Bronchoscopic procedures for emphysema treatment
7
Review Bronchoscopic procedures for emphysema treatment Federico Venuta * , Erino A. Rendina, Tiziano De Giacomo, Marco Anile, Daniele Diso, Claudio Andreetti, Francesco Pugliese, Giorgio F. Coloni Universita` di Roma ‘‘La Sapienza’’, Cattedra di Chirurgia Toracica, Policlinico Umberto I, V.le del Policlinico, 00100 Rome, Italy Received 19 July 2005; received in revised form 28 November 2005; accepted 5 December 2005 Summary Emphysema is a debilitating lung disease continuing to be a major source of morbidity and mortality in the developed countries. Medical treatment is the mainstay of therapy and consists of smoking cessation, pulmonary rehabilitation, administration of bronchodilators and, when indicated, steroids and supplemental oxygen. Various surgical procedures have been promoted in the past to relieve dyspnoea and improve quality of life in patients with advanced emphysema; whilst early results were often encouraging, a sustained objective functional improvement was rarely achieved and most of those procedures were progressively abandoned. Despite controversies, LVRS has been shown to be beneficial to selected patients with end-stage emphysema when medical therapy has failed. There is no doubt that LVRS allows a significative functional improvement in a selected group of patients; however, it still carries a substantial morbidity, even if mortality is low at the centres with the larger experience. Patients with a most advanced functional deterioration show a higher surgical mortality and less impressive functional results, suggesting that LVRS should be considered more carefully in these situations. Bronchoscopic alternatives to the surgical approach have been recently proposed and some of them may play an important role in the future; in particular, the airway bypass and bronchoscopic lung volume reduction with one-way valves are certainly one step beyond on their way to clinical application. We hereby report the initial experimental and clinical experience with these new treatment options. # 2006 Published by Elsevier B.V. Keywords: Lung volume reduction; Emphysema; Bronchoscopy 1. Introduction Emphysema is a debilitating lung disease continuing to be a major source of morbidity and mortality in the developed countries. Estimates suggest that as many as two million people are affected in the United States; many of them develop severe dyspnoea and subsequent deterioration in quality of life [1—4]. Emphysema is characterized by permanent and anatomi- cally irreversible enlargement of air spaces distal to the terminal bronchiole, accompanied by destruction of their walls, and without obvious fibrosis [5]. This definition is probably the only concept about emphysema that has not been modified over the last 50 years. In fact, the clinical approach along with the therapeutic policy have been progressively changed to reach the current state. Medical treatment is the mainstay of therapy and consists of smoking cessation, pulmonary rehabilitation, administration of bronchodilators and, when indicated, steroids and supple- mental oxygen. From the functional point of view, a considerable degree of emphysema is suspected when the forced expiratory volume in 1 s (FEV 1 ) is significantly decreased, the total lung capacity (TLC) and residual volume (RV) are increased and single breath carbon monoxide diffusion capacity (DLCO) is reduced. The regional severity of emphysema within each lung or between both lungs may significantly vary; hetero- geneity refers to the regional variation of severity of emphysema throughout the parenchyma. Patients having ‘target areas’ of severe emphysema among areas of relatively mild or moderate disease are said to possess a high degree of heterogeneity. Heterogeneity may exist within the same lobe, between different lobes of the same lung or between the two lungs. When the emphysematous destruc- tion is diffused throughout the lungs with all regions similarly affected, the disease is defined homogeneous. Heterogeneity can be assessed with chest radiographs, computed tomo- graphy and lung scans [6]. Major pathophysiological consequences of this disease can be attributed to a loss of elastic recoil resulting in static and dynamic hyperinflation. The loss of elasticity results in a progressive enlargement of the lung and thoracic diameters; the rib cage expands to an abnormal position and the diaphragm becomes flattened. This results in severely impaired respiratory mechanics with consequent dyspnoea; www.elsevier.com/locate/ejcts European Journal of Cardio-thoracic Surgery 29 (2006) 281—287 * Corresponding author. Tel.: +39 06 4461971; fax: +39 06 49970735. E-mail addresses: [email protected], [email protected] (F. Venuta). 1010-7940/$ — see front matter # 2006 Published by Elsevier B.V. doi:10.1016/j.ejcts.2005.12.009
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Bronchoscopic procedures for emphysema treatment

Review
Bronchoscopic procedures for emphysema treatment
Federico Venuta *, Erino A. Rendina, Tiziano De Giacomo, Marco Anile,Daniele Diso, Claudio Andreetti, Francesco Pugliese, Giorgio F. Coloni
Universita di Roma ‘‘La Sapienza’’, Cattedra di Chirurgia Toracica, Policlinico Umberto I, V.le del Policlinico, 00100 Rome, Italy
Received 19 July 2005; received in revised form 28 November 2005; accepted 5 December 2005
Summary
Emphysema is a debilitating lung disease continuing to be a major source of morbidity and mortality in the developed countries. Medicaltreatment is the mainstay of therapy and consists of smoking cessation, pulmonary rehabilitation, administration of bronchodilators and, whenindicated, steroids and supplemental oxygen. Various surgical procedures have been promoted in the past to relieve dyspnoea and improvequality of life in patients with advanced emphysema; whilst early results were often encouraging, a sustained objective functional improvementwas rarely achieved and most of those procedures were progressively abandoned. Despite controversies, LVRS has been shown to be beneficial toselected patients with end-stage emphysema when medical therapy has failed. There is no doubt that LVRS allows a significative functionalimprovement in a selected group of patients; however, it still carries a substantial morbidity, even if mortality is low at the centres with the largerexperience. Patients with a most advanced functional deterioration show a higher surgical mortality and less impressive functional results,suggesting that LVRS should be considered more carefully in these situations. Bronchoscopic alternatives to the surgical approach have beenrecently proposed and some of them may play an important role in the future; in particular, the airway bypass and bronchoscopic lung volumereduction with one-way valves are certainly one step beyond on their way to clinical application. We hereby report the initial experimental andclinical experience with these new treatment options.# 2006 Published by Elsevier B.V.
Keywords: Lung volume reduction; Emphysema; Bronchoscopy
www.elsevier.com/locate/ejctsEuropean Journal of Cardio-thoracic Surgery 29 (2006) 281—287
1. Introduction
Emphysema is a debilitating lung disease continuing to bea major source of morbidity and mortality in the developedcountries. Estimates suggest that as many as two millionpeople are affected in the United States; many of themdevelop severe dyspnoea and subsequent deterioration inquality of life [1—4].
Emphysema is characterized by permanent and anatomi-cally irreversible enlargement of air spaces distal to theterminal bronchiole, accompanied by destruction of theirwalls, and without obvious fibrosis [5]. This definition isprobably the only concept about emphysema that has notbeen modified over the last 50 years. In fact, the clinicalapproach along with the therapeutic policy have beenprogressively changed to reach the current state. Medicaltreatment is the mainstay of therapy and consists of smokingcessation, pulmonary rehabilitation, administration ofbronchodilators and, when indicated, steroids and supple-mental oxygen.
* Corresponding author. Tel.: +39 06 4461971; fax: +39 06 49970735.E-mail addresses: [email protected], [email protected]
(F. Venuta).
1010-7940/$ — see front matter # 2006 Published by Elsevier B.V.doi:10.1016/j.ejcts.2005.12.009
From the functional point of view, a considerable degreeof emphysema is suspected when the forced expiratoryvolume in 1 s (FEV1) is significantly decreased, the total lungcapacity (TLC) and residual volume (RV) are increased andsingle breath carbon monoxide diffusion capacity (DLCO) isreduced. The regional severity of emphysema within eachlung or between both lungs may significantly vary; hetero-geneity refers to the regional variation of severity ofemphysema throughout the parenchyma. Patients having‘target areas’ of severe emphysema among areas ofrelatively mild or moderate disease are said to possess ahigh degree of heterogeneity. Heterogeneity may exist withinthe same lobe, between different lobes of the same lung orbetween the two lungs. When the emphysematous destruc-tion is diffused throughout the lungs with all regions similarlyaffected, the disease is defined homogeneous. Heterogeneitycan be assessed with chest radiographs, computed tomo-graphy and lung scans [6].
Major pathophysiological consequences of this disease canbe attributed to a loss of elastic recoil resulting in static anddynamic hyperinflation. The loss of elasticity results in aprogressive enlargement of the lung and thoracic diameters;the rib cage expands to an abnormal position and thediaphragm becomes flattened. This results in severelyimpaired respiratory mechanics with consequent dyspnoea;

F. Venuta et al. / European Journal of Cardio-thoracic Surgery 29 (2006) 281—287282
the work of breathing is markedly increased and the amountof air moved in and out of the chest with each breath is quitelimited. The main symptom for patients with severeemphysema is shortness of breath during minimal physicalactivity.
Despite all the available therapies, the course of thedisease is progressively disabling with a significant increase inmorbidity and mortality. Over the past 50 years, manyinvestigators have attempted to determine which factorsinfluence survival of patients with COPD: when the FEV1 islower than 30% of the predicted value, less than 50% ofpatients will survive for 3 years [7,8] notwithstanding optimalmedical therapy; thus, medical treatment certainly showssome limitations in the most advanced phases of the disease.
Various surgical procedures have been promoted in thepast to relieve dyspnoea and improve quality of life inpatients with advanced emphysema [9,10]; whilst earlyresults were often encouraging, a sustained objectivefunctional improvement was rarely achieved and most ofthose procedures were progressively abandoned. Bullectomyis the only operation that has stood the test of time. Lungtransplantation and lung volume reduction surgery (LVRS) arenow established treatment modalities in selected patients.
Despite controversies, LVRShas been shown tobebeneficialto selected patients with end-stage emphysemawhenmedicaltherapy has failed [11,12]. This operation was rescued andpopularized by Cooper et al. in 1995 [13] and progressivelygained worldwide acceptance. The basic principle of thisprocedure is that removal of the most diseased parts of thehyperinflated lungshelps to remodel and restore the chestwalland diaphragmatic mechanics during respiration. There is nodoubt that LVRS allows a significative functional improvementin a selected group of patients; however, it still carries asubstantial morbidity, even if mortality is low at the centreswith the larger experience [14]. Patientswith amost advancedfunctional deterioration show a higher surgical mortality andless impressive functional results, suggesting that LVRS shouldbe considered more carefully in these situations [15]. Inparticular, patients with very low FEV1 and either homo-geneous emphysema or a very low DLCO are at high risk ofdeath, and the most recently published data have indicatedthat patients with non-upper lobe disease have a higheroperative mortality.
Bronchoscopic alternatives to the surgical approach havebeen recently proposed and some of them may play animportant role in the future; in particular, the airway bypassand bronchoscopic lung volume reduction (BLVR) with one-way valves are certainly one step beyond on their way toclinical application.
2. Airway bypass
This endoscopic procedure is based on the concept of‘collateral ventilation’, first described by Van Allen et al. in1930 [16]. Collateral ventilation is defined as the ability ofgas tomove from one part of the lung to another through non-anatomical pathways. Originally, it was used the term‘collateral respiration’ to explain how gases may enter onelobule from another without resorting to known anatomicalpathways. Hogg et al. [17] demonstrated that resistance to
collateral airflow in post-mortem emphysematous humanlungs was low in comparison to normal lungs, concluding thatcollateral channels may be important ventilatory pathways inemphysema. Terry et al. [18] studied collateral ventilation innormal and emphysematous subjects. In young normalpersons they found that resistance to collateral ventilationis high at functional residual capacity and they concludedthat there was a negligible role for collateral channels in thedistribution of ventilation in these subjects. However,patients with emphysema had lower resistance throughcollateral channels than through the airways. Thus, collat-eral ventilation is present in normal lungs but it does not playan important role; in emphysematous lungs the destructionof alveolar septa creates a preferential route for collateralairflow. Gunnarsson et al. [19] looked in detail at patientswith COPD undergoing general anaesthesia; they describedsignificantly less atelectasis and shunt when compared to thepopulation with normal lungs. Three levels of collateralventilation have been described in human lungs. Kohn firstdescribed intra-alaveolar pores over a century ago [20]; in1955, Lambert [21] described accessory bronchiolar—alveo-lar connections; interbronchial channels were described byMartin in dogs, and have been subsequently verified inhumans [22]. Morrell et al. [23] discovered that segmentalcollateral ventilation occurred to a much greater extent inthe emphysematous lung than in the normal lung. Utilizingcareful dissection techniques and selective lobar intubation,Hogg et al. [17] noted complete upper/lower lobe fissures inonly three out of eight normal lungs and one of eightemphysematous lungs, with substantial flow across theincomplete fissures. Rosenberg and Lyons [24] examined 13isolated lungs from patients with various diseases, includingone patient with emphysema and pneumonia with significantcrosslobar flow; their microscopic analysis of the regionsadjacent to the fissures where interlobar collateral flow hadbeen seen demonstrated lobar/alveolar pores, potentiallyvariants of the pores of Kohn. Such interlobar flow andcommunications were not observed in paediatric lungs. It hasbeen speculated that pathologic collaterals may representinflammatory or sheer force damage between airways andthe parenchyma and serve to even out areas on inhomo-geneity [23].
Macklem [25] suggested that creating extra-anatomicpathways through the chest wall, between the surface of thelung and the skin, might alleviate hyperinflation and improverespiratory mechanics; in fact, ‘bypassing’ the smallobstructed airways should allow trapped gas to exit fromthe hyperinflated emphysematous lung. The extensivecollateral ventilation present in emphysematous lungs canbe demonstrated at the time of lung volume reductionsurgery. The portion of the lung to be removed remainsdistended after suspension of ventilation to that lung.Compression of the lung will not significantly deflate the lobebecause of the collapse of the small airways. However, a1 mm puncture on the surface of the lung will lead to rapidcollapse of the lobe because of the extensive collateralventilation from other parts of the lobe to the lobule that hasbeen punctured [26]. The procedure proposed by Macklemwas certainly a great idea; however, it could create someproblems of acceptance and management in the clinicalsetting.

F. Venuta et al. / European Journal of Cardio-thoracic Surgery 29 (2006) 281—287 283
The concept of bypassing the small obstructed airwayswas recently rescued and simplified by the group of theWashington University in St. Louis [26]. They proposed thatthe creation of artificial communications between lungparenchyma and segmental bronchi would facilitate lungdeflation and improve expiratory airflow and respiratorymechanics. In fact, on inspiration the regular airways canopen, allowing air passage through normal channels; onexpiration, the new passageways provide escape pathwaysbypassing the obstructed small airways. This procedureshould be particularly indicated for patients with a homo-geneous distribution of the disease to maximize expiratorydeflation.
The airway bypass procedure has been initially performedby bronchoscopically puncturing the wall of segmentalbronchi with a radiofrequency catheter and inserting aspecially designed stent to keep open the internal bronch-opulmonary communications. The first step to evaluate thepotential for this procedure was performed in the labora-tories of the Washington University School of Medicine in St.Louis [26]. A specially designed ventilation chamber wasprepared to evaluate the improvement obtained by creatingairway bypass in emphysematous lungs resected for lungtransplantation. Twelve lungs were closed in the chamberand connected to a pneumotachygraph to measure theairflow. The baseline FEV1 was measured and then flows weremeasured again after creation of stented passages. As aresult of this study, the FEV1 increased from an average of245 ml at baseline to 447 ml after the creation of threestented passages in each lung and to 666 ml after six stentedpassages. The experimental procedure was repeated innormal lungs harvested but not used for lung transplantation:after three stented holes the FEV1 did not differ frombaseline, confirming that the modifications in emphysema-tous lungs and probably the presence of collateral ventilationwere the base of the modifications observed in the first partof the experiment.
The improved flow rates observed in this simple ex vivomodel with emphysematous lungs were encouraging andwarranted further exploration. The second step has beendesigned to assess safety of the procedure and ability toavoid injury to the adjacent blood vessels. A speciallydesigned Doppler probe (Bronchus Technologies, Inc.,Mountain View, CA, USA) was used to map the extra-bronchial vessel distribution [27]. This probe can beintroduced through the operating channel of the flexiblebronchoscope and used to scan from the inner surface of thebronchus the bronchial and pulmonary vessels locatedoutside it. A preliminary safety study was performed inpatients undergoing lobectomy for lung cancer and lungtransplantation for emphysema. In this group of patients,after selecting the target site, the Doppler probe waswithdrawn and a radiofrequency catheter was advanced tocreate a passage through the bronchial wall into the lungparenchyma. Twenty-nine passages were performed in thelobectomy patients with only two episodes of mild bleeding,and 18 passages in patientswith emphysemaundergoing lungtransplantation. No major complications were observed.Further laboratory observations and preliminary clinicalwork (personal unpublished data) subsequently demon-strated that the new pathways progressively close within
2—3weeks after the procedure, and that stents derived fromintracoronary devices can prolong patency only for a limitedperiod of time. The radiofrequency probe has the disadvan-tage of injuring adjacent tissue because of the radial spreadof heat and of penetrating too deeply, with potentialhaemorrhage and pneumothorax. For this reason thetechnique was subsequently simplified [28]. Once theappropriate site within the airway was identified, theDoppler probe was exchanged for a 22-gauge transbronchialneedle that was advanced through the bronchial wall tocreate a small passage into the lung parenchyma. Aspirationthrough the needle was performed as it was slowly with-drawn out of the bronchial wall. An angioplasty catheterwith an expandable balloon diameter of 2.5 mm and a lengthof 30 mm was then inserted into the fenestration anddilated. A 3 mm long � 3 mm wide balloon expandablestainless steel stent covered with a sleeve of silicone rubberwas placed into the dilated passage. To avoid, or at leastdelay obstruction by granulation tissue, mitomycin C(concentration 1 mg/ml) was delivered over the stent. Thisis an anti-inflammatory and antifibrotic agent that has beenreported to be useful in the treatment of airway stenosis[29]. Four episodes of minor and brief bleeding occurredduring stent placement. These were treated with dilutedtopical epinephrine solution and resolved without incident.Also, one pneumothorax and one episode of leucopoeniadeveloped. Control stents, without drug application, wereall occluded at the first week bronchoscopic follow-up. Incontrast, mitomycin C-treated stents had a prolongation ofpatency, and the duration of stent patency was alsoassociated with the number of once-weekly topical mito-mycin application, reaching 20 weeks for dogs treated for 9weeks with topical application of the drug.
A combined needle-and-balloon device has subsequentlybeen developed to overcome the disadvantages encounteredwith the separate needle and balloon devices used in thisstudy. To further improve patency avoiding multiple druginstillations within the airway a drug eluting stent has beenproposed and experimented in an animal model. Onehundred and seven controlled release Paclitaxel stents havebeen implanted in dogs and compared with 50 control stentswith no impregnation; the follow-up at 12 weeks demon-strated that 65% of the Paclitaxel stents were patent while nocontrol stent was patent [30].
The experimental studies previously reported [27,28]demonstrate that the creation of bronchial fenestration isfeasible and safe in normal and severely emphysematouslungs. However, this information will certainly require pilotclinical studies and trials to be confirmed. The functionalimprovement probably can last only until the new passage-ways stay open; the use of anti-inflammatory, antifibrotic orantiblastic agents topically instilled or stent-eluted maysignificantly contribute to prolong patency; this willprobably bring this procedure in the clinical arena aftertesting in multicentre trials which are not yet available inthe international literature. However, based on thephysiological principles on which the procedure is based(the need of a wide collateral ventilation), we can postulatethat in the future the best indication for airway bypassshould be homogeneous emphysema with chronic respira-tory failure.
F. Venuta et al. / European Journal of Cardio-thoracic Surgery 29 (2006) 281—287284
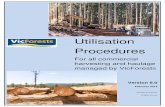
Fig. 1. First-generation endobronchial valve (EBV) designed to both controland redirect airflow.
3. Bronchoscopic lung volume reduction withone-way valves
The airway bypass is not the only endoscopic procedureproposed to improve symptoms and quality of life in patientswith emphysema. Other procedures have been describedboth experimentally and in selected clinical settings with theuse of occlusive stents, synthetic sealants and unidirectionalvalves [31—35]. These procedures were all designed toreduce hyperinflation and obtain atelectasis of the mostdestroyed functionless parts of the emphysematous lungs(heterogeneous emphysema). They have been evaluated tofind safe alternatives to LVRS, especially for patients with themost advanced disease; this group of patients, as mentionedbefore, showed a higher surgical mortality suggesting thatLVRS may not be suitable for all of them.
It has been postulated that blocking an airway supplyingthe most over-inflated emphysematous parts of the lungcould cause atelectasis of these regions and contribute toalleviate symptoms. This has been experimentally demon-strated by Ingenito et al. in 2001 [35]. They studied threegroups of sheep with papaine-induced emphysema andcompared the effectiveness of surgical lung volume reduc-tion, bronchoscopic lung volume reduction performed byoccluding lung segments with a synthetic sealant and a shamprocedure that was a simple bronchoscopy. The results of thisexperimental work showed that with this model, broncho-scopic lung volume reduction could produce the samefunctional results as LVRS.
Instead of sealants, other authors have used endobron-chial devices working as one-way valves. These devices allowair to exit from the lung parenchyma but not to enter andshould also allow a sufficient clearance of bronchialsecretions.
There are basically two devices under clinical evaluation:the Spiration umbrella and the Emphasys one-way valve(Fig. 1). These devices are placed in the segmental orsubsegmental bronchi to obtain lobar exclusion. The goal ofthe procedure is deflation of the target area in patients withheterogeneous emphysema, mimicking surgical lung volumereduction.
The Umbrella Implantable Intrabronchial Valve (IBVIM)(Spiration, Inc., Redmond, WA, USA) is a one-way valvedesigned for placement in the bronchi via flexible broncho-scopy. The valve is made of nitinol (nickel—titanium)framework with five anchors that seat distally, engagingthe airway without perforation, and providing stability. Theproximal portion is made up of six support stents that expandradially. These struts are covered by a synthetic polymer,forming an umbrella shape that conforms to the airway wall.The flexible membrane and struts allow conformation to theairways to improve sealing with minimal pressure on themucosa. The valve is designed to limit airflow distally, but themembrane and support stents allow mucociliary clearance,air and mucous to flow proximally past the valve in order toallow decompression of collateral ventilation and to reducethe hazards of mucous impaction and obstruction pneumo-nia. The valve design includes a proximal centre rod thatallows repositioning or removal if required. This device iscurrently under evaluation in a North American multicentretrial, but yet no clinical data are available in the literature.
The Emphasys endobronchial valve (EBV) (Emphasys,Redwood City, CA, USA) is an endobronchial prosthesisdesigned to control and redirect airflow. It is a one-way,polymer, duckbill valve that is mounted inside a stainlesssteel cylinder which is attached to a nickel—titanium (nitinol)self-expanding retainer. It prevents air entering the targetlung but allows air and mucous to exit. The EBV is provided inthree sizes, each intended for a different range of targetbronchial lumen diameters: 4.0—5.5 mm (inner—outer dia-meter), 5.0—7.0 mm and 6.5—8.5 mm; the valve is 10 mmlong. These valves are usually placed in the operating room,with the patient intubated under intravenous anaesthesia(Propofol infusion) and spontaneous assisted ventilation.After the patient is intubated, the flexible bronchoscope isadvanced into the endotracheal tube and the target bronchiaare chosen. They correspond to the most hyperinflated partof the lung affected by heterogeneous emphysema. Thevalves are usually placed in the segmental bronchi, butsubsegmental orifices can also be stented to obtain completelobar occlusion. A guide wire is inserted through theoperating channel of the bronchoscope and left in placewhile the bronchoscope is withdrawn; a flexible deliverycatheter is guided to the target bronchus by the guide wire.Local anaesthesia is generously administered before insertingthe valves to prevent coughing. The fiberoptic bronchoscopeis reinserted after the advancement of the delivery catheter;the tip of the delivery catheter containing the valve is pushedwith a gentle rotation in the selected bronchial orifice, andthe valve is delivered. Fiberoptic bronchoscopy performed

F. Venuta et al. / European Journal of Cardio-thoracic Surgery 29 (2006) 281—287 285
Fig. 2. Zephyr new-generation endobronchial valve.
after removal of the delivery catheter confirms the correctplacement of the valve. Gentle suction through thebronchoscope ensures the correct opening of the valve toallow deflation of the lung and clearance of secretions. Thevalves can be removed easily if placement is not satisfactoryusing a rat-tooth grasper through the working channel of thebronchoscope. The EBV can be clearly seen at chest X-ray.
The first generation of EBV have been extensivelyemployed in several prospective, non-randomized, singlecentre longitudinal pilot studies to evaluate safety andshort-term efficacy with promising results in a selectedgroup of patients with heterogeneous end-stage emphysema(Table 1).
A new generation of EBV is ready and is currently underevaluation in a multicentre prospective trial: the Zephyrendobronchial valve (Fig. 2). This new valve is a deviceincorporating a one-way valve supported by a stent-like self-expanding retainer that secures the EBV in place during allphysiological conditions, including coughing. The retainer is aself-expanding tubular mesh structure that is cut from nitinol(nickel—titanium) superelastic alloy tubing and processed toits final expanded dimensions. It is covered with silicone inorder to create a seal between the implant and the bronchial
Table 1Worldwide experience with bronchoscopic lung volume reduction
Authors
Yim et al. [39] Toma et al.
No. pts 21 8Valves/pts 4 3
FEV1 pre (l) 0.73 0.79FEV1 1 month (l) 0.84 1.06p value ns 0.028
RV pre (l) 4.98 6.82RV 1 month (l) 4.85 NAp value ns NA
TLC pre (l) 7.03 NATLC 1 month (l) 6.5 NAp value ns NA
DLCO pre 8.00 3.05DLCO 1 month 9.18 3.92p value ns 0.01
FVC pre (l) 1.94 NAFVC 1 month (l) 2.12 NAp value ns NA
6MWT pre (m) 251.6 NA6MWT post (m) 306.3 NAp value 0.01 ns
FEV1: forced expiratory volume in 1 s; RV: residual volume; TLC: total lung capacity; D6-min walking test. NA: not available; ns: not statistically significative; No. pts: nu
wall; the silicone membrane is formed integrally with thestruts of the self-expanding retainer component. When theEBV is delivered into the target bronchus, the retainerexpands to contact the walls of the lumen. Also, this valvehas been designed to allow air to be vented from the isolatedlung segment while preventing air from refilling the isolatedlung area during inspiration: it vents during expiration andcloses when flow is reversed during inhalation. The ZephyrEBV is provided in two sizes: the EBV 4.0, designed forbronchial lumens with diameters of 4.0—7.0 mm, and theZephyr EBV 5.5, designed for bronchial lumens withdiameters of 5.5—8.5 mm. The previous version of thedevice, as mentioned before, was provided in three differentsizes for the same overall treatable lumen diameter rangeof 4.0—8.5 mm. The Zephyr valve can be easily seen at chestX-ray (Fig. 3).
The performance of the valve is different according to thetype of valve (first generation vs second generation of EBV),and to the size of the device itself. In other words, thecracking pressure, and thus flow resistance, was higher forthe EBV of the first generation when compared to the Zephyrvalve. On the other side, within the two different models ofvalves, flow resistance is lower for valves of the largerdiameter. In other words, air expiratory flow is much higherfor large valves of the second generation.
A flexible delivery catheter is used also to place thissecond-generation EBV valve to the targeted bronchiallumen. The catheter is constructed of a flexible stainlesssteel and polymer composite shaft. It has an actuation handleon the proximal hand and a retractable polymer housing forcontaining the compressed Zephyr EBV on the distal end. Abronchial diameter measurement gauge made of flexiblepolymer is attached to the proximal end of the distal housing.
[37] Venuta et al. [40] Snell et al. [36]
13 104 6.7
0.75 0.721.1 0.740.01 ns
5.3 4.24.8 4.20.01 ns
7.9 6.817.1 6.720.04 ns
33% 7.4745% 8.260.01 0.04
1.86 2.332.3 2.34ns ns
223 340375 3460.005 ns
LCO: carbon monoxide diffusion in the lung; FVC: forced vital capacity; 6MWT:mber of patients; valves/pts: mean number of valves per patients.

F. Venuta et al. / European Journal of Cardio-thoracic Surgery 29 (2006) 281—287286
Fig. 3. Chest X-ray showing the Zephyr EBV in place in the right upper lobe.
This measurement gauge allows the user to visually(bronchoscopically) measure the diameter of the bronchiallumen prior to device deployment to verify that the sizegauge of the valve is appropriate for the target lumen. Themeasurement gauge consists of two sets of flexible gauges.On the delivery catheter for the Zephyr EBV 4.0, the largergauge spans a 7 mm diameter and the smaller gauge spans a4 mm diameter, indicating the maximum and minimumtreatable bronchial diameters, respectively, for this size ofdevice. On the delivery catheter for the Zephyr EBV 5.5, thetwo gauges are sized to span diameters of 8.5 and 5.5 mm.The EBV is compressed into the retractable distal housing bythe operator using a specifically designed EBV loader system.The loaded catheter is advanced to the target location andthe valve is deployed by actuating the deployment handle,which retracts the distal housing and releases the EBV. Thedelivery catheter is designed to be inserted through a 2.8 mmdiameter working channel of a flexible bronchoscope. Thus,this new generation of valves can be placed under localanaesthesia since the deployment manoeuvre is muchsimpler.
After a series of animal experiments, more than 100patients have been treated so far in pilot studies performedat several centres worldwide, with selection criteria similarto those for LVRS (Table 1). The inclusion criteria in thesepilot studies were similar to those for surgical lung volumereduction: heterogeneous emphysema, FEV1 less than 30%,DLCO higher than 20%, no pulmonary hypertension, nohypercapnia. Heterogeneous emphysema was chosen sincethis type of disease shows less collateral ventilation than thehomogeneous one; thus, it should be easier to achievevolume reduction and even atelectasis. The first 10 patientstreated with a first-generation type of EBV were reported bySnell et al. [36]. They demonstrated that that type ofbronchoscopic prosthesis could be safely and reliably placedinto the human bronchi; however, symptomatic improvement
was observed only in four patients, with no major change inradiographic findings, lung function, or 6-min walk distanceat 1 month, although gas transfer improved from 7.47 �2.0 ml/(min mmHg) to 8.26 � 2.6 ml/(min mmHg) andnuclear upper lobe perfusion fell from 32 � 10% to27 � 9%. Toma et al. [37] subsequently reported on eightpatients undergoing unilateral volume reduction with asecond generation of EBV. Five patients had emphysemajudged too severe for volume reduction surgery and threerefused the operation. After valve placement there was a 34%increase in FEV1 and 29% difference in DLCO; CTscans showeda substantial reduction in regional volume in four of the eightpatients. The same group also reported that in a subgroup ofpatients in whom invasive measurements were performed,improvement in exercise capacity was associated with areduction of lung compliance and isotime oesophagealpressure—time product [38]. Other two series of patientstreated with EBV have been reported [39,40] with encoura-ging functional results. Along with the functional improve-ment (Table 1) there was also a subjective improvementbenefit reported by most of the patients, even if a dyspnoeascore was not available in all the series. Overall, all patientstolerated the treatment well. Between three and five valveswere placed in the target lobe and most of them receivedunilateral treatment. It has been demonstrated that theprocedure can be safely performed with encouraging short-term results. Up to now the data available for this techniqueare still extremely limited and the follow-up is too short to becompared with other therapies.
In our experience [40] with the first generation of EBVvalves, we have observed one contralateral and two bilateralpneumothorax out of 17 treatments (two-staged bilateral);this complication has been experienced also by other authors[39]. However, with the second generation of EBV valves (fivepatients, unpublished data) we have not observed thiscomplication any more. Three of our patients showedgranulation tissue obstructing one or more of the valves;this complication occurred with the first-generation valves 6months after placement. One patient had pneumonia in thenon-treated lobe; this complication was easily managed withthe administration of broad-spectrum antibiotics. Thefunctional improvement was statistically significant; inparticular FEV1 markedly improved and the residual volumedecreased: at 3 months more than 50% of the patients stillshow at least a 30% functional improvement; most of themrequired less supplemental oxygen and 7 out of 15 were ableto stop it. Wewere not able to observe a complete atelectasisof the lobe where valves where implanted, even if it has beendescribed by other authors; however, in most of the patients,the shape of the chest was redesigned. Exercise tolerancewas also improved and remained stable after 3 months offollow up. Contralateral BLVR could be attempted to obtain asecond functional improvement when pulmonary functiontests start to deteriorate again, as it is done for LVRS [41]. Acontralateral BLVR was performed in two of our patients, butneither was required for functional reasons: both patientshad pneumothorax on the contralateral side and valves wereplaced with the aim of stopping the air leak; this result waseasily obtained, along with further functional improvement.With more experience, simultaneous bilateral insertion ofthe valves could be attempted. One of the advantages of the

F. Venuta et al. / European Journal of Cardio-thoracic Surgery 29 (2006) 281—287 287
endobronchial lung volume reduction is that the procedurecan be reversed and other treatments tried if necessary.
The short-term results with BLVR are encouraging, butlong-term follow-up is certainly required, as well as multi-centre trials, to evaluate the therapeutic potential of thisprocedure. Even if it is certainly too early to speculate aboutthe potential clinical implications of these new techniques,we can postulate that airway bypass could be indicated forpatients with homogeneous emphysema while BLVR withone-way valves should be indicated for patients with anheterogeneous distribution of the disease. However, it couldbe more likely that in the future both systems could beemployed in each patients to optimize results.
References
[1] Feinleib M, Rosenberg H, Collins J, Delozier JE, Pokras R, Chevarley FM.Trends in COPD morbidity and mortality in the United States. Am RevRespir Dis 1989;140(Suppl.):S9—18.
[2] Guyatt G. Measuring health status in chronic airflow limitation. Eur RespirJ 1988;1:560—4.
[3] Higgins M, Keller J. Trends in COPD morbidity and mortality in Tecumseh,Michigan. Am Rev Respir Dis 1989;140(Suppl.):S42—8.
[4] McSweeney A, Grant I, Heaton R, Adams KM, Timmes RM. Life quality ofpatients with chronic obstructive pulmonary disease. Arch Intern Med1982;142:473—8.
[5] Russi EW, De Wever W, Decramer M. Surgery for emphysema: medicalaspects. In: Verleden GM, Van Raemdonck D, Leryt T, Demedts M, editors.Surgery for non neoplastic disorders of the chest a clinical updateEuropean Respiratory Society monograph 29, vol. 9. 2004. p. 129—38.
[6] Stone RM, Gierada DS. Radiology of pulmonary emphysema and lungvolume reduction surgery. Semin Thorac Cardiovasc Surg 1996;8:61—82.
[7] Anthonisen NR, Wright EC, Hodgkin JE, IPPB Trial Group. Prognosis inchronic obstructive pulmonary disease. Am Rev Respir Dis 1986;133:14—20.
[8] Ries AL, Kaplan RM, Limberg TM, Prewitt L. Effects of pulmonary reha-bilitation on physiologic and psychosocial outcomes in patients withchronic obstructive pulmonary disease. Ann Intern Med 1995;122:823—32.
[9] Cooper JD. The history of surgical procedures for emphysema. Ann ThoracSurg 1997;63:312—9.
[10] Deslauriers J. History of surgery for emphysema. Semin Thorac Cardio-vasc Surg 1996;8:43—51.
[11] Yusen RD, Lefrak SS, Gierada DS, Davis GE, Meyers BF, Patterson GA,Cooper JD. A prospective evaluation of lung volume reduction surgery in200 consecutive patients. Chest 2003;123:1026—37.
[12] Ciccone AM, Meyers BF, Guthrie TJ, Davis GE, Yunes RD, Lefrak SS,Patterson GA, Cooper JD. Long term outcome of bilateral lung volumereduction in 250 consecutive patients with emphysema. J Thorac Cardi-ovasc Surg 2003;125:513—25.
[13] Cooper JD, Trulock EP, Triantafillou AN, Patterson GA, Pohl MS, DeloneyPA, Sundaresan RS, Roper CL. Bilateral pneumectomy (volume reduction)for chronic obstructive pulmonary disease. J Thorac Cardiovasc Surg1995;109:106—19.
[14] Fishman A, Martinez F, Naunheim K, Piantadosi S, Wise R, Ries A,WinmannG, Wood DE, National Emphysema Treatment Trial Research Group. Arandomized trial comparing lung volume reduction surgery with medicaltherapy for emphysema. N Engl J Med 2003;348:2059—73.
[15] National Emphysema Treatment Trial Research Group. Patients at highrisk of death after lung volume reduction surgery. N Engl J Med 2001;345:1075—83.
[16] Van Allen CM, Lindskog GE, Richter HT. Gaseous interchange betweenadjacent lung lobules. Yale J Biol Med 1930;2:297—300.
[17] Hogg JC, Macklem PT, Thurlbeck WM. The resistance of collateral chan-nels in excised human lungs. J Clin Invest 1969;48:421—31.
[18] Terry PB, Traystman RJ, Newball HH, Batra G, Menkes HA. Collateralventilation in man. N Engl J Med 1978;298:10—5.
[19] Gunnarsson L, Tokics L, Lundquist H, Brismar B, Strandberg A, Berg B,Hedenstierna G. Chronic obstructive pulmonary disease and anaesthesia:formation of atelectasis and gas exchange impairment. Eur Respir J1991;4:1106—16.
[20] Cordingley JL. Pores of Kohn. Thorax 1972; 27:433—41.[21] Lambert MW. Accessory bronchoalveolar communications. J Pathol Bac-
teriol 1955;70:311—4.[22] Mitzner W. Collateral ventilation. In: Crystal RG, editor. The lung:
scientific foundations. New York, NY: Raven Press; 1991. p. 1053—63.[23] Morrell NW, Wignall BK, Biggs T, Seed WA. Collateral ventilation and gas
exchange in emphysema. Am J Respir Crit Care Med 1994;150:635—41.[24] Rosenberg DF, Lyons HA. Collateral ventilation in excised human lungs.
Respiration 1979;37:125—34.[25] Macklem PT. Collateral ventilation. N Engl J Med 1978;298:49—50.[26] Lausberg HF, Chino K, Patterson GA, Meyers BM, Toeniskoetter PD, Cooper
JD. Bronchial fenestration improves expiratory flow in emphysematoushuman lungs. Ann Thorac Surg 2003;75:393—8.
[27] Rendina EA, De Giacomo T, Venuta F, Coloni GF, Meyers BF, Patterson GA,Cooper JD. Feasibility and safety of the airway bypass procedure forpatients with emphysema. J Thorac Cardiovasc Surg 2003;125:1294—9.
[28] Choong CK, Haddad FJ, Gee EJ, Cooper JD. Feasibility and safety ofairway bypass stent placement and influence of topical mitomycin C onstent patency. J Thorac Cardiovasc Surg 2005;129:632—8.
[29] Correa AJ, Reinisch L, Sanders DL, Huang S, Deriso W, Dunacavage JA,Garrett CG. Inhibition of subglottic stenosis with mitomycin C in a caninemodel. Ann Otol Rhinol Laryngol 1999;108:1053—60.
[30] Choong CK, Phan L, Massetti P, Haddad FJ, Roschak EJ, Cooper JD. Patencyof airway bypass stents is prolonged with use of drug eluting stents.American Association for Thoracic Surgery 85th Annual Meeting, April 10—13, 2005, San Francisco, CA. Paper F20, p. 160.
[31] Snell GI, Smith GA, Silovers AJ. Bronchoscopic volume reduction: a pilotstudy. ACCP Meeting 2001; Paper 25.
[32] Ingenito EP, Berger RJ, Henderson AC, Reilly JJ, Tsai L, Hoffman A.Bronchoscopic volume reduction using tissue engineering principles.Am J Respir Crit Care Med 2003;167:771—8.
[33] Sabanhatan S, Richardson J, Pieri-Davies S. Bronchoscopic lung volumereduction. J Cardiovasc Surg 2003;44:101—8.
[34] Fann JI, Berry GJ, Burden TA. Bronchoscopic approach to lung volumereduction using a valve device. J Bronchol 2003;10:253—9.
[35] Ingenito EP, Reilly JJ, Mentzer SJ, Swanson SJ, Vin R, Keuhn H, Berger RL,Hoffman A. Bronchoscopic volume reduction: a safe and effective alter-native to surgical therapy for emphysema. Am J Respir Crit Care Med2001;164:295—301.
[36] Snell GI, Halsworth L, Borrill ZL, Thomson KR, Kalff V, Smith JA, WilliamsTJ. The potential for bronchoscopic lung volume reduction using bron-chial prosthesis: a pilot study. Chest 2001;124:1073—80.
[37] Toma TP, Hopkinson NS, Hiller J, Hansell DM, Morgan C, Goldstraw PG,POlkey MI, Geddes DM. Bronchoscopic volume reduction with valveimplants in patients with severe emphysema. Lancet 2003;361:931—3.
[38] Hopkinsons NS, Toma TP, Hansell DM, Goldstraw P, Maxham J, Geddes DM,Polkey MI. Effect of bronchoscopic lung volume reduction on dynamichyperinflation and exercise in emphysema. Am J Crit Care Med 2005;171:423—4.
[39] Yim AP, Hwong TM, Lee TW, Li WW, Lam S, Yeung TK, Hui DS, Ko FW, SihoeAD, Thung KH, Arifi AA. Early results of endoscopic lung volume reductionfor emphysema. J Thorac Cardiovasc Surg 2004;127:1564—73.
[40] Venuta F, De Giacomo T, Rendina EA, Ciccone AM, Diso D, Perrone A,Parola D, Anile M, Coloni GF. Bronchoscopic lung volume reduction withone way valves in patients with emphysema. Ann Thorac Surg 2005;79:411—7.
[41] Soon SY, Saidi G, Ong ML, Syed A, Codispoti M, Walker WS. Sequential VATSlung volume reduction surgery: prolongation of benefits derived after theinitial operation. Eur J Cardiothorac Surg 2003;24:149—53.