts 233–234throat infect ions 262–263thym ic cysts 202thyroarytenoid m uscle 147, 149thyroglossal cysts 200–201, 245thyroglossal duct carcinom a 201thyroid cancer 185–189
paediat ric 246prognost ic factors 186–187referral guidelines 187–188staging 187t reatm ent 188–189
thyroid car t ilage 147t raum at ic injury 193, 194
thyroid cytology, classi cat ion 183, 276thyroid disease, benign 180–182thyroid eye signs 277–278thyroid m ass, paediat r ic 188thyroid nodule 183–184thyroid storm 181thyroid tum ours 185–189t innitus 27–29, 69t innitus-related neural act ivit y (TRNA) 27tongue
base, tum ours 207carcinom a/tum ours 175, 176, 177, 178, 215 ssured 173hairy 173taste percept ion 123–124, 124
tonsillectomy 256–257, 271tonsillit is 255–256tonsillogenic infect ion 198, 198tonsils 255–257
Brodsky classi cat ion 257, 257, 277paediat ric pathology 255–256palat ine 255tum ours 207, 208, 215
toxoplasm osis 205, 230t rachea
foreign bodies 251paediat ric pathology 242–244stenosis 195t raum at ic injuries 194
t racheit is 263t racheobronchom alacia 242, 250t racheoesophageal stula (TOF) 242–243, 279
t racheostomy 192paediat ric 249–251
t racheostomy tubes, paediat ric sizes 250, 278–279
t ransit ional cell papillom a, sinonasal see inver ted papillom a, sinonasal
t ransposit ion aps 140–142, 141–142t raum a 38–40, 193–196Trautm ann t riangle 5Treacher–Collins syndrom e 229, 237t rench m outh 262t ricyclic ant idepressants 266t rigem inal neuralgia 112t risomy 21 (Dow n syndrom e) 230, 236–237t test 268tuberculosis 78, 151
cervical adenit is 204, 204–205Tullio sign 58, 60tuning fork tests 42, 43, 44t ym panic m em brane (TM) 4, 8
in am m atory disorders 10perforat ions 13ret ract ions 13–14, 272traum at ic injuries 38
t ym panic neuralgia 41t ym panom etry 45, 45, 232t ym panoplasty 16, 17t ym panosclerosis 13t ype I/t ype II errors 268
Uuncinate process 74, 74–75Unterberg stepping test 61, 61upper airway resistance syndrom e (UARS) 118upper airway t raum a 193–196Usher syndrom e 229
VVACTERL associat ion 242vagus nerve 162vascular m alform at ions 245, 258vasculit ides 83–86, 84verrucous carcinom a, larynx 159ver t igo 54
benign paroxysm al posit ional (BPPV) 40, 54–55
m igrainous 57–58vest ibular aqueduct , w idened 227vest ibular disorders 54–63
exam inat ion 60–61
Philpott_9783131662316_BM.indd 297 02/05/14 3:55 PM

298
Index
invest igat ion 61–63vest ibular evoked myogenic potent ials
(VEMPs) 59, 63vest ibular failure, acute 57vest ibular neuronit is 57vest ibular schwannom a 30–32, 31, 69–70vest ibular system 5, 8–9, 9
congenital anom alies 227traum a 40
vest ibulit is, nasal 78vest ibulo-ocular re ex (VOR) 9, 60
caloric test ing 62suppression test 61
vest ibulospinal response, test ing 61Veterans A airs Laryngeal Cancer Study 220vidian nerve 64, 77Vincent angina 255vincrist ine/vinblast ine 218viral infect ions
facial nerve palsy 65–66hearing loss 20, 23m iddle ear 13oral cavity/pharynx 170–171, 263salivary glands 165sinonasal 87, 262tonsils 255
visual acuit y, dynam ic 61vitam in B12 de ciency 170vitam in C de ciency 170
vocal fold palsy 162–164bilateral 164paediat ric 239unilateral 162–164, 163
vocal folds (vocal cords) 148, 149classi cat ion of endoscopic resect ion
222–223, 224, 277 xat ion, carcinom a 158nodules 152–153, 153paradoxical m ovem ent 152polyps 154–155, 155
vocal process granulom as 154, 155voice disorders 151–152Voice Handicap Index (VHI) 163–164Voice Sym ptom Scale (VoiSS) 164vom eronasal organ 121, 122–123
WWaardenburg syndrom e 229Waldeyer ring 213, 255Warthin tum our 168wax, ear 11Weber test 42, 43Wegener granulom atosis see granulom atosis w ith
polyangiit isWilcoxon test 269Winkler nodule 11
Philpott_9783131662316_BM.indd 298 02/05/14 3:55 PM