Bereavement Support in an Acute Hospital: An Irish Model
20
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [UDST - Death Studies] On: 4 September 2008 Access details: Access Details: [subscription number 790425462] Publisher Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Death Studies Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713657620 Bereavement Support in an Acute Hospital: An Irish Model Trish Walsh a ; Maeve Foreman a ; Philip Curry a ; Siobhan O'Driscoll b ; Martin McCormack b a School of Social Work and Social Policy, Trinity College Dublin, Ireland b Social Work Department, Beaumont Hospital, Dublin, Ireland Online Publication Date: 01 September 2008 To cite this Article Walsh, Trish, Foreman, Maeve, Curry, Philip, O'Driscoll, Siobhan and McCormack, Martin(2008)'Bereavement Support in an Acute Hospital: An Irish Model',Death Studies,32:8,768 — 786 To link to this Article: DOI: 10.1080/07481180802289788 URL: http://dx.doi.org/10.1080/07481180802289788 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Bereavement Support in an Acute Hospital: An Irish Model
PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [UDST - Death Studies]On: 4 September 2008Access details: Access Details: [subscription number 790425462]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Death StudiesPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713657620
Bereavement Support in an Acute Hospital: An Irish ModelTrish Walsh a; Maeve Foreman a; Philip Curry a; Siobhan O'Driscoll b; Martin McCormack b
a School of Social Work and Social Policy, Trinity College Dublin, Ireland b Social Work Department,Beaumont Hospital, Dublin, Ireland
Online Publication Date: 01 September 2008
To cite this Article Walsh, Trish, Foreman, Maeve, Curry, Philip, O'Driscoll, Siobhan and McCormack, Martin(2008)'BereavementSupport in an Acute Hospital: An Irish Model',Death Studies,32:8,768 — 786
To link to this Article: DOI: 10.1080/07481180802289788
URL: http://dx.doi.org/10.1080/07481180802289788
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

BEREAVEMENT SUPPORT IN AN ACUTEHOSPITAL: AN IRISH MODEL
TRISH WALSH, MAEVE FOREMAN, and PHILIP CURRY
School of Social Work and Social Policy, Trinity College Dublin, Ireland
SIOBHAN O’DRISCOLL and MARTIN MCCORMACK
Social Work Department, Beaumont Hospital, Dublin, Ireland
In the first Irish study to examine a hospital-based bereavement care program,1 year’s cohort of bereaved people was surveyed. A response rate of over 40%provided 339 completed questionnaires from bereaved next-of-kin. The findingssuggest that a tiered pyramid model of bereavement care (the Beaumont model)may be functional in a number of ways. The outreach aspect of the service issuccessful in providing additional support and information through telephoneand postal contact to people at a distance or with mobility difficulties. Thosebereaved by sudden death are twice as likely to access the service as those for whomdeath was expected. These, and other findings, are discussed.
Falling mortality rates, less exposure to death, and increased lifeexpectancy are all facts of life in contemporary Ireland leadingto changed attitudes toward death, dying, and bereavement (VanDoorslaer & Keegan, 2001). Although home is seen as the idealplace to die, the reality is that most people die elsewhere. Almost30,000 people die annually in Ireland (Health Services Executive,2005) and up to 66% of deaths take place in some form of hospitalor institution, with 40% occurring in acute hospitals (Irish HospiceFoundation [IHF], 2006).
Death, when it occurs, brings to an end for a range of hospitalstaff their role in that individual fight for life. With the urgency of
Received 22 October 2007; accepted 16 March 2008.We acknowledge with gratitude the guidance and support offered by Orla Keegan of
the Irish Hospice Foundation, Erna O’Connor, and Shane Butler of Trinity College Dublinand Dr. Regina Quillan of Beaumont Hospital. This article is dedicated to the memory ofSiobhan O’Driscoll, an inspired and inspiring social work practitioner and teacher, who diedin December 2007.
Address correspondence to Trish Walsh, PhD., School of Social Work and SocialPolicy, Trinity College Dublin, Dublin 2, Ireland. E-mail: [email protected]
768
Death Studies, 32: 768–786, 2008Copyright # Taylor & Francis Group, LLCISSN: 0748-1187 print/1091-7683 onlineDOI: 10.1080/07481180802289788
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

need and the pressure on beds that often exists, staff must move onquickly to the next patient, the next critical situation, the nextemergency. But what of the bereaved? How are they dealt within such situations, and how many of them see the hospital as a con-tinued source of support and help? How valid is the concept of ahospital-based bereavement care service?
In this article, a report is provided of a study evaluating ahospital-based bereavement service in an inner-city area of Dublin,Ireland. Beaumont Hospital is a large acute general hospital with750 beds and the national referral center for neurosurgery, neurol-ogy, renal and pancreatic transplantation and cochlear implan-tation. It serves an increasingly diverse local population of250,000 in an urban area with a high degree of social disadvantage.In this hospital there are approximately 1,050 deaths per year(O’Driscoll, 2004). Beaumont’s bereavement care service is uniqueamong acute hospitals in Ireland in offering an extensive outreachprovision to named ‘‘next-of-kin’’.
The objectives of this article are firstly to review relevant inter-national literature relating to services in acute hospitals, secondlyto locate this specific service within its Irish context, thirdly todescribe the service model itself, and finally to present and discussfindings from a study that elicited feedback from bereaved next-of-kin and hospital staff. The findings discussed here primarily relateto next-of-kin. The findings regarding hospital staff will be reportedmore fully separately. This article is not an attempt to measure theefficacy of the services offered nor does it claim to do so.
Literature Review
Contemporary holistic theorists call for a move to ‘‘normalize’’grief and for more community education to improve the socialsupport systems that people already have (N. P. Field & Friedrichs,2004; Klass, Silverman, & Nickman, 1996; Neimeyer, 2001, 2005;M. Stroebe & Schut, 1999). Although much research in the1970s–1990s focused on issues of pathology and risk assessment,it is now generally accepted that most people will recover overtime from normal bereavement experiences without any profes-sional interventions or with low-level interventions only (Bonanno,Wortmann, & Nesse, 2004; Prigerson, 2005; W. Stroebe & Stroebe,1987). Evidence does not support the provision of routine
An Irish Model of Bereavement Support 769
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008
specialized therapeutic interventions to all. Clinical interventionsoffer most benefit when they are of a high quality, delivered byspecially trained professionals and targeted at the 5 to 20% of spe-cific groups who may experience complex or complicated grief(Nucleus Group, 2004; Wimpenny et al., 2006). Different grievingstyles and experiences require a choice of intervention approachesthat should be responsive to individual need. Interventions shouldbe flexible and customized to suit different genders, cultures, ages,coping styles, and perceived individual need ( Jordan & Neimeyer,2003). The argument is made by some for a public health approachwith a view to developing a seamless health care response towardthe human experiences of death, dying and loss, includingbereavement care (International Work Group on Death, Dyingand Bereavement, 2005; p. 159). Greater community awarenessof grief and bereavement is seen to increase people’s preparationfor death and the community’s capacity to support individuals(Nucleus Group, 2004). Strategies such as self-help=support groupsmight be particularly relevant where cultural barriers haveprevented particular groups from accessing traditional servicemodels (e.g., indigenous or immigrant minority groups; NucleusGroup, 2004).
Acute Hospitals and Bereavement Care
Although benefits are hard to quantify, indications are thatbereavement services located within the acute hospital help thegrieving process, give a positive image of the hospital, and arebeneficial to staff. Benefits identified by next-of-kin include receiv-ing medical information, being told of the death in a compassion-ate way, and having good communication and emotional support(Billings & Kolton, 1999; Burke & Gerraughty, 1994; Williams,Harris, Randall, Nichols, & Brown, 2003). Aspects of care thatare particularly valued include sensitive facilitation of viewingthe body, privacy, belongings returned considerately, written infor-mation on bereavement and available support services, correspon-dence concerning hospital records and procedures, sympathycards from staff, phone calls, and referrals to community serviceswhere needed (Browne, O’Mahony, & McEochaidh, 2005; Fauri,Ettner, & Kovacs, 2000). In the United States (Demmer, 2003)and England (D. Field, Reid, Payne, & Relf, 2004), social workers
770 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008
and nurses are the primary providers of bereavement care. InEngland, volunteers, who have often experienced a bereavementthemselves, also play a role (Farrelly, 2005; McGinley, 2005). Itcan be argued that a range of professionals have a role to play ineffective bereavement care; however, there is no direction fromresearch to date as to whether one professional group should takethe lead in this role or whether a more flexible multi-disciplinaryteam approach is indicated.
The Adequacy of Bereavement Care in Acute Hospitals
A review of bereavement care in emergency rooms some years ago(British Association for Accident and Emergency Prevention,1995) found that follow-up support was limited, information pro-vided was mainly practical, facilities provided for families werepoor, and staff training was limited. Recommendations for dedi-cated services in acute hospitals internationally include trainingfor medical and nursing staff; multidisciplinary teamwork; earlyinterventions commencing before loss; the provision of infor-mation on procedures; expressions of concern through sympathycards or personal contact; education on the grief process, copingstrategies and available support services through written infor-mation, meetings, and support groups; and follow-up support inperson or by telephone (Fauri & Grimes, 1994; Kent & McDowell,2004; LeBrocq, Charles, Chan, & Buchanan, 2003; Williams et al.,2003). Assessment of, and the provision of targeted services to, thenewly bereaved in the acute hospital is particularly problematicwhere the death is sudden or traumatic, when the bereaved doesnot have an existing relationship with the hospital, or where theyreside at some distance from the hospital. The literature suggeststhat the education and support of key hospital personnel in theidentification of those most at risk of complicated grief reactionsand the co-ordination across the disciplines of a whole hospitalapproach to bereavement care is indicated (Nucleus Group,2004; Wimpenny et al., 2006).
The Timing of Interventions
Both Neimeyer (2001) and Schut, Stroebe, Bout, and Terheggen(2002) suggested that interventions offered too soon after death
An Irish Model of Bereavement Support 771
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

have less effect (than those offered later) or may even be counter-productive. They suggest the critical window of time when peopleare most able to use formal support services may be 6 to 18 monthsafter the loss. Renzenbrink (2002) pointed out that it is difficult toknow how long support should be provided after bereavementbecause of the multitude of secondary losses that can occur (per-sonal, social, economic). Current British guidelines recommendthat those assessed as being at risk should be engaged with proac-tively (e.g., by phone call or letter) around eight weeks after theirbereavement (National Institute for Health and Clinical Excel-lence, 2004). Yet although initial contact can take place at an earlystage, bereaved people may not access services, or feel the need forsupport services, for months or even years later. If this is the case,the provision of an annual schedule of ritualized events, widelypublicized and available to all, may have their place in both invit-ing contact and establishing the potential for future contact.
The Case for Outreach Services
The concept of outreach preventive screening is now common-place in developed health care systems; less so that of outreachbereavement care support. Outreach may be needed to reachthe bereaved who are not likely to improve with time and informalsupport but who are unwilling or unable to access professional sup-port. Field et al. (2005) found that the bereaved accessed supportfrom voluntary bereavement organizations, general medical practi-tioners, and churches. Those who declined bereavement supportservices either had enough support from other sources or preferredto cope on their own. Feedback from a study evaluating an emerg-ency room phone service following death, as well as six weekslater, was positive (Williams et al., 2003). The specific needs ofcaregivers for the dying or bereaved, both formal and informal,are increasingly emphasized (Harding & Leam, 2005; Papadatou,2006). Quin, Clarke, Murphy-Lawless, Hickey, & Browne (2005)pointed out that caring for the caregivers is now regarded aspart of good quality health care. Dyregrov (2005) suggestedthat the needs of those who comprise support networks, and theimpact of providing such support post-bereavement have beenoverlooked.
772 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

Irish Bereavement Services
Factors that have driven the development of bereavement servicesin both Ireland and its nearest neighbor, Britain, have been three-fold. Firstly, both Britain and Ireland have a long tradition of hos-pice, stretching back to the 18th century, specifically in Ireland thecare provided by Our Lady’s Hospice, Dublin, and MarymountHospice, Cork. Modern palliative care has developed in Irelandwith the statutory and voluntary sectors working together, withservices available in different settings, including teams in acutehospitals. The presence of a very active and influential hospicefoundation in Ireland has driven the agenda of improved palliativeand bereavement care for all.
Secondly, following public outcries over organ and tissue reten-tion scandals, whereby bereaved relatives had not always been con-sulted or even informed in situations where retention took place, aseries of public inquiries were held. One such was The Royal Liver-pool Children’s Inquiry in 2001. The Irish Madden Inquiry (D. Mad-den, 2006) recommended the appointment of hospital-based liaisonofficers countrywide to offer practical help and support to bereavedfamilies, as well as to staff caring for those families; a role in liaising withpathology departments and families; and mandatory training on griefand bereavement for all patient care staff. Hospitals here and in Britainhave appointed social workers, nurses or administrative staff, or a com-bination of all three as their dedicated bereavement officers.
Thirdly, Irish social workers have a long tradition of bereave-ment work in community, hospital and hospice settings (Farrelly,2005; Harmey & Price, 1992; Kearney, 1977; McCormack, 2002;H. Madden, 1977). The upturn in Ireland’s economy in the early1990s allowed for an increase in hospital-based social workposts and an expansion in their capacity to provide more supportand therapeutic services to patients and their families (Horne &O’Connor, 2005).
Research on Irish Bereavement Services
Although some dissatisfaction with dying in hospital has beenrecorded in Ireland (Browne et al., 2005; Keegan et al., 1999),many report a good experience, based on end-of-life care receivedand compassion of staff (Keegan et al., 1999; Quin et al., 2005).
An Irish Model of Bereavement Support 773
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

Positive features such as offering choice, and good communicationwith patients, increased with palliative care team involvement. Inan Irish nationwide survey on death and dying, only 11% listedbeing in a private space as one of the three things considered mostimportant (IHF, 2004). Being surrounded by people they lovedand being free from pain were considered most important.
Following a review of families’ experiences after sudden infantdeath, one Dublin children’s hospital instituted new interdis-ciplinary procedures and a parents’ booklet explained the roles ofeach professional. The prompt provision of information and ongoingliaison with hospital staff ensured a more sympathetic, honest, andinformative system, and a claimed reduction in long-term unresolvedgrief problems (Ward, 1997). A recent Irish study into the palliativecare needs of children (Quin et al., 2005) found most families werepositive about quality of care although some voiced concern aboutpoor physical conditions, poor communication, and a lack of psycho-logical support. Families identified the period immediately afterdeath as particularly difficult, and a time they would welcome coun-seling and support, both from professionals and other bereaved par-ents. Ironically this was the time when most, if not all, services werewithdrawn. Very few were offered counseling, but those that didfound it helpful. Despite the fact that the majority of social workersinterviewed (n ¼ 14 in all) said that they provided informational,psychological, and practical support, families’ reported experienceswere very different, indicating at best, gaps in these services. Quinet al. (2005) concluded that hospitals needed to provide more com-prehensive care in the immediate postdeath phase, and furthermore,also extend support beyond this period. The provision of annualremembrance services was seen to be particularly beneficial.
The Beaumont Model of Service Delivery
Beaumont Hospital in Dublin is the only Irish acute hospital toprovide a comprehensive outreach service to all bereaved next-of-kin. Conceptualized as a pyramid and based on a philosophyof open access, this model (established in 2001, consolidatingpre-existing initiatives) incorporates psycho-educational activities,peer support and normalizing rituals and events to supportrelatives, the local community, and hospital staff. In addition itensures the provision of more specialized interventions either fromwithin the hospital or from other bereavement services. Although
774 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008
tiered approaches to bereavement care were identified by Schutet al. (2002), and by the Irish National Advisory Committee onPalliative Care (NACPC, 2001), these ideal models are rarelyactualized in practice and examples of their use in acute settingswere not found in the literature. The Beaumont service predatesmore recent local initiatives, most notably the national Hospice-Friendly Hospitals project (IHF, 2007). The conceptual frameworkdevised for this service (O’Driscoll, 2002, 2004) is outlined.
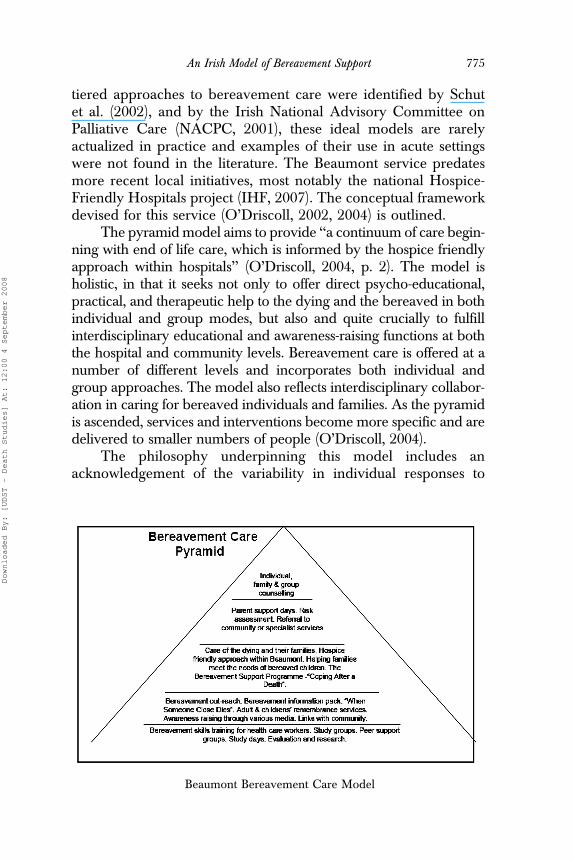
The pyramid model aims to provide ‘‘a continuum of care begin-ning with end of life care, which is informed by the hospice friendlyapproach within hospitals’’ (O’Driscoll, 2004, p. 2). The model isholistic, in that it seeks not only to offer direct psycho-educational,practical, and therapeutic help to the dying and the bereaved in bothindividual and group modes, but also and quite crucially to fulfillinterdisciplinary educational and awareness-raising functions at boththe hospital and community levels. Bereavement care is offered at anumber of different levels and incorporates both individual andgroup approaches. The model also reflects interdisciplinary collabor-ation in caring for bereaved individuals and families. As the pyramidis ascended, services and interventions become more specific and aredelivered to smaller numbers of people (O’Driscoll, 2004).
The philosophy underpinning this model includes anacknowledgement of the variability in individual responses to
Beaumont Bereavement Care Model
An Irish Model of Bereavement Support 775
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

bereavement; adoption of a strengths approach rather than a focuson pathology; a targeted approach focused on providing appropri-ate services at the right time to those in need; promotion of thedevelopment of psycho-educational and preventative services;the utilization and valuing of mutual help or peer support in ser-vice provision. In addition, the aims are to support existing familyand community networks; make a positive contribution to the localcommunity; recognize and acknowledge the impact of socialfactors (e.g., poverty, social exclusion) and include a commitmentto training, evaluation, and research (O’Driscoll, 2004).
Study Design
The study was commissioned by the hospital and received ethi-cal approval as a quality assurance project aimed at improvingpractice. Although the Beaumont model had been in operationsince 2001, it had not been evaluated externally before this study.To this end the aims of the study were firstly, to carry out a reviewof the service’s original objectives, ethos and service frameworkagainst what constitutes best practice. Secondly, to carry out a sur-vey of bereaved next-of-kin noting patterns of uptake, exploringlevels of satisfaction with both hospital care and the bereavementservice and attempting to establish if there were any statisticallysignificant relationships between such variables as geographicdistance from the hospital and likelihood of service-uptake.Finally, we set out to assess hospital staff’s experiences of, andviews on, the service and its importance within the wider hospitalcommunity.
A mixed methodology generating quantitative and qualitativedata was considered most appropriate given the aims as outlinedabove. A census of one year’s deaths in the hospital, and a postalsurvey of one year’s cohort of bereaved (1 November 2003 to31 October 2004) provided a baseline profile of deaths and infor-mation on a range of demographic features, bereavement experi-ences and patterns of support used. Sufficient quantitative datawere generated to allow for multivariate statistical analysis using astandard SPSS program. Two focus-groups were attended by 20self-selected hospital staff from a range of disciplines and levels, attimes designed to facilitate those working different shifts. The find-ings relating to hospital staff will be reported in a separate article.
776 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

Ethical and Methodological Considerations
Given the sensitivity of the topic and the risk of causing distress,great care was taken to provide several opt-out points for respon-dents. Firstly, the hospital manager made contact with all potentialrespondents, alerting them to the study and offering them thechoice of opting out at that point. Secondly, questionnaires weresent with a cover letter assuring the respondents of their anonymityas contact details remained with the hospital, in compliance withlocal Data Protection legislation. In addition, respondents wereinvited to make contact with the principal investigator, and over20 did so, some to withdraw from the survey, others to recountin more personal detail their narratives of loss.
Social workers were excluded from the focus groups, as theywere centrally involved in the delivery of the service. No physi-cians participated in the two staff focus groups. A third focus groupscheduled specifically for physicians attracted no participants.Informal feedback suggested that although individual physicianshad hoped to attend, the general population of physicians weresimply too busy.
A cause for concern with all surveys is that people who do notrespond may be different from those who do and that this will biasthe results. The hospital database provided information for thesurvey population on eight variables: deceased’s gender; age;location of death; length of stay in hospital; the next-of-kin’saddress; relationship to next-of-kin; and if the death was a cor-oner’s case or required no post-mortem. On each variable, therewas no significant difference between the people who respondedto the survey and those who did not, which is some limitedevidence for the unbiased nature of the results.
Findings
Of the 934 people who died in Beaumont hospital during the1-year period, 839 named next-of-kin were eligible to take partin this survey. Of this 839, some were not contactable or had diedin the intervening period. In total, 335 completed questionnaireswere returned, amounting to a response rate of 40% of the eligiblepopulation.
An Irish Model of Bereavement Support 777
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008
A Profile of the Respondents
The majority of respondents was female, older, had lower formaleducation levels, attended a religious service weekly, and lived inDublin’s suburbs. Respondents, in general, had lived at their cur-rent addresses for many years and the vast majority had friendsand=or family living nearby. Over 90% of respondents believedtheir relationship with the deceased to be very positive or positive.Since this original bereavement, 101 (31.2%) had experiencedanother bereavement in the intervening time.
One hundred thirty-four respondents (41%) believed thedeath in Beaumont was unexpected, 99 (30%) thought it wassudden, and 95 (29%) respondents had expected the death tooccur at that time. It is likely that deaths that came as a shock wererecorded in the ‘‘sudden’’ category.
Family disputes were the most common unresolved legalproblems existing at the time of the survey with 32 reporting these.An additional 25 respondents reported legal issues to do withinquests, financial problems, litigation, or criminal investigations.A further 14 reported ‘‘other’’ legal issues not covered by this list.No one reported litigation involving the hospital.
Over 73% of respondents reported that their social network offamily and friends was most helpful to them in coping with theirbereavement. In descending order, respondents identified familydoctors (6%), pets (5%), priests=spiritual advisers (5%), books orfilm media (4%) or other professionals (2%) as the single mostimportant source of help for them in coping with their bereavement.
In common with previously cited studies, the three most fre-quently cited complaints regarding hospital care were poor standardsof information and communication, lack of privacy for the dyingpatient and family, and poor conditions in the emergency room.
Bereaved Next-of-Kin Perspectives on the Service
Two hundred six (65%) found it a comfort to receive the initialletter from the bereavement service 10 to 12 weeks followingtheir loss. Only 6 (2%) were not pleased to have received thisletter, stating that it was an unwelcome intrusion. Over 60% ofrespondents found the enclosed information booklet useful forthemselves and=or other family members.
778 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

The majority of respondents, 152 (57%) felt they receivedinformation at the right time. Following further analysis, it tran-spired that women would have preferred to receive informationearlier, and men would have preferred to receive it later. Respon-dents who contacted the service felt the information came at theright time. However, one-third of respondents would have likedthe invitation to make contact at a different time (either earlieror later) and a substantial proportion of one-fifth would have likedto receive the information later. That these preferences were con-sistent for those who did and did not make contact with the serviceindicated that there is an interaction between these two variablesthat warrants further investigation.
Following on from the contact letter and information bookletfrom the bereavement service, 78 (25%) of those surveyed con-tacted the service, and 234 (75%) did not. Over 90% found it easyto contact the service. Only a very small number, 4 (7%) of respon-dents, were prompted to seek help by a professional. The servicemost frequently accessed (48 respondents) was that of telephoneor postal advice; followed by the peer support programs(n ¼ 32), remembrance services (n ¼ 27), and counseling (n ¼ 26).Services were in the main accessed on more than one occasion.Fifty-two people used bereavement services not provided by thehospital, primarily masses or services of remembrance, supportgroups, or counseling. Over a third of this group learnt about thesesources of support through the hospital.
Feedback was overwhelmingly positive on the range of ser-vices offered: postal or telephone advice and support; peer supportprograms; public lectures, remembrance services, and face-to-facecounseling. The three most helpful aspects of the bereavementcare service cited were (a) information and advice, 117 (49%);(b) speaking to someone about their feelings, 63 (26%); and(c) sharing of experiences with other bereaved people, 47 (20%).
Respondents were asked to identify one aspect of the servicethat they would like changed. Of the 65 (18%) who replied, 9 wishedto see the service extended to pre-death contact; 7 would have likedto use the service but geographical distances were too great. Fourrespondents reported that although they had not used the service,it was a comfort to know that it was there; and 3 respondents didnot avail of the service as they could not face returning to the hospi-tal because of the association with the death of their loved one.
An Irish Model of Bereavement Support 779
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

Perspectives on General Hospital Care
Compared with an earlier Irish nationwide study (IHF, 2004) thatfound that 41% of respondents who had experienced the deathof a significant person in the previous two years described care asexcellent, 52% of this sample described it as such; and a significantmajority of over 80% were satisfied with the care receivedcompared with a total of 75% in the IHF study in 2004. At the sametime, nearly 1 in 10 had serious enough concerns to want issuesaddressed ‘‘urgently’’. These can be summarized under 10 cate-gories: information=communication; privacy around dying anddeath; conditions in the emergency room; problems with staff, bothindividuals and groups; bed shortages and over-crowding; hygieneand cleanliness; facilities for families; staffing shortages and inex-perience; respect for patient=family; and a miscellaneous category.
Findings of Particular Significance
A significant (i.e., greater than chance) relationship was foundwhen looking at the age of the deceased and likelihood of contact-ing the bereavement service. The average age of the deceased wassignificantly lower (Mdn. ¼ 62.9 years of age; SD ¼ 16.9) for thosewho contacted the service than those who had not (Mdn. ¼ 71.4years of age; SD ¼ 15.8); t(307) ¼ 4, p < .001.
A significant relationship was also found between making con-tact with the service and whether the death was sudden, expected,or unexpected. Whereas only 15% of respondents who expectedthe death made contact with the service; twice as many (30%)who did not expect the death made contact with the service. Afurther 26% of respondents who believed the death was suddencontacted the service. It can therefore be suggested that the serviceis particularly successful in establishing contact with those forwhom a death has been sudden or unexpected.
Contrary to expectation, the 78 respondents who contactedthe service (25% of the total) represented roughly the samepercentage from each of the geographic regions, regardless ofdistance: 45 respondents from Dublin city (25% of the total fromthat region); 16 respondents from the county Dublin area, (28%of that population), and 17 who made contact from outside theDublin city and county area (25% of the total from that region).
780 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008
It can therefore be suggested that the service acts as a successfuloutreach service regardless of geographical distance from thehospital. The finding that the traumatically bereaved (by suddendeath) responded to the hospital’s outreach without the benefit ofa relationship with staff is surprising and suggests that the tone ofthe hospital’s outreach service is working. Given the calls for anincrease in community education, it is a positive finding that of thosewho received written information in the post, 25% looked for more.
Summary of Survey Findings
These findings confirm that each experience of bereavement isunique. Death in an acute hospital setting is often traumatic, unexpec-ted, and distressing for family and friends. Physical conditions andissues of communication play an important part in the experienceof death in an acute hospital. For some, if the experience has beenparticularly distressing they may be disinclined to make contact witha hospital-based bereavement service; however for others it appearsthat post-death contact can help to resolve distress or to facilitate theprocess of meaning-making. For most, the outreach bereavementcare approach is welcomed even if there are wide variations in viewson the right timing for initial contact. The provision of a written infor-mation booklet fulfils the recommendation made by Sque, Long, andPayne (2004) and others of the need to avoid pathologizing normalgrief reactions and the presumption that counseling may be needed.Despite the fact that Beaumont’s quality of general care is rated some-what more highly in this study than that of hospitals nationally (IHF,2004), the accounts and responses of those surveyed suggest only oneaspect of care to be found wanting for the whole experience to becontaminated with a negative and bitter aftertaste. Yet, concurrently,sensitivity and kindness and a display of respect on the parts of keystaff are warmly welcomed and remembered.
Discussion
Although some Irish data existed that had reviewed relatives’experience of palliative care and death in another acute hospital(Keegan et al., 1999), sudden death and the death of those residentover 60 miles from the hospital were excluded in that study.This study is therefore the first Irish one that has conducted a
An Irish Model of Bereavement Support 781
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

comprehensive survey of one year’s cohort of bereaved next-of-kinto elicit service-user feedback.
Overall the research message from this study is that thisbereavement service is being used appropriately in that outreachcontact and information provision is welcomed by the majorityand large numbers are not coming forward for specialist or coun-seling services—a quarter of our sample proceeded to make use ofthe service following the initial outreach letter. Higher proportionsof those who described the death as sudden or unexpected (twiceas many as those for whom death was expected) made contact withthe service further suggesting appropriate use of this aspect of thebereavement care service.
The outreach aspect of the service is successful in providingadditional support and information through telephone and postalcontact, suggesting that this aspect can be effective in meetingsome needs of those at a distance or with mobility or transportdifficulties. Both respondents in the survey and hospital staff spokeof the importance of the annual public lectures and memorialservices as an aid to processing their grief.
Limitations of the Study
The use of the ‘‘next-of-kin’’ category does not allow access to thefull range of people affected by a single death and in particularmay be problematic in not reflecting the diversity of relationshipsthat can exist, nor in capturing fully the needs of bereaved peoplewhere family discord or conflict exists. In particular it is likely toexclude friendship networks and the impact loss has in this con-text. It also masks the number of young people (under 18 yearolds) affected by a death.
A very small number of the survey population (n¼12) hadaddresses outside Ireland. These were excluded because they werenot offered the service. This is acknowledged as a significant omis-sion as the foreign national population in Ireland increases andshould not be taken as an indication of lack of regard for theirneeds. In the recommendations of our report (Walsh, Foreman, &Curry, 2007), the needs of this group are specifically addressed.
The absence of feedback from physicians is another signifi-cant gap. This issue will be discussed more fully in a future articlefocused on hospital staff’s experience of the service.
782 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

Finally, the reader is reminded that this study did not set outto establish the efficacy of this service per se, rather it was toestablish some baseline information about take-up rates andservice-users experiences as well as hospital staff perspectives.
Conclusions
Although the palliative care movement has greatly enhanced theconcept of a ‘‘good death’’, acute hospitals will always face chal-lenges in relation to the large number of sudden and unexpecteddeaths with which they have to contend. Those with nationalspecialist centers such as neurosurgery will have increased num-bers of traumatic deaths following workplace accidents, car acci-dents, assaults, and suicides. Some patients will have kin atwidely dispersed geographical locations, who are more prone tocomplicated grief reactions where the circumstances are traumatic,more likely to occur in emergency rooms, and for whom there maybe complicated legal and procedural issues following death.
The Beaumont model of service delivery (O’Driscoll, 2002,2004) provides a flexible multi-tiered outreach bereavement careservice, available to all and apparently successful in supportingsome bereaved both locally and at a geographic distance. In thecase of sudden and unexpected death this service is being accessedby a particularly vulnerable bereaved group.
Overall, on the basis of these findings, we believe that a cau-tious endorsement of this service delivery model is indicated, andthat if positive outcomes for such tiered models are confirmed,they should be considered as one possible template for this difficultarea of service provision. Future developments need to moreactively consider the needs of those bereaved ‘‘at a distance’’(i.e., resident outside the specific nation), given the high mobilityof many migrant working groups in our globalized economies.More creative strategies for reaching those at a geographical dis-tance, those with mobility problems, and particularly vulnerablegroups (such as adolescents bereaved through tragedies, such as sui-cide and accidents) can possibly be developed by harnessing thepower of the internet in addition to offering local opportunitiesfor communal grieving, as well as more specialized interventionsfor the minority who do not self-recover from their loss.
An Irish Model of Bereavement Support 783
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

References
Billings, J. A. & Kolton, E. (1999). Family satisfaction and bereavement carefollowing death in the hospital. Journal of Palliative Medicine, 2, 33–49.
Bonanno, G. A., Wortman, C. B., & Nesse, R. M. (2004). Prospective patterns ofresilience and maladjustment during widowhood. Psychology and Aging, 19,260–271.
Browne, M., O’Mahony, A., & MacEochaidh, G. (2005). Focus group discussionswith staff of Our Lady of Lourdes Hospital, Drogheda: A report prepared for the Careof People Dying in Hospitals Project. Dublin: Irish Hospice Foundation=HealthService Executive, North East.
British Association for Accident and Emergency Prevention. (1995). Bereave-ment care in accident and emergency medicine. London: Royal College ofNursing.
Burke, C. & Gerraughty, S. M. (1994). An oncology unit’s initiation of a bereave-ment support program. Oncology Nurses Forum, 21, 1675–1680.
Demmer, C. (2003). A national survey of hospice bereavement services. Omega,47, 327–341.
Dyregrov, K. (2005). Experiences of social networks supporting traumaticallybereaved. Omega, 52(4), 339–358.
Farrelly, M. (2005). The bereavement journey: The Irish experience. In J. Ling &L. O’Siorain (Eds.), Facing death: palliative care in Ireland (pp. 95–108).Basingstoke, England: Open University Press.
Fauri, D. P., Ettner, B., & Kovacs, P. J. (2000). Bereavement services in acute caresettings. Death Studies, 24, 51–64.
Fauri, D. P. & Grimes, D. R. (1994). Bereavement services for families andpeers of deceased residents of psychiatric institutions. Social Work, 39,185–190.
Field, D., Reid, D., Payne, S., & Relf, M. (2004). Survey of UK hospice andspecialist palliative care adult bereavement. International Journal of PalliativeNursing, 10, 569–576.
Field, D., Reid, D., Payne, S., & Relf, M. (2005). Adult bereavement support in fivehospices in England. Sheffield: University of Sheffield.
Field, N. P. & Friedrichs, M. (2004). Continuing bonds in coping with the death ofa husband. Death Studies, 28, 597–620.
Harding, R. & Leam, C. (2005). Clinical notes for informal carers in palliativecare: Recommendations from a random patient file audit. Palliative Medicine,19, 639–642.
Harmey, N. & Price, B. (1992). Groupwork with bereaved children. GroupworkSpecial Issue: Group work in Ireland, 5, 19–27.
Health Service Executive. (2005). National Service Plan for 2006. Dublin, Ireland:Author.
Horne, M. & O’Connor, E. (2005). An overview of the development of health-related social work in Ireland. In N. Kearney & C. Skehill (Eds.), A historyof social work in Ireland (pp. 163–183). Dublin, Ireland: Institute of PublicAdministration.
784 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008

Irish Hospice Foundation. (2004). Survey of attitudes to death and dying in Ireland.Dublin, Ireland: Author.
Irish Hospice Foundation. (2006). A baseline study on the provision of hospice=specialistpalliative care services in Ireland. Dublin, Ireland: Author.
Irish Hospice Foundation. (2007). Launch of hospice-friendly hospitals project.IHF Newletter, 13, 4.
International Work Group on Death, Dying and Bereavement. (2005). Charterfor the normalisation of dying, death and loss, Mortality, 10, 157–161.
Jordan, J. R. & Neimeyer, R. A. (2003). Does grief counselling work? DeathStudies, 27, 765–786.
Kearney, S. (1977, December 8). Care of the dying child. In Dying and Bereave-ment, Papers from Irish Association of Social Workers Seminar (pp. 11–25). Dublin,Ireland: Irish Association of Social Workers.
Keegan, O., McGee, H., Brady, T., Kunin, H., Hogan, M., O’Brien S., &O’Siorain, L. (1999). Care for the dying: Experiences and challenges. Dublin,Ireland: Irish Hospice Foundation.
Kent, H. & McDowell, J. (2004). Sudden bereavement in acute care settings.Nursing Standards, 19, 38–42.
Klass, D., Silverman, P. R., & Nickman, S. L. (Eds.) (1996). Continuing bonds: Newunderstanding of grief. Philadelphia: Taylor and Francis.
LeBrocq, P., Charles, A., Chan, T., & Buchanan, M., (2003). Establishing abereavement program: Caring for bereaved families and staff in the emerg-ency department. Accident and Emergency Nursing, 11, 85–90.
Madden, D. (2006). Report of Dr. Deirdre Madden on Post Mortem Practice and Proce-dures. Dublin, Ireland: Government of Ireland. www.dohc.ie/publications/pdf/madden (accessed November 2006).
Madden, H. (1977). Casework with newly bereaved widows. Papers from IrishAssociation of Social Workers Seminar: Dying and Bereavement (pp. 1–10). Dublin,Ireland: Irish Association of Social Workers.
McGinley, E. (2005). Milford Care Centre Bereavement Support Service–serving hospice andcommunity. 7th International Conference on Grief and Bereavement, London.
National Advisory Committee on Palliative Care. (2001). Report of the NationalAdvisory Committee on Palliative Care. Dublin, Ireland: Department of Healthand Children.
National Institute for Health & Clinical Excellence. (2004). Improving supportiveand palliative care for adults with cancer: Research evidence. London: Universityof London.
Neimeyer, R. (2001). Searching for the meaning of meaning: Grief therapy andthe process of reconstruction. Death Studies, 24, 541–558.
Neimeyer, R. (2005). Grief, loss and the quest for meaning: Narrative contribu-tions to bereavement care. Bereavement Care, 24, 27–30.
Nucleus Group. (2004). Review of specific grief and bereavement services: Final report.Melbourne, Australia: Department of Human Services, Victoria.
O’Driscoll, S. (2002, Summer). Responding to trauma and bereavement in anacute hospital. Eisteach, 15, 5–11.
O’Driscoll, S. (2004). Responding to bereavement in the acute care setting – Ajourney in service development. In L. Cruz (Ed.), Making sense of dying and
An Irish Model of Bereavement Support 785
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008
death. Oxford, England: The Inter-Disciplinary Press. www.interdisciplinary.net/publishing//idp/eBooks (accessed 2006).
Papadatou, D. (2006). Caregivers in death, dying and bereavement situations.Death Studies, 30, 649–663.
Prigerson, H. (2005). Complicated grief when the path of adjustment leads to adead end. Healthcare Counselling & Psychotherapy Journal, 5(3), 14–15.
Quin, S., Clarke, J., Murphy-Lawless, J., Hickey, L., & Browne, P. (2005). Reporton a research study of the palliative care needs of children in Ireland. Dublin,Ireland: Department of Health & Children=Irish Hospice Foundation.
Renzenbrink, I. (2002). Foundations of bereavement support in hospice and palliativecare. Dublin, Ireland: Irish Hospice Foundation.
Schut, H., Stroebe, M., van den Bout, J., & Terheggen, M. (2002). The efficacyof bereavement interventions: Determining who benefits. In W. Stroebeet al. (Eds), Handbook of bereavement research: Consequences, coping and care(pp. 705–737). Washington, DC: American Psychological Association.
Sque, M., Long, T., & Payne, S. (2004). From understanding to implementation:Meeting the needs of families and individuals affected by post mortem organretention. Accessed online, Nov 2006: http://eprints.soton.ac.uk/9789/01/finalexecutivesummary.pdf
Stroebe, M. & Schut, H. (1999). The dual process model of coping with bereave-ment: Rationale and description. Death Studies 23, 197–213.
Stroebe, W. & Stroebe, M. (1987). Bereavement and Health: Psychological and physicalconsequences of partner loss. New York: Cambridge University Press.
The Royal Liverpool Children’s Hospital Inquiry Report. (2001). London: CrownPublications.
Van Doorslaer, O. & Keegan, O. (2001). Contemporary Irish attitudes towards death,dying and bereavement. Dublin, Ireland: Royal College of Surgeons in Ireland.
Walsh, T., Foreman, M., & Curry, P. (2007). Bereavement Care in Acute Hospitals: Anevaluation of the Beaumont Hospital Bereavement Care Service. Dublin, Ireland:Beaumont Hospital=Trinity College Dublin.
Walter, T. (1996). A new model of grief: Bereavement and biography. Mortality, 1,7–25.
Ward, O. (1997). A study of bereavement care after a sudden and unexpecteddeath. Archives of Disease in Childhood, 76, 79.
Williams, R., Harris, S., Randall, L., Nichols, R., & Brown, S. (2003). A bereave-ment after-care service for intensive care relatives and staff. Nursing CriticalCare, 8, 109–115.
Wimpenny, P., Unwin, R., Dempster, P., Grundy, M., Work, F., Brown, A., &Wilcock, S. E. (2006). Literature review on bereavement and bereavement care.Aberdeen, Scotland: Joanna Briggs Institute=Robert Gordon University.
786 T. Walsh et al.
Downloaded By: [UDST - Death Studies] At: 12:00 4 September 2008