Blood Physiology Blood Physiology
38
Blood Physiology Blood Physiology Blood Physiology Lecture 1 Dr. A-M Zagrean
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Blood Physiology Blood Physiology

1
Blood PhysiologyBlood Physiology
Blood Physiology Lecture 1Dr. A-M Zagrean
2
Blood Physiology - Syllabus
Lecture 1 Functions of the blood Composition and physico chemical- Functions of the blood. Composition and physico-chemical
properties of blood. The hematocrit. Blood volume. HematopoiesisLecture 2
- Erythrocytes. Respiratory gases transportation. Blood groups. Lecture 3Lecture 3
- Physiology of Immune System. Function of specific defense. Lymphocytes. Function of nonspecific (cellular) defense. Leukocytes.
Lecture 4- Function of maintaining the fluid- coagulant balance. Hemostasis. Fibrinolysis. Therapeutic uses of blood. Transfusions.

3
Blood = ?
- component of the internal medium
internal medium - Cl. Bernard - 1865
- component of the circulatory system
- liquid tissueq

4
Functions of the blood1) Because of the blood volume and pressure, blood flow,
tissue perfusion and capillary exchanges are maintained.
2) Transport through the body of:2) Transport through the body of: -oxygen and carbon dioxide -food molecules (glucose, lipids, amino acids) -ions: Na+, Ca2+, HCO3−
-wastes (e.g., urea) -hormones -heat
3) Defense of the body against infections and other foreign materials. All the WBCs participate in these defenses.
4) Acid-base buffering power RBC: CA HCO3-; Hb (>deoxyHb); phosphate; plasma proteins (polyanions at plasmatic pH)
5) Wound repair… blood clotting…

5
Blood components1 - blood cells / cell fragments – hematocrit
1) red blood cells (RBCs) or erythrocytes) ( ) y yThe fraction occupied by the red cells is called the hematocrit. Normally it is
approximately 45%. Values much lower than this are a sign of anemia.2) platelets or thrombocytes3) five kinds of white blood cells (WBCs) or leukocytes
- 3 kinds of granulocytest hilneutrophils
eosinophilsbasophils
- 2 kinds of leukocytes without granules in their cytoplasm lymphocytesmonocytes
2 – plasma - plasmatic volumePlasma is the non-cellular part of the blood and communicates continuouslywith the interstitial fluid through pores of the capillary membranes
monocytes

6
Blood (5 l or 7%BW)= 60% plasma (ESF) + 40% blood cells (ICF)

7
Composition of Blood

8
Plasma (mOsm/l H2O) Interstitial (mOsm/l H2O) Intracellular (mOsm/l H2O)N + 142 139 14
Plasma composition: comparison with other fluid compartments
Na+ 142 139 14K+ 4.2 4 140Ca++ 1.3 1.2 0Mg+ 0.8 0.7 20Cl- 108 108 4HCO-
3 24 28.3 10HPO4
-,H2PO-4 2 2 11
Amino acids 2 2 8Creatine 0.2 0.2 9Lactate 1.2 1.2 1.5Glucose 5.6 5.6Proteins 1 2 0 2 4Proteins 1.2 0.2 4Urea 4 4 4Others 5.3 4.4 70Total mOsm/l 301.8 300.8 301.2

9
Osmotic pressure of the plasma
• Relation between osmotic pressure – osmolarity ex: albumin, glucose, NaCl
• Van’t Hoff’s law for osmotic pressure (Π)Π = CRT
C = concentration of solutes (osmoles/L)R = ideal gas constantT= absolute temperature (Kelvin degrees)
Π (mmHg) = 1 osm/L x R x (37+273) = 19,300 mmHg1 mosm/L 19.3 mmHg
10
Plasma Proteins : albumin (oncotic press), globulin (Ig), and fibrinogen (clotting).
Essentially all the albumin and fibrinogen of the plasma proteins, as well as 50 -80 % of the globulins, are formed in the liver (30 g/day). The remainder of the globulins (mainly the gamma globulins) are formed in the lymphoid tissue.
Conditions that cause rapid loss of plasma proteins: severe burns that denude large surface areas of the skin; severe renal disease;denude large surface areas of the skin; severe renal disease; cirrhosis of the liver, large amounts of fibrous tissue develop among the liver parenchymal cells, causing a reduction in their ability to synthesize plasma proteins this leads to decreased plasma colloid osmotic pressure, which causes generalized edema.
Pl P t i S f A i A id f th TiPlasma Proteins as a Source of Amino Acids for the Tissues.Protein tissues depletion – plasmatic proteins pinocytosis by macrophages intracell split into amino acids that are transported back into the blood (plasma proteins function as a labile protein storage medium)

11
Hematocrit (packed red cell volume)- definition: fraction of the blood composed of RBCp- functional significance- methods of determination: centrifuging blood in a calibrated ‘hematocrit tube’- values ~ 35% – 45%;
~ up to 10% in severe anemia up to 10% in severe anemia~ up to 65% in polycytemia
- corrected Ht = 0,96 Ht (3-4% from the measured Ht is represented by entrapped plasma)
- venous vs. arterial hematocrit …l ti h t it bl d i it- relation hematocrit – blood viscosity…
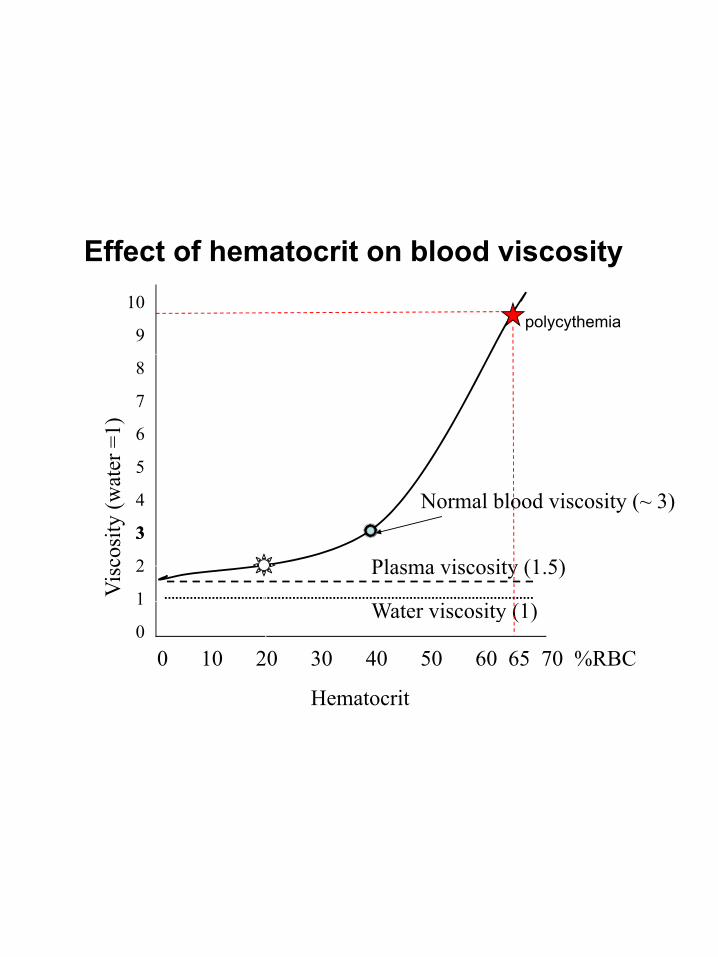
12
Effect of hematocrit on blood viscosity10
9polycythemia
8
7
6
5ater
=1)
4
33
2
1Vis
cosi
ty(w
a
Plasma viscosity (1.5)
Normal blood viscosity (~ 3)
1
00 10 20 30 40 50 60 65 70 %RBC
Hematocrit
Water viscosity (1)

13
From Guyton, 2006

14
The erythrocyte sedimentation rate (ESR)- commonly used, inexpensive, but non-specific laboratory test (Westergren, 1921)
measures the speed of sedimentation of RBC/RBC aggregates in- measures the speed of sedimentation of RBC/RBC aggregates in plasma over a period of 1 hour in a vertical column of anticoagulated blood under the influence of gravity
- sialic acid-rich glycoproteins on cell surface membranes contribute to g y pcreating a negative charge on the cells’ surface cellular repel …
- a raised ESR is assoc with marked rouleaux formation of RBCs- mainly depends on plasma concentration of large proteins (fibrinogen, Ig)
- ESR raised in systemic inflammatory & neoplastic diseases; useful in chronic diseases, for monitoring disease activity/response to therapy

15
The basic factors influencing the ESR- increased ESR
with elevated fibrinogen (e.g., pregnancy, collagen vascular diseases, malignancy).
decreased albumin conc.anemia (hematocrit is reduced, red blood cell aggregates fall
faster); macrocytic red cells also settle more rapidly.
– a decreased ESR is associated with:hypofibrinogenemia, hypergammaglobulinemia associated with
dysproteinemia, and hyperviscosity blood diseases in which RBC have an irregular or smaller shape
that causes slower settling; increased albumin concentration polycythemia
– an abnormal value remains a nonspecific finding

16
ESR normal valuesAdults mm/hrAge < 50 years
– Men 1 - 15 – Women 5 - 15
Age > 50 years – Men up to 20 – Women up to 30
ESR increases in inflammatory & neoplastic diseases; >100mm.hr in chronic infections (e.g., tuberculosis)
17
Blood volume
- values: 5000 ml; 65-70 ml/kg; 7-8% BW- changes:
1. physiological: pregnancy, water loss/gain 2. pathological: hemorrhage
- circulating blood volume, ‘stagnant’ blood volume - blood volume: plasma volume and cell volume

18
Determination of blood volume
- Dilution method:- volume = mass of substance injected / concentration
- plasmatic volume -T1824 (Evans Blue ), I125 albuminbl d l C 51 k d RBC- blood volume - Cr 51 marked RBC
- Blood volume = plasma volume / (1 – Ht)

19
Blood cells

20
Red blood cells are seen as biconcave disks

21
E
WBC - LeukocytesThi h t h i hil (E) d t hil (N) R f RBCThis photo shows an eosinophil (E) and a neutrophil (N). R for RBCs.The eosinophil is distinguished by its red granules and bilobed nucleus.

22
WBC – LeukocytesA basophile is characterized by a lobed nucleus and it is filled by large blue-blackp y y ggranules that sometimes cover the nucleus.Here you can see the distinct granules against the purple nucleus.

23
Monocytes are phagocytic and may have vacuoles in the cytoplasm.They also have a horseshoe shaped nucleus or in immature monocytesThey also have a horseshoe shaped nucleus or, in immature monocytes, they may have an indented nucleus.

24
Lymphocytes are only slightly larger than red blood cells and they havea relatively large nucleus / cytoplasm ratio.Note that the lymphocyte in the above photo has only a thin rim of light purple cytoplasm around the dense nucleus.

25
Fibrin clot with platelets and red blood cells
26
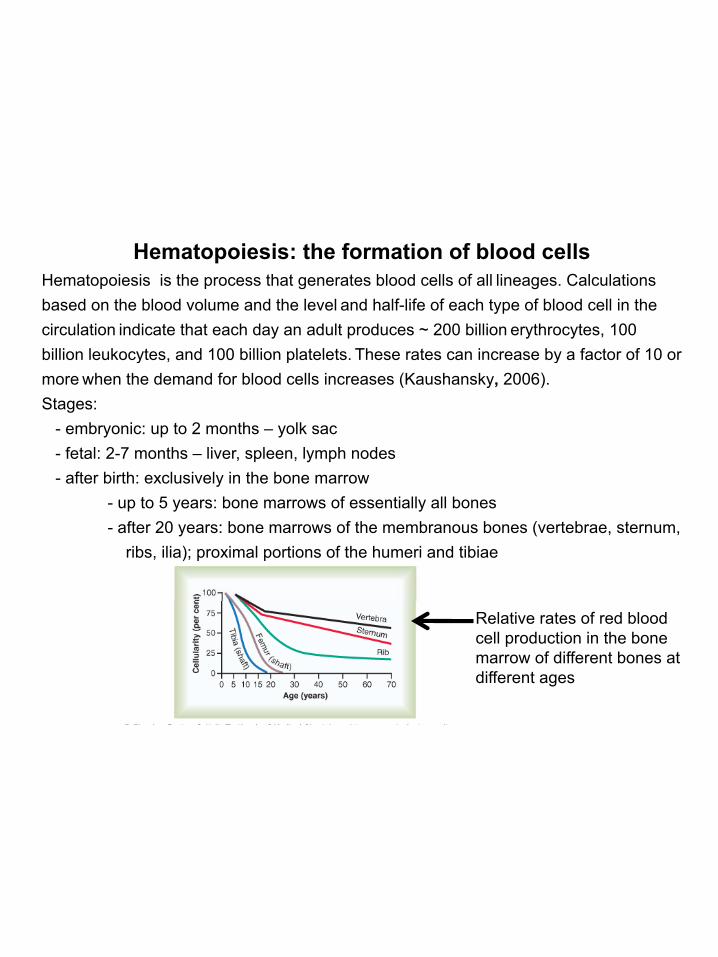
Hematopoiesis: the formation of blood cellsHematopoiesis is the process that generates blood cells of all lineages. Calculations based on the blood volume and the level and half-life of each type of blood cell in the circulation indicate that each day an adult produces ~ 200 billion erythrocytes, 100 billion leukocytes and 100 billion platelets These rates can increase by a factor of 10 orbillion leukocytes, and 100 billion platelets. These rates can increase by a factor of 10 or more when the demand for blood cells increases (Kaushansky, 2006).Stages:
- embryonic: up to 2 months – yolk sac- fetal: 2-7 months – liver, spleen, lymph nodes
after birth: exclusively in the bone marrow- after birth: exclusively in the bone marrow- up to 5 years: bone marrows of essentially all bones- after 20 years: bone marrows of the membranous bones (vertebrae, sternum,
ribs, ilia); proximal portions of the humeri and tibiae
Relative rates of red blood cell production in the bone marrow of different bones at different ages

27
Hematopoiesis in the bone marrow

28
All the various types of blood cells:
the formation of blood cellsHematopoiesis:
All the various types of blood cells:- are produced in the bone marrow - arise from a single type of cell called a pluripotential hematopoietic stem cell (PHSC)- the path that is taken, to a committed stem cell, is regulated by the p , , g yneed for more of a certain type of blood cell which is, in turn, controlled by grows inducers (cytokines: IL-3, IL-7, IL-11, etc.) - committed cells colony forming units (CFU): CFU erythrocytes (E)/ granulocytes & monocytes (GM)/ megakaryocytes (M)- differentiation inducers then act on CFUs final adult blood cells-hypoxia, infectious diseases: control grows & differentiation inducers

29
Pluripotential hematopoietic stem cell
- attached (probably by adherens junctions) to osteo-blasts lining the inner surface of bone cavities;
- produce, by mitosis, two kinds of progeny:produce, by mitosis, two kinds of progeny:1) more stem cells (a mouse that has had all its blood
stem cells killed by a lethal dose of radiation can besaved by the injection of a single living stem cell !).
2) cells that begin to differentiate along the pathsleading to the various kinds of blood cells.
- their number decrease with age;

30
CFU-B CFU-E Erithrocytes
Committed stem cells
Pluripotential hematopoietic
t ll
Colony forming unit(CFU)
CFU-GM Granulocytes
Monocytes/Macrophages
CFU-M Megakaryocytes platelets
stem cell(PHSC)
Lymphoid stem cell(LSC)
T Lymphocytes
B LymphocytesPHSC (LSC) B Lymphocytes

31
Hematopoiesis
s dPr
edom
inan
t for
ms
circ
ulat
ing
in b
lood

32
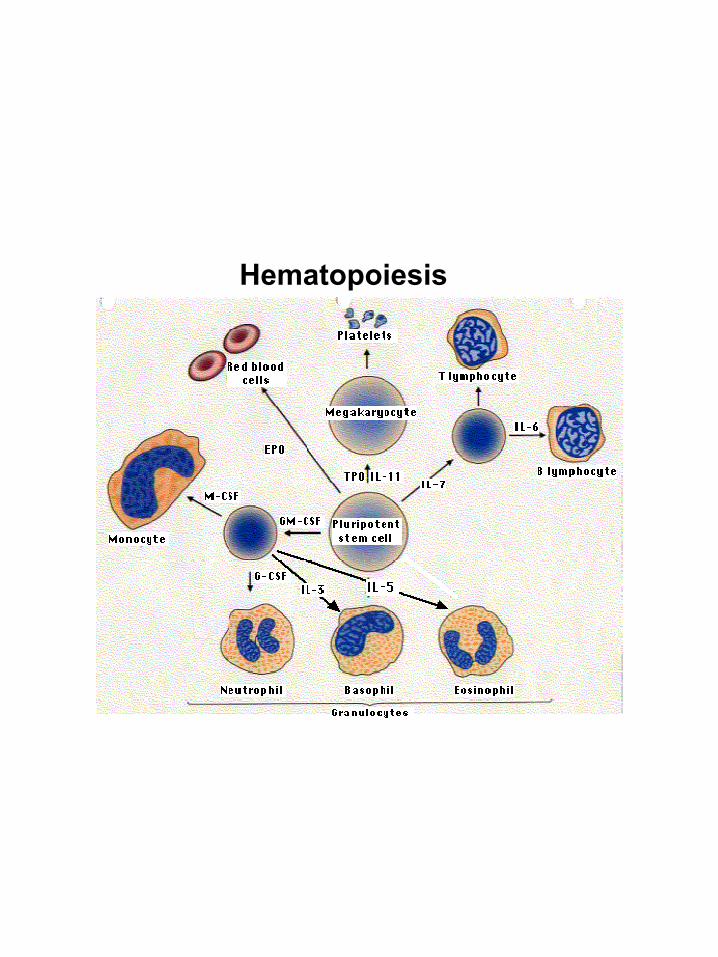
Growth and differentiation inducers (cytokines, hormones) for the formation of blood cells …
Interleukin-3 (IL-3) promotes growth of most of the different types of stem cellstypes of stem cells
Interleukin-7 (IL-7) - major cytokine in stimulating bone marrow stem cells to start down the path leading to the various lymphocytes(mostly B cells and T cells).
Erythropoietin (EPO), produced by the kidneys, enhances the production of red blood cells
Thrombopoietin (TPO/ megakaryocyte growth and development factor)Thrombopoietin (TPO/ megakaryocyte growth and development factor), assisted by Interleukin-11 (IL-11), stimulates the production of megakaryocytes. Their fragmentation produces platelets.
Granulocyte-monocyte colony-stimulating factor (GM-CSF), as its name suggests, sends cells down the path leading to both those cell types. In due course, one path or the other is taken. - Under the influence of granulocyte colony-stimulating factor (G-g y y g (
CSF), they differentiate into neutrophils. - Further stimulated by interleukin-5 (IL-5) they develop into
eosinophils. - Stimulated by macrophage colony-stimulating factor (M-CSF)
the granulocyte/macrophage progenitor cells differentiate into monocytes, the precursors of macrophages.
33
Hematopoiesis

34
35
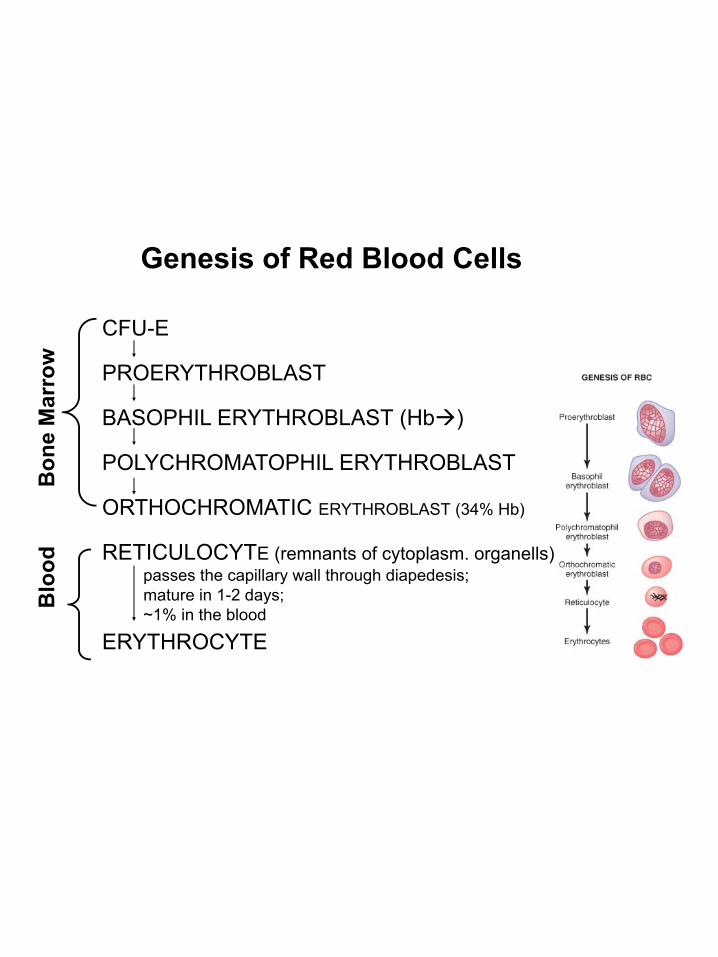
Genesis of Red Blood Cells
CFU-E
w
PROERYTHROBLAST
BASOPHIL ERYTHROBLAST (Hb )
POLYCHROMATOPHIL ERYTHROBLAST
Bon
e M
arro
w
ORTHOCHROMATIC ERYTHROBLAST (34% Hb)
RETICULOCYTE (remnants of cytoplasm. organells)
BB
lood passes the capillary wall through diapedesis;
mature in 1-2 days;
ERYTHROCYTE
B y ;~1% in the blood

36
Regulation of RBC genesisRBC precursors mature in the bone marrow closely attached to a macrophage. Time for the transition from proerythroblast to reticulocitocyte:
5 days (2 days in anemic stress macrocytes with >25 % HbF)Erythropoiesis rate: 5 x 104 RBC / day / µl, stimulated by erythropoietin (EPO)
Reticulocytes in the blood: 0,5 –1%
RBC life-time: 120 days
6. Low atm O2 /High altitude

37
ErythropoietinGlycoprotein, MW = 34.000, T1/2 = 6 - 9 hoursMechanism of action:
↑↑ the committment of stem cells to proerythroblasts↑ the differentiation of erythroblastic stages
Synthesized - 90% kidneys (renal tubular* epithelial cells?),the rest of 10% formed mainly in the liver- stimulus = renal hypoxiayp
↑ in EPO conc. after minutes to hours, with a maximum level after 24 h
after 3 - 5 days: ↑ RBC number. 10 x- other non-renal hypoxia sensors act through E NE PG (+) EPO productionE, NE, PG (+) EPO production
Regulation of erythropoietin control mechanism…Therapeutically used: 50 – 300 U / kg, 3 times / week
in kidneys diseases, transplant, anemia, pulmonary diseases, blood loss…

38
B12 Vitamin & Folic acid
Act on the final maturation of RBC.B th ti l f DNA th i th h th f ti fBoth are essential for DNA synthesis through the formation of an essential DNA building block, thymidine triphosphat
B12 Vitamin:- the body uses 1-3 µg/day of B12 vitamin
h i 1000 3000- hepatic stores amounts 1000-3000 µg (enough for 3-4 years…)- intrinsic factor needed for absorption …
Vit. B12 & folic acid deficiency proliferation & maturation failure:
- pernicious anemia macrocytes (large, oval, fragile) short life - causes: atrophic gastric mucosa intrinsic factor deficiency no B12 absorption