
Automaattisten segmentointialgoritmien analysointi - Jultika
19
Automaattisten segmentointialgoritmien analysointi Fysiikan kandidaatti opinnäytetyö Arttu Cowell 28.12.2019
-
Upload
khangminh22 -
Category
Documents
-
view
8 -
download
0
Transcript of Automaattisten segmentointialgoritmien analysointi - Jultika
Automaattisten segmentointialgoritmien analysointi
Fysiikan kandidaatti opinnäytetyö
Arttu Cowell
28.12.2019
Oheisessa tekstissä käsittelen viittä eri automaattista segmentointialgoritmia. Algoritmeja analysoitiin
Matlab skriptillä, joka laski Dice Similarity Coefficientit (DSC) ja ruston paksuus poikkeamista verrattuna
manuaalisesti segmentoiduista polvien magneettikuvista. DSC mittaa kuvien yhtäläisyyssuhdetta pikseli
kohtaisesti, kombinoituna paksuus analysoinnilla sain kvantitatiivisesti mitattua algoritmien pätevyyden ja
vertasin vastaavan tyyppisten tutkimusten tuloksiin. Saadusta datasta huomasin automaattisten
algoritmien potentiaalin laajassa kliinisessä polven nivelrikko -tutkimuksessa pienen lisäoptimoinnin
jälkeen.
Projekti alkoi Oulun yliopistollisen sairaalan Reasearch Unit of Medical Imaging, Physics and
Technology antamana ja ohjaamana kesätyöprojektina, mutta kahden kuukauden aikainen työaika ei
riittänyt suorittamaan projektia loppuun, joten sovittiin, että teen työn loppuun kandityönä. Projektia
ohjasi Eveliina Lammentausta ja työssä käytetty analysointi algoritmi oli Mikael Juntulan kirjoittama.
Paperissa kirjoitetut tekstit, johtopäätökset datasta, kuvat, kaaviot ja analysointiskriptin käyttö ovat kaikki
omaa tuotostani.

Evaluation of multiple automatic knee cartilage
segmentation algorithms
Abstract
Commonly in osteoarthritis studies, large
amounts of MRI data are acquired and cartilage is
manually delineated from the MRI data. We
investigate automatic segmentation frameworks
in order to obtain quantitative data on articular
cartilage morphology. We cover Mokkula, a
manual segmentation framework, atlas-based
automatic segmentation methodologies and a
patch-based technique comparing their
respective segmentation accuracies. Using
Laplace’s equation to calculate cartilage thickness
error (LTE), a vector thickness error method (VTE)
and Dice Similarity Coefficient (DSC) to assess the
accuracy of these techniques. The most accurate
segmentations reached DSC of 0,87 on both the
Femur and Tibia. The thickness analysis gave
avarage errors of 0,32mm over the Femur and
0,36mm over the Tibia. We feel these values are
reaching high enough stantards to be used in
large studies.
Introduction
Osteoarthritis (OA) is a joint disease affecting
significant populations worldwide [1]. Symptoms
of OA include swelling, pain, discomfort, and
locking of the joint [2]. It has been hypothesized
that OA is the result of multiple factors, e.g.
biomechanical stress and joint injury, eventually
leading to the degeneration of cartilage [3].
Cartilage has a limited ability to regenerate and
repair itself. This ability becomes less effective as
an individual ages making OA common amongst
the elderly [4]. Currently it is not understood
what causes OA to develop in young individual,
but genetics and obesity have been speculated to
have an effect [5][6]. Treatment of OA is highly
limited but knee joint replacement surgery can
help relieve pain and recover mobility [7]. The
use of Magnetic Resonance Imaging (MRI) in
clinical diagnosis of OA has increased recently
because MRI has the ability to detect signal and
morphologic changes of articular cartilage in 3D
[8].
Using MRI to study articular
cartilage is not straightforward. In order to study
the progression of OA one needs to follow the
cartilage borders closely. Morphological changes
in cartilage thickness are small in the span of a
few years, which means that the cartilage surface
changes its shape very slowly in a normal aging
patient [9].
Having a high contrast to noise ratio and high
signal to noise ratio (SNR) is important to
distinguish the bone-cartilage interface [10].
Turning the MR images into quantifiable research
data is a challenge. Segmenting articular cartilage
is currently performed manually by trained
experts. This process of manual segmentation can
be laborious and could take hours with 3D MRI
protocols. Recent studies have shown that
automatic segmentation methods, where a
computer analyses reference data to perform
segmentation using machine learning, for
instance, is a much faster process [11]. Automatic
segmentation methods could help in gathering
quantitative data in order to research and
development treatments for OA.
International workshop on
osteoarthritis imaging (IWOAI) Nordic segment
organized the knee cartilage segmentation
challenge in Oulu, Finland 2016, receiving entries
from five separate development teams. All
entries were atlas-based segmentation methods
and performed segmentation without expert
supervision. In this paper, we evaluated the
accuracy of these algorithms using manually
segmented images as the reference data.
Materials and Methods
Dataset
We gathered 44 knee MR images from the Oulu
Knee Osteoarthritis (OKOA) study [12] with the
criteria that the patients must have a Kellgren –
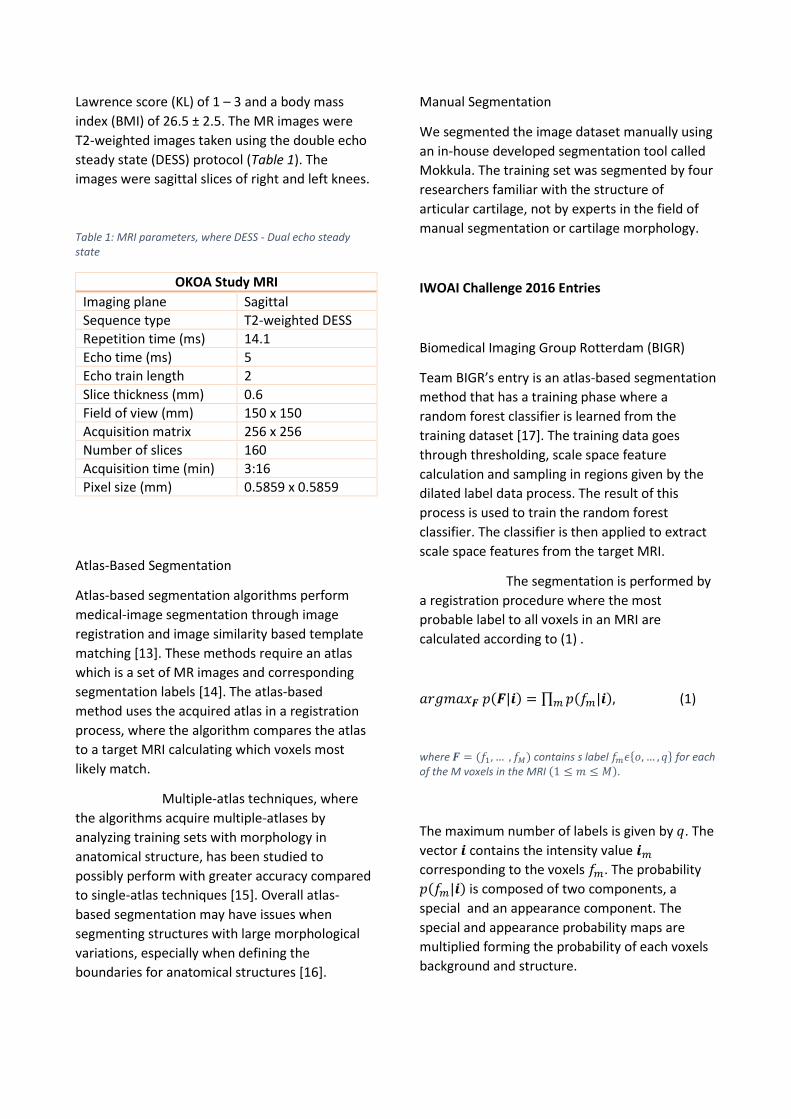
Lawrence score (KL) of 1 – 3 and a body mass
index (BMI) of 26.5 ± 2.5. The MR images were
T2-weighted images taken using the double echo
steady state (DESS) protocol (Table 1). The
images were sagittal slices of right and left knees.
Table 1: MRI parameters, where DESS - Dual echo steady state
OKOA Study MRI
Imaging plane Sagittal
Sequence type T2-weighted DESS
Repetition time (ms) 14.1
Echo time (ms) 5
Echo train length 2
Slice thickness (mm) 0.6
Field of view (mm) 150 x 150
Acquisition matrix 256 x 256
Number of slices 160
Acquisition time (min) 3:16
Pixel size (mm) 0.5859 x 0.5859
Atlas-Based Segmentation
Atlas-based segmentation algorithms perform
medical-image segmentation through image
registration and image similarity based template
matching [13]. These methods require an atlas
which is a set of MR images and corresponding
segmentation labels [14]. The atlas-based
method uses the acquired atlas in a registration
process, where the algorithm compares the atlas
to a target MRI calculating which voxels most
likely match.
Multiple-atlas techniques, where
the algorithms acquire multiple-atlases by
analyzing training sets with morphology in
anatomical structure, has been studied to
possibly perform with greater accuracy compared
to single-atlas techniques [15]. Overall atlas-
based segmentation may have issues when
segmenting structures with large morphological
variations, especially when defining the
boundaries for anatomical structures [16].
Manual Segmentation
We segmented the image dataset manually using
an in-house developed segmentation tool called
Mokkula. The training set was segmented by four
researchers familiar with the structure of
articular cartilage, not by experts in the field of
manual segmentation or cartilage morphology.
IWOAI Challenge 2016 Entries
Biomedical Imaging Group Rotterdam (BIGR)
Team BIGR’s entry is an atlas-based segmentation
method that has a training phase where a
random forest classifier is learned from the
training dataset [17]. The training data goes
through thresholding, scale space feature
calculation and sampling in regions given by the
dilated label data process. The result of this
process is used to train the random forest
classifier. The classifier is then applied to extract
scale space features from the target MRI.
The segmentation is performed by
a registration procedure where the most
probable label to all voxels in an MRI are
calculated according to (1) .
𝑎𝑟𝑔𝑚𝑎𝑥𝑭 𝑝(𝑭|𝒊) = ∏ 𝑝(𝑓𝑚|𝒊)𝑚 , (1)
where 𝑭 = (𝑓1, … , 𝑓𝑀) contains s label 𝑓𝑚𝜖{𝑜, … , 𝑞} for each of the M voxels in the MRI (1 ≤ 𝑚 ≤ 𝑀).
The maximum number of labels is given by 𝑞. The
vector 𝒊 contains the intensity value 𝒊𝑚
corresponding to the voxels 𝑓𝑚. The probability
𝑝(𝑓𝑚|𝒊) is composed of two components, a
special and an appearance component. The
special and appearance probability maps are
multiplied forming the probability of each voxels
background and structure.

Biomediq Shape and Texture
The Biomediq texture and shape teams used the
knee image quantification (KIQ) framework for
segmentation which combines rigid multi-atlas
registration, supervised voxel classification and
shape modeling in a multi-structure setting
[18][19]. The voxel classification step includes an
ROI analysis and feature selection step for each
structure. Before using the KIQ framework, some
pre-processing steps are taken, the manual
cartilage compartments from the training dataset
is sub-divided into medial and lateral sub-
compartments approximately at the trochlea. The
quality-assurance steps of the KIQ framework
removed two knees from their training dataset,
noticing a very low SNR on their MRI’s and some
misplaced manual segmentation.
The statistical shape model was
trained analyzing the training dataset and using
the pre-processed manual masks. The shape
model parameters were optimized using the
Bootstrap framework. In post-processing the
medial and lateral cartilage sub-compartments
are merged to form a singular tibial and femoral
compartment.
Combinostics
The Combinostics team submitted their multi-
atlas brain segmentation algorithm to our
challenge. This method uses non-rigid
registration, multi-atlas selection, and multi-atlas
combination [11]. Non-rigid registration is often
formulated as a maximization or minimization
problem of the cost function (2).
𝐸 = 𝐸𝑑𝑎𝑡𝑎 + 𝛾𝐸𝑚𝑜𝑑𝑒𝑙 (2)
Here Edata represents similarity or dissimilarity
between atlas and target image, Emodel is a
regularization term that constrains the
transformation that maps the atlas to the target
image denoted by 𝐓 = 𝐓(x, y, z) to be smooth
and γ is a user-defined weight that determines
the trade-off between both terms.
Combinostics used an intensity-
based selection method which calculates
normalized mutual information (NMI). The NMI
value was computed by dilating the binary
segmentations of the structure and using the
resulting binary image as a mask for NMI
computation. The dilation was used for including
the structure borders and their surroundings into
the mask.
The Combinostics team’s algorithm
was designed and optimized for brain
segmentations. The team sent us their algorithm
and we used it on the challenge data without
extensive optimization of the algorithm for knee
cartilage segmentation.
Deep In Progress
The Deep In Progress team used a patch-based
voxel classification technique that employs a 3D
convolutional neural network (CNN) for
supervised segmentation [20]. The neural
network was developed by Deep In Progress and
was trained through back- and forward
propagation of the network with labelled sample
data. In the network training technique, the
training set was turned into patches of various
sizes and fed into the neural network and all
voxels labelled in the reference masks as cartilage
were included.
Inverse distance transform called
taxicab was used to compute sample voxel
distances to cartilage in order to gather all voxels
with a three-voxel radius from a labelled voxel to
include in the training of the network. For each
sampled voxel they extracted two patches of
9x9x9 and 5x5x5 with the voxel and the patches
(x, y, z) coordinates were fed in three separate
CNNs in order to be classified, the output from
each CNN was then concatenated.
The training periods were divided
into epochs, where batches of 150 voxels were
fed into the network, until all sampled voxels had
been used for training. Voxels were then
resampled in the same way, before training was
continued. From every fifth epoch the
parameters were saved and the best match
image used for evaluation. An optimal set of
parameters was then used to segment the full set
of training images and evaluation images. The
Deep In Progress team noticed issues in two of
the training set masks we provided and didn’t use
them in their segmentation training procedure.
The segmented images went
through post-processing where the training MRIs
were registered onto the evaluation MRIs. The
segmented images are then processed by a
largest connected component (LCC) method in
order to select three largest connected segments.
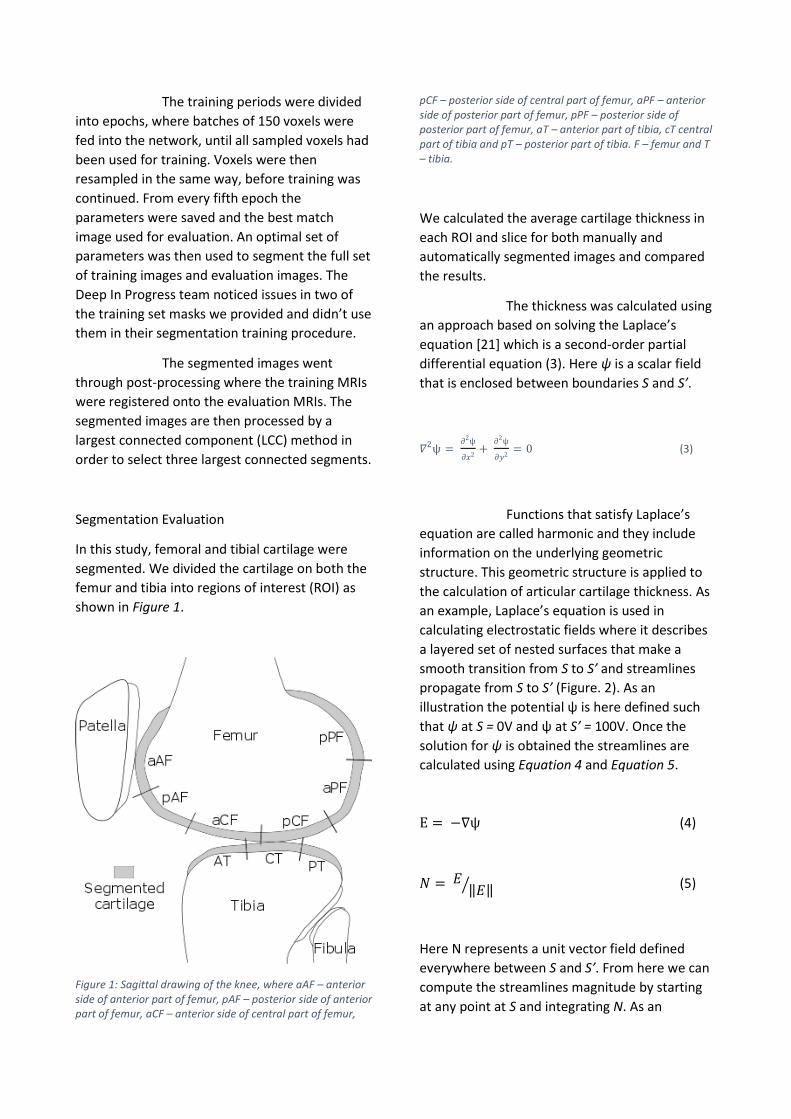
Segmentation Evaluation
In this study, femoral and tibial cartilage were
segmented. We divided the cartilage on both the
femur and tibia into regions of interest (ROI) as
shown in Figure 1.
Figure 1: Sagittal drawing of the knee, where aAF – anterior side of anterior part of femur, pAF – posterior side of anterior part of femur, aCF – anterior side of central part of femur,
pCF – posterior side of central part of femur, aPF – anterior side of posterior part of femur, pPF – posterior side of posterior part of femur, aT – anterior part of tibia, cT central part of tibia and pT – posterior part of tibia. F – femur and T – tibia.
We calculated the average cartilage thickness in
each ROI and slice for both manually and
automatically segmented images and compared
the results.
The thickness was calculated using
an approach based on solving the Laplace’s
equation [21] which is a second-order partial
differential equation (3). Here ѱ is a scalar field
that is enclosed between boundaries S and S’.
𝛻2ѱ = 𝜕2ѱ
𝜕𝑥2+
𝜕2ѱ
𝜕𝑦2= 0 (3)
Functions that satisfy Laplace’s
equation are called harmonic and they include
information on the underlying geometric
structure. This geometric structure is applied to
the calculation of articular cartilage thickness. As
an example, Laplace’s equation is used in
calculating electrostatic fields where it describes
a layered set of nested surfaces that make a
smooth transition from S to S’ and streamlines
propagate from S to S’ (Figure. 2). As an
illustration the potential ѱ is here defined such
that ѱ at S = 0V and ѱ at S’ = 100V. Once the
solution for ѱ is obtained the streamlines are
calculated using Equation 4 and Equation 5.
E = −∇ѱ (4)
𝑁 = 𝐸‖𝐸‖⁄ (5)
Here N represents a unit vector field defined
everywhere between S and S’. From here we can
compute the streamlines magnitude by starting
at any point at S and integrating N. As an
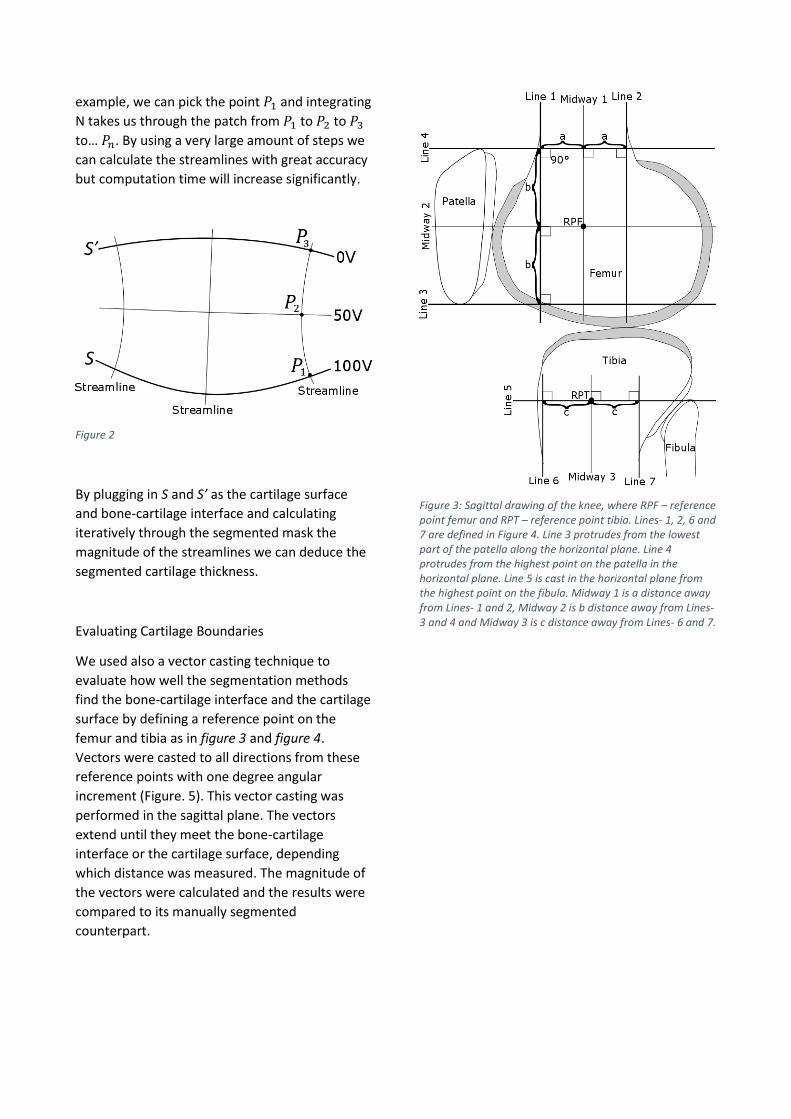
example, we can pick the point 𝑃1 and integrating
N takes us through the patch from 𝑃1 to 𝑃2 to 𝑃3
to… 𝑃𝑛. By using a very large amount of steps we
can calculate the streamlines with great accuracy
but computation time will increase significantly.
Figure 2
By plugging in S and S’ as the cartilage surface
and bone-cartilage interface and calculating
iteratively through the segmented mask the
magnitude of the streamlines we can deduce the
segmented cartilage thickness.
Evaluating Cartilage Boundaries
We used also a vector casting technique to
evaluate how well the segmentation methods
find the bone-cartilage interface and the cartilage
surface by defining a reference point on the
femur and tibia as in figure 3 and figure 4.
Vectors were casted to all directions from these
reference points with one degree angular
increment (Figure. 5). This vector casting was
performed in the sagittal plane. The vectors
extend until they meet the bone-cartilage
interface or the cartilage surface, depending
which distance was measured. The magnitude of
the vectors were calculated and the results were
compared to its manually segmented
counterpart.
Figure 3: Sagittal drawing of the knee, where RPF – reference point femur and RPT – reference point tibia. Lines- 1, 2, 6 and 7 are defined in Figure 4. Line 3 protrudes from the lowest part of the patella along the horizontal plane. Line 4 protrudes from the highest point on the patella in the horizontal plane. Line 5 is cast in the horizontal plane from the highest point on the fibula. Midway 1 is a distance away from Lines- 1 and 2, Midway 2 is b distance away from Lines- 3 and 4 and Midway 3 is c distance away from Lines- 6 and 7.

Figure 5: Sagittal drawing of the knee, where α – angle at which vectors are cast from RPF and φ – angle at which vectors are cast from RPT.
Dice Similarity Coefficient
The Dice similarity coefficient (DSC) is a
quantitative tool in validating segmentation
accuracy [22]. We used it to measure the overlap
between automatic and manual segmentations.
The DSC value range from 0 to 1 with 0 denoting
no overlap and 1 denoting total overlap (6). We
calculated the DSC for the entire segmentation of
tibia, femur, and for each ROI.
𝐷𝑆𝐶 = 2𝑁(𝐴∩𝑀)
𝑁(𝐴)+𝑁(𝑀) (6)
where A – automatic mask, M – manual mask and N – number of points in mask.
Results
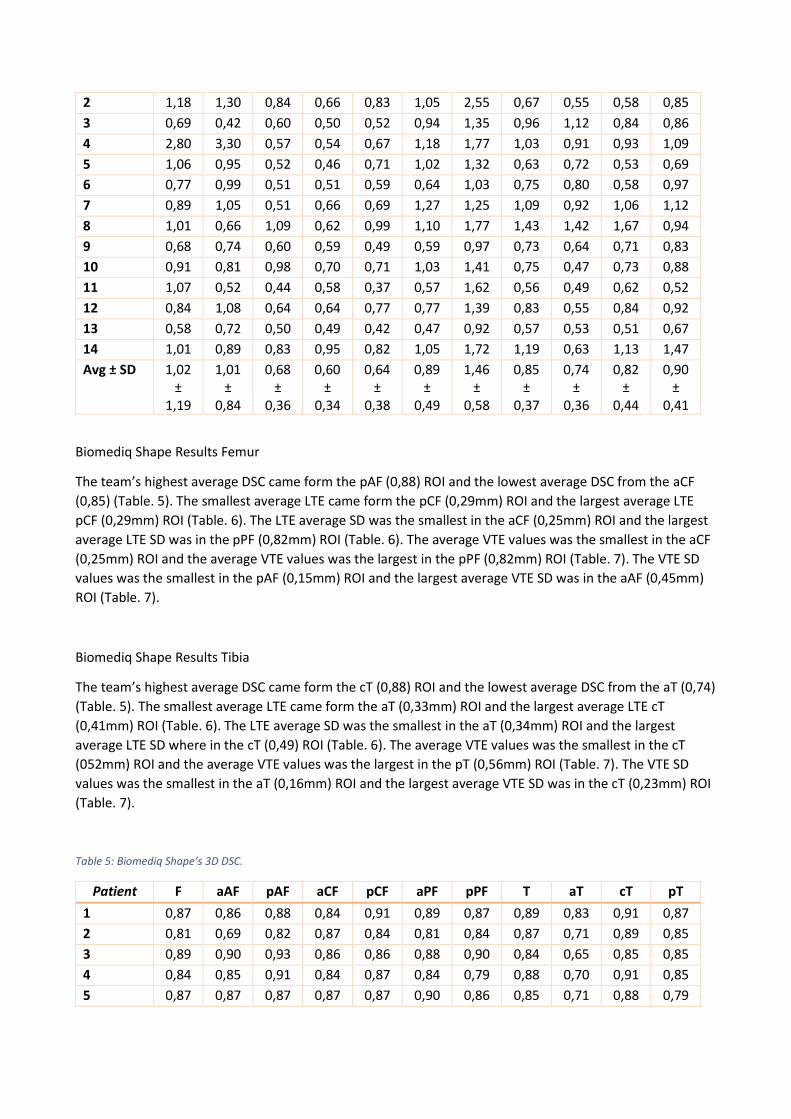
BIGR Results Femur
The team’s highest average DSC came from the pCF (0,81) ROI and the lowest average DSC from the pPF
(0,62) (Table. 2). The smallest average Laplace Thickness Error (LTE) came from the aCF (0,36mm) ROI and
the largest average LTE (0,58mm) from aPF (Table. 3). The LTE Standard Deviation (SD) was the smallest in
the aCF (0,33mm) ROI and the largest LTE SD in the aAF (0,75mm) ROI (Table. 3). The average Vector
Thickness Error (VTE) value was the smallest in the aCF (0,6mm) ROI and the average VTE value was the
largest in the pPF (1,02mm) ROI (Table. 4). The VTE SD values was the smallest in the aCF (0,34mm) ROI and
the largest average VTE SD was found in the aAF (0,84mm) ROI (Table. 4).
BIGR Results Tibia
The team’s highest average DSC came from the cT (0,78) ROI and the lowest average DSC from the aT (0,71)
ROI (Table. 2). The smallest average LTE came from the (0,37mm) ROI and the largest average LTE pT (0,43)
ROI (Table. 3). The LTE average SD was the smallest in the aT and pT (0,44mm) ROI and the largest average
LTE SD was in the cT (0,54mm) ROI (Table. 3). The average VTE values was the smallest in the aT (0,74mm)
ROI and the average VTE values was the largest in the pT (0,9mm) ROI (Table. 4). The VTE SD values was the
smallest in the aT (0,36mm) ROI and the largest average VTE SD was in the cT (0,44mm) ROI (Table. 4).
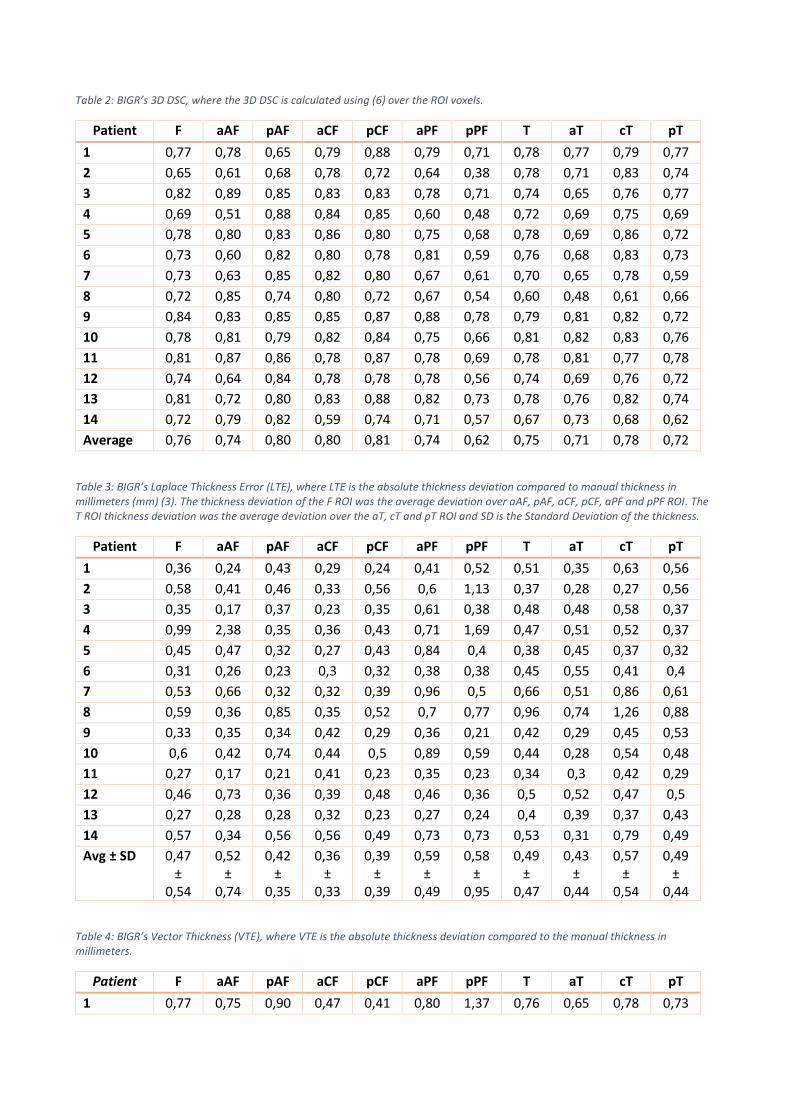
Table 2: BIGR’s 3D DSC, where the 3D DSC is calculated using (6) over the ROI voxels.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,77 0,78 0,65 0,79 0,88 0,79 0,71 0,78 0,77 0,79 0,77
2 0,65 0,61 0,68 0,78 0,72 0,64 0,38 0,78 0,71 0,83 0,74
3 0,82 0,89 0,85 0,83 0,83 0,78 0,71 0,74 0,65 0,76 0,77
4 0,69 0,51 0,88 0,84 0,85 0,60 0,48 0,72 0,69 0,75 0,69
5 0,78 0,80 0,83 0,86 0,80 0,75 0,68 0,78 0,69 0,86 0,72
6 0,73 0,60 0,82 0,80 0,78 0,81 0,59 0,76 0,68 0,83 0,73
7 0,73 0,63 0,85 0,82 0,80 0,67 0,61 0,70 0,65 0,78 0,59
8 0,72 0,85 0,74 0,80 0,72 0,67 0,54 0,60 0,48 0,61 0,66
9 0,84 0,83 0,85 0,85 0,87 0,88 0,78 0,79 0,81 0,82 0,72
10 0,78 0,81 0,79 0,82 0,84 0,75 0,66 0,81 0,82 0,83 0,76
11 0,81 0,87 0,86 0,78 0,87 0,78 0,69 0,78 0,81 0,77 0,78
12 0,74 0,64 0,84 0,78 0,78 0,78 0,56 0,74 0,69 0,76 0,72
13 0,81 0,72 0,80 0,83 0,88 0,82 0,73 0,78 0,76 0,82 0,74
14 0,72 0,79 0,82 0,59 0,74 0,71 0,57 0,67 0,73 0,68 0,62
Average 0,76 0,74 0,80 0,80 0,81 0,74 0,62 0,75 0,71 0,78 0,72
Table 3: BIGR’s Laplace Thickness Error (LTE), where LTE is the absolute thickness deviation compared to manual thickness in millimeters (mm) (3). The thickness deviation of the F ROI was the average deviation over aAF, pAF, aCF, pCF, aPF and pPF ROI. The T ROI thickness deviation was the average deviation over the aT, cT and pT ROI and SD is the Standard Deviation of the thickness.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,36 0,24 0,43 0,29 0,24 0,41 0,52 0,51 0,35 0,63 0,56
2 0,58 0,41 0,46 0,33 0,56 0,6 1,13 0,37 0,28 0,27 0,56
3 0,35 0,17 0,37 0,23 0,35 0,61 0,38 0,48 0,48 0,58 0,37
4 0,99 2,38 0,35 0,36 0,43 0,71 1,69 0,47 0,51 0,52 0,37
5 0,45 0,47 0,32 0,27 0,43 0,84 0,4 0,38 0,45 0,37 0,32
6 0,31 0,26 0,23 0,3 0,32 0,38 0,38 0,45 0,55 0,41 0,4
7 0,53 0,66 0,32 0,32 0,39 0,96 0,5 0,66 0,51 0,86 0,61
8 0,59 0,36 0,85 0,35 0,52 0,7 0,77 0,96 0,74 1,26 0,88
9 0,33 0,35 0,34 0,42 0,29 0,36 0,21 0,42 0,29 0,45 0,53
10 0,6 0,42 0,74 0,44 0,5 0,89 0,59 0,44 0,28 0,54 0,48
11 0,27 0,17 0,21 0,41 0,23 0,35 0,23 0,34 0,3 0,42 0,29
12 0,46 0,73 0,36 0,39 0,48 0,46 0,36 0,5 0,52 0,47 0,5
13 0,27 0,28 0,28 0,32 0,23 0,27 0,24 0,4 0,39 0,37 0,43
14 0,57 0,34 0,56 0,56 0,49 0,73 0,73 0,53 0,31 0,79 0,49
Avg ± SD 0,47 ±
0,54
0,52 ±
0,74
0,42 ±
0,35
0,36 ±
0,33
0,39 ±
0,39
0,59 ±
0,49
0,58 ±
0,95
0,49 ±
0,47
0,43 ±
0,44
0,57 ±
0,54
0,49 ±
0,44
Table 4: BIGR’s Vector Thickness (VTE), where VTE is the absolute thickness deviation compared to the manual thickness in millimeters.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,77 0,75 0,90 0,47 0,41 0,80 1,37 0,76 0,65 0,78 0,73
2 1,18 1,30 0,84 0,66 0,83 1,05 2,55 0,67 0,55 0,58 0,85
3 0,69 0,42 0,60 0,50 0,52 0,94 1,35 0,96 1,12 0,84 0,86
4 2,80 3,30 0,57 0,54 0,67 1,18 1,77 1,03 0,91 0,93 1,09
5 1,06 0,95 0,52 0,46 0,71 1,02 1,32 0,63 0,72 0,53 0,69
6 0,77 0,99 0,51 0,51 0,59 0,64 1,03 0,75 0,80 0,58 0,97
7 0,89 1,05 0,51 0,66 0,69 1,27 1,25 1,09 0,92 1,06 1,12
8 1,01 0,66 1,09 0,62 0,99 1,10 1,77 1,43 1,42 1,67 0,94
9 0,68 0,74 0,60 0,59 0,49 0,59 0,97 0,73 0,64 0,71 0,83
10 0,91 0,81 0,98 0,70 0,71 1,03 1,41 0,75 0,47 0,73 0,88
11 1,07 0,52 0,44 0,58 0,37 0,57 1,62 0,56 0,49 0,62 0,52
12 0,84 1,08 0,64 0,64 0,77 0,77 1,39 0,83 0,55 0,84 0,92
13 0,58 0,72 0,50 0,49 0,42 0,47 0,92 0,57 0,53 0,51 0,67
14 1,01 0,89 0,83 0,95 0,82 1,05 1,72 1,19 0,63 1,13 1,47
Avg ± SD 1,02 ±
1,19
1,01 ±
0,84
0,68 ±
0,36
0,60 ±
0,34
0,64 ±
0,38
0,89 ±
0,49
1,46 ±
0,58
0,85 ±
0,37
0,74 ±
0,36
0,82 ±
0,44
0,90 ±
0,41
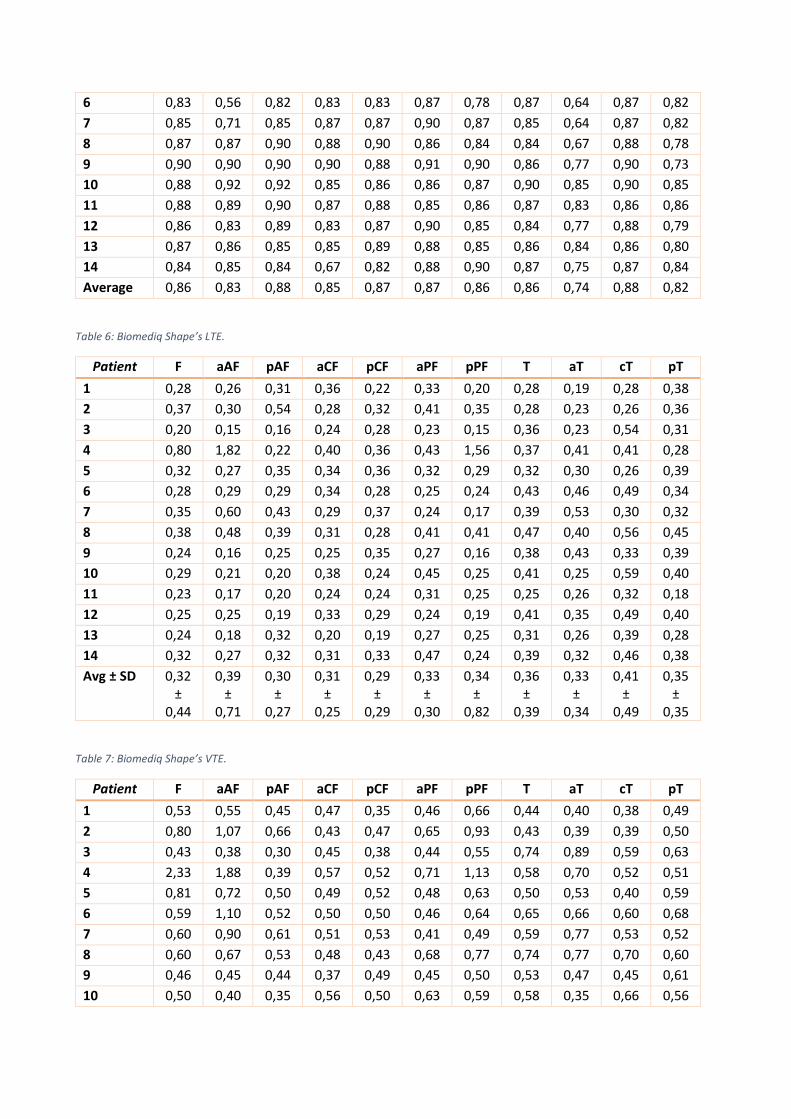
Biomediq Shape Results Femur
The team’s highest average DSC came form the pAF (0,88) ROI and the lowest average DSC from the aCF
(0,85) (Table. 5). The smallest average LTE came form the pCF (0,29mm) ROI and the largest average LTE
pCF (0,29mm) ROI (Table. 6). The LTE average SD was the smallest in the aCF (0,25mm) ROI and the largest
average LTE SD was in the pPF (0,82mm) ROI (Table. 6). The average VTE values was the smallest in the aCF
(0,25mm) ROI and the average VTE values was the largest in the pPF (0,82mm) ROI (Table. 7). The VTE SD
values was the smallest in the pAF (0,15mm) ROI and the largest average VTE SD was in the aAF (0,45mm)
ROI (Table. 7).
Biomediq Shape Results Tibia
The team’s highest average DSC came form the cT (0,88) ROI and the lowest average DSC from the aT (0,74)
(Table. 5). The smallest average LTE came form the aT (0,33mm) ROI and the largest average LTE cT
(0,41mm) ROI (Table. 6). The LTE average SD was the smallest in the aT (0,34mm) ROI and the largest
average LTE SD where in the cT (0,49) ROI (Table. 6). The average VTE values was the smallest in the cT
(052mm) ROI and the average VTE values was the largest in the pT (0,56mm) ROI (Table. 7). The VTE SD
values was the smallest in the aT (0,16mm) ROI and the largest average VTE SD was in the cT (0,23mm) ROI
(Table. 7).
Table 5: Biomediq Shape’s 3D DSC.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,87 0,86 0,88 0,84 0,91 0,89 0,87 0,89 0,83 0,91 0,87
2 0,81 0,69 0,82 0,87 0,84 0,81 0,84 0,87 0,71 0,89 0,85
3 0,89 0,90 0,93 0,86 0,86 0,88 0,90 0,84 0,65 0,85 0,85
4 0,84 0,85 0,91 0,84 0,87 0,84 0,79 0,88 0,70 0,91 0,85
5 0,87 0,87 0,87 0,87 0,87 0,90 0,86 0,85 0,71 0,88 0,79
6 0,83 0,56 0,82 0,83 0,83 0,87 0,78 0,87 0,64 0,87 0,82
7 0,85 0,71 0,85 0,87 0,87 0,90 0,87 0,85 0,64 0,87 0,82
8 0,87 0,87 0,90 0,88 0,90 0,86 0,84 0,84 0,67 0,88 0,78
9 0,90 0,90 0,90 0,90 0,88 0,91 0,90 0,86 0,77 0,90 0,73
10 0,88 0,92 0,92 0,85 0,86 0,86 0,87 0,90 0,85 0,90 0,85
11 0,88 0,89 0,90 0,87 0,88 0,85 0,86 0,87 0,83 0,86 0,86
12 0,86 0,83 0,89 0,83 0,87 0,90 0,85 0,84 0,77 0,88 0,79
13 0,87 0,86 0,85 0,85 0,89 0,88 0,85 0,86 0,84 0,86 0,80
14 0,84 0,85 0,84 0,67 0,82 0,88 0,90 0,87 0,75 0,87 0,84
Average 0,86 0,83 0,88 0,85 0,87 0,87 0,86 0,86 0,74 0,88 0,82
Table 6: Biomediq Shape’s LTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,28 0,26 0,31 0,36 0,22 0,33 0,20 0,28 0,19 0,28 0,38
2 0,37 0,30 0,54 0,28 0,32 0,41 0,35 0,28 0,23 0,26 0,36
3 0,20 0,15 0,16 0,24 0,28 0,23 0,15 0,36 0,23 0,54 0,31
4 0,80 1,82 0,22 0,40 0,36 0,43 1,56 0,37 0,41 0,41 0,28
5 0,32 0,27 0,35 0,34 0,36 0,32 0,29 0,32 0,30 0,26 0,39
6 0,28 0,29 0,29 0,34 0,28 0,25 0,24 0,43 0,46 0,49 0,34
7 0,35 0,60 0,43 0,29 0,37 0,24 0,17 0,39 0,53 0,30 0,32
8 0,38 0,48 0,39 0,31 0,28 0,41 0,41 0,47 0,40 0,56 0,45
9 0,24 0,16 0,25 0,25 0,35 0,27 0,16 0,38 0,43 0,33 0,39
10 0,29 0,21 0,20 0,38 0,24 0,45 0,25 0,41 0,25 0,59 0,40
11 0,23 0,17 0,20 0,24 0,24 0,31 0,25 0,25 0,26 0,32 0,18
12 0,25 0,25 0,19 0,33 0,29 0,24 0,19 0,41 0,35 0,49 0,40
13 0,24 0,18 0,32 0,20 0,19 0,27 0,25 0,31 0,26 0,39 0,28
14 0,32 0,27 0,32 0,31 0,33 0,47 0,24 0,39 0,32 0,46 0,38
Avg ± SD 0,32 ±
0,44
0,39 ±
0,71
0,30 ±
0,27
0,31 ±
0,25
0,29 ±
0,29
0,33 ±
0,30
0,34 ±
0,82
0,36 ±
0,39
0,33 ±
0,34
0,41 ±
0,49
0,35 ±
0,35
Table 7: Biomediq Shape’s VTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,53 0,55 0,45 0,47 0,35 0,46 0,66 0,44 0,40 0,38 0,49
2 0,80 1,07 0,66 0,43 0,47 0,65 0,93 0,43 0,39 0,39 0,50
3 0,43 0,38 0,30 0,45 0,38 0,44 0,55 0,74 0,89 0,59 0,63
4 2,33 1,88 0,39 0,57 0,52 0,71 1,13 0,58 0,70 0,52 0,51
5 0,81 0,72 0,50 0,49 0,52 0,48 0,63 0,50 0,53 0,40 0,59
6 0,59 1,10 0,52 0,50 0,50 0,46 0,64 0,65 0,66 0,60 0,68
7 0,60 0,90 0,61 0,51 0,53 0,41 0,49 0,59 0,77 0,53 0,52
8 0,60 0,67 0,53 0,48 0,43 0,68 0,77 0,74 0,77 0,70 0,60
9 0,46 0,45 0,44 0,37 0,49 0,45 0,50 0,53 0,47 0,45 0,61
10 0,50 0,40 0,35 0,56 0,50 0,63 0,59 0,58 0,35 0,66 0,56
11 0,90 0,43 0,36 0,37 0,38 0,46 0,84 0,41 0,40 0,44 0,35
12 0,50 0,51 0,40 0,50 0,46 0,37 0,63 0,63 0,45 0,58 0,64
13 0,44 0,41 0,44 0,39 0,37 0,37 0,63 0,46 0,35 0,46 0,50
14 0,59 0,54 0,59 0,77 0,63 0,55 0,52 0,62 0,53 0,59 0,60
Avg ± SD 0,72 ±
0,67
0,72 ±
0,45
0,47 ±
0,15
0,49 ±
0,18
0,47 ±
0,19
0,51 ±
0,23
0,68 ±
0,25
0,56 ±
0,17
0,55 ±
0,16
0,52 ±
0,23
0,56 ±
0,17
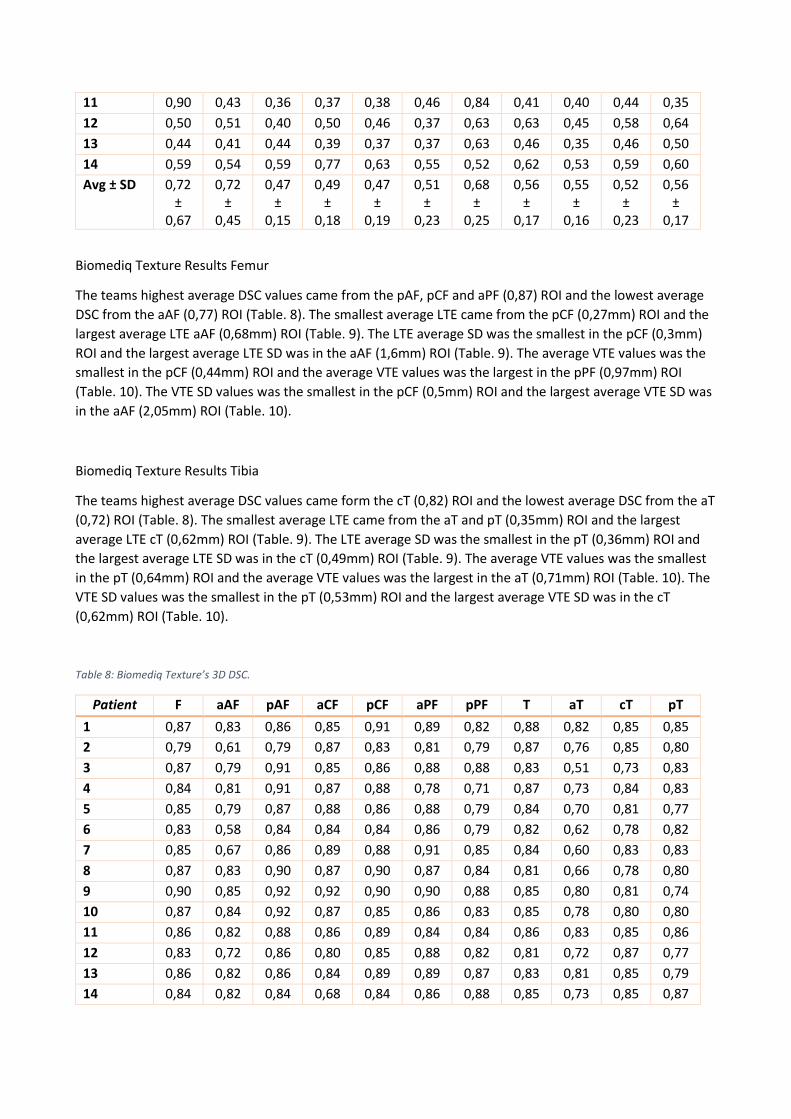
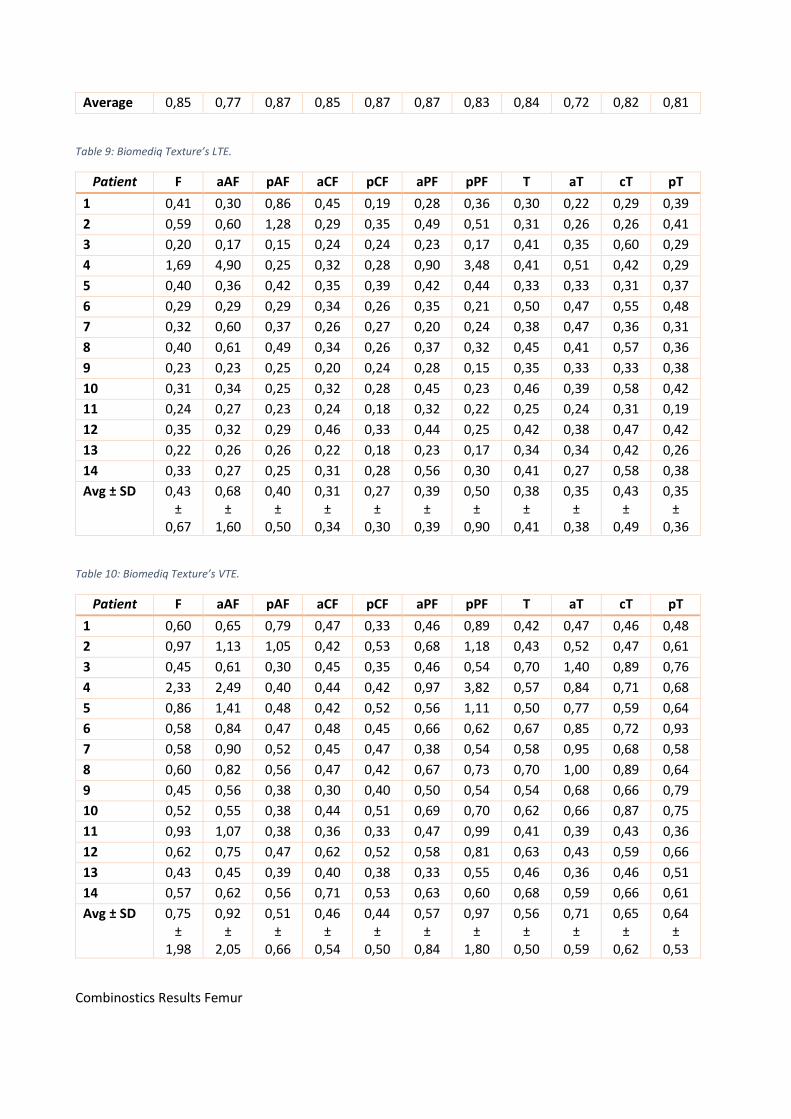
Biomediq Texture Results Femur
The teams highest average DSC values came from the pAF, pCF and aPF (0,87) ROI and the lowest average
DSC from the aAF (0,77) ROI (Table. 8). The smallest average LTE came from the pCF (0,27mm) ROI and the
largest average LTE aAF (0,68mm) ROI (Table. 9). The LTE average SD was the smallest in the pCF (0,3mm)
ROI and the largest average LTE SD was in the aAF (1,6mm) ROI (Table. 9). The average VTE values was the
smallest in the pCF (0,44mm) ROI and the average VTE values was the largest in the pPF (0,97mm) ROI
(Table. 10). The VTE SD values was the smallest in the pCF (0,5mm) ROI and the largest average VTE SD was
in the aAF (2,05mm) ROI (Table. 10).
Biomediq Texture Results Tibia
The teams highest average DSC values came form the cT (0,82) ROI and the lowest average DSC from the aT
(0,72) ROI (Table. 8). The smallest average LTE came from the aT and pT (0,35mm) ROI and the largest
average LTE cT (0,62mm) ROI (Table. 9). The LTE average SD was the smallest in the pT (0,36mm) ROI and
the largest average LTE SD was in the cT (0,49mm) ROI (Table. 9). The average VTE values was the smallest
in the pT (0,64mm) ROI and the average VTE values was the largest in the aT (0,71mm) ROI (Table. 10). The
VTE SD values was the smallest in the pT (0,53mm) ROI and the largest average VTE SD was in the cT
(0,62mm) ROI (Table. 10).
Table 8: Biomediq Texture’s 3D DSC.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,87 0,83 0,86 0,85 0,91 0,89 0,82 0,88 0,82 0,85 0,85
2 0,79 0,61 0,79 0,87 0,83 0,81 0,79 0,87 0,76 0,85 0,80
3 0,87 0,79 0,91 0,85 0,86 0,88 0,88 0,83 0,51 0,73 0,83
4 0,84 0,81 0,91 0,87 0,88 0,78 0,71 0,87 0,73 0,84 0,83
5 0,85 0,79 0,87 0,88 0,86 0,88 0,79 0,84 0,70 0,81 0,77
6 0,83 0,58 0,84 0,84 0,84 0,86 0,79 0,82 0,62 0,78 0,82
7 0,85 0,67 0,86 0,89 0,88 0,91 0,85 0,84 0,60 0,83 0,83
8 0,87 0,83 0,90 0,87 0,90 0,87 0,84 0,81 0,66 0,78 0,80
9 0,90 0,85 0,92 0,92 0,90 0,90 0,88 0,85 0,80 0,81 0,74
10 0,87 0,84 0,92 0,87 0,85 0,86 0,83 0,85 0,78 0,80 0,80
11 0,86 0,82 0,88 0,86 0,89 0,84 0,84 0,86 0,83 0,85 0,86
12 0,83 0,72 0,86 0,80 0,85 0,88 0,82 0,81 0,72 0,87 0,77
13 0,86 0,82 0,86 0,84 0,89 0,89 0,87 0,83 0,81 0,85 0,79
14 0,84 0,82 0,84 0,68 0,84 0,86 0,88 0,85 0,73 0,85 0,87
Average 0,85 0,77 0,87 0,85 0,87 0,87 0,83 0,84 0,72 0,82 0,81
Table 9: Biomediq Texture’s LTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,41 0,30 0,86 0,45 0,19 0,28 0,36 0,30 0,22 0,29 0,39
2 0,59 0,60 1,28 0,29 0,35 0,49 0,51 0,31 0,26 0,26 0,41
3 0,20 0,17 0,15 0,24 0,24 0,23 0,17 0,41 0,35 0,60 0,29
4 1,69 4,90 0,25 0,32 0,28 0,90 3,48 0,41 0,51 0,42 0,29
5 0,40 0,36 0,42 0,35 0,39 0,42 0,44 0,33 0,33 0,31 0,37
6 0,29 0,29 0,29 0,34 0,26 0,35 0,21 0,50 0,47 0,55 0,48
7 0,32 0,60 0,37 0,26 0,27 0,20 0,24 0,38 0,47 0,36 0,31
8 0,40 0,61 0,49 0,34 0,26 0,37 0,32 0,45 0,41 0,57 0,36
9 0,23 0,23 0,25 0,20 0,24 0,28 0,15 0,35 0,33 0,33 0,38
10 0,31 0,34 0,25 0,32 0,28 0,45 0,23 0,46 0,39 0,58 0,42
11 0,24 0,27 0,23 0,24 0,18 0,32 0,22 0,25 0,24 0,31 0,19
12 0,35 0,32 0,29 0,46 0,33 0,44 0,25 0,42 0,38 0,47 0,42
13 0,22 0,26 0,26 0,22 0,18 0,23 0,17 0,34 0,34 0,42 0,26
14 0,33 0,27 0,25 0,31 0,28 0,56 0,30 0,41 0,27 0,58 0,38
Avg ± SD 0,43 ±
0,67
0,68 ±
1,60
0,40 ±
0,50
0,31 ±
0,34
0,27 ±
0,30
0,39 ±
0,39
0,50 ±
0,90
0,38 ±
0,41
0,35 ±
0,38
0,43 ±
0,49
0,35 ±
0,36
Table 10: Biomediq Texture’s VTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,60 0,65 0,79 0,47 0,33 0,46 0,89 0,42 0,47 0,46 0,48
2 0,97 1,13 1,05 0,42 0,53 0,68 1,18 0,43 0,52 0,47 0,61
3 0,45 0,61 0,30 0,45 0,35 0,46 0,54 0,70 1,40 0,89 0,76
4 2,33 2,49 0,40 0,44 0,42 0,97 3,82 0,57 0,84 0,71 0,68
5 0,86 1,41 0,48 0,42 0,52 0,56 1,11 0,50 0,77 0,59 0,64
6 0,58 0,84 0,47 0,48 0,45 0,66 0,62 0,67 0,85 0,72 0,93
7 0,58 0,90 0,52 0,45 0,47 0,38 0,54 0,58 0,95 0,68 0,58
8 0,60 0,82 0,56 0,47 0,42 0,67 0,73 0,70 1,00 0,89 0,64
9 0,45 0,56 0,38 0,30 0,40 0,50 0,54 0,54 0,68 0,66 0,79
10 0,52 0,55 0,38 0,44 0,51 0,69 0,70 0,62 0,66 0,87 0,75
11 0,93 1,07 0,38 0,36 0,33 0,47 0,99 0,41 0,39 0,43 0,36
12 0,62 0,75 0,47 0,62 0,52 0,58 0,81 0,63 0,43 0,59 0,66
13 0,43 0,45 0,39 0,40 0,38 0,33 0,55 0,46 0,36 0,46 0,51
14 0,57 0,62 0,56 0,71 0,53 0,63 0,60 0,68 0,59 0,66 0,61
Avg ± SD 0,75 ±
1,98
0,92 ±
2,05
0,51 ±
0,66
0,46 ±
0,54
0,44 ±
0,50
0,57 ±
0,84
0,97 ±
1,80
0,56 ±
0,50
0,71 ±
0,59
0,65 ±
0,62
0,64 ±
0,53
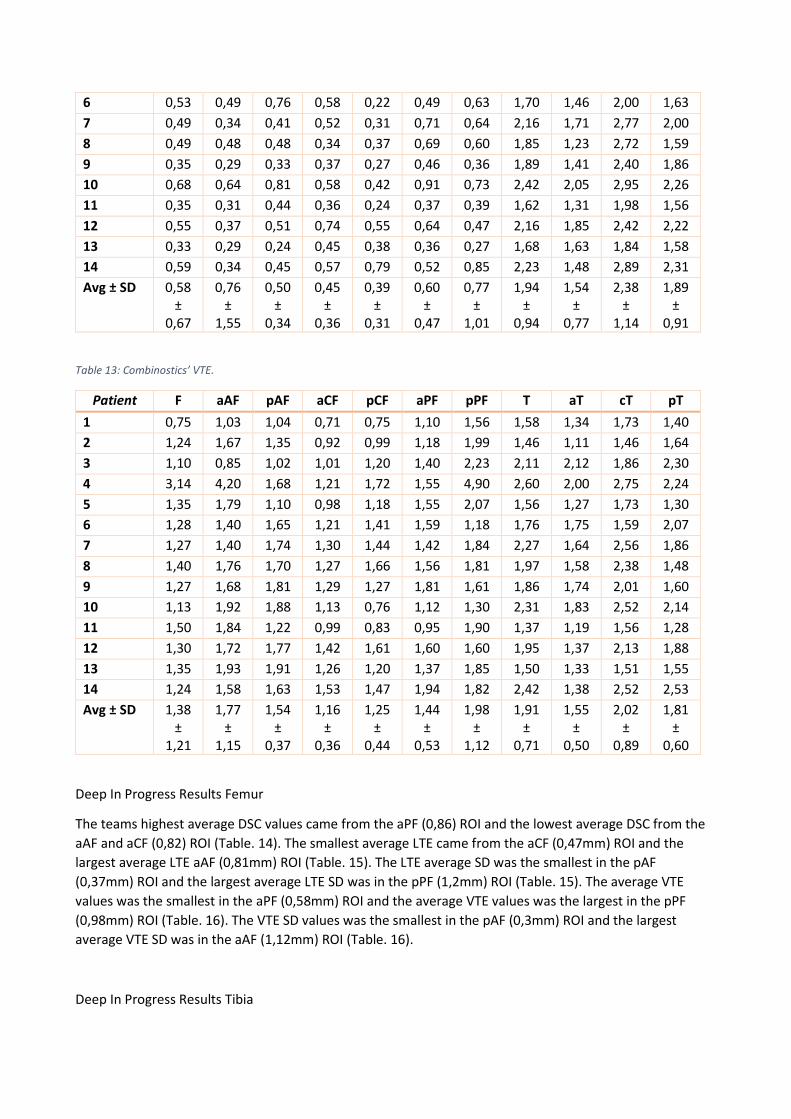
Combinostics Results Femur
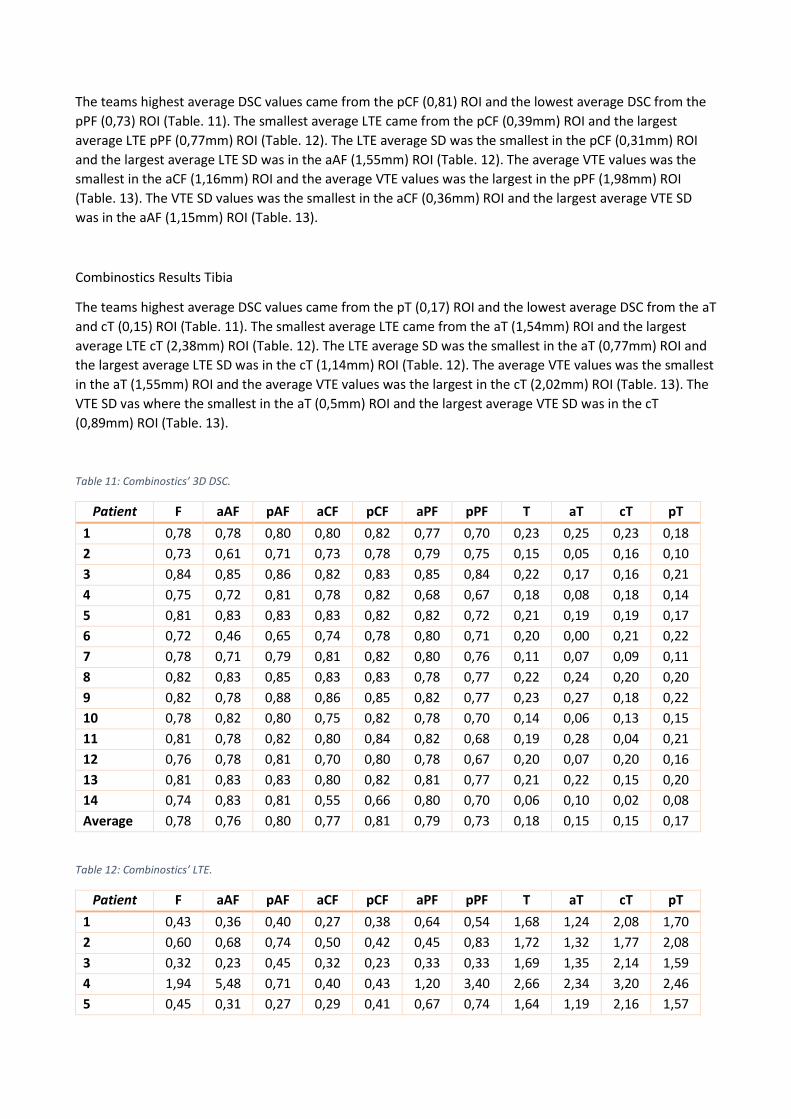
The teams highest average DSC values came from the pCF (0,81) ROI and the lowest average DSC from the
pPF (0,73) ROI (Table. 11). The smallest average LTE came from the pCF (0,39mm) ROI and the largest
average LTE pPF (0,77mm) ROI (Table. 12). The LTE average SD was the smallest in the pCF (0,31mm) ROI
and the largest average LTE SD was in the aAF (1,55mm) ROI (Table. 12). The average VTE values was the
smallest in the aCF (1,16mm) ROI and the average VTE values was the largest in the pPF (1,98mm) ROI
(Table. 13). The VTE SD values was the smallest in the aCF (0,36mm) ROI and the largest average VTE SD
was in the aAF (1,15mm) ROI (Table. 13).
Combinostics Results Tibia
The teams highest average DSC values came from the pT (0,17) ROI and the lowest average DSC from the aT
and cT (0,15) ROI (Table. 11). The smallest average LTE came from the aT (1,54mm) ROI and the largest
average LTE cT (2,38mm) ROI (Table. 12). The LTE average SD was the smallest in the aT (0,77mm) ROI and
the largest average LTE SD was in the cT (1,14mm) ROI (Table. 12). The average VTE values was the smallest
in the aT (1,55mm) ROI and the average VTE values was the largest in the cT (2,02mm) ROI (Table. 13). The
VTE SD vas where the smallest in the aT (0,5mm) ROI and the largest average VTE SD was in the cT
(0,89mm) ROI (Table. 13).
Table 11: Combinostics’ 3D DSC.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,78 0,78 0,80 0,80 0,82 0,77 0,70 0,23 0,25 0,23 0,18
2 0,73 0,61 0,71 0,73 0,78 0,79 0,75 0,15 0,05 0,16 0,10
3 0,84 0,85 0,86 0,82 0,83 0,85 0,84 0,22 0,17 0,16 0,21
4 0,75 0,72 0,81 0,78 0,82 0,68 0,67 0,18 0,08 0,18 0,14
5 0,81 0,83 0,83 0,83 0,82 0,82 0,72 0,21 0,19 0,19 0,17
6 0,72 0,46 0,65 0,74 0,78 0,80 0,71 0,20 0,00 0,21 0,22
7 0,78 0,71 0,79 0,81 0,82 0,80 0,76 0,11 0,07 0,09 0,11
8 0,82 0,83 0,85 0,83 0,83 0,78 0,77 0,22 0,24 0,20 0,20
9 0,82 0,78 0,88 0,86 0,85 0,82 0,77 0,23 0,27 0,18 0,22
10 0,78 0,82 0,80 0,75 0,82 0,78 0,70 0,14 0,06 0,13 0,15
11 0,81 0,78 0,82 0,80 0,84 0,82 0,68 0,19 0,28 0,04 0,21
12 0,76 0,78 0,81 0,70 0,80 0,78 0,67 0,20 0,07 0,20 0,16
13 0,81 0,83 0,83 0,80 0,82 0,81 0,77 0,21 0,22 0,15 0,20
14 0,74 0,83 0,81 0,55 0,66 0,80 0,70 0,06 0,10 0,02 0,08
Average 0,78 0,76 0,80 0,77 0,81 0,79 0,73 0,18 0,15 0,15 0,17
Table 12: Combinostics’ LTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,43 0,36 0,40 0,27 0,38 0,64 0,54 1,68 1,24 2,08 1,70
2 0,60 0,68 0,74 0,50 0,42 0,45 0,83 1,72 1,32 1,77 2,08
3 0,32 0,23 0,45 0,32 0,23 0,33 0,33 1,69 1,35 2,14 1,59
4 1,94 5,48 0,71 0,40 0,43 1,20 3,40 2,66 2,34 3,20 2,46
5 0,45 0,31 0,27 0,29 0,41 0,67 0,74 1,64 1,19 2,16 1,57
6 0,53 0,49 0,76 0,58 0,22 0,49 0,63 1,70 1,46 2,00 1,63
7 0,49 0,34 0,41 0,52 0,31 0,71 0,64 2,16 1,71 2,77 2,00
8 0,49 0,48 0,48 0,34 0,37 0,69 0,60 1,85 1,23 2,72 1,59
9 0,35 0,29 0,33 0,37 0,27 0,46 0,36 1,89 1,41 2,40 1,86
10 0,68 0,64 0,81 0,58 0,42 0,91 0,73 2,42 2,05 2,95 2,26
11 0,35 0,31 0,44 0,36 0,24 0,37 0,39 1,62 1,31 1,98 1,56
12 0,55 0,37 0,51 0,74 0,55 0,64 0,47 2,16 1,85 2,42 2,22
13 0,33 0,29 0,24 0,45 0,38 0,36 0,27 1,68 1,63 1,84 1,58
14 0,59 0,34 0,45 0,57 0,79 0,52 0,85 2,23 1,48 2,89 2,31
Avg ± SD 0,58 ±
0,67
0,76 ±
1,55
0,50 ±
0,34
0,45 ±
0,36
0,39 ±
0,31
0,60 ±
0,47
0,77 ±
1,01
1,94 ±
0,94
1,54 ±
0,77
2,38 ±
1,14
1,89 ±
0,91
Table 13: Combinostics’ VTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
1 0,75 1,03 1,04 0,71 0,75 1,10 1,56 1,58 1,34 1,73 1,40
2 1,24 1,67 1,35 0,92 0,99 1,18 1,99 1,46 1,11 1,46 1,64
3 1,10 0,85 1,02 1,01 1,20 1,40 2,23 2,11 2,12 1,86 2,30
4 3,14 4,20 1,68 1,21 1,72 1,55 4,90 2,60 2,00 2,75 2,24
5 1,35 1,79 1,10 0,98 1,18 1,55 2,07 1,56 1,27 1,73 1,30
6 1,28 1,40 1,65 1,21 1,41 1,59 1,18 1,76 1,75 1,59 2,07
7 1,27 1,40 1,74 1,30 1,44 1,42 1,84 2,27 1,64 2,56 1,86
8 1,40 1,76 1,70 1,27 1,66 1,56 1,81 1,97 1,58 2,38 1,48
9 1,27 1,68 1,81 1,29 1,27 1,81 1,61 1,86 1,74 2,01 1,60
10 1,13 1,92 1,88 1,13 0,76 1,12 1,30 2,31 1,83 2,52 2,14
11 1,50 1,84 1,22 0,99 0,83 0,95 1,90 1,37 1,19 1,56 1,28
12 1,30 1,72 1,77 1,42 1,61 1,60 1,60 1,95 1,37 2,13 1,88
13 1,35 1,93 1,91 1,26 1,20 1,37 1,85 1,50 1,33 1,51 1,55
14 1,24 1,58 1,63 1,53 1,47 1,94 1,82 2,42 1,38 2,52 2,53
Avg ± SD 1,38 ±
1,21
1,77 ±
1,15
1,54 ±
0,37
1,16 ±
0,36
1,25 ±
0,44
1,44 ±
0,53
1,98 ±
1,12
1,91 ±
0,71
1,55 ±
0,50
2,02 ±
0,89
1,81 ±
0,60
Deep In Progress Results Femur
The teams highest average DSC values came from the aPF (0,86) ROI and the lowest average DSC from the
aAF and aCF (0,82) ROI (Table. 14). The smallest average LTE came from the aCF (0,47mm) ROI and the
largest average LTE aAF (0,81mm) ROI (Table. 15). The LTE average SD was the smallest in the pAF
(0,37mm) ROI and the largest average LTE SD was in the pPF (1,2mm) ROI (Table. 15). The average VTE
values was the smallest in the aPF (0,58mm) ROI and the average VTE values was the largest in the pPF
(0,98mm) ROI (Table. 16). The VTE SD values was the smallest in the pAF (0,3mm) ROI and the largest
average VTE SD was in the aAF (1,12mm) ROI (Table. 16).
Deep In Progress Results Tibia
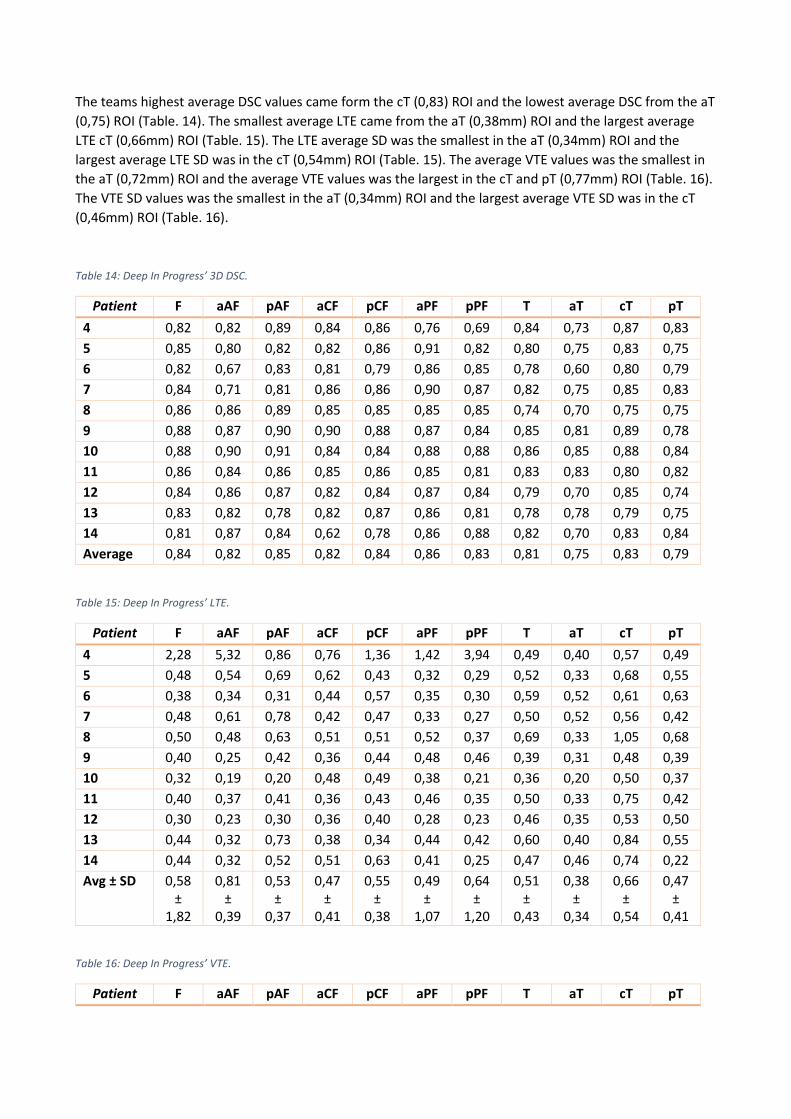
The teams highest average DSC values came form the cT (0,83) ROI and the lowest average DSC from the aT
(0,75) ROI (Table. 14). The smallest average LTE came from the aT (0,38mm) ROI and the largest average
LTE cT (0,66mm) ROI (Table. 15). The LTE average SD was the smallest in the aT (0,34mm) ROI and the
largest average LTE SD was in the cT (0,54mm) ROI (Table. 15). The average VTE values was the smallest in
the aT (0,72mm) ROI and the average VTE values was the largest in the cT and pT (0,77mm) ROI (Table. 16).
The VTE SD values was the smallest in the aT (0,34mm) ROI and the largest average VTE SD was in the cT
(0,46mm) ROI (Table. 16).
Table 14: Deep In Progress’ 3D DSC.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
4 0,82 0,82 0,89 0,84 0,86 0,76 0,69 0,84 0,73 0,87 0,83
5 0,85 0,80 0,82 0,82 0,86 0,91 0,82 0,80 0,75 0,83 0,75
6 0,82 0,67 0,83 0,81 0,79 0,86 0,85 0,78 0,60 0,80 0,79
7 0,84 0,71 0,81 0,86 0,86 0,90 0,87 0,82 0,75 0,85 0,83
8 0,86 0,86 0,89 0,85 0,85 0,85 0,85 0,74 0,70 0,75 0,75
9 0,88 0,87 0,90 0,90 0,88 0,87 0,84 0,85 0,81 0,89 0,78
10 0,88 0,90 0,91 0,84 0,84 0,88 0,88 0,86 0,85 0,88 0,84
11 0,86 0,84 0,86 0,85 0,86 0,85 0,81 0,83 0,83 0,80 0,82
12 0,84 0,86 0,87 0,82 0,84 0,87 0,84 0,79 0,70 0,85 0,74
13 0,83 0,82 0,78 0,82 0,87 0,86 0,81 0,78 0,78 0,79 0,75
14 0,81 0,87 0,84 0,62 0,78 0,86 0,88 0,82 0,70 0,83 0,84
Average 0,84 0,82 0,85 0,82 0,84 0,86 0,83 0,81 0,75 0,83 0,79
Table 15: Deep In Progress’ LTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
4 2,28 5,32 0,86 0,76 1,36 1,42 3,94 0,49 0,40 0,57 0,49
5 0,48 0,54 0,69 0,62 0,43 0,32 0,29 0,52 0,33 0,68 0,55
6 0,38 0,34 0,31 0,44 0,57 0,35 0,30 0,59 0,52 0,61 0,63
7 0,48 0,61 0,78 0,42 0,47 0,33 0,27 0,50 0,52 0,56 0,42
8 0,50 0,48 0,63 0,51 0,51 0,52 0,37 0,69 0,33 1,05 0,68
9 0,40 0,25 0,42 0,36 0,44 0,48 0,46 0,39 0,31 0,48 0,39
10 0,32 0,19 0,20 0,48 0,49 0,38 0,21 0,36 0,20 0,50 0,37
11 0,40 0,37 0,41 0,36 0,43 0,46 0,35 0,50 0,33 0,75 0,42
12 0,30 0,23 0,30 0,36 0,40 0,28 0,23 0,46 0,35 0,53 0,50
13 0,44 0,32 0,73 0,38 0,34 0,44 0,42 0,60 0,40 0,84 0,55
14 0,44 0,32 0,52 0,51 0,63 0,41 0,25 0,47 0,46 0,74 0,22
Avg ± SD 0,58 ±
1,82
0,81 ±
0,39
0,53 ±
0,37
0,47 ±
0,41
0,55 ±
0,38
0,49 ±
1,07
0,64 ±
1,20
0,51 ±
0,43
0,38 ±
0,34
0,66 ±
0,54
0,47 ±
0,41
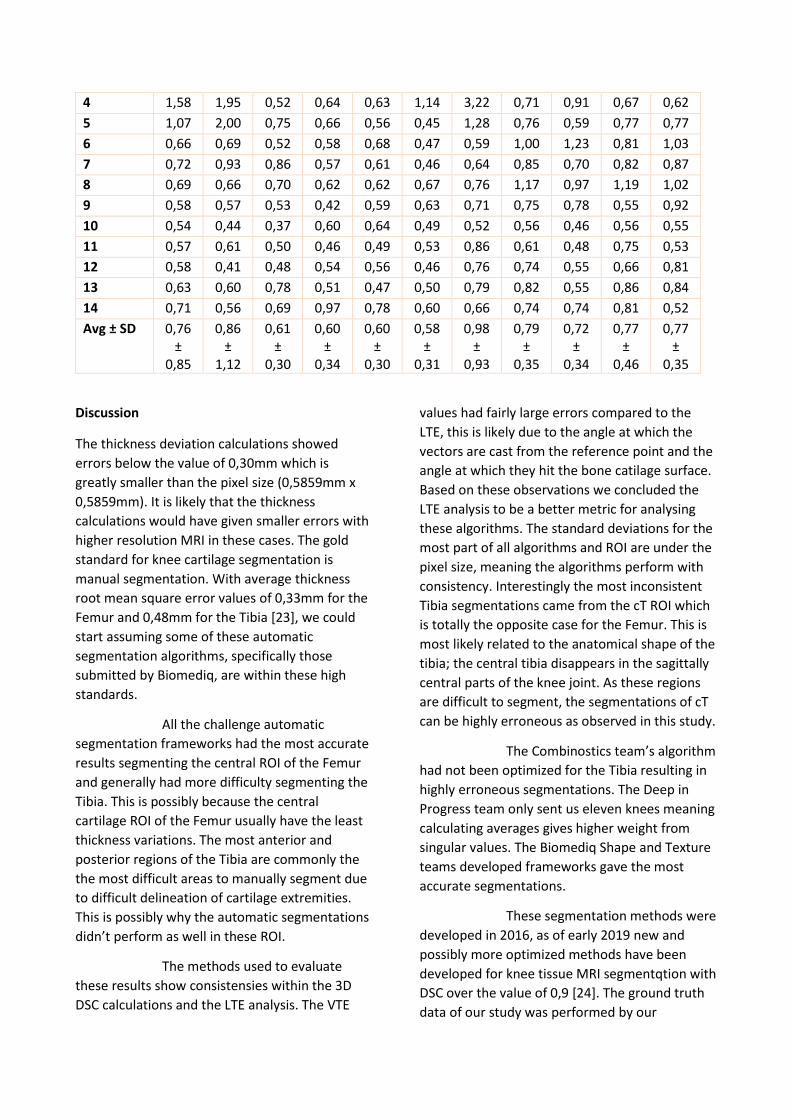
Table 16: Deep In Progress’ VTE.
Patient F aAF pAF aCF pCF aPF pPF T aT cT pT
4 1,58 1,95 0,52 0,64 0,63 1,14 3,22 0,71 0,91 0,67 0,62
5 1,07 2,00 0,75 0,66 0,56 0,45 1,28 0,76 0,59 0,77 0,77
6 0,66 0,69 0,52 0,58 0,68 0,47 0,59 1,00 1,23 0,81 1,03
7 0,72 0,93 0,86 0,57 0,61 0,46 0,64 0,85 0,70 0,82 0,87
8 0,69 0,66 0,70 0,62 0,62 0,67 0,76 1,17 0,97 1,19 1,02
9 0,58 0,57 0,53 0,42 0,59 0,63 0,71 0,75 0,78 0,55 0,92
10 0,54 0,44 0,37 0,60 0,64 0,49 0,52 0,56 0,46 0,56 0,55
11 0,57 0,61 0,50 0,46 0,49 0,53 0,86 0,61 0,48 0,75 0,53
12 0,58 0,41 0,48 0,54 0,56 0,46 0,76 0,74 0,55 0,66 0,81
13 0,63 0,60 0,78 0,51 0,47 0,50 0,79 0,82 0,55 0,86 0,84
14 0,71 0,56 0,69 0,97 0,78 0,60 0,66 0,74 0,74 0,81 0,52
Avg ± SD 0,76 ±
0,85
0,86 ±
1,12
0,61 ±
0,30
0,60 ±
0,34
0,60 ±
0,30
0,58 ±
0,31
0,98 ±
0,93
0,79 ±
0,35
0,72 ±
0,34
0,77 ±
0,46
0,77 ±
0,35
Discussion
The thickness deviation calculations showed
errors below the value of 0,30mm which is
greatly smaller than the pixel size (0,5859mm x
0,5859mm). It is likely that the thickness
calculations would have given smaller errors with
higher resolution MRI in these cases. The gold
standard for knee cartilage segmentation is
manual segmentation. With average thickness
root mean square error values of 0,33mm for the
Femur and 0,48mm for the Tibia [23], we could
start assuming some of these automatic
segmentation algorithms, specifically those
submitted by Biomediq, are within these high
standards.
All the challenge automatic
segmentation frameworks had the most accurate
results segmenting the central ROI of the Femur
and generally had more difficulty segmenting the
Tibia. This is possibly because the central
cartilage ROI of the Femur usually have the least
thickness variations. The most anterior and
posterior regions of the Tibia are commonly the
the most difficult areas to manually segment due
to difficult delineation of cartilage extremities.
This is possibly why the automatic segmentations
didn’t perform as well in these ROI.
The methods used to evaluate
these results show consistensies within the 3D
DSC calculations and the LTE analysis. The VTE
values had fairly large errors compared to the
LTE, this is likely due to the angle at which the
vectors are cast from the reference point and the
angle at which they hit the bone catilage surface.
Based on these observations we concluded the
LTE analysis to be a better metric for analysing
these algorithms. The standard deviations for the
most part of all algorithms and ROI are under the
pixel size, meaning the algorithms perform with
consistency. Interestingly the most inconsistent
Tibia segmentations came from the cT ROI which
is totally the opposite case for the Femur. This is
most likely related to the anatomical shape of the
tibia; the central tibia disappears in the sagittally
central parts of the knee joint. As these regions
are difficult to segment, the segmentations of cT
can be highly erroneous as observed in this study.
The Combinostics team’s algorithm
had not been optimized for the Tibia resulting in
highly erroneous segmentations. The Deep in
Progress team only sent us eleven knees meaning
calculating averages gives higher weight from
singular values. The Biomediq Shape and Texture
teams developed frameworks gave the most
accurate segmentations.
These segmentation methods were
developed in 2016, as of early 2019 new and
possibly more optimized methods have been
developed for knee tissue MRI segmentqtion with
DSC over the value of 0,9 [24]. The ground truth
data of our study was performed by our
reaserchers who are not experts in the field of
manual segmentation.
Conclusion
The gap in the accuracy between segmentations
produced by automatic methods and experts has
been narrowing. The leaps in automatic
segmentation methods, i.e. deep learning, have
been great in the recent years, emphasizing their
future potential in the clinical realm. In this
study, the Biomediq Shape framework reached
accurate cartilage delineation with DSC values of
0,86 for Femur and Tibia, with thickness
quantification error falling below the pixel size of
the used MR protocol. We feel that the Biomediq
Shape framework has reached the accuracy
standards to be used in large knee osteoarthritis
studies. In order to gather further and more
accurate data about these types of methods we
need to start using higher resolution MRI images
as the ground truth data.
References
[1] A. M. Ogunbode, L. A. Adebusoye, O. O. Olowookere, and T. O. Alonge, “Physical functionality and self-rated health status of adulute patients with knee osteoarthritis presenting in a primary care clinic.”
[2] J. A. Buckwalter, H. J. Mankin, and A. J. Grodzinsky, “ArticuIarCartiIage and Osteoarthritis,” pp. 465–480, 2005.
[3] J. A. Buckwalter and J. A. Martin, “Osteoarthritis,” Adv. Drug Deliv. Rev., vol. 58, no. 2, pp. 150–167, 2006.
[4] G. S. Dulay, C. Cooper, and E. M. Dennison, “Knee pain, knee injury, knee osteoarthritis & work,” Best Pract. Res. Clin. Rheumatol., vol. 29, no. 3, pp. 454–461, 2015.
[5] H. Bliddal, A. R. Leeds, and R. Christensen, “Osteoarthritis, obesity and weight loss: Evidence, hypotheses and horizons - a scoping review,” Obes. Rev., vol. 15, no. 7,
pp. 578–586, 2014.
[6] F. J. Blanco, “Osteoarthritis year in review 2014: We need more biochemical biomarkers in qualification phase,” Osteoarthr. Cartil., vol. 22, no. 12, pp. 2025–2032, 2014.
[7] D. Dere, “Effect of body mass index on functional recovery after total knee arthroplasty in ambulatory overweight or obese women with osteoarthritis,” ACTA Orthop. Traumatol. Turc., vol. 48, no. 2, pp. 117–121, 2014.
[8] F. Cicuttini, J. Hankin, G. Jones, and A. Wluka, “Comparison of conventional standing knee radiographs and magnetic resonance imaging in assessing progression of tibiofemoral joint osteoarthritis,” Osteoarthr. Cartil., vol. 13, no. 8, pp. 722–727, 2005.
[9] Y. Li, X. Wei, J. Zhou, and L. Wei, “The age-related changes in cartilage and osteoarthritis,” Biomed Res. Int., vol. 2013, 2013.
[10] T. M. Link, Cartilage imaging : significance, techniques, and new developments. Springer, 2011.
[11] J. M. Lötjönen et al., “Fast and robust multi-atlas segmentation of brain magnetic resonance images,” Neuroimage, vol. 49, no. 3, pp. 2352–2365, 2010.
[12] J. Podlipská et al., “Erratum: Comparison of Diagnostic Performance of Semi-Quantitative Knee ULTErasound and Knee Radiography with MRI: Oulu Knee Osteoarthritis Study,” Sci. Rep., vol. 6, no. March, p. 33109, 2016.
[13] L. Shan, C. Zach, C. Charles, and M. Niethammer, “Automatic atlas-based three-label cartilage segmentation from MR knee images,” Med. Image Anal., vol. 18, no. 7, pp. 1233–1246, 2014.
[14] S. Egmentation, D. L. Pham, C. Xu, and J. L. Prince, “C m m i s,” 2000.
[15] T. Sekine et al., “Multi-Atlas-Based Attenuation Correction for Brain 18F-FDG
PET Imaging Using a Time-of-Flight PET/MR Scanner: Comparison with Clinical Single-Atlas- and CT-Based Attenuation Correction,” J. Nucl. Med., vol. 57, no. 8, pp. 1258–1264, 2016.
[16] C. Wachinger, K. Fritscher, G. Sharp, and P. Golland, “Contour-Driven Atlas-Based Segmentation,” IEEE Trans. Med. Imaging, vol. 34, no. 12, pp. 2492–2505, 2015.
[17] N. M. Hansson, H. Achterberg, A. Opbroek, and S. Klein, “IWOAI Challenge 2016 : Combined muLTEi-atlas and appearance segmentation model ( Team BIGR ),” pp. 1–9, 2016.
[18] E. B. Dam, “Knee Cartilage Segmentation Challenge Team : Biomediq Shape,” pp. 3–6.
[19] E. B. Dam, “Knee Cartilage Segmentation Challenge Team : Biomediq Texture,” pp. 2–3.
[20] D. I. Progress, “Tibial and Femoral Cartilage Segmentation with Deep 3D Convolutional Neural Networks.”
[21] A. I. Jones S.E., Buchbinder B.R., “Three-dimensional mapping of cortical thickness using Laplace's Equation” Hum. Brain Mapp., vol. 11, no. 1, pp. 12–32, 2000.
[22] N. H. Foley et al., “NIH Public Access,” Cell, vol. 18, no. 7, pp. 1089–1098, 2012.
[23] Zohara A. Cohen, Denise M. McCarthy, S. Daniel Kwak, Perrine Legrand, Fabian Fogarasi, Edward J. Ciaccio and Gerard A. Ateshian, ”Knee cartilage topography, thickness, and contact areas from MRI: in-vitro calibration and in-vivo measurements” Osteoarthritis and Cartilage (1999) 7, 95–109.
[24] Zhou Z, Zhao G, Kijowski R, Liu F. “Deep convolutional neural network for segmentation of knee joint anatomy.” Magn Reson Med. 2018 Dec;80(6):2759-2770. doi: 10.1002/mrm.27229. Epub 2018 May 17.










