Avoiding Lumbar Spine Injury During Resistance Training
9
Avoiding Lumbar Spine Injury During Resistance Training Christopher J. Durall, DPT, SCS, LAT, CSCS University of Wisconsin–LaCrosse, LaCrosse,Wisconsin Robert C. Manske, CSCS, MPT, MEd, ATC, SCS Wichita State University,Wichita, Kansas Via Christi Sports and Orthopedic Physical Therapy,Wichita, Kansas © National Strength and Conditioning Association Volume 27,Number 4,pages 64–72 Keywords: lumbar spine; injury; resistance training L umbar spine injury is extremely pervasive and can be extraordinar- ily debilitating. It has been esti- mated that up to 80% of adults eventu- ally will develop some form of low back pain (12). In addition, it has been esti- mated that 10–15% of all sporting in- juries involve the spine (21, 35–37). The compressive, shear, tensile, and tor- sional forces on the lumbar spine during resistance training may be sufficient to cause injury, especially if these forces are concentrated by virtue of the exerciser’s mechanics. In this article we will review briefly the anatomy and pathologic me- chanics of common lumbar spine in- juries during weight training and discuss strategies for injury prevention. Our in- tent is not to provide an exhaustive re- view of lumbar spine pathologies, nor is it to enable strength and conditioning professionals to diagnose and to treat lumbar spine injuries. Instead, we hope to raise awareness of common resistance exercises that putatively are more likely to cause lumbar spine injury. In addi- summary In this manuscript, the injury risk to the lumbar spine during common resistance exercises is discussed. Al- ternative, theoretically less risky ex- ercises are presented. 64 August 2005 • Strength and Conditioning Journal Figure 1. Anterior and posterior aspects of the lumbar spine. (a) anterior aspect of lum- bosacral spine. 1, anterior longitudinal ligament; 2, intervertebral foramen; 3, spinous process; 4, spinal nerve; 5, inferior facet; 6, superior facet; 7, interverte- bral disk; 8, sacrum; and 9, coccyx. (b) posterior aspect of lumbosacral spine. 1, superior facet; 2, transverse process; 3, inferior facet; 4, intervertebral disk; 5, posterior longitudinal ligament; 6, pars interarticularis; 7, spinous process; 8, lamina; 9, facet joint capsule; 10, sacral ala; 11, sacral foramina; and 12, coccyx. With permission from J.A. Nicholas and E.B. Hershman (29). a b
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Avoiding Lumbar Spine Injury During Resistance Training

Avoiding Lumbar Spine InjuryDuring Resistance TrainingChristopher J. Durall, DPT, SCS, LAT, CSCSUniversity of Wisconsin–LaCrosse, LaCrosse,Wisconsin
Robert C. Manske, CSCS, MPT, MEd, ATC, SCSWichita State University,Wichita, KansasVia Christi Sports and Orthopedic Physical Therapy,Wichita, Kansas
© National Strength and Conditioning AssociationVolume 27, Number 4, pages 64–72
Keywords: lumbar spine; injury; resistance training
Lumbar spine injury is extremelypervasive and can be extraordinar-ily debilitating. It has been esti-
mated that up to 80% of adults eventu-ally will develop some form of low backpain (12). In addition, it has been esti-mated that 10–15% of all sporting in-juries involve the spine (21, 35–37).The compressive, shear, tensile, and tor-sional forces on the lumbar spine duringresistance training may be sufficient tocause injury, especially if these forces areconcentrated by virtue of the exerciser’smechanics. In this article we will reviewbriefly the anatomy and pathologic me-chanics of common lumbar spine in-juries during weight training and discussstrategies for injury prevention. Our in-tent is not to provide an exhaustive re-view of lumbar spine pathologies, nor is
it to enable strength and conditioningprofessionals to diagnose and to treatlumbar spine injuries. Instead, we hope
to raise awareness of common resistanceexercises that putatively are more likelyto cause lumbar spine injury. In addi-
s u m m a r y
In this manuscript, the injury risk to
the lumbar spine during common
resistance exercises is discussed. Al-
ternative, theoretically less risky ex-
ercises are presented.
64 August 2005 • Strength and Conditioning Journal
Figure 1. Anterior and posterior aspects of the lumbar spine. (a) anterior aspect of lum-bosacral spine. 1, anterior longitudinal ligament; 2, intervertebral foramen; 3,spinous process; 4, spinal nerve; 5, inferior facet; 6, superior facet; 7, interverte-bral disk; 8, sacrum; and 9, coccyx. (b) posterior aspect of lumbosacral spine. 1,superior facet; 2, transverse process; 3, inferior facet; 4, intervertebral disk; 5,posterior longitudinal ligament; 6, pars interarticularis; 7, spinous process; 8,lamina; 9, facet joint capsule; 10, sacral ala; 11, sacral foramina; and 12, coccyx.With permission from J.A. Nicholas and E.B. Hershman (29).
a b

tion, we will discuss alternative, presum-ably less-risky, exercises. It is importantto acknowledge that our advice is basedon general biomechanical informationand that biomechanical data are notavailable for all exercises that either di-rectly or indirectly affect the lumbarspine. In spite of this, we believe thatcareful exercise selection and instructionbased on knowledge of pathologic lum-bar spine mechanics will reduce the inci-dence of lumbar spine injury.
Overview of Lumbar SpineAnatomyThe lumbar spine consists of 5 separatevertebrae, which increase in size fromsuperior to inferior (Figure 1) (3). Thelumbar vertebrae are the largest in thespinal column, enabling them to beartremendous compressive loads. Betweeneach pair of lumbar vertebrae is an inter-vertebral disc comprising a central nu-cleus pulposus, a series of fibrocartilagi-nous rings known as the annulusfibrosis, and a pair of cartilaginous end-plates at the disc/vertebral body inter-faces. The nucleus pulposus acts like agelatinous cushion that disperses spinalcompressive forces to the annulus andend-plates. The annulus acts like a liga-ment, resisting shear (sliding), tensile(stretching), and torsional (rotational)forces imparted to the lumbar spine,while restraining the nucleus and con-necting the vertebral bodies. The annu-lus fibrosis is thinner posteriorly thananteriorly in the lumbar spine. The ver-tebral end-plates, sandwiched betweenthe disc and the vertebral body, permitdiffusion of nutrient and waste materialbetween the disc and vertebral body.The end-plates are thinnest and weakestin their centers adjacent to the nucleuspulposus (Figure 2) (3).
The bony posterior vertebral arch andvertebral body together form the neuralarch, which envelops and protects thespinal cord (3). Small processes situatedon each side of the arch articulate withadjacent vertebrae (Figure 1). These ar-ticulations are known as zygoapophyseal,
or facet, joints. The portion of the neuralarch located between the superior and in-ferior articular processes is known as thepars interarticularis. The pars interarticu-laris is a common site for a stress fracturein the posterior vertebral arch (9).
The ligamentous restraints of lumbarspine movement are typically dividedinto anterior and posterior portions.These ligaments restrain spinal move-ments in all directions, but we will focuson their roles in limiting lumbar flexionand extension. The anterior longitudi-nal ligament becomes taut during thespine extension, whereas the posteriorligaments (posterior longitudinal liga-ment, ligamentum flavum, interspinousligament, facet capsules, supraspinousligaments) become taut during flexion(Figure 2) (3). The anterior longitudinalligament is thicker and stronger anteri-orly in the lumbar spine than in otherregions of the spine; consequently, ante-rior ligamentous disruptions are rare.The posterior longitudinal ligament isconsiderably narrower and weaker thanthe anterior longitudinal ligament, butstill provides support for the central pos-terior aspect of the intervertebral disc.
The posterior lateral portions of the in-tervertebral disc, however, are not wellprotected by the posterior longitudinalligament (3).
Kinesiology of the LumbarSpineLumbar spine movement occurs in 6 di-rections, including left and right rota-tion in the transverse plane, around avertical axis; left and right side bending(or lateral flexion) in the frontal plane,around an anterior/posterior axis; andforward bending (flexion) and backwardbending (extension) in the sagittal plane,around a medial/lateral axis (3). We havechosen to focus our discussion of lumbarspine kinesiology on flexion and exten-sion, because these are the primarymovements in this region of the spine(28). All lumbar spine movements in-volve vertebral rolling (or tilting) andshearing (or sliding). During flexion, thesuperior vertebral segment rolls (or tilts)forward around a frontal plane axis, andit shears (or slides) forward, essentiallyalong the transverse plane (3). The facetsof the superior vertebral segments slidesuperiorly and anteriorly during flexion,while the posterior fibers of the annulus
65August 2005 • Strength and Conditioning Journal
Figure 2. Axial section of the lumbar vertebrae. 1, spinous process; 2, lamina; 3, facet;4, transverse process; 5, pedicle; 6, spinal nerve; and 7, intervertebral disk.With permission from J.A. Nicholas and E.B. Hershman (29).
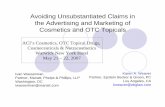
pulposus and the posterior ligaments(ligamentum flavum, interspinous liga-ment, facet capsules, supraspinous liga-ments, posterior longitudinal ligament)become taut. During lumbar spine ex-tension, the superior vertebral segmenttilts and shears backward, while thefacets of the superior vertebral segmentsslide inferiorly due to the posteriorrolling of the segments. The spinousprocesses approximate while the anteriorannular fibers of the intervertebral discand the anterior longitudinal ligamentare stretched (Figure 3).
Several groups of muscles control move-ment of the lumbar spine and act to stiff-en the spine, thereby providing resis-
tance to injury. These include the ab-dominals (rectus abdominus, internaland external obliques, transversus ab-dominus), the erector spinae (iliocostal-is, longissimus, spinalis), the deep intrin-sic spinal muscles (multifidus, rotatores,semispinalis), and the quadratus lumbo-rum (8, 11, 20). When these muscles areactive, they function like guy wires to in-crease the stiffness (or rigidity) of thelumbar spine “mast” (8, 31). Some ofthese muscle groups, along with others(e.g., diaphragm, levator ani), also helpto increase lumbar spine stiffness whenthey increase pressure in the abdominalcavity (10). As the stiffness of the spineincreases, the spine becomes more stable,and presumably less vulnerable to injury
(8). It is therefore imperative that themuscles that act to stiffen and to stabilizethe spine have excellent strength and en-durance. Advice on training these mus-cles is offered in the sections below.
Common Mechanisms of Lumbar Spine Injury During Resistance TrainingMost lumbar spine injuries that occurduring resistance training, fortunately,are thought to be simple muscle strainsand/or ligament sprains (4, 34, 39). Inone study of male Olympic weight-lifters, nearly 75% of weightlifting-re-lated back injuries were diagnosed asmuscle strains (4). In our experience,muscle strains are often the result of im-proper exercise loads, improper rest in-tervals (i.e., fatigue), and/or improperlifting technique. Obviously, these fac-tors can readily be adjusted with properexercise guidance to reduce the risk ofmuscle strain.
Though muscle strains are often not seri-ous injuries, injuries involving the inter-vertebral disc, pars interarticularis, orvertebral end-plate may have more seri-ous consequences. As discussed above,the inherently weak posterior annulus fi-brosis is under greater tensile stress dur-ing lumbar flexion (6, 13). Not surpris-ingly, most lumbar disc injuries occurwhen the spine is flexed (6, 13). Exam-ples of resistance exercises that may in-volve full lumbar flexion include goodmornings, dead lifts, rows, and sit-ups.
As mentioned previously, the posteriorvertebral elements of the lumbar spineare compressed when the spine is extend-ed. Repetitive, forceful end range of mo-tion lumbar extension (e.g., during theend of a dead lift) or forceful shearing ofthe vertebrae can lead to compression in-jury of the facet joints and/or fatigue andfailure of the pars interarticularis (9).Fracture of the pars interarticularis(known as a spondylolysis) may lead toforward slipping of the superior verte-brae on the inferior (known as a spondy-lolisthesis). In a sample of competitive
66 August 2005 • Strength and Conditioning Journal
Figure 3. Flexion and extension of the lumbar spine. (a) posterior longitudinal liga-ment is stretched during forward flexion of the vertebral column and isslack and may be compressed during extension. (b) anterior longitudinalligament is slack in forward flexion of the vertebral column and in exten-sion of the vertebral column, the ligament is stretched.With permissionfrom C.C. Norkin and P.K. Levangie (30).
a
b

weightlifters, 36% were found to have aspondylolysis on radiograph (27). Fortu-nately, fractures account for a small per-centage of all weight-training injuries.
Another structure that may be injuredwith resistance training is the vertebralend-plate. With compressive loading(e.g., during a squat or leg press), the ver-tebral end-plate will fail before the inter-vertebral disc (24). Fissures in the end-plate lead to migration of the nucleuspulposus into the vertebral body, a loss ofdisc height, and an alteration of vertebralsegment mechanics. End-plate fracture isalways a potential risk during heavycompressive loading. It would be sensi-ble to increase compressive loads gradu-ally over time to encourage tissue adapta-tions that reduce the likelihood of injury.
Modifying Common ResistanceExercises to Reduce the Risk ofLumbar Spine InjuryAs discussed above, the lumbar spine ismore likely to be injured when loadedwhile flexed or extended. The posteriorvertebral elements may be injured whenthe lumbar spine is loaded while fullyextended, whereas the posterior inter-vertebral disc annulus appears to bemost vulnerable when the spine isloaded while flexed. The corollary ofthis observation, then, would suggestthat the structures of the lumbar spineare less likely to be damaged when thespine is in the middle of the availablerange of motion. The middle portion ofthe available range of motion has previ-ously been described as the neutral range(15). The neutral range also has beenpurported to be advantageous for pre-venting injury and for enhancing athlet-ic performance (16). Herring and Wein-stein (16) suggest that the neutral rangeis close to the center of reaction and al-lows for quick movements into bothflexion and extension. Because the neu-tral lumbar spine range appears to be rel-atively safe and may enhance athleticperformance, it is sensible to performstrengthening and stretching exercisesfor the extremities with the lumbar
spine in the neutral range. To help yourclients find their neutral position, havethem fully flex, then fully extend theirlumbar spine in a supine position; theneutral range is midway between thesetwo extremes.
Once a client is able to assume the neu-tral range, he or she should be chal-lenged to maintain this range during re-sistance exercises. The strength andconditioning professional should devel-op the skill to identify when a client failsto maintain a neutral range and shouldprovide verbal and/or tactile cueinguntil the neutral spinal range is adopted.For instance, the bench press is typicallyperformed with the feet resting on thefloor, which may place the hips in an ex-tended position. If the hip flexors areshort or inflexible, the lumbar spine willbe forced to extend when the hips are ex-tended, due to the attachment of thepsoas muscle on the lumbar discs andvertebrae. If the lifter pushes throughthe legs and arches the lumbar spine togain leverage during a bench press, lum-bar spine extension will increase further,
resulting in increased compressive load-ing of the posterior bony elements. Thestrength and conditioning professionalshould make appropriate adjustments toavoid excessive lumbar extension andadverse compressive loading of the pos-terior spinal structures. For example,improving extensibility of the hip flex-ors will reduce lumbar extension whenthe feet are placed on the floor. Alterna-tively, placing the feet on the benchthroughout the lift reduces the tensionon the psoas muscle. Exercises thatrepetitively load the posterior arch mayoverstress the weak pars interarticularisand result in a spondylolysis, or progressa spondylolysis into a spondylolisthesis(9). Clients with a spondylolysis orspondylolisthesis should be advised toavoid exercises that involve end range-of-motion lumbar extension.
The squat and the leg press are standardtraining exercises used to increase thestrength of the entire lower-extremitykinetic chain, which can be problematicfor those with back injuries. Proper formis essential to the correct execution of
67August 2005 • Strength and Conditioning Journal
Figure 4. Abnormal squat posture due to tight gastrocnemius/soleus complex.

these exercises. One of the authors(R.M.) has rehabilitated several weight-lifters following lumbar disc rupture oc-curring during the performance of the
squat or leg press exercises. In all of thesecases, the exercisers were injured whenthey executed the squat with a flexedlumbar spine. Excessive forward trunk
flexion during the squat increases in-tradisc pressure and tensile loads on theposterior annulus (6, 13). A flexed pos-ture during the squat also shifts the loadanteriorly, relative to the lumbar spine(25). The effect of this load shift is alengthening of the load’s lever arm andan increase in the torque applied to thelumbar spine. Maintaining a neutrallumbar spine will help the exerciser keepthe external load and the upper body di-rectly over the hips and torso, and thusshorten the load’s lever arm, decreasingthe external torque on lumbar spine.
Clients who have difficulty maintaininga neutral lumbar spine during the squatmay have greater success by using a self-spotting rack initially. A self-spottingrack should promote a more erect posi-tion during both the descent and ascentphases of the squat exercise. Clients withinflexible ankle plantar flexors (gastroc-nemius/soleus/Achilles tendon complex)may flex their trunk to compensate fortheir inability to dorsiflex their anklesduring the descent phase of the squat(Figure 4). In this case, placing a smallwedge under the exerciser’s heels will de-crease the amount of dorsiflexion neededduring that phase. This should improvethe exerciser’s ability to maintain a neu-tral lumbar spine position throughoutthe exercise (Figure 5), until the flexibili-ty of their plantar flexors improves.
When performing the leg press, it is im-portant that the exerciser maintain aneutral spine to modulate the lumbarspine injury risk. The strength and con-ditioning professional should be able toobserve for excessive lumbar spine flex-ion during the beginning and end of theleg press exercise (Figure 6). The rangeof motion during the exercise may needto be limited, depending on the flexibil-ity in the exerciser’s hip extensors, toavoid full lumbar spine flexion.
As discussed above, the posterior annulusis vulnerable to injury when the spine isflexed. Individuals recovering from pos-terior intervertebral disc injury would be
68 August 2005 • Strength and Conditioning Journal
Figure 6. Leg press with hips posteriorly rotated.
Figure 5. Normal squat posture with block under heel.

well advised to avoid lifts that involvelumbar flexion (e.g., good-mornings,stiff-legged dead lifts, bent-over rows).Exercisers with posterior intervertebraldisc injury should maintain a neutrallumbar spine range to reduce tension onthe posterior annulus. The importance ofa proper warm-up and light stretching toreduce the risk of sprain or strain is famil-iar to most strength and conditioningspecialists and therefore does not warrantfurther discussion.
Exercises to Reduce the Risk ofLumbar Spine InjuryAddressing strength deficits in the mus-cles that help stabilize the lumbar spineis a logical step toward reducing the riskof injury. In the authors’ experience, theposterior spinal muscles (iliocostalis,longissimus, spinalis, multifidus, rota-tores, semispinalis) are the most oftenneglected muscles in strength trainingroutines. In a 5-year prospective study ofthe general population, individuals withlow back pain were found to have a sig-nificantly lower ratio of trunk extensorto trunk flexor strength (20). This trunkextensor strength deficit proved to be themost sensitive predictor of future occur-rence of low back pain; that is, individu-als with relative weakness of the lumbarspine extensors were more likely to expe-rience subsequent episodes of low backpain. In another study, extensor strengthwas significantly lower than flexorstrength in patients recovering fromspinal surgery (22). Several investigatorshave found that the multifidus muscle isparticularly affected by back pain or in-jury (17, 18, 32). The multifidus hasbeen found to atrophy quickly followingback injury (17, 18), and to remain atro-phied after back pain subsides (17).
Callaghan and colleagues found that sin-gle-leg extension in quadruped (i.e.,hands and knees position) is a relativelysafe exercise for the extensor muscles (5).This exercise also can be performed proneover an exercise ball. The exercise can beprogressed to include simultaneous exten-sion of the contralateral arm or by per-
forming the movement from a prone po-sition, lying with the spine in a neutralrange (Figure 7). If tolerated, lumbar ex-tension can be performed on a selector-ized machine. When using a selectorizedmachine, the pelvis should be stabilized tolimit substitution by the gluteals andhamstrings (14). Even such limited range-of-motion lumbar extension trainingshould result in strength gains through alarger range of motion (14, 33).
Lateral stability of the lumbar spine ap-pears to be largely attributable to theoften-overlooked quadratus lumborummuscles (1, 25). Activity in the quadra-tus lumborum muscles has been foundto increase significantly when the lum-bar spine is loaded, suggesting that thismuscle is important in stabilizing thelumbar spine (25). The isometric hori-zontal side-support exercise (Figure 8)has been shown to effectively challenge
69August 2005 • Strength and Conditioning Journal
Figure 7. Prone single-leg extension exercise.
Figure 8. Isometric horizontal side-support exercise.

these muscles while imparting relativelylow levels of spinal compression (2).
Many exercises have been suggested toenhance performance of the abdominalmuscles in the interest of improvinglumbar spine health. Training of thetransversus abdominus muscle has beenadvocated in particular, because aber-rant performance of this muscle hasbeen found in patients with low backpain (19). Clients with a history of lowback injury should utilize a regimen ofabdominal exercises that create mini-mal lumbar spine compression andshear. Routine exercises such as thebent-knee sit-up involve high levels ofspinal compression and may be con-traindicated for certain clients (2, 23).Axler and McGill examined the safetyof several abdominal exercises by com-paring muscle activity with lumbarcompressive loading (2). Four abdomi-nal exercises were found to have a highratio of muscle challenge to spine com-pression: the curl-up with feet unsup-ported, the curl-up with feet anchored,the dynamic cross-knee curl-up, andthe hanging straight-leg raise. The curl-up exercise (feet free or fixed) had thehighest ratio of muscle activity to lum-bar spine compression, making this arelatively safe abdominal exercise. Sev-eral exercises were not recommendedbecause they involve a high level ofspinal compression. These were thesupine bilateral straight-leg raise, bilat-eral bent-leg raise (supine and hang-ing), and isometric cross-knee curl-up(pushing against elevated knee) (2).
It is sensible to perform isolatedstrengthening exercises at the end of aworkout for the muscles that supportthe lumbar spine. Exercising these mus-cles at the beginning of a workout willtemporarily fatigue them and may im-pair dynamic spinal stabilization duringthe initial phase of the exercise session.High-repetition resistance exerciseshould be used with these muscles topromote greater endurance for lumbarspine stabilization.
In addition, muscle groups that help con-trol pelvic position, hamstrings, quadri-ceps, iliopsoas, rectus femoris, gastrocne-mius and soleus, and the associated hiprotators also should be strengthened ifdeficits are present (16). The lumbarspine requires a stable lower extremityand pelvic base of support to function ef-fectively (21). Weakness in these musclegroups may require compensatory activi-ty in the lumbar spinal muscles, predis-posing the lumbar muscles to fatigue andan increased risk of injury.
The Use of Lifting Belts to Reduce Lumbar Spine InjuryDuring Resistance TrainingNo article on lumbar spine injury dur-ing resistance training would be com-plete without a discussion of liftingbelts. Although commonly used, there isno conclusive evidence that lifting beltsare effective in preventing lumbar spineinjury. However, lifting belts have beenshown to increase intramuscular stiff-ness in the erector spinae muscles (26)and spinal stiffness in general (7).Whether or not increased erector spinaeintramuscular stiffness increases spinalstiffness is unknown. Despite the in-crease in intramuscular stiffness, erectorspinae electromyogram activity has beenshown to decline when a lifting belt isworn (7, 38). It remains to be seen if thedecline in erector spinae muscle activa-tion is offset by the increase in muscularstiffness, thus increasing injury resis-tance during tasks that require an exten-sor moment, such as lifting from a flexedposition (e.g., dead lift). We have ob-served many exercisers wearing beltsduring these lifts, with the intent of re-ducing spinal injury.
Although the extent to which a liftingbelt can provide lumbar stabilization isunclear, a lifting belt does provide tactilebiofeedback. This feedback may assist thelifter in making protective postural ad-justments (e.g., maintaining a neutrallumbar spine) during a lift. We encouragestrength and conditioning professionalsto stay abreast of research in this area; fu-
ture research may provide more definitiveconclusions on the use of weightliftingbelts to reduce lumbar spine injury riskduring resistance training.
ConclusionStrength and conditioning specialistsneed to be cognizant of factors that con-tribute to lumbar spine injury in orderto formulate safe exercise regimens fortheir clients. Avoidance of lifting with ahyperextended or hyperflexed spinemay reduce lumbar spine injuries dur-ing resistance training. Maintaining aneutral lumbar spine range allows forcesborne on either the upper or lower por-tions of the body to be appropriatelydispersed across the tissues of the lum-bar spine. Performance of the trunkmuscles that stabilize the lumbar spineshould be improved to enhance dynam-ic stabilization of the spine during load-ing. When in doubt about the safety of aparticular exercise for a client recover-ing from lumbar spine injury, consultwith the appropriate health careprovider. ♦
References1. Andersson, E.A., L.E. Oddsson, H.
Grundstrom, J. Nimsson, and A.Thorstensson. EMG activities of thequadratus lumborum and erectorspinae muscles during flexion-relax-ation and other motor tasks. Clin. Bio-mech. (Bristol, Avon). 11:392–400.1996.
2. Axler, C.T., and S.M. McGill. Lowback loads over a variety of abdominalexercises: Searching for the safest ab-dominal challenge. Med. Sci. Sports.Exerc. 29:804–810. 1997.
3. Bogduk, N. Clinical Anatomy of theLumbar Spine and Sacrum. (3rd ed.).New York: Churchill Livingston,1997. pp. 5–13, 35, 58.
4. Calhoun, G., and A.C. Fry. Injuryrates and profiles of elite competitiveweightlifters. J. Athl. Train. 34:232–238. 1999.
5. Callaghan, J.P., J.L. Gunning, andS.M. McGill. The relationship be-tween lumbar spine load and muscle
70 August 2005 • Strength and Conditioning Journal

activity during extensor exercises. Phys.Ther. 78:8–18. 1998.
6. Callaghan, J.P., and S.M. McGill. In-tervertebral disc herniation: Studies ona porcine model exposed to highlyrepetitive flexion/extension motionwith compressive force. Clin. Biomech.(Bristol, Avon). 16(1):28–37. 2001.
7. Cholewicki, J., K. Juluru, A. Rade-bold, M.M. Panjabi, and S.M. McGill.Lumbar spine stability can be aug-mented with an abdominal belt and/orincreased intra-abdominal pressure.Eur. Spine. J. 8:388–395. 1999.
8. Cholewicki, J., M.M. Panjabi, and A.Khachatryan. Stabilizing function oftrunk flexor-extensor muscles arounda neutral spine posture. Spine.22:2207–2212. 1997.
9. Chosa E., Totoribe K., Tajima N. Abiomechanical study of lumbarspondylolysis based on a three-dimen-sional finite element method. J Orthop.Res. 22(1):158–63. 2004.
10. Cresswell, A., P. Blake, and A.Thorstensson. The effect of an intra-abdominal muscle training programon intra-abdominal pressure. Scand. J.Rehabil. Med. 26:79–86. 1994.
11. Crisco, J.J., and M.M. Panjabi. The in-tersegmental and multisegmental mus-cles of the lumbar spine: A biome-chanical model comparing lateralstabilizing potential. Spine. 16:793–799. 1991.
12. Frymoyer, J.W. Back pain and sciatica.N. Engl. J. Med. 318:291. 1988.
13. Gordon, S.J., K.H. Yang, P.J. Mayer,A.H. Mace Jr., V.L. Kish, and E.L.Radin. Mechanism of disc rupture. Apreliminary report. Spine. 16(4):450–456. 1991.
14. Graves, J.E., D.C. Webb, M.L. Pol-lock, J. Matkozich, S.H. Leggett,D.M. Carpenter, D.N. Foster, and J.Cirulli. Pelvis stabilization during re-sistance training: Its effect on the de-velopment of lumbar extensionstrength. Arch. Phys. Med. Rehabil.75:210–215. 1994.
15. Hart, D.L., T.J. Stobbe, and M. Jaraie-di. Effect of lumbar posture on lifting.Spine. 12:138–145. 1987.
16. Herring, S.A., and S.M. Weinstein.Assessment and nonsurgical manage-ment of athletic low back injury. In:The Lower Extremity and Spine InSports Medicine (2nd ed.). J.A.Nicholas and E.B. Hershman, eds. St.Louis: Mosby Year Book, Inc., 1995. p.1189.
17. Hides, J.A., C.A. Richardson, andG.A. Jull. Multifidis recovery is not ap-propriate after resolution of acute,first-episode low back pain. Spine.21:2763–2769. 1996.
18. Hides, J.A., M.J. Stokes, M. Saide,G.A. Jull, and D.H. Cooper. Evidenceof lumbar multifidus muscle wastingipsilateral to symptoms in patientswith acute/subacute low back pain.Spine. 19:165–172. 1994.
19. Hodges, P.W., and C.A. Richardson.Inefficient muscular stabilization oflumbar spine associated with low backpain. Spine. 21:2640–2650. 1996.
20. Lee, J., Y. Hoshino, K. Nakamura, andY. Ooi. Trunk muscle imbalance as arisk factor of the incidence of low backpain. J. Neuromusculoskeletal Syst.7:97–101. 1999.
21. Maxwell, C., and A. Spiegal. The re-habilitation of athletes followingspinal injuries. In: The Spine in Sports.S.H. Hochschuler, ed. Philadelphia:Hanley and Belfus, 1990. pp. 281–292.
22. Mayer, T.G., H. Vanharanta, R.J.Gatchel, V. Mooney, D. Barnes, L.Judge, S. Smith, and A. Terry. Com-parison of CT scan muscle measure-ments and isokinetic trunk strength inpostoperative patients. Spine 14:33–36.1989.
23. McGill, S.M. The mechanics of torsoflexion: Sit-ups and standing dynamicflexion manoevres. Clin. Biomech.(Bristol, Avon). 10:184–192. 1995.
24. McGill, S.M. The biomechanics oflow back injury: Implications oncurrent practice in industry and theclinic. J. Biomech. 30:465–475.1997.
25. McGill, S.M. Distribution of tissueloads in the low back during a vari-ety of daily and rehabilitation tasks.
J. Rehabil. Res. Dev. 34:448-458.1997.
26. Miyamoto, K. N. Iinuma, M. Maeda,E. Wada, and K. Shimizu. Effects of ab-dominal belts on intra-muscular pres-sure, intra-muscular pressure in theerector spinae muscles and myoelectri-cal activities of trunk muscles. Clin.Biomech. (Bristol, Avon). 14:79–87.1999.
27. Namey, T.C., and J.C. Carek. Powerlifting, weight lifting and body-building. In: Sports Injuries: Mecha-nisms, Prevention, Treatment. F.H. Fuand D.A. Stone, eds. Baltimore:Williams & Wilkins, 1994. pp.515–529.
28. Ng, J.K., V. Kippers, C.A. Richard-son, and M. Parnianpour. Range ofmotion and lordosis of the lumbarspine: Reliability of measurement andnormative values. Spine. 26(1):53–60.2001.
29. Nicholas, J.A., and E.B. Hershman,eds. The Lower Extremity and Spinein Sports Medicine (2nd ed.). St.Louis, MO: Mosby Year Book, Inc.,1995.
30. Norkin, C.C., and P.K. Levangie. JointStructure and Function: A Comprehen-sive Analysis (2nd ed.). Philadelphia:F.A. Davis, 1992.
31. Panjabi, M. Symposium on the lum-bar spine. Orthop. Clin. North. Am.8:169–179. 1977.
32. Parkkola, R., U. Rytokoski, and M.Kormano. Magnetic resonance imag-ing of the discs and trunk muscles inpatients with chronic low back painand healthy control subjects. Spine.18:830–836. 1993.
33. Pollock, M.L., S.H, Leggett, J.E.Graves, A. Jones, M. Fulton, and J.Cirulli. Effect of resistance training onlumbar extension strength. Am. J.Sports Med. 17:624–629. 1989.
34. Risser, W.L., J.M. Risser, and D. Pre-ston. Weight-training injuries in ado-lescents. Am. J. Dis. Child. 144:1015–1017. 1990.
35. Spencer, C.W., and D.W. Jackson.Back injuries in the athlete. Clin.Sports. Med. 2:191–216. 1983.
71August 2005 • Strength and Conditioning Journal

36. Stinson, J.T. Spine problems in theathlete. Md. Med. J. 45:655–658.1996.
37. Tall, R.L., and W. DeVault. Spinal in-jury in sport: Epidemiologic consider-ations. Clin. Sports. Med. 12:441–448.1993.
38. Thomas, J.S., S.A. Lavender, D.M.Corcos, and G.B. Andersson. Effect oflifting belts on trunk muscle activationduring a suddenly applied load. Hum.Factors. 41(4):670–676. 1999.
39. Zemper, E.D. Four-year study ofweight room injuries in a nationalsample of college football teams.Strength. Cond. J. 12:32–33. 1990.
Christopher J. Durall is the Director ofthe Student Health Center Physical Thera-py Department and a Graduate Facultymember at the University of Wisconsin-LaCrosse.
Robert C. Manske is an assistant profes-sor in the Department of Physical Therapyat Wichita State University. He also prac-tices clinically for Via Christi Sports andOrthopedic Physical Therapy and for ViaChristi Sports Medicine.
72 August 2005 • Strength and Conditioning Journal
Durall
Manske