Asystole with Syncope Secondary to Hyperventilation in Three Young Athletes
8
Asystole with Syncope Secondary to Hyperventilation in Three Young Athletes GIANFRANCO BUJA,* ANTONIO F. FOLINO,* MARINA BITTANTE,** BRUNO CANClANi,* BORTOLO MARTINI,* MANUELA MIORELLI,* DANIELA TOGNIN,** DOMENICO CORRADO,* and ANDREA NAVA* From the Department of Cardiology* and Sport Medicine Center.** University of Padua, Medical School BUJA, G., ET AL.: Asystole with syncope secondary to hyperventilation in three young athletes. We describe three athletes who had syncope after (case 1} or during (cases 2, 3) hyperventiiation. During the episode, ECG showed prolonged sinus arrest. Clinicai datn and noninvasive investigations were normaJ and the phenomenon was not reproducible. EJectrophysioJogicaJ study after autonomic blockade allowed a prolonged intrinsic heart rate in case I, and abnormal corrected sinus node recovery time in cases 1 and 2. During foUow-up, symptomatic sinus arrest provoked by deep inspiration occurred in case 3. These cases document prolonged asystole of unknown etiology, secor)dary to hyperventilation, and probably caused by different vagally-mediated mechanisms. (PACE, Vol. 12, March, 1989) hypervenliJation, sinus arrest, syncope Introduction Hyperventilation causes hypocapnia, alka- losis. increased cerebrovascular resistance, and decreased cerebral blood flow,^ which often pro- duce symptoms of giddiness and faintness, but rarely syncopal attack. In this report we describe three well-trained athletes who manifested syn- cope with convulsion secondary to voluntary hy- perventilation while undergoing screening for competitive sport activity. The electrocardio- gram, during the episode showed prolonged sinus arrests promptly terminated by a chest thump. After all the examinations, the origin of the phe- nomenon remains unexplained, but a reflex car- diac asystole is supposed to be the more probable mechanism. Case Report Case 1 An 18-year-old asymptomatic and well- trained man underwent routine cardiac evalua- AddrBss for rRprints: Gianfranco Biija. M.D,, [)K|)artmf;nt of Cardiology. University of Padua. Medical School, via Ciusti- niaiii. 2. 35100 Padovii, Italy, Received ]uly 21. 198B\ revision October 11. 1988: revision November 29, 1988; accepted November 30. 1988. tion to take part in a competitive sport (soccer). The protocol included: physical examination, standard electrocardiogram, chest x-ray, and ex- ercise stress test. Prior to the effort test, he was instructed to hyperventilate for about 45 seconds in the sitting position, and his electrocardiogram was simultaneously recorded; blood pressure was also checked before, during (15-30 seconds), and after cessation of maneuver. The resting heart rate was 60 bpm, and a normal increase was ob- served up to a maximum of 100 bpm; blood pres- sure was constant (125/75). Immediately after hyperventilation, a sudden decrease in heart rate appeared (65 bpm), followed by a sequence of prolonged sinus arrests lasting 4320 msec, 4240 msec, and 15840 msec. Each arrest was inter- rupted by isolated sinus beats (Fig. 1). The subject complained of syncope and convulsion, and sev- eral chest thumps restored a stable junctional rhythm of 50 bpm. About 20 minutes later, a blood test showed normal electrolyte (Na, K, Ca, Mg) levels, and acid-base balance. The hyperven- tilation maneuver and deep inspiration were re- peated the next day, but no bradyarrhythmias were observed. The previous noninvasive tests and 24-hour Holter monitoring, including a pe- riod of sport activity, as well as M-mode and 2D echocardiogram were normal. Holter monitoring 406 March 1989 PACE, Vol. 12
Transcript of Asystole with Syncope Secondary to Hyperventilation in Three Young Athletes

Asystole with Syncope Secondary toHyperventilation in Three Young Athletes
GIANFRANCO BUJA,* ANTONIO F. FOLINO,* MARINA BITTANTE,**BRUNO CANClANi,* BORTOLO MARTINI,* MANUELA MIORELLI,*DANIELA TOGNIN,** DOMENICO CORRADO,* and ANDREA NAVA*
From the Department of Cardiology* and Sport Medicine Center.** University of Padua,Medical School
BUJA, G., ET AL.: Asystole with syncope secondary to hyperventilation in three young athletes. Wedescribe three athletes who had syncope after (case 1} or during (cases 2, 3) hyperventiiation. During theepisode, ECG showed prolonged sinus arrest. Clinicai datn and noninvasive investigations were normaJand the phenomenon was not reproducible. EJectrophysioJogicaJ study after autonomic blockade allowed aprolonged intrinsic heart rate in case I, and abnormal corrected sinus node recovery time in cases 1 and 2.During foUow-up, symptomatic sinus arrest provoked by deep inspiration occurred in case 3. These casesdocument prolonged asystole of unknown etiology, secor)dary to hyperventilation, and probably caused bydifferent vagally-mediated mechanisms. (PACE, Vol. 12, March, 1989)
hypervenliJation, sinus arrest, syncope
Introduction
Hyperventilation causes hypocapnia, alka-losis. increased cerebrovascular resistance, anddecreased cerebral blood flow,^ which often pro-duce symptoms of giddiness and faintness, butrarely syncopal attack. In this report we describethree well-trained athletes who manifested syn-cope with convulsion secondary to voluntary hy-perventilation while undergoing screening forcompetitive sport activity. The electrocardio-gram, during the episode showed prolonged sinusarrests promptly terminated by a chest thump.After all the examinations, the origin of the phe-nomenon remains unexplained, but a reflex car-diac asystole is supposed to be the more probablemechanism.
Case Report
Case 1
An 18-year-old asymptomatic and well-trained man underwent routine cardiac evalua-
AddrBss for rRprints: Gianfranco Biija. M.D,, [)K|)artmf;nt ofCardiology. University of Padua. Medical School, via Ciusti-niaiii. 2. 35100 Padovii, Italy,
Received ]uly 21. 198B\ revision October 11. 1988: revisionNovember 29, 1988; accepted November 30. 1988.
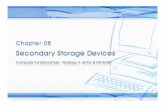
tion to take part in a competitive sport (soccer).The protocol included: physical examination,standard electrocardiogram, chest x-ray, and ex-ercise stress test. Prior to the effort test, he wasinstructed to hyperventilate for about 45 secondsin the sitting position, and his electrocardiogramwas simultaneously recorded; blood pressure wasalso checked before, during (15-30 seconds), andafter cessation of maneuver. The resting heartrate was 60 bpm, and a normal increase was ob-served up to a maximum of 100 bpm; blood pres-sure was constant (125/75). Immediately afterhyperventilation, a sudden decrease in heart rateappeared (65 bpm), followed by a sequence ofprolonged sinus arrests lasting 4320 msec, 4240msec, and 15840 msec. Each arrest was inter-rupted by isolated sinus beats (Fig. 1). The subjectcomplained of syncope and convulsion, and sev-eral chest thumps restored a stable junctionalrhythm of 50 bpm. About 20 minutes later, ablood test showed normal electrolyte (Na, K, Ca,Mg) levels, and acid-base balance. The hyperven-tilation maneuver and deep inspiration were re-peated the next day, but no bradyarrhythmiaswere observed. The previous noninvasive testsand 24-hour Holter monitoring, including a pe-riod of sport activity, as well as M-mode and 2Dechocardiogram were normal. Holter monitoring
406 March 1989 PACE, Vol. 12
ASYSTOLE SECONDARY TO HYPERVENTILATION
4320 riK
ttsec
4240m6
1S840ms
Figure 1. Case I. Confinuoiis eJectrocartJiographic sfrip in L2 recordejd inimedicileiy ofier cessa-(ion (45 seconds) o/ hypi^rventiitilion maneuver. A sinus rhylhm o/ 60-65 bpm is followed hyprolonged sinus arresfs [4320, 3560. 4240, 15840 msec) inferrupted by three isolated sinus beats.After two chest thumps, a stable junctional rhythm of 50 bpm appeared dissociated hy a sinusrhyfhni a( a s)ightly lower rate. Paper speed: 25 mm/sec.
showed an average heart rate of 65 bpm in theawake period, and 45 bpm during sleep; a mini-mum of 38 bpm was also recorded at night. Elec-trophysiological study (EPS), performed with thestandard protocol,^'' showed normal correctedsinus node recovery time (CSNRT), and sino-atrial conduction time (SACT by Narula method;the sum total of conduction times into and out ofthe sinus node was used to calculate the SACT),as well as intranodal-infrahisian conductiontimes [Table 1). Hyperventilation, deep inspira-tion, carotid sinus massage (CSM), eyeball com-pression (EBC) and Valsalva maneuver (VM) wereperformed in the supine position during sinusrhythm and atrial pacing at the rate of 100 ppm. Inthe course of sinus rhythm, a slight decrease inheart rate (from 60 to 40 bpm) was recorded.
mostly during EBC. while during atrial pacing noconduction disturbances appeared. These proce-dures were repeated with passive upright tilting(60°) with no significant variation in the electro-cardiogram. Simultaneous blood pressure record-ing using a cuff sphygmomanometer showed a fallin the systolic value in the upright position (from125/75 to 120/75). Sinus node function was alsoevaluated after complete sympathetic and para-sympathetic autonomic blockade, achieved uti-lizing the following protocol; i.v. propranolol (0.2mg/Kg body weight] at a rate of 1 mg/min; after10 minutes, i.v. atropine sulfate (0.04 mg/Kg bodyweight) for 1 minute. The ten shortest consecu-tive sinus cycles after atropine infusion were usedto determine the intrinsic heart rate (IHR). Fiveminutes after atropine, the standard protocol for
PACE. Voi. 12 March 1989 407

Case
1
2
3
HR
60
75
65
AH
100
80
80
HV
40
45
40
WP
380
350
400
BUJA, ET AL.
Table 1.
Electrophysiologic Data
CSNRT
330
460
450
SACT
130
300
280
VAG
negr -
negr =
negr =
IHRp
107.992.7-123103.3
88.8-11795.9
82.5-109
.1
.8
.3
IHR
85
100
97
CSNRT*
300
360
230
SACT*
120
280
70
Abbreviations: HR = Resting heart rate. WP = Wenckenbach point. CSNRT = Maximum corrected sinus noderecovery time. SACT = Sino-atrial conduction time (Narula method). VAG = Vagai maneuvers. IHRp = Intrinsicheart rate predicted after autonomic blockade. IHR = Intrinsic heart rate observed after autonomic blockade, r= normal range for IHRp. * = Values after autonomic blockade. The HR, IHRp and the IHR are in bpm. The othervalues are in msec.
CSNRT and SACT evaluation was repeated (Table1). The predicted intrinsic heart rate (JHRp) wasdetermined by means of the linear regressionequation derived by Jose and Collison:^ JHRp= 118.1 - (0.57 X age); for young individuals (<40year), the 95% confidence limits are ±14%. Afterautonomic blockade, heart rate was higher thanthe control (85 bpm vs 60 bpm) but significantlyslower than the IHRp (85 bpm vs 107.9 bpm= -21%) (Table 1). Both CSNRT and SACT werereduced, but the former was higher than normalvalues (Table 1).^ After 30-month follow-up,which included 24-hour Hoiter monitoring withdeep inspiration, hyperventilation, and stresstesting, this subject is asymptomatic and no ar-rhythmias have been detected.
Case 2
A 26-year-old man underwent routine car-diac examination to qualify for competitive activ-ity (canoeing). All the above mentioned noninva-sive cardiological tests gave normal results. Hy-perventilation was performed as described. Theresting heart rate was 75 bpm, and gradually in-creased to 100 bpm; 15-20 seconds after the startof this maneuver, a junctional rhythm (45 bpm]suddenly appeared followed by two episodes ofsinus arrest lasting 2040 msec and 6600 msec, re-spectively, with the interposition of two ventricu-lar escape beats (Fig. 2). Three consecutive chestthumps were delivered, and were followed once
again by two brief sinus arrests lasting 3000 msecand 2640 msec, respectively; a junctional escapebeat was recorded between the two arrests (Fig.2). Blood pressure before and during the maneu-ver was normal and unchanged. The patientmanifested syncope and convulsion and a stablejunctional rhythm at a rate of 70 bpm was re-corded after another chest thump. Electrolyte(Na, K, Ca, Mg) levels, as well as the acid-basebalance were normal. On the next day, hyper-ventilation associated with deep inspiration failedto induce bradyarrhythmias. The average heartrate during 24-hour Hoiter monitoring was 65bpm (waking period) and 50 bpm (sleeping pe-riod), with a minimum of 38 bpm. Some days laterthe subject underwent electrophysiological studyfollowing the protocol described above. Hyper-ventilation. deep inspiration, and vagal maneu-vers (CSM, EBC, VM) produced a decrease inheart rate from 75 to 50 bpm during sinus rhythmand no conduction disturbances during atrialpacing (100 ppm). A change in body position from0° to 60° did not induce significant electrocardio-graphic variations, while systolic blood pressurefell from 120/70 to 110/70. After autonomicblockade, the IHR was increased while CSNRTand SACT were reduced, compared to controlvalues (Table 1). In this case, CSNRT after auto-nomic blockade was higher than the normalvalues (Table 1).*̂ The IHR was slightly slowerthan the IHRp (100 bpm vs 103.3 bpm = -3.2%)(Table 1). After 15-month follow-up, this athlete is
408 March 1989 PACE, Vol. 12

ASYSTOLE SECONDARY TO HYPERVENTILATION
L.hyper
ventilation15 Msec
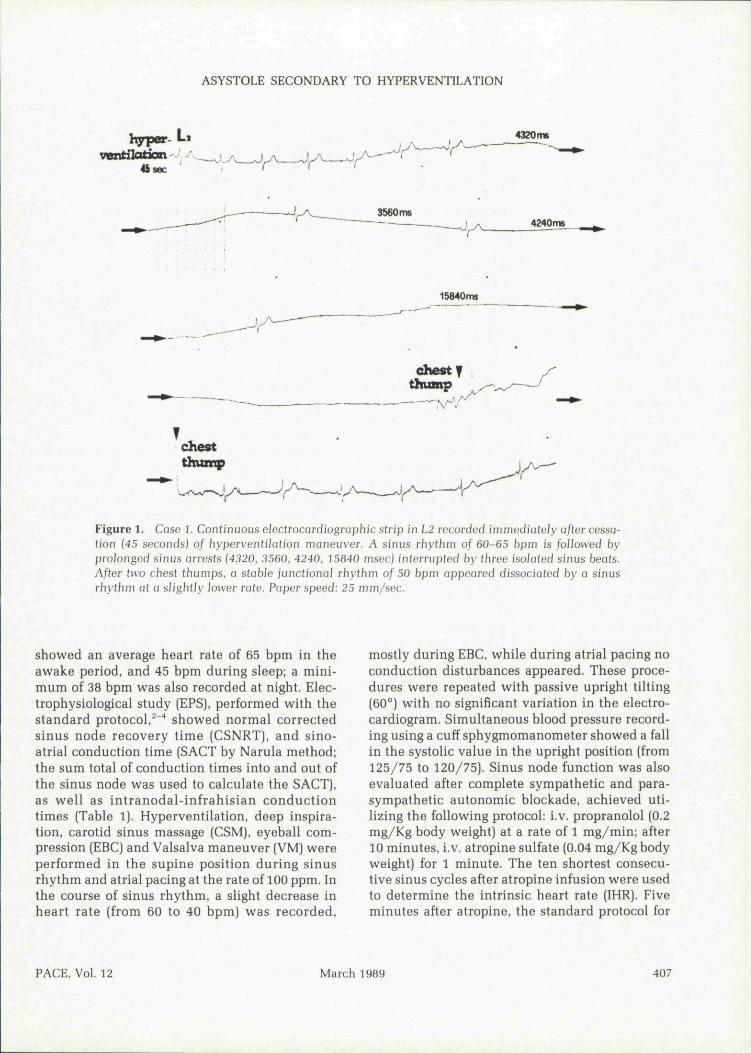
Figure 2. Case 2. Continuous electrocardiograpbic strip in L3 recorded 15-20 seconds after thestart of hypervenliJalion. A junctional rbytbm of 45 bpm is followed by a first brief sinus arrestlasting 2040 msec interrupted by Hvo escape beats. A prolonged sinus arrest then appeared lasting6600 msec. Three consecutive chesl (humps ivere given hu( two more sinus arrusis occurred (3000msec, 2640 msec) inlerrupled by sponlaneous escape beats. Finally, after anofher chesi thump, astable juncd'onal rhylhm, al a rafe of 70 bpm wos recorded. Tbe artifacts are caused by tbeconvulsion. Paper speed; 25 mm/sec.
still asymptomatic and Hoiter monitoring, in-cluding a period of sport activity and deep inspira-tions, as well as tbe exercise stress test did notshow any arrhythmias.
Case 3
A 39-year-old man, a well-trained mountainclimber, was evaluated before participating in anexpedition. Physical examination, electrocardio-gram, chest x-ray, 24-hour Hoiter monitoring, ex-ercise stress test, echocardiogram, and respiratorytests were normal. Hyperventilation was per-formed as described. The resting heart rate beforethe maneuver was 65 bpm, and reached a maxi-mum of 130-135 bpm after 30 seconds when a
sudden decrease (60 bpm) and a prolonged sinusarrest lasting 4080 msec were recorded. After twoescape beats, the following sequence appeared: afirst sinus arrest of 6040 msec; three escape beats;a second asystole lasting 7600 msec; two escapebeats; a third sinus pause of 4320 msec, and anisolated escape beat followed by a last arrest of3680 msec (Fig. 3). Blood pressure before this epi-sode was normal and remained unchanged. Theathlete manifested syncope and convulsion, andafter a chest thump, a junctional bradycardia of30 bpm was recorded for seven beats followed bya normal rhythm of 60 bpm. In this case as well,blood tests were normal, and hyperventilation aswell as deep inspiration repeated on the followingday failed to reproduce the previously observed
PACE, Vol. 12 March 1989 409

BUJA, ET AL.
glg-
tu jr. ^ ~ ^
a o o c— aCD
a3
Q) O
0) -Q
w O QJ ."a > a .c 5 aP =. u
J p w j ^
- E ^ ~ .2=0 O
oCO a ,
ca
-c 1:: aCL o -a° w c«) 5 g.2 -5 oj- Q en en
- a au ^ wO .-Q ~-̂Q) Q ~ QJ
g .P o a
C<U
cp
D O
a CJ
QJ • -
e*s. r_ CO = t i ;
D O -=;£ —oc -Si t.. o •
410 March 1989 PACE. Vol. 12

ASYSTOLE SECONDARY TO HYPERVENTILATION
bradyarrhythmia. Holter monitoring demon-strated an average heart rate of 60 bpm (wakingperiod) and 40 bpm (sleeping period), with a min-imum of 35 bpm. Hyperventilation, deep inspira-tion, and vagal maneuvers (CSM, EBC, VM) per-formed during sinus rhythm and atrial pacing(100 ppm) showed a decrease in heart rate from 65to 45 hpm, with no conduction disturbances. Achange in body position (from 0° to 60°) did notlead to significant electrocardiographic variationsduring the maneuvers, but blood pressure fellfrom 130/80 to 120/75. The EPS showed a higherheart rate after autonomic blockade and sborterCSNRT-SACT, compared to control values (Table1). Moreover, the IHR was slightly faster than theIHRp (97 bpm vs 95,9 bpm = +1.2%) (Table 1).After a follow-up of 24 months, the last Holtermonitoring recorded some prolonged sinus pausesassociated with dizziness. The patient noted in hisdiary that during these pauses he was inspiringdeeply (Fig, 4). Deep breathing was then repeatedin the supine position and the occurrence of sinusarrest was confirmed. A permanent pacemakerwas proposed, but was refused by the patient,who was consequently advised against strenuousclimbing at high altitudes.
Discussion
Three athletes without overt heart diseasehad unexpected, prolonged asystole secondary tothe hyperventilation maneuver. This phenome-non is rarely reported' and, in our experience,was found in four cases out of 1100 investigationscarried out in 2 years. It is worth stressing thatthese subjects were top-level, well-trained ath-letes with periods of bradycardia during Holtermonitoring; asystole appeared after cessation of
the maneuver in case 1, and during hyperventila-tion in case 2 and case 3 (15-20 seconds and 30seconds after the beginning, respectively). Whilethis suggests a possible role of the parasympa-thetic system in determining the phenomenon,different mechanisms may be working in eachcase. During EPS performed some days later, dif-ferent vagal maneuvers in the supine or uprighttilt position (60°) during sinus rhythm or atrialpacing failed to demonstrate in all the athletes anabnormal response and a significant vasodepres-sor component could not be evidenced eitherduring the event or the EPS. Moreover, the analy-sis of sinus node function before and after theautonomic blockade does not show abnormalitiesin patient 3. The normal results of these investi-gations do not allow to identify the underlyingetiology responsible for asystole in case 3. Someauthors^"^" have reported isolated cases with syn-copal attack due to postexercise vagal reactionand experimental animal studies seem to indicatethat exercise-induced enhancement of sympa-thetic activity results in release of acetylcholinefrom parasympathetic nerves." Likewise a sud-den, momentary fall in sympathetic activity asso-ciated with a strong, temporary vagal predomi-nance occurring immediately after the hyperven-tilation maneuver may be suspected in case 1.Interestingly an abnormal vagally-mediated re-sponse to deep breathing was documented duringthe follow-up (24 months later) in this case withprolonged sinus pauses and dizziness. It is sur-prising that this patient did not show abnormalresponses to vagal stimulation originating fromdifferent sites. Therefore, an exaggerated car-dioinhibitory response following pulmonarystretch receptors stimulation^^"^" associated withan enhanced vagal tone can be postulated. To-
deep fnsplratJon?
Figure 4, Case 3. Electrocardiographic strip during 24-hour Holter moniforing. Two prolongedsinus arrests lasting 4440 and 3800 msec, associated with dizziness, are recorded at 4:05 PM whilethe patient was spontaneously deep breathing. Paper speed: 25 mm/sec.
PACE, Vol. 12 March 1989 411

BUJA, ET AL.
gether with the above mentioned normal investi-gations cases 1 and 2 showed some abnormal elec-trophysiological data: case 1 had significantlyslower IHR (-21%) than that predicted for age,associated with an abnormal CSNRT after auto-nomic blockade; case 2 presented only a pro-longed CSNRT after autonomic blockade. Thesefindings might reflect initial intrinsic abnormali-ties of the sinus node, but they do not explain theprevious asystole with syncope. Therefore, also inthese cases, we were not able to identify an evi-dent etiology, Parasympathetic reflexes inducedeither by cerebral ischemia secondary to vaso-
constriction or emotional stress might be in-volved.^'
The inability to reproduce the asystole, to-gether with the absence of symptoms and docu-mented bradyarrhythmias at the first control andduring the follow-up suggest a benign prognosis incases 1 and 2 who were considered eligible forcompetitive activity. On the contrary, in consid-eration of the sport activity (climbing) of the lastathlete, the spontaneous, symptomatic sinuspauses were judged potentially dangerous and theimplantation of a permanent pacemaker was ad-vised.
References1. Adams RD, Martin |B. Faintness, syncope and sei- 9.
zures. In RG Petersdorf et al. (eds); Harrison's Prin-ciples of Internal Medicine. Japan: McGraw HillBook Company, 1983; p. 79. 10.
2. Naruia OS. Electrophysiology of normal impulsepropagation. In Gardiac Arrhythmias. Philadel-phia: Williams & Wilkins, 1979; p. 57.
3. Narula OS, Shanta N, Narula LK, et al. Glinical 11.and electrophysiological evaluation of sinus nodefunction. In Gardiac Arrhythmias. Philadelphia:Wiliiams & Wilkins, 1979; p. 176.
4. Narula OS, Shanta N, Vasquez M, et al. A new 12.method for measurement of sinoatrial conductiontime. Circulation 1978; 58:706.
5. Jose AD, Gollison D. The normal range and deter- 13.minants of intrinsic heart rate in man. GardiovascRes 1970: 4:160.
6. Alboni P, Malacarne G, Pedroni P, et al. Electro-physiology of normal sinus node with and without 14.autonomic blockade. Girculation 1982; 65:1236.
7. Pinelli G, Alberici S, Manini G, et al. Episodi sin-copali in giovani atleti sani. G Ital Gardioi 1982; 15.12:445.
8. Schlesinger Z. Life-threatening "vagal reaction" tophysical fitness test. J Am Med Assoc 1973;226:1119.
Fleg JL, Asante AVK. Asystole following treadmillexercise in a man without organic heart diseases.Arch Intern Med 1983; 143:1821.Hirata T, Yano K, Okui T. et al. Asystole withsyncope following strenuous exercise in a manwithout organic heart disease. J Electrocardiol1987; 20:280.Leaders FE. Local cholinergic-adrenergic interac-tion: mechanism for the biphasic chronotropic re-sponse to nerve stimulation. I Pharmacol ExpTher 1963; 142:31.Aviado FM, Schmidt GF. Reflexes from stretch re-ceptors in blood, heart and lungs. Physiol Rev1955; 35:247.Glick G, Wechsler AS, Epstein SE, et al. Reflexcardiovascular depression produced by stimula-tion of pulmonary stretch receptors in the dog. JGlin Invest 1969; 48:467.James TN, Urthaler F, Hageman GR. Reflex heartblock. Baroflex and bronchopulmonary reflexcauses. Am J Gardioi 1980; 45:1182.Berne RM, Levy MN. Gontrol of the heart. In Car-diovascular Physiology. Saint Louis: G. V. MosbyGompany, 1972; p, 139.
412 March 1989 PAGE, Vol. 12