
Bereavement as a Psychosocial Transition: Processes of Adaptation to Change
13
Journal of Social Issues, Vol. 44, No. 3. 1988, pp. 53-6s Bereavement as a Psychosocial Transition: Processes of Adaptation to Change Colin Murray Parkes The London Hospital Medical College There are many ways of construing the psychology of loss. This paper describes one such model, which enlightens some, but not all, aspects of bereavement and needs to be used alongside other models. Loss is one aspect of psychosocial transition, the psychological change that takes place whenever people are faced with the need to undertake a major revision of their assumptionsabout the world. The paper focuses on the ways in which people change or fail to change their internal model of the world in the face of emergent even?s. Examples are taken from bereavement, loss of a limb, and the succession of losses that mark the course of terminal illness. implicationsfor identifyingpeople at risk and mitigat- ing that risk are outlined. People are fascinating because of their individuality; no two problems are alike because no two people are alike. This tempts some people to reject theories of human behavior. There are none that can be expected to predict or explain more than part of a person, and it seems mechanistic to attempt to force people into preconceived models. Yet we must have some frame of reference if we are to be of use to those who cannot cope with life’s vicissitudes. It is not enough for us to stay close and to open our hearts to another person’s suffering; valuable though this sympathy may sometimes be, we must have some way of stepping aside from the maze of emotion and sensation if we are to make sense of it. One might say that our central nervous system has been designed to enable us to do just that. Human beings, to a greater extent than other species, have the capacity to organize the most complex impressions into internal models of the world, which enable us to recognize and understand the world that we experience and to predict the outcome of our own and others’ behavior. Psychological Correspondence regarding this article should be addressed to Colin Murray Parks, The London Hospital Medical College, University of London, Turner Street, London El 2AD, England. 53 0022-4537/88109M)dO53~~00/l 0 1988 The Society for he Psychological Study of Social Issues
Transcript of Bereavement as a Psychosocial Transition: Processes of Adaptation to Change
Journal of Social Issues, Vol. 44, No. 3. 1988, p p . 53-6s
Bereavement as a Psychosocial Transition: Processes of Adaptation to Change
Colin Murray Parkes The London Hospital Medical College
There are many ways of construing the psychology of loss. This paper describes one such model, which enlightens some, but not all, aspects of bereavement and needs to be used alongside other models. Loss is one aspect of psychosocial transition, the psychological change that takes place whenever people are faced with the need to undertake a major revision of their assumptions about the world. The paper focuses on the ways in which people change or fail to change their internal model of the world in the face of emergent even?s. Examples are taken from bereavement, loss of a limb, and the succession of losses that mark the course of terminal illness. implications for identifying people at risk and mitigat- ing that risk are outlined.
People are fascinating because of their individuality; no two problems are alike because no two people are alike. This tempts some people to reject theories of human behavior. There are none that can be expected to predict or explain more than part of a person, and it seems mechanistic to attempt to force people into preconceived models. Yet we must have some frame of reference if we are to be of use to those who cannot cope with life’s vicissitudes. It is not enough for us to stay close and to open our hearts to another person’s suffering; valuable though this sympathy may sometimes be, we must have some way of stepping aside from the maze of emotion and sensation if we are to make sense of it.
One might say that our central nervous system has been designed to enable us to do just that. Human beings, to a greater extent than other species, have the capacity to organize the most complex impressions into internal models of the world, which enable us to recognize and understand the world that we experience and to predict the outcome of our own and others’ behavior. Psychological
Correspondence regarding this article should be addressed to Colin Murray Parks, The London Hospital Medical College, University of London, Turner Street, London El 2AD, England.
53
0022-4537/88109M)dO53~~00/l 0 1988 The Society for h e Psychological Study of Social Issues

54 Parka
theories are one way of doing this, and the measure of their success is their usefulness.
This article describes a theory that the writer has found useful in explaining certain aspects of the human reaction to loss. Other theories are useful in explain- ing other aspects; these include theories about the nature of attachments, anxiety, family dynamics, and the psychophysiology of stress. Each of these adds some- thing to our understanding of loss, and they do not conflict with each other. Aspects of most of these are considered elsewhere in this issue.
The theory that follows is simple in essence but complex and wide-ranging in its implications. It is not possible, in the space available here, to give more than an outline of its scope, inevitably condensed and shorn of detail. For a more extended treatment, see my forthcoming book, Loss and Health Care: Psycho- social Transitions in Medicine.
Reactions to Life Events
Bereavement by death is a major psychological trauma and usually takes place in the presence of members of the caring professions; consequently, it has been much studied. In fact, one sometimes gets the impression that “grief” and “mourning” (the public face of grief) are confined to this type of loss, but there are some bereavements that are not a cause for grief and many griefs that have causes other than bereavement by death.
What, then, defines a loss? How can we distinguish grief from the other emotions that arise in the face of life events? Why is it that some life events menace our sanity while others are an unmitigated blessing? These questions are more easily asked than answered.
Grief is essentially an emotion that draws us toward something or someone that is missing. It arises from awareness of a discrepancy between the world that is and the world that “should be.” This raises a problem for researchers because, though it is not difficult to discover the world that is, the world that should be is an internal construct; hence each person’s experience of grief is individual and unique. Two women who have lost husbands are not the same. One may miss her husband greatly, while the other’s grief may arise less from her wish to have her husband back (for she never did like him as a person) than from loss of the status and power that she achieved in marrying an important man. Clearly, grief is not a unitary phenomenon.
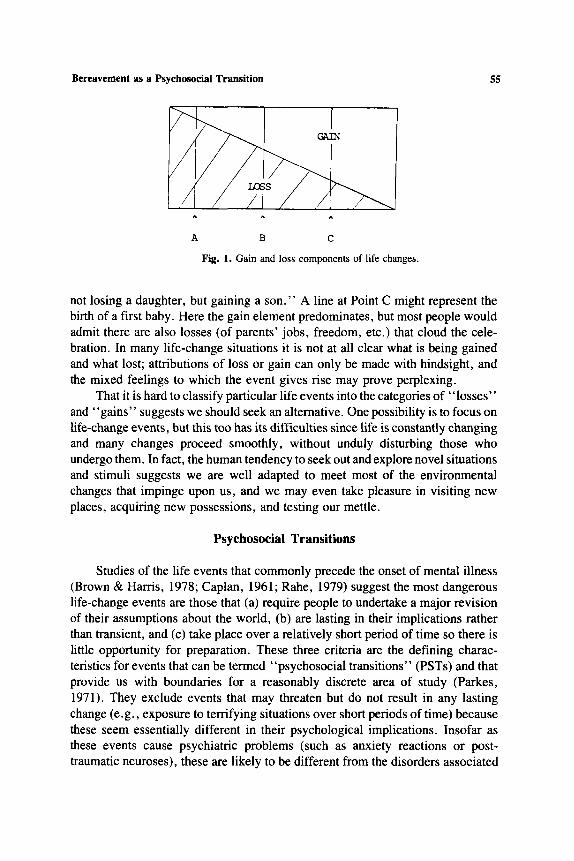
The situation is further complicated by the fact that there are many life- change events that bring about both loss and gain. The death of a loved person might be represented by a line at Point A in Fig. I. Here the main component is one of loss, but the honest person will admit there are certain consequences of the death that add something wanted. Point B is more ambiguous, for here loss and gain may balance out, as in the case of the bride’s mother who is told, “You are
Bereavement as a Psychosocial Transition 55
A B C
Fig. 1. Gain and loss components of life changes.
not losing a daughter, but gaining a son.” A line at Point C might represent the birth of a first baby. Here the gain element predominates, but most people would admit there are also losses (of parents’ jobs, freedom, etc.) that cloud the cele- bration. In many life-change situations it is not at all clear what is being gained and what lost; attributions of loss or gain can only be made with hindsight, and the mixed feelings to which the event gives rise may prove perplexing.
That it is hard to classify particular life events into the categories of “losses” and “gains” suggests we should seek an alternative. One possibility is to focus on life-change events, but this too has its difficulties since life is constantly changing and many changes proceed smoothly, without unduly disturbing those who undergo them. In fact, the human tendency to seek out and explore novel situations and stimuli suggests we are well adapted to meet most of the environmental changes that impinge upon us, and we may even take pleasure in visiting new places, acquiring new possessions, and testing our mettle.
Psychosocial Transitions
Studies of the life events that commonly precede the onset of mental illness (Brown & Harris, 1978; Caplan, 1961; Rahe, 1979) suggest the most dangerous life-change events are those that (a) require people to undertake a major revision of their assumptions about the world, (b) are lasting in their implications rather than transient, and (c) take place over a relatively short period of time so there is little opportunity for preparation. These three criteria are the defining charac- teristics for events that can be termed “psychosocial transitions” (PSTs) and that provide us with boundaries for a reasonably discrete area of study (Parkes, 1971). They exclude events that may threaten but do not result in any lasting change (e.g., exposure to terrifying situations over short periods of time) because these seem essentially different in their psychological implications. Insofar as these events cause psychiatric problems (such as anxiety reactions or post- traumatic neuroses), these are likely to be different from the disorders associated

56 Parkes
with PSTs. The criteria also exclude gradual changes, such as those associated with maturation, unless these are associated with more rapid changes that “bring home” implications of the more gradual change. Thus the physical changes associated with sexual maturation do not constitute a PST, but they may bring about rapid attachments or disappointments that are PSTs.
One other characteristic of those life-change events that commonly predict illness is a tendency to be evaluated in a negative way. This criterion, while predictive in practice, has been excluded from the definition of PST because, as we have seen, it tends to be made with hindsight. It is tautologous to claim that negative or stressful events are causes of mental distress when it is the mental distress that has caused us to define the event as stressful! Furthermore, there are many events initially greeted as positive, such as having a baby, being promoted at work, or marrying the mate of one’s dreams, that may subsequently tax our adaptive capacity to the limit.
The Assumptive World
The internal world that must change in the course of a PST consists of all those expectations and assumptions invalidated by the change in our life space (that is, the part of the world that impinges upon us-Lewin, 1935). These expectations constitute part of an organized schema or ‘‘assumptive world,” which contains everything that we assume to be true on the basis of our previous experience. It is this internal model of the world that we are constantly matching against incoming sensory data in order to orient ourselves, recognize what is happening, and plan our behavior accordingly.
Waking in the morning, we can put on the light, get out of bed, and walk to the bathroom because we have an assumptive world that includes assumptions about the presence and layout of the doors, windows, light switches, and rooms in our home, and assumptions about the parts of the body that we must use in turning the light on, getting out of bed, walking across the floor, etc. If as a result of some life event we lose a limb, go blind, lose our memory, move to a new house, or have the electricity cut off, we must revise our assumptive world in order to cope with the numerous discrepancies that arise.
The death of a spouse invalidates assumptions that penetrate many aspects of life, from the moment of rising to going to sleep in an empty bed. Habits of action (setting the table for two) and thought (“I must ask my husband about that”) must be revised if the survivor is to live as a widow.
The Pain of Change
Such changes are easier said than done, for not only does a major PST require us to revise a great number of assumptions about the world, but most of

Bereavement as a Psychosocial Transition 51
these assumptions have become habits of thought and behavior that are now virtually automatic. The amputee knows very well that he has lost a limb, but this knowledge does not prevent him from leaping out of bed in the morning and sprawling on the floor because he has med to stand on a leg that is not there. Likewise, the blind person “looks” toward a sudden noise, and the widow “hears” her husband’s key in the lock. Each is operating on a set of assumptions that have become habitual over many years. Grief following bereavement by death is aggravated if the person lost is the person to whom one would turn in times of trouble. Faced with the biggest trouble she has ever had, the widow repeatedly finds herself turning toward a person who is not there.
These examples begin to explain why PSTs are so painful and take so much time and energy. For a long time it is necessary to take care in everything we think, say, or do; nothing can be taken for granted any more. The familiar world suddenly seems to have become unfamiliar, habits of thought and behavior let us down, and we lose confidence in our own internal world.
Freud (1917) called the process of reviewing the internal world after be- reavement “the work of mourning,” and in many ways each PST is a job of work that must be done if a person is to adapt to the requirements of the real world. But the mind that is doing the reviewing is also the object that is being reviewed. A person is literally lost in his or her own grief, and the more disor- ganized one’s thinking the more difficult it is to step aside from the disorganiza- tion and to see clearly what is lost and what remains.
Since we rely on having an accurate assumptive world to keep us safe, people who have lost confidence in their world model feel very unsafe. And because anxiety and fear cloud our judgment and impair concentration and mem- ory, our attempts to make sense of what has happened are likely to be fitful, poorly directed, and inadequate.
Coping and Defense
Of course, people are not completely helpless when the level of anxiety becomes disorganizing. We have a variety of coping mechanisms that usually reduce the level of tension or at least prevent it from rising any higher. Hence people in transition often withdraw from the challenges of the outside world, shut themselves up at home, and restrict their social contacts to a small group of trusted people. They may avoid situations and chains of thought that will bring home the discrepancies between inside and outside worlds; they may fill their lives with distracting activities, or deny the full reality of what has happened. The complete range of psychological defense mechanisms can be called into play to protect someone from too painful a realization of a loss. These defenses will often succeed in preventing anxiety from becoming disorganizing, but they are also likely to delay the relearning process.

58 Parkes
Taking Stock
The magnitude of a PST is such that it includes simultaneous dysfunctions in several areas of functioning. Thus the loss of a spouse may produce any or all of the following: (1) loss of sexual partner, (2) loss of protection from danger, (3) loss of reassurance of worth, (4) loss of job, (5) loss of companionship, (6) loss of income, (7) loss of recreational partner, (8) loss of status, (9) loss of expecta- tions, (10) loss of self-confidence, (1 1) loss of a home, (12) loss of a parent for one’s children, and many other losses. It may also produce (a) relief from responsibilities, (b) entitlement to the care of others, (c) sympathy from others and an increase in tenderness (or at least inhibition of hostility and competition), (d) attributions of heroism, (e) financial gains, and (f) freedom to realize poten- tialities that have been inhibited. These latter consequences, too, involve change in the life space and require that assumptions be modified, but since they also serve to assist those modifications (e.g., by providing time and opportunity for introspection, and by keeping people safe from threat during that time), they are more likely to facilitate than to impair the transition.
PSTs thus emerge as a complex interweaving of psychological and social processes, whose implications are far from clear to the person who undergoes them and even less clear to the would-be helper. Only in the most general terms can anyone else be said to “understand.” But this does not mean we cannot help. By encouraging those who are in transition to help us understand, by talking about their situation, we help them take stock, review, and relearn their assumptive world.
Resistance to Change
Although minor changes are often embraced, major changes are more usu- ally resisted. Resistance to change is seen as an obstacle by planners, but it is not always so irrational or so harmful as it seems. We can bring to the appraisal of new situations only the assumptions that arise out of old situations. Our old model of the world may be imperfect, but it is the best we have, and if we abandon it we have nothing left. Our first effort, in the face of change, must therefore be to interpret the change in the light of our old assumptions. To throw over old models of the world the moment they appear discrepant with the new is dangerous and often unnecessary. Closer scrutiny will sometimes reveal that our initial appraisal of the situation was incorrect and that the discrepancy was more apparent than real. Thus, a person who is told by a doctor that he has a terminal illness may be wise to ask for a second opinion before preparing himself to die.
Refusing to accept change also gives us time to begin rehearsing in our minds the implications of the change, should it come about. Thus, the patient who refuses surgery may need time to talk through its implications with his
Bereavement as a Psychosocial Transition 59
doctor and his family before changing his mind. While he does this, he is preparing a new model of the world, which will help ensure that the transition proceeds smoothly when, eventually, it comes about.
On the other hand, there may come a time when it is more dangerous to resist change than to accept it. Because the person in transition has no models of thought and behavior to meet the new situation, he or she will eventually feel helpless and in danger. Three things are needed: emotional support, protection through the period of helplessness, and assistance in discovering new models of the world appropriate to the emergent situation. The first two of these may need to be provided before the person can begin to feel safe enough to accept the third. Thus, people whose sight has failed often refuse to learn blind skills until they have been supported in their helplessness and reached a point where they feel safe enough to accept the help of guide dogs, white canes, and all the other means by which blind people can rebuild their model of the world.
Implications of Transition Theory for Various Transitions
Despite points of similarity between the reactions to various life-change events, there are also important differences. No one would pretend that the death of a wife or child is the same kind of event as the loss of a limb or the anticipated loss of one’s own life. It is instructive to study the differences as well as the similarities between the reactions to these events.
Bereavement
The death of a loved person evokes a characteristic emotion-pining for the lost person (or “separation anxiety”)-which is largely independent of the magnitude of the life change that will result. Thus, the death of a child may lead to very little change in the mother’s model of the world, whereas the death of a spouse inevitably leads to a major upheaval. Yet it has been claimed that the emotional reaction of a mother to the death of a child is as great or greater than the typical reaction to the loss of a spouse (Fulton & Owen, 1971). This suggests it is the nature and quality of the attachment that determines the intensity of grief, rather than the magnitude of the psychosocial transition that results. This does not mean the PST is unimportant, but it does seem overshadowed, during the early phase of bereavement, by the pangs of grief, which are more easily ex- plained in terms of attachment theory than transition theory. John Bowlby (1982) has shown how the bonds between human beings arise out of deep-seated innate mechanisms, which have evolved in order to ensure survival. The child’s tie to the mother and the mother’s tie to the child are biologically determined, and their very strength is a reflection of their survival value. Although derived from an inborn tendency, the child’s attachment to its mother is influenced by its experi-

60 Parkes
ence of its parents, and thus attachments may become secure or insecure. Basic trust arises out of these early attachments and then influences all later attach- ments, including those the child will make to his or her own children in years to come.
From this point of view, it is reasonable to suppose one’s reaction to loss of a person will be determined as much by the biological significance of that person as by the magnitude of the life change resulting from the loss. In other respects, however, loss of a person resembles loss of other objects.
Amputation
The amputation of a limb is a cause of distress, and some of the reactions to it resemble the reaction to death of a person (Parkes, 1972). Both commonly evoke feelings of numbness and disbelief followed by anxiety and anger. The amputee, like the bereaved, goes over and over the events leading up to the loss as if it could still be prevented. Both ask the question, “Why should this happen to me?” Even the phantom limb, a strong sense of the presence of the lost limb, has its equivalent in the sense of the presence of a dead partner, which is reported by over 50% of widows. But the amputee does not pine for the lost limb in the same way that a widow pines for her lost husband. If pining is experienced at all, it is likely to be for the workmates and social relationships lost along with the limb. As one amputee put it, “I don’t miss my leg like I missed my father” (Parkes, 1972).
Even so, amputees may have the same difficulty in accepting the implica- tion of their loss that is reported by widows, and delayed reactions are not uncommon. For example, a roof tiler who had been “the hero of the ward” and had impressed everyone by his stoicism was readmitted in a very distressed state a month after breaking his remaining leg by falling from a roof.
Terminal Illness
Elizabeth Kubler-Ross’s (1969) “phases of dying”-denial, bargaining, anger, despair, resignation, and acceptance-bear a close resemblance to Bowlby’s “phases of grief‘ ’ (numbness, pining, disorganizationldespair, and reorganization-Bowlby & Parkes, 1970), and the link between dying and griev- ing was made by Kubler-Ross’s former professor of psychiatry, C. Knight Al- dritch (1963) in a paper titled “The Dying Patient’s Grief.” The consistency and even the occurrence of these “phases” have been questioned, and it would certainly be unwise to set them up as “norms” through which each dying patient should be expected to pass. But to those who work with late-stage cancer pa- tients, they are very familiar even if they do not always occur in the sequence and manner that Kubler-Ross described. What these phases seem to reflect is a tendency for seriously ill patients to move from a state of relative ignorance of,
Bereavement as a Psychosocial Transition 61
and reluctance to accept, the facts of their illness toward awareness and accep- tance. Along the way they may try to strike bargains (“If I accept surgery, then I shall live to see my grandchild born”), express anger (“It’s not fair”), or despair (“I give up”). These kinds of phenomena are also commonly found in amputees and other disabled people, and they are best viewed as typical components of a PST. However, cancer patients undergo, not one, but a number of PSTs in the course of long and varied illnesses. Their psychological reactions are correspon- dingly unpredictable.
Cancer often takes a stepwise course as each new crop of symptoms appears and is treated. Each step is likely to involve some loss-of employment, mobili- ty, strength, good looks, etc.-and each confronts the patient with a need to give up one set of assumptions about the world and to develop another. Lacking any clear basis for planning, most patients tend to be as optimistic about their future as they dare, and this optimism is fostered by their doctors and nurses, who prefer to “look on the bright side.” Consequently, they are often unaware of the full implications of those cancers that will end fatally.
Even if they are informed and aware of the likely ending, it is rare for them to feel prepared for an outcome that, for most of us, is a step into the dark. None of the great religions is really clear as to what lies beyond life, and there are no training courses for the afterlife. It follows that the transition from life to death must be made without rehearsal and without any of the provisional models that, however inadequate, we bring with us to other situations.
Strange to say, this ignorance seems to mitigate anxiety, and most patients claim to be more afraid of dying than of being dead. Dying is envisaged as a projection of everything bad about illness. As the illness gets worse the symp- toms will get worse, and “death agonies” are assumed to be an ultimate horror. The fact that, given a decent quality of care, it should be possible for medical attendants to relieve the physical distress of the dying makes it all the more important for them to relieve mental distress by communicating that fact (Parkes, 1978).
Preventive Intervention
Many of the problems arising in the course of a PST can be mitigated if those who are at risk receive appropriate counseling and support. To plan this effectively, a sound knowledge of risk factors and methods of intervention is needed.
Determinants of Outcome
Studies of a variety of types of transition and of the variation of response to each of these not only.throw light on the nature and dynamics of PSTs, but also enable us to identify people and situations that involve special risk. The identifi-

62 Parkes
cation of risk is, of course, an important step toward prevention of ill health, and studies of bereavement by death suggest that those most vulnerable to this type of loss can be recognized before or at the time of bereavement, and that members of this group will benefit from counseling. The wide range of empirical studies contributing to our knowledge of vulnerability in the face of a range of PSTs include the circumstances of the life-change event (e.g., anticipation, massive or multiple changes, brutal or violent events), the personality and previous experi- ence of the bereaved person (e.g., self-confidence, success or failure of resolu- tions of earlier PSTs), and factors impinging after the event (e.g., social sup- ports, opportunities for new roles and status). These studies are treated in more detail elsewhere in this issue (e.g., by Sanders, this issue). They indicate that the outcome of a PST is related to the magnitude of the PST, the extent to which it has been correctly anticipated, and the supports and opportunities available. Such findings enable us to make predictions regarding the probable outcome of many PSTs.
Prediction of outcome is also improved from observation of the initial reaction to the event. Thus, severe and lasting distress, as well as excessive denial or delay in reacting emotionally, may presage later problems.
Intervention
Knowledge of risk factors is of value when planning intervention. If antici- pation is important, then any activity that helps people to prepare themselves for an event is likely to reduce the risk. Similarly, those who cope by avoiding may need help in facing up to a transition, while those who are overwhelmed may need permission to escape for a while by taking a holiday or by the judicious use of psychotropic medication. But these expedients only provide a temporary solution, and we must also guard against the misuse of medication, be it alcohol or other tranquilizers. People of low self-esteem or dependent personality may need forms of help that build on their strengths and wean them from undue reliance on others, including the providers of health care.
Up to the present time, the only settings where these principles have been widely adopted are hospices and bereavement services. Although neither hospices nor bereavement services are universally successful in relieving the suffering of those they serve, there are a number of well-conducted studies indicating that the right help given to the right people at the right time can reduce physical and mental symptoms and improve the quality of life before and after bereavement (Mor, 1987; Parkes, 1981; Raphael, 1977).
If this is so, then we have to ask ourselves whether similar interventions might help people through the other major PSTs of their lives. Since doctors, priests, nurses, and social workers are likely to be in contact at such times and may be the only care givers to whom these people will turn for help, it follows
Bereavement as a Psychosocial Transition 63
that they should develop the knowledge base needed and organize their services in an appropriate way. Whether we like it or not, we are agents of change, midwives at the birth of new identities.
What, then, are the essential resources for this new midwifery, and how can they be provided within the constraints of a shrinking economy? The resources are, of course, properly trained people with the necessary time and skills. To some extent these are the same people who have always cared for the sick. Psychosocial medicine has been around for a long time, but it used to be called “tender loving care.” It relied on the communication skills and life experiences of the care givers and was none the worse for that. However, it frequently seems to get displaced by other, “more important” priorities.
Yet the whole history of medicine tells us that prevention is more eco- nomical than cure. If, in fact, preparing someone for major surgery reduces the chances of postoperative complications and, as some studies have shown, gets people out of the hospital sooner (Egbert, Battit, Welch, & Bartlett, 1964), then it is likely to be an economical use of our time. Hospices are no more expensive than the service that they replace (Mor, 1987), and even the provision of support during the transition of leaving prison has been shown to save money by reducing the chances of recidivism (Shaw, 1974; Sinclair, Shaw, & Troop, 1974).
Furthermore, much of the support that people need at times of transition can and should be given by volunteers. Volunteers who have been carefully selected and trained to act as counselors, or whose own experience of the transition in question provides them with inside knowledge (although it is important to ensure that they have come through it and are not trying vicariously to solve their own problems), are often the best people to help others in transition. Not only are they less expensive, but they are often seen as less threatening because they are not “experts,” and they have the one thing that professionals often lack-time to listen. These volunteers can be organized in specialized counseling services (e.g., Ostomy Associations or Bereavement Services), or they can take a wider frame of reference and offer counsel to anyone in crisis or distress (e.g., Sa- maritans, Good Neighbor Schemes, etc.). These services will be much more effective if they are backed by and integrated with the services provided by members of the caring professions. This enables the professionals to discover their true value, facilitates referrals, and ensures that the volunteers receive the expert help that they need in training counselors and dealing with individuals whose problems require professional skills.
Social workers and other primary care givers in the community are in a good position to identify people in transition, to assess their vulnerability, and where necessary, to provide the support needed or refer them to those who can. They should receive proper training in this field of study. Hospital and other institu- tional staff may also have important roles to play if they are involved in the diagnosis or care of people with life-threatening or chronic diseases.

64 Parkes
Support for the Supporters
Because transitions of one sort or another affect us all, we cannot come close to people who are facing them without, to some degree, sharing their feelings. We too suffer their losses and frustrations, and it is only by “hanging in” and seeing them come through to a new life that we will be rewarded for the pains we share. But not everybody who seeks our help will come through, and sometimes their pain sparks off pain in us that we thought we had forgotten, reminding us too vividly of our own losses. At such times we too need the help and understanding of a counselor. If it is all right for our clients to grieve, it should also be acceptable for us to express the sorrow and frustration to which our work gives rise. Any caring team must, therefore, take account of the need for support to the supporters, for in the end the only difference between carer and cared-for is in the roles assigned to us.
Conclusion
Societies have always had their elders, doctors, shamans, priests, and coun- selors. Most of these have a dual role-to provide wise counsel and to perform rituals. The rituals mark the rites of passage (Van Gennep, 1909). They identify people in transition, induct them into a temporary status (as “client,” “moum- er, ” “initiate,” “patient,” etc.), and then, after sufficient time has elapsed, mark the end of the transition to a new identity (as “widow,” “adult,” “dis- abled person,” etc.). The rites performed by doctors include the provision of sickness certificates, prescriptions, and a range of other procedures (some of them bloody) through which patients pass on the way to their new life.
The success of scientific medicine in finding cures for many diseases has distracted many members of the caring professions from their traditional respon- sibility to care for people in transition. As a result, medicine and its allied professions find themselves faced with the need to change, to face a psychosocial transition of their own, whose implications penetrate all aspects of our work. We can expect similar difficulties in revising our models of the world, like those experienced by the bereaved, the disabled, and the dying when faced with irreversible changes in their lives. Social workers and counselors are likely to find it less difficult than medical personnel to make use of a theory of transition because much of their existing work is carried out from a similar viewpoint. Consequently, they may need to take the lead in educating doctors, nurses, and other health care workers. It is hoped that the theory presented here will facilitate this transition.
References
Aldritch, C. K. (1963). The dying patient’s grief. Journal ofthe AmericanMedical Association, 184, 329-33 I .

Bereavement as a Psychosocial Transition 65
Bowlby, J. (1982). Attachment and loss: Vol. I , Attachment. London: Hogarth. Bowlby, J. , & Parkes, C. M. (1970). Separation and loss. In E. 3. Anthony & C. Kopernick (Eds.),
The child in his family, Vol. 1 of The international yearbook of child psychiatry. New York: Wiley.
Brown, G. W., & Hanis, T. (1978). Social origins of depression: A study ofpsychiatric disorder in women. London: Tavistock.
Caplan, G. (1961). An approach to community mental health. London: Tavistock. Egbert, L. D. , Battit, G. E., Welch, L. E., & Bartlett, M. K. (1964). Reduction of post-operative
pain by encouragement and instruction of patients. New England Journal of Medicine, 270, 825-827.
Freud, S. (1917). Mourning and melancholia. In The complete psychological works of Sigmund Freud (Vol. 14). New York: Norton.
Fulton, R., & Owen, G. (1971, October). Adjustment to loss through death: A sociological analysis. Center for Death Education and Research, University of Minnesota.
Kubler-Ross, E. (1969). On death and dying. New York: Macmillan. Lewin, K. (1935). A dynamic theory of personality. New York: McGraw-Hill. Mor, V. (1987). Hospice care systems: Structure, process, costs and outcome. New York: Springer. Parkes, C. M. (1971). Psycho-social transition: A field for study. Social Science & Medicine, 5 ,
Parkes, C. M. (1972). Components of the reaction to loss of a limb, spouse or home. Journal of
Parkes, C. M . (1978). Psychological aspects. In C. M. Saunders (Ed.), The management of terminal
Parkes, C. M . (1981). Evaluation of a bereavement service. Journal of Preventive Psychiatry, 1 ,
Rahe, R. H. (1979). Life events, mental illness: An overview. Journal ofHuman Stress. 5 (3). 2-10. Raphael, B. (1977). Preventive intervention with the recently bereaved. Archives of General Psychi-
atry, 34, 1450. Shaw, M. J. (1974). Social work in prison: An experiment in the use of extended contact with
offenders. London: HMSO. Sinclair, I. A. S., Shaw, M., &Troop, J. (1974). The relationship between introversion and response
to care work in a prison setting. British Journal ofSocial and Clinical Psychology, 23, 51- 60.
Van Gennep, A. (1909). Les rites de passage. (1960). English translation, The rites of passage. London.
101-105.
Psychosomatic Research, 16, 343-349.
disease. London: Arnold.
179.
COLIN MURRAY PARKES is Senior Lecturer in Psychiatry, The London Hospital Medical College, an Honorary Consultant Psychiatrist at St. Christopher’s Hospice, Sydenham, and a member of the research staff at the School of Family Psychiatry, The Tavistock Institute of Human Relations. His many works on bereavement include The First Year of Bereavement, with I. Glick and R. Weiss, and Recovery from Bereavement, with R. Weiss.




















