Bipolar disorder: recent clinical trials and emerging therapies for depressive episodes and...
9
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and emerging therapies for depressive episodes and maintenance treatment, Drug Discov Today (2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010 Drug Discovery Today Volume 00, Number 00 July 2014 REVIEWS Bipolar disorder: recent clinical trials and emerging therapies for depressive episodes and maintenance treatment Ricardo P. Garay Q1 1,2 , Pierre-Michel Llorca 3 , Allan H. Young 4 , Ahce `ne Hameg 2 and Ludovic Samalin 3 1 INSERM U999, Universite ´ Paris-Sud et Ho ˆ pital Marie Lannelongue, Le Plessis-Robinson, France 2 Craven, Villemoisson-sur-Orge, France 3 Psychiatry Service, CHU Clermont-Ferrand, EA 7280, Auvergne University, Clermont-Ferrand, France 4 Centre for Affective Disorders, Institute of Psychiatry, Kings College London, De Crepisgny Park, London, UK Bipolar disorder (BD) is one of the world’s ten most disabling conditions. More options are urgently needed for treating bipolar depressive episodes and for safer, more tolerable long-term maintenance treatment. We reviewed 30 recent clinical trials in depressive episodes (eight tested compounds) and 14 clinical trials in maintenance treatment (ten tested compounds). Positive results in Phase III trials, regulatory approval and/or new therapeutic indications were obtained with some of the developing drugs, particularly for depressive episodes. The current BD pipeline is encouraging with promising new compounds, acting on novel pharmacological targets and on specific aspects of bipolar depression. Introduction Bipolar disorder (BD) is a chronic, severe and recurring illness (typically manic episodes alternate with episodes of depression), which affects 3% or more of the population and is associated with substantial morbidity and mortality [1]. The mortality rate of those with BD is two-to-three-times higher than the rate in the general population, owing particularly to suicide but also to accidents, medical illness and substance abuse [2]. Indeed, BD is one of the world’s ten most disabling conditions and one of the greatest public health problems [3]. BD refers to a continuum of disorders [4], including: (i) the tradi- tional bipolar I subtype (BD-I), which includes episodes of full-blown mania and major depression; (ii) BD type II (BD-II) depressive and hypomanic episodes; (iii) cyclothymic disorder (depressive and hy- pomanic symptoms); and (iv) BD not otherwise specified. The cause of BD is unknown, but genetic and environmental risk factors are believed to have a role [5,6]. Treatment commonly includes mood-stabilizing medication and supportive and educa- tional therapy [7–12]. The treatment of mania is provided for by the available treatments: (i) mood stabilizers including lithium and anticonvulsants (valproate, carbamazepine) that are effective in treating acute manic episodes and preventing relapses; and (ii) some atypical antipsychotics (olanzapine, quetiapine, risperidone, aripiprazole) initially used to treat schizophrenia, which have also been found to be efficacious for managing mania. Generally speaking, the periods of depression far exceed those of mania in terms of frequency and duration [13,14]. BD patients commit or attempt suicide mostly during severe depressive epi- sodes, but very rarely during states of euphoric mania or euthymia [2]. Quetiapine and an olanzapine–fluoxetine combination (OFC; a single capsule containing the atypical antipsychotic olanzapine and the selective serotonin reuptake inhibitor fluoxetine) are used to treat bipolar depressive episodes [10], but they are not exempt from adverse effects in long-term treatment (e.g. weight gain, dyslipidaemia and/or sedation or somnolence). Because of discor- dant data concerning lithium and valproate, these two drugs are placed either as first- or as second-line treatment for bipolar depression [12,15]. Unmet treatment needs in the management of BD include more options for treating bipolar depressive episodes and safer, more-tolerable medications for long-term maintenance treatment [8,16]. This review summarizes a selected number of recent clinical trials in bipolar depressive episodes and in long- term maintenance treatment and also discusses important ongo- ing trials. Reviews POST SCREEN Corresponding author: Garay, R.P. ([email protected]) 1359-6446/06/$ - see front matter ß 2014 Published by Elsevier Ltd. http://dx.doi.org/10.1016/j.drudis.2014.07.010 www.drugdiscoverytoday.com 1
Transcript of Bipolar disorder: recent clinical trials and emerging therapies for depressive episodes and...

Q1
Reviews�POSTSCREEN
Drug Discovery Today � Volume 00, Number 00 � July 2014 REVIEWS
Bipolar disorder: recent clinical trialsand emerging therapies for depressiveepisodes and maintenance treatment
Ricardo P. Garay1,2, Pierre-Michel Llorca3, Allan H. Young4,Ahcene Hameg2 and Ludovic Samalin3
1 INSERM U999, Universite Paris-Sud et Hopital Marie Lannelongue, Le Plessis-Robinson, France2Craven, Villemoisson-sur-Orge, France3 Psychiatry Service, CHU Clermont-Ferrand, EA 7280, Auvergne University, Clermont-Ferrand, France4Centre for Affective Disorders, Institute of Psychiatry, Kings College London, De Crepisgny Park, London, UK
Bipolar disorder (BD) is one of the world’s ten most disabling conditions. More options are urgently
needed for treating bipolar depressive episodes and for safer, more tolerable long-term maintenance
treatment. We reviewed 30 recent clinical trials in depressive episodes (eight tested compounds) and 14
clinical trials in maintenance treatment (ten tested compounds). Positive results in Phase III trials,
regulatory approval and/or new therapeutic indications were obtained with some of the developing
drugs, particularly for depressive episodes. The current BD pipeline is encouraging with promising new
compounds, acting on novel pharmacological targets and on specific aspects of bipolar depression.
IntroductionBipolar disorder (BD) is a chronic, severe and recurring illness
(typically manic episodes alternate with episodes of depression),
which affects 3% or more of the population and is associated with
substantial morbidity and mortality [1]. The mortality rate of those
with BD is two-to-three-times higher than the rate in the general
population, owing particularly to suicide but also to accidents,
medical illness and substance abuse [2]. Indeed, BD is one of the
world’s ten most disabling conditions and one of the greatest
public health problems [3].
BD refers to a continuum of disorders [4], including: (i) the tradi-
tional bipolar I subtype (BD-I), which includes episodes of full-blown
mania and major depression; (ii) BD type II (BD-II) depressive and
hypomanic episodes; (iii) cyclothymic disorder (depressive and hy-
pomanic symptoms); and (iv) BD not otherwise specified.
The cause of BD is unknown, but genetic and environmental
risk factors are believed to have a role [5,6]. Treatment commonly
includes mood-stabilizing medication and supportive and educa-
tional therapy [7–12]. The treatment of mania is provided for by
the available treatments: (i) mood stabilizers including lithium
and anticonvulsants (valproate, carbamazepine) that are effective
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and e(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
Corresponding author: Garay, R.P. ([email protected])
1359-6446/06/$ - see front matter � 2014 Published by Elsevier Ltd. http://dx.doi.org/10.1016/j.drudis.2014.
in treating acute manic episodes and preventing relapses; and (ii)
some atypical antipsychotics (olanzapine, quetiapine, risperidone,
aripiprazole) initially used to treat schizophrenia, which have also
been found to be efficacious for managing mania.
Generally speaking, the periods of depression far exceed those of
mania in terms of frequency and duration [13,14]. BD patients
commit or attempt suicide mostly during severe depressive epi-
sodes, but very rarely during states of euphoric mania or euthymia
[2]. Quetiapine and an olanzapine–fluoxetine combination (OFC;
a single capsule containing the atypical antipsychotic olanzapine
and the selective serotonin reuptake inhibitor fluoxetine) are used
to treat bipolar depressive episodes [10], but they are not exempt
from adverse effects in long-term treatment (e.g. weight gain,
dyslipidaemia and/or sedation or somnolence). Because of discor-
dant data concerning lithium and valproate, these two drugs are
placed either as first- or as second-line treatment for bipolar
depression [12,15]. Unmet treatment needs in the management
of BD include more options for treating bipolar depressive episodes
and safer, more-tolerable medications for long-term maintenance
treatment [8,16]. This review summarizes a selected number of
recent clinical trials in bipolar depressive episodes and in long-
term maintenance treatment and also discusses important ongo-
ing trials.
merging therapies for depressive episodes and maintenance treatment, Drug Discov Today
07.010 www.drugdiscoverytoday.com 1

SCC���
��
��
�
DW
lo
s�
�
�
��
REVIEWS Drug Discovery Today � Volume 00, Number 00 � July 2014
DRUDIS 1467 1–9
T
In
F
A
A
N
a
b
c
d
eQ9f Fg
h
i Tj A
2
Review
s�P
OSTSCREEN
election criterialinical trial eligibilitylinical trials were selected on the basis of the following criteria.
The primary outcome was at least one of the following:
efficacy in bipolar depressive episodes;
long-term efficacy for relapse prevention or residuals symp-
toms;
status as a long-term safety trial.
The clinical trial was recruiting or active (not recruiting), or
completed in 2012 or later.
It was a Phase II, III or IV trial.
It was a randomized trial, or an open trial versus placebo and/or
a comparative compound.
Compound development was not discontinued.
ata sources and searche identified clinical trials in bipolar depressive episodes and
ng-term BD maintenance treatment using the following main
ources.
The clinical trials databases of the NIH (National Institutes of
Health; http://www.clinicaltrials.gov/), the European Medicines
Agency (EMA; EU Clinical Trials Register; https://www.clinical-
trialsregister.eu/ctr-search/search;jsessionid=sa0a1Jq2IuPPzCa-
QoIpaEOkYugzkgm_2UA9T_Bmp3ks9p4LXbe5D!-895578838)
and WHO (World Health Organization International Clinical
Registry Platform; http://apps.who.int/trialsearch/).
Records from the EMA (http://www.ema.europa.eu/ema/) and
FDA (http://www.fda.gov/).
Medical journals, using PubMed, Science Direct and Google
Scholar.
Conferences and meetings on psychiatry.
Websites of pharmaceutical and biotech companies active in
the field of BD-targeted therapies.
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
ABLE 1
vestigational compounds for bipolar depressive episodes and mai
amily Compound Main
typical antipsychotics+antidepressant Quetiapine D2 an
Olanzapine D2 an
Paliperidone D2 an
Lurasidone D2 anAsenapine D2 an
Aripiprazole D2 an
OFCa D2 an
nticonvulsants Lamotrigine Sodium
ew investigational compounds Armodafinil Unkno
Ramelteon Melato
Lisdexamfetamine TAAR1
Cariprazine D2 anScyllo-inositol Amylo
Mifepristone Proge
Olanzapine–fluoxetine combination.
Dopamine D2 and serotonin 5-HT2A antagonist (see ref. for other actions on neurotransm
Dopamine D2 and D3 partial antagonist (see ref. for other actions on neurotransmitter re
Selective serotonin reuptake inhibitor.
Progesterone and glucocorticoid receptor antagonist.
DA and/or EMA approval status before 2012 is given in Figs 1,2.
Treatment-resistant depression.
Cariprazine is currently under investigation for the treatment of BD and schizophrenia an
race-amine-associated receptor 1.
ttention deficit hyperactivity disorder.
www.drugdiscoverytoday.com
Identification of clinical trials and compoundsClinical trials are given with their proper name or a
literature reference, or the ClinicalTrial.gov identifier, in decreas-
ing order of priority. Compounds are given with their generic
name and the biotech or pharmaceutical company in charge of
development. Trade name is indicated when available.
Compound classificationCompounds reviewed here are divided into FDA- and/or EMA-
approved compounds (for the bipolar depressive episodes, for BD
maintenance treatment or for other psychiatric disorders) and new
investigational compounds (for the treatment of bipolar depres-
sive episodes and/or for maintenance treatment). Finally, the
phase of development is indicated together with its status.� With results.� Completed.� Ongoing, with the estimated study completion date.
Recent clinical trials in bipolar depressive episodesOur search identified 30 eligible clinical trials in bipolar depres-
sive episodes (accessed between 19th February and 7th May
2014) corresponding to eight developing compounds.� The olanzapine–fluoxetine combination (OFC, Symbyax1, Eli
Lilly) – for review of previous studies see [17].� Quetiapine extended-release (XR) (quetiapine XR, Seroquel
XR1, AstraZeneca) [18].� Asenapine (Saphris1, Forest, USA; Sycrest1, Lundbeck, EU) [19].� Lurasidone (Latuda1, Sunovion) [20].� Armodafinil (Nuvigil1, TEVA) [21].� Ramelteon (Rozerem1, Takeda Pharmaceuticals, Japan) [22].� Lisdexamfetamine dimesylate (Vyvanse1, Shire Pharmaceuti-
cals, UK) [23].� Cariprazine (Forest Laboratories, USA) [24].
emerging therapies for depressive episodes and maintenance treatment, Drug Discov Today
ntenance treatment of bipolar disorder (BD) reviewed in this article.
receptor actions Main medication usesf Refs
d 5-HT2A antagonistb BD and schizophrenia [18]
d 5-HT2A antagonistb BD and schizophrenia [33]
d 5-HT2A antagonistb BD and schizophrenia [35]
d 5-HT2A antagonistb BD and schizophrenia [20]d 5-HT2A antagonistb BD and schizophrenia [19]
d D3 partial agonistc BD and schizophrenia [34]
d 5-HT2A antagonistb + SSRId Bipolar depression and TRDg [17]
channel blocker BD, epilepsy and seizures [32]
wn (dopamine suspected) Sleep disorders [21]
nin MT1/MT2 agonist Insomnia [22]i activator ADHDj disorder [23]
d D3 partial agonistc Under investigationh [24]id antiaggregation agent Under investigationh [36]
sterone and glucocorticoide Abortifacient and contraceptive [38]
itter receptors).
ceptors).
d scyllo-inositol is under investigation for the treatment of Alzheimer’s disease.
Drug Discovery Today � Volume 00, Number 00 � July 2014 REVIEWS
DRUDIS 1467 1–9
FDA- and/or EMA- approval status before 2012Compounds in clinical trials for
bipolar depression in 2012 or later
• Olanzapine-fluoxetine combination (OFC)
• Quetiapine
• Lurasidone• Asenapine
New investigationalcompounds
Compoundsapproved inpsychiatricindications
Other
Bipolardepressiveepisodes
• Armodafinil• Ramelteon• Lisdexamfetamine• Cariprazine
Drug Discovery Today
FIGURE 1
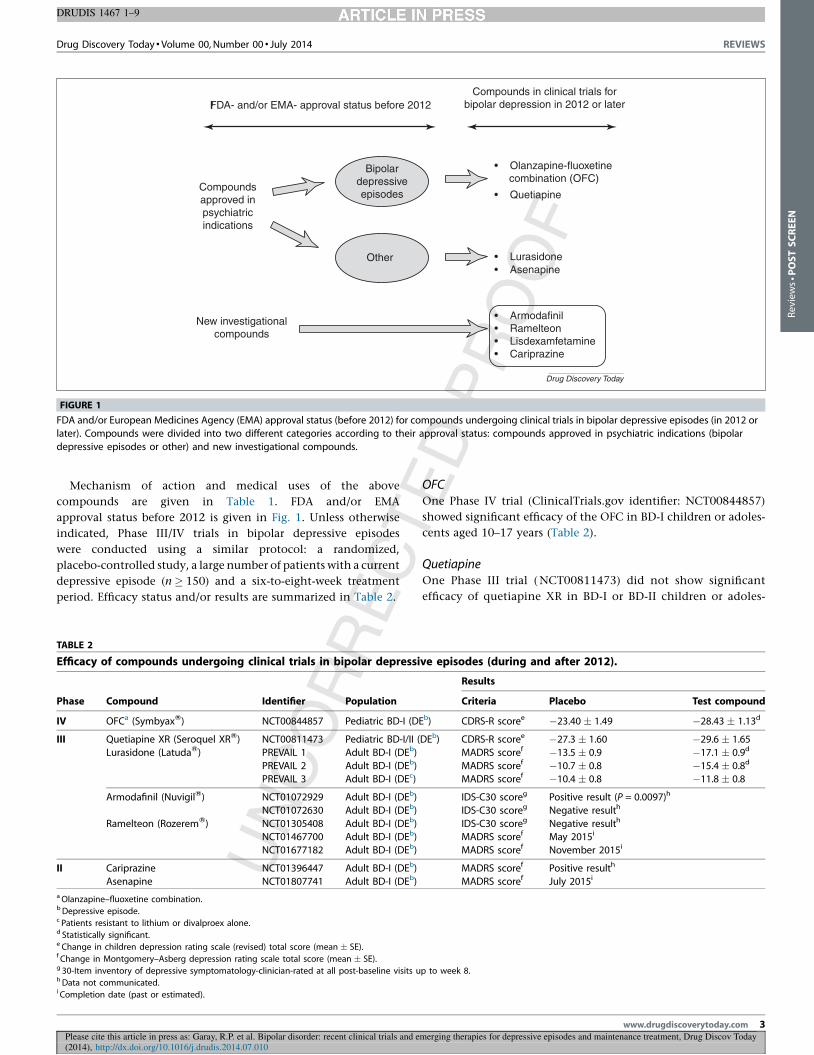
FDA and/or European Medicines Agency (EMA) approval status (before 2012) for compounds undergoing clinical trials in bipolar depressive episodes (in 2012 or
later). Compounds were divided into two different categories according to their approval status: compounds approved in psychiatric indications (bipolar
depressive episodes or other) and new investigational compounds.
Reviews�POSTSCREEN
Mechanism of action and medical uses of the above
compounds are given in Table 1. FDA and/or EMA
approval status before 2012 is given in Fig. 1. Unless otherwise
indicated, Phase III/IV trials in bipolar depressive episodes
were conducted using a similar protocol: a randomized,
placebo-controlled study, a large number of patients with a current
depressive episode (n � 150) and a six-to-eight-week treatment
period. Efficacy status and/or results are summarized in Table 2.
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and e(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
TABLE 2
Efficacy of compounds undergoing clinical trials in bipolar depressi
Phase Compound Identifier Population
IV OFCa (SymbyaxW) NCT00844857 Pediatric BD-I (DE
III Quetiapine XR (Seroquel XRW) NCT00811473 Pediatric BD-I/II (
Lurasidone (LatudaW) PREVAIL 1 Adult BD-I (DEb)
PREVAIL 2 Adult BD-I (DEb)
PREVAIL 3 Adult BD-I (DEc)
Armodafinil (NuvigilW) NCT01072929 Adult BD-I (DEb)
NCT01072630 Adult BD-I (DEb)
Ramelteon (RozeremW) NCT01305408 Adult BD-I (DEb)
NCT01467700 Adult BD-I (DEb)
NCT01677182 Adult BD-I (DEb)
II Cariprazine NCT01396447 Adult BD-I (DEb)
Asenapine NCT01807741 Adult BD-I (DEb)
a Olanzapine–fluoxetine combination.b Depressive episode.c Patients resistant to lithium or divalproex alone.d Statistically significant.e Change in children depression rating scale (revised) total score (mean � SE).f Change in Montgomery–Asberg depression rating scale total score (mean � SE).g 30-Item inventory of depressive symptomatology-clinician-rated at all post-baseline visits uhData not communicated.i Completion date (past or estimated).
OFCOne Phase IV trial (ClinicalTrials.gov identifier: NCT00844857)
showed significant efficacy of the OFC in BD-I children or adoles-
cents aged 10–17 years (Table 2).
QuetiapineOne Phase III trial ( NCT00811473) did not show significant
efficacy of quetiapine XR in BD-I or BD-II children or adoles-
merging therapies for depressive episodes and maintenance treatment, Drug Discov Today
ve episodes (during and after 2012).
Results
Criteria Placebo Test compound
b) CDRS-R scoree �23.40 � 1.49 �28.43 � 1.13d
DEb) CDRS-R scoree �27.3 � 1.60 �29.6 � 1.65
MADRS scoref �13.5 � 0.9 �17.1 � 0.9d
MADRS scoref �10.7 � 0.8 �15.4 � 0.8d
MADRS scoref �10.4 � 0.8 �11.8 � 0.8
IDS-C30 scoreg Positive result (P = 0.0097)h
IDS-C30 scoreg Negative resulth
IDS-C30 scoreg Negative resulth
MADRS scoref May 2015i
MADRS scoref November 2015i
MADRS scoref Positive resulth
MADRS scoref July 2015i
p to week 8.
www.drugdiscoverytoday.com 3

c
s�
�
r
d
p�
�
�
�
�
�
a�
�
�
AIn
e
d
p
LT
B
II
lu
a
a
d
g
t
lu
s
c
t
REVIEWS Drug Discovery Today � Volume 00, Number 00 � July 2014
DRUDIS 1467 1–9
4
Review
s�P
OSTSCREEN
ents aged 10–17 years (Table 2). We can also mention two pilot
tudies.
NCT00671853, showing small effects on bipolar depressive
episodes and co-morbid generalized anxiety disorder (no
statistical analysis was provided to ClinicalTrials.gov).
A small pilot study in 42 patients with bipolar depression
showing that quetiapine XR monotherapy was more effective
than lithium and suggested that quetiapine XR can improve
subjective and objective sleep quality [25].
A large number of other studies are now ongoing or were
ecently completed with quetiapine and quetiapine XR in bipolar
epression in specific populations. Six of these studies were com-
leted, but the results were not posted to ClinicalTrials.gov.
NCT00232414 – quetiapine in BD-I depressive episodes in
children and adolescents (Phase III study).
NCT01527448 – quetiapine XR in BD-II women with postpar-
tum depression (open-label study).
NCT01195363 – adjunctive quetiapine XR in mixed states of BD
(Phase IV study).
NCT00186043 – quetiapine for the treatment of dysphoric
hypomania in BD-II patients (Phase IV study).
NCT00608296 – brain structure, function and chemistry of BD
patients who are receiving quetiapine or lithium.
NCT00751504 – psychotic features of depression under
quetiapine treatment (pilot study, n = 20).
Three other studies were communicated to ClinicalTrials.gov
nd are currently recruiting participants:
NCT00817323 investigates whether quetiapine exerts its
antidepressant activity in bipolar disorder through altering
either serotonergic or catecholinergic activity.
NCT01213121 examines within-subject changes in neurophys-
iologic parameters in patients with bipolar depression treated
with quetiapine.
NCT01357967 – this Phase IV study investigates quetiapine XR
in depressive patients showing aberrant N100 amplitude slope
(the N100 amplitude slope is used as a marker of central
serotonergic activity).
senapine September 2013 a Phase II trial ( NCT01807741) was initiated
valuating the efficacy of asenapine versus placebo in BD-I
epressive episodes (Table 2). This study is currently recruiting
articipants.
urasidonehe efficacy of lurasidone for the acute treatment of adults with
D-I depression was established in two placebo-controlled Phase
I trials: PREVAIL 1 (NCT00868452) investigating adjunctive
rasidone in patients treated with either lithium or valproate;
nd PREVAIL 2 (NCT00868699) testing lurasidone as monother-
py (Table 2) [26] (http://www.latuda.com/). In these two trials,
iscontinuation rates as a result of adverse events in the lurasidone
roup were small (<7%) and were not different from those of
he placebo group. The most common adverse events in the
rasidone group were headache, nausea, somnolence and akathi-
ia. The changes in lipid profiles, weight and parameters of gly-
emic control were minimal, and these findings were in-line with
hose observed in schizophrenia trials.
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
www.drugdiscoverytoday.com
In a third Phase III study (Prevail 3, NCT01284517) of patients
with BD-I depression, who were nonresponders to lithium or
divalproex alone, adjunctive lurasidone showed no significant
differences with a placebo (Table 2). Other Phase III/IV studies
are planned or in progress in children and adolescents with bipolar
disorder (NCT01932541, NCT02046369).
ArmodafinilA Phase II study showed that adjunctive armodafinil significantly
improved depressive symptoms over a placebo in patients with
bipolar depression [21]. Three Phase III trials of armodafinil were
recently completed in adults with major depression associated
with BD-I: 3071 (NCT01072929), 3072 (NCT01072630) and
3073 (NCT01305408). Two out of the three Phase III trials did
not reach statistical significance in their primary endpoint (Table
2) (http://ir.tevapharm.com). Interestingly, armodafinil reached
statistical significance in several important secondary endpoints,
such as responder rate and remission.
RamelteonA small pilot study in ambulatory BD-I with insomnia showed that
ramelteon improved the global rating of depressive symptoms
[27]. Recently, two Phase III studies were initiated for sublingual
adjunctive ramelteon in bipolar depressive episodes:
NCT01467700 and NCT01677182 (Table 2).
LisdexamfetaminePilot Phase IV studies suggested that lisdexamfetamine can miti-
gate depressive symptom severity in BD (NCT01051440) [23]. In
2010, a 30–36-month Phase III trial was initiated evaluating lis-
dexamfetamine as an adjunctive treatment of bipolar depression
(NCT01093963, NCT01131559). The sponsor halted both studies
in March 2014 (http://article.wn.com/view/2014/02/08/Shire_-
scraps_Vyvanse_for_depression_after_failed_trials/).
CariprazineForest and Gedeon recently completed their Phase IIb trial in
patients with bipolar depression and announced positive results
(http://news.frx.com/press-release/r-and-d-news/forest-laborato-
ries-inc-and-gedeon-richter-plc-announce-positive-phase-ii), but
at time of writing the results had still not been communicated
to ClinicalTrials.gov (Table 2).
Therapeutic advances and future perspectives inbipolar depressionThe atypical antipsychotic lurasidone demonstrated efficacy in
reducing depressive symptomatology in adult BD-I (Table 2) and
received FDA approval for this indication in 2013, either as
monotherapy or as adjunctive to lithium or valproate Q2(http://
www.accessdata.fda.gov/drugsatfda). Lurasidone is a dopamine
D2 receptor (D2R) and serotonin 5-HT2A receptor (5-HT2AR)
antagonist, which can be differentiated from other available
atypical antipsychotics by a strong antagonist activity at 5-HT7
receptors (5-HT7R) and partial agonist activity at 5-HT1A recep-
tors (5-HT1AR), compatible with favorable effects on cognitive
function and an antidepressant action. By contrast, lurasidone
has a low affinity for adrenergic a1R, a2cR and 5-HT2cR, and no
affinity for histamine H1R or muscarinic M1R, suggesting a
emerging therapies for depressive episodes and maintenance treatment, Drug Discov Today

Q3
Drug Discovery Today � Volume 00, Number 00 � July 2014 REVIEWS
DRUDIS 1467 1–9
Q8
Reviews�POSTSCREEN
better tolerability profile than other second-generation antipsy-
chotics.
The OFC combination showed efficacy in pediatric BD-I
depressive episodes (Table 2) and received FDA approval in
2013 for this indication (http://www.accessdata.fda.gov/drug-
satfda). Further development of OFC in bipolar depression
should consider the well-known adverse effects of long-term
OFC treatment in adults with schizophrenia (weight gain, dys-
lipidaemia and somnolence) [28].
Conversely, quetiapine XR, which was already FDA- and EMA-
approved for the treatment of adult bipolar patients, failed to
demonstrate a statistically significant difference with a placebo
in pediatric BD-I and/or BD-II depressive episodes (Table 2). The
antidepressant mechanism of quetiapine is poorly understood,
and several trials are ongoing to understand its effects in humans.
Data were also obtained with armodafinil, which showed
negative results in two out of the three Phase III trials
(Table 2). The compound reached statistical significance in
several important secondary endpoints, such as responder rate
and remission, but Teva decided not proceed with regulatory
filings in this therapeutic indication.
The antipsychotic cariprazine recently completed a Phase IIb
trial in patients with bipolar depression (Table 2) and Forest and
Gedeon announced positive results (http://news.frx.com/press-
release/r-and-d-news/forest-laboratories-inc-and-gedeon-richter-
plc-announce-positive-phase-ii), but at time of writing the results
had still not been communicated to ClinicalTrials.gov. Caripra-
zine is a dopamine D2 partial agonist, similar to aripiprazole, but
with preferential affinity for dopamine D3 receptors [24].
Ramelteon is the first in a new class of sleep agents that
selectively binds to the MT1 and MT2 receptors in the suprachias-
matic nucleus [22,29–31]. Two Phase III studies were initiated for
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and e(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
FDA- and/or EMA- approval status before 20
Compoundsapproved inpsychiatricindications
New investigationalcompounds
Other
BDmaintenance
treatment
FIGURE 2
FDA and/or European Medicines Agency (EMA) approval status (before 2012) for
disorder (BD) (in 2012 or later). Compounds were divided into two different categ
indications (maintenance treatment or other) and new investigational compound
sublingual ramelteon in adult BD-I patients with acute depressive
episodes (Table 2). The rational of these studies is supported by
studies showing that abnormalities in circadian rhythms are
prominent features of bipolar disorder [29] and by a small pilot
study in ambulatory BD-I with manic symptoms and insomnia
showing that ramelteon improved the global rating of depressive
symptoms [27].
Recent clinical trials in maintenance treatmentA total of 14 clinical trials fulfilling our selection criteria were
identified in the above databases (accessed between 19th Febru-
ary and 7th May 2014). These corresponded to ten compounds
active in clinical trials for maintenance treatment in 2012 or
later.� Lamotrigine (Lamictal1, GlaxoSmithKline) – for review of
previous studies see [32].� Olanzapine (Zyprexa1, Lilly) [33].� Quetiapine (Seroquel1, AstraZeneca) [18].� Aripiprazole (Abilify1, Otsuka) [34].� Lurasidone (Latuda1, Sunovion) [20].� Paliperidone extended release (ER, Invega Sustenna1 in USA,
Xeplion1 in Europe, Janssen), the primary active metabolite of
the older antipsychotic risperidone [35].� Ramelteon (Rozerem1, Takeda Pharmaceuticals) [22].� Cariprazine (Forest Laboratories) [24].� Scyllo-inositol (ELND005, AZD-103, Elan Pharmaceuticals)
[36].� Mifepristone (Mifeprex1, Korlym1) [37,38].
Mechanism of action and medical uses of the above compounds
are given in Table 1. FDA and/or EMA approval status before 2012
is given in Fig. 2. Efficacy status and/or results are summarized in
Table 3.
merging therapies for depressive episodes and maintenance treatment, Drug Discov Today
12Compounds in clinical trials for
bipolar depression in 2012 or later
• Ramelteon• Cariprazine• Scyllo-inositol• Mifepristone
• Lurasidone• Paliperidone extended release
• Lamotrigine• Olanzapine• Quetiapine• Aripiprazole
Drug Discovery Today
compounds undergoing clinical trials in maintenance treatment of bipolarories according to their approval status: compounds approved in psychiatric
s.
www.drugdiscoverytoday.com 5

LO
v
e
c
n
QS
q
B
p�
a�
�
�
AO
ic
w
p
z
LS
o
(T�
REVIEWS Drug Discovery Today � Volume 00, Number 00 � July 2014
DRUDIS 1467 1–9
TABLE 3
Compounds undergoing clinical trials for maintenance treatment of bipolar disorder (during and after 2012).
Condition Phase Compound Identifier or ref. Results
Relapse prevention IV Lamotrigine versus olanzapine NCT01864551 Completed in September 2012
III Paliperidone ER (InvegaW) [39] Significant for MEa, not for DEb
III Quetiapine (FK949E) NCT01725308 October 2016c
III Aripiprazole (AbilifyW) NCT01567527 February 2016c
III Lurasidone (LatudaW) PERSIST May 2015c
III Ramelteon (RozeremW) NCT01467713 February 2015c
II Quetiapine (FK949E) NCT01737268 October 2016c
II Scyllo-inositol (ELND005, AZD-103) NCT01674010 August 2014c
Safety trial III Lurasidone (LatudaW) NCT00868959 Completed in February 2013
III PERSISTxt August 2015c
III Cariprazine NCT01059539 Completed in March 2012
Not specified Quetiapine XR (Seroquel XRW) NCT01447082 Completed in December 2012
Cognitive function II Mifepristone (MifeprexW, KorlymW) [38] Memory improvement
aManic episode.b Depressive episode.c Estimated completion date.
6
Review
s�P
OSTSCREEN
amotrigine versus olanzapinene Phase IV trial ( NCT01864551) compared lamotrigine
ersus olanzapine for relapse prevention of depressive
pisodes (time frame = 12 months) (Table 3). The trial was
ompleted in 2012, but at time of writing the results were
ot posted to ClinicalTrials.gov.
uetiapineome studies are now ongoing or were recently completed with
uetiapine and quetiapine XR in the maintenance treatment of
D. One of these studies was completed, but the results were not
osted to ClinicalTrials.gov:
NCT01447082 – epidemiological safety study of quetiapine XR
(estimated time frame is 1.5 years).
Three other studies were communicated to ClinicalTrials.gov
nd are currently recruiting participants:
NCT01725308 – quetiapine (FK949E) in BD-I or BD-II patients
with major depressive episodes;
NCT01737268 – quetiapine (FK949E) in elderly BD patients
with major depressive episodes (open-label study, 52 weeks);
NCT01938859 – quetiapine, lithium or shuganjieyu capsules
(Chinese medicine) in bipolar patients currently suffering from
depressive episodes.
ripiprazolene Phase III study (NCT01567527) was communicated to Clin-
alTrials.gov and is currently recruiting participants. The trial
ill assess the time to recurrence of any mood episode in BD-I
atients who have maintained stability on intramuscular aripipra-
ole for at least 8 weeks.
urasidoneeveral long-term studies are in progress to assess the efficacy
f lurasidone in the maintenance treatment of BD-I depression
able 3).
NCT00868959. A 24-week extension study of PREVAIL 1
and 2 trials. The primary outcome of this study is to
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and em(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
www.drugdiscoverytoday.com
evaluate safety and tolerability of lurasidone. This study was
recently completed. Of 813 participants analyzed, 529
participants with serious and nonserious treatment-emergent
adverse events completed 24 weeks of extension study
treatment.
PERSISTExt (NCT01575561). A 12-week extension study of the
PREVAIL 3 trial. The primary outcome of this open-label study
is to evaluate treatment-emergent adverse events. At the time of
writing, this study was currently recruiting participants.
�
� PERSIST (NCT01358357). This is a 28-week, Phase III study
designed to evaluate the efficacy and safety of lurasidone (in
combination with lithium or divalproex) for the maintenance
treatment of BD-I. This study was currently recruiting
participants.
Paliperidone ERBerwaerts et al. [39] conducted a Phase III study of paliperidone
extended release Q4(ER) as maintenance treatment in adult BD-I
patients with manic or mixed episodes who achieved remission
with flexibly dosed paliperidone ER (3–12 mg/day) or olanzapine
(5–20 mg/day) (NCT00490971). Responders to paliperidone ER
were randomized (1:1) to a fixed-dose paliperidone ER (n = 152)
or a placebo (n = 148); those on olanzapine continued to receive it
at a fixed dose (n = 83) (maintenance phase). Median time to
recurrence of any mood symptoms (primary endpoint) was 558
days (paliperidone ER) and 283 days (placebo) and not observed
with olanzapine (<50% of patients experienced recurrence). Time
to recurrence of any mood symptoms was significantly longer with
paliperidone ER than the placebo (P = 0.017); the difference was
significant for preventing recurrence of manic, but not depressive,
symptoms. Treatment-emergent adverse events (maintenance
phase) occurred more often in the olanzapine group (64%) than
in the placebo (59%) or paliperidone ER (55%) groups.
RamelteonA Phase III study of ramelteon was recently initiated for
the maintenance treatment of BD-I in adults (NCT01467713)
erging therapies for depressive episodes and maintenance treatment, Drug Discov Today

Drug Discovery Today � Volume 00, Number 00 � July 2014 REVIEWS
DRUDIS 1467 1–9
Reviews�POSTSCREEN
(Table 3). The primary endpoint is the time from randomization to
relapse over 9 months.
Scyllo-inositolIn 2012, a Phase II trial was initiated for the adjunctive mainte-
nance treatment of BD-I with scyllo-inositol (NCT01674010), as
compared with placebo, lamotrigine or valproic acid (Table 3).
The primary endpoint is the time to recurrence of any mood
episode up to 48 weeks.
CaripiprazineThe NCT01059539 study evaluated the long-term safety, tolera-
bility and pharmacokinetics of cariprazine in patients with bipolar
I disorder (n = 403, time frame = 16 weeks). The study was com-
pleted in March 2012 (Table 3). No results were posted at time of
writing to ClinicalTrials.gov.
MifepristoneWatson et al. [38] examined the longer-term efficacy of 600 mg/
day of mifepristone as an adjunctive treatment for one week in a
placebo-controlled, randomized, double-blind trial in 60 patients
with bipolar depression, with spatial working memory (SWM) as
the primary outcome measure. Mifepristone treatment was asso-
ciated with a sustained improvement in SWM performance. The
magnitude of this neuropsychological response was predicted by
the magnitude of the cortisol response to mifepristone. The re-
sponse occurred in the absence of a significant improvement in
depressed mood.
Therapeutic advances and future perspectives inmaintenance treatmentPaliperidone ER significantly prevented relapse in clinically stable
bipolar patients. Interestingly, the compound was efficacious for
preventing recurrence of manic but not depressive symptoms
(Table 3). Paliperidone ER is not approved for the treatment of
BD-I in the USA or the EU.
Extension studies with lurasidone are testing its long-term
tolerability and safety in bipolar patients (Table 3). Positive results
are expected because lurasidone differs from the other second-
generation antipsychotics by having a good tolerability profile, in
particular for cardio-metabolic tolerability [20,40]. However, lur-
asidone seems to have a significant although moderate link with
the occurrence of akathisia, extrapyramidal symptoms and hyper-
prolactinemia at the start of treatment [20]. Lurasidone should be
tested for its long-term tolerability and safety in BD in comparative
studies versus quetiapine or olanzapine.
Several trials are ongoing with quetiapine for maintenance
treatment of BD (Table 3). Further head-to-head trials of quetia-
pine versus other drug regimens that are effective in bipolar
depression would be of considerable interest.
One interesting Phase IV trial compares olanzapine versus
lamotrigine in the prevention of depressive episodes (Table 3).
The investigators hypothesized that olanzapine will be superior to
lamotrigine in the prevention of any kind of recurrence of bipolar
disorder. By contrast, the lamotrigine group will have better
prevention of depressive episodes than the olanzapine group.
The study was completed, but at time of writing results were
not posted to ClinicalTrials.gov.
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and e(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
Long-term maintenance treatment does not only imply relapse
prevention but also improvement of residual symptoms. In this
respect, ongoing studies with ramelteon will decide if the com-
pound mitigates insomnia. Similarly, there is hope that mifepris-
tone will confirm preliminary results on cognitive function.
Ramelteon has a strong rational to be tested in this indication.
Disrupted circadian rhythms are associated with an increased risk
of relapse in bipolar disorder, and a Phase IV pilot study (n = 83)
showed that patients treated with ramelteon were approximately
half as likely to relapse as patients treated with a placebo through-
out a 24-week treatment period [29].
Scyllo-inositol is an amyloid beta peptide aggregation inhibitor
under investigation for the treatment of Alzheimer’s disease (AD)
and BD. The drug has been shown to prevent, reduce and reverse
AD processes, such as amyloid beta load and loss of cognitive
function in animal models. By contrast, the cognitive, affective
and functional impairment in BD could be difficult to differenti-
ate from those in elderly patients with Alzheimer’s disease [41].
Moreover, both diseases show response to lithium treatment [41].
An ongoing Phase II study with scyllo-inositol will indicate if the
compound reduces relapse in BD.
Remaining treatment needsBesides bipolar depression and long-term maintenance, there are
other unmet needs of BD, like comorbidities, residual symptoms
and cognition. Although this topic is out of the scope of our study,
it is interesting to mention that lisdexamfetamine reduced
attention deficit hyperactivity disorder (ADHD) symptom severity
(in comorbid BD) in a pilot Phase IV study (NCT01051440) [23]
and that mifepristone improved cognition [38]. Adjunctive psy-
chosocial interventions are providing substantial progress in the
management of BD [8], and their combination with the new
pharmacological treatments warrants further clinical research.
Drug development limitations in BDDrug development in BD is hampered by the scarce knowledge of
basic disease mechanisms and the unconvincing animal models
[8]. The advances in pathophysiological [8] and diagnostic aspects
of BD [42,43] could contribute to define therapeutic targets and
treatment options of BD better. One successful example is the
study by Watson et al. [38] suggesting that mifepristone could
enhance spatial working memory in bipolar depression by a per-
sistent enhancement of hippocampal mineralocorticoid receptor
function.
More treatment outcome research is needed in BD. Comparative
studies are lacking, particularly for long-term tolerance. Clinical
trials of adjunctive therapies for treatment refractory cases are also
lacking [9]. Patients in clinical trials usually differ from those in
real life who are frequently poly-medicated and suffer multiple
comorbidities. Randomized, controlled research is needed to pro-
vide guidelines for possible use of mood stabilizers and/or anti-
psychotics in patients with comorbidities [44].
Concluding remarksA great deal of work is going on in the area of BD-targeted
therapies. We identified 30 recent clinical trials testing eight
compounds in depressive episodes. Among these, lurasidone
showed efficacy and was approved by the FDA for adult BD-I
merging therapies for depressive episodes and maintenance treatment, Drug Discov Today
www.drugdiscoverytoday.com 7

d
p
m
c
r
II
t
b
c
a
r
a
o
t
R
1
1Q6
1
1
1
1
1
1
1
1
2
2
2
REVIEWS Drug Discovery Today � Volume 00, Number 00 � July 2014
DRUDIS 1467 1–9
8
Review
s�P
OSTSCREEN
epressive episodes. OFC showed efficacy and was approved for
ediatric BD-I depressive episodes.
Fourteen other recent clinical trials tested ten compounds in
aintenance treatment. Paliperidone ER prevented relapse in
linically stable patients. A Phase III trial with the melatonin
eceptor agonist ramelteon is ongoing in BD-I in adults. A Phase
study suggested that the progesterone and glucocorticoid recep-
or antagonist mifepristone improves spatial working memory in
ipolar depression. A large number of other clinical trials should be
ompleted in the near future.
Recent clinical trials reviewed here are providing therapeutic
dvances, particularly for depressive episodes. Moreover, the cur-
ent pipeline is encouraging with promising new compounds,
cting on new pharmacological targets and on specific aspects
f bipolar depression. After years of slow development and with
he help of governments and public organizations, we hope that
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
www.drugdiscoverytoday.com
current research will lead to advances that mean that BD will lose
its status as one of the top ten disabling conditions.
Conflict of interestThe authors have received no payment in preparation of this
manuscript. Ricardo Garay and Ahcene Hameg are members of
a non-profit association for therapeutic innovation (Craven, Vil-
lemoisson-sur-Orge, France), and have no conflicts of interest to
declare concerning this study. Pierre-Michel Llorca declares grants,
consulting, expertise and conferences from Astra-Zeneca, Eli Lilly,
Lundbeck, Bristol-Myers Squibb and Otsuka. Ludovic Samalin has
received honoraria for conferences and consulting from AstraZe-
neca, Bristol-Myers Squibb, Eli Lilly, Lundbeck and Otsuka. Allan
Young declares paid lectures and advisory boards for all major
pharmaceutical companies with drugs used in Q5affective and related
disorders.
eferences
1 Fagiolini, A. et al. (2013) Prevalence, chronicity, burden and borders of bipolar
disorder. J. Affect. Disord. 148, 161–169
2 Gonda, X. et al. (2012) Suicidal behavior in bipolar disorder: epidemiology,
characteristics and major risk factors. J. Affect. Disord. 143, 16–26
3 Kupfer, D.J. (2005) The increasing medical burden in bipolar disorder. J. Am. Med.
Ass. 293, 2528–2530
4 Phillips, M.L. and Kupfer, D.J. (2013) Bipolar disorder diagnosis: challenges and
future directions. Lancet 381, 1663–1671
5 Craddock, N. and Sklar, P. (2013) Genetics of bipolar disorder. Lancet 381,
1654–1662
6 Alloy, L.B. et al. (2005) The psychosocial context of bipolar disorder: environmental,
cognitive, and developmental risk factors. Clin. Psychol. Rev. 25, 1043–1075
7 APA (2002) American Psychiatric Association. Practice guideline for the treatment
of patients with bipolar disorder (revision). Am. J. Psychiatry 159 (Suppl. 4), 1–50
8 Geddes, J.R. and Miklowitz, D.J. (2013) Treatment of bipolar disorder. Lancet 381,
1672–1682
9 Keedwell, P.A. and Young, A.H. (2014) Emerging drugs for bipolar depression: an
update. Expert Opin. Emerg. Drugs 19, 25–36
0 Mc Intyre, R.S. et al. (2013) A review of FDA-approved treatment options in bipolar
depression. CNS Spectr. 18 (Suppl. 1), 4–20
1 NICE Bipolar Disorder (2006) Clinical Guidance no. 38. Available at: http://
www.nice.org.uk/guidance/CG38
2 Samalin, L. et al. (2011) Lithium and anticonvulsants in bipolar depression.
Encephale 37 (Suppl. 3), 203–208
3 Baldessarini, R.J. et al. (2010) Bipolar depression: overview and commentary.
Harvard Rev. Psychiatry 18, 143–157
4 Leboyer, M. and Llorca, P.M. (2011) Bipolar depression. Encephale 37 (Suppl. 3),
161–162
5 Selle, V. et al. (2014) Treatments for acute bipolar depression: meta-analyses of
placebo-controlled, monotherapy trials of anticonvulsants, lithium and
antipsychotics. Pharmacopsychiatry 47, 43–52
6 Ketter, T.A. (2010) Nosology, diagnostic challenges, and unmet needs in managing
bipolar disorder. J. Clin. Psychiatry 71, e27
7 Silva, M.T. et al. (2013) Olanzapine plus fluoxetine for bipolar disorder: a systematic
review and meta-analysis. J. Affect. Disord. 146, 310–318
8 Sanford, M. and Keating, G.M. (2012) Quetiapine: a review of its use in the
management of bipolar depression. CNS Drugs 26, 435–460
9 Stoner, S.C. and Pace, H.A. (2012) Asenapine: a clinical review of a second-
generation antipsychotic. Clin. Ther. 34, 1023–1040
0 Samalin, L. et al. (2011) Clinical potential of lurasidone in the management of
schizophrenia. Ther. Clin. Risk Manag. 7, 239–250
1 Calabrese, J.R. et al. (2010) Adjunctive armodafinil for major depressive
episodes associated with bipolar I disorder: a randomized, multicenter, double-
blind, placebo-controlled, proof-of-concept study. J. Clin. Psychiatry 71, 1363–
1370
2 Miyamoto, M. (2009) Pharmacology of ramelteon, a selective MT1/MT2 receptor
agonist: a novel therapeutic drug for sleep disorders. CNS Neurosci. Ther. 15,
32–51
23 Mc Intyre, R.S. et al. (2013) The effect of lisdexamfetamine dimesylate on body
weight, metabolic parameters, and attention deficit hyperactivity disorder
symptomatology in adults with bipolar I/II disorder. Human Psychopharmacol. Clin.
Expl. 28, 421–427
24 Citrome, L. (2013) Cariprazine in bipolar disorder: clinical efficacy, tolerability, and
place in therapy. Adv. Therapy 30, 102–113
25 Kim, S.J. et al. (2014) Effect of quetiapine XR on depressive symptoms and sleep
quality compared with lithium in patients with bipolar depression. J. Affect. Disord.
157, 33–40
26 Woo, Y.S. et al. (2013) Lurasidone as a potential therapy for bipolar disorder.
Neuropsychiatr. Dis. Treat. 9, 1521–1529
27 Mc Elroy, S.L. et al. (2011) A randomized, placebo-controlled study of adjunctive
ramelteon in ambulatory bipolar I disorder with manic symptoms and sleep
disturbance. Intl. Clin. Psychopharmacol. 26, 48–53
28 Leucht, S. et al. (2013) Comparative efficacy and tolerability of 15 antipsychotic
drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet 382,
951–962
29 Norris, E.R. et al. (2013) A double-blind, randomized, placebo-controlled trial of
adjunctive ramelteon for the treatment of insomnia and mood stability in patients
with euthymic bipolar disorder. J. Affect. Disord. 144, 141–147
30 Liu, J. and Wang, L.N. (2012) Ramelteon in the treatment of chronic insomnia:
systematic review and meta-analysis. Int. J. Clin. Practice 66, 867–873
31 Krystal, A.D. (2005) Q7Ramelteon. Hypnotic agent targets delayed sleep onset. Curr.
Psychiatry 4, 11
32 Reid, J.G. et al. (2013) Lamotrigine in psychiatric disorders. J. Clin. Psychiatry 74,
675–684
33 Tohen, M. et al. (2013) Efficacy of olanzapine monotherapy in acute bipolar
depression: a pooled analysis of controlled studies. J. Affect. Disord. 149, 196–201
34 McKeage, K. (2014) Aripiprazole: a review of its use in the treatment of manic
episodes in adolescents with bipolar I disorder. CNS Drugs 28, 171–183
35 Canuso, C.M. et al. (2009) Paliperidone extended-release for schizophrenia: effects
on symptoms and functioning in acutely ill patients with negative symptoms.
Schizophrenia Res. 113, 56–64
36 Ma, K. et al. (2012) Scyllo-inositol, preclinical, and clinical data for alzheimer’s
disease. Adv. Pharmacol. 64, 177–212
37 Swica, Y. et al. (2013) Acceptability of home use of mifepristone for medical
abortion. Contraception 88, 122–127
38 Watson, S. et al. (2012) A randomized trial to examine the effect of mifepristone on
neuropsychological performance and mood in patients with bipolar depression.
Biol. Psychiatry 72, 943–949
39 Berwaerts, J. et al. (2012) A randomized, placebo- and active-controlled
study of paliperidone extended-release as maintenance treatment in patients
with bipolar I disorder after an acute manic or mixed episode. J. Affect. Disord. 138,
247–258
40 Citrome, L. et al. (2014) Clinical assessment of lurasidone benefit and risk
in the treatment of bipolar I depression using number needed to treat,
number needed to harm, and likelihood to be helped or harmed. J. Affect. Disord.
155, 20–27
emerging therapies for depressive episodes and maintenance treatment, Drug Discov Today

Drug Discovery Today � Volume 00, Number 00 � July 2014 REVIEWS
DRUDIS 1467 1–9
41 Besga, A. et al. (2012) Discovering Alzheimer’s disease and bipolar disorder white
matter effects building computer aided diagnostic systems on brain diffusion tensor
imaging features. Neurosci. Lett. 520, 71–76
42 Angst, J. et al. (2014) DSM-IV diagnosis in depressed primary care patients with
previous psychiatric ICD-10 bipolar disorder. J. Affect. Disord. 152–154, 295–298
Please cite this article in press as: Garay, R.P. et al. Bipolar disorder: recent clinical trials and e(2014), http://dx.doi.org/10.1016/j.drudis.2014.07.010
43 Parker, G. et al. (2013) Differentiation of bipolar I and II disorders by examining for
differences in severity of manic/hypomanic symptoms and the presence or absence
of psychosis during that phase. J. Affect. Disord. 150, 941–947
44 Azorin, J.M. et al. (2010) Possible new ways in the pharmacological treatment of
bipolar disorder and comorbid alcoholism. Neuropsychiatr. Dis. Treat. 6, 37–46
merging therapies for depressive episodes and maintenance treatment, Drug Discov Today
www.drugdiscoverytoday.com 9
Reviews�POSTSCREEN







![[CONFERENCE PAPER] Bipolar Bozuklukta BDT](https://static.fdokumen.com/doc/165x107/63328d1f4e0143040300b9b3/conference-paper-bipolar-bozuklukta-bdt.jpg)