Board paper January 2012 - Agenda - North Bristol NHS Trust
154
Any identifiable information reported within an Agenda or Minutes will be discussed under a “Part B” section of a meeting and will be Exempt under this Act where Personal or Sensitive information is discussed. Board Meeting Thursday 26 January 2012 Board Room, Trust Headquarters, Frenchay Hospital AGENDA FOR PUBLIC SESSION 1. APOLOGIES 2. TO RECEIVE QUESTIONS FROM MEMBERS OF THE PUBLIC 3. TO RECEIVE QUESTIONS FROM LINKS REPRESENTATIVES 4. MINUTES Minutes of the Trust Board meeting held on 24 November 2011 Enc 5. MATTERS ARISING 5.1 Medication Errors Data (Minute 219/11 refers) MNO 6. GOVERNANCE, QUALITY AND SAFETY 6.1 Quality Report MNO/Enc 6.2 Safeguarding Adults MNO/Enc 6.3 Histopathology Action Plan CB/Enc 7. STRATEGY 7.1 NBT Redevelopment Project Highlight Report DP/Enc 7.2 Foundation Trust Update RB/Verbal 8. SERVICE DELIVERY AND PERFORMANCE 8.1 Cerner Update MB/Enc 8.2 Management Information Reports 8.2.1 Activity and Performance SWa/Enc 8.2.2 Emergency Access Performance SWa/Enc 8.2.3 Workforce Strategy & Organisation Development HH/Enc 8.2.4 Infection Control Report CB/Enc 8.2.5 Finance Report SWe/Enc 9. COMMUNICATIONS 9.1 Chairman’s Report PR/Verbal 9.2 Chief Executive’s Report RB/Verbal P.T.O. This Agenda and Minutes may be made available through the Freedom of Information Act 2000, Publication Scheme.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Board paper January 2012 - Agenda - North Bristol NHS Trust

Any identifiable information reported within an Agenda or Minutes will be discussed under a “Part B” section of a meeting and will be Exempt under this Act where Personal or Sensitive information is discussed.
Board Meeting
Thursday 26 January 2012 Board Room, Trust Headquarters, Frenchay Hospital
AGENDA FOR PUBLIC SESSION
1. APOLOGIES 2. TO RECEIVE QUESTIONS FROM MEMBERS OF THE PUBLIC 3. TO RECEIVE QUESTIONS FROM LINKS REPRESENTATIVES 4. MINUTES Minutes of the Trust Board meeting held on 24 November 2011 Enc 5. MATTERS ARISING 5.1 Medication Errors Data (Minute 219/11 refers) MNO 6. GOVERNANCE, QUALITY AND SAFETY 6.1 Quality Report MNO/Enc
6.2 Safeguarding Adults MNO/Enc 6.3 Histopathology Action Plan CB/Enc
7. STRATEGY 7.1 NBT Redevelopment Project Highlight Report DP/Enc 7.2 Foundation Trust Update RB/Verbal 8. SERVICE DELIVERY AND PERFORMANCE 8.1 Cerner Update MB/Enc
8.2 Management Information Reports 8.2.1 Activity and Performance SWa/Enc 8.2.2 Emergency Access Performance SWa/Enc 8.2.3 Workforce Strategy & Organisation Development HH/Enc 8.2.4 Infection Control Report CB/Enc 8.2.5 Finance Report SWe/Enc 9. COMMUNICATIONS 9.1 Chairman’s Report PR/Verbal 9.2 Chief Executive’s Report RB/Verbal
P.T.O.
This Agenda and Minutes may be made available through the Freedom of Information Act 2000, Publication Scheme.

This Agenda and Minutes may be made available through the Freedom of Information Act 2000, Publication Scheme.
Any identifiable information reported within an Agenda or Minutes will be discussed under a “Part B” section of a meeting and will be Exempt under this Act where Personal or Sensitive information is discussed.
10. INFORMATION
10.1 Trust Board Forward Plan RB/Enc 10.2 Building our Future Programme – Executive Summary HH/Enc
10.3 Research & Innovation Strategy Status Report 2011-12 Quarter 3 HH/Enc 10.4 GRMC Report RB/Enc 10.5 Declarations of Interest 2011-12 MB/Enc 11. ANY OTHER BUSINESS 12. NEXT MEETING The next meeting will be held on Thursday 23 February 2012 in the Board Room,
Trust Headquarters, Frenchay Hospital.
13. RESOLUTION
That representatives of the press and other members of the public be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest (section (2) Public Bodies (Admission to Meetings) Act 1960)

North Bristol NHS Trust Minutes of the North Bristol NHS Trust meeting held on 24 November 2011
Present: Mr P Rilett (Chair) Mr M Bell Ms M-N Orzel Mrs R Brunt Mr N Patel Dr C Burton Mr D Powell Mr K Guy Mrs S Watkinson Mr H Hayer Prof A Waterman-Pearson Mr S Hughes Mr S Webster Mr R Mould Mr S Wood Observers: Ms L Baber, PWC Ms G Maw, LINkS Mr J Britton Mr R Storer, Deloittes Mr R Farrow, NBT Mr I White, Deloittes Ms V Mathias, BEP In Attendance: Mr N Baker Ms S Lewis Mr M Lawton Apologies: Mr S Webster
ACTION 215/11 QUESTIONS FROM THE PUBLIC There were no questions from the public. 216/11 QUESTIONS FROM LINKS Ms Maw enquired about difficulties in getting patient pathology
results from multidisciplinary teams. Dr Burton stated that this had been monitored closely and waits longer than 2 weeks had been significantly reduced. Ms Maw cited the case of one patient who had to wait 2 weeks and did not know who to speak to. Dr Burton asked for more information on this so he could investigate it.
217/11 MINUTES The minutes of the meeting held on 27 October 2011 were
approved as a correct record.
1

ACTION 218/11 MATTERS ARISING (i) Research Strategy 2012-2016
(Minutes 176/11 and 191/11 refer)
It was noted that the Strategy had previously been received by the
Board in draft format and the final version had been approved by TMT with very few changes. Mr Hayer would supply a list of these to Professor Waterman-Pearson. Mrs Brunt had attended a BRIG-H workshop earlier in the week and a paper on AHSC would be brought to the Board in February.
HH RB
(ii) Cancer Peer Review – Other Hospitals’ Results
(Minute 196/11 refers)
Dr Burton reported that NBT was broadly in line with the national
reporting of MDTs and was second in line only to Taunton in the South West for the new reporting measures.
(iii) Peer Review on Dementia Feedback (Minute 209/11 refers) The visit to both sites had provided positive feedback, especially
the fact that a Non-Executive Director had been involved. The key message was to maintain momentum and this would be monitored by the Board.
(iv) Industrial Action – 30 November 2011 – Update Mr Hayer reported that 6 out of 8 unions had confirmed strike
action and picket lines were expected at all entrances of both hospitals which could slow traffic down. A Q&A briefing had gone to all staff. The strike would run from midnight to midnight, and NBTXtra would be extending its opening hours. Outpatient and elective lists had been revised to reduce activity on the day, and there would be an impact on staff due to closure of schools etc. Liaison with the ambulance service and essential services would be maintained. Staff had been asked to volunteer to help out if necessary. Both restaurants would close but the nursery would remain open. A central control unit would be set up and communications given to the public. The Board were assured that the Trust was prepared for any ice and snow which had been forecast for that day.
219/11 QUALITY REPORT Mr Mould commented that the decrease in the number of falls was
positive. It was clarified that the total number of cardiac arrest calls were included. These will include those that may be false alarms and/or those that occur outside of the ward or department areas. It
2

ACTION was noted that although there had been a recent rise in the number of cardiac arrest calls this was still below the national average. The missing data for medication errors would be clarified.
MNO
220/11 AUDIT COMMITTEE REPORT It was agreed that the Terms of Reference should take account of
the Finance Committee recommendation from Deloittes. MB
221/11 CQC REPORT ON GENERAL COMPLIANCE AT SOUTHMEAD The Trust had been found to be fully compliant overall, with a few
areas of minor concern noted. Comments on being short staffed were not backed up by any evidence of impact on patient care. In answer to a query, Ms Orzel confirmed that a role for volunteers would be developed to support dementia patients in hospital. It was noted that those patients at potential risk would be recorded on Cerner when patients were admitted and this would be taken into consideration.
222/11 EQUALITY OBJECTIVES These had been requested at the last meeting and were noted. Mr
Powell queried how achievement of the objectives would be gauged. It was agreed that the 2011/12 Equality Annual Report would measure progress against these objectives.
223/11 NBT REDEVELOPMENT PROJECT HIGHLIGHT REPORT Mr Powell reported that the project was on programme and work
was being undertaken on the internal part of the building. NHS Supplies had changed their trolleys so that they would fit the robots. The fitting out would now be closely monitored. There would be liaison with the PCT regarding provision of community hospital beds in the PFI.
DP
224/11 FT STATUS REPORT Mrs Brunt reported that the Private Board had discussed the
outcome of the consultation, which had 2500 responses. As a result, the membership age would remain at 16 but the minimum age for a Governor would be raised to 18. 2 additional Governors would be appointed, from North Somerset Council and UWE, making a total of 23. A further 2 elected public Governors would therefore also be needed. The results would be widely publicised in a leaflet.
3

ACTION Specific issues relating to young people and children’s services would be addressed by setting up a Youth Council. Governor elections would take place in summer 2012 following approval from the Department of Health.
225/11 WORKFORCE & OD STRATEGY 2012-2017 Mr Hayer reported that this had been approved by TMT and
directorates would actively use it as a framework for the approach to workforce and organisation development. It was agreed that a five year operational framework was needed, with a timetable. This would come to the February Board. There may be some minor changes to the Strategy after discussion with the staff side and the Board agreed this could be signed off in December following Executive approval.
HH HH
226/11 PATHOLOGY INTEGRATION PROJECT Mrs Brunt reported that a different project structure would be in
place for the next phase of this work. Some resource would come from the Healthy Futures Programme Board. There would be a single Executive lead and a full time Project Director. The Board approved all the recommendations on P.11 of the report. The first draft of the detailed business case would be brought to the February Board. Mrs Brunt and Dr Burton were meeting with pathology staff in all 4 organisations to discuss the changes.
CB
227/11 ACTIVITY AND PERFORMANCE REPORT Mrs Watkinson explained that reporting on Frenchay and
Southmead was now separate, and Yate would be coming on line. She confirmed that Ward 12 had opened on 1 November and Ward 106 had become a 28 bedded medical ward. She highlighted an error under the cancer figure, which should state that 3 of the targets had been maintained, not 2.
228/11 WORKFORCE STRATEGY & ORGANISATION DEVELOPMENT The report was noted. There was a table missing on page 3 of the
report relating to e-learning and this would be included in the next report. The uptake of flu vaccinations had been good this year. The question of whether DNAs in Occupational Health should be
HH
4

ACTION charged for was raised, and information would be included in the next report.
HH
229/11 INFECTION CONTROL REPORT MRSA and C Diff numbers had reduced from the last quarter and
there was a generally improved position on infection control. It was noted that MSSA was much more common than MRSA and numbers had reduced in the Trust this year. Measurement of MRSA non-elective screening was sometimes complicated, providing some explanation for why the target had not been achieved, but there had been improvement through the year.
230/11 FINANCE REPORT Mr Webster reported that the year end figures were still on track.
The likely cost of the strike was still approximate. Non-pay analysis had been undertaken over the previous three months to try and understand the overspend. Mrs Brunt and Mr Webster met monthly with the most challenged directorates and had specifically looked at some of the detail behind this.
231/11 CHAIRMAN’S REPORT Professor Ian Cumming had been appointed as CEO of NBT on 11
November 2011 and would begin to spend time at the Trust ahead of his commencement in April. There had been significant involvement from the organisation with this recruitment and it had been a well run process.
232/11 CHIEF EXECUTIVE’S REPORT The Director of Operations post was currently being recruited and
Professor Cumming would be on the interview the following week, with four candidates attending. The Operating Plan for the new hospital was being discussed with specialties and they had drawn up pathways to present to Dragons’ Dens, which included GPs. There was confidence that this would define how our patients would receive care and treatment in the future. The Board would be kept updated. There had been no consultant appointments since the last Board but two interview panels were soon to be held.
233/11 BUILDING OUR FUTURE EXECUTIVE SUMMARY The report was noted.
5

6
ACTION 234/11 G&RMC REPORT The report was noted. The Trust had passed Level 2 of CNST and
LARMS the previous week and the standard had increased since the last inspection. Level 3 could not be achieved for at least another year.
235/11 ANY OTHER BUSINESS Mr Wood reported that the Trust had won a Green Apple award for
sustainability. He and two members of the Environmental Management Unit had gone to the Houses of Parliament to receive it. This ‘NHS Champion’ award was one of the two top awards given that day recognising NBT’s efforts and improvements across waste management, and the Treading Lightly Campaign.
236/11 NEXT MEETING The next meeting would be held on Thursday 26 January 2012 in
the Board Room, Trust Headquarters, Frenchay Hospital.
RESOLUTION That representatives of the press and other members of the public
be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to other public interest (section (2) Public Bodies (Admission to Meetings) Act 1960.

This document may be made available via the Freedom of Information Act 2000. Any identifiable information reported within this document to be discussed under a ‘Part B’ section of the meeting and is Exempt under the FOI Act 2000, where personal/sensitive information is discussed.
1
Report to the Trust Board – January 2012
Title: Quality Report to Board Purpose of paper: To inform the Board on progress with measures of the quality of
clinical services provided by the Trust and progress with priorities set out in the Trust’s Quality Account.
For Information
Executive Summary: HSMR rate continues to be below the national average of 100 with a rolling mean of 88.1 using the Dr Fosters age adjusted casemix. Work continues on the Trust priorities for improvement as set out in the Quality Account and CQUINs; Preventing deterioration – There were 18 calls in November - a decrease of 27 from the previous month. The rolling (12 month mean) is 1.74 per 1000 discharges. This remains well below the national average of 2.5. Patient Safety Days have been organised in March 2012 to launch the Deteriorating Patient Ward Change Package. The aim is to reduce the number of cardiac arrests within ward areas by an overall target of 30% from 2010/11 baseline figures within 1 year. Falls –There have been five Grade 3 and one grade 4 falls in November - an increase of 5 since last month. In December there were four grade 3 falls, a decrease of 2, with no Grade 4’s. The CQUIN measure requires a reduction in overall falls by Qtr 4 - a 10% reduction would require no more than 152 falls per month for Jan-March 2012. On the current trajectory it is not likely to achieve the reduction required by year end Pressure Ulcers – There were no grade 3 or 4 pressure ulcers for November. Overall incidence for November has increased from 14.1 to 17.6 patients per 10,000 bed days, with a total of 51 patients reported with Grade 2 pressure ulcers. All directorates have seen an increase in the number of ulcers reported. Wards with high incidence now have a daily review by Tissue Viability Nurse. Provision of pressure relieving equipment including seating and protective footwear has increased. A mandatory patient safety event is being held in March for all Senior Nurses within the Trust, Pressure Ulcer Prevention will be a key component of this. NQAT scores – Over 87% of wards audited are achieving either silver or gold score with patients giving their experience a score over 97%. Work is commencing in February to review NQAT over the last 12 months and to review weighting of questions used, to ‘raise the bar’ on standards required. Nutrition - The number of wards rated silver or gold in November for nutritional element of NQAT audits is 74% an increase of 3% from October. The target for 90% of wards to be rated as silver or gold by year end is on track to be achieved - extra support is being provided to target those wards underperforming. Trust-wide nutritional screening is currently at 71% - this is being severely impacted upon by the Cerner issues. Action Required: The Trust Board is asked to note the contents of this report. Key Risks: Non-achievement of CQUIN targets would prevent the Trust from accessing incentive payments and result in the Trust receiving financial penalties.

This document may be made available via the Freedom of Information Act 2000. Any identifiable information reported within this document to be discussed under a ‘Part B’ section of the meeting and is Exempt under the FOI Act 2000, where personal/sensitive information is discussed.
2
Impact on Patients: All measures relate to the delivery of patient care, achievement of gateways/CQUIN targets helps to build confidence in Trust service provision and assure the public/other key stakeholders that the organisation is meeting quality and safety standards. CQC Outcomes:, O16 – assessing & monitoring quality of services Responsible Committees: Quality Committee, GRMC Financial Issues considered: As indicated in regard to incentive payments/penalties Equality Impact Assessment: Equality and diversity is considered throughout Legal Issues : Legal issues are considered throughout. Sustainability Assessment Completed: No Presented by: Marie-Noelle Orzel – Director of Nursing Prepared by: Lesley Le-Pine – Head of Clinical Governance, Phil Martin – Information Analyst

North Bristol NHS Trust - Quality Indicators
Due to data quality issues related to the Cerner implementation, accurate bed day information for December is not currently available therefore the following indicators which require this as a denominator have not been updated:-Cardiac Arrest CallsPressure UlcersNutritionPatient experience and overall NQAT score
There was an improvement in November from 68% to 83% scored correctly, with a slight drop to 80% in December.
There were 18 calls in November - a decrease of 27 from the previous month. The rolling (12 month mean) is 1.74 per 1000 discharges.This remains well below the national average of 2.5
In November 9 out of 17 cases were completed correctly. In December 3 out of 12 cases reviewed were correct. Action is being taken to ensure nurses do not put up oxygen unless prescribed
In November there were - 6 cases were assessed correctly. In December there were 3 applicable cases and 3 were assessed correctly according to protocol. There is an overall shift in more cases being assessed correctly.
There were 164 falls in November, a reduction of 14 from October figures. However this increased to 180 falls in December.
There were five grade 3 (moderate) falls in Novermber with one grade 4 (serious) falls. There were four Grade 3 falls in December with no grade 4's.
0
0.5
1
1.5
2
2.5
3
3.5
01/
12/
201
0
01/
01/
201
1
01/
02/
201
1
01/
03/
201
1
01/
04/
201
1
01/
05/
201
1
01/
06/
201
1
01/
07/
201
1
01/
08/
201
1
01/
09/
201
1
01/
10/
201
1
01/
11/
201
1
Preventing Deterioration Cardiac Arrest calls Rate per 1000 discharges
0%
20%
40%
60%
80%
100%
Apr
-11
Ma
y-1
1
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
Dec
-11
Preventing Deterioration Oxygen Correctly prescribed (source NQAT)
Actual Target
0%
20%
40%
60%
80%
100%
Apr
-11
Ma
y-1
1
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
Dec
-11
Preventing Deterioration (source NQAT) EWS correctly recorded
Actual Target
0%
20%
40%
60%
80%
100%
Apr
-11
Ma
y-1
1
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
Dec
-11
Preventing Deterioration High EWS assessed to Protocol (source NQAT)
Actual Target
0
50
100
150
200
250
2011
-04
2011
-05
2011
-06
2011
-07
2011
-08
2011
-09
2011
-10
2011
-11
2011
-12
nu
mb
er o
f fa
llsTotal Falls - All severity Levels
(Target be 10% reduction in Q2 level)
0
2
4
6
8
10
12
2011
-04
2011
-05
2011
-06
2011
-07
2011
-08
2011
-09
2011
-10
2011
-11
2011
-12
Nu
mb
er o
f 3+
fal
ls
Severe Falls (Level 3 +)

North Bristol NHS Trust - Quality Indicators
Due to data quality issues related to the Cerner implementation, accurate bed day information for December is not currently available therefore the following indicators which require this as a denominator have not been updated:-Cardiac Arrest CallsPressure UlcersNutritionPatient experience and overall NQAT score
97% of wards surveyed through NQAT have achieved silver of gold for the patient experience rating based on patient questionnaires.This is on target to meet the CQUIN measure for patient experience
This chart shows overall achievement including documentation & patient observations. In November, of wards surveyed - 87% are achieving silver or gold
HSMR is rebased using data from 2001 onwards. There has been a further drop with NBT's rolling mean now at 88.1 - well below the national average.(Dr Foster publish data 3 months in arrears)
There were no grade 3 or 4 pressure ulcers for November.Overall incidence for November has increased from 14.1 to 17.6 patients per 10,000 bed days, with a total of 51 patients reported with grade 2 pressure ulcers.
There has been an increase in the number of wards rated silver or gold from 71% in October to 74% in November. December data not availble due to Cerner (see footer)
0
5
10
15
20
2011
-04
2011
-05
2011
-06
2011
-07
2011
-08
2011
-09
2011
-10
2011
-11
2011
-12
2012
-01
2012
-02
2012
-03
Cquin -Tissue
Viability -Patients/10
,000 beddays
0%
20%
40%
60%
80%
100%
2011
-04
2011
-05
2011
-06
2011
-07
2011
-08
2011
-09
2011
-10
2011
-11
2011
-12
2012
-01
2012
-02
2012
-03
Cquin - Nutrition (source NQAT Survey)
Actual Target
0%
20%
40%
60%
80%
100%
2011
-04
2011
-05
2011
-06
2011
-07
2011
-08
2011
-09
2011
-10
2011
-11
2011
-12
2012
-01
2012
-02
2012
-03
CQ2.2 - Patient experience - local MeasuresActual Target
0%
20%
40%
60%
80%
100%20
11-0
4
2011
-05
2011
-06
2011
-07
2011
-08
2011
-09
2011
-10
2011
-11
NQAT - Percentage of wards schieving Silver or Gold Overall
Actual Target

SAFEGUARDING ADULTS
ANNUAL REPORT NORTH BRISTOL NHS TRUST 2011
1 Introduction
This paper outlines the work undertaken by North Bristol NHS Trust (NBT) in relation to the Safeguarding Adult Agenda for 2011. It identifies a number of recommendations for taking forward the work into 2012 to further disseminate, reinforce and make implicit North Bristol NHS Trust’s duty of care to safeguard those adults who are unable to protect themselves from harm or exploitation. This work now spans a range of areas (illustrated in Appendix 1) to meet the needs of those patients with dementia, or a learning disability, as well as those who may be vulnerable1 as a result of their social, physical and mental needs.
2 Background 2.1 All NHS organisations are required to provide the systems and
processes to identify and support patients who may be vulnerable or at risk of harm. There are a number of relevant national guidelines and these are shown at Appendix 2.
2.2 The CQC state that ‘the term safeguarding, whether it is used in
relation to health or social care, refers to an organisation’s responsibility to protect people whose circumstances make them particularly vulnerable to abuse, neglect or harm.’
2.3 Organisations that work with vulnerable adults share a commitment to
safeguard adults against abuse and to work with other agencies to respond to allegations of abuse. The groups of patients that are specifically covered by these strategies are:
Vulnerable adults – a person over 18 years old who is or may be in
need of community care services by reason of mental or other disability, age or illness and who is or may be unable to take care of themselves or unable to protect him or herself against significant harm.
1 The Care Quality Commission defines vulnerable adults as ‘adults receiving care at home and
those with physical, sensory or mental impairments, or a learning disability’.
Page 1 17 January 2012

Learning disability (LD) – is a classification of several disorders where a person has a difficulty in learning in a typical manner usually caused by an unknown factor or factors.
Dementia – A progressive and largely irreversible clinical syndrome that is characterised by a widespread impairment of mental function.
2.4 The requirements on organisations are outlined in the Care Quality
Commission (CQC) – Essential Standards of Quality and Safety (March 2010):-
Safeguarding service users from abuse (Regulation 11) (1) The registered person must make suitable arrangements to ensure that service users are safeguarded against the risk of abuse by means of: (a) Taking reasonable steps to identify the possibility of abuse and
prevent it before it occurs; and (b) Responding appropriately to any allegation of abuse. (2) Where any form of control or restraint is used in the carrying on of the regulated activity, the registered person must have suitable arrangements in place to protect service users against the risk of such control or restraint being: (a) Unlawful; or (b) Otherwise excessive. (3) For the purposes of paragraph (1), “abuse”, in relation to a service user, means: (a) Sexual abuse; (b) Physical or psychological ill-treatment; (c) Theft, misuse or misappropriation of money or property; or (d) Neglect and acts of omission which cause harm or place at risk
of harm. (Regulation 11 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010)
2.5 In 2009 a national review of the ‘No Secrets’ policy (published in 2000)
was carried out. Further to this a number of documents and best practice guidance have since been issued (also listed in Appendix 2). The final recommendations arising from this review are still to be published.
3. Operational Management 3.1 The NBT safeguarding team is made up of the following roles and
individuals – a reporting structure is attached at Appendix 3:
Page 2 17 January 2012

Role Title Postholder Board Executive Lead Director of Nursing Marie-Noelle Orzel Non-Executive Lead Nick Patel Operational Lead for Adult Safeguarding
Head of Care Management
Diana Porter (Reporting to the Director of Operations)
Clinical Lead Consultant Nurse for Older People and Safeguarding Adults
Aileen Fraser: (0.2 WTE). A joint post with Bristol Community Health reporting to the Operational Lead
Operational Support Safeguarding Adults and Children Manager
Sean Collins (1.0 wte). Appointed December 2010 and reporting to the Deputy Director of Nursing
3.2 Within Clinical Directorates the management team of General
Manager, Clinical Director and Head of Nursing are responsible for the dissemination and monitoring of compliance to Trust policies in their areas. They are responsible for ensuring that their directorate is represented at relevant meetings.
4. Governance and Assurance 4.1 NBT has a number of policies that outline the processes for staff to
follow if they have concerns and/or are caring for patients who may be vulnerable. These policies include:
CG 43 Policy and procedure for raising concerns over services.
Whistle Blowing Policy CG 15 Safeguarding Adults Policy – revised and awaiting
ratification CP 7I Policy for Assessment of Mental Capacity and Best Interests
– revised and awaiting ratification CP 7 J Deprivation of Liberty Safeguards Policy - revised and
awaiting ratification CP 7 K Restriction and Restraint Policy (Adults) - to be reviewed
Jan 2012 4.2 During 2011, processes and training have been established within the
Advice and Complaints and Risk Management Teams to ensure early identification of Safeguarding concerns that come through the Trust Complaints process, Serious Incident reporting and the e-AIMS
Page 3 17 January 2012

reporting system. Additional work will be undertaken to further develop the links with Human Resources and the whistle-blowing process.
4.3 The implementation and effectiveness of the policies and procedures is
overseen by the Safeguarding Adult Operational Group. Membership includes representatives from directorates, Local Authority Safeguarding Co-ordinators, hospital Social Work teams, LD Liaison Nurses and Training. The attendance at the Operational Group over 2011 has improved. The Operational Group reports directly to the Trust Board through the Governance, Risk Management Committee via the Executive Board Lead and to the Safeguarding Boards (SAB) in Bristol and South Gloucestershire. The reporting structure is shown at Appendix 4
4.4 Attendance at the Bristol and South Gloucestershire Safeguarding
Boards is now managed within the Safeguarding Team with provision for the Safeguarding Manager to deputise if either the Consultant Nurse for Older People or the Operational Lead for Adult Safeguarding is not available to attend.
4.5 In 2011 NBT Internal Audit reviewed Safeguarding compliance for
2010/11 against national standards and criteria. The overall Internal Audit opinion of ‘the design and operation of controls relating to Safeguarding and Protection of Vulnerable Adults’ within NBT is amber. Both the objectives and a summary of the findings together with the latest (December 2011) update position and risk rating are attached at Appendix 5.
4.6 A detailed work plan has been developed to address all areas arising
from the Internal Audit report. Since the audit was undertaken in June 2011, progress has been made against all the recommendations (with the exception of domestic violence) and each is planned to be fully addressed by 31st March 2012. The recommendation relating to domestic violence remains ‘red’ as progress in this area is dependent on a wider piece of work which is currently being lead by NHS Bristol on behalf of the BNSSG community. The NBT Safeguarding Manager is a member of the working group associated with this. The objective of the working group is to produce a single BNSSG wide policy for domestic violence which will include links to Safeguarding procedures and specific guidance for adults without children.
4.7 During 2010/11 NBT was inspected on 3 occasions by the CQC. A
summary of the visits and the findings on each visit is given below. More detailed information about the findings is provided in Appendix 6.
Site/Date Visit Type Finding Frenchay, March 2011
Full Overall finding: ‘We found that Frenchay was meeting all the essential standards of quality and safety we reviewed but, to maintain this, we suggested that some
Page 4 17 January 2012

improvements were made.’ Outcome 7:Safeguarding people who use services from abuse - Compliant
Southmead, May 2011
Only ‘Dignity and Nutrition for Older People’
Overall finding: ‘We found that Southmead Hospital was meeting both of the essential standards of quality and safety we reviewed but, to maintain this, we suggested that some improvements were made.’ Outcome 1: People should be treated with respect, involved in discussions about their care and treatment and able to influence how the service is run - Compliant Outcome 5: Food and drink should meet people’s individual dietary needs - Minor concerns
Southmead, September 2011
Full Overall finding: ‘Southmead Hospital was meeting all the essential standards of quality and safety but, to maintain this, we have suggested that some improvements are made.’ Outcome 7: Minor concerns ‘Systems were in place to ensure people were protected from harm with improved reporting mechanisms in place to ensure that information was shared swiftly with the appropriate people. However, not all staff were aware or had an understanding of adult safeguarding principles and processes.’
Although Frenchay was found to be compliant, Southmead’s assessment noted ‘Minor Concerns’. As a result, further work is required and this has been incorporated in the detailed work plan (mentioned in section 4.6) in relation to staff training, access to guidance and revision of current (and creation of new) policies.
5 Training 5.1 Safeguarding training for adults has been mandatory in NBT since
2009. This has required the development of an intensive programme to ensure all staff have access to training and support. The training is provided internally by both the Consultant Nurse for Older People and the Safeguarding Manager. There are 3 levels of training provided currently.
Level 1: Basic awareness training for all staff at induction Level 2: Safeguarding vulnerable adults training for clinical staff
Page 5 17 January 2012

Level 3: Safeguarding vulnerable adults training for senior and on-call managers
To support the training programme, an e-learning programme for Safeguarding Children and Adults is being reviewed for implementation in the Trust during 2012.
5.2 As Safeguarding encompasses a wide range of legal responsibilities
and types of patient - as shown at Appendix 1 - the Safeguarding Adult training sessions also include coverage of:
Mental Capacity Act, Deprivation of Liberty Caring for patients with a Learning disability Caring for patients with Dementia Addressing issues around dignity.
5.3 From March 2012 all non-clinical staff will be required to attend
mandatory training in adult safeguarding (combined with dementia awareness and infection control – known as S.I.D training – to be refreshed after 3 years).
5.4 The Level 3 training sessions are aimed at managers and/or senior
staff who are required to support individuals who raise an alert of potential abuse. A number of incidents that have occurred in 2011 have highlighted a need for more advanced training for this group of staff in how to manage issues more effectively. This is particularly key in situations where a crime may have been committed to ensure that the process for alerting police, preserving evidence and not prejudicing any criminal investigation are understood and implemented. To date, two training sessions have been run with 19 staff (approximately 25% of this staff group) trained in total so far. Further sessions have been scheduled for 2012 to reach 100% of staff in this group.
5.5 The recording of training has become consistent over the last 6 months
and the latest figures (to November 2011) show that 75.16% of clinical staff at NBT are compliant with adult safeguarding training requirements. The training figures are shown at Appendix 7. Whilst there has been a steady increase in the percentage of staff trained, this has plateaued during quarter 4 as Cerner training has taken priority. (Refresher training for all levels of Safeguarding Adults training is required after 3 years).
6 Safe Recruitment 6.1 All staff employed within the Trust since 2009 have been subject to a
Criminal Records Bureau (CRB) Check. For staff employed before 2009, Human Resources have a plan to ensure all those staff obtain and/or renew their CRB checks. The priority focus for this work has been on the staff within the Women & Children’s Health directorate in
Page 6 17 January 2012

6.2 To date, 89% of the staff within the Women & Children’s Health
directorate hold a current CRB check. 100% of staff within the Emergency departments hold a current CRB check.
7 Serious Case Reviews (SCRs), Internal Safeguarding incidents 7.1 Serious Case Reviews take place where there are major concerns
about adult protection working or system failures or where there is a death of a vulnerable adult. Any professional can request a serious case review by the Safeguarding Board.
There were no SCRs in 2010/11 for Bristol however there is a current SCR ongoing for South Gloucestershire Local Authority (Winterbourne View) due to report in 2012.
7.2 An electronic referral system for patient safeguarding concerns was
established in April 2011 using the Clinical Information System Suite (CISS) and this has ensured rapid referrals and accurate transmission of data directly to Social Services.
7.3 The referrals to hospital social work teams for 2011 (Apr-Nov inc) were:
A total of 28 referrals recorded using the new electronic database Of these, 24 were assessed as appropriate safeguarding concerns
(i.e. that significant harm had occurred and that the adult was accurately assessed as vulnerable)
7.4 The Annual Safeguarding Adults report for 2010 highlighted significant
concerns relating to the application of the Mental Capacity Act and the Deprivation of Liberty Safeguards by staff across the Trust. Over the year action has been taken to address this risk area which, if exercised incorrectly, could lead to criminal prosecution. Training for medical staff has been put in place and all key staff provided with decision making flowcharts. All applications for DoLS are now monitored by the Safeguarding Manager and this year, there has been a low refusal rate. Further awareness work is required however to ensure that appropriate applications are made in all necessary cases.
7.5 During 2011 there were 16 applications by the Trust for DoLS. Over
the year 3 e-AIMs forms were received in relation to the Mental Capacity Act.
7.6 Following the linking of the Trust reporting systems to Safeguarding, a total of 6 safeguarding concerns were raised via the complaints process.
Page 7 17 January 2012

8 The Safeguarding Adult Agenda for the next 12 months 8.1 Policy Development 8.1.1 The Safeguarding Adults policy (CG15) has been reviewed by the
Safeguarding Adults Operational Group and now incorporates new guidance issued from the Department of Health for organisations to develop links between serious incident processes and Safeguarding. This will involve each serious incident being reviewed to consider whether Safeguarding processes need to be instigated prior to root cause analysis (RCA) being carried out. The policy is scheduled for ratification in January 2012. The Mental Capacity Act and the Deprivation of Liberty Safeguards policies have also been revised and are awaiting ratification.
8.1.2 The Restraint Policy is planned for review from January 2012. 8.1.3 External work has begun to review legislation around domestic
homicide and this will mean tighter links with the Multi-Agency Risk Assessment Conference (MARAC). An internal policy on ‘Domestic Violence’ will be a key development for 2012 and work on this will proceed in line with the BNSSG forum (referred to in section 4.6).
8.2 The staff structure to support Adult Safeguarding is currently under
review and future structure proposals aim to simplify and centralise Safeguarding within the Clinical Governance Directorate.
8.3 From January 2012 work will take place to develop a dedicated intranet
page for staff containing a variety of resources and information to support safeguarding processes. A key feature will be easy access for staff to policy flowcharts.
8.4 Further work is to take place in early 2012 on developing the
Safeguarding database to facilitate monitoring of referrals and regular reporting on safeguarding activity
8.5 The process to link serious incident reporting with Safeguarding Adult
processes has been incorporated within the NBT Safeguarding Adults policy and this will be further strengthened with the new Serious Incident Policy (to be issued in early 2012).
8.6 Formal monitoring and reporting of Adult Safeguarding training will be
set up in early 2012. Whilst the basic awareness training at induction already reaches 100% of new staff, further work is needed to confirm which staff require the level 2 training within the NBT Staff Training Database. Monitoring will continue for staff requiring level 3 training and the aim is for 100% of relevant staff to be trained by 30th September 2012.
8.7 A new e-learning programme for Safeguarding Children and Adults is
under review for implementation during 2012.
Page 8 17 January 2012

8.8 Focused work is to take place on embedding links with Human
Resources and whistle blowing processes 8.9 NHS South West has proposed the development of a single South
West policy for Safeguarding Adults (similar to the London multi-agency Safeguarding Adults policy). A number of work groups have been established to progress this and the Safeguarding Manager is involved in this process.
Page 9 17 January 2012

Appendix 1
Mental C
Mental Health Act
1983
Deprivation of Liberty Safeguard
(2009)
Restraint
Domestic Violence
Safeguarding Adults
apacity Act 2005 (2007)
Diagram to show the inter-relatedness of:
Safeguarding Adults Mental Capacity Act 2005 (2007) Deprivation of Liberty Safeguards (2009) Mental Health Act 1983 (2009) Restraint Domestic Violence
within North Bristol NHS Trust
Page 10 17 January 2012

Appendix 2 National Guidance relating to Safeguarding Vulnerable Adults
Care Quality Commission standards. Outcome 7 Safeguarding Adult and Children.
Association of Directors of Adult Social Services 2005. A national framework of standards of good practice.
Dept of Health 2000. No Secrets. Guidance on developing and implementing policy and procedures to protect vulnerable adults from abuse.
Safeguarding adults: report on the consultation on the review of No Secrets (DH 2009)
Safeguarding Adults: The role of Health service practitioners (DH 2011)
Clinical governance and adult safeguarding: an integrated process (DH 2010)
Healthcare Standards. Safety Domain, C2 and Governance C10. MENCAP. Death by Indifference, 2007. Independent inquiry commissioned by the Secretary of State for
Heath. Healthcare for All. 2008 Ombudsman. Six Lives, the provision of public services to people
with learning difficulties. 2009 National Institute for Health and Clinical Excellence, Dementia –
Supporting People with Dementia and their Carers in Health and Social Care. 2006
National Dementia Strategy, Living Well with Dementia. 2009 Dept of Health. Quality Outcomes for People with Dementia:
building on the work of the national dementia strategy. 2010 National Patient Safety Agency; (2010) National Framework for
reporting and learning from serious incidents requiring investigation Safeguarding Vulnerable Groups Act (2006)
.
Page 11 17 January 2012

Appendix 3
Organisational Structure – Adult Safeguarding
Director of Operations
Director of Nursing
Deputy Director of Nursing
Safeguarding Manager
Consultant Nurse - Older People and Safeguarding Adults
Head of Care Management and Operational Lead for Adult Safeguarding
Key ___ Direct line mgt ----Responsible to
Page 12 17 January 2012

Appendix 4
Safeguarding Assurance and Reporting Structure – agreed April 2011
Trust Safeguarding Committee
Page 13 17 January 2012
Sub-Groups’ responsibilities are defined as:
Producing, Monitoring & Intelligence Reports for Safeguarding Committee Process Design Operational Action Plans Development Identifying Education / Training Needs Reviews Identifying Themes Audits Working with Partner Agencies Reviewing Complaints
The Safeguarding Adults (Operational) Group also reports to the Safeguarding Adults Board (SAB) for Bristol and South Gloucestershire Local Authorities respectively. The Trust Safeguarding Committee (which meets quarterly) receives reports from the monthly/bi-monthly meetings of the sub-groups. The Trust Safeguarding Committee reports to the Governance and Risk Management Committee (GRMC), which reports to the Trust Board.
MembershipChair – MNOChairs of Sub GroupsEducation RepSimon Wood/Security RepIT AnalystEquality RepNon-Executive
MembershipNamed ProfessionalsDirectorate RepsPartner AgenciesTrainerOperational Reps
MembershipNamed ProfessionalsDirectorate RepsPartner AgenciesTrainerOperational Reps
MembershipNamed ProfessionalsDirectorate RepsPartner AgenciesTrainerOperational Reps
MembershipNamed ProfessionalsDirectorate RepsPartner AgenciesTrainerOperational Reps
Overarching Committee with Responsibilities for;• Strategic Planning / Horizon Scanning• Board Assurance• CQC Outcomes – Monitoring• Identifying / Resolving Trust Issues• Reporting Trustwide Themes• Risk Assessment• Holding Sub-Groups to Account• Maintaining Actions Plans
SafeguardingChildren Group
SafeguardingAdults Group
Dementia Steering Group
MH OperationalGroup
LD Group
MembershipNamed ProfessionalsDirectorate RepsPartner AgenciesTrainerOperational Reps

Page 14 17 January 2012
Appendix 5 Internal audit report: Safeguarding Vulnerable Adults June 2011
AUDIT SCOPE AND OBJECTIVES
The overall objective of this review was to provide assurance to the Audit and Assurance Committee that the Trust has implemented a sound system of internal control surrounding the Safeguarding Vulnerable Adults system. Specific Audit Objectives were: Objective 1 - The Trust has provided staff with sufficient information, guidance and support to allow them to
successfully execute their responsibilities regarding Safeguarding Vulnerable Adults in line with relevant legislation and national guidance.
Objective 2 - Appropriate reporting arrangements at an Executive Level are in place. Objective 3 - Staff are trained to be confident and competent in carrying out the Safeguarding Vulnerable Adults. Objective 4 - Staff are compliant with the ‘No Secrets’ Safeguarding Adults Multi-Agency Policy and procedures
when a concern regarding a possible vulnerable adult is raised. Objective 5 - All staff are aware of the appropriate procedures to use when restraining vulnerable adults. Objective 6 - Accurate record keeping is maintained when an alert has been made and that the monitoring
surrounding the alerts is robust. Objective 7 - Correct procedures are followed when accusations of abuse are made against members of staff. Objective 8 - Processes are in place within the Trust’s A&E Department, Cotswold Ward and Maternity
Department for dealing with patients who present with possible domestic violence concerns. Objective 9 - The Trust effectively communicates with all departments within the Trust and external agencies. RECOMMENDATIONS IN BRIEF
Recommendations Risk
Rating
Dec 2011
position
Use safeguarding activity information to measure compliance with Trust policy and legislation. Red (16) Green (16)
An AIMS form should be completed for each identified case of non-compliance with the Mental Capacity Act.
Red (15) Green (15)
Develop new policies and revise existing policies to reflect new national guidance, re-distribute interim guidance and ensure staff access to all policies, regardless of status.
Red (12) Amber (12)
Ensure Safeguarding Adults training is incorporated in Junior Doctors’ mandatory training programmes. Red (12) Green (12)
Formalise the SLA with AWP to provide professional advice and administration. Red (12) Amber (12)
Create alert to inform staff on re-admission of patients that have disclosed they are domestic abuse victims and liaise with HR regarding staff that are victims.
Red (12) Red (12)
Update job descriptions to reflect Safeguarding responsibilities. Approve an honorary contract for the funded post with Trustwide safeguarding responsibilities.
Amber (9)
Green (9)
Evaluate and improve the quality of evidence embedded in the PCAT. Amber (9)
Green (9)
Define the reporting requirements for the Safeguarding Committee and its sub-groups. Amber (9)
Amber (9)
Document and seek approval for the Safeguarding Adults training strategy. Amber (9)
Amber (9)
Within Trust policies state when to complete an AIMS form. Amber (9)
Green (9)
Develop an audit programme to measure staff practice against Trust policy. Amber (9)
Amber (9)
Develop a process, ideally within existing patient recording systems, that informs the Safeguarding Team when restraint is used.
Amber (9)
Amber (9)
Consider Use of Restraint / Safe Holding technique training for staff. Develop an improvement plan for attendance at Conflict Resolution training.
Amber (9)
Amber (9)
Develop a Safeguarding intranet page to provide inter alia out of hours contact details. Amber (8)
Amber (8)
Develop a referral process to the Safeguarding Team from Whistleblowing concerns from HR advisors regarding allegations made against staff
Amber
(8)
Amber
(8)
Write a policy for Use of Restraint of children in hospital that specifies procedure when ‘children’ (i.e. 16-17 year olds) are on adult wards.
Amber (8)
Amber (8)
Develop a protocol for transition of protected children that will or are highly likely to be vulnerable adults. Amber (6)
Amber (6)

Page 15 17 January 2012
Recommendations Risk
Rating
Dec 2011
position
Increase the frequency of attendance at local Safeguarding Boards to demonstrate commitment to implementing recommendations from serious case reviews as well as benefitting from shared learning and resource.
Amber (6)
Green (6)
Two recommendations were made that were of low risk, these are included in the detailed findings of the report; review externally-provided training and input to MLE reconcile referral source data with Safeguarding data
Green (4) Green (4)
Green (4) Green (4)

Page 16 17 January 2012
Appendix 6
Outcome 7: Safeguarding people who use services from abuse What the outcome says This is what people who use services should expect. People who use services:
Are protected from abuse, or the risk of abuse, and their human rights are respected and upheld.
What we found Our judgement
The provider (Frenchay) is compliant
Our findings
What people who use the service experienced and told us:
We did not consult people using the service about this outcome area.
Other evidence
The Trust declared compliance with this outcome area in information received as part of this review and in their application to register with the Care Quality Commission in April 2010.
Staff told us that they were aware of the safeguarding processes, that they knew who to report it to and where to find information to confirm the processes. Nursing staff told us that they had received training in safeguarding for children and for the protection of vulnerable adults.
However, three junior doctors told us that they had not received training in the protection of vulnerable adults however they confirmed they had completed safeguarding for children. We have received evidence from the trust which demonstrates that junior doctors have received training in this and this was completed during their induction. The Trust should ensure that the training is clear that it relates to vulnerable adults.
Staff spoken with during the visit said that they had all received training in the
Mental Capacity Act 2005 and Deprivation of Liberty Safeguards.
Where Deprivation of Liberty Safeguards were discussed with staff they were not clear about who would take the lead if an application needed to be made and said that it would be discussed at the multi disciplinary team meeting.
A member of nursing staff said they had safeguarding training before they joined the Trust 18 months ago. They were aware where the trust policy was kept. They were aware of who to talk to if they had safeguarding concerns. They would talk to their manager first and depending on the situation, the matter could be escalated.
The Trust provided us with evidence that there was a rolling programme of safeguarding training and they had exceeded their target to ensure that 85% of the workforce had completed the training. All staff we spoke with confirmed they had attended the training. We were told this was completed via e-learning with an assessment at the end.
The Trust gave us assurances as part of this review that policies and procedures were in place to guide staff. There were named staff within the hospital that have the overall lead for safeguarding. There were systems in place to audit the effectiveness of the processes that were in place.
The Trust had identified an area that requires improvement to ensure ongoing compliance in respect of making applications for a Deprivation of Liberty. This included the recording of the information, completing the application, training for staff and the notifying the Care Quality Commission in accordance with the Health and Social Care Act 2008. We will continue to

Page 17 17 January 2012
monitor this at future visits to the Trust.
Our judgement
Suitable arrangements are in place to ensure people can be confident that safeguards are in place to protect them from harm. The Trust has developed an improvement plan to ensure that processes are in place and the staff have the skills where an application is made in respect of Deprivation of Liberty Safeguards.
____________________________________________________ Outcome 07: Safeguarding people who use services from abuse What the outcome says This is what people who use services should expect. People who use services: Are protected from abuse, or the risk of abuse, and their human rights are respected and upheld.
What we found Our judgement
There are minor concerns with Outcome 07: Safeguarding people who use (Southmead) services from abuse
Our findings
What people who use the service experienced and told us:
We visited eight wards during our three day visit to Southmead Hospital. These included maternity services, a stroke ward, general medicine, a surgical, a cardiac ward, a dementia care unit and a day assessment unit. We looked at how the hospital was meeting the health needs of the older person with dementia both on the wards and in a specific ward for people who have a diagnosis of dementia. We spoke with at least two members of staff working on each ward, doctors where we were able and the ward manager. We spoke with patients and visiting relatives. Southmead hospital has a security system in place to ensure the protection of the mother and their new born babies. We observed the maternity wards having strict visiting times in relation to the number of visitors. This included all visitors being named prior to them visiting. A security guard was in situ 24 hours a day and visitors were issued with an identification tag prior to entering the unit. We observed that all visitors must sign in prior to entering the maternity suite. In addition where babies were at risk of harm then specialist equipment was provided to enable the staff to track the movement of the baby whilst in their cot. People told us on the maternity units that they felt safe and whilst they felt the visiting restrictions were strict they could understand why they were in place to ensure the safety of the baby Other evidence The Trust provided us with evidence that there was a rolling programme of safeguarding training for staff and at all levels throughout the organisation. They told us they had exceeded their target to ensure that 85% of the workforce had completed the training. However, we requested a further break down of the adult safeguarding training figures for each ward that we visited. Areas we visited varied from 61%, 81%, 85% and one ward had achieved 100%. We spoke to a number of staff including health care assistants, registered nurses, ward managers and clinical matrons about their understanding of safeguarding and protecting people from abuse and the policies that were in place. It was evident that ward managers and clinical matrons had a good knowledge of what constituted abuse and the reporting mechanisms that were in place. However, this was not always apparent with some of the registered nurses and

Page 18 17 January 2012
health care assistants that we spoke with. Where the Trust had stated they were 100% compliant two staff told us they had not received adult safeguarding training and when questioned about whether they had attended training stated "[I am] unsure if I have attended training- safeguarding is about monitoring people if unwell, they may need 'specialing'". The Trust told us that the reporting of adult safeguarding concerns and incidents to the local authority safeguarding team was a relatively new process of reporting in relation to safeguarding adults in the NHS acute services and that historically investigations took place internally rather than working with the local authority. The Trust also have a responsibility to report to the Strategic Health Authority and the Care Quality Commission on this area with reporting mechanisms in place. On the maternity units the staff we spoke with demonstrated a good understanding of safeguarding and periodic training updates were organised regularly. It was evident the staff were equipped with the understanding of what constituted abuse and the process of reporting to ensure women and children were protected from abuse and neglect. There were clear lines of communication between community services and the hospital staff in protecting the mother and the unborn baby. We discussed safeguarding processes and training with the safeguarding manager for the Trust and a Bristol City Council team leader for adult social care, who confirmed that safeguarding was a high priority for the Trust and improvements were continually being made. This included reporting, policies and procedures and training. Systems had recently been introduced where all complaints were being reviewed by the NBT's safeguarding team to establish if any of the concerns were about potential abuse. Where this was found they would report and share the information with Bristol City Council or South Gloucestershire Council in accordance with Department of Health's No Secrets guidance. In addition all electronic notifications that had been coded by staff as abuse was forwarded to the safeguarding manager to ensure safeguarding processes were followed to ensure the appropriate agencies were involved in any investigation. The Trust gave us assurances as part of this review that policies and procedures were in place to guide staff. We were informed by the safeguarding manager that these were being reviewed and updated. The Trust identified (in February 2011) an area that required improvement to ensure ongoing compliance in respect of making applications for a Deprivation of Liberty Safeguard (DoLS). This included the recording of the information, completing the application, training for staff and notifying the Care Quality Commission in accordance with the Health and Social Care Act 2008. From our discussions with the safeguarding manager it was evident that much progress had been made in this area. Matrons and ward managers had a good knowledge of the process for making applications where required for an authorisation of a Deprivation of Liberty Safeguard ensuring people were protected. The Trust continues to monitor this. We were aware from our visit that DoLS applications had been made from talking to the safeguarding manager and ward staff. However, we were not being notified in accordance with the Health and Social Care Act 2008. We were also informed that an audit was being completed of a sample of people with a learning disability who had been admitted to hospital ensuring that the correct protocols had been followed in relation to consent to treatment, mental capacity and the Deprivation of Liberty Safeguards. We were told this would be fed back to the board and if any shortfalls were identified an action plan would be developed. Our judgement Systems were in place to ensure people were protected from harm with improved reporting mechanisms in place to ensure that information was shared swiftly with the appropriate people. However, not all staff were aware or had an understanding of adult safeguarding principles and processes.

Page 19 17 January 2012
Appendix 7 Adult Safeguarding Training Compliancy Report for 2011 - 2012
Topic Jan
-11
Feb
-11
Mar
-11
Qtr
1 2
011
Ap
r-11
May
-11
Jun
-11
Qtr
2 2
011
Jul-
11
Au
g-1
1
Sep
-11
Qtr
3 2
011
Oct
-11
No
v-11
Dec
-11
Qtr
4 2
011
Yea
r to
d
ate
Ave
rag
e
Saf
egu
ard
ing
C
om
plia
nt
68% 69% 69% 68.80% 69% 81% 76% 75.11% 76% 77% 83% 78.72% 79% 77% - 78.00% 75.16%

Report to the Trust Board – January 2012
Title: Safeguarding Adults Annual Board Report 2011
Purpose of paper: To provide the Trust Board with an overview of the activities and work relating to the safeguarding of adults during 2011 and how this has informed a work plan for 2012
For Information
Executive Summary: This Safeguarding Adult work is evolving in accordance with national guidance. Whilst significant progress has been made over the year (and in the last 6 months in particular), there is growing demand in this area to further develop the systems, processes and training to support clinical staff in practice. Internal audit reviewed Adult Safeguarding within the Trust and, further to
an overall amber rating, a detailed work plan has been put in place. Of the 20 key areas of assessment there is now only one area assessed as at a ‘red risk’ rating. Delivery of this key area (domestic abuse policy and guidance for staff) is under development through the BNSSG (led) community. It is anticipated that all areas of the work plan will be complete by 31 March 2012.
CQC assessments of Adult Safeguarding (Outcome 7 Safeguarding
people who use services from abuse) at NBT over the course of the year delivered a ‘compliant’ assessment for Frenchay. For Southmead the assessment was ‘minor concerns’ which reflects the outstanding work required (further to the Internal Audit review).
Staff training has developed to cater to the variety of staff group needs
with new mandatory training in place for non-clinical staff to start from March 2012. Training compliance levels have increased steadily over the year. A key priority for 2012 is to train senior and on-call managers to be able to deal effectively with safeguarding concerns (particularly those arising out of hours).
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under
a 'closed section' of any meeting. 1
Safeguarding reporting structures have been reviewed and re-defined for greater clarity and to ensure effective monitoring. Monitoring reports are under development and clear links have been created to ensure that Safeguarding concerns are identified and reported across a range of sources (e-AIMs, Complaints, Serious Incidents).

This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under
a 'closed section' of any meeting. 2
Action Required: The Trust Board is asked to:
Note the report, the progress to date and the recommendation for further work in 2012 to further embed and develop the safeguarding systems
Key Risks:
The Trust is at risk of not maintaining/achieving full compliance on CQC standards (outcome seven) where staff awareness and understanding is not consistent and comprehensive
Impact on Patients: Delays in identification of suspected abuse can hamper investigation both
for adult community care services and the police. Achieving prosecutions in this area is difficult and early identification and involvement of the police can ensure that witness statements and evidence collection are robust.
Patient discharge is delayed if safeguarding processes have not been commenced in a timely manner and there are concerns about the safety of returning to home or nursing home.
CQC Outcome: 7 Responsible Committee: Safeguarding Adults Operational Group Financial Issues considered: Staff training costs Equality Impact Assessment Completed: To be completed at next Safeguarding
Adults Operational Group Legal Issues Considered: As detailed in report Sustainability Assessment Completed: To be completed at next Safeguarding
Adults Operational Group Presented by: Marie-Noelle Orzel, Director of Nursing Prepared by: Diana Porter, Operational Lead for Adult
Safeguarding Nicola Alfonsi - Operations Directorate

Report to the Trust Board – January 2012
Title: Action plan following Independent Inquiry into Histopathology services at University Hospitals Bristol FT.
Purpose of paper: To provide the Trust Board with an update
Executive Summary:
This is an update since the last report to the board in October 2011
The Medical Director of NBT continues to meet with the MD of UHBristol, the joint clinical lead for histopathology and Director of Governance at NHS Bristol to review progress with implementation of the Inquiry recommendations.
The action plan is shown in appendix 1 with outstanding actions at the start of
the document and completed actions identified.
1.2. progress has been made with joint working at management level with unified approaches agreed. Individual managers remain site specific as the majority of their work load relates to a specific laboratory. Common KPIs require further work with recent helpful guidance from the RCPath having been published and work on this issue continuing through the BNSSG pathology project.
1.7 benchmarking of consultant staffing against the RCPath guidance has
been completed. Further benchmarking has also been completed using Keele benchmarking activity data. The Clinical Lead is close to completion of individual consultant job planning. Once this information is available the two Trusts will be able to make a judgement about any changes to consultant staffing that may be required. A meeting is being arranged for relevant executives from each organisation to meet and decide an appropriate response.
13.1 The Clinical Lead has contacted the RCPath and they have on going
discussions with respect to the recommendation on specialist reporting.
13.2 There are two areas remaining where there is a single specialist histopathologist – these are oral/maxillofacial cancer and paediatric cardiology. A business case is being developed for appointment to an oral/maxillofacial post. Paediatric cardiology pathology is a rare requirement and it would not be appropriate to have two individuals in Bristol with this specialism. The risk associated with single handed practice in this area is being managed by arranging a partnership with a paediatric cardiac specialist in another Trust.
The configuration of cellular pathology in Bristol continues to be evaluated as
part of the North Bristol NHS Trust lead provider for Pathology project.

South Gloucestershire Health Overview and Scrutiny Select Committee Histopathology Evidence day This event took place on 4th January 2012 following a request to the council from South West Whistleblowers Health Action Group. Councillors were asked to consider submissions from SWWHAG suggesting that the Independent Inquiry into Histopathology services at UHBristol had not provided adequate assurance that cellular pathology services were safe. The council stated that it would listen to evidence relating to areas not covered by the inquiry but were not prepared to re-open the inquiry or question its findings. Three members of the public and a retired paediatric surgeon from UHBristol spoke on behalf of SWWHAG. The Chief Executive of UHBristol FT provided a reply addressing the questions raised by SWWHAG and demonstrating the regulatory reviews of the service that had taken place in addition to the independent inquiry. The Medical Director from NBT, The joint Clinical Lead for Histopathology and the Lead for Governance at NHS Bristol were in attendance to answer questions. Councillors noted that the Trusts accepted the findings of the Independent Inquiry and that it had identified significant concerns about culture and behaviour of leaders and clinicians in both organisations. Councillors sought further reassurance that the actions taken by the Trusts were addressing the cultural issues. They specifically asked questions with respect to double reporting of cellular pathology specimens and how Bristol compared to other pathology providers nationally with respect to this practice. NHS Bristol stated that they would continue to provide assurance by performance managing the Trusts against the quality of the pathology services they provided. The HOSC agreed to consider whether they wished to recommend any actions to NHS organisations at their next meeting on 8th February 2012. Action Required: The Trust Board is asked to note progress with implementation
of the action plan and note the S Glos HOSC evidence day.
Impact on Patients: Pathology services are crucial to the work of many other specialties and patients need assurance that the service is of high quality.
CQC outcomes: 1, 2, 4, 6, 12, 13, 14, 16, 17, 20 Presented by: Dr Chris Burton, Medical Director Prepared by: Dr Chris Burton, Medical Director

Appendix 1
V24 12/12/2011 1
Recommendations from Histopathology Inquiry – Action Plan
Actions not yet due
Ref No Actions Timescale Responsible person
Progress Complete Evidence
Section 1 Section Lead: Rob Pitcher
Overarching recommendation A: A single Histopathology Service should be established for Bristol with the potential to be one of the leading service and academic centres.
1.2 Develop Service Structure and Proposition for integrated cellular pathology service Agreed sub-milestones:
Integration of the management tier beneath Clinical Lead
Common reporting template for each speciality
Agreement of specialist and team roles & profiles
Common KPI suite and associated metrics agreed and in place
31 Dec 2011
Rob Pitcher These issues are being considered as part of the Pathology Services Review being led by NHS Bristol. Clinical Lead for Cellular Pathology is feeding into the review accordingly. Meanwhile, a governance structure has been put in place.
Revised management structure/Job Descriptions.
Reporting template.
Specialist and team role profiles.
KPI suite.

Appendix 1
V24 12/12/2011 2
Ref No Actions Timescale Responsible person
Progress Complete Evidence
1.7 Review consultant staffing levels in accordance with the Royal College of Pathologists' "Guidelines on staffing and workload for histopathology and cytopathology departments" (2nd edition) June 2005, and, if necessary, adjust to ensure they are sufficient for a safe, timely and reliable service. Further milestones:
Complete comprehensive Job Planning process for all Consultants working in Cellular Pathology across both UHB and NBT.
Complete skill mix exercise to determine what work currently performed by Consultants could be carried out by other staff.
Review outcome of the Job Planning and skill mix exercises and, if necessary, adjust staffing configuration to ensure sufficient support for a safe, timely and reliable service.
Review 31 Aug 11.
Rob Pitcher The review is complete. A paper has been produced to include recommending an in depth Job Planning and skill mix exercise.
Review paper.
30 Nov 2011 30 Nov 2011 29 Feb 2012
Rob Pitcher Rob Pitcher Sean O’Kelly/ Chris Burton.
Complete. Process in place and job planning underway to be completed by end February 2012. Skill mix exercise underway.
Agreed process.
Skill mix exercise outcome.
As above.

Appendix 1
V24 12/12/2011 3
Ref No Actions Timescale Responsible person
Progress Complete Evidence
1.9 Identify short term and longer term location plan for department.
31 Oct 11
Rob Pitcher The Inquiry recommended that the service should for the time being remain on two sites. The longer term plan is subject to the outcome of the Pathology Services Review. See actions for 1.2.
Linked to 1.2.
Section 10 Section Lead: Alison Moon
Overarching recommendation I: Patients and Histopathology For information: The Royal College of Pathologists has an active programme to inform the public about histopathology. Next year is designated National Pathology Year.
10.2 Implement PPI strategy – Year 2 (Expansion of Year 1 approach into Outpatients – pending identification of funding)
31 Mar 12 Alison Moon Year 2 funding obtained. Two major internal surveys of outpatients to complement the National Outpatients Survey are taking place in 2011/12. Comments Cards are being implemented in Outpatients Departments and plans for surveys using hand held devices are currently under discussion.
On track
Minutes and papers of Patient Experience Group and its predecessor.
Six monthly PPI strategy update to the Board October 2011.
10.4 Develop proactive and constructive working relations with new ‘Local HealthWatch’, including its proposed responsibilities for patient advocacy (detail has yet to be
DH expects HW to be “up and
Tony Watkin Bristol LINk is a national pathfinder for
HealthWatch status and is attending the Trust’s
Patient Experience Group in November 2011 to
On-going
Notes of meeting.

Appendix 1
V24 12/12/2011 4
Ref No Actions Timescale Responsible person
Progress Complete Evidence
announced by the DH). running by 2012”
present its plans.
UH Bristol representation on Bristol LINks Acute
Hospital Group to facilitate operational activity.
UH Bristol workshop with Bristol and South
Gloucester LINks has taken place to inform
2010/11 Quality Account.
Robert Woolley has met with Chair of Bristol LINk
to provide assurance of positive working
relations.
Two new pieces of Patient and Public
Involvement work relating to histopathology
have commenced:
1. Interviewing patients in named UH Bristol outpatient clinics about their experiences of having tests and receiving results.
Minutes of LINks Acute Hospital Group
Third party comments from LINks on UHB Quality Account.
Survey outcomes.

Appendix 1
V24 12/12/2011 5
Ref No Actions Timescale Responsible person
Progress Complete Evidence
2. Supporting NHS Bristol in broadening participation of parents and carers of young people in the “What Patients Want” document which identifies four key themes which matter to patients regarding histopathology services: quality, timeliness, convenience of access and communication.
In addition, we have added questions about tests and results to our monthly in-patient survey, outpatient survey and bi-monthly ward based surveys. The outcomes of which provide both assurances about our services and areas for patient led service improvements.
“What Patients Want” document. In electronic evidence files.
Inputs from UH Bristol and outputs from the partnership involvement work. As above.
Section 13 Section Lead: Rob Pitcher

Appendix 1
V24 12/12/2011 6
Ref No Actions Timescale Responsible person
Progress Complete Evidence
13.1 The Royal College of Pathologists should review its guidance on specialist histopathology with the intention of making it more explicit where possible.
For RC Path to determine
RC Path Rob Pitcher has met informally with the President
of the Royal College of Pathologists.
There is a current Royal College of Pathologists document in existence and the College Histopathology Specialist Advisory Committee have been asked to comment on whether further work is required.
To be advised by Royal College.
13.2 There should be at least two specialist histopathologists in each subspecialist area to allow proper review and to provide cover for meetings and periods of leave.
Dependent on the outcome of 1.2
Rob Pitcher Linked to action 1.2.

Appendix 1
V24 12/12/2011 7
Completed Actions
Ref No Actions Timescale Responsible person
Progress Complete Evidence
Section 1 Section Lead: Rob Pitcher
Overarching recommendation A: A single Histopathology Service should be established for Bristol with the potential to be one of the leading service and academic centres.
1.1 Appoint Clinical Lead for Cellular Pathology 30 Jun 11 Jane Luker/ Chris Burton
Complete. Clinical Lead in post as of 3 May 11.
Job Description and staff in post.
1.3
Short term Consultants should work across both sites when necessary to provide the optimum service to patients.
31 Mar 11 Jane Luker/ Chris Burton
Agreed and implemented where appropriate. Cross site working in place for haemato-malignancy, Head and Neck, Lung and Her 2 Breast pathology. Further work underway to develop greater cross site working in line with planned service reconfiguration.
Letter of expectation sent to pathologists by Acting Medical Director. Honorary contracts in place. In pathologists’ HR files.

Appendix 1
V24 12/12/2011 8
Ref No Actions Timescale Responsible person
Progress Complete Evidence
1.4 Put in place honorary contracts for cellular pathologists with reciprocal trust.
31 Mar 11 Philippa Finch/ Tracy Smallwood
Honorary contracts issued to pathologists to be signed and returned by 17 Jun 11. UH Bristol and NBT pathologists have all signed their honorary contracts.
Honorary contracts in place. In pathologists’ HR files. Letter from Acting Medical Director to pathologists March 2011.
1.5 All new cellular pathology appointments to be joint
31 Dec 10
Jane Luker/ Chris Burton
Agreed. March 11: Two new adult pathologists appointed on 50:50 contracts
Appointment process documentation i.e. Job Description and advert.
Contracts for new staff. In pathologists’ HR files.
1.6 Clarify roles and responsibilities of Heads of Division, Lead Doctor and Specialty Lead
31 Dec 10
Robert Woolley
Complete. Communications to relevant staff and revised job descriptions completed. This will be evidenced through Job Planning and appraisal. The UH Bristol Medical Director team will conduct an initial assessment of compliance with the clarified responsibilities.
Letters from CEO to Heads of Division.
Lead Doctor Job Descriptions.

Appendix 1
V24 12/12/2011 9
Ref No Actions Timescale Responsible person
Progress Complete Evidence
Written confirmation from divisions.
1.8 Identify areas of urgent staffing need and produce action plan
31 May 11
Rob Pitcher Complete. Necessary measures in place to manage current workload, including outsourcing.
Specialist working overview.
1.10 Develop process to ensure service changes are fully supported by Histopathology
31 Oct 11 Rob Pitcher The Bristol Cellular Pathology Forum described is part of developing the wider team ethos and will include discussions with clinical teams on issues such as service reconfiguration, standards etc.
Minutes of meetings.
Section 2 Section Lead: Mark Callaway
The MDTs in both Trusts should be reviewed to promote collaboration.
2.1 Complete MDT reviews 31 May 11
Mark Callaway/ Chris Burton/Rob Pitcher
UH Bristol MDT review for pathology completed. NBT review has been completed and a report received by their Board in June 2011.
MDT review report and meeting minutes.
2.2 Agree a plan for on-going development of joint MDT
31 July 11 Mark Callaway/ Chris Burton/Rob Pitcher
A joint UH Bristol and NBT meeting took place on 16th June to agree a joint approach for MDT development going forward. A joint report was produced by the end of July 2011.
Joint Report.
Minutes of meetings SDG 25/07/2011.

Appendix 1
V24 12/12/2011 10
Ref No Actions Timescale Responsible person
Progress Complete Evidence
Minutes of Cancer Board.
2.3 Ensure slides are available at MDTs.
30 Mar 11
Lis Kutt
Complete. The MDT outcome records indicate where a patient referred in from another Trust is deferred to the next meeting if their slides are not yet available from the referring trust.
June 2011 spot check slide audit report.
MDT audit results.
On-going results presented to SDG.
2.4 Agree and implement process to ensure patients are aware that a diagnosis given pre MDT may be refined at the MDT meeting.
30 May 11
Teresa Levy/ Dany Wells
Cross Trust patient information leaflet finalised and being piloted. The pilot is due to be completed by the end of August 2011.
Patient Information Leaflet.
Evaluation of pilot.
Section 3 Section Lead: Rob Pitcher
Quality Assurance For information: The Royal College of Pathologists is working on a set of Key Performance Indicators for pathology.

Appendix 1
V24 12/12/2011 11
Ref No Actions Timescale Responsible person
Progress Complete Evidence
3.1 Agree audit programme 2011/12 for Histopathology
30 April 11
Lis Kutt
Complete and shared with NBT 5 audits are planned, of which 3 are underway:
An audit of the double reporting protocol (not yet started)
An audit of reporting systems (not yet started).
Review of supplementary reports after multi-disciplinary team meeting (started August)
High grade serous carcinoma of endometrium-network audit (started August)
Correlation of breast tumour grading between core biopsies and resection specimens in a screened population (started July)
UH Bristol Clinical Audit Forward Plan 2011/12.
Joint Histopathology Audit Programme
3.2 Develop joint audit plan across both Trusts 30 June 11
Rob Pitcher Complete. Joint Histopathology Audit Plan.
3.3 Ensure current involvement in all appropriate EQAs and CPD to develop specialisation
31 Mar 11 Lis Kutt
UHB EQA involvement identified. All specialist pathologists have an appropriate EQA programme. Relevant UH Bristol pathologists are registered for the regional lung EQA.
EQA Matrix.

Appendix 1
V24 12/12/2011 12
Ref No Actions Timescale Responsible person
Progress Complete Evidence
3.4 Develop full joint EQA and CPD programmes
31 Aug 11
Rob Pitcher The interviews with consultants demonstrated the current position on EQA. This information is held within the consultants' appraisal folders and reviewed annually as part of their appraisal. The Bristol Cellular Pathology Service in its policy statement on the recognition of specialist roles in cellular pathology recognises the need for pathologists to partake in appropriate EQA schemes. This will be monitored on an annual basis
Updated EQA Matrix.
Section 4 Section Lead: Lis Kutt
Upgrade Histopathology Department
4.1 Upgrade work to be completed 31 Jul 11
Sven Howkins
Complete. Site visit
Works Project Plan.
Section 5 Section Lead: Rob Pitcher
Double Reporting For information: There is a current Royal College of Pathologists document in existence about double-reporting. The College Histopathology Specialist Advisory Committee is meeting in June 11 and will be asked to comment on whether further work is required.
5.1 Agree and implement a revised joint double reporting protocol
31 May 11
Rob Pitcher Complete. Protocol has been finalised and disseminated.
Double Reporting Protocol.

Appendix 1
V24 12/12/2011 13
Ref No Actions Timescale Responsible person
Progress Complete Evidence
Section 6 Section Lead: Rob Pitcher
Overarching Recommendation E: Raising Concerns about diagnostics Any concerns about the standard of pathology reporting should be thoroughly, rapidly and, where appropriate, independently investigated and the results made available to all those involved. Concerns should be dealt with at the lowest possible level and not escalated unnecessarily. The pathologist(s) involved should be consulted directly.
6.1 Agree and implement a revised raising concerns protocol
31 May 11
Rob Pitcher Complete. Protocol has been finalised and disseminated.
Raising Concerns Protocol..
Section 7. Section Lead Sarah Pinch
Overarching recommendation F: Whistleblowing The Department of Health should review advice on whistleblowing to ensure that local policies include clear guidance on raising concerns about the work of a pathologist or any other clinician who works for a different Trust from the Trust employing the person raising the concern.
7.1 Strengthen UHB Whistleblowing policy
31 May 11
Sarah Pinch Complete. Policy agreed and confidential staff helpline in place.
Revised policy.
Evidence of advertising this to staff
Section 8 Section Lead: Sarah Pinch
Overarching recommendation G: Media Relationships. Relationships with the media should be proactive with an emphasis on openness, honesty and the involvement of senior managers and clinicians Relationships with the media should reinforce positive relationships with patients. Service change should be explained including the Chief Executive

Appendix 1
V24 12/12/2011 14
Ref No Actions Timescale Responsible person
Progress Complete Evidence
8.1 The Trust Board will approve the revised communications strategy and plan in light of the report’s recommendations
30 June 11
Sarah Pinch
The Communications Strategy was approved by the Board on 28 June 2011.
Revised Communications Strategy. Evidence in June 2011 Board papers and minutes.
8.2 The Trust’s media protocols will be revised in light of the report’s recommendations and will include consultation with relevant staff groups. The revised protocol will then be reissued to all staff. The protocol will be included in the revised communications strategy.
31 Mar 11
Sarah Pinch
Complete. Revised media protocols approved 13 April 11.
Revised Media Protocols. Evidence in TEG papers and minutes 13 April 2011.
8.3 The Trust’s website is currently being redeveloped and will deliver a more responsive, interactive up-to-date tool for Trust communications, direct to patients, staff, FT members and the media.
30 June 11
Sarah Pinch
The new website was launched on 1st July 2011.
New website.
Section 9 UHB Section Lead: Lis Kutt
Overarching recommendation H: Paediatric and Perinatal Pathology Paediatric and perinatal pathology should be valued and supported by managers, pathologists and other clinicians. The minimum level of staffing should be one paediatric pathologist, one perinatal pathologist and one pathologist trained in both paediatric and perinatal pathology.

Appendix 1
V24 12/12/2011 15
Ref No Actions Timescale Responsible person
Progress Complete Evidence
9.1 Recruit and permanently appoint to proposed staffing levels demonstrating full commitment to the service
31 Jul 11 Lis Kutt/ Rob Pitcher
Interviews held Feb 2011. No appointment made. Further interviews were held 23 June 11 and an offer has been made subject to references and employment checks. Anticipated start date end of September. Interim outsourcing provision in place.
Staff in post. Recruitment update in November 2011 minutes of Bristol Cellular Pathology Forum
9.2 CEO to write to Southampton and Oxford to seek opportunities for joint working in principle
31 Dec 10
Robert Woolley
Complete. Positive responses received from Southampton CEO and Oxford MD.
Letters between Trusts.
9.3 Establish joint working arrangement
31 Jul 11 Sean O’Kelly UH Bristol Medical Director has met with the Medical Directors from Southampton and Oxford to explore networking opportunities for paediatric pathologists. Agreement in made in principle, an operational specification is being drawn up.
Operational Specification.
Section 10 Section Lead: Alison Moon
Overarching recommendation I: Patients and Histopathology For information: The Royal College of Pathologists has an active programme to inform the public about histopathology. Next year is designated National Pathology Year.

Appendix 1
V24 12/12/2011 16
Ref No Actions Timescale Responsible person
Progress Complete Evidence
10.1 Implement PPI strategy – Year 1 (Inpatient feedback systems)
31 Mar 11 Alison Moon Complete. Inpatient feedback mechanisms in place and providing timely information on the quality of patients’ experiences, the results of which are being acted upon within the Trust.
Minutes and papers of Patient Experience Group and its predecessor.
Six monthly PPI strategy update to the Board October 2011. In Board papers and minutes.
10.3 Devise and delivery four UH Bristol patient focus groups to explore current awareness and future involvement in the on-going development of histopathology at UH Bristol
30 Apr 11 Tony Watkin \ Lis Kutt
Complete. The report from the focus groups has been finalised and has been shared with the Pathology Services Review.
Focus Group Outcome report..
10.5 Agree process to promptly inform patients of diagnostic errors
31 Jan 11 Jane Luker Complete. Staff Support and Being Open Policy 2009 is already in place. Next update will make link to diagnostic errors more explicit.
Current policy. on DMS.
Policy due for review by end December 2011
10.6 Explore options for providing service users with information about the purpose of role and multi-disciplinary cancer teams and team meetings.
31 Mar 11 Teresa Levy Cross Trust leaflet finalised and being piloted. The planned date for completion of the pilot is 31 August 2011.
Patient Information Leaflet..

Appendix 1
V24 12/12/2011 17
Ref No Actions Timescale Responsible person
Progress Complete Evidence
10.7 Where a patient‘s care is going to be discussed at a multidisciplinary team meeting, patients should not be given information contained in histopathology reports until the reports have been considered by the multidisciplinary team.
The Trusts have agreed that implementing this recommendation could lead to a delay in patients being given information concerning their diagnosis and could put clinicians in the position of having to withhold important information from patients. The Trusts’ ability to run one-stop clinics would also be compromised. Instead the Trusts propose that patients should be given information appropriate to their care, with an explanation of the diagnostic and treatment decision process by the Multidisciplinary Team.
N/A N/A
Section 11 Section Lead: Rob Pitcher
Training
11.1 Trainees should have supervised involvement in the full range of specimens, including the most complex cases, in accordance with their seniority
Nov 10 Lis Kutt Complete. Trainees are supervised by individual consultants as befits their experience and seniority. The number of educational supervisors has been increased from 1 to 4 to further improve monitoring of progress with subsequent adjustments to individual learning plans as required.
Annual report to Severn Deanery.

Appendix 1
V24 12/12/2011 18
Ref No Actions Timescale Responsible person
Progress Complete Evidence
11.2 Training plans to be adjusted to provide access to all levels of case
30 Nov 10 Lis Kutt Complete. Training plans for the trainees have been revised by Dr Mohammed Sohail. A written training plan has been in use since the January 2011 which advises on the type of case mix trainees should expect to see to ensure that they have opportunities to work with a broad range of specimens of varying complexity.
Training Plan
Section 12 Section Lead: Steve Aumayer
Overarching recommendation L: The histopathologists should be given whatever support they need to face the aftermath of this Inquiry including skilled facilitation.

Appendix 1
V24 12/12/2011 19
Ref No Actions Timescale Responsible person
Progress Complete Evidence
12.1 Develop detailed organisational development plan to support the move towards an integrated cellular pathology service
31 Aug 11 Steve Aumayer/ Rob Pitcher
Integrated Cellular Pathology Service:
Joint Trust Monthly formal business meetings in place (Meeting 3 in September)
Joint Trust workshop programme enabling discussion on key issues – resulted to date in:
o The recognition of specialist roles in cellular pathology
o Definitions of Lead Roles in Cellular Pathology
o Policy on the content of the reports from the Bristol Cellular Pathology Service
Educational activities including case discussion, audit presentations, research, feedback from external educational activities being planned
A series of workshops is planned to examine at specialist team level what cellular pathology service is required on which site to support the clinical service – commencement date TBA
Working with NHS Improvement
Launch event 5th September for a core team who will be working on LEAN review of processes across sites.
Programme supported by site visits, the purpose of which to see how others provide integrated services to more than one acute Trust and to look at the work to improve efficiency (LEAN) that some have done.
Training resources, attendance records and notes of meetings.

Appendix 1
V24 12/12/2011 20
Ref No Actions Timescale Responsible person
Progress Complete Evidence
12.2 Provide Counselling and Occupational Health support to affected staff
31 Dec 10
Steve Aumayer
Complete. Some staff have accessed this
Letter from Acting Medical Director to pathologists March 2011
12.3 Provide facilitation and mediation
As required
Lis Kutt
Facilitation and mediation are available to staff should this be required. Externally facilitated event took place in Jan 11 with NBT and meetings of the Bristol Cellular Pathology Forum continue.
Letter from Head of Division to pathologists Jan 2011.
Agenda, minutes and papers of Bristol Cellular Pathology Forum.
12.4 Support to assist in development of single service
On-going. Lis Kutt/ Rob Pitcher
As for completed action 12.1 and ongoing. On-going
Section 14 Section Lead: Rob Pitcher
Pathology reports

Appendix 1
V24 12/12/2011 21
Ref No Actions Timescale Responsible person
Progress Complete Evidence
14.1 Review style of reporting and implement any changes if deemed appropriate
To be agreed
Rob Pitcher The Bristol Cellular Pathology Forum has topics already identified to be built into its work programme. These topics for discussion, debate and development into policy and procedure include pathology reporting. A draft policy is in development.
Reporting policy.

Report to the NBT Trust Board 26 January 2012
Title: Southmead Hospital Redevelopment Update
Purpose of paper: To provide an overview of issues and risks associated with the Southmead Hospital Redevelopment project.
To note
Executive Summary: The bulk of the design process has been completed. Some M&E designs are outstanding as
well some Phase 2 works A meeting was held just before Christmas to agree timescales for all outstanding works on the
staff multi-storey car park. A detailed programme is expected soon. Carillion’s awaited claim for unidentified asbestos, which is a standard contractual
requirement, has been agreed but not yet formally documented. No claims have been received by the Trust. No variations have been issued by the Trust to date, although Variation Enquiry 1 has been
submitted by the Trust in relation to Skirtless canopies in theatres and this is in hand. David Powell and Phil Morgan served bacon baps to the Carillion staff in their canteen one
lunchtime in December to celebrate the achievement of 1 million man hours since the last RIDDOR accident – see photographs below
As part of the collaboration between Carillion and NBT to work together on community programmes, the Horfield CE Primary School choir of 3 - 6 year olds gave carol concerts in the Carillion canteen and in the Richard Bright Renal Unit. The children sang beautifully and were well received in both venues.
Action Required: The Trust Board is asked to Note the issues identified. Key Risks: The key risks identified for the period include:
Changes identified as a result of reviewing clinical areas or clinical practice developments could lead to variations but the current flexible design has proved successful to date.
Service transfers between Trusts not proceeding to agreed timescales. Contingency plans are being developed in the event that services are unable to transfer.
Staff not having sufficient time to engage with the service redesigns and workforce planning for development of the commissioning plan for the new hospital. The forthcoming major projects which could compete with resources are planned to peak prior to the new hospital commissioning process.
Impact on Patients: Emerging costs that have not been allowed for could reduce available funding for patient care or could result in additional savings being required. A successfully delivered design should bring significant benefits to patients, visitors and staff in terms of environment and functionality. CQC Outcome: 10 and 26 Responsible Committee: North Bristol Trust Redevelopment PB Financial Issues considered: Yes Equality Impact Assess’t Completed: Yes Legal Issues Considered: Yes Sustainability Assess’t Completed: No Presented by: David Powell, Director of Projects Prepared by: Martin Warren, Project Manager
C:\Documents and Settings\nbc2068\Desktop\January 2012\7.1 NBT Redevelopment Project Highlight Report Summary.doc

Celebrating 1 Million man hours since last RIDDOR accident
C:\Documents and Settings\nbc2068\Desktop\January 2012\7.1 NBT Redevelopment Project Highlight Report Summary.doc

Decisions Required:
Key Issues:
Programme 2011/12 A S O N D J F M A M J J A S O NWard block envelopes G G G G G GClinical block envelopes G G G G G GWard block fit outs G G G G G GClinical block fit outs G G G G G GClinical (C-sheets) G GEquipping G G G G G GConcourse Roof G GCommissioning G GRisk/Cost impacts RAGSummary: GType No. Mitigation Score
Operational G1
The Trust has minimised this risk through extensive and consistent involvement of clinical staff at all stages of the design. This development of departmental requirements, clinical output specifications, 1:200 plans, 1:50 plans, C Sheets and the schedule of accommodation was also overseen and co-ordinated by senior clinicians and the Project Team. The incorporation of zonal accommodation, standard layouts and standard rooms should ensure the building is fit for purpose in the future.
15
Commissioning P10The Trust is actively planning the immediate priority projects including Cerner, BoF, Operational Planning and FT application. It is essential that there is sufficient resource and engagement from 2012 on what is needed to transform the services and to commission the new building.
15
Operational A6Generic space planning allows for temporary mix changes and closure programme around Frenchay could be managed to allow time to resolve service transfer issues. Maintain close liaison with UHB and other organisations to ensure early warning signs are picked up and seek share of risk of delay with new host organisation.
12
Quality RAGSummary: GDesign GClinical/functionality GTechnical GArts GSustainability GComms/involvement GAsbestos/Ground Conditions
Cost £000 RAG
Unexpected ground conditions
0 G
Unidentified asbestos 200 (anticipated and allowed for in budget) GVariations Cost £000 RAGError Corrections: 0 GStrategic Decisions: 0 G
Southmead Hospital Redevelopment Project
Southmead Highlight Report
The quality of design submissions and samples continue to meet the Trust requirements and expectations
0
Author: Martin Warren
None
On programmeStone cladding to block 6 is nearing completion and windows nearly complete on block 2Terracotta panel installation has continued to blocks 2 - 5Works have continued as planned with pre fit out to block 5 complete and toilet pod deliveries have continued throughout the period
SRO: David Powell
Trust requirements change and building does not accommodate all requirements
Staff unable to allocate sufficient time to engage with commissioning new building and delay the opening
Date: 13/01/12
Report Number:
Period: 10/12 - 9/01
91
Design has generally maintained position and the construction work is on programme overall
Risk
Pre fit out works continued to blocks 5 & 6 and fit out to blocks 1 - 3 has continued as planned
Allocation of sufficient staff time to engage with service redesign and workforce planning is critical to development of a commissioning plan
Revised theatre and burns designs are now in hand with Carillion's architects
Several community events were held jointly with Carillion including some children's carol concertsNumber
Service transfers out from NBT do not proceed as planned
Carillion's risk assessment of the main concourse installation is awaited before concluding the detailed designTotal waste quantities remained relatively static at 247 tonnes for the period, of which 96% was reused or recycled
0
Number0
1 (Phase 1 demolitions)
With the skirtless canopies issues settled the C sheets for theatres are now awaitedGenerally on programme. Carillion are investigating alternative suppliers for skirtless theatre solution
The critical care workshop highlighted 5 key areas for further detailed work and Carillion's submissions are awaitedSkirtless canopy design proposals are progressing well following agreement on the principles
External cladding to northern windcatcher has continued but was disrupted by high winds during the periodA workshop with Carillion was held to identify issues to be covered in the development of the Joint Commissioning Plans
7.1 NBT Redevelopment Project Highlight Report

Report to Trust Board – January 2012
PUBLIC SESSION
Title: Implementation of new Patient Administration System and Electronic Patient Record.
Purpose of paper: Update on the implementation of Cerner Millennium – the progress made, and the issues arising.
For Information Executive Summary: North Bristol has been implementing a new electronic patient record system and patient administration system (Cerner Millennium) that went live on 8th December 2011 and replaced our previous, two, old patient administration systems. Implementation across the Trust We have implemented the Cerner system across the entire Trust: The Emergency Department and our two Minor Injuries Units (Southmead
and Yate) has gone to plan with the ‘expected‘ types of issues following a large and complex implementation. ED and MIUs are working well.
Overall our 65 wards has gone to plan again with some of the ‘expected’ issues for a very large and complex implementation in an organisation of our size, on some wards. The wards are working well and using the new system.
All Theatres are using Cerner. Some theatres have experienced problems relating to patient data migration causing delays with the result of rescheduling some operations. We expect theatres to be back to normal by this Board meeting. Parallel systems have been introduced to ensure optimum safety of each patient, including the manual checking of theatre lists while any issues have been corrected. With these final corrections in place, theatres will be working normally.
The area where we have experienced the most significant problems is in outpatient clinics. These problems have been caused by the incorrect configuration of clinic lists and data migration of existing appointments. As a result, there have been problems with how we are interacting with Choose & Book; patients receiving the wrong appointment dates, no confirmation or cancellation letters and patients being booked into incorrect clinics.
1

2
This has caused disruption and frustration for our patients, and we have apologised publicly for this. It has also placed extra workload on our staff, who nevertheless remain dedicated to ensuring the best possible patient care during this period, and managing the issues that the Trust faces. We have a robust plan in place to “re-launch” all the outpatient clinic areas by the week of February 13th. Around 90% of areas will be working properly on Cerner by the end of January, and at the time of writing (19th January), 57% of outpatient activity is now being successfully processed via Cerner. We are looking at all ways we can to ensure this process if re-launching the outpatient clinics correctly is carried out as fast as we can. Minimising disruption to out-patient appointments We are currently going through a process of correcting the issues with outpatient clinics. To support GPs and their patients we wrote to them on Monday 16 January to advise them as follows: ”We would like to reassure you that all patients who have been referred to us either through Choose & Book, fax or Fast Track are within our appointments system. We are also working through all existing referrals in chronological order and contacting patients, either by phone or letter, advising them of their current appointment slot. “If you have any outstanding queries about your patients’ appointments please ring the appointments helpline, from Monday 16 January, on 0117 323 3700 (Monday to Friday 7am to 8pm and Saturday 10am to 4pm) or alternatively email us at [email protected]. We are very happy for you to provide this telephone number or email address to your patients if they would prefer to contact us directly. “In addition to following your normal route of referral into NBT, if you have any specific concerns about a particular patient’s appointment, from Monday 16 January until Friday 2 March 2012, we have set up a dedicated fax line for you to send through a duplicate referral. This fax number is 0117 323 5450.” Correcting the problems We have apologised to all those patients and GPs affected, recognising the anxiety, frustration and inconvenience caused by the current situation, which we recognise is an unacceptable level of service. We are doing whatever is necessary to resolve the problems as quickly as possible, and have a robust plan to return all outpatient clinics to normal by the middle of February, with 90% plus being returned to normal by the end of January. Our priority is always clinical safety and there is no indication that this has in any way been compromised. In implementing additional safeguarding processes to minimise further disruption to out-patient appointments we will keep the helpline service running until we return to business as usual in February.

3
Our Information Management & Technology Team, supported by our suppliers, BT and Cerner, have been working very hard to sort out these initial issues and we are already seeing improvements. We remain confident that once the new system is fully implemented, it will significantly improve services for our patients and better equip us to meet future challenges. Trust Board is asked to:
Note the significant impact that the implementation of Cerner in outpatients has had on patients and staff.
Note the steps taken to correct and recover this position, and resolve the problems.
Note the progress of the implementation in ED, MIUs, Wards and Theatres.
Key Risks:
Ensuring that patient care is continued and the impact on patient experience is minimised during this transition period.
Ensuring staff are suitably supported during this period, and onto the new system.
Impact on the ability of the Trust to report all information. Ensuring external stakeholders and partners are aware of the position
and progress being made. Impact on Patients:
The implementation of Cerner directly impacts patients. In the medium-long term, across the whole Trust, this will be for the good. However, the unexpected problems in outpatients has impacted on some patients, and the Trust has apologised for this, and taken steps to minimise the impact at this time.
Quality and Safety Standards:
All standards, although Records specifically. Financial Issues:
Have been considered as part of this implementation. Equality Impact Assessment:
Has been completed for this programme.

4
Legal Issues:
Have been considered for this programme. Sustainability Assessment:
Have been considered as part of this programme. Presented by: Martin Bell, Director of Information Management &
Technology. Prepared by: Martin Bell, Director of Information Management &
Technology.

C:\Users\nbe0360\Desktop\trust board downloaded\8.2.1 Activity and Performance Report.doc
Report to the Trust Board – 26th January 2012
Title: Activity and Performance Report
Purpose of paper: To present the current Trust position against new and existing performance targets/indicators to the Board
For Information
Executive Summary: Emergency Access – There remains to be significant issues in relation to the 4 hour emergency department access target. This is largely due to unavailability of medical beds. This has had a knock on effect to the surgical specialties as there have been significant numbers of medical patients in surgical / neuroscience beds. Activity Data – due to some system reporting issues, some areas of performance reporting is behind schedule. It is anticipated that this will be remedied within the next few weeks. Cancer - Cancer targets are being met, however a final data validation will take place over the next 2 weeks to confirm the NBT position in December. Monitor Framework – Attached is the monitor framework for compliance with the governance standards. Action Required: No action required. The Trust Board is asked to: Note the content of the report. Key Risks: Financial penalties associated with performance indicators. Impact on Patients: There is a consistent drive to improve all access targets irrespective of whether they are being met or not. Timely access to clinical opinion and on going care has been identified by patients as being of upmost importance.
C:\Users\nbe0360\Desktop\trust board downloaded\8.2.1 Activity and Performance Report.doc
CQC Outcome: Performance indicators. Responsible Committee: PPFC Financial Issues considered: Yes Equality Impact Assessment Completed: No Legal Issues Considered: Yes Sustainability Assessment Completed: No Presented by: Sue Watkinson, Director of Operations Prepared by: Dan Bates, Information Analyst


Explanation of operational performance targets and associated financial penalties Target Target Description Contract measure Financial
penalty per target
Total possible financial penalty per 12 months
Admitted 18 weeks 90% of all admitted patients for an elective operation/ procedure (pathway) should be treated within 18 weeks from referral.
Contract penalty Up to £3,000,000
Up to £3,000,000
Admitted median The middle patient out of all admitted 18 week pathways should wait no longer than 11.1 weeks
Contract penalty Up to £3,000,000
Up to £3,000,000
Admitted 95th percentile
The patient at 95% out of all admitted 18 week pathways should not be waiting longer than 23 weeks
Contract penalty Up to £3,000,000
Up to £3,000,000
Non-admitted 18 weeks
95% of all non-admitted patients should wait no longer than 18 weeks.
Contract penalty Up to £3,000,000
Up to £3,000,000
Non-admitted median The middle patient out of all the non-admitted 18 week pathways should wait no longer than 6.6 weeks
Contract penalty Up to £3,000,000
Up to £3,000,000
Non-admitted 95th percentile
The patient at 95% out of all the non-admitted pathways should not wait longer than 18.3 weeks.
Contract penalty Up to £3,000,000
Up to £3,000,000
Incomplete pathway 95th percentile
The patient at 95% of all incomplete pathways should not wait longer than 28 weeks
Contract penalty Up to £3,000,000
Up to £3,000,000
Incomplete pathway median
The middle patient out of all the incomplete pathways should wait no longer than 7.2 weeks
Contract penalty Up to £3,000,000
Up to £3,000,000
TWW GP referrals 93% of all patients with suspected cancer will be see from date of referral within 2 weeks
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group

TWW Breast symptoms
93% of all patients with suspected cancer will be see from date of referral within 2 weeks
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group
62 day First treatment from GP referral
85% of all patients with a cancer diagnosis will receive their first treatment within 62 days from being referred by their GP
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group
62 day First treatment from Consultant screening
90% of all patients with a cancer diagnosis following routine screening will have their first treatment within 62 days of referral
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group
62 day First treatment from Consultant Upgrade
90% of all patients with a cancer diagnosis following a routine consultant referral will have their first treatment within 62 days
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group
31 day First treatment from diagnosis
96% of all patients following a cancer diagnosis will be have their first treatment within 31 days
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group
31 day Secondary AntiCancer Drug Treatment
98% of patients will have cancer drug treatments within days for second or subsequent treatments
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group
31 day Secondary Surgery Treatment
94% of patients wait no more than 31 days for second or subsequent surgical cancer treatment
Contract penalty 2% of the value of all activity associated with this patient group
2% of the value of all activity associated with this patient group
31 day Secondary 94% of patients wait no more than 31 days for Contract penalty 2% of the value 2% of the value

Radiotherapy Treatment
second or subsequent radiotherapy cancer treatment
of all activity associated with this patient group
of all activity associated with this patient group
31 day Secondary Palliative Care
94% of patients wait no more than 31 days for second or subsequent palliative care
Internal target No financial penalty
No financial penalty
31 Day Secondary Active Monitoring
94% of patients wait no more than 31 days for second or subsequent active monitoring
Internal target No financial penalty
Cancelled Operations for non-clinical reasons
Provider cancellation of Elective Care operation for non-clinical reasons either before or after Patient admission – 0.8% of all elective admissions
Contract penalty £15k per quarter breached
£60k
Cancelled Operations re-booking within 28 days
95% of same-day cancellation to be re-booked within 28 days
Contract penalty Provider must pay for the relevant Patient’s treatment by another provider of the Patient’s choice
Provider must pay for the relevant Patient’s treatment by another provider of the Patient’s choice
A&E total time 95th percentile (4 hours)
95% of patients to spend no longer than 4 hours in department
Contract penalty 2% of value of A&E activity for period
2% of value of A&E activity for period
A&E unplanned re-attendance rate
Less than 5% of patients to re-attend unless planned
Contract penalty Penalty to be decided
Penalty to be decided
A&E left department without being seen
Less than 5% of patients leave department without being seen
Contract penalty Penalty to be decided
Penalty to be decided
A&E Initial assessment 95th percentile (15 mins)
95% of patients have initial assessment within 15 minutes
Contract penalty Penalty to be decided
Penalty to be decided
A&E time to treatment median (60 mins)
The middle patient of all patients waiting treated within 60 minutes
Contract penalty Penalty to be decided
Penalty to be decided

A&E Ambulance Handover times >2 hours
No ambulance handovers taking longer than 2 hours
Contract penalty Penalty to be decided
Penalty to be decided
A&E ambulance handover times >45 mins
No ambulance handovers taking longer than 45 minutes
Contract penalty £95 per breach £95 for each breach
Length of stay measures
Local targets set for improved productivity Internal target No financial penalty
No financial penalty
Readmissions within 30 days – emergency re-admissions following elective admission
With the exception of specific patient groups, emergency re-admission following an elective admission within 30 days is not paid for
Contract limiter No re-admission activity is paid for
No re-admission activity is paid for
Readmissions within 30 days – emergency re-admissions following emergency admission
2% reduction on 2010/11 levels of emergency re-admissions following emergency admissions
Contract limiter Activity not paid for if reduction is less than 2%
Activity not paid for if reduction is less than 2%
DNA rates “Did not attend” rates to be less than 5% Internal target No financial penalty
No financial penalty
6 week diagnostic waits
99.5% of diagnostic waits to be less than 6 weeks
Contract penalty £10k / month breached
£120k
Revascularisation – 11 weeks
100% of revascularisation within 11 weeks National target No financial penalty
No financial penalty
Choose & Book sufficient appointment slots
Failure to ensure that “sufficient appointment slots” are made available on the Choose and Book system – 96% availability
Contract penalty £10k / month breached
£120k
18 week direct access audiology
95% of Patients seen within 18 weeks for direct access audiology treatment
Contract penalty £10k per month breached
£120k
Stroke management 90% on stroke unit
80% of stroke patents who spend at least 90% of their time on a stroke unit.
Contract penalty £30,000 per quarter
£120,000
Stage of Treatment – 26 week inpatient
No patient waiting longer than 26 weeks from referral to admitted treatment
National target No specific financial
No specific financial

breaches penalty penalty Stage of Treatment – 13 week outpatient breaches
No patient waiting longer than 13 weeks for an outpatient appointment from referral
National target No specific financial penalty
No specific financial penalty
Delayed Transfers Delayed transfers of care to be maintained at a minimal level. Target set at 20% reduction on 2010/11 levels
Contract penalty No financial penalty
No financial penalty
Daycase Rates 72.7% of specific procedures to be carried out as a daycase
Internal target No financial penalty
No financial penalty
Performance against SLA
Performance against SLA
Monitor Compliance Framework
Monitor Compliance Framework

Performance against SLA 2011/12 : DATA SOURCE = WAREHOUSE
Directorate / Specialty = ALL
0
5000
10000
15000
20000
25000
30000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
New Outpatient AttendancesActual 10/11 Outturn SLA
0
5000
10000
15000
20000
25000
30000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
FUp Outpatient Attendances Actual 10/11 Outturn SLA
0
50
100
150
200
250
300
350
400
450
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Regular Attenders Actual 10/11 Outturn SLA
0
500
1000
1500
2000
2500
3000
3500
4000
4500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Day Cases Actual 10/11 Outturn SLA
0
500
1000
1500
2000
2500
3000
3500
4000
4500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Elective Inpatient Spells Actual 10/11 Outturn SLA
0
500
1000
1500
2000
2500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Emergency Short Stay Spells Actual 10/11 Outturn SLA
0
500
1000
1500
2000
2500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Emergency Long Stay Spells Actual 10/11 Outturn SLA
0
200
400
600
800
1000
1200
1400
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outpatient ProceduresActual 10/11 Outturn SLA

North Bristol NHS TrustMonitor Compliance Framework
Service Performance Score Risk Rating
Number Target Weighting Target Threshold YTD Q1 Q2 Q3 Q4 Notes <1 Green
1 Infection Control ‐ C.Diff Infections Against Trajectory 1.0 < or = trajectory 52 29 23 4Trajectory: Q1 29; Q2 28; Q3 28; Q4 28
0.0 ≥ 1.0 ‐ < 2.0 Amber‐green Score and ratings tables taken from Monitor Compliance Framework 2011/12
2 Infection Control ‐ MRSA Bloodstream Cases Against Trajectory 1.0 < or = trajectory 9 8 1 0Trajectory: Q1 2; Q2 2; Q3 2; Q4 2
0.0 ≥ 2.0 ‐ < 4.0 Amber‐red Service Performance Score ‐ Diagram 11, p25
3a Cancer ‐ 31 Day Diagnosis To Treatment (Subsequent ‐ Drug) 98% 100.0% 100.0% 100.0% 100.0% ≥ 4.0 Red Red Override Rating ‐ Diagram 12, p28
3b Cancer ‐ 31 Day Diagnosis To Treatment (Subsequent ‐ Surgery) 94% 98.2% 98.9% 97.1% 100.0%
3cCancer ‐ 31 Day Diagnosis To Treatment (Subsequent ‐ Radiotherapy)
94% 100.0% 100.0% No Cases No Cases Red Override Rating
4a Cancer 62 Day Referral To Treatment (Urgent GP Referral) 85% 89.0% 89.2% 87.6% 87.1% Indicator Monitor may apply a red governance risk rating and escalate an NHS foundation trust for consideration as to whether it is insignificant breach if the trust:
4b Cancer 62 Day Referral To Treatment (Screenings) 90% 97.7% 94.4% 100.0% 91.7% Meeting the MRSA objective Has greater than six cases in the year to date, and either:
5Referral to treatment time for admitted patients (95thpercentile) ‐ in weeks 1.0 23.0 20.6 20.3 20.7 20.0 0.0 • breaches the cumulative trajectory for three successive quarters and has greater than six cases in the year‐to‐date; or
6Referral to treatment time for non‐admitted patients (95th percentile) ‐ in weeks 1.0 18.3 13.0 13.0 13.1 13.3 0.0 • breaches its full year objective.
7 Cancer ‐ 31 Day Diagnosis To Treatment (First Treatments) 0.5 96% 97.9% 98.9% 96.8% 96.4% 0.0 Meeting the Clostridium Difficile o• breaches the cumulative trajectory for three successive quarters; or
8a Cancer ‐ Urgent Referrals Seen In Under 2 Weeks 93% 93.8% 93.4% 94.0% 93.6% • breaches its full year objective.
8b Cancer ‐ Symptomatic Breast in Under 2 Weeks 93% 97.4% 97.1% 95.5% 98.1% Referral to Treatment (RTT) • breaches either the admitted OR non‐admitted waiting time measure for a third successive quarter.
9 A&E Total time in A&E 4 hours (95th percentile) Q1 only 1.0 95% 97.0% 97.6% Not scored in Q2 A&E clinical quality indicators • fails to meet the A&E target twice in any two quarters over a twelve month period and fails the indicator in a quarter during
9a A&E Total time in A&E 4 hours (95th percentile) Q2‐4 95% N/A 96.3% 95.0% the subsequent nine‐month period or the full year.
9b A&E Time to initial assessment (95th percentile) ‐ in minutes 15 78.0 82.0 80.0 • "failure" is defined as either:
9c A&E Time to treatment decision (median) ‐ in minutes 60 55.0 56.0 54.0 • failing the A&E 4‐hour waiting time target in any quarter prior to Q2 2011/12; or from Q2 2011/12, failing 3 or more A&E clinical quality indicators
9d A&E Unplanned reattendance rate (within 7 days) 5% 4.3% 4.6% 4.3% Cancer waiting times • breaches either:
9e A&E Left without being seen 5% 2.6% 2.7% 2.3% • The 31‐day cancer waitingtime target for a third successive quarter; or
10 Stroke indicators ‐ to be confirmed 0.5To be confirmed
(TBC)N/A Not scored • The 62‐day cancer waitingtime target for a third successive quarter.
11Self certification against healthcare for patients withlearning disabilities (year‐end compliance)
0.5See LD Action Plan
Oct 11 Ambulance response times • breaches either:
0.5• the category A 8‐minute response time target for a third successive quarter; or
Please note: Service Performance Score, Risk Rating and Override Rating are derived from Monitor Compliance Framework ‐ details are on the next page GREEN • the category A 19‐minute response time target for a third successive quarter.
RED All other indicators weighted 1.0 breaches the indicator for three successive quarters.Override Rating
Q1 Forecast
Risk Rating
Standards to be confirmed
Service Performance Score
1.0
1.0
0.5
0.5 (failing 2 or fewer)
1.0 failing 3 or more)
Q3 Service Performance Score
Quarterly Performance
Not scored in Q1
0.0
0.0
0.0
0.5

CQC – ACCESS TO HEALTH CARE FOR PEOPLE WITH A LEARNING DISABILITY
All LD inpatients to have LD Risk Assessment carried out within 48 hours. CQUIN 7.2
Random audit of 8 sets of notes monthly.
90% compliance
JY Monthly
Community services informed if LD patient discharged from ED.
Working party formed August 2011.
ED records demonstrate liaison with LD services for all LD patients.
JR/MC November
NQAT includes LD related questions
1. Does the trust have a mechanism in place to identify and flag patients with learning disability and protocols that ensure that pathways of care are reasonably adjusted to met the health needs of these patients.
All LD patients to be identified on PAS.
As LD patients become known to LD nurses they are entered onto PAS. Alert email to LD Nurses if admitted. Currently 60% demonstrating month on month improvements
Clinical alert sent for 100% LD patients that are known to NBT.
ImplementedAW/SB
Indicator Action Progress Measure
Routine nursing quality audit tool identifies staff
All LD questions answered
DateLead
Review quarterly.
All LD patients to be coded
LD increasingly being coded by
100% of all patients
DM
EG/JR
Review quarterly

Develop NQAT reportsRed napkins/ Malnutrition screening tool
Audit. KL/GH
Accessible menu’s
Available in inpatient areas
Nutrition steering
Easy Read Leaflets and letters -
Available on intranet and in public areas.
Pre admission information pack
Audit by LD Leads.
Communication folder in all areas
Pharmacy card is easy read.Leaflets available on intranet:
Compliments and Complaints
X RayGoing to HospitalHealthy eatingLD Nurses
Under development
General Anaesthetic
September
Nutrition and hydration needs met
2. In accordance with the Disability Equality Duty of the Disability Discrimination Act (2005) does the trust provide readily available and comprehensible information?
Accessible information to be developed and available to patients, carers and staff:
EG/JR/SH
knowledge of LD correctly.

Pre Assessment AOCEmergency DepartmentDischarge
NBT external website to include links to leaflets
Leaflets available via LD page
JK Aug-11
Carers Policy draft
AW October
Reports.Carers badge roll out Trust wide- to enable increased access, subsidised meals and discounted parking.
AW Sep-11
3. Does the trust have protocols in place to provide suitable support for family carers who support patients with learning disabilities, relevant legislation, and carers rights
Carers to be supported and involved as partners in care

Carers Strategy Group minutes.
Carers feedback project
Report TS/AW Sep-11
Matrix being developed
AW/JH
Capture training on MLEDevelop e learning package
Minutes LD group
HoN’s Jun-10
Directorate leads established
Comms evidence
AW Jul-11LD Awareness week delivered
December LD Advisors to be recruited across the Trust to support LD patients and staff
AW
Good Practice Stories
LD Group minutes
EG/JR Ongoing
Resource folder and communication pack available in all clinical areas.
EG/JR Jun-10
4. Does the Trust have protocols in place to routinely include training on learning disability awareness, relevant legislation, human rights, communication techniques for working with people learning disability and person centred approaches in their staff development and/or induction programmes for all staff.
All staff to receive awareness/training at appropriate level

Accessible information re specific conditions e.g cancer & diabetes
EG/JR 2010People with a learning disability have a voice and are able to influence NBT services.
People with a learning disability to be included within FT consultation process and membership recruitment.
Easy read leaflet to be developed
NBT LD Nurses are regular members of local LD partnership groups.
Minutes of meetings.
EG/JR On going
11.7.2011 Tour
Annual tour.
Individual case studies
Individuals tours as required.
5. Does the trust have protocols in place to encourage representation of people with learning disability and their family carers within Trust Boards, local groups and other relevant forums, which seek to incorporate their views and interests in the planning and development of health services.
Evidence of involvement/visits to local LD groups.
JW November
LD people are welcomed into the Trust and given tours to meet staff.
EG/JR

Easy read ward feed back card
Pilot JW August
Service user feedback system
PDSA AW October
Develop LD Strategy
Published AW December
LD group reports to Safeguarding Committee which reports to Trust Board.
Implemented
Executive and non- Executive leads
IdentifiedReview policies related to MCA, Safeguarding, Restraint and Mental Health.
Policies published
MCA training include reference to LDRaise awareness of IMCA’s
Use of IMCA’s records
Central safeguarding data base developed
October
6. Does the trust have protocols in place to regularly audit its practices for patients with learning disability and to demonstrate the findings in routine public reports.
Robust Safeguarding framework enables LD to be discussed at Trust Board regularly.
Meeting minutes
MNO
Robust MCA and safeguarding policies.
SC

All incidents and complaints are recorded in Trust wide electronic systems that automatically alert the Safeguarding Manager when vulnerable adults are involved; he liaises with the LD Nurses.
AIMS records
SC In place
Any complaints made to ACT involving LD patient will be referred to LD Nurses within 24 hours for opinion.
Complaints records
SS In place
Audit of consent compliance
Report MNO September
System for flagging serious incidents or complaints involving LD patients to LD nurses promptly.
Outcomes for LD patients
LD admissions and deaths, by speciality, reported weekly on Trust information service.
On IT system
PM In place

Fortnightly report from IT of all OPD DNA’s and re admissions.
Put information on ILD Nurses follow up all DNA’s.
Feedback to community teams
6 monthly meetings – Sept.6 monthly reports inform action plan.
Jun-11
2013
IT system PM
Confidential Enquiry into the deaths of people with learning disabilities.
GH
CQC – ACCESS TO HEALTH CARE FOR PEOPLE WITH A LEARNING DISABILITY Indicator Action Progress Measure Lead Date
All LD patients to be identified on PAS.
As LD patients become known to LD nurses they are entered onto PAS. Alert email to LD Nurses if admitted. Currently 60% demonstrating month on month improvements
Clinical alert sent for 100% LD patients that are known to NBT.
EG/JR Review quarterly.
All LD patients to be coded
LD increasingly being coded by medical staff. Awareness raising by coders of extra payments for LD as a co-morbidity April 2011.
100% of all patients with an LD to be coded.
DM Review quarterly
All LD inpatients to have LD Risk Assessment carried out within
Random audit of 8 sets of notes monthly.
90% compliance JY Monthly
1. Does the trust have a mechanism in place to identify and flag patients with learning disability and protocols that ensure that pathways of care are reasonably adjusted to met the health

48 hours. CQUIN 7.2 y
Community services informed if LD patient discharged from ED.
Working party formed August 2011. ED records demonstrate liaison with LD services for all LD patients.
JR/MC November
Routine nursing quality audit tool identifies staff knowledge of LD
NQAT includes LD related questions Develop NQAT reports
All LD questions answered correctly.
AW/SB Implemented
needs of these patients.
Nutrition and hydration needs met
Red napkins/ Malnutrition screening tool Accessible menu’s
Audit. Available in inpatient areas
KL/GH Nutrition steering
2. In accordance with the Disability Equality Duty of the Disability
Accessible information to be developed and available to patients, carers and staff:
Easy Read Leaflets and letters - Pre admission information pack Communication folder in all areas Pharmacy card is easy read.
Available on intranet and in public areas. Audit by LD
EG/JR/SH

Medical Directorate Action Plan – January 2012
Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Supporting Targets Who & When
Confidential Page 1 of 5
Generic Issues Understand whole bed management system and promote clinical team engagement.
Arrange a facilitated process mapping event to include representation from teams throughout the patient pathway
Event
Identify bottlenecks and get team agreement on how these will be addressed.
Nicola Alfonsi February 2012
Designate operational clinical lead to lead directorate approach to improvement of performance
Reorganisation of matron responsibilities to allow release of senior nurse.
The directorate recognises the importance of senior clinical leadership in introducing and managing change in relation to patient quality indicators.
4 Hour patient access target
Jan McIntyre January 2012
Raise awareness of impact of delayed transfers of Care
Daily reporting of delays on sit rep
Discharge and delay information available at Trust bed meetings,
Reduced length of stay.
Care Management team Feb 2012
All Southmead specialties to ensure that they have process in place to ‘pull’ specialty patients into the appropriate bed.
AGM, Matron and Specialty Lead to identify criteria and work with designated clinical operational lead to embed a process.
Increase the number of ‘right patient, right bed, first time.
Directorate big 5 objective
AGM, Matron, Specialty Lead and Directorate Operational Lead Feb 2012

Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 2 of 9
Undertake profile of the Emergency ‘take’ to ensure correct distribution of specialty beds and consultant bed base
Develop an audit tool to capture information to inform the directorate.
Understanding the bed profile
Right patient, right bed.
Nicola Alfonsi Feb 2012
Remove steps in the patient pathway which extend LOS
Profile patient intervention and movements
Evidence to support patient transfer policy and performance manage the systems in place. Correct decision making process followed.
Right patient, right bed. To achieve Trust and directorate objective on patient moves.
Nicola Alfonsi Feb 2012
Introduce early morning ward rounds to see ‘New, Sick and Dischargeable patients’ on selected wards
PDSA. Profile current discharge rate by day and time against pilot period.
Improvement in early discharge.
No waits no, delays AGM’s, Matrons and Specialty Leads Feb 2012
Access to Pharmacy out of hours
Liaise with Core Clinical Services to extend pharmacy opening hours.
Availability of TTA’s. Reduced length of stay and improved weekend discharges.
Director of Operations General Manager- Core Clinical Services.
ITU bed availability
Improve access to ITU beds from ED
4 Hour patient access target.
Right patient, right bed. Director of Operations General Manager- Core Clinical Services.

Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 3 of 9
Length of Stay
Clinical analyst to highlight directorate ‘hot spots’.
Evidence that correct discharge processes followed.
Reduced length of stay.
Information Analyst GM and CD Medicine Feb 2012
Respiratory
Engagement with senior clinicians to ensure that priority patient list maintained, to allow ‘pull’ of appropriate patients from Frenchay
Ward consultant of the day will liase with AAU and other colleagues to allow respiratory wards to keep a priority list
List available and profile of patient movement will improve
Right patient, right bed. No waits, no delays
AGM, Matron and Specialty Lead
Infectious Diseases
ID to develop education to facilitate recognition of appropriate patients by AAU junior Drs and Nurses
Daily liaison between ID SpR* and AAU coordinator to identify patients suitable for transfer
List available and profile of patient movement will improve
Right patient, right bed. No waits, no delays
AGM, Matron and Specialty Lead
Gastro
Build on ‘productive ward methodology using white board rounds to facilitate timely management of pts by MDT
Ensure consistency of practice by MDT
Improvement in safe and timely discharge
Right patient, right bed.
AGM, Matron and Specialty Lead

Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 4 of 9
Palliative Care Consultant Palliative care Consultants and Nurse practitioners to join AAU ward handover daily to identify patients appropriate for the service and to be available each morning to assist in rapid assessment and treatment of these.
Reorganisation of job plans. Palliative Care team to work with AAU to develop education and practice
Patients will receive earlier input and therefore a better experience. Macmillan Unit beds will be used earlier and appropriately
Better patient experience. Right patient Right bed
AGM, Matron and Specialty Team
Care of the Elderly
Expand admission avoidance and OPALS team through QIPP schemes
Develop and promote the Rapid Access and OPALS model
Decrease admission numbers and reduction in 0-48 hours LOS
Monitor delay report AGM, Matron and Specialty Lead
Cardiology
Clinical model of care
tbc
Risks
No SPR currently in ID service Medicine currently carrying 6 SpR gaps

Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 5 of 9
Emergency Department Reduce/eliminate breaches that occur in see and treat at Frenchay
1 additional ENP on every shift in See & Treat at Frenchay (5.5wte band 6/7) Treatment nurse on every shift in See & Treat at Frenchay (5.54wte band 5)
ENP shifts recruited to. Provide consistency and senior decision making in see and treat avoiding peaks and troughs in activity associated with Junior Doctor changes. Release Junior Doctors to concentrate on the majors admitted and not admitted patient population. Treatment nurse shifts recruited to. Maximise the efficiency of the see & Treat clinicians by undertaking treatments such as suturing plastering. This will ensure that flow is maintained through see and treat. In times of increased demand the seen and treat nurse will
Reduction in overall waiting time of patients across the department at Frenchay and therefore contribute to a reduction in ambulance handover delays Reductions in overall waiting time of patients in see and treat at Frenchay. Time to analgesia target will improve.
Juliette Hughes (once funding /recruitment approved) Juliette Hughes (once funding /recruitment approved)

Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 6 of 9
be able to provide a double triage facility.
Standardisation of Shift Coordination
Shift Coordinators to be supernummary (at present is included in the department numbers and therefore carries out direct patient care at times). (5.54wte band 4) Continue to educate shift coordinators on the benefits realisation of Cerner millennium in the Emergency Department.
This will enable accurate coding, accurate breach recording, and accurate time stamping of bed requests and prompting effective escalation to CSM team.
Reduction in overall breach numbers having reduced the anxiety levels around breach reporting.
Juliette Hughes & Matt Crabtree(once funding /recruitment approved) Juliette Hughes & Matt Crabtree
Meet the initial assessment clinical indicator and improve ambulance handover times
Substantively recruit to Initial Assessment Nurse (IAN) post (currently done on a bank basis which often is left unfilled) (5.54wte band 5 Short term funding source identified)
IAN shifts recruited to. Maximise the efficiency of the department by streaming patients to the most appropriate area within the Emergency Department at Frenchay. Contribute to the reduction in time to analgesia clinical indicator.
Reductions in overall waiting time of patients in see and treat at Frenchay. Time to analgesia target will improve.
Juliette Hughes & Matt Crabtree(once funding /recruitment approved)

Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 7 of 9
Dedicated ED porters 24 hours a day. With the facility to call on the lodge at times of high activity.
Substantively recruit. Currently have agency porters from 10 am to 2am. Agency porters are expensive as well as lacking the commitment and consistency that is required. These posts can help in the department with log rolling, stocking up etc.
Porter’s shifts recruited to. Maximises the efficiency of the department by transferring patients for their diagnostic tests and to wards in a timely manner
Reductions in overall waiting time of patients across the Emergency Department at Frenchay.
Mo Swinscoe & Nicola Hughes
Acute Assessment Unit Specialty wards to actively pull patients from the AAU
AAU to assist in this process by identifying the specialty that the patient requires (this will be put onto the whiteboard) Each Specialty to hold a prioritised TCI list of all patients requiring a bed on their ward(s). This list will be kept up-to-date at all times, this will be used by the bed management team and Clinical Site Team.
All patients on the AAUs will have a specialty destination allocated. List exists for each specialty and is shared with the bed management team.
Denver McCrum Specialty Matrons
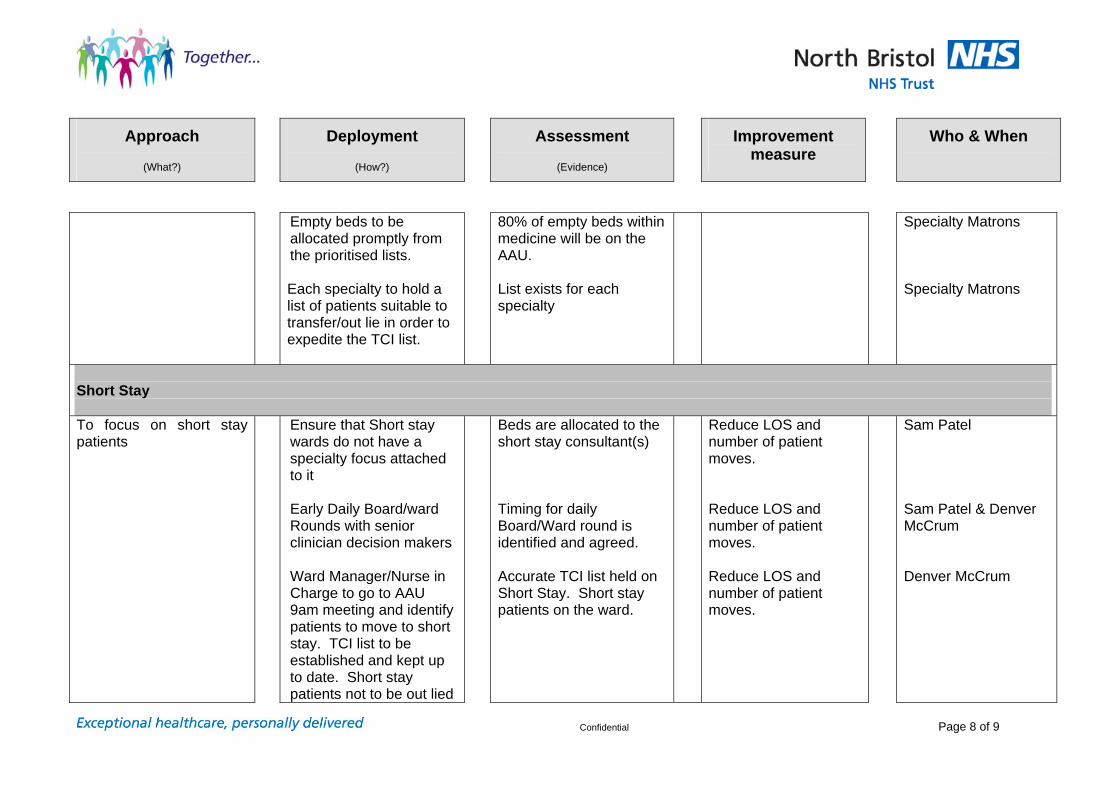
Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 8 of 9
Empty beds to be allocated promptly from the prioritised lists. Each specialty to hold a list of patients suitable to transfer/out lie in order to expedite the TCI list.
80% of empty beds within medicine will be on the AAU. List exists for each specialty
Specialty Matrons Specialty Matrons
Short Stay To focus on short stay patients
Ensure that Short stay wards do not have a specialty focus attached to it Early Daily Board/ward Rounds with senior clinician decision makers Ward Manager/Nurse in Charge to go to AAU 9am meeting and identify patients to move to short stay. TCI list to be established and kept up to date. Short stay patients not to be out lied
Beds are allocated to the short stay consultant(s) Timing for daily Board/Ward round is identified and agreed. Accurate TCI list held on Short Stay. Short stay patients on the ward.
Reduce LOS and number of patient moves. Reduce LOS and number of patient moves. Reduce LOS and number of patient moves.
Sam Patel Sam Patel & Denver McCrum Denver McCrum

Approach
(What?)
Deployment
(How?)
Assessment
(Evidence)
Improvement measure
Who & When
Confidential Page 9 of 9
as this compromises patient flow and length of stay. Golden patient model to be fully implemented.
Empty beds on the AAU every morning by 10am
Reduce LOS and number of patient moves.
Denver McCrum
Anne Morris Nicola Hughes Judith French Pauline Roost Juliette Hughes Denver Mccrum

CONFIDENTIAL
Report to the Trust Board – January 2012
Title: Emergency Access Performance
Purpose of paper: To present to the Board the current emergency access performance issues and the recovery plan to improve performance.
For Information
Executive Summary: The emergency department access target at Frenchay is not being achieved mostly due to a lack of medical beds in the system. This has serious implications for Monitor compliance. As a direct result of medical patient flow problems, and an increase in length of stay, associated targets such as 4 hour patient access target, cancelled operations and 18 weeks admitted are all being compromised. Action Required: For the Board to review, discuss and if appropriate, agree the
recommendations in the attached report. The Trust Board is asked to: Agree the approach outlined in the report. Key Risks: The key risks to the organisation are as follows:- Inability to proceed to become a Foundation Trust Financial penalties associated with non delivery key performance and
quality indicators. Reputational damage to the Trust Lack of confidence from our patients and external stakeholders Inability to proceed with Major Trauma designation.
Trust Board Jan 2012 AM

Impact on Patients: Poor outcome and experience as a result of cancelled operations and timely access to emergency care. CQC Outcome: Performance indicators. Responsible Committee: PPFC Financial Issues considered: Yes Equality Impact Assessment Completed: No Legal Issues Considered: Yes Sustainability Assessment Completed: No Presented by: Sue Watkinson, Director of Operations Prepared by: Anne Morris, General Manager, Medicine
Trust Board Jan 2012 AM

Report into Access Targets 1. Background 1.1 This paper is to advise the Trust Board and Trust Management Team of the
current status of North Bristol NHS Trust’s operational performance relating to the Emergency Department quality indicators and the steps being undertaken to improve performance and patient experience. It concentrates mainly on the actions being undertaken in the Directorate of Medicine although will provide an overview of issues relating to other directorates and external agencies.
1.2 Since September 2011, performance the 4 hour patient access target has
consistently not been met. Other access targets are at risk of being compromised, such as cancelled operations, rebooking within 28 days and length of stay.
2. Diagnostics 2.1 In order to understand the reasons behind the fall in performance a full
diagnostic investigation has been undertaken. There have been many high impact changes in the Medicine directorate over the last year. It is not possible to completely link each event to a single impact due to the complexity of systems and processes. Each of these events has had an impact and it is likely that the volume of system changes concentrated within a time period have caused complicated effects and possibly exaggerated effects a single change might have made.
2.2 The changes that have impacted on patient flow through the organisation
include:-
The amalgamation of the two medical admissions units on the Frenchay site in May 2011 although direct admissions to the AAU remain consistent pre and post move.
Performance has shown that the ‘cross site’ transfer process can deliver the
volume of patient transfers needed as indicated from the MAU project modeling. However, the data raises a concern with the time of transfer. This may indicate an improvement is needed in bed management and the management of transfers. A reactive “push” rather than proactive “pull” system is currently operating.
Implementation of the common approach. Phase 1 of the project went live as
of 3 May 2011. Phase 1 includes the common approach portal acting as the portal through which all referrals from GPs and community practitioners to secondary care for medicine are sent. Phase 2 commenced as of 1 September 2011 and the core of this is redirection of appropriate patients from ED back to primary care via dedicated “hot slots” in GP practices across South Gloucestershire. Those patients not accepted by the common approach now attend ED.
The average monthly number of ambulances presenting at ED has increased,
there are approximately 60 more ambulances a month attending ED since April 2011. Anecdotally patients attending with “Dear Doctor” letters increased after August. All of this may mean GPs are using ED rather than the Common Approach portal but this analysis requires further scrutiny.
Trust Board Jan 2012 AM

The emergency department is busier autumn 2011 compared to autumn 2010 and it would appear that more emergency attendances are being turned around rather than admitted. 233 more majors attended ED this September compared to September 2010.
The MAU move does not have a clear impact on breaches as a percentage of
admits but this relationship gets noticeably worse for all specialties from September. Breaches as a percentage of admits showed a steep increase for all specialties from September. This could suggest one of the September changes has impacted on performance.
There are fewer direct admissions than expected to the Southmead site.
These patients are being admitted directly to Frenchay instead. Respiratory analysis and the opportunity to increase direct admissions is complicated by hot clinic admission avoidance.
Reduction in bed base on ward 104 (burns) for infection control reasons. In
addition, a new criteria for patient admissions to this ward has resulted in empty beds that cannot accommodate other patients.
An increased length of stay for medical and surgical patients. There has been
an increased number of staying patients in Medicine in autumn 2011 compared to autumn 2010, causing a constraint on bed availability. This has impacted on patient flow. The current nature of delays data makes analysis of the reasons challenging however Cerner should improve this.
Average length of stay has increased however short stay activity has
reduced. This may mean that length of stay for the patients who are admitted is actually quite stable but the average has skewed by the reduction in short stay activity.
Single sex accommodation requirements resulted in 15% less reduction in
CDU capacity and less flexibility of available beds. CDU bed changes have impacted patient flow at a level of 20 patients per week; this is likely to be linked to ED breaches.
From September 2011 Bed managers have been managed centrally rather
than in directorates
There has been a shift in peak activity times to much later in the day with many direct admissions to AAU taking place out of hours. Anecdotally this is due to transport issues.
Plain film x-rays are taking longer compared to the same time period in 2010.
This can be seen in the AAU and across the General Medicine category. Plain film requests are likely to be affecting AAU length of stay. The time to scan will have been affected by the increased request volume at the Frenchay site. Once time to “report” is considered this is likely to have a significant impact on the AAU length of stay. Plain film requests are taking longer for “Gen Med” patients. For 438 patients “request to scan” took longer than 8 hours in a 3 month period. This is 91 more patients than the same time last year.
Trust Board Jan 2012 AM

Trust Board Jan 2012 AM
The Stroke service moving to Neurosciences, with an expected increase in direct stroke admissions demonstrate a decrease in Medicine ED attendances. This has not been seen. Further understanding is required to establish the issues.
3. Action Plan 3.1 Following a meeting with the Chief Executive and the Director of Operations in
early January a fresh action plan has been drawn up by the Medicine Directorate.
3.2 The Emergency Intensive Support team have been informally approached and
are visiting the Trust on 26th January 2012 to carry out an initial independent review of our systems and processes.
3.3 In the meantime the following actions are currently being undertaken:-
Staffing review in ED of ENP’s, shift co-ordinators, treatment room nurses and initial assessment nurses to improve reduction in ‘see and treat’ wait times, overall department wait times and ambulance off load times.
Staffing review of ED porters to reduce reliance on agency staff, provide dedicated ED Porters and maximise efficiency of transfer for diagnostic tests and to ward beds
Specialty wards to actively ‘pull’ patients from the AAU. All patients in AAU to have allocated specialty destination. 80% of empty beds in medicine to be in the AAU.
Improved efficiency of ‘short stay’ beds with daily board/ward rounds and accurate patient transfer lists held.
Patient flow review in progress by AGM. Clinical Operational lead in place working with central bed management
team and reviewing patient flow with AGM. Central bed management team have allocated senior bed manager to
Medicine to improve consistency. All specialties within medicine have contributed to an action plan to improve
performance with both generic and specialty measures in place. Daily telephone conferences with the PCT in place to review all patients
awaiting repatriation to other hospitals Daily delayed transfer of care lists being sent to the PCT for review Reviewing with GWAS patient flows into the organisation. Root cause
analysis to be undertaken following a 2 week audit of GWAS activity through the ED. This will be carried out jointly by NBT, GWAS and South Glos PCT.
OPALS pilot scheme to be launched end of Jan 2012. Directorate analyst providing information on ‘hot spot’ areas with rising or
extended length of stay. 4. Recommendation 4.1 That the Trust Board reviews the approach outlined in this paper for
consideration and approval. Sue Watkinson Director of Operations

Report to Trust Board – January 2012
Title: Workforce & Organisation Development Report
Purpose of paper: To provide the Trust Board with an update on current workforce and organisation development issues.
For Information Action Required: Trust Board is asked to NOTE the attached paper.
Key Risks: Financial and performance-related risks
Impact on Patients: The Trust’s workforce and organisation development strategy
and associated matters directly affect the provision of patient care and treatment
CQC Outcome: CQC Outcomes 12,13,14 Responsible Committee: Workforce Strategy & Governance Committee Financial Issues considered Yes Equality Impact Assessment Completed: Yes where applicable Legal Issues Considered: Yes Sustainability Assessment Completed: Not Applicable Presented by: Harry Hayer, Director of Organisation, People & Performance Prepared by: Senior HR Management Team
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
1

This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
2
Workforce & OD Report
January 2012 1) National issues: The Secretary of State has announced a new ‘Whistleblowing’ helpline for NHS staff who
have concerns and are unsure how to raise them or would like free, independent and confidential advice. The helpline is also open to employers for good practice advice.
The new number (08000 724725) is available weekdays between 8.00am and 6.00pm with an ‘out of hours’ answering service on weekends and public holidays. NBT is considering how to communicate the new helpline number to staff and will ensure it is embedded within the existing Whistleblowing Policy.
The NHS pension scheme undertook a consultation on proposals for member contribution increases in 2012, following the Government's announcement in last year's Spending Review that public sector workers would be asked to contribute an average of 3.2 per cent more for their pensions, phased in over three years from 2012.
The outcome of the consultation has been announced, relating to delivering savings in the first year (financial year, 2012/13). The changes will come into effect on 1 April 2012. The details of the new arrangements are set out in the table below.
Full-time 2010/11 pay
2010/11 contribution (gross)
2012/13 contribution (gross)
Contribution increase (gross)
Up to £15,000 5.0% 5% 0% £15,001 to £21,175
5.0% 5% 0%
£21,176 to £26,557
6.5% 6.5% 0%
£26,558 to £48,982
6.5% 8.0% 1.5%
£48,983 to £69,931
6.5% 8.9% 2.4%
£69,932 to £110,273
7.5% 9.9% 2.4%
Over £110,273 8.5% 10.9% 2.4%
Under this new structure, the Government Actuary’s Department (GAD) estimates that the number of employees who will pay nothing extra in 2012/13 will be 630,000. This represents approximately 48% of the total NHS Pension Scheme membership. The Department has prepared draft NHS Pension Scheme regulations which will implement the changes to contribution rates. A copy of the draft Regulations are available on the NHS Pensions website.
2) Local issues :
2.1) Learning and Development (L&D) :
A second cohort of Maternity Care Assistants has been commissioned from L&D by Womens & Childrens Health after launching a successful first group on a ‘fast track programme’ of which the taught element will complete in 9 months.

This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
3
A new E-learning module on ‘falls prevention’ developed by NBT subject matter experts and clinicians in partnership with UWE has been successfully integrated on the NBT MLE and is now available for all clinical staff.
Mandatory and Statutory Training shows the anticipated drop in % in core topics, due to the focus being on other training to implement Cerner, and also large number of staff being due for update at the same time, as we meet anniversaries of new programmes being implemented 2 years ago:
Based on the 5.12.11 report : o Fire 66% o Manual handling 66% o Health & Safety 63% o Infection Control 75% o Child protection 88%
The following shows the use of e-learning as a percentage of all module attendance for the top current issues:
o Fire 19% o Manual handling 21% o Health & Safety 28% o Infection Control 8%
Individuals have the option of doing e-learning on alternate update ‘anniversaries’. It is possible therefore that in future 50% of all updates will be by e-learning once the full cycle is complete for every individual.
In response to the fall in infection control compliance, and as part of the ongoing initiative to give people access to core training, a new programme will launch from February 2012 including an Infection Control update for non-clinical staff together with two further essential modules in response to new requirements, Dementia Awareness and Safeguarding Adults Level 1 Awareness. Staff at all levels are also encouraged to get involved as a ‘Dementia Champion’ and in raising awareness of training/update opportunities for our staff.
Leadership and management development – Institute of leadership and management
accredited programme through the NBT centre (ILM), 20th December saw the awards ceremony for over 100 successful participants who achieved ILM qualifications during 2011 in team leading, first line management and Certificate in Management. L&D are launching a new ILM new Coaching Award, and a Level 5 certificate in Management from April.
2.2) Workforce issues
NBT successfully TUPEd in 20 staff from a privately-run Dialysis Unit (South Bristol), in December, which will now be run as a satellite unit. This has always been part of Renal Directorate’s workforce plan as growth and will affect finances in a positive way.
Starting in January, there will be a transition to a new laundry contract provided by Sunlight, with the consequent closure of the Blackberry Hill Laundry at the end of March. This will lead to the redundancy of about 26 staff, with a further 12 having been identified for re-deployment.
Revised terms of reference have been prepared for the Workforce & OD Strategy &
Governance Committee, a working group of the Trust Board, with the role of chair moving from the Chief Executive to a Non-Executive Director (Nick Patel). The purpose of the Committee has been redefined as being to :-

This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
4
‘oversee the development and implementation of the NBT Workforce & Organisation Development Strategy, whilst ensuring that appropriate and effective governance, measurement, compliance and assurance processes are in place’.
The first meeting of the newly constituted Committee takes place on the 6 February 2012.
The Workforce Report in November showed significant DNAs for medical review at Occupational Health. Consideration has been given as to whether these should be charged (as with non-attendance at training events).
Two key factors need resolving before this is considered, firstly, there is no indication in the figures if staff did not attend because they were too ill on the day; secondly, there are some known problems with staff receiving notification in time. This latter point has led to the recent introduction of trying to text appointments to individuals, and the effectiveness of this needs to be monitored.
Charging is not therefore being pursued at this time, but this will be kept under close review.
2.3) Industrial Action – 30 November 2011
In response to government proposals to reform public sector pensions, a dispute between public sector workers trade unions and the government has been on-going, and a number of public service unions called upon their members, following a legal ballot, to take legal industrial action in the form of a strike on 30 November 2011. The strike was called from midnight to midnight.
Within NBT, UNITE; GMB; Unison; Society of Radiographers; Society of Physiotherapists; Society of Chiropodists and Podiatrists; UCATT were involved with a membership which meant that potentially 2000 staff could have taken action.
A Silver Command structure was established, which oversaw the actual day on 30 November throughout the Trust, which passed trouble free, thanks to pre-planning and information distributed. Whilst a number of staff did take action, and there were pickets on the main entrances to the hospitals, these were in the main held with a common sense approach, and without overt pressure to stop staff attending work.
Following the day of action, a management debrief was held by Emergency Planning, regarding in particular the operation of Silver Command.
Key success features included:
Excellent communications and relationships between Trust, HR&D and the Unions, and on the day the picket lines.
Work undertaken by staff who volunteered to cover those services affected, and the overall teamwork throughout the Trust
Set up arrangements of Silver Command Areas for improvement included : Some equipment failures in Silver Command Obtaining information on staffing numbers Confusion on relationships between Silver and Bronze Command
These issues are contained in an Action Plan for improvement.

WORKFORCE & OD Metrics Summary
Target Last month Current Month Data Used Performance
Staff in Post (wte) n/a 7358 7372 Dec-11
Sickness Absence (%) 3.8% 4.09% 4.09% Rolling 12 month
Mandatory Training H&S (%) 85% 73% 63% Nov-11
Mandatory Training Manual Handling (%) 85% 63% 66% Nov-11
Mandatory Training Fire Training (%) 85% 66% 66% Nov-11
Mandatory Training Child Protection (%) 85% 88% 88% Nov-11
Mandatory Infection Control (%) 85% 75% 75% Nov-11
KEY Sickness Jun-11 3.69%Shading indicates performance against plan Jul-11 3.97% Aug-11 3.90%Grey = above target Sep-11 3.93%White = target achieved/no target set Oct-11 4.25% Nov-11 4.34%Arrow indicates performance trend compared to last month Dec10-Nov11 4.09%
Improving
Deteriorating Similar
Page 1

TRAINING AND APPRAISALS
HR Board Report
Health & Safety - CompliantManual Handling -
CompliantFire Training - Compliant
Child Protection -Compliant
Infection Control -Compliant
June-2011 75% 68% 63% 86% 85%September-2011 72% 62% 64% 84% 78%November-2011 63% 66% 66% 88% 75%Target 85% 85% 85% 85% 85%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Mandatory Training Compliance (%) 1. DESCRIPTION
1.1 Mandatory Training
As one of the top 3 Workforce Risks within the Trust, this datapage is included to assure the Board of the progress being made to ensure that the Top 5 mandatory training issues are being constantly monitored, and improvements developed to ensure compliance,
Comparison of top 5 mandatory training issues showing end of quarter compliance for periods June 2011, September 2011 plus the latest months figures.
2. COMMENTARY
2.1 Mandatory Training
The figures shown on the graphs represent the % of all staff on the Trust payroll.
Infection control is the biggest concern – staff must be encouraged to undergo update training. There are a number of people who are moving into non compliance at the same time as such a large number were trained at the same time 2 years ago.
Work is currently on-going within the BNSSG community to rationalise the identity of e-learning modules, with the aim of soon being able to auto-generate, from MLE, an email reminder to staff when their previous courses expire.
Page 2

TEMPORARY STAFFING
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
160.00
180.00
200.00
Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10
Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11
Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11
HCSW 105.46 120.90 113.76 133.91 132.25 125.02 132.16 145.75 142.46 122.69 116.83 107.23 105.85 131.00 117.22 124.77 116.11 128.55 125.65 149.92 161.84 137.94 138.89 121.02 118.61
Registered Nurses 125.83 147.65 150.91 178.48 151.52 145.62 150.54 151.85 137.39 129.09 116.88 109.62 94.49 117.75 115.05 134.93 108.26 116.11 123.93 129.50 126.19 132.16 142.26 113.93 101.97
Temporary Staffing - Qualified Nurses & HealthCare Support Workers (WTE) 1. DESCRIPTION
The two charts show the shifts covered by NBT eXtra during the preceding 2 years on a month by month basis. This excludes local banks which are not managed through NBT eXtra.
This data needs to be considered alongside sickness absence, and staff in post, as an indicator of the trends in staffing levels overall.
1.1 - shows the trends for Qualified Nurses, and Healthcare Support Workers over a 25 month period.
1.2 - shows the trends for remaining staff groups, and agency usage through NBT eXtra over a 25 month period. 'Other' includes ancillary and other professional groups (eg pharmacy).
Information is shown on the basis of whole time equivalent, based on hours worked.
2. COMMENTARY
2.1 - Total Bank Nurse usage in December was 221 wte,14 wte down on the previous month. This remains however HIGHER than the bank nursing staff used in the equivalent period in 2010.
2.2 - Use of Clerical Bank and Other staff has shown an overall reduction of 19% on the previous month. The figures for 'Other' staff group shows significantly increased levels since April 2011. Much of this is not an overall increase to the Trust, but a transfer of responsibility to NBT eXtra for booking Facilities bank staff, and hence now included in these figures. 52% of 'Other ' staff bookings are in Facilities.
Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11
Clerical Bank 71.19 67.77 69.64 83.66 71.81 69.82 85.22 86.71 76.77 72.16 62.52 63.02 54.61 59.45 60.52 64.94 52.41 61.25 65.63 65.59 71.41 71.31 72.32 81.60 67.07
Other 11.61 11.80 12.78 14.04 11.20 8.52 13.08 13.56 14.89 14.48 10.31 10.10 9.76 9.43 9.78 12.72 11.90 17.76 24.50 28.99 29.53 28.61 31.13 32.44 28.92
WLI 9.18 10.14 11.01 14.46 6.83 11.29 9.58 11.30 4.93 6.53 8.14 9.09 6.18 10.38 9.10 11.10 10.89 10.50 14.18 16.60 7.90 11.99 13.30 12.06 7.58
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
Temporary Staffing - Other Staff Groups Usage through NBT eXtra (WTE)
Page 3

SICKNESS ABSENCE
HR Board Report
Month YTD Rolling Year
Directorate Nov-11 Apr-Nov-11Dec10-Nov11
Staff Group Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Capital Projects 0.99% 1.19% 0.87%
Clinical Governance 4.28% 3.80% 3.48%
Registered Nursing & Midwifery 4.65% 5.35% 4.72% 4.08% 4.04% 4.12% 3.89% 3.57% 3.90% 3.72% 3.82% 4.27% 4.28% Chief Executive 1.18% 4.50% 1.38%
Allied Health Professionals 2.19% 3.21% 3.77% 3.09% 2.85% 1.65% 0.99% 1.35% 1.92% 1.83% 1.58% 1.62% 1.89% Renal and Transplant 4.70% 4.47% 4.24%
Add Prof, Sci & Technical 3.45% 2.82% 2.63% 3.53% 2.45% 2.71% 3.39% 2.65% 2.54% 2.17% 3.29% 5.34% 5.86% HR&D/R&I/BOF 1.42% 2.73% 2.99%
Healthcare scientists 4.11% 3.95% 2.99% 3.23% 2.03% 2.01% 2.21% 2.06% 1.71% 2.10% 2.37% 2.41% 3.28% South Glos 2.75% 3.40% 3.40%
Ancillary & estates 6.03% 5.37% 6.57% 5.86% 5.81% 5.75% 3.61% 4.68% 5.79% 7.64% 7.35% 7.65% 6.78% Women and Childrens 4.32% 3.79% 3.88%
Admin & Clerical 4.28% 5.69% 4.52% 4.43% 4.56% 3.84% 3.27% 3.73% 4.06% 3.98% 3.94% 4.16% 4.50% Finance 4.80% 3.59% 4.34%
Additional Clinical Services 6.47% 7.35% 7.42% 5.94% 6.02% 5.59% 5.72% 6.91% 6.97% 6.07% 6.15% 6.35% 6.43% Core Clinical Services 4.23% 3.47% 3.74%
Medical & Dental 1.47% 1.55% 1.31% 1.24% 1.40% 1.12% 1.29% 1.24% 1.27% 1.00% 1.08% 1.25% 1.17% Surgery 3.86% 3.42% 3.66%
Medicine 4.65% 4.01% 4.09%
Information Management 4.12% 3.28% 3.67%
Operations 2.63% 4.67% 4.53%
Musculoskeletal 5.08% 4.90% 5.25%
Neurosciences 4.06% 4.14% 4.43%
Facilities 7.13% 6.16% 6.07%
TRUST TOTALS 4.34% 3.91% 4.09%
April May June July August September October November December January February March2009/10 3.41% 3.92% 3.99% 4.32% 4.18% 4.0% 4.73% 4.61% 4.59% 4.83% 4.23% 4.33%2010/11 3.98% 3.61% 3.66% 3.82% 3.65% 4.0% 4.05% 4.40% 5.05% 4.77% 4.34% 4.12%2011/12 3.75% 3.43% 3.68% 3.97% 3.87% 3.93% 4.25% 4.34%11/12 rolling 4.09% 4.08% 4.06% 4.07% 4.08% 4.1% 4.09% 4.09%Target 11/12 3.80% 3.80% 3.80% 3.80% 3.80% 3.8% 3.80% 3.80% 3.80% 3.80% 3.80% 3.80%
-0.50%
0.50%
1.50%
2.50%
3.50%
4.50%
5.50%
6.50%
Staff Sickness Absence (%)
1. DESCRIPTION
Data is provided to show levels of sickness against the Trust's target of 3.8% by year end.
1.1Sickness Absence : Comparison of sickness levels against Trust target - showing month by month levels within current and previous financial year. The dashed black line shows 12 month rolling average absence. across the Trust.
1.2 Sickness Absence by Staff Group: This shows month on month achievement by each staff group against the Trust's target of 3.8%.
Note:-Add Prof Sci and Technical group includes: - Pharmacists, Technical staff, Clinical Psychologists etcAdditional Clinical Services group includes: - HCAs, Technical Instructors, Medical Laboratory Assistants etc
1.3 Sickness absence by Directorate: This shows current month and rolling year sickness levels by each Directorate.
Key to shaded code in Charts 1.2 and 1.3 White = on or below TargetGrey = above target
2. COMMENTARY
2.1 Sickness Absence : Rolling 12 month sickness data remains at 4.1%, 0.3% above target. This is likely to remain high through the winter, due to the level of sickness in those preceding autumn and winter months. In month, this was the lowest November % for 3 years.
2.2 Sickness Absence by Staff Group: The majority of staff groups are above target in month. 'Additional Professional, Scientific and Technical,' continue to exceeded 4%, with a figure of 5.86%. This staff group includes Pharmacists, Operating Department Practitioners and other qualified technical staff.
2.3 Sickness Absence by Directorate: Year to date figures are just over target, following the levels of sickness in August and November. While many Directorates remain below target, Year to Date, the level of sickness in Facilities, now at consistently over 7% has increased the Trust's average.
Page 4

STAFF IN POST TURNOVER
HR Board Report
1. DESCRIPTION
1.1 Staff in Post : Comparison of Whole Time Equivalent (wte) Staff in Post, showing month by month levels within current and previous financial years.
1.2 Turnover : Turnover for all staff groups (except Medical Staff) for the 12 month periods ending on the months shown, comparing 2010/11 with 2011/12. Figures are calculated on Whole time Equivalent.
2. COMMENTARY
.2.1 Staff in Post : Staffing figures in December include the TUPE transfer of Staff from the South Bristol Dialysis Unit to NBT.
2.2 Turnover : Staff turnover remains relatively stable, and slightly lower than this time last year.
April May June July August September October November December January February March
2009/10 7184 7198 7211 7210 7215 7271 7303 7317 7314 7265 7281 7272
2010/11 7220 7203 7189 7179 7208 7186 7230 7226 7211 7150 7155 7127
2011/12 7498 7474 7419 7366 7402 7342 7357 7358 7372
6900
7000
7100
7200
7300
7400
7500
7600
Staff In Post (WTE)
April May June July August September October November December January February March
2010/11 12.45% 12.30% 12.17% 12.33% 11.99% 11.5% 11.32% 11.14% 11.40% 10.96% 10.73% 10.50%
2011/12 10.15% 10.33% 10.5% 10.2% 10.4% 11.0% 11.0% 11.0%
0.0%
3.0%
6.0%
9.0%
12.0%
15.0%Turnover WTE 2010 - 2012 (%) excludes junior doctors
Page 5

DESCRIPTION1 - Redeployment - This graph reflects the number of NBT staff on the formal Risk Register as at the 1st of each month. It also reflect the number of staff who have commenced a trial period during the proceeding month and those successfully redeployed.
2. Staff On Risk Register By Directorate - This graph reflects the Directorate split of staff on the Risk Register as at the 1st of each month.
COMMENTARY
Trust Position - The number of staff on the 'At Risk' register increased during the December, although the majority of cases not being due to Organisational Change. One member of staff was permanently redeployed during their trial period.
CG CCS Fac IM&T Med MS Neuro Ops R&T Surg W&C HREdu, Res& Dev1
Finance NBT ExtraSouthGlos
1st October 2011 0 2 0 0 4 3 0 0 0 0 1 0 0 0 0 1
1st November 2011 0 2 2 0 4 3 0 0 0 0 2 0 0 0 0 1
1st December 2011 0 2 2 0 4 2 0 0 0 0 1 0 0 0 0 1
1st Jan 2012 0 1 2 0 3 5 0 0 0 0 1 0 0 0 0 1
0
1
2
3
4
5
6
Sta
ff N
um
ber
s
Directorates
Staff On Risk Register By Directorate
1st Aug 2011 1st Sep 2011 1st Oct 2011 1st Nov 2011 1st Dec 2011 1st Jan 2012
At Risk 14 12 11 14 12 13
On Trial (During Previous Month) 3 3 2 2 3 2
Successfully Redeployed (During previous month) 4 1 0 1 0 1
0
2
4
6
8
10
12
14
16
Sta
ff N
um
ber
s
Measurement Points
Redeployment

HR Support Services Monthly Performance Measures - February to December 2011
Recruitment Activity Feb March April May June July August Sept Oct Nov DecNBT Live Vacancies (Non-Medical) 31 33 78 91 110 66.31 81.04 38.84 93.43 111 87NBT Live Vacancies (Medical) 9 26 23 16 10 14 8 8 12 18 40Number of posts advertised externally 0 0 0 0 0 1 1 1 2 1 4Number of posts advertised outside of NBT via NHS Jobs (Non-Medical)
20 23 60 70 72 57 84 54 70 95 86
External Acceptance Rate (Posts accepted by the applicant)
100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Benchmark Acceptance Rate 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94%
Performance Measures
Time to Hire - Days (Medical) 29 36 29 29 47 28 36 42 42 20Time to Hire - Days (Non-Medical) 28 28.7 30 37.1 38 36 36 39 41 40


Trust Board Infection Report December 2011
0
5
10
15
20
25
Ap
r-08
May-0
8Jun
-08
Jul-0
8A
ug
-08
Se
p-0
8O
ct-
08
Nov-0
8D
ec-0
8Jan
-09
Feb-0
9M
ar-
09
Ap
r-09
May-0
9Jun
-09
Jul-0
9A
ug-0
9S
ep-0
9O
ct-
09
Nov-0
9D
ec-0
9Jan
-10
Feb-1
0M
ar-
10
Ap
r-10
May-1
0Jun
-10
Jul-1
0A
ug-1
0S
ep-1
0O
ct-
10
Nov-1
0D
ec-1
0Jan
-11
Feb-1
1M
ar-
11
Ap
r-11
May-1
1Jun
-11
Jul-1
1A
ug
-11
Se
p-1
1O
ct-
11
Nov-1
1D
ec-1
1
cases
C.Difficile Cases: Trust Attributable April 2008 to December 2011
Trust Attributable Cdiff SHA Performance Target
0
2
4
6
8
10
Ap
r-08
May-0
8Jun
-08
Ju
l-0
8A
ug-0
8S
ep-0
8O
ct-
08
Nov-0
8D
ec-0
8Jan
-09
Feb-0
9M
ar-
09
Ap
r-09
May-0
9Ju
n-0
9Jul-0
9A
ug-0
9S
ep-0
9O
ct-
09
No
v-0
9D
ec-0
9Jan
-10
Feb-1
0M
ar-
10
Ap
r-10
May-1
0Jun
-10
Ju
l-1
0A
ug-1
0S
ep-1
0O
ct-
10
Nov-1
0D
ec-1
0Ja
n-1
1F
eb-1
1M
ar-
11
Ap
r-11
May-1
1Ju
n-1
1Jul-1
1A
ug-1
1S
ep-1
1O
ct-
11
Nov-1
1D
ec-1
1
cases
MRSA Cases: Trust Attributable April 2008 to December 2011
Trust Attributable MRSA Limit Gateway
0
5
10
15
20
Ap
r-08
May-0
8Jun
-08
Jul-0
8A
ug-0
8S
ep-0
8O
ct-
08
Nov-0
8D
ec-0
8Jan
-09
Feb-0
9M
ar-
09
Ap
r-0
9M
ay-0
9Jun
-09
Jul-0
9A
ug
-09
Se
p-0
9O
ct-
09
Nov-0
9D
ec-0
9Jan
-10
Feb-1
0M
ar-
10
Ap
r-1
0M
ay-1
0Jun
-10
Jul-1
0A
ug
-10
Se
p-1
0O
ct-
10
Nov-1
0D
ec-1
0Jan
-11
Feb-1
1M
ar-
11
Ap
r-1
1M
ay-1
1Jun
-11
Jul-1
1A
ug
-11
Se
p-1
1O
ct-
11
Nov-1
1D
ec-1
1
cases
MSSA Cases: Trust Attributable April 2009 to December 2011
Trust Attributable MSSA
*validated from January 2011
0
5
10
15
20
25
30
Ap
r-08
Ma
y-0
8Jun
-08
Ju
l-0
8A
ug-0
8S
ep-0
8O
ct-
08
Nov-0
8D
ec-0
8Jan
-09
Feb-0
9M
ar-
09
Ap
r-09
May-0
9Jun
-09
Jul-0
9A
ug-0
9S
ep-0
9O
ct-
09
No
v-0
9D
ec-0
9Ja
n-1
0F
eb-1
0M
ar-
10
Ap
r-10
May-1
0Jun
-10
Jul-1
0A
ug-1
0S
ep-1
0O
ct-
10
Nov-1
0D
ec-1
0Jan
-11
Feb-1
1M
ar-
11
Ap
r-11
Ma
y-1
1Jun
-11
Ju
l-1
1A
ug-1
1S
ep-1
1O
ct-
11
No
v-1
1D
ec-1
1
cases
ECOLI Cases: Trust Attributable April 2009 to December 2011
Trust Attributable ECOLI
*validated from June 2011

Trust Board Infection Report December 2011
50%
60%
70%
80%
90%
100%
Ap
r-09
May-0
9
Jun
-09
Jul-0
9
Au
g-0
9
Se
p-0
9
Oct-
09
Nov-0
9
Dec-0
9
Jan
-10
Feb-1
0
Mar-
10
Ap
r-10
May-1
0
Jun
-10
Jul-1
0
Au
g-1
0
Se
p-1
0
Oct-
10
Nov-1
0
Dec-1
0
Jan
-11
Feb-1
1
Mar-
11
Ap
r-11
May-1
1
Jun
-11
Jul-1
1
Au
g-1
1
Se
p-1
1
Oct-
11
Nov-1
1
Hand Hygiene Overall NBT Compliance
Compliance (Combined) Target
40%
50%
60%
70%
80%
90%
100%
Jul-1
0
Au
g-1
0
Se
p-1
0
Oct-
10
Nov-1
0
Dec-1
0
Jan
-11
Feb-1
1
Ma
r-1
1
Ap
r-11
May-1
1
Jun
-11
Jul-1
1
Au
g-1
1
Se
p-1
1
Oct-
11
Nov-1
1
Dec-1
1
% a
dm
issio
ns s
cre
en
ed
MRSA Elective pre-Screening within 18 weeks for BNSSG patients seen in pre-op
Elective IP/DC Target
40%
50%
60%
70%
80%
90%
100%
Jul-1
0
Au
g-1
0
Se
p-1
0
Oct-
10
Nov-1
0
Dec-1
0
Jan
-11
Feb-1
1
Mar-
11
Ap
r-11
May-1
1
Jun
-11
Jul-1
1
Au
g-1
1
Se
p-1
1
Oct-
11
Nov-1
1
Dec-1
1
% a
dm
issio
ns s
cre
en
ed
MRSA Non-elective screening within 24 hours of admission Excludes admissions not staying overnight
Non-Elective IP Target

Title: Finance Report to the Trust Board for the nine months ended 31st December 2011.
Purpose of paper: To report the year to date financial position and to highlight key issues.
For Information
Executive Summary: The overall position for the Trust for the first nine months of the year is a surplus of
£7.1m before impairment, which is on plan. This is after releasing reserves of £3.0m to offset capacity reductions not achieved.
PCT income is above plan by £2.3m.
Other income is £0.3m adverse year to date but £0.02m favourable in month.
Pay is £0.3m adverse year to date, £0.2m adverse in month.
Non-pay is £2.8m adverse year to date with an adverse movement in-month of £0.5m.
Efficiency savings are £0.2m adverse, £0.3m favourable to phased plan in month.
The forecast surplus for the year of £9.0m before impairment remains as per the
plan Action Required: The Trust Board is asked to note the key risks and issues as
follows:
Non pay expenditure is now overspent by £2.8m for 9 months and Directorates are reviewing this to take action where necessary.
The backlog of activity needs to be brought up to date so income can be billed satisfactorily.
Impact on Patients: Failure of the Trust to achieve its target surplus will have a negative impact on the Trust. CQC Outcome: 26-Financial Position Responsible Committee: Finance Committee Financial Issues considered: Yes Equality Impact Assessment Completed: No Legal Issues Considered: Yes
Sustainability Assessment Completed: No Presented by: Steve Webster Director Finance & Information Prepared by: Mark Ross, Financial Controller Nigel Baker, Deputy Director of Finance
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 1

NORTH BRISTOL NHS TRUST
FINANCE REPORT TO TRUST BOARD
APRIL 2011 to DECEMBER 2011
1. Summary Financial Performance
KPIs
Retained Surplus Before Impairment (£m) Green
Capital Expenditure Green(£m)
Debt repayment (£m) Green
Better payment performance Amber
Financial risk rating Green
Year to date
Notes on scoring: Retained surplus. This is the bottom line on the Trust’s income and expenditure account excluding
impairment. Green is ahead of the £9m plan, amber is adrift in the year to date position but forecasting an outturn on plan, red is adrift in the year to date with a high risk of not achieving the year end plan.
Capital expenditure. This is capital expenditure compared with plan. Green is on plan or underspent,
amber is overspent in the year to date but forecasting an outturn on plan or underspent. Red is adrift in the year to date with a high risk of overspending the year end plan.
Debt repayment. Whether the trust is on track with making its debt repayments. Either green, red or
amber according to the level of risk. Payment performance. The total number of invoices paid within 30 days expressed as a % of the total.
Green is 95% or above, amber 80% to 95%, and red is below 80% Overall risk rating under the FT rating system. Green is a risk rating of 3 or above for the year to date and
plan. Amber is less than 3 year to date but a planned 3 or above. Red is a 2 or 1 risk rating year to date and plan. The calculation of risk rating scores is set in table 9.
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 2

2. Overall position The profile shows planned I&E deficits in the first two months, followed by variable levels of surplus in the following 10 months. As the graph below shows, the actual position for the first 9 months is in line with the plan.
(3)
(2)
(1)
0
1
2
3
4
5
6
7
8
9
10
Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12
£m
Month
Retained Surplus (Before Impairment) Actual vs Budget
Plan Actual
£'000 % E000's %
Income (120) (0.3%) (2,019) (0.5%)
Pay 152 0.6% 322 0.1%
Non-pay 533 4.5% 2,838 2.7%
Variance to planned savings (252) n/a 196 n/a
Demand dependant cost reductions 339 n/a 3,028 n/a
Reserves released (333) n/a (3,000) n/a
Depreciation & financing (332) (12.0%) (1,400) (5.7%)
Retained surplus (12) (1.4%) (35) (0.5%)
In month variance before impairment
Year to date variance before impairment
(Fav)/ adv(Fav)/ adv
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 3

2.1 Income PCT income analysis is not yet complete for month 9 due to the slightly earlier Board meeting date.
It is more difficult than usual to assess the likely position due to gaps in the activity data following the implementation of CERNER. It is likely that activity, and hence income, will be below the SLA (pre-QIPP) as a consequence of the strike at the end of November and some impact on activity levels during the CERNER implementation. We have included some provision for these issues against the favourable variance that arises from the QIPP plan. 2.2 Pay expenditure Pay expenditure is £0.2m adverse to plan in December, giving an adverse overall variance of £0.3m. The figures include an estimate of £0.3m in respect of outstanding Christmas and New Year unsocial payments.
24.5
25.0
25.5
26.0
26.5
27.0
27.5
28.0
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
£m
Month
Trust Total Pay
Actual 2010/11 Actual 2011/12
A breakdown of variances across staff groups is shown below and a more detailed analysis by Directorate in Table 3a.
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 4

Staff groups In-month % of total pay budget forvariance
£000's £000's
the year to date by staff group
Medical staff (63) 416 0.7%
Qualified Nursing & Midwifery 75 (130) (0.2%)
Healthcare Assistants (15) 532 3.1%
Waiting list initiatives 78 417 n/a
Other staff 77 (913) (1.0%)
Total staff 152 322 0.1%
Year to date variance (Fav) / Adv
0.00%
5.00%
10.00%
15.00%
Apr-11
May-11
Jun-11
Jul-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
Jan-12
Feb-12
Mar-12
Cumulative Bank and Agency Nursing and Healthcare Assistants Spend as Percentage of Total Nursing Spend
Nursing Agency Spend
Healthcare Assistant Bank Spend
Qualified Nursing and Midwifery Bank spend
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 5

2.3 Non-pay expenditure Non pay expenditure is £533k adverse to plan in-month with £245k in Core Clinical (including £100k of recharges below plan, showing favourable in other Directorates) £125k in Surgery and £118k in Womens and Children’s. The table below shows a Directorate based analysis of the cumulative variance of £2.8m. £0.9m of this relates to expenditure recovered through PCT income. A significant proportion of the balance relates to clearly identifiable or one-off issues (such as the specialist breast issue in Core Clinical Services) and as can be seen in the table below there are a number of remaining areas where the Directorates are required to look further.
Reason
Directorate month 9 total
varianceDirectorate Directorate reason as at month 9 £000 £000
Core Clinical Services Specialist breast issue 295
Growth on external contract work - laboratory chemicals 86Other 286
667
Medicine Drugs & M&S across various headings 153Blood products 61Other 65
279
MusculoskeletalDrugs and blood product overspends recovered through PCT income 165Other -20
145
NeurosciencesSpinal cord stimulators and coils - cost per case recovered through income 390Other 39
429
Surgery Change of accounting practice 123Correction of stock figure 131Use of the private sector 252Genreral overspends recovered through income 113Budget setting error 73Prosthesis overspend 58Other 247
997
Womens & Childrens Drugs - change of product mix 32Various overspends 185
217
Total of above 2,734
Other Directorates 104
YTD month 9 total adverse non-pay variance 2,838
This document could be made public under the Freedom of Information Act 2000.
Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
6

The graph below shows the pattern of actual spend over the last 21 months.
8.0
9.0
10.0
11.0
12.0
13.0
14.0
Apr-10
May-10
Jun-10
Jul-10
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-11
May-11
Jun-11
Jul-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
£m
Month
Trust Total Non-Pay
Actual 2010/11 Actual 2011/12
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 7

2.4 Efficiency Savings To date we have identified £30.8m against a target of £29.8m target, with £29.8m implemented to date. The shortfall against the phased plans has reduced in month by £0.3m.
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
Apr‐
11
May‐
11
Jun‐
11
Jul‐11 Aug‐
11
Sep‐
11
Oct‐
11
Nov‐
11
Dec‐
11
Jan‐
12
Feb‐
12
Mar‐
12
£m
Month
Total Trust Total CRES position
Further work
Possibles
Likely to beimplemented
Implemented
Target
Gross Savings
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
£m
Month
Trust Total phased CRES plan vs actual
Forecast Actual Gap Plan
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 8

3. Forecast Detailed forecasts have been prepared by Directorates based on their year to date positions. Overall the forecast surplus remains at £9.0m as planned. Risks against this are:
Other expenditure overspends Backlog in activity due to CERNER
9 months to December variance
Year end forecast variance
(Fav) / adv (Fav) / adv£000's £000's
Income PCT income for activity done (2,324) (3,486)Other Income 305 374
Total Income (2,019) (3,113)
Expenditure Directorate Pay 322 908Directorate Non Pay 2,838 4,564Capacity reductions not achieved 3,028 4,035Reserves released (3,000) (4,000)CRES 196 0
Total Expenditure 3,384 5,507
EBITDA 1,365 2,395
Capital charges and financing costs (1,400) (2,406)
(35) (11)Variance to planned surplus
As in previous months, the forecast above excludes the impact of the write down of the Frenchay site.
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 9

4. Capital and balance sheet December expenditure fell below plan as with most previous months but there was increased expenditure on Cerner, and is expected to bring full year expenditure back up to the current forecast as shown in table 5. The forecast outturn expenditure is £2.3m below plan although this includes an overspend of £0.9m on IT because of CERNER.
-
200
400
600
800
1,000
1,200
1,400
1,600
Apr May June July August Sept Oct Nov Dec Jan Feb March
£'00
0
Month
Capital expenditure against plan
Planned spend Actual Spend
The cash position has improved since last month and against plan, principally due to a reduction in payments to creditors. There is a small element within this of delays to payments caused by the Christmas break (see BPPC performance below), but mainly this is caused by delays in receiving invoices from suppliers, and creditors being composed of a larger proportion of accruals than expected. The capital underspend highlighted above is reflected in the forecast cash balance which is £2.1m higher than plan. This is expected to be a temporary increase as the capital underspend is attributable to slippage on schemes.
I&E movementsstock
Debtors
Creditors
Capital PDC Loans
Total variance
0
5,000
10,000
15,000
1
£0
00
Cash flow variance against plan - December 2011
(10,000)
(5,000)
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 10

Performance against the Better Payment Practice code in December fell to 91.67%. This is a normal pattern that we see in December each year, caused by the number of invoice approvers who take leave over Christmas, and the delays in payment runs that the number of bank holidays cause. We also normally see a dip in performance in January as invoices delayed in the system are cleared and paid. The cumulative performance has only fallen from 93.64% to 93.42%.
80.00
90.00
100.00
Dec-10
Jan-11
Feb-11
Mar-11
Apr-11
May-11
Jun-11
Jul-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
%
Better payment practice code performance Paid within30 days
Target
In month
A new table (7a) has been added to the financial tables which is a rolling 12 month cashflow forecast. This information has been prepared as part of our forward planning and forms part of the Financial Modelling for the Foundation Trust application process. It is considered best practice to include this and is a useful addition to the monthly reporting information. 5. Financial risk ratings There has been an improvement in the trusts projected financial risk rating score as an improvement in liquidity means that the restriction of the overall score to two has been lifted, and the weighted average becomes 3.25.
This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 11

This document could be made public under the Freedom of Information Act 2000. Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed
section' of any meeting. 12
FINANCE TABLES INDEX Table 1 Summary Income and Expenditure Statement Table 2 Variance Analysis by Directorate - Year to Date Table 3a Pay Variance Analysis Table 3b Whole Time Equivalents (WTEs) Analysis Table 4 Savings by Directorate Table 5 Capital Expenditure & Funding Table 6 Balance Sheet Table 7 Current Year Cash Flow Table 7a Rolling Cash Flow Forecast Table 8 Debtors Analysis Table 9 Financial Risk Ratings

Table 1Finance Report December 2011 - Summary Income & Expenditure Statement
DescriptionVariation from
budget In-month
Plan Budget ActualAdverse /
(Favourable)Adverse /
(Favourable)£'000 £'000 £'000 £'000 £'000
Income
429,551 PCT Income 321,104 323,428 (2,324) (96)77,198 Other Operating Income 59,732 59,427 305 (24)
506,749 Total Income 380,836 382,855 (2,019) (120)
Expenditure
322,425 Pay 244,358 244,680 322 152142,568 Non Pay 105,000 107,838 2,838 533
Variance to planned savings (196) 196 (252)Capacity reductions not achieved (3,028) 3,028 339Reserves released 3,000 (3,000) (333)
464,993 349,134 352,518 3,384 439
41,756 Earnings before Interest & Depreciation 31,702 30,336 1,365 319
22,073 Depreciation & Amortisation on Purchased Assets 16,555 15,918 (637) (70)1,148 Depreciation on Donated Assets 861 861 0 0(25) Interest receivable (19) (34) (15) (2)
1,311 Interest payable on loans 1,019 1,019 0 08,269 PDC Dividend 6,202 5,454 (748) (260)
8,980 Net Surplus / (Deficit) 7,084 7,119 (35) (12)
4,552 Fixed asset impairments 69,559 69,559 0 0429 Below the line effect of IFRIC 12 322 322 0 0
3,999 Surplus /( Deficit) after impairments (62,797) (62,762) (35) (12)
North Bristol NHS Trust
Position as at 31st December

Table 2
Overall Variance by Directorate for the Nine Months Ended 31 December 2011
(Favourable) / Adverse
M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12 YTD
Core Clinical Services 118 117 345 348 116 (372) (126) (297) 44 293
Medicine (10) (11) 199 434 656 738 373 (16) 385 2,748
Musculo (116) (115) 446 214 (109) (13) 191 176 (135) 539
Neuro (10) (10) 142 73 (94) (93) 481 147 38 674
Renal 107 108 (290) 470 123 79 262 (106) (206) 547
South Glos Community HS 0 (1) (104) 8 16 (187) (78) 11 (54) (389)
Surgery (60) (60) 201 614 527 (15) 722 302 242 2,473
Womens & Childrens 173 172 67 238 (236) 31 (245) (42) 90 248
Facilities 26 26 (14) 186 176 141 (38) 43 103 648
Corporate Directorates 50 50 43 35 30 4 (43) (39) 62 192
Other (292) (291) (1,055) (2,587) (1,214) (292) (1,495) (201) (581) (8,008)
Total (15) (16) (20) 33 (9) 21 4 (22) (12) (35)
= > 2 % adverse variance
= Adverse to plan by up to 2% adverse variance
= On plan or favourable
£000's

Pay Variance Analysis Table 3a
Months 1 to 9 2011/12 Month 9 2011/12
Adverse / (Favourable) Adverse / (Favourable)
MedicalQualified Nursing HCAs Other
Waiting list payments Total Medical
Qualified Nursing HCAs Other
Waiting list payments Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Core Clinical Services (154) (447) (65) (201) 66 (801) Core Clinical Services (132) (62) 1 (36) 40 (189)
Medicine 308 406 342 (209) 26 873 Medicine 25 149 1 (29) 1 147
Musculo 2 270 89 (31) (62) 268 Musculo 24 77 (8) (18) (26) 49
Neuro (46) (125) 625 (166) 131 419 Neuro (14) 17 59 (44) 22 40
Renal (57) (196) 90 (5) 0 (168) Renal (26) (28) (6) 0 0 (60)
South Glos Adult Community 33 38 (59) (291) 0 (279) South Glos Adult Community 21 3 (29) (8) 0 (13)
Surgery 68 244 (79) (346) 228 115 Surgery 19 (11) (10) (34) 41 5
Womens & Child 262 (320) (411) 477 28 36 Womens & Child 20 (70) (23) 29 0 (44)
Other Directorates (141) (141) Other Directorates 0 0 0 217 0 217
Totals 416 (130) 532 (913) 417 322 Totals (63) 75 (15) 77 78 152

Table 3b
Whole Time Equivalents (WTEs) Analysis
Worked WTE by Directorate
Worked Worked Worked Worked Worked Worked Funded VarianceJul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 WTE WTE
Core Clinical Services 1,942 1,938 1,946 1,953 1,977 1,966 2,007 (41)Medicine 964 963 948 948 951 983 931 52Musculoskeletal 445 455 446 453 446 441 425 16Neurosciences 474 485 478 480 495 480 473 7Renal Services 267 270 262 265 260 274 292 (18)South Glos Community Health Services 336 338 329 331 326 335 350 (15)Surgical Services 658 656 637 661 668 659 661 (2)Women and Childrens 1,307 1,307 1,294 1,267 1,267 1,267 1,300 (33)
Clinical Directorates Sub-Total 6,393 6,412 6,339 6,358 6,390 6,404 6,439 (35)
Chief Executive 18 20 20 21 19 19 19 (0)Clinical Governance 44 52 53 53 53 54 60 (6)Facilities 796 796 783 775 775 770 803 (33)Finance 141 140 139 141 141 141 146 (5)HR 230 230 231 234 240 240 235 5Information Management 215 212 207 206 209 208 210 (2)Operations 98 98 100 103 80 82 76 6Projects 11 11 11 12 13 11 11 (0)Ring Fenced Funding 34 34 34 29 29 29 30 (1)
Total 7,979 8,003 7,916 7,930 7,949 7,959 8,030 (71)
Transfer into Renal Directorate of South Bristol Renal Satellite Unit from existing private provider in December 2011
Transfer of Outpatients from Operations Directorate to Core Clinical Services in November 2011
Trend : WTE Current Month : Dec-11
7,300
7,400
7,500
7,600
7,700
7,800
7,900
8,000
8,100
8,200
Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11
WT
Es
Month
TREND TOTAL WORKED AND FUNDED WTEs
Funded
Worked

NORTH BRISTOL NHS TRUST Table 4Savings by Directorate as at December 2011
2011-2012
Total Probability ProbabilityGross Adjusted adjusted
Directorate Savings Target (2011/12) Savings Savings
gap
% of Target % of Target
£000 £000 £000 £000 £000 £000 % £000 £000 £000 £000 £000 % £000
Core Clinical Services 5,304 4,192 91 44 20 4,346 82% 4,192 81 23 4 4,300 81% 1,004 Medicine 3,562 3,251 50 152 - 3,453 97% 3,251 41 76 - 3,368 95% 194 Musculo-skeletal 3,401 3,314 38 - - 3,352 99% 3,314 33 - - 3,347 98% 55 Neurosciences 2,301 2,236 56 - - 2,293 100% 2,236 56 - - 2,292 100% 9 Renal 801 802 24 - - 826 103% 802 21 - - 823 103% (22) South Glos Community HS 519 535 - - - 535 103% 535 - - - 535 103% (16) Surgery 2,751 2,583 42 23 - 2,647 96% 2,583 36 11 - 2,630 96% 121 Women and Children's Health 4,402 4,340 52 - - 4,392 100% 4,340 47 - - 4,388 100% 14
Clinical Directorates 23,042 21,253 353 218 20 21,844 95% 21,253 315 110 4 21,682 94% 1,360
Chief Executive 54 54 - - - 54 99% 54 - - - 54 99% 0 Clinical Governance 228 228 - - - 228 100% 228 - - - 228 100% 0 Facilities 2,822 1,705 252 483 - 2,441 86% 1,705 207 231 - 2,144 76% 679 Finance 324 324 - - - 324 100% 324 - - - 324 100% 0 Human Resources 372 372 - - - 372 100% 372 - - - 372 100% (0) IM&T 773 525 97 165 - 786 102% 525 87 83 - 694 90% 78 Operations 265 244 - - - 244 92% 244 - - - 244 92% 21 Central Projects 1,899 5,053 - - - 5,053 266% 5,053 - - - 5,053 266% (3,154)
Non-clinical Directorates 6,736 8,505 349 648 - 9,502 141% 8,505 294 314 - 9,112 135% (2,376)
Total 29,778 29,757 702 866 20 31,345 105% 29,757 609 424 4 30,794 103% (1,016)
In-progress
Further
Total
Gross Savings Recurring & Non Recurring
Probability Adjusted Savings Recurring & Non Recurring Im
plemented
Most Likely
In-progress
Further
Total
Implem
ented
Most Likely

Table 5
CAPITAL EXPENDITURE MONITORING REPORT 2011/12 - December 2011
Full year CAPITAL EXPENDITURE PLAN Project Plan Actual Variance ForecastPlan Director to December to December from plan Outturn£'000 £'000 £'000 £'000 £'000
Expenditure
2,242 Cossham Renal Dialysis Unit D Powell 1,000 620 380 1,2421,000 Pathology Ph IIA/Learning & Research D Powell 225 38 187 2501,205 Childrens community services N Curtis 925 562 363 925590 Frenchay site preparation D Powell 150 21 129 150450 Directorate schemes S Watkinson 295 55 240 112
3,463 IM&T M Bell 2,367 3,552 (1,185) 4,3431,600 Medical equipment (excluding leasing) C Burton 750 620 130 1,500800 Facilities expenditure S Wood 525 522 3 800500 Car parking S Wood 0 17 (17) 50350 Contingency CPMG 320 214 106 490300 Donated assets 225 176 49 300
1,066 Other 1,148 275 873 1,105
13,566 TOTALGROSS CAPITAL EXPENDITURE 7,930 6,672 1,258 11,267
Funding
20,816 Purchased assets depreciation (excl car park) 15,612 15,612 0 21,164500 Land sales 0 0 0 0300 Donations 150 169 19 300
21,616 Total funding 15,762 15,781 19 21,464
8,050 Surplus of capital funding 7,832 9,109 1,277 10,197
520 Capital loan repayments 0 0 520
7,530 Cash surplus from capital items 7,832 9,109 1,277 9,677

Table 6
Variance ForecastFull year Plan Actual from plan Mar-12
Plan £'000 £'000 £'000 £'000 £'000
Non Current Assets296,490 Property, Plant and Equipment 226,626 224,562 2,064 220,9031,853 Intangible Assets 1,508 1,508 0 1,853
298,343 Total non-current assets 228,134 226,070 2,064 222,756
Current Assets6,655 Inventories 6,956 8,758 (1,802) 7,5815,903 Trade and other receivables NHS 3,752 9,878 (6,126) 5,82014,629 Trade and other receivables Non-NHS 22,026 22,908 (882) 12,62212,820 Cash and Cash equivalents 10,265 14,107 (3,842) 14,96240,007 Total current assets 42,999 55,651 (12,652) 40,986
0 Non-current assets held for sale 0 0 040,007 Total Current assets 42,999 55,651 (12,652) 40,986
338,350 Total assets 271,133 281,721 (10,588) 263,742
Current Liabilities (< 1 Year)4,607 Trade and Other payables - NHS 6,969 7,517 (548) 4,39438,239 Trade and Other payables - Non-NHS 37,212 47,918 (10,706) 36,4689,970 Borrowings 9,735 9,735 0 9,9701,205 Provisions 1,205 920 285 1,3202,894 Other liabilities 2,894 2,229 665 3,94256,915 Total current liabilities 58,015 68,319 (10,304) 56,094
(16,908) Net current assets/(liabilities) (15,016) (12,668) (2,348) (15,108)
281,435 Total assets less current liabilites 213,118 213,402 (284) 207,648
2,396 Trade and other payables 2,396 2,317 79 2,17120,061 Borrowings 24,939 24,728 211 19,7421,744 Provisions 1,744 1,434 310 1,564
257,234 TOTAL NET ASSETS 184,039 184,923 (884) 184,171
CAPITAL & RESERVES209,644 Public Dividend Capital 209,644 209,644 0 209,644(59,086) Income and expenditure reserve (43,513) (47,113) 3,600 (47,113)
3,999 Income and expenditure account - current year (62,797) (62,762) (35) (68,717)87,104 Revaluation reserve 80,705 85,154 (4,449) 90,35715,573 Donation reserve 0 0 0 0
257,234 TOTAL CAPITAL & RESERVES 184,039 184,923 (884) 184,171
NORTH BRISTOL NHS TRUSTSTATEMENT OF FINANCIAL POSITION AS AT 31 DECEMBER 2011

Table 7
Variancefrom plan Forecast
£'000 Plan ActualCash inflow
/(outflow) Mar-12£'000 £'000 £'000 £'000
40,499Earnings Before Interest, Depreciation and Amortisation 31,702 30,337 (1,365) 38,653
0 Less Transfer from donated reserve 0 0 0 0
1,000 (Increase)/Decrease in Stock 700 (1,103) (1,803) 74(1,149) (Increase)/Decrease in Debtors (6,395) (13,403) (7,008) 941
28 Increase/(Decrease) in Creditors (2,811) 11,194 14,005 (456)0 Increase/(Decrease) in Provisions (500) (595) (95) (65)
40,378Net Cash Inflow/(Outflow) from Operating Activities 22,696 26,430 3,734 39,147
25 Interest received 19 34 15 34(1,305) Interest Paid on Long Term Loan (715) (715) 0 (1,331)
(1,280)Net Cash Inflow/(Outflow) from Returns on Investment and Servicing of Finance (696) (681) 15 (1,297)
(13,416) Cash payments for Capital Purchases (7,757) (7,723) 34 (10,963)425 Cash receipts from Asset Sales 425 495 70 0
(8,269) Dividends paid / payable (4,135) (4,146) (11) (6,907)17,838 Net Cash Inflow Before Financing 10,533 14,375 3,842 19,980
Financing0 Donated Capital Receipts 0 0 0 00 Temp PDC Drawn Down 0 0 0 00 Temp PDC repaid 0 0 0 0
(9,500) Loans Repaid (4,750) (4,750) 0 (9,500)
(9,500) Net Cash Inflow From Financing (4,750) (4,750) 0 (9,500)
8,338 Increase (decrease) in Cash 5,783 9,625 3,842 10,480
4,482 Opening cash balance 4,482 4,482 0 4,482
12,820 Closing cash balance 10,265 14,107 3,842 14,962
NORTH BRISTOL NHS TRUSTSTATEMENT OF CASH FLOWS AS AT 31ST DECEMBER 2011
Full year Plan

Table 7a
Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12£000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000
Opening Balance 14,107 21,114 19,086 14,962 26,094 27,481 23,793 21,743 25,791 24,683 26,249 29,941
EBITDA 2,388 2,821 7,105 6,330 2,657 3,500 2,486 2,532 3,244 2,561 3,358 1,270
Operating cash flows before movements in working capital 2,388 2,821 7,105 6,330 2,657 3,500 2,486 2,532 3,244 2,561 3,358 1,270
Movement in working capital 5,817 (3,650) (1,497) 6,001 (420) (6,078) (3,293) 3,158 5,856 474 2,071 (2,401)
Net cash inflow/(outflow) from operating activities 8,205 (830) 5,608 12,332 2,237 (2,578) (807) 5,689 9,101 3,036 5,430 (1,131)
Cash flow from investing activitiesCapex spend (1,149) (1,149) (1,457) (1,174) (830) (1,090) (1,220) (1,619) (1,950) (1,450) (1,720) (1,890)
Cash receipt from asset sales - - - - - - - - - - - -
Net cash inflow/(outflow) from investing activities (1,149) (1,149) (1,457) (1,174) (830) (1,090) (1,220) (1,619) (1,950) (1,450) (1,720) (1,890)
CF before Financing 7,056 (1,978) 4,152 11,158 1,407 (3,668) (2,027) 4,070 7,151 1,586 3,710 (3,021)
Cash flow from financing activitiesDividends paid - - (2,761) - - - - - (2,787) - - -
Interest (paid) on loans and leases - - (715) - - - - - (467) - - -
Interest element of PFI Unitary Charge (52) (52) (52) (47) (47) (47) (47) (47) (47) (47) (47) (47)
Interest received on cash and cash equivalents 2 2 2 20 27 26 24 25 27 27 29 30
Drawdown of loans and leases - - - - - - - - - - - -
Repayment of loans and leases - - (4,750) - - - - - (4,985) - - -
Movement in Other grants/Capital received - - - - - - - - - - - -
Net cash inflow/(outflow) from financing (49) (49) (8,275) (26) (20) (20) (23) (22) (8,259) (20) (17) (17)
Net cash outflow/inflow 7,006 (2,028) (4,124) 11,131 1,387 (3,688) (2,050) 4,048 (1,108) 1,566 3,692 (3,038)
Closing Balance 21,114 19,086 14,962 26,094 27,481 23,793 21,743 25,791 24,683 26,249 29,941 26,903
NORTH BRISTOL NHS TRUSTCASHFLOW FORECAST FOR 12 MONTHS FROM 31ST DECEMBER 2011

Debtors Graphs Table 8
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11
Val
ue
£000
ANALYSIS OF RECEIVABLES (£000)
InvoicesRaised
TotalReceivables
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11
NORTH BRISTOL NHS TRUST - AGEING ANALYSIS OF NON-NHS RECEIVABLES (£000)
Over 12 Months
6 to 12 months
3 - 6 Months
1 - 3 months
Less than 1month
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11
NORTH BRISTOL NHS TRUST - AGEING ANALYSIS OF NHS RECEIVABLES (£000)
Over 12 Months
6 to 12 months
3 - 6 Months
1 - 3 months
Less than 1month
0
500
1,000
1,500
2,000
2,500
3,000
Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11
NORTH BRISTOL NHS TRUST - INVOICES OVER 3 MONTHS OLD (£000)
Invoices over3 months

NORTH BRISTOL NHS TRUST Table 9
Finance Report Dec 2011 - Key Financial Performance Indicators
Actual Actual PlanIndividual scoring
required
Mar-11 Dec-11 Mar-12for overall rating
of 3Financial Metrics - Indicators used to derive financial risk rating
EBITDA margin % 7.9 7.9 8.0 5.0EBITDA % achieved % 94.0 95.7 100.0 70.0
Return on Capital Employed % 6.5 7.3 6.8 3.0
I&E Surplus margin (net of dividend)
% 1.6 1.9 1.8 1.0
Liquidity Ratio Days 3.0 13.0 10.5 15.0
Weighted Average 3.0 3.3 3.3 3.0Overall FRR 2 3 3
Items Highlighted fail to achieve the Threshold required for the Trust to achieve Foundation Trust status

TRUST BOARD – FORWARD PLAN – JANUARY TO DECEMBER
Month
Report Executive
JANUARY Major Capital Projects (including Frenchay PQQ evaluation report) David Powell Cerner Follow Up/Progress Martin Bell GRMC and Risk Register Martin Bell Building our Future – Executive Summary Harry Hayer Bristol Health Partners – Quarterly Review Harry Hayer Safeguarding Adults Marie-Noelle Orzel Research and Innovation Performance/KPI – Quarterly Report Harry Hayer Foundation Trust Ruth Brunt Urology Chris Burton Building Our Future Quarterly Review Harry Hayer 2012/13 Contracting Update Steve Webster MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report SWa Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster FEBRUARY Project Performance and Financial Control Steve Webster Private Patients’ Project Update and Approvals Steve Webster Workforce & OD Strategy – Operational Plan Harry Hayer NBT/UHB Partnership Programme Board Harry Hayer 2012/13 Contracting Update Steve Webster Assurance Framework Martin Bell
Revised January 2012 1

Month
Report Executive
Building our Future – Executive Summary Harry Hayer Major Trauma – Update (2012 only) Harry Hayer Foundation Trust Ruth Brunt Patient Survey (possible) Marie-Noelle Orzel Annual GRMC Report Martin Bell MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster MARCH Major Capital Projects (including Learning and Research phase 2 FBC) David Powell Quality Account – Priorities Marie-Noelle Orzel Equality & Diversity – Annual Objectives Harry Hayer Learning Disabilities Marie-Noelle Orzel Budget Steve Webster Operating Plan David Powell Objectives Ruth Brunt NHS Constitution Ruth Brunt Building our Future – Executive Summary Harry Hayer GRMC and Risk Register Martin Bell Annual Staff Survey Results (potential movement) Harry Hayer Foundation Trust Ruth Brunt MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster APRIL Annual Performance Sue Watkinson
Revised January 2012 2

Month
Report Executive
NBT/UHB Partnership Programme Board Harry Hayer Assurance Framework 2011/12 and 2012/13 Martin Bell Board Effectiveness Assessment Ian Cumming Building our Future – Executive Summary Harry Hayer Major Trauma Implementation (2012 only) Harry Hayer Research and Innovation Performance/KPI – Quarterly Report Harry Hayer Bristol Health Partners – Quarterly Review Harry Hayer Building our Future Quarterly Review Harry Hayer Foundation Trust Ian Cumming MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster MAY Major Capital Projects (including Frenchay bidder shortlist) David Powell Project Performance & Financial Control Steve Webster Security Simon Wood NBT Leadership Development Programme Harry Hayer Pay Strategy Harry Hayer 2012/13 Operating Plan and Updated MTFP Steve Webster Building our Future – Executive Summary Harry Hayer GRMC and Risk Register Martin Bell Information Governance Martin Bell Freedom of Information Martin Bell Use of Trust Seal Ian Cumming Foundation Trust Ian Cumming Annual Accounts Steve Webster MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson
Revised January 2012 3

Month
Report Executive
Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster JUNE Quality Account Sign Off Marie-Noelle Orzel Dementia Marie-Noelle Orzel Health and Safety Simon Wood Building our Future – Executive Summary Harry Hayer Cancer Annual Report Chris Burton NBT/UHB Partnership Programme Board Harry Hayer Charitable Funds and Fundraising Steve Webster Foundation Trust Ian Cumming Statement of Internal Control Steve Webster Emergency Planning Annual Report Simon Wood MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster JULY Major Capital Projects David Powell Research Annual Report Harry Hayer Bristol Health Partners – Quarterly Review Harry Hayer GRMC & Risk Register Martin Bell Research and Innovation Performance/KPI – Quarterly Report Harry Hayer Infection Control Annual Report Chris Burton Building our Future – Executive Summary Harry Hayer Building our Future Programme - Quarterly Review Harry Hayer Complaints Marie-Noelle Orzel Foundation Trust Ian Cumming Clinical Excellence Awards Chris Burton
Revised January 2012 4

Month
Report Executive
MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster AUGUST NO MEETING SEPTEMBER Major Capital Projects David Powell Project Performance & Financial Control Steve Webster Building our Future – Executive Summary Harry Hayer GRMC and Risk Register Martin Bell NBT/UHB Partnership Programme Board Harry Hayer Overview & Scrutiny Committees – Annual Report Harry Hayer Foundation Trust Ruth Brunt Safeguarding Children Marie-Noelle Orzel MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster OCTOBER Research and Innovation Performance/KPI – Quarterly Report Harry Hayer Annual Audit Letter Ken Guy Bristol Health Partners – Quarterly Review Harry Hayer Capital schemes: Frenchay Preferred Bidder Approval David Powell Building our Future – Quarterly Review Harry Hayer MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson
Revised January 2012 5

Revised January 2012 6
Month
Report Executive
Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster NOVEMBER GRMC and Risk Register Martin Bell NBT/UHB Partnership Programme Board Harry Hayer Learning and Research Phase 2 SOC David Powell Building our Future – Executive Summary Harry Hayer Workforce & OD Strategy – Review Harry Hayer Post PPFC Summary Steve Webster Major Capital Projects David Powell Foundation Trust Ian Cumming MONTHLY REPORTS Quality Report Marie-Noelle Orzel Activity and Performance Report Sue Watkinson Workforce & OD Strategy Report Harry Hayer Infection Control Report Chris Burton Finance Report Steve Webster DECEMBER NO MEETING

Trust Board – January 2012
Title: Building our Future Programme – Executive Summary
Purpose of paper: This paper outlines progress on the Building our Future Programme up to January 2011. The Trust Board is asked to NOTE this report.
For Information 1. Key Progress Highlights: 1.1 Planning
The Operating Plan project has resubmitted its revised project PID. The Long Term Conditions PID was submitted and approved. Two projects have submitted change control requests; Non Pay and Outpatients.
1.2 Theatres
The Productive Operating Theatre (TPOT) initiated first two steps of the process. The ‘Visioning Workshop’ was held and attended by over 80 staff members from various staff groups. Theatres Advisory Board agreed a draft set of measures which all theatre suites will use to monitor performance to achieve the vision. 1.2 Bed reconfiguration
Stroke bed move was completed as planned. Communication sent pre and post move to all Trust users advising of planned moves. Thank you ‘walkaround’ undertaken on wards 12, 18 & 19. 1.3 Nursing
Productive Ward agreed the ‘Patient Status at a Glance’ boards funding through the charitable funds committee.
A group has been set up to review the scope of clinical nurse specialists and nursing practioner roles in NBT.
1.4 Non-Pay
Inaugural Clinical Procurement Group meeting was held with good attendance. Spend analytical demonstrations held with preferred provider identified. Decision to procure agreed. 1.5 Outpatients
Continuing to support East Central Community Paediatrics’ with their achievement of reducing DNA rate from 20% to 8.9% by devising and implementing a phone call and letter reminder based system to remind patients to attend clinics. Discussions are being had to roll out to other localities. Barnardo’s are sharing the work nationally.
This document could be made public under the Freedom of Information Act 2000.
Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
1

This document could be made public under the Freedom of Information Act 2000.
Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
2
Final draft of the Orthopaedics Capacity and Demand Study has been shared with the project team. Next steps for directorate will be to look at identified opportunities clinic by clinic to see where capacity can be rescheduled to increase utilisation and where it can be potentially released. The business case for a Trust wide third party patient reminder service has been signed off by the Trust Management Team 2. Key Risk Highlights:
Low levels of staff engagement causing projects to be delayed
Lack of ownership in Directorates limiting the ability to achieve full financial and quality benefits
3. Key Priorities Highlight - Month Ahead
3.1 Theatres
The Productive Operating Theatre (TPOT) will be completing the sign-off vision for theatres and a standard set of measures to be used in the project Theatres Redesign - a session will be arranged for process mapping the key processes for theatres in the new hospital.
3.2 Bed reconfiguration
The project will continue with directorate engagement to agree bed and Length of Stay reductions.
3.3 Nursing
Work on Phase 2 and 3 benchmarking (renal, neurosurgery, paediatric and maternity) to progress.
3.4 Non-Pay:
Agree remedial plan for directorates spend reviews. Appointment process underway for Procurement Relationship Manager pilot.
3.5 Outpatients
The project will be handing over-capacity and demand data and recommendations to the MSK directorate. Partnering with Diabetes will commence. Follow up request to share East Central/ Barnardo’s. Continue Patient reminder service work.

This document could be made public under the Freedom of Information Act 2000.
Any person identifiable, corporate sensitive information will be exempt and must be discussed under a 'closed section' of any meeting.
3
Impact on Patients: The ‘Building our Future’ Programme will be central to improving patient safety, quality and experience. CQC Outcome:
Responsible Committee: Building our Future Programme Board
Financial Issues considered: N/A
Equality Impact Assessment Completed: Each programme of work in ‘Building our Future’ will require an equality impact assessment.
Legal Issues Considered: N/A
Sustainability Assessment Completed: N/A Presented by: Harry Hayer, Director of Organisation, People & Performance Prepared by: Building our Future Programme Team

Sheet 1 - R&I Strategy Status ReportNorth Bristol NHS Trust
Summary of Progress in Quarter 3:Research & Innovation Strategy Status Report 2011-12 -Quarter 3
Training courses held for Researchers:12 Researchers attended a follow up date for Successful Research Delivery
22 researchers attended introduction to GCP8 People attended a Refresher to GCP14 Researchers attended various training in the field of Statistics 23 Researchers attended a one day monitoring course, with an aim to raise standards, and develop skills in monitoring.We have invested a total of £7,822 in equipment for researchers in this quarter
and finally invested a total of £3,243 in conference attendance, University modules, specific research training courses for six individual researchers.
R&I KPI metrics indicate targets are being met or exceeded in terms of study numbers, recruitment and income.
The NBT Small Grant Scheme funding panel met on the 19th Decemeber and have made 8 awards to a total of £103,000
An NIHR briefing paper has beeen released that outlines a renaming of the Flexibility and Sustainability Funding to Research Capability Funding with effect from April 2012. A Q&A document is due for publication imminently which will further explain the new and extended scope of the funding.
The inaugral PPI Forum will be held in January at NBT for South West Researchers who are actively involved in PPI to share best practice.An R&I communication plan is currently being developed to raise awareness to patients and the public in research involvement at North Bristol NHS Trust.The 'Innovation Health & Wealth: accelerating adoption and diffusion in the NHS' and 'Strategy for UK Life Sciences' report was published in December. The relevance of this for NBT is as follows:• Stratified Medicine is prominent as an innovative area in the UK Life Sciences Strategy and the Innovation Manager is working with BGL to build on its work in this area.• Modern Apprenticeships are to become more widespread. NBT is actively encouraging this via membership of the SWATPro consortium. Skills for Health are keen on this new business model, the first of its kind in the country. The Innovation Manager has worked with the Head of L&D to ensure appropriate contracts are in place to secure current core business and growth opportunities. • A new Innovation Strategy will be developed over the coming quarterIn November Dr Shea Palmer (UWE) was awarded an NIHR HTA grant (amount TBC).The development of the grant was supported by NBT FSF (Dr Emma Clark, co-applicant) and was submitted through NBT.
A pipeline deal has been set up with Wiley Blackwell to publish nurse education books from an NBT Practice Development Trainer author.Licenced images taken by BUI PhD student are being supplied to the Wellcome Image Library.The NBT Small Grant Scheme funding panel met on the 19th Decemeber and have made 8 awards to a total of £103,000 to support small /pilot research projects within NBT. These projects will support future NBT-led NIHR/portfolio eligible grant applications.R&I have been successful in a bid to secure £35,998 in 2011/12, £86,395 in 2012/13 and £50,397 in 2013/14 from the WCLRN to increase research capacity / infrastructure in cancer services.
Learning and Research Phase 2 planning continues, a planning application will be submitted in Jan/Feb 2012.A Clinical research facilities group has been established to consider other facilities required for research outside Learning and Research and main clinical areas.
Strategic Aim 4: Strategic aim 4: Develop research and innovation infrastructure, providing access to protected space and facilities 4.1 Establish a Clinical Trials Unit (CTU) 4.2 Scope the Potential for establishing Clinical Research Facilities
Objectives:
4.3 Scope the potential for a BioTechnology Incubator
Strategic Aim 2: Increase high quality research and innovation activity by improving and developing new opportunities for engagement 2.1 Support and Increase National Institute for Health Research (NIHR) Portfolio Research 2.2 Develop and Lead New Research 2.3 Increase Patient and Public Involvement (PPI)
Objectives:
2.4 Develop Innovation Activities
Strategic Aim 1: Support our leading clinical researchers and develop new talent 1.1 Provide Protected Time for Research 1.2 Develop Research Capacity
Objectives:
1.3 Develop Engagement with Clinical Research Networks
Strategic Aim 3: Increase income arising from research and innovation and use that income in support of our strategic aims 3.1 Maximise External Income 3.2 Develop the Internal Funding Scheme
Objectives:
3.3 Develop Best Practice in Financial Management

Research & Innovation Highlights
Arrows
Target Currently met, AND..
Target NOT met this quarter although on target overall, AND..
Target NOT met this quarter and NOT on target overall, AND..
This quarter IMPROVED on preceding quarter
This quarter IMPROVED on preceding quarter
This quarter IMPROVED on preceding quarter
This quarter SAME as preceding quarter
This quarter SAME as preceding quarter
This quarter SAME as preceding quarter
This quarter DOWN on preceding quarter
This quarter DOWN on preceding quarter
This quarter DOWN on preceding quarter
Two linked reports were published in early December - 'Innovation Health & Wealth: accelerating adoption and diffusion in the NHS' and 'Strategy for UK Life Sciences'. The relevance of the second report for NBT is as follows:• no new call will be made for Academic Health Science Centres (AHSC) but BRIG-H intends to pursue its plans under the new brand of Bristol Health Partners. The Innovation Manager is a member of the Innovation Working Group of BRIG-H which has a key role in shaping BHP.
The panel for the Small Grants Scheme sat in December, awards have been made.The NBT Small Grant Scheme funding panel met on the 19th Decemeber and have made 8 awards to a total of £103,000 to support small /pilot research projects within NBT. These projects will support futureNBT-led NIHR/portfolio eligible grant applications.
Dr Shea Palmer (UWE) was awarded an NIHR HTA grant (amount TBC) to study the effects of a comprehensive physiotherapy intervention for adults with joint hyermobility.
NIHR Flexibility and Sustainability Funding will be renamed as Research Capability Funding from April 2012 and the scope for applicable funding widened.
Strategic Aim 5: Work with partners to deliver the NBT strategic aims and develop a pan-Bristol research and innovation strategy
5.1 Tackle priorities for research through partnership 5.2 Develop a pan-Bristol Research and Innovation Strategy
Objectives:
5.3 Support the development of Regional Research and Enterprise

Sheet 2 - Key Performance Indicators
IndicatorTOTAL 2009-10
TOTAL 2010-11 Q1 Q2 Q3 Q4
Target (where appropriate) Progress
Non-commerical studies active - ALL (No.) 342 473 385 430 482 N/A
Non-commerical studies active - NIHR Portfolio only (No.) 84 204 172 196 221 N/A
NIHR Programme Grants for Applied Research led by NBT active (No.) 2 3 3 3 3 3
Other NIHR grants led by NBT active (No.) 3 7 7 8 9 6
Commercial studies active - ALL (No.) 51 74 51 52 52 N/A
Commercial studies active - NIHR Portfolio only (No.) 8 21 15 19 19 N/A
Patients Recruited - NIHR Portfolio only (No.) 5467 6519 2204 3481 3807 4388
Income - NIHR Delivery funding (justified by activity) £1,065,204 £2,674,942 £700,000 £1,337,631.00 £2,166,752 £2.9million
Total grant income administered by NBT - NIHR Grants only (£) £4,565,580 £6,478,650 £6,487,064 £6,719,412 £6,719,412 N/A
Net contribution to NBT's existing embedded research costs £1,000,000 £1.456million £1,360,000 £1,495,000 £1,495,000 £1.49million
Commercialised products (No.) 3 3 0 0 2 N/A
Product innovation projects active (No.) 45 34 15 7 28 N/A
Royalties from licensed products before royalty sharing £109,784 £65,250.51 £18,863.40 £37,418.00 £37,418.00 TBC
North Bristol NHS Trust
Key Performance Indicators
Q3 2011-12

Sheet 3
KPI Definition/Relevance Target
Commercial studies active The Research Committee will agree a localtarget
Patients recruited The target for the number of patients recruitedhas been determined by the R&I finance plan.
NIHR Research for Patient Benefit(RfPB)
NIHR Programme Grants forApplied Research (PGAR)
Other NIHR grants
Income - NIHR Delivery Funding NIHR Delivery funding is allocated to NHS Trustsbased on the number of patients the Trust recruitsinto NIHR Portfolio studies each year. The WesternComprehensive Local Research Network (WCLRN)determinesand provides the NHS Trusts' allocationsin the South West region.
Based on 2009-10 activity, the WCLRN hasprovisionaly allocated £2.679million to NBT tosupport the delivery of NIHR portfolio studies.
Total grant income administeredby NBT
This represents the total value of all NIHRgrants held by NBT for this financial year.
There is no target agreed for this KPI.
Description of the metrics used
Non-commercial studies active The Research Committee will agree a localtarget
The number of studies active and number of patients recruited into those studies (sometimes referred to as ‘accruals’) is a useful high level indicator of the overall size of NBT research portfolio. These KPIs are routinely used in regional and national comparisons between organisations (particularly NIHR Portfolio studies) and are also used in any activity/formula based funding allocations made by Department of Health or research networks. Commercial research also generates a) profit for NBT (in that commercial direct costs are changed) and b) capacity building income (20% of direct costs) which is directed to the Innovation Seed Fund (see below).
Please note: All figures are cumulative totals
Attracting NIHR Grants (where NBT is the lead NHSOrganisation) is of particular importance asadditional Department of Health income (Flexibility &Sustainability Funding (FSF)) is paid in directproportion to NIHR Grant Income to NBT in theprevious calendar year. FSF is used to fund thedevelopment of future NIHR Grants and therefore avirtuous cycle can be maintained. The main NIHRgrants are included in the KPIs and will be reportedannually due to the varying timescales throughoutthe year at which these grants are awarded.The 'other NIHR Grants' refer to funding streamssuch as Health Technology Assessment (HTA),Invention for Innovation (I4I) and Service Delivery &Organisation (SDO).
The target for the number of successful NIHRgrants has been determined by the R&Ifinance plan.

Commercialised products The number of different products invented by NBTstaff that have been commercialised.
Local target – yet to be agreed.
Product Innovation projects active The number of product innovation projects that arecurrently active provides a high level indicator of theNBT innovation activity
Local target – yet to be agreed.
Royalties from licensed productsbefore royalty sharing
This is royalties from licensed intellectual propertyrights before royalty sharing accrording to our IPPolicy takes place between the inventor, theirdepartment and the trust. This does not includeincome from sales of products developed andproduced in-house.
Local target defined within the business casedrafted in 2007 to support NBT continuingwith the Trust Innovation Lead role. Thistarget will be reviewed and amended afterlocal discussions have taken place.
Glossary of terms
NIHR
FSF
Embedded FSF
Accruals
Portfolio
Commercial studies
Non-commercial studies
WCLRN
WCLRN - One of 25 Comprehensive Local Research Networks (CLRNs) as part of a national research network infrastructure. All NHS organisations in Avon, Gloucester, Wiltshire, Dorset and Somerset are members of the Western CLRN.
y p gy'Best Research for Best Health'
Flexibility and Sustainability Funding - funding provided by the NIHR for use in developing new grant applications and/or plugging the gaps of NIHR Investigators' salaries in-between grants
Research development time which already exists within individuals' job plans
Number of patients recruited to a studyThe NIHR's list of adopted studies. Studies that are funded through major funders (NIHR, Research Councils, Charities etc) via peer reviewed open national competition are eligible for inclusion on the NIHR Portfolio. Other studies are also adopted on a case by case basis. Funding from CLRNs is provided to support NIHR portfolio adopted studies. Some Commercial research is also adopted
Commercial studies - Research funded AND sponsored (i.e. contracted) by commercial companies e.g. pharmaceutical company; medical device company
Non-commercial - All other research. Funded by a non-commercial organisation such as the NIHR, a research council or charity or local funding. Also includes studies funded by a grant from a commercial company but sponsored by a non-commercial organisation.

GRMC
Clinical RiskClinical
EffectivenessPatient Experience
Group
Workforce Governance
Infection ControlInformationGovernance
Health & SafetySafeguarding
CNST4.9 LARMs2.8 Hand hygiene trainingCQCOutcome 8 infection control
CNST4.4 record keeping4.1 - Patient ID1.8 Management of
RecordsCQCoutcome21 records
CNST3.1Secure environment3.2 slips trips staff3.4 moving & handlingCQCOutcome 10 Safety/suitability
of premises
CNST 5.2 incident reporting5.4 claims5.5 investigations3.9 support for incidents4.1 Patient info & Consent5.10 being openCQC Outcome 2 consent
CNST 5.8 - Best practice NICE5.9 – Best practice NCEPOD
CQCOutcome 17 ComplaintsOutcome 1 –Respecting &
involving people using services
Outcome 4 – Care & Welfare
CNST3.2 - Sickness absence1.10 employment checks1.9 professional
registrationCQCOutcome 13 Sufficient staffing & skill mixOutcome 12 – req of staff
CNST3.3 – Adults
CQC Outcome 7Safeguarding
Falls GroupDrugs & Therapeutic
Committee
Learning & Dev Committee
Patient Records Committee
Violence & Aggression
CNST3.3 Slips, trips , falls(patients)
Resuscitation Committee
CNST 4.7 - resuscitation
Blood Transfusion
CNST–4.6 transfusion
Medicines Governance
CNST 4.5 Medicines manCQC- Outcome 9medicines
VTE Committee
CNST4.8 - VTE
CNST2.1 Corporate induction2.2/2.3 Local induction2.5- Risk training2.6 Training needs
analysis2.7 Medical devices
training2.8 hand hygiene training2.9 Moving/handling
training2.4 Supervision of medical staff in training2.10 Consent trainingCQC – Outcome 14 Supporting workers
Equalities Committee
Sharps Group
CNST3.5 - inoculation
incidents
Staff Wellbeing
CNST3.7 - bullying/harassment3.10 - stress
GRMC Sub Committees – Showing CNST/CQC Responsibilities
CNST3.8 - violence +
Aggression
Nutrition Group
CQC – Outcome 5 meetingNutritional needs
Medical Devices Management Group
Trust Care Management Forum
CNST3.6 Maintenance ofmedical devices
& equipmentCQCOutcome 11 Safety,availability & suitability
of equipment
CNST4.10 Discharge of patients 4.9 Transfer of patientsCQCOutcome 6 Co-operating with other providers
CNST 1.1 risk strategy, 1.2 policy on policies, 1.3 Risk Cttees,1.4 Risk training for Snr Mgmt 1.5 risk process, 1.6 risk register, 1.7 responding to external recommendations 5.3 Complaints 5.4 claims 5.6 analysis 5.7 improvementCQCOutcome 16 – quality of service
CNST4.2 Health record keeping standards4.3 screening Procedures4.4 diagnostic testing procedures
CQC – Outcome 4Equality diversity ofpatient & staff
Clinical Audit Committee
CNST5.1 – Clinical Audit
Committees – not reporting through to GRMC
3.1 –
Appendix 2

Report to Trust Board – January 2012
PUBLIC SESSION
Title: Governance and Risk Management Committee Report Purpose of paper: To report the key decisions, assurances and risk issues
addressed at the meeting of the Governance and Risk Management Committee (G&RMC) held on 13th January 2012.
For Discussion and Information
Executive Summary: A summary of the meeting is attached as an appendix to
provide the Trust Board with assurance that the G&RMC is conducting its business in a robust manner. It also provides opportunity for board members to triangulate the assurance and risk issues covered with information received directly at the Board, or within the normal course of their duties.
Key areas discussed included;
Outpatient Survey – the Committee reviewed a summary of the Outpatient Survey and agreed actions to be monitored through the Patient Experience Group and reported back through its highlight report. Patient & Public Involvement Strategy – this was approved based upon a recommendation received from the Patient Experience group. Risk Reporting – the proposed approach to reviewing existing procedures was approved and specific recommendations will be made to the next G&RMC meeting.
Action Required: Trust Board is requested to:
Review the work of the Governance and Risk Management Committee and discuss any appropriate issues.
Key Risks: Demonstration of an adequate process for ensuring the Board that
objectives can be achieved and governance processes and compliance issues are dealt with is important for the safety of patients, the Trust’s own health as an organisation and for those outside bodies with statutory obligations to oversee health care providers. Failure to follow adequate procedures could bring financial penalties.
Impact on Patients: Indirect impact on the safety of patients and demonstration to patients and the public of the Trust’s ability to maintain that safety.
1

2
Quality and Safety Standards:
Impacts on all CQC registration and other bodies’ standards.
Financial Issues considered:
There are no extra financial issues.
Equality Impact Assessment:
None Undertaken
Legal Issues Considered as part of compliance issues.
Sustainability Assessment Completed:
An inherent part of the assurance process.
Presented by: Ruth Brunt, Chief Executive & Chair of G&RMC Prepared by: Nick Stibbs, Corporate Services Manager & Paul Cresswell, Head of
Compliance

3
Summary of Governance and Risk Management Committee Meeting
13 January 2012
1. Decisions Made / Requested
Exec. lead
The Committee approved;
a) the Trusts updated Patient & Public Involvement Strategy following detailed review and recommendation from the Patient Experience Group.
b) The review process and timescales proposed to strengthen the existing risk management systems and associated governance.
No requests for Board approvals are being made from this meeting.
MNO MB
2. Assurance Reports Directly reviewed by GRMC
Exec. lead
The Outpatient Survey showed the Trust had improved significantly on four questions and worse on only one. Nine areas were identified as needing action which will be progressed through directorates and performance monitored by the Patient Experience Group.
MNO
A report was received on the achievement of Level 2 LARMS assessment in November. The next meeting will consider an outline plan for achieving Level 3 in November 2013 and the relative values of the cost of doing so and the savings achieved.
MNO
All sub-committees have been mapped to show their CNST and CQC responsibilities. Appendix A illustrates the current position.
MNO
The quarterly report on Central Alerts showed that no reports were outside of their deadline for completion and six remained still within their deadline.
MNO
3. Assurances Received from Sub-Committees Exec.
lead Quality Committee Cardiac arrest calls are now below the national average and there was a 10%
drop in falls incidences in October. Medication errors have fallen by 10%.
MNO
Clinical Risk Committee Reporting from the CRC sub-groups is now more robust and the backlog of
incidents to be reported to the National Patient Safety Agency has been cleared.
CB
Health and Safety Committee Attendance at fire training has increased to 72% and the achievement of
Level 2 NHS Litigation Authority risk management standards included 90% on the criterion that includes health and safety. 17 items on the Non-clinical risk register were reviewed, two of them being reviewed again in three months. One item was removed from the register.
SW

4
Clinical Effectiveness Committee Performance on NICE Technology Appraisal Guidelines, NICE guidance and
Venous Thrombosis Event prophylaxis remain rated at Green. CB
4. Key Risk Areas Discussed:
Exec. lead
The Committee received an update on preparations for the CNST Maternity assessment for Level 3 in June 2012.
MNO
Complaints in the second quarter have risen 23% above last year’s figure and compliments have fallen 59%. Advice is being taken from the Parliamentary and Health Service Ombudsman to improve communication and reduce premature complaints to the PHSO.
MNO
The issues with the implementation of the Cerner Millennium system may impact on the data mapping between e-aims and the NRLS.
MB
Following an Internal Audit report a local audit on the use of consent forms for Learning Disabled patients will be carried out in March and a broader consent audit tool is being devised. A Learning Disability Strategy is being circulated for review by staff and a proactive measurement tool to ensure Do Not Attempt Resuscitation documents are completed appropriately is being developed. Follow-up actions from the IA report will be reported to the Audit Committee.
MNO
Clinical Audit Committee Recruiting local leads and identifying available middle grade doctors is
making it difficult for the Trust to participate in national audits and to devise local action plans regarding published audits. These issues will be discussed by the Medical Director with the Chair of the Clinical Audit Committee.
CB
Quality Committee The overall incidence of pressure ulcers is static although there have been no
grade 3 or 4 incidences for some months. Staff from U Ward and Ward 104 are helping the poorer performers.
MNO
Clinical Risk Committee The risk of drug shortages has been escalated to the Risk Register and
across the UK regional procurement specialists have advised all pharmacy procurement staff to do this. Training for Root Cause Analysis/report writing has been arranged for March and will include input from Beachcrofts on the legal elements of report writing.
CB
Clinical Effectiveness Committee The Committee remains concerned that the Document Management System
needs to be replaced with a system that is easier to access by staff. .
MB
18/01/12

NORTH BRISTOL NHS TRUST
TRUST BOARD 26th JANUARY 2012 Declaration of Interest 2011/2012 This report is presented to the Trust Board for information. Introduction Under the Standards of Business Conduct for NHS Staff, the Codes of Conduct and Accountability and to help comply with the Bribery Act 2011 all members of the Trust Board must declare any relevant and material interest and those declarations must be recorded in the Public Minutes. The following declarations (including ‘nil responses’) have been made.
BOARD MEMBER
INTEREST DECLARED
1. Mr Peter Rilett Chairman
1. Non-Executive Director of: Watts of Lydney Ltd Bordeaux Quay Ltd 2. Trustee of: St. Monica’s Trust 3.. Adviser to: Centaur Services Ltd 4. Chairman of Governors of: Bristol Grammar School
2. Mr Robert Mould Non-Executive
1. Trustee of: Hopes Place Charity
3. Mr Nick Patel
None
4. Mr Stephen Hughes Non-Executive Director
1. Trustee and Company Secretary of Great Western Air Ambulance Charity Ltd. 2. Partner of Bevan Brittan LLP, Solicitors
5. Professor Avril Waterman-Pearson Non-Executive Director
1. Senior member of academic staff of University of Bristol

6. Mr Ken Guy Non-Executive Director
1. Trustee of:
Milestones Trust 2. Independent Member of Bristol City Council Audit Committee
7. Mr Andrew Nield Non-Executive Director
1. Director/Shareholder in Nield Enterprises Ltd 2. Finance Director, University of
Bristol 3. Director of a number of subsidiary University of Bristol companies 4. Trustee of University of Bristol Pension and Assurance Scheme
8. Mrs Ruth Brunt Chief Executive
None
9. Mr. Stephen Webster Director of Finance and Information
None
10. Miss Marie-Noelle Orzel Director of Nursing
None
11. Dr Christopher Burton Medical Director
None
In addition I can confirm that Declarations of Interest, including nil returns, have been made by all Corporate Directors, Clinical Directors, General Managers, second-in line officers of the Trust and other relevant staff. These forms are available for inspection from the secretary to the Trust Board. Presented by: Mr Martin Bell, Director of Assurance, Information and
Technology Prepared by: Nick Stibbs, Corporate Services Manager
17.01.12