ASHA AP Report
74
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of ASHA AP Report


Evaluation of Accredited Social Health Activist (ASHA) in
Andhra Pradesh
Commissionerate of Family Welfare GoAP, Hyderabad – 500 095
Indian Institute of Health and Family Welfare Vengalrao Nagar, Hyderabad – 500 038
February, 2009

ACKNOWLEDGEMENTS
The core strategy of the NRHM is to have a female Accredited Social Health Activist (ASHA) for every
village with a 1000 population to act as an interface between the community and the public health systems.
ASHA receives performance-based compensation for promoting a variety of primary health care services
for institutional deliveries, universal immunization, DOTS treatment for Tuberculosis etc.
The Government of Andhra Pradesh also incorporated the ASHA volunteer scheme in the Program
Implementation Plan (PIP) since 2005-06. The First Common Review Mission of NRHM (2007) adjudged
the quality of ASHA training and methodology as of very high standard. The Government of Andhra
Pradesh placed about 55,400 ASHA workers in the state as a first referral for any small ailments in the
villages. Andhra Pradesh was the first state which completed training of ASHA volunteers, and their
deployment in their respective villages. The present study is an attempt to review the training strategy,
evaluate the knowledge and practices of ASHAs, their work performance and to identify existing lacunae
and incorporate mid-term revision of the NRHM initiative.
We would like to thank Commissionerate of Family Welfare, Department of Medical, Health and Family
Welfare, Government of Andhra Pradesh for funding this study.
We sincerely acknowledge the studies of CORT (UNFPA) on ASHA and JSY in different states which
was a source of inspiration in the preparation of questionnaire and draft. Special thanks are due to Dr M.
Prakasamma, Director and Mr.G.S. Chowdhary, Training Coordinator, Academy of Nursing Studies,
Hyderabad, for their active interest in the project and for providing timely guidance as well as sharing their
views during preparation of questionnaire. We wish to express our thanks to Dr M. Srinivasa Rao,
Additional Director, Dr G. Srinivas Rao, Project Officer and Mr. B. Brahmanandam, Deputy Director
(Demography) of the Commissionerate of Family Welfare, Govt. A.P for offering useful comments to
finalize the survey instruments and their active participation in the dissemination workshop.
Special mention and thanks are due to Dr. N.V. Rajeswari, Dr. K. Anand Reddy and Mr. Ch.V.S.
Sitarama Rao, faculty IIHFW and Mrs. Prameela for sharing their views and enriching our knowledge on
the training and other aspects. We also extend our thanks to the investigators for completing field work in
record time.
We appreciate the immense help received from the computer staff (Mr. PSVN. Kumar, Mr. Mir Wajahat
Ali and Mr. K. Ravindra Babu, Mr. K. Santhosh and Mr. K. Vijay) in developing the software package
and carrying out data cleaning, data entry, data processing and preparation of tables. We thank our
respondents-officers at the district and PHC level, ANMs, community members, ASHAs and the JSY
beneficiaries for their cooperation.
AuthorsAuthorsAuthorsAuthors

CONTENTS
S.No. Topic Page
Chapter 1
1.1 Introduction 1
1.2 National Rural Health Mission 2
1.3 Need for the study 4
1.4 Objectives of the study 5
1.5 Presentation of the Report 5
Chapter 2 - Data and Study Design
2.1 Questionnaires
A. ASHA Questionnaire 6
B. Beneficiary questionnaire 7
2.2 Sample Design 8
2.3 Field work 9
2.4 Data Editing and Analysis 9
Chapter-3- Training Strategies of ASHA in Andhra Pradesh
3.1 Training Strategy 10
3.2 Training of ASHA Volunteer in Andhra Pradesh 11
3.3 Training Strategy 12
3.4 Training Process 12
3.5 Methods & Materials 13
3.6 Monitoring Systems 13
3.7 Training Programme Outcome 13
Chapter-4 - ASHA Intervention in Andhra Pradesh
4.1 ASHA intervention 17
4.2 Background Characteristics of ASHA 18
4.3 ASHA Selection and Motivation factors for joining
Working status before joining as ASHA 19
Training of ASHAs 19
Payments during training 20
Use of reading material / Drug kit 21
Knowledge of ASHA Volunteers 21
Knowledge about Newborn Care 22
Knowledge about role and responsibilities 23
Organization of work by ASHAs 24
Record updation 25
ASHAs clientele 25
Perceptions of ASHA 26
Cash remuneration received by ASHAs 27
Monitoring System 29
Cash incentives to ASHAs 29
Chapter-5 - Beneficiaries of ASHA for Delivery Care
5.1 Respondent profile 39
5.2 Awareness about JSY 39
5.3 Knowledge on JSY Aspects 40
5.4 Utilization of ANC Services by JSY Beneficiaries 41
5.5 Role of ASHA in Micro-Birth planning: 41
5.6 Intention and Actual Place of Delivery: 42
5.7 Process of Arranging Transport 42
5.8 Motivation for Institutional delivery. 43
5.9 Quality of services available at the place of delivery 43
5.10 Impact of JSY on institutional delivery 44
5.11 JSY beneficiaries – place & type of delivery 44
5.12 Role of ASHA in JSY 44
Chapter-6 – Summary and Recommendations Recommendations 50
Policy 50
Programme Management 50
Demand Generation 51

LIST OF TABLES
S. No. Topic Page No.
Table 4.1 Profile of ASHA functionaries 31
Table 4.2 Motivation for being an ASHA 31
Table 4.3 Topics Covered in the Training of ASHA 32
Table 4.4 Expected follow-up action on recognition of signs of complications in pregnant
women by ASHA 33
Table 4.5 ASHA’s Knowledge about Common Complications during delivery that could
Result in Maternal Mortality 33
Table 4.6 Knowledge about Likelihood of Neonatal mortality 33
Table 4.7 ASHA’s Awareness about their Responsibilities 34
Table 4.8 Networking of ASHA with other Stakeholders 34
Table 4.9 Working Situation of ASHA 35
Table 4.10 Suggestions for further strengthening the work of ASHAs 36
Table 4.11 Challenges faced by ASHAs 37
Table4.12 Reasons for Delay in Incentive Payments 37
Table 4.13 Expected Monthly salary by ASHA as Worker Remuneration 38
Table 4.14 Awareness of ASHA Day Attendance and TA and DA on ASHA Day 38
Table 4.15 Expected Incentives of ASHAs for other Activities 38
Table 5.1 Profile of Respondents (ASHA Beneficiaries) 45
Table 5.2 Place and Source of Information Regarding JSY 45
Table 5.3 Stage of Pregnancy and Place of Registration for ANC 46
Table 5.4 Micro-Birth Planning of JSY Beneficiaries 46
Table 5.5 Responses of JSY Beneficiaries about Intended and Actual Place of Delivery 46
Table 5.6 Motivational factors for JSY beneficiaries for opting institutional delivery 47
Table 5.7 Shift in the place of delivery before & after JSY 47
Table 5.8 Place of delivery of JSY beneficiaries 47
Table 5.9 Type of delivery of JSY beneficiaries 48
Appendix
S. No. Topic Page No.
Appendix 1 The list of villages Selected in the Survey 15
Appendix 2 Mandal-wise PHC and Sub centre in the selected Districts 54

EXECUTIVE SUMMARY
The ‘omnibus approach’ of NRHM is to provide accessible, accountable, affordable, effective
and reliable primary health care, especially to the poor and vulnerable sections in the community. The
NRHM has been envisaged as a focal point of all the earlier health interventions programs after wide
deliberations of various field experts, adaptations of the successful best practices and learning from
the failures in the past, all have made the NRHM a different program.
The NRHM aims to have a village-based female ASHA to act as the interface between the
community and the public health system and negotiate health care for poor women and children. The
Indian Institute of Health and Family Welfare (IIHFW), based at Hyderabad conducted this evaluation
of ASHA and beneficiary perceptions to understand the implementation of NRHM programme for
Commissionerate of Family Welfare, Government of Andhra Pradesh. This report is based on the
quantitative and qualitative assessment of ASHA intervention and beneficiaries covering the three
regions of the state.
Using the semi structured study tools, 941 ASHAs and 1121 JSY women beneficiaries were
interviewed by 30 well-trained investigators. Information also collected from key stakeholders at
district level, PHC level and village leaders.
The Government of Andhra Pradesh adopted an innovative training approach, and initiated 21
days in-house training in every district headquarters covering around 180-200 ASHAs every month. The
Academy of Nursing Studies (ANS), an NGO, was entrusted the responsibility of selection of trainers,
conducting of TOTs, deployment of trainers, facilitator’s guide and audio-visual support for conducting
training in a record period of 18 months time frame.
Training was designed to be participatory and adult learning oriented, with overall
personality development, empowerment, self confidence and orientation to health as the main
objectives. All trainees were reviewed daily in the morning (about previous day’s activity) and evening
review (to recapitulate the day’s activities) followed by weekly reviews and written examination and
role plays by involving all trainees.
The Andhra Pradesh training model (21 days residential) was successful in completing the
training of all ASHAs in the state within the stipulated time schedule laid down by the NRHM time-
frame. All the ASHAs working in the field were well acquainted with their job schedule.
The training strategies adopted in Andhra Pradesh taken as a role model and suitable
modifications/ actions can be initiated by other states in overcoming teething problems of selection,
quality training etc, Whatever the training methodology we had chosen, it is very important to deploy
the ASHA volunteers in all villages and really bring about the change that is expected by the NRHM
visionary.

Involvement of ASHA and JSY beneficiaries
About half of the ASHAs indicated that they were selected by ANM and about one-fifth (21
percent) were recommended by Sarpanch/Politician, followed by 10 percent who were
approved/selected by Gram panchayat. The Gram panchayat approved the selections of ASHAs and
nominated them for training at district headquarters.
Eighty-nine percent of ASHAs indicated they preferred to be ASHA in order to serve the
community, earning extra money for the family was indicated by 58 percent followed by 30 percent
stating the purpose to save the children and bring awareness on health issues.
More than a half (55 percent) of ASHAs are house wives / economically active women and less
than one third (31 percent) are agriculture laborers followed by less than 3 percent of ASHAs reporting
their association with ANM/AWW or participation in the health programs of Indira Kranthi Patham ( a
program to eradicate poverty, introduced in Andhra Pradesh).
Among the selected districts, 82-97 percent of ASHAs appreciated the training centre logistics
like seating arrangements and 82-95 percent appreciated size of the room as ‘big’ and ‘good’. More
than eighty percent (79-96 percent) of ASHAs appreciated food arrangements and accommodation
facilities.
Knowledge of ASHA on high risk of pregnant women was assessed by six components (Short
stature, Low age <18 years and above 34 years of age for delivery, first pregnancy, birth order four
and above, High BP/Diabetic symptoms and Anemia). ASHAs had good practical knowledge of
identifying high risk pregnancy and knew where to shift the pregnant women in case of emergencies.
The familiarity of tasks indicated by ASHAs were immunization services (98 percent) provision
of ANC care (97 percent), accompanying delivery cases (85percent), family planning operations
(71percent), working as DOT provider for TB cases (59percent).
Ninety-eight percent of ASHA volunteers organized their work regularly and coordinated with
the ANM and Anganwadi center activities in the village. The respondents unanimously indicated that
they used to meet ANM/AWW during the weekly immunization sessions and called all the pregnant
women for timely ANC check-up and helping in organizing of Village Nutrition Day at AW center.
Thirty-seven percent of ASHAs in the survey revealed that they maintained records regularly
(23-24 percent in Kurnool and Mahabubnagar districts and 63 percent in East Godavari district). The
weekly updating of records varied between 29-53 percent across districts. Thus the survey indicated
that 66-80 percent of ASHA volunteers update their records within seven days.
Ninety-eight percent of ASHAs handled a JSY case for delivery in hospital and the last JSY client
was accompanied 24 days prior to the date of interview. Seven out of ten (71 percent) of ASHAs stayed
for one day, 15 percent stayed for two days along with the JSY beneficiary for delivery services.
The common suggestions for improving the ASHA intervention were mainly related to
enhancing the cash assistance for making timely money payments, provision of complete information

and practical trainings. Propagation of the NRHM schemes by the lady medical officer, doctors and
nurses helping ASHA to propagate healthy practices easily in the community.
The ASHAs, on an average earned about Rs. 545/- (range of Rs. 200 – 1875; calculated on the
basis of cases motivated for RCH activities in the reference period of three / one month) prior to the
survey. ASHAs received higher incentives for accompanying institutional delivery (36 percent), post
natal care (19 percent), one ANC with MBBS doctor (13 percent), Measles and Vitamin-A ((11 percent)
respectively. Only one-fifth of ASHAs (19 percent) were satisfied with incentive they had received
(more than state average recorded in Karimnagar 32 percent) followed by Kurnool (28 percent). Sixty-
seven percent of ASHAs were not satisfied with the cash assistance commenting on ‘too much work
with too little payment’ followed by delays in receipt of payment.
Ninetynine percent of ASHAs were aware of monthly ASHA Day meetings and equal number
attending regularly, obtaining counseling from district program officers, PHC staff along with NGOs
(Table 4.14). Ninetyeight percent of ASHAs indicated the usefulness of the ASHA Day.
Beneficiaries of ASHA for Delivery Care
The mean age of the respondent was 22.8 years. Only 3 percent of respondents were aged
more than 30 years. Nine out of ten women respondents were in the age group of 20-29 years. In the
sample, less than 11 percent of respondents had passed intermediate and higher education level. Less
than sixty percent (58 percent) of JSY respondents belonged to BC community (with BPL white card)
and remaining 42 percent were from SC and ST community. The average household monthly income
was Rs.2034/- and varied between Rs.1840/- in Karimnagar and a high of Rs. 2271/- in Mahabubnagar
district respectively. About 65 percent of respondents (residing in the ASHA volunteers locality) were
providing the services in the SC/ST and BC colonies respectively.
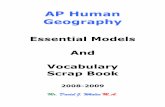
Regarding the source from where they heard of JSY, about 82 percent mentioned ASHA
volunteer and 66 percent as ANM. Around 20 percent of beneficiaries indicated other sources of
information like T.V, Radio, Relatives and Gram panchayat (Table 5.2). The knowledge regarding JSY
scheme in the state was mainly disseminated through interpersonal communication rather than mass-
media channels.
Majority of beneficiaries had interactions with ASHA on the Micro-Birth planning issues.
Eighty-four percent (84 percent) of beneficiaries informed about the date of next check-up, sixty-eight
percent had received information on place of delivery, forty-six percent advised on expected date of
delivery (EDD) but lower than one-fifth of beneficiaries indicated that ASHA informed them about the
referral place to visit in case of any emergency. Birth planning is one of the key elements taken up
during the refresher training and ANMs and AW workers interaction sessions
Sixty-nine percent of beneficiaries reported safety to mother and child for choosing institution
delivery followed by 63 percent due to monetary benefits offered under JSY scheme. Twenty-eight
percent of beneficiaries were motivated ‘due to better access of service at medical institution in the
nearest locality’ and ‘support provided by ASHA’. Less than ten percent were motivated due to
compulsion like ‘the previous birth in hospital’ and ‘availability of transport’ for availing services from
medical institutions.

The JSY beneficiaries were asked about place of delivery of the last child born prior to the
index child of JSY beneficiaries interviewed. Out of 1145 total beneficiaries only 745 had history of
previous child birth. Data from these 745 beneficiaries was cross tabulated by place of delivery of
previous child with that of the index child. In other words, the analysis would indicate a shift in place
of delivery before and after introduction of JSY. It was observed that 610 JSY beneficiaries in the
preceding index child birth had an institutional delivery while the remaining 135 (18 percent) were
home deliveries. ). In case of index pregnancy, 730 (98 percent) births were institutional and only 15
(2 percent) births were home deliveries. It may however be mentioned here that this can not be
generalized as the sample had been confined to only those who had availed JSY. The results may be
considered as indicative of their change in behavior.
Andhra Pradesh: Shift in the Place of Delivery before and After JSY
Particulars For last but one child For last (JSY) child
Place of delivery
Institutional 82 (610) 98 (730)
Home 18 (135) 2 (15)
Number of beneficiaries with two or more children : 745
ASHAs briefed women about the JSY. ASHAs informed the JSY beneficiaries about early
registration in first trimester, hospital delivery and postnatal care. Higher percentage of JSY belonged
to SC/ST and BPL group availed the benefits and was satisfied about the role played by ASHA. This is
evident from the beneficiary assessment wherein it was found that they were supportive right from
pregnancy to child birth in three-fourth of deliveries. The ASHA role in motivating beneficiaries for
institutional delivery services and accompanying them to institutions has emerged significantly.

CHAPTER 1
1.1 Introduction
AIDS can kill by stigma even when lifesaving medical treatment is available. Until
recently, an HIV-infected woman in Sauri, Kenya, was discouraged by her husband, also
HIV-infected, from seeking medical care because of his fear of stigma. All too often, death
quickly ensues in such cases. But not in this one. Husband and wife were saved by Mary
Wasonga, a fellow villager recently trained to be a community health worker by the
Millennium Village Project, which is helping more than 400,000 people in dozens of
African communities fight extreme poverty, hunger and disease. Wasonga visited the
couple and encouraged them to get home-based HIV testing and counseling, and then
helped them enroll in a treatment program. Indeed, she and the 82 other community
health workers in Sauri have helped thousands of villagers do the same.
These workers also attend to women in labor who need urgent transport to a
delivery room, individuals too weakened by cholera to get to a clinic, children with
malaria and many others. They do this with one year of on-the-job training that builds on
at least some secondary education. That basic training is enough to save lives in vast
numbers”. Thorough training is sufficient to facilitate the multiple task-shifting and task-
sharing.
Jeffrey D. Sachs, TIME, 28th August, 2008
Across the globe, programs are under way that are reminiscent of China's successful
barefoot doctors initiated a few decades ago. The mother of all community health efforts is
India's National Rural Health Mission initiated by Prime Minister Manmohan Singh in 2005. In
just over three years, the mission has mobilized more than half a million new community
health workers, each known as an ASHA - short for "accredited social health activist," and the
Hindi word for hope”. The ‘omnibus approach’ of NRHM is to provide accessible,
accountable, affordable, effective and reliable primary health care, especially to the poor and
vulnerable sections in the community. The NRHM has been envisaged as a focal point of all
the earlier health interventions programs after wide deliberations of various field experts,
adaptations of the successful best practices and learning from the failures in the past, all
have made the NRHM a different program. Moreover, no government program was as
meticulously prepared or planned as NRHM since Independence (Lahariya, Khandekar and
Prasuna, 2007). In order to achieve the National Health Policy goals and health-related
Millennium Development Goals (MDGs), the mission adopted convergence among the sectors
of health, family welfare, AYUSH, nutrition and sanitation. The NRHM emphasized the result-
based management approach in order to attain different health goals: Millennium
Development Goal (MDG, 2000), National Health Policy (NHP, 2002) and Tenth Plan Goals
(last two years of plan period) and Eleventh Plan (2007-12) through provision of right number
of service providers with right skills at right place and at right time beginning from village to
state level (Satpathy and Venkatesh, 2006).

According to a study, the health facilities at PHC, CHC have fallen short of people’s
needs both in quantitative and qualitative terms. The NRHM is an architectural correction in
tackling available optimum fund utilization, higher accountability and better utilization of
resources. The availability of an appropriately trained residential health care provider in
every village reduces loss of human days due to absence of timely first contact care by the
village community. In view of the failure of official Community Health Worker (CHW) scheme
launched in 1978 identifying the flaws in that program, the NRHM reconceptualised the
ASHA program (Jan Swasthya Abhiyan, 2006).
In the health care system, sub-center is the most peripheral level of contact with the
community covering a 3000 population in rural areas, but effectively in Andhra Pradesh it is
serving 4424 population on an average. Out of the existing 12522 sub-centers in the state,
about 84 percent of sanctioned positions of MPHA (F) were filled (RHS, 2007), but slightly
less than half (48 percent) of sanctioned positions of MPHA (M) are vacant. It is one of the
crucial bottlenecks hindering the implementation of vertical National Health Programs and
outreach services in the rural areas. The Anganwadi centers in the villages, under the
Integrated Child Development Scheme (ICDS) are engaged in organizing supplementary
nutrition programmes and other supportive activities. The posting of additional MPHA
(F)/ANM at the sub-centers could not completely address problems in the provision of basic
health facilities at the village level. Thus a new brand of community health functionaries,
named as Accredited Social Health Activist (ASHA) was introduced in the existing rural health
care delivery system.
1.2 National Rural Health Mission
The thrust of the NRHM is to establish a fully functional, community-owned,
decentralized health delivery system with an emphasis on inter-sectoral convergence with
sanitation, water, education, nutrition, social and gender equality besides strengthening all
health facilities with Indian Public Health Standards (IPHS). Although NRHM covers all the
States of India, special focus was laid on 18 EAG states that have weak public health
indicators and/or weak health infrastructure facilities.
Technological companies and foundations extended support under Public private
partnership by providing Mobile phone for training, reporting of vital statistics and calling
ambulances. The Emergency Management Research Institute (EMRI, Hyderabad) under Public-
private partnership with the Andhra Pradesh State Government has been providing
emergency-response coverage for 84 million people for maternal and child care, accidents
and other related emergency services.

Andhra Pradesh is a non-focused and high performance state. The State has to
adhere to mutually agreed milestones of NRHM objectives by signing MOU with the GOI. The
Andhra Pradesh State NRHM Mission proposed a budget of Rs. 888.9 crores (about 15.3%
State Government share of NRHM allocation to A.P) for the year 2008-09. After two years of
NRHM, different interventions/ infrastructure developed including the following (PIP 2007-
08):
• About 70,700 ASHAs (Women Health Volunteers1) are trained and positioned in
their respective villages tribal areas for working towards the betterment of
women and children
• Implementation of Janani Suraksha Yojana (JSY) for encouraging the institutional
deliveries by SC/ST and BPL groups
• Strengthening of 151 CEMONC centers
• 800 round-the-clock MCH centers
• 299 urban health centers in municipalities of towns
• 160 Neonatal Intensive Care Units
• 92 Mobile units in remote rural and tribal areas
• 502 Rural Emergency Health Transport Services (108 of EMRI)
ASHA volunteers programme is the one of the core strategies from the first Andhra
Pradesh Programme Implementation Plan (2005-06). ASHA will be the first port of call for any
health related demands of deprived sections of the village community. In the state there are
about 51,200 ASHAs in rural villages (remaining in urban and tribal areas) at the rate of 1 for
1000 population. As an honorary volunteer, ASHA receives performance-based compensation
for promoting a variety of primary health care services in general and reproductive and child
health services in particular. Andhra Pradesh is the first state in the country that successfully
completed the selection, training and placement of ASHAs in all villages as per the NRHM
guidelines. The State government attempted to complete the training of ASHA within first
two years (as per the Guidelines of NRHM), so that they could have five more years to
perform; and in cases required, mid-course corrections have been undertaken for sustainable
implementation of the program. The Government of Andhra Pradesh implemented in
conjunction with the initiative of ASHA, the demand-driven, intertwined programme of Janani
Suraksha Yojana2 (JSY) from late 2005-06.

BOX-1 Roles and responsibilities of ASHA
• Create awareness and provide information to community on determinants of health
(nutrition, basic sanitation & hygienic practices, healthy living and inform on health
services and need for timely utilization of health and Family Welfare services.
• Counsel women on Antenatal care – birth preparedness, importance of safe delivery,
breastfeeding and complementary feeding, immunization, contraception and
prevention of common infections, RTI/STI and care of young children.
• Mobilize the community and facilitate in accessing health and health-related services
available at village/sub-centre/PHC such as immunization, ANC checkup, Post natal
checkup, ICDS and sanitation.
• Work with the Village Health and Sanitation Committee of the Gram Panchayat to
develop comprehensive Village Health Plan.
• Escort/accompany pregnant women & children requiring treatment/ admission to the
nearest pre-identified health facility in PHC/CHC/FRU.
• Provide primary medical care for minor ailments such as diarrhea, fever and first aid
minor injuries and reduce man hours lost in attending a PHC or a health facility. She is
also a provider of Directly Observed Treatment Short-course (DOTS) under RNTCP.
• A depot holder for ORS, IFA tablets, chloroquine, oral pills and condoms.
• Inform about births and deaths in her village and any unusual health problems/
disease outbreaks in the community to SC/PHC.
1.3 Need for the study
The cornerstone of the NRHM program is positioning a trained community link
worker (ASHA for every 1000 population) in all villages in the country. Most states have
demonstrated remarkable enthusiasm in scaling up ASHA activities of identification, selection,
training and placement in their respective villages. However, the impact of ASHA volunteer in
the community depends on proper selection, training (knowledge, inter-personal
communication skills), due recognition from health and other staff at local levels as well as
from the family members) and timely payment of incentives etc. The twenty-one days’
residential ASHA training in Andhra Pradesh was adjudged as the best strategy in the country
(NRHM First Common Review Mission, 2008). The present evaluation conducted after two
years of their placement in their respective villages to examine the knowledge levels and
views of ASHA volunteers about the scheme, problems faced in discharging responsibilities
towards health staff and community is necessary for sustainability of program. Further it is
worthwhile to know the extent of benefit community experienced, from the ASHA program at
local level. Andhra Pradesh being the first state with trained ASHAs working in the field, it is

also required to identify and note suggestions and common complaints in order to make any
mid course corrections.
1.4 Objectives of the study
The specific objectives of the study are to
a) Study the adherence with guidelines for ASHA selection in the villages
b) Review the training strategy including design, material development and
implementation, quality of training and post-training follow-up
c) Analyze work performance and support of health system to ASHA
d) Study the satisfaction of ASHAs with the delivery of scheme, suggestions and
comments including compensation / reimbursement
e) Map community perceptions of Janani Suraksha Yojana beneficiaries with whom
the ASHAs accompanied to institution for delivery
1.5 Presentation of the Report
The report has five chapters; the present one gives a brief introduction NRHM and
study objectives of the evaluation. Chapter 2 elucidates the study design and survey
instruments used and sample methodology. Chapter 3 discusses training strategy and
implementation of the ASHA programme in Andhra Pradesh. ASHA’s profile, selection
criteria, training, knowledge about different aspects of NRHM (RCH) and other related issues
are discussed in chapter 4. Chapter 5 covers the evaluation of JSY beneficiaries on the ASHA
work performance and their perceptions. The last chapter 5 is on programmatic
interventions for enhancing ASHA intervention and strengthening JSY scheme.

CHAPTER 2
DATA AND STUDY DESIGN
The data used for the study has been collected through a combination of quantitative
and qualitative evaluation techniques. Detailed structured questionnaires were developed in
collaboration with the CFW program officers, Academy of Nursing Studies (training agency)
and canvassed among the ASHA volunteers and beneficiaries in the five selected districts. The
questionnaires and study sample design are discussed in the following sections.
2.1 Questionnaires
Two types of questionnaires were developed for the present study: the ASHA
schedule and the Beneficiary schedule. The overall content and format of the questionnaires
were designed keeping in mind the objectives of the study. The preliminary draft
questionnaires prepared after three meetings between the training agency and IIHFW faculty
were field tested in Keesara PHC, Ranga Reddy district. After obtaining feedback, the
questionnaires were pre-tested in Shamirpet PHC, Ranga Reddy district. Following the
approval of the final questionnaires and methodology from the Commissionerate of Family
Welfare (funding agency) it was decided to select about 700 ASHA volunteers (slightly more
than 10%) and an equal number of beneficiaries for the selected districts.
A. ASHA Questionnaire
The ASHA questionnaire was designed to identify the topics covered in the training,
spontaneous responses on RCH aspects of compensation /incentives and suggestions for
program sustainability.
Section-1 Identification
Identification particulars such as name of the mandal, PHC, sub-center, name of the
ASHA volunteer, age, qualification, marital status, work experience before joining, area and
population covered by ASHA
Section-2 Training component
This part of the questionnaire covered information on logistic arrangements made in
the training centers in the districts and different topics covered in the 2-day in-house training
Section-3 Knowledge of ASHA about NRHM
This section deals with ASHA perceptions and spontaneous responses of knowledge
levels based on a) different components of Antenatal care, danger signs pregnancy,

symptoms of high risk pregnancies, factors causing maternal mortality and causes for infant
deaths etc.
Section-4 Functions of ASHA volunteers
The coordination of ASHA volunteer with health and other department personnel are
highlighted in this section. The section includes place and periodicity of the meeting with
ANM/AWW as well as information on the frequency of updating the records and periodicity
of births and deaths registration with village panchayat etc.
Section-5 Working aspects by ASHA
This section includes the general profile of the last client who availed the ASHA
services, mean days of last service provided to the client, type of service availed, escorting
the JSY beneficiary by ASHA for hospital delivery, mode of transport arranged to shift the
pregnant woman for delivery, mean days of ASHA’s stay at the hospital etc. Information was
also collected on the receipt of cash incentive, satisfaction about the incentive provided to
various activities and likely amount expected by ASHA as a monthly remuneration.
Section-6 Work and Remuneration
This section includes the supply and re-filling of ASHA drug kit and remuneration
received under different schemes by SC/ST and BPL groups besides the incentive for
promotion of family planning sterilization.
B. Beneficiary questionnaire
The draft Report of the NRHM Common Review Mission (2007-08) highlighted that
ASHA are actively involved in majority of the states and their main work was linked with their
accompanying the JSY beneficiary, immunization and promotion of sterilization acceptors
rather than attending eight tasks of ASHA as given in the NRHM Guidelines (First Common
Review Mission, 2008). In this section we enquire about the background information of
respondent beneficiary, delivery information of last child (in case of 1 or more children),
when they come to know about the scheme, details of ANC, counseling by ASHA/ANM, place
of delivery, receipt of timely incentive etc.
Section-1 Identification of beneficiary
This section includes identification particulars such as name of the beneficiary/
respondent, age, caste, number of children, white card status and monthly income etc.
Section-2 Knowledge of JSY
Information is included in this section regarding when the beneficiary heard about
the JSY scheme, source of information etc.

Section-3 Prenatal and Natal care of JSY beneficiary
Information sought includes time of ANC registration, place of JSY registration,
counseling about ANC etc.
Section-4 Satisfaction of JSY beneficiaries
Information is sought from the beneficiaries about mode of transport for shifting the
pregnant woman for delivery, arrangement of transport, satisfaction of the services obtained
at the health facility, opinion/value added due to the accompaniment of ASHA to the hospital
during delivery and post- natal care etc.
2.2 Sample Design
It was decided by the CFW to that the survey be conducted in five districts of Andhra
Pradesh. The selection of districts (high performance and low performance) was based on
District Human Development Index (CESS, 2007) as well as monthly program reports. It was
also decided to select one district from Rayalaseema region and two districts each from the
Coastal and Telangana regions of Andhra Pradesh.
The two selected districts were East Godavari and Srikakulam from Coastal Andhra
region, Karimnagar and Mahabubnagar form Telangana region and Kurnool district from
Rayalaseema region. The survey adopted a multi-stage-systematic sampling design. In each
district, the PHCs (mandals) were selected in the first stage using systematic random
sampling. In the second stage, all the villages in the PHC were ranked depending on the
number of ASHA workers (a proxy for population proportion to size) and six villages selected
by using Systematic random sampling procedure. In the final stage, all ASHA volunteers in
the selected village were interviewed. Information was also sought from local panchayat
sarpanch / panchayat member/ local committee members /ANM about their perceptions and
views about ASHA’s work and opinion and performance by beneficiaries (the pregnant (JSY)
women who were accompanied by ASHA to the institution for delivery).
The overall sample size was initially fixed at 700 (10% of the 70,700 ASHA volunteers
in the state). The study covered about 941 ASHA volunteers and 1100 ASHA beneficiaries
who availed the services from the ASHA volunteers (for accompanying delivery to a health
institution) during recent past. Thus in each district, from the 70-80 PHCs, about 15 PHCs
were selected randomly and then from each PHC area, six villages were selected. All the
ASHA workers and one or two beneficiaries who delivered under JSY scheme and who were
accompanied by ASHA were interviewed by using an in-depth questionnaire. The list of
villages selected in the survey is given in Appendix-1. The survey design is given below:

SURVEY DESIGN
Number of Mandals / PHCs selected 75 Number of Sub centers selected 387
Number of Villages selected 532 Number of ASHAs interviewed 941
Number of Beneficiaries interviewed 1121
2.3 Field work
About 36 interviewers with experience in Health/Demographic surveys were
recruited. They were provided intensive training both by coordinators and program officers
on various aspects of conducting quality field work and different NRHM interventions. The
training consisted of instructions in interviewing techniques and field procedures, a detailed
review of each item in the questionnaires, mock interviews among participants in the class
room situation and practice interviews conducted in the Keesara and Shamirpet PHC villages
of Ranga Reddy district. The field work of the study was carried out during November 2008
by four teams of 8 interviewers and 4 supervisors. All the completed questionnaires were
verified manually for internal consistency.
2.4 Data Editing and Analysis
The data were entered in EPI-INFO package developed by internal computer faculty
and SPSS 16.0 package utilized for cross-tabulation analysis.
Coastal
Andhra
Rayalaseema Telangana
Srikakulam East Godavari Kurnool Mahabubnagar Karimnagar
15 PHCs 15 PHCs
78 Sub
Centers
80 Sub
Centers
127 villages
102 villages
15 PHCs
74 Sub
Centers
93 villages
15 PHCs
79 Sub
Centers
97 villages
15 PHCs
76 Sub
Centers
113 villages
Andhra Pradesh

CHAPTER-3
TRAINING STRATEGIES OF ASHA IN ANDHRA PRADESH
The positioning of trained community link workers in all villages is one of the core
strategies of the mission and most states have demonstrated remarkable enthusiasm in
scaling up implementation activities. The present chapter covers broad areas of selection of
ASHA, training, logistics of training adopted, topics covered etc. The primary role of ASHA is
to create awareness on health and its social determinants and mobilize the community
towards local health planning and increase utilization and accountability of the existing
health services. The eight tasks of ASHA are Village planning, Linkages with health staff,
Village water and sanitation, IEC and counseling, Primary medical care, Timely referral, Depot
holding and Record keeping. Training is an important element of the ASHA programme since
it goes a long way in determining its effectiveness.
Box 3.1 Key Activities of NRHM
The Accredited Social Health Activist is called by the acronym ASHA. She must be a
primary resident of the village with formal education up to the eighth class, and
preferably in the age group of 25-45 years. She would be selected by the Gram Sabha
through an intense community mobilization process, and provided with training. She
would also be equipped with a drug kit. After selection, ASHA will be given induction
training for 23 days spread over a period of 12 months. Training manuals have been
prepared. ASHA will be given periodic training, re-training and on-the-job training. She
will act as a mobilizer, facilitator and a link between ANM at the sub-centre, Anganwadi
worker and the community, and play a major role in forging ownership of the
community for the health programme. ASHA will be first port of call for any health-
related demands of deprived sections of the population, especially women and
children, who find it difficult to access health services. She will ensure better access to
universal immunization, safe delivery, newborn care, and prevention of water-borne
and other communicable diseases, nutrition, and sanitation. She will be accountable to
the panchayat, and will be entitled to receive performance-based compensation for
providing health services.
3.1 Training Strategy
The Ministry proposed the training of ASHAs for 23 days’ duration spread over five
rings/exposures in one year period. The first round of induction training consists of seven
days to provide preliminary knowledge on eight tasks of ASHA. The responsibility of ASHA
training and monitoring was given to the State Institutes of Health and Family Welfare along
with a reputed NGO with working experience in health area. The trainings conducted in the
states of Uttar Pradesh, Rajasthan, Jharkhand, Bihar and Orissa showed discouraging

experience of identification, selection, induction training and subsequent rounds of ASHA
trainings (Garg and Nath, 2007).
The Government of Andhra Pradesh adopted an innovative approach, and initiated
21 days in-house training in every district headquarters covering around 180-200 ASHAs
every month. After prolonged deliberations concerning training experience and extensive
planning, the huge task of ASHA training in the State run (Department of Women and Child
Welfare, GoAP) training centers in each district was initiated. The Academy of Nursing
Studies (ANS) was entrusted the responsibility of selection of trainers, conducting of TOTs,
deployment of trainers, development of manual, facilitator’s guide and other audio-visual
support for conducting the 21 days training in a record period of 18 months from early 2006.
3.2 Trainings of ASHA Volunteer in Andhra Pradesh
In order to train massive number of ASHA volunteers, it was proposed to conduct
the training in all the 22 districts (except in Hyderabad urban district) covering around 3500-
4000 volunteers every month. This task was fulfilled successfully with the close co-ordination
and cooperation and monitoring among the three agencies. The process of selection and
approval and timely deputation of ASHA volunteers for the training was closely monitored by
the Commissionerate of Family Welfare. The Andhra Pradesh State Women Finance
Corporation (a wing of Department of Women and Child Welfare) provided accommodation,
food and other training arrangements in their ‘Mahila Pranganams’ (training center for
empowering women groups). The task of developing training manual, Facilitator’s training
manual, Demonstration material were under taken by the Academy of Nursing Studies (ANS),
Hyderabad, a reputed NGO in the state.

3.3 Training Strategy
The Academy of Nursing Studies developed the necessary manuals and audio-visual
aids in a record time. In response to a paper advertisement, the ANS selected more than 350
trainers (ANMs with additional educational qualifications) along with a commitment to work
for 12-15 months period. A fifteen days TOT was conducted for these selected trainers who
subsequently provided with quarterly refresher trainings. The Women Finance Corporation
(WFC) has spacious training centers (Mahila Pranganams) located in every district
Headquarters capable of accommodating about 200 female trainers. The lodging, boarding,
class room availability and other training requirements in each district were taken care of by
the District Manager (a female officer), WFC and supporting staff.
Research studies related to training of health personnel, showed that majority of the
National Health Program initiatives started with training and ended with training activities
without proper evaluation to assess the success of the initiated programme. It is necessary to
ensure that training of ASHA is completed within first two years of NRHM so that they have 5
years’ period to perform and, if required, mid-course correction can be undertaken in the
implementation. (Umesh Kapil, 2006).
3.4 Training Process
The NRHM Mission directorate, the WFC authorities and the ANS decided to train
180-200 volunteers per district in a month. Two batches were conducted simultaneously for
a duration of 21 days at the training centre and five days in the field and another 2 days at
their respective PHCs for providing feedback on the training in order to strengthen linkages
between them and the PHC staff.

3.5 Methods & Materials
Training was designed to be participatory and adult learning oriented, with overall
personality development, empowerment, self confidence and orientation to health as the
main objectives. The ANS training adopted discussions, practical experience, reviews, quiz
programmes, songs, video shows, yoga and folk arts during training period. All trainees were
reviewed daily in the morning (about previous day’s activity) and evening review (to
recapitulate the day’s activities) followed by weekly reviews and written examination and
role plays by involving all trainees.
3.6 Monitoring Systems
The key for the success of Andhra Pradesh model of ASHAs / WHVs training in a
record period (18 months) was attributed to the triangulation of coordination among the two
government departments and the NGO. The District training manger (a senior DPHNO)
monitored the nomination, field training, review and the distribution of kits and
remuneration aspects. The regional coordinators of ANS staff monitored the training
programme. The State level monitoring was conducted by DM & HO and other program
officer in-charge. The CFW in collaboration with ANS appointed a state level coordinator to
monitor timely nominations, conducting the training as per the norms indicated in the PIP
according to the ASHA guidelines.
3.7 Training Programme Outcome
The pre-test and post-test evaluations and other weekly evaluations and the
responses of the trainees indicated remarkable difference in their behavior (especially in
their dressing, inter-personal communication (talking, increased participation in discussions)
by the end of first week of training. It is interesting to observe that a small percentage
(below two percent) of ASHAs discontinued the 21 day residential training due to health
reasons and family problems indicating that well planned and designed training programs
will falsify common perceptions that women may not prefer long duration trainings. The
State Government ASHA training strategy, also successfully completed the refresher-training
course in all the districts successfully.
Bajpai et al (2008) reported that the crash course of ASHA trainings in Andhra
Pradesh was inadequate in terms of quality training and allocation of time for different
training aspects. The authors pointed to the need for an on-going short-duration training of
ASHA at regular intervals throughout the year and the need to share the rich experience of
ANMs in the training sessions as per the GOI guidelines. Bang (2007) advocated for extending
training days from 23 days per annum to 150-180 days over a period of 3-5 years. The Rural

Health Watch Survey conducted interviews with 250 ASHAs in around 80 districts and
reported that most of ASHAs had yet to initiate work (Rajyalakshmi, 2007). Sharma (2007)
observed in Rajasthan that the ASHA trainings were inadequate with reference to tasks
performed and that ASHA volunteers had poor knowledge about JSY related concepts,
components and provisions. Moreover, ASHAs in Rajasthan preferred longer initial training in
the first round from 7 days (Sharma, 2007).
It is interesting to observe that the Andhra Pradesh training model (21 days
residential) was successful in completing the training of all ASHAs in the state within the
stipulated time schedule laid down by the NRHM time-frame. All the ASHAs working in the
field were well acquainted with their job schedule. The refresher training course, Monthly
ASHA Day meetings helped ASHAs to strengthen the skills. This rich experience of Andhra
Pradesh may be extended to other NRHM states which are lagging in selection and
completion of five rounds of training and finding other teething problems.
The CARE agency under the Integrated Nutrition Health Project (INHP) developed a
training program of 6 days of three hours duration on the convergence ASHA Day with a
stipulated period of 6 months duration. The organization developed a module and started
the intervention through DPHNO /Nodal officers in the PHC area under the guidance of
Mission Director, Government of Andhra Pradesh since October 2008. Some of the
monitoring reports indicated the need a) to strengthen newborn care with IYCF knowledge
to the DPHNO/ Nodal officers, b) strengthening of monitoring ASHA Day by district / PHC
programme officers; and c) ASHAs in many PHCs expressed that inputs provided by CARE on
ASHA Day were useful and expressed qualitative improvement in outcome indicators.5
To sum up, the training strategies adopted in Andhra Pradesh serve as a role model
and suitable action should be initiated by other states in overcoming teething problems of
selection, quality training on different aspects.
Whatever the training methodology we had chosen, (5 rounds of 4-5 days duration in
a span of one year period or 21 days in-house training), to achieve the goals of NRHM
initiatives, it is very important to deploy the ASHA volunteers in all villages and really bring
about the change that is expected by the NRHM visionary.

Appendix- 1
Matrix indicating broad Training strategies adopted by GOI and AP Model
GOI norms of ASHA training Andhra Pradesh ASHA Training
Duration of training
Twenty-three days of training in five
rings/exposures spread in 12-18 months.
Seven days induction training.
Twenty-one days residential training and
seven days of practical field training in
respective PHC area.
Operational difficulties in conducting four
or five rounds training. Difficult to sustain
same motivation in all rounds and
operational difficulties.
Cost-effective in conducting twenty-one days
training at district headquarters under Govt.
training centre ‘Mahila Pranganam’ under
Dept. of Women and Child Welfare, Andhra
Pradesh.
Method of training
Interactive techniques including pictorial
materials, story telling, role plays, folk
media (Kalajathas) and local radio
programs.
Interactive techniques covering pictorial
materials, group discussion, melodious folk
songs composed with health messages, role
plays, skits and special health education
video shows.
Module
Reading material in the form of five books.
First book provides preliminary knowledge
on major ASHA themes. Aspects covered
step by step from module one to module
five. Flexibility to delete and add topics
according to local needs by States.
ASHA training module, Facilitators Guide and
Demonstration Aids prepared in the initial
year 2005-06 in local language. Reviewed
periodically and additional topics included
from time to time by the NGO on the request
of Health department.
Periodic training
After completion of seven days induction
training, periodic training for 2 days in
every alternate month at appropriate level.
After completing twenty-one days of
induction training, Refresher Training for 3
days twice in a year conducted for updating
skills and knowledge. On ASHA day of every
month CARE INDIA conduct convergence
meeting in pilot districts.
On-the-Job –Training
As ASHA needs On-the-Job support after
induction and other periodic trainings, it is
proposed to provide on-the-job training
during immunization days and out reach
service days by ANM and on monthly
nutrition day by AWW.
ANM and AWW provide on-the-job training
to ASHA during out reach service days.
Author’s field experience indicates that
ASHAs are in a position to question the non
availability (absenteeism) of ANM in the
village.

GOI norms of ASHA training Andhra Pradesh ASHA Training
Venue of Training
PHC or Panchayat Bhavan or other facility
closer to their habitation. Empirical
evidence indicates that trainings are not up
to the mark in terms of training quality and
quantitative rounds of training.
Government Women and Child Welfare
Department ‘Mahila Pranganams’ which
accommodate 180 participants at a time with
good quality boarding & lodging and training
center facilities. In 18 months time, all ASHA
trainings could be completed in the State.
Selection of ASHA
It is proposed that every State government
should ensure that at least 40% of the
induction training is completed in first year
and rest of ASHAs training may be
subsequently completed in second and
third year of NRHM (by 2008-09).
All ASHA workers trainings completed in
Andhra Pradesh by end of 2007 and Ninety
percent of ASHAs completed refresher
training
ASHA is the main stakeholder and higher
attrition rate of ASHA may take one year for
selecting and replacement in the village.
Five rounds of training of one year duration
may increase operational costs.
In case of attrition of ASHAs, new volunteers
may be selected and placed within a span of
3 months with cent per cent replacement.
Operational Problems
Timely communication to the volunteers
about the batches/rounds, availability of
time and their inability to get away from
work or sickness or domestic problems
may cause poor turnout for training
program.
Operational problems can be managed.
ANMs involved from recruitment of ASHA.
She personally brings the deputed volunteer
from the sub-center village to the training
center and introduces them to the trainers
on the first day of training.
Chance of dropout rate from induction to
5th round of training due to various
operational and personal reasons.
Dropout cases may be effectively tackled
with less operational cost.
The NRHM trainings of ASHA preferred in
five rounds due to shortage of initiation
and development of modules for the
training. The retaining capacity of the
trainees may cause a serious block in this
cascade approach.
Trainers are evaluated on a daily/weekly
basis by training coordinators /district
manager. The CARE agency trainings on
ASHA Day, refresher trainings enrich the
coordination of knowledge update.

Chapter-4
ASHA INTERVENTION IN ANDHRA PRADESH
4.1 ASHA intervention
The government of India formulated guidelines on roles and responsibilities of ASHA,
institutional mechanisms, selection and training of ASHAs, work arrangements and linkages
with ANMs and Anganwadi workers, incentives to ASHA on work performance etc. In the
previous chapter, we elaborately discussed issues related to the ASHA selection, training
procedures adopted in Andhra Pradesh. The District Medical & Health Officer (DM & HO) and
District Programme Management Unit (DMPU) of NRHM are implementing and reviewing the
district level monitoring of ASHA intervention programme .The PHC medical officers, ANMs
directly monitor the performance, on-the-job guidance, payment of incentives and
convergence with other departments. Strenuous efforts are made by Gram Panchayat,
Sarpanch, PHC / SC staff, ANM, Women Health Group members and AWWs for motivating the
village women with necessary criteria as ASHA workers. The PHC staff indicated that in
majority of the places women had not shown any interest due to lower educational
qualifications, lack of interest to work in SC /BC colonies by forward caste and vice versa and
low and uncertain incentives, unfavorable comments from the family members etc. In some
places the ANM and AW workers and Village Sarpanch had taken personal interest along with
the PHC Medical Officers for motivating the women.
The State of Andhra
Pradesh adopted national
guidelines of selecting ASHA
volunteers but provided
relaxation in education
qualification from 8th
standard to 7th standard
pass. The selection
procedure guidelines were
translated into Telugu
language and were
transmitted to the district
and PHC level officers for effective implementation. A series of workshops was organized by
the State Mission Directorate in all districts and for familiarizing objectives and mechanism
of selection of ASHA volunteers. The State level program officers in turn conducted and
monitored the block level and PHC level workshops. The DWCRA (Women Help Groups) in
every village acted as a catalyst and helped the village level selection of ASHA Volunteer. The
10035
41166
7816 8054
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
2005-06 2006-07 2007-08 2008
Trained ASHAs in Andhra Pradesh

Triangulation of efforts by the three agencies namely DM&HO representative (senior DPHNO)
and district manager of the Women Finance Corporation and ANS enabled massive training
of 70,700 ASHA volunteers in a record time of 18 months. As indicated in the methodology
section we selected five districts in Andhra Pradesh and about 75-80 PHCs and around 990
ASHA workers in the PHC villages. An equal number of beneficiaries who availed the services
of ASHA recently in the village were also selected.
In the following paragraphs we would discuss the Socio-demographic profile of
ASHAs, the motivating factors to take up ASHA volunteership, the selection process, training
and gauging of retention of training knowledge regarding antenatal and child care aspects.
Their roles and responsibilities, ways of motivate clients and service assurances were also
discussed. Information on ASHA’s last clientele (to understand the nature and type of
interactions), networking with key stakeholders, cash assistance received by ASHAs, their
suggestions and bottlenecks for the sustenance of the program is presented below.
4.2 Background Characteristics of ASHA
The survey covered a sample of 941 ASHAs (a maximum of 224 in East Godavari and a
minimum of 165 in Mahabubnagar district) from five districts of Andhra Pradesh. The ASHAs
interviewed were young with a mean age of 28 years (ranging between 19-50 years) and
about eighty-six percent of the ASHAs had above 7th standard of school education (Table 4.1).
Eight out of ten ASHAs interviewed were currently married women, 13 percent un-married
and remaining seven percent were divorced / widowed / separated. More than half (57
percent) of ASHAs belonged to scheduled caste/ scheduled tribe groups followed by 35
percent from backward castes and the remaining 7 percent were upper caste Hindus. One
percent of the ASHAs belonged to Christian / Muslim communities. All ASHAs were residing
in their respective villages. With regard to the experience, three-fourth (76 percent) ASHAs
had completed more than 18 months of work experience in the field and less than one-fifth
(18 percent) had completed below one year. All the ASHAs had completed 21 days of
residential training in their respective district head quarters. It was also observed that nine
out of ten (92 percent) had attended three days refresher training in the early months of
2008. The ASHA volunteers welcomed the refresher trainings, twice per annum along with
the on-the-job-training of monthly convergence meeting on ASHA Day (last Tuesday of every
month). Most (87 percent) of the ASHAs had children and the average number of living
children was 1.9. While answering the question of the age of last child of ASHA, 54 percent
of ASHAs had their last child born more than 60 months earlier and only 20 percent of ASHAs
have last child born within one year prior to the survey.

4.3 ASHA Selection and Motivation factors for joining
The Commissinerate of Family Welfare conducted dissemination workshops in all the
districts and sub-regions and at lower levels and communicated selection process and ASHA’s
role and responsibilities to the Village Gram panchayat. It is important for the village
community to understand the process and selection of appropriate person as ASHA within
the NRHM framework. More than half of the ASHAs came to know about ASHA selection from
ANMs and Anganwadi workers. About half of the ASHAs indicated that they were selected by
ANM and about one-fifth (21 percent) were recommended by Sarpanch/Politician, followed by
10 percent who were approved/selected by Gram panchayat. The Gram panchayat approved
the selections of ASHAs and nominated them for training at district headquarters. Eighty-nine
percent of ASHAs indicated they preferred to be ASHA in order to serve the community,
earning extra money for the family was indicated by 58 percent followed by 30 percent
stating the purpose to save the children and bring awareness on health issues (Table 4.2).
Working status before joining as ASHA
The Survey collected information from the ASHAs about the work they usually
attended to before becoming an ASHA. More than a half (55 percent) of ASHAs are house
wives / economically active women and less than one third (31 percent) are agriculture
laborers followed by less than 3 percent of ASHAs reporting their association with
ANM/AWW or participation in the health programs of Indira Kranthi Patham ( a program to
eradicate poverty, introduced in Andhra Pradesh).
Training of ASHAs
As per the norm, every ASHA was supposed to attend 21 days residential induction
training and 7 days of field based (at PHC/SC) training. All ASHAs interviewed had attended
the induction training program in their respective district headquarters. Contrary to the GOI
guidelines of ASHA followed in other states in a phased manner, all aspects were highlighted
in the ASHA training by way of group discussions, communication skills, story telling, songs
with health messages in local language, video shows, clearing of doubts in the morning
during assembly and evening between 4-6 pm during training programme.
ASHAs who had attended the residential training were questioned about the topics
covered. The spontaneous responses included maternal and child health, eight tasks of
ASHAs, nutrition and HIV/AIDS. Aspects related to community health and sanitation, curative
care was also included. A special emphasis was made to include aspects of interpersonal
communication (IPC), methods of organizing community meetings, skills to discuss with
higher authorities etc. which were taught and practically demonstrated in the training
program (Table 4.3). The training team used to invite some of the ASHAs of previous batches

and working in the field to the
training program in order to share
the experiences. The training
aspects covered in ASHAs training
was assisted by series of 13
questions. Each correct response
was given a score of one mark and
equal weightage was given. Later,
the scores were categorized into
Grade A- 9-13 correct responses,
Grade B- 6-8 correct responses and
Grade C- 1-5 correct responses.
Eleven percent of the ASHAs scored
Grade A, 50 percent of ASHAs
scored Grade B and 35 percent
scored Grade C. In other words, sixty eight percent of ASHAs had reasonably good
knowledge of training topics. This indicated the need to emphasize some of the aspects in
refresher training programme.
The ASHAs were further asked about the logistic arrangements during their training
period. Training of ASHAs was held in a training institute ambience ‘Mahila Pranganams’ at
the district head-quarters. ASHA trainings were conducted in other states mostly at PHC /
CHC and schools which have relatively poor ambience for training environment for village
women to learn about the health aspects (CORT, 2007). Among the selected districts, 82-97
percent of ASHAs appreciated seating arrangements and 82-95 percent appreciated size of
the room as ‘big’ and ‘good’. More than eighty percent (79-96 percent) of ASHAs appreciated
food arrangements and accommodation facilities. The IIHFW faculty observed during the
field work excellent facilities in majority of training centers though a few complained about
the need for more number and clean toilet and bathroom facilities. All the training centers
were constructed on the outskirts of district head-quarters; the health officials felt difficulty
to monitor daily proceedings of ASHA trainings (IIHFW, Annual Report, 2007-08).
Payments during training
The project officer (District training team, DTT) from the DM&HO office used to
disburse the payments at the end of the last day of training. Each ASHA used to get payments
as per the guidelines. Discussion with the trainers of NGO and the WFS personnel revealed
smooth flow of funds from the CFW to all district training centers in regular intervals.
Scoring Knowledge of Training
Grade B
50.3%
Grade C
38.7%
DK
0.3% Grade A
10.7%
DK Grade A Grade B Grade C

Use of reading material / Drug kit
ASHAs were given reading material ‘ASHA Margadarshini’ in local language on the first
week of training. All ASHA trainees received the manual and used to answer the questions,
exercises on filling the blanks provided at the end of each lesson. About eighty-one percent
of ASHAs indicated that they were provided with ASHA drug-kit during training.
Knowledge of ASHA Volunteers
a) Component of Antenatal services
Knowledge of ASHAs on
antenatal care services was assessed
through seven types of ANC checkups
(Measurement of weight and height, BP
checkups, Blood sample and Hb, Urine
sample examination, HIV Test, Medical
examination / Abdominal Checkup and
Blood grouping). Each correct response
was given a score of one mark,
otherwise zero. They were divided into
Group –A correct answers of 5-7 score;
Group-B correct answers of 3-4 and Group-C below 2 correct answers. Interestingly,
fiftyseven percent of ASHAs knew all aspects of Antenatal services and fortythree percent
reported 3-4 correct answers. The aspects of Antenatal Checkups are widely popular and the
field experience indicates that ASHA worker were requesting for additional incentive for
accompanying the pregnant women for HIV test. More than sixty percent of score was
recorded in East Godavari and Karimnagar districts.
b) Recognizing pregnancy complications
The major signs of complications included in the scoring pattern pertained to those
that required: i) immediate reference to the nearest FRU, ii) request the patient to consult
ANM/PHC, iii) refer to Govt. / Private accredited hospital and iv) call 108 Ambulance. About
sixtyfive percent of ASHAs reported that they advise to shift the patient to the nearest FRU.
Eightytwo percent of ASHAs indicated a call to 108 ambulances for immediate shifting of
patient / pregnant women (Table 4.4).
Score of ASHAs Knowledge on
Antenatal Care
Grade A
56.6%
Grade B
43.4%
Grade A Grade B

c) High risk of pregnant women
Knowledge of ASHA on high risk of pregnant women was assessed by six components
(Short stature, Low age <18 years and above 34 years of age for delivery, first pregnancy,
birth order four and above, High BP/Diabetic symptoms and Anemia). Each correct response
was given a score of one mark,
otherwise zero. We made three groups,
Grade- A correct answers of 4-6 score,
Grade-B correct answers of 1-3 score
and Grade-C zero score. Below one
percent of ASHAs scored Grade- C,
sixtyfour percent of ASHAs scored
Grade-B and thirtysix percent indicated
Grade-A. In other words, ASHAs had
good practical knowledge of identifying
high risk pregnancy and knew where to
shift the pregnant women in case of
emergencies.
d) Complications during delivery
Regarding the complications which can result in maternal mortality at the time of
delivery, ASHAs indicated excessive bleeding (86 percent), blood pressure problem (53
percent), convulsions / fits (53 percent), abnormal position of the foetus (47 percent), and
tetanus (44 percent) respectively. Less than 25 percent of ASHAs mentioned abdominal pain,
foetus died in mother womb and placenta problems (Table 4.5). There is a great need to
reinforce during refresher training and convergence meetings of CARE in the pilot districts
and by department in non-CARE focus districts the knowledge of ASHAs on the factors that
can cause maternal deaths.
Knowledge about Newborn Care
Less than forty percent (38 percent) of the ASHAs said that newborn are most likely
to die between 3-4 weeks of birth, followed by thirtyone percent of the ASHAs who reported
it could be soon after the birth/first day birth and about 23 percent mentioned a period
within one week of birth. Another 20 percent of ASHAs indicated ‘Don’t know’ (Table 4.6). A
lower percent of ASHAs with lack of knowledge about Neonatal death varied (4-5 percent) in
Mahabubnagar and Karimnagar districts of Telangana regions.
Score on High Risk Pregnancy
Grade B
63.8%
Grade A
35.6%
DK
0.6%
DK Grade A Grade B

Knowledge about role and responsibilities
The evaluation study explored ASHAs familiarity with their roles and
responsibilities (tasks). The aspects included: help in bringing children for immunization,
accompanying delivery cases to health facility, health awareness activities, providing ANC
counseling, working with
Anganwadi worker, registration of
births and deaths, motivating and
mobilizing community on health
and sanitation aspects, family
planning information, Village
health planning, counseling
villagers on health aspects,
promotion of good health
practices, treatment of minor
elements, timely referrals,
participation in National
programme and working for DOTS. Each of these fifteen tasks of ASHA volunteers was scored
as one mark for correct response and equal weightage was given for incorrect answer. Later
the scores were categorized into three Grades, Grade-A 12 -15 correct responses, Grade-B 8-
11 correct responses and Grade-C for 4-7 correct responses. About a half of the respondents
were in Grade B (8-11 correct responses) followed by 42 percent in Grade C (4-7 correct
responses).
A comparison of individual tasks of ASHA volunteers is presented in Figure-1. The
familiarity of tasks indicated by ASHAS were immunization services (98%) provision of ANC
care (97%), accompanying delivery cases (85%), family planning operations (71%), working as
DOT provider for TB cases (59%). A lower number of ASHAs indicated counseling (13%) and
work with AWW/Dai (17%) as their responsibilities in (Table 4.7). A few ASHA volunteers
stated that they promote good health facilities, counseling and timely referrals as their other
responsibilities. These are the core areas which need emphasis during refresher training,
CARE-INDIA convergence meetings on ASHA Day and the on-the-job trainings.
Score of ASHA responsibilities
Grade C
42.2%
Grade B
50.1%
Grade A
7.7%
Grade A Grade B Grade C

Figure 1 – ASHA’s awareness about their responsibilities
98.3
84.8
46.3
97.4
16.7
50.1
31.8
71.3
30.1
13.5
21.5
55.8
28.9
55
44.1
58.6
0 20 40 60 80 100 120
Help in immunization program
Accompanying delivery cases
Create awareness on health
Provide ANC Care
Work with Anganwadi Worker/Dai
Registration of birth and death
Motivating & mobilizing community
Family Planning
Village health planning
Counselling
Promote good health practices
Treatment of minor ailments
Make timely referrals
Increase in Institutional delivery
Participating in National Health Program
Working as DOT provider for TB cases
Organization of work by ASHAs
Ninety-eight percent of ASHA volunteers organized their work regularly and
coordinated with the ANM and Anganwadi center activities in the village. The respondents
unanimously indicated that they used to meet ANM/AWW during the weekly immunization
sessions and called all the pregnant women for timely ANC check-up and helping in
organizing of Village Nutrition Day at AW center. Field experience indicates that majority of
ASHA volunteers were highly dependent on ANM and AW workers. The roles and
responsibilities and the work organization of ASHA indicates that the ASHA was acting as
assistant to the ANM/AWW rather than a village health activist.
Research studies indicated that the work performance of ASHA is highly linked to JSY
beneficiaries accompanying to hospital for delivery, Family Planning operations and bringing
children for immunization rather than attending to other tasks. A potent program like ASHA
was being used for merely escorting women to the hospital and assisting the ANM and AWW.
This requires a re-look at the activities and ensures that ASHA gets sufficient role in the
NRHM as envisaged in the document.

Record updation
Thirtyseven percent of ASHAs in the survey revealed that they maintained records
regularly (23-24 percent in Kurnool and Mahabubnagar districts and 63 percent in East
Godavari district). The weekly updation of records varied between 29-53 percent across
districts. Thus the survey indicated that 66-80 percent of ASHA volunteers update their
records within seven days. It should be emphasized that cent percent of births and deaths
registration in the village be done immediately or within one week. A combined effort of all
ASHAs in every village may provide a timely and reliable estimate of infant deaths and
maternal deaths at district level (Table 4.8).
ASHAs clientele
ASHA volunteers indicated that they provided services to the client, on an average
six days prior to the survey date (the model / mode of average days reported was two days).
CORT research studies indicated that the provision of services by ASHAs to the clientele was
on an average 28 days in Orissa, 25 days in Bihar (CORT, 2007). It is also very heartening that
the services provided to the clients were accompanying for institutional deliveries of JSY (94
percent), Family planning operations (80 percent), Diarrhea/ARI cases (31 percent) and
Accident/Born cases (19 percent) respectively. It is also observed that a small percent of
ASHAs indicated that they are accompanying the client to PHC/CHC for other health related
purposes including ANC Check up, HIV test for pregnant women, distribution of DEC, eye
operations, and Thyroid care.
Less than half of
the clientele of ASHA
belonged to Scheduled
Caste and Tribe
communities followed
by forty-seven percent
of backward caste (BPL
group) remaining were
of general category
(10%). The grading of
the eleven types of
services provided by
ASHA to the clients is
presented in (Table 4.9). Each correct response was given a score of one mark and equal
weightage was given. Later, the scores were categorized into Grade- A 8-11 correct answers,
Grade-B 5-7 and Grade-C 5 or less correct answers. In all only 11% of the ASHAs scored Grade-
Scoring knowledge of services provided to clients
Grade C(<5)
46.8%
Grade B(5-7)
42.6%
Grade A(8-
11)
10.6%
Grade A(8-11) Grade B(5-7) Grade C(<5)

A, 43 % scored Grade-B, and 47% Grade-C. The purpose of clients who visited ASHA for the
purpose of collecting medicines, for fever, back pain and vomiting (82 percent), child
immunization (77per cent), antenatal care advice (64 percent), and registration of pregnant
women for ANC (59 percent).
Ninety-eight percent of ASHAs handled a JSY case for delivery in hospital and the last
JSY client was accompanied 24 days prior to the date of interview. Ninety-three percent of
ASHAs stayed with the client at the place of delivery and average number of days of stay was
1.87 (the number recorded 2.19 in East Godavari and 2.25 days in Mahabubnagar districts).
Seven out of ten (71 percent) of ASHAs stayed for one day, 15% stayed for two days along
with the JSY beneficiary for delivery services.
Perceptions of ASHA
The informal qualitative information from the selected village leaders, panchayat
members and elders and ANMs indicated that the ASHA programme intervention has value
added as observed by higher turnout of mothers for child immunization, ANC checkups and
preference of institutional delivery as compared to home deliveries. In Ahobilam PHC of
Kurnool district, the ASHA worker daily visited S.C colony for monitoring the consumption
tablets provided under DOTS programme. The important suggestions reported by ASHA were
timely (monthly) payment of incentives (91 percent), having a dress for ASHA for easy
identification (71 percent), timely supply of drug kits and drugs replacement (56 percent),
arrangement for transport / Bus pass for attending hospitals for delivery of JSY beneficiaries
(51 percent), increase in cash incentives / equal remuneration for all communities (43
percent), improvement of facilities at village or at hospital to ASHA (33 percent) are the
major suggestions (Table 4.10). A meager percentage of ASHAs reported higher interaction of
lady doctors/doctors/ Nurse with JSY beneficiaries, higher propagation in media regarding the
NRHM (ASHA and JSY), good behavior of hospital staff towards ASHA and no doctors/ANM
not demanding perks for timely payment of incentives.
The common suggestions for improving the ASHA intervention were mainly related
to enhancing the cash assistance for making timely money payments, provision of complete
information and practical trainings. Propagation of the NRHM schemes by the lady medical
officer, doctors and nurses helping ASHA to propagate healthy practices easily in the
community.
A half of the ASHAs mentioned the complaints of JSY beneficiaries about untimely
payments, staying long hours away from home, un-timely schedules, dislike of the
husband/family for her job (29 percent), reluctance among families and women to go for
institutional delivery (25 percent), reluctance of women to consume IFA tablets (16 percent)

which constituted major challenges faced by ASHA volunteers in delivering the services3
(Table 4.11).
Cash remuneration received by ASHAs
ASHAs were asked about
the delay in cash incentives received
by them. The JSY incentive received
by ASHA varied substantially from
one day (3 percent) to more than
one month (56 percent). The various
reasons for the delay are given in
Table 4.12. Thirty-eight percent of
ASHAs indicated delay in the
approval process of incentives, and
27 percent mentioned lack of
advance money at the medical
facility. Less than ten percent of
ASHAs indicated non-availability of
signing authority or delay in obtaining Sarpanch signature etc.
The ASHAs were asked about the case incentives received by them. Eighty percent of
ASHAs received remunerations for child immunization, 74-79 percent for escorting delivery
(of JSY beneficiary) followed by family planning cases and antenatal care. About 42 percent of
ASHAs had received remuneration for National Health Programs and 19 percent for DOT
services.
Regarding duration of work as ASHA it was found that 60 percent had worked for
more than two years and marginal variations were reported in the selected districts. More
than 64 percent had completed two years of work as ASHA in Srikakulam, East Godavari and
Karimnagar districts. On the other side, about 40 percent in Kurnool and 29 percent in
Mahabubnagar districts indicated below 18 months of work experience. Ninety-eight
percent of ASHA volunteers had received incentives during three months preceding the
reference period. The government of Andhra Pradesh developed a special work and
remuneration record sheet for ASHA workers. Based on the performance, the ASHA will enter
the details and that will be counter signed by ANM after verification and endorsement by the
sarpanch. The different items covered are a) Number of pregnant women registered in the
first trimester (SC family cases only); b) 3 ANC received from ANM / Other health staff (SC
family only); c) Pregnant women received at least one ANC from doctor (SC and BPL families);
d) institutional deliveries (SC and BPL families); e) Post natal care by home visit (SC and BPL
Score of Remuneration by ASHA
>3 Months
18.4%
After 1
Month
59.6%
Below 1
Month
19.0%
Same day
3.0%
Same day Below 1 Month
After 1 Month >3 Months

families); e) infants who received vaccinations (both SC and BPL families); f) children who
received Measles and Vitamin - A (both SC and BPL families); g) registration of birth with birth
weight below 2000 grams (both SC and BPL families); h) family planning methods (both SC
and BPL families and other than the general RCH activities) respectively.
Out of 919 ASHA volunteers who indicated the incentives, only 74 percent
mentioned information of items (a) to (h) and the remaining 242 respondents stated family
planning incentive and the total amount only. The ASHAs, on an average earned about Rs.
545/- (range of Rs. 200 – 1875; calculated on the basis of cases motivated for RCH activities in
the reference period of
three / one month) prior to
the survey. ASHAs received
higher incentives for
accompanying institutional
delivery (36 percent), post
natal care (19 percent), one
ANC with MBBS doctor (13
percent), Measles and
Vitamin-A ((11 percent)
respectively4. From the
responses, the average
figure recorded for RCH
activities was Rs. 467/- (a
range of Rs. 300 – 1100).
Only one-fifth of ASHAs (19 percent) were satisfied with incentive they had received
(more than state average recorded in Karimnagar 32 percent) followed by Kurnool (28
percent). Sixty-seven percent of ASHAs were not satisfied with the cash assistance
commenting on ‘too much work with too little payment’ followed by delays in receipt of
payment. ASHA is one of the main actors in the Mission, and the woman responsible for a
variety of tasks, but she does not have a fixed remuneration (Rajyalakshmi, 2008). The study
also enquired the respondents to mention the ‘willingness to receive’ or the expected salary
of remuneration. Thirty seven percent of ASHAs viewed the salary between Rs. 1500-2000
and slightly lower than 32 percent indicated Rs. 1000/- as a fixed remuneration (Table 4.13).
The mean salary expected was RS. 1600/- and the model salary (indicated by majority of
ASHAs) expected was Rs. 2000/ respectively.
INCENTIVES RECEIVED BY ASHA
Newborn <
2000 gms
0.7%
Measles &
Vit.A
11.5%
Immunization
7.4%
Postnatal Care
19.5%Institutional
Delivery
36.1%
One ANC by
Doctor
13.4%
3 ANC by ANM
7.1%
ANC in first
trimester
4.3%
ANC in f irs t t rimester 3 ANC by ANM
One ANC by Docto r Inst itut io nal D elivery
P ostnatal C are Immunizat ion
M easles & Vit .A Newbo rn < 2000 gms

Monitoring System
All ASHA volunteers reported proper maintenance of record book (including
information a) on pregnant woman particulars, b) information on child immunization
coverage, and c) record of health services provided and particulars on remuneration
received). Field experience indicates that ASHAs were updating information on regular basis
in all the districts. Ninetynine percent of ASHAs were aware of monthly ASHA Day meetings
and equal number attending regularly, obtaining counseling from district program officers,
PHC staff along with NGOs (Table 4.14). Ninetyeight percent of ASHAs indicated the
usefulness of the ASHA Day. However, when it came to payment of TA/DA of RS.40/- towards
attending ASHA Day, the matter required close monitoring by program officers. Srikakulam
district results indicate that 97 percent of payments of TA & DA followed by 73-80 percent in
East Godavari, Mahabubnagar, and Karimnagar districts. Sixty percent of volunteers reported
timely payment of TA&DA in Kurnool district which requires improvement in regular
monitoring.
Some of the ASHA’s stated that special incentives were required namely for
conducting survey work (72 percent), increase of PPI incentive (37 percent) followed by
assisting School Health Program (35 percent) (Table 4.15). The CARE organization
intervention through training ASHAs in IYCF aspects improved their knowledge levels on
newborn care in the eight districts.
Moreover the ‘Supplementary Nutrition Model’ initiated by Andhra Pradesh
government under NRHM was a role model for other states to emulate. Under the program
daily nutritious / iron-rich food supply starts from fourth month of pregnancy for all pregnant
women on a daily basis at village-level through self-help groups. A pilot project showed on a
sample of 2150 pregnant mothers, no single case of maternal mortality and the birth weight
of babies were above 2.75 kilograms (The Hindu, 15th December 2008).
Cash Incentives to ASHAs
Almost all ASHAs received cash incentive money for RCH services and FP services.
Majority of ASHAs received incentives for escorting JSY beneficiary for delivery to a hospital
(36 percent) followed by postnatal care (19 percent), at least one ANC by a MBBS doctor (13
percent) and Measles and Vitamin A to the children below one year (11 percent) respectively.
The mean monthly amount received by ASHA volunteer was Rs. 574/- (ranging between Rs.
493 in Karimnagar and Rs. 669 in Mahabubnagar districts). Seven out of ten ASHAs were
unsatisfied with cash incentives as it was ‘too much work with little incentive money’ or
‘because of delays in payments’ respectively.

To sum up, the training strategy of 21 days and 7 days of field training of ASHAS
rendered it possible to deploy them in their villages and we can assess the performance of
ASHAs, as well as suggestions and corrections to be taken up by the mission. ASHA’s
knowledge on various reproductive and child health aspects was good; however, there is a
need for strengthening their knowledge about registration of ANC in first trimester,
consumption of IFA tablets and nutritious food, counseling during ANC on best practices,
new born care etc. ASHAs are coordinating their work with ANM and AW centers and helping
them on immunization day and monthly nutrition days. ASHAs mentioned areas of
strengthening that could be incorporated in refresher training, monthly on-the-job trainings
in the convergence meetings by CARE and NGOs. Timely payment of incentives and dress
code to ASHA are welcomed. The incentives limited to SC and ST groups may be extended to
all pregnant women from other communities who are economically backward.

Table 4.1 – Andhra Pradesh: Profile of ASHA Functionaries
Profile SKLM EG KRL MHBN KRM All
Total number of ASHAs interviewed 176 224 179 165 197 941
Age of ASHA (in completed years)
Below 19 years 1.7 1.3 2.8 6.7 1.0 2.6
20 – 24 years 25.6 15.2 21.2 32.1 35.0 25.4
25 – 29 years 42.0 42.0 34.6 36.4 40.1 39.2
30 – 34 years 19.3 21.4 20.7 17.6 18.3 19.6
35 years & above 11.4 20.1 20.7 7.3 5.6 13.3
Mean (in years) 27.54 29.50 28.97 26.32 26.65 27.88
Year of schooling completed
No formal education 0.6 1.3 1.1 1.8 0.0 1.0
Studied up to 5th class 13.6 17.9 13.4 10.9 7.1 12.8
7th standard 20.5 16.1 17.9 15.8 23.9 18.8
Secondary ( 8 – 10 standard) 60.8 58.5 58.1 65.5 62.4 60.9
Inter and above 4.5 6.3 9.5 6.1 6.6 6.6
Mean (years of schooling) 3.55 3.50 3.61 3.63 3.69 3.59
Caste / Tribe of ASHA
Scheduled Caste & Tribe 48.3 74.1 50.8 40.0 64.0 56.7
Backward Caste 46.0 18.8 36.3 49.1 31.0 35.1
Other Community 5.7 6.7 9.5 9.1 4.1 6.9
Minority 0.0 .4 3.4 1.8 1.0 1.3
Table 4.2 – Andhra Pradesh: Motivation for being an ASHA
Profile SKLM EG KRL MHBN KRM All
Total number of ASHAs interviewed 176 224 179 165 197 941
Means of Selection
Selected/approved by Gram Panchayat 23.9 32.1 6.7 16.4 12.7 18.9
ANM got me selected 32.4 37.5 78.2 64.2 46.7 50.9
Was working as Anganwadi Worker 3.4 0.4 1.7 0.6 2.5 1.7
VHSC 0.6 1.3 0.0 0.0 0.5 0.5
Because of my good nature 0.0 0.0 0.6 1.8 0.0 0.4
Because of Politician / Sarpanch 39.8 26.3 6.7 10.9 17.3 20.5
Mahila Samithi / by PHC members 0.0 1.3 3.9 1.8 3.0 2.0
Others 0.0 0.9 2.2 4.2 17.3 5.0

Profile SKLM EG KRL MHBN KRM All
Reasons for wanting to be an ASHA*
Serving / helping the community 92.6 97.8 81.0 85.5 86.8 89.2
Earning money 78.4 60.3 43.6 47.3 59.9 58.1
To remove misconceptions 5.7 4.9 2.2 9.7 4.6 5.3
Bring awareness on health issues 23.3 38.4 27.4 33.3 23.4 29.4
Save children from dying / for benefit of
children 25.6 46.4 13.4 40.6 11.2 27.8
Others 0.0 0.9 6.1 2.4 1.5 2.1
* Multiple responses
Table 4.3 – Andhra Pradesh : Topics Covered in the Training of ASHA
Profile SKLM EG KRL MHBN KRM All
Total number of ASHAs interviewed 176 224 179 165 197 941
Topics covered during training program for
ASHA*
Women and Health (ANC, breast-
feeding) 100.0 98.7 100.0 95.8 96.4 98.2
Infant and Child Care (Immunization) 97.7 98.2 97.2 98.2 93.4 96.9
ASHA (my eight tasks) 21.0 9.8 18.4 21.2 8.6 15.3
Reproductive and Sexual Health
problems 18.2 17.9 11.7 13.9 16.8 15.8
Aspects on safe drinking water 23.9 33.5 50.8 31.5 31.5 34.2
Disposal of waste water / clean drainage 46.0 56.7 62.6 39.4 55.8 52.6
Nutrition 77.8 70.1 62.0 52.1 69.0 66.6
HIV and AIDS 73.9 81.7 59.2 66.7 82.2 73.4
Curative Care 27.8 62.5 30.2 27.9 42.6 39.6
Organizing a group meeting 6.3 12.5 2.8 14.5 6.1 8.5
Adolescent health education of girls 11.9 46.9 28.5 29.7 36.0 31.6
Management of Diarrhea and
Pneumonia 30.1 33.0 9.5 21.2 25.9 24.4
Family Planning methods 85.2 57.6 39.7 58.2 68.5 61.7
Percent mentioned logistics arrangements at
training were adequate / good
Sitting arrangements 96.6 87.5 82.7 81.8 86.3 87.0
Size of the room 94.9 82.1 86.0 89.1 85.3 87.1
Accommodation facilities 96.0 79.0 83.2 87.9 87.8 86.4
Arrangements for food 91.5 78.6 83.8 73.9 89.8 83.5
* Multiple responses

Table 4.4 – Andhra Pradesh: Actions Supposed to be Taken if ASHA
Recognize Signs of Complications in Pregnant Women*
Profile SKLM EG KRL MHBN KRM All
Immediately refer to the nearest FRU (CHC) 60.8 62.9 61.5 57.0 80.7 64.9
Ask her to consult the ANM the next day 52.8 50.9 31.3 38.2 20.8 39.0
Refer to Govt. accredited hospital 26.1 17.0 28.5 33.3 18.3 24.0
Refer to Private hospital 4.0 4.9 3.9 7.9 12.7 6.7
Call 108 91.5 84.4 72.1 81.2 81.7 82.3
* Multiple responses
Table 4.5 – Andhra Pradesh: ASHA’s Knowledge about Common
Complications during Delivery that could Result into Maternal Mortality
Profile SKLM EG KRL MHBN KRM All
Total number of ASHAs interviewed 176 224 179 165 197 941
Common complications during pregnancy /
delivery that can result into death of a woman*
Excessive bleeding 96.0 95.5 72.1 86.1 77.7 85.8
Tetanus 30.1 73.7 29.1 27.3 50.3 44.0
Blood pressure problem 40.3 52.2 64.8 60.0 46.2 52.5
Abdominal pain 34.1 22.3 8.4 33.3 23.9 24.1
Abnormal position of the foetus 19.9 67.0 34.6 41.2 62.9 46.7
Convulsions / fits 75.6 41.1 46.4 40.6 60.9 52.6
Foetus dies in mother’s womb 13.6 9.8 26.8 32.7 60.4 28.4
Fever 57.4 25.9 37.4 21.8 30.5 34.2
Placenta problems 7.4 6.3 14.5 13.3 11.2 10.3
* Multiple responses
Table 4.6 – Andhra Pradesh: Knowledge about Likelihood of
Neonates Dying after Birth
Profile SKLM EG KRL MHBN KRM All
Total number of ASHAs interviewed 176 224 179 165 197 941
Period (in life) when newborns are most likely
to die
Soon after birth / first day of birth 18.8 20.1 33.5 47.9 36.5 30.7
Within one week of birth 40.9 21.0 22.3 18.8 12.7 22.8
Between one to two weeks of birth 11.4 5.8 4.5 4.2 3.0 5.7
Between 3 – 4 weeks of birth 29.0 53.1 37.4 25.5 43.1 38.7
Others 0.0 0.0 2.2 1.8 3.6 1.5
Don’t Know 0.0 0.0 0.0 1.8 1.0 0.5

Table 4.7 – Andhra Pradesh: ASHA’s Awareness about their Responsibilities
Profile SKLM EG KRL MHBN KRM All
Help in immunization program 100.0 99.1 100.0 98.2 94.4 98.3
Accompanying delivery cases 88.1 90.6 91.1 70.9 81.2 84.8
Create awareness on health 30.7 51.8 49.2 42.4 54.8 46.3
Provide ANC Care 99.4 99.6 97.8 93.9 95.9 97.4
Work with Anganwadi Worker/Dai 27.8 8.5 14.5 24.2 11.7 16.7
Registration of birth and death 80.1 53.1 25.7 50.3 41.6 50.1
Motivating & mobilizing community 39.2 26.3 23.5 26.7 43.1 31.8
Family Planning 84.1 70.1 50.3 66.7 84.3 71.3
Village health planning 27.8 20.5 35.2 37.6 32.0 30.1
Counseling 5.7 23.2 14.0 13.3 9.1 13.5
Promote good health practices 9.7 28.1 27.9 24.2 16.2 21.5
Treatment of minor ailments 39.2 73.7 44.7 41.2 72.6 55.8
Make timely referrals 23.3 34.8 37.4 23.6 23.9 28.9
Increase in Institutional delivery 69.3 59.8 47.5 40.0 56.3 55.0
Participating in National Health Program 63.1 72.3 8.4 33.3 36.5 44.1
Working as DOT provider for TB cases 48.9 72.3 43.6 53.3 69.5 58.6
Table 4.8 – Andhra Pradesh: Networking of ASHA with other Stakeholders
Profile SKLM EG KRL MHBN KRM All
Meet ANM / AWW regularly 98.9 99.6 99.4 99.4 100.0 99.5
Frequency of meeting ANM/AWW in
Village immunization sessions 99.4 100.0 98.3 98.8 98.5 99.0
Help in conducting village surveys 81.8 96.9 89.4 87.9 98.0 91.3
Call ANM/AWW for Nutrition day /
camps 78.4 89.7 89.4 86.7 92.4 87.6
Call all pregnant women for timely ANC 96.0 98.7 96.6 94.5 86.8 94.6
Updating Records
Daily once 30.1 62.9 24.0 23.0 35.5 36.7
Weekly once 35.8 28.6 53.1 48.5 45.2 41.6
Fortnightly 15.3 3.1 5.0 6.1 2.0 6.1
Once in a month 15.3 2.7 14.0 17.6 16.2 12.6
Less frequently 2.3 1.8 0.0 4.2 0.0 1.6
Incomplete 1.1 0.9 3.9 0.6 1.0 1.5

Table 4.9 – Andhra Pradesh: Working Situation of ASHA
Profile SKLM EG KRL MHBN KRM All
Working days back the client availed ASHA services
Mean 4.78 5.73 8.42 8.15 3.50 6.02
Median 4.00 3.00 5.00 5.00 2.00 4.00
Mode 5 2 3 1 2 2
Caste of the client
SC 31.3 35.3 34.6 37.0 52.8 38.4
ST 12.5 12.9 5.0 11.5 1.5 8.7
BC 52.8 30.8 43.0 47.9 41.1 42.4
General 3.4 21.0 17.3 3.6 4.6 10.5
Reasons for interaction or ASHAs contact with them*
Collect medicines for fever, backpain,
vomiting 96.6 88.4 74.9 60.0 88.3 82.4
Pregnant woman for registration 65.9 46.4 71.5 36.4 76.1 59.3
Antenatal care / advise 72.7 67.4 69.3 43.6 64.5 64.0
IFA tablet distribution 55.1 33.0 55.3 37.6 58.9 47.6
Delivery / advice about place of delivery 61.9 48.7 39.1 24.8 27.9 40.8
Helping mother to get JSY for BPL 50.0 27.2 13.4 10.9 26.4 25.8
Postnatal care 52.8 38.8 30.2 20.6 36.0 36.0
Immunization 84.7 81.3 80.4 43.0 90.9 77.0
Information about FP methods 48.3 19.2 25.1 11.5 42.6 29.3
Procuring Mala D and condom 8.5 3.1 3.9 4.8 8.6 5.7
Treatment / advise for pain in lower
abdomen 5.1 4.5 7.8 9.7 4.1 6.1
No. of days since ASHA last accompanied a
woman for delivery 25.46 17.55 28.60 25.46 23.98 23.87
Number of ASHAs who had handled a JSY
case 98.9 99.1 99.4 97.6 95.9 98.2
Percent of ASHAs who stayed with JSY
beneficiary at the place of delivery 99.4 97.7 95.5 82.6 88.4 93.1
Average Days ASHA stayed with JSY beneficiary
at place of delivery 1.77 2.19 1.66 2.25 1.48 1.87

Table 4.10 – Andhra Pradesh: Suggestions ASHAs Work
Profile SKLM EG KRL MHBN KRM All
Suggestions made by ASHA for improving the scheme*
Should get monthly payment 98.9 95.1 70.4 92.7 94.9 90.6
Cash assistance should be more 47.2 50.0 23.5 44.2 49.7 43.4
Some officials / doctors / nurse should
come and talk about JSY 15.9 17.0 5.6 15.2 3.6 11.5
Should give complete information 17.0 25.4 18.4 18.8 36.0 23.6
Lady doctor should be there 7.4 4.0 2.2 10.9 24.9 9.9
Arrangement of transport / bus pass 65.3 55.4 28.5 49.7 57.4 51.5
ASHA should have a dress code 75.0 89.3 46.4 52.7 85.8 71.3
Should get good / practical training for
ASHA 38.6 37.9 26.8 29.7 20.3 30.8
Facilities should be improved 40.9 40.2 14.0 30.3 35.5 32.6
Should use posters, role play for training
ASHA 4.0 12.5 5.6 4.8 2.5 6.2
More incentive for sterilization 38.6 18.8 1.7 21.8 30.5 22.2
More propagation / advertise on TV / Paper 2.3 1.8 3.9 8.5 14.7 6.2
Good behaviour with woman at the place
of delivery 6.8 14.7 4.5 12.7 5.6 9.0
Should get drug or medicine kit 64.8 75.4 36.9 35.2 58.9 55.6
People should recognize me as ASHA 49.4 22.3 10.6 23.0 14.2 23.6
Health systems should deal with myths and
misconceptions 1.1 2.2 0.6 3.6 5.6 2.7
Cash assistance should be given timely,
doctors / ANM should not demand money 6.3 2.7 3.4 7.9 0.5 3.9
Others 6.8 29.0 36.3 9.7 19.8 20.9
* Multiple responses

Table 4.11 – Andhra Pradesh: Challenges faced by ASHAs
Profile SKLM EG KRL MHBN KRM All
Village people are not ready for
institutional delivery 34.7 21.9 15.1 32.1 25.4 25.5
I do not get money on time 45.5 57.6 35.2 52.1 52.8 49.1
Woman do not listen regarding
immunizing child 11.4 9.8 17.9 17.0 7.6 12.4
Opposition from community / illiterate
people 9.1 21.0 6.7 13.3 27.9 16.2
Women are not ready to take IFA tablets 14.2 12.9 5.6 24.2 21.3 15.5
Women do not listen regarding weighing
the baby 4.5 3.1 2.8 8.5 6.1 4.9
ANM does not allow to work 0.0 1.3 1.1 3.0 2.0 1.5
Sterilization cases motivated by us are
registered by ANM 5.7 3.6 2.2 7.3 4.6 4.6
My husband / family do not like my job 38.1 22.3 12.8 23.0 50.8 29.5
Others / doctors says if woman dies it will
be ASHA’s responsibility / other ASHAs take
away my cases
1.1 1.3 3.4 4.8 1.0 2.2
No distinction of incentives for ASHA
working in SC colony and other areas 6.3 9.8 0.6 6.1 14.2 7.7
Table 4.12 – Andhra Pradesh: Reasons for Delay in Incentive Payments
Profile SKLM EG KRL MHBN KRM All
Lack of advance money at the facility 38.6 25.0 11.7 19.4 38.1 26.8
Got money after 2 – 3 months 22.2 29.0 2.8 20.6 32.0 21.9
Delay in payment by ANM 7.4 4.9 1.1 1.8 1.5 3.4
Not getting amount as per entitlement 0.0 0.9 3.4 12.7 1.0 3.3
Delay in approval process 18.2 39.3 73.7 39.4 22.3 38.4
Signing authority not available 0.0 0.0 0.6 2.4 1.5 0.9
Sarpanch not signing 0.6 0.4 1.1 1.2 0.0 0.6

Table 4.13 – Andhra Pradesh: Salary Expected per Month by
ASHA Volunteer as Remuneration
Salary Amount (Rest) SKLM EG KRL MHBN KRM All
<1000 18.8 28.6 56.4 30.3 26.4 31.9
1001-1500 33.0 22.8 17.9 21.2 25.4 24.0
1501-2000 40.9 39.7 19.6 36.4 45.7 36.8
>2001 7.4 8.9 6.1 12.1 2.5 7.3
Total 100.0 100.0 100.0 100.0 100.0 100.0
Mean salary expected is 1600/-
Median salary expected is 1500/-
Mode salary expected is 2000/-
Table 4.14 – Andhra Pradesh: Awareness of ASHA Day Attendance and TA and DA
Awareness SKLM EG KRL MHBN KRM All
Awareness of ASHA day 99.4 100.0 97.2 98.8 100.0 99.1
Attending regularly ASHA day 99.4 100.0 98.9 99.4 99.0 99.4
Usefulness of ASHA day 99.4 100.0 98.9 93.3 98.5 98.2
Receipt of TA/DA for attending ASHA day 97.7 76.3 59.8 80.6 73.1 77.3
Table 4.15 – Andhra Pradesh: ASHAs Expect Incentive for the Activities*
Profile SKLM EG KRL MHBN KRM All
Doing survey work 86.4 84.4 52.5 70.3 62.4 71.6
Assisting school Health prog. 61.9 41.1 20.7 37.6 14.7 35.0
Conducting health Camps 47.2 31.7 14.0 27.3 12.7 26.5
Covering >1000 Population 22.7 10.7 3.9 12.7 16.2 13.2
Increase PPI incentive 42.6 29.9 7.3 28.5 73.6 36.9
Processing to get JSY benefits 26.1 14.3 11.2 13.9 3.6 13.6
Others 3.4 12.9 16.2 9.1 4.1 9.2
*-Multiple responses

CHAPTER-5
BENEFICIARIES OF ASHA FOR DELIVERY CARE
The selection, training, work performance, cash incentives, and suggestions for
improvements were discussed at length in the previous chapter. We have highlighted that
more than eighty percent of clients/ beneficiaries availed ASHA services for escorting delivery
in the medical institution.
The second important intervention after ASHA under NRHM is the Janani Suraksha
Yojana (JSY) all over the country to promote safe delivery practices. Cash assistance is
integrated with antenatal care during the pregnancy period, institutional care during delivery
and immediate post partum period in health continue by establishing a system of
coordinated care by field level health worker.
In the beneficiary survey we interviewed about 1440 JSY beneficiaries in all the
villages who had availed the services of ASHA in the recent past prior to the survey.
Awareness of the programme, complete information, understanding of program, eligibility
criteria of beneficiaries, cash assistance etc play a crucial role in the success of the
intervention.
5.1 Respondent profile
The respondent profile of JSY beneficiaries is presented in Table 5.1. The mean age
of the woman respondent was 22.8 years. Only 3 percent of respondents were aged more
than 30 years. Nine out of ten women respondents were in the age group of 20-29 years.
Forty percent of respondents had no formal education and the figure varied across districts
of Mahabubnagar (64 percent) and Kurnool (51 percent) respectively.
In the sample, less than 11 percent of respondents had passed intermediate and
higher education level. Less than sixty percent (58 percent) of JSY respondents belonged to
BC community (with BPL white card) and remaining 42 percent were from SC and ST
community. The average household monthly income was Rs.2034/- and varied between
Rs.1840/- in Karimnagar and a high of Rs. 2271/- in Mahabubnagar district respectively. About
65 percent of respondents (residing in the ASHA volunteers locality) were providing the
services in the SC/ST and BC colonies respectively.
5.2 Awareness about JSY
The JSY beneficiaries were enquired about how and when they had heard about the
scheme. More than a half (55 percent) of respondents knew about JSY scheme during the
pregnancy and slightly more than
one third (36 percent) of
respondents had heard of it before
being pregnant / before ANC
registration. Regarding the source
from where they heard of JSY, about
82 percent mentioned ASHA
volunteer and 66 percent as ANM.
Around 20 percent of beneficiaries
indicated other sources of
information like T.V, Radio,
Relatives and Gram panchayat
(Table 5.2). The knowledge
regarding JSY scheme in the state
was mainly disseminated through interpersonal communication rather than mass-media
channels.
5.3 Knowledge on JSY Aspects
The JSY beneficiaries were enquired about the details regarding JSY scheme which
they were told. More than sixty percent (66 percent) of the beneficiaries understood that
they would get some money for availing JSY services and thirty six percent (36 percent) heard
JSY as a scheme for promotion of institutional delivery (Table 5.2). About Thirty percent (30
per cent) mentioned the free institutional delivery for poor pregnant women and twentysix
percent (26 per cent) stated that the scheme was intended to improve the intake of
nutritional food for the benefit of
pregnant women. A few
respondents viewed that JSY is for
population control and did not
know about the scheme. Wide inter-
district variations were recorded
regarding the purpose of JSY. It is
essential that correct message is
communicated before ANC
registration. Better BCC is required
to focus correct and consistent
message is disseminated about the
scheme.
Time when Beneficiary heard about JSY
After
Delivery
9.4%
During
pregnancy
54.7%
Before
being
pregnant
35.9%
Before being pregnant During pregnancyAfter Delivery
Score of Beneficiaries heard about JSY
Grade O
10.3%
Grade A
71.6%
Grade B
18.1%
Grade O Grade A Grade B

An attempt was made to score the knowledge levels of JSY beneficiaries. The five
items regarding JSY included were: a) provision of cash incentive for hospital delivery b)
promoting institutional delivery c) family planning d) free institutional delivery for poor
women and e) nutritional benefit and transportation. Each correct response was given one
mark. Responses were categorized into three Grades. Grade O-Don’t Know, Grade A- 1-2
correct responses and Grade B 3- 5 correct responses. Seventytwo percent (72 percent) of
beneficiaries indicated 1-2 correct responses and Eighteen percent (18 per cent) indicated 3-
5 correct responses.
5.4 Utilization of ANC Services by JSY Beneficiaries
The beneficiaries were asked about the month and place of registration for ANC.
Sixty percent of beneficiaries registered for ANC during first trimester. Wide variation was
reported across districts. More than three fourth (79-88 percent) of beneficiaries in East
Godavari and Karimnagar registered for ANC in their first trimester of pregnancy. Less than
half of respondents (46-48 percent) registered in first trimester in Srikakulam and
Mahabubnagar districts followed by 39 percent in Kurnool districts. Three percent of
beneficiaries indicated ‘Don’t Know’ / ‘No contact’. In order to reduce the pregnancy
complications, ASHA volunteers must ensure cent per cent of ANC coverage in first trimester
(Table 5.3). The respondents availed ANC services for the index child from PHC/ Sub centre
(49 percent), private accredited hospitals (32 percent) and Sub-district/CHC (16 percent)
respectively. On an average, four ANC checkups (ranging 1 - 9) were reported during their
pregnancy period by JSY beneficiaries in the selected districts.
5.5 Role of ASHA in Micro-Birth planning
The Micro-Birth planning
includes counseling and informing
the date and place of next check-up,
place of delivery, expected date of
delivery and place of referral in case
of any complications (CORT, 2007).
Majority of beneficiaries had
interactions with ASHA on the
Micro-Birth planning issues.
Eightyfour percent (84 percent) of
beneficiaries informed about the
date of next check-up, sixtyeight
percent had received information
Score of Mocro-Birth Planning
Grade C
26.4% Grade A
12.1%
Grade O
6.1%
Grade B
55.4%
Grade O Grade A Grade B Grade C

on place of delivery, fortysix percent advised on expected date of delivery (EDD) but lower
than one-fifth of beneficiaries indicated that ASHA informed them about the referral place to
visit in case of any emergency. Birth planning is one of the key elements taken up during the
refresher training and ANMs and AW workers interaction sessions (Table 5.4). The responses
of beneficiaries on the aspects of micro-birth planning were scored and data presented. Each
correct response was given one mark for all questions. Responses were categorized into four
Grades. The categorization was Grade O- Don’t Know, Grade A- All correct aspects, Grade B-
2-3 correct aspects and Grade C- only one aspect. It was surprising to find that only twelve
percent of beneficiaries stated all the four aspects, fifty five percent of beneficiaries knew 2-3
aspects and six percent don’t know any of the above. This could be an area that needs
strengthening and can be linked as part of Micro-Birth planning along with other aspects.
5.6 Intention and Actual Place of Delivery
The respondents were asked to state about the place where they intended to deliver
and the place where they actually delivered. Information was cross tabulated and analyzed in
Table 5.5. Eightyeight percentage of beneficiaries interviewed were intending to deliver in an
institution (56 percent in public and 30 percent in private) and remaining, at home. Out of 13
percent of beneficiaries who had intended to deliver at home changed their opinion and
preferred medical institution (11 percent). Among institutional deliveries, majority of
beneficiaries delivered at the private medical institutions as compared to public institutions.
The motivating factors for institutional deliveries are given in Table 5.6. Sixtynine
percent of beneficiaries reported safety to mother and child for choosing institution delivery
followed by 63 percent due to monetary benefits offered under JSY scheme. Twentyeight
percent of beneficiaries were motivated ‘due to better access of service at medical institution
in the nearest locality’ and ‘support provided by ASHA’. Less than ten percent were motivated
due to compulsion like ‘the previous birth in hospital’ and ‘availability of transport’ for
availing services from medical institutions.
5.7 Process of Arranging Transport
Some of the major delays in accessing health services during delivery were time
taken in recognizing the problem, arranging the transport, travelling time and delay in
getting services after reaching the place of delivery. The Andhra Pradesh Government as part
of the NRHM intervention introduced 108 emergency rural medical health ambulances
throughout the state and the field experiences indicate that people were very quite familiar
with the scheme and availing the services.

In the case of ninetytwo percent of JSY beneficiaries, transport facility for shifting
from home to medical institution was arranged by family members. The ASHA volunteer
arranged transport for 16 percent of beneficiaries while ANM, AWW/SHG and relatives also
played a role (10 percent) in arranging transport. Regarding time of reaching the place of
delivery, it can be observed that 64 percent beneficiaries reached the facility during the day
(between 6 am and 6 pm) followed by 24 percent during late evening (between 6 pm to 12
am) and the remaining 12 percent, at early hours.
Concerning accompanying of beneficiaries to health facility, it was reported that
mother of the beneficiary, husband and other family members were commonly cited. Seven
out of ten were accompanied by mother, followed by husband 56 percent and mother–in-law
32 percent. In the selected districts, about 49 percent in Kurnool and a maximum of 66
percent in East Godavari districts, ASHA volunteers accompanied the JSY beneficiary for
delivery. The field observations indicated that presence of ASHA in the hospital provided a
physical assurance to the family members and the beneficiaries also indicated that they
received timely services due to the presence of ASHA at the time of delivery.
5.8 Motivation for Institutional Delivery
The monetary benefits offered under JSY (63 percent) and for safety of mother and
child (69 percent). Twentyeight percent of beneficiaries (Table 5.6) of JSY were motivated
because ASHA support in natal and at delivery time. One interesting observation of the study
is that ASHA volunteers were also playing crucial role in decision making for institutional
delivery on par with the mother-in-law and husband and other family members. The role of
ASHAs was very significant in decision making regarding institutional delivery and
discouragement of home deliveries.
5.9 Quality of Services Available at the Place of Delivery
The study attempted to ascertain the quality of services at the place of delivery like
promptness in attending on the delivery case, waiting time, persons attending on the
delivery etc. On an average, the study found that it took 12 minutes to complete the
administrative process at the hospital. About 94 percent of JSY beneficiaries were admitted
in the health facility between 10- 30 minutes of duration by the hospital staff. The time taken
to attend on the delivery was below 10 minutes as indicated by 48 percent of beneficiaries
and 30 minutes as indicated by 11 percent after reaching the hospital respectively. About 70
percent of deliveries were normal, 2 percent were assisted and 29 percent were caesarean
deliveries.

5.10 Impact of JSY on Institutional Delivery
The JSY beneficiaries were asked about place of delivery of the last child born prior
to the index child of JSY beneficiaries interviewed. Out of 1145 total beneficiaries only 745
had history of previous child birth. Data from these 745 beneficiaries was cross tabulated by
place of delivery of previous child with that of the index child. In other words, the analysis
would indicate a shift in place of delivery before and after introduction of JSY. It was
observed that 610 JSY beneficiaries in the preceding index child birth had an institutional
delivery while the remaining 135 (18 percent) were home deliveries (Table 5.7). In case of
index pregnancy, 730 (98 percent) births were institutional and only 15 (2 percent) births
were home deliveries. It may however be mentioned here that this can not be generalized as
the sample had been confined to only those who had availed JSY. The results may be
considered as indicative of their change in behavior.
5.11 JSY beneficiaries- Place and type of delivery
The study tried to ascertain the place of delivery and type of delivery in the selected
districts. Almost 98 percent of beneficiaries delivered at medical institutions in all the five
selected districts. Fiftyone percent of deliveries were conducted in public institutions and 47
percent in private nursing homes and private hospitals (Table 5.8). A comparison of inter-
district variations of JSY beneficiary deliveries indicated that 32-49 percent of deliveries were
conducted in private hospitals (except 82 percent in Karimnagar district). The JSY beneficiary
deliveries indicating that 66 percent were normal and 32 percent caesarian sections followed
by assisted deliveries (2 percent). The caesarian sections varied from 22-26 percent in
selected four districts and recorded more than fifty percent in Karimnagar district (Table 5.9).
5.12 Role of ASHA in JSY
ASHAs briefed women about the JSY. ASHAs informed the JSY beneficiaries about
early registration in first trimester, hospital delivery and postnatal care. Higher percentage
of JSY belonged to SC/ST and BPL group, availed the benefits and was satisfied about the role
played by ASHA. This is evident from the beneficiary assessment wherein it was found that
they were supportive right from pregnancy to child birth in three-fourth of deliveries. The
ASHA role in motivating beneficiaries for institutional delivery services and accompanying
them to institutions has emerged significantly. The deliveries conducted in both public and
private institutions were almost equal in all districts except in the case of Karimnagar district.
Why the beneficiaries in Karimnagar district were more inclined towards private institutions
for ANC, delivery care require further probing.

Table 5.1 – Andhra Pradesh: Respondents’ Profile of ASHA Beneficiaries
Profile SKLM EG KRL MHBN KRM All
Age(Completed years)
Below 19 4.0 7.0 8.7 7.2 4.9 6.4
20-24 69.0 72.9 72.6 64.6 57.0 67.9
25-29 25.2 18.6 15.2 23.6 34.8 22.9
30 years or more 1.8 1.5 3.5 4.6 3.3 2.8
Education
No formal education 37.4 19.5 50.6 63.7 32.8 39.7
Up to 5th 20.2 27.7 19.7 10.5 22.5 20.6
Passed 7th 9.2 12.8 8.7 4.6 12.7 9.8
Studied 8 to 10th 26.1 28.7 17.1 12.7 25.8 22.8
Passed Intermediate & above 7.1 11.3 3.9 8.4 6.1 7.4
Religion
SC\ST 39.0 58.8 33.5 45.31 32.0 42.1
Others 61.0 41.2 66.5 54.9 68.0 57.9
Table 5.2 – Andhra Pradesh: Place and Source of Information Received about JSY
Profile SKLM EG KRL MHBN KRM All
Source of JSY information
ASHA 98.5 83.2 72.6 77.2 73.0 81.7
AWW/center 35.0 4.6 5.2 19.8 18.9 16.5
MPHA(F) 92.0 50.0 70.0 55.3 56.1 65.7
Television 17.8 10.1 3.2 2.1 1.6 7.6
Doctor 25.2 11.0 20.3 17.7 3.7 16.1
Relative 15.0 6.1 5.2 6.3 2.5 7.3
Other JSY Beneficiary 44.8 10.4 28.7 19.4 7.4 23.0
Radio 3.7 0.9 0.6 1.3 - 1.4
Gram Panchayat 1.5 6.4 1.9 3.4 - 2.8
Information heard about JSY
Get cash incentive for Hospital deliveries 93.9 59.5 60.6 73.4 39.3 66.4
Promotion of Institutional Deliveries 43.9 50.3 31.0 34.6 17.2 36.5
Family Planning 40.5 19.2 11.9 14.3 9.8 20.1
Free intuitional delivery services for poor
women
28.8 37.5 35.5 26.2 18.0 30.0
For intake of nutrition food 8.0 39.3 19.4 14.8 54.1 26.4
For rich & influential families 1.8 6.1 0.6 1.7 0.8 2.4
Population control/take care of Newborn
care
1.2 3.7 0.6 1.7 2.5 1.9
Do not know/can’t say 0.3 1.5 3.5 4.6 6.1 3.0

Table 5.3 – Andhra Pradesh: Stage of Pregnancy and Place of Registration for ANC
Stage of Pregnancy of Woman for
Registration SKLM EG KRL MHBN KRM All
First Trimester 48.8 88.4 39.0 45.6 78.7 60.2
Second Trimester 46.9 7.6 49.7 45.1 14.3 32.8
Third Trimester 3.7 2.7 9.7 6.3 1.2 4.8
After delivery 0.3 - - - - 0.1
Do not know 0.3 1.2 1.6 3.0 5.7 2.1
ANC services for index child
PHC/Sub Centre 66.3 59.8 40.3 50.6 21.3 49.1
Dist Hosp/CHC 22.0 11.3 21.9 15.6 5.3 15.8
Private accredited Hospital 11.7 25.9 35.8 28.4 65.6 31.8
AW Centre - 0.3 1.0 3.8 - 0.9
Other - 2.7 1.0 1.6 7.8 2.4
Total 100 100 100 100 100 100
Table 5.4 – Andhra Pradesh: Micro-Birth Planning of JSY Beneficiaries
Information on ANC SKLM EG KRL MHBN KRM All
Date of next check up 98.5 77.4 82.3 82.3 79.9 84.4
Date of expected delivery 57.5 40.9 42.6 50.2 38.1 46.1
Place of delivery 88.3 59.1 77.7 61.2 44.7 67.6
Place of referral in case of complications 16.3 7.6 21.3 17.7 18.4 16.0
Table 5.5 – A.P: Responses of JSY Beneficiaries about
Intended and Actual Place of Delivery
District
Home Delivery Govt. Hospital Private Hospital Percentage change between
intended & actual
Intended Delivery
took place Intended
Delivery
took place Intended
Delivery
took place Home
Govern-
ment
Hospital
Private
Hospital
Srikakulam 15.6 0.6 69.4 66.4 14.7 33.0 -96.1 -4.3 124.9
East Godavari 5.2 0.9 57.6 49.8 37.2 49.2 -83.1 -13.5 32.3
Kurnool 16.8 1.9 59.7 58.8 23.5 39.3 -89.0 -1.5 67.2
Mahabubnagar 17.7 6.5 63.3 56.7 19.0 36.8 -63.0 -10.4 93.7
Karimnagar 11.5 2.2 26.2 17.5 62.3 80.3 -80.9 -33.2 28.9
ALL 13.1 2.2 56.4 51.4 30.4 46.4 -83.2 -8.9 52.6

Table 5.6 – Andhra Pradesh: Factors Motivated
JSY Beneficiary for Opting Institutional Delivery
Factors SKLM EG KRL MHBN KRM All
Money available under JSY 71.7 64.6 43.9 67.9 39.8 62.6
Better access to Institutional delivery
services
30.1 26.6 37.1 29.5 16.0 28.4
For safety of child /mother 68.4 57.0 79.0 65.0 78.7 69.3
Support provided by health personnel 14.1 15.5 14.8 11.8 19.7 15.2
Had health problems 21.8 17.4 17.4 13.1 29.5 19.7
Support provided by ASHA 15.0 19.2 14.5 25.3 10.2 28.0
Previous child born in hospital 12.8 5.5 5.8 7.6 19.7 10.0
Availability of transport assistance 17.2 4.9 2.3 8.0 21.7 10.4
Previous caesarean, miscarriage 0.9 18.0 3.2 3.4 3.7 6.2
Table 5.7 – Andhra Pradesh: Shift in the Place of Delivery Before and After JSY
Particulars For last but one child For last (JSY) child
Place of delivery
Institutional 82 (610) 98 (730)
Home 18 (135) 2 (15)
Number of beneficiaries with two or more children : 745
Table 5.8 – Andhra Pradesh: Place of Delivery of JSY Beneficiaries
Place of delivery
District Home Public Private All
Srikakulam 0.9 66.7 32.4 100.0
East Godavari 1.8 48.9 49.2 100.0
Kurnool 1.0 58.4 40.6 100.0
Mahabubnagar 5.6 54.5 39.8 100.0
Karimnagar 0.9 17.5 81.7 100.0
All 1.9 50.9 47.2 100.0

Table 5.9 – Andhra Pradesh: Type of delivery of JSY Beneficiaries
Type of Delivery
District Normal Assisted Caesarian All
Srikakulam 76.9 0.9 22.2 100.0
East Godavari 73.2 2.5 24.3 100.0
Kurnool 75.3 1.3 23.4 100.0
Mahabubnagar 72.7 0.9 26.4 100.0
Karimnagar 42.3 5.7 52.0 100.0
All 65.9 2.1 32.0 100.0

CHAPTER 6
SUMMARY AND RECOMMENDATIONS
In this evaluation study an attempt has been made to understand the process
adopted for operationalization of ASHA intervention in the state of Andhra Pradesh. ASHA
volunteers were interviewed to assess their awareness of topics in the training, work
performance, suggestions and cash incentives. Besides, the study also interviewed ASHA
beneficiaries (who were JSY beneficiaries and availed institutional delivery) from the same
villages where the ASHAs were working. The study as a whole yielded better understanding
of the implementation of ASHA and the ways to improve the programme.
The Government of Andhra Pradesh adopted an innovative approach, and initiated 21
days in-house training in every district headquarters covering 180 – 200 ASHAs every month
differing from the GOI - proposed training of 23 days duration spread over five exposures in
a year period. The key for the success of Andhra Pradesh model of ASHAs training in a
record period of 18 months was attributed to the triangulation of coordination among the
two government departments and the NGO (Academy of Nursing Studies). A negligible
percentage (below two percent) of ASHAs discontinued the residential training due to health
reasons and family problems indicating that well planned and designed training programs
will discount the common perceptions that women may not prefer long duration training.
The revised training strategy in the State enabled to train all the ASHA Volunteers (one per
1000 population) who could be deployed in their respective villages within two years of
introducing NRHM.
In general the ASHAs were selected as per norms in terms of age, education
qualification, residence in village etc. ASHAs were questioned about the topics covered in the
training. The spontaneous responses for the aspects of women health, infant and child care,
eight tasks of ASHA, nutrition and HIV/AIDS were satisfactory. As majority of ASHAs had 18 –
24 months of service, there is a need to strengthen knowledge on the above aspects in the
refresher training, CARE ASHA Day convergence meetings and on-the-job trainings.
In executing their role as ASHAs, they were networking with various stakeholders
other than Anganwadi Workers and ANMs and the community started recognizing the work
of ASHA. Performance-based cash incentives to ASHAs were untimely and there were delays
in payment. Majority of ASHAs were dissatisfied with the incentives and felt receiving ‘less
money’ for ‘higher work load’.
About JSY, inter-personnel communication played a vital role in disseminating
information regarding JSY. Around 48 percent of the beneficiaries belonged to SC/ST and 52
percent had BPL card. Most of the beneficiaries (55 percent) heard about JSY during

pregnancy through ASHA and ANMs, but their knowledge about different aspects of the
scheme was inadequate. Aspects pertaining to micro-birth planning by ASHAs to the
beneficiaries require improvement in order to help reduce MMR and IMR. The JSY along
with ASHA schemes have brought awareness among poor and socially disadvantaged
population. The preliminary observations of place of delivery of the last child prior to the
index child of JSY beneficiaries interviewed showed a shift from home to institutional
deliveries.
As for the private sector in JSY, almost 40 – 50 percent deliveries were conducted in
private nursing homes / hospitals. In Karimnagar district more than three-fourth of JSY
beneficiaries availed ANC, delivery from the private sector institutions. However the rate of
Caesarian sections (more than 50 percent) in the district is alarming and require further
probe.
Recommendations
Important recommendations stem from an analysis of the findings and discussions
with stakeholders. These findings are organized in three groups namely policy, programme
related and demand-side issues.
Policy
The Commissionerate of Family Welfare and the Academy of Nursing Studies have
mainly shouldered the implementation of ASHA intervention. At the field level, monitoring,
supervising and providing support of ASHA is the need of the hour.
1. The Senior DPHNOs who are actively involved during training should be made
in-charge at district level to monitor and supervise ASHA. The ASHA Day and
convergence meeting must be monitored by senior DPHNO by provision of
vehicle for 8 – 10 days a month.
2. The PHC DPHNOs / Nodel Officers knowledge on IYCF required updation in order
to train the ASHA on these aspects during ASHA Day.
Programme Management
1. ASHA Resource Centre / State Health Resource Centre should pay more attention
to monitoring, supervising, re-training and improving knowledge of ASHAs in the
different PHCs in the State.

2. Continuing education is an important component and has to be supplemented in
all districts of IYCF aspects by CARE and NGOs.
3. Timely release of incentives for all sections of population.
4. Provision of the Iron and nutrition supplements implemented in the pilot
districts has been a success and needs to be extended to all districts in order to
achieve NRHM goals.
Demand Generation
There is a need to develop programme-related communication at different levels.
Communication interventions were limited to disseminating guidelines in the form of
circulars and media activities like radio / TV programmes, posters etc. The recent attempts
namely :
a) Scrolling on TV channels made an impact on Family Planning and this must be
extended to propagate good healthy practices messages.
b) State should conduct re-orientation programmes for medical and health
department for effective dissemination of ASHA and JSY.
Notes:
1. According to the State PIP (2005-06), under the Maternal Health Interventions at
village level the Mission Director, RCH-II (later named as NRHM) initiated the
village level Women Health Volunteers Programme. The purpose is to identify,
train and position Women Health Volunteers (WHV) in the Gram Panchayats in
the state to act as health resource persons-of- first-resort in all Panchayats on all
maternal and child health matters in the villages, and to act as link-persons
between the community and the service providers in these villages. The WHVs
will be identified and selected by the village community through interactive
process in which all the members of village Mahila Swastha Sangh, Micro-credit
group leaders, women ward members of Gram Panchayat etc.
2. The NRHM launched Safe Motherhood interventions in the form of Janani
Suraksha Yojana (JSY) for reducing maternal and neo-natal mortality. In availing
institutional delivery services, the client needs escort and transport to reach the
institution and in case of complications, referral services are required. The
scheme considered all these elements and made provision for transport including
referral and escort and at the same time invested in improving public health
institutions and services through the Reproductive and Child Health (RCH)
Programme interventions. This scheme was started during the year 2005-06 with
an objective to encourage pregnant women for institutional delivery in
Government / Private Institutions in A.P. Under this scheme Rs.1000/- (Rs.700/-
under JSY (GOI) + Rs.300/- under Sukhibhava (State) scheme) is being paid to

rural BPL woman who undergoes an institutional delivery. From 1st April 2006,
JSY has been extended to BPL urban families also. 3.06 lakh beneficiaries have
been covered under JSY scheme during financial year 2007-08 (up to Dec-2007).
3. Field experience in certain tribal PHCs indicated that the tribal women/ families
are not interested to choose institutional delivery even after persistent
counseling by ASHA. They respect the customs rather than preferring
institutional deliveries.
4. The average incentive of Rs. 462 includes only for RCH services and did not
include incentive of RS. 150/- provided for accompanying family planning
operation cases.
5. CARE agency in Andhra Pradesh spread their activities in eight districts
(Srikakulam, Vizianagaram, Visakhapatnam, Khammam, Warangal, Karimnagar,
Nizamabad and Medak) and started the three hour convention session on ASHA
Day (last Tuesday of the month) and helping the ASHAs improve their knowledge,
skills and capacity building activities. ASHAs are supposed to visit newborn
houses and advise on infant feeding and other aspects using the home visit
planner developed by the agency.

References
Accredited Social Health Activist (ASHA) - Guidelines (2005), Ministry of Health & Family
Welfare, Government of India.
Ashtekar S (2008),’ The National Rural health Mission: A Stocktaking’, Economic and Political
Weekly, September 13, 2008, pp. 23-26.
Bajpai N, R.H.Dholakia and J D Sachs (2008), ‘Scaling up Primary Health Services in Rural
India: Public Intervention Requirements and Health Sector Refors: Case Studies of Andhra
Pradesh and Karnataka’, CGSD Working Paper No.33, The Earth Institute at Columbia
University, www.earth.columbia.edu
CORT (2007), ‘Assessment of ASHA and Janani Suraksha Yojana in Orissa’, Centre for
Operations Research& Training, Wadodara.
Indian Institute of Health and Family Welfare (2008 Annual Report 2007-08. IIHFW,
Hyderabad
National Rural health Mission (2005), Meeting people’s health needs in rural areas,
Framework for Implementation 2005-2012. Ministry of Health and Family Welfare,
Government of India.
Premchand Babu and K. Anand Reddy (2006),’ Training of Women Health Volunteers, A.P
experience’, Health Action, 23-25, Health Action, June 2006.
Rajyalakshmi, TK (2008),’Health Care –Gaps in a Mission, downloaded from Website
Satpathy, S.K and S. Venkatesh (2006), ‘Human Resources for Health in India’s National Rural
Health Mission: Dimensions and Challenges’, Regional health Forum, Vol. 10, No.1, 2006
Sharma, R (2007),’ Janani Suraksha Yojana: A Study of the Implementation Status in Selected
Districts of Rajasthan, Population Research Centre, Mohanlal Sukhadia University, Udaipur
Srinivasa Rao, M.S (2007), ‘Training of Women ‘NRHM Newsletter, Vol.2, No.3, March, 2007
Suneela Garg and Anita Nath (2007), ‘Current Status of National Rural health Mission’, Indian
Journal of Community Medicine, Vol. 32, No.3, July 2007
The Hindu ’Emulate Andhra Pradesh Model’, National Rural Health Mission lauds
supplementary nutrition for pregnant women. (15th December 2008)
Umesh Kapil (2006), ‘NRHM: Training of Health Functionaries’, (letter to the Editor), Indian
Journal of Pediatrics, Vol.73, March 2006.
Satpathy, S K and S. Venkatesh (2006),’ Human Resources for Health in India’s National Rural
Health Mission: Dimensions and Challenges’, Regional Health Forum, Vol. 10, No.1, 2006.

APPENDIX-2
SRIKAKULAM DISTRICT
Code Mandal PHC Code Sub centre Name of the village
1 Ranasthalam Ptharlapally 1 1.Kothapalem 1.Kothapalem 2. Jeerupalem
2 S.R.puram 3. S.R.Puram 4. Garikapalem
3 Pydi Bhimavaram 5. Pydi Bhimavaram
4 Kammesigadam 6. Velupurai 7. Arjunuvasala
5 Thippavalasa 8. Thippavalasa
2 Amadalavalasa Thogaram 6 Korlakota 9. Korlakota
7 Thogaram 10.Muddadpet
8 Buddadpet 11. PS Pet
9 Vedullavalasa 12. Vedullavalasa
13. Thurakapeta
10 Edurulavalasa 14. Bobbilipeta
11 Akkulapeta 15. Mondigam 16. SRC peta
12 Chittivalasa 17. Ponnana Peta
18. Gajulakullivalsa
3 Veeragattam Bittiwada 13 Hussanpuram 19. Konchali 20. Hussanpuram
14 Vandava 21. Adaru 22.Vanduva 23. Judi
15 Bittivada 24. Palametta 25. Bittivada
16 Neelanagaram 26. Neelanagaram
4 Seethampet Seethampet 17 Sanegendi 27. Sanegendi
18 Goidi 28. Goidi 29. Pattikagude
19 Devanapuram 30. Devanepuram
31. Sankkilligude 32. Pedaram
20 Seethampeta 33. Seethampeta 34.Vaiageoda
35. Kariguda
5 Rajam Pogiri 21 Polapeta 36. Rucchimpeta
22 Rajam 2 37.Mallikarjuna Colony
38. GayatriColony
23 Guravam 39. V.R. Agraharam 40. Guravam
24 Pogiri 41. Pogiri
6 Laxminarayapeta Laxminarayapeta 25 Ravichandra
42. Danukuvada
43. Ravichandra
26 Siddantham 44. Siddantham
45. Samanthapuram
27 Chorling 46. Pusam
28 Dabbapadu 47. Dabbapadu
29 Lommuvalasa 48. Moduguvalasa
49. Kommuvalasa
30 Laxminarayanapet 50. Laxminarayanapet

Code Mandal PHC Code Sub centre Name of the village
7 Sarubujjali Sarubujjali 31 Purushothapuram
51. Peddapalem/Chinnapalem
52. Purushothapuram
32 Galantri 53. Galantri
33 Sarubujjali 54. Marripadu 55. Vennilavalasa
34 Kothakota 56. Kothakota
35 Yaragam 57. LPM Agraharam
58. Pathapadu
36 Rottavalasa 59. Rottavalasa
37 Peddalavelapuram 60. Buridilavala nagar colony
8 Srikakulam Singupuram 38 Mavarambad 61. Mavarambad
39 Karimillapeta 62. Karimillapeta
40 S S valasa 63. Byrivanipeta
41 Eappli 64. Balivada
42 Peddapadu 65. Peddapadu
43 Singupuram 66. Singupuram
9 Echerla Echerla 44 S N puram 67. Lingalpeta
45 Kusalpuram 68. Kusalpuram
46 Allinagaram 69. Chilakalapalem
47 Pudivalasa
70. Venkatapuram
71. Sanapanvanipet
72. Pudivalasa
48 Jarjam 73. Jarjam
10 Hiramandalam Hiramandalam 49 Thulagam 74. Thulagam
50 Kittlapadu 75. Kittlapadu 76. Rillivalasa
51 Patha
Hiramandalam
77. Chinnakollivalasa
78. Patha Hiramandalam
52 Pedasakili 79. Subalari Colony- 2
53 Hiramandalam 80. Hiramandalam
54 Solipi 81. Padali
11 Saravakota Saravakota 55 Navathala 82. Savarabonthu 83. Patouru
56 Saravakota 84. Vaddinevalasa 85. Garibanda
86. Pedda Ratyba 87. Saravakota
57 Chinnagujjuwada 88.Saravabejji
89. Chinnagujjuwada
58 K S palli 90. Marripadu 91. K S palli
59 C N K paidu 92. Ryaveda 93, Burijavada
12 Kanchili Kanchili 60 P Shesanam 94. P Shesanam 95. J Shesanam
61 N S colony 97. S Baramali
98. Manikyapuram 99. Bugabelli
62 Kattivaram 100. Kattivaram 101. Peddatula
63 Kanchili 102.Purshothamapuram
103.Kanchili 104.Golla Kanchili

Code Mandal PHC Code Sub centre Name of the village
13 Palasa Rentikota 64 Chinnabandam
105. Garuda Khandi
106. Guralapuram
65 B Tharala 107. B Tharala
66 Rangoli 108. Rangoli 109.Manedimatu
67 Savagangaripuram 110. Sanagangaripuram
68 Kasibugga 111. Kasibugga
14 Tekkali Konasalakothur 69 Nawpada 112. Nawpada
70 Nawathala 113. Nawathala 114. Jandapeta
71 Ranivalasa 115. Jolusurepally
116. Bagovanpura
72 Pedasane 117. Polavaram
73 Jaganathapuram 118. Narasingapally
74 Tekkali 119. Tekkali
15 Nandigama Nandigama 75 Nandigama
120. Kottavalasa 121. Swamypeta
122. Pallavalasa
76 Raipuram 123. Raipuram 124. Belchi kolla
77 K Thambur 125. Devapuram
126. K. Thumbur
78 Haridasupuram 127. Haridasupuram
EAST GODAVARI DISTRICT
Code Mandal PHC Code Sub centre Name of the village
1 Rajanagaram Rajanagaram 1 Kalaracherla 1.Kalaracherla
2 Thokada 2. Thokada
3 Srirampuram 3. Srirampuram
4 Konda Guntur 4. Konda Guntur
5 Punya Shatram 5. Bhupalapatnam
6 Chekradwarabandham 6. Chekradwarabandham
2 Gandepalli Gandepalli 7 Gandepalli
7. NT Rajapuram
8. Singarampalem
8 8. Neeladrirao pet 9. Neeladriraopet
9 Yellamilli 10. Borrampalem
10 Surampalem 11. Surampalem
11 Mallepalli 12. Mallepalli
3 Razole Tatipaka 12 Kadali 13. Kadali
13 B Savaram 14. Palagummi 15. B. Savaram
14 Konavaram 16. Mulikipalli
15 Katrenipadu 17. Katrenipadu
16 Vegivaripalem 18. Vegivaripalem

Code Mandal PHC Code Sub centre Name of the village
4 Mamidikuduru Nagaram 17 Appanapalli 19. Appanapalli
18 Magatapalli 20. Magatapalli
19 Pasarlapudi lanka 21. Pasarlapudi Lanka
20 Mamidikuduru 22. Mamidikuduru
21 Magallakuduru 23. Geddada
22 Edarada 24. Makanapalem
5 P Gannavaram Gannavaram 23 Modupu lanka 25. L Gannavaram
24 P Gannavaram 26. Y S Palem
25 Narendrapuram 27. Narendrapuram
26 K Manjavaram 28. K Manjavaram
27 Vadrevupalli 29. Vadrevupalli
28 Udimudi 30. Udimudi
6 Ambajipet Ambajipet 29 Pulletukuru 31. K V Lanka
30 Moosampally 32. Irusumanda
31 G Agraharam 33. G. Agraharam
32 Nandapudi 34. Nandhapudi
33 K Pedapudi 35. K Pedapudi
34 Mukkamala 36. Mukamala
7 Amalapuram Bandarulanka 35 Batnavilli 37. Reddipally
36 Sakurru 38. Sakurru
37 Rollapalem 39. Rollapalem
38 Janipalli 40. Janipalli
39 Samanasa 41. Samanasa
40 Eedharapalli 42. Eedharapalli
8 Mummidivaram KothaLanka 41 Kotha Lanka 43. Karrivani revu
42 Thane lanka 44. Pallavari palem
43 Annampalli 45. Annampalli
44 Mummidivaram 46. Mummidivaram
45 Rajupalem 47. Rajupalem
46 Ananthavaram 48. Ananthavaram
9 Seethanagaram Seethanagaram 47 Chinakondupudi
49. Chinakondupudi
50. Cheepurupalli
48 Vangalapudi 51. Singavaram
49 Mulaka Lanka 52. MulakaLanka
50 Lankuru 53. Lankuru
51 Munikudali 54. Katavaram
10 Rampachodavaram Pedageddada 52 Pedageddada
55. Chinageddada
56. Sokulagudem
53 Lankapakalu 57. Peerukonda 58.Thiragathi
Rollu 59.Yarlamamidi

Code Mandal PHC Code Sub centre Name of the village
54 Kakawada
60. Annampalli
61. Chelakaveedhi
62. Suvarlawada
55 Musurumilli 63. Bornagudem 64.
ChinaBarangi 65. PedaBarangi
11 Y. Ramavaram Chavitidibbalu 56 P V padu 66. Tunikalapadu 67. Dalipadu
57 Bandigadda 68. Rachapalem
58 Yarlagadda 69. Vankabusi 70. Vattigadda
71. P Yerragonda
59 Chaviti Dibbalu 72. Thotakurapalem
73. Devaramadugu
60 Panasalapalem 74. Kokita Gondhi
75. Varnamamidi Gondhi
61 Y Ramavaram 76. Chinta Karrapalem
77. Chamagadda
12 Korukonda Kotikesavaram 62 Butchampet
78.Butchampet
79. Gummaluru
63 Bolladdupalem 80. Bolleddupalem
81. Raghavapuram
64 Kotikesavaram 82. Koti
65 S R Patnam 83.Sri Rangpatnam
13 Kirlampudi Kirlampudi 66 Rajupalem 84. Mukkollu 85. R.K puram
67 Srungarayunipalem 86. SrungaRayunipalem
68 Chillangi 87. Chillangi
69 Tamarada 88. Ramachandrapuram
70 Somavaram 89. Krishnavaram
14 Anaparthi Ramavaram 71 Ramavaram 90. Ramavaram
72 Polumuru 91. Polumuru
73 Anaparthi 3 92. Anaparthi savaram
74 Anaparthi 4 93. A. Kothuru
75 PRC puram 94. Peera Ramachandrapuram
95. Dumpalapudi
15 Rayavaram Machavaram 76 Chelluru 2
96. Buttayapet
97. Battulavari savaram
77 Venturu 98. Naralapet 99. Challangipet
78 Machavaram 100. Machavaram
79 Pasalapudi 1 101. Naralapalem
80 Chelluru 1 102. Chelluru

KURNOOL DISTRICT
Code Mandal PHC Code Sub centre Name of the village
1 Owk Owk 1 Singampalli 1. Singampalli
2 Uppalapadu 2. Uppalapadu, 3. Kanukunta
3 Peddakottalu 4. G. Singaram,
5. Peddakottalu
4 Cherlopalli 6. Sangapatnam
2 Atmakur Bairutla 5 Nallakaluva 7. Rudrakodurugudem
6 Byrutla 8. Siddapuram
7 Siddapalli 9. Musrapalli
8 Karivena 10. Charaka colony
9 Venkatapuram 11. Krishnapuram.
12 Venkatapuram
10 Atmakur 6 13. Atmakur 6
3 Nandyla Chapirevula 11 Chapirevula
14. Chapirevula,
15. Bapujinagar
12 Poluru 16. Venkateswapuram
13 Pusuluru 17.Pusuluru
14 Kanala 18. Kanala
15 Peddakottla 19. Peddakottla
4 Gonegandla Gonegandla 16 Gonegandla 20. Gonegandla
17 Gonegandla 2 21. Bc colony
18 Korur 22. Bodepadu
19 Alwada 23. Alwada,
24. Peddamarrireddy
20 Ontedidinne 25. Yernabadu
5 Adhoni Peddathumbalam 21 Narayanapuram 26. Chagi, 27. Dhanapuram
22 Arekallu 28. Arekallu
23 Kadhithota 29. Kadhitota
24 Peddathumbalam 1 30. Peddathumbalam 1
25 Virupapuram 31. Rajivnagar
6 Bandiatmakur Bandiatmakur 26 G.Lingapuram 32. G.Lingapuram,
27 G.C. Palem 33. G.C. Palem,
34. Navallakunta
28 Singavaram 35. Singavaram
29 Narayanapuram 36. Narayanapuram,
37. Chinnadevurapuram
7 Banaganipalli Pulukur 30 Palukuru 1 38. Devanagar
31 Palukuru 2 39. Palukuru 2
32 Nandivargam
40. Nandivargam,
41. Thimmapuram
42. Padlapuram
33 Berval 43. Berval

Code Mandal PHC Code Sub centre Name of the village
8 Aspara Aspara 34 Yettakal 44. Yteekal
35 Thagaradhone 45. Thagaradhone
36 Aspari 1 46. Aspari 1
37 Bingari 47. Bingari
38 Billakal 48. Putakalamarri
39 Aspari 2 49. Chirumanidoddi
9 Allagadda Ahobilam 40 Bachipalli 50. Kodampalli
41 Allagadda 2 51. Allagadda 5 Ward
42 Nallagatta 52. Nallagatla
43 Chinnakandukur 53. Chinnakandukuru
44 Allagadda 4 54. Gubagudem, 55. Ward- 4
10 Kalluru Ulindakonda 45 Kongapadu
56. Kollampalli thanda
57. Kongampadu
46 Chinnatekuru 58. Chinnatekuru,
59. Thadamkampalli
47 Bastipadu 60. Basthipadu, 61. Bollaram
48 Ulindakonda 62. Ulindakonda
11 Sirivella Sirivella 49 Sirivella 4 63. Sirivella 4
50 Sirivella 3 64. Sirivella 3
51 Gangavaram 65. Chennooru
52 Gamparamamididdne 66. Jennepalli
53 Kotapadu 67. Kamirinenipalli
54 Maharadevarapuram 68. Boilakunta
12 Done Kothaburuju 55 Udumulapadu
69. Jagadarthi,
70. Udumulapadu
56 Devarabanda 71. Rekulakunta
57 Dharapalli 72. Dharapalli
58 Done 1 73. Done1
59 Done 4 74. Done 4
13 Koilakunta Revanuru 60 Revanuru
75. Revanuru, 76. Muppaluru,
77. Yallampadu
78. Lingala
61 Peddakopparla 79. Kalagatta,
80. Peddakopparla
14 Bethamcherla Bethamcherla 62 Emboy 81. Seetharampuram
63 Buggaripalli 82. Buggaripalli
64 Gorlagutta 83. Hanumannagar
65 Bethamcherla 1 84. Bethamcherla 1
66 Bethamcherla 2 85. Bethamcherla 2
67 Bethamcherla 3 86. Bethamcherla 3
68 Bethamcherla 4 87. Bethamcherla 4

Code Mandal PHC Code Sub centre Name of the village
15 Chagalamarri Chagalamarri 69 Chagalamarri 2 88. Chagalamarri 2
70 Chagalamarri 3 89. Chagalamarri 3
71 Madduru 90. Madduru
72 Muthyalapadu 91. Muthyalapadu
73 Mallavemula 92. Mllavemula
74 Chagalamarri 1 93. Chagalamarri 1
MAHABUB NAGAR DISTRICT
Code Mandal PHC Code Sub centre Name of the village
1 Farooq Nagar Burgula 1 Kammadanam 1. Solpur
2 Burgula 2. Kasireddiguda
3 Dosakal 3. Dosakal
4 Veldnada 4. Buchiguda
5 Annaram 6. Peddchilakamarri
6 Madurapur 7. Devunibanda thanda
2 Kondadurg Kondadurg 7 Srirampur 8. Srirampur 9. Pullapraguda
8 Choudariguda 10. Choudariguda
11. Indiranagar
9 Peddayelikacherla 12. Peddayelikacherla
13. Veerannapeta
10 Pedmaram 14. Chegireddi Ghanpur
11 Venkirala 15. Old Agirala
3 Velidanda Velidanda 12 Cherukur 16. Cherukur
13 Peddapur 17. Peddapur
14 Kotra 18. Kotra
15 Ballampalli 19. Ballampalli
16 Jupalli 20. Jupalli
17 Tandra 21. Tandra
4 Tadoor Tadoor 18 Gunthakurudu
22. Yadireddipalli
23. Guntakuduru
19 Ithale 24. Ithole 25. Sivatharada
20 Kummera 26. Thummalasagar
27. Kummera
5 Bijinepally Palem 21 Allipur
28. Allipur 29. Salkarpeta
30. Khanapur
22 Palem 31. Palem
23 Kundlalavara 32. Kundlanlavara
24 Vasanthapur 33. Vasanthapur
6 Amrabad Mannanur 25 Macharam
34. Macharam
35. Mukamamidi
26 Venkateshwarabai 36. Venkateshwarabai

Code Mandal PHC Code Sub centre Name of the village
27 Amarabad 37. Telugubili
38. Jangamreddipalli
28 Mannanur 39. Mannanur
40. Prashanth Nagar
7 Balamur Balamur 29 Barala 41. Ramujupalli
30 Anthavaram 42. Narasaipalli thanda
31 Kondalagula 43. Thodalagadda
32 Jinkuntla 44. Kodepalli
33 Polisethipalli 45. Polisethipalli
34 Godal 46. Godal
8 Uppunuthala Uppunuthala 35 Kasanpalli 47. Thirumalapur
36 Penumella 48. Guvvalolipalli
37 Uppunuthala 49. Jayaram thanda
38 Ventoor 50. Ventoor
39 Kortikal 51. Kortikal
40 Upparpalli 52. Upparpalli
9 Panagal Panagal 41 Kethapalli 53. Kethapalli
42 Panagal 54. Pangal
43 Mandapur 55. Kothapeta
44 Annaram 56. Devajpalli
45 Telarallapalli 57. Telarallapalli
58. Tellarallapalli thanda
46 Gajapur 59. Madavaraopalli
10 Gopalpet Gopalpet 47 Gopalpet 60. Gopalpet
48 Palakapadu 61. Palakapadu
49 Edutla 62. Edutla
50 Tadipatri 63. Tadipatri
51 Kesampeta 64. Chakalapalli
52 Buddaram 65. Buddaram
11 Koilkonda Manikonda 53 Malkapur 66. Rampur
54 Garlapahad 67. Garlapahad
55 Parepalli 68. Parepalli
56 Burugupalli 69. Kagipur
57 Manikonda 70. Manikonda
58 Kesavapur 71. Perikivadu thanda
12 Damaragidda Damaragidda 59 Sajanapur 72. Maddalaveedu
60 Kanukurthi 73. Gadimunkampalli
61 Lokurthi 74. Hasanpalli
62 Itlapur 75. Ulligudem
63 Mogullamadaka 76. Annasagaram
64 Damaragidda 77. Damaragidda
Code Mandal PHC Code Sub centre Name of the village
13 Nawabpet Nawabpet 65 Nawabpet 78. Gurukunta
66 Yanamangandla 79. Yanamangandla
80. Chennreddipalli
67 Eppatur 81. Eppature 82. Karoor
68 Karukonda 83. Thigalapalli
69 Rudraram 84.Kakarlapadu 85. Rudraram
14 Amangal Amangal 70 Mysigandi 86. Mysigandi
71 Chennapalli 87. Chennapalli
72 Vittaipalli 88. Vittaipalli
73 Mangalpalli 89. Meddigadda thanda
74 Kadathal 90.Kadathal
91. Puligundathanda
15 Devarakadra Devarakadra 75 Devarakadra 92. Gokulapur
76 Devarakadra (B) 93. Gurukonda
77 Basavapalli 94. Basavapalli 95. Hagalapur
78 Nagaram 96. Pedda Rajamoor
79 Venkataipalli 97. Gaddaguduru.
KARIMNAGAR DISTRICT
Code Mandal PHC Code Sub centre Name of the village
1 Jullapalli Jullapalli 1 Vadkapur 1. Vadkapur 2. Kummarikunta
2 Narsapur 3. Narsapur 4. Raikaldevpally
3 Venkatroopalli 5. Venkarroopalli 6. Kachapur
4 Dulikatte 7. Muppidipally
5 Jullapalli 8. Jullapalli
6 Sulthanpur 9. Sulthanpur
2 Manakondur Veldi 7 Ootur 10. Ootur
8 Pachunoor 11. Pachnoor
9 Vefurupally 12. Vegurupally
10 Laxmapur 13. Laxmapur
11 Devampally 14. Pochampally 15. Kellada
16. Lalithapur 17. Devanpally
12 Lingapur 18. Jaggaiah pally 19.Lingapur
3 Kamalapur Kamalapur 13 Vangapalley 20. Vangapally
14 Ambala 21. Srirampally 22. Ambala
23. Sriram
15 Kanparthy 24. Shambunipally 25. Deshrajpally
16 Marripallygudem 26. Marripallygudem
4 Bejjanki Thotapalli 17 GannewVarma 27. Gannawvarma
18 G. Kondapur 28 Gundlapally

Code Mandal PHC Code Sub centre Name of the village
19 Thotapalli 29. Thotapally 30. Veerapur
20 Jangapally 31. Jangapally 32. Hannajpally
33. Gotlamitla
21 Khasimpet 34. Paruvella
5 Koheda Koheda 22 Samudrala 35. Samudrala
23 Basvapur 36. Posiddipally 37.Basvapur
24 Koheda 38. Koheda
25 Vinjampally 39. Vinjampally 40. Gotlamitla
26 Shanigaram 41. Shanigaram
6 Sulthanabad Garepalli 27 Gattepally 42. Gattepally 43. Neerukulla
28 R M Kunta 44. R M Kunta
29 Garepally 45. Garrepally 46. Bupathipur
30 Kodurupally 47. Kodurupak 48. Devunipally
31 Togarrai 49. Kadampur
7 Karimnagar Kothapally 31 Magnoor 50. Magnoor 51. Takerpet
32 Asifnagar 52. Asifnagar
33 Elagundla 53. Elagundla
34 Chanapally 54. Chamanpally
35 Kamanpur 55. Baddipally
8 Ibrahimpatnam Ibrahimpatnam 36 Ibrahimpatnam 56. Thimmapur
37 Thimmapur 57. Thimmapur
38 Dabba 58. Dabba
39 Varshakonda 59. Varshakonda
40 Godhur 60. Godhur
41 Vemulakurthy 61. Mularampur
42 Medipally 62. Rajeshwaraopet
9 Gambhirraopeta Gambhirraopet 43 Gambhirraopet 63. Ghambhirraopet
44 Gambhirraopet 2 64. Gambhirraopet 2
45 Gajasingaram 65. Gajasingaram
46 Dammanapet 66. Nagampeta 67. Dammanapet
47 Mallareddypeta 68. Mallareddypeta
10 Mallala Mallala 48 Mallala 69. Mallala 70. Gudipeta
49 Thatipally 71. Sarvapur 72. Kothapally
73. Balvanthapur 74. Thatipally
50 Takkalapally 75. Lambadipally
11 Vemulavada Vemulavada 51 Subhashnagar 76. Vemulavada
52 Nukalamarry 77. Nandigundlapally
78. Nukalammay
53 Vemulavada 79. Vemulavada
54 Mallaram 80. Mallaram
55 Marripallem 81. Pochatipalli

Code Mandal PHC Code Sub centre Name of the village
12 Medipally Medipally 56 Mannegudem 82. Dammanapeta
57 Kondapur 83. Kondapur
58 Venkatraopet 84, Oddada 85. Rajojipeta
86. Venkartropet
59 Porumalla 87. Porumalla
60 Kalvakota 88. Kalvakota
13 Metpally Jaggasagar 61 Jaggasagar
89. Ramchalpet 90. Kondrikarla
91. Jaggasagar
62 Metpally Urban 92. Metpally Urban
63 Metpally
Indranagar 93. Metpally Urban
64 Ambedkar Nagar 94. Metpally
65 Vellula 95. Vellula
66 Gajullapalley 96. Metpally Urban
67 Kalanagar 97. Metpally Urban
68 Mushimpura 98.Metpally
14 Boinpally Boinpally 69 Karem
99. Karem 100. Dandrapalli
101. Ananthapalli 102. Stambanpally
70 Boinpally 103. Boinpally 104. Ramamapet
105. Burgupally
71 Takakonda 106. Tadakonda 107. Malkapur
15 Sarangapur Sarangapur 72 Nagnur 108. Nagnur
73 Pembatla 109. Pembetla
74 Laxmidevipally 110. Laxmidevipally
75 Sarangapur 111. Potharam 112. Sarangapur
76 Beerpoor 113. Narsimhulupally 114. Beerpoor.
����