Are patterns of cortical hyperexcitability altered in catamenial epilepsy?
15
ORIGINAL ARTICLE Are Patterns of Cortical Hyperexcitability Altered in Catamenial Epilepsy? Radwa A. B. Badawy, MBBCh, PhD, 1,2,3 Simon J. Vogrin, BApplSc, 1 Alan Lai, BEng, PhD, 4 and Mark J. Cook, MBBS, MD 1,2 Objective: We used transcranial magnetic stimulation to determine menstrual cycle-related changes in cortical excit- ability in women with and without catamenial epilepsy and investigated whether these changes differed between ovulatory and anovulatory cohorts. Methods: Healthy nonepilepsy women and women with generalized and focal epilepsy were investigated during ovu- latory (n 5 11, 46, and 43, respectively) and anovulatory (n 5 9, 42, and 41) cycles. Patients were divided based on seizure pattern into catamenial (C1 5 perimenstrual, C2 5 periovulatory, C3 5 luteal seizure exacerbation), noncata- menial, and seizure free. Cortical excitability was assessed using motor threshold (MT) and paired pulse stimulation at short (2–15 milliseconds) and long (100–300 milliseconds) interstimulus intervals twice, at the (1) late follicular and (2) mid luteal phases of the menstrual cycle. Results: In controls, cortical excitability was greatest in the follicular study, where intracortical facilitation was increased (p < 0.05). The opposite was seen in women with epilepsy, where intracortical facilitation was greatest and intracortical inhibition was least in the luteal studies (p < 0.05). There were no differences between the ovulatory and anovulatory groups in any of the cohorts. No changes were observed in MT. Interpretation: Nonhormonal factors are involved in the cyclicity of cortical excitability across the menstrual cycle. Normal menstrual cycle variations in cortical excitability are altered in a similar pattern in ovulatory and anovulatory women with epilepsy regardless of seizure patterns. The underlying neural changes associated with epilepsy may al- ter responses to sex hormones. This may be an important underlying mechanism for catamenial seizure clustering. ANN NEUROL 2013;74:743–757 S eizure clustering in relation to the menstrual cycle is a common phenomenon that is found in a significant proportion (35%) of women with epilepsy. 1,2 Many mechanisms have been proposed to explain this associa- tion. The most established hypothesis is that it is due to neuroactive properties of sex hormones and cyclic varia- tions in their serum levels. 1,2 In ovulatory cycles, estrogen increases late in the follicular (preovulatory) phase and then gradually declines during the luteal (premenstrual) phase, whereas progesterone is low prior to ovulation and increases during the luteal phase. Evidence for this hypothesis comes from numerous clinical reports of changes in seizure patterns in relation to puberty, preg- nancy, and menopause, 3–5 as well as periodical hormonal fluctuations across the menstrual cycle. 1,2 It also comes from animal data demonstrating a seizure threshold- lowering effect with estrogen 6,7 and depressed neuronal firing as well as decreased epileptiform discharges with progesterone. 7–9 This evidence is indirect, and although the anticonvulsant effects of progesterone are a common finding, there is contradictory evidence on the effects of estrogen both in clinical reports that do not link this hormone to seizure exacerbation 10 and in many animal studies that do not find it to have a proconvulsant effect. 11–13 Furthermore, even if these competing proper- ties were a proven feature, if seizure exacerbation in women with epilepsy was only linked to fluctuations in sex hormone levels, then raised seizure risk would be pre- dicted when the estrogen=progesterone ratio increases. This would either be right before or during ovulation, when estrogen levels are at their highest, or right before and during menstruation, when progesterone declines. View this article online at wileyonlinelibrary.com. DOI: 10.1002/ana.23923 Received Feb 4, 2013, and in revised form Apr 13, 2013. Accepted for publication Apr 26, 2013. Address correspondence to Dr Badawy, Department of Medicine, University of Melbourne, 41 Victoria Parade, Fitzroy, Victoria 3065, Australia. E-mail: [email protected] From the 1 Department of Clinical Neurosciences, St Vincent’s Hospital, Fitzroy, Australia; Department of 2 Medicine and 3 Electrical and Electronic Engineering, University of Melbourne, Parkville; and 4 Bionics Institute, East Melbourne, Victoria, Australia. V C 2013 American Neurological Association 743
Transcript of Are patterns of cortical hyperexcitability altered in catamenial epilepsy?

ORIGINAL ARTICLE
Are Patterns of Cortical HyperexcitabilityAltered in Catamenial Epilepsy?Radwa A. B. Badawy, MBBCh, PhD,1,2,3 Simon J. Vogrin, BApplSc,1
Alan Lai, BEng, PhD,4 and Mark J. Cook, MBBS, MD1,2
Objective: We used transcranial magnetic stimulation to determine menstrual cycle-related changes in cortical excit-ability in women with and without catamenial epilepsy and investigated whether these changes differed betweenovulatory and anovulatory cohorts.Methods: Healthy nonepilepsy women and women with generalized and focal epilepsy were investigated during ovu-latory (n 5 11, 46, and 43, respectively) and anovulatory (n 5 9, 42, and 41) cycles. Patients were divided based onseizure pattern into catamenial (C1 5 perimenstrual, C2 5 periovulatory, C3 5 luteal seizure exacerbation), noncata-menial, and seizure free. Cortical excitability was assessed using motor threshold (MT) and paired pulse stimulationat short (2–15 milliseconds) and long (100–300 milliseconds) interstimulus intervals twice, at the (1) late follicular and(2) mid luteal phases of the menstrual cycle.Results: In controls, cortical excitability was greatest in the follicular study, where intracortical facilitation wasincreased (p< 0.05). The opposite was seen in women with epilepsy, where intracortical facilitation was greatest andintracortical inhibition was least in the luteal studies (p<0.05). There were no differences between the ovulatory andanovulatory groups in any of the cohorts. No changes were observed in MT.Interpretation: Nonhormonal factors are involved in the cyclicity of cortical excitability across the menstrual cycle.Normal menstrual cycle variations in cortical excitability are altered in a similar pattern in ovulatory and anovulatorywomen with epilepsy regardless of seizure patterns. The underlying neural changes associated with epilepsy may al-ter responses to sex hormones. This may be an important underlying mechanism for catamenial seizure clustering.
ANN NEUROL 2013;74:743–757
Seizure clustering in relation to the menstrual cycle isa common phenomenon that is found in a significant
proportion (!35%) of women with epilepsy.1,2 Manymechanisms have been proposed to explain this associa-tion. The most established hypothesis is that it is due toneuroactive properties of sex hormones and cyclic varia-tions in their serum levels.1,2 In ovulatory cycles, estrogenincreases late in the follicular (preovulatory) phase andthen gradually declines during the luteal (premenstrual)phase, whereas progesterone is low prior to ovulation andincreases during the luteal phase. Evidence for thishypothesis comes from numerous clinical reports ofchanges in seizure patterns in relation to puberty, preg-nancy, and menopause,3–5 as well as periodical hormonalfluctuations across the menstrual cycle.1,2 It also comesfrom animal data demonstrating a seizure threshold-
lowering effect with estrogen6,7 and depressed neuronalfiring as well as decreased epileptiform discharges withprogesterone.7–9 This evidence is indirect, and althoughthe anticonvulsant effects of progesterone are a commonfinding, there is contradictory evidence on the effects ofestrogen both in clinical reports that do not link thishormone to seizure exacerbation10 and in many animalstudies that do not find it to have a proconvulsanteffect.11–13 Furthermore, even if these competing proper-ties were a proven feature, if seizure exacerbation inwomen with epilepsy was only linked to fluctuations insex hormone levels, then raised seizure risk would be pre-dicted when the estrogen=progesterone ratio increases.This would either be right before or during ovulation,when estrogen levels are at their highest, or right beforeand during menstruation, when progesterone declines.
View this article online at wileyonlinelibrary.com. DOI: 10.1002/ana.23923
Received Feb 4, 2013, and in revised form Apr 13, 2013. Accepted for publication Apr 26, 2013.
Address correspondence to Dr Badawy, Department of Medicine, University of Melbourne, 41 Victoria Parade, Fitzroy, Victoria 3065, Australia.E-mail: [email protected]
From the 1Department of Clinical Neurosciences, St Vincent’s Hospital, Fitzroy, Australia; Department of 2Medicine and 3Electrical and ElectronicEngineering, University of Melbourne, Parkville; and 4Bionics Institute, East Melbourne, Victoria, Australia.
VC 2013 American Neurological Association 743

These patterns are seen in some women with catamenialepilepsy.2,14 However, seizure exacerbation during theentire second half (luteal phase) of the cycle when pro-gesterone levels are expected to be high is also commonlyreported.15,16 In some, this may be due to an inadequateluteal phase, with insufficient rise in progesterone levelsto be protective against seizures in these women.15,16
Clinical data indicating that the catamenial pattern ofseizure exacerbation is more often observed in womenwith temporal lobe epilepsy,17 where reproductive endo-crine disorders such as anovulatory cycles and oligome-norrhea are also commonly present,18–20 support thisproposition, but it is not a universal finding,21 nor is itapplicable to all seizure types experienced by thesewomen.19 Furthermore, whereas perimenstrual and perio-vulatory seizure clustering was found to be much morefrequent in women with ovulatory than those with anov-ulatory cycles, luteal phase clustering was evenly distrib-uted among both cycle types.15 It is thus possible thatepilepsy-related factors influence the response of neuronalcircuits to sex hormone. This interaction may be reflectedas a disturbance in cortical excitability and could underlieincreased seizure susceptibility in women with epilepsy.
Transcranial magnetic stimulation (TMS) is a safeand sensitive measure of both excitatory and inhibitoryfunctions of motor cortical neurons that has a well-estab-lished role in studying cortical excitability changes in epi-lepsy.22–26 Variations in cortical excitability were recentlyreported in relation to the sleep–wake cycle,27,28 sleep de-privation,29–31 and seizures32,33 in patients with epilepsy.There are also reports of variations across the menstrualcycle in normal ovulatory34,35 and anovulatory women36
and in a small group with catamenial epilepsy.37
In the current study, we used TMS in a largecohort of women with ovulatory and anovulatory cyclesto determine whether there are variations in corticalexcitability across the menstrual cycle in women with epi-lepsy. We asked whether these changes differ fromhealthy women without epilepsy, and whether they arelinked to fluctuations in sex hormone levels across themenstrual cycle. We also investigated whether this differ-ence relates to seizure patterns, such that each of theknown catamenial patterns of seizure clustering wouldhave specific cortical excitability changes that would bedifferent compared to those observed in other womenwith refractory seizures and those who are on seizuremedication.
Subjects and Methods
Study PopulationsThe participants (nonepilepsy controls and patients) were consec-utively recruited until a minimum of 8 women per group
completed the study. This was based on power calculations andwas done to ensure evenly distributed groups. The patients wererecruited through (1) the Outpatient Epilepsy Clinic and (2)screening the databases of the Epilepsy Clinic and Epilepsy Sur-gery Program at St Vincent’s Hospital in Melbourne. These aretertiary referral centers; the first provides the management ofpatients with epilepsy, and the latter aims for the characterizationand presurgical evaluation of patients with refractory focal epi-lepsy. The diagnoses were made by at least 2 experienced epilep-tologists who were unaware of the study based on clinical history,electroencephalogram (EEG), and imaging findings.
The study protocol was approved by the St Vincent’sHospital Human Research Ethics Committee, and writteninformed consent was obtained from each participant.
Participants were grouped according to (Table 1):
Ovulatory=Anovulatory CyclesAll participants (nonepilepsy controls and patients) were di-vided based on their menstrual cycle profile into ovulatory andanovulatory. This was verified by asking each participant beforethey were included to maintain menstrual diaries for 3 monthsprior to the onset of the study. Women with regular menstrualcycles and with progesterone levels >5ng=ml in the luteal phase(serum levels were measured 7 6 1 days before the onset ofmenstruation16) were classified as ovulatory. Women wereassumed to have anovulatory cycles if progesterone levels didnot rise above 5ng=ml during that phase (Table 2).
Clinical FeaturesThe patients were further categorized based on (see Table 1):
Syndrome:
" “Genetic” (previously named idiopathic) generalizedepilepsy syndromes including juvenile myoclonic epi-lepsy, juvenile absence epilepsy, and generalized epi-lepsy with tonic–clonic seizures alone." Focal epilepsy syndromes including temporal lobe and
extratemporal lobe epilepsy.
Seizure FrequencyOur previous studies showed that TMS measures differ depend-ing on whether the patients are studied at onset prior to expo-sure to antiepileptic drugs (AEDs), and whether they continueto have refractory seizures or become seizure free.38 Conse-quently, we divided our patient groups into:
PATIENTS WITH REFRACTORY SEIZURES. Patientswere considered refractory if they continued to have seizures forat least 3 years despite trials of at least 2 different AEDs attherapeutic doses.39,40 This included generalized or secondarilygeneralized tonic–clonic seizures, absences, myoclonic seizures,focal seizures with loss of awareness, and unequivocal focal seiz-ures comprising visual, auditory, motor, sensory, or autonomicmanifestations with retained awareness. Isolated infrequent non-specific vague feelings, uneasiness, or brief d!ej"a vu were notconsidered seizures. Those patients were divided into:
ANNALS of Neurology
744 Volume 74, No. 5

TA
BLE
1.
Dem
og
rap
hic
so
fP
arti
cip
ants
Incl
ud
ed
inE
ach
Gro
up
Gro
up
Sub-
grou
pN
um
ber
Mea
nA
gein
year
s(r
ange
18-4
0in
all)
Age
ofO
nse
tin
year
s(r
ange
)
Mea
nC
ycle
Len
gth
ind
ays
(ran
ge25
-30
inal
l)
Seiz
ure
Freq
uen
cy;
all
typ
es(r
ange
)
AE
Ds
Les
ion
son
MR
I(n
um
ber)
Non
-Epi
lep
syC
ontr
ols
Ovu
lato
ry11
23—
29—
——
An
ovu
lato
ry9
24—
29—
——
Gen
eral
ized
Ep
ilep
sy
Ovu
lato
ry
Cat
amen
ial
Ep
ilep
syC
19
2620
(14-
23)
286/
mon
th(2
-12)
VPA
,L
EV
,LT
G,
TP
M—
C2
925
18(1
2-24
)29
6/m
onth
(3-1
1)V
PA,
LE
V,
LTG
,T
PM
—C
39
2718
(12-
24)
278/
mon
th(2
-16)
VPA
,L
EV
,LT
G,
TP
M—
Non
-cat
amen
ial
924
18(1
1-22
)29
6/m
onth
(2-1
4)V
PA,
LE
V,
LTG
,T
PM
—Se
izu
refr
ee10
2516
(11-
21)
30-
VPA
,L
EV
,LT
G,
TP
M—
An
ovu
lato
ry
Cat
amen
ial
Ep
ilep
syC
18
2417
(11-
23)
288/
mon
th(3
-10)
VPA
,L
EV
,LT
G,
TP
M—
C2
822
18(1
4-22
)29
7/m
onth
(2-1
2)V
PA,
LE
V,
LTG
,T
PM
—C
39
2516
(12-
24)
296/
mon
th(4
-11)
VPA
,L
EV
,LT
G,
TP
M—
Non
-cat
amen
ial
825
18(1
3-24
)27
8/m
onth
(2-1
5)V
PA,
LE
V,
LTG
,T
PM
—Se
izu
refr
ee9
2316
(11-
21)
27-
VPA
,L
EV
,LT
G,
TP
M—
Foca
lE
pil
epsy
Ovu
lato
ry
Cat
amen
ial
Ep
ilep
syC
18
2523
(11-
29)
305/
mon
th(3
-11)
CB
Z,
GB
P,L
AC
,L
EV
,LT
G,
OX
C,
TP
M,
VPA
1co
rtic
aldy
spla
sia,
1hi
ppoc
ampa
lsc
lero
sis
C2
827
20(1
3-27
)27
6/m
onth
(2-1
0)C
BZ
,G
BP,
LA
C,
LE
V,
LTG
,O
XC
,T
PM
,V
PA
1hi
ppoc
ampa
lsc
lero
sis
C3
926
22(1
1-30
)28
6/m
onth
(2-1
1)C
BZ
,G
BP,
LE
V,
LTG
,O
XC
,T
PM
,V
PA1
cort
ical
dysp
lasi
aN
on-c
atam
enia
l9
2824
(13-
32)
275/
mon
th(3
-12)
CB
Z,
LE
V,
LTG
,O
XC
,T
PM
,V
PA1
hipp
ocam
pal
scle
rosi
sSe
izu
refr
ee9
2322
(14-
29)
29-
CB
Z,
LA
C,
LE
V,
LTG
,O
XC
,T
PM
,V
PA—
Annals of Neurology Vol 73 No 6 June 2013: Badawy et al: Cortical Excitability
November 2013 745

TA
BLE
1.
(Co
nti
nued
)
Gro
up
Sub-
grou
pN
um
ber
Mea
nA
gein
year
s(r
ange
18-4
0in
all)
Age
ofO
nse
tin
year
s(r
ange
)
Mea
nC
ycle
Len
gth
ind
ays
(ran
ge25
-30
inal
l)
Seiz
ure
Freq
uen
cy;
all
typ
es(r
ange
)
AE
Ds
Les
ion
son
MR
I(n
um
ber)
An
ovu
lato
ry
Cat
amen
ial
Ep
ilep
syC
18
2323
(11-
26)
305/
mon
th(2
-10)
CB
Z,
GB
P,L
AC
,L
EV
,O
XC
,T
PM
,V
PA—
C2
826
20(1
7-30
)29
6/m
onth
(4-1
3)C
BZ
,L
EV
,LT
G,
OX
C,
TP
M,
VPA
1oc
cipi
tal
glio
sis
C3
924
24(1
1-31
)27
4/m
onth
(2-1
0)C
BZ
,G
BP,
LA
C,
LE
V,
LTG
,O
XC
,T
PM
,V
PA
1co
rtic
aldy
spla
sia
Non
-cat
amen
ial
826
25(1
4-32
)28
5/m
onth
(2-1
1)C
BZ
,G
BP,
LA
C,
LE
V,
LTG
,O
XC
,T
PM
1hi
ppoc
ampa
lsc
lero
sis
Seiz
ure
free
824
22(1
3-29
)28
-C
BZ
,L
EV
,L
AC
,LT
G,
OX
C,
TP
M,
VPA
1fro
ntal
cyst
a Ran
ge5
18–4
0ye
ars
inal
l.bR
ange
525
–30
days
inal
l.A
ED
5an
tiep
ilept
icdr
ug;
C1
5pe
rim
enst
rual
patt
ern
ofse
izur
eex
acer
bati
on;
C2
5pe
riov
ulat
ory
patt
ern
ofse
izur
eex
acer
bati
on;
C3
5lu
teal
patt
ern
ofse
izur
eex
acer
bati
on;
CB
Z5
carb
amaz
epin
e;G
BP
5ga
bape
ntin
;L
AC
5la
cosa
mid
e;L
EV
5le
veti
race
tam
;LT
G5
lam
otri
gine
;M
RI
5m
agne
tic
reso
nanc
eim
agin
g;O
XC
5ox
carb
azep
ine;
TP
M5
topi
ram
ate;
VPA
5so
dium
valp
roat
e.
ANNALS of Neurology
746 Volume 74, No. 5

" Catamenial epilepsy: Defined as doubling of seizurefrequency in relation to the menstrual cycle observedfor at least the past 12 months. These patients werefurther subdivided based on the known 3 patterns ofcatamenial epilepsy16 into:
" Perimenstrual (C1): Seizure exacerbation on day 23to day 3 (day 1 being the first day of menstrualbleeding)." Periovulatory (C2): Day 10 to day 213 (day 214
being mid cycle or the day of ovulation in ovulatorycycles)." Luteal (C3): Day 212 to day 24.
" Noncatamenial epilepsy: Women with refractory epi-lepsy but with no history of seizure exacerbation inrelation to the menstrual cycle.
SEIZURE-FREE PATIENTS. Patients were included in thisgroup if they did not experience any form of the seizuresdescribed above for at least 12 months prior to the TMS test.
Inclusion CriteriaInclusion criteria included the following:
" Eighteen to 40 years of age." Regular menstrual cycle of 25 to 30 days during the
last 6 cycles." Normal neurological examination." Generalized epilepsy, that is, generalized epileptiform
abnormalities (3.5–5Hz spike-wave) on at least 1 EEGrecording and a history of generalized tonic–clonicseizures, myoclonic, absence seizures." Focal epilepsy, that is, seizure symptomatology (specifi-
cally characteristics of the aura when consistently pres-ent) and the EEG showed either a left-sided or right-sided lateralization. The EEG was considered localizingonly if definite and prominent sharp-slow dischargeswere seen consistently lateralized to 1 region. Patientswith temporal intermittent rhythmic delta activity wereincluded only if the activity was consistently recordedover 1 hemisphere. Nonspecific slowing or sharp waveswere not considered lateralizing or localizing even ifonly recorded on 1 side. Further localizing signs werefound on brain magnetic resonance images. (Imagingwas only routinely performed on patients thought tohave focal epilepsy. The findings were available for allpatients and are summarized in Table 2.)
Exclusion CriteriaExclusion criteria for all participants included the following:
" Fluctuation in cycle length of >1 day." Menstrual-related affective disorders.
" Use of hormonal contraceptive methods throughoutthe study period or the preceding 6 months." Pregnancy or lactation." History of ovariectomy ." Suffering from any medical condition at the time of
the study, particularly endocrinal abnormalities or hor-monal disturbances." Previous cortical resections or craniotomies." Cardiac pacemaker, vagal nerve stimulator, or intracra-
nial metal implants.
Exclusion criteria for nonepilepsy controls included thefollowing:
" History of seizures, migraine, or any other neurologi-cal condition." History of head trauma or skull fractures." Previous exposure to AEDs." Currently taking any medication of any kind.
Exclusion criteria for patients included the following:
" Suspicion of nonepileptic events (psychogenic nonepi-leptic seizures, migraine, parasomnias, etc)." Patients with an undetermined epilepsy syndrome (not
clear whether generalized or focal epilepsy)." Seizure foci originating in the vicinity of the motor
area (seizure semiology or on imaging)." Bilateral seizure foci." Any change to the AED regimen during the study or
at any time in the 6 months preceding it.
Timing of the StudiesTMS was performed on all participants (nonepilepsy controlsand patients) twice, 12 to 15 days apart (Fig 1).
In women with ovulatory cycles, 1 study was in the latefollicular phase (day 12 6 2, 1–2 days preovulation, whenestrogen is at its highest level) and the other was in the midluteal phase (day 27 6 2, 7 days premenstruation, when theprogesterone level is at its peak). In women with anovulatorycycles, the follicular and luteal studies were timed to coincidewith approximately the same phases, the first being 1 to 2 daysbefore mid cycle and the second 5 to 10 days prior to theexpected time of menstruation.
The timing of the 2 studies was calculated for eachparticipant based on the duration of her menstrualcycles. Plasma estrogen and progesterone levels were measuredat the time of each study to verify the phase of the menstrualcycle.
To avoid any hypothetical order effect, the follicularphase study was randomly performed before the luteal phasestudy in half the participants in each group, and the order wasreversed in the others.
In all groups, care was taken to perform both TMS stud-ies for each participant between 10 AM and 3 PM so as to
Annals of Neurology Vol 73 No 6 June 2013: Badawy et al: Cortical Excitability
November 2013 747

increase the repeatability of the measurements. Care was alsotaken to avoid clustering of any of the participants in a groupto a particular time, and the studies were spread evenly overthis time interval in all groups. All participants were asked tomaintain regular sleep patterns, with 7 to 9 hours of sleep thenight before each study. The results were only analyzed after a2-day seizure-free period was confirmed (based on seizure dia-ries) on either side of the study. If seizures were reported withinthis time frame, the study was repeated. No patients wereexcluded due to seizures.
Transcranial Magnetic Stimulation ParadigmBoth hemispheres were studied in each participant (patientsand controls). During TMS, the participants sat in a comfort-able, reclining chair. Surface electromyographic (EMG)recordings were made from the abductor pollicis brevis mus-cle. Stimuli were delivered to the contralateral cerebral hemi-sphere by applying the appropriate direction of coil currentflow (anticlockwise for left cortical stimulation and clockwisefor right cortical stimulation), using a flat circular 9cm-diame-ter magnetic coil (14cm external diameter) with the center ofthe coil positioned over the vertex and held in a plane tangen-tial to it using a pair of Magstim 200 magnetic stimulators(Magstim, Whitland, UK). Paired stimulation at various inter-stimulus intervals (ISIs) was performed using a BiStim module(Magstim) to connect 2 stimulators to the coil.
The motor evoked potentials (MEPs) were recorded anddigitized online via a CED 1401 interface (Cambridge Elec-tronic Design, Cambridge, UK) and stored on computer foroffline analysis. Signal software (Cambridge Electronic Design)was used for automated acquisition and marking of therecorded MEPs. Filters for the acquisition were set to a low fre-quency of 10Hz and a high frequency of 5KHz. Sweep speedfor threshold determination and paired pulse TMS at short ISIswas 100 milliseconds, and the sensitivity was set to100lV=division. For longer ISIs the sweep was adjusted to 500milliseconds and sensitivity to 2mV=division. The MEP ampli-tude was measured from peak to peak.
The experimental session lasted for 60 to 90 minutes,and the following parameters were recorded:
Motor ThresholdMotor threshold (MT) was determined in all tested hemi-spheres while the participant was at rest, verified by continuousvisual and auditory EMG feedback. Stimulation commenced at30% of maximum output and increased in 5% increments untilthe MEP was established. One-percent changes in intensitywere then used to measure the threshold value. Motor thresholdwas defined as the lowest level of stimulus intensity that pro-duced a MEP in the target muscle of peak-to-peak amplitude>100lV on 50% or more of 10 trials.41
Intracortical Inhibition and FacilitationCortical recovery curves were derived using paired pulse TMS.For the short ISIs of 2, 5, 10, and 15 milliseconds, the firststimulus was given at 80% of MT and the second stimulus at
20% above MT. Ten stimuli at 20% above MT without a pre-conditioning stimulus were also given. For longer ISIs, thestimulation intensity was 20% above MT using paired stimuliin 50-millisecond increments at ISIs of 100 to 300 millisec-onds. A minimum interval of 15 seconds was kept between thedelivery of each pair of stimuli. Stimuli were given at randomlyselected ISIs until a total of 10 at each ISI was achieved.
Recovery curves at short ISIs (2–15 milliseconds) wereconstructed for each hemisphere using the ratio of the meanpeak-to-peak amplitude of the response (termed test response[TR]) at each ISI following the conditioning stimulus givenbelow MT expressed as the percentage of the mean MEP whenthe test stimulus was given alone without a preconditioningstimulus (TR=MEP%).
Recovery curves at longer ISIs (100–300 milliseconds)were constructed for each hemisphere using the ratio of themean peak-to-peak amplitudes of the response to the secondstimulus termed the TR and the response to the first stimulustermed the conditioning response (CR) at each ISI measured asa percentage (TR=CR%).
Each participant was given a unique alphanumeric code.This was the only identifying feature on the TMS dataacquired. The analysis was performed after all participants hadbeen tested. This ensured that the investigator analyzing theTMS results was blinded to clinical information during theanalysis.
Statistical AnalysisIn nonepilepsy controls and generalized epilepsy, theresults were analyzed according to hemisphere dominanceassessed according to the Edinburgh handednessinventory.42
In focal epilepsy, the results were analyzed accord-ing to the ipsilateral and contralateral hemisphere (the ip-silateral hemisphere is defined here as the hemispherewith the presumed seizure focus). This was based on sei-zure semiology and EEG findings.
Correlation of clinical features (age, age at onset ofseizures, seizure type, and frequency) and AED (type andserum levels) with change in cortical excitability was per-formed using Pearson correlation coefficient as well asthe chi-square test.
For cortical excitability measures (MT and ISIs),a 2-way repeated measures analysis of variance wasused. Each test had a within-participant factor (timingof the study [the dependent variable was the change;follicular minus luteal value at each measure]) and abetween-participants factor “group” (menstrual cycletype, type of epilepsy; seizure pattern, nonepilepsycontrols). This was performed for each hemisphere ineach group.
A 1-way analysis of variance test was used to compareplasma estrogen and progesterone levels measured in eachgroup at the time of the follicular and luteal studies.
ANNALS of Neurology
748 Volume 74, No. 5

For all analyses, p< 0.05 was chosen as the signifi-cance level. Fisher protected least significant differencepost hoc tests for correction of multiple comparisons
were performed as appropriate. The analysis was per-formed on SPSS 15.0 for Windows (IBM, Armonk,NY).
TABLE 2. Plasma Hormone Levels in Each Group Measured on the Day of the Transcranial Magnetic Stimula-tion Test (Mean 6 Standard Deviation)
Group Subgroup Follicular LutealEstrogen, pg/ml Progesterone, ng/ml Estrogen, pg/ml Progesterone, ng/ml
Nonepilepsy controls
Ovulatory 199.7 6 60.4 0.7 6 0.4 77.8 6 17.2 8.2 6 3.9
Anovulatory 54.8 6 15.7 0.6 6 0.4 49.4 6 12.4 1.1. 6 0.3
Generalized epilepsy
Ovulatory
Catamenial epilepsy
C1 193.4 6 52.7 1.1 6 0.3 79.1 6 12.7 12.0 6 3.9
C2 186.1 6 68.1 0.7 6 0.5 89.4 6 15.4 9.4 6 4.1
C3 190.0 6 59.1 0.9 6 0.4 84.5 6 19.6 8.7 6 4.8
Noncatamenial epilepsy 180.9 6 66.4 1.2 6 0.4 79.5 6 19.1 11.7 6 5.3
Seizure free 197.1 6 39.4 0.9 6 0.3 85.3 6 20.3 9.4 6 5.0
Anovulatory
Catamenial epilepsy
C1 55.7 6 14.9 0.9 6 0.2 44.2 6 11.8 1.2 6 0.5
C2 64.1 6 14.6 0.8 6 0.5 55.8 6 12.9 0.9 6 0.2
C3 49.5 6 19.3 0.8 6 0.3 41.3 6 10.9 0.8 6 0.2
Noncatamenial epilepsy 38.9 6 17.9 1.0 6 0.5 32.7 6 11.2 0.9 6 0.5
Seizure free 50.6 6 12.7 0.8 6 0.3 46.8 6 9.4 0.8 6 0.3
Focal epilepsy
Ovulatory
Catamenial epilepsy
C1 204.1 6 44.2 0.7 6 0.5 79.7 6 24.2 8.9 6 5.0
C2 188.9 6 39.2 1.2 6 0.2 86.7 6 16.8 9.9 6 6.2
C3 189.5 6 57.1 1.0 6 0.2 89.2 6 14.6 12.4 6 4.8
Noncatamenial epilepsy 200.2 6 45.1 0.8 6 0.6 84.6 6 22.1 10.2 6 4.9
Seizure free 185.2 6 67.3 0.8 6 0.5 79.9 6 16.9 11.2 6 5.6
Anovulatory
Catamenial epilepsy
C1 57.4 6 18.4 1.0 6 0.3 50.1 6 10.9 0.9 6 0.2
C2 42.7 6 17.2 0.9 6 0.4 35.3 6 9.1 0.7 6 0.5
C3 54.3 6 19.3 0.7 6 0.5 39.2 6 11.8 0.7 6 0.3
Noncatamenial epilepsy 61.3 6 11.1 0.9 6 0.6 44.2 6 15.1 0.8 6 0.2
Seizure free 44.3 6 10.0 1.0 6 0.4 35.3 6 13.1 0.8 6 0.5
C1 5 perimenstrual pattern of seizure exacerbation; C2 5 periovulatory pattern of seizure exacerbation; C3 5 luteal pattern ofseizure exacerbation.
Annals of Neurology Vol 73 No 6 June 2013: Badawy et al: Cortical Excitability
November 2013 749

The effect size was calculated for the significant results(mean MTand mean value at each ISI) using the formula:
effect size 5 mean of luteal values - mean of follicular values
= ðstandard deviation of follicular values
1 standard deviation of luteal valuesÞ - 2
Effect size 0.2 was considered small, 0.5 was consideredmedium, and %0.8 was considered large.43
ResultsThere were no significant differences between the groupsin the average cycle day of testing in the follicular orluteal phases.
Hormonal ChangesTable 1 shows the mean plasma estrogen and progester-one levels measured on the day of each TMS test in eachgroup. Other than the expected changes in hormone lev-els between the 2 phases in each group, the only signifi-cant differences observed were lower estrogen levelsduring the follicular phase and lower progesterone levelsduring the luteal phase in all groups with anovulatorycycles compared to those with ovulatory cycles. No othersignificant intergroup hormone level differences wereobserved.
Cortical Excitability MeasuresInterstudy variability in cortical excitability did not corre-late with age, age at seizure onset, or frequency or typeof seizures in any of the subgroups. It also did not corre-late with the number of AEDs used or their differentcombinations or serum levels.
There were no interhemispheric differences in anyof the groups in any of the studies. Consequently,although the results from both hemispheres were ana-lyzed, only the results from the dominant hemispherefor nonepilepsy controls and generalized epilepsy andthe ipsilateral hemisphere for focal epilepsy arepresented.
There were no differences in MEP sizes to teststimuli at 120% between the groups.
MOTOR THRESHOLD. There were no differences inmean MT comparing the follicular and luteal values inany of the groups (Table 3).
INTRACORTICAL INHIBITION AND FACILITATION.
Menstrual Cycle Variations in Cortical Excitability.
Nonepilepsy controls:
" Nonepilepsy controls:
" In nonepilepsy controls, there was increased corticalexcitability evidenced by higher intracortical facilita-tion (10- and 15-millisecond ISIs) in the follicularstudy compared to the luteal study (F 5 4.98,p< 0.05, effect size 5 0.4). There were no changesin short (2- and 5-millisecond ISIs) or long (100–300-millisecond ISIs) intracortical inhibition com-paring the 2 studies (Fig 2).
Women with epilepsy:
" Catamenial refractory seizures:
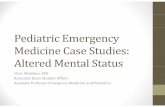
" Perimenstrual (C1): There was no differencebetween the follicular and luteal studies at any ofthe ISIs in either group with generalized or focalepilepsy (Figs 3A, B and 4A, B). There was also nodifference between the ovulatory and anovulatorygroups in either study." Periovulatory (C2): Similar to the groups with C1 cata-
menial patterns, no difference was found between thefollicular and luteal studies at any of the ISIs in thegroups with generalized or focal epilepsy (see Figs 3C,D and 4C, D). There was also no difference betweenthe ovulatory and anovulatory groups in either study." Luteal (C3): A pattern opposite to that seen in con-
trols was found. Cortical excitability was higher inthe luteal study compared to the follicular one. Thiswas present in both groups with generalized (see Fig3E, F) and focal (see Fig 4E, F) epilepsy and wassignificant at the short ISIs of 10 and 15 millisec-onds (F 5 4.56–5.92, p< 0.05, effect sizerange 5 0.3–0.5) and all the long ISIs (F 5 5.31–16.73, p< 0.05, effect size range 5 0.4–0.9), beingmaximum at the 300-millisecond ISI and greater ingeneralized epilepsy. Cortical excitability was higher
FIGURE 1: Timing of transcranial magnetic stimulation (TMS) studies in relation to the menstrual cycle. [Color figure can beviewed in the online issue, which is available at www.annalsofneurology.org.]
ANNALS of Neurology
750 Volume 74, No. 5

in the luteal study in a similar fashion in both theovulatory and anovulatory groups, with no differ-ence between them.
" Noncatamenial refractory seizures: A pattern identicalto that observed in patients with the C3 catamenialpattern was found, but with smaller effect sizes.
TABLE 3. Menstruation-Related Variation in MT in the Dominant Hemisphere in Nonepilepsy Controls andGeneralized Epilepsy, and the Ipsilateral Hemisphere in Focal Epilepsy (Mean 6 Standard Deviation)
Group Subgroup Follicular MT,stimulus intensity %
Luteal, MTstimulus intensity %
Nonepilepsy controls
Ovulatory 53.9 6 5.4 55.1 6 4.9
Anovulatory 54.1 6 4.9 53.4 6 5.2
Generalized epilepsy
Ovulatory
Catamenial epilepsy
C1 54.2 6 5.3 55.2 6 5.2
C2 56.2 6 4.8 55.6 6 6.3
C3 51.8 6 7.9 53.2 6 5.3
Noncatamenial epilepsy 53.2 6 5.2 54.6 6 6.1
Seizure free 56.3 6 4.7 56.3 6 4.8
Anovulatory
Catamenial epilepsy
C1 55.7 6 4.5 53.9 6 6.4
C2 54.2 6 5.4 55.1 6 4.5
C3 53.9 6 7.2 55.3 6 6.1
Noncatamenial epilepsy 54.1 6 5.7 53.4 6 6.3
Seizure free 56.1 6 4.9 55.1 6 6.2
Focal epilepsy
Ovulatory
Catamenial epilepsy
C1 58.4 6 4.2 59.0 6 3.2
C2 57.1 6 3.4 57.6 6 6.2
C3 55.3 6 6.9 55.9 6 6.5
Noncatamenial epilepsy 57.3 6 6.5 56.8 6 6.9
Seizure free 59.2 6 6.3 59.9 6 6.7
Anovulatory
Catamenial epilepsy
C1 54.9 6 8.4 55.2 6 3.8
C2 56.3 6 5.4 56.1 6 5.4
C3 56.8 6 5.6 55.6 6 6.3
Noncatamenial epilepsy 55.9 6 6.2 55.2 6 6.5
Seizure free 57.1 6 5.1 57.9 6 6.2
C1 5 perimenstrual pattern of seizure exacerbation; C2 5 periovulatory pattern of seizure exacerbation; C3 5 luteal pattern ofseizure exacerbation; MT 5 motor threshold.
Annals of Neurology Vol 73 No 6 June 2013: Badawy et al: Cortical Excitability
November 2013 751

Cortical excitability was higher (F 5 4.01–5.64,p< 0.05, effect size range 5 0.3–0.4 at the 10- and15-millisecond ISIs, and F 5 3.97–10.31, p< 0.05,effect size range 5 0.3–0.7 at the long ISIs) in theluteal study compared to the follicular study in bothpatients with generalized and patients with focal epi-lepsy (see Figs 3G, H and 4G, H). Again, the changeswere similar in both the ovulatory and anovulatorygroups." Seizure free: Cortical excitability was also higher in
both groups with generalized and focal epilepsy in theluteal study compared to the follicular study (see Figs3I, J and 4I, J). The differences were significant at theshort ISIs of 10 and 15 milliseconds (F 5 3.90–4.13,p< 0.05, effect size range 5 0.2–0.3) and the long ISIsof 250 and 300 milliseconds only (F 5 4.06–6.48,p< 0.05, effect size range 5 0.3–0.5), being maximumat the 300-millisecond ISI. This was greater in gener-alized epilepsy, where a significant difference was alsoobserved at the 150-millisecond ISI (F 5 3.59,p< 0.05, effect size 5 0.3). Here too the changes werethe same in both the ovulatory and anovulatorygroups.
Comparisons with Nonepilepsy Controls. Intergroupcomparisons confirmed our previously reported increasein cortical excitability in patients with epilepsy comparedto controls, which relied on whether they were refractoryor seizure free.38 The magnitude of this depended on the
phase of menstruation studied. Comparison of follicularstudies between patients and controls showed signifi-cantly higher cortical excitability in both ovulatory andanovulatory patients with generalized and focal epilepsyat the short ISIs of 2 and 5 milliseconds (F 5 5.49–6.08,p< 0.05, effect sizes 5 0.5 and 0.6) and all the longISIs (F 5 12.21–19.91, p< 0.05, effect size range 5 0.9–1.4) in patients with refractory seizures and only at the250- and 300-millisecond ISIs (F 5 5.57–7.26, p< 0.05,effect sizes range 5 0.4–0.6) in seizure-free cohorts.
Effect sizes were larger at these same ISIs when thesame comparison was performed for the luteal studies(range 5 0.5–1.7). In addition, cortical excitability wasalso significantly higher in both ovulatory and anovula-tory generalized and focal epilepsy with refractory seiz-ures at the 10- and 15-millisecond ISIs (F 5 4.52–8.14,p< 0.05, effect size range 5 0.3–0.7) compared to con-trols in the luteal studies. These changes were observedin all the refractory groups (catamenial and noncatame-nial), with no differences between them.
Discussion
The current study shows that normal variations in corti-cal excitability during the menstrual cycle are altered inwomen with epilepsy regardless of clinical presentation,or type of cycle (ovulatory or anovulatory). Corticalexcitability is highest in healthy, nonepileptic womenduring the follicular phase. In women with epilepsy, the
FIGURE 2: Short and long interstimulus interval (ISI) recovery curves for the dominant hemisphere in nonepilepsy controls ateach of the studied phases of the menstrual cycle. Ratios <100% indicate inhibition, and ratios >100% indicate facilitation. Thebars represent standard error. CR 5 conditioning response; MEP 5 motor evoked potential; TMS 5 transcranial magnetic stim-ulation; TR 5 test response. [Color figure can be viewed in the online issue, which is available at www.annalsofneurology.org.]
ANNALS of Neurology
752 Volume 74, No. 5
FIGURE 3: Short and long interstimulus interval (ISI) recovery curves for the dominant hemisphere in each group with general-ized epilepsy at each of the studied phases of the menstrual cycle. C1 5 perimenstrual pattern of seizure exacerbation; C2 5periovulatory pattern of seizure exacerbation; C3 5 luteal pattern of seizure exacerbation. Ratios <100% indicate inhibition,and ratios >100% indicate facilitation. The bars represent standard error. The upper boundary of the gray shaded area repre-sents the mean of nonepilepsy controls during each phase. CR 5 conditioning response; MEP 5 motor evoked potential; TMS5 transcranial magnetic stimulation; TR 5 test response. [Color figure can be viewed in the online issue, which is available atwww.annalsofneurology.org.]
Annals of Neurology Vol 73 No 6 June 2013: Badawy et al: Cortical Excitability
November 2013 753

FIGURE 4: Short and long interstimulus interval (ISI) recovery curves for the ipsilateral hemisphere in each group with focal epi-lepsy at each of the studied phases of the menstrual cycle. C1 5 perimenstrual pattern of seizure exacerbation; C2 5 periovu-latory pattern of seizure exacerbation; C3 5 luteal pattern of seizure exacerbation. Ratios <100% indicate inhibition, andratios >100% indicate facilitation. The bars represent standard error. The upper boundary of the gray shaded area representsthe mean of nonepilepsy controls during each phase. CR 5 conditioning response; MEP 5 motor evoked potential; TMS 5transcranial magnetic stimulation; TR 5 test response. [Color figure can be viewed in the online issue, which is available atwww.annalsofneurology.org.]
ANNALS of Neurology
754 Volume 74, No. 5

pattern is reversed, and cortical excitability is highest dur-ing the luteal phase.
Changes in Cortical Excitability inNonepileptic WomenIncreased intracortical facilitation (10 and 15-millisecondISIs) was seen during the follicular phase in normal ovulat-ing women compared with the luteal phase. This findingreplicates that published in 2 previous TMS studies per-formed in groups of healthy ovulating women across themenstrual cycle.34,35 Intracortical facilitation is not clearly apurely intracortical phenomenon; there may be both corticaland segmental contributions.44 Despite the complex natureof its underlying substrate, increased intracortical facilitationmay be taken to imply increased glutamate-mediated neuro-nal excitability45 and possibly also decreased c-aminobutyricacid (GABA)A-mediated inhibition46 during the follicularphase in normal nonepileptic women. A lowering ofGABAA-mediated inhibition during the follicular phase isfurther supported by the reported reduction in intracorticalinhibition at the short (<5 milliseconds) ISIs47,48 in 2 previ-ous studies,34,35 although we did not find this in the currentstudy. We also found no evidence of change in long intra-cortical inhibition. Long intracortical inhibition is mainlythought to reflect GABAB-mediated inhibition,49–51
although this has only been pharmacologically confirmed atthe 100-millisecond ISI. If hormonal fluctuations are an im-portant factor underlying variations observed in corticalexcitability, then higher excitability during the follicularphase of ovulatory cycles could be explained by increasedlevels of estrogen associated with decreased levels of proges-terone during the follicular phase, or it could be due to areduction in cortical excitability in the luteal phase resultingfrom increased levels of progesterone. The cyclical variabilitycould also reflect the interplay of both factors at each phaseof the cycle. Hormonal fluctuations, however, do not explainwhy cortical excitability was higher during the follicularphase in women with anovulatory cycles as well. It is knownthat anovulatory cycles do not show the same variations inhormonal levels.16 In addition, there is a report of increasedintracortical inhibition in the luteal phase in women withanovulatory cycles compared to those with ovulatory cyclesdespite the high levels of progesterone in the latter group.36
Our direct human data clearly shows a lack of differencebetween the women with ovulatory cycles and those withanovulatory cycles. Although this contrasts with conclusionsdrawn from indirect evidence based on pharmacologicalstudies mostly performed on ovariectomized animals,6–9 it issupported by others,11–13 particularly the report that hormo-nal fluctuations during rats estrous cycle do not correspondat all with increased excitability measured as progression intopilocarpine-induced status epilepticus.13 This underscores the
need for more studies to clarify the physiological nature ofthe neuronal–hormonal interaction. It also suggests that non-hormonal factors may be involved in the cyclicity of corticalexcitability changes across the menstrual cycle.
Changes in Cortical Excitability inWomen with EpilepsyParadoxically, cortical excitability was highest (increasedintracortical facilitation and decreased long intracortical in-hibition) during the luteal phase of the cycle in our cohortof ovulatory and anovulatory women with both generalizedand focal epilepsy. That this occurs in ovulatory women aswell implies that C3 patterns are not solely explained byhormonal disturbances in anovulatory cycles as suggestedby clinical observations.1,2 Anovulatory cycles are character-ized by an abnormal absence of a substantial increase inprogesterone secretion during the luteal phase despite thelate follicular estrogen surge that results in a high ratio ofneuroexcitatory estrogen to neuroinhibitory progesteronethroughout the luteal phase.15,16 This disturbance does notapply to ovulatory women. Furthermore, luteal phase sei-zure exacerbation cannot be fully attributed to the rapidwithdrawal of the antiseizure effects of progesterone,because cortical excitability was found to be high at a timewhen progesterone levels were very high (confirmed by themeasurements obtained on the day of testing in ourcohorts). Another intriguing finding is that increased corti-cal excitability in the luteal phase was not limited towomen with C3 patterns. It was found in all women withepilepsy whether or not they suffered from catamenial epi-lepsy and even in those who were seizure free, although itwas not statistically significant in the cohorts with the C1and C2 patterns. Again, there was a lack of differencebetween ovulatory and anovulatory women. Normal sexhormone levels were also reported despite increased corticalexcitability during the luteal phase in a TMS study of ovu-latory women with known catamenial epilepsy.37 Thisoccurred in women with all 3 patterns of seizure exacerba-tion (C1, C2, and C3), although the numbers were verysmall. Furthermore, we also found luteal phase hyperexcit-ability in a different cohort of women with new onset epi-lepsy who did not have a definite history of catamenialseizure clustering.52 None of those patients was takingAEDs. All these findings show a striking reversal of thenormal pattern of cortical excitability changes over themenstrual cycle in women with epilepsy that seems tooccur soon after the onset of epilepsy and is present regard-less of clinical presentation and use of AEDs.
The results of the present study provide noveldirect human evidence that the changes in cortical excit-ability cannot be solely explained by hormonal fluctua-tions across the menstrual cycle. This is in contrast to
Annals of Neurology Vol 73 No 6 June 2013: Badawy et al: Cortical Excitability
November 2013 755

previous observational and clinical studies on this topic,which only associated and linked periodical clustering ofseizures to the hormonal changes. The findings alsounderscore the complexity of the effects of sex hormoneson neuronal excitability, seizures, and seizure-induceddamage. This is likely to be due to the multifacetedaction of steroid hormones, which include modulation ofmultiple genes by their up- or downregulation and acti-vation of membrane orphan G-protein–coupled receptorsor specific membrane hormone receptors, or by directbinding to neurotransmitter receptors.53 Alterations inGABAA (decreased short intracortical inhibition47,48) andGABAB (decreased long intracortical inhibition49–51) cir-cuits have been suggested as a mechanism for theincreased cortical excitability observed in numerous TMSstudies of epilepsy.22–26 These changes may alter theresponse of intracortical circuits to all the factorsinvolved in cyclicity of cortical excitability across themenstrual cycle (hormonal and nonhormonal) and causeneurons to interact in an atypical way with circulatingsex hormones. There is evidence that the effects of estro-gen can be influenced by the region or neurotransmittersystem involved, the seizure type or animal model used,and the specific expression of individual estrogen receptortypes.54 There are also distinct modulatory effects ofestrogens on the neurotransmitter system involved in sei-zure genesis.54 It is also known that progesterone metab-olites function as potent positive modulators of theGABAA receptor,8,9 which in the setting of chronic ill-nesses such as epilepsy can cause changes in GABAA re-ceptor subunit composition to compensate for sustainedlevels of inhibition due to periods of prolonged exposureand withdrawal.55 The changes in subunit compositionhave been shown to profoundly alter GABAA receptorstructure and function,56 and subsequently the responseto hormones. Although these conclusions are predomi-nantly based on pharmacological studies on animal mod-els and involve noncortical structures that may not beapplicable to the cortical excitability changes we observedhere, they nevertheless suggest there may be disturbancein the way neurons in general react. This interaction isalso likely to be affected by the use of AEDs and seizurecontrol. It would therefore appear that the final result ofthe cascade of effects initiated by sex hormones on corti-cal excitability and seizure risk is influenced by many fac-tors, but this may express itself at the whole brain levelas increased excitability at a time that corresponds to thetiming of seizure worsening. Clearly, more work isneeded to delineate the nature of all factors involved inthis interaction. Further clarification of the effects of sexhormones on healthy neurotransmitter systems and howthey are altered in epilepsy is also important, as this is a
significant factor in seizure control unique to womenwith epilepsy.
Acknowledgment
We thank Drs W. D’Souza, M. Tan, and K. Fuller fortheir help in recruiting the patients and facilitating accessto their electroclinical and imaging findings; A. Iwasiwfrom JLM Accutek Health Care for providing the TMSequipment; Dr D. Flanagan for his support during allphases of the study; S. Cook, Dr D. Grayden, T. Nelson,R. Balson, N. Beattie, and D. Freestone for the adminis-trative and technical support they provided throughoutthe study; and the participants for their time.
Potential Conflicts of Interest
None.
References1. Klein P, Herzog AG. Hormonal effects on epilepsy in women. Epi-
lepsia 1998;39(suppl 8):S9–S16.
2. Herzog AG. Catamenial epilepsy: definition, prevalence patho-physiology and treatment. Seizure 2008;17:151–159.
3. Klein P, van Passel-Clark LM, Pezzullo JC. Onset of epilepsy at thetime of menarche. Neurology 2003;60:495–497.
4. Tomson T, Battino D. Pregnancy and epilepsy: what should wetell our patients? J Neurol 2009;256:856–862.
5. Harden CL, Pulver MC, Ravdin L, Jacobs AR. The effect of meno-pause and perimenopause on the course of epilepsy. Epilepsia1999;40:1402–1407.
6. Woolley CS. Estradiol facilitates kainic acid-induced, but not flur-othyl-induced, behavioral seizure activity in adult female rats. Epi-lepsia 2000;41:510–515.
7. Scharfman HE, MacLusky NJ. The influence of gonadal hormoneson neuronal excitability, seizures, and epilepsy in the female. Epi-lepsia 2006;47:1423–1440.
8. Lan NC, Gee KW. Neuroactive steroid actions at the GABAA re-ceptor. Horm Behav 1994;28:537–544.
9. Kokate TG, Svensson BE, Rogawski MA. Anticonvulsant activity ofneurosteroids: correlation with gamma-aminobutyric acid-evokedchloride current potentiation. J Pharmacol Exp Ther1994;270:1223–1229.
10. Jacono JJ, Robertson JM. The effects of estrogen, progesterone,and ionized calcium on seizures during the menstrual cycle of epi-leptic women. Epilepsia 1987;28:571–577.
11. Veliskova J. The role of estrogens in seizures and epilepsy: thebad guys or the good guys? Neuroscience 2006;138:837–844.
12. Hoffman GE, Moore N, Fiskum G, Murphy AZ. Ovarian steroidmodulation of seizure severity and hippocampal cell death afterkainic acid treatment. Exp Neurol 2003;182:124–134.
13. Scharfman HE, Goodman JH, Rigoulota M, et al. Seizure suscepti-bility in intact and ovariectomized female rats treated with theconvulsant pilocarpine. Exp Neurol 2005;196:73–86.
14. Foldvary-Schaefer N, Falcone T. Catamenial epilepsy: pathophysi-ology, diagnosis, and management. Neurology 2003;61(6 suppl2):S2–S15.
ANNALS of Neurology
756 Volume 74, No. 5

15. Herzog AG, Fowler KM. Sensitivity and specificity of the associa-tion between catamenial seizure patterns and ovulation. Neurol-ogy 2008;70:486–487.
16. Herzog AG, Klein P, Ransil BJ. Three patterns of catamenial epi-lepsy. Epilepsia 1997;38:1082–1088.
17. Herzog AG, Harden CL, Liporace J, et al. Frequency of catamenialseizure exacerbation in women with localization-related epilepsy.Ann Neurol 2004;56:431–434.
18. Morrell MJ. Effects of epilepsy on women’s reproductive health.Epilepsia 1998;39(suppl 8):S32–S37.
19. Herzog AG, Fowler KM, Sperling MR, et al. Variation of seizurefrequency with ovulatory status of menstrual cycles. Epilepsia2011;52:1843–1848.
20. Herzog AG. Disorders of reproduction in patients with epilepsy:primary neurological mechanisms. Seizure 2008;17:101–110.
21. Murri L, Galli R. Catamenial epilepsy, progesterone and its metab-olites. Cephalalgia 1997;17(suppl 20):46–47.
22. Reutens DC, Berkovic SF. Increased cortical excitability in general-ised epilepsy demonstrated with transcranial magnetic stimulation.Lancet 1992;339:362–363.
23. Werhahn KJ, Lieber J, Classen J, Noachtar S. Motor cortex excitabil-ity in patients with focal epilepsy. Epilepsy Res 2000;41:179–189.
24. Hamer HM, Reis J, Mueller HH, et al. Motor cortex excitability infocal epilepsies not including the primary motor area—a TMSstudy. Brain 2005;128(pt 4):811–818.
25. Manganotti P, Bongiovanni LG, Zanette G, Fiaschi A. Early andlate intracortical inhibition in juvenile myoclonic epilepsy. Epilep-sia 2000;41:1129–1138.
26. Badawy RA, Curatolo JM, Newton M, et al. Changes in corticalexcitability differentiate generalized and focal epilepsy. Ann Neu-rol 2007;61:324–331.
27. Badawy RA, Macdonell RA, Jackson GD, Berkovic SF. Why doseizures in generalized epilepsy often occur in the morning? Neu-rology 2009;73:218–222.
28. Salih F, Khatami R, Steinheimer S, et al. A hypothesis for hownon-REM sleep might promote seizures in partial epilepsies: atranscranial magnetic stimulation study. Epilepsia 2007;48:1538–1542.
29. Manganotti P, Bongiovanni LG, Fuggetta G, et al. Effects ofsleep deprivation on cortical excitability in patients affected byjuvenile myoclonic epilepsy: a combined transcranial magneticstimulation and EEG study. J Neurol Neurosurg Psychiatry2006;77:56–60.
30. Scalise A, Desiato MT, Gigli GL, et al. Increasing cortical excitabil-ity: a possible explanation for the proconvulsant role of sleep de-privation. Sleep 2006;29:1595–1598.
31. Badawy RA, Curatolo JM, Newton M, et al. Sleep deprivationincreases cortical excitability in epilepsy: syndrome-specificeffects. Neurology 2006;67:1018–1022.
32. Badawy R, Macdonell R, Jackson G, Berkovic S. The peri-ictalstate: cortical excitability changes within 24 h of a seizure. Brain2009;132(pt 4):1013–1021.
33. Wright MA, Orth M, Patsalos PN, et al. Cortical excitability pre-dicts seizures in acutely drug-reduced temporal lobe epilepsypatients. Neurology 2006;67:1646–1651.
34. Smith MJ, Keel JC, Greenberg BD, et al. Menstrual cycle effectson cortical excitability. Neurology 1999;53:2069–2072.
35. Smith MJ, Adams LF, Schmidt PJ, et al. Effects of ovarian hor-mones on human cortical excitability. Ann Neurol 2002;51:599–603.
36. Hattemer K, Knake S, Reis J, et al. Excitability of the motor cortexduring ovulatory and anovulatory cycles: a transcranial magneticstimulation study. Clin Endocrinol (Oxf) 2007;66:387–393.
37. Hattemer K, Knake S, Reis J, et al. Cyclical excitability of themotor cortex in patients with catamenial epilepsy: a transcranialmagnetic stimulation study. Seizure 2006;15:653–657.
38. Badawy RA, Jackson GD, Berkovic SF, Macdonell RA. Corticalexcitability and refractory epilepsy: a three-year longitudinal trans-cranial magnetic stimulation study. Int J Neural Syst2013;23:1250030.
39. Kwan P, Brodie MJ. Early identification of refractory epilepsy.N Engl J Med 2000;342:314–319.
40. Kwan P, Arzimanoglou A, Berg AT, et al. Definition of drug resist-ant epilepsy: consensus proposal by the ad hoc Task Force of theILAE Commission on Therapeutic Strategies. Epilepsia2010;51:1069–1077.
41. Rossini PM, Barker AT, Berardelli A, et al. Non-invasive electricaland magnetic stimulation of the brain, spinal cord and roots: basicprinciples and procedures for routine clinical application. Reportof an IFCN committee. Electroencephalogr Clin Neurophysiol1994;91:79–92.
42. Oldfield RC. The assessment and analysis of handedness: TheEdinburgh inventory. Neuropsychologia 1971;9:97–113.
43. Cohen JB. Statistical power analysis for the behavioral sciences.New York, NY: Academic Press, 1969.
44. Di Lazzaro V, Pilato F, Oliviero A, et al. Origin of facilitation ofmotor-evoked potentials after paired magnetic stimulation: directrecording of epidural activity in conscious humans. Neurophysiol-ogy 2006;96:1765–1771.
45. Ziemann U. Pharmacology of TMS. Suppl Clin Neurophysiol2003;56:226–231.
46. Fedi M, Berkovic SF, Macdonell RA, et al. Intracortical hyperexcit-ability in humans with a GABAA receptor mutation. Cereb Cortex2008;18:664–669.
47. Kujirai T, Caramia MD, Rothwell JC, et al. Corticocortical inhibitionin human motor cortex. J Physiol 1993;471:501–519.
48. Boroojerdi B. Pharmacologic influences on TMS effects. J ClinNeurophysiol 2002;19:255–271.
49. McDonnell MN, Orekhov Y, Ziemann U. Suppression of LTP-likeplasticity in human motor cortex by the GABAB receptor agonistbaclofen. Exp Brain Res 2007;180:181–186.
50. Florian J, Muller-Dahlhaus M, Liu Y, Ziemann U. Inhibitory cir-cuits and the nature of their interactions in the human motorcortex: a pharmacological TMS study. J Physiol 2008;586:495–514.
51. Mott DD, Lewis DV. The pharmacology and function of centralGABAB receptors. Int Rev Neurobiol 1994;36:97–223.
52. Badawy RA, Macdonell RA, Berkovic SF, Jackson GD. Corticalexcitability and the menstrual cycle: reversal of normal patterns innew onset epilepsy [abstract]. Clin Neurophysiol 2010;121:S197.
53. Vel!ı#skov!a J, DeSantis KA. Sex and hormonal influences on seizuresand epilepsy. Horm Behav 2013;63:267–277.
54. Veliskova J. Estrogens and epilepsy: why are we so excited? Neu-roscientist 2007;13:77–88.
55. Smith SS, Shen H, Gong QH, Zhou X. Neurosteroid regulation ofGABA(A) receptors: focus on the alpha4 and delta subunits. Phar-macol Ther 2007;116:58–76.
56. Maguire J, Mody I. Neurosteroid synthesis-mediated regulation ofGABA(A) receptors: relevance to the ovarian cycle and stress. JNeurosci 2007;27:2155–2162.
Annals of Neurology Vol 73 No 6 June 2013: Badawy et al: Cortical Excitability
November 2013 757