Barriers and Bridges to Prevention and Control of Dengue: The Need for a Social–Ecological...
18
Barriers and Bridges to Prevention and Control of Dengue: The Need for a Social–Ecological Approach Jerry Spiegel, 1 Shannon Bennett, 2 Libby Hattersley, 3 Mary H. Hayden, 4 Pattamaporn Kittayapong, 5 Sustriayu Nalim, 6 Daniel Nan Chee Wang, 7 Emily Zielinski-Gutie ´rrez, 8 and Duane Gubler 2 1 Liu Institute for Global Issues, University of British Columbia, 203-6476 N.W. Marine Drive, Vancouver, British Columbia, Canada V6T 1Z2 2 Asia-Pacific Institute of Tropical Medicine and Infectious Diseases, University of Hawaii, Honolulu, HI 3 Global Health Research Program, University of British Columbia, Vancouver, British Columbia, Canada 4 CU Trauma Center, NISSC, University of Colorado, Colorado Springs, CO 5 Center for Vectors and Vector-Borne Diseases and Department of Biology, Faculty of Science, Mahidol University, Bangkok, Thailand 6 Vector and Reservoir Control Research Unit, National Institute of Health Research and Development, Central Java, Indonesia 7 National Environment Agency, Singapore, Singapore 8 Division of Vector-Borne Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, GA Abstract: This article critically examines how programs for the prevention and control of dengue fever have been conducted in the absence of an integrated approach, and considers the social and ecological factors influencing their effectiveness. Despite recognition of dengue fever as the most important arboviral disease affecting humans, and in spite of a greater emphasis on community-based control approaches, the burden placed on the communities, countries, and regions affected by this disease continues to rise. In considering historical experience in the Americas and the Asia-Pacific region, as well as the global forces that are exerting new pressures, the important elements of successful control programs are identified as community ownership, partnership with government, leadership, scalability, and control of immature mosquitoes. The key barriers to the exchange of knowledge and the transdisciplinary cooperation necessary for sustainable dengue control are rooted in differences in values among policy-makers, citizens, and scientists and are repeatedly expressed in technical, economic, cultural, geographic, and political dimensions. Through consideration of case studies in Cuba, Guatemala, Singapore, Thailand, Indonesia, and Vietnam, the limitations of control approaches that fail to take into account the complexities of ecological and social systems are presented. Bridges to effective control are identified as the basis for adaptability, both of control programs to the mosquito vector’s changing behavior and of education programs to public, regional and local particularities, as well as transdisciplinarity, com- munity empowerment, the ability to scale local experiences up to the macro-level, and the capacity to learn from experience to achieve sustainability. Key words: dengue fever, Aedes aegypti mosquitoes, social and ecological systems, driving forces, community- based, partnership Published online: November 4, 2005 Correspondence to: Jerry Spiegel, e-mail: [email protected] EcoHealth 2, 273–290, 2005 DOI: 10.1007/s10393-005-8388-x Ó 2005 EcoHealth Journal Consortium
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Barriers and Bridges to Prevention and Control of Dengue: The Need for a Social–Ecological...

Barriers and Bridges to Prevention and Control of Dengue:The Need for a Social–Ecological Approach
Jerry Spiegel,1 Shannon Bennett,2 Libby Hattersley,3 Mary H. Hayden,4 Pattamaporn Kittayapong,5
Sustriayu Nalim,6 Daniel Nan Chee Wang,7 Emily Zielinski-Gutierrez,8 and Duane Gubler2
1Liu Institute for Global Issues, University of British Columbia, 203-6476 N.W. Marine Drive, Vancouver, British Columbia, Canada V6T 1Z22Asia-Pacific Institute of Tropical Medicine and Infectious Diseases, University of Hawaii, Honolulu, HI3Global Health Research Program, University of British Columbia, Vancouver, British Columbia, Canada4CU Trauma Center, NISSC, University of Colorado, Colorado Springs, CO5Center for Vectors and Vector-Borne Diseases and Department of Biology, Faculty of Science, Mahidol University, Bangkok, Thailand6Vector and Reservoir Control Research Unit, National Institute of Health Research and Development, Central Java, Indonesia7National Environment Agency, Singapore, Singapore8Division of Vector-Borne Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, GA
Abstract: This article critically examines how programs for the prevention and control of dengue fever have
been conducted in the absence of an integrated approach, and considers the social and ecological factors
influencing their effectiveness. Despite recognition of dengue fever as the most important arboviral disease
affecting humans, and in spite of a greater emphasis on community-based control approaches, the burden
placed on the communities, countries, and regions affected by this disease continues to rise. In considering
historical experience in the Americas and the Asia-Pacific region, as well as the global forces that are exerting
new pressures, the important elements of successful control programs are identified as community ownership,
partnership with government, leadership, scalability, and control of immature mosquitoes. The key barriers to
the exchange of knowledge and the transdisciplinary cooperation necessary for sustainable dengue control are
rooted in differences in values among policy-makers, citizens, and scientists and are repeatedly expressed in
technical, economic, cultural, geographic, and political dimensions. Through consideration of case studies in
Cuba, Guatemala, Singapore, Thailand, Indonesia, and Vietnam, the limitations of control approaches that fail
to take into account the complexities of ecological and social systems are presented. Bridges to effective control
are identified as the basis for adaptability, both of control programs to the mosquito vector’s changing behavior
and of education programs to public, regional and local particularities, as well as transdisciplinarity, com-
munity empowerment, the ability to scale local experiences up to the macro-level, and the capacity to learn
from experience to achieve sustainability.
Key words: dengue fever, Aedes aegypti mosquitoes, social and ecological systems, driving forces, community-
based, partnership
Published online: November 4, 2005
Correspondence to: Jerry Spiegel, e-mail: [email protected]
EcoHealth 2, 273–290, 2005DOI: 10.1007/s10393-005-8388-x
� 2005 EcoHealth Journal Consortium

INTRODUCTION AND BACKGROUND
Dengue fever (DF), the most important arboviral disease
affecting humans, is an increasingly significant cause of
morbidity and mortality in tropical and subtropical re-
gions around the world. Over half of the global human
population lives in areas of risk, and more than 100
countries are experiencing DF and/or dengue hemorrhagic
fever (DHF) epidemics in the early 21st century (Guha-
Sapir and Schimmer, 2005). Each year, there are an esti-
mated 50 to 100 million new dengue infections globally
(Gubler, 1998a, 2004), of which 500,000 are DHF, and
25,000 are fatal (Gubler, 1998a; Guzman and Kouri, 2002;
Guha-Sapir and Schimmer, 2005), although marked
underreporting results in the notification of far fewer
cases (Gubler, 1998b) (Fig. 1). The disease is endemic in
the Americas, southeast Asia region (SEAR), western Pa-
cific region (WPR), Africa, and the eastern Mediterranean,
with the major disease burden falling into the first three
regions (Guzman and Kouri, 2002; Renganathan et al.,
2003) (Fig. 2).
The clinical presentation and epidemiology of DF, an
acute viral disease caused by infection with any one of four
dengue virus serotypes (DENV-1, DENV-2, DENV-3,
DENV-4), is well understood and has been recently re-
viewed (Rigau-Perez et al., 1998; Guzman and Kouri,
2002). The dengue viruses are single-stranded RNA viruses
belonging to the family Flaviviridae, and are transmitted
principally in an urban cycle involving humans and Aedes
aegypti mosquitoes (Guzman and Kouri, 2002). In the ab-
sence of a vaccine, the emphasis has been on mosquito
control to prevent and control dengue epidemics (Rigau-
Perez et al., 1998). Although there have been some tem-
porary successes achieved in controlling dengue, these have
not persisted, partly because the single approach so often
taken, spraying against mosquitoes, is too costly to be
sustainable. While new and more effective approaches to
prevention and control are urgently required (Gubler,
1989), our scientific understanding of the factors that
influence success in this domain remains minimal.
Today’s climate of emerging infectious diseases amid
extensive global socio-economic change increasingly calls
Figure 1. Average annual number of dengue fever/
dengue hemorrhagic fever cases reported to the World
Health Organization, 1955–2003.
Figure 2. World distribution of Aedes
aegypti, 2005.
274 Jerry Spiegel et al.

for integrative, adaptive approaches that recognize the
complexities inherent in intertwined and constantly
evolving social-ecological systems (SES) (Wilcox and Gu-
bler, 2005; Gunderson et al., 1995). This requires building
bridges between disciplines and decision-makers not tra-
ditionally in the ‘‘disease control’’ network, so that the
driving forces that produce vulnerability to disease can be
altered ‘‘upstream’’ from where effects are manifest, rec-
ognizing the fundamental institutional and knowledge-re-
lated barriers that must be overcome to achieve the needed
intersectoral collaboration. The failure of previous linear
modes of understanding and their policy prescriptions
(such as a reliance on mosquito spraying), for example,
challenges us to broaden our understanding of the behav-
iors of complex natural systems, including their resilience
in the face of changing pressures (Levin, 1999; Holling,
2001), and how social institutions must comparably re-
spond (Gunderson, 2002; Gunderson et al., 1995). The SES
approach to dengue control accordingly applies multiple
methodologies to target the mosquito vector at all life-
stages, as well as continuous community engagement at all
levels to ensure adaptive intervention.
This article is the result of a workshop, Social–Ecolog-
ical Systems and Emerging Infectious Diseases, hosted by the
East-West Center and the University of Hawaii’s Asia-
Pacific Institute of Tropical Medicine and Infectious Dis-
eases in Honolulu, March 2005. Its purpose was to facilitate
interdisciplinary integration as part of National Institutes
of Health (NIH) Roadmap initiative Research Teams of the
Future (Lewis, 2005), applying a coupled, human–natural
systems approach to emerging infectious diseases (Wilcox
and Colwell, 2005); in this case, to the dengue virus. The
specific purpose of this article is thus to critically examine
approaches for preventing and controlling DF/DHF,
drawing lessons from a variety of community case studies
from the Americas and Asia, to identify barriers and
bridges to effective intervention, and to recommend new
strategies and approaches for effectively controlling this
disease. Knowledge and organizational requirements for
sustaining success will be emphasized, with regard to both
ecological and social systems.
Historical Overview of Dengue Control
DF/DHF has never been effectively contained in the Asia-
Pacific region, with the notable exception of Singapore. In
the Americas, on the other hand, epidemic dengue was
successfully controlled from 1945 until the late 1970s,
with the exception of sporadic DF epidemics in the
Caribbean islands (Gubler and Trent, 1993; Gubler, 1997).
The highly successful program, spearheaded by the Pan
American Health Organization (PAHO) amid yellow fever
epidemic concerns (Guzman and Kouri, 2003), was based
on A. aegypti larval control in domestic water storage and
collection containers and emphasized insecticide use
(particularly DDT). It was a vertically structured, para-
military approach, without community involvement
(Soper, 1943; Schliessman and Calheiros, 1974). As a re-
sult of this program, epidemic dengue transmission was
prevented in most of the tropical American region for 30
years (Guzman and Kouri, 2003). It was, however, a
classic example of success breeding failure, eventually
being disbanded in the early 1970s (Gubler, 1998b) when,
in the absence of DF/DHF epidemics, there was no longer
a perceived need for such an expensive program (Gubler,
1989).
Amid competing priorities for resources, major policy
changes at this time included the merging of dengue and
yellow fever control with malaria control, and the use of
ultra-low-volume adulticides as the recommended method
to control A. aegypti, and thus DF. Both these decisions
were major policy failures and ultimately ineffective in
preventing the reemergence of epidemic DF and the
emergence of DHF in the region (Gubler, 2005).
During the 1970s and 1980s, A. aegypti reinfested most
of the countries from which it had been eliminated (WHO,
1997). Generally, within a few years of reinfestation, these
countries experienced epidemic DF, followed by hyperen-
demicity and the emergence of DHF (Gubler, 1997; Pin-
heiro and Corber, 1997). Alarm-bells were sounded,
however little has been accomplished to reverse the trend of
increasing epidemic activity, and, in a short period of 20
years, this disease went from virtual nonexistence to one of
the region’s most important public health problems at the
dawn of the 21st century (Gubler, 2002; Guzman and
Kouri, 2002).
During the 1980s, in an effort to achieve sustainable
A. aegypti control, the emphasis was shifted from a top-down
to a bottom-up approach (Gubler, 1989). The goal was to
convince people living in the homes in which most trans-
mission was occurring to take ownership of household and
neighborhood mosquito control. The term ‘‘bottom-up’’
refers to an integrated community-based approach to mos-
quito control by environmental management, with increased
emphasis placed on health education, and community-
ownership (Gubler, 1989; WHO, 2001; Renganathan, 2003).
Prevention and Control of Dengue 275

This public health approach, combining active surveillance,
emergency response, case management, and community-
based A. aegypti control (Gubler and Casta-Velez, 1991)
received wide acceptance in the 1990s, became the basis for
the World Health Organization (WHO) global strategy for
prevention and control of DF/DHF (WHO, 2001) and was
echoed regionally in declarations and programs in the
Americas (PAHO, 1994) and Asia Pacific region (WHO,
1999). Today, A. aegypti control programs based on active
community participation have been developed in numerous
countries worldwide (Parks et al., 2004). Nevertheless, suc-
cessful program implementation has remained a significant
challenge, and the spread of epidemic DF/DHF persists
(Fig. 3).
Global Driving Forces
Dengue’s progressive expansion and increasing impact on
vulnerable communities has accompanied a number of
trends in global human influences: rapid and unplanned
urbanization; population growth; increasingly inadequate
municipal services; increased use of nonbiodegradable
products (bottles, plastic, cans, tires, etc.); and an unprec-
edented growth in the movement of people and com-
modities via travel and commerce, all amid largely
ineffective mosquito control efforts (Gubler, 1989; Gubler,
1997; Gubler, 1998a; WHO, 2001). Above all, as A. aegypti
is a highly domesticated urban mosquito, the public health
problem posed by DF is particularly important in cities in
the tropical developing world, where aides to human–
mosquito interaction, such as unscreened housing, dense
residential areas with large numbers of household breeding
sites (such as containers and tires), and absence of waste
management, sewer, and water systems produce ideal
conditions for mosquito breeding in the domestic envi-
ronment. Thus, large populations of mosquitoes are living
in intimate contact with crowded human populations. In
addition, dengue endemic areas are spatially well-con-
nected, undermining the feasibility of eradication in iso-
lated locales. Furthermore, the public health capacity of
states was fundamentally weakened by fiscal restraints in
the 1970s, 1980s, and 1990s (Gubler, 1989; Rigau-Perez,
1998), creating even greater challenges to effective pre-
vention and control. Therefore, local circumstances have
been subject to driving forces that extend across both
spatial and temporal scales, well beyond the capacity of
local control efforts, and thus strategies are required that
reflect this.
ELEMENTS OF A SUCCESSFUL AND
SUSTAINABLE CONTROL PROGRAM
Through the experience of failed control efforts, we have
learned that the coupled human–natural interaction of
humans and dengue behaves as a complex adaptive system
that has undergone repeated phases of management ef-
forts from local to regional scales, much as described by
the ‘‘adaptive cycle’’ metaphor (i.e., Gunderson and
Holling, 2002), from ephemerally stable periods of mos-
quito control through to destabilized periods of release
and reorganization due to economic constraints, mosquito
recolonization, and rapid human expansion. Such man-
agement experiences have stimulated policy-makers and
researchers to review successes and failures, and consider
barriers to success and sustainability in dengue control.
Figure 3. Aedes aegypti distribution in
the Americas.
276 Jerry Spiegel et al.

Given the need for broad synthesis and collaboration,
critical ‘‘barriers’’ can best be regarded as those that
fundamentally arise from differences in values among
policy-makers, citizens, and scientists and interfere with
the exchange of knowledge and the transdisciplinary
cooperation necessary for sustainable dengue control
(Gunderson et al., 1995). As a result, piecemeal policies
have developed, favoring the targeting of single elements
in an inefficient and unsustainable fashion (Holling,
1995), historically giving rise to vertically structured
intervention programs and approaches that have relied
almost exclusively on using insecticide application to
break the transmission cycle, proven to be incapable of
achieving sustainable control. Our review identifies the
following program elements as being critical to success
because they require bridging disciplines and the divergent
short-term objectives of the various interested parties in-
volved: (i) focus on immature mosquito control; (ii)
community ownership; (iii) partnership with government;
(iv) leadership; (v) scale; and (vi) adaptability.
Immature Mosquito Control
Programs that solely or primarily rely on eliminating adult
mosquitoes in crisis situations are doomed to failure
(Gubler, 1989; Newton and Reiter, 1992). While such
intervention plays an important contingency role in a
comprehensive program, and certainly generates the
greatest public satisfaction, it nonetheless entails consid-
erable and avoidable economic cost and ecological impact,
and should be strategically minimized. Therefore, the
emphasis should be on interrupting the transmission cycle
at an early phase through immature mosquito control. This
can only be achieved through an integrated approach that
addresses the complex, nonlinear behavior of the SES in
which the dengue virus exists (Gunderson et al., 1995;
Wilcox and Gubler, 2005).
Community Ownership
Community-based programs are increasingly being touted
as the key to successful control programs (Gubler and
Clark, 1996; Rifkin, 1996; Parks and Lloyd, 2004; Parks
et al., 2004), recognizing the fundamental importance of
mobilizing and channeling household-level behaviors and
capacities in eliminating mosquito breeding sites, reducing
exposure, and targeting efforts. What is actually meant by
‘‘community’’ must, of course, take into account social,
geographical, and political factors specific to a local con-
text, fully recognizing multi-cultural complexity (e.g., rur-
al–urban migration; diversity in norms and practices).
Above all, community engagement is best achieved through
creating and reinforcing local ownership of efforts, not
merely passively conveying information developed outside
of the community itself.
Partnership with Government
Community-based programs have often been viewed as an
economical alternative to government intervention.
However, the role of government in coordinating efforts
cannot be underestimated. Without a coordinated ‘‘top-
down’’ and ‘‘bottom-up’’ approach, successful imple-
mentation of control programs is unlikely to be achieved
and sustained (Gubler, 1989). Because dengue is only one
among many health problems faced by residents, gov-
ernment support is essential if coordination of control
efforts and stimulus to participate is to be maintained. For
example, visible concern on the part of government af-
firms the serious nature of the threat and validates the
need to continue source-reduction efforts at the local
level. The likelihood of success is further enhanced if a
wide range of local and regional partners are engaged in
the effort (Halstead, 2000), and government is in an
excellent position to facilitate and broadly extend this
process, especially to ensure coordination with clinical-
epidemiological recognition and management of dengue
cases in the context of timely feedback of information on
DF and vector incidence.
Leadership
Leadership at a local level guides the successful establish-
ment and follow-through of intervention programs. Those
executing the control project must take the time to identify
and enlist local leaders who have the credibility to ensure
buy-in by members of the community. Formal and infor-
mal local leaders have necessary insider knowledge of
neighborhood practices, and, as such, may be better able to
control mosquito breeding sites using environmental
management by enlisting community participation.
Investment of time and effort must go into the identifica-
tion of mosquito breeding sites, which may vary among
neighborhoods. Educational campaigns need to be targeted
locally and adapted seasonally to potentially changing
ecologies, both human and vector.
Prevention and Control of Dengue 277

Scale
An important caveat to the above discussion is the stability
of the social structure at all scales. In this sense, what may
work in ideal circumstances may not necessarily lend itself
to wider application. Communities beset by insecurity,
influx of recent immigrants and/or extreme poverty may
lack the cohesion to work on source-reduction as a
concerted effort, and individuals may be hard-pressed to
focus daily efforts on reducing breeding sites. Under such
conditions, government agencies must still be held
responsible for mounting control efforts, although they
may be realistically able to respond only when necessary to
avoid an outbreak. The question remains as to the feasi-
bility of extending the local-level scale of successful com-
munity participation in immature mosquito control to a
‘‘macro’’ regional, national, or cross-border level.
Adaptability
In recognizing the dengue problem in the context of complex
social and ecological systems, the capacity to adapt becomes
an undeniable emergent property. Mosquitoes rapidly
recolonize sprayed territory. Female mosquitoes adapt to
utilize new breeding habitats, from disposable containers to
manhole covers, as old breeding sites are eliminated and new
ones become available. Any successful control strategy needs
to be similarly adaptable through a built-in monitoring
component that provides feedback to respond and adjust
with rapidly executable control measures. This adaptability
requires such changes be neither costly nor require major
changes in the infrastructure needed to execute them.
BARRIERS AND THEIR EXPRESSION
Fundamental differences in the value systems and short-term
objectives of the different sets of actors involved in man-
agement of dengue transmission form the bedrock for the
‘‘barriers’’ (Gunderson et al., 1995) that impede a transdis-
ciplinary and therefore adaptive and sustainable control
program. As a result, failed management strategies are often
directed towards single targets, policies are piecemeal, the
scale of focus is myopic in both time and space, and there is
an over-reliance or confidence that ignores the plasticity of
the system (Holling, 1995). How such approaches have failed
at effective dengue control can be readily observed by
examining the range of contexts in which they have been
manifest and expressed, while critically assessing each from
the perspective of the complex, integrated cycle that ulti-
mately impacts on the functional and adaptive capacities of
social and ecological systems (Gunderson et al., 1995).
Technical Cure-alls
Despite the unequivocal targeting of A. aegypti as the
principal vector of interest, an over-reliance on technical
management ‘‘solutions’’ is costly, unsustainable, falsely
lulls citizens into a state of complacence, and ultimately
leads to failure of control and resurgence when control
programs are dropped. Application of chemical insecti-
cides, for example, remains only minimally effective in
ultimately restricting human exposure to the vector. A. ae-
gypti is primarily an indoor-resting mosquito, greatly
reducing the potential of typical insecticide spraying to
penetrate resting sites. In addition, the residual effect of
most insecticides used today is limited, making periodic
application necessary, and thus effective vector control too
costly for most countries. Insecticide resistance, which oc-
curs in mosquito vector populations after continued
application of the same chemical compounds, or when
insecticides become freely used by several communities
with a lack of collaboration and technical skill, serves as
another significant impediment to sustainable control.
Persistence of insecticide application as an option is a
result of barriers to the exchange of knowledge required for
integrated mosquito control and cooperation among agen-
cies planning and implementing application regimes. Over-
coming these barriers requires bridging the gaps in inter-
agency communication, between individuals with different
disciplinary training, among other factors. For example,
when an understanding of the evolutionary ecology of
mosquito populations is integrated with that of the physio-
logical mechanisms of chemical controls used, sustainable
control measures become apparent. In the case of dengue,
insecticide application to control adult mosquitoes should be
limited to emergency response during disease epidemics, and
guidelines for monitoring insecticide use and insecticide
resistance should be continually updated. Reduction of
insecticide use could be achieved by integrating it with other
control approaches, such as lethal ovitraps and pyrethroid
impregnated curtains and bednets, although more research is
needed to assess the efficacy and feasibility of these measures.
In addition, research suggests that knowledge of mosquito
preference for certain containers can help to target and in-
crease the effectiveness of control of immatures.
278 Jerry Spiegel et al.

Surveillance for both DF/DHF cases and vectors is also
of critical importance. However, dengue case reporting is
frequently delayed relative to time of transmission, nor
does it achieve anything near full coverage, hampering
control efforts. While an ideal on-line electronic case
reporting system could be a solution to this problem, this is
far from the reality of most developing country health
systems. Surveillance can fail at numerous stages: less severe
cases may never seek care, care providers may elect not to
collect a sample, samples collected may not arrive in suit-
able condition for analysis, and even laboratories with the
means for testing may lack sufficient supplies to fully
analyze all samples. Thus, in many countries, the resulting
surveillance data may reflect only a fraction of actual cases.
Unfortunately, surveillance for dengue mosquito vec-
tors has furthermore not routinely been effective because
vector indices and dengue epidemics have not always been
correlated. For example, the pupal index may be more
closely correlated with dengue transmission than the more
familiar larval indices (Focks, 2003). Research is still
ongoing to search for better vector indices and to achieve
agreement regarding their use.
False Economies
It is ironic that economically expensive approaches to
dengue control are favored when less costly government and
community cooperatively based programs would do, par-
ticularly since dengue afflicts poverty-stricken communities
greatest, where there is a lack of reliable disease-burden
estimates; i.e., who becomes clinically ill with DF/DHF and
what happens to them (clinic visits, hospitalizations, days
off work, etc.). Impoverished communities will only adopt
interventions when they can clearly see the economic ben-
efits, however lack of data currently makes it difficult to
demonstrate such benefits. Burden estimates are available
(Meltzer et al., 1998; Gubler and Meltzer, 1999) but these
are typically based on extrapolations from small datasets.
While resources are often expended during a dengue out-
break, the burden imposed by dengue during nonoutbreak
periods could be considerable, albeit ignored (Meltzer et al.,
1998; Gubler and Meltzer, 1999). Furthermore, there are
very few cost–benefit estimates available for existing inter-
ventions (e.g., larvae control) (Shepard et al., 2004).
Cultural Insensitivity or Gross Oversimplification
Given the necessary reliance on community mobilization
strategies to achieve larval mosquito control, programs that
ignore or gloss over the ‘‘cultural,’’ social structure or
heterogeneity across different scales will not succeed in
dengue transmission prevention. A first consideration must
be which unit of ‘‘community,’’ and therefore which as-
pects of culture, are being examined. The householder/
family, the neighborhood, the broader social units and,
indeed, the culture of the public health workforce and of
policymakers must all be considered.
Household
At the household level, the perceived risk for dengue, and
therefore motivation for taking action, may be low
(Fig. 4). People may not identify fevers as pertaining to
dengue infection, and laboratory diagnosis may be
unavailable. Dengue is frequently ‘‘invisible’’ during inter-
epidemic periods, and the seasonality of the disease can
further affect mobilization efforts. It is difficult to ask
people to prioritize dengue among other acute health and
environmental concerns, and the reduction in fatalities
due to advances in DHF treatment may reduce perceived
severity. Tragic fatalities do, sadly, serve to motivate
community action, though often too late to intervene in
the trajectory of the outbreak (Kouri et al., 1986; Deitz
et al., 1996).
Larval control activities typically focus on household
breeding sites, often taking the form over many years of a
broader focus on ‘‘cleanliness.’’ This approach may ulti-
mately prove inefficient by diverting attention away from
the most productive breeding sites, which may be out-of-
view or ‘‘acceptable’’ by cleanliness standards. Of course,
some items identified as disposable by researchers may in
fact have household function and are being saved for future
use. Though source reduction campaigns increasingly rec-
ognize this issue, control of these useful containers can
remain a problem.
It can also be challenging to engage householders in
prevention (and, arguably, may be epidemiologically
pointless) when vector breeding continues unabated in
neighboring households, commercial sites such as tire
shops, and ‘‘unregulated’’ sources such as informal dumps.
This highlights the need to consider the local human
ecology as a whole, rather than focusing on individual
actions.
Another household factor is the availability of indoor
climate control (air-conditioning), which was protective
during a dengue outbreak on the US–Mexico border
(Reiter et al., 2003). This ‘‘adaptation’’ of more affluent
Prevention and Control of Dengue 279

populations, living in ‘‘sealed’’ environments where vec-
tor issues are reduced, is seldom available to the wider
population. Less income-dependent factors, such as
‘‘open’’ housing styles, adapted for and preferred in the
tropics, may also be a factor contributing to indoor
exposure to mosquitoes and these demand consideration
when developing interventions to reduce human–vector
contact.
Community
Level of community integration is an important factor to
consider when implementing a dengue transmission
control program. Areas with networks of volunteers and
institutions (such as churches and schools) present
greater opportunity for mobilization than newly urban-
izing zones with high levels of poverty and large numbers
of new migrants. In such communities, there may be few
households with intact families, limited relationships be-
tween neighbors, and large numbers of people working at
the subsistence level, with little time to participate in
mobilization efforts. Communities in regions of conflict,
likewise, are not suited to traditional mobilization ap-
proaches. Formative research prior to an intervention is
therefore critical, and has major implications for project
scale-up.
As already noted, rapid urbanization and other changes
in land-use also contribute to vast areas without adequate
services or infrastructure. Household water-storage is
widespread and, in expanding peri-urban areas, is com-
bined with massive numbers of people drawn into close
quarters. These areas often lack infrastructure to deal with
refuse, exacerbating the problem of potential breeding sites.
The influence of global consumer culture further adds to
this risk with disposable but nonbiodegradable water-
holding containers, vector breeding sites, proliferating
widely (Gubler, 1989).
Policy and Intervention Culture
Finally, the ‘‘culture’’ of interventions themselves is highly
relevant. Government-sponsored vector control is still
practiced in many dengue endemic areas, complicating
attempts to create community ownership of dengue control
programs. Educational interventions more directly,
including pre-testing of community-directed messages, can
be rare due to limited time and personnel. A tendency
toward the inertia of previously used messages and cam-
paigns can prevail regardless of proof of their efficacy. For
example, dispersing the broad message to ‘‘keep the patio
clean’’ and ‘‘control all household breeding sites,’’ despite
indications that a more limited number of containers may
house the majority of mosquito breeding sites, represents a
potential misdirection of community efforts.
Geographical
Migrating populations in search of work (and travelers in
general) have the potential to carry the dengue virus with
them, as does global shipping. Exponential growth in such
global interconnectivity highlights the importance of wider,
regional approaches to control. The rapid dissolution of the
dengue virus’ geographic impediments to transmission also
emphasizes the need to establish scalable and sustainable
Figure 4. Knowledge (left) and attitude (right) on dengue and vector control in Thailand.
280 Jerry Spiegel et al.

adaptive approaches to dengue prevention and control, as
opposed to focusing on eradication.
Political
Dengue epidemics give rise to serious public concern and
alarm, as hundreds to thousands of new infections can arise
every week. The public must be kept informed, however,
heightened awareness further exacerbates the level of
concern. It is natural, therefore, that the public will turn to
the government for a solution, and yet, ironically, it will be
the government that must turn to the public to solve the
problem.
Despite the ineffectiveness of chemical control and its
potential collateral effects on nontarget organisms, insec-
ticides remain the leading dengue vector control method in
most developing countries. A significant contributing rea-
son for this is that adulticiding is a highly visible, and
therefore politically popular, method of control which
demonstrates that a government is responsive. While
adulticiding may provide some ‘‘psychological satisfaction’’
for both public health authorities and householders, this
can also create a false sense of security among both gov-
ernment officials and the public (Gubler, 1989).
In fact, the control of dengue can only be effective
when the entire community agrees to accept responsibility
to prevent A. aegypti from breeding. The government needs
to forge an alliance with the community and, in doing so,
provide the leadership and coordination for an integrated
effort. Such leadership, however, does not usually exist in
most affected communities, and a lack of trust in public
authorities rapidly undermines the feasibility of a govern-
ment–community alliance. To overcome this, local gov-
ernment must be a full partner and provide competent
leadership in initiating control activities, and encouraging
and facilitating community participation (and not solely
for dengue control).
Equally important is that governments forge an alli-
ance at the regional level, sharing surveillance information
and pooling resources in order to better cope with DF/
DHF outbreaks. Dengue transmits easily through travelers
moving from country to country. Therefore, no matter
how well equipped a country may be, it will not be able to
prevent epidemic transmission unless all other countries
in the region participate in serious DF/DHF control
efforts.
Ultimately, the greatest political barrier to DF/DHF
prevention and control in most endemic countries is lack of
political skill and the will to develop and maintain effective
programs.
CROSS-COUNTRY COMMUNITY CASES
In the context of the preceding assessment of barriers to
dengue control and elements critical to its success, the
experiences of a range of affected countries have been
examined. Table 1 provides a summary of these cases for
comparative purposes, however a brief description of each
setting is also provided in the text below.
Cuba
A strong vertically structured control program was rein-
forced in Cuba in 1981 following the first and largest DHF
epidemic in the Americas (Kouri et al., 1986), notably
including regular home visits by environmental inspectors.
Amid the outbreak itself, there was heavy reliance on pesti-
cide use. Despite the program’s recognized efficacy (Gubler
and Clark, 1994), and after more than 15 years without re-
ported dengue activity, serious outbreaks reoccurred in 1997
(Guzman et al., 1999) and 2001–2002 (Spiegel et al., 2002).
This prompted a strong interest and commitment to alter-
native strategies that placed greater emphasis on intersectoral
coordination beyond just the health sector, as well as com-
munity participation in vector control (Sanchez et al., 2005).
Cuba’s strong health care infrastructure plays a key role
in dengue control in this country. At the local level, family
medicine centers provide free and accessible health care for
120 families each, enabling effective clinical-epidemiologi-
cal surveillance through rapid detection and isolation of
cases. These centers reinforce the efforts of Health Area
Teams, which serve between 10,000 and 30,000 inhabitants,
and provide a platform for working on health promotion
matters with each district’s Popular Council of elected
officials and community organizations. They further com-
plement national strengths in laboratory analysis and vector
control capacity. Another element critical to the 2001–2002
dengue campaign was a great mobilization of people to
identify and eliminate breeding sites, clean up high-risk
areas, and conduct comprehensive adulticide spraying.
Although this enabled effective containment of what be-
came an uncontrolled epidemic in other countries in the
region, authorities deemed it too costly to be sustainable.
In 2003, pilot projects were initiated in two commu-
nities in the City of Havana to explore how integrated
Prevention and Control of Dengue 281

Tab
le1.
Co
mp
arat
ive
Sum
mar
yo
fSi
xC
ross
-co
un
try
Co
mm
un
ity
Cas
eSt
ud
ies
Co
un
try
Sum
mar
yO
utc
om
eA
ttri
bu
tes
Ch
alle
nge
s
Cu
ba
Ave
rtic
alco
ntr
ol
pro
gram
,w
ith
hea
vyre
lian
ce
on
ho
use
ho
ldin
spec
tio
nan
du
seo
fp
esti
cid
es
inep
idem
icsi
tuat
ion
ssu
cces
sfu
lu
nti
l20
01
Lin
kto
stro
ng
clin
ical
-ep
idem
iolo
gica
l
surv
eill
ance
and
pri
mar
yca
ren
etw
ork
wit
h
com
pre
hen
sive
com
mu
nit
yco
vera
ge
Pil
ot
pro
ject
sin
itia
ted
in20
03in
two
Hav
ana
com
mu
nit
ies
top
rom
ote
inte
grat
edsu
rvei
llan
ce
and
com
mu
nit
yp
arti
cip
atio
n
Inte
rsec
tora
lco
llab
ora
tio
nan
dco
mm
un
ity
mo
bil
izat
ion
incr
isis
situ
atio
nen
able
d
effe
ctiv
eco
nta
inm
ent
of
wh
atw
asan
un
con
tro
lled
epid
emic
ino
ther
cou
ntr
ies
inth
ere
gio
n,
bu
td
eem
edto
oco
stly
tob
esu
stai
nab
le
Em
ph
asis
on
dev
elo
pin
gm
ore
effe
ctiv
e
surv
eill
ance
Stro
ng
hea
lth
infr
astr
uct
ure
Tra
nsd
isci
pli
nar
y
Em
po
wer
men
t
Par
tici
pat
ory
Soci
alm
ob
iliz
atio
n
Stro
ng
po
liti
cal
wil
lin
cris
is
Sust
ain
abil
ity
Gu
atem
ala
DH
Fo
utb
reak
in19
96le
dto
init
iati
on
of
a
com
mu
nit
y-b
ased
pro
ject
inP
acifi
cco
asta
lar
ea
Inco
rpo
rate
dco
mm
un
ity,
loca
lo
ffici
al,
and
hea
lth
-car
e
wo
rker
par
tici
pat
ion
,p
hys
icia
no
utr
each
,m
ass
med
ia,
and
trai
nin
go
fco
mm
un
itie
sto
con
du
ctin
spec
tio
ns
of
nei
ghb
ors
’h
ou
ses
Go
vern
men
tst
aff
invo
lved
inp
roje
ct
reas
sign
edel
sew
her
ew
hen
USA
IDfu
nd
ing
ran
ou
t
No
ou
tbre
aks
du
rin
gp
roje
ct
Man
yh
ou
seh
old
pra
ctic
esim
pro
ved
Th
ree-
year
po
st-e
valu
atio
nfo
un
dd
ecli
ne
in
som
ekn
ow
led
gein
dic
ato
rs,m
ain
ten
ance
or
imp
rove
men
tin
man
yh
ou
seh
old
pre
ven
tio
np
ract
ices
,b
ut
ove
rall
incr
ease
inla
rval
infe
stat
ion
Rec
ent
visi
tsb
yh
ealt
ho
rve
cto
r
con
tro
lw
ork
ers
no
tfo
un
dto
hav
ea
sign
ifica
nt
po
siti
veas
soci
atio
nw
ith
pre
ven
tio
np
ract
ices
or
larv
aein
fest
atio
n
Ho
use
ho
ldvi
sits
by
nei
ghb
ors
fou
nd
tosi
gnifi
can
tly
red
uce
larv
aein
fest
atio
ns
Tra
nsd
isci
pli
nar
y
Par
tici
pat
ory
Lo
cal
sen
siti
vity
Soci
alm
ob
iliz
atio
n
Sust
ain
abil
ity
Lac
ko
f
po
liti
cal
wil
l
Sin
gap
ore
Nat
ion
alst
rate
gyb
ased
for
man
yye
ars
on
stro
ng
surv
eill
ance
,p
ub
lic
edu
cati
on
cam
pai
gns,
and
stri
ct
enfo
rcem
ent
Ove
rall
AH
Ire
du
ced
toar
ou
nd
2%;
bu
tgr
eate
rth
an5%
ince
rtai
nar
eas.
KA
Psu
rvey
resu
lts:
Kn
ow
led
gele
vels
hig
h,
bu
tat
titu
de
very
po
or
Nat
ion
alst
rate
gyre
vise
dto
emp
has
ize
com
mu
nit
yre
spo
nsi
bil
ity,
gove
rnm
ent
faci
lita
tio
n
rath
erth
anre
gula
tio
n,
and
inte
rsec
tora
lco
ord
inat
ion
Sign
ifica
nt
red
uct
ion
inn
um
ber
of
mo
squ
ito
bre
edin
gsi
tes
Imp
rove
din
tera
ctio
nb
etw
een
gove
rnm
ent
and
com
mu
nit
y
Cu
rren
tly,
the
maj
or
issu
eis
sust
ain
abil
ity
Inte
rsec
tora
l
Par
tici
pat
ory
Soci
alm
ob
iliz
atio
n
Go
vern
men
tco
mm
itm
ent
Ad
apta
bil
ity
Tra
nsl
atin
g
kno
wle
dge
into
atti
tud
ean
d
beh
avio
ral
chan
ge
Sust
ain
abil
ity
(Con
tin
ued
)
282 Jerry Spiegel et al.

Tab
le1.
(Con
tin
ued
)
Co
un
try
Sum
mar
yO
utc
om
eA
ttri
bu
tes
Ch
alle
nge
s
Th
aila
nd
WH
O-f
un
ded
pil
ot
pro
ject
inea
ster
nre
gio
nu
sin
g
com
bin
atio
no
fto
p-d
ow
nan
db
ott
om
-up
app
roac
hes
,w
ith
coll
abo
rati
on
bet
wee
nlo
cal
auth
ori
ties
,h
ou
seh
old
ers,
pu
bli
ch
ealt
hvo
lun
teer
s,
and
sch
oo
lch
ild
ren
Gen
eral
edu
cati
on
cam
pai
gn,
foll
ow
edb
ysp
ecifi
ctr
ain
ing
inth
eu
sean
d
pro
du
ctio
no
flo
cal
vect
or-
con
tro
lm
ater
ials
Cle
an-u
pca
mp
aign
and
dis
trib
uti
on
of
con
tro
l
mat
eria
lsco
nd
uct
edp
rio
rto
rain
yse
aso
n
Wee
kly
garb
age
pic
kup
du
rin
gra
iny
seas
on
Sign
ifica
nt
red
uct
ion
inb
oth
mo
squ
ito
vect
or
po
pu
lati
on
san
dse
rolo
gica
lly
con
firm
edd
engu
eca
ses
in
no
n-c
on
tro
lar
eas
com
par
edto
con
tro
lar
eas
(pre
-in
terv
enti
on
:
265.
25vs
.21
7.86
per
100,
000
po
pu
lati
on
;p
ost
-in
terv
enti
on
:0
vs.
332.
23p
er10
0,00
0p
op
ula
tio
n)
KA
Psu
rvey
:kn
ow
led
gele
vels
mo
der
atel
yh
igh
;b
ut
atti
tud
eu
nch
ange
d;
den
gue
no
tra
nke
das
ah
igh
-pri
ori
ty
dis
ease
Em
po
wer
men
t
Par
tici
pat
ory
Lo
cal
sen
siti
vity
Sust
ain
abil
ity
Scal
ing-
up
toth
e
nat
ion
alle
vel
Tra
nsl
atin
g
kno
wle
dge
into
atti
tud
ean
d
beh
avio
ral
chan
ge
Ind
on
esia
Ext
ern
ally
fun
ded
pro
ject
init
iate
din
1997
tod
esig
na
com
mu
nit
yed
uca
tio
nca
mp
aign
and
con
du
ctw
eekl
y
ho
use
ho
ldin
spec
tio
ns
Sign
ifica
nt
red
uct
ion
inD
HF
case
s
Man
yC
BO
sev
olv
edfr
om
the
pro
ject
,in
clu
din
gth
e‘‘
Das
awis
ma’
’
(ten
-ho
use
)gr
ou
ps
Wee
kly
insp
ecti
on
pro
gram
has
bee
n
mai
nta
ined
CD
Cin
Fo
rtC
oll
ins,
thro
ugh
WH
O,
has
con
tin
ued
tosu
pp
ort
the
pro
gram
Lo
cal
sen
siti
vity
Ad
apta
bil
ity
Sust
ain
abil
ity
Vie
tnam
Co
llab
ora
tive
com
mu
nit
y-b
ased
pro
gram
init
iate
d
in19
95
Key
acti
viti
es:
com
mu
nit
ym
ob
iliz
atio
nan
d
edu
cati
on
cam
pai
gns,
bre
edin
gan
du
se
of
loca
lco
pep
od
pre
dat
ors
,an
dm
on
ito
rin
g
of
vect
or
po
pu
lati
on
san
dh
ou
seh
old
beh
avio
rs
KA
Pan
dve
cto
rsu
rvey
su
sed
tota
ilo
rp
rogr
amto
loca
lco
nd
itio
ns
An
nu
alev
alu
atio
ns
and
on
goin
gm
on
ito
rin
g
use
dto
mea
sure
pro
gres
s,ad
dre
ssis
sues
,an
d
adju
stac
tivi
ties
2000
:F
ull
vect
or
con
tro
lac
hie
ved
infi
ve
ou
to
fsi
xco
mm
un
es,
and
pro
po
rtio
n
of
ho
use
ho
lds
rate
das
sho
win
gan
exce
llen
to
rgo
od
leve
lo
fp
reve
nti
on
pra
ctic
esh
add
ou
ble
dto
94%
2003
:L
arva
lp
op
ula
tio
ns
red
uce
db
y
99.6%
–10
0%in
fou
rco
mm
un
es.
Fu
rth
erp
rogr
amex
pan
sio
nac
hie
ved
con
tro
lin
32o
ut
of
37co
mm
un
es
Soci
al
mo
bil
izat
ion
Beh
avio
rch
ange
Inte
rsec
tora
l
Lo
cal
sen
siti
vity
Ad
apta
bil
ity
Sust
ain
abil
ity
AH
I,A
edes
ho
use
ind
ex;
CB
Os,
com
mu
nit
y-b
ased
org
aniz
atio
ns;
CD
C,
Cen
ters
for
Dis
ease
Co
ntr
ol
and
Pre
ven
tio
n;
DH
F,
den
gue
hem
orr
hag
icfe
ver;
KA
P,
Kn
ow
led
ge,
Att
itu
de
and
Pra
ctic
e;U
SAID
,U
S
Age
ncy
for
Inte
rnat
ion
alD
evel
op
men
t;W
HO
,W
orl
dH
ealt
hO
rgan
izat
ion
.
Prevention and Control of Dengue 283

surveillance and community participation can form the
basis for sustainable control and prevention of dengue
(Spiegel et al., 2004). This study includes a case-control
examination of factors associated with the presence of
breeding sites in homes in a nonoutbreak period.
Guatemala
In 1997, a dengue prevention project based on community
mobilization was carried out on the Pacific coast of Gua-
temala by the Ministry of Public Health and Social Assis-
tance, the Guatemalan Institute of Social Security, and the
Institute for Nutrition of Central America and Panama
(part of the Pan-American Health Organization), with
funding from the US Agency for International Development
(USAID). The project was in response to DHF cases iden-
tified in 1996, and in recognition of the potential for further
DHF cases. A variety of ‘‘best practices’’ were employed,
such as involving the community through children’s events,
talks given by Public Health employees, collaboration with
local officials, outreach to physicians, mass media and, in
some sectors, the training to conduct neighboring house-
hold visits to look for mosquito breeding sites.
There was no outbreak during the project and many
household prevention practices increased from the baseline
assessment. Local officials and health workers were exten-
sively involved in the implementation of the program, al-
though funding primarily came from outside the national
government, and when funds were no longer available
many staff were reassigned to other activities.
A 3-year post-evaluation was conducted to examine
lasting effects of the project in 2000 (Zielinski-Gutierrez,
2002). Cross-sectional surveys were undertaken with resi-
dents who had lived in the intervention communities since
before the project period. While some knowledge indicators
declined in the intervening 3 years, many household pre-
vention practices for control of breeding sites had, in fact,
continued or even increased. Entomological indices of
larval infestation had, however, increased in almost every
category of container. In this instance, the remaining pre-
vention practices were not sufficient to hold down vector
populations.
Factors such as recent interactions with health or
vector control workers were not significant in their asso-
ciation with positive prevention practices or the presence of
mosquito larvae. Interestingly, however, multivariate anal-
ysis suggested that households in areas that received visits
from neighbors during the 1997 intervention (vs. areas
where only mass media and community-wide events were
carried out) were significantly less likely to become Aedes
larvae-infested over time. While a whole range of caveats
could explain this association, it may suggest that further
evaluation of the effects of direct neighbor-to-neighbor
interaction is warranted, and bolster other case studies
discussed in this article.
Singapore
For many years, Singapore’s strategy for the prevention and
control of DF was based on a strong surveillance capability,
an extensive public education program, and a strict
enforcement regime.
The Aedes House Index (AHI) was reduced to
approximately 2%, which was considered below the
threshold level of epidemic transmission, but there were
many occasions when some neighborhoods registered an
AHI of more than 5, which increased the risk of a localized
outbreak. Evidence from surveillance indicated that female
mosquitoes quickly adapted to control measures by
switching breeding sites, even to such unlikely places as
manhole covers, requiring the need for constant vigilance
and adaptive responses at all levels.
It became clear that while public education served to
raise awareness, it did not spur action. Surveys have shown
that while the knowledge content was extremely high,
attitudes were very poor. Enforcement did not change
people’s attitude. Four years ago, Singapore revised its
strategy, with emphases given to winning the community
over and getting them to take responsibility for the dengue
problem. Working very closely with the private, public, and
people (3-P) sectors, the government was able to raise the
level of ownership of the dengue control program among
residents, who volunteered their time to help carry out
surveillance and conduct public education programs.
The government, on the other hand, openly displayed
full commitment to join in the battle with the community.
It strengthened its surveillance system and started a re-
search facility to study dengue. Internally, the government
also initiated a program to change the mindset of its field
staff and provided training to employees in facilitation
rather than regulation.
In 2005, the Singapore government had succeeded in
establishing a closer rapport with the community and, in
many of the campaigns organized with grassroots support,
the number of breeding sites has declined significantly (Ooi
et al., 2005). The major challenge now is sustainability.
284 Jerry Spiegel et al.

Thailand
Dengue vector control in Thailand has not had much
impact in reducing dengue transmission at the national
level. To find an effective strategy to control this disease, a
pilot intervention project, funded by the WHO, was re-
cently conducted in eastern Thailand using a combination
of top-down and bottom-up approaches [Kittayapong et
al., unpublished data]. Implementation was initiated by
local administrative authorities, including public health
and school officials in collaboration with householders,
public health volunteers, and school children. The local
public health volunteers are mostly women who do not
work outdoors and have more free time at home. As
volunteers for public health activities, they usually bene-
fited from their public health service. Local public health
volunteers and students were the key persons for con-
ducting control activities at homes and schools, respec-
tively. An educational series for students and public health
volunteers was organized in both schools and communi-
ties. General education in dengue, vector biology, and
vector control was followed by specific training in vector
control methodologies and production of local vector
control materials, which were then distributed following a
clean-up campaign prior to the rainy season.
The strategy combined source-reduction campaigns
with appropriate vector-control technologies applied only
in the foci where dengue cases were clustered, within 100
meters around those foci, and within schools attended by
children from the control areas. Vector control measures by
local government authorities included the source-reduction
campaign noted above, followed by a routine weekly gar-
bage pickup during the rainy season. Integrated vector-
control methodologies used in this campaign included lo-
cally made screen covers designed to fit tightly over the
opening of clay water-storage jars, a combination of locally
produced Bti, local predaceous copepods, and locally
constructed lethal ovitraps. The success of this intervention
was evidenced by a significant reduction in both dengue
mosquito vector populations and serologically confirmed
dengue cases in control areas compared to noncontrol areas
(pre-intervention: 265.25 vs. 217.86 per 100,000 popula-
tion; post-intervention: 0 vs. 332.23 per 100,000 popula-
tion).
Even though cost-effective suppression of dengue
transmission was clearly demonstrated, it was a challenge
for this pilot program to be maintained and scaled-up. The
main reason for the reluctance to accept this environ-
mentally friendly approach was related to the psychological
satisfaction of insecticide spraying. It was concluded that
the key factors for program sustainability are the change in
attitude and behaviors of both communities and public
health authorities; they must accept and promote the
community-based approach with minimal use of insecti-
cides and integrate locally appropriate control methodol-
ogies. The Knowledge, Attitude and Practice (KAP) survey
showed that background knowledge on dengue and its
mosquito vectors among householders was moderately
high, but knowledge alone did not translate to control
action; dengue did not rank as a high priority disease to
Thai’s in most communities (Fig. 5).
The key person with leadership standing in each
community is also an important driving force for the
development and maintenance of an effective and sus-
tainable community dengue control program. A remaining
challenge is the adoption of a national policy for dengue
control to include an integrated community-based ap-
proach aimed at controlling larval mosquito vectors, as well
as to promote environmental management and source
reduction.
Indonesia
A dengue control project was initiated in Indonesia in 1997,
with support from the Rotary Foundation of Rotary
International. Rotary Indonesia, ‘‘PKK’’ (Family Welfare
Movement) at the national level and the Department of
Health at the national and local levels, collaborated to de-
sign a community education program on topics such as the
mosquito life cycle, mode of DF/DHF transmission, and
ways in which the community can protect itself. Weekly
household inspections, both indoors and outdoors, were
conducted in every village (kelurahan) as a means of edu-
cating and motivating communities. Many community
organizations have since evolved, including farmers’
groups, neighborhood groups, and women’s groups. One
of these is the ‘‘Dasawisma’’ (ten-house) groups, the
smallest unit of the national ‘‘PKK,’’ initiated through the
Interior Department.
The Department of Health and local government
officials were requested to continue motivating the com-
munity through repeated visits. Rotary has initiated the
‘‘Jumantik’’ (surveyor of mosquito larvae) in the 13 cities
where the weekly inspection program was first initiated.
Continuous supervision by local PKK members (including
the Mayor’s wife in one city) and local health officials
Prevention and Control of Dengue 285
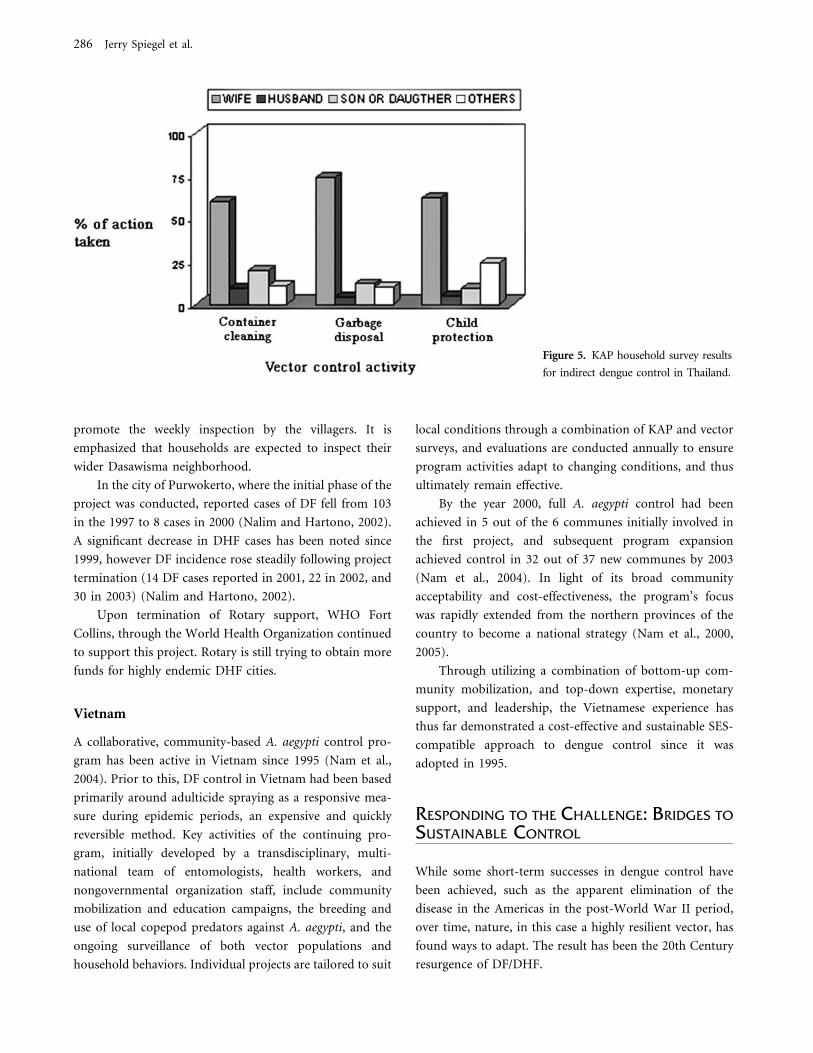
promote the weekly inspection by the villagers. It is
emphasized that households are expected to inspect their
wider Dasawisma neighborhood.
In the city of Purwokerto, where the initial phase of the
project was conducted, reported cases of DF fell from 103
in the 1997 to 8 cases in 2000 (Nalim and Hartono, 2002).
A significant decrease in DHF cases has been noted since
1999, however DF incidence rose steadily following project
termination (14 DF cases reported in 2001, 22 in 2002, and
30 in 2003) (Nalim and Hartono, 2002).
Upon termination of Rotary support, WHO Fort
Collins, through the World Health Organization continued
to support this project. Rotary is still trying to obtain more
funds for highly endemic DHF cities.
Vietnam
A collaborative, community-based A. aegypti control pro-
gram has been active in Vietnam since 1995 (Nam et al.,
2004). Prior to this, DF control in Vietnam had been based
primarily around adulticide spraying as a responsive mea-
sure during epidemic periods, an expensive and quickly
reversible method. Key activities of the continuing pro-
gram, initially developed by a transdisciplinary, multi-
national team of entomologists, health workers, and
nongovernmental organization staff, include community
mobilization and education campaigns, the breeding and
use of local copepod predators against A. aegypti, and the
ongoing surveillance of both vector populations and
household behaviors. Individual projects are tailored to suit
local conditions through a combination of KAP and vector
surveys, and evaluations are conducted annually to ensure
program activities adapt to changing conditions, and thus
ultimately remain effective.
By the year 2000, full A. aegypti control had been
achieved in 5 out of the 6 communes initially involved in
the first project, and subsequent program expansion
achieved control in 32 out of 37 new communes by 2003
(Nam et al., 2004). In light of its broad community
acceptability and cost-effectiveness, the program’s focus
was rapidly extended from the northern provinces of the
country to become a national strategy (Nam et al., 2000,
2005).
Through utilizing a combination of bottom-up com-
munity mobilization, and top-down expertise, monetary
support, and leadership, the Vietnamese experience has
thus far demonstrated a cost-effective and sustainable SES-
compatible approach to dengue control since it was
adopted in 1995.
RESPONDING TO THE CHALLENGE: BRIDGES TO
SUSTAINABLE CONTROL
While some short-term successes in dengue control have
been achieved, such as the apparent elimination of the
disease in the Americas in the post-World War II period,
over time, nature, in this case a highly resilient vector, has
found ways to adapt. The result has been the 20th Century
resurgence of DF/DHF.
Figure 5. KAP household survey results
for indirect dengue control in Thailand.
286 Jerry Spiegel et al.

Past experience has vividly demonstrated the ineffec-
tiveness of approaches to dengue control that have failed to
take into account the complex behaviors of ecological and
social systems, and, in this sense, have failed to build
adequate ‘‘bridges,’’ the term employed by Gunderson
et al.(1995) to refer to the potential linkages between social
actors dispersed across various disciplines and institutions,
who are all called upon to contribute to both an under-
standing of complexity and a construction of effective
interventions capable of achieving impact.
Insights gained have also underscored the importance
of developing and reinforcing community capacity to play a
pivotal role in control efforts. This capacity encompasses
the ability of communities to identify risks and undertake
interventions, as well as their agility to recognize and adapt
to changes in the social–ecological systems. Thus, the above
failure analysis provided using this coupled human–natural
systems perspective provides insight into the key elements
of a sustainable dengue control program. Bridges built by
the social actors in the relevant arenas are thus necessary to
enable the development of each of these elements.
Adapt Control Programs to the Mosquito’s
Changing Behavior
In pursuing vector control in the absence of a vaccine, a
strategy must be developed that is fully cognizant of how
A. aegypti adapts to interventions, including pesticide
resistance and breeding-site selection. An understanding of
this adaptative response to habitat change or other control
measures is necessary to target and modify control strate-
gies accordingly. In this sense, campaigns focusing on the
same breeding sites year-after-year may not be effective.
Adapt Education Programs to the Public
In DF/DHF affected areas, wide-ranging needs must be
balanced among scarce resources. In this sense, knowledge
must be regarded as a two-way street, where ‘‘experts’’
must develop technical approaches and solutions that
correspond to social realities. Social realities themselves
must be acknowledged as dynamic and constantly in flux,
and other stakeholders, from policy-makers to community
representatives, must be engaged to support sustainable
and effective dengue control practices.
Regional and Local Focus
Local social realities vary regionally. Recognizing that the
control of dengue cannot be geographically isolated, and
that there is much interaction of both vectors and infected
humans among countries and regions, strategies must ac-
count for both regional and local factors. This calls for a
more profound understanding of political, economic, so-
cial, and ecological similarities and differences among
countries in a region, and for continued efforts at regional
and international communication of epidemiological,
entomological, and laboratory information.
Transdisciplinarity
The challenge of understanding complex social and eco-
logical systems calls for building transdisciplinary capacity
that recognizes the interplay between social and ecological
systems. The entomologist must collaborate with the epi-
demiologist and the anthropologist. And all must work in
close collaboration with communities, policy-makers, and
other stakeholders who are intimately involved in the
success of control efforts.
Empowerment
Failures of previous top-down efforts have demonstrated
that all segments of the community must play an active
and conscious role. To carry out this role, however,
communities must have access to the information and
resources they need, reinforced by governments who are
better placed to consolidate and disseminate information,
and facilitate this support. Note that empowering com-
munities may mean that dengue control will become one
among many environmental health goals pursued by
communities which choose to focus on wider sanitary
and/or water access issues. Programmatic goals and
mechanisms may need to be adjusted to reflect these less
direct projects.
Scalability
While pilot projects play an essential role in developing
effective methods, progress cannot be made unless the
approaches can be scaled up to the national and regional
level. This calls for a commitment to go beyond the
‘‘learning’’ phase at the local level and engage in a new level
of learning at the macro, indeed the global, level.
Adaptability
Sustainable dengue control, above all, calls for the will-
ingness to adapt to new information and create ‘‘learning
Prevention and Control of Dengue 287

systems.’’ In this sense, surveillance capacities play an
important role in real-time management of evolving situ-
ations, but they must also constantly reevaluate their
effectiveness. The overall success of global DF/DHF control
calls for forging transdisciplinary capacities to share lessons
and adapt to inevitable changes.
Sustainability
Sustainability of dengue control remains a continued
challenge, and realistic expectations for, and indicators of,
sustainability must be defined according the characteristics
of each specific setting. Community participation ap-
proaches have often been seen by governments as
‘‘inexpensive alternatives’’ to vector control. This is unre-
alistic in the short-term, but may succeed in the long-term.
Short-term, project-focused funding from bilateral aid
agencies is unsustainable due to its lack of ongoing support.
Sustainable, effective long-term DF/DHF control must
begin with a combination top-down/bottom-up program
that provides initial success, followed by a gradual transi-
tion to integrated, community-owned programs.
The level of control that can be locally sustained at any
given time may need to be adjusted to reflect local capac-
ities and resources. For example, reduction of A. aegypti
populations below transmission levels may be achievable in
some settings, whereas readiness to detect and respond to a
pending outbreak may be an achievable goal elsewhere.
CONCLUSIONS
To effectively and sustainably protect human populations
from dengue fever, we must be prepared to dynamically
translate our understanding of social-ecological systems
into effective actions. The failure to appreciate how
complex systems interact has ultimately prevented sus-
tainable solutions from being adopted. Dengue provides
an ideal terrain for evaluating how successfully we are
able to take on this challenge, as despite our growing
understanding of the problem, we have witnessed a
pandemic increase of this disease. Here we have consid-
ered dengue transmission in an SES framework, as a
coupled human–natural system of elements separated by
value-based barriers demanding transdisciplinary solu-
tions. Ultimately, what is required is a transformation of
the control effort itself, to extend beyond the barriers that
reinforce compartmentalized visions and, through the
catalyst of implementation for the benefit of vulnerable
communities and the application of an integrated SES
approach, to forge bridges among the myriad of social
actors who heretofore have followed separate agendas.
ACKNOWLEDGMENTS
Ideas for this article were developed during a working
meeting on social–ecological systems and emerging infec-
tious diseases, hosted by the Asia-Pacific Institute of
Tropical Medicine & Infectious Diseases and the East-West
Center in Honolulu, Hawaii (March 9–11, 2005). This
meeting was supported by a grant to promote methodo-
logical innovation in interdisciplinary health research from
the National Institutes of Health (R13 TW007300) and
funded by the Fogarty International Center and Office of
Behavioral and Social Sciences under the NIH Roadmap
initiative ‘‘Research Teams of the Future.’’ We acknowledge
the efforts of the meeting organizers, and especially other
colleagues who played a full role in these discussions that
produced the core ideas for the article, including Martin
Meltzer, Eileen Shea, and Rainer Sauerborn. Special thanks
to Mayee Wong for her valuable contributions to the
working group discussions.
REFERENCES
Dietz V, Gubler DJ, Ortiz S, Kuno G, Casta-Velez A, Sather GE,et al. (1996) The 1986 dengue and dengue hemorrhagic feverepidemic in Puerto Rico: epidemiology and clinical observa-tions. Puerto Rico Health Sciences Journal 15:201–210
Focks DA (2003) A review of entomological sampling methods andindicators for dengue vectors. Geneva, Switzerland: World HealthOrganization, p 11. Available: http://www.who.int/tdr/publica-tions/publications/Pdf/dengue_review.pdf. [accessed August 16,2005]
Gubler DJ (1989) Aedes aegypti and Aedes aegypti-borne diseasecontrol in the 1990s: top down or bottom up. American Journalof Tropical Medicine and Hygiene 40:571–578
Gubler DJ, Casta-Valez A (1991) A programme for preventionand control of epidemic dengue and dengue haemorrhagic feverin Puerto Rico and the U.S. Virgin Islands. Bulletin of the PanAmerican Health Organization 25:237–247
Gubler DJ, Trent DW (1993) Emergence of epidemic dengue/dengue hemorrhagic fever as a public health problem in theAmericas. Infectious Agents and Disease 2:383–393
Gubler DJ, Clark GG (1994) Community-based integrated controlof Aedes aegypti: a brief overview of current programs. AmericanJournal of Tropical Medicine and Hygiene 50(Suppl):50–60
Gubler DJ, Clark GG (1996) Community involvement in thecontrol of Aedes aegypti. Acta Tropica 61:169–179
288 Jerry Spiegel et al.

Gubler D (1997) Dengue and dengue hemorrhagic fever: its his-tory and resurgence as a global public health problem. In:Dengue and Dengue Hemorrhagic Fever, Gubler D, Kuno G(editors), Wallingford, UK: CAB International, pp 1–21
Gubler D (1998a) Dengue and dengue hemorrhagic fever. ClinicalMicrobiology Reviews 11:480–496
Gubler DJ (1998b) Resurgent vector-borne diseases as a globalhealth problem. Emerging Infectious Diseases 4:442–450
Gubler DJ, Meltzer MI (1999) The impact of dengue/denguehemorrhagic fever on the developing world. Advances in VirusResearch 53:35–70
Gubler DJ (2002) Epidemic dengue/dengue haemorrhagic fever asa public health, social and economic problem in the 21st cen-tury. Trends in Microbiology 10:100–103
Gubler DJ (2004) Cities spawn epidemic dengue viruses. NatureMedicine 10:129–130
Gubler DJ (2005) The emergence of epidemic dengue fever/den-gue hemorrhagic fever in the Americas: a case of failed publichealth policy. Pan American Journal of Public Health 17:221–224
Guha-Sapir D, Schimmer B (2005) Dengue fever: new paradigmsfor a changing epidemiology. Emerging Themes in Epidemiology2:1-10; DOI:10.1186/1742-7622-2-1 [accessed May 2, 2005]
Gunderson LH (2002) Adaptive dancing: interactions betweensocial resilience and ecological crises. In: Navigating Social-ecological Systems: Building Resilience for Complexity andChange, Berkes F, Colding J, Folke C (editors), Cambridge, UK:Cambridge University Press, pp 33–52
Gunderson LH, Holling CS, Light SS (editors) (1995) Barriers andBridges to the Renewal of Ecosystems and Institutions, New York:Columbia University Press, pp 3–35
Gunderson LH, Holling CS (2002) Panarchy: UnderstandingTransformations in Human and Natural Systems, Washington,DC: Island Press
Guzman MG, Alvarez M, Rodriquez R, Rosario D, Vazquez S,Vald L, et al. (1999) Fatal dengue hemorrhagic fever in Cuba,1997. International Journal of Infectious Diseases 3:130–135
Guzman MG, Kouri G (2002) Dengue: an update. Lancet Infec-tious Diseases 2:33–42
Guzman MG, Kouri G (2003) Dengue and dengue hemorrhagicfever in the Americas: lessons and challenges. Journal of ClinicalVirology 27:1–13
Halstead SB (2000) Communicable diseases: successes and failuresin dengue controlglobal experience. Dengue Bulletin 24. WorldHealth Organization, Regional Office for South-East Asia.Available: http://w3.whosea.org/en/Section10/Section332/Sec-tion522_2509.htm [accessed April 20, 2005]
Holling C (1995) What barriers? What bridges? In: Barriers andBridges to the Renewal of Ecosystems and Institutions, GundersonLH, Holling CS, Light SS (editors), New York: ColumbiaUniversity Press, pp 3–35
Holling C (2001) Understanding the complexity of economic,ecological and social systems. Ecosystems 4:390–405
Kouri G, Guzman MG, Bravo J (1986) Hemorrhagic dengue inCuba: history of an epidemic. Bulletin of the Pan AmericanHealth Organization 20:24–30
Levin SA (1999) Fragile Dominion: Complexity and the Commons,Reading, MA: Perseus Books Group
Lewis ND (2005) Is the social-ecological framework useful inunderstanding infectious diseases? The case of HIV/AIDS.EcoHealth 2 (DOI: 10.1007/s10393-005-8477-x, this issue)
Meltzer MI, Rigau-Perez JG, Clark GG, Gubler DJ (1998) UsingDALYs to assess the economic impact of dengue in Puerto Rico:1984–1994. American Journal of Tropical Medicine and Hygiene59:265–271
Nalim S, Hartono B, Suskamdani dan SW (2002) Communitypartnership in vector control for dengue. Journal Ekologi Kes-ehatan 2:19–24
Nam VS, Yen NT, Holynska M, Reid JW, Kay BH (2000) Nationalprogress in dengue vector control in Vietnam: survey for Mes-ocyclops (Copepoda), Micronecta (Corixidae), and fish asbiological control agents. American Journal of Tropical Medicineand Hygiene 62:5–10
Nam VS, Kay B, Yen NT, Ryan P, Bektas A (2004) Communitymobilization, behaviour change and biological control in theprevention and control of dengue fever in Viet Nam. DengueBulletin 28(Suppl):57–61
Nam VS, Yen NT, Phong TV, Ninh TU, Mai LQ, et al. (2005)Elimination of dengue by community programs using Mes-ocyclops (Copepoda) against Aeges Aegypti in central Viet-nam. American Journal of Tropical Medicine and Hygiene 72:67–73
Newton EA, Reiter P (1992) A model of the transmission ofdengue fever with an evaluation of the impact of ultra-lowvolume (ULV) insecticide applications on dengue epidemics.American Journal of Tropical Medicine and Hygiene 47:709–720
Ooi EE, Goh KT, Gubler DJ (2005) Singapore’s 35 year experiencewith dengue prevention: is vector control effective? EmergingInfectious Diseases (in press)
PAHO (1994) Dengue and Dengue Haemorrhagic Fever in theAmericas: Guidelines for Prevention and Control, ScientificPublication No. 548, Washington, DC: World Health Organi-zation/Pan American Health Organization 548
Parks WJ, Lloyd LS (2004) Planning Social Mobilization andCommunication for Dengue Fever Prevention and Control: a Step-by-Step Guide, Geneva: World Health Organization
Parks WJ, Lloyd LS, Nathan MB, Hosein E, Odugleh A, Clark GG,et al. (2004) International experiences in social mobilization andcommunication for dengue prevention and control. DengueBulletin 28(Suppl):1–7
Pinheiro FP, Corber SJ (1997) Global situation of dengue anddengue hemorrhagic fever, and its emergence in the Americas.World Health Statistics Quarterly 50:161–169
Reiter P, Lathrop S, Bunning M, Biggerstaff B, Singer D, Tiwari T,et al. (2003) Texas lifestyle limits transmission of dengue virus.Emerging Infectious Diseases 9:86–89
Renganathan E, Parks W, Lloyd L, Nathan MB, Hosein E, Odu-gleh A, et al. (2003) Towards sustaining behavioural impact indengue prevention and control. Dengue Bulletin 27:6–12
Rifkin SB (1996) Paradigms lost: towards a new understanding ofcommunity participation in health programs. Acta Tropica61:79–92
Rigau-Perez JG, Clark GG, Gubler DJ, Reiter P, Sanders EJ,Vorndam AV (1998) Dengue and dengue hemorragic fever.Lancet 352:971–977
Sanchez L, Perez D, Perez T, Sosa T, Cruz G, Kouri G, et al. (2005)Intersectoral coordination in Aedes aegypti. A pilot project inHavana City, Cuba. Tropical Medicine and International Health10:82–91
Schliessman DJ, Calheiros LB (1974) A review of the status ofyellow fever and Aedes aegypti eradication programs in theAmericas. Mosquito News 34:1–9
Prevention and Control of Dengue 289

Shepard DS, Suaya JA, Halstead SB, Nathan MB, Gubler DJ,Mahoney RT, et al. (2004) Cost-effectiveness of a pediatricdengue vaccine. Vaccine 22:1275–1280
Soper FS, Wilson DB, Servulo L, Waldemar SA (1943) TheOrganization of Permanent Nationwide anti-Aedes aegypti Mea-sures in Brazil, New York: The Rockefeller Foundation
Spiegel JM, Yassi A, Tate R (2002) Dengue in Cuba: mobilizationagainst Aedes aegypti. Lancet Infectious Diseases 2:207–208
Spiegel JM, Bonet M, Tate GM, Ibarra AM, Tate RB, Yassi A(2004) Building capacity in Central Havana to sustainablymanage environmental health risk in an urban ecosystem.EcoHealth 1(Suppl 2):120–130
WHO (1997) Dengue Haemorrhagic Fever: Diagnosis, Treatment,Prevention and Control, 2nd ed., Geneva: World Health Orga-nization
WHO (1999) Prevention and Control of Dengue and DengueHaemorrhagic Fever – Comprehensive Guidelines. WHO RegionalPublication, SEARO No. 29. New Delhi: WHO Regional Officefor South-East Asia
WHO (2001) Report of the Consultation on Key Issues in DengueVector Control, toward the Operationalization of a Global Strat-egy, Geneva: World Health Organization
Wilcox BA, Colwell RR (2005) Emerging and re-emerging infec-tious diseases: biocomplexity as an interdisciplinary paradigm.EcoHealth 2 (DOI: 10.1007/s10393-005-8961-3, this issue)
Wilcox BA, Gubler DJ (2005) Disease ecology and the globalemergence of zoonotic pathogens. Environmental Health andPreventive Medicine 10:263–272
Zielinski-Gutierrez E (2002) Evaluating the Sustainability of aCommunity-based Prevention Intervention in Escuintla, Guate-mala, New Orleans, LA: Tulane University
290 Jerry Spiegel et al.