Attachment insecurities and identification of at-risk individuals following the death of a loved one
24
Article Attachment insecurities and identification of at-risk individuals following the death of a loved one Angelique M. Jerga 1 , Phillip R. Shaver 2 , and Ross B. Wilkinson 1 Abstract We examined variables that might identify at-risk individuals following the death of a significant other. Previous research indicates attachment anxiety is associated with more intense grief, while avoidant individuals seem to cope with loss as well as secure individuals. Participants in this study (368 adults aged 17–49) completed an online survey measuring general and relationship-specific attachment insecurities, relationship charac- teristics, loss circumstances, and typical and prolonged grief symptoms. General attachment anxiety and avoidance were related to prolonged grief symptoms but not to typical symptoms. Relationship-specific anxiety was positively related to grief symp- toms, while specific avoidance was negatively related. The results support the distinc- tion between general and specific attachment insecurities and between normative and prolonged grief reactions. Keywords adjustment, attachment, bereavement, coping, death, grief, loss, prolonged grief 1 Australian National University, Australia 2 University of California, Davis, USA Corresponding author: Angelique M. Jerga, Department of Psychology, College of Medicine, Biology and Environment, Building 39, The Australian National University, Canberra, ACT, 0200, Australia Email: [email protected] Journal of Social and Personal Relationships 28(7) 891–914 ª The Author(s) 2011 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/0265407510397987 spr.sagepub.com J S P R at UNIV CALIFORNIA DAVIS on February 9, 2015 spr.sagepub.com Downloaded from
Transcript of Attachment insecurities and identification of at-risk individuals following the death of a loved one

Article
Attachment insecuritiesand identification ofat-risk individualsfollowing the deathof a loved one
Angelique M. Jerga1, Phillip R. Shaver2, andRoss B. Wilkinson1
AbstractWe examined variables that might identify at-risk individuals following the death of asignificant other. Previous research indicates attachment anxiety is associated withmore intense grief, while avoidant individuals seem to cope with loss as well as secureindividuals. Participants in this study (368 adults aged 17–49) completed an online surveymeasuring general and relationship-specific attachment insecurities, relationship charac-teristics, loss circumstances, and typical and prolonged grief symptoms. Generalattachment anxiety and avoidance were related to prolonged grief symptoms but notto typical symptoms. Relationship-specific anxiety was positively related to grief symp-toms, while specific avoidance was negatively related. The results support the distinc-tion between general and specific attachment insecurities and between normative andprolonged grief reactions.
Keywordsadjustment, attachment, bereavement, coping, death, grief, loss, prolonged grief
1 Australian National University, Australia2 University of California, Davis, USA
Corresponding author:
Angelique M. Jerga, Department of Psychology, College of Medicine, Biology and Environment, Building 39,
The Australian National University, Canberra, ACT, 0200, Australia
Email: [email protected]
Journal of Social andPersonal Relationships
28(7) 891–914ª The Author(s) 2011
Reprints and permissions:sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0265407510397987spr.sagepub.com
J S P R
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

For most people love is the most profound source of pleasure in our lives, while the loss of
those whom we love is the most profound source of pain. Hence, love and loss are two sides
of the same coin. We cannot have one without risking the other. (Parkes, 2006, p. 1)
The loss of a loved one is a potentially traumatic experience that everyone is likely to face at
some point. Although the majority of bereaved people recover following a loss (e.g.,
Bonanno, 2004; Bonanno, Moskowitz, Papa, & Folkman, 2005; Bonanno et al., 2002),
Raphael and Minkov (1999) estimated that approximately 9% of bereaved individuals
experience chronic grief. Little is known, however, about how to identify individuals who
are at risk for chronic grief after losing a loved one. Stroebe and Schut (2001) listed the
following kinds of risk factors that affect bereavement outcomes: (a) the bereavement sit-
uation; (b) the person; and (c) the interpersonal context. Attachment insecurities are among
the personal risk factors associated with bereavement outcomes, but they have not yet been
thoroughly researched (see Shaver & Fraley, 2008, for a review).
One of the newest and most promising models of bereavement is the Dual-Process
Model of Coping with Bereavement (Stroebe & Schut, 1999; Stroebe, Schut, & Stroebe,
2005). This model, which includes both painful thoughts about a loss (‘‘loss orienta-
tion’’) and future-oriented thoughts about accepting the loss, adjusting, and building a
reorganized life (‘‘restoration orientation’’), incorporates elements of attachment theory
and makes predictions about how people with different attachment patterns are likely to
differ in their grief reactions (Stroebe et al., 2005). A few studies have supported the pro-
posed inclusion of aspects of attachment theory in bereavement models by finding that
attachment insecurity is a risk factor for more intense grief reactions (Field & Sundin,
2001; Fraley & Bonanno, 2004; van Doorn, Kasl, Berry, Jacobs, & Prigerson, 1998;
Waskowic & Chartier, 2003; Wayment & Vierthaler, 2002). It seems likely that attach-
ment theory can provide a useful framework for understanding different patterns of grief
following losses of various kinds.
Attachment theory
Since its inception, Bowlby’s (1973, 1980, 1982) attachment theory has been focused
on separation and loss. Bowlby’s (1944) early work on maternal separation and
loss provided the basis for his three-volume work, Attachment and Loss (Vol. I,
Attachment, first published in 1969 and revised and republished in 1982; Vol. II,
Separation, 1973; Vol. III, Loss, 1980). As early as 1948, Bowlby and his colleague
James Robertson identified three phases that children go through following separation
from a parent: protest, despair, and detachment. Bowlby and Parkes (1970) later
became aware of similarities between the responses of children to separation from
a parent and the responses of adults who lost an important relationship or relationship
partner. They modified the phases of grief to include an initial phase of numbness, and
eventually Bowlby (1980) reformulated ‘‘detachment’’ as ‘‘reorganization.’’ This
change fit better with the emphasis in attachment theory on ‘‘internal working mod-
els’’ of self, partners, and relationships; it also fits better with subsequent research on
‘‘continuing [mental] bonds’’ with deceased attachment figures (summarized by
Field, 2008, and Shaver & Fraley, 2008).
892 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

In all three volumes of the Attachment and Loss series, Bowlby discussed individual
differences in attachment to caregivers and, later, to adult relationship partners. In these
discussions, Bowlby often contrasted anxious attachment with what was eventually
called avoidant attachment (e.g., Ainsworth, Blehar, Waters, & Wall, 1978; Mikulincer
& Shaver, 2007). These were the two main kinds of insecurity that Ainsworth et al.
(1978) identified with their famous Strange Situation laboratory assessment procedure
for infant–parent dyads, and they are the two main kinds of insecurity operationalized by
personality and social psychologists in studies of adolescent and adult attachment (e.g.,
Brennan, Clark, & Shaver, 1998; Fraley & Shaver, 2000). People who score relatively
high on measures of anxious attachment are anxious about separations, abandonment,
lack of love and support, and deficiencies in themselves. People who score relatively
high on measures of avoidant attachment are wary of intimacy and dependency, and are
likely to suppress rather than express emotions and other signs of need or vulnerability.
Bowlby (1980) described two disordered variants of grieving: chronic mourning and
the prolonged absence of conscious grieving (also called absent, delayed, inhibited, or
suppressed grief). He described adults who show a prolonged absence of conscious
grieving in ways that correspond with current conceptions of avoidant attachment,
describing them as ‘‘normatively self-sufficient people, proud of their independence and
self-control, scornful of sentiment; tears they regard as weakness’’ (p. 153), while people
with chronic grief were described in ways that correspond with attachment anxiety.
Bowlby (1980) described how people who fail to mourn loss may go on to feel deeply
dissatisfied with their lives, experiencing emptiness in personal relationships, as well
as depersonalization and a sense of unreality.
The Dual-Process Model
According to the Dual-Process Model (DPM; Stroebe & Schut, 1999; Stroebe et al.,
2005), most bereaved individuals oscillate between painful thoughts about their loss,
reminiscent of the psychoanalytic notion of ‘‘working through’’ a loss and consistent
with Bowlby’s ideas about anxious attachment, and thoughts about adjusting, changing,
and getting on with life, reminiscent of Bowlby’s ideas about secure and avoidant attach-
ment. The DPM interprets difficulties in the grieving process as either a lack of oscillation
or a disturbance in the oscillation process.
Stroebe and Schut (1999) related three kinds of grief complications – chronic, absent/
delayed or inhibited, and traumatic grief – to different coping strategies. In addition,
Stroebe et al. (2005) predicted that people with a ‘‘preoccupied’’ attachment style (low
on avoidance and high on anxiety; Bartholomew & Horowitz, 1991) would be most
likely to experience chronic grief, a state in which they remained focused on – and highly
preoccupied with – a loss orientation. Stroebe et al. predicted that people with a dis-
missing attachment style (low on anxiety and high on avoidance; Bartholomew &
Horowitz, 1991) would be most likely to experience delayed or inhibited grief, a con-
dition in which they focused mainly on the tasks of restoration and moving on while
avoiding processing the loss (i.e., avoiding loss-oriented reminders and stressors). They
predicted that people with a disorganized attachment style (high on both anxiety and
avoidance; Bartholomew & Horowitz, 1991) would be more likely to experience a
Jerga et al. 893
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

disturbance of the oscillation process, experiencing both intense and persistent periods of
confrontation with the loss, on the one hand, and an inability to confront or reorganize
thoughts and feelings about it, on the other.
Empirical evidence
There is some evidence that a person’s attachment ‘‘style,’’ or characteristic pattern of
cognition, emotion, emotion-regulation, and behavior in close relationships, has an effect
on experiences and behavior following the loss of a close relationship (Field & Sundin,
2001; Fraley & Bonanno, 2004; Wayment & Vierthaler, 2002). People with a secure
attachment style tend to fare better after the loss of a loved one than people with an inse-
cure attachment style. However, there can be different reactions as a function of the dif-
ferent kinds of insecurity – anxiety and avoidance.
Studies investigating attachment and bereavement have often found an association
between attachment anxiety and grief symptoms, but little or no association between
avoidant attachment and symptoms (Field & Sundin, 2001; Fraley & Bonanno, 2004;
Wayment & Vierthaler, 2002). Fraley and Bonanno (2004), for example, investigated
attachment insecurities and intensity of grief and found that participants with a pre-
occupied or fearful attachment style (i.e., the two styles characterized by high attachment
anxiety) experienced more intense grief over time, while those with a secure or dis-
missing attachment style (i.e., those who scored relatively low on attachment anxiety)
were more resilient. This latter finding (i.e., little difference between secure and dis-
missing individuals) contradicts widely held beliefs that people with a dismissingly
avoidant attachment style are likely to experience grief complications in the form of a
delayed grief response (e.g., Belitsky & Jacobs, 1986; Parkes, 1965; Rando, 1992;
Worden, 1982). Other studies support these findings, with attachment anxiety being
positively related to grief symptoms, and avoidant attachment having little or no rela-
tionship with grief symptoms (Field & Sundin, 2001; Wayment & Vierthaler, 2002).
Studies investigating attachment styles and romantic dissolution, another important kind
of loss, have yielded similar findings (Davis, Shaver, & Vernon, 2003; Sprecher,
Felmlee, Metts, Fehr, & Vanni, 1998). Two studies have even revealed a significant
negative association between avoidant attachment and post-breakup distress (Feeney &
Noller, 1992; Simpson, 1990). In fact, Feeney and Noller (1992) found that avoidant
individuals reported being ‘‘quite’’ relieved after their relationship ended.
Wijngaards-de Meij et al. (2007) are the only investigators who found a positive asso-
ciation between avoidant attachment and grief symptoms following loss. They con-
ducted a study of bereaved parents and showed that both anxious and avoidant
attachment were related to grief and depression symptoms following the death of their
child. This study, however, concerns the loss of a caregiving relationship rather than
an attachment relationship, as defined in attachment theory, and therefore is a loss of
a different kind than examined in most other studies (e.g., loss of a parent, grandparent,
romantic partner, or friend).
In summary, in studies of losses of attachment figures, a positive association between
attachment anxiety and grief symptoms has been observed, whereas no association and
sometimes even a negative association has been found between avoidant attachment and
894 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from
grief symptoms, whether following a loss caused by death or one caused by the dis-
solution of a romantic relationship. These findings contradict common beliefs of
bereavement theorists and clinicians (e.g., Belitsky & Jacobs, 1986; Parkes, 1965;
Rando, 1992; Worden, 1982), who expect avoidant defenses applied early in the
bereavement process to portend a later, delayed grief response. Traditional bereavement
theory postulates that failure to work through a loss, including the emotional pain of the
loss, may result in a delayed grief reaction.
With this background in mind, we designed a study to examine relations between
attachment insecurities and adjustment to loss, but with the special goal of understanding
more about the divergence between theoretical notions of delayed or inhibited grief and
the lack of empirical support for it. There are a few reasons why avoidant attachment
may have been unrelated to grief symptoms in previous bereavement research (Field &
Sundin, 2001; Fraley & Bonanno, 2004; Wayment & Vierthaler, 2002).
Firstly, previous research did not assess grief symptoms in line with current concep-
tions of prolonged or complicated grief. Prigerson (e.g., Prigerson et al., 2009) has pio-
neered the creation of a diagnostic category, complicated grief, which is now called
Prolonged Grief Disorder (PGD). It has been proposed for inclusion in the DSM V, and is
best represented by the Prolonged Grief Inventory (PG-13; Prigerson et al., 2009). The
eight symptoms of grief assessed by Fraley and Bonanno (2004) covered only four of the
11 symptoms in the PG-13 (yearning, trouble accepting the loss, life as empty and mean-
ingless, and interpersonal difficulties), leaving aside over 60% of the items in the PG-13
(intense sorrow, avoiding reminders, shock, role confusion, bitterness, trouble moving
on, emotional numbness). Wayment and Vierthaler (2002) and Field and Sundin (2001)
used the 13-item Texas Revised Inventory of Grief (TRIG; Faschingbauer, Zisook, &
DeVaul, 1987), which included the contents of only one item from the PG-13 (trouble
accepting the loss). Previous studies on attachment and loss, while assessing grief symp-
toms, have failed to assess symptoms of prolonged or complicated grief. It may be that
avoidant attachment is related only to more complicated or prolonged grief symptoms,
which indicate the difficulties some people have in reinvesting in the world after a loss.
Secondly, previous research has been inconsistent with respect to the con-
ceptualization and measurement of attachment patterns. For example, Fraley and
Bonanno (2004) and Wayment and Vierthaler (2002) assessed attachment generally,
whereas Field and Sundin (2001) assessed attachment specific to the relationship with
the deceased. While general (or global) and specific attachment insecurities are related
conceptually, they are not interchangeable and should be assessed and discussed sepa-
rately. A variety of attachment measures have been used in previous research, with
Fraley and Bonanno (2004) using the Relationship Styles Questionnaire (RSQ; Griffin &
Bartholomew, 1994) to create the two attachment dimensions of avoidance and anxiety,
whereas Wayment and Vierthaler (2002) used the Attachment Style Questionnaire
(ASQ; Feeney, Noller, & Hanrahan, 1994) to derive three attachment styles: secure,
anxious-ambivalent, and avoidant. Field and Sundin (2001) used the Compulsive
Care-Seeking scale from the Reciprocal Attachment Questionnaire (RAQ; West &
Sheldon-Keller, 1994) to indicate attachment anxiety, even though it loaded only .49
on the anxiety factor in Brennan, Clark, and Shaver’s (1998) factor analytic study of
attachment items.
Jerga et al. 895
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

Thirdly, participants in previous attachment and loss studies were aware, when they
agreed to participate, that the study was designed to investigate grief and bereavement
(e.g., Fraley & Bonanno, 2004, disseminated information about the study to recently
bereaved people, and Wayment & Vierthaler, 2002, recruited bereaved people through
hospices), making it evident that the investigators were interested in loss. This may
have biased the sample, causing people to choose whether or not to participate based on
whether they were struggling to integrate the loss or were using an avoidant strategy to
keep from thinking about it. Bowlby (1980) mentioned that we may know less about
people who are ‘‘independent of affectional ties’’ (i.e., avoidant) than about other kinds
of people because ‘‘individuals disposed to assert emotional self-sufficiency are pre-
cisely those who are least likely to volunteer to participate in studies of the problem’’
(p. 211).
Fourthly, previous research has not always controlled for the closeness of the rela-
tionship with the deceased or the strength of the attachment relationship. It is possible
that people high on attachment-related avoidance report losses of a less significant nature
than those reported by other study participants. If so, the lack of a relationship between
avoidant attachment and grief symptoms might be partly a function of the kind of rela-
tionship that was lost rather than a result of avoidant coping following the loss.
Finally, previous studies have often involved small participant samples and may not
have had sufficient statistical power to detect an effect between avoidant attachment and
grief symptoms.
The present study is an attempt to address these problems and improve upon past
research by: measuring both manifestations of typical grief and symptoms of prolonged
grief; assessing attachment both generally and with respect to the particular relationship
that was lost; using measures of the two major dimensions of attachment insecurity,
anxiety and avoidance; disguising the nature of the study in the beginning to avoid
sampling biases; controlling for relationship closeness and degree of attachment; and
involving a large sample.
Hypotheses
A number of hypotheses were proposed with regard to relations between attachment and
prolonged versus typical grief. Firstly, consistent with the literature on general attach-
ment styles (i.e., not specific to a particular relationship), we expected that general
attachment anxiety would be associated with both typical and prolonged grief symptoms.
Also consistent with previous findings, general avoidant attachment was expected not to
be related to typical grief symptoms. However, based on our argument that generalized
avoidant working models would lead to a failure to resolve a loss over the longer term,
we expected that there would be an association between general avoidant attachment and
prolonged grief symptoms.
With regard to relationship-specific attachment insecurities, previous research has
shown that relationships characterized by anxious attachment (i.e., involving conflict,
ambivalence, or dependency) are associated with more intense grief symptoms and pro-
blematic adjustment to loss. Thus, we expected relationship-specific attachment anxiety
to be associated with manifestations of both typical grief and prolonged grief symptoms.
896 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

In the case of avoidant attachment, previous studies have failed to find an association
between relationship-specific avoidance and manifestations of grief, and we expected
to replicate this finding. In contrast to the predictions for general avoidant attachment,
however, because relationship-specific avoidant attachment may indicate a weaker emo-
tional bond with the lost relationship partner, we expected either no association between
relationship-specific avoidance and grief symptoms or a negative association, if
relationship-specific avoidance went with lower relationship strength.
In addition, we expected that stronger bonds, greater relationship conflict, greater
care experienced in the relationship, and the traumatic nature of the loss would be
associated with both typical and prolonged grief symptoms. Given the likely healing
effects of time on grief, we expected that time since loss would be associated with less
intense typical and prolonged grief symptoms. No predictions were made concerning
participant age or gender.
Method
Participants and design
Three hundred seventy-two undergraduate students from the University of California,
Davis (250 women and 122 men), aged 17–49 years (M ¼ 19.6, SD ¼ 2.59), completed
an online survey for class credit, and within the survey there were questions about a sig-
nificant death loss. More students than we are discussing here completed the online sur-
vey, reporting no loss or a non-death loss, but here we discuss only the data for students
who reported a death loss. Students were not aware in advance that the study was focused
on interpersonal losses. They were informed through the consent form that they would be
asked questions about their relationships, coping strategies, and current functioning.
They were also warned that they would be asked personal questions about their life and
that there was a chance that they might feel some sadness during or after completing the
survey. Students were told they could withdraw from the study at any time without pen-
alty and that there were alternate ways of obtaining research credit, including other
research studies or writing a short paper. Students who reported a loss were provided
with a debriefing statement at the end of the online questionnaire and were encouraged
to contact the researchers if they had any questions about or problems with the study. The
study was approved in advance by the Ethics Committee at the Australian National
University and the Institutional Review Board at the University of California, Davis.
Procedures and measures
Participants completed the online survey without time pressure. To begin, they answered
demographic questions and questions relating to general attachment insecurities (anxiety
and avoidance). They then answered questions about past losses and designated their
most significant loss (if no loss was reported, they moved on to the end of the survey).
The remainder of the survey dealt with this loss. Participants completed a narrative
writing task in which they described their ‘‘deepest thoughts and feelings’’ about the loss
and then answered questions about their relationship with the deceased and any recent
grief symptoms related to this loss.
Jerga et al. 897
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

Demographics. Questions were asked about the participant’s gender, age, ethnicity, first
spoken language, religion, and relationship status.
General attachment. General attachment insecurities, measured along the two dimensions
of anxious and avoidant attachment, were assessed with the Experiences in Close
Relationships Scale (ECR; Brennan, Clark & Shaver, 1998). Instructions focused on how
the participant generally feels and behaves in close relationships. Attachment anxiety
and avoidance were each assessed with 18 questions answered on a seven-point Likert
scale ranging from 1 (strongly disagree) to 7 (strongly agree). In past studies both scales
have been internally reliable, as indicated by high alpha coefficients, and they were again
reliable in the present study, as reported in the Results section. The item scores were
averaged to obtain each scale score, yielding means that could range from 1 to 7.
Past losses. This measure was created by the authors and includes questions regarding
past losses, including death and non-death losses. Participants answered specific ques-
tions about their most significant loss, including how the loss occurred, the circum-
stances surrounding the loss (including how traumatic it was, how prepared the
participant was, and how expected the loss was), age at the time of the loss, time since
the loss, length of the relationship with the deceased, and whether the participant had
received counseling in relation to the loss. Although participants could have chosen
either a death or a non-death loss to report as their most significant loss, here we pres-
ent only data related to a death loss.
Traumatic loss. The traumatic nature of the loss was assessed by asking, ‘‘Were the cir-
cumstances surrounding the loss traumatic?’’ The question was answered on a five-point
scale ranging from 1 (not at all) to 5 (a great deal).
Next, participants completed a narrative writing task in which they wrote con-
tinuously for five minutes about their deepest thoughts and feelings about the loss. They
then completed the following measures with reference to that particular loss.
Specific attachment. Specific attachment insecurities, both anxiety and avoidance, were
assessed with the short form of the ECR (ECR-Short Form; Wei, Russell, Mallinckrodt,
& Vogel, 2007). Instructions focused on the past relationship with the deceased. Attach-
ment anxiety and avoidance were each assessed by six items rated on a seven-point
Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). The item scores
were averaged to obtain each scale score, yielding means that could range from 1 to 7.
Attachment strength. To measure the strength of the attachment to the deceased, eight
items were adapted from the Attachment Network Questionnaire (ANQ; Doherty &
Feeney, 2004). Instructions were based on the relationship with the deceased. Two items
were included for each of four attachment functions: safe haven (e.g., I would turn to this
person if I felt upset or down), secure base (e.g., I felt that I could always count on this
person, no matter what), proximity seeking (e.g., I enjoyed spending time with this
person), and separation protest (e.g., I did not like to be away from this person). Ratings
were made on a seven-point Likert scale ranging from 1 (strongly disagree) to
898 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

7 (strongly agree), and the scores were averaged to obtain a scale score, yielding a mean
that could range from 1 to 7.
Relationship quality. Two scales were used from the Relationship Rating Form (RRF;
Davis, 2001) to assess aspects of the relationship to the deceased: care and conflict. The
care scale includes 11 items and comprises three subscales: giving the utmost (e.g.,
Could you count on this person to give the utmost on your behalf?), championing (e.g.,
Could you count on this person to support you in an argument or dispute with others?),
and assistance (e.g., Could you count on this person to come to your aid when you
needed help?). The conflict scale includes three items (e.g., I would fight and argue with
this person). Items on the RRF are usually answered on a nine-point Likert scale. To
maintain response-scale consistency with the other relationship measures, the rating
scale was changed in the present study to a seven-point Likert scale ranging from
1 (strongly disagree) to 7 (strongly agree). The item scores were averaged to obtain each
scale score, yielding means that could range from 1 to 7.
Prolonged grief symptoms. Prolonged grief symptoms were measured with the PG-13
(Prigerson et al., 2009), which was designed to assess symptoms of prolonged grief and
to screen for people with PGD. Neimeyer and Hogan (2001) explained how the Inven-
tory of Complicated Grief (ICG; Prigerson et al., 1995), an earlier version of the PG-13,
‘‘was designed to distinguish between ‘normal’ grief and its more ‘pathological’ forms’’
(p. 98). Eleven questions assess the severity of prolonged grief symptoms (rated on a
five-point Likert scale), and two questions assess whether the symptoms have been
present for longer than six months and whether the person has experienced a significant
reduction in functioning (based on a yes/no response scale). The questionnaire was used
in the present study to assess the severity of prolonged grief symptoms (and not to screen
for PGD) and was therefore based on the 11 questions assessing the severity of grief
symptoms. The first two questions asked about separation distress (e.g., How often have
you felt yourself longing or yearning for the person you lost?), and the other nine ques-
tions asked about cognitive symptoms (e.g., How often have you tried to avoid reminders
that the person you lost is gone?), emotional symptoms (e.g., Do you feel emotionally
numb since your loss?), and behavioral symptoms (e.g., Do you feel that moving on
(e.g., making new friends, pursuing new interests) would be difficult for you now?). The
11 items were averaged, resulting in a mean score that could range from 1 to 5.
Manifestations of more typical grief. Manifestations of normal, or typical, grief were
measured with the Core Bereavement Items (CBI; Burnett, Middleton, Raphael, &
Martinek, 1997). This scale was designed to measure core bereavement phenomena as
experienced by a community sample of people reporting different types of losses. The
items in the scale are considered to be central to the construct of grief as conceptualized
in Western society and to represent manifestations of normal grief that are commonly
experienced by bereaved individuals and generally decline significantly over time. This
is distinguished from a more ‘‘complicated’’ or ‘‘prolonged’’ grief response, which is
better assessed using the PG-13, as previously mentioned. In a chapter describing a
variety of grief scales, Neimeyer and Hogan (2001) said that the CBI is best suited to
Jerga et al. 899
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

the study of ‘‘normal’’ grief responses, rather than more complicated grief trajectories (p.
98). The CBI includes 17 items that can be assembled into three subscales: images and
thoughts (e.g., Do you experience images of the events surrounding the loss?), acute
separation (e.g., Do you find yourself pining for/yearning for the person you lost?), and
grief (e.g., Do reminders such as photos, situations, music, places, etc, cause you to feel
longing for the person you lost?). The first subscale includes seven items, whereas the
second and third subscales each include five items. Items on the CBI are usually
answered on a four-point Likert scale. To maintain response-scale consistency with the
prolonged grief measure, the rating scale was changed in the present study to a five-point
Likert scale ranging from 1 (not at all) to 5 (all the time). The 17 items were averaged,
resulting in a mean score that could range from 1 to 5.
Results
A total of 372 people provided information about a death loss in the online survey. The
data were screened for missing values, violations of univariate and multivariate nor-
mality, outliers, homoscedasticity, and multicollinearity. Univariate outliers were
detected using a criterion of jzj > 3.29. Once detected, their influence was reduced by
altering the associated raw score so that it was less deviant than before. That is, scores
were manually adjusted so there was less difference between them and the closest score
that did not violate the criterion of jzj > 3.29 (see Tabachnick & Fidell, 2001). Altered
scores were only used for the regression analyses. Four multivariate outliers were
detected using the Mahalanobis distance measure in SPSS software and were deleted.
Multicollinearity and singularity were not present in the regression analyses. Homo-
scedasticity was observed in the bivariate scatterplots, but due to the large sample size it
was not considered problematic for the regression analyses.
The average age of members of the final sample of 368 (247 women, 121 men) was 19.6
years (SD ¼ 2.6). Most participants reported English as their first language (67.1%) and
were Christian (47.6%) or Agnostic (14.1%), followed by a group that chose no specific
religion (11.1%), Buddhists (9.8%), other (7.9%), Atheist (5.7%), and Jewish (3.8%). About
half of the participants (49.7%) were in a romantic relationship at the time of the study;
20.9% were in a relationship that had lasted for up to 12 months, and 28.8% had been in a
relationship for longer than a year. Of the death losses reported, the majority of the deceased
were grandparents (54.1%), followed by friends (13.0%), parents (12.8%), other relatives
(12.2%), other losses (4.3%), siblings (1.9%), and romantic partners (1.6%).
Due to the large correlation of .80 between the two grief measures, a decision was
made to factor analyze all 28 grief items to see if the two scales actually measured
distinct constructs, as intended. All 28 items were entered into an analysis using principal
axis factoring. The data were initially assessed to see if they were suitable for factor
analysis, and they were according to a Kaiser–Meyer–Olkin value of .959, a statistically
significant value for the Bartlett Test of Sphericity (Bartlett, 1954), and many coeffi-
cients greater than .30 in the correlation matrix. Cattell’s (1966) scree test indicated a
two-factor solution, as did Horn’s parallel analysis (Horn, 1965). Both a two- and a
three-factor solution, based on direct oblimin rotation, were computed. The two-factor
solution was the most interpretable and fit the data best. Items were chosen that best
900 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

discriminated between the two factors. Loadings had to exceed .50 and cross-loadings
had to be lower than .32. Based on these criteria, six items from the CBI scale were
removed (CBI6, CBI11, CBI12, CBI14, CBI15, CBI17). Besides not meeting our cri-
teria, all of these six items had mean values that were lower than the overall mean value
for the CBI, indicating that they were not strongly endorsed by participants. The removal
of these items left 22 items, with 11 items on each of the two scales. The remaining 22
items were re-analyzed, using principal axis factoring and direct oblimin rotation (see
Table 1 for the final solution). Factor 1 included mostly items from the CBI, with only
two items from the Prolonged Grief Scale. All of the items assess typical grief symptoms,
such as thinking about the deceased, missing the deceased, being reminded of the
deceased, and longing and yearning for the deceased. Factor 2 included mostly items
from the PG-13, with only two coming from the CBI. The two items from the CBI had
the lowest means of the remaining CBI items, indicating that they were not frequently
endorsed by participants. The items on Factor 2 concern difficulties reinvesting in the
world, such as difficulty trusting people, feeling that life is empty, and feeling emotion-
ally numb. The first factor, which we will call, for present purposes, typical grief symp-
toms, accounted for 48.10% of the item variance. The second factor, which we will call
prolonged grief symptoms, accounted for 7.64% of variance. Unit-weighted scores were
computed for the two factor-based scales. The reliability of the first scale, typical grief
symptoms, was .94 and the reliability for the second scale, prolonged grief symptoms,
was .91. The first scale was correlated .96 with the CBI (Burnett et al., 1997), and the
second scale was correlated .97 with the PG-13 (Prigerson et al., 2009), supporting the
naming of these two scales. The correlation between the two scales was .70.
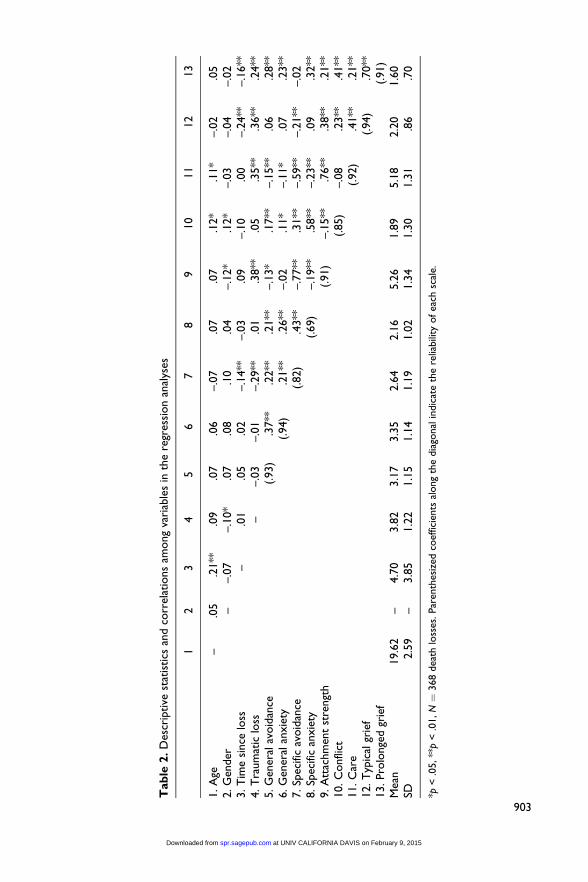
The correlations among the variables used in the regression analyses are presented in
Table 2. The scale reliabilities are reported in parentheses along the diagonal of the table
and range from .69 to .94. The means and standard deviations are presented in the last
two rows of the table.
The two general attachment dimensions were significantly correlated (r ¼ .37), as
were the two specific attachment dimensions (r ¼ .43). General and specific attachment
dimensions were all significantly correlated with each other (see Table 2). With respect
to typical grief symptoms, neither general attachment anxiety nor specific attachment
anxiety was related to typical grief symptoms, contrary to expectations. As predicted,
general avoidant attachment was not significantly related to typical grief symptoms.
However, specific attachment avoidance was negatively associated with typical grief
symptoms (r ¼ –.21). In addition, the following variables were significantly correlated
with typical grief symptoms as expected: attachment strength, relationship conflict and
care, the traumatic nature of the loss, and prolonged grief symptoms. Time since loss
was, as expected, negatively correlated with typical grief symptoms.
With respect to prolonged grief symptoms, as hypothesized, both general and specific
attachment anxiety, and general but not specific avoidant attachment, were associated
with more intense prolonged grief symptoms. Other variables were significantly corre-
lated with prolonged grief symptoms, as predicted, including attachment strength,
relationship care, relationship conflict, the traumatic nature of the loss, and typical grief
symptoms. Time since loss was, as expected, significantly and negatively correlated with
symptoms of prolonged grief.
Jerga et al. 901
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

All four attachment dimensions were significantly correlated with relationship
conflict (in the lost relationship), with specific attachment anxiety correlating most
highly (r ¼ .58). All four attachment dimensions were also significantly, negatively
correlated with relationship care (the degree of care in the relationship with the
deceased), with specific avoidant attachment correlating most strongly in the negative
Table 1. Pattern matrix for final two-factor solution with 22 items
Factor 1 Factor 2
CBI4: Do you think about X? .933 –.161CBI8: Do you find yourself missing X? .905 –.156CBI9: Are you reminded by familiar objects (photos,
possessions, rooms etc) of X?.802 –.053
CBI2: Do thoughts of X come into your mindwhether you wish it or not?
.684 .201
PG1: In the past month, how often have you feltyourself longing or yearning for the person youlost?
.680 .147
CBI16: Do reminders of X such as photos, situations,music, places, etc, cause you to feel sadness?
.666 .123
CBI1: Do you experience images of the events sur-rounding the loss of X?
.658 .170
CBI13: Do reminders of X such as photos, situations,music, places, etc, cause you to feel longing for X?
.646 .177
CBI10: Do you find yourself pining or yearning for X? .594 .276CBI7: Do you find yourself thinking of reunion with
X?.590 .052
PG2: In the past month, how often have you hadintense feelings of emotional pain, sorrow, orpangs of grief related to the lost relationship?
.544 .300
PG11: Do you feel emotionally numb since your loss? –.063 .829PG8: Has it been hard for you to trust others since
your loss?–.177 .828
PG12: Do you feel that life is unfulfilling, empty, ormeaningless since your loss?
–.054 .793
PG9: Do you feel bitter over your loss? .125 .663PG4: In the past month, how often have you tried to
avoid reminders that the person you lost is gone?.064 .660
PG10: Do you feel that moving on (e.g., making newfriends, pursuing new interests) would be difficultfor you now?
.012 .659
PG6: Do you feel confused about your role in life orfeel like you don’t know who you are (i.e., feelingthat a part of yourself has died)?
.123 .593
PG5: In the past month, how often have you feltstunned, shocked, or dazed by your loss?
.226 .571
CBI5: Do images of X make you feel distressed? .177 .550CBI3: Do thoughts of X make you feel distressed? .215 .539PG7: Have you had trouble accepting the loss? .210 .528
902 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from
Tab
le2.
Des
crip
tive
stat
istics
and
corr
elat
ions
among
vari
able
sin
the
regr
essi
on
anal
yses
12
34
56
78
910
11
12
13
1.A
ge–
.05
.21**
.09
.07
.06
–.0
7.0
7.0
7.1
2*
.11*
–.0
2.0
52.G
ender
––.0
7–.1
0*
.07
.08
.10
.04
–.1
2*
.12*
–.0
3–.0
4–.0
23.T
ime
since
loss
–.0
1.0
5.0
2–.1
4**
–.0
3.0
9–.1
0.0
0–.2
4**
–.1
6**
4.T
raum
atic
loss
––.0
3–.0
1–.2
9**
.01
.38**
.05
.35**
.36**
.24**
5.G
ener
alav
oid
ance
(.93)
.37**
.22**
.21**
–.1
3*
.17**
–.1
5**
.06
.28**
6.G
ener
alan
xie
ty(.94)
.21**
.26**
–.0
2.1
1*
–.1
1*
.07
.23**
7.Sp
ecifi
cav
oid
ance
(.82)
.43**
–.7
7**
.31**
–.5
9**
–.2
1**
–.0
28.Sp
ecifi
can
xie
ty(.69)
–.1
9**
.58**
–.2
3**
.09
.32**
9.A
ttac
hm
ent
stre
ngt
h(.91)
–.1
5**
.76**
.38**
.21**
10.C
onfli
ct(.85)
–.0
8.2
3**
.41**
11.C
are
(.92)
.41**
.21**
12.T
ypic
algr
ief
(.94)
.70**
13.Pro
longe
dgr
ief
(.91)
Mea
n19.6
2–
4.7
03.8
23.1
73.3
52.6
42.1
65.2
61.8
95.1
82.2
01.6
0SD
2.5
9–
3.8
51.2
21.1
51.1
41.1
91.0
21.3
41.3
01.3
1.8
6.7
0
*p<
.05,**
p<
.01,N¼
368
dea
thlo
sses
.Par
enth
esiz
edco
effic
ients
along
the
dia
gonal
indic
ate
the
relia
bili
tyofea
chsc
ale.
903
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

direction (r ¼ –.59). General avoidant attachment, specific avoidant attachment, and
specific attachment anxiety were all significantly negatively correlated with attachment
strength (the strength of the attachment relationship with the deceased), with specific
avoidant attachment correlating most negatively (r ¼ –.77).
Prediction of typical grief
A hierarchical regression analysis was conducted to see whether general and specific
attachment insecurities were related to typical grief symptoms after controlling for the
other major predictors (see Table 3). The final model was significant F (11, 356) ¼18.94, p < .01, and accounted for 36.9% of the variance in typical grief symptoms. In the
first step, age, gender, time since loss, and the traumatic nature of the loss were entered
as predictors, resulting in R2 ¼ .19, F (4, 363) ¼ 21.46, p < .01. The traumatic nature of
the loss was a significant positive predictor of typical grief symptoms (b¼ .36, p < .001)
and time since loss was a significant negative predictor (b ¼ –.25, p < .001). Age and
gender did not significantly predict typical grief symptoms.
In step 2, general attachment anxiety and avoidance were entered as predictors, with
the result that R2 ¼ .20, F (6, 361) ¼ 15.09, p < .05, and an additional 1% of the
variance was explained, which was a non-significant contribution to the model. Neither
avoidance (b ¼ .06, p ¼ .245) nor anxiety (b ¼ .06, p ¼ .253) made a unique and sig-
nificant contribution to the model.
In step 3, specific attachment anxiety and avoidance were added to the model, R2¼ .25,
F (8, 359) ¼ 14.96, p < .01, and this resulted in a significant increment in variance
explained (R2D ¼ .05; see Table 3). Specific attachment anxiety was associated with
typical grief symptoms (b¼ .16, p < .01) and specific avoidant attachment was negatively
associated with these symptoms (b ¼ –.26, p < .001).
In step 4, attachment strength was added to the model, yielding R2 ¼ .31, F (9, 358) ¼17. 46, p < .01, and a further significant increase in explained variance (R2D ¼ .055;
see Table 3). Strength was positively associated with typical grief symptoms (b ¼ .40, p <
Table 3. Multiple regression analysis predicting typical grief
Betastep 1
Betastep 2
Betastep 3
Betastep 4
Betastep 5 F D
Age .01 .00 –.03 –.03 –.08 21.46**Gender –.02 –.03 –.03 –.01 –.05Time since loss –.25** –.25** –.28** –.27** –.23**Traumatic loss .36** .36** .29** .23** .19**General avoidance .06 .08 .09 .08 2.09General anxiety .06 .06 .02 .06Specific avoidance –.26** .06 .01 11.86**Specific anxiety .16** .11* .02Attach. strength .40** .19* 28.34**Conflict .23** 18.10**Care .25**
R2 ¼ 0.191** R2 D¼ 0.009 R2 D¼ 0.050** R2 D¼ 0.055** R2 D¼ 0.064** R2 ¼ 0.369**
*p < .05, **p < .01, N ¼ 368 death losses.
904 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from
.001), and its inclusion in the regression model reduced the beta coefficient for specific
avoidant attachment to non-significance, suggesting that the significant negative association
between specific avoidant attachment and typical grief symptoms was due to the weaker
strength of avoidant individuals’ attachment bond with the lost person.
In step 5, with relationship conflict and care added to the model, R2¼ .37, F (11, 356)
¼ 18.94, p < .01, and there was a further significant increment in variance explained
(R2D ¼ .064; see Table 3). Relationship conflict and care were both significant pre-
dictors of typical grief symptoms (b ¼ .23, p < .001 and b ¼ .25, p < .001, respectively),
and the beta coefficient for specific attachment anxiety was no longer significant, sug-
gesting that conflict and care may have mediated the association between specific
attachment anxiety and typical grief symptoms.
In the final regression model, the following variables were positively associated with
typical symptoms: traumatic nature of the loss, attachment strength, and relationship
conflict and care. Time since loss was negatively associated with symptoms, and specific
attachment insecurities were no longer significantly related to symptoms.
Prediction of prolonged grief
A hierarchical regression analysis was conducted to see whether general and specific
attachment insecurities were uniquely related to prolonged grief symptoms after controlling
for the other major predictors (see Table 4). The final regression model was significant,
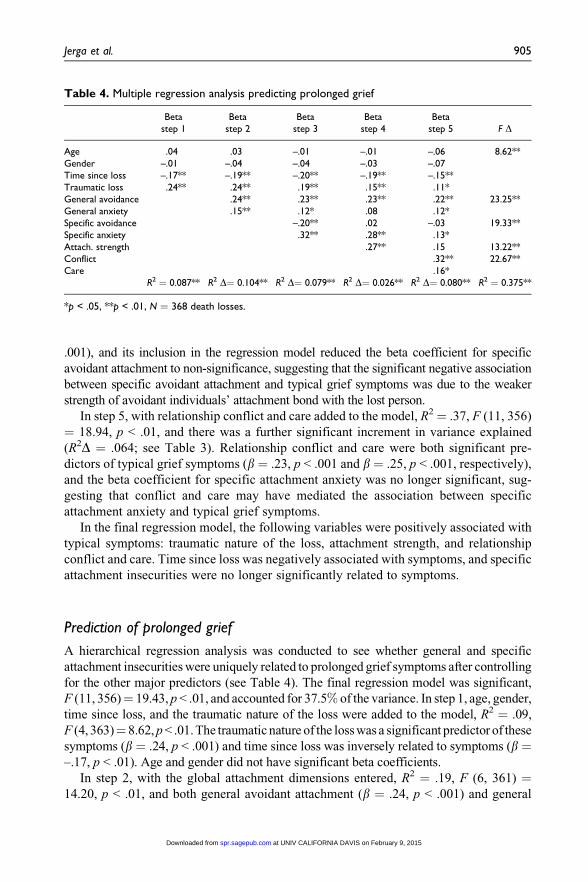
F (11, 356)¼ 19.43, p < .01, and accounted for 37.5% of the variance. In step 1, age, gender,
time since loss, and the traumatic nature of the loss were added to the model, R2 ¼ .09,
F (4, 363)¼ 8.62, p < .01. The traumatic nature of the loss was a significant predictor of these
symptoms (b ¼ .24, p < .001) and time since loss was inversely related to symptoms (b ¼–.17, p < .01). Age and gender did not have significant beta coefficients.
In step 2, with the global attachment dimensions entered, R2 ¼ .19, F (6, 361) ¼14.20, p < .01, and both general avoidant attachment (b ¼ .24, p < .001) and general
Table 4. Multiple regression analysis predicting prolonged grief
Betastep 1
Betastep 2
Betastep 3
Betastep 4
Betastep 5 F D
Age .04 .03 –.01 –.01 –.06 8.62**Gender –.01 –.04 –.04 –.03 –.07Time since loss –.17** –.19** –.20** –.19** –.15**Traumatic loss .24** .24** .19** .15** .11*General avoidance .24** .23** .23** .22** 23.25**General anxiety .15** .12* .08 .12*Specific avoidance –.20** .02 –.03 19.33**Specific anxiety .32** .28** .13*Attach. strength .27** .15 13.22**Conflict .32** 22.67**Care .16*
R2 ¼ 0.087** R2 D¼ 0.104** R2 D¼ 0.079** R2 D¼ 0.026** R2 D¼ 0.080** R2 ¼ 0.375**
*p < .05, **p < .01, N ¼ 368 death losses.
Jerga et al. 905
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

attachment anxiety (b ¼ .15, p < .01) were significantly related to prolonged symptoms,
accounting for 10.4% of the variance (see Table 4).
In step 3, specific attachment anxiety and avoidance were entered, and R2¼ .27,
F (8, 359) ¼ 16.56, p < .01, with an additional 7.9% of the variance in symptoms being
accounted for (see Table 4). Specific attachment anxiety significantly predicted pro-
longed symptoms (b ¼ .32, p < .001) and specific avoidant attachment was negatively
associated with them (b ¼ –.20, p < .001).
In step 4, attachment strength was added as a predictor, and R2 ¼ .30, F (9, 358) ¼16.69, p < .01, resulting in a significant increment in R2 (R2D ¼ .026, see Table 4).
Attachment strength was positively associated with prolonged symptoms (b ¼ .27, p <
.001), and its inclusion in the model reduced the beta coefficient for specific avoidant
attachment to non-significance (similar to step 4 of the regression analysis predicting typ-
ical grief symptoms). This suggests, again, that the negative association between specific
avoidance and grief symptoms was mediated by strength of attachment.
In step 5, relationship conflict and care were entered, and R2 ¼ .38, F (11, 356) ¼19.43, p < .01, with there being a significant increment in variance explained (R2D¼ .08,
see Table 4). Relationship conflict and care were both positively associated with pro-
longed grief symptoms (b ¼ .32, p < .001 and b ¼ .16, p < .05, respectively). The beta
coefficient for specific attachment anxiety, although still significant, was reduced from
.28 to .13, suggesting that conflict and care within the relationship partially mediated the
association between relationship-specific attachment anxiety and prolonged symptoms.
In the final regression model the following variables were significant predictors of pro-
longed grief symptoms: traumatic nature of the loss, general attachment anxiety and
avoidance, specific attachment anxiety, and relationship conflict and care. Time since loss
was negatively associated with prolonged symptoms. Relationship-specific avoidant attach-
ment and attachment strength were unrelated to prolonged grief symptoms in the final model.
We were interested in testing whether the attachment variables would remain sig-
nificant predictors of prolonged grief symptoms once normal manifestations of grief,
represented by typical grief symptoms, entered the model. The three attachment vari-
ables remained significant predictors of prolonged grief symptoms, as did relationship
conflict, but relationship care, time since loss, and traumatic nature of the loss became
non-significant. Thus, attachment and relationship conflict contributed to a person’s
moving beyond typical grief symptoms to prolonged adjustment difficulties.
We were also interested in determining whether there were any significant interac-
tions between the general attachment scores and the specific attachment scores, for both
grief outcome variables. Interactions were tested with and without the control variables
(age, gender, time since loss, and traumatic nature of the loss) and none were found to be
significant. Thus, only the main effects will be discussed.
Discussion
The main purpose of this study was to examine associations between general and specific
attachment insecurities, on the one hand, and experiences of grief following a death loss,
on the other. General attachment anxiety, reflecting general working models of
relationships characterized by conflict and ambivalence, was expected to be associated
906 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

with both ‘‘normal,’’ or typical, manifestations of grief and prolonged grief, the latter
state having been associated in the past with failure to resolve feelings and issues related
to the deceased. This hypothesis was partially supported, in that general attachment
anxiety was correlated with a measure of prolonged grief symptoms (closely related to
Prigerson et al.’s, 2009, measure of these symptoms) and predicted these symptoms in a
regression analysis, even after measures of specific relationship factors were statistically
controlled. General attachment anxiety was not significantly correlated with our measure
of more typical, or normative, grief symptoms and did not predict these symptoms in a
regression analysis. These findings suggest that people who are generally anxious in
close relationships are vulnerable to prolonged grief symptoms, even though they do not
necessarily experience more intense normative grief symptoms.
Turning to avoidant attachment, we expected that general avoidant attachment would
predict prolonged grief symptoms but not typical grief symptoms. This hypothesis was
confirmed by a significant correlation between general avoidant attachment and pro-
longed grief symptoms, but not typical or normative grief symptoms. The hypothesis was
also supported in all steps of a regression analysis. This finding suggests that people who
are generally avoidant in close relationships experience long-term difficulties adjusting
to the loss of a loved one, even though they do not necessarily experience more intense
typical grief symptoms, a lack of relationship that had been found in previous studies.
In relation to specific attachment insecurities in the relationship with the deceased,
attachment anxiety was expected to be related to both typical and prolonged grief
symptoms. Specific avoidance, however, was expected to be unrelated, or possibly
negatively related, to either kind of symptoms. The first of these hypotheses was largely
supported. Specific attachment anxiety was correlated with prolonged grief symptoms,
and significantly predicted prolonged grief symptoms in every step of a regression
analysis. Specific attachment anxiety was not significantly correlated with typical grief
symptoms, and although it was a significant predictor in steps 3 and 4 of a five-step
regression analysis, it became non-significant in the fifth step when relationship conflict
and care were statistically controlled. These results indicate that people who were more
anxiously attached to the deceased individual experienced more intense grief after the
person’s death, but this may have happened because they had experienced more conflict
with the person and received more care from him or her. This kind of ambivalence (want-
ing care but provoking conflict) is characteristic of people who score high on attachment
anxiety (Mikulincer, Shaver, Bar-On, & Ein-Dor, 2010).
Our predictions regarding relationship-specific avoidance were also largely sup-
ported. Relationship-specific avoidance was not significantly correlated with prolonged
grief symptoms, but it was negatively correlated with typical grief symptoms. It was also
unrelated to both prolonged and typical grief when other relationship variables were
included in a regression analysis. Specific avoidance was negatively related to both pro-
longed and typical grief symptoms when it was entered into the regression analyses, but
when attachment strength was included in the model predicting either typical or pro-
longed grief symptoms, the association with avoidance became non-significant. These
results fit with previous studies of attachment insecurities and romantic dissolution,
which have found a negative association between avoidant attachment and post-
breakup distress (Feeney & Noller, 1992; Simpson, 1990). Our results suggest that the
Jerga et al. 907
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from
specific bond to the deceased may not have been as strong for more avoidant individuals,
leaving less to grieve about in comparison with people who were emotionally close to the
people they lost. The strong negative correlation between specific avoidant attachment
and attachment strength to the deceased (r ¼ –.77) clearly supports this idea.
Our results also support the predictions made regarding the remaining relationship
factors. Attachment strength, relationship conflict, and relationship care were correlated
with manifestations of typical grief and prolonged grief symptoms and were significant
predictors of these variables in regression analyses (with the exception of attachment
strength in the final step of the prolonged grief model). These results indicate that the
greater the strength of the attachment bond with the deceased, the greater the degree of
care in the relationship with the deceased, and the greater the degree of conflict in the
relationship with the deceased, the greater was the grief experienced after the loss. As
expected, time since loss was negatively correlated with both typical and prolonged grief
symptoms and was inversely related to both outcome variables in the regression anal-
yses, confirming, as expected, that grief declines in intensity over time. The loss being
traumatic was correlated with both kinds of grief symptoms and was a significant pre-
dictor of both, even when attachment variables and relationship quality were statistically
controlled. Age and gender were unrelated to grief symptoms of either kind.
We were interested in distinguishing, to the extent possible, general attachment
insecurities from relationship-specific attachment insecurities. The two have often been
confused or conflated in previous research on attachment and loss. By measuring the two
kinds of attachment insecurity separately and measuring both typical and prolonged grief
symptoms, we hoped to shed light on previous studies that have not found an association
between avoidant attachment and grief symptoms.
Two important findings emerged when examining the different outcomes of general
and specific attachment insecurities. First, there was a difference between general and
specific avoidant attachment when predicting prolonged grief symptoms. General
avoidant attachment was positively associated with prolonged grief symptoms, but
specific avoidant attachment was not, and in fact specific avoidant attachment was
negatively related to these grief symptoms even after controlling for general attachment
in a regression analysis. Second, the association between general avoidant attachment
and grief symptoms was present only in the case of prolonged or complicated grief
symptoms, and not with respect to normative or typical grief. These two findings help to
explain why previous studies have failed to find a significant association between
avoidant attachment and reactions to loss (Field & Sundin, 2001; Fraley & Bonanno,
2004; Wayment & Vierthaler, 2002). In relation to the first point, Field and Sundin
(2001) investigated the association between specific avoidant attachment to the deceased
and grief symptoms, based on the assumption that the specific attachment to the
deceased spouse was an expression of the bereaved individual’s general attachment
style. As shown in the present study, however, global and specific avoidant attachment
are not related in the same way to grief symptoms. In relation to the second point,
previous investigators have measured grief in different ways. As mentioned in our
Introduction, Fraley and Bonanno (2004) included four of the 11 prolonged grief
symptoms in their study, while Wayment and Vierthaler (2002) and Field and Sundin
(2001) included only one of the 11 prolonged grief symptoms. It is possible that
908 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

previous studies have assessed mainly manifestations of normal grief, inadvertently
resulting in a failure to find an association between avoidant attachment and experi-
ences of prolonged grief.
Wijngaards-de Meij et al. (2007), although assessing a caregiving rather than an
attachment relationship with the deceased, were the only previous investigators who
found a relation between avoidant attachment and grief symptoms. Interestingly, they
used the ICG (Prigerson et al., 1995) – an early version of the PG-13 used in our study.
Previous research may have underestimated the importance of distinguishing between
normal and prolonged grief symptoms. Other factors that may have affected previous
findings include small sample sizes, the transparent nature of the studies in the eyes
of participants, failing to assess strength of the attachment to the deceased individual,
and assessing grief symptoms closely following the loss.
Turning to attachment anxiety, both general and specific attachment anxiety were
associated with prolonged grief symptoms, making it less critical that previous studies
failed to differentiate between the two types or levels of attachment. General attachment
anxiety did not predict manifestations of normal grief, however, and specific attachment
anxiety predicted these symptoms only in the initial steps of a regression analysis, sug-
gesting that the apparent main effects were mediated by care and conflict. The finding that
general attachment anxiety was unrelated to normal grief symptoms seems inconsistent
with previous research findings on attachment and loss (Fraley & Bonanno, 2004; Way-
ment & Vierthaler, 2002). This inconsistency may be related to the different samples, with
the other studies using much older samples and where a number of people reported the loss
of a spouse, a loss reported by less than 2% of people in the current study.
So, why are general attachment anxiety and avoidance related to prolonged grief
symptoms but not to more normative manifestations of grief? When describing the
effects of disordered mourning, Bowlby (1980) wrote about the impact on relationships
as well as one’s ability to organize one’s life.
Disordered variants of mourning lead to many forms of physical ill health as well as of
mental ill health. Psychologically they result in a bereaved person’s capacity to make and
to maintain love relationships becoming more or less seriously impaired or, if already
impaired, being left more impaired than it was before. Often they affect also a bereaved per-
son’s ability to organize the rest of his life. (p. 137)
Normative manifestations of grief include missing and yearning for the deceased, but
do not usually include a person’s level of functioning in daily life. The symptoms of
prolonged grief assessed in the present study included difficulties experiencing emo-
tions, forming and maintaining close relationships, and reinvesting in the world and
organizing one’s life. It is possible that the items in the prolonged grief measure are able
to detect the impact of loss on avoidant people’s lives to an extent that other measures do
not. Bowlby (1980) discussed these research difficulties:
First, it is in the nature of the condition that, to an external eye, their mourning should often
appear to be progressing uneventfully. As a result, in all studies except those using the most
sophisticated of methods, it is easy to overlook such people and to group them with those
whose mourning is progressing in a genuinely favourable way. (p. 211)
Jerga et al. 909
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

Another goal of our study, beyond examining attachment and loss, was to identify
factors that helped to predict and explain prolonged grief symptoms. Around 9% of
people are likely to exhibit a chronic grief response, and it is important to understand
who is at risk for this disabling experience. Attachment insecurities accounted for over
10% of the variance in prolonged grief symptoms, and the nature of the specific
attachment relationship accounted for an additional 8% of the variance. Other rela-
tionship variables (relationship strength, care, and conflict) accounted for an additional
11% of the variance, and circumstances surrounding the loss accounted for 9% of the
variance. Attachment insecurities, both general and specific to the relationship,
accounted for over 18% of the variance. It may be useful to consider attachment issues
and other variables when identifying people who may be at risk for psychological
problems following the loss of a loved one.
Limitations and future research
Although we consider our results to be both enlightening and clinically useful, several
limitations should be considered. First, and perhaps most importantly, we cannot be sure
that a person’s attachment orientation after a loss is the same as it was before the loss. It
is possible that people who experienced a difficult loss became more avoidant or anxious
as a result. With respect to specific attachment insecurities, it is possible that a person’s
view of his or her relationship with the deceased was affected by the loss, resulting in
either idealization or minimization of its importance. In addition, if the relationship
ended long before our study, it is possible that a person’s description of it was affected by
memory errors or biases.
Another possible limitation of our study is the heterogeneous nature of the losses.
Because of our participants’ youth, most of their losses were of parents and grandparents.
Loss of a romantic partner, the kind of loss most often studied previously, was rare in our
sample. The type of loss may help to explain why general attachment anxiety did not
have as strong an association with manifestations of normal grief as had been reported in
several previous studies.
The relative youth of our sample is also a limitation of the study. Most of the par-
ticipants were between the ages of 18 and 25, with an average age of 19.6 years, and all
were university students living in the United States. The sample is not representative of
the general population, even of the United States, which may limit the generalizability of
the results.
Future research can benefit from separately assessing general and specific attachment
insecurities and from using a variety of measures to assess adjustment to a loss. Given the
multiple factors associated with grief, many probably having relatively small effect
sizes, it is important that future research in this area employs adequately large samples.
Moreover, methods will need to be employed that allow for the investigation of different
kinds of relationship losses. Finally, to enable the detection of delayed grief symptoms,
future research should extend the length of time considered following a loss and include
measures of prolonged grief symptoms that are indicative of problematic adjustment to
the loss.
910 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

Conclusions
Although previous research has generally supported the view that people with an
avoidant attachment style cope well with loss, the present study questions this view by
finding that general avoidant attachment is significantly related to prolonged grief
symptoms. Although theorists have written about avoidant attachment as a precursor of
delayed or inhibited grief responses, previous research seemed not to support this
clinically based understanding. Our results suggest that the hypothesis should continue to
be entertained, and that it deserves to be studied with adequately complex measures and
research designs.
Conflict of interest statement
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of
this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or
not-for-profit sectors.
References
Ainsworth, M. D. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of attachment: A psy-
chological study of the Strange Situation. Hillsdale, NJ: Erlbaum.
Bartholomew, K., & Horowitz, L. M. (1991). Attachment styles among young adults: A test of a
four-category model. Journal of Personality and Social Psychology, 61, 226–244.
Bartlett, M. S. (1954). A note on the multiplying factors for various chi square approximations.
Journal of the Royal Statistical Society, 16 (Series B), 296–298.
Belitsky, R., & Jacobs, S. (1986). Bereavement, attachment theory, and mental disorders. Psychia-
tric Annals, 16, 276–280.
Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human
capacity to thrive after extremely aversive events? American Psychologist, 59, 20–28.
Bonanno, G. A., Moskowitz, J. T., Papa, A., & Folkman, S. (2005). Resilience to loss in bereaved
spouses, bereaved parents, and bereaved gay men. Journal of Personality and Social Psychology,
88, 827–843.
Bonanno, G. A., Wortman, C, B., Lehman, D. R., Tweed, R. G., Haring, M., Sonnega, J., et al.
(2002). Resilience to loss and chronic grief: A prospective study from pre-loss to 18 months
post-loss. Journal of Personality and Social Psychology, 83, 1150–1164.
Bowlby, J. (1944). Forty-four juvenile thieves: Their characters and home life. International
Journal of Psychoanalysis, 25, 19–52, 107–127.
Bowlby, J. (1969/1982). Attachment and loss: Vol. 1. Attachment (2nd ed.). New York: Basic Books.
Bowlby, J. (1973). Attachment and loss: Vol. 2. Separation: Anxiety and anger. New York: Basic
Books.
Bowlby, J. (1980). Attachment and loss: Vol. 3. Loss: Sadness and depression. New York: Basic
Books.
Bowlby, J., & Parkes, C. M. (1970). Separation and loss within the family. In E. J. Anthony (Ed.),
The child in his family (pp. 197–216). New York: Wiley.
Jerga et al. 911
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult romantic
attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment
theory and close relationships (pp. 46–76). New York: Guilford Press.
Burnett, P., Middleton, W., Raphael, B., & Martinek, N. (1997). Measuring core bereavement
phenomena. Psychological Medicine, 27, 49–57.
Cattell, R. B. (1966). The screen test for the number of factors. Multivariate Behavioral Research,
1, 245–276.
Davis, D., Shaver, P. R., & Vernon, M. M. (2003). Physical, emotional, and behavioral reactions to
breaking up: The roles of gender, age, emotional involvement, and attachment style.
Personality and Social Psychology Bulletin, 29, 871–884.
Davis, K. E. (2001). The Relationship Rating Form (RRF): A measure of characteristics of roman-
tic relationships and friendships. In J. Touliatos, B. Perlmutter, & G. Holden (Eds.), Handbook
of family measurement techniques (Vol 1, 2nd ed.). Thousand Oaks, CA: Sage.
Doherty, N. A., & Feeney, J. A. (2004). The composition of attachment networks throughout the
adult years. Personal Relationships, 11, 469–488.
Faschingbauer, T., Zisook, S., & DeVaul, R. (1987). The Texas Revised Inventory of Grief.
In S. Zisook, (Ed.), Biopsychosocial aspects of bereavement (pp. 111–124). Washington,
DC: American Psychiatric Press.
Feeney, J. A., & Noller, P. (1992). Attachment style and romantic love: Relationship dissolution.
Australian Journal of Psychology, 44, 69–74.
Feeney, J. A., Noller, P., & Hanrahan, M. (1994). Assessing adult attachment. In M. B. Sperling
& W. H. Berman (Eds.), Attachment in adults: Clinical and developmental perspectives
(pp. 122–158). New York: Guilford Press.
Field, N. (2008). Whether to relinquish or maintain a bond with the deceased. In M. Stroebe,
R.O. Hansson, H. Schut, & W. Stroebe (Eds.), Handbook of bereavement research and
practice: Advances in theory and intervention (pp. 113–132). Washington, DC: American
Psychological Association.
Field, N. P., & Sundin, E. C. (2001). Attachment style in adjustment to conjugal bereavement.
Journal of Social and Personal Relationships, 18, 347–361.
Fraley, R. C., & Bonanno, G. A. (2004). Attachment and loss: A test of three competing models on
the association between attachment-related avoidance and adaptation to bereavement. Person-
ality and Social Psychology Bulletin, 30, 878–890.
Fraley, R. C., & Shaver, P. R. (2000). Adult romantic attachment: Theoretical developments,
emerging controversies, and unanswered questions. Review of General Psychology, 4, 132–
154.
Griffin, D., & Bartholomew, K. (1994). Metaphysics of measurement: The case of adult attach-
ment. In K. Bartholomew & D. Perlman (Eds.), Advances in personal relationships, Vol. 5:
Attachment processes in adulthood (pp.17–52). London: Jessica Kingsley.
Horn, J. L. (1965). A rationale and test for the number of factors in factor analysis. Psychometrika,
30, 179–185.
Mikulincer, M., & Shaver, P. R. (2007). Attachment in adulthood: Structure, dynamics, and
change. New York: Guilford Press.
Mikulincer, M., & Shaver, P. R., Bar-On, N., & Ein-Dor, T. (2010). The pushes and pulls of close
relationships: Attachment insecurities and relational ambivalence. Journal of Personality and
Social Psychology, 98, 450–468.
912 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from

Neimeyer, R. A., & Hogan, N. S. (2001).Quantitative or qualitative? Measurement issues in the
study of grief. In M. S. Stroebe, R. O. Hansson., W. Stroebe, & H. Schut (Eds.), Handbook
of bereavement research: Consequences, coping, and care (pp. 89–118). Washington, DC:
American Psychological Association.
Parkes, C. M. (1965). Bereavement and mental illness. British Journal of Medical Psychology, 38,
388–397.
Parkes, C. M. (2006). Love and loss: The roots of grief and its complications. London and
New York: Routledge.
Prigerson, H. G., Horowitz, M. J., Jacobs, S. C., Parkes, C. M., Aslan, M., Goodkin, K., et al.
(2009). Prolonged grief disorder: Psychometric validation of criteria proposed for DSM-V and
ICD-11. PLoS Med, 6(8). doi: 10.1371/journal.pmed.1000121
Prigerson, H. G., Maciejewski, P. K., Reynolds, C. F., Bierhals, A. J., Newsom, J. T., Fasiczka, A.,
et al. (1995). Inventory of Complicated Grief: A scale to measure maladaptive symptoms of
loss. Psychiatry Research, 59, 65–79.
Rando, T. (1992). The increasing prevalence of complicated mourning: The onslaught is just
beginning. Omega: Journal of Death and Dying, 26, 43–59.
Raphael, B., & Minkov, C. (1999). Abnormal grief. Current Opinion in Psychiatry, 12, 99–102.
Shaver, P. R., & Fraley, R. C. (2008). Attachment, loss, and grief: Bowlby’s views and current
controversies. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research,
and clinical applications (2nd ed., pp. 48–77). New York: Guilford Press.
Simpson, J. A. (1990). Influence of attachment styles on romantic relationships. Journal of
Personality and Social Psychology, 59, 971–980.
Sprecher, S., Felmlee, D., Metts, S., Fehr, B., & Vanni, D. (1998). Factors associated with distress
following the breakup of a close relationship. Journal of Social and Personal Relationships, 15,
791–809.
Stroebe, M., & Schut, H. (1999). The dual process model of coping with bereavement: Rationale
and description. Death Studies, 23, 197–224.
Stroebe, W., & Schut, H. (2001). Risk factors in bereavement outcome: A methodological and
empirical review. In M. S. Stroebe, R. O. Hansson., W. Stroebe, & H. Schut (Eds.), Handbook
of bereavement research: Consequences, coping, and care (pp. 349–371). Washington, DC:
American Psychological Association.
Stroebe, M., Schut, H., & Stroebe, W. (2005). Attachment in coping with bereavement: A theore-
tical integration. Review of General Psychology, 9, 48–66.
Tabachnick, B.G., & Fidell, L.S. (2001). Using multivariate statistics (4th ed.). Boston, MA: Allyn
& Bacon.
van Doorn, C., Kasl, S. V., Berry, L. C., Jacobs, S. C., & Prigerson, H. G. (1998). The influence of
marital quality and attachment styles on traumatic grief and depressive symptoms. The Journal
of Nervous and Mental Disease, 186, 566–573.
Waskowic, T. D., & Chartier, B. M. (2003). Attachment and the experience of grief following the
loss of a spouse. Omega: The Journal of Death and Dying, 47, 77–91.
Wayment, H. A., & Vierthaler, J. (2002). Attachment style and bereavement reaction. Journal of
Loss and Trauma, 7, 129–149.
Wei, M., Russell, D. W., Mallinckrodt, B., & Vogel, D. L. (2007). The Experiences in Close
Relationship Scale (ECR)-Short Form: Reliability, validity, and factor structure. Journal of
Personality Assessment, 88, 187–204.
Jerga et al. 913
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from
West, M. L., & Sheldon-Keller, A. E. (1994). Patterns of relating: An adult attachment perspec-
tive. New York: Guilford Press.
Wijngaards-de Meij, L., Stroebe, M., Schut, H., Stroebe, W., van den Bout, J., van der Heijden, P. G.,
& Dijkstra, I. (2007). Patterns of attachment and parents’ adjustment to the death of their child.
Personality and Social Psychology Bulletin, 33, 537–548.
Worden, J. W. (1982). Grief counseling and grief therapy: A handbook for the mental health
practitioner. New York: Springer.
914 Journal of Social and Personal Relationships 28(7)
at UNIV CALIFORNIA DAVIS on February 9, 2015spr.sagepub.comDownloaded from