
Block 2 Abnormal Pregnancy - eGyanKosh
166
2 ABNORMAL PREGNANCY UNIT 5 Pregnancy with Abnormal Fetus 5 UNIT 6 Complications in Early Pregnancy 31 UNIT 7 Complications in Late Pregnancy I : Hypertensive Disorders in Pregnancy 60 UNIT 8 Complications in Late Pregnancy-II: Antepartum Haemorrhage 85 UNIT 9 Complications in Late Pregnancy-III: PROM, Preterm Labour, Postmaturity and Hydramnious 110 UNIT 10 Complications in Late Pregnancy-IV : Rh Incompatibility, Intra Uterine Infection 136 UNIT 1 1 Pain during Pregnancy 151 Block MME-302 Reproductive Health Indira Gandhi National Open University School of Health Sciences
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Block 2 Abnormal Pregnancy - eGyanKosh
2ABNORMAL PREGNANCY
UNIT 5
Pregnancy with Abnormal Fetus 5
UNIT 6
Complications in Early Pregnancy 31
UNIT 7Complications in Late Pregnancy I : HypertensiveDisorders in Pregnancy 60
UNIT 8Complications in Late Pregnancy-II: AntepartumHaemorrhage 85
UNIT 9
Complications in Late Pregnancy-III: PROM,Preterm Labour, Postmaturity and Hydramnious 110
UNIT 10
Complications in Late Pregnancy-IV : RhIncompatibility, Intra Uterine Infection 136
UNIT 11Pain during Pregnancy 151
Block
MME-302Reproductive Health
Indira GandhiNational Open UniversitySchool of Health Sciences

BLOCK PREPARATIONTEAM
CO-ORDINATION
PRINT PRODUCTION
March, 2019
© Indira Gandhi National Open University, 2019
ISBN-
All rights reserved. No part of this work may be reproduced in any form, by mimeograph or any other means, without permission in writing from the Indira GandhiNational Open University.
Further information about the School of Health Sciences and the Indira Gandhi National Open University courses may be obtained from the University’s office at MaidanGarhi, New Delhi-110 068, India.
Printed and published on behalf of the Indira Gandhi National Open University, New Delhi, by Prof. S. B. Arora, Director, School of Health Sciences.
Lasertypeset by : Rajshree Computers, V-166A, Bhagwati Vihar, (Near Sec. 2, Dwarka), Uttam Nagar, New Delhi-110059
Printed at:
Dr. S. B. AroraProfessor & Director, SOHSIGNOU, New Delhi
Mr. Ajit KumarSection Officer (Pub.), SOHS IGNOU, New Delhi
Dr. T.K. JenaProfessor and Programme CoordinatorSOHS, IGNOU, New Delhi
Wri ters
Unit 5-9Dr. Ashok KumarDirector Professor,Deptt. of Obst. & GynaeMAMC, New Delhi
Unit 11Dr. Nidhi GuptaAssistant ProfessorDeptt. of Obst. & GynaeJamia Hamdard
Format Editing
Dr. T.K. JenaProfessor and ProgrammeCoordinatorSOHS, IGNOU, New Delhi
COURSE REVISION TEAM (3rd Revision)
PROGRAMME CORE TEAM
COURSE REVISION TEAM (1st Revision)
COURSE REVISION TEAM (2nd Revision)
Dr. Ruchika KubaCourse CoordinatorSOHS, IGNOU, New Delhi
Dr. I.C. TiwariSr. Consultant, UNICEFNew Delhi
Dr. S.C. ChawlaDirector Professor and Head ofPSM Deptt., LHMC, New Delhi
Dr. (Mrs.) Kamala GaneshDirector Professor and Head ofO&G Deptt., MAMC, New Delhi
Dr. Sidharth RamjiProfessor, Deptt. of PaediatricsMAMC, New Delhi
Dr. L.N. BalajiChief, Planning DivisionUNICEF, New Delhi
Prof. (Col.) P.K. DuttaProgramme CoordinatorSOHS, IGNOU, New Delhi
Dr. S.B. AroraCourse CoordinatorSOHS, IGNOU, New Delhi
Dr. T.K. JenaCourse CoordinatorSOHS, IGNOU, New Delhi
Dr. T.K. JenaProfessor and ProgrammeCoordinatorSOHS, IGNOU, New Delhi
Dr. Sunita MittalProfessor & Head ofO&G Deptt.AIIMS, New Delhi
Dr. Nita YajnikEx. Professor, O&G Deptt.B.J. Medical College,Ahmedabad
Dr. S. B. AroraProfessor & Director, SOHSIGNOU, New Delhi
Dr. (Mrs.) Kamala GaneshEx. Director Professor andHead of O&G Deptt.MAMC, New Delhi
Dr. Reva TripathiProfessor of O&G Deptt.MAMC, New Delhi
Dr. A.K. AgarwalProfessor, SOHS, IGNOU,New Delhi
Dr. Chitra RaghunandanProfessor of O&G Deptt.LHMC, New Delhi
Dr. H. BhusanAssistant Commissioner (MCH)MOHFW, New Delhi
Dr. T.K. JenaReader and ProgrammeCoordinatorSchool of Health Sciences,IGNOU, New Delhi
Dr. (Mrs.) Kamala GaneshEx. Director Professor andHead of O&G Deptt.MAMC, New Delhi
Dr. Nita YajnikEx. Professor, O&G Deptt.B.J. Medical CollegeAhmedabad
Dr. Asha OumachuigiEx. Professor and Head ofO&G Deptt., JIPMERPondicherry
Dr. A.K. AgarwalDirector,School of Health Sciences,IGNOU, New Delhi
Unit 10Dr. Sumedha SharmaAssistant ProfessorDeptt. of Obst. & GynaeJamia Hamdard
Dr Himanshu BhushanNHSRC, NIHFW Campus,Munirka, New Delhi
Dr. T.K. JenaProfessor, School of HealthSciencesIGNOU, New Delhi
Dr. Manju PuriDirector ProfessorDeptt. of Obst. & Gynae, LHMC,New Delhi
Dr. Shyama KanungoProfessor and Head,Deptt. of Obst. & GynaeSCB Med. College, Cuttack
Dr. Pratima MittalProfessor and Head,Deptt. of Obst. & Gynae,VMMC, New Delhi
Dr. A.K. JainSenior ConsultantDeptt. of Obst. & GynaeVMMC, New Delhi
Dr. Sunita MittalEx-Professor and Head,Deptt. of Obst. & Gynae,AIIMS, New Delhi
Dr. Gokul Chandra DasProfessor and Head,Deptt. of Obst. & Gynae,Guwahati Medical College, Assam

BLOCK 2 INTRODUCTION
Safe motherhood is a concern for all the health managers. While everyattempt is being aimed at preventing the maternal morbidity and mortality,doctors must remain prepared to deal with the emergencies and complicationsarising during the course of pregnancy. In the previous block, you have learntabout the antenatal care and its importance in timely detection ofcomplications of pregnancy. In this block, we will discuss the complicationsarising during different stages of pregnancy.
There are seven units in this block. While Unit 6 deals with complicationsarising in early pregnancy, Unit 7, 8, 9 and 10 deal with complications arisingin the later part of pregnancy. Pregnancy Induced Hypertension (PIH) hasbeen dealt in Unit 7 and the antepartum haemorrhage have been dealt in Unit8. Unit 9 deals with complications related to the maturity and growth of thefoetus e.g. PROM, Post maturity, etc. Other important complicationsincluding the Rh incompatibility have been discussed in Unit 10.Anew unit(Unit 11) has been added to discuss issues related to pain during pregnancy.
In India, where 70% people live in rural area, management of the pregnancyrelated complications in peripheral health institutions need a lot of attention.Therefore, you as a physician working in peripheral health institutions have animportant role not only in preventing but also in managing pregnancy relatedcomplications both in the clinic and community health set-ups. Yourendeavour in this regard will go a long way in preventing the maternalmorbidity and mortality at the national level.

Abnormal Pregnancy

5
UNIT 5 PREGNANCY WITHABNORMAL FETUS
Structure
5.0 Objectives
5.1 Introduction
5.2 Intrauterine Fetal Death (IUFD)5.2.1 Incidence
5.2.2 Aetiology and Risk Factors
5.2.3 Diagnosis
5.2.4 Systemic Approach to Evaluation
5.2.5 Management
5.2:6 Complications
5.2:7 Post delivery Management
5.2.8 Preconception / Initial Prenatal Visit
5.3 Foetal Growth Restriction (FGR)5.3.1 Classification of FGR
5.3.2 Aetiology
5.3.3 Pathology
5.3.4 Fetal Complications
5.3.5 Diagnosis
5.3.6 Management
5.3.7 Long Term Sequalae
5.4 Let Us Sum Up
5.5 Key Words
5.6 Answers to Check Your Progress
5.0 OBJECTIVES
After going through the contents of this unit, you will be able to:
diagnose a case of IUFD;
enumerate the causes of IUFD;
evaluate mother and baby;
manage a case of IUFD after delivery;
make a decision as to when and how to terminate the pregnancy;
screen and identify pregnancies complicated by FGR;
differentiate early and late FGR;
identify complications of FGR;
provide appropriate antenatal care by careful monitoring of fetal growthand its wellbeing; and
make a balanced decision for management at various stages i.e. duringpregnancy.

Abnormal Pregnancy
6
5.1 INTRODUCTION
The terms foetal death, foetal demise, stillbirth, and stillborn all refer to thedeliveryof a fetus with no signs of life. The terms are used interchangeably.Intrauterine death is an unfortunate incidence. Many of the causes areunknown. It is a challenge to handle such situation both for the treatingphysician/obstetrician and parents. Careful counselling is required. FetalGrowth Restriction (FGR) is a major problem with the fetus. You willrealize that careful monitoring of fetal growth and wellbeing is extremelyimportant as birth weight is a significant determinant of perinatal mortalityand morbidity and later childhood morbidity. In India, about 30% of thebabies are growth retarded. Improving maternal nutrition, avoidingpregnancy during adolescence and lactation and increasing the intervalbetween pregnancies to more that 2 years will help in reducing small fordate babies. Biomedical technology especially, ultrasonography has helpedus monitor fetal wellbeing especially in guiding us to plan the delivery ofmother suffering from FGR.
5.2 INTRAUTERINE FETALDEATH (IUFD)
Foetal death means death prior to complete expulsion or extraction from themother of a foetus irrespective of duration of pregnancy and which is not aninduced termination of pregnancy. Intrauterine foetal death refers to babieswith no signs of life in utero. Foetal death can occur before onset oflabour(antepartum death) or during labour (intrapartum death). Thedefinition of intrauterine foetal death (IUFD) varies and takes intoconsideration the gestational age and birth weight. eg. An infant deliveredwithout signs of life after 20 weeks of gestation or weighing >500 g whengestation age is not known.
5.2.1 Incidence
Stillbirth (SB) is common, with 1 in 200 babies born dead. This compareswith one sudden infant death per 10 000 live births. Still Birth Rate is a ratioof number of SBs / one thousand births. It complicates 1 % of pregnanciesand the cause is unknown in 50% of cases. Still birth rate is
4.5 to 6.5(2.95) per thousand births in US
22.1 per thousand births in India (2009)
18.9 / thousand births (Worldwide)
National Centre for health statistics USA divides foetal death into 3 categories:-
1. Early : <20 weeks
2. Intermediate: between 20-27 weeks
3. Late :>28 weeks
5.2.2 Aetiology
Unknown in 25-35% of cases
Known causes (%)
1. Maternal: 5-10

7
2. Foetal: 25-40
3. Placental: 20-35
4. Unexplained: 15-35
i) Maternal Risk Factors
Obesity (>30kg/m2): proven, modifiable, highest ranking
Maternal age (>35years)/paternal age
Race
Low educational status
Smoking/Alcohol/Drugabuse
Infections (malaria, hepatitis, influenza, syphilis,Toxoplasma, sepsis)
Medical disorders(DM,HT, Thyroid Diseases)
Pre-existing diseases (Heart Disease,Anaemia, Epilepsy)
Autoimmune Disorders (APS, SLE)
Rhincompatibility
Multiplepregnancy
Post term pregnancy
Previous historyof still birth
Hyperpyrexia
Thrombophilia
Trauma
Cholestasis of pregnancy
Obstetric causes (Abruption, PPROM)
Labour related (preterm, dystocia, uterine rupture)
INFECTIONS
Still Birth due to infections usuallyoccurs in foetuses weighing less than 1000 gm(<28weeks). The important causes are
1. Viral–Parvovirus B 19, CMV
2. Bacterial – Listeria monocytogenes, E.coli, B streptococcus and ureaplasmaurealyticum.
3. Protozoal – malaria is also a cause of still birth in developing countries
THROMBOPHILLIAS
Earlier studies showed a strong association between inherited and acquiredthrombophillias and adverse pregnancy outcome like recurrent pregnancyloss and stillbirth. There is a small absolute increased risk of late pregnancy loss in
Pregnancy withAbnormalFetus

Abnormal Pregnancy
8
women with factor V Leiden (4.2% versus 3.2%) although there was noassociation of factor V Leiden with preeclampsia or foetal growth retardation.
The current evidence seems to suggest that inherited or acquired thrombophilliasare associated with a increased risk of thromboembolism, but whether theyadverselyaffect other pregnancyoutcome includingpregnancyloss, placentalabruption, severe preeclampsia, and still birth are controversial. Routine screeningfor thrombophillias in women with obstetrics complications like preeclampsia,foetal growth restriction (FGR) and stillbirth is therefore, not required.
ii) Foetal Risk Factors
Multiple gestations
FGR
Congenital anomalies
Infections
Hydrops fetalis (immune & non-immune)
G6PD deficiency
Birth Defects
iii) Placental Causes
Abruption
Cord accidents
Placental insufficiency
Placenta previa
Twin transfusion syndrome (TTTS)
Chorioamnionitis
PROM
Feto-maternal haemorrhage
iv) Iatrogenic Causes
External CephalicVersion,
Drug overdoses
5.2.3 Diagnosis
a) Symptoms:
Absence of foetal movements
b) Signs:
Gradual retrogression of the height of the uterus
Uterine tone is diminished
Foetal movement are not felt during palpation
Foetal heart sound is not audible.
Auscultation of the foetal heart byPinard stethoscope or Doppler ultrasound isinsufficientlyaccurate for diagnosis. In a series of 70 late pregnancies in whichfoetal heart sounds were inaudible on auscultation, 22 were found to have viable

9
foetuses.Auscultation can also give false reassurance; maternal pelvic blood flowcan result in an apparently normal foetal heart rate pattern with external Dopplerauscultation and cardiotocographyshould not be used to investigate suspectedIUFD. Real-time ultrasonography is essential for the accurate diagnosis of IUFD.A second opinion should be obtained whenever practicallypossible. Mothersshould be prepared for the possibilityof passive foetal movement. If the motherreports passive foetal movement after the scan to diagnose IUFD, a repeat scanshould be offered. Real-time ultrasound allows direct visualisation of the foetalheart. Imaging can be technicallydifficult, particularly in the presence of maternalobesity, abdominal scars and oligohydramnios, but views can often be augmentedwith colour Doppler of the foetal heart and umbilical cord.
c) Ultrasonographic features of IUFD:-
Absent foetal heart beat
Robert’s sign : Appearance of gas shadow within heart or greatvessels (in 12 hours)
Spalding sign: Overlapping of skull bones (usually appears 7 daysafter)
Ball sign : Hyperflexion of the spine (by 3 to 4 weeks)
Helix sign : Gas in umbilical arteries
Crowding of the ribs shadow(by 3 to 4 weeks)
Gross distortion of foetal anatomy (maceration)
Soft tissue oedema: skin >5 mm
Associated features can be noted (oligohydramnios, hydrops)
Parents should be offered written information to supplement discussions.Many strategies have been described for discussing bad news. IUFD posesparticular difficulties as it is often sudden and unexpected. A crucialcomponent is to determine the emotional feelings and needs of the motherand her companions. This empathetic approach seeks to identify andunderstand women’s thoughts and wishes but without trying to shape them.Women with an IUFD and their partners value acceptance and recognition oftheir emotions highly. Empathetic techniques, which can enhance recovery,can be learned and retained as a skill. Pregnancy loss can quickly result invulnerability; imposing care can worsen the psychological impact.
5.2.4 Systemic Approach to Evaluation
I. History
II. Gross examination
SB infant
Umbilical cord
Placenta
Amniotic fluid
III. Foetal autopsy& karyotyping
Pregnancy withAbnormalFetus

Abnormal Pregnancy
10
IV. Placental investigations
V. Maternal Investigations
i) HISTORY
a) Family History
Recurrent abortions
Congenital anomalies
Abnormal karyotype
Hereditaryconditions
Developmental delay
b) Maternal History
DM
HPT
Thrombophilia
Autoimmune disease
SevereAnaemia
Epilepsy
Consanguinity
Heart disease
c) Past Obstetrical History
Babywith congenital anomaly /hereditarycondition
FGR
Gestational Hypertension with adverse sequele
Placental abruption
IUFD
Recurrent abortions
ii) MATERNALINVESTIGATIONS
Hb, complete blood counts,ABO and Rh grouping, electrophoresis
Diabetes testing (HbA1c, Fasting and postprandial Blood Sugar)
Thyroid function test, renal and liver function test
Additional Tests

11
Kleihauer Betke -Women who are rhesus D (RhD)-negative should be advised tohave a Kleihauer test undertaken urgently to detect large feto–maternalhaemorrhage (FMH) that might have occurred a few days earlier.Anti-RhDgammaglobulin should be administered as soon as possible after presentation. Ifthere has been a large FMH, the dose of anti-RhD gammaglobulin should beadjusted upwards and the Kleihauer test should be repeated at 48 hours toensure the fetal red cells have cleared. If it is important to know the baby’s bloodgroup; if no blood sample can be obtained from the baby or cord, RhD typingshould be undertaken using free fetal DNA (ffDNA) from maternal blood takenshortlyafter birth. Persistent positivityof the Kleihauer is often because the baby’sgroup is also RhD-negative, but might occur with very large RhD-positive FMHs.If it is important to distinguish between the two, the baby’s blood group can betyped using conventional serology on cord blood. Major FMH is a silent cause ofIUFD and a Kleihauer test is recommended for all women to diagnose the causeof death.
SerologicalTests (TORCH, Syphilis, Parvovirus) :if clinical findings suggestintrauterine infection (i.e., those with FGR, microcephaly)
MATERNAL BACTERIOLOGY
1. Blood cultures
2. Midstream urine
3. Vaginal swabs
4. Cervical swabs
MATERNAL SEROLOGY
1. Viral
2. Syphillis
3. Tropical infections
Antiphospholipid antibodies: Lupus Anticoagulant(LA),Anticardiolipin antibody (ACA), Antiplatelet Ab if ICHdetected, antiRho and antiLa antibody in case suspected autoimmunedisease.
Thrombophilias screening (6 weeks postpartum) - factor V Leidenmutations & deficiencies, antithombin III, protein C & S
Bile acids (Cholestasis of pregnancy)- important cause, recurrence in80% cases
Urine for casts and pus cells and toxicology screening (cocaine,amphetamines are associated with abruption)
iii) FETAL AND PLACENTAL INVESTIGATIONS
i) Foetal blood: Cord or cardiac blood (if possible)
Foetal viral serologyfor detecting viral infections
ii) Placental swabs for microbiology
Pregnancy withAbnormalFetus

Abnormal Pregnancy
12
iii) Foetal and placental tissues
Send several foetal samples for cell cultures/ DNA based methods forkaryotyping, deep foetal skin, foetal cartilage (patella), placenta cultureand biopsy.
Autopsy: External examination, birth weight and length measurementskeletal X-rays and histopathological examination of placenta,membranes and cord.
iv) GROSS DESCRIPTION
a) Infant description
Malformation
Skin staining
Degree of maceration
Colour: pale, plethoric
b) Umbilical cord
Prolapse
Entanglement-neck, arms, legs
Hematoma or stricture
Number of vessels
Length
c) Amniotic fluid
Colour-meconium, blood
Volume
d) Placenta
Weight
Staining
Adherent clots
Structural abnormality
Velamentous insertion
Oedema/ hydropic changes
e) Membranes
Stained
Thickening

13
5.2.5 Management
Recommendations about labour and birth should take into account the mother’spreferences as well as her medical condition and previous intrapartum history.Women should be stronglyadvised to take immediate steps towards delivery ifthere is sepsis, preeclampsia, placental abruption or membrane rupture, but amore flexible approach can be discussed if these factors are not present. Wellwomen with intact membranes and no laboratory evidence of DIC should beadvised that they are unlikely to come to physical harm if they delay labour for ashort period, but theymaydevelop severe medical complications and suffergreater anxiety with prolonged intervals. Women who delaylabour for periodslonger than 48 hours, should be advised to have testing for DIC twice weekly. If awoman returns home before labour, she should be given a 24-hour contactnumber for information and support.
More than 85% of women with an IUFD, labour spontaneouslywithin threeweeks of diagnosis. Vaginal birth can be achieved within 24 hours ofinduction of labour for IUFD in about 90% of women. Vaginal birth carriesthe potential advantages of immediate recovery and quicker return to home.Caesarean birth might occasionally be clinically indicated by virtue ofmaternal condition.
If active approach is adopted, induction of labour is done as follows:
Foetal death <28weeks
Mifepristone 200 mg followed by Misoprostol 400μg, 4 - 6 hourly mosteffective with shortest interval-delivery interval.
Foetal death >28weeks
Cervical ripening (mechanical or chemical by PGE2)followed byoxytocin induction. Mechanical methods of induction might increasethe risk of ascending infection in the presence of IUFD.
Misoprostol in IUFD cases
Misoprostol (PGE1) can be given either vaginally or orally. Vaginalroute is as effective asoral route but associated with fewer adverseeffects.
IUFD at term: 25 μg 6 hourly 2doses, if noresponse increase to 50μg 6hourly, do not exceed 4 doses.
Do not use Oxytocin within 8hours of using Misoprostol
IUFD <26 weeks:100μg 6hrly (max 4 doses)
IUFD >27 weeks:25-50μg 4hrly (max 6 doses)
Contraindicated in previous caesarean cases
Use of Prostaglandins is associated with increased risk of uterine rupture incases of previous scar. The woman should be closely monitored for featuresof scar rupture. Foetal heart rate abnormality, usually the most common earlysign of scar dehiscence, does not apply in this circumstance. Other clinical
Pregnancy withAbnormalFetus

Abnormal Pregnancy
14
features include maternal tachycardia, atypical pain, vaginal bleeding,haematuria on catheter specimen and maternal collapse.
Membranes should not be ruptured as long as possible
Pain management should be offered
Keep watch on signs of infection, leucocyte count, coagulation profile,
Active management of III stage of labour
Keep blood and blood products ready
5.2.6 Complications
Infection is a common association of late IUFD infection and the mother candevelop severe sepsis from a wide range of bacteria, including severesystemic chlamydial. Women with sepsis should be treated with intravenousbroad-spectrum antibiotic therapy (including antichlamydial agents).Routine antibiotic prophylaxis should not be used. Intrapartum antibioticprophylaxis for women colonised with group B streptococcus is notindicated. Regardless of the primary cause of death, the foetus can act as afocus for severe secondary sepsis, including gas-forming clostridial species,which can result in severe DIC.
The important complications are:
Infections
PPH
Retained placenta
Abruption
DIC
Shock, renal failure
Sepsis
Maternal death
5.2.7 Post Delivery Management
- Women should be routinely assessed for thromboprophylaxis, but IUFDis not a risk factor. If the woman has DIC, heparin thromboprophylaxisshould be discussed with a haematologist.
- Emotional support &Counselling as they are at increased risk ofpostpartum depression
- Keep in non maternity ward
- Suppression of lactation - Women should be advised that dopamineagonists successfully suppress lactation in a very high proportion ofwomen and are well tolerated by a very large majority. Oralcabergoline( 1mg single dose) is superior to bromocriptine. Dopamineagonists should not be given to women with hypertension or pre-eclampsia.Estrogens should not be used to suppress lactation

15
- Counsel for future pregnancy, earlyANC visit, preconception testing
Risk of recurrence is 7-10 / 1000 birth
- Assurance in cases of non recurring causes
- Contraceptive counselling
5.2.8 Preconception / Initial Prenatal Visit
Detailed medical and obstetric history
Evaluation and workup of previous stillbirth
Determination of recurrence risk
Smoking cessation
Weight loss in obese women (preconception only)
Genetic counselling if familygeneticcondition exists
Medical problems like Diabetes, hypothyroidism should be managed prior toconception
Thrombophilia workup:antiphospholipid antibodies(onlyif specificallyindicated)
Support and reassurance
Check Your Progress 1
1) Define IUFD
.................................................................................................................
.................................................................................................................
2) Enumerate three maternal causes of IUFD.
.................................................................................................................
.................................................................................................................
3) Enumerate three ultrasonographic signs of IUFD.
.................................................................................................................
.................................................................................................................
4) What is the main complication known to occur if the dead fetus isretained inside?
.................................................................................................................
.................................................................................................................
Pregnancy withAbnormalFetus

Abnormal Pregnancy
16
5.3 FOETALGROWTH RESTRICTION
Fetal growth restriction (FGR) is defined as estimated birth weight less than 10th
percentile of the average for the gestational age associated with doppler changes.Growth restriction can occur in preterm, term and post-term babies. Small forgestation (SGA) and FGR are too often used synonymously although there is adegree of overlap. SGA fetus is not necessarily growth restricted. The baby maybe constitutionallysmall simplybecause of normal biological factors and itsperinatal outcome is similar to those of normal fetuses. Fetus reacts differently at aspecific age of gestation.
It is essential to adjust for physiological variation in order to identify those babieswho are pathologicallysmall. Maternal height, weight, parity, ethnic origin and thebaby’s gender have all been found to be significantlyassociated with normalvariation in birth weight. These variables need to be adjusted for to calculate thetrue growth potential, which can be represented as individuallycustomized fetalgrowth curves and birth weight percentiles.FGR is associated with doppler signssuggesting hemodynamic redistribution as a reflection of fetal adaptation to undernutrition/hypoxia.
5.3.1 Classification of FGR
Two phenotypes of FGR are identified: early and late, based on moment of onset(cutoff is 32 weeks of gestation), evolution, doppler parameter modifications andpostnatal outcome (Table 1). Earlyonset FGR is associated with high impedanceutero-placental perfusion which in turn leads to elevated umbilical arterybloodflow resistance once villous damage exceeds 30%.
Table1.:Summaryof the main differences between early- and late-onset forms ofFGR.
Early-onset FGR Late-onset FGR
CHALLENGE: MANAGEMENT CHALLENGE: DIAGNOSIS
Prevalence: ~1% Prevalence: 3e5%
Severe placental disease: UA Doppler Mild placental disease: UA Dopplerabnormal, highassociation with PEnormal, low association with PE
Severe hypoxia ++ :systemic Mild hypoxia: central CVCV adaptation adaptation
Tolerance to hypoxia. Natural history Low tolerance: no natural history
High mortalityand morbidity. Lower mortality (but common causeof late stillbirth).
Abbreviations: PE: preeclampsia CV: cardiovascular.
With the use of the sonographicallydetermined head-abdomencircumference ratio, growth restricted fetuses can be differentiated intosymmetrical or asymmetrical FGR. Those who were symmetrical wereproportionately small(normal HC: AC and FL: AC ratios) and those who areasymmetrical had disproportionately lagging abdominal growth (high FL:AC

17
ration).Symmetric FGR accounts for one third of all cases of FGR and is due tolow genetic growth potential. The symmetrical growth restricted fetus is affectedvery early in the phase of cellular hyperplasia and are caused by chromosomal orstructural abnormalities or congenital infection (TORCH). The pathologicalprocess is intrinsic to the fetus and therefore all organs/parts are involveduniformly. Postnatal catch up of growth is poor and long term prognosis isunfavourable. The asymmetrical growth restricted fetus is affected in later half ofpregnancy during the phase of hypertrophy. The growth is restricted because ofrestriction in the uteroplacental blood flow or oxygen or nutrient (uteroplacentalinsufficiency).The infant has a long, thin and wasted appearance. Head size isproportionatelybigger than trunk size. These infants have a normal postnatal catchup and long term prognosis is good.
5.3.2 Aetiology of FGR
Causes can be divided into maternal, fetal and placental.
i) Maternal factors:
Preeclampsia, chronic hypertension
Renal disease
Diabetes with vasculopathy
Autoimmune disorders- Antiphospholipid antibody syndrome,Systemic lupus erythematosus.
Thrombophilia
Cyanotic heart disease
Haemoglobinopathy
Smoking, alcoholism, substance abuse like cocaine.
Malnutrition
Therapeutic agents like anticancer drugs.
ii) Foetalfactors:
Aneuploidies- Trisomy 13, 18, 21 ortriploidy.
Genomic imprinting and uniparental disomy
Malformations- heart disease, diaphragmatic hernia, gastroschisis,omphalocoele.
Multiple gestations.
Fetal infections- Malaria, Cytomegalovirus, Toxoplasmosis,Herpes.
iii) Placentalfactors:
Placenta previa, Placenta accreta
Abruptio placenta
Placental infarction
Pregnancy withAbnormalFetus

Abnormal Pregnancy
18
Hemangioma
Circumvallate placenta.
Risk factors and Etiologies
As you have studied earlier in the physiologyof pregnanacy, all optimal placentalfunction is essential for fetal growth and well being. Risk factors for impaired fetalgrowth include potential abnormalities in the mother, fetus and placenta.Constitutionallysmall mothers have smaller newborns. Both pre-pregnancyweightand gestational weight gain modulate this risk. In a women of average or lowBMI, poor weight gain throughout pregnancy may be associated with fetal-growth restriction. The infants of those women who received the nutritionsupplement had lower risks of early infant mortalityand low birth weight and hadimproved childhoodmotor and cognitive abilitiesemphasizing that maternalnutrition has an impact on fetal growth. The effect of social deprivation on birthweight is interconnected to the influence of associated life style factors such assmoking, alcohol or other substances and poor nutrition. In India, by far the mostcommon conditions are pre-eclampsia in primigravidae (10-12%), malnutrition,advanced cardiac disease especially rheumatic heart disease and chronichypertension. Drugs like Phenytoin can cause teratogenic injuryand fetal growthretardation. Chronic renal disease is frequentlyassociated with underlyinghypertension and vascular disease and thus causes FGR. Fetal growthrestriction in women with diabetes is due to congenital malformations or asa result of substrate deprivation from advanced maternal vascular disease.Conditions associated with uteroplacental insufficiency like pre eclampsia,chronic hypertension, asthma, smoking cause growth restriction of fetus.Thrombophillias and APLA syndrome cause placental thrombosis andconsequent growth restriction. Maternal and fetal infections promotecalcifications that are associated with cell death and consequent growthrestriction.
Fetal conditions are responsible in 10-20% cases and abnormalities ofchromosomal origin in at least 1/3rd of cases like autosomal trisomies,genetic defects like phenyl ketonuria etc. However, in 10% of the cases fetalgrowth retardation occurs due to infection. We must be aware that theseinfections are acquired by the mother during pregnancy and are transmittedto the fetus; or the mother may be the carrier when she conceives eg. viralinfection like rubella, protozoal infections like toxoplasmosis, bacterialinfections like Listeria Monocytogens and malaria.
Fetal congenital malformations account for 20% of fetal causes of FGR.Congenital heart disease, microcephaly are obviously associated withgrowth retardation.
5.3.3 Pathology
In case of symmetrical growth restriction, an early pregnancy insult couldresult in a relative decrease in cell number and size. For example, globalinsults such as from chemical exposure, viral infection or cellularmaldevelopment with aneuploidy may cause a proportionate reduction ofboth head and body size. Asymmeetrical growth restriction might follow alate pregnancy insult such as placental insufficiency from hypertension. As aresult of which diminished glucose transfer and hepatic storage would primarily

19
affect cell size and not number and fetal abdominal circumference, which reflectsliver size is reduced. Such somatic growth restriction is proposed to result frompreferential shuntingof oxygen and nutrients to the brain. This allows normal brainand head growth, that is brain sparing.
5.3.4 Foetal Complications
The complications can take place during antepartum, intrapartum or neonatalperiod,
a) Antepartum
Still Birth
There isa definite relationship between intrauterine malnutrition andstill births. It has been recorded in the literature that FGR isresponsible for 20-30% of all cases of still, births. Fetal death in FGRmay occur at any time, but occurs more frequently after 35 weeks ofgestation.
Oligohydramnios
Oligohydramnios as you will appreciate is common, especially, insevere FGR, In fact the degree of oligohydramnios is being consideredas an important factor in the prognosis of fetal outcome. It is possiblethat oligohydramnios in FGR is caused due to the decreased fetalurinary output as a result of decreased renal blood flow caused byredistribution of blood flow with preferential shunting of blood to thebrain.
b) Intrapartum FetalAcidosis
If you happen to perform an electronic fetal monitoring and if there isacidosis, you will record late decelerations, severe variable decelerations,decreased beat to beat variability and frequent episodes of bradycardia.Acidosis is said to manifest during labour or in about 40% of cases resultingin high incidence of caesarean delivery.
c) Neonatal Complications
The diagnosis of FGR is confirmed when the fetal weight is below 10thpercentile. The typical picture of an FGR infant is loose skin with very littlesubcutaneous fat. Most of the time, the head circumference is larger thanabdominal circumference.You must appreciate at this point that the neonatalcourse of an FGR infant is different from that of a constitutionallysmallbaby.
The most important complications are related to:
1) Perinatal asphyxia and acidosis: Meconium aspiration syndrome andhypoxic ischaemic encephalopathy
2) Metabolic disturbances: Hypoglycemia, hypocalcemia, hyperviscosity,hypothermia
3) Specific causes of fetal growth restriction: Infection, chromosomalabnormalities
Pregnancy withAbnormalFetus

Abnormal Pregnancy
20
5.3.5 Diagnosis
Fetal growth restriction is identified byestablishment of gestational age,ascertainment of maternal weight gain and careful measurementof uterine fundalgrowth throughout pregnancy in low risk women. In a woman with risks, serialsonographic evaluation is considered.
Before making a diagnosis of FGR, wrong dates should be rules out.
Clinical Examination
Poor maternal weight gain in second half of pregnancymay lead to suspicion.Obstetric examination for fundal height, liquor volume and fetal weight isperformed.Alag of 4 cm or more between symphsis fundal height measurementand gestational age suggests FGR. Similar trends will be observed withabdominal girth. Therefore, serial measurements are important rather than anabsolute value for diagnosis of FGR.
Investigations
Investigations include routine haemogram, blood group, testing for HIV, syphillis,hepatitis B, glucose challenge test. Haemoglobin electrophoresis to rule out sicklecell anemia which maycause FGR. Urine routine, microscopy, culture andsensitivity,TORCH test(Toxoplasma, Rubella, Cytomegalovirus, Herpes andothers), screen forAPLAantibodies, kidneyfunction and liver function tests,thyroid function test. PCR for fetal viral infections in earlyonset FGR with normalamniotic fluid index (AFI) and doppler studies with maternal TORCH testpositivity. Fetal karyotype is needed to rule out aneuploidies. Chromosomalanomalies maybe found in 20% of fetuses with abdominal circumference andestimated fetal weight less than fifth centile.
Ultrasonography
Biometry of fetus is done to estimate the gestational age. Biparietal diameter(BPD), femur length (FL), abdominal circumference (AC), head circumference(HC) are used to calculate various ratios and also for fetal weight. Normally HC:AC exceeds 1.0 before 32 weeks, 1.0 between 32 to 34weeks and less than 1.0after 34 weeks of gestation. FLis not affected by asymmetric FGR.Amniotic fluid
volume is reduced in cases with uteroplacental insufficiency(asymmetric FGR).Anatomic surveyof the fetus is also done for anomalies/ structural defects.
Fetal biometry to confirm FGR, repeated every 2 weekly to monitor fetal growth.Fetal abdominal circumference and estimated fetal weight are measuredspecifically. Fetal echo can be done to rule out congenital heart disease. Dopplerflow studies of umbilical arteryare performed weekly if normal and biweekly incase of compromised blood flow. Doppler examination is based on thehaemodynamics of blood circulation, involving speed, turbulences, vascularreactivityand resistance. The doppler examination is extremelyuseful for theevaluation of the fetal arterial circulation, of the cardiac function and of the venoussystem permitting a better characterization of the fetal status. Doppler ultrasoundtogether with the biophysical profile, amniotic fluid index and cardiotocographyhas an important role in the follow-up of FGR babies.

21
FGR :on the basis of doppler changes
1. Early: umbilical arterypulsatility index >95thpercentile
2. Late : cerebro-placental ratio < 5thpercentile estimated fetal weight <3rdpercentile uterine artery pulsatility index > 95thpercentile.
i) Uterine artery doppler is predictor of FGR, providing a moreaccurate prediction when performed in the second trimester than inthe first trimester.
ii) Umbilical artery (UA) doppler is the only measure that providesboth diagnostic and prognostic information for the management ofFGR( Fig 1). It identifies different degrees of impaired placentalfunction. Early-onset FGR is associated with high impedance uteroplacental perfusion which in turn leads to elevated umbilical arteryblood flow resistance once villous damage exceeds 30%.
Fig. 5.1: UmbilicalArtery Doppler
Umbilical arterydoppler shows different degrees of impaired placental function.Absent end diastolic flow (AEDF) or reversed end diastolic flow (REDF) areextreme abnormalities in waveforms and flow resistance and associated withsignificantperinatalmorbidityand mortality.
REDF velocity isan extreme abnormality in waveform and resistance andassociated with perinatal mortality of 50%, significant perinatal morbidityand higher incidence of long-term permanent neurologicdamage. AEDF orREDF, UA Doppler, have been reported to be present on average 1 week
before the acute deterioration.
iii) Middle cerebral artery Doppler (MCA):
A condition of chronic hypoxia determines blood flow redistribution thatmanifests as vasodilatation in the brain circulation. It is considered assurrogate marker of hypoxia (Fig 2). There is reduction in the MCApulsatility index ( PI).
Pregnancy withAbnormal Fetus

Abnormal Pregnancy
22
Fig. 5.2: Middle CerebralArtery Doppler
Fig. 5.2 a: Mild Vasodilatation of MCA
Fig. 5.2 b: Marked Vasodilatation of MCA
iv) Cerebro-placental ratio (CPR)
Normal CPR Ratio is MCA PI : UA PI >1. It is useful for assessmentof vascular cerebral hemodynamics in pregnancies complicated withFGR (brain sparingeffect). It determines quantification of redistribution ofcardiac output.CPR<1 associated with a poor perinatal outcome.Abnormalcerebroplacental ratio is superior to biophysical profile for the prediction ofadverse pregnancy outcome in early FGR.

23
v) Changes in Venous Circulation
Ductusvenosus( DV) Doppler studies are performed to find out changes invenous circulation. This finding is associated with worseningof fetal hypoxiaand academia. It precedes abnormalities in fetal heart rate. Reverse flowvelocity waveform at the DV leads to fetal death.
Abnormal DV precedes the loss of short-term variability in cCTG(computerized cardiotocography) in about 50% of cases. It is abnormal48 to 72 hours before BPP (biophysical profile) in about 90% of cases.
Late FGR
It is suspected whenthe individual fetal growth curve slows down or even becomeflat. Undetected late FGR in the third trimester of pregnancyrepresents the maincause of unexplainedstillbirths in low-risk pregnancies. These fetus have inabilityto tolerate hypoxia. There are either no or mild placental abnormalities (lessimpact upon placental resistance). UA Doppler fails to identify fetal compromiseand fetuses mayreact with decreased MCA impedance in response tohypoxemia.Abnormal CPR is associated with increased risk of fetal distress inlabor. Doppler indices of UAare mainly normal. Thus, the doppler evaluation ofthe MCA is mandatory and the CPR must be calculated.
5.3.6 Management
i) Depending on the cause, various therapies have been applied.
Patient is admitted, daily fetal movement record, weeklysymphysio-fundal height, weekly weight check is done.
Advised for adequate bed rest.
Steroid cover is given depending on the gestational age.
Weekly doppler of umbilical artery, biweekly biophysical profile isdone.
Antihypertensive for blood pressure control in hypertensivedisorders of pregnancy.
Lifestyle modifications like smoking cessation, cessation of alcohol orillicit drug usemaybe useful.
Diagnosis and treatment of fetal viral and parasitic infections isimportant for prognosis and neonatal management.
Combined aspirin and heparin therapymaybenefit fetal outcome inwomen withAPLA.
ii) After confirming thediagnosis you will learnabout management duringpregnancybyfetal monitoring and decision making about when to terminatepreganancy.
Antepartum Fetal Surveillance
You will surelyagree that there is a need for veryclose antepartum fetalmonitoring in a case of FGR which includes monitoring of both fetal growth andfetalwellbeing.
a) Fetal Growth Monitoring
Pregnancy withAbnormalFetus

Abnormal Pregnancy
24
Besides clinical examination of SF height, fetal weight and size and amount ofamniotic fluid, serial biometry is important. BPD growth of < 2 mm per weekbetween 13-34 weeks or < 1 mm per-week between 35-40 weeksindicates poor fetal growth.
b) FetalWellbeing
Methods to assess fetal wellbeing include fetal kick count, Fetal Heart Rate(FHR) monitoring, Non stress test (NST), Biophysical Profile Score (BPS)and amniotic fluid Index (AFI).
iv) Management duringPregnancy
By now, you must haverealised that all cases where FGR is confirmed,should be admitted to the hospital.Attempts should be made to controlunderlying factors like hypertension.You will appreciate that bed restespecially in left lateral position improves placental perfusion therebyhelpingfetal growth. Drugs like progestogens, betasympathomimetics and low doseaspirin have been administered in the hope of improving fetal prognosis.However, their value has not be proven definitely. One of the serious fetalcomplication was meconium aspiration syndrome; some studies have shownthat aminoinfusion not onlyreduces the risk of this complication, but alsocontributes to fetal growth.
Meanwhile, it is essential to reconfirm the period of gestation, monitor fetalgrowth and fetal wellbeing using more than one test and doing the testsseriallyand interpreting the results carefullyin the light ofclinical findings.
We have already discussed the complications that can occur in a case ofFGR. In order to avoid them, a careful antepartum fetal surveillance plays acrucial role.You will need to assess the fetal growth and the fetal wellbeing.
v) ManagementDuringDelivery
a) Factors Governing Decision for Termination
You will realise that management of labour and deliveryform an essentialcomponent of the care of the FGR fetus. Once you have taken care toexclude fetal malformations, intrapartum asphyxia is the most frequent causeof fetal morbidityand mortality.As a rule, no patient with FGR should beallowed to go beyond term; the principle underlying this should be clear toyou.Abiophysical profile and scoring can be done, but at this point wewould like to reiterate that more importance should be given toAFI, NSTand fetal breathing movements.You will recollect that low scores indicate animmediate termination of pregnancy. However, before resorting tointervention, you must ensure the facilities available for care of preterm andgrowth retarded babies. In most institutions, in our country babies of 34weeks of gestation survive quite well.With these facts in mind, you maycommence performing a biophysical profile byabout 32 weeks of gestation.
Besides the dictates of scores of biophysical profile, deterioration in maternalcondition (e.g. persistent hypertension) is another indication for terminationof pregnancy. In last few years, management plan has seen a significantchange internationallyand stage based management is empahsised for FGRon the basis of Doppler changes in the fetus. However, one should not forgetthe scenario of local resources and NICU facility in our country.

25
b) Timing of Delivery
Early FGR
The timing of deliveryshould be chosen taking into account the gestational age,umbilical Doppler, MCADoppler, ductusvenosus doppler, cardiotocography andbiophysical profile.
If gestation is more than 26 weeks, a detailed surveillance protocol integratingfetal ductusvenosus doppler and computerized CTG allows better outcomes anddeliveryonlywhen one or both become abnormal.
Late FGR
The UA Doppler is usuallywithin normal range. The cerebral vasodilatation beingthe first reaction of the fetus to hypoxia, therefore MCA doppler is the mostvaluable examination tool for this condition. The fetal cerebral resistance tohypoxia is inferior to the cardiac one, so it is possible to have major fetalaccidents before cardiac and ductusvenosus doppler modification appears. Theseare cases with severe fetal distress, with pathologic CTG but without venousmodifications.
Late FGR fetuses with brain sparring effect should be delivered because it ispredictive of acidosis at birth. After 34 weeks, the risk of serious morbidity andof mortality is low and the deliveryof the fetuses with late FGR will minimize thelong term sequelae. MCA PI < p5 is considered a marker of cerebralvasodilatation ( predictive for acidosis at birth) even in the presence of a normalUAPI & useful to time delivery.
It is important to identifysmall babies, and then differentiate them into FGRand SGA. FGR babies are then subdivided into early and late depending onthe onset, evolution, doppler parameters and stage based management isdone.
Stage based classification and management of FGR (Fig 3):
Stage 1:
Characterised bymild placental insufficiencywith earlydoppler changes.
Weeklymonitoring is done.
Termination of pregnancydone at 37 weeks by labour induction.
Stage 2:
Characterised bysevere placental insufficiency.
Doppler of umbilical arteryshows absent end diastolic flow.
Biweeklymonitoringis done.
Termination is done at 34 weeks by caesarean section
Stage 3:
Characterised by low suspicion fetal acidosis with umbilical arteryshowingreversal of diastolic flow.
Frequent monitoring is done, every 1-2 days.
Pregnancy termination planned at 30 weeks by caeserean.
Pregnancy withAbnormalFetus

Abnormal Pregnancy
26
Stage 4:
Characterised byhigh suspicion fetal acidosis with doppler changes inductusvenosus.
Aggressive fetal monitoring is done every12 hourly.
Termination of pregnancy after 26 weeks by caesarean, according to the patientprofile and her informed consent, NICU facilityand local resources.
Fig. 5.3: Stage wise management of FGR as follows:
c) Mode of Delivery
The mode of delivery, as you can conclude depends on:
Degree fetal compromise
Presence of other risk factors
Fetal presentation
Favourabilityofcervix

27
Availabilityof facilitiesfor intrapartummonitoring
If labour has been induced and prognosis satisfactory, you should ensure thefollowing:
Anepisiotomy
Cutting short of 2nd stage of labour
Earlycord clamping in order to avoid circulation overload
Presence of a neonatologist
d) Indications for Caesarean Section
It is important for you to remember that perinatal mortalityhas improvedtremendouslywith the liberal use of caesarean section.You mayadopt themode of termination of pregnancywhen you encounter anyof the followingsituations:
- Obstetrical complication like Preeclampsia,Antepartum Haemorrhage
- Period of gestation less than 35 weeks
- Unfavourablecervix
- Absent end diastolic flow in umbilical arterydoppler
e) IntrapartumMonitoring
As you know intrapartum asphyxia is the leading cause of fetal death. Hence,you will agree that these patients require intensive intrapartum monitoring.Continuous fetal monitoring using CTG and / or scalp electrode and scalpblood sampling is recommended. In the absence of these facilities, FHR ismonitored every15 minutes during first stage and every five minutes in thesecond stage.
f ) Neonatal Care
As discussed earlier, special neonatal problems in FGR babies arehypoglycemia, hypocalcemia, hypocalcemia,hyperviscosityand necrotizingenterocolitis.You must appreciate that a small for gestational age infant(SGA) fare better than an appropriate for gestational age infant having sameweight.
Almost 2/3rd of SGA infants suffer from hypoglycemia as glycogen stores ofthese infants are poor. Hypoglycemia can lead to polycythemia andhyperviscosity. Hyperviscositymay lead to reduced cerebral perfusionfurther complicating the effect of a reduced arterial concentration. Perinatalasphyxia causes vasoconstriction in gastrointestinal tract resulting innecrotizing enterocolitis. Prolonged perinatal asphyxia canresult inneurodevelopmental disorders. Hence the neonatal care should include:
i) Resuscitation
There is all increased risk of perinatal asphyxia in SGA infants. Resuscitationstarts at delivery table with adequate suction. Meconium staining of liquor iscommon in FGR leading to meconium aspiration syndrome. This is takencare of by timely suction through a laryngoscope. Oxygen as well asintubation facilityshould be available. If respiratoryeffort is poor, continuouspressure ventilation (CPAP) helps in assisted ventilation.
Pregnancy withAbnormalFetus

Abnormal Pregnancy
28
ii) Supportive Care
This includes attention to ventilation, oxygenation, cardiac output, tissueperfusion and glucose, fluid, electrolyte and acid-base balance.
iii) Maintenance of Temperature
Both cold and heat put a stress on metabolic and physiologic homeostasis.Thermal neutrality is the temperature zone at which infant oxygenconsumption is minimum. Generallythis correlatedwith skin temperaturebetween 36 to 36.5 degree centigrade. During winter months, delivery placeas well as infant crib should be kept warm before the arrival of infant toprevent sudden fall in temperature. Undue exposure of the infant should beavoided:
iv) Prevention of Infection
It is important for you to remember that these infants are nursed with allbarrier nursing principles as the host defence mechanisms are poor. Risk ofinfection is more if patient had premature rupture of membranes or somemanipulation was required. If gastric lavage indicates in utero infection,prophylactic antibiotics are given.
v) Nutrition
You must realise the importance of close monitoring of glucose levels of thebaby and need for immediate feeding of the baby to avoid hypoglycemia.The lower acceptable limit for glucose concentration is 40-45 mg/dl. If levelis not beingmaintained with oral feeding, intravenous glucose infusion isgiven. In a preterm SGA infant glucose infusion is routinelygiven soon afterbirth.
vi) Polycythemia
Venous haematocrit of more than 60 % is present in 50% SGAinfants.These infants mayhave neurologic, pulmonaryor cardiac symptomsincluding lethargy, jitteriness, poor feeding, respiratorydistress, cyanosis andoccasional, seizures. The infants are also more prone to hyperbilirubinemia.Partial plasma exchange is carried out in symptomatic infants.
vii) Treatment of Congenital Infection
There maybe congenital infection with rubella, CMV toxoplasma etc. whichhad caused IUGR initially.The infants born maybe completelyasymptomaticbut should be screened for the presence of infection and treated.
5.3.7 Long Term Sequalae
It is found that FGR babies have an increased risk of subsequent adulthypertension, atherosclerosis, type 2 diabetes and other metabolic derangements.It has been hypothesized that poor health in adulthood is mainlymodulated by lowbirth weight, postnatal compensatory growth or an interaction of both the factors.Fetal growth restriction mayaffect organ development, particularly that of heart.Adults born preterm have persistent structural remodeling and thus reducedsystolic and diastolic function. Fetal growth restriction is also associated withpostnatal structural and functional renal changes like disordered nephrogenesis,renal dysfunction, chronic kidneydisease and subsequent hypertension.

29
Check Your Progress 2
I) What are the parameters included in assessing the Biophysical score?
.................................................................................................................
.................................................................................................................
.................................................................................................................
2) Apatient has undergone a Non Stress Test (NST). There is a rise of 15beats/min above baseline with fetal movement.
The test is said to be…………………………………...................
3) Can a patient with IUGR be allowed to go beyond term?
.................................................................................................................
.................................................................................................................
.................................................................................................................
4) List four complications that a growth retarded infant is prone to develop.
.................................................................................................................
.................................................................................................................
.................................................................................................................
5.4 LET US SUM UP
We have learnt that when an infant delivered without signs of life after 20 weeksof gestation or weighing >500 g when gestation age is not known, then it is IUFDand not an abortion.Anumber of maternal, placental and fetal causes can causeIUFD and in 25-35% of cases, no cause can be found. Prostaglandins are usedto deliver these babies.Asystemic approach is adopted to evaluate mother, fetus,placenta and membranes and infant after delivery.
In the section of FGR, you have learn about definitions, aetiology andclassification of FGR.You should suspect FGR clinicallyduring pregnancyandconfirm your diagnosis with the help of several ultrasound parameters.Antenatalfetal monitoringhas made a big dent in obstetric management of high riskpregnancy as in FGR cases.You have learn about several tests to monitor fetalgrowth and wellbeing; interpret them and correlate the results with expected fetaloutcome. Management of FGR has been highlighted with clear cut guidelines.Monitoringduring labour and judicious deliveryalso improves fetal survival byreducing intrapartum hypoxia.You have also learnt about special neonatalproblems.
5.5 KEY WORDS
IUFD : Intrauterine Foetal Death
APS : Antiphospholipid Syndrome
BPS : Biophysical Profile Score
FMH : Foetomaternal Haemorrhage
CMV : Cytomegalovirus
Kick Count : Counting fetal movement perceived bymother
NST : Non stress test of fetal well being
Pregnancy withAbnormalFetus

Abnormal Pregnancy
30
Perinatalperiod : Pertaining to period from 28 weeks of gestation tillone week after delivery
SGA : Small forgestational age infant
5.6 ANSWERS TO CHECKYOUR PROGRESS
Check Your Progress 1
1) an infant delivered without signs of life after 20 weeks of gestation orweighing >500 g when gestation age is not known, then it is IUFD
2) —Infections (malaria, hepatitis, influenza, syphilis,Toxoplasma, sepsis)
—Medical disorders (DM, HT, Thyroid Diseases)
—Pre-existing diseases (Heart Disease,Anaemia, Epilepsy)
3) —Absentfoetal heart beat
—Robert’s sign :Appearance of gas shadow within heart or great vessels
—Spalding sign: Overlappingof skull bones
4) DIC
Check Your Progress 2
1) Non Stress Test (NST),
Fetal Breathing Movements (FBM),
Gross BodyMovements (GBM),
Fetal tone
AmnioticFluidVolume.
2) Reactive
3) No (preferably should be terminated at 37-38 weeks).
4) Asphyxia
Hypocalcemia
Hypoglycemia
Infection

31
UNIT 6 COMPLICATIONS INEARLY PREGNANCY
Structure
6.0 Objectives
6.1 Introduction
6.2 Bleeding During Early Pregnancy
6.2.1 Causes of Bleeding in Early Pregnancy
6.2.2 Definitions
6.2.3 Aetiology
6.2.4 Guidelines for Clinical Assessment
6.2.5 Differential Diagnosis
6.2.6 Management
6.3 Rapid Initial Assessment and Rapid Initial Management
6.4 Recurrent Abortions
6.5 Hyperemesis Gravidarum
6.6 Retention of Urine
6.7 Let Us Sum Up
6.8 Key Words
6.9 Answers to Check Your Progress
6.0 OBJECTIVES
After reading this unit, you will be able to:
list complications of early pregnancy resulting into foetal loss;
diagnose and differentiate the different types of abortions; and
manage early pregnancy complications effectively so that you can
contribute in reducing maternal morbidity and mortality.
6.1 INTRODUCTION
Pregnancy is a physiological process but it can become pathological or
high risk and add to maternal and foetal morbidity and mortality.
Vaginal bleeding and pain in lower abdomen in early pregnancy are
causes for concern. Vaginal bleeding in early pregnancy may be due to
pregnancy related complications like abortion, ectopic pregnancy and
hydatidiform mole which lead to foetal loss, or causes unrelated to

Abnormal Pregnancy
32
pregnancy like cervical erosion, polyp and cervical malignancy. Similarly
pain in lower abdomen in early pregnancy can be due to pregnancy
related complications like abortions, ectopic pregnancy or twisted
ovarian and other surgical and medical conditions unrelated topregnancy. Around 10 to 15% ofall pregnancies diagnosed after sixweeks amenorrhoea end in spontaneous abortion in first trimester. In1% of women, pregnancy failure is due to ectopic pregnancy.Approximately 1 in 400 pregnancies in India result in hydatidiformmole. Haemorrhage due to ectopic gestation and abortion and sepsisdue to abortions are important causes of maternal mortality (seematernal mortality) and morbidity in India. Besides abortions, ectopicpregnancy and vesicular mole during 1st trimester, the woman mayhave hyperemesis gravidarum and retention of urine. In this unit youwill learn about complications of early pregnancy.
6.2 BLEEDING DURING EARLY PREGNANCY
Vaginal bleeding in early pregnancy is a cause for concern. You will bereading about is in the following sections.
6.2.1 Causes of Bleeding in Early Pregnancy
Bleeding can be due to pregnancy related complications or not relatedto pregnancy.
Pregnancy related causes are:
Abortions
Ectopic pregnancy
Hydatidiform mole
Non-Pregnancy related causes are:
DUB / Delayed periods (delay in periods is taken as amenorrhoeadue to pregnancy)
Cervical polyp
Cervical erosion
Cervical malignancy
6.2.2 Definitions
a) Abortion
Abortion is defined as loss of pregnancy at a period of gestationbefore the stage of viability i.e. 20 weeks of gestation (or foetalweight of < 500gms.)
Spontaneous abortion is when pregnancy loss is spontaneous. Thestages of spontaneous abortion include:
Threatened abortion (the pregnancy may continue);

33
Inevitable abortion (the pregnancy will not continue and willproceed to incomplete / complete abortion);
Incomplete abortion (the products of conception are partiallyexpelled).
Complete abortion (the products of conception are completelyexpelled).
Missed abortion (the embryo is dead and retained in uterusfor weeks or months.
Induced abortion is defined as a process by which the pregnancyis deliberately terminated before foetal viability.
Unsafe abortion is defined as an induced abortion performed eitherby persons lacking the necessary skills or in uncertified facilities,or both.
Septic abortion is defined as abortion complicated by infection.Sepsis may result from infection if the organisms ascend from thelower genital tract following either a spontaneous or an unsafeabortion. Sepsis is more likely to occur if there are retainedproducts of conception and evacuation has been delayed. Sepsis isa frequent complication of unsafe abortion involving instrumentation.
b) Ectopic Pregnancy
Ectopic pregnancy is defined as implantation of fertilised ovumoutside the endometrial cavity. The most common site of ectopicpregnancy is fallopian tube. Other sites are uterine cornu,undeveloped horn of a bicornuate uterus, cervix, ovary andabdomen. It is one of the causes of maternal mortality.
c) Hydatidiform Mole
Hydatidiform mole is defined as the condition resulting fromabnormal proliferation of the trophoblast. Chorionic villi aretransformed into grape like vesicles. Gestational trophoblasticdisease is the term used for spectrum of diseases resulting fromabnormal proliferation of trophoblast. The diseases are vesicularmole, invasive mole and choriocarcinoma.
6.2.3 Aetiology
a) Abortion
The causes which lead to one or two spontaneous abortions varywidely. The reasons for these may be unrelated and just chancehappenings in an individual.
Causes of first trimester abortions:
1) Choromosomal anomalies:
Complications in EarlyPregnancy

Abnormal Pregnancy
34
Aneuploidy (autosomal trisomy or monosomy)
Polyploidy (triploidy, tetraploidy)
Structural abnormalities
Majority of abortions in first trimester are due to chromosomalabnormalities.
2) Endocrinal factors.
Progesterone deficiency - Corpus luteum defect
Rarely thyroid disorders
3) Immunological factors
4) Infection.
- Rubella and cytomegalovirus produce gross congenitalanomalies in first trimester and abortion
- Influenza and hepatitis virus cause death of foetus andexpulsion
- Parasitic infection - Malaria and toxoplasma
5) Hyperpyrexia and hypoxia can lead to abortion.
Causes of second trimester abortion:
1) Cervical incompetence (congenital or acquired)
2) Uterine anomalies (Mullerian fusion defects)
3) Uterine synaechae
4) Low lying placenta, twins
5) Maternal systemic illness-chronic hypertension, diabetes.
b) Ectopic Pregnancy
Causes of ectopic pregnancy are
1) Chronic pelvic inflammatory disease
2) Surgery on tube - Tubal recanalisation
Tubal ligation
Plastic surgery on tube for tubal diseases
Induction of ovulation
IVF, GIFT, ZIFT
3) Following MTP, IUCD
4) Low dose progesterone- Minipill, hormonal implants, injectables
5) Distortion of tube due to congenital developmental errors.
c) Hydatidiform Mole (Vesicular mole)
1) Faulty nutrition
2) Disturbed maternal immune mechanism

35
3) Incidence is more common in women with AB or A group withgroup O partner.
4) Incomplete mole -chromosomes of paternal origin (originalchromosomes of ovum being absent or inactivated)
5) In partial mole -Karyotype is triploid with 2 paternal and onematernal haploid complements.
6.2.4 Guidelines for Clinical Assessment
Table 6.1: Guidelines for complete clinical assessment of awoman with spontaneous abortion
Complete clinical assessment
History (Ask about Period of amenorrhoea (ask the date of her
and record THE LMP )
information) Bleeding (duration and amount)
abdominal cramping (duration and severity)
Foul-smelling vaginal discharge
Abdominal or shoulder pain
Allergy to drugs
H/o passage of the products of conception/foetus/blood clot
H/o inserting something into the vagina(suggestive of an illegal abortion)
Routine physical Check the vital signs (temperature, pulse,examination respiratory rate, blood pressure)
examine the general condition of the woman(malnourished)
Look for pallor
examine the respiratory system, cardiac systemand extremities
Abdominal Auscultate for bowel sounds (absent inexamination peritonitis due to septic abortion)
Check whether the abdomen is distended(hydatidiform mole, ectopic pregnancy)
Assess the presence, location and severity ofpain
Palpate for abdominal rigidity (tense and hard)and guarding (peritonitis, ectopic pregnancy)
Palpate for rebound tendernessa
Complications in EarlyPregnancy

Abnormal Pregnancy
36
Assess for abdominal mass(molar/ectopicpregnancy)
Pelvic examination External Genitalia and vaginal examination :
Look for lacerations outside the vagina orover the external genitalia
Assess the amount of bleeding (light/heavy)
Look for protruding products of conceptionlying inside or outside the vaginal canal
P /S examination
Look for :
Any visible product of conception protrudingfrom the cervical os or visible in the vaginalcanal
Foul –smelling vaginal/cervical discharge
Cervical lacerations(indicative ofinstrumentation; may be suggestive of illegalabortion)
Foreign bodies in the vagina
P/V examination
Assess the amount of bleeding (light/heavy)
Check whether the cervical os is open orclosed (to determine the stage of abortion)
Bimanual examination
Estimate the size of the uterusb
Palpate for any pelvic masses
Examine for pelvic pain (note severity,location, and what causes the pain : is itpresent at rest; does it occur/increase withtouch and pressure; does it occur/increaseon moving of the cervix).
Investigation The woman’s blood group, especially her Rhstatus, should be a part of routineinvestigations during the clinical assessment incases of abortion.
a To check for rebound tenderness, keep a hand over the abdomen and press gently.Then suddenly remove your hand to release the pressure rapidly. If removal of thehand causes pain or worsens it, there is rebound tenderness. Rebound tendernessis a sign of peritoneal inflammation.
b In this document, the uterine size is measured by weeks passed after the lastmenstrual period (LMP) (the uterine size is equivalent to a pregnant uterus of a
given number of weeks since LMP) rather than by gestational weeks.

37
6.2.5 Differential Diagnosis
Table 2 lists the symptoms and signs for differential diagnosis of vaginalbleeding during early pregnancy.
Table 6.2: Symptoms and signs for the differentialdiagnosis of bleeding during early pregnancy
Symptoms and signs Symptoms and signs Probable
typically present sometimes present
diagnosis
Light bleedinga Cramping/lower abdominal pain
Threatened
Closed cervix Uterus softer than normal abortion
The size of the uterus
corresponds to the
gestational period and
presence of fetal heart
activity
Heavy bleedingb Cramping/lower abdominal pain Inevitable
Dilated cervix No expulsion of the products of abortion
The size of the uterus conception
corresponds to the The uterus is tender
gestational period
Heavy bleedingb Cramping/lower abdominal pain
Incomplete
Dilated cervix History of partial expulsion abortion
The size of the of the products of conception
uterus is smaller than
that expected for the
gestational period
Light bleedinga Light cramping/abdominal pain Complete
Closed cervix History of expulsion of the abortion
The size of the products ofconception
uterus is smaller than
that expected for the
gestational period
Uterus softer than normal
Light bleedinga Amenorrhoea/irregular bleeding Ectopic
Abdominal pain, Fainting
pregnancy
may be severe
Closed cervix Presence of tender adnexal
The size of the mass
uterus is slightly Tenderness on moving the
larger than normal cervix
Uterus softer than normal
Complications in EarlyPregnancy

Abnormal Pregnancy
38
Heavy bleedingb Nausea/vomiting Molar
Partial expulsion of
pregnancy
the products of Spontaneous abortion
conception which
resemble Grapes and Cramping/lower abodminal pain
Dilated cervix Presence of ovarian cysts
The size of the uterus (easily ruptured)
is larger than that
expected for the Early onset of pre-eclampsia
gestational period No evidence of a foetus
Uterus softer than normal
a Light bleeding : Takes five minutes or longer for a clean pad or cloth to be soaked
b Heavy bleeding : Takes less than five minutes for a clean pad or cloth to be soaked
6.2.6 Management
i) Management of threatened abortion
Ultrasonography (preferably transvaginal) to confirm foetal viabilityand to record gestational age. It also gives an opportunity toevaluate any uterine or adnexal pathology
Medical treatment is usually not required. Tablet folic acid 5mgper day is prescribed and the patient is observed for amount ofvaginal bleeding.
Advise the woman to avoid strenuous activity and sexualintercourse; complete bed rest is, however, not mandatory.
If the bleeding stops, follow up in an antenatal clinic. Reassess ifthe bleeding recurs.
If the bleeding persists, reassess for foetal viability (ultrasound) orectopic pregnancy. Persistent bleeding, particularly in the presenceof a uterus larger than expected, may indicate twins or molarpregnancy. Such cases should be referred to an FRU.
NOTE : Do not give medications such as hormones (e.g. oestrogens orprogestins) or tocolytic agents (e.g. salbutamol or indomethacin) as theywill not prevent miscarriage.
ii) Management of inevitable abortion
If the pregnancy is less than 12 weeks;
- Plan for evacuation of the contents of the uterus (see Annexure18 : “Procedure for manual vacuum aspiration forincomplete abortion”)
- Give Misoprostol 400 mcg (2 tablets of 200 mcg each) orally.Repeat once after 4 hours, if necessary.
- Arrange for evacuation as soon as possible.

39
If the pregnancy is more than 12 weeks;
- Await spontaneous expulsion of the products of conception andthen evacuate the uterus to remove any retained products ofconception.
- If necessary, augment uterine contractions or expulsion of theproducts of conception by Oxytocin 20 U in 500 ml of R/L @40 drops/minute;
OR
- Admnister Tab. Misoprostol, 800 mcg (4 tablets of 200 mcgeach), intravaginally. Give 2 tablets (400 mcg) again after 4 hoursif the woman has not expelled the products of conception tillthen.
iii) Management of incomplete abortion
If the bleeding is light to moderate and the pregnancy is less than12 weeks, use your fingers or a pair of ring (or sponge) forceps toremove the products of conception protruding through the dilatedcervix.
If the bleeding is heavy and the pregnancy is less than 12 weeks,evacuate the uterus.
- Manual vacuum aspiration (MVA) is the preferred method ofevacuation. Do not carry out evacuation by sharp curettage.
- If evacuation is not immediately possible, give tab. Misoprostol400 mcg orally (repeated once after 4 hours, if necessary)
If the pregnancy is more than 12 weeks.
- Start an Oxytocin drip, i.e. 20 U of Oxytocin in 500 ml of R/L@ 40 drops/minute until the produces of conception are expelled.
- If necessary, give Tab. Misoprostol 200 microgm vaginally every4 hours until the products of conception are expelled ; do notadminister more than a total of 800 mcg.
- Evacuate any remaining products of conception from the uterus.
After 12 weeks of pregnancy the foetus is usually expelled in totobut the placenta may be retained, which has to be delivered.
- If the placenta does not deliver normally, and there is nobleeding, start an oxytocin drip (as in the case of a delayedthird stage of labour with retained placenta). You can keep thepatient at the PHC for about 2 hours after starting the Oxytocindrip, waiting for the placenta to be expelled, however, if bleedingoccurs, refer immediately to an FRU.
- If the placenta is still retained, and the woman is bleeding, sheneeds immediate referral to the FRU. Establish an IV line, startthe Oxytocin drip and refer
Complications in EarlyPregnancy

Abnormal Pregnancy
40
- In rare cases, even after expulsion of the placenta, the womanmay bleed. Such patients too need to be referred to an FRU.
Ensure post-abortion follow up of the woman after treatment [seebelow].
iv) Management of complete abortion
Evacuation of the uterus is usually not necessary as all the productsof conception have been expelled.
Observe for heavy bleeding. If bleeding continues, refer to an FRU.
Ensure post-abortion follow up of the woman after treatment[seebelow].
In all such cases, it is important to document byultrasonography that uterus is empty and there are no productsof conceptions remaining inside the uterus.
v) Management of Missed Abortion
There is risk of developing disseminated intravascular coagulation and
hypofibrinogenemia after fetal death. Therefore early evacuation ofuterus is undertaken. If few weeks have passed, prothrombin time andpartial thromboplastin time is done prior to any intervention.
If size of uterus less than 12 weeks,
- Suction evacuation can be done under sedation and paracervicalblock or general anesthesia, or
- Misoprostol 800 microgram is kept in the posterior fornix. Itachieves expulsion within 48 hours.
If uterus is more than 12 weeks size,
- Misoprostol 200 microgram can be given by vaginal or sublingualor buccal route, every 4-6 hour, maximum of five doses.
- Oxytocin drip is started as 10 units of oxytocin in glucose salineand after every 100 ml, 10 units of oxytocin is added till patientstarts pains or oxytocin concentration of 100 units is reached.Intake and output chart should be maintained and drip should bediscontinued for at least six hours in a day.
- Vaginal suppository of prostaglandin E2, 20 mg 3hourly for fourdoses can be given
- Injection 15 methyl PG F2 alpha (carboprost) can be given IMin doses of 250 microgm, 3 hourly for maximum of 10injections. It can cause vomiting and diarrhea; this complicationcan be minimized by loperamide (2 mg tablet), 2 tabs threetimes daily.
After this, ultrasonography should be done to document that theuterus is empty.

41
vi) Septic Abortion
Investigations like Hb, TLC, ABO, Rh typing, blood urea, serumelectrolytes, liver function tests and coagulation profile are done. Incase of respiratory difficulty, blood for acid, base and gas analysisshould be sent. Urine should be examined microscopically and foralbumin and sugar. Blood, cervical swab and urine are sent forculture. It will help in identifying the infecting organisms anddetermining sensitivity of these to antibiotics.
Chest X-ray and Plain X-ray of abdomen and pelvis in sitting andlying position (to demonstrate gas under diaphragm following uterine orgut perforation and air – fluid levels in gut) are taken. Absence ofgas under diaphragm does not rule out perforations. Ultrasonographycan be done to demonstrate any free fluid in abdomen (blood orpus) or seeing any products in uterus or collection of fluid (pus orblood) in Pouch of Douglas.
The woman is hospitalized. Broad spectrum antibiotics like ampicillin500mg IV/IM six hourly plus gentamycin 80 mg twice daily andmetronidazole 500mg 8 hourly is given to patient. Pulse rate, B.P.central venous pressure (normal is 0-5 cm of water) and intakeoutput chart is maintained.
Urine output of 30ml/hour shows adequate blood circulation and tissueperfusion. Prophylactic anti-Gas gangrene serum (8000 units) and anti-Tetanus serum (3000 units) are given to illegal abortion cases.
Analgesics and sedatives can be given and appropriate antibiotics canbe prescribed following culture and sensitivity reports if patient is notresponding to antibiotics started initially.
If patient is toxic or looks very ill, then higher antibiotics like 3rdgeneration caphalosporins can be started (Inj Ceftriaxone 1- 2 gm IV12 hourly and Inj Clindamycin 600 mg, IV 8 hourly). Intravenousdrip is given and blood transfusion is given to severely anaemicpatients. Evacuation of uterus is done after starting antibiotics in gradeI septic abortion. One should be very gentle and sharp curettage
should be avoided to prevent perforation and spread of infection.
Patient should be watched for complications like
- Haemorrhage
- Spread of infection outside uterus (pelvic peritonitis, generalized,peritonitis, septicaemia)
- Renal failure (due to toxic cortical necrosis or tubular nephrosis)
- Thrombophlebitis and embolisation
- Coagulation failure
Complications like renal shut down occurs due to release ofthromboplastins from damaged placenta and coagulation failure is due
Complications in EarlyPregnancy

Abnormal Pregnancy
42
to consumptive coagulopathy. Jaundice and hepatic failure due to useof hepatotoxic drugs for inducing abortion or due to CI. Welchiiinfection. Approximately 20% of maternal mortality may be due tothese complications
Late complications of septic abortion are:
1. Secondary infertility due to tubal block
2. Chronic ill health and pelvic pain
3. Chronic pelvic inflammatory disease
4. Endometritis
In case of excessive vaginal bleeding, immediate evacuation is to bedone. If infection has gone beyond uterus and the patient is notresponding to the conservative management in 48 hours thenintervention should be done. In pelvic abscess, needling throughposterior fornix to diagnose abscess followed by colpotomy (incisionin posterior fornix to drain pus) is done. Malecot catheter is leftthrough colpotomy incision for 24 hours to facilitate drainage.
All grade II and III cases should be kept on intravenous fluid andhigher antibiotics. Laprotomy is indicated when there are features ofgeneralized peritonitis to drain pus. If no improvement on medicaltreatment or there is deteriorating condition, then gangrenous andinfected uterus is removed or perforation site is stitched and intestinalinjury is repaired; and foreign bodies removed. Inferior vena cava isligated in case of repeated embolization.
To sum up, management of septic abortion include (1) medicaltreatment in form of antibiotics, adequate fluid therapy for correctionof blood volume and electrolytes, steroid therapy and vasopressoragents for ensuring adequate tissue perfusion and (2) appropriatesurgical treatment depending upon diagnosis to control haemorrhage,removal of infected products and to prevent extension of sepsis.
vii) Ectopic Pregnancy
Keeping a high index of suspicion for ectopic pregnancy,specially in high risk cases, helps in early diagnosis.
A positive pregnancy test without ultrasonogrphic evidences ofintrauterine pregnancy, after a missed period is almost conclusive ofectopic pregnancy. Serum β HCG level can be measured byradioimmuno assay. In normal pregnancy, level of beta HCG in serumdoubles in 48 hours and the lowest normal value for this increase is66%. If there is failure in this rate of increased beta HCGproduction, it is suggestive of ectopic pregnancy.
Transvaginal sonography (TVS) can pick up pregnancy by 5th or 6thweek in intrauterine site or suspect pregnancy in adnexal region.Besides this the most important is the maternal mortality can beprevented in this group if ectopic can be diagnosed in early stages.

43
Diagnosis of ectopic is based usually on clinical examination, urinepregnancy test and TVS. If needed, serial serum beta HCG levelscan be done 48 hours apart. Culdocentesis will confirm only rupturedectopic pregnancy. In culdocentesis, needling is done through pouch ofDouglas and blood with small clots can be aspirated in ectopicpregnancy with blood in peritoneal cavity. In unruptured ectopic, it willbe negative if there is no free blood in abdominal cavity. Whenectopic is strongly suspected negative culdocentesis should not deterthe gynaecologist from doing laparoscopy or laparotomy.
When in doubt, laparoscopy is indicated to reach at diagnosis. Freeblood is seen in peritoneal cavity or blue mass is seen at ectopic siteon laparoscopy.
Treatment
Patient should be hospitalized in case suspicion of ectopic. If sheis collapsed, give her sedation, raise foot end, set up I.V. dripwith Ringer lactate, send blood for cross matching and don’t dovaginal examination. Transfusion with blood or plasma may be lifesaving. If patient is at home, rapid infusion may bring the bloodpressure up and then she should be transferred to centre wherefacility for laparotomy under general anesthesia is there. If she isin hospital, operation theatre should be arranged simultaneouslyand one should not wait for blood pressure to come up.Intravenous fluids and blood should be pushed rapidly by settingtwo or three I.V. fluid lines.
Treatment of acute ruptured ectopic is laparoscopy/laparotomyand salpingectomy (excision of fallopian tube) of affected side.Other tube and ovary should be seen before sacrificing the tubeas sometimes conservative surgery by removal of rupturedsegment is possible if other tube is absent or diseased andtuboplasty can be undertaken at later date. In chronic cases also,laparoscopy or laparotomy is required. Blood clots may becovered by intestines and pseudosac due to deposit of fibrinousmaterial. Adhesions are usually flimsy. After reaching the sac,clots are taken out and salpingectomy or salpingoophrectomy isdone on diseased side. Improvements in diagnostic techniques likeserum beta HCG estimation and transvaginal sonography hasrevolutionized the treatment of ectopic and in unruptured ectopicpregnancy instead of salpingectomy, one can do conservativesurgery like salpingostomy, salpingectomy or segmental resectionand anastomosis of tube to improve future fertility.
Medical management by Inj Methotrexate can also be done. Thecriteria for medical management are:
Haemodynamically stable
Able to comply with post treatment followup
Ectopic pregnancy is unruptured and has a size of less than 3-4 cmwith no foetal cardiac activity
Complications in EarlyPregnancy

Abnormal Pregnancy
44
hCG levels<5000 mIU/ml
- The contraindication for medical therapy are:
Signs of impending rupture
Associated hematological, renal, hepatic or pulmonary disease
Immunodeficiency
Coexistant intrauterine pregnancy (which is rarely seen)
Unwilling or unable to comply with post therapeutic monitoring
Routine of Administration of methotrexate:
1. Systemically: Intramuscular injection is the most commonlyused route.
2. Direct local injection into the gestation sac throughlaparoscopic or guided by ultrasound
Single dose protocol: Single dose of 50mg/m2 of body surfacearea is given and beta HCG is repeated on D4 and D7 whereD1 is the day of injection. Fall in serum beta HCG between D4& D7 of less than 15 percent requires a repeat dose of 50mg/m2 IM on D7. The above monitoring is repeated again after thesecond dose.
Post treatment Surveillance phase consists of weekly hCGmeasurement till it is negative. If the fall is less than 15% fromprevious level, then an additional dose is given.
viii) Hydatidiform Mole (Vesicular Mole)
Once diagnosis of hydatidiform is made, the pregnancy is to beterminated as no useful purpose is being served by its continuationand profuse bleeding may occur at any time. Patient is examined toassess degree of anaemia, toxaemia and to exclude congestive cardiacfailure. Hb, haematocrit, total and differential count and X-ray chest torule out secondaries should be done. Urine is examinedmicroscopically and tested for albumin and sugar. In case of moderateto severe anaemia blood transfusion is given and congestive cardiacfailure is controlled before undertaking active treatment.
In case of molar pregnancy is in process of abortion, spontaneousexpulsion can be encouraged by concentrated oxytocin drip using 5-10 units oxytocin in 500 ml ringer solution. Alternatively prostaglandinscan also be used if there are no contraindications to its use.
If mole is diagnosed before spontaneous expulsion begins, it should beevacuated by suction evacuation, after setting up 10 units oxytocinintravenous drip in ringer lactate. Blood should be kept arranged. Anysize of uterus can be evacuated by suction evacuation. Afterevacuation, size of uterus becomes smaller and bleeding stops. 10units oxytocin infusion helps in controlling bleeding. Uterus can easily
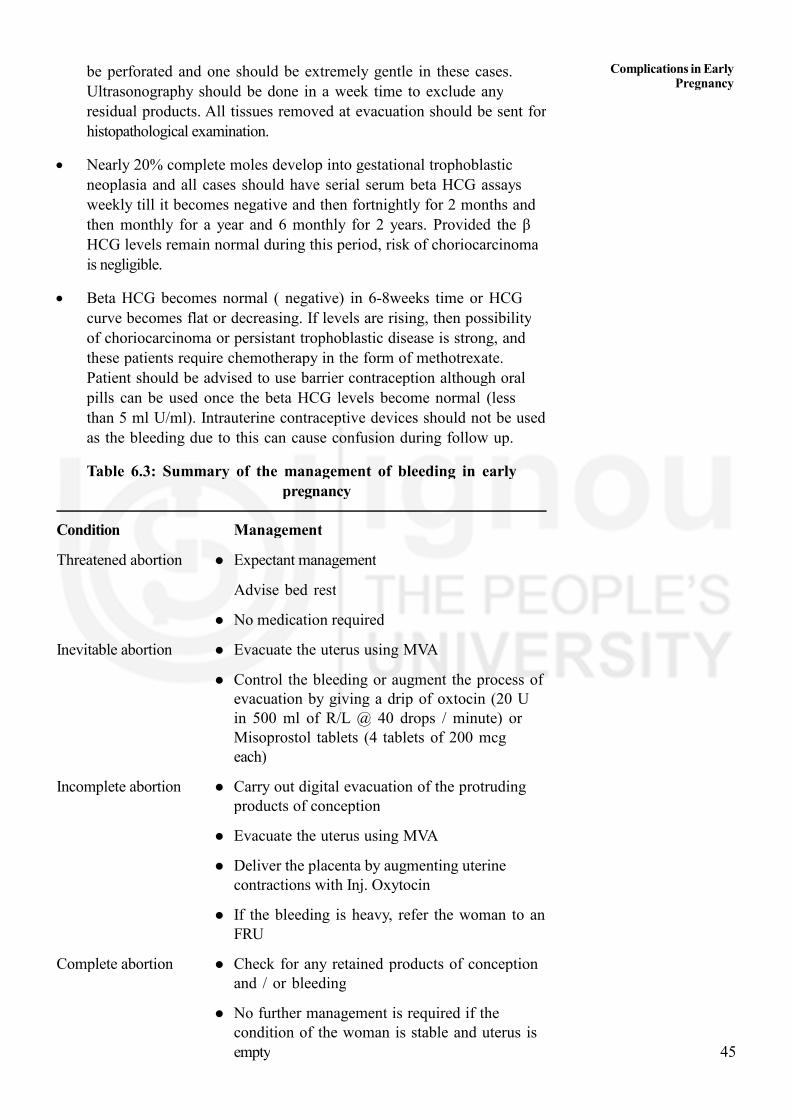
45
be perforated and one should be extremely gentle in these cases.Ultrasonography should be done in a week time to exclude anyresidual products. All tissues removed at evacuation should be sent forhistopathological examination.
Nearly 20% complete moles develop into gestational trophoblasticneoplasia and all cases should have serial serum beta HCG assaysweekly till it becomes negative and then fortnightly for 2 months andthen monthly for a year and 6 monthly for 2 years. Provided the βHCG levels remain normal during this period, risk of choriocarcinomais negligible.
Beta HCG becomes normal ( negative) in 6-8weeks time or HCGcurve becomes flat or decreasing. If levels are rising, then possibilityof choriocarcinoma or persistant trophoblastic disease is strong, andthese patients require chemotherapy in the form of methotrexate.Patient should be advised to use barrier contraception although oralpills can be used once the beta HCG levels become normal (lessthan 5 ml U/ml). Intrauterine contraceptive devices should not be used
as the bleeding due to this can cause confusion during follow up.
Table 6.3: Summary of the management of bleeding in earlypregnancy
Condition Management
Threatened abortion Expectant management
Advise bed rest
No medication required
Inevitable abortion Evacuate the uterus using MVA
Control the bleeding or augment the process ofevacuation by giving a drip of oxtocin (20 Uin 500 ml of R/L @ 40 drops / minute) orMisoprostol tablets (4 tablets of 200 mcgeach)
Incomplete abortion Carry out digital evacuation of the protrudingproducts of conception
Evacuate the uterus using MVA
Deliver the placenta by augmenting uterinecontractions with Inj. Oxytocin
If the bleeding is heavy, refer the woman to anFRU
Complete abortion Check for any retained products of conceptionand / or bleeding
No further management is required if thecondition of the woman is stable and uterus isempty
Complications in EarlyPregnancy

Abnormal Pregnancy
46
Septic abortion Give Paracetamol (1 tablet of 500 mg) tocontrol fever (temperature>380C)
Examine for the presence of any foreign bodyin the vagina
Thoroughly irrigate the vagina to remove anyherbs, local medications or caustic substances
Give the following antibiotics:
- Inj. Ampicillin 2 g IV, every 6 hours PLUS
- Inj. Gentamicin 60-80 mg, IV, every 8-12hours PLUS
- Inj. Metronidazole 500 mg IV, every 8hours, until the woman has no fever for 48hours.
(To avoid phlebitis, change the infusion siteevery three days or at the first sign ofinflammation).
Or
- Inj. Ceftriaxone 1- 2 g IV, every 12 hoursPLUS
- Inj. Metronidazole 500 mg IV, every 8hours, until the woman has no fever for 48hours.
(Gentamycin is avoided in patients withabnormal renal function tests)
If the bleeding is minimal, evacuate the uteruswithin 24 hours following antibiotic coverage;preferably use MVA.
If the bleeding is more than 200 ml or there aresymptoms and signs of local injury/ peritonitis, referthe woman to an FRU.
Missed abortion Refer to FRU to confirm diagnosis andmanagement.
Ectopic pregnancy Start IV drip with Ringer’s lactate.
Collect blood for grouping and cross matching.
Refer to FRU for laparotomy and bloodtransfusion.
Molar pregnancy Evacuation of uterus.
Blood transfusion.
Follow up with serum beta hCG level.
Then refer to FRU.

47
General treatment of vaginal bleeding in early pregnancy
Universal Measures
Monitor the woman’s vital signs and general condition. When complicationsexist, it is important to take steps to continue stabilizing the woman’scondition, before giving specific management for abortion. If the conditionof the patient suddenly worsens, reassess for shock or other complicationsand treat as appropriate.
Oxygen
If the woman is stable and there are no life-threatening complication (i.e.she is not in shock and the vital signs are normal), oxygen is NOTrequired. If she is being given because of a complication, continue oxygenas directed in the relevant chapter (s) related to the complication(s).
Fluids
If the woman is stable and there are no complications (i.e. she is not inshock and the vital signs are normal), IV fluids are NOT required. If sherequires IV fluids because of a complication, continue treatment according
to the relevant chapter(s) related to the complication(s)
Medicines
Oral medicines may be given if the woman is stable and there are no life-threatening complication. The IV or IM routes of administration are theONLY acceptable routes for giving medicines if the woman is in shock. Ifshe is also being treated for a life-threatening condition, follow thetreatment guidelines for that condition.
i) Antibiotics : Antibiotics should preferably be given intravenously. If anevacuation is needed, start antibiotics before carrying out theevacuation. In case of a septic abortion, give the woman an antibioticcover and perform uterine evacuation within 24 hours.
ii) Tetanus toxiod : If there is a possibility that the woman was exposedto tetanus (if the abortion was not performed with sterile instruments,and/for or if there was any contamination of the instruments or woundwith dirt, as may be the case in an unsafe abortion, there is achange of exposure to tetanus), and her vaccination history isuncertain, give her Inj. TT (0.5 mg IM) and tetanus antitoxin.
iii) Pain control:For the control of pain, along with verbal reassurance andrelaxation, injection promethazine 25-50mg IM and injection pentazocin30 mg IV or injection diclofenac sodium 75mg IM can be givenbefore the procedure. Alternatively, paracervical block with 10-20 mlof 1% lidocaine can be given.
Additional measures
The woman’s Rh status should be routinely assessed in pregnancy, andespecially so in cases of abortion. If the patient is non-sensitised Rh Dnegative give a dose of anti-D globulin (IgG 250 IU IM) as soon aspossible or within 72 hours of uterine evacuation.
Complications in EarlyPregnancy

Abnormal Pregnancy
48
Complications of abortion
Patients who bleed in early pregnancy may also present with complicationsof abortion. In these cases there will invariably be a history of inducedabortion at the hands of unqualified personnel. Table 4 gives the diagnosisand management of complications of abortion.
Table 6.4: Diagnosis and management of complications of abortion
Complications Symptoms and signs Management
a Give Amplillin 2 g IV every 6 hours PLUS Gentamincin 5 mg/kg body weight IV every 24
hours PLUS Metronidazole 500 mg IV every 8 hours until the woman is fever free for 48 hours.
Follow-up of woman who have had an abortion
Before discharge, tell a woman who has had a spontaneous abortion that :
Spontaneous abortion is common and occurs in at least 15% (1 in 7) ofclinicallyrecognizedpregnancies.
The changes of subsequent successful pregnancy are good unless there hasbeen sepsis or cause of abortion is identified, which mayhave an adverseeffect on future pregnancies (this is rate).
It is better to delay the next pregnancy till the woman has completelyrecovered(preferably for 3-6 months), even though she maywant to becomepregnant soon having an abortion.
InjuriesUterine, vaginal, urinarybladder or bowel(if left unattended,these injuries can getinfected and lead tosepsis)
Infection/sepsis (mightresult from septictechniques andinterventions, or mightoccur asa furthercomplication of theinjuries mentionedabove)
Symptoms
Signs
Symptoms
Signs
Abdominal pain/cramping
Shoulder pain Nausea/vomiting Vaginal bleeding Retention of urine or
dysuriaor incontinence
Fever (if associated withinfection/sepsis)
Distended abdomen Rigid (tense and hard)
abdomen Rebound tenderness Vaginal haematoma
Pain in the lowerabdomen
Malaise Prolonged bleeding Foul-smelling vaginal
discharge Fever Rebound tenderness
uterus is tender Purulent cervical
discharge Tenderness on moving
thecervix.
Start an IV linesinfuse R/L as amaintenance drip.
Refer to an FRU.Ensure that facilitiesfor conducting anoperation areavailable at the FRU.
Start an IV line&infuse R/L.
Give antipyretic suchas Paracetamol tocontrol the fever.
Begin antibioticsa assoon as possiblebefore attemptinguterine evacuation byMVA (in cases ofincomplete abortionand heavy bleeding).
If you cannotperform MVA, or thebleeding continues,or the conditiondeteriorates, refer thewoman immediatelyto an FRU.

49
Contraceptive counseling
Depending on the reproductive decision of the couple, contraceptivecounseling should be offered. This is especially important for women whohave had an unsafe abortion. If pregnancy is not desired, certain methodsof family planning can be started immediately (within 7 days), provided :
- there are no severe complication requiring further treatment and
- the woman receives adequate counseling to help her select the mostappropriate family planning method (see Table 5).
Table 6.5: Family planning methods advisable after an abortion
Type of contraceptive Advise to start
Hormonal (pills, Immediately
injections, implants)
Condoms Immediately
Intrauterine device Immediately
If infection is present or suspected, delayinsertion till it is cleared
If the level of haemoglobin (Hb) is lessthan 7 g/dl, delayuntil the anaemiaimproves
Provide an interim method (e.g. condom)
Voluntarytubal ligation Immediately
If infection is present or suspected, delaysurgeryuntil it is cleared
If the Hb level is less than 7 g/dl, delayuntil anaemia improves. Provide aninterim method (e.g. condom)
6.3 RAPID INITIALASSESSMENTAND RAPIDINITIALMANAGEMENT
When a woman of childbearing age presents with a problem of bleedingin early pregnancy, identify the underlying obstetric condition and rapidlyassess her condition to determine her degree of illness. This is known asRapid Initial Assessment. To minimize the delay in diagnosis, Table 4will guide you about what to ask, for what danger signs you have to lookand examine and what to assess if such danger signs are present. Rapidinitiation of treatment requires immediate recognition of the specific problemand quick action. This is known as Rapid Initial Management.
Rapid Initial Assessment:
When you are doing rapid initial assessment, encourage the woman andher family to speak honestly and completely about events surrounding thecomplication. Listen to what the woman and her family have to say andencourage them to express their concerns; try not to interrupt. Respect thewoman’s sense of privacy and modesty by closing the dooror drawingcurtains around the examination table. Let the woman know that she isbeing listened to and understood. Use supportive nonverbal communication
Complications in EarlyPregnancy

Abnormal Pregnancy
50
such as nodding and eye to eye communication. Answer the woman’squestions directly in calm, reassuring manner. Explain what steps will betaken to manage the situation or complication. Ask the woman to repeatback to you, the key points to assure her understanding.
In a case of bleeding in early pregnancy, you must ask certain importantpoints of history e.g.duration of amenorrhoea, severity and type of pain,amount of bleeding, products passed, and appearance of products passed.In case of excessive bleeding, severe pain, severe pallor, quickly youshould assess her circulatory system for hypovolaemic shock, give primarymanagement and without other delays, refer her to appropriate place.
Table 6.6: Rapid initial assessments for what and forwhich complication:
Problem Quick history andExamination Consider Assess what
and whichcomplications/life threateningcondition
Vaginal bleeding Associated with:Pain Inevitable Circulatory Systemearly in in lower abdomen Abortion for Hypovolaemicpregnancy & Some fleshy mass ShockAmenorrhoeaupto (products) passed20 weeks
Pain in abdomen IncompleteSome fleshy mass Abortion(products) passed
Pain in abdomen Grape Molarlike products passed Pregnancyvaginally
Severe pain in abdomen RupturedSlight vaginal bleeding EctopicFainting Severe pallor Pregnancy
History of interference Septic Abortion Circulatory SystemPain in abdomen for Septic ShockFullness of abdomenFoul smelling discharge
Once you know the problem, probable obstetric/medical underlying condition, andthink of complication developed or likely to develop, you should rapidly assesscardiovascular system to start primary treatment to save life of woman. Table 5shows how to assess cardiovascular system.
Table 6.7: Rapid initial assessment of circulatory system
Assess Danger signs Consider
Circulation Skin: cool and clammy Hypovolaemic shock(signs of shock) Pulse: fast (more than 110) Septic shock
and weakB.P.: low, systolic less than
90 mm of Hg
Rapid Initial Management:
You should also know the four important steps of Rapid Initial Management
1. Stabilization

51
2. Administration of medicine
3. Management of a case
4. Referral to appropriate health facility
1. Stabilization:
Important steps for stabilization in hypovolaemic shock are:
Intravenous fluid therapy
Maintenance of body temperature
Intravenous fluid therapy is one of the important life saving step. MO atPHC can do it. Use isotonic solution (0.9 % NaCl) or compoundsolution. Glucose solution, without saline does not provide salt to restorefluid balance. Use large bore needle, preferably 16-18 gauge. Even 20gauge is acceptable. Infuse rapidly in shock , 500 cc to 1 liter in 15 to20 minutes helps to stabilize condition. Once fluid loss is replaced, slowdown the drip to 30 drops per minute. Record pulse, BP andtemperature. For maintaining body temperature, cover the woman withblankets. Do not use hot water bottles by the side of the woman.
2. Administration of medicines
Different need based medicines during an emergency are:
i) Drugs to control uterine bleeding: In case of heavy bleeding dueto inevitable abortion and incomplete abortion, one can give injectionmethergin I.M. This will contract the uterus and bleeding can becomeless. If you have facility to start intravenous infusion, add 5 units ofoxytocin in it to contract the uterus.
ii) Drugs to control sepsis: Consider antibiotics in case of septicabortion (unsafe abortion), and septic shock. Preferred route ofadministration is intravenous to help delivery of antibiotics speedily ataffected site. Broad spectrum antibiotics are effective against Gram –ve, Gram +ve, anaerobic organisms and Chlamydia. Combination ofantibiotics is ideal to achieve broad coverage of multiflora. Table 6will give you an idea of recommended dose of various antibiotics andtheir coverage.
Table 6.8: Recommended dose of antibiotics and their coverage
Antibiotics Dose and Route of CoverageAdministration
Ampicillin 1 gm I.V. 4 to 6 hourly, Broad Spectrum500 mg orally 6 hourly
Benzyl Penicillin 10 million units 4 hourly, I.V. Limited effect onGram+ve Cocciand Gonococci
Gentamycin 1.5 mg/Kg body weight, Gram –ve e.g. E.8 hourly Coli
Doxycycline 100 mg I.V. 12 hourly Adulate for GramGram –ve, Chlamydia, +ve andGood with Metronidazole
Metronidazole 1 gm. I.V. two times day or Good Gram –vecoverage and 500 mg IV 8 hourly anaerobic coverage
400mg 8 hourly orally
Complications in EarlyPregnancy

Abnormal Pregnancy
52
iii) Drugs to control septic shock: Injection Efcorline 100 mg.intravenously will help to minimise septic shock. If required you canrepeat the dose, if condition worsens.
iv) Drugs to prevent/control tetanus: Required in a woman havingunsafe abortion. If she is fully immunised in last 5-10 years, givebooster dose of Tetanus Toxoid. If not, give one injection of TetanusToxoid as well Tetanus Anti Toxin 250 IU. If she is a establishedcase of tetanus, she will need 3000 to 6000 IU Tetanus Anti ToxinInjection.
While administering medicines consider
Safety
Route of administration
Dose
Side effect
Antidot
Please enter time of giving medicine with dose, and route of administrationin referral note.
3. Evacuation of the uterus
Over and above medicines mentioned above, as Medical officer you canmanage a case of inevitable abortion, incomplete abortion and completeabortion. As mentioned earlier, you can do evacuation of uterus undersedation in case of inevitable and incomplete abortion. This will help tocontrol the bleeding.
You can do evacuation of uterus in a case of septic abortion undercoverage of antibiotics.
You can also evacuate uterus having hydatidiform mole after taking allprecautions.
You should refer the case to higher level, if she needs
1. Blood transfusion in case of hypovolaemic shock due to excessivebleeding
2. Surgical management in case of Ruptured Ectopic pregnancy, unsafeabortion
3. Management of Septic Shock.
4. Referral at appropriate health facility:
Referral means, sending patient to a place where better facilities areavailable than parent place, to save patient from morbidity/mortality.Procedure of referral involves two steps.
a. Discuss need for referral with decision makers in family & arrange forvoluntary blood donors.

53
b. Referral note.
a. Discuss need for referral with decision makers in family & arrange forvoluntary blood donors: Emergency situations are often very disturbingfor all concerned and evoke a range of emotions that can havesignificant consequences. While discussing the situation developed andneed for referral, speak in a calm, quiet manner and assure thewoman that it is for her benefit. Be sensitive to any cultural orreligious considerations and respect her views. Use local language andshort sentences. Give some time to think. Decision makers getconvinced earlier for need of referral, if as a preventive measure,warning signs are told to woman, her family members and decisionmakers during pregnancy well in advance. Also convince them to take2-3 young boys along with a referred woman.
These young boys may be helpful for supply of blood, in case of anobstetric emergency having severe bleeding (post abortal, ruptured ectopic,severely anaemic woman etc.)
b. Referral note:
Whenever you refer a pregnant woman, you must write a referralnote or fill up referral form. This note/form should accompany referredwoman. It should be handed over to doctor in charge of that referralcentre. Note will help that doctor to know about the place ofreference, why the reference is done, clinical condition ofwoman, what medicines have been given at what time, and in whichdose, what procedures have been performed etc.
Referral form/note must include
Identification data of the woman
History
Clinical condition
Initial treatment (Medicines)
Interventions
Time of reference
Referred from
Referred by
Date of reference
Signature of referring person
You can avoid or minimize these delays by different actions.
Delay in decision taking for transfer to a better place can also prove fatal.Once you have completed rapid initial assessment and you have come toa conclusion that she needs further help, which you cannot provide, sheneeds to be sent at a place where comprehensive surgical as well

Abnormal Pregnancy
54
obstetric care facilities are available. Always discuss the situation byexplaining the condition, its seriousness, type of ntervention needed tosave woman’s life, and where such are available. Also tell the approximatetime required to reach that place. If a woman must undergo a surgicalprocedure, explain to her the nature of the procedure and its risks andhelp to reduce her anxiety. Women who are extremely anxious have amore difficult time during surgery and recovery.
Discuss these issues with decision makers of the family usually, husband,mother in law and father in law. Use simple local language. Use shortsentences. Answer their all queries. Give some time to think.
6.4 RECURRENT ABORTION
Recurrent spontaneous abortion (miscarriage) is defined by the RoyalCollege of Obstetricians and Gynaecologists and the European Society ofHuman Reproduction and Embryology, as three or more consecutivepregnancy losses less than 20 weeks of gestation, and by the AmericanSociety of Reproductive Medicine as two or more pregnancy losses.
Primary recurrent abortion refers to women with no prior successfulpregnancy, whereas secondary refers to pregnancy losses following a livebirth. The risk of recurrence of an abortion increases with the number ofsuccessive losses. Women who had experienced miscarriage twice, 3 times,and 4 times in the past are likely to lose the next pregnancy with aprobability of 43.7%, 44.6%, and 61.9%, respectively.
The etiologies for recurrent pregnancy loss are parental chromosomalabnormalities, untreated hypothyroidism, uncontrolled diabetes mellitus,certain uterine anatomic abnormalities, and antiphospholipid antibodysyndrome. Other possible etiologies include heritable and/or acquiredthrombophilias, immunologic abnormalities, infections, and environmental
factors. The cause of recurrent abortion cannot be determined in almost50% of cases. Immunologic factors might be the causative factorsresponsible for unexplained RSM.
When patient aborts spontaneously repeatedly 2 times or more, it is acause of worry and patient should have detailed investigation, to diagnosethe cause. If the abortions have taken place at same period of gestationand in similar fashion, then the underling recurrent cause is the onlypossibility.
Along with supportive measures, including ‘tender loving care’,pharmacological options include administration of progesterones.Progesterone stimulates the production of PIBF (progesterone inducedblocking factor), which induces a Th2 response and down-regulates NKcells activity, thus exerting an anti-abortive effect. In this condition,dydrogesterone 10mg orally twice daily can be given after confirming foetalheart activity ultrasonographically. Defective germ plasma can be responsiblein some cases where karyotyping of parents should be done to detectchromosomally balanced translocation.

55
In secondary recurrent abortion, cervical incompetence caused by cervicaltear is a strong possibility and should be excluded. Second trimesterabortion may result from previous obstetric trauma, forceful surgicaldilatation, cone biopsy or cervical amputation and congenital cause resultinginto cervical incompetence. In non-pregnant state, it can be diagnosed byhysterosalpingogram in premenstrual phase showing funnel shaped cervicalshadow or easy passage of 8 No. Hegar dilator through internal os.
During pregnancy, recurrent abortion due to cervical incompetence issuspected on basis of history of mid trimester loss which is almostpainless following spontaneous rupture of membranes. On examinationduring the current pregnancy, findings like cervical tear going up to intervalos, shortening of cervical length with patulous os and membranes buldgingthrough os suggest incompetent os. By USG, dilated os, funneling ofmembranes into os will help in diagnosing incompetent os. It is treated byinsertion of purse string suture of non-absorbable material in the thicknessof wall of the cervix at the level of internal os(Shirodkar operation) afterpushing the bladder up or putting the stitch below internal os (Macdonaldstitch). Preoperatively patient should have injection proluton depot 500 mg
I.M. which is then continued postoperatively biweekly for one week.Patient should be kept sedated for 24 hours afterwards. Stitch is removedat 38 weeks or at onset of labour, whichever is earlier. Failure to removestitch will cause obstructed labour or annular detachment of cervixposteriorly (bucket handle tear) and bleeding. Patient should be toldabout this risk. Complications like slipping or cutting through the suture,intrauterine infection, rupture of membranes and abortion can take place.Contraindications to stitch application are leaking, features of amnionitis,bleeding and uterine irritability/contractions.
Congenital anomalies of uterus may require operative correction;myomectomy may be required for submucous fibroid; chronic maternaldiseases like diabetes, hypertension and thyroid dysfunction may requireappropriate treatment. Infections like syphilis, toxoplasmosis, listerioses mayrequire proper diagnosis and treatment. These patients should ideally beinvestigated during interconceptional period before attempting nextpregnancy. Treatment will vary according to cause and proper treatmentshould be given before starting next pregnancy.
During pregnancy, a close watch is kept on the length of the cervix bytransvaginal ultrasonography in suspected cases of incompetence. In caseswhere no cause is detected, general advice regarding balanced diet,abstinence during critical period and assurance is given to patient. She maybe hospitalised during time of previous abortions.
Check Your Progress 1
1) Fill in the blanks:
a) Complications of early pregnancy are:
i) ........................... ii)............................ iii)...............................
b) Commonest cause of first trimester abortion is..........................

Abnormal Pregnancy
56
c) One of the commonest cause for second trimester abortionand recurrent abortion is.......................................
d) When patient aborts .....................................times, it is calledhabitual abortion.
e) Habitual abortion due to incompetent os can be diagnosed duringinterconceptional period by passing ......................... No. Hegardilator through os.
f) .........................................stitch is applied in the cervix forincompetent os at the level of internal os.
g) Serious complications of septic abortion are:
i)...................... ii)........................... iii)......................iv)......................
2) Tick the right answer.
i) Gut perforation is diagnosed by:
a) Features of generalised peritonitis
b) Absent bowl sounds
c) Gas under diaphragm
d) All of above
ii) Features of pelvic peritonitis with pelvic abscess are:
a) Tenesmus and muscusdiarrhoea
b) High grade temperature
c) Tenderness and guarding lower abdomen
d) Cystic fullness in pouch of Douglas
e) All of above
6.5 HYPEREMESIS GRAVIDARUM
You have already read about vomiting in pregnancy in Unit 1, Block 1 ofthis course. When the vomiting is excessive, the woman is unable to retainanything taken orally and develop metabolic acidosis. This condition isknown as hyperemesis gravidarum. This is more commonly seen inprimigravida, multiple pregnancy and vesicular mole. On examination, youwill find she is dehydrated (dry tongue, loss of elasticity of skin, oliguria).Tachycardia may be present and urine shows presence of ketone bodies(acetone). These women need admission in a hospital, IV fluids,reassurance and counseling. IV fluids given are ringer lactate and dextrosesaline. Urine examination is repeated every 4 hours till it becomes negativefor ketone bodies. Occasionally, antiemetic injection stemetil 5 mg IM, 8hourly (24-48 hours) or injection metoclopramide 10 mg IM, 8 hourly orinjection ondansetron 4 mg may be required to control vomiting. Once the

57
vomiting stops and dehydration is corrected the woman may be dischargedafter 24 hours, with advice to take small frequent carbohydrate meals.
Excessive vomiting may also be caused by jaundice, meningitis, diabetesand uraemic coma and also by peritonitis caused by induced septicabortion. Hence, exclude these conditions by thorough history, clinicalexamination and investigations wherever required.
6.6 RETENTION OF URINE
Retention of urine during late first trimester of pregnancy is usually causedby retroverted gravid uterus. Usually, retroverted gravid uterus does notcause any symptoms and after 12 weeks, spontaneous correction ofretroversion occurs and uterus rises above the pelvic brim and becomespalpable per abdomen. When it remains retroverted at 12 weeks ofgestation, retention of urine occurs due to stretching of urethra. Onexamination, a cystic tender swelling in the lower abdomen. arising fromthe pelvis is palpable (sometimes the swelling may reach above umbilicus).On pelvic examination, the cervix is high up behind the pelvic symphysisand is directed downwards and forwards. Uterus is retroverted, 12 weeksin size and is felt below the cervix. A cystic mass is felt in the anteriorfornix.
A self retaining urinary catheter (preferably Foleys catheter) is insertedtaking all aseptic and antiseptic precautions and urine is drainedcontinuously for 48 hours. Urine is examined for infection and is treatedaccording to the culture and sensitivity report. The woman is advised tolie prone. These measures allow the uterus to rise above the pelvic brim.Once the uterus is palpated above the pubis symphysis, catheter can beremoved. Ensure that the woman can pass urine on her own.
Check Your Progress 2
Mark True (T) or False (F):
1) Transvaginalsonography (TVS) can pick up pregnancy by5th or 6th week in intrauterine site. (T/F)
2) Abnormal proliferation of trophoblast cause hydatidiformmole. (T/F)
3) Ultrasonography findings is a better diagnostic test than quantitativeassay of hCG for diagnosing hydatidiformmole. (T/F)
4) Retroverted uterus with 12 weeks of pregnancy never causes retentionof urine. (T/F)
6.7 LET US SUM UP
Vaginal bleeding in early pregnancy is always a cause for concern. Theimportant pregnancy related complications causing bleeding are abortion,ectopic and hydatidiform mole. History and clinical examination will settlethe diagnosis most of the time although pregnancy test is positive in allthese complications. USG specially transvaginal ultrasonography is an

Abnormal Pregnancy
58
important diagnostic aid to differentiate these from each other and otherdifferential diagnosis. If these cases are managed properly, maternalmorbidity and mortality can be prevented although foetal loss cannot beavoided in all circumstances. Antenatal care, timely identification ofproblems, blood transfusion, antibiotics, modern diagnostic aids andappropriate surgical management have revolutionised the management andhave gone a great way in reducing the complications of these mishaps ofearly pregnancy which are not entirely preventable. Pregnancy is theprimary cause of these complications and so contraception and avoidingunwanted pregnancy is the reasonable solution. Hyperemesis gravidarumand retention of urine are other problems that you may encounter duringfirst trimester and management of these conditions are described.
6.8 KEY WORDS
Aneuploidy : Gain or loss of one or more chromosomes or partsthereof. Individuals with extra chromosomes are knownas trisomic and those with one chromosome missing areknown as monosomic. This occurs due to
nondysjunction during meiosis or mitosis.
Hysterotomy : Taking out the products of conception before 28 weeksof pregnancy by incising the uterus.
Polyploidy : Simple multiple of basic haploid number which results inkaryotype of 69 (Triploidy) or 92 (Tetraploidy)chromosomes. This can result from double fertilisation orfrom abnormal cell division in either the egg or spermwhereby either can contribute 46 chromosomes insteadof 23.
Salpingotomy : Longitudinal incision is made on antimesentric border of
tube over ectopic pregnancy. Products are removed andincision site is closed with 7-0 vicryl suture.
Salpingostomy : Linear incision on antimesentric border of tube onpregnancy site is given. Products are removed,haemostasis is obtained and tube is left unstitched.
6.9 ANSWERS TO CHECK YOUR PROGRESS
Check Your Progress 1
1) a) i) Abortion ii) ectopic pregnancy iii) Hydatidiform mole
b) chromosomal disorders.
c) incompetent os.
d) consecutively more than three
e) 8

59
f) Shirodkar
g) i) Peritonitis ii) Septicaemia
iii) Renal failure iv) Coagulation failure
2) i) d ii) e
Check Your Progress 2
1) T
2) T
3) F
4) T
Abnormal Pregnancy
60
UNIT 7 COMPLICATIONS IN LATEPREGNANCY-I:HYPERTENSIVE DISORDERSIN PREGNANCY
Structure
7.0 Objectives
7.1 Introduction
7.2 Hypertensive Disorders of Pregnancy
7.3 Preeclampsia and Eclampsia
7.3.1 Preeclampsia
7.3.2 Eclampsia
7.3.3 Post-Partum Care
7.3.4 Rapid Initial Assessment and Rapid Initial Management.
7.4 Let Us Sum Up
7.5 Key Words
7.6 Answers to Check Your Progress
7.7 Further Readings
7.0 OBJECTIVES
After going through this unit, you should be able to:
diagnose preeclampsia early and institute treatment;
provide essential care in eclampsia before referring to a tertiaryhealth care centre;
list the complications of eclampsia;
advise women with preeclampsia and eclampsia regarding theimportance of postnatal care;
7.1 INTRODUCTION
This unit deals with the hypertensive disorders in pregnancy which isa common medical complication during pregnancy. The importantcomplications of preeclampsia, eclampsia, which are important causesof maternal mortality, will be highlighted. Though preeclampsia ispreventable, eclampsia cannot be prevented but early identification ofpreeclampsia and prompt management help in avoiding the seriouscomplications of eclampsia. You will learn about the diagnosis andappropriate management of these conditions at various levels of healthcare in this unit.

61
7.2 HYPERTENSIVE DISORDERS OFPREGNANCY
Pre-eclampsia, a multisystem disorder, usually begins after 20 weeksof pregnancy in a woman whose blood pressure had been normal. Itcan lead to serious, even fatal, complications for both mother andbaby.There may be no symptoms.
The revised classification for hypertensive disorders in pregnancy (theInternational Society for the Study of
Hypertension in Pregnancy, 2014) is as follows :
1. Chronic hypertension.
2. Gestational hypertension.
3. Pre-eclampsia – de novo or superimposed on chronichypertension.
4. White coat hypertension.
1. Hypertension
Pre-eclampsia and gestational hypertension are characterized by thenew onset of hypertension (systolic >140 mmHg or diastolic >90mmHg) after 20 weeks gestation . It is important to document normalblood pressure either pre-pregnancy or at least in earlypregnancybefore there has been much pregnancy-relateddecrease inblood pressure.
When women present with hypertension in pregnancyafter 20 weeksgestation and the earlier blood pressure is unknown, the womanshould be managed as if she has gestationalhypertension or pre-eclampsia and appropriate investigations should be done afterpregnancy to determineif she has underlying chronic hypertension.
2. Proteinuria
The gold standard for diagnosing abnormal proteinuria in pregnancy isa 24-h urinary protein equal to or more than 300 mg per day. A spoturine protein/creatinine ratio equal to or more than 30 mg per mmol(=0.26 mg/mg, usually ‘rounded’ to 0.3 mg/mg) represents significantproteinuria.
3. HELLP
The combination of haemolysis, elevated liver enzymes andthrombocytopenia is often referred to as the HELLP syndrome. Thisconstellation of abnormalities signifies a more serious part of thespectrum of this disorder of preeclampsia.
4. Oedema
Pitting oedemaover ankles of the patients, after 12 hours of best restor rapid weight gain in a week may be the earliest sigh ofpreeclampsia.Oedema over the hands and face that persists even afteradequate rest may be associated with preeclampsia. Dependent oedema
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
62
that disappears in the morning may be associated with normal pregnancy.Some amount of pedal edema is common in pregnancy due to obstructionof venous return by gravid uterus.
5. Chronic hypertension
Chronic hypertension refers to high blood pressure predatingthepregnancy.Most of the times, chronic hypertension is due toessentialhypertension, usually accompanied by a family historyofhypertension and associated with obesity. Othersecondary causes ofhypertension are less common and inthis age group. It may beunderlying primary renal parenchymaldisorders (such as refluxnephropathy or glomerulonephritis), renal arteries stenosis or primaryhyperaldosteronism.
6. Gestational hypertension or Pre-eclampsia
When de novo hypertension is present after20 weeks gestation, thenext decision is whether this represents
pure gestational hypertension or pre-eclampsia.
Preeclampsia is diagnosed by hypertension and the coexistence ofoneor more of the following new-onset conditions:
i) Proteinuria (spot urine protein/creatinine>30 mg/mmol [0.3 mg/mg]or >300 mg/day or at least 1 g/L or ‘2 + ’ on dipstick testing)
ii) Other maternal organ dysfunction:
renal insufficiency (creatinine>90 umol/L; 1.02 mg/dL)
liver involvement (elevated transaminases – at leasttwiceupper limit of normal with or without right upper quadrantorepigastric abdominal pain)
neurological complications (eclampsia, altered mental status,blindness, stroke,or more commonly hyperreflexia whenaccompaniedby clonus, severe headaches when accompaniedbyhyperreflexia, persistent visual scotomata)
haematological complications (thrombocytopenia –plateletcount below 150,000/dL, DIC, haemolysis)
Gestational hypertension is usually benignand hypertension resolves by12 weeks postpartum. However, it can progress to pre-eclampsia inabout 25% of cases, especially when the hypertension presents before32 weeks.
iii). Uteroplacental dysfunction
foetal growth restrictio
This means that ideally all asymptomatic women withless than severehypertension (140–159/90–109 mmHg) and no dipstick proteinuriashould have the appropriatelaboratory investigations done to excludematernal organ dysfunction. Without these, it will be impossible toexcludepre-eclampsia.
63
Pre-eclampsiasuperimposed on chronic hypertension should not bediagnosed on the basis of a rise in blood pressure alone. For patientswith underlying essentialhypertension, superimposed pre-eclampsia canbe diagnosedwhen one or more of the above features ofpreeclampsiaoccur in addition to the hypertension.
7. White-coat hypertension
About 25% of patients with elevated clinic or officeblood pressurehave white coat hypertension.It is believed that the phenomenon isdue to anxiety experienced during a clinic visit. This diagnosis can beeliminated partly by having clinic or officeblood pressures recorded bya nurse or paramedical worker, rather than a doctor,preferably usingrepeated blood pressure readings.
Upto 50% will develop true gestational hypertension or pre-eclampsia.If a diagnosis of white coat hypertension is confirmed,pregnant womencan be managed with regularhome blood pressure assessments andantihypertensivescan be avoided, at least up to blood pressure levelsof160–170/110 mmHg. If home blood pressure monitoring is notavailable, maternal blood pressure should bechecked regularly,preferably weekly, by a healthcare worker, to reduce the likelihood ofawhite-coat effect.Increased surveillance is required throughoutpregnancyto detect the emergence of pre-eclampsia.
7.3 PREECLAMPSIA AND ECLAMPSIA
Reading this Section will help you understand the principles ofmanagement of preeclampsia and eclampsia. A peripheral hospital isnot equipped to adequately treat eclampsia and we have made aneffort to help you to decide when to refer patients to better equippedhospital.
7.3.1 Preeclampsia
Preeclampsia is the development of hypertensionand the coexistence ofone or more of the following new-onset conditions: proteinuria orevidence of organ dysfunction as mentioned above, after the 20thweek of gestation and sometimes earlier in presence of hydatidiformmole.
a) Pathophysiology
Why do women develop preeclampsia? Exact etiology of thiscondition is still controversial. Preclampsia is multifactorial, polygenic,disorder. There is 20- 40 % risk of preeclampsia in daughters ofpreeclampticmothers, 11-37 % risk in sisters of eclamptic women and22-47 % risk in twin sisters.
In normotensive pregnancy, there is trophoblastic invasion into thewalls of spiral arterioles of uterine bed. This transforms the spiralarterioles into a low resistance, low pressure high flow system. Inpreeclampsia, there is incomplete trophoblastic invasion of spiralarteries and deficient blood supply to placenta. However the mainbasic problem in this condition is uteroplacental arterial insufficiency
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
64
causing placental ischaemia and hypoxia. ‘Vasospasm’ is basic to thepathophysiology of preeclampsia. Vascular constriction causes aresistance to blood flow and accounts for the development of arterialhypertension. Diminished perfusion and a hypoxic environment lead torelease of placental debris into the maternal circulation,thereby incitingsystemic inflammatory response.
Women with preeclampsia have an increased vascular reactivity toangiotensin II which precedes the onset of hypertension. Moreoverangiotensin II appears to have a direct action on endothelial cellscausing them to contract. These factors lead to inter endothelial cellleaks through which blood constituents including platelets andfibrinogen are deposited subendothelially. The vascular changestogether with local hypoxia of the surrounding tissues presumably leadto hemorrhage, necrosis and other end organ disturbances that havebeen observed at times with preeclampsia.
The imbalance of prostaglandins occurs due to deficiency ofvasodilator, namely PGI2 (prostacyclin) from vascular endothelium andincreased synthesis of vasoconstrictor namely TXA2 (thromboxane) inplatelets.
The vasospasm occurs due to endothelial dysfunctionalso.Endothelialcell dysfunction may result from an extreme activated state ofleukocytes in the maternal circulation. Systemic endothelial cell injurypromotes interstitial leakage, and blood constituents, including plateletsand fibrinogen, are deposited subendothelially. Cytokines such astumor necrosis factor-α (TNF-α) and the interleukins may contribute tothe systemic oxidative stress associated with preeclampsia. This ischaracterized by reactive oxygen species and free radicals that lead toformation ofself-propagating lipid peroxides. These peroxides in turngenerate highly toxic radicals that injure systemic vascular endothelialcells, modify nitric oxide production by these cells, and interfere withprostaglandin balance. Otherconsequences of oxidative stress includeproduction of the lipid-laden macrophage foam cells seen in placentalatherosis, activation of systemic microvascular coagulation manifestedby thrombocytopenia, and greater systemic capillary permeabilityreflected by edema and proteinuria.
Angiogenic imbalance describes excessive amounts of antiangiogenicfactors, which are thought to be stimulated by worsening hypoxia atthe uteroplacental interface. Trophoblast of women destined to developpreeclampsia overproduces at least two antiangiogenic peptides thatenter the maternal circulation.
1.Solublefms-like tyrosine kinase 1 (sFlt-1) is a receptor for VEGF.Elevated maternal sFlt-1 levels inactivate and reduce circulating freeplacental growth factor (PlGF) and VEGF concentrations, leading toendothelial dysfunction. sFlt-1 levels begin to risein maternal serummonths before preeclampsia is evident. These high levels in thesecond trimester are associated with a doubling of the risk forpreeclampsia
2. A second antiangiogenic peptide, soluble endoglin (sEng), inhibits

65
varioustransforming growth factor beta (TGF-β) isoforms from binding toendothelialreceptors. Endoglin is one of these receptors. Decreased bindingto endoglin diminishes endothelial nitric oxide-dependent vasodilatation.Serum levels of sEng also begin to rise months before clinical preeclampsiadevelops.
The pathology in preeclampsia is not restricted to the placenta. A numberof changes occur in other systems of the body and these contribute to theclinical manifestations.
i) Cardiovascular Changes
There is a virtual absence of pregnancy induced hypervolemia inpreeclampsia. The causes could be:
a) Generalised vasoconstriction
b) Increased vascular permeability leading to less fluidintravascularly and marked excess extravascularly. -
Therefore these women are extremely sensitive to even normalblood loss at delivery.
ii) Hematological Changes
a) Intravascular coagulation
b) Thrombocytopenia
c) Evidence of erythrocyte destruction in the form of hemolysis,hemoglobinuria
d) Reduced antithrombin III
iii) Endocrine Changes
Reduced serum angiotensin II and aldosterone.
iv) The Kidney
Diminished glomerular filtration
Proteinuria
Microscopic picture includes
Glomerular capillary endothelial swelling
Sub endothelial deposits of protein material
These together constitute capillary endothelial changes.
v) The Liver
Serum liver enzyme elevation due to periportalhaemorrhagicnecrosis in the periphery of the liver lobule.
Bleeding may extend beneath hepatic capsule and form asubcapsular hematoma giving rise to epigastric pain in severepreeclampsia.
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
66
vi) The Brain
Cerebral oedema, hyperemia, focal anemia, thrombosis and hemorrhagemay be seen in cases of severe preeclampsia.
Preeclampsia is not preventable but can be detected early by goodantenatal care.
Women with mild preeclampsia are usually asymptomatic. Thus itsearly detection demands careful observation at appropriate intervals.Measurement of blood pressure is the only way to detect it.
Pregnant women should be examined every 2 weeks from theseventh month and weekly in the 9th month or more often ifblood pressure rises.
At these visits, the woman is weighed and careful blood pressuremeasurements are made. Rapid weight gain any time during thelatter half-of pregnancy or an upward trend in the diastolic bloodpressure, even while still in the normal range should be takenserious note of. Mild to moderate high blood pressure (140-159mm Hg systolic or 90-159 mm Hg diastolic measured on twooccasions at least four hours apart) warrants close evaluation andmonitoring. The patient should have frequent re-evaluation forsevere features of the disease.
Evidence shows organ problems with the kidneys and liverscan occur without signs of protein and amount of protein inthe urine does not predict how severely the disease willprogress.
Woman with severe preeclampsia may have the following symptoms
a) Headache
is usually frontal
is not relieved by ordinary analgesics
severe headache usuaIly precedes the first convulsion
b) Epigastric Pain or Right Hypochondriac Pain
is a symptom of severe preeclampsia
may be indicative of imminent convulsions
is due to stretching of liver capsule by oedema orhemorrhage
c) Visual Disturbances
may range from slight blurring of vision to partial orcomplete blindness
occur due to ischaemia of retina or occipital cortex
Effect of Hypertension on Pregnancy
Effect of Preeclampsia on mother and foetus is given below:

67
On mother ;
Eclampsia
Abruptio Placentae
Pulmonaly edema
Cerebralhaemorrhage
Acute Renal Failure
DIC (DissemninatedIntravasular Coagulation)
On Foetus :
FGR
Foetal distress
Prematurity
IUFD (Intra Uterimefetal Death)
Management
Management of preeclampsia will depend upon the severity of eclampsia.Preeclampsia is classified into severe and non-severedepending upon thefollowing clinical and laboratory features.
Severe Features of Preeclampsia (Any of these findings): ACOG
1. Hypertension: systolic >160 or diastolic >110 on two occasions atleast 4 hours apart while the patient is on bed rest (unlessantihypertensive therapy is initiated before this time).
2. Thrombocytopenia (platelet count <100,000).
3. Impaired liver function (elevated blood levels of livertransaminases to twice the normal concentration), severe persistentRUQ or epigastric pain unresponsive to medication and notaccounted for by alternative diagnoses, or both.
4. New development of renal insufficiency (elevated serum creatininegreater than 1.1 mg/dL, or doubling of serum creatinine in theabsence of other renal disease).
5. Pulmonary edema.
6. New-onset cerebral or visual disturbances
All the above features need not be present to classify preeclampsia assevere. The following examples will illustrate this.
1) A woman with BP of 140/90 withsevere headache would beclassified as severe preeclampsia although the blood pressure is inthe range of mild preeclampsia.
2) A diastolic blood pressure of more than 11 0 mmHg irrespectiveof the presence or absence of other clinical or biochemicalparameters is classified as severe preeclampsia.
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy
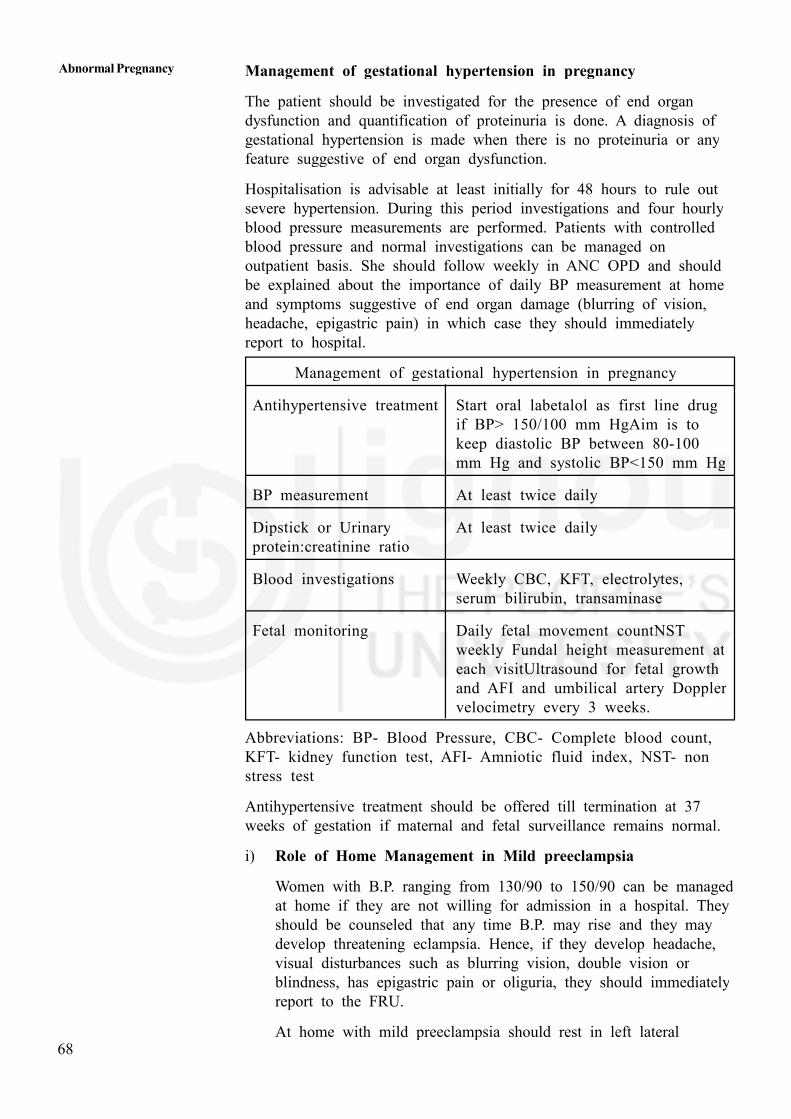
Abnormal Pregnancy
68
Management of gestational hypertension in pregnancy
The patient should be investigated for the presence of end organdysfunction and quantification of proteinuria is done. A diagnosis ofgestational hypertension is made when there is no proteinuria or anyfeature suggestive of end organ dysfunction.
Hospitalisation is advisable at least initially for 48 hours to rule outsevere hypertension. During this period investigations and four hourlyblood pressure measurements are performed. Patients with controlledblood pressure and normal investigations can be managed onoutpatient basis. She should follow weekly in ANC OPD and shouldbe explained about the importance of daily BP measurement at homeand symptoms suggestive of end organ damage (blurring of vision,headache, epigastric pain) in which case they should immediatelyreport to hospital.
Management of gestational hypertension in pregnancy
Antihypertensive treatment Start oral labetalol as first line drugif BP> 150/100 mm HgAim is tokeep diastolic BP between 80-100mm Hg and systolic BP<150 mm Hg
BP measurement At least twice daily
Dipstick or Urinary At least twice dailyprotein:creatinine ratio
Blood investigations Weekly CBC, KFT, electrolytes,serum bilirubin, transaminase
Fetal monitoring Daily fetal movement countNSTweekly Fundal height measurement ateach visitUltrasound for fetal growthand AFI and umbilical artery Dopplervelocimetry every 3 weeks.
Abbreviations: BP- Blood Pressure, CBC- Complete blood count,KFT- kidney function test, AFI- Amniotic fluid index, NST- nonstress test
Antihypertensive treatment should be offered till termination at 37weeks of gestation if maternal and fetal surveillance remains normal.
i) Role of Home Management in Mild preeclampsia
Women with B.P. ranging from 130/90 to 150/90 can be managedat home if they are not willing for admission in a hospital. Theyshould be counseled that any time B.P. may rise and they maydevelop threatening eclampsia. Hence, if they develop headache,visual disturbances such as blurring vision, double vision orblindness, has epigastric pain or oliguria, they should immediatelyreport to the FRU.
At home with mild preeclampsia should rest in left lateral
69
position, their daily B.P. is to be checked. If B.P. monitoring is notpossible, they may be called to the health centre after 2-3 days. Ifthere is no improvement or it has gone up, she may be admitted inPHC for B.P. monitoring and to ensure bed rest. If B.P. becomesless or remains the same, they may be kept in PHC. Maternal andfoetal conditions are monitored daily. They require referral to a FRUif B.P. goes up, they develop features of severe preeclampsia or theyhave completed 37 weeks of gestation.
ii) Management in hospital
Management of preeclampsia may be discussed under the followingheadings:
General management
Specific management
- Drug treatment
- Termination of pregnancy
Management of Severe Preeclampsia
A patient of severe preeclampsia or with mild preeclampsia who do notrespond to out patient treatment needs hospitalization.
a) General Management
The general management includes:
1) An appropriate history and general physical examination followed bydaily search for the development of signs and symptoms such asheadache, visual disturbances, epigastric pain and rapid weight gain.
2) Blood pressure reading every 4 hours except between midnight andmorning.
3) Abdominal girth and fundal height record.
4) Weight measurement at admission and every 2 days thereafter.
5) Bed rest throughout much of the day.
6) Diet with adequate protein and calories.
7) Sodium and fluid intake should be neither limited nor forced.
8) Urine test for protein at admission.
9) Measurements of plasma creatinine, uric acid, hematocrit, platelets andserum liver enzymes.
10) Serial sonography for biometry and well being. Doppler studies, ifrequired.
b) Drug Treatment of Hypertension
Antihypertensives are required to optimize blood pressure control and
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
70
allowing timely delivery of the baby.The role of antihypertensive therapy inmild to moderate hypertension is controversial.
The target of blood pressure control is to maintain Systolic BP below150mm Hg andDiastolic BP between 80-100 mm Hg.
If in any 24 hour period, two measurements reach the threshold, thetreatment is started.
A sudden rise in blood pressure requires a smooth and sustainedreduction. Acute onset severe hypertension which is persistent for 15 minor more is considered a hypertensive emergency. The following drugs maybe used. The target is not to normalize BP but to keep the systolic BPbetween 140-150 mmHg and diastolic BP between 90-100 mmHg. Startfetal surveillance also if fetus is viable.
i) Labetalol is the drug of choice. It is a combined alpha and betaadrenergic blocking agent. It lowers blood pressures smoothly andrapidly without causing headache. It acts by decrease in peripheralvascular resistance. The drug is given intravenously for hypertensiveemergencies- 20 mg initial dose for more than 2 min followed by 40mg after 20 minutes until the therapeutic response is achieved. If BPthreshold is not achieved in next 20 min, 80 mg IV labetolol is given.If BP is still high after 20 min, administer hydralazine 10 mg IV andrepeat BP after 20 min. Consult specialist for further control of BP.
Max dose for treatment cycle is 220 mg.
To initiate orally, give 100 mg. bd, and increase by 100 mg. bd perdayupto a maximum oral dose of 2400mg per day, if required.Usually, need is 200 - 400 mg. bd per day.
ii) Nifedipineis given orally. This orally administered calcium-channelblocking agent has become popular because of its efficacy to controlacute pregnancy-related hypertension. A 10-mg initial immediate-releaseoral dose to be followed in 20 minutes with 20 mg if necessary. IfBP threshold not achieved in next 20 min, 20 mg oral nifedipine isgiven. If BP is still above threshold level after 20 min, giveinjlabetolol 40mg IV over 2 min and consult specialist for control ofblood pressure..
If threshold of BP achieved, , repeat BP measurements every10 min for one hr then every 15 min for one hr, then every 30min for one hr and then every hr for 4 hrs.
Maximum dose which can be given in a day is 90 mg per day.
Headache, facial flushing and tachycardia are the side effects. As perneed, oral dose varies from 5 to 20 mg. tds. Close monitoring ofblood pressure should be done.Sublingual administration is avoided asit causes sudden hypotension and death.
iii) Hydralazine may be given by intravenous/intramuscular route.Hydralazine is administered intravenously with a 5 or 10-mg initial

71
dose, and this is followed by10-mg doses at 20-minute interval until asatisfactory response isachieved.If BP is still above threshold after 20min, give injlabetolol 40mg IV over 2 min. If BP is high after 20min, give 40 mg IV labetolol and consult specialist for control ofblood pressure.If threshold of BP achieved, , repeat BP measurementsevery 10 min for one hr then every 15 min for one hr, then every30 min for one hr and then every hr for 4 hrs.Its onset of action isin 20-30 minutes. Side effects are headache, tachycardia, fetaldistress.
iv) Methyldopais centrally acting adrenergic agonist. It is given in aloading dose of 500-1000 mg followed by 250-500 mg four times aday can control the blood pressure within 6-12 hours. Tiredness andpostural hypotension may occur. Its safety in pregnancy has been wellestablished.
v) Diuretics: Potent loop diuretics can further compromise placentalperfusion. Immediate effects include redistribution of the intravascularvolume, which most often is already reduced in severe preeclampsia .Therefore, before delivery, diuretics are not used to lower bloodpressure.Diuretics during pregnancy is only given for the managementof heart failure and pulmonary edema.
c) Magnesium Sulfate
To prevent eclampsia (seizures), magnesium sulfate is given in cases ofsevere preeclampsia i.e.
-BP : 160/110 or higher.
-BP < 160/110 and severe symptoms that usually precede seizures.
Magnesium sulphate is also neuroprotective for the preterm infant(<37 weeks) and useful in preventing cerebral palsy.There is acohort of women with mild to moderate pre-eclampsia who do notmeet maternal indications for magnesium sulphate but in whom, forfetal reasons, preterm delivery is necessary. It is appropriate now togive those women magnesium sulphate for fetal neuroprotection.
d) Termination of Pregnancy
The cure for preeclampsia is delivery. In mild controlled preeclampsiapregnancy may be continued till 37 weeks when the foetus has a betterchance of survival. Uncontrolled or severe preeclampsia should preferablybe managed in a bigger hospital with facilities for intensive maternal andfetal care. These women require immediate termination of pregnancy underthe care of a specialist gynaecologist.
e) Expectant management
It has been tried in women remote from term without compromisingmaternal condition for better fetal outcome. It is useful between 28 to 34weeks of gestation in a tertiary care hospital with intensive fetal andmaternal monitoring. Antihypertensive gents are given for blood pressure
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
72
control and a course of antenatal corticosteroids is given for fetal lungmaturity. Prophylactic anticonvulsant therapy with magnesium sulphate maybe required. Prompt delivery is indicated in the following conditions:
Maternal Indication
1. Persistent severe headache or visual changes
2. Uncontrolled hypertension despite maximum dose of twoantihypertensive drugs.
3. Progressive renal insufficiency ( serumcreatinine>1.1 mg/dl or doublingof serum creatinine absence of other renal disease)
4. Elevated liver enzymes with persistent severe epigastric pain or rightupper quadrant pain
5. Persistent thrombocytopenia or HELLP syndrome.
6. Eclampsia
7. Pulmonary edema
8. Abruption placentae.
Fetal Indications
1. Severe fetal growth restriction (estimated fetal weight<5th percentiles)
2. Persistent oligohydraminos (maximum vertical pocket<2cm)
3. Reversed or absent umbilical artery end-diastolic flow
4. Biophysical profile <4 on at least two occasions 6 hours apart.
5. Recurrent variable or late decelarations during non stresstest(NST).
Prevention of Preeclampsia
Low-dose aspirin (150 mg/day) prophylaxis is recommended in women athigh risk of preeclampsia and should be initiated between 12 weeks and28 weeks of gestation (optimally before 16 weeks) and continued dailyuntil 36 weeks of pregnancy.
If dietary calcium is low in a population, then oral calcium supplementationduring pregnancy between 1500-2000mg per day can also preventoccurrence of preeclampsia.
Check Your Progress 1
1) The basic pathophysiology in preeclampsia is
.................................................................................................................
2) Which organ systems of the body manifest changes of preeclampsia?
.................................................................................................................
3) What are the hematological changes in preeclampsia?
.................................................................................................................
73
4) How is hypertension in pregnancy classified?
.................................................................................................................
5) List the main clinical features of the preeclampsia
.................................................................................................................
6) Name the drugs used for acute control of hypertension.
.................................................................................................................
7) Name the drugs used for long term control of hypertension.
.................................................................................................................
8) The cure for preeclampsia is ..................................................................
7.3.2 Eclampsia
You have just read about preeclampsia. If a pregnant woman withpreeclampsia is not treated properly or despite treatment continues toworsen, this may lead to eclampsia. Eclampsia is characterised bygeneralized tonic clonic convulsions in addition to other features ofpreeclampsia.
Eclampsia is regarded with particular concern due to its associated highmaternal and fetal mortality. Hence we shall now discuss thepathophysiology diagnosis, management and complications of this condition.
Pathophysiology
What causes the convulsions of eclampsia?
The cause of convulsion is not exactly known. The cerebral irritation maybe due to anoxia, cerebral edema and cerebral dysrhythmia. The spasm ofcerebral vessels is responsible for anoxia. Nonspecific electroencephalographic abnormalities can usually be demonstrated for some timeafter eclamptic convulsions. The most common findings on computedtomography are hypodense cortical areas that correspond to petechialhemorrhage and infarction sites. The principal post mortem cerebral lesionsare oedema, hyperemia, focal anemia, thrombosis and haemorrhage.
Why all women with preeclampsia do not have convulsions?
This is difficult to explain, perhaps the brain like the liver and kidney maybe more involved in some women than in others and the extent ofischaemia and petechial subcortical lesions further altered by an inherentseizure threshold, influences the incidence of eclampsia.
Diagnosis
Eclampsia characterised by convulsions may occur in the antenatal period(antepartum 50%), duringlabour (intrapartum 25%) or after delivery(postpartum 25%). Eclampsia is most common in the last trimester andbecomes increasingly more frequent as term approaches. Nearly all casesof postpartum eclampsia develop within 24 hours of delivery. Almostwithout exception, eclampsia is preceded by warning features ofhypertension, proteinuria, headache, visual disturbance and epigastric orright upper quardrant pain.
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
74
The convulsion consists of four stages:
i) Premonitory stage: It begins with facial twitching and onset ofunconsciousness and lasts for about 30 seconds.
ii) Tonic stage: The whole body becomes rigid in a generalized muscularcontraction. This phase lasts for 15 to 20 seconds. Respiration ceasesand cyanosis appears.
iii) Clonic stage: All the voluntary muscles undergo alternate contractionand relaxation starting from the jaw. The tongue may be bitten andthe woman may be thrown out of the bed. Blood tinged froth mayexude from the mouth. This state lasts for one minute.
iv) Stage of coma: Gradually the movements become less frequent andthe woman lies motionless.
Throughout the seizure the woman is apneic. The breathing is resumedafter a long deep inhalation. Coma follows a convulsion and may last fora few minutes or persist from one convulsion to another.
After a convulsion, the respiratory rate becomes fast. There may becyanosis and fever which is a poor prognostic sign. Proteinuria andoedema are almost always present. Oliguria and haemoglobinuria may alsobe seen.
Differential Diagnosis
The dictum is ‘Until other causes are excluded, all pregnant womenwith convulsions should be considered to be eclamptics’.
The other causes of convulsion in pregnancy include epilepsy, encephalitismeningitis, cerebraltumour, ruptured cerebral aneurysm and even hysteria.These should be borne in mind whenever convulsion or coma developsduring pregnancy.
Management
It should be emphasised that a patient of eclampsia requires intensive carein a specialised obstetric unit. The patient should be referred to thetertiary centre at the earliest after giving preliminary first aid. A medicalpersonnel should accompany the patient to the referral centre. If anobstetric flying squad is available it is the ideal one to shift the patient.
Transport of a patient:
BP should be stabilized and convulsion should be controlled.
Magnesium sulfate loading dose of 4 gm IV and 10gm IM is given
Labetolol 20mg IV is given to control blood pressure
Diuretic (Furosemide) is give if pulmonary oedema is present
All maternal records and detailed summary including details of drugsadminister to the patient should be sent along with a medical personnel toa higher tertiary care centre.
During transport, air passage is kept clear, oxygenation is maintained, injuryto patient and recurrence of convulsions are avoided and blood pressure ismonitored.

75
Treatment of eclampsia consists of:
General care of the unconscious
Control of convulsions
Blood pressure control
Delivery after control of convulsion
General Care
a) The patient should be nursed in a lateral position on a railed cot inan isolated room.
b) After the patient is sedated IV line is started. Total fluid intake shouldnot exceed 2 litres in 24 hours.
c) The air passage is to be cleared of mucus, vomitus and secretions atfrequent intervals with a suction catheter.
d) A gag is placed between the teeth to prevent tongue bite.
e) Oxygen 8-10 L/min by mask should be given. Oxygenation ismonitored by pulse oximeter.
f) Antibiotics should be given to prevent infection.
g) Bladder should be catheterized and hourly urine output is monitored.
h) Blood pressure, pulse and respiration to be recorded 1/2 hourly.
i) Intake-output record to be maintained.
Control of Convulsions
Various regimes have been used to treat convulsion in eclampsia. Two ofthem are described below.
1) Magnesium Sulphate
This is the recommended regime by the Govt. of India and is commonlypracticed. Initial loading dose consists of 4 gm of magnesium sulphategiven intravenously as 20 ml of 20% solution at a rate not to exceed1gm/min. This should be followed by 10 gm of 50% solution (5gm ineach buttock) injected deeply. If convulsions persist after 15 minutes, 2gm more may be given intravenously as a 20% solution at a rate not toexceed 1 grn/min.
Every 4 hours thereafter 5 gmas 10ml of 50% solution may be injecteddeep intramuscularly but only after ensuring that:
a) the patellar reflex is present
b) respiration is not depressed ( RR >14 per minute)
c) urine output in the previous 4 hours exceeds 100 ml ( >30 ml perhour)
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy
Abnormal Pregnancy
76
Therapeutic level of magnesium is 4 – 7 meq / l .
Depression of patellar reflex occur at serum level of 8-10meq/l and isearliest sign og magnesium toxicity.
Respiratory depression occur at 12-14 meq/l.
Cardiac arrest occur at 25-30meq/l.
If respiratory depression develops, stop magnesium sulphate and givecalcium gluconate 10% ml iv slow over 3 mins.
Magnesium sulphate is continued for 24 hours after delivery or lastconvulsion, whichever is later. For recurrence of seizure, another 2 gm IVbolus is given over 5 minutes.
Alternatively, loading dose of magnesium sulfate is given as 4gm ivfollowed by iv infusion of 1gm per hour until 24 hours delivery.
Blood Pressure Control
If the blood pressure remains more than 150/100 mmHg,anithypertensives(labetalol, nifedepine, hydralazine) should be given asmentioned in severe preeclampsia.
Delivery after Control of Convulsion
In eclampsia, labour often starts spontaneously or can be inducedsuccessfully even if the woman is remote from term. Serious morbidity isless common during puerperium in women delivered vaginally. Hencevaginal delivery is attempted and is quite often successful. The women witheclampsia lack normal pregnancy hypervolemia and are thus much lesstolerant of blood loss than a normotensive pregnant woman.
Complications
Many organ systems are affected in patients of eclampsia since it is amulti system disorder. The complications include the following:
i) Aspiration pneumonia follows inhalation of gastric contents ifvomiting accompanies convulsion and airway is not adequatelymaintained.
ii) Pulmonary oedema may be the result of the combination of severehypertension and vigorous intravenous fluid administration. If nottreated promptly, it is associated with a poor prognosis.
iii) Hemiplegia may be caused by cerebral haemorrhage.
iv) Comaor altered sensorium may follow seizures. It may be caused bycerebral oedema or ruptured vessels and requires supportivemanagement.
v) Blindness may be due to retinal detachment or occipital lobeischaemia. In either case, the prognosis for return of normal vision isgood and usually complete within a week.
vi) Psychosis: The patient may become violent following seizures. Thestate may last up to two weeks and has a good prognosis.

77
vii) Renal failure requires supportive treatment and the renal functionusually returns to normal.
viii) Sudden Death: Sudden death may occur along with a convulsion orshortly thereafter usually as a result of massive cerebral haemorrhage.Pulmonary oedema is another important cause of maternal death ineclampsia.
7.3.3 Postpartum Care
After delivery, there is usually rapid improvement of blood pressure andproteinuria.
However, the patient should be closely monitored for at least 48 hours.One must remember that convulsions may occurupto 48 hours afterdelivery.
Apart from the routine postpartum care the following regime should befollowed: During hospital stay
i) Blood pressure should be checked every two hours.
ii) Antihypertensives should be given if diastolic BP is > 100 mmHg.
iii) If patient appears restless, she should be sedated.
iv) Anticonvulsant regimes if started before delivery should be continuedfor at least 24 hours after delivery or last convulsion, whichever islater
v) The dose of antihypertensive should be reduced according to BPrecords.
vi) Patient should be kept in the hospital till BP is brought down to safelevels and proteinuria disappears.
After discharge from hospital
i) The patient is reevaluated 2 weeks later. Most often hypertensioninduced by pregnancy dissipates spontaneously during the first 2weeks postpartum. If hypertension persists, a beta blocker ornifedipne may be prescribed. .
ii) Hypertension persisting 6 weeks after delivery usually signifies chronicvascular disease, often essential hypertension. Basic investigations likeurine protein, microscopic examination, blood urea, serum creatinine,chest X-ray and ultrasound of kidneys should be done. The patientshould be followed closely to ascertain the cause of hypertension andwhether the antihypertensives should started or continued. It may bebetter to refer the patient to a specialist for further evaluation.
Contraception
The patient should be advised to avoid pregnancy for at least one year.Intrauterine contraceptive devices are an effective method of contraception.Double barrier (condom and spermicide) are an alternative. Oralcontraceptives are not contraindicated if the BP comes back to normalafter delivery though they should be avoided during lactation
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
78
Check Your Progress 2
1) What are the warning symptoms that precede eclampsia?
.................................................................................................................
2) What are the stages of an eclamptic convulsion?
.................................................................................................................
3) What are the prerequisites before repeating a dose of magnesiumsulphate?
.................................................................................................................
4) List the complications of eclampsia.
.................................................................................................................
7.3.4 Rapid Initial Assessment and Rapid InitialManagement
As severe preeclampsia and eclampsia is one of the major causes forhigh maternal mortality and morbidity, it is very important for you toassess and manage such case rapidly for lowering maternal morbidityand mortality.
Rapid Initial Assessment
Table will help you to do rapid initial assessment to diagnose thesevere preeclampsia andeclampsia
Presenting Symptoms Symptoms and Probableand other symptoms signs sometimes Diagnosisand signs present
Typically present
Diastolic blood pressure Hyperreflexia Severemore than 110mm of Hg Headache (increasing Preeclampsiaor more after 20 weeks of frequency, unrelieved bypregnancy regular analgesicsProteinuria 3 + or more Clouding of vision
Ologuria (passing lessthan 400 ml. per24 hours)Upper abdominal pain
(Epigastric pain or painin right upper quadrant)
Convulsions Coma (Unconscious) EclampsiaOther signs and Other signs andsymptoms of severe symptoms of severepreeclampsia preeclampsia

79
Diastolic blood pressure alone is an accurate indicator ofhypertension in pregnancy.
When woman develops severe preeclampsia, there is risk of developingconvulsions at any time. Prior to convulsions some danger signsappear in woman. This condition is known as imminent eclampsia.
Danger signs of imminent eclampsia are
1. Severe headache (increasing frequency, unrelieved by regularanalgesics)
2. Visual disturbances, clouding of vision.
3. Upper abdominal pain (Epigastric pain or pain in right quadrant)
4. Oliguria (passing less than 400 ml of urine in 24 hours)
5. Hyper-reflexia
6. Diastolic blood pressure 110 mm of Hg
7. Proteinuria 3 + or more.
Rapid Initial Management
Imminent eclampsia and eclampsia are to be managed similarly withthe exception that delivery must occur within 12 hours of onset ofconvulsions in eclampsia. Both require active management.
Management during imminent eclampsia and eclamsia
Principles of management:
1. Give anticonvulsant drugs.
2. Gather equipment (airway, suction, mask and bag, oxygen) andgive oxygen at 8 to 10L per minute (if available at your place).If nothing is available, put the handle of spoon or mouthgag in themouth, between teeth, to avoid injury to the tongue.
3. Protect the woman from injury but do not actively restrain her.
4. Place the woman on her left side to reduce the risk of aspiration ofsecretions, vomiting and blood.
5. After the convulsion, aspirate the mouth and throat as necessary. Ifyou have no facility to suck out the secretions, clean the mouth andturn the face on one side.
6. Catheterise the bladder soon after convulsion or after anticonvulsantdrug.
Anticonvulsive Drugs:
A key factor in anticonvulsive therapy is adequate administration ofanticonvulsive drugs. Convulsions in hospitalised woman are mostfrequently caused by inadequate dose.
Magnesium Sulphate is the drug of choice for preventing andtreating convulsions in severe preeclampsia and eclampsia.
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
80
In your emergency kit, keep syringes and needles, ampoules ofnormal saline for dilution, Magnesium Sulphate and CalciumGluconate (antidote to Magnesium Sulphate)
Magnesium sulfate:
Magnesium sulfate schedules for severe pre-eclampsia and eclampsia:
Loading dose:
Magnesium sulfate 20% solution, 4 g IV over 5 minutes.\
Follow promptly with 10 g of 50% magnesium sulfate solution, 5 g ineach buttock as deep IM injection with 1 mL of 2% lignocaine inthe same syringe. Ensure that aseptic technique is practiced whengiving magnesium sulfate deep IM injection. Warn the woman that afeeling of warmth will be felt when magnesium sulfate is given.
If convulsions recur after 15 minutes, give 2 g magnesium sulfate(50% solution) IV over 5 minutes.Refer the woman to CHC/FRU for further management. If youare in such a set up where you can not refer her to CHC/FRU, be ready to help her.
You should repeat the maintenance dose of magnesium sulphate afterproper monitoring.
You should hasten the delivery and manage her during labour
Maintenance dose of magnesium sulfate:
5 gm of Magnesium sulfate (50% solution) + 1 mL lignocaine 2% IMevery 4 hourly into alternate buttocks.
Continue treatment with magnesium sulfate for 24 hours after deliveryor the last convulsion, whichever occurs last.
Before repeating Magnesium Sulphate, ensure that
Respiratory rate is atleast 16 per minute.
Patellar reflexes are present.
Urinary output is atleast 30 ml. per hour over last 4 hours.
Withhold or delay the drug if
Respiratory rate falls below 16 per minute.
Patellar reflexes are absent.
Urinary output falls below 30 ml. per hour over preceding 4 hours.
Keep Antidote ready.
In case of respiratory arrest,
Assist ventilation (Bag and mask, anaesthesia apparatus, intubation)
Give Calcium Gluconate 1 gm. (10 ml.of 10 % ) IV slowly untilrespiration begins to antagonise the effects of Magnesium Sulphate.

81
Diazepam:
If Magnesium Sulphate is not available, use Diazepam as anticonvulsiveagent. As drug passes freely through placenta, there is risk of respiratorydepression in newborn. Usually single dose of Diazepam, to controlconvulsion does not cause neonatal respiratory depression.
Use Diazepam only if Magnesium Sulphate is not available.
Diazepam schedule for severe preeclampsia and eclampsia:
Loading dose:
Intravenous administration of 10 mg. IV slowly over 2 minutes.
Repeat the dose, if convulsions recur.
Mantainance dose:
Diazepam 40 mg. in 500 ml IV fluids (Normal Saline or Ringer Lactate)titrated to keep woman sedated but rousable.
General management
Never leaver the woman alone. A convulsion followed by aspiration ofvomit may cause death of woman as well asfoetus.
Catheterise the bladder to monitor urinary output as well proteinuria.
Observe vital signs, reflexes and foetal heart sounds hourly.
Counsel family members for transfer and arrange for transportsimultaneously.
Meanwhile, if facility is available, start IV infusion and infuse IVfluids.
Maintain a strict fluid chart and monitor the amounts of fluidadministered and urine output to ensure that there is no fluidoverload.
If diastolic blood pressure remains above 110 mm of Hg, giveantihypertensive drugs. Reduce the diastolic blood pressure below100 mm of Hg but not less than 90 mm of Hg.
If urinary output is less than 30 ml per hour, with hold Magnesiumsulphate and infuse IV fluids (Normal Saline or Ringer Lactate), at 1L in 8 hours.
Auscultate the lung bases hourly for rales indicating pulmonaryoedema. If rales are heard, withhold IV fluids and give Frusemide40 mg IV once.
Management during labour :
Delivery should take place as soon as woman’s condition getsstabilised. Delaying delivery to increase foetalmaturity will as risk thelives of both, mother as well foetus. Deliveryshould occur regardlessof gestational age.
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy
Abnormal Pregnancy
82
In Imminent eclampsia, delivery should take place within 24 hoursof onset of symptoms.
In eclampsia, delivery should take place within 12 hours of onset of
convulsions.
For assessing woman for vaginal delivery,
Assess the cervix
If cervix is favourable, (soft, thin, partially dilated), rupture the
membrane with amniotic hook or Kocher’s forceps, and induce labour
with oxytocin drip for vaginal delivery.
If vaginal delivery is not anticipated within 12 hours in eclampsia, or 24
hours in case of severe preclampsia, refer the woman to CHC/FRU.
Postpartum care:
Mantain anticonvulsive therapy for 24 hours after delivery or last
convulsion, whicheveroccurs last.
Continue antihypertensive therapy till diastolic blood pressure is 110
mm of Hg or more.
Continue to monitor urinary output.
Do not give Ergometrine to cases of severe preeclampsia, eclampsia
or high blood pressure as it increases the risk of convulsions and
cerebro vascular accidents. If needed, you can give inj. syntocinon10
units IM.
Referral for tertiary level care:
Oliguria that persists for 48 hours after delivery
Coagulation failure e.g. coagulopathy or haemolysis, Elevated liver
enzymes, and low platelet count (HELLP Syndrome)
Persistent coma, lasting for more than 24 hours after convulsion.
7.4 LET US SUM UP
Reading this unit will make you realise how you could prevent the serious
complication of eclampsia by diagnosing preeclampsia early and managing
the patient properly.
Essential features of preeclampsia include hypertension, oedema and
proteinuria. In eclampsia convulsions occur apart from these features. Early
diagnosis of this condition can be made by good antenatal care.
7.5 KEY WORDS
Amniotomy : Rupture of membranes
ARM : Artificial Rupture of Membranes

83
7.6 ANSWERS TO CHECK YOUR PROGRESS
Check Your Progress 1
1) Vasospasm
2) Placenta
Cardiovascular system
Hematoloical system
Endocrine system
Kidney
Liver
Brain
3) Intravascular coagulation
Thrombocytopenia
Hemolysis
Reduced antithrombin III
4) Pregnancy induced hypertension
Pregnancy aggravated hypertension
Coincidental hypertension
5) High blood pressure
Excessive weight gain
Oedema
Proteinuria
6) Nifedipine
Hydralazine
Labetalol
7) Mthyl.dope
.Betablockers
8) Delivery
Check Your Progress 2
1) Headache
Visual disturbances
Epigastric or right upper quadrant pain
2) Premonitory stage
Tonic stage
Complications in LatePregnancy-I :
Hypertensive Disordersin Pregnancy

Abnormal Pregnancy
84
Clonic stage
Stage of coma
3) Patellar reflex is present
Respiration is not depressed
Urine output in previous 4 hours is 100 ml
4) Aspiration pneumonia
Pulmonaryoedema
Hemiplegia
Coma
Blindness
7.7 FURTHER READINGS
Arias, Fernando (1993).Practical Guide to High Risk Pregnancy andDelivery, Mosby year book, 09: 162-182.
Chamberlain, Geoffrey (ed.) Turnbull’s Obstetrics, 2nd edition,Churchill Livingstone.
Cunningham (1993).Williams Obstetrics, Appleton & Lange, 37:819-851
Donald, Ian (1994). Practical Obstetrics Problems, B.I. Publications(P) Ltd., 15:420-480

85
UNIT 8 COMPLICATIONS IN LATEPREGNANCY-II:ANTEPARTUMHAEMORRHAGE
Structure
8.0 Objectives
8.1 Introduction
8.2 Antepartum Haemorrhage (APH)
8.2.1 Placenta Praevia
8.2.2 Abruptio Placentae
8.2.3 Other Causes of APH
8.2.4 Rapid Initial Assessment and Rapid Initial Management.
8.3 Let Us Sum Up
8.4 Key Words
8.5 Answers to Check Your Progress
8.6 Further Readings
8.0 OBJECTIVES
After going through this unit, you should be able to:
define the terms antepartum haemorrpage, placenta praevia,abruptio placentae, vasa praevla;
list the causes of antepartum haemorrhage;
describe the diagnostic features of abruptio placentae, vasapraevia, placenta praevia and indetermininate bleeding; and
discuss the management of placenta praevia, abruptio placentae,vasa praevia and indeterminate bleeding.
8.1 INTRODUCTION
This unit deals with the important complications of antepartumheamorrhage, which is an important causes of maternal mortality.Ante-partum haemorrhage includes mainly placenta praevia andabruptio placentae, which contributes to a large extent to the deathscaused by haemorrhage. You will learn about the diagnosis andappropriate management of these conditions at various levels of healthcare in this unit.
8.2 ANTEPARTUM HAEMORRHAGE (APH)
Antepartum haemorrhage is defined as haemorrhage from the genitaltract after 28 weeks of pregnancy (bleeding before 28 weeks ofpregnancy is called abortion).

Abnormal Pregnancy
86
Causes
Bleeding from the genital tract after 28 weeks of pregnancy can occurbecause of the following conditions:
Placenta praevia
Abruptio placentae
Vasa praevia
Extra placental incidental causes
Indeterminate causes
Incidence of antepartum haemorrhage among hospital deliveries variesfrom 2-3%. In 2/3 of the cases, the causes is either placenta praeviaor abruptio placentae. Vasa praevia and extra placental incidentalcauses like cervical and vaginal lesions are rare. In about 1/3 of thecases, no cause can be found and these form the unclassified orindeterminate bleeding (Table 8.1).
Table 8.1: Causes of Antepartum Haemorrhage
Placental Bleeding Unexplained ExtraplacentalOr Causes
Indeterminate
Local Cervical Lesions
Placenta Abruptio Cervival Polyp
Praevia Placentae Carcnoma Cerivx
Varicose Viens
Vasa Previa
8.2.1 Placenta Praevia
The placenta is implanted partially or completely over the loweruterine segment.
Lower uterine segment
Lower uterine segment has been defined in different ways:
Anatomical definition: It is that part of the uterus which lies belowthe level at which the peritoneum on the anterior surface of theuterus ceases to be intimately applied to the uterus.
Metric definition: It is that portion of the uterus which, towardsterm, lies within three inches (7.5 cm.) from the cervical os. Itrepresents the distance over which the uterine cavity can be exploredby the examining finger passed through the cervix during vaginalexamination.
Physiological definition: It is that part of the uterus which passivelystretches and acts as a receptacle in labour and takes hardly anyactive contractile part in the expulsion of foetus.

87
Histological definition: It arises from the anatomical os of the cervix.
a) Incidence
Placenta praevia occurs in about I in 200 deliveries. The frequency withwhich the zygote implants in lower part of the uterus is much higher butmany of these pregnancies end in abortions. In many others, the placentamigrates and comes to lie in the upper uterine segment. Only in fewcases, where it is implanted over the os, it persists as placenta praevia.
b) Aetiology and Associated Conditions
Aetiology
Placenta praevia is caused by implantation of the blastocyst at a site lowin the uterine cavity but what causes this low implantation is not known.There are certain factors which predispose to placenta praevia and theseare:
Multiparity: Multiparity somehow predisposes to placenta praevia. Theincidence of placenta praevia is much higher, about 5% in grand multiparaas compared to 0.2% in nulliparous.
Advanced Maternal Age: Placenta praevia is 2-3 times more common inwomen after 35 years as compared to women less than 20 years.
Placental Size: Incidence of placenta praevia is higher in twin pregnancy,presumably because of large placental size.
Uterine Scars and Pathology: Placenta praevia is found more commonly incases with previous caesarean section, previous dilation and curettage,myomectomy and endometritis.
Placental Pathology: Marginal or velamentous cord insertions, succinturatelobes, bipartite placenta and fenestrated placenta are more commonly foundin placenta praevia.
Smoking: Smoking at any time increases the risk of developing placentapraevia. Compensatory placentalenlargement due to carbon mono oxidehypoxaemia could be the cause.
Associated Conditions
Abnormal Placentation: Placenta accreta and percreta may be associatedwith placenta praevia specially if there is a caesarean scar. The decidua ispoorly developed in the lower uterine segment and therefore the placentamay get morbidly adherent to the uterus and give rise to third stagecomplications. .
Malpresentations: In placenta praevia, the bulk of the placenta in the loweruterine segment may prevent the engagement of foetal head and predisposeto malpresentation. Therefore, if high floating head, breech presentation,oblique or transverse lie is present, one should suspect the possibility ofplacenta praevia.
Congenital Anomalies: Incidence of congenital anomalies is higher inplacenta praevia. The reason is not known.
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
88
c) Classification
There are four types of placenta praevia depending on the degree ofextension of placenta into the lower uterine segment (Fig. 8.1).
Fig. 8.1: Types of Placenta Praevia
Type I (Low lying placenta): Placenta encroaches on the lower uterinesegment (it lies within 7.5 cm of the internal os ) but does not extend tothe internal os.
Type II (Marginal placenta praevia): Placenta reaches the internal osbut does not coverit.
Type III (Partial placenta praevia): Placenta covers the os but ceasesto do so as the cervix dilates.
Type IV (Total placenta praevia): Placenta covers the internal os evenwhen the cervix is fully dilated.
The placenta can be on the anterior or posterior wall. Type I and IIanterior are called mild degree and Type II posterior, Type III andType IV placenta previa are called major degree placenta previa.
d) Clinical Features
Symptoms
The only symptom of placenta praevia is vaginal bleeding. Thebleeding is sudden in onset, painless, apparently causeless and recurrent.The bleeding may vary from being slight to profuse. The first bout ofbleeding may not be alarming and it usually but not always ceasesspontaneously, only to recur later. Bleeding in some cases may not occurtill the onset of labourand then it may be profuse.
Signs
The general condition of the patient is proportionate to the amount ofblood loss. If the bleeding has been profuse, all the signs of shock maybe present. These include pallor, cold and clammy skin, dyspnoea,restlessness, agitation, syncope, anxiety, confusion, falling blood pressure,tachycardia and oliguria or anuria.On abdominal examination, size of the

89
uterus corresponds to period of gestation. Uterus is relaxed, soft andwithout any areas of tenderness. The foetal parts are palpable, presentingpart is high up, foetus may present in oblique or transverse lie. Foetalheart sounds are present unless there is major degree of placentalseparation, hypovolaemic shock or cord accident.
e) Diagnosis and Differential Diagnosis
Diagnosis
The antepartum diagnosis of placenta praevia is confirmed bytransabdominal, transperineal and transvaginal ultrasound.
Vaginal Examination must not be doneas it can provoke furtherseparation of placentawith torrential bleeding. Vaginal examination is doneonly in the operation theatre prior to termination of pregnancy and isdiscussed in the management. Speculum examination after bleeding hasstopped for 48 hour to exclude local cause is also discussed inmanagement.
The accuracy of transabdominal ultrasound in the diagnosis of placentapraevia is excellent with false positive and false negative rates of 7% and8% respectively. This accuracy is even higher when a vaginal probe isused. Both transabdominal and transvaginal ultrasound are safe techniqueswith minimal or no risk for mother and foetus. The precaution to takenduring transvaginal ultrasonography is not to touch cervix and probe iskept in the middle part of the vagina. If there is central placenta previaand risk of bleeding is very high, then transperineal ultrasonography is anequivalent option.
It is also important to look for features of placenta accrete whileperforming ultrasonography in cases of placenta previa. Color flow Dopplerstudies help in establishing the diagnosis.
Differential Diagnosis
Placenta praevia has to be distinguished from other causes of antepartumhaemorrhage specially the abruptio placentae. The differentiating features ofplacenta praevia and abruptio placentae are:
Criteria Placenta Praevia Abruptio Placentae
Nature of Painless, causeless and Painful, oftenbleeding recurrent localised to start
with and laterbecomesgeneralised,attributed topreeclampsia ortrauma and iscontinuous
Bleeding is always Bleeding isreveled revealed,
concealed orusually mixed
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
90
General Proportionate to blood loss Out ofproportion to the visiblecondition and blood loss inanaemia concealed variety
Features of Not relevant Present in one thirdpreeclampsia of cases
Height of Proportionate to gestational May beuterus age dispproportionately
enlarged in concealedtype
Feel of uterus Soft and relaxed May be tense, tenderand rigid
Malpresentation Common. The head Unrelated, the headis high and floating may be engaged
FHS, foetal Usually present Usually absent,heart sound specially in concealed
type
Localisation Placenta felt in lower Placenta in upperof placenta segment segment
Vaginal Placenta felt in lower Placenta is not felt inexamination segment lower(not tobe done segment is ready)unless OT
Local lesions in cervix and vagina can be ruled out by doingspeculum examination but the placenta praevia may coexist with them.
e) Management
All cases of antepartum haemorrhage should be regarded as due toplacenta praevia unless proved otherwise. All efforts should be madeto obtain the location of placenta through antenatal ultrasonography.
There are two principles of management of antepartum haemorrhage:
1) All women with antepartum haemorrhage must be evaluated in ahospital capable of managing massive haemorrhage and with allthe facilities for operative delivery.
2) A vaginal or rectal examination must not be performed till allpreparations for immediate caesarean section and blood transfusionare available.
Ultrasound diagnosis of Placenta Previa
Transvaginal ultrasonography between 18-24 weeks identifies the inferior-most aspect of the placenta and determines the distance between it andthe internal os. If the placental edge reaches (touches) the internal os, thediagnosis is marginal placenta previa. Low-lying placenta is diagnosed whenthe distance between the internal cervical os and the placental edge is

91
between 1 to 20 mm. If the distance between the internal cervical os andthe placental edge is more than 20 mm, the patients should be managedas per routine because there is no increased risk for cesarean delivery dueto hemorrhage. The ultrasound should be repeated in third trimester tolocalize placenta.
The use of MRI in the diagnosis of placenta previa is limited to afew specific cases, and MRI should be used only after sonographyfails to provide adequate information or in cases of posteriorplacenta previa.
Management at Home
A woman who starts bleeding at home must be instructed to remain inbed and if she is still bleeding when first seen, 15 mg of morphine shouldbe given intra muscularly and intravenous fluids should be started. A quickassessment of blood loss is made. Pulse, blood pressure is recorded andabdomen is palpated gently mainly to exclude any area of uterinetenderness or hardness suggestive of abruptio placentae. Fundal height ismarked to detect any increase later on. F.H.S. is auscultated. Vulva isexamined for any bleeding and no vaginal examination is done. All patientsof A.P.H. must be admitted to hospital. This is important because theinitial bleeding may be small and may cease spontaneously but it can recurat any time and may be life threatening.
Management in Hospital
On admission, an overall assessment of the patient is made. History istaken and complete examination except vaginal examination is done.Blood samples are taken for haemoglobin, grouping and crossmatching and coagulation studies. Routine urine examination foralbumin sugar is done. Intravenous line is established with atleast 16gauze needle. Further management of placenta praevia will depend onthe amount of bleeding, maturity of foetus and whether patient is inlabour.
In cases with preterm live foetus, with minimal bleeding expectantline of treatment is given. Active management of patient is done incases where bleeding is excessive or it continues, or where foetus ismature or patient is in labour.
Expectant Treatment
Expectant management with close observation is indicated in situationswhere the fetal gestational age is less than 36weeks of gestation aslong as reassuring fetal monitoring is present and vaginal bleeding hasresolved or significantly decreased. Administration of betamethasoneshould be provided if gestational age is less than 34weeks. If bleeding issevere or non-reassuring fetal monitoring is present then emergencycesarean delivery is indicated.
Expectant line of treatment is always at the hospital. Absolute bedrest is given for atleast 5 days after the bleeding stops. Careful monitoringof pulse, blood pressure, fundal height, foetal heart and vaginal bleeding isdone. Rh-ve woman should be given Anti-D immunoglobulin. Ultrasound
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
92
examinations is done to localise placenta and to exclude any foetalmalformation. When bleeding stops, perspeculation examination is done toexclude incidental causes. Antianaemic treatment is given and patient iskept in hospital, under observation.
Aim of expectant treatment is to continue pregnancy till 38 weeks i.e tillthe foetus is clinically viable. Active management is termination ofpregnancy which is described below.
Active Management
Active management is indicated in following conditions:
1) In cases who have been on expectant treatment and reach 38 weeksof pregnancy.
2) In cases who are admitted with severe bleeding.
3) Where bleeding recurs and continues with expectant management.
4) Where on admission, pregnancy is more than 38 weeks.
5) In patients who are in labour.
6) Where foetus is dead or congenitally malformed.
In cases where placental location remains uncertain, a double setupexamination is done. One management team is prepared for vaginalexamination and an uneventful vaginal delivery, and a second team isprepared for an immediate cesarean delivery, as needed.
In cases who have no bleeding or minimal bleeding, active managementincludes examination of patient in operation theatre with all preparations foran immediate caesarean section and blood transfusion. A gentle perspeculum examination is done, if not already done, to exclude localincidental causes in the cervix and the vagina like polyps, varicose veinsetc. A vaginal examination is carefully done, first through the fornices andif no bogginess is felt, then finger is introduced through the os to feel forplacenta. If no placenta is felt, the finger is swept above the os in aconcentric fashion till whole of the lower segment is explored. If noplacenta is felt or it is type I or type II anterior, rupture of membranes is
done and patient is monitored for vaginal delivery. Oxytocin drip, if notcontraindicated is given.
If placental edgetocervical os distance is greater than 2 cm from theinternal cervical os, a trial of labor can be offered to the patient. Ifdistance is less than 2 cm, cesarean delivery is done.
In type II posterior, type III, type IV placenta praevia or in cases wherebleeding continues following rupture of membranes or foetal distress isdetected, caesarean section is done. In cases where bleeding is excessiveor there are associated factors like malpresentation, caesarean section isindicated without a prior per vaginal examination.
In cases with hypovolaemic shock, two intravenous infusions with largecaliber should be established to allow rapid transfusion of blood and fluids

93
but caesarean must not be deferred, unless, patient has already stoppedbleeding when restorative measures may be carried out before startingcaesarean section.
Lower segment caesarean section is preferred. In cases where placenta isimplanted anteriorly, the placenta is separated manually to reach themargin, membranes are ruptured and baby delivered. Alternatively one maycut through the placenta and deliver the baby. In both these conditions,the cord must be clamped promptly to prevent further foetal blood loss.New born must be monitored carefully and it may require bloodtransfusion.
Management of Third Stage
Postpartum haemorrhage is common in cases of placenta praevia. Even asmall amount of blood loss in third stage may lead to a shock in analready exsanguinated patient. The effects of bleeding are more marked inplacenta praevia but postpartum haemorrhage is most likely to occurbecause of following reasons:
1) Placental site is in lower uterine segment which does not contract andretract as efficiently as the upper segment.
2) Placenta is larger and thinner and may not separate completely.
3) Placental site is larger.
4) There may be morbid adhesions of placenta.
Blood should, therefore, be always available and prophylactic measuresmust be adopted to minimise the third stage bleeding. High dosesyntocinon infusion andmethergin soon after the second stage is sufficient inmost cases.
Serious postpartum haemorrhage should be managed with injcarboprost(
125-250 microgm IM 15 methyl prostaglandin F2 alpha), manual uterinecompression and uterine packing. If these fail, internal iliac artery ligationor hysterectomy may be required especially in cases of placenta accreta.Before hysterectomy, haemostatic sutures in the placental bed may betried. In case the general condition of the patient is not good,hysterectomy must not be delayed.
f) Complications
Placenta praevia is one of the most common complications of pregnancy.Maternal and foetal mortality and morbidity can be very high unless timelyproper management is given to the patient.
Maternal Complications
Severe antepartum haemorrhage, shock and death may result from placentapraevia. Death may also occur as a result of intra partum and postpartumhaemorrhage, operative trauma orinfection. Placenta accreta is a seriouscomplication and may add to the mortality and morbidity of placentapraevia.
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
94
Foetal Complications
Prematurity accounts for 60% of the perinatal mortality in placenta praevia.Intrauterine asphyxia, birth injury, congenital anomaly and foetalhaemorrhage are the other causes of foetal death in placenta praevia.
g) Prognosis
Maternal
With good management, it has been shown that maternal mortality can bebrought down to zero. This is achieved because of the availability ofblood, timely caesarean section, safe anaesthesia and antibiotics. Good antenatal care with elimination of anaemia and routine diagnosis of placentapraevia on ultrasound also contributes to lowered mortality.
Foetal
The perinatal mortality inspite of the expectant management and availableresources still remains high. In most of the centres it ranges from 10-20%.
Check Your Progress 1
1) List the diagnostic features of placenta praevia.
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
2) In which cases of placenta praevia, vaginal examination is notindicated even in the operation theatre?
.................................................................................................................
.................................................................................................................
.................................................................................................................
3) Give two basic principles of management of placenta preavia.
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
4) In which cases of placenta praevia expectant management should notbe given?
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................

95
5) Why is postpartum haemorrhage more likely to occur in cases ofplacenta praevia?
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
8.2.2 Abruptio Placentae
Abruptio plecentae is also known as placental abruption and accidental-heamorrhage. An Abruptio placenta is the premature separation of anormally situated placenta and accounts for 30% of cases of ante partumhaemorrhage.It occurs in about 1 % of deliveries, the severe formoccurring in about 1 in 500 deliveries.
a) Aetiology
Tile exact cause of separation of normally situated placenta is often difficultto ascertain. Following are some of the conditions which lead to abruptioplacentae.
External trauma —fall or blow on abdomen or external cephalicversion may lead to placental separation.
Acute decompression of polyhydramnios —sudden diminution ofsurface area of uterus where placenta is attached results inplacental separation.
Preterm rupture of membranes may lead to abruptio placentae.Hypertension has been found to be the most commonly associatedcondition with placental separation. In severe abruption, pregnancyinduced or chronic hypertension was found in 50 percent of thecases. In milder form of abruption, the incidence of hypertensionis not high.
Other predisposing factors include advanced maternal age,multiparity, uterine leomyoma, smoking and previous history ofabruption. Folic acid deficiency though implicated, has not provedto be the cause of abruptio.In many cases, no cause is found.
b) Varieties—Concealed and Revealed
Two principal forms of the premature separation of placenta may berecognised depending on whether the haemorrhage is concealed orrevealed.
Concealed Form
This is a severe form of abruptio placentae, seen in about 20% of thecases. Following the separation of the placenta, the blood does notescape out but is retained behind the placenta within the uterinecavity. Foetal death is common and coagulation disorders and othermaternal complications are also more common.
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
96
Revealed Form
The blood from the separated placenta drains out through the cervix. Theplacental detachment is usually incomplete and complications are fewer andless severe. The revealed form of abruptio placentae is more common andis found in approx. 80% of the cases.
c) Clinical Features
Vaginal bleeding is the predominant feature and is found in about 80% ofthe cases. Uterine tenderness and rigidity is present in most of thesecases. Back pain and uterine contractions may be observed in somecases. Foetal distress is found in about 50% of the cases and foetal deathoccurs in about 15% of the cases. In severe form of concealedhaemorrhage, no vaginal bleeding may be observed but the uterus is foundto be tender and hard and foetal heart is usually absent. There may be aclinically significant amount of disseminated intravascular coagulationassociated with depletion of fibrinogen as well as other clotting factors.The patient may develop a haemorrhagic diathesis leading to activebleeding from all the sites. Hypovolaemic shock and renal failure maydevelop.
Small separation of placenta may present as APH and may not produceany signs. It may be diagnosed only after delivery. Ultrasound rarely helpsin diagnosing abruptio placentae because many a times it may not reveal aretroplacental clot. Ultrasound may be helpful in excluding placenta praeviain milder forms of abruptio where clinical signs of tense and tender uterusare not present.
Clinical Classifications
Depending upon the degree of abruption and its clinical effects, the casesare graded as follows:
Grade I
Clinical features suggestive of placental separation are absent, the diagnosisis made retrospectively. No vaginal bleeding to mild vaginal bleeding,slightly tender uterus, normal maternal BP and heart rate, no coagulopathy
no fetal distress. Retro placental clot volume is about 150 ml. Foetus isusually not at risk.
Grade II
In this grade, antepartum haemorrhage is accompanied by classic featuresof abruptio placentae and the foetus is alive. Retro placental clot is about500 ml. Maternal tachycardia with orthostatic changes in BP and heartrate. The uterus is tense and tender and foetal heart abnormalities arepresent.
Grade III
Along with the features of grade II, there is foetal death. Maternal shock,very painful tetanic uterus and hypofibrinogenemia (ie, < 150 mg/dL) are
97
the characteristics. It has associated maternal shock, coagulation failure orrenal failure.
d) Pathology
Placental abruption is initiated by haemorrhage into the decidua basalis. Asthe decidual haematoma expands, it separates and compresses theplacenta. The blood then separates the membranes and escapes giving riseto revealed type I abruptio placentae. In early stages, there may not beany clinical features. Only on inspection of the placenta after delivery, acircumscribed depression with dark clotted blood is found. Recentlyabrupted placenta may however show no evidence of separation.
In concealed variety, the placental margins or the membranes remainadherent to the uterine wall and blood keeps collecting behind theplacenta. Blood may enter the amniotic cavity after breaking through themembranes. In some cases, the head which is closely applied to thecervix may prevent the blood to escape.
Couvelair Uterus (Utero Placental Apoplexy)
In the more severe form of placental abruption, widespread extravasationof blood occurs into the uterine musculature and beneath the serosa givingrise to couvelair uterus which appears ecchymotic, purplish and hard andcan be seen only on laparotomy. These myometrial haematomas do notinterfere with uterine contractions and do not warrant hysterectomy.Retroplacental blood may penetrate through the thickness of the uterinewall into the peritoneal cavity. The myometrium in this area becomesweakened and may rupture with increased intrauterine pressure duringcontractions. A myometrium rupture immediately leads to a life-threateningobstetric emergency.
e) Management
Management of abruptio placentae depends on the severity of the caseand on the condition of the mother and the foetus.
Management of severe abruptio placentae with foetal death
If the abruption of placeta is severe enough to cause foetal death, theaverage intrapartum blood loss has been shown to be about 2500ml.These patients, therefore, require prompt and adequate transfusion of fluidsand blood. Two intravenous lines should be established to allow rapidadministration of fluids and blood.Haemotocrit and coagulation studiesshould be done. Indwelling urinary catheter should be put and vital signsmonitored. Haematocrit should be maintained at 30% or more, to sustainthe oxygen carrying capacity of the patient. Urinary output of atleast 30ml per hour signifies effective intravascular volume. Acute tubular orcortical necrosis, the most common cause of maternal mortality in abruptioplacentae is avoided by maintaining adequate urine output. Central venouspressure may be monitored by putting a catheter in internal jugular veinand this should be maintained at 10cm of water. This helps in infusingcorrect volume of fluids. Lung bases also must be auscultated for signs of
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
98
overload along with other clinical signs.
Patients with foetal death should be delivered vaginally. Amniotomy shouldbe done as soon as possible and oxytocin drip started. Careful monitoringof vital signs, coagulation profile and urinary output is done. Oxytocin dripand uterine massage is usually sufficient to prevent postpartumhaemorrhage.
Ceaserean section may be required if there is malpresentation,disproportion or some contraindication to vaginal delivery. Coagulationdisorder, if present, must be treated before doing caesarean section.
Management of Coagulopathy
In severe abruption acute disseminated intravascular coagulation may occurleading to fall in fibrinogen levels below 150 mg per dl. and drop inplatelet count along with prolongation of partial thromboplastin time (P. T.T.) and prothrombin time ( P. T.) The blood does not clot and allvenepuncture start oozing blood.
Table 8.2: Normal Values for D.I.C. Profile
Test Normal Results
B.T. 1-3 min
C.T. 3-7 min
Fibrinogen 150 to 600 mg/dl
PT 11 to 16 seconds
PTT 22 to 37 seconds
Platelet count 120,000 to 350,000/cu.mm
FDP (Fibrin Degradation Products) < 10 micrograrn/dl
Bedside Investigations:
In absence of facilities for these tests a simple bed side clot observationtest is invaluable in managing these cases. A venous blood sample isdrawn and is placed in a clean dry testtube. It is observed for clotformation and clot lysis. Failure of clot formation within 5-10 minutes ordissolution of a firm clot when the tube is gently shaken at the end of anhour suggests clotting deficiency due to lack of fibrinogen and platelets.Bleeding time is also determined at bedside. The venipuncture site wouldbe oozing if bleeding time is prolonged (Table 8.2).
Treatment of coagulopathy will depend on the amount of bleeding andanticipated route of delivery. Fresh whole blood is best for treating clottingdeficiency and replacing blood loss. Cryoprecipitates can be given as theycontain all necessary coagulation factors and are free of hepatitis B virus.10 -20 units can be given. Fibrinogen deficiency usually corrects itself butif required fresh frozen plasma or fibrinogen can be transfused. Platelettransfusion in a bleeding patient is indicated if count is below 40,000 per

99
cubic rom. and in patients with counts of 20,000 per cubic mm. even ifthere is no abnormal bleeding. Coagulation defect has to be treated ifcaesarean section or episiotomy carried out.
Management of Renal Failure
Acute renal failure is rare with lesser degrees of placental abruption but isseen in cases when there is delayed or incomplete treatment ofhypovolaemia. The possibility of renal cortical or tubular necrosis must beconsidered if oliguria persists after an adequate volume has been restored.An attempt should be made to improve renal circulation and promotediuresis by increasing fluid volume (under close monitoring). If renal failurepersists dialysis is indicated.
Management of Abruptio Placentae with Live Foetus
There are two sub-groups:
1) Those with Hypertonic Uterus
2) Those with Soft Uterus
If the foetus is alive and the uterus is rigid, the abruption is large but isless than 50%. The chances of foetal distress are high and thereforepatient should be prepared for immediate caesarean section unless there ismaternal shock or previable foetus. Blood coagulation studies are doneand blood arranged before taking the patient for caesarean section. If theuterus is soft and abruptio is present, the pregnancy should be terminatedby induction of labour with low rupture of membranes and oxytocin. Ifuterus becomes rigid and foetal distress develops caesarean section shouldbe done. In very mild cases of abruptio placentae where foetus ispretenm, expectant treatment can be given under very close supervision.Ultrasound is done for placental localisation.
Remember that complications are more when abruption and deliveryinterval is more. Hence the aim is to terminate pregnancy and deliver thefoetus without delay.
Management of abnormal placentae is summarized in Fig. 8.2.
f) Prognosis
Maternal - Maternal mortality in abruptio placentae ranges from 0.5% to5%. Haemorrhages D.I.C, cardiac and renal failure are responsible for highmortality. A high degree of suspicion, early diagnosis and definitive therapyresults in lowered maternal mortality.
Foetal - Foetal mortality ranges from 50% to 80%. Live born infantshave a high morbidity due to hypoxia, birth trauma and prematurity.
Indications for caesareans section in abruptio placenta are:
1) When foetus is live.
2) When maternal complication sets in. They are corrected and caesareandone.
3) Inspite of adequate blood transfusions, bleeding continues and patient’sB.P. continues to fall or does not come up.
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
100
Is the Foetus Alive?
YesNo
Fig. 8.2: Management of Abruptio Placentae
Mild or Moderate Abruptio( 80 % of cases)
Severe Abruptio Placenta( 20 % of cases)
Mild or Moderate Abruptio
Is the Uterus hard with noapperant relaxation betweencontractions ?
Is there any contraindicationfor vaginal delivery ?
No Yes Yes No
Is there aCoagulation Defect?
Is there aCoagulation Defect?
* Mantain organperfusion
* Amniotomy* Oxytocin
Induction* Vaginal Delivery
Yes Yes No
Correct Coagulation Defect withPlasma and Cryoprecipitate
Correct Coagulation Defect withPlasma and Cryoprecipitate orFresh Blood
CAESAREANSECTION
*Oxytocin Inductionof Labour*Electronic FoetalMonitoring
Normal FoetalMonitoring
AbnormalFoetal
Monitoring
VaginalDelivery
4) Inspite of ARM and syntocnion drip, delivery does not take place in12-16 hours.
8.2.3 Other Causes of A P H
Besides placenta praevia and abruptio placentae, antepartum haemorrhage iscaused by incidental causes, marginal placenta and Vasa Praevia.

101
a) Local Lesions of Cervix
These include cervicitis, cervical erosion, polyps, varicose veins invagina or cervix and cancer cervix. Per speculum examination willreveal these but they may coexist with other causes of antepartumhaemorrhage which should, therefore, be excluded.
b) Vasa Pearvia
This is a rare condition occurring in one in two thousand to threethousand deliveries. Vaginal blood tested for foetal haemoglobin incases of A.P.H. showing foetal distress may reveal this condition.Caesarean section is indicated if foetal bleeding is detected.
c) Indeterminate Bleeding
Many cases of antepartum haemorrhage have no evidence of placentapraevia or abruption and speculum examination is negative.Ultrasonography shows upper segment placenta. Perinatal mortality ishigh in this group.
The cause of bleeding in these cases is not known. It can be marginalseparation of placenta or excessive show. The bleeding is usually slight.The management of these patients is expectant in pregnancy less than 38weeks. At 38 weeks, vaginal examination is done and if placenta is notfelt, low rupture of membranes is done, oxytocin drip is given and closefoetal monitoring is required.
8.2.4 Rapid Initial Assessment and Rapid InitialManagement in case of APH
Now you know that APH is one of the life threaten obstetric emergency.You should be very alert and competent to handle such case. Your mainactivities in such circumstances should include
1. Rapid initial assessment and primary management of shock dueto profuse bleeding.
2. Management of abruption placentae
3. Management of placenta praevia
1. Rapid initial assessment and primary management of shock dueto profusebleeding :
When a woman of childbearing age presents with a problem of bleedingin late pregnancy, identify the underlying obstetric condition and rapidlyassess her condition to determine her degree of illness. This is known asRapid Initial Assessment. To minimize the delay in diagnosis, Table 8.3will guide you about what to ask, for what danger signs you have to lookand examine and what to assess if such danger signs are present.Rapidinitiation of treatment requires immediate recognition of the specific problemand quick action.
When you are doing rapid initial assessment, encourage the woman andher family to speak honestly and completely about events surrounding the
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
102
complication. Listen to what the woman and her family have to say andencourage them to express their concerns; try not to interrupt. Respect thewoman’s sense of privacy and modesty by closing the door or drawingcurtains around the examination table. Let the woman know that she isbeing listened to and understood. Use supportive nonverbal communicationsuch as nodding and eye to eye communication. Answer the woman’squestions directly in calm, reassuring manner. Explain what steps will betaken to manage the situation or complication. Ask the woman to repeatback to you the key points to assure her understanding.
While taking history or asking or any information, use communicationtechniques.
In a case of bleeding in late pregnancy, you must ask certain importantpoints of history e.g.duration of amenorrhoea,, amount of bleeding, bleedingassociated with pain or without pain, if pain, severity and type of pain,presence of fetal movements. Look or signs symptoms of pre-eclampsiai.e. oedema on feet; blood pressure may not be high as it can fall due toheavy bleeding. In case of excessive bleeding, severe pain, severe pallor,quickly you should assess her circulatory system for hypovolaemic shock,give primary management and without other delays, refer her toappropriate place. (Table 8.4)
Table 8.3: Rapid initial assessments for what and for whichcomplication
Problem Quick History Consider Assess what andand Examination for which life
threateningcondition
*Vaginal - Painless Placenta CirculatoryPraevia System for
Bleeding HypovolaemicShock in Late
- With Pain in Abruptioo PlacentaePregnancy Abdomen after 20 weeks
In case of heavy bleeding, and if you are alone,
SHOUT FOR HELP. Urgently mobilize all available personnel.
Make a rapid evaluation of the general condition of the woman includingvital signs (pulse, blood pressure, respiration, temperature). Do not performper vaginal examination. Per vaginal examination can give rise to furtherseparation of placenta previa and more bleeding. This will worsen thecondition of the woman. Table 8.4 will help you for assessment ofcirculatory system for diagnosis of hypovolaemic shock.

103
Do not do a vaginal examination at this stage.
Table 8.4: Rapid initial assessment of circulatory system
Assess Consider
Circulation (Signs of shock) HypovolaemicShock
Skin: cool and clammy Septic ShockPulse: fast (110 or more)and weakBlood pressure: low(systolic less than 90 mm Hg)
If shock is suspected, immediately begin treatment. Even if signs ofshock are not present, keep shock in mind as you evaluate thewoman further because her status may worsen rapidly. If shockdevelops, it is important to begin treatment immediately.
Primary management of shock due to profuse bleeding in latepregnancy:
You may be already aware, primary management of shock due toprofuse bleeding in late pregnancy should include
Stabilization of the patient
Referral at appropriate health facility
Stabilization:
Important steps for stabilization in hypovolaemic shock are:
Intravenous fluid therapy
Maintenance of body temperature
Intravenous fluid therapy is one of the important lifesavingstep. Staffnurse, ANM at PHC can do it. Use isotonic solution (0.9 % NaCl orRinger’s lactate solution). Glucose solution, without saline does notprovide salt to restore fluid balance. Use large bore needle, preferably16-18 gauge. Infuse rapidly in shock. 500 cc to 1 liter in 15 to 20minutes helps to stabilize condition. Once fluid loss is replaced, slowdown the drip (30 drops per minute). Record pulse, BP andtemperature.
For maintaining body temperature, cover the woman with blankets. Donot use hot water bottles by the side of the woman.
Referral to appropriate health facility:
In a case of placenta previa, bleeding occurs in bouts. After first bout ofbleeding, when second bout of bleeding will occur is not definite. Due toheavy first bout of bleeding, woman may need blood transfusion. Ifbleeding of first bout or subsequent bouts is heavy, she may needtermination of pregnancy. In case of placenta covering internal os of thecervix, will require abdominal surgery. Looking to all such possibilities, it ismost advisable to refer the woman to nearby CHC/FRU with referralnote.
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
104
In a case of abruption placentae, pregnancy must be terminated as earlyas possible. One more danger in case of abruption of placenta isdevelopment of hypofibrinogenaemia and disseminated intravascularcoagulopathy. Most of the fibrinogen of the body gets utilized in clotting ofretroplacental blood. Toxins liberated due to separation of placenta, leadsto DIC. Hence such case should also need transfer at a health facilityhaving specialist, Operation Theater, anaesthetist, blood transfusion facility,laboratory facility, i.e. at CHC/FRU.
As delay in decision of transfer can become fatal due to haemorrhagicshock and delay in the treatment, you should explain the seriousnessof the case to woman as well her family members. This will help inquick action from family members. Ideally, you have told warningsigns to woman and her family members during antenatal visits onlyand family members are mentally ready to face the situation.Convince family members to take young adults, in case of need forblood transfusion. It is better, if you accompany the woman to takecare on the way. You should also write appropriate referral note. Suchnote is very informative to treating doctor.
2. Management of abruption placentae:
Abruptio placentae is the detachment of a normally located placentafrom the uterus before the fetus is delivered. Blood gets collectedretroplacentally. Huge clot is formed which utilizes large quantity offibrinogen from the body. This leads to hypofibrinogenaemia. Clottingtime gets disturbed and blood does not clot for long time. Separated,damaged placental tissue liberates thromboplastin, which can lead tocoagulopathy.
Major principles of management of abruption placentae are:
1. Termination of pregnancy at earliest
2. Management of shock
3. Management of coagulopathy, hypofibrinogenaemia, if developed
In your health set up, you cannot provide these managements but youcan guide the woman as well as her family members. Main steps atyour level should include:
By rapid initial assessment, assess the circulatory system for signs andsymptoms of shock.
Cover her with blanket
Start intravenous infusion.
Counsel woman, family members for quick decision of taking womanto a health facility having surgical, laboratory and blood transfusionfacility.
Counsel/arrange for transport
Request to take young adults for blood donation

105
Write appropriate referral note
Give proper address of health facility and guide for shortest route toreach there.
If possible, accompany the woman.
3. Management of placenta previa:
As a Medical Officer, your management should include
Assess the amount of bleeding
Assess circulatory system
Restore blood volume by infusing IV fluids (normal saline or Ringer’slactate).
Cover her with clothes
Counsel woman herself if in good condition and family members forquick decision of taking her to CHC/FRU,
Arrangement for transport and money.
Convince two or three young adults to accompany for blood donation
Write a referral note
Give proper address of health facility and suggest shortest route andaccompany the woman
In a case of placenta previa, bleeding occurs in bouts. After first bout ofbleeding, when second bout of bleeding will occur is not definite. Due toheavy first bout of bleeding, woman may need blood transfusion. Ifbleeding of first bout or subsequent bouts is heavy, she may needtermination of pregnancy.
Check Your Progress 2
1) What are the varieties of abruptio placentae?
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
2) List the features of abruptio placentae which distinguish it fromplacenta praevia.
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
106
3) What are the two basic principles in management of abruptioplacentae?
.................................................................................................................
.................................................................................................................
.................................................................................................................
4) What is couvelair uterus?
.................................................................................................................
.................................................................................................................
.................................................................................................................
5) In which condition of abruptio placentae is vaginal delivery indicated’?
.................................................................................................................
.................................................................................................................
.................................................................................................................
8.3 LET US SUM UP
Reading this unit will make you realise how you could prevent the seriouscomplication of eclampsia by diagnosing preeclampsia early and managingthe patient properly.
Placenta praevia accounts for one-third cases of A.P.H. and occurs inabout one in two hundred delivery. Bleeding in placenta praevia ispainless, causeless and recurrent. General condition of the patientcorresponds to the amount of blood loss, Uterus is soft, non-tender,presenting part may be high up, malpresentations are common.Diagnosis is confirmed by ultrasound or vaginal examination in theoperation theatre prior to termination of pregnancy. Expectant treatmentis given if bleeding is slight or it stops, pregnancy is less than 38week foetus is live and there are no congenital malformations.Termination of pregnancy is indicated if bleeding is excessive andcontinues, pregnancy is more than 38 weeks, foetus dead ormalformed.
Vaginal delivery is allowed in placenta praevia type I and II anterior.Caesarean section is done in type II posterior, type III and type IVplacenta praevia or if bleeding is excessive if there are associatedindications for caesarean sections. Maternal complications areantepartum, intra partum and postpartum haemorrhage, shock, retainedplacenta and puepereal sepsis. Perinatal mortality ranges from 10-25% andis due to prematurity, asphyxia, birth injury, haemorrhage and congenitalmalformations.
Abruptio placentae is the separation of normally situated placenta andoccurs in about I % of deliveries. Bleeding in abruptio placentae isassociated with pain. Uterus is tense andtender, foetal parts are noteasily made out and foetal heart may be absent. In concealed variety of

107
abruptio placentae, there is no external bleeding but patient may be inshock with all the other signs of abruptio placentae. Severe haemorrhage,shock, coagulation failure and renal failure may be present in severe cases.Prompt and adequate administration of fluid and blood, early delivery withcareful monitoring of vital signs, urinary output and coagulation profile arelifesaving. Vaginal, delivery is preferred with careful foetal monitoring inmild cases with relaxed, uterus and in cases with dead foetus. Longuneffaced cervix is not an indication for doing caesarean section. In mostcases of abruptio placentae, cervix dilates rapidly after amniotomy andoxytocin induction. Caesarean section is indicated where immediate deliveryis not imminent, foetus is alive, uterus is hard and in cases with associatedconditions requiring caesarean section. Coagulation disorder, if present, mustbe corrected before surgical procedure. Maternal mortality ranges from 0.5-5% and foetal mortality from 50 to 80%.
8.4 KEY WORDS
Amniotomy : Rupture of membranes
ARM : Artificial Rupture of Membranes
Succinturate Lobe : Lobe of placenta away from the placentalmargin with communicating blood vessels.
Velamentous placenta : The cord is attached to the membranes andvessels traverse in the membranes beforeentering the placenta.
8.5 ANSWERS TO CHECK YOUR PROGRESS
Check Your Progress 1
1) The diagnostic features of placenta praevia are:
i) Bleeding is painless, causeless and recurrent.
ii) Uterus is relaxed and non tender.
iii) Foetal parts are easily palpable.
iv) Presenting part is high up and malpresentation may bepresent.
v) On ultra sound, placenta is located in the lower uterinesegment
2) Vaginal examination is contraindicated in:
i) Patients in exsanginated state.
ii) Diagnosed cases of major degrees of placenta praevia.
iii) Associated complicating factors which are self indications forcaesarean section-example-contracted pelvis.
3) Principles of management of placenta praevia are:
i) All patients must be hospitalised.
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
108
ii) No vaginal examinations to be done till facilities of caesareansection and anaesthesia are available in O T.
4) In following conditions of placenta praevia expectant managementshould not be given
i) In cases who are admitted with severe bleeding.
ii) In cases where bleeding recurs or continues with expectantmanagement.
iii) In cases who reach 38 weeks of pregnancy with expectantmanagment.
iv) Where on admission pregnancy is more than 38 week
v) In patients who are in labour
vi) Where foetus is dead or congenitally malformed.
5) Postpartum haemorrhage is more likely to occur in cases ofplacenta praevia because :
i) Placental site is in lower uterine segment which doesefficiently as the upper segment.
ii) Placenta is larger and thinner and may not separatecompletely
iii) Placental site is larger.
iv) There may be morbid adhesions of placenta.
Check Your Progress 2
I) There are two varieties of abruptio placentae:
i) Concealed
ii) Revealed
2) Abruptio placentae can be distinguished from placenta praevia byfollowing features :
i) Bleeding is associated with pain.
ii) Uterus is tense and tender.
iii) Foetal heart is usually absent.
iv) On ultrasound placenta is not low.
3) Two principles in management of abruptio placentae are:
i) To correct hypovolaemia with fluids and blood transfusion.
ii) To deliver the patient, preferably, by vaginal route.
4) What is Couvelair uterus (utero placental apoplexy )?
In the more severe form of placental abruption, widespreadextravasation of blood occurs into the uterine musculature and

109
beneath the serosa giving uterus which appears ecchymotic, purplishand hard and can be seen only on laparotomy. These myometrialhaematomas donot interfere with and donot warrant hysterectomy.
5) Vaginal delivery in abruptio placenta is indicated in :
i) Mild abruptio placentae where uterus is relaxed, but closematernal and foetal monitoring is required.
ii) When placental separation is mild to extensive but the foetus isdead
8.6 FURTHER READINGS
Arias, Fernando (1993).Practical Guide to High Risk Pregnancy andDelivery, Mosby year book, 09: 162-182.
Chamberlain, Geoffrey (ed.) Turnbull’s Obstetrics, 2nd edition,Churchill Livingstone.
Cunningham (1993).Williams Obstetrics, Appleton & Lange, 37:819-851
Donald, Ian (1994). Practical Obstetrics Problems, B.I. Publications(P) Ltd., 15:420-480
Complications in LatePregnancy II: Haemorrhage

Abnormal Pregnancy
110
UNIT 9 COMPLICATIONS IN LATEPREGNANCY-III: PROM,PRETERM LABOUR,POSTMATURITY ANDHYDRAMNIOUS
Structure
9.0 Objectives
9.1 Introduction
9.2 Premature Rupture of Membranes9.2.1 Aetiology
9.2.2 Diagnosis
9.2.3 Complication
9.2:4 Management
9.2:5 Role of PHC doctor in PROM
9.3 Preterm Labour9.3.1 Definition
9.3.2 Aetiology
9.3.3 Diagnosis
9.3.4 Investigation
9.3.5 Management
9.3.6 Recent Advances
9.3:7 Role and Responsibilities of PHC Doctor in a case of Preterm Labour.
9.4 Postmaturity9.4.1 Definition
9.4.2 Aetiology
9.4.3 Management
9.5 Disorders of Amniotic Fluid Volume9.5.1 Hydramnios
9.5.2 Oligohydramnios
9.6 Let Us Sum Up
9.7 Key Words
9.8 Answers to Check Your Progress
9.9 Further Readings
9.0 OBJECTIVES
After going through the contents of this unit, you will be able to:
diagnose a case of premature rupture of membranes (PROM) anddecide the type of management in each;
enumerate and diagnose complications due to PROM;
diagnose and manage a case of preterm labour;
institute measures for prevention of PTL;
diagnose post term pregnancy and identify the etiological factors;

111
make a decision as to when and how to terminate the pregnancy;
diagnose polyhydramnios; and
enumerate causes and complications of polyhydramnios.
9.1 INTRODUCTION
In the previous unit, you have read about preeclampsia, eclampsia andAPH. Another common problem encountered is premature labour withor without rupture of membrane. As delivery of a term baby ensuresbetter child survival, you as a doctor should be able to prevent andmanage a case of preterm labour.
Post maturity may be another problem, if not managed in time, mayresult in fetal death or severely asphyxiated baby. So this unit dealswith problems of maturity and their management. Amniotic fluidvolume abnormalities polyhydramnios and oligohydramnios areassociated with congenital malformations of fetus and may result inadverse pregnancy outcome and complications.
9.2 PREMATURE RUPTURE OF MEMBRANES
Premature rupture of membranes (PROM) is a common complicationin the third trimester of pregnancy. It is defined as spontaneousrupture of amniotic membranes before onset of labour. In the normalcourse of events, membranes rupture during labour or just beforeonset of labour pains.
You must be aware that under normal circumstances fetal membranesrupture during the active phase of labour. Whenever you come acrossa patient who complains of watery discharge per vagina before theonset of labour, in all likely hood, you are dealing with a case ofPROM.
PROM complicates about 10% of all cases and very often you maynot be able to find any cause. Following rupture of membranes ifdelivery occurs within 12 hours, the risk of infection to mother andfetus are minimal. In those cases where delivery does not occur for12 hours or more, bacteria which are normally present in the vaginastart ascending up to cause infections in the mother and the fetus. Inthose cases, where pregnancy has reached about 34 weeks or moreone would like to induce labour to prevent infection. Clinical problemarises when pregnancy is 34 weeks or less where induction of labourresults in a premature baby associated with the risk of respiratorydistress syndrome and other complications.
You must appreciate the fact that PROM is responsible for 30% ofcases of preterm labour. The functions of amnitoic fluid are:
a) Protective medium from external trauma
b) Media for excretion and deglutination
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
112
c) Permits fetal movement and fetal growth
d) Prevents cord compression
9.2.1 Aetiology
PROM may occur without any apparent cause. However factors thatreduce the tensile strength of fetal membranes have been implicated.
i) Apparent causes
a) Over distention of uterus (twins, polyhydramnios)
b) Cervical incompetence
c) Uterine anomalies
d) External cephalic version
e) Direct trauma to the uterus
f) Infection( chorioamnionitis, urinary tract infection, vaginalinfection)
g) Stress
ii) Inapparent Causes
At this point, it isimportant to note that in more than halfnumber of cases, no obvious cause can be found. In these casesinfection of amniotic membranes has been implicated.
Bacteria which are normally present in vagina and otherpathogenic bacteria can cause ascending infection, if pH of vaginachanges or cervical os is dilated. In some studies, it has beenfound that infection of membranes weakens them and predisposesto premature rupture.
9.2.2 Diagnosis
It is extremely important for you to recognise the presence of PROM.In most cases, it is quite easy especially when you find on speculumexamination amniotic fluid coming through cervical canal. At thisstage you can look for signs of vaginitis and cervicitis. Inspection ofsanitary pad used by the patient appears wet and odourless. There willbe situations where the diagnosis is not clear and could be due tostress incontinence or vaginal infection. It is essential in such cases toproceed with the following laboratory investigations.
a) Nitrazene Test
Normally vaginal secretions are acidic whereas amniotic fluid isslightly alkaline. Checking pH of fluid with a litmus paper mayhelp in differentiating vaginal secretions from amniotic fluid.Nitrazine paper turns from yellow to blue at pH> 6. (Normal pHof vagina during pregnancy 4.5 to 5.5)

113
b) Fern Test
A drop of fluid can be put on a slide, dried and seen undermicroscope for ferning pattern. Amniotic fluid will show a fernpattern whereas vaginal secretions will not show such a pattern
9.2.3 Complications
Once there is suspicion of PROM you must know the complicationsthat may ensue.
a) Intrauterine infection
After rupture of membranes, bacteria which are normally presentin vagina ascend up and cause infection of amniotic membranes,fetus and even uterine wall. Bacteria responsible for infection aregroup B Streptococcus, peptostreptococcus, E.coli, fusibacterium.Like in any other infections, investigations like total leucocytecount and cultures should be carried out.
b) Preterm labour
After rupture of membranes, majority of patients go into labour.Approximately 50-60% with in the first 12-24 hours and as manyas 80-90% deliver with in 7 days. If at the time of birth,maturity of the baby is less than 34 weeks, a number ofproblems can develop in such babies, most important beinghyaline membrane disease. In such cases glucocorticoids like inj.Dexamethasone or inj. Betamethasone 12 mg intramuscularly 2doses in 12 hours apart is indicated to accelerate the lungmaturity.
c) Cord prolapse
Occasionally one loop of umbilical cord may prolapse at the timeof PROM which can cause fetal death if not detected. WhenPROM occurs with the fetal parts not fitting into pelvis, chancesof cord prolapse are high. You must make it a point to look fora loop of umbilical cord and when detected the condition callsfor immediate delivery of the baby.
d) Abruptio placentae
This complication can occur following PROM, especially if thepregnancy is complicated by polyhydramnios. Leakage of amnioticfluid leads to decrease in uterine size. This results in decrease insurface area of placental attachment. As a result, some bloodvessels get open and there is formation of retroplacentalhaematoma.
9.2.4 Management
Let us now proceed to the management of a case of PROM. Themanagement depends on gestational age, any evidence ofchorioamnionities, neonatal intensive care facility, if delivery occursand patient in labor or not.
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
114
In a given case of PROM we have two models of treatment namely:
Conservative management
Termination of pregnancy
a) Conservative Management
You must appreciate the fact that conservative line of management willprolong the pregnancy. Your aim should be to attempt to achieve a periodof gestation of about 35 -36 weeks, keeping in mind of course the riskof infection. When PROM occurs before 34 weeks of gestation, this lineof management is indicated. The conservative treatment consists of :
i) Bed rest
ii) Use of sterile vulval pads
iii) Antibiotics: Ampicillin. Cephalaxin. Garamycin or Erythromycin ispreferred. Antibiotics may be changed as required.
iv) Tests to detect infections of amniotic fluid : Total leucocytecount, cervical swab culture and sensitivity. In recent yearsultrasound is being used to asses the liquor volume periodically.
v) Injection Betamethazone 12 mg. IM, and repeat the dose after 12hours to increase the lung maturity. If pregnancy is continuedsafely, repeat the dose after one week.
vi) Amnioinfusion: At tertiary level, amnioinfusion has beenperformed in order to prevent cord compression; solutions such asRinger lactate or normal saline are infused into the amnioticcavity either transabdominally or transcervically. Repeatedinfusions may be needed at weekly interval till delivery.
b) Termination of Pregnancy
You must consider termination of pregnancy in the followingsituations as there will be no purpose served by continuing pregnancyeither from maternal or fetal point of view.
i) Pregnancy 34 weeks or more duration. The gestation at which,pregnancy to be terminated depends on profile of patient andlocal neonatal intensive care facility.
ii) Those already in labour: Cervix 75% or more effaced, more than3 cm dilated as these patients are unlikely to respond toconservative management.
iii) Those with signs of intrauterine infection: Fever (37.8 degreeCentigrade), maternal tachycardia, fetal tachycardia (>180/min),foul smelling vaginal discharge or uterine tenderness or significantleucocytosis in the mother.
iv) Those with intrauterine fetal death or severe congenitalmalformation incompatible with life.
115
9.2.5 Role of PHC doctor in patients of PROM
You must consider a case of PROM for specialized care whenever youfind PROM before 34 weeks of gestation. You should do
1. Rapid Initial Assessment for
i) Accuracy for duration of pregnancy. You should ask about woman’slast menstrual period. Clinical examination of abdomen will also helpyou to estimate duration of pregnancy.
ii) Presence of rupture of membrane and it’s duration.
iii) Development of any complication due to rupture of membrane fromhistory and examination.
When a woman approaches you with pregnancy (without painful uterinecontractions), and watery discharge per vagina, you should confirmdiagnosis of PROM. Use a high-level disinfected speculum to assess vaginaldischarge (amount, colour, and odour) and exclude urinaryincontinence. Thetypical odour of amniotic fluid confirms the diagnosis. If you have nospeculum, you should look at her pad/cloth kept at perineum.
If rupture of membrane is not recent or when leakage is gradual,confirming the diagnosis may be difficult. In such case,
Place a vaginal pad over the vulva and examine it an hour latervisually and by odour.
Use a high-level disinfected speculum for vaginal examination:(Those who have facility for high level disinfection and perspeculum examination)
Fluid may be seen coming from the cervix or forming a poolin the posterior fornix;
Ask the woman to cough; this may cause a gush of fluid.
Do not perform a digital vaginal examination as it does not helpestablish the diagnosis and can introduce infection.
If available, do tests:
The nitrazine test depends upon the fact that vaginalsecretions and urine are acidic while amniotic fluid isalkaline. Hold a piece of nitrazine paper in an artery forcepsand touch it against the fluid pooled on the speculum blade.A change from yellow to blue indicates alkalinity (presenceof amniotic fluid). Blood and some vaginal infections givefalse positive results;
For the ferning test, spread some fluid on a glass slide andlet it dry. Examine it with a microscope. Amniotic fluidcrystallizes and may leave a fern-leaf pattern. False negativesare frequent (possible at PHC).
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
116
If the woman complains of bleeding in later pregnancy (after 22 weeks),do not do a digital vaginal examination.
Table 1 will help you to arrive at diagnosis as in some cases; womanmay approach with similar complaints in case of discharge due tovaginitis or cervicitis, or at onset of labour. If discharge is bloody,you should also keep in mind, abruption of placenta.
Table 9.1: Diagnosis of vaginal discharge
Presenting Symptom and Symptoms and Signs ProbableOther Symptoms and Sometimes Present DiagnosisSigns Typically Present
Watery vaginal Sudden gush or Prelabourdischarge intermittent leaking rupture of
of fluid membranes Fluid seen at introitus
Foul-smelling vaginal Itching Vaginitis/discharge No history of loss cervicitisx
of fluid
Frothy/curdish discharge
Dysuria
Blood-stained mucus Cervical dilatation and Possible termof watery vaginal effacement labour, Possibledischarge (show) Painful uterine preterm
Contractions labour
Bloody vaginal Abdominal pain Antepartumdischarge Loss of fetal haemorrhage
movements
Excessive vaginalbleeding
X - Determine cause and treat accordingly.
Diagnosis of Complications of PROM:
Amnionitis:
One of the commonest complications of PROM is infection ofamniotic fluid. It is known as amnionitis. When delivery does notoccur within 12 hours after PROM, bacteria normally present invagina, start ascending up to cause infection of amniotic fluid.Amnionitis is dangerous for mother as well fetus. It can lead to intrauterine death. If live fetus is born, fetus can develop respiratorydistress syndrome, pneumonitis. Table 2 will help you with signs,symptoms and probable diagnosis of amnionitis.

117
Table 9.2: Signs, symptoms and probable diagnosis of amnionitis
Presenting Symptom and Symptoms and Signs ProbableOther Symptoms and Sometimes Present DiagnosisSigns Typically Present
Foul-smelling watery History of loss of fluid Amnionitisvaginal discharge after Tender uterus22 weeks Rapid fetal heart rate
Fever/chills Lighta vaginal bleeding Abdominal pain
a Light bleeding: takes longer than 5 minutes for a clean pad orcloth to be soaked.
2. Rapid Initial Management:
1. If there are no signs of infection and the pregnancy is lessthan 37 weeks (when fetal lungs are more likely to beimmature), consider transfer at CHC/FRU for care of thenewborn. Mention about name of antibiotic, dose, route ofadministration and time of administration.
At this time of pregnancy, fetal lungs are immature, and as thereis possibility of delivery, to improve fetal lung maturity, if youhave with you, give corticosteroids to the mother to improve fetallung maturity:
a. betamethasone 12 mg IM, two doses 12 hours apart; or
b. dexamethasone 6 mg IM, four doses 6 hours apart.
Mention about dose, route and time of administration ofcorticosteroids given by you in referral note. Corticosteroidsshould not be used in the presence of frank infection.
2. If there are no signs of infection and the pregnancy is 37weeks or more:
If the membranes have been ruptured for more than 18hours, give prophylactic antibiotics, in order to help reduceGroup B streptococcus infection in the neonate. Antibiotics ofchoice are ampicillin 2 g IV every 6 hours, until delivery. If youdo not have facility for intravenous antibiotics, give oralantibiotics.
If delivery is not likely to occur immediately i.e. if the cervix isunfavourable (firm, thick, closed),transfer woman to near by CHC/FRU with proper referral note.
If delivery is likely to occur, i.e. if the cervix is favourable (soft,thin, partly dilated), conduct the delivery. If there are no signs ofinfection after delivery, discontinue antibiotics.
If there is vaginal bleeding with intermittent or constant abdominalpain, suspect abruption placentae. Transfer woman to CHC/FRU
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
118
If there are signs of infection (fever, foul-smelling vaginal discharge), giveantibiotics as for amnionitis and transfer her to CHC/FRU.
If there are palpable contractions and blood-stained mucus discharge,suspect preterm labour. If delivery is not likely to occur immediately,transfer woman to CHC/FRU. If delivery is imminent, conduct the deliveryand refer both mother and baby to CHC/FRU for care of baby.
If you suspect amnionitis, give combination of antibiotic, ampicillin 2 g IVevery 6 hours; PLUS gentamicin 5mg/kg body weight IV every 24 hours.Transfer to CHC/FRU with referral note.
Check Your Progress 1
1) Define PROM.
.................................................................................................................
.................................................................................................................
.................................................................................................................
2) Enumerate three clinical conditions that are associated with PROM?
.................................................................................................................
.................................................................................................................
.................................................................................................................
3) Enumerate three complications that occur in premature rupture ofmembranes.
.................................................................................................................
.................................................................................................................
.................................................................................................................
4) What are the antibiotics of choice in PROM?
.................................................................................................................
.................................................................................................................
.................................................................................................................
9.3 PRETERM LABOUR (PTL)
9.3.1 Definition
It is important for you to appreciate that preterm labour is a veryimportant clinical problem, responsible for 50-75% of all the newborndying within 7 days after birth. PTL accounts for 75% of alladmissions to neonatal nursery. These babies need specialised neonatalcare which is extremely costly and difficult. Many of the survivorsmay have long term sequelae.
Preterm labour (PTL) is defined as onset of labour before 37 weeks of

119
gestation. Ten per cent of all pregnancies are complicated by PTL. It maybe higher among poor socio- economic strata especially in women of lessthan 17 years or more than 35 years of age.
9.3.2 Aetiology
It is useful for us to categorise causes of PTL into maternal, fetal andplacental causes.
Maternal causes
a) Hypertension during pregnancy: When blood pressure is uncontrolled,labour may needs to be induced or patient may spontaneously go intolabour.
b) Renal disease
c) Diabetes mellitus
d) Anaemia
e) Heart disease
t) Cervical incompetence
g) Uterine anomalies: bicornuate, unicornuate etc.
h) Asymptomatic bacteruia or recurrent urinary tract infections
Fetal causes
a) Congenital malformation of fetus
b) Intrauterine death
c) Multiple pregnancy
Placental causes
a) Abruptio placentae
b) Placenta praevia
c) Hydramnios
Let us be aware of the fact that in 30-40% of cases, no obvious causecan be found.
Predisposing Factors
As we proceed, it is interesting to know some of the predisposing factorsin cases of PTL.
a) Age of mother: <17 or >35 years
b) Low socio-economic status
c) Occupation: manual workers, doctors, nurses etc.
d) Smoking and drug addictions
e) Parity: primi or grand multipara
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious
Abnormal Pregnancy
120
f) Previous history of abortion or preterm delivery.
g) Pregnancy following assisted reproductive techniques
9.3.3 Diagnosis
History of labour pains before 37 weeks of gestation should make onesuspect PTL. On examination, regular uterine contractions can be felt,at least one in 10 minutes, (or more frequently, coming every 3-4minutes and lasting for 35-40 seconds). Vaginal exanimation revealscervix to be dialated more than 2 cm and effaced 80% or more. Insome cases, membranes may also be ruptured. In threatened pretermlabour, the uterine contractions are not associated with cervicalchanges. It may be associated with excessive mucous discharge andthe head may have gone into the pelvis.
9.3.4 Investigation
It is important to investigate a case of pretermlabour thoroughly.While investigating, you will try to detect the cause of PTL as far aspossible. The results of investigations will help us to make a decisionas to cases in which medical or surgical intervention is likely to bebeneficial to the patient. However, infection has been implicated incases where no obvious cause has been found. Most of the times, theetiology is multifactorial. Therefore, the complete haemogram , urineculture and vagulal swab culture should be performed. You can detectchorioamnionitis by performing the following tests on amniotic fluidobtained by amniocentesis i.e. Gramstain, bacterial cultures, leucocytecount.The presence of fetal fibronectin, interlukins 6 and 8 and tumornecrosis factor –alpha in cervicovaginal secretions predict pretermlabor.
9.3.5 Management
As you are already aware, a baby born before 34 weeks of gestationis prone tor dangerous neonatal complications. Hence you will agreethat every effort must be made to prevent/ arrest PTL. If pregnancy isalready 36 weeks or more, labour may be allowed to take place.
In order to arrest PTL you must ensure:
a) Admission to hospital
b) Bed rest in lateral position
c) Infusion of I.V. fluids in initial 30 minutes
d) Administration of uterine relaxants (tocolytic agents) i.e. drugsthat reduce uterine contractions.
Tocolytic agents
Short term tocolytic therapy is given to delay delivery for at least 48hours for corticosteroids therapy to mother to enhance fetal lungmaturity and for in utero transfer of the patient to an advancedneonatal intensive care unit.

121
a) Nifedepine
This drug used to treat hypertension is also used to treat PTL. It isgiven initially as 30 mg tablet, orally followed by 10-20 mg 6- 8hourly. When given orally, it does not cause much of hypotension butyou must be on look out for headache which is a common sideeffect of Nifedepine.
b) Magnisium sulfate
It is given as 4 gm IV bolus followed by infusion of 1-2 gm perhour. It requires careful and active monitoring of the patientand awatch is kept on patellar reflex, hourly urine output andrespiratory rate
c) Beta mimetic drugs (isoxuprine, salbutomol, ritodrine etc.)
Isoxuprine is the most commonly used drug in India. It can begiven orally as one tablet (10 mg) four times daily and it canalso be given as intramuscular injections 10 mg intramuscularevery 6th hourly) or as intravenous infusion (40 mg dissolved in500 ml of dextrose or Ringer lactate). Intravenous infusion shouldbe started at 10-15 drops/minute and dose should be increasedonly after checking pulse rate and blood pressure. If pulse ratebecomes more than 120/minute or BP falls below 90/60 mm ofHg, infusion should bestopped or should be made very slow. Ifcare is not taken, isoxuprine drip can cause heart failure,pulmonary edema or even death.
Once the uterine contractions are arrested, I. V drip should bestopped and intramuscular injections started. When there are nouterine contractions for more than 24 hours, oral isoxuprine canbe started.
d) Atosiban
This is a new drug and blocks myometrial oxytocin receptors (oxytocin antagonist). An initial bolus of 6.75 mg followed by IVinfusion 300microgm/minute is given, followed by 100 microgmper minute upto 45 hours.
Contraindications for Tocolysis
You should not use tocolysis in the following situations:
a) Pregnancy> 34 weeks
b) Intrauterine death
c) Malformed uterus
d) PROM
e) Abruptio placentae
t) Cervical dilatation> 4 cms
g) Cervical effacement >80 %
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
122
Role of glucocorticoids
You are aware that Respiratory Distress Syndrome (RDS) is the mostdangerous complication in babies born with PTL. RDS developsbecause of lack of pulmonary surfactants, a factor which preventsalveoli from collapsing during expiration. Normally this appears after34 weeks of gestation. Administration of glucocorticoids to the motherin the form of inj. Dexamethasone or inj. Betamethasone 12 mg I.M.2 doses 12 hours apart helps in acceleration of lung maturity due toincreased production of surfactants in the baby there by reducing thechances of baby developing RDS.
Referral
If after starting treatment, it appears that labour will not stop andbaby born will be premature, it is better to shift such patients to ahospital with facilities for nursery care. In those cases where deliveryis expected before patient reaching large hospital, delivery can beconducted but baby may have to be transferred to referral hospital. Itis always better to deliver a woman with PTL in the hospital wherefacilities for good neonatal care are available.
Intrapartum care
Following points need to be taken care of when you conduct deliveryin a PTL case, so as to reduce injury to fetus.
Episiotomy should be given
Cord clamped after pulsations are stopped
Cover the baby in a warm dry towel immediately after birth toprevent hypothermia.
Caesarean section may be better than vaginal delivery when thepreterm fetus presents as breech
Neonatal Management
You are aware that babies born as premature may develop a numberof problems but most common and serious complication is respiratorydistress syndrome due to lung immaturity. The following are thecomplications of preterm newborn:-
a) Hyaline Membrane Disease (HMD): It leads to RDS which aswe have discussedearlier, can be prevented by administration ofglucocorticoids to mother. Babies with RDS will need ventilatorsupport and surfactant therapy.
b) Hypothermia: Due to lack of subcutaneous fat, these babies maydevelop hypothermia. It can be prevented by using room heaters,drying the baby and covering the baby with a warm towel.Keeping the baby hugged close to mothers chest is another wayof keeping the baby warm.
c) Infections: Premature babies are more prone for infections suchas pneumonia, meningitis, septicemia. Antibiotics are given totreat such infections.

123
d) Feeding: Due to poor suckling reflex, newborn babies may havedifficulty in sucking milk from breast nipple. Often feeding withspoon may have to be tried. Precaution should be taken toprevent regurgitation and aspiration of milk.
e) Jaundice: Premature almost always have jaundice in the firstweek of life. If bilirubin levels are more than 15 mg%,phototherapy and exchange transfusion may be needed. Thesebabies may develop kernicterus if jaundice is not properly treated.
f) Necrotising enterocolitis.
g) Intraventricular haemorrhage.
9.3.6 Recent Advances
For babies born prematurely, artificial surfactant are given bynebulisers. This treatment is very costly and available in only fewcenters. It helps to prevent RDS due to hyaline membrane diseases.
For prevention of preterm labor in high risk women, progesterone canbe given as micronized progesterone 200 mg twice in a day orally orvaginally or injection 17 hydroxy progesterone caproate IM 250 mgonce a week.
9.3.7 Role and Responsibilities of MOs in a Case ofPreterm Labour
Woman having preterm labour needs either
Control of uterine contractions to prevent preterm delivery or
Help for her preterm delivery.
Control of uterine contractions to prevent preterm delivery:
As preterm delivery is dangerous for newborn, if possible, one shouldattempt to arrest preterm labour in selected cases. This can be doneby drugs which control/reduce uterine contractions and keep uterus inrelaxed condition. This management is known as tocolysis. Drugs usedfor this treatment are known as tocolytic agents.
Tocolytic drugs should not be given in cases having:
Cervical dilatation more than 4 cms.
Cervical effacement more than 80 %
Intrauterine death
Pregnancy more than 34 weeks
Abruptio placenta
PROM
The woman having preterm labour and in need of tocolytic drugs,needs to be hospitalized. You should refer such case to CHC/FRU.Woman on tocolytic drug needs monitoring for its side effects.
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
124
Help for her preterm delivery:
One has to help woman for her preterm delivery in cases having:
Cervical dilatation more than 4 cms.
Cervical effacement more than 80 %
Intrauterine death
Pregnancy more than 34 weeks
Abruptio placenta
PROM
OR when tocolytic drugs should not be given e.g.
any fetal anomaly incompatible with survival;
there is amnionitis or pre-eclampsia.
Allow labour to progress if
gestation is more than 34 weeks;
the cervix is more than 3 cm dilated;
there is active bleeding;
the fetus is distressed, dead or has anomaly
As baby born will be premature, it is better to refer woman at CHC/FRU having facilities for care of preterm baby.
If delivery is imminent and you have to conduct preterm delivery,
Give episiotomy to prevent head injury to fetus
Clamp the umbilical cord after stoppage of pulsations This willallow more blood to newborn
Wipe the baby gently and cover in dry, warm cloth to preventhypothermia
Refer woman and baby to CHC/FRU having facility for care ofpreterm newborn.
Check Your Progress 2
1) Define Preterm Labour (PTL).
................................................................................................................
................................................................................................................
................................................................................................................
2) To what extent PTL contributes to perinatal mortality?
................................................................................................................
................................................................................................................
................................................................................................................

125
3) What are the essential investigations you will do in a case of pretermlabour?
................................................................................................................
................................................................................................................
................................................................................................................
................................................................................................................
4) Name the tocolytic agents that you could use in PTL.
................................................................................................................
................................................................................................................
................................................................................................................
................................................................................................................
9.4 POSTMATURITY
In the previous section, you have seen the risks associated with pretermlabour. As pregnancy progresses beyond 40 weeks, it has been found thatthere is a gradual decline in the placental function leading to fetal distressand occasionally fetal death. Therefore, in such cases there is need torecognise fetal jeopardy and terminate the pregnancy.
9.4.1 Definition
Pregnancies which are 42 weeks duration or more are defined as postmature pregnancy You must recall that only 4.5% pregnant womendeliver on their expected date of delivery About 30-40% womendeliver before completion of 40 weeks. Similarly 45-55% womendeliver after their Expected Date of Delivery (EDD). About 2-4% ofpregnancies are post term. It is important to realise the significance ofpost dated pregnancies as the placenta function declines in suchpregnancies resulting in less blood flow to fetus whereas fetarequirement increases due to increasing size. In some cases, whereplacental blood flow not adequate fetus suffers from fetal distress andmay die in uterus. It is difficult to say for how many days after termin a particular pregnant woman the fetus can safely grow inside theuterus. Therefore, whenever a pregnant woman completes 40 weeks,she needs careful monitoring of her pregnancy.
In our country as in some others, many women do not remember thedate of their last menstrual period (LMP) and hence the EDD cannotbe calculated correctly. You may recall in some other instances inwhich it may not be possible to calculate the EDD correctly e.g.irregular cycles, conception during lactational amenorrhoea or wheneverthe woman had been on oral contraceptives. It is mandatory to takethe menstrual history in sufficient detail and also make efforts to gothrough her previous records which may help you to assess the periodof gestation. If you do not care to document the above facts, you arelikely to make a wrong diagnosis of past dates / post term pregnancy.
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
126
9.4.2 Aetiology
You will not find any definite cause for a woman to go post term.
A familial tendency has been recorded in some women; in yet others(50%) there is previous history of post term pregnancies. Someconditions, you will note are particularly associated with prolongedpregnancies. For example, anencephaly, fetal adrenal hypoplasia,absence of fetal pituitary, placental sulphatase deficiency etc. Theseclinical conditions show a common feature i.e. lack of high level ofestrogen seen in normal pregnancy.
In a post term pregnancy, the fetus continues to grow, often to anunusually large size. Besides manifestation due to decline in theplacental function, fetus passes meconium in uterus. Large babies canbe responsible for cephalopelvic disproportion. Shoulder dystocia isclassically associated with a large baby. Subsequently there is theincreased hazard of instrumental delivery and caesarean section.
We have already discussed the complication of fetal distress due touncompromised placental function. Fetus passes meconium in uterusthereby increasing the chances of meconium aspiration syndrome.Beyond 42 weeks, oligohydramnios occurs and can predispose to fetaldistress due to cord compression. Depending on the decrease in bloodflow, fetal growth retardation can set in leading to loss ofsubcutaneous fat.
9.4.3 Management
From the discussion so far you have gathered that even in theabsence of recognisable maternal complications, there remains littledoubt that fetuses who continue their intrauterine existance beyond 42weeks, suffer from serious morbidity and mortality. Unfortunately wecannot make the decision straight away because:
Assessment of gestational age is often inaccurate.
It is difficult to identify precisely the fetus which will developserious morbidity.
Many of the fetuses are healthy even when post term.
Induction of labour may not always be successful.
Caesarean section increases the risk of maternal morbidity
In view of the above, you must have definite plan of managementwhich includes proper fetal surveillance and institute an appropriateintervention. Pregnancy associated with medical or obstetriccomplication should NEVER be allowed to go postterm.
Perinatal morbidity and mortality increases when pregnancy continuesbeyond 41 weeks. Induction of labor is considered at or beyond 41weeks in uncomplicated pregnancies because timely delivery reducesthe chances of stillbirth. Increase fetal surveillance (NST or BPS isdone twice weekly) is maintained during conservative management.

127
Management of postmaturity includes :
i) Fetal surveillance
ii) Induction of labour
iii) Intrapartum care
i) Fetal Surveillance
In fetal surveillance, the following tests as many of them as possible/feasible should be performed.
a) Fetal kick count
Pregnant woman is asked to count movements of fetus for one hourafter lunch and one hour after dinner. Whenever movements reduce by50% or more or there are less than 3 movements per hour, there isrisk to fetus.
Cardiff count to 10
If foetal movements are less than 10 in 12 hour working period, thewoman requires further investigation.
b) Non Stress Test (NST)
Normally after fetal movement, fetal heart rate increases by 15beats/minute and this rise persists for 15 seconds. If there is noincrease in fetal heart rate after movement or increase is lessthan 15 beats, such a fetus may be at risk of fetal distress. Sucha situation may require confirmation by another test. Fetal heartmay be heard with a stethoscope or with an electronic machineor with doppler.
c) Biophysical Profile Score (BPS)
This is a fetal assessment score designed by Manning et al. in1980. They combined real time ultrasound and NST to have ascoring system to evaluate fetal well being. This is called theBiophysical Profile Score (BPS) or Manning Score. Variousparameters included in BPS are :
1) NST
2) Fetal Breathing Movements
3) Gross Body Movements (GBM)
4) Fetal Tone
5) Amniotic Fluid Volume
Interpretation of Biophysical Profile
We have familiarized ourselves with component of fetal biophysicalscore. The scoring is made as shown in Table 9.1
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
128
Table 9.3: Components and their Scores of the Biophysical ProfileScored over a 30 minute period
Variable Score = 2 Score = 0
Fetal Breathing At least one FBM FBM of < 30 Sec.Movements (FBM) of > 30 Sec. or no FBM
Fetal Movements 3 or more discrete <3 GBM(GBM) GBM (body/limb
movement)
Fetal Tone At least1 episode of No limb movement orfetal limb/trunk slow extension,extension with return movement of limb inof flexion full extension
Reactivity of fetal 2 or more FHR No or < 2 FHRheart rate ( FHR) acceleration (15 or accelerations or
more beats /min) in acceleration of < 1520 min, each lasting beats/min in 20 min>15 sec associatedwith fetal movement
Qualitative 1 or more pocket of Largest best pocket< 1Amniotic > 1 cmdepth in two cm in twoperpendicularFluid Volume perpendicular planes planes
Such a scoring system gives a guideline which will help you inmanaging pregnancy logically. Manning et al. (1987) tested over19,000 pregnancies using bioprofile interpretations and management isshown in the following Table 9.2.
Table 9.4: Management based on Biophysical Profile Score(BPS)
Biophysical Interpretation RecommendedProfile Score Management
10 Normal fetus, No fetal indication fornonasphyxiated intervention;
Repeat test weeklyexcept in Diabetic patientand postmaturity (Twice
8 Normal fetus, No fetal indication forNormal nonasphyxiated. intervention;Amniotic Repeat testing as per Fluidprotocol
8 Chronic fetal asphyxia DeliverDecreased suspectedAmnioticfluid

129
6 Possible fetal asphyxia If Amniotic fluid volumeabnormal, Deliver
If normal fluid at > 36weeks with favourablecervix, Deliver
If<36 weeks or Lecithin- Repeat test in 24 hoursSphingomyelin< 2/1 orcervix unfavourable,
If repeat test, 6 or less Deliver
If repeat test > 6, observe and repeat as perprotocol
4 Probable fetal asphyxia Repeat testing same day,if biophysical profile scoreis 6 or less, deliver
0 to 2 Almost certain fetal Deliverasphyxia
Protocol for management as per BPS:
A score of 10 is considered normal and its management isconservative. Repeat BPS is done after 3 days or 1 weekdependingupon high risk factors present in pregnancy.A score of 8 is managedsimilarly except if liquor is less or it is a post date pregnancy. Ascore of 6 is considered equivocal and BPS should be repeated in 24hours and if persists, the patient should be evaluated for delivery. Ascore of 4 or less is abnormal and immediate delivery is plannedunless the fetus is grossly immature.
d) Amniotic Fluid Index (AFI)
Amniotic fluid is measured with the four quadrant technique i.e.measuring the largest part of fluid found in each of the fourquadrants of uterus. The measurements are added. The result is theAFI. The fluid is decreased if the AFI is less than 8cms andmarkedly decreased if less than 5 cms.
ii) Induction of Labour
Before induction, it is necessary for you to do a per vaginalexamination to assess the favourability of the cervix. A firm, long,uneffaced cervix with a closed os is unlikely to respond to inductionof labour. In such cases cervix is made favourable by instillingprostaglandin( dinoprostone) gel into the cervix or dinoprostonevaginal pessary or by giving oxytocin drip. If cervix is favourable(soft, effaced, dialated),labour can be induced by artificial rupture ofmembrane followed by the syntocinon drip. ARM reveals the amountand the colour of the liquor and presence of meconium. If it ismeconeum stained, C.S. is indicated.
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
130
iii) Intrapartum Care
Once labour sets in, it should be monitored very carefully. Uterinecontractions and fetal heart should be monitored every 30 minutes asfetal distress and incoordinate uterine actions are more common in thethese pregnancies.
At the time of delivery, if meconium is present, suction of nose andmouth should be done immediately after the delivery of the head butbefore the delivery of trunk.
If during labour, fetal heart becomes slow or meconium is noted andthere, is no chance of delivery within few hours, caesarean section iswarranted. As you know that the babies tend to be larger and chancesof shoulder dystocia are high, it should be managed by using amanure to depress the anterior shoulder.
Check Your Progress 3
1) Define postmature pregnancy.
...............................................................................................................
...............................................................................................................
...............................................................................................................
2) Name three complications of post mature pregnancy.
...............................................................................................................
...............................................................................................................
...............................................................................................................
3) ................................% of pregnant women deliver after 40 weeksof gestation.
...............................................................................................................
...............................................................................................................
...............................................................................................................
4) What are the advantages of induction of labour by ARM in postmature pregnancy?
...............................................................................................................
...............................................................................................................
...............................................................................................................
9.5 DISORDERS OF AMNIOTIC FLUID
You may be aware that amniotic fluid increases in volume to onelitre till 37 weeks and thereafter there is a gradual decrease to about800 ml at 40 weeks. In post mature pregnancines, it is furtherreduced.

131
9.5.1 Hydramnios
When the amniotic fluid is 1500 ml or more, it is known as hydramniosor polyhydramnios. Presence of excessive liquor is diagnosed on USGwhere routine ultrasound testing is done.
a) Causes of Hydamnios
i) Foetal
Foetal abnormalities
Open neural tube defects - anencephaly, spina bifida,meningomyelocele, encephalocele, oesophageal atresia. Others areomphalocele, polycystic kidneys etc.
Monozygotic twins
Hydropsfoetalis
Chorioangioma of placenta
ii) Maternal
Diabetes mellitus
Severe eclampsia
Severe heart disease
iii) Idiopathic
b) Types of Hydramnios and Clinical Features
i) Acute
Hydramnios develops quickly usually around 24-30 weeks. Acuteabdominal pain, a feeling of abdomen about to burnt are thesymptoms. There may be associated vomiting.
Abdominal skin is glazed, abdominal wall oedema may be present ,fresh striae are seen. Uterus is tense and tender and may be mistakenfor accidental haemorrhage. Shock is absent in acute hydramnios.
ii) Chronic
Development of hydramnios is gradual and in the last trimester. Thesymptoms are due to the bulk and weight of uterus. The woman hasdyspnoea, discomfort, oedema feet, increase in haemorrhoids andvaricose veins, There may be abdominal pain. The symptoms dependon amount of fluid. On examination, you find the size of the uterusmore than the period of amenorrhoea, foetal parts are not identifiedeasily, foetus is balloted, fluid thrill is present, FHS may not beheard or heard distantly and faintly.
c) Differential Diagnosis
Any condition causing size of uterus greater than the period ofamenorrhoea forms the differential diagnosis such as:
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
132
Twins
Ovarian cyst
Hydatidiform mole
Full bladder
d) Complications
Preterm labour
Malpresentation, unstable lie
Premature rupture of membranes
Cord prolapse
Abruptio placentae
Uterine inertia
PPH
Increased perinantal morality
e) Management
Ultrasonography is useful to diagnose foetal abnormalities. AFI more than25 cm or single largest pocket of amniotic fluid (echo free) should bemore than 8 cm to confirm diagnosis of polyhydramnios. It also confirmsthe multiple pregnancy and helps in distinguishing differential diagnosis.ABO and Rh grouping is required because Rhesus isoimmunisation maycause hydropsfetalis. Glucose tolerance test is done for the diagnosis ofgestational diabetes mellitus must be excluded. Hydramnios should bemanaged in a FRU (CHC) District Hospital.
For acute hydramnios, the patient is given Fowler’s position and oxygeninhalation. Abdominal amniocentesis with very slow drainage of liquor isdone to relieve respiratory embarrasement. If patient goes in labour,controlled artificial rupture of membranes is done, if the lie is longitudinalwith cephalic presentation. The amniotic fluid is drained slowly so as toprevent premature separation of placenta and cord prolapse.
9.5.2 Oligohydramnios
Oligoydramnios is the condition when there is abnormal decrease in thevolume of amnioticfluid. At term, it may be 300-500 ml. If diagnosedduring first half of pregnancy, renal agenesis or potters syndrome (foetalpulmonary hypoplasia) has to be excluded. If diagnosed before 37 weeks,it may be because of foetal abnormality, preterm premature rupture ofmembranes, intrautrine growth retardation and postmaturity.
Diagnosis is made when uterus size is smaller than the expected period ofgestation, foetus is felt easily, foetus is small and head feels more maturefor the size of foetus (unlike preterm foetus). USG will confirm thediagnosis.
Foetus may be affected by oligohydraminos. Foetal skin is dry, leathery,face may look pinched with flattening of nose, micrognathia, talipes or

133
tortocoliis because of placental insufficiency and IUGR, meconium stainedliquor and meconium aspiration may occur.
Management is to refer such women to referral centres for furtherinvestigations and treatment.
Check Your Progress 4
1) List common causes of hydramnios.
...............................................................................................................
...............................................................................................................
2) Acute hydramnios is to be differentiatedfrom ...................................
3) Enumerate four complications of hydramnios.
...............................................................................................................
...............................................................................................................
9.6 LET US SUM UP
We have learnt that 10% of all pregnancies end before 37 weeks ofgestation and a number of maternal and fetal causes can cause PTL.Sometimes no cause can be fond. If pregnancy is < 34 weeks,attempt should be made to stop labour contractions by giving drugssuch as duvadilan or nifedepine. In those cases where contractions donot stop, glucocorticoid should be administered to the mother withaim of accelerating fetal lung maturity. As far as possible, delivery ofpremature baby should occur in a place where newborn nursery isvailable. Babies born prematurely can have a number of problems likehyaline membrane diseases, hypothermia, infections etc. prematurebaby.
In pregnancies of more than 34 weeks duration at the time ofdiagnosis of PROM, termination of pregnancy is indicated. In thosecases where pregnancy is less than 34 weeks duration, conservativemanagement should be considered. Conservative management aims atcontinuation of pregnancy till 35 weeks so as to avoid risks ofprematurity. Conservative treatment comprises of bed rest, use ofantibiotics and detection of infection at an early stage. However, inmajority of cases patients deliver within first 7 days after onset ofPROM. It is better to transfer the fetus in utero rather than afterdelivery as the fetal salvage is much better.
If a pregnancy goes beyond 40 weeks, fetuses are at a risk of fetaldistress and intrauterine death. Whenever any test indicates fetaldistress, labour should be induced. During labour, fetal heart rateshould be counted carefully every half hourly. If meconium is notedat the time of delivery, suction of nose and mouthof the baby shouldbe done to prevent meconium aspiration.
In the disorders of amniotic fluid section, causes of hydraminios andoligohydramnios have been discussed so that timely referral could preventthe complications.
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious
Abnormal Pregnancy
134
9.7 KEY WORDS
Amniocentesis : Puncture of amniotic sac to obtain amniotic fluid
ARM : Artificial Rupture of Membrane
BPS : Biophysical Profile Score
EDD : Expected Date of Delivery
Kick Count : Counting fetal movement perceived by mother
NST : Non stress test of fetal well being
Perinatal : Pertaining to period from 28 weeks of gestation tillone week after delivery
PTL : Preterm Labour
SGA : Small for gestational age infant
9.8 ANSWERS TO CHECK YOUR PROGRESS
Check Your Progress 1
1) Spontaneous rupture of membrane before onset of labour.
2) — Over distention of uterus
— Cervical incompetence
— Ascending lnfection from vagina
3) — Preterm labour
— Cord prolapse
— intrauterine infection
4) Ampicillin, Cephalexin, Garamycin, Erythromycin. Anyone of the fourcould be used.
Check Your Progress 2
1) Labour before 37 completed weeks of gestation.
2) 50-75% of new born dying within 7 days after birth are due to PTL.
3) Complete Haemogram, Urine culture, Vaginal swab culture.
4) Beta mimetic, Nifedepin, Indomethacin
Check Your Progress 3
1) Pregnancy of 42 completed weeks duration or more.
2) — Fetal distress
— Cephalo Pelvic Disproportion
— Meconium Aspiration Syndrome

135
3) 45-55% women
4} To note meconium stain of liquor and the quantity of liquor
Check Your Progress 4
1) a) Foetal abnormalitities (open neural tube defects)
b) Monozygotic twins
c) Hydropsfoetalis
d) Diabetes Mellitus
2) accidental haemorrhage.
3) Any four from :
a) Preterm labour
b) Malpresentation
c) abruption placenae
d) PPH
e) Uterine inertia
f) Cord prolapse
g) Unstable lie
9.9 FURTHER READINGS
Arias, F., Practical Guide to High Risk Pregnancy. and Delivery. 2ndEdition, St. Louis, Mosby Year Book, 1993.
Cunningham, G., Williams Obstetrics. 19th Edition, Connecticut,Prentice Hall International, 1993.
Complications in LatePregnancy-III:PROM,
Preterm Labour,Postmaturity and
Hydramnious

Abnormal Pregnancy
136
UNIT 10 COMPLICATIONS IN LATEPREGNANCY-IV: RHINCOMPATIBILITY,INTRAUTERINEINFECTION
Structure
10.0 Objectives
10.1 Introduction
10.2 Rh-incompatibility
10.2.1 Classification of Rhesus Factors and Isoimmunization
10.2.2 Pathological Changes in Haemolytic Disease of Newborn
10.2.3 Management of Rh-ve Non-immunized Pregnancy Women
10.3 Maternal Infection Affecting Fetus and Neonate
10.3.1 Viral Infection
10.3.2 Protozoal Infection
10.3.3 Bacterial Infection
10.4 Let Us Sum Up
10.5 Key Words
10.6 Answers to Check Your Progress
10.7 Further Readings
10.0 OBJECTIVES
After reading this unit, you should be able to:
describe the importance of blood grouping and Rh tying duringpregnancy;
provide immuoprophylexis against Rh-isoimmunization;
enumerate the organism causing intrauterine infection with the sequel;and
manage appropriately pregnancy and labour in women with intrauterineinfections.
10.1 INTRODUCTION
This unit deals with miscellaneous topics on Rh incompatibility andcongenital infection during pregnancy. Immunoprophylaxis with “anti D”immunoglobulin has greatly reduced Rh-isoimmunization in pregnant women.In section on intrauterine infection, you will read about various types ofinfection and the resulting complications. Pain in abdomen is a common

137
problem for which pregnant women seek care. In majority of cases, it isdue to pregnancy related or incidental physiological causes and you canmanage them. Life threatening conditions also may present with painabdomen and may be due to obstetric, gynaecological, surgical or medicalcauses. You should be able to diagnose them and refer to FRU/CHC/District Hospital after primary care.
10.2 RH-INCOMPATIBILITY
In this section, you will be reading about presentation of hemolytic diseaseof newborn caused by Rhesus incompatibility. Rhesus incompatibility is thecommonest cause of hemolytic disease. ABO incompatibility can also causehemolytic disease but it is rare.
10.2.1 Classification of Rhesus factor andIsoimmunization
In every individual, Rhesus genes are carried on two chromosomes one ofwhich is passed on to the succeeding generation. There are six mainRhesus genes, three carried in each chromosome. Of the six, 3 aredominant genes and 3 are recessive genes. The 3 dominant genes are C,D and E and the recessive genes are c, d and e. Each chromosome hasa locus for C, D and E which may be occupied by either dominant orrecessive gene of the particular type.
In Rh-incompatibility, the dominant D gene is the most important. Theindividual possessing D gene is one or both chromosome is known asRh+ve. When dominant D gene is absent in both chromosomes, theperson is known as Rh-negative.
When a Rh negative women marry a Rh positive man, the offspring willbe Rh positive if the man is homozygous positive and can either be Rh-negative or Rh positive if he is heterozygous. If the man is also Rhnegative, the offspring will be Rh negative and there will be noincompatibility.
In India, prevalence of Rh D antigen varies from 90 to 95%, lower inSouth India compared to North India. It is important to remember thatCE antigen other than D have low immunogenicity and not very importantexcept on few occasions. Therefore, all the pregnant women should beroutinely screened for D (Rh) antigen on erythrocytes.
Fetomaternal hemorrhage is the transmission of fetal blood cells into thematernal circulation. Some amount of FMH is known to occur in most
pregnancies, usually in small amounts. 90% of the FMH occurs in the
antenatal period and around 10% occurs intrapartum. Most studies have
defined FMH >30mL to be clinically significant.
Oncean Rh negative mother carries a Rh positive fetus, FMH leads to
primary immune response in the mother to the D antigen. This primary
response occurs over 6 weeks to 12 months in the form of IgM antibody
production. These antibodies are unable to cross the placenta. Therefore,
Complications in LatePregnancy-IV : RH
Incompatibility,Intrauterine Infection

Abnormal Pregnancy
138
the first pregnancy is not at much risk. In subsequent pregnancies, when
re-exposure occurs, the secondary response generated is in the form of
IgG antibodies. This response is more rapid and IgG antibodies can cross
the placenta. Theycoat the fetal RBC’s and result in their removal
(hemolysis)by the reticuloendothelial system of the fetus.
Fortunately, erythroblastosis fetalis occurs in very few pregnancies because
of ABO incompatibility between mother and fetus. If the mother and fetus
are ABO incompatible, the fetal red cells are destroyed immediately and
no sensitization for Rh D antigen occurs. If they are ABO compatible, the
fetal red cells persist in maternal circulation and sensitization occurs
resulting in antibody formation.
10.2.2 Pathological Changes in Hemolytic Disease ofthe New Born
We are aware of the basic concept of isoimmunization. But, it is important
to know the pathologic changes in the organ system of the new born in
the hemolytic disease of the new born. In a D-positive fetus, maternal
antibodies (IgG) are both adsorbed to D-positive erythrocytes and exist
unbound in fetal serum. The absorbed antibodies act as haemolysins
leading to an accelerated rate of red cell destruction. Maternal antibodies
detectable in fetal serum at birth gradually disappear from infants circulation
over a period of I to 4 months, to some extent influenced by exchange
transfusion.
a) Immune Hydrops
The hall mark of Rhisoimmunization is hemolysis in fetus leading to
hydrops fetalis or hyperbilirubinemia in neonatal period. The affected fetus
shows severe anemia due to hemolysis leading to hydrops fetalis. Marked
tissue edema will be seen in the affected fetus as well as effusion into the
serous cavities (Hydrops fetalis).
The placenta is markedly enlarged boggy, with prominent cotyledons.
Excessive extra medullary hematopoiesis results in massive
hepatosplenomegaly. Histological examination of liver shows fatty
degenerative parenchymal changes as well as deposition of hemosiderin and
engorgement of hepatic canaliculi with bile. There may be cardiomegaly
and pulmonary haemorrhage. The ascites along with hepatosplenomegaly
may result in severe dystocia. The fetus with hydrops may die in utero
from profound anemia and circulatory failure. The live born hydropic infant
appears pale, edematous and limp at birth; often requiring resuscitation.
Dyspnea and circulatory failure are common.
b) Hyperbilirubinemia
The less severely affected infants appear well at birth and becomes
jaundiced within few hours. The fetus does not develop jaundice in utero
because unconjugated bilirubin resulting from fetal hemolysis freely crosses

139
the placenta and enters maternal circulation where it is disposed by
maternal liver. But at birth, newborn especially premature liver is not
mature enough to metabolize high levels of unconjugated bilirubin resulting
in hyperbilirubinemia. The unconjugated bilirubin crosses the blood brain
barrier and enters central nervous system resulting in degeneration of the
basal ganglia and hippocampus. This complication occurs more often in
premature, hypoxic, acidotic infants. Surviving infants show spasticity,
muscular in co-ordination and varying degree of mental retardation. There
is a positive correlation between serum unconjugated bilirubin and
Kernicterus above 18-20 mg/dl, although Kernicterus can develop at lower
concentrations.
10.2.3 Management of Rh-ve Pregnant Woman
Routine screening of all pregnant women for the blood group and Rh
typing at 1st prenatal visitis of utmost importance. If the woman is Rh
negative, the husband’s blood group with Rh typing should be done. The
chances of Rh isoimmunization depends on Rh blood type of the father. If
the father is Rh negative, there are no chances of Rh isoimmunization. If
the father is Rh positive, the baby has the chance of 50% being Rh
positive (Heterozygous) and 100% being Rh positive (Homozygous).
Now a days, the option of non-invasive prenatal diagnosis (NIPD)can be
used to determine the fetal Rh typing. If the fetus is Rh negative, no
further monitoring for Rh isoimmunization is required. If, however, the fetus
is Rh positive, then the pregnancy needs to be monitored for Rh
isoimmunization. But, still NIPD is a very costly procedure and not
affordable for most women in India.
Once the pregnant Woman is identified as Rh negative, with an Rh +ve
husband, the next step is to screen for anti-Rh antibodies to rule out
sensitization which is done by indirect Coomb’s test (ICT). Indirect
Coomb’s test detects maternal antibodies (i.e., IgG; incomplete antibodies)
by Coomb’s serum, which contains anti IgG immunoglobulin. The IgG
antibodies (Anti Rh antibodies) cannot agglutinate red blood cells
themselves at 37 degree centigrade but they do so in presence of albumin
or Coomb’s serum.
Management of Rh-ve non-immunized pregnancy
Indirect Coomb’s test is done at 1st prenatal visit and if negative repeated
at 20, 24 and 28 weeks of gestation. If any time the indirect Coomb’s
test is positive it is managedas Rh isoimmunized pregnancy. If indirect
Coomb’s test is negative by 28 weeks, anti-D prophylaxis given and
indirect Coomb’s test is discontinued. In cases where excessive feto
maternal haemorrhage is suspected (e.g. abruptio placenta, caesarean
section, manual removal of placenta), Kleihauer-Betke’s test is used toquantify the amount of fetal erythrocytes in maternal circulation and amountof anti D required is calculated. The approach to a Rh negative non-
Complications in LatePregnancy-IV : RH
Incompatibility,Intrauterine Infection

Abnormal Pregnancy
140
immunized pregnant women can be schematically represented as follows:
Negative Management asnormal Pregnancy
Father Antibody Screening Manage as RhRh factor screening at 20, + ve sensitised pregnancy
Positive 24 & 28 weeks Screening Anti D at 28 weeks 2nd- ve dose at delivery
PROPHYLAXIS
The effective maternal prophylaxis against Rh isoimmunization with anti Dwas developed by Finn and associates and Freda and co-workers 1963.Anti D immunoglobulin (lgG) when given to mother, coats the fetalerythrocytes in maternal circulation leading to enhanced destruction of fetalerythrocytes in maternal reticuloendothelial system and prevents exposure ofanti D antigen sites to maternal immune system.
Each dose of anti D contains 300 microgram of anti D which provides
protection for next 12 weeks for 15 ml of fetal erythrocytes (30 ml ofcord blood).
The Rh negative, non sensitized(ICT negative) should be administered 300microgram anti-D at 28 weeks gestation to account for the fetomaternalhemorrhage that takes place in utero.
Immediately post delivery, if the baby born is Rh positive, another 300microgram Anti-D should be given intramuscularly within 72 hours ofdelivery. If the dose could not be given within 72 hours, it should still begiven as beneficial effect has been documented till 28 days after delivery.
Without RhD immune globulin prophylaxis, the risk of alloimmunization withthe first Rh D-positive pregnancy is approximately 16 percent. Routine
antenatal administration of anti D given at 28 weeks along with the seconddose at immediate post partum period (within 72 hours) brings down theRh sensitization to less than 0.07%.
There are certain conditions which increase the chances of feto maternalhemorrhage warranting the need for Anti- D :
Spontaneous abortion
Elective abortion
Threatened abortion
Ectopic pregnancy
Invasive procedures- Amniocentesis, Chorionic villus sampling, Fetalblood sampling
Hydatiform mole
Placenta previa with bleeding
Suspected abruption

141
External cephalic version
Intrauterine fetal demise
Blunt trauma to the abdomen
The dose of Anti-D for all events at less than 12 weeks is 50-100microgram and for more than 12 weeks gestation 300 microgram.
Anti-D prophylaxis may not be protective against Rh isoimmunizationwhen amount of fetal erythrocytes in maternal circulation exceed15mL (fetomaternal haemorrhage exceeds 30 ml). Excessive fetomaternal haemorrhage (as in Abruptio placenta, manual removal ofplacenta, Caesarean section)makes it necessary to quantify the exactamount of fetal erythrocytes in maternal circulation which is done byusing Kleihauer-Betke test (Acid elusion test). The principle behindKleihauer-Betke test is that when treated with acid the maternalhemoglobin will be driven out of maternal erythrocytes, giving them‘ghost’ cell appearance, which does not happen with fetal erythrocytes.Fetal erythrocytes identified by Kleihauer-Betke test can be quantified anddose of anti D can be calculated.
Timing of delivery and management in labour
Pregnancy in non-immunized women is allowed to go to term - forspontaneous labor. They have to be induced if they go beyond 40weeks.
During labor, certain precautions need to be taken:
avoid stripping of membrane
avoid oxytocin(prefer ARM for induction of labor)
no fundal pushing in 1st or 2nd stage of labor
avoid uterine massage or uterine grasp and squeeze in 3rd stage
don’t clamp the cord from maternal side
let the placenta be delivered spontaneously using control cordtraction without squeezing the uterus
no active management of third stage of labor
immediate cord clamping after delivery of baby
avoid manual removal of placenta
protect the vaginal and perineal wounds and laceration from beingexposed to the fetal blood spilled from cord
During caesarean section
Use abdominal packs in the sides of the uterus before opening thelower segment to prevent spilled blood from the placenta to enter theperitoneal cavity.
After delivery, cord is clamped immediately after birth to the fetomaternaltransmission cord. Blood is collected and sent for blood group (ABO,
Complications in LatePregnancy-IV : RH
Incompatibility,Intrauterine Infection

Abnormal Pregnancy
142
Rh), coomb’s test, Hb and serum bilirubin. Anti D (300ug) is givenintramuscularly as early as possible within 72 hours if baby’s blood groupis Rh +ve.
Management of Rh isoimmunized pregnancy
Rh –ve isoimmunised women are to be referred to specialized centres forfurther management, but one should be aware of the management forprognostication and timely referral. This section deals with management ofRh isoimmunized pregnancies in brief.
If at any time during the course of pregnancy, the ICT is reported aspositive, then, ICT titres should be done. If the ICT titre>1:16 (criticaltitre), then it is labelled an Rh isoimmunized pregnancy.ICT titre less thanthe critical titre need to be followed with repeat ICT titres at fortnightlyor monthly intervals. Once they cross the critical titre more intensive carewould be required.
ICT more than the critical titre indicates that there are antibodies in themother’s serum which can cross to the fetal side, coat the fetal RBC’sresulting in their removal by the reticuloendothelial systemThe fetus is likelyto have anemia and further complications like heart failure, hydrops fetalis.
One management option is to get the fetal Rh status by NIPT usingmaternal blood. Only fetuses that are Rh +ve need to be followed for thedevelopment of fetal anemia and its consequences. If this is not possible,then, the fetus should be monitored for fetal anemia with a non-invasivetechnique like MCA-PSV(middle cerebral artery-peak systolic velocity). Ithas been found that as anemia develops in the fetus, the velocity of bloodflow in the middle cerebral artery rises. The increased velocity of blood inthe MCA is due to decreased viscosity of the anemic fetal blood andsecondly, becauseof cerebral autoregulation in anemia. The MCA has beenfound to be easily imaged on ultrasound. Based on studies, there arecharts of variations in MCA-PSV with gestational age. If the MCA-PSVe”1.5 MoM at any gestational age, it indicates moderate-severe fetalanemia. Such women would require cordocentesis for fetal Hb levels andif Hb< 10 gm%, then intrauterine blood transfusion. There are otherfeatures in ultrasound that help in predicting fetal anemia like amniotic fluidvolume, liver and spleen length or thickness, placental thickness, increasedbowel echogenicity and the cardiac biventricular diameter.
Earlier, women with Rh isoimmunized pregnancies had to undergo repeatedamniocentesis for spectrophotometry but with advent of non invasivemonitoring with MCA-PSV, invasive procedures are limited tocordocentessis when MCA-PSV is raised.
Check Your Progress I
1) Who is called an Rh +ve individual?
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................

143
2) Give 4 clinical signs that suggest that suggest hydrops fetalis.
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
3) What is Anti-D ?
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
4) Anti-D must be given to RH negative mother with in............. hour ofdelivery?
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
5) KlehauerBetke test is use for detecting
.................................................................................................................
.................................................................................................................
.................................................................................................................
6) Give three conditions when Anti ‘D’ must be administered to mother?
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
.................................................................................................................
10.3 MATERNAL INFECTION AFFECTINGFETUS AND NEONATE
Intra uterine infection and vertical transmission to fetus (congenital infection)can occur at any time during pregnancy. Severity of infection depends ontheir virulence of the organism, route of infection, gestational age atinfection and susceptibility of fetus. These infections result in increasedperinatal mortality and morbidity and occasionally delayed symptoms andsigns. Infection can be viral, protozoal, bacterial or fungal.
Complications in LatePregnancy-IV : RH
Incompatibility,Intrauterine Infection

Abnormal Pregnancy
144
10.3.1 Viral Infections
You must know that besides the fetus being affected, the pyrexia causedby any viral infection can cause abortion, preterm labor or start term laborpains. Viral infection can cause congenital defects, abortions, preterm births,IUGR, still births, early or late neonatal complications or even latecomplications due to persistence of the virus in various organs. Importantviral infections affecting the fetus is given below:
i) Rubella
ii) Cytomegalovirus (CMV)
iii) Herpes Simplex Virus (HSV)
iv) Human Immunodeficiency Virus (HIV)
v) Varicella Zoster (Chickenpox Virus)
vi) Hepatitis B Virus (HBV)
vii) Human Papilloma Virus (HPV)
1. Rubella
It is an RNA virus. It is transmitted via respiratory droplet exposure.Infection may be silent or clinically evident. The clinical features are facialrash, postauricular lymphadenopathy, flu like symptoms, arthralgia or arthritisof small joints. The incubation period is 2-3 weeks. After an infection, theimmunity acquired is long.
If infection occurs in early pregnancy (<12 weeks), the risk of fetalinfection is very high (80%). The pregnancy may end in abortion or thefetus may be born with congenital rubella syndrome i.e. cataract, deafnessand congenital heart disease. Psychomotor retardation, fetal and neonatalgrowth retardation and hepatosplenomegaly may be present.
Methods for in utero diagnosis include fetal blood sampling formeasurement of rubella-specific IgM, rubella-specific reversetranscriptase polymerase chain reaction (RT-PCR), and virusisolation from amniotic fluid or products of conception.
With maternal infection in first trimester, MTP should be offered. There isno specific therapy for congenital rubella, so treatment is mainly supportive.
MMR vaccination at 9 months age protects the girl child from futureinfection. When not sure of MMR vaccination, school girls in their teensmay be vaccinated routinely against rubella. Those adults who have noantibodies (immunity) may be given vaccination but should avoid pregnancyfor 3 months. If no antibodies are found during pregnancy, the mothershould protect herself from exposure to rubella infection and get vaccinatedin the postpartum period.
2. Cytomegalovirus (CMV)
CMV infection is the commonest intrauterine infection and is an importantinfectious cause of mental retardation and congenital deafness.

145
The transmission of CMV may be from person to person via saliva, bloodand transplanted organ, through sexual transmission and vertical transmissionthrough placenta.Vertical transmission occurs in 30% cases but the fetus issymptomatic in only 10% cases.
Many women are asymptomatic during infection. Symptomatic women maypresent with fatigue, infectious mononucleosis like symptoms – malaise,lymphadenopathy, hepatosplenomegaly
Fetus with congenital CMV infection presents with hepatosplenomagaly,petechiae and purpura, growth restriction and mental retardation. Abnormalneurological findings may be microcephaly, microphthalmia, intracranialcalcifications, late sequel of CMV infection is deafness, mental retardationand visual defects. In recurrent infection, because of protection by maternalantibodies, chances of baby being affected is less and sequel is also lesssevere.
Diagnosis is by detection of specific IgM or a four fold increase in IgGlevels. If the pre pregnancy serological status is not
3. Herpes Simplex Virus (HSV)
It is a DNA virus and like CMV has the ability to persist throughout life,with recurrent infection. HSV-II affect genital tract and HSV Ioropharyngeal areas, due to orogenital contact and contact by fingers tomouth and face. Neonatal infection can occur with both HSV II and I,but infection with HSV II is more common. Adult infection may beasymptomatic or present with genital lesion. The lesions are seen in labiaand other parts of vulva. Shedding of virus occurs between one week and3 months of appearance of lesions.
Fetal or neonatal infection may cause abortion, prematurity or disseminatedHSV infection from intrapartum transmission. Babies with disseminatedinfection usually have symptoms of lethargy, irritability, hypotonia whichappear between 9-11 days. This is followed by seizure, heart failure, liverinvolvement and death.
Acyclovir is the treatment for primary or recurrent infection. It is categoryB drug and can be given during pregnancy safely though data of use infirst trimester is limited. If clinically visible lesions are present at the timeof labor, caesarean delivery is advised. If no lesions are present, vaginaldelivery is allowed.
4. Varicella Zoster (Chickenpox) Virus
It is a DNA virus, once infected, it give life long immunity. When infectionoccurs in a pregnant women, it causes significant maternal and fetalmorbidity and mortality. The fetus is infected through transplacental route.Infection is severe in adults as compared to children. When it affectspregnant mothers, it becomes serious with development of pneumonia,which occurs 2-3 days after cutaneous lesions appear. They may developadult respiratory distress syndrome (ARDs). A rare complication is maternalencephalitis.
Complications in LatePregnancy-IV : RH
Incompatibility,Intrauterine Infection
Abnormal Pregnancy
146
Congenital infection is diagnosed when the symptoms develop before 10th
day after birth or when born with developmental abnormalities such asvaricella embryopathy. Congenital varicella syndrome (CVS) is characterizedby dermatomal scarring; ocular abnormalities such as cataracts,chorioretinitis, and microphthalmia, low birth weight, cortical atrophy, andmental retardation. Most cases occur in infants whose mothers wereinfected between 8 and 20 weeks of gestation.
When mother has infection in later third trimester and new born developvaricella, the infection is severe with pneumonitis, hepatitis and disseminatedintravascular coagulation. It is seen that babies born 5 days or more aftermaternal disease develops are protected and are also those babiesdeveloping neonatal varicella between birth and 5 days of age. Mortality ismore in those babies who develop rash between 5-10 days after birth.After 10 days of birth, neonatal infection that develop is mild.
Women who are exposed to varicella infection can be protected by givingvaricella zoster immunoglobulin (VZIG) in a single dose (IM ng) within 4days of exposure. Varicella appear, watch for complications. Those whodevelop complications are admitted in the hospital and treated withacyclovir. Women with varicella in late 3rd trimester should be monitoredfor preterm labor.
Hepatitis B: You may refer to Block 1, Unit 4, Section on Jaundice.
HIV: Again you may refer to Block 5, Unit 22 on RTI and STJ.
Parvovirus B19: Parvovirus B19 is a DNA virus. It may be
asymptomatic infection or cause arthralgia in adults and may have a role indevelopment of rheumatoid arthritis. It may also cause hemolytic anemia.This virus is important to maternal care providing since infected motherstransmit to fetus causing non immune hydrops fetalis. Fetal loss is higherwhen infection occurs before 20 weeks of gestation.
Human Papilloma Virus
It is sexually transmitted in women. Baby gets the infection during vaginaldelivery while passing through infected birth canal.
In the adults, HPV causes condylomatous lesion over vulva, vagina andcervix. Neonatal infections cause laryngeal papillomas. Maternal infection isdiagnosed by southern blot by hybridization, papsmear and colposcopy.
The aim of treatment is to reduce pain and bleedings, prevent secondaryinfection, prevent excess hemorrhage or obstructed labor from vaginallesions and prevent infection of neonate during delivery. Topicalpodophyllum and 5FU are contra indicated in pregnancy. Application oftrichloroacetic acid, surgical excision, cryosurgery and laser surgery orelectrocautery is the management during pregnancy.
10.3.2 Protozoal Infection
Protozoal infection of mother that can cause congenital infection are
Toxoplasmosis—toxoplasma gondii

147
Malaria—plasmodia
You have already read about malaria in Block 1, Unit 4 hence onlytoxoplasmosis will be dealt in this section.
Toxoplasma
As already mentioned above, it is a protozoal infection. Cat acts as host.Infection may occur from ingestion of new or partly cooked meat, directcontact with contaminated infection may be asymptomatic or produce mildsymptoms, such as fatigue and lymphadenopathy. Congenital transmission ofparasite may occur during acquired acute maternal infection resulting inabortions, still births or congenital toxoplasmosis with characteristic cerebralcalcification, choriorctinitis, hydrocephalus. Infected asymptomatic neonatemay develop mental retardation, visual impairment and other neurologicsequelae late in life.
Acute toxoplasmosis is diagnosed by serological tests. IgM indicates acuteinfection and IgG positivity indicates chronic infection. IgM and IgG levelsare measured in 2 samples, 4 weeks apart for a four fold increase intiters is significant. Another method to differentiate acute and chronicinfection is IgG avidity testing. Higher avidity is seen with long standinginfection.Spiramycin 3g/day should be started after maternal infection isdocumented. If PCR testing of amniotic fluid confirms fetal infection, thenpyrimethamine/sulfadiazine should be added.
10.3.3 Bacterial Infection
You will be reading about 4 bacterial infection in mother affecting the fetusand neonate. They are
l Syphilis
l Gonococci
Chlamydia
Group B streptococci (GBS)
Syphilis
You are already aware that syphilis is caused by a spirochete calledTreponema pallidum. Primary, secondary, latent and tertiary syphilis aredifferent stages of disease progressing from the beginning of infection. It isa sexually transmitted disease. The test routines done to diagnose diseaseis VDRL in both partners. Primary and secondary syphilis can bediagnosed by demonstration of organism on dark ground illumination. T.Pallidum can cross the placenta and infect the fetus at any time duringpregnancy. The infection can result in stillbirth, preterm labor, IUGR, fetalhydrops and congenital syphilis. Baby may have vascular bullous lesions onthe skin mainly palm and soles or look healthy at birth. Symptoms andsigns appear in 3-4 days after birth. Iritis, signs of meningeal irritation,rhinitis, pharyngitis, generalized lymphadenopathy and splinting of arms andlegs due to arthralgia may be present. Rash appears all over the body. Asymptomatic babies may develop the disease later in life. The more recent
Complications in LatePregnancy-IV : RH
Incompatibility,Intrauterine Infection

Abnormal Pregnancy
148
the maternal infection, the more severe the congenital disease. Severity alsodepends on the gestational age of fetus at the time of infection. Syphilis istreated by Benzathine penicillin G. NACO guidelines for treatment ofsyphilis is given in Block 5, Unit 22.
Gonococci
Gonorrheal infection in mother is often asymptomatic. Infection istransmitted to the baby during labor and gonococcal ophthalmia developsin 3-4 days. Routine prophylaxis against ophthalmia neonatorum is notpracticed any longer. Only when symptoms and signs develop, treatment isstarted. Mother and her partner is also treated. Refer to block 5, unit 22for more details.
Chlamydia
Chlamydia trachomatis is the organism and it is sexually transmitted. In nonpregnant woman, it may be asymptomatic or causes symptoms and signslike frequency and burning micturition, pain and enlargement of bartholinsgland and mucopurulent cervicitis. When upper genital tract is involved, it
causes PID and infertility. LGV (lymphogranuloma venerum) is another typeof lesion caused by chlamydia. Infected mother during vaginal delivery maytransmit infection to the bay and neonatal conjunctivitis result. Pneumoniawith prominent respiratory symptoms may follow in some cases. Chlamydialinfection isdiagnosed by Elisa test and since the test is expensive, it is notcommonly done. For more, refer Unit 22 of Block 5.
Group B Streptococci (GBS)
Group B Streptococci causes severe congenital infection and alsochoroamnionitis, post partum endometritis, wound infection and sepsis inmother and is an important cause of intrauterine asphyxia. High riskmothers likely to transmit the infection to baby are with preterm rupture ofmembranes, preterm labor, intrapartum fever, prolonged induction andrepeated pelvic examination. Early neonatal sepsis occurs and has a highmortatlity rate. Universal screening of all pregnant mothers is notrecommended in our country. Prophylactic antibiotic – Inj ampicillin 500mg QID till delivery followed by oral route for 7 days) is administered to
all high risk woman.
Fungal (candida albicans)
Candidiasis is caused by c albicans and is an infection of skin, mucosaand rarely of internal organs. It is an important opportunist endogenousinfection. Skin lesions are seen in folds of skin. The sites are groin,perineum, axilla and infra mammary folds where skin is macerated byperspiration. Nails may be affected when hands and feet are frequentlyimmersed in water. Mucosal lesions are vaginitis seen frequently inpregnancy, diabetes mellitus, women on oral pills or steroid therapy, etc.you may refer to block 5, unit 19 and 22.
During vaginal birth, the baby may acquire infection. Oral thrush followscharacterized by creamy white patches on buccal mucosa and tongue.Read more about it in problems of new born.

149
Check Your Progress 2
1. List the viral infection that produce (a) life long immunity and (b)those that cause recurrent infection.
................................................................................................................
................................................................................................................
2. How can you prevent congenital rubella infection?
................................................................................................................
................................................................................................................
3. a) Parvovirus B19 infection in mother cause …………………..
b) Human papilloma crus cause …………….. in the neonate.
4. List the organisms producing neonatal conjunctivitis.
...............................................................................................................
...............................................................................................................
...............................................................................................................
10.4 LET US SUM UP
In this unit, you read about Rhesus isoimmunisation, pathology ofhaemolytic disease of newborn screening of pregnant woman for Rhcompatibility against Rh isoimmunisation. You also read about variousorganisms causing intrauterine infection of foetus, the complicationsdue to infection and how to diagnose them.
10.5 KEY WORDS
RNA : Ribonucleic acid
DNA : Deoxyribonucleic acid
Congenital Infection : Infection acquired during intrauterine life
Vertical Transmission : Transmission from mother to foetus
IgM antibodies : Antibodies produced during active infection
IgG antibodies : Antibodies persisting after infection
Topical Application : Local application on the affected part
10.6 ANSWERS TO CHECK YOUR PROGRESS
Check Your Progress 1
1) Rh factor is rhesus antigen i.e. a type of antigen found in red boodcells of human beings identical to those found in rhesus monkeys. Aperson who lacks this antigen is called Rh negative.
2) 5-10%
Complications in LatePregnancy-IV : RH
Incompatibility,Intrauterine Infection

Abnormal Pregnancy
150
3) Positive fetal red blood cells cross placenta and sensitise mother whoin turn produce antibodies which cross placenta and cause fetalhaemolysis and its consequences.
4) — Variable antigenicity
— Insufficient amount of antigen
— Variability of maternal response
— Protection due to ABO incompatibilities
— Insufficient antibody transfer across placenta.
Check Your Progress 2
1) a) Rubella, varicalla zoster
b) Cytomegalovirus, Herpes Simplex Virus
2) Giving MMR vaccination 9 months of age
– Immunizing school going girls who have no antibodies
– By protecting mothers from exposure to rubella infection andimmunizing mothers who have no antibodies in the postpartum period.
3) i) hydrops foctalis ii) larigngeal papillomes
4) 1) gonococcus 2) chlamydia trechomatis
10.7 FURTHER READINGS
Arias F (Indian Reprint 1997) Practical Guide to High Risk Pregnancyand Delivery, Second Edition, Harcourt Brace and Company Asia PTELtd.
Miller A, Govan A and Callander R (1989) Obstetrics Illustrated, 4th
Edition Churchill Livingstone.
Bennet V.R., Brown L.K.(2000) Myles Textbook for Midwives, 13th
Edition Churchill Livingstone.

151
UNIT 11 PAIN DURINGPREGNANCY
Structure
11.0 Objectives
11.1 Introduction
11.2 Causes of Pain During Pregnancy
11.2.1 Minor Ailments
11.2.2 Major Ailments
11.3 Approach to Pain During Pregnancy
11.4 Diagnosis and Management in Emergency
11.4.1 Attending an Emergency Situation in an Appropriate Way
11.4.2 Avoid Delay
11.4.3 Management on the Way
11.5 Diagnosis and Management in Hospital
11.6 Let Us Sum Up
11.7 Answers to Check Your progress
11.8 Further Readings
11.0 OBJECTIVES
After going through the unit, you will be able to:
enumerate the causes of pain during pregnancy;
diagnose the cause of pain abdomen during pregnancy, and
mange pain abdomen during pregnancy in emergency or hospitalsetting.
11.1 INTRODUCTION
You may be already aware from your past experience that pain inabdomen during pregnancy is a common symptom. Heartburn is thecommonest problem. Pain could be due to obstetrical, gynaecological,medical or surgical causes. In advanced pregnancy, diagnosis or non-obstetric causes in difficult. You must remember while counseling thatlaparotomy for other abdominal condition is never combined withcaesarean section unless there is an obstetric indication.
Pregnancy is one of the few experiences that sounds at once beautifulas well as alarming. Abdominal pain in pregnancy is very common.Many of the complications of pregnancy present with some form ofabdominal pain. There are several causes of abdominal pain duringpregnancy, some being directly related to pregnancy while others areunrelated medical or surgical conditions.

Abnormal Pregnancy
152
11.2 CAUSES OF PAIN DURING PREGNANCY
Causes can be many. Pains may be caused by physiological andpathological reasons. Some of the causes are not life threatening whileother are life threatened and need urgent treatment. The causes ofpain abdomen given below:
1. Pregnancy related
i) Physiological
— Round ligament pain
— Braxton-thick contractions
— Miscellaneous pain due to uterine muscle stretching
ii) Pathological
a) Early pregnancy
— Abortion including induced abortion
— Ectopic pregnancy
— Cystitis
— Retention of urine
b) Late pregnancy
— labour pains which can be false or true in nature
— Severe preeclampsia
— Accidental haemorrhage
— Rupture uterus
— Acute hydramnios
— Acute pyelitis/pyeloneptisitis
2. Incidental causes
i) Physiological
— Heart burn
— Excessive vomiting
— Constipation
ii) Pathological
a) Gynaecological
— Red degeneration in forbroid
— Torsion of ovaries cyst
b) Surgical
— Acute appendicitis
153
— Acute Cholecystitis, gall stones
— Urinary stones
— Intestinal obstruction
c) Medical
— Acute pancreatitis
— Peptic ulcer
— Colitis
— Diarrhoea, dysentery
11.2.1 Minor Ailments
There are some minor ailments leading to pain in pregnant women that istroublesome but will barely need any major intervention.
i) Round ligament pain
This can be characterized by a sharp stabbing pain while changingpositions, or it can also be an achy, dull, lingering pain. Roundligament pain is caused by the two large ligaments that run from youruterus to your groin. As the uterus grows, these ligaments arestretched and create discomfort due to the fact that the growing uterusputs traction on bands and ligaments. This pain is generally reportedin the second trimester, and considered to be harmless.
ii) Leg pain or cramps
Due to the physiological changes in pregnancy, there will behaemodilution leading to hypoproteinaemia and anaemia. Due to thepressure from the enlarging uterus on venous system, there will bedecrease venous return and lymphatic drainage resulting in swellingand pressure in lower extremities causing leg cramps. Plenty of fluidswith electrolytes, avoidance of prolonged standing, foot elevation andfoot massage will be the required management.
iii) Lower back pain
Due to temporary changes in spinal curvature, weight shifts can causemuscle spasms and soreness in lower back of pregnant female. Alongwith calcium supplements, applying heat, trying one of the supportbelts, and sitting down whenever possible to relieve some of thetension on back can be a helpful management.
iv) Braxton Hicks contractions
Braxton Hicks feel like a tightening of the uterine muscles so yourabdomen feels firm or hard. It is important to differentiate BraxtonHicks from true contractions. True contraction will be closer together,last for a longer period of time, and are painful. True contractionswill take your breath away, so a general rule of thumb is that if youare able to carry on your normal activities, then it is most likelyBraxton Hicks. Also, doctors report that Braxton Hick can be caused
Pain during Pregnancy

Abnormal Pregnancy
154
by dehydration, so drinking plenty of water can help eliminate thisproblem.
v) Gas pain and Constipation:
Gas during pregnancy is caused by increased levels of progesterone.As more of this hormone is released, your gastrointestinal tract slowsdown, which makes food travel more slowly. Plus, a lot of prenatalvitamins have iron, and your growing uterus makes it harder for yourbowels to move things along, both of which can cause theseconditions.
Drinking plenty of water, eating fibre rich foods, exercising, and usingstool softeners are excellent ways to combat excessive gas andconstipation.
vi) Pain in Breast
Under the influence of hormones like oxytocin, progesterone, andprolactin, breast can swell and become tender. There may be somedischarge from the nipples. Nothing much is to be done except warmbath or hot fomentation, breast support and pain reliever may help.
vii) Accommodation pain
A sharp, stabbing pain that feels like your baby is punching you inthe vagina. Regardless of the baby’s position, if something’s pressingon your cervix, it can stimulate the nerves there. Pain might be dueto varicose veins during pregnancy. There is increasing pressure fromthe enlarging uterus, so the blood from everything below it doesn’tmake its way effectively upward as it typically does. That pressurechanges cause dilation of those veins. Your veins usually have valvesthat stop blood from flowing backwards, but because of all thatpregnancy-induced pressure in the area, they might not work as wellas usual. Hence, varicose veins that can cause tingly pain in yournether regions.
11.2.2 Major Ailments
Although many women who experience abdominal pain have healthypregnancies, there are times when abdominal pain can pose a seriousrisk.
i) Ectopic Pregnancy:
Occurring in 1 out of 50 pregnancies, an ectopic pregnancy is whenthe pregnancy is implanted anywhere other than the uterus. Mostoften, the it is implanted in the fallopian tube. Women at increasedrisk for an ectopic pregnancy include those who have had an ectopicpregnancy in the past or have had endometriosis, pelvic inflammatorydisease etc. See chapter on ectopic pregnancy for further details.
ii) Placental abruption:
Placental abruption is a life-threatening condition in which theplacenta separates from the attachment in uterus before the baby isborn. One symptom of placental abruption is constant pain with or

155
without bleeding per vaginum. Additional symptoms include tendernessin abdomen, back pain, or leaking that includes traces of blood.
iii) Miscarriage:
15 to 20 percent of pregnancies end in miscarriage making it the mostcommon form of pregnancy loss. Sometimes referred to as “spontaneousabortion,” miscarriage most often occurs in the first 13 weeks ofpregnancy. Signs of a miscarriage include mild to severe back pain, truecontractions (happening every 5-20 minutes), brown or bright red bleedingwith or without cramps, tissue or clot-like material passing from thevagina, and a sudden decrease in other signs of pregnancy.
iv) Urinary Tract Infection:
While easily treated during pregnancy, if ignored, a urinary tract infectioncan cause complications. Most often recognized by pain, discomfort, and/orburning while urinating, UTIs can also produce lower abdominal pain. OralAntibiotics according to urine culture analysis should be given. If leftuntreated then infection will spread to kidneys causes pyelonephritis leadingto lumbar pain, fever and other symptoms. Injectable antibiotics are to begiven to prevent the further complications.
v) Gastroenteritis:
This may be due to the infection of gastrointestinal system leading todiarrhoea, vomiting and abdominal pain mostly crampy in nature.Infection can be bacterial, viral or protozoal. Appropriate managementincluding antibiotics if needed. Hydration should be maintained. Ifappropriate management is not given timely it can lead to dehydrationand ketosis affecting the mother and fetus.
vi) Preeclampsia:
Preeclampsia is a condition in pregnancy characterized by high bloodpressure and protein in the urine after 20 weeks gestation. Upperabdominal pain, usually under your ribs on the right side, canaccompany other symptoms used to diagnose preeclampsia. Nausea,vomiting and increased pressure on your abdomen are additionalsymptoms that will affect your abdomen. This may be due to thesubcapsular hematoma under the liver capsule.
Check Your Progress 1
1. List four causes of pregnancy related physiological causes of painabdomen.
..................................................................................................................
..................................................................................................................
..................................................................................................................
..................................................................................................................
..................................................................................................................
..................................................................................................................
Pain during Pregnancy

Abnormal Pregnancy
156
2. Mention 2 salient features of pain in Placental abruption
..................................................................................................................
..................................................................................................................
..................................................................................................................
..................................................................................................................
..................................................................................................................
..................................................................................................................
..................................................................................................................
11.3 APPROACH TO PAIN ABDOMENDURING PREGNANCY
Take a detailed history and do a thorough physical examination.
i) HISTORY TAKING
Onset and progression of pain.
Localization of pain: where is the maximum point, where does itradiate, what makes it better or worse.
Character of pain: is it sharp or dull, continuous or intermittent,deep or superficial?
Associated symptoms: nausea, vomiting, bloating, abdominaldistention, constipation, diarrhoea, dysuria, hypotension, fever,vaginal bleeding.
Last menstrual period, regularity of cycle. Was the last periodregular or unexpected; was it heavier or lighter than normal?
Obstetric history.
Contraceptive history: actual contraception, desire for children.
Gynecological history: recent vaginal discharge, other gynecologicaldiseases (e.g. fibroids), problems conceiving.
Previous abdominal surgery: specifically ask about appendectomy.
Medical history: sickle cell trait, thalassemia, porphyria.
ii) MEDICAL EXAMINATION
General physical examination including physical appearance: verysick, in pain, pale, sweating, weak, pale, level of consciousness.In a ruptured ectopic pregnancy with severe blood loss, patientmay be unconscious.
Cardiorespiratory system: respiration rate, pulse/ heart rate, blood
pressure.
157
Abdominal examination: physical appearance, if distended, flat,
tenderness, palpable masses, percussion note and bowel sounds.
Tenderness at McBurney’s point and Rovsing’s sign may imply
appendicitis. Abdominal muscle guarding: appendicitis, ectopic
pregnancy, torsion of ovarian tumor. Rebound and percussion
tenderness is an indication of appendicitis, ectopic pregnancy or
torsion of ovarian tumor.
Speculum examination is also very important. It may reveal
products of conception in the vagina or at the cervical os found
in incomplete abortion. It may reveal frank blood in ectopic
pregnancy. Uneventful speculum examination does not rule out
the suspected disease.
Bimanual palpation/digital vaginal examination is used to elucidate
the enlargement of the uterus, cervical excitation test etc.
Proper history taking and medical examination will guide further
investigations.
Make a list of differential diagnosis from the history and clinical feelings if
necessary, review the history and rule out life threatening conditions. Try
to make a provisional diagnosis. Observe the patient closely. Usually the
clinical picture become clear and a diagnosis can be made in a few
hours. The clinical picture and diagnosis of obstetrics conditions has
already been dealt with in their respective units. Diagnose of red
degeneration of fibroid is not difficult. When pain and tenderness is
localized in nature not spreading to the other areas of uterus and there is
no sign of shock. Fibroid may have been diagnosed previously before
pregnancy. This can be elicited from history. It could have been
diagnosed earlier in this pregnancy on clinical examination or by
ultrasound. Diagnosis of torsion of ovarian cyst is difficult clinically but
USG will help in diagnosis. Appropriate laboratory investigation and USG
help in making the diagnosis in other conditions.
11.4 DIAGNOSIS AND MANAGEMENT INEMERGENCY
Pregnancy & childbirth are natural process but they are by no means risk
free. Any woman can develop complication at any time during pregnancy.
As a service provider, if you are in periphery, having limited facilities, or
provide only basic obstetric care, you will have to refer that woman to a
place, where she can get comprehensive emergency obstetric care. This
section will give you an idea about different important points to be
remembered and followed, while attending emergency for pain in abdomen
during pregnancy and referring woman to a place where she can get
services to save her life and her baby’s life, without delay or minimizing
delays.
Pain during Pregnancy

Abnormal Pregnancy
158
Points to be remembered while attending obstetric emergency:
Attending an emergent situation in an appropriate way:
Avoid delay
Management on the way
11.4.1 Attending an Emergent Situation in anAppropriate Way
As Medical cofficer(MO), you are well aware that complications related topregnancy and childbirth are killing or giving sufferings to large number ofmothers. We should make all possible efforts to reduce such deaths andsufferings. One of the essential functions of the MO is to identify obstetricemergencies, i.e. Rapid Initial assessment, and do Rapid Initial Managementby making efforts to stabilize the conditions by maintaining vital functions,give first doses of need based medicines and to refer the mother promptlyto the appropriate place if you are not in position or equipped for furthermanagement.
General principles of attending an emergency situation in an appropriateway include:
i) Rapid initial Assessment
ii) Rapid Initial Management.
a. Stabilizationb. Administration of need based medicines such as:
Antibiotics
Sedatives and analgesics
Tetanus Toxoid
iii) Referral.
i) Rapid initial Assessment
Emergency means development of life-threatening condition. You havealready learned in previous units about different types of obstetricemergencies. When a woman of childbearing age presents with a problem,or you are called at the time of emergency, you should identify theunderlying obstetric condition and rapidly assess her condition to determineher degree of illness. This is known as Rapid Initial Assessment. Tominimize the delay in diagnosis, Table 1 will guide you about what to ask,for what danger signs you have to look and examine and what to assessif such danger signs are present. Rapid initiation of treatment requiresimmediate recognition of the specific problem and quick action.
Three important steps to keep in mind for Rapid Initial Assessment are:
a) History taking according to obstetric problem
b) Consideration of situation
c) Assess what and for which life-threatening condition

159
While taking history, encourage the woman and her family to speakhonestly and completely about events surrounding the complication. Listento what the woman and her family have to say and encourage them toexpress their concerns; try not to interrupt. Respect the woman’s sense ofprivacy and modesty by closing the door or drawing curtains around theexamination table. Let the woman know that she is being listened to andunderstood. Use supportive nonverbal communication such as nodding andeye to eye communication. Answer the woman’s questions directly incalm, reassuring manner. Explain what steps will be taken to manage thesituation or complication. Ask the woman to repeat back to you the keypoints to assure her understanding.
While taking history or asking for any information, use communicationskills. use of communication skills willhelp you a lot for carrying outyour work
Table 11.1: Rapid Initial Assessment
Problem Quick history Consider Assess what and forand Examination which Complication/
Life threateningcondition
Abdominal Sudden Onset Twisted Needs Surgerypain Ovarian Cyst
Localised tenderness Red degeneration Conservativeat site of fibroid of fibroid management
With Vomitting Acute Needs Surgeryand Fever Appendicitis
Antibiotics
Guidiness Ruptured Needs SurgeryPallor Ectopic Blood TransfusionLow B.P. Pregnancy Fast Pulse
Pregnancy Amnionitis AntibioticsTemperature Termination of(38 degree C) PregnancyLeaking Membranes Care of Newborn
Pregnancy with Abruptio Assess circulatoryvaginal bleeding Placenta system for
HypovolaemicshockNeeds terminationof Pregnancy
Labour Pain Onset of Labour Needs help fordelivery
Prolonged labour Rupture Uterus Assess Circulatorysystem forhypovolaemic Shock
Needs Surgery
Pain during Pregnancy

Abnormal Pregnancy
160
ii) Rapid Initial Management
In previous units, you have already learnt how to access circulatory systemrapidly and manage hypovolemic shock. For other assessment andmanagement of other causes, one has to follow guidelines given below.
The woman also needs prompt attention and top priority for prompttreatment, if she has any of the following signs:
Blood-stained mucus discharge (show) with palpable contractions;
Ruptured membranes;
Pallor;
Weakness; Fainting
Low temperature
Fast and low volume pulse
Low blood pressure
a) Stabilization
Depending upon presence of signs, important steps for stabilizationare:
Intravenous fluid therapy
Maintenance of body temperature
Intravenous fluid therapy is one of the important life-saving steps. Ifavailable, use isotonic solution (0.9 % NaCl) or compound solution.Glucose solution; without saline do not provide salt to restore fluidbalance. Use large bore needle, preferably 16-18 gauge. Even 20gauge is acceptable. Infuse rapidly in shock. 500 cc to 1 liter in 15to 20 minutes helps to stabilize condition. Once fluid loss is replaced,slow down the drip (30 drops per minute). Record pulse, BP andtemperature.
For maintaining body temperature, cover the woman with blankets. Donot use hot water bottles by the side of the woman.
b) Administration of medicines:
Different need-based medicines during an emergency are:
Antibiotics: Consider antibiotics in case of septic abortion (unsafeabortion), acute appendicitis, premature rupture of membranes,prolonged labour, obstructed labour, and septic shock. Preferred routeof administration is intravenous to help delivery of antibiotics speedilyat affected site. Broad spectrum antibiotics are effective against Gram–ve, Gram +ve, anaerobic organisms and Chlamydia. Combination ofantibiotics is ideal to achieve broad coverage of multiflora. Table 3will give you an idea of recommended dose of various antibiotics andtheir coverage.
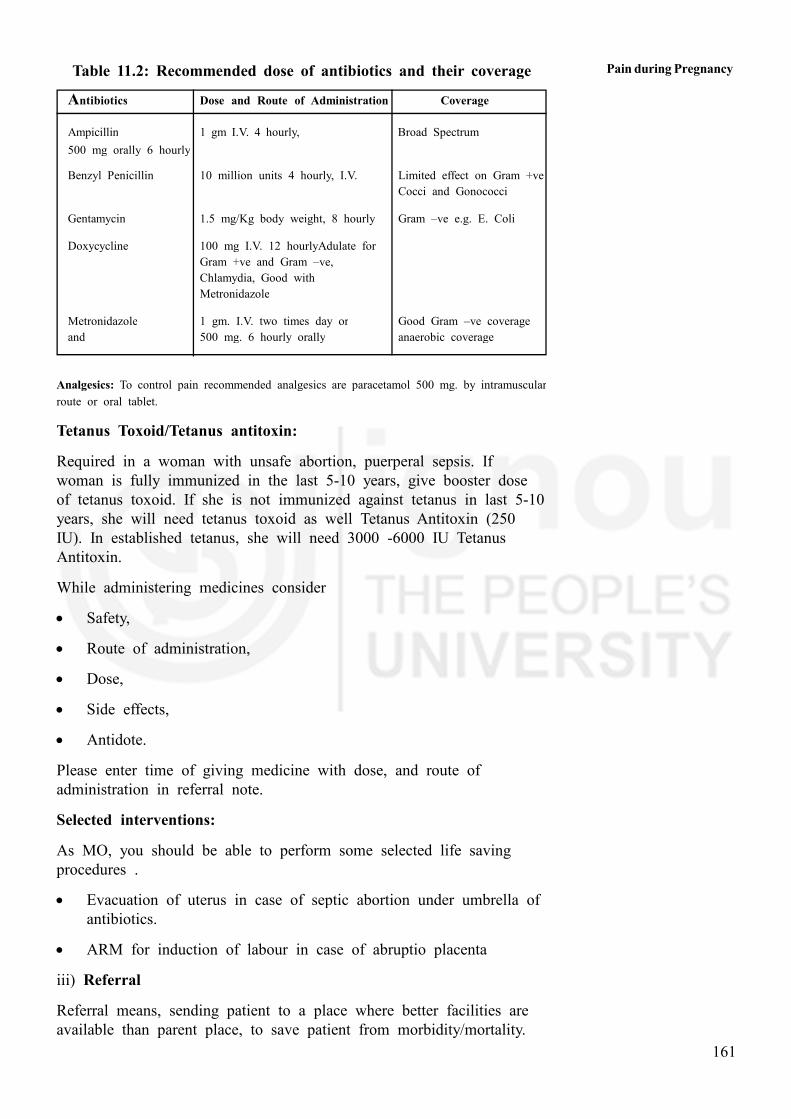
161
Table 11.2: Recommended dose of antibiotics and their coverage
Antibiotics Dose and Route of Administration Coverage
Ampicillin 1 gm I.V. 4 hourly, Broad Spectrum
500 mg orally 6 hourly
Benzyl Penicillin 10 million units 4 hourly, I.V. Limited effect on Gram +ve
Cocci and Gonococci
Gentamycin 1.5 mg/Kg body weight, 8 hourly Gram –ve e.g. E. Coli
Doxycycline 100 mg I.V. 12 hourlyAdulate for
Gram +ve and Gram –ve,
Chlamydia, Good with
Metronidazole
Metronidazole 1 gm. I.V. two times day or Good Gram –ve coverage
and 500 mg. 6 hourly orally anaerobic coverage
Analgesics: To control pain recommended analgesics are paracetamol 500 mg. by intramuscular
route or oral tablet.
Tetanus Toxoid/Tetanus antitoxin:
Required in a woman with unsafe abortion, puerperal sepsis. Ifwoman is fully immunized in the last 5-10 years, give booster doseof tetanus toxoid. If she is not immunized against tetanus in last 5-10years, she will need tetanus toxoid as well Tetanus Antitoxin (250IU). In established tetanus, she will need 3000 -6000 IU TetanusAntitoxin.
While administering medicines consider
Safety,
Route of administration,
Dose,
Side effects,
Antidote.
Please enter time of giving medicine with dose, and route ofadministration in referral note.
Selected interventions:
As MO, you should be able to perform some selected life savingprocedures .
Evacuation of uterus in case of septic abortion under umbrella ofantibiotics.
ARM for induction of labour in case of abruptio placenta
iii) Referral
Referral means, sending patient to a place where better facilities areavailable than parent place, to save patient from morbidity/mortality.
Pain during Pregnancy

Abnormal Pregnancy
162
Procedure of referral involves two steps.
Discuss need for referral with decision makers in family & arrange forvoluntary blood donors.
Referral note.
a) Discuss need for referral with decision makers in family &arrange for voluntary blood donors:
Emergency situations are often very disturbing for all concerned andevoke a range of emotions that can have significant consequences.While discussing the situation developed and need for referral, speakin a calm, quiet manner and assure the woman that it is for herbenefit. Be sensitive to any cultural or religious considerations andrespect her views. Use local language and short sentences.
Delay in decision taking for transfer to a better place can also provefatal. Once you have completed rapid initial assessment and you haveconcluded that she needs further help, which you cannot provide, sheneeds to be sent at a place where comprehensive surgical as wellobstetric care facilities are available. Always discuss the situation byexplaining the condition, its seriousness, type of intervention needed tosave woman’s life, and where such interventions are available. Alsotell the approximate time required to reach that place. If a womanmust undergo a surgical procedure, explain to her the nature of theprocedure and its risks and help to reduce her anxiety. Women whoare extremely anxious have a more difficult time during surgery andrecovery
Discuss these issues with decision makers of the family usually,husband, mother in law, and father in law. Use simple local language.Use short sentences. Answer their all queries. Give some time tothink.
Decision makers get convinced earlier for need of referral, if as apreventive measure, warning signs are told to woman, her familymembers, and decision makers during pregnancy well in advance.
Also convince them to take 2-3 young boys along with a referredwoman. These young boys may be helpful for supply of blood, incase of an obstetric emergency having severe bleeding(post abortal,ruptured ectopic, rupture uterus, severely anaemic woman etc.)
b) Referral note
Whenever you refer a pregnant woman, you must write a referral noteor fill up referral form. This note/form should accompany referredwoman. It should be handed over to doctor in charge of that referralcentre. Note will help that doctor to know about the place ofreference, why the reference is done, clinical condition of woman,what medicines have been given at what time, and in which dose,what procedures have been performed etc.
Referral form/note must include
Identification data of the woman

163
History
Clinical condition
Initial treatment (Medicines)
Interventions
Time of reference
Referred from
Referred by
Date of reference
Signature of referring person
You can avoid or minimize these delays by different actions.
11.4.2 Avoid Delays
You have already learned about “Delays” responsible for maternal mortalityand morbidities. You can avoid or minimize these delays by differentactions.
i) Organization of transport & finance
Though family members agree for referral, if transport and finance are notorganized, same will further make delay in reaching to referral hospital.During birth preparedness only, these points should be highlighted. This willhelp family to keep ready some vehicle or inquire about availability ofvehicle at the time of emergency, to take woman to referral hospital.Neighbors can also help for transport. PHC vehicle can also be utilized.
Sarpanch of the village is also given some money by state government forarrangement of transport. ASHA worker can also be helpful for the same.
Ask family members to keep money for expense like, transport, medicines,blood transfusion etc. Highlighting this point during birth preparedness willnot put family in tension. Preplanned saving can be utilized at this time.
While organizing transport, give details about address of referral center,information about shortest route of reaching to referral center, availabletransport services and approximate fare, telephone no. of referral center, towhom to meet etc.
Emergencies with heavy external/internal bleeding, surgical emergencies,women with severe pallor, may require blood transfusion. For voluntaryblood banks, voluntary donors are needed to replace the blood. It is notnecessary that for replacement of same group of blood is required. Onreplacing blood of any group, in the voluntary blood bank, bank willsupply blood of same group as of patient’s group. So it is always betterto send 2 to 3 young people along with woman, to donate blood ifrequired.
Pain during Pregnancy

Abnormal Pregnancy
164
ii) Information to referral center
To avoid delay in receiving treatment, it is better that referral center isaware about arrival of mother in advance, about woman is having whattype of problem. This will take care of 1. Availability of staff (Doctor,Anesthetist, Staff nurses, class III & IV staff),2. Readiness of operationtheatre
For performing this responsibility, you should keep with you, telephonenumbers of all nearby hospitals and name of persons working at referralcenter.
iii) Preparation of supplies & drugs for use in transport
As far as possible, you should accompany the mother while transferringher to referral hospital. She may need some medicines, observations onthe way. Keep your bag ready with all equipment required.
Common equipment’s necessary are, BP instrument, stethoscope, syringes,needles, spirit swabs, gloves, IV cannula, drip set sticking plaster, mouthgag, rubber bulb, catheter, urobag, gauze pieces, paper, pen etc.
As far as drugs are concerned,
Woman having hypovolemic shock or likely to go in hypovolemicshock need IV transfusion in form of normal saline, or RingerLactate.
Woman having excessive bleeding after abortion need drugs foruterine contraction. (Syntocinon in drip, Methergin)
11.4.3 Management on the Way
It is better if you accompany with woman when she is referred forsurgical or obstetric emergency. On the way to referral hospital,woman having such emergency may need help. She needs monitoringand management for
her vital signs,
worsening of the problem,
See the effect of drugs given
Continue intravenous therapy
Administration of 2nd dose of medicine
Maintain position important to maintain vital signs and preventingworsening of mother’s condition.
Removing secretions from mouth
Monitoring urinary output
Your presence will help a lot to woman on the way to referral hospital.

165
11.5 DIAGNOSIS AND MANAGEMENT INHOSPITAL
At hospital there is facility of medical as well surgical management.Following table will help you to understand different type of managementsaccording to cause of pain in abdomen along with pregnancy.
Table 11.3: Diagnosis and management for Acute Abdomenin Hospital
Condition Management
Septic Abortion AntibioticsEvacuation of uterusLaparatomy, repair of uterine/intestinalinjury, drainage of pelvic abscess, ifinjury/pelvic abscess suspected,
Red degenerationof fibroid Conservative management
Twistwed Ovarian cyst Laparotomy & removal of twistedovarian cyst
Inj. Prolutan Depo ortocolytic drugs to avoidabortion or preterm labourAcute Appendicitis Antibiotics
Laparatomy and AppendicectomyInj. Prolutan Depo or tocolytic drugsto avoid abortion or preterm labour
Ruptured Tubal Ectopic LaparatomySalphingostomy or SalphingectomyBlood transfusion if required
Abruptioo Placentae Termination of Pregnancy by ARM ifcervix is partly dilated or LSCS if cervix is closed
Treatment of Coagulopathy if developedTreatment of PIH
Preterm Labour Inj. Dexona 12 mg. IM at 12 hoursinterval for fetal lung maturity, if pregnancy is between 32to 36 weeks Antibiotics
Tocolytic drugs till decision for termination
Termination of pregnancy by augmentationor LSCS as per situation.Care of newborn by neonatologist
Labour pains Assist for delivery
Rupture Uterus LaparotomyRemoval of fetusRepair of uterine tear orRepair of tear and tubectomy orSubtotal HysterectomyLigation of Internal Illiac Artery ifrequired
Pain during Pregnancy

Abnormal Pregnancy
166
Check Your Progress 2
1. List four life threatening obstetric conditions causing painabdomen.
................................................................................................................
................................................................................................................
2) Describe diagnosis of red degeneration of fibroid duringpregnancy.
................................................................................................................
................................................................................................................
11.6 LET US SUM UP
Pain in abdomen is a common symptom during pregnancy. Many otherobstetric, gynaecologic, surgical and medical causes of pain abdomenduring pregnancy including life threatening condition presenting with painabdomen have been described.
11.7 ANSWERS TO CHECK YOUR PROGRESS
Check Your Progress 1
1) i) Round ligament pain
ii) Braxton–Hicks contraction
iii) Severe uterine torsion
2) i) constant pain with or without bleeding per vaginum
ii) tenderness in abdomen, back pain, or leaking that includes tracesof blood
Check Your Progress 2
1) i) Ectopic pregnancy
ii) Accidental haemorrhage
iii) Severe preeclampsia
iv) Rupture uterus
2) Diagnosis of red degeneration of fibroid during pregnancy
i) n/o pain in abdomen which is located in there is no sign ofshock
ii) n/o diagnosed fibroid uterus
iii) Diagnosis of fibroid during ……. Antenatal examination or duringUSG exam
iv) Diagnosis of fibroid by USG when the women has come withpain abdomen during pregnancy.
11.8 FURTHER READINGS
Miller A, Govan A and Callander R (1989) Obstetrics Illustrated, 4th
Edition Churchill Livingstone.
Bennet V.R., Brown L.K.(2000) Myles Textbook for Midwives, 13th
Edition Churchill Livingstone.




















