
Balance and gait improved in patients with MS after physiotherapy based on the Bobath concept
14
Physiotherapy Research International Physiother. Res. Int. 11(2) 104–116 (2006) Published online in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/pri.327 104 Physiother. Res. Int. 11: 104–116 (2006) Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri Balance and gait improved in patients with MS after physiotherapy based on the Bobath concept TORI SMEDAL National Multiple Sclerosis Competence Centre, Department of Neurology, and Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway HILDEGUNN LYGREN Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway KJELL-MORTEN MYHR National Multiple Sclerosis Competence Centre, Department of Neurology, Haukeland University Hospital, Bergen and Department of Clinical Medicine, Section for Neurology, University of Bergen, Norway ROLF MOE-NILSSEN Department of Public Health and Primary Health Care, Section for Physiotherapy Science, University of Bergen, Norway BENTE GJELSVIK Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway OLAV GJELSVIK Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway LIV INGER Strand Department of Public Health and Primary Health Care, Section for Physiotherapy Science, University of Bergen, Norway ABSTRACT Background and Purpose. Patients with multiple sclerosis (MS) tend to have movement difficulties, and the effect of physiotherapy for this group of patients has been subjected to limited systematic research. In the present study physiotherapy based on the Bobath concept, applied to MS patients with balance and gait problems, was evaluated. The ability of different functional tests to demonstrate change was evaluated. Method. A single-subject experimental study design with ABAA phases was used, and two patients with relapsing–remitting MS in stable phase were treated. Tests were performed 12 times, three at each phase: A (at baseline); B (during treatment); A (immediately after treatment); and A (after two months). The key feature of treatment was facilitation of postural activity and selective control of movement. Several performance and self-report measures and interviews were used. Results. After intervention, improved balance was shown by the Berg Balance Scale (BBS) in both patients, and improved quality of gait was indicated by the Rivermead Visual Gait Assessment (RVGA). The patients also reported improved balance and gait function in the interviews and scored their condition as ‘much improved’. Gait parameters, recorded by an electronic walkway, changed, but differently in the two
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Balance and gait improved in patients with MS after physiotherapy based on the Bobath concept
Physiotherapy Research InternationalPhysiother. Res. Int. 11(2) 104–116 (2006)Published online in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pri.327
104
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
Balance and gait improved in patients with MS after physiotherapy based on the Bobath concept
TORI SMEDAL National Multiple Sclerosis Competence Centre, Department of Neurology, and Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway
HILDEGUNN LYGREN Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway
KJELL-MORTEN MYHR National Multiple Sclerosis Competence Centre, Department of Neurology, Haukeland University Hospital, Bergen and Department of Clinical Medicine, Section for Neurology, University of Bergen, Norway
ROLF MOE-NILSSEN Department of Public Health and Primary Health Care, Section for Physiotherapy Science, University of Bergen, Norway
BENTE GJELSVIK Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway
OLAV GJELSVIK Department of Physiotherapy, Haukeland University Hospital, Bergen, Norway
LIV INGER Strand Department of Public Health and Primary Health Care, Section for Physiotherapy Science, University of Bergen, Norway
ABSTRACT Background and Purpose. Patients with multiple sclerosis (MS) tend to have movement difficulties, and the effect of physiotherapy for this group of patients has been subjected to limited systematic research. In the present study physiotherapy based on the Bobath concept, applied to MS patients with balance and gait problems, was evaluated. The ability of different functional tests to demonstrate change was evaluated. Method. A single-subject experimental study design with ABAA phases was used, and two patients with relapsing–remitting MS in stable phase were treated. Tests were performed 12 times, three at each phase: A (at baseline); B (during treatment); A (immediately after treatment); and A (after two months). The key feature of treatment was facilitation of postural activity and selective control of movement. Several performance and self-report measures and interviews were used. Results. After intervention, improved balance was shown by the Berg Balance Scale (BBS) in both patients, and improved quality of gait was indicated by the Rivermead Visual Gait Assessment (RVGA). The patients also reported improved balance and gait function in the interviews and scored their condition as ‘much improved’. Gait parameters, recorded by an electronic walkway, changed, but differently in the two

Physiotherapy in MS 105
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
patients. Among the physical performance tests the BBS and the RVGA demonstrated the highest change, while no or minimal change was demonstrated by the Rivermead Mobility Index (RMI) and Ratings of Perceived Exertion (RPE). Conclusion. The findings indicate that balance and gait can be improved after physiotherapy based on the Bobath concept, but this should be further evaluated in larger controlled trials of patients with MS. Copyright © 2006 John Wiley & Sons, Ltd.
Key words: balance, gait, multiple sclerosis, physical performance tests, physiotherapy, the Bobath concept
INTRODUCTION
Gait and balance disturbance caused by weakness, spasticity and ataxia are com-monly seen in patients with multiple sclero-sis (MS) and may lead to problems in activities of daily living (Oligati et al., 1998; Rodgers et al., 1999; Thompson, 2001). Gehlsen et al. (1986) reported reduced range of motion in the lower legs and walking with slow speed and short, quick steps in a study of 11 MS patients. The probability of manag-ing without walking aids after 15 years is about 70% (Myhr et al., 2001).
The large heterogeneity of the disease requires comprehensive management by a multidisciplinary rehabilitation team (Ko Ko, 1999; Freeman, 2001). Different types of interventions are recommended at differ-ent stages of the disease (Thompson, 2001). Physiotherapy is commonly recommended, and tentative evidence suggests that it may be helpful to improve physical functioning or prevent deterioration (Lord et al., 1998a; Solari et al., 1999; Freeman and Thompson, 2001; Wiles et al., 2001). There is, however, limited evidence to guide the therapist in choosing the most effective approach (Freeman and Thompson, 1997; Lord et al., 1998a).
There are methodological challenges when undertaking rehabilitation trials of patients with MS. When designing interven-tion studies, homogeneity of study popula-
tion and intervention is usually recommended. However, the heterogeneous manifestations and unpredictable course of MS call for an intervention tailored to each individual (Freeman and Thompson, 1997). In line with the World Health Organization (WHO) International Classification of Functioning, Disability and Health (WHO, 2001) the choice of outcome measures should also be carefully considered to capture various aspects of functioning and disability.
The aim of the present study was to investigate whether physiotherapy based on the Bobath concept could improve gait and balance for two patients with MS. We also wanted to evaluate the usefulness of differ-ent functional tests.
METHOD
Study design
A single-subject experimental study design, with ABAA phases, was used to get thor-ough and repetitive information about the patients. Several registrations at baseline and during treatment make it possible to evaluate whether treatment has an effect beyond normal variability in the condition, and each patient was, accordingly, their own control. The patients received individualized tailored physiotherapy and were followed closely by assessments once a week, in four three-weeks periods:

Smedal et al.106
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
• A: baseline (weeks 1–3).• B: treatment (weeks 4–6).• A: early follow-up (weeks 7–9).• A: late follow-up (weeks 15–17).
All assessments were undertaken in the same sequence and at the same time of day by an independent physiotherapist. During the treatment period, the patients had phys-iotherapy for one hour a day, five times a week. Patients were treated by different physiotherapists, one patient each. Written, informed consent was obtained, and the regional ethics committee approved the study.
Subjects
Two patients with MS were recruited from the National Multiple Sclerosis Competence Centre, Norway. Inclusion criteria were relapsing–remitting MS without any new relapses during the last year, gait problems attributed to spastic paraparesis or ataxia and capability of walking for 10 minutes, with pauses if needed. Exclusion criteria were progressive MS or cognitive dysfunc-tion and excessive fatigue that could pre-clude the testing procedures. Mrs A was a 48-year-old woman diagnosed with MS at the age of 20, and Mr B was a 32-year-old man diagnosed at the age of 17.
Intervention
The intervention was based on the Bobath concept (Lennon, 1996; Lennon, 2001; Gjelsvik, 2002) as interpreted and applied by two International Bobath Instructors Training Association (IBITA) approved Bobath instructors. Treatment was individu-ally tailored to the patients, based on the physiotherapists’ examination. In this approach, reduced postural control, abnor-
mal co-ordination of movement patterns, weakness and abnormal tone are considered the main cause of the movement problem for people with central nervous system (CNS) disease. The treatment aims to improve function through motor learning, emphasiz-ing the individual’s own control. Hands-on therapy is used when necessary, to enhance an optimal postural alignment and thereby muscle function. Analysis of movement in functional activity determines which com-ponent of movement dysfunction (impair-ment) is most central to the patient’s limitation of activity. The principle underly-ing treatment is that the CNS has the capac-ity to learn. ‘Neuroplasticity’ refers to the ability of the CNS to change both its struc-ture and function as a response to changing demands (Nudo, 2003).
Mrs A had Expanded Disability Status Scale (EDSS) (Kurtzke, 1983) equal to 6.0. She had pronounced spastic paraparesis and ataxia, and was depending on visual fixation for balance. Based on functional assessment, treatment was focused on postural stability and orientation. The aim was to improve adaptability of the patient’s feet in relation to the base of support, alignment of the trunk in relation to the pelvis, and recruitment of trunk and pelvic activity. The patient was treated in different postures and through transfers (for example, sitting to standing) to allow the experience of demands from changing relationships between the body and the environment.
Mr B had EDSS equal to 6.0. He had spastic paraparesis and trunk instability consistent with weakness of trunk muscles. He had clawing of toes in standing, inver-sion of feet in walking and hypersensitivity to muscle stretch (clonus) during floor contact. The treatment was focused on mobi-lization of ankles, feet and toes in order to prepare for weight-bearing and facilitate

Physiotherapy in MS 107
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
abdominal and low back muscles to activate selective activity against gravity.
Assessments
Physical performance measures, as follows.
• The Berg Balance Scale (BBS) consists of 14 standardized sub-tests scored on five-point scales (0–4), with a maximum (best) score of 56 (Berg et al., 1992). Reliability and validity have been dem-onstrated in elderly people (Berg et al., 1989; Berg et al., 1992; Berg et al., 1995), and scores below 45 may indicate increased risk of falling for elderly people (Thorban and Newton, 1996).
• Gait parameters were assessed by GAITRite; a 5-metre long computerized electronic mat for automated measure-ment of gait parameters. Maximum gait velocity, step-length (SL) and double stance phase (DS) (percentage of gait cycle) were registered when walking on the mat. Walking was performed three times at different speeds: normal, slow and maximum. SL and DS were regis-tered for each speed. By interpolation, a point estimate was calculated for each of the two variables at a normalized speed representative for that subject. Thus com-parisons between test occasions could be done without the confounding effect of walking speed (Moe-Nilssen, 1998). Before testing, the patients walked once on the mat to get comfortable with the test. Results from the GAITRite have shown strong test–retest reliability and concurrent validity for healthy adults (Bilney et al., 2003).
• ‘Timed Up & Go’ (TUG) measures the time while the patient stands up from a standard arm chair, walks a distance of 3 metres, turns, walks back and sits down
again. Performance of the test in less than 20 seconds has been suggested to indicate independent mobility (Podsiadlo and Richardson, 1991). The test has been shown to be reliable and valid for elderly people (Podsiadlo and Richardson, 1991).
• The Rivermead Visual Gait Assessment (RVGA) consists of two observations of the arms at swing and stance phases of gait and 18 observations of the trunk and lower limb: 11 observations during stance phase and seven during swing phase. The assessor watches the patient during walking. A four-point scale is used to quantify the degree of abnormality for each of the component items. A global score is calculated by summing the total numbers of scores, which range from 0 (normal gait) to 59 (grossly abnormal gait). The RVGA can be applied to measure change over time for patients with neurological disease and is sensitive to gait impairment. Reliability and valid-ity has been shown in patients with MS (Lord et al., 1998b), and it is suggested that a six-point change on the global score is clinically relevant (Lord et al., 1998a).
Self-report measures, as follows.
• Visual analogue scale (VAS): the patients estimated their perceived amount of gait problem on a scale from 0 mm to 100 mm, anchored by ‘No problem’ and ‘Worst imaginable problem’. A mean reduction of 10 on a scale from 0 to 100 has previ-ously been proposed as a clinically sig-nificant improvement (Kaasa and Lode, 2004).
• Ratings of perceived exertion (RPE) was scored after walking four times on the GAITRite mat, by a 15-point graded scale from 6 (no exertion) to 20 (maximal

Smedal et al.108
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
exertion) (Borg, 1970). The scale values correlate well with exercise variables such as heart rate, ventilation, percentage VO2 max and workload (ACSM, 1998).
• The Rivermead Mobility Index (RMI) is a measure of activity domain with focus on body mobility. It consists of 14 ques-tions and one observation of the ability to perform activities, from turning in bed (as the easiest) to running (as the most advanced) (Collen et al., 1991). Increase by two points or more has been regarded as clinically significant (Lord et al., 1998b).
• The Patient Global Impression of Change (PGIC) or the Clinical Global Impression of Change (CGIC) are graded on a seven-point scale, from 1 (very much improved) to 7 (very much worse). A score of 4 means no change (Farrar et al., 2001).
Interviews
Semi-structured interviews were used focusing on bodily function, activities of daily living (ADL), experiences in the body and comments from family and friends. The interviews were tape-recorded and transcribed.
The PGIC was applied once after the treatment and the follow-up periods, and the CGIC was applied after the treatment period. The interviews were done once after treat-ment, once three weeks after and once two months after. The other tests were used at each assessment. The tests were performed once before baseline, to reduce the learning effect. Before each testing, the patients were asked to report special events that could have influenced their functioning.
The tests have been validated for other populations, but almost none for patients with MS. However, many of them have been used in studies with MS patients.
Data analysis
Visual analysis of the graphs was used. The 2 SD deviation band method was also used, defining a statistically significant change if at least two consecutive data points after the baseline phase fell outside the 2 SD range (Noubakhsh and Ottenbacher, 1994). Calcu-lation of effect size, (mean change) / [(SD follow-up + SD baseline) / 2] was used to compare sensitivity to change in the different measures as effect size is a unit-less term, allowing direct comparison between mea-sures. A summary of the semi-structured interviews was made.
RESULTS
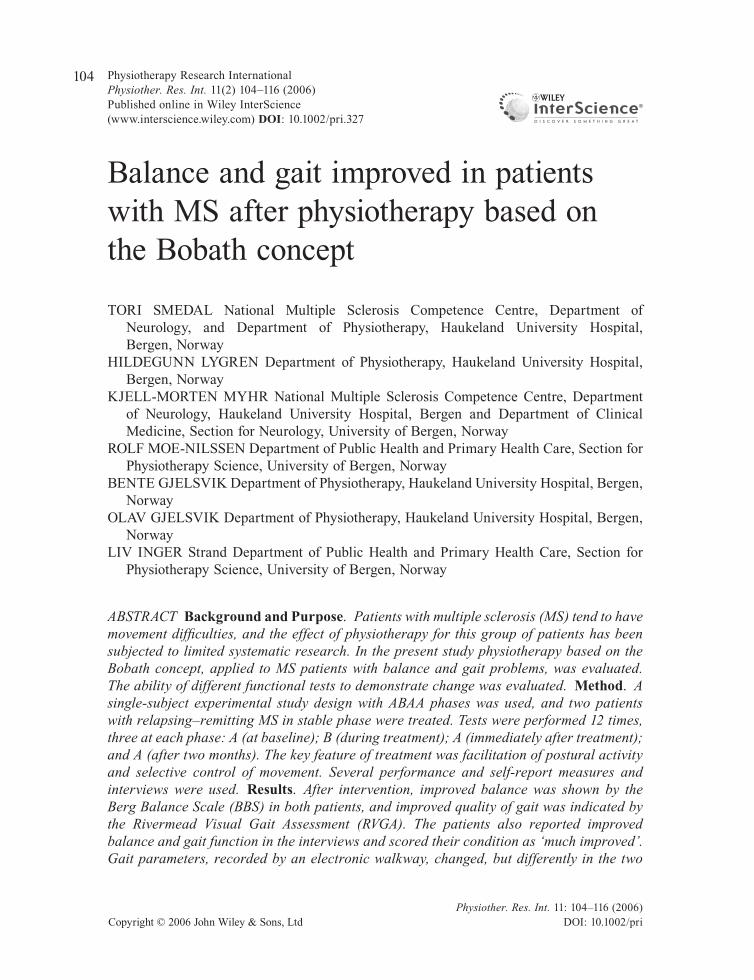
Both patients were stable, without new relapses during the study period, and EDSS improved from 6.0 to 5.5 for both. However, Mrs A experienced gastrointestinal symp-toms during the first half of the study period and Mr B experienced a short period of fatigue at the time of first testing during late follow-up. Test data (mean, SD) of both patients are shown in Table 1.
Mrs A
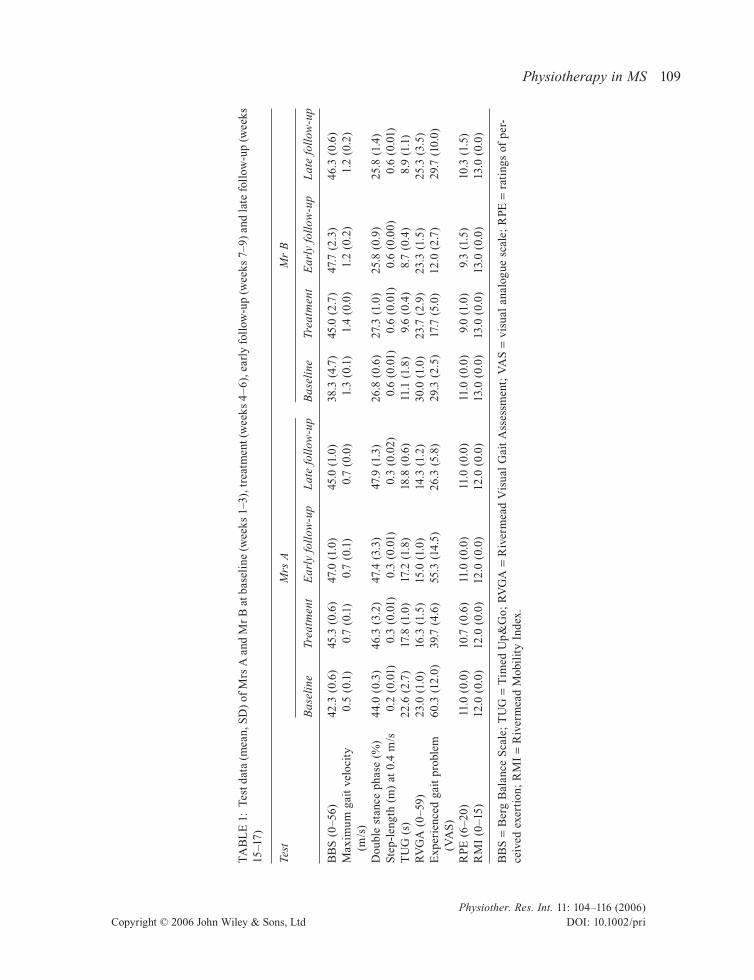
The BBS scores at baseline (<45) indicated increased risk of falling, but significant improvement was shown in connection with treatment (Figure 1). The RVGA scores, reflecting quality of movement during gait, also improved (Figure 2). Maximum gait velocity assessed by GAITRite was low at baseline: 0.5 m/s (normal reference value 2.10 m/s; Bohannon, 1997), but improved somewhat during treatment. Double stance (DS) as well as step-length (SL) increased. Some clinical important improvement was demonstrated by the TUG test as <20 s is suggested to be the limit for independent
Physiotherapy in MS 109
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1TA
BL
E 1
: Te
st d
ata
(mea
n, S
D)
of M
rs A
and
Mr
B a
t bas
elin
e (w
eeks
1–3
), t
reat
men
t (w
eeks
4–
6), e
arly
fol
low
-up
(wee
ks 7
–9)
and
late
fol
low
-up
(wee
ks
15–1
7)
Test
M
rs A
M
r B
B
asel
ine
Trea
tmen
t E
arly
fol
low
-up
Lat
e fo
llow
-up
Bas
elin
e Tr
eatm
ent
Ear
ly f
ollo
w-u
p L
ate
foll
ow-u
p
BB
S (
0–5
6)
42.3
(0.
6)
45.3
(0.
6)
47.0
(1.
0)
45.0
(1.
0)
38.3
(4.
7)
45.0
(2.
7)
47.7
(2.
3)
46.3
(0.
6)M
axim
um g
ait
velo
city
0.
5 (0
.1)
0.7
(0.1
) 0.
7 (0
.1)
0.7
(0.0
) 1.
3 (0
.1)
1.4
(0.0
) 1.
2 (0
.2)
1.2
(0.2
)
(m/s
)D
oubl
e st
ance
pha
se (
%)
44.0
(0.
3)
46.3
(3.
2)
47.4
(3.
3)
47.9
(1.
3)
26.8
(0.
6)
27.3
(1.
0)
25.8
(0.
9)
25.8
(1.
4)S
tep-
leng
th (
m)
at 0
.4 m
/s
0.2
(0.0
1)
0.3
(0.0
1)
0.3
(0.0
1)
0.3
(0.0
2)
0.6
(0.0
1)
0.6
(0.0
1)
0.6
(0.0
0)
0.6
(0.0
1)T
UG
(s)
22
.6 (
2.7)
17
.8 (
1.0)
17
.2 (
1.8)
18
.8 (
0.6)
11
.1 (
1.8)
9.
6 (0
.4)
8.7
(0.4
) 8.
9 (1
.1)
RV
GA
(0
–59)
23
.0 (
1.0)
16
.3 (
1.5)
15
.0 (
1.0)
14
.3 (
1.2)
30
.0 (
1.0)
23
.7 (
2.9)
23
.3 (
1.5)
25
.3 (
3.5)
Exp
erie
nced
gai
t pr
oble
m
60.3
(12
.0)
39.7
(4.
6)
55.3
(14
.5)
26.3
(5.
8)
29.3
(2.
5)
17.7
(5.
0)
12.0
(2.
7)
29.7
(10
.0)
(V
AS
)R
PE (
6–2
0)
11.0
(0.
0)
10.7
(0.
6)
11.0
(0.
0)
11.0
(0.
0)
11.0
(0.
0)
9.0
(1.0
) 9.
3 (1
.5)
10.3
(1.
5)R
MI
(0–1
5)
12.0
(0.
0)
12.0
(0.
0)
12.0
(0.
0)
12.0
(0.
0)
13.0
(0.
0)
13.0
(0.
0)
13.0
(0.
0)
13.0
(0.
0)
BB
S =
Ber
g B
alan
ce S
cale
; T
UG
= T
imed
Up&
Go;
RV
GA
= R
iver
mea
d V
isua
l G
ait
Ass
essm
ent;
VA
S =
vis
ual
anal
ogue
sca
le;
RPE
= r
atin
gs o
f pe
r-ce
ived
exe
rtio
n; R
MI
= R
iver
mea
d M
obil
ity
Inde
x.
Smedal et al.110
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
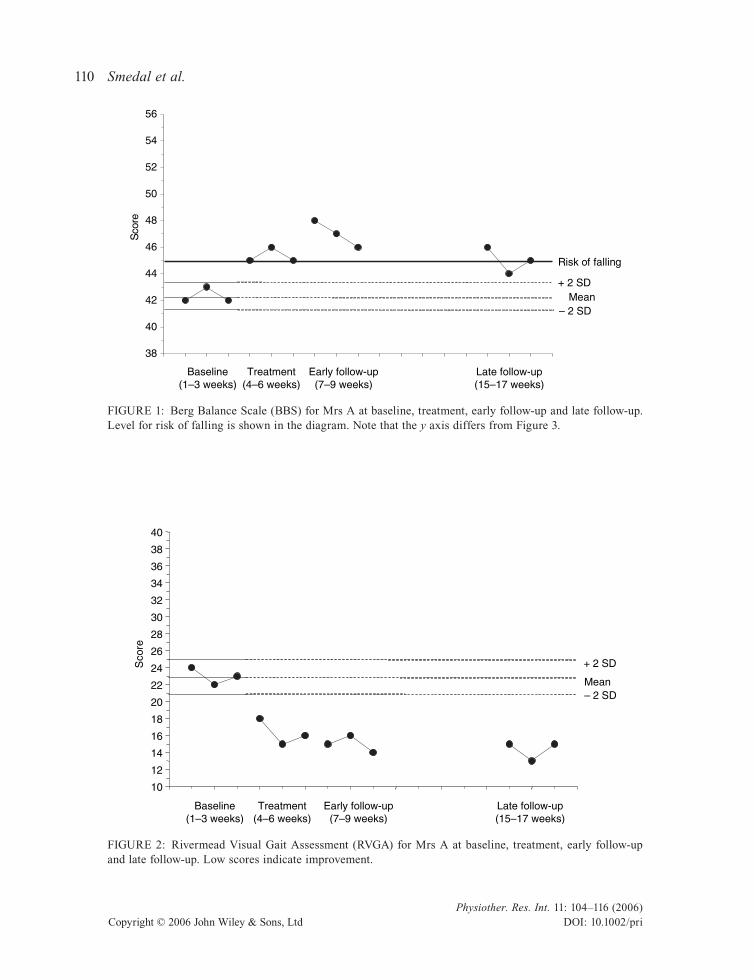
FIGURE 1: Berg Balance Scale (BBS) for Mrs A at baseline, treatment, early follow-up and late follow-up. Level for risk of falling is shown in the diagram. Note that the y axis differs from Figure 3.
38
40
42
44
46
48
50
52
54
56
erocS
Risk of falling
+ 2 SD
– 2 SDMean
Baseline(1–3 weeks)
Treatment(4–6 weeks)
Early follow-up(7–9 weeks)
Late follow-up(15–17 weeks)
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
erocS + 2 SD
– 2 SDMean
Baseline(1–3 weeks)
Treatment(4–6 weeks)
Early follow-up(7–9 weeks)
Late follow-up(15–17 weeks)
FIGURE 2: Rivermead Visual Gait Assessment (RVGA) for Mrs A at baseline, treatment, early follow-up and late follow-up. Low scores indicate improvement.
Physiotherapy in MS 111
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
walking (Podsiadlo and Richardson, 1991). The change was, however, not statistically significant.
Substantial gait problems were reported at baseline, but the scores were improved from 60.3 (VAS) at baseline to 26.3 (VAS) at late follow-up. Minor exertion was reported on RPE during baseline and almost no change was demonstrated during the study. Similarly, no change was demon-strated by the RMI. The PGIC was reported as ‘much improved’, ‘very much improved’ and ‘much improved’ after treatment and at early and late follow-up, respectively. Simi-larly the physiotherapists reported ‘much improved’ (CGIC).
Mr B
The BBS scores at baseline indicated increased risk of falling. Improved BBS scores after baseline were demonstrated, but the mean change was not statistically signifi-
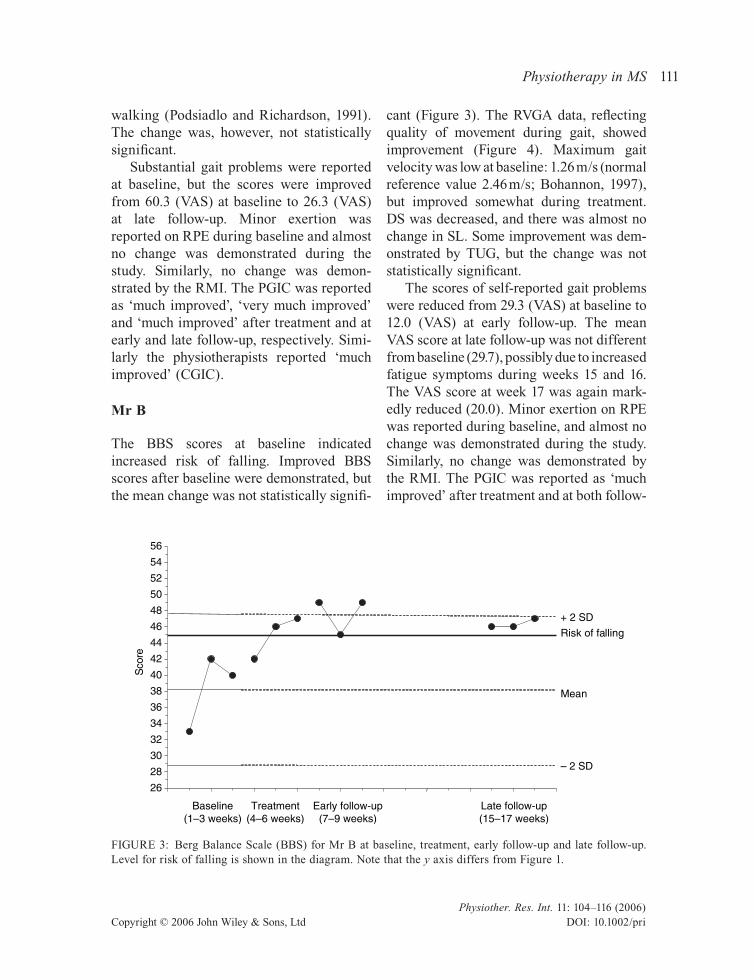
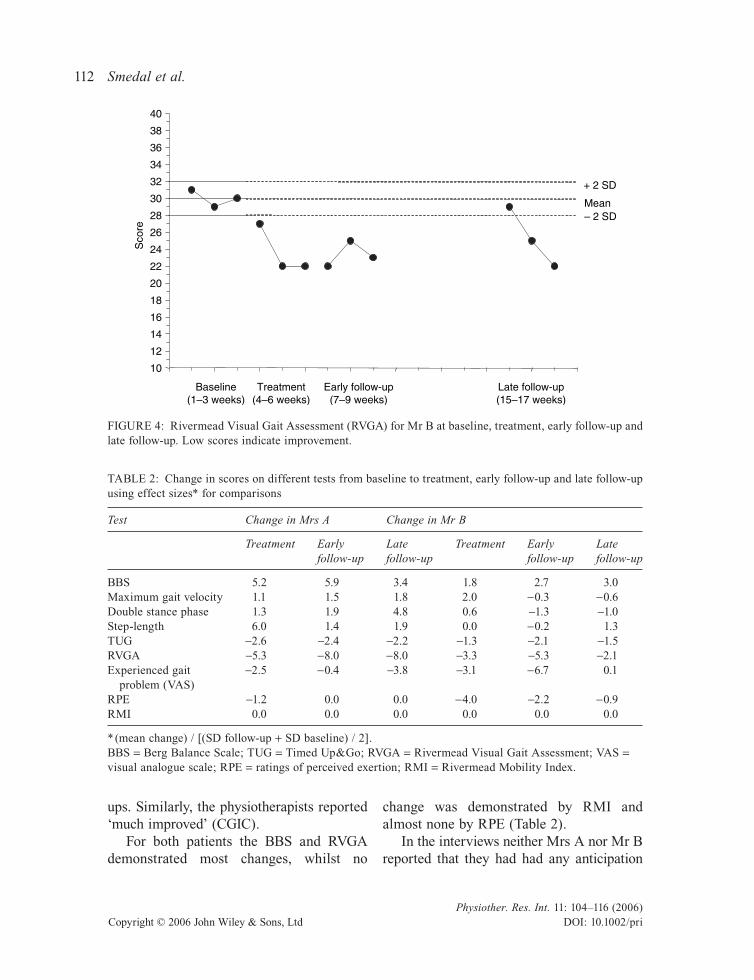
cant (Figure 3). The RVGA data, reflecting quality of movement during gait, showed improvement (Figure 4). Maximum gait velocity was low at baseline: 1.26 m/s (normal reference value 2.46 m/s; Bohannon, 1997), but improved somewhat during treatment. DS was decreased, and there was almost no change in SL. Some improvement was dem-onstrated by TUG, but the change was not statistically significant.
The scores of self-reported gait problems were reduced from 29.3 (VAS) at baseline to 12.0 (VAS) at early follow-up. The mean VAS score at late follow-up was not different from baseline (29.7), possibly due to increased fatigue symptoms during weeks 15 and 16. The VAS score at week 17 was again mark-edly reduced (20.0). Minor exertion on RPE was reported during baseline, and almost no change was demonstrated during the study. Similarly, no change was demonstrated by the RMI. The PGIC was reported as ‘much improved’ after treatment and at both follow-
26
28
30
32
34
36
38
40
42
44
46
48
50
52
54
56
erocS
Risk of falling
+ 2 SD
– 2 SD
Mean
Baseline(1–3 weeks)
Treatment(4–6 weeks)
Early follow-up(7–9 weeks)
Late follow-up(15–17 weeks)
FIGURE 3: Berg Balance Scale (BBS) for Mr B at baseline, treatment, early follow-up and late follow-up. Level for risk of falling is shown in the diagram. Note that the y axis differs from Figure 1.
Smedal et al.112
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
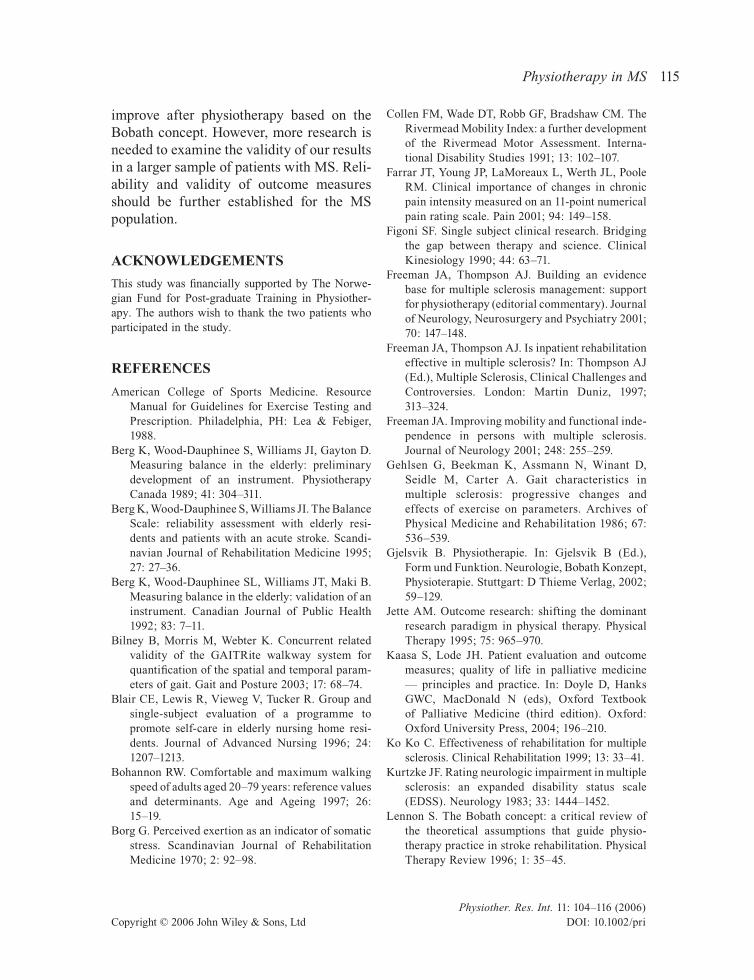
ups. Similarly, the physiotherapists reported ‘much improved’ (CGIC).
For both patients the BBS and RVGA demonstrated most changes, whilst no
change was demonstrated by RMI and almost none by RPE (Table 2).
In the interviews neither Mrs A nor Mr B reported that they had had any anticipation
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
erocS
+ 2 SD
– 2 SDMean
Baseline(1–3 weeks)
Treatment(4–6 weeks)
Early follow-up(7–9 weeks)
Late follow-up(15–17 weeks)
FIGURE 4: Rivermead Visual Gait Assessment (RVGA) for Mr B at baseline, treatment, early follow-up and late follow-up. Low scores indicate improvement.
TABLE 2: Change in scores on different tests from baseline to treatment, early follow-up and late follow-up using effect sizes* for comparisons
Test Change in Mrs A Change in Mr B
Treatment Early Late Treatment Early Late follow-up follow-up follow-up follow-up
BBS 5.2 5.9 3.4 1.8 2.7 3.0Maximum gait velocity 1.1 1.5 1.8 2.0 -0.3 -0.6Double stance phase 1.3 1.9 4.8 0.6 -1.3 -1.0Step-length 6.0 1.4 1.9 0.0 -0.2 1.3TUG -2.6 -2.4 -2.2 -1.3 -2.1 -1.5RVGA -5.3 -8.0 -8.0 -3.3 -5.3 -2.1Experienced gait -2.5 -0.4 -3.8 -3.1 -6.7 0.1 problem (VAS)RPE -1.2 0.0 0.0 -4.0 -2.2 -0.9RMI 0.0 0.0 0.0 0.0 0.0 0.0
* (mean change) / [(SD follow-up + SD baseline) / 2].BBS = Berg Balance Scale; TUG = Timed Up&Go; RVGA = Rivermead Visual Gait Assessment; VAS = visual analogue scale; RPE = ratings of perceived exertion; RMI = Rivermead Mobility Index.

Physiotherapy in MS 113
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
concerning the effect of physiotherapy. However, both patients reported improve-ments in connection with treatment. Mrs A found it easier to walk and to dress. Family and friends had noticed that she walked better, and they did not find it necessary to ‘give her a hand’. When starting treatment Mrs A walked with a crutch outdoors, but after treat-ment she walked with a cane. Mr B experi-enced better ability to walk and improved balance after treatment. He found it easier to dress and ‘to take the pizza in and out of the oven’, and his legs felt stronger. He reported an increased feeling of well-being and refresh-ment in his body, and family and friends commented that he walked much better. Both patients reported that the improvement still lasted two months after the treatment.
DISCUSSION
We have shown that physical functioning improved after individualized physiotherapy based on the Bobath concept for two patients. Both patients had BBS scores <45 at base-line, indicating increased risk of falling. After treatment, the scores were >45. This improvement of balance seems to be clini-cally significant (Thorban and Newton, 1996). Improvement in quality of movement during walking was demonstrated in both patients by the RVGA. The patients also reported improved balance and gait function in the interviews, and reported much improvement on the PGIC, confirmed by the therapist’s evaluations using the CGIC.
Both patients had more than a six-point improvement on the RVGA scale, which has been suggested to indicate a clinically rele-vant change (Lord et al., 1998a). The RVGA focuses on impairments consistent with the focus of the Bobath concept. This may explain why the RVGA was the most respon-sive to change among the assessment scales.
However, the BBS scores improved indicat-ing that the patients achieved better function in the activity domain as well. Thus improve-ment after physiotherapy based on the Bobath concept seemed to be related to the domain of activity, as well as the domain of impairment.
After treatment, Mr B had reduced maximum gait velocity walking on the mat. However, he walked faster when performing the TUG test, which appears to be a contra-dictory result. Walking on the mat seemed to make Mr B focus on achieving correct footsteps, whereas he concentrated more on walking at a fast speed when performing the TUG test, knowing that the tester used a stopwatch.
Mrs A had ataxic gait with short step-length (SL) during the baseline phase. After treatment velocity increased, and she reported better balance and ability to walk, as well as demonstrating increased SL and double stance (DS). The longer steps accom-panied by longer DS may possibly be explained by improved postural control, reducing the ataxia and thereby lengthening the DS. It is plausible that changes in RVGA and gait parameters after treatment for both patients is a result of changed underlying motor control strategies. If this is the case, the patients may have learnt new movement strategies. The changes seemed to imply long-term learning as they lasted beyond the immediate effect of treatment (Shumway-Cook and Wollacott, 2000).
Physiotherapy research needs to include assessment tools at different functional domains, and the relationship between them should be investigated (Jette, 1995). The present study included outcome measures of impairments as well as of activities. While the BBS measures ability to perform various physical activities that demand balance, the RVGA registers quality of performance.

Smedal et al.114
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
From our results, it seems likely that improved balance in daily activities is associated with improved quality of movement. However, this needs to be further investigated.
The intention was also to examine which assessment scales were the most sensitive to change. Among the physical performance tests, the BBS and RVGA showed the great-est change. However, a substantial effort was made to obtain a sufficient inter-rater reli-ability of RVGA scores prior to the study.
The single-subject experimental study design (SSED) is considered appropriate to assess the effectiveness of individualized treatment (Figoni, 1990; Ko Ko, 1999). Using results from randomized controlled studies may not always be helpful to guide treatment of individual patients (Mant, 1999). It was decided therefore to use SSED where treatment was tailored to the individ-ual’s needs (Ottenbacher, 1992; Ko Ko, 1999). Because of the variable and unpre-dictable nature of MS, the opportunity to follow each patient thoroughly and fre-quently through different phases is a great advantage of this design (Figoni, 1990; Blair et al., 1996; Polit and Hungler, 1999).
The visual analysis of the graphs is insen-sitive to weak treatment effects (Nourbakhsh and Ottenbacher, 1994), ensuring that only treatment effects with obvious changes were reported. We further used the two-standard deviation band method, which is reported to be sensitive to changes in variability across phases of a SSED study, although the few data in each phase made it impossible to confirm normality in distribution (Nourbakhsh and Ottenbacher, 1994). This method made it possible to evaluate whether change during treatment superseded vari-ability in a non-treatment phase.
Self-report measures and physical perfor-mance tests with different degrees of objec-tivity were employed. Although the gait
parameters are more objectively registered using the GAITRite system, the RVGA is dependent on the testers’ subjective opinion. It was impossible to blind the tester. The results showed, however, the same tendency in most tests containing different aspects of objectivity. In addition, what the patients reported, confirmed positive functional changes after treatment.
If the tests had been done more than three times at each period, we would have more thorough data, but we found this too strenu-ous for the patients. A treatment period of three weeks may also seem short, but this was in accordance with rehabilitation stays in our department.
The demonstrated improvement may be attributed to the effect of treatment, but might also be explained by multiple testing. However, analysis showed that most of the baseline data were rather stable. Thus it is likely that the observed changes during treatment were not simply due to repetitive assessments. The improvement could also be explained by an eventual spontaneous improvement. However, we would not expect this, as the patients had had their diagnosis for many years without any new relapses the last years.
Although the present study shows that physical functioning in two patients with MS improved after individualized Bobath treat-ment, the results cannot be generalized to a broad population of MS patients, and the effect should therefore be further examined in larger MS samples. Further validation of balance and gait measures is needed in neurological disorders (Perennou et al., 2005), and this seems particularly applicable in MS.
IMPLICATIONS
The implication of the present study is that balance and gait in patients with MS may
Physiotherapy in MS 115
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
improve after physiotherapy based on the Bobath concept. However, more research is needed to examine the validity of our results in a larger sample of patients with MS. Reli-ability and validity of outcome measures should be further established for the MS population.
ACKNOWLEDGEMENTS
This study was financially supported by The Norwe-gian Fund for Post-graduate Training in Physiother-apy. The authors wish to thank the two patients who participated in the study.
REFERENCES
American College of Sports Medicine. Resource Manual for Guidelines for Exercise Testing and Prescription. Philadelphia, PH: Lea & Febiger, 1988.
Berg K, Wood-Dauphinee S, Williams JI, Gayton D. Measuring balance in the elderly: preliminary development of an instrument. Physiotherapy Canada 1989; 41: 304–311.
Berg K, Wood-Dauphinee S, Williams JI. The Balance Scale: reliability assessment with elderly resi-dents and patients with an acute stroke. Scandi-navian Journal of Rehabilitation Medicine 1995; 27: 27–36.
Berg K, Wood-Dauphinee SL, Williams JT, Maki B. Measuring balance in the elderly: validation of an instrument. Canadian Journal of Public Health 1992; 83: 7–11.
Bilney B, Morris M, Webter K. Concurrent related validity of the GAITRite walkway system for quantification of the spatial and temporal param-eters of gait. Gait and Posture 2003; 17: 68–74.
Blair CE, Lewis R, Vieweg V, Tucker R. Group and single-subject evaluation of a programme to promote self-care in elderly nursing home resi-dents. Journal of Advanced Nursing 1996; 24: 1207–1213.
Bohannon RW. Comfortable and maximum walking speed of adults aged 20–79 years: reference values and determinants. Age and Ageing 1997; 26: 15–19.
Borg G. Perceived exertion as an indicator of somatic stress. Scandinavian Journal of Rehabilitation Medicine 1970; 2: 92–98.
Collen FM, Wade DT, Robb GF, Bradshaw CM. The Rivermead Mobility Index: a further development of the Rivermead Motor Assessment. Interna-tional Disability Studies 1991; 13: 102–107.
Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001; 94: 149–158.
Figoni SF. Single subject clinical research. Bridging the gap between therapy and science. Clinical Kinesiology 1990; 44: 63–71.
Freeman JA, Thompson AJ. Building an evidence base for multiple sclerosis management: support for physiotherapy (editorial commentary). Journal of Neurology, Neurosurgery and Psychiatry 2001; 70: 147–148.
Freeman JA, Thompson AJ. Is inpatient rehabilitation effective in multiple sclerosis? In: Thompson AJ (Ed.), Multiple Sclerosis, Clinical Challenges and Controversies. London: Martin Duniz, 1997; 313–324.
Freeman JA. Improving mobility and functional inde-pendence in persons with multiple sclerosis. Journal of Neurology 2001; 248: 255–259.
Gehlsen G, Beekman K, Assmann N, Winant D, Seidle M, Carter A. Gait characteristics in multiple sclerosis: progressive changes and effects of exercise on parameters. Archives of Physical Medicine and Rehabilitation 1986; 67: 536–539.
Gjelsvik B. Physiotherapie. In: Gjelsvik B (Ed.), Form und Funktion. Neurologie, Bobath Konzept, Physioterapie. Stuttgart: D Thieme Verlag, 2002; 59–129.
Jette AM. Outcome research: shifting the dominant research paradigm in physical therapy. Physical Therapy 1995; 75: 965–970.
Kaasa S, Lode JH. Patient evaluation and outcome measures; quality of life in palliative medicine — principles and practice. In: Doyle D, Hanks GWC, MacDonald N (eds), Oxford Textbook of Palliative Medicine (third edition). Oxford: Oxford University Press, 2004; 196–210.
Ko Ko C. Effectiveness of rehabilitation for multiple sclerosis. Clinical Rehabilitation 1999; 13: 33–41.
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 1983; 33: 1444–1452.
Lennon S. The Bobath concept: a critical review of the theoretical assumptions that guide physio-therapy practice in stroke rehabilitation. Physical Therapy Review 1996; 1: 35–45.

Smedal et al.116
Physiother. Res. Int. 11: 104–116 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
Lennon S. Gait re-education based on the Bobath concept in two patients with hemiplegia following stroke. Physical Therapy 2001; 81: 924–935.
Lord SE, Wade DT, Halligan PW. A comparison of two physiotherapy treatment approaches to improve walking in multiple sclerosis: a pilot ran-domized controlled study. Clinical Rehabilitation 1998a; 12: 477–486.
Lord SE, Halligan PW, Wade DT. Visual gait analysis: the development of a clinical assessment and scale. Clinical Rehabilitation 1998b; 12: 107–119.
Mant D. Can randomised trials inform clinical deci-sions about individual patients? Lancet 1999; 353: 743–746.
Moe-Nilssen R. A new method for evaluating motor control in gait under real-life environmental con-ditions. Part 2: Gait analysis. Clinical Biome-chanics 1998; 13: 328–335.
Myhr KM, Riise T, Vedeler C, Nordtvedt MW, Gron-ning M, Midgard R et al. Disability and prognosis in multiple sclerosis: demographic and clinical variables important for the ability to walk and awarding of disability pension. Multiple Sclerosis 2001; 7: 59–65.
Nourbakhsh MR, Ottenbacher KJ. The statistical anal-ysis of single-subject data: a comparative examina-tion. Physical Therapy 1994; 74: 768–775.
Nudo RJ. Adaptive plasticity in motor cortex: impli-cations for rehabilitation after brain injury. Journal of Rehabilitation Medicine 2003; 41: 7–10.
Oligati R, Burgunder JM, Mumenthaler M. Increased energy cost of walking in multiple sclerosis: effect of spasticity, ataxia, and weakness. Archives of Physical Medicine and Rehabilitation 1998; 69: 846–849.
Ottenbacher KJ. Analysis of data in idiographic research. Issues and methods. American Journal of Physical Medicine and Rehabilitation 1992; 71: 202–208.
Perennou D, Decavel P, Manckoundia P, Penven Y, Mourey F, Launay F et al. Evaluation of balance in neurologic and geriatric disorders. Annales de Réadaptation et de Médecine Physique 2005; 48: 317–335.
Podsiadlo D, Richardson S. The timed ‘Up&Go’: a test of basic functional mobility for frail elderly
persons. Journal of the American Geriatrics Society 1991; 39: 142–148.
Polit D, Hungler B. Qualitative research design and approaches. In: Polit D, Hungler B (eds), Nursing Research: Principles and Methods (sixth edition). Philadelphia, PA: Lippincott, 1999; 239–255.
Rodgers MM, Mulcare JA, King DL, Mathews T, Gupta SC, Glaser RM. Gait characteristics of individuals with multiple sclerosis before and after a 6-month aerobic training program. Journal of Rehabilitation Research and Development 1999; 36: 183–188.
Shumway-Cook A, Woollacott MH. Physiological basis of motor learning and recovery of function. In: Shumway-Cook A, Woollacott MH (eds), Motor Control, Theory and Practical Applications (second edition). Baltimore, MD: Lippincott Williams & Wilkins, 2000; 91–109.
Solari A, Filippini G, Gasco P, Colla L, Salmaggi A, Mantia LL et al. Physical rehabilitation has a posi-tive effect on disability in multiple sclerosis patients. Neurology 1999; 52: 57–62.
Thompson AJ. Symptomatic management and reha-bilitation in multiple sclerosis. Journal of Neurol-ogy, Neurosurgery and Psychiatry 2001; 71: 22–27.
Thorban LDB, Newton RA. Use of Berg Balance Scale to predict falls in elderly persons. Physical Therapy 1996; 76: 576–582.
World Health Organization. International Classifica-tion of Functioning, Disability and Health: ICF, Geneva: WHO, 2001.
Wiles CM, Newcombe RG, Fuller KJ, Shaw S, Furnival-Doran J, Pickersgill TP et al. Controlled randomised crossover trial of the effects of physiotherapy on mobility in chronic multiple sclerosis. Journal of Neurology, Neurosurgery and Psychiatry 2001; 70: 174–179.
Address correspondence to: T Smedal, Department of Physiotherapy, Haukeland University Hospital N- 5021 Bergen, Norway (E-mail: [email protected]).
(Submitted June 2005; accepted November 2005)





















