aviation safety letter - Transports Canada
38
COPA Corner: Can GPS Get You Lost? NAV CANADA Online Store Reduces Costs, Boosts Convenience and Safety Single-Pilot Resource Management (SRM) Competencies Scenario-Based CRM Case Study: Stall Warning Device Event The Flight Safety Foundation’s ALAR Tool Kit Maintenance: Winter Operation Woes Maintenance of Small Non-Commercial Aircraft The Suspension or Cancellation of Canadian Aviation Documents Due to “Incompetence” DON’T WALK OUT... Stay in the Prime Search Area Learn from the mistakes of others; you’ll not live long enough to make them all yourself ... In this issue… TP 185E Issue 4/2012 aviation safet y letter
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of aviation safety letter - Transports Canada

COPA Corner: Can GPS Get You Lost?
NAV CANADA Online Store Reduces Costs, Boosts Convenience and Safety
Single-Pilot Resource Management (SRM) Competencies
Scenario-Based CRM Case Study: Stall Warning Device Event
The Flight Safety Foundation’s ALAR Tool Kit
Maintenance: Winter Operation Woes
Maintenance of Small Non-Commercial Aircraft
The Suspension or Cancellation of Canadian Aviation Documents Due to “Incompetence”
DON’T WALK OUT... Stay in the Prime Search Area
Learn from the mistakes of others; you’ll not live long enough to make them all yourself ...
In this issue…
TP 185E Issue 4/2012
aviation safety letter

2 Table of Contents ASL 4/2012
Table of Contents
Guest Editorial .............................................................................................................................................................................3Pre-Flight ..............................................................................................................................................................................4Flight Operations .........................................................................................................................................................................7Answers to the 2012 Self-Paced Study Program ..............................................................................................................16Maintenance and Certification ...........................................................................................................................................17Recently Released TSB Reports ........................................................................................................................................20Accident Synopses ..............................................................................................................................................................31Regulations and You .............................................................................................................................................................. 34Debrief: DON’T WALK OUT... Stay in the Prime Search Area ......................................................................................362012 Self-Paced Study Program .............................................................................................................................. Tear-off
The Aviation Safety Letter is published quarterly by Transport Canada, Civil Aviation. The contents do not necessarily reflect official government policy and, unless stated, should not be construed as regulations or directives.
Letters with comments and suggestions are invited. All correspondence should include the author’s name, address and telephone number. The editor reserves the right to edit all published articles. The author’s name and address will be withheld from publication upon request.
Please address your correspondence to:
Paul Marquis, Editor Aviation Safety Letter Transport Canada (AARTT) 330 Sparks Street, Ottawa ON K1A 0N8 E-mail: [email protected] Tel.: 613-990-1289 / Fax: 613-952-3298 Internet: www.tc.gc.ca/ASL
Copyright:Some of the articles, photographs and graphics that appear in the Aviation Safety Letter are subject to copyrights held by other individuals and organizations. In such cases, some restrictions on the reproduction of the material may apply, and it may be necessary to seek permission from the rights holder prior to reproducing it.
To obtain information concerning copyright ownership and restrictions on reproduction of the material, please contact:
Public Works and Government Services Canada Publishing and Depository Services 350 Albert Street, 4th Floor, Ottawa ON K1A 0S5 Fax: 613-998-1450 E-mail: [email protected]
Note: Reprints of original Aviation Safety Letter material are encouraged, but credit must be given to Transport Canada’s Aviation Safety Letter. Please forward one copy of the reprinted article to the editor.
Electronic distribution:To subscribe to the Aviation Safety Letter e-Bulletin notification service, visit: www.tc.gc.ca/ASL.
Print-on-Demand:To purchase a Print-on-Demand (POD) version (black and white), please contact:
The Order Desk Transport Canada Toll-free number (North America): 1-888-830-4911 Local number: 613-991-4071 E-mail: [email protected] Fax: 613-991-2081 Internet: www.tc.gc.ca/Transact
Sécurité aérienne — Nouvelles est la version française de cette publication.
© Her Majesty the Queen in Right of Canada, as represented by the Minister of Transport (2012). ISSN: 0709-8103 TP 185E
section page

ASL 4/2012 Guest Editorial 3
I am pleased to have this opportunity to introduce myself to all our stakeholders as the new director of the Standards Branch in the Civil Aviation Directorate at Transport Canada.
In this editorial, I would like to briefly discuss some of the principles that I think are integral to building a robust aviation safety program.
Ultimately, it is Canadian aviation document holders who are responsible for staying safe. This is achieved by complying with the Canadian Aviation Regulations (CARs) and its associated Standards and, more specifically, by proactively identifying, assessing and managing risks. In this context, Transport Canada’s role is to develop regulations that meet the public interest of improving aviation safety and to oversee compliance with those regulations. We do this by taking a risk-based approach, collaborating with stakeholders and looking at issues holistically and comprehensively.
Promoting the safe transportation of people and goods by air requires a risk-based approach. This means accepting that risk cannot be eliminated; it does not, however, mean that we blindly accept risk. Rather, a strong aviation safety program is built upon the identification, assessment and management of risks. As the nature of risk varies throughout the aviation industry, applying a risk-based approach allows us to adapt our program to different sectors of the aviation industry, allowing for a more effective mitigation of risks—one size does not always fit all. It also means applying our resources, whether in developing or overseeing regulations, to the areas of greatest risk—those areas where an investment in safety will produce the greatest benefit in terms of reducing risk.
Collaboration with all stakeholders is critical to identifying, developing and implementing the most effective approaches to improving safety. Those who operate and work in the aviation industry have unique knowledge and expertise from which we, at Transport Canada, need to benefit. We gather this information through formal and informal consultation with stakeholders. These exchanges must be based on mutual respect and a willingness to engage and listen. Given different roles and responsibilities, we may not always agree, but your views and knowledge are taken seriously when we make decisions and recommendations to the Minister.
It is rare that the response to any given safety issue is confined to the organizational boundaries that we all create for ourselves. For example, an effective response to many safety issues involves a number of different disciplines, including training, licensing, flight operations, maintenance, and aircraft design and certification. That is one of the reasons why Transport Canada has re-organized the Civil Aviation Directorate—to break down silos. As a result of this effort, all rule-making activities were pulled together into a single branch—Standards. This allows us to develop more effective safety solutions by ensuring a more holistic and comprehensive approach to program development and implementation.
In summary, I believe that an effective aviation safety program is built upon a clear understanding of roles and responsibilities; a risk-based approach; program development through collaboration with all stakeholders; and a holistic and comprehensive approach.
Finally, I look forward to meeting and working with you. As I have suggested, I find it useful to hear from all stakeholders to learn what are considered the challenges and opportunities that we face together. I firmly believe that it is only through meaningful dialogue and effective co-operation between stakeholders and regulators that we can build an effective, balanced and risk-based approach to aviation safety.
Aaron McCrorie Director, Standards Civil Aviation
Guest Editorial
Aaron McCrorie

4 Pre-Flight ASL 4/2012
COPA Corner: Can GPS Get You Lost?by Dale Nielsen. This article was originally published in the “Chock to Chock” column of the August 2007 issue of COPA Flight, and is reprinted with permission.
The answer is yes.Many of us have become very dependent on these little gadgets. They provide a lot of information and are very accurate. They can however, fail. They can lose satellite coverage and batteries in portable units can die.
One B.C. pilot on a flight from Vancouver to Nelson, B.C. had to fly low through the valleys due to cloud cover. He was unable to use his GPS as satellite coverage was sporadic throughout the flight. He didn’t get lost but he had to rely on map reading, at which he had become very rusty.
We should always be in a position to navigate by means other than GPS—such as by map, VHF omnidirectional range (VOR) or automatic direction finder (ADF). This means that we must always know where we are on a map, VFR or IFR.
When the GPS stops giving us information, the natural tendency is to play with it to try to get some of the GPS information back. While we are doing this, we are not paying attention to where we are. When we revert to map reading, nothing looks familiar.
A PA 28-160 Warrior was flying in the Yukon when his GPS stopped giving him information. He became disoriented while trying to locate his position on a map and started to run low on fuel. His radio transmissions were heard by a PA 31 Navajo pilot who relayed the call for help through the nearest flight service station (FSS).
The Navajo pilot also cancelled his IFR clearance and tried to locate the Warrior pilot. The Warrior pilot eventually found a highway and landed on it.
In Canada’s far north, airports can be a long way apart. Time spent searching for a position fix can deplete the fuel supply to where the destination can no longer be made. Highways and roads that may be suitable for landing an aircraft are also few and far between.
A C-172 pilot in southern Ontario neglected to carry spare batteries with him and became disoriented as to his position after his GPS lost power. He was able to transmit his distress to an FSS where the specialist gave him a Toronto area control centre (ACC) frequency. The Toronto area controller provided radar vectors to an airport for a safe landing.
When the GPS stops giving us information, the natural tendency is to play with it to try to get some of the GPS information back.
While we are doing this, we are not paying attention to where we are. When we revert to map reading, nothing looks familiar.
A PA 28-140 in northern Ontario lost satellite coverage for his GPS and became concerned as to his position. He was able to contact an FSS by radio and request a VHF direction finding (VHF DF) steer to the airport. He was asked to give the FSS specialist a 10 count so the specialist could home in on his radio signals with direction finding equipment and give him a heading to the airport. Not all FSSs and control towers have this equipment.
There have been enough GPS failures in IFR flight that many IFR pilots keep their VORs and ADFs tuned to the nearest VOR and non-directional beacon (NDB) frequencies so they can switch means of navigation quickly. It is a good practice for VFR pilots as well if VOR or ADF equipment is installed in their aircraft.
Pre-FlightCOPA Corner: Can GPS Get You Lost? .............................................................................................................................. page 4NAV CANADA Online Store Reduces Costs, Boosts Convenience and Safety ...................................................................... page 5Transporting Bulk Fuel in compliance with the Certificate of Airworthiness ........................................................................ page 6

ASL 4/2012 Pre-Flight 5
The VOR or ADF can be used to home or track directly to a VOR station or to an NDB. You can also use the VOR radial or NDB track from the station to help locate yourself on a map.
ADFs can be tuned into any AM radio station as well as NDBs. Local AM radio stations are often indicated on VFR navigation chart (VNC) maps.
If you need navigational assistance and you are unable to contact a flight information centre (FIC), FSS, control tower or ACC, climb as high as the weather allows and keep trying. You can select 7700 on your transponder and monitor 121.5 and someone will contact you. Make some calls for assistance on 126.7 as well, aircraft flying in the vicinity may hear your transmission and relay your request for assistance.
If the worst happens and you become “uncertain of your position” (it would never do to admit you were lost), note the time you last knew exactly where you were. Estimate the distance you would have flown in the time since then and draw an arc on your map across your approximate track. You should be somewhere close to this arc.
Look on the map for readily identifiable features and then look outside to locate one (watch, map, ground). If you try to look at the ground first for a feature and then the map, you won’t know where to look on the map as you don’t know where you are and you will just confuse yourself further.
None of us want to admit to being disoriented or lost, but the sooner we ask for help, the more fuel we will have to get to a safe place to land. FIC specialists, FSS specialists, tower controllers and ACC controllers are there to help. Use them if you need them.
You are never lost if you don’t care where you are. Most of us though, do care.
Dale Nielsen is an ex-Armed Forces pilot, air charter and flying school owner/operator, corporate pilot, bush pilot, medevac pilot, airline pilot and aerial photography pilot. He lives in Abbotsford, B.C., and currently manages a small airline and teaches part-time for a local aviation/university program. Nielsen is also the author of eight flight training manuals published by Canuck West Holdings. To know more about COPA, visit www.copanational.org.
NAV CANADA Online Store Reduces Costs, Boosts Convenience and Safetyby Janelle Denton, Manager, Customer Contact Centre and Aeronautical Publications, NAV CANADA
NAV CANADA is now offering a fast and easy way for pilots to purchase the essential documents they need to fly safely to their destinations.
The NAV CANADA Online Store went operational in early 2011. Today, customers can either order or download a range of NAV CANADA aeronautical publications with just a few clicks of the mouse.
With 7 000 active customer accounts, NAV CANADA has seen steady demand for its publications over the Web. More recently, with the added option of downloading some of its key publications in PDF format, the company is anticipating significant growth in the number of customers taking advantage of this service.
Available for download, for example, are all seven volumes of the Canada Air Pilot (CAP), the Restricted Canada Air Pilot (RCAP) and the Canada Water Aerodrome Supplement (WAS). Customers can purchase these products and then print their required pages. These products are official aeronautical publications and are suitable for air navigation purposes.
To meet customer demand, NAV CANADA plans to increase the number of titles available for download in the near future. One attraction is the cost. Downloaded products are priced 20 percent less than their paper equivalents. Customers also save on shipping and handling costs.
To date, the Web-based store has nearly 1 000 registered users, and about 20 percent of all NAV CANADA publications are now ordered online. The company believes that number will eventually grow to 75 percent of all orders.
Improving customer service may be the raison d’être of the Online Store, but not to be discounted is the safety benefit.
By providing immediate access to downloadable aeronautical publications, pilots planning their flights can obtain the most up-to-date information in a timely manner. Moreover, the publications are made available a full 10 days prior to their effective date.
Also available at the Online Store, at no additional charge, are the CAP General pages and a CAP Changes page that allows customers to quickly identify all the aeronautical changes made from one publication cycle to the next.
Before accessing the Online Store, all NAV CANADA customers—including those with existing accounts—must first register to obtain a User ID and password. Once registered, customers can order all the publications they need from the convenience of their desktop or laptop computer. To maximize service, ordering these publications by phone or fax will remain an option.

6 Pre-Flight ASL 4/2012
Over the years, NAV CANADA has invested in an aeronautical database system that has strengthened its focus on managing aeronautical data, while providing a digital production platform for documents and charts, and enabling more flexible product delivery.
This includes a national inventory of more than 20 publications and chart titles, including over 1 700 instrument procedures
and data for 1 800 airports across Canada, as well as charts, maps, CDs, books and other documents.
To access the NAV CANADA Online Store go to: http://products.navcanada.ca.
If you have any questions about ordering aeronautical publications online, please contact AEROPUBS at 1-866-731-PUBS (7827).
Transporting Bulk Fuel in compliance with the Certificate of Airworthinessby Micheline Paquette and Roger Lessard, Compliance and Response Branch, Transport Dangerous Goods, Transport Canada
The following article is meant to clarify the requirements of the Transportation of Dangerous Goods (TDG) Regulations for transporting dangerous goods in large means of containment by aircraft.
The TDG Act and Regulations contain requirements for handling, offering for transport or transporting dangerous goods to, from or within Canada for all modes of transport (i.e. road, rail, marine and air). The TDG Act and Regulations do not permit the handling, offering for transport or transport of dangerous goods in large means of containment by aircraft unless an exemption applies. A large means of containment is defined as any container with a capacity greater than 450 litres.
Section 12.9 of the TDG Regulations, Limited Access, provides three exemptions that only apply to Class 3 Flammable Liquids:
• a tank, a container or an apparatus that is an integral part of the aircraft or that is attached to the aircraft in accordance with the Certificate of Airworthiness issued under the Canadian Aviation Regulations;
• a cylindrical collapsible rubber drum that is transported in or suspended from an aircraft and that is constructed, tested, inspected and used in accordance with MIL-D-23119G; or
• a collapsible fabric tank that is transported suspended from a helicopter and that is constructed of material and seamed in accordance with MIL-T-52983G.
Section 12.12, Aerial Work, provides similar exemptions for all classes of dangerous goods that are essential for aerial work activities.
In both cases, a designated airworthiness representative or an aircraft certification engineer at Transport Canada must issue a Supplemental Type Certificate (STC) or a Limited Supplemental Type Certificate (LSTC) for each aircraft in order for a tank, a container or an apparatus to be considered an integral part of the aircraft or to be attached to the aircraft.
When compliance with the TDG Regulations is impossible or impractical, an operator may apply for an Equivalency Certificate from the TDG Directorate in order to handle, offer for transport, or transport dangerous goods in a manner that will provide a level of safety at least equivalent to that provided through compliance with the TDG Act and Regulations.
Air operators may not load and secure a tank, container or apparatus to the aircraft floor without a STC, a LSTC or an Equivalency Certificate.
The International Civil Aviation Organization (ICAO) has announced updates to the content of the internationally utilised flight plan with a worldwide implementation date of November 15, 2012. For details visit: http://onboard-abord.ca/flight-plan-2012/.

ASL 4/2012 Flight Operations 7
Single-Pilot Resource Management (SRM) Competenciesby Dr. Suzanne Kearns
As a follow-up to the article written by Alexander Burton, entitled “Single-Pilot Resource Management (SRM)” and published in Aviation Safety Letter (ASL) 3/2012, this article discusses SRM competencies. As mentioned in the previous article, aviation has entered a curious time when the aircraft we fly are statistically safer than the pilots who fly them. The reality is that, following a mechanically caused aviation accident, it is possible to identify a faulty component and then fix the flaw on all operational aircraft. Following an accident caused by pilot error, it is relatively complex to identify why the human being made the mistake and then “fix” the flaw in all operational pilots!
However, that is the ultimate goal of SRM—to understand the characteristics and limitations of the human mind and body and how these factors can lead to poor performance and, eventually, accidents. SRM training is based on a large body of work gathered by aviation safety researchers and accident investigators.
Although it can be hard on a pilot’s ego to be reminded of their limitations, it is not something to be embarrassed by. Think of it this way: everyone knows that it would be unreasonable if a chief pilot asked a new hire to go out to the ramp, pick up an aircraft, and carry it inside the hangar. Clearly, a pilot would not have enough physical strength to carry out this ridiculous request. It is easy to understand human physical limitations.
However, the same chief pilot may ask a new-hire pilot to complete a trip that would require the pilot to stay awake for a 24-hr period. This situation would cause fatigue, which could result in increases in pilot errors. Yet, when it comes to mental limitations such as fatigue, we often expect a pilot to tough it out. The reality is that human beings are limited in their ability to stay awake and alert for an extended period
of time. This limitation is a natural part of being human. It is important to recognize and understand these limitations, just as we understand the limitations of our physical strength.
SRM competencies are elements of pilot performance that are impacted by natural human limitations. Broadly, some SRM competencies include situational awareness, workload management, fatigue management, and decision making. It is helpful to understand these factors, as they can help us make safer choices in the air and on the ground—which is the goal of SRM training.
Situational awareness Situational awareness refers to a pilot’s ability to 1) perceive things in their environment, 2) understand their meaning, and 3) predict how they will impact the flight. For example, was the pilot aware of the high terrain? Did they understand how dangerous it was? Were they able to predict a collision with terrain?
Situational awareness can be thought of as a pilot’s mental picture of their environment. Researchers assess a pilot’s situational awareness in a simulator by pausing mid-flight, asking the pilot to close their eyes, and having them describe elements of their environment by memory. This can be replicated during your flights (with a co-pilot, of course) if you close your eyes and challenge yourself to recall as many details about your environment as possible.
Unfortunately, pilots sometimes lose situational awareness. This can lead to a specific type of accident called controlled flight into terrain (CFIT) (pronounced “see-fit”).
Flight OperationsSingle-Pilot Resource Management (SRM) Competencies ................................................................................................... page 7Scenario-Based CRM Case Study: Stall Warning Device Event ........................................................................................ page 10The Flight Safety Foundation’s ALAR Tool Kit ................................................................................................................. page 15Answers to the 2012 Self-Paced Study Program ................................................................................................................ page 16
Focus on CRMThe following two articles continue our campaign to promote Crew Resource Management (CRM) concepts and principles, in the overall context of extending contemporary CRM Training to all commercial pilots. The first one, entitled “Single-Pilot Resource Management (SRM) Competencies” is from Dr. Suzanne Kearns, an assistant professor teaching Commercial Aviation Management at the University of Western Ontario. The second one is a typical scenario-based airline case study for CRM training programs.

8 Flight Operations ASL 4/2012
A CFIT accident occurs when a pilot unintentionally flies a perfectly good airplane into the ground. Unfortunately, CFIT accounts for nearly 20 percent of all general aviation accidents.
How can a pilot lose situational awareness? Unlike a computer, human memory has a limited capacity. You can only remember a certain number of things in your environment before items begin to slip by unnoticed. Generally, researchers suggest that humans can remember approximately seven, plus or minus two, chunks of information. However, under high-stress conditions, this capacity shrinks to about two or three chunks of information.
Everyone has experienced the frustration of forgetting something. Most of the time, the impact of this slip is minor. However, when a pilot is forced to make a snap decision and they don’t have an accurate mental picture of their environment, it can lead to an accident such as CFIT. When flying, remember that your memory is limited. If you encounter a stressful situation or get behind the aircraft, your ability to maintain a mental picture of your environment will be reduced. Don’t be shy about asking for help, informing air traffic control (ATC) about your situation, or climbing to a higher altitude until you mentally catch up with the aircraft.
Workload managementThe amount of work a person can manage at a given time is influenced by another human characteristic that has a limited capacity: attention. Similar to memory, the number of things we can pay attention to is limited. You can think of workload capacity as a bucket—it can only hold so much before it begins to overflow. With your mental bucket, as you begin to take on more tasks, the bucket fills. Eventually your mental bucket will reach capacity and then spill over. When you have exceeded your capacity, you will begin to make mistakes. What is less understood is where you will make those mistakes—though it is expected that you will make mistakes on the tasks you place at the lowest priority.
For this reason, when teaching pilots how to manage their mental workload, we introduce prioritization strategies. The best-known strategy is known as ANCS, which stands for aviate, navigate, communicate, and manage systems. This strategy is meant to serve as a reminder, when your mental bucket is full, to focus your attention on flying the aircraft. It doesn’t matter if you precisely manage the onboard systems if you fail to fly the aircraft safely!
Fatigue managementThe nature of aviation is that pilots are prone to sleep disruptions from jet lag, long duty days, or a lack of quality sleep while on the road. However, only relatively recently has the industry come to appreciate the risk associated with fatigue. As an example, the following was reported anonymously to the U.S. National Aeronautics and Space Administration’s (NASA) Aviation Safety Reporting System (ASRS):
In March of 2004, the captain and first officer of an Airbus 319 headed to the Denver International Airport both fell asleep. The pilot reported that he flew a red-eye (overnight) flight, after two previous red-eye flights, and after only a one-hour break, immediately started the seven-hour flight back to Denver. In the last 45 min of the flight, he fell asleep and so did the first officer. He missed all of the calls from ATC, crossing a navigational intersection 16 000 ft too high and 350 NM/h too fast. The captain eventually woke up, although he wasn’t sure what awoke him, and heard frantic calls from ATC. He then woke up the first officer and they were able to land the aircraft without further incident.
Although falling asleep while flying is an extreme example, fatigue imposes other threats. Researchers have identified that, when fatigued, people have a greater tolerance for risk. For example, fatigued drivers stop checking their blind spot—not because they have forgotten how to properly drive a car, but because fatigue is causing them to accept this risk. It is expected that, when piloting an aircraft, fatigue will result in similar corner cutting, which leads to increased errors.
Overall, humans are naturally effort conserving. This means that it is in our nature to try and accomplish a task with as little effort as possible. When we are fatigued, this is more pronounced and can lead to very dangerous behaviour. In fact, fatigue can impair a person’s performance similar to alcohol intoxication. Once a person has been awake for 18–24 hr, their
You can think of workload capacity as a bucket—it can only hold so much before it begins to overflow.

ASL 4/2012 Flight Operations 9
performance may be impaired similar to a blood alcohol concentration (BAC) of 0.1 percent. This BAC would be experienced if an average-sized man drank six beers in an hour.
Understanding that fatigue is directly linked to an increase in pilot error is important. This means that no one can choose to tough it out and avoid the fatigue-related dip in performance. It is important to be aware of your level of fatigue and appreciate that it increases risk, so that you can make informed decisions about when it is safe for you to fly.
Decision makingEven the best-trained pilots are prone to making poor decisions in the heat of the moment. This SRM skill focuses on strategies to help pilots make the most effective decisions in the cockpit. Everyone likes to think of themselves as a rational decision maker. However, this is not always true.
For example, consider being in a checkout line at a store, waiting to purchase a package of computer paper for $11. While in line, the person behind you says that there is a big sale at an office store 15 min away where you can get the same package of paper for only $4. Would you drive the 15 min to save the money? Most people in this situation would choose to leave and purchase the more affordable pack of paper.
In another situation, if you were lined up in a store to purchase a new suit for $590 and a fellow shopper said you could travel to another suit store 15 min away and buy the suit for $583, would you leave the store? Most people would choose to stay and buy the $590 suit.
Consider for a moment if this decision is logical. In either case, you would be saving $7. Logically, you are giving 15 min of your time for $7 in both situations. However, when $7 is just a small piece of a large purchase, people value the dollars less. Another example of this is during negotiations to purchase a house, where people who would otherwise pinch pennies are easily willing to barter with thousands of dollars without blinking an eye.
In an aviation context, it is important to understand human bias in decision making as most decisions are not based on a logical weighting of all options—as we would like to believe. Similar to the $7 example, the amount of risk a pilot is willing to accept varies depending on their situation and environment. For example, your decision of whether or not to report a fellow pilot skipping their walk-around may vary depending on whether you are used to a flight school with a perfect safety record and an open safety culture or a school that continually
cuts safety corners. Human decisions are heavily influenced by environment and past experiences.
In addition, human beings anchor on previous decisions. This means that, after we have made one decision, it becomes much easier for us to make the same decision in the future. If a student pilot chose to complete training at the flight school with poor safety standards, it would be easier for them to accept low levels of safety throughout their entire professional career. Research suggests that a single decision can impact decision making years in the future. It is important that we critically evaluate our decisions and consider how our habits were formed in the first place—particularly in relation to safety.
The following is an example of bad decision making in action:
A story was in the media a while ago about a pilot who was flying his Piper Tri-Pacer from the Modesto Airport with a passenger who had never flown in an airplane before. Unfortunately, he had to make an emergency landing due to smoke coming out of the engine.
After the pilot performed an inspection, he determined that a problematic hose clamp was to blame. He went to his local Wal-Mart to get a replacement, and then “fixed” the problem himself. No mechanic was called in to check the work.
The pilot took off again and, unfortunately, the cockpit began to fill with smoke a second time. An emergency was declared and the pilot executed a second landing. When the pilot investigated, he determined that the
hose had a hole in it. He replaced the hose and then took off a third time.
Not surprisingly, this time the engine caught fire and the pilot was forced to make a third emergency landing. The aircraft was damaged by the hard landing, and the subsequent fire destroyed the aircraft. The poor passenger was so frightened that, during the landing, she threw herself from the aircraft onto the runway and had to be taken to the hospital.
This example of bad decision making is rather ridiculous. It is easy for us to consider the pilot crazy and dismiss the implications of this event. However, if we knew more about the pilot’s past experiences, these poor decisions were probably linked to those experiences. For example, if fellow pilots in his club exhibited similar decision making, or if he had acted in a similar way in the past without incident, it could have led to this situation.
Ultimately, it is important to understand the biases that influence our decision making and to critically consider whether or not our choices are based on logic.
Understanding that fatigue is directly linked to an increase in pilot error is important.

10 Flight Operations ASL 4/2012
Improving SRM skillsAfter exploring examples of SRM, the question becomes how these skills can be improved. Traditionally, the aviation industry has relied on pilots naturally developing SRM skills by spending time building hours in the real world. The perspective is that, while building experience, pilots will be exposed to and manage enough threats and errors that they will naturally develop SRM skills.
However, there is a major challenge with the traditional approach to building SRM skills. With the predicted pilot shortage on the horizon, future pilots will begin to progress into senior positions more quickly, with less time building skills naturally during the hours-building phase of their career.
To compensate for this, the burden will fall on aviation training organizations to identify methods of improving SRM skills within a training environment. Many airlines around the world develop safety training by using an observational strategy, called a line operations safety audit (LOSA). Within a LOSA, a company gathers data by hiring a trained observer pilot to sit in the jump seat behind crews and write down all the threats and errors that are faced. However, it can be difficult or impossible to conduct a LOSA within general aviation operations as the cost would be prohibitive, operations vary significantly, and many aircraft lack jump seats altogether.
However, there is a more convenient option—hangar talk stories. Stories are a powerful medium for learning. Storytelling is the fundamental way knowledge has been passed down from generation to generation—far preceding humans’ ability to produce written word. Research has demonstrated that stories are an extremely popular method of conveying information across all cultures.
We often take what people learn from stories for granted because it is something that happens naturally outside of a classroom. However, junior pilots can develop SRM skills by listening to the experiences of senior pilots. If you listen closely when a senior pilot is chatting about a situation they faced, which challenged their skills and required them to think creatively to maintain flight safety, you may realize that they utilized SRM skills. In a recent study, we examined 130 hangar talk stories. Pilots were asked to describe a situation they encountered which challenged them, and required them to think outside the box to maintain flight safety. After analysis, it was revealed that 39 percent of the stories involved decision-making skills, 26 percent communication skills, 20 percent situational awareness, and 15 percent task-management skills.
General aviation companies can gather this data in-house through simple “hangar talk surveys” that ask pilots to share their experiences. The results of hangar talk surveys can be used to create scenario-based exercises within a simulator that target specific SRM skills. Through this approach, it may be possible to accelerate the development of SRM skills without having to gather thousands of flight hours in the real world and lead to SRM training becoming a standard component of initial and recurrent pilot training.
Dr. Suzanne Kearns is an assistant professor teaching Commercial Aviation Management at the University of Western Ontario. Dr. Kearns is also a commercial airplane and helicopter pilot and an aviation safety researcher. Her most recent project is the development of a pilot safety app called “m-Safety” which is available through iTunes. She can be reached at [email protected].
Scenario-Based CRM Case Study: Stall Warning Device EventThe following event, which occurred in Australia in March 2011, was recommended as an excellent case study for scenario-based crew resource management (CRM) training programs. Operators are therefore encouraged to consider it for that purpose. The Aviation Safety Letter (ASL) will include more of these examples, as we strongly believe the discussions generated by this training method yield great benefits for the crews involved. This report has been slightly shortened and de-identified for use in the ASL. Click on Report AO-2011-036 to read it in full.
SummaryOn March 1, 2011, a Bombardier DHC-8-315 was conducting a regular public transport flight from Tamworth Airport to Sydney Airport, New South Wales, Australia. The crew were conducting a Sydney Runway 16L area navigation global navigation satellite system [RNAV (GNSS)] approach in vertical speed (VS) mode. The aircraft’s stick shaker stall warning was activated at about the final approach fix (FAF). The crew continued the approach and landed on Runway 16L.
The stick shaker activated at a speed 10 kt higher than was normal for the conditions. The stall warning system had computed a potential stall on the incorrect basis that the
aircraft was in icing conditions. The use of VS mode as part of a line-training exercise for the first officer meant that the crew had to make various changes to the aircraft’s rate of descent to maintain a normal approach profile.
On a number of occasions during the approach, the autopilot pitched the aircraft nose up to capture an assigned altitude set by the pilot flying. The last recorded altitude capture occurred at about the FAF, which coincided with the aircraft not being configured, the propeller control levers being at maximum RPM, and the power levers at a low power setting. This resulted in a continued speed reduction in the lead-up to the stick shaker activation.

ASL 4/2012 Flight Operations 11
Each factor that contributed to the occurrence resulted from individual actions or was specific to the occurrence. The Australian Transport Safety Bureau (ATSB) is satisfied that none of these safety factors indicate a need for systemic action to change existing risk controls. Nevertheless, the operator undertook a number of safety actions to minimize the risk of a recurrence.
In addition, the occurrence highlights the importance of effective CRM and of the option of conducting a go-around should there be any doubt as to the safety of the aircraft.Transport Canada, which regulates the aircraft manufacturer, advised that it would publish a summary of this occurrence and recommend that operators consider using it in their scenario-based CRM training programs.
Factual information Sequence of events At about 18:10 local time on March 1, 2011, the flight crew conducted the approach to land at Sydney using the Runway 16L RNAV (GNSS) approach. The instrument landing system (ILS) approach that was normally used for an approach and landing on this runway was not operative at the time. The captain was the pilot not flying (PNF), and the first officer was the pilot flying (PF).
Both pilots stated that an approach brief was completed and that it included an overview of the approach chart procedure, the missed approach procedure and the identification of any additional restrictions or requirements. The approach was conducted with the autopilot engaged and using the flight director in VS mode, rather than the vertical navigation (VNAV) mode. The VNAV mode uses a higher level of automation than the VS mode, which maintains a constant descent profile to an assigned altitude entered by the crew1. When the assigned altitude is reached, the aircraft flight director and autopilot automatically levels the aircraft off unless another, lower altitude has already been entered.
The flight crew reported that the approach was commenced in instrument meteorological conditions (IMC) but as it progressed, the conditions became visual and the approach was operated in visual meteorological conditions (VMC) until landing.
The captain stated that, approaching the initial approach fix (IAF), the crew had started to feel some time pressure to complete all of the necessary checklist items and actions for 1 The VNAV mode utilizes the aircraft’s flight management system to
fly a pre-determined profile which conforms to the published approach procedure, while the VS mode maintains a constant rate of descent to an assigned altitude entered by the crew.
the approach. It was at this point that the captain identified that the aircraft was no longer in icing conditions and so turned off the ice protection switch, without informing the first officer. During this action, the captain did not turn off the increased reference speed switch. That switch is selected ON for flight in icing conditions and sets the stall warning to activate at a lower angle of attack (thus raising the speed at which the stall warning activates).
The captain reported initially being high on profile during the approach; however, by the ‘SYDLI’ intermediate fix (Figure 1), the aircraft was back on profile but, as a result, needed to slow down. In response, the captain selected the propeller control levers to maximum RPM, which changed the pitch of the propellers and effected a significant slowing of the aircraft. In addition, the first officer reported that
the power levers were retarded to flight idle from about the SYDLI position fix until the FAF. The use of maximum RPM at this point in the approach, rather than at the FAF, was not considered normal practice by the operator.
The first officer reported that, despite approaching the FAF, they had not yet configured the aircraft for landing with flaps extended or the landing gear down. In contrast, the captain stated that the landing gear was down prior to the FAF but the flaps were not extended.
The first officer adjusted the assigned altitude in the flight director system during the approach; however, the captain indicated that these adjustments were not happening fast enough to allow a continuous descent, and that the autopilot kept capturing the assigned altitude and levelling off.
Prior to the FAF, the captain noticed the airspeed was decreasing through 130 kt and called “airspeed”. The recorded flight data showed that at about this time the autopilot commenced pitching the aircraft up in anticipation of capturing the preselected altitude set by the first officer. This further reduced the airspeed to around 114 kt, the stick shaker activated, and the autopilot disconnected.
The captain called “stick shaker”, took over as PF and momentarily advanced the power levers before continuing the descent. The first officer reported assuming the role of PNF and conducted the checklist items in preparation for landing, including selecting flaps to 15°.
The aircraft continued on the approach and the crew reported they were stable by 500 ft, in accordance with the operator’s stable approach procedure. They then conducted a landing on Runway 16L. After landing, the first officer noticed the increased reference speed switch was still in the ON position.
It was at this point that the captain identified that the aircraft was no longer in icing conditions and so turned off the ice protection switch, without informing the first officer. During this action, the captain did not turn off the increased
reference speed switch.

12 Flight Operations ASL 4/2012
PilotsBoth the captain and first officer were properly licensed and qualified for the flight. The captain had several thousand hours on type, while the first officer had a total of 3 250 hours, with about 26 on type. Those hours were line training and had occurred within the last two weeks. The training notes from the first officer’s endorsement indicated there had been a recurring issue with speed, descent and power management during approaches, and those exercises were successfully repeated before undertaking the next training session. The first officer satisfactorily completed the endorsement training program.
As part of the company’s training program, all pilots initially completed CRM as well as threat and error management (TEM) training as part of the induction program. CRM and TEM training then formed part of flight crew’s annual recurrent training. CRM is a strategy for pilots to use all available resources effectively (including other crew, air traffic control [ATC], equipment and information)2.
2 Salas E., Wilson, K.A. & Burke C.S (2006). “Does Crew Resource Management Training Work? An Update, an Extension, and Some Critical Needs”. Human Factors, 48(2) 392-412.
Approach procedures The operator’s standard operating procedures (SOPs) required that, when conducting an instrument approach, the relevant aircraft speed and configuration should be accomplished prior to a defined position in the approach. For an RNAV (GNSS)approach, the crew was required to achieve a speed reduction to 180 kt by the IAF. From the IAF, the aircraft was to be slowed further to a speed below 163 kt and then to 150 kt, with the PF expected to achieve a target speed of 120 to 130 kt by the FAF.
Before the aircraft passed the FAF, the operator’s SOPs required that the PF would request the PNF to select the gear down, set the flaps to 15° and initiate the landing checklist. The crew reported that the aircraft’s speed was not stable and the configuration was not finalized prior to reaching the FAF.
At the FAF, the propeller control levers were to be advanced to provide maximum RPM, the landing checklist was to be completed and the speed reduced to Vref
3+5 to Vref+20 kt by 500 ft above ground level (AGL). If these conditions were not met by 500 ft AGL, a go-around was to be conducted. Additionally, according to the operator’s flight administration manual (FAM):
Flight crew are encouraged to perform a missed approach whenever any doubt exists as to the safe continuation of an approach and landing.
Previous stick shaker occurrences prompted the operator to issue a safety alert and safety investigation bulletins to all operating crew. These notices highlighted the importance of crews following SOPs and monitoring all stages of the approach. They also highlighted the need for crews to adhere to the SOPs for ceasing the use of all ice protection systems after exiting icing conditions. In addition, the safety alert detailed strategies for profile management and aids for maintaining situational awareness.
With regard to the use of automation, the company’s DHC-8 flight crew operating manual (FCOM) stated:
Use of the autopilot is encouraged for all RNAV (GNSS) approaches to reduce workload...
The autopilot can be used with the flight director in either VNAV or VS mode for an RNAV approach.
Stall warning system Based on the aircraft’s weight, and using data available in the operator’s FCOM, the flap 15° stalling speed of the aircraft at the time of the occurrence was 81 kt. In contrast, the flap 0° stalling speed was 99 kt.
3 Vref: Reference speed that is commonly used to determine an aircraft’s approach speed. Vref is Vs multiplied by a factor of 1.3. Vs is the minimum indicated airspeed at which the airplane exhibits the characteristics of an aerodynamic stall.
Figure 1.

ASL 4/2012 Flight Operations 13
The aircraft’s stall warning system consisted of two stall warning computers, an angle of attack (AOA) vane on each side of the forward fuselage, a stick shaker on each control column, and a stick push actuator.
The aircraft’s two stall warning computers received AOA data from the respective AOA vanes, as well as true airspeed, flap angle and pitch rate information. The computers used that information to determine a compensated angle which, if greater than the stall warning threshold angle, would activate the stick shaker. That activation occurred at a speed of 6 to 8 kt above the computed stall speed.
If action was not taken by the flight crew in response to the stick shaker, and an aerodynamic stall was encountered, the stall warning computer would activate a stick push actuator to drive the control column forward. This would decrease the aircraft’s AOA to aid in the recovery from the stall.
According to the operator’s SOPs, the recovery action following a stick shaker was to simultaneously:
• Call “stick shaker”; • Advance power levers to within 10 percent of maximum
take-off power (MTOP), then adjust for maximum power; • Select flap 15 if flap 35 is extended; • Gear up with positive rate of climb; • Select flap zero when indicated airspeed (IAS) is above
flap retraction speed. The aircraft manufacturer advised that recent updates to the aircraft flight manual (AFM) include an immediate reduction in pitch attitude in response to a stick shaker activation, as well as stating that no configuration changes should be made.
Human factors The first officer reported that, after passing the IAF, there was an increase in workload, predominantly due to conducting an unfamiliar approach as PF and commencing the approach in IMC. In addition, the approach was being conducted in VS mode, which the first officer had reportedly not used for an approach during line flying. Use of the VS mode required more mental calculations and data entry inputs by the PF to meet the descent profile targets than would be necessary using VNAV mode (where data entry is done before descent and the autopilot flies the required descent path).
The captain reported that the use of VS mode was to increase the first officer’s awareness of ground speed and vertical speed. The aim was to increase the first officer’s skill at maintaining a vertical profile without the use of VNAV mode.
The captain also stated that, as a result of previous flights with the first officer, he anticipated an increase in his own workload due to the need to monitor the approach and the actions of the first officer. Both flight crew reported that the clearance to conduct an RNAV (GNSS) approach caught them by surprise as they were expecting another approach type.They both commented that this increased the time pressure, as they had to re-brief unexpectedly for the RNAV (GNSS) approach.
The first officer and captain both reported inter-personal communication issues with the other pilot prior to the commencement of the approach. The first officer reported not feeling comfortable speaking up in the line-training environment. As a result, the first officer had been scheduled to fly with another line-training captain, which was to take effect in the days following the occurrence.
Both of the flight crew also reported issues during the approach. The use of non-standard phraseologies by the first officer, and the fact that the captain was not aware the first officer was feeling overloaded, affected the conduct of the approach.
When learning a new skill, individuals move from what is known as knowledge-based performance to skill-based performance4. Skill-based actions are possible once an individual is very familiar with a task and they have repeated it to an extent that the actions become predominantly automatic and do not need conscious oversight. Knowledge-based performance is typical during unfamiliar or novel situations and, by contrast to skill-based performance, requires more conscious oversight and typically uses greater mental resources, increasing mental workload.
Analysis The stick shaker activation was because the aircraft’s speed had slowed to the computed stall reference speed. In this case, due to the increased reference speed switch being left on, the stick shaker activated 10 kt higher than normal for the aircraft’s configuration. The aircraft was not configured in accordance with the operator’s SOPs for the approach. This also contributed to the stick shaker activating at a higher reference speed than if the aircraft was appropriately configured.
In addition, the target airspeed range of 120 to 130 kt for this stage of flight was not met and the action of the auto flight system’s altitude capture feature, which raised the aircraft’s nose to maintain altitude, resulted in a further decrease in airspeed. This speed reduction also contributed to the stick shaker activating.
4 Rasmussen, J. (1983). “Skills, Rules, and Knowledge; Signals, Signs, and Symbols, and Other Distinctions in Human Performance Models”. IEEE Transactions on Systems, Man & Cybernetics, SMC; 13(3).

14 Flight Operations ASL 4/2012
Following the stick shaker activation at around the FAF, the aircraft was not configured for landing and the speed was not stable. According to the operator’s SOPs, if the safe continuation of the flight is in doubt, a go-around is to be conducted. Given a stick shaker activation is an indicator of an impending stall, which could affect the safety of the flight, a lower risk option for the crew was to have conducted a go-around.
The first officer’s training in the simulator had identified performance issues with speed, descent and power management during the approach and landing phase. While the first officer was successfully re-trained in the simulator during the endorsement, some of these issues reappeared during the approach.
The use of VS mode for the approach was a deliberate decision by the captain to make the first officer consider the vertical profile and power management. While this technique had reportedly helped other first officers in this situation, it would appear that for this first officer’s level of training and experience, the use of VS mode was not appropriate and unnecessarily increased the workload of both flight crew.
The flight crew reported feeling time pressured during the approach, which increased their workload. As a result, the captain turned off the ice protection system without informing the first officer. While this action was done as a result of the captain identifying and completing a required action, it was not conducive to a shared understanding of the system state by both crew. There is a need for clarity in operating roles and close adherence to SOPs during normal operations and this is particularly important in the line-training environment, given the first officer’s level of experience.
Despite the mismanagement of the speed and power during the approach by the first officer, which necessitated the selection of maximum RPM by the captain in order to slow down, the captain did not take over prior to the stick shaker activation, nor was a go-around initiated when the activation occurred. Although the decision of the captain to continue with the approach did not result in a further incident, the lower risk option is for flight crew to discontinue an approach or landing if at any stage there is any doubt as to the safe continuation of the flight.
The inter-personal communication issues reported by both crew appears to have affected their interactions and the learning opportunities for the first officer in the line-training environment. This was supported by the fact that despite having completed CRM training, the first officer reported feeling unable to report feeling overloaded to the captain at the beginning of the approach. The first officer’s performance during the approach may have affected the captain’s decision to continue following
the stick shaker activation, as conducting a missed approach or go-around with the first officer overloaded may have further increased the workload of both flight crew.
The reported workload of the first officer during the approach, combined with the level of unfamiliarity of both the approach and the aircraft’s automation, is typical of knowledge-based performance. That is, the first officer’s performance was
indicative of increased mental effort and workload, as opposed to the predominantly automatic actions used when conducting a highly familiar task.
As set out below, the investigation identified a number of factors that contributed to the occurrence. Each resulted from individual actions or was specific to the occurrence. The ATSB has assessed each of these safety factors and is satisfied that none of them
indicated a need for organizational or systemic action to change existing risk controls. However, the investigation did highlight the importance of effective CRM and of the option of conducting a go-around should there be any doubt as to the safety of the aircraft.
Findings The ATSB issued the following findings:
Contributing safety factors • The stick shaker system activated during the approach as a
result of the increased reference speed switch being in the ON position, the associated computed reference speed being reached, and the aircraft not being configured in accordance with SOPs.
• A lack of communication and ineffective CRM between the flight crew and non-adherence to the operator’s SOPs adversely affected crew actions and coordination.
• Due to time pressure, inadequate CRM and the increased workload of both flight crew, the RNAV approach was not flown in accordance with SOPs.
Other safety factors • Despite being aware that at the FAF the aircraft was not
appropriately configured, and the resulting stick shaker activation, the crew did not initiate a go-around/missed approach as recommended by the operator’s guidance material.
• The conduct of the approach in VS mode rather than VNAV mode increased the workload of the first officer and captain.
Safety action Operator The operator has advised that, as a result of this incident the following action was taken:
Although the decision of the captain to continue with the approach did not result in a further incident, the lower risk option is for flight crew
to discontinue an approach or landing if at any stage there is any doubt as to the safe continuation of the flight.

ASL 4/2012 Flight Operations 15
• Relevant sections of the training and checking manual have been reviewed and will, subject to Civil Aviation Safety Authority approval, be revised as a result of this incident.
• The aircraft mechanical checklist was amended to include an item known as “ice protection” to confirm the status of the ice protection system.
• A procedure was implemented to identify and heighten flight crew awareness of the minimum speed for the environmental and aircraft configuration state.
• The Standards Department and Procedures Review Group conducted a review of approach workload and submitted the findings to the Flight Standards Review Group. These included better clarity and role definitions within documented
procedures; and expanded timing and sequencing procedures to aid in management during high workload periods.
• A group/industry workshop forum was organized to share experiences and best practices in regard to situational awareness on the flight deck. The workshop identified additional human factors competencies that the operator intends to incorporate into its training program.
Transport Canada Transport Canada advised that given its current focus on contemporary CRM training for all commercial pilots, once the final report has been released, it will publish a summary of the occurrence in the ASL, with a recommendation for operators to consider using it in their scenario-based CRM training programs.
The Flight Safety Foundation’s ALAR Tool KitThe aim of this article is to build awareness of the Flight Safety Foundation (FSF) Approach and Landing Accident Reduction (ALAR) Task Force recommendations, and the associated FSF ALAR Tool Kit, and to encourage its use by Canadian operators and pilots.
Background on the FSF ALAR Task Force The FSF created the “FSF ALAR Task Force” in 1996 as another phase of its controlled flight into terrain (CFIT) accident reduction initiatives, launched in the early 1990s. The task force final working group reports were presented in November 1998 through a 288-page special issue of the FSF Flight Safety Digest1, at the joint meeting of the FSF 51st International Air Safety Seminar, the International Federation of Airworthiness 25th International Conference, and the International Air Transport Association (IATA), in Cape Town, South Africa. The task force issued detailed recommendations targeting the reduction and prevention of the approach and landing accidents (ALAs). The FSF ALAR Task Force recommendations have been recognized internationally as practical tools for mitigating the risks of ALAs.
Further to those recommendations, the FSF ALAR Tool Kit was developed and distributed by the FSF as an aid to education and training, and as a resource that could be used by a variety of aviation professionals in company management, flight operations and air traffic control. The tool kit, which was updated in 2010, consists of a multimedia resource on a compact disc (CD), and contains the report of the FSF ALAR Task Force, conclusions and recommendations, the FSF ALAR Briefing Notes, videos, presentations, hazard checklists, and, lastly, other documentary notes and products designed to prevent ALAs, the leading causes of fatalities in commercial aviation.
1 Special Issue of the FSF Flight Safety Digest, “Killers in Aviation: FSF Task Force Presents Facts About Approach-and-landing and Controlled-flight-into-terrain (CFIT) Accidents”. November-December 1998 / January-February 1999.
Fundamental components of the tool kit are the 33 FSF ALAR Briefing Notes. They were produced to help prevent ALAs, including those involving CFIT. The briefing notes are based on the data-driven conclusions and recommendations of the FSF ALAR Task Force, as well as data from the U.S. Commercial Aviation Safety Team (CAST), the Joint Safety Analysis Team ( JSAT) and the European Joint Aviation Authorities Safety Strategy Initiative ( JSSI).
Generally, each briefing note includes the following:
• Statistical data related to the topic;• Recommended standard operating procedures;• Discussion of factors that contribute to excessive deviations
that cause ALAs;• Suggested accident prevention strategies for companies and
personal lines of defense for individuals;• Summary of facts;• Cross-references to other briefing notes;• Cross-references to selected FSF publications; and• References to relevant ICAO standards and recommended
practices, U.S. Federal Aviation Regulations and European Joint Aviation Requirements.
The briefing notes include key topics such as automation, approach briefings, human factors, crew resource management, altitude deviations and terrain avoidance manoeuvres, to name just a few. As examples, check out Briefing Note 2.1 on
16 Flight Operations ASL 4/2012
1. Regional TSB office; a NAV CANADA ATS unit
2. 2 200; AGL; controlled.
3. white or yellow X’s
4. 10
5. poor
6. the operator of the aircraft
7. takeoff, climb, approach and landing
8. Thunderstorm
9. The surface wind is forecast to be from the east (090° true) with a speed of 35 kt.
10. 040° at 15 kt, gusting to 25 kt.
11. 2 SM, temporarily 6 SM
12. greater than 6 SM visibility, no significant weather, 2 000 ft overcast
13. 3 400
14. As per Comparison Table.
15. Moderate turbulence between 8 000 ft and 2 000 ft during descent; 18:30Z.
16. “have numbers”; runway; wind; altimeter
17. Report departure intentions prior to moving onto the take-off surface; report departing from the aerodrome traffic circuit
18. minutes
19. level; good; very low
20. 5; 5
21. 20 to 40
22. When specified in a replacing or cancelling NOTAM.
23. The FIR NOTAM file.
24. 5 years.
25. potential hazards to air navigation; 500; 300
26. 20
27. clothing and equipment; exposure
28. insufficient rest; lack of sleep; overexertion
29. The AIC number according to the Web site.
30. 60 minutes
31. 62.9 litres; 2.787 hours or 2 hours 46 minutes
32. light on the ground; adequate celestial illumination
33. life preserver
34. The rotor will flap and the gyroplane will become uncontrollable.
35. decreases; decreases
36. slack; under tension
37. same
38. A propane leak at the valve stem.
39. 105 ft
Answers to the 2012 Self-Paced Study Program
Human Factors, which expands on the human factors which could be involved in ALAs, and Briefing Note 2.2 on Crew Resource Management, which touches on critical aspects of crew coordination and cooperation. All 33 briefing notes are equally useful in preventing ALAs, and they are available for free download on the FSF Web Site.
The IATA has endorsed the FSF ALAR Tool Kit and has recommended that its members use it. In 2001, ICAO stated
that the FSF ALAR Tool Kit contained extremely valid accident prevention information and that member states should consider incorporating the material into their training programs. ICAO then purchased and distributed 10 000 copies of the tool kit at its 33rd Assembly in the fall of 2001. To date, approximately 40 000 copies of the tool kit have been distributed worldwide. The FSF ALAR Tool Kit on CD is available for online sale from FSF in English, Spanish and Russian, at a cost of $95.00 for FSF members or $200.00 for non-members.

ASL 4/2012 Maintenance and Certification 17
Winter Operation WoesThis article was originally published in Aviation Safety Maintainer Issue 4/1992.
What differences should we be aware of with winter operations? Why do we need extra vigilance? Here are a few accidents where winter conditions were a contributing factor. I hope the results remind AMEs that, no matter how small or how large the aircraft, it is often the very simple things that cause the most serious problems.
LubricationEveryone knows that grease and oil thicken up with the onset of colder weather. Well, almost everyone. Take the case of an Enstrom helicopter operating in -30° conditions, where the pilot was unable to maintain control during takeoff. The subsequent accident investigation revealed that the manufacturer had not taken into account the fact that the grease used to lubricate the flight controls lacked properties necessary for cold weather operations. As a result, the manufacturer was alerted to the problem, and Transport Canada issued an Airworthiness Directive CF-89-17, forbidding the use of Almagard 3751 and Almaplex 1275 lubricants in the Enstrom flight control system.
Engine lubricating oil can be a source of trouble if the oil system is not properly winterized. Winterization includes changing to the correct winter weight oil, then checking that the oil lines or oil tank are lagged (insulated), as specified by the manufacturer’s manual, and that oil cooler doors operate correctly and freely.
The pilot of a Cessna 310 was proceeding en route in -30° temperatures when he noticed the oil pressure rising on the right engine and oil on the cowling. The pilot feathered the right engine and diverted toward the nearest airport. A few minutes later the left engine displayed similar problems. Oil pressure increased, then dropped to zero as the oil supply was forced overboard by excessive, crankcase pressure, and the left engine was feathered. The right engine was restarted and sufficient power was obtained to stabilize the flight. Fortunately, a second aircraft appeared on the scene and managed to direct the troubled pilot to a nearby airstrip, where he landed safely with smoke and oil pouring from the engine. The oil supply for both engines had been depleted due to ice formation blocking the inside of each engine crankcase breather line. Most aircraft maintenance manuals refer to special holes or other alternate crankcase breather methods that should be in place to counter ice accumulation in these lines during winter operations.
Fuel systemsThe condition of the carburetor heat system and fuel system are major concerns when preparing aircraft for winter operations. The Cessna 150 is most susceptible to carburetor icing and fuel system ice. The following accidents illustrate some problems in this area.
The pilot of a Cessna 182Q was flying from Resolute Bay, N.W.T., at 11 500 ft and above cloud, when the engine started running rough and stopped despite the application of full carburetor heat. The temperature and humidity were conducive to the formation of carburetor ice. After the forced landing, investigators found that, although the pilot applied carburetor heat properly, the engine could not respond because of a malfunctioning carburetor heat valve. The carburetor heat shroud was found split and separated where nine of the 12 shroud rivets had sheared. As a result, the carburetor heat system was unable to counter the carburetor icing. Maintenance personnel must ensure that the carburetor heat system works according to specifications.
Maintenance and CertificationWinter Operation Woes .................................................................................................................................................... page 17Maintenance of Small Non-Commercial Aircraft .............................................................................................................. page 18
Aircraft parked unprotected from ice and snow as shown above, require inspection for possible damage and for the presence of ice in the
tailcone or elevator assembly prior to flight.

18 Maintenance and Certification ASL 4/2012
A Cessna 150G was climbing out from St. Francois Xavier, Manitoba airstrip, when the engine stopped. The pilot made a successful force landing and no injuries occurred. Examination of the fuel drain fitting located in the centre fuselage belly area revealed signs of ice covering the fitting port. Since no other cause could be determined, it is assumed that this area iced over or became blocked with ice crystals suspended in the fuel, preventing fuel flow. Numerous warnings and articles have been published about the belly fuel drains on Cessna aircraft. Some models of the Cessna 150 are particularly vulnerable. This unobtrusive little drain cap, or set screw, should be removed at every inspection, and the line drained for a few seconds to remove any accumulated water or debris. This is particularly important in the fall before freezing temperatures are encountered.
UndercarriageThere are many cases on record where slush has frozen inside wheel pants, locking the wheels and causing the aircraft to nose over on landing. AMEs should also pay particular attention to oleos and brakes because rubber seals and “O” rings tend to leak and break down in extremely cold temperatures. Retractable gear may require servicing with
winter weight grease and the removal of corrosive salts or other contaminants from the mechanism if it is to continue to function safely during winter.
Cabin heatersExhaust type cabin heaters must be monitored for exhaust leakage into the cabin (see AD CF-90-03 for mandatory requirements). The exhaust system should be inspected for leaks at the beginning of the winter season. Janitrol type heaters should be checked for correct operation and serviced at the beginning of each winter season. A little preventive maintenance is the best protection against in-flight explosion of gas heaters or carbon monoxide impairment of the crew from exhaust type heaters.
Cold weather operations are a fact of life in Canada, and can be performed safely if everyone, including pilots, AMEs and ramp attendants remain vigilant in detecting and correcting winter operational differences before they cause big trouble during flight.
Last but not least, do not forget to remove the obvious hazard such as ice, snow, or freezing precipitation adhering to the aircraft surfaces and possibly inside the turbine inlet ducts prior to flight.
Maintenance of Small Non-Commercial Aircraftby Joel Virtanen, Civil Aviation Safety Inspector, Operational Airworthiness, Standards Branch, Civil Aviation, Transport Canada
Section 605.86 of the Canadian Aviation Regulations (CARs) requires that all aircraft be maintained in accordance with a maintenance schedule that is approved by the Minister and that meets the requirements of Standard 625—Aircraft Equipment and Maintenance Standard. However, there are exceptions; CAR 605.86 does not apply to ultralight aeroplanes and hang gliders.
Maintenance schedulesMost small aircraft owners use a maintenance schedule found in Standard 625, Appendix B, that is considered to be approved by the Minister. Anyone using the maintenance schedule in Appendix B needs to make an entry in the aircraft technical record that the aircraft is maintained to that maintenance schedule. Appendix B lists the areas that are to be inspected, but it is not a checklist for the inspection.
Standard 625, Appendix C, is part of the maintenance schedule for every aircraft. It lists the maintenance requirements for specific equipment that are due at intervals specified in the Appendix. Annual review of Appendix C items is required to ensure that the equipment listed is inspected at the proper intervals.
Inspection checklistIn respect of an aircraft, “owner” means the person who has legal custody and control of the aircraft. The aircraft owner must develop a detailed inspection checklist that covers all areas included in Standard 625, Appendix B, as the Appendix in itself is not an inspection checklist. The owner can use the manufacturer’s inspection checklist for the aircraft, where the manufacturer has provided one. Where the manufacturer has not provided an inspection checklist, the owner must develop one.
It is important to review the checklist to ensure that it contains all items included in Standard 625, Appendix B. Manufacturers’ checklists may be deficient for several reasons. For example, the manufacturer’s checklist may be out of date with reference to the current standard. A checklist should also include items covering any modifications carried out on the aircraft. An inspection checklist should be detailed enough to cover all wear items on the aircraft in order to maintain the aircraft in a safe flying condition until the next inspection.

ASL 4/2012 Maintenance and Certification 19
Airworthiness directivesThe most important thing to remember about airworthiness directives is that compliance with them is mandatory for all aircraft, except those in the owner-maintenance and amateur-built classifications. It is the owner’s responsibility to determine which airworthiness directives are applicable to the aircraft, and to make them available to the maintenance provider. A list of airworthiness directives that could be applicable to your aircraft or equipment can be found on the Transport Canada Web site. If you are not familiar with airworthiness directives, ask your maintainer for help.
Life-limited partsSome aircraft have life-limited parts that have to be replaced when they reach their life limit based on elapsed time, calendar time or operating cycles. Most turbine engines and helicopter drive systems have parts that are life-limited. It is the owner’s responsibility to ensure that these parts are replaced at proper intervals. Life limits do not apply to aircraft operated under a special certificate of airworthiness, to owner-maintained aircraft or to amateur-built aircraft.
Inspection intervalsMost small aircraft owners are familiar with the 100-hr inspection or the annual inspection. In 2007, Standard 625.86(2)(a) was modified with respect to the meaning of “interval”. The “annual” inspection is no longer due 12 months from the last inspection, but rather on the last day of the 12th month. This means that if the last
“annual” inspection was carried out on January 1, 2011, the next inspection is not due until January 31, 2012. In this case, the effective inspection interval is 13 months less one day. This applies to any interval that is stated in months in the Standard. If the interval is stated as “annual”, it means 365 days. As tolerances are not permitted for aircraft maintained under Standard 625, Appendix B, the inspection interval cannot be exceeded.
Logbook entriesIn some cases, all items with respect to the maintenance work done on the aircraft are entered in the aircraft journey log. This is permitted in the case of a balloon or a glider, or an aircraft operated under a special certificate of airworthiness in the owner-maintenance or amateur-built classification. In all other cases, only maintenance items listed in CAR 605, Schedule I, must be recorded in the aircraft journey log.
CAR 571.03 requires that the details of all maintenance and elementary work be recorded in the aircraft technical record. No logbook entry is required for servicing. An entry must be made in the aircraft journey logbook for the date, air time, operating cycle or landing at which the next scheduled maintenance action is required. In this way, the pilot is kept informed of the next maintenance action to be performed.
For more information on recreational aircraft in Canada, visit the Transport Canada recreational aircraft Web site at www.tc.gc.ca/eng/civilaviation/standards/maintenance-aarpe-recreational-menu-2753.htm.
2012-2013 Ground Icing Operations Update In July 2012, the Winter 2012–2013 Holdover Time (HOT) Guidelines were published by Transport Canada. As per previous years, TP 14052, Guidelines for Aircraft Ground Icing Operations, should be used in conjunction with the HOT Guidelines. Both documents are available for download at the following Transport Canada Web site: www.tc.gc.ca/eng/civilaviation/standards/commerce-holdovertime-menu-1877.htm.
If you have any questions or comments regarding the above, please contact Doug Ingold at [email protected].
Worth Watching—Again! The FAA In-Flight Fire Fighting VideoDeveloped by the United States Federal Aviation Administration (FAA) with assistance from Transport Canada Civil Aviation (TCCA) and other aviation authorities, this excellent video addresses how to prevent, react and deal with in-flight fires. It’s time well spent!

20 Recently Released TSB Reports ASL 4/2012
The following summaries are extracted from final reports issued by the Transportation Safety Board of Canada (TSB). They have been de-identified and include the TSB’s synopsis and selected findings. Some excerpts from the analysis section may be included, where needed, to better understand the findings. For the benefit of our readers, all the occurrence titles below are now hyperlinked to the full TSB report on the TSB Web site. —Ed.
TSB Final Report A09W0021—Loss of Power and Collision with Terrain
On January 30, 2009, a Robinson R44 helicopter was en route from Grande Prairie, Alta., to Grande Cache, Alta., with one pilot and one passenger on board. At approximately 17:02 Mountain Standard Time (MST), while climbing over rising terrain, the helicopter lost engine power and main rotor RPM. The pilot turned downhill in an effort to regain main rotor RPM. When this failed, he carried out a forced landing into the trees where the aircraft came to rest on its right side. The pilot was seriously injured when the passenger fell on top of him during impact. The passenger sustained no injury. They spent more than 15 hr on site before being rescued. The emergency locator transmitter (ELT) did not activate during the impact sequence, thus delaying the search and rescue (SAR) response.
AnalysisThe weather at the time of the accident was conducive to the formation of carburetor icing. The pilot had spent most of his career flying turbine-powered helicopters, in which carburetor icing is not a concern. The carburetor heat lever can move away from the required position through movement of the collective arm in flight. The reported loss of power was likely the result of carburetor icing, which could not be corrected by the pilot in the time available.
The different SPOT satellite GPS messenger functions activated by the passenger, coupled with uncertainty among family members during discussions with the joint rescue coordination centre (JRCC), contributed to the delay in the SAR response.
The lack of a common communication frequency among SAR responders also contributed to the delay in rescue. Faster clarification of the accident location and coordination of tasks would have shortened rescue time. The risk of serious injury and death increases as SAR response time increases.
Finding as to causes and contributing factors1. It is likely that carburetor ice formed resulting in the loss
of engine power and main rotor RPM from which the pilot was unable to recover.
TSB Final Report A09O0207—Collision with Terrain
On September 21, 2009, a Robinson R22 Alpha helicopter departed Toronto City Centre Airport, Ont., on a short flight to the pilot’s private helipad in the rural town of Norval, Ont. At 20:00 Eastern Daylight Time (EDT), in the hours of darkness, the helicopter crashed 1.8 NM northeast of the final destination. The helicopter erupted into flames on impact and was partially consumed by a post-crash fire. The pilot was fatally injured.
AnalysisExamination of the helicopter engine indicates that it was not running on impact and that the helicopter struck the ground in a 50° nose-down attitude, suggesting an in-flight loss of control. Although the helicopter was extensively damaged, there were no signs of any pre-impact mechanical failure or system malfunction that could have contributed to this accident. As a result, this analysis focuses on possible scenarios for what
Recently Released TSB Reports

ASL 4/2012 Recently Released TSB Reports 21
caused the engine to stop running and why the helicopter departed controlled flight and collided with terrain.
While it was not possible to determine accurately the position of the carburetor heat control before impact, the mixture control knob was found out and bent. With the push-button locking feature, it is unlikely that the mixture control moved during the impact. It was, therefore, likely in the idle cut-off position on impact.
Two scenarios were considered as to why the pilot inadvertently pulled the mixture control to the idle cut-off position, causing the engine to shut down:
• On approaching destination and in preparation for descent, the pilot attempted to apply carburetor heat.
• The meteorological conditions were conducive to moderate carburetor icing during cruise and descent. The Robinson R22 governor can easily mask carburetor icing by automatically increasing the throttle to maintain engine RPM, which will also result in a constant manifold pressure. It is possible that the helicopter’s engine developed carburetor ice en route, causing performance degradation or a total power loss. To correct this situation, the pilot would have attempted to apply carburetor heat.
The mixture control knob is shaped differently than the carburetor heat knob. To reposition the mixture control, the pilot needs to action the push-button locking feature. In addition, to prevent its inadvertent actuation, the manufacturer also requires that a cylindrical plastic guard be placed over the mixture control knob from the time the engine is started until such time as the engine is shut down. This plastic guard would make it difficult to inadvertently action the mixture control
and would also provide tactile feedback that the pilot was attempting to move the wrong control knob. In order for the pilot to be able to pull the mixture control knob to the idle cut-off position, it is likely that the plastic guard had not been placed over the mixture control knob as required.
Mixture control pushed in to full rich with guard installed
Mixture control pulled out to idle cut-off with guard removed
In the Robinson R22, the pilot must take immediate action following a loss of power to ensure that rotor RPM is maintained. Failure to do this can lead to a low rotor RPM and rotor stall from which recovery may not be possible. The Robinson R22 pilot operating handbook (POH) emergency procedures for a power loss above 500 ft in part instructs the pilot to immediately lower the collective to maintain rotor RPM and enter a normal autorotation. A restart may be attempted at the pilot’s discretion if sufficient time is available. If unable to restart, the pilot should turn off unnecessary switches and shut off the fuel.
Approximately 40 s before the crash, the helicopter started to turn to the right, then immediately started turning sharply to the left and climbed 300 ft. Approximately 20 s before the crash, the helicopter began a rapid descent from 1 800 ft above sea
Centre pedestal with mixture control (upper right) and carburetor heat control (lower right)

22 Recently Released TSB Reports ASL 4/2012
level (ASL) to the crash site at 650 ft ASL; this equates to a descent rate of approximately 3 450 ft/min. According to Robinson Helicopter Company Safety Notices SN-18 and SN-26, helicopters have less inherent stability and much faster roll rates than airplanes. Loss of the pilot’s outside visual references, even for a moment, can result in spatial disorientation, wrong control inputs and an uncontrolled crash.
With a lack of visual reference at night, limited visibility due to weather and the pilot’s relative inexperience, the pilot likely became spatially disoriented while dealing with the power loss emergency. Unable to determine the correct attitude of the helicopter without visual reference, the pilot lost control, resulting in uncontrolled flight into the terrain.
Findings as to causes and contributing factors1. It is likely that, while attempting to apply carburetor heat,
the pilot inadvertently pulled the mixture control knob to the idle cut-off position, causing the engine to shut down.
2. It is likely that the plastic guard had not been placed over the mixture control knob, resulting in the pilot being able to pull the control to the cut-off position.
3. Following the engine shutdown, the rotor RPM was allowed to decay, resulting in a loss of control and uncontrolled flight into the terrain.
4. With few visual references, the pilot likely became spatially disoriented, contributing to the inability to maintain control.
Other findings1. The helicopter was being operated in Canada without
liability insurance as required by the Canadian Aviation Regulations (CARs).
2. The helicopter had not been registered in Canada as required by the CARs.
TSB Final Report A09P0397—Loss of Control—Collision with Water
Note: The TSB investigation into this occurrence resulted in a major report, with extensive discussions, analysis and recommendations on emergency egress from floatplanes and the wearing of personal floatation devices. Therefore we could only publish selected parts of the report in the ASL. Readers are invited to read the full report, hyperlinked in the title above. —Ed.
On November 29, 2009, a de Havilland DHC-2 MK 1 was departing Lyall Harbour, Saturna Island, B.C., for the water aerodrome at the Vancouver International Airport, B.C. After an unsuccessful attempt at taking off downwind, the pilot took off into the wind towards Lyall Harbour. At approximately 16:03 Pacific Standard Time (PST), the aircraft became airborne, but remained below the surrounding terrain. The aircraft turned left, then descended and collided with the water. Persons nearby responded immediately; however, by the time they arrived at the aircraft, the cabin was below the surface of the water. There were eight persons on board—the pilot and an adult passenger survived and suffered serious injuries; the other six occupants drowned inside the aircraft. No signal from the emergency locator transmitter (ELT) was heard.
AnalysisThe DHC-2 Beaver was originally certified without a stall warning system. One had been installed on the occurrence aircraft, but was later rendered unserviceable. The absence of a functioning stall warning system, coupled with the known benign stalling characteristics of the Beaver, precluded any warning of an impending stall. Furthermore, the stall warning horn had been filled with silicone to make it less noisy. It is therefore possible that a horn would not be heard during periods of loud engine noise, thereby increasing the risk of inadvertent stalls.
The conditions in Lyall Harbour at the time of the occurrence were conducive to the development of mechanical turbulence and mountain waves. The turbulence associated with these

ASL 4/2012 Recently Released TSB Reports 23
phenomena likely contributed to vertical gusts, which subjected the aircraft to temporary, but significant, increases in aerodynamic load.
Following takeoff, after the initial climb, the pilot commenced a left turn out of the harbour. The aircraft encountered down flowing air, restricting its ability to gain altitude. As the aircraft turned, it drifted towards terrain, causing the pilot to increase the bank angle. To maintain altitude while banking, the pilot likely had to increase the angle of attack, thereby increasing the load factor and the speed at which the aircraft would stall. While the use of flap may have increased the wing area and consequently decreased its loading, it was likely insufficient to counteract the combined loads brought about by the atmospheric conditions and increase in bank.
Lyall Harbour with flight route and winds
A float-equipped Beaver with the flaps set in the landing position was demonstrated to stall in straight and level flight at 54 mph. In this occurrence, the combined effects of the reduced airspeed during the climb, the bank angle during the turn and the atmospheric conditions increased the load factor of the aircraft to the point of aerodynamic stall.
The aircraft was under its maximum gross takeoff weight, but loaded such that its centre of gravity (CG) was beyond the aft limit for floatplane operations. The aircraft levelled off prior to impact, indicating the pilot had initiated stall recovery.
Full recovery was compromised by the aft CG. Controllability notwithstanding, the altitude from which recovery was made was insufficient to arrest the descent, causing the aircraft to strike the water.
The damage to the pilot’s seat rendered the restraint system ineffective and contributed to the pilot’s injuries. These injuries,
which included a brief loss of consciousness, caused a delay in the pilot’s egress and limited his ability to provide assistance to the passengers.
With the exception of one adult, all passengers undid their seatbelts, indicating that they likely remained conscious after impact. Following the impact, the passengers would have had a few seconds to locate a suitable egress point, release their seat belts and exit the aircraft.
In this occurrence, the aircraft was not equipped with jettisonable doors or windows. As a result, the only possible egress points were the four doors on the aircraft. However, impact damage jammed two of the four doors and restricted egress from the sinking aircraft, which meant all seven passengers and the pilot would have had to exit via one of two usable egress points. Rather than deliberately attempting to open a door, the surviving passenger exited through the door that had opened as a result of impact forces. It is likely that the pilot’s recent egress training contributed to him being able to open the door and escape from the aircraft. The lack of alternate emergency exits, such as jettisonable windows, increases the risk that passengers and pilots will be unable to escape a submerged aircraft due to structural damage to primary exits following an impact with the water.
Seeing as the impact forces experienced by all onboard were considered survivable, the issue of timely escape contributed to the passengers drowning. Many persons could improve their chances of survival by identifying the possible exits and mentally rehearsing their actions, including identifying alternate exits in the event of an accident. If passengers are not provided with explicit safety briefings on how to egress the aircraft when submerged, there is increased risk that they will be unable to escape following an impact with the water.
Given the time involved in conducting a rescue, in cases when an individual is successful in escaping an aircraft following an impact, continued survival is a significant concern. This is particularly true if the individual has been injured. Since it is unlikely that persons faced with the urgency of escape in water will retrieve life vests stored in the aircraft, passengers and pilots not equipped with some type of flotation device prior to an impact with the water are at increased risk of drowning once they have escaped the aircraft.
Findings as to causes and contributing factors1. The combined effects of the atmospheric conditions
and bank angle increased the load factor, causing an aerodynamic stall.
2. Due to the absence of a functioning stall warning system, in addition to the benign stalling characteristics of the Beaver, the pilot was not warned of the impending stall.

24 Recently Released TSB Reports ASL 4/2012
3. Because the aircraft was loaded in a manner that exceeded the aft CG limit, full stall recovery was compromised.
4. The altitude from which recovery was attempted was insufficient to arrest descent, causing the aircraft to strike the water.
5. Impact damage jammed two of the four doors, restricting egress from the sinking aircraft.
6. The pilot’s seat failed and he was unrestrained, contributing to the seriousness of his injuries and limiting his ability to assist passengers.
Findings as to risk1. There is a risk that pilots will inadvertently stall aircraft
if the stall warning system is unserviceable or if the audio warnings have been modified to reduce noise levels.
2. Pilots who do not undergo underwater egress training are at greater risk of not escaping submerged aircraft.
3. The lack of alternate emergency exits, such as jettisonable windows, increases the risk that passengers and pilots will be unable to escape a submerged aircraft due to structural damage to primary exits following an impact with the water.
4. If passengers are not provided with explicit safety briefings on how to egress the aircraft when submerged, there is increased risk that they will be unable to escape following an impact with the water.
5. Passengers and pilots not wearing some type of flotation device prior to an impact with the water are at increased risk of drowning once they have escaped the aircraft.
Safety action takenOperatorThe operator has equipped each aircraft with hand-held baggage scales to allow pilots to make more accurate weight and balance calculations.
The operator has ordered new door latch release and window modification kits from Viking Air Limited, the aircraft type certificate holder.
The operator has enhanced its pre-flight safety briefing by now including an independent demonstration of where to find the life vests, what they look like and how to put them on. A mannequin located at the operator’s Vancouver and Nanaimo docks is used to perform this safety demonstration. Enlarged photographs from the safety briefing cards are displayed on the mannequin stand. A briefing is provided to passengers before they head down to the aircraft at the dock and a second safety briefing is provided once they are at the aircraft.
Viking Air LimitedViking Air Limited, the aircraft type certificate holder, has made push-out window and cabin and cockpit door latch kits available for installation on Beaver aircraft.
Transport CanadaSince this accident, Transport Canada (TC) completed a number of initiatives:
- TC facilitated a meeting of floatplane operators in October 2010, which resulted in the formation of an industry-led safety association of B.C. floatplane operators.
- TC ran an updated floatplane safety promotional campaign during the summer of 2011, which included: • publishing articles in the Aviation Safety Letter to promote
egress training and effective passenger briefings; • developing posters and pamphlets for distribution to
floatplane passengers to increase awareness of their role in safety;
• tasking its inspectors to ensure floatplane operators receive the latest safety promotion materials, to emphasize the importance of egress training and better passenger briefings during their visits, and to conduct follow-up telephone surveys of floatplane operators to verify that they are using the safety promotion materials;
• developing a Web portal to centralize floatplane safety information for use by operators and passengers and encouraging floatplane operators to provide a link to the portal from their Web sites;
• producing a video for use by operators promoting best practices and lessons learned in floatplane operations; and
• producing a video for use by floatplane passengers on their role in safety.
- TC issued a Civil Aviation Safety Alert (CASA) on June 6, 2011, with its focus on commercial and private floatplane operators and pilots, recommending the following best practices in relation to floatplane safety:• Upper body restraints to be used by front seat occupants; • Passenger briefings on the proper usage of floatation
devices during emergency egress; • Underwater emergency egress training for flight crew; and • Aircraft safety design improvements facilitating egress.
In August 2011, TC held a focus group with selected members of industry to determine the most effective means of addressing the TSB recommendations related to rapid egress and the mandatory use of personal floatation devices (TSB Recs A11-05 and A11-06). This process is ongoing.
TSB Final Report A09Q0203—Controlled Flight into Terrain (CFIT)
Note: The TSB investigation into this CFIT occurrence resulted in a major report, with extensive discussions, analysis and recommendations on instrument approach design, instrument approach depiction, instrument approach techniques, approach and landing accidents, and approach and landing accident reduction (ALAR) initiatives. Therefore we could only publish
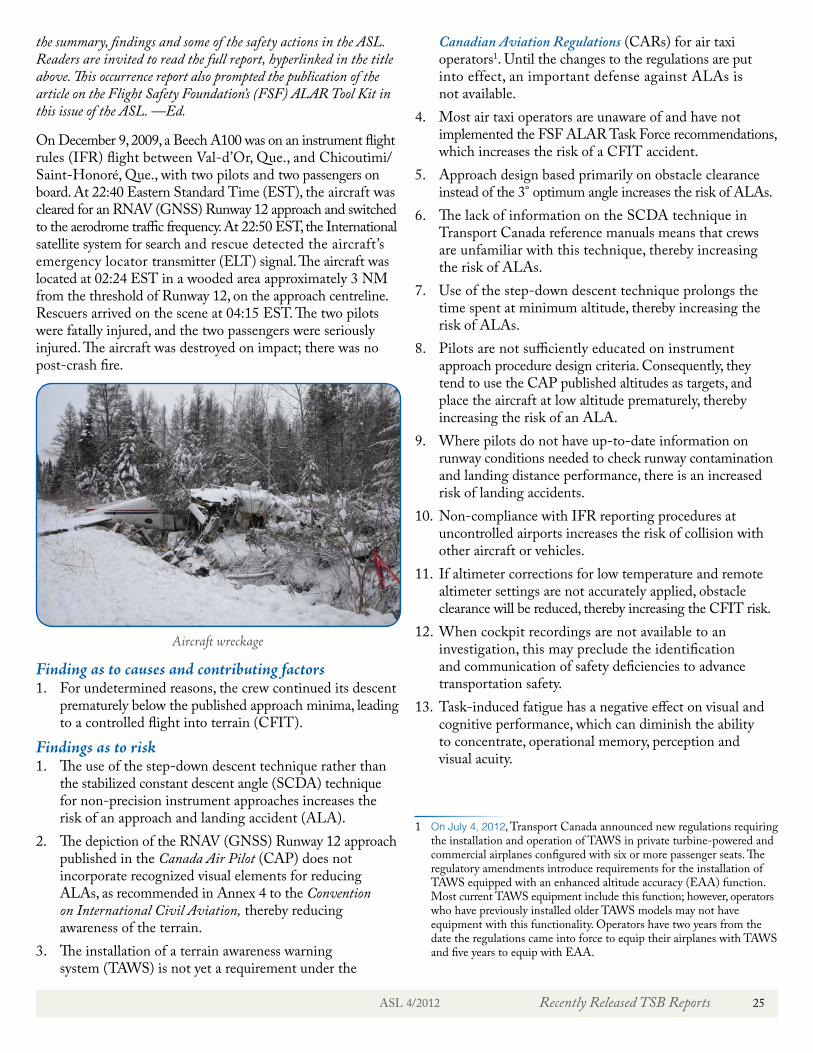
ASL 4/2012 Recently Released TSB Reports 25
the summary, findings and some of the safety actions in the ASL. Readers are invited to read the full report, hyperlinked in the title above. This occurrence report also prompted the publication of the article on the Flight Safety Foundation’s (FSF) ALAR Tool Kit in this issue of the ASL. —Ed.
On December 9, 2009, a Beech A100 was on an instrument flight rules (IFR) flight between Val-d’Or, Que., and Chicoutimi/Saint-Honoré, Que., with two pilots and two passengers on board. At 22:40 Eastern Standard Time (EST), the aircraft was cleared for an RNAV (GNSS) Runway 12 approach and switched to the aerodrome traffic frequency. At 22:50 EST, the International satellite system for search and rescue detected the aircraft’s emergency locator transmitter (ELT) signal. The aircraft was located at 02:24 EST in a wooded area approximately 3 NM from the threshold of Runway 12, on the approach centreline. Rescuers arrived on the scene at 04:15 EST. The two pilots were fatally injured, and the two passengers were seriously injured. The aircraft was destroyed on impact; there was no post-crash fire.
Aircraft wreckage
Finding as to causes and contributing factors1. For undetermined reasons, the crew continued its descent
prematurely below the published approach minima, leading to a controlled flight into terrain (CFIT).
Findings as to risk1. The use of the step-down descent technique rather than
the stabilized constant descent angle (SCDA) technique for non-precision instrument approaches increases the risk of an approach and landing accident (ALA).
2. The depiction of the RNAV (GNSS) Runway 12 approach published in the Canada Air Pilot (CAP) does not incorporate recognized visual elements for reducing ALAs, as recommended in Annex 4 to the Convention on International Civil Aviation, thereby reducing awareness of the terrain.
3. The installation of a terrain awareness warning system (TAWS) is not yet a requirement under the
Canadian Aviation Regulations (CARs) for air taxi operators1. Until the changes to the regulations are put into effect, an important defense against ALAs is not available.
4. Most air taxi operators are unaware of and have not implemented the FSF ALAR Task Force recommendations, which increases the risk of a CFIT accident.
5. Approach design based primarily on obstacle clearance instead of the 3° optimum angle increases the risk of ALAs.
6. The lack of information on the SCDA technique in Transport Canada reference manuals means that crews are unfamiliar with this technique, thereby increasing the risk of ALAs.
7. Use of the step-down descent technique prolongs the time spent at minimum altitude, thereby increasing the risk of ALAs.
8. Pilots are not sufficiently educated on instrument approach procedure design criteria. Consequently, they tend to use the CAP published altitudes as targets, and place the aircraft at low altitude prematurely, thereby increasing the risk of an ALA.
9. Where pilots do not have up-to-date information on runway conditions needed to check runway contamination and landing distance performance, there is an increased risk of landing accidents.
10. Non-compliance with IFR reporting procedures at uncontrolled airports increases the risk of collision with other aircraft or vehicles.
11. If altimeter corrections for low temperature and remote altimeter settings are not accurately applied, obstacle clearance will be reduced, thereby increasing the CFIT risk.
12. When cockpit recordings are not available to an investigation, this may preclude the identification and communication of safety deficiencies to advance transportation safety.
13. Task-induced fatigue has a negative effect on visual and cognitive performance, which can diminish the ability to concentrate, operational memory, perception and visual acuity.
1 On July 4, 2012, Transport Canada announced new regulations requiring the installation and operation of TAWS in private turbine-powered and commercial airplanes configured with six or more passenger seats. The regulatory amendments introduce requirements for the installation of TAWS equipped with an enhanced altitude accuracy (EAA) function. Most current TAWS equipment include this function; however, operators who have previously installed older TAWS models may not have equipment with this functionality. Operators have two years from the date the regulations came into force to equip their airplanes with TAWS and five years to equip with EAA.

26 Recently Released TSB Reports ASL 4/2012
14. Where an ELT is not registered with the Canadian Beacon Registry, the time needed to contact the owner or operator is increased, which could affect occupant rescue and survival.
15. If the tracking of a call to 9-1-1 emergency services from a cell phone is not accurate, search and rescue efforts may be misdirected or delayed, which could affect occupant rescue and survival.
Other findings1. Weather conditions at the alternate airport did not meet
CARs requirements, thereby reducing the probability of a successful approach and landing at the alternate airport if a diversion became necessary.
2. Following the accident, none of the aircraft exits were usable.Safety action takenOperatorTo minimize the risks of ALAs, the operator implemented SCDA in its standard operating procedures (SOPs).
A program was set up to progressively install radio altimeters on the company aircraft.
The company CFIT training was reviewed to integrate the recommendations of the FSF ALAR Task Force.
The following measures have been, or will be, taken by the operator to reduce the operational risks:
• A review of all departments related to flight operations. • A complete review of SOPs. • A review of operational limitations of the charter operations
(i.e. new restrictions for new captains and first officers as well as equipment restrictions).
• All flying personnel will redo the company CFIT course. • A risk analysis file is available to the flight crew to review
the level of risk associated with approaches in instrument meteorological conditions (IMC) for all destinations. This file is based on the FSF program.
• A flight safety awareness campaign called “Objectif Zéro” was set up to involve all company employees. The aim is to allow all employees to have a positive impact on flight safety via the company safety management system (SMS).
TSB Final Report A10P0147—Loss of Control—Collision with Water
On May 29, 2010, a float-equipped Cessna 185F took off from Tofino, B.C., at 12:00 Pacific Daylight Time (PDT) for a flight to Ahousat, B.C., with a pilot and three passengers. The short flight was being carried out under visual flight rules (VFR) at about 500 ft above sea level (ASL). About 2 NM from Ahousat, while in cruise flight, the aircraft descended in a steep nose-down attitude until it hit the water in Millar
Channel and overturned. Attempts to secure the aircraft failed and it sank. There were no survivors. The emergency locator transmitter (ELT) functioned but its signal was not received until the wreckage was brought to the surface two days later.
AnalysisThe weather was suitable for the VFR flight; the wind direction and speed would not have caused downdrafts or severe turbulence on the flight route. There was no evidence to suggest that any mechanical or environmental issue played a role in this occurrence.
The aircraft struck the water at an angle and speed consistent with a deliberate dive, or a loss of control. Based on the pilot’s demeanour, there was no reason to dive to the point of impact with the water. Therefore, the TSB concluded that the pilot lost control of the aircraft.
The aircraft was trimmed for level cruising flight. Had the pilot simply released the controls, the aircraft would have remained more or less in level cruising flight, and it would not have pitched down abruptly or to an angle of 45°. To sustain a descent at a 45° angle from level attitude, a high and continued pressure would have had to have been placed on the control column.
The passengers were intoxicated at the time they boarded the aircraft, and had previously been argumentative. The final location of some beer cans and fragments of the beer case indicate that the case of beer was in proximity to the passengers just before impact.
It is not known if all the passengers were wearing their seat belts at the start of the flight, but the physical evidence shows that the seatbelts of the passenger in the right front seat (beside the pilot) and of the passenger in the left rear seat (behind the pilot) were not fastened at impact.

ASL 4/2012 Recently Released TSB Reports 27
What was happening in the cabin moments before the pilot lost control cannot be accurately determined. However, the TSB concluded that this probably involved activity by the unsecured passengers that interfered with the pilot and his control of the aircraft.
The pilot’s broken right wrist and the bent V brace suggest that the pilot was bracing or trying to resist a force imposed from behind. The broken ankles of the passenger behind the pilot are consistent with that person bracing with both feet, or pushing forward with both feet, at the time of impact. It is possible the passenger seated behind the pilot kicked the pilot’s seatback forward and held it there, pushing the pilot into the instrument panel and the controls forward, thereby inducing a dive.
Because there was no locking mechanism on the pilot’s seatback, and because the pilot was not wearing his shoulder strap, he would have been unable to prevent his upper body from being forced onto the instrument panel.
When aircraft controls are accessible to passengers there is a risk of inadvertent control manipulation and a risk of the pilot losing control of the aircraft at a critical time of flight operations.
It is also possible the level of the passengers’ intoxication impaired their ability to recognize the gravity of the situation and stop their interference in time for the pilot to regain control of the aircraft before impact.
Findings as to causes and contributing factors1. It is likely that passenger interference caused the pilot to
lose control of the aircraft, whereupon it descended in a steep nose-down attitude until it struck the water.
2. It is possible the passengers’ level of intoxication contributed to their inability to recognize the gravity of the situation and stop the interference in time for the pilot to regain control of the aircraft before impact.
3. Because there was no locking mechanism on the pilot’s seatback, and because the pilot was not wearing his shoulder strap, he would have been unable to prevent his upper body from being forced onto the instrument panel.
Findings as to risk1. When controls are accessible to passengers there is a risk
of inadvertent control manipulation and a risk of the pilot losing control of the aircraft.
2. When upper body restraint systems are not used, there is a risk of serious head injury in the event of an accident.
3. When cargo or passengers’ baggage is not restrained, there is a risk of unsecured items injuring persons on board in the event of sudden aircraft stoppage or encounters with severe turbulence.
Other finding1. Post-impact survival issues such as egress and flotation
were not relevant in this accident. Safety action takenBritish Columbia Coroners ServiceThe British Columbia Coroners Service has made the following recommendation to Transport Canada as a result of its investigation into the deaths of the four individuals:
It is recommended that all commercial air operators be required to establish a policy, procedure, and training (based on the Canadian [Aviation] Regulations) for all personnel, to assist them in identifying inappropriate behaviour in passengers, and take the necessary action to mitigate risk where there are reasonable grounds to believe that the person’s faculties are impaired by alcohol or drugs.
This recommendation is currently under review by Transport Canada officials. In the meantime, we strongly encourage all operators to review CAR 602.4 Alcohol or Drugs – Passengers.
TSB Final Report A10Q0218—Engine Failure and Hard Landing
On December 9, 2010, a Bell 206B, equipped with high skid landing gear, departed Matane, Que., on a visual flight rules (VFR) flight with the pilot and four passengers on board. The aircraft was flying northeast at low altitude over the south shore of the Saint Lawrence River so that the passengers could evaluate and document damage caused by high tides. At 11:31 Eastern Standard Time (EST), approximately 27 min after takeoff, the helicopter experienced an engine (Rolls-Royce 250-C20B) failure. The pilot did an autorotation with a right turn of more than 180°. The aircraft landed hard on the beach, breaking the landing gear, and came to rest on its belly. One of the occupants was seriously injured, two had minor injuries and two were unharmed in the accident.

28 Recently Released TSB Reports ASL 4/2012
AnalysisThe No. 2 bearing assembly in the engine broke down due to the fatigue failure of its cage. Because this bearing served as a thrust bearing, its failure caused the compressor to move forward, which in turn brought the impeller into contact with the shroud. The resulting friction led to significant deceleration and a loss of power. The propulsive movement of the compressor caused it to stall, as demonstrated by the bangs it produced.
The breaking of a gearbox stud, the crack in the compressor scroll and the fatigue failure of three fingers in the vibration damper may suggest that the damage was caused by abnormal engine vibration. However, after the stud and scroll were repaired, the engine was tested on a test bench, and no anomalies or vibrations outside of the limit were noted. This suggests that it is unlikely that engine vibration caused the anomalies. It can also be concluded that the vibration damper was not fractured at the time of the inspection on the test bench. Consequently, the successive fractures of the damper fingers occurred during the last 30 flight hours.
Because three fingers had fractured less than 30 flight hours before the accident, the vibration damper was less effective. It cannot be concluded beyond all doubt that the broken damper caused the No. 2 bearing assembly to fail. However, the partial failure of a component intended to absorb engine vibration cannot be ruled out; it could have altered the vibration load of the compressor, increasing the load on the No. 2 bearing assembly and causing its cage to sustain a fatigue failure.
Although the gearbox had been disassembled three times less than 35 flight hours before the accident, no anomalies were observed. The ball bearings and the vibration damper were not examined because the disassembly of the gearbox was not meant to verify their condition. Therefore, the engine may have been rebuilt with components that needed to be replaced.
The engine was equipped with a working chip-detection system, but the pilot did not notice the warning light before the loss of power, while significant spalling was generated by the slippage of the ball bearings in the No. 2 bearing assembly. However, 3.2 flight hours before the accident, the chip detectors detected metallic debris in smaller quantities from the engine ball bearings, which were starting to break down. Consequently, the ENG CHIP warning light may have been illuminated without the pilot noticing.
According to the height/speed chart, the loss of power occurred in an operating range within which a safe emergency landing was possible. At the time of the failure, there were three operating conditions posing a greater challenge than usual for the pilot. Given the height of the aircraft, the pilot had little time to lower the collective, perform a 180° turn into the wind, and begin the descent before landing on a slope. The power loss caused a rapid drop in rotor RPM to the point where the low
rotor RPM warning horn sounded during the descent. It can be concluded that the collective was off the down stop and that the rotor RPM fell below 90 percent.
Findings as to causes and contributing factors1. The No. 2 bearing assembly in the engine broke down
due to the fatigue failure of its cage. The failure of the bearing assembly caused the engine to lose power.
2. The power loss caused a rapid drop in rotor RPM to the point where the LOW ROTOR RPM warning horn sounded during the descent. It can be deduced that the collective was not completely lowered and that rotor RPM dropped below 90 percent. This caused a hard landing.
Findings as to risk1. Although the aircraft was operated outside of the high-risk
“to avoid” zone on the height/speed chart, the autorotation resulted in a hard landing. Because of operating factors other than speed and height, the operation of the helicopter at low altitude posed a risk to safe landing in the event of an engine failure.
2. Operating an aircraft outside of the weight and balance limits set by the manufacturer can reduce aircraft performance and cause a power surge, in turn causing major damage to the engine, airframe and power train.
3. The aircraft can attain the performance figures in the height/speed chart when it is loaded with its limit weight. Operating the aircraft at a higher weight compromises the success of an autorotation following an engine failure.
Other finding1. The wear on the ball bearings and the vibration damper
was not observed when the gearbox was examined because the three engine teardowns performed within the 31 flight hours before the accident did not expose them and were not intended to verify their condition.

ASL 4/2012 Recently Released TSB Reports 29
TSB Final Report A10A0122—Controlled Flight Into Terrain
On December 14, 2012, at 19:41 Atlantic Standard Time (AST), a Cessna 310R departed the Montréal/St-Hubert Airport, Que., on a night instrument flight rules (IFR) flight to the Pokemouche Airport, N.B. Between 21:56 AST and 21:58 AST, three transmissions were received from the occurrence aircraft’s 406 MHz emergency locator transmitter (ELT); however, the signal terminated before the location could be determined. The wreckage was located two days later in a wooded area, approximately 5.5 NM west-northwest of the Pokemouche Airport. The aircraft was destroyed by the impact and post-crash fire. The lone occupant was fatally injured.
AnalysisOn the day of the occurrence, the departure altimeter setting for St-Hubert was 29.61 in. Hg and the arrival altimeter setting for Bathurst, N.B., was 29.41 in. Hg. If the Bathurst altimeter setting was not applied prior to the commencement of the instrument approach, the aircraft’s actual altitude would have been 200 ft lower than indicated on the altimeter. While an altimeter error of this nature would reduce safety margins, levelling off at the minimum descent altitude with the incorrect altimeter setting of 29.61 in. Hg would still provide several hundred feet of clearance between the aircraft and the terrain. As a result, it is unlikely that the aircraft impacted the ground simply because the altimeter had not been switched to the current Bathurst altimeter setting.
This occurrence involved several of the most common factors associated with controlled flight into terrain (CFIT) accidents. In particular, it involved flight conditions that would make it nearly impossible to see the approaching terrain and it involved an instrument approach procedure with multiple step-down altitudes. As a result, each time that a descent is commenced, the pilot must remain vigilant to ensure that the aircraft does not descend below the appropriate minimum safe altitude, which during this portion of the approach was 1 000 ft above sea level (ASL). The combination of a non-precision instrument approach, conducted at night, with low ceilings and limited visibility significantly increases the risk of CFIT.
The operator was not authorized to conduct GPS approaches on revenue flights, and there was no evidence of the pilot undergoing the required training for conducting GPS approaches. While familiar with the aircraft and operating environment around Pokemouche, the pilot was inexperienced with the newly installed equipment. As a result, trying to use the new and unfamiliar GPS with a terrain awareness feature and audio panel in adverse weather at night would have increased pilot workload and made it difficult to maintain situational awareness. Based on the heading and location of the aircraft at the time of the impact, it is likely that the pilot was attempting to carry out the area navigation (RNAV) approach to Runway 13 and inadvertently flew into terrain.
The pilot elected to return to Pokemouche on the evening of December 14, 2010, so the aircraft would be available for an unexpected charter flight booked for the following morning. This influenced the pilot’s decision to depart, despite the pilot’s lack of familiarity with the new GPS and unfavourable weather at the destination. The pilot, under self-imposed pressure, likely elected to carry out a GPS approach to Runway 13 in IFR weather that was at or below landing limits. The other two approaches available were on Runway 31, both having the same landing limits as the approach to Runway 13.
Currently, there is no requirement for smaller Canadian-registered aircraft to be equipped with terrain awareness and warning systems (TAWS). Although Transport Canada has proposed new regulations which will require TAWS for commercially operated turbine-powered aircraft with six or more passenger seats, the regulation will not require TAWS to be installed on commercially operated turbine-powered aircraft with less than six passenger seats. The lack of regulation requiring TAWS on all commercially operated passenger aircraft places flight crew and passengers travelling on those aircraft at increased risk of CFIT.
The occurrence aircraft was fitted with a terrain awareness feature which would visually warn the pilot of the aircraft’s proximity to terrain if it got too low during an instrument approach. This type of equipment is an example of recent advances in technology designed to improve a pilot’s situational awareness and reduce the risk of CFIT. However, in order for its full potential to be realized, pilots must be properly trained in the use of the terrain awareness feature.
In this occurrence, the pilot received a brief familiarization session on the GPS, avionics, and terrain awareness feature that had been newly installed in the aircraft. It is unknown whether the terrain awareness feature was activated during

30 Recently Released TSB Reports ASL 4/2012
the RNAV approach to Runway 13. It is possible that the terrain awareness feature was activated and that the pilot did not understand the information that was being presented. The lack of adequate training on newly installed equipment, such as a GPS with a terrain awareness feature, increases the risk of improper use during flight.
It took two days for search and rescue (SAR) personnel to locate the aircraft. This is due to the 406 MHz ELT, which was not equipped with GPS encoding, only transmitting briefly before it was rendered inoperative. If 406 MHz ELTs are not GPS-encoded, there is increased risk that SAR services will be delayed unnecessarily if the ELT is rendered inoperative following an occurrence.
Aircraft flight path to Pokemouche Airport
Findings as to causes and contributing factors1. The pilot, under self-imposed pressure to meet an
unexpected charter request the next day, likely elected to carry out an RNAV approach in IFR weather that was at or below landing limits.
2. It is likely that the aircraft was inadvertently flown into terrain while the pilot was attempting to carry out the RNAV approach to Runway 13.
3. Attempting to use a new and unfamiliar GPS, terrain awareness feature and audio panel in adverse weather at night would have increased pilot workload, making it difficult to maintain situational awareness.
Findings as to risk1. The combination of a non-precision instrument approach,
conducted at night, with low ceilings and limited visibility significantly increases the risk of CFIT.
2. The lack of regulation requiring TAWS on all commercially operated passenger aircraft places flight crew and passengers travelling on those aircraft at increased risk of CFIT.
3. The lack of adequate training on newly installed equipment, such as a GPS with a terrain awareness feature, increases the risk of improper use during flight.
4. If 406 MHz ELTs are not GPS-encoded, there is increased risk that SAR services will be delayed unnecessarily if the ELT is rendered inoperative following an occurrence.
Other finding1. It is unlikely that the aircraft impacted the ground simply
because the altimeter had not been switched to the current Bathurst altimeter setting.
The winter season is just around the corner… …are you prepared?
Got something to say? The Civil Aviation Issues Reporting System (CAIRS) provides our stakeholders, including our clients and the public, with a means to raise issues (concerns, complaints, compliments, and suggestions for improvement) to the Civil Aviation Program of Transport Canada. Check it out!

ASL 4/2012 Accident Synopses 31
Note: The following accident synopses are Transportation Safety Board of Canada (TSB) Class 5 events, which occurred between February 1, 2012, and April 30, 2012. These occurrences do not meet the criteria of classes 1 through 4, and are recorded by the TSB for possible safety analysis, statistical reporting, or archival purposes. The narratives may have been updated by the TSB since publication. For more information on any individual event, please contact the TSB.
— On February 10, 2012, a Diamond DV-20 aircraft was on a VFR time-building flight from Moncton International (CYQM) to Bathurst (CZBF) airports. The aircraft lost control on landing and impacted a snow bank. The crew and passenger sustained minor injuries and the aircraft was substantially damaged. TSB File A12A0017.
— On February 11, 2012, a privately registered Cessna 150, converted to a tail dragger, was operating on a sandbar in the Fraser River north of Chilliwack Mountain, B.C. The aircraft came into contact with water during the take-off run, overturned, and came to rest partially submerged. There was only the pilot on board and he was not injured. The pilot was rescued by two other aircraft that landed at the same site. TSB File A12P0019.
— On February 11, 2012, a privately registered ultralight Beaver RX550 with one person on board was reported to have crashed near Rosa Lake, B.C., 20 NM south of Williams Lake VORTAC (YWL). A post-impact fire occurred. The pilot was rescued and transported to hospital with serious injuries. TSB File A12P0020.
Despite constant reminders, warnings, and on-the-job training, marshallers sometimes forget about turning propellers.
— On February 13, 2012, a de Havilland DHC-8-100 was operating from Cambridge Bay, Nun., to Yellowknife, N.W.T. On arrival, the aircraft was marshalled in to parking spot 9 on the main apron. The left engine was shut down and the right engine was feathered. The marshaller moved from the nose of the aircraft towards the right main landing gear area with wheel
chocks in hand and was struck by the propeller. The flight attendant provided immediate first aid and fire rescue personnel responded within one minute. The marshaller sustained serious injuries but was stable enough for MEDEVAC transportation to Edmonton. TSB File A12W0013.
— On February 14, 2012, a Cessna 150, with one pilot on board, was used to conduct a local VFR flight from the Montréal/St-Hubert Airport (CYHU), Que., without authorization. After takeoff, the aircraft climbed over the airport, nosed down, and struck the ground approximately 1 200 ft east of the Runway 24R threshold. The pilot was fatally injured and the aircraft was destroyed. TSB File A12Q0022.
— On February 17, 2012, a Cessna T206H on amphibious floats was about 10 NM from Springbank Alta., descending through 6 000 ft on approach when smoke was noticed coming from under the instrument panel. The pilot requested priority for landing and was cleared to the threshold of Runway 25. After advising the tower, the electrical system was shut down, but the smoke continued to become thicker. On short final the throttle control failed, and the aircraft landed in the grass about 140 ft short of the runway. The aircraft rolled onto the pavement and came to rest just before Taxiway Delta, on the south side of the centreline. The pilot and two passengers evacuated without injury, and the airport operations staff contained the fire. Maintenance determined that the turbocharger “V” clamp failed due to corrosion and the hot exhaust gasses initiated a fire in the engine compartment that breached the firewall. The aircraft had about 1 000 hr TTSN, most of which had been float operations on and over salt water. TSB File A12W0014.
— On March 5, 2012, a Lockheed 188A had departed from Goose Lake, N.W.T for Yellowknife. After takeoff, the right main landing gear jammed in a partially retracted position. Several attempts were made to lower the right main landing gear with alternate extension methods, but with no success. An emergency was declared and the aircraft landed on Runway 34 with the left main landing gear and nose landing gear extended. The aircraft departed the right side of the runway and came to rest in the airport infield. There were no injuries to the six flight crew members and no post-occurrence fire. The outboard gear door strut is suspected to have jammed the gear mechanism during landing gear retraction after takeoff. TSB File A12W0020.
Accident Synopses

32 Accident Synopses ASL 4/2012
— On March 5, 2012, a Cessna 182RG, was on a VFR training flight from the Chicoutimi/St-Honoré Airport (CYRC), Que., with one pilot and one instructor on board. During a touch-and-go on Runway 12, the aircraft landed on its belly and came to a stop on the runway. There was friction damage to the aircraft’s belly and propeller blades. There were no injuries. TSB File A12Q0031.
— On March 11, 2012, a Hughes 369D helicopter was transporting three passengers to a seismic survey site about 60 NM southwest of Anchorage, Alaska. After landing on snow the helicopter experienced a dynamic rollover and was substantially damaged. The pilot and passengers were not injured. The emergency locator transmitter (ELT) automatically activated during the incident. TSB File A12F0023.
— On March 14, 2012, a Eurocopter EC 130-B4 helicopter was conducting low-level wildlife management work in a heavily wooded area near the Ameson (VOR) (YAN) in Northern Ontario. While manoeuvring, the helicopter’s tail rotor struck a tree. The helicopter became uncontrollable and collided with the ground. The pilot and two crew members sustained minor injuries and were airlifted to safety by another helicopter. TSB File A12O0032.
— On March 17, 2012, a Citabria was conducting circuits at Prince George Airport (CYXS), B.C., when the aircraft touched down and ground-looped. The aircraft veered off the runway and overturned in the snow. The aircraft was substantially damaged. The pilot was the sole person on board and was unharmed. TSB File A12P0044.
— On March 17, 2012 a private Helio Courier H-391B was attempting a takeoff with a crosswind from Langley Airport (CYNJ), B.C., when the aircraft veered hard and ground-looped. The aircraft came to rest off the runway surface in a soft field with the wheels sinking into the mud. The right wing and horizontal stab contacted the ground causing extensive damage. TSB File A12P0043.
— On March 18, 2012, an amateur-built Super Ben 160 was on a local flight on skis from a private property. During the flight, fog formed on the ground, and the pilot turned back. He recognized Lac Louvier and decided to conduct a precautionary landing. The lake’s surface, measuring about 1 500 ft, was frozen. The aircraft did not slow down as anticipated and came to a stop in the trees at the far end of the lake. The aircraft impacted the trees at a reduced speed. The engine cowl and the left wing were damaged. The pilot and the passenger were uninjured. TSB File A12Q0037.
— On March 20, 2012, a Cessna 172N had taken off from the St-Frédéric Airport (CSZ4), Que., to conduct a circuit. This was the first solo flight for the student pilot. When landing on Runway 23 with wind blowing from 300° at 10 kt, the student pilot did not sufficiently deflect the ailerons against
the wind. The aircraft went off course to the left, the left wheel struck a runway edge light and the left landing gear collapsed. The aircraft spun 180° while sliding on the slope at the edge of the runway. The propeller touched the ground and the left wing crumpled, the rear fuselage folded in, and the stabilizer was bent out of shape. The student pilot was not injured and the emergency locator transmitter (ELT) was not activated. TSB File A12Q0040.
— On March 22, 2012, a Hughes 500 helicopter had taken off from Lac-à-la-Tortue (CSL3), Que., for Trois-Rivières, Que. At approximately 1.5 NM from its destination, the engine (Rolls-Royce, Allison C20B) shut down in flight. The pilot conducted an autorotation toward a railroad track. Upon landing, the skids slid next to the track and the aircraft tipped onto its side. The aircraft was assessed and no anomalies were found. The engine was placed on a test stand and showed no operating anomalies under any operating conditions. TSB File A12Q0043.
— On March 22, 2012, a Grob G120A was completing a practice forced landing and experienced a hard landing at Portage la Prairie Airport (CYPG), Man. The right main wheel detached from the aircraft. The crew elected to overshoot and returned to land on a different runway. On touchdown the left main landing gear partially collapsed. The aircraft departed the runway to the right and came to rest beside the runway in the grass. The crew was uninjured. Both main landing gear assemblies were damaged. TSB File A12C0030.
— On March 24, 2012, an Air Création XPGT582S ultralight on wheels took off from a field in Bury, Que., for a recreational flight, with the pilot and one passenger on board. About 15 min later, while cruising at low altitude, the left wing pointed towards the ground and the aircraft nosed down. The ultralight crashed into a forest and was severely damaged. The pilot did not survive and the passenger was seriously injured. The TSB is collaborating with the Quebec coroner’s office, which is conducting an investigation. TSB File A12Q0044.
— On March 25, 2012, a private Cessna 170 on wheels was attempting to land on a frozen lake 15 NM east of Smithers, B.C. The aircraft touched down prior to the threshold of the snowmobile compacted strip and nosed over onto its back. There were no injuries to the sole occupant. The 406 emergency locator transmitter (ELT) activated and was shut off by the pilot. TSB File A12P0041.
— On March 27, 2012, a privately operated Cessna A185F was on a local pleasure flight from the Cooking Lake Airport (CEZ3), Alta. The wind was from the south-southeast for arrival on Runway 10 with an estimated crosswind component of 5-8 kt. The initial touchdown was smooth but as the tail came down the aircraft swerved to the right resulting in the left wing tip scraping the runway. The aircraft departed the

ASL 4/2012 Accident Synopses 33
right side of the runway and the left wheel dislodged a conduit access cover and fell into the conduit. The aircraft came to rest on the left wing tip resulting in significant damage to the wing tip and left landing gear strut and wheel assembly. The pilot and three passengers were not injured. TSB File A12W0032.
— On March 31, 2012, the pilot-owner of a Kangook Th powered parachute was flying in the vicinity of Saint-Henri-de-Taillon, Que. When the powered parachute was at a very low altitude, the pilot was unable to avoid hitting a tree. The pilot sustained minor injuries and the aircraft was substantially damaged. TSB File A12Q0050.
— On April 5, 2012, a Van’s RV-6A had landed at a private airstrip near Leask, Sask. While taxiing off the runway, the aircraft’s nosewheel sank into a soft depression in the grass taxiway. The aircraft overturned and its fuselage, propeller, and vertical stabilizer were substantially damaged. The pilot was not injured. TSB File A12C0032.
— On April 12, 2012, a Piper PA-18-150 Supercub was landing on Runway 34 at Mackenzie Airport (CYZY), B.C. The aircraft was observed descending steeply and touched down at the mid-point of the runway at an estimated airspeed of 45-50 mph. There was a crosswind at 310° and 8 kt. The aircraft bounced and the pilot regained control with full throttle application. The aircraft was pointing straight down the runway when a wind gust reportedly picked up the left wing. It subsequently stalled with a right wing drop; the aircraft punched through a perimeter fence to the right of the runway, impacted a small berm, and flipped over. The pilot of this tandem-seating plane was in the front wearing a seat belt restraint system with shoulder harness, and the passenger was wearing a lap belt. Both occupants extricated themselves from the aircraft. The passenger was taken to hospital for observation. The aircraft was substantially damaged. TSB File A12P0050.
— On April 14, 2012, the pilot of a Piper PA-14 Family Cruiser was performing circuits on Runway 25 at Boundary Bay Airport (CZBB), B.C. On its third landing, the aircraft touched down, bounced and porpoised before veering off to the right side of the runway and into the grass. The pilot shut off the engine, fuel valve, and electrics as the aircraft was rolling but it entered a ditch and nosed over before coming to a full stop. It came to rest inverted in the ditch. The pilot was wearing only a lap seat belt and was able to exit the aircraft uninjured. The aircraft was substantially damaged, and fuel was leaking into the ditch. The aircraft was righted in short time to prevent further contamination and the risk of fire. TSB File A12P0052.
— On April 14, 2012, a Bellanca 7ECA Citabria tow plane was landing beside Runway 06 at Pemberton Airport (CYPS), B.C., when it flipped over. The pilot
was on the first approach to land for the season. The aircraft was low and slow on final and touched down in the grass area abeam the runway near the end, in an area with standing water; there was no braking action but it decelerated rapidly in the standing water and overturned. The pilot was wearing a seat belt restraint system with shoulder harness and extricated with minor leg scrapes. TSB File A12P0053.
— On April 15, 2012, a Schweizer SGS 2 33A glider landed short of Runway 36 at Oliver Airport (CAU3), B.C., in a peach tree orchard. The solo pilot was apparently not injured, but taken to hospital for observation. The aircraft damage was limited to the wings. TSB File A12P0054.
— On April 15, 2012, a Taylorcraft BC12-DX was hand started at Finlay Air Park (CDH3), N.S. Once started, the engine RPM continued to increase. Before the pilot could enter the cabin, the unoccupied aircraft jumped the chocks and impacted the side of a hangar. The hangar sustained minor damage while the aircraft was substantially damaged. The pilot was uninjured. It is likely that the throttle resistance was not adjusted properly which allowed the engine power to increase above idle. TSB File A12A0041.
— On April 15, 2012, a privately operated Kitfox Model 1 crashed after an attempted takeoff from a grass strip 10 MN east of Manning, Alta. The pilot and passenger sustained minor injuries. TSB File A12W0040.
— On April 18, 2012, a privately operated Grumman Tiger AA-5B was on a local VFR training flight from the Lachute Airport (CSE4), Que., with an instructor and a student on board. While practicing touch-and-goes, the aircraft bounced on the nose wheel during one of the landings, and when the wheel touched down again the aircraft momentarily left the runway and drove on the grass before pulling back onto the runway. There were no injuries; the damage to the aircraft was mainly to the propeller, which had made contact with the runway. TSB File A12Q0055.
— On April 20, 2012, a privately owned Bellanca 7KCAB tail-dragger aircraft was landing in crosswind conditions. Shortly after touchdown the pilot lost directional control and the aircraft ground-looped. The right-hand side wing, wing strut, and landing gear were substantially damaged. TSB File A12O0053.
— On April 28, 2012, an Aeronca 7BCMX on floats was taking off from Pelican Lake in the vicinity of Sioux Lookout, Ont., when a float strut bracket broke and the left strut collapsed. The pilot aborted the takeoff immediately and the aircraft remained upright. The aircraft was towed to shore. There were no injuries and the damage was confined to the float and strut assembly. TSB File A12C0042.

34 Regulations and You ASL 4/2012
The Suspension or Cancellation of Canadian Aviation Documents Due to “Incompetence”by Jean-François Mathieu, LL.B., Chief, Aviation Enforcement, Standards, Civil Aviation, Transport Canada
Previous issues of the ASL have contained articles that described the recently published staff instructions SUR-014, 015 and 016—the Transport Canada Civil Aviation (TCCA) internal guidance material related to the suspension or cancellation of a Canadian aviation document (CAD) or revocation of managerial positions approved by the Minister. The first article introduced these TCCA staff instructions, and indicated that future articles would delve further into the legal authorities that the Minister has for “certificate action”, i.e., the suspension or cancelation of CADs, such as licences or certificates. The second article in this series detailed the suspension of a CAD under the authority of section 7.(1) of the Aeronautics Act (the Act), which enables a TCCA inspector to respond to an “immediate threat to aviation safety”. This article will focus on the Minister’s authority to take certificate action when “the holder of the document is incompetent.”
Section 7.1(1) of the Act specifies that the Minister may take certificate action for safety reasons other than a situation that poses an immediate threat to aviation safety. The three reasons are listed in paragraphs 7.1(1)(a), (b) and (c) of the Act:
a. the holder of the document is incompetent; b. the holder or any aircraft, airport or other facility in respect
of which the document was issued ceases to meet the qualifications necessary for the issuance of the document or to fulfil the conditions subject to which the document was issued; or
c. the Minister is of the opinion that the public interest and, in particular, the aviation record of the holder of the document or of any principal of the holder, as defined in regulations...warrant it.
The meaning of “incompetent”—in terms of paragraph 7.1(1)(a) of the Act—is a fundamental concept that must be clearly understood. This key term is not specifically defined in the Act or in the Canadian Aviation Regulations (CARs). For guidance, we can consider dictionary definitions, as well as past determinations of the Transportation Appeal Tribunal of Canada (TATC).
The Concise Oxford Dictionary, Eighth Edition, defines “incompetent” as:
• not qualified or able to perform a particular task or function • showing a lack of skill• not able to perform its function.1
1 The Concise Oxford Dictionary, Eight Edition, Oxford University Press, Oxford, U.K. 1990, p. 598
The definition for “incompetent” in Merriam Webster’s Collegiate Dictionary, Tenth Edition, includes: • inadequate to or unsuitable for a particular purpose• lacking the qualities needed for effective action• unable to function properly”.2 In this context, “incompetence” refers to the inability to perform required activities. Therefore, it is an inability to comply rather than an unwillingness to comply.
The TATC3 has previously rendered decisions on the concept of “incompetence” and has adhered to a set of principles that were enumerated in Mason v. The Registered Nurses’ Association of British Columbia:
1. The particular definition placed upon the word ‘incompetency’ should be molded by the object of the enactment in which the word appears.
2. All the definitions of ‘incompetency’ focus on the lack of ability, capacity or fitness for a particular purpose.
3. The want of capacity, ability or fitness may arise from a lack of physical or mental attributes. However, a person not lacking in physical or mental attributes may nonetheless be incompetent by reason of a deficiency of disposition to use his or her abilities and experience properly.
4. Negligence and incompetence are not interchangeable terms. A competent person may sometimes be negligent without being incompetent. However, habitual negligence may amount to incompetence.
5. A single act of negligence unaccompanied by circumstances tending to show incompetency will not of itself amount to incompetence.4
The TATC has also further amplified the first principle: “The object of the enactment in which incompetence appears (i.e., Aeronautics Act) is aviation safety.”5
Evidence that collectively demonstrates an inability to comply with the regulations and standards, over a reasonably lengthy period of time, demonstrates a state of incompetence; one or two incidents do not constitute sufficient grounds to substantiate incompetence. The evidence used by the Minister to support certificate action is itemized in the Notice of Suspension (NoS) or Notice of Cancellation (NoC) served to the document holder. The burden of proof rests with the 2 Merriam Webster’s Collegiate Dictionary, Tenth Edition, Merriam-Webster,
Springfield, MA, 1996, p. 5883 TATC File No. C-3128-214 Mason v. Registered Nurses’ Assn. of British Columbia, 102 D.L.R. (3d) 225.5 CAT File No. A 1789 25, p. 9
Regulations and You

ASL 4/2012 Regulations and You 35
Minister, who must prove on the balance of probabilities [subsection 15.(5)] of the Transportation Appeal Tribunal of Canada Act, that certificate action is warranted.
There are often similar characteristics or an interrelationship between the circumstances and criteria cited to support certificate action under the various provisions of section 7.1(1) of the Act. For example, a significant history of non-compliance may result in certificate action under Section 7.1(1)(a) (incompetence), or Section 7.1(1)(c) (public interest). In order to support a certificate action taken under Section 7.1(1)(a) —based on the incompetence of a CAD holder—it must be demonstrated that the repetitive non-compliant acts are the result of an inability to comply rather than an unwillingness to comply. In contrast, repetitive non-compliant behavior—which was not based on incompetence, but instead conducted to further other needs such as a business or financial goals—would support certificate action under Section 7.1(1)(c), for reason of public interest. In consideration of the available evidence, TCCA will determine the appropriate course of action to be taken.
There are a number of legislative requirements in both the Act and the CARs that specify the form and content of an NoS or NoC. Certificate action under any of the provisions of section 7.1(1) of the Act is not taken in response to an immediate threat to aviation safety (section 7.(1) of the Act deals with immediate threats to safety). Therefore, because an immediate threat to aviation safety is not present, the CAD holder is provided an
effective date of the suspension or cancellation that is a later date than the date of service of the notice (typically 30 days). The notice will include a clear and accurate description of the nature of the alleged incompetence. In the case of suspension, because suspensions under the authority of this section of the Act are intended to deal with safety related matters, no duration for the suspension will be stipulated. However, an NoS will include the conditions necessary to resolve or rectify the incompetence (there may be more than one) in order to terminate the suspension.
Due to the nature of “incompetence” as defined above, certificate action for this reason is only applicable to an individual; it does not apply to a corporation.
The NoS or NoC will include a notification that the recipient must return the CAD to the Minister immediately after the suspension or cancellation takes effect. This is a requirement of section 103.03 of the CARs. Refusal (or failure) to return the CAD to the Minister following a suspension or cancellation constitutes a contravention of this section of the CARs.
This type of certificate action is subject to review by the TATC. Any person who has been served with an NoS or NoC for “incompetence” may request a review of the Minister’s decision before the TATC.
For more information on the subject, please refer to Staff Instruction SUR-014.
TC AIM Snapshot: Monitoring 126.7 MHz and Position Reporting En route
Pilots operating VFR en route in uncontrolled airspace when not communicating on an MF, or an ATF, or VFR on an airway should continuously monitor 126.7 MHz and whenever practicable, broadcast their identification, position, altitude and intentions on this frequency to alert other VFR or IFR aircraft that may be in the vicinity. Although it is not mandatory to monitor 126.7 MHz and broadcast reports during VFR or VFR-OTT flights, pilots are encouraged to do so for their own protection.
(Ref: Transport Canada Aeronautical Information Manual (TC AIM), Section RAC 5.1)
Invest a few minutes into your safe return home this winter... ...by reviewing section AIR 4.13 of the Transport Canada Aeronautical Information Manual (TC AIM), titled “First Aid
Kits on Privately Owned and Operated Aircraft.”

36 Debrief ASL 4/2012
DON’T WALK OUT... Stay in the Prime Search AreaThis is a slightly updated version of an article originally published in Aviation Safety Letter Issue 1/1997. Good advice!
Walking, they say, is as good as running. But not always. If you’re trying to stay in shape, walking can indeed be as good as running. But if you’re trying to get your shape back to the jungle we call civilization, walking can be hazardous to your health.
Years ago, when luckless aviators found themselves contemplating a wrecked biplane zillions of miles from the nearest outpost, they had no choice but to walk out. But it was at least 50 years ago when such teaching went out of style. With the advent of search and rescue (SAR), radios, emergency locator transmitters (ELT) and, more lately, GPS, the advice is to stay with the aircraft.
Why? Because when SAR starts looking for people, it goes to the last known point, then follows the proposed track. Although they’re really looking for the people inside the airplane, they have long since learned that the aircraft is easier to see than the people. Thus the search tends to concentrate on that area between the last known point and the proposed destination.
The search isn’t confined to that area, but it does start there, and initially concentrates there. During the search, SAR and Civil Air Search and Rescue Association (CASARA) crews look for anything unusual. You might think that a person wandering through the woods in a passionate purple T-shirt and bright yellow stretch pants would stand out, but such targets are pretty small. Even the larger remnants of, say, a single-engine Cessna or Piper are hard to see. But they are bigger than the average person.
Thus, SAR organizes the searches to find the downed aircraft. What does this mean to restless campers who think that walking out is showing admirable initiative? Unless they are retracing their proposed flight route, it means that they are moving away from the primary search area; away from possible detection.
Once in a while, there are valid reasons to move away from the crash site. If the aircraft slides underwater, you shouldn’t go much farther than the nearest shore. If you’re in the middle of a forest fire, you’d probably want to move to the upwind side.
Most of the time, you should stay with or in proximity to the wreckage. If you can get at the ELT, move its function switch to ON. Then leave it there. The SAR tech who comes to your rescue can make any further switch selections.
Of course, you want to make yourself visible to SAR or CASARA crews. During the day, smoke gets attention. Your campfire, covered with pine boughs, will have local environmentalists on your case in no time. You can also add a touch of oil from the engine crankcase, just to make the smoke smokier.
Shiny bits from the aircraft can make signalling mirrors that you can use to attract the attention of SAR crews. Or, as one pilot did recently, you can arrange larger chunks of aircraft in a nearby clearing to make it show up better for airborne searches.
Search efforts taper off at night, as SAR crews are not wild about flying into mountains. However, there are overflights, and most pilots are pretty good about reporting fires in areas where no fires had trodden before. Thus, an especially exuberant signal fire should get attention.
If you’re an incorrigible Type A and think you must walk out—don’t. Not unless you can see the lights of a nearby town, and the road connecting you to it. Even then, remember that distances are deceiving. If you must leave, leave a message of some sort. Let SAR know that you survived, and that you are walking northeast to salvation.
Salvation is fine. Too often however, it becomes eternity.
Stay with your aircraft.
Debrief

2012 Flight Crew Recency RequirementsSelf-Paced Study Program
Refer to paragraph 421.05(2)(d) of the Canadian Aviation Regulations (CARs).
This questionnaire is for use from November 1, 2012, to October 31, 2013. Completion of this questionnaire satisfies the 24-month recurrent training program requirements of CAR 401.05(2)(a). It is to be retained by the pilot.
All pilots are to answer questions 1 to 29. In addition, aeroplane and ultralight aeroplane pilots are to answer questions 30 and 31; helicopter pilots are to answer questions 32 and 33; gyroplane pilots are to answer question 34 and 35; glider
pilots are to answer questions 36 and 37; and balloon pilots are to answer questions 38 and 39.
Note: References are at the end of each question. Many answers may be found in the Transport Canada Aeronautical Information Manual (TC AIM). Amendments to that publication may result in changes to answers or references, or both.
The TC AIM is available on-line at: www.tc.gc.ca/eng/civilaviation/publications/tp14371-menu-3092.htm
1. Reportable aviation accidents and incidents, and missing aircraft are to be reported to the _______________________ or alternatively through _____________________, which will forward the report. (GEN 3.3.5)
2. A low level airway extends upwards from _______ ft ASL/AGL above the surface of the earth and is controlled/uncontrolled airspace. (GEN 5.1, RAC 2.8.5)
3. When a section of a runway or a heliport is closed, it is marked with _______________________________________. (AGA 5.6)
4. A dry Transport Canada standard wind direction indicator blowing at an angle of 5° below horizontal indicates a wind speed of ___ kt. (AGA 5.9)
5. In communications checks, “strength 2” means ________________________________________________________. (COM 5.10)
6. The onus for determining if passenger-operated electronic devices will cause interference is placed on _____________. (COM Annex B 2.0)
7. Portable electronic devices, other than two-way radiocommunication devices, may be used on board aircraft except during ________________________________________________________________________________________.
(COM Annex B 3.1)8. What does the following symbol on a graphic area forecast (GFA) represent? _____________________________.
(MET 3.3.5)9. What does the following symbol on a GFA mean (direction and speed)? _____________________________
______________________________________________________________________________________________. (MET 3.3.11)
TAF CYOW 231438Z 2315/2412 02012G22KT 6SM -RA BR SCT005 OVC015 TEMPO 2315/2321 3SM -RA BR BKN005 OVC015 BECMG 2315/2317 04015G25KT FM232200 07015KT 2SM -SHRA BR BKN005 OVC010 TEMPO 2322/2402 6SM -SHRA BR OVC010 BECMG 2400/2402 20012KT FM240200 20010G20KT 5SM -SHRA BR FEW003 BKN010 OVC040 TEMPO 2402/2408 P6SM NSW OVC020 FM240800 18010KT P6SM BKN010 OVC040 RMK NXT FCST BY 231800Z=10. According to the aerodrome forecast (TAF) above, what will the wind be at 1700Z on the 23rd? _________________.
(MET 3.9.3)11. According to the TAF above, what is the visibility at 2200Z on the 23rd? ____________________________________.
(MET 3.9.3)12. According to the TAF above, from 0200Z to 0800Z on the 24th there will be temporary periods of _______________.
(MET3.9.3)METAR CYXU 032000Z 22015KT 5SM HZ SCT010 BKN025 12/09 A3000 RMK CU3SC2 SLP161=13. While flying over London (CYXU), field elevation 912 ft, a pilot would expect to encounter the ceiling at an altitude
of approximately _____ ft ASL. (MET 3.15.3)14. State four (4) differences between human observations and automated weather observation system (AWOS)
observations. _________________________________________________________________________________________________________________________________________________________________________________.
(MET 3.15.5)UACN10 CYQB 291835 UL UA/OV CYQB /TM 1830 /FLDURD /TP DH8 TB MDT 080-02015. What is reported in the above pilot weather report (PIREP) and at what time was it reported?_________________________________________________________________________________________________.
(MET 3.17)16. To assist in reducing frequency congestion, pilots are encouraged to use the phrase ____________ on the initial call to a
ground station to indicate that they have received ____, ____, and ______ information from the previous aerodrome advisory. (RAC 4.5.6)

17. What two radio transmissions are mandatory when departing from an uncontrolled aerodrome within a mandatory frequency (MF) area? ____________________________________________________________________________.
(RAC 4.5.7, CAR 602.100)18. Where possible, pilots are required to report at least five _______ prior to entering an MF area.
(RAC 4.5.7, CAR 602.101)19. Wire-strikes account for a significant number of low-flying accidents. A number of these accidents occur over
__________ terrain, in ____ weather and at ________ altitudes. (RAC 5.4)20. Every few months, or as recommended by the manufacturer, pilots should test their emergency locator
transmitter (ELT). Testing of a 121.5/243 MHz ELT must be conducted only during the first ___ minutes of any UTC hour and restricted in duration to not more than ___ seconds.
(SAR 3.8, CARs Standard 571 Appendix G)21. Raising a portable ELT from ground level to 2.44 m (8 ft) increases its range by ________ percent.
(SAR 3.6)120059 CYKZ TORONTO/BUTTONVILLE MUNICIPAL CYKZ RWY 33 CLSD 1210101900 TIL APRX 121012170022. When does the above NOTAM expire?_______________________________________________________________.
(MAP 5.6.1)23. Closure of airspace due to forest fires can be found under which NOTAM file? ______________________________.
(MAP 5.6.8)24. For how long is an aviation document booklet valid? ___________________________________________________.
(LRA 1.2, CAR 401.12)25. Structures assessed as _____________________________________ are required to be marked. Special high intensity
strobe lighting is required for all structures ____ ft AGL and higher. The majority of aircraft collisions with man-made structures occur at levels below ___ ft AGL. (AIR 2.4)
26. Severe turbulence may extend up to ___ NM from severe thunderstorms. (AIR 2.7.1)27. In the event of a forced landing in sparsely settled areas, survival will depend on preparations and knowledge. The
need to carry ______________________ that will provide protection from insects in the summer and ________ in the other seasons cannot be overstressed. (AIR 2.14)
28. The most common causes of fatigue are ________________, _____________, and ____________________________. (AIR 3.8)
29. Go to the NAV CANADA Aviation Weather Web Site (www.flightplanning.navcanada.ca/cgi-bin/CreePage.pl?Langue=anglais&NoSession=NS_Inconnu&Page=forecast-observation&TypeDoc=html).
From the “Forecasts and Observations” page, open the AIC page and bring yourself up-to-date. Record the number of the latest AIC here: _____________________________________________________________________________.
Aeroplane-specific questions (including ultralight)30. On flights from Canada to the U.S., the U.S. Customs and Border Protection (CBP) requires a passenger manifest no
later than ___________ before an aircraft departs. (FAL 2.3.2)31. How many litres is 100 lbs of AvGAS at 15° C?_____. Your aircraft burns 6 U.S. gallons per hour, how long can you
fly on 100 lbs?_______. (RAC 3.5.8, Canada Flight Supplement [CFS] General Section—Fuel and Oil Weights)Helicopter-specific questions32. Most rotorcraft flight manuals state in the limitation sections that at night the pilots must maintain visual reference to
the ground by one of the following means: ___________________ or ______________________________________.(Rotorcraft flight manuals, rotorcraft references)
33. For an extended over-water flight, you should consider wearing your ________________ because preparation and knowledge are paramount to survival in ditching events.
(Aviation Safety Letter [TP 185] 3/2010 “Take Five”, helicopter references)Gyroplane-specific questions34. What could happen if the gyroplane experiences “zero G”? ______________________________________________.
(Gyroplane references)35. When a low rotor RPM produces an excessive coning angle, the disc area increases/decreases and the rotor thrust
increases/decreases. (Gyroplane references)Glider-specific questions36. The release-hook check should be made twice: once with the launch cable _____ and once with the launch cable ____
______________________________________________________________________________________________. (Glider references)
37. When joining another glider in a thermal, you are to circle in the opposite/same direction as the other glider. (Glider references)Balloon-specific questions
38. If frost develops at a propane tank valve stem, what should you suspect is the cause? _________________________________________________________________________________________________.
(Balloon references)39. To launch an 84-ft balloon within a built-up area, the diameter of the launch site may be no less than ____________.
(CAR 602.13)Answers to this quiz are found on page 16 of ASL 4/2012.