Bed- and sofa-sharing practices in a UK biethnic population
22
1 1 Bed and sofasharing practices in a UK biethnic population 2 Helen L. Ball, PhD, MA, BSc. Professor of Anthropology, ParentInfant Sleep Lab & Medical 3 Anthropology Research Group, Durham University, Durham, DH1 3LE. (Corresponding author 4 and guarantor: T: +44 191 334 1602; F: +44 191 334 1615; E: [email protected]) 5 Eduardo Moya, LMS, MRCPCH. Consultant Pediatrician & Honorary Senior Lecturer, Bradford 6 Teaching Hospitals NHS Foundation Trust, Bradford Royal Infirmary, Bradford, BD9 6RJ 7 Lesley Fairley, MSc, BSc. Statistician, Bradford Institute for Health Research, Bradford Royal 8 Infirmary, Bradford, BD9 6RJ 9 Janette Westman, RM, BSc, MCGI, IBCLC . Midwife/Infant Feeding Advisor, Maternity Unit, 10 Bradford Royal Infirmary, Bradford, BD9 6RJ 11 Sam Oddie, MBBS, MRCP (Paed), FRCPCH. Consultant Neonatologist, Bradford Neonatology, 12 Ward M1, Bradford Royal Infirmary, Bradford, BD9 6RJ 13 John Wright, MB, ChB, BSc, FFPHM, FRCP. Director of Research, Bradford Institute for Health 14 Research, Bradford Royal Infirmary, Bradford, BD9 6RJ 15 16 Abbreviations used: SIDS (Sudden Infant Death Syndrome); SUDI (Sudden Unexpected Death 17 in Infancy); BiB (Born in Bradford); BradICS (Bradford Infant Care Study). 18 19 Keywords: Bedsharing, sofasharing, SIDS, infant care, Bradford Infant Care Study, 20 breastfeeding, infant sleep, Born in Bradford (BiB). 21 22 The authors have no financial disclosure or conflicts of interest to declare. The project was 23 funded by the Foundation for the Study of Infant Deaths (FSID), UK. 24 Word count 3200 words, 4 Figures, 4 Tables 25 26
Transcript of Bed- and sofa-sharing practices in a UK biethnic population

1
1
Bed and sofa-‐sharing practices in a UK bi-‐ethnic population 2
Helen L. Ball, PhD, MA, BSc. Professor of Anthropology, Parent-‐Infant Sleep Lab & Medical 3
Anthropology Research Group, Durham University, Durham, DH1 3LE. (Corresponding author 4
and guarantor: T: +44 191 334 1602; F: +44 191 334 1615; E: [email protected]) 5
Eduardo Moya, LMS, MRCPCH. Consultant Pediatrician & Honorary Senior Lecturer, Bradford 6
Teaching Hospitals NHS Foundation Trust, Bradford Royal Infirmary, Bradford, BD9 6RJ 7
Lesley Fairley, MSc, BSc. Statistician, Bradford Institute for Health Research, Bradford Royal 8
Infirmary, Bradford, BD9 6RJ 9
Janette Westman, RM, BSc, MCGI, IBCLC . Midwife/Infant Feeding Advisor, Maternity Unit, 10
Bradford Royal Infirmary, Bradford, BD9 6RJ 11
Sam Oddie, MBBS, MRCP (Paed), FRCPCH. Consultant Neonatologist, Bradford Neonatology, 12
Ward M1, Bradford Royal Infirmary, Bradford, BD9 6RJ 13
John Wright, MB, ChB, BSc, FFPHM, FRCP. Director of Research, Bradford Institute for Health 14
Research, Bradford Royal Infirmary, Bradford, BD9 6RJ 15
16
Abbreviations used: SIDS (Sudden Infant Death Syndrome); SUDI (Sudden Unexpected Death 17
in Infancy); BiB (Born in Bradford); BradICS (Bradford Infant Care Study). 18
19
Keywords: Bed-‐sharing, sofa-‐sharing, SIDS, infant care, Bradford Infant Care Study, 20
breastfeeding, infant sleep, Born in Bradford (BiB). 21
22
The authors have no financial disclosure or conflicts of interest to declare. The project was 23
funded by the Foundation for the Study of Infant Deaths (FSID), UK. 24
Word count 3200 words, 4 Figures, 4 Tables 25
26
2
Contributor’s Statement 1 2 3 Helen L. Ball is corresponding author and guarantor. She was involved in all aspects of study 4 design and funding application, was a member of the BradICS steering committee that 5 oversaw project management and analysis; she was principal author of the submitted 6 manuscript. 7
Eduardo Moya conceived of the initial project, was involved in all aspects of study design 8 and funding application, chaired the BradICS steering committee that oversaw project 9 management and analysis; he contributed to and approved the submitted manuscript. 10
Lesley Fairley designed the analysis plan in collaboration with the BradICS steering 11 committee, conducted all statistical analyses, drafted the methods and analysis sections of 12 the manuscript and approved the submitted manuscript. 13
Janette Westman served as BradICS project manager, was involved in all aspects of study 14 design and implementation, was a member of the BradICS steering committee, and 15 contributed to and approved the submitted manuscript. 16
Sam Oddie was involved in all aspects of study design and funding application, was a 17 member of the BradICS steering committee that oversaw project management and analysis, 18 and contributed to and approved the submitted manuscript. 19
John Wright provided liaison with the larger BiB cohort study, was involved in all aspects of 20 study design and funding application, was a member of the BradICS steering committee that 21 oversaw project management and analysis, and contributed to and approved the submitted 22 manuscript. 23
24 The authors have no financial or competing interests to declare 25 26 27 The project was funded by the Foundation for the Study of Infant Deaths (FSID), UK. 28
3
1
2
3
What’s known 4
Parent-‐infant bed-‐sharing is a common behavior of breastfeeding mothers, and various 5
ethnic groups. Under certain circumstances it is associated with an increased risk of sudden 6
infant death. Blanket prohibitions against bed-‐sharing conflict with breastfeeding promotion 7
and inhibit safe bed-‐sharing discussion. 8
9
What’s new 10
Bed-‐sharing and sofa-‐sharing were almost mutually exclusive. Pakistani families avoided 11
sofa-‐sharing and hazardous bed-‐sharing and have a very low rate of Sudden Infant Death 12
Syndrome. White British families were more likely to smoke, drink alcohol and sofa-‐share 13
with their baby. 14

4
Abstract 1
Objective: To describe the prevalence and associations of bed and sofa-‐sharing in a bi-‐2
ethnic UK birth cohort. 3
Methods: We surveyed 3082 participants in the Born in Bradford birth cohort study by 4
telephone when infants were aged 2-‐4 months. We asked families about sleep surface 5
sharing behaviors, and other sudden unexpected death in infancy (SUDI)-‐related behaviors. 6
Results: 15.5% of families ever bed-‐shared, 7.2% of families regularly bed-‐shared, and 9.4% 7
of families ever sofa-‐shared with their infants. 1.4% reported both. Regular bed-‐sharers 8
were more commonly Pakistani (adjusted odds ration [aOR] = 3.02, 95% confidence interval 9
[CI] 1.96-‐4.66), had more education (aOR = 1.62, 95% CI 1.03-‐2.57), or breastfed at least 8 10
weeks (aOR = 3.06, 95% CI 2.00-‐4.66). The association between breastfeeding and bed-‐11
sharing was greater among White British than Pakistani families. Sofa-‐sharing occurred in 12
association with smoking (aOR = 1.79, 95% CI 1.14-‐2.80); breastfeeding at least 8 weeks 13
(aOR = 1.76, 95% CI 1.19-‐2.58); and was less likely in Pakistani (aOR = 0.21, 95% CI 0.14-‐14
0.31), or single parent families (aOR = 0.50, 95% CI 0.29-‐0.87). 15
Conclusions: The data confirm that bed-‐sharing and sofa-‐sharing are distinct practices, 16
which should not be combined in studies of unexpected infant deaths as a single exposure. 17
The determinants of sleep-‐surface sharing differ between the UK Pakistani and UK majority 18
communities, and from those of US minority communities. Caution is needed in generalizing 19
SUDI/SIDS risk factors across populations with differing risk factor profiles, and care should 20
be taken in adopting SUDI/SIDS reduction guidelines from other contexts. 21
22
23
5
Background 1
In many countries parent-‐infant bed-‐sharing (sleeping together on the same surface) is 2
common among breastfeeding mother-‐infant dyads,1-‐6 and a long-‐standing cultural practice 3
for one or more minority groups.7-‐12 Studies have demonstrated an increased risk of SIDS 4
(Sudden Infant Death Syndrome) associated with bed-‐sharing for infants of parents who 5
smoke,13,14 no risk associated with bed sharing with mother ± father, irrespective of 6
maternal smoking status,11 while the European Concerted Action on SIDS (ECAS) 7
investigation found a significantly increased risk of SIDS among the infants aged under 9 8
weeks of non-‐smoking mothers who bed-‐shared.15 In the Netherlands the risk was increased 9
only for infants under 2 months of age.16 Gessner et al estimate the maximum potential risk 10
for bed-‐sharing infants of non-‐smoking mothers to be <1/10000.17 Research has recently 11
begun to document more closely the particular parental behaviors and shared sleep surfaces 12
that present risks to infants.18 13
14
Although the evidence linking parent-‐infant bed-‐sharing with increased risk of SIDS or 15
accidental infant death is inconsistent and contested,19,20 international guidelines have been 16
dominated by recommendations to avoid bed-‐sharing. These guidelines have been heavily 17
influenced by authorities in the United States (e.g. Consumer Product Safety Commission21; 18
American Academy of Pediatrics22) who have advised against parents sleeping with their 19
infants. This advice has been adopted in countries with different ethnic compositions, 20
cultural practices, and SIDS profiles than the United States,23-‐25 even though other 21
researchers have cautioned against imposing particular cultural values upon diverse ethnic 22
groups.3,26 23
24
Given the lack of agreement regarding which practices are associated with increased 25
SUDI/SIDS-‐risk when parents and infants sleep together, and the suggestion from previous 26
6
studies that parent-‐infant sleep sharing may be practiced in different ways according to 1
ethnic and socio-‐demographic characteristics, it is imperative to have data on the actual 2
sleep-‐sharing practices within any given community for whom guidance to parents is issued. 3
The aim of this paper is therefore to describe parent-‐infant sleep sharing (bed-‐sharing and 4
sofa-‐sharing) in a multi-‐ethnic urban population in the UK, to determine similarities and 5
difference from bed-‐sharing practices in the United States and elsewhere, and to discuss 6
implications for the formulation of infant ‘safe sleep’ recommendations. 7
8
Participants and Methods 9
The Born in Bradford (BiB) and Bradford Infant Care Study (BradICS) have been described 10
elsewhere in detail.27,28 Briefly, the Born in Bradford birth cohort study includes 14000 11
pregnant women who gave birth in Bradford between May 2007 and May 2011. Women 12
were recruited at 26-‐28 weeks gestation and completed a baseline questionnaire. The 13
BradICS study reports on 3082 women who gave birth at the Bradford Royal Infirmary 14
between June 2008 and September 2009. 4131 mothers were contacted by telephone when 15
their baby was 2 to 4 months of age and 3082 completed a telephone interview on infant 16
care practices; 84% of women completing the telephone survey had complete baseline 17
survey data (80% of the BiB sample completed the baseline survey). Analysis is this paper is 18
restricted to White British and Pakistani women who completed the BradICS telephone 19
survey, the BiB baseline questionnaire, and had a singleton birth at the Bradford Royal 20
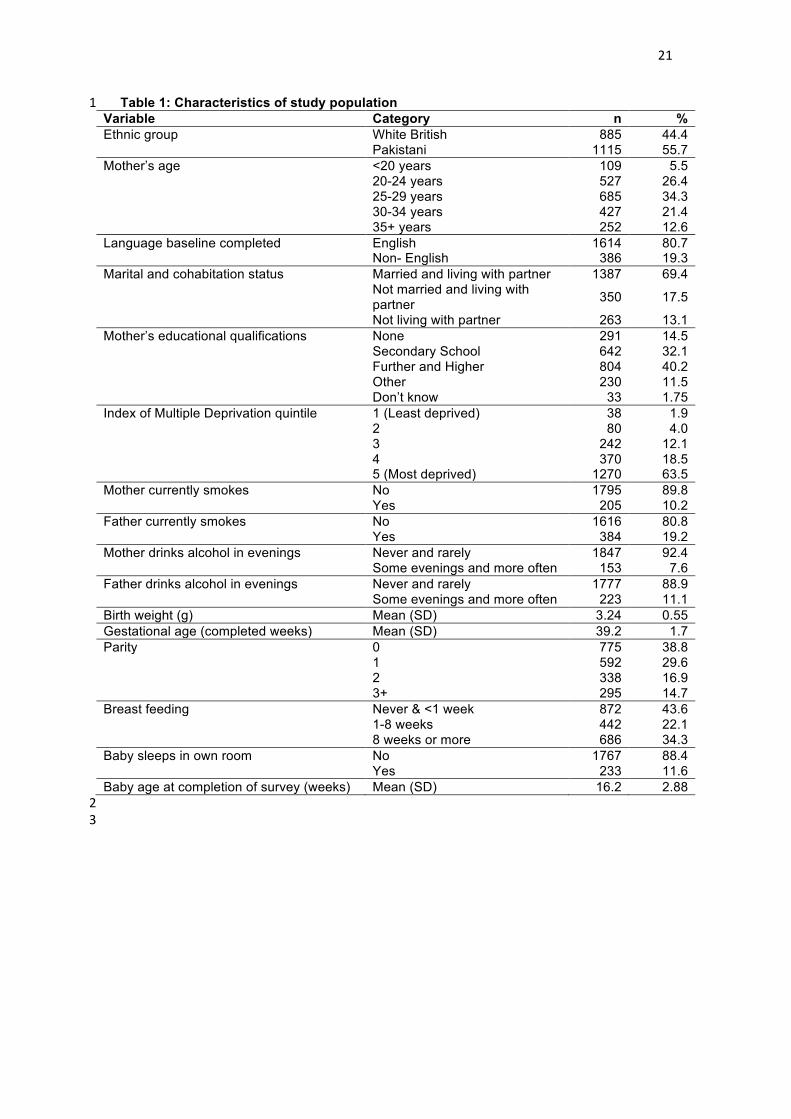
Infirmary (N=2180). The characteristics of the sample can be found in Table 1. 21
TABLE 1 22
23
Outcome measures 24
Three self-‐reported outcome measures were used: ever bed-‐share, regular bed-‐share and 25
ever sofa-‐share. All mothers were asked “Does your baby sleep in your bed when you are 26

7
asleep?” If the mother responded “Rarely (once or twice)”, “Occasionally (less than once a 1
week)”, “Regularly (twice or more per week)” or “Every night” then they were classified as 2
ever bed-‐share. Regular bed-‐share was defined as responding “Regularly” or “Every night” to 3
this question. Mothers were asked “Has the mother ever fallen asleep with the baby on a 4
sofa or armchair?” Women were defined to ever sofa-‐share if they responded “Once”, 5
“Occasionally” or “Regularly”. Mothers were excluded from analysis if the response to either 6
of these questions was missing (n=7). 7
8
Potential risk factors 9
Several co-‐variables, available from the baseline questionnaire, the hospital birth record or 10
the BradICS telephone survey, were included as potential risk factors in our analysis. The 11
variables included were those previously shown to be associated with bed or sofa-‐sharing 12
and SUDI/SIDS-‐risk in other populations. Ethnicity was self-‐defined by the mother when 13
completing the baseline questionnaire. Other variables from the baseline questionnaire 14
include; language questionnaire completed, marital and cohabitation status, mother’s 15
highest education qualification, Index of Multiple Deprivation based on postcode of 16
residence at registration to the study (an area-‐based measure of average deprivation where 17
areas are assigned scores based on measures in seven domains. Participant postcodes are 18
mapped directly to IMD scores for the area). Variables from the birth record include; 19
maternal age at delivery, parity, baby’s birth-‐weight and gestational age. Potential risk 20
factors reported as part of the BradICS study were: mother currently smokes, father 21
currently smokes, mother drinks alcohol in the evenings, father drinks alcohol in the 22
evenings, breastfeeding duration, baby sleeps in own room and baby’s age at completion of 23
questionnaire. If data were missing on any of the potential risk factors they were excluded 24
from analysis (n=173); this resulted in 2000 mothers being included in the analysis, (885 25
(44.3%) White British and 1115 (55.8%) Pakistani). We did not have access to data regarding 26

8
maternal prenatal smoking. In general, less than 4% of Pakastani women smoked before 1
pregnancy. 2
3
Statistical analysis 4
Univariable logistic regression was used to investigate the association between each of the 5
potential risk factors and the three outcomes (ever bed-‐share, regular bed-‐share and ever 6
sofa-‐share). 7
8
Multivariable models were constructed using backwards stepwise procedure. All variables 9
with a significance level of p<0.05 were included in the multivariable model and variables 10
with a significance level of p>0.1 were removed from the model. The final model was chosen 11
when no further variables were eligible for entry to or removal from the model. 12
13
We hypothesized that there would be ethnic differences in the association between 14
breastfeeding and co-‐sleeping based on previous reports that bed-‐sharing is a general 15
cultural practice among South Asians,29 but is principally associated with breastfeeding 16
among White British mothers.1 We tested this hypothesis by assessing the interaction of 17
ethnicity and breastfeeding duration in the final models for each of the outcomes. 18
19
Results 20
In this UK bi-‐ethnic sample, with a mean infant age of 16.2 weeks (SD 2.88 weeks), 15.5% of 21
mothers ever bed-‐shared, 7.2% of mothers regularly bed-‐shared, and 9.4% of mothers ever 22
sofa-‐shared with their infant (Table 2). Only a very small proportion of mothers both bed-‐ 23
and sofa-‐shared (1.4%). 24
[TABLE 2] 25

9
The prevalence of bed-‐sharing (ever and regular) was greater for the Pakistani than the 1
white British mothers, and the prevalence of sofa-‐sharing was lower (Figure 1). Logistic 2
regression analyses indicate that those mothers who bed-‐shared with their infant were 3
different from those who sofa-‐shared. 4
[FIGURE 1] 5
Ever bed-‐share 6
Univariable analyses (Table 3) demonstrated that mothers who ever bed-‐shared were more 7
likely to a) be Pakistani (OR=1.92, 95%CI 1.48-‐2.48), b) have further or higher educational 8
qualifications (OR=1.62, 95%CI 1.21-‐2.18), c) be primiparous (OR=1.40, 95%CI 1.03-‐1.90) or 9
grand-‐multiparous (OR=1.60, 95%CI 1.10-‐2.35), and d) have breastfed for more than a week 10
(OR=1.48, 95%CI 1.03-‐2.13) or at least 8 weeks (OR=3.51, 95%CI 2.63-‐4.69). These mothers 11
were less likely to a) be under 20 years of age (OR=0.50, 95%CI 0.25-‐0.98), b) not be living 12
with a partner (OR=0.55, 95%CI 0.36-‐0.84), c) have their baby sleep in a room alone 13
(OR=0.59, 95%CI 0.38-‐0.92). 14
15
Adjusted odds ratios (Table 4) indicate that mothers who ever bed-‐shared with their infants 16
were more likely to a) be Pakistani (OR=2.09, 95%CI 1.47-‐2.97), b) be living with a partner 17
(not married) (OR=1.59, 95%CI 1.01-‐2.51), c) be first-‐time mothers (OR=1.46, 95%CI 1.06-‐18
2.02), and d) have breastfed for at least 8 weeks (OR=3.17, 95%CI 2.34-‐4.30). 19
[TABLES 3 & 4] 20
Regular bed-‐share 21
Mothers who regularly bed-‐shared are a sub-‐set of those who ever bed-‐shared. Univariable 22
analyses reflect many of the characteristics of the larger ever bed-‐share group in terms of 23
ethnicity, maternal age, education, high parity, greater breastfeeding duration and infant 24
sleep location (see Table 3). In addition mothers who regularly bed-‐shared were more likely 25
to be a) non-‐English speakers (OR=2.19, 95%CI 1.52-‐3.17), and less likely b) to be unmarried 26
10
but living with a partner (OR=0.39, 95%CI 0.21-‐0.71), and c) for the father to consume 1
alcohol on a regular basis (OR=0.45, 95%CI 0.22-‐0.94) (Table 3). 2
3
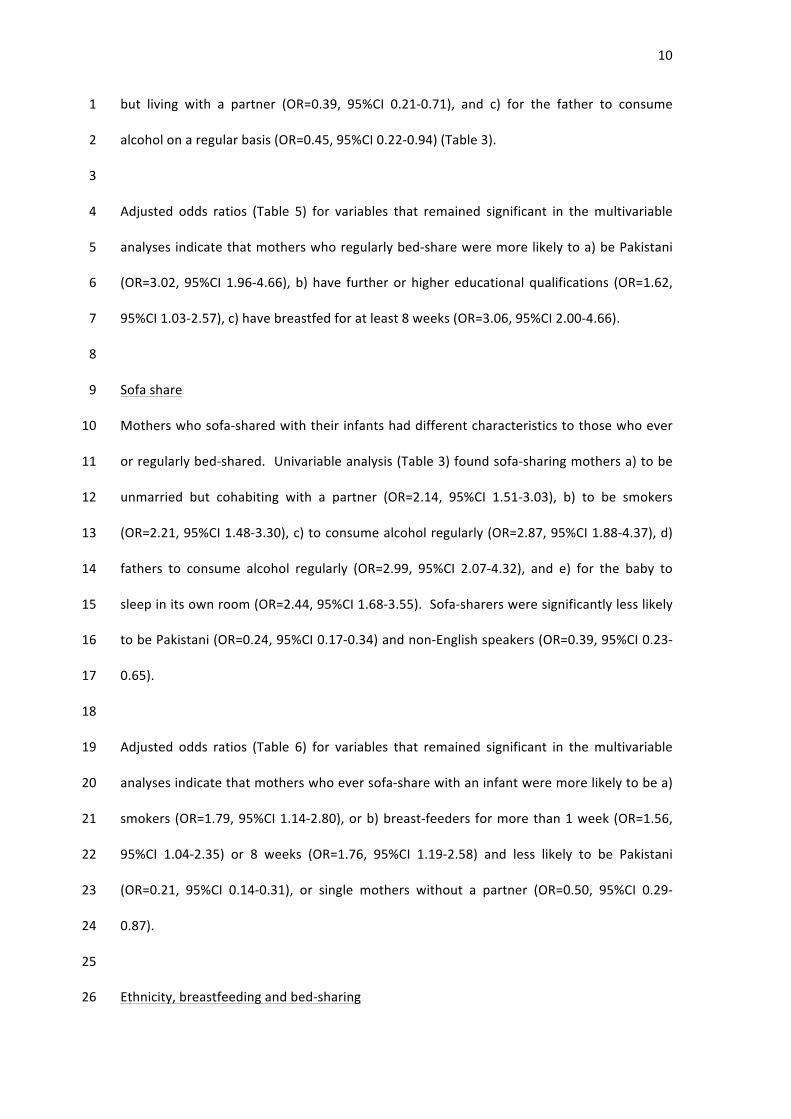
Adjusted odds ratios (Table 5) for variables that remained significant in the multivariable 4
analyses indicate that mothers who regularly bed-‐share were more likely to a) be Pakistani 5
(OR=3.02, 95%CI 1.96-‐4.66), b) have further or higher educational qualifications (OR=1.62, 6
95%CI 1.03-‐2.57), c) have breastfed for at least 8 weeks (OR=3.06, 95%CI 2.00-‐4.66). 7
8
Sofa share 9
Mothers who sofa-‐shared with their infants had different characteristics to those who ever 10
or regularly bed-‐shared. Univariable analysis (Table 3) found sofa-‐sharing mothers a) to be 11
unmarried but cohabiting with a partner (OR=2.14, 95%CI 1.51-‐3.03), b) to be smokers 12
(OR=2.21, 95%CI 1.48-‐3.30), c) to consume alcohol regularly (OR=2.87, 95%CI 1.88-‐4.37), d) 13
fathers to consume alcohol regularly (OR=2.99, 95%CI 2.07-‐4.32), and e) for the baby to 14
sleep in its own room (OR=2.44, 95%CI 1.68-‐3.55). Sofa-‐sharers were significantly less likely 15
to be Pakistani (OR=0.24, 95%CI 0.17-‐0.34) and non-‐English speakers (OR=0.39, 95%CI 0.23-‐16
0.65). 17
18
Adjusted odds ratios (Table 6) for variables that remained significant in the multivariable 19
analyses indicate that mothers who ever sofa-‐share with an infant were more likely to be a) 20
smokers (OR=1.79, 95%CI 1.14-‐2.80), or b) breast-‐feeders for more than 1 week (OR=1.56, 21
95%CI 1.04-‐2.35) or 8 weeks (OR=1.76, 95%CI 1.19-‐2.58) and less likely to be Pakistani 22
(OR=0.21, 95%CI 0.14-‐0.31), or single mothers without a partner (OR=0.50, 95%CI 0.29-‐23
0.87). 24
25
Ethnicity, breastfeeding and bed-‐sharing 26
11
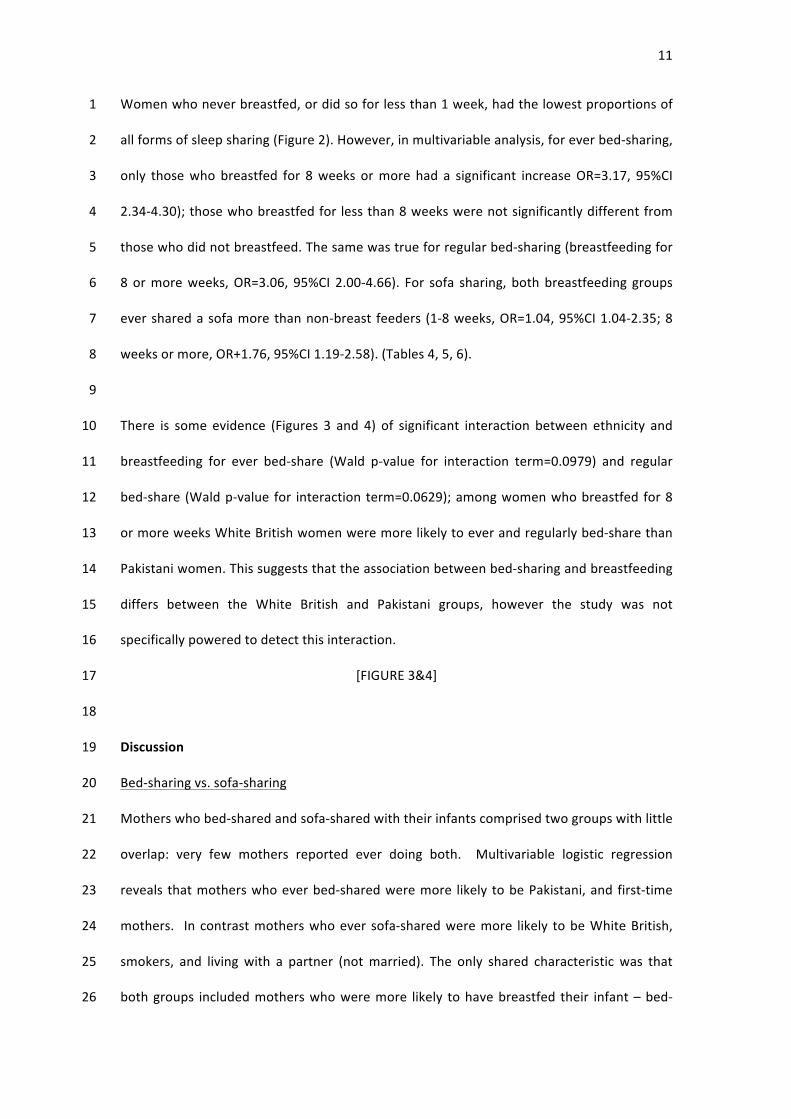
Women who never breastfed, or did so for less than 1 week, had the lowest proportions of 1
all forms of sleep sharing (Figure 2). However, in multivariable analysis, for ever bed-‐sharing, 2
only those who breastfed for 8 weeks or more had a significant increase OR=3.17, 95%CI 3
2.34-‐4.30); those who breastfed for less than 8 weeks were not significantly different from 4
those who did not breastfeed. The same was true for regular bed-‐sharing (breastfeeding for 5
8 or more weeks, OR=3.06, 95%CI 2.00-‐4.66). For sofa sharing, both breastfeeding groups 6
ever shared a sofa more than non-‐breast feeders (1-‐8 weeks, OR=1.04, 95%CI 1.04-‐2.35; 8 7
weeks or more, OR+1.76, 95%CI 1.19-‐2.58). (Tables 4, 5, 6). 8
9
There is some evidence (Figures 3 and 4) of significant interaction between ethnicity and 10
breastfeeding for ever bed-‐share (Wald p-‐value for interaction term=0.0979) and regular 11
bed-‐share (Wald p-‐value for interaction term=0.0629); among women who breastfed for 8 12
or more weeks White British women were more likely to ever and regularly bed-‐share than 13
Pakistani women. This suggests that the association between bed-‐sharing and breastfeeding 14
differs between the White British and Pakistani groups, however the study was not 15
specifically powered to detect this interaction. 16
[FIGURE 3&4] 17
18
Discussion 19
Bed-‐sharing vs. sofa-‐sharing 20
Mothers who bed-‐shared and sofa-‐shared with their infants comprised two groups with little 21
overlap: very few mothers reported ever doing both. Multivariable logistic regression 22
reveals that mothers who ever bed-‐shared were more likely to be Pakistani, and first-‐time 23
mothers. In contrast mothers who ever sofa-‐shared were more likely to be White British, 24
smokers, and living with a partner (not married). The only shared characteristic was that 25
both groups included mothers who were more likely to have breastfed their infant – bed-‐26

12
sharers for at least 8 weeks and sofa-‐sharers for at least a week. That smokers may sofa-‐1
share is not surprising given that they are specifically advised not to bed-‐share. That a group 2
of breastfeeding mothers slept with their babies on sofas is consistent with the suggestion 3
that some breastfeeding mothers are doing so in an attempt to avoid bed-‐sharing and 4
inadvertently ending up sleeping with their babies in more hazardous situations.18 5
6
In the UK researchers confirmed that bed-‐sharing in combination with smoking was 7
associated with an increased risk of SIDS (OR=12.35, 95%CI 7.41-‐20.59) but found no 8
increase in risk for infants of parents who did not smoke (OR 1.08, 95%CI 0.45-‐2.58).18 In 9
2006 the same team reported that over a 20-‐year period in the UK, the proportion of 10
children who died from SIDS while sleeping with their parents, rose from 12% to 50%, while 11
the absolute number of SIDS deaths in the parental bed halved,30 and deaths of infants 12
sleeping with their parents on a sofa increased, suggesting the most dangerous forms of 13
sleep-‐sharing occur on sofas. A subsequent study on hazardous sleeping environments 14
identified a significant interaction between sleep-‐sharing deaths and recent parental use of 15
alcohol or drugs, and an increased proportion of SIDS infants who died while sleep-‐sharing 16
on a sofa.18 The results of the present study support the conclusion that bed-‐sharing and 17
sofa-‐sharing are practiced by different families under different circumstances. This 18
heterogeneity would imply that bed-‐ and sofa-‐sharing should not be combined in studies on 19
infant sleep safety and SIDS, and casts doubt on the validity of previous studies where bed-‐ 20
and sofa-‐sharing have been combined. 21
22
Bed-‐sharing, ethnicity and socio-‐demographics 23
Parents who ever, or regularly, bed-‐shared in the present study were different from those 24
who are characterized as bed-‐sharers in US studies of infant care. Our data show that infants 25
of teenage mothers, single mothers, and fathers who consumed alcohol were the least likely 26

13
to bed-‐share, while being the infant of a highly educated mother, a first-‐time mother, being 1
breastfed, or being of Pakistani origin was associated with being more likely to bed-‐share. In 2
the US Infant Feeding Practices Survey II non-‐Hispanic black mothers were more likely to 3
bed-‐share, as were lower income women, unmarried women, breast-‐feeders and smokers.31 4
Other US studies report the prevalence of bed-‐sharing in the US is higher among mothers 5
who are younger, never married, have less than a high school education, lower household 6
incomes, are of Black or Asian ethnicity, living in Southern states.2,12 McCoy et al (2004) 7
reported that breastfeeding was associated with bed-‐sharing throughout the 1st 6 months of 8
life; breastfeeding was significantly associated with bed-‐sharing among White non-‐Hispanic 9
and Asian mothers, but not among Black and Hispanic mothers.2 Young maternal age and 10
unmarried status were associated with bed-‐sharing among Black non-‐Hispanic mothers. In 11
the US, therefore, bed-‐sharing is often characterized as being practiced by young, 12
unmarried, poorly educated mothers from minority ethnic groups living in circumstances of 13
socio-‐economic deprivation, and by mothers who breastfeed. 14
15
In the UK, as in US and New Zealand, bed-‐sharing is a cultural practice among particular 16
ethnic minority groups. Associations between bed-‐sharing and SIDS are clearly 17
demonstrated in particular cultures and circumstances: for example in New Zealand bed-‐18
sharing is a common practice for both Maori and Pacific Islanders, however only among the 19
Maori population is bed-‐sharing linked with an increased risk of SIDS.8 The NZ Cot Death 20
study revealed that bed-‐sharing was a SIDS-‐risk in Maori families among whom maternal 21
smoking was common, but not for Pacific Islanders who bed-‐share but do not smoke.8,13,32 In 22
contrast, although the SIDS rate in the 1990s for US Black infants were twice those for white 23
infants, the Chicago Infant Mortality Study found no interaction between bed-‐sharing and 24
maternal smoking either during pregnancy or postpartum; only bed-‐sharing with individuals 25
other than parents was identified as a SIDS-‐risk factor in multivariate analysis.3 South Asian 26

14
infants in UK generally,33 and Bradford specifically, have a lower SIDS rate than White British 1
infants (0.2/1000 vs. 0.8/1000 per annum, 2003-‐2008, Bradford and Airedale District, 2
compiled by Moya, Bradford SUDI pediatrician, based on unpublished data from births and 3
deaths registry). Pakistani-‐origin mothers in Bradford rarely smoke and neither mothers nor 4
fathers consume alcohol.34 Pakistani infants were much more likely to bed-‐share than sofa-‐5
share. Ethnic minority practices with regard to sleep-‐sharing in UK are therefore different 6
from those defined among minority groups in NZ and US. It should not be assumed that 7
families who bed-‐share have similar characteristics or outcomes across different geographic 8
locations and care should be taken in generalizing the findings across different minority 9
ethnic groups 10
11
Bed-‐sharing and breastfeeding 12
Multiple studies have documented an association between bed-‐sharing and breastfeeding.1-‐13
6,30,34-‐36 The present study reinforces this association and suggests that the interaction 14
between breastfeeding and bed-‐sharing (especially regular bed-‐sharing) is greater for White 15
British than Pakistani mothers who breastfeed for more than 8 weeks. It is beyond the scope 16
of this study to determine causality or conclude that less bed-‐sharing would lead to less 17
breastfeeding. 18
19
Although no case-‐control studies have calculated odds ratios for SIDS-‐risk among breast-‐20
feeders who bed-‐share, breastfeeding has generally been found to reduce the risk of 21
SIDS.25,37 Data from the Alaska PRAMS survey suggest a maximum potential risk of bed-‐22
sharing related SIDS among non-‐smoking mothers is likely to be <1 in 10 000.38 Caution 23
should therefore be taken in making sweeping recommendations regarding the avoidance of 24
bed-‐sharing which does not appear to carry the same risk for all families, and may lead to 25
unintended consequences such as reduced breastfeeding, or adoption of more risky 26

15
strategies such as sofa-‐sharing. The American Academy of Pediatrics position on bed-‐sharing 1
reflects the characteristics of mothers who sleep-‐share with infants in the US and how they 2
do so,22 yet not all sleep sharing is inherently risky, even within the US; data from Alaska led 3
researchers to conclude: “Among parents who do not use tobacco, alcohol or other drugs, 4
sleeping with their infant is a perfectly reasonable and potentially beneficial option” 5
(p.990).38 6
7
We are aware of the limitations of telephone survey methods, and the cross-‐sectional 8
nature of our data,28 however this study also presents a major strength as the largest study 9
of Pakistani families in the UK, who comprise the second largest minority ethnic group in the 10
UK (after Indian). Infants belonging to the highest SIDS-‐risk categories are under-‐11
represented in the sample,28 and we may therefore have underestimated the extent of the 12
relationship between some behaviors. While we examined who was most likely to bed-‐13
share, we did not ask operational questions about bed-‐sharing such as firmness of 14
mattresses, and types of bedding used. While Pakastani families in the UK have an increased 15
prevalence of bed-‐sharing and a lower incidence of SIDS, it is beyond the scope of this study 16
to determine if there are specific differences in the practices of bed-‐sharing that contribute 17
to this association. We also cannot address reports that younger infants may be more 18
vulnerable to bed-‐sharing related SIDS than older infants as we did not question families 19
about the age of infants when sleep-‐sharing began.16 20
21
The present study supports the conclusions of previous studies that in the UK emphasis on 22
unsafe sleep sharing should predominantly target sofa-‐sharing and parental behaviors such 23
as smoking and alcohol consumption.18 24
25

16
Our data lead us to challenge the notion that assumptions and guidance about infant care 1
practices can or should be exported from one cultural setting (such as the US) to another 2
(such as the UK). Evidence regarding the nature and extent of parent-‐infant sleep contact 3
and related behaviors is crucial in ascertaining whether infants are at risk in shared-‐sleep 4
scenarios, and in tailoring advice to parents. 5
6
Conclusions 7
This study supports the view that bed-‐sharing and sofa-‐sharing are distinct practices, which 8
ought not to be combined in studies of unexpected infant deaths as a single exposure. Sleep 9
surface sharing practices in the UK Pakistani community differ from those of the UK majority 10
community, and from those of minority communities in the US. Health policy makers should 11
exercise caution in generalizing SUDI/SIDS risk factors across populations with differing risk 12
factor profiles. Care should therefore be taken in adopting SUDI/SIDS reduction guidelines 13
from other contexts. 14
15

17
1. Ball HL. Breastfeeding, bed-‐sharing and infant sleep. Birth. 2003;30(3):181-‐188. 1
2. McCoy RC, Hunt CE, Lesko LM, et al. Frequency of bed sharing and its relationship to 2
breastfeeding. J Dev Behav Pediatr. 2004;25(3):141. 3
3. Lahr M, Rosenberg K, Lapidus JA. Maternal-‐Infant Bedsharing: Risk factors for bedsharing 4
in a population-‐based survey of new mothers and implications for SIDS risk reduction. 5
Matern Child Health J. 2007;11(3):277-‐286. 6
4. Santos IS, Mota DM, Matijasevich A, Barros AJD, Barros CFC. Bed-‐Sharing at 3 Months 7
and Breast-‐Feeding at 1 Year in Southern Brazil. J Pediatr. 2009;155:505-‐509. 8
5. Tan KL, Ghani SN, Moy FM. The prevalence and characteristics associated with mother-‐9
infant bed-‐sharing in Klang District, Malaysia. Med J Malaysia. 2009;64(4):311-‐315. 10
6. Blair PS, Heron J, Fleming PJ. Relationship between bed sharing and breastfeeding: 11
Longitudinal, population-‐based analysis. Pediatrics. 2010;126(5):e1119-‐e1126(doi: 12
10.1542/ peds.2010-‐1277) 13
7. Farooqi S, Perry IJ, Beevers DG. Ethnic differences in infant-‐rearing practices and their 14
possible relationship to the incidence of Sudden Infant Death Syndrome (SIDS). Paediatr 15
Perinat Epidemiol. 1993;7:245-‐252. 16
8. Tuohy PG, Smale P, Clements M. Ethnic differences in parent/infant co-‐sleeping 17
practices in New Zealand. NZ Med J. 1998;111:364-‐366. 18
9. Eades SJ, Read AW. Infant care practices in a metropolitan aboriginal population 19
Bibbulung Gnarneep Team. J Paediatr Child Health. 1999;35(6):541-‐544. 20
10. Paterson J, Tukuitonga C, Butler S, Williams M. Infant bed-‐sharing among Pacific families 21
in New Zealand. NZ Med J. 2002;115(1154):241-‐243. 22
11. Hauck FR, Herman SM, Donovan M, et al. Sleep environment and the risk of Sudden 23
Infant Death Syndrome in an urban population: The Chicago infant mortality study. 24
Pediatrics. 2003;111:1207-‐1214. 25

18
12. Willinger M, Hoffman HJ, Wu KT, Hou JR, Kessler RC, Ward SL, et al. Factors associated 1
with the transition to non-‐prone sleep positions of Infants in the United States: the 2
National Infant Sleep Position Study. JAMA. 1998;280:329-‐335. 3
13. Scragg R, Mitchell EA, Taylor BJ, et al. Bed sharing, smoking, and alcohol in the Sudden 4
Infant Death Syndrome. Br Med J. 1993;307:1312-‐1318. 5
14. Blair PS, Fleming PJ, Smith IJ, et al. Babies sleeping with parents: case-‐control study of 6
factors influencing the risk of the sudden infant death syndrome. Br Med J. 7
1999;319:1457-‐1461. 8
15. Carpenter R G, Irgens L M, Blair P S, England P D, et al. Sudden unexplained infant death 9
in 20 regions in Europe: case control study Lancet 2004;363:185–91 10
16. Ruys JH, de Jonge GA, Brand R, Engelberts AC, Semmekrot BA. Bed-‐sharing in the first 11
four months of life: a risk factor for sudden infant death. Acta Paediatr. 12
2007;96(10):1399-‐1403. 13
17. Gessner BD, Ives GC, Perham-‐Hester KA. Association Between Sudden Infant Death 14
Syndrome and Prone Sleep Position, Bed Sharing, and Sleeping Outside an Infant Crib in 15
Alaska. Pediatrics. 2001;108(4):923-‐927. 16
18. Blair PS, Sidebotham P, Evason-‐Coombe C, Edmonds M, Heckstall-‐Smith EMA, Fleming 17
P. Hazardous cosleeping environments and risk factors amenable to change: case-‐18
control study of SIDS in south west England BMJ. 2009; 339:doi:10.1136/bmj.b3666 19
19. Horsley T, Clifford T, Barrowman N, et al. Benefits and harms associated with the 20
practice of bed sharing. Arch Pedatr Adolesc Med. 2007;161:237-‐245. 21
20. Blabey MH, Gessner BD. Infant bed-‐sharing practices and associated risk factors among 22
births and infant deaths in Alaska. Pub Health Reports. 2009;124:527-‐534 23
21. Nakamura S, Wind M, Danello MA. Review of Hazards Associated with Children Placed in 24
Adult Beds. Arch. Pediatr. Adolesc. Med. 1999;153:1019-‐1023. 25
19
22. American Academy of Pediatrics. The Changing Concept of Sudden Infant Death 1
Syndrome: diagnostic coding shifts, controversies regarding the sleeping environment, 2
and new variables to consider in reducing risk. Pediatrics. 2005;116:1245-‐1255. 3
23. Alm B, Lagercrantz H, Wennergren G. Stop SIDS – sleeping solitary supine, sucking 4
soother, stopping smoking substitutes. Acta Paediatr. 2006;95:260-‐262. 5
24. Mitchell EA. Sudden Infant Death Syndrome: Should Bed Sharing be Discouraged? Arch 6
Pediatr Adolesc Med. 2007;161:305-‐306. 7
25. Vennemann MM, Bajanowski T, Brinkman B, et al. Does Breastfeeding Reduce the Risk 8
of Sudden Infant Death Syndrome? Pediatrics. 2009;123(3):e406-‐e410. 9
26. Pelayo R, Owens J, Mindell J, Sheldon S. Bed sharing with unimpaired parents is not an 10
important risk for Sudden Infant Death Syndrome: to the editor. Pediatrics. 11
2006;117:993-‐994. 12
27. Born in Bradford Collaborative Group. Born in Bradford, a cohort study of babies born in 13
Bradford, and their parents: Protocol for the recruitment phase. BMC Public Health. 14
2008; 8:327. 15
28. Ball HL, Moya E, Fairley L, Westman J, Oddie S, Wright J. Infant care practices related to 16
Sudden Infant Death (SIDS) in South Asian and White British families in the UK: the 17
Bradford Infant Care Study (BradICS). Paediatr Perinat Epidemiol. 2011; Online First 18
doi:10.1111/j.1365-‐3016.2011.01217.x 19
29. Gantley M, Davies D, Murcott A. Sudden Infant Death Syndrome: Links with infant care 20
practices. Br Med J. 1993;306:16-‐20. 21
30. Blair PS, Sidebotham P, Berry PJ, Evans M, Fleming PJ. Major epidemiological changes in 22
sudden infant death syndrome: a 20-‐year population-‐based study in the UK. Lancet. 23
2006;367:314-‐319. 24
31. Hauck FR, Signore C, Fein SB, Raju TNK. Infant Sleeping Arrangements and Practices 25
during the First Year of Life. Pediatrics. 2008;122:s113-‐s120. 26

20
32. Mitchell EA, Tuohy PG, Brunt JM, et al. Risk Factors for Sudden Infant Death Syndrome 1
Following the Prevention Campaign in New Zealand: a prospective study. Pediatrics. 2
1997;100(5):835-‐840. 3
33. Office of National Statistics. Infant mortality by ethnic group, England and Wales. ONS 4
Online Edition. 2005; www.statistics.gov.uk. 5
34. Ball HL. Reasons to bed-‐share: why parents sleep with their infants. J Reprod Infant 6
Psychol. 2002;20(4):207-‐222. 7
35. Blair PS, Ball HL. The prevalence and characteristics associated with parent–infant bed-‐8
sharing in England. Arch Dis Child. 2004;89:1106-‐1110. 9
36. Kendall-‐Tackett KA, Cong Z, Hale TW. Mother-‐infant sleep locations and nighttime 10
feeding behaviors: U.S. data from the Survey of Mothers’ Sleep and Fatigue. Clinical 11
Lactation. 2010;1:27-‐36. 12
37. Hauck FR, Thompson JMD, Tanabe KO, Moon RY, Vennemann MM. Breastfeeding and 13
Reduced Risk of Sudden Infant Death Syndrome: A Meta-‐analysis Pediatrics. 2011; 14
peds.2010-‐3000; doi:10.1542/peds.2010-‐3000 15
38. Gessner BD, Porter TJ. Bed sharing with unimpaired parents is not an important risk for 16
sudden infant death syndrome. Pediatrics. 2006;117(3):990-‐991; author reply 994-‐996. 17
18
19
21
Table 1: Characteristics of study population 1 Variable Category n % Ethnic group White British 885 44.4 Pakistani 1115 55.7 Mother’s age <20 years 109 5.5 20-24 years 527 26.4 25-29 years 685 34.3 30-34 years 427 21.4 35+ years 252 12.6 Language baseline completed English 1614 80.7 Non- English 386 19.3 Marital and cohabitation status Married and living with partner 1387 69.4 Not married and living with
partner 350 17.5
Not living with partner 263 13.1 Mother’s educational qualifications None 291 14.5 Secondary School 642 32.1 Further and Higher 804 40.2 Other 230 11.5 Don’t know 33 1.75 Index of Multiple Deprivation quintile 1 (Least deprived) 38 1.9 2 80 4.0 3 242 12.1 4 370 18.5 5 (Most deprived) 1270 63.5 Mother currently smokes No 1795 89.8 Yes 205 10.2 Father currently smokes No 1616 80.8 Yes 384 19.2 Mother drinks alcohol in evenings Never and rarely 1847 92.4 Some evenings and more often 153 7.6 Father drinks alcohol in evenings Never and rarely 1777 88.9 Some evenings and more often 223 11.1 Birth weight (g) Mean (SD) 3.24 0.55 Gestational age (completed weeks) Mean (SD) 39.2 1.7 Parity 0 775 38.8 1 592 29.6 2 338 16.9 3+ 295 14.7 Breast feeding Never & <1 week 872 43.6 1-8 weeks 442 22.1 8 weeks or more 686 34.3 Baby sleeps in own room No 1767 88.4 Yes 233 11.6 Baby age at completion of survey (weeks) Mean (SD) 16.2 2.88
2 3

22
Table 2: Prevalence of co-sleeping variables 1
Outcome n %
Ever bed share 310 15.5
Regularly bed share 143 7.2
Ever sofa share 188 9.4
Ever bed share and ever sofa share 27 1.4
2