AquaDios-Med™ Proactive Preventive Medicine Is • Solution To HealthCare Crisis • AquaDios Corp
607
A 21 st Century Immersion Environment for Advanced Fitness & Accelerated Healing AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION • To The Manufactured • Man-Made Healthcare • Crisis Research • Solution • Analysis • Answers By Dr. Alan Jensen www.AquaDios.com [email protected] P.O. Box 2228 Malibu, CA 90265 310-897-5055 Dr. Alan Jensen • Founder • CEO • Creator • • AquaDios-Med™ • Copyright © 1985 • 2008 • 2012 • 2013 AquaDios TM / AquaDios-Med TM AquaDiosMed TM All Rights Reserved AquaDios-Med™ PPM • Healthcare Crisis • Solution
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of AquaDios-Med™ Proactive Preventive Medicine Is • Solution To HealthCare Crisis • AquaDios Corp

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION • To
The Manufactured • Man-Made Healthcare • Crisis
Research • Solution • Analysis • Answers
By Dr. Alan Jensen
www.AquaDios.com [email protected]
P.O. Box 2228
Malibu, CA 90265 310-897-5055
Dr. Alan Jensen • Founder • CEO • Creator •
• AquaDios-Med™ •
Copyright © 1985 • 2008 • 2012 • 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
AquaDios-Med™ PPM • Healthcare Crisis • Solution
A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is
AquaDios-Med Proactive Preventive Medicine
By Dr. Alan Jensen
Over View • Summary • Research
Evidence Based Deep-Water Running Immersion Therapy
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
[email protected] www.aquadios.com diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Healthcare Crisis • Manufactured • Man-Made AquaDios-Med™ Proactive Preventive Medicine Is • Solution
Research • Deep-Water Running Immersion Therapy • Mind-Body Medicine Part I Thru Part IX • Overview • Summary
Many years ago I set out to create and develop the most innovative and complete preventive medicine procedure imaginable, a process that relied on the two basic and historically proven healing capacities and abilities for all people, from children to geriatricians. Western civilization research indicates that safe sustained vigorous exercise will, in itself, establish a physical fitness and rejuvenation level that will establish healthy homeostasis equilibrium consistent to what Hans Selye MD references in his General Adaptation Syndrome -- GAS
The late Hans Selye, a Hungarian endocrinologist died in 1982, was the first to give a scientific explanation for biological stress with a model based on physiology and psychobiology – GAS; an event that threatens an organism’s well-being -- a stressor leads to a three-stage bodily response of Alarm – Resistance - Exhaustion. This theory is fundamental to the practical understanding, etiology and diagnosis of most all medical illness – disease symptoms – syndromes. Exhaustion is the stage of physiological and psychobiological distress that may breakdown the mind - body. Research has confirmed that when this psychophysiological is just beginning to interfere with a person’s normal function, safe sustained vigorous exercise can re-establish healthy homeostasis equilibrium.
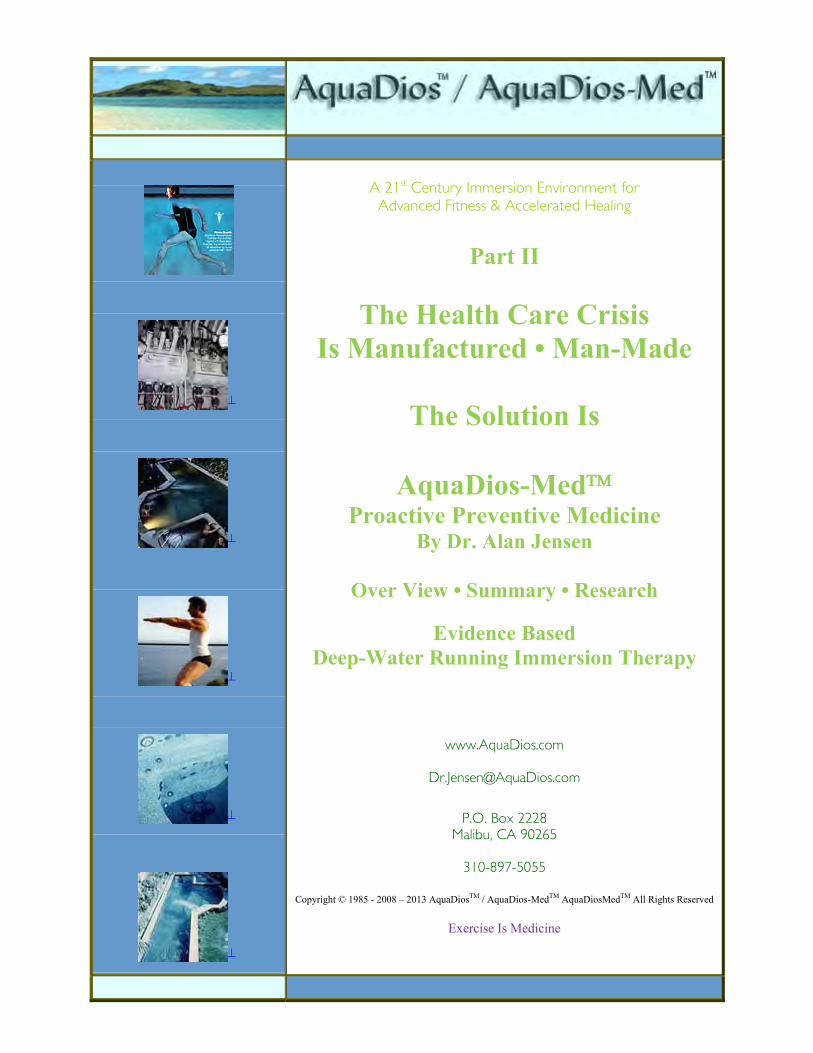
Dr. Ken H. Cooper stressed the necessity for providing epidemiological data to support the
benefits of regular exercise and health early in his career. Cooper’s data from thousands of individuals became the foundation for his aerobic concepts. Aerobics, released in 1968, sent a powerful message to the American people - to prevent the development of chronic diseases, exercise regularly and maintain high fitness levels throughout life. Dr. Cooper’s message, programs and ideas established the model from which fitness has proliferated up to modern time; unfortunately this scientific knowledge seems to have little to no influence on how the modern hospital medicine system works
Dr. Ken H. Cooper advocated a philosophy that shifted away from disease treatment to one of
disease prevention … It is easier to maintain good health through proper exercise, diet, and emotional balance than it is to regain it once it is lost … In 1970 he opened The Cooper Institute, and today is widely recognized as The Father of the Modern Fitness Movement. Cooper is generally credited with encouraging more individuals to exercise than any other individual in history.
By the 1980’s cutting edge research showed the mind played an immense role in serious and chronic diseases suggesting people could be taught how to regulate their psycho-physio-biology to prevent dis-ease while sports enthusiasts learned ideal performance states. Sweden was the first country to apply a process of self-hypnosis to the general population, known as Inner Mental Training – IMT and millions of Swedes showed remarkable long term health and decreased need on modern medicine; a preventive process.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
This program was made possible by Dr. Uneståhl, Sweden. During this period I collaborated with Uneståhl and we discussed how IMT should be taught to people worldwide as a part of all cultures. Simultaneously I became active in Psychoneuroimmunology -- PNI research that verified thoughts, experience, sensations, sounds, taste, visual perceptions and much more can and does influence physiology in both positive and negative ways – Mind the Healer - Slayer. About the same time I began research safe exercise modalities, at the time running – jogging and power walking were popular but the impact trauma was causing more than many people injury and sending them to doctors’ offices with pain, suffering and need for rehabilitation. Most all of these people were attempting to accomplish physical fitness with Cooper aerobic concepts and deep-water immersion therapy consisted mainly of the high temperature water for increased healing. This was about the time Glen McWaters who had worked with rehabilitation of American miler Steve Scott and developed Deep-Water Running with a Wet Vest to continue workouts during injury and overcome any cardiovascular training loss. At the time I was running between 4 and 16 miles daily, usually two 4-mile runs per day, am – pm combined with two eight-mile runs per week and one 16-mile run per week. This rigorous exercise program resulted in innumerable aches, pains, sprains of the ankle, feet, knees, hips, lower back etc. McWaters, inventor of the WetVest and only expert in Deep-Water Running Immersion Therapy at the time, was kind enough to consult with me by phone to discuss the many physiological healing properties that were accelerated by DWRIT and, I most instances the DWRIT exercise could be accomplished – while injured to accelerate healing. I did extensive research beginning with the International Society Medical Hydrology – Climatology Association -- ISMH, Rehabilitation Centers, and SPAS to find DWRIT practices but found Deep-Water Immersion Therapy was limited, at the time to a few advance elite runners such as Steve Scott. All Rehabilitation Facilities relied on deep-water immersion, but only in warm-hot temperatures of 86°- 93 ° F. No DWRIT exercise in any of these rehab facilities through the US, Europe, Canada, Australia; I visited more than many of these centers in the western world and found there to be what I coined as a Rehabilitation and Spa Culture; only hot-warm water with limited to no exercise as it is not advised to exercise in hot-warm water immersion. By 1987 I had developed the innovative DWRIT with multiple immersion chambers, each with its own unique temperature starting at 98 ° F for warm up and power massage and then mild DWRIT training in 88 ° F for a few minutes followed by about 35 minutes of sustained vigorous DWRI in 70° F with a few minutes DWRI in cold 63° F. Research physiology show the multiple immersion chambers and temperature together with power massage to maximize the human healing capacities. When PNI – Mind body Medicine MBM – Inner Mental Training - IMT was added to the healing equation it showed the human healing response could accelerated beyond all expectations especially when Rehabilitation Pain was integrated – a just noticeable difference – JND between injury pain and rehabilitation pain. The DWRI work of Selye, Cooper, McWaters and others united together with the known principles found in PNI- MBM- IMT became my innovation known as AquaDios-Med™ Proactive Preventive Medicine. But, to bring this process into the real world a medical prototype had to be built with the multiple immersion chambers each with its own specific temperature. Unfortunately, I have been unable to locate any research on studies with multiple temperature immersion or sustained DWR though anecdotal accounts have been cited when possible; most often in the sports world.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
Mind-Body Medicines • Deep-Water Running Immersion Therapy • Research AquaDios-Med™ Proactive Preventive Medicine • Evidence Based
AquaDios-Med™ Proactive Preventive Medicine is patient-centered evidence based scientific
medical process that integrates physiological aspects of Medical Hydrology, Deep-Water Running Immersion Therapy and Aquatics. The ADM™ PPM innovative process takes place in unique Proprietary Deep Immersion Chambers with Multiple Temperatures, Proprietary Power Massage with Proprietary Safety Handles. Patients learn correct Deep-Water Running posture to sustain safe vigorous exercise together with Psychoneuroimmunology – PNI, Mind Body Medicine -- MBM; Inner Mental Training – IMT; Physiological Self-Regulation -- PSR and Medical Hypnosis to accelerate healing when sick or injured, manage -- control pain, manage -- control symptoms and to establish physical fitness, increase the speed of rejuvenation to maintain normal healthy chemical balance and establish natural homeostasis equilibrium specific to Hans Selye’s, MD General Adaptation Syndrome -- GAS.
Emphasis of AquaDios-Med™ PPM is to teach each patient how to use mental skills to alter
and control positive physiology and how to accomplish safe sustained vigorous exercise to build endurance, stamina, a strong Immune System, to improve vitality and a establish a healthy psychophysiological state; a process that will establish a healthy mental and physical state, independent from drugs and most surgeries.
Research shows the American Healthcare Crisis is a factual Manufactured Man-Made Crisis
created and contrived by an unscrupulous deceitful for-profit culture found in in the U.S. Congress, the FDA, the pharmaceutical-medical device makers, the American Medical Association -- AMA, the American Hospital Association – AHA -- Modern Hospital Medicine practices and the entire healthcare industry. This industry spends hundreds of billions of dollars lobbying Congress to shelter incredibly, stupendous and colossal profits. For that reason, the American Healthcare Crisis is nothing more than an artificial politicized hypothetical construct, a Franklin D. Roosevelt quote is relevant here … In politics, nothing happens by accident. If it happens, you can bet it was planned that way. For this culture the HealthCare System design is to manipulate one of the most important and absolutely necessary socio-medico-system, one that all people need and depend on from birth to death for healthcare. Consequently, hospitals and modern medicine are both manipulated and directly complicit in the fraud of selling iatrogenic medicine with unnecessary services such as surgeries, medicines, procedures, tests, examinations, all of which are profit-centered and dangerous, some causing serious debilitating and lasting side effects and too often death.
If your car had a tire low on air, all it needed was a little air, but you took it to an unscrupulous
mechanic, one who convinced you there was a serious problem needing expensive diagnostics that eventually led to replacing enumerable parts, none of which needed replacement, at a cost of thousands of dollars; and those parts were installed incorrectly leading to breakdowns – this activity, very similar to that which takes in hospitals daily, would be ruled as criminal and prosecuted. This kind of fraud would not be tolerated; the car would be protected, but that same protection does not apply to patients entering hospitals for evaluation and honest treatment.
The perverse nature of this culture, made up of the richest, most powerful Americans, makes it
next to impossible to change anything in this system because it is purposely designed – created, to make enormous amounts of money with no concern for healthcare whatsoever. This one-per-center culture will never tolerate smaller profits in exchange for a patient-centered healthcare system built on the noble principles of medicine that decreases pain and suffering.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
Example • Hospital -- Doctor Profit-Centered Patient-Centered A 64 year old doctor was suffering visual problems [nearly blind in one eye] and went to a
respected Ophthalmologist for examination and diagnosis. What he found was both perplexing and frustrating. First, he never received a valid diagnosis. Second, each of the many scheduled and rescheduled appointments, all with the same repeated tests, already given many times, were again repeated. Third, when he complained about the recurrent, unnecessary testing he was chastised by the Ophthalmologist Expert. Fourth, after calling a nationally recognized University Eye Clinic he was told by the Department Head to inquire about the machine used for eye surgery and gave me the name and model of the newest his department used. Fifth, when he approached the Ophthalmologist Expert he was insulted and when he asked about the medical equipment [it was the older model, less reliable model] and suggested he have the surgery ASAP. Instead, he traveled about 460 miles to the University Hospital and within 2 minutes, literally 2 minutes, the Department Head identified the problem, gave a diagnosis and asked questions to establish the etiology and learned the visual problem was an injury suffered from the impact of a traffic accident. The first doctor NEVER gave a diagnosis nor etiologically determined the cause of the visual problem while requiring more than many repeated appointments and repeated tests – all of which were being charged to Medicare and all but one were unnecessary – all along padding the bill – income – profit. Whereas, the University doctor immediately determined the visual problem and helped to discover how it occurred, schedule the surgery and within two weeks the near blindness in that one eye was gone – a medical miracle.
The point here is that technical medical equipment together with examinations and evaluations
are all needed and a part of modern hospital medicine practices, but many procedures are repeated or completely unnecessary for patient care. Had the above patient not been a doctor it is unlikely there would have been such a positive result; a visual miracle as described by the patient-doctor. This one life example is duplicated hundreds of thousands of times in modern medicine, but not with such a positive outcome and is the basis of the healthcare crisis; the first doctor profit-centered, the second patient-centered. The first medical procedure was part of the crisis, the second part of a miracle.
Another example -- same doctor-patient, as a child he had nasal-throat congestion with possible
allergies and was told he must have a tonsillectomy; a popular but proven to be an unnecessary surgery 80 to 90% of the time; he never got over that surgery, he’s still troubled with the same nasal-throat and allergy congestion.
AquaDios-Med™ PPM can become a competitive system or a part of the existing healthcare
system, but it will likely never be more than an ideo, an ideology that will never be acknowledged and put into practice unless the 400 world wide Billionaires step up to the plate with approximate $ 15 Billion it will take to establish AquaDios-Med™ PPM Health Centers across America. It is likely that only then will modern hospital medicine either change or and abandon the ChargeMaster Price System and become patient-centered hospitals. This would be the kind of hospital culture that would never order necessary surgeries, or prescribe unneeded drugs, or order unnecessary procedures. And it would be a medicine practiced with reasonable income -- profits, not just for the big profit, it would always include the patient’s needs.
In order to prove AquaDios-Med™ PPM is a legitimate evidence base health procedure it is
necessary to attempt to pinpoint some of the major research in deep-water running, which unfortunately is mostly directed toward the athlete recovering from injury. Nevertheless, research has demonstrated how valuable deep-water running can be to eliminate or reduce symptoms for those suffering from chronic disease and specific ailments.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
I believe, and I’m certain you’ll agree the research in this supports the fact that exercise is medicine. This is preventive medicine that only the patient or person can produce as a consequence of safe daily exercise as advocated by AquaDios-Med™. The research supports the fact that the impaired become repaired with safe daily exercise; just as AquaDios-Med™ states.
Research Summary Deep-Water Running Immersion Therapy • Mind-Body Medicine
AquaDios-Med™ Proactive Preventive Medicine
Physiological Fundamentals • Scientific Benefits • Deep-Water Immersion To Neck
• Physiologic changes accelerate removal of metabolic waste • Improved cardiac function • Lower blood pressure • Assists the body in healing the tissues
Circulatory System • Cardiac volume increases • cardiac output is increased 32 percent at rest
Most ideal Aerobically efficient cardiovascular conditioning medium available Pulmonary System The total work of breathing increases by 60 percent • Maximized respiratory system efficiency Musculoskeletal System
Blood flow to muscle tissue Increased • 225 percent resting muscle blood flow Increase Kidneys Increase • urine production • sodium and potassium excretion •
• Eliminates toxins which cause disease and inhibit the natural healing processes of the body •
AquaDios-Med™ PPM • Evidence Based Treatment Fundamentals • Summary AquaDios-Med™ Multiple Immersion Chambers • Depths • Temperatures • Hot • Cold
Maximizes healing • Rejuvenation • Re-establishes Healthy Homeostasis - Equilibrium Each Chamber • Therapeutic Power Massage •Buoyant Massage •Exercise Immersion • Helps injured • sore • tender areas to become active •
Physiological Self-Regulation • PSR Accelerated Healing • Rehabilitation
Introduces • Rehabilitation pain • Re-Injury Pain • Maximized Injury Recovery • Accelerated rehabilitation • differentiate • re-injury pain • rehabilitation pain.
Exercise Physiologist’s Rate Benefits • Deep Cool Water Immersion Exercise Highest
• Safest of all physical activities • More than 40 benefits Research • cold immersion to neck increases hemoglobin • oxygen production in blood • enhances cell production • healing capabilities • immune system • accelerates rebuilding the cell
structure • sustained vigorous exercise • in cool water • stimulates • immune system to • aids removal of toxins that build up body • enhances healing properties of blood • rapid recovery • rejuvenation Deep-Water exercise • multiple temperatures • pathway to release safe inner medicine • inner medical doctor • to acquire peak performance • stimulates immune system • establish • balanced healthy homeostasis • physiological self-regulation for accelerated healing • Highest Aerobic Cardiovascular Value • All Exercise • Safest • Bone-Mass Density • Strength Increased • Reverses Aging
Exercise is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
Isokinetic Muscle Contraction Isokinetic Muscle Movements • A product of Deep Water Exercise • Deep Water Movements Produce • Isokinetic Muscle Movements • Only Exercise Possible When Injured • The Safest Exercise for all walks of life • Physiologists recognize isokinetic activity as a speed • strength • power relationship • Best • Most Durable Muscle Structure • Connective tissue
Necessary Deep-Water Running Equipment • WetVest • AquaJoggeer
Integrated • Inner Mental Training • IMT • Mind Body Medicine • MBM • Brief History Mind Body Medicine MBM • Inner Mental Training IMT • Cognitive • Emotional Skills
•Attitudes Wellness • Physical fitness •Health •Pain Management • Physiological Self-Regulation PSR • Safe Rapid Healing • Rehabilitation
Summary AquaDios-Med™ Proactive Preventive Medicine • Inner Mental Training Positive Psychology • Mind Body Medicine • Psychoneuroimmunology • Clinical Hypnosis
• Hospital • Out Patient • Research This research explores and confirms the powerful human capacities that have been included in the AquaDios-Med™ Proactive Preventive Medicine maximized healing and healthcare design with its Mind Body Medicine • MBM • Psychoneuroimmunology • PNI • Altered State of Conscious • ASC • Clinical Hypnosis • All Evidence • Science Based Healthcare Practices
Research • The Ideal Performing State • IPS • ASC • Hypnotic State for Healthcare The autonomic nervous system ASC response to warm water immersion is equivalent to how the
ASC responds to meditation, or other relaxation states • Warm water immersion aids autonomic nervous system maintain positive control of body’s vital functions • Heart Rate, Digestion, Respiration, Salivation, Circulation • Sexual Arousal • Adapt to changes in environment •sympathetic nervous system, SNS accelerates body’s system under stress • parasympathetic nervous system, PNS promotes calm • becomes balanced when body immersed in warm water • These positive physiological changes reduce risk of cardiovascular disease, improves memory, enhances cognitive processes and increases concentration.
Re-Visit Problematic Dangers • Medicine • Pharmaceuticals • $8.2 Million Study • 2008 Proactive Preventive Medicine • Problem Solving
The AquaDios-Med™ Philosophy
• A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing • • EXERCISE IS MEDICINE • THE IMPAIRED BECOME REPAIRED • • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD • • YOU GROW OLD BECAUSE YOU STOP EXERCISING • • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race •
Copyright © 2008 – 2012 – 2013 2nd Edition AquaDios-Med™ • AquaDios Corp.
All rights reserved Exercise is a weapon against Disease

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is
AquaDios-Med Proactive Preventive Medicine
By Dr. Alan Jensen
Research
Deep-Water-Immersion Therapy Mind Body Medicine • Inner Mental Training Positive Psychology • Psychoneuroimmunology
Evidence Based AquaDios-Med™ Proactive Preventive Medicine Deep-Water Running Immersion Therapy
65 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California 90265 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
www.aquadios.com
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
SOLUTION To • Man-Made Healthcare Crisis AquaDios-Med™ Proactive Preventive Medicine 65 Pages
Introduction — The Body Naturally Heals Itself
The human body is designed to heal itself, and it does that very well, given favorable conditions. Unfortunately, with its practice of cutting, drugging and irradiating patients, traditional medicine produces conditions that actually inhibit the body’s self-healing capabilities.
It is in large measure because of this that healthcare costs in the United States are so high (see “The Healthcare – Crisis Manufactured – Man-Made). The solution to the high cost of healthcare is therefore found in providing modalities of treatment that support the body in healing itself when it gets sick, and preventing disease in the healthy body.
An Effective Alternative Healing Modality
Fortunately, modalities that help the body heal itself are well known scientifically. One such modality, with both centuries of historical use and modern confirmation of effectiveness, is deep-water immersion. Traditional deep-water immersion has been refined by AquaDios-Med™ to even more effectively aid the body in healing itself. The latest research on the benefits of physical activity while immersed to the neck in water is described in Considering the Biologic Aspects of Water, Cole, Andrew J. MD - Becker, Bruce E. MD, April 1995;“Water therapy exercise program; Water therapy pain relief; December 27, 2006; American College Sports Medicine, 2006, Advance for Directors in Rehabilitation. Dr. Becker has researched, published, and taught extensively on aquatics. The following points are summarized from his and other research. An Efficient Preventive Medicine Healing • Exercise Modality
Water is the oldest rehabilitation modality known to mankind. Few understand the magnitude, variety, and rapidity of its healing properties. Physical activity while immersed up to the neck in water promotes physical fitness, rapid healing, pain management, and more. Much research over the centuries confirms these properties, and recent research adds further understanding. For example, physical activity while immersed to the neck in water produces physiologic changes that accelerate the removal of metabolic waste, improve cardiac function, and lower blood pressure, thus assisting the body in healing the tissues.
The Circulatory System
Immediately upon immersion, water begins to exert pressure on the body. This aids the circulatory system. For example, central venous
pressure rises with immersion to the chest and increases until the body is completely immersed. Cardiac volume increases by nearly one-third with immersion to the neck. Since the ultimate purpose of the heart is to pump blood, its measure of performance is the amount of blood pumped per unit of time. This is called “cardiac output” and submersion in water to the neck increases cardiac output 32 percent at rest. Research shows structured deep-water exercise is the most ideal, aerobically efficient cardiovascular conditioning medium available.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
The Pulmonary System Like the circulatory system, the pulmonary system experiences profoundly positive effects by
immersion of the body to the thorax. Part of the effect is due to the shifting of blood into the chest cavity, and part is due to compression of the chest wall. The combined effect creates a positive alteration of pulmonary function, increasing the work of breathing and changing respiratory dynamics. In fact, reserve lung capacity decreases by 75 percent at neck immersion, with vital capacity decreasing only slightly. The combined effects of these changes increase the total work of breathing by 60 percent. When water-training time is sufficient, this challenge can markedly improve the respiratory system’s efficiency. The Musculoskeletal System
Deep-water immersion positively affects the musculoskeletal system as well, particularly with vasoconstriction. On land, for instance, sympathetic vasoconstriction tightens the vessels of skeletal muscle to resist blood pooling. But in water, immersion pressure removes the biologic need for vasoconstriction, thus increasing blood flow to muscle tissue. In fact, resting muscle blood flow increases by 225 percent during neck immersion. The Kidneys Aquatic immersion creates many effects upon renal blood flow and the renal regulatory systems. For instance, the flow of blood to the kidneys increases immediately upon immersion, which produces an increase in urine production, as well as sodium and potassium excretion. Sodium excretion also increases as a function of depth due to the shifting of circulating central blood volume. The result of these physiological changes is the elimination of toxins which both cause disease and inhibit the natural healing processes of the body.
Deep-Water Running
Deep-water running while immersed to the neck is often utilized for its conditioning effect. Although opinions vary about the optimal exercise program for people who need joint off-loading during a recovery period, it is known that deep-water aquatic exercise can indeed increase conditioning in that population. In fact, water running equals land running in its effect upon maximal oxygen uptake when training intensities and frequencies are matched.
Similarly, when maximum gains in oxygen uptake during aquatic exercise are compared with equivalent land-based exercise in unfit individuals, the aquatic exercise achieves equivalent results. And water-based exercise programs may be used to sustain or increase aerobic conditioning in people who need joint offloading.
All of the physiological changes described above, and many more, combine to assist and accelerate the body’s natural healing processes, thus providing the body with the conditions most favorable for rejuvenation and self-healing.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
AquaDios-Med™ • State -of-the-Art • Deep-Water Immersion Therapy
AquaDios-Med™ is a specially developed, state-of-the-art, deep-water immersion therapy whose
potential has only begun to be exploited. This unique healing modality represents a fusion of time-tested hydrologic healing practices and modern medical research. It goes beyond any hydrology-based healing modality thus far devised to offer superior healing potential.
The AquaDios-Med™ process is conducted in four stages utilizing four chambers filled with water
at different temperatures, each with powerful jet massage to achieve healing effects above and beyond that of historical or traditional deep-water immersion practices.
Stage one provides a proactive, full-body, therapeutic massage and warm-up. In this chamber, the
temperature is held at a constant 98-99° F (the warmest immersion temperature recommended).
Physiological Self-Regulation • PSR
The autonomic nervous system ASC response to warm water immersion is equivalent to how the ASC responds to meditation, or a number of other relaxation states. Research shows warm water immersion aids the autonomic nervous system maintain positive control of the body’s vital functions of heart rate, digestion, respiration, salivation, circulation and even sexual arousal to adapt to changes in environment. This means that the sympathetic nervous system, SNS which accelerates the body’s system under stress, and the parasympathetic nervous system, PNS which promotes calm, becomes balanced when the body is immersed in warm water. This positive, natural physiological change reduces the risk of cardiovascular disease, improves memory, enhances cognitive processes and increases concentration.
The average person will spend three to five minutes here undergoing water massage of all areas of the body. This station is designed to increase circulation and encourage blood flow into all the muscles, thus relaxing stiff or sore areas and enabling healing to begin. Those with more severe injuries or aches and pains may take a few minutes longer, concentrating the massage on the specific areas requiring additional attention.
Stage two is a deep vertical chamber. This is where structured deep-water rehabilitation exercise
begins. Its temperature is held within a range of 83-88° F. This chamber is designed to accomplish lower-extremity stimulation through powerful therapeutic massage and exercise. Its 8-foot depth frees the skeletal joints and muscles of all compression forces, thus “unloading” all body weight so healing can take place most efficiently. This stage is highly therapeutic for the very sick or aged cardiac patients, people with skeletal problems such as arthritis, those with broken limbs and spinal problems, and the “couch potato” whose health is compromised by inactivity. The average person will spend about five minutes in this chamber doing deep-water running and getting additional deep power massage. Actual therapeutic exercise begins here.
Stage three is the main chamber where sustained, structured, deep-water rehabilitation exercise
takes place. The temperature in this chamber is held at a cool 65-68° F. Sustained exercise in cool water stimulates the immune system, facilitates the removal of toxins built up in the body, and enhances the healing properties of the blood for rapid recovery and rejuvenation. This chamber has therapeutic massage stations at various depths and power levels, plus a Swim Gym, which simulates the currents of a river, allowing the user to swim continuously without interruption. The average person will spend 40 to 55 minutes here doing sustained vigorous exercise and deep tissue massage, to facilitate the removal of disease toxins.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
Research shows that cold immersion to the neck increases hemoglobin and oxygen production in the blood which further enhances cell production and the healing capabilities of the immune system; thereby accelerating rebuilding of the cell structure. Thus, sustained vigorous exercise, in cool water, stimulates the immune system to aid in the removal of toxins that build up in the body, and to enhance the healing properties of the blood for rapid recovery and rejuvenation. Deep-Water exercise in multiple temperatures is the pathway to release one’s safe inner medicine and inner medical doctor, acquire peak performance, to stimulate ones immune system to establish a balanced, healthy homeostasis for physiological self-regulation and for accelerated healing.
Stage four is the cold work chamber. This is the final phase of the process and begins immediately
upon conclusion of the sustained exercise in stage three, just before a cool-down-relaxation period. The temperature here is held at a cool 56-60° F. The average person will spend from three to fifteen minutes here, depending on his or her specific goals and medical needs. This “cold immersion” bath increases hemoglobin and oxygen in the blood and further enhances the healing capabilities of the immune system, thereby accelerating rebuilding of the cell structure. This “cold” process is followed by a quick “first phase hot immersion” for less than one minute, then a return to stage three.
AquaDios-Med™ procedures and processes stimulate dynamic immune system function, eliminate
disease toxins, prevent swelling, advance rapid healing, and reduce psychological obstacles to healing such as anxiety or depression. AquaDios-Med™ is the cutting edge of healing technology because it combines modern therapeutic practices and engineering science together with potent healing sources found in the psychoneuroimmunology mind-body sciences.
The AquaDios-MedTM innovative prototype and programs evolve from the physiology of
Rehabilitation Pain, an innovative term originally coined by Dr. Jensen to describe how accelerated rehabilitation requires differentiating between re-injury pain versus rehabilitation pain. One objective was to create a safe immersion environment where structured, mild-to-rigorous exercise activity can stimulate the inherent, natural capacities within the immune system to accelerate cell structure production. This immune mediation in turn speeds up recuperation, healing, rehabilitation, vitality, strengthening, and endurance for all walks of life. This includes simple well-being and physical fitness. See http://www.aquadios.com/sportmedicine.html
"Rehabilitation pain" is a term Dr. Jensen coined decades ago to describe the difference
between proactive physical activities while injured and the more common, do-nothing, "use-plenty-of-pain-medication" approach to recovery. The downside to proactive or aggressive rehabilitation is that re-injury pain is very similar to rehabilitation pain. Many argue that purposely produced pain is masochistic or self-destructive.
To achieve one's exercise or athletic best and to surpass that level of best -- e.g. if one can lift five pounds five times before fatigue and or pain sets in -- it is that very pain (the tearing down of tissues) that rebuilds tissues and allows one to soon lift ten pounds ten times. Thus, today's best becomes a warm-up activity to the future or new best, a potential endless spectrum of greater achievement; this principle applies in safe, rapid or accelerated rehabilitation.
Injury and injury pain has an automatic internal unconsciousness to prevent re-injury.
Rehabilitation pain is similar to the above example. The problem with pain medication is that it suppresses healing at the injury/trauma site where the mind is capable of establishing pain management and rapid repair - rehabilitation. People are able to heal more quickly and completely when willing to experience rehabilitation pain, particularly at the trauma site, and to learn to distinguish between rehabilitation pain and re-injury pain.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
Rapid accelerated rehabilitation healing involves learning to discriminate safe pain or rehabilitation pain from re-injury pain; this is not a sadomasochist pursuit of pain, it is a complex self-awareness, one which involves self-empowerment, self-improvement, not suffering. It is the act of setting a limit today, a threshold that cannot be crossed today. But tomorrow or the day after, it will be easily delivered.
AquaDios-Med™ PPM • Evidence Based Treatment Fundamentals • Summary
AquaDios-MedTM includes therapeutic massage in each buoyant stage of exercise immersion to
help injured, sore or tender areas to become active. The AquaDios-Med™ physical hard-work exercise phase is a cold immersion to establish
individual tolerance for self-determined physical movement and exercise. The last AquaDios-Med™ phase begins recognition of Rehabilitation Pain or safe exercise
movement activities without causing further or new injury. Click here Rehabilitation Pain AquaDios-Med™ deep-water exercise permits people to distinguish between re-injury and
acceptable non-injury physical activity to further accelerate healing. Rehabilitation Pain during these immersions expedites a much higher cell-production repair rate than normal. Click here to see AquaDios-MedTM Videos.
For decades in Russia, then in Sweden, this type of special therapy was secretly reserved only for
top athletes to promote soft tissue healing such as tendons and nerve tissue as well as bone fractures and other injuries. Around the world, similar procedures are commonly used on prize thoroughbred racing horses and other animals to aid in healing spinal and leg injuries.
AquaDios-Med™ proactive preventive medicine combines these procedures with Mind Body
Medicine science and structured deep-water exercise immersion in one process.
Exercise physiologists rate benefits of deep, cool-water exercise, while immersed to the neck, highest of all physical activities because of the following facts:
Activation of approximately 90% of the major muscle groups results in superior cardiovascular
conditioning; Elimination of high body heat, and neuromuscular trauma to the joints, ligaments, tendons, and
muscles; A heart rate of 10 to 20 beats less per minute allows the heart muscle to grow stronger during
water exertion than on dry land; Hemoglobin oxygen in the blood is increased; Improved body tissue oxygen extraction from blood; Arterial venous difference allows a greater volume of oxygen consumption; Vital air capacity in lungs increases;
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
Bone mass density strength and regeneration is increased; Lactic acid is higher and dissipates faster; Isokinetic water resistance increases strength, endurance, balance, coordination and flexibility; Warm- to hot-water immersion at 90 to 100 degrees F dilates vessels, engorges the body with
blood, and accelerates flexibility, mobility; The autonomic nervous system ASC response to warm water immersion is equivalent to how the
ASC responds to meditation, or a number of other relaxation states. Research shows warm water immersion aids the autonomic nervous system maintain positive
control of the body’s vital functions of heart rate, digestion, respiration, salivation, circulation and even sexual arousal to adapt to changes in environment.
The sympathetic nervous system, SNS which accelerates the body’s system under stress, and the
parasympathetic nervous system, PNS which promotes calm, becomes balanced when the body is immersed in warm water, positive, natural physiological changes reduce the risk of cardiovascular disease, improves memory, enhances cognitive processes and increases concentration.
Cool-water immersion at 68 to 72 degrees F increases hemoglobin and oxygen within the cell
structure. Cold-water immersion 48 to 58 degrees F accelerates immune system production of hemoglobin and oxygen extraction inside the blood for rapid construction and repair of body tissue. AquaDios-Med™ pre-exercise immersion environment is substantially cooler than standard hydrotherapy temperature.
Deep Water Running has the highest aerobic cardiovascular value of all exercise with minimal risk
of injury; is the safest exercise [requires specific training]. Bone-mass density and strength is increased with deep cool-water immersion exercise, as this
activity creates increased body-fluid exchange at porous bone areas and synaptic response to stimulate bone regeneration.
Typical conservative treatment takes about 70% longer to rehabilitate to pre-injury levels of
functionality and in general is much less effective than the more aggressive applied procedures of AquaDios-Med™. AquaDios-Med™ has formulated methods for multiplying concentrations of oxygen and other vital nutrients for cell production repair within the blood.
AquaDios-Med™ technologies and procedures unite the most powerful methods to activate and
accelerate natural individual immune system capacities. Research confirms that circulation and engorgement of blood is stimulated by hot immersion, and by alternating with cold immersion the production of hemoglobin and oxygen in the blood is additionally increased. AquaDios-Med™ multiple temperature immersion programs are calculated to accelerate rehabilitation, recuperation and recovery by access to multiple exercise immersion temperatures. Thus, AquaDios-Med™ technologies actively and spontaneously accelerate the individual's natural immune system functions.
Psychoneuroimmunological, psychophysiological and psychobiological research demonstrates
applied clinical hypnosis and behavior medicine help mediate immune system functions to facilitate therapeutic mind/body healing.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
An AMA (American Medical Association) ten-year study on aging concluded that aging is the equivalent of inactivity, not passage of time, and nutrition with proper exercise can delay or reverse the aging process.
AquaDios-Med™ is an ingenious fusion of health wisdom found all through ancient civilization to the present combined with modern computerized biomechanical science.
AquaDios-Med™ produces only positive results. There are no downsides or negative side effects.
Daily AquaDios-Med™ immersion in this preventative medicine and physical fitness tool boosts immune system cell production required to rejuvenate and accelerate healing. This, in itself, is worth hundreds of millions of dollars to our economy.
Brief History • AquaDios-Med™
Proactive Preventive Medicine System
As an entrepreneur, doctor and scientist I am committed to eliminating the healthcare problem by expanding awareness of the AquaDios-Med™ proactive preventive medicine system, because in my opinion, it is the only genuine innovative healthcare technology that is capable of changing the face of healthcare; my the goal is to launch AquaDios-Med™ PPM across the US
AquaDios-Med™, is a Spanish acronym, to both express the proactive preventive medicine
methods and the process I developed from my life experience to accelerate recovery from serious injury, rehabilitation, rejuvenation, and to honor and respect the cadre of Mexican laborers who helped to construct the AquaDios-Med™ prototype. Symbolizing the divine presence within, the name advocates that all people have, within them, the capacity to be well, healthy and strong with just 45 minutes of deep-water running a day when combined with inner mental training.
Water or aqua exercise, in multiple temperatures of water, is the pathway to release one’s
natural, safe inner medicines and inner medical doctor, which most often completely replaces the need for pharmaceuticals, while awakening natural, positive, healthy homeostasis balance to acquire peak performance, stimulate the immune system and to establish a balanced, healthy platform for physiological self-regulation and for accelerated healing.
The autonomic nervous system ASC response to warm water immersion is equivalent to how
the ASC responds to meditation, or a number of other relaxation states. Research shows warm water immersion aids the autonomic nervous system maintain positive control of the body’s vital functions of heart rate, digestion, respiration, salivation, circulation and even sexual arousal to adapt to changes in environment. This means that the sympathetic nervous system, SNS which accelerates the body’s system under stress, and the parasympathetic nervous system, PNS which promotes calm, becomes balanced when the body is immersed in warm water. This positive, natural physiological change reduces the risk of cardiovascular disease, improves memory, enhances cognitive processes and increases concentration.
Research also shows that cold immersion increases hemoglobin and oxygen production in the
blood which further enhances the healing capabilities of the immune system, thereby accelerating rebuilding of the cell structure. Thus, sustained vigorous exercise, in cool water, stimulates the immune system to aid in the removal of toxins that build up in the body, and to enhance the healing properties of the blood for rapid recovery and rejuvenation. Water or aqua exercise in multiple temperatures is the pathway to release one’s safe inner medicine and inner medical doctor, acquire peak performance, to stimulate ones immune system to establish a balanced, healthy homeostasis for physiological self-regulation and for accelerated healing.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
Dios or God signifies the hidden healing powers in aqua – water and within the body, especially, when strenuous aquatic exercise is done with faith and belief of the power within to heal, no matter the circumstance, within the water and within self. This includes the aptitude to learn mind body medicine to sustain safe exercise, to exercise at peak performance, to rapidly recover from injury or simply recuperate from toxins acquired during the day of work for rejuvenation, physical fitness and to be at one’s best. St. Paul in Romans 12:2 is a biblical source … willfully being transformed in the renewing of mind-body as a positive metamorphosis to something healthy, lasting and enduring, the change of one's organic and substantial change of who we are in life …
AquaDios-Med™, PPM is based on evidence that multiple hot – cold water temperatures,
together with safe sustained vigorous physical activity, while immersed to the neck in cool water, produces natural physiologic changes that cannot be duplicated any other way to speed up the removal of metabolic waste, improve cardiac function, lower blood pressure, learn pain management and assist the body to heal and rebuild tissues. These natural physiological changes result in the elimination of toxins that cause disease and inhibit the natural healing processes of the body. AquaDios-Med™, PPM is designed to be the safest, quickest, most complete natural detoxification procedure for complete, total rejuvenation, healthy homeostasis and a foundation to achieve peak health, wellness and balance.
As a professional, with more than 30 years of private practice and hospital health experience
and an entrepreneur I researched and developed the AquaDios-Med™, PPM health project for more than two decades. Research constantly shows that safe daily exercise, a balanced stress-free mind and body, together with sensible healthy eating habits can eliminate 80 percent or more of the U. S. HealthCare problem and related costs.
The long term research of Bruce Becker, MD, Medical Director at St. Luke’s Rehabilitation
Institute in Spokane Washington has studied the effects of aquatic activities on athletes and people recovering from injuries and ailments. Becker and Andrew Cole, MD wrote a most valuable book, Comprehensive Aquatic Therapy 3rd Edition. Becker also wrote Water therapy exercise program; Water therapy pain relief; while Mary E. Sanders, Ph.D., University Nevada School of Medicine and Public Health research is more focused on physical fitness and aquatic exercisers. Also, I have written an unpublished research document The Health Care Problem: Research of the Crisis; The Solution Is AquaDios-Med™ A Proactive Preventive Medicine Process, available in PDF.
The AquaDios-Med™ proactive preventive medicine process I’ve worked on for so long
assimilates safe structured deep water running exercise with Mind Body Medicine and Psychoneuroimmunology. This unified process forms an Integrated Mental Training (IMT) of Cognitive, Emotional Skills and Attitudes toward wellness, health and pain management. In essence AquaDios-Med™, PPM is designed to facilitate and produce a homeostatic bio-physiology balance that eliminates the dependence on and the abuse of biopharmaceuticals, as well as many surgeries and hospital stays. I estimate AquaDios-Med™, PPM can reduce the need for Pharmaceuticals and biopharmaceuticals by approximately eighty percent.
AquaDios-Med™, PPM combines Mind Body Medicine, through an Inner Mental Training
(IMT) of Cognitive, Emotional Skills and Attitudes toward wellness, health and pain management. IMT or MBM is combined together with sustained, safe structured deep water exercise utilizing Four separate proprietary chambers, each with its own temperature from 100 degrees F; 80 degrees F; 68 degrees F; 64 degrees F and with proprietary power massage - see video demonstration at http://www.aquadios.com/dvd.html or go to http://www.aquadios.com/
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
IMT • Integrated or Inner Mental Training • Brief History
In essence the AquaDios-Med™, PPM design integrates the safest, most well-established, vigorous deep-water exercise together with the most robust deep-rooted and proven physiological self-regulation. The Inner Mental Training - IMT program has been adapted from the work of Dr. Uneståhl, Sweden and Dr. Barrios, USA, and helps patients to learn Physiological Self-Regulation, PSR. Aquadios-Med™, PPM is designed to produce safe rapid healing, pain management, rejuvenation, physical fitness, rehabilitation and has had very good success with cancer patients and other serious medical issues as well as great benefits with professional athletes and all walks of life; see http://www.aquadios.com/mbs.html
The innovative and original IMT has demonstrated its efficacy as a systematic and long-term
training of physiological self-regulation since the 1970’s by Dr. Lars-Eric Uneståhl in close cooperation with the Swedish National and Olympic Teams. The Training System was based on principles from Uneståhl´s research about positive mental training and Mind- Body relations at Uppsala University during the 1960’s.
In Sweden, IMT is used in Schools, Corporations, Business, large Organizations and for
Personal Growth becoming popular in the 1980’s. Emphasis in the 1990’s gradually turned more and more to Health and Clinical areas, but had been involved in Sport, Performing Arts and Education. Today more than 3 million Swedes are involved in the practices of IMT. The four main application areas are: Sport- and Stage performance; School and education, from first grade to University; Business and Public Administration and used by most major international and national companies.
Summary • AquaDios-Med™ Proactive Preventive Medicine • Inner Mental Training • Mind Body Medicine • Psychoneuroimmunology • Clinical Hypnosis
Positive Psychology • Research Aquadios-Med™ or ADM proactive preventive medicine is A 21st Century Immersion
Environment for Advanced Fitness & Accelerated Healing. It is built on the Philosophy that Exercise Is Medicine! The Impaired Become Repaired! You Don't Stop Exercising Because You Grow Old; You Grow Old Because You Stop Exercising! Its design is to produce safe, rapid: healing, pain management, rejuvenation, physical fitness, rehabilitation and has very good success with cancer and other serious medical issues as well as great benefits with professional athletes and all walks of life.
ADM combines Mind Body Medicine, an Integrated Mental Training IMT of Cognitive,
Emotional Skills and Attitudes toward wellness, health and pain management with sustained, safe structured deep water exercise in 4 separate proprietary chambers, each with its own temperature from 98 degrees F; 80 degrees F; 68 degrees F; 64 degrees F and with proprietary power massage - see video demonstration at http://www.aquadios.com/
The combined activities of this specific physical and mental exercise will create a lasting,
healthy, homeostatic bio-physiology balance; one that eliminates the dependence on and the abuse of biopharmaceuticals, many surgeries and hospital stays. See unpublished manuscript titled "The Healthcare Problem and the Solution; AquaDios-Med™ proactive preventive medicine” at http://www.aquadios.com/aquadiosmovies.html
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination. - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
ADM preventive medicine design is based on long term research in two areas. One that shows structured deep-water exercise while immersed to the neck in water is the safest, most well established, proven vigorous exercise because this exercise naturally produces positive physiologic changes that accelerate the removal of metabolic waste, improve cardiac function, and lower blood pressure, all of which accelerate the body in rebuilding and healing the tissues to accelerate healing, rehabilitation and well-being. Over decades the other research area has confirmed that physical or emotional stress - anxiety automatically causes a detrimental mind - body interaction that spontaneously releases hormones that negatively affect all physical systems and organs, which disrupts the body's natural homeostatic balance, the heart, immune function, and diminishes the capacity to heal.
Psychoneuroimmunology is a relatively new discipline that interlinks psychological,
autonomic, immune, and nervous system functioning "psycho" for psychology; "neuro" for neurology, or nervous system; and "immunology" for immunity, and is often referred to as Mind Body Medicine, Psychosomatic Medicine, Non-Invasive Medicine, Medical Hypnosis and Inner Mental Training, these positive medical procedures can be taught to the patient to interrupt dysfunction. ADM has been developed through the proven scientific practices cited herein.
Psychoneuroimmunology, Mind Body Medicine, Psychosomatic Medicine, Non-Invasive
Medicine, Medical Hypnosis and Inner Mental Training all use the same basic principles and all rely on natural positive occurring human events scientifically identified as Altered State of Conscious or ASC and is based on the scientific research that shows all people naturally experience ASC daily; the idea is to make this a positive state for well-being.
The ASC familiarity leads to other naturally occurring positive human experiences to develop
what is scientifically identified as a heightened state of focused concentration, a wilful process of being … “transformed in the renewing of your mind…” and referred to as the Inner Mental Room. This IMT process is common to applications of Mind Body Medicine MBM and will eventually lead to the beginning of psychophysiological self-regulation PSR for positive purpose of well-being. This training in turn leads to development of a practice similar to a self-induced and purposeful self-suggestion, autosuggestion or autohypnosis carried out by means of the learned IMT routine and techniques. The IMT progression begins with physiological conditioning, muscle relaxation, breathing control and heart rate control and advances to psychic conditioning through mental imagery, acoustic therapy and more. ADM has been developed through the proven scientific practices cited herein.
The innovative and original IMT has proven its efficacy as a systematic and long-term training of physiological self-regulation. Its process was developed during the 1970’s in Sweden by Dr. Lars-Eric Uneståhl and under the name Self-Programmed Control or SPC, by Dr. Alfred Barrios in the USA. IMT has been used by more than 3 million of the Swedish population. The main application areas are: Sport and Stage performance; School and education, from first grade to University; Business and Public Administration, Hospitals and used by most major international and national companies. The emphasis in the 1990’s gradually turned more and more to Health and Clinical areas.
One part of the ADM healthcare program is structured deep-water exercise while the other is
within the principles of Mind Body Medicine MBM, Inner Mental Training IMT and Psychoneuroimmunology PNI. In essence AquaDios-Med™ proactive preventive medicine combines the most robust, well-established and proven vigorous, safest exercise together with the most forceful well-established and proven physiological self-regulation, Inner Mental Training IMT to establish Physiological Self-Regulation PSR to facilitate and produce a lasting homeostatic bio-physiology balance that eliminates the dependence on and the abuse of biopharmaceuticals, many surgeries and hospital stays.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
Evidence Based • AquaDios-Med™, PPM Deep-Water Immersion • Preventive Medcine AquaDios-Med™, PPM is evidence based, research shows immersion to the neck in multiple
hot – cold water temperatures together with safe sustained vigorous physical activity, in cool water, natural healthy physiologic changes are generated that cannot be duplicated in any other way. These immersions to substantially increase the speed of the body’s ability to remove metabolic waste -- to improve cardiac function – to lower blood pressure – to learn pain management -- to maximize body healing and rebuilding tissues. These natural physiological changes result in the elimination of toxins that cause disease and inhibit the natural healing processes of the body. AquaDios-Med™, PPM is designed to be the safest, quickest, most complete natural detoxification procedure for complete, total rejuvenation, healthy homeostasis and a foundation to achieve peak health, wellness and balance
Recently research physiologists acknowledged cold water immersion to the neck boosts the
immune system because, in simple terms, this purposeful sudden and drastic cold water immersion temperature change represents an assault that fools the body to significantly increase white blood cell counts and several other positive factors that maximize immune system function. Cold water immersion is a designed stressor to automatically stimulate neurotransmitter’s to produce endorphins, the body’s natural analgesics or pain killers. Endorphins also create a euphoric natural high accompanied by a positive and energizing outlook on life. Simultaneously the parasympathetic nervous system, releases dopamine and serotonin, these neurotransmitters are responsible for rest and repair which further increases positive immune system function.
Current research shows hot water immersion brings a stable balance to the autonomic nervous
system and the sympathetic nervous system, similar to the process of meditation and associated with a reduction in the risk of cardiovascular disease, improved memory, enhanced cognitive processes and increased concentration; this means heart rate, digestion, respiration, salivation, circulation, calm and sexual arousal are normalized
Combined Hot Cold Immersion • Positive Blood Transformation
Hot water immersion brings blood to the surface while cold immersion moves blood to your
organs; these immersion extremes effortlessly cause the heart to increase blood flow – for healing. These alternating immersions help to flush blood circulation pushing blood through all the capillaries, veins and arteries; this exfoliates skin and flush impurities from it, helping complexion and some say it stops cellulite. Evidence shows the General Adaptation Syndrome at work – the body adapts to the hot - cold immersions with repeated exposure and this improves circulation, particularly to the extremities. Researchers also found increased production of testosterone and estrogen in men and women respectively, enhancing libido in both sexes; these hormones also play an important role in fertility. Cold water immersion exercise makes the body work twice as hard to keep warm and burns more calories in the process, a benefit for weight control -- for this exercise, fat is your body’s primary source of energy and the increased work rate will increase your metabolism in the long run
Colder water immersion 64° • 68° F • Coldest water immersion 51° • 58° F •Accelerates Healing
Physiologists confirm Cool – Cold water immersion 68 to 72 degrees F triggers the body to
increase hemoglobin oxygen which improves body tissue oxygen extraction from blood, this allows more rapid – complete cell production with a high density lipoprotein increase to reduce arteriosclerosis -- the heart is stronger with better blood supply with increased stroke volume due to the effects of immersion. Further research shows Colder Water immersion 48° to 58° F accelerates hemoglobin oxygen, the blood's oxygen transportation and extracts even more oxygen from the blood.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
Another physiological benefit of deep-water immersion exercise is that 80-90% of the major muscles groups are used -- especially the gluts, quadriceps and hamstrings to improve posture. There is a total blood volume increase for better oxygen transport; Vital air capacity of the Lungs increases to improve longevity; Warm to Hot water immersion dilates vessels, engorges blood, and accelerates flexibility, mobility; there is No Impact Trauma; Physical movement in the water requires Isokinetic muscle contractions -- an even tension, constant speed, full range of motion – this is the strongest most durable connective tissue and helps reflexes, while quicker movement’s increases water resistance. Water running in Cool water immersion is a Full regime of cardiovascular fitness providing joint motion, flexibility, strength, balance, and coordination. Colder Water Immersion from 51° – 68° F has a powerful healing capacity, but utilized most often only by athletes.
Historical Research • Deep-Water Immersion • Temperature • Therapeutics Research on the cultural use of Deep-Water Immersion Therapy shows the evolution from
before 2000 B.C. For thousands of years Deep-Water Immersion Therapy has been a part of cultures around the world. Even in ancient times the distinctive thermodynamic properties of Water, with its markedly different therapeutic effects at different temperatures has been known and applied for healing.
Hot water is above body at temperature 100° to 103° F, is stimulating, raises the body temperature slightly, very relaxing and dispersing, especially to the muscles, joints and blood vessels. It opens the pores, induces sweating, and penetrates the skin and muscles quite deeply. Hot water can also ripen latent boils, abscesses or skin eruptions and bring them to the surface for release. Hot water draws the body's circulation outwards, opening up the pores and capillaries. Prolonged hot water immersion is not recommended.
Warm water 96° – 99° F, about body temperature or slightly cooler, is gently relaxing,
stimulates appetite – digestion and activity of the digestive organs when done about an hour before eating. Warm water, particularly water that's almost lukewarm -- called tepid is best for general bathing purposes -- warm water is harmonizing and balancing.
Cool water 82° – 88° F is good for soothing heat and inflammation, and for cooling the body on
hot summer days; cool water immersion is good for bringing down fevers. Cold water immersion 72° – 74° F for short periods of time, act as a bracing, stimulating tonic;
after bathing in the hot water pools, Romans would go for a quick dip in the frigidarium, or cold water bath, to brace their skin and close back up their pores.
Sebastian Kneipp a German priest in the 1800s is recognized as the originator – promoter of
cold water therapy in the modern Western world. He was pronounced terminally ill with lung disease and his self-treatment included daily baths in the icy Danube River for just a few minutes; in a year he was cured. He developed a system of hydrotherapy with treatments of alternating hot and cold water therapies for many different health complaints. Today the Kneipp Association has a network of treatment and training centers throughout Europe and in South Africa.
Hot water 100° – 103° F relaxes, disperses, and thrusts blood circulation out to the body's
exterior -- cold water 72° – 74° F stimulates, consolidates and shunts blood circulation inwards towards the core and internal organs. Cold water constricts the blood vessels, stimulates circulation, digestion and metabolism, and awakens the appetite, having an exhilarating effect. Cold water compresses reduce swelling and inflammation. Passive Cold water immersion should only be for a maximum of about 3 to 4 minutes.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
Alternating Hot and Cold water immersions is a particularly powerful technique. The hot water draws old, stagnant blood out of the internal organs or the body’s interior, and the cold water drives fresh blood back into the internal organs and the body's core. With alternating hot and cold immersion, the circulation is powerfully increased, the affected area begins to throb and pulsate -- a sign of healing and regeneration; Hot immersion -- about 3 to 4 minutes -- followed by cold immersion of 1 to 2 minutes. Repeat this two or three time or more, but always end on a short hot or warm application to remove or neutralize any remaining chills.
Summation • AquaDios-Med™ Proactive Preventive Medicine • Design
Deep-Water Running Immersion Therapy • Mind Body Medicine
The evidenced based AquaDios-Med™, PPM is a robust design that integrates the safest, most well established, vigorous deep-water immersion exercise, known to maximize immune system function, together with the most robust deep-rooted and proven physiological self-regulation , a process that interlinks psychological, autonomic, immune, and nervous system functioning.
These physical and mental exercise programs rely on natural positive occurring human events, that of scientific physiology together with that of identified Altered State of Conscious or ASC; scientific research shows all people naturally experience ASC daily – the two activities combined produce a natural positive state of psychophysiological self-regulation.AquaDios-Med™ proactive preventive medicine design is to facilitate and produce a lasting homeostatic bio-physiology balance that eliminates the dependence on and the abuse of biopharmaceuticals, many surgeries and hospital stays.
Research shows structured deep-water exercise while immersed to the neck in water is the
safest, most well established, proven vigorous exercise because this exercise naturally produces positive physiologic changes that accelerate the removal of metabolic waste, improve cardiac function, and lower blood pressure, all of which accelerate the body in rebuilding and healing the tissues to maximize healing, rehabilitation and well-being.
• END Summary
•
AquaDios-Med™ Proactive Preventive Medicine
Inner Mental Training • Positive Psychology • Mind Body Medicine
Psychoneuroimmunology • Clinical Hypnosis •
END Summary •
Exercise Is Medcine
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
14
Begin
Proprietary Innovations
Intellectual Property
AquaDios-Med™
Created By Dr. Alan Jensen
AquaDios-Med™ Proactive Preventive Medicine
Proprietary Innovations • Intellectual Property
Deep Immersion Chambers
• Overhead Views
• AquaDios-Med™ • Medical Prototype
Main Exercise Chamber Deep Strider
Lounge Spa Chamber
Designed • Built • By Dr. Jensen
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
15
AquaDios-Med™ Medical Prototype With multiple Deep-Water Immersion Chambers
The 98 “F” Degree Lounge Spa Chamber The 80 “F” Degree Deep Strider Chamber The 68 “F” Degree Main Exercise Chamber [Cold Chamber not shown]
• AquaDios-Med™ • Multiple • Immersion • Chambers
• AquaDios-Med™ Main Exercise Chamber • Deep Strider • Lounge Spa Chamber
Main Exercise Chamber >>>
• Proprietary Multiple • Depths
• Proprietary Flat Bottom Surfaces
• Proprietary Safety Handles
• Proprietary Dam Walls
• Proprietary Easy Access
• Proprietary Immersion • Chambers

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
16
Proprietary Deep Water
• Main Exercise • Chamber • Proprietary Safety Handles
• Entire • Perimeter
• Swim Gym
• Proprietary Variable Depths
• Proprietary Flat Bottom Surface
• Multiple Jacuzzi Jets • Proprietary Power Massage • Proprietary Safety Handles
Proprietary Deep Strider Chamber Design • People Who Cannot Exercise • Injury • Where Structured Deep Water Running Taught To All People.
• Deep Strider Chamber • • Proprietary Safety Handles • Teaching Correct Posture • Deep Water Running Teaches patients how to perform Safe daily structured deep-water running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
17
Proprietary
Deep Strider Chamber
Multiple Jacuzzi Jets
Proprietary Power Massage
Numerous Proprietary
Safety Handles
Various Standing Locations
Ergonomic Design
Comfort Safety
Lounge Spa Chamber
Multiple Depths
Jacuzzi Jets
Power Massage
Lounge Spa
Chamber
Multiple
Proprietary
Handles
• Safety • Assist
• Power Massage
• All Body Areas

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
18
AquaDios-Med™ Lounge Spa Chamber
Multiple Depths • Jacuzzi Jets • Proprietary Safety Handles Massage • Head • Neck • Shoulders • Lower Back • Thighs • Knees • Calves • Ankles • Feet
AquaDios-Med™ Lounge
Spa Chamber
Patients learn how to perform Safe Power Massage
with Proprietary Safety Handles

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
19
AquaDios-Med™ Proprietary Plenums
Proprietary Plenums Absolutely Necessary To
Supply Sufficient Water Pressure Forces For
Power Massage To Numerous Jacuzzi Jets
AquaDios-Med™ Proprietary Safety Handles

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
20
AquaDios-Med™ Proprietary Safety Handles
AquaDios-Med™ Proprietary Computer Power Center Controller for
Multiple Plenums and Numerous Jacuzzi Jets
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
21
Dr. Jensen Demonstrating Curative - Healing Yoga Poses
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
22
AquaDios-Med™ Pictures – Graphs
Dr. Jensen Deep-Water Running in a Wet Vest Steve Scott Deep-Water Running
In a Wet Vest Correct Posture Deep-Water Running
The AquaDios-Med™ Philosophy • EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING!
AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
23
Borg’s RATING OF PERCEIVED EXERTION (RPE)
0 nothing at all
1 very, very weak
2 very weak
3 weak
4 somewhat weak
5 moderate
6 somewhat hard
7 hard
8 very hard
9 very, very hard
10 maximal (all-out effort)
AquaDios-Med - Rehabilitation Pain
RATINGS OF PERCEIVED PAIN
0 nothing at all No Pain
1 very, very weak Minimal Discomfort
2 very weak Minor Pain
3 weak Experienced Discomfort
4 somewhat weak Low Grade Pain
5 moderate Tolerable Pain
6 somewhat hard Uncomfortable Pain (Safe) 7 hard Moderate Pain (Safe-Marginal)
8 very hard Severe Pain (UNSAFE)
9 very, very hard Unmanageable Pain (DANGEROUS)
10 maximal (all-out effort) - Intractable Pain (UNSAFE-RE-INJURY)
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
24
AquaDios-Med™ Dr. Alan Jensen
TABLE 2 • AEROBIC ACTIVITIES • ADVANTAGES • DISADVANTAGES ACTIVITY ADVANTAGES DISADVANTAGES RUNNING Convenient. Extremely hard on joints, muscles bones Provides aerobic benefits in short period of time Decreases flexibility.
Causes muscle imbalance. Low skill level required
Increases speed, endurance. Most of activity performed by lower body.
SWIMMING Reduced pressure on joints 80-90% of activity-performed bones. by upper body. Eliminates neuro- Possible ear - eye infections muscular trauma. Sinus - other problems Allows extended exercise High skill level required
Increases endurance. Pool - immersion water required CROSS- Many muscles involved. High altitude. COUNTRY Provides vigorous workout Cold. SKIING Limited season. Overload principle. Limited access. Increases endurance. High skill level required DEEP WATER Nearly all muscles involved. Pool or body of deep water required RUNNING Provides vigorous workout. Overload principle. Reduced pressure on joints, bones. Eliminates neuro-muscular trauma. Allows extended exercise. Provides aerobic benefits in short
period of time. Low skill level required. Maintains or increases flexibility. Prevents muscle imbalance. Increases speed, endurance.
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
25
Isokinetic Contraction Isotonic Contraction
Eccentric Contraction Isometric Contraction
Controlled Breathing Through BRACEDVE:
a) Breathing e) Energy
b) Relaxation f) Detachment
c) Attention g) Visual Imagery
d) Concentration h) Equilibrium-Balance-Being Centered
Deep-Water Running Nearly All Muscles Involved Deep-water running exercise uses all the upper and lower body muscles -- the safest and best
aerobic exercise for developing cardiovascular capacity – also - best safest for muscular strength -- endurance because it is isokinetic exercise. Edward Fox, in Sports Physiology … From a physiology viewpoint, isokinetic training programs are the best for improving athletic performance ... Muscles can undergo four basic types of contractions: isokinetic, isotonic, eccentric, and isometric:

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
26
Isokinetic Contraction Isokinetic - - same speed contractions are positive muscle contractions -- occur when a muscle is subjected to an even amount of tension at a constant speed over the full range of motion. Isokinetic activities maintain an equal amount of tension on the muscle throughout the range of motion. A bicep curl is performed in water at a constant speed using only the resistance of the water -- the muscle receives equal amounts of tension -- the more quickly the arm moves, the more resistance it encounters. Isotonic Contraction
Isotonic -- meaning same weight -- are positive contractions -- occurs when a muscle shortens under tension such as a bicep curl. Isotonic exercises require a weight that can be moved the full range of motion because the velocity of the weight carries it through the range where the muscles are otherwise too weak.
Eccentric Contraction
Eccentric contractions -- muscles lengthen under tension is a -- negative contraction -- opposite of isotonic contractions -- occurs when you lower the dumbbell from the shoulder to the starting position in a bicep curl -- takes effort to control the weight as it is lowered.
The more slowly the weight is lowered, the more pronounced the exercise becomes. Eccentric Contraction - A 50- pound weight is lowered slowly from the shoulder to the starting position.
Isometric Contraction
Isometric -- same length contraction -- muscle is
subjected to tension without changing length -- contraction occurs when you attempt to lift a weight that is too heavy to lift, as illustrated – you strain with the weight for several seconds before deciding -- you cannot lift it -- this straining period -- is an isometric exercise. The muscle does not move, but it is subjected to tension. A bicep curl is attempted with more weight than the subject can lift. The muscle is subjected to tension but does not move.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
27
Necessary Deep-Water Running Equipment WetVest • AquaJoggeer
AquaJogger Buoyancy Belt
Wet Vest – Hydrotone Structured Deep Water Running AquaJogger Buoyancy Belt >>>>
Deep Water Running Wet Vest
Structured Deep Water Running AquaJogger Buoyancy Belt <<<<<
WetVest

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
28
Correct Posture • Deep-Water Running • Graphs
Deep-Water Running Examples

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
29
Aquatic Exercise Examples

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
30
Advanced Aquatic Exercise Equipment
Hydratone Aquatic Equipment Advanced Athlete
In-Water Aquatic Equipment

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
31
Isokinetic resistance
Isokinetic resistance is an even
opposition to power ratio, it builds the most durable, elastic and strong connectivity for muscle to bone.
Sustained vigorous intense power water running is the safest way to build physical fitness and both muscle and skeletal strength. It is the only exercise possible when injured; making it the safest exercise for all walks of life. Physiologists recognize isokinetic activity as a speed – strength - power relationship
As speed of movement in the water is accelerated a certain level of strength is required and this repeated action builds Isokinetic resistance muscle power --
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
32
Equipment Needed • Deep-Water Immersion Running AquaJogger • Wet Vest • Hydrotone
ISOKENITIC PURPOSE See picture >>>
Wet vest is a lightweight, snug fitting, training aid for superior conditioning and fitness specifically designed for deep-water exercise. During immersion its design comfortably allows total freedom of movement while keeping the head above water for easy breathing and visibility. There is no risk of injury because there is no impact trauma in deep water. Aqua-Jogger Belt – see picture>> Each movement is isokinetically opposed by water's natural soothing resistance. It takes about 3 times more energy to run in deep water compared to dry land. Superior conditioning with increased cardiovascular safety is possible because during immersion heart rate averages are around 10 to 20 beats less per minute. Waters added resistance requires more neuromuscular activation at the lower back, stomach wall, upper back and chest to maintain the correct walking-running position.
STRUCTURED DEEP WATER RESISTANCE EXERCISE
The Wet Vest or Aqua-Jogger allows body immersion up to the neck in a safe and comfortable manner. Joints and muscles can then become easily aligned. During immersion active exercise motion takes place with no pressure or distress on the body. Muscles are soothed and pain and fatigue are reduced while healthy aerobic cardiovascular strengthening and endurance are stimulated. Structured Deep Water Resistance Exercise-running Physiotherapy is safe and has virtually no disadvantages when use of the WET VEST is integrated with practical assistance, Behavior Medicine, and Applied Clinical Hypnosis for creative healing and performance imagery.
Physiologist’s rate benefits of Deep Cool water exercise Highest!
Exercise physiologists rate benefits of structured deep cool water resistance exercise while immersed to the neck highest of all physical activities because of the following facts: ***Approximately 90% of the major muscle groups are activated resulting in superior cardiovascular conditioning; ***arterial venous difference allows a greater volume of oxygen consumption; ***bone mass density strength and regeneration increases; ***lungs vital air capacity increases; ***lactic acid is higher, dissipates faster; ***at the same RPE, rate of perceived exertion, heart rates are 10 to 20 beats less per minute in water than dry land, heart muscle can grow stronger during exertion ; ***elimination of high body heat, and neuromuscular trauma to joints, ligaments, tendons, muscles; ***hemoglobin oxygen in the blood is increased; improved body tissue oxygen extraction from blood; ***water resistance increases strength, endurance, balance, coordination, and flexibility.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
33
Nearly All Muscles Involved
Deep-water exercise involves use of a large number of muscles. Swimming is a good exercise, but upper body muscles, primarily the shoulder muscles, do 80 to 90 percent of the work. Running on land is just the opposite; lower body muscles do nearly all the work. Deep water running exercise uses all these muscles, both upper and lower body. Yet another reason safe deep-water exercise is the best exercise for developing muscular strength and endurance is that DWR is an isokinetic exercise.
AquaDios-Med™ Proactive Preventive Medicine Mind Body Medicine MBM Psychoneuroimmunology PNI
Inner Mental Training IMT • Evidence Based
1. Psychoneuroimmunology- Mind Body Medicine – Inner Mental Training is a disciplined use of natural Altered State of Conscious - - Attention, which approaches peak concentration capacity as related to an individual’s unique use of his or her own Neurophysiology, and helps to establish a common language relevant to treatment goals.
2. Psychoneuroimmunological; Mind Body Medicine capacity perceived as natural human trait 3. Psychoneuroimmunological - Hypnotic Induction Profile: one practical clinical method to measure Mind Body Medicine compliance relevant to treatment goals – Teach Self-Hypnosis.
4. Lay hypnotists, stage hypnotists and minimally trained professionals can be dangerous, cause confusion for the public and medical-psychological professions.
5. Psychoneuroimmunological, Psychophysiological and Psychobiological Research Demonstrates Mind Body Medicine and Inner Mental Training help mediate immune system functions to facilitate therapeutic mind body healing.
6. BRACEDVE, an Ideal Performance State acronym for athletes and wellness: (Breathing, Relaxation, Attention, Control, Energy, Detachment, Visual-imagery, EQUILIBRIUM) 7. 70 to 90 percent of Disease and other related medical or psychological maladies can be eliminated or controlled with psychoneuroimmunological mediation. 8. Discrimination between Rehabilitation pain and re-injury pain is an essential subjective discrimination to accelerate healing, improve rehabilitation while cultivating balanced strength.
9. Wet Vest is a lightweight snug fitting training aid for immersion in deep water conditioning. 10. Hydrotone is durable space age lightweight equipment designed to cube the resistance of
specific water movement velocity. 11. It takes more than three times the energy to run in the water than on dry land. 12. Deep Water-Running has the highest aerobic cardiovascular value of all Exercise with minimal risk of injury.
13. Range of Deep water resistance varies from 4 to 52 times greater than on dry land depending on exertion level used.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
34
14. Exercise physiologists rate benefits of deep cool water exercise while immersed to the neck highest of all physical activities because of the following 10 facts: a. activation of approximately 90% of the major muscle groups results in superior cardiovascular conditioning; b. elimination of high body heat, and neuromuscular trauma to the joints, ligaments, tendons, and muscles; c. a heart rate of 10 to 20 beats less per minute allows the heart muscle to grow stronger during water exertion than on dry land at the same RPE (rate of perceived exertion); d. hemoglobin oxygen in the blood is increased; e. improved body tissue oxygen extraction from blood; f. arterial venous difference allows a greater volume of oxygen consumption; g. vital air capacity in lungs increases; h. bone mass density strength and regeneration is increased; i. lactic acid is higher and dissipates faster; j. isokinetic water resistance increases strength, endurance, balance, coordination - flexibility;
15. Sport physiologists theorize training programs requiring isokinetic muscle contractions are
best suited for improving athletic performance.
16. Isokinetic muscle contractions are made with even tension, constant speed and a full range of motion. 17. With a foot stroke of 800 to 1,000 pounds (or more), per square inch running creates maximum neuromuscular trauma to the whole body precipitating a new medical vocabulary: runners knee, Achilles tendentious, plantar fasciitis, illiotibial band friction syndrome, and joggers nipple.
18. An AMA (American Medical Association), ten-year study on aging concluded aging is the equivalent of inactivity not passage of time, and nutrition with proper exercise can delay or reverse aging process.
19. Aging is a complex process when breathing capacity declines, heart vigor decreases, reflexes slow, and capacity for work lessens.
20. Age is not a limiting factor in exercise.
21. Cooper's Cardiovascular System Physical Activity Scale:
A. Higher number equals greater demand and increased benefit: B. Injury correlates to highest point value:
1.) Long distance road Running and high impact aerobics is most injurious through neuro-muscular trauma caused by impact
C. Deep water exercise while immersed to neck HAS Highest point value, highest aerobic value, WITH no injury;
1.) Equivalent exertion is 4 to 52 times greater as land; 2.) Each cell of every muscle HAS increased work load, superior cardiovascular conditioning
(strength, endurance); 3.) Deep-water extremity pressure forces blood to heart faster; 4.) Combined water buoyancy + WET vest decreases gravitational pull;
5.) Joints, muscles, tendons, ligaments trauma eliminated; 6.) Reduced heart rate 10 to 20 beats per minute less.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
35
22. Cooper's aerobic training effect for total wellness: A. Positive physical changes deep water immersion include:
1.) Maximum muscle use (80-90% major muscles groups) especially: gluts; quadriceps; hamstrings (improves posture); 2.) No impact trauma;
3.) Total blood volume increase = better oxygen transport; 4.) Lungs Vital air capacity increases, improves longevity; 5.) Process of oxygen consumption: Mitochondria (cells' power plant) Increases oxygen
extraction; volume of oxygen consumed; arterial venous difference (endurance energy)
23. Cool water immersion 68 to 72 degrees F Increases hemoglobin oxygen: a. Improves body tissue oxygen extraction from blood; b. Heart is stronger with better blood supply; c. Increased stroke volume; d. High density lipoprotein increase manifests reduced arteriosclerosis. 24. Cold water immersion 48 to 58 degrees F accelerates hemoglobin oxygen, blood's oxygen transportation, extracts even more oxygen from the blood. 25. Warm to Hot water immersion 90 to 102 degrees F dilates vessels, engorges blood, and accelerates flexibility, mobility. 26. ISOKENETIC (same speed) muscle contractions are from Even tension, constant speed, full range of motion, helps reflexes while quicker movement’s increases water resistance. 27. Cool water immersion 68 to 72 degrees "F" is a Full regime of cardiovascular fitness providing joint motion, flexibility, strength, balance, and coordination.
28. Rating of perceived exertion/pain (RPE & RPP): (Gunnar Borg Scale) 0 to 10 scale (0 = neutral 10 = maximal).
29. Research shows Lactic acid causes Muscle fatigue (not soreness) a. Same group compared water running to treadmill at RPE 6 the Water group Lactic acid higher, dissipated faster with a lower heart rate (10-20 beats per minute), had no soreness or fatigue. 30. Bone mass density and strength increased with deep Cool water immersion exercise Activity creates increased body fluid exchange at porous bone areas, and a synapse to stimulate bone regeneration. 31. Swimming is PERCEIVED as too difficult with minimal benefits, freestyle (crawl), common stroke the Body is flat on water surface, hyper-extends back muscles, increase intradiscal pressure CAUSES tension, pain and Activates 80-90% upper body muscles, but MINIMAL LOWER BODY.
32. Road Running has Maximum impact trauma to whole body with Foot strike 800 to 1000 pounds per square inch, Major muscles exercised gluts, quadriceps hamstrings.
33. American Medical Association (AMA) 10 year study on aging state Aging is equivalent to
inactivity, not passage of time and Exercise, nutrition can delay or reverse aging. 34. Aging is a complex process, defined (Dr. Agress) Maximum breathing capacity decline,
heart vigor decrease, reflexes slow, capacity for work lessens.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
36
AquaDios-Med AquaDios CORP. Dr. Alan Jensen
Table 2. Aerobic Activities: Advantages, Disadvantages
Activity Advantages Disadvantages Running Convenient. Extremely hard on joints, muscles bones Provides aerobic benefits fits in short period of time Decreases flexibility. Causes muscle imbalance. Low skill level required Most of activity performed by lower body. Increases speed, endurance. Swimming Reduced pressure on joints 80-90% of activity-performed by bones. upper body. Eliminates neuro- Possible ear - eye - sinus infections muscular trauma. - other problems Allows extended exercise High skill level required
Increases endurance. Pool - immersion water required Cross- Many muscles involved. High altitude - Cold Country Provides vigorous workout Skiing Limited season. Overload principle. Limited access. Increases endurance. High skill level required Deep Water Nearly all muscles involved. Pool or body of deep water required Running
Provides vigorous workout. Overload principle. Reduced pressure on joints, bones. Eliminates neuro-muscular trauma. Allows extended exercise. Provides aerobic benefits in short period of time. Low skill level required. Maintains or increases flexibility. Prevents muscle imbalance. Increases speed, endurance.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
37
Part I AquaDios-Med™ Proactive Preventive Medicine
Inner Mental Training •Positive Psychology Adapted from Lars-Eric Uneståhl, Ph.D. – Sweden
Inner Mental Training • Psychoneuroimmunology • Mind Body Medicine • Clinical Hypnosis
AquaDios-Med™ Inner Mental Training or ADM - IMT is a is a systematic proactive preventive medicine procedure designed to purposely cultivate in people the naturally occurring state of mind referred to as an Altered State of Consciousness or ASC and defined as a heightened state of focused concentration. It is a psychophysiological mental training for people to recognize and to become familiar with purposely, wilfully being transformed in the renewing of your mind as referenced by St. Paul in Romans; a positive metamorphosis to something healthy, lasting and enduring, the change of one's organic and substantial change of who we are in life. This is developed through a positive Self-Hypnotic process to manage demands of life from a learned ideal performance state; a process synonymous with the practice of Mind Body Medicine, psychoneuroimmunology and ASC. This workshop will focus on the short term benefits and practices in healthcare with little reference to sports.
AquaDios-Med™ Inner Mental Training or ADM – IMT is a proactive process of Cognitive, Emotional Skills and Attitudes toward wellness, health and pain management with sustained. One primary goal of the [ADM] - IMT is to deemphasize or minimize the over reliance of modern medicines on pharmaceutical medications and surgeries because both have ghastly side effects. Instead, utilize the patient, the person as the main source for remission of the illness. The ADM - IMT process is designed to produce safe rapid healing, rehabilitation, pain management, distinguish between rehabilitation pain and re-injury pain, rejuvenation, physical fitness; this procedure has had very good success with cancer patients and other serious medical issues as well as great benefits with professional athletes and all walks of life.
AquaDios-Med™ IMT is a robust well-established and proven psycho-physiological self-
regulation or Inner Mental Training IMT to establish, to facilitate and to produce a lasting homeostatic bio-physiology balance that eliminates the dependence on and the abuse of biopharmaceuticals, many surgeries and hospital stays.
IMT • Inner Mental Training • Brief History
The innovative and original IMT has proven its efficacy as a systematic and long-term training
of physiological self-regulation and was developed in the 1970’s by Dr. Lars-Eric Uneståhl in close cooperation with the Swedish National and Olympic Teams. The Training System was based on principles from Uneståhl´s research about positive mental training and Mind- Body relations at Uppsala University during the 1960’s. In Sweden IMT is used in Schools, Corporations, Business, Hospitals, large Organizations, for Personal Growth since being popularized in the 1980’s. The emphasis in the 1990’s gradually turned more and more to Health and Clinical areas. IMT is today used by more than 2.5 Million people of the Swedish population. The four main application areas are: Sport- and Stage performance; School and education, from first grade to University; Business and Public Administration, used by most major international and national companies.
Exercise is a weapon against disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
38
The goal of IMT is for the person to learn to identify the desired ASC - to experience a heightened state of focused concentration, a wilful process of being … “transformed in the renewing of your mind…” and referenced as the Inner Mental Room. This IMT process can be referenced to as applications of Mind Body Medicine - MBM and to eventually lead to the beginning of psychophysiological self-regulation; which in turn leads to the development of a practice similar to a self-induced and purposeful self-suggestion, autosuggestion or autohypnosis. This is carried out by means of the learned IMT routine and techniques through a progression of physiological conditioning, muscle relaxation, breathing control and heart rate control and advances to cognitive conditioning through mental imagery, acoustic therapy and more.
Most patients who are stressed or lack self-esteem can be taught IMT techniques which induce deep relaxation and strengthen self-esteem. Specifically, once the patient learns to enter the ASC the doctor - therapist can communicate messages to the patient to allow self-induced relaxation; strengthening and self-empowerment practice’s to occur so that audio recordings can be introduced.
IMT is the only risk-free childbirth anesthetics and can effectively help pregnant women in
labor to alleviate pain. Common methods include Glove Anesthesia or learning to numb the hand then placing it upon a painful region to remove the pain sensation there; Time Distortion: Perceiving periods of time accompanied by pain as shorter in length and those free of pain as longer lasting; Imaginative Transformation: Viewing the pain as a non-threatening, acceptable sensation, such as merely mild pressure that causes no trouble or pain.
In general, IMT starts with the basics of Muscular relaxation ASC- Self-Hypnosis followed by specific interventions and applications and a more general personal development system with Self- and Goal-Image Training, Attitude- and Mental Toughness Training, Training of specific Mental Skills like Concentration, Creativity etc., and finishing with Emotional- and Life Quality Training.
Myth • ASC • Hypnotic Susceptibility • Personality Trait • Medical Concern
Hypnotic Susceptibility is a term used to identify those people that medicine believed to be able
to allow the ASC known as a heightened state of focused concentration experience. The amount of this capacity or susceptibility became a concern of medical practioners who felt that ASC or hypnosis was a remarkable asset for patient care, but it seemed not all people could develop ASC or be treated with ASC – MBM - hypnosis. This led to the development of standardized tests like the Hypnotic Induction Profile, Harvard Group Scale of Hypnotic Susceptibility, the Stanford Hypnotic Susceptibility Scales, concluding people had low, medium or high hypnotic skills.
This early research caused a myth that ASC - Hypnotic Susceptibility, as measured by standard
tests is a stable personality trait; meaning some people are not susceptible to developing ASC or the hypnotic state. However, many experts in clinical hypnosis, including this author and Unestahl demonstrated that hypnotic capacities, abilities and skills can, in fact, be learned and improved through ASC education and training; just like any other physical and mental skill. Thus, those people who measured as low ASC or non-hypnotizable can learn and adapt to these heightened states of focused concentration referred to as Altered States of Consciousness ASC or hypnotic susceptibility. Thus, all people can learn to benefit from ASC and IMT. This conclusion is based on the obvious fact that all people naturally experience ASC daily.
The AquaDios-Med™ Inner Mental Training - IMT is designed to purposely develop in people awareness and experience of these naturally occurring states of mind as an Altered State of Consciousness, ASC, or a heightened state of focused concentration that will become the platform for learning and applying the ideal performance state. This IMT expedites people’s recognition and familiarization with ASC to purposely develop a positive ASC or Self-Allowed Hypnotic like process to better manage the demands of life from their ideal performance state.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
39
Research shows that all ASC or hypnosis, especially where the person is willfully receiving an hypnotic induction in order to become involved with ASC or hypnotized is indeed self-hypnosis and the person – subject actually controls the ASC experience of the suggested hypnotic effects. However, ASC or hypnotic training is necessary in order for the subject to be able to take over and understand the control; the subject must know that he is in control and how to take control.
Inner Mental Training • Positive Psychology • IMT Evidence Based
Psychology has traditionally focused on dysfunction, problems or on people with mental illness
or other psychological problems. IMT replaces the traditional clinical and problem-based negative model with a solution-based and life-long developmental model referred to as Positive Psychology. In IMT Goals are identified instead of problems as is creating your own future. Change is related to satisfaction instead of dissatisfaction and direction is changed from away from to towards. In other words, observe, understand, and confront that which is feared.
Inner Mental Training develops positive personal development through the acquisition of
mental skills, using relaxation, visualization and other hypnosis - ASC techniques. Unestahl’s 1973 research demonstrated two fundamental points, that self-hypnosis, in Sweden, using pre-recorded material could be as effective as having a hypnotist present (hetero-hypnosis), and that regular ASC practice increased hypnotic effectiveness. The first mental training programs were licensed for prescription by doctors in Sweden for stress in 1970. In the first year 27,000 prescriptions were issued and because there were no reported side effects, IMT was removed from the requirements of prescription, and has been freely available in all pharmacies in Sweden since then.
IMT is based on the use of Alternative States of Consciousness (ASC1), which is operationally
defined as the Inner Mental Room (IMR). Continued ASC practice makes it possible to use: Alternative Systems of Control (ASC2) like triggers and Images; Alternative Systems of Change (ASC3) are practiced from very structured training based changes akin to cybernetic programming or using user feedback to improve results.
Training • Psychoneuroimmunology • Mind Body Medicine • Hypnosis
IMT can be developed and effectively utilized with ASC training methods. As referenced
above, ASC, hypnosis or hypnotic capacity, as based on the induction of positive altered states of consciousness has been regarded by some research as a stable personality trait. Some modern textbooks indicate there is only a percentage of the population that can experience deep, medium, light ASC or hypnosis. Research shows that Hypnotic Capacity can be improved and learned with IMT. Thus, a low ASC hypnotizable person can be trained to become highly hypnotizable.
The degree of ASC or hypnotic depth is also situation specific and varies with the hypnotist,
the method used, motivation, the expectation, etc. Even inter-individual variations in ASC hypnotic responses when the same hypnotist and the same method is used there is no proof for claiming that these differences in hypnotic susceptibility should be regarded as a stable personality trait. It could as well be regarded as lack of training.
In a number of experiments in the 1960’s Unestahl research showed that there are significant
increases in hypnotic susceptibility scores (Stanford scales) after 6 months of hypnotic training and that there are significant increases of imaginary capabilities after 6 months of imagery training. Thus, the interesting question is not if he or she is a good hypnotic subject but instead, what training methods could be used to develop a good hypnotic capability in this person in so short time as possible?

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
40
OBJECTIVE
Inner Mental Training is based on 35 years of scientific research conducted in Sweden by Dr Lars-Eric Unestahl, Sports Psychologist, founding President of the Scandinavian International University, Orebro University. Dr Unestahl was also the founding president of the International Society for Mental Training and Excellence (ISMTE). This method is used with Olympic gold medal athletes, schools, the medical field, organizations, and for many social issues, including empowerment for the homeless.
AquaDios-Med™ IMT participants will learn the basic methods of Muscular relaxation; Mental Relaxation; Use of triggers (clues) to reach goals and reduce stress. The visual art process requires no previous art experience or ability and uses art materials to create concrete images through color, shapes, or lines. This process will use the 7 C's (Confidence, Calmness, Concentration, Commitment, Creativity, Cheerfulness, and Control) as topics for capacities important to life. This program currently is used in Swedish schools for fifteen minutes three times weekly as part of the curriculum from kindergarten through high school graduation resulting in mental focus, improved grades, increased self-esteem, and stress reduction.
The Ideal Performing State (IPS) an ASC - Hypnotic State
One line of investigation which led to the development of IMT and to its applications in Sport,
Stage and Work Performance were studies where Unestahl investigated the relation between IPS and Hypnosis. It was possible to show that both states were almost identical in areas like amnesia, perceptual changes, trance logic, change of control system etc.
RESEARCH • HEALTH and CLINICAL Areas •Evidence Based
Investigations of the Alternative State of Consciousness (in IMT called the inner mental room
shows a change of brain activity quantitative as well as qualitative. EEG shows the biggest differences on the theta level (4-7 c/s) with a significant increase in the ”mental room” The qualitative change could be described as a leveling out of the activity with the same activity in each of the four quarters of the brain (change of operative system).
Systematic IMT-training changes the hormonal level. Examples are decrease of cortisol levels
and increase of betaendorphin levels. Three different studies have all showed an improvement of the immune defense (measured with
T4/T8 cells) after Mental Training. The decrease of the immune defense in connection with hard training and overtraining could be prevented by Mental Training. The last study showed that the improved immune defense could be related to one part of IMT – the Life Quality Training.
Biological aging (measured with the DHEAS-hormone) stopped in connection with 6 month
IMT-training. The experimental group instead became 7 years younger.
Research • Pain Control • Physiological • BODY CHANGES • IMT EEG-studies of the Self-Hypnotic state, used in the Basic Inner Mental Training, called the
Mental Room, showed a quantitative as well as qualitative change of brain activity. The biggest change could be seen in the theta level (4-7 c/s). The qualitative change could be described as a leveling out of the activity with the same low activity in each of the four quarters of the brain and show the cortex begins to work as a holistic unit which changes the informational pathways.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
41
Systematic IMT-training affected the endocrinal system and the production of a variety of hormones, for instance decrease of cortisol levels and increase of beta-endorphin levels; significant decrease of cortisol and increase of betaendorphin levels are common effects after a number of weeks of regular IMT-training.
A number of studies showed an improvement of the immunological system (measured with T4/T8 cells) during and after Mental Training. The decrease of the immune defense in connection with hard training and overtraining could also be prevented by Mental Training. One study also showed that the improved immune defense mainly came through one part of IMT – the Life Quality Training. Significant immunological positive changes have been shown in 3 different IMT-investigations. A further analysis showed that it was the Life Quality-Emotional Training that gave the most positive changes.
300 cancer patients were divided into two similar groups through matching. The experimental group combined the hospital treatment with IMT. There was a significant lower mortality rate in the experimental group receiving IMT. Most research since year 2000 has been made by Uneståhl and his mental training students.
70 tinnitus patients had 15 minutes of IMT-training every day for 4 months (Sahlgrenska hospital). Very few got rid of the sound and noise but almost everyone could learn to lower or remove the disturbance.
Chronic Pain studies made at the hospital in Helsingborg show that even if the chronic pain was still there the IMT-patients had learned to dissociate and detach from the pain and concentrate on the important things in Life. The same positive effect was shown in Hans Olssons work with Mental Training for chronic pain patients, the most common effects have to do with moving and reframing the pain and learning to ignore and refocus to establish Pain Control Management.
A number of sleep studies (Motala), overweight (Lund), asthma (Åre) etc. show that regular
IMT-training gives positive effects independent of the medical area. Thus, IMT is both an alternative and a complementary medicine. Studies show IMT has had positive effects on areas to improve Sleep and overcome sleep disturbances, Weight of control of the ability to stop Smoking.
Using IMT- audio-tapes during general anesthesia (orthopedic surgery at Örebro hospital) have
shown positive effects during operation and less postoperative complications. Relaxing music and positive hypnotic and posthypnotic suggestions improved the conditions during and after 70 surgeries compared with a control group with white sound.
A jet-lag study with the Swedish National Swimming Team in connection with the preparation
for the Sydney Olympics showed better effects on sleep and performance of IMT compared with Melatonin, Placebo and Control.
Biological aging (measured with the DHEAS-hormone) stopped in connection with 6 month
IMT-training. The experimental group instead became “7 years younger”. In a recent study the aging process could be reversed through 6 months of mental training.
The Swedish National Team in swimming was divided in a control group and 3 experimental
groups (mental training, melatonin, and placebo) in a jet lag study before the Sydney Olympics. The Mental Training group showed the best results in the measured variables (Sleep quality and Performance ratings).
In a number of studies the effects of IMT on areas like Sleep, Weight, Smoking etc. have been
shown. The best results are shown if the training starts with the basic mental training (learning self-hypnosis) before starting with the specific application.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
42
Life skills training is under investigation in a number of schools from primary to high school level, containing Basic Mental Training, Mental Training, Lifestyle training, Communication and Teamwork, Emotional and Mental Toughness training, Parent ship and Leadership Training, but the results have not been released.
In Sweden, at the University level, continuous evaluation is made from those professional
related academies (The Police Academy, Music Academy, etc. where Mental Training is an integrated part of the studies), to those Universities having specific courses like Humor and Health, Learning to learn, ”Mental Training and Project Leadership” over to the private Scandinavian Internationa University, which specialize in using Mental Training, NLP and Coaching for education to a number of new professions, like Licensed Mental Trainers, Stress Coaches, Health Coaches etc.
Inner Mental Room – IMR
Investigations of the Inner Mental room (IMR) showed the biggest EEG changes in the theta band, more than in the alpha band, in which a lower part increase and higher part decrease can be seen. IMR was also related to a hemispheric shift with a similar activation of left and right holistic brain.
In one pilot study a world champion in archery was compared with an athlete of lower level.
Ten seconds before each shot the situation was the same with a higher left hemispheric activity. However, the world champion had the skill to go into a hypnosis-like state or an altered state of consciousness with a hemispheric shift. The shot was released when both hemispheres were inside the optimal zone of activation. Asked how she knows when to shoot she answered, I don´t but my body knows. I do not shoot, my body does. In this Ideal Performance State (IPS) the release of the shot is done by an ideomotor response, which is much smoother and stable compared with a voluntary release.
IMR also seemed to be related to Section divine, the ratio 1.618 the old classical ratio for beauty and harmony. This ratio was found both in the measurement of various cortical points of IMR-activation and also in the ratio between EEG frequencies (beta 1/beta 2, alpha/beta 1, theta/alpha, delta/theta). Thus, the holistic brain concept could be complemented with the harmonious brain.
COURSE CONTENT AND METHODS OF TEACHING
This AquaDios-Med™ workshop is effective because it empowers the individual by putting the power in the hands of the person rather than the professional. Each exercise begins by clenching the left fist, taking a deep breath, holding and then releasing, which demonstrates the difference between tension and relaxation.
Progressive Relaxation is learning to use each muscle group by tensing and relaxing from head to toe. Autogenic Training utilizes feelings of warmness and heaviness. Triggers are cues which the individual decides are the most effective for obtaining goals. For example, placing your hand over your watch might trigger "time to focus", on the edge of your glasses to signal "seeing the situation clearly" and imaging yourself doing what you need to do prior to proceeding toward your goal. You create your own trigger and image.
Training Benefits • Everyone
The benefits of the AquaDios-Med™ IMT have been addressed by the research; it is a truly holistic and effective method of treatment, which has had very positive outcomes for patients. We are able to offer simple training to any group of health professionals who can than supervise the use of the CD’s by patients. This can become is a self-help program with minimal supervision required, availability is the key, in office hours, after the first assessment our patients only required occasional phone calls.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
43
IMT • ASC • Mind Body Medicine • Psychoneuroimmunology • Research Research shows that every person - every patient has more than an 80% chance of learning psychophysiological self-regulation sufficiently enough with training to decrease and or eliminate medications and pharmaceuticals and some surgeries. This is important because there are negative and dangerous side effects to most all pharmaceuticals and surgeries whereas MBM has no negative side effect, only positive outcomes to accelerate healing or decrease the time needed for rehabilitation and complete recovery. Thus, all people should be taught these inner mental skills. Because studies consistently show that ASC are naturally occurring human events the premise or presupposition held by AquaDios-Med™ proactive preventive medicine is that all physical human biology – physiology, through IMT, that all patients can learn to manage to manipulate their physiology in a learned, positive psychophysiological self-regulation toward symptom management. Thus, Inner Mental Training, ASC – Psychoneuroimmunology - Mind Body Medicine are all methods to help foster positive homeostatic immune function.
Conceptually or hypothetically the common illness or disease is, to some degree, the outcome of suppressed, subconscious negative, destructive cognitive mechanisms occurring in the patient that is too often below one’s threshold of awareness and too often with a negative, dysfunctional outcome. Below are a few, not all, common medical conditions that can be successfully treated with IMT with a minimum of modern medical procedures --
Accelerated healing and recovery from surgery or injury, addictions, allergies, Alopecia areata
[patches of hair loss], AIDS, anesthesia - non-pharmacological, anxiety and panic disorders, arthritis, asthma, atopic dermatitis, skin disorders - acne, psoriasis, eczema, bedwetting, breast enhancement, burns, cancer, chronic low back pain, chronic illness, chronic pain, childbirth, chemotherapy reactions, dealing with negative people, diabetes, eating disorders, enuresis, fibromyalgia, headaches, hypertension, indigestion (dyspepsia), irritable bowel syndrome, healing and recovery from surgery or injury, headaches, hemophilia, hepatitis C, hypertension, insomnia, impotence, interstitial cystitis, incontinence, menstrual problems, migraines, neurological problems, pain - pain relief – management, peptic ulcer, peak performance, problem solving techniques, stress-related neurological problems, phobias, pregnancy problems - labor and delivery, PTSD, tinnitus, warts; weight loss, treatment of coronary artery disease (cardiac rehabilitation), headaches, tension headaches; insomnia – sleep disturbance - disorders, incontinence, , disease and treatment-related symptoms of cancer, and improving postsurgical outcomes; hypertension and arthritis; And many ore conditions that haven’t been studied yet to examine all the benefits of IMT. It is safe to say that any every person has the ability to control any condition occurring in their own body.
Physical problems worsened • Stress • Anxiety • Depression
IMT – ASC works directly with the sub-conscious patterns of thinking and reacting so that a
person becomes calmer and more positive, no matter what is going on physically. While in the ASC the sub-conscious mind has direct positive effects on the autonomic nervous system and hormones. Positive suggestions given in the IMT – ASC sessions can directly change bodily functions including blood flow, allergic responses, gut activity and decrease stress hormones. Research shows that physical or physiological sensations are perceptions or observations. Since perceptions, observations or sensitivities can be changed, physiological sensations, such as pain can be altered by the mind. The human brain literally doesn’t know the difference between what is "real" and what is imagined. Through your powerful imagination you can change your perception of pain and feel more comfortable and relaxed.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
44
IMT improves your motivation to take good care of yourself. By befriending yourself and changing eating, exercise, sleeping and smoking habits you feel better. And your body says, "Thank you! Now I have better chance to heal!" With IMT – ASC self-hypnosis you continue these good feelings and lifestyle changes.
IMT – training in ASC is used in a variety of settings -- from emergency rooms to dental
offices to outpatient clinics. Clinical studies that IMT improves immune function, increases relaxation, decreases stress, and eases pain and feelings of anxiety, reduces the fear and anxiety that some people feel before medical or dental procedures, learning a significantly higher threshold for pain. Also improves recovery time and reduce anxiety and pain following surgery.
Clinical trials on burn patients show that IMT decreases pain well enough to replace pain
medication and speeds healing. Generally, clinical studies show that using IMT reduces ones need for medication, improves patient mental and physical condition before an operation, and reduces the time it takes to recover. Dentists can also use IMT to control gagging, bleeding and for dental anesthesia.
IMT can teach physiological self-regulation skills. For instance, someone with arthritis may
learn to turn down pain like the volume on a radio and to also be used to help manage chronic illness. IMT can enhance a sense of control, which is often lacking when someone has a chronic illness. Clinical studies on children in emergency treatment centers show that IMT reduces fear, anxiety, and discomfort. There is considerable evidence of efficacy showing IMT to be as effective as conventional medical treatment, as the treatment of choice, for an array of mind-body therapies that can be used and be as effective for a number of common clinical conditions. Thus, IMT can be considered as the primary treatment choice rather than just an adjunct to conventional medical treatment.
Common Questions - Answers - IMT - ASC – MBM; Medical Treatment
You’ll be surprised at how widely IMT - ASC – MBM is used for medical conditions
Which medical conditions might improve with IMT – ASC- MBM? Scientific evidence shows that IMT – ASC- MBM can be effectively used with positive results
for most all medical conditions. Can IMT - MBM help real medical problems?
Definitely; Research shows that IMT – MBM – ASC can help many types of illnesses and symptoms and in some instances replace common medical treatment.
How can this be possible if the problem is in the physical body?
Because the mind and body are not separate; the "mind" (thoughts, perceptions, beliefs, feelings, habits, memories, etc…) is directly connected through nerves and hormones to the entire body. And anything that happens to the body is relayed back to the mind.
How does IMT - ASC – MBM help physical conditions?
The physical - mental state called IMT – ASC- MBM is healing all by itself. In this natural relaxed state blood pressure and pulse lower, muscles relax, pain decreases, the immune system is enhanced, elevated blood sugar decreases and intestinal activity come back towards normal. Most all physical medical problems are worsened by stress, anxiety and depression.
IMT – ASC- MBM works directly with the sub-conscious patterns of thinking and reacting so that you are calmer and more positive, no matter what is going on physically.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
45
The sub-conscious mind directly affects the autonomic nervous system and hormones. Suggestions given in the IMT – ASC- MBM sessions can directly change such bodily functions as
blood flow, allergic responses and gut activity and decrease stress hormones. Research shows that physical sensations are only perception.
The human brain literally doesn’t know the difference between what is "real" and what is imagined, therefore the imagined can be just as powerful as the real. For example, through your powerful imagination you can change your perception of pain.
IMT – ASC- MBM improves motivation to take good care of yourself.
By befriending yourself and changing eating, exercise, sleeping and smoking habits you feel
better. And your body says, "Thank you! Now I have better chance to heal!" With IMT • ASC • MBM you continue these good feelings and lifestyle changes. Which medical conditions might improve with IMT • ASC • MBM
Scientific evidence shows that IMT – ASC- MBM can be effectively used with positive results
for most all medical conditions.
There are several stages of IMT • ASC • MBM
Reframing the problem Becoming relaxed, then absorbed (deeply engaged in the words or images presented by a suggestion) Dissociating (letting go of critical thoughts) Responding (complying with positive IMT – ASC- MBM suggestions) Returning to usual awareness Reflecting on the experience
What illnesses or conditions respond well to IMT • ASC • MBM IMT – ASC- MBM is used in a variety of settings -- from emergency rooms to dental offices
to outpatient clinics. Clinical studies show that IMT – ASC improves immune function, increases relaxation, decreases stress, and eases pain and feelings of anxiety.
IMT • ASC • MBM can reduce the fear and anxiety that some people feel before medical or dental procedures. For example, studies show that dental patients who underwent hypnosis had a significantly higher threshold for pain than those who were not hypnotized. IMT – ASC- MBM may also improve recovery time and reduce anxiety and pain following surgery. Clinical trials on burn patients suggest that hypnosis decreases pain (enough to replace pain medication) and speeds healing. Generally, clinical studies show that using IMT – ASC- MBM may reduce your need for medication, improve your mental and physical condition before an operation, and reduce the time it takes to recover. Dentists also use hypnotherapy to control gagging and bleeding.
AquaDios-Med™ IMT • ASC • MBM can teach you self-regulation skills. For instance,
someone with arthritis may learn to turn down pain like the volume on a radio. Hypnotherapy can also be used to help manage chronic illness. Self-hypnosis can enhance a sense of control, which is often lacking when someone has a chronic illness. Clinical studies on children in emergency treatment centers show that hypnotherapy reduces fear, anxiety, and discomfort.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
46
Generally speaking healing is a natural occurrence and involves removing the toxin or disease from the body and this is done through three basic body functions: urination, defecation, and perspiration. Thus, drinking plenty of fluids and exercise is important to help in the evacuation of toxins from the body by stimulating the many different glands specific to urination, defecation, and perspiration.
End Part I
AquaDios-Med™ Proactive Preventive Medicine Inner Mental Training • Positive Psychology
Adapted from Lars-Eric Uneståhl, Ph.D. – Sweden
Copyright © 2008 – 2013
AquaDios-Med™ • AquaDios Corp.
All rights reserved.
See References References • Part I ADM™ PPM IMT PP – End
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
47
– Part II - AquaDios-Med™ Proactive Preventive Medicine
Inner Mental Training - Positive Psychology - Brief History Adapted from Lars-Eric Uneståhl, Ph.D. • Alfred A. Barrios, Ph.D.
I began working with Lars-Eric Uneståhl, Ph.D. in 1976 when he first presented his original
Inner Mental Training process which he based on a number of his studies in Sweden, from the 1960’s and he operationalized in the early 1970’s. Starting with the National and Olympic Teams and the Swedish School System IMT has been used by more than 4 million Swedish people and over 35 years it has been applied to most areas of the Swedish Society. This systematic training is designed for people to recognize, become familiar with and to purposely develop a positive Self-Hypnotic process to manage demands of life from a more ideal performance state.
In Sweden IMT is seen as a systematic Self-Hypnotic training for people to recognize and
become familiar with developing and utilizing ASC, a naturally occurring state of mind, defined as a heightened state of focused concentration. Alfred A. Barrios, Ph.D. developed Self-Programed-Control, SPC, a similar process of self-hypnosis he shared with Uneståhl in the late 1960’s and early 1970’s. Barrios and I have also worked together since about 1978. AquaDios-Med™ Inner Mental Training combines these two approaches and much more.
In general, IMT starts with the basics of Muscular relaxation and Self-Hypnosis followed by
specific interventions and applications with a more general personal development system for Self and Goal-Image Training, Attitude and Mental Toughness Training, Training of specific Mental Skills like Concentration, Creativity etc., and finishing with Emotional and Life Quality Training.
Today, for practical purposes the process of IMT is considered synonymous with
psychoneuroimmunology, Mind Body Medicine and ASC. Also, the original IMT is based on long term training whereas this AquaDios-Med™ IMT – ASC workshop will focus on the short term benefits and practices in healthcare and preventive medicine.
AquaDios-Med™ Inner Mental Training is a highly effective program for giving individuals
greater control over all aspects of their lives and mind-body function. This includes: Health & Wellness, Stress, Bad Habits, Addictions, Immuno-Deficiency Diseases; Learning Capabilities and Relationships. There are two basic reasons the program has proven so effective. First, it provides the two key components necessary for positive change: (1) Self-Efficacy or the means for increasing belief in one’s capabilities; and (2) The Positive Guidance and tools for achieving one’s goals. The former provides the all-important ingredient for facilitating change. The basic problem with most people is that it is very hard to change, and belief is a most powerful catalyst for change. The guidance component provides some good ideas for what changes to make. The second reason for the program’s effectiveness is the immediate positive feedback provided, and that’s what the techniques provide in all aspects of the program, immediate positive results, making the belief factor all the more powerful.
The person learns methods combined with auto-suggestion to enable them to self-program
being happy, productive, getting to work on time, not let life circumstances get him down, to picture success in one's mind and eventually achieve it. Most importantly, it teaches a person to rebound quickly from mistakes or failures and to be smarter the second or third time. These techniques are for demonstrating the power of one’s mind and how to more effectively tap into this inner power. These techniques involve a series of suggestions such that each positive response increases the belief factor even more, so that at the end of the series of steps a person is going to be much more.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
48
Belief can be defined as concentration on a thought to the exclusion of any contradictory thoughts -- the stronger the belief, the more effectively the negative contradictory thoughts will have been blocked out. The person begins by first Writing down one’s goals; and then begins learning how to effectively program in one’s goals through visualization. For the goal of stress control you would want to visualize yourself or imagine yourself in a typical stressful situation reacting calmly or able to automatically calm yourself down -- desensitization. Additional key goals, beside stress control, is Breaking Free of Bad Habits & Addictions, this includes drugs, alcohol, smoking, and weight problems through the Development of Greater Willpower, Stress Control and Providing More Constructive Sources of Pleasure. A weakness in one or more of these areas underlies most addictions.
Greater Health & Wellness - The Stress Diseases - Bad Habits – Addictions
Etiology of immune-deficiency diseases including, cancer is based on the premise that (1) the body has natural defenses against cancer and that certain psychological factors, in particular hopelessness, can interfere with these defenses and the IMT - ASC program can eliminate these psycho-physiological factors as well as eliminating cancer causing habits like smoking and in particular eliminating two major sources of hopelessness; Positive Mental Attitudes must be systematically incorporated to assist a balanced homeostasis to empower and awaken healthy immune system function. Developing positive attitudes will further insure achieving many of the goals since many of the goals will most likely be influenced by these positive attitudes. Stress Control is a perfect example of breaking free of a bad habit like smoking, or overeating or drinking, etc. For school students it could be exam anxiety. Or it could be anger control, or it could be certain people that stress you out. Or you may want to program in one of the positive attitudes that will lessen stress. It is important to choose one or two goals with reminders to not to program everything in all at once.
IMT • Background • Positive Psychology (PP) • Ideal Performance States The focus of Positive psychology is on what makes life most worth living, happiness, making
the lives of normal people fulfilling, its concern is with strength, building the best things in life and examines positive emotions, strengths-based character, healthy institutions and how ordinary people can become more fulfilled; whereas, Psychology traditionally focused on dysfunction—on people with mental illness or other psychological problems and how to treat them. Inner Mental Training (IMT) is based on the same philosophy and is using the same principles as Positive Psychology (PP).
Developmental Ideal Performance States is based on the philosophy the same principles as Positive Psychology and Integrated Mental Training (IMT). IMT – ASC- differences are more in methods of learning and development, the emphasis is more on Action Learning and Learning through feedback, while Positive Psychology is a Reflective Learning and IMT an Unconscious Learning. Positive Psychology looks at human beings as self-organizing, self-directed, adaptive entities and wants psychology to focus on two neglected areas, one is to develop ordinary people to increased Productivity and Well-being, the other is using personal development of resources for Problem prevention and empowerment.
Knowledge • Life Competence
Because studies show no correlation between success in School or University and success in Life, Mental Training becomes the most important method to transform abstract knowledge into real competence in dealing with life. IMT is future oriented, solution focused, action directed and experiential based. IMT for development of one’s own well-being or one’s ability to facilitate healing, pain management, symptom reduction – management, Childbirth Anesthesia, is the integration that has been made between IMT and hospitalized as well as out-patients participation in their medical treatments in the last decade.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
49
IMT • ASC Development Versus • Focus on Problem
The IMT • ASC approach presumes the client – patient needs to develop new resources, skills, and behavior in order to reach the goal, say of pain management without pharmaceuticals, for example. This developmental skill presumes the patient can be satisfied with the present and still want - and be working and training- to reach a better situation; pain management without the dependence on the pharmaceutical and all the negative – dangerous side effects.
In the problem - solution model, people want to change because of a problem or crisis. So in
the problem - solution model the direction of change is away from the problem, meaning that sometimes the result can still be worse; out of the metaphorical frying pan into the Integrated Mental Training and Positive Psychology fire where one learns to develop the skills needed to master pain management without the dependence on the pharmaceutical and its negative – dangerous side effects.
In the practice of modern hospital – private practice medicine it is common to rely or over-rely
on pharmaceuticals in pain management without ever considering the patient capacity to participate directly in the medical process. This establishes a child – parent type of relationship, where the patient is the child and the doctor is the omniscient, well intended parent.
Dental surgery commonly relies on anesthetics commonly delivered via a hypodermic syringe
needle into the gums. The pain of this injection is as painful as the dental surgery which negatively impacts the patient, leaving them drowsy, and lethargic, making it dangerous to drive while also causing the patient loss of sensation to the tongue, lips and mouth making it difficult to talk or eat.
Conversely, applied dental hypnosis or IMT – ASC allows the full dental procedure to proceed
with no negative side effects and at conclusion of the dental surgery patients feel invigorated and engage in their day with a new found enthusiasm because they produced endorphins; this type of team work is possible for more than many medical procedures.
Re-Visit Medical Dangers • Iatrogenic Complications
The Inner Mental Training of AquaDios-Med™ proactive preventive medicine is based on the
premise that modern hospital medicine underutilizes the healing power of the patient while exploiting unnecessary medical events and procedures that are invasive and most often not be necessary; this practice is considered as part of the iatrogenic picture. The AquaDios-Med™ approach is to focus on developing patient awareness to IMT and etiology to first determine whether the patient has sufficient control over all aspects of their lives and mind-body function.
Attention to unnecessary medical events is very important because any medical procedure that
is invasive and may not be necessary must be considered as part of the larger iatrogenic picture otherwise cause and effect go unmonitored. The figures on unnecessary medical events represent “patients” who are thrust into a dangerous healthcare system. In 2001, each one of these 16.4 million lives was affected in a way that could have had a fatal consequence. Simply entering a hospital can result in a serious adverse drug reaction (186,000); a hospital-caused infection (489,500); iatrogenic injury or medical error with adverse drug reactions (1.78 million); and procedure error (1.3 million). Over a ten year period researchers project 7.8 million iatrogenic hospital deaths; more than all the casualties from wars that America has fought in its entire history.
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
50
Re-Visit Problematic Dangers • Medicine • Pharmaceuticals • $8.2 Million Study • 2008
There is an osteoporosis study called Scoop for prevention of fracture, it is led by respected scientists from Universities in the UK. Women aged 70 to 85 were recruited from communities close to the seven universities. This study is a good example of how patients will be thrust into a treacherous and irresponsible healthcare system. The “high-risk” group were offered bone scans and given bisphosphonate drugs, which is said to be a preventive medicine because it prevents bone thinning and can reduce the risk of fracture by 50 percent. Nevertheless, there are almost always serious side effects from pharmaceutical drugs. In this case, oral bisphosphonates stay in the bone for many years and cause osteonecrosis, or bone death, years after the drug is stopped. Bisphosphonate drugs are not at all preventive medicine; rather they iatrogenically cause osteonecrosis, a medical condition worse than osteoporosis, but this side effect is not discussed or shared with the patients and the drug is disguised as preventive medicine.
Research shows that Oral bisphosphonates, like Fosamax, cause jawbone death, or jaw rot, a
form of jawbone decay. This can be very painful and may lead to complications such as infection, breakdown of the jawbone, ulcerations in the mouth, non-healing wounds, and osteomyelitis (inflammation of bone marrow). Once necrosis begins, it is irreversible. Common symptoms of osteonecrosis of the jaw are pain, swelling, gum infections, loose teeth, poor healing of gums after dental work and numbness, or a heavy feeling in the jaw. Approximately 3 million women in the U.S. take the drug and numerous class action legal suits have been initiated.
Research shows Osteoporosis leads to 86,000 debilitating hip fractures. The “Scoop” study
received $8.2 million funding from the Medical Research Council (MRC) and the Arthritis Research Campaign (ARC) and has the backing of the National Osteoporosis Society (NOS). But this study failed to investigate proactive preventive medicine such as AquaDios-Med™, by far a most effective “remedy” for osteoporosis.
Why does an 8.2-million-dollar osteoporosis study for prevention of fracture fail to include safe
exercise, like “deep-water running,” a proactive preventive medicine treatment, while failing to include any form of IMT – ASC or Mind Body Medicine; proactive preventive medicine care was never considered.
Hospital Healthcare Can Cause Death • Re-Visited
Research shows that the modern healthcare hospital system is the leading cause of death in America. Doctors themselves are not to blame, the entire modern healthcare system is to blame, for allowing, and promoting, so many unnecessary procedures, drugs and mishaps, not to mention the infections which plague hospitals and attack patients opportunistically. Government health statistics show that some American medicine practices can cause more harm than good. In-hospital, adverse drug reactions (ADR) to prescribed medicine is listed at 2.2 million. Dr. Richard Besser, of the CDC, said the number of unnecessary antibiotics prescribed annually for viral infections was 20 million in 1995. Years later, in 2003, Dr. Besser referred to tens of millions of unnecessary antibiotics. Unnecessary antibiotics not only tax the healthcare system with the unnecessary costs of these drugs and their administration, they also make disease-causing microbes resistant to treatment, thereby causing further disease and the incurring further costs of treatment. The number of unnecessary medical and surgical procedures performed annually is more than 7.5 million. The number of people exposed to unnecessary hospitalization annually is more than 8.9 million.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
51
In 2001The total number of iatrogenic deaths (those deaths induced inadvertently by a physician or surgeon or by medical treatment or diagnostic procedures) was reported at more than 783,936; heart disease annual death rate was 699,697 and annual cancer death rate, 553,251. In 2001, the American Medical Hospital System was the leading cause of death and injury in the United States by more than 84,000; those numbers have increased substantially through 2012.
Proactive Preventive Medicine • Problem Solving
The AquaDios-Med™ proactive preventive medicine process assimilates safe structured deep
water running exercise with IMT – ASC - Mind Body Medicine and Psychoneuroimmunology. This unified process forms an Integrated Mental Training (IMT) of Cognitive, Emotional Skills and Attitudes toward wellness and health. In essence AquaDios-Med™ proactive preventive medicine is designed to facilitate and produce a homeostatic bio-physiology balance that eliminates the dependence on and the abuse of biopharmaceuticals as well as most surgeries and hospital stays.
It is believed that the proactive preventive medicine process of AquaDios-Med™ can reduce
surgeries and prescribed Pharmaceuticals - biopharmaceuticals by approximately eighty percent. AquaDios-Med™ proactive preventive medicine can help to simultaneously raise the level of health in Americans and bring down the high cost of healthcare in the United States and can reduce American healthcare costs.
Decades of research confirms physical or emotional stress - anxiety causes the body to release
hormones that negatively affect all physical systems and organs disrupting heart and immune function to diminish the body's natural capacity to heal. IMT – ASC or Psychoneuroimmunology is a relatively new discipline that interlinks psychological, autonomic, immune, and nervous system functioning "psycho" for psychology; "neuro" for neurology, or nervous system; and "immunology" for immunity.
Research shows Mind Body Medicine practices fight disease and promotes health by "training"
a state of "focused concentration" where people learn to improve their complete health and wellness. Because energy is the underlying pattern of the universe this science of consciousness – unconsciousness merges psychology, physiology and physics. Early Kirlian photography research of the human energy Aura by Thelma Moss, PhD, UCLA showed a definite energy exchange between care givers – healer to patient.
Ainslie Meares, MD, Australian psychiatrist, medical hypnosis scholar, authority on stress, and
a prolific author including best-seller Relief without Drugs believed human beings are part of an interconnected, universal energy field; his cancer patients reversed cancer. Meares did not involve mental imagery or visualization as did Oncologist Carl Simonton, MD in "Getting Well Again", 1978. Drug-free alternatives to health with non-chemical and non-mechanical medicine or surgery is one key to management of stress - anxiety induced medical illness.
IMT – ASC - Mind-Body Medicine uses the power of thoughts and emotions to influence positive
physical health. Hippocrates wrote, "The natural healing force within each one of us is the greatest force in getting well." This is IMT – ASC mind-body medicine in a nutshell. Mind Body Medicine is based on the doctor and patient recognizing the relationship of the body's innate healing potential, and the partnership of patient and healer in restoring the body to health. IMT – ASC for development looks at life as a journey with continuous improvement necessary stimulation and challenge important for high quality of life.
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
52
Pro-action • Prevention • Problem Solving Method Proactive preventive medicine is action oriented and has its basis in learning by doing; tasking
construct experiences, which through feedback provides adequate changes. While the goal in problem centered medicine is to return to a “pre-problem” situation, (mostly with the help of retroactive actions), IMT – ASC for development uses proactive methods to create a situation which is not only better than the present but also better than the pre-problem conditions. This includes “problem solving” but without having to work on the problems.
Our brain is more easily caught by problem thoughts and images. There are three reasons: An
evolutionary survival mechanism; the emotional components (emotions like fear catch our mind very easily); Problems are often more concrete than goals. In order to change this perception, IMT – ASC for development works to decrease fear and other negative emotions and make goals clear and attractive. One part of that is to learn to think and talk in positive ways and to replace problem words with developmental ones. In order to make even better progress IMT – ASC for development combines the use of Mental Training tasks with goal programming.
While Problem oriented medicine stops when the clients’ goals are clear and value based, IMT
– ASC for development translates the intellectual goals to images, after which the goals are integrated and programmed. This seems to start an automatic process. The client often reports being more creative, that they get solutions in an effortless way without conscious problem solving. They reach goals without knowing what took them to the goals.
Positive Inner Mental Training is a system of personal development through the acquisition of
mental skills, using relaxation, visualization and other hypnosis ASC techniques, and that regular ASC practice increased ASC or hypnotic effectiveness. The first mental training programs were licensed for prescription by doctors in Sweden for stress in 1970. In the first year 27,000 prescriptions were issued and because there were no reported side effects, IMT was removed from the requirements of prescription, and has been freely available in all pharmacies in Sweden since then.
IMT is based on the use of Alternative States of Consciousness (ASC1), mostly on Self-
Hypnosis, which is operationally defined as the Inner Mental Room (IMR). This makes it possible to use: Alternative Systems of Control (ASC2) like triggers and Images; Alternative Systems of Change (ASC3) from very structured and training based changes over to cybernetic programming or using user feedback to improve results.
Training • Psychoneuroimmunology • Mind Body Medicine • Hypnosis
IMT can be developed and effectively utilized and easily learned by most all people and hospital patients regardless of standardized tests suggesting some people have little or no Hypnotic Capacity to accomplish medical or health goals. Some erroneous research shows that hypnotic capacity, as based on the induction of positive altered states of consciousness and has been regarded as a stable personality trait. Even some modern textbooks indicate there is only a percentage of the population that can experience deep, medium, light hypnosis etc. However, as stated above, other research shows that Hypnotic Capacity can be improved and learned with IMT. Thus, a low hypnotizable person can be trained to become highly hypnotizable.
Exercise is a weapon against disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
53
Standard tests designed to measure hypnotic capacity simply identify those who need training before successful, dependable medical hypnosis or ASC can be included in hospital or out-patient treatment. The Hypnotic Induction Profile is a standard hypnotic capacity tests and is used to determine what the patient may need to successfully participate in and learn IMT – ASC. These skills and capacities can be learned by training; just like many other skills. For example, a person capable of bench pressing only twenty pounds can, with training, learn to bench press hundreds of pounds. Or a person with seemingly no math skills can learn complicated mathematics just as a person that cannot play the piano can learn to be a competent musician or a non-swimmer can learn to swim. There is no proof that hypnotic susceptibility - low or no hypnotic susceptibility is a stable personality trait or that measured low hypnotizability can as well be regarded as lack of mental training; only speculation.
Ideal Performing State (IPS) • Altered State of Conscious • Hypnotic State
Recent research shows that a deeply focused attention or absorbed concentration is a conscious state in humans that has been scientifically confirmed. For, example, great athletes are known to enter this state while in fierce sport competition, but also the entertainer, singer, pianist, dancer, race car driver all enter this state to achieve maximum performance. Thus, the IPS is a human capacity or aptitude that can be learned and applied, much like hitting a baseball or playing the piano without interference caused by distraction, stress or anxiety; an anxiety-less state, a state of absolute, maximized freedom and self-control. One line of investigation which led to the development of IMT and to its applications in Sport, Stage and Work Performance were studies where Unestahl investigated the relation between IPS and Hypnosis. It was possible to show that both states were almost identical in areas like amnesia, perceptual changes, trance logic, change of control system etc.
Inner Mental Room IMR • Research • Health
Investigations of the Alternative State of Consciousness in IMT called Inner Mental room (IMR) showed a change of quantitative and qualitative brain activity. EEG shows the biggest differences on the theta level with a significant increase in the inner mental room. The qualitative change could be described as a leveling out of the activity with the same activity in each of the four quarters of the brain – a change of operative system. The biggest EEG changes are seen on the theta band, more than in the alpha band, in which a lower part increase and higher part decrease can be seen. IMR was also related to a hemispheric shift with a similar activation of left and right holistic brain.
Regular IMT-training changes the hormonal level and shows a decrease of cortisol levels and
increase of betaendorphin levels. IMR also seemed to be related to Section divine, the ratio 1.618 the old classical ratio for beauty and harmony. This ratio was found both in the measurement of various cortical points of IMR-activation and also in the ratio between EEG frequencies (beta 1/beta 2, alpha/beta 1, theta/alpha, delta-theta). Thus, the holistic brain concept could be complemented with the harmonious brain.
Three different studies have all showed an improvement of the immune defense (measured with
T4/T8 cells) after Mental Training. The decrease of the immune defense in connection with hard training and overtraining could be prevented by Mental Training. The last study showed that the improved immune defense could be related to one part of IMT – the Life Quality Training. Biological aging (measured with the DHEAS-hormone) stopped in connection with 6 month IMT-training. The experimental group instead became 7 years younger.
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
54
Positive IMT • ASC Biologic • Physiologic Changes
Research shows significant decrease of cortisol and an increase of betaendorphin levels are common effects after a number of weeks of regular IMT-training. Research also shows significant immunological positive changes, measured with T4/T8 cells, have been shown in 3 different IMT- investigations. A further analysis showed that it was the equivalent of Life Quality Training (Emotional Training) that gave the most positive changes. Other research shows that 300 cancer patients were matched into a control and experimental group. The difference between the control and the mental training group was largest in the terminal ill group; more survivors with IMT. Auditory research showed 70 tinnitus patients who had inner mental training for 3 months reduced or got rid of the disturbance, though only a few were able to get rid of the sound.
Hans Olssons research showed that IMT for chronic pain patients at Helsingborgs hospital
learned effective pain management by moving and reframing the pain and learning to ignore and refocus. And, research with 70 surgery patients compared with a control group with white sound showed that relaxing music and positive suggestions with hypnotic and posthypnotic suggestions improved the conditions during and after surgery. In a recent study, the aging process (measured with DHEAS) could be reversed through 6 months of mental training.
Positive stress
As stress is a normal reaction on being stimulated, stress really is an essential part of life; without stress there is no life. Selye, the originator of the notion of stress, specifically pointed out the difference between negative stress (distress) and positive stress (eustress). When we say that one of the important tasks of Mental Training is to reduce stress, we mean the "negative stress". Reducing negative stress
Is it possible to reduce stress and how is it done? One way is reducing the experienced level of stress and increasing the tolerance against stress. Research has repeatedly shown that after a few weeks of Mental Training this really occurs. This has been verified, among other things, by observing a reduction of cortizole level (our most common stress hormone). This reduction is partly caused by the Muscular Relaxation Training, which not only reduces the general level of tension and the level of experienced stress, but also makes you calm and sure of yourself. This makes you worry less about the future, at the same time making you perform your tasks in a calmer and more relaxed way. Stress
Patients who are stressed or lack self-esteem can be taught IMT techniques which can induce deep relaxation and strengthen self-esteem. Specifically, once the patient enters the ASC the doctor can communicate messages to the patient, allowing the self-induced relaxation and strengthening process to occur so that audio recordings can be introduced. When teaching self-hypnosis, a word or phrase should be stated to the patient for them to repeat. This will not work unless the patient deliberately uses the word or phrase to hypnotize them self.
Autogenic Training Autogenic training is a relaxation technique developed by the German psychiatrist Johannes
Schultz and first published in 1932. Schultz based his approach on the work of the German hypnotist Oskar Vogt. The technique involves a step-by-step progression that begins from physiological conditioning, such as muscle relaxation, breathing control and heart rate control. Then it advances to psychic conditioning through mental imagery, acoustic therapy, etc.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
55
Self‐Hypnosis•ASC•SPC•IMT•Stress
Patients who are stressed and/or lack self-esteem can be taught self-hypnotic techniques which can induce relaxation and/or strengthen their self-esteem. Specifically, once the patient is in a self-hypnotic state the therapist can communicate messages to the patient, allowing the relaxation and strengthening process to occur. When teaching self-hypnosis, a word or phrase should be stated to the patient for them to repeat. This will not work unless the patient deliberately uses the word or phrase to hypnotize them self.
ChildbirthAnesthesiaSelf-hypnosis can effectively help laboring women alleviate their pain. In fact, Joseph DeLee, a
well-known obstetrician, stated in the early 20th century that hypnosis was the only risk-free childbirth anesthetic. Common self-hypnotic techniques include:
Glove Anesthesia: Pretending the hand is numb and placing it upon a painful region to remove the sensation there.
Time Distortion: Perceiving periods of time accompanied by pain as shorter in length and
those free of pain as longer lasting. Imaginative Transformation: Viewing the pain as a non-threatening, acceptable sensation
(perhaps merely pressure) that causes no trouble. Comparisons of self-hypnosis with more traditional 'hetero-'hypnosis show that they are highly
correlated. At the same time, Kihlstrom questions the extent to which most self-hypnosis qualitatively resembles the experience of traditional hetero-hypnosis.
Self-hypnosis ("autohypnosis") is a form of hypnosis which is self-induced, and normally makes use of self-suggestion ("autosuggestion"). Listening to pre-recorded audio or other media is often mistaken for self-hypnosis, but is just another form of hypnosis. Self-hypnosis is used extensively in modern hypnotherapy. It can take the form of hypnosis carried out by means of a learned routine. Research • Pain Control • Physiological • Body Changes • IMT
EEG-studies of the Self-Hypnotic state, used in the Basic Inner Mental Training, called the
Mental Room, showed a quantitative as well as qualitative change of brain activity. The biggest change could be seen in the theta level (4-7 c/s). The qualitative change could be described as a leveling out of the activity with the same low activity in each of the four quarters of the brain and show the cortex begins to work as a holistic unit which changes the informational pathways.
Create your own future
The goal of Mental Training is to increase your quality of life, where an important part is to
learn how to live in the present moment; concentration, engagement, focusing, flow etc. are different terms for this. I have at times asked people to which extent they really live. Most of them arrive at numbers below 10 percent.
What stops us from living in the present moment is of course thoughts which either are about
the past or about the future. If you divide your life into the present, the future and the past, most of us agree upon that the present moment is the most important and that the past is the least important.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
56
Why do we then think more about the past that about the future? Well, you say, the past has happened, while the future we know nothing about. It is a fact that there are researchers specializing in trend analysis and in creating prognosis statements about the future using extrapolations of past events, but the rate of change in our society is so high that any monkey very well could be better qualified in foreseeing stock exchange rates than the so-called experts.
Relaxed spontaneous efficiency
We all want to be efficient, but the negative side of this is that efficiency is still associated with hard work and the expenditure a lot of energy; sweating. The term efficiency has officially been changed from quantity to quality, from "doing as much as possible" to "doing the right things", not to work harder, but to work smarter, e.g. Ti Chi requires only efficient, deliberate focused movements that improve well-being. Inner Mental Room • (IMR)
IMR implies a self-hypnotic state of mind or a self-absorbed state of mind where you will be
able to learn how to relax, how to regain energy after hard work and how to rebuild your energy assets. The Mental Room is also the base you will be using in work with your self-image, which I will describe in the next section. You are more competent than (if) you believe you are. A person's self-image constitutes ether base that can block or create success in life.
The notion of self-image is a combination of self-esteem, self-confidence, respect for oneself
and self-assurance. Numerous research reports have shown the importance of the self-image for performance levels in areas like sports, education and professional life. Edgar Borgenhammar and others have also pointed out the importance of self-assurance and self-confidence in the area of health.
Blocked self-image
Most of us have resources we never use. Seligman's research about "learned helplessness" has
shown that this is often a result of limitations in our self-image, built up early in our lives. Measurements of the level of self-assurance in pre-school children have shown higher levels than measurements after a couple of years in school. We often hear how people regard themselves in negative ways: I am no good in math, or I can't handle that. This sort of comment is most often a self-fulfilling prophecy that leads to negative goal images and negative expectations, which influence the end result. One gets "proof" of one's insufficiency, and as a consequence one becomes more and more uncertain whether one really has what it takes to cope with the situations in life.
In this way many of us go through life believing things about our-selves that really are completely untrue. Therefore, an important question you should ask yourself is: What kind of inner resources do I have, that I have not yet discovered? Through Mental Training you will embark on an exciting journey of discovery. Self-image Training
The self-image cannot be changed through logical reasoning; it has to be altered from the inside. By receiving positive information while residing in your Inner Mental Room, an inner process will start that slowly will reconstruct self-image. Mental Training suits everybody, including Self-image Training. To spend time developing ones self-image is not egoistic, on the contrary - everyone around you will benefit. A poor self-image often leads to different forms of asserting oneself like arrogance, boasting, etc. Trying to show, both oneself and others, how important, big and clever one is.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
57
OBJECTIVE: IMT • MBM Inner Mental Training, a specific Mind Body Medicine, is based on 35 years of scientific research conducted in Sweden by Dr Lars-Eric Unestahl, Orebro University and many others. Dr Unestahl is the founding president of the International Society for Mental Training and Excellence (ISMTE). This method is used with Olympic gold medal athletes, schools, the medical field, organizations, and for many social issues, including empowerment for the homeless.
AquaDios-Med™ IMT participants will learn the basic methods of Muscular relaxation; Mental Relaxation; Use of triggers (clues) to reach goals and reduce stress. The visual art process requires no previous art experience or ability and uses art materials to create concrete images through color, shapes, or lines. This process will use the 7 C's -- Confidence, Calmness, Concentration, Commitment, Creativity, Cheerfulness, Control -- as topics for capacities important to life. A similar program currently is used in Swedish schools for fifteen minutes three times weekly as part of the curriculum from kindergarten through high school graduation resulting in mental focus, improved grades, increased self-esteem, and stress reduction.
The AquaDios-Med™ Philosophy
• EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING! • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race.
End Part II
AquaDios-Med™ Proactive Preventive Medicine Inner Mental Training - Positive Psychology - Brief History
Adapted from Lars-Eric Uneståhl, Ph.D. Alfred A. Barrios, Ph.D.
Copyright © 2008 – 2013
AquaDios-Med™ • AquaDios Corp.
All rights reserved.
AquaDios-Med™ Proactive Preventive Medicine
Inner Mental Training - Positive Psychology - Brief History
Adapted from Lars-Eric Uneståhl, Ph.D. Alfred A. Barrios, Ph.D.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
58
Summation
These professional research documents explore the U. S. Healthcare Problem and the Solution. They demonstrate how Aquadios-Med™, PPM Healthcare Innovations, together with its intellectual properties, has the capability to save the U.S. as much as $ 2 Trillion should Aquadios-Med™, PPM be accessible across the nation in what I call the Medical McDonalds model of pragmatic healthcare. The premise is that every population capable of supporting a McDonald’s, KFC or Kentucky Fried Chicken, etc. must have an Aquadios-Med™ proactive preventive medicine Health Center open to the public for a minimum of 20 hours a day. The other PDF offers greater depth, insight and understanding to the Mind Body Medicine, IMT process.
I've spent more than twenty years researching and developing AquaDios-Med™ proactive preventive medicine health process because I believe it is the only system capable of eliminating more than $2 Trillion from US Healthcare Costs while returning many thousands of people to the workforce and wellness.
Mind Body Medicine • Psychoneuroimmunology • Non-Invasive Medicine
AquaDios-Med™ Proactive Preventive Medicine
AquaDios-Med™ proactive preventive medicine process has been developed through scientific research of Mind Body Medicine, MBM – Psychoneuroimmunology PNI Psychosomatic Medicine, Non-Invasive Medicine and structured deep-water exercise. In 1969, Dr. Lars-Eric Uneståhl of Sweden conceptualized the process of Inner Mental Training. AquaDios-Med™ has combined accelerated healing, performance and pain control practices with structured deep-water running and immersion. Research shows Structured deep-water running alone produces positive healing and rejuvenation through physiological changes described in detail below. This sustained exercise, when combined with Mind Body Medicine, the body’s natural healing process is accelerated, providing the body with the most favorable conditions for rapid, complete and natural self-healing.
Mind-Body Medicine uses the power of thoughts and emotions to influence physical health.
Hippocrates wrote, "The natural healing force within each one of us is the greatest force in getting well." This is mind-body medicine in a nutshell. Mind Body Medicine is based on the doctor and patient recognizing the relationship of the body's innate healing potential, and the partnership of patient and healer in restoring the body to health.
My personal injuries and rehabilitation motivated me to create an innovative rapid healing
method where rehabilitation pain and re-injury pain are differentiated from original injury pain to accelerate rapid healing. I concluded my rapid healing was the product of the combined process of Mind Body Medicine and the deep water exercise. My professional training and these injuries became the creative force to help motivate me to research and build a medical prototype I named AquaDios-Med™ at a cost to me of more than $1 Million of my own money.
Research of healthcare practices shows AquaDios-Med™ proactive preventive medicine use of structured deep water exercise, combined with Mind Body Medicine, Inner Mental Training, was indeed a process that safely accelerates healing and rejuvenation as well as a physical fitness tool for all people. Research shows AquaDios-Med™ proactive preventive medicine can be a boon to lower healthcare costs when implemented throughout the U.S.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
59
AquaDios-Med™ Deep-Water Running Case Abstracts Confirms Efficacy
The following case results were obtained through treatment with the AquaDios-Med™ Deep-
water running process with no inner mental training. Each of these cases represents healing speed and effectiveness well beyond what can be obtained with traditional medical treatment. They demonstrate conclusively that deep-water immersion therapy in general and specific to AquaDios-Med™ can significantly reduce the time and costs of traditional medical intervention:
A married 55-year-old Swedish dentist from Stockholm had a stroke and with just five home
training treatments with AquaDios-Med™ returned to work in his practice within less than a year. An unmarried 68-year-old obese woman with severe cardiac and back problems prepared for by-
pass surgery and rehabilitated completely in less than 90 days following surgery. A 58-year-old German doctor visiting a colleague in Canada with his family developed a serious
painful phlebitis, interfering with his ability to walk. The whole family participated in the AquaDios-Med™ deep-water running and family consultations and treatments. Walking returned to normal and pain brought under control by the third treatment.
A married, 44-year-old Canadian mother of three, diagnosed with severe lower back syndrome and
disabled for over a year, reported never feeling better after four AquaDios-Med™ home training treatments and returned to work within three months.
A 42-year-old married woman diagnosed with depression, alcoholism, multiple personality
disorder and recent surgery to both knees rehabilitated from her surgery, recovered from the pain, and returned to normal activities, while controlling her emotional difficulties, in less than 90 days.
A married 43-year-old woman just completing hysterectomy surgery, suffering severe pain, and diagnosed with lumbar and disc problems rehabilitated after five treatments with an AquaDios-Med™ “home pool program.”
An obese (312 pounds) 44-year-old mother of two, diagnosed as addicted to pain medications with severe pain, depression, phobias, and lumbar, hip, knee and disc pathology, with recommended surgery, returned to work after 53 treatments 125 pounds lighter and free of both pain and pain medication without surgery; continued to follow self-directed home treatment.
A 28-year-old professional football player with severe chronic lower back and lumbar disc
pathology was able to continue his career without loss of playing time with four treatments and a self-directed home treatment plan.
A 26-year-old female professional tennis player was able to overcome chronic knee, ankle and
hamstring injuries with 16 treatments and a self-directed home treatment plan. A 78-year-old married man with a recent hip transplant suffering chronic pain was pain free with
normal ambulation after four treatments and a self-directed home treatment plan combined with a YMCA aquatics class.
An obese (375 pounds) 55-year-old divorced great grandmother was able to avoid knee implant surgery and eliminate/control back and knee pain in six treatments and a self-directed home treatment plan combined with available aquatics classes.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
60
A 41-year-old mother of two, the victim of a rear-end traffic accident resulting in chronic intractable pain and neck and lumbar disc pathology, was pain free and fit in eight treatments and a self-directed home treatment plan.
A 26-year-old single man with recommended back surgery, addicted to pain medications for
lumbar and disc pathology, was completely free of both pain and pain medications without surgery in four treatments and a self-directed home treatment plan.
A 27-year-old athletic actress fell at high speed on the concrete bike path while Rollerblading.
The injury was diagnosed as a four-to-six week injury, with severe pain, likely rendering the patient unable to walk for several days post injury and an expected hematoma the size of a fist. After just two days of AquaDios-Med™ treatment, a bad, colorful bruise was noted but she had no pain and continued with all normal daily activities, walked normally; no hematoma developed and she continued her daily life without interruption.
The personal injuries of Dr. Jensen helped motivate him to develop the innovative deep-water
immersion treatment he used on himself to accelerate healing and physical recovery when injured or fatigued. When he broke a leg and ankle, was fitted with a toe-to-hip cast, and faced a projected 10-month healing period. He made special arrangements with his orthopedic surgeon and cut the cast in half (where the inseam and outer seam would be for a pair of slacks). The cast was removed twice daily for hot cold Jacuzzi and mild deep-water immersion exercise. In six weeks he passed a physical and shortly thereafter was skiing.
When Dr. Jensen took up long distance running—four to sixteen miles with an average of eight
miles per day—he utilized his Mind-Body Medicine and daily power Jacuzzi with deep-water immersion exercise to overcome the usual sprained ankles, twisted knees and hips to never miss a run in over 10 years.
J. Glenn McWaters Case Abstracts • Confirms Effectiveness of Deep-Water Running
The following case abstracts represent just a fraction of the results obtained through treatment with
J. Glenn McWaters’ Wet Vest (pictured on page 1). Each of these cases represents healing speed and effectiveness beyond what can be obtained with traditional medical treatment. Note: These healing benefits were obtained with exercise only. The multi-temperature immersion therapy offered by AquaDios-Med™ multiplies the effectiveness of exercise alone:
The Philadelphia Eagles drafted Keith Byers of Ohio State as their number one draft choice in
1986. Although he had been one of the most outstanding collegiate running backs for several years, Keith had suffered a severe fracture in his foot and some people felt he would never play football again. The Eagles had Keith run in deep-water on a daily basis. After several months of deep-water running, Keith was pronounced fit to play and had a fine rookie season.
Bob Slusarek, owner of the Northwest Athletic Club in Springdale Arkansas, reports on the
healing effects of deep-water exercise on his members: “In the first two months, we had runners, two cardiac rehabilitation patients, swimmers, pregnant women, numbers of grossly overweight, elderly men and women, coaches, a boy with cerebral palsy, and two members with knee rehabilitation.”
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
61
Mary Carol developed lymphedema (an inflammation of the lymph glands) six years prior to this report. After four major operations, the addition of surgical tubing to her lymphatic system, and the use of a compression machine, she was told not to run again. Deep-water immersion therapy resolved this problem. She says, “I am enjoying the deep-water running beyond words! The thrill of using muscles that I haven't been able to use in over five years was unbelievable!”
Larry Walton, a multiple sclerosis patient in Culver City, California, reports: “After deep-water
running for two weeks I have found my energy level raised and, as a multiple sclerosis patient in remission, I have found that I walk with a far greater 'spring in my step' and am generally in far better shape than I was prior to deep-water running.”
Don Gambril, head swim coach of the University of Alabama and 1984 U.S. Olympic swim coach
underwent a heart bypass operation to clear four clogged arteries a few years before this report. Coach Gambril, who had noted several of the university runners frequenting the pool to do deep-water running, realized that he could overcome his cardiac problem with deep-water running. His cardiologist, Dr. William A. Hill, remarked that it was a shame that most cardiac patients could not swim. Dr. Hill, a non-swimmer himself, became excited about the possibilities for his patients and adopted a deep-water running program even though he could not swim.
Like millions of Americans, composer Burt Bacharach suffers from back pain. He has discovered
that the key to keeping these problems under control is daily deep-water running. This activity has been instrumental in reducing the occurrence of back pain.
A neurosurgeon specializing in back pain, Dr. Gerard Sava of Stamford, Connecticut is one of the
top neurosurgeons in the country. Before performing surgery, Dr. Sava explores other possibilities for overcoming back pain. Dr. Sava uses deep-water workouts to strengthen the back in an attempt to avoid surgery, and is successful in many cases. When surgery is required, Dr. Sava uses deep-water exercises to rehabilitate the patient quickly and effectively.
AquaDios-Med™ • Healing Conclusion •
The human body is designed to heal itself, given favorable conditions. Traditional medical
intervention typically creates conditions antagonistic to self-healing. The specially designed, multi-temperature deep-water immersion therapy offered by AquaDios-Med™ can create such favorable conditions, thereby helping sick people to heal faster and more effectively than traditional medical intervention. Furthermore, healthy people can prevent disease by regular deep-water immersion and exercise. The result of this will be a significant reduction in the costs of healthcare and a healthier, happier populace.
For Further Information
Research into the healing effects of deep-water immersion—how and why it works—is extensive,
and much more information is available upon request. Dr. Jensen has authored a an unpublished and yet to be edited professional manuscript with over 1,000 references of the many studies and research in the field of preventive medicine including deep-water immersion, mind body medicine and much more.
Exercise is a weapon against disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
62
Additionally, some proprietary details and design of operation of the AquaDios-Med™ process
and facility is made available in picture format below. Specific proprietary details of the design and operation of the AquaDios-Med™ process and
facility will be made available on a confidential basis upon request and non-disclosure agreement.
Contact Dr. Alan Jensen can be reached by email at [email protected] or by phone at 310-897-5055 - USA. Dr. Alan Jensen is Founder & CEO of AquaDios-Med™, a 21st Century Immersion Environment
for Advanced Fitness & Accelerated Healing. He has a Ph.D. in Professional Psychology, a Masters in Rehabilitation Psychology, two Bachelor Degrees from accredited universities, and has been a member of MENSA since 1978.
Dr. Jensen’s private practice spanned more than 25 years and included staff privileges and close
associations at numerous hospitals in Southern California. As a long-term member and faculty of the American Society of Clinical Hypnosis and the Society for Clinical Experimental Hypnosis, he taught Clinical Hypnosis to physicians and psychologists throughout the United States, Europe, Australia, and Canada. Dr. Jensen has enjoyed membership in many professional associations and has lectured at numerous venues, including the International Society of Medical Hydrology & Climatology in Istanbul, Turkey on the benefits of AquaDios-Med™.
Dr. Jensen offers the world the wisdom of his experience both as a healer and as the developer of
AquaDios-Med™. Visit at http://www.aquadios.com/
Trademark/Copyright Dr. Jensen's corporation, AquaDios-Med™ Corp. is on the books with variations of AquaDios™
and AquaDios-Med™. These terms and trademarks are equitable and legally binding. These terms and trademarks are descriptive of the process associated with the medical prototype invented and built between 1985 and 1994 by Dr. Jensen.
The AquaDios-Med™ Corp. and its trademarks AquaDios™ and AquaDios-Med™ and
AquaDiosMed™ refer to a process defined and identified in multiple articles Dr. Jensen has written and professionally presented to universities, hospitals and organizations.
Brief History – Education - Dr. Alan Jensen - AquaDios™ - Aquadios-Med™ As a 3 year old Dr. Jensen was abandoned to an orphanage then foster homes. He put himself
through college – university studies while working menial jobs, with scholarships, stipends and loans. When he qualified as a Mensa Society member he knew one reason for his success was that he had high intelligence and was uniquely innovative; this is combined with his strong motivation and desire to succeed. Late President Kennedys’ famous statement, ask not what your country can do for you, but what you can do for your country has been his driving force to bring something great to his country and to the world.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
63
Dr. Jensen developed a passionate thirst for understanding human healing capacities starting with his own childhood accidents and injuries including a lacerated Achilles heel, a hand held fishing spear accidentally thrust into his biceps, a broken leg and fractured ankle. These injuries led him to study paranormal phenomenon and achieve the Diplomate in Pain Management, while being board eligible for the Diplomate in psychological hypnosis since 1980. A few of his certifications include applied clinical hypnosis and neuro-linguistic programming; he is the founder/creator of Aquadios-Med™ - AquaDios™.
After graduating with a Master of Science he had an accident that resulted in a fractured fibula and
ankle stirrup; prognosis was a 10 to 12 month healing interval with a hip to toe cast. The orthopedic surgeon agreed to cut the cast where trousers seems would be for its removal and refitting. Once the cast was off an X-Ray reveled the ankle stirrup was fractured as well; had the cast not been removed the ankle joint would have become immovable causing a sever limp.
He applied his rapid healing mental techniques together with daily hot – cold Jacuzzi and deep
water walking. In 6 weeks he passed a physical for his first college teaching position and was skiing shortly thereafter. This accidental injury and rehabilitation became the stimulus to invent his innovative and unique proactive preventive medicine process he named AquaDios-Med™. The AquaDios-Med™ medical prototype cost him more than $1 Million of his own money to build with countless dollars for research and development. Simply put, AquaDios-Med™ PPM is a combination of safe, sustained physical exercise in deep-water immersions, mental training and correct eating. The prototype and mush more can be seen at http://www.aquadios.com/
The AquaDios-Med™ research and development demands were so excessive and demanding he
re-tired from private practice, teaching and hospital work of nearly 3 decades to focus his life energy on his passion, AquaDios-Med™; he continued to consult with individuals and groups.
His membership in professional medical societies spans more than two decades during which his
activities and involvement have been both national and international. As a faculty member in these societies, he presented multiple workshops and lectured to a broad spectrum of professionals, including physicians, surgeons, dentists, psychologists and more. His expertise began in the of preventative medicine fields such as clinical hypnosis, sports and behavioral medicine, psychosomatics, rehabilitation, physiotherapy, hydrology, health and fitness, coaching and psychoneuroimmunological mediation. He has taught at the university, college and medical school level and served on hospital medical staff.
He has been on the cutting edge of medical treatment recognized in the early 1990’s by the
scientific term psychoneuroimmunological mediation, a procedure known to bolster patient immune system function and accelerate healing. It combines doctor-patient activities and procedures once limited to early practices in medical/clinical hypnosis and mind body medicine.
His formal education is from several universities and includes post- graduate degrees with a
Ph.D. in Professional Psychology [two physicians stood on his doctoral committee], emphasizing the treatment of disease with mind body medicine, applied medical hypnosis, the forerunner of the hospital practice of behavioral medicine, and other alternatives; an M.S. in Rehabilitation Psychology, the psychological/medical aspects of severe, and sometimes permanent traumatic injury; a B.A. in philosophy (logic) & psychology; and a B.S. in criminology, psychology and forensics.
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
64
The spectrum of his private practice embraced treatment of children, families, adults, Olympic and professional athletes. Some of these patients/athletes suffered severe disease, such as cancer, serious drug addiction and difficult-to- break habits, as well as common family, emotional, medical physical maladies. His treatment was based on the belief that a positive attitude, physical fitness and re-creation through sustained exercise are the cornerstone of wellness and healing.
He abides by the premise that he would not prescribe something to anyone that he would not do
for himself. He has healed from many of the maladies and injuries that have also worked to help his patients. He has been one of his own most used test subject in the development of his programs.
"The driving force to create both the AquaDios™ process and the AquaDios™ prototype is a
common world-wide belief that, at some level, we all want to be the best and get the best that life has to offer. To achieve this goal we must first feel abundant energy together with an unfailing sense of peace and well-being before the stream of growth can flow into all areas of life. A successful outcome requires being in charge of your life and unlocking or letting go of whatever bothers you, regardless of your circumstances." Dr. Alan Jensen
Professional Societies - Affiliations
American Psychological Association; American Academy Pain Management; American Medical Athletic Association; American Society Clinical Hypnosis; American Holistic Medical Association; American Medical Hydrology Climatology Association; Academy Psychosomatic Medicine; Society Clinical Experimental Hypnosis; International Hypnosis Society; Southern California Society Clinical Hypnosis; Los Angles Academy Clinical Hypnosis; Group Psychotherapy Association; Southern California, and more.
Professional Teaching - Faculty USA
U.S. International University San Diego; Antioch University Los Angles CA.; Los Angeles Community College District; Pepperdine University Malibu CA; American Society Clinical Hypnosis; International Hypnosis Society, Southern California Society Clinical Hypnosis, Los Angeles Academy Clinical Hypnosis.
He has participated as an ambassador, in international relations, on the speaker’s bureau, in
education and practice and more for some of these societies and associations. He has been on faculty, staff and an associate with many hospitals. He has taught at the national
level for the American Society Clinical Hypnosis across the U. S. Canada, Europe, and Australia. He is an expert trained in forensic hypnosis and helped to establish a program for the Los
Angeles County Sheriff Department designed to assist eye witnesses and victims of crime in the recovery of facts and reduce or eliminate trauma.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
65
FORENSIC HYPNOSIS Team Member - AMERICAN SOCIETY CLINICAL HYPNOSIS – established Los Angeles County Sheriff Department Program 1976-1978; Ambassador: American Society Clinical Hypnosis; Speakers Bureau International Relations; Education and Practice 1976 – 1990
End Part I HealthCare • Crisis
SOLUTION • Man-Made Healthcare Crisis AquaDios-Med™ Proactive Preventive Medicine
AquaDios-Med™ Proactive Preventive Medicine • Evidence Based
Deep-Water Running Immersion Therapy • Mind-Body Medicine • Research Brief History
AquaDios-Med™ Proactive Preventive Medicine AquaDios-Med™ Inner Mental Training
Positive Psychology
The AquaDios-Med™ Philosophy • EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING! • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race.
Copyright © 2008 – 2012 – 2013 2nd Edition
AquaDios-Med™ • AquaDios Corp.
All rights reserved. Respectfully,
Dr. Alan Jensen (Alan) Founder • CEO • Creator, AquaDios-Med™ http://www.aquadios.com/ A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing Phone 310-897-5055 - Email: [email protected] - P.O. Box 2228 Malibu, Ca. 90265
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section II
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
AquaDios-Med™ Proactive Preventive Medicine Deep-Water Immersion Therapy • Safest • Healthiest Exercise
Mind Body Medicine • Inner Mental Training Accelerated Healing • Rehabilitation Pain
Evidence Based Deep-Water Running Immersion Therapy
143 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California 90265 • 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
www.aquadios.com
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Research Deep Water Immersion Therapy
An Answer To • Man-Made Manufactured • Healthcare • Crisis
Is AquaDios-Med™ Proactive Preventive Medicine 143 Pages
Part One Solution -- presented research to show that the human body natural healing capacities are often ignored, even damaged by modern hospital medicine, in favor of powerful pharmaceutical drugs, most all of which have dangerous side effects and order unnecessary invasive tests, most with negative side effects, and order unnecessary surgeries, many of which disable patients or worse cause death.
Other research studies showed that AquaDios-Med™ Proactive Preventive Medicine reliance
on deep-water immersion therapy combined with Mind Body Medicine is a substantiated evidence based safe medical that all walks of life can learn and apply while remaining free of harmful pharmaceutical drugs and dangerous surgeries.
Research studies repeatedly show Physiological Self-Regulation • PSR when combined with
the deep-water immersion therapy as a capable method of managing most symptoms while improving immune system function and physical fitness. Research showed how the autonomic nervous system ANS works with the sympathetic nervous system, SNS and the parasympathetic nervous system, PNS positive, natural physiological change reduces the risk of cardiovascular disease, improves memory, enhances cognitive processes and increases concentration.
Detailed Images of the AquaDios-Med™ Proactive Preventive Medicine immersion chambers
were presented as well as Videos of the process with detailed information on the physical exercise and mental training. Research confirmed that cold immersion to the neck increases hemoglobin and oxygen production in the blood which further enhances cell production and the healing capabilities of the immune system; thereby accelerating rebuilding of the cell structure to acquire peak performance, to stimulate ones immune system to establish a balanced, healthy homeostasis for physiological self-regulation and for accelerated healing.
Part Two will expand the research and evidence based values in AquaDios-Med™ Proactive
Preventive Medicine deep-water immersion therapy and Mind Body Medicine to further substantiate ADM™ PPM is the safest and healthiest procedure that all walks of life can learn and apply while remaining free of harmful pharmaceutical drugs and dangerous surgeries.
More details will identify the value of Isokinetic Muscle movements, training effects, pain
management, injury and accelerated healing and why many experts regard the process as secret weapons to health, fitness, stamina, endurance and longevity.
Exercise is a weapon against disease Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
Summary AquaDios-Med™ Deep-Water Immersion Therapy AquaDios-Med™ is a scientific application of aquatic hydrology rehabilitation medicine
producing a verifiable re-creation or transformed rejuvenation. Its applications and procedures decrease injury -- rehabilitation recovery time by 75 percent or more.
These positive psychophysiological results are byproducts of natural body chemistry; these same positive results can be produced by healthy people who can eliminate or decrease the common contemporary tension, stress, anxiety, syndromes leading to 70% of our nation's medical problems. It can also address drug/alcohol abuse.
AquaDios-Med™ re-creation programs improve conditioning, strength, endurance, and reaction time. It also accelerates recovery from the physical pounding found in competitive sports. It eliminates or greatly reduces pain expected with and inherent in competition, decreases or eliminates a high percentage of future injuries, and can provide a positive addition to training of the professional or university athlete or performer. AquaDios-Med™ deep-water exercise permits people to distinguish between re-injury and acceptable non-injury physical activity to further accelerate healing. Rehabilitation Pain during these immersions expedites a much higher cell-production repair rate than normal. To see AquaDios-MedTM videos go to http://www.aquadios.com/aquadiosmovies.html
Rehabilitation Pain - Sport Medicine
Sport Medicine is another, more glamorous name for the science and application of physical rehabilitation following minor to serious injury trauma from accidents, sport and other manners of trauma. The ultimate goals of sport medicine are rapid healing and preventative medicine – or preventative injury in sport – physical activities designed for physical fitness.
Rehabilitation Pain is a term Dr. Jensen coined decades ago to describe the difference between proactive physical activities – while injured and the then more common – do nothing – use plenty of pain medication approach to recovery. The downside to proactive – or – aggressive rehabilitation is that re-injury pain is very similar to rehabilitation pain. Many argue that purposely-produced pain is masochistic or a self-inflected pain - a pleasurable arbitrative event, or self-destructive. However, to achieve one’s best and to surpass that level of best, e.g. if one can lift 5 pounds 5 times before fatigue and or pain sets in, it is that very pain – the tearing down of tissues - that rebuilds itself - to soon allow one to lift 10 pounds ten times. Thus, today’s best becomes a warm up activity to pursuing the future or new best, a potential endless spectrum of greater achievement. Re-injury pain is an automatic internal awareness to prevent re-injury. Rehabilitation pain is similar to the above example. The problem with pain medication is that it suppresses healing while the mind is capable of establishing pain management at the injury – trauma site. Healing is more complete and faster when one is willing to experience the trauma site and distinguish between re-injury and rehab pain. Thus, rapid healing is not a pursuit of pain, but rather a-higher order self-awareness, one which involves self-empowerment or self-improvement not suffering. It is setting a limit today, a threshed that cannot – today be crossed, but tomorrow or the day after, soon will be easily passed. Dr. Jensen has worked with many individual and team athletes, some at the elite – Olympic – professional level, some gold – silver – bronze medalists’. Each individual and each team member was taught to deal with personal pain – work out and competition pain – to rise to the level of excellence within their potential. Many of these athletes were injured in their sport, during training or competition or in traffic accidents and other common traumas that befall all of us. In every case those that considered retirement from competition prior to treatment went on to even greater success at their respective level whether it be at the university, Olympic, professional or physical fitness levels. Thus, their injuries became a corner stone for greater success.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
Injury and Pain Relief AquaDios-Med and Mind Body Medicine techniques directed at specific altered states of
consciousness is a wonderful tool for the use of pain relief. [See above specific to rehabilitation pain] One has only to clench a tight fist and pinch its skin, then relax the same hand while maintaining that pinch to notice how the simple act of relaxation lessons the pain.
Sports Medicine is glamorous name for physical rehabilitation following minor to serious injury trauma from accidents, sports and other manners of suffering. The ultimate goal of sports medicine is rapid healing and preventative medicine or preventative injury in sports with physical activities designed for physical fitness.
"Rehabilitation pain" is a term I coined decades ago to describe the difference between proactive physical activities while injured and the more common, do-nothing, "use-plenty-of-pain-medication" approach to recovery. The downside to proactive or aggressive rehabilitation is that re-injury pain is very similar to rehabilitation pain. Many argue that purposely-produced pain is masochistic or self-destructive. However, the injured athlete, working mother, father or child who may be suffering from an injury may need to achieve their best effort to rehabilitate. Or, one may simply be working hard at physical fitness and concentrate on one's best and to surpass that level of best during workouts. -- e.g. if one can lift five pounds five times before fatigue and or pain sets in -- it is that very pain (the tearing down of tissues) that rebuilds tissues and allows one to soon lift ten pounds ten times. Thus, today's best becomes a warm-up activity to the future or new best, a potential endless spectrum of greater achievement. The same is true in rehabilitation activities and healing.
Injury has an automatic internal unconsciousness to prevent re-injury. Rehabilitation pain is
similar to the above example. The biggest problem with pain medication is that it suppresses healing at the injury/trauma site where the mind is capable of establishing pain management and rapid repair. One is able to heal more quickly and completely when one is willing to experience rehabilitation pain, particularly at the trauma site, and to distinguish between re-injury pain and rehabilitation pain. Thus, rapid healing is not a pursuit of pain, but rather a higher order of self-awareness one, which involves self-empowerment or self-improvement, not suffering.
It is the act of setting a limit today, a threshold that cannot be crossed today. But tomorrow or the day after, it will be easily passed. To be successful preventive medicine and Mind Body Medicine must teach each individual to deal with personal pain, workout and physical conditioning pain, and to rise to the level of excellence within his or her potential for healing.
Many people are injured in sport, during physical fitness training in traffic accidents and other common traumas that befall all of us. In every case, those that considered this body awareness treatment went on to even greater success at their respective level, whether at the university, professional or physical fitness levels. Thus, their injuries became a cornerstone for greater success.
Usual treatment for injury is extended rest, which iatrogenically contributes to the syndrome by the development of scar tissue within the adjacent muscular and soft tissues. Pain management teaches patients to master pain by the experience of painful but safe, necessary physical body exercise movements for rapid healing, conditioning, strength and endurance by full body activation.
Immune systems normally act automatically to preserve the integrity of the body, but symptomatic pain can become an active process of unconscious learning that contributes negative patient energy to illness and symptomatic process. Agitated depression and somatic pain are often dynamically linked to hostile anger and veiled rage. Legitimate anger is manifest by being a victim of accident, injury or disease. One treatment focus is to help differentiation of legitimate anger and pain from sadomasochistic projection caused by the victim’s tragic ordeal.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
AquaDios-Med treatment relies on a Prescription Intervention Plan, a treatment contract agreement signed and dated by the patient stipulating their required treatment responsibilities and cooperation with the treatment staff during consult. It requires their compliance to assist the treatment team exploration of secondary symptomatic gains, essential to depotentiate relapse and encourage patients to participate in a daily health regime, including proper use of medication, surgery, and social support to facilitate and integrate health. It is incumbent on the patient to learn enough responsibility to establish and maintain wellness during rehabilitation. By so doing, most symptoms may be significantly reduced and clinical medicine can thus rely less upon medication or surgery and more on the patient.
PERCEIVED EXERTION RATINGS
Exercise requires energy, effort or exertion. Subjective estimate of how much effort it takes to perform a given task is called "perceived exertion". "Ratings of Perceived Exertion" (RPE) charts are a categorical rating scale established by the scientific community. Borg and McWaters developed similar scales to establish "Ratings of Perceived Exertion" based on the fact that exercise requires energy, effort or exertion.
In 1982, Dr. Borg once again refined the RPE scale to a 10-point categorical scale.
RATING OF PERCEIVED EXERTION (RPE)
0 nothing at all
1 very, very weak
2 very weak
3 weak
4 somewhat weak
5 moderate
6 somewhat hard
7 hard
8 very hard
9 very, very hard
10 maximal (all-out effort) Rehabilitation objectives or any process to maximize performance must first teach sustained correct breathing with focused command of exercise activation while the patient accurately rates the subjective quality of perceived exertion or pain. Perceived Pain Ratings between 7 and 10 carry the greatest healing potential but paradoxically also encompass the most dangerous re-injury potential. This gray area is a fine line of patient motivation and compliance with minimal scientific control and maximal rapport between patient treatment team personnel and physical therapy.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
Successful accelerated rehabilitation treatment seems to rely on patients actually experiencing minor re-injury pain before the "just notable differences" (JND'S), co-exist to establish the compliance foundation necessary for hard work and focus in this treatment. Re-injury pain during controlled accelerated rehabilitation is unwelcome, but with guidance and support motivated patients can learn its physical manifestation, find it is not too traumatic and that it is almost always followed by an accelerated learning curve with a sense of confidence self-mastery and desire to be less dependent on physical therapy.
AquaDios-Med • REHABILITATION PAIN
Rate of Perceived Pain (RPP) scale looks identical to the Rate of Perceived Exertion scale because it has a range from 0 to 10, but the Rate of Perceived Pain (RPP) scale is measuring rehabilitation pain with ranges from 0 to 10.
AquaDios-Med PPM and Rehabilitation Pain
RATINGS OF PERCEIVED PAIN
0 nothing at all No Pain
1 very, very weak Minimal Discomfort
2 very weak Minor Pain
3 weak Experienced Discomfort
4 somewhat weak Low Grade Pain
5 moderate Tolerable Pain
6 somewhat hard Uncomfortable Pain (Safe) 7 hard Moderate Pain (Safe-Marginal)
8 very hard Severe Pain (UNSAFE)
9 very, very hard Unmanageable Pain (DANGEROUS)
10 maximal (all-out effort) Intractable Pain (UNSAFE-RE-INJURY)
CARDIOVASCULAR BENEFITS
Reduced Heart Rate • Oxygen Consumption
The body's transportation and extraction of oxygen is improved IN DEEP WATER EXERCISE! During sub-maximal exercise, heart rate is about 10 to 20 beats per minute less in water than on land, at the same perceived exertion level (RPE). The heart does not work as hard yet produces a superior cardiovascular conditioning workout with superb muscular strength and muscular endurance because the body is completely surrounded and buoyed by a fluid. Water can generate between 4 to 52 times greater resistance force against each body movement than air depending on exertion level -- how fast you move your arms and legs -- Isokinetic.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
The personal injuries of Dr. Jensen, the founder of AquaDios-Med, helped to motivate him to develop the inventive deep-water immersion treatment he used on himself to accelerate healing and physical recovery when injured or fatigued. The most profound instance was when he broke a leg and ankle and was fitted with a toe to hip cast; a projected 10- month healing.
Dr. Jensen made special arrangements with his orthopedic surgeon and cut the cast in half; where the inseam and outer seam would be for a pair of slacks. The cast was removed twice daily for Jacuzzi and mild deep-water immersion exercise; in 6 weeks he passed a physical. When Dr. Jensen took up long distance running, 4 to 16 miles with an average of 8 miles per day he utilized his Mind Body Medicine and daily power Jacuzzi with deep-water immersion exercise to overcome the usual sprained ankles, twisted knees and hips to never miss a run in over 10 years.
Pain Management
Pain is a warning that something is wrong, so the first step is consulting a professional to learn
its cause. Once you learn what the cause of your pain is, only then should you ever use a program like this. Once you begin this program, you will be able to eliminate any painkillers you have been using, or at the very least reduce the amounts drastically so that you can enjoy life coherently. Pain doesn't have to stop you in your tracks preventing you from enjoying life. Get a grip on it, and control whatever is bothering you.
As a hypothetical construct, pain is composed of not only the present experience, but in
addition, is greatly enhanced by memories of past pain, and fears of future pain. This allows for many possibilities in the lessening and/or complete obliteration of the pain experienced with hypnotic techniques. For example, a classical study was done decades ago by pairing the noise of an electronic shock with pain. Unbeknownst to the subjects the electric shock was disconnected and when the noise associated with the shock was heard the subjects re-experienced the same level of pain as the “real” electric. This imagined pain was measured to be equal in strength to the “real” pain. Thus, the “sound” of the electric shock became the electric.
Mind Body Medicine deals with pain management and control by looking upon pain
analytically that is that, pain has certain temporal, emotional, psychological, and somatic significance's and therefore can lean to be altered, managed and controlled by the subject.
Pain is a hypothetical construct composed of three parts; past remembered pain, the present
pain experience, and the anticipation of future pain. Thus, immediate pain is amplified by past pain and is further enhanced by thoughts of future possibilities of pain. The immediate stimuli are only a central third of the entire experience. Nothing so much intensifies pain as the fear that it will be present in the near future. It is likewise increased by the realization that the same or similar pain was experienced in the past, and this and the immediate pain render the future even more threatening. Because pain is complex, it is more readily vulnerable to Mind Body Medicine management and dealing successfully with it, than it would be were it simply an experience of the present.
To understand pain further, one must think of it as a neuro-psycho-physiological complex
characterized by various understandings of tremendous significance to the sufferer. Pain, as an experience is also rendered more susceptible to memory because it varies in its nature and intensity, and hence, through life experiences, it acquires secondary meanings resulting in varying interpretations of the pain.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
Mind Body Medicine procedures are very successfully used for pain relief and pain control and include: direct suggestion, indirect suggestion for symptom alleviation; amnesia for eliminating past pain; which in turn would control fears of future pain; analgesia, and anesthesia for eliminating immediate pain, replacement or substitution of psychosomatically induced pain; displacement of pain, which increases a patient’s sense of pain control; dissociation for long-term chronic care, and the reinterpretation of pain, which helps reorganize one’s learning’s, along with time distortion techniques to lessen the perceived time span of unpleasant experiences, and increase the perception of times of comfort.
The question now is how do we begin to help someone suffering pain, and how do we focus their attention long enough to apply hypnotic techniques to help eliminate, reduce, or control the pain experience.
Mind Body Medicine relaxation techniques can automatically reduce about one third of the pain experience. A large part of the pain experience is due to tensions within the body and most often produced by the person “trying” to control what hurts; but in fact compounding the pain effect. Relaxing, one of the main benefits in Mind body Medicine causes the pain to automatically diminish. It is important that Mind body Medicine techniques can relax a person who is all tensed up. One method is called “pacing the experience”. Providing an acknowledgement of what is happening, will further establish a “yes set”, to help lead the individual into the abstraction experience. From there, you can learn to ask for an intricate description of the pain from 0 – 10, 10 being the worst pain and 0 being no pain.
Discussing what kind of pain it is helps to gain control, is it a sharp pain, dull, stabbing, piercing pain, etc? This gets a person to identify what is happening so that they can confirm within themselves when something changes. Furthermore you can ask for the specific location, and how much of the area, the specific times, duration, and frequency. This will provide you with information that you can use to help the person control what is going on. From this point on, any number of the hypnotic techniques mentioned above can be used.
Milton Erickson, MD recommended time distortion as one the most useful pain control
techniques. It is accomplished by having the patient remember how time flies when they are having fun, and yet slows right down and almost stops, when waiting for a kettle to boil. From this point on, you would use suggestion to have the good parts of the day appear to last longer, the person would go into a deep relaxed state during painful episodes, and if suggestions for amnesia had been learned or accepted, the patient will tend forget to remember having had the pain, and we know how we can distort time as it is, but we can distort it into a very, very short time. Putting all this together could help someone with the most extremes of pain tremendously.
To summarize, pain is a subjective experience. Pain; during lives experience serves to establish body learning, associations, and conditionings that constitute a source of potentials permitting the use of hypnosis for the study and implementation of pain relief.
Training Effect • Positive Physical Changes • Aerobic Exercise
Evidence Based
In his book, The Aerobics Program For Total Well-Being, Cooper defines "training effect" as "the positive physical changes that accompany aerobic exercise": 1. Strenuous physical activity increases total blood volume; the body transports more oxygen and has more endurance; 2. Capacity of the lungs increases, and this increase in `vital air capacity’ is associated with a greater longevity;

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
3. Heart muscles grow stronger, are better supplied with blood, and with each stroke the heart pumps more blood, increased stroke volume; 4. "High density lipoprotein (HDL) increases, the total cholesterol HDL ratio decreases, reducing risk of developing atherosclerosis, or hardening of the arteries."
In 1974 Aerospace Medicine reported A. Crittenden and associates discovered the blood's
capacity to carry oxygen increases when the body is submerged in water cooler than body temperature. The cooler the water, the more affinity hemoglobin seems to have for oxygen. Hemoglobin, the blood's oxygen transportation system, thus carries more oxygen when it is cooled. Research found ability of the body's tissues to extract oxygen from the blood improves in cool water because of reduced gravitational pull on the heart and extremities experience more pressure in deep water. The increased pressure forces venous blood from the extremities back to the heart at a faster rate, more blood is available to be pumped by the heart. Mitochondria are a cell's power plants and produce most of the cell's endurance energy through oxygen extraction and utilization. The more mitochondria in a cell, the more oxygen that cell can extract and use. According to McWaters, the volume of oxygen consumed (VO2) is equal to cardiac output (Q) multiplied by arterial venous difference (A-V difference) or: VO2 = Q x (A-V difference).
Cardiac output (Q), the amount of blood pumped with each heartbeat, is the central component of the equation and is composed of heart rate time’s stroke volume. Arterial Venous Difference (A-V Difference), the peripheral factor in the equation, basically describes mitochondria in the cells. Sport physiologists theorize training programs requiring isokinetic muscle contractions are best suited for improving athletic performance -- isokinetic muscle contractions are made with even tension, constant speed and a full range of motion. The blood's capacity to carry oxygen increases when the body is submerged in water cooler than body temperature. The cooler the water, the more affinity hemoglobin seems to have for oxygen. Hemoglobin, the blood's oxygen transportation system, thus carries more oxygen when it is cooled.
Research found ability of the body's tissues to extract oxygen from the blood improves in cool
water because of reduced gravitational pull on the heart and extremities experience more pressure in deep water. The increased pressure forces venous blood from the extremities back to the heart at a faster rate, more blood is available to be pumped by the heart.
Lactic Acid • Training Effect Enhanced
Science thought lactic acid build-up was the cause of muscle soreness during the first few days after exercise, but learned compression trauma not lactic acid causes soreness. Isokinetic Deep Water Running exercise quickly dissipates Lactic acid build-up after treadmill running exercise. Earlier research was explored by Exercise Physiologist, K. J. Cureton, and Ph.D., who determined exercise activity perceived, as "somewhat hard" is the point where lactic acid begins to accumulate. This intensity level is equivalent to RPE 6 on the Borg/McWaters scale. If exercise is too hard, at an REP above 6, then muscles will feel fatigued to the point of not being able to continue, this means the lactate level is too high. Lactic acid doesn't cause soreness, only muscle fatigue.
Researchers compared lactic acid samples from persons after Wet Vest water running to samples from these same individuals after running on a treadmill. The subjects ran at the same RPE level in the water and on the treadmill. Heart rates were significantly lower during water running, but the lactic acid levels were actually higher, indicating that the muscles worked harder and achieved a better overall workout in the water, even though the heart rate was 10 to 20 beats per minute less!

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
Lactic acid was dissipated much more quickly after water running than after treadmill exercise. Further, none of the subjects experienced soreness or fatigue the day or two following a Wet Vest workout, while they all suffered soreness and fatigue after running on the treadmill. Running at the equivalent exertion level in water as on land creates a minimum of 12 to 14 times greater resistance force against each body movement and subjects every cell of every muscle submerged below water to an increased work load. Physiologists rate isokinetic training programs best suited for improving athletic performance, developing muscular strength - endurance and rank Deep Cool Water Running as the highest aerobic cardiovascular value of all exercise. When the body is submerged to the neck in water substantially cooler than body temperature, the blood's capacity to carry oxygen increases, hemoglobin oxygen in the blood is increased to accelerate body tissue regeneration; colder water increases hemoglobin affinity for oxygen. Patients gain training effects of a higher heart rate but sustain a lower heart rate while building the heart muscle stronger because Heart Rate is up to 20 beats per minute less in deep water at the same perceived exertion level (RPE) of exercise intensity and "High density lipoprotein (HDL) increases, the total cholesterol HDL ratio decreases, reducing risk of developing atherosclerosis, or hardening of the arteries". Exercising in deep cold water provides superior cardiovascular conditioning, superb muscular strength and endurance because the body is completely surrounded and buoyed by a cold fluid. Water resistance creates increased venous return with less demand to the heart.
AquaDios-Med Rehabilitation and Strengthening program is realistic alternative to surgery or hip replacement. ADM™ improves conditioning, strength, endurance, reaction time and accelerates recovery from emotional – physical stress and physical soreness found in injury, disease and pain problems.
For competitive sports it eliminates or greatly reduces pain suffered in competitions, decreases future injuries, provides a positive addition to pre-season training, the season’s competition and post-season conditioning. It is ideal for physical fitness, for elite athletes, sports figures, dancers or entertainers who must rely on their physical and emotional prowess for their livelihood.
Nearly All Muscles Involved
Swimming is a good exercise, but primarily the shoulder muscles do 80 to 90 percent of the work. Running on land is just the opposite; lower body muscles do nearly all the work. Deep-water running uses all these upper and lower body muscles. Another reason deep-water exercise is the best exercise for developing muscular strength and endurance is that it is an isokinetic exercise. Muscles can undergo four basic types of contractions: isokinetic, isotonic, eccentric, and isometric. Isokinetic Contraction Isokinetic ("same speed") contractions are positive contractions, which occur when a muscle is subjected to an even amount of tension at a constant speed over the full range of motion. Unlike isotonic contractions, which vary the tension on the muscle, isokinetic activities maintain an equal amount of tension on the muscle. A bicep curl is performed in water at a constant speed using only the resistance of the water. The muscle receives equal amounts of tension. The more quickly the arm moves, the more resistance it encounters.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
Isotonic Contraction
Isotonic (meaning same weight), are positive contractions and occurs when a muscle shortens under tension such as a bicep curl. Isotonic exercises require a weight that can be moved the full range of motion because the velocity of the weight carries it through the range where the muscles are otherwise too weak.
Eccentric Contraction Eccentric contractions occur when the muscles lengthen under tension. These are "negative" contractions, the opposite of isotonic contractions. For example, this type of contraction occurs when you lower the dumbbell from the shoulder to the starting position in a bicep curl. It takes effort to control the weight as it is lowered.
The more slowly the weight is lowered, the more pronounced the exercise becomes. Eccentric Contraction - A 50- pound weight is lowered slowly from the shoulder to the starting position. Isometric Contraction
In an isometric ("same length") contraction, the muscle is subjected to tension without changing length. This type of contraction occurs when you attempt to lift a weight that is too heavy for you to lift, as illustrated here. You may strain with the weight for several seconds before deciding that you cannot lift it. During this straining period, you are performing an isometric exercise. The muscle does not move, but it is subjected to tension.
A bicep curl is attempted with more weight than the subject can lift. The muscle is subjected to tension but does not move.
Exercise • Weapon Against Disease • Training Effect
The New England Journal of Medicine recently suggested exercise is a weapon against disease; Aerobic exercise lowers risk of coronary artery disease, high blood pressure, stroke, obesity, diabetes, osteoporosis, and depression. .
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
AquaDios-Med™ • Solution Healthcare • Crisis • Evidence Based One primary goal of this research is to validate the power of AquaDios-Med™ proactive preventive medicine-- ADM™ PPM a process integrating Psychoneuroimmunology, Mind Body Medicine, together with deep-water running -- multiple immersion chambers, each with individual temperature and function, leading to rapid healing, symptom management – control – remission and individual patient empowerment. It is easy to state a belief or even a fabrication as if it is a fact; prosecutors in court rooms throughout the U.S. make these ploys to juries with the expectation that prosecutorial belief or worse fabrication is fact. But legitimate authentic preventive medicine -- PM is not and should not be like courtroom banter between prosecution and defense. PM is a process with many professional medical studies to demonstrate the benefits of Mind Body Medicine and vigorous safe exercise as it relates to health, physical fitness and that safe daily exercise is the only treatment that will eliminate the many chronic diseases that maul the American population. Unfortunately research consistently confirms modern hospital medicine practices rely on their own fabrications – beliefs with ChargeMaster Prices, ordering unnecessary surgeries more than 60% of the time, admission of about 16.5 million patients without discernible pathology – PWDP, exposing millions of patients to needless pain and suffering, iatrogenic disease medicine, adverse events and many thousands of deaths; with profit as the motive, not healthcare. This perverse culture has been discussed in the SCOOP osteoporosis research where the advertised preventive medicine was prescribing the drug Fosamax, known to cause osteonecrosis of the jaw bone, a condition far worse than osteoporosis; this is iatrogenic disease medicine, not legitimate preventive medicine as utilized and discussed in the AquaDios-Med™ PPM. The medical researchers of SCOOP believed – fabricated a preventive medicine process and by so doing exposed that innocent population to a serious danger. Research confirms that many horrific facts about main stream hospital medicine, the pharmaceutical companies and their abuse of medications and surgeries as treatments, while avoiding the one process that works; the kind of preventative medicine and safe daily exercise as advocated by the process of AquaDios-Med™. What I believed was missing was sufficient research data to verify for the reader that the principles of AquaDios-Med™ were in fact supported by scientific evidence and not just “belief”. Just because this author knows the facts and the tremendous values of preventive medicine as it is integrated into AquaDios-Med™, the reader does not.
The task therefore was to expand the research in all areas of deep-water running treatments including rehabilitation for injured athletes as well as for physical fitness for the sedentary non athlete and for people with medical problems. The question to answer is can the principles of AquaDios-Med™ be supported as a procedure that can in fact eliminate or substantially decrease the healthcare crisis and its more than $ 2.8 Trillion costs? Obviously this author believes a nationalized AquaDios-Med™ program where an AquaDios-Med™ health center is made available to every
community across America, is the answer to the healthcare crisis and its more than $ 2.8 Trillion expense; not to mention the lives and lost man hours this method of healthcare has tragically provoked.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
Too often professionals are the only one’s well versed in medical research, which is often very technical. More than 30 years of research has led me to know enough about the human capacities that I spent more than $ 1 Million dollars building a medical prototype I’ve named AquaDios-Med™ and presented in this book.
Remember, the core process of AquaDios-Med™ is its proactive preventive medicine program that has combined safe daily exercise together with Mind Body Medicine in such a way that it is believed almost anyone can be free of most prescribed medications with 45 minutes of its structured deep-water exercise and MBM in 90 days. To prove to the American public and to the powers of our great democracy this book must provide the facts that AquaDios-Med™ is a genuine healing, rehabilitation and physical fitness process. Those facts are found in medical research, sport medicine research, deep-and water running research, psychoneuroimmunology and mind body medicine research. This segment of the book goes deeper into the facts of exercise and physical fitness research and its history as it relates to wellness and its ability to prevent chronic disease. Forty five minutes of safe daily exercise is an activity that produces the body’s natural medicine, homeostatic equilibrium; especially for those American’s suffering from the many chronic diseases debilitating our population. One idea is for those with chronic disease to participate in forty five minutes of safe daily exercise to reverse, eliminate and or substantially decrease the debilitating effects or symptoms of chronic disease. This book is not an attack on organized mainstream medicine or hospital medicine; our nation needs the most comprehensive hospital and medical doctors possible. Nor, is it an attack on pharmaceuticals and the advancement of drug therapy. On the other hand, both must defer to the facts at hand and that is that 45 minutes of safe daily exercise will keep the human body physically fit and free of chronic diseases killing and insulting our populace. If there is a problem with main stream medicine it is the fact that primary care is profit-based with ChargeMaster-Prices not patient-centered with a perverse reliance on unnecessary procedures,
surgeries, drugs whether in-patient or out-patient rather than what all contemporary research pinpoints and all patients need; safe daily exercise of for at least 45 minutes as is advocated by AquaDios-Med™. In other words, patient protocol should first assign patients to 90 days of safe daily exercise for at least 45 minutes as is advocated by AquaDios-Med™ before medications or surgeries are considered. Of course
there are instances where short term medication is required and necessary; this is to be continued. Much of the present evidence based format is often somewhat technical to demonstrate to the reader, especially to the U. S. Congress and or the U. S. Senate as these studies are sophisticated and rely on advanced machinery as well as complicated and complex mathematics and statistics. For example, exercise physiology measures oxygen capacity, heart rate blood lactate and many other physiological parameters; and this is complex. It demands specific calibrations made by expensive and technical machines and analyzed by highly educated professionals.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
Safe Daily Exercise Methods • Eliminate • Manage Disease Aqua-Dios-Med™ • Deep • Water Immersion Training • Arthritis
Laurie Udesky is a frequent contributor to Consumer Health. Udesky health reporting has appeared in numerous newspapers and trade publications, including TB Monitor and AIDS Alert, and has aired on National Public Radio. Udesky has written an article for the Arthritis Foundation aquatics class. She says it is important to bear in mind that aquatics therapy teachers are nothing like aerobics instructors, who push you to work harder. Certified aquatics instructors frequently remind classes that nobody should extend beyond his or her own comfort level; she addresses the science of moving in water and introduces the outcomes of many research studies. Experts say that if people with arthritis spent more time in the water, they'd be able to move better with less pain. Dr. Robert Gilbert, an orthopedic surgeon and clinical professor of orthopedics at University of California San Francisco Medical Center because states that in water, a person who has trouble moving on land with gravity and surfaces can move in ways they would never be able to do out of the water; this is important to the arthritic. Physical therapist Donna Everix reminds us that in waist-deep water, you bear about 50 percent of your weight. Walk in chest deep and you've shaved away another 25 percent of your body weight. You're lighter in water, there's less weight going through the joints, so it doesn't hurt as much and you can tolerate more, explains Everix, who specializes in rheumatology and aquatics at Mills-Peninsula Health Services in Burlingame, California. Numerous experiments have proven the benefits of water exercise. In a study published in the journal Arthritis Care Research, researchers compared the benefits of warm-water exercises to the advantages of sitting in warm water, exercise on land, and general relaxation techniques. The 139 patients studied, all suffering from rheumatoid arthritis, were randomly assigned to try one of the four techniques twice weekly for 30-minute sessions over the course of one month. All patients improved physically and emotionally, but those assigned to the hydrotherapy group showed significantly greater improvement in joint tenderness. It’s a pity this study did not offer AquaDios-Med™ safe daily exercise for an additional comparative population. But, what’s important is that water submersion exercise proved the greatest health benefits. A small study comparing land and water exercise for people between the ages of 45 and 70 with osteoarthritis of the knee found no difference in the strengthening benefits of either form of exercise. However, subjective pain levels were significantly less in the aquatic group, according to the results published in the Journal of Strength Conditioning Research. Once again here is another study that did not offer AquaDios-Med™ safe daily exercise for an additional comparative population. But, what’s important is that water submersion exercise proved the greatest health benefits. Apart from making one feel lighter and experience less pain in the pool, aquatic therapy can also buoy one's spirits. Nevarez became such an enthusiastic aquatic therapy student that the Arthritis Foundation recruited her to teach the class. She knows well how difficult it can be even to make it to the class, so she uses her own brand of humor as encouragement. I tell them, 'take your pain, put it under your arm and get your como se llama into the pool!'
AquaDios-Med™ Safe Exercise • Health Cross Training • Athletes Mandas and Einhorn published research on “Aquatic Exercise Program as an Effective Alternative Method of Cross Training for Cross Country and Track Athlete” of Los Alamitos Orthopaedic & Sports Physical Therapy. Mandas and Einhorn say many times, athletes are advised to seek alternative source of conditioning while recovering from injury. An aquatic cross training program can provide treatment for the injury, maintenance of aerobic capacity and sport specific cross training.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
14
The properties of water provide support, resistance and assistance in the athlete's training session. Buoyancy devices can further reduce the undesirable effects of weight bearing on an injured extremity. At the same time, athletes can increase the work expenditure during exercise and maximize the cardiovascular conditioning required for competition. An aquatic training program can decrease compression forces, vibration forces and torsional forces that an athlete may endure while training on land. The effects of gravity play a significant role in the overuse syndromes athletes suffer; gravity can also limit and slow a well-designed rehabilitation program for the injured athlete. Pain is something many athletes learn to ignore, however, pain from injury should rarely be ignored, since it can lead to longer disability. Rehabilitation is much more effective when early intervention is available. Properties of water make an aquatic training program center extremely important when it comes to early intervention following injury. Early intervention in the athlete's injury can mean a speedier return to competition. It has been well-documented that performing certain structured therapeutic exercises in water can be used successfully when treating injury. Physiological effects include increased circulation to muscles, increased joint viscoelasticity and decreased joint pain. Muscles can get stronger with less strain and cardiovascular training is accomplished. The physical properties of water have been utilized in aquatic therapy to decrease gravitational forces placed on a weakened extremity and increase body movements. These aquatic exercise programs can produce rapid results in an athlete where land activities are aggravating the present symptoms. Shallow and deep water training can produce sport specific results which can easily carry over to land-based activities or more traditional exercise formats.
Conditioning • Exercise Tool • Athlete An aquatic training program is an effective form of cardiovascular exercise combining both deep (gravity eliminated) and shallow (buoyancy assisted) water exercises. This unique workout greatly amplifies the natural resistance of water, while maintaining a "target heart rate." Deep and shallow water exercise accommodates high intensity cardiovascular training, while reducing the risks that accompany high impact loading
Buoyancy Assistive • Resistive Exercise Training in water enables the athlete to improve upper or lower body strength and cardiovascular endurance while utilizing buoyancy to decrease weight bearing. Standing in neck-deep water reduces lower extremity body weight to about 10%. Standing in chest-deep water reduces weight bearing to 25-30% of body weight. Standing in waist deep water translates to a 50% reduction in the athlete's body weight. Buoyancy allows the athlete to exercise while reducing the effects of gravity. In addition, buoyancy assistive devices (vests) can be used in shallow water to reduce body weight or in deep water training. Buoyancy resistive devices (cuffs or fins) may be used to create additional resistance and increased cardiovascular intensity. Water provides an accommodating variable resistance which automatically adjusts to the degree of force applied. The degree and resistance encountered during aquatic exercise is directly related to the speed and direction at which the equipment is moved through the water. Aquatic exercise provides a true form of isokinetic resistance proportionate to the square of the velocity during movement. For example, moving an extremity at three times the speed generates nine times the resistance. Cross training exercises are conducted in both deep water (6 feet or more) and shallow water (3 1/2 - 4 1/2 feet) levels. Five minute deep water warm up is conducted prior to stretching exercises. The quadriceps femoris muscles, hip flexors-extensors, gastrocnemius, lumbar spine flexors and extensors all require stretching.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
15
Deep • Shallow Water Training Initial deep water cross training exercises are conducted for one minute. As the athlete's endurance and techniques improve, the exercise is extended for five minutes. Buoyancy assistive and resistive devices are used to help maintain the athlete above water and increase the exercise intensity. After completing a deep water routine, shallow water exercises are performed. The shallow water exercises are typically conducted for 30-60 seconds. Buoyancy assistive devices can be used if lower extremity pain is present.
Deep Water Running • Non-weight bearing exercise • Maintenance • Land-based Running Performance
In May 2000 a study was released to Association of Military Surgeons of the United States titled Deep water running: “An effective non-weight bearing exercise for the maintenance of land-
based running performance.” Deep water running (DWR) has become a well-recognized form of cardiovascular conditioning for injured athletes and has been used successfully to maintain running performance. DWR provides for decreased stress and weight bearing to injured tissue and joints, allows for maintenance of cardiovascular fitness and a training effect, and offers greater specificity of exercise in relation to running. During a 22-month period, 181 active duty Army soldiers, placed on temporary profiles for injuries that precluded them from their regular weight bearing physical fitness activities, participated in a DWR program. Injuries to the back, knee, and ankle were the most common reasons for referral to the program. This article reviews the physiological characteristics of DWR, specifics of DWR program design, DWR mechanics, and the
advantages of DWR over other aerobic forms of exercise to maintain land running performance in military personnel on temporary non-weight bearing profiles. DWR is an ideal exercise alternative to swimming or cycling for the injured soldier on a non-weight bearing profile because of the similar mechanics to land-based running. Unlike swimming or cycling, there is evidence that run performance can be maintained or improved with DWR. DWR also offers a good alternative form of exercise to prevent injuries occurring from excessive land weight bearing exercise. DWR is an ideal exercise for maintaining conditioning and land running performance in military personnel who are on a temporary non-weight bearing profile. It is a safe and well-tolerated form of exercise that is more specific for land running than alternative forms of exercise. Although previous reports support the notion that DWR participants will be able to return to full active duty at a comparable level of performance, prospective studies performed on a military population are needed to objectively measure preinjury and postinjury run times as well as the impact on recovery time required for a return to full active duty.
Water Therapy • Pain Relief Water therapy exercise programs (sometimes called pool therapy, hydrotherapy, or aquatic therapy) consist of a variety of aquatic-based treatments and exercises that are designed for back pain relief, to condition and strengthen muscles. Water therapy exercise offers many of the same benefits associated with a land-based exercise program, including development of a treatment plan that is carefully tailored to the individual.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
16
Water therapy exercise is especially helpful in cases where a land-based exercise program is not possible due to pain, decreased bone density, disability or other factors. As such, water therapy is a versatile exercise and is particularly good for people with conditions such as: Osteoarthritis -- Advanced osteoporosis (with susceptibility to and/or pain from fracture) -- Muscle strain or tears In addition to those conditions, water therapy is frequently recommended as one form of exercise therapy to treat those with diabetes as well as individuals with high blood pressure. Both conditions can improve and become more manageable with aquatic exercise. All of these conditions can make it uncomfortable or painful to exercise on a hard or even padded surface, or while standing. Water provides a much gentler, welcoming environment.
Benefits • Water Exercise Therapy • Evidence Based The physical properties of water make it a highly desirable medium in which to exercise to treat back pain and other musculoskeletal injuries. Some of the most important properties of water that make exercise easier are: Buoyancy: water counteracts gravity and helps to support the weight of the patient in a controlled fashion as the patient is immersed. This can aid the development of improved balance and strength. Viscosity: water provides resistance by means of gentle friction, allowing strengthening and conditioning of an injury, while reducing the risk of further injury due to loss of balance. Hydrostatic pressure: there are powerful effects produced by hydrostatic pressure that improve heart and lung function, making aquatic exercise a very useful way to maintain and strengthen heart and lung function. This pressure effect also aids in improving muscle blood flow. Together, these properties allow development of an exercise regimen that minimizes the weight placed on the spine (axial load) and risk of injury due to unintended movements during exercises. For example, individuals with osteoarthritis in the neck (cervical spine) and shoulder could practice arm circles or shoulder rolls in water to improve their range of motion and strength. Because the water provides both mild resistance and support through buoyancy, the person would most likely not experience the pain caused when a tired arm drops suddenly, as it can do at the end of land-based exercises. For many back pain patients, water-based exercises should only be performed under the guidance of a qualified health professional. About.com Health's Disease and Condition content is reviewed and approved by Kate Grossman, MD. Aquatic therapy or pool therapy consists of an exercise program that is performed in the water. It is a beneficial form of therapy that is useful for a variety of medical conditions. Aquatic therapy uses the physical properties of water to assist in patient healing and exercise performance.
Physiological Effects • Aquatic Exercises • Deep Water Running (DWR) • Properties of Water Fitness • Evidence Based
The properties of water, such as buoyancy, hydrostatic pressure, viscosity (resistance), surface tension, and heat dissipation can have several advantages over land-based programs. Buoyancy – any object, wholly or partly immersed in a fluid, is buoyed up by a force equal to the weight of the fluid displaced by the object. In simpler terms, buoyancy lets participants experience a partial floating feeling when they enter the pool. When a person is in water, the water will naturally want to push the person up (this is particularly valuable for a person who does not want to place their whole body weight on an affected joint or body part). The deeper the person goes in the water, the less weight they will have to support with their own body.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
17
The buoyancy of water can reduce the “weight” of a person by about 90 percent depending on body composition, size, muscular structure and depth of water, which reduces stress on joints and connective tissues. For exercisers with lower body or spinal injuries, pregnant exercisers, and participants with physical limitations, the buoyancy of the water is a welcome benefit. The buoyancy also adds a challenge to exercisers to maintain control of their body position while in the water. Buoyancy can also be used to aid or resist exercises. Exercises that move towards the surface of the water (such as bicep curls or hip flexion) are assisted by buoyancy. Exercises that move away from the surface of the water (such as triceps extensions) are resisted by the buoyancy.
Hydrostatic Pressure • Healing
Hydrostatic pressure is the pressure exerted by water on an object immersed in the water. It is an equal amount of pressure on all surfaces of the object at a given level of immersion. The deeper an object is submerged, the more pressure there is on that object (this property is especially useful for patients who have excessive edema or swelling in certain areas). Hydrostatic pressure is also beneficial for breathing. The pressure of the water on the chest wall resists muscles that expand the chest for breathing. In this way, these muscles are strengthened and can more efficiently expand the chest to allow a greater volume of air to be inhaled when performing everyday tasks on land (for the same reason, it is inadvisable for people with respiratory problems to exercise in the water). The increased hydrostatic pressure of the water helps to take the lactic acid out of the cells and delivers it to the liver more efficiently, so the exercised muscles do not feel as sore. Viscosity (resistance) – Viscosity is a type of resistance that occurs between the molecules of a liquid, effecting how a liquid flows. It is the property of water that makes water resistant. It can also be thought of as a measure of a fluid's resistance to flow. Liquids of high viscosity, such as syrup, flow slowly. Liquids of a low viscosity flow fast, such as mercury. Water is 790 times more viscous, or thicker, than the air we normally walk around in. This allows for a variety of ways to create resistance to an exercise that will not overload muscles or joints involved. As an exerciser moves through the water, he or she drags along with him/her the water molecules that are not only stuck to his/her body, but also the molecules that are trying to stick to each other. If the surface area of a body part is increased by a piece of equipment, more force is required to move the amount of water in front of it. Also, if the speed is increased, the force required to perform the exercise is also increased. A good way to measure progress of an exercise is to see how many repetitions of an exercise can be performed in a minute. A greater number of repetitions that can be performed means that greater force is overcome by the muscle. This, in turn, means that the muscle is getting stronger. Also, as the muscle tires, it will automatically slowdown, which automatically decreases the amount of force to be overcome. This helps to prevent further injury while performing an exercise. Another effect of the viscosity of water is the creation of an equal amount of resistance in all planes of motion. When performing an exercise on land to strengthen muscles of the knee, usually only one muscle group can be strengthened at a time with a given exercise due to gravity. Either the muscles that extend the knee are strengthened with an exercise such as the knee extension machine, or the muscles that flex the knee are strengthened, such as occurs on a hamstring curl machine. In the water, because of the viscosity, both of these muscles groups can be worked at the same time with the same amount of resistance with one exercise. This can help to create a better balance between the muscle groups so that one group does not overcome its opposing group.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
18
The properties of viscosity and drag resistance that works so well in a training environment are a swimmer's biggest enemy. Swimmers attempt to move as fast as they can through the water with the least resistance possible. Every effort is made to streamline the body and its movement. The goal of aquatics exercise is the opposite. To increase the intensity of the water exercise every effort is made to increase surface space and use non-efficient physical movements. That means using a lot of space and moving a lot of water to create turbulence. The water offers 12 times the resistance of air. This means that an exerciser will have to apply more force to the water in order to move as opposed to the same movement out of the water. Instead of gravity as resistance, water exercisers have water. The water is a dynamic resistant force, meaning that the more force that is applied in the aquatic environment, the more resistance it will offer. This is a huge benefit that affords many different fitness and skill level participants to exercise together, modifying the movement to meet their individual needs. Also, because of the resistance, movements in the water tend to be slower and more controlled, which lessens the risk of injury. This constant resistance helps to promote muscular balance. Surface tension – surface tension refers to the water resistance at its surface. The cohesiveness among water molecules is responsible for surface tension. Ever wonder why when you pour a full glass of water the water will actually fill to above the rim of the glass? This represents the water molecules holding onto one another. The water molecules on the surface do not have other water molecules surrounding them completely. This creates a surface membrane that makes moving an object through the surface more difficult than moving an object that is completely underwater. For the purposes of aquatic exercise, instructors should be aware of this phenomenon and consider how they are incorporating out-of-the-water arm movements. Heat dissipation – this refers to the process of water absorbing the heat generated from exercising bodies. This could be a good or bad thing. On the positive side, as exercise intensity increases so does a student's core body temperature. This heat is “dissipated” or transferred to the water. This allows the student to maintain a high intensity without the risk of overheating. On the other hand, some students must be very careful about how they regulate their core temperature and may not want the cooling effects of the water. One unique factor associated with water is our ability to regulate its temperature. While it is not always feasible to request a certain temperature for a particular aquatics class, it is a good idea to be aware of the impact the water's temperature may have on the participants. Typically, the water temperature for exercise is between 80 degrees and 86 degrees Fahrenheit. Water that is below 78 degrees F may not be appropriate for group exercise classes. Most students will get cold and not be able to maintain a comfortable body temperature even with rigorous aerobic movements. Pools can be too warm as well. Pool temperatures above 88 degrees F may feel too warm to some students. If you are faced with this challenge, consider altering the class's movement plan and avoid any intense aerobic movements. Water exercise is low- or no-impact, depending on the water’s depth. Water’s buoyancy counters the downward pull of gravity and takes the weight and strain off joints. Water also helps with balance and removes the fear of falling, which makes the pool an excellent environment for people who are overweight, pregnant or elderly as well as those who have arthritis or multiple sclerosis.
According to aquatic exercise experts, water provides about 12 times the resistance of air. Working against the resistance of water has a strengthening effect, much the same way using iron dumbbells strengthen muscles. Those who want an extra strengthening effect can add resistance by using equipment designed for water workouts, such as webbed gloves, wrist and ankle weights and aquatic dumbbells.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
19
“People exercising in a pool should avoid the tendency to stay on their tiptoes,” said Dr. Bob Keith, an Extension nutritionist and fitness expert at Auburn University. “Instead, walk all the way through the foot, stepping heal to toe when walking forward and toe to heel when walking backward. It’s also a good idea to vary how you walk. Walk forward, backward and sideways or march with knees held high.
Therese Iknoian and Deep Water Running From
Therese Iknoian is an award-winning and internationally published fitness/sports journalist, has consulted on educational programs for the likes of Nike, and has written numerous books, including Mind-Body Fitness For Dummies, Tai Chi For Dummies, and Fitness Walking. She is an exercise physiologist and former nationally ranked race walker, and has partnered with her journalist-husband, Michael Hodgson. Therese Iknoian is a huge fan of deep water running. She believes DWR to be an ideal injury rehabilitation tool and she uses DWR as a regular part of her training to prevent injuries, receive an inexpensive massage, and increase running ‘mileage’ without the risk of overdoing it on the roads. Thus, Therese Iknoian is not only aware of the “preventive medicine” properties in DWR; she includes this activity in her own daily exercise. Iknoian varies between a ‘running stride’ and a ski stride and also mixes in steady effort and interval effort work. She cannot over stress the value of using pool running as part of your training (or, be adventurous and find a pond! Keep in mind the Therese Iknoian audience is the athlete, not the sedentary couch potato or person-patient in need of a safe daily exercise and even though she points to DWR as the best “preventive medicine” she is not a doctor. As for equipment, you can do water running as a minimalist with nothing more than a bathing suit and a deep end of a pool. However, she has found the equipment to be very helpful in keeping cadence and heart rate more similar to running and to make the experience a lot more enjoyable. Therese says her ideal set-up is the AQX Zero Gravity Water Running Suit, Webbed Water Gloves, and AQX Sports Aquatic Shoe. She finds that this combination provides optimal flotation, resistance, and comfort and all last a long time. You can also replace the Zero Gravity running suit
with an AquaJogger Belt and get a more than acceptable buoyancy, though Therese believes the AquaJogger Belt is just a bit less running specific and not as well dispersed.
Injured - Why deep water running? Aqua-Jogger - AQX-Sports resources offer information on deep-water running. Depending on your specific injury, you may be able to cycle, row, or use a cross
country skiing simulator. If you can do these activities, without interfering with your recovery, then by all means, include them in your cross training program. A number of running injuries are aggravated by these other types of exercise - with most running injuries you can safely run in the water. Deep water running with a flotation vest provides an excellent training stimulus, and more closely simulates land running than most other cross training options. Also, deep-water running is a total body exercise, excellent for physical fitness and it works your legs, trunk, and arms, and positively stresses your cardiovascular system.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
20
Many studies have verified that deep water running can be used by sedentary people, patients, and to accelerate healing from injuries as well as to maintain fitness of the athlete and runners. Investigators from Florida State University coerced a group of trained male runners to run in the water while another group continued regular training. The runners were tested for VO2 max, lactate threshold, and running economy before and after 6 weeks of water running. The water running group fully maintained their aerobic fitness over the 6 weeks; with one bid advantage, no impact trauma. Similarly, a study by Ed Eyestone and colleagues at Brigham Young University found no change in 2 mile run time after runners trained in the water for 6 weeks. Additional support for the fitness benefits of water running is provided by a study from the exercise physiology lab at the University of Toledo, in which trained runners ran in the water 5 to 6 days per week for 4 weeks. These runners had no change in 5 km performance time, VO2 max, lactate threshold, or running economy after 4 weeks of water running. To an athlete not training, but participating in deep-water running “no change in performance” is a godsend. The common denominator in athletic based research of deep-water running is the fact that “while injured” athletes are able to continue a viable intense exercise to maintain their fitness level. As pointed out many times in this book this valuable “athletic” research applies to the common sedentary person or patient especially those on daily medications whose fitness level is so low they have medical problems and rely on medications. This population of “injured” by “inactivity” is one of the biggest American populations that AquaDios-Med™ can address.
What’s so special about water?
Although various forms of water exercise have been used for centuries, space age research now documents more reasons than ever to take training and recovery programs into the water. One of the most important benefits to deep-water running is its buoyancy that allows “No” impact running exercise. Your body weighs about 10% of its land weight when immersed in water up to your neck in water. If you weigh 200 lbs. when standing on land, you weigh only 20 lbs. in water. With the addition of a buoyancy belt like the AquaJogger®, you can run with your head comfortably out of water, breathe normally, and accomplish most of the same workouts you perform on land. In the water your musculo-skeletal system is no longer bearing weight, so it can be recovering from all the pounding of your land based programs while you focus your conditioning on the cardio-pulmonary
system. No pounding … no impact. For the above reasons deep-water running is the safest daily exercise for all people, including children, pregnant mothers, patients on medications, geriatricians and the injured or disabled.
Aerobic and Anaerobic Conditioning A decade of research by a variety of sources has shown that the training effect of water running can be equal or greater than the same level of effort on land. Improve your cardio-pulmonary conditioning while giving your weight-bearing joints and muscles a day off.
Water – Buoyant –Resistance
Water creates resistance to movement in all directions through a full range of motion; this Isokinetic resistance. Increase or decrease the intensity by changing the speed of your movements. Being submerged in water is like having an adjustable weight machine surrounding your body.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
21
Water – Massage
Water massages your muscles with every movement of your arms and legs. This action increases circulation, promotes relaxation, and helps remove stress and tension.
Up to your neck Immersion - physiological changes
Being up to your neck in water produces physiological changes in your body that help remove metabolic waste, improve cardiac function, lower blood pressure, and assist the body in tissue healing. Start thinking about how you can use these changes to accelerate your recovery from competition, training sessions, and injuries. For the sedentary person or non-athlete person or patient that does not exercise it is important to note the many health benefits from deep-water immersion and running listed above. Immersion in the water to your neck helps to remove metabolic waste, improve cardiac function, lower blood pressure, and assist the body in tissue healing. Much of what you know about land-based conditioning and fitness programs applies to water exercise.
Water Running Technique
Water running technique is an area of some debate. Some coaches insist that you try to simulate land running form as closely as possible. While that is a nice ideal, Therese Iknoian believes that the most important consideration is to maintain your training intensity to the degree possible, and if your form needs improvement, so be it. Regardless of your running form, your stride rate will be slower during water running due to the increased resistance of moving your legs through water. If you try to simulate land running too closely, your stride rate will be even slower. For that reason, don’t worry if your leg isn’t brought behind the body to the same degree as in land running-find a happy compromise with decent form and a reasonable rate of leg turnover.
What Therese Iknoian is attempting to communicate to the athlete applies to the common
person or patient, the difference being those that do not participate in daily exercise will have more difficulty to learn about “stride rate” and even correct stride, but this book has provided many pictures of deep-water running. The best and most correct form of deep-water running, are the pictures of Steve Scott and Dr. Jensen, both wearing the Wet Vest, but the correct form can just as easily be accomplished with the AquaJogger belt.
Some athletes move forward while running in the water, and actually do laps during their workouts. Whether you move forward or remain relatively still
depends on subtle changes in body position. Therese Iknoian recommends a relatively upright posture during water running because this posture will work your trunk muscles and result in only a slight tendency to move forward through the water.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
22
Iknoian indicates that Deep-Water Running in the Cross Country Style of DWR looks qualitatively more like land-based running due primarily to the increased horizontal displacement (position) of the ankle. This increased movement of the ankle allows for a greater range of motion to be achieved and thus maintains the normally elliptical appearing gait pattern found in land-based running and increases the muscular benefit. The AQx was specifically designed to be used with this style of DWR.
What Therese Iknoian is getting at is what has been described earlier in this book, and is commonly referred to, is the ankle – foot rotation or “foot flap”. Remember the import of this book is to reach hospital based medicine, doctors and insurance companies to establish “preventive medicine” and to communicate to the common person or patient that does not or has not included safe daily exercise in their day. For the latter group it is important to learn a correct posture for your daily safe DWR because your body will “work smarter” not harder to promote your physical fitness and overall health. The ankle-foot rotation or “foot flap” insures a more biomechanically correct motion for the lower extremities and this affects the overall exercise the body receives.
Therese Iknoian Key points for DWR
1. The water should be at shoulder level below the chin with the head held in a neutral position facing forward. 2. The body leans slightly forward of a vertical position. This is important because if you lean too far backwards your knees will come up too high in the front and you will be practicing the high-knee version of DWR
(which looks more like stair-stepping). 3. The arm carriage should be relaxed and identical to land-based running. Your arms will primarily move from the shoulder joint (relatively stable) with elbows flexed at approximately 90º. 4. The hands are held in a slight or half clinched-fist position with your thumb resting lightly on your forefinger to decrease the likelihood of using a dog-paddling - type motion. 5. The legs will actually follow a pattern that is VERY similar to a faster type running motion like interval training where: a) The knee comes up toward the surface of the water until the hip reaches a position of approximately 60-80º (hip flexion), followed by full extension (not hyperextension) of the leg toward the bottom of the pool. b) The foot moves from approximately 0º dorsiflexion at full hip flexion (imagine your foot in the same position as if you were standing on the ground in a normal position) to approximately 50-70º of plantarflexion (toes pointed slightly at the bottom of the pool) when the leg is fully extended. A good imagery is to imagine or think of your foot touching the bottom of the pool when your leg is fully extended, then moving your foot back toward the edge of the pool as far as possible without rotating your hips; then the foot moves under your butt, and finally lifting the knee up to allow the foot to continuously move through the gait pattern [see picture]. c) The major differences between the high-knee and cross-country styles of DWR are that the high-knee style leg action is primarily in a vertical plane with the legs moving straight up and down in a piston-like movement pattern with very little horizontal displacement present (imagine marching or stair-stepping) while the cross country style has a much greater range of motion which elicits more muscular involvement [picture is high knee-piston like].

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
23
Iknoian suggests the Deep-Water Cross (X) Country Ski-like motion or style of skiing in deep-water looks qualitatively very similar to its’ land (snow)-based counterpart. This is an excellent activity for runners, but also works very well for anyone interested in an alternative exercise that will benefit the whole body.
Therese Iknoian Key points for DW Ski Motion
1. The water should be at shoulder level below the chin with the head held in a neutral position facing forward (just like in DWR). 2. The body leans slightly forward of a vertical position, but you might notice that you don’t have to lean forward as much as in DWR. 3. The arm carriage should be relaxed and relatively straight swinging from the shoulders with your hands extended to increase drag (resistance). 4. The legs will stay relatively straight with knees slightly bent. Focus on moving the leg backwards until you feel the gluteals (butt) contract and then simply swing the leg forward until your foot starts to lift toward the surface. 5. The feet will stay in somewhat of a neutral position (imagine yourself standing on the ground again). You will not need to point your toes toward the bottom of the pool like in DWR (Cross Country skiers don’t point their toes either). This is the best position to take advantage of the AQx’s increase in resistance, particularly while moving the foot backwards (pay attention to the gluteals and hamstrings during this part of the motion).
Gauging • Effort • RPE
Therese Iknoian and many others indicate you will not be able to achieve as high a heart rate running in the water as running on land. A study from the famed Karolinska Institute in Stockholm found that heart rate is 8-11 beats per minute lower for the same oxygen uptake when running in the water compared to normal running. This study also found maximal heart rate on average to be 16 beats per minute lower during all-out water running compared to land running. Lower heart rates during water running are primarily due to the pressure of water on the body which makes more blood return to the heart so more blood is pumped with each heart beat; deep-water running makes the heart work smarter not harder. A useful rule of thumb is that heart rates during water running are about 10% lower than during land running. If you get your heart rate up to 140 beats per minute during deep-water running, that is roughly equal to 154 beats per minute during normal running. Also, the temperature of the water affects your heart rate during deep water running. Your heart rate will be lower in cool water and higher in warm water and this author strongly recommends “all” deep-water running must be done in water between 68 and 70 degrees F to obtain the best results. In addition, two studies have found that women have slightly lower heart rates and oxygen consumption than men during deep water running. This is thought to be due to women’s generally higher body fat content and resultant greater buoyancy than men. Therese Iknoian reports that the Karolinska study found that perceived exertion is higher during water running for a given heart rate or level of oxygen consumption. So, in order to get a beneficial workout in the water, you will feel that you are working harder than during land running. For this reason, she prefers a 9-week schedule to emphasize interval workouts in the water.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
24
She also states that if you just do steady water running sessions your effort won’t be high enough to maintain your fitness. A study on water running by former 800 meter runner Tim Quinn, Ph.D., and colleagues at the University of New Hampshire concluded that for runners to maintain fitness during water running it is necessary to include intervals, tempo, and or fartlek [Swedish speed-play] training.
Water Running Shoes • Water Training Jogging Silent Running Exercise
Whether it is the heat of summer and you're looking for a cool alternative to running or you've been injured and want to keep in shape or you just want to add a new element to your running routine, water jogging can help. The basic idea is that you are running, suspended in water, so you use all the same muscles as running, but without the impact and wear 'n tear on your body. You can get started water jogging in 5 easy steps. Warm Up: Get in the water - swim (tread water) for 2-3 minutes to get your body warmed up. Laps: In deep water, where you cannot touch, simulate running with your flotation device worn as instructed. Think about your form. As in running, you should not be leaning forward much or be hunched over. Keep your shoulders back and your head and eyes looking toward the horizon. Do laps this way for 10 min. Sprints: Continue doing laps as before, but make your motions bigger. Kick your feet up to your buttocks on the back swing. Extend your leg forward as far as you can to the front. Swing your arms bigger, but keep the movement forward and back and not diagonally or side-to-side. Do laps this way for 5 min. Laps (Part 2): Return to doing laps as you did in step 2. Remember to concentrate on your form. Do laps this way for 10 more min. Cool Down: Take off your flotation device and swim comfortably for 2-3 minutes to cool down.
Injured • Use Deep-water Running To Heal • Matt Russ
Matt Russ has coached and trained elite athletes from around the country and internationally for over ten years. His expert licenses include: USA Triathlon, USA Cycling (Elite), and he is a licensed USA Track and Field Coach and he works with athletes of all levels full time. He is a free-lance author and his articles are regularly featured in a variety of magazines such as Inside Triathlon, and Triathlete. Coach Matt Russ suggests that if you develop an impact related injury there are not a lot of alternatives to running. Treatment usually means time off from training and loss of fitness. Water running is a good stop gap for this. With the use of a flotation belt and a good program you can use deep water running as an effective means of run training while you let your body heal. Coach Russ says the first rule of training is specificity and you want to attempt to mimic your run stride and form while immersed under water to your neck. The advantage of water training is that you will perform the water run under more resistance than you would normally. This can help train the appropriate muscles without lower extremity stress. Coach Russ states you can use your heart rate monitor to supervise your intensity, but realize your heart rate will be lower due to water temperature and hydrostatic pressure. Coach Russ recommends that it is best to start off slowly; you may only be able to perform 20-30 min. initially. Take a rest break every 15 minutes if needed. As you become adapted you may perform intervals and sprints after warm up. With a well devised plan you can offset the loss of fitness and even increase strength and stamina.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
25
Injured Athlete • Heal with Deep-Water Running
Lance Watson is a professional writer for Professional Coaching Inc. and he writes about deep-water running for the athlete. Watson starts with the example of Greg Bennett, a talented Aussie short courser who became ranked No. 1 in the world by the ITU. Throughout much of the early fall of 2003, Bennett was sidelined by a minor foot injury that prevented him from running. But less than two weeks after resuming his run training, Bennett won the Treasure Island ITU race in San Francisco, taking the victory over top American Hunter Kemper and five-time ITU world champion Simon Lessing. To speed his recovery and maintain fitness during his injury, Bennett included deep-water pool running in his training program. As the injury healed, he decreased the pool sessions and increased outdoor running -- and was soon able to return to his pre-injury level of fitness.
What is Pool Running
Some coaches discuss pool running as the involvement of the simulation of running technique in deep or shallow water for a low- or no-impact run session. Most pool runners do their workouts in deep water while wearing a flotation belt specifically designed for water running. With the belt, you can maintain proper body position and focus on duplicating true running form. Do not forgo the flotation belt, because your running form will be altered by non-running movements used to stay afloat, using unnecessary muscles and you will get less of a workout; even though you will likely achieve a higher heart rate. Most pool runners do their workouts in deep water while wearing a flotation belt specifically designed for water running.
Plan an interval workout: To make a pool-running workout effective, plan ahead. As with all workouts, if you have a plan the time will go by quickly and you will get better results. Use time and heart rate to measure your effort in the pool. Try a series of challenging intervals such as: 10 x 2 minutes @ 85% effort. Follow each work interval with equal rest consisting of easy water running. Most workouts should be kept to less than 45 minutes in length. A shorter and more intense workout is more effective, mentally and physically, than an extended low-intensity session. Build sport-specific strength: The added resistance provided by the water will help you increase your running strength. Normally easy movements, such as arm recovery, become more difficult in water. Increased resistance can allow you to feel stronger and more fluid when the resistance is removed in an outdoor run. Some athletes prefer to do deep-water running in old running shoes. Doing so provides slightly more resistance and gives your foot a sense of pressure on the bottom, a subtle platform to better heighten awareness of the normal “impact” run feel. Improve range of motion: Water running can improve range of motion. Participate in drills where you run with a long stride -- longer than you would be able to perform on land. Increased range of motion is especially important for slower runners who shuffle along without adequate stride length. Fitting it in-Deep-water pool running is an attractive option when you are traveling. If you find yourself in a strange city that doesn't have safe or scenic runs near the hotel, get in the water, for a short and intense running session. In 20 minutes, you can get in an effective and safe workout.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
26
Pool running offers triathletes an endless array of workouts that will increase running performance. If you are creative and focused on the task, pool running can become one of the most enjoyable workouts of your week. At the very least, pool running will make you healthy, stronger and more motivated to get outside. If you love running, the pool may hold the key to your longevity in the sport.
DEEP WATER RUNNING A SECRET WEAPON • Glenn Venturini
Glenn Venturini, a coach and sports – athletic writer points out that an in-season injury can be devastating for a runner, especially if the athlete is told they can’t run during the early stages of the rehabilitation process. Some types of injuries do not allow athletes to run or perform other types of cardiovascular training because of pain, decreased weight bearing on the injured leg, casts or surgery. As a result, the runner begins to lose conditioning and falls behind the pack. On the other hand a non-athlete or patient has injured themselves with no conditioning at all; the only thing they have to lose is daily medications or a surgery. Their approach is similar to the injured athlete and that is learning to accomplish a correct deep-water running posture with a running cadence level high enough to achieve physical fitness. Venturini believes deep water running is an underutilized training and physical fitness exercise especially when an injury prevents land training. But this author has a much stronger stance and that is deep-water running, as practiced by AquaDios-Med™ is the safest exercise activity possible for all humans and must be included as the primary “preventive medicine” acknowledged by hospital medicine and doctors. Venturini further believes many times the cardiovascular conditioning exercises performed in the water are not achieving maximum benefit for the athlete because even the athlete must be coached on how to train in deep water. Although Venturini statements are mostly specific to the athlete or the injured athlete they can be directed to the non-athlete or common person-patient that has not included safe daily exercise or the important awareness of physical fitness or daily exercise is to health. Venturini suggest that previous treatment practices in rehabilitation have focused on biking, cross country skiing, swimming, elliptical machines, stair climbing and other forms of low impact training to help maintain conditioning if the athlete is injured but these same exercises can also accommodate those people or patients who have excluded daily exercise form their life. While these types exercise provide good cardiovascular benefits and are good ways to attempt to maintain some level of conditioning during rehabilitation or the acquisition of physical fitness, they are not the same as deep water running and the athlete may find themselves in a de-conditioned state when they return to their daily athletic training practice; the non-athlete or patient simply needs to awaken to the fact physical fitness can be achieved by daily safe deep-water exercise. Venturini states that in order to maintain or improve your "running shape" you must run. The specificity of training principle indicates athletes must train the way they compete to maximize conditioning for competition; Lance Armstrong trains by cycling, Alan Webb trains by running, Ian Thorpe trains by swimming. In simple terms, the way you choose to train (running, biking or swimming) produces specific changes in your muscles for the chosen activity. If your physician tells you land running is on hold, ask about deep water running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
27
Deep water running has been used by many injured world class runners and other athletes who participate in sports that require running. The benefits of deep water running include; decreased stress to the injury site, enhancement of cardiovascular and peripheral (legs and arms) fitness level, ability to perform resistive exercises in the water to strengthen the injured area and an opportunity to improve running form or economy. Deep-water running is excellent for the injured athlete while it is an ideal daily safe exercise for the common person or patient who has avoided exercise most all their life. Venturini makes some examples for the athlete about training in deep water and includes duplicating some land workouts. For example, let’s say the cross country coach had planned for 6 repeat 800’s to be run in 3 minutes with a 3 minute slow jog recovery. You would run in the water for the same amount of time and perform the same recovery. If the coach calls for a long steady run of 30-45 minutes you can do the same in the water. However, for the common person or patient their safe daily deep-water exercise objective is a minimum 45 minute workout with a running stride cadence target rate of between 84 to 96 strides per minute. Venturini indicates deep water running is challenging because every movement an isokinetic push against the resistance of water. Since there is no foot impact you can train hard in the water 2 days in a row; but this author recommends that 5 to 7 days a week is safe and healthy for the athlete or non-athlete. Venturini suggests it is best for the athlete to match their effort of land training to deep water running. And, points out fatigue will be overwhelming if the athlete attempts to match land running speed with deep water running speed of movement. Your coach, athletic trainer and /or physical therapist together can assist developing a custom program for you to continue training and rehab the injury at the same time. While it has been uncommon to note rehabilitation of an injury and “physical training” in the same sentence nowadays it is occurring regularly because now it is possible to recover from an injury and continue athletic training. Things to be aware of Before deep-water running 1. A lifeguard should be present. 2. Wear a flotation device, such as the Aqua Jogger. 3. Run in deep enough water your feet do not touch the bottom. 4. Run in place with high knees, do not bike pedal in the water, 5. Lean slightly forward while running, 6. Keep hands in a thumbs-up position with half closed palms. 7. Run as many days in the water as you would have on land if you were training with your team or 5 to 7 days a week if you’re a non-athlete or patient. Venturini recommends the athlete must give themselves time to adjust to deep water running, and suggests that when they return to daily training practice they may find themselves in front of, instead of behind the pack! Venturini is of course implying that an athlete using deep-water running to rehabilitate from an injury may be stronger and faster than those participating in usual “training”.
What is Deep Water Running Exercise • DWRE Venturini explains that Deep water running or exercise is exactly what the name would imply—training while immersed in water to your neck and deep enough to avoid contact with the bottom of the pool with your feet and while keeping your head above the water's surface. In other words, it is like following an exercise routine while suspended in a buoyant body of water. This unique environment of cool buoyancy and isokinetic resistance gives Deep Water Running Exercise (DWRE) the capacity to rehabilitate injured elite level athletes as well as the potential to improve performance; and this applies to any non-athlete or patient willing to become involved with DWR.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
28
Because the athlete or person is not in contact with the underlying surface, DWRE is a completely non-weight bearing form of exercise while it is the most isokinetic because of waters proportional resistance to movement. Some athletes, particularly runners, but not many non-athletes or patients, may already be familiar with deep water running. Water Works Performance has expanded that concept to include "Deep Water Skating", which is the training technique employed with hockey players. The principles of DWRE can be successfully applied to a variety of sports and exercise activities. Due to the non-weight bearing nature of DWRE, an athlete, non-athlete or patient can often perform high intensity training in the water — while unable to bear even their own body weight when standing on land.
How Deep Water Exercise Works
Venturini notes that the stresses imposed by bearing our own body weight on land are significant. For example: the impact force generated while running is about 3 to 5 times our body weight. These stresses often result in both acute and chronic injury. By replicating weight-bearing exercise in the buoyant non-weight bearing environment of deep water immersion to the neck, the athlete, non-athlete or patient will realize its benefits Increased physical fitness and training loads or resistance to improve performance; Unloading of all vertebrae, skeletal and joints to avoid injury because Water can act to assist, to resist or to support; Maintaining training loads and performance while recovering from injury or simply developing physical fitness; Accelerated rehabilitation during recovery from injury, for both the athlete, no-athlete or simply rapid development of physical fitness for the non-athlete or patient; and without the stresses imposed by land based, weight bearing exercise.
Deep Water Running • Speed • Strength
In June 2007 Joyce Rankin, wrote an article titled “Deep Water Running for Speed and Strength” for the Aspen Club and Spa and its Triathlon Training Session. Joyce Rankin suggests that Deep Water Running is usually thought of as a form of rehabilitation following an injury or surgery. However, she notes Deep Water Running also has great benefits for the fit athlete for use as cross training or as a way to improve speed and strength without impact on the muscles used in a primary sport. And, can and should be used for non-athletes or patients as part of a “preventive medicine” program. Rankin relates an example of this can be found when coaches of long distance runners get their athletes in the pool for various workouts on a day prior to a long even paced run. The athlete can work on speed while doing a “deep water interval session” which will be beneficial not only to increase speed but also rid the legs of lactic acid and allow for fresher legs/muscles for the workout the next day. Rankin notes that deep-water running also forces opposing muscles to work equally due to the isokinetic resistance caused by movement in water.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
29
Isokinetic Resistance • Aggressive Movement in Water
While immersed to the neck in water and move your arms and legs fast enough to perform a running cadence the water resists the movements, in both directions causing you to get a greater strength workout for muscles on both sides of the legs and arms. Rankin recommends for athletes to get a workout at an even higher intensity to not use a flotation device such as AquaJogger. In order to work out without floatation a person must know how to swim and tread water. Cross country skiing or easy treading is used as a recovery with actual simulated running form used in the tempo and interval training. However, this author would not comply with Rankin for safe exercise of an injury or for physical fitness. On the other hand, a coach might want an athlete to enhance performance and strength in this manner. Rankin concludes that form and technique are very important when working out in the water. He suggests a coach or trainer is recommended to observe and correct any improper form.
Rankin •Tips • Running Technique
Rankin recommends that it is best to use your legs to metaphorically kick or power the water back behind you with a flexing of the ankle [see picture]. Lower stride cadence is acceptable since water offers more resistance, but the target for a continuous nonstop 45 minute workout should be between 84 to 96 stride cadences per minute in cool water 68 to 72 F degrees. Rankin recommends the Rate of Perceived Exertion [RPE] rather than pulse when working out in the water. She notes that your pulse will be approximately 15 BPM slower while immersed in water to the neck and doing deep-water running. RPE will help you become more aware of the amount of energy you are expending; Level 10 RPE is the highest with level while 1 being that of a TV watcher! Rankin recommends doing your best effort to use your normal running style and help yourself by Visualizing yourself running on land. Rankin says, Remember: It may take a few sessions for you to become comfortable in the water doing something other than swimming. In a short time your deep-water running will become as comfortable as your land running and the deep-water running benefits will amaze you. The non-athlete or patient can learn to become comfortable with deep-water running practiced by AquaDios-Med™ almost as easy as an athlete.
Wet Set • Deep-Water Running
In July 2006 the Diet Detective Editorial Staff, contributed to an internet group article titled “Join the Wet Set: Deep-Water Running” The writers indicate that for cross training or getting over an injury, it’s tough to beat a jog in the pool. And, what's the next best thing to walking on water? It’s “Running” in it. They say Deep-water running is a great way to get the cardiovascular benefits of running without the impact that's part of running on dry land. That's why it's often prescribed for runners sidelined by injury and obviously should be a prescribed “preventive medicine” by hospital medicine. Mindy Solkin, owner of The Running Center in New York City, claims deep-water running is a better substitute than other forms of cross training for the athletic because it's more like regular running. She points out that while deep-water running immersed to your neck, you run more or less in place, but in water deep enough so that your feet don't touch the bottom of the pool.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
30
A good floatation belt like AquaJogger must be used to keep your head comfortably above water so you can breathe, but body, below the neck, your arms and legs remain submerged. Depending on your exercise stride cadence, "You do sort of travel a bit, floating this way and that," says Solkin. She continues, "You don't stay in one place. You sort of stay in your own little area." But, this is not accurate for a stride cadence of 84 to 96 per minute which will cause you to slowly travel through the water and across the pool. How does the workout compare to your usual run? "It's harder in terms of the effort because of the resistance of the water," says Solkin, "but there's no impact trauma, so it's safe in terms of injury prevention." It is not advisable to get your heart rate as high in the water as you would on land because you can't turn your legs over as fast and the heart rate in deep-water running, while immersed to the neck, is about 17 beats per minute slower. The one downside to deep-water running is that usually there's not a lot of variety involved-no changing scenery, no hills or turns as there is inland running. You can add some variety by angling your body differently, pumping your arms higher, shortening your stride or increasing your stride cadence rate. But really Solkin says "the most you can do is go slower or faster”. And, it's really tough to go fast in deep-water running while in the correct position due to the isokinetic resistance properties of water. Solkin notes that you're basically running in place, probably without the distractions of the treadmill, such as headphones or television so use of mental imagery is important. This author agrees with the imagery but not that you’ll be running in place.
Dr. Weil • Running In Water
In March 2005 Andrew Weil, M.D is asked “What are the advantages of deep water running?” and he says deep water running is just what it sounds like – being immersed to your neck and deep-water running in a pool instead of on land. Weil declares Deep-water running was designed for injured runners and that this pool-based exercise can provide a good non-impact cardiovascular workout and an option for staying in shape if you have to stop running on land temporarily. According to Glen McWaters, inventor of the Wet Vest, Weil is correct. McWaters developed
the Wet Vest to rehabilitate elite injured runners and probably had no idea that deep-water running would be as useful as a preventive medicine process. In fact, this author consulted with McWaters while building the AquaDios-Med-™ prototype seen at http://aquadios.com/ Weil continues that deep-water running offers the advantage of safe but effective cardiovascular exercise for persons with stress fractures or muscle tears that would keep them off the track or treadmill. Deep water running is also a good exercise option for people who are overweight and those who have lower back pain or nerve damage to the feet that might be worsened by the impact of
running on land. And it can serve as a nice change of pace in any exercise program.
Dr. Weil • Healthy Aging • Fitness
Dr. Weil proclaims “It's never too late to get fit”! Promote a healthy weight, increase your energy, encourage better rest and feel great with a regular exercise program designed for your needs and capabilities. The Dr. Weil on Healthy Aging
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
31
Dr. Weil notes an article in the September/October 2004 issue of Health & Fitness Journal that reports you can maintain or improve cardiovascular fitness with deep water running as long as you do it with sufficient intensity. Weil does not yet know, however, how effective deep water running is for weight loss. Weil suggests it doesn't matter if you run in place or move through the water. However, you do need to use a flotation device like an AquaJogger to help keep you upright and in the vertical running position, prevent your feet from hitting the pool bottom and enable you to keep your head and mouth out of the water. Otherwise, you just run exactly as you would on land, with the same arm motion and hip flexion. Of course the pool you use has to be deep enough to accommodate your deep water running.
Who benefits from Aqua Running • Dr. Garry Killgore
Dr. Garry Killgore, Professor of biomechanics, head track and field coach at Linfield College, Oregon, USA and founder of AQx Sports has come up with a concept and a product to take aqua running or deep water running - that step further. Dr. Killgore claims that every athletic runner can benefit from Aqua or deep water Running, it is the answer to your injury prayers and allows you to run while injured! Dr. Killgore explains Aqua or deep-water running is really a fantastic way to keep training while injured or to cross train. Killgore gives workshops that verify water is a unique environment for training and for rehabilitation because Water can act to assist, to resist or to support.
Killgore verifies that when we run on dry land the major form of resistance is air or gravity, but water is 775 times denser than air, and when you 'run' in the water your biomechanical weaknesses are exposed and this can be problematic as well for the non-athlete, sedentary person or patient. Killgore states that research has shown that running form and the mechanics of running on land and in water immersed to your neck are very different. But, running in water will improve your running technique on land. And it doesn't end there. Deep water running does have many advantages and is the "secret weapon" of many world class athletes including Lornah Kiplagat, 2007 Woman's World Cross Country Champion, who used deep water running while injured during September 2006, between 10th through the 16th September 2006. On 17th September Lornah broke the 10 mile road record. Athletes are prone to injury and aquatic deep-water running will give you the opportunity to add extra miles without adding risk of injury.
Prescribed Aqua Running • Anecdote
An athlete was told by his doctor that he was guilty of enjoying his running too much to the point of ignoring the early warning signs of an injury. The doc said absolutely no running for 8 weeks and then only a gradual return. The athlete felt he was sentenced to 8 weeks off from running because his injury was a big one a stress fracture of the tibia. The athlete asked for a cross-training plan that would keep him fit and preserve his sanity while his stress fracture recovered. Most all athletes are frustrated and worried that they will rapidly lose fitness. Just as importantly, the athlete’s usual form of stress relief will be missing. The challenge for the athlete is to obtain a training schedule hard enough to maintain fitness for a well-trained runner, but not so hard that he would become discouraged and quit before the injury was fully healed.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
32
Research shows that most of the benefits of training are reversible and is referred to as de-training or the state most non-athletes or patients are in. Cardiovascular fitness decreases measurably after 2-3 weeks without training. Studies have shown, however, that with reduced training you can maintain your fitness at almost the same level for several months. The intensity and specificity of cross training workouts are most important in determining how much fitness you lose when you take time off from running. Research shows that you must do some training above 70% of VO2 max in order to maintain your aerobic fitness and racing performances. Of course, you’ll need to a method of cross training that will allow your injury to heal like deep-water running. Deep-Water running in the deep end of the pool is quite advantageous as an alternative workout for run training or just getting physically fit for the non-athlete or patient. There are a few reasons why deep-water running is recommended in an athlete’s training plan and should be a part of every person daily safe exercise. One of the primary reasons is if the athlete, non-athlete or patient has an injury or medical problem that will not allow him or her to run on a hard surface. For the athlete these injuries are Achilles tendonitis, ankle sprains, soreness in the knees, lower back pain, etc, but for the non-athlete or patient with a medical problem must have a safe daily exercise such as is offered in AquaDios-Med™ where there are scheduled deep-water running workouts as recovery workouts following a long run or bike session. Another benefit to deep-water running is that an athlete can do interval workouts in the pool that could be substituted for road intervals or track work. Many athletes get injured doing intense interval running on a hard surface. If done in a structured manner, the benefits of an interval workout in the pool can provide similar benefits as that of an interval workout on land. Athletes, non-athletes or patients must wear a flotation vest or AquaJogger for their deep-water running workouts as this will help with proper form while completing the workout. Stride Cadence is a great way to monitor your workout in the pool, about 76 to 80 cycles per minute with each leg will help duplicate land running and when you’re ready to work harder – increase the intensity accelerate to 84 to 96 and more cycles per minute. On land the recommended cadence is about 88 to 90 cpm, but due to water resistance the equivalent in the water is about 10 cpm less.
It is also important to have the athlete, non-athlete or patient to wear a heart rate monitor. After warming up, a good range to work in is heart rate zones depending on the type of workout scheduled. Keep in mind that due to buoyancy heart rate is 10 to 15 beats per minute lower than it would be on land for the same effort. When the workout is over the athlete, non-athlete or patient will know they did some good hard work in the pool and will see some positive fitness results.
Dr. Garry Killgore • Kidney Transplant Surgery
Dr. Garry Killgore wrote another article titled “Time-to-Run Cape Town - Running in the Deep End”. He suggests whenever the athlete gets injured and is unable to run, the first thing he or she thinks is - that's it, I can't run, what can I do to keep my fitness. Typically they rush to the gym hop on the bike or the cross trainer and go mad training, next thing they know they have another injury!
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
33
The obvious question is Why not do aquatic deep-water running? Killgore has confidence the athlete or non-athlete will get out of the pool after deep-water running fitter and stronger than when they got in and they won’t have to worry about the pain cause by each foot strike and the impact trauma. Killgore confirms aquatic deep-water running is really a fantastic way to keep training while injured or to cross train. At his workshops he explains that water is a unique environment for training and for rehabilitation. Water can act to assist, to resist or to support the body. Aquatic deep-water running already boasts many big names amongst its clients including the England Rugby Football Union, Chelsea,
Blackburn Rover, Aston Villa and Everton football clubs, Elite Marathon Runners, it's a well-known fact that Paula Radcliff does Aqua Running to maintain fitness when injured and for recovery. And it doesn't end there.
Thousands of runners rave about aqua running but few can be as evangelical as Terry Nelson, former Liverpool Player. Deep-water running submerged to the neck in deep water helped Terry to a gold medal at the World Transplant Games and then saw him through 11 years of Kidney Dialysis. Terry now owner of Aquatic Training Specialists, Aqua Running Ltd and AQx Sports International is no stranger to sports injuries, in the early 80’s; his football career was ended with Liverpool AC by repetitive injuries. However, Terry's real challenges began a few years later, he was told his kidneys had failed and he would live 6 months without a transplant; his brother saved Terry's life by giving him transplant. Terry went on to run the London Marathon and to made a decision to become the best transplant runner in the world.
After months of training Terry swept the board at the British Transplant Games in 1992 after which he was selected for the World Transplant Games but with weeks to go broke his foot. Terry ordered his first AquaJogger belt and transferred all his usual sessions to the pool. When Terry returned to running 6 weeks later he was lighter on his feet, more flexible and his running form was greatly improved. Terry went on to win the 5,000m gold medal at the World Games. Unfortunately Terry's kidney failed again and he waited 11 years for another transplant, during this time Terry kept his fitness by pool running. With his enthusiasm for pool running Terry is now providing the most cutting edge training and products for aqua running in the UK.
Catherina McKiernan, Muriel Haire & Grainne Butler are now bringing the concept of Aquatic deep-water running to Ireland and are holding workshops in 2008 in the National Aquatic Centre. AQx have designed two key products to boost the training effect and to mirror the demands of dry land running in water.
The 'deep water running shoe' is really a running shoe that you wear to 'run' in water, even though the foot never touches the bottom of the pool, it will provide more neuromuscular feedback via the shoe and which increases the runner's sensation of running
on land. The shoes also does increase the amount of work the runner does and so have great potential to help you hold onto fitness during rehab or to increase fitness while you cross-train. The shoes have been designed to improve running economy and reduce the risk of injury.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
34
AQx have gone one step further and developed their "Zero Gravity Suit" modeled on the speed suits used by triathletes and runners, it's designed to provide better overall comfort, proper buoyancy distribution, additional resistance, warmth and a much more natural range of motion. The principle of the suit is that it distributes buoyancy appropriately around the body to enable the correct biomechanical posture while in the water and so allows a much better running action in the water.
One might ask if the pool is such a great training environment then why does it not feature far more prominently in our athlete's rehabilitation or in “preventive medicine” or used by hospital medicine and doctors for recovery of medical problems for non-athletes and conditioning sessions for the athlete. Although the extent to which pool training is used will vary from country to country, the unavoidable reality is that most sports support professionals and doctors fail to use water workouts as physical conditioning, a rehab or training tool for many reasons, one of which they don't know its value.
That is why AQx Sports International has been invited to Dublin to give professional
Workshops and open up a whole new way for athletes to train, but it would be even more dramatic when this deep-water running healing process, as advocated by AquaDios-Med™ is nationalized for all people, the sedentary, the patient, the injured, the geriatrician and the athlete.
Killgore implies that everyone-from children through elite athletes, non-athletes and patients to
the burgeoning group of active over-50s- must become aware of the extreme benefits of aquatic deep-water exercise and its “preventive medicine” capacities. He states that in the not too distant future water may well become as vital a component in our sporting and hospital activities as it is to our very existence. This author goes one step beyond believing hospital medicine and doctors must learn that “preventive medicine” like AquaDios-Med™ is a vital healthcare component oppressed by both American hospital medicine and the pharmaceutical companies.
Wet Workout Basics • Elizabeth B. Krieger
On June 12, 2000, Elizabeth B. Krieger, an associate editor at WebMD published an article titled “Wet Workout Basics - WebMD Feature”. Krieger points out that both water-walking and deep-water running offer numerous fitness benefits and are catching on with competitive and recreational athletes alike. Too bad hospital medicine and doctors do not advocate “preventive medicine” like those used by AquaDios-Med™.
Water Walking
Krieger says water walking is about as simple as it sounds. You just take your walk into the water. The deeper the water, the harder your workout will be. Find out which depth works for you and start there. Most people choose a water level between the bellybutton and the neck. You don't need a flotation belt to water-walk, but nonslip pool shoes or old tennis shoes may help.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
35
Krieger recommends that you swing your arms in broad sweeping motions to push and pull the waters resistance. For more of an upper-body challenge, wear webbed gloves. This increases the surface area of your hands, and thus, increases the resistance. Stand tall, keeping your abdominal and back muscles tight. To burn more calories, vary your direction: go backwards, sideways, or change directions suddenly. And remember, even though you don't see sweat, you are losing water. Keep a bottle
of water nearby and drink early and often.
Deep-Water Running • Equipment • Procedure
Krieger suggests that if you choose to participate in deep-water running, seek out water deep enough so that your feet don't touch the bottom. And to keep your body vertical or upright and your head and mouth out of the water, you'll need a flotation belt like the AquaJogger. Make sure it fits snugly around your waist and doesn't ride up. This belt will keep you floating at about the shoulder line. Keep your abdominal muscles tight and your chest lifted as you mimic your land-based running motion. Your elbows should be at a 90-degree angle; try to lift your knees higher than you normally would on land. As you run, your body should naturally lean slightly forward. You might
want to try alternating between pointing your toes and pressing your heels down, to work your calves and hamstrings.
Krieger suggests alternating long, exaggerated strides with shorter
sprint-like ones. If you find yourself in a less-than-Olympic-sized pool, tether yourself to a ring at the edge of the pool and run in place; you can find specially made tethers at swim shops or sporting goods stores. In fact, with a tether holding you in place, you'll get a higher-intensity workout. Just try to ignore the fact that you look like a dog.
Liverpool Centre • Aquatic Excellence On January 12, 2008 Neil Hodgson wrote an article in the Liverpool Echo titled, “Liverpool in
the running to become a centre of aquatic excellence”. Hodgson claims LIVERPOOL will become a center for European Deep-Water Running excellence and a revolutionary training regime to train and produce Olympic champions. Aqua running involves both deep-water running and water running in more shallow depths that utilize the pool bottom as described by AquaDios-Med™. Aqua-running also uses special gravity suits and aquatic training shoes for athletes to train in swimming pools.
Deep-water running eliminates the impact trauma on muscles and joints from the foot strike on land and helps injured athletes heal more quickly and achieve fitness more rapidly.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
36
Hodgson did not include the modern history of Deep-water running. DWR was first established in the late 1970’s by Glen McWaters inventor of the Wet Vest. In the 1980’s American Dr. Alan Jensen built a medical prototype he named AquaDios-Med™ with multiple immersion chambers, each with different temperatures ranging from 98 to 64 F and all have powerful Jacuzzi massage stations. The main exercise chamber has several flat, non-slip surfaces for more shallow workouts requiring foot contact with the pool surface bottom. AquaDios-Med™ has many proprietary components identified in this book. The AquaDios-Med™ process makes use of deep-water immersion exercise, power massage and proactive use of Mind Body Medicine; see pictures this book or go to http://aquadios.com/ and view the videos and many pictures. A system utilizing variations of aqua-running was marketed by American professor Garry Killgore, who licensed the British and European rights to former Liverpool FC reserve Terry Nelson. Mr. Nelson runs Aqua Running, renamed AQx International, from his base in Silvester Street, Everton, and has developed many pieces of aquatic equipment including the aquatic running suit and aquatic running shoes and more. His clients include Aston Villa and the England rugby union side. Mr. Nelson is looking for FA and British Olympic approval, and he hopes to create British gold medal winners at the 2012 London Olympics. Nelson aims to make Liverpool the European centre of excellence for aqua running. Mr Killgore, a professor of human performance and bio-mechanics traveled to Europe from Oregon to accompany Mr. Nelson on a European tour of leading sporting organizations interested in signing up to their system. Their schedule included trips to Liverpool FC and clinics for athletes and physiotherapists in Dublin and Belfast. They met Sir Clive Woodward, head of elite performance at the British Olympic Association.
Running Suit • Shoe • Deep-Water • Running Exercise
AQx has already marketed their AQX Running Suit and a patent is pending for an invention that relates to a water running shoe during the exercise known as deep water running (DWR) to help simulate the land running strides. Mr. Nelson claims approximately 30 million Americans participate in running as a form of general exercise for physical fitness and health. It has also been estimated that up to 70% of this “fitness” population will incur a running-related injury. Nelson says that land based running has been described as "essentially a series of collisions with the ground, and these collisions typically exhibit vertical ground reaction forces
(VGRF) of 1.5 to 3 times the runner's body weight.” These traumatic foot strike impact forces combine with the person’s training errors and result in escalating the total volume of mileage too rapidly and or excessive mileage; which is at least partially responsible for the cause of many running-related injuries. A known method of decreasing the running impact forces and the negative effects of excessive mileage is to supplement a runner's training program with deep-water running (DWR) in a pool. This mode of training allows the runner to incorporate the terrestrial running style in the pool while typically using a buoyancy device, e. g., AquaJogger, to support the runner's weight.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
37
It has been reported that the DWR training method decreases spinal and joint compressive loading, because the properties of water can act to assist, to resist or to support the body which eliminates the likelihood of incurring running-related injuries. Despite the increasing use of DWR for rehabilitation and more recently as training to supplement a normal regimen, very little research focuses on the DWR technique, especially for the sedentary non-athlete or patient addicted to multiple medications. Several sources describe "proper" DWR techniques, but it appears that the most common DWR style is characterized by a high-knee or piston-like leg action. In contrast, the cross-country style is intended to be more like land-based running. The specificity-of-training principle suggests that the movement pattern of DWR should be closely aligned with that of terrestrial running to maximize the benefit to the runner. The cross-country style of DWR is the one most like terrestrial running, particularly in terms of the horizontal ankle displacement. A rationale for deep- water running (DWR) is that it allows the untrained sedentary person or runner to exercise or train with movements very similar to that found on land running without incurring the traumatic impact forces, which greatly reduces the repetitive loading and compression of the musculoskeletal system. Rehabilitation after injury, rather than prevention, is the most common use of deep water running. But, a reasonable person would put more effort into prevention of injury rather than becoming injured through “over-use” and abuse during training as well as the prevention of serious medical problems most of which can be eliminated with safe daily exercise prescribed by AquaDios-Med™.
Deep-water Running AQx Shoe INVENTION The AQx new shoe is particularly designed for use in DWR exercise to enhance the effects of the accommodating resistance provided by the water when the foot is moving from the anterior (front) to the posterior (back) portion of the stride gait. The unique construction of the shoe allows the athletic runner to maintain proper running technique throughout the normal range of stride motion and to benefit from enhanced resistance in the appropriate planes of motion and minimal drag when appropriate. This author would not recommend this new AQx Shoe for the sedentary, non-athlete or patient until they have mastered the kind of form demonstrated by the many pictures of Steve Scott performing deep-water running. The AQx shoe utilizes the accommodating resistance properties of water by increasing or decreasing
drag to maximize resistance in the appropriate planes of motion inherent in a stride running gait while immersed to the neck in water. The AQx shoe is designed to increase overall benefit to the athletic runner and to improved "feel" of the DWR exercise as it is achieved. AQx research suggests that wearing a shoe during DWR enhances kinesthetic perception and further helps the athletic runner achieve a gait during DWR that is more similar to that of land-based running. Thus, it is ideal for a “runner” but likely to advance for the sedentary.
AQx design is to enhance resistance by its proprietary three small scoops on each side of the shoe at the
forefoot, mid-foot, and heel areas of the shoe. Thus, the scoops create fluid drag, and the size, configuration, and placement of the scoops are important to the effective operation of the shoe in DWR. The objective for AQx is to provide an Aqua-Running shoe that helps the athlete to be more perceptive of water movements and to help simulate land - based running. Another object of this invention is to provide a shoe for use in DWR exercising when contact with the pool bottom is required. A further object of this invention is to provide a shoe having several elements that create fluid arranged on a shoe for creating drag simulating land - based running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
38
Physiology • Deep-water Running • Evidence Based
In 2003 Thomas Reilly, Clare N. Dowzer and N. T. Cable et al published a research study in the Journal of Sports Sciences, London titled “The Physiology of Deep-water Running”. The authors are on staff at the Research Institute for Sport and Exercise Sciences, Liverpool John Moores University and Academic Unit of Psychiatry and Behavioural Sciences, University of Leeds. Reilly, Dowzer and Cable concluded that Deep-water running must be performed while immersed to the neck in the deep end of a swimming pool, deep enough the participant will not be able to touch the bottom of the pool with their feet while in the “stride cadence” of running and use of the AquaJogger, Wet Vest or similar device. These researchers identify deep-water running as a safe physical exercise used for purposes of preventing injury and promoting recovery from strenuous exercise and as a form of supplementary training for cardiovascular fitness; therefore AquaDios-Med™ procedures prevent injury for the physically fit while providing those dependent on medications to rid themselves of most all medications. Other research shows structured deep-water exercise is the most ideal, aerobically efficient cardiovascular conditioning medium available; therefore AquaDios-Med™ procedures is ideal for all cardiac and coronary artery disease patients. For example, physical activity while immersed to the neck in water produces positive physiologic changes that accelerate the removal of metabolic waste, improve cardiac function, and lower blood pressure, thus assisting the body in healing the tissues. The physiological effects of deep-water immersion include increased circulation to muscles, increased joint viscoelasticity and decreased joint pain. Increased joint viscoelasticity means the body’s natural skeletal joint space is enlarged as is the synovial fluids of the joints. Synovial fluid reduces friction between the articular cartilage and other tissues in joints to lubricate and cushion them during movement. These specific healthy body improvements are caused by the absence of gravitational body
weight compression. Also, muscles can get stronger with less strain while cardiovascular training is accomplished. The physical properties of water have utilized in aquatic therapy decrease gravitational forces placed on a weakened extremity and increase body movements, especially for the non-athlete, the sedentary or patients. Deep-water running has a positive health effect on the cardiovascular system especially the heart. In 1995 Dr. Becker showed that Cardiac volume increases by nearly one-third with immersion to the neck. Since the ultimate purpose of the heart is to pump blood, its measure of performance is the amount of blood pumped per unit of time. This is called “cardiac output” and submersion in water to the neck
increases cardiac output 32 percent at rest.
During deep-water running the pulmonary system undergoes profoundly positive effects by immersion of the body to the thorax. Part of the effect is due to the shifting of blood into the chest cavity, and part is due to compression of the chest wall. The combined effect creates a positive alteration of pulmonary function, increasing the work of breathing and changing respiratory dynamics. In fact, expiratory reserve volumes decrease by 75 percent at neck immersion, with vital capacity decreasing only slightly. The combined effects of these changes increase the total work of breathing by 60 percent. When water-training time is sufficient, this challenge can markedly improve the respiratory system’s efficiency.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
39
Deep-water immersion has positive health effects of the musculoskeletal system as well, particularly with vasoconstriction. On land, for instance, sympathetic vasoconstriction tightens the vessels of skeletal muscle to resist blood pooling. But in water, immersion pressure removes the biologic need for vasoconstriction, thus increasing blood flow to muscle tissue. In fact, resting muscle blood flow increases by 225 percent during neck immersion.
Aquatic immersion creates many effects upon renal blood flow and the renal regulatory systems. For instance, the flow of blood to the kidneys increases immediately upon immersion, which produces an increase in urine production, as well as sodium and potassium excretion. Sodium excretion also increases as a function of depth due to the shifting of circulating central blood volume. The result of these physiological changes is the elimination of toxins which both cause disease and inhibit the natural healing processes of the body.
When maximum gains in VO2 during aquatic exercise are compared with equivalent land-based exercise in unfit individuals, the aquatic exercise achieves equivalent results. And water-based exercise programs may be used to sustain or increase aerobic conditioning in people who need joint offloading.
All of the these positive physiological health changes and many more, combine to assist and accelerate the body’s natural healing processes, thus providing the body with the conditions most favorable to self-healing. This evidence verifies deep-water running as proposed by AquaDios-Med™ is a genuine authentic “preventive medicine”. The Reilly, Dowzer and Cable research confirms the heart is positively affected during deep-water immersion water running, because both stroke volume and cardiac output increase occurs during water immersion with an average reduced heart rate of 15 to 18 beats per minute. Simultaneously there is an increase in blood volume which largely offsets the cardiac decelerating reflex at rest. Deep-water running allows the heart to “work smarter” not harder. Research shows that at submaximal exercise intensities, blood lactate responses to exercise during deep-water running are elevated in comparison to treadmill running at a given oxygen uptake VO2 [DWR increases blood lactate]. Research shows that Lactic acid starts to accumulate in the muscles once you start operating
above your anaerobic threshold. This is normally somewhere between 80% and 90% of your maximum heart rate (MHR) in trained athletes or non-athletes. While VO2, minute ventilation and heart rate are decreased under maximal exercise conditions in the water, deep-water running nevertheless can be justified as providing an adequate stimulus for cardiovascular training of the athlete and non-athlete. Responses to training programmes
have confirmed the efficacy of deep-water running, although positive responses are most evident when measured in a water-based test. Aerobic performance is maintained with deep-water running for up to 6 weeks in trained endurance athletes; sedentary individuals benefit more than athletes in improving maximal oxygen uptake. There is some limited evidence of improvement in anaerobic measures and in upper body strength in individuals engaging in deep-water running. A reduction in spinal loading constitutes a role for deep-water running in the prevention of injury, while an alleviation of muscle soreness confirms its value in recovery training.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
40
Further research into the applications of deep-water running exercise as therapy for athletes' training and non-athletes or patients taking daily prescribed medicine is recommended to demonstrate its benefits as “preventive medicine”. Although the Reilly, Dowzer and Cable research is from 2003 it holds significant evidence that “preventive medicine” programs like AquaDios-Med™ can and will eliminate today’s healthcare crisis. First, their research shows unequivocally that deep-water running is a safe method of daily physical exercise and is to be used for the purpose of preventing injury while accelerating rehabilitation and promoting recovery from strenuous exercise; while being an excellent activity for cardiovascular fitness. Second, sedentary individuals benefit more from deep-water running than athletes in improving maximal oxygen uptake. Thus, non-athletes and patients taking daily medical prescriptions, and who make up the bulk of the population within the healthcare crisis can gain tremendous health benefit from deep-water running. Third, Deep-water running while immersed to the neck causes a reduction in spinal loading which constitutes a powerful role for deep-water running in the prevention of injury, while an alleviation of muscle soreness confirms its value in accelerating rehabilitation recovery.
Fourth, the physiological changes caused by deep-water running, while immersed to the neck, accelerates the elimination of toxins which both cause disease and inhibit the natural healing processes of the body.
Fifth, all of the physiological changes produced by deep-water running while immersed to the
neck combine to assist and accelerate the body’s natural healing processes, thus providing the body with the conditions most favorable to self or natural-healing.
The Reilly, Dowzer and Cable research, along with many other studies demonstrates “why” preventive medicine” practices like AquaDios-Med™ is needed to be nationalized to end the healthcare crisis and its colossal $2.5 Trillion albatross of suffering to the American economy and manpower. American hospital medicine and doctors must stop the abuse of prescribed medications for illness and disease that can be better managed by daily safe deep-water running exercise as recommended by AquaDios-Med™ with it Mind Body Medicine principles. Certainly the Research Institute for Sport and Exercise Sciences, Liverpool and John Moores University and Academic Unit of Psychiatry and Behavioural Sciences, University of Leeds believes exercise is medicine.
Marc Bloom Running • Fitness • WATER WORKOUTS
Runner's World Senior Contributor and award-winning NY Times writer Marc Bloom is one of the nation's foremost authorities on running, fitness and youth sports. Author of the new "God on the Starting Line" and other books, Marc was formerly editor-in-chief of "The Runner" and is long-time publisher of "The Harrier" high school cross-country and distance running magazine.
Marc Bloom states deep-water running and all aquatic training or running prevents injury and
keeps you in great shaped. If as a runner you've not yet learned about deep-water running, you're missing out on an increasingly popular and foolproof method of training with water workouts.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
41
Marc Bloom says that deep-water running in a pool with the aid of a flotation belt has entered the fitness mainstream with classes at virtually every health club in the country, from Asphalt Green in New York City to the Incline Village Recreation Complex in Lake Tahoe, California. It's no wonder because runners find that the buoyancy of the water helps them recover from hard running and prevent injury, and that the resistance of the water offers a no-impact, relaxing workout that taxes the body, increasing heart rate and results in ideal cardiovascular exercise.
W.E.T. Workout • Dr. Katz
"The magic of the water," and deep-water running says Jane Katz, Ph.D, a former Olympic
swimmer, coach and author of many aquatics books including "The W.E.T. Workout", "extends the life of your land based running by providing comfort, safety and a greater range of motion." When immersed in water to the neck the water deep-water pressure is 12 times greater than air pressure. A pool therefore provides two extremes at once--the resistance to stress the body and the liquid density to protect it.
Dr. Katz confirms that runners of the stature of world champion Mary Slaney and Olympic champion Joan Samuelson did deep-water pool workouts during the height of their careers. Both women used deep-water pool running mainly for fitness when injured.
Dr. Katz says that now runners and coaches, always on the lookout for new strategies, are
taking deep-water pool workouts to the next level. Using the prescription of the American College of Sports Medicine and other groups, they seek muscle-building strength work along with aerobic benefits for optimum training effect and overall health. These goals have led to weight training in the water, as well water dance, water yoga, water bicycling, and an expanding array of water gear to facilitate these activities.
Dr. Katz points out the fact that almost any form of exercise done on land can be done in a
swimming pool with deep and shallow. While classes help and provide group support, you can always learn-by-doing and train on your own.
Dr. Katz says that while I can't walk on water, I can walk in it. I'm a frequent water-trainer and
when I've found myself in a small, shallow hotel pool, I've gotten a good workout from simply walking laps with the water up to my waist. One study done at New York's Nicholas Institute of Sports Medicine found that walking at 3 miles per hour in mid-thigh water depth burned twice the calories of walking at the same speed on land. Of course, this type of exercise can be accomplished by all non-athletes and patients taking daily medications.
Dr. Katz believes that all people, whatever their fitness goals, can get in great shape by learning deep-water running and offers the following advice.
Deep-Water RUNNING • Fitness
1. Staying Afloat - Dr. Katz states that to run or do other exercise in deep water, all people need a light flotation
belt to remain upright; it's best to have your own. Chains like Sports Authority and Brookstone carry popular models or you can order a belt through AquaJogger, an originator of the concept (800 922-9544, www.aquajogger.com), or from swim-product companies like Speedo (800/847-8770). Cost runs about $50. New York City pool running coach Doug Stern uses a more streamlined flotation belt with four cubes as opposed to one thick piece. It folds up and travels well.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
42
2. Recovery Running - Dick Brown, a noted coach and exercise physiologist in Eugene, Oregon, who helped develop
the AquaJogger, recommends two types of workouts--easy, L.S.D.-type running for recovery from intense land based exercise or if you're injured and accelerated running to enhance conditioning. For recovery, once a week, do 30 minutes in the pool. "The hydrostatic effect of the water helps blood pump," says Brown. "There's a massaging effect on the muscles. Even if you're totally healthy, you should be in the water to stimulate recovery."
3. If You're Injured - Brown says that most injuries that prevent you from road running can be accommodated by the
deep-water running, where there is no impact; like a stress-fracture in the tibia, or lower leg. However, an illiotibial band injury in the knee area could be aggravated by movement in water. "The rule," says Brown “is to do only the speed and range of motion that does not elicit pain."
4. Training Effects - Any type of "quality training," from tempo runs to speed-work, can
be replicated in the water. For example, you can alternate faster leg action for 2 minutes with 2 minutes of easy striding. Or you can go hard for 10 minutes, easy for 5, and then repeat. Studies show you get virtually the same benefit as running "on-land" but with less wear-and-tear on the body.
5. Going The Distance – Some runners may not know that heart rate during deep-water running is about 16 beats a
minute slower or believe that pool running doesn't get pulse rate high enough. But that's because, at the outset you may have forgotten about the lower rate in deep-water running or experienced fatigue early and fail to sustain an entire workout. Give it time. Progress gradually. In water, when you double your speed, your legs encounter a four-fold increase in resistance.
6. Stride Length – Dick Brown suggests that the water is also an ideal environment to do running drills that tend
to batter your body on land. The water's buoyancy permits a greater range of motion. Try knee lifts, but keep your leg straight, not bent. World-class athletes he's worked with, says Brown, find their strides lengthen because of water-strengthened Posas muscles in the groin that act as levers during running.
Psoas Muscle • Hip • Spinal Column
The psoas muscle, pronounced "so - az", primarily flexes the hip
and the spinal column. At about 16 inches long on the average, it is one of the largest and thickest muscles of the body. This powerful muscle runs down the lower mid spine beginning at the 12th thoracic vertebrae connecting to all the vertebral bodies, discs and transverse processes of all the lumbar vertebrae down across the pelvis to attach on the inside of the top of the leg at the lesser trochanter. The lower portion combines with fibers from the iliacus muscle, which sits inside the surface of the pelvis and sacrum, to become the Iliopsoas muscle as it curves over the pubic bone and inserts on the lesser trochanter.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
43
7. Water Form – While running, keep your body perpendicular to the pool. Your legs, however, should not flow
as in typical running, according to methods used by the New York water guru Stern. To attain the greatest amount of resistance and smoothness, says Stern, "sweep" your legs forward, from toes to hips, with minimal knee lift. This form, “similar” to the movement done on a cross-country ski machine, uses the entire leg to drive against the water.
8. Faster Times – This sweep style, says Stern, will cause you to work the legs from the upper thigh, increasing
flexibility in the hips and lengthening your stride (and improving speed) on land. "Without exaggeration," says Stern, "100 percent of runners in my deep-water running classes get faster on the roads."
9. Cooling Off – After hard running on land, even with a cool-down jog, your muscles may be stiff and achy. A
1999 study of runners' cool-downs at Cal-State Northridge University showed that being in the water hastened elimination of muscle-fatiguing lactic acid, as compared with running on a treadmill. In addition, following a land run with deep-water running, the athletes report feeling more fully recovered.
10. Pregnant Pause – Deep-water Pool running is ideal and the safest exercise for pregnant
women, whose shifting center of gravity, is stabilized in the water. "Running in the water is better than swimming," says Stern, who has seen an increase in the number of pregnant women in his New York classes, "because it keeps the women in a vertical position. He says the women do the same workout as anyone else, using perceived exertion as their guide.
WATER BICYCLING
11. Spinning Your Heels, Biking in a pool? This novel idea was created by an Italian bike manufacturer, who developed a lightweight, rust-proof titanium bike that could be submerged in water. Clubs like Crunch Gym (in New York City, Chicago and Atlanta) ran with it. They adapted their bike spinning classes to the water. Hydro-spinning was born. "It's a really intense class," says T.J. Cris of Crunch in New York.
12. Total Body Workout: Hydro-spinning is
intense because it not only works the legs hard but the upper-body too, picking up on a water exercise trend that stresses upper- and lower-body at the same time. While pedaling, you also move your arms,
pressing your hands against the water for upper-body muscle toning. The bikes have no gears. Leg resistance comes solely from pedaling against the water, which is up to your waist. The club provides aqua-shoes, featherweight booties, and suggests you wear bike shorts as opposed to a bathing suit.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
44
WATER STRETCHING • STRENGTHENING
13. Going Both Ways - Using the full-body idea, clubs like Manhattan Plaza of New York have new stretch-and-strengthen classes combining cardiovascular and muscle work. Participants use kickboards, Styrofoam water barbells, ankle weights (actually weightless but add to resistance) and "noodles" (long Styrofoam stringbeans) in a circuit-training workout. At Atlanta's Peachtree Athletic Club, the water running classes include use of Styrofoam dumbbells and such at the same time.
14. Stepping Up - Many clubs have aqua-step classes in which various forms of aerobic dance
have been transferred from the studio to the pool. Wearing a flotation belt and holding weights for upper-body work, you move on and off a 2-to-4 inch step in chest-high water. Speed of movement determines intensity. You can buy your own step and train solo.
15. Stronger Abs - In New York, Stern,
responding to runners' requests, has expanded his upper-body repertoire. When you exercise your arms near the water's surface, says Stern, by doubling the speed of movement you multiply the resistance eight-fold. Stern achieves chest and back strength by having runners move their arms across their bodies with palms open. He achieves abdominal strength with water crunches in which the runners, wearing flotation belts, lean forward to form a "V" and bring knees to chest.
16. Board Benefits - Jane Katz suggests getting the feel of water exercise with a kickboard, available at most pools. KickBoards provide resistance and buoyancy. "Create a waterfall," says Katz, "by raising and lowering the board above shoulder level." If you have weakness on one side of your body, you can emphasize those muscles in the positioning of the board.
17. Developing a Kick: Also use a board for its main purpose--kicking. Extend your trunk and legs; hold the board shoulder-width apart, with head just above the surface. For the flutter kick effect, which enables you to move through the water, point your toes so your soles face upward and kick up and down from the hips. This is excellent exercise in and of itself, if you can manage several laps, as well as groundwork for proper free-style lap swimming. Runners usually need some time to get the hang of kicking and prevent heavily-muscled legs from sinking. You can practice while grasping the end of the pool.
18. Ribbing It Up - Most workouts neglect the intercostal muscles in the rib area. To stretch these, do a trunk twist while standing in chest-deep water with arms extended parallel to the water surface. Inhale as you twist your body to one side (moving your arms with you for added resistance), and exhale as you return to the starting position. Repeat on opposite side.
19. Yes, You Can-Can - Water dance includes the can-can, offered in the book "Water Exercise," by Martha White, director of aquatic therapy at Texas Medical Center in Houston. Stand in chest-high water and hold a barbell in each hand out to the sides, just above the surface. While keeping arms extended, alternate raising the knees to a 90-degree angle while turning the lower leg inward. Keep abs and buttocks tight to stabilize the trunk.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
45
20. Breathing Lessons - Inhale on the recovery or rest phase of your exercise, exhale on the power phase, says Jane Katz. Rhythmic breathing increases oxygen flow, giving water exercise a calming, meditative quality.
21. Water Yoga: Fitness Swimmer magazine called it "Woga," yoga-style movements in water.
Using a noodle, you can do an exercise like the "swan," by lying face down in a "chest float," bending the knees upward and placing a noodle in front of your ankles. Then grab the noodle with hands stretched backwards and your head above the water. You'll look like a relaxed pretzel while stretching the hips and quadriceps and strengthening the back and gluteals. AquaJogger (800, 922-9544, Speedo (800/847-8770), Water Gear (800/794-6432), Hydro-Fit (800/346-7295). www.aquajogger.com)
Summarizing Water Training Benefits For Sedentary
Non-Athletes Patient and Runners
No-Impact Aerobic Exercise; Provides Physical Fitness; Helps Prevent Injury; Exercise Options While Injured; Hard Training in Protective Environment; Recovery From Running
Sedentary Life style – Patient’s Workout Variety; Relaxation and Stress Relief: Total Body Workout
Coach Doug Stern's 5 Rules of the Pool Deep-water Running 1. Form: Keep posture erect and body perpendicular to the water by looking straight ahead,
with chin slightly down, pulling shoulder blades back and keeping hips positioned under your shoulders.
2. Intensity: Use a system of 1 to 10 in which 1 is the easiest effort and 10 the hardest. Most running should be in the 4 to 8 range. 4-5 is a recovery workout, 6-8 is interval workout or a sustained hard pace.
3. Rest: Because of the cooling effect of the water and the fact that it's non-weight bearing, you recover faster in the pool than on land. If you do intervals, you can take short rests. For example: 10 x 45 seconds with a 15-second rest, but these rests are better when you continue to deep-water run at a slightly lower pace.
4. Hydration: People think they don't sweat in the pool, but they do. Keep a water bottle on the pool deck. This is another benefit of pool training: you can sip fluids during training, which is harder to manage on land.
5. Training Mix: it is best to alternate land running with deep-water pool running and DWR can be an occasional substitute for running on land--fitness without the pounding--not an extra workout. It is best if you maintain regular on-land mileage with a cool down of deep-water running, but it is not recommended to add a full schedule of deep-water running to land running because you'll be risking fatigue.
Two Testimonials About Aquatics • Deep-Water Running
A dentist mother of six young children, including twins, and a 1992 Olympic marathoner, does pool exercise twice a week while running 20 to 40 miles a week. She does lap swimming and aqua-jogging, mainly for recovery. She always tells people pool work can be the most benign form of exercise. She did aqua-jogging through all her pregnancies, when it was a huge part of her exercise. And with her busy schedule when she is too tired to run, she jumps in the pool and feels energized for the whole day.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
46
A social worker from New York, NY does a weekly pool workout in addition to running 12 to 18 miles a week along with bicycling. "she had a back injury leading up to her first marathon at New York a few years ago. Though skeptical, she started pool running. She stayed in the deep-water running for 6 weeks. After that, her back felt fine and when she resumed regular running she was amazed that she had not lost any fitness. She ran the marathon in 3:24. Now she uses pool training mainly as recovery from hard workouts, for overall well-being and physical fitness.
Aquatic Exercise Gaining • Popularity
On June 12, 2000 Elizabeth B. Krieger, an associate editor at WebMD.com wrote an article titled “Power in Resistance - Workouts with water. Krieger believes Aquatic exercise is growing in popularity within the fitness industry. She says, in past years, water exercise was done mostly by older adults, but now people of all ages are working out in the pool.
Krieger confirms that Sports medicine experts have used aquatic exercise for years as a way for injured athletes to maintain cardiovascular fitness while rebuilding strength and flexibility in a low-stress environment without the joint-jamming impact of land-based activity.
Krieger says water exercise is a low - or no-impact, depending on the water’s depth and
whether the pool bottom is used. Water’s buoyancy counters the downward pull of gravity and takes the weight and strain off joints. Water also helps with balance and removes the fear of falling, which makes the pool an excellent environment for people who are overweight, pregnant or elderly as well as those who have arthritis or multiple sclerosis.
Some of the more popular exercises are water walking, deep-water running, kickboxing, cardio/toning, circuit training, yoga and tai chi. And of course, there is lap-swimming.
According to aquatic exercise experts, water provides about 12 times the resistance of air. Working against the resistance of water has a strengthening effect, much the same way as using strong rubber bands as dumbbells strengthen muscles. Those who want an extra strengthening effect can add resistance by using equipment designed for water workouts, such as webbed gloves, wrist and ankle weights and aquatic dumbbells or Hydrotone.
Chest-deep water is recommended for aquatic exercise, but if this is too difficult, walking in hip- or waist-deep water is acceptable.
“People exercising in a pool should avoid the tendency to stay on their tiptoes,” said Dr. Bob Keith, an Extension nutritionist and fitness expert at Auburn University. “Instead, walk all the way through the foot, stepping heal to toe when walking forward and toe to heel when walking backward. It’s also a good idea to vary how you walk. Walk forward, backward and sideways or march with knees held high.”
Even in the water, warm-up and cool-down stretching are important. Take about five minutes to warm up before starting your water routine and another five minutes to cool down at the end of your routine. Doing so will help prevent muscle cramps and soreness.
Aquatic exercise is not a quick fix for losing weight, but it is a fun way to get some exercise and tone muscles.
A So-So Relationship with Water
On March 19, 2007, Robert P. Wilder, M.D modified an Article from The Charlottesville & Albemarle Observer, October 18, 2000. Dr. Wilder starts by saying he’s always had a so-so relationship with water. At summer camp in Maine, he remembers desperately clinging to the docks until the very last moment, when his frustrated swim counselor nearly drop-kicked him into the icy lake. Summer after summer, he was grouped with the tadpoles and the guppies, never the dolphins or sharks.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
47
So it was no surprise that as an adult he gravitated towards land-based activities like running. But about many years ago, his back rebelled, which wreaked havoc on his 6-mile-a-day jogging habit. He couldn’t imagine giving up on running. Luckily, he’d just read in a fitness magazine that working out in water was as good as doing it on land. So he slapped on his old Speedo and took to the water.
Walking onto the pool deck that first day, wearing a big blue aqua running belt that would keep
him buoyant in the deep water, he scanned the pool for other aqua exercisers. There were some silver-haired ladies schmoozing by the stairs and the usual lines of lap swimmers, but there were no other water runners. He says he slunk over to the slow lane and slipped in. As he began his soggy jog to nowhere, he said he felt vaguely ridiculous and overly aware of curious glances.
But after about an hour, his legs were tired, his heart was racing, and his back didn't hurt. So he
kept at it. When his back finally got better, and he laced up his sneakers again, his heart and muscles felt strong, and he hadn't lost a step.
Changing the Way People See Water Exercise
Before Dr. Wilder started this routine, he thought of aqua exercise as something that might be
fine for his grandmother, but way too wimpy for him. "That's wrong," says Mary E. Sanders, MS, professor of health ecology at the University of Nevada, Reno, and creator of many aquatics programs. "While water exercise can be great for older and overweight people, it's equally good for serious -- even competitive -- athletes." What's more, if you're pressed for time, water exercise is a great way to squeeze an intense workout into a short period.
Sanders should know. Besides looking the part of someone who's discovered a terrific workout,
she's done numerous studies comparing water exercise to its land-based counterparts. Time and again she's found that the wet workouts are as good as or better than dry ones in terms of fat and calorie burning, cardiovascular efficiency, and endurance.
In one of her studies, water walkers who water-trained for four months increased their on-land
walking speeds by more than 16% and their stride lengths by 10%. And check out these numbers: a 130-pound person burns about 6 calories per minute by aerobic dancing. The same person running in deep water at an 11-minute-per-mile pace burns about 11 calories per minute.
Wilder has noticed that more and more people are using aquatics and deep-water running for
exercise. This includes world-class athletes such as Carl Lewis deep-water exercise and of course just ordinary folks can achieve healthy physical fitness.
Deep-water running and pool workouts give athletes bodies a break between grueling land sessions, while helping to increase speed and sharpen form. "Active recovery," they call it. College runners and basketball and volleyball players also can routinely be found training in water.
The Unbearable Lightness of Water
Wilder asks, So what makes water so great? First, its natural viscosity, or thickness, challenges
your body with a constant state of resistance. To generate greater resistance you have several options: for instance, if you wear gloves or hold your fingers closed, you'll find it harder to move your hands through the water. Pushing yourself to go faster creates more resistance. Current and depth can also make your workout harder. Ever try to swim in choppy ocean waters?

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
48
Deeper you go • the tougher the work
For the injury-prone, injury-wary, or already-injured person, water is an extremely forgiving environment. During a run on land, your foot strikes the ground between 800 and 2,000 times per mile, each time at a force of up to four times your body weight, says David Brennan, aqua running expert and assistant clinical professor of physical medicine and rehabilitation at Baylor College of Medicine in Houston.
Your knees, ankles, and back take the brunt of this pounding, but in water your joints and skeleton are cushioned. You can work as hard and as fast as you want, but without the impact-related problems. Skiers, dancers, need to work on your balance? Dive in, says Sanders. The muscles you use for balance and posture are all challenged by the constant push-pull of water. Try a one-legged squat in waist-deep water, she suggests. Not hard enough? Do it with your eyes closed and try to stay balanced. Strength work, too, can be done in water, with foam dumbbells. Think about a biceps curl, says Sanders. On land, this movement only works the biceps, whereas in water, you'll also target the triceps as you fight the dumbbell's buoyancy to lower your arm.
Choosing Your Workout - Go Solo or Join a Class
You don't have to memorize a complicated routine to get a good pool workout. Most YMCAs or health clubs with pools offer some sort of aquatic exercise class nowadays, says Sanders. Some focus on endurance, some on strength, and some on moves that will help you in your specific sport.
However, water walking or running are physical exercise activities that anyone can effectively
do alone. If you're going to be running in the deep end, all you need is your own bright blue flotation belt; for walking, a pair of nonslip shoes or old tennis shoes can help you grip the bottom of the pool. (Of course, if you haven't been exercising regularly, you should get your doctor's approval before you start.) For more tips on proper water walking and running techniques, see Wet Workout Basics.).
As for Dr. Wilder he’s back to being a landlubber -- most of the time. But whenever his back acts up, or he needs a change of pace, he’s back in the water in a flash. He says he has gotten his money's worth out of his big blue belt and, summer-camp indignities aside, he’s made peace with the water. He says he thinks he’s finally graduated from guppy to dolphin.
Most Deep -Water Running Research - Rehabilitation – Athlete
On March 19, 2007 and October 18, 2000 Dr. Robert Wilder wrote an article for The Charlottesville
& Albemarle Observer titled “Deep Water Running for Athletic Rehabilitation”.
Wilder states that resting or not participating in daily training routine can be particularly frustrating for the runner or other athlete while they undergo the treatment of “rest - no physical activity” for an injury. Not long ago this meant no exercise at all. However, today the athlete or person whose daily
routine calls for daily exercise has deep water running as an option to continue training during almost any injury.
What is truly sad about the healthcare crisis is that modern hospital medicine
and doctors in general, do not consider the benefits of “preventive medicine” like AquaDios-Med™ which advocates deep-water running as the only safe daily exercise activity. Especially for those who pursue “intense” powerful workouts; which everybody on the planet needs to learn for genuine health.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
49
One problem Wilder mentions is that deep-water running has not been a popular activity which is regrettable because deep-water running is one of the safest and most useful exercise for almost everybody.
Dr. Wilder indicates deep water running is the most biomechanically specific form of cross training for
the runner or running athlete; therefore the best, safe exercise for non-athletes and patients. This means that deep water running more closely simulates actual running than other forms of exercise and it is so safe it can be done while injured. This also means that the athlete or any person interested in physical fitness will gain better fitness benefits from this form of exercise than from other forms.
What Dr. Wilder fails to mention is that the average person does not exercise daily, let alone participate
in significantly intense workouts, which is possible for almost all people, injured, young, old, pregnant, or those suffering medical problems and on daily medications.
Daily DEEP WATER RUNNING • Cross Training
In 2007 Doug Stern wrote an article for Total Fitness Network, tilted “DEEP WATER RUNNING”. Stern begins by stating deep water running is the best cross training venue for runners. It will allow you to train if you are injured and speed up the recovery process. It will enhance your speed if you are healthy and provide a whole body workout which will increase your joint range of motion strengthen postural muscles. Thus, Deep-Water Running can and should be an exercise activity employed by everybody every day; when this occurs the healthcare crisis will be over. Second, Stern points out the water has certain properties, which lend itself to non-weight bearing resistance training when immersed to the neck. The most obvious benefit of water is its buoyant effect on the body. People float at or near the surface of the water. People can run in the water without any pounding or impact on feet or joints. Also, the water is viscous or thicker than air. As people move their arms and legs gently through water while immersed to the neck they encounter little or no resistance but as the speed and power is increased there will be a tremendous resistance. Stern verifies Deep-water running is a non-weight bearing activity that accelerates rehabilitation when injured and provides a whole body work out that strengthens postural muscles; this certainly sounds like a “preventive medicine” process.
Isokinetic Resistance
Isokinetic resistance is referred to as a resistance that increases proportionally; as the speed or power of movement in the water increases. Physiologists have determined isokinetic resistance is perhaps the most “healing” virtue of water submersion and is the reason it can be used to repair and strengthen muscles and joints; even while injured. The faster you move your arms and legs through the water the greater the resistance you will encounter and therefore the harder, more intense the workout, the greater the strength and aerobic gain. Sterns point is that when submerged in water to the neck, the properties of water exert greater pressure on bodies than air or gravity does. Stern also indicates that running in the water while submerged to the neck allows people to do more exercise bouts with less recovery time than a similar workout done on land. The water buoyancy and pressure coupled with the lack of gravity acting on the body, plus the water’s cooling affect allows for faster recovery from strenuous exercise. The pressure of the water cause the Venous blood to flow back to the heart faster which increases “cardiac output” with less cardiac effort and the body remains substantially cooler while submerged in the water than on land. All of these deep-water running benefits place it as the exercise of choice especially as a “preventive medicine” treatment.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
50
Equipment for Deep Water Running
Stern mistakenly indicates that any device that keeps your body afloat and in an upright position will be alright for deep-water running, but this author does not recommend this approach at all. We must be aware that “correct” posture during deep water running is critical to learning how to obtain the genuine benefits of DWR. For example, people should use “running” shoes to run, not tennis shoes; each is designed for a specific purpose.
It is recommended that DWR be attempted only with a Wet Vest or AquaJogger buoyancy belt. Whichever equipment is chosen be sure it is snug.
Aquatic Equipment
Kudlacek states that individuals with JRA can use aquatic equipment such as Hydrofit dumbbells or floatation devices, running belt, water resistance gloves, water shoes to reduce risk of slipping and provide skin protection, kick board or water "noodles". Music is strongly recommended. The
music should be age appropriate and motivating for the participants.
Stern recommends concentration should be focused first on the Legs – Start with very straight legs. Point your toes as if you are a ballet dancer and sweep your legs back and forth. Use your upper thigh to create the movement. Feel the water on the tops of your toes and your leg moves forward and on the bottom of your feet as they move backward. Make no attempt to bend of lift your knees.
Arms - With your arms gently by your sides, palms of hands facing backward, elbows slightly bent, leading with your elbows, move your arms back in coordination with your leg movements (left leg-right arm and vice versa). Let your thumb almost graze your thigh as it swings in each direction. Make sure your arms move directly forward and back. Head and eyes - Feel as if a string is supporting your head above your shoulders. LOOK STRAIGHT AHEAD with your chin angled toward your neck, mouth open and jaw relaxed. Shoulders – Press your shoulders back and down slightly. They should be loose and relaxed. Chest - Press forward and up (it allows for easier breathing and an erect body position) Hips - keep them under your shoulders.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
51
Deep Water Defined
When submerged up to the neck, water depth must be enough that your feet cannot touch the bottom while you’re in an up-right-vertical running position. Individuals can hit the pool for serious results or cross train using a “surf and turf” approach, alternating wet and dry workouts for balance. However, they need to learn the proper deep-water-running techniques to optimize training.
The following studies reflect lessons learned from investigations targeting participants who were under 50 years of age. More research needs to be conducted on non-athletes and patients as well as the older populations exercising with deep-water running, but there is data to roughly estimate the energy costs for seasoned athletes. Frangolias, Rhodes and Tauton (1996) suggest that water skills are important to maximizing results. The subjects in their study who were “water trained” achieved higher intensities than those who were not strong enough or those who did not know how to perform within the water’s resistance effectively. Sanders says it’s important to keep in mind that water running is a learned skill, similar to other sports such as tennis and that an individual must have good body alignment while running in the water.
Deep-water running form is patterned as closely as possible to running on land. Wilder and Brennan (1997) suggest the following tips for good wet-running biomechanics.
The participant should wear a buoyancy (flotation) belt that brings the water line at the neck just above the shoulder level, with the mouth comfortably above the surface.
The body should be slightly forward of a vertical position, with the spine in a neutral position (ears, shoulders, hips lined up). Arm motion is similar to land, with the primary action at the shoulder. Hip flexion should reach 60–80 degrees. As the hip is flexed, the leg is extended at the knee from a flexed position. Finally, the ankle works as it would on land. The participant should think about the bottom of the feet and toes as he or she moves through the ankle foot rotation or “foot flap” action. 2 equip -425
Deep Water running Technique Concentrate and image your normal running style. Don't 'paddle'- Keep your hands in a half
open position with fingers touching, and let your arms and legs move you forward with each stride and arm motion. The harder you pull with your arms, the greater exercise delivered to the upper body, chest and back.
Please remember the normal “foot- flap” or ankle – foot rotation in running and walking, allow your ankles to rotate your heal and toe completely as you do naturally when running and walking. Allow the bottoms of your feet to be involved, especially the reach of the toes in the forward stride. Usually short, quick strides are best for beginners with a fast cadence to intensify the physical activity of the workout; and when you’re ready make the stride bigger – longer with more power.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
52
Expect a lower stride cadence, that is, you will not travel very far with each stride because water is more resistant than air and your forward pace or travel will decrease accordingly; the faster – harder the stride the greater the resistance, your speed of travel through the water will be very slow, though your cadence or running speed may be very fast, intense and powerful. Your heart rate will be about 10 percent lower than at the same intensity on land; this is a good thing – increased cardiac output with fewer heart beats [see pages xx]. It will take some practice to get the hang of water running, but when you concentrate on your form, just
as you would while running on land, you will pick it up quickly.
Deep Water running Technique
Concentrate and image your normal running style. Don't 'paddle'- Keep your hands in a half open position with fingers touching, and let your arms and legs move you forward with each stride and arm motion. The harder you pull with your arms, the greater exercise delivered to the upper body, chest and back.
Please remember the normal “foot- flap” or ankle – foot rotation in running and walking, allow your ankles to rotate your heal and toe completely as you do naturally when running and walking. Allow the bottoms of your feet to be involved, especially the reach of the toes in the forward stride. Usually short, quick strides are best for beginners with a fast cadence to intensify the physical activity of the workout; and when you’re ready make the stride bigger – longer with more power.
Expect a lower stride cadence, that is, you will not travel
very far with each stride because water is more resistant than air and your forward pace or travel will decrease accordingly; the faster – harder the stride the greater the resistance, your speed of travel through the water will be very slow, though your cadence or running speed may be very fast, intense and powerful.
Your heart rate will be about 10 percent lower than at the same intensity on land; this is a good
thing – increased cardiac output with fewer heart beats [see pages xx]. It will take some practice to get the hang of water running, but when you concentrate on your form, just as you would while running on land, you will pick it up quickly.
Deep-Water Running • Physical Fitness
Anne Asher writes for About.Com, a division of the New York Times and has written an article
about the ‘Benefits of Water Exercise”. She is an expert in Back and Neck Pain having worked for clinics, fitness centers, schools and in her own business. She has created and taught therapeutic exercise programs for patients with back and neck problems, and has delivered presentations to members of the medical profession including.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
53
Asher states that deep-water running is great for physical fitness, rehabilitation for injury and athletic training. People of all ages of life including the sedentary, pregnant women, children, geriatricians or athletes of all sorts can attain the benefits of deep water running. It is also a great form of cross training for athletes and an excellent way for all people to be physically fit and to deal with and prevent injuries.
Deep-water running allows all people the safest form of exercise there is and those that are injured, including the athlete, to recover without losing fitness. It can also help with improving running form and decreasing risk of sustaining injuries by decreasing the “impact” stress from running on hard surfaces. The most popular form of aqua training devices among water runners is
the AquaJogger. Made from EVA foam it looks like a belt that you strap around your waist; another is the
Wet Vest >>> The goal is to keep your body buoyant and afloat while immersed to the neck while allowing
you to perform a running motion while immersed to the neck without stress to the body. Submerged in the water to your neck you will have resistance or water pressure on all sides; this pressure forces opposing muscles to work equally. As you move your arms and legs against the resistance of the water you will get a great cardiovascular, as well as, strength training workout. By adding additional hydro devices,
such as a “aqua-socks”, dumbbells, and 'gloves' allows you to vary your effort and intensity. In addition to increasing the extremities resistance to increased speed of movement, being in the water decreases the stress on your joints, while increasing your range of motion. Because there is no impact, a common patient or an injured athlete can train in the water and develop physical fitness or remain fit while injuries heal.
Sedentary and uninjured people and most all medical patients can use water running for
physical fitness while athletes can use it as a cross training method, to work on technique, increase resistance while reducing mileage and risk of injury.
Shallow and Deep Water Exercise Responses 317
Treadmill running is considered the ‘gold standard’ exercise modality to which all other modalities are compared. Studies comparing treadmill to other modalities such as cycling, simulated cross-country skiing, rowing, and stepping have shown treadmill running to elicit the highest energy expenditure and oxygen consumption (Thomas, Ziogas, Smith, Zhang, & Londeree, 1995; Zeni, Hoffman, & Clifford, 1996). It therefore can be assumed that water exercise comparisons to treadmill running will have similar findings. However, the true relationship of water exercise to treadmill running (and other forms of land exercise) can only be determined through experimental research.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
54
Knowledge of the acute physiological responses of aquatic exercise programs helps the applied professional make correct decisions on safe and effective programming for participants. Part II of this aquatic review will summarize the responses to shallow and deep water exercise.
Comparisons of Submaximal Land and Water Exercise in Waist –To - Chest Deep Water
A pioneer aquatic investigation examined the oxygen consumption and heart rate responses of
walking and jogging in waist deep water and on land with six males (21 - 42 yr) (Blanche, Evans, Cureton, & Purvis, 1978). Water temperature was 86°F to degrees 88°F. In waist deep water, walking and jogging produced similar heart rate responses to land while oxygen consumption was higher in water. It was concluded that the water resistance in waist deep water while walking and jogging results in high levels of energy expenditure with relatively little strain on the lower extremities.
Hered et al. (1997) compared aquatic exercise using the arms and legs, and legs only, on land and in chest deep water at four different intensity levels with 12 females (mean = 20 yr). Results indicated that heart rates were lower in water than on land while oxygen consumption at 2 of the 4 intensities were significantly higher in water. Subjects incorporating both the arms and legs had the highest heart rates regardless of the environment (land or water). This study substantiates that adding the arms to leg exercise in chest deep water increases the energy expenditure cost of the aquatic activity. One investigation studied the effect of walking on land and in water, at a matched cadence of 103 bpm, with and without an external elastic resistance belt, in ten male and eight female college-aged participants (Robert, Jones, & Bobo, 1996). The elastic belt (tubing) allowed for more resistance to be applied to the arms and shoulders during exercise. Water temperature ranged from 72°F to degrees 78°F.
Treadmill walking had significantly higher oxygen consumption and kilocalorie expenditure than matched exercise in chest-deep water. The resistance belt was did not affect the oxygen cost or caloric cost of the exercise on land and in water.
Comparison of Aerobic Exercise on Land to Water
In a comparison of identical aerobic exercise routines on land and in water with ten female subjects (mean = 43 yr),
land exercise produced significantly higher oxygen consumption results (Heberlein, Perez, Wygand, & Connor, 1987). However, the cardiovascular stimulus for the hydroaerobics program was within ACSM guidelines for the improvement of cardiovascular endurance. Having the subjects perform the same exact aerobic exercise routines on land and water may have impaired the participant responses due to the varying effects of water density (800 times greater) compared to land. Cassady and Nielsen (1992) evaluated heart rate and oxygen consumption of 40 subjects (20 males, 20 females, mean = 25 yr) performing upper extremity and lower extremity exercise on land and in water, at three different cadences.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
55
The oxygen consumption responses were greatest during water exercise, whereas heart rate, expressed as a percent of age-predicted heart rate maximum was highest on land, attributable in part to the hydrostatic pressure of water.
Maximal Intensity Land and Water Exercise 318
Comparisons in Chest Deep Water
One investigation compared maximal oxygen consumption (VO2max), maximum heart rate (HRmax) and ratings of perceived exertion (RPE) of treadmill running to aquatic exercise (in chest deep water) with 19 males and 11 females (Hoeger, Hopkins, Barber, & Gibson 1992). The aquatic exercise consisted of arm and leg work which was gradually increased by speeding up the movement to attain maximal work output. Maximal treadmill exercise elicited a significantly higher response in VO2max, HRmax and RPE. This is not surprising since treadmill exercise has been shown to produce higher VO2max values when compared to other modalities (Thomas et al., 1995).
Comparison • Bench Stepping • Land • Water
Evans and Cureton (1996) compared oxygen consumption, heart rate and perceptual response of bench stepping on land and in chest-deep water. Ten women completed 5-minute trials of aqua bench stepping (29 steps/minutes) at three different bench heights (0, 7 in, 12.5 in) using a traditional stepping pattern and an arms and legs stepping pattern (water only). Water temperature varied between 29 degrees C (84°F) and 32 degrees C (90°F). Heart rates and oxygen consumption were lower in the water, although the perceived exertion response was very similar for stepping in water and on land. The added use of arms to legs increased oxygen consumption demands of the
movement to 48%, 58%, and 78% of VO2peak, for the step heights 0, 7 in, and 12.5 in, respectively. Thus, bench stepping with the use of the arms in water meets ACSM guidelines for the improvement of aerobic capacity (50% to 85% VO2max).
Heart Rate Oxygen Consumption - Shallow Water Exercise
Eckerson and Anderson (1992) explored the energy expenditure of shallow water aquatic exercise. In approximately 1 meter of water, 16 college females (20 yr) performed shallow water exercise routines. Maximal metabolic and cardiovascular data for the subjects was also obtained from land tests on a treadmill. When compared to treadmill effort, shallow water exercise resulted in mean heart rate responses that were 74% of heart rate reserve and 82% of HRmax, while VO2 was 48% of VO2max (minimally meeting ACSM guidelines). Subjects burned an average of 5.7 kilocalories per minute during the aquatic exercises. Another investigation studied the effects of rhythmic aquatic calisthenics (stretching, jogging in place, modified lap swimming, simulated crawling, and treading water) on heart rate and oxygen consumption, at three different intensities (Vickery, Cureton, & Langstaff, 1983). The researchers found heart rates of 70% to 77% and oxygen uptakes of 51% to 57% (meeting ACSM guidelines) of maximal values. The caloric expenditure ranged from 5.9 to 6.5 kilocalories per minute for the various programs.
Physical Fitness Is Preventive Medicine Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
56
Deep Water Running Studies Treadmill Walking - Running vs. Deep Water Walking/Running
Coad et al. (1987) studied the energy costs of treadmill walking and running versus matched speeds of deep water walking and running with 14 subjects. Subjects wore wet vests while exercising in the water. Results indicated that deep water walking required significantly greater metabolic costs than treadmill walking. Deep water running and treadmill running were very similar in energy expenditure. DeMaere et al. (1997) compared five-minute trials of deep water running to treadmill running at 60% and 80% of VO2peak in eight cross-country runners. Deep water running and treadmill walking at similar intensities resulted in similar energy expenditure values.
Svedenhag and Seger (1992) compared running on land to vest-supported deep water running with 10 trained male runners (26 yr). Subjects ran at heart rates of 115, 130, 145, 155-160 bpm and also exercised to maximal exercise intensity. Maximal oxygen uptake (4.03 vs 4.60 l/min) and maximal heat rate (172 vs 188 bpm) was lower during water running. The authors suggest the lower maximal heart rates may be attributable to an increase in heart blood volumes, while the influence of different test procedures in the water vs. land may partially explain the differences in VO2max. RPE values were higher for deep water running as were the blood lactate concentrations at any given VO2. These responses may be due to a decreased blood flow in the legs during deep water running as well as the altered leg muscle activation patterns of deep water running. An investigation by Glass, Wilson, Blessing and Miller (1995) compared the maximal
physiological costs of deep water running to treadmill running using ten male and ten female subjects (26 yr). Treadmill running produced higher VO2 and heart rate values. However, heart rate was measured by palpation, and water temperatures were reported to be 24°C (75°F), which has been shown to be associated with a lowered exercise heart rate response. Treadmill running elicited higher metabolic training intensities than deep water running when equated for the same level of RPE.
The authors suggested that due to the density of water, subjects utilized more anaerobic energy because of the increased challenge to the exercising muscles, and thus had lower VO2 and heart rate values. In addition, the use of the arms and legs against the water resistance contributed to higher lactate levels for deep water running as compared to treadmill running. Frangolias, Rhodes, and Taunton (1996) compared the cardiovascular responses of maximal deep water running to treadmill running utilizing 22 endurance runners (8 female, 14 males, ages 21 to 35 yr) who were divided into experienced and inexperienced deep water running groups and given maximal exertion tests on the treadmill and in the water. Experienced deep water runners were classified as those doing at least 6 deep water running workouts per month for 6 months prior to the study. Results indicated that the more familiar subjects were with deep water running, the smaller the difference in maximal oxygen uptake values between water and land running. Experienced deep water runners had VO2max values on land and in water that were within 3.8 ml/kg/min whereas the difference in the inexperienced deep water runners was 10.3 ml/kg/min.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
57
Underwater video analysis revealed that inexperienced deep water runners were unable to maintain upright positions in the water and more likely to cup the water with their hands, propelling themselves slightly forward. Leg patterns of the inexperienced deep water runners adapted to a shorter stride cycle, similar to a swimming kick motion, which increased the contribution of the upper body. Maximal heart rate results indicated no significant differences in maximal heart rate in land vs. water in the experienced deep water runners. The researchers concluded that the more familiar individuals are with deep water running, the more closely matched the physiological responses of the two exercise mediums. In another study using experienced deep water runners, Frangolias and Rhodes (1995) found higher maximal metabolic values on land compared to deep water running with 13 distance runners (21-35 yr). Experienced deep water runners were defined as those who incorporated at least 6 DWR workouts per month into their training program for six months prior to the study. Maximal VO2 and heart rate values were approximately 8% lower in water as compared to land. Also, lower ventilatory threshold (which is a marker for the body’s production of lactic acid) values were noted for DWR as compared to treadmill running at the same RPE and respiratory exchange ratio; the ratio of carbon dioxide produced and oxygen consumed levels. However, when ventilatory threshold was expressed as a percentage of the respective DWR or treadmill VO2 values, there was no statistical difference. This suggests that factors dampening the effect of maximal effort also appear to be factors limiting VO2 at the ventilatory threshold. The authors suggest that the differences observed in maximal values in land versus water are most likely related to hydrostatic responses, gravitational effects, and running styles in the different mediums. It is noted that during exercise in water there is a tendency for breathing frequency to be higher and tidal volume lower in submaximal (80% of VO2max) and maximal exercise (Sheldahl et al., 1987). This suggests that the cost of breathing in DWR increases and a larger portion of oxygen is consumed by the respiratory muscles during water exercise as compared to land. Researchers also reported similar blood lactate responses during submaximal, maximal and recovery periods in land and water. This implies that variations in arm and leg actions (DWR technique) as well as the recruitment patterns in the deep water running that may limit oxygen consumption also contribute to the onset of blood lactate. Michaud et al. (1995) compared the physiological, perceptual and metabolic responses of peak and moderate intensity deep water running to treadmill running with six trained male runners (mean = 25 yr). Peak oxygen consumption and heart rate were 12% and 8% greater for treadmill running than deep water running At similar relative and absolute exercise intensities, blood lactate and respiratory exchange ratio were significantly greater during deep water running. No significant difference was found in submaximal heart rate responses between trials. Subjects in this study were inexperienced DWR and received only three familiarization trials in deep water running. Water temperature was maintained at approximately 84°F to 86°F. Submaximal trials were 75% of treadmill VO2peak on treadmill (TM 75%), 70% of deep water running VO2peak in water (DW 70%), and 75% of treadmill VO2peak in water (TM 75%-W). Oxygen consumption at 75% of deep water running VO2peak was significantly lower than the other trials. No difference in heart rate occurred between trials. For both blood lactate and respiratory exchange levels, the water responses were significantly higher than land. At the same absolute exercise intensity, RPE values were higher in deep water running. The authors suggest that the mechanics of DWR are not as similar to land running as has been suggested. Butts, Tucker and Smith (1991) investigated the maximal responses to treadmill and deep water running in 12 high school female cross country runners (mean = 15 yr). Subjects were taught DWR technique prior to testing, but had no previous experience with this form of training. Peak heart rate and oxygen consumption was higher on the treadmill than in water by 9% and 13%, respectively.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
58
The authors suggest the lower DWR metabolic responses may be attributable to a number of factors, including the cooling effect of the water temperature 84°F, the hydrostatic forces exerted by water, the low body fat of the subjects (mean = 17.6%), and mechanical differences observed in deep water running due to the buoyancy effect of water. It was concluded that DWR provided numerous rehabilitation and training possibilities for athletes.
Maximal Gender Responses - Treadmill - Deep Water Running
Any investigation comparing maximal physiological responses between women and men is complicated by differences in body composition, physical size, and level of training. The larger percentage of body fat observed in women is a chief contributing factor to the lower cardiorespiratory observations (Pate & Kriska, 1984). These differences in body composition may also facilitate buoyancy, possibly resulting in a reduced metabolic response in women when compared to men, making the water exercise more economical for women (Brown, Chitwood, Beason, & McLemore, 1997). Butts, Tucker and Greening (1991) compared maximal physiological responses to treadmill running and deep water running in 12 trained men (mean = 20.6 yr) and 12 trained women (mean = 21.9 yr). Subjects were familiarized prior to testing with treadmill and deep water running exercise. Water temperature was 29°C (84°F). Men and women had significantly lower maximal VO2 and heart rate responses in water. The DWR VO2max values in water for men and women were 9% and 16% lower, respectively. The DWR maximal heart rate values in water for men and women were 5% lower. Respiratory exchange ratio was similar in both the water and on land. The authors concluded that the magnitude of these differences in water exercise and treadmill running is not different from that comparing treadmill running to other modalities and in no way precludes deep water running as an effective training technique. Brown et al. (1997) explored the physiological differences to deep water running and treadmill running and differentiated them by gender with 12 untrained 21 yr. old men and 12 untrained 20 yr old women. This investigation matched running cadences at a wider range of intensities to compare the two modalities. Subjects were familiarized to DWR with at least 2 DWR practice sessions prior to testing. Water temperature averaged 85°F. At all submaximal intensities, with running cadences matched in water and on land, deep water running resulted in higher VO2 responses. The authors concluded that at matched cadences in submaximal exercise, subjects were working harder during DWR. Heart rate was not significantly different between genders on land or in water, although heart rate on the treadmill was 6% and 10% higher than DWR for men and women. Men had significantly higher VO2max responses compared to women and treadmill VO2max values were 13% and 24% higher for men and women than in deep water running. A very interesting finding of this study was that at matched running cadences, submaximal physiological responses for men and women were higher during DWR as compared to treadmill running.
Submaximal Energy Expenditure
An investigation with 8 male competitive runners (18 to 42 yr) running at a submaximal pace for 30 minutes showed deep water running incurred higher oxygen consumption values, respiratory exchange ratios, and RPE levels than normal treadmill running and road running (Richie &, 1991) . Heart rates were similar in the three experimental conditions. When subjects exercised at a self-selected ‘hard’ pace on the treadmill, metabolic values were higher than in deep water running. It was concluded that submaximal exercise can be sufficiently and effectively completed in deep water.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
59
Differences in Deep Water and Treadmill Running Mechanics
It has been suggested that there is greater involvement of the anaerobic energy system during water exercise because of the additional recruitment of smaller muscle groups (Michaud et al., 1995). Subjects have reported more fatigue in the arms, shoulders, hips, and legs during DWR, with potentially greater use of the upper body and less use of the lower body (Michaud et al., 1995). The propulsion mechanics of the muscles in the legs when running are different than water, where the body is suspended and not working against gravity. In deep water running there is no weight-bearing and hence no push-off phase against a hard surface. Therefore, although deep water running mimics running on land, several important factors differentiate the two activities.
Met levels are a unit of measurement frequently used to designate the energy costs of exercise programs. One MET equals 3.5 ml/kg/min. This table will provide MET data for various aquatic exercise programs. Due to variation in fitness levels of subjects and gender, these values are best used as approximations for the aquatic activity. From this review of literature on the cardiovascular and energy expenditure responses to aquatic exercise, the following is a summary of findings: Adding arms to leg exercise in chest deep water significantly increases the energy cost of the workout. This may equal or exceed matched exercise performed on land depending only on the amount of effort and intensity applied in deep-water running. Water jogging and running in waist-deep water results in equal or even greater cardiovascular responses compared to similar exercise on land. Aqua exercise routines can meet ACSM guidelines for the improvement of cardiorespiratory endurance. However, the ACSM guidelines for improvement of cardiovascular fitness may need to be adapted for aquatic training, since current standards prescribe only for land- based exercise. Bench stepping exercise in water, using the arms, meets ACSM guidelines for the improvement of cardiorespiratory endurance. Water exercise using elastic resistance with the upper body does not significantly increase energy expenditure. Investigations have found the cardiorespiratory responses of deep water running to be less than, similar, and greater than treadmill running on land. Blood lactate levels in deep water running have been shown to be higher and lower to land exercise which may reflect variations in arm and leg actions and exercise protocols. Ratings of perceived exertion for DWR appear to be elevated due to higher blood lactate levels and upper extremity muscular fatigue. The hydrostatic pressure and altered running style (due to different muscle activity patterns of DWR) contribute to a greater involvement of the anaerobic energy system during deep water running.
There is an increase in breathing frequency and cost of breathing during water exercise which leads to the respiratory muscles consuming more oxygen. This may function to limit the oxygen available for the legs. The more familiar subjects are to DWR, the smaller the difference between VO2max values between land and water. Exercise heart rate and oxygen consumption comparisons of teenage females in land and water exercise appear to result in similar responses to those seen in adults.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
60
This section of the book brings the reader a short history of exercise and its effects on and health. This includes studies on exercise and addresses how chronic disease is killing sedentary American’s that could have healthy quality lives with safe daily exercise offered by AquaDios-Med™ exercise. Len Kravitz, Ph.D. the program Coordinator of Exercise Science and Researcher at the University of New Mexico, wrote an article titled “The 25 Most Significant Health Benefits of Physical Activity and Exercise” together with Jonathan N. Mike, MS, a doctoral student at the time in the exercise science program in the Department of Health, Exercise, and Sport Science at the University of New Mexico, Albuquerque. Kravitz and Mike state that recent research shows that people of all ages can improve the quality of their lives and reduce the risks of developing coronary heart disease, hypertension, some cancers, and type 2 diabetes with ongoing participation in moderate, safe, daily physical activity and exercise such as deep-water running 45 minutes a day as recommended by AquaDios-Med™. Safe, daily physical activity with sustained exercise will also enhance one’s mental well-being and promote healthy musculoskeletal function throughout life. Kravitz and Mike indicate that routine physical activity is an attainable goal to a healthier life, but only 48% percent of all American adults currently get 30 minutes of moderate intensity exercise per day on at least 5 days a week according to Center for Disease Control, 2005. A formidable challenge facing doctors and many personal trainers and health and fitness professionals is finding new approaches to motivate people to improve their well-being with consistent participation in physical activity and exercise. In fact, significant health benefits can be obtained by including moderate amounts of physical activity accumulated on most, preferably all days of the week. Fitness programs involving progressively increasing intensities of exercise will elicit even greater cardioprotective benefits according to the research of Swain and Franklin, 2006. There is a growing understanding of how levels of physical activity may positively affect cardiovascular, musculoskeletal, respiratory, endocrine function, and mental health. This section of this book will bring to realization the evidence on 25 significant benefits linking physical activity to health enhancement. Some health benefits have been grouped together because of their physiological or metabolic associations.
Research • More than Half Insured American’s Take Daily Prescriptions
On May 14, 2008, Linda A. Johnson, writer for the
associated press reported on a recent new study indicating that more than half of all insured Americans are taking prescription medicines regularly for chronic health problems. This author believes and 100’s of studies show that most all of these same people, within 90 days could safely stop their medications, if for those 90 days, they participated in AquaDios-Med™ daily safe structured deep-water running and Mind Body Medicine programs. The research shows that the most widely used drugs are those to lower high blood pressure and cholesterol; medical problems most often linked to heart disease, obesity and diabetes. Simultaneously, this book has repeatedly shows studies that these very “dis-eases” are treatable with safe daily exercise; to the point of reversing the dis-ease and no longer requiring medication.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
61
Johnson reports that Medco Health Solutions Inc. manages prescription benefits for about one in five Americans and gathered those numbers in 2007. Dr. Daniel W. Jones, a heart specialist, Dean of the University of Mississippi's medical school and president of the American Heart Association stated that “Unless we do things to change the way we're managing health in this country ... things will get worse instead of getting better". This author agrees with Dr. Jones and the … “change of managing healthcare” … must be to aggressively utilize preventive medicine programs like AquaDios-Med™ as the first and primary treatment of choice for most all medical problems. Johnson’s report indicates the pharmaceutical industry's relentless advertising is causing too many people, as well as hospitals and doctors to think most medical problems are best resolved when treated by their drugs. Johnson information indicates that medical experts say the data indicate there is a worsening public health and better medicines for chronic conditions that are more aggressive treatment by doctors. Dr. Jones points out that more people are now taking blood pressure and cholesterol-lowering medicines because they need them, which may be true, but not because these same people are participating in safe daily exercise. This author and most all research studies make it crystal clear that hospital medicine and current healthcare mentality is the reason people need medicine. Dr. Jones fails to point out that aggressive treatment by doctors is commonly more prescribed medications and surgery, rarely is there ever an “aggressive” treatment demanding safe daily exercise as is prescribed in the AquaDios-Med™ program. Johnson reports that with these myopic hospital medical factors and dependence on aggressive medications, the healthcare crisis is unlikely to change. In fact, her report indicates that doctors today say the proportion of Americans on chronic medications can only grow unless this attitude of “overmedicating” patients and under using “preventative medicine” continues.
Johnson cites Dr. Robert Epstein, chief medical officer at Franklin Lakes, N.J.-based Medco who believes a big part of the problem is caused by obesity, because people have become a couch potato culture (and) it's a lot easier to pop a pill than to exercise regularly or eat nutritional healthy meals. Dr. Epstein points out that medical research has turned fatal diseases into chronic ones, including AIDS, some cancers, hemophilia and sickle-cell disease. But, ironically Epstein notes the biggest jump in chronic medication use was in the 20- to 44-year-old age group; at 20 percent over six years and these are adults in the prime of life. Data show that the drugs “overused” or abused are for depression, diabetes, asthma, attention-deficit disorder and seizures. Antidepressant use has become the biggest prescription for teens and working-age women. Doctors concluded this fact is due to more stress in daily life and to family doctors, including pediatricians, prescribing more and newer antidepressants. The research studies in this book once again make it clear these “medical problems” are effectively handled with “preventive medicine” programs like AquaDios-Med™ that require safe daily exercise.
Johnson reveals Medco's data show that last year, 51 percent of American children and adults were taking one or more prescription drugs for a chronic condition, up from 50 percent the previous four years and 47 percent in 2001. Most of the drugs are taken daily, although some are needed less often. Medco’s data was from prescription records from 2001 to 2007 from a sample of 2.5 million customers including newborns to the elderly. Records indicate Americans buy much more medicine per person than any other country. But, Johnson states data were not available for Europe, for instance.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
62
Medco’s statistics show that medication use for chronic problems was seen in all demographic groups including two-thirds of women 20 and older, one in four children and teenagers, 52 percent of adult men and three out of four people 65 or older. And, among seniors, 28 percent of women and nearly 22 percent of men take five or more medicines regularly. Johnson identifies a 57 year old full-time nurse who takes 18 prescription medicines daily. This person is a “classical” example of the average patient who has become a victim of the healthcare crisis and today’s hospital medicine practices of “over-medicating”. She takes prescribed medications for high blood pressure, diabetes, chronic back and shoulder pain, asthma and the painful muscle disorder fibromyalgia. This author believes this patient could be off all medications within a 90 day period if she included the safe daily exercise in the AquaDios-Med™ program.
The woman’s 69-year-old husband medicines include four daily pills for arthritis and heart disease, plus two inhalers for lung problems. Her husband is also a candidate for the AquaDios-Med™ program with a similar prediction; free of medications within 90 days of the AquaDios-Med™ program. Johnson’s news update includes a statement from Dr. Sidney Wolfe; Public Citizen's Health Research Group who reveals that Americans increased use of medications is traced to pharmaceutical companies who heavily advertise drugs for chronic conditions because most patients will take them for a long time. Dr. Wolfe also blames doctors for not spending the time to help patients with “preventive medicine” programs like AquaDios-Med™ where they can safely exercise daily and remove excess weight and make other healthy changes before writing a prescription. Johnson explains the study shows that many more children use medicines to treat weight-related problems and other illnesses previously considered adult problems. Medco estimates about 1.2 million American children now are taking pills for Type 2 diabetes, sleeping troubles and gastrointestinal problems such as heartburn. This author has faith in the many studies included in this book, all demonstrating the value of “exercise” for health. Most of the research identifies that only “moderate” exercise improves and I have so much in the safe daily deep-water running of the AquaDios-Med™ program I have confidence these children can be free of “all” medications within 90 days. Dr. Jones states the great concern is that children’s body weights are much higher in general and he concludes that this means the American population is going to have larger numbers of adults who develop high blood pressure, abnormal cholesterol or diabetes at an earlier age. Dr. Richard Gorman, an American Academy of Pediatrics expert on children's medicines, said more children are taking medicines for "adult conditions" partly because pharmaceutical manufacturers now provide pediatric doses, liquid versions or at least information to determine the right amount of the drug for a child. It does not take a mental giant to conclude that preventive medicine programs like AquaDios-Med™ can free hundreds of thousands of children and adults from being “patients” dependent on prescribed medication. The Medco study found that among boys and girls under age 10, the most widely used medication switched from allergy drugs to asthma medicines between 2001 and 2007. Dr. Gorman believes this is because over the last decade, asthma care has gone from treating flare-ups to dependence on inhaled steroids regularly to prevent flare-ups and hospitalizations.
Deep -Water Running Research Rehabilitation – Athletes Dr. Wilder believes deep water running is perfect for cross training which has traditionally been used
for several purposes such as alternative training during an injury and supplementing a regular exercise program to gain greater fitness without excessive impact; this author concurs.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
63
Dr. Wilder’s opinion is in the category of most doctors who may regard “deep-water running” only as a benefit for the injured athlete or as excellent for “cross training” but not a “preventive medicine” treatment for the average patient cited in the Medco study above.
Wilder’s myopic view is consistent with “hospital medicine” mentality, a narrow minded view
that at best DWR is a primary form of training for a multi-sport athlete such as a triathlete while providing variety to a training regimen to enhance enjoyment. And, this bias is held only by “sports medicine” doctors while most doctors know nothing of deep-water running or its benefits. Wilder utterly avoids discussing “preventive medicine” programs like AquaDios-Med™ or that safe daily deep-water running is the primary treatment of choice for those patients who have become victims of the healthcare crisis and who will have greater health benefits than an injured athlete.
Dr. Wilder discloses a variety of injuries such as stress fractures and muscle tears mandate the injured person refrain from running or weight bearing exercise while rehabilitating from the injury. This author would like to extrapolate these facts to the common patient told to avoid all weight bearing exercise and take these medications instead. Preventative medicine programs like AquaDios-Med™ need to be included as primary treatment of choice before medication and sedentary rest.
Many people and patients including athletes are able to participate in deep water running; this deep-water running activity allows the injured athlete or the patient suffering from one or more of “today’s” common medical problems to
establish or enhance fitness during the time in which the injury or medical problem is healed by the exercise. Thus, safe daily exercise as is recommended by AquaDios-Med™ must be the first choice of care.
Dr. Wilder suggests Aqua running is synonymous with deep-water running, an activity of simulated running in the deep end of a pool aided by a floatation device (vest or belt) that maintains the head above water.
This author believes that Dr. Wilder’s statement is too constricted and one reason why so many hospitals, doctors and people in general are unaware that deep-water running is the safest exercise for all walks of life for mothers, fathers, children, pregnant
women, geriatricians, the athlete, the sedentary, the general patient, the injured and disabled .
Deep-water running is not a “simulated” exercise; it is a genuine and tricky to learn physical activity which requires deep concentration and focus to become skilled and to develop the correct vertical running position while fully immersed to the neck in water. Deep-water running is difficult to learn because the “runner” never touches the surface of the pool bottom. Thus, Wilder’s “simulated running”, is running but without the common “heel strike” or impact to register to the brain that a running stride has begun. This “fantasy” impact is indeed difficult to learn, but not too complex. Because the mind knows the millions of steps or strides we have taken and all are registered in the mind, it knows exactly when the “heel strike” will or should occur. The heel strike is the beginning of the “foot flap” or rocking motion at the ankle and foot.
The task is of deep-water running involves some imagery to adjust to the lack of impact to register the full natural stride experienced on land. But, like Astronauts learning to adapt to weightlessness the aquatic runner learns to accommodate to the buoyancy with some training and concentration.
This author prefers to expand Dr. Wilder’s narrow view of deep water running and say that to obtain the genuine factual deep water running physical benefits of deep-water running the correct running posture in the water “must” be very similar to the gait and physical strides taken in “dry-land running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
64
The reason this stride cadence in deep-water running is important is that most people have difficulty maintaining the complete upright vertical running position in water because the water’s resistance increases as the “power” of each stride increases and this tends to make the “foot-flap” more difficult. This inadvertently causes most people to revert to a “bicycle” motion rather than the correct vertical running stance. Incorrect running posture>>>>> <<<<Correct Running Posture
The new “water runner” may choose to be held in one location by a tether cord, essentially running in place, or
may actually run through the water across the width of the pool. The tether is useful to serve as an increase resistance as well and to facilitate monitoring of exercise by a physician, therapist, or coach.
No foot contact or impact is made with the bottom of the pool; this eliminates all impact and “opens” all
skeletal joint cavities because there is no weight bearing on the skeleton or joints at all. Cavaties between bones in synovial joints are filled with synovial fluid and these “cavities” receive no impact or compression allowing the joint and cavity to be free to heal and rejuvenate from the exercise without impact or compression of the joint.
Synovial joints allow much more movement than cartilaginous joints which are joints in which the bones are attached by cartilage. These joints allow for only a little movement, such as in the spine or ribs. Cavaties between bones in synovial joints are filled with synovial fluid. This fluid helps lubricate and protect the bones and it is the Bursa sacks that contain the synovial fluid and absorb the impact of running on land; but in deep-water running the bursa sac and synovial fluid receive no trauma.
The elimination of weight bearing on the skeleton and joints makes deep-water running the safest exercise for almost all people, especially those with medical problems and it is an ideal method for rehabilitating or conditioning injuries for all walks of life including the athlete, particularly those people with foot, ankle, or knee injuries for whom running on land is contraindicated.
Dr. Wilder continues that the form of running in water is patterned as closely as possible after that used
on land; it is the safest possible exercise for all walks of life including the runner or any athlete whose sport requires running.
Wilder contends that aqua or structured deep-water running is the most biomechanically specific means of conditioning during a
rehabilitation program or when supplementing regular training. Thus, it is ideal as a “preventive medicine” activity as advocated by AquaDios-Med™.
Dr. Wilder believes this has special importance because the effects of deep-water running exercise includes a vast improvement in cardiac and pulmonary performance as well as improvement in those muscle groups being used that undergo enzyme changes, capillary density
changes, as well as other important positive physiological changes.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
65
Compared to land-based running, the elimination of weight bearing and the traumatic impact from each stride together with the addition of the water’s resistance in deep-water running there is change to the relative contribution of each muscle group. Every effort must be made, therefore, to reproduce the running form used on land and to ensure the incorporation of those muscle groups that are used in land-based running; especially the foot flap.
See Picture – Foot Flap>>> Dr. Wilder believes certain guidelines will assist people maintaining
proper form during aqua running. First, the water line is best when right at the shoulder level. Your chin
will be just an inch or so above the water and the bottom of your chin will likely get wet.
For comfortable breathing the mouth must be comfortably above the water without having to tilt the head back. It is best to keep the head looking straight ahead, not down. The body position is best when it is slightly forward of the vertical, with the spine maintained in a neutral position [see pictures].
Arm motion is identical to that used in land running, with primary motion at the shoulder. It is best to keep the hands held half open with fingers together; this will help when your running intensifies to get good chest and upper body exercise. Hip flexion should reach approximately 60 to 80 degrees. As the hip is being flexed, the leg is extended at the knee, from the flexed position. When end hip flexion is reached, the lower leg should be perpendicular to the horizontal. The hip and knee are then extended together, the knee reaching
full extension when the hip is in neutral or “0” degrees of flexion. As the hip is extended, the leg is flexed at the knee. The cycle then repeats itself.
Dorsiflexion and plantarflexion
Dorsiflexion is the movement which decreases the angle between the foot and the leg. Plantarflexion is the movement which increases the angle between the foot and the leg, as when depressing an automobile pedal. The word "Plantar" translates as "toward the sole" or "Planta".
Dorsiflexion and plantarflexion occur throughout the cycle and make up the “foot flap” or ankle foot rotation. Wilder explains that the ankle is in a position of dorsiflexion when the hip is in neutral and the leg is extended at the knee. Plantarflexion is assumed as the hips are extended and the leg flexed. Dorsiflexion is reassumed as the hip is flexed and the leg extended. Underwater viewing has shown us that inversion and eversion will accompany dorsiflexion and plantarflexion, as it does with land-based running. In kinesiology Inversion is the movement of the sole towards the median plane, same as when an ankle is twisted while Eversion is the anatomical term of motion denoting the movement of the sole of the foot away from the median plane. In simple terms water running becomes almost identical to land based running with a little practice and concentration.
People seeking physical fitness as well as those that are sedentary, runners, athletes and non-athletes do not often get the scientific evidence that demonstrates deep-water running results in a sufficient training response in order to positively affect physical fitness and enhance athletic improvement. This has been further documented by studies that have shown maintenance of exercise and performance in even competitive distance runners while training strictly with deep water running for periods up to six weeks long.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
66
This means that deep-water running is scientifically proven to produce positive physical fitness for the sedentary, non-athletes and patients as well as maintain a competitive runner’s athletic performance.
Additionally, running in the water allows the patient or athlete to maintain proper form and technique,
and maintain quick turnover during a period of which they may have had compromise in these factors. This means injured athletes heal faster and will get back to usual training faster with daily safe deep-water running, and of course this applies to physical fitness for the sedentary, non-athletes and patients as well.
Dr. Wilder suggests that while training with deep water running it is best for the athletes to perform
workouts that closely mimic the workouts that they would do on land. If an athlete would normally be running a long distance run, perhaps one hour at a moderate pace on land, then they would perform one hour of running at a moderate pace in the water. If the athlete were doing track intervals, they would then in the water do shorter intervals at a very high intensity and turnover rate with rest periods of easy water jogging in between. Applying this logic to sedentary people or patient’s means they can begin deep-water running and use the Borg Scale of Perceived Exertion to easily determine the exercise pace.
Wilder comments that he oftentimes has athletes measure their heart rates and count their cadence because that is the number of times that they turnover per minute as measures of their exercise intensity as well. This same intensity and variation can be practiced by all people seeking physical fitness as well.
Dr. Wilder points out that properly performed deep-water running is a viable form of cross training for
the athlete who cannot run due to injury or for the person or patient who desires a low impact or no impact form of aerobic exercise; not to mention those millions of sedentary people and patients not exercising at all. Deep-water running has been proven to demonstrate training effects for rehabilitation and fitness by regular programs in deep water running, but this powerful and inexpensive “preventive medicine” activity is not considered by hospital medicine or most doctors for the more than many patients that can benefit from this safe daily exercise.
Biomechanical Comparison • Deep Water and Treadmill Running
John A. Mercer, Ph.D. is Assistant Professor of Biomechanics and Graduate Coordinator at the University of Nevada Las Vegas. In 2005 he authored a study titled “Biomechanical Comparison of Deep Water and Treadmill Running”. Biomechanics uses the principles of mechanics to investigate biological systems. It is a science
that investigates motion and the effects of both internal and external forces that occur during the actions performed by living organisms. Mercer’s presentation of deep water running mechanics has been broken down into the sections of biomechanical significance. Mercer includes work by Robin Horne titled “The Physiology of Deep Water Running as a Training Program - Proposition for Debate”
The Physiology of Deep Water Running as a Training Program
Mercer’s focus is that of a “Sport Medicine” specialist, in this case on running and its related common injuries frequently due to overuse. Mercer notes the prescription of an appropriate training protocol to maintain an injured athlete-s cardiovascular and muscular fitness is a major challenge for the treating clinician. This author would like to apply Mercer’s statement of fact to the common patient on daily prescribed medications. In this context the injured athlete is the common layman who eats, uses alcohol incorrectly and does not exercise. Ironically should the average person see a coach instead of a doctor “preventive medicine” could be put into motion?

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
67
The point here is the cardiovascular and muscular fitness of the person-patient has not become a major challenge for the treating clinician because treatment of choice is daily medications rather than daily exercise.
Doctors have learned prescribing exercise is dangerous because most all patients will injure themselves in the process unless they are directed to a “preventive medicine” program that employs safe daily exercise as is the case with AquaDios-Med™.
For the athlete part of the treatment program often involves reducing or discontinuing exercise-training. This inactivity can result in a significant loss of cardiovascular fitness (Coyle 1984). Research has shown that a six- week break from training can result in a 14-16% decrease in maximal oxygen uptake (VO2max), a significant indicator of aerobic performance (Coyle 1984).
Let’s extrapolate from Coyle’s data from the athlete to the average non-exercising patient or person. First, look at the statistics of inactivity, a “significant loss of cardiovascular fitness” and a “decrease in maximal oxygen uptake” of 15 percent in just 6 weeks. Second, recognize the average patient or person has suffered such cardiac and pulmonary loss to dramatically and negatively impact the immune system. Certainly no medication in the world will ever improve the cardiovascular, pulmonary system or immune system, but daily exercise will; exercise is medicine. Dr. Mercer’s description of the injured athlete treatment program is focused on reducing or discontinuing training, which is the treatment of choice but just the opposite for the average person who is not exercising enough or at all. Mercer’s treatment is to reduce “training” or the exercise of running while the average persons “injury” is to their cardiovascular system and more, from lack of exercise and proper nutrition; but the treatment is the same – deep water running. Ironically the couch potato and the athlete rehabilitate with the same treatment. Mercer points out that injured athletes are required to avoid full weight-bearing activities and often forms of non-weight bearing exercise, such as swimming or cycling, is prescribed to maintain fitness levels. On the other hand, the average person’s doctor does not prescribe or treat the patient with “preventive medicine” or exercise that has no weight bearing even though these people are injured, one by too much exercise, and the other by too little exercise. The injured runner must avoid running and most often all weight bearing exercise. However, Deep
water running (DWR) is running while being suspended in deep water by the use of a floatation device. This essentially weightless environment eliminates the impact with the ground and the reactive traumatic force associated with heel strike and eliminates all “impact” traumas. Thus, DWR is “safe” and the only exercise for the injured athlete as well as the average patient on daily medications. DWR is also the safest exercise for the general population including pregnant women, children, the average “hospital patient and includes geriatricians. Mercer’s research shows that DWR has gained popularity in the rehabilitation of injured runners as it is seen to have high specificity by simulating
the same muscle groups in a similar movement pattern to running on land (Hamer and Morton 1990). However, hospitals and private doctors still don’t recognize “preventive medicine” such as the programs of AquaDios-Med™ which specifies daily safe deep-water running for all people, including most all “medical patients” and the athlete.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
68
Mercer points out that the research to support the theory that DWR can heal injured runners has often been of poor experimental design with low subject numbers and of course he does not mention DWR as a treatment of choice for most all infirmities, illness or disease as is recommended in AquaDios-Med™. Mercer’s research will only examine the available literature in an attempt to evaluate the efficacy of DWR as an alternative to running on land. He does not examine the safest and therefore the only exercise for the general populations like the sedentary, injured, diseased or well.
Mercer examines parameters such as frequency, intensity and duration of exercise – training with regard to their effect on maintaining cardiovascular fitness and strength. There is little to no research on frequency, intensity and duration of exercise – training with regard to DWR effect on cardiovascular patients other than some reports by this author McWaters.
Aerobic Performance • DWR Mercer points to the obvious difference between the “average” patient and the injured athlete and that is that following injury most athletes are concerned regarding their loss of aerobic fitness during the recovery process. The average patient has no aerobic fitness or awareness of how this healthy process works – through exercise; because the average person-patient does not exercise. Mercer posits that “If” DRW is to be prescribed as an alternative to land running it is important to examine the effect of this exercise on maintaining or improving aerobic ability. Here, of course is where American Research is crippled by the healthcare crisis; there is no research on “general patients” health after 90 days of DWR. Mercer notes the Hamer and Morton (1990) study that examined DRW with regard to aerobic, anaerobic and muscular parameters where twenty untrained subjects were randomly allocated into a DWR and a control group. The DRW group underwent an eight-week interval- training program with 20-45 minutes per
session three times per week. Aerobic performance parameters measured were maximum oxygen [O2] consumption or (VO2max), maximal oxygen pulse (O2 pulse max), maximal ventilation (VE max) and sub-maximal and maximum heart rate (HR max). These twenty untrained subjects were measured on an incremental treadmill test to volitional exhaustion. Muscular endurance was examined by measuring knee flexor and extensor torque output on a Cybex II. A graded exercise test was performed by the DWR group to determine VO2max and the relationship between HR and oxygen consumption during running in water. Training was performed three times per week and target HR's increased from 60% (wks. 1-2) to 70% (wks. 3-6) to 80%VO2max (wk. 6-8).
This means that untrained subjects or “non-athletes” like the sedentary person or average patient, participated in DWR sessions of 20 to 45 minutes three times a week for eight weeks and their maximum heart rate and oxygen consumption improved dramatically; and this health statistic is based on relatively mild exercise only 3 days a week! Mercer emphasizes that the scientific data shows significant increases in VO2max and O2 pulse occurred in the DWR group that were not found in the treadmill control group. Significant decreases occurred in HR max of the DWR group compared to the treadmill control;

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
69
This is a good thing because a lower heart rate protects the heart while increased maximal oxygen means there is more oxygen to make the body and its immune system healthier and stronger. The DWR group also demonstrated a 13% increase in anaerobic peak power, anaerobic mean power and anaerobic total work. This means DWR increased endurance, power and strength of twenty untrained subjects. Mercer notes that most other studies and research found lower heart rates (6-12b/min) at VO2max and O2 pulse max measured while DWR compared with treadmill running. Thus, DWR produces a lower rate with improve cardiac output. Hamer and Morton (1990) concluded that the six-week training protocol used demonstrated DWR to effectively increase both aerobic and anaerobic fitness. This is a good thing and is the reason “why” cardiovascular infirmities can be cured or eliminated with very hospital medicine with its care of prescribed medications. Physiological responses when exercising to maximal aerobic capacity was compared between twenty male subjects while DWR and Treadmill Running (Nakanishi et al 1999).
Oxygen consumption (VO2), ventilation, respiratory quotient (RQ), HR, rate of perceived exertion (RPE) and blood lactate were measured. Responses to DWR compared with TR indicated significantly lower VO2max (2.68 vs. 3.4 ml/kg/min), HR max (171 vs.190 b/min) maximal minute ventilation and peak blood lactate levels. It was suggested that the hydrostatic effects of immersion in water and altered muscle recruitment patterns of DWR attributed to the lower VO2max and HR max values compared with TMR; but Dr. Becker has shown that deep-water running benefits from the venous blood returning with greater ease because of the immersion to the neck. These healthy responses were found to be similar in young and middle aged subjects. In a similar study, maximal physiologic responses were compared between DWR and TMR using 24 subjects (Butts et al 1991). Again, VO2max and HR max were found to be significantly lower with DRW, with similar responses found in both sexes. The observation was made that these differences were similar in magnitude to those found between TMR and cycling ergometry. It was recommended that DWR should be considered a useful training technique. Again caution was advised in using land based HR's to determine training intensity for a DWR program because DWR heart rates are 1bout 15 beats per minute slower. Davidson (2000) examined the ability of deep water running training to improve cardiovascular fitness in a young sedatory population. Ten untrained female subjects were allocated into a DRW and road running (RR) group. They each underwent a four- week training program consisting of progressive aerobic interval training, three days a week. A ten-week detraining program followed this training. A four-week training program in the alternate exercise was then completed. Subjects underwent pre-test VO2max testing which was repeated after each training program. Results indicated both methods produced a significant increase in VO2max compared with the pre-test without a significant difference between the two. The finding that a DWR regime may be equally as effective as road running in improving cardiovascular fitness in an untrained population has important clinical implications. Specifically for those with musculoskeletal disorders that may exclude the possibility of RR, it is important to be able to prescribe exercise in a non-impact environment, which produces similar physiological effects. Thus, DWR such as prescribed by AquaDios-Med™ is at least as effective as land running, with one huge difference; it is safe.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
70
Mercer suggests that during a long rehabilitation phase it may be useful to compare current aerobic fitness with pre-injury levels. A sub-maximal DWR test could be used if it was able to provide a valid VO2max estimate. Decisions regarding training intensity based on comparisons between the water and land tests could then be safely made. In order to develop a DWR field test for estimating VO2max a study was performed by Sherman and Mitchaud (1997). A maximal treadmill test was used to determine VO2max in thirty subjects. A 15-minute sub-maximal DWR test was then performed at a self-selected cadence. A regression model using cadence, PPE, body weight and gender was developed which was found to accurately predict VO2max. Therefore, based on the results of this study, and using a similar young healthy population, the model developed could be used to accurately determine VO2max during a rehabilitation phase. Adjustments to the intensity of the athlete's current training regime could be made accordingly. Mercer’s idea accommodates a “preventive medicine” model that can be and must be used by hospital medicine and doctors to influence them to prescribe safe exercise as is practiced by the programs in AquaDios-Med™.
Frequency and Intensity of Exercise
Mercer states that intensity of training is an important parameter in exercise prescription. Commonly target HR ranges are used as an indicator of intensity in road running (RR). The relationship therefore between the parameters of HR, cardiac output (Q) and stroke volume (SV) while DWR and RR need to be examined if accurate prescription of intensity of exercise in water is to be achieved. And, this accurate “exercise prescription” can easily become the “preventive medicine” model for the average person or patient. Mercer cites the McClung et al (1998) study performed on five endurance athletes to examine cardiac output [Q] and stroke volume [SV] at a similar heart rate [HR] and oxygen consumption [VO2] when DWR and treadmill running (TMR). Results indicated cardiac output Q and stroke volume SV to be significantly higher in TMR as compared to DWR respectively. It was concluded that while heart rate HR was lower while deep-water running DWR compared with tread mill running TMR other physiologic parameters must be examined in order to prescribe intensity. However, it is a scientific fact that heart rate is always lower with deep-water running and land or treadmill heart rate is always higher by 10 to 18 beats per minute so that DWR heart rate and tread mill running heart rate will be acknowledged as different with land running a higher rate and therefore more dangerous than deep-water running DWR. Mercer cites Eyestone et al (1993) who compared the effectiveness of DWR, cycling and running in maintaining VO2max and 2 mile run performance using a six-week training protocol. Thirty-two trained athletes underwent a 4-week pre-training course of 30 minutes running three days per week. VO2max and 2-mile run performance was measured after the pre-training and post intervention.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
71
Maximum Volume of Oxygen or VO2 max criteria was expiratory ratio, the oxygen carbon dioxide ratio per breath, plateau of VO2 and achievement of heart rate HR max. Following the two-mile run subjects were stratified into low, medium and high performance levels and randomly allocated into a cycling, DWR or LR group and trained for six weeks. Training frequency was 3x/week (wk. 1), 4x/week (wks. 2-5) and 5x/week (wk. 6). Length of training was increased from 20mins to 30mins and the intensity from 70% to 80% HR max. All groups showed a slight decrease in 2-mile run times though this was statistically insignificant. A slight decrease in VO2max also occurred in all groups with insignificant differences between groups. Mercer indicates that this study shows that an injured runner who adopted a DWR or cycling protocol at an intensity, duration and frequency similar to pre-injury could maintain the near normal acquired athletic VO2max and 2-mile run times over a six-week period. This means that “while injured” anyone can increase physical fitness while an athlete can maintain the acquired plateau of fitness prior to injury. Therefore, structured deep-water running as prescribed by AquaDios-Med™ is indeed a viable, safe preventive medicine for the non-athlete, the sedentary or the patient. While this study maintained frequency and duration of training other research found that if training intensity was maintained frequency could be reduced by 67% for up to 15 weeks with no loss of performance (Hickson et al 1995). Thus, greater intensity of exercise for the athlete will produce sufficient improvement that fewer training days are necessary to retain fitness. This correlates to the sedentary and patient populations suggesting that once they are free of medications and have become physically fit they can enjoy “more intense” exercise with fewer exercise days to maintain their new health standard.
Rate of Perceived Exertion – Borg Often while exercising athletes will estimate their intensity by using perceived exertion rather
than a HR. A scale that correlates rate of perceived exertion (RPE) and HR has been developed. Borg in 1982 demonstrated a strong linear relationship between RPE and HR with incremental exercise intensity. Hamer and Slocombe (1997) examined the relationship between heart rate HR and rate of perceived exertion RPE for deep-water running DWR and treadmill running TMR. Twelve subjects were used and performed six sub-maximal incremental work intensities running on the treadmill and in water. At each incremental exercise level the subject provided a RPE between 3 (very, very light) and 9 (very, very hard) to reflect total body fatigue. This scale was
developed to correspond approximately to HR's ranging from 60 to 200 beats/min.
Results indicated that running in water with an RPE the same as on the treadmill produced a HR which was on average 17 beats/min lower. This is due to increased cardiac output by an increased stroke volume produced by shunting of blood from the periphery. This occurred due to the hydrostatic pressure of the water properties increasing venous return and in turn stroke volume. Therefore, at similar sub-maximal exercise levels HR's were lower in the water due to an increase in cardiac output.
This means that the heart works smarter rather than harder when the body is immersed in water up to the neck. The “pressure” of the water increases “return” of venous blood which increases “output”. This research data verifies one reason why DWR is the safest exercise for all people, including average, out of shape people and those with health problems.
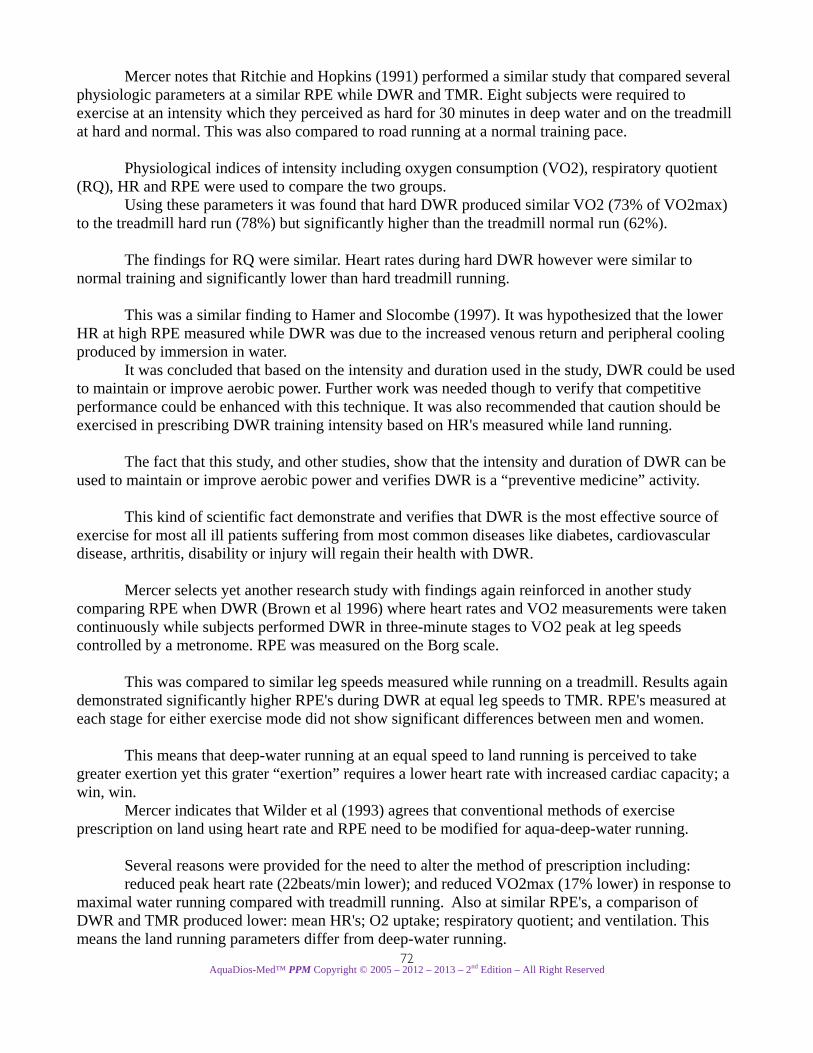
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
72
Mercer notes that Ritchie and Hopkins (1991) performed a similar study that compared several physiologic parameters at a similar RPE while DWR and TMR. Eight subjects were required to exercise at an intensity which they perceived as hard for 30 minutes in deep water and on the treadmill at hard and normal. This was also compared to road running at a normal training pace. Physiological indices of intensity including oxygen consumption (VO2), respiratory quotient (RQ), HR and RPE were used to compare the two groups. Using these parameters it was found that hard DWR produced similar VO2 (73% of VO2max) to the treadmill hard run (78%) but significantly higher than the treadmill normal run (62%). The findings for RQ were similar. Heart rates during hard DWR however were similar to normal training and significantly lower than hard treadmill running. This was a similar finding to Hamer and Slocombe (1997). It was hypothesized that the lower HR at high RPE measured while DWR was due to the increased venous return and peripheral cooling produced by immersion in water. It was concluded that based on the intensity and duration used in the study, DWR could be used to maintain or improve aerobic power. Further work was needed though to verify that competitive performance could be enhanced with this technique. It was also recommended that caution should be exercised in prescribing DWR training intensity based on HR's measured while land running. The fact that this study, and other studies, show that the intensity and duration of DWR can be used to maintain or improve aerobic power and verifies DWR is a “preventive medicine” activity. This kind of scientific fact demonstrate and verifies that DWR is the most effective source of exercise for most all ill patients suffering from most common diseases like diabetes, cardiovascular disease, arthritis, disability or injury will regain their health with DWR. Mercer selects yet another research study with findings again reinforced in another study comparing RPE when DWR (Brown et al 1996) where heart rates and VO2 measurements were taken continuously while subjects performed DWR in three-minute stages to VO2 peak at leg speeds controlled by a metronome. RPE was measured on the Borg scale. This was compared to similar leg speeds measured while running on a treadmill. Results again demonstrated significantly higher RPE's during DWR at equal leg speeds to TMR. RPE's measured at each stage for either exercise mode did not show significant differences between men and women. This means that deep-water running at an equal speed to land running is perceived to take greater exertion yet this grater “exertion” requires a lower heart rate with increased cardiac capacity; a win, win. Mercer indicates that Wilder et al (1993) agrees that conventional methods of exercise prescription on land using heart rate and RPE need to be modified for aqua-deep-water running. Several reasons were provided for the need to alter the method of prescription including:
reduced peak heart rate (22beats/min lower); and reduced VO2max (17% lower) in response to maximal water running compared with treadmill running. Also at similar RPE's, a comparison of DWR and TMR produced lower: mean HR's; O2 uptake; respiratory quotient; and ventilation. This means the land running parameters differ from deep-water running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
73
Mercer reports on a study performed to investigate if a correlation existed between cadence and heart rate (Wilder et al 1993). It was assumed that as HR and O2 uptake are linearly related and that to produce a training effect an exercise level between 55% and 90% of HR max was desirable. Twenty subjects underwent an exercise test that matched running rhythm in the deep water to a cadence set by a metronome. Twelve incremental cadences were used and heart rates at each increment taken. It was demonstrated that a high correlation existed between cadence and heart rate. The conclusion drawn was that cadence could be used as a standard measure for exercise prescription for deep water running.
Age and Gender Physiologic Variations
Mercer refers to research by Brown et al (1997) who investigated the physiological responses to DWR and TMR between males and females. Twenty-four subjects (12 males and 12 females) performed tethered DWR at incremental leg speeds matched to metronome cadences. VO2 peak was recorded when the subject could no longer match the cadence. Subjects then performed a treadmill running test with cadences matched to the DWR test. When the
final DWR cadence was reached the treadmill grade was incrementally increased 5% every two minutes until VO2max was reached. Significant gender differences averaged across all DWR measurement standards occurred, but these variations were not found for HR, VO2 ml/kg/LBW/min or respiratory exchange ratio (RER) which is a measurement of one breathe. Normally in one
breathe we breathe in more molecules of oxygen than we breathe out molecules of carbon dioxide. The ratio between these CO2 and %O2 is the RER. Gender differences for TMR were not found. TMR compared with DWR showed significant difference for HR, VE, VO2 ml/kg/min, VO2 ml/kg/LBW/min and RER. This appeared consistent with the other studies comparing the two exercise mediums. Mercer concludes that these results would indicate that when DRW is matched to TMR by stride cadence the positive physiological responses during DWR are significantly greater for health and fitness. Women appear to respond with less physiologic stress to DWR compared with males though are similar during TMR. Thus, Dr. Mercer concludes that women will benefit the most form DWR and this is significant according to a new research study.
Exercise Protects Girls From Future Breast Cancer On May 13, 2008, Lauran Neergaard wrote an article for the Associated Press titled “Exercise May Protect Girls From Future Breast Cancer”. Neergaard begins by emphatically stating get your daughters off the couch because new research shows exercise during the teen years, starting as young as age 12, can help protect girls from breast cancer when they're grown. Middle-aged women have long been advised to get active to
lower their risk of breast cancer after menopause, but what this new research shows is that starting regular exercise as young as 12 and younger helps to prevent breast cancer in later years.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
74
Dr. Graham Colditz of Washington University School of Medicine in St. Louis, the study's lead author, states “this research really points to the health benefits of sustained physical activity from adolescence through the adult years, to get the maximum benefit". Dr. Colditz statement is consistent with the treatment practice of AquaDios-Med™ and helps to verify the AquaDios-Med™ program as a powerful preventive medicine. Neergaard reports the researchers tracked nearly 65,000 nurses’ ages 24 to 42 that enrolled in a major health study. They answered detailed questionnaires about their physical activity, dating back to age 12. Within six years of enrolling, 550 were diagnosed with breast cancer before menopause. A quarter of all breast cancer is diagnosed at the younger ages, when it's typically more aggressive. Researchers report in the Journal of the National Cancer Institute that the research shows women who were physically active as teens and young adults were 23 percent less likely to develop premenopausal breast cancer than women who grew up sedentary. And this fact also verifies the AquaDios-Med™ treatment of safe daily exercise. Dr. Colditz indicates this “exercise” group is not the extreme athlete because the biggest positive health impact group is those with regular exercise from ages 12
to 22, and not athletes in training. These women at lowest risk reported doing only 3 hours and 15 minutes of running or other vigorous activity a week and for the less athletic, 13 hours a week of walking was reported. Typically, the teens reported more strenuous exercise while during adulthood, walking was most common. Will this moderate exercise help prevent breast cancer? A big point of exercise in middle age and beyond is to keep off the pounds. After menopause, fat tissue is a chief source of estrogen. In youth, however, the theory is that physical activity itself lowers
estrogen levels. This conclusion is based on studies of teen athletes that shows very intense exercise can delay onset of menstrual cycles and cause irregular periods. Dr. Alpa Patel, a cancer prevention specialist at the American Cancer Society praised the new research while he also believes the moderate exercise reported in this study was nowhere near enough for those big positive health changes. But, it probably was enough to cause slight yet still helpful hormone changes, and apparently enough to prevent breast cancer.
This research and its conclusion that moderate exercise prevents breast cancer supports the AquaDios-Med™ premise that exercise is medicine; and that safe daily intense exercise for the greater part of the American life will end the healthcare crisis. When hospital medicine and doctors look to preventive medicine programs like AquaDios-Med™ it is predicted the healthcare crisis will begin to decline rapidly and eventually stopped. Dr. Colditz added that while the study examined only premenopausal breast cancer, it’s highly probable that the protection from youthful exercise will condition the body’s health system to positively affect more common postmenopausal breast cancer. And Dr. Patel indicates that if you were a female bookworm as a teen, it's not too late, start exercising today. Other research on the middle-age benefits of exercise shows mom should join her daughters for that bike ride or game of tennis or at least a daily walk around the block to help prevent breast cancer. To help defeat breast cancer a woman can certainly participate in safe daily exercise and encourage her daughters to do the same.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
75
Dr. Patel stressed that even though the exercise benefit is modest, physical activity and body weight are risk factors that women can control. She indicated mothers and daughter must be getting off the couch to protect their health because women who engage in physical activity not only during adolescence but during adulthood lower their risk of breast cancer. Getting back to Dr. Mercer, his study recognizes the Brown et al (1998) research which also explored physiological parameters in older adults while DWR. The relationship between HR as a percentage of HR peak and VO2 as a percentage of VO2 peak were examined in twenty-three healthy older adults aged 50 to 70 years. The protocol involved DRW at three-minute incremental stages at leg speeds matched to a cadence. Oxygen uptake and HR were monitored continuously during the task until VO2 peak was reached. Using linear regression the relationship between %VO2 peak and %HR peak was found to be significantly different. Similar differences were also found between males and females and would appear to support the gender differences revealed in the previous study by Brown et al (1997). And that is that women adapt to deep-water running easier and show more positive physiological changes than do men.
Deep-water running Injured Runners Rehab
Dr. Mercer concludes that Deep water running has become an extensively used training option for the rehabilitation of runners. And, this author agrees with Dr. Mercer, but points to the travesty caused by modern hospital medicine and doctors because they do not recognize AquaDios-Med™ as the primary treatment of choice for a minimum of 90 days prior to considering treatments of medications or surgery. Dr. Mercer presumes the research presented would suggest that a water-based running programme could be confidently implemented in the short or long term as a substitution for land running. This verifies that AquaDios-Med™ safe daily exercise is ideal for patient populations. Mercer determines that DWR satisfies the principles of specificity of training for running as effective maintenance and improvement of both aerobic and anaerobic fitness have been demonstrated. This confirms that AquaDios-Med™ safe daily exercise is ideal for patient populations. Mercer determines the research verifies that submaximal DWR tests can be used to accurately determine current fitness levels. Target HR's should be set on average 17 b/min. lower to account for the effect of the water. If land RPE scores are used to set intensity, expect HR's to be lower compared to land running. It is suggested the athlete use a similar training frequency and intensity to pre-injury to maintain fitness though there is the indication that frequency may be reduced if the intensity is maintained. Thus, Dr. Mercer confirms the DWR research clarifies that heart rate is lower during intense DWR, on average 17 beats less per minute making it ideal for most patient populations.
Mercer research Supports “preventive medicine” Even though most of research was performed on “athletes”, the preponderance being “runners” it is very clear these are “people” who exercise regularly, some too often suffering “over-use” injuries. The practical applications of preventive medicine utilized by the methods and process of AquaDios-Med™ rely on these studies to prove the “safest” physical exercise activity is deep-water running and it produces the best results. The “while injured” aspect of the “runner” or “athlete” can be compared to the typical sedentary or out of shape average person or the patient who has abused their body by under use and overeating, especially the wrong food high in cholesterol.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
76
One main objective of “preventive medicine” programs like AquaDios-Med™ is to treat those patients suffering diseases that are caused by physical inactivity, incorrect eating habits, stress, anxiety, alcohol, prescribed medications, and recreational drugs; this includes those injured or disabled. The research Mercer reports on is significant to “preventive medicine” and must be expanded to “actual” hospital patients and “outpatients” with common medical problems. When this is done the healthcare crisis will begin to be reversed. That is, when the healthcare system insists safe daily exercise such as AquaDios-Med™ is the treatment of “first” choice. And, will continue for at least 90 days before dangerous drugs, surgery and hospitalization are considered; at best no higher than “second” choice of treatment.
Pre-Habilitation • Rehabilitation • Preventive Medicine
Stew Smith is a graduate of the U.S. Naval Academy, a former Navy SEAL, and author of several fitness and self-defense books. Smith wrote an article he titled “Prehabilitation” a term defined by the National Institute of Health where doctors use pre-hab to prepare a patient for the inactivity associated with post-surgical procedures. The addition of functional exercises prior to surgery will help a patient rebound more quickly. Generally speaking, a pre-hab program consists of warming-up, stretching to full range of motion, a cardiovascular component like walking, swimming or deep-water running with a resistance training component mixed with functional tasks. Smith indicates many physical therapists and athletic trainers are using pre-hab as part of a daily program to help prevent nagging injuries as well as the larger ones that require surgery. To be specific, a pre-hab program to prevent injuries focuses on a person's body imbalances. Most imbalances occur in the following regions of the body.
Abdominal region / lower back
Many people work their stomach muscles but neglect their lower back causing an imbalance that can lead to injury in both sports and daily life. In deep-water running the stomach muscles and lower back is work simultaneously, this is why DWR is so effective at relieving back pain. Prehabilitation or preventive medicine can be accomplished with safe daily deep-water running so long as the proper – correct up right vertical position is achieved. DWR exercises help strengthen the upper back and deltoids especially when the stride cadence is above 86 strides per minute with an RPE of about 8.
Chest and Upper back / Rear Shoulder
Many young athletes try to bench press a truck but neglect their upper back and rear deltoids, which can lead to shoulder injuries and a sloping of the upper back. Deep-water running in the proper – correct up right vertical position exercises the upper back and deltoids especially when the stride cadence is above 86 strides per minute with an RPE of about 8.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
77
Thighs and Hamstrings
Smith believes a very delicate combination of exercises is needed for the hamstrings or the back of the legs (hamstrings) so they do not get under worked. A hamstring injury usually occurs when running sprints or jumping. Usually the upper side of the hamstring receives the injury so a smart stretching plan that incorporates the top and bottom of the hamstring connections is critical. However, Smith forgets that deep-water running activates the hamstring muscles with each and every stride. Thus, correct deep-water running posture with intense Swedish Fartlek sessions included in each workout is highly recommended as are many Yoga poses. There are many other natural imbalances in the body. Basically, for any movement your body makes there are two or more groups of muscles or joints that are stretching (or flexing) to make (or oppose) that motion. Injuries occur all the time but can be easily avoided by training smarter - not necessarily harder! Thus, rely on safe daily exercise with AquaDios-Med™.
What is Prehab?
Kenneth L. Johnson a Team 2002 Sports Therapist wrote an article for the Therapist Specialist of Sports Injury prevention, Management, Evaluation and Prehabilitation. Johnson states that Prehab is a personalized exercise program that continually evolves. It provides sports specific focused exercises and activities for athlete's needs. The philosophy is simple. Prevent injuries. The development and execution of an effective program can be complex. The practice of prehab and its success relies greatly on an athlete's ability to commit to prevention. The development of the program needs to be progressive and periodically re-evaluated to change with the athlete's needs. Johnson’s prehab is very similar to the concept of “preventive medicine”. Generally speaking, preventive medicine is the part of medicine engaged with preventing disease rather than curing it. It can be contrasted not only with curative medicine, but also with public health methods (which work at the level of population health rather than individual health). In the United States, preventive medicine is a medical specialty, one of the 24 recognized by the American Board of Medical Specialties (ABMS). It encompasses three areas of specialization, General preventive medicine and public health, Aerospace medicine, Occupational medicine. However, this book hopes for the reader to recognize “preventive medicine” as it is meant in the AquaDios-Med™ format. The position AquaDios-Med™ has taken regarding “preventive medicine” is that the process of Mind Body Medicine combined with safe daily exercise, such as deep-water running advocated by the AquaDios-Med™ treatments can prevent many common diseases and prevent injuries as well as cause remission or substantial management of the related symptoms and may in some cases cause a cure; the outcome is said to be dependent on the patient. AquaDios-Med™ is said to be both a public health method, which works at the level of population health and is directly related to individual health. By this, the author of this book, and the inventor of AquaDios-Med™, means to say that “individual health” and “population health” can be improved by 75 percent or more over the current healthcare crisis in America.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
78
This dramatic health improvement can be accomplished by the “nationalizing” of AquaDios-Med™ as a health center available to everyone within a population of 350,000. This of course will require the current hospital medicine practices to relinquish medications and surgeries as “primary treatment of choice” and make the treatment of AquaDios-Med™ and its “preventive medicine” practices the “primary treatment of choice” in at least 80 percent of all medical cases. Health Insurance Management companies must of course reimburse for the common methods of “preventive medicine” and even give major discounts to those who become physically fit and free of the need for any daily prescribed medications.
Who Should Prehab?
Johnson’s considers only athletes but no non-athletes when he mentions all levels of athletes as those who should include a prehab program in their training. He comments that the more advanced the athlete, the greater the need for a prehab program. On the other hand, and at the other end of the continuum is the non-athlete or patient who’s dependent on daily medications; this population of people need “prehab” more than a trained athlete. Johnson suggests that as an athlete's body matures within a sport, their body adapts to the physical demands of training. But too often repetitive movements and the daily stresses of life as well as stresses of training cause negative effects within the athlete’s bodies. This impact of stressors and limited training technique often cause tightness of muscle groups, imbalances of strength, coordination or muscle stabilization.
These imbalances occur naturally with physical activity and are reinforced with each workout. These imbalances are often the root of many training injuries and may predispose athletes to greater risk of injury during training and competition; Johnson has hit the nail on the head because all of these athlete issues can be managed very effectively with the safe daily deep-water running practices of AquaDios-Med™. Thus, prehab is AquaDios-Med™.
Johnson makes a good point that includes all people and that is that the stressors of life can have a negative influence on people. The athlete or recreationist has physical activity as a means to relieve life stressors, but the non-active couch potato has no way out of the stress and this is often the person on multiple medicines. Obviously too much exercise in not good, but 45 minutes a day of safe daily exercise as recommended by AquaDios-Med™ is not too much.
How to Prehab
Johnson advocates a personalized Prehab program must address total body balance and consider sports specific needs for the athlete, but this is not required for the non-athlete or patient dependent on medications. Johnson contends a Prehab program balances the range of motion, strength, coordination and stabilization. Comparing left to right, front to back, and upper to lower body is the basic premise. Exercises and sports specific skills and drills are focused on an athlete's weaknesses. The majority of prehab programs should focus on coordination and stabilization of the hips, stomach and back "core". Core instability is common and is often due to the lack of a proper training program. Many athletes and coaches use traditional protocols of upper and lower body lifting or basic sprinting and lifting routines, outside of regular practice drills. This leaves the core without a direct focus or training routine. This author believes variations of intense deep-water running will assist the athlete as well as the non-athlete and patient taking daily medication.
Exercise is a weapon against Disease
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
79
Continual Progress
Johnson recommends a Prehab program should be constantly updated to match the athlete's progress. Activities in a prehab routine can be a subtle focused exercise or a complex sequence of movements designed for dynamic stabilization or to improve an athlete's skill. Adding dimensions of skill, 1 on 1 competition or scoring values can stimulate an athlete's focus and improve the success of a program. Using tools from traditional sports and physical therapy programs can add options. Tools like a foam roll, balance boards, weighted and exercise balls can also make a program unlimited in design. Once again, this author contends that the athlete will benefit from regular deep-water exercise and other aquatic exercises following intense workouts and the non-athlete or patient dependent on daily medications needs only to master a 45 to 50 minute a day safe daily deep-water running.
When to Prehab Prehab by definition is physical exercise before an injury and designed to prevent injury. Unfortunately, it often takes an athlete and staff many injuries to decide to initiate a prehab program. Depending on an athlete's training cycle, prehab can be done within a practice session, such as deep-water running or deep-water running as an independent workout. Certainly Yoga is an excellent “Prehab or preventive medicine approach but it often takes the time of a full workout. Johnson suggests including three or four different mild exercises in a warm up or cool down or a few different mild exercises while resting or waiting a turn in practice, or a detailed tedious workout focusing on an athlete's weaknesses. Full workouts can be designed for off days or active rest days. Mini prehab workouts are great for team travel and recovery days. In any case, a prehab program should be a regular part of an athlete's training routine. Likewise, a prehab program or “preventive medicine” program must be a daily activity, preferably 50 minutes of deep-water running.
Where to Get Help with Prehab Program Design Johnson recommends that athletes need be screened for imbalances. Objective measurements of active range of motion and strength, biomechanical observations, past medical history, present health status and input from support staff should all be considered when designing a program. Such screenings can be performed by professionals like an Athletic Trainer, Athletic Therapist, Sports Therapist or a Physical Therapist with additional sports training. The non-athlete or patient dependent on daily medications will not need to see so many specialists to start a safe daily deep-water running program, you can begin AquaDios-Med™ programs on your own but it recommended you have someone to assist you in your initial learning.
Research Deep-Water Running – Rehab and Prehab Elizabeth Quinn is an exercise physiologist - fitness consultant who has been writing and
editing sports medicine and health information content while working with athletes for over a decade. Quinn says that Sports medicine has a reputation of being reserved for professional athletes, but anyone who is active can benefit from understanding the basics of sports medicine. She recently wrote an article titled “Deep Water Running: When your training should land you in deep water“. Quinn says that at its simplest deep-water running (DWR), or 'Aquajogging', mimics its land-based equivalent, except that it is performed in water deep enough to prevent your feet from making contact with the bottom of the pool. In recent years this deep-water running technique has become more utilized and increasingly popular with coaches and practitioners from a variety of sporting disciplines.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
80
Deep-water running is both a rehabilitative method that allows participants to avoid the negative effects of detraining, and it can also be used as an adjunct to normal training, reducing the risk of injury because of the much more 'forgiving' environment that water provides. Despite its current popularity with coaches and athletes, DWR is still not understood and incorrectly used by many while it is not accepted by hospital medicine, doctors and insurance companies. Quinn describes Basic DWR technique as similar to a natural running motion. You have to reach out with your leading stride leg and pull through the water strongly and evenly to end the stride. The correct deep-water running stride is for the front foot to 'land' where the metaphorical “impact” would take place on land or begin its stride in front of the body's centre with a reduced hip flexion and keeping knees slightly lower than in ‘normal' running. The trailing leg should be actively pulled forward because of the increased resistance of the water and actively flexed at ‘take off' [see picture of Steve Scott].
Quinn does not mention that one if the major difficulties in learning correct deep-water running mechanics is that the feet and the rest of the body has no impact from “land” to tell the brain a foot strike has begun nor is there any “land” for the foot to “push” you forward. This complete lack of impact
trauma has powerful healing properties for the body and is similar to running in air.
But confounded by the fact the more muscle power you use to run faster in the water the greater is the water’s isokinetic resistance, another healing and endurance factor.
Deep-water running mechanics involve using mental imaging to envision where your specific foot strike would be on land as well as to visualize where the land would be for your foot that is land based to drive you forward. This visualizing is based on your life time of the strike force impact of every step or running stride you’ve ever taken in your life and this means your brain knows exactly where your foot stride and forward driving foot force would be on land. However, the resistance of the water is completely “new” to the natural stride cadence on land and you must learn to appreciate these two healing properties of your water immersion buoyancy. On April 1, 2008 Ross Tucker and Jonathan Dugas wrote an article for The Science of Sport
titled “Running technique: The Footstrike Heel vs. Midfoot vs. Forefoot: How do elite runners land?” Tucker and Dugas suggest that for the athlete, the landing of the foot during road running involves focusing on only one of many aspects and particularly, whether the elite runner tends to land on the heel, the midfoot, or the forefoot. This is a less important issue for the non-athlete or patient only because they will have less “unlearning” to do as the athlete has spent much more time running. The overwhelming
majority of coaches and experts were advocating that heel-striking was the most effective technique, simply because most athletes did it.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
81
Tucker and Dugas concluded the vast majority (75%) of the elite runners land on the heel and about 1 in four (24%) runners landed on the mid-foot, while only 4 out of 283 runners landed on the forefoot. For deep-water running this author recommends the “heel landing” method because it will automatically generate the correct and natural biomechanics of the foot-ankle rotation found in walking and running. Also, the “heel landing” gives the deep-water runner an easier visualization to envision the location of the “missing impact” of the heel landing. Visual imagery of the heel of the foot reaching forward, just before the “heel strike”, is included and makes adapting to deep-water running easier to learn. Remember that you are deep-water running, not swimming, it is best for the palms of the hands to be half closed and turned inward, so there is a partial cupping of the water as your arm goes move back toward your body to complete the arm related running motion. As well as helping to maintain nearly correct land running mechanics, this will also increase upper body work with each stride. In addition to these purely mechanical issues, Quinn recommends the deep water runner needs to learn how best to apply muscle power throughout the range of stride cadence motion. She indicates bobbing and moving backwards in the water are two obvious markers of improper stride application. She states that bobbing occurs if the application of power is mostly vertical and or performed only with the driving leg, while backward movement is a sign that power is being applied only during the recovery phase, with little applied to the driving leg. This means the full arm and leg stride motion must have sufficient and equal power to slowly move the runner forward through the water. Quinn says that initially, the resistive properties of the water may, at first hinder deep-water running mechanics and that all beginners will need a lot of feedback about correct running posture and form. But is this any different from learning any new complex skill? With practice, there should eventually be little difference between your land and water technique.
Flotation Devices • Tethers
Quinn relies on two kinds of flotation devices with her athletes - 'belts' and 'lifejackets'. Both of these are designed to suspend the deep water runner in a vertical, head-above-water position and both have their pros and cons. The AquaJogger buoyancy belt is convenient and easy to wear, but is less
effective for larger, heavier performers because of its constant buoyancy factor. The picture shows a Deep-water runner wearing the AquaJogger with Aqua-shoes and Aqau-dumbells to increase the intensity of the workout. Quinn prefers the buoyancy belt over the lifejacket, which tends to fit badly and restrict arm movement. This author believes only the AquaJogger type buoyancy belt or Wet Vest should be used because a “lifejacket” is designed to keep you afloat in an emergency and not designed for the correct posture of deep-water running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
82
The great advantage of the flotation devices is that they enable performers to perfect their running style and control the intensity of the activity; but they do need to be worn tightly, which some people feel restricts their breathing.
Quinn indicates that some athletes perform DWR without a flotation device (known as free DWR), although in this situation just staying afloat becomes the primary concern. Also, it takes much more strength and strength endurance to deal with the increased amount of stress placed on the core and legs to keep the body stable and upright. These difficulties can, of course, provide further training stimulus for the athlete. However, I would always advocate that athletes become fully proficient with flotation-assisted DWR before attempting a 'free' session. This author always recommends deep-water running be done only with a Wet Vest or AquaJogger type buoyancy belt as both are specifically designed for deep-water running and because water running form is critical to accomplish the true benefits of sustained DWR. Quinn reminds us that another piece of useful equipment is a tether, which can be attached to the flotation device (or the runner) to anchor them to the pool side. This provides increased resistance, helps the athlete to maintain a near-vertical posture, allows for monitoring of the activity by a coach or trainer and maximizes space in the pool. However, in Quinn’s experience, athletes do not like this 'hamster' approach and prefer to have the freedom of the pool. Research to date suggests that DWR provides suitable training for maintaining aerobic performance when used as a substitute for normal land-based running. In one study competitive runners were reported to have maintained both their VO2max [maximum oxygen] and their 5k run time following four weeks of DWR training. Another research team found VO2max [maximum intake of oxygen] and ventilatory threshold responses unchanged following a six week DWR programme.
Ventilatory Threshold measures exercise intensity. As the exercise progressively increases in intensity, the air into and out of the respiratory tract (called ventilation), increases linearly or similarly. As the intensity of exercise continues to increase, there becomes a point at which ventilation starts to increase in a non-linear fashion. This point where ventilation deviates from the progressive linear increase is called the ventilatory threshold. The ventilatory threshold corresponds (but is not identical) with the development of muscle and blood acidosis (Brook 1985). Blood buffers, which are compounds that help to neutralize acidosis, work to reduce the muscle fibers acidosis. This leads to an increase in carbon dioxide, which the body attempts to eliminate with the increase in ventilation (Neary et al 1985). Because increased ventilation occurs with increasing blood lactate values and acidosis, scientists originally believed this was an indication that the ventilatory and lactate threshold occur at similar exercise intensities. This interpretation is appealing because measuring the ventilatory threshold is non-invasive compared to the lactate threshold. And while numerous studies have shown a close correlation between the thresholds, separate studies have demonstrated that different conditions, including training status and carbohydrate nutritional supplementation, can cause thresholds in the same individual to differ substantially (Neary et al 1985). This scientific data of VO2max [maximum intake of oxygen] ventilatory threshold are important to the elite or professional athlete and mostly indicate for the non-athlete that intense deep-water running is a safe and proven activity to accelerate healing and develop physical fitness.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
83
Quinn cites that two groups of investigators also reported that DWR had effectively sustained running economy. Unfortunately, no research has been conducted into the effects of DWR training on more power-related performance indicators, such as sprinting and jumping, and this may be an area of future research for the athlete but not necessary for the recreational but non-athlete or patient seeking physical fitness as a safe method to stop daily medications.
Does DWR boost performance?
Quinn states that however, actual improvement in athletic performance indicators have been demonstrated only with young runners and untrained subjects. Consequently, she prescribes DWR to elite performers not as an additional training stimulus, but only for rehabilitation or injury prevention purposes. This author believes that Quinn is over relying on scientific data because proper Aquatic deep-water running training will improve performance of the athlete, but increased athletic performance is not the purpose for this book, it is for providing the reader as well as hospital medicine – doctors and health insurance companies sufficient “logic” from research based sources that prove deep-water running is the one best and safest preventive medicine as is used in AquaDios-Med™. Quinn reminds us that a correct training prescription and monitoring is essential with any mode of physical activity. Heart rate monitoring is popular with land based activity, but its use with DWR is contentious. Studies have shown that hydrostatic pressure exerted on the chest while the body is immersed in deep water produces different, and more healthy circulatory responses than those associated with land-based running. Dr. Bruce Becker has documented the positive effects of being immersed in water to the neck and the increased pressure on the chest wall or pulmonary system. Quinn’s research shows that the deep-water immersion itself causes physiological changes like a redistribution of blood volume away from the extremities, with greater amounts of blood in the thorax region. This central shift in blood volume, together with the venous blood being “pushed” back to the heart by the water pressure and physical activity together with the “coolness” of the water leads to an increase in the hearts stroke volume and a compensatory reduction in heart rate.
Some call this increased “cardiac output” because the heart works smarter not harder in deep-
water immersion. That is even though the heart is “coasting” along at about 15 beats less per minute it is supplying the equivalent amount of blood as a faster heart rate. This heart rate economy is one of the primary reasons that deep-water immersion running can be so beneficial for non-athletes and patients dependent on daily medications.
Research consistently shows Heart Rater responses are reported to be approximately 10 to 18 beats lower than those achieved during land based running at matched sub-maximal intensities. Quinn shows that some investigators have observed differences in HR between exercise modes; factors such as altered running technique and differences in water temperature are thought to be the cause of this disparity between research findings. This author would like all studies on deep-water running to demand a stride cadence of between 84 to 96 and a water temperature no warmer than 72 degrees F to determine dependable research study replications.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
84
Quinn cites Wilder and Brennan who prescribed the use of an auditory metronome as an external cue to regulate DWR exercise, by recording heart rate responses to varying levels of cadence. This allowed them to design DWR sessions using timed intervals with anticipated physiological responses for particular cadence levels. However, this type of training prescription is clearly specific to the individual.
Quinn feels that the key factors influencing DWR prescription are Familiarity; The accuracy with which a performer's water technique reflects their land based running style; the athlete's or non-athlete aerobic development. Quinn shows that research demonstrates that at sub-maximal intensities experienced performers achieve similar rate of perceived exertion (RPE) values to those associated with treadmill running, although this does not appear to apply to 'unfit', inexperienced, non-athletes or patient DWR performers. Consequently, Quinn prescribes active recovery DWR sessions only when she is completely satisfied that the athlete or non-athlete is able to perform a land-based running style, so making HR monitoring a viable method of monitoring the exercise. This author recommends RPE be taught and utilized as a point of reference for intensity and performance.
The sessions Quinn prescribes mirror land based workouts with the performers instructed to work at the upper end of their HR intensity zones. Whatever prescription is used, Quinn says it is worth remembering that, as with any 'new' training stimulus, the risk of delayed onset muscle soreness (DOMS) is increased, so the prescription needs to be gradual.
Why Recovery from Intense DWR is Shorter
Quinn notes that recoveries between DWR sessions can be shorter than for land-based running. Quinn’s empirical studies show that once athletes are proficient in the DWR technique and the stimulus has been progressive, they can cope with greater intensities and longer durations; yet perceive fatigue levels associated with much less intense land-based sessions. Quinn is simply saying that DWR at verified levels of “high intensity” are experienced as easier than land exercise. She posits this must be due primarily to the lack of impact trauma and the consequent reduced stress on the body. She also considers that other contributory factors may be the reduced eccentric contraction in the 'landing' phase of the running stride (remember that the knees are lower than in normal running) and increased thermal dispersion in the surrounding water.
Quinn fails to mention the importance of the “cool” water temperature as most all pool temperatures are much cooler than ambient temperature and this contributes to a more rapid recovery. Another factor she has not evaluated is the natural soothing massage effect cool water has when exercising intensely. This author finds most every pool is consistently higher in temperature than the ideal exercise water temperature recommended by AquaDios-Med™ a cool 72 degrees F and for the most intense workout 65 to 68 degrees F.
Quinn reminds us of the importance of flotation devices and that they may give deep water runners a sense that their breathing is restricted; this feeling can be amplified by water pressure, causing some performers to breathe only with the upper portion of their lungs. But, as performers become familiar with DWR techniques, they need encouragement from their trainers to increase use of the lower portion of their lungs, or they may become short of breath.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
85
Quinn reports that returning to 'normal' training from a total DWR programme required a careful approach. Some athletes reported they felt sluggish and slow when they return to land, a problem which can be overcome to some extent by incorporating more advanced techniques into pool sessions during the final phases of pool-based rehab. These include:
1. 'High tempo' - moving as fast as possible, with short strides landing behind the body's centre of gravity and a sprinting-style arm action;
2. 'Bum flicks' - keeping upper leg still while flexing the lower leg (moving backwards is allowed for this one);
3. 'High knees' - a slight forward lean, driving the lead leg up as high as possible, little emphasis on the trailing leg and very active arms.
Quinn reminds us that it is important to ensure that the basic technique has been mastered before these variations are attempted, as this allows for correction of faults and optimizes the effectiveness.
In summary, Quinn states that with minimal equipment and properly-designed workouts, DWR can be a valuable adjunct to the training of both fit or injured athletes and non-athletes - even if they do have to constantly explain to a bemused general public what they are doing!
DWR offers an effective means of continuing training during rehabilitation. Maintaining a rapid leg turnover and coordinated movements between arms and legs facilitates the speediest return to full training. However, Quinn notes that athletes and coaches should not wait until injury strikes before considering DWR. As an alternative to the repetitive strain of hard training, it has been shown to preserve performance variables such as VO2max, ventilatory threshold and running economy. And using this low-stress alternative as part of your periodisation plan helps to prevent injury in the first place.
What Defines a Periodised Routine - Fartlek?
A Periodised Routine is a training plan which changes your workouts systematically over time. It involves manipulating training variables such as the number of reps, type of exercise performed, the intensity of the set, and the amount of rest taken between training sessions. In deep-water running it can be as simple as increasing your heart rate by intensifying the stride cadence from 84 to 96 strides per minute to 96 to 108 strides per minute.
Fartlek is a Swedish word meaning "speed play" (fart=speed, lek=play). It is a modified form of continuous training involving regular changes of pace. A deep-water running with the Swedish Fartlek might be something like beginning at a moderate pace to a very intense maximum pace with incremental spurts of maximum effort. Such as, starting the session at a Rate of Perceived Exertion or RPE at 3 to 5 and within 5 minutes increasing the RPE 5 to 8 for 5 minutes and then alternating between an RPE of 7 to 9 and 5 to 8; this is best achieved by simultaneously increasing the stride cadence accordingly. In this example the stride cadence would start about 72 strides per minute and peak at 96 to 108 strides per minute. The objective will be to hold the 108 strides per minute for one minute.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
86
During land running these changes in pace may occur as a result of natural obstacles, such as sand of hills on a cross country run, or involve deliberate bursts of speed every 2 or 3 minutes during a session. Incorporating these Fartlek changes of pace increases the involvement of the an-aerobic energy systems, while primarily using the aerobic system. Fartlek is a form of conditioning which puts stress mainly on the aerobic energy system due to the continuous nature of the exercise. The difference between this type of training and continuous training is that the intensity or speed of the exercise varies, meaning that aerobic and anaerobic systems can be put under stress. Most fartlek sessions last a minimum of 45 minutes and can vary from aerobic walking to anaerobic sprinting. Fartlek training is generally associated with running, but can include almost any kind of exercise.
Questionable Effects of maximal exercise on the brain
The field of sports psychology is awash with research on how the brain can affect physical performance. But how does intense exercise affect brain function? That’s the question that US scientists have been looking at in a study on how maximal treadmill running affects subsequent cognitive function in recreational athletes. In other words, how does the brain of an untrained non-athlete function immediately after intense exercise? In the study, 102 male and female athletes were recruited and then split into two groups; the exercise group performed a 15-minute incremental treadmill run right up to the limit of their maximum oxygen uptake, to exhaustion. The control group meanwhile simply rested for 15 minutes. Immediately before and following these two experimental conditions, all the subjects were asked to perform a neuropsychological test battery called ‘Immediate Post-Concussion Assessment and Cognitive Testing’ (ImPACT), which measures neurocognitive function and fatigue symptoms. The verbal memory scores in the running group decreased following the VO2max test; in particular, immediate recall memory and delayed recall memory were significantly worse after the test compared to the controls; A prolonged memory effect was also shown to occur as it took three days for the running group to fully recover their baseline scores; No significant differences between the runners and controls were found for visual memory, motor processing speed and reaction times. These results are somewhat surprising as you might expect motor processing speed and reaction times rather than memory to be adversely affected following maximal exercise, but this doesn’t appear to be the case. This author acknowledges “temporary loss of memory” after intense exercise as one of the positives because stress and anxiety are memory based and intense exercise eliminates these anxiety provokers; one of the benefits. Hypothetically one can posit that for athletes the best time for learning new skills, particularly where verbal tuition forms part of the process may not be after high-intensity training sessions or competition, but instead well away from these times in a well-rested state.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
87
Without follow up studies to exam this phenomena this author believes the study results means very little but agrees that the best time to learn verbal skills is not immediately after intense exercise. On the other hand one can infer that short intense exercise relaxes the mind enough to lose some verbally social necessities.
Successful Prehab
Johnson concedes that the ability to challenge and motivate an athlete is the difference between success and failure with respect to a tailored prehab program. Knowledge of the chosen sport, the athlete's needs and open communication are the keys to success with Prehabilitation. And, non-athletes or patients are no different, they must be motivated to participate in a program like AquaDios-Med™. The practice of prehab or preventive medicine and its success rely greatly on a person’s ability to commit to prevention.
Does deep-water running Reduce Exercise • Induced Breast Discomfort
On May 29, 2007 Wendy Lynne Gilleard published a research article in the British Journal of
Sports Medicine titled “Does deep water running reduce exercise-induced breast discomfort? Gilleard’s study was aimed at determining whether exercise-induced vertical breast displacement and discomfort in women with large breasts were reduced during deep water running compared to treadmill running.
The research population involved sixteen women with an age range of 19 to 43 years; weight range of 134 to 251pounds with a height range of 5’2 to 5.7 feet, who were professionally sized to wear a C+ bra cup. Gilleard concluded these 16 women were recruited as representative of
women with large breasts. After extensive familiarization, Gilleard quantified vertical breast motion of the participants as these 16 women ran at a self-selected stride rate on a treadmill and in 7’ 8 feet deep water. Immediately after running, the subjects rated their breast discomfort or breast pain by the visual analogue scale and their perceived rate of exertion; the Borg RPE scale. Breast discomfort, breast pain, perceived exertion, vertical breast displacement and vertical breast velocity were compared between the two experimental conditions.
Gilleard concluded that exercise-induced breast discomfort was significantly less and perceived exertion was
significantly greater during deep-water running relative to treadmill running. Although there was no significant between-condition difference in vertical breast displacement, mean peak vertical breast velocity was significantly less during deep water running compared to treadmill running. 31113_Exrcs_Heal IMF_MBM_PNI_ Pg. 75_90
Gilleard verified that Deep-water running was perceived by these women as a more strenuous but more comfortable exercise mode, especially for women with large breasts. Increased comfort was attributed to reduced vertical breast velocity rather than reduced vertical breast displacement. Thus, large breasted women are able to get a more strenuous exercise during deep-water running with no associated breast discomfort experienced in land exercises.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
88
Burnin’ the fat in deep water Mary E. Sanders, PhD, FACSM, is an associate professor in the Department of Internal
Medicine’s Division of Medical Nutrition in the School of Medicine at the University of Nevada, Reno. Dr. Sanders is also an adjunct professor with the Department of Health Ecology in the University’s School of Public Health. She is also the associate editor of ACSM’s Health & Fitness Journal for the American
College of Sports Medicine; and editor/coauthor of YMCA Water Fitness for Health. She also developed the WaterFit and Speedo® Aquatic Fitness. Dr. Mary E. Sanders wrote an
article for The Journal on Active Aging in April 2007, titled “Burnin’ the fat in the water”. In it she describes that Deep-water running may offer an effective option for older adults who want to exercise safely at higher intensities, for weight loss. Among water’s greatest benefits for exercisers is that its natural resistance can stimulate both cardiorespiratory and muscular endurance conditioning.
Sanders cites training studies conducted in shallow water indicate significant body fat loss, and significant muscular strength and endurance gains (D’Acquisto et al., 2001; Nagle et al., 2003; Sanders, 2006; Pöyhönen et al., 2002; Takeshima et al., 2002). Documented benefits of exercising in deep water for older adults are less clear. However, the practical benefits include zero impact, for a low-joint stress, high-intensity cardio workout with some crossover muscular conditioning.
If weight loss is the goal of a program and time is limited, participants should exercise safely at as high an intensity as tolerable, to expend as much energy during their allotted time—somewhere in the range of about 96 to 106 strides per minute. Deep-water running provides a safe and effective environment for older adults to run at higher intensities, without some of the risks associated with impact on the land.
Guideline - weight control - body composition 426 > 427
When Dr. Sanders is asked, What are the guidelines for training targeting weight control? She responds that the minimum training threshold for weight loss, as published by the American College of Sports Medicine (ACSM, 2006), follows: Initially the Frequency is 3 to 7 days per week, depending on functional capacity, health, age, preference, goals and tolerance to training. Intensity of the workout must be high enough to obtain a stride cadence of 84 to 96 per minute or higher and or a RPE. Sanders relies on The Journal on Active Aging, 2007 is used to determine the type or mode for cardiorespiratory fitness. The best workout time for success is 60 minutes or more per day to achieve an energy expenditure of 2,000 calories a week; which has been found successful for both short- and long-term weight-control. It is recommended a heart rate monitor be worn and used to track heart rate for safety and intensity of work output. The stride cadence of 84 to 96 per minute or higher with a RPE of 6 to 8 for most of the workout is recommended.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
89
When emotionally and physically ready, participants can be encouraged to move to the upper end of the intensity range, a stride cadence of 96 to 106 per minute or higher with heart rate monitoring throughout. Sanders notes that Deep-water running is a non-impact, high-intensity workout; it is a safe, effective and comfortable alternative to land-based walking or running. This type of water activity may also offer a non-impact option for vigorous exercise, contributing to total exercise energy expenditure for weight management, cardiorespiratory conditioning, and muscular endurance—all in one session.
Deep-Water Running for Neck and Back Pain
In an article about back pain for About.Com - the New York Times, Ann Asher states that Aquatic Therapy Helps Reduce Back Pain. Asher identifies the special properties of water that supply people with excellent health benefits especially for those who want to heal a back injury. She points out that being submerged in water to your neck provides a safe
environment for working out your muscles and stretching your body without any pain. The submersion also allows injured people to do more than they could on land by eliminating the constraints imposed by gravity and being buoyant.
She notes that beneficial water exercise can be done in shallow, mid-deep and deep water, depending upon the person’s level of conditioning and the goals of their workout. However, this author recommends
full body immersion to the neck for deep-water running with intense strong powerful cadence to eliminate the usual back problems.
Muscle Strengthening Asher indicates water exercise or deep-water immersion exercise can strengthen back, ab and
hip muscles, all key for a healthy spine. The buoyancy and viscosity of water causes a greater resistance as physical movement is accelerated and functions similarly to weight training: it gets your muscles strong. Weight training, on the other hand can cause severe strain on joints and connective tissue whereas the exponential resistance of water is an isokinetic resistance and develops the most desirable connective tissue for the body.
Isokinetic water resistance with intense power movements in the water produces a resistance such that no matter how much effort is exerted, the movement takes place at a constant speed. In simple terms, as the “power” of the movement increases against the water; an equal or slightly greater opposing force is developed.
Isokinetic resistance is an even opposition to power ratio, it builds the most durable, elastic and strong connectivity for muscle to bone.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
90
As a result, intense “power” running is the safest way to build physical fitness and both muscle and skeletal strength. It’s also the only exercise possible when injured; making it the safest exercise for all walks of life. Physiologists recognize this isokinetic activity as a speed – strength - power relationship; as speed of movement in the water is accelerated a certain level of strength is required and this repeated action builds muscle power.
To develop “power” strength and endurance an applied isokinetic exercise is “ideal” because the maximum force of which the muscle is capable of producing throughout the range of motion can be accomplished while immersed in the water to your neck; utilizing almost all the muscles in the body.
Being immersed in water to the neck places the water’s pressure all over your body and the pressure or force against the body increases with each 12 inches of 1 foot of submersion. To build power, strength and endurance, you must work your muscles hard enough to create the “water’s” opposition against this pressure of the body.
The deeper immersed in the water you are, the more pressure will be exerted by the water, and the harder the workout will be. Beginners might consider staying close to the water level where they can barely touch the bottom when desired. If you feel insecure around deep-water stay close to where the floor or surface of the pool bottom and sides of the pool unite, this will provide you with greater stability and confidence. Exercise physiologists strongly recommended that anyone who wants to learn deep-water running exercise in deep-water must wear a flotation device such as the Wet Vest [seen to the left] or a buoyancy belt like the AquaJogger, seen to the right,
to help you learn the challenge of structured deep-water running. Increasing Joint Range of Motion The buoyancy of the water helps take the load off your joints. It creates a significant degree of
weightlessness, allowing you to perform slow movements with ease but fast movements with great opposition or resistance. To develop range of motion, the goal is to take each body part through its full path of motion. However, even with the weightlessness provided by the water, it is best to begin gently and slowly to avoid re-injury.
Core Stabilization Exercise Deep water such as what you’ll find at most swimming pools is a great place to work on low back and core strengthening. In water AquaCycle>>>>
Exercises that work the hips are good for stabilizing the low back. Water walking, bicycling, deep water only, kicks and ab exercises are common. In water Aqua-TreadMill >>> In general, trunk stabilization is accomplished by first establishing a neutral spine, and then moving legs and arms while the spine stays where it is. Any water depth will provide benefits. Aquatic equipment such as the AquaCycle and Aqua-TreadMill pictured here are available. The floatation belt and the dumbbells are very inexpensive and can support you in such a way as to accentuate access to the core muscles that stabilize body posture.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
91
Another way to develop trunk stabilization in the water is by working on your balance. You can position yourself on certain pieces of aquatic equipment such as in water parallel bars or Aquatic Parallel Bars, kickboards or swim bars (long dumbbells) and try to stay there. You can do your best to sit, or kneel, or even stand. Balance exercises in the water will cause all muscles in your trunk to work to hold you upright. Aquatic-Parallel-Bars are available
and they allow for one of the best “back” exercises to heal backs along with deep water running.
Working out in water is relaxing. For many people it is pleasant and even fun. The buoyancy of water takes weight and load off of the joints, which can result in decreased joint pain. Together these benefits of working out in water result in longer and more frequent workouts, providing improved results in the healing or managing of back problems.
Stay Fit or Get Fit While You Heal Your Back Injury
Has your doctor or physical therapist advised you to avoid weight bearing and or high impact
exercise until your back heals? Many active people who are injured fret over lost time at the gym. Others just worry about healing and getting rid of the pain.
The Athlete can substitute normal routine with water workouts, and can minimize the loss of
fitness due to the reduced activity, while the “non-athlete” can rehabilitate the back while becoming physically fit. When either the athlete or the “couch potato” is determined to learn structured deep-water running both will actually increase their fitness while rehabbing. You can also use the opportunity to get strong in the right places, such as ab, back and hip muscles.
Intense Deep-Water aerobics keeps your heart and lungs fit. Deep water exercises wearing a flotation device and using other pieces of aquatic equipment as seen above can help you continue to get strong even
through periods of reduced or no weight bearing activity. Because you are not doing weight bearing exercises when you work out in the water, the chances of aggravating your injury is greatly reduced especially when you learn to identify “rehab pain” from “re-injury pain”.
Deep-water exercise - Decreased Pain
When you work out in water remain as completely immersed in this supportive medium as
possible to take advantage of movement without pain. The immersion minimizes joint pain because the “joints” are un-weighted or “unloaded” and this makes it easy to move slowly until you are ready to increase the intensity. Deep-water immersion is especially helpful for people with arthritis.
Australian researchers compared water exercise to land based exercise with 60 people who had low back pain, and found that both types of exercise significantly reduced pain in participants, but this author believes the “back pain patient” should avoid dry land exercise until the pain is gone by using intense deep-water running. There is a section in this book devoted to “pain management” and the value of “rehabilitation pain”, if you’re interested look it up in the contents.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
92
Juvenile Rheumatoid Arthritis In 1999 Martin Kudlacek, Doctoral Student in Adapted Physical Education at Texas Woman's University, wrote an article "Aquatics for Special Populations". Init Kudlacek indicates that Juvenile Rheumatoid Arthritis (JRA) is an inflammatory disease of the connective tissue, usually affecting the joints that affect children. The primary joints involved are usually the hips, knees, elbows, ankles and neck; the condition onsets between 2 and 5 years.
Aquatic Exercise – Arthritis
Kudlacek states that the aquatic environment is a safe and stimulating environment for the Arthritic patient in which individuals suffering from JRA can safely exercise. With the buoyancy of the water these patients can exercise with little or no pain, while enjoying the benefits of systematic cardiovascular exercise. Kudlacek mentions many community centers; YMCA's and YWCA's have water exercise classes developed for people with arthritis. But he points out that these classes need to be modified for students with JRA by adding playful activities for the children sufferers.
Kudlacek believes that deep-water exercise can be used by adapted physical educators, physical and occupation therapists, or therapeutic recreation specialists in school, hospital, or community-based programs. And, that a quality deep-water exercise program for arthritis sufferers can reduce joint pain and stiffness, increase flexibility, muscle strength and endurance as well as cardiovascular fitness. Kudlacek notes that because of the buoyancy of water it helps support the body and “unloads” its weight while the arthritis victim is able to move their joints through the full range of motion.
The buoyancy of the water places less stress on the hips, knees, and spine and other joints, as well. Individuals with JRA can enjoy swimming, shallow and deep-water aerobics, deep water running or specially designed classes.
Types of Exercise in Aquatics
Kudlacek says that Aquatics offer an excellent combination of following three recommended types of activities. Range of Motion exercises help maintain normal joint movement and relieve stiffness. This type of exercise helps maintain and increase flexibility. Examples:
Slow kicking movements and walking in shallow or deep water aerobics; Extending arms in breaststroke or backstroke motions.
With deep water running there is no impact of gravity. Strengthening exercises help maintain or increase muscle strength. Strong muscles help support and protect joints affected by arthritis.
Examples: Kicking, controlled jumping, walking, jogging, sculling and special strengthening exercise in aqua aerobics. Participants work, essentially, with 30% of body weight affected by gravity. Therefore, there is minimal impact on joints.
Aerobic Endurance exercises improve cardiovascular endurance, help control weight, and improve overall body function. Some studies show that aerobic exercise can reduce inflammation in some joints.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
93
Examples: shouldn't do all your training in the pool running and swimming are extraordinary programs that can improve aerobic endurance while putting little stress on joints. 427 > 430
Swimming
Kudlacek believes swimming can also be a type of exercise for students with juvenile
rheumatoid arthritis because it puts very little strain on the joints. Students can join their peers and improve their fitness levels. This may also contribute to the improvement of self-esteem. Access to the pool: Make sure the participant can comfortably enter and leave the pool. Assess these needs and keep them in mind for programming. Schedule swimming for later hours when the individual does not suffer from typical morning stiffness. Kudlacek recommends Warm water of 86 to 90 F and states aquatic exercise can help to relax muscles, decrease pain, and increase circulation. However, this author believes a “warm-up” is good in the
warmer water and is good to have available but the exercise activity water is best when cool at 72 to 76 degrees F.
DURATION OF ONE UNIT (80KCAL) DURING TREADMILL WALKING IN WATER • Diabetes
Research by Kumiko Ono, Kazuki Nishimura et al at the Graduate School, Kawasaki University of Medical Welfare, Kurashiki, show that the number of Japanese people diagnosed with diabetes has been increasing. Epidemiological and intervention studies of endurance exercise training strongly support its efficacy for improving diabetes. The purpose of the present study was to make clear the difference of duration per expended one unit (80kcal) during treadmill walking in water between younger and older people. The authors collected the standard data by using non
diabetes people. Ten healthy young men and eight healthy women participated in this study. Subjects walked at .6; 1.24 and 1.86 mph in 86°F water. The duration of exercise that expended one unit of energy was calculated from VO2. There was no difference due to the difference of the age in one unit. It might be suggested that it becomes possible to prescribe underwater exercise for older diabetes patients by using the young’s one unit index. The authors believe research shows that in Japan 7.4 million people are suspected of having diabetes in 2002. Moreover, recently the number of Japanese people diagnosed with diabetes has been increasing
and may be as high as 8.5 million or more in 2008. Many diabetes patients suffer from complications, for example diabetic renal disease, retinopathy and neurosis. As for diabetic renal disease, it is the number one cause of artificial dialysis in Japan. Many diabetes patients also suffer from obesity. Epidemiological and intervention studies of endurance exercise training strongly support its efficacy for improving diabetes.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
94
But exercise on land causes kidney blood flow to reduce. It will not be good for the diabetic patient’s kidney. In water, the amount of kidney blood flow is maintained during exercise. And by the action of buoyancy the weight which is loaded on the joint of the legs decreases. This means daily deep-water running is ideal for the diabetic patient. The remedy for diabetes consists of diet, exercise and medication. For diet, the unit conversion
which designates 80kcal as one unit has been used in Japan. For diabetes patients, by using this kind of unit conversion, they can take the calorie which is easily decided in detail (intake per a day divided by nutrition). The authors calculated the duration when one unit (80kcal) is expended in young people during underwater treadmill walking. As for diabetes, it can recognize the increase of morbidity in older people. The purpose of the present study was to make clear the difference of duration per expended one unit (80kcal) between younger and older people during treadmill walking in water, and whether or not
one unit index of the young can be adapted to older.
Aquatic Methods • Diabetics
In this study, in order to accomplish the above mentioned purpose, the authors gathered standard data which is intended for people who are not diabetes as the subject. Ten healthy young men and eight healthy women participated in this study. The authors conducted informed consent following the Helsinki declaration for participation in this experiment. In order to enter the water, subjects wore a swimming suit. They took a rest by standing before walking for 5 minutes each on land and then in water. Subjects walked at 3 velocities ranging from just over ½ mile per hour to 1.86 mph on a treadmill in water. On the 1st day, young subjects were walking in water for 15 minutes at one velocity. They walked the other two velocities on the other days. On the other hand, older subjects completed three consecutive 7-minute walks at progressively increasing velocity. So they walked for 21 minutes in water. Water level was set to Trochanter major. Heart rate (HR) and oxygen uptake (VO2) were measured. HR was measured by bipolar lead chronologically. And the authors recorded for each minute. Exhaled gas was gathered to calculate VO2. The authors set 5 points to gather, rest on land for 5 minutes, rest in water for five minutes and walking in water for 2 minutes by each velocity. The duration of exercise that expended one unit of energy was calculated from oxygen uptake. Energy used per liter of expended oxygen is about 5 kcal, so we used the following formula (duration of one unit=16/VO2). Water temperature was 86 to 89 degrees F room temperature and was about 80 degrees F. The young people’s average HR at rest was 72.2±8.6 bpm on land and 64.3±8.2 bpm in water. Older people’s average HR at rest was 81.2 ±10.4 bpm on land and 76.2±9.3 bpm in water. Average HR for older people was significantly higher than the young’s on land and in water respectively. Older people’s average HR during walking was significantly higher than the young’s at all velocities. Older people’s VO2 was not significantly different from the “young’s”. On the other hand, older people’s relative VO2 was significantly lower than the young’s. Older people’s relative VO2 was not significantly different to the young’s.
Physical Fitness Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
95
Another way to develop trunk stabilization in the water is by working on your balance. You can position yourself on certain pieces of aquatic equipment such as in water parallel bars or Aquatic Parallel Bars, kickboards or swim bars (long dumbbells) and try to stay there. You can do your best to sit, or kneel, or even stand. Balance exercises in the water will cause all muscles in your trunk to work to hold you upright. Aquatic-Parallel-Bars are available
and they allow for one of the best “back” exercises to heal backs along with deep water running.
Working out in water is relaxing. For many people it is pleasant and even fun. The buoyancy of water takes weight and load off of the joints, which can result in decreased joint pain. Together these benefits of working out in water result in longer and more frequent workouts, providing improved results in the healing or managing of back problems.
Stay Fit or Get Fit While You Heal Your Back Injury
Has your doctor or physical therapist advised you to avoid weight bearing and or high impact
exercise until your back heals? Many active people who are injured fret over lost time at the gym. Others just worry about healing and getting rid of the pain.
The Athlete can substitute normal routine with water workouts, and can minimize the loss of
fitness due to the reduced activity, while the “non-athlete” can rehabilitate the back while becoming physically fit. When either the athlete or the “couch potato” is determined to learn structured deep-water running both will actually increase their fitness while rehabbing. You can also use the opportunity to get strong in the right places, such as ab, back and hip muscles.
Intense Deep-Water aerobics keeps your heart and lungs fit. Deep water exercises wearing a flotation device and using other pieces of aquatic equipment as seen above can help you continue to get strong even
through periods of reduced or no weight bearing activity. Because you are not doing weight bearing exercises when you work out in the water, the chances of aggravating your injury is greatly reduced especially when you learn to identify “rehab pain” from “re-injury pain”.
Deep-water exercise • Decreased Pain
When you work out in water remain as completely immersed in this supportive medium as
possible to take advantage of movement without pain. The immersion minimizes joint pain because the “joints” are un-weighted or “unloaded” and this makes it easy to move slowly until you are ready to increase the intensity. Deep-water immersion is especially helpful for people with arthritis.
Australian researchers compared water exercise to land based exercise with 60 people who had low back pain, and found that both types of exercise significantly reduced pain in participants, but this author believes the “back pain patient” should avoid dry land exercise until the pain is gone by using intense deep-water running. There is a section in this book devoted to “pain management” and the value of “rehabilitation pain”, if you’re interested look it up in the contents.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
96
Juvenile Rheumatoid Arthritis In 1999 Martin Kudlacek, Doctoral Student in Adapted Physical Education at Texas Woman's University, wrote an article "Aquatics for Special Populations". Init Kudlacek indicates that Juvenile Rheumatoid Arthritis (JRA) is an inflammatory disease of the connective tissue, usually affecting the joints that affect children. The primary joints involved are usually the hips, knees, elbows, ankles and neck; the condition onsets between 2 and 5 years.
Aquatic Exercise – Arthritis
Kudlacek states that the aquatic environment is a safe and stimulating environment for the Arthritic patient in which individuals suffering from JRA can safely exercise. With the buoyancy of the water these patients can exercise with little or no pain, while enjoying the benefits of systematic cardiovascular exercise. Kudlacek mentions many community centers; YMCA's and YWCA's have water exercise classes developed for people with arthritis. But he points out that these classes need to be modified for students with JRA by adding playful activities for the children sufferers.
Kudlacek believes that deep-water exercise can be used by adapted physical educators, physical and occupation therapists, or therapeutic recreation specialists in school, hospital, or community-based programs. And, that a quality deep-water exercise program for arthritis sufferers can reduce joint pain and stiffness, increase flexibility, muscle strength and endurance as well as cardiovascular fitness. Kudlacek notes that because of the buoyancy of water it helps support the body and “unloads” its weight while the arthritis victim is able to move their joints through the full range of motion.
The buoyancy of the water places less stress on the hips, knees, and spine and other joints, as well. Individuals with JRA can enjoy swimming, shallow and deep-water aerobics, deep water running or specially designed classes.
Types of Exercise in Aquatics
Kudlacek says that Aquatics offer an excellent combination of following three recommended types of activities. Range of Motion exercises help maintain normal joint movement and relieve stiffness. This type of exercise helps maintain and increase flexibility. Examples:
Slow kicking movements and walking in shallow or deep water aerobics; Extending arms in breaststroke or backstroke motions.
With deep water running there is no impact of gravity. Strengthening exercises help maintain or increase muscle strength. Strong muscles help support and protect joints affected by arthritis.
Examples: Kicking, controlled jumping, walking, jogging, sculling and special strengthening exercise in aqua aerobics. Participants work, essentially, with 30% of body weight affected by gravity. Therefore, there is minimal impact on joints.
Aerobic Endurance exercises improve cardiovascular endurance, help control weight, and improve overall body function. Some studies show that aerobic exercise can reduce inflammation in some joints.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
97
Examples: shouldn't do all your training in the pool running and swimming are extraordinary programs that can improve aerobic endurance while putting little stress on joints. 427 > 430
Swimming
Kudlacek believes swimming can also be a type of exercise for students with juvenile
rheumatoid arthritis because it puts very little strain on the joints. Students can join their peers and improve their fitness levels. This may also contribute to the improvement of self-esteem. Access to the pool: Make sure the participant can comfortably enter and leave the pool. Assess these needs and keep them in mind for programming. Schedule swimming for later hours when the individual does not suffer from typical morning stiffness. Kudlacek recommends Warm water of 86 to 90 F and states aquatic exercise can help to relax muscles, decrease pain, and increase circulation. However, this author believes a “warm-up” is good in the
warmer water and is good to have available but the exercise activity water is best when cool at 72 to 76 degrees F.
DURATION OF ONE UNIT (80KCAL) DURING TREADMILL WALKING IN WATER – Diabetes
Research by Kumiko Ono, Kazuki Nishimura et al at the Graduate School, Kawasaki University of Medical Welfare, Kurashiki, show that the number of Japanese people diagnosed with diabetes has been increasing. Epidemiological and intervention studies of endurance exercise training strongly support its efficacy for improving diabetes. The purpose of the present study was to make clear the difference of duration per expended one unit (80kcal) during treadmill walking in water between younger and older people. The authors collected the standard data by using non
diabetes people. Ten healthy young men and eight healthy women participated in this study. Subjects walked at .6; 1.24 and 1.86 mph in 86°F water. The duration of exercise that expended one unit of energy was calculated from VO2. There was no difference due to the difference of the age in one unit. It might be suggested that it becomes possible to prescribe underwater exercise for older diabetes patients by using the young’s one unit index. The authors believe research shows that in Japan 7.4 million people are suspected of having diabetes in 2002. Moreover, recently the number of Japanese people diagnosed with diabetes has been increasing
and may be as high as 8.5 million or more in 2008. Many diabetes patients suffer from complications, for example diabetic renal disease, retinopathy and neurosis. As for diabetic renal disease, it is the NO. 1 cause of artificial dialysis in Japan. Many diabetes patients also suffer from obesity. Epidemiological and intervention studies of endurance exercise training strongly support its efficacy for improving diabetes.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
98
But exercise on land causes kidney blood flow to reduce. It will not be good for the diabetic patient’s kidney. In water, the amount of kidney blood flow is maintained during exercise. And by the action of buoyancy the weight which is loaded on the joint of the legs decreases. This means daily deep-water running is ideal for the diabetic patient. The remedy for diabetes consists of diet, exercise and medication. For diet, the unit conversion
which designates 80kcal as one unit has been used in Japan. For diabetes patients, by using this kind of unit conversion, they can take the calorie which is easily decided in detail (intake per a day divided by nutrition). The authors calculated the duration when one unit (80kcal) is expended in young people during underwater treadmill walking. As for diabetes, it can recognize the increase of morbidity in older people. The purpose of the present study was to make clear the difference of duration per expended one unit (80kcal) between younger and older people during treadmill walking in water, and whether or not
one unit index of the young can be adapted to older.
Aquatic Methods • Diabetics
In this study, in order to accomplish the above mentioned purpose, the authors gathered standard data which is intended for people who are not diabetes as the subject. Ten healthy young men and eight healthy women participated in this study. The authors conducted informed consent following the Helsinki declaration for participation in this experiment. In order to enter the water, subjects wore a swimming suit. They took a rest by standing before walking for 5 minutes each on land and then in water. Subjects walked at 3 velocities ranging from just over ½ mile per hour to 1.86 mph on a treadmill in water. On the 1st day, young subjects were walking in water for 15 minutes at one velocity. They walked the other two velocities on the other days. On the other hand, older subjects completed three consecutive 7-minute walks at progressively increasing velocity. So they walked for 21 minutes in water. Water level was set to Trochanter major. Heart rate (HR) and oxygen uptake (VO2) were measured. HR was measured by bipolar lead chronologically. And the authors recorded for each minute. Exhaled gas was gathered to calculate VO2. The authors set 5 points to gather, rest on land for 5 minutes, rest in water for five minutes and walking in water for 2 minutes by each velocity. The duration of exercise that expended one unit of energy was calculated from oxygen uptake. Energy used per liter of expended oxygen is about 5 kcal, so we used the following formula (duration of one unit=16/VO2). Water temperature was 86 to 89 degrees F room temperature and was about 80 degrees F. The young people’s average HR at rest was 72.2±8.6 bpm on land and 64.3±8.2 bpm in water. Older people’s average HR at rest was 81.2 ±10.4 bpm on land and 76.2±9.3 bpm in water. Average HR for older people was significantly higher than the young’s on land and in water respectively. Older people’s average HR during walking was significantly higher than the young’s at all velocities. Older people’s VO2 was not significantly different from the “young’s”. On the other hand, older people’s relative VO2 was significantly lower than the young’s. Older people’s relative VO2 was not significantly different to the young’s.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
99
Duration of Expending One Unit (80kcal) Treadmill Walking in Water
It was made clear that older people’s heart rate HR on land at rest was higher, the rate of decease in HR in water at rest was lower and the rate of increase in HR while exercising was higher than the young’s. From this, it was suggested that older people’s Venous return could prevent promotion by comparison with the young. The aerobic ability of older people has decreased by comparison with the young. As a result, the authors thought that older people’s absolute VO2 became the same as the young’s. So the authors will have to consider the duration of exercise for the patient whose body weight deviates from these subjects.
For example, if patient’s weight is too high when compared with the young subjects’ the study authors will change the duration by decreasing it. When introducing exercise the authors reason it is important to start at lower durations, too. The Ministry of Health, Labor and Welfare in Japan advises that diabetes patients should exercise easily enough to sweat a little while having a conversation with their neighbor for about 30 minutes per day. Based on this wisdom the authors can say that the index for this study is fit for these patients.
As said in the introduction it is clear that exercise on land reduces the renal blood flow rate but that in water it is maintained. By exercising on land or in water our muscles can use glucose easily and glucose metabolism is improved; so diabetics should exercise. Including diabetes patients that may develop diabetic renal disease, the authors say that for diabetes patients exercise in water is the best choice of training for preventing deterioration caused by diabetes. Almost all Japanese people live on rice. The energy of a half cup of rice is about 80 kcal. So, in the diet of diabetics in Japan, the unit conversion which designates 80 kcal as one unit has been used. It suggests that the index calculated
in this study is useful for the patients exercising by themselves, too. The authors calculated the duration of water level that is at Processus xiphoideus, too; this is the cartilage at the lower end of the sternum. If the water level goes up to the Processus xiphoideus, the duration for expending one unit becomes long. It is showed that the strength of the exercise is lower than at Trochanter major. So introducing exercise for the patients it is recommended to start at the Processus xiphoideus or the lower end of the sternum level. 432
Deep-water Exercise for Diabetics – Conclusion In this study the authors calculated the duration of expending one unit (80kcal) of energy during treadmill walking in water to obtain the standard data to improve diabetes. Older people’s one unit data was equal to the young’s. We could expect to prevent the health of those with aggravation of diabetes or improve it using the one unit index. Using this index, we can connect it to the quality of life QOL maintenance or the improvement of life for patients with diabetes patients who also are at an advanced age.
Physical Fitness Is Preventive Medicine
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
100
Swimming Movement Analysis in Coronary Artery Disease CAD-PATIENTS Otto von Guericke, Lutz Schega1, and Daniel Daly did a study at the University Magdeburg,
Institute of Sport Science, Germany 2K.U. Leuven, Department of Rehabilitation Sciences, Belgium. The authors set out to measure changes in movement parameters under various load conditions during breaststroke swimming in Coronary Artery Disease (CAD) patients.
Kinematic analysis of time- discrete and time-continuous characteristics and timing of the swim-movement was made during a breaststroke “load-steptest” in a flume for 26 male CAD-patients. The path of hands, feet and hips, the pause between propulsive phases and the angle of attack of hip-shoulder-water surface are of crucial importance in patients with CAD. These findings are supported by the factor analysis where comparable parameters were found to be of relevance. Results did indicate large individual variations in time-continues characteristics. The importance of physical activity in patients with Coronary Artery Disease (CAD) is undisputable. The aim of sport related rehabilitation is to develop an optimal specific program depending on the current condition of the individual. Nevertheless such programs focus primarily on physiological adaptations although it is well known that changes in the movement may influence this. The physiological adaptation to immersion in various water temperatures and the duration of immersion, have often been investigated in this population. Few scientific reports, however, provide information on the actual swimming movement in patients with cardiac disease. Some studies have provided indications of the influence of movement changes on physiological responses from a qualitatively point of view, for example by Bücking et al. and Meyer & Bücking. No quantitatively analysis has been reported however. The goal of this study, therefore, was to assess the changes in movement parameters of CAD patients under different load conditions during breaststroke swimming. Two-dimensional movement analysis was made during a flume “load-step-test” in breaststroke of 26 male CAD-patients: age, 51 to 59, infarct age, 2 to 14yrs. Weight 172 to 193 pounds. The test consisted of three 3 minute swims at the same mean swimming speed with added, subtracted or no extra load. One video camera was placed outside the flume perpendicular to the swimming direction at 3.5-m from the swimmer. The actual camera view in the swimming plane was 4-m x 3-m. At the start of each video session a 1-m calibration ruler was placed in both the vertical and horizontal direction and recorded. Reference makers were set at eight points on the left side of the body: toe, ankle, knee, hip, shoulder, elbow, wrist and top middle finger. Recordings were made during each step, in order to analyze 10 movement cycles in the middle of each step. Sampling frequency was 50 Hz. Digitizing was done using the SIMI-Motion“ software package 6.1 and analysis was based on the breaststroke phase model of Wiegand et al.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
101
Based on the time-discrete findings 9 parameters were found to be relevant to describe the changes in swimming movement of the CAD-patients examined. These 9 parameters showed a frequency of change of more than 5. All in all only one patient demonstrated no significant changes over the increasing load steps. On average 31 parameters changed. Only one patient actually demonstrated an ideal velocity-time regime of the hip according to Costill et al. or Schramm. In total a marked divergent regime in horizontal hip
velocity was observed in this population: 12 arm-swimmers, 4 leg-swimmers and 10 change-swimmers. There conditions. Six patients showed significant changes of the use of their arms. The other 20 patients did not change time-continuous characteristics with increasing loads. The calculated values of the leg movements changed significantly in 10 patients whereas 16 patients showed no adaptation during the step-test.
ADAPTED SWIMMING SPORTS AND REHABILITATION As a result of factor analysis 4 factor-components of relevance provide indications for organizing swim rehabilitation programs with a special view to movement co-ordination. The variance of the factor-components are: 30% for time-structure, 18% for velocity-regime, 10% posture of upper part of the body, 8% for angle of attack of thigh. The verification of reliability of the factors showed good internal consistencies (Cronbachs Alpha from .62 to .89). All main items may be evaluated as strong to very strong regarding selectivity and being greater than the limiting value. Based on Kinematic analysis of time-discrete parameters during breaststroke in patients with CAD the movement path of the arms and legs and of the hip, the duration of pause between the movements of the extremities and the angle of attack of hip-shoulder-water surface are of crucial importance to forward speed. These findings are supported by the findings of factor analysis where comparable parameters were found to be of relevance. Results indicated large individual variations in time continuous characteristics. The authors had a good predictor for load specific adaptations related to movement co-ordination. When compared to the findings on healthy volunteers from Blaser or for elite swimmer by Witte different values were observed. The values in CAD-patients are usually larger with no differences between arms and legs. Therefore the majority of CAD-patients are not able to react to increasing loads adequately. Patients who were not able to change the load values under increasing external loads might be increasing their cardiac stress. The movement patterns of CAD-patients react in diverse ways to increased loads. Based on these findings the importance of movement analysis in swimming of CAD-patients was underlined in order to guarantee an adapted sport-specific rehabilitation program as an additional way to control the load-stress situation and to develop movement skills.
LOWER LIMB MUSCLES ACTIVITIES - DEEP-WATER RUNNING INTERVENTION EFFECTS ON BALANCE ABILITY - THE ELDERLY
Researchers Kaneda, Wakabayashi and Nomura from the University of Tsukuba, Ibaraki, Japan investigated the thigh-muscle activity during deep-water running (DWR), along with the effects of intervention with upright-floating (UF) or deep-water running exercise on balance ability in elderly. The study included nine healthy 25 year old males who performed DWR and water walking (WW).

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
102
The authors placed surface electromyogram (EMG) electrodes on the rectus femoris (RF) and biceps femoris (BF). The mean electromyogram (mEMG) of the BF during the DWR showed significantly higher values than that during the Water Walking. The authors then began the second experiment with fourteen healthy elderly persons ranging in age from 56 to 66 years who participated in a once-a-week water exercise program of 12 weeks. They were separated into a normal and an Upright Floating group or deep-water running. The UF group improved both their body-sway area with eyes open and tandem walk time by 10 steps. It was considered that the high
stimulus of the biceps femoris BF during DWR affected the improvement of the balance ability in UF. Various water exercises exist for rehabilitation or fitness maintenance. In water, buoyancy acts against the body to reduce the load at the joints and prevents impact trauma while water viscosity requires the subject to exert greater force than when moving on land.
An upright-floating or DWR situation in a water environment with feet separated from the swimming pool floor is hard to experience in any other exercise environment. The typical form of uprightfloating (UF) exercise in water is deep-water running (DWR). The advantages of this exercise are that it eliminates the impact stress for lower limb joints while immersed to the neck and maintains aerobic fitness. Studies have investigated motion analysis and aerobic fitness during DWR and suggested its characteristics. Moening et al. described that when comparing DWR and treadmill running, the subject leans forward in the DWR at the trunk to counteract the buoyancy effect on the lower
limbs. They also described that the DWR is an open kinetic chain compared to the closed kinetic chain of treadmill running. Another study of DWR reported that the maximal oxygen uptake ( O2)
and the heart rate (HR) were lower than those for running on land, but the ratings of perceived exertion (RPE; legs and breathing) and the respiratory exchange ratio (RER) were greater during submaximal, whereas ventilation (l/min) was similar with younger males. However, no studies have investigated thigh muscle activity during DWR and its intervention effects for elderly persons. This study was intended to investigate lower limb muscle activity during DWR and the effects of intervention of upright floating UF exercise on balance abilities of elderly persons. The authors established two experiments to explore these issues mentioned above. The first
experiment investigated thigh muscle activity during DWR in young males. The second experiment conducted short-time water exercise intervention for elderly persons and investigated their balance ability before and after intervention. Nine healthy young males participated in experiment one as subjects. Their respective mean age, height, weight and % fat were 25 years of age, 5’ 6” height and 155 pounds. Subjects practiced to familiarize themselves with water walking (WW) and DWR before the experiment. The subjects underwent WW and DWR at their comfortable speeds for 8 sessions with two repetitions.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
103
An aqua jogger (Aqua Jogger; Excel Sports Science Inc., Japan) was attached to the subject’s waist during DWR. The left thigh muscle activities of rectus femoris (RF) and biceps femoris (BF) were measured during trials using surface electromyography (EMG). The skin cuticle was removed carefully using a blood lancet (Blood Lancet; Asahi Polyslider Co. Ltd., Japan) and cleaned with alcohol wipes so that the inter-electrode impedance was less than 20 kΩ. A pair of surface EMG electrodes was placed in the middle of the belly of the RF and BF. Electrodes were covered with transparent film for waterproofing. The EMG signals were telemetered via a multi-channel telemetry system (WEB-5500 Nihon Kohden multi-telemeter system; Nihon Kohden Corp., Japan) using a time constant of 0.03 s, 2 kHz sampling rate, and 500 Hz hi-cut filter.
The trials were videotaped with synchronization to the EMG. A digital video camera was placed on the left side of the subject; it allowed coverage of one cycle at a 30 Hz frame rate. Data were collected from one cycle of the videotaped picture, from heel contact to the next heel contact in WW and from the maximum knee drive (as a maximal hip flexion) to the next maximum knee drive at DWR. Then, the mean electromyogram (mEMG) was calculated during one cycle. The water temperature was set at 81°F and the water depth was set at 4.3 feet throughout the experiment. In experiment two Fourteen healthy elderly volunteers persons ranging in age from 56 to 66 years who 2 males and 12 females were separated into two groups: a normal water exercise group (NW, n = 7: 1 male and 6 females) and an deep-water running or “upright-floating” exercise group (UF, n = 7: 1 male and 6 females). Their mean height, weight and BMI were respectively 5’ 0” to 5’ 2” ft., 124 to 147 pounds and 24.5 ±3.2 in Normal Water NW, 4’ 8” to 5’ 3” feet, 119 to 151 pounds. They had already become accustomed to water exercise, but did not engage in other water exercise programs. Subjects participated in a 60 min water exercise program, including 30 min divided into two groups in one session, once a week, for 12 weeks. The NW participants underwent water walking WW, resistance training and other ordinary water exercises using a kick board. The UF participants performed locomotive motions, mainly DWR
with feet separate from the bottom of the swimming pool, using a water noodle. The pool depth was 3’ 6” feet deep and was 27.3 yards long and 2.8 yards wide, with water temperature maintained at 86°F throughout the 12 weeks. A body sway test for static balance ability and a tandem walk test for dynamic balance ability were conducted before and after 12 weeks. The body-sway test was conducted using a posturo-graphic meter. Once again this author notes the 86°F water temperature referred to as “warm-up” temperature by AquaDios-Med™ and is about 10 too hot to expect intense work out.
ADAPTED Deep-Water Running - REHABILITATION
Subjects stood silently on the posturographic meter staring at a point marked on the wall, distance was 3 meters forward, height was 1.5 meters with their feet bared and kept together. Tests were conducted for 30 subjects with eyes open. Body-sway distance and body-sway area were analyzed in this study. A tandem walk test was conducted for two trials. Subjects were required to walk heel to toe along a 10-step line as quickly as they could without mis-stepping. A misstep occurred when subjects stepped completely off the line or failed to follow a heel-to-toe pattern. The 10-step tandem walk time measured using a stopwatch of two trials without mis-stepping was then averaged.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
104
Wilcoxon’s signed-rank test was used to detect differences in the two tests, taken by each group and for the conditions before and after 12 weeks. A Mann-Whitney U-test was used to assess differences in the two tests between two groups before and after 12 weeks. The first objective of this study was to compare the thigh muscle activities of WW and DWR. For that purpose, the first experiment was designed to collect the RF and BF activity data using surface EMG and mEMG during 1 cycle at each trial and compare them. The
mEMG of BF was significantly higher in DWR than that of WW, but the mEMG of RF was similar. No studies have compared water-walking WW to Deep-water running DWR directly in motion analysis. Moening et al. described that trunk flexion was larger for DWR than for treadmill running on land. In addition, the joint angle of hip maximum flexion in the knee drive was about 60° greater in DWR than that in treadmill running. At the knee joint, the range of motion from the back swing to the knee drive was about 55° greater in DWR than that in treadmill running. Hip and knee flexion are greater in DWR than that in treadmill running. Miyoshi et al. reported that the range of motion at the hip joint in WW was similar to land walking at comfortable speed, and that the range of motion at the knee joint in WW was smaller than that of land walking. Regarding treadmill walking and running, Nilsson et al. reported that the net hip angle was somewhat larger during walking than running at the same speed. The net amplitude of the hip joint was four times larger during running than walking when the speed was changed from low to high. They also reported a significantly larger net knee flexion amplitude during running than during walking. This study measured the rectus femoris RF and biceps femoris BF muscle activities and compared WW to DWR. The RF activates hip flexion and knee extension. The BF activates hip extension and knee flexion. The authors hypothesized that muscle activities of RF and BF were higher in DWR than in WW, but this study showed a similar value on RF activity, probably because buoyancy served to assist hip flexion, although maximum flexion in the knee drive was greater in DWR than in WW. The higher muscle activity of BF in DWR than in WW was attributable to the greater range of motion at the knee joint in DWR. Experiments of motion analysis that are synchronized to EMG are required to elucidate this aspect more precisely.
Deep-water running - Rehabilitation for the Elderly The second objective of this study was investigation of the intervention effects of DWR or upward floating UF exercise on balance ability in elderly. For that purpose, we designed a once-a-week water exercise program lasting 12 weeks and established normal water NW and upright floating UF exercise groups. The body-sway distance and area were increased in NW, but the body-sway area was decreased in UF and the tandem walk time of 10 steps was decreased in UF. It is widely acknowledged that body-sway as a static balance ability reflects the center of gravity (COG) during standing. Tandem walking is often used as dynamic balance ability. In the present study, the static balance declined in NW, but static and dynamic balance improved in UF. No studies have reported the decline of body-sway through exercising for the elderly.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
105
Simmons et al., who reported enhancement of functional reach in water exercise group, explained two characteristics during water exercise. First, the buoyancy provided by water can be considered destabilizing because it will tend to lift a subject up. Second, because water exercise was conducted in a group, this created turbulence, which might have increased the variability of the factors influencing each participant’s movement. Destabilizing buoyancy and turbulence that occurred during water exercise might have affected the increased body-sway distance and area in NW. Improvement of body-sway in women with lower extremity arthritis was demonstrated in water exercises, and this is a positive result. In the present study, Deep-water running or UF improved in the body-sway area. Tandem walking also improved but only for the UF group.
Experiment 1 revealed that BF mEMG increased significantly in DWR compared to WW. The high stimulus of the BF during DWR was inferred to improve the balance ability in UF. Other possibilities are coordination between the legs and body or adjustment of body balance, as seen in Tai Chi Chuan, but further research is required. The static and dynamic balance ability improved in deep-water running in the present study. In general, the balance ability declines with age; it is an important function that prevents fall accidents because it is associated with postural control. Results of the present study suggest that DWR exercise might be useful for elderly persons to prevent fall accidents because the balance ability was improved after 12 weeks’ intervention. This study suggests that DWR exercise can improve the balance abilities of elderly persons. It might be affected by the high muscle activity of BF during DWR. Furthermore, because balance abilities were improved after 12 weeks, DWR exercise might be useful to prevent elderly persons’ fall accidents. It is of great interest that this research suggests that elderly fall accidents may be eliminated or lessened with deep-water running.
Deep-water running - a safe exercise for elderly people with mobility limitations
On May 6, 2006 Broman, Quintana, Lindberg, Jansson and Kaijser presented a research study to the Department of Sports and Health Sciences, Stockholm University College of Physical Education and Sports, Stockholm, Sweden which was designed to evaluate deep-water running as a safe exercise for elderly people with mobility limitations. The study was Published online August 22, 2006. Their research concluded that Deep water running with a Wet Vest is a safe form of exercise for elderly people with mobility limitations. However, the study did not calculate aerobic capacities and the study does not conclude to what extent the participants aerobic power may have been improved. Broman and Quintana et al aim was to assess the effects of high intensity deep water interval training with the Wet Vest in elderly women. Twenty-nine healthy women 65 to 73 years old participated in the study.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
106
The participants performed a graded maximal exercise test on the cycle ergometer and were randomly assigned to a control or to a training group. A submaximal exercise test on the cycle ergometer was executed only by the training group. The group trained in deep water running and water walking wearing a the Wet Vest two times a week for 8 weeks. Their target heart rate was 75% of maximal heart rate and the training consisted of several short working periods and resting intervals. After the intervention the heart rate at rest was
8% lower for the training group. Their heart rate at submaximal exercise was 3% less, their maximal oxygen uptake was raised by 10%, and their maximal ventilation was increased 14%. The values for the control group were unaltered after the period of intervention. In conclusion, high intensity deep water running with the Wet Vest improves submaximal work capacity, maximal aerobic power, and maximal ventilation with the effects transferable to land-based activities in elderly women.
Deep water running • recovering from injuries Older runners - Hurt
In 2000, Carol Newman wrote an article published in the Journal of Strength and conditioning Research, Deep water running - for those recovering from injuries and older runners. She says don't let a metatarsal fracture, iliotibial band syndrome, patellar tendinitis, Achilles tendinitis or just about any other lower body injury keep you from your regular run. A non-weight bearing prescription doesn't have to stop you. All you need is shoulder high or deeper water and a buoyancy device to simulate road running and you can preserve virtually all your training gains made before you were injured. She claims that study after study has confirmed that deep water running provides comparable cardiovascular benefits to road running and treadmill running without the impact that must be avoided when you're injured. "Stop running while your injury heals" doesn't have to mean "stop running." Just take your workout to the pool. In one study, four weeks of deep water training was substituted for the usual running workouts of well trained, competitive male runners. All before and after tests of fitness and performance confirmed that training gains were maintained. In a published case study of an elite male runner with a metatarsal fracture of the right foot, deep water running was used for training during rehabilitation. At the end of 24 weeks, all pre-injury fitness and performance measures were maintained. Six months of injury rehabilitation resulted in no deconditioning whatsoever. These and dozens of other published reports confirm that deep water running can keep you running strong, during injury rehab.
How is a Water-Run Different? Newman claims your cardiovascular system doesn't really care how you make it work. It performs on demand to the extent that you exert yourself to the heart it is of no consequence whether you are kickboxing, bicycling, or running. But in chest deep water, the heart's work is made a bit easier by the pressure of the water and its cooling effects. The same effort is not likely to produce as high a heart rate in the water, usually about ten beats per minute slower. The pressure of the water on your body makes the blood return to the heart more easily, and your body weighs only 10% of its land weight in deep water, which also eases the load on the heart. Finally, the water is cooling your body as you work, again easing the demands on the heart. The result is that you will feel as though you are working harder than your heart rate indicates.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
107
As for your body, the effort is real work, closely mimicking the muscular demands of land running effectively. At the same time, water pressure is massaging your muscles, cushioning your joints, and increasing the circulation around injured tissues. Not only are you getting the muscular and cardiovascular benefits of your regular workout, the water is also enhancing the healing process for your injury.
Beyond Recovery
Newman says that although there are disputes among the experts, deep-water running may not only allow you to maintain fitness while injured, it might help improve your running performance when healthy. The benefits of water training may allow you to train harder without the limitations of injury risk. This may be especially true for older runners whose training hours and intensity may be limited by a less durable skeletal system. At least some quality training can be done in the pool, allowing training benefits to accrue without the impact of land running. Deep water running doesn't just have to be slogging it out at a steady, tedious pace. All types of quality training can be employed in the water--intervals, fartlek, sprints, long runs, threshold runs and whatever else you might do on the trails or track. Women runners in the later stages of pregnancy can reap the benefits of strenuous training without worry of the extra mechanical burden of third trimester weight. In addition to the training benefits, the hydrostatic pressure of the water reduces lower extremity swelling. As a cross training method deep water running has a great advantage--it is directly transferable to ground running. For a runner, that is an important consideration. You can reduce the wear and tear of running extra miles while still gleaning all the training specificity of running. A day off from running can be substituted for a day in the pool without anything lost in the translation. Deep water running shouldn't give you an excuse to over-train or skip rest and recovery but it can certainly reduce the burdens of hard training on your musculoskeletal system.
The Downside
Newman states that deep-water running seems to have no critics. Many injured runners have recovered from injury and then kept right on training in deep water due to its advantages. But unless you are injured, you certainly shouldn't do all your training in the pool since your body will need to be conditioned to the effects of land running if you plan to continue to run on land. If you have used deep water running for rehabilitation of an injury, you will need gradually to reintroduce gravity and ground impact forces in order to avoid re-injury.
HOW To Do • Deep-Water Running
Newman states that deep water running is made possible by a water walker-basically a Styrofoam belt that keeps your bottom half and top half in an upright
position in the water. The buoyancy of the belt keeps your feet off the bottom surface and allows you to move your arms and legs in a close simulation of land running movements. You can run essentially free of the effects of gravity. In
addition, the water provides 12 times the resistance of air so that although your movement speed is slower, the exertion needed for the movement is increased.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
108
Your objective in the water is to closely mimic the movements you make on land. Arms, body position, and leg motion should appear to be slow motion running. Your head should be positioned upright without any awkward forward tilt. This sounds easier on paper than it is likely to feel--you'll need to experiment and practice, maybe even get the help of an instructor to get it right. But once you get the position, the motion, and a comfort level in the water, your training can proceed with your normal running routine.
Cardiovascular disease Abnormal Cholesterol research reveals the leading health-related cause of mortality for men and women in the U.S is cardiovascular disease (CVD) even though meaningful cardiovascular health benefits can be easily attained with long-term participation in cardiovascular exercise. To properly address the question of “how much exercise is enough,” the American College of Sports Medicine ACSM has recognized the need for physical activity and exercise, and updated its position stand on the recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults (ACSM, 2006). This author, inventor of the deep-water running and Mind Body Medicine of AquaDios-Med™ believes 45 minutes a day of deep-water running, for 90 days, will be a long enough time period for doctors and scientists to accurately measure the health benefits of the individuals. The second 90 days will show the eliminating of symptoms with no need to continue on daily medications for those on such prescriptions. But, the exercise program must be a lifelong activity fir the results to carry forward throughout the years. Kravitz and Mike say the research of Myers et al., 2004 shows that higher levels of cardiovascular fitness are associated with a 50% reduction in risk of coronary artery disease CVD in men. Myers and colleagues demonstrated that increasing physical activity to 1000 kilocalories per week is associated with a 20% reduction of mortality in men. Hu and colleagues in 2004 showed that physically inactive middle-aged women who engaged in less than 1 hour of exercise per week doubled their risk of mortality of CVD as compared to their physically active female counterparts. It should be emphasized that Haskell in 2003 notes that CVD is a multifactor process and that “not smoking, being physically active, eating a heart healthy diet, staying reasonably lean, and avoiding stress and depression are the major components of an effective CVD prevention program.
Diabetes, Insulin Sensitivity and Glucose Metabolism Research in 2005, by Stumvoll, Goldstein and van Haeften, showed that diabetes has reached endemic proportions, affecting 170 million individuals worldwide; and many more today. One unfortunate health consequence of a sedentary and physical inactive life is the weakening of the body’s insulin regulatory mechanisms. Elevated insulin and blood glucose levels are characteristic features involved in the development of non-insulin-dependent diabetes mellitus. The Steyn et al., 2004 research shows that when insulin function starts breaking down there is a rise in the body’s blood sugar levels, with the eventual onset of ‘pre-diabetes’ and then type 2 diabetes. Diabetes is a growing disease in youth and adults, largely as a result of obesity and inactivity. Regular aerobic exercise meaningfully increases insulin sensitivity and glucose metabolism, which means the body’s cells, can more efficiently transport glucose into the cells of the liver, muscle and adipose tissue. In 2001, Pollock et al. showed that improvements in glucose metabolism with strength training, independent of alterations in aerobic capacity or percent body fat. Although the mechanisms for improvement are not fully understood, it appears that both resistance training and aerobic exercise offer a strong protective role in the prevention of non-insulin-dependent diabetes mellitus. This research alone is sufficient to state that any diabetic participating in deep-water running 45 minutes a day for 90 days will no longer show the signs or symptoms of diabetes.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
109
Hypertension - major health problem
Health research has concluded that elevated systolic and diastolic blood pressures are associated with a higher risk of developing coronary heart disease (CHD), congestive heart failure, stroke, and kidney failure. There is a one-fold increase in developing these diseases when blood pressure is 140/90 mmHg according to Bouchard & Despres, 1995. It may be necessary for American’s to personal trainer and fitness professionals on the daily news to educate local people that reducing weight and lowering alcohol and salt intake in their diet also helps reduce elevated blood pressure. Even moderate-intensity aerobic exercise (40%-50% of VO2max), performed three to five times per week for a 30 to 60 minute session appears to be effective in blood pressure reduction, when elevated. In 2002, Whelton et al. indicated the evidence that higher intensity exercise is more effective in managing hypertension, but scientists say there is inconsistent data to project this to all people. In a recent meta-analysis, a statistical technique that combines the results of several studies, of 54 clinical aerobic exercise intervention trials, findings, in hypertensive men and women, included a reduction in systolic blood pressure and diastolic blood pressure. Fagard in 2001 concludes that although routine aerobic exercise usually will not affect the blood pressure of normotensive [normal blood pressure] individuals, routine aerobic exercise may be protective against the increase in blood pressure commonly seen with increasing age. Once again this author relies on the 90 day rule of AquaDios-Med™ that is 45 minutes a day of intense deep-water running will show a marked improvement of blood pressure when accompanied by nutritional foods. During resistance exercise, systolic and diastolic blood pressures may show steep increases, which indicates that caution should be observed with persons with known cardiovascular disease or risk factors however this is not the case with deep-water running because these increases in blood pressure are dependent on the intensity of the contraction, the length of time the contraction is held, and the amount of muscle mass involved in the contraction. In deep-water running the stride cycle is a continuous isokinetic activity. In 2001, Pollock et al. demonstrated that more dynamic forms of resistance training, such as circuit training, that involve moderate resistance loads and high repetitions with short rests are safe and associated with reductions in blood pressure. Although there is relatively little research on blood pressure and resistance exercise as compared to aerobic training and blood pressure studies, in 2005 Cornelissen and Fagard, dis a meta-analysis in resistance exercise intervention trials and found a decrease for systolic and diastolic blood pressure.
Blood Triglycerides, HDL-Cholesterol, and LDL-Cholesterol In 2003 Neiman established the link between cholesterol and CHD had been well established through long-term studies of individuals with high levels of blood cholesterol and the incidence of CHD. High-density lipoprotein cholesterol (HDL-C) the good cholesterol levels are inversely and independently associated with reduced risk of CHD. Research has established that a sedentary lifestyle contributes significantly to the development of CHD and unfavorable elevation of blood fats and cholesterol levels; physical activity plays an important role in decreasing these health risks. In 2002, Durstine determined the exercise thresholds established from longitudinal and cross-sectional training studies indicate 15 to 20 miles a week jogging or brisk walking, which is equivalent to 1200 to 2200 kilocalories of energy expenditure, may decrease blood triglycerides by 5 to 38 mg/deciliter. That same threshold of exercise has been shown to elevate HDL-C, a positive alteration.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
110
Durstine and colleagues continue that exercise training studies rarely show a decrease in total cholesterol or LDL-C, the bad cholesterol, unless there is a loss of body weight or dietary fat is decreased or both. In 1998 Stefanick et al., concluded the serum level of LDL-C has been shown to be significantly reduced among women and men randomly assigned to a diet-plus-exercise group, as compared with to a control group. Although some studies have shown favorable impact of resistance training on blood lipids, others have reported no change. It may be that the resistance programs that best modify blood lipid profiles incorporate larger muscle mass and multi-segment exercises with a high total volume (reps x sets x load) prescription. Additional research needs to be conducted which controls for body composition changes, day-to-day variations in lipoproteins, dietary factors, and possible other training adaptations, to provide a more credible summary of the effect of resistance training on blood lipids and lipoproteins. This author is positive the Aquadios-Med™ process is ideal for this kind of proof.
Lowering the risk of stroke in men and women
Physical activity exerts at positive effect in lessoning the risk of stroke in men and women. According to Sacco et al. in 2006 moderate to high physically active individuals have a lower risk of stroke incidence as compared to those persons accumulating little exercise. Statistics show that those who are moderately active have a 20% lower risk of stroke while those who are highly active have a 27% lower risk of stroke. Sacco and colleagues suggest that these levels of physical activity tend to lower blood pressure (if high), reduce body weight (if over fat), enhance vasodilation of blood vessels (widening of inside of blood vessels), improve glucose tolerance (how body breaks down glucose) and promote cardiovascular health. The implementation of progressive aerobic exercise (for cardiovascular health) and strength training (for mobility and balance) is recommended to reduce the risk of stroke or recurrent stroke (Sacco et al., 2006).
Colon, breast, lung and multiple myeloma cancer
Physical activity and exercise are correlated with a lower incidence of colon cancer and breast cancer in men and women, respectively. Lee, in 2003, reports that moderate-to-vigorous physical activity has a greater protective effect than lower intensities of physical activity. She notes that physically active men have a 30% to 40% reduction of relative risk to colon cancer as compared to their inactive counterparts. It seems that about 30-60 minutes of moderate-to-vigorous exercise per day is needed for this decreased risk, with higher levels of exercise showing even lowered risk. In addition, Lee states that physically active women have a 20% to 40% reduction in relative risk of breast cancer as compared to their inactive counterparts. It also appears that the 30-60 minutes of moderate-to-vigorous exercise per day is needed to elicit this risk reduction in breast cancer for women. Although more research is needed, it appears that physically active individuals may also have a lower risk of lung cancer, although lung cancer is relatively uncommon in non-smokers. In 2007, Robert-McComb, research showed that multiple myeloma cancer is more common in persons after the age of 50 yrs. Robert-McComb explain that with multiple myeloma there is genetic damage to plasma cells, transforming them into malignant or myeloma cells. Chronic fatigue is frequently reported and a distressing side effect of many cancers, including multiple myeloma. However, patients doing 3-5 days of walking for 15-30 minutes per session and light resistance exercise (2-3 times per week) have demonstrated an increased overall quality of life.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
111
The research is clear that there is no association with the incidence of rectal cancer and exercise (Lee, 2003). The data is also somewhat inconsistent whether exercise can have a positive influence on lowering the risk of prostate cancer in men. Clearly, the present research on physical activity and cancer prevention indicates that exercise has a different association with various site-specific cancers. However, it is believed that safe daily deep-water running exercise with AquaDios-Med™ will demonstrate positive results for both rectal cancer and prostate cancer in men.
Osteoporosis - degenerative disease - loss of bone mineral density
Physical activities that stimulate bone growth need to include progressive overload, variation of load, and specificity of load. According to Kohrt et al., in 2004 and this author it is believed the intense deep-water running of AquaDios-Med™ is adequate to reverse osteoporosis. Specificity of load refers to exercise that directly place a load on a certain region of the skeleton. With osteoporosis, a degenerative disease characterized by a loss of bone mineral density resulting in a susceptibility to bone fractures and health problems, it appears resistance training and weight bearing aerobic exercise may provide the needed stimulus for bone formation (Kohrt et al., 2004). Some research suggests a progressive overload is necessary so the bone and associated connective tissue do not exceed the critical level that would place them at risk. Exercise programs to maintain and increase bone growth should be full-body in nature, including exercises such as squats and lunges, which direct the forces through the axial skeleton and allow for greater loads to be utilized. In addition, evidence does suggest that moderate weight-bearing activity, such as brisk walking done regularly, and for a long-term basis, is effective in averting age-related bone loss. Harder relative intensities of effort and greater volume of physical activity are more effective in increasing bone density. Kohrt and colleagues recommend doing weight-bearing endurance activities 3 to 5 times per week and resistance exercise 2 to 3 times per seek for a total of 30 to 60 minutes per day to preserve bone health during adulthood.
Musculoskeletal Health and Sarcopenia
In 2003 Marcell determined muscle mass, strength; power and endurance are essential contributing factors for the improvement in musculoskeletal health and the enhancement of movement capabilities. Although these components of musculoskeletal health show substantial decreases with age, it has been suggested that this is due largely to a decrease in physical activity, and not solely age. Therefore, safe daily deep-water running must continue to the old age. Sarcopenia is the age-related loss of muscle mass and strength (Marcell, 2003). Marcell adds that the rate of muscle loss with age is relatively consistent, approximately 1-2% per year starting at age 50. He notes that there is a linear relationship with loss of muscle strength and loss of independence, contributing to falls, fractures and admissions into nursing homes. In addition, there is a decrease in metabolic rate and maximal oxygen consumption (due to the loss of muscle mass). Improved musculoskeletal health may allow elderly persons to more effectively perform activities of daily living and with less effort (ACSM, 2006). The 2006 ACSM Resistance Training Guidelines for elderly persons suggest performing at least one set of 8 to 10 exercises that use all of the major muscle groups. Each set should include 10 to 15 repetitions that elicit a somewhat hard intensity for the active older exerciser. For sarcopenia prevention, the selection of multi-joint exercises on machines is recommended, because this requires less skill, and may allow the user to more easily control the exercise range of motion.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
112
Body Composition and Obesity Obesity has risen to epidemic levels in the U.S., with over 65% of the U.S adults being overweight and 31% obese (ACSM, 2006). According to the Centers for Disease Control (CDC, 2007), overweight and obesity are associated with increased risk for hypertension, osteoarthritis, abnormal cholesterol and triglyceride levels, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, sleep apnea, respiratory problems and some cancers (endometrial, breast, and colon). The most favorable approach to weight loss is one that includes committed endurance exercise, resistance exercise, and caloric restriction within a sound behavioral modification delivery program. Weight loss achievements are most effective with increasing cardiovascular exercise up to 200 to 300 accumulated minutes of moderate-intensity (somewhat hard) exercise throughout 5 to 7 days per week (which is equivalent to expending &Mac179;2,000 kilocalories per week exercising) (ACSM, 2006). Resistance training and circuit training research has shown meaningful changes in body composition (Marx et al., 2001). Thus, one of the noteworthy benefits of resistance exercise, as it relates to body composition, is the positive impact of maintaining, or increasing fat-free body mass while encouraging the loss of fat body weight in a progressive overload resistance training program.
Arthritis refers to 100 rheumatic diseases In 2004 Maes and Kravitz research identify arthritis as a broad term referring to greater than 100 rheumatic diseases. Of the many types of arthritis, osteoarthritis (a degenerative joint disease) and rheumatoid arthritis (an inflammatory disorder affecting multiple joints) are the two most prevalent. Arthritis is a health problem commonly characterized by stiffness, pain, and loss of joint function that affects people of all ages, genders and ethnic groups. It may imperil the physical, psychological, social and economic well-being of individuals, depriving them of their lifestyle independence. Physicians commonly prescribe exercise for the treatment of arthritis. In 2003 Finckh, Iversen and Liang, research shows consistent exercise improves aerobic capacity, muscle strength, joint mobility, functional ability, and mood, without apparent increases in joint symptoms or disease. Exercise has shown to have a pain-relieving effect similar to that of a pharmacological treatment for some people. However, Finckh and colleagues suggest guarded caution in the exercise design of patients who have significant joint damage, especially in their weight-bearing joints. The authors Maes and Kravitz, 2004 continue that high-impact exercise is contraindicated in many cases of arthritis and should be replaced with swimming, aquatic exercise, aquatic walking, and biking, which are much safer on the weight bearing joints. Exercise programming for clients with arthritis should focus on gradually increasing cardiovascular conditioning, progressively overloading resistance exercise, increased flexibility, and steadily increasing flexibility and joint stability. Thus deep-water running is a godsend to those with arthritis.
Stress - psychological well-being - distress A growing body of research over the last 10 years substantiates that physical activity and exercise also improves psychological well-being (Dubbert, 2002). It is important to clarify that much of the research presented here is correlational, which means that the scientists studied the associations that exist between exercise and mental health variables, and not the causal relationships. Published investigations conclude that individuals with improved levels of fitness are capable of managing stress more effectively than those who are less fit (Hassmen, Koivula & Uutela, 2000). The data suggest an inverse relationship: higher physical fitness is associated with lower levels of stress.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
113
It appears that the method of exercise that most benefits stress reduction is cardiovascular exercise such as the deep-water running of AquaDios-Med™. Studies describe the role of exercise as a “preventive intervention” in managing stress as opposed to a corrective intervention. The research indicates that moderate intensity aerobic exercise, performed three times a week (sessions lasting over 20 minutes) for up to 12 weeks, has the most influence on stress management. Although the specific mechanisms explaining the improved stress levels from aerobic exercise are unclear at this time, it appears that possible theories include the involvement of physiological, biochemical and psychosocial factors (Callaghan, 2004).
Mood State
Frequently, personal trainers and fitness professionals hear clients say that they exercise because it “feels good.” Because mood state is influenced by psychosocial, psycho-physiological, biochemical, and environmental factors, explaining the exercise-induced mechanism is quite difficult. However, it appears that cardiovascular and resistance exercise can positively affect different mood states including tension, fatigue, anger and vigor (a psychological variable defining vitality or energy) in normal and clinical populations (Lane & Lovejoy, 2002; Fox, 1999). In addition, even acute bouts of exercise may improve a person’s present mood state. It has been shown that a single bout of 25-60 minutes of aerobic exercise (at low, moderate or high intensities) increases positive mood feelings while also decreasing negative mood feelings. Implications from these data denote the incorporation of regular exercise in a person’s lifestyle for the enhancement of a positive mood state. The use of resistance training to improve mood state requires further research.
Depression Eliminated by Exercise
The antidepressant action is one of the most commonly accepted psychological benefits of exercise. Individuals with clinical depression tend to be less active than healthy active adults and have a reduced capacity for physical exertion (Fox, 1999). As such, it is challenging for the personal trainer and fitness professional to introduce physical activity to this population, as people suffering from depression are not predisposed to participating in exercise. However, patients diagnosed with depression have credited exercise as being a most important element in comprehensive treatment programs for depression (Dunn et al., 2002). Cardiovascular and resistance exercise seem to be equally effective in producing anti-depressive effects (Brosse, Sheets, Lett, & Blumenthal, 2002). Therefore, the inclusion of resistance exercise, circuit training, calisthenics, as well as different modes of aerobic exercise should be encouraged. It also appears that both acute exercise bouts and chronic exercise training programs have a positive effect on people with clinical depression (Dunn et al., 2002). The research does infer, though, that the greatest anti-depressive effects seem to occur after 17 weeks of exercise, although observable effects begin after 4 weeks (Scully et al., 1998). In addition, the effects of exercise on depression seem equivalent in both genders and are uninhibited by age or health status. Although no research guidelines exist for an actual exercise prescription, the evidence suggests following the ACSM guidelines for the recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness and flexibility in healthy adults.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
114
Anxiety • Distress Eliminated by Exercise
Anxiety can be defined as “distress or uneasiness of mind caused by fear of danger or misfortune.” It is a state of apprehension. The results of over 30 published papers substantiate a link between acute and chronic exercise and the reduction of anxiety (Scully et al., 1998). Most of the research on exercise and anxiety involves aerobic training regimens. The few studies involving resistance training and flexibility have also shown a slight decrease in anxiety, but additional research in this area is needed. However, the data does indicate that aerobic exercise is more beneficial for the reduction of anxiety. In reference to the actual aerobic exercise prescription, there appears to be much debate about whether low-intensity, moderate-intensity, or high-intensity exercise is most beneficial. For participant adherence, exercise intensity should be set at an adjustable level agreed upon by the individual in consultation with a personal trainer or fitness professional. It appears that even short bursts of 5 minutes of cardiovascular exercise stimulate anti-anxiety effects. The research also indicates that individuals who train for periods of 10 to 15 weeks receive the greatest beneficial effects.
Self-Esteem • Improved by Exercise
In 2004 Callaghan research determined exercise has a positive influence on improving self-esteem. The effect of exercise also appears to be more potent in those who have lower self-esteem. Studies indicate that aerobic exercise may have a more pronounced effect than anaerobic exercise, but that may be because there is little research available on resistance training exercise and self-esteem. However, self-esteem is quite complex and studies suggest that certain subcomponents contribute to a person’s self-esteem, including perceived sport competence, physical condition, body image and strength (Scully et al., 1998). Because of the many variables that influence self-esteem, it is important to note that a person may highly value his/her physical condition and yet have a negative evaluation of his/her body. Current research provides little direction regarding the type of exercise and dose recommendation for improved self-esteem. In relation to exercise, it is interesting to note that important factors influencing a person’s self-esteem are perceptions of their body attractiveness and physical condition (McAuley et al., 2000).
The “Weekend Warrior”
All position statements on physical activity surround their messages around the importance of consistent physical activity and exercise throughout the course of the week. Yet, a sub-population of exercisers are those who do 1 or 2 bouts of exercise a week (perhaps because of time or choice), who have been ‘affectionately’ labeled ‘weekend warriors.’ Although many hypothesis and suppositions have been suggested about the health of this subpopulation of exercises, most recently a rather large scientific investigation revealed some interesting findings. I-M Lee and colleagues (2004) found that ‘weekend warrior exercisers’ who had no major risk factors (and expended at least 1,000 kilocalories in this sporadic exercise pattern) had a lower risk of dying as compared with their sedentary counterparts. However, individuals with one or more risk factors to CHD may not benefit from this sporadic approach to physical activity, and should be encouraged to get their physical activity and exercise throughout the course of most days of the week.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
115
Directions for Future
As personal trainers and health and fitness professionals expand their professional direction, the core model of the programs developed and endorsed will surely be engrossed in the enhancement of health for people. As well, with the rapid growth of the computer and communication technologies, more education and information about health, fitness and quality of life issues is easier to disseminate to our interested and growing audience. All professionals need to combine creative capabilities in exercise programming with highly developed technologies and utilize these research applications into designing new strategies to get more people, of all ages, physically active and exercising.
Interval Training • Safe for coronary artery disease CAD
Len Kravitz, Ph.D., Program Coordinator of Exercise Science and Researcher at the University of New Mexico and Jonathan N. Mike, M.S., doctoral student Department of Health, Exercise, and Sport Science at the University of New Mexico, Albuquerque (UNM) published research titled “Effectiveness of high-intensity interval training for the rehabilitation of patients with coronary artery disease” in 2004 with the American Journal of Cardiology. According to the American Heart Association in 2004, over 79 million Americans have one or more forms of cardiovascular disease (CVD). One in three deaths in the U.S. is attributable to CVD (AHA, 2004). As well, CVD deaths are listed as the top deadliest diseases in the world. The overall objective of cardiac rehabilitation is to restore and maintain physiological, psychological, social, and occupational status in patients with coronary artery disease (CAD) which is a narrowing of the coronary arteries that supply blood and oxygen to the heart. This intervention also seeks to assist patients with their resumption of daily recreational activities. Traditionally, continuous aerobic activities have been the primary methods of training patients enrolled in cardiac rehabilitation in order to improve and maintain aerobic fitness. High-intensity interval training has been employed and shown to be an effective exercise modality to improve maximal aerobic power in healthy active populations of men and women. Warburton and colleagues note that preliminary data on interval training with some patients with cardiac disease has also led to improved health benefits. Despite the wide-ranging usage of interval training in healthy populations, few studies have evaluated the effect of interval training on the health status of patients with cardiovascular disease. Therefore, the purpose of this study was to examine the underlying benefits of interval training with highly functional patients with CAD. The 14 volunteers in this study were men, average age of 56 years; average weight 190 lbs., who had undergone bypass surgery or an angioplasty (a medical procedure in which a balloon is used to open narrowed or blocked blood vessels of the heart) and were 6 months post-surgery. The subjects were identified in stable condition and highly functional, with peak aerobic capacities. The researchers grouped the subjects by age, weight and aerobic capacity into one group (n=7) of traditional aerobic training and another group (n=7) of interval training. Both training groups were required to train two days a week of the 16-week study. The traditional aerobic group completed a 10-minute warm-up followed by 30 minutes of continuous aerobic exercise at 65% heart rate reserve (heart rate reserve is the difference between resting heart rate and maximum heart rate), which is also equivalent to 65% of their VO2 reserve; the subjects also performed a standardized resistance training program, which was followed by a 10-minute cool-down.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
116
The interval training group performed the same warm-up, resistance training and cool-down segments as the traditional group. However, the interval training group’s aerobic workout consisted of 2-minute high-intensity bouts at 90% heart rate reserve followed by 2-minute low-intensity bouts at 40% heart rate reserve, for the 30-minute cardiovascular bout. Both groups training sessions utilized three different types of exercise modes, including combined arm and leg ergometry, treadmill and stair stepping. All subjects were also encouraged to participate in three additional training sessions per week of continuous aerobic exercise at 65% of their heart rate reserve. The researchers confirmed that the volume of the exercise (aerobic and resistance training) performed by both groups in this study was the same. The traditional aerobic and interval training groups showed statistically significant and similar improvements in aerobic capacity during this 16-week training study as measured by a maximal treadmill test (subjects were pre- and post-tested commonly employed in cardiac rehabilitation programs). However, the interval training group showed a significantly greater treadmill time to exhaustion by exercising twice as long as the traditional aerobic group in a specific treadmill test to exhaustion. In this exhaustion test, the subjects exercised at 90% of their heart rate reserve until they voluntarily stopped. This test is valuable for measuring endurance capacity, with the later minutes of the test demonstrating anaerobic capacity markers. Warburton and colleagues explain that as subjects near the end of their aerobic capacity, in the exhaustion test, they will recruit energy from the anaerobic energy systems. Though improvement did occur, no statistically significant changes were observed with either group in systolic and diastolic blood pressure, pulse pressure (which is the difference between systolic and diastolic pressure and a function of stroke volume), artery compliance (extensibility of arteries to facilitate blood flow), or rate-pressure product which is a measurement of the heart muscle’s oxygen consumption and is calculated by multiplying the heart rate times the systolic blood pressure.
Practical Application With the pervasiveness of heart disease in all societies throughout the world, fitness professionals and personal trainers should be very familiar with the risk factors to CAD. This investigation demonstrates that functional CAD male patients, with poor aerobic capacities can perform interval training in addition to a continuous cardiovascular exercise program. However, care should always be taken as some patients will possess higher functional abilities than others. Therefore, it is imperative that proper screening, extensive health evaluations, and physician approval be taken to ensure adequate safety precautions during exercise. Fartlek Perhaps the most notable finding of this study was the significantly greater time to exhaustion observed in the interval training group. As the authors highlight, “it does appear to lead to adaptations that allow for a greater tolerance to a strenuous exercise challenge. These adaptations would be of particular benefit for the performance of many activities of daily living.” The bottom line message personal trainers and fitness professionals can share with their physically active and stable CAD clients is that the inclusion of interval training programming will result in them being able to function more efficiently during the day and for lengthier periods of time. This next section is a short history of exercise and its effects on health. This includes studies on exercise and addresses how chronic disease is killing sedentary American’s that could have healthy quality lives with exercise.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
117
BACK PAIN RELIEF
Primary concern is avoiding a potential lower back surgery syndrome. Treatment of choice for a large percentage of back surgery candidates is a structured deep-water exercise program, and many cases are complicated and there is frankly no other efficacious treatment choice.
The number one cause of missing work is painful lower back syndrome and CHRONIC INTRACTABLE PAIN of the lower back. Many BACK PATIENTS with herniated discs, tendentious, arthritis of the spine, or once devastated with pain are now happily living normal lives. Treatment of choice is AquaDios-Med Rehabilitation pain management and Strengthening program that will accelerate healing, quicken bone mass density strength and regeneration by SPECIFIC PHYSICAL activation within the waters resistance.
This program does not replace physical therapy but it will increase reflexes, strength, endurance, balance, coordination, flexibility, and improve conditioning, reaction time, and accelerate recovery from physical pounding found in athletics and professional sports; and decrease PT dependency.
Ninety days of intense AquaDios-Med Treatment improves overall conditioning, strength, endurance, reaction time and accelerates recovery stress caused pain manifest of injury in professional sports like football and injuries thereof. The program helps to eliminate or greatly reduce pain so the patient can be better prepared for return to work. Disc Pathology may involve torsional compression injury with resultant extensive inflammatory reactions and chronic pain. Often MRI and other differential diagnosis procedures are unable to isolate the injury site adequately while the patient is unable to develop balanced muscular strength and conditioning to eliminate physical fatigue and tissue aggravation, which contributes to torsion-compression injury of the thoracolumbar fascia.
Usual treatment for this condition is extended rest, which in itself may iatrogenically contribute to the syndrome by scar tissue development within the disc and adjacent muscular and soft tissues.
Iatrogenic or doctor caused problems may ironically contribute in these cases but can be controlled and eliminated by a carefully designed Structured Deep Water Resistance Exercise Program to balance and strengthen the injury site while controlling the pain. The treatment plan is dependent on patient compliance, daily exercise (some of which is painful, fatiguing and frustrating), to develop disciplined practice to build endurance and stamina for daily life or any sport. Pain management teaches patients full body activation, to classify and discriminate differences between re-injury and rehabilitation pain, motivation to master pain by experience of safe, painful physical body exercise movements necessary for correct healing, conditioning, strength and endurance.
BACK PATIENT COMPLIANCE TREATMENT SUCCESS
Treatment plan success is dependent on critical daily patient exercise movements and activities designed so the patient can easily differentiate between REHABILITATION PAIN AND RE-INJURY PAIN and learn one is dangerous while the other necessary to return to health without a disability. Back patients are very threatened by the injury, too often expect others to make the pain go away, avoid dynamic treatment and may be found crowding Chiropractors, Physical Therapy or Psychiatrists offices. Successful accelerated rehabilitation is dependent on daily patient exercise activities and patient willingness to follow directions.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
118
Even when medical CatScan identifies damage to lumbar disc herniation and Lateral protrusions it is possible to establish a foundation for pain management without medication. Primary concern is alternative treatments to surgery for the lower back syndrome, pain management, decrease medication dependence, independence from physical therapy and a program to help body conditioning and strength while managing the pain. Treatment relies on IN VIVO BEHAVIOR MEDICINE-MODIFICATION Mind Body Medicine COMBINED WITH prescribed structured resistance hydrology exercise for reduction of chronic pain, control of joint pain, swelling, back pain, anxiety, neuromuscular strengthening of the damaged herniated discs and tissues while building stamina, endurance, muscle tone, and self-control.
Physiological self-regulation and pain management is simultaneously taught with daily clinical
consultation, behavior medicine, and structured deep-water resistance exercise hydrology.
ARTHRITIS VICTIMS
Arthritis, a painful disease, cripples people worldwide. Researchers estimate 360 million people are victims and more than 250,000 children in the United States suffer from this debilitating affliction. One out of three families is touched or about 10 percent of the population. AquaDios-Med helps ARTHRITIS casualties with pain relief, increased range of motion, mobility, muscle and bone stimulation that contributes to remission or control of this disease. Medical research has proven exercise stresses the bones, causing them to bend slightly increasing both bone mass and density. This bending stimulates the flow of body fluids into porous areas where exchanges occur between the fluids and the bones. A small electrical current created by physical activity stimulates the bone, causing it to regenerate itself. Without this flow of electrical current, deterioration of the bone occurs. Waters viscosity and natural isokinetic resistance found in Deep Water Exercise Running creates more flexing, elongation, increased innerspace of the joints and with no trauma to the bones. Bones become stronger, the joints less inflamed, pain is decreased, mobility improved and accelerated healing is noted thus preventing or delaying osteoporosis onset. Arthritis victim need to use as many muscles as possible, especially in the lower body. The Wet Vest allows patients to walk or run in deep water without touching the bottom and to use more of the major muscles, without the traumatic effects of touching the bottom. Swimming is a highly skilled good exercise, but impossible for most Arthritic patients because of their chronic neck, shoulder, and lower back, pain prohibits swimming very well and mostly uses upper body muscles. When Arthritics swim they do not get much exercise because they are limited to leg scissoring on their side and paddling the hands to avoid pain. Mild dry land exercise developed for the Arthritic and taught by a physical therapist can be safe, improve circulation and morale, lower inflammation and decrease pain. However, most doctors discourage arthritis victims from exercise because land exercise produces increased inflammation and pain of the joints. Even mild exercise for healthy body tissue increases pain, causes muscles to become more tense and compounds the problem. Conversely, no exercise or movements of arthritic joints leads to deterioration of the body and further degeneration of the joints.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
119
Structured Deep and Shallow Water Resistance Exercise naturally relaxes the muscles and helps to eliminate pain while performing isokinetic movements. AquaDios-Med Deep Water Exercise Treatment helps patients to learn management of the condition with a higher or improved quality life. Exercise will not cure arthritis but supervised water exercise does help soothing, healing and relief. Research indicates many arthritics are able to manage chronic pain and within a few months show dramatic improvement of their conditions.
CARDIOVASCULAR DISEASE PATIENTS
Structured Deep Water Resistance Exercise is Safest for Cardiac Patients because arrhythmias occur with elevated heart rate. Running in water provides a better workout than comparable dry land activities, WITH A REDUCED HEART RATE. Water resistance creates increased venous return with less demand to the heart. Cardiac patients gain training effects of a higher heart rate but sustain a lower heart rate while building the heart muscle stronger; they begin with water walking then running while improving cardiovascular healing.
WEIGHT Management – CONDITIONING
Research confirms a minimum of 40 % more energy is normally expended in deep water exercise, approximately 1,000 calories per hour, compared to dry land running activities, which burn about 600 calories per hour. Even without restricting diet tremendous weight loss can be achieved because water resistance opposes every movement in deep water running.
LIFE EXPECTANCY AND EXERCISE
Research confirms exercise alone can add years to survival, with improved quality of life, and proper nourishment with supervised exercise can arrest the aging process even high risk groups (smokers, high blood pressure), can increase life expectancy and have fewer hospitalizations.
SUCCESSFUL AGING – GERIATRICS
Research has shown the brain is dynamic, adaptable well into middle age and beyond. Aging itself is not uniform, the brain has a quality called redundancy or enough extra neurons to function well with losses in some areas and the brain retains its capacity to grow new anatomical connections for
learning. Some people in their 70's and older retain their energy, physical aliveness and zest for live. Geriatric aging may be a misnomer; a redefinition like "successful aging" may be applied because some people are vigorous at age 80 and others old at 60. Regular vigorous exercise improves the sense of well-being, produces physiological benefits, reduces incidence of chronic disease, improves cardiovascular fitness, respiratory capacity, strength, lowers blood pressure, raise in HDL (GOOD) cholesterol, relieves emotional distress, delays or prevents osteoporosis, weight management, helps preserve neurological functioning and enhances the neurology of the sedentary.
An editorial in Annals of Internal Medicine states, "functional aerobic age is lowered by the conditioning effect of repeated exercise, meaning EXERCISE MAKES YOU YOUNGER!"

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
120
Research demonstrates regular vigorous exercise can improve brain function in older people and produces "successful aging". A 10-year AMA (American Medical Association) study on aging concluded age is not a limiting factor in exercise. Aging is the equivalent of inactivity not passage of time and nutrition with proper exercise can delay or reverse the aging process. Aging is a complex process, breathing capacity declines, heart vigor decreases, reflexes slow, and capacity for work lessens.
AGING AND THE ELDERLY
The AMA Committee on aging studied the phenomenon of old age for ten years and didn't find one physical or mental condition that could be attributed directly to the passage of time, concluding the effects of aging are indistinguishable from the result of inactivity. Old age is not a natural body deterioration according to Dr. Agress, author of Energetics, who defines aging as a "complex process during which maximal breathing capacity declines, heart vigor diminishes, capability for work lessens, and reflexes become slower." E. L. Smith, Ph.D., a biogerontology researcher states "Age should never be viewed as a limiting factor in developing an exercise program". The British Journal of Sports Medicine, stresses strengthening of all muscle groups and cautions exercise programs for the elderly should include exercises to increase strength, endurance and flexibility to counteract muscle atrophy and loss of joint motion associated with aging.
Research data supports daily exercise with proper nutrition delays, or reverses premature aging. Deep-water exercise and other forms of aerobic conditioning such as running, walking, cycling and swimming will add year’s longevity. Professionals in Health Science believe physical activity is essential for everyone but is especially important for older women, as it can enhance quality of life and make the eliminate over-dependence.
Research consistently demonstrates human athletic capacity is maximized between 18 to 25 years of age and begins to decline with age. It was believed the aging process included:
Loss of Aerobic Capacity (Lung Capacity Decrease); Maximum Heart rate Decrease; Heart
Output Reduction; Weakened Muscle (As Muscle Converts to Fat we get flabbier, weaker), Lose Coordination and Ability to Maintain Balance, Reaction Time Slows Down, Backs Become Slumped, We become Shorter (at age 40 an eighth and 50 another three quarters of an inch), Discs of spine compress, girth increase of 20 or more pounds, the kidneys, eyes, hearing and brain are affected negatively. According to Research the losses listed above are the effects of a sedentary life more than of the aging process.
STUDY OF SKIERS
Studies of physical fitness indicate superiority is maintained by personal desires and motivation for activation of the nervous system, which builds constant improvement of technique and accumulated skill. Research of accomplished lifelong Skiers who have stayed active their entire life with disciplined workouts and practice claim to be as good as ever. They claim to even ski better because they have another 20 or 30 years’ experience and ski with greater efficiency. Disciplined Workouts is a process of learning a demanding active focus or mastery of a physical task with desire for improved performance outcome accented by growth, challenge and achievement.
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
121
THE INVERTED PYRAMID
After a certain point in training, practice and performance the possibility to improve has horizons of infinite expansion. These lifelong ski athletes develop communications relevant to sensations felt in their joints and muscles like arcing, slicing, flowing, guiding, with clean, fluid, minimal movements for optimal advantage for performance. Hippocrates postulated more than 2,000 years ago the body must be used to develop health for strength and endurance. By taxing the limits endurance and stamina is improved because deliberate stress on muscle groups creates strength to handle the stress. Master athletes who continue disciplined physical exercise do not become deconditioned and stay youthful because the training effect immunizes against the aging process and its effects listed above. Recent research with improved designs at the Center for exercise, University Florida reveals no reduction in aerobic capacity to age 65 for master athletes provided they maintain their training and only a slight decline after 65. Other studies at the University revealed reaction time of aging athletes do not slow down if they maintain their training. University Research of the national ski team for 20 years and showed no loss of reaction time but an unrecoverable decrease in quickness is measured when training is discontinued. Old poorly designed research falsely presumed Aerobic Capacity dropped about 10 percent per decade after the age of 25 for the general population while master athletes decline was less than 4 percent per decade. In fact, people in their 70's are able to increase muscle strength at about the same rate as those in their 20's. Ronald Reagan, Past President, exercised with nautilus and added so much muscle his suits would not fit. Some 80 year olds have tripled their muscle mass with training. Isokinetic Exercise in deep water is gentle on the body and offers a full fitness regimen of cardiovascular fitness, flexibility, strength, balance, and coordination. Heart rate levels in water activities are lower than for the same intensity level on land. Exercise at a particular heart rate on land, can be adjusted downward by 10 to 20 beats per minute for water exercises at the same perceived exertion rate (RPE). The heart gets a better workout with less work because of the continued buoyancy of the water with use of the Wet Vest or AquaJogger and other facts previously discussed, which allow the heart muscle to be strengthened rather than fatigued.
AQUADIOS-MED AND PREGNANCY Many physicians worry about the possibility of congenital defects in infants due to increased body temperature during prolonged aerobic conditioning and advise their pregnant patients to avoid raising their body temperatures by more than two degrees Fahrenheit during the first trimester. Running or cycling outdoors in hot or humid weather can cause a woman's body temperature to rise quickly. Many obstetrician-gynecologists, believe pregnant women who were normally physically active prior to pregnancy should continue muscle toning exercises, but restrict aerobic activities to those which avoid high body temperatures for no more than 30 minutes a day. The one exercise a physically active woman can do before after and during pregnancy is deep-water training. Fitness can be achieved while the fetus benefits. Some women use swimming as an exercise during pregnancy. Although swimming is an excellent form of exercise, it is still not ideal. If a pregnant woman tries to swim the freestyle, she must hyperextend her back to keep her body stretched out on top of the water. This hyperextension can add to the problems of an already overstressed back. Most pregnant women, trying to swim, go to the sidestroke or the breaststroke.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
122
To swim the freestyle (or crawl), the most common stroke, a person must try to keep the body flat on the surface of the water. Maintaining this position requires the back to be hyper-extended. The lower back muscles must exert a great deal of effort to keep the feet trailing behind on top of the surface. This effort increases the intradiscal pressure, tension, and may cause pain in the lower back; very few lower back patients find swimming to be a beneficial activity. None of the swimming strokes use the major muscles of the body, the gluts (buttocks), quadriceps (thighs), and hamstrings (inner thighs) as do running. Swimming uses 80 to 90 percent upper body muscles, while running uses primarily lower body muscles. Swimming may also irritate the eyes or cause sinus and/or ear infections. Although running on land uses the large muscles of the lower body, the continuous pounding creates an excessive amount of trauma on the already overtaxed body of the expectant mother. Running before pregnancy may have produced a foot strike of 400 to 500 pounds per square inch; running while carrying an extra 20 pounds can increase that pressure to 600 to 800 pounds per square inch. Additionally, hormones produced during pregnancy cause connective tissue to soften, which can lead to injury of the joints and ligaments brought on by excessive stretching or pounding.
NON-SWIMMERS • DWR
Even non-swimmers can participate in deep water rehabilitation benefits because the Wet Vest or AquaJogger keeps the head above water preventing your face going into the water so breathing is easy while deep-water exercising.
Sport Psychologist Sports Psychiatry Imagery and Injury
In March 1991 Ievleva and Orlick published an article titled “Mental Links to Enhanced Healing: An Exploratory Study” in the Sport Psychologist. The authors confirm research shows that it is possible to speed up healing by using specific mental skills and techniques including visualization imagery, Mind Body Medicine and self-hypnosis combined with deep-water running such as offered by AquaDios-Med™.
What is Imagery • How to Use it
Ievleva and Orlick discuss imagery, sometimes called guided imagery, visualization, mental rehearsal, or self-hypnosis that refers to specific techniques often used by psychologists to help individuals visualize or mentally rehearse a desired event. It involves using all of the senses to create an imagined experience that feels real. By using all your senses you create a very real experience of having the desired outcome. Ievleva and Orlick say the first time you experience imagery it's helpful to have a skilled facilitator or practitioner walk you through the process. This is referred to as guided imagery. You can also use CDs or tapes, or record your own script to use as your guide. AquaDios.Com or this link http://aquadios.com/aquadiosmovies.html will take you to a video labeled “View Mind-Body Medicine Video” (Guided), but before viewing the video please first read the information about the DVD and the Spiral. This video can give you some good practice. After you are comfortable with the technique, it's easy to practice these techniques on your own.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
123
Sit in a comfortable “private” place where you won’t be interrupted. Relax your body and take several long, slow breaths. Close your eyes and create a vivid and convincing image. This image can be one you've previously experienced, or one you simply desire. It’s beneficial to visualize one of your three favorite places. Should you become distracted or find you are thinking about something else, simply acknowledge it and let it go. Focus on your breathing should you lose the image or if there is competition with your preferred imagery. Maintain a positive attitude. Imagine the sights, sounds, tastes, feelings, and even smells of the experience. Take note of as much detail of the scene as possible. What are you wearing, who is there, what are you hearing, how do you feel? If your imagery session is not going the way you want it to, simply open your eyes and start over with your breathing. Ievleva and Orlick say it is always best to end an imagery session with a positive image.
Imagery – Sports – Life
Ievleva and Orlick believe athletes have many opportunities to try the various imagery or self-hypnosis techniques. From injury recovery to improved sports performance, these techniques are showing promise as a standard part of an athlete's training program. Of course everyone can benefit from developing Mind Body Medicine skills to improve their life, health and welfare.
Coping with a Sports Injury – patience On March 8, 2008 Elizabeth Quinn wrote an article on About.com titled, “Coping with a Sports Injury - patience”. Quinn reveals that athletes frequently react to injuries with a wide range of emotions including denial, anger, and even depression. She says a sport related injury often seems unfair to the athlete who has been physically active and otherwise healthy. Although all people’s feelings are real, she says it’s important to move beyond the negative and find more positive strategies to cope with this setback. In many cases dealing gracefully with an injury will make you a more focused, flexible, and resilient athlete and person. Quinn offers some suggestions for coping with an injury which can be considered by the non-athlete as well as the patient who have neglected physical fitness activities.
Learn About Your Injury
Quinn says to learn as much as possible about the cause, treatment and prevention of your injury, illness or disease. Not fully understanding an injury illness or disease can cause fear or anxiety. Learn how to talk to your doctor. Ask the following questions of your doctor, trainer, coach or therapist until you know exactly what you can do to heal quickly and fully.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
124
What is my diagnosis what type of injury illness or disease do I have? How long will recovery take? What is the purpose of the treatments I am receiving? What should I expect during rehab? What alternative workouts can I safely do? What are the warning signs that I am getting worse?
Quinn says that by understanding the injury and knowing what to expect during the rehabilitation process, you will feel less anxiety and a greater sense of control.
Accept Responsibility for Your Injury – Health Problem
Quinn believes you must not blame yourself or become involved with guilt, responsibility is not saying that the injury is your fault. What this means is that you must accept that now you have an injury, sickness or disease and you are the only one that can truly determine how to manage your outcome. Quinn says that by taking on the responsibility for your recovery process you will find a greater sense of control and will quickly progress in recovery, rather than dwelling on the past or blaming the injury on an outside factor.
Monitor Your Attitude Quinn says to heal quickly you must be committed to overcoming your injury by showing up for your treatments, working hard, and listening and doing what your doctor and/or athletic trainer tells you to do. You also must monitor what your “self-talk” is and what you are thinking and saying to yourself regarding the injury and the rehab process.
Your self-talk is important.
Are your thoughts negative and self-defeating?
To get the most out of your daily rehab, work hard and maintain a positive attitude. Remain focused on what you need to do.
Use the Mind to Heal the Body
Quinn notes there is growing research that shows it is possible to speed up the healing process by using specific mental skills and techniques such as imagery, visualization and self-hypnosis. Imagery techniques use all of the senses to create mental images, feelings and sensations related to a desired outcome as though it is happening now or has already happened.
Get Support
A common response after an injury is to isolate yourself from teammates, coaches, and friends. Quinn believes that is important to maintain contact with others as you recover from your injury. Your teammates, friends and coach can listen when you need to vent some anger, or can offer advice or encouragement during the rehab process. Just knowing you don't have to face the injury alone can also be a tremendous comfort. So, go to practice; remain around the locker room and the weight room. Be visible by being an active member of the group.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
125
Set Goals
Just because you are injured doesn't mean you stop planning or setting goals. Rather than viewing the injury as a crisis, make it another training challenge. You goals will now focus on recovery rather than performance. This will help keep you motivated. By monitoring your goals you will also be able to notice small improvements in the rehab of your injury. You will feel more confident that you are getting better and improving. Remember to work closely with your therapist or doctor. They can help you set realistic goals that are in line with each stage of your rehab. Most athletes have a tendency to try to speed-up the recovery by doing too much too soon. It is important to accept that you are injured and know your limits.
Maintain Your Fitness While Injured
Depending upon the type of injury, illness or disease you have, you may be able to modify your training or add alternate forms of training to maintain cardiovascular conditioning or strength. Work with your trainer, therapist or physician to establish a good alternative workout program. If you can't run, you can always learn deep-water running, cycle or swim. Work on relaxation training and flexibility. Create a modified strength training program, do a limited amount of exercise to maintain cardiovascular fitness or focus on better nutritional health. With the right knowledge, support and patience an injury, illness or disease can be overcome without turning your whole world upside down. By taking things slow, setting realistic goals and maintaining a positive, focused approach most athletes can overcome minor injuries quickly and major injuries in time. Make sure you see your doctor for a proper diagnosis and treatment plan for any injury.
Knee - Pelvis - Foot Fractures Joint Pain Treatment
Bone Fractures A broken bone, or a bone fracture, is a term used to describe a crack or a break in a bone. A fracture can be complete or partial. If the broken bone punctures the skin, it is called an open or compound fracture.
What Causes a Fracture
Fractures commonly occur from a high impact or trauma to the bone, although some diseases can weaken bones and cause them to break. Very small cracks in the bone called stress fractures can be caused by overuse. The most common causes of stress fracture are caused by: High impact sports injuries, Traumatic, forceful and unnatural movements, Overuse - prolonged long-distance walking or running, Falls, Accidents, Osteoporosis, Tumors growing near the bone.
The Symptoms of a Fracture
Out-of-place or misshapen limb or joint; Swelling, bruising or bleeding; Intense pain; Numbness and tingling; Limited mobility or inability to move a limb.
Bone Fractures Types and Descriptions
Simple — the bone is broken in one place Closed — the skin over the broken bone has not been pierced Comminuted — the broken bone has three or more bone fragments

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
126
Open or Compound; the skin over the fracture has been pierced and the broken bone is exposed Undisplaced — the broken bone pieces are aligned Displaced — the broken bone pieces are not aligned Transverse fracture - the fracture is at a right angle to the long axis of the bone. Greenstick fracture; the fracture is on one side of the bone, causing a bend on the other side of the bone .
Immediate Treatment for a Fracture
If you suspect you have a fractured bone, you should seek immediate emergency medical care. X-rays are often used to located and assess fractures. The broken pieces may need to be put back in place and then immobilized until the bones can heal as new bone forms around the break. You may need to wear a cast or splint, or possibly have surgery to put in plates, pins or screws to keep the bone in place.
Bone Healing
Immediately after a bone fracture the body forms a protective blood clot and callus or fibrous tissue to protect the injured area. New bone cells start forming at the edges of fracture site and grow toward each other. Over time the fracture closes completely and the bony callus is absorbed. Treatment for Fractures The type of treatment will depend on the kind of fracture and the specific bones involved. Casting — After the broken bones have been manipulated back into their proper positions, a plaster or fiberglass cast is applied to keep the bones from moving while they heal. External fixation — Pins or wires are set into the bone through the skin above and below the fracture. These are connected to a ring or a bar outside the skin that holds the pins in place. After the bones have healed, the pins are removed. Internal fixation — In a surgical procedure, metal rods, wires, or screws are inserted in the bone fragments to keep them together.
Rehabilitation for Fractures
Fractures usually heal in about four to six weeks, but some can take several months depending on the extent of the injury and how well you follow rehab instructions. Casts or braces are often removed before complete healing to prevent joint stiffness. Pain usually decreases before the fracture is solid enough to handle a complete return to sports, so working with a therapist on a rehab protocol is important to avoid further injury. Once the bone is healed and strong, it's safe to begin muscle building. During the disuse, the muscles will have atrophied and be extremely weak. Tendons and ligaments may also be stiff from a lack of use. Rehabilitation involves flexibility, balance and strengthening exercises and a gradually increase of activity. Physical therapy is the preferred method of safely getting back into sports.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
127
Enhanced - Accelerated Healing
Lydia Ievleva and Terry Orlick recently published a study titled “Mental Links to Enhanced Healing: An Exploratory Study”. The purpose of the study Ievleva and Orlick study was to determine whether athletes who healed very rapidly demonstrated greater evidence than did slower healing athletes of psychosocial factors thought to be related to enhanced healing. Ievleva - Orlick used a survey format to measure the following factors – positive attitude, outlook, stress and stress control, social support, goal setting, positive self-talk, and mental imagery-as well as related items about beliefs and recommendations for enhanced healing.
Thirty-two former sports medicine clinics with either knee or ankle injuries participated in the study. Some 19% of these athletes had exceptionally fast recoveries. These subjects’ evidenced high scores on all variables tested; while those in the slowest healing group evidenced low scores. The most significant results were found in the more action related factors of goal setting, positive self-talk, and the use of healing imagery. This is particularly encouraging for those working in an applied setting, as these factors are within one's potential control. Thus, Ievleva and Orlick have demonstrated that “when injured” one’s attitude, stress control, positive self-talk, and use of mental imagery accelerates healing; not drugs.
DWR Examples Rheumatoid arthritis Abstract
Rheumatoid arthritis (RA) is a chronic, systemic, autoimmune, inflammatory disorder of unknown etiology and is the most common type of inflammatory arthritis. The disease is most often characterized by morning stiffness, tenderness, and swelling. Other systemic symptoms, such as anemia, increased free radical production, muscle atrophy, and weakness, also occur. Most likely, a combination of these factors contributes to physical inactivity as well, which, in turn, reinforces the muscle wasting. Despite these barriers, it is now becoming recognized that patients with well-controlled RA can tolerate increased physical activity under carefully supervised conditions and that there are many benefits to exercise. This article reviews the effects of various types of physical activity on RA, with particular emphasis on studies that have examined the use of strength training in clinical practice for the management of RA. Without exception, the studies have shown that increased physical activity in patients with RA improves physical capacity without exacerbating disease activity. Important criteria to consider when recommending an exercise program for patients with RA are outline.
Swimming Pool Exercises - Cost-Effective Help in Fibromyalgia
On February 22, 2008 Charles Bankhead a Staff Writer for MedPage wrote an article titled Swimming Pool Exercises May Offer Cost-Effective Help in Fibromyalgia.; reviewed and approved by Robert Jasmer, MD, an Associate Clinical Professor of Medicine, University of California, San Francisco for accuracy. Bankhead identifies a study reported in CACERES Spain where supervised exercises in a waist-deep pool of warm water proved to offer a cost-effective adjunctive therapy for fibromyalgia. The researchers suggested that doctors need to explain to patients that an aquatic exercise program may be a cost-effective treatment for patients with fibromyalgia, even though the study involved a small number of patients.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
128
Narcis Gusi, University of Extremadura, and Pablo Tomas-Carus, of the University of Evora in Portugal, reported online in Arthritis Research & Therapy that despite adding to the cost of usual care for fibromyalgia, three hourly aquatic exercise sessions weekly for eight months fell well within economic standards for cost-effectiveness. The cost per quality-adjusted life year (QALY) was 3,947 Euros (about $5,800) from a healthcare perspective and €7,878 (about $11,700) from a societal perspective. The investigators' analysis suggested the aquatic exercise program would still be cost-effective if each QALY cost three to four times more than the estimated cost. The authors concluded this Aquatic program enhances the health-related quality of life in women with fibromyalgia, but remained cautious in their assessment of the exercise program because the characteristics of the facilities (distance from patients' homes and the number of patients that can participate per session) are major concerns that have to be considered before a health manager decides to invest in such a program. Several studies have shown that physical therapy has a positive effect on health-related quality of life and fitness. In particular, short-term (six months) physical exercise in warm water has been shown to reduce pain and minimize mechanical impact associated with exercise, the authors noted. In a previous study involving patients with fibromyalgia, Gusi and Tomas-Carus found that the benefits of a 12-week aquatic exercise program disappeared with a similar period of inactivity. The results suggested the need for longer-duration programs or maintenance programs, neither of which had proven efficacy. The two investigators sought to determine the economic feasibility of an eight-month program of aquatic exercise for women with fibromyalgia. They compared usual care with or without the addition of an aquatic exercise program. The study involved 33 fibromyalgia patients, who were randomly assigned to usual care or the same care plus swimming-pool exercises. Patients assigned to the aquatic group met three times weekly for an hour. Each session consisted of supervised exercises in warm 92 F waist-deep water; which is way too hot for exercise. The sessions were held at a facility with a pool with room for 20 people at a time. The primary outcomes were healthcare costs and the number of QALYs gained. Sensitivity analyses examined the effects of variations in staff salary, number of women attending the sessions, and the time spent traveling to the pool. During the eight-month study, the exercise program added € 517 in healthcare costs and € 1,032 in societal costs per patient to the cost of usual care. The mean incremental QALY associated with the intervention was 0.131. Cost-effectiveness acceptability curves revealed a 95% probability that the addition of the aquatic exercise program to usual care would remain cost-effective up to a ceiling of inversion of €14,200/QALY (~$21,000) from a healthcare perspective and €28,300/QALY (~$42,000) from a societal perspective. Patients randomized to the aquatic exercise program had a greater increase in score on a validated health status instrument. The between-group difference emerged at three months and persisted through the end of the study. In general, the sensitivity analyses found the cost-effectiveness of the exercise program to be robust across variations in staff salaries and the number of participants per session. However, in a worst-case scenario that included minor improvements in cost utilities and a low number of participants per session, the exercise program exceeded the boundaries for cost-effectiveness (healthcare and societal). The authors acknowledged the small sample size and omission of other fibromyalgia therapies as limitations of the study.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
129
LEADING CAUSES OF DEATH
The Center for Disease Control says that more than 450,000 deaths a year in the U.S. are due to a lack of regular physical activity. A specialist in preventive medicine says that for every hour you exercise, you extend your life by two hours. Failure of a regular daily physical activity and sustained exercise is the cause of Heart diseases; Cancer (lung, colorectal, breast, prostate); Cerebrovascular disease; Chronic obstructive pulmonary disease; Pneumonia and influenza. A vital preventive medicine prescription is to think of exercise as a medicine.
The U.S. Surgeon General's Office and the American College of Sports Medicine recommend "moderate" activity for at least 30 minutes most days while AquaDios-Med™ recommends 45 minutes a day of intense, safe daily exercise like structured deep-water running. Ted Mitchell, M.D., a respected internist, director of the Wellness Program at the renowned Cooper Clinic in Dallas and a member of the Texas State Board on Aging believes “exercise is medicine” and he prescribes a “dose” of this most powerful and natural medicine of at least 30 minutes exercise most days, for his patients, that means five days a week minimum. Dr. Mitchell stipulates that if you underdose, you don't get the full benefits; if you overdose, there are toxic side effects like exhaustion and injuries.
So, what's enough safe daily exercise? AquaDios-Med™ and research confirms that 45 minutes of structured deep-water running 5 to 7 days a week is adequate to keep the body fit and the immune system strong and vital and that when American’s accomplish this the healthcare costs will lower by more than 50 % or about $ 1.2 Trillion. Dr. Mitchell, a health expert, says that older people are national treasures who deserve our preventive medicine efforts to improve the quality of their lives; Exercise Is Medicine, The Impaired become Repaired; YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; YOU GROW OLD BECAUSE YOU STOP EXERCISING!
Education - Research Health Insurance Company
Pumps Physical Fitness On July 22, 1996 Gray Weaver wrote an article for the Central New York Business Journal titled "My Heart Couldn't Take It". Weaver states that physical fitness, considered to be preventive medicine by many, continues to gain corporate converts in Central New York, including such major players as Bristol-Myers Squibb, Carrier Corp., and Welch Allyn. To help meet this need for personal well-being, Group Health Inc. (GHI), the largest not-for-profit health-services and insurance firm operating state-wide in New York, and with an office in East Syracuse, is promoting its concepts about exercise and nutrition. A nationally known fitness trainer and nutritionist, GHI consultant Donna Davidge, explains that many people (employers and employees) feel too busy to give physical fitness and proper nutrition the priorities they deserve. Paying attention to these vital elements of modern life can mean less time lost from illness and. as a result, lower insurance costs. Davidge, a blonde, radiant former model and cum laude university graduate in dietetics, encourages business owners to inspirit their employees to prepare themselves for the normal stresses of the workplace by taking short breaks during the day for quick pick-me-ups. She declares that just three minutes for a good stretch and deep, relaxed breathing (through the nose) will help clear the mind, relax the muscles, and sharpen concentration.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
130
Deep breathing and healthy breathing exercise is one of the priority health mechanisms and begins with determining your baseline respiration cycle, the number of inhalations and exhalations per minute. It is determined by counting each time you inhale and exhale per minute, usually a 30 second count, doubled. The objective is to teach yourself slow, calm and relaxed breathing. This is done by lowering the respiration cycle. If it is 20 per minute learn to lower it by 50 % or to 10 cycles per minute. This longer slower respiration cycle will dilate the vessels and veins lowering the heart rate while bring bringing more oxygen to the system. Moderate exercise three or four times a week is much more beneficial in maintaining general health and alertness, according to Davidge. And a brisk 20-minute walk will fit into a lunchtime schedule. But even this moderate-exercise regimen cannot substitute for a safe daily sustained exercise like deep-water running and a good night's sleep. Davidson warns an nutritious breakfast is important. Don't skip breakfast and make do with coffee and a doughnut or Danish. Too much coffee can actually cause midmorning slump. Be sure to eat a variety of nutritional foods and take fruit juice and a vitamin supplement. When you're serious about keeping fit while losing weight, consider six small meals a day to help take off pounds more readily than the proverbial three square meals.
The combination of moderate exercise and proper nutritional foods can give you extra energy and fewer health problems, Davidge concludes. It will help you feel better, look better, and work better.
Older Women's Beliefs About Exercise Benefits and Risks
Sandra O'Brien Cousins and Toni Antonucci, PhD reviewed research and wrote an article titled “Older Women's Beliefs About Exercise Benefits and Risks”, Physical Education and Recreation, University of Alberta, Edmonton. This research determined daily physical activity is advocated by various federal health agencies for reducing many of the health risks affecting old age, but older women are generally not heeding the message. The Health Belief Model proposes that sedentary living occurs when people believe that the risks of exercising exceed the benefits. To clarify the beliefs that act as incentives and barriers to more active living, the author asked 143 independent-living women aged 70 and older to respond to open-ended questions on their beliefs about benefits and risks for 6 fitness activities: brisk walking, Aquacise, riding a bike or cycling, stretching slowly to touch the toes, modified push-ups from a kneeling position, and supine curl-ups. Content analysis organized perceived risks into 19 categories and perceived benefits into 6 categories providing original data on the conceptions that older women hold about the utility of various types of physical activity. Respondents generally recognized broad health benefits to fitness activities, but beliefs about risks were strong, anatomically specific, and sometimes sensational in description. The findings suggest that many older women feel physically vulnerable, are unsure about their actual risks and benefits in exercise settings, and, in the face of that uncertainty, report medical reasons why they should be excused from fitness-promoting exercise. The profound result of this study shows that the elderly are afraid to exercise from fear they’ll become injured and supports the need for a safe daily exercise like the AquaDios-Med™ structured deep-water and Mind Body Medicine.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
131
Older People's Views of Falls-Prevention Interventions Six European Countries
On March 18, 2001Yardley and Bishop et al published an article in the Gerontologist Society of America titled “Older People's Views of Falls-Prevention Interventions in Six European Countries”. The study identified factors common to a variety of populations and settings that may promote or inhibit uptake and adherence to falls-related interventions. They began with semi-structured interviews to assess perceived advantages and barriers to taking part in falls-related interventions and carried this out in six European countries with 69 people aged 68 to 97 years. The sample was selected to include people with very different experiences of participation or nonparticipation in falls-related interventions, but all individuals were asked about interventions that included strength and balance training. The study concluded that the attitudes were similar in all countries and contexts. People were motivated to participate in strength and balance training by a wide range of perceived benefits (interest and enjoyment, improved health, mood, and independence) and not just reduction of falling risk. Participation also was encouraged by a personal invitation from a health practitioner and social approval from family and friends. Barriers to participation included denial of falling risk, the belief that no additional falls-prevention measures were necessary, practical barriers to attendance at groups (e.g., transport, effort, and cost), and a dislike of group activities. The study also found that because many older people reject the idea that they are at risk of falling, the uptake of strength and balance training programs may be promoted more effectively by maximizing and emphasizing their multiple positive benefits for health and well-being. A personal invitation or prescription from a health professional to participate is important, and it also may be helpful to provide home-based programs for those who dislike or find it difficult to attend groups.
Exploring the aging phenomenon
A century ago the average life expectancy for an American was less than 60 years. Leading causes of death were pneumonia, influenza, tuberculosis and infectious diarrhea. "Preventive" medicine in those days basically meant quarantine. Because we had no antibiotics to treat infections when people became ill they were removed to a "sick room." People under age 50 probably don't recall such epidemics, but many older people may remember people who were sent to tuberculosis sanatoriums or quarantined for other infectious diseases and some off to a leper colony. There was no leprosy treatment at the time, and because the disease was considered horrid these patients were not even allowed to get out to vote! Back in 1928, British bacteriologist Alexander Fleming first noted the action of a natural substance in killing bacteria. A decade later, other scientists concentrated this substance, developing the antibiotic we know as penicillin. This revolutionized medicine. For the first time, an effective tool was available to destroy the bacteria responsible for so many deaths. Penicillin derivatives and other antibiotics were developed in the 1940s and '50s. Even today, scientists constantly work to develop new means of destroying microbiological marauders.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
132
With the advent of the antibiotic era, we saw two things occur.
First, deaths from infections dropped dramatically and life spans grew significantly longer. The Census Bureau projects that an American who is 60 today has 22 years, or more of life ahead!
The second effect of antibiotics was less cheery. Americans were living longer but dying from chronic illnesses; the most common causes of death are heart disease, stroke and cancer. This early medical treatment of prescribing antibiotics treatment was then referred to as preventive medicine and it now has to change into a procedure that prescribes safe daily exercise and proper nutrients. Fifty years ago, physicians didn't explain much to a patient, but simply prescribed a therapy. But in 2008, the more you know about risks for chronic illness, the more capable you are of making lifestyle changes to improve long-term health. Research continues to reveal that most all our illnesses are related to our unhealthy or “bad” habits. To some degree physicians must become counselors, this is where a program like AquaDios-Med™ can be so beneficial.
A 7-step action Health plan for everyone Do you want to live a long, healthy life; with a little vim and vinegar in the old machinery? Whether you are 35 and feeling great or 75 and feeling the weight of the years, there are many things you can do to help enjoy the time you have to the fullest. Exercise is the key ingredient to living longer and living better. Just look around and you’ll notice that older people who exercised consistently through their lives all look better, have brighter twinkles in their eyes and take on life with passion. Studies also have shown this phenomenon. A wonderful study published in 1998 in the New England Journal of Medicine looked at a group of men and women starting in 1962. At the time, the group was about age 40. The researchers followed these people up until the 1990s, when they were in their 70s. They study examined three lifestyle risks -- physical activity, obesity and cigarette smoking. The group that had the "low-risk" lifestyle not only was living longer, but more important, had what the researchers called "compression of morbidity." That means they did not develop significant illnesses until the very end of their lives (in the study, until their final 12 months). The "high-risk" group not only died earlier, but had increasing health problems over the last several years of life. There is more on exercise in this book on pages 10 and 12. Don't smoke! Most people, when they think of cigarette smoking, think only of lung cancer. But smoking also raises the risk for other cancers, including mouth, tongue, throat, esophagus, pancreas and kidney. Smoking substantially increases the risk of heart disease and stroke. And it is a significant cause of chronic lung disease (emphysema, chronic bronchitis), an absolutely horrific illness. Volumes have been written about the detrimental health effects of smoking cigarettes. Like any habit, it is hard to break and the best thing to do is never start. If you are a smoker don't give up hope because the ill effects on the cardiovascular system may be temporary. Once people have kicked the habit, their risk for heart attack and stroke drops off dramatically in the next couple of years. Unfortunately, the cancer risk lingers, and long-term studies indicate it takes 10 to 15 years before risks get close to that of the non-smoking population. Some people have the attitude that that says, OK, I am 60 and I smoke. If I stop now, does that mean that I have to live until I am 70 or 75 before my risk for cancer even gets close to that of non-smokers? If that is so, why would I want to quit?"

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
133
Studies show the answer to that question is because people are statistically more likely to die from cardiovascular disease than from cancer, and that risk improves almost as quickly as you quit smoking! Some people smoke like a chimney and do not plan to quit. In those cases they can at least cut back the number of cigarettes to reduce their long-term risks, and take on a safe daily exercise like the AquaDios-Med™ plan. Do your best to manage your weight. Imagine somebody who weighed 180 pounds being asked to carry around a 40-pound backpack constantly. The effect is immediate and obvious. So is the effect of obesity. Unfortunately, 1 in 3 American adults is obese and at increased risk of high blood pressure, high cholesterol and diabetes. Obesity is associated with increased fatigue, sweating, sleep disturbance (obstructive sleep apnea) and gastroesophageal reflux (associated with heartburn). Pain in the hips, knees, back, ankles and feet are all common in people who are overweight. Most of the common problems seen in common medicine could be helped, if not eliminated, by maintaining appropriate weight and participating in safe daily exercise recommended by the AquaDios-Med™ plan. What is an appropriate weight? Unfortunately, many height and weight charts aren't useful, because they don't consider body type. Knowing someone's appropriate weight is kind of like looking at good art, but for a "guesstimate," you can use the body mass index (BMI). An ideal exercise program will include safe daily structured deep-water running prescribed by AquaDios-Med™ and some gentle stretching, maybe some light weight or resistance training and learning Yoga. Lifting weights will increase your lean body mass. Beginners should work with a personal trainer to avoid injuries and maximize results.
Simple weight-training advice
Do strength-training exercises two, three or days a week. Include eight to 10 exercises involving all large muscle groups of the upper and lower body. Lift a comfortable weight, because you should complete 12 to 15 repetitions per set. Do your best to complete at least one (preferably, two) sets per exercise session. Forty five minutes a day of structured deep-water running will provide the greatest health benefits. Getting older? Your doctor should look for this in your regular checkups
EXERCISE WEIGHT LIFTING - 1998 (National Geographic)
Getting old is part genetics and partly your own fault. Even the very elderly can retain as well as regain mobility and agility. Some subjects who found it difficult to climb stairs were put on a specially designed weight lifting regimen. It was shown that even 90 year weaklings can regain the strength and vitality they had 30 years earlier. And they can do it with simple exercises around their own homes. In one study of hundreds of nursing home residents age 72 to 98 went through ten weeks of weight training and more than doubled the participants muscle strength and increased walking speed and their ability to climb stairs. Another study of 40 mostly sedentary women ages 50 to 70 involving just twice a week exercises led to substantial increases in muscle mass, strength, balance and bone density.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
134
KEEP ON TRUCKING - NY Times 1996
Do you want to stay physically active till your 90+? You can by just keeping your weight down with safe daily exercise. Studies show that every extra pound of body weight adds four pounds of pressure to the kneecap. When climbing stairs, that single pound adds 20 pounds of stress; when running or doing aerobics, it adds about 25 pounds of stress. It's much cheaper budgeting for running shoes than a wheel chair and a nurse, but you need to act while you are younger.
EXERCISE 1997 UC Berkeley study
In a UC Berkeley study, it stated that doing the same exercise when you were younger will not stave off weight gain. Men will have to exercise harder or longer as they age if they want to maintain their weight. The study showed that per decade, the average 6 foot tall runner gained about 3.3 pounds and about 3/4 inch around the waist. That means that 50% more runners will end up in the moderately overweight category by the time they reach their late 40's." They said one would have to increase physical activity by 240% between age 30 and 40 to maintain weight all others things being equal. You can only do so much exercise before your body breaks down unless it is the safe daily exercise of deep-water running advocated by AquaDios-Med™. It is not practical to land run an extra 10 miles per day, but you can be aware of nutrition and watch your diet. Put the two together and it works. Dr. Mollenkopf says that if you are over 80 years of age, you are a prime candidate for falling down and hurting yourself and must work on weight training or deep-water running immediately. You must recognize that you will have to do a safe daily exercise such as structured deep-water running for the rest of your life.
Exercise - USA Today 2004
Regular exercise, including walking at an easy pace, seems to protect the aging brain from erosion in thinking ability — and even from Alzheimer's. Research shows that older women who were physically active, including those who walked at a leisurely pace two to three hours a week, performed much better on tests of memory and thinking ability than inactive women. Those who exercised more did even better. The study team found that women who were the most active — for example, those who walked at least six hours a week — had a 20% reduced risk of doing poorly on the same tests of cognitive ability. Relatively sedentary older men — those who walked less than one-quarter of a mile each day — had nearly twice the risk of developing dementia as men who walked more than 2 miles each day.
EXERCISE the Mind?
Most people think of physical exercise when the word exercise is mentioned, but mental exercise is even more a concern particularly as we get older. Study after study has shown that both are absolutely necessary to maintain any sharpness in later years. Done properly, safe daily exercise can extend the healthy life span and push chronic diseases out toward the end according to the director of Health Watch. An ASF Chronicle article noted that people who held onto their intellectual prowess in later years tended to exercise their brains. Studies have also shown that intellectual stimulation helped older people adopt better health behaviors as well. They made positive decisions about exercising and eating right.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
135
Researchers also used education to reverse declines in mental ability. In a study of 228 people over 65, 40% regained lost intellectual ability when they received five hours of mental training. Another study of 10,000 people over age 55, only 45% of women who rarely walked maintained their mobility over four years compared to 58.8% of frequent walkers. Among men, 57.4% of frequent walkers maintained their mobility versus 46.6% of those who never walked. Exercise allows people to live healthier and even longer. But the key is more vitality when you really need it. One Doctor commented that there is no drug in current or prospective use that holds as much promise for sustained health as a lifetime of physical exercise. Studies have shown that "perpetual athletes" are two or three decades younger physically than their contemporaries.
They have also shown that the competitive runner loses only 5% in speed and endurance with every decade while the average jogger loses only inactive 30 year old will have equal physical work capacity. Dr. Robert Leach of the U.S. Olympic team commented that most people who last a long time really do look after themselves. I don't think there is any question that if you are careful, your body can keep a high level of performance.
WEIGHT LIFTING - 1998 National Geographic As stated numerous times, getting old is part genetics and part your own fault. Even the very elderly can retain and regain mobility and agility. Some subjects who found it difficult to climb stairs were put on a specially designed weight lifting regimen. It was shown that even 90 year weaklings can regain the strength and vitality they had 30 years earlier. And they can do it with simple exercises around their own homes. In one study of hundreds of nursing home residents age 72 to 98, ten weeks of weight training more than doubled the participants muscle strength and increased walking speed and their ability to climb stairs. Another study of 40 mostly sedentary women ages 50 to 70 involving just twice a week exercises led to substantial increases in muscle mass, strength, balance and bone density.
AGING IS JUST A BY PRODUCT OF INACTIVITY POOR NUTRITIONTAKE A HIKE • 1998 University of Virginia
Earlier studies that indicated that walking may not have been that beneficial for health are probably wrong. In a 12 year study of the elderly in their '60s '70s and '80s who walked just two miles a day, they cut risk of death almost 50%. Additionally every extra mile they walked per day lowered their death rate by 19%. Nonetheless medical experts note that 60% of Americans don't get enough regular activity to improve their health and even worse for the elderly.
EXERCISE AND THE POOR – 1999 According to the American Medical Association poor people have a death rate three times that of other groups but it is more due to lack of medical care, stress of poverty, dangerous jobs, and polluted homes and bad neighborhoods. Stopping smoking, eating better, exercising, etc. might reduce the death rate by 13% or more. The biggest killers were still - heart disease and cancer.
EXERCISE - 1999 The Journal of American Medical Association noted that only about 22 % of Americans get enough exercise to do themselves any good. Vigorous walkers had a 43 % reduced risk of premature death when compared to those who did no exercise at all. Even occasional exercise led to a 29 % reduced risk of premature death.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
136
Exercise studies verify that exercise is shown to improve energy, reduce feelings of stress, anxiety and Depression, improve sleep, improve concentration, enhance self-esteem, help one lose weight, reduce the risk of heart disease, increases good cholesterol and lower triglycerides, reduces the risk of colon cancer, lowers high blood pressure and the risk of stroke and improves bone density and lowers the risk of osteoporosis.
ALZHIMERS AND EXERCISE 1999
Studies from 1991 by the American Academy of Neurology and the University of Cleveland indicate that people who exercise regularly during their lifetime are at a lower risk of Alzheimers. The findings agree with previous studies suggesting that staying active physically, mentally and socially helps protect against the disease. And to repeat from the book: "How We Die", the two worst ways to die are from AIDS and Alzheimers. How you live today IS a direct factor on how you die later on.
MORE GET OFF YOUR DUFF • J. Andrew Doyle, PhD 1999
Weight lifting can improve self-confidence according to a study of 16 sedentary women in their 70s found that both their strength and their confidence in their physical abilities increased significantly after they lifted weights three days a week for 10 weeks. Subjects used Nautilus weight machines, performing 11 different exercises, three sets of each exercise at 50%, 60% and 70% of individual maximum weight for that exercise. Declining physical powers tend to decrease people's self-confidence as they age, contributing to depression. What the article did not state is what happened after the study finished. In previous accounts of elderly patients who improved dramatically after weight training, most simply reverted to doing NOTHING thereafter and "regained" past ailments.
Harvard-affiliated Brigham • Women's Hospital in Boston – 2000
The health care costs that result from inactivity costs the national healthcare bill, conservatively, more than $24.3 billion in 2000. All of those costs could be avoided if people who are inactive now did the minimum recommended by the federal government - 30 minutes of moderate activity on most days of the week. Inactivity accounted for 22% each of coronary heart disease, colon cancer and osteoporotic fractures, as well as 12% of diabetes.
EXERCISE, EXERCISE, EXERCISE! 2000 AP Harvard School of Public Health
In 2000 a Harvard School of Public Health study of more than 70,000 women found that exercise- even brisk walking - can reduce the risk of developing adult-onset diabetes. The study of women participating in the Nurses’ Health Study found that moderate to vigorous exercise was associated with a 46% lower risk.
Exercise • (2000)
You can teach a dog new tricks- at least make them healthier. Leg muscle increased 84% for men ages 60 – 75 who did weight training type exercises. In fact, they gained muscle mass in the same proportion as young exercisers in their 20s. The elderly also gained endurance.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
137
Not that much exercise is necessary
A study in the Journal of the American Medical Association tracked heart disease in some 40,000 female health professionals aged 45 year plus, over several years starting in the early 1990s. By 1999, the group developed 244 cases of heart disease. Risk was reduced by 47% in those who engaged in vigorous activity. But surprisingly, walking only 2 or more hours a week saw risk levels drop by 52%.
EXERCISE – 2001
Young men who jog regularly build strong bones and may be less likely to develop the brittle bone disease osteoporosis, a new study finds. Researchers report in the American Journal of Public Health that men in their 30s who jog at least nine times a month develop a bone density that is at least 5% higher than that of men who jog less. For couch potatoes, men who do little or no exercise, the bone density of joggers was almost 8% better.
Exercise: 2002
Obese people who exercise have half the death rate of trim people who don't exercise. Imagine, however, someone that was trim AND fit. “I don’t need to exercise anymore! I’m too old to work out! What can I do at my age anyway?” (2002)
Exercise: (2003)
A British medical journal found that only vigorous exercise — such as jogging, hiking, climbing stairs, racket sports and swimming — seems to help lower the risk of early death from heart disease. Other research has shown moderate exercise helps. They found that activities considered to provide mild exercise — such as walking, bowling and sailing — as well as pursuits of moderate intensity — such as golfing, dancing and brisk walking — did not lower the risk of early death. That flies in the face of other studies that have promoted the benefits of mild exercise. However, this information corresponds to what AquaDios-Med™ and that is the safe daily exercise of deep-water running. Only vigorous exercise was linked with a reduction in the risk of death from heart disease or any other cause within the 10 years of the study. The more heavy exercise the men did, the less their chances of dying during the study. Those who did the most exercise were 40% less likely to die than those who did the least, the researchers found.
Strength Training - (2004)
In 2004 The Centers for Disease Control and Prevention (CDC) released another issue of its series on Public Health and Aging featured in the Morbidity and Mortality Weekly Report. This study is entitled “Strength Training Among Adults Aged 65 and over.” It finds that only 11 percent of people aged 65 and older regularly perform any sort of strength training. Strength training is important at any age, and is recommended for older adults as a way to decrease the risk of falls and fractures and to promote independent living. The results of the CD survey indicate the need for older people to engage in more strength training.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
138
National Blueprint Increasing Physical Activity Among Adults Age 50 and Older
In 2004 Feifei Wang did a study on “Just a little exercise” and reported it in the Journal of Occupational and Environmental Medicine at the University of Michigan. The study involved 23,500 workers at General Motors and estimated that getting the most sedentary obese workers to exercise would have saved about $790,000 a year, or about 1.5 percent of health-care costs for the whole group. Company-wide, the potential savings could reach $7.1 million per year. Of the whole group of workers, about 30 percent were of normal weight, 45 percent were overweight, and 25 percent were obese. Annual health-care costs averaged $2,200 for normal weight, $2,400 for the overweight, and $2,700 for obese employees. But among workers who did no exercise, health-care costs went up by at least $100 a year, and were $3,000 a year for obese employees who were sedentary. It would be interesting to learn what the programs of AquaDios-Med™ would produce in a similar study.
Physical Activity – 2004
A study in the July, 2004 issue of the American Journal of Preventive Medicine found that even occasional physical activity can increase the life expectancy of people aged 65 and over. It tracked over 3,000 people aged 65 and over for 12 years and found that those who exercised just once a week reduced their risk of early mortality by up to 40 percent. Physical activity reduces the likelihood of death by lowering the risk of heart disease and other ailments. The researchers note that efforts to provide older people with more opportunities for physical activity are important in enhancing their health and well-being. In October 2004, The NY Times commented that exercise, including strength training can help even the very old. A Tufts University study found that people in the 80's and 90's that pump iron are able to walk faster, climb more stairs, and, in some cases, give up walkers for canes." This study follows a groundbreaking study started four years ago. They indicated that the main reason many elderly grow chair bound is that their muscles are weak from lack of exercise. The study involved 100 men and women in a nursing home. The exercising residents increased their walking speed by 12% and their ability to climb stairs by 26%. The people who worked out were less depressed and more likely to walk around on their own and take part in nursing activities. Unfortunately, previous studies also showed that once the survey was over, many went back to doing nothing and became the sick couch potatoes they were before. The National Institute for Aging and the University of Iowa found another advantage to exercise. Scientists report that moderate exercise three times per week can cut the risk of severe bleeding in the digestive tract by a third. Gastrointestinal hemorrhaging accounts for 200,000 hospital admissions of people over 65 who are five times more likely to suffer from the potentially fatal problem than those of middle age. And we're not necessarily talking about major sweat. In reviewing 8,205 people over 65, those that exercised vigorously or even walked or gardened were 30% less likely to develop gastrointestinal hemorrhaging probably because exercise helps promote blood circulation.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
139
EXERCISE: (Who says Retirement Has to be Boring?)
Exercise is the closest thing we have to an anti-aging pill says Dr. Leaf of the Harvard Medical School. Research shows that many of the problems once attributed to aging as slowing down, declining muscle strength and fatigue are actually the result of a sedentary lifestyle. Eighty percent of the health problems once associated with aging are now thought to be preventable or postponable if a person keeps fit. Exercise strengthens the heart and lungs, increases circulation, reduces body fat, relieves stress, keeps bones strong and lowers blood pressure. It strengthens and tones your muscles and keeps joints, tendons, and ligaments flexible, allowing you to move more easily. Exercise increases your energy level, aids digestion, helps you sleep better, improves your appearance and overall sense of well-being.
Following an exercise program gives you a sense of self-reliance, self-mastery, power, control, and an opportunity to set and achieve goals. You don't have to be a marathon runner to achieve results. A study conducted by the Institute for Aerobics Research and Cooper Clinic in Dallas shows that moderate exercise can substantially reduce your chance of dying of heart disease or cancer.
For those many of you that say you" don't have the time, you're too busy, work is hectic, etc., etc."- that may be O.K. if you live in Cuba, Haiti, Somalia or some other third world country. But because you do live in the U.S., you have time through the freedom of life that is provided here. Take advantage of that right by committing yourself to being better both mentally and physically; if not for yourself, at least set an example for your children.
EXERCISE – Reduces Breast Cancer
Continuing study on the benefits of exercise now show that there is up to a 58% reduction in the risk of breast cancer for women under 40 years of age if they exercise at least 4 hours per week.
EXERCISE Stanford University
Stanford University compared the health of 451 members of the 50 Plus Fitness Association who exercised at least four hours per week with that of 330 people 50 to 72 who have never maintained a jogging or aerobic program for as long as a month. They concluded: people over 50 who run regularly live longer and are slower to develop age related illnesses than their non-running sedentary counterparts. Further, the average cost in medical expenses and time off from work was 24% less for the active group. Over the eight year period of the study, 7% in the non-active group died while only 1.5% in the active group did. Male runners had 40% less disability rates- women's rates were 80% LESS than the non-runners and are now that male female ratio as well.
EXERCISE: Harvard
A Harvard Medical School Study of frail and institutionalized volunteers between ages 86 and 96 did leg lifts for 45 minutes three times per week. After 8 weeks the size of leg muscles increased as much as 13.5% and walking speed by nearly 50%. In another study, active women over the age of 60 were placed on a 24 week weight training program. They increased their weight lifting capacity from 5% to 65% and they significantly increased their lean muscle mass while decreasing body fat.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
140
EXERCISE: Lower Risk Heart attack
Another study on 73,029 women shows that those who were the most active had about a 40% lower risk of a heart attack. Another study of men showed that those that did any exercise at all had a 21% less risk than a sedentary one. Those who exercised the hardest had a 29% lower risk than the sedentary man. A third study showed that postmenopausal women who exercised reduce their risk of a heart attack by 60%.
Lack of Exercise -250,000 deaths a year
The Center for Disease Control says that 250,000 deaths a year in the U.S. are due to a lack of regular physical activity. A specialist in preventive medicine says that for every hour you exercise, you extend your life by two hours.
EXERCISE: Multiple Health Benefits
A 1995 study showed that regular exercise can decrease heart disease and stroke by reducing the risks 50 %. Exercise also lowers blood pressure, raising the level of HDL, reducing the risk of developing blood clots and diabetes and countering weight gain.
Exercise reduced the risk of colon cancer and exercise lowered the risk of osteoporosis by increasing bone density and reduced the risk of fractures. The exercise does not have to be weight bearing - stationary cycling and water aerobics and deep-water running worked as well. Research consistently shows that older people who exercise increase balance, strength, coordination and flexibility and all this exercise helps to prevent falls and the common fractures that follow. Safe daily exercise can perhaps eliminate 80 % of the diabetes case because regular exercise increases sensitivity of cells to insulin which lowers blood sugar and the need for insulin. Exercise is known to assist in weight control since exercise reduces fat and increases muscle. Exercise enhances the immunity to disease since exercise increases circulation that helps fight infections and tumors. Exercise reduces arthritis proven by studies indicating even moderate exercise combined with stretching has been shown to reduce pain and the need to medicate Exercise is known to stop gastrointestinal bleeding since studies show physical activity decrease severe gastrointestinal hemorrhaging in older people, probably through increase circulation to the digestive tract. Exercise improves memory through increased circulation and the fact that the person is more active and involved with living to begin with. Exercise also improves sleep since activity- though not immediately before bedtime - has been shown to allow people to enter sleep faster and sleep more deeply.
Preventive Medicine - Preventive Care - Exercise and Health Safe daily exercise has many benefits, both physical and mental. It helps to minimize the risk of cancer, stroke, heart disease, diabetes, and premature aging. Safe daily exercise also reduces anxiety, fatigue, and tension. Regular exercise has been shown to effectively manage stress, which helps prevent acne and the occurrence of tension headaches. Exercise helps people sleep better, which, in turn, contributes to a stronger immune system and greater ability to fight illness and infection. In general, people who exercise enjoy a higher energy level than others, and are better able to concentrate at school or at work.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
141
A physically fit person is more likely to recover quickly from illness and injury and from surgery. By safe daily exercising, a person will strengthen his or her heart and muscles and improve the flexibility of the joints. Aerobic exercise, which raises the heartbeat, improves the condition of other organs as well as the heart, and increases one's overall conditioning and endurance. Women who exercise are at a decreased risk of developing osteoporosis, a degenerative bone disease.
AquaDios-Med™ EXERCISING SAFELY AquaDios-Med™ believes the human body requires safe daily exercising, for about forty minutes five to seven times a week. AquaDios-Med™ advocates the exercise should be structured deep-water running for the general population including non-athletes, the sedentary and patients, especially those prescribed daily medications. The activity of deep-water running is an aerobic activity that raises the heartbeat, adds flexibility and muscle-strengthening. The safe daily exercise by AquaDios-Med™ will provide enough physical activity for a healthy person of any age and includes the majority of people injured and many that may be handicapped as well as those infirmed or suffering from chronic diseases. Research has proven that safe daily exercise can help heart disease and stroke by reducing the risks by more than 50 % and when the AquaDios-Med™ process is followed the problems may be eliminated. Safe daily exercise lowers blood pressure, raising the level of HDL, reducing the risk of developing blood clots and diabetes and countering weight gain. Research has shown deep-water running to be the best and safest exercise and this is why AquaDios-Med™ believes everybody must enjoy its health benefits to lower the $ 2.5 Trillion healthcare cost and to improve their quality of life. Research has shown safe daily exercise lowers, and sometimes eliminates cancer and is specific to reducing the risk of colon cancer. Safe daily exercise increases bone density and reduces the risk of fractures and reduces or eliminates osteoporosis. The exercise does not have to be weight bearing- stationary cycling, water aerobics and deep-water running are very effective. Safe daily exercise for older people increases their balance, strength, coordination and flexibility- all that help prevent falls, the most common reason for hospitalization.
Exercise and Health A good rule of thumb is to try to exercise for about thirty minutes three times a week. Exercise should include a variety of activities, including aerobic activities that raise the heartbeat, stretching and flexibility exercises, and muscle-strengthening activities. Usually, participation in sports, either at school or with friends, provides enough physical activity for a healthy young person.
Exercise's Effects on Bones and Muscles New York Times May 26, 2008 – Health Guide
Exercise is critical for strong muscles and bones. Muscle strength declines as people age, but studies report that when people exercise they are stronger and leaner than others in their age group.
Exercise helps kids lower their risk of chronic pain in the future. Research has shown that it helps them prevent back and neck pain. The more flexible men are as teenagers, the lower their risk of neck tension in the future, according to a study published in the February 2006 British Journal of Sports Medicine. The same report found that women who had the greatest endurance strength as teenagers had a lower risk of tension neck than those with lower teenager endurance strength. However, men with the greatest endurance strength had higher rates of knee injuries later on.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
142
Joints are complex structures. They are designed to bear weight and move the body. Above the
knee is the femur (thigh bone). Below the knee is the tibia (shin bone) and fibula. The kneecap is also called the patella. It rides on top of the lower portion of the femur and the top portion of the tibia. The muscles and ligaments connect these bones, and the space between them is cushioned by fluid-filled capsules (synovia) and cartilage. When you exercise, the muscles pull on the bones, strengthening them. The range of motion of a joint represents how far it can be flexed (bent) and extended (stretched).
Effects of Exercise on Osteoarthritis
Joints require motion to stay healthy. Long periods of inactivity cause the arthritic joint to stiffen and the adjoining tissue to weaken. A moderate exercise program that includes low-impact aerobics, power, and strength training has benefits for osteoarthritic patients, even if exercise does not slow down the disease progression. Many patients who start an exercise program report less disability and pain. They are also better able to perform daily chores, and remain independent longer than their inactive peers. Older patients and those with medical problems should always check with their doctor before starting an exercise program.
Effect of Exercise on Back Pain
People who do not exercise regularly face an increased risk for low back pain, especially during times when they suddenly have to perform stressful, unfamiliar activities. These activities may include shoveling, digging, or moving heavy items. Although no definitive studies have been done to prove the relationship between lack of exercise and low back pain, sedentary living is probably a primary nonmedical cause contributing to this condition. Exercise -- Obese people who exercise have half the death rate of trim people who don't exercise. Imagine, however, someone that was trim AND fit. “I don’t need to exercise anymore! I’m too old to work out! What can I do at my age anyway?”
The Council of State and Territorial Epidemiologists Chronic Disease
Chronic diseases account for seven of the 10 leading causes of death in the U. S. including the three leading causes of preventable death (tobacco use, improper diet and physical inactivity, and alcohol use). In addition, 70% of health-care costs in the United States are for chronic diseases. Seven of every 10 U.S. residents who die each year (>1.7 million persons) do so as a result of a chronic disease. Chronic diseases affect the quality of life of 90 million U.S. residents (1) and the cost of medical care for persons with these diseases accounts for 70% of total medical care expenditures Chronic diseases are among the most common and costly health problems, they are also among the most preventable. Adopting healthy behaviors -- eating nutritious foods, being physically active, avoiding tobacco use -- can prevent or control the effects of these diseases. In addition, quality of life is enhanced when chronic diseases are detected and treated early. Regular screening can reduce morbidity and mortality from cancers of the breast, cervix, colon, and rectum. Clinical preventive services can prevent the debilitating complications of diabetes and cardiovascular disease. Of the 92 indicators, 24 are for cancer; 15, cardiovascular disease; 11, diabetes; 7, alcohol; 5 each, nutrition and tobacco; 3 each, oral health, physical activity, and renal disease; and 2 each, asthma, osteoporosis, and immunizations. The remaining 10 indicators cover such overarching conditions as poverty, education, life expectancy, and health insurance.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
143
UNDERSTANDING THE CHALLENGE OF OBESITY IS THE KEY TO ITS SOLUTION
To summarize a bit .... I trust we understand the serious challenge of Obesity in America. The fact that almost 35% of Americans are obese and amazingly over 50% of Black women are classified as Obese. We should be clear to know the prevalent serious widespread health risks of being Obese include: High Blood Pressure, Heart & Artery Disease, Diabetes, Osteoarthritis, Cancer, Sleep Disorders, Breathing Disorders, Gastrointestinal Problems, Depression, Anxiety, Low Self-Esteem, etc.
The U.S. spends $70 billion annually on these Obesity-related illnesses just enumerated. And while the U.S. Government frivolously states its so-called goals of decreasing Obesity to 20% of Adults (instead of the current 35%).... The actual truth is that Obesity is increasing at an Alarming Rate in Adults as well as children. And, the Statistics clearly reveal that most people are unsuccessful in their Weight Loss quest and gain any weight loss back very quickly. Therefore, obesity is an illness that requires continued public education, understanding, support, and compassion. Let’s finally be clear that the major contributors of the proliferation of Obesity in America is FAST Food, Junk Food, and tremendous Media Advertisements to support the same, Food Processing, Poor Nutrition, Lack of Good Exercise, Emotional Triggers, and Stress Management. So, we must understand that Obesity is a pervasive public health problem and can be difficult to treat. It is multi-factorial and really involves appetite regulation, energy metabolism, genetics, psycho-social, environmental, economic, as well as cultural factors.... I cannot overemphasize the need for compassion and understanding and support for those suffering with obesity.... Unfortunately, the lay public, healthcare providers, as well as insurance companies often view Obesity as simply a problem of willful misconduct --- eating too much and exercising too little. The truth is that Obesity is a remarkable disease in terms of the effort required by an individual to manage it and the extent of discrimination its victims SUFFER....
Alternative Medicine
Alternative Medicine may be defined as any form of medicine that is outside the main stream of western medicine or allopathy (allopath/ allopathic) or orthodox medicine. It find in all cultures to some extent and It is also called as indigenous medicine, traditional medicine (tm), folk medicine etc... These Alternative Medicines date back even thousands of years depending on the country and culture. 2/3rd of the world population relies solely on such therapies. The World Health Organization (WHO) encourages such traditional medicines across the globe. The adaptations of traditional medicines are called as Complementary or Complementary and Alternative Medicine. Energy Medicine has opened new horizons for scientific research on the nature of human psychology and consciousness. And of course science is now beginning to understand the mystery of healing. Quantum physics shows us that we are all energy fields moving and interacting with other energy fields. Scientific studies have revealed that energy healing produces immediate biochemical effects such as a rise in the hormone levels that protect the body against major illnesses, and an increase in the activation of cells associated with the immune system. It is confirmed that healing treatments positively affect hemoglobin, human hormone and enzyme levels and discourage the growth of bacteria and cancer cells.

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section III
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
Mind Body Medicine • Psychoneuroimmunology Physiological Self-Regulation • Preventive Medicine
Evidence Based
AquaDios-Med™ Proactive Preventive Medicine 94 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Preview • Mind-Body Medicine • Research AquaDios-Med™ Proactive Preventive Medicine • Evidence Based
Part III • 94 Pages AquaDios-Med™ Proactive Preventive Medicine is patient-centered evidence based scientific
medical process that integrates physiological aspects of Medical Hydrology, Deep-Water Running Immersion Therapy together with Psychoneuroimmunology – PNI, Mind Body Medicine – MBM – known as Inner Mental Training – IMT -- Physiological Self-Regulation -- PSR and Medical Hypnosis.
ADM™ PPM teaches patients to accelerate healing when sick or injured, to manage -- control pain, manage -- control symptoms and to establish physical fitness, increase the speed of rejuvenation to maintain normal healthy chemical balance and establish natural homeostasis equilibrium specific to Hans Selye’s, MD General Adaptation Syndrome -- GAS.
Part III research concentrates on Psychoneuroimmunology -- PNI Mind-Body Medicine – MBM, Mind Body Healing • Mind Body Wisdom • Clinical Hypnosis • Physiological Self-Regulation -- PSR • Visual Imagery and much more. A key element in all of these comparable modalities is the work of David Cheek, MD -- Leslie LeCron, Psychologist -- Ideomotor Finger Techniques to establish Ideomotor Signaling - Mind Body Medicine communications and to help eliminate, manage and or control symptoms with their Seven-Keys. Dr. Ernie Rossi discusses Milton Erickson, MD, father medical hypnosis in an Interview with French publication Le Journal des Psychologues, October 1994.
Research studies -- examines Self-Healing Behavior -- Etiology Distress - Dis-Ease -
Psychoneuroimmunology -- Empowered Patients -- How Dis-ease may have SECONDARY GAIN • Preventive Medicine - Holistic Medicine -- Alternative Medicine -- History – Philosophy –
Methods Mind Body Medicine • Dealing with Chronic Pain • Mind Body Solution • Imagery – Guided Imagery – Visualization • Biofeedback • Medical Hypnosis • Cognitive-Behavioral Therapy (CBT) • Meditation • Back Pain • Headaches • Arthritis • Other Musculoskeletal Pain • Managing Stress to Improve Immune Functions - Thoughts • Heal Your Body - Live longer, better wiser • Alternative Medicines • Uterine Fibroids • Prayer • Health • Psychoneuroimmunology - Guided Imagery – Mind Body Medicine Preventive Medicine Preventive Care • Simonton's Work – Cancer Remissions • Neuroendocrine Interaction • Immune System • Selye General Adaption Model • Adrenal Cortical Hormones • Stress Hormones • Heart Attack • Stroke Prevention Program • Dermatology Skin Disorders – Psychosomatic MBM • Psychoneuroimmunology • AFFIRMATIONS Prayer •Neurolinguistic Programming •Allergy Relief MBM •Weight Loss- Mind Body Medicine • Natural Breast Enlargement • Optimal Healing Environment • Chronic Low-Back Pain • Primary Care • Anesthesia MBM Surgery MBM • Natural Healing – Brief History PREVENTIVE Medicine FOR TYPE 2 DIABETES MELLITUS • For Coronary Artery Disease CAD • For Breast Cancer
Patients learn correct Deep-Water Running posture to sustain safe vigorous exercise AquaDios-Med™ PPM teaches each patient how to use mental skills to alter and control positive physiology and how to accomplish safe sustained vigorous exercise to build endurance, stamina, a strong Immune System, to improve vitality and a establish a healthy psychophysiological state; a process that will establish a healthy mental and physical state, independent from drugs and most surgeries.

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 Aquadios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Part Three • Mind Body Medicine • Research • Answers Healthcare • Crisis Manufactured • Man-Made
AquaDios-Med™ Proactive Preventive Medicine • Evidence Based Mind-Body Medicine • Research • Summary • Part III • 94 Pages
SOLUTION To • Man-Made Healthcare Crisis
Is AquaDios-Med™ Proactive Preventive Medicine
MIND-BODY MEDICINE Research AquaDios-Med™ Proactive Preventive Medicine is patient-centered evidence based scientific
medical process that integrates physiological aspects of Medical Hydrology with Deep-Water Running Exercise Therapy and Aquatics. ADM™ PPM has developed Proprietary Deep Immersion Chambers, access to Proprietary Multiple Temperatures, Proprietary Power Massage together with Mind Body Medicine – MBM, Inner Mental Training – IMT, Psychoneuroimmunology – PNI, in order for patients to learn and apply Physiological Self-Regulation – PSR, Medical Hypnosis, to accelerate healing when sick or injured, manage and control pain, manage and control symptoms establish physical fitness and increase the speed of rejuvenation and establish homeostasis.
Emphasis of AquaDios-Med™ PPM is to teach each patient how to develop and use natural individual mental skills to alter and control positive physiology and how to accomplish safe sustained vigorous exercise to build a strong Immune System, improve endurance, vitality and a establish a healthy state of homeostatic equilibrium; a process that will establish a healthy mental and physical state, independent from drugs and most surgeries.
The American Healthcare Crisis has been shown to be a Man-Made -- Manufactured Crisis created by a for-profit culture found in in the U.S. Congress, the FDA, the pharmaceutical-medical device makers, the American Medical Association -- AMA, the American Hospital Association – AHA Modern Hospital Medicine practices and the entire healthcare industry.
The perverse nature of this culture, made up of the richest, most powerful Americans, makes it
next to impossible to change anything in this existing system because it is purposely designed – created, to make enormous amounts of money with no concern for healthcare whatsoever. These one-per-centers will never tolerate smaller profits in exchange for a healthcare system built on the noble principles of medicine that decreases pain and suffering.
AquaDios-Med™ PPM can become a competitive system or a part of the existing healthcare system, but it will likely never be more than an ideo, an ideology that will never be acknowledged and put into practice unless the 400 world wide Billionaires step up to the plate with approximate $ 15 Billion it will take to establish AquaDios-Med™ PPM Health Centers across America. It is likely that only then will modern hospital medicine either change its method or abandon the ChargeMaster Price System and become patient centered hospitals. This would be the kind of hospital culture that would never order necessary surgeries, or prescribe unneeded drugs, or order unnecessary procedures. And it would be a medicine practiced with reasonable income- profits, but not just for big profits, it would include the patient’s needs.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
In order to prove AquaDios-Med™ PPM is a legitimate evidence base health procedure it is necessary to present major research and history in Mind Body Medicine - MBM, Inner Mental Training – IMT, Psychoneuroimmunology – PNI, to demonstrate patients can and do learn to apply Physiological Self-Regulation – PSR, Medical Hypnosis, to accelerate healing when sick or injured, manage and control pain, manage and control symptoms establish physical fitness and increase the speed of rejuvenation and establish homeostasis.
This research supports the fact that exercise is medicine; a preventive medicine that only the patient or person can produce as a consequence of safe daily exercise in the AquaDios-Med™ format. The research supports the fact that the impaired become repaired with safe daily exercise; just as AquaDios-Med™ states. This research also shows that age, longevity and a high caliber quality of life is something most all people can enjoy. The research shows that you don’t stop exercising because you grow old; you grow old because you stop exercising.
Further, the vast medical literature is filed with research that demonstrates the genuine capacity
of all people to heal when helped with proven methods of Psychoneuroimmunology -- PNI; Mind Body Medicine -- MBM; Inner Mental Training – IMT; Physiological Self-Regulation -- PSR and Medical Hypnosis; all confirmed methods to accelerate healing when sick or injured, manage and control pain, manage and control symptoms establish physical fitness and increase the speed of rejuvenation and establish homeostasis. Some of this Mind Body Medicine research is presented forthwith to help establish a better understanding the why and how these procedures are integrated and combined within the AquaDios-Med™ process with the result of its safe daily exercise with such a powerful healing force.
Modern Hospital Medicine • Mind-Body Medicine (MBM) Psychoneuroimmunology [PNI] Mind Body Healing • Mind Body Wisdom • Mind Body Medicine
Reference has been previously made to the groundbreaking 1981 research of Dr. R. Ader, who
has authored more than two hundred research articles. The New York, Academic Press report confirmed what experts in Medical Hypnosis have known for more than many decades, the mind – body process of medical illnesses and established Psychoneuroimmunological Mediation. Decades of research has shown a strong relationship between the nervous system and immune inflammatory responses. Ader’s study makes it clear the immune system communicates with the neuroendocrine system and that imbalances in the neuroendocrine–immune circuitry are relevant to host defenses. This knowledge is the basis of the scientific discipline called psychoneuroimmunology.
What may be the benefactor of this groundbreaking research is that there is now a scientific
term to classify what Medical Hypnosis experts do to treat the many serious dis-ease etiologies without or with very little medication or surgery and given birth to a pleasant socio-medical term almost anyone can identify with, and feel good about – Mind Body Medicine. This positive name recognition will both popularize the process and eliminate the many negative attitudes held by some when it was referred to as hypnosis.
Psychoneuroimmunology – PNI is by far the most scientifically accurate, but it is a long complicated term that defines a process, which combines patient – doctor activities and procedures designed to cause a positive influence on the entire physiology – immunology, and to some degree authority over the immune system; a mediation to intervene, initiate the activate a treatment team interaction between patient, doctor and healing -- Mind Body Medicine -- MBM.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
The AquaDios-Med™ proactive preventive medicine process for healing, health, well-ness and physical fitness is entrenched teaching patients through PNI – MBM to establish and facilitate positive homeostasis and physiological-self regulation – PSR, but refers to the process as Inner Mental Training a method first developed in the Sports Field to develop ideal performance states in competition.
We humans do, in fact, influence our minds and bodies daily in positive and negative ways.
The objective is to eliminate or decrease the negative or dis – ease and increase the positive to ease toward wellness – balance – well-being – homeostatic balance. In healthcare the ideal performance state is emphasis on healthy natural homeostasis equilibrium and balance to eliminate- control symptoms of medical illness, pain or suffering to develop physical fitness. Physiological self-regulation -- PSR becomes a learned mind – body interaction to sustain a healthy body and mind. For a more in depth cancer and other disease related scientific data, go to http://www.aquadios.com/ and http://www.stresscards.com/cancerabst.htm
Mind Body Healing
Research of Dr. Ader might be heralded as one of the most important scientific contributions to
modern hospital medicine, because there no longer remains a defensible reason for hospitals to not have a cadre of Mind body Medicine – MBM experts on staff to lower the approximate 20 million admissions of patients without discernible Pathology - - PWDP. This step alone would protect more than 6.7 million patients from suffering adverse events, iatrogenic medicine and death by hospitalization.
When hospitals employ sufficient MBM experts they will have to insist, the AMA’s select RUC committee of 29 members, the American Hospital Association – AHA, Centers for Medicare and Medicaid Services –CMS, establish Mind Body Medicine services amongst the more than 10,000 physician services for reimbursements. Remember, the AMA over sees a 29 member RUC committee - - Specialty Society Relative Value Scale Update Committee. The RUC advises the Centers for Medicare and Medicaid Services. Medicare reimbursements for physician services come from a $ 60 Billion budget controlled by CMS a government agency that relies on the AMA special 29 member RUC committee to advise who to pay and how much.
It is estimated that as much or more than $ 300 Billion can be saved from the healthcare budget
by modern hospital medicine with this one intelligent recommendation to add Health Center’s staffed with experts in Mind Body Medicine. This of course involves change to the AMA reimbursement system process in place with its representative RUC advisory committee and the CMS that would allow the types of suggestions being made here – the patients without discernible Pathology - - PWDP would all but disappear. Psychoneuroimmunology - - Mind Body Medicine is an evidence based and proven scientific process and must become an integral of each and every hospital across America – this must be accepted as the valuable preventive medicine treatment that it is to streamline healthcare.
Research studies will be presented to demonstrate and give examples of how most all medical
illness, ailments and disease -- disorders with physical symptoms originate etiologically from, and with mental or emotional causes, and therefore the first line of treatment should be with MBM followed by the modern hospital medicine approach; not the other way around. Research is leading us into the greater science of how our thoughts affect us physically and how our mind may be producing serious physical ailments and dis-ease. Dis-ease is considered the absence of natural function at the cell level and in as much as 80% of all cases; the patient can learn symptom management, control and or remission.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
Maurice Kouguell, Ph.D. Emeritus of Harvard medical states Mind Body Medicine - - MBM originates from ancient healing practices, yet is still active in modern medical treatment; just not often enough, it should be utilized in all cases as part of the medical history. Mind Body Science - - MBS approaches may include professional clinical hypnosis, healing and cures through suggestion, imagination, imagery, placebo effect, expectancy and the self-determination and motivation of the patient.
Medical science demonstrates the human immune system to be labile yet governed by what is conceptually recognized in science as the unconscious part of the human brain, and that mind, part of the body science mediation, can ingeniously instruct the immune system. Medical science also demonstrates the human body's response to traumatic injury or the insult of surgery is automatic and governed by each individual's immune system.
Mainstream approaches fail to capitalize on the individual's independence and capacity to
utilize their internal mind-body capacities to manifest pain management, monitor re-injury pain and to remain functional from the moment of injury or disease.
Research dating back to the scientific importance of physiological homeostasis shows that people and their perceived reality may cause negative reaction to stresses which can trigger more than 90% of their ailments with everything from psychosomatic illnesses through the most disastrous of physically handicapping cancers. Homeostasis is the physiological ability or tendency of an organism or cell to maintain internal equilibrium by adjusting its physiological processes. Psychosomatic illness is a powerful example of how our subconscious mind, can cause serious illness.
Research confirms this extreme negative human power can be caused by our own repressed
anger or guilt. See Cheek and LeCron’s 7 Keys -- COMPISS (1) Conflicts, (2) Organ Language, (3) Motivations - Masochism, (4) Past Experiences (5) Identification, (6) Self-Punishment and (7) Suggestion. These very forceful emotional states have the ability to cause mass physiological damage when released; and may be extremely self-destructive.
The experience or repression of strong emotions can be a mental – body reaction. Unbridled
emotion can cause the homeostasis or balance of our body to automatically release chemicals, endorphins, adrenaline, and a myriad of other physiological changes in our body. These chemicals are designed to provide us with whatever we may perceive as real or imagined need at the time and to give us the particular strength(s) we require to overcome those real or imagined challenges, and reach our desired outcomes. These powerful chemicals can be released into our system initially by the power of our real world demand or by our wonderful and extreme imagination.
When reality demands these chemicals we take action with accelerated speed, power and
authority to accomplish a desirable outcome. However, too often reality is in the eyes of the beholder, a perceived perception, more imaginal than structural, yet, in some ways more dangerous as we are left to stew in our juices of dis-ease, soon to be diagnosed as a medical anomaly.
When imagination demands production of these chemicals we have no real outlet to act upon
and we may produce a real illness, but caused by our imagination; most often a pre-conscious brain activity or sub-threshold to awareness. On the other hand, Mind Body Medicine or Sport Medicine training can prepare the athlete for improved performances in difficult and demanding circumstances of sport. But, this un-harnessed and instantaneous chemical production can both help and simultaneously have the power to destroy us. Thus, Mind Body Medicine training can eliminate psycho emotionally produced somatic body ailments.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
One crusade of civilized Man has been to harness the power of these human chemicals and recreate them in a controlled setting of sport for the ideal performance state in competition or life itself while pharmaceutical companies attempt to make a pill to be ingested or an injection of appropriate chemicals. For example, in a healthy focused altered state of consciousness -- ASC one may simply imagine past examples of pleasure to cause levels of serotonin to rise causing mental and physical orgasms. With the simple yet complex imagination harnessed, and the power of Mind Body Medicine these countless wonders can be recreated all on one’s own; with some Inner Mental Training or Self-Programmed Control, both MBM approaches.
When emotions are suppressed, or our expressions are prohibited, our mind – body will
produce chemicals to be released into our systems, and without an external release, they manifest in different forms continuing to grow until recognized and calmed, or the manifestation becomes an illness of dis-ease.
Certain strong emotions may cause extreme negative mind-body effects. These emotions are
most often fear, anger, pain, sadness, that of guilt and more. These emotions if not dealt with lead to an incredible number of medical problems, ailments and disease, because they are often suppressed and continue on either being ignored, or unreleased in any fashion. As with any emotion, certain chemicals are created and released, yet if not used by specific body actions they build up and create a serious illness – dis-ease.
Unresolved fear can be the driving force of phobias and anxiety. Research suggests that most
emotional distress results from our unconscious mind that has recorded a problem that hasn’t been solved and one that may not be identified within the person. Phobias can be like an internal recording that is triggered by a similar association to an original memory that is at the unconscious level. This “phobia” effectively immobilizes the sufferer without revealing any direct connection of its source. This “phobia” can be the result of an “overly literal interpretation by the subconscious mind”, in its confused state of comprehension of the outside world.
Clinical Hypnosis
Mind Body Medicine DEFINED
David Cheek, M.D. and Milton Erickson, M.D. define Clinical Hypnosis as permissive, coercive, transitory depotentiation of an earlier learned set of symptom beliefs. Pain symptoms are often a learned limitation, a value imposed by either the patient's or physicians primary belief system or prejudice. Cheek's permissive, coercive term is defined as: "permissive", allowing the patient's behavior to be acknowledged as acceptable, thereby depotentiating any negative set of learned limitations; "coercive", a subtle manipulating of the patient's abilities by gradually supporting each patient's actions, gently taking control and guiding him/her into a state of increased receptivity (trance), toward health.
Rossi and Erickson refer to an -- MBM altered state of conscious - - ASC trance as an inner directive experience, free from most of the learned limitations of previous history and training, a natural free period of inner discovery, exploration, and realization of natural personal potential. Fundamental to this ASC is realizing that patients have symptoms or problems because of their personal learned limitations or those of their physicians. The objective is to relax patient and physician learned limitations, clinically disrupt the cognitive neurochemical circuits of the patient's usual frames of reference, and help previously unrecognized patient potentialities to surface.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
Deconditioning the victim attitude is facilitated by ideo-motor-finger-movement and Behavior Medicine to teach assertiveness, improved life coping skills, learning what myths the patient may be using to dignify disease and uncovering possible self-destructive tendencies that may cause Iatrogenic Complications (controlled relapses) or signs of improvement and remission. This -- MBM treatment approach relies on directness and moves quickly to the symptom source and may contribute to a clinical, iatrogenic patient energy, commonly referred to as resistance, acting out, aberration, and temporarily worsened symptoms; all a part of symptom management.
Professional awareness and management of the patient’s human energy in a controlled manner can make healing surprisingly easy and natural while mismanagement may contribute to disaster. Treatment utilizes clinically induced ASC to help patients relearn sub-cortical brain activity then to alter (self-talk) to counterattack symptoms. Research suggests 70 to 90 % of symptomatic etiology is rooted in natural, critical life events, resulting in destructive, subconscious psychophysiological phenomena of medical symptomatology.
Mind Body Medicine • Behavioral Medicine
Merging behavioral medicine with Mind Body Medicine has advantages because civilization and medicine has cultural inhibitors, which contribute to any disease, injury or accident. Treatment attempts to determine degree of symptom management potential each patient possesses. A problem facing the professional is how to determine the degree of unconscious aspects of symptom etiology while maintaining rapport with family and physician. Mind Body Medicine combined with Behavior Medicine helps to mobilize patient healing forces to their maximum power but does not replace Physical Therapy, but AquaDios-Med™ has power massage to reduce PT needs. By so doing, most symptoms may be reduced significantly and clinical medicine can thus rely upon less physical therapy, less medication and more on the patient.
PSYCHONEUROIMMUNOLOGICAL Mediation: Physiological Self-Regulation (PSR)
Dr. Kay Thompson, DDS in a 1983 BBC Documentary taught Hemophiliacs Physiological Self-Regulation (PSR), allowing them access to surgical intervention and dental treatment then filmed in surgery, to prove, even they can control bleeding and pain. Distress produces a particular destructive process in the body, which absorbs and decreases immune system energy. An embarrassing social situation may have sufficient distress to alter skin color, raise body temperature, produce perspiration, cause changes in the delicate internal chemical state, alter heart rate, increase acidity, drastically alter vision, hearing, smell, balance, and a host of other physical changes. Immune systems normally act automatically to preserve the integrity of the body. Research indicates that the majority of illness and disease is preceded by distress, either of a conscious or an unconscious nature, which produces a particular destructive process in the body, which absorbs and decreases immune system energy. Research supports - -ASC capacity as a natural human trait and demonstrates applied clinical hypnosis and behavior medicine mediates immune system function to facilitate therapeutic mind body healing. In Russia, Rosen reports some diabetics can improve their condition.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination. - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
Normal people can alter blood sugar levels by imagining eating candy fruit or vegetables. ASC – PSR are a disciplined use of a natural altered state of conscious attention which approaches peak concentration capacity, as related to an individual’s unique use of their own Neurophysiology, and helps to establish a common language relevant to treatment. Physiological Self-Regulation (PSR) is most effective when applied before the primary administration of medicines and before the competitive season for the athlete. Ideally, the best time to begin the program is just before surgery, or during treatment of an injury and for the athlete before pre-season training camp. Mental training programs have been adapted to improve economic performance in business while lowering stress-related disease, illness, accident, and malingering. It has also been adapted to assist actors, dancers, and entertainers. Actually, all learning can be accelerated through this approach, especially character actor’s parts and language learning. Programs are also designed to simply help make life easier and more fulfilling with decreased stress and anxiety. AquaDios-Med specific, dynamic psychophysical training requires time to learn even when applied by competent professionals. Modern Mind Body Medicine facilitates symptom removal, healing and cures through suggestion, imagination, imagery, expectancy and motivation of the patient. At the university student level it involves far-reaching sociocultural identity including the family, physician, alumni, student body, fans, administration budget and finance.
Mind Body Medicine – Teamwork
Techniques for improving performance by the patient are simply application of behavior principles related to human situations. This is technically referenced by four principles in psychology: (1) Applied behavior analysis as rooted in operant conditioning developed by Dr. B.F. Skinner. The basic tenet is that much of our behavior is modified by direct consequences that either "turn us on", "turn us off", or have no effect. (2) A second theory is the learning conditioning model popularized by Dr. Joseph Wolpe and colleagues. His approach relies on respondent conditioning developed by Russia's Dr. Pavlov in 1927 and learning theories of Drs. Hull and Guthrie formulated between 1935 and 1952. These combined methods are widely used to eliminate phobias and maladaptive habits.
(3) Dr. Bandura and colleagues, from 1969 to the present, formulated the social learning theory which today in practice relies on cognitive interpretations of mediation, antecedent stimuli and consequences. This technical jargon in simple terms means future behavior is somewhat dependent on how each person perceives his/her immediate role models and specific environmental reality. (4) Between 1974 and 1977, Drs. Mahoney and Meichenbaum expanded a specific cognitive behavior modification. This means first identifying the self-talk inside the mind that is faulty or irrational, then purposefully eliminating these destructive thoughts with constructive adaptive approaches within the inner dialogue to life.
Physiological Self-regulation (PSR) - Improved Concentration
Physiologic Self-Regulation (PSR) relies on applications of MBM – ASC – IMT procedures to
facilitate learning the regulation of physiology. AquaDios-Med uses Specific Mental Imagery to help patients stimulate and direct neuro-transmitter substances of the brain, accelerate rehabilitation, healing and pain management. This process facilitates acceleration of neuromuscular responsivity of prior Ideal Performance States - - IPS, helps to mobilize hidden reserves and become more integrated and active in the rehabilitation, healing process. This procedure can accomplish a rapid healing and also eliminate phobic-type fear for the patient or athlete.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
Other objectives of the mental training are to expand awareness of the limits of the patient and athlete's optimum physical fitness and consistent performance in both accelerated rehabilitation, competitive and non-competitive sports.
Mind Body Medicine Training
Mind Body Medicine Training is similar to Self-Hypnosis training through refractionation (a profound hypnotic state), to help patients learn self-management of some physical functions even though complex and complicated. Clinically produced MBM is an altered state of consciousness to help patients change rigid, imprisoning molds another may have cast, and to free them from this symptomatic, learned bondage.
PHYSIOLOGICAL SELF-REGULATION
1.) The psychology of attention in exercise or competition
2.) Narrow versus broad focus of attention
3.) Stimulation of concentration through "Think Training"
4.) Controlled Breathing Through BRACEDVE:
a) Breathing e) Energy
b) Relaxation f) Detachment
c) Attention g) Visual Imagery
d) Concentration h) Equilibrium-Balance-Being Centered
5.) Developing Energy Awareness:
a) Positive, Relaxed Attitudes
b) Muscular and Mental Relaxation;
c) Encourage Meditation, Visualizations;
d) Creating Altered States of Consciousness
OVERVIEW: TREATMENT OBJECTIVES 1) Unique Stress Factors for Pain Patients
2) Handling Superstitions and Phobias
3) Dealing with Family or Social Pressure
4) Dealing with Denial, Mental Blocks, Depression
5) Regulation of Arousal Levels Before – During Performance
6) The Roles of Tension and Task Difficulty

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
VISUAL IMAGERY
Research indicates symptom-bound energy provokes and distorts Intrapsychic perceptions and sensations causing severely disturbed biochemical mutation. Clinical visual imagery by the patient helps to return physiology to a natural state. ASC – MBM – IMT - is more direct and useful simply because it is regarded as a natural human capacity. Erickson and Kroger cite ASC as direct because a person in an altered state of consciousness is more easily approached and influenced to accept a healthier viewpoint rather than their symptom or complaint as a solution.
Ideomotor Techniques In 1954 and 1961 LeCron utilized ideomotor techniques to uncover symptom manifestations.
He used the Chevreul pendulum together with ideomotor finger movements during hypnosis with people suffering psychosomatic disorders. LeCron also organized the methods for ideomotor search and psychosomatic sensitizing and precipitating events under the categories of (1) Conflicts, (2) Motivations, (3) Identification, (4) Organ Language, (5) Suggestion, (6) Masochism or Self-Punishment and (7) Past Experiences; See Cheek and LeCron COMPISS acronym – same terms.
David Cheek, MD illustrated ideomotor questioning and subconscious review with a number of
case examples in 1962. Cheek - LeCron expanded the use of the pendulum and ideomotor finger signals. They felt these nonverbal techniques permitted accessing preverbal and nonverbal memories. Cheek - LeCron also elaborated on the Seven Keys to detecting causative factors for problems.
(1) Conflict was described as "I want" colliding with "you can't". (2) Motivation dealt with the
symptom or problem serving some purpose or secondary gain. (3) Identification related to a similar problem that a parent, sibling, or other significant person had had. (4) Masochism or Self-Punishment was unconsciously self-damaging behavior due to strong guilt feelings. (5) Imprints or Suggestion were single high-impact events, engrams, or fixed ideas similar to Pavlovian conditioning. (6) Organ Language made a figure of speech into a literal psychosomatic problem, such as "I felt stabbed in the back" becoming a chronic backache. (7) Past Experiences could be emotionally charged imprints or traumatic events.
In 1968 Cheek and LeCron mentioned skin diseases associated with sexual difficulties. For women they included acne, psoriasis, neurodermatitis, recurrent genital herpes, and pruritus vulvae while for men they listed psoriasis, neurodermatitis, and recurrent genital herpes.
Cheek collaborated with Ernie Rossi, Ph.D. and wrote a revised expanded edition (Cheek,
1994) in which he added considerable clinical case material. He also expressed the law that Pessimism Overrides Optimism during times of distress or threat (Cheek, 1994, p. 49). He used the pendulum only for pre-hypnosis demonstration of ideomotor activity to skeptical patients, preferring the "yes", "no", and "I don't want to answer" finger signals in clinical work. He eliminated the "I don't know" finger signal because too many of his patients used it to avoid answering. The "I don't know" finger signal is important to retain in hypnotic legal work where leading questions must be carefully avoided. Cheek noted that animal research on imprints showed that epinephrine both imprinted the memory and produced amnesia for it, correlating with and explaining the findings in humans of amnesia on the conscious level for traumatically imprinted memories.
Barnett discussed some problems in performance and interpretation of ideomotor finger responses (Barnett, 1980). While the finger technique is easily established and interpreted in the majority of patients, resistance may produce slight or no finger response or more than one finger may lift. Barnett discussed this further in his 1989 book.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
He also used transactional analysis and related the conscious state to the conscious part of the adult ego state and the subconscious ideomotor finger signals to the parent ego state, where resistance usually resides, or to the even deeper subconscious child ego state. He mentioned self-excoriating skin disorders with no organic cause as an example of self-punishment for guilt, reflecting a parent/child ego state conflict (Barnett). Ewin reported a series of 41 cases of warts resistant to standard wart therapies including hypnotic suggestion, with 33 cures using ASC with ideomotor signaling (Ewin, 1992). Ewin and Eimer expanded and standardized the process of ideomotor signaling for psychosomatic ASC (Ewin & Eimer, 2006).
Cheek recommends the practice of specific finger ideomotor signaling and use of the
mnemonic COMPISS for LeCron's seven keys for detecting causative factors: Conflict, Organ language, Motivation, Past experiences, Identification, Self-punishment, and Suggestion outlined in the ideomotor finger responses described.; same terms different order for acronym. Detection of significant initiating, sensitizing, and/or precipitating factors can be indicated by ideomotor signaling and brought to consciousness by imaging the memories and verbalizing them. With ideomotor signals, preverbal memories can be detected and subsequently brought to conscious memory. Each of the seven COMPISS factors should be checked to assure diagnostic completeness, as more than one factor can be involved. If one or two categories are involved and one initiating event can be recalled and emotionally neutralized, amelioration or cure of the problem can usually occur in one to three treatment sessions.
Therapeutic reframing options are mentioned for uprooting or neutralizing emotionally charged
factors uncovered by the ideom otor signals. They give case examples of resolution of a plantar wart neurodermatitis, penile warts, recu rrent herpes simplex labialis, urtic aria, and a one-visit cure of hypersensitivity to touch in a scar . Dr. Ewin has stated that alm ost anything you can treat with cortisone or antihistamine will probably respond to MBM and personal communication.
Cheek • LeCron Seven-Keys
There are seven keys or seven factors involved in the cause of any set of symptoms, according
to Leslie LeCron and David Cheek, MD, the first to bring medical hypnosis to the medical community, and developers of the use of ideomotor signaling. Through using a pendulum or other ideomotor signaling response, along with a specific list of questions, it is possible to identify the cause or causes for any particular problem by working through all seven keys.
This involves setting up a means of rapid and direct communication with the unconscious part of the mind must. In response, obtaining from it replies to questions by means of unconsciously controlled signals.
The Keys laid out by Cheek and LeCrone are motivation, masochism, identification, imprinting, conflict, organ language, and past experience.
Once the relevant keys have been pinpointed, it is then a simple matter of using the ideomotor signaling system to achieve a quick release of the problem that has been blocked and causing distress.
Mind Body Medicine • eliminate effects of Negative "Imprints"
LeCron’s ingenious questions --The Seven Keys and his ideomotor finger technique is a
process in which the client develops an altered state of consciousness -- ASC. And told that each of four fingers, preferably on one hand, will indicate a different response depending upon which one rises in response to a question. For example, the forefinger might stand for "yes," the middle finger for "no," the ring finger for "I do not know," and the little finger for "I do not wish to answer."
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
LeCron makes it clear that it is important for the unconscious to have the option of not revealing something for which the conscious mind is not ready to be aware of or hear.
Cheek and LeCron demonstrate how powerful negative words can be on children. What we
term as failure can be attributed to negative imprinting that people have been exposed to since birth. LeCron designed a series of resourceful questions [The Seven Keys] that this book teaches the
student reader to enable them self with the use age-regression or the return to an earlier time in life, being regressed back to the time of the experience. Leslie LeCron’s, book "Self-Hypnosis:
The Technique and its use in Daily Living and The Complete Guide to Hypnosis identify how unconscious self-talk may be sabotaging people’s lives. It is important for the reader to become aware of their negative Self-talk, to develop positive visualization, quiet sitting time and common sense to not compromise learning of self-empowerment through Mind Body Medicine.
The author of this book hopes you will be surprised and pleased at how comfortable you can
become by finding yourself breathing slower and deeper, as well as feeling calmer as you read each page. But there's no magic, this is just a book that will help to enable you to get to learn your own comfort with Mind Body Medicine naturally and with trust.
THE SEVEN KEYS Cheek • LeCron
The late David Cheek, M.D., and the late Leslie LeCron, authors of “Clinical Hypnotherapy”
(1968), believed there are seven keys or seven factors involved in causing any set of symptoms. Cheek states … With these seven keys, the door to the understanding of these ailments can be opened and insight gained into the patient symptom helping the patient to gain control over its negative life impact.
Cheek and LeCron have established Ideomotor Question Techniques to help patients cure or manage symptoms. These principles are the basis that all Mind Body Medicine self-empowerment comes from altered states of consciousness. Cheek and LeCron - Seven Keys:
1. Motivation 5. Conflict 2. Masochism 6. Organ Language 3. Identification 7. Past Experiences
4. Imprinting Motivations like those cited here are generally deeply unconscious but can often be quickly and
easily identified by the ideomotor questioning technique; insight alone may be enough to overcome the condition. 1 – Motivation
Have you ever heard of the Chicken soup syndrome? An illness or symptom can serve a purpose to gain sympathy, attention, even power and most often this motivation is unconscious and immature; like the child being sick to avoid a test at school. Most of us have immaturities along some lines.
A motive in hysterical blindness could be that the condition prevents the person from seeing something unpleasant or could serve as punishment for having seen something, which causes profound guilt.
As an unconscious means of escaping from hated housework, a woman might have a motivation to develop an allergy to detergents.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
The motive behind a symptom or illness is frequently defensive with the condition acting as a protection.
An example would be migraine headaches, which are used as a defense against unacceptable feelings of hostility and aggression, emotions almost invariably are found in migraine patients.
Motivations are sometimes deeply hidden but much more often can quickly be located through the questioning technique. Often insight alone is enough to overcome the condition. 2 – MASOCHISM- Self-punishment
Masochism is a form of unconscious Self-punishment or self-destructiveness, believed to be caused by strong unconscious guilt feelings and can lead to suicide or fatal illness – often a factor in painful diseases.
Self-punishment from strong guilt feelings can be a common form of unconsciously damaging one’s self. Masochism may include self-destruction. People with an overgrown conscience will punish themselves severely, often over minor transgressions or unacceptable thoughts. One part of the subconscious can compel a person to behave in an unacceptable way while another part then demands punishment for the offense.
The alcoholic frequently uses drinking as a means of self-destruction while there is an instinctive need for self-preservation; sometimes the will to die overcomes it. Many of these people do not want to get well and refuse therapy.
Research has shown that 80 per cent of accidents occur to 20 per cent of the personnel. Many accidents can be unconsciously self-induced or intentional. The housewife who often cuts or burns herself can be punishing herself.
In painful psychosomatic diseases, masochism can be a factor in their origin and can often be uncovered by questioning in such conditions as migraine, chronic headache of other types, in arthritis and bursitis, slipped disc, dysmenorrhea, neuralgias, and other painful conditions.
When self-punishment is located as a cause, insight is seldom enough to end the symptom. The
reasons for guilt feelings need to be explored. These guilt feelings often center on sex and we must learn to reassure an understanding that the feelings of guilt are probably unwarranted. No one wears a halo and everyone does things he regrets and has thoughts, which are not acceptable.
Help yourself to understand that self-punishment not only harms you and may also punish
everyone in the family at the same time. For example your illness may worry and upset the family and may be expensive, causing family hardship, which is unfair to innocent people.
3 -IDENITIFICATION
Symptoms caused by Identification are generally a process of Dramatization. In early childhood we all identify with parents and those close to us – it is normal to copy and emulate parents or other, most often this is an unconscious trait or even illness that may be inherited or is merely a result of identification.
Children tend to imprint or copy their parents and emulate them. In early childhood we all identify with those close to us; some can carry this into adult life. Identification is a process of dramatization. It may be difficult to know whether some trait or even illness is inherited or is merely a result of identification. If a mother, or father, is greatly overweight, the children probably will tend to be fat. There may be some hereditary tendency for obesity, but certainly identification plays a role.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
Love is a strong motive to identify with parents and a hated parent may be the object of identification. Often the child wishes to be like the parent to be big and strong and powerful, as the parent seems to be. A child may be told repeatedly they are just like one parent and that they take after that side of the family, this acting as a powerful suggestion. Identification with the father is common when a boy is named Jr. -- John Jones, Jr. Calling a boy Junior can promote feelings of inferiority. 4 – IMPRINTS
An Imprint is an idea, which has become fixed in the subconscious part of the mind and carried out exactly the same way as a posthypnotic suggestion. Suggestion can be the cause of single impact imprints, of great importance to the symptom syndrome.
Suggestion can be the cause of single impact imprints, which often can explain the cause of a
symptom. An imprinted experience may seem consciously trivial but most often of great importance to the symptom syndrome. An imprint is an idea, which has become fixed in the subconscious part of the mind and carried out exactly the same way as a posthypnotic suggestion.
Herbert Spiegel, M.D. points out many neuroses may be imprints with a compulsion to act out
behavior for which the causative stimulus is forgotten. Spiegel also has a logical statement as a powerful altered state of consciousness - suggestion, encouraging the person to repeat it as necessary …”Anxiety is a poison to my body … I need my body to live … I owe my body this respect and protection”.
Strong emotion causes people to become very suggestible. Something said at the time of high emotion may cause the subconscious to handle it as a post-hypnotic suggestion because people experiencing strong emotion slip spontaneously into a hypnotic state and thought processes become childlike and literal just as in hypnosis; this is why you need to learn about your altered states of consciousness.
Emotionally charged imprints or “engrams” unconsciously affect everyone. Depending on their wording, they can be very beneficial, but at other times they are extremely detrimental. They can affect behavior, cause illnesses, and some types of imprint or "prestige suggestions" may prevent recovery from disease or prevent the loss of some symptom.
Cheek and LeCron labeled damaging imprints as a field of semantics or "command statements" worded something like: "You’ll never get over this," "You'll have to learn to live with this condition," "Nothing does any good," "It can’t be helped."
The physician speaks with prestige or superior knowledge and years of experience. For example a discouraged or frustrated physician may make such a statement when the patient is in surgery or is very likely to be in a frightened or discouraged state to be hyper suggestible and may cause an iatrogenic complication.
When these types of imprinted ideations are set up, personal growth is most often unsuccessful until the imprint is removed. Such phrases may not have any effect if the person were not under a strong emotion when it is said.
5 – Conflict
Conflict is said to be an “I want colliding with I can't” and commonly revolves around sex with strong guilt feelings. Emotional conflict can be the presence of different and opposing subconscious emotions relating to a situation that has recently taken place or is in the process of being unfolded, accompanied at times by a physical discomfort and in particular by tension headaches.
Inner emotional conflicts can cause physical discomfort or pain, often in the form of tension headaches, the duration of which can range from a few minutes to days and in some cases even months, but would normally be a few hours.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
14
Tension headaches can be episodic or chronic, with episodic normally occurring less than 15 days a month, and chronic occurring 15 days or more a month, sometimes stretching over a few months. The pain associated with Tension headaches is normally mild to moderate, but can be severe.
Situations that cause emotional conflicts can be everyday occurrences which might seem
unimportant; as in the case of having to decide whether or not to accept an invitation to dinner, where a person we don't like or wish to see is likely to be, but where another person whom we do wish to see is likely to be as well, or when there is an underlying anger against a friend or a family member that we are unable or afraid to express for fear of hurting their feelings, and therefore repress, or when we are doing something we don't like and resent having to do.
One way of dealing with underlying emotional turmoil and anxiety is by using self-hypnosis to become aware of the real life conflict that triggered the symptom.
Simply relax yourself, calm down, and focus on what recent experience or event could have been the cause of the inner conflict.
Bring any underlying conflict to awareness, by rationally looking at and dealing with the conflicting desires and needs, a gradual dissipation and relief of the pain is possible.
6 - ORGAN LANGUAGE
Organ Language is a physical condition, something unpleasant from a thought like "That's a headache to me," "That makes me sick to my stomach," "I can't swallow that," "It's a pain in the neck to me," 'that gives me a pain."
A source of physical difficulty can be caused by "organ language". The actual physical condition mentioned may develop from such an idea. Many a chronic headache, nausea, pains, etc., seem to arise from organ language including cases of dermatitis, the person "itching" to do something. A breaking out of the skin can appear because something is "irritating," the skin being one's outside.
7 - PAST EXPERIENCES
Past experiences may house guilt feelings and unacceptable ideas that originate in the past. Often a sexual trauma is combined with verbal suggestions and traumatic or frightening events.
Past Experiences may be involved with some of the other of the Cheek and LeCron seven keys.
In the case of torticollis, the past experiences with his secretary were a part of his conflict and the motivation for the symptom. When an imprint is established, a past experience is involved. We believe guilt feelings and unacceptable ideas originate in the past.
A different type of experience is one, which was traumatic. A great fright may be responsible
for the development of a phobia or may produce many other effects. Often a sexual trauma combined with verbal suggestions was the source of difficulty.
In a case of child stutterers the patient’s had been sexually molested by an adult and had been told, "If you ever tell, I’ll kill you," which was the command statement. The molester in each case meant he would kill the boy if he told of the attack but literally "If you ever tell" means about anything, if you speak at all.
With the subconscious carrying out this idea, if he talks he will die. It doesn't matter if the threat was made years ago and there is no present danger, the threat hangs over him like the sword of Damocles. The subconscious does not view this logically. A need to talk collided with the fear of being killed if he talked, so there is blocking and stuttering.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
15
There can be many reasons for stuttering, but this one stutterer quickly found he could speak normally after the trauma had been brought out and the imprint removed. Strangely most stutterers are good hypnotic subjects and most do not stutter if they talk while in hypnosis. When awakened the speech difficulty returns.
This fact is of help in the therapy of stuttering. Some other command statements may also be
active with a stutterer. One is where a stern parent has repeatedly told a child to "shut up" or "be quiet" "shut your mouth" or some similar exclamation. Difficulties may develop from other kinds of traumas. When a past experience is located, the person can learn age regression to the time and the effects then remove them.
Highly charged emotion may be tied up in the trauma experience. The first time the person is returned to the trauma there may be overwhelming strong emotion.
Desensitizing and getting control of this powerful energy involves a reality base in the present
with knowledge that going back over the trauma again will bring more control. Generally a third review will reduce the emotional energy greatly, and by a fourth or fifth time all emotional trauma will disappear. The object of such a regression is to gain insight and to discharge the pent-up emotions tied to the experience. It is important to revisit this “old trauma” until a finger response says all emotion has been discharged. This may be done in a single session.
It is important for all people to rely on a professionals trained in Mind Body Medicine or
Clinical – Medical Hypnosis to regress themselves to a traumatic event and first obtain an affirmative answer to the question "Is it all right for me to return to this event?"
The causes of many psychosomatic illnesses will be found to be very superficial and easily remedied, though other cases may be very complicated, so deep-seated that require special consultations. Often in one session of only 30 or 40 minutes the apparent roots of the matter can be uncovered with a rapid clearance of symptoms.
Permanent benefits can be expected from these symptom removals procedures. In many cases the causes may have been superficial. Long suffering usually crystallizes many constellations of triggering causes for distress. It takes longer to effect cure and one may have to settle for mitigation of distress.
The cases cited here by the author are taken from examples of Cheek and LeCron and are typical in showing how ideomotor answers to questions can bring out apparent causes for psychosomatic ailments. Almost any illness can be handled in the same general way.
In the authors experience a large percentage of common illnesses can be cleared up in a very
few sessions, indicating the superficiality of the case. These can usually be handled readily by a non-psychotherapist. Others may take much longer, and there will be failures with some. Resistances and repressions can prolong treatment.
“Giving Misery the Finger - Ideo-Motor-Response (IMR) for Mind-Body Medicine (MBM)” Mind Body Wisdom
This book involves use of Ideo-Motor-Finger-Response (IMFR), "ideomotor finger signals"
and explores use of the Ideo-motor-response (IMR) to broaden the reader better understanding of methods in Mind-Body Medicine (MBM). Remember, Ideo-motor-response (IMR) includes "ideomotor finger signals". All we need for "ideomotor finger signals" are the fingers on our hands - no materials or props to take care of.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
16
Long ago Cheek and LeCron established the fact that the human unconscious holds the answers to our human suffering and that with their properly and purposely designed questions with "ideomotor finger signals" we can compel our unconscious to address our own inner Mind Body Wisdom to assist us in our wellness and quality of life. Thus, our inherent Mind Body Wisdom is capable of “Giving Misery the Finger".
Mind Body Therapy has professionally become a new buzz word nowadays; it is coupled together with "ideomotor finger responses" and mind-body healing methods in hypnosis. Just before David Cheeks untimely death he co-authored his last book in 1994 with Ernie Rossi, Ph.D. titled Mind-Body Therapy: Methods of Ideodynamic Healing in Hypnosis. The author remembers David complaining to him about the Santa Barbara to Malibu roundtrip drive to meet with Ernie, his neighbor because Dave had night vision problems, which interfered with his ability to drive at night.
Ideomotor Signaling - Mind Body Medicine
Rossi and Cheek demonstrate that the ideodynamic finger signaling method of mind-body
communication and healing in hypnosis has evolved into a safe and flexible general approach to psychotherapy and the coauthors believe the readers of this book can learn to use these techniques for their own self-improvement. Two decades ago this thinking was merely a pioneering peek at the mind body process, but today this book explores different facets of the use of communication, suggestion and MBM in medical situations to support the information about the power of the human mind-body relationship. Cheek was an Ob/Gyn who regularly used medical hypnosis in his practice. Rossi an ally, student and collaborator of the late, famous Dr. Milton Erickson, is a theorist, a psychologist and specialist in Clinical Hypnosis and he is a clear-thinking, research-driven psychobiologist.
Work with medical patients show the profound and binding impact of experience on the health
of the body. Processes of communication are used to explore past experiences of patients (usually consciously forgotten) that had a dramatic impact on current reproductive health with a look at many different facets of the mind in medical situations. Leslie LeCron's ideomotor signaling dates back to the 1930’s, which he formalized in the 1950’s. By 1964 LeCrone published his book, "Self-Hypnotism". LeCron taught ideomotor signaling; including use of a pendulum to professionals in medicine in the 1950’s and it has become surprisingly effective when doing auto hypnotic "uncovering" work.
I am excited at the prospect of discussing clinical applications of the technique because I
collaborated with Cheek and of course Cheek consulted and co-authored with LeCron; I also collaborated with Rossi who worked together with Milton Erickson. Mind Body Medicine is proving to be an opportunity to empower the individual patient.
This discussion will present a comprehensive framework for understanding the process of mind-body communication to better understand the importance of ideomotor finger signals in Mind body Medicine help. This section will help gain access to the importance of state-dependent memories and learning that is not otherwise readily accessible to consciousness but nevertheless adversely impacting one's functioning at emotional and physiological levels.
This book discusses the use of ideomotor finger signals to uncover unconscious material and
also helps one to actively facilitate its therapeutic resolution, often with minimal if any processing at the conscious level. The coauthors contend that when using ideomotor signals, formally inducing trance becomes unnecessary because establishing the signals facilitates a trance. It is important to know doctors and specialists are trained to be proficient at using ideomotor signaling more frequently and confidently when working with patients learning about mind body medicine.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
17
The author's discussion of "imprinting" aims for synthesis in the context of traumatic experiences and subsequent emotional, psychosomatic and general medical illness, injury and pain. Remember, the presence of great emotional or physical stress is indistinguishable from that of hypnosis and might be referred to as spontaneous hypnosis. The unconscious response to injury is similar to the effect of a strongly given posthypnotic suggestion. Unlike ordinary learning by repetition, this memory is completed learned in one trial.
Finger movement and, ideodynamic signals indicate the accessing of memory at an
unconscious level, with verbal reporting of the experience following. The authors have added this section on "ideomotor finger signals" because it will help to bring the reader audience to more completely recognize that "today's" approach for our "mind body" issues is a responsible "self-help" way to eliminate and or decrease symptoms of illness and disease.
A modern hero of Medical Hypnosis is Dabney Ewing, MD, past president of the American
Society Clinical Hypnosis, who has “tongue in cheek” spoke of giving "m isery the finger”. In 2006 Ewin presented an article titled "Giving Misery the Finger: Ideomotor Signals for Diagnosis and Healing" and the authors want you, the reader to learn about "Giving Misery the Finger" to improve your quality of life.
Case Report
A 44-year-old, obese Caucasian female patient was a demonstration subject, with Dabney Ewin, M.D. illustrating his ideomotor signals for rapid hypnoanalysis technique. She had a 9-year history of biopsy proven erythema nodosum, tender red subcutaneous nodules on her arms and legs, predominantly on the left side, with no associated physical conditions. She had seen the author periodically for about 8 years and had experienced only partial responses to several anti- inflammatory therapies. About 2 months prior to participating in the demonstration she had experienced another flare of her inflammatory erythema nodosum nodules. At that time she had expressed frustration that the conventional medical treatments had not successfully suppressed and resolved the painful and tender inflammatory nodules. She agreed when questioned that there might be an emotional component involved in triggering the flares of the inflammatory nodules, and she expressed a willingness to explore the emotional factors. She had a past medical history of a cholecystectomy at age 28 and a hysterectomy at age 29. At the onset of the erythema nodosum, at age 35, she was caretaking for her mother who had emphysema and her father who had Alzheimer's dementia. Both parents are now deceased. She was not on supplemental estrogen or other medications that could trigger the erythema nodosum. Isoniazid treatment for a positive tuberculin test during the first year of her erythema nodosum failed to improve the erythema nodosum and precipitated a peripheral neuropathy with some residual permanent neuropathy post isoniazid treatment.
In response to questioning during the intake interview at the demonstration she said that the
most frightened she had ever been was at age 6 when her mother told her that her 21-year-old sister had been carjacked and raped. The worst thing that had ever happened to the patient was finding out at age 30 that her father had sexually abused her 12-year-old daughter. The most embarrassed the patient had ever been was with her overweight problem in grammar school.
During the ideomotor review in trance, her fingers answered "no" to Conflict; "yes" each to
Organ language, Motivation (excused from caretaking when so many people in her family got sick), Past experiences (her sister's rape), Identification (mother had a skin rash) and Self-punishment; and "I'm not ready to answer that yet" to Suggestion.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
18
When asked if she sensed that she could let her skin come to normal like 10 years ago, she signaled, "I'm not ready to answer that yet". Dr. Ewin gave her positive reframing suggestions for each of the five positive and the one "I'm not ready to answer that yet" factors. She was seen by the author in clinic 5 days later and had improved, with only one tiny fading erythema nodosum lesion remaining on her left upper arm. However, 2 weeks later a few new lesions appeared. Since it was apparent from her history and ideomotor signaling that she was on chronic emotional overload and that some of it pertained to the history of her sister's and daughter's sexual abuse, she was referred to a psychotherapist who specializes in that area and is well trained in hypnosis. However, she did not follow through to call for an appointment and was not seen by the psychotherapist.
A month later she still had a few fading lesions, and at 2 months she still had a few minimally
active lesions. By 10 weeks after the demonstration her erythema nodosum lesions had fully resolved, and she has since remained clear of these lesions. This clearing likely was a result of the Hypnoanalysis, since it followed temporally in a patient where other treatment measures had failed.
Discussion
This case illustrates the diagnostic value of using Mind Body Medicine approaches with
ideomotor signaling to screen for psychosomatic factors related to skin disorder triggering or exacerbation. It is possible to rule out a psychosomatic component to the skin disorder if the focused history and ideomotor questioning for all seven factors are all negative.
If only one or two factors are positive and are related to only one or two initiating events that
can be identified, treatment with positive reframing suggestions may be sufficient to neutralize the negative associated emotions and alleviate or resolve the psychosomatic component of the skin disorder. This may result in a permanent uprooting and weeding out of the problem. On the other hand, if the focused history is extensively positive and many of the seven factors are positive as in this case, this degree of complexity is an indicator for referral to an appropriate psychotherapist for treatment. In this case, the patient experienced clearing of her lesions despite noncompliance with the recommended further psychotherapy.
Mind Body Therapy – Ideodynamic Another View Historically, ideodynamic feeling is reported to have appeared as far back as one thousand B.C.
Through the use of altered states and expectancy, the practice of magical interventions through incantations and rituals brought about healing. Maurice Kouguell, Ph.D., believes Ideodynamic communication describes all the relationships between ideas, thoughts and the dynamic or physiological responses of the body to the thought.
In the 18th Century, Anton Mesmer, followed by Chevreul, believed that unconscious knowledge could affect minimal movements and the muscles. Shortly after this Bernheim described hypnosis as basically an ideodynamic process in which ideas are transformed into acts. He describes the process of hypnosis as thoughts into action, vision and movement, which occur so rapidly that it circumvents the critical factors of the subject. Bernheim used the patients’ own inner resources, which later on was adopted by Erickson in his naturalistic approach to hypnosis.
This author refers to the most significant realization in psychobiology that memory, learning
and behavior are influenced by neuromodulators capable of recording information in the brain; thus imprinting traumatic events. These memories are often imprinted on a non-verbal level thus making ideomotor response the vehicle of choice to recover these memories.
The true sign of intelligence is not knowledge but imagination. - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
19
The experience of hypnosis and ideodynamic signaling allows the patient to re-examine, organize, re-evaluate his physiological problems using his own abilities, capabilities and potentials, to reach a satisfactory resolution.
LeCron and Cheek used Chevreul’s pendulum as a vehicle to access the unconscious by watching how accurately the pendulum moved. Using a similar procedure, the patient is then introduced to the finger signaling method.
A valid ideodynamic signal is repetitive and is hardly visible. One needs to observe changes in
respiration, pulse rate and emotionality. All these have to occur prior to the finger signaling. When the finger lifts, the patient is not fully aware of the experience itself. This is just an anticipatory period, sometime reflected by a discomfort. It is the repertoire of the patients’ unconscious creative resources that is continuously being accessed in order to bring about healing.
Mind body Medicine - Credibility
Ernie Rossi, Ph.D. – Milton Erickson, M.D. Psychoneuroimmunology - Mind Body Medicine
Interview - Ernie Rossi, Ph.D., Co-Author “Mind-Body Therapy: Methods of Ideodynamic Healing in Hypnosis”
French publication Le Journal des Psychologues, October 1994
You have worked with the outstanding pioneering psychotherapist Milton Erickson and edited his writings. Will you present a colorful portrait of Erickson?
Well, perhaps the most important story I can tell about Erickson is how he discovered hypnosis when at the age of 17 he lay acutely ill with polio for the first time. This was in the frontiers of Wisconsin around 1918 before there were any hospitals or modern medical understanding of the problem. Erickson reports overhearing the doctor tell his mother just outside of his bedroom that he thought the boy would be dead in the morning. The young Erickson felt so angry that anyone should tell an American mother that her son would die in the night that he was determined to stay alive to see the dawn. He weakly asked his family to rearrange the dresser with its large mirror so that he could see from his bed the next day’s sunrise reflected in the mirror. He did manage to stay alive all night but when he saw the morning’s sun reflected in the mirror he fell into a coma for three days and three nights. When he awoke he found he was paralyzed but he could move his eyes and his hearing was unusually acute.
Life had to get back to normal at the farm. Every morning before breakfast they would lift him out of the bed and tie him into a rocking chair with a hole cut in the bottom, with a pot underneath so he could move his bowels while they went about the first chores of the day. Well one day as misfortune would have it, they forgot to come and untie him from the rocking chair and put him back into bed. So there he was in the middle of the room tied in the rocking chair wishing that he could look out the window and at least see what was going on in the farm. As he looked longingly at the window he suddenly realized that the rocking chair was slowly beginning to rock; how could this be he thought to himself. If my body is truly paralyzed how come the rocking chair is moving? Could it be he reasoned to himself that some of my muscles are still capable of movement and just by wishing is unconsciously causing the chair to rock?
Thus the young boy without knowing it of course had rediscovered the basic principle of hypnosis described as ideomotor movement by one of the fathers of hypnosis 100 years earlier. "Ideomotor" simply means that an idea can automatically give rise to a motor movement. Erickson continued to access his sensory memories to recover most of his normal muscle movements throughout his body. He would ask himself, for example, how did my fingers hold a spoon while staring at his fingers? After a week or so of this exercise he was rewarded with a small movement in his finger.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
20
Gradually he thus acquired movements of his fingers, hands, and arms, and finally the rest of his body by reviewing real sense memories. This became one of his revolutionary contributions to the theory and technique of hypnosis. Hypnosis is really not suggestion in the sense of putting something into a person’s mind or programming a person, although it can be used in that bazaar sort of way by the unscrupulous. Therapeutic hypnosis by contrast, helps a patient access their own inner creative resources for problem solving.
Mind-Body Healing is about the inter-dependence of the physical body, the mind, and the emotions. Would you discuss the emergence and the development of the mind-body inter-relationship?
Erickson often wrote about the psycho-neuro-physiological basis of hypnosis. However when I
asked him what he meant by that exactly he would just sing me the old Negro spiritual song where the words go "the foot bone is connected to the ankle bone, and the ankle bone is connected to the leg bone, and the leg bone is connected to the hip bone," etc. He was in his 70's when I studied with him in the last decade of his life, so I felt, well, perhaps I got here too late. I gradually came to understand, however, what he was trying to tell me by singing that song: Everything in mind and body are connected somehow. It is the task of our generation to learn exactly how everything is connected. When I began to update his writings in the area of psychosomatic medicine I was profoundly shaken to learn that modern molecular biology did in fact enable us to trace out a complete cybernetic loop of information flow between mind and body right down to the genetic level.
Most people, for example, still think that genes are simply the units of heredity. They are
unaware that genes are also receiving messages from our psychosocial environment so that they turn on and off to help us adapt to continually changing life circumstances. This is what I call the mind-gene connection in many of my papers and books. This, I believe, is the true scientific foundation of the new science of Psychosocial Genomics (how the psychological experiences we call "mind" can modulate gene expression as well as visa-versa in mind-body relationships) that can be measured in the test tube and eventually described with differential equations. In the recent 12th international congress on clinical and experimental hypnosis in Israel last year, for example, I introduced the first mathematical model of hypnosis in mind-body healing.
Do you believe that the concepts that you are developing about therapeutic hypnosis are revolutionizing therapeutic practice?
Well, no one could say these new concepts are revolutionizing therapeutic practice. At least not yet! They are, however, introducing new paradigms for theory and research. But, you must be careful to separate me from the revolution. The true revolutionaries were Watson and Crick who got the Nobel Prize in the early 1950's for discovering the informational basis of life in the DNA code.
Most people, however, still believe that genes determine human behavior. They are not yet
aware that the reverse can be true as well. That our behavior states can determine the moment-by-moment changes in our gene expression profiles. This is now called "Behavior state-related gene expression." The behavioral state of being awake has a gene expression profile, for example, that is very different from gene expression during sleep and dreaming. I believe that states of creativity and emotional arousal typical of optimal sessions of psychotherapy and therapeutic hypnosis will eventually be found to alter our gene expression profiles as well. I discuss much recent research and future prospects in this area in my recent books such as:
Dreams, Consciousness, Spirit: The Quantum Experience of Self-Reflection and Co-creation, (2000). Phoenix, Arizona: Zeig-Tucker & Theisen - www.ZeigTucker.com The Psychobiology of Gene Expression: Neuroscience and Neurogenesis in Hypnosis and the Healing Arts - W. W. Norton Professional Books, New York.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
21
I am simply exploring the implications of this new informational conception of the basic nature of life on the biological as well as psychological level. Physics, psychology, and biology are now united by this common denominator of information.
One of the most interesting developments in this area is the new mathematical science of Complex Adaptive Systems, at the Santa Fe Institute in New Mexico, where over the past decade some of the most innovative minds in all the sciences have been exploring this new informational foundation of life. Up to now psychology has been based on the various psycho-cultural environments of its leading practitioners such as Freud, Jung, etc.
Psychology has been something of a stepchild in science up to this time because it has not been connected with the other sciences. With the new informational basis of psychology it can become an integral part of all the sciences as well as the humanities. I explore the possibilities of using the non-linear dynamics of Complex Adaptive Systems to reformulate the foundations of hypnotherapy on a more scientific foundation in my book, The Symptom Path to Enlightenment: The New Dynamics of Self-Organization in Hypnotherapy
For several years you have been teaching your mind-body therapeutic approach at the Milton Erickson Institute of Paris, under the direction of D. Jean Godin. Who are the practitioners who attend your seminars and what are their responses to your mind-body approach? Additionally, to what extent do they believe that you are on the "right track?"
Well, of course, I would like to believe that the psychiatrists, psychologists, nurses, social workers, etc., who attend my seminars are among the most brilliant of the new wave of the French intellectual world. We are currently exploring the radical idea that "suggestion" and so-called "programming" are not the essence of hypnotherapy.
What is conventionally called "suggestion" is actually the psychobiological entrainment the healing power that takes place naturally at various phases of our mind-body rhythms. Every hour and a half, for example, we go through peaks and troughs of mental, emotional and physical activity. Every night, when we are asleep these rhythms continue so that we dream every hour and a half, and then we sink deeper into sleep where certain hormones flow, the immune system is potentiated and many healing processes take place.
I believe my new approach to hypnosis and mind-body healing entrains and facilitates many of these natural healing processes. At a recent conference sponsored by du Comite National De La Recherche Scientifique (CNRS) at the Salpetriere in November 1992 I proposed the type of psychoneuroimmunological research that is now needed to explore this new model of healing on all levels from mind to gene.
To what extent do I believe I am on the "right track?" Only future research can tell. But, for the first time we have something worth researching in hypnosis and mind-body healing besides old wives tales and anecdotes. And, as I mentioned earlier, for the first time in its 200-year history we at least can begin to speculate about what a mathematical model of hypnotherapeutic work and mind-body healing might be in terms of leading edge molecular biology and physics. In the broadest sense we may be approaching a new resolution of the classical mind-body problem: How do thoughts, emotions and stress communicate with the body and visa-versa?
As you know, in France psychoanalysis is taught at the university, and psychoanalytic theory has dominated the practice of psychiatrists and psychotherapists, even if they are non-confirmed. Would you explain your mind-body approach vis-a-vis psychoanalysis?
In the first place, let me say that I was originally trained in Freudian psychoanalysis by the
great psychosomatic specialist Franz Alexander. I later completed my training as a Jungian analyst. So I have full respect for all the major psychoanalytic traditions and methods. But, after all, psychoanalysis comes out of 19th century science and, as you say, this theory is very difficult to validate in the original terms of its creators.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
22
In my book, Dreams and the Growth of Personality: Expanding Awareness in Psychotherapy back in 1972 (2nd Edition, Brunner Mazel, 1985), I used the classical psychoanalytic approach of free association and the analysis of the transference and resistance. It seemed to me that I was discovering entirely new patterns in the evolution of consciousness that Freud and Jung could never have dreamed of just a generation or two earlier. I now believe the psyche and its laws of development and growth actually change with the evolution of consciousness over the generations. The new science of mind-body healing based as it is in the new informational worldview uniting physics, psychology and biology now requires new approaches to facilitating healing development and consciousness.
My last question - Does the mind-body connection have anything in common with the
religious feelings so prevalent in American Culture? (For example, some groups pray for healing, and some even practice the laying on of hands to heal a "patient.")
This question actually goes to the heart of the matter. Recent research has shown that under
stress medical students, for example, suppress their own immune system. On a molecular-genetic level it has been found that their stress inhibits the expression of their interleukin-2 messenger molecules of their immune system. These molecular messengers are the same ones that Stephen Rosenberg, M.D., Ph.D., at the National Cancer Institute, is using to fight cancer on a purely medical basis. In other words, psychosocial stress may inhibit our immune system by blocking the same molecular messenger molecules that medical science is seeking to amplify to cure cancer on a purely biological level.
This is a clear example of how biological and medical science are using many of the same
molecular messengers that we now realize are also modulating memory, learning, emotions and behavior. These messenger molecules make up a complex system of mind body communication that psychology now needs to learn more about to facilitate the resolution of psychological problems associated with emotions, stress and trauma - many of the posttraumatic stress syndromes, for example.
I believe that whenever faith healing actually worked in the past, it was because hope, faith and religious passion could in some way activate these same messenger molecules. The mind-brain, the brain-body (the neuroendocrine system), and the cell-genetic level are all connected with many such families of messenger molecules that facilitate mind-body communication in health and illness.
Current research at the cellular-genetic level documents that, with the experience of novelty
and emotional arousal on the psychological level, many different genes are expressed. The Hypnotherapist s and faith healers of the past did not understand these specifics of molecular biology, psychoimmunology and gene expression as we are beginning to learn about them today.
The new revolution that I am attempting to explore in mind-body healing integrates the best of
the past and these new informational sciences that are uniting medicine and psychology at the molecular-genetic level. * End Rossi Interview
Self-Healing Behavior
The scientific medical definition of “Healing” shows it to be an innate natural dynamic process
of recovery, repair, restoration, renewal and transformation that increases resilience, coherence and wholeness. Healing is a naturally emergent process of the person’s whole system which includes the physical, mental, social, spiritual and environmental. It is a unique personal and communal process and experience that may or may not involve curing or any contact with doctors or hospitals; it is a natural response to injury, illness and disease.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
23
The American Journal of Health Promotion defines preventive medicine or health promotion as the science and art of helping people change their lifestyle to move toward a state of optimal health. Optimal health is defined as a balance of physical, emotional, social, spiritual, and intellectual health. Lifestyle change can be facilitated through a combination of efforts to enhance awareness, change behavior and create environments that support good health practices. Of the three, supportive environments will probably have the greatest impact in producing lasting change. This definition applies equally well to overtly healthy people and people with acute and chronic diseases.
In 2004 Michael O’Donnell, M.B.A., M.P.H., Ph.D. reported on “Health-Promotion Behaviors
That Promote Self-Healing” for the JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE, and for Mary Ann Liebert, Inc. Dr. O’Donnell noted there is a lot of scientific evidence that shows health-promotion programs in smoking cessation, stress management, fitness, nutrition, weight control, and medical self-care to successfully help many people improve their health practices and related health conditions. He however points out programs that promote self-healing among people with acute and chronic diseases is absent.
It is not surprising all “Healing” studies point to the positive results of health behaviors that include regular exercise, eating nutritious foods, managing stress, and avoiding toxic substances such as tobacco and alcohol. O’Donnell states that people who have established this kind of relationship with well-being reduce morbidity and increase longevity. For science to understand health behaviors that promote self-healing provided to overtly healthy people is simple. However, science does not seem to be able produce health practices for people with chronic illness.
All of these studies rely on very little exercise yet it is exercise which produces the highest and
most steady result of lasting improved health. This is why AquaDios-Med™ factually states “Exercise is Medicine” and when daily safe exercise such as structured deep-water running is manifest in every person’s daily activities the “health crisis” will be over.
Anger
Anger is a normal human emotion, but it becomes crippling when its expression is prohibited
from becoming an action. "Anger” can be repressed but most often it is not eradicated without professional training. Anger can seek release by expressing itself in an abnormal, and most often disguised and or confused manner”. Examples of repressed anger could be migraines, peptic ulcer, back pain, hypertension, obesity and more.
Pain and Sadness
The deep wound and the sadness of rejection may be central to the genesis of most emotional
pain and resultant illnesses. The earlier the deep pain of rejection occurs, the more devastating its effect can be. For a child who has never experienced acceptance, pain may destroy internal resources with which to deal with later rejection. Mother is most often the person who plays the greatest part in the creation of a child’s emotional-mental and physical health. A mother’s acceptance enables a child to have self-acceptance. Rejection by the mother can be so acutely painful and frightening that the child will have serious developmental traumas.
A child’s pain of rejection can often be too severe to tolerate on a conscious level and therefore becomes repressed, below conscious awareness. The pain does not go away, however, no matter how unaware the individual is of its existence. This “pain” becomes a constant demand to be expressed in some form or other and often results in a physical or emotional disturbance or a combination of both such as asthma, depression, drug addiction, alcoholism, excessive smoking and more.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
24
Guilt
Guilt plays an interrelated role with fear, anger, and pain. Guilt is identified as a consistently potent factor in the production of most emotional illnesses. Guilt can be the source of impotence, frigidity, obesity, skin diseases, and the ultimate of hostile acts, “suicide”. Blood flow plays a central role in a wide variety of acute and chronic illnesses. It has been hypothesized that altering blood flow by directed thinking, imaging, imagining, and feeling is a common factor in most methods of mind body healing. Behind the process of mind body communication mediating blood flow at the mind-brain level, the brain-body level, and the cellular-molecular level.
The mind-brain level of modulating blood flow can be illustrated by common metaphors in everyday speech. Everyone knows what is meant when we say that we feel "warm" or "cool" about a person or situation. Biofeedback research shows these feelings of warmth and coolness are linked with actual dilation or constriction of blood vessels, which either increase or decrease blood flow accordingly. This blood vessel change takes place because of a positive response at the cognitive-emotional level is associated with positive life experiences of warmth on a sensory level. The thought of warmth also has an actual emotional, sensory, and physical experience of warmth.
The brain-body level of blood flow modulation takes place in the limbic-hypothalamic system.
The hypothalamus is located in the brain and has some of the major control centers for regulating the autonomic nervous system. The autonomic nervous system, through its sympathetic and parasympathetic systems, can mediate the alarm response that contributes to the psychosomatic aspects of surgical emergencies and critical illnesses. For example, the ANS sympathetic branch can signal the adrenal medulla to secrete epinephrine and norepinephrine into the blood, where they function as information substances that can regulate blood flow by signaling the receptors on vessels in the skeletal muscles and liver to dilate or constrict the diameter of the arterials in other parts of the body. This chemical action can and does take place either from a “real world” demand, imagination or emotion. Thus, our MBM guided imagery has the capacity alter our physiology in positive and healthy ways.
Our cellular-molecular level is illustrated through the action of a number of information substances on the receptors of the capillaries of the cardiovascular system that carry the blood through all the tissues of the body. In a study on "changes in tissue vulnerability induced during hypnotic suggestion", Chapman, Goodell, and Wolff concluded, "proteolytic enzymes and a bradykinin-like polypeptide are implicated in these enhanced reactions."
Bradykinin also causes contraction of most smooth muscles and has a very potent action in
dilating certain blood vessels. Its function, which is not yet completely scientifically established, may be to regulate the rate of blood flow or to participate in the inflammatory response of an injury. "It is now known that the formation and metabolism of bradykinin is interwoven with the metabolic processes that mediate the conversion of angiotensionogen to angiotensin I and II.
The interrelationships of the kinins, histamine, and angiotensins in regulating blood flow at the cellular level suggests how all the information substances may be modulating blood flow in well-coordinated communication patterns on all levels from mind to molecule. The conventional view has been that while all these substances may be coordinated in their activity, this coordination takes place on an entirely mechanical, involuntary, or unconscious level."
Bradykinin is a kinin that is formed locally in injured tissue, it acts in vasodilation of small
arterioles, is considered to play a part in inflammatory processes, and is composed of a chain of nine amino acid residues. Bradykinin is involved in many physiological and physiopathological processes such as pain, allergies, chronic and acute inflammation and some cardiovascular diseases.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
25
These molecules may help in defining the role of hormones in general and bradykinin in particular in certain physiological or pathological processes.
Pharmaceutical companies look at these molecules to possibly be used for drug design: a bradykinin antagonist, for example, may relieve pain, allergies, low blood pressure, or even cranial trauma. An agonist may be used as an adjuvant for cancer treatment to increase the permeability of the hemato-encephalic barrier to the anti-cancer drugs.
There is a safe way to repair damage done to your body by your mind and the cure is created by
Mind Body Medicine techniques to use our own mind in a healthy way. MBM techniques provide a doorway into the realm of one's responsibility to take a healthy control of your mind, so with care and a little bit of desire, what you may have unconsciously created can be undone. Feel free to go to http://www.aquadios.com/ to read and view the videos.
ETIOLOGY DISTRESS - DIS-EASE
PSYCHONEUROIMMUNOLOGICAL MEDIATION
Deese and Holse define spontaneous hypnotic trance as paradoxically accurate for symptom bondage indicating at least a percentage of all symptoms are an active process of unconscious learning experiences without awareness or control of the process and implies the passage to awareness is through altered states of consciousness common in clinical hypnosis. Literature indicates the majority of illness and disease is preceded by distress, either of a conscious or an unconscious nature. Whether the individual is aware or not, distress produces a particular destructive process in the body which absorbs and decreases immune system energy.
For example, an embarrassing social situation has sufficient "distress" to alter skin color, raise body temperature, produce perspiration, cause changes in the delicate internal chemical state, alter heart rate, increase acidity, drastically alter vision, hearing, smell, balance, and generate a host of other physical changes. Words and sounds may be internalized to produce distress, depending upon the circumstances and the situational demands. Often, just thoughts stimulate physical change. Imagine cutting a ripe, juicy, yellow lemon; imagine the juice running down the knife to your fingertips, imagine the cool juice touches your finger and you lick it off, experiencing the strong, tart liquid exploding in your mouth, producing uncontrollable mouth-watering. If you experienced increased saliva just from (reading) the words then the suggestions helped to alter physiology.
"Dis-Ease"
Immune systems as a rule act automatically to preserve integrity of the body but an upsetting, distressing event may develop sufficient distress to disturb normal function of the nervous system and cause "dis-ease"; the absence of physical or psychological ease. Therapeutic practical mind body healing found in AquaDios-Med Treatment and Exercise techniques combine to activate psychoneuroimmunological mediation with deep or shallow water in variable water temperature, gentle to strong current or Jacuzzi force. Treatment reinforces patients to RE-ESTABLISH DIGNITY, INTEGRITY to be FREE of the SICK ROLE, accommodate family and friends and teach them to improve CONTROL OF THEIR LIFE AND HEALING. It is important for treatment strategies to create an inner directive experience for the patient, free from so many previous learned limitations about pain, recent history or training.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
26
A natural free period of inner discovery, exploration, and realization of natural personal potential for healing must be explored with personal curiosity and positive regard.
Rehabilitation emphasis is focus on activities patients can control, in their own world to enable
return to normal life as soon as possible and liberate or integrate genuine psychophysiological motivation to correct immune deficiencies, overcome, resolve, potential deep seated internalized guilt, inappropriate self-blame for the accident, injury, disease or life circumstance. Signed treatment contract, Dated Prescription Intervention Plan stipulating treatment is required. Professional consultation, observation, treatment, and psychological testing objectively verifies personality profile of the high-risk poor prognosis patient.
SECONDARY GAIN
Iatrogenic Complications or controlled relapses are accepted as signs of symptomatic remission. Rehabilitation emphasis is to focus on activities patients can control in their own world to enable return to normal life as soon as possible. Professional athletes, as well as sports-minded individuals, respond favorably to applied clinical hypnosis with improved performance and endurance. Special equipment includes HYDROTONE bells-boots and a WET VEST or Aqua - Jogger. AquaDios-Med preventive treatment relies on a signed agreement/contract by the patient to work with the treatment staff, assist the treatment team, including proper use of medication, surgery, and social support to facilitate and integrate health. Exploration of secondary symptomatic gains is essential to depotentiate relapse and encourage patients to participate in a daily health regime.
MIND-BODY MEDICINES Research
In November 2002 Authors C. Norman Shealy, MD, PhD, Patricia A. Norris, PhD, and Steven L. Fahrion, PhD discuss guidelines and resources for education about mind-body medicines and the scientific and clinical basis for their usage. The mind-body medicine learning is presented for the reader to better understand the effect of thought and attitude upon physiology and health and have knowledge about the benefits of engaging in meditation and guided imagery. It is important the reader be aware of the principles of biofeedback and remembers the differences between placebo and nocebo and the effects physicians can evoke.
After reading this book it is anticipated the reader will be able to intelligently discuss evidence and the value for prayer, mind-body medicine and psychoneuroimmunology and be aware of the value of
simple relaxation breathing exercises. It is hoped all the readers will incorporate the importance of mind-body practices into their own lifestyle as part of self-care and role modeling for family members and friends.
Preventive Medicine - Holistic Medicine Alternative Medicine
People usually think of medicine as something to be taken to make a person well after he or she has gotten sick. Preventive medicines are things a person can take or do as a physical exercise activity when well to help prevent becoming sick or developing common diseases. A well-balanced diet of fruits, vegetables, whole grains, lean meat, fish or poultry should contain most, if not all, of the vitamins and minerals necessary to maintain health.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
27
The World Health Organization (WHO) encourages traditional Alternative Medicine medicines across the globe. The adaptations of traditional medicines are called as Complementary or Complementary and Alternative Medicine; any form of medicine that is outside the main stream of western medicine or orthodox medicine. It is found in all cultures to some extent and it is also called indigenous medicine. These Alternative Medicines date back thousands of years depending on the country and culture and 2/3rd of the world population relies solely on such therapies. Alternative medicine is the practice of techniques to treat and prevent disease that are not generally accepted by conservative modern Western medicine. Although some of these forms such as yoga, meditation, acupuncture and hydrotherapy have been practiced for centuries in many cultures, the U.S. medical community has been slow to acknowledge their benefits. With an increased emphasis on disease prevention in recent years, many people have looked to alternative forms of medicine for drug-free approaches to achieving and maintaining good health. Alternative medicine allows people a measure of participation and control in their own well-being, as many of the practices can be taught and self-administered. Some people have turned to alternative medicine in search of treatment or cures for illnesses such as cancer, AIDS (acquired immunodeficiency syndrome), arthritis, and heart disease and much more.
Preventive Medicine Preventive Care
Illnesses and injuries affect everyone at some point in life. That is why it is important to think about how to prevent getting sick or injured. There is a saying: "An ounce of prevention is worth a pound of cure." This means that even a small amount of prevention will save a lot of time lost from getting sick or injured; such as the safe daily exercise mandated by AquaDios-Med™. Amazingly, there is a wide variety of ways that each individual can try to protect her or his own health and well-being. Starting in childhood, a person can establish a healthy diet and physical fitness program and begin other healthy habits that will greatly reduce the likelihood of future illnesses and injuries.
Mind Body Medicine Definitions
Mind-body medicine and preventive medicine evolved in the early 1970s from the Humanistic Psychology Movement; the earliest biofeedback work of Dr. Elmer Green and his wife, Alyce; the meditation and relaxation studies of Dr. Herb Benson; and the psychoneuroimmunology work of Dr. George Solomon and Dr. Candace Pert. Mind-body medicine is a term that demonstrates physical, chemical, mental and spiritual interconnectedness, and currently encompasses a wide variety of techniques.
These include biofeedback, relaxation training, autogenic training, psychosynthesis, meditation, guided imagery, spiritual healing, prayer, Logotherapy, Gestalt therapy and many other short-term psychotherapeutic interventions.
History – Philosophy – Methods Mind Body Medicine
Research suggests separation of mind and body originated with Rene Descartes. Prior to his contributions, medicine, science, philosophy and spirituality were commonly considered aspects of the whole person. With his influence in the 1600’s, the separation of mind and body occurred with mind being the purview of religion and metaphysics and body being the purview of science and medicine.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
28
In the late 18th century, Anton Mesmer began the trend to re-examine the connection of body and mind. Although rejected by most of his contemporaries, Mesmer’s work, said by Benjamin Franklin to be only a suggestion of the effect of the mind, spawned the concept of hypnosis, which was introduced by James Braid and James Eisdale after Dr. John Elliotson demonstrated in the 1840’s that surgery could be performed on mesmerized patients with no pain, no anesthesia and rapid healing. Hypnosis was highly controversial for over 100 years but led to the beginning of modern psychiatry. Sigmund Freud is said to have been such a poor hypnotist that he retreated to psychoanalysis. In the early 20th century, the French pharmacist, Emil Coue, was reported by physicians to have cured thousands of patients with his famous statement, “Every day in every way I am getting better and better.” It is important to note, in spite of his tremendous positive results Coue was ridiculed by the American Medical Association when he visited this country. This author notes that many a physician had to treat patients with medical hypnosis in secret as early as the 1970’s for fear of being charged as a charlatan especially when many patients had reversed cancer.
Jan Smuts, former Prime Minister of South Africa, wrote in the 1920s the most elegant integration of all aspects of science, philosophy, and psychology in his book, Holism and Evolution. This was essentially the foundation of what is now called Holistic Medicine. William James discussed ‘Mind Cures’ extensively in his landmark book, The Varieties of Religious Experience, perhaps still the most in-depth study of religion and spirituality. In 1929, Dr. Edmund Jacobsen published his landmark book, Progressive Relaxation, in which he demonstrated physiological homeostasis with his practical technique of focused systematic muscle contraction and relaxation. He demonstrated that 80% of patients with “psychosomatic illness” were cured with this approach. It was never embraced by the medical profession. Meanwhile, Dr. J.H. Schultz of Germany had begun a specific form of self-hypnosis called autogenic training. His first book was published in 1932. By 1969, the six volumes on autogenic therapy were published by Schultz and Luthe. With some 2800 scientific references, they reported that 80% of “psychosomatic” illnesses were adequately treated with autogenic training. Meanwhile, Dr. Hans Selye had demonstrated the major effect of stress and anxiety on health in general and maladaptation to stress as the basis of most disease. He emphasized the physiologic similarities of physical, chemical, and emotional stress. In 1954, the American Society of Psychosomatic Medicine was founded. It was, and remains, primarily a psychiatrically oriented concept. Unfortunately, the term psychosomatic, which could be called mind-body, has been considered by most patients and physicians to mean “all in the head.”
Meanwhile placebo, which has been the standard since the beginning of modern scientific medicine, has been both used and abused and is poorly understood by both physicians and the public. Interestingly, the vast majority of drugs are only a few percent better than placebo, which in most controlled studies averages 35% efficacy. Almost no drugs are 70% efficacious. In the 1960s, Dr. Abraham Maslow and Dr. Carl Rogers began the reintegration of spirit and mind, founding Humanistic Psychology. Dr. Roberto Assagioli meanwhile had integrated all of his concepts, as well as Carl Jung’s concepts of symbology, into his technique of psychosynthesis.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
29
In 1970, Dr. Elmer Green and his wife, Alyce, introduced the concept of autogenic feedback training, which became biofeedback. Their earliest work proved that 84% of migraineurs and 80% of patients with hypertension were remarkably improved and adequately controlled with temperature biofeedback training. Since that time, it has been demonstrated that every physiological response, which can be measured and fed back to the patient visually or audibly, is capable of being brought under voluntary control. In the 1970s, Dr. Herbert Benson first reported on the physiologic homeostatic benefits of meditation and later recognized that the basic benefit was deep relaxation, soon to become known as the Relaxation Response. Benson’s work proved what Jacobson had shown fifty years earlier. Most striking was Benson’s demonstration that individuals who did 20 minutes of deep relaxation twice a day had a 50% decrease of both catecholamine production and insulin requirement for the entire 24-hour period. The work of Benson and Jacobson is instrumental for several reasons, first is the reluctance of American Medicine to accept a successful treatment or practice not involving medicine or surgery and another is this myopia is consistent today in the lack of hospital medicine and doctors utilizing the many “preventive medicine” programs available like AquaDios-Med™. In the early 1980s, George Solomon introduced the major field of psychoneuroimmunology, which has provided the greatest evidence of the complete interconnectedness of body, mind and attitude. Most remarkable is the finding that virtually every neurochemical produced in the brain is also produced in white blood cells and usually in the intestines. To some extent, the field of psychoneuroimmunology has suggested that the “mind” is part of every cell. Candyce Pert’s discovery of beta endorphin, the natural opioid, was the first major step in demonstrating what Buryl Payne had introduced in “Getting There Without Drugs” in the 1970s. It now appears that the mind can produce a wide variety of mind-altering chemicals, ranging from anandamide to neurotensin with analgesic, neuroleptic, and hallucinogenic effects. Ultimately, mind-body medicine is the foundation for virtually all modalities.
Major Clinical Applications
The wide array of mind-body therapies have been reported to be effective in pain control, migraine, rheumatoid arthritis, ADHD, epilepsy, hypertension, peptic ulcer, anxiety, depression, diabetes and much more. For instance, 84% of migraineurs can control their headaches when they learn temperature control of the index finger, the least difficult biofeedback technique. In many chronic disorders mind-body medicine is the approach of choice in stress illnesses and at the very least, a major adjunct even when pharmaceuticals are necessary. A few Scientific Evidence-based approaches include relaxation for GERD, Gastroesophageal reflux disease, hypnosis for irritable bowel syndrome, biofeedback and guided imagery for headaches, meditation and guided imagery for pain, and prayer for coronary artery disease.
Interface - Complementary Alternative Medicine CAM
Ultimately, as Sir William Osler said over 100 years ago, “More important than what the physician does, is the patient’s belief and the physician’s belief in what the physician does.” Benson, for instance, demonstrated that every 20th century treatment for angina pectoris, when subjected to double blind controls was no better than placebo. The recent article “The Emperor’s New Drugs” has emphasized the remarkably minimal effect of antidepressants, compared with placebo.
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
30
Faith and belief appear to be key elements in all therapy. A positive attitude not only improves outcome but also positively affects quality of life. Even outcome of surgery is positively influenced by proper mental preparation. Ultimately, to a significant degree, the mind- body connection influences all therapy.
Mind Body Medicine Research Summary
There are well over 100,000 scientific articles emphasizing the effects of mind on body and of body on mind. The fields of hypnosis, biofeedback, relaxation training, psychoneuroimmunology, faith and prayer and spirituality have solid scientific studies at this time. More and more, the medical community prescribes complementary therapies for many types of conditions. Since complementary treatments have become more common, The National Institutes of Health has developed a department called The National Center for Complementary and Alternative Medicine (NCCAM) that is dedicated to the study of these treatments. You can learn more about complementary therapy at the NCCAM website, http://nccam.nih.gov.
The Mind-Body Connection
American patriot Benjamin Franklin said “A cheerful face is nearly as good for the individual as healthy weather” and Alexander von Humboldt stated “True enjoyment comes from activity of the mind and exercise of the body; the two are ever united”. Many of us frequently experience the connection between our state of mind and our physical health. Too often however, it comes in the form of mental stress impacting how we feel. Over 200 years ago, Benjamin Franklin and Alexander von Humboldt noticed the connection between our state of mind and our physical health. Whether we are aware of it or not, many of us frequently experience this connection. For example, have you ever found yourself feeling that you were on the verge of becoming sick or tired— and decided to fight it? Probably, you kept telling yourself over and over, “I don’t feel sick” or “I don’t have time to be tired. What happened next? My guess is that some of you went on to become sick or tired and others did not. While there are physical factors such as genetics, our immune system, and overall physical health that can account for this difference, other factors, including our emotional state and beliefs about health and illness, come into play as well. Scientists have studied the placebo effect for many years and more than many pages of this
book examined the process. As the reader already knows, a placebo is any treatment that does nothing to alleviate symptoms or disease, but somehow causes a positive effect. The positive effect results from the patient’s belief in the medicine’s efficacy, not from the medicine itself. While testing the effectiveness of a certain drug one group of patients is given the drug the other is given a placebo, which is often a sugar pill. At the end of the trial period, the group receiving the placebo experiences an improvement in symptoms or, on the other hand, feels worse or suffers side effects.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
31
Studies show that between 60 to 90 percent of all physician visits are for stress-related complaints. For over 30 years, Dr. Herbert Benson, the founder of the Mind/Body Medical Institute in Boston and author of The Relaxation Response (2000), has studied how mind/body medicine can help treat stress-related conditions, including joint pain, hypertension, diabetes, migraine headaches, asthma, and allergies. Dr. Benson explains that stressful thoughts lead to the secretion of stress hormones that impede our natural healing capabilities. These hormones send the body into a state of arousal, causing metabolism, heart rate, blood pressure, breathing rate, and muscle tension to increase. The relaxation response which produces a physical state of deep rest is a simple breathing and concentration technique that is practiced for only 10 - 20 minutes a day. Dr. Benson’s research shows that it reduces the harmful effects of the stress hormones. What are some other ways to combat stress? Regular physical exercise helps. Yoga and meditation do, too. Although these methods are effective, they can take time and money for instruction and often may not be practical in the midst of a stressful situation. So what else can we do? First, stop and take a deep breath—or two or even three! Turn your focus toward using the mind-body connection to produce a positive effect. For example, try using affirmations on a regular basis. Or, practice mindfulness. Affirmations are a way of turning negative self- talk, which leads to stress, into positive, life-affirming statements. They are always stated in the present tense— I am, I have, I choose —and they reflect what we wish to experience. Think back to what we say when we might be getting sick or feeling tired: “I don’t feel sick” or “I don’t have time to be sick.” What do both of these statements have in common? They are negative and focus on what we do not want to happen. More positive and effective statements are, “I feel energetic and healthy,” or “I am relaxed and have plenty of time to do what needs to be done.” At first it may feel silly to state over and over the exact opposite of what you are feeling. But with regular practice, you will notice a change. The inner world of your thoughts and feelings will be in line with the outer world of your experience. Your mind and body will work together to produce a positive result. In her book Emotional Alchemy, Tara Bennett-Goleman (2001) describes mindfulness as a “meditative awareness that cultivates the capacity to see things just as they are from moment to moment.” In other words, we become fully aware, in a nonjudgmental way, of our thoughts, body sensations, and feelings as we experience them. For example, when you are showering, instead of allowing your mind to wander and worry about the busy day ahead, focus on the sensation of the water and the smell of the soap. When walking from the parking lot to your office, instead of anticipating the piles of paperwork you must wade through, listen to the sounds of your feet touching the pavement, smell the air, and feel the warmth of the sun. By practicing mindfulness regularly, we can live in the moment, feel content and peaceful, and experience joy in the process of doing all that we do. We use our minds to produce the positive results that we want. Children approach whatever they are doing with joy and how they focus intently on their involvement. When they feel ready to do something else, they turn their attention and energy to that. “Whenever I wake up and think it is going to be a bad day, I tell myself over and over it is a good day. And before you know it, it really is.” I learned an important lesson from Melanie that day.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
32
Dealing with Chronic Pain: The Mind Body Solution
Dr. Hilary Tindle is assistant Professor of Medicine, University of Pittsburgh School of Medicine and has researched persistent and chronic pain. She says that when medical professionals talk about "persistent" or "chronic pain," they are referring to debilitating, day-in-and-day-out pain that is difficult or impossible to live with and cure. Research shows that persistent and chronic pain affects approximately 30% of the United States population; for a significant portion of them, the pain is centered on the back, joints or other part of the musculoskeletal system. While this kind of pain remains a frustrating and difficult-to-treat condition, our understanding of what pain is and how it works has advanced greatly in recent years, leading to innovative and effective treatments. Many of these are so-called "mind body" therapies that aim to help people to control their own pain response. The groundbreaking gate control theory of pain in 1962 helped explain how psychological factors influence pain perception. Gate control theory says that physical pain is not a direct result of an assault from the outside on the pain producing neurons, (as is the case when you bang your elbow or break a leg), but rather the result of interaction between different parts of the brain and nervous system. The bottom line is that the brain controls the perception of pain quite directly, and has a proven ability to moderate or even turn on and off certain forms of pain. In earlier theories of neurochemistry, the role of the brain had not been taken into account; pain was thought to be a sort of one-way "alarm system" that always responded in the same way to the same stimuli. Also, in accordance with the biopsychosocial model of disease, a late 20th-century alternative to the traditional ("biomedical") model of disease, in which medical conditions are seen as having biological, psychological and sociological aspects, there is now increasing attention on pain as not only a physiologic, but also a psychological phenomenon. This broader understanding of the complex interaction of mind and body has resulted in new approaches to pain treatment.
Advantages of Mind Body Medicine in Treating Pain
In 1996, the NIH Consensus Panel on the Integration of Behavioral and Relaxation Approaches Into the Treatment of Chronic Pain and Insomnia recommended the use of mind body therapies for chronic pain. Since that time, increasing evidence has supported the use of mind body therapies. In addition, many mind body therapies are relatively inexpensive. When used appropriately, mind body therapies are generally safe. Finally, to the extent that mind body therapies emphasize self-care, they are economical and result in decreased utilization of the health care system.
Mind Body Medicine – Brain – Body – Behavior
Mind body medicine defined by National Center for Complementary and Alternative Medicine (NCCAM) "focuses on the interactions among the brain, mind, body, and behavior, and the powerful ways in which emotional, mental, social, spiritual, and behavioral factors can directly affect health." Mind body medicine is one of the five major domains of complementary and alternative medicine, and mind body therapies are some of the most commonly used CAM therapies among US adults.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
33
Mind Body Therapies
Mind body therapies are characterized by NCCAM as "techniques designed to enhance the mind's capacity to affect bodily function and symptoms." Common examples include relaxation techniques such as deep breathing, progressive muscle relaxation and the relaxation response, guided imagery, biofeedback, hypnosis, cognitive behavioral therapy and mediation.
Meditation is further divided into several sub-types, the two most commonly studied being transcendental meditation and mindfulness meditation; mindfulness meditation is also referred to as attentional training or metacognitive awareness. There is substantial overlap between different mind body therapies. For example, many guided imagery exercises begin with progressive muscle relaxation and involve deep breathing and meditation, while various forms of meditation incorporate breathing exercises and imagery. This reference does not provide an exhaustive list of Mind body Medicine but rather provides basic information on common mind body therapies.
Description of common Mind Body Therapies and Relaxation techniques include a variety of practices intended to affect a state of relaxation or reduced sympathetic arousal. The goal of these therapies is to allow patients to perform self-relaxation at will.
Imagery – Guided Imagery – Visualization
Guided imagery involves the process of visualized image generation for the purpose of improving health. There are active styles of guided imagery, where the patient mentally creates the image(s), as well as more passive styles in which the guide describes the images using a script, while the patient listens intently. Visualization and guided imagery are additional relaxation techniques that involve focusing the mind on specific images. With eyes closed, the person pictures in his mind a peaceful image or scene and concentrates on the sights, sounds, and smells that make the image soothing. Visualization is sometimes used as a supplemental treatment for patients with cancer or other serious and painful diseases. Guided by a therapist, the patient may visualize his body fighting the disease. This technique has been credited with bringing about physical healing in some cases. Guided Imagery is the use of imagined pictures, sounds, or sensations for generalized relaxation or for specific therapeutic goals, such as the reduction of pain. These images can be initiated by the patient or guided by a practitioner. The sessions in which imagery is used can be individual or group. More than half the studies of visual imagery for pain, postoperative pain, cancer pain, chronic low back pain, burns, and migraine headache--report significant relief from the procedure (Eller, 1999). In a review of laboratory research on coping strategies for pain control, visual imagery has been the most effective in relieving pain (Eller, 1999). Many of these studies, however, evaluate imagery together with other interventions such as hypnosis, cognitive behavioral therapy and relaxation techniques. Nonetheless, the preponderance of evidence suggests the usefulness of guided imagery in reducing the sensory and emotional components of pain. The Agency for Health Care Policy and Research recommends the use of imagery for reduction of pain intensity and distress for cancer pain and for the management of mild to severe acute pain (AHCPR, 1992).
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
34
Biofeedback
Biofeedback utilizes a device to amplify normal physiological processes e.g., muscle tension to make them more easily perceptible. Patients then receive feedback regarding their physiologic state (e.g., tension in a given muscle group) and learn to manipulate their own physiology (e.g., decreasing muscle tension), guided by cues. Biofeedback is the process and use of electronic monitoring instruments to provide patients with immediate feedback on heart rate, blood pressure, muscle tension, or brain wave activity. This allows the patient to learn how to influence these bodily responses through conscious control and regulation. Electromyographic (EMG) biofeedback, for example, can teach patients how to relax a particular muscle or how to achieve more generalized relaxation for stress reduction. Biofeedback has been shown to be effective in
the management of migraine headaches, fibromyalgia, temporomandibular disorders, and rheumatoid arthritis (Barkin, 1996), Raynaud's disease, tension headaches (DePalma, 1997), headaches in children (Serration, 2000) and the pain associated with irritable bowel syndrome (Leafy, 1998). Many other applications of biofeedback continue to be studied.
Medical Hypnosis
The Hypnosis state is often identified as a highly relaxed individual and internal state of focused concentration in which the conscious or rational part of the brain is temporarily tuned out through a focus on relaxation and non-attention to distracting thoughts. During the hypnotic intervention, changes like those found in meditation can occur, such as a slowing of the pulse and respiration, and an increase in alpha brain waves. The person may become more open to specific suggestions and therapeutic goals such as pain reduction. In the post-suggestion phase, the continued use of the new behavior after the hypnosis session is reinforced. Medical hypnosis has been shown to be helpful in reducing both acute and chronic pain (Holyroid, 1996). A National Institutes of Health panel found hypnosis to be effective in alleviating the pain associated with cancer (NIH, 1996). A 1997 review of the literature on hypnosis in pain control, which evaluated all controlled scientific studies comparing hypnosis to other psychological interventions for pain, showed hypnosis to be equally or more effective in reducing suffering and possibly even reducing pain sensation (Holyroid, 1996). Other studies have shown effectiveness of hypnosis for pain associated with burns, cancer, and rheumatoid arthritis (DePalma, 1997) (Sellick, 1998) and pain and anxiety reduction related to surgery (Lang, 2000). Clinical evidence supports the use of hypnosis in reducing pain in a wide variety of acute and chronic pain conditions for a substantial number of patients. Similar to passive style guided imagery, described by expert David Spiegel as "a natural state of aroused, attentive focal concentration coupled with a relative suspension of peripheral awareness." The hypnotic state includes three main components: absorption (in an object of concentration), dissociation (from ordinary conscious perception) and suggestibility.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
35
Medical Hypnosis is the use of hypnosis to help a person gain control over stress, pain, and bad habits such as smoking and overeating. It is also sometimes used in medicine to block the sensation of pain during medical procedures and in psychotherapy to assist patients in recalling traumatic events. Under the guidance of a hypnotherapist, the person enters a trancelike state during which his subconscious mind responds to the suggestions of the therapist. The person can be taught to recreate the deeply relaxed state he experienced while under hypnosis and to use it on his own to overcome pain, control eating and smoking habits, and reduce stress.
Cognitive-Behavioral Therapy (CBT)
Cognitive behavioral therapy is composed of cognitive and behavioral techniques that address the role of maladaptive cognitions and behaviors in disease. Cognitive therapy emphasizes correcting negative thinking patterns through a process called cognitive restructuring, while behavioral therapy rewards behaviors that are beneficial. While most mind body therapies are considered to be part of complementary and alternative medicine, cognitive behavioral therapy is an example of a mind body therapy that has gone main stream. Like other mind body therapies, cognitive behavioral therapy addresses the associated cognitive and emotional issues that accompany or enhance pain symptoms, such as a person's feelings of helplessness or associated depression. CBT has proven to be effective in reducing pain and disability when it is used as part of a therapeutic strategy for chronic pain. CBT addresses the psychological component of pain, including attitudes and feelings, coping skills, and a sense of control over one's condition. It can provide educational information and diffuse feelings of fear and helplessness. It can help a patient look at ways in which their attitudes contribute to inaccurate and unrealistic expectations, and can help them find a more realistic and balanced view of the problem. CBT may include training in various types of relaxation approaches, which can help people in chronic pain lower their overall level of arousal, decrease muscle tension, control distress, and decrease pain, depression and disability (Barkin, 1996). Relaxation imagery or pain-management imagery may also be taught to promote relaxation and changes in pain intensity or quality (Fernandez, 1989). Finally, CBT may include the teaching of life skills and coping skills that can assist the patient in productive problem solving and the prevention or minimization of future pain episodes. CBT has been found to be effective as part of a treatment regimen for a variety of pain conditions including episodic migraine and chronic daily headache (Lake, 2001), chronic musculoskeletal pain (Haigh, 1999), pain in the well elderly (Manetto, 1996), chronic cancer pain (Thomas, 2000), rheumatoid arthritis and osteoarthritis (Bradley, 2002), fibromyalgia (Berman, 1999), myofascial temporomandibular disorders (Sherman, 2001), chronic low back pain (van Tulder, 2001), carpal tunnel syndrome pain (Feuerstein, 1999), and chronic pelvic pain (Reiter, 1998). It has been suggested to benefit patients with chronic fatigue syndrome, irritable bowel syndrome (Kroenke, 2000), and anxiety (Ketterer, 1999). Although research into the use of CBT in children is in the early stages, it holds promise for reducing pain-related distress in children (Chen, 2000).
Meditation
When used in clinical settings, meditation is the practice of consciously focusing one's attention on inner experience. It may also be described as the self-regulation of attention. Two main forms of meditation interventions that have been extensively studied for health conditions are transcendental meditation, in which practitioners silently repeat a word or phrase (mantra), and mindfulness meditation, which involves non-judgmental attention to internal events such as thoughts, emotions and physical sensations on a moment-to-moment basis.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
36
Like other mind body therapies, meditation often brings about a hypometabolic state, or overall slowing down of bodily systems.
Meditation is a specific type of relaxation intervention that also can have an effect on pain. Results suggest that meditation can result in a higher tolerance to pain; decreased anxiety, stress and depression; increased activity levels; decreased use of pain-related medications; and increased levels of self-esteem (Mills, 1981; Kabat-Zinn, 1985; Harmon, 1999). The meditative technique based on increased awareness and staying in the moment, called mindfulness meditation, has been successfully used in treatment programs to reduce pain and improve mood in patients with chronic pain from a
variety of conditions, including facial pain, coronary and noncoronary chest pain, gastrointestinal pain, low back, neck and shoulder pain and headache (Kabat-Zinn, 1982). Complementary and alternative therapies such as Qi Gong, Tai Chi and yoga share many of the features of mind body therapies (e.g., the use of imagery and breathing techniques) but are not always classified as such. For the purposes of this article, we will focus on the more classical mind body therapies in Table 1. Similarly, prayer also meets the criteria for a mind body therapy and is widely used by U.S. adults for health reasons. However, in research studies of mind body therapies and health, prayer is often considered separately because the characteristics of respondents who pray and the reasons for use of prayer may differ from those of other mind body therapies.
How do People Receive Mind Body Therapies?
Mind body therapies may involve group or one-on-one therapy, but they also lend themselves well to self-care. For example, many forms of relaxation techniques combine practitioner-based instruction, often on video or CD, with a home-study program. There are no hard and fast rules for types of mind body therapies to avoid, because they are generally safe. Therapies such as guided imagery or meditation may not be appropriate for those with untreated psychiatric conditions, (such as uncontrolled depression or active hallucinations), although one recent study safely used a mindfulness-based therapy for people with active depression and anxiety.
Mind Body Therapies Are in Widespread Use
According to three large, nationwide surveys, the use of mind body medicine by U.S. adults is surprisingly common. In 1997, one study surveyed 2,055 individuals and found that 16.3% used relaxation techniques such as meditation or the relaxation response. Chronic pain was the third-most common reason (19.5%) to use mind body therapies and was reported to be "very useful" for that condition by 55% of users. Chronic pain may lead people to seek out mind body therapies. The 1999 and 2002 National Health Interview Surveys (NHIS) were conducted by the Census Bureau for the National Center for Health Statistics. In 1999, 30,801 U.S. adults were asked if they had persistent joint pain during the past year and if they had used a mind body therapy (including relaxation techniques, guided imagery, hypnosis and biofeedback) during the past year. People with musculoskeletal pain were almost twice as likely as those without pain to use mind body medicine and prayer. The 9% who used mind body medicine represents about 3.5 million U.S. adults.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
37
Effectiveness of Mind Body Therapies for Musculoskeletal Pain Back Pain
Back pain is an area where we are beginning to have some data on the effectiveness of alternative therapies for pain. One study of behavioral therapy (such as cognitive behavioral therapy) for chronic low back pain in people ages 18 - 65 was conducted to determine if behavioral therapies were effective, and which therapies were most effective. The results suggested that there was strong evidence to support respondent therapy (e.g., relaxation techniques or guided imagery) for a medium effect on pain. There was moderate evidence suggesting that progressive relaxation had a large effect on both pain and behavioral outcomes, but only in the short term. Interestingly, there was no evidence that one behavioral therapy was more effective than another for pain-related outcomes.
Breath therapy -- mind body therapy integrates body awareness, breathing, meditation and movement for treatment of chronic low back pain was about as effective as physical therapy both in the short and in the long term in one study. Mindfulness meditation resulted in significant improvements in pain acceptance and physical function in a study of 37 older adults with chronic low back pain.
Headaches, Arthritis and Other Musculoskeletal Pain
Mind body therapies appear to be effective for some types of headache. Relaxation training,
electromyography (EMG) biofeedback (the recoding of muscle activity at rest and while contracting) and a combination of the two therapies reduced the severity of tension headaches by half. Relaxation and biofeedback were as effective as the drug propranolol for the treatment of migraine. Fibromyalgia is one area where mind body therapies have not been yet shown to be effective, or to have very limited effectiveness. Several mind body therapies have also been used for arthritis (both rheumatoid and osteoarthritis). The Arthritis Self-Management Program uses cognitive therapy and relaxation
techniques. People who used this self-management program had reduced pain and disability, though a study reviewing the overall results of over 20 trials of mind body therapies for rheumatoid arthritis found significant effects in the short-term on pain, functional disability, and psychological status and coping with pain; follow up only moderate effectiveness for psychological status and coping with pain.
How Mind Body Therapies Treat Pain The mechanism by which mind body therapies alleviate pain is not well understood, but it may result from their effect of increasing sufferers' sense of self control, which is known to influence how pain is experienced. Similarly, there is emerging evidence that mind body therapies facilitate a sense of empowerment. Mind body therapies may also modify the cognitive and emotional components of pain perception known as pain unpleasantness and pain affect; these are distinct from pain sensation and contribute significantly to suffering. The emotional components of pain often have the effect of magnifying pain severity.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
38
Pain • Complex Sensory Experience Pain is not only sensory; it has a very powerful and unpleasant emotional effect. Pain researcher Troels Statehelin Jensen underscores the complexity of pain when he asks, "What is pain: a sensation, an experience, a symptom, or even a disease?" Mind body therapies are generally safe, inexpensive and already used widely by the U.S. public. Despite this, the effectiveness of most mind body therapies for pain has not been well tested and studied. While their effectiveness for musculoskeletal pain appears to be limited to moderate when used alone, when applied in combination with standard therapies, they may be considerably more useful. Further study is needed to understand more fully how hypnosis and other mind body therapies for pain work in general and in particular. Some experts in the field have argued that the demonstrated effectiveness of many mind body therapies is more or less a "placebo effect." More studies need to be done to determine if this is the case, and to find the brain areas that are more or less active when mind body therapies are applied.
Finally, mind body therapies may be particularly suitable to certain populations, such as the elderly, where there is a higher risk of medication interactions, or in populations who prefer to use alternative therapies. This latter population is substantial, considering that in 2002 about 29 million people used relaxation techniques.
Managing stress • improve immune function
In July 2007 Sheri Kaplan wrote a brief article about managing stress with mind body medicine and improving immune system functions. Dr. Kaplan explains Mind Body Medicine techniques decrease stress and anxiety, which can physically affect the body. The basic premise of mind body medicine is that our thoughts, feelings, and mental states influence our bodies at the physical level and express themselves in our health. The brain has often been called the organ of the mind because it connects to the immune system through nerve fibers that reach into all of the organs and systems. When you experience stress, the nervous system becomes hyperactive and provokes the effects of the immune systems over and over again. This causes the body to move into a state commonly called “fight or flight”. In this state, the immune system becomes weakened and the adrenal glands become exhausted causing the body to feel weak and lethargic. You can also experience dizziness, headaches, memory loss, irritability, allergies, cold and flu symptoms and more serious illnesses. Studies have shown that people with high levels of social support and intimate relationships have stronger immune systems and fewer illnesses. Research at Southern Methodist University in Dallas has shown that confiding thoughts and feelings about traumas -- if only by writing them down -- improves immune function. Seeking a support group in your area can reduce stress and benefit overall health.
Safe Daily Exercise
Each day the body must have a minimum of one-half hour of enjoyable exercise that causes sweating, because “sweat” signals the removal of waste from the body and possibly the reduction of virus replication. Cardiovascular fitness can strengthen the heart and circulatory system. This is done by simply increasing one’s heart rate about 20 percent more than resting heart rate, and keeping it up for at least 20 minutes, at least six times per week. More and more, the medical community prescribes complementary therapies for many types of conditions. Since complementary treatments have become more common, The National Institutes of Health has developed a department called The National Center for Complementary and Alternative Medicine (NCCAM) that is dedicated to the study of these treatments.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
39
Thoughts Heal Your Body • Live longer • better • wiser
Robert Moss wrote an article for PARADE Magazine and in it he states that our thoughts can make us sick, and they can help us get well. That may seem like New Age thinking, but medical research increasingly supports the role played by the mind in physical health. Dr. Herbert Benson, founder of the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital states that people have been seeking healing through prayer and intention since Paleolithic times. What’s new is our detailed scientific knowledge of how the mind-body connection operates. Scientists first proved a link between stress, anxiety and disease in the early half of the last century. Since then, researchers have examined old and new practices including biofeedback, meditation, guided imagery, spiritual healing and deep breathing.
The fast-expanding field of psychoneuroimmunology examines how the neurological and immune systems interact and is providing new clinical evidence of the connection between thoughts and health. Mary Jo Kreitzer, director of the Center for Spirituality & Healing at the University of Minnesota says that we now can measure changes in immune cells and the brain in ways that give us objective scientific proof of the connection between them. Some people still are surprised to discover that thoughts can control physical sensation. Larry Dossey, a physician and an advocate for mind-body study since the 1980s explains that the body responds to mental input as if it were physically real. Images create bodily changes—just as if the experience were really happening. For example, if you imagine yourself lying on a beach in the sun, you become relaxed, your peripheral blood vessels dilate, and your hands become warm, as in the real thing. Similarly, under clinical hypnosis, someone who is told he is being touched by a red-hot object often will produce a burn blister, even though the object touching him was at room temperature. Brain scans show that when we imagine an event, our thoughts “light up” the areas of the brain that are triggered during the actual event. Sports psychologists have done pioneering work in this area. In one study, skiers were wired to EMG monitors which record electrical impulses sent to the muscles while they mentally rehearsed their downhill runs. The skiers’ brains sent the same instructions to their bodies whether they were doing a jump or just thinking about it. The “placebo effect” is an example of how the connection between brain and body works in healing. It has been demonstrated that when a patient believes something will relieve pain, the body actually releases endorphins that do so. In a recent study, Parkinson’s patients who were given fake surgery or fake drug treatments produced dopamine, a chemical their bodies lack in quantities similar to those they might have received in a genuine intervention. Medical research has suggested that 30% to 70% of successful treatments may be the result of the patient’s belief that the treatment will work. Lorenzo Cohen, director of the Integrative Medicine Program at the M.D. Anderson Cancer Center in Houston explains there is ample evidence that negative thoughts and feelings can be harmful to the body. Stress is known to be a factor in heart disease, headaches, asthma and most all chronic illnesses.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
40
Studies by Janice Kiecolt-Glaser and Ronald Glaser at Ohio State University demonstrate how even minor psychological stress that of newlyweds having their first fight or of students facing an exam, can compromise the immune system. The researchers found that a marital spat delays wound-healing and that the stress of caring for an Alzheimer’s patient leaves the caregiver more vulnerable to illness even years later. When the body fights a virus or heals a wound, it releases cyto–kines (literally, “moving cells”)—chemical messengers that call in immune agents. The Glasers’ research showed that stress and anxiety distracts these cytokines from doing their proper work, instead sending them ranging wildly through the bloodstream. Kiecolt-Glaser explain that when the cyto-kines are misdirected, they produce something you don’t want—a prolonged inflammatory response that far exceeds what is needed with infection. Just as our thoughts can make us ill, they also can help us heal, say those who practice mind-body therapies. There is growing clinical evidence that imagery is beneficial in treating skin disease, diabetes, breast cancer, arthritis, headaches and severe burns, among other conditions. Imagery also has been helpful in managing pain. “The mind is our most potent weapon in the battle for health,” says Lyn Freeman, a researcher of mind-body therapies for chronic diseases. “It can be both slayer and healer.”
What To Do For Health
Adjust your mind-set to promote good health. Take a deep breath. Hold it, exhale - then repeat for 10 minutes. Take a walk, preferably in nature. Breathe in the fresh air. Laugh! When you do, you pump more oxygen into your lungs, improve blood flow and boost your immune system. Keep a journal. Writing about emotionally charged events helps us deal with them mentally and physically.
Pain Management Conventional Approaches Psychological • Mind-Body Therapies
Psychological factors are important contributors to the intensity of pain and to the disability associated with chronic pain. Pain and stress are intimately related. There may be a vicious cycle in which pain causes stress, and stress, in turn, causes more pain. Mind/body approaches address these issues and provide a variety of benefits, including a greater sense of control, improved coping skills, decreased pain intensity and distress, changes in the way pain is perceived and understood, and increased sense of well-being and relaxation. These approaches may be very valuable for adults and children with pain (Rusy, 2000). For pain specialists, the therapies that are psychological, or focused on the relationship between mind and body, are considered mainstream; for many others in the health professions, and for the public at large, the same therapies might be considered complementary or alternative. The evidence in support of these approaches is very strong and how they are labeled is less important than their acceptance as necessary treatments.
Prayer and Health
Prayer is not usually considered a mind-body or a psychological approach, but it is worthwhile considering it in this context of mind/body treatments. Changes in the concept of health and illness, a broadening view of healing and curing, and interest in other cultural systems of medicine have created a growing openness to the spiritual dimensions of health. There are many anecdotal reports of the power of prayer and its effects on health.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
41
This has led to a substantial number of scientific research studies. As of 1992, there were at least 131 controlled trials that evaluated the effect of prayer on humans, microorganisms, plants, cancer cells and animals; 56 of these studies found significant effects (Targ, 1997). In human trials, prayer had a positive effect on levels of stress, depression, hypertension and substance abuse, illness-related complications, and life satisfaction (Targ, 1997). In a systematic review of randomized trials of distant healing, 57% of 23 trials showed a positive treatment effect (Astin, 2000). A recent study of the effects of direct and distant healing on chronic pain, however, showed no specific effect after eight weekly 30 minute treatments (Abbot 2001). This is an area that clearly warrants further study.
Alternative Medicines for Uterine Fibroids
Dr. Jon Kaiser of Integrativehealthconsulting.com writes that Fibroids are noncancerous tumors in the muscular wall of the uterus. Fibroids can be as small as a pea or as large as a grapefruit. The body's level of the estrogen hormone seems to play a role in the condition as fibroids tend to grow during pregnancy and shrink after menopause. Several alternative therapies offer ways to reduce estrogen levels naturally. The hope is to forestall or eliminate the need for a hysterectomy.
Mind/Body Medicine for Uterine Fibroids
For women with fibroids, mind/body medicine focuses on significantly reducing stress. This is vital because stress can interrupt the development and release of eggs (a process called ovulation). When this process doesn't happen, the body's level of estrogen remains unnecessarily high, precipitating fibroid development. Mind/body medicine offers many therapies that teach relaxation and how to lower stress levels, including: Forms of guided imagery and creative visualization include meditation yoga (including breathing exercises and stretches), biofeedback, dance therapy, hypnotherapy, and spirituality.
Here's an example of a relaxation breathing exercise that would be part of a guided imagery regimen: Wearing loose clothing, lie down or sit in a comfortable chair. Slowly close your eyes. Begin breathing deeply and slowly. When exhaling, imagine tension effortlessly flowing out of your body with each breath. As you inhale, picture yourself filling your body with fresh air and energy. Continue the slow, deep breathing for as long as you are comfortable.
Hydrotherapy for Uterine Fibroids
Hydrotherapy directed at the lower abdomen can stimulate blood circulation, which delivers nutrients and other beneficial substances to the cells and cleans away waste products. These treatments can also provide pain relief. Castor oil, made from the leaves of the castor oil plant, is commonly applied to the lower abdomen as a warm pack. The cold-pressed oil contains a substance that boosts the action of cells important to the immune system. Alternating hot and cold sitz baths can also be effective.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
42
Nutritional Therapy for Uterine Fibroids
According to nutritional therapy, diet and supplements can stabilize or even lower the levels of estrogen in the body. As estrogen amounts drop, existing fibroids should shrink and new ones can be prevented. Diet and supplements may also reduce some of the symptoms of fibroids. One of the liver's roles in the body is to break down estrogens. Therefore, the diet should allow the liver to do its work and not include foods that can tax this organ. These taxing foods to be avoided include: sugar, meat, dairy products, alcohol. Meat and dairy products can be a source of hormones (including estrogen) from livestock. Because they are also high in fat and estrogen is stored in fat cells, these foods may cause additional problems for women with fibroids. Instead, focus on eating fresh vegetables and fruits, whole grains, nuts, and raw seeds. These steps should also result in a diet that's high in fiber and low in fat. The B vitamins also aid the liver and are recommended. They can be added in the form of whole foods (such as lentils, rice bran, and blackstrap molasses) or supplements. Vitamin B6, in particular, enhances the breakdown and removal of estrogen from the body. Natural plant estrogens, called phytoestrogens, can actually compete with human estrogen in the body, resulting in an overall lower level of estrogen. Soybeans are a good food source of this substance and can be used as a whole cooked bean or in its other forms, including tofu, tempeh, and soy milk. Researchers have linked heavy menstrual bleeding with low levels of vitamin A in the blood. One study gave women doses of vitamin A for 15 days, after which time menstrual bleeding was reduced in about 90 percent of the patients. To achieve proper levels of vitamin A in the body, most practitioners of nutritional therapy recommend eating foods rich in beta-carotene (such as carrots and sweet potatoes) or taking beta-carotene supplements. A naturopathic physician may recommend a program of several supplements to normalize estrogen levels, including B vitamins; vitamin E; beta-carotene; cysteine, methionine, choline, inositol (to help the liver metabolize estrogen and other substances more efficiently); and iron (if the fibroids cause heavy menstrual bleeding and anemia). Dietary recommendations include adopting a low-fat, high-fiber diet and avoiding meat, dairy products, eggs, refined sugar, and caffeine.
Other Therapies for Uterine Fibroids
Acupressure for Uterine Fibroids -- Points along the liver and spleen channels are often targeted for symptom relief. Acupressure, also called shiatsu in Japan, is an ancient Chinese method of improving a person's health by applying pressure to specific points on the body. Acupressure uses the same channels of energy flow as acupuncture but does not break the skin. Instead, the acupressure practitioner applies pressure using the fingertips or knuckles to loosen muscles and improve circulation. Herbal Medicine for Uterine Fibroids -- Some herbs that can ease the symptoms of fibroids are blue cohosh, dong quai, and wild cherry. Homeopathy for Uterine Fibroids -- Remedies for short-term relief of symptoms can be very effective, but a careful diagnosis by a professional is necessary to tailor a long-term remedy for fibroids. Detoxification, Fasting, and Colon Therapy for Uterine Fibroids -- Several types of treatments can remove toxins and prevent certain organs (such as the liver) from being overworked. These therapies can also alleviate constipation and hemorrhoids related to fibroids.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
43
Mind Body Medicine • Psychoneuroimmunology
The next research will focus on psychoneuroimmunology which is a separate process but nevertheless included in Mind Body Medicine practices as is Medical Hypnosis and many other alternative medicines. What’s important for the reader is assimilate the multiple values to non-pharmacological and non-surgery treatments. The logic to follow is that should the most successful and least intrusive treatments fail then the pharmaceuticals and surgery options are always open. It is important for main stream medicine to make its primary treatment a preventive medicine approach as is advocated in AquaDios-Med™ because all of research supports safe daily exercise as the one most powerful treatment for mankind.
Psychoneuroimmunology - Guided Imagery – Mind Body Medicine Preventive Medicine Preventive Care
For practical reasons this author considers terms like Mind Body Medicine,
Psychoneuroimmonlgy, psychosomatic medicine and preventive medicine, medical hypnosis as synonyms even though these practices differ their procedures and outcomes are very similar. The Center for Evidence Based Physiotherapy says the word psycho-neuro-immunology refers to the positive health effect that visualization can have on the mind, the nervous system, and the immune system. Psychoneuroimmunology, often referred to as PNI, is the study of interactions between ones perception of the world around them, their behavior, the way their brain functions, and their immune system. The field of PNI studies the measurable interaction between psychological and
physiological processes. The psychological portion is the Psycho aspect, the central nervous system aspect is the Neuro aspect, there is an endocrine system aspect, and the body's defense against external infection and aberrant cell division is the Immunology aspect. The medical use of visualization and imagery can produce a positive effect on the body that is much like programming your computer to produce the tasks you direct. The use of visualization and imagery has become increasingly widespread over the past few years. Athletes visualize their performance and successes before they achieve them. Successful people visualize achieving their goals, and reach them. AquaDios-Med™ especially likes to use guided imagery and structured deep-water running to help people facilitate their own healing; especially while learning to wean themselves for prescribed medications. The Mind Body Medicine process can also be used to help change people’s habits and achieve and goals, such as weight loss or the cessation of smoking, for example. There are several studies supporting a positive relationship between the ability of the mind to modulate mental and physical illness. The Center for evidence based physiotherapy indicates the field of psychoneuroimmunology, emerged in the 1940s and established the fact that there is a brain-body connection in which the mind can impact the immune system in its fight against the body's foreign invaders (e.g., bacteria, viruses). Psychoneuroimmunology explains a brain-body connection in which the limbic-hypothalamic system of the brain converts electrical neural impulses into the hormonal messengers of the body.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
44
The hypothalamus is the brain's control center for all the major regulatory systems of the body: the autonomic, endocrine, immune systems, and the neuropeptide psychosomatic network as described by Dr. E. Rossi in 1988. Thus, psychoneuroimmunology offers one possible explanation for the link between spiritual beliefs and psycho-biological phenomena such as consciousness, emotions, moods, and memory.
Simonton's Work • Cancer Remissions
Carl O. Simonton, MD et al. in 1978 demonstrated a relationship between spirituality, not religiosity but matters regarding humankind's ultimate nature and purpose, not only as material biological organisms, but as beings with a unique relationship to that which is perceived to be beyond both time and the material world. Holistic ideas of health and healing is grounded in more than biology, and healing may often entail genuine belief coupled with guided imagery to overcome serious diseases such as cancer and that a good practice of medicine depends upon physicians' awareness of both their patients' and their power of belief.
In the late 1970’s Dr. Simonton, an Oncologist began to treat cancer patients with severe physical illness diagnosed with medically incurable cancer malignancies. The group participated in a six week
program of theory presentation and application of topics related to spirituality such as the interrelatedness of mind, body, and emotions, relaxation, positive mental imagery, and physical exercise. The average survival time of participants, still living at the time data were being collected was 24.4 months, twice that of national norms for persons with similar conditions. The average survival time of the subjects who had died was 20.2 months, one and a half times the national norm.
While there are now literally thousands of studies and case histories regarding PNI that could be presented at this point, none is as dramatic as is the work of Dr. O. Carl Simonton and his wife Stephanie Matthews-Simonton.
While working with cancer patients who were considered to be incurable and terminal, the Simonton's started a program which educated them and helped them reduce their fears and stress about cancer. They instructed these patients that cancer is really a weak and malleable process, and not the strong overwhelming process that the medical profession and the general public usually think it to be.
The Simonton’s taught these sever cancer patients a process of positive visual imagery in which they "saw" their immune system attacking and destroying cancer cells. This activated their immune systems and caused the natural defense of the body which had apparently been "turned off" or "impaired" to be reactivated and attack and destroy their cancer cells. The Simonton's presented their patients with a new model for recovery over their cancer. Using this new model many were successful in overcoming their cancers and other health problems.
Simonton’s Important Breakthroughs
Patients who were previously told that they were incurable, by using the Simonton program were able to stimulate their immune systems to reverse their cancer and in many cases eliminate the cancer entirely. Unfortunately American Medicine now better recognizes the role of beliefs, thoughts and emotions especially negative thinking, resentment, anger and rage in causing cancer and how resolving conflict or changing it to a positive, can promote reversal of illness and healing.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
45
We have established that the body's defense mechanisms can be activated and that white blood cells, lymphocytes, killer cells and other messenger factors associated with the healing response can be stimulated to act against cancer and other illnesses.
Importance to Preventive Medicine
This research and the way that it is capable of changing hospital medicine is important to all of us; if main stream medicine will only listen. Fritjov Capra in his book The Turning Point suggested that we are now in process of changing from the presently accepted paradigm, which we refer to generally as Modern Western Medicine, to a new paradigm. This new paradigm, while yet without a name, is fueled by movement away from the concepts involved with the Cartesian-Newtonian construct that underlies present medical thought of treating medical problems with medications and surgeries. The new paradigm is based on the present new understanding of the universe laid down by Albert Einstein, Werner Heisenberg, Nils Bohr, David Bohm and many others. It is this author’s professional opinion is that the paradigm referenced here is not new at all, it is old and its name is “preventive medicine”. The American healthcare crisis and its $ 2.5 Trillion cost has been caused by poor decisions of main stream medicine insisting the treatment of choice is to begin with prescribed medications that most often have side effects as bad or worse than the medicine or surgeries rather than prescribe what most all of the health studies research has determined and that is “safe daily exercise” is the best medicine. Preventive medicine is based in Systems Theory which suggests that everything is interconnected, and that there is an interrelatedness and interdependence of all phenomena. While the Newtonian-Cartesian paradigm suggests that to understand something medicine had to break it into its component pieces and separate them one from the other, the new paradigm tells us that Systems, such as the human body a reintegrated wholes whose properties cannot be reduced to smaller units. While medicine can look at each component separately, it is impractical in reality to separate one from the other. Human beings and the environment are dependent upon each other and their interrelatedness is integral to their ability to function appropriately; this emphasizes basic principles of organization. Hence, we are in a sense one and the same as our environment and we respond to it based not only on how we work, but also on how it works. In summary, more than many studies verify that there is a connection between beliefs, mental and physical health. More studies are needed in order to explore the structure of beliefs and process by which belief and health transformation can take place. In the meantime scientific research has repeatedly proven that safe daily exercise with Mind Body Medicine as offered by AquaDios-Med™ is the best medicine; with no negative side effects.
Dualistic Medical Systems -Body – Mind – Soul
Today the immune system is no longer regarded as autonomous and separated from the mind and external events. With the emergence of PNI we begin to see the rise of a new paradigm such as practical “preventive medicine” relating to the practice of medicine. This new paradigm for the first time integrates the previously dualistic concepts of mind and body. It introduces a new concept where mind and body interact as one, each affecting the other.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
46
Substantial scientific evidence regarding this mind-body-immune system interaction has been collected with regard to the role of nerve fibers in lymphatic tissues, the sympathetic and parasympathetic nervous systems, the effects of brain lesions on the immune system, the interplay of neurotransmitters, hormones and immunotransmitters. It is being used in research and treatment of AIDS, cancer and bacterial and viral infectious processes.
Researchers are looking at its effects in classic learning and conditioning, the development of the immune system, the impact of experimental and naturally occurring stressors on the immune system, the immune modulating effects of personality characteristics, life style and psychodynamic processes. Research will extend into many new areas including psychotherapy, pregnancy, illness prevention and healing to name only a few. PNI goes beyond the present narrow biological perspectives of illness to consider behavioral components as an integral part of health and disease. The conceptualization of the role of human behavior and how it interacts with the central nervous system and the immune system are central issues. Psychoneuroimmunology is thus an arena in which questions about the mind, body and person in context of each other come to the fore. Research is often driven by attempts to define the extremely complex and non-linear relationships between behavioral and biological dimensions of 'immune system.' Today researchers operate under disciplinary, institutional, and funding constraints, which tend to work against PNI research. These tend to maintain the status quo, as well as inhibit the development of competing and radical models within the field psychoneuroimmunology itself. This slows research down and tends to keep it out of the mainstream of medicine. Over the last 30 years, the body of knowledge in PNI has emerged and in the last 10 years has flourished. PNI is still in its infancy; there is growing evidence that it is and will continue to be an important discipline in medicine.
Bidirectional Feedback Loop
The Center for Evidence Based Physiotherapy says that disciplines as diverse and different as anatomy to psychology have demonstrated that the immune system is the target of signals from both the brain and the endocrine system. Findings also suggest that a bidirectional feedback loop exists between the brain, the body, its tissues, the stress mechanism and the immune system. This means that ultimately our past experiences, our present behavior, what we think and believe all have impact on the body, and its immune system and vice versa; and this can have a positive or negative impact on individual health. The existence of this bidirectional communication pathway between the brain, the body and the immune system is maintained by neuron activity, neurochemicals, hormones and various other molecules such as peptides, endorphins, enkephalins and cytokines. They carry messages from the brain to the immune system and from the immune system back to the brain
Characteristics of PNI
The overall implications are that processes can alter immune functions and those events that occur as part of immune responses can modulate our behavior. Evidence for influences in both of these directions is presently being collected and evaluated. The psychological modulation of immunity generally focuses on classical conditioning and stress, whereas that of immune modification of behavior highlights behavioral effects produced by substances released from the immune system. The ultimate implication of this work suggests that we are due for a major shift in the way we think, and the practice medicine and the healing arts. Whether in the medical, psychological, social or behavioral realm, PNI either is already affecting you or will in the near future.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
47
Neuroendocrine Interaction with the Immune System
The Center for evidence based physiotherapy indicates that one of the primary areas of study is the relationship between stress and the immune, defensive, repair and healing systems of the body. It is this area which is probably best understood at this time. For example, when we get angry, our entire body responds, it instantaneously becomes tense and we move toward Fight or Flight. When we are happy, our entire body becomes happy and balanced. In our old system of thinking such responses were thought to start off as electrical impulses from the brain to various parts of the body. That is, instructions in the form of electrical impulses were sent by means of the nervous system to innervate various tissues. It was, and in fact, still is believed that the nerve ending or synapse played the largest role in this process by releasing chemicals which are ultimately responsible for all changes which occur in anatomy and physiology. While this concept has not really changed, PNI has added to it. We now know that the process is more complex then this alone. Besides electrical stimulation there is also release of neurochemicals that travel along nerve tissues, other neurochemicals are released into the blood stream, our hormonal system also plays a significant role, and other chemical and yet undetermined messengers appear to have specific tasks of carrying messages to every part of the body. To simplify the language of all of the various ways that the body can communicate with itself these various mechanisms shall be referred to as messenger pathways and messengers regardless of what these processes or pathways are. These messengers and their specific pathways have some important properties that tell us that something quite remarkable is occurring. We know that they are not simply "neutral actions." That is, these messengers are not simply general messengers that bring chemical or electrical stimulation from one place to another. They are quite specific. There are messengers which transmit happiness, joy and positive feelings and there are messengers that transmit fear, activate the Stress Mechanism, or create depression. The old model of too much of one chemical or another causing a particular effect will likely be replaced by a more complex model of interaction between the various stimulating and inhibiting messengers. In a sense the body, mind and psychology are the result of a symphony, and not simply a three or four-piece ensemble. This concept was known by the ancient healers who talked about it in the form of spirits, of various shades of good and evil. It can also be seen clearly in the humoral concept or the typical body fluids, especially blood serum of that held sway on the healing arts for hundreds of years. Man was seen as responding to interaction of various humors or temperaments. They accounted for changes in emotion, for anger, rage, for love, caring, melancholia and depression, for humor and for illness. Almost anything could happen when the humors were out of balance. While these humors did not entirely answer what we needed to know, they were an attempt to understand how and why we acted the way we did. In a sense they were not entirely wrong, for we are a blending of the interaction of many chemical, electric and other processes that ultimately make us the sum total of who and what we are. We have come a long way since belief in the humoral concepts of healing, yet as things often have a tendency to make complete circles we are now once again recognizing that we are not linear but rather a more integrated or Holistic, as many people are now calling it, construction.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
48
The interaction of mind, our thoughts and the sense of how we think it is supposed to be, can be called our "picture of the experience," come together along with body chemistry to create us to be what we are at any given moment. In this example, I am mixing positive, negative and neutral simply to be able to introduce these concepts all at the same time. In real life, however, most of what we experience is a combination of these three types of emotions.
Body chemistry creates our Persona
Center for evidence based physiotherapy describes how experience and body chemistry works. An external event occurs ---> through our memories of the past, prior decisions and beliefs we have already, and automatically created a picture of the way we expect things to be. When the external events either support or conflict with this picture which we have already accepted as real ---> Positive or negative messengers are released to inform the entire body ---> There is a physical, mental, emotional and possibly even spiritual response to these events which is mediated by our past experience, what we think and what we believe. When this process relates to an event which is external to us, and when it is negative, we refer to it as a stressor. This stressor can also come from within and be an internal stress or such as a thought, a remembrance, a fear or a faulty belief system. Remember, stress can be both positive and negative so a reaction can also arise from something that is happening to us that is positive. For example, a pleasurable feeling, getting what we desire or even an internal joke. We hold a significant number of specific and general pictures, sets of belief systems, of how we desire or expect things to be. When an event (or stressor) occurs we will likely react to it in either positive or negative way or somewhere in between. Our mind-brain and not the actual event, makes the decision as to what the unfolding event means to us and then tells our body how to respond to it. In the example, the question was whether the shadowy figure was or was not a friend. When you thought the figure to be a friend, positive messengers were released. When you thought the figure to be a menace, negative messengers were released and the Stress Mechanism was activated. In any case, the entire body was being informed about what was happening and it was waiting, as you and I were, to find out who the figure really was. The picture of the way we expect things to be already exists ---> an event occurs and depending upon whether the event is positive or negative ---> it causes the release of messengers ---> there is a physical, mental, emotional and spiritual response to the event. In the first case presented the event occurred randomly without our being ready for it. It just happens. In the second case, we were already expecting something to happen and we had a preconceived notion of what we wanted to happen. In both situation what happens, happens and we are left to deal with it through already set pathways using the PNI mechanism and at times the Stress Mechanism, if it is perceived as a threat. What then is actually happening? To understand this process let’s look at one more schematic of the events: Our past experiences and memories ---> Cause us to create beliefs or a picture of the way we expect things to be ---> this affects our ultimate mind/brain interaction ---> and hence our mind, body response.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
49
Responding to Our Internal Environment
The Center for evidence based physiotherapy says research verifies that we respond to life and the environment depending on our beliefs and memories. When the event is perceived as a threat, we experience fear, apprehension and the Stress Mechanism may be activated. If the event is perceived as positive, we experience an entirely different set of feelings, emotions and body responses. The key point to remember is that the immune system is also simultaneously affected. The immune system is turned on and off, activated and deactivated depending on the variables we have already outlined. When messages are mixed the response of the immune system, may well also become mixed and its ability to respond, confused.
The Bodies Systems – Their Involvement
Nervous System (Brain, Memories, Past Experiences, Future Projections, Belief Systems) Neurochemical System (Neuro-peptides, Neurohormones, Endorphins, Signaling Neurotransmitters, Neuroreceptors) Hormonal/Endocrine System (Entire Hormonal/Endocrine System - Principally Corticosteriods) Immune, Repair and Healing Systems (Stress Mechanism, Primary, Secondary and Tertiary defensive Systems) Adequate Nutrition and Normal Body Chemistry: We know that when there is inadequate nutrition, illness, mental instability, or chemical imbalances this can affect the process described above and create faulty responses at all levels including within the immune system. Our state of physical being can affect the direction of these interactions and the end result of what is perceived and how we act.
Feedback from Body Tissues - Cells and Organs What is Stress and How Does It relate To the PNI Process?
The Center for evidence based physiotherapy indicates one of the focal points of this fledgling branch of science is its ability to link stress and disease. However, this author believes that “stress” can be a healthy response toward action and it is not debilitating until stress becomes chronic and turns into a perpetual “distress” capable of altering our physiology. Science can now pinpoint changes in hormonal flow as well as the various messengers and messenger pathways within the body to and from immune system cells. We can also associate these phenomena with specific responses involved in both the creation and healing of many illnesses. The stress hormones can change immune cell behavior and the activity of the entire immune system. The immune system cells actually have receptors which as Margaret Kemeny a Professor of Psychiatry at UCLA says, "hear" the signals and allow nervous, endocrine and immune systems to "talk" with each other and the rest of our body.
What is Stress • Anxiety • Distress
Stress is an inborn biologic mechanism which exists in all living creatures. Its purpose is to protect the organism and to ensure its survival and the survival of our species. The Stress Mechanism, also thought of as the survival instinct, operates through a concept which is often referred to as Fight or Flight. When threatened, more than stress, the individual may have little or no time to think or plan. Nature understood this and gave us the ability to either turn or fight the threat, or to run from it. In our modern society threats are everywhere, however, we are rarely able to attack or run.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
50
Hence, we most often respond by creating what we think of as stress and now we know that stress can and does affect our body and our immune system in both positive and negative ways unless we take an action to correct the perception.
Selye General Adaption Model
The term stress was first coined in response to the work of Hans Selye and his General Adaption Model. Selye had noticed that when humans were stressed for prolonged periods without a release or solution over time they demonstrated characteristic internal responses affecting the hormonal system and the stomach, thymus glands, lymphoid tissues and white blood cells. These are the organs of stress. Notice the similarity between Selye's General Adaption Model and what we have talked about PNI so far. The only difference is that PNI tells us that these organs and cellular components communicate back with the brain.
The Stress Cascade - There are three major aspects to stress
First, is the stressor event which poses a real or imagined threat to our internal or external well-being; when this is effectively dealt with the stress is reduced. The event can be life threatening or can instead be only interpreted by the individual as life threatening. That is, it is interpreted as a threat to our picture of the way we see our life. For example, a pile of bills can act to be threatening to the way an individual sees his or her future. Second, there is a complex series of internal chemical, neurologic and hormonal changes that are automatically set in motion which is called the Stress Cascade. Again, notice the similarity to what has already discussed. These events occur below the level of our awareness or control and result in physical, emotional and mental alterations which are directed at preparing the individual for self-defense. Once initiated, this process can only be stopped by eliminating the threat. Only then can the Stress Mechanism be released come to a natural conclusion. The Stress Mechanism can also be released when the individual is able to recognize that the events in question are no longer or never were life threatening. Since the overall goal of the Stress Mechanism is to ensure our survival, when any event (threatening or not) occurs in our direct life space, the very first thing our body/mind does is to check all past experiences, including our genetic codes (our species specific and collective unconscious memories) and our personal learned experiences to determine whether the event occurring is a threat. If it is threatening in any way, the Stress Mechanism is triggered. If it is not, we may never even know that the event took place. This cycle of action can be named the Survival Center. This may be where all PNI phenomena begin and ultimately end. The neuro/electric, hormonal, and biochemical aspects of the Stress Mechanism are the same as those of the PNI response. You could essentially say they are the same mechanism.
Stress Hormones
Science supports this by looking at the stress organs, and their hormones. Once again, notice the similarities to the PNI mechanism. The Stress organs are the Hypothalamus and Pituitary gland, Adrenal Glands, Thyroid, Thymus and Reproductive glands. They communicate through hormonal feedback systems and there is sympathetic and parasympathetic nervous system involvement.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
51
The Adrenal Cortical Hormones
Specifically, the Stress Hormones, Adrenalin (epinephrine) and Cortisol, they prepare the individual for Fight or Flight and are responsible for the Primary Stress Response. Adrenalin turns on the Inflammatory System, the Defensive Systems and Immune Systems of the body to prepare it for external invasion and possible injury. The inflammatory mechanism is the first step of repairing any injury that might occur should an injury result from Fight or flight. Cortisol, on the other hand, stimulates the Anti-Inflammatory mechanism which turns off the Inflammatory mechanism once healing and repair are in process. These two hormones also affect sugar metabolism and the blood clotting mechanisms of the body. They also have an effect on the blood pressure control mechanisms of the body, cholesterol manufacturing, renal function, blood flow to the digestive and muscular systems, as well as many cardiovascular functions including blood pressure, heart rate and rhythm. They affect the primary systems which are responsible for the creation of illness, healing, repair and housekeeping activities of our body. Establishment medicine and physicians are now integrating concepts of acupuncture, biofeedback, nutrition, prayer work, religion, spirituality and exercise into their medical practices. Not always because they totally believe in it, often because economic pressures are pushing them toward these old proven practices “called” new.
Psychoneuroimmunobiology (PNI) - Mind-Body-Spirit Healing Mind Vs Body Vs Spirit
In June 2006 the Center for evidence based physiotherapy stated that for the past 100 years the
rule of medicine has been to separate mind from body, and mind and body from spirit. The problem with this is that no matter how much the present modern western medical system wants to tell us that this is right, or that it should be this way, even though most physicians have been trained and disciplined into believing that this is the way it should be -- many of us are having difficulty reconciling the fact that each person comes to us with a body, a mind, and a spirit. Because the present medical system and the training to become part of the medical system have been the way they presently are for many generations, it is easy for most physicians to accept the body, most even accept the mind, but many still are unwilling to admit that the two are not
only connected but inseparable. To cut the mind (not just the brain) away from the body, means loss of consciousness and in many cases even death.
No matter how hard it is to admit it recognizing that there is something that animates us, something that gives us life and it is not just the personality nor the will, is hard for most physicians. In many cases it is even difficult for physicians who are themselves, religious people. But the fact is, when we die--something leaves us, something that appears to be crucial to our existence as a sentient being. We can try as we may to ignore it, we can try to think of it as chemical, energetic or even as neurologic, but in the long run it transcends all of these.
The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
52
For several hundred years this concept worked. Then modern scientists like Albert Einstein, Werner Heisenberg, Nils Bohr and later David Bohm began to tell us that something existed beyond what we could see, taste, smell or touch. Einstein wrote about modern science, he was specifically talking about physics but did extend it to all "modern science," definitely proves the existence of God. Bohm, a disciple of Einstein, and a more recent major force in modern physics, goes even further and says, "God is proven mathematically." Heisenberg--as part of his Uncertainty theorem created a rift in the concepts presently held by Western modern science when he told us that scientific experiment can't prove anything for the way an experiment is set up, who does the experiment, what they believe, and what they are looking for, all influence the outcome of the end result. Therefore, scientific experimentation is always biased and at best can only be used as a tool and never as a rule. Today there is a group of scientists from many disciplines who are coming together under a banner of Psychoneuroimmunobiology. They have transcended the past linear approach of Western medicine, but not with the intention of destroying it. They are adding a new and much needed dimensions to the practice of medicine, they are integrating mind and body and in many cases mind, body and spirit. Fritjov Capra, in his books the Tao of Physics and the Turning Point, refers to this movement as a "new paradigm." He suggests that it is acting on all of Western society. Capra includes not only physics and medicine, but also psychology, economics, politics, and even reality itself. This new study of the body, mind and spirit connection is demonstrating that there are some
dramatic new ways of looking at wellness and illness. One of the areas which is becoming very meaningful is the role of thought and stress on the immune system and the physiology of the body. We can now better understand the role of specific events on blood pressure and other body physiology. We can now look at how prayer and visual imagery can affect the course of an illness. Through them we are now seeing that multiple internal factors are involved in the creation of illness, healing and maintenance of wellness. Illness is no longer simply an extension of the Germ Theory--our present concept of infection being the end result of exposure to a germ, but is expanded to include the ability of the
body and its immune system to resist and destroy invading organisms, the Stress Mechanism, the environment, nutrition and all those factors that are involved with defending and protecting our self from illness. Understanding that nothing operates in a vacuum means that wellness, illness, healing and even death, are the end results of a number of complex interrelationships between who and what we are, our thoughts, the stress Mechanism and the complex interactions between our mind, our body and our spiritual selves. Many physicians feel threatened; many feel that if what has been done cannot be proven scientifically, it can't be accepted at all. Some simply suggest that these healings are simply "lucky." They generally tell us that the "initial diagnosis must have been wrong,” what happened, happened because of "placebo effect." They dismiss the work of these non-traditional healers as "parlor tricks," "flim-flam," and on occasion as "spontaneous miracles." However, they often add what happened was not scientific and cannot be accepted without proof and scientific scrutiny. Thus, when a person is healed by their own internal motivating forces such as exercise and imagery but not a medicine, doctors dismiss the results.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
53
Neuropsychoimmunobiology is a part of the medical sciences; it has already contributed important understandings to the practice of medicine. We now have clear evidence that thought can change body chemistry. We know that when we have good (positive) thoughts we create positive neurochemical messengers that are released not only into local brain tissues but to the entire body. We now also know that our thoughts cannot only create or change our mood, but they can actually change our chemistry. We also know that they affect how we see ourselves and the world around us. We also know that our thoughts can affect our physiology. Thinking that your hand is cold can lower the temperature of your hand; more specifically thinking the right hand is cold and the left hand is hot can lower the temperature of the right hand and raise the temperature of the left hand. We know that the mind is not only connected to the body, but that it is intimately related to it and that for all practical purposes, they are one and the same. We have learned that no physical disease can occur without a mental, emotional or spiritual component. We are now also recognizing that the after-emotions caused by an illness are often preceded by one or more pre-emotions which are related directly to the cause of the illness. It is rapidly becoming clearer that most illnesses have a mental or thought component aspect to them. As I like to think of it, a conflict exists which is not only associated with the illness itself, but frequently is part of the cause of the illness. How can this information be used in medical practice? This is a highly complex area and it is clear that nothing is going to replace the present interventive medical system. No one is advocating replacing it or doing away with it. The current medical construct involving diagnosis and treatment will always be needed. In the end, the healer never heals the patient, the patient must heal themselves, they may use the help and assistance of the healer to do this; the meaning of the symptoms or the disease process is personal to the patient. It is more correct to suggest the patient helps the doctor to help themselves, like a “life” coach. For example, arthritis - can be the body's way of communicating that the individual is losing his or her grip on their life. Recurrent headaches may well be trying to tell the individual that something or someone in their life is a headache. Consider the possibility that cancer is a clue that "something is eating" at the person. How often do we say or think that something in our life is "eating at us" or "eating us up alive?" Sound far-fetched, yet research has repeatedly demonstrated that cancer is associated with unresolved anger and rage.
About Treatment Programs
Today this presents a major dilemma. The medical profession and to a great degree the laws of our states and country have made it necessary that a physician operate and treat patients in "a manner which is consistent with the standard of the (specific) community." On the surface this is a wonderful law, one which protects many people from unnecessary surgery and poor medical treatment. On the other hand, it is responsible to hundreds of thousands of unnecessary hospital deaths and infinite suffering. If mind, body, spirit medicine is not the standard of the community than physicians will shy away from it. They will fear legal problems and being ostracized by the medical community. In spite of this however, there is a growing trend of bold and adventurous physicians to recognize that standard medicine is not working for most of their patients. In many people simply treating illnesses with drugs and surgery often either makes it worse or does little or nothing to help.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
54
Many physicians recognize that standard medicine often leaves people less than whole, on medications, with their symptoms and little resolution. Without finding the cause of the illness one cannot really expect to heal it. If the cause is in the interactions of mind, body and spirit then traditional medical treatments will often fail. Many physicians are also recognizing that the medications they prescribe often lead to new and different problems compounding the distress their patient already experience. Many physicians are also recognizing that treatment of early illnesses is not really protecting their patients from ultimately developing chronic diseases. Attempts are being made on the part of physicians and patients alike to find solutions Bernie Siegel and Leo Bassiglia teaches about love being the new medicine, Kenneth Pellitier writes about Mind as Healer Mind as Slayer, Arnold Fox writes and lectures on the relationship of the immune system to wellness. We have acupuncture, biofeedback, bioenergetics, pyramid energy, macrobiotics, radionics, autogenic training, transcendental meditation, somatography, aromatherapy, biodynamic psychology to name only a few new disciplines that are now competing with standard medical thought and practice. Remember, exercises medicine and it is the one thing most all patients can do as advocated by AquaDios-Med™. It is important for those physicians who are enlightened to recognize that if they are not able to help their patient get well with conventional medical treatment they must send the patient to someone else who can. This means not just to another conventional medical doctor, but to someone who can really help them even if they are not using standard or conventional interventive medical techniques such as the methods and practices found in AquaDios-Med™. It truly is ironic that primary care refuses to prescribe safe daily exercise last instead of first.
Physician • Healer Working Together In many cases today patients go to their regular medical doctor for problems which require drugs and surgery but for problems which do not they may go to modern body, mind, spirit healers to find the underlying mind-body (mental or emotional conflict) or spiritual conflict that are causing their physical, mental or emotional problems and illnesses. However, this author posits that treatments like AquaDios-Med™ with its safe daily exercise must be considered primary treatment of choice over most medications for at least a 90 day period to determine if the medication is still recommended. In this process the patient helps the doctor help the patient. Often the healer can better support the patient and treat the spiritual and mental aspects of their illnesses better, while the physician treats the physical manifestations of the conflict. Most medical doctors would be negative to cooperating with non-traditional medical or non-medical practitioners. If the patient is already seeing a non-traditional practitioner, he or she frequently keeps it a secret from their medical doctor. If only the medical doctors could get past their biases and work together with the non-traditional practitioners, that is work together as a team, the interests of the patient would be much better served. Patients might be healed, instead of kept on medications for the rest of their life, and allowed to develop chronic diseases. Preventive medicine is what our nation must nationalize to end the horrible waste of human life and the $2.5 Trillion healthcare disaster.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
55
Summary • stress • anxiety • distress When we experience conflict, guilt, threat, fear, anger, rage, hostility, negativity the stress mechanism is activated at first this is good for once activated it prepares the healing and repair systems of the body for first fight or flight and next, for potential injury. Initially this same response also activates the immune system as the immune system and the stress mechanism are essentially one and the same things. If these conflicts, threats, guilt, anger, rage or hostility are not resolved the stress mechanism/immune system soon become exhausted and overwhelmed and over time parts of the immune system are shut down and illness is allowed to enter into it (bacterial, viral or parasitic infection) or is caused by one part of the body attacking another part of the body (autoimmune diseases). As we suggested earlier the underlying conflict, what we feel guilty about what we feel we have sinned over select out the organs that will most likely become involved. Mind-body medicine is an extension of the concept of the physician as the healer. Many may think of it as the horse and buggy doctor, whether you accept or reject this depends on you. Certainly, there is much more that can be said on both sides. Only you can decide what is true for you. In Hawaiian it is said, Malama ola pono, "May your life be in balance."
Self-control • Better Health
In May 2002 Steven Solberg wrote an article for the Center for evidence based physiotherapy about emotional stress, distress and anxiety and other psychological factors that can influence physical health. Research in this field of psychoneuroimmunology (PNI) is proving what the world's spiritual healers and holistic medical practitioners have been saying for thousands of years: Our thoughts, moods, state of being and feelings are powerful influences on our health and immune system. A University of Miami study of HIV-positive individuals showed that the belief system of an HIV-positive person plays an important role in influencing the strength of his or her immune system and its ability to fight HIV. Thus, changing thoughts, beliefs and behavior may affect the body's ability to fight disease. UCLA AIDS Institute research showed that stress enables HIV to spread more quickly in HIV-positive persons and impairs antiretroviral drugs from restoring the immune system. Depression and negative attitudes have also been linked to lowering the immune system. Another study found that even being "closeted" or hiding gay identity leads to a decline in the immune system and more rapid progression to AIDS, possibly suggesting that the stress of having to hide one's gay identity may be stressful to the immune system. Thoughts and the various body systems don't work in isolation. They work together as a whole system. Through chemicals, called neurotransmitters, they are constantly trading information back and forth. These neurotransmitters travel along pathways within the brain and body to provide messages to nearby systems and cells, including our immune system. Neurotransmitters are responsible for sensation, feelings, dreams, thinking, memory, emotions and all the physical and mental activities that make up our inner universe. Without them, we would be unable to relate to the outer world through sound, smell, taste, touch and light. Thus, these chemical exchanges of information received through our senses deliver that information to the mind and body.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
56
Working on the body affects the mind just as working on the mind affects the body. Doing this with the intention of healing is called Mind-Body Medicine. Mind-Body Medicine includes exercise, meditation, shamanism, biofeedback, yoga and guided imagery. It also includes hypnosis, dream work, and various kinds of psychotherapy. Some of these systems have been around for centuries. Only recently, however, have scientists begun to map out mind-body medicine on a molecular level. This is not to suggest that HIV itself can be controlled or eliminated. However, mind-body medicine can help an individual take control, reframe and impact beliefs about HIV. This, in turn, will affect their health, well-being and the body's ability to fight the virus. The meditation on these pages can be done with the eyes opened or closed, or even as a focused walking meditation in nature once it has become familiar. It can help reduce stress, connect you to healing energies in the natural world, and increase energy and magnetism. Take a few minutes and start out the day with this for a week or so and notice how it affects your state of being. Then once you've got it down you can take a few moments aside and practice anytime and almost anywhere. The breathing should be slow, gentle and focused. Repeat each element concentration four times.
Healing • Treatment
The term healing is frequently misused in our standard Western medical system. Most physicians’ rarely use the word healing. In fact it is often considered a dirty term one that is used by faith healers, shaman and fakes. The physician more commonly talks about treating because in medicine most medical problems are rarely ever healed. When a patient is seen by a physician and talks about healing, the physician will frequently tune out. However, when a patient says that he or she has been healed by a physician this same physician will often take credit and say that it was the medications or surgery he performed that healed this patient. When the average person thinks about healing they usually have two definitions. One is that the disease or illness disappeared and everything returned to normal. The other is that their symptoms are under control and they feel better. In the first case, the individual wants, expects or has experienced a complete return to normal. Their symptoms are gone, their disability is gone and they are living the life they lived before they became ill. In the second case the disease is still present but the symptoms that made them uncomfortable or unhappy, caused pain and/or suffering are either gone, or much better, or at least tolerable. When we talk about healing we imply that the disease or illness process has been mastered. That in fact, it has been accepted and the individual has either eliminated the illness process or has learned to live with it in a kind of peace and harmony. As you will see we do not think of illness as something that happens from outside of us, rather we think of illness as a result of unresolved conflict within the body-self. This unresolved conflict alters body chemistry, impairs or undermines the immune and defensive systems and the healing-repair systems of the body. We think of illness as an intelligent communication from the body to the individual letting him or her know that they have one or more unresolved conflicts which must be looked at and dealt with. Healing is the process of resolving these conflicts and learning, growing and evolving because of them. We believe that life is a learning process and illness is the indication that we are not learning or that we have made mistakes that require correction. Using this approach illness and healing take on entirely different meanings. They cannot be truly affected by drugs and while drugs can either lessen or cover up symptoms they cannot entirely heal the individual.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
57
While it may often appear that drugs and medications help the healing process (and in some cases they do for example when the immune system is not functioning and a bacteria invades and causes an infection antibiotics can help fight the infection and "cure" it), but in fact in most cases it is the fact that the individual took some sort of action, this may be taking the medication, or that they decided that they were doing something to help themselves that was the real source of the resolution of the illness. It might be that they consciously or unconsciously resolved or solved their conflict.
More Relaxation Techniques
Relaxation techniques help promote sleep, reduce stress, and alleviate pain. Controlled breathing is the simplest form of relaxation and consists of sitting or lying in a quiet place and breathing slowly in through the nose and out through the mouth. An advantage of this technique is that, if needed, it can be performed at any time, in any location, to produce relaxation. Hypnotherapy or Clinical Hypnosis is the use of a natural human capacity to help a person gain control over stress, pain, and bad habits such as smoking and overeating. It is also sometimes used in medicine to block the sensation of pain during medical procedures and in psychotherapy to assist patients in recalling traumatic events. Under the guidance of a hypnotherapist, the person enters a focused state or a detachment from one's physical surroundings, as in contemplation or daydreaming, some describe it as a very comfortable semiconscious state, as between sleeping and waking during which his subconscious mind responds to the suggestions of the therapist. The person can be taught to recreate the deeply relaxed state he experienced while under hypnosis and to use this “self-hypnosis” on his own to overcome pain, control eating and smoking habits, and reduce stress. Visualization and guided imagery are additional relaxation techniques that involve focusing the mind on specific images. With eyes closed, the person pictures in his mind a peaceful image or scene and concentrates on the sights, sounds, and smells that make the image soothing. Visualization is sometimes used as a supplemental treatment for patients with cancer or other serious and painful diseases. Guided by a therapist, the patient may visualize his body fighting the disease. This technique has been credited with bringing about physical healing in some cases. Acupressure, also called shiatsu in Japan, is an ancient Chinese method of improving a person's health by applying pressure to specific points on the body. Acupressure uses the same channels of energy flow as acupuncture but does not break the skin. Instead, the acupressure practitioner applies pressure using the fingertips or knuckles to loosen muscles and improve circulation.
Prevention
AquaDios-Med™ and its position on safe daily exercise is like the proverbial valuable ounce of prevention. Nowhere is this more true than with our American medical and healthcare problems. Being sick not only saps us of energy and is financially a drain, but it also creates a host of problems which can not only affect us personally, but our entire family, our job and even our society. How then can we prevent becoming sick? In our society this is rarely taught and commonly ignored or discounted. We often take much better care of our pets or our cars than we do of ourselves. The answer to how we prevent illness is understanding what causes illness. In school and by inference through our Western medical culture we are often told that bacteria, viruses, radiation, or other people are more often than not to blame for our getting sick. Nothing in fact could be farther from the truth.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
58
Your wellness or lack of wellness is almost entirely in your hands. It’s generally controlled by factors of how you live your life, your lifestyle, whether you smoke, get sufficient sleep, what you eat and what you do not eat, the stress you experience, whether you get safe daily exercise, than almost any other factor. Other factors such as mental attitude, what you believe and do not believe, the amount of exercise you get, where you live, how you conduct your life plays a role in health. While it is true that bacteria and viruses and other parasites do exist, whether or not they invade your body, take up residence are cause disease is more often controlled by those factors above which in turn determine how effective your body is in resisting them, how competent you immune system is in fighting them and how your healing and repair systems are working to provide healing and repair of injury they may cause.
Illness Prevention
Experts agree there are many things a person can do to keep from getting ill. Many common illnesses are usually caused by living organisms—bacteria, parasites, fungi, or viruses—that are transmitted from one person to another. A healthy person's immune system usually can attack and destroy these organisms before the person becomes ill, but when this system is weakened by factors such as poor nutrition or stress, sickness or disease may be the result. However, many “diseases” are caused a sedentary lifestyle and by the lack safe daily exercise.
People can take many actions that can help guard their bodies against infections and build up their immune systems to make them strong and resistant to illness; especially by safe daily exercise. These actions include good habits like eating well, getting plenty of exercise and sleep, managing stress, practicing good hygiene, and getting frequent physical checkups and complete immunizations. FIBER multiple whole grains - fruits, vegetables, and legumes In general, a person should concentrate on eating a diet high in fiber. Sufficient dietary fiber intake helps prevent colon cancer and irritable bowel syndrome, as well as constipation, hemorrhoids, and diarrhea. Fiber also promotes bowel regularity. Research has shown that eating enough fiber regularly lowers cholesterol and, in diabetics, slows the absorption of sugar, which may decrease the need for insulin. Foods high in fiber include whole grains, fruits, vegetables, and legumes (peas, beans), but some people prefer to take fiber supplements available at grocery and drug stores.
FRUITS – VEGGIES
Everyone has heard: "an apple a day will keep the doctor away," or "eat your vegetables, they're good for you!" Fruits and vegetables are good for everyone, but many people find it hard to eat enough of them. They benefit a person's health in many ways. One group of vegetables, called cruciform, includes broccoli, cauliflower, Brussels sprouts, kale, kohlrabi and Swiss chard. Eating vegetables from this group helps prevent the development of stomach, colorectal (large intestine and rectum), and lung cancers. Dark green and deep yellow vegetables like spinach, carrots, sweet potatoes, cantaloupes, and apricots are good sources of vitamin A. Oranges, grapefruit, strawberries, and green and red peppers contain vitamin C. Vitamins A and C are antioxidants, which are important vitamins that help neutralize harmful molecules called free radicals in the body. Free radicals damage normal cells and can cause cancer, as well as cataracts, diabetes, heart disease, high blood pressure, and both Alzheimer's and Parkinson's disease.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
59
Heart Attack Stroke Prevention Program Psychoneuroimmunology
Heart disease and heart attacks are the #1 killer of adults in the U.S. Stroke is the #3 killer. If you are a diabetic your risk is even higher than the general population. The good news is that heart disease, heart attack and stroke are often easy to prevent. The problem is that if you wait until you have symptoms of heart disease, high blood pressure, chest pain, angina or heart attack you have waited much too long. Currently the allopathic medical profession concept of heart disease and heart attack prevention is statins and eating a low salt diet. To date we have some evidence that some of the statins actually do work, but only in 10% to 50% of the people who use them. This leaves 50% to 90% of you vulnerable to heart disease, heart attack and stroke. Many people either do not want to take statins or cannot take statins due to severe and problematic side effects. What do these people do to help themselves? The answer is simple, you use the basic concepts your grandparents did to protect you from heart disease, heart attack and stroke, healthy foods and exercise. To this prescription we can add supplements and nutritional products with proven protective effects. This psychoneuroimmunology and Mind Body Medicine research demonstrates why AquaDios-Med™ combined with safe daily exercise is so potent in accelerating rehabilitation and eliminating common symptoms of chronic disease. Research illuminates procedure for dermatological treatment, but this author believes it can be used on all medical problems with high success.
Mind Body Medicine • Practical Applications • Dermatology
Most people are not aware that the largest organ of the body is the skin, the outer surface which covers the body. In November 1998 Michael R. Bilkis, MD, MSC; Kenneth A. Mark, MD published a research in the Archives of Dermatology titled “Mind-Body Medicine - Practical Applications in Dermatology”. The study of Dr. s Bilkis and Mark, though focused on the skin is applicable to all medical and or living matters in life. Their approach should not be limited to just the skin. The authors claim that it is only recently that Western physicians are rediscovering the link between thought and health. They state that the spectrum of causative factors in inflammatory dermatoses or skin problems, are often multifactorial. Dr.’s Bilkis and Mark say that stress and negative thoughts are major factors in dermatologic conditions and this author believes this is the case in all medical problems. The authors give some basic information on the ways that thoughts affect health and provide some practical methods of intervention including meditation, journal writing, affirmations, prayer, biofeedback, and hypnosis.
It is this author’s opinion that mainstream medicine must take a similar approach to Dr.’s Bilkis and Mark and add the one missing ingredient – safe daily exercise advocated by AquaDios-Med™. Have you ever wondered how your thoughts affect your health? Did you know that you can improve your health by changing the way you think and respond to events in your life? The basics of several different techniques in mind-body medicine are easy to learn. Dr.’s Bilkis and Mark present 2 pathways that represent the ways thoughts can affect health. Metaphors are used to help explain certain principles and treatments.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
60
It is extremely important for all people especially physicians to have an understanding of the basic principles of mind-body interactions because it has been shown that there are direct connections between the central nervous system and the immune system. Through research Dr.’s Bilkis and Mark conclude that the immune system is influenced by
thoughts and other functions of the brain and determine that most of the common dermatologic problems such as adult acne, rosacea, eczema, psoriasis, and other nonspecific inflammatory disorders may be directly influenced by a person’s thoughts and emotions. While most dermatologic problems are multifactorial in origin, Dr.’s Bilkis and Mark only discuss the causative role of thoughts and emotions in the development of disease. In some patients, this may be the primary causative component, while in others it may be a tertiary or minor component. In all cases, however, knowledge of mind-body interactions and mind-body interventions can be useful in improving a patient’s dermatologic
condition and, in most cases, their quality of life. This author believes this approach is applicable to all human medical conditions. Dr.’s Bilkis and Mark suggest it is important to construct a picture in your mind that sees every human being as consisting of 3 distinct bodies: physical, mental, and emotional. The 3 are intimately connected and changes in one will produce changes in the others.
The authors suggest that the body of every human being vibrates at different energetic frequencies; therefore any changes in these bodies will occur at its specified rate. For example, the mind operates at the highest frequency. Throughout the day, the mind creates many thoughts and most people will quickly jump from one thought to the next and back again without much difficulty.
Dr.’s Bilkis and Mark state the emotional body operates at a lower vibrational rate than the mind, and changes of state in the emotional body occur at a slower rate than in the mental body. A good example of the ease with which shifts occur in the emotional body is a child. If the child is happily playing and something occurs that upsets the child, he/she will freely express displeasure, usually by crying. A few moments later, tears are replaced by a smile.
Whereas, the physical body operates at the lowest vibrational rate and changes in the physical body occur at a much slower rate than changes in the other two. To understand this concept better, consider the reaction of a person who sees a car heading straight for him/her and almost gets hit by it. The first reaction probably is the thought, “Oh no!” Fear quickly follows the recognition of danger, which releases hormones, including adrenaline, and the person moves out of the way. Once the event is over, the person may think, “I am OK” and the fear may slowly be replaced by feelings of gratitude. Finally, slowest of all, the physical body begins to return to a relaxed parasympathetic state. Normally, all 3 bodies respond to and easily return to baseline following changes from external stimuli. Pathologic manifestation occurs when there is a problem with the ease in which the mental body returns to baseline. Thus, a pathway develops that may explain how negative thoughts can lead to pathologic changes in the physical body. A negative thought form can be metaphorically thought of as a “demon” who has taken up residence in a person’s consciousness. It constantly makes itself known and whenever the person acknowledges it and feeds into it, the demon grows stronger.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
61
For many people, this thought eventually grows so strong that they may develop the belief that it is true and unchangeable. As thought forms become beliefs, emotions become frozen in a negative state, and the body enters a chronic sympathetic state often termed stress or distress. As a result, the normal homeostatic mechanisms fail and dis-ease or the absence of ease appears. The type of disease that manifests is dependent on the degrees of change in the body and the genetic predisposition of the individual. Negative thoughts are one of the more prevalent contributors to stress - distress. Stress is the result of a person’s response to external stimuli and not the events themselves. From the viewpoint of traditional Chinese medicine, when stress is internalized, the flow of vital life energy throughout all 3 bodies is impeded. This vital life energy is called chi in Chinese, ki in Japanese, and prana in Sanskrit (India). To better understand the effects of stress on a person’s chi, imagine that a healthy person is like a deep river, flowing smoothly on its course. A person on the shore throwing rocks of all different sizes into the river represents stressful events. As the number of rocks increases, the river’s flow becomes more turbulent. This corresponds to turbulence in the flow of chi and the appearance of physical problems. Therefore, treatment plans must include a method of preventing the accumulation of more stress and, moreover, a plan for removing the stress that is already in place.
There are many different techniques in mind-body medicine for achieving these goals. People can be taught a pathway for reversing the disease process and creating health. In dermatology, disease usually falls into several major categories such as acquired inflammatory dermatoses, congenital dermatoses, and non-inflammatory dermatoses - tumors. Dr.’s Bilkis and Mark state that their many observations in practice stress appears to be one of the most prevalent components in the cause and severity of most inflammatory skin conditions. Through the use of mind-body techniques for the reduction of stress,
most inflammatory dermatologic conditions can be helped to some extent. Acquired inflammatory dermatoses are the most amenable to mind-body techniques because their life cycle is one that waxes and wanes. Other dermatologic problems can also improve, to some degree, with mind-body techniques. In all cases, however, the quality of life of the patient can be greatly improved with mind-body techniques. Dr.’s Bilkis and Mark divide mind-body techniques into 2 major categories: techniques practiced by the patient and techniques used by the practitioner with the patient. The first category includes meditation, affirmations, journal writing, prayer, exercise, reading spiritual books, and biofeedback. The second category includes hypnosis and Neurolinguistic Programming (NLP, explained later). The techniques listed above that are practiced by the patient represent the categories of the mind-body techniques that are easy to do and readily available. There are many classes and books available that list a myriad of other techniques and spiritual practices.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination. - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
62
MEDITATION
Meditation is the practice of bringing one’s total focus into the present moment. The first reports in American literature of the physical effects of meditation were made by Herbert Benson, MD, a cardiologist at Harvard Medical School, Boston, Mass. Benson observed that after 20 minutes of meditation participants’ heart rate, breathing rate, blood pressure, oxygen consumption, carbon dioxide production, and serum lactic acid levels all decreased, while skin resistance increased and blood flow was altered. He called this phenomenon the “relaxation effect.”4 Similar physiological responses have been found to occur with other techniques such as hypnosis, progressive muscular relaxation, and autogenic training. One of the simplest forms of meditation involves sitting
comfortably and focusing on the breath. For most Westerners, this means sitting in a chair with the feet flat on the floor and the hands in the lap. A word or phrase is then repeated over and over for a specified length of time. This word or phrase is called a mantra. Most people will find that their mind will wander at times and they will begin thinking of different things. It is important that, when one becomes aware of the wandering, he/she lets go of the superfluous thoughts and returns to following the breath and repeating the mantra. A Meditator must be willing to let go of extraneous thoughts, without judgment, and return to his/her point of focus. Since focus is the key to meditation, it can take many forms— sitting quietly, painting, playing an instrument, participating in a sport, or working out at the gym. During any of these activities, the person’s mind becomes clear of everything but what he/she is doing at that specific moment. The goal of meditation is to bring one’s full awareness into the present moment and simply be. When this occurs, not only can a person induce relaxation but he/ she also can begin to bring the benefits of meditation into all aspects of his/her life.
AFFIRMATIONS
Affirmations are statements made in the present tense, containing only positive statements, and expressed in the first person singular. The use of affirmations provides a simple and effective vehicle to access the “thought-healing pathway”. Many of our dermatology patients look at themselves in the mirror and have decided that their problem is so awful that they are embarrassed to go out in public. Some of these patients may even have a minor skin problem, yet they refuse to believe that the problem is minor or that it is safe to be seen in public. These beliefs started out as repetitive negative thoughts. The use of affirmations occupies the consciousness with positive thoughts, leaving no room for negative thoughts; by repetitively using affirmations, the patient is unable to subvocalize the 2 opposing thoughts at the same time. With time, the patient’s neurologic pathways shift and the positive thoughts can predominate. For example, a patient who has spider veins states that she is disfigured and cannot wear shorts. One possible affirmation for her to say may be, “I am beautiful in every way.” It is not important for her to believe what she is saying; the belief comes later.
The important thing is for her to say the positive words. Our advice to our patients is to use the affirmation every morning and also whenever they become aware of the presence of the negative thoughts. The repeated use of affirmations provides a powerful tool for eliminating negative self-talk, which is a major contributor to stress and turmoil in people’s lives. Herbert Spiegel, M.D. has a valued affirmation; stress and anxiety are poisons to my body, I need my body to live, I owe my body this respect and protection.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
63
JOURNAL WRITING
Journal writing is the next, most simple technique to use for self-help. As with affirmations, writing in a journal requires no classes and the only skills needed are reading and writing. Patients are instructed to set aside the same time each day for their journal writing. At the start of a session, it is important to sit quietly for a few moments and take some breaths to become centered. The next step is to write whatever comes to mind, without stopping to think about what is being written. The final step is to read over the entry. Writing in a journal helps unlock the unconsciousness and bring repressed emotions and thoughts up into consciousness. It also creates a new perspective for the patient to approach his/her challenges. Studies of college students and executives have shown that immune function can be improved through the use of a journal. In addition, when the test subjects stopped writing in their journals, their immune function returned to the prestudy baseline after about 6 months. The following comments were made by 2 patients regarding their journal writing experience. “Whenever I write in my journal, I feel like the problems I was having are no win my book and no longer in my body.” “I feel lighter . . . like a load has been lifted from me.”
PRAYER Dossey in his book Healing Words defines prayer as communication with the Absolute (this is the name he chose to represent God). In this book, he states that there are more than 300 experiments using prayer involving living organisms, from microbes to humans, and that about half of the studies show that prayer can cause a statistically significant change in the test subjects. The studies he quotes in his book show that all types of prayer are equally effective, including prayers that specify an outcome vs nonspecific types of prayer such as, “Thy will be done.” The studies showed differences in an individual’s ability to evoke a positive effect from prayer. In essence some people were better “prayers” than others. It appears that the more effective prayers were more able to alter their state of consciousness and enter a more meditative or prayerfulness state than those who were less effective prayers. It is helpful to suggest to patients that prayer be approached like a meditation, in which the object of the meditation is the prayer itself. With this approach the prayer experience can be intensified. Most studies on prayer have been performed with microscopic organisms like bacteria and fungi. One of the most profound studies of prayer and health was reported
by cardiologist Byrd. In his study, a computer assigned the 393 patients admitted to the coronary care unit to either a group that was prayed for by outside prayer groups or to a control group. This study was done according to a strict double-blind protocol. The results of this study showed that the prayed for patients differed significantly from the control group in the following areas: They were 5 times less likely than the control group to require antibiotics (3 compared with 16 patients).
They were 3 times less likely to develop pulmonary edema (6 compared with 18 patients). None of the prayed-for group required intubation while 12 in the control group did. Fewer patients in the prayed-for group died, although this was the only result that was not statistically significant.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
64
While the results seem difficult to believe, the study was well designed. If the focus of the study were from a medication, then it might be heralded as a new miracle drug. This study had some flaws, which Dossey discusses in Healing Words. The flaws, however, are overshadowed by the positive implications, if even part of the study’s results are true.
BIOFEEDBACK Biofeedback is a technique that uses machinery to measure autonomic functions such as heart
rate or muscle tension. The patient uses various imagery exercises and learns how to consciously alter these autonomic functions. In the rheumatology literature, the use of biofeedback has been shown to be beneficial in the treatment of Raynaud disease and phenomenon. In this study, patients were taught biofeedback first as a relaxation technique and then as a method of increasing the skin temperature in their fingers. All patients in the study were able to elevate their baseline fingertip temperature. The results suggested that biofeedback is useful in the treatment of Raynaud disease and phenomenon, and that “further studies were required to completely evaluate the efficacy and clinical significance of biofeedback.”
Clinical Hypnosis and NLP
The essential goal of both hypnosis and NLP (Richard Bandler & Associates Seminars Group International, Hopatcong, NJ) is to help a patient access resources that he/she has available in his/her subconscious and use them to change his/her behavior. Milton Erickson, M.D. is considered to be the father of modern clinical hypnosis and was a firm believer that everyone is born possessing all the resources needed to create new behaviors. The problem is that most people have set up conscious and unconscious blocks that thwart their healing process. Erickson used hypnosis to help his patients bypass these blocks and overcome their problems. Richard Bandler and John Grinder studied the works of Erickson and other therapists who had the reputation of being miracle workers when it came to curing patients with behavioral disorders. They found that Erickson and other therapists used certain language patterns when working with their patients. Bandler and Grinder developed specific language models based on their study that achieved success for various mental conditions. In the 1970s, they began to teach these models in conjunction with hypnosis and called their new technology.
Neurolinguistic Programming
Neurolinguistic Programming is a process-oriented science as opposed to the content-oriented science of traditional psychotherapy. This means that an NLP practitioner only needs to know the type of problem that the patient is having and what the patient desires as the outcome of the session. The actual details of the situation and the patient’s history is unimportant to make therapeutic changes. One of us (M.R.B.), for instance, had a patient who became very stressed at work and her acne flare up corresponded with the start of a new job. During the session, he
helped the patient create a relaxed state and associate this relaxed state with events that previously triggered her stress. The specific details of what caused her stress at work were not important to help her overcome and feel better about the situation.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
65
The first author (M.R.B) has used hypnosis and NLP for several types of problems: treatment of neurogenic skin problems, stress reduction, improvement of self-image and quality of life as a result of a skin problem, and as anesthesia for minor surgical procedures and sclerotherapy. The following are examples of treatments with the NPL techniques that the first author used with some of his patients. The explanations of the actual procedures have been simplified and, for the sake of brevity, examples of the language patterns used are not included. Patient 1, an aspiring actress and model in her middle 20s, complained of constantly picking at her skin that created marks and scars. This problem was distressing to her. She denied any pruritus. The essence of the first author’s work with his patient was to suggest that she develop new behaviors that provided the same benefit as the unwanted behavior. Moreover, it was suggested that these new behaviors be fully evaluated by her subconscious so that the negative aspects are minimized. All negative behaviors have some sort of reward for the person engaged in that behavior. If we simply “command” the person to stop the unwanted action, then they may develop an even worse behavior or resume the old one. After 1 session with her, the patient completely stopped picking at her skin. This remission lasted for about 1 year when she returned complaining that the problem was back. Once again, hypnosis was used and the condition resolved itself after 1 hypnosis session. Patient 2, a 30-year-old white woman, complained of a scar on her left thigh. The scar was flat, brown. Objectively, this was not a terrible problem. Subjectively, however, she stated that the scar was so horrible and disfiguring that she could not expose it in public. For example, she stated that if she needed to use a communal dressing room, she would either wait until it was empty or stand in a corner with her hip facing the wall before removing her pants. A common reaction to a patient with this type of problem might be to try to convince her that the scar is barely noticeable and she should stop obsessing about it. Had that been done, she would have looked for a new physician because her point of view would not have been acknowledged. Instead, it was acknowledged how awful this problem was for her and NLP techniques were used to neutralize her emotional reaction to the scar. On the follow-up visit 1 month later, she said that while she did not like having the scar, she no longer had any problems exposing it in public. In this case, the use of NLP did not improve the appearance of the problem; it did, however, greatly improve the patient’s quality of life.
Patient 3 (a woman) was treated with sclerotherapy and patient 4 (a woman) was treated for multiple electrodessicated and curreted dermatosis papulosa nigra. In both cases, a hypnotic induction was done and suggestions of anesthesia were given. Patient 3 stated that there was no pain compared with the severe leg cramping she had experienced during previous sclerotherapy sessions. Patient 4 also experienced no pain while the procedure was performed. A 1.5-cm seborrheic keratosis was even electrodessicated and curreted from her cheek without any memory of it ever happening. As an aside, patient 4 has had many sessions for the treatment of her dermatosis papulosa nigra and on her all subsequent visits hypnotic anesthesia was induced in less than 1 minute.
Stress – distress – Anxiety – exacerbate medical problems
Dr.’s Bilkis and Mark have offered illustrations of how a person’s health and thoughts are connected and how stress, dis-stress and anxiety plays a role in the origin and exacerbation of health medical problems. The old mechanistic viewpoint of health and disease, started by Rene Descartes, is now known to be obsolete. The connection between our thoughts and health has been well established thanks to the work of many health care practitioners, including Larry Dossey, MD, Bernie Seigal, MD, Herbert Benson, MD, Dean Ornish, MD, Jon Kabat-Zin, PhD, Joan Borysenko, MD, and others.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
66
The field of mind-body medicine is vast and offers the medical practioner an opportunity to treat his/her patients on more levels than simply prescribing medications for symptomatic relief. Responsibility as physicians is to promote health in addition to combating disease. In almost all cases, the medications we prescribe will help alleviate the symptoms, yet they do little to induce a remission. Through the use of mind-body medicine, improved nutrition, exercise, and general improvement in lifestyle, physicians can play a pivotal role in teaching patients how to be healthy.
Skin Disorders • Psychosomatic MBM
The skin and the nervous system are intimately connected from their side-by-side
developmental beginnings in the early embryo, and this connection persists throughout life. Psychosomatic modulation occurs in many types of skin disorders. Mechanisms include alterations in blood flow, biochemical signaling via neurons, immune response, scratching, and other factors.
Skin disorders include abnormal formation from genetic or congenital defects, inflammatory
conditions in response to trauma, exposure, infection, allergy, autoimmune, or other processes, and tumors benign and malignant. It is the inflammatory disorders that are most affected by negative emotional impacts, imprints or conditioning of past events (Griesemer, 1978).
Nervous system disorders that are "felt" in the skin include itching, burning, formication (feels
like bugs crawling on the skin), and pain. Weeding the psychocutaneous garden becomes necessary when pruning the issues with direct suggestion in hypnosis and posthypnotic suggestion is not enough. Locating the weeds through psychosomatic hypnoanalysis and uprooting the negative emotional impact component can permit healing of skin disorders that had been resistant or unresponsive to standard dermatological care.
A study reported in 2007 by Philip D. Shenefelt, M.D. indicates many skin disorders have a significant psychosomatic component. The study focused on history-taking coupled with Mind Body Medicine Techniques to induce hypnosis while using ideomotor finger signals to detect positive responses to one or more of 7 common triggering or exacerbating factors; This process permitted systematic diagnosis of the presence or absence of a significant psychosomatic component.
If no factor is positive, a psychosomatic component to the skin disorder can likely be excluded. If one or two of the 7 factors are positive and it is possible to identify the initiating event, treatment by refraining with suggestions in hypnosis may succeed in defusing the associated negative emotional impact associated with the psychosomatic component of the skin disorder. This may be sufficient to uproot and weed out the problem. However, if a multiple of the 7 factors are positive as in the included case report, referral to an appropriate psychotherapist is recommended.
“Psychocutaneous Hypnoanalysis: Detection and Deactivation of Emotional and Mental Root Factors” December 2007 - Keywords: Skin, psychosomatic, hypnoanalysis, dermatology. Scott in his book, Hypnosis in Skin and Allergic Diseases, used direct suggestion in hypnosis and posthypnotic suggestion for symptomatic relief of cutaneous itching, burning, pain, compulsive habits affecting the skin, anxiety related to skin disorders, and insomnia (Scott, 1960). Scott did discuss hypnoanalysis for skin disorders and described its use in cases of herpes simplex reactivation, rosacea, and neurotic excoriations.
Elman in 1964 reports use of hypnoanalysis to uncover the root factor for a patient with urticaria (hives). He described the application of hypnoanalysis for psychosomatic problems and talked about pinpointing the sensitizing event and the precipitating events.
Schneck also wrote about hypnoanalysis and mentioned ideomotor hand levitation as had been discussed by Erickson in 1961. Schneck (1965) did not however mention ideomotor signaling or psychosomatic skin disorders.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
67
Allergy Relief MBM
Allergies can cause serious headaches and be a real pain in the nose and eyes to say the least, and at times can even be life threatening. I used to have serious allergies for the greater part of my life until I discovered how to rid myself of those discomforts. I have rid myself of about 90% of the uncomfortable allergic discomforts such as sneezing, runny nose, tearing, itchy and watering eyes, using a hand syringe to wash out the sinus cavities with a warm saline solution and applied methods found in this book about Mind Body Medicine techniques such as imaging, relaxation, breathing techniques and yoga.
One theory of allergies is that the person has developed a hypersensitivity to the stimulus or offending trigger object. Often the source or situation responsible for this allergic response trigger can be identified by the Cheek and LeCrone Seven Keys and ideomotor responses.
This approach coupled with a genuine desire to become free of the trigger and the afore
mentioned symptoms is “irrigation of the sinus cavities with a warm saline solution that will provide substantial relief and symptom management. Often the environment must be considered so that it is kept reasonably free of the common types of allergen, this may mean more vacuuming, dusting and washing of drapes, etc.
Dave Elman's theory of allergies suggests most psycho-neurological symptoms have an initial point in time as a cause in the person’s history. Elman’s "Hypnotherapy" book effectively deals with allergies. Elman postulates that many allergies; those of which cause symptoms similar to actions produced when crying [runny nose, teary eyes, difficulty breathing], have associations to some past experience in which the person wanted to cry; and past experience is included in the Cheek and LeCrone Seven Keys.
Elman labels this the “crying syndrome” and associates it to hay fever and many other allergies. Elman believes that allergies are naturally present, and that at some point in time, the allergy becomes triggered due to stress, and manifests itself, thus “stress” is the trigger. Elman utilizes a similar approach of Cheek and LeCron to regresses the person to attempt to pinpoint a period in which similar symptoms are recognized; this approach eliminates the allergy for some while others will need ongoing self-help for symptom management.
Doctors and the scientific community agree that cancer cells commonly exist in the most
everybody, but some people begin treating the cancer cells as if they are “life sustaining” and build these cells into growing into a serious health problem. Robert Dilts’, in his book “Beliefs: Pathways to Health and Well-being”, suggests that allergies manifest once a person is exposed to normally safe agent/s, when either run down, or excessively stressed, and the body’s immune system over-reacts, and the agent becomes harmful. Once triggered, the immune system maintains a memory of the agent and continues to attack it whenever present, in turn causing the symptoms. This is a common element with Elman’s theory where “stress” is viewed as the trigger. Dilts’ process when compared to Elman’s is much simpler. All one needs to do, is take a memory of symptom causes, and anchor an association to something similar, yet pleasant without allergic reactions; this may eliminate the allergic response for some.
This procedure may seems to be overly simple, but in a matter of a few days many people find they no longer have allergic reactions to cats, which they find to be amazing. Some readers of the book of the procedure naturally remember their own allergy and may follow the procedure while reading. Some allergic reactions like adverse reactions to dairy products can be considered to be pathological. Dilts’ allergy relief process is much very useable because it can even be applied covertly as directed in his most wonderful book “Beliefs”.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
68
Weight Loss- Mind Body Medicine MBM
Weight management with Mind Body Medicine or hypnosis and cigarette cessation has been at the forefront of treatment for years.
The fact is you can remove the excess weight you desire, and develop a mindset that will help you keep the weight off ensuring the you remain healthy, sexy, and full of life enhancing energy and learn how you can respect and help yourself.
There are some very basic and simple things you can do to help you help yourself. 1. Eliminate all butter, salt, sugar and alcohol form your food intake. 2. Agree to not eat “deep fried” food. 3. Remind yourself to “always” drink a full glass of water before each and every meal or snack. 4. Snacks or deserts can be fresh raw vegetable, preferably carrots, celery and cucumbers and
or fresh raw fruit of choice, apple, orange, pear, banana, all berries and plain yogurt. 5. Your eating style must include this reminder to yourself to take half sized bites and “always”
place your fork or spoon down in between each and every bite. And, to take a sip of water after you have swallowed each bite. 6. Be sure the served portion is less than half as much as you feel you need and leave some of that on the plate, to throw it away. For example, a normal restaurant serving is to be split in half. 7. Remind yourself to “masticate” or chew your food very well; you can actually count each mastication, up to 30 or more per bite of food before swallowing. 8. Slow your eating down; take it slow enough to “taste” the food. 9. Use diluted soy sauce – 3 parts water one part soy sauce for flavoring while cooking and eating. 10. For hydration mix Cranberry or Raspberry-Cranberry and or any fruit juice with 66 % water and drink a full glass before each meal. Drink at least enough so that your urine is almost clear. 11. Include at least three vegetables that grow in the ground and 3 vegetables that grow above the ground in each meal other than breakfast. Breakfast can be any berries you like and or fruit with a small bowl of oatmeal cooked with about 1/3 of the volume being raisins. Use soymilk or non-fat milk. Two pieces of dry toast, preferably OroWheat – Winter Wheat; a multigrain bread. 12. Your main meals must include a good source of protein like simply prepared chicken, fish, pork and occasionally beef. 13. Lunch and dinner must include a mixed garden salad with vinegar and oil and or lemon dressing; low fat cottage cheese is ok. 14. Always carry with you a snack of fresh fruit, carrots, celery and cucumber with a container of your mixed fruit or vegetable juice; be sure it is kept cold. Notice that the above is not a diet, it is a way of eating; it includes a broad range of fruits, vegetables, juice and grains for proper nutrition.
Adjustment of eating habits
First split your meals up into smaller portions to a frequency of five times a day. One major factor in fat loss or storage is insulin. The pancreas produces insulin, and its functions are to drive fat and sugar through your bloodstream and into the fat storage cells. It is also the most powerful profat hormone and the primary promoter of “fat preservation”. Large meals cause the production of large doses of insulin to be dumped into the system promoting fat storage. Small mini-meals cause small production of insulin promoting easy digestion, and faster burning of calories.
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination. - Albert Einstein

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
69
Super-hydration of water and or diluted fruit juice
This consists of sipping a gallon of ice water throughout the day. a) High volume of diluted juices flushes the system.
b) diluted juices promote digestion, and c) diluted juices have very few calories. d) cold diluted juices have the effect of causing the body to constantly work, to reheat the body. Work means a transfer of energy to heat, causing the constant burning of calories.
In effect, one is putting into the body a substance of zero calories (water) and causing the burning of calories approximately 8 calories per glass of ice water. Nice formula: zero calories in = 8 calories out. e) As the body ages, it dries out. Dehydration causes headaches, eye irritation, back pains, and body numbness. Water combats all this and helps promote healthy, young looking skin, and improves overall health. Education -- Set a little time aside each week to learn about nutrition from foods and vitamins.
Rest --The body and mind need rest. Too much work on the body (exercise) causes muscle atrophy and undeserved stress on the system. Adequate sleep is necessary for muscle recuperation and subconscious mind processing to evaluate and work on things. Repeat daily that you are achieving your desired weight and form.
Think positively, and in your self-induced hypnotic state provide positive affirmations. In summary of all that has been stated, when dealing with obesity, a patient’s desired results are
often difficult to achieve, but these needs are best met with the use of hypnotherapeutic measures due to the ability of reorganizing one’s thought patterns as elaborated upon above.
The many uses of Mind Body Medicine and hypnosis allow a person to reorganize old thinking patterns, as well as develop strong motivational factors. Triggers, or anchors that have at one time directed a person towards food can be altered towards healthier measures of fulfilling the need desired, weight loss.
To successfully overcome obesity you’ll need to combine Mind Body Medicine with safe exercise like deep water as long term maintenance requires periodic re-evaluation along with new learning, and your willingness to practice these procedures and exercise daily – weekly – monthly and yearly to maintain strong motivational health goals in order to continue achieving or maintaining your desired results of weight maintenance, and control. Feel free to go to http://www.aquadios.com/ and view the videos whenever necessary.
Natural Breast Enlargement
We in the Western World live in a “breast” culture with morays, which promote serious sexuality problems for both sexes and many psychosomatic as well as serious dis-eases, and illnesses which modern medicine often routinely treats by surgery. Both men and women seek the perfectly shaped “breast” and for this reason plastic surgery is becoming common for both sexes. Life is naturally sustained for infants of both sexes by breast-feeding which provokes many serious psychosexual problems for both sexes. Too often a man or woman holds an undesirable or unrealistic Body image. Many marriages suffer after having children, the woman rejecting her body should her breasts be less than “perky”.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
70
And, for good reason, the male sees all those “playful” breasts on younger women and is no longer aroused by his wife “saggy” or pendulous breasts. Some women surgically augment their breast to overcome this problem and others rely on the simple benefits of proper eating and exercise before, during and after pregnancy and childbirth.
Since the beginning of time humans have had the desire to somehow augment or change something about their body; everything from breast enlargement through building extra muscle to changing facial features, as well as many other augmentations such as penis enlargement, and more sexual enhancements. When thinking about such changes one might wonder how could something genetic be changed with simply the power of our minds?
The evidence is ever present in a number of scientifically organized research papers. There is much proof positive that Mind Body Medicine techniques and hypnosis helps with altering all parts of the body. Incredible feats such as that of Milton Erickson in fact having clients with incredible breast growth, and believe it or not, doctor Erickson even had a client grow a handicapped leg an entire twelve inches to match the other.
"Is it possible, to change one's physical appearance with exercise, a positive self-image and self-efficacy, Mind Body Medicine practices and hypnosis? " The answer is "yes", and not only because of the research already present, but from my own personal experience patients of my own. Below is a small sampling of the prominent research done in the field of natural breast growth.
Willard Study – Breast Enlargement
At the end of 12 weeks, 28% had reached the goal they had set at the beginning of the program and desired no further breast enlargement. There were 85% who could tell a significant enlargement in their breasts had been accomplished, and 46% found it necessary to buy a larger brassiere. Forty-two percent had a loss in weight of greater than 4 pounds and still had enlargement of their breasts. The average increase in circumference was 1.37 inches; the average increase in the vertical measurement was 0.67 inches and the average increase in horizontal measurement was 1.01 inches. Please note: the study was continued past 12 weeks to let those who hadn't reach their goals to do so.
In this study, 63% of the subjects had had children and complained of pendulous breasts defined as asymmetrical sagging breasts where often one breast is hanging lower than the left. Medical experts say this is perfectly normal after breast-feeding. And, those that say “ladies, quit worrying about your breast size and shape just don’t understand our “breast” culture society. Certainly “breasts” do not determine what you are as a person, but a woman with “perky” breasts may lure a married man away with nothing more than “lively” breasts. These subjects expressed a desire to reclaim the fullness and contour of their breasts before pregnancies. All of these subjects reported they were very pleased with the increase in fullness and firmness of their breasts at the end of the study.
The only two subjects, who subjectively felt there had been no significant increase in breast enlargement, did have a measurable increase in size. Both subjects had difficulty obtaining the visualizations. All of the subjects reported an increase in firmness of their breasts. All of the subjects who began the study with one breast smaller than the other found them to be equal in size at the end of the twelve weeks.
Scientific Research - Natural Breast Enlargement By Hypnosis
1. Peter H.C. Mutke, M.D., UCLA performed the first study. He presented his results as a research paper to the Department of Neuropsychiatry, University of California Los Angeles on February 28, 1971. As of 1994, Dr Mutke was still with UCLA and has been active in the American Council of Hypnotist Examiners.
2. Williams, J.E., Stimulation of breast growth by hypnosis Journal of SexResearch, 1974. His thirteen volunteer’s averaged 2.11-inch increase in the circumference of their breasts; equal to 2-cup sizes).

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
71
3. Staib, A.R., and Logan, D.R., "Hypnotic Stimulation of Breast Growth", The American Journal of Clinical Hypnosis, 1977 repeated Dr. Williams' tests with similar results. They also found women's waist size decreased by 1.4 inches. Their follow up study showed that 81 % of the breast enlargement was retained several months after the women stopped their visual imagery.
4. Willard, R. D., Breast enlargement through visual imagery and hypnosis. "The American Journal of Clinical Hypnosis," 1977, used a different technique than Dr. Williams, who used age regression and age progression, and achieved an average 1.44-inch increase in breast size for his 22 volunteers. Every woman had an increase in her breast circumference.
5. Wilson, Donald L. MD, "Natural Bust Enlargement With Total Mind Power" How to use the other 90% of your brain to increase the size of your breasts, 1979. This Book has the scripts and a great bibliography. Dr Wilson ran a clinic in California with great success. This book, a small hardback, is available thru Hypnosis Institute of Texas.
6. Beran, M.D., Roy, a neurologist at Adelaide Children's Hospital, England presented the results of his study to the February 1979 National Convention of Hypnotherapist ‘s in Adelaide. Dr. Beran showed that the breast volume (he measured the breast's cubic displacement of water) more than doubled during the three-month hypnosis program.
Optimal Healing Environment
Chronic Low-Back Pain Primary Care Dr’s Cherkin and Sherman research focuses on the use of a new protocol to evaluate the effect
of an “optimal healing” environment for low back injury and pain on a variety of important patient and clinician outcomes. Their optimal healing environment has three major components:
(1) The health care environment in which the primary care team works; (2) The cognitive, technical, clinical and organizational skills of the team; (3) The healing skills of the team members, particularly the primary care physician. Many elements of Optimal Healing for chronic back pain seen in primary care settings would
also be relevant for the other 98% of primary care visits.
Optimal Healing Environment for Chronic Lower Back Pain
A primary care environment has “Four” major components: (1) The health care environment in which the patient works with the primary care team; (2) The cognitive, technical, clinical, and
organizational skills of the team; and (3) The healing skills (and abilities) of the
patients and team members, particularly the primary care physician (PCP).
(4). The environment or the physical attributes of the healing space in which the patient and provider encounter occurs.
Specific aspects of the AquaDios-Med™ health care environment that affect the healing experience involve access to all health care.
This optimal healing environment for chronic lower back pain will include those developed by AquaDios-Med™ because it logically includes easy and responsive access to the immersion chambers.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
72
Cognitive, technical, clinical, and organizational skills of AquaDios-Med™ includes every imaginable safety in and around the immersion chambers including ergonomic and physical comfort, safety handles and instruction on use and benefits of its “power massage” see http://aquadios.com/ and http://aquadios.com/aquadiosmovies.html
Research shows that patients of family physicians who were more confident of their abilities to manage low-back pain effectively were more satisfied with the information they received about their back problem than patients of less confident physicians and at AquaDios-Med™ confidence is very high as there is just no other process that will strengthen the lower back and eliminate pain simultaneously.
It is important to rule out “red flags” (e.g., tumors, infections, fractures, substance abuse). Primary Care must collect relevant medical history including information about the effectiveness of the treatments the patient has used in the past for their back pain and conduct an appropriate physical examination to reassure the patient that their back has been adequately examined.
It is important to identify risk factors for chronicity (e.g., patient is applying for or receiving compensation, psychologic distress) because this information might influence treatment decisions. For the great majority of patients with CLBP lacking evidence of serious spinal pathology, the PCP would then determine if the patient is willing to participate in safe daily structured deep-water running exercise treatments; it is this author’s belief that AquaDios-Med™ is the preferred treatment of choice for most all human ailments.
There are no medical contraindications or substantial risks for patient treatment with AquaDios-Med™ but currently the treatment might not be available or covered by the patient’s health insurance, even though there is compelling evidence that AquaDios-Med™ treatment is the most effective and cost effective treatment available.
Research shows there is scarcity of clearly effective treatments for low back pain other than AquaDios-Med™ treatments. The treatment plan will include safe daily structured deep-water running treatments to break the cycle of chronic pain.
Spinal manipulation, massage, acupuncture, physical therapy, will accommodate the specific AquaDios-Med™ exercise program as will methods to increase body awareness and efficiencies of movement (e.g., Alexander technique, bodywork massage education, yoga classes).
Self-care strategies to maintain back health or enhance self-awareness and coping (e.g. safe daily exercise, relaxation, mindfulness training, yoga [see above], stress reduction, psychotherapy, and writing therapy as described by Pennebaker)
High-quality educational resources such as books, videotapes, and Web sites help patients understand how to take appropriate advantage of social and family support without being a burden on family and friends.
AquaDios-Med™ consistently encourages learning self-care strategies that can help the patient better cope with back pain as well as with other problems that might be caused or exacerbated by life’s stresses. There is regular follow – up’s to reassure the patient that they will never reach a dead end in their search for relief of their back pain and that they will never be abandoned so long as continue to participate in safe daily exercise such as deep water running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
73
Dr’s Cherkin and Sherman point to a recent research that shows physician behaviors most strongly associated with patient trust were caring and comfort, technical competency and communication. AquaDios-Med™ includes only physicians and staff who are capable of facilitating healing and ensuring that the fundamental physical and emotional needs of the patients are being met. An unhappy, stressed, and preoccupied patient or physician is unlikely to be a very effective at the complex task of healing.
Dr’s Cherkin and Sherman identify a recent research that shows the full range of important outcomes include measures of the effect of treatment on outcomes of greatest concern to patients (e.g., social and physical functioning, pain), and future use and costs of health care for back pain relief. Since AquaDios-Med™ includes techniques that may take a month to learn (e.g., stress reduction techniques, yoga, safe sustained daily exercise), it is best to measure outcomes at least 6 to 12 months after initiation of treatment.
Dr’s Cherkin and Sherman identify research that shows persons with back pain caused by tumors, infections, unstable fractures, or other specific diseases generally need comprehensive daily evaluations when participating in mechanical back pain exercises such as AquaDios-Med™. Care is taken to ensure that persons with special contraindications for specific treatments (e.g., heart pacemaker for acupuncture, eczema for massage, osteoporosis for high velocity spinal manipulation) are carefully evaluated for any AquaDios-Med™ treatments.
Chronic Back Pain and Other Health Problems
The primary care settings should apply equally well to other common nonspecific chronic
musculoskeletal conditions (e.g., neck pain, headache, shoulder pain) that collectively comprise a substantial fraction of primary care practice. In fact, most of the design, implementation and evaluation elements are directly applicable to chronic illness care in general, and many elements would also apply to acute and preventive care.
Creation of an optimum healing in primary care will only succeed with adequate support from a
health care organization that is committed to exploring innovative ways of transforming health care. Once such an organization is found, the next major challenge would be to develop a curriculum that would fundamentally transform the members of the primary care team and the organizational structures within which they practice. To the extent possible, the curriculum should be at least guided by or preferably based on the relevant evidence that exists in the medical, psychological, organizational, business and other literatures.
It is particularly important to provide clinicians with an evidence-based rationale for recommending or withholding specific treatments from their patients (e.g., massage, acupuncture, stress reduction courses). Preparation for major change might be facilitated by training the entire clinical team in mindfulness and stress-reduction techniques at the beginning of the change process (e.g., the mindfulness-based stress-reduction course). In addition to promoting a more open and thoughtful approach to the change process and opportunities for bonding among team members, such training could provide physicians with a valuable coping skill for use in their own lives and with a profound understanding of the value of a tool that might benefit many of their patients.
Implementation of the curriculum might require removing the clinicians from their practices for
a period of time (e.g., up to 1 day per week for 3 months), and exposing them to different ways of interacting with patients. This group process might be enhanced by participation of selected practitioners who could model their unique and often more patient-friendly approaches to care. Furthermore, this would expose conventional clinicians to the skills that of sensitive practitioners have to offer, and would prepare the physicians for more informed and appropriate referrals.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
74
To benefit from their new awareness of what genuinely concerned practitioners and other resources (e.g., stress reduction training, health clubs) can offer their patients, physicians would need the organizations in which they work to permit, support and facilitate such referral options.
Dr’s Cherkin and Sherman may be overly optimistic when they say that they believe there are
enlightened health care organizations that would be interested in partnering and supporting preventive medicine programs such as AquaDios-Med™ with philanthropic organizations to devise, implement and evaluate the development of optimal healing environments like AquaDios-Med™ to be include in primary care facilities.
Dr’s Cherkin and Sherman optimism continues when they say that given the high levels of
stress and dissatisfaction now endemic in the physician community and the deep chasm between what the American health care system provides and its full potential, forward-looking organizations are hungering for innovative solutions in the preventive medicine field such as AquaDios-Med™ to make fundamental changes in medical practice.
The challenge for these organizations is to meld their commitment to change with the skillful,
sensitive, and scientifically rigorous development, implementation, and evaluation of a new environment that more fully realizes its potential for facilitating true healing as does AquaDios-Med™ treatment and programs.
The uniqueness of AquaDios-Med™ proprietary deep immersion chambers is represented by pictures. The overhead views show the AquaDios-Med™ medical prototype designed and built by Dr. Jensen and include the Main Exercise Chamber, Deep Strider and Lounge Spa Chamber.
Anesthesia MBM
The advantages to the use of Mind Body Medicine as an adjunct to chemical anesthesia are
many, but first I will define the difference between anesthesia, and analgesia. Anesthesia refers to one's ability to lose sensation in one or more parts of the body. Analgesia
diminishes rather than eliminates sensation, in other words pain can be eliminated, but sensation such as feeling a pressure when touched in the area will be recognized.
The first notable advantage to using Mind Body Medicine as an adjunct to chemical anesthesia
is that it calls for far less amounts of chemical anesthesia than normally required. This in turn has the effect of reducing deaths in surgery due to chemical incompatibilities with patients. The Mayos have had an unbroken record of about seventeen thousand cases without any fatalities due to the anesthetic ever since employing the use of Mind Body Medicine procedures.
Additionally, patients have far more energy and vitality left after surgery for recuperation, and
Mind body Medicine suggestions and practices include quick recovery and rehabilitation have also been used to help with great success.
Joseph Barber, Ph.D. in his book Hypnosis and Suggestion in the Treatment of Pain: A Clinical Guide, 1996, pg. 248 – 249, states that hypnoanesthesia is very effective and quite necessary in the relief of pain for burn victims, in which the use of chemical anesthesia could possibly be quite dangerous. Barber also suggests that simply pre-operative suggestions via the use of hypnosis are quite effective for speedy recovery after surgery. Learn more about hypnosis for surgery. Learn more about hypnosis for pain relief.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
75
Dabney Ewin, MD, a clinical professor of surgery and psychiatry at Tulane University School of Medicine, has demonstrated that when methods of Mind Body Medicine can be administered within hours of the incident in severe burn cases that such care can slow or even stop the inflammation and blistering that can cause permanent damage with relatively little scarring. Ewing has a series of examples showing burns in which early intervention prevented serious, lifelong injuries.
Crasilneck, Ph.D. in Clinical Hypnosis: Principles and Applications, 1975 provides advantages
of Mind Body Medicine methods to produce “natural” anesthesia in situations where chemical agents are considered dangerous due to respiratory, cardiac, or other diseases. He also states that the repeated use of anesthetics have a debilitating effect upon the recovery of burn patients, and that in certain cases, such as chemopallidectomy, it is desirable to have the patient conscious in order to respond to questions.
Karen Olness, M.D. and Kohen’s Hypnosis and Hypnotherapy with Children, 3rd edition, 1996 reports that in a controlled study by Gaal, Goldsmith and Needs, 1980, on the effects of hypnosis on anxiety and pain in children, those that received Mind Body Medicine preparation before surgery required only one fifth as much post-operative pain medication.
Andre Weitzenhoffer, Ph.D. in his book “The Practice of Hypnotism,” Second Edition, states
that hypnoanesthesia for major surgery is only effective for about 10 percent of the population, but that the effectiveness using hypnosis as an adjunct to chemical anesthesia is great.
Some of the primary benefits include, Mind Body Medicine anesthesia in obstetrics, which
allows more control over the birth movements, and also eliminates all the ill effects of chemical anesthesia on the infant. Mind Body Medicine is an excellent preoperative tool, allowing for relief of preoperative fear and anxieties, and works as an alternative to preoperative sedation.
Benefits postoperatively are many including the control of constipation, hiccups, coughing,
retching, and for eliminating all sorts of postoperative pains in turn leading toward speed of recovery. Weitzenhoffer helped to pioneer Mind Body Medicine anesthesia for major surgery and identifies it requires a preparatory period, a maintenance phase, and a postoperative phase for greatest success.
There is a caution for those who will be or have been, or are soon to be under the effects of
chemical anesthesia. During unconsciousness established by surgical anesthesia or trauma, the last human resource
maintaining contact with the external environment may be that of hearing. Research discovered long ago that it is a grave error to consider the anesthetized patient as being unable to hear or understand simply because the person may have no conscious memory for events during the period of unconsciousness.
Meaningful sounds, silence, and meaningful conversation during these unconscious moments are registered in the mind and may have a strong influence on the patient’s behavior during surgery and for many years after, possibly indefinitely, since these memories are recorded at a deep level of consciousness. This is known due to several cases which have been uncovered and the events recalled by David Cheek, M.D. who used Mind Body Medicine techniques that produced age regressions.
"Fears originating during an earlier surgical operation have been found to reappear as the
subject's later re-experienced the surgical anesthesia using hypnotic techniques. These fears produce changes in heart rate and respiration." This indicates that the utmost of cautions should be taken to protect patients to prevent cardiac arrest and other associated problems in the operating room."

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
76
Cheek makes it clear that patients under surgical anesthesia are as aware of deceit, and attempts to avoid the truth as are patients with malignancy or a critical illness. Most importantly the patient's unconscious records and associates communications in a most literal way.
Unconscious mental activity of deeply anesthetized surgical patients Human thought processes
continue independently at both a conscious level and a more child-like, literal, subconscious level while awake. Objective type thinking may be blocked in states of serious illness, fear, and during unconsciousness. A remark such as, "Don't worry about this operation, Mrs. Jones, it will be all over in hour-and-a-half", may be understood as thoughtful and reassuring by the conscious mind. But, at the unconscious level the patient may misunderstand this and believe there will be a sudden death in 90 minutes after the beginning of surgery!
Study of the mind shows the unconscious mind puts together associations of thought that are
senseless to the conscious mind. For example, treating someone badly might bring awful guilt if the other person dies, which would leave blame on oneself even though the incidents had nothing to do with each other.
Reassurance usually given by physicians and relatives is often quite useless. Often, disturbing secondary questions are aroused such as, "I wonder why he said, this operation carries practically no risk? Could it be that he is really worrying about me?" People recognize lies, and this could trigger unconscious setbacks.
Indirect reassurance by implication is almost always accepted at an unconscious level of mind, and this is the strongest weapon the anesthesiologist, specialist in Mind Body Medicine, hypnotist, or doctor has against potentially dangerous fears. Most anesthesiologists seem to sense this fact, and will talk calmly about the preparation for anesthesia, and also about what the patient is to do when he awakens. This becomes an assurance that the patient will survive.
Altered States of Consciousness similar to Hypnosis may occur spontaneously in the presence of fear, sensory of postural disorientation, and in loss of consciousness, during which time the auditory capacity has been shown to remain operative.
The unconscious mind is able to perceive pain without necessarily passing the awareness along
to the conscious mind. Hyperemia, edema, and muscle guarding may occur so long as the unconscious mind knows that trauma is being produced, regardless of whether or not there is conscious pain.
It is possible to help the mind reject the unconscious awareness of pain, and to maintain a lack
of attention for stimuli coming from traumatized tissue with simple hypnotic suggestions to recalling a previous experience of numbness centered in the operative area.
In addition to suggesting the hallucination of numbness or lack of pain, it is possible to dissociate awareness. Dentists and anesthesiologists frequently use this method when working with children. In Dave Elman's Hypnotherapy he offers hypnotic suggestions that the patient hold on tight with both hands to a pencil, and to concentrate on holding the pencil tight; Another suggestion would be for the patient to imagine themselves swimming for a nice relaxing hour.
Surgery MBM
Before undergoing any surgery it is highly recommended you get three separate opinions one of
which is preventive medicine oriented such as AquaDios-Med. Research indicates that as many as 75 percent of the surgeries can be eliminated with aggressive preventive medicine where the person is taught the differences of rehabilitation and re-injury pain see http://www.aquadios.com/

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
77
James Esdaile, M.D. is recognized for his use of hypnosis in surgery, though his method found
much better reception in India. Modern day Mind Body Medicine and hypnotists have modified techniques developed by Esdaile, Elliotson, Parker, Cloquet and other pioneers in the filed over the last century. The most significant developments in this area include the use of autohypnosis, hypnotic suggestions to improve the postoperative period, glove anesthesia and autogenic training (which employs a practice run of the intended surgery). This type of conditioning protects the patient against surprise, fear, and apprehension. Using these techniques to “block” the neurophysiologic paths that transmit the painful afferent impulses can automatically raise a person’s pain threshold.
Hypnoanesthesia has been used successfully for many major and minor surgical procedures.
Since the use of hypnosis allays fear and tension, hypnotic anesthesia is easily facilitated, anoxemia is reduced and, because of the profound relaxation, less analgesia and chemical anesthesia are required. In some patients the traditional preoperative administration of narcotics can be eliminated even in those who are presently able to enter the light stages of hypnosis.
Postoperatively, Mind Body Medicine and hypnosis is of inestimable value when it is used with
suitable patients. For instance, when surgical patients wake up, they are usually afraid to cough because of excessive pain, especially those having upper abdominal operations. In good subjects, trained to enter quickly into hypnosis, fear, and often pain, may be eradicated in a matter of seconds by posthypnotic suggestion.
The chief disadvantage of MBM - hypnosis is its unpredictability and its effectiveness; not every patient responds as expected. Unless the hypnotic conditioning is performed in a group, the procedure can be time-consuming, and several hours of preparation may be required. However, since hypnosis is seldom utilized as the anesthetic agent per se, the unpredictability is not a deterrent – even if only partially successful, its advantages outweigh its disadvantages.
Pharmacological analgesia and anesthesia, with their ease of administration and effectiveness, are the methods of choice over pure hypnoanesthesia for major surgery because of its reliability, and primarily because people are generally lazy, most often preferring that things are done for them. However, where there is a definitive contraindication to all types of chemoanesthesia, hypnoanesthesia is indicated.
A pain expert, Joseph Barber, Ph.D. "Hypnosis and Suggestion in the Treatment of Pain" states,
"The single most dramatic use of hypnosis for acute medial situations is for burn patients. Hypnotic intervention can dramatically improve the patient's experience of his injury, treatments, and recovery, and is very useful for pain control and improving nutrition and activity. Hypnoanesthesia eases the numerous necessary painful treatment procedures. Ideally, hypnotic treatment begins as early as the patient's arrival in the emergency room and extends throughout his hospital stay and into eventual reconstructive surgery and rehabilitation."
Though the mechanism of hypnoanesthesia is as yet poorly understood, current research
indicates that the pain, perceived in the tissues, does not reach the pain receptors in the higher brain centers during hypnosis. With the higher cortical centers inhibited during deep hypnosis, the reticular formation and other subcortical centers prevent the intrusion of painful impulses into awareness. This raises the adaptive responses of the organism to them (painful stimuli). From an operational standpoint, a subject is relieved of pain when he becomes “relatively inattentive and unconcerned about all stimuli to which the hypnotist does not specifically direct his attention.” If the readiness to respond is minimized, “the sensation of pain” is no longer “painful”, it is an isolated “sensation” unaccompanied by pain.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
78
Mind Body Medicine and hypnosis are very similar and are considered to be multifaceted tools; effectiveness can be enhanced when it is employed in conjunction with other medical procedures. All physician involved with Mind Body Medicine or hypnotists who use hypnoanesthesia recognize the limitations of this modality will not try to operate on every patient without careful selection, preparation, with the availability of chemical anesthesia.
Dave Elman a layman and specialist in hypnosis was another at the forefront of the medical
community promoting hypnosis before Mind Body Medicine and its use to medical personnel caught on. Elman suggests that the “coma” or “Esdaile state” is the level of hypnosis, which can be used for surgery. Elman’s reasoning behind this is twofold: firstly, physical anesthesia is automatic even without suggestion, and secondly, physical mobility is not possible even with suggestion. Elman suggests a pre-conditioning for the use of hypnosis before surgery.
Introduce the idea that the upcoming procedure can be accomplished painlessly and comfortably, naturally, via the Esdaile state. At the time he suggested not using the term hypnosis, but I feel that it is fairly safe, and probably more respectable to use proper terminology in this day and age.
If a desire is present, then introduce the patient to the trance state by guiding her into trance,
most specifically into the somnambulistic state. While in this state, the patient is to be spoken to about the benefits of having the procedure done in the state of hypnosis, as well as how easily it will go, that the patient will do well throughout it, and that recovery will be quick and easy. The patient is also asked to practice this type of relaxation until the time of surgery.
Guide the patient into the Esdaile state for the experience, and continue talking about how well
the surgery will go, and that she will be in better health than the present. Pregnancy
Mind Body Medicine • Natural Healing • Brief History
The process of healing was the primary approach to disease and illness before the arrival of scientific medicine. The enhancement of healing has been one primary pursuit for humans since the beginning recorded history. Each culture has its own special rituals, techniques and preparations to support and stimulate healing. Most ancient medical systems consider spiritual, energetic and physical forces as integral to illness and journey of healing.
Ancient healing has relied on specific rituals and the induction of altered states of
consciousness to enter, manipulate or remove spiritual forces thought to be the cause of many illnesses and restore beauty to the individual and their group.
Chinese Medicine is based "life energy", or "bioenergy", the life force responsible for health, illness and recovery." Indian cultures rely on the belief of "universal consciousness" that if properly entered through meditation and intention restores order and health to the dysfunctional person and society.
Researchers define “Healing” as a dynamic process of recovery, repair, restoration and transformation of the mind, body and soul on the path to becoming more whole." And, “Healing” occurs at many levels of the human system-mental, physical, emotional and spiritual.'
The Hippocratic School of medicine in ancient Greece considered several approaches to the treatment of disease. These included removal of primary causes to supporting natural recovery capacities as integral to a physician's duty.''
Florence Nightingale the nurturing and caring nurse-healer captures the fundamentals of empathy, compassion, warmth, trust, credibility, and respect that are felt to be essential to healing of mind, body and spirit in the West.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
79
Healing is the dynamic process of recovery, repair, restoration, renewal and transformation that increases resilience, coherence and wholeness. Healing is an emergent process of the person's whole system - physical, mental, social, spiritual and environmental." It is a unique personal and communal process and experience that may or may not involve curing.
Mind Body Medicine involves the using intention and education of the patient to increase
awareness and to establish hope, belief and expectation in the possibility of wholeness and well-being and positive change.
Healing energy refers to a deep emotional presence to enhance recovery and repair; a physical and emotional wholeness from which deep personal engagement, caring and communication emerge to facilitate "bioenergy" toward deep healing to be accumulated, stored and transmitted for life. This “healing” energy is said to derive from spiritual sources and to arise from the cultivation of compassion and altruism.
Healing relationships consist of the therapeutic alliance between doctor patient and staff that facilitate mutually desired health. Proper healing includes the social involvements in the household, family, friends, support groups and community; elements and degrees to provide a sense of belonging, caring and coherence to the patient's life.
Proper “healing” involves empathy, compassion, beneficence, mindfulness, demeanor, caring, hope, love, inspiration, reassurance, comfort, warmth, trust, confidence, credibility, honesty, expectation, courtesy, respect, harmony, challenge and genuine communication.
Health promoting behavior also demands adequate amounts and types of safe daily exercise,
healthy nutrition, relaxation, creative outlets, social service and support, and spiritual development. This category includes patient and family education programs dedicated to forming cognitive skills through modeling optimistic and positive behaviors.
Preventive medicine treatment such as AquaDios-Med combines science, safe daily exercise,
an accounting of proper daily nutritional experience and requires a dynamic, trusting interaction to identify the best treatment for individual situations. Genuine healthcare includes nutrition from Low-fat, high-fiber, high fruit and vegetable, whole-food as these foods, in moderation have proven to lower incidences of cardiovascular disease, cancer, hypertension, diabetes, stoke, obesity and other common conditions."
AquaDios-Med “Healing” treatments are designed from methods that stimulate the body's healing processes and repair with a focus on disease management and a goal of cure when appropriate.
Initially these modalities do not include surgery and drugs, and primarily focus on safe daily
exercise together with healthy dietary changes and supplements as well as transformative psychological and social therapies, and physical – mental activities and treatments that stimulate repair and recovery processes.
Conventional approaches such as psychotherapy, physical therapy, nursing care and complementary medicine approaches include acupuncture; massage, homeopathy, manipulation and electromagnetic treatments provide examples of treatments. Healing may include the physical environment, including visual esthetics, sound, music, smell, taste, lighting, air, art, water, horticulture, architecture and conditioning processes that support and stimulate recovery and repair processes. Surgery, pharmacology and prescribed drugs are considered last, not first. The belief and focus of AquaDios-Med is that with proper safe daily exercise together with healthy nutritional foods and a genuine participation with Mind Body Medicine and a desire to be well the patient will produce their “homeostasis” for correct biochemistry.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
80
Classic studies by Arthur Kleinman of how and why healers from different cultures are often so successful illustrate the importance of meaning, context and environment for the delivery of effective healing. Lifestyle and behavioral medicine because it is now well established that health-supporting behaviors can both prevent and help reverse chronic disease. Low-fat, high-fiber, high fruit and vegetable, whole-food diets are associated with lower incidences of cardiovascular disease, cancer, hypertension, diabetes, stoke, obesity and other conditions."
Regular daily aerobic exercise has beneficial effects on general health and other conditions
including improved mental and physical health. The regular use of mind-body medicine interventions or self-care practices such as relaxation and stress management techniques, and the pursuit of creative outlets, are also important for maintaining health and well-being. Healing relationships, social support, and spiritual and religious practices are a second important component of healing. Deep self-disclosure to another person, either in a medical, religious or social context can induce profound preventive and recuperative processes.
Both individual and collective intention and mental attitude contribute to healing and well-being. There is increasing evidence from research in mind-body medicine that consciousness, in the form of belief, expectation and intention plays a central role in healing. A person's self-perception of health is a major correlate of future health." Hardiness, a type of self-perception, is a mental state of commitment, coherence and control that enhances resilience to both social and physical stresses.
Practices such as mindfulness, yoga and transcendental meditation contribute to improved
health, function and well-being. Mental control of specific physical functions with methods such as biofeedback, conditioning and other techniques demonstrate our ability to enhance and control self-healing capacities. The breadth of such capacity has been explored in placebo research where expectation and the role of the meaning and context of therapy is profound and widespread, affecting almost every major condition known to humanity.
Lifestyle practices and health outcomes
Dr. O’Donnell, notes there is an abundance of high-quality scientific evidence supporting the
simple relationship between health practices and health outcomes the most important of which is exercise. There is little question or disagreement that health behaviors have a huge impact on health outcomes. In 2004, approximately 40% of all premature deaths in the United States, at least 900,000 deaths annually, are the result of unhealthy lifestyle choices such as tobacco use, poor diet, a sedentary lifestyle, misuse of alcohol and drugs, and accidents. Other early death contributors include genetic predisposition (30%), social circumstances (15%), poor access to quality medical care (10%) and environmental exposures (5%).
O’Donnell verifies that unhealthy lifestyle is the primary cause for the six leading causes of death in the United States including heart disease, cancer, stroke, respiratory diseases, accidents, and diabetes, and collectively accounts for 75% of all deaths. More than two thirds of American adults are overweight or obese, more than 60% of the population do not get enough physical activity, 25% are completely inactive, and only 23% eat recommended amounts of fruit and vegetables. This information alone is substantial enough to support the nationalization of AquaDios-Med™ programs across America.
Scientific studies like that of O’Donnell continuously show that people with healthier lifestyles live an average of 6 to 9 years longer, postpone disability by 9 years, and compress disability into fewer years at the end of life. The devastating impact of lifestyle on the population is clear, and the burden is made worse by the fact that lifestyle diseases disproportionately affect racial and ethnic minorities, poor people and older adults.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
81
The Surgeon General’s Report on Health Promotion and Disease Prevention, published in 1979, called for a second public health revolution in the history of the United States to address problems related to lifestyle. The revolution never occurred because the federal government has invested minimal resources and finances in this area, forcing health-prevention programs to emerge in the private sector such as AquaDios-Med™. But, without federal, state and county governments, along with health insurance carriers subsidizing preventive medicine programs like AquaDios-Med™ the more than $ 2.2 Trillion healthcare costs will continue to rise causing millions of American’s to suffer needlessly and be unavailable for the work force.
The workplace offers a unique environment to provide programs like AquaDios-Med™ because people spend a large portion of their waking hours at work, and the employer has a financial incentive to keep its employees healthy and medical utilization low. As such, approximately 90% of employers with 50 or more employees have offered some type of health promotion program, but none offer preventive medicine programs like AquaDios-Med™.
Most health related programs intend to address alcohol and drug abuse, exercise, human immunodeficiency virus - acquired immune deficiency syndrome (HIV/AIDS), hypertension, hypercholesterolemia, nutrition, seat belt use, smoking control, stress management, weight control, and health risk appraisals. And, positive results occur in 75% of the experimental studies, 88% of the quasiexperimental studies and 100% of the nonexperimental studies. But none of health related programs have ever offered the public a preventive medicine program like AquaDios-Med™ let alone a validated “study” to prove the benefits of preventive medicine programs like AquaDios-Med™.
These narrow focus programs have been successful in changing knowledge, attitudes,
behaviors, and health conditions on a short-term basis. Long-term impacts were typically not measured. Studies showed people decreased their symptoms of hypertension, stress management, smoking control, nutrition, hypercholesterolemia, and improved exercise, seat belt use. But, weight control and alcohol and drug abuse showed no improvements. There has never been an established comprehensive preventive medicine program to show the benefits of AquaDios-Med™ practices for just one year, or any program that instituted daily safe exercise.
There are no government standards or guidelines for high-quality preventive medicine programs such as AquaDios-Med™, but there is widespread agreement that education on the benefits of healthy lifestyle is not enough; we humans have to become engaged in safe daily exercise activities as is offered in AquaDios-Med™. The most successful programs offer people opportunities to engage in behavior change processes that include health assessment, goal setting, and ongoing opportunities to acquire knowledge and build skills and receive feedback on progress.
There is increasing recognition of the importance of creating supportive environments that encourage good health practices. These environments provide smoke-free air, access to nutritious foods, opportunities for daily physical exercise and activities as part of the routine day as well as fitness facilities, and protection from stress inducing situations and safety hazards; all of this and much more is available in the AquaDios-Med™ program.
HEALTH- PROGRAMS TO PROMOTE SELF-HEALING AMONG ILL PEOPLE
Comprehensive Preventive Medical programs such as AquaDios-Med™ are just not offered to
people suffering from major causes of death related to lifestyle factors, such as functionality and disability symptoms, quality of life, medical care utilization, recovery, mortality, intervention focus, safe daily exercise, stress management, smoking cessation, nutrition, weight control, and degree of illness or wellness of the populations. However, there is at least one effort to review the impact of a wide range of preventive services from a clinical standpoint.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
82
The U.S. Preventive Services Task Force was convened by the Public Health Service in 1984 to perform this function; it published its first Guide to Clinical Preventive Services in 1989. But, like so many “good ideas” its management has avoided strong support of comprehensive preventive medicine programs like AquaDios-Med™.
The second edition was published in 1996. The content details the value of screening for 53
different health conditions of major categories including cardiovascular diseases, neoplastic diseases, metabolic, nutritional and environmental diseases, infectious diseases, vision and hearing disorders, prenatal disorders, congenital disorders, musculoskeletal disorders, mental disorders and substance abuse. For each of the 53 screenings, there is a summary comment on the quality of evidence supporting a recommendation to conduct the screening, burden of suffering, accuracy of screening tests, effectiveness of early detection, recommendations of other groups and a brief description of the screening protocol.
When the AquaDios-Med™ preventive medicine program is nationalized I am certain evidence will show just how effective it can treat and progressively eliminate those 53 different health conditions identified in the Clinical Preventive Services Guide.
The third edition of the Clinical Preventive Services Guide is published in booklet form and is
available online as installments are completed. Two installments have been completed. This series of guides is an excellent resource, but provides insufficient information on the literature to give a clear sense of the most important research priorities or why preventive medicine programs like AquaDios-Med™ have not been economically supported.
O’Donnell reports on studies of three of the most prevalent chronic diseases in the United
States: type 2 diabetes mellitus, coronary artery disease (CAD), and breast cancer.
Preventive Medicine Mind Body Medicine and Healing
In the United States, holistic healing practices, indigenous medical systems, and alternative
forms of medicine have been transferred to the sideline of modern, scientifically oriented medicine. This has included any form of healthcare, modern or ancient, that rests on a vitalistic or "energy" based philosophy and approach. Yet, these practices are used widely in the world and increasingly used in the West.
Patients and the public find them attractive precisely because they offer approaches that emphasize self-healing with their affiliated increase in individualized, holistic, and high-touch care, and their potential for reduction in side effects, medical dependence and cost.
In addition, scientific data from research on vitalistic traditions is beginning to emerge.
Evidence of efficacy for medical practices that stimulate healing such as homeopathy," acupuncture," and energy medicine are gradually accumulating. Interestingly, the scientific investigation of these systems is converging with modem concepts in biology such as complexity, chaos and self-organization in living systems.
There is a science pertinent to healing processes. In 1987, Antovofsky used the term
"salutogenesis" to describe the process of healing that strives toward human growth and development. We think it should be used more broadly to refer to the science of Mind Body Medicine. The will serve an important comparison and contrast to "pathogenesis", the processes by which disease is generated.
Exercise is a weapon against Disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
83
Modem science is already face of the joint epidemics of chronic illness, emergent infections and rising healthcare costs, but urgent development and expansion is needed for dealing with whole system complexity in cell biology, immunology, epidemiology, cardiology, nursing:' psychiatry, and neuroscience, are helping us develop a scientific basis for understanding the biology of healing. Data emanating from molecular and cellular biology reveal the complex and redundant nature of repair and recovery. For example, stress proteins are a complex system of cellular protection and repair responsive to multiple toxins and environmental stressors." DNA repair is a redundant process with factors essential to organism survival and reproduction.
The principles of evidence-based medicine require the application of rigorous clinical research protocols with valid measurements to evaluate the components and impact of optimal healing environments in our current healthcare system. The ample anecdotal experiences in which a patient attains well-being or is successfully healed after a therapeutic encounter are insufficient proof.
A recent publication has described emerging definitions and guidelines for healing research
useful in primary care for investigating the impact of healing in medicine. Since individuals spend more time at work than sleeping and employers have an inherently
vested interest in their health, performance, and productivity, the worksite is an essential optimal healing environments node. Additionally, the private corporate sector is second only to the US government in its role as a payor for healthcare.
Over 115 studies to date have demonstrated both the clinical and cost effectiveness outcomes of worksite-focused interventions. These studies yield insights into some dimensions of optimal healing environments. Within these communities, there are multiple pathways and multiple systems to achieve both healing of individuals and of their relationships. Thus, there is a creative tension and dynamic change in healing environments and no signal pathway to health may emerge as best in all situations.
PREVENTIVE Medicine FOR
TYPE 2 DIABETES MELLITUS
There are more than 13 million deaths from Diabetes mellitus in the U.S. population; it is one of the leading causes of U.S. mortality and ranked 6th most likely cause of death. Yet, exercise alone can reverse the symptoms of diabetes. This excludes undiagnosed cases that are estimated to increase the prevalence by approximately 35%. In 2003 diabetes mellitus increased by 14.8% in 4 years, representing a preventable epidemic among the 90% - 95% of diabetics classified as type 2.
Thus, lifestyle interventions that reduce the incidence of type 2 diabetes mellitus among those
with impaired glucose tolerance (IGT), promote glucose control and cardiovascular risk factor reduction in diagnosed type 2 diabetics, and benefit the long-term vascular complications of type 2 diabetes mellitus in established diabetics offer significant opportunities for self-healing.
It is believed that within one year these approximate 14 million people can be educated and
taught a lifestyle by AquaDios-Med™ preventive medicine techniques that will reverse this epidemic and harness the symptoms of diabetes.
The effectiveness of AquaDios-Med™ reducing the incidence of type 2 diabetes mellitus includes those with Impaired Glucose Tolerance (IGT). This is the name given to define blood glucose levels that are higher than normal, but below the level of a person with diabetes. IGT is a combination of Impaired Secretion of insulin with reduced insulin sensitivity (insulin resistance). In people with IGT, the rise in blood glucose that occurs after consuming 75g glucose is greater than normal although not as great as in people with type 2 diabetes.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
84
Fasting blood glucose levels are normal or moderately raised. IGT carries a high risk of progressing to type 2 diabetes, leading to it being referred to as ‘pre-diabetes’ by, among others, the American Diabetes Association. It is believed that safe daily exercise offered by AquaDios-Med™ programs would all but reverse this “pre-diabetic” medical condition. This is supported by the evidence study in Da Qing China. The Da Qing IGT and diabetes study in China was the first randomized, controlled trial to show that interventions of diet alone, physical activity alone, or diet and physical activity reduced the incidence of type 2 DM among those with IGT by 25% to 50% in a group of 110,660 participants over 6 years.
Daily safe exercise as provided by AquaDios-Med™ practices for one year or less will improve glucose control and cardiovascular risk factors in diagnosed type 2 diabetics, and it is believed that AquaDios-Med™ mind body medicine activities will support self-healing of macrovascular complications, such as Coronary Artery Disease (CAD). CAD is a condition in which plaque (plak) builds up inside the coronary arteries. See Graph of Artery>>>
These arteries supply your heart muscle with oxygen-rich blood. Plaque is made up of fat, cholesterol, calcium, and other substances found in the blood. When plaque builds up in the arteries, the condition is called atherosclerosis. AquaDios-Med™ process will not only reverse CAD it will largely reduce or eliminate stroke and peripheral vascular disease which account for 80% of diabetic mortality, and microvascular complications such as damaged retina or retinopathy, Kimmelstiel -Wilson syndrome a progressive kidney disease caused by angiopathy or diseased vessels and capillaries in the kidney and caused by longstanding diabetes mellitus; it is a prime cause for dialysis in many Western countries.
Dr. Boule and colleagues found in analysis of 14 controlled clinical trials involving type 2 diabetics, that physical activity with and without diet changes significantly decreased high blood sugar or hemoglobin A1c (HbA1c) by approximately 0.66%, which was near the average 0.9% difference between the conventionally treated control and intensive pharmacologically treated intervention groups in the United Kingdom Prospective Diabetes Study (UKPDS).
Although the UKPDS metformin arm showed only a 0.6% decrease in blood sugar problems [HbA1c] compared to the control group, there was a 32% reduction in diabetes-related complications. These and many other scientific results repeatedly show the evidence to controlling diabetes is daily exercise and AquaDios-Med™ programs have established the safest daily exercise to be structured deep-water running.
The Finnish Diabetes Prevention Study Group conducted a randomized, controlled trial of 522 subjects with IGT followed for an average of 3.2 years, and showed a 58% reduction in the incidence of type 2 Diabetes using a diet with 30% total fat, 10% saturated fat, and 15 grams of fiber per 1000 kcal, plus 30 minutes of daily physical activity to increase muscle strength and aerobic fitness. These results were consistent with those of the Diabetes Prevention Group, which followed patients without diabetes with IGT for an average of 2.8 years in a randomized, controlled trial showing a 58% reduction in type 2 Diabetes with lifestyle intervention, including a minimum of 7% weight loss and 150 minutes of weekly physical activity, versus a 31% reduction using metformin compared to the control group. What do you think the results would be with daily AquaDios-Med™ programs with the safest daily exercise of structured deep-water running?

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
85
For 8 years the National Health Interview Survey followed 2,896 participants with diabetes that demonstrated a 34% lower cardiovascular mortality rate with just 2 hours of weekly walking. The group was controlled for gender, age, race, body-mass index, smoking and comorbid conditions. Can you imagine the improvements if the group participated in daily safe exercise with AquaDios-Med™ proactive preventive medicine?
A Nurses Health Study subgroup of 6,547 women with type 2 diabetes followed for 20 years showed a 7.7 times greater risk for developing CAD among women with diabetes who smoked 15 or more cigarettes daily than women without diabetes who never smoked, and the relative risk for CAD among diabetic women 10 years after smoking cessation was comparable to women with diabetes who had never smoked. Obviously smoking is a killer.
The Japan Diabetes Complications Study of 2,205 subjects with established type 2 diabetes
examined the effects of comprehensive lifestyle intervention on the long-term macrovascular and microvascular disease complications. During the initial 3 years, the intervention group showed small but significantly increased glycemic control.
Dr. Surwit and investigators also demonstrated small but significant glycemic control
improvements in the first randomized study using a simple, cost-effective group stress management program in 108 subjects with type 2 diabetes over 1 year.
There just are no studies of a proactive preventative medicine program such as the process of
AquaDios-Med™ and what it has to offer, so it is not surprising the results demonstrating improved health are minimal at best.
Because Diabetes is an independent predictor of using complementary and alternative medicine such as meditation and lifestyle diets such as those designed by Pritikin and Ornish, what is the efficacy of the broad range of these treatments? And, what if the AquaDios-Med™ preventive medicine programs, which are far more complete that those mentioned above, were instituted as the treatment of choice for diabetic related syndromes to improve glycemic control for various target subgroups and levels of stress? Research has established that people with diabetes are simply less responsive to common medical treatments which have been effective in managing cardiovascular disease in the general population, so why not get them on a comprehensive AquaDios-Med™ program?
And diabetics in general are resistant to lifestyle intervention so it is difficult to address the cardiovascular morbidity and mortality seen in people with type 2 diabetes unless they are involved with a daily AquaDios-Med™ program which can include biofeedback assisted relaxation training in reversing the accelerated atherosclerosis seen in people with type 2 diabetes. It is obvious that brief, customized, practical, self-management interventions for improving compliance and sustaining lifestyle changes just does not work.
Preventive Medicine For Coronary Artery Disease CAD
In 1999, heart disease, the foremost cause of U.S. mortality, 20 affected 21.5 million or 11.0%
of the U.S. population, including 10.7 million or 5.4% of the U.S. population with Coronary Artery Disease - CAD. Thus, to be truly effective health practices must promote preventive medicine behaviors to support CAD healing, risk factor reduction, reversal or prevention of atherosclerotic stenosis progression and or decreased morbidity and mortality through safe daily exercise as is offered in AquaDios-Med™; a nationalized AquaDios-Med™ program will have the potential to significantly impact this major public health burden and simply eliminate more than 90 percent of the suffering and deaths it causes.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
86
Dr. O’Donnell reports there is rigorous evidence to support the effectiveness of health promotion behaviors in healing CAD, including clinical trials examining the effects of comprehensive lifestyle change on CAD and those demonstrated by Dr. Ornish and colleagues, whose work demonstrates the possibilities, though not necessarily the practicality, for CAD reversal using comprehensive lifestyle changes. When Ornish and colleagues studied intervention and control patients with ischemic heart disease in a randomized, controlled trial using stress management and a vegan diet for 24 days, they found a 21% mean plasma cholesterol decrease, a 44% mean exercise capacity increase and a 91% mean decrease in the frequency of anginal episodes.
The Ornish study was the first to successfully demonstrate atherosclerotic constrictions in free-
living, highly motivated CAD patients over 1 year using comprehensive lifestyle modifications, including low-fat vegetarian diet, smoking cessation, stress management, and moderate physical activity. The “study” group atherosclerotic constrictions decreased substantially, [vessels less clogged] while the control group lesions enlarged or worsened. Lipid-lowering drugs were not used, and 82% of the intervention group showed an average positive health change. Further, a 5-year follow-up showed continuing significant differences between the study group improvement and control group. Keep in mind, this group participated in only “mild exercise”, not safe daily intense exercise as is a part of AquaDios-Med™.
Dr. Manchanda and colleagues demonstrated significant atherosclerotic improvement with prevention of increased artery blockage in a small, study group of 42 male participants using a comprehensive yoga diet, physical activity, and stress management intervention over 1 year without lipid-lowering drugs.
The severity of disease was greater in this study than the Lifestyle Heart Trial because 81% of the participants had triple vessel disease. Participants were asked to pursue a diet with low cholesterol per day and few calories from fats versus the Lifestyle Heart Trial’s 5 mg cholesterol per day and 10% of calories from fats. This group suffered significantly fewer cardiac events such as revascularization procedures in the intervention versus the control group, a finding Ornish and colleagues also reported during their five year follow-up, but no data were available for the 1-year Lifestyle Heart Trial.
Dr. Wallner and colleagues recruited 60
patients after successful percutaneous transluminal coronary angioplasty (PTCA); this is a type of balloon angioplasty in which the catheter is inserted through the skin and through the lumen of the vessel to the site of the narrowing See Graph >>>
The expanded balloon presses against a “narrowed” site in an artery
Dr. Wallner and colleagues set out to test the effect of comprehensive lifestyle changes,
including American Heart Association (AHA) step II diet, physical activity and smoking cessation, on the rate of clinical restenosis or narrowing of the artery and necessity for revascularization or restoring the vessels procedures.
This study cannot claim the prevention of blocked arteries through comprehensive lifestyle intervention at the end of the one year trial because repeat angiography [pictures of the vessels] was not performed, but there was an overall 74% reduction in such vascular procedures through comprehensive lifestyle modification. Thus, once again modification of life style is again the primary “healer” whereas the AquaDios-Med™ “Exercise is Medicine” through daily safe exercise was not employed.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
87
Dr. Singh and associates conducted a study of 406 patients with suspected myocardial infarction [heart attack] that demonstrated a significantly lower occurrence of cardiac events and all-cause mortality over 1 year when a low-fat, high-fiber diet with abundant fruits and vegetables was started within 72 hours after acute myocardial infarction (AMI).
Dr. Hambrecht and colleagues in a study of 62 male patients, with stable angina, who altered
their diet to an average of 2200 kcal per week over 1 year showed significant artery improvements without lipid lowering drugs.
Dr. Diehl performed a study with 304 free-living participants with CAD enrolled in the initial Coronary Health Improvement Project (CHIP), and found significant coronary risk factor improvements, over one month, in total cholesterol, LDL cholesterol, high density lipoprotein (HDL) cholesterol, blood pressure, weight, and body mass index.
Dr. O’Donnell documents patients have demonstrated startling success in studies using only a
low-cost 40-hour hospital-based educational program to improve dietary habits, physical activity, smoking cessation, and stress management in combination with 30 minutes of daily walking and adherence to the Optimal Diet focusing on complex carbohydrates.
It is obvious that coronary artery disease can be all but eliminated through moderate nutritional
food intake together with a comprehensive preventive medicine program offering daily safe exercise program as in AquaDios-Med™. There is sufficient evidence today that physical activity has independent positive effects on coronary artery disease and atherosclerotic stenosis and it is believed that preventive medicine programs like AquaDios-Med™ , will significantly decrease the risk coronary artery disease and extend the lives of patients with CAD.
Preventive Medicine for Breast Cancer
Dr. O’Donnell reports that in 1999 malignant neoplasms – Cancer accounted for 13 million
U.S. deaths and was the second leading cause of death or 6.5% of the U.S. population. This includes 2.2 million or 1.1% of all women who are diagnosed with breast cancer, which is the second leading cause of cancer deaths among women after lung cancer. Thus, preventive medicine health promotion behaviors that support self-healing among cancer patients and cancer survivors have unique opportunities to influence an important burden of illness through impacting the lives of individuals who are often highly motivated to make lifestyle changes.
Dr. O’Donnell reports there is considerable research data on lifestyle change and cancer,
including studies on primary prevention and survival, and many of the few studies on the effects of lifestyle change on cancer survival have focused on breast cancer.
Studies support an association between body weight and breast cancer prognosis. When Rock
and Demark-Wahnefried reviewed 40 published epidemiologic studies, they found moderate evidence that obesity at the time of diagnosis is associated with recurrent breast cancer and or decreased survival. The studies supporting this association indicated that the risk of death increased by 30% to 40% for higher levels of obesity, and that the effect may be magnified in patients first diagnosed with early stage breast cancer and women with estrogen receptor-positive disease.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
88
When Dr. Tretli and colleagues followed 8,427 breast-cancer survivors from the Cancer Registry of Norway for over 4 years, they found a 1.7 relative risk of all-cause death for stage I and 1.4 for stage II disease in both premenopausal and postmenopausal women in the highest quintile versus the lowest quintile of body mass. No similar associations were seen for stage III and IV participants.
Some studies suggest that post diagnostic weight gain is associated with poorer patient
outcomes. In an exploratory study of weight change over 60 weeks of chemotherapy, Dr. Camoriano and associates monitored post-treatment weight changes in 646 node-positive breast-cancer survivors over a median of 6.6 years. They found that premenopausal women who gained more than the treatment median of 5.9 kg during follow - up had a one and one half relative risk of recurrent disease and 1.6 relative risk of breast-cancer death.
Nutrition studies have focused on investigating the relationships between nutritional factors and breast-cancer recurrence and survival. Although cancer survivors have used many types of diets, such as the macrobiotic diet, scientific evidence is lacking on the effectiveness of these diets in extending survival in cancer patients. However, controversial evidence using self-reported intakes suggests that post diagnostic dietary fat, unadjusted for energy intake in many studies, may be associated with recurrence or decreased survival in breast-cancer patients.
When Dr. Rohan and investigators followed 412 breast-cancer survivors from the South Australian Central Cancer Registry for almost 6 years, they found a 1.4 relative risk of breast-cancer death for those in the highest quintile compared to the lowest quintile of fat intake after energy intake adjustment. In contrast, Dr. Holmes and associates found no survival differences for post diagnostic low-fat intake after energy intake adjustment during the average 13-year follow-up of 1,982 breast-cancer survivors from the Nurses’ Health Study.
In addition, although the evidence is variable, some studies suggest that vegetable-related intake may have a modest protective effect in breast-cancer survivors. In the study noted above by Dr. Rohan the investigators also found a 0.78 relative risk of death for b-carotene and corresponding 0.76 for vitamin C among those in the highest quintile of beta-carotene and vitamin C intakes.
A second category of experimental studies investigates the effects of physical activity and stress
reduction on quality of life for breast-cancer survivors. According to a research review by Dr’s Courneya and Friedenreich, preliminary evidence from studies shows that physical activity may improve functional quality of life in breast-cancer survivors. In the 14 studies reviewed, physical activity to increase cardiovascular and or muscle strength showed overall beneficial effects on quality of life indicators, including improvements in cardiovascular function, pulmonary capacity, muscular strength, loss of lean muscle mass, nausea, fatigue and sleep problems.
In one of the larger physical activity intervention studies to date, Dr. Mock and investigators
randomly assigned stage I and II university hospital patients with breast cancer using a two-group pretest and post-test design. They found improved functional capacity and diminished fatigue, anxiety, and sleep problems compared to the usual care control group using a home-based, self-paced walking program for 20 to 30 minutes 4 to 5 times weekly over 6 weeks of radiation therapy.
A limited number of stress reduction interventions have also demonstrated improved quality of
life in patients with breast cancer. When Dr. Carlson and associates studied 49 patients with breast cancer through pre-intervention and post intervention assessments using an 8-week mindfulness-based stress reduction (MBSR) program including relaxation, meditation, gentle yoga, and daily home practice, they found significant improvements in quality of life, stress symptoms, and sleep quality, as measured by the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire, the Symptoms of Stress Inventory and a Health Behaviors Form.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
89
An internet support group entitled Bosom Buddies has also been moderately effective in decreasing depression, perceived stress and cancer-related trauma as demonstrated by Dr. Winzelberg and colleagues in a randomized, clinical trial of 72 breast-cancer survivors over 12 weeks.
There are two noteworthy studies currently in progress that examine the effects of nutrition on
breast-cancer recurrence and survival. The Women’s Intervention Nutrition Study (WINS) began in 1987 and includes 2,500 postmenopausal stage I and II breast-cancer survivors with resected disease who are testing the effect of a 15% or less dietary fat intake on breast-cancer recurrence and survival over a mean of at least 6 years of follow-up. The basis for conducting WINS comes both from laboratory data suggesting that dietary fat promotes breast-cancer progression and cross-cultural data indicating an association between levels of fat intake and breast-cancer survival.
The Women’s Healthy Eating and Living (WHEL) Study began in 1995 and tests the effect of a
plant-based, high-fiber, low-fat diet on recurrence and survival over a mean of 6 years for 3,100 breast-cancer survivors diagnosed with stages I, II and IIIA within 4 years prior to study entry and previously treated with conventional therapy. The WHEL intervention diet provides 2 to 3 fruits per day, 3to 5 vegetables per day with 16 ounces of vegetable juice per day, 30 g of dietary fiber and 15% to 20% of daily energy from fat.
Dr. O’Donnell research concludes that Lifestyle is the primary contributor to the six leading
causes of death in the United States: heart disease, cancer, stroke, respiratory diseases, accidents and diabetes collectively account for almost 72% of all deaths, and is a secondary factor for seven of the next nine causes, e.g. Alzheimer’s disease, kidney diseases, suicide, liver disease, essential hypertension, and assaults, which account for an additional 9% of deaths.
Dr. O’Donnell states that Health-promotion interventions might include any of the dimensions
of optimal health including preventive medicine safe daily physical exercise, nutrition, weight control, smoking cessation, emotional (including stress management), social (including building social support and relationship training), spiritual, or intellectual interventions.
Dr. O’Donnell believes that for many diseases lifestyle interventions can and do impact the
positive changes in the progression of the deadly disease, especially safe daily exercise and healthy nutritious foods.
The missing link in American Health Care is AquaDios-Med™ and its regime of mind body
medicine combined with safe daily structured deep-water running.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
90
AquaDios-Med™ Multiple Immersion Chambers AquaDios-Med™ Main Exercise Chamber - Deep Strider Chamber and Lounge Spa Chamber
The Deep Strider Chamber was designed to accommodate severely handicapped patients whether it is due to accident, injury, diabetes, arthritis, obesity, age, or any disabling cause while it is also used for physical fitness and deep water running training for the athlete.
AquaDios-Med™ Deep Strider Chamber
Multiple Proprietary safety handles ergonomic sitting and standing positions
AquaDios-Med™ Deep Strider Chamber
Deep Strider Chamber was designed to accommodate those incapable of using their body for exercise whether due to accident, injury or disability or disease.
Power jets at bottom

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
91
AquaDios-Med™ Deep Strider Chamber two large power jets very bottom pointing in an
upward direction. These jets assist the physically incapacitated or disabled to obtain the benefits of deep water movement and undulation.
Please note “power jets” at bottom
^^ ^^

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section IV
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research Placebo Effect • Guided Placebo
Maximizing Immune System Without Pharmaceuticals Symptom Management • Control • Remission
Preventive Medicine
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
24 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ • [email protected] diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Placebo Research History • Consolidated Solution • Healthcare Crisis • Introduction • Summary • Part IV
Research on the placebo effect has tremendous impact on patient healing as it attempts to
identify the importance of subject-expectancy effects or the effect that occurs when a patient's symptoms are altered - alleviated by a non-treatment; the positive result or placebo effect is due to only the individuals expectation or belief that it will work; an uninhibited maximized immune system.
The placebo effect occurs when a patient takes an inert substance (sometimes called a "sugar
pill") in conjunction with the suggestion from an authority figure or from acquired information that the pill will aid in healing and the patient’s condition improves. This effect has been known since the early 20th century and is a valuable tool in learning more about the natural capacity of all patients healing, especially as it applies to preventive medicine.
Science is often unwilling to give credit to the person who believes they will heal and they do,
by maximizing their immune system without pharmaceuticals. Some research experts suggest that placebo research can determine what is valuable in empirical based medical evidence that emphasizes a therapeutic meaning response to medical procedures. The objective review of the importance of these effects could change how medicine is practiced bringing greater importance to preventive medicine procedures such as Mind Body Medicine and the universal expansion of patient healing capacities.
Placebo research is opening the door to patient healing and the self-healing capacities of the person, a fact normally neglected by research. The objective of preventive medicine is to maximize healing by harnessing these factors in any therapeutic context. The real issue is that every patient has power over their psychologic processes and social contexts that can facilitate hope, expectation, belief, positive feelings, relief of anxiety, anticipation of improvement and complete healing; each patient is able to truly affect physiologic processes, and contribute to healing without pharmacologically mediated processes.
The placebo effect is also part of the human potential to react positively to a healer. A patient's
distress may be relieved by something for which there is no medical basis. A Band-Aid put on a child can make the child feel better by its soothing effect, though there is no medical reason it should make the child feel better.
Placebos have measurable physiological effects, when subjects are told they have taken a
stimulant they can speed up pulse rate, increase blood pressure, and improve reaction speeds. Placebos have the opposite physiological effects when participants are told they have taken a sleep-producing drug.
This healing response arises from the interaction between the external environment and the internal conditions of each individual, their history, social circumstances, individual predilections, expectations and belief to heal and be well. These facts bring into focus the importance of individuality in medicine and therapy. And, it makes plausible why one and the same situation, for instance surgery, may arouse hope in one patient and induce fright in another with completely different physiologic reactions and clinical outcomes.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
The scientific study of the placebo effect is dated to the pioneering paper published in 1955, The Powerful Placebo by anesthesiologist Henry K. Beecher. Research on the Placebo Effect shows that expectation; belief, faith, hope, prestige, imagination, response expectancies and suggestibility are all important variables. A reference to the Talmud of rabbinical thought says … Where there is hope, there is life. And hope is positive expectation …
Placebo effect is a medical science term applied to the therapeutic and healing effects of inert,
non-drug, medicines and may be combined with ritualistic or faith healing practices as well as medical hypnosis or Mind Body Medicine; positive suggestion can be combined to create a powerful patient healing expectation and belief.
Placebo research is providing critical information for how the mind-body heals for developing
a science of healing and is expanding awareness of the importance of Mind Body Medicine healing practices in all medical interventions. These facts have long been known by preventive medicine programs like AquaDios-Med™.
Placebo research indicates that in general, people have previously been conditioned to accept,
at face value, the statements of an authority, one with prestige, a doctor or nurse in medicine; their statements, commands or suggestions of a person are said to cause greater expectations and tend to be questioned less while producing more positive results. Research shows that suggestions – statements given by a doctor or person of authority works in the same way as hypnotic suggestion, because most all patients are in a heightened state of belief.
Research shows that religious faith increases belief and that the Power of Religious faith
increases the development of belief. Foundations of belief can be traced to the fulfillment of religious predictions, expectations or prophecies such as fulfillment of religious prophecies, miracles produced through the powers of the religion’s prophet; positive responses to prayers to God; and positive occurrences in one’s life resulting from following the religion’s guidelines.
Research has repeatedly shown that Cleary the immune system communicates with the
neuroendocrine system and that imbalances in the neuroendocrine–immune circuitry are relevant to patient defenses. This knowledge is the basis of the scientific evidence based discipline of psychoneuroimmunology.
Also, when a patient is given a substance or treatment aimed at healing, the prescribing of the
medicine by doctor – nurse, in itself, is a powerful healing contributor, with both verbally and non-verbally essentially saying, you will be healed. This scenario dramatically raises the probability of a powerful cognitive stimulus healing that is triggered together with its attendant immune associated response (e.g. release of t-cells, macrophages, etc.); as well as the inhibitory set that eliminates any doubt about the treatment’s effectiveness.
The Ader research links directly to the Unified Placebo Theory. Ader demonstrates the placebo
need not be words dependent on suggestions and cognitions as you can see by the Ader research where the placebo, or the nocebo was sweet water, therefore almost any sensory stimulus such as sound, smell, taste, visual experience, pressure, imagination, belief, faith, suggestion etc. can produce, enhance the placebo effect.
Exercise is a weapon against disease
There is nothing as deceptive as an obvious fact

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
Research shows the healing powers in the placebo effect can be like taking a powerful magic pill that is effective as much as 68% of the time. The healing cannot be from the fake inert pill because it has no ingredient to heal at all. The pill becomes metaphoric, symbolic of potent aggressive curative capacities. And, each time it is taken this healing power is released, not by the pill, but by the patient’s uninhibited maximized immune system.
Research shows that for a placebo to have the power to heal as described above it must be
presented to the patient by an esteemed doctor or known healer, with noble bed side manner who also develops a relationship of trust, confidence and positive expectation in that patient. This revered person, with specific language of suggestion talks to the patient about the healing power within the pill, building faith and belief in the patient about the fake medication. It is this faith and belief that is identified in hypnotic healing, but in this instance with a fake pill; considered positive bedside manner.
Research shows through the ages the main weapon to use against disease by doctors is the
Placebo because the placebo effect is present in all treatments. Placebo, another name for suggestion, expectation, faith, belief, goes unrealized by most doctors, though present whenever any treatment is prescribed. With any treatment and proper bed-side-manner, the doctor is saying … this will help you get or feel better – this form of suggestion is one of his most potent tools in medicine and healing. The physician carries a tremendous amount of prestige in the eyes of most all patients and his presence or image can take on hypnotic-like qualities and guided healing suggestions can be especially powerful and helpful when used correctly.
Direct evidence placebos produce real physiological responses was reported by a team of
researchers at UC San Francisco medical school by Levine in 1978. The study showed that placebos given for pain relief produced a release of natural painkilling compounds in the brain called endorphins which are chemically similar to morphine.
Research verifies when a doctor gives a patient an injection to kill the pain; the suggestion is …
this is going to ease your pain. Research shows the actual pain relief occurs even when the injection is an inert saline solution because of two factors associated with suggestion -- the cognitive stimulus pain relief, with its associated endorphin -- the body’s natural pain killing substance is released into the bloodstream automatically. And, the inhibitory set of the suggestion is evoked that would inhibit anything that might interfere with the cognitive stimulus, such as any doubts about the doctor’s skills, or doubts about the pain killer’s effectiveness, or even the sensory pain stimulus itself.
Nocebo can be negative suggestions or doubts like a doctor who felt it was his duty to be open
with his patients and telling them they had cancer … you will die but perhaps the chemotherapy will extend your life somewhat … this powerful negative suggestions may be why all this doctors patients die; the equivalent of iatrogenic disease medicine. In 1960 Pavlov said … Speech, on account of the whole preceding life of the adult, is connected up with all the internal and external stimuli which can reach the cortex, signaling all of them and replacing all of them, and therefore can call forth all those reactions of the organism which are normally determined by the actual stimuli themselves.
Mind Body Medicine - Preventive Medicine methods for therapeutic cancer treatment have
always been present such as cancer treatments; Hoxey's Treatment, Laetrile and Krebiozen. Unfortunately the medical profession has labeled non-traditional approaches as quackery and dismissed the often very real cures as cases of spontaneous remission or mis-diagnosis.
Exercise is a weapon against disease Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
The expectation, the belief, the hope of being cured could very well have momentarily revitalized the body's own natural defenses against cancer. In 1957 Klopfer cited a captivating case of such a placebo effect in action and cited by Achterberg, 1976; the miracle cure was Krebiozen:
… This patient with far advanced lymphosarcoma begged to be entered into a study of
Krebiozen - a drug claimed to have cancer curative properties. Upon the initial administration of Krebiozen, his tumor masses 'melted like snowballs on a hot stove' and having previously required an oxygen mask to breathe, he became fully active and flew his plane at 12,000 feet with no discomfort. When clinical reports appeared announcing the ineffectiveness of the drug, he returned to his bedridden state. His physician then, in a last attempt to offer him life, told him that the preparation deteriorated upon standing and that it would be given to him at a double strength. Actually the injection was water. The man again evidenced rapid disease remission, until it was announced to the press that the AMA and FDA had found Krebiozen to be a worthless preparation. He died within a few days...
Long ago the placebo was the main tool of the physician, going back to the shamans and witch
doctors. The modern importance of the placebo has been recognized and documented by numerous researchers. Shapiro (1959), Whitehorn (1958) and Benson (1975), among others, all are persuaded that the placebo effect is still the principal factor in the success of modern medicine. And according to Beecher (1961) this includes surgery. Moseley, J.B., et.al. (2002) found that placebo (sham) knee surgery for alleviating the pain of osteoarthritis was just as effective as the regular surgery.
Barrios, says … when it comes to cancer many of the standard treatments of today – radiation,
a burning, surgery a cutting, and chemotherapy a poisoning -- will someday be looked upon the same way as the bleeding and leeching treatments of yesteryear…
In 1997 Block cited the U. S. Office of Technology Assessment … only 10 to 20 percent of
mainstream medicine procedures for cancer have been shown to be successful by controlled trials. Research seems to confirm that a major, if not the main, reason for the success of many conventional Western medical treatments is the placebo or faith factor. With its profit-centered approach it is unlikely the medical profession will investigate the possibilities of maximizing the placebo factor especially in combination with the appropriate positive life style changes needed to insure a long term cure - and this of course is what the ADM™ PPM program for health is all about.
Placebo researchers Wickramasekera, 1980, Knowles, 1963, Hernstein, 1962, Gliedman, 1957,
all agree that the conditioning explanation is what is behind the placebo response; it is from a form of first-order classical conditioning ... when a person or animal is injected a number of different times with a pain killing medication, the stimuli associated with the injection - the syringe, the person giving the injection, etc. -- are the conditioned stimuli -- the CS. Pain relief -- the UCR produced by the actual pain killer -- morphine -- the UCS, becomes associated with the CS such that the CS can eventually produce a conditioned response -- CR -- pain relief. This CR illustration helps to explain the placebo response – in this case produced through first order conditioning.
A 1995 extinction trials study by Montgomery and reported by Kirsch, 1997found that instead
of extinguishing the placebo effect it [extinction trials] the placebo effect actually increased over the course of 10 extinction trials. This is inconsistent with classical conditioning, models of placebo effects, but is consistent with clinical data indicating that placebo effects can be remarkably persistent.
Exercise is a weapon against disease There is nothing as deceptive as an obvious fact

5 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
In 1985 Barrios cites Timeless Healing: The Power and Biology of Belief, 1996 by Herbert Benson, and a section on placebos in Cousins’ book Head First, 1989)… Although strong belief of being healed can be very effective in producing at least temporary improvement in one’s health, by allowing for a stronger immune response and creating greater peace of mind at least for the moment, in order for this improvement to remain permanent, the belief factor must also be used to help fully absorb the guidance factor … making post hypnotic suggestion more effective by adding a guidance factor so that the immuno-suppressive psychological factors can be more likely to be permanently removed … one way of differentiating between the concept of belief and the concept of faith is to point out that faith … needs the addition of a guided belief or belief in a certain way of life…
Research supports the need for guided placebo, and though it may be of interest, it is not important to determine the effective difference between faith and belief alone in affecting permanent healing. The placebo literature, the positive effects of the placebo can be long lasting with guided placebo and continued follow-up treatment such as AquaDios-Med™ Proactive Preventive Medcine when lifestyle changes may take place.
For decades placebo research pondered how an inert or a non-medicine can produce remarkable
healing in many patients. Long term research of the Placebo Effect reveals a simple scientific definition -- a process that maximizes the human immune system allowing it to become unencumbered to perform the natural healing available in most all people. This natural and powerful healing is not considered or utilized in modern medicine practices nor do hospitals develop methods to manifest this powerful natural healing – Why -- because there is way less profit. Research shows Mind Body Medicine combined with multiple immersions with structured deep-water running can maximize most people’s immune system to reverse disease and need for surgery70 to 80 percent of the time.
The AquaDios-Med™ Philosophy
• EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING! • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race.
Copyright © 2008 – 2012 – 2013 2nd Edition
AquaDios-Med™ • AquaDios Corp. All rights reserved.
Respectfully,
Dr. Alan Jensen (Alan) Founder • CEO • Creator, AquaDios-Med™ http://www.aquadios.com/
A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing Phone 310-897-5055 - Email: [email protected] - P.O. Box 2228 Malibu, Ca. 90265
The true sign of intelligence is not knowledge but imagination - Albert Einstein
Exercise is a weapon against disease

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Placebo Research • Consolidated • Problem Solution • Healthcare Crisis • Part IV • Placebo • 18 Pages
Power of the Guided Placebo
Research confirms the Guided Placebo Effect that maximizes natural human healing and pain
relief capacities is Robust with a 70% positive effect for healing – pain relief; this is based on suitable guided administration -- induction – suggestion by a doctor – nurse at time of administrating the placebo. This is possible because the immune system communicates with the neuro-endocrine system and imbalances in the neuroendocrine–immune circuitry are relevant to patient defenses.
Moguls in the field of medicine say placebo … can bring the old and forgotten power of proper
bedside manner back into modern hospital medicine practices and Evidence Based Medicine. Placebo theorems link Psychoneuroimmunology PNI – Mind Body Medicine MBM to the research of Dr. Ader. The placebo - nocebo, effect of Ader’s sweet water and immune response is broadly examined as a basis for power of the placebo; although almost all environmental stimuli can contribute to or become the causality of either.
Placebo research shows that every attempt at a medical treatment is given within a context of a
doctor - patient interaction. The classic placebo effect concept is that patients should feel better after receiving the placebo – pill, injection or salve. Research also shows many factors can contribute to the perceptions of the placebo response such as verbal context, visual perspective, olfactory, tactile and auditory stimulation, nearly anything and everything can lead to patient interpretation or misinterpretation that a medical treatment is being performed.
The presence of a physician - nurse -- with a syringe, pills or salve automatically triggers, in
most patients, a non-verbal suggestion -- this will relieve pain. When doctor or nurse simultaneously give verbal suggestion … this will relieve your pain … the verbal context, visual, olfactory, tactile and auditory stimulation, especially the perceptible sensation taking a pill or of the needle entering the skin -- no matter if the substance is just an inert saline solution or a real drug, there is a better than 70% placebo effect to enhance complete rapid pain relief or healing.
Research indicates the guided placebo effect is equivalent to a hypnotic product -- the presence
of physicians, therapists, their prestige -- strong authority positions – can automatically arouse a state of heightened belief, faith and expectation for healing – pain relief. The Scientific Evidence is based on components associated with this Guided Placebo Delivery:
Cognitive stimulus aroused by the visual presence of the doctor – nurse with pill or syringe; Verbal suggestion stimulates the cognitive stimulus -- pain relief; The stimuli evoke automatic release of endorphins -- endogenous opioids into the bloodstream; This triggers the inhibitory set to eliminate any doubt about the doctor's skills or effectiveness
of the painkiller substance; Exercise Is Preventive Medicine

2 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Stimuli includes verbal context -- belief, faith, expectation -- olfactory, tactile perceptible and auditory stimulation, especially sensation – process of taking and swallowing the pill or of the needle entering the skin contribute to the Placebo Production – pain relief -- you will be healed.
The word or healing suggestion comes to be associated with the immune response and both
events occur as a result of the process of higher-order conditioning. In 1927 Pavlov said … words - speech and thoughts -- inner speech can affect physiology of the human body … in 1928 the Thomas Theorem, formulated as a fundamental Law of Sociology stated … if men define situations as real, they are real in their consequences.
How we define something depends on current knowledge, common sense, beliefs, values, and
also on scientific evidence. We ourselves can make those stimuli perceptions become very real, very powerful, to become a magic reality. Such a reality can be achieved through the heightened state of belief which is defined as a state of mind, in the placebo process, often evoked by words, whereby there is concentration on a thought. Guided Placebo utilizes verified theoretical constructs and research studies to show how important this is in the delivery of medical healthcare services.
This placebo knowledge is the basis of the scientific evidence based discipline of Inner Mental
Training, a psychoneuroimmunology process. AquaDios-Med™ process is evidence based with Emphasis of this never ending mind – body interaction -- we humans do influence our minds and bodies in positive and negative ways. The objective is to eliminate or decrease negative or dis – ease and increase the positive to ease or wellness – balance – well-being – healthy homeostatic equilibrium.
The American Hospital Association AHA confirms healthcare costs were about $1.5 Trillion
for the year 2011, with the addition of Guided Placebo it is possible to extrapolate gross savings of about $ 750 Billion from positive placebo effects; even if it cost $250 Billion to administer Guided Placebo three is still nearly $500 billion in healthcare savings. An even greater savings is possible when Evidence Based AquaDios-Med™ practices are factored into the hospital healthcare equation with its Psychoneuroimmunology and Mind Body Medicine practices to facilitate and sustain physiological self-regulation and its Deep-Water Running Therapy together with Guided Placebo about $ 1 Trillion can be saved; even with the added expense of $250 Billion for the ADM™ PPM – Guided Placebo there remains a savings of $ 750 Billion.
Ground Breaking Placebo Research – 2012 Unified Placebo Theory [UPT]
Pgs. 1,3-6,10,20,30,36,49-51,92,101,106,108,115-124 A 2012 placebo research titled - Everything out of Nothing or Anything You Want - The
(R)evolution (With)in the (R)evolution: The Unified Placebo Theory (UPT) BY Dr. Rado Gorjup and Dr. Alfred Angel Barrios, has for the first time, with elegant clarity, succinctly identified the, how, why and power of the placebo effect with proven theoretical constructs and research studies. The Unified Placebo Theory (UPT) is a complete, accurate scientific and medico cultural view – definition – of the placebo process to date.
The Unified Placebo Theory -- UPT is consistent with the most scientific view of Placebo, the
language used is essential to adequately explain the how, why, power and the reason Placebo is not more widely used and respected in modern hospital medicine. Robust placebo studies, utilizing a similar approach indicate a 70% healing value of placebo; the 70% positive effect – healing is based on suitable administration or the induction – suggestion at the time of giving the placebo. This Guided Placebo concept is explained in Unified Placebo Theory – UPT below.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
The Unified Placebo Theory with a goal of enlightening acceptance in the field of Evidence Based Medicine is certainly an essential step toward a better understanding of humane medical treatment. Experts in the field of medical hypnosis might say UPT can bring bed side manner back into medicine and can return the power of proper bed side manner in hospital medicine practices.
Certainly any genuine application of Unified Placebo Theory, honestly accepted and applied in
the field of Evidence Based Medicine would make a dramatic difference in healthcare; possibly leading to the empowerment of the old and forgotten empathetic and compassionate patient-centered methods surging back into medicine.
Most studies rely on positive context to produce a reduction of symptoms (placebo effect) and
negative context to reverse the result (nocebo effect). In 2002 research looked to better explain, clarify and bring insight to the placebo mystery phenomena. This research focused on how the patient internalized meaning that interacts with both illness and healing to better understand the positive or negative impact on physiological or psychological effects of treatment towards getting a human well or ill again.
In his book, The Powerful Placebo Shapiro points out ... If the non-specificity of the placebo effect can be rendered specific and its strength can be unleashed, the terms placebo and placebo effect can appropriately disappear into medical history.... Variables impacting the placebo response are vast because everything within the body – mind and mind - body inter-communicates with everything else in the healing environment. The generally accepted medical equation implies that both specific and nonspecific factors are essential components for the patient to get well or ill again.
For positive placebo effect UPT places great importance on acknowledgement of how the
individual patient is a unique entity independent from the symptoms, disease or illness that may or may not be the same for numbers of patients; and recognizes this viewpoint may be a clear distinction from the classical medical paradigm; an abscence of the power within the positive, empathic bedsie manner.
The UPT theorum is an ecclectic scientific consolodiation of proven reserch principles and studies some explaining the placebo effect as the hypnotic effect of physicians and therapists due to their prestige and strong authority positions, a state of heightened belief as well as differentiation between the mind – body and the body – mind, the conditioning and the expectancy theory, psychobiological explanatory gap together with modern hypnosis theroy and much more.
UPT discusses a common medical procedure or discussion can carry with it a complexity of
meaning such as merely giving an injection for pain relief. Just the presence of the physician - nurse automatically triggers in the patient a suggestion like this will relieve your pain, should the doctor or nurse simultaneously give the verbal suggestion, this will relieve your pain, the verbal context, olfactory, tactile perceptible and auditory stimulation, especially the perceptible sensation of the needle entering the skin, no matter if the substance is just an inert saline solution or a real drug has a better than 70% placebo effect to enhance the chance of complete rapid pain relief.
Also, when a patient is given a substance or treatment aimed at healing, the prescribing of the
medicine by doctor – nurse, in itself, is a powerful healing contributor, with both verbally and non-verbally essentially saying, you will be healed. This scenario dramatically raises the probability of a powerful cognitive stimulus healing that is triggered together with its attendant immune associated response (e.g. release of t-cells, macrophages, etc.); as well as the inhibitory set that eliminates any doubt about the treatment’s effectiveness.
There is nothing as deceptive as an obvious fact

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
Similarly UPT explains how the words and thoughts pain relief come to be associated with endorphin secretion. And how the word or thought healing comes to be associated with the immune response and both events occur as a result of the process of higher-order conditioning. Obviously, for man, speech provides conditioned stimuli which are just as real as any other stimuli… Speech, on account of the whole preceding life of the adult, is connected up with all the internal and external stimuli which can reach the cortex, signaling all of them and replacing all of them, and therefore it can call forth all the reactions of the organism which are normally determined by the actual stimuli themselves; healing. The science of compassionate care in every treatment is critical as is the Guided Placebo because of the subjective nature and interpretation response is much more powerful and long lasting than placebo alone.
The Ader research links directly to the Unified Placebo Theory. Ader demonstrates the placebo
need not be words dependent on suggestions and cognitions as you can see by the Ader research where the placebo, or the nocebo was sweet water, therefore almost any sensory stimulus such as sound, smell, taste, visual experience, pressure, imagination, belief, faith, suggestion etc. can produce, enhance the placebo effect. Some researchers say the placebo effect is the same as hypnotic suggestion when Hypnotic Induction is defined as the giving of two or more suggestions in succession, so that a positive response to one increases the probability of responding to the next one.
In simple language a positive placebo result is dependent on a respected doctor that
communicates the aura, language and behavior of compassionate care who can guide the patient with suggestions specific to the power of the medicine that are internalized by the patient; this process is foreign to the practice of today’s modern medicine, but common in the field of medical hypnosis, Psychoneuroimmunology, Mind Body Medicine and possibly the returning medicine to patient-centered practice.
Consider this paradox: with the pharmaceutical companies bribery of FDA official, doctors,
hospitals, society in it’s never ending advertising - media blasts of its drugs, UPT explains how this process of deception just might raise the success of bad drugs with horrible side effects in some patients, while others manage to get well without the side effects.
Placebo effect is referred to more than many times throughout this research dedicated to
illuminate, identify, locate and observe the complex and complicated nature that makes up the whole of the healthcare crisis. The Ground Breaking Placebo Research identified as Unified Placebo Theory is the most complete, noble and elegant documentation of the vast placebo research while being the most accurate and scientific. Current and earlier placebo research has not yet been privy to the Unified Placebo Theory; consequently the difference in terminology from UPT is simply due to the rapid pace and changes within science and research.
Heart Frauds by Charles T McGee MD, page 32 … Thomas A. Preston, professor of medicine
University of Washington, Seattle, an outspoken critic, claims one half of all cabbage surgeries performed in the United States are unnecessary. He says that survival rates are basically the same as with medical management, except for a well-defined minority of patients, and in most cases cabbage surgery is no more effective than a placebo … page 35 … Race has been found to play a role in who gets cabbaged and who does not. Nationally the rate of having a cabbage surgery runs 27.1 per 10,000 whites per year, and only 7.6 per 10,000 blacks. Hospital admission rates for coronary artery disease for the two races are the same.
Exercise Is Preventive Medicine There is nothing as deceptive as an obvious fact

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
The authors conclude racial prejudice appears to influence cabbage surgery rates. Black people with coronary artery disease are being spared a lot of unnecessary heart surgery because of racial discrimination.
I also noted SCOOP did not offer placebo trails to demonstrate or compare the drug use
outcome to placebo or offer a combined trial that be divided into two separate groups. I pointed out the study did not include any evidence based alternative such as AquaDios-Med™ safe vigorous exercise, like deep-water running, a proactive preventive treatment. The AquaDios-Med™ group could be divided into 2 groups, one with no drugs and the second AquaDios-Med™ group with placebo drugs. This suggested addition to the study would add important research data and it would also protect some of the patients from the Fosamax drug side effects.
The SCOOP administrators only said the study was going forward as is, no placebo, no
AquaDios-Med™. My deep concern was identified with research facts demonstrating that a study of this magnitude not only failed to employ effective and safe preventive medicine it was promoting iatrogenic disease medicine and was about to unleash an iatrogenic time bomb by prescribing dangerous Fosamax, a bisphosphonate drug.
As cited many times herein classical research studies do not include any process similar to
AquaDios-Med™ Proactive Preventive Medicine as part of the study, nor did they offer a comparative group or groups with placebo together with AquaDios-Med™, an evidence based process that avoids all medications, when possible, and engages the patient, to enhance and accelerate the natural healing within almost all people of any age; with no negative side effects only positive outcomes of improved stamina, strength, endurance, physical fitness, improved sleep, mood, attitude and more.
As has been stated, had the SCOOP study included a separate population of patients who
received a placebo together with AquaDios-Med™ Proactive Preventive Medicine and compared the results to patients who received Fosamax would shine the light of enlightenment on healing without drugs; without the dangerous side effects of jawbone necrosis. In this instance, research shows deep-water running strengthens and builds bone a treatment like AquaDios-Med™ should have been included.
In July 2012 GlaxoSmithKline LLC (GSK), a Global health care giant Plead Guilty to
criminal felony charges and Paid a $3 Billion fine for Failure to Report Safety Data, for bribery and paying kickbacks. GSK agreed to resolve its dishonest conduct and stop (1) promoting the drugs Paxil, Wellbutrin, Advair, Lamictal and Zofran for off-label, non-covered uses and paying kickbacks to physicians to prescribe those drugs as well as the drugs Imitrex, Lotronex, Flovent and Valtrex; (2) making false and misleading statements concerning the safety of Avandia; and (3) reporting false best prices and underpaying rebates owed under the Medicaid Drug Rebate Program. Research of the $11.3 billion antidepressant industry shows the drug Prozac with 17 million Americans currently taking some form of the drug, is less effective than a placebo.
On February 19, 2012 60 Minutes Lesley Stahl investigated
The Placebo Effect - Antidepressants The question asked was Do antidepressants work? Perhaps a more profound question is that of
the healing powers in the placebo effect which research shows can be like taking a powerful magic pill that is effective as much or more than 68% of the time. The healing is not from the fake inert pill because it has no ingredient to heal at all.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
The pill becomes metaphoric, symbolic of potent aggressive curative capacities. And, each time it is taken this healing power is released, not by the pill, but by the patient’s expectation, belief and faith to alter their physiology and immune system for health. Mind Body Medicine, Psychoneuroimmunology and medical hypnosis are proven and similar methods of healing without the fake pill.
Since the introduction of Prozac in the 1980s, prescriptions for antidepressants have soared 400 percent, with 17 million Americans currently taking some form of the drug, with the drug companies having spent billions over the years advertising them
Harvard scientist Irving Kirsch says the difference between the effect of a placebo and the effect of an antidepressant is minimal for most people. The $11.3 billion antidepressant industry is very concerned at the Kirsch research and the work of others in this area. Irving Kirsch the associate director of the Placebo Studies Program at Harvard Medical School says that his research challenges the very effectiveness of antidepressants because the medication is less effective than a placebo. For 36 years Irving Kirsch has studied the placebo effect or the taking of a dummy pill without any medication in it that creates an expectation and belief of healing that is so powerful, symptoms are actually alleviated more than 60 % of the time. Studies show placebos, known as sugar or fake pills of an inert substance work miracles; this is the placebo response.
Today, the drug industry and the FDA essentially work in tandem to get dangerous, but highly-profitable, drugs and medical devices to market. It is a win-win situation for both groups as the FDA gets kickbacks in the form of exorbitant new drug and medical device application fees, and the drug industry rakes in billions of dollars for blockbuster drug and device products that would never have been approved had science and facts been legitimately factored into the equation.
In 2009, the FDA's own doctors and scientists came forward that they are routinely threatened by their superiors to cover up unfavorable study data, and promote corrupt and distorted information to the public. This same deception is inherent within food and drug firms as well [a certified signed affidavit by Government authorities verify the letter is in fact written by FDA doctors and scientists].
On March 23, 2009 a Federal District Court Judge reported wrongdoing by the head of the
FDA, their decisions arbitrary and capricious. FDA’s scientists at the Center for Drug Evaluation and Research (CDER) testified that they didn’t have a choice, and would be fired if they didn’t agree to ignore the science and the law so they didn’t follow the science or the law. The judge ruled FDA’s decision was from political pressure not health and safety concerns. FDA physicians and scientists wrote that there is an atmosphere at FDA in which the honest employee fears the dishonest employee. Honest employees committed to integrity and the FDA mission cannot act without fear of reprisal.
On March 6, 2009 Senator Grassley told top FDA leaders and top FDA attorneys they had
concealed the fact of conflict of interest; two of the authors of a major publication presented support of a knee implant device, had affiliations with the device manufacturer. Dr. Larry Kessler, former Director of the Office of Science and Engineering Laboratories at FDA, who had direct knowledge of the advisory committee meeting and process, characterized the process as the FDA at its worst.
Treating Depression Is there a placebo effect • 60 Minutes Lesley Stahl investigates • Expanded Version • February 19, 2012
Research shows the healing powers in the placebo effect can be like taking a powerful magic
pill that is effective as much as 68% of the time. The healing cannot be from the fake inert pill because it has no ingredient to heal at all. The pill becomes metaphoric, symbolic of potent aggressive curative capacities. And, each time it is taken this healing power is released, not by the pill, but by the patient’s immune system.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
Research shows that for a placebo to have the power to heal as described above it must be presented to the patient by an esteemed doctor or known healer, with noble bed side manner who also develops a relationship of trust, confidence and positive expectation in that patient. This revered person, with specific language of suggestion talks to the patient about the healing power within the pill, building faith and belief in the patient about the fake medication. It is this faith and belief that is identified in hypnotic healing, but in this instance with a fake pill.
Mind Body Medicine, Psychoneuroimmunology and medical hypnosis are proven and similar methods of healing without the fake pill. However, the fake pill takes on a post hypnotic value of tremendous healing which is repeated each time the pill is ingested. Ironically, these fake pills carry negative side effects if and when they are known or given to the patient.
Research shows that when the placebo is given by esteemed doctor or known healer, with poor
bed side manner, who may or may not develop a relationship of trust and confidence in that patient, the power or effectiveness of the placebo can be as low as 15%. This effectiveness range 15% to 68% or greater seems to be in the belief and faith of the patient, that is, when the patient has low positive expectation, little faith and belief the fake pill has a lower effect. Harvard scientist Irving Kirsch says the difference between the effect of a placebo and the effect of an antidepressant is minimal for most people. The $11.3 billion antidepressant industry is very concerned at the Kirsch research and the work of others in this area.
Irving Kirsch the associate director of the Placebo Studies Program at Harvard Medical School says that his research challenges the very effectiveness of antidepressants because the medication is less effective than a placebo. Studies show people get better when they take the drug. But it's not the chemical ingredients of the drug that are making them better. It's largely the placebo effect, the faith, belief, expectation of getting better.
For 36 years Irving Kirsch has studied the placebo effect or the taking of a dummy pill without
any medication in it that creates an expectation and belief of healing that is so powerful, symptoms are actually alleviated more than 60 % of the time. Studies show placebos, known as sugar or fake pills of an inert substance work miracles; this is the placebo response.
Studies show placebos are great for treating a number of disorders: irritable bowel syndrome,
repetitive strain injuries, ulcers, Parkinson's disease and much more. Even traumatic knee pain. In a clinical trial some patients with osteoarthritis underwent knee surgery. Others had their knees merely opened and then sewn right back up. In terms of walking and climbing, the people who got the placebo surgery actually did better-- And that lasted for a year. At two years after surgery, there was no difference at all between the real surgery and the sham surgery.
Placebo effects are not all in your head because the placebos can also affect your body. When
you take a placebo tranquilizer, you're likely to have a lowering of blood pressure and pulse rate. Placebos can decrease pain. And we know that's not all in the mind because we can track that using neuro-imaging in the brain as well. Proper studies show that the doctors who prescribe the pills become part of the placebo effect, as described above. A clinician who cares, who takes the time, who listens, who asks questions about your condition and pays attention to what you say, that's the kind of care that can help facilitate a placebo effect over 68%.
Studies show that it almost didn't matter what kind of pill doctors gave patients. Even drugs
that are not considered antidepressants: tranquilizers, barbiturates had the same effect as the antidepressants.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
Kirsch was so surprised by his initial findings he did a second study - using data not only from the drug companies' clinical trials that had been published in medical journals. This time he got the data that weren't published but had been submitted to the FDA, which he got through the Freedom of Information Act. These are studies that showed there was no benefit of the antidepressant over the placebo. The drug companies' showed only the more successful studies to publish, and did not publish unsuccessful studies. The Kirsch study put all the trials together and evaluated patients who took the drug and patients who took the placebo.
For the patients and the psychiatrists, it's clear why they would say the drug works. They take
the drug; they get better. Our data show that as well; they got better. The reason they get better is not because of the chemicals in the drug, it’s because if the faith, belief and expectation. The statistical difference between drug and placebo is very, very small and in 50% of the studies non-existent. The Kirsch studies triggered a furious counterattack - mainly from psychiatrists, who are lining up to defend the use of antidepressants like Dr. Michael Thase, a professor of psychiatry at the University of Pennsylvania School of Medicine, who has been a paid consultant to many of the drug companies.
Dr. Walter Brown is a clinical professor of psychiatry at Brown University's Medical School.
He has co-authored two studies that largely corroborate Kirsch's findings. The number of antidepressant prescriptions over the last decade has increased and most troublesome, the biggest increase is in the mildly depressed, who are the ones who are least likely to benefit from them. However, studies show these drugs do work for the severely depressed, but Dr. Brown questions the widely held theory that depression is caused by a deficiency in the brain chemical called serotonin, which most of these pills target. Experts in the field now believe the theory is a gross oversimplification and probably is not correct; the whole idea of antidepressants is built around, what is thought to be a false theory.
To approve any drug, the Food and Drug Administration merely requires that companies show
their pill is more effective than a placebo in two clinical trials, even if many other drug trials failed. The FDA for antidepressants has a fairly low bar. A new drug may be no better than placebo in 10 trials, but if two trials show it to be better, it gets approved.
Dr. Tim Kendall, a practicing psychiatrist and co-director of the commission that did the review
says that like Irving Kirsch, he was surprised by what they found in the drug companies' unpublished data; the published data significantly overestimated the effectiveness of these drugs and underestimated the side effects. This is a multibillion dollar industry. I doubt that they are spending $10 million per trial to come up with a poor methodology.
What characterizes the unpublished studies is that the outcome is negative for the drug. And,
research experts believe that the drug company method is valid in these unpublished studies. The drug companies refuse to believe or accept that the placebo study outcome, showing placebo as good as or better than the drug is just not suitable from the company's point of view.
Because of the review, new public health guidelines have been issued. Now drugs are given
only to the severely depressed as the first line of treatment. For those with mild to moderate depression the British government is spending nearly half a billion dollars training talk therapists. Physical exercise is another treatment prescribed for the mildly depressed. By the end of 10 weeks, you get just as good a change in their depression scores, as you do with an antidepressant.
There is nothing as deceptive as an obvious fact

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
None of the drug companies was willing to go on camera, but Eli Lilly told 60 Minutes in an email that drug trials show antidepressants work better than placebos over the long term and that numerous studies have shown that patients on placebos are more likely to relapse back into depression. The industry's trade association, PhRMA, wrote us: antidepressants have been shown to be tremendously effective. If Irving Kirsch has his way, the drug companies will have to completely rethink their $11.3 billion business. The problem for the drug company is that studies show you can get more benefit without the drugs. This evidence is beginning to be more accepted and its possible things have begun to change in perception of these drugs.
In addition, research on mind-body interactions, the mechanism of action of the placebo effect,
and purposeful investigation of healing elements in complementary and alternative medical systems can all contribute to our understanding of healing and its role in our healthcare system. Preventive Medicine and scientific medicine must concentrate on whole person healing, the patient's recovery and the restoration of balance as the primary outcome, the improvement in function or dissipation of symptoms as the secondary outcome and cure as the third; an increased focus on health promotion and prevention, such an orientation will produce positive outcomes on chronic disease and costs in healthcare.
Practices such as mindfulness, yoga and transcendental meditation contribute to improved health, function and well-being. Mental control of specific physical functions with methods such as biofeedback, conditioning and other techniques demonstrate our ability to enhance and control self-healing capacities. The breadth of such capacity has been explored in placebo research where expectation and the role of the meaning and context of therapy is profound and widespread, affecting almost every major condition known to humanity.
In July 2001, Merck filed a report with the FDA saying that out of the roughly 1,000 people in each "arm" of the study, 29 who were taking Vioxx died, compared with 17 taking a placebo. An internal and hidden Merck document months earlier, reported -- 34 deaths in the Vioxx group compared with 12 deaths in the placebo group.
The Placebo Effect • Powerful Human Healing [See UPT]
Placebo work supported by the Samueli Institute, Newport Beach, CA. leading to the 2004
published research study titled Placebo Research: The Evidence Base for Harnessing Self-Healing Capacities in THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE and Mary Ann Liebert, Inc. by HARALD WALACH, Ph.D., and WAYNE B. JONAS, M.D. - - Their primary statement is that research that involves placebo provides critical information for how the mind, body, and culture heal for developing a science of healing; a fact long known by preventive medicine programs like AquaDios-Med™. Placebo effect is a medical science the term applied to the therapeutic and healing effects of inert medicines [non-drug] and or ritualistic or faith healing practices. Thus, positive “suggestion” can be combined to create a powerful patient healing expectation and belief.
When referring to medicines, a placebo is a preparation which is pharmacologically inert but
which may have a therapeutic or healing effect based solely on the power of suggestion, patient expectation and believe. Placebo may be administered in any of the ways in which pharmaceutical products are administered and concealed as a powerful healing drug.
Sometimes known as non-specific effects or subject-expectancy effects, a placebo effect or the
nocebo effect, occurs when a patient's symptoms are altered in some way -- alleviated or exacerbated by an otherwise inert treatment, due to the individual expectation or belief that it will work.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
The placebo effect occurs when a patient takes an inert substance (sometimes called a "sugar pill") in conjunction with the suggestion from an authority figure or from acquired information that the pill will aid in healing and the patient’s condition improves. This effect has been known since the early 20th century.
Too often scientific medical researchers regard “Placebo” effects as irrelevant and unimportant at best and a nuisance at worst for determining what is valuable in medicine. Dr’s Walach and Jonas propose a new definition of placebo should be therapeutic meaning response; they review empirical evidence that emphasizes the importance of these effects.
These researchers believe that the effects resulting from the individual meaning of an “intervention” are an important factor of any therapeutic approach. And, they attempt to maximize these therapeutically desirable factors to which to base these healing interventions.
Until recently, many authors dealing with placebo effects were not interested in the placebo
effect as such, or in conceptual clarity. Rather, they combined a number of possible confounding factors such as spontaneous remission, measurement artifacts, and regression to the mean, all under the heading of placebo.
This unfortunate practice has fueled a debate and obscured the real issue, namely, whether psychologic processes and social contexts that facilitate hope, expectation, belief, positive feelings, relief of anxiety, anticipation of improvement and complete healing are able to truly affect physiologic processes, and contribute to healing over and above pharmacologically mediated processes.
Placebo controlled clinical trials have been unable to distinguish between “true therapeutic
response” and other confounding factors to determine the magnitude and power of the placebo effect as it relates to patient healing. Evidence from the psychologic literature, and from experiments especially targeting the question of mechanisms of placebo effects, are beginning to clarify the message that behind the facade of what we normally call placebo effects are the “self-healing capacities of the person”, a fact normally neglected by research. The objective of preventive medicine is to maximize healing by harnessing these factors in any therapeutic context.
Brief HISTORY • PLACEBO THE MEANING RESPONSE
The term placebo derives from the Latin psalm verse, placebo Domino in regione vivorum
(Psalm 116:6 modern counting): I shall please the Lord in the land of the living. This psalm was part of the prayers offered at the deathbed in the Middle Ages. At later times, it was customary to pay others to sing the rites. Hence the connotation of placebo emerged as a fraudulent replacement of the real.
Placebos were popular in the era of medicine when effective pharmacologic interventions were
scarce and often fraught with horrible side effects; tough today drugs are not scarce, they are often loaded with negative, deadly side effects. Some studies tagged the placebo as all those “unreal” effects that were not the result of pharmacologic interventions; which is absurd.
The Department of Environmental Medicine and Hospital Epidemiology together with Samueli
Institute for Information Biology, University of Freiburg, Freiburg, Germany and the Samueli Institute for Information Biology, Alexandria, VA. all agree that today, placebos normally mean inert substances that are given to subjects, mostly in the context of a scientific study, to control for psychologic and social or nonspecific effects of treatment.
Scientific attempts to define placebo effects all have one thing in common; they all define placebo effects as a negative when in fact “placebo is a positive”.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
Placebo is regarded as either the psychologic (side) effect of an intervention, as an unintended effect or as nonspecific effect; even as effects caused by a pharmacologically inert substance. Too often science is unwilling to give credit to the person who “believes” they will heal and they do, thus maximizing their immune system without pharmaceuticals.
Dr’s Moerman, Jonas and Brody define Placebo as the response - to the effect - that is due to the meaning of a therapeutic intervention for a particular patient and context. This translates to a person’s positive healing response to a specific therapeutic process.
This new conceptual definition of “placebo” has two virtues. It is a semiotic definition or a
study of how the meaning of “placebo” is constructed and understood. And it acknowledges that humans are not deterministic machines reacting to mechanical causes (e.g., pharmacologic agents). Rather, they are responding to signs and the meaning those signs generate in a highly complex, often self-determined and sometimes unpredictable fashion such as facilitating powerful healing immune responses to suggestion and belief.
This “healing response” is not fully determined by the external stimuli themselves, but arises
from the interaction between the external environment and the internal conditions of persons, their history, their social circumstances, their individual predilections, their expectations and their belief to heal and be well. These facts bring into focus the importance of individuality in medicine and therapy. And, it makes plausible why one and the same situation, for instance surgery, may arouse hope in one patient and induce fright in another with completely different physiologic reactions and clinical outcomes.
ARE PLACEBO EFFECTS “REAL” CLINICAL TRIALS
Dr’s Walach and Jonas researched many “placebo studies” and found that most all those investigations showed the studies suffered from poor design making it nearly impossible to show the result of placebo effect. However, their research into these studies did show that there is a scientific basis that shows beneficial effect of placebo administration in the context of clinical trials over and above natural history and spontaneous remission.
It is a fact that treatments can be more effective than their placebos or vice versa depending on
those context factors. An example is the study by Dr. Bergman and colleagues in which the same trial was conducted twice. Patients with cancer who regularly received naproxen as a routine analgesic [drug to alleviate pain] were either given their normal bedside medication or a placebo. Some patients knew they were part of a trial, and some were informed about the trial and knew that they would be randomized to either naproxen or placebo.
Informed patients who received the active medication had the greatest pain relief, followed by
their placebo counterparts. Patients who had received placebo in the formal trial had greater pain relief than the patients who had received the normal naproxen medication without knowing that they were part of the trial. The logical conclusion here is that expectation and belief of potential effects is vitally important to the patients healing responses.
Another trial illustrates how expectancy and belief are factors mediating a meaning response. In
a study comparing the experimental drug to sumatriptane, an established drug and placebo, the ethics committee insisted that the randomization ratio to placebo should be 16:1, because it is known that triptanes are effective and hence as few patients as possible should be exposed to the risk of placebo.
There is nothing as deceptive as an obvious fact

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
This study was unable to show superiority of any of the two active drugs against placebo. This means the placebo or no-drug was as effective as the pharmaceutical. The active medication showed an effect in 42% of the cases, and the placebo an effect in 38%.
The conclusion drawn by the researchers is that because patients in the placebo group knew the
randomization ratio, they had a strong hope, expectation and belief of actually receiving active treatment, and it was this expectation and belief that contributed to the strong positive “placebo” effect.
An analysis of all triptane studies showed that studies that had a randomization ratio to placebo
different from 1:1, and hence provided a greater likelihood for patients to expect real treatment, yielded higher placebo response rates than studies with symmetrical randomization; this result adds to the concept that expectation and belief are powerful healing forces.
Dr’s Walach and Jonas concluded that ethical requirements threaten scientific progress if they
require unsymmetrical randomization ratios, which in turn drive patient’s expectations, which again inflate placebo response rates due to these expectations.
To explore the question whether more frequent application of placebos yields larger effects Dr’s
Walach and Jonas compared interventions of acid blockers in ulcers. Earlier drugs had to be taken four times per day, while the newer drugs had to be taken only twice a day. They compared the placebo response rates in 51 studies with a regimen of four times per day dosage with 28 studies with a twice daily dose.
They learned that more frequent application of a drug raises different expectations than an application twice daily to the point of needing to treat more patients with a twice per day regimen to obtain the same effect as a four times per day regiment.
Perhaps one of the most direct proofs for the power of expectation is a recent experimental
study on irritable bowel syndrome. Thirteen (13) patients received an experimental rectal distention and heat stimulus as a pain stimulant to test different analgesic interventions. Apart from the natural history of the pain, each patient received in randomized order all of the following interventions: rectal lidocaine, oral lidocaine, rectal placebo (a lubricant) with the suggestion of improvement, and rectal placebo with the suggestion of potential aggravation (i.e., a nocebo intervention).
Desire for pain control and expectation of pain reduction were also measured. There was a
highly significant effect for the placebo intervention, the oral and the rectal lidocaine compared to natural history.
While neither the rectal nor the oral lidocaine were distinguishable from the placebo, the nocebo or the subject's pessimistic belief and expectation that the inert drug would produce harmful, injurious, unpleasant, or undesirable consequences and intervention produced a nonsignificant increase in pain perception.
Research shows that the desire and expectation of pain control explains 77% of the variance in
pain ratings for placebo and 81% for lidocaine. Thus, expectation and belief was the most important factor in this study, even for the effectiveness of the pharmaceutically active agent.
Dr’s Walach and Jonas underline that it was probably important that the same physician who
treated the patients in a normal context was responsible for the experimental interventions, and thus these effects might depend on a good relationship between the patients and the physician.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
The same conclusions can be drawn from a recent clinical trial of massage, acupuncture, and self-education in 262 patients with chronic low-back pain. This trial showed massage and self-education to be superior to acupuncture after a year. This trial also assessed general and specific expectation and belief of patients and reanalyzed the data according to expectations. Those patients who had the largest expectation of change for a specific treatment had the largest therapeutic benefit.
When all other factors were controlled statistically, specific expectation alone showed that
patients with high expectation and belief had a fivefold chance of benefiting from the treatment, all other things being equal. Dr’s Walach and Jonas underline that this effect of expectation and belief was larger than the treatment effect in comparable low-back pain trials.
Taken together, these data show that expectation and belief is probably the most important “meaning” factor of a treatment, and can be more powerful than a specific pharmacologic intervention. It is plausible, then, to suppose that the meaning response is nourished to a large extent by the expectation and belief a specific treatment raises in patients.
Placebo • SUGGESTION • EXPECTATION
Imagination • Faith • Belief • Hope
Expectations and beliefs may be indirectly altered or manipulated directly by suggestion. The power of suggestion historically was brought to the attention of the scientific community by the investigation of Mesmerism in Paris, 1784. These studies showed that the claims made by the followers of Mesmer, at least in formal studies, were largely the result of suggestions, as the effects could only be seen when therapist and subject had visible contact, allowing subtle communication. The interest in suggestion waned with the rise of behaviorism and later cognitive therapy. Interest in suggestion now is increasing, as the neurosciences are able to measure and better understand the intricate complexities of subconscious and preattentive processes.
Suggestion and the subconscious processes it triggers may be the link between the meaning of
an external situation and physiologic responses. In many ways placebo effects are akin to therapeutic hypnosis, with the difference being that in hypnosis a patient actively and willingly agrees to the procedure. The clarifying psychological literature is vast and has been reviewed elsewhere. However, there are relevant aspects that highlight the mechanisms of healing.
In a convincing piece of evidence for the physiologic effectiveness of suggestions, Dr’s Butler
and Steptoe gave a water aerosol as an inhalant to 12 subjects with asthma using a balanced, crossover experimental study.
Initially subjects were told the aerosol was a bronchodilator and would relieve asthma
symptoms. In later sessions the same inert “water aerosol” was described as a new powerful bronchoconstrictor, making asthma symptoms worse. The placebo, given with the suggestion it was bronchodilation, was able to reverse the suggested bronchoconstrictive effect; and both compared to the control situation and the baseline reference measurement. This means expectation and belief altered or reversed the effect of the placebo depending on suggestion.
Psychologic research has studied several pharmacologically active substances, such as caffeine,
alcohol, or cannabis, comparing their pharmacologic to psychological properties in balanced placebo design. This design balances substance and expectation with one factor being the substance versus placebo.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
14
The other factor manipulates “meaning” or importance by giving either correct or misleading information. This design allows for a separation of pharmacological and psychological effects of substances, and the demonstration of the effects of suggestion.
The first review showed the strong effects of expectancy and belief can be observed and vary by the setting. For instance, in studies on sexual arousal subjects either received alcohol or an appropriate placebo (normally tonic with a few drops of vodka sprinkled on top) and expectancy manipulations [suggestions], and then they would view stimulating visual material.
Here, expectancy of receiving alcohol produces strong effects, independent of the substance actually ingested. Measures in these studies were objective measures of sexual arousal, such as penile erecti•on or vaginal blood flow that address social desirability.
MECHANISMS • ENDORPHINS CONDITIONING • CENTRAL PROCESSES
Dr. Levine and colleagues published findings on the reversal of placebo analgesia by the
administration of naloxone. Patients given naloxone reported significantly greater pain than those given placebo. The researchers thought they had solved the placebo puzzle. In these studies, patients suffering from either postoperative or experimental pain received either a placebo infusion without their knowledge through a covered indwelling line, or naloxone, an opiate antagonist. With their knowledge, they then received another placebo injection that was claimed to be either a potent analgesic or a control substance. Dr. Levine and colleagues observed that the opiate antagonist reversed or attenuated a placebo analgesia produced by the suggestion of administering an alleged painkiller.
They concluded that the substances responsible for this effect must be endogenous opiates, which mediate centrally modulated pain and analgesia. These data are consistent with the hypothesis that endorphin release mediates placebo analgesia for dental postoperative pain. A paper reviewing this evidence concludes that the effects are real and mediated by endogenous opiates. The same conclusion was reached indirectly by Dr’s Lichtigfeld and Gillman, with the addition of the central role of nitric oxide to the placebo response.
These researchers conducted studies on the effects of nitric oxide in post withdrawal depression of alcoholics. When titrated or analyzed to be chemically correct and administered in low doses such that patients remain conscious, nitric oxide, normally a potent narcotic, relieves withdrawal depression quickly and effectively.
This psychotropic analgesic nitric oxide (PAN) is superior to placebo (air) even though the response rate to this placebo can be as high as 50% of cases. Because PAN is effective in alleviating 95% of the cases of post withdrawal depression, the authors conclude that the endogeneous opiate system is be involved.
Because medical air and oxygen have the same effect in many cases, this effect must be the
result of activation of the endogenous opiate system. This is also suggested by Dr. Stefano and colleagues who imply that endogenous nitric oxide is the hub around which both the immunologic and the affective effects of placebo revolve.
Expectancy Versus Conditioning
Is this system of placebo production activated by expectancy or by conditioning, or both?
Autonomous processes can be subject to conditioning has been uncontested since Ader’s groundbreaking studies on conditioning immune responses in rats. These studies make plausible that autonomous processes, such as the activation of the immune system or a neurotransmitter system, could be reinforced by operant conditioning or by a keying stimulus as in classic conditioning.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
15
Thus, placebo effects could be conceived of as conditioned reactions. On the other hand, social cognitive theorists suggest that the placebo effect is controlled by response expectancies. That is that when a response is expected by an organism, it is more likely to happen, thus expectation produces the anticipated result. There are studies supporting a conditioning model, as well as studies supporting expectancy models.
Current evidence suggests that the conditioning effect is mediated by expectancies. Dr.
Benedetti and colleagues have presented evidence both for the reality and clinical relevance of placebo effects and their mechanisms through different neurotransmitter systems.
There are some pertinent points relevant to healing effects in these complex experiments. First,
natural history control groups were run, showing that the effects in the placebo groups are clearly different from the effects in no treatment control groups. Thus, the effects of placebo are not merely artifacts. Second, these studies show that not only are endogenous opiate systems involved in placebo analgesia, but so is the specific information and meaning given to a patient who can modulate specific receptor families involved in producing analgesia and direct those effects to certain areas of the body.
For instance, cholecystokinine (CCK) antagonizes morphine effects that operate via opiate
receptors. Proglumide is an antidote to CCK, and therefore acts synergistically with opiates. It was shown that proglumide; the antidote not only potentiates placebo-mediated analgesia, but also operates via different receptor systems independently from those that are affected by naloxone. And, these opiate dependent effects can be targeted toward specific body parts, a finding that supports the expectancy hypothesis. There are also objective effects (i.e., depression of lung function).
Such objective opiate-dependent effects cannot be explained by expectancy, and likely are
conditioned. There seem to be two systems active, both of which are mediated by endogenous opiates. One operates via expectancies, and the other operates via conditioning. Additionally, there seem to be conditioned effects which are not dependent on opiates.
Response expectancies are also effective in clinically relevant settings such as postoperative
pain. The effect of expectancy was determined by open (unblinded) or hidden (blinded) administration of analgesics to patients, postoperatively or experimentally, without administering placebo. Open administration involved an arousal of expectancies and produced significantly stronger effects. Similar findings were found with patients suffering from Parkinson’s disease, who had had subthalamic electrodes implanted to stimulate dopaminergic neurons. In one condition, they were told about the actual stimulation levels and their reduction. In another condition, they expected the stimulation to be active but it was in fact reduced.
After 30 minutes, significantly different effects in motor tasks were seen, indicating that
endogenic processes were activated by the expectation. The most recent study has shown a clear effect of expectation in a pain model while heart rate variability measures were also taken. Given as an alleged analgesic, placebo reduced pain and the low-frequency power spectrum component of heart rate variability caused by sympathetic activation. This effect was antagonized by naloxone, again supporting evidence that endogenous opioids are responsible for the mediation of this expectancy effect. It remains to be seen which class of opioids influencing the parasympathetic system is responsible for these effects. There seem to be several processes that mediate meaning responses, depending on the paradigm and the context. It is reasonable to assume that neurotransmitters such as the endogenous opioids have a role. It is also likely other systems like dopaminergic pathways mediate these effects.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
16
If central neurotransmitter systems are active in mobilizing expectation effects, it is also plausible that many other effects in addition to pain alleviation or antidepressant responses are mediated by those systems. It is well-known, for example, that practically every neurotransmitter, including endogenous opioids and serotonin have immunomodulatory effects.
Imaging Placebo Effects
There are two primary opiate networks in the brain, one in the brainstem, and one in the cortex, involving the rostral anterior cingulate cortex, (rACC) and the ventromedial prefrontal cortex, respectively. In an experiment nine subjects received heat or warmth, followed by opiate or placebo, while their regional cerebral blood flow was monitored. It could be demonstrated that in placebo responders, the same areas are active during placebo analgesia as with opiates, namely the nuclei in the rACC. Nuclei in the pons covaried with the activities of the rACC. Notably, the activation of the rACC was only seen in placebo responders.
Another part of the puzzle has been illuminated by a positron emission tomography (PET), this is a nuclear medicine imaging technique which produces a three-dimensional image or map of functional processes in the body; this imaging study was able to determine the effects of apomorphin and placebo on dopamine release in patients with Parkinson’s disease.
The study utilized the competition of radioactively marked raclopride (RAC) and endogenous dopamine. The authors observed a 17% and 19% diminution of RAC by placebo administration in the nucleus caudatus and the putamen, respectively. Both areas contain many dopamine producing neurons. This finding suggests that patients expecting dopaminergic pharmacological effects will produce dopamine. Dopamine is an important neurotransmitter which activates the reward system, and is important in learning. Thus, this finding illustrates how placebo may produce effects beyond pain relief and influence areas such as affect, learning and motivation.
An imaging study of placebo effects in an antidepression study using the selective serotonin reuptake inhibitor (SSRI) fluoxetine showed a clear overlap of areas activated in placebo responders and drug treatment responders.
While activation of the thalamus was reduced in both groups and activation of prefrontal areas enhanced, fluoxetine showed enhanced activity in the pons and reduced activity in the hippocampus and striatum. These findings were not seen with placebo. Fluoxetine effects were generally more pronounced overall, but activation of the right prefrontal cortex was more pronounced in placebo responders. This finding is qualified by another recent antidepressant imaging study that used high-resolution quantitative electrocardiogram (EEG) to locate areas of higher or lower electrical activity.
In this study, it was found that placebo responders, drug responders, and nonresponders had distinctive activation patterns. While placebo responders showed increased activity in the prefrontal cortex, drug responders showed decreased activity, and nonresponders showed no change. This seems to show that the importance or “meaning” produced specific areas of altered brain metabolism and activity. These findings are the first of their kind and replications are called for to help confirm and clarify our understanding of the mechanisms of meaning effects. They have already dispersed doubt about the reality of meaning and it importance to response effects in healing and medicine.
Preventive Medicine • Natural Healing
Harnessing Placebo Effects
This review has highlighted a selective list of findings; it has illustrated a number of issues about healing and its mechanisms.
1. Meaning and healing effects are real and can be quite strong. 2. If conceived as an individual response to the meaning of an intervention, many paradoxes
inherent in traditional usages of the concept of placebo disappear.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
17
3. This latter usage of the concept can also contribute to a broader understanding of healing responses, which seem to be triggered by central processes, either through expectation, or through conditioning, or both, and can involve multiple central mechanisms and neurotransmitter pathways.
4. Placebo analgesia is mediated by endogenous opiate systems which are similar to those activated by exogenous opiates.
5. Other systems besides the endogenous opiate system are involved, such as the dopaminergic system. It is time to change our perspective on placebo and meaning effects in research and medicine. Rather than viewing the placebo effect as an enemy that hampers clinical trials, it should be seen as a ubiquitous healing response mediated by expectations and conditioning. Thus, it can be utilized to enhance or interfere with healing in many clinical settings.
By understanding the meaning response, we might understand how optimal healing can be
fostered. Complementary and alternative medical (CAM) therapies may be elegant, efficient and comparatively harmless ways to harness healing processes. We should view that possibility as a virtue rather than a vice. But CAM is not the proprietor of all meaning responses. These responses are ubiquitous and occur in every healing context. Here are many ways to enhance healing with any therapy derived from the research literature on placebo effects. In addition, evidence points to the following suggestions on how to harness these optimal healing processes:
1. Always work with and not against patients expectations. If patients expect an intervention to
be harmful, dangerous, fraught with side-effects, and not curative, they are likely to experience just that. Thus, it should be mandatory for every physician and therapist to find out about those expectations and move them in a positive direction. If multiple treatment choices are available always use the one which is most conforming to the patient’s expectations for improvement. For instance, when a patient expects to get better from a natural product rather than from a chemical one, it is likely that this preference has clinically important influences.
2. If patient’s expectations are unhealthy or harmful, work to change them first before jumping from intervention to intervention. Although modern day patients are sometimes surprisingly educated, they also sometimes cling to outdated or faddish beliefs. It is likely that interventions are unsuccessful or less effective if patient’s expectations are not fulfilled. In addition, it is likely that going against expectations will reduce compliance, a factor central to any therapeutic success.
3. Talking can induce a response toward cure. Rapport between doctor and patient is an
important vehicle for suggesting therapeutic effects and enhancing expectations. Dr. Frank, in his seminal work on meaning in medicine, made the effects produced by the general ambience of treatment the most important of therapeutic factors.
4. One of the greatest skills of a doctor, and a topic often left out of the debate around evidence-based medicine, is individualization. It is in the subtle changes to therapy and how they are delivered by a skilled healer that the meaning response is harnessed to its fullest. It is expected that any therapist who individualizes his treatment will have better results, because he can harness the meaning response.
5. Raising hope and alleviating anxiety in a credible way is one of the most therapeutic acts. It
has been shown empirically that a simple act, such as giving a clear diagnosis and prognosis, improves outcome. If patients receive clear and positive communications conveyed with trust, credibility, and confidence, complete healing is more likely. This must be mastered in a world in which knowledge is transitory, and changes quickly and frequently contradicts previous knowledge. Truth and integrity are integral components of a trusting relationship; however, the patient should not be made the primary target for transferring our insecurity.
There is nothing as deceptive as an obvious fact

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
18
6. A frequent assumption is that only specific causal effects count, like those produced by drugs or surgery. But this placebo research makes it plausible that other effects also count. Believing that one has a potent therapeutic agent at one’s command may be the single most important ingredient for producing a broad spectrum of meaning responses. For it is only when a physician believes in what he uses that he can fully convey competence and positive expectations. Thus, applying interventions which patients demand without real conviction is not an evidence-based healing strategy.
7. Giving placebos is not identical to using the meaning response therapeutically. One need not
give sugar pills. However, in some cases the use of nonactive or minimally active drugs might be a better option than continuous medication of toxic but effective therapies. Should the patient respond favorably, it would be a mistake to attribute the problems to psychologic problems. The meaning response teaches us that there is not a clear divide between the mental and physical.
8. Therapeutic rituals might be helpful in eliciting the meaning response. A significant portion
of the effects from modern devices used in both conventional and complementary medicine may be caused by such effects. It may be useful to develop one’s own rituals with patients, like taking a drug after a morning bath, in a special room, before or with prayer, or having it administered by a friend.
Taken together, Walach and Jonas have demonstrated that placebo effects, reframed as meaning
responses, can evoke powerful healing and should be cherished rather than chided. The meaning response is ubiquitous, exists and can be used or abused in any therapeutic context. To ignore it is to risk having it produce random and possibly harmful effects. To understand it and use it intelligently is to increase therapeutic benefit. Placebo research can and should be directed toward providing the evidence base for developing optimal healing environments.
The AquaDios-Med™ Philosophy
• EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING! • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race.
Copyright © 2008 – 2012 – 2013 2nd Edition AquaDios-Med™ • AquaDios Corp.
All rights reserved. Respectfully,
Dr. Alan Jensen (Alan) Founder • CEO • Creator, AquaDios-Med™ http://www.aquadios.com/ A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing Phone 310-897-5055 - Email: [email protected] - P.O. Box 2228 Malibu, Ca. 90265
Exercise Is Preventive Medicine
There is nothing as deceptive as an obvious fact

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section V
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
Physical Exercise • History Physical Fitness • Preventive Medicine
Section V
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
20 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
[email protected] www.aquadios.com
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
History • Research • Physical Exercise • Introduction Solution • Healthcare Crisis • Part V • 14 Pages
The History and research of Physical Exercise is significant to health, physical fitness and ultimately to a better understanding of its importance to Preventive Medicine. Primitive man in 10,000 B.C. had little documentation to what is referred to as physical fitness; in that time it is likely the Darwinian principle of power, strength and intelligence ruled and probably continued through the Neolithic Agricultural Revolution from about 8,000 - 10,000 B.C. Ancient civilizations in China and India from 2500 - 250 B.C. shows a definite movement toward physical exercise in China through the philosophical teachings of Confucius that encouraged participation in regular physical activity including archery, badminton, dancing, fencing, wrestling and Cong Fu. For more than 5000 years in India Yoga began to develop despite the repressive beliefs of Buddhism. Through the Hindu priests practices that strive to develop the body, mind, and spirit characterized by discipline and meditation this Hindu Philosophy grew through exercises in physical posture and breathing patterns known today as Hatha Yoga. Today in the United States, there is an estimated 14 million individuals regularly participating Yoga.
The Near East Countries such as Egypt, Palestine, Persia, and Syria between 4000-250 B.C. were mostly interested in building armies, not exercise for health; they trained youth in hunting, marching, riding, and javelin throwing. Fitness training to improve strength and stamina was not intended for health benefits it was to create more able soldiers to help expand the Empire. Ancient Greek Civilization from 2500 to 200 B.C. Athens - Greece – was perhaps like no other civilization and held physical fitness in high regard. The idealism of physical perfection was one that embodied ancient Greek civilization. The Greeks believed development of the body was equally as important as development of the mind. Physical well-being was necessary for mental well-being, with the need for a strong, healthy body to harbor a sound mind; exercise for the body and music for the soul. Gymnastics, running, jumping, and wrestling were practiced regularly. Sparta or Northern Greece primary interest was military strength; fighting skills were highly correlated with physical fitness levels to personally develop the body, mind, and spirit. The military-dominated culture of Sparta resulted in one of the most physically fit societies in the history of mankind.
Roman Civilization - 200 B.C.-476 A.D. was a military based training activities such as running, marching, jumping, discus and javelin throwing. This lifestyle resulted in strong, fit people who conquered nearly all the Western World. Fitness Roman’s declined as wealth, entertainment, Materialistic acquisition and excess became higher priorities than physical condition. Roman civilization fell to the physically superior Barbarian tribes from Northern Europe.
In the Dark 476-1000 and Middle Ages 900 – 1400 fitness experienced a revival. But, the
Renaissance 1400-1600 saw growth by Martin Luther (religious leader), John Locke (philosopher), Vittorino da Feltra, John Comenius, and Richard Mulcaster (physical educators) who maintained that high fitness levels enhanced intellectual learning. Greece recognized School curriculums involving physical education fostering physical education throughout Europe.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
The National Period in Europe - 1700-1850 – Germany – Sweden - Denmark – England saw educational, military, and medical gymnastics, all with strong medical background and recognized that exercise was necessary for all persons. In Great Britain, medical benefits of fitness and regular exercise became important especially the scientific components of fitness; which are remarkably similar to present-day exercise recommendations and the importance of progression of exercise.
Colonial America from 1700-1776 left physical fitness behind due to the demands and nature of
settlement, farming and cattle ranches that took up all the time. But the National Period - 1776 to 1860 -- Early Physical Education in the United States - United States – post-Civil War from 1865-1900 saw Physical Education grow as many immigrants brought these activities with them. Benjamin Franklin recommended regular physical activity, including running, swimming, and basic forms of resistance training for health purposes. President Thomas Jefferson acknowledged fitness, saying … Not less than two hours a day should be devoted to exercise and the weather shall be little regarded. If the body is feeble, the mind will not be strong... Dr. J.C. Warren, Harvard University, was a major proponent of physical activity and the necessity for regular exercise, such as gymnastics and calisthenics. Catherine Beecher's programs of the mid-nineteenth century bear remarkable similarities to modern-day aerobics.
The Industrial Revolution resulted in widespread cultural changes, advancement in industrial
and mechanical technologies replaced labor-intensive jobs. Rural life changed to an urban lifestyle, decreasing levels of physical activity. In 1900 the most common causes of death were from influenza, polio, rubella, and other infectious diseases. Risk of disease and mortality from infectious diseases were alleviated with the discovery of Penicillin.
The cost of industrialization and urbanization became glaringly apparent starting in the 1950s
and 1960s. An epidemic of hypokinetic diseases – sedentary lifestyle, including cardiovascular disease, cancer, and Type II diabetes, never before prevalent, began to be leading causes of disease and death. The lifestyle improvements brought in part by the Industrial Revolution had come with an unwanted and alarming cost to health.
The 20th Century was a new era of fitness leaders such as Theodore Roosevelt who led the
nation into the new century with the importance of exercise and physical activity, and encouraged America to be physically active. His desire for physical fitness evolved out of his childhood battle with asthma, which he overcame with a rigorous exercise program. He encouraged multiple forms of physical activity including hiking, horseback riding, and other outdoor endeavors. However, when the U. S. joined World War I in 1917 one in three drafted was unfit for combat and many of those drafted were highly unfit prior to military training. Government legislation ordered improvement of physical education programs in the public schools. The heightened interest and concern for physical fitness would be short-lived as the United States entered the 1920s and the Depression.
The Roaring Twenties, Great Depression and World War II took a toll on physical education.
But, in the 1950s Jack LaLanne became a pioneer of fitness. Throughout his life, LaLanne preached the value of preventive lifestyle habits. On television, LaLanne developed fitness programs including aerobics, water aerobics, and resistance exercise. He also introduced numerous pieces of exercise equipment including the first cable-pulley machine, the safety system for doing squats called the Smith machine, and the first leg extension machine. LaLanne preceded the modern fitness movement by three decades but his fitness ideology and exercise programs were correct in approach when judged by modern research.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
Research • Support Exercise is Medicine In 1956 President Eisenhower formed the President's Council on Youth Fitness and the
President's Citizens Advisory Committee on the Fitness of American Youth. Numerous organizations took initiative in educating the general public about promoting physical fitness including the American Health Association (AHA), the American Medical Association (AMA), the American Association for Physical Education, Recreation, and Dance (AAPHERD), and the President's Council on Youth Fitness. The American College of Sports Medicine (ACSM) was formed in 1954, and has proved to be one of the premier organizations in the promotion of health and fitness to American society and worldwide. Throughout its history, ACSM has established position stands on various exercise-related issues based on scientific research. These organizations would provide merit and legitimacy to the coming fitness movement.
In the 1960s - United States President John F. Kennedy, a major proponent of fitness and
health-related benefits established the President's Council on Physical Fitness to guide the need for American citizens to improve their fitness levels. He also wrote an article in Sports Illustrated entitled "The Soft American. Where he said … We are under-exercised as a nation; we look instead of play; we ride instead of walk ... Kennedy prompted the federal government to become more involved in national fitness promotion and started youth fitness programs. Kennedy's commitment to fitness is summarized by his quote … Physical fitness is the basis for all other forms of excellence…
Professional Organizations • Support Exercise is Medicine
A common mission for these groups is to forge a strong, collective voice for sport medicine; to
be a leader in advancing the art and science of sport medicine, including health promotion and disease prevention, for the benefit of all people through advocacy, education, research and service.
The American College of Sports Medicine (ACSM) Founded in 1954 is the largest and most
prominent sports medicine and exercise science organization in the world. ACSM has more than 45,000 International, National and Regional Chapter members. Since its founding ACSM members have applied their knowledge, training and dedication in sports medicine and exercise science to promote healthier lifestyles for people around the globe.
American Orthopaedic Society for Sports Medicine (AOSSM) The American Orthopaedic
Society for Sports Medicine is a world leader in sports medicine education, research, communication, and fellowship. Founded in 1972, AOSSM is an international organization of Orthopaedic surgeons and other allied health professionals dedicated to sports medicine. Essentially every professional and collegiate team has a team physician who is a member of the AOSSM. [1]
Canadian Academy of Sport and Exercise Medicine The Canadian Academy of Sport and
Exercise Medicine (CASEM) is an organization of physicians committed to excellence in the practice of medicine as it applies to all aspects of physical activity. http://www.casm-acms.org/
American Medical Society for Sports Medicine (AMSSM) Founded in 1991 is a multi-
disciplinary organization of physicians whose members are dedicated to education, research, collaboration and fellowship within the field of Sports Medicine. It now comprises over 2100 Sports Medicine Physicians whose goal is to provide a link between the rapidly expanding core of knowledge related to sports medicine and its application to patients in a clinical setting. http://www.amssm.org/
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
National Athletic Trainers' Association (NATA) Founded in 1950 with the mission to enhance the quality of health care provided by certified athletic trainers and to advance the athletic training profession.
Canadian Athletic Therapists' Association (CATA) Founded in 1965 is an organization devoted
to the comprehensive health care of an individual at any level of physical ability by Certified Athletic Therapists. http://www.athletictherapy.org/en/index.aspx
American Medical Association (AMA) Recognized Athletic Training(AT) as an allied health
profession in 1990. American Academy of Podiatric Sports Medicine (AAPSM) Sports Medicine Australia (SMA) Australasian Academy of Podiatric Sports Medicine (AAPSM) American Osteopathic Academy of Sports Medicine (AOASM) http://aoasm.org/
Lessons From History • Sweat • Hydration
The mind-body concept and preventive medicine dates to before the Greek society ideal that a sound mind can only be found in a healthy body. History also supports exercise for the body and music for the soul; music is a distinctive component to the aerobics exercise experience.
The Ideal Sport Performance or Ideal Performance State was perhaps most glorified by the
Russian Olympic teams and later by the development of Inner Mental Training in Sweden by Lars-Erik Uneståhl in the 1970’s and later. These cultural activities eventually led to the development and practice of Sport Medicine and Sport Psychology. Sweden is the only country that has introduced Inner Mental Training throughout is culture as well as in Sport.
In recent years Western societies continued to recognize the importance of daily exercise and
the health dangers of sedentary life style with no or little physical exercise. Research shows that Physical inactivity, in itself, is cause for most medical problems today. The U. K. has made efforts within the Public Health community to encourage the nation to become more physically active; to reflect this is the new specialty of Sport & Exercise Medicine – SEM. Since 2007 the U. K. postgraduate medical education has established exercise training programmes in addition to supporting professional development across the UK in SEM, and recurrent funding for 50 National Training Numbers (NTN’s) is available. Unfortunately this same patient-centered health practice is not being advanced in the U.S. with the same enthusiasm.
Also, in October 2007 the U. K. Foresight Report issued by the Government Office for Science,
highlighted the unsustainable health and economic costs of its nation that continues to be largely sedentary. It predicts the incremental costs of physical exercise inactivity will be about $15.2 billion per year by 2050 and with bigger costs to society and businesses it will be about $ 76 Billion. Lack of daily exercise or Physical Inactivity leads to ill-health and the cost of paying for this unnecessary expense will be unsustainable in the future; and boldly states … No existing group of medical specialists is equipped with the skills and training to deal with this challenge.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
SEM Physicians are able to evaluate medical patient’s co-morbidities, perform exercise testing and provide an exercise prescription, together with a motivational programme and exercise classes. The concept of that Daily Physical Exercise is a Health Tool; a Preventive Medicine Health Tool is becoming increasingly important.
On June 20, 1996 the American Heart Association published a study titled Statement on
Exercise: Benefits and Recommendations for Physical Activity Programs for All Americans … by 13 separate experts in medicine. This American Heart Association published Statement was aimed at Health Professionals by the Committee on Exercise and Cardiac Rehabilitation of the Council on Clinical Cardiology. The most important message is a simple verifiable reality -- Physical inactivity is one of the biggest risk factor leading to coronary artery disease and a host of other common disease.
These experts cited more than 100 research studies and found that most beneficial effects of
physical activity on cardiovascular disease mortality can be attained through moderate-intensity activity. They also determined that Medical Professionals become more engaged in the fact that physical exercise is a Preventive Medicine activity and they should be attending to these services because preventive medicine through physical exercise is an important component of the national health agenda … Physicians have the opportunity and responsibility to promote regular physical activity because it is drug free and will reduce high blood pressure, improve weight control, help in the management of abnormal blood lipids, and helps in prevention and cessation of smoking … providing preventive services, the physician must set and support the agenda to deliver preventive services and defines the physical exercise as medically appropriate ... Physical activity counseling protocols that require only a few minutes. And, the experts say … Medical schools, residency, and fellowship training programs should prepare physicians to recommend exercise ... An individual's customary physical activity level should be an integral part of a comprehensive medical history.
The research presented emphasized that exercise is a primary activity in the prevention of
cardiovascular disease -- benefits of regular aerobic exercise are well known including blood pressure–lowering hypertensive groups. Regular aerobic physical activity can control diabetes, and obesity. Physical inactivity is an independent risk factor for the development of coronary artery disease. The greatest potential for reduced mortality is in the sedentary who become moderately active
This research showed that children must be introduced to the principles of regular physical
exercise and recreational activities at an early age. Schools at all levels must develop and encourage positive attitudes toward physical exercise, providing opportunities to learn physical skills and perform physical activities, especially those that can be enjoyed for many years. The school curriculum should not overemphasize sports and activities that selectively eliminate children who are less skilled. Schools must teach the benefits of exercise and the development and maintenance of exercise and exercise conditioning throughout life.
Research included that Employers, Community Groups and Insurance Industry must all
participate in the simple focus on daily exercise and perhaps most importantly said … The insurance industry, including managed care, and the medical community must engage in a collaborative effort to provide policyholders with exercise programs that meet American Heart Association standards and the Agency for Health Care Policy and Research Guidelines for Cardiac Rehabilitation.
A study titled, Physical Inactivity: Associated Diseases and Disorders by Joseph A. Knight M.D, Department of Pathology, University Utah School of Medicine, Department of Pathology, University of Utah School of Medicine demonstrates that sedentary lifestyle is a very serious worldwide problem, especially in North America and Europe.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
Knight’s study indicates that over several decades there has been a decrease in exercise and more physical inactivity being responsible for numerous diseases – disorders in the U. S. including cancer, diabetes, hypertension, coronary - cerebrovascular diseases, overweight – obesity; all of these - cause diseases - disorders and add tremendously to healthcare costs, premature mortality and death. Knight concludes that unless there is a reversal of this sedentary lifestyle, the incidence of these diseases/disorders will increase, life expectancy will decrease, and medical costs will continue to rise.
Another study published by the American Heart Association in December 2012 Physical
Activity Prevents Progression for Cognitive Impairment and Vascular Dementia was from Department of Neurosciences, University Lisbon, Santa Maria Hospital, Portugal and it determined regular physical activity delays and can prevent the onset of cognitive impairment and dementia in the elderly, especially in women. The study concluded that physical activity reduces the risk of cognitive impairment, mainly vascular dementia, in older people.
Mind-Body Medicines • Deep-Water Running Immersion Therapy • Research
AquaDios-Med™ Proactive Preventive Medicine • Evidence Based Emphasis of AquaDios-Med™ PPM is to teach each patient how to use mental skills to alter
and control positive physiology and how to accomplish safe sustained vigorous exercise to build endurance, stamina, a strong Immune System, to improve vitality and a establish a healthy psychophysiological state; a process that will establish a healthy mental and physical state, independent from drugs and most surgeries.
Research shows the American Healthcare Crisis is a factual Manufactured Man-Made Crisis
created and contrived by an unscrupulous deceitful for-profit culture found in in the U.S. Congress, the FDA, the pharmaceutical-medical device makers, the American Medical Association -- AMA, the American Hospital Association – AHA -- Modern Hospital Medicine practices and the entire healthcare industry. This industry spends hundreds of billions of dollars lobbying Congress to shelter incredibly, stupendous and colossal profits. For that reason, the American Healthcare Crisis is nothing more than an artificial politicized hypothetical construct, a Franklin D. Roosevelt quote is relevant here … In politics, nothing happens by accident. If it happens, you can bet it was planned that way. For this culture the HealthCare System design is to manipulate one of the most important and absolutely necessary socio-medico-system, one that all people need and depend on from birth to death for healthcare. Consequently, hospitals and modern medicine are both manipulated and directly complicit in the fraud of selling iatrogenic medicine with unnecessary services such as surgeries, medicines, procedures, tests, examinations, all of which are profit-centered and dangerous, some causing serious debilitating and lasting side effects and too often death.
In order to prove AquaDios-Med™ PPM is a legitimate evidence based health procedure it is
necessary to attempt to pinpoint some of the major research in deep-water running, which unfortunately is mostly directed toward the athlete recovering from injury. Nevertheless, research has demonstrated how valuable deep-water running can be to eliminate or reduce symptoms for those suffering from chronic disease and specific ailments.
I believe, and I’m certain you’ll agree the research in this supports the fact that “exercise is
medicine”. This is the kind of medicine that only the patient or person can produce as a consequence of safe daily exercise as advocated by AquaDios-Med™. The research supports the fact that the “impaired become repaired” with safe daily exercise; just as AquaDios-Med™ states. This research
Exercise Is Preventive Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Research • Physical Exercise • History • Part V History • Physical Fitness • Preventive Medicine 13 pages
This section of the book will briefly focus on the history of physical fitness and its impact on
the many health benefits safe sustained intense exercise can accomplish in fighting chronic deadly disease. Deep-water running and other forms of Aquatic exercise is discussed as well. The hope is to bring to the reader a short history of physical exercise and its continuous positive effects on health. This includes studies on exercise and addresses how chronic disease is killing sedentary American’s that could have healthy quality lives with exercise. Lance C. Dalleck and Len Kravitz, Ph.D. discuss exercise as we enter the 21st century and call
it one of the greatest accomplishments to be celebrated is the continuous pursuit of fitness since the beginning of man’s existence. Dalleck and Kravitz say that throughout prehistoric time, man's quest for fitness has been driven by a desire to survive through hunting and gathering. Today we are no longer driven by subsistence requirements, but physical fitness remains dominant in the quest for health, well-being and a high quality of life. The historical events of physical fitness and its impact on over all general health is examined together with the highlight of
influential individuals who have helped shaped the history of fitness beginning with primitive man up to the foundation of the modern fitness movement.
Primitive man and fitness 10,000 B.C
Primitive nomadic lifestyles required the continual task of hunting and gathering food for survival. Tribes commonly went on one or two day hunting journeys for food and water. Regular physical activity apart from that necessary for hunting and gathering was also a principal component of life. Following successful hunting and gathering excursions, celebration events included trips of six to 20 miles to neighboring tribes to visit friends and family, where dancing and cultural games often lasted several hours. This Paleolithic pattern of subsistence pursuit and celebration, demanding a high level of fitness and consisting of
various forms of physical activity, defined human life. Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
The Neolithic Agricultural Revolution - 10,000-8,000 B.C. The Neolithic Agricultural Revolution marked the conclusion of primitive lifestyle and signified the dawn of civilization. This historic period was defined by important agricultural developments including animal and plant
domestication, and the invention of the plow. These human advancements made it possible for hunting-gathering tribes to obtain vast amounts of food while remaining in the same area, thus transforming primitive man into an agrarian (agriculture and farming) society.
This era in history symbolizes the beginning of a more sedentary lifestyle, as man began to alleviate some hardships of life while simultaneously decreasing daily physical activity.
Ancient Civilizations • China • India 2500 • 250 B.C. In China, the philosophical teachings of Confucius encouraged participation in regular physical activity. It was recognized that physical inactivity was associated with certain diseases, referred to as organ malfunctions and internal stoppages, which sound similar to heart disease and diabetes were preventable with regular exercise for fitness.
Cong Fu gymnastics was developed to keep the body in good, working condition. Cong Fu exercise programs consisted of various stances and movements, characterized by separate foot positions and imitations of different animal fighting styles. In addition to Cong Fu gymnastics, other forms of physical activity existed throughout
ancient China including archery, badminton, dancing, fencing, and wrestling.
India In India, individual pursuit of fitness was discouraged as the religious beliefs of Buddhism and
Hinduism emphasized spirituality and tended to neglect development of the body. Consequently, the importance of fitness within society in general was relatively low. However, an exercise program similar to Chinese Cong Fu gymnastics developed, while still conforming to religious beliefs, known as Yoga. Though it’s exact origin has yet to be identified, Yoga has existed for at least the past 5000 years. Translated, Yoga means union, and refers to one of the classic systems of Hindu philosophy that strives to
bring together and personally develop the body, mind, and spirit. Yoga was originally developed by Hindu priests who lived frugal lifestyles characterized by discipline and meditation. Through observing and mimicking the movement and patterns of animals, priests hoped to achieve the same balance with nature that animals seemed to possess. This aspect of Yoga, known as Hatha Yoga, is the form most Westerners are most familiar and is defined by a series of exercises in physical posture and breathing patterns.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
Bedsides balance with nature, ancient Indian philosophers recognized health benefits of Yoga including proper organ functioning and whole well-being. These health benefits have also been acknowledged in the modern-day United States, with an estimated 12 million individuals regularly participating in Yoga.
The Near East • 4000-250 B.C.
Early political and military leaders within the civilizations of Assyria, Babylonia, Egypt, Palestine, Persia, and Syria, realizing the importance of fitness to the efficiency and performance of military forces, encouraged fitness throughout society. Perhaps the best example of a civilization utilizing fitness for political and military purposes is the Persian Empire. Persian leaders demanded strict physical fitness in its people; accomplished through the implementation of rigid training programs. At age six, boys became property of the Empire and underwent training which included hunting, marching, riding, and javelin throwing. Fitness training to improve strength and stamina was not intended for health benefits, but rather to create more able soldiers to help expand the Empire. The Persian Empire during its height, with its policy and emphasis on high fitness, eventually encompassed all of the Near East. However, emphasis on fitness levels throughout the Persian civilization decreased as affluence and corruption entangled political and military leaders. The downfall and collapse of the Persian Empire occurred at a time when society could largely be characterized by an overall lack of fitness.
Ancient Greek Civilization • 2500-200 B.C. Athens - Perhaps no other civilization has held fitness in such high regard as ancient Greece. The idealism of physical perfection was one that embodied ancient Greek civilization. The appreciation for beauty of the body and importance of health and fitness throughout society is one that is unparalleled in history. The Greeks believed development of the body was equally as important as development of the mind. Physical well-being was necessary for mental well- being, with the need for a strong, healthy body to harbor a sound mind. Many founding medical practitioners facilitated the growth of fitness throughout ancient Greece, including the likes of Herodicus, Hippocrates, and Galen. Gymnastics, along with music, was considered to be the most important classroom topic. A common saying in ancient Greek times was "exercise for the body and music for the soul". Gymnastics took place in palaestras, which were sites of physical education for young boys. The palaestra consisted of an indoor facility for gymnastics, in addition to an outdoor area for running, jumping, and wrestling. When adulthood was reached, typically between the ages of 14 and 16, the site for fitness training switched from palaestras to gymnasiums. Exercise in the palaestra and gymnasium was supervised by the paidotribe, who is similar to the modern fitness trainer. This idealistic fitness situation existed most strongly within Athens, which has been characterized as a democratic society most similar to the United States.
Sparta The Spartans of Northern Greece valued fitness even more than the Athenians. However, the heightened interest in fitness within Spartan culture was primarily for military purposes. During this era, Greek states were frequently at war with each other. Fighting skills were highly correlated with physical fitness levels, making it imperative for individuals to maintain high fitness levels. Spartan society required males to enter special fitness programs at the age of six. From this point until adulthood, the government was responsible for the child’s upbringing and training. This upbringing consisted of rigorous training programs that ensured all boys would grow into highly fit adult soldiers.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
Females were also required to maintain good physical condition for the purpose of being able to have strong offspring who could serve the state. The military-dominated culture of Sparta resulted in one of the most physically fit societies in the history of mankind.
Roman Civilization • 200 B.C. 476 A.D.
The Roman Empire was the antithesis of the ancient Greek civilization with the overall physical fitness condition of the Roman civilization highest during its time of conquest and expansion. During this period, all Roman citizens between the ages of 17 and 60 were eligible for the military draft. Therefore, it was imperative for all citizens to maintain good physical condition and be prepared for service. Military training consisted of activities such as running, marching, jumping, and discus and javelin throwing. This lifestyle resulted in strong, fit people who conquered nearly all of the Western World. However, the fitness levels of the general Roman population declined as individuals became enamored with wealth and entertainment, such as the gladiator battles. Materialistic acquisition and excess became higher priorities than physical condition. The lavish lifestyle and physical decay eventually took its toll as the
Roman civilization fell to the physically superior Barbarian tribes from Northern Europe.
The Dark 476 A.D. • 1000 and Middle Ages 900 – 1400
The crumbling of the Roman Empire, which was conquered by Barbarians from Northern Europe, symbolized the beginning of a millennium of intellectual standstill. However, these occurrences were beneficial with respect to fitness. The lavish lifestyles of the Romans had resulted in the complete deterioration of the society's fitness level. The barbaric tribes from Northern Europe possessed similar characteristics to primitive people. Their lifestyle consisted of hunting and gathering food, and tending to cattle. Physical activity and fitness were prerequisites for survival. Therefore, despite the cultural setbacks that occurred with the fall of the Roman Empire, fitness experienced a revival during the Dark and Middle Ages.
The Renaissance 1400-1600
Following the Dark and Middle Ages, the rebirth of cultural learning from the ancient Greek and Roman civilizations gave rise to the Renaissance. Accompanying this time period was a renewed interest in the human body. Once again, the ancient Greek ideals, which glorified the human body, gained widespread acceptance. Many individuals, including Martin Luther (religious leader), John Locke (philosopher), Vittorino da Feltra, John Comenius, and Richard Mulcaster (physical educators) maintained that high fitness levels enhanced intellectual learning. Civilizations that recognized the importance of fitness needed an avenue to convey this knowledge to their people. Therefore, fitness and physical education share a common bond. Physical education became the tool used to spread the value and benefits of fitness throughout society. School programs, primarily in ancient Greece, had previously recognized the necessity for curriculums involving physical education. The renewed appreciation for human life, which evolved during the Renaissance, created an environment which was ready for the widespread development of physical education throughout Europe.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
National Period in Europe • 1700-1850
Continental Europe underwent numerous cultural changes following the Renaissance. Fitness remained important and continued to follow trends initiated during the Renaissance. Physical education programs expanded within emerging nations of Europe. Intense feelings for nationalism and independence created the atmosphere for the first modern fitness movement, which came in the form of gymnastics programs. Gymnastics enjoyed immense popularity during this era, becoming especially prevalent in Germany, Denmark, Sweden, and Great Britain.
Germany
The growth of gymnastics in Germany can be primarily attributed to the
work of two physical educators: Johann Guts Muths and Friedrich Jahn. Guts Muths is generally referred to as the "Grandfather of German Gymnastics." He invented numerous exercise programs and the equipment upon which they were performed. His lifetime works and achievements are found in two books - Gymnastics for the Young and Games.
Friedrich Jahn earned the title of Father of German Gymnastics for his
long-lived work. It was early during Jahn's lifetime that Napoleon conquered much of Europe, including Germany. With its downfall to France, Germany was subsequently divided into separate states. Jahn's passion for German nationalism and independence became the driving force behind his creation of gymnastic programs. He believed future susceptibility to foreign invasion could be prevented through physical development of the German people. Shortly thereafter, exercise facilities that housed apparatuses designed for running, jumping, balancing, climbing, and vaulting called Turnvereins developed throughout Germany.
Sweden
Per Henrik Ling developed and introduced his own gymnastics program to Sweden which
consisted of three different areas: 1) educational gymnastics, 2) military gymnastics, and 3) medical gymnastics. Ling had a strong medical background and recognized that exercise was necessary for all persons. He maintained that exercise programs should be devised based on individual differences. Ling also believed physical educators must possess knowledge of the effects of exercise on the human body. Ling used science and physiology to better understand the importance of fitness.
Denmark
Frank Nachtegall, who initially started teaching out of his home, introduced and helped popularize gymnastic programs throughout Denmark. He was especially concerned with development of gymnastic programs within school systems. Childhood interest in physical activity sparked Nachtegall’s fascination with fitness. Eventually he taught in a private facility, which was devoted entirely to physical training and later became director of a program designed to prepare future fitness instructors called Training Teachers of Gymnastics.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
England
Within Great Britain, medical student Archibald Marclaren spread the word on the benefits of fitness and regular exercise. Marclaren, like Per Henrik Ling of Sweden, was fascinated in the scientific components of fitness. His lifetime works in these areas are recorded in National Systems of Bodily Exercise and Training in Theory and Practice. Marclaren made several observations based on his work, which are remarkably similar to present-day exercise recommendations. Marclaren believed the cure for weariness and stress was physical action. He noted recreational exercise found in games and sport was not sufficient for attaining adequate fitness levels. Finally, Marclaren realized both growing boys and girls required regular physical exercise. In agreement with Ling, Marclaren also recognized the need for individual variation in fitness training programs. Furthermore, he documented the importance of progression of exercise.
America – Colonial Period - 1700-1776
Hardships of colonial life ensured that regular physical activity continued to be a lifestyle priority, however during this period no organized exercise or fitness programs existed. Colonial America remained an undeveloped country characterized by much unexplored land and wilderness. Lifestyles during this era consisted largely of plowing the land for crops, hunting for food, and herding cattle. This lifestyle provided sufficient levels of physical activity with no additional need or demand for exercise to maintain fitness levels.
United States - National Period - 1776 to 1860
Fitness in the United States during the National Period was influenced by European cultures. Immigrants brought many aspects of their heritage to the United States, including German and Swedish gymnastics. Constant threats to independence and nationalism from foreign invasion were dynamics prevalent in Europe and not the United States. German and Swedish gymnastic programs failed to attain the same levels of popularity as in Europe. Early leaders in the United States were conscious of the need for exercise and fitness. Benjamin Franklin recommended regular physical activity, including running, swimming, and basic forms of resistance training for health purposes. President Thomas Jefferson acknowledged the necessity for fitness, although maybe to a somewhat extreme measure: “Not less than two hours a day should be devoted to exercise and the weather shall be little regarded. If the body is feeble, the mind will not be strong".
Early Physical Education in the United States
Within Europe, schools had been an important medium for spreading the need for fitness to society through physical education programs. However, in the United States, the educational process focused primarily on intellectual matters. Schools concentrated on teaching traditional subjects including reading, writing, and arithmetic. Physical education remained missing from the public education system for the better part of the nineteenth century. Despite the relative lack of interest in fitness existing during this era, J.C. Warren and Catherine Beecher made significant contributions to the future of fitness in America.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
Dr. J.C. Warren, a medical professor at Harvard University, was a major proponent of physical activity. Warren’s medical background gave him a clear understanding of the necessity for regular exercise, with his recommendations including exercises such as gymnastics and calisthenics.
Warren began devising exercises for females. Catherine Beecher specifically devised fitness programs to meet the needs of women. Among her many different programs was a system of calisthenics performed to music. Though not formally recognized in name, Beecher's programs of the mid-nineteenth century bear remarkable similarities to modern-day aerobics.
United States • Post-Civil War • 1865-1900
One of the most important events with respect to modern fitness in the United States was the Industrial Revolution, which resulted in widespread cultural changes throughout the country. Advancement in industrial and mechanical technologies replaced labor-intensive jobs. Rural life changed to an urban lifestyle. The new city life generally required less movement and work compared to rural life, consequently decreasing levels of physical activity. At the turn of the century, the most common causes of death were from influenza, polio, rubella, and other infectious diseases. Risk of disease and mortality from infectious diseases were alleviated with the discovery of Penicillin. The cost of industrialization and urbanization became glaringly apparent starting in the 1950s and 1960s. An epidemic of hypokinetic diseases including cardiovascular disease, cancer, and Type II diabetes, never before prevalent, began to be recognized as the leading causes of disease and death. The lifestyle improvements brought in part by the Industrial Revolution had apparently come with an unwanted and alarming cost to health.
Physical Education
Following the end of the Civil War in 1865, Swedish and German Gymnastics enjoyed a moderate growth in popularity. However, the most popular form of gymnastics during this time period was “The New Gymnastics,” introduced by Dioclesian Lewis. Individuals who played important roles in the development of fitness during this time period were Edward Hitchcock, William Anderson, and Dudley Sargent. Hitchcock recognized the desired outcome of his fitness programs, a combination of gymnastics and calisthenics, was improved health. He also introduced the concept of utilizing anthropometric measurements to assess fitness progress. Sargent added scientific research to fitness instruction and developed organized instructor teaching methodologies. The lifetime work of Anderson focused on physical education instruction, with his greatest contribution being its development into a professional organization.
An interesting argument developed during the post-Civil War period that still exists today. Many physical education instructors believed firmly in the value of incorporating exercise programs that would improve health-related fitness. However, sports were also gaining popularity in the United States during this era. Consequently, the majority of physical education programs focused on sports and games. The debate between health-related fitness and skill-related fitness physical education programs continues to exist.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
The 20th Century
The 20th century symbolized the beginning of a new era of fitness leaders: the Presidents of the United States. Theodore Roosevelt, perhaps the most physically fit President to occupy the oval office, also led the nation into the new century. He recognized the importance of exercise and physical activity, and had the power to encourage the citizens of America to be physically active. President Roosevelt held an infatuation for fitness similar to the ideology of ancient Greece. His desire for physical fitness evolved out of his childhood battle with asthma, which he overcame with a rigorous exercise program.
As President, he engaged in multiple forms of physical activity including hiking, horseback riding, and other outdoor endeavors. Although not all the presidents following Roosevelt have held fitness in the same high regard, they recognized that the position required a commitment to the fitness of the citizens of the United States.
World War I
In Europe, the First World War started in August of 1914, with the entrance of the United States occurring three years later in 1917. With the United States' entry into the battle, hundreds of thousands of military personnel were drafted and trained for combat. After the war was fought and won, statistics were released from the draft with disturbing data regarding fitness levels. It was found that one out of every three drafted individuals was unfit for combat and many of those drafted were highly unfit prior to military training. Government legislation was passed that ordered the improvement of physical education programs within the public schools. However, the heightened interest and concern for low fitness levels would be short-lived as the United States entered the 1920s and the Depression.
The Roaring Twenties • Great Depression
Heightened interest in fitness dissipated throughout the decade. A pattern that had been familiar throughout history is that after a war is fought and won, the tendency is for society to relax, enjoy life, and exercise less. The Roaring Twenties earned the label for a reason, as society lived more frivolously than at any other time in history. Priorities centered on eating, drinking, partying, and other forms of entertainment. In October of 1929, the stock market crashed, signaling the beginning of what would be a decade of economic depression. The economy failed to recover until the United States entered World War II in 1941. Along with many other aspects of life, fitness levels declined during the Depression. The gains that physical education programs made through the passage of legislation following the WW I were short-lived. Funding for these programs became limited and eventually was exhausted as emphasis in the poor economy was forced to shift elsewhere. Despite the setbacks which fitness suffered during the Great Depression, Jack LaLanne, who would eventually be recognized as a guiding pioneer of fitness, began his lifetime career as a media fitness instructor. Throughout his life, LaLanne preached the value of preventive lifestyle habits. In the 1950s, The Jack LaLanne Show began airing on television, preceding the appearance of Richard Simmons and Jane Fonda by 25 years. LaLanne developed fitness programs including aerobics, water aerobics, and resistance exercise.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
LaLanne also introduced numerous pieces of exercise equipment including the first cable-pulley machine, the safety system for doing squats called the Smith machine, and the first leg extension machine. Although LaLanne is often referred to as the originator of the "jumping jack movement", history suggests the real inventor was John “Black Jack” Pershing, a tactical officer from West Point in World War I. Though LaLanne preceded the modern fitness movement by some three decades, his fitness ideology and exercise programs were correct in approach when judged by modern research.
World War II
Throughout world history, military conflicts have had major impacts on the state of fitness. The Second World War and its aftermath in the United States would be no different. Essentially, the modern fitness movement evolved out of the influence of World War II and subsequent development of the Cold War. The United States entered World War II with the bombing of Pearl Harbor on December 7, 1941. With the declaration of war came the necessity to draft military personnel. However, as more men were drafted, it became embarrassingly clear that many of them were not fit for combat. When the war was over, it was reported that nearly half of all draftees needed to be rejected or were given non-combat positions. These disturbing statistics helped gain the attention of the country with regards to the importance of fitness. Important contributions to fitness came during the 1940s, specifically from Dr. Thomas K. Cureton at the University of Illinois. Cureton introduced the application of research to fitness, which improved exercise recommendations to individuals. Cureton not only recognized the numerous benefits of regular exercise, he strived to expand the body of knowledge regarding physical fitness. He wanted to answer questions such as how much exercise was healthy and what types of exercise were most effective. More importantly, Cureton wanted to know how physical fitness could best be measured within an individual. Among his most important contributions were developing fitness tests for cardiorespiratory endurance, muscular strength, and flexibility. His research resulted in multiple recommendations for the improvement of cardiorespiratory fitness, including the identification of exercise intensity guidelines necessary for improved fitness levels. His suggestions became the fundamental basis behind future exercise programs.
1950s • United States
The Cold War, Baby Boomer era was marked by the development of an important factor influencing the modern fitness movement known as the "Minimum Muscular Fitness Tests in Children" by Kraus-Hirschland. This study utilized the Kraus-Weber tests to measure muscular strength and flexibility in the trunk and leg muscles. It was reported that close to 60 percent of American children failed at least one of the tests. In comparison, only nine percent of children from European countries failed one of the tests. During the Cold War, these startling numbers launched political leaders into action to promote health and fitness. When results of the Kraus-Hirschland studies were reported to President Eisenhower by Senators James Kelly and James Duff, he responded by holding a White House Conference in June of 1956. Out of these meetings came two important results: 1) the formation of the President's Council on Youth Fitness and 2) the appointment of the President's Citizens Advisory Committee on the Fitness of American Youth. This was an important first step in helping to gain the nation’s attention concerning her fitness levels.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
During the 1950s, numerous organizations took initiative in educating the general public about the consequences of low fitness levels. Several agencies that have been involved in fitness promotion since the mid-1950s include the American Health Association (AHA), the American Medical Association (AMA), the American Association for Physical Education, Recreation, and Dance (AAPHERD), and the President's Council on Youth Fitness. These organizations would provide merit and legitimacy to the coming fitness movement.
The American College of Sports Medicine (ACSM) was formed in 1954, and has proved to be one of the premier organizations in the promotion of health and fitness to American society and worldwide. Throughout its history, ACSM has established position stands on various exercise-related issues based on scientific research.
1960s • United States
President John F. Kennedy was a major proponent of fitness and its health-related benefits to the American people. He furthered the development of the President’s Council on Youth Fitness, appointing Bud Wilkinson as head of the council. The name was also changed to the President's Council on Physical Fitness. Kennedy spoke openly about the need for American citizens to improve their fitness levels; including writing an article in Sports Illustrated entitled "The Soft American." He said, "We are under-exercised as a nation; we look instead of play; we ride instead of walk". Kennedy prompted the federal government to become more involved in national fitness promotion and started youth pilot fitness programs. Kennedy's commitment to fitness can best be summarized when he said, "Physical fitness is the basis for all other forms of excellence." Dr. Ken H. Cooper, widely recognized as "The Father of the Modern Fitness Movement", is generally credited with encouraging more individuals to exercise than any other individual in history. Cooper advocated a philosophy that shifted away from disease treatment to one of disease prevention. … It is easier to maintain good health through proper exercise, diet, and emotional balance than it is to regain it once it is lost... Early in his career, Cooper stressed the necessity for providing epidemiological data to support the benefits of regular exercise and health. Data from thousands of individuals became the foundation for his aerobic concepts. Aerobics, released in 1968, sent a powerful message to the American people - to prevent the development of chronic diseases, exercise regularly and maintain high fitness levels throughout life. Dr. Cooper’s message, programs and ideas established the model from which fitness has proliferated up to modern time.
Lessons From History
The history of fitness portrays some fascinating themes that relate closely to the 21st century. One commonality is the strong association of military and political might with physical fitness throughout mankind’s advancement. In many ways, this shows how impacting our world leaders can be on health and fitness. The mind-body concept has had a tenuous development. At times, some cultures prescribed spirituality at the expense of the body where as others, such as Greek society, upheld the ideal a sound mind can only be found in a healthy body. Another interesting development from history is the concept of exercise for the body and music for the soul. Present day fitness programs have evolved this concept harmoniously, with music being a distinctive component to the exercise experience.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
It appears that as societies become too enamored with wealth, prosperity and self-entertainment that fitness levels drop. In addition, as technology has advanced with man, the levels of physical fitness have decreased. History offers little insight how to prevent or turnaround these recourses. Thus, this is a resolution we are challenged with in today’s society. Perhaps utilizing all of the extensive research completed on health and fitness in combination with the creative minds now in the fitness industry, we now can solve this part of the fitness puzzle. This section covers common questions about exercise and gives worthwhile information about what happens during exercise.
Staying Cool When Your Body is Hot
Chantal A. Vella, M.S and Len Kravitz, Ph.D. say that maintaining ample hydration can be challenging for participants in outdoor and indoor aquatic exercise classes. Sustaining hydration is essential for normal bodily functions and for peak exercise performance. Many of your students do not associate aquatic exercise with any potential risk of dehydration; however, this is a fundamental issue in aquatic exercise. This overview will discuss and explain some of the key physiological concepts of body temperature regulation and hydration for aquatic exercise professionals. In addition, specific recommendations for optimal hydration during exercise and aquatic exercise are provided.
How does the body regulate body temperature?
The human body regulates temperature by keeping a tight balance between heat gain and heat loss. Your temperature regulation system is more analogous to the operation of a home furnace, as opposed to the function of an air conditioner. Humans regulate heat generation and preservation to maintain internal body temperature or core temperature. Normal core temperature at rest varies between 97.7 to 99.5 °Fahrenheit (°F). Core temperature is regulated by the hypothalamus (in the brain), which is often called the body’s thermostat. The hypothalamus responds to various temperature receptors located throughout the body and makes physiological adjustments to maintain a constant core temperature. For example, on a hot day, temperature receptors located in the skin send signals to the hypothalamus to cool the body by increasing the sweat rate. During all types of exercise the body’s ability to thermoregulate is challenged. Heat is produced as a bi-product of metabolism; metabolism is defined as all of the reactions that occur in the human body. However, the human body is only 25% efficient; therefore you lose approximately 75% of energy as heat. During exercise, heat is produced mainly from working muscle contractions and core temperature can go above 104 °F.
How does the body lose heat
As previously discussed, the body regulates temperature like a furnace. It is constantly producing heat and then dispersing it through various processes. Heat can be lost through the processes of conduction, convection, radiation, and evaporation. Conduction is the process of losing heat through physical contact with another object or body. For example, if you were to sit on a metal chair, the heat from your body would transfer to the cold metal chair. Convection is the process of losing heat through the movement of air or water molecules across the skin. The use of a fan to cool off the body is one example of convection.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
The amount of heat loss from convection is dependent upon the airflow or in aquatic exercise, the water flow over the skin. Radiation is a form of heat loss through infrared rays. This involves the transfer of heat from one object to another, with no physical contact involved. For example, the sun transfers heat to the earth through radiation. The last process of heat loss is evaporation. Evaporation is the process of losing heat through the conversion of water to gas (evaporation of sweat). The primary heat loss process for aqua enthusiasts is convection, however, in an outdoor pool on hot day evaporation will also play a primary role in heat loss.
How much water • in the Body
Water makes up approximately 60% of your total body composition. In addition, 73% of lean body mass or muscle is composed of water. It is the essential nutrient for survival and is required for all cell functions. Water is also an important constituent in thermoregulation, because it is a major component of blood volume. It is mainly lost through sweat, respiration, and waste. However, when the body is dehydrated, most of the water lost is from the blood.
Sweat Basics
The average person has 2.6 million sweat glands. Sweat is made up of water and electrolytes such as sodium, chloride, and potassium. When the hypothalamus senses an increase in core temperature it will act by increasing blood flow to the skin, stimulating the sweat glands. The result is an increase in the rate of water lost through sweating. During low- to moderate-intensity exercise of less than one hour, there are minimal electrolyte losses because the body reabsorbs most of the electrolytes from the sweat. However, during moderate- to high-intensity exercise of greater than one hour, the electrolyte loss in sweat becomes significant and the sweat rate is too fast for re-absorption of electrolytes.
Water • lost during Exercise
During high-intensity exercise, a person can lose up to 2.0 liters of water per hour! However, 1.0 liter of water per hour is more common. Sweat rate can vary depending on the environmental temperature, humidity, type of clothing worn during exercise, intensity of exercise, fitness level of the individual and acclimation of the individual to the environment. Replacing fluids during and after exercise is very important for staying hydrated and preventing dehydration. Signs of dehydration include dark colored urine (urine should be the color of water with a splash of lemon); muscle cramps, decreased sweat rate, and increased fatigue.
Best way to stay hydrated
According the American College of Sports Medicine (ACSM), before, during and following exercise, water or a carbohydrate electrolyte drink is recommended to stay hydrated. The drink of choice should be cold in temperature and taste good to the individual. If it’s more palatable to the person, more will be ingested! ACSM makes the following general recommendations for the amount and type of fluid that should be ingested before, during and after exercise:
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
*Approximately 24 hours before exercise, an individual is recommended to consume fluids and foods to promote hydration. Fruits, vegetables, and carbohydrates are examples of foods that promote hydration. In addition, avoid too much alcohol and caffeine, as these fluids can cause water loss and promote dehydration.
*Two hours before exercise, 16 ounces (2 cups) of fluid should be ingested to promote hydration and allow time for excretion of excess water. *During exercise of less than an hour, it is recommended to ingest water every 15 minutes to prevent dehydration. Electrolyte loss is negligible; therefore a carbohydrate drink is not necessary. *During exercise of greater than an hour, it is recommended to ingest a carbohydrate and electrolyte drink every 15 minutes. *Never restrict fluids during exercise! Quite the contrary. Encourage your students to take water breaks during the class. Many aquatic exercise professionals actually plan the hydration breaks into the structure of the class. *After exercise ingest a carbohydrate and electrolyte solution. The carbohydrate will replenish glycogen stores (muscle carbohydrate stores) and the electrolytes will replenish sodium, chloride, and potassium lost in sweat. In addition, avoid carbonated drinks, as they make you feel full and decrease fluid intake.
Specific Suggestions - Aqua Instructor
As aqua instructors it is essential to promote fluid intake before, during and after exercise. Many individuals do not associate dehydration with exercise in the pool. However, in a hot humid environment, dehydration is a potential risk to your aqua exercise students. During a 60 to 90 minute class, encourage participants to take a water break every 15 minutes. In hot, humid weather a carbohydrate and electrolyte drink is preferable to water. However, in cool to moderate weather, water is sufficient to maintain hydration during exercise. Following each class, remind students to continue to re-hydrate throughout the day. Advise your students to drink 1-2 glasses of water at least one hour before each exercise class begins. For the health, safety and enjoyment of your students, aquatic exercise professionals are encouraged to develop teaching strategies that educate students about correct and appropriate hydration before, during and after exercise. In the long run, this will help your students realize their fitness goals. The unique and innovative exercises in Aquatics are explored including deep-water running and other deep to shallow water exercises. This includes more information and research on the positive physiological effects of Aquatic exercises. The AquaDios-Med™ Philosophy
• EXERCISE IS MEDICINE • THE IMPAIRED BECOME REPAIRED • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD • • YOU GROW OLD BECAUSE YOU STOP EXERCISING! • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race.
Copyright © 2008 – 2012 – 2013 2nd Edition AquaDios-Med™ • AquaDios Corp.
All rights reserved. Exercise Is Preventive Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section VI
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
History • Introduction • Spas 2000 B.C. • Present
Physical Fitness • Preventive Medicine Section VI
Evidence Based
AquaDios-Med™ Proactive Preventive Medicine 11 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
History • Introduction • Spas Solution • Healthcare Crisis • Part VI
Brief Ancient World History • Evolution Deep-Water Immersion • 2000 B.C • Present The Mission of AquaDios-Med -- seize the natural evolution provided by Ancient World
History healing and transport it into the new millennium. History -- research show that healing centers with therapeutic immersion chambers to advance healing and decrease suffering have existed throughout the world • India before 2000 BC • 1350 BC Egypt • For Centuries: Turkey, Iran, Japan • used deep-water immersion for healing • 5th Century BC, Greek - Roman special immersion chambers for physical exercise - healing • Ancient deep-water immersion exercising • hot • warm • cool • cold temperatures • steam bath • 18th -- 19th century Americans • natural medicinal • hot springs for health • England, France, Germany, New York luxury hotels, grew up around the baths
Spa logic is similar to modern hospital medicine, disregards the simple fact Exercise is Medicine --- seen instead as sport or leisure -- not critical to health. The Spa concept is built on fundamental passive Balneology -- therapeutic use of thermal baths, a place to relax, be pampered, de-stress. Spa Medicine • Balneology – Hydrology • Medical science study physicochemical properties of immersion in mineral waters •Long tradition Europe, Israel, Japan • Predominantly for chronic diseases -- no exercise, let alone sustained vigorous exercise • No Mind Body Medcine, Inner Mental Training, Psychoneuroimmunology -- immersions are warm to hot – no cool or cold
Balneology – Hydrology - Hydrotherapy research • Warm water relaxes spasm • Treat muscular strains and sprains • muscular fatigue • backache • Heat with massage • other manipulative -- stimulative treatments -- whirlpool bath • Sitz baths (sitting in hot water) treatment -- painful hemorrhoids • Physical Therapy -- Water Immersion Buoyancy allows exercise in a buoyant medium – patients can move weak parts of their bodies without contending with the strong force of gravity Water treatments in general are called hydrotherapy
European Spas employ German Cure System (KUR) -- patient is sent to a spa village for 2 to 4 weeks where the climate and altitude have a positive impact in a stress free environment -- Since the 1960s Insurance companies pay for these cure stays.
Studies cite 60% drop in sick days -- 66% decrease prescription drug consumption -- long-term physical, mental, spiritual, and emotional improvements. This healthcare is a better system than the U.S. but is not proper and lasting treatment – akin to Kwan-Tzu … Give a man a fish and he eats today … Teach a man to fish and he can feed himself for the rest of his life. AquaDios-Med™ Proactive Preventive Medicine and research show – Spa Concept • too passive no patient daily exercise • The 60 to 66 percent improvement is nearly identical to expected outcomes with placebo. Nationalized AquaDios-Med™ programs are what are needed to reverse the American over dependence on invasive hospital tests, drugs and surgeries.
AquaDios-Med™ submits a simple basic human fact that safe daily proactive Exercise is Medicine for all people eighty percent of the time. In other words, only 20 percent of the hospital patient admission population needs hospitalization or in-patient care because 80 percent of all ailments can be resolved and managed by the kind of safe daily Exercise is Medicine and Mind Body Medicine offered in AquaDios-Med™ programs.
The U.S. Spa Industry reported revenues of $13.4 billion U.S. dollars at the end of 2011.

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Spas History • Research • Solution • Healthcare Crisis • Part VI Historical Research Deep-Water Immersion • Temperature • Therapeutics Research on the cultural use of Deep-Water Immersion Therapy shows the evolution from
before 2000 B.C. For thousands of years Deep-Water Immersion Therapy has been a part of cultures around the world. Even in ancient times the distinctive thermodynamic properties of Water, with its markedly different therapeutic effects at different temperatures has been known and applied for healing.
Hot water is defined as above body temperature 100° – 103° F, is stimulating, raises the body temperature slightly, very relaxing and dispersing, especially to the muscles, joints and blood vessels. It opens the pores, induces sweating, and penetrates the skin and muscles quite deeply. Hot water can also ripen latent boils, abscesses or skin eruptions and bring them to the surface for release. Hot water draws the body's circulation outwards, opening up the pores and capillaries. Prolonged hot water immersion is not recommended.
Warm water 96° – 99° F, about body temperature or slightly cooler, is gently relaxing, stimulates appetite – digestion and activity of the digestive organs when done about an hour before eating. Warm water, particularly water that's almost lukewarm -- called tepid is best for general bathing purposes -- warm water is harmonizing and balancing.
Cool water 82° – 88° F is good for soothing heat and inflammation, and for cooling the body on hot summer days; cool water immersion is good for bringing down fevers.
Cold water immersion 72° – 74° F for short periods of time, act as a bracing, stimulating tonic; after bathing in the hot water pools, Romans would go for a quick dip in the frigidarium, or cold water bath, to brace their skin and close back up their pores.
Sebastian Kneipp a German priest in the 1800s is recognized as the originator – promoter of
cold water therapy in the modern Western world. He was pronounced terminally ill with lung disease and his self-treatment included daily baths in the icy Danube River for just a few minutes; in a year he was cured. He developed a system of hydrotherapy with treatments of alternating hot and cold water therapies for many different health complaints. Today the Kneipp Association has a network of treatment and training centers throughout Europe and in South Africa.
Hot water 100° – 103° F relaxes, disperses, and thrusts blood circulation out to the body's exterior -- cold water 72° – 74° F stimulates, consolidates and shunts blood circulation inwards towards the core and internal organs. Cold water constricts the blood vessels, stimulates circulation, digestion and metabolism, and awakens the appetite, having an exhilarating effect. Cold water compresses reduce swelling and inflammation. Passive Cold water immersion should only be for a maximum of about 3 to 4 minutes.
Alternating Hot and Cold water immersions is a particularly powerful technique. The hot water draws old, stagnant blood out of the internal organs or the body’s interior, and the cold water drives fresh blood back into the internal organs and the body's core. With alternating hot and cold immersion, the circulation is powerfully increased, the affected area begins to throb and pulsate -- a sign of healing and regeneration; Hot immersion -- about 3 to 4 minutes -- followed by cold immersion of 1 to 2 minutes. Repeat this two or three time or more, but always end on a short hot or warm application to remove or neutralize any remaining chills.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
Brief Ancient World History • Evolution Deep-Water Immersion • 2000 B.C • Present AquaDios-Med • Comprehensive Preventive Medicine
The Mission of AquaDios-Med has been to seize the natural evolution provided by Ancient World History healing and transport it into the new millennium. Healing centers have existed throughout the world which included therapeutic immersion chambers to advance healing and decrease suffering. Ancient World Excavations prove that in India before 2000 BC, there was common use of deep-water immersion for health purposes; and from about 1350 BC in Egypt. Centuries ago places like Turkey, Iran, and Japan also used deep-water immersion for healing. By the late 5th Century BC, Greek and Roman cities had huge gymnasium facilities with rooms where special immersion chambers were located for physical exercise and healing.
These deep-water immersion activities involved people exercising in hot, cool and cold temperatures and incorporated a steam bath. In the 18th and 19th century Americans relied on natural medicinal or hot springs for health while resorts in England, France, Germany, and New York flourished. Notably, luxury hotels, fine shops, concert halls, and casinos grew up around the baths as is true today.
Historically deep water immersion chambers used for health benefits were located in rooms or
buildings containing facilities for physical exercise of the body while immersed into hot, cool and cold temperatures. Roman immersion health centers in Pompeii were built in about the 2nd century BC for health and exercise. The layout included the apodyterium, or dressing room; the calidarium, or hot room, containing the alveus, or hot immersion and the laconicum, a hot or steam bath; the tepidarium, or warm immersion; and the frigidarium, or cold immersion; shops, lecture halls, elaborate gymnasiums, gardens, and libraries were included.
In Northeastern Europe, Finns and Russians developed steam baths Water thrown on heated
rocks created dense clouds of steam, in which bathers sweated then splashed with cold water and plunged into snow or an icy stream.
History shows one worldwide priority of Ancient Health Practices Centered on Physical Exercise in Immersion Chambers with hot, cool and cold temperatures.
In Rome, 952 of these health facilities were in operation by the 4th century BC. It has been
estimated that one immersion chamber contained space for 1600 users. These health centers were huge with vaulted interior ceilings and contained immersion chambers, swimming pools, lecture halls, lounges, and other exercise facilities.
Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
AquaDios-Med is the new age philosophy that the safe process of Mind Body Medicine
combined with deep-water running is a legitimate procedure based on proven health practices of more than 2000 years. AquaDios-Med is a proactive preventive Heal Yourself concept and includes, Heal Your Family; Heal Your World as a reality. The Synergy of Medicine can be defined as the
cooperative action of two or more drugs, muscles, or organs. And the synergy of AquaDios-Med is the cooperative action of the mind and body producing the right drugs by proper muscle and organ use.
Generally the term synergy is applied to drugs whose combined action is more powerful than their simple effects added together. The challenge faced by the human immune system is to recognize and destroy non-self- substances - such as foreign microbes and damaged or abnormal cells—while recognizing and leaving healthy cells and tissues intact; this daunting task is being confronted by Mind Body Medicine and Psychoneuroimmunological Mediation.
AquaDios-Med is designed for its practices and procedures of physical exercise immersions, within a Health Center. It is a modernized version fitting the basic path of the 4th century BC Greek-Roman models similar to those facilities found in Pompeii. To achieve AquaDios-Med accelerated healing the integrity and versatility of the individual immersion chamber is important. Each Chamber has an integral and little different, yet essential alternative dynamic required for exercise-therapy and healing.
Hydrotherapy has a number of uses. Warm water will relax spasm; thus, hydrotherapy has been useful in treating such conditions as muscular strains and sprains, muscular fatigue, and backache. Heat is often used in conjunction with massage or other manipulative or stimulative treatments, such as the whirlpool bath. Sitz baths (sitting in hot water) are effective in the treatment of swollen, painful hemorrhoids. Water is also useful in physical therapy because patients who exercise in a buoyant medium can move weak parts of their bodies without contending with the strong force of gravity.
Bath (hygiene) in medicine and many of the numerous systems for submerging all or part of the human body in water for therapeutic purposes is the treatment for various conditions and illnesses. The use of baths for such purposes as well as for religious purification, personal cleanliness, and private or social relaxation (see Baths) dates from at least the time of ancient Greece. Water treatments in general are called hydrotherapy; in this article, particular kinds of baths are discussed: hot and cold, medicated, and mineral.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
Spa • Optimal Healing
Gary J. Frost, Ph.D. wrote an article for Mary Ann Liebert, Inc. which was published in the JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE, Volume 10 in 2004 titled The Spa as a Model of an Optimal Healing Environment.
Most important of Frost’s work is the practice of medical doctors in Germany and their
specialized postmedical education and the study of climatology, balneology, and natural therapies. This training promotes the use of these natural therapies before resorting to medical drugs or surgeries. This author believes the U. S. must abolish the modern hospital medical practices of demanding invasive procedures, prescription of dangerous, often deadly pharmaceuticals, the over reliance on surgery and make preventive medicine programs such as AquaDios-Med™ the primary focus of all modern hospital medicine.
The AquaDios-Med™ mantra cannot be refuted … Exercise is Medicine … the Impaired Become Repaired. Studies continue t show that daily safe sustained proactive human exercise will provide the person with the proper biochemical homeostasis in about 80 percent of all presenting cases. Akin to the age old metaphor … give a man fish for dinner will feed him for one day, but teach a man to fish and he can eat the rest of his life. The proper medicine for 80 percent of the population is within them but it cannot be utilized without sustained safe exercise as in deep-water running.
Spa’s, like modern hospital medicine do not regard Exercise as Medicine they regard it as sport
or leisure and not critical to health. Further, the concept of Spa is passive. AquaDios-Med™ submits a simple basic human fact that safe daily proactive Exercise is Medicine for all people eighty percent of the time. In other words, only 20 percent of the hospital patient admission population needs hospitalization or in-patient care because 80 percent of all ailments can be resolved and managed by the kind of safe daily Exercise is Medicine and Mind Body Medicine offered in AquaDios-Med™ programs.
This author has been to European Spas and observed the German Cure System (KUR) utilized by physicians who have previously explored more conventional means, or when the patient is not sick enough to go to a hospital. This method involves the patient being sent to a spa village for 2 to 4 weeks where the climate and altitude are believed to have a positive impact and is stress free. Insurance companies in Germany have been paying for these cure stays since the 1960s.
They cite a 60% drop in sick days, a 66% decrease in prescription drug consumption, and long-
term physical, mental, spiritual, and emotional improvements. Although this is a better system than that used in the U.S. it misses the mark of proper and lasting treatment – it is akin to the metaphor, Give a man a fish and he eats today. Teach a man to fish and he can feed himself for the rest of his life. — Kwan-Tzu What this author means is that this approach is too passive and requires very little activity and very little daily exercise form the patient. Furthermore, the 60 to 66 percent improvement is identical to expected outcomes with placebo. Nationalized AquaDios-Med™ programs are what are needed to reverse the American over dependence on invasive hospital tests, drugs and surgeries.
Historic Origins • Spa • Deep-Water Immersion • Hydrotherapy • Differs
Spa is an acronym for salus per aqua - “health through water” and there approximately 10,000
Spas in the United States; most focus on eating and weight programs, including sports activities and nutrition, but none has a comparable program to AquaDios-Med™.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
Common use of Spas is primarily for stress reduction, with some specific medical and health issues, eating and weight loss, rest and relaxation, fitness – mild exercise, pampering and beauty. I’d say the biggest draw is pampering and beauty applications. Frost indicates the three most critical factors in creating an optimal healing environment in a spa venue are --
(1) a dedicated caring staff at all levels (2) a mission driven organization that will not compromise (3) a sound business model and leadership that will ensure permanency
The problem I have with factors two and three is that the organizations mission may be like
hospitals and be driven by the dollar rather than the outcome of health while a sound business plan may be to focus on income rather than health benefits.
AquaDios-Med™ has it focus on what works for more than 80 percent of the population and
that is simply the fact that Exercise is Medicine and that with safe daily exercise such as deep-water running the Impaired will become Repaired. This is supported and repeated in study after study – the human being must participate in safe daily exercise to be healthy and those with impairments do in fact heal or repair themselves with the same safe daily exercise.
J. Paul De Vierville traces the origin of the word spa to the early Latin verb spargere, which
means to pour forth. His research indicates the modern word spa found its way into the English language through the old Belgian Walloon word, espa, which referred to a fountain. The English derived spaw from espa. The outgrowth of Spa occurred simultaneously in different parts of Europe and Asia, where mineral springs and thermal mud were used for soothing and healing. Taking the waters for cleansing and purification prior to marriage and other religious ceremonies were practices in several cultures.
The presence of spas in Bath, England, Baden Baden, Germany, and other sites in Switzerland, Austria, Italy, Belgium, and the Czech Republic proves just how widespread the movement was. Thalassotherapy, which is healing by using ocean waters, exists in many cultures from the Red Sea to Europe and Japan.
According to the European Spa Association, representing Spas in 20 nations, there are more
than 1200 spas and health resorts throughout Europe. They are promoted as places of therapy and cure, rather than the pampering connotation that this author holds and that prevails in the United States. Alternative names for Spas throughout Europe are beauty farms, wellness hotels, vital hotels, dream hotels, and fitness hotels.
Unlike the U.S. where Spas are not supported as “health” practices European countries are the beneficiaries of a government social health policy that provides lengthy stays for workers to heal and rejuvenate. Scandinavian countries, The Netherlands, and Germany have been sending citizens throughout Europe for spa vacations for decades.
The word spa leads to a variety of interpretations in the United States, none of which include
any reference to places of healing. The following descriptions illustrate this point: 1. Club Spa - a facility, the primary purpose of which is fitness, which offers a variety of
professionally administered spa services on a day-use basis.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
2. Cruise Ship Spa - a spa onboard a cruise ship providing spa services, fitness, and often spa-cuisine menu choices.
3. Day Spa a spa offering a variety of spa services on a day-use basis. The emphasis is on pampering services such as facials and body scrubs, not fitness.
4. Mineral Springs -- a spa with an onsite source of natural mineral springs or seawater -- used
in hydrotherapy treatments. 5. Resort/Hotel SpaÑa spa located within a resort or hotel environment that provides spa
services, fitness activities, spa-cuisine menu choices, and perhaps some wellness components. 6. Medi-SpaÑa center where medical and spa professionals offer some wellness care in
addition to spa services, most often in the area of cosmetic procedures. 7. Destination SpaÑa facility, the sole purpose and mission of which is to provide guests with
opportunities for lifestyle improvement and health enhancement through professionally administered spa services, fitness and educational programming, onsite accommodations, and a variety of health and healing services. Healthy cuisine is served exclusively.
UNITED STATES SPA INDUSTRY • Details
Spas are estimated to number at least 10,000 in the United States. The largest grouping is day
spas, comprising approximately three quarters of the spas. Resort/hotel spas are the second most numerous, with destination spas being the smallest group with only 25 listed in North America.
In 2001, there were approximately
156,000,000 visits made to spas; 68% of these were to day spas. Currently, the spa industry in the United States has 100,000,000 square feet under roof. Almost 50% of the space is occupied by treatment rooms (massage, body treatments as examples), and slightly more than 20% is designated as beauty space. The annual revenue in this industry is approximately $11 billion. More than 50% of the revenue is derived from treatment
rooms, with beauty and retail sales accounting for about 36%.5 There are nearly 285,000 people employed, of whom approximately 65% are fulltime. Wages and salaries in 2001 accounted for more than $5 billion. In 2012, the U.S. spa industry reported revenues of $13.4 billion U.S. dollars for 2011.
This author believes the process of AquaDios-Med™ which includes its “teaching” patients to perform their own “power massage “ is a far more economical practice than the above identified treatment room “space” for massage – body treatment. In fact I believe that if AquaDios-Med™ facilities were equivalent to the above and dispersed throughout the U.S. the approximate $ 2.2 Trillion Healthcare costs would be reduce by at least 50 percent of $1.1 Trillion.
The evolution of the spa movement of today in the United States has had three major markers: (1) Rancho La Puerta in Tecate, Mexico, in the 1940s (2) The Golden Door in southern California in the 1950s (3) Canyon Ranch in Tucson, AZ, in 1979.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
These three have become models for spa development over the past five decades. Rancho La Puerta modeled a return to nature and minimalism, with an emphasis on healthy eating and fitness. The Golden Door set the standard for small intimate centers of pampering and relaxation, with a high premium on aesthetic beauty. Canyon Ranch emerged at the end of the 1970s when the founders, the Zuckermans, chose to add to what these two institutions had established by bringing integrated health and healing into the Ranch menu of opportunities. But, none has its focus on daily safe deep-water exercise as is found in AquaDios-Med™.
The largest health resort in the country based on the “number” in attendance, staff, and services
provided focus on nutrition, mild exercise, and health education. To this author the statement that the practicing Spa’s concept of valid integration of traditional and credible nontraditional healing modalities, with prevention at the forefront relies is valid in “Spa Logic” but in reality it is a “passive” coddling and “pampering” of patients completely leaving out “proactive” daily safe aerobic exercise such as sustained deep-water running found in AquaDios-Med™.
Medical Requirements for Health AquaDios-Med™
It is this authors opinion that board certified Physiatrists or rehabilitation physicians are best
qualified to be “Chief of Staff” for AquaDios-Med™ or at all hospitals because they or experts at preventive medicine, non-pharmaceuticals and non-surgical treatments. They are also experts in diagnosing and treating pain, teaching patients how to restore maximum function lost through injury, illness or disabling conditions because they treat the whole person, not just the problem area. Physiatrists are capable in leading a team of medical professionals explain medical problems and treatment plans in simple easy to understand language.
Rehabilitation physicians are excellent communicators who prize prevention and healthy
lifestyle as a framework from which to counsel patients who may have suffered nerve, muscle or bone injuries and they treat all injuries or illnesses that affect how people move. Rehabilitation physicians have completed training in the medical specialty physical medicine and rehabilitation (PM&R). Physiatrists treat a wide range of problems from sore shoulders to spinal cord injuries. Their goal is to decrease and manage pain and enhance performance without surgery.
Physiatrists are physicians that take the time needed to accurately pinpoint the source of an
ailment. They then design a treatment plan that can be carried out by the patients themselves or with the help of the rehabilitation physician’s medical team. This medical team might include other physicians and health professionals, such as neurologists, orthopedic surgeons, and physical therapists. By providing an appropriate treatment plan, rehabilitation physicians help patients stay as active as possible at any age. Their broad medical expertise allows them to treat disabling conditions throughout a person’s lifetime.
This author believes the ideal hospital or AquaDios-Med™ staff would be led by Physiatrists and a staff of podiatrists, chiropractors, physical therapists, and acupuncturists, as needed to complement registered nurses with advanced training and qualifications in various modalities, including healing touch. The AquaDios-Med™ health services will be integrated, and stress a holistic or integrated approach while recommending each patient participate in a minimum of 50 minutes for individual daily safe deep-water running exercise.
Exercise Is Medicine Exercise is a weapon against disease

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
The staff should include qualified Nutrition experts including registered dieticians to assist in how and what food is to be eaten as well as advising patients on the relationships between food and health, fitness, and weight issues. Their information would include the latest scientific data on food, and addresses the frequently contradictory information put forth in the media. The nutrition staff will work closely with the behavioral staff members in addressing the changing of eating habits on a permanent basis. Nutritional medicine and vitamin and mineral supplement consultations will be performed by a team comprising a physician and a nutritionist.
Behavioral
Behavioral health professionals and clinical psychologists will be included on staff to offer
consultations in sleep management, positive psychology, habit change, anger management, stress management, hypnotherapy, biofeedback, guided imagery, grief counseling, and relationship counseling to facilitate helping people evaluate what changes they want to make and how it best fits into their lifestyles.
Exercise physiology
Exercise physiologists must be a part of the AquaDios-Med™ staff to help organize the deep-water exercise program that fosters and maintains vitality and stamina. Their emphasis includes issues of weight loss, weight maintenance, biomechanics, motor learning, strength training, and exercise adherence.
Fitness AquaDios-Med™ is primarily a rehabilitation and fitness process with focus on physical
therapy of deep-water running to help them feel more energetic, decrease stress, enhance general wellbeing and increase self-esteem. In addition, AquaDios-Med™ includes instruction in meditation and yoga specialists. The ultimate goal is to help people find a way to add movement into their lives.
Aquatic and movement therapy
The AquaDios-Med™ movement and aquatic staff provide instruction in Pilates, gyrotonic, Feldenkrais, dance therapy, watsu, and other aquatic therapies. Drawn from dance, body work, somatics, martial arts and meditation, the focus is on helping the person find a modality that responds to his or her needs.
The physical environment
The physical facility (environment) plays a role in promoting optimal healing. Elaborately detailed landscaping plans can be implemented with a vision of a stress-free environment to assist people in the healing process. The buildings can be set to create small pockets of privacy, one building from the other and to maximize views. Good design on its own cannot heal, but it can make science work better. Lighting, offices, public and private spaces, finishes, wall coverings, acoustics, outdoor seating areas, a meditation path, and water artwork can be designed to impact positively as people enjoy the change of their lifestyles.
SPA CULTURE • TREATMENTS • OTHER HEALING ENVIRONMENTS
The Price Waterhouse Coopers study commissioned by the spa industry in September 2002
identified several key points about its growth: People no longer see the spa as purely pampering, but as a prerequisite to staying healthy and
looking good. Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
Spas are offering a growing number of self-awareness and self-improvement activities. Most now focus on eating and weight programs with subcategories of sports activities and nutrition.
There has been a marked growth in the inclusion of health and medically oriented services into
certain spas in the past 3 years. Given the frantic schedules of most individuals today, the spa industry has responded by
offering shorter stays to encourage more frequent visits. Health organizations, residential communities, hospitals, and community centers, among
others, have begun to capture a vast market of people who are willing to purchase services to “feel and look better.” For many of these organizations, it is a way to enhance their mission and create healthier environments. Some health care systems executives have recognized that the billions of dollars individuals are willing to spend out of pocket on modalities and body treatments such as massage, acupuncture and healing touch, for example, are deeply valued by the customer. These types of services currently are available at health organization locations such as:
Life Enhancement Center focusing on living a healthier lifestyle, an integrative approach to
optimal well-being, lectures, group workshops, and individual consultations. One-week residential program in the Life Enhancement Center; integrative approach to specific
health conditions (arthritis, aging, diabetes, midlife journey, healthy heart); partner with specialists from University of Arizona, Joslin Clinic, in addition to Canyon Ranch faculty.
The spa industry also has learned that significant opportunities exist when they add medical and
other health services into their spa environments. On the surface, combining health care and spa services addresses one of the factors guests see as valuable, namely, having everything they desire under one roof. Some current examples of this approach are:
Greenbrier Resort, White Sulphur Springs, WV La Quinta Resort, Palm Springs, CA La Costa Resort, Carlsbad, CA Health care organizations integrating spa services into its offerings hold greater potential for
success than health services in a spa setting. The two factors that determine this are the public’s perception of the credibility of the sponsoring organization and the financial reality. It is much easier to incorporate moderately priced body workers into the health care financial structure than it is to employ a medical doctor, registered dietician or doctor of philosophy into a spa setting. However, what could undermine this potential for future success is the philosophy and organization of traditional health care systems that have been devoted to the pure science and technology of treating the sick individual, rather than building staff and programs oriented to prevention and optimal health. It is not that this process cannot be accomplished.
Rather, it must be done in a way that does not create a caste system among staff and services
while implementing a massive turning of the direction of the enterprise. This undertaking requires commitment and investment rather than the superficiality of public relations or corporate statements. Given the amount of money being spent, it is clear that the public has unmet needs. Therefore, the health educators, practitioners and others who are well trained, have high ethical standards, and are willing to expand the boundaries of their professions, can capture this vast market.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
Otherwise, it will fall to the charlatans, snake-oil salesmen, and others praying on the health and aging phobias of the public. For long-term financial remedies to make this model available to greater numbers of people, it is critical to obtain the recognition of an integrative preventive model of health for reimbursement by the health insurance industry.
The mission is to help people live a healthier life by making the necessary lifestyle changes;
there is a need to quantify what is effective beyond anecdotal data. Several of the most pressing hypotheses that need testing are:
1. The combination of specific educational programs, medical, behavioral, nutritional and exercise consultations, spa treatments, and first-hand practice with healthy behaviors leads to an increased feeling of individual empowerment and well-being, and improved emotional and physical well-being.
2. The small, integrated group focused residential Life Enhancement Center environment produces significant lifestyle changes in a shorter time interval than in a back-home setting.
3. The immersion and reflective time given to guests during a stay translates into more sustained lifestyle changes than comparable work attempted in the home or work setting.
4. The ability for guests to have continued interaction with their health practitioners by telephone or electronically after they leave a health spa will enhance the positive and lasting benefits of their experience.
5. Interaction between the guest and staff prior to arrival will positively impact the quality of care provided, the timeliness of the treatments and acceptance by the guest.
6. Identifying facilities in the guest’s locale for maintaining an ongoing health link once they return home will enhance the likelihood of permanent change.
7. Assigning a guide/coach to each guest from prearrival to departure will enable the guest to select more focused treatments and services and help them navigate through the healing environment with greater ease and less stress.
8. Creating an environment that takes into consideration the research on the impact of color, light, sound, texture and the environment in making a positive impact on the healing process will result in healthier staff and guests.
9. Organizational activities that create a positive staff culture will pay dividends to the organization in lower staff turnover and greater guest satisfaction.
10. Scholarship guests will experience the same degree of lifestyle change and awareness that the traditional paying guest experiences.
11. The opportunity to interact with other individuals with similar issues and concerns in a variety of structured educational and recreational settings will bring about lasting health changes.
12. The integration of spa services, such as massage and water treatments, combined with medicine, nutrition, exercise and behavioral expertise will produce a healthier individual.
13. Spirituality can be effectively taught as part of the guests experience at a health spa in a variety of formats. In summary, the three most critical factors in creating an optimal healing environment at any price point are: -- (1) a dedicated, caring staff at all levels, (2) a mission driven organization that will not compromise who they are, and (3) a sound business model and leadership that will ensure permanency. Dr. Jesse Williams in the 1930s provided an excellent description of a health philosophy that emphasizes these three points:
It’s of value to think of health as that condition of the individual that makes possible the highest
enjoyment of life. Health, when thought of simply as the absence of disease, is a standard of mediocrity, but when thought of as a quality of life is a standard of inspiration and ever-increasing achievement. Jesse F. Williams, M.D.

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section VII
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
History • Introduction • Research • Hospital Healthcare Crisis • Survey 2012 • Chargemaster Prices
Section VII
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
Patients Without Discernible Pathology 28 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
[email protected] aquadios.com diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Introduction • Research • Hospital • History • Solution • Healthcare Crisis • Part VII
Hospitals Most Recent Survey 2012
According to American Hospital Association AHA records in 2011there were more than 10,600 registered and community hospitals in the U.S. About 72 million admitted patients are reported in these two hospital groups alone, with expenses of about $ 1.5 Trillion; this does not include income or profit figures. This means there were more 72 million patients admitted to these hospitals. Debt.Org states the 2011 healthcare costs were $2.7 Trillion. The CDC reports 48 million surgeries with a reported $166 Billion in surgical costs at non-federal hospitals and other research shows 24 million of those surgeries was unnecessary as was $83 Billion in healthcare costs.
Recent research shows that in 2011, of the more than 72 million patients admitted to hospitals,
about 36 million were unnecessary hospitalizations because 50 % or more of those admitted were patients without discernible pathology PWDP and 33 % of these patients suffered iatrogenic disease medicine and many died. About 36 million patients were hospitalized with no logical health or medical rationale or reason.
Global Trigger, a new medical research method show Adverse Events occurred in more than
33% of admissions. Of the approximate 72 million admitted patients in 2011—about 24 million of the admitted patients in 2011 will suffer from a hospital mistake, error or negative side effect caused by treatment, surgery or prescribed drug. Doctors and or hospital staff make morbidity errors about one third of the time; thus causing disease, illness, injury and sickness to 1 out of 3 patients admitted to a hospital.
Conservative analysis of these statistics predict AquaDios-Med™ practices could eliminate about 50 Million patients from hospitalization admission if AquaDios-Med™ practices were prescribed for 90 days instead of admission to the hospital.
The AHA identifies 2011 Healthcare costs at about $1.5 Trillion for roughly 72 million patients
and when 50% or 36 Million patients are removed from admissions this extrapolates to a savings of about $750 Billion when Evidence Based AquaDios-Med™ practices are factored into the hospital healthcare equation. It would take less than 50% of that savings or about $375 Billion to effectively treat the 36 million patients with AquaDios-Med™ Proactive Preventive Medicine an overall cost savings of $375 Billion; while eliminating all of the adverse events, iatrogenic disease medicine, pain and suffering and deaths. See The Healthcare • Crisis Is Manufactured • Man-Made AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION this research.
If AquaDios-Med™ PPM practices were instituted the approximate 36 million PWDP or
patients without discernible pathology patients would never be admitted to the hospital or face iatrogenic medicine and the healthcare cost could be reduced by as much as $375 Billion. Research indicates one reason for the large amount of patients being admitted to hospitals is the profit driven culture and has nothing to do with healthcare or patient care. This is why the Healthcare Crisis Is Manufactured -- Man-Made and AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
Hospitals Most Recent Survey 2012 Presuppose there are about 36 million fewer patients admitted to hospitals, these are people
who need proactive preventive medicine healthcare and now there is a reserve or a savings of $750 Billion. Should half or $375Billion of that saved healthcare money be reinvested into an out-patient evidence based process such as AquaDios-Med™ Proactive Preventive Medicine, a system built on known health outcomes and practices, there would be 36 million more physically fit people with minimal to no hospital medicine needs. The remaining $375Billion savings could be earmarked for honest, noble pharmaceutical drugs and devices – a Win-Win.
Cost Issues • Hospitals • ChargeMaster Prices
Routine Care • Outrageous Bills
New research reports the U.S. Congress keeps healthcare costs both astronomically high by supporting a hospital chargemaster price system bill up to be 15 times higher than actual cost while authorizing Drug Company–Device Makers unlimited profits, some over 300 percent of cost. The study shows this to be leading causes of the $750 Billion Americans overspend each year on health care. Research reveals the entire consolidated healthcare industry spends about $ 500 Billion on lobbyists before Congress where there seems to be a quid-pro-quo. Congress allows Hospitals to bill at incredibly high ChargeMaster Prices; Congress prevents Medicare from establishing a fair market value for drugs and medical devices; Congress allows drug-medical device makers profits 300 times or more than the cost to produce the drug-device; the FDA threatens to fire their own scientists if they do not approve a drug-device with known dangers, if it is a high profit drug-device
Non-Profit Hospital • Produces More Profit • Deceitful Billing • Dishonest Claims The American Hospital Association has run daily ads on Mike Allen’s Playbook, a popular
Washington tip sheet, urging that Congress not be allowed to cut hospital payments because that would endanger the $39.3 Billion in care for the poor that hospitals now provide. Analysis shows that $39.3 Billion is deceitful because it is calculated on the basis of chargemaster prices, the equivalent of double books.
Hospitals • Spas • Preventive Medicine • Deepak Chopra, MD • Research shows modern hospital medicine has distorted the true meaning of preventive medicine, let alone the concept of proactive preventive medicine. Advertised preventive medicine can be prescribing drugs like Fosamax with dangerous side effects -- necrosis of the jawbone. This distorted, corrupted and inferior characterization lowers the genuine quality and true and noble meaning of preventive medicin; optimal health, disease resistance through safe sustained vigorous exercise, a process that increases muscle mass, bone density, strength, energy and aerobic capacity, elevates mood, improves sleep, reduces blood sugar, cures diabetes, reduces body fat, enhances immunity and decrease the frequency of illness, improve the cholesterol profile, accelerates wound healing, protects against cancer and heart disease and improves skin tone for just a few of the positive outcomes. Good health requires pro-active participation. Geneticists say over 60 percent of healthcare can be safe daily exercise. AquaDios-Med™ Proactive Preventive Medicine never confuses prescribed drugs; with negative – dangerous side effects for the quality preventive medicine received in the process of it robust program involving the most cutting edge programs of Mind Body Medicine together with Deep-Water Running Immersion Treatment; all the side effects of ADM™ PPM are positive and life sustaining.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
Modern hospital medicine is filled with daily miracles with its engineering, technology and science, yet it is also a system bursting with profit-centered and not patient-centered incentives, and too often replicating the SCOOP phenomena of dangerous and sometimes deadly iatrogenic medicine. Modern society needs and depends on hospitals for emergency care when injured or with serious illness, for necessary surgery, it is a place for Childbirth, Maternity Wards Intensive Care and much more; but the system needs to return to its noble patient-centered roots and abandon the profit motives. This section will explore types of Hospitals and Services Provided, including Length of Stay, Ownership of Hospitals, not-for-profit hospitals, profit hospitals; and Proprietary, or for-profit, hospitals owned by corporations to make money.
It is better to risk saving a guilty man than to condemn an innocent one … Voltaire
The AquaDios-Med™ Philosophy
• EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING! • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race.
Copyright © 2008 – 2012 – 2013 2nd Edition
AquaDios-Med™ • AquaDios Corp.
All rights reserved. Respectfully,
Dr. Alan Jensen (Alan) Founder • CEO • Creator, AquaDios-Med™ http://www.aquadios.com/ A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing Phone 310-897-5055 - Email: [email protected] - P.O. Box 2228 Malibu, Ca. 90265
Exercise Is Preventive Medicine The true sign of intelligence is not knowledge but imagination - Albert Einstein

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California 90265 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
www.aquadios.com
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Hospital • History • Research • Introduction Solution • Healthcare Crisis • Part VII 25 Pages
Hospitals Most Recent Survey 2012
On January 3, 2013 the American Hospital Association AHA reported hospital admissions and costs, but for only the more than 10,600 registered and community hospitals in the U.S. About 72 million admitted patients are reported in these two hospital groups alone, with costs of about $ 1.5 Trillion. Debt.Org states the 2011 healthcare costs were $2.7 Trillion. The CDC reports 48 million surgeries with a reported $166 Billion in surgical costs at non-federal hospitals.
The most recent American Hospital Association [AHA] research shows that more 36.5 million patients were admitted to registered hospitals with another 35 million to community hospitals in 2011 and more than 36 million of those 72 million were unnecessary patient hospitalizations. Other research shows that 50 % or more of those admitted were PWDP, patients without discernible pathology and 33 % of these patients needlessly suffered iatrogenic disease medicine and many died. This indicates there were about 36 million patients hospitalized for no logical health or medical rationale or reason.
Global Trigger research methods by Dr. David C. Classen show Adverse Events occurred in
more than 33% of admissions. This means about 24 million of the admitted patients in 2011 will suffer from a hospital mistake, error or negative side effect caused by treatment, surgery or prescribed drug. And another approximated 36 million falsely admitted patients without discernible pathology – PWDP will also suffer from the same iatrogenic medicine diseases. Research confirms doctors and or hospital staff make morbidity errors one third of the time; causing disease, illness, injury and sickness.
Conservative analysis of the American Hospital Association - AHA research statistics predicts
AquaDios-Med™ practices could subtract about 36 Million patients from hospital admission and save about $ 750 Billion to $1.35 Trillion in costs if AquaDios-Med™ practices were prescribed for 90 days instead of admitting the 36 Million patients to the hospital without discernible pathology.
The AHA identifies 2011 Healthcare costs to be about $ 1.5 Trillion for roughly 72 million admitted patients. By deducting 36 Million PWDP patients from admissions this extrapolates to a savings of about $750 Billion when Evidence Based AquaDios-Med™ practices are factored into the hospital healthcare equation. The estimated cost to effectively treat the 36 million PWDP patients with AquaDios-Med™ Proactive Preventive Medicine is less than 50% of that $ 750 Billion savings, a price of about $375 Billion, with an overall cost savings of $375 Billion; and ADM™ PPM will eliminate all the adverse events, iatrogenic disease medicine, pain - suffering and deaths. See The Healthcare • Crisis Is Manufactured • Man-Made •AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION this research.
Another derivative from this same data predicts that about 50 Million patients could participate in AquaDios-Med™ PPM practices at a savings of $ 1Trillion. The costs of the ADM™ PPM practices are calculated to be 50% of the $ 1Trillion saved. This number is derived by taking 70% of the total admissions and providing them with the ADM™ PPM practices. The basis of 70% is taken from the projection that ADM™ PPM will reduce 70 % of the patients admitted to hospitals when every new admission is evaluated for and referred to ADM PPM for 90 days prior to major invasive diagnostic procedures.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
The same 70 % number of 50 Million patients is arrived at by taking the 50% or PWDP patients without discernible pathology – those who have no medical reason to be admitted and add 20 % of the original total population of admitted patients. The 70 % savings derivation calculates to the $ 1Trillion in healthcare savings. This means more than 50 Million people would not be exposed to pain, suffering and death caused by healthcare mistakes and iatrogenic disease medicine. It is likely modern hospital medicine would never tolerate such an efficient patient-centered practice such as ADM PPM because they would not want to give up the $1Trillion.
Decades of Placebo research illustrates that Placebo Effects are stable at 70 % when the prescribed placebo is given to the patient by a respected doctor who makes positive verbal suggestion designed to enhance or elevate belief, imagination, expectation and faith in the drug. An integral part of evidence based AquaDios-Med™ PPM is Psychoneuroimmunology – PNI, Mind Body Medicine – MBM, Inner Mental Training – IMT, combined with the most advanced Deep-Water Running Immersion Therapy DWRIT practices to facilitate and sustain Physiological Self-Regulation – PSR with an expected success rate of 80%, slightly above the Placebo Effects but without the placebo. Success being described as symptom management and or remission with limited or no use of prescribed drugs; because the healing chemicals are naturally and internally produced by the patient.
Consequently, it is pragmatic to estimate AquaDios-Med™ PPM can be attributed to a 70 % reduction in patient admission with an equal 70 % cost savings in the healthcare equation. This means that when seventy percent is used as a constant in the AquaDios-Med™ healthcare equation the AHA documented hospital expenses of about $1.5Trillion for the year 2011 extrapolates to a savings of about $ 1Trillion when Evidence Based AquaDios-Med™ practices are factored into the hospital healthcare cost equation. The most optimistic prediction, in simple language, means hospital profits could decrease by $ 1Trillion and admissions would decrease by 36 million patients while AquaDios-Med™ PPM patient population would increase by about 50 million patients with patient costs of $525 Billion, hospitals costs would be down to about $500 Billion; a combined healthcare cost of $ 1.025 Trillion or a total savings of about $475 Billion; and this package eliminates many thousands of patient’s pain and suffering and countless deaths.
Healthcare Costs Savings Summary
Based on hospital expenses for the year 2011 the AHA estimates Healthcare costs to be about $1.5Trillion. When Evidence Based AquaDios-Med™ practices are factored into the hospital healthcare equation a savings of about $475 Billion is estimated. Seventy Percent is used as a constant in this AquaDios-Med™ equation. ADM™ PPM predicts an 80% success rate with its integrated Psychoneuroimmunology PNI -- Mind Body Medicine – MBM training practices used to facilitate and sustain physiological self-regulation – PSR together with proprietary Deep-Water Running Immersion Therapy -- DWRIT with its positive physiologic changes that accelerate removal of metabolic waste, enhanced cardiac function, lowered blood pressure and increased body production of healing -- rejuvenation of tissues. The Elements of placebo power is to enhance or elevate belief, imagination, expectation and faith in a drug while the Inner Mental Training -- IMT is the self-empowerment of these capacities for health, symptom control and physical fitness. Consequently AquaDios-Med™ PPM practices are far more powerful and lasting than placebo effects. Simply stated the $1.5Trillion healthcare costs can be reduced by 70%, a savings of about $ 1Trillion. This figure is derived by deducting $ 1Trillion, the 70% savings, from the $1.5Trillion actual costs and then adding the AquaDios-Med™ PPM treatment costs of $525 Billion for a total annual savings of about $475 Billion. See The Healthcare • Crisis Is Manufactured • Man-Made AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION; this research.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
The healthcare savings scenario sighted above saves money protects patients and saves lives.
Simply stated if AquaDios-Med™ PPM practices were instituted for the approximate 36 million PWDP -- patients without discernible pathology would not be admitted to the hospital or face iatrogenic medicine and the healthcare cost could be reduced by as much as $750 Billion. Research indicates one reason for the large amount of patients being admitted to hospitals is the profit driven culture and has nothing to do with healthcare or patient care. This is why the Healthcare Crisis Is Manufactured • Man-Made; AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION.
Presuppose there are about 36 million fewer patients admitted to hospitals, all people who need
healthcare; this is a savings of about $750 Billion. Should half or $375 Billion of that saved healthcare money be reinvested into an out-patient evidence based process such as AquaDios-Med™ Proactive Preventive Medicine, a system built on known health outcomes and practices, there would be 36 million more physically fit people with minimal to no hospital medicine needs. The other $375 Billion could be earmarked for honest, noble pharmaceutical drugs and devices – a Win-Win.
Cost Issues • Hospitals • ChargeMaster Prices
Routine Care • Outrageous Bills
New 2013 research reports the U.S. Congress keeps political control of healthcare costs both artificially and astronomically high by allowing hospital over pricing through a hospital chargemaster price system that allows billing to be 15 times higher than actual cost while sanctioning Drug Company–Device Makers unlimited profits. Research discloses the Hospital ChargeMaster prices have a minimal mark-up of about 15 times the cost; designed to negotiate prices 30% to 50% above the common Medicare rates. The study shows these out of control hospital prices are high enough to make hospital costs a leading cause of the $750 Billion Americans overspend each year on health care.
Non-Profit Hospital • Produces More Profit • Deceitful Billing • Dishonest Claims Studies show that hospitals use their sympathetic nonprofit status to drive their interests. The
American Hospital Association has run daily ads on Mike Allen’s Playbook, a popular Washington tip sheet, urging that Congress not be allowed to cut hospital payments because that would endanger the $39.3 Billion in care for the poor that hospitals now provide. Analysis shows that $39.3 Billion is deceitful because it is calculated on the basis of chargemaster prices, the equivalent of double books.
Research reveals the entire consolidated healthcare industry spends about $ 500 Billion on
lobbyists before Congress where there seems to be a quid-pro-quo. Congress allows Hospitals to bill at incredibly high ChargeMaster Prices; Congress prevents Medicare from establishing a fair market value for drugs and medical devices; Congress allows drug-medical device makers profits 300 times or more than the cost to produce the drug-device; the FDA threatens to fire their own scientists if they do not approve a drug-device with known dangers, if it is a high profit drug-device
Hospitals • Spas • Preventive Medicine • Deepak Chopra, MD • As has been noted in the first part of this research modern hospital medicine has extremely distorted the true meaning of preventive medicine, let alone the concept of proactive preventive medicine. In 2008 the U. K. SCOOP study advertised preventive medicine by prescribing the drug Fosamax with the dangerous side effects of necrosis of the jawbone. This distorted, corrupted and inferior characterization lowers the genuine quality and true and noble meaning of preventive medicine.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
The true meaning of preventive medicine is optimal health, disease resistance through safe sustained vigorous exercise, a progressive physical fitness with evidence-based solutions that simply enhance quality of life extend the potential life span. A process that increases muscle mass, bone density, strength, energy and aerobic capacity, elevates mood, improves sleep, reduces blood sugar, cures diabetes, reduces body fat, enhances immunity and decrease the frequency of illness, improve the cholesterol profile, accelerates wound healing, protects against cancer and heart disease and improves skin tone for just a few of the positive outcomes. Good health is not an accident; it requires pro-active participation. Geneticists agree that over 60 percent of what happens to us is within our own control. And since your health is a most-treasured asset, it should never be put on the "backburner."
AquaDios-Med™ Proactive Preventive Medicine never confuses prescribed drugs; with negative – dangerous side effects for the quality preventive medicine received in the process of it robust program involving the most cutting edge programs of Mind Body Medicine together with Deep-Water Running Immersion Treatment; all the side effects of ADM™ PPM are positive and life sustaining.
Modern hospital medicine is filled with daily miracles with its technology, engineering, technology and science, yet it is also a system bursting with profit-centered and not patient-centered incentives, and too often replicating the SCOOP phenomena of dangerous and sometimes deadly iatrogenic medicine. Modern society needs and depends on hospitals for emergency care when injured or with serious illness, for necessary surgery, it is a place for Childbirth, Maternity Wards Intensive Care and much more; but the system needs to return to its noble patient-centered roots and abandon the profit motives. This section will explore types of Hospitals and Services Provided, including Length of Stay, Ownership of Hospitals, not-for-profit hospitals, profit hospitals; and Proprietary, or for-profit, hospitals owned by corporations to make money.
Preventive Medicine – Deepak Chopra, MD
DEEPAK CHOPRA, M.D. is a board-certified in internal medicine and endocrinology and is
now chairman and co-Founder of the Chopra Center for Wellbeing in Carlsbad, California. He is one of the world's leaders in the field of mind body medicine.
Chopra has taught at Tufts University and Boston University Schools of Medicine, and became the Chief of Staff at the New England Memorial Hospital (later the Boston Regional Medical Center) in Stoneham, Massachusetts. Chopra also established a large private practice before turning to Mind Body Medicine as the treatment of choice.
Chopra teaches an annual update in Internal Medicine at Beth Israel Deaconess Medical Center, a teaching hospital of Harvard Medical School, where his younger brother, Sanjiv, is Professor of Medicine and Faculty Dean for Continuing Medical Education. Also, Physicians' continuing medical education through the Chopra Center has been certified by the American Medical Association.
Dr. Chopra is a critic but not an enemy of conventional hospital medicine, and he is invested in Mind Body Medicine as is this author and this research in both cases.
In 1981, Chopra became a leader in the Transcendental Meditation movement and a spokesman for mind-body treatment including, in 1993, the position of executive director of the Sharp Institute for Human Potential and Mind–Body Medicine, affiliated with Sharp Healthcare, in San Diego.
Chopra is the co-founder of the Chopra Center, which he founded in 1996 in La Jolla with Dr. David Simon.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
In 2002 the Center moved its official headquarters to La Costa Resort & Spa in Carlsbad, California with a branch in New York City.
Chopra is a staunch advocate of the interconnection between mind and body, advocating meditation, self-awareness and Yoga as primary factors in both illness and healing.
Dr. Chopra deepened these themes in “Quantum Healing” (1989), where he examined the mysterious phenomenon of spontaneous healing of cancer. Here he introduced quantum physics as a means of understanding the mind-body connection, arguing -- as he would in many other books -- that consciousness is the basic foundation of nature and the universe.
In 1998, Chopra was awarded the satirical Ig Nobel Prize in physics for "his unique interpretation of quantum physics as it applies to life, liberty, and the pursuit of economic happiness."
Approaches of mind body medicine and preventive medicine has attacked one of the most brilliant and educated minds in the world. The Journal of the American Medical Association (JAMA) attacked Chopra and his co-author and in response two Transcendental Meditation groups and Chopra sued the author, Andrew Skolnick, JAMA's editor Dr. George Lundberg, and the AMA for $194 million in July 1992.
Pursuant to a settlement agreement, in 1993 the suit was
dismissed by the judge at the request of the plaintiffs, with the option of reinstating pending completion of the settlement.
Deepak Chopra, M.D. continues to transform the
understanding of the meaning of health, preventive medicine and mind body medicine; he has written more than 40 books.
Hospital’s Accept - Preventive Medicine
In the case of hospitals, the AMA, researchers and the pharmaceutical industry preventive
medicine may produce a “fear” response because the treatment approach would cost these populations billions of income dollars.
Most dictionaries and Behavioral Medicine agree that “Fear” is a common human emotional
response to tangible and realistic dangers, and fear may generated by fantasy at a subconscious level. Fear is often distinguished from anxiety, an emotion that often arises out of proportion to the actual threat or danger involved, and can be subjectively experienced without any specific attention to the threatening object. People who are experiencing fear are said to be "scared", often when people get scared they hide away, a man named Samuel Bishop often gets scared at the first sign of danger and retires to his bed where he feels more secure.
Most fear is usually connected to pain like the fear of heights because a person falls; they may
suffer severe injury or even die upon landing. Behavioral theorists, like Dr. Watson and Dr. Ekman, have suggested that fear is one of several very basic emotions like joy and anger. Fear is conceived as a survival mechanism, and usually occurs in response to a specific negative stimulus.
This concept is seen in the mind body medicine and preventive medicine attack of Deepak
Chopra, MD, one of the most brilliant and educated minds in the world. In July 1992 this attack against Chopra cause a $194 million lawsuit to be filed by Chopra against the attacking author the JAMA's editor and the AMA. Is “fear” what causes attacks rather than acceptance of medical information that may simply treatment or must we presume the altruistic value of human health just does not exist because today’s healthcare is driven by dollars not by health and wellness?

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
In any case because Chopra did have the economical and personal fortitude to “take on” the establishment to protect preventive medicine and mind body medicine from continued sufferance as do blacks in a society of prejudice.
This author has spent decades and millions of dollars proving the AquaDios-Med™ concepts and
procedures are valid, though basically simple and can reverse the more than $ 2.2 Trillion HealthCare deficit. Does this mean I will have to sue big hospitals, the pharmaceutical companies and the AMA because the principles of AquaDios-Med™ are too good and will extinguish too much cash flow to these industries?
Hospitals – Preventive Medicine - Spas
In a comprehensive research article for Microsoft® Encarta® Online Encyclopedia 2007, author Karen Sandrick, Contributing Editor, Diagnostic Imaging Magazine and Writer, Oncology News International has accumulated and disseminated vast information about hospitals in the U.S.
This 2007 research article points out that today there are 6,021 hospitals in the United States and have well over 1 million hospital beds; 770 of those hospitals are “for-profit: institutions; these hospitals are typically part of large investor-owned hospital chains. U.S. hospitals annually admit more than 34 million patients who are assigned a bed and receive medical or surgical treatment as inpatients. Hospitals also provide outpatient treatment in clinics or other walk-in, or ambulatory, settings for an additional 483 million patients every year or service to more than 513 million patients in 2007.
There are approximately 300 hospitals that are university-based academic medical centers that offer both medical training and opportunities for medical research.
Spas on the other hand number about 10,000 in the United States. This includes day spas, Resort
hotel spas and destination spas. And in 2001, there were 156,000,000 visits made to spas, mostly to day spas. The spa industry in
the United States has more than 100,000,000 square feet under roof with 50% of the space occupied by treatment rooms for massage and body treatments with about 20% designated as beauty space.
The annual Spa industry income was about $11 billion in 2001 with more than 50% of the revenue derived from treatment rooms, with beauty and retail sales accounting for about 36%.
By combining the 6,021 hospitals with the approximate 10,000 Spas there are more than 16,000 U.S. health facilities that are capable of accommodating the 513 million patients and more than 180 million Spa users; a total of about 793 million people.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
What’s missing at hospitals is a department of preventive medicine such as that of AquaDios-Med™ and its immersion chambers. And what’s missing at Spa’s is a department of preventive medicine such as that of AquaDios-Med™ and its immersion chambers. The common error of the American hospital and the Spa is the same, no proactive safe daily deep water running exercise.
There are at least two intriguing aspects of the American population, it wants to be pampered and Spas will provide more than $ 11 Billion in pampering service to their clients; and that Americans want to make hospitals
responsible for their health. In both cases, the responsible party, the person, has vacated the
premise of responsibility and made the hospital accountable. Here the hospital, like the Spa accommodates the patients as best it can with as many reimbursable, tests, treatments and diagnostic procedures allowed by the insurance industry, even when not needed or required.
This author has read more than many health and medical research studies, all of which state the same thing over and over, a healthy diet and regular exercise will eliminate the medical symptoms, the suffering, the pain, the surgeries, the need for prescribed pharmaceuticals and the deaths of American’s.
Because this is true what is stopping insurance companies from reimbursing American hospitals for preventive medicine practices such as those of AquaDios-Med™.
Certainly if we as a nation can populate more than 16,000 health facilities that generate more
than $ 2.2 Trillion in HealthCare costs then we Americans are not utilizing these facilities or the intelligent staff available at these facilities correctly or efficiently.
The human body is much like the automobile, let it sit without using it and it will deteriorate
wore than if you exercised it vigorously every day. Where the automobile and the body differ is the human body replenishes itself with intense aerobic cardiovascular exercise that will
produce perspiration; unless it is done in the safest environment known to mankind and that is in deep water immersion to the neck with an AquaJogger or a WetVest as is practiced in the AquaDios-Med™ programs.
This author believes the proactive process of AquaDios-Med™ which includes its “teaching” patients to perform their own safe daily exercise and “power massage “is a far
more economical health practice than any Spa treatment. I believe that when AquaDios-Med™ facilities are
included as required daily exercise in the combined number of hospitals and Spas throughout the U.S. the approximate $ 2.8 Trillion Healthcare costs would be greatly reduce by 100’s of Billions of dollars.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
Preventive Medicine advocates who believe in treatments practiced and offered by AquaDios-Med™ programs also accept as true that about 415 million of these patients would not need “in-bed-patient” care when the AquaDios-Med™ “preventive practices” are utilized for 90 days prior to admitting hospital “in-bed-patient”. In this authors view about 80 % of those admitted to modern hospital inpatient care can and will be better served by principles practiced by AquaDios-Med™ programs.
Hospitals can be defined as an institution that provides a broad range of medical services to sick,
injured, or pregnant patients. But, they could provide “preventive services too. Hospitals employ medical, nursing, and support staff to make available inpatient care to people who require close medical monitoring and outpatient care to people who need treatment but not constant medical attention. Here is where the preventative medicine can play such a large role in the American economy especially with focus on safe daily exercise.
Hospitals offer diagnosis and medical treatment of physical and mental health problems, surgery, rehabilitation, health education programs, and nursing and physician training. Many hospitals also serve as centers for innovative research and medical technology. And this advancement of research and technology is absolutely necessary.
Hospital • Types
Hospitals in the United States are classified by the services they provide (general or specialized), the length of stay they offer patients (short stay or long-term care), and by their ownership (not-for-profit, proprietary, or government owned). Does the reader understand the political and economic problems in getting hospitals to be classified with a preventive medicine department and then the political upheaval when a cost-effective health care insurance carrier that saw the merit of preventive medicine.
Today Insurance Giants advertise “good hands” but refuse to pay for most important and required treatments for those most in need. Why not search out a political and economic band wagon that presents only simple facts about health, such as that only safe daily deep water exercise and a daily nutritional intake of food will empty the hospitals?
Of course this must be combined with a vast decrease in most prescribed medications. It is projected that after just 90 days of treatment in the AquaDios-Med™ program more than 50 percent of the patients would no longer need their medications or would need a decreased amount and within 180 days be free of almost all medications, especially those with such toxic side effects.
Although most U.S. hospitals are classified as not-for-profit, any one hospital will fall into
several of the above categories. For example, Methodist Hospital in Houston, Texas, with more than 300,000 sq. m (3 million sq. ft.) of space, is one of the largest short-stay, not-for-profit, general hospitals in the country.
Services Provided • Hospitals
General hospitals, regardless of their size, provide patients with a wide range of services wide range of services, including emergency treatment, surgery, and medical and nursing care, but no preventive medicine. Why?

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
Specialized hospitals, in contrast, may concentrate on a particular group of patients, such as children, or a disease, such as cancer. Some specialized hospitals combine treatment and research, but still not preventive medicine. For instance, Roswell Park Cancer Institute in Buffalo, New York, offers 37 specialized cancer treatment centers, including centers for acquired immunodeficiency syndrome (AIDS)-related cancers, brain tumors, and ovarian cancer, and provides state-of-the-art treatments for these cancers that are not generally available in other hospitals.
And, these special hospitals need to continue their great service, but they must also offer
preventive medicine. The institute also conducts research on new cancer drugs and procedures, such as photodynamic therapy, which uses a laser to activate cancer-killing chemicals inside tumors; and it is a must this research continues.
Some general and specialized hospitals also function as ancillary care centers, treating the most
difficult and complex cases or the most seriously ill patients. These may include patients who need heart, lung, or liver transplants. Even these patients can benefit from the deep immersion chambers of AquaDios-Med™ and some may even demonstrate complete recovery.
This author concedes that these great medical centers must continue on with special focus on
advancement of technology but they must put what works best, first for the American population and that is daily healthy foods and daily safe exercise.
Although preventive medical health centers do not exist yet they could someday represent 65 to
75 percent of all U.S. health centers in the U.S. and care for about 75 percent of all patients nationwide because they would serve as community “wellness centers” and for those in need for specialized consultation or for advanced diagnostic and therapeutic procedures for patients in wide regional areas.
The Medical McDonalds Model to HealthCare would place an AquaDios-Med™ Health Center
into every American population with a McDonald’s fast food. And, this author believes that when the AquaDios-Med™ Health Center concept is practiced in every elementary school, mid school, high school and college across America the HealthCare problem will be over.
Many hospitals that serve as teaching institutions train residents such as medical school
graduates who are doing postgraduate training in general medicine or specialty areas. Teaching hospitals also train others interested in a health care career, including nurses and laboratory specialists and this certainly must continue.
Although some of these hospitals are relatively small and train only a few doctors in teaching
programs that are affiliated with medical schools, there are more than 300 university-based academic medical centers that are active in medical training and medical research and we Americans need these trained doctors and innovative research for our future health care. Micro Surgery >>>>
Academic medical centers are usually massive urban
hospitals linked closely with major medical schools. Although academic medical centers represent only 6 percent of all U.S. hospitals, they care for only about 20 percent of all patients nationwide because their main goal is to serve as referral centers for specialized consultation or for advanced diagnostic and therapeutic procedures for patients in wide regional areas.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
The Medical Center of the University of California at San Francisco annually admits almost 27,000 patients and treats about 340,000 outpatients in its clinics and 53,000 patients in its emergency room and trauma center.
Length of Stay
The American Hospital Association (AHA), a national organization that promotes organizational and legislative issues of interest to hospitals, classifies hospitals by the length of stay they offer patients. AHA categorizes hospitals as short-stay or acute-care centers if their patients receive 30 days or less of inpatient treatment. In contrast, AHA classifies hospitals as long-term care institutions if their patients require more than 30 days of treatment, as is available in rehabilitation facilities or nursing homes.
AHA makes the distinction between short-stay and long-term care facilities to reflect not only the
difference in length of stay but also the scope and intensity of services provided by an institution. Short-stay hospitals are geared for quick intervention and constant monitoring of serious, often
life-threatening illnesses. These hospitals provide immediate attention until a patient is stabilized enough to be treated at home or in a health care setting that can provide a longer stay. However, preventive medicine is a short stay approach and needs to be included in all 6,017 hospitals across the US.
Long-term care institutions treat physical diseases or injuries that are debilitating and require
prolonged medical intervention or physical therapy and regular skilled nursing care. Some long-term care facilities are psychiatric institutions for the mentally ill who cannot be cared for at home. And these facilities need the service of preventive medicine as well.
Ownership of Hospitals
Not-for-profit, or voluntary, hospitals, which represent about 84 percent of the hospitals in the
United States, are charitable institutions that exist to serve the best interests of their communities. Although not-for-profit hospitals do not receive funding from tax dollars, they are exempt from local, state, and federal taxation. Many not-for-profit hospitals were founded and continue to be run by religious groups, such as members of the Catholic Church, Presbyterian or Methodist ministries, or Jewish organizations.
A small number of private charitable hospitals were spearheaded by individuals. Probably the
best known of these is the Mayo Clinic in Rochester, Minnesota, established by American physician William Mayo and his two physician sons (see Mayo [family]). Most not-for-profit hospitals, however, were established by members of their local community and continue to be governed by community representatives.
Proprietary, or for-profit, hospitals are owned by corporations and their shareholders. Although only about 770 U.S. hospitals are for-profit institutions, these hospitals are typically part of large investor-owned hospital chains. For instance, Hospital Corporation of America (HCA), the largest for-profit hospital chain in the United States, has more than 200 hospitals in its network.
HCA is listed on the New York Stock Exchange, just as any other
for-profit company; company executives seek to reward shareholders who invest in the company by applying standard corporate management techniques, likely to yield corporate profits, to hospital administration.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
A health maintenance organization (HMO) pays for and provides medical care to enrolled patients. For a fixed payment, HMOs deliver health services by establishing panels of doctors and hospitals that provide all the treatment their members require. The first HMO in the country, not-for-profit Kaiser Permanente of Oakland, California, has operated ten hospitals in California since the late 1980s. Although some HMOs, like Kaiser, purchase the hospitals they use, other HMOs only contract with hospitals to treat HMO patients. When a hospital contracts to meet the health care needs of an HMO’s patients, it retains its ownership status.
Cities, counties, states, and the federal government also own hospitals. About 1,000 public hospitals are owned by their cities or counties and are supported by local tax dollars. The vast majority of city hospitals are in small or moderate-size communities, and they offer services that are similar to those provided in small, general, and not-for-profit hospitals.
About 150 municipal or county hospitals are found in major cities, such as Cook County Hospital in Chicago, Illinois. These large, urban, public institutions provide most of the care for the poor in their communities.
They also often offer comprehensive, high-tech care for certain categories of gravely ill patients, such as trauma and burn victims seen in the picture, as well as intensive care for newborns who are premature or who have severe birth defects. In contrast to the many city and county hospitals in the United States, only a small number of hospitals are run by state governments, and most of these are long-term psychiatric or chronic care institutions.
Federal hospitals care for specific types of government program beneficiaries, such as the hospitals on reservations that care for Native Americans. Walter Reed Army Medical Center, in Washington, D.C., and other military hospitals provide treatment for military personnel and high-ranking members of the government, including the president of the United States.
Hospitals run by the Department of Veterans Affairs are located throughout the United States and
treat illnesses of military veterans and their dependents. It is the Federal Hospital that a reasonable person would logically think preventive medicine would flourish, but it does not, yet.
Licensing • Accrediting Hospitals
Each hospital, regardless of its classification, must be licensed by the state in which it operates, a procedure that assesses a hospital’s compliance with public health standards governing, for example, cleanliness and overcrowding. In addition to being licensed, hospitals seek accreditation from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), a private quality-measurement organization.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
JCAHO sets 700 national standards for hospitals covering every area of their operation, such as clinical care, social services, administration, and financial services. Teams of inspectors evaluate a hospital’s compliance with these standards once every three years. JCAHO has established several categories of accreditation, including full accreditation for institutions that meet the vast majority of its standards and provisional accreditation for institutions that must correct specific lapses before they can be accredited. Only about 5 percent of all hospitals surveyed by JCAHO are accredited with commendation for meeting top levels of achievement in all 28 areas of measurement. One such hospital is the University of Washington Medical Center in Seattle, Washington, a 450-bed teaching hospital that also has specialty centers for research on Alzheimer’s disease, women’s health, and diabetes, and offers over 80 outpatient clinics.
Hospital Organization and Staff
A hospital is a complex institution that coordinates the skills of doctors, nurses, and support care personnel to provide health services, but not preventive medicine services. A hospital also has administrative departments to ensure the efficient and financially sound operation of the institution. Large not-for-profit general hospitals, the most common hospital type, have several levels of organization that include a board of trustees, chief administrative officer, chief of the medical staff, administrative and medical department heads, and a director of nursing.
A hospital’s board of trustees oversees the operation of the hospital by evaluating its financial health and its strategic growth and development. One of the board’s major responsibilities is to hire and assess the performance of the hospital’s chief administrative officer; another is to approve the appointment and retention of the hospital’s physicians.
Board members also participate in fund-raising and other philanthropic activities and in community outreach activities that seek to improve the health of the community. Not-for-profit hospitals are charitable institutions that are expected to meet the needs of their communities and their boards of trustees are typically made up of representatives from local businesses and community groups.
The chief administrator of a not-for-profit general hospital is known as the chief executive
officer, president, or administrator, depending on the size and complexity of the hospital’s organization. As the hospital’s top executive, the chief administrator plans for the ongoing financial health of the institution, considering such issues as whether the hospital should remain independent or merge with another institution; expand or reduce specific health services, such as high-cost trauma care; develop relationships with groups of physicians, HMOs, or clinics; or create satellite facilities in nearby cities or towns.
The chief of the medical staff is a physician appointed to direct the work of all the doctors who treat patients in the hospital and to supervise the procedures for adding doctors to the hospital staff. Also called privileges, these procedures define the qualifications needed by doctors and the specific treatments each doctor may perform in the hospital, but still no preventive medicine.
The chief of the medical staff takes disciplinary action against doctors who do not follow the
rules and regulations of the hospital, and reviews the work of committees of doctors who evaluate the quality of medical care in the hospital and the use of hospital resources.
Vice presidents, sometimes called directors, of administrative departments are responsible for the
daily operation of a hospital. The vice president of finance directs the work of a hospital’s admissions, budget, and cashier’s offices, overseeing the general accounting and internal auditing of the hospital’s finances. Although responsibilities vary in individual institutions, the vice president of materials management usually buys, stores, and maintains supplies, while the vice president of clinical engineering buys and maintains hospital equipment, including high-tech instruments and machines; here is where preventive medicine may get a foothold?

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
The vice president of environmental services supervises the laundry, power plant, and the hospital at large and ensures the safety and security of all staff and patients.
A physician heads each of the many medical departments found within most not-for-profit
general hospitals. Most hospitals have separate departments organized by medical specialties, including internal medicine, surgery, pediatrics, obstetrics and gynecology, radiology and diagnostic testing, pathology, anesthesiology, and sometimes psychiatry or neurology; we just have to get a specialist in preventive medicine.
The director of nursing supervises the work of nurses, the hospital’s largest group of health care providers, to ensure the quality and efficiency of the care they provide patients. Nurses provide round-the-clock care that includes giving patient’s medication, monitoring health status, and maintaining personal hygiene. Nurses also care for hospital outpatients in the emergency department, ambulatory surgery center, and clinics. They provide specialized services in intensive care units, surgical suites, and trauma units, but no preventive medicine.
In addition to medical, surgical, and nursing care, a hospital also provides many other
professional services, all of which have a department head who reports to the hospital’s chief administrator.
Dietary or nutrition staff ensures that hospitalized patients receive food or dietary supplements that maintain and improve health. The pharmacy dispenses the medications that are ordered by doctors and advises doctors on alternative drug regimens for individual patients.
The social services department links patients with agencies and professionals inside and outside
the hospital that can provide patients with financial help, counseling, long-term care, or assistance in the home. Educational outreach programs not only acquaint community members with the direct services offered by the hospital, they also teach individuals about disease prevention and health maintenance, but no preventive medicine.
Hospital Departments
Hospitals are typically organized into medical departments, or units, such as an emergency room, surgical suites, intensive care units (ICUs), pediatric and maternity wards, and departments of radiology, anesthesiology, pathology, and rehabilitative medicine.
A hospital’s emergency department is staffed 24 hours a day by doctors and nurses who have
been trained to diagnose health problems quickly. In pre mature births incubators or intensive care units are required for the “preemie”. These doctors and nurses perform medical or surgical treatments that stabilize a patient’s condition so that the patient can be moved to another part of the hospital for additional care. When the emergency room is crowded with patients, emergency department staff identify and respond immediately to the most seriously ill or injured patients, a medical approach called triage.
Childbirth
The surgical suites include the actual operating rooms, where surgical procedures are performed, and postoperative recovery rooms. All operating rooms have an operating table that can be adjusted to accommodate the surgical procedure and facilitate the use of sophisticated monitoring equipment. Instruments and equipment, such as lasers or television screens, are brought into the operating room as needed. After surgery, patients are taken to the postoperative recovery room, adjacent to the operating room, so they can be monitored as they awaken from anesthesia.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
14
Many hospitals offer two types of ICUs—one for patients who have had surgery and one for patients with dangerous medical conditions, usually involving the heart.
Some hospitals also have ICUs for newborns or burn patients. Intensive care units use monitoring equipment that transmits data on a patient’s condition directly to the nurses’ station. ICUs also have on hand technology and medications that are specific to the medical needs of the patients they serve. Newborn ICUs have equipment that is specifically designed to deliver oxygen to premature births or tiny babies, while burn units have special ventilation systems, as seen in the picture, to reduce the chance that patients will be exposed to infection.
The pediatric unit admits only children and is equipped with
instruments and machines that are suitable for the small size of its patients. Hospitals often prepare children for a hospital stay by allowing them
to visit before being admitted so that the surroundings will seem less frightening during their stay. Some hospitals allow a parent to stay in the child’s room during a hospital stay. Pediatric wards often have playrooms for their young patients and organize special activities such as parties to cheer children who are hospitalized during holidays.
Maternity Ward – childbirth avoids Meditation – Mind Body Medicine
The maternity ward, also found in many hospitals, offers homelike labor and delivery rooms
where a pregnant woman and her family can gather for the birth of her baby. It also may have a separate surgical area for difficult deliveries requiring a cesarean section,
sometimes needed when the baby is not in the normal head-down position or when there are multiple babies.
Most maternity wards have a central area where newborns spend most of their time until they are ready to be released from the hospital with their mother.
Childbirth - Meditation – Not Hospitals
Robert Bruce Newman is the developer of Calm Birth and he wrote several books one titled
“Calm Birth: New Method for Conscious Childbirth, North Atlantic Books, October 2005 and Calm Healing: Methods for a New Era of Medicine North Atlantic Books, November 2006. He Published articles include: The Emergence of Mind/Body Medicine, Sentient Times, August, 1999.
Newman has worked with doctors, childbirth educators, midwives, nurses, for years and doulas, has come a new childbirth method.
Doulas is the term describing an experienced, non-medical assistant who provides physical, emotional and informed choice support in prenatal care, during childbirth and during the postpartum period. It is based on Newman’s more than 20 years of apprenticeship with Tibetan meditation teachers and doctors, methods he learned and was authorized to teach.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
15
Newman has presented more than 90 hospital and conference training seminars in the Calm Birth method since 1997. He has presented the method twice at the world congress of the Association of Pre and Perinatal Psychology and Health (2002, 2005), at the University of Michigan Medical School (3/04), and at Bastyr University (2005). He has taught at the University of Colorado, Naropa University, and the City University of New York.
Newman’s research sites Verny in 2002 stating that biological and psychological benefits of meditation are transmitted to a womb child through the pregnant woman’s bloodstream and through sympathetic resonance. This practice involves the
woman communicating with the child telepathically and energetically, influencing the production of beneficial neurohormones and neurotransmitters. Thus, postnatal benefits will be transmitted to the child through lactation and breast-feeding and through sympathetic resonance. Before and after birth, meditation benefits are dual, inseparably benefiting the woman and the child.
Biological Benefits of Meditation
With respect to direct influence and quality of prenatal and perinatal health, Newman will focus
primarily on hormonal balance and immune system enhancement. Newman points out that anxiety causes an overproduction of the hormones adrenaline and
cortisol, suppressing important biological functions in order to shift energy into muscle systems. He notes that anxiety suppresses immune system function, but childbirth meditation brings adrenaline and cortisol levels down, restoring normal immune function for birth. Meditation strengthens the immune system with major hormones, melatonin and DHEA, to give a vital basis for life and to cope with the side effects of medical birth.
Newman indicates research shows that anxiety pushes tolerance of pain to low levels; meditation
restores normal tolerance of pain and produces endorphines, pleasure agents in the nervous system, so important for childbirth, reducing physical pain.
Newman verifies that the chemical or drug treatment of anxiety in pregnancy can be risky, while childbirth meditation is a safe, proven antidote to anxiety. Childbirth meditation reduces the need for medical interventions during labor, and brings biological enrichment.
DHEA (dehydroepiandrosterone)
Newman indicates that research shows DHEA to be a life-enhancing hormone, was one of the
first biological benefits of meditation to be observed. DHEA is produced in the adrenal glands, just above the kidneys. Issuing from the same glands that produce the stress hormones, elevated levels of DHEA involve reduced production of restrictive cortisol and adrenaline.
DHEA has a variety of health-impacting benefits. It is an immune enhancement agent that has been proven to be beneficial in the prevention and treatment of cancer, cardiovascular disease, diabetes, lupus and other conditions.
DHEA stimulates the production of monocytes (T cells and B cells), potent immunity bio-chemicals that cause the production of other immune system agents. Research shows T cells or white blood cells produced in the bone marrow produce two powerful immune system agents: interleulin-2 and gamma-interferon.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
16
These are intelligent defense agents that help maintain health. DHEA is good for the bones, muscles, blood pressure, vision and hearing. It is the substance from which the male and female hormones are developed and it is the source of vitality and youthfulness. DHEA is a mood elevator that makes people feel and look better. It enhances brain biochemistry and growth.
Anxiety and stress lower normal DHEA levels in the bloodstream. Meditation elevates DHEA levels. Thus meditation during pregnancy, in offering potentially ideal hormonal function, conveys elevated levels of vivifying DHEA to the womb child, and, through lactation and breast- feeding, to the child after birth.
Melatonin versatile antioxidant
Research shows the fact that meditation produces elevated levels of melatonin, the hormone secreted by the pineal gland located at the center of the brain, was first disclosed by research conducted at the University of Massachusetts Medical Center. The pineal gland has drawn the attention of human insight for a long time. In sacred literature more than 2,500 years old, the Vedas of India, the pineal gland was envisioned.
“The [pineal] gland was portrayed as one of the seven chakras, or centers of vital energy, which
are arranged along the central axis of the body. The pineal gland was thought to be the supreme or crown chakra…the ultimate center of spiritual force.” (Reiter, 1995, p.131).
In the 17th century AD, Descartes, in his famous Treatise of Man, called the pineal gland the seat of the human psyche, the principal location of self-awareness. Though the above insights may be inspiring concerns for people interested in meditation, current world-wide interest in melatonin, evident in the presence of hundreds of research papers and books, is focused on its biological benefits, particularly concerning the remarkable effects of melatonin on the human immune system.
Melatonin many be the most potent and versatile antioxidant. It directly stimulates interleukin
(IL-2) activity which in turn stimulates the increase of all the various cells of the immune system, in a pervasive, global optimization of immune function. Melatonin directly restores and increases T-helper cell production in bone marrow.
In stress-inducing times, which tend to cause detrimental hormonal imbalances, strong levels of melatonin in the bloodstream, naturally induced by pregnant women, are a sign that they are engaged in effective prenatal care. Melatonin is renowned as a sleep-aid. Especially when produced naturally to elevated levels, it helps establish normal sleep and rest even in challenging situations. Melatonin is known to have a calming effect, bringing contentment and improved mood.
Summary of Benefits
The natural production of elevated levels of melatonin in meditation conveyed to the womb child
through the woman’s prenatal bloodstream, and then through postnatal lactation and breast-feeding, gives woman and child remarkable immune enhancement and overall health benefits.
Though the extensive research in melatonin benefits has been concentrated almost entirely on the above, there are probable intelligence enhancement benefits warranting research.
Endorphines
Deepak Chopra writes that Meditation is known to produce endorphines, peptides secreted
throughout the nervous system that have a very strong pain-relieving and pleasure-inducing effect, similar to that of morphine.
“Thus the brain [and nervous system in general] produces narcotics up to 200 times stronger than anything you can buy . . . with the added boon that our own pain-killers are nonaddictive.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
17
Morphine and endorphines both block pain by filling a certain receptor on the neuron and preventing other chemicals that carry the message of pain from coming in, without which there can be no sensation of pain, no matter how much physical provocation is present.”
Newman identifies that in 1994 Michel Odent observed that the longer and more challenging the labor the higher the level of endorphines. Also, the more time devoted to the practice of prenatal meditation the higher the level of endorphines at birth. A woman who practices prenatal meditation will tend to be less afraid of pain, less disturbed by it, and will experience more joy.
Endorphine production is important to a woman in avoiding the risks of medical interventions and in gaining confidence in her natural abilities in childbirth. In 1997 Pert writes about her third childbirth . . . my magic bullet had been breathing, which is a surefire, proven strategy for releasing endorphines and quelling pain.
Obviously, this is what previous generations of women, in the days before I V drips and synthetic painkillers, had relied on. Both they and their babies must have been better off for the experience, as I certainly felt myself to be says Pert.
Psychological Benefits – Meditation
In 1999 Murphy & Donovan reported on extensive research conducted at the UMMC that
another important benefit derived from meditation is increased tolerance of pain based on psychological factors. The study demonstrated statistically significant reductions in present moment pain, negative body image, inhibition of activity, mood disturbance, anxiety and depression, and the need for pain-related drug utilization. The implications for childbirth are evident.
Murphy and Donovan describe published research in the following psychological benefits of meditation: Extended Perceptual Ability;
Quick Alert Reaction Time; Field Independence
Concentration; Empathy; Creativity; Self-Actualization In a pregnant woman, the above benefits of meditation entrain the womb child, through
sympathetic resonance, to develop these inherent traits. Hopefully research will seek to observe these traits developed in children though childbirth meditation methods.
Childbirth Meditation - Pre-Eclampsia
Newman reposts that one of the first important health effects of meditation to be discovered by
modern medicine was that it lowers blood pressure. Today there is strong evidence that meditation helps lower blood pressure and heart rate. The findings have been replicated in many studies according to Murphy and Donovan, “The Physical and Psychological Effects of Meditation”, IONS, 1999.
Childbirth meditation directly reduces blood pressure and heart rate, lowering the risk of preeclampsia and potential preterm brain damage.
Attention Gain Entrained in Utero
With the alarming pandemic of attention deficit disorders in children, it’s good to see how
childbirth meditation can help. Mindfulness meditation, known and respected in the medical establishment, is a practice of attention. It strengthens attention. It increases attention. In childbirth meditation, the woman’s shift of attention from mind to awareness entrains the womb child to be aware, to orient better. It is speculated that this can only help prevent attention deficit problems which might arise from hospital birth medications.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
18
Other observed benefits of childbirth meditation: In 1996 Benson observed Meditation to be helpful with depression and insomnia. Benson also
observed cesarean section surgery reduced by 56% and epidural anesthesia use reduced by 85% among meditators.
Altogether, increased attention to the child, increased pain management skills, increased levels of endorphines and important hormones, and this should be important incentives for women who don’t want to risk chemicals and anesthesia in childbirth.
Newman believes that as we discover more and more dimensions of physiological and psychological function and as mind/body methods become more and more a part of childbirth medicine and the focus of research, we’ll learn
more about the potential benefits of meditation in childbirth. However, these “preventive medicine” medicine practices and their benefit are rarely if ever
allowed in certified hospitals and it is unlikely that any large HMO or insurance carrier will pay or reimburse payment cost of these wonderful human and beneficial treatments; not for just the mother but for the fetus and newborn.
A reasonable person will logically presume that the physiological benefits described above are “better” and normal for both the fetus and the mother. Natural Child Birth produces all of nature’s natural chemicals for both the mother and newborn.
David Cheek, MD has written about the fact that natural childbirth is superior to all other means of childbirth; in books and presented these facts to thousands of doctors across the U.S., Canada and Europe. Yet, for malpractice protections hospitals will order and prefer caesarean birth with epidurals for pain management which has negative effects on the fetus, mother and new born.
In fact, for decades, thousands of brilliant doctors across the U.S. Canada, Europe and Australia have been ostracized, criticized and abandon as quacks by their professional medical associations if they dared to practice Clinical Hypnosis, Mind Body Medicine or such natural techniques for pain management, treatment for cancer and many other medical problems.
It is no wonder Deepak Chopra, MD had to file lawsuits against those in “main stream” hospital
medicine attempting similar attacks; keep in mind Chopra won a large settlement! Preventive medicine including techniques of meditation are powerful “medical” treatments and must become a part of the hospital department and staff. When preventive medicine treatment, techniques and approaches are a part of “every” hospital staff the American HealthCare Crisis will be on the road to extermination.
Hospital departments
Hospitals also have departments that assist in the treatment of patients but that are not involved
in their day-to-day care. The department of radiology provides internal images of the body to diagnose and treat disease; the anesthesiology department works with physicians to provide the safest type of anesthesia for a patient during surgery and pain relief after surgery; and the pathology department examines body tissues in a laboratory to diagnose disease.
AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
19
Some hospitals help patients in their recovery by providing the services of a department of rehabilitative medicine, which is often headed by a doctor and staffed by physical and occupational therapists. These professionals help patients regain normal physical function following surgery and relearn muscular control and coordination in resuming everyday tasks. But, there are no Preventive Medicine Departments.
Cost Issues – Hospitals
Hospital costs have increased steadily over the last 30 years, largely because of the way health care is paid for in the United States. For many years, both private health insurance companies and government agencies, referred to as payers, paid more for treating insured patients in hospitals than in outpatient settings.
In response to this reimbursement strategy, many hospitals expanded their facilities and added the latest in high-tech equipment, spreading the cost of these expensive improvements to every hospitalized patient.
Since the mid-1980s, however, private and public payers have tried to reduce the skyrocketing costs of hospital care that resulted from the facility improvements of the preceding two decades. The federal government has cut the budgets for both Medicare, which covers health costs for people over age 65, and Medicaid, which provides similar coverage to the poor (see Medicare and Medicaid). Further, both public and private payers increasingly are opting for an approach to the delivery of health care called managed care, which controls not only the cost but the number of services patients receive.
As a result of these trends, hospitals are receiving less money from government programs and
have had to reduce their own spending because of the cost-control activities imposed by managed care. Despite tighter budgets, hospitals continue to provide treatment to an increasing number of
uninsured Americans, whose ranks swelled from 33.5 million to 44 million between 1988 and 1998. These changes have affected some hospitals more dramatically than others. Public hospitals,
which treat large percentages of Medicaid patients and uninsured individuals, have been hit the hardest, often receiving no payment for roughly 13 percent of the care they provide.
Because many city and state governments have cut taxes, public hospitals do not receive
adequate tax dollars to cover their deficits. The financial constraints facing public hospitals have forced some to close their doors, such as the 112-bed Polk County Florida Hospital, and others to downsize, including the District of Columbia General Hospital, which eliminated 160 of its 410 beds and laid off 260 employees in 1995.
The financial health of private, not-for-profit hospitals has largely depended on their location. Hospitals in areas where much of the population is enrolled in managed care plans have had to cut their costs by examining and redefining the most efficient ways of treating patients while ensuring the best medical results.
A program at Boston’s Massachusetts General Hospital ensuring that patients receive prompt physical therapy, for example, has decreased by 22 percent the average length of stay for patients having hip or knee replacements. In most instances, maybe as high as 70 percent of all hip or knee replacements can be avoided and the need for surgery delayed or postponed indefinitely with proactive AquaDios-Med™ structured deep-water running treatments. The cost for the surgery would of course be eliminated.
However, it’s good to know the cost of hospital hip or knee replacements surgeries has been
decreased by 17 percent; the result of this program is not only cost reduction, but also faster recovery for patients and earlier release to home or to a health care setting for further rehabilitation.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
20
Another cost-cutting strategy is to merge not-for-profit hospitals with other hospitals to become part of multihospital systems, some of which are for-profit companies. In 1994, 251 of the 308 nonprofit hospitals that changed hands were acquired by for-profit hospital chains.
The biggest hospital cost cutting strategy is that of preventive medicine and programs like Aqua-Dios-Med™ because it will reduce the 80 percent of “inpatient” population to outpatient while eliminating as much as 80 percent of today morbidities.
Canadian hospitals also are facing financial challenges, although their challenges differ from
those that U.S. hospitals must address. Whereas the number of uninsured Americans is increasing each year, Canada has no uninsured individuals because it provides all citizens with health insurance. However, this health insurance is financed through taxes that provincial governments are reluctant to increase, despite the increased demand for medical services among Canada’s aging population.
In addition to making tax decisions that affect the financial health of many of Canada’s hospitals,
provincial governments also make decisions that govern how hospitals operate, even if a hospital is not in the public sector. Examples of decisions made by provincial governments in their efforts to minimize health care costs include prohibiting hospitals from acquiring new technology and rationing nonemergency services by placing patients on long waiting lists for treatment.
It is not unusual for Canadian patients to wait as long as three months for a hip replacement and
eight months for gall bladder surgery. In contrast, elective surgery in the United States is delayed by only the days, or at most weeks, required for an insurer or managed care company to approve the requested surgical procedure.
It is astonishing that Canada and America suffer the same syndrome of no preventive medicine.
The one constant in all of this research is that safe daily exercise and healthy nutritional foods
will prevent most all serious medical problems such as the treatment of preventive medicine practices in AquaDios-Med™ with its requirement of safe daily structured deep-water exercise and Mind Body Medicine.
Some Author Background - Summary – Overview This Book
As a child, long ago this author’s opinion and personal experience of doctors and hospitals began its journey from the formative years to old age. In that span of approximately 5 decades I feared hospitals, especially surgeons and dentists.
Hospitals and surgeons were to be avoided because hospitals allowed surgeons to cut into the body, known as an “insult” that causes pain and suffering. Dentists were to be avoided because their work caused the utmost pain.
I have learned “pain” is an important human message like a phone call that must be answered and its message listened to. I have gotten over my “fear” of dentists and enjoy all dental procedures with no anesthetic to numb the surgery. I leave the dentist office with an uplifting feeling and no numbness in my mouth, cheeks or tongue, likely because I produced endorphines and other positive chemicals during the procedure.
To me hospitals and surgery was and still is a paradox; to improve a person’s health a surgeon
must cause “pain” to eliminate the suffering of injury, sickness or disease. This means almost any complication, even death can be iatrogenic or brought forth by the physician, procedure, surgery or nursing staff. Thus, a reasonable person will logically conclude that “surgery” is dangerous and should be the last resort not the first choice of procedures.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
21
My personal injuries were a “godsend” because I learned that sometimes hospitals, surgery and dentists were an absolute necessity for me to go on with a normal life; and that “pain” was a part of healing. As the victim of a “free diving accident” I had to have a “fish spear” surgically removed from my biceps. The surgeon had “good bedside manner” and told me I would completely recover but only if I was willing to face pain twice a day; that was removing my wounded arm from the sling to “break loose” the forming scar tissue.
I learned this “rehabilitation pain” was very similar to “re-injury pain”; one generated growth
and repair the other caused a failure to heal. Too often patients, hospitals and doctors rely on pharmaceuticals to prevent pain, but this practice is more dangerous than the pain for several reasons. Pain is nature’s way of telling the person to stop. But, most people do not understand that after they stop use of the body part in pain their job is to relax and identify the severity of the injury; this often requires a doctor’s diagnosis and opinion. Once this is established a decision must be made as to what the healing protocol is and what is required of the injured or ill person.
Unfortunately hospitals and doctors have a tendency to overuse and even abuse pain
medications. This is dangerous because some of these medications can be addicting and because the medications stop, delays or slows the natural healing response. Thus, the patient faces a longer recovery period and may become a hospitalized “inpatient” rather than released as an outpatient.
The above scenario is one of the failures of modern hospital medicine because it is to the patients
disadvantage to be an “inpatient” while it is advantageous to the hospital, doctor and staff. Thus, the patient is stuck in a very expensive and dangerous hotel.
Hospitals are not dangerous because I say so, research and facts presented in this book make it
very clear that hospitals make mistakes, cause “iatrogenic” or doctor – staff caused complications, they demand invasive tests when not required or necessary, they have bacteria that is deadly and resistant to all drugs – antibiotics and indeed patients die that should not. Therefore, a reasonable person must logically say themselves, my visit to the hospital shall be as short as possible and I will seek trustworthy advocates to help protect me.
Hospitals, doctors and staff are absolutely necessary, but often “run up” the tab when a more simple approach may be best for the patient, such as a 30 to 90 day “preventive medicine” program, one that requires the patient to be responsible for safe daily exercise as is in the AquaDios-Med™ treatment and a nutritious daily diet.
This book has given the reader deliberate and factual information based on research studies of
the major medical “killers” in our society and one of the most dangerous killers is the hospital itself. This is not an opinion, it is a fact based on research evidence collected by scientists. However, we cannot throw out the baby with the bath water, hospitals are absolutely necessary for our communities and nation.
It is imperative for the American population to recognize the medical crisis, its horrific healthcare costs of more than $ 2.2 Trillion just does not work as it is managed and has been managed over the past several decades.
Research repeatedly shows the power of the “placebo effect”, when a respected doctor at an
esteemed hospital tells a patient that medicine has a “new” and wonderful pill that is designed to eliminate their presenting medical problem; even though the pill is an inert “placebo”, the patient has a miraculous recovery. This is no miracle, it is the phenomenon of belief and expectancy allowing the human immune system to do its work; and that is to heal. The “placebo effect” has a remission rate of about 68%.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
22
Dr’s Petr Skrabanek and James McCormick identify the placebo effect as the physician's belief in the treatment and the patient's faith in the physician to exert a mutually reinforcing effect; the result is a powerful remedy that is almost guaranteed to produce an improvement and sometimes a cure.
It is this premise that “preventive medicine” is built on. Research presented in this book shows
that the patient will do the healing not the doctor or the hospital and the most aggressive healing with no negative side effects is intense safe daily exercise as is a process of AquaDios-Med™ combined with principles of Mind Body Medicine to assure the person is “intent” on healing.
The substantial research reviewed in this book make it crystal clear that most people do not know
what “safe” daily exercise is nor do hospitals and doctors. Too often only “mild” exercise 3 or 4 days a week is reported, and ironically this paltry amount shows vast health improvement.
In my private practice I encouraged patients to take daily exercise but those that did became
injured and lame in a short period of time which led me to develop AquaDios-Med™ first for myself; I assure you it works. My premise is that if it works for me it will also produce the same result for the entire population. It is certain that the human body is made to take safe daily exercise and eat nutritious foods. These two activities alone can eliminate the healthcare crisis and it’s more than $ 2.5 Trillion costs.
I believe that when AquaDios-Med™ health centers are made available to each community with a population of 350,000 residents the healthcare crisis will be over. This simplistic approach will also require that all schools from elementary through high school, including Junior College, College and University to provide a minimum safe daily exercise in the form of structured deep-water running. Simultaneously all hospitals will be required to have a “health center” offering AquaDios-Med™ preventive medicine treatments.
It does not take a mental giant to logically conclude the human body “must” partake in safe daily exercise and the only method of exercise that is truly safe is structured deep-water running as seen in AquaDios-Med™.
I researched and developed what I believed to be the only system that meets the human bodies needs when I built the medical prototype AquaDios-Med™. This was not done as a project to corner the medical market, it was done as a by-product of finding ways to heal rapidly when injured, to remain active when injured, to be as healthy as possible without having the need to see doctors or go to hospitals. I have treated broken bones, sprains and strains, eye disease, lower back pain and much more with the methods and practice I’ve include in AquaDios-Med™.
I hope this book will help to nationalize AquaDios-Med™ the
only program I know of that is capable of eliminating the healthcare crisis and returning so many sick and disabled people to an active and full life.
The research in this book verifies the leading cause of death in America is the healthcare system itself, while research studies qualifying for multi-million dollar grants are found to include prescribing dangerous pharmaceuticals also identified in this manuscript; but no preventive medicine. I also include the fact that the Center for Disease Control – Prevention confirmed more than 85 percent of all disease has an emotion - stress manifestation yet “preventive medicine” is excluded from hospital departments and HMO’s refuse to reimburse for the expense of these most successful treatments. The CDCP established the fact that emotion and belief are responsible for most “dis-ease” yet there is still no national “preventive medicine” program available in hospitals.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
23
Diabetes and diseases caused by diabetes all have a very easy fix, and that is safe daily exercise with nutritional foods; this is true for heart disease, stroke, most arthritis, and nearly all diseases that kill Americans including cancer. Remember, this is not a fact because I say so, scientific research has proven this to be true.
Hospital medicine treats most diseases with pharmaceuticals all of which have adverse effects, some severe enough to cause death, yet these same hospitals do not provide “preventive medicine” programs as treatment of choice. AquaDios-Med™ (see “The Healthcare Solution,” page 8), combined with a healthy diet of five servings of fruits and vegetables a day, moderate alcohol consumption and no smoking, will decrease the need for medical intervention, and thus reduce exposure to the adverse effects thereof.
The miracle of human body is that it heals itself, and it does that very well, given favorable conditions. With its practice of surgery, drugging and irradiating patients, traditional medicine produces conditions that inhibit and sometimes prevent the body’s natural self-healing capacity.
Centuries of historical research prove deep-water immersion and structured deep-watering
running is confirmed to be the safest most effective exercise for the human body as is refined in the form of AquaDios-Med™ to even more successfully aid the body in healing itself.
Not long ago “Mind Body Medicine” practices and treatment were accepted by only a few
Avant guard practioners but recent research has proven that Mind Body Medicine, an outgrowth of psychoneuroimmunological mediation is a very powerful and effective human capacity. This procedure falls under the procedure of preventive medicine practices which is still excluded from most hospital primary care and likely not reimbursed by most HMO’s, yet it is the most effective treatment for all people?
This book has been organized in such a way to first show the medical facts presented to the reader to make a factual statement that modern medicine, as practiced today, is dangerous to the patient. I then examine a proven preventive medicine method AquaDios-Med™ and show its basic procedures are cultivated from proven ancient practices then combined with modern techniques and proprietary innovations that can make AquaDios-Med™ successful to almost the entire American population.
Modern scientific studies verify the positive physiological effects that daily safe exercise by
structured deep-water has on the human body and answers the “why” and “how” of accelerated healing; and documents agedness is related more to lack of exercise than it is to passage of time through ageing. Research data supports that daily exercise, with proper nutrition, delays or reverses premature aging; and that deep-water exercise; may be the one “best” exercise for pregnant mothers and the developing fetus.
Pain management is an inherent human condition and this book gives the reader an opportunity
to learn how to avoid all pain medications so long as the person is willing to acknowledge “pain” “re-injury pain” and “rehabilitation pain”. As discussed in the pages of this book “rehabilitation pain” is very similar to “re-injury pain” with one major difference; it shortens rehabilitation and accelerates healing. Thus, the majority of pain medication can be avoided as can its negative side effects.
Several sections of this book discusses obesity and the many diseases associated with it and a
practical down to earth method of eating and nutrition is documented as possible for almost anyone. It can be as simple as avoiding all sugar, butter, salt and fried foods while relying on salads, whole grains, lean meat, fish or poultry in small portions.
Scientific proof shows how natural “breast enlargement” is possible and even discussed as is allergy and skin rash control.
These confirmed research medical studies and facts demonstrate causes of the healthcare crisis.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
24
It is unfortunate but true that politics and avarice play a far too important role in the healthcare crisis. Research shows that hospitals rely on drugs and surgery while both are most often unnecessary and dangerous as shown by the high percentage of adverse events and iatrogenic disease medicine. The profit-centered hospital avoids any patient-centered primary treatment of choice such as preventive medicine practices which includes safe daily intense exercise such as that found in AquaDios-Med™ procedures and which proves to work more effectively than anything else in a high percentage of the cases. Research studies show that as little as 30 days of mild exercise has a dramatically positive effect on cardiac patients and continuously point to the power of a daily healthy nutritious food; this is pretty simple.
The history and underpinning of ancient world deep-water immersions for health shows the reason why AquaDios-Med™ is so powerful and effective with its modern applications, proprietary innovations and physiological changes derived from the process itself.
The more than $ 12 Billion Spa industry is discussed; and recognized as a business with too
much pampering to have long term effects on healthcare. However, the concept of Spa is factually very close to the more productive deep-water immersion and structured deep-water running found in the historical AquaDios-Med™ foundations. Simply put Spa is adequate for stress and anxiety reduction and a place to absorb quality “pampering”.
Specific research is dedicated in this part of the book to the preventable hospital deaths caused
by avoidable hospital mistakes and errors. This includes medications mix-ups and adverse effects to medicine often resulting in death. This brings the reader to the recent issues with Dennis Quads newborns and the serious hospital medicine errors that nearly killed the newborns. Pain killer drugs are briefly discussed here, as well as are the danger of hospitals after 11:00 pm, when the death rates spike from what should be “preventable deaths”.
Specific current problems with the FDA and drugs are cited as is more about “medical error” and patient responsibilities to avoid death while in the hospital.
A large part of the book looks at the research studies proofing how chronic cardiovascular
disease and hypertension can be prevented with “preventive medicine” procedures, but these departments cannot be found in hospitals. Once again there is a simple cure, safe daily exercise and daily nutritional foods in small quantity. This takes in to account stress management interventions.
Because diabetes has become such a powerful killer with its multifaceted diseases more time is
spent with studies that are designed to control the disease and maybe eliminate it. Ironically diabetes can be cured by the daily safe intense exercise and daily nutritional foods as well; truly “exercise is medicine”.
Studies have focused on what is called “Optimal Healing Environments” and a good deal of this book deals with this concept. In general the wisdom of these studies points to the fact that “healing” is done by the patient and not the doctor or hospital. Thus, providing the patient with the most relaxed environment with staff to encourage them seems to produce the most complete and rapid healing. This of course relies on daily exercise and nutritional foods.
This book digresses to more studies that demonstrate the healthcare crisis is caused by the
healthcare system because of its many errors of practice and because preventive medicine is not included as the first and primary treatment of choice.
A more comprehensive fact finding mission exposes the more than $ 200 Billion a year pharmaceutical industry and its “fraud” with its appalling lack of ethics or morals when it comes to marketing its product regardless if the drugs may cause serious disabling adverse effects or death. This section ends with methods of preventive medicine as a way to avoid the addiction to medical drugs.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
25
One most important research is study of the placebo effect and how powerful human healing can be with just a little guided suggestion, expectation, belief, faith and support from doctors and hospital staff. It is incredible that 68% of the time or more – placebo – natural healing performs better than the medicine. This means the placebo or no-drug was as effective or more so that the pharmaceutical. What is astounding is, the verified, positive drugs, the human can naturally produce to accelerate healing. It is this approach that is the foundation of AquaDios-Med™, finding ways for the patient to produce the immune systems natural healing responses; Placebo should be major part of modern hospital medicine. Preventive medicine is so powerful - works because PM harnesses the placebo effect while producing treatments that precipitate, activate and maximize the natural human production of the immune system and our capacity to produce natural healing physiology.
The low back problem is re-addressed as a serious dredge on our American economy pointing
out it can be all but eliminated by AquaDios-Med™ daily deep-water running and power massages as can 80 % of all disease, medical problem or injury.
A part of this segment deals with self-healing, a focus on preventive medicine and the
AquaDios-Med™ approach including this treatment for diabetes, coronary artery disease, breast cancer, pediatric rehabilitation and disabilities. It deals more specifically with childhood obesity and the value of the pediatric societies which of course includes basic safe daily exercise and daily nutritional foods.
One of the last parts of the book deals with hospitals and preventive medicine. It points to one of America’s prolific Mind Body Medicine specialists, Deepak Chopra, MD who had to file a $ 194 million lawsuit, settled in his favor over issues of Mind Body Medicine.
Including “preventive medicine” in hospitals would change the healthcare crisis and in this
authors opinion would eliminate it. The basic philosophy of hospital logic is “in patient” or patient in hospital bed; while preventive medicine is based in the “outpatient” model where the patient goes to work, home and participates in safe daily exercise. This author uses analogy that would combine the more than 6,000 hospitals and the more than 10,000 Spas in the US to make the point that when AquaDios-Med™ facilities were built into each of these approximate 16,000 health care service locations there would be no healthcare crisis.
Hospitals are absolutely necessary for society to function, but they and Spas must include preventive medicine services like AquaDios-Med™ to genuinely meet the healthcare needs of America.
A segment given special attention is that of Child Birth, something each person in the world experiences. Hospitals prefer the caesarian surgery childbirth as it makes things orderly and predictable and all but eliminates mal practice. But, anesthetics given the mother have a strong negative impact on both the mother, fetus and new born. Here, the book discusses Meditation or similar mind body medicine methods that focus on natural childbirth which produces natural powerful positive chemicals such as endorphines that have a benefiting effect on the mother and newborn.
The last segment deals with the importance of Population Health Management and Optimal
Healing. The basic premise of preventive medicine programs which must find their way into hospitals to become reimbursable treatments by HMO’s.
For those of you who feel AquaDios-Med™ is a preventative medicine program that can and
will help to eliminate the healthcare crisis please contact your local, state and federal leaders as well as your hospitals and doctors to help spearhead its installation in your community.
Exercise Is Preventive Medcine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section VIII
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
Introduction • Research • Fibromyalgia Treatment • DWRIT • Deep Water Running
Clinical Effectiveness • Aquatic Exercise • Section VIII
Evidence Based
AquaDios-Med™ Proactive Preventive Medicine
26 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Research • Fibromyalgia Treatment DWRIT • Solution • Healthcare Crisis • Part VIII Fibromyalgia
AquaDios-Med™ Proactive Preventive Medicine • Evidence Based • Introduction
HOW Do You Do • Deep-Water Running • Water Exercise Benefits Fibromyalgia
Research studies confirm Fibromyalgia and Water Running are like ham and eggs; made to
order. Any Water exercise program is essential to fibromyalgia treatment -- aquatic therapy is one of the best forms of exercise, particularly for fibromyalgia patients. When immersed to the neck in water it takes almost no effort to move your arms and legs slowly. But, water has an isokinetic resistance as the speed of arm and leg movement’s increase, this resistance is proportional to the effort or muscular power of the movement and promotes strength, enhances balance and endurance. Deep-water immersion to the neck also reduces pain perception and aids in relaxation. A mild exercise done in deep-water water will be both easier to perform and more beneficial than the same exercise done on land while the more intense exercise is far more difficult providing improved strength, cardiovascular benefits and the healing benefits of no impact trauma.
Fibromyalgia patients reduced pain, improved functionality and emotional health. All of the studies showed long-term benefits from water exercise. Jentoft and Saltskar concluded that physical capacity can be increased by exercise, even when the exercise is performed in a warm-water pool; Aquatic programs have additional positive effects on symptoms management. Fibromyalgia Patients Exercise • Why Water Works • Fibromyalgia DWRIT Deep-water running immersion therapy DWRIT to the neck – positive physiological effects • increased circulation to muscles • increased joint viscoelasticity • decreased joint pain • body’s skeletal joint space is enlarged • synovial joint fluids increased • friction between articular cartilage tissues lubricate • cushion with movement • absence of gravitational body weight compression • muscles get stronger • less strain • cardiovascular training increased • aquatic therapy fibromyalgia patient improvements. Deep-water running studies consistently produce more people that improve and feel much better. Aquadios-Med™ Proactive Preventive Medcine recommends warm Jacuzzi massage prior to deep-water running exercise using cool 72 to 75 degree F water for the DWR exercise rather than warmed water and conducting the DWR exercise daily or a minimum of 5 days a week. Research concludes DWRIT is more effective than Land Based Exercise in treating patients with FM regarding pain, and advantageous regarding emotional aspects. Deep-Water Running is a dominant source of aerobic exercise for patients with FM and for any person or patient whose weight bearing activity may be limited. Additionally, exercise in a pool is a pleasant stimulus for exercise compliance.
One key factor in treatment of Fibromyalgia Patients with Deep-Water running Immersion Therapy is the water’s isokinetic resistance.
Exercise Is Preventive Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Research • Fibromyalgia Treatment DWRIT Mind-Body Medicine • Deep-Water Running Immersion Therapy
• Solution • Healthcare Crisis • Part IX Fibromyalgia AquaDios-Med™ Proactive Preventive Medicine • Evidence Based
HOW Do You Do • Deep-Water Running
Newman states that deep-water running is made possible by a water-walker; basically a Styrofoam belt that keeps your bottom half and top half in an upright position in the water. The buoyancy of the belt keeps your feet off the bottom surface and
allows you to move your arms and legs in a close simulation of land running movements. You can run essentially free of the effects of gravity. In addition, the water provides 12 times the resistance of air so that although your movement speed is slower, the exertion
needed for the movement is increased. Your objective in the water is to closely mimic the movements you make on land. Arms, body position, and leg motion should appear to be slow motion running. Your head should be positioned upright without any awkward forward tilt. This sounds easier on paper than it is likely to feel--you'll need to experiment and practice, maybe even get the help of an instructor to get it right. But once you get the position, the motion, and a comfort level in the water, your training can proceed with your normal running routine.
Water Exercise Benefits Fibromyalgia
Kate Grossman, MD wrote an article titled Fibromyalgia and Water Running for About.com and Dr. Grossman explains that summer is a great time to begin a water exercise program. Exercise is an essential component of any fibromyalgia treatment program and aquatic therapy is one of the best forms of exercise, particularly for fibromyalgia patients.
Fibromyalgia • Why Water Exercise is Beneficial
Dr. Grossman begins by noting the buoyancy of water is important because it substantially
decreases the effects of gravity when a person is immersed up to the neck with a buoyancy belt so it takes almost no effort to move your arms and legs slowly. But, water has an isokinetic resistance as the speed of arm and leg movement’s increase, this resistance is proportional to the effort or muscular power of the movement and promotes strength, enhances balance and endurance. Deep-water immersion to the neck also reduces pain perception and aids in relaxation. A mild exercise done in deep-water water will be both easier to perform and more beneficial than the same exercise done on land while the more intense exercise is far more difficult providing improved strength, cardiovascular benefits and the healing benefits of no impact trauma.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
Exercise sessions may be individual or in groups. Start slowly with 20 to 30 minute sessions two or three times a week. Gradually work up to sessions that last 45 minutes to an hour. Know your limitations. If you become tired anytime during the workout, stop exercising and just relax in the water or leave the pool. Do not push through the pain. If you experience new or increased pain, stop or slow down. Listen to your body. Have fun! Enjoy the freedom of movement water gives you.
Research Supporting Water Exercise As a Treatment
Multiple studies have shown that water exercise benefits fibromyalgia patients both physically and emotionally and this author believes every American including patients on daily medications can benefit enough with Aqua-Dios-Med™ to end the healthcare crisis.
In 2006 a study in Brazil looked at the effectiveness of deep water running on fibromyalgia
patients and [FM] symptoms, while in Spain researchers evaluated FM patients exercising in waist-high warm water. A 2001 Norway study compared the effects of land-based and pool-based aerobic exercise on women with FM.
In these studies, fibromyalgia patients experienced reduced pain, improved functionality and better emotional health. The comparative study found that both forms of exercise resulted in physical improvements but in the pool-based group improvements were also found in the number of days of feeling good, self-reported physical impairment, pain, anxiety and depression. All of the studies also showed long-term benefits from water exercise. Once again, this author believes Aqua-Dios-Med™ is the treatment of choice for about 80 percent of the American patient population including those with daily medications.
Fibromyalgia • chronic muscle pain • Exercise
In February 2001 Jentoft, Eva Saltskar, et al. published a research study titled “Effects of pool based and land-based aerobic exercise on women with fibromyalgia and chronic widespread muscle pain” in the journal Arthritis and Rheumatism. The study was done at the Haugesund Sanitetsforening Rheumatism Hospital, Norway.
The objective of the study was to examine the effects of pool-based or pool exercise (PE) and land-based (LE) or land exercise programs on patients with fibromyalgia. The outcomes were assessed by the Fibromyalgia Impact Questionnaire, the Arthritis Self-Efficacy Scale, and tests of physical capacity.
Eighteen subjects in the pool exercise PE group and 16 in the land exercise LE group performed a structured exercise program. After 20 weeks, greater improvement in grip strength was seen in the LE group compared with the PE group. The Jentoft and Saltskar study showed statistically significant improvements were seen in both groups in cardiovascular capacity, walking time, and daytime fatigue. In the PE group improvements were also found in number of days of feeling good, self-reported physical impairment, pain, anxiety, and depression. The results were mainly unchanged at 6 months follow-up. Jentoft and Saltskar concluded that physical capacity can be increased by exercise, even when the exercise is performed in a warm-water pool. They also stated that Aquatic programs may have some additional positive effects on limiting symptoms.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
Fibromyalgia Patients Exercise Why Water Works • Fibromyalgia DWR
On Jan. 13, 2008 Mary Essert wrote an article titled Why Water Works for the Aquatic Resources Network. Essert’s article is based on the research work of Assis, Marcos Renato, et al. titled A randomized controlled trial of deep water running: Clinical effectiveness of aquatic exercise to treat fibromyalgia reported in Arthritis and Rheumatism February 2006 and Gusi, N., et al. Exercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgia. Essert states summer is a great time to begin a water exercise program especially because exercise is an essential component of any fibromyalgia treatment program and aquatic therapy is one of the best forms of exercise, particularly for fibromyalgia patients.
Why Water Exercise is Beneficial for fibromyalgia patients
Essert relies on research that show the buoyancy of water decreases the effects of gravity so it takes less effort to slowly move through the water. However, water provides increased resistance as movements increase in intensity and in speed, which promotes strength and enhances balance. Immersion to the neck in deep-water also reduces pain perception and aids in relaxation. An exercise done in water will be both easier to perform and more beneficial than the same exercise done on land. Essert forgets to mention that the properties of water also provide support, resistance and assistance. In deep-water immersion the buoyancy of the water eliminates all impact and this decreases compression forces, vibration forces and torsional forces that a patient may endure while on land. This “unloading” of the joints prevents undesirable and often painful effects of weight bearing of the extremities. The physiological effects of deep-water immersion include increased circulation to muscles, increased joint viscoelasticity and decreased joint pain. Increased joint viscoelasticity means the body’s natural skeletal joint space is enlarged as is the synovial fluids of the joints. Synovial fluid reduces friction between the articular cartilage and other tissues in joints to lubricate and cushion them during movement. These healthy body improvements are caused by the absence of gravitational body weight compression. Also, muscles can get stronger with less strain while cardiovascular training is accomplished. The physical properties of water have utilized in aquatic therapy decrease gravitational forces placed on a weakened extremity and increase body movements, especially for the fibromyalgia patients.
How to Get Started Fibromyalgia Patients • Others
Exercise sessions may be individual or in groups, but Essert recommends that you start slowly with 20 to 30 minute sessions two or three times a week. Gradually work up to sessions that last 45 minutes to an hour 5 days a week. Essert reminds fibromyalgia patients must know their limitations and recommends that if you become tired anytime during the workout, decrease the intensity of your exercising and if necessary just relax in the water. Essert recommends fibromyalgia patients to not push through the pain. If you experience new or increased pain, stop or slow down. And listen to your body. Have fun! Enjoy the freedom of movement water gives you.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
More Fibromyalgia Research Supporting Water Exercise
As previously cited many recent studies show that deep-water exercise improves fibromyalgia patient symptoms physically and emotionally. This author notes that the general fibromyalgia patient has demonstrated a high psychological component to their conditions and symptoms. Nevertheless the process outlined by the daily safe deep-water running exercise of AquaDios-Med™ is believed to be very effective in getting these patients back into a normal life process so long as their motivation and confidence is kept high.
Effectiveness of Aquatic Exercise to Treat Fibromyalgia Arthritis Care and Research
In 2006 Assiss, Silva and Alves et al studied fibromyalgia and arthritis care and they published
a research article titled The Effectiveness of Aquatic Exercise to treat Fibromyalgia and Arthritis. The purpose of their study was to compare the effects of a water-based and a land-based aerobic exercise program in women with Fibromyalgia (FM). The authors also looked at adverse events, aerobic conditioning, and the relationship between improvements in symptoms and aerobic gain. The study population included 336 women who were screened and sixty sedentary women who fulfilled the American College of Rheumatology classification criteria for FM. These women were recruited from the Rheumatology
outpatient clinic of the Federal University of Sao Pauol. The patients were randomly assigned to either deep water running (DWR) in the warmed swimming pool or land based exercise (LBE) consisting of walking or jogging on a treadmill. This author believes warm water immersion is problematic for deep-water running as it is too hot for correct intensity, but adequate for warm-up. Both groups exercised for 60 minutes, 3 times a week for 15 weeks. Deep-Water Running
consisted of simulated running in the deep end of the pool aided by a floatation device. Pain, response to therapy, depressive symptoms, physical functioning, symptom severity, heart rate and peak oxygen uptake were all assessed. Both groups improved significantly at week 15 compared to baseline. Fifty percent of the patients from the land based running [LBE] group rated themselves as clinically improved at week 8 vs. seventy percent from the DWR group.
Only the DWR showed improvements in the section of the short form health survey that addresses limitations in usual role activities because of emotional problems. This means that deep-water running helped these women physically and emotionally to improve their quality of life and a willingness to participate in social activities. The authors concluded that DWR is as effective as or more effective than LBE in treating patients with FM regarding pain, and may be even more advantageous regarding emotional aspects. Deep-Water Running is a dominant source of aerobic exercise for patients with FM and for any person or patient whose weight bearing activity may be limited. Additionally, exercise in a warmed pool may be a pleasant stimulus for exercise compliance.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
This author believes this is a good study to replicate with some changes, first by having the participants start with a warm Jacuzzi massage prior to deep-water running exercise as recommended by AquaDios-Med™ and second using cool 72 to 75 degree F water for the DWR exercise rather than warmed water and last by conducting the DWR exercise daily or a minimum of 5 days a week.
Randomized Controlled Trial • Deep Water Running • Clinical Effectiveness
Aquatic Exercise • Treat Fibromyalgia
In 2006 Assiss, Silva and Alves, et.al., conducted another and similar research on fibromyalgia to compare the clinical effectiveness of aerobic exercise in the water with walking-jogging for women with fibromyalgia (FM). Sixty sedentary women with FM, ages 18–60 years, were randomly assigned to either deep water running (DWR) or land-based exercises (LBE). Patients were trained for 15 weeks at their anaerobic threshold AT. The AT is an extremely reliable and powerful predictor of performance in aerobic exercise. The anaerobic threshold (AT) is also called the lactate threshold or the level of exertion where your body must switch from aerobic metabolism to anaerobic metabolism.
Aerobic metabolism burns oxygen and produces carbon dioxide as a by-product. Your lungs provide the oxygen and get rid of the CO2. Muscles "burn" glucose two ways, aerobically or "with oxygen" and anaerobically, "without oxygen". Both systems generate a temporary energy store for the muscles, called ATP, which in turn produces the ability for sustained exercise.
The Visual analog scale of pain, Fibromyalgia Impact Questionnaire (FIQ), Beck Depression Inventory, Short Form 36 Health Survey (SF-36), and a patient’s global assessment of response to therapy (PGART) were measured at baseline, week 8, and week 15. Statistical analysis included all patients. Assiss, Silva and Alves reported that four patients dropped out from each group. Both groups improved significantly at week 15 compared with baseline, with an average 36% reduction in pain intensity. Forty percent of the DWR group and thirty percent of the LBE group assessed themselves much better at post treatment therapy. Thus, deep-water running produced more people that improved and “felt much better”. The DWR group was both significantly faster to demonstrate less Fibromyalgia symptoms and less depression than the land based group and kept on improving as measured by the cited tests. And, only the DWR group showed significant improvements in their emotional role testing. Thus, deep-water running proved to be more effective in reducing common physical and emotional symptoms of the patients. These researchers concluded that DWR is a safe exercise that has been shown to be more effective than LBE regarding pain. And, deep-water running brings more advantages related to positive emotional aspects. Aerobic gain was similar for both groups, regardless of symptom improvement. Therefore, DWR could be studied as an exercise option for patients with FM who have problems adapting to LBE or lower limbs limitations.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
Fibromyalgia Expanded Research • DWR
Fibromyalgia (FM) is a widespread musculoskeletal pain syndrome with patients suffering a diminished pain threshold. Many studies have now demonstrated abnormal sensory processing in individuals with FM, further supporting the organic nature of the abnormal central pain processing in FM. Sedentary lifestyle and unfitness are factors that can trigger this illness in which reduced tolerance and sympathetic response to exercise are found. Regular physical exercise has been proven to be useful in treating patients with FM. Thus, Fibromyalgia can be associated as one very negative side-effect cause by sedentary lifestyles with no daily sustained exercise. Several studies have demonstrated a reduction in pain and fatigue and improvements in sleep and mood quality. Many mechanisms of exercise benefits can be attributed to tissue oxygenation improvements, increased muscle endurance, and high energy phosphate levels. Most studies provide the scientific evidence of the therapeutic effects of exercise using aerobic training by walking or running. These studies do not clarify the exact duration and intensity needed, nor do they clarify the relationship between aerobic gain and symptom improvement. AquaDios-Med™ has several exercise goals for patients. First is integrating the correct running posture. Second is learning to tolerate cool water of 72° 75° F for 45 minutes and to allow a stride cadence of 84 to 96 strides per minute. A hot in water power massage in 99 F water as warm-up and cool down is recommended for fibromyalgia patients.
Individualized prescription based on fitness assessment and monitoring with frequency meters may favor exercise performance with enough intensity for aerobic gain. The anaerobic threshold seems to be a physiologic limit and may be the best outcome measure of an ergometric evaluation because it is less influenced by pain.
Several modalities of aerobic training can benefit patients with FM. However, pool exercises can bring some advantages due to the effects of the biophysical properties of immersion: buoyancy, hydrostatic pressure gradient, water viscosity, specific heat of water, and controlled temperature. Deep-water immersion eliminates all Weight-bearing impact and facilitates tactile, and thermal stimulation as well as the inertial effect of the movement leads to greater relaxation, joint overload and eccentric effort reduction, vasodilatation by warming, and analgesia. When the immersed limbs move faster, reaching a critical level of speed, water turbulence occurs. This situation creates a hydrodynamic force that offers isokinetic resistance to body movement. Also, a wide repertoire of movement is possible, allowing proprioception, body balance, strength, and aerobic exercises. Although standard hydrotherapy is widely used in general practice, there are few studies related to FM. However, standard hydrotherapy relies on water that is too hot to provide intense deep-water running; hot water must be used only for warm-up. But, even this poorly designed Aquatic exercise seems to be useful for improvement in FM symptoms, but none of the water-based studies used standardized evaluation, prescription, and training. Improvement due to galvanic baths has been demonstrated in 2 studies.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
Mixed exercises (aerobic, endurance, and flexibility), on land and in water, were effective in 2 studies, one of which demonstrated an association between relaxation and education. Patients who underwent deep-water immersion pool exercises associated with education showed better results, which were maintained after 2 years, than controls. Only Jentoft et al compared pool-based and land-based exercises (LBE) in a randomized clinical trial. The Jentoft et al study involved thirty-four patients who completed a 20-week training program consisting of exercise sessions 2 times a week with mixed exercises. For 20 minutes they maintained 60–80% of the maximum heart rate. Within-group improvements in symptoms and cardiovascular capacity were noted for both groups. The warm-water pool group achieved greater reduction in pain, anxiety, and depression; however, a small sample of patients was studied and 22.7% dropped out. Jentoft et al state that the scientific evidence favors aerobic training and verifies there are
advantages of water-based exercises because it is a safe modality of aerobic conditioning and has proposed deep water running (DWR). In DWR, the patient must learn to perform a deep-water running movement while immersed in water to the neck in the pool while wearing a snug AquaJogger buoyancy belt. The pool water must be deep enough that the participants stride motion cannot make any contact with the bottom of the pool. This deep-water immersion process eliminates all impact traumas because the participant never has any contact with the pool bottom. The absence of foot strike is however problematic which requires
training and relearning for the participant to overcome this new phenomena of no foot impact with each stride. The other “new” learning for the patient is the adjustment to the water’s isokinetic resistance with arm and leg motions used in running; this resistance is present for both cycles of the stride cadence. The author’s aim of this study was to compare two aerobic exercise programs in women with Fibromyalgia or FM, specifically the effects of deep-water running - and land
based running exercises and measure the aerobic difference between the two methods of exercise. These researchers also studied any adverse events, aerobic conditioning, and any relationship between improvements in symptoms and aerobic gain. Jentoft et al studied a total of 60 sedentary women who fulfilled the American College of Rheumatology classification criteria for FM. All were recruited from the rheumatology outpatient clinic of the Federal University of Sa˜o Paulo. From September 2000 to December 2001 these same patients received a minimal level of care from the clinic. All patients were screened for entry into the study by just
one investigator who was blind to forthcoming patients’ allocation. All patients who were included were required to be literate, age 18–60 years old, and kept in an unchanged drug regimen for at least 4 weeks before starting the study. Patients with symptomatic cardiac failure, uncontrolled thyroid disturbances, body mass index of 40, infectious contagious skin diseases, coronary disease, pulmonary disease, neurologic disease, and rheumatic disease limiting or hindering their ability to exercise, and those who had performed regular physical activity in the 6 weeks before the trial were excluded. The inability to swim was not an exclusion criterion.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
The 60 patients were randomly assigned to either DWR in a warmed swimming pool of 84 to 90F or Land Based Exercise, LBE (walking or jogging). Patients were allocated to treatment groups by simple randomization according to drawing lots. Folded pieces of paper in which the interventions’ label were written (LBE and DWR) were contained in a set of sealed envelopes. One of the investigators took the envelopes out of a container to see who would go to which group. He remained unaware of screening and assessments of the patients during the randomization process. Patients performed supervised training at their anaerobic threshold determined by a graded treadmill exercise test with spirometric analyses. Anaerobic threshold (AT) is a frequently used term that sometimes causes a little confusion. The AT is an extremely reliable and powerful predictor of performance in aerobic exercise like land based running or deep-water running. A brief, oversimplified, review of physiology shows that muscles "burn" glucose two ways, aerobically ("with oxygen") and anaerobically ("without oxygen"). Both systems generate a temporary energy store, called ATP, which in turn allows the production of mechanical work by the person. An all-out sprint requires a great deal of power output in a short period of time and uses the anaerobic system. The energy is quickly available, but the anaerobic pathways are not very efficient; short term energy stores are rapidly depleted, lactic acid builds up, and exercise soon comes to a halt. After a brief rest, the system recharges itself and is ready for the next sprint. Distance running, which requires a steady power output over a long period of time, uses the aerobic system. These pathways can't generate the speed of the anaerobic, but they do possess a great deal more efficiency and endurance. Depending upon the distance, and effort, the body can use different proportions of both of these systems. For example the 800 meter run is too long to be a sprint, but too short to qualify as a distance run. Thus, the 800 meter run is right at the cross-over between the aerobic and anaerobic systems. Untrained non-athlete individuals have a low Anaerobic threshold AT of approximately 55 % of VO2 max, while elite endurance athletes; have a high AT approximately 80 to 90% of VO2 max. A higher VO2 max means you have more oxygen available to feed your muscles for exercise. Thus, sedentary or non-athletes average nearly 50% less Anaerobic threshold. All the assessments of both groups and the deep-water running pool-based exercises were performed in the Sports and Physical Medical Center (CEMAFE) of UNIFESP. LBEs took place in a local city park. The Ethics Committee of UNIFESP approved the study. Patients were required to sign a written consent form to be able to participate.
Procedures for the Fibromyalgia Study
Patients were interviewed to complete a set of questionnaires, and afterwards they underwent a spiroergometric test which gives a value in the evaluation of cardiorespiratory function prior to intervention at weeks 8 and 15 (week 0, 8, 15). Patients were randomized after the initial assessment. All the assessments were performed by the same investigator who remained unaware of the allocation throughout the trial. Both groups exercised for 60 minutes, 3 times a week for 15 weeks, following the 1998 American College of Sports Medicine guidelines. For both groups, each session was composed of a 10-minute stretching warm-up, followed by aerobic training according to the desired intensity for 40 minutes and after that a 10-minute relaxation period.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
The exercise prescription was based on the heart rate at the anaerobic threshold (HRAT) determined at the initial assessment. Heart rate (HR) was readjusted after week 8 based on the second test. The HR variation in deep water immersion to the neck is influenced by water temperature and exercise intensity; therefore, the DWR group trained at 9 beats per minute lower than the LBE group. This was based on previous studies of sub maximum deep-water water exercise while immersed to the neck in temperatures from 83 to 90 F [ADM™ PPM states this is too hot]. All sessions were supervised by 2 physical therapists that alternated groups weekly; neither of them was involved in the clinical and fitness assessments. The HR of the patients was registered in 10-minute intervals with a pulse watch recorder model A1 Polar (Polar, Helsinki, Finland). An adaptation interval with low-intensity exercises lasted 2 weeks, emphasizing the learning of the new movements. Afterwards, the patients were asked to exercise at the HRAT. In case of pain while exercising, the patients were instructed to reduce the intensity for a short time for pain relief. After that they were expected to reach the target HR again. The patients’ drug regimen was unaltered throughout the study. Acetaminophen, up to 3 gm/day, was allowed as rescue medication. Patients from the LBE group were instructed to begin walking and maintain their paces to achieve the target HR. Each patient should set a controlled regular speed based on individualized prescription rather than keeping pace with another patient. If the exercise intensity was not found to be within the desired limits, the patient could jog or run in the training area near the supervisor, without talking to other patients. Patients in the DWR group were submitted to adaptation to the underwater medium because some of them had never entered a swimming pool before or were not able to swim. DWR consisted of deep-water running in the deep end of a pool aided by a AquaJogger buoyancy device that maintained the head above the water.
Patients were instructed in the following DWR technique: 1) an upright posture with spine maintained in a neutral position; 2) running in place, held in one location by a tether cord; 3) water line kept at shoulder level; 4) upper limbs alternating shoulder flexion-extension movements, with elbows in right angle, moving hands from the waist level to 5 cm below the water surface; 5) hands held tightly clenched; 6) lower limbs in a bicycling action; 7) end of hip
flexion at _70° with lower leg being perpendicular to the horizontal; and 8) throughout the cycle, ankle dorsal flexion and eversion occurring during the lower leg flexion and plantar flexion and inversion during the extension. Patients from the DWR group were also instructed to keep a regular speed to achieve the prescribed HR.
DWR Clinical outcomes • Fibromyalgia
The primary outcome was a visual analog scale of pain (VAS) graded from 0 to 10, with 0 being no pain and 10 being the worst imaginable pain.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
Secondary outcomes included patient global assessment of response to therapy (PGART) on a 5-point scale; Short Form 36 Health Survey (SF-36) a generic health status questionnaire that is widely used and has been validated into Portuguese, with calculation of the physical and mental components summary; Beck Depression Inventory (BDI), a 21-item inventory measuring depression that has been validated into Portuguese, recommended for the assessment of changes induced by exercise; and Fibromyalgia Impact Questionnaire (FIQ), a brief 10-item instrument that measures physical functioning and symptom severity, developed and validated for an FM population.
Physical fitness outcomes • Fibromyalgia
Patients performed an increasing load protocol on a quality treadmill. Life Fitness (Life Fitness, Franklin Park, IL) Heart Rate HR was recorded at the end of each stage. The expired gas was collected by a transparent silicone mask, which covered the nose and mouth. A computerized metabolic system, Mini Vista CPX Turbofit Vacuumed, Ventura, CA, was used to analyze the data obtained in 30-second intervals. The following outcomes of physical fitness were obtained: peak oxygen uptake (peak VO2); anaerobic threshold, determined using the slope point on the curve of the oxygen ventilatory equivalent, which corresponds to lactic acidosis increase; peak HR; and HRAT. Anaerobic threshold was considered the mean value of 2 blind investigators’ independent readings.
Sample size • Nonpharmacologic Fibromyalgia Study • Pain
To achieve an improvement in visual analog scale VAS pain a minimum of 23 patients per group was necessary. However, 30 patients were randomized as a previous compensation for the possible 20% loss at follow-up.
Statistics • Results Nonpharmacologic Fibromyalgia Study
A total of 276 patients were screened, of whom 60 were included in the study after initial assessment. Four participants in each group dropped out during the intervention, leaving 56 participants at midline and 52 participants at the final assessment. The alleged reasons for leaving the study were related to personal problems and incompatibility with patients’ work schedules; thus, adverse events were not indicated as a cause of interruption. Patients who left treatment refused to undergo other evaluations; for these patients, any missing data were replaced with the last known value, even if this was the baseline value. There were no statistically significant differences between study groups in demographic and physical fitness data between patients who dropped out and those who remained in the program, except for age (mean age 35 years versus 43 years). The completers performed at least two-thirds of the sessions, and no one missed more than 3 consecutive sessions. Among the patients who completed the program, there were 10 adverse events in the DWR group and 16 in the LBE group, with no significant difference. In case of pain, training intensity was reduced, but the duration of the session was maintained. Four patients in the DWR group reported muscle pain and 1 reported tinea pedis.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
Tinea pedis is a foot infection due to a dermatophyte fungus. Tinea pedis thrives in warm humid conditions and is most common in young adult men. Dermatophyte fungi are the ringworm fungi (tinea). They depend on their host, which may be an animal ("zoophilic") or a human ("anthropophilic") and need to spread from one host to another to survive. Dermatophytes may also prefer to live in the soil ("geophilic"). There were 12 patients in the LBE group who reported muscle pain. One of them presented an impingement syndrome (on the right side); another presented bilateral ankle arthritis; and a third presented a Baker cyst.
Fibromyalgia Nonpharmacologic Study Discussion
Nonpharmacologic interventions in FM have been used with success in different trials, either in combination with other therapies or as isolated treatment. In 1976, Moldofsky and Scarisbrick showed that induction of diffuse muscle pain by sleep deprivation was delayed and intensity was reduced in fit subjects, which led exercise to be proposed as a treatment. Physical exercise is relatively easy to do and offers a lower risk of adverse effects when correctly performed. Studies have shown that aerobic exercises have beneficial effects in terms of quality of life and pain reduction in patients with FM. Therefore, exercise is routinely indicated in clinical practice. Walking is a cheap, easily accessible and safe exercise that has been used as the standard aerobic exercise to treat FM, whereas aquatic or deep-water running exercise had not been extensively studied. Therefore, the study’s authors proposed an aquatic exercise modality that is the most similar to walking, i.e., the deep water running. The use of 2 therapists allowed both groups to be trained simultaneously. The interchange of the 2 therapists was thought to avoid a confounding effect, a better outcome attributable to one of the therapists. The study results showed that clinical endpoints, including pain, mood, function, and quality of life, improved to a similar degree after both land- and water-based exercises. There were no serious side effects in the groups, confirming that patients with FM can undergo physical training without damage and this outcome suggest most all patient or sedentary populations can benefit from safe daily deep-water running as AquaDios-Med™ recommends. This Nonpharmacologic study with aquatic exercise differs from previous studies because of its larger sample size, excellent compliance, and individualized, strictly controlled and supervised exercise program with higher training frequency and intensity. According to a recent meta-analysis, only the study by Wigers et al with aerobic exercise on land demonstrated an 11.4% pain decrease against 1.6% in the control group. The patients in this study had the highest VAS pain score. Among validated pain scores, the visual analog scale (VAS) score is the most widely used, in both clinical practice and therapeutic trials. The visual analogue score VAS is a standardized measure of pain and quality of life used to determine meaningful pain relief and to evaluate treatment effects. Both groups showed improvements in quality of life with less pain and regarded their treatments as beneficial. This effect was comparable only with Valim et al’s work, in which the VAS pain decreased 45% in the aerobic exercise group against 26% in the stretching exercise group. Previous studies that have shown modest or nonsignificant improvements in pain and or functional outcomes prescribed very low-intensity exercise with short training and assessment periods. In both works by Van Santen et al, no important benefit in VAS was reported, even in the high-intensity physical conditioning group, which was not superior to the low-intensity group.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
On the contrary, exceeding a certain training intensity could increase adverse effects; patients in the high-intensity group claimed to have pain and difficulty during their training. In another study, the high-intensity group, reaching 85% of peak HR, worsened in the 20th week. Many patients reported worsening and abandoned a program that used aerobic dance. This author believes aerobic dance is likely an exercise with too much impact for the fibromyalgia patient. In the study by Mannerkorpi et al, the planned intensity of exercise was reduced because many patients reported increased pain after the training sessions. In another study, 17% of the patients reported symptom worsening and intolerance to the level of exercise prescribed. This confirms the concept that excessive effort leads to a worsening of symptoms when impact is involved but this pain increase is believed likely to be avoided in deep-water running especially with the AquaDios-Med™ approach which includes hot, warm and cold water together with mind body medicine. In this study the exercise intensity was lower than that used in the study by Meyer and Lemley, but higher than that used in the study by Van Santen et al. In spite of this, there were no frequent complaints, and the final results were better in this study. Three important differences between these previous studies and this study justify the results: the authors set a 2–3-week adaptation period to prevent pain due to exercise in sedentary individuals, we tolerated a temporary reduction of training intensity in patients who reported pain, and they trained the patients for a longer period. These adjustments in training intensity in the adaptation phase and during the worsening appear to be a fundamental strategy to carry out the exercise program successfully. No adverse events were cause for discontinuation. Higher intensity exercise might lead to better results as long as it remains below the pain and fatigue threshold. The authors believe the best results are obtained when the exercise program follows some exercise prescription principles such as to minimize muscular trauma and central sensitization, avoid important increase in pain; increase auto efficacy, allowing a sense of body control; and individualize prescription. The patients of this study had improved PGART in the first and second halves of the study, showing that the benefit continues with time. If we consider only the best response of the PGART in the last assessment of this study, at least 70% of the groups showed high or moderate improvement, results that are more expressive than those found in the study by Richards and Scott. Most outcomes showing improvement did so as early as week 8 and kept improving up to week 15. Valim et al’s study has also shown that several outcomes continue to improve after 10 weeks, implying that trials should be held for longer periods as others have stated. Several randomized trials with exercise have demonstrated improvement in FIQ total score related to control groups. However, a significant difference between 2 types of intervention was seen only in the study by Valim et al, which compared 20 weeks of aerobic exercise with stretching. In this study, the authors demonstrated not only an FIQ total score improvement for both groups, but also superiority of the DWR group over the LBE group at the middle and the last assessments. In 2001, Gowans et al reported improvements in depression according to the Mental Health Inventory and the BDI after the first 6 weeks of exclusively deep-water exercise. FIQ depression improved in the study of aquatic exercise by Jentoft et al, but not in the land-based exercises group. In this study statistical analysis showed that groups equally improved in BDI. However, a significant difference favoring the DWR group was seen in FIQ depression after 8 and 15 weeks.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
Also, the tests of role emotional activities showed within group improvements only for aquatic exercise. The authors of this study caution they must be careful to conclude an advantage of aquatic exercise in improving emotional aspects because this study was not designed to test this hypothesis, and the 2 analyses of BDI did not show between-group differences. Nonetheless, we cannot ignore that 2 other outcomes of this study and Jentoft et al’s study are pointed toward the same direction. The authors made use of pulse watch recorders, similar to other studies. This ensured that patients maintained an HR equal to or higher than that prescribed, from week 3 on. An intensity reduction for adverse painful events was necessary for no more than 3 consecutive sessions. Wigers et al allowed resting breaks during sessions when necessary and also obtained symptom improvements and physical fitness. Some studies used the same prescription for all patients, whereas others considered maximum HR. In this study, the intensity of the exercise program was individualized based on spiroergometric tests such as that in Valim et al’s study. It was prescribed at the HRAT, and the accomplishment of the intensity ensured the minimum suggested to obtain physical fitness. The authors recommend that Aquatic Exercise is best for Fibromyalgia specific patients, because the treadmill test is practically identical to the LBE but differs from the DWR. Analysis of categorical outcome data showed no significant difference in the other physical fitness outcomes between the groups. There was not a significant association between clinical improvement and aerobic gain, suggesting the benefits are not necessarily a consequence of better physical fitness as noted in a previous study. Every program must consider strategies to maintain patient compliance which is fundamental to the success of the treatment, as observed by many authors. Deep-water running while immersed to the neck in water had a fairly easy adaptation, even for patients who were not able to swim. Furthermore, some individuals would rather exercise in water, and this modality was shown to be an effective option to walking or running. This randomized trial comparing aerobic training in water with a largely supported modality of aerobic exercise on land shows DWR to be effective and safe. Although this study followed the patients for 3 months, it is also very important to study long-term benefits of physical training, considering the chronic nature of FM; the exercise effects usually disappear when exercise is discontinued. Walking is a practical type of exercise for most individuals; however, some individuals are limited even for simple physical tasks due to comorbidities, such as knee or hip arthritis, hindering their own weight-bearing ability. For these individuals, land-based physical activity can be difficult and painful, worsening their symptoms. Several aerobic exercise modalities in warm water could be as beneficial as walking, especially for persons with lower limb limitations. The authors conclude that aerobic exercise in a warmed swimming pool was as effective as a land-based program in treating patients with FM regarding pain. And, deep-water running brings advantages regarding emotional aspects because it is a pleasant stimulus for exercise compliance. Aerobic gain was similar in the 2 groups and did not correlate with clinical improvement. When properly performed, DWR is a safe and viable form of low-impact aerobic exercise for patients with FM.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
14
Fibromyalgia Deep-water running Treatment Cost
On February 22, 2008 Gusi and Tomas-Carus published a research study in Arthritis Research & Therapy titled “Cost-utility of an 8-month aquatic training for women with fibromyalgia: a randomized controlled trial”. The authors recognize that physical therapy in warm water has been effective and highly recommended for persons with fibromyalgia, but its efficiency remains largely unknown. For example the question: Should patients or health care managers invest in this therapy? The aim of the current study was to assess the cost-utility of adding an aquatic exercise program to the usual care of women with fibromyalgia. Costs to the health care system and to society were a primary consideration in this study that included 33 participants, randomly assigned to the experimental group of 17 or a control group of 16. The intervention in the experimental group consisted of a 1hour supervised, water-based exercise session, three times per week for 8 months. The main outcome measures were the health care costs and the number of quality-adjusted life-years (QALYs) using the time trade-off elicitation technique from the EuroQol EQ-5D instrument. Sensitivity analyses were performed for variations in staff salary, number of women attending sessions and time spent going to the pool. The cost effectiveness acceptability curves were created using a non-parametric bootstrap technique. The mean incremental treatment costs exceeded those for usual care per patient by 5 euros for health care costs and 10 euros for societal costs. The mean incremental quality-adjusted life-years QALY associated with the intervention was significant. The statistics showed a 95% probability that the addition of the water-based programme is a cost-effective strategy from a health care perspective and from a societal perspective due to the quality-adjusted life-years. The addition of an aquatic exercise programme to the usual care regime for fibromyalgia in women is cost effective in terms of both health care costs and societal costs. However, the characteristics of facilities (distance from the patients' homes and number of patients that can be accommodated per session) are major determinants to consider before investing in such a programme. This conclusion supports the Medical McDonalds Model offered by AquaDios-Med™ which is that population suburbs of 350,000 residents must have access to the AquaDios-Med™ health center.
Controlled trials • Fibromyalgia Fibromyalgia Deep-water running Treatment Cost
Fibromyalgia (FM) is a chronic disorder of widespread pain in combination with tenderness of at least 11 of 18 specific tender points. FM affects approximately 2–3% of the general population, and more than 90% of patients are female. The estimate of the U.S. population was in July 2007 was 301,139,947; extrapolation suggests there are 81 million American women suffering from Fibromyalgia. The average yearly cost updated to 2005 using a 5% annual inflation for service utilization among patients with FM is approximately $ 7,091.10 US and the societal cost is $ 14,119.17 US for an annual healthcare cost of about $ 1.8 Billion.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
15
These costs are largely due to the frequent use of medical services such as consultations (approximately 10 per year) and medication, and the health system and societal expenses of disability from work. Patients with FM consume health care resources to a similar extent as patients with other chronic diseases such as diabetes mellitus and hypertension. Patients with FM also incur about twice the health care costs as the general population, and are absent from work approximately twice as much as other employees. Studies reported in scientific literature have demonstrated evidence of the benefits of physical therapy on health-related quality of life and fitness. In particular, physical exercise in warm water has been effective in short-term programmes (less than 6 months) and is highly recommended to reduce pain and minimize mechanical impact during exercise. However, in our earlier study of patients with FM we found that most of the gains in health-related quality of life and physical fitness achieved in 12 weeks of water-based exercise were lost after a subsequent similar period of physical inactivity. These findings suggest the need for longer programmes or maintenance programmes, but the effectiveness of such programmes remains unknown. Unfortunately most all physical therapy hydrotherapy in done in “warm water” and boarding on hot water of a temperature of 89 degrees F which is too hot for intense exercise, but just right for warm-up, relaxation and hydro-massage. Likewise research of physical exercise with patients, is conducted in warm water rather than the four temperatures recommended by AquaDios-Med™; although some patient populations would not likely be able to tolerate the cold temperature until there was a remission in their symptoms.
The research heads of this fibromyalgia study advocate for deep-water programs like AquaDios-Med™ must be considered in light of limited health system resources and the horrific healthcare cost of more than $ 2. 6 Trillion.
Health system managers or decision-makers frequently select the treatment strategies based on the lowest cost per quality-adjusted life-year (QALY). Cost utility is the ratio of the incremental effectiveness of one strategy compared to another (e.g. standard medical practice), and is measured in QALYs divided by the incremental cost. To our knowledge, there is no cost-utility or cost-effectiveness study of these exercise programmes for patients with FM, but when AquaDios-Med™ is nationalized the costs will be minimal; at least 60 % less than the currents costs. The researchers suggest that cost-effectiveness may be studied from a health service perspective by including the costs to the health care system or from a societal perspective by adding to the health care costs those borne by the patients and society. These additional societal costs include time spent, travel costs, lost work hours, etc. The approach from a health service perspective can help inform decisions about adding services to the current health care system. The purpose of this study was to assess the cost utility of adding an 8-month, supervised, warm water exercise programme to the usual care of Public Health Service for women with FM. The population of the catchment area comprised women who were in a local FM association. Eligible women were those who had FM diagnosed by a rheumatologist in accordance with the diagnostic criteria of the American College of Rheumatology (ACR). A total of 40 potentially eligible participants responded and sought further information.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
16
Once the study protocol was explained, 38 people gave their written informed consent. The following exclusion criteria were applied: history of severe trauma, frequent migraines, peripheral nerve entrapment, inflammatory rheumatic diseases, severe psychiatric illness, other diseases that prevent physical loading, pregnancy, participation in another psychological or physical therapy programme, or engaging in regular physical exercise more than once a week for 30 min or longer during a 2-week period in the last 5 years. The participants in our study of a 12-week aquatic program were excluded from the current trial to avoid the influence of re-training. Participants' clinical conditions were checked and a rheumatologist confirmed the diagnosis of FM. After excluding 5 candidates due to their participation in other therapies, 33 female patients, aged 37 to 71 years of age, were selected to participate. They were randomly assigned to either the exercise group (EG; n = 17) or a control group (CG; n = 16). Two patients in the “EG” failed to attend at least 95% of the treatment sessions due to personal reasons. Nevertheless, these patients were included in the current study to apply an intent-to-treat analysis. The trial was exclusively developed and performed at the facilities of the University of Extremadura, Spain, with the approval of the Committee on Biomedical Ethics of the University and following the updates of the Declaration of Helsinki. Usual care and the addition of a water-based exercise programme were compared in the CG and EG, respectively. The usual care included standard medical attention in the public system (hospital and outpatient clinic including primary care) and the social support of the local FM association. This care could be considered the average standard of care or better for patients with FM. The intervention added an exercise programme in a waist-high pool of warm water 91 F. A qualified exercise leader instructed and trained the intervention group three times a week for 1 hour per session over a period of 8 months. Each session included 10 min of warming up with slow walking and easy movements of progressive intensity, 10 min of aerobic exercises at 60–65% of maximal heart rate, 20 min of overall mobility and lower limb strength exercises using water resistance, another set of 10 min of aerobics at 60–65% of maximal heart rate, and 10 min of cooling down with low intensity exercises. Heart rate was monitored using a pulse meter (Polar Accurex Plus, Kempele, Finland). During this 8-month period participants in the control group continued their daily activities, which did not include any form of physical exercise similar to that in the programme. This programme was designed without reference to any explicit behavioral model or theory, and was intended as a pragmatic intervention that could be easily organized for a large population. Participants completed questionnaires, including the EuroQol EQ-5D health status instrument at the beginning of the programme and after 3 and 8 months. During the same period, private and public health care was recorded, including hospital stays, drug usage, and secondary and primary care appointments.
Unit costs for DWR treatment
The expense and time needed for travel from the patient's residence to the rehabilitation pool varied, because this facility is a scarce health resource serving a large area. To allow for a range in such additional costs, we performed two economic analyses, one from a health service perspective and another from a societal perspective. The first perspective is recommended by the National Institute for Clinical Excellence (NICE) in the UK to inform decisions on health care policy for an expensive condition.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
17
This perspective could help to decide whether to finance the addition of the programme to the health system. The second perspective is recommended to consider the combination of the burden to the patient and the health care system. The unit costs are expressed in Euros (€) based on prices in 2005. Costs were not adjusted or discounted for changes in currency value over time, as we focused solely on effects over less than 1 year. The program's cost was calculated based on the following: salaries at the level for a university graduate, cost of staff to run the programme, salaries at minimum wage for the patient's time (based on the 2005 official bulletin of the regional government), cost of renting a pool at a university at public prices without a grant, public bus prices, and private external management costs of the programme (insurance, monthly retrievals from patients and withdrawals to employees). Health care prices (consultations, etc.) were based on the 2005 official bulletin of the regional government. Drug prices were obtained from the Spanish version of Vademecum International.
Health outcomes • Benefits
The EQ-5D was used to assess five dimensions of health related quality of life: (1) mobility, (2) self-care, (3) daily activities, (4) pain and discomfort, and (5) anxiety or depression. The scale for each dimension is from 1 to 3 (with 1 no problems, 2 some problems, and 3 extreme problems). Using a combination of these dimensions, a total of 243 possible health states exist. Each health state has been previously defined using the time trade-off method of utility analysis based on the response of a sample of the Spanish population. This total score of utility was scaled from 1 = fully functional quality of life to 0 = death. The quality-adjusted life years (QALYs) that participants experienced over the 8-month period were estimated by calculating areas under health utility curves. To avoid bias, data were adjusted by regression analysis for differences in baseline EQ-5D scores .
Cost utility analysis
First, the authors estimated the incremental mean costs of the water-based programme and the mean QALYs added by the programme from a health care and societal perspective. Secondly, the incremental cost effectiveness ratio for the water-based programme was calculated by dividing the incremental costs by incremental QALYs. To report the uncertainty due to sampling variation, we calculated the 95% confidence interval using the non-parametric bootstrapping technique (1,000 replicates re-sampled with replacement from treatment and control populations) and plotted a cost effectiveness acceptability curve. This curve shows the probability that the intervention is cost effective compared with the alternative, across the range of values that decision makers are willing to pay to achieve an additional QALY. The "investment ceiling" is the level of spending that should not be exceeded, even assuming unlimited funding availability. For the health care system in Spain, the 2005 adjusted investment ceiling was set at € 34,729/QALY. Decision makers should compare this upper limit of acceptable payment with estimated incremental cost effectiveness ratios to determine whether a given treatment is cost effective relative to the alternatives. For the health system and societal perspectives, seven sensitivity analyses were performed to explore the robustness of the estimates and how dependent the results were on estimates of participants' unit costs and efficacy. From the health system perspective, the first analysis examined the influence of participation rate in the programme as this could influence the productivity by affecting the number of participants per unit of time provided by the technician.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
18
A second analysis explored the variations due to the salary changes of the technician, since this is a major source of variability in economic studies. From a societal perspective, in addition to two previous analyses the third analysis estimated the cost of increasing the mean distance (in terms of time spent and the number of bus tickets purchased) from the patient's residence to the rehabilitation pool. Finally, from both perspectives, the robustness of cost effectiveness was examined by exploring scenarios combining the influence of the variations in staff salary, rate of participation, distance to the facility and effectiveness, from the lowest to the highest limit of the 95% confidence interval.
There were incremental costs, to the health care system, and to society, of implementing the exercise programme. The main cost was associated with renting the pool and the difference between perspectives was mainly attributed to the cost of time spent for travel and the intervention programme.
There was an incremental cost per patient who participated in three sessions per week in a pool with a capacity for 20 persons. Participants in the EG and CG did not report changes in the number of physician consultations (1 primary care visit per month; 0.3 specialist visit per month, and no hospitalizations). A total of 10 women in the EG and 5 in the CG reported changes in medication. Seven women in the EG stopped their doses of medication of amitriptyline (n = 7), cyclobenzaprine for sleeping (n = 2) or paracetamol (n = 1). However, two of these seven women started to take ibuprofen and another began to take cyclobenzaprine. In the CG, three women stopped the doses of medication (hydroaltesona, ibuprofen and citalopram). Over the 8 months, the weekly cost of medication increased above baseline by € 5.4 in each group as a whole; however, no remarkable incremental costs of intervention group compared to control group for medication or consultation were observed.
Health Benefits DWR Cost Outcome
The water-based programme was associated with a greater increase in the EQ-5D utilities than the usual care during the first 3 months and this difference was preserved during the subsequent 5 months. The cost utility analyses from both perspectives, the health service perspective and the Spanish Health System Efficiency Threshold was set at € 23,153/QALY for 8 months by multiplying the published threshold of 34,729 for 12 months by 8/12. From the health service perspective, each additional QALY gained by the exercise group cost in average € 3,947. However, the cost effectiveness acceptability curves (Figure 2) showed a 95% probability that the addition of the water-based programme is a cost effective strategy if the ceiling of inversion is € 14,200/QALY and a 97.5% probability if the ceiling is set at € 21,233/QALY. Probability curves that the addition of the aquatic training to usual care is cost-effective. From a societal perspective, the mean cost per QALY was € 7,878/QALY and there is a 95% probability that the addition of the aquatic training is cost effective if the ceiling of inversion is € 28,300/QALY. A 97.5% probability requires an inversion higher than € 42,000/QALY. The sensitivity analyses showed the robustness of the conclusion that the water-based therapy is the best alternative compared to usual care to the variations of staff salaries and the number of participants attended per session. Nevertheless, in the worst case scenario, with a combination of minor improvements in cost utilities and a low number of clients per session, warm water exercise would be inefficient (more than € 23,000/QALY) from both perspectives. The main source of variation was observed by changing the staff salaries, effectiveness in QALYs, and the distance to the facility.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
19
Principal findings fibromyalgia Study – Costs
Previous studies reported the efficacy of aquatic training on patients with fibromyalgia and the cost-utility of a 2.5 week spa treatment, but to our knowledge the present study is the first to report cost-utility. The major finding of this study was that the water-based programme was a cost-effective addition to usual care from both health system and societal perspectives. More precisely, an investment in this aquatic training for a similar population (sedentary women with FM) has a greater than 95% probability of being efficient according to the investment ceiling in Spain.
Strengths and weakness
The acceptable efficiency threshold, investment ceiling or maximum willingness to pay for each gained QALY varies among countries or societies because of differences in salaries, priorities, etc. The current study applied the commonly lower threshold of € 34,729 (€ 23,153 for 8 months) used in the Spanish literature, but similar conclusions about the efficiency of the addition of aquatic training to usual care could be achieved using the threshold updated to year 2005 (annual inflation of 5%) often reported in American literature]($ 50,000 to $ 60,000) or Dutch literature (€ 28,940). The retention rate of patients in the our programme (88%) was similar to rates previously reported in community group-based exercise programmes in fibromyalgia (70–90%); however, aquatic training programmes usually report lower retention rates (55–75%). The social support provided by physicians, research teams, and peers with FM from the local association may have contributed to this high retention rate and the improvement in the psychosocial dimensions of health related quality of life and QALY in the exercise group. Particularly, the patient's affiliation with the local FM association brought them additional care (social support, information, etc.) in comparison to what is offered by the Public Health Care System. In this sense, the care received by the control group could be considered better than usual. By contrast, care that combines the study program with other therapies may be even better than the programme alone. This issue could not be addressed in the current study because patients were excluded if they used other therapies (standardized behavioral or physical therapies such as massages, etc.). The small sample size led us to use non-parametric bootstrapping techniques to treat the confidence intervals and probability curve. Health economists recommend bootstrapping techniques, rather than standard deviation-based methods, for treating the uncertainty of cost-effectiveness ratios. The small sample, the fact that subjects were self-selected according to bioethics requirements and the catchment throughout local patient associations may limit the generalization of our findings to treatment of less motivated patients.
Use of health care • fibromyalgia
The current study did not find any evidence for decreased use of health care services during the study period. However, the lack of change in the ratio of frequency (consultations/month) can be explained partially by the limits of supply and the management of free appointments in the general practices of the National Health System in Spain. A study in a non-limited supply setting could address the question of whether an aquatic programme could reduce the use of other health care services. The increase in the medication cost in both groups may be partly explained because the perception of pain is slightly increased in the summer in persons with fibromyalgia; with a change in the average temperature in Extremadura from 57F at baseline to 71°F at the end of program.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
20
By contrast, the aquatic training in facilities with warm water was a cost-effective addition to usual care but it was not compared to other physical therapies that could reduce geographic inequalities (e.g., land-based therapies such as low-impact aerobics, walk-based exercise, tai chi, etc.) because their facilities are cheaper and easier available in more municipalities. An 8-month aquatic training programme is a cost-effective addition to the usual care provided by the Public Health System. This programme enhances the health-related quality of life in women with FM. However, the characteristics of facilities (distance from patients' homes and the number of patients that can participate per session) are major determinants that have to be considered before a health manager decides to invest in such a programme.
Perceived exertion Critical Velocity Deep water running The linear relation between exercise intensity and the increase rate of the neuromuscular activity assessed by electromyography allows the estimation of the fatigue threshold, which would be the intensity that could be maintained indefinitely without presenting increase on the electromyography signals a long time. It has been hypothesized that the subjective perception of exertion would behave similarly to the neuromuscular activity and that a perceived exertion threshold (PET) identified similarly to the electromyographic fatigue threshold could coincide with the critical velocity (CritV). Thirteen individuals from both genders 21 to 25 years of age, in a 49 feet long x 8.2 feet deep swimming pool performed three deep water running exhaustive tests for the determination of the parameters of the critical velocity model, reporting the perceived exertion in Borg scale, each 20 feet. For the PET identification, the straight lines inclination coefficients of the increase on the perceived exertion in time (ordinate) and the velocities used (abscissa) were adjusted into a linear function that provided a point in the velocity axis where, theoretically, the perceived exertion would be indefinitely stable. The CritV was estimated through the equations used in the critical velocity model. For comparison purposes of the CritV and PET estimations and their associations, the repeated measures analysis of variance ANOVA was used and the Pearson correlation was calculated. These results suggest that the PET seems to represent the maximum exercise intensity in which the physiological and psychophysical variables would attain stability and that this index may be used in the CritV determination. Perceived exertion scales were created with the objective of establishing relations between the subjective perception of exertion and the external load or physiological stress objective data. According to Borg, the exertion perception is a result of the integration of afferent signals originated from both the skeletal muscles (peripheral) and from the cardiorespiratory system (central). During the performance of high-intensity exercises, in other words, exercises performed at intensities above the critical power (CritP), the metabolic acidosis seems to be an etiological agent common to both types of sensorial activities. The decrease on the tissue pH causes muscular fatigue and the decrease on the blood pH is associated with a ventilation increase. Both responses require higher afferent neuromotor activity for both skeletal muscles and ventilatory muscles, which would be subjectively perceived by the individual as a progressive effort to maintain the same muscular work rate. Thus, it seems that the exertion perception involves both feedback and feed forward.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
21
Studies show that the electromyographic activity of the knee extensor muscles undergoes progressive increase along time in high-intensity exercises in cycle ergometer. The electromyographic activity increase rate is proportional to the exercise intensity. The linear relation between exercise intensity and electromyographic activity increase rate allows the estimation of the fatigue threshold, which is the intercept of the linear regression in the intensity axis. The fatigue threshold would be the exercise intensity that could be maintained indefinitely without alterations on the neuromuscular activity, in other words, without increases on the electromyographic signals a long time. In the present study, it has been hypothesized that the subjective perception of exertion would behave similarly to the neuromuscular activity objective data. Thus, a perceived exertion threshold could be estimated through procedure similar to the electromyographic fatigue threshold. Le Chevalier et al. suggest that the fatigue threshold coincides with the CritP determined through the inclination of the work-time linear relation in ergometer adapted for unilateral knee extension exercise. This intensity was originally described as that in which the exertion of isolated muscles is maintained without exhaustion. Moritani et al.(9) extended this concept to the cycle ergometer. In modalities such as running and swimming, the work is replaced by distance and the power by velocity. One adopts, through this conversion, a linear relation between the respective pairs of variables. Thus, the critical velocity may be estimated (CritV). The CritV corresponds to a limit exertion intensity that could be maintained with VO2 and lactate steady state. Above this intensity, these variables reach peak values, thus predicting the exhaustion occurrence. The occurrence of exhaustion in running at supra-CritV coincides with the full exhaustion of the anaerobic running capacity (AnaerRC). The AnaerRC is described as the maximum distance to be covered at the expense of the anaerobic metabolism. As the anaerobic metabolism mobilization is the main source of H+ ions accumulation in tissues and hence the decrease on the pH in the organism, one may infer that the AnaerRC exhaustion rate would be the responsible for the increase on the perceived exertion in high-intensity exercises. Thus, the maximum intensity able to be maintained without increases on the perceived exertion along time should coincide with the CritV. Therefore, the objective of the present study is to compare CritV obtained in the deep water running with the perceived exertion threshold (PET) that we have proposed as alternative way to determine the maximal exercise intensity that allows stabilization of the physiological and psychophysical variables. Thirteen young individuals from both genders with 21 to 25 years of age, participated in this study. All individuals signed the free consent form in order to participate in the study. None of them presented previous experience with deep water running. None of them had familiarization with deep water running or the Borg scale. The swimming pool used in this study was 15 m long and 2.5 m deep, with water temperature kept near to 84F. It was considered as favorable for the deep water running practice because the individuals could not touch the pool floor while maintaining their heads out of water.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
22
The volunteers underwent two to four sessions of deep water running familiarization. These sessions were aimed at instructing them the correct deep water running technique with the objective of presenting reliable results during tests for the determination of the parameters of the critical velocity model and PET. The deep water running technical instructions were given by two appraisers. One of them remained out of the swimming pool while the other monitored movements in the underwater environment. Once participants wore floating vests like the AquaJogger their relaxed bodies tended to be positioned vertically, in relation to the bottom of the swimming pool; with heads above the surface. During running, the trunk should simulate traditional running in order for the body to start dislocating. The incursions amplitude of hip, knees and ankles joints should be large and fingers should be united in the sagittal plane in order to simulate swimming strokes. Their elbows should lie along their trunks. Each familiarization session lasted about 20 minutes. The exercise intensity was selected by the participant himself. They were advised to select a comfortable intensity. At the end of each session, shortly after a rest period, the participants were asked to cover 60 m at maximum water displacement velocity. When the deep water running technique seemed to be effective and the performance in both consecutive 60-m tests was not over than 5% different, the participants were able to start the tests to determine CritV, AnaerRC and PET. Still during familiarization, instructions about the use of the Borg 15-points scale were given to be used in further stage. The scale was presented to participants during the deep water running practice, and they attributed a numerical value in the corresponding scale to their general exertion perception in that moment. The scale presents verbal attributes next to the numbers to facilitate the selection so that participants would familiarize with the use of the scale and memorize the relation between the verbal attributes and the numerical values they should report (example: 3-very, very light; 8-very intense).
Tests to determine CritV and AnaerRC
All tests used to determine the parameters of the critical velocity model were performed in different days. Before each test, the participant performed quick warm-up exercise in rhythm freely selected. The tests intensities were established individually, so that exhaustion would only occur within range of one to ten minutes. In order to control velocity, cones were placed at the border of the swimming pool each 5 m. Sound signals, performed with the aid of a whistle, indicated the moment in which the individual should be aligned with the cone. When reaching the end of the swimming pool, the participant turned around to perform the same exercise all the way back with no interruption. The voluntary abdication or the incapacity of maintaining the rhythm indicated for more than two cones were considered as exhaustion. In case two consecutive errors of rhythm were made, the participant was encouraged to correct them in the next cone. If the errors were successfully corrected, the test was carried out until one of the exhaustion criteria occurred. If a participant could not correct the rhythm requested, the distance covered by the last two cones (10 m) was deduced from the total distance covered. This variable, the test total time and the mean velocity were adjusted to the equations predicted through the critical velocity model in order to estimate CritV and AnaerRC. These equations are described below.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
23
During the three exhaustive tests, the individuals were instructed to report the perceived exertion according to the Borg RPE points scale, each 20 yards covered. The angular coefficient of the linear regression between time as independent variable and individual perceived exertion values attributed during each test was determined through linear regression. The angular coefficients of all straight lines (perceived exertion increase rate) obtained with this procedure were used to estimate the parameters of the linear regression in function of the mean velocity of the three tests. PET was identified through the projection of this straight line on the velocity axis (x), in other words, it corresponded to the velocity in which the perceived exertion increase rate was “0”. Figures 1 and 2 exemplify these procedures in a representative individual. There are no published studies that estimated CritV and Anaer-RC in deep water running in literature. Most works on the modality, unlike the present study, use the static deep water running model, in which the individual remains attached to the border through the floating vest, and the exertion intensity is controlled by the steps frequency or through physiological markers, such as the heart rate. To review these studies, Wilder and Brennan, and Reilly et al. are recommended. The parameters of the critical velocity model were determined in modalities related to the deep water running and their physiological meaning was established. According to Wakayoshi et al. and Kokubun, the CritV obtained in swimming is not different from the anaerobic threshold, calculated through fixed concentration of 4 mM of blood lactate in test with progressive velocities.
The correlation between both variables in the studies mentioned was high. Besides, the CritV seems to be coincident with the maximal lactate steady-state directly measured. In running, Sid-Ali et al. and Hill and Ferguson found similar results.
Increase on the perceived exertion along time in three exhaustive rectangular tests from a representative subject Borg scale results with regard to the meaning of CritV. In the second study, it was additionally demonstrated that the CritV is the maximal intensity possible to be maintained without the elevation of the VO2 up to its maximum value. The meaning of AnaerRC is not fully clear, once the expected correlation between this index and the peak plasma lactate after exhaustive test was not confirmed by Housh et al. Still, the AnaerRC would theoretically be an indicative of anaerobic capacity. Albuquerque da Silva (data not published) showed that, in the deep water running, the CritV is not significantly different from the anaerobic threshold, determined through the fixed concentration of 3.5 mM in incremental test. The correlation between these variables ranged from 0.79 to 0.90, depending on the equation used in the CritV estimation. Therefore, the physiological meaning of CritV in the deep water running seems to agree with that established in other modalities. The CritV estimations are not different from each other in the present study. Besides, the mean SEE ranged from 2 to 10% of the CritV. According to Hill, these are important conditions in which the parameter’s validity and accuracy are assured. However, a significant difference was observed between the AnaerRC estimations. The SEE associated to this variable ranged from 14 to 23%. Both factors made the AnaerRC validity and accuracy infeasible as indicative of anaerobic capacity, according to criteria elaborated by Hill and Smith. Still, the adjustment of the experimental data to all equations was satisfactory, considering the high values of r2, above 0.96 on mean.
Exercise Is Preventive Medicine

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
24
Much has been discussed on the neurophysiological mechanisms responsible for the exertion perception. Cafarelli summarizes the discussion into three thinking lines with their respective explanatory hypotheses. Hypothesis 1 supports the feed forward primacy and the theory that a “copy” of the motor impulses is transmitted to the sensorial cortex, carrying the information about the degree of muscular activation. This information would be the main constituent of the exertion perception. Hypothesis 2 supports that the feedback coming from chemical and mechanical receptors in the joints, tendons, parts of the cardiorespiratory system and the skeletal muscles would produce the peripheral sensation, translated into exertion perception in high levels of the central nervous system. Hypothesis 3 proposes that the afferent muscles would be compared to the efferent motors and that this comparison of information would cause immediate compensations by counterbalancing the fatigue. This hypothesis supports that the sensorial cortex monitors both the efferent and the afferent signals in order to generate the exertion perception. Several works have attempted to establish perceptive responses to exertion performed at metabolic thresholds (ventilatory, lactate), to regulate lactacidemia in tests with variable loads through perceived exertion, and also to control other variables such as the heart rate and exercise intensity with the use of perceived exertion scales. Particularly, about the determination of the metabolic thresholds that has been objective of this study, the use of the exertion perception has presented some problems. The results from Mahon et al. indicate that the perceived exertion rated by the Borg RPE scale at the ventilatory threshold intensity presents significant inter-individual variability, besides being significantly different when children and adults were compared. However, a study by Hill et al. demonstrated that the training affects the ventilatory threshold in adults, but does not modify the associated exertion perception. Weltman gathered findings that emphasize that the 14 and 16-17 exertion perception is associated to the blood lactate fixed concentrations of 2.0 and 4.0 mM, frequently indicated as indicative of lactate and anaerobic thresholds, respectively. The approach presented in this study is different from the works mentioned above with regard to the detection of one of the thresholds – CritV – once we did not intend to establish a fixed value for the perceived exertion at this intensity. The proposal was to search for an original application for the Borg RPE scale, which takes into consideration the perceived exertion variation rate as alternative to the CritV individualized determination. Indeed, as verified in our results, the perceived exertion value may change along a rectangular exercise, what invalidates the attempt of establishing a fixed value associated to the exertion intensity in high-intensity exercise. For the same step frequency, the perceived exertion is significantly higher in the deep water running than in the field running. This probably occurs because in this situation, the VO2 and the heart rate are quite higher in the deep water running. Both variables seem to be relevant in the prediction of the perceived exertion in deep water running through the multiple regression analysis. Other important variables are the minute-ventilation and ventilatory frequency (central) and the legs movement velocity (peripheral). This information, integrated in the sensorial cortex and in the respiratory centers, probably determines the evolution of the perceived exertion in exhaustive rectangular tests and, thus, would influence the PET estimation. In the present study, PET provided good CritV indirect estimation, once both presented values close to each other, and the correlation between each other ranged from 0.85 to 0.88. It was presupposed that the perceived exertion would be increased in exhaustive tests along with the use of the AnaerRC. Therefore, the maximum intensity in which, theoretically, no increase on the perceived exertion would occur, would coincide with the intensity in which AnaerRC would not be used. In this context, the PET was determined based on the intersection of the linear regression of the relation between the perceived exertion increase rate and the velocity used in exhaustive tests.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
25
One presupposes that the regions from the central nervous system responsible for the organism’s perceptive representation, is sensitive to the anaerobic reserve depletion, represented by the AnaerRC. In fact, this hypothesis is in agreement with Caffareli, Kostka and Cafarelli, and Robertson et al., who established through their findings that H+ accumulation, both in the exercised muscles and blood, would be the main responsible for the increase on the perceived exertion. Most H+ accumulation in exercise is direct result of the anaerobic metabolism mobilization. The role the feed forward plays in the perceived exertion manifestation cannot be ignored, once the electromyographic activity that indicates the motor drive for the muscular activation increases along high-intensity rectangular exertions. This increase may be attributed to the incapacity of the motor stimuli at the beginning of the exercise to remain effective until the end of the exercise due to alterations on the peripheral cellular environment (ADP and H+ accumulation). The increase on the electromyographic activity would be a result of the communication between efferent and afferent information, whose comparison and integration would modulate the perceived exertion. The coincidence between the fatigue threshold and CritP reinforces this hypothesis. From the practical point of view of the use of metabolic thresholds for the prescription of aerobic exercises, the PET identification seems to be promising, once the results of this study suggest that the increase on the exertion perception would somehow be determined through the use of the anaerobic capacity. A limitation of this study was the lack of an objective measure of the use and depletion of the anaerobic energetic supplies concomitantly to the perceived exertion data collecting. Although the PET identifies the same metabolic threshold already described through other methods based on the heart rate, ventilation and on the blood lactate concentration, it showed to be a useful tool for the prescription and control of the aerobic training. The use of any equipment or the employment of invasive procedures would be useless. However, its physiological meaning and applicability on the aerobic training deserve further investigations. The results of the present study suggest that the perceived exertion may be used in the CritV determination. The PET was not significantly different in relation to the CritV. Besides, the correlations between both variables were quite high (r = 0.85 to 0.88). Thus, PET seems to represent the maximum exercise intensity where physiological and psychophysical variables would find stability. New studies must be conducted in order to assess the PET validity in other experimental conditions. All the authors declared there is not any potential conflict of interests regarding this article.
Exercise Is Preventive Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section IX
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
Introduction • Research • Introduction • Optimum Healing Pediatric • History • Treatment
Section IX
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
25 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055 AquaDios.Com
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Introduction • Research • Optimum Heal Pediatric • History Solution • Healthcare Crisis • Part IX
Pediatric Rehabilitation and Optimal Healing
Research studies are specific to Pediatric Rehabilitation to minimize disability and improve the
quality of life for people with disabilities and their families. Cure may not be possible for many rehabilitation patients, but rehabilitation medicine is particularly well-suited to the philosophy of healing. Recent research study shows that rehabilitation of persons with catastrophic illnesses or injuries is a complex, labor-intensive interaction between patients and caregivers. Experiences of overwhelming loss and suffering evoke strong emotions that shape the behavior of both patients and staff during the rehabilitation process. Each patient’s unique experience together with mutual compassion, caring and other humanistic qualities of the effective the caregiver and patient help create an optimal healing environment.
REHABILITATION MEDICINE • Scientific • Social Advances
Dr.’s Geller and Warren point out that over the past three decades, there have been significant scientific advances in the field of rehabilitation medicine. Biomedical knowledge has grown exponentially, particularly in the areas of genetics, neuroscience, and developmental neurobiology thereby affecting our understanding of neurodevelopment and related disabilities.
Research shows the ability to minimize disability and improve the quality of life for people with disabilities and their families is impressive -- cure is still not possible for many rehabilitation patients. Inability to cure renders the field of rehabilitation medicine particularly well-suited to achieving a balance between scientific, humanistic and preventive medicine programs like AquaDios-Med™ that are highly receptive to the development and implementation of optimal healing.
Relationship between Rehabilitation – Healing
The definition of rehabilitation is remarkably similar to the definition of healing. Dr. Jennings
defines rehabilitation as the restoration of the power or capacity for living, where living does not signify mere biologic life and function. It is the qualitative dimension of living well and living meaningfully that rehabilitation seeks to restore. Healing is defined as: Those physical, mental, social or spiritual processes of recovery, repair, renewal, and transformation that increase wholeness, and often but not invariably, order and coherence in one’s life.
In contrast to curing, which is aimed at removing or reversing a disease process, both
rehabilitation and healing are meant to enhance all aspects of well-being and facilitate the creation of life’s meaning. The appropriate goals of rehabilitation are the restoration of integrity to the person and the preservation of a meaningful life and self-identity with self-efficacy. Dr.’s Geller and Warren insist the transformative process that occurs in the context of rehabilitation is borne of caring rather than curing.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
This author believes physiatrists are the key to complete and comprehensive rehabilitation which may or may not lead to a cure, because the approach of the physiatrist will lead to a compassionate development of the patients desire to be the best they can be given what Is.
Optimal Healing • Pediatric Rehabilitation
The conventional rehabilitation literature is calling for several major changes in priority that is aligned with the goals of healing research. First, in its statement of research priorities, the National Center for Medical Rehabilitation Research (NCMRR) calls for a shift in the focus of research from cause and cure to functional limitations. The NCMRR task force argues that, the scientific enterprise needs to turn its attention to the functioning of the whole person within our society.
Techniques such as song-writing and improvisation can influence the child’s level of participation by providing opportunities for children to express their feelings, communicate appropriately and identify strengths that restore a sense of self-worth and dignity and improve self-esteem. Studies have repeatedly shown that music in itself, just listening to it, having it as a part of daily life has curative and relaxing benefits on all walks of life.
Impairment and activity levels can be altered by playing musical instruments that encourages use of arms, reach, grasp, coordination, strength of upper limbs and shoulder stability. Similarly, rhythmic auditory stimulation (RAS) can facilitate long-term gait training in patients with traumatic brain injuries
Management of Childhood Obesity
In 2004 Dr’s Freedman and Stern published a research study titled “The Role of Optimal
Healing Environments in the Management of Childhood Obesity” in the Journal of Alternative and Complementary Medicine and Mary Ann Liebert, Inc. The research identifies subsequent risks for type 2 diabetes and premature coronary artery disease. Other important complications and associations include pulmonary (asthma, obstructive sleep apnea syndrome, Pickwickian syndrome, sleep-related breathing disorders), orthopedic (genu varum, slipped capital femoral epiphysis, lower bone mass), and gastrointestinal hepatic complications (nonalcoholic steatohepatitis, cholecystitis). Dr’s Barlow and Dietz have generated a complete list and approximate prevalence of obesity-associated conditions in children.
Healing intentionality is the effort by one or more persons to improve the health status of another person (or oneself) through conscious, purposeful actions. In the treatment of childhood obesity, pediatricians, members of the health care team, and children are all involved in this process. Importantly, parents must be willing to be part of the treatment as well, and be supported in their efforts.
Healing relationships, previously defined as the quality and characteristics of interactions
between healer and healee that facilitate healing occur in nonclinical social supportive interactions and/or the therapeutic alliance (the doctor and nurse patient/family relationship). Although there is published research regarding the therapeutic alliance as it pertains to treating adult obesity, there are few published data with respect to this relationship in treating pediatric obesity. Nevertheless, this component of an optimal healing is critical, and should be emphasized.
Healthier behaviors are designed to persist throughout development and into adulthood. Comprehensive lifestyle changes, including diet modification, exercise (physical activity), and behavior modification are an integral part of any intervention program aimed at weight control in children.
Physical activity -- reducing sedentary behavior among children -- adolescents is important. To
provide a baseline assessment of physical activity levels among children ages 9 - 13, Centers for Disease Control Prevention (CDC) conducted the Youth Media Campaign Longitudinal Survey (YMCLS).

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California
90265 • 310.897.5055
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
[email protected] aquadios.com diAquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Research • Optimum Heal • Pediatric History Solution • Healthcare Crisis • Part IX • 23 Pages
Pediatric Rehabilitation • Optimal Healing
In 2004, Dr.’s Geller and Warren conducted a study titled “Toward an Optimal Healing
Environment” and published it in the Journal of Alternative and Complementary Medicine and for Mary Ann Liebert, Inc. Their research was specific to Pediatric Rehabilitation to minimize disability and improve the quality of life for people with disabilities and their families; noting “cure” is still not possible for many rehabilitation patients. This inability, they say, to “cure” renders the field of rehabilitation medicine particularly well-suited to the philosophy of healing.
Dr.’s Geller and Warren point out that curing is aimed at removing or reversing a disease process
-- both rehabilitation and healing, are meant to enhance all aspects of well-being; to restore integrity to the person, while facilitating the creation of meaning. Pediatric rehabilitation is the interface of rehabilitation medicine and pediatrics, and is associated with unique characteristics that provide a natural context for exploring the optimal healing environment.
Dr.’s Geller and Warren argue to establish a systematic integration and evaluation of healing
interventions among children with developmental disabilities and their caregivers (parents, health care practitioners, and teachers). They say the ultimate goal of these interventions would be to improve all levels of the children’s functioning in their homes, schools, and community environments by reducing their impairment while increasing activity and participation.
Dr.’s Geller and Warren research study shows that rehabilitation of persons with catastrophic illnesses or injuries is a complex, labor-intensive interaction between patients and caregivers. Experiences of overwhelming loss and suffering evoke strong emotions that shape the behavior of both patients and staff during the rehabilitation process. Each patient’s unique experience together with mutual compassion, caring and other humanistic qualities of the effective the caregiver and patient help create an optimal healing environment.
REHABILITATION MEDICINE • Scientific • Social Advances
Dr.’s Geller and Warren point out that over the past three decades, there have been significant
scientific advances in the field of rehabilitation medicine. Biomedical knowledge has grown exponentially, particularly in the areas of genetics, neuroscience, and developmental neurobiology thereby affecting our understanding of neurodevelopment and related disabilities.
Whole new classes of disease have been delineated in the past 10 years. Major interventions in medical, surgical, behavioral, and technological sciences have resulted in a much broader choice of therapeutic options, with increasing scientific support for the effectiveness of certain interventions.
Societal changes in the past 30 years have been equally striking. We have witnessed a major movement toward accepting people with disabilities and respecting their integrity and wholeness. This is reflected, in part, by the almost complete disappearance of terms such as cripple, imbecile, deaf and dumb, and a rejection of the phrase disabled people in favor of people with disabilities.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
2
In addition, the classification used to describe the functional limitations associated with disability and assess the progress of people with disabilities was modified. In the late 1990s, the World Health Organization (WHO) and the International Classification of Functioning and Disability (ICFD) changed the categories “disability” and “handicap” to activity and participation. These modifications reflect a more positive, optimistic, and holistic orientation toward the evaluation process.
In addition, society has moved from an institutional model of care toward community-based
models of care. Federal mandates ensure that people with disabilities have adequate health coverage and full access to their work and community environments, and families are increasingly being seen as partners in the care of their loved ones with disabilities.
The Americans with Disabilities Act (ADA) of 1990 provides civil rights protections to people with disabilities. Since 1975, and the implementation of the Education of the Handicapped Act (in 1990 renamed IDEA, Individuals with Disabilities Education Act), many rehabilitation services required for the child to participate in the educational setting are provided within the school system, and typically in the classroom, with educational funding.
Research studies show ability to minimize disability and improve the quality of life for people with disabilities and their families is impressive -- cure is still not possible for many rehabilitation patients. This inability to cure renders the field of rehabilitation medicine particularly well-suited to achieving a balance between scientific, humanistic medicine, and preventive medicine programs like AquaDios-Med™ that are highly receptive to the development and implementation of optimal healing.
Relationship Between • Rehabilitation • Healing
The definition of rehabilitation is remarkably similar to the definition of healing. Dr. Jennings
defines rehabilitation as the restoration of the power or capacity for living, where living does not signify mere biologic life and function. It is the qualitative dimension of living well and living meaningfully that rehabilitation seeks to restore.
Healing is defined as: Those physical, mental, social or spiritual processes of recovery, repair, renewal, and transformation that increase wholeness, and often but not invariably, order and coherence in ones life.
In contrast to “curing”, which is aimed at removing or reversing a disease process, both rehabilitation and healing are meant to enhance all aspects of well-being and facilitate the creation of life’s meaning. Dr. Jennings argues that in rehabilitation, disease or disability cannot be seen as an external enemy to be defeated with the assistance of medical technology and expertise. Nor is the “Sick” role the proper lens through which to view the situation of the person with a long-term disability. Instead, the appropriate goals of rehabilitation are the restoration of integrity to the person and the preservation of a meaningful life and self-identity with self-efficacy.
Dr.’s Geller and Warren insist the transformative process that occurs in the context of rehabilitation is borne of caring rather than curing. In the face of disability or disabling injury, transformation can only take place in and through relationships of mutual giving and interdependence. In addition to tending to the physical needs and limitations of their patients, rehabilitation professionals tend to a wounded human, a person whose feelings of self-worth are shattered. By tending to these emotional and psychological wounds, the caregiver often develops an awareness of his or her own grief, loss, and sorrow; those who are aware of their own wounds,
Dr.’s Geller and Warren believe that “Wounded” healers are the most effective healers. It is their compassionate knowing and understanding that empowers and leads to the thousands of undocumented, selfless acts of caring and compassion that assist in genuine and authentic healing. Thus, the “open” caregiver is, as the witness, who allows the patient to say, if you can accept me in all the ways that I am wounded, and then maybe, just maybe, I can and will accept myself.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
3
In pediatric rehabilitation, self-acceptance is vital to recovery for both the child and the parent. There are different strategies for promoting self-acceptance and self-efficacy; some are main stream and some are unconventional. However, fundamental to all such strategies is the importance of becoming more mindful about and focused on the present.
Dr.’s Geller and Warren define “mindfulness” as moment to moment nonjudgmental awareness. By being in the present time, participants can remain hopeful without attachment to or expectation of a particular outcome. It is this balance between hope, expectation and belief that is likely to facilitate the healing process and of course is critical to development of an altered state of consciousness used to release the patients full recovery powers; absent of secondary gain.
Yet, in rehabilitation, it is easy for patients and their support circle to ignore or forget about the
present while they nostalgically remember the past or long for a better future, thus their “now” is cancelled. Caregivers can help family members and the child learn to accept the child exactly as he or she is. Making use of the present moment with acceptance have healing qualities not because they reduce a disability, but because they impart a sense of worth, deepen hopes, and honor the personhood of each patient.
In addition to the inherently transformative nature of rehabilitation, there are several quite
tangible characteristics of the inpatient rehabilitation setting that promote healing. First, the process of rehabilitation is highly physical, helping to diminish a sense of physical isolation that can be brought on by disability. Patients get up early every morning, they shower and dress, and follow an active schedule and meet with several different therapists in one day. They have to move from their rooms to the therapy areas. Some of the therapies take place in groups and some are individual.
Either way, there are always one or more individuals who encourage the patient. Moreover,
throughout the day there is a considerable amount of touching and body contact. Unlike the physical contact that takes place in acute care medical settings, which is usually centering on physical examinations, withdrawal of body fluids, administration of medication or painful procedures, much of the physical interaction in rehabilitation involves being held and touched.
Another factor that facilitates healing in rehabilitation is quality care that is highly individualized
and interdisciplinary. Because deficits resulting from multisystem neurologic disease or injury are medical, physical, functional, communicative, behavioral, cognitive and social, therapeutic interventions aimed at all of these areas to necessitate having a team of professionals available. This healing “team” includes, at a minimum, pediatricians, physiatrists, physical therapists (PT), occupational therapists (OT), speech language pathologists, psychologists and social workers.
This author believes physiatrists are the key to complete and comprehensive rehabilitation which may or may not lead to a cure, because the approach of the physiatrist will lead to a compassionate development of the patients desire to be the best they can be given what Is.
All of these rehabilitation factors demand an interdisciplinary team, a vibrant and supportive environment, a focus on the present moment may have a healing effect not only on the patients but on the caregivers themselves. It is highly plausible that the levels of burnout, so prevalent among health professionals in other settings, are not as commonly observed among clinicians in rehabilitation settings. Unfortunately, the national data that exist on staff retention, burnout and turnover rates are either flawed by low response rates or categorized by type of professional rather than type of setting.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
4
Special characteristics • Pediatric Rehabilitation
Pediatric rehabilitation represents the interface of rehabilitation medicine and pediatrics, the combination of which results in some unique characteristics. First, the goal in pediatric rehabilitation is not simply to restore the child to premorbid levels of functioning, but rather to facilitate development for the remainder of childhood and attain optimal functioning and quality of life into adulthood.
The Commission on Accreditation of Rehabilitation Facilities (CARF) describes pediatric
rehabilitation as family centered, culturally sensitive, interdisciplinary, coordinated, and outcome oriented, where the outcomes are focused on preventing further impairment, reducing activity limitations, and minimizing participation restrictions while maximizing growth and development. The achievement of these goals will depend on the nature of the child’s disease, disability and genuine authentic desire to rehabilitate”; this often is determined by the willingness to identify and participate in “rehabilitation pain” described and practice by AquaDios-Med™.
The second unique characteristic relates to the population served by pediatric rehabilitation, most of whom are children with neurologic deficits. Within neurorehabilitation, there are predominately three distinct groups of children. In the first group are children with developmental disorders.
Some of these disorders are clearly congenital, such as spina bifida and Down’s syndrome.
Others, such as cerebral palsy, may be congenital or acquired during the perinatal period. Still others, such as autism, may not be apparent until the preschool years and will have lifelong consequences.
The services provided to children with developmental disabilities are described as habilitative. They are focused not on regaining lost skills, but on learning ways to foster developmentally appropriate skills with whatever impairment or activity limitation the children might have.
In the second group, children are born healthy and grow up normally until they experience a
traumatic event such as a brain or spinal cord injury. These events completely disrupt family life as it was previously known. Services provided to children with acquired injury are focused on regaining lost skills. This goal fits the truest sense of rehabilitation.
Nevertheless, according to Dr. Ylvisaker, meaningful rehabilitation for a child after brain injury extends far beyond the treatments, equipment, and restorative exercises of medical rehabilitation. He states that it is a long-term success in a child’s life, years after the injury. It is in large measure a function of supports provided in family, school and social contexts. It is also developed from the child’s skill and knowledge acquired in and applied to the many specific settings, tasks and activities that children encounter over the course of their development.
The third population of children; less prevalent than the other two, are those, who have degenerative disorders.
These children seem to develop normally for a period of time. Then they begin to lose skills and eventually die at an earlier than expected age. Degenerative disorders include muscular dystrophy, Rett syndrome and adreno-leukodystrophy.
Rehabilitation for these children focuses on slowing the loss of function and helping the child and family cope with the disease process. The nature of the child’s disorder, whether developmental, acquired, or degenerative, is likely to influence the child’s and/or the primary caretaker’s level of hope and expectation.
For example, a 12-year-old child with cerebral palsy has only known himself or herself that way. Although the child still may have hopes of being different, the child has no lived experience of how else life could be. By contrast, a child with an acquired brain injury or degenerative disorder has an image of himself or herself without any impairment and, therefore, a set of expectations about returning to that previous state.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
5
Similarly, a parent of a child with an acquired injury may have more difficulty letting go of the image they had for their child’s future than a parent who gives birth to a child with a developmental disability. In the latter case, after grieving the loss of the child they did not have, these parents can focus on the as yet unknown potential of the infant and developing child they do have. Interventions aimed at developing an optimal healing therefore need to take account of the nature of the child’s disorder and its impact on hope and expectation.
The third distinguishing characteristic is the role of the parent-caretaker and other significant
family members in all aspects of care delivery. Children with disabilities, like all children, are dependent on others in their world to provide care and direction during their developing years.
Although family members are usually involved in other areas of pediatric medicine, in pediatric
rehabilitation, designated family members, usually self-selected, become the healers and are taught to carry out the therapeutic program in everyday life. In contrast to the dyadic nature of the healing relationships in the context of clinical nursing practice or clinical medicine, caregiving in pediatric rehabilitation is always three-way.
Dr’s Ylvisaker and Feeney refer to an unpublished study in Brazil where indirect rehabilitation
services carried out by well-trained parents produced superior outcomes to those carried out by rehabilitation specialists.
Family members not only influence the well-being of the child with a disability, but having a
child with a disability in the family can influence the well-being of family members. Some families, particularly those with deep religious faith, may feel Blessed to have a child with a disability; others may not. Some research indicates that divorce and stress on siblings are more prevalent in this group of families.
Fourth is the longitudinal nature of much of pediatric rehabilitation, especially for children with
developmental disabilities. In any pediatric population, the need for and intensity of services will change over time as the child develops. In the pediatric rehabilitation population, because many children are not “cured” they need attention throughout their lifetimes. However, the type and intensity of service must change to reflect not only where the child is in life, but the particular needs of the child’s condition and the interaction between the two. Moreover, the needs of the family change over time. For example, a parent at the time a child is diagnosed with cerebral palsy has very different needs than that same parent as the child is making the transition from school to work.
Less is known about the needs of parents during the latter stages of a child’s recovery from
traumatic injury. This is an important time point to evaluate because it coincides with a decreased access to rehabilitation professionals, and because the adult studies have suggested that parent’s unmet needs may increase over time.
Fifth, not only do needs change throughout development, but so also do the team players. For
example, teachers become increasingly important in the child’s life because he will spend the majority of his waking hours in the school setting. The longitudinal nature of pediatric rehabilitation also influences the delivery of health care in two distinct but related ways. The first has to do with the inevitable involvement of sites other than the hospital where rehabilitation may be conducted or continues after discharge from the hospital such as medical day program, outpatient, and homebased services.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
6
The second implication concerns the continuity of care. Some children may continue to see their hospital - based team of therapists on an outpatient basis. Most children, however, will transition to a new community outpatient or school-based team. Although significant efforts are made to make this transition as seamless as possible by identifying the new team prior to discharge, ensuring communication between caregivers at different sites and encouraging adoption of the same treatment approach and style in the new setting, challenges associated with transfer of training are well documented.
Less well-documented are the implications of transition on the healing relationships that family members have formed with the inpatient team of therapists and or with a particular therapist in an outpatient setting.
A sixth variable, always present in the rehabilitation process, is the degree of personal resilience that the specific child brings with him or her. Because of the developing nature of the child, his or her strengths and weaknesses are not as set in stone as they might be with an adult.
Dr.’s Geller and Warren define “Resilience” as a dynamic process encompassing positive adaptation within the context of significant adversity; that is daily rekindling of hope, faith, expectation and belief to overcome.
The resilience literature has focused on the identification of underlying protective factors that mediate children’s reaction to stressful experiences and chronic adversity. These factors may be within the individual (temperament, self-esteem, locus of control), within the family environment (e.g., caregiving styles or parenting) or within the community (e.g., a strong role model or a supportive friend).28 It is not known whether resilience or adaptability is an immutable personality trait or whether it can be modified or enhanced by a healing environment.
One of the potential obstacles to positive adaptation, and another common characteristic of pediatric rehabilitation, is the tendency toward learned helplessness or secondary gain. Dr. Ylvisaker and Feeney argue that, in a rehabilitation context, clinicians and parents are disposed to intensify their control over children and adolescents with neurologic impairment, thereby potentially increasing the probability that the children will become increasingly helpless.
Rehabilitation programs in which clinicians fail to work collaboratively with and empower parents, and in contrast direct the parents in a unilateral manner, may unwittingly promote learned helplessness in the parents. Learned optimism is the antidote to learned helplessness and provides a useful outcome against which to measure the impact of a healing intervention.
Optimal Healing • Pediatric Rehabilitation
The conventional rehabilitation literature is calling for several major changes in priority that is
aligned with the goals of healing research. First, in its statement of research priorities, the National Center for Medical Rehabilitation Research (NCMRR) calls for a shift in the focus of research from cause and cure to functional limitations. The NCMRR task force argues that, the scientific enterprise needs to turn its attention to the functioning of the whole person within our society.
The goal of improving independent living for people with disabilities depends on the
development of a science that recognizes that the whole is greater than the sum of individual parts. Two of NCMRR seven research priorities, behavioral adaptation and whole-body response, include factors that are directly related to components of optimal healing. For example, NCMRR suggests that future behavioral adaptation research explore ways to facilitate the process of positive adjustment and full participation including community integration of both children and adults with disabilities. Similarly, NCMRR encourages a research focus on whole body adaptive mechanisms developed in response to chronic pain and an exploration of the body’s ability to heal from within.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
7
Second, the NCMRR also has identified the need to develop standardized measures of subjective well-being. Some existing scales developed in other fields examine subjective well-being, but the sensitivity of such scales in rehabilitation in general, and pediatric rehabilitation in particular, requires exploration. For example, the concept of quality of life which is defined as the perceived differences between an individual’s hopes and expectations and their present experience, is directly relevant to pediatric rehabilitation. However, most research on this topic has focused on illness rather than disability, and hospitalized children rather than children in the community. Furthermore, although measures of resilience and self-efficacy have been used in the context of pediatric rehabilitation research, the distinctions between some of these concepts are not clear in relation to quality of life.
Third, there has been a shift in emphasis within the standard classification system established by
the WHO ICIDH. This system identifies and describes three levels of functioning: impairment, activity and participation.
Impairment focuses on the loss or deviation of body function (e.g., paralysis or spasticity of an extremity).
Activity refers to functional tasks that one needs to perform on a daily basis, such as walking and eating.
Participation refers to one’s ability to engage in daily life situations such as going to school, work, or church, or whatever other activities are a meaningful part of that individual’s life.
In recent years, the focus of rehabilitation research has changed from an emphasis on measures
of impairment and activity to measures of participation. This shift was motivated by the need to capture the highly individualized nature of rehabilitation. For example, two individuals could have the same impairment and activity restriction (e.g., leg paralysis and inability to walk unassisted) and yet have different levels of participation. One could use a wheelchair and fully participate in a meaningful life, and the other could choose not to do so.
When assessing the impact of an optimal healing, one should consider whether the intervention
is appropriately targeting the level of participation. Moreover, more sensitive measures of participation may need to be developed because identifying and assessing the components of participation, motivation, passion and interest is challenging. This focus on societal participation has also been identified as a research priority for the American Occupational Therapy Foundation.
Fourth, both the American and the Canadian occupational therapy literature highlight the
importance of caring, hope, and spirituality in relationships with patients. Although spirituality has been a part of the Canadian written practice guidelines since 1983, it remains unclear how this translates into practice. Survey research among American’s also demonstrates uncertainty about the role of spirituality in practice and a lack of educational training in this area, as well as concern about whether caring oversteps appropriate patient boundaries.
More research is needed to explore rehabilitation therapist’s attitudes, beliefs and practices
regarding caring, hope, and spirituality. Although each of the other specialties (physical therapy, speech language pathology, Physiatry, etc.) has a robust literature describing interventions and outcomes among specific populations in pediatric rehabilitation, most of this research does not shed light on the components of an optimal healing.
The research literature in less conventional specialties that are not consistently part of the rehabilitation team, such as music and art therapy, suggests significant alignment with the goals of optimal healing. Music therapy has been shown to be effective in meeting the diverse needs of the child involved in rehabilitation, regardless of the level of functioning.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
8
Impairment and activity levels can be altered by playing musical instruments that encourages use of arms, reach, grasp, coordination, strength of upper limbs and shoulder stability. Similarly, rhythmic auditory stimulation (RAS) can facilitate long-term gait training in patients with traumatic brain injuries.
Techniques such as song-writing and improvisation can influence the child’s level of
participation by providing opportunities for children to express their feelings, communicate appropriately and identify strengths that restore a sense of self-worth and dignity and improve self-esteem. Studies have repeatedly shown that music in itself, just listening to it, having it as a part of daily life has curative and relaxing benefits on all walks of life.
Consideration of Disabilities
School-age children with traumatic brain injury (TBI) will likely experience intensive inpatient
services followed by transition to outpatient and school-based services all in a relatively short time. By contrast, children with developmental disabilities such as cerebral palsy except when and if
they are hospitalized for an acute rehabilitative need, will experience a more stable team of caregivers. Another measurement challenge when studying children with TBI is how to differentiate normal
developmental variations from functional manifestations of disability. With cerebral palsy and autism, classification of severity poses significant research challenges that do not typically exist with spinal cord injury or spina bifida.
Interventions will sometimes be more appropriately targeted to the parent. In this case, the design of healing-oriented research needs to consider the nature and timing of the intervention. For example, when children are newly diagnosed, parents are likely to be in a state of crisis. Depending on the nature of the intervention, this may or may not be an appropriate time to involve parents.
To the extent that parents are in crisis, and that unmet parental needs and poor family functioning
influence the outcome for children with TBI and other neurologic disorders, an appropriate intervention might be aimed at healing the parent and the family together. Whether the target of the intervention is the parent or another of the child’s healers (e.g., clinician or teacher), the goal of such an intervention might be to enhance self-care and wholeness. In this case, appropriate and highly sensitive outcome measures, such as improvement in, or balance of, energy, can be developed.
Dr.’s Geller and Warren believe priority should be given to the intrapersonal and interpersonal elements of optimal healing and assessments of their impact on a child’s level of participation. Intention, wholeness and compassionate, trusting relationships between children and their caregivers and among caregivers, form the basis of any transformative, healing experience.
Healing intention – Awareness
Because healing is an inherent goal of rehabilitation, we assume that rehabilitation therapists and
teachers intend to be Healers albeit to varying degrees. Therefore, an intervention in this category may be most powerfully aimed at the parent or significant caretaker.
Such an intervention might focus on assisting parents to let go of expectations where expectation is defined as attachment to a particular outcome, and determining whether a shift in participants hope and expectation creates greater Ease between parent and child. Change in Ease might be operationalized by a change in the nature of the Stories parents tell about their children. With certain disabilities, particularly acquired injury or degenerative disease, the parent may be so devastated that the child may become the most likely focus of an intervention to enhance healing intention.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
9
Dr. Ylvisaker and associates describe a very individualized model for working with children following brain injury that focuses on positive supports, empowering the child and real-life participation. For example, one can imagine participating in a community service-oriented process in which the child-participant assumes the role of Healer by systematically providing gifts or services to those individuals who are most important in the child’s life. Goals and outcomes should focus on increased self-efficacy, greater initiation (particularly meaningful in children with frontal-lobe injuries), and increased attention to task and participation in school; and always consider the age of the child.
Questions and Rehabilitation
What is the impact of an intervention aimed at shifting parental hope and expectation in the level of ease in the relationship between parent and child; on the child’s attention; level; on parental grief and acceptance; on the child’s motivation and participation in school?
What is the impact of offering qigong, yoga or drumming to parents, teachers and or clinicians on their energy levels and balance (measured objectively) and mindfulness; on the child’s level of participation?
What is the impact of offering parents, teachers and/or clinicians an educational intervention about the healing relationship on the child empowerment/self-efficacy; on the child’s motivation and participation in school?
What is the impact of a healing environment (e.g., designing patient or treatment rooms according to Feng Shui principles) on treatment outcome; level of participation in therapy?
What is the impact of offering energy healing or acupuncture to children on their pain/spasticity -- On their functional magnetic resonance imaging; on their levels of participation?
What is the impact of seated massage, qigong, or yoga for clinical staff on their use of sick days/annual health care costs?
Management of Childhood Obesity
In 2004 Dr’s Freedman and Stern published a research study titled “The Role of Optimal Healing Environments in the Management of Childhood Obesity” in the Journal of Alternative and Complementary Medicine and Mary Ann Liebert, Inc.
Dr’s Freedman and Stern research identifies the prevalence of childhood and adolescent obesity has increased steadily over the past three decades such that obesity is now a major worldwide pediatric health risk factor.
Their research verifies that pediatric obesity is associated with significant health problems, and is an important early risk factor for adult morbidity and mortality. They focus on the role and components of optimal healing that may be useful in the management of childhood obesity: healing intention, healing relationships, health promotion and disease prevention, and healing spaces. Diet, physical activity, and behavior modification strategies used in the treatment of childhood obesity.
Dr’s Freedman and Stern research indicates childhood and adolescent obesity has increased steadily over the past three decades such that obesity is now a major pediatric health risk factor, not only in the United States but worldwide.
Freedman and Stern confirm that Pediatric obesity is associated with significant health problems and is an important early risk factor for adult morbidity and mortality. Medical problems are common in obese children and adolescents, and affect the cardiovascular system (hypercholesterolemia and dyslipidemia, hypertension) and endocrine system (hyperinsulinemia, insulin resistance, impaired glucose tolerance, type 2 diabetes, menstrual irregularities, and early sexual maturation).

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
10
Dr. Cook and associates recently reported that a metabolic syndrome phenotype might exist in perhaps 4% of the U.S. adolescent population and almost 30% of overweight adolescents.
Freedman and Stern suggest that childhood obesity interventions include the home, school and primary care settings. This involves the educating of parents on eating and lifestyle modification to significantly reduce the obesity in their children. They found that holding classroom lessons on nutrition and physical activity improves fitness and body fat levels.
The delivery of programs through primary care has received little formal assessment, and its
potential role seems to be undervalued and underused. Although all three settings may be part of optimal healing we have chosen to focus on the role of the health care provider, working with patients and their families, to prevent and treat childhood obesity.
Health care providers, in conjunction with their patients (and other family members), form the therapeutic alliance. This alliance is an important component of healing in health care settings and falls under the category of healing relationships as defined by the Samueli Institute.
Healing relationships may occur in nonclinical social supportive interactions and or the
therapeutic alliance. With respect to childhood obesity, social supportive interactions may include family members, friends, support groups (clubs, camps, both for children and parents), school and after school environments (including recreational activities), religious institutions, and the community at large. The therapeutic alliance includes the doctor and nurse patient/family relationship.
Dr’s Freedman and Stern hypothesize that the therapeutic alliance can play an important role in prevention, treatment, and management of childhood obesity. The American Academy of Pediatrics strongly advocates support for development and testing of primary prevention strategies, such as preventive medicine programs, for the primary care setting, and investment of substantial resources for development of effective treatment approaches. Although there is a scarcity of published research in this area, we believe that navigating through these relatively uncharted waters may lead to innovative approaches to managing this serious issue.
ASSESSMENT OF OBESITY
Body mass index (BMI) is the ratio of weight in kilograms to the square of height in meters
(kg/m2). BMI is widely used to define overweight and obesity, because it correlates well with measures of body fatness and is derived from the Department of Nutrition, University of California Davis, Davis, CA. from commonly available data, weight, and height.
The pediatric growth charts for the U.S. population, which include BMI for age and gender, are readily available (www.cdc.gov/ Growth charts), and allow longitudinal tracking of BMI.
In children, BMI between the 85th and 89.9th percentile for age and gender is considered at risk of overweight, and BMI at or about the 95th percentile is considered overweight or obese. There is no category for obesity that avoids stigma. Until more definitive recommendations are established, the American Academy of Pediatrics Committee on Nutrition recommends that children and adolescents with BMI greater than or equal to the 95th percentile for age and gender should undergo in-depth medical assessment and treatment unless some contraindication is found. This percentile is used because it not only identifies children with a significant likelihood of adult obesity, but in older adolescents, it is associated with elevated blood pressure and lipid profiles that increase the risk of obesity related disease and mortality.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
11
A child who’s “BMI” falls between the 85th and the 95th percentile for age and gender should be evaluated carefully, with attention to secondary complications of obesity; such as hypertension and dyslipidemias. Evaluation and treatment should also be prompted by a recent large increase in BMI.
SCOPE OF THE PROBLEM
The prevalence of obesity among children and adolescents has been increasing steadily since the
mid-1960s. Between the 1960s and 1988 - 1994, prevalence among 6- through 11-year-old children increased from 4% to 11%. During this same time period, prevalence among 12- through 19-year-olds increased from 5% to 11%. In 2004 15.% of 6- through 11-year olds, and 16 % of 12- through 19- year olds meet the criteria for obesity.
Recent data suggest that overweight and obesity is more common among specific population subgroups, including African Americans and Hispanics. For example, prevalence of overweight for non-Hispanic black children 6 - 11 years of age is 20%; for Mexican Americans, it is 24%. In contrast, 12% of non-Hispanic white children in this age range are overweight. The prevalence of overweight among males was not significantly different than among females, although among Mexican American adolescents a nonsignificant trend toward an increase in males was seen.
These racial - ethnic trend disparities remained large and statistically significant after controlling
for family income and other confounding variables. In fact, keeping adolescents in their same environment and changing only family income and parental education had a limited effect on the disparities in overweight prevalence. It may be that cultural attitudes about body weight and food are more important than socioeconomic status (SES). This appears to be the case in Caucasians as well.
The literature on ethnicity and body size in children is inconsistent. A study of 219 Mexican
children (6- to 12-years old) from affluent families indicated that children are more likely to be obese if they are boys, from small households with few or no other children, and more permissive, less authoritarian parents. The value placed on children, especially sons, in smaller middle-class Hispanic families can result in indulgent feeding because food treats are a cultural index of parental caring, and parent’s value child fatness as a sign of health. Interestingly, these obese Mexican children had no greater social or psychologic problems than their non-obese peers.
African American females, as contrasted with white females, have been reported to have an
aesthetic preference and physical tolerance for increased adiposity or fat cells, and less dissatisfaction with body weight. Black adolescent girls were much more likely than white girls to be satisfied with their body size, to describe themselves as thinner than other girls, and to say they were not overweight.
In contrast, in a study of 969 third-grade northern California public school children where overweight concerns and body dissatisfaction were highly prevalent among girls and boys across ethnicity and SES, young Latina and African American girls manifest equivalent or higher levels of disordered eating attitudes and behaviors than white and Asian Americans girls.
Finally, a study of more than 1200 Asian, Hispanic, black, and white men and women indicated ethnicity, independent of age, education, and body weight, does not influence preference for female and male shapes or tolerance for obesity. Dr’s Freedman and Stern recommend future research in the cross-cultural aspects of body dissatisfaction, overweight, and obesity needs to continue.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
12
HEALTH IMPLICATIONS CHILDHOOD OBESITY
Obese children may be at higher risk for the metabolic syndrome in adulthood and the subsequent risks for type 2 diabetes and premature coronary artery disease. Other important complications and associations include pulmonary (asthma, obstructive sleep apnea syndrome, Pickwickian syndrome, sleep-related breathing disorders), orthopedic (genu varum, slipped capital femoral epiphysis, lower bone mass), and gastrointestinal hepatic complications (nonalcoholic steatohepatitis, cholecystitis). Dr’s Barlow and Dietz have generated a complete list and approximate prevalence of obesity-associated conditions in children.
There is a strong link between obesity during childhood and adolescence and obesity in adults.
Dr. Whitaker’s research team showed that the odds of being obese as an adult were 1.3 for obesity at ages 12 years and increased to 18 for obesity at ages 15 - 17 compared to not being obese at these ages. Dr. Kvaavik research concluded that tracking of BMI from adolescence into adulthood was substantial. In fact, it has been estimated that the risk of adult obesity is 20% at age 4, but rises to approximately 80% by adolescence. Numerous comorbidities seen in obese adolescents will likely persist into adulthood.
When physicians talk to and care for children who are overweight, sensitivity and compassion are paramount. In many obese children and adolescents, a widespread consequence of obesity is psychologic. Obese children may already be suffering from depression, low self-esteem, and social marginalization.
A modest association between depressive symptoms and BMI was found for overweight girls (but not boys) in third grade, explained by an excess of overweight concerns in these children. Despite increased prevalence of obesity, stigmatization of obese children has gotten worse, and obese children suffer greater rejection than in the past. Fifth- and sixth-grade children ranked a picture of an obese child lower than that of a child holding crutches with a brace on one leg, a child sitting in a wheelchair with a blanket covering both legs, a child with no left hand, and one with a facial disfigurement. This may explain the lower self-esteem and greater shame, humiliation, and teasing experienced by an overweight child, compared to their non-obese peers.
Consequences of stigma persist into early adolescence and adulthood. Schwimmer and
colleagues reported that even in the absence of comorbid disease, obese children and adolescents (ages 5 – 18 years) have lower health related quality of life (QOL) (which assesses physical, emotional, social, and school functioning) than children and adolescents who are healthy, and similar QOL as those diagnosed as having cancer. Dr. Friedlander and colleagues reported similar findings in children 8 -11 years of age. A practitioner who understands the psychologic significance of a child’s or adolescent’s obesity will be able to focus concerns on health, not self-worth, or to refer for counseling if necessary.
Basic’s in Childhood Obesity
Components of optimal healing most readily incorporated into the management of childhood obesity include healing intention, healing relationships, health promotion and disease prevention, and healing spaces.
Healing intention
Dr’s Freedman and Stern research shows that healing intentionality is the effort by one or more persons to improve the health status of another person (or oneself) through conscious, purposeful actions. In the treatment of childhood obesity, pediatricians, members of the health care team, and children are all involved in this process. Importantly, parents must be willing to be part of the treatment as well, and be supported in their efforts.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
13
Proposed Contract Physician – Patient
Dr’s Downey and Stern believe a patient contract is absolutely necessary for success: I, your doctor, am concerned about the growing problem of obesity among my patients. I am
more concerned that many of you find it difficult to talk to me about your weight. You might feel this way. Therefore, I promise: (1) to keep up to date on the latest scientific and medical understanding of causes and treatments of obesity; (2) to work with my office staff to make sure everyone is comfortable and respected in my office; (3) to commit to work with you on your weight issues, if any, and if you want to; (4) to research community resources that might be helpful to you; (5) to make appropriate referrals if you need greater expertise than those I can provide; and (6) to work with you to obtain insurance coverage and to help with discrimination you face because of your weight.
I, the patient, agree: (1) that my weight is an important part of my health; (2) to provide you with a history of my family’s weight, my weight, and my efforts to lose weight; (3) to work with you on a plan for weight loss or weight maintenance, and improving my fitness; and (4) agree that, if you do your homework, I will work as hard as I can to follow your recommendations.
AMERICAN ACADEMY OF PEDIATRICS THERAPY
Dr. From Barlow and Dietz have formulated a check list for the successful treatment of obesity. Intervention should begin early. The family must be ready for change. Clinicians should educate families about medical complications of obesity. Clinicians should involve the family and all caregivers in the treatment program. Treatment programs should institute permanent changes, not short term diets or exercise
programs aimed at rapid weight loss. As part of the treatment program, a family should learn to monitor eating and activity. The treatment program should help the family make small, gradual changes. Clinicians should encourage and empathize and not criticize. A variety of experienced professionals can accomplish many aspects of a weight management
program. Dr’s Freedman and Stern point out that the decision to attempt weight loss treatment should take
into account the patient’s readiness to make necessary lifestyle changes, because patient motivation is critical to the success of an obesity treatment program. Motivational readiness can be determined by understanding stages of change.
In the precontemplation stage, patients have no intention to change. If a parent brings a child to
the doctor for a routine physical, immunization, or medical problem (e.g., sore throat), he or she is not likely to be thinking about their child’s body weight. But that does not mean the physician should lose this opportunity to discuss body weight with patient and parent (see Healing relationships section for more information on physician and patient communication about weight). At this stage, the goal for patients (and their family members) is to begin thinking about changing behavior.
June 200, Daniel Delgado, M.D. reported personal communication of the physician must engage
the child (and family members) in contemplating change. When the child is in the room, the provider has a captive audience and an opportunity to educate the child and parent and motivate further action. Parents in denial about their child’s weight will not make the extra effort to bring the child back unless they are aware of the importance of follow-up. At the very least, clinicians need to gather objective data; including blood pressure, height, and weight. The child’s BMI should always be calculated and plotted.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
14
The Contemplation Stage
The contemplation stage is characterized by an intention or willingness to change. During this stage, barriers as well as benefits of change must be assessed. In adults, one barrier may be the patient’s belief that losing weight and exercising is stressful, difficult, painful, or even hopeless, as evidenced by the high relapse rate among dieters. There are few data regarding these perceptions in children. One study reported a family-based approach resulted in a higher percentage of weight reduction and better maintenance of weight loss compared to a child-centered approach.
Success was attributed to a lower level of resistance to change by children because weight-loss
related decisions were not theirs. In the control group, although children were encouraged to seek their parents help if needed, any change in weight was a result of their own efforts (e.g., self-control and exercise). Many of these children claimed they felt stressed and frustrated when they failed to achieve or maintain weight loss.
For optimal healing of obesity empathy, validation, praise, and encouragement on the part of the physician is particularly necessary during the contemplation stage. The way in which clinicians discuss body weight with patients (and their family members) may affect receptivity to counseling. Clinicians should communicate with a nonjudgmental attitude that distinguishes between the weight problem and the patient with the weight problem.
A new contract between physicians and patients, proposed by Downey and Stern (see “Contract Between Physician and Patient”) provides a model that can be used in clinical practice, and supports many aspects of the healing relationship including trust, credibility, honesty, expectation, courtesy, respect and communication. This is a model for approaching adult obesity that should be modified for children and adolescents (see Healing relationships section for further discussion).
Patients reach the preparation stage when they are ready to make a specific change. At this point,
a program individually suited to their needs will be devised and other health care professionals will join the treatment team (see Health promotion and disease prevention section for further discussion).
As the patient’s determination to change increases, he or she may experiment with small but inconsistent changes. For example, a child may watch fewer hours of television once per week as he or she attempts to decrease physical inactivity. At this stage, physicians or other members of the health care team should encourage patients to address the barriers to changing this behavior on a more regular basis (e.g., watching fewer hours of television every day).
Patients reach the action stage when they perform a behavior regularly for 6 months. Any such action taken by patients should be praised because it demonstrates the desire for lifestyle change. The health care team should continue to ask about successes and difficulties and be generous with praise and admiration. The final stage of maintenance is reached when changes are sustained. It is not uncommon, however, for patients to find themselves moving through stages of change several times before change becomes truly established. By identifying a patient’s position in the change process, physicians can intervene as necessary and help patients move along these stages of change.
Healing relationships
Healing relationships, previously defined as the quality and characteristics of interactions
between healer and healee that facilitate healing occur in nonclinical social supportive interactions and/or the therapeutic alliance (the doctor and nurse patient/family relationship). Although there is published research regarding the therapeutic alliance as it pertains to treating adult obesity, there are few published data with respect to this relationship in treating pediatric obesity. Nevertheless, this component of an optimal healing is critical, and should be emphasized.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
15
The first step in developing a therapeutic alliance is for physicians to take a more active role in the identification and treatment of their overweight or obese patient, including those who are at risk for overweight and obesity. Adult patients who were counseled by a physician and told specifically to lose weight were significantly more likely to report attempts at weight loss compared to those who were not.
Achieving and maintaining weight loss in adults is more likely to be successful when there is a
physician-patient partnership that provides the support and motivation for the patient’s effort to initiate and maintain a healthy body weight. We hypothesize a similar result is likely in the pediatric population.
Weight counseling patterns of U.S. pediatricians are inconsistent. Miller et al. reported that pediatricians frequently referred mildly underweight children but not moderately obese and overweight children for nutritional work-ups. Many physicians are reluctant to initiate treatment in overweight children with no associated medical conditions.
In a survey of physicians regarding their attitudes and practices related to the treatment of pediatric obesity in a primary care setting in which 28% of adolescents and 23% of children were assessed as overweight, the frequency with which physicians addressed weight issues in both groups increased incrementally with the patient’s level of overweight. In a recent study of pediatricians, approximately 50% reportedly always counseled about maintaining a healthy weight. Those who always counseled were more likely to be women and to spend more time with patients during well-care visits.
When addressing obesity, 25% of physicians think they are not at all or only slightly competent,
while 20% report feeling not at all or only slight comfortable. In some clinical cases, providers feel uncomfortable bringing up the issue, and in other cases, they do not want to make the patients feel uncomfortable. This issue is compounded by discussion with overweight parents about their overweight children.
Physicians may have similar prejudices that society holds, and often blame the obese patient for being obese, thinking the solution to obesity is a simple one, eat less and exercise more. These findings suggest physicians would benefit from additional training and education regarding safe and efficacious intervention strategies for pediatric obesity, to effectively integrate discussion of weight issues into the primary care setting. A survey of pediatricians, pediatric nurse practitioners, and dietitians indicated high interest in additional training in the use of behavioral management strategies, guidance in parenting techniques, and addressing family conflicts. With no training in obesity counseling, physicians discussed weight with 42% to 47% of their patients. With training, this number increased to 89%.
Other cited barriers to physician involvement include lack of reimbursement, lack of parent
involvement, lack of patient motivation and compliance, lack of support services, time available for counseling and pessimism about treatment outcomes. Among those who do address dietary issues with their patients, the time spent discussing weight management has been reported to be 5 minutes or less. Interestingly, pediatricians report similar barriers to prevention and treatment of type 2 diabetes.
Even when physicians are interested in taking an active role in this area, they need to consider how to broach the topic of overweight and obesity in their patients, and act with sensitivity and compassion. Obesity is one of the few conditions still actively discriminated against by the public and health care providers. Historically, the public has used the words obese and fat in a pejorative manner as in you’re fat. . . . Numerous studies show that obese individuals, whether children or adults, are subjected to pervasive prejudice and discrimination. Health care professionals themselves seem to share society’s negative attitudes toward obesity, often stereotyping them as weak-willed, ugly, and awkward and lacking in self-control and lazy.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
16
More than 50% of physicians viewed obese adults as awkward, unattractive, ugly, and noncompliant. Despite these views, obese women, when asked about their physician’s weight management attitudes and practices, did not report being treated disrespectfully or routinely alienated by physicians making critical or offensive remarks about weight. It is unknown whether pediatricians have a similar attitude toward obese children, or, if these children (or their parents) feel disrespected by pediatricians when discussing weight.
Dr’s Wadden and Didie surveyed obese men and women to determine terms that obese
individuals find undesirable or desirable for their doctors to use to describe excess weight. Fatness and obesity were rated as undesirable to very undesirable descriptors for doctors to use in discussing body weight. Physician’s use of such terms could abruptly halt a needed discussion of an important topic.
By contrast, the descriptors weight, excess weight, and BMI were rated neutral to desirable. Of
these three, weight was the most desirable term, probably because it is nonjudgmental and easily understood. Thus, it is essential to determine what terms are most acceptable to overweight and obese children and their parents so that when pediatricians initiate conversations about body weight, all are receptive to the discussion.
This may be particularly true for parents who have different perceptions about obesity than do
heath care professionals. An anonymous questionnaire was distributed during well-care visits involving children 4 to 8 years of age at a pediatric faculty practice. Of 83 parents surveyed, 23% had overweight children. These parents did not differ from other parents in their level of concern about excess weight as a health risk or in their knowledge of healthy eating behaviors. But the two groups of parents did differ in the accuracy of their perceptions about their children’s weight. Only 11% of parents of overweight children perceived their child’s weight accurately compared to 60 % of other parents.
Parents of overweight children invariably underestimated their children’s weight. Considering
the key role of parents in treatment outcomes it would be important to understand underlying bases for parental attitudes regarding their child’s body weight, especially in sociocultural contexts.
Without this understanding, communication between health care providers and parents may be
ineffective. Third, physicians need to develop trust with their patients. Research conducted in Canada over 20 years found the more trust-based and patient-centered an encounter between physician and patient, the better the outcome for the patient. Therefore, Canada’s physician education program emphasizes building a trusting physician patient relationship.
A confrontational approach is far more likely to result in hurt feelings than weight loss.
According to Johnson: Practitioners who insist they are breaking through patient’s denial by calling them obese should realize what they are more probably breaking is the patient’s trust and desire to return for further care. Trust must also be developed between practitioners and family members. Studies of preadolescent children have demonstrated improved long-term outcome when a parent participates in the treatment program.
A survey of pediatricians, pediatric nurse practitioners, and registered dietitians indicated that
nearly all respondents involved a parent or the entire household in the treatment of preschool and school-aged children. The Expert Committee of the American Academy of Pediatrics recommends practitioners engage the entire household in the eating and activity changes to create a healthy environment.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
17
Finally, personal characteristics of practitioners, such as their own body-weight status, eating habits, and exercise habits might affect their approach to the management of obesity. These characteristics might also influence their effectiveness in counseling and serving as role models for children and adolescents with obesity problems and their parents. This subject needs further study.
A key aspect optimal healing for the management and treatment of childhood obesity is figuring
out the best way to present these materials to children and their parents via the therapeutic alliance.
Health promotion and disease prevention The primary goal of childhood obesity interventions is regulation of body weight and fat with
adequate nutrition for growth and development. For long-term weight maintenance, old eating and exercise behaviors must be replaced with new, healthier behaviors, thereby allowing healthier behaviors to persist throughout development and into adulthood. Comprehensive lifestyle changes, including diet modification, exercise (physical activity), and behavior modification are an integral part of any intervention program aimed at weight control in children.
The American Academy of Pediatrics recommended approach to therapy
The literature on treatment of pediatric overweight has already been extensively reviewed, and
concludes that Epstein’s four long-term family based studies provide the basis for much of our current understanding of treating pediatric obesity. His target group (children ages 6 - 12 years) is similar to our proposed study group (children 8 - 12 years of age) and his program integrates diet, physical activity, and behavior modification strategies.
Diet – Nutritional Foods
Dietary goals for patients and their families are well balanced, healthy meals and a healthy approach to eating. Because parents can control access to, and model behaviors involving, food purchasing, preparation, and consumption, particularly among young children, the involvement of the family in dietary modification is important. Key findings from the 10-year follow-up treatment of 143 families showed that the program was significantly improved when the intervention was aimed at the parents as well as the child. Other research supports parents as the exclusive agents of change in the treatment of childhood obesity. Furthermore, Family-based approaches provide the additional benefits of improving parental diet and physical activity patterns and reducing parental obesity.
Different approaches to healthy eating have been proposed. One approach is following the Food
Guide Pyramid for Young Children (see www.usda.gov/fcs/cnpp.htm). Another is the Stoplight Diet. The latter has been used in research and clinical settings for the treatment of childhood obesity. It encourages consumption of low-calorie green foods and moderate calorie yellow foods over high-calorie red foods. No foods are forbidden. Recently, a reduced glycemic load diet was reported to be a promising alternative to a conventional diet in obese adolescents, but there are no current data to support the use of this diet in children. Ultimately, the best dietary approach is one that the patient and their family members will follow with a high level of compliance.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
18
Physical activity
National health objectives for the year 2010 include increasing levels of physical activity and reducing sedentary behavior among children and adolescents. To provide a baseline assessment of physical activity levels among children ages 9 - 13, the Centers for Disease Control and Prevention (CDC) conducted the Youth Media Campaign longitudinal Survey (YMCLS).
Data from this survey of children and their parents indicate that 62% of
children in this age range do not participate in any organized physical activity during non-school hours and 23% do not engage in any free-time physical activity. Fewer children reported involvement in organized sports (39%) than in free-time physical activity (78%) during the 7 days preceding the survey.
Non-Hispanic black and Hispanic children were significantly less
likely than white children to report involvement in organized activities, as were children with parents who had lower incomes and education levels.
Barriers to participation in physical activities, regardless of the child’s age and gender include
concerns about transportation, opportunities in their area, and expense. Overall, parents with lower incomes and education levels reported more barriers.
Physical activity is essential to long-term maintenance of weight control in children, and
interventions aimed at either increasing physical activity or decreasing physical inactivity (sedentary behaviors) are useful in treating pediatric obesity.
The majority of exercise programs have focused on aerobic exercise. However, there has been
very little research on the best way to implement aerobic exercise programs to maximize weight loss and adherence.
Several other important issues needing study include: Can resistance
training be used safely in a pediatric population to maximize the development of lean body mass and increase total energy expenditure?
Is it better to focus on one activity or is cross training better? And, is
the combination of aerobic and resistance training better than aerobic exercise alone? The structure of the program may also be important for developing active lifestyles in treating obesity. Data from several trials incorporating moderate to intense aerobic exercise suggest that school-based exercise interventions may be a promising approach to treating childhood obesity. In addition, the family is important to structure and support activity, as parent activity level is a strong predictor of child activity.
In the health care setting, interventions focused on increasing physical activity should be
delivered in a nurturing, non-intimidating environment. Obese children respond differently physiologically and emotionally to exercise than do normal-weight children, and experience negative consequences to participation in activities considered appropriate for normal-weight children.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
19
In clinical settings, specialized exercise programs that include specific recommendations for obese children have been shown to enhance safety, efficacy, and compliance during treatment. Optimal results may be achieved by combining programs to reduce sedentary behaviors with those that increase physical activity, such as walking or biking to school instead of riding. An OHE for the treatment of childhood obesity should examine and modify, as necessary, the home environment as it pertains to physical activity. Some children spend more time in front of the television and playing video games than doing any other activity other than sleeping. Watching television often decreases the amount of time spent performing physical activities, and is also associated with increased food consumption either during viewing or as a result of food advertisements.
In a study of sixth - and seventh-grade students, time spent watching television along with the
number of soft drinks consumed were significantly associated with obesity. Latinos spent more time watching television and consumed more soft drinks than did non-Hispanic whites or Asian students. Children who watched 4 or more hours of television per day had significantly greater BMI, compared to those watching less than 2 hours per day. Furthermore, having a television in the bedroom has been reported to be a strong predictor of being overweight, even in preschool-aged children.
The American Academy of Pediatrics has recommended limitation of television to 1 or 2 hours
per day. The results of a randomized trial to decrease television viewing for school-aged children has
provided the strongest evidence to support the role of limiting television in prevention of obesity. In this study, decreasing media use without specifically promoting more active behaviors in the intervention group resulted in a significantly lower increase in BMI at the 1-year follow-up, compared to the control group. Additional support for the importance of decreasing television viewing comes from controlled investigations that demonstrated that obese children who were reinforced for decreasing sedentary activity (and following an energy restricted diet) had significantly greater weight loss than those who were reinforced for increasing physical activity.
Behavior Modification strategies
Behavior modification strategies that have been used in the treatment of childhood obesity
include self-monitoring of activity and eating, use of praise and contracts with nonfood and nonmonetary rewards, stimulus control to make the home environment more conducive to a healthy lifestyle, role-modeling of healthy behaviors by parents, and avoidance of over regulation of children’s food consumption.
Children are widely exposed to television advertisements for ready to eat sugared cereals to
Happy Meals from McDonalds. Even though children do not drive themselves to fast-food restaurants or to grocery stores, they often influence adult food purchasing behavior. The question, Who is the boss? is often answered I am by a young child who has manipulated their tired or stressed parent into purchasing ready-to-eat foods, easily accessibly on supermarket shelves or near the checkout stand, that may be high in fat and sugar. Furthermore, parental efforts to limit children’s intake of sweet snacks and drinks are being undermined by their child’s access to money.
Because parents institute the changes needed for successful treatment, they need support and guidance in basic parenting skills. The American Academy of Pediatrics recommends the following parenting skills in the management of eating and activity behaviors:

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
20
(1) find reasons to praise the child’s behavior; (2) never use food as a reward; (3) parents can ask for rewards for children in exchange for the changes in their own behavior; (4) establish daily meal and snack times; (5) determine what food is offered and when but allow the child to decide whether to eat; (6) offer only healthy options; (7) remove temptations; (8) be a role model; (9) be consistent. Although progress has been made in the treatment of childhood obesity, most pediatric obesity
interventions are marked by small changes in relative weight or adiposity and substantial relapse. It is premature to assume there are efficacious standardized treatments. Research is needed to improve treatment outcome and maintenance of treatment effects.
Obesity is a chronic disease, and chronic diseases require long-term treatment. For childhood
obesity treatments to be effective long-term, explicit change on the part of the patient, family members, and health care practitioners is necessary. In addition, changes in the school and after-school environment, community, and even state and local government e.g., legislation may be necessary, Currently there are many programs being conducted throughout all sectors of American society to reverse the rapidly increasing prevalence of overweight and inactivity among children and adolescents.
Shaping Americas Youth is a nationwide initiative to identify and centralize this information see:
wwwshapingamericasyouth.com. Ultimately, information on local and regional programs that may be outside the healthcare system may be helpful to primary care physicians working with obese patients.
Healing spaces Brownell and Horgen have coined the term toxic environment to illustrate what
most U.S. adults and children experience almost every waking hour of every day of every year, namely an abundance of food, and very little reason to move our bodies.
The food is available 24 hours per day, accessible in restaurants, machines, and stores as never
before, sold in places previously unrelated to eating (e.g., gas stations, drugstores), inexpensive, promoted heavily and sometimes deceptively, and designed to taste really good and keep people coming back for more. Between 56% and 85% of children in school consume at least one soft drink daily, with the highest amount consumed by adolescent males. On a typical day, 30% of children and adolescents ages 4 to 19 years old consume fast food.
The second half of the energy equation, physical activity, has also been affected adversely.
According to Dr’s Brownell and Horgen: Few children walk or bike to school, and often have little physical education. Computers, video games, and televisions keep children inside and inactive, and parents are
reluctant to let children roam free to play. Each of these potentially healing spaces home, school, and community environments contributes
to childhood obesity, and each of these eventually must play a role if the problem of childhood obesity is to be solved.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
21
The physical environment that exists in the health care professional office also should be addressed. The space should communicate support to patients and their family members. As such, it should be accommodating, accessible and comfortable to overweight and obese patients. Although this may be less of an issue for obese children compared to obese adults, stairs, doorways, hallways, restrooms, and waiting room chairs should be evaluated for their suitability to meet the needs of the large patient.
In addition, specialized equipment (e.g., blood-pressure cuffs, private scales, large gowns, tape
measures, step stools) is necessary to consider when looking at components of optimal healing spaces. There is no research to direct recommendations regarding nature, light, fresh air, color, aroma,
music, fine arts, and architecture with respect to healing spaces and the management of childhood obesity. A bowl of fresh fruit, rather than a bowl of candy, to welcome patients enforces the message of healthful eating. Rewards of stickers, pencils or toys may be given to patients instead of the usual sweet treat. The environment should be child-friendly and promote comfort and caring, rather than anxiety or distress.
Fundamental Research: Hypothesis
Despite the growing prevalence of childhood obesity, there are few, if any, successful models of optimal healing for these children. We have chosen to focus on the therapeutic alliance, and hypothesize that creating optimal healing for patients and their family members through the therapeutic alliance will allow health care providers to initiate treatment, which ultimately results in a beneficial outcome. The treatment for obesity patients will receive all necessary materials and training to facilitate the development of a therapeutic alliance.
In addition to age and BMI, criteria for obesity may include a positive family history of obesity, increased blood pressure, increased total cholesterol levels, a large change in BMI, or concern about weight. An in-depth medical assessment of all children needs to be conducted. These criteria are based on the American Academy of Pediatric Expert Committee Recommendations.
Exclusion factors
Identifiable exogenous causes of obesity are rare. However, children with organic causes of
obesity, such as Prader-Willi syndrome, Turner syndrome, Cushing’s syndrome, or hypothyroidism will be excluded. Children with clinical depression or an eating disorder identified by the Diagnostic and Statistical Manual of Mental Disorders, 4th edition revised (DSM-IV-R) need specific treatment.
A managed care environment includes the primary care pediatrician and other health care
providers (e.g., nurses, dietitians, exercise trainers, behavior therapists, and psychologists) who work together with the patient/family. A multidisciplinary treatment program provides the most flexible, individualized, and effective strategy.
Even if a pediatrician in private practice had access to other health care providers, obtaining their
services is impossible for many patients because they lack insurance coverage. One study found that only 11% of pediatrician ordered treatments for obesity were reimbursed. The lack of reimbursement for treating obese patients is the leading barrier to providing care, even when health care providers acknowledge their leading role for overweight and obesity prevention and treatment efforts. Lack of reimbursement should never be a problem in the health management organization (HMO) setting.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
22
However, possible barriers to the managed care approach include whether or not and to what extent HMOs cover the treatment of obesity. Care varies from state to state and from health plan to health plan. In California, the basic language is that health plans provide all basic, medically necessary health services. But it is not clear what constitutes medically necessary service for an overweight or obese child, or even one at risk for overweight or obesity. Beyond surgery for morbid obesity, HMOs benefit packages are relatively silent on obesity management.
Outcome measures
Behavioral, medical, and weight goals as described by the American Academy of Pediatrics,
Committee on Nutrition will serve as major outcome measures. Dr’s Freedman and Stern point out the primary behavioral goal of a program to manage
uncomplicated obesity is healthy eating and daily safe physical activity and exercise, not achievement of ideal body weight. The medical goal is aimed at children with secondary complications of obesity. It includes the improvement or resolution of the complication such as abnormal blood pressure or lipid profile.
With respect to weight, the first step is maintenance of baseline weight, followed by prolonged weight maintenance that allows a gradual decline in BMI as the child grows in height. For children older than 7 years with BMIs between the 85th and 95th percentile and no secondary complications of obesity, prolonged weight maintenance is an appropriate goal.
However, weight loss is recommended if a child in this age and BMI range has a non-acute
secondary complication of obesity, or a BMI at the 95th percentile or above. An appropriate weight goal for all obese children is a BMI below the 85th percentile although such a goal should be secondary to the primary goal of health eating and activity.
In the context of a optimal healing it is important to determine what effect, if any, the therapeutic
alliance has on the treatment of childhood obesity, and the achievement of the health goals. It is important to determine what aspects of the therapeutic alliance are beneficial, and what aspects are potentially detrimental to the outcome. What tools are needed to help physicians feel more comfortable in assessing and treating children (and their family members) who are overweight or obese? Can these tools be standardized and serve as a template for others? The answers to these questions will help further the management of childhood obesity in the context of optimal healing.
Obesity Summary
The prevention, treatment, and long-term management of childhood obesity are serious
challenges facing health care professionals. Considering the high risk that an obese adolescent will become an obese adult and the high personal and societal cost of obesity, it is incumbent to examine creative solutions to this serious public health crisis. Designing an optimal healing for managing childhood obesity may provide some hope for children and their parents who are at risk for, or already suffering from overweight and obesity.
Dr’s Freedman and Stern belief that the solution to the obesity crisis will take a concerted effort
not only on the part of individuals and their family members, but schools, health care professionals, communities, local, state, and federal governments and regulatory agencies, professional and scientific organizations, the food industry and the media. There is not a simple solution to this complex problem, but if we can work to send a person to Mars, perhaps we can solve the problem of obesity here on earth.

AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
23
There is not doubt AquaDios-Med™ is the treatment of choice to manage obesity by teaching safe daily exercise of structured deep-water running. The Deep Strider Chamber is ideal for the treatment of the obese.
AquaDios-Med™ Deep Strider Chamber
Designed for people who cannot exercise due to injury, obesity, disability; this chamber is where structured Deep Water Running is taught.
AquaDios-Med™ Deep Strider Chamber
Note use of Proprietary Safety Handles in the teaching correct posture for Deep Water Running
Deep Strider Chamber – Note Multiple Jacuzzi Jets for Power Massage; numerous safety handles; various standing positions; Ergonomic design for comfort and safety.
The Deep Strider Chamber design is to accommodate severely handicapped patients whether it is due to accident, injury, diabetes, arthritis, obesity, age, or any disabling cause while it is also used for physical fitness and deep water running training for the athlete.
AquaDios-Med™ Deep Strider Chamber
Note - two large power jets at the very bottom pointing in the upward position. These jets assist the physically incapacitated or disabled to obtain the benefits of deep water movement and undulation.

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section X
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
Magic of the Mind Mind Body Medicine Practice
AquaDios-Med™ Proactive Preventive Medicine Experiential • DVD
Section X
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
5 pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Magic of the Mind
AquaDios-Med Proactive Preventive Medicine
Mind Body Medicine Practice By Dr. Alan Jensen
www.AquaDios.com [email protected]
310-897-5055 P.O. Box 2228
Malibu, CA 90265
Dr. Alan Jensen • Founder • CEO • Creator •
• AquaDios-Med™ •
Copyright © 1985 – 2008 – 2012 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California 90265
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
310•897•5055 www.aquadios.com [email protected] AquaDios-Med™ MBM PPM Copyright © 2005 – 2012 – 2013 2nd Edition
Mind-Body Medicine – Psychoneuroimmunology DVD - Video Please read the information below before using the MBM Videos
Please view videos to the end - credits for the full experience
Mind-Body Medicine Practices DVD
Individual genetics and the environment dictate how each of us becomes susceptible to disease; that is, the absence of ease (health) at the cellular level. Our immune systems are capable of overcoming very formidable dis-ease and health problems, even those as severe as cancer. At one extreme, medical research shows that with practiced, positive visualization, the immune system can rise to the challenge of stopping the aberrant cancer cell from reproducing. One of the simplest, most basic, and universally applicable self-training methods for creating positive effects is the use of a special spinning spiral.
For many years, a large number of scientific studies have shown a direct connection between the mind and the immune response and medically defined dis-ease, including cancer. A 1993 book titled The Type C Connection by L. Temoshok & H. Dreher identifies a series of studies in the early 1970s by Dr. Robert Ader that helped put mind/body science on the map.
Ader and his group found that by following a Pavlovian conditioning paradigm they
could condition a group of rats to suppress their immune response. Ader gave the rats a drug that suppressed their immune system at the same time they were fed saccharin- sweetened water. Later, when the rats were given only the sweet water, the immune functions plummeted, just as if they had been given the immune- suppressing drug.
Ader concluded the brain is involved in immunity. How else could a rat learn to suppress
its own immune system? Dr. Ader coined the term psychoneuroimmunology (PNI) to describe the mind/body connection affecting such dis-eases as cancer; and opened the door verifying the mind is a powerful healing tool and may in fact have unconsciously contributed to the disease, much like the sweetened water causing immune problems.
Mind-Body Medicine uses the power of thoughts and emotions to influence physical
health. Hippocrates wrote, "The natural healing force within each one of us is the greatest force in getting well." This is mind-body medicine in a nutshell. Mind Body Medicine is based on the doctor and patient recognizing the relationship of the body's innate healing potential, and the partnership of patient and healer in restoring the body to health.
Individual genetics and the environment dictate how each of us becomes susceptible to
disease; that is, the absence of ease (health) at the cellular level. Our immune systems are capable of overcoming very formidable dis-ease and health problems, even those as severe as cancer. At one extreme, medical research shows that with practiced, positive visualization, the immune system can rise to the challenge of stopping the aberrant cancer cell from reproducing. One of the simplest, most basic, and universally applicable self-training methods for creating positive effects is the use of a special spinning spiral. http://www.aquadios.com/dvd.html

2 AquaDios-Med™ - MBM - PPM Copyright © 2005 – 2012 – 2013 2nd Edition
By focusing one’s total attention on the spinning spiral while simultaneously receiving suggestions for relaxation, most people—young and old—are able to enter into this natural, positive state of empowerment and learn to use it to enhance their lives. This practice can enhance wellness, productivity, physical fitness and the elimination of dis-ease. To help people experience positive self-change using this special spinning spiral, a demonstration has been produced and exhibited on the AquaDios web site, and a DVD has been professionally produced.
This program combines narration and classical music to assist the participant in
accessing this positive state of relaxation. It is recommended that in the beginning you use these tools in uninterrupted privacy until you feel comfortable about your experience. Concentration and the Spinning Spiral
One of the most universally dramatic tools for achieving powerful concentration is the special spinning spiral. The spinning spiral shows most clearly how focused and responsive the mind can become with simple concentration on this rotating shape.
To achieve the greatest value from this practice, it is best to remain focused on the
spinning spiral throughout the exercise, except as instructed. At one point the auditory instructions ask you to look away at any object of choice. The object can be almost anything, but the experience is most profound when the object is small enough to be seen in its entirety in one glance, such as a lamp, a potted plant, a picture, or a painting on the wall. Some locations may have wall clocks, which are ideal. The Spinning Spiral Experience
To perform the practice, first focus your eyes on the center of the spiral. A common perceptual change is a fuzziness or waviness in the lines of the spiral. This is a positive sign that your mind is becoming more focused. Another common perceptual change may be the appearance of a yellowish, fluorescent-like fringe on the edges of the lines. As you continue to focus on the spinning form, you may occasionally perceive the spiral to grow larger, especially when looking toward the edges. It may even almost seem to come out at you.
While the spiral is spinning, you can give yourself the suggestion that the spinning shape is exhibiting three-dimensional effects. By suggesting to yourself that the spiral is a funnel or a whirlpool, you may experience these perceptions manifesting right before your eyes.
Now and again, the spiral may seem to be unwinding, much like the spring of a giant clock. Continued concentration on the spinning shape may also produce the appearance of dark rays spinning off the edges of the figure.
These are all positive signs that your mind is becoming progressively more
focused and your imagination and mental capacities are coming more under your control. As one suggestion while focusing on the spinning spiral, you might consider
telling yourself that you are in a spiral tunnel that is speeding away from you. Can you imagine yourself in a train traveling through a tunnel and looking out the rear window?

3 AquaDios-Med™ - MBM - PPM Copyright © 2005 – 2012 – 2013 2nd Edition
Whiling focusing on the spinning spiral, can you imagine yourself looking up at the top of a deep well? Can you allow yourself to feel as though you are sinking into the deep, spiral well as you continue to look up at the top? After experiencing these sensations, can you reverse this perception? Can you give yourself the suggestion that you are looking down at the bottom of a well and feel the experience of rising out of it?
From the moment you first began gazing at the spinning spiral, have you wondered about the possibility that your mind could become increasingly focused on positive suggestions, feelings, and sensations? Can you imagine how your life might improve by purposefully allowing yourself this kind of highly focused ability? Can you allow yourself to know that your mind can become increasingly powerful with each beat of your heart, with each blink of your eyes, especially thoughts for superior health and good will?
At some point during the practice, you can demonstrate to yourself that there has been a positive change within your perceptions. For a brief moment, look away from the spinning spiral at some particular object. Can you see how enjoyable your new experience, your new perceptions, can be? Do you see the changes in your perception as you gaze at that object? Inner Peace and Enhanced Living
As you continue to focus on the spinning spiral, you may be pleased to feel a sense of inner peace gradually coming over your body. As this inner peace grows, allow yourself to sink into a deep state of relaxation, and become even more deeply relaxed with each breath you take. Gradually, as you contemplate how much more relaxed you can become, permit your eyes to close. Can you allow your body to feel comfortably warm, especially your hands, as if you were in a nice, warm, comfortable bath or Jacuzzi?
After beginning to feel these states of relaxed comfort, allow yourself to internally count backward from 20 with each exhalation. You may also imagine this counting to be preparing you for your own positive self-suggestions, whatever they are or will be, as you become more empowered with your natural abilities to focus your mind on your health and welfare in all of your life’s pursuits.
For example, if you wish to lose weight, can you suggest to yourself that you will become satisfied with smaller amounts of more healthful food, and that you will learn to eat more slowly and to chew longer before swallowing?
If you wish to stop smoking, can you give yourself the suggestion that you will recognize the health hazards of smoke, nicotine, tars and other toxic debris found in the smoke of cigarettes? You might imagine recovering your early memories of how cigarette smoke made you cough, caused yours eyes to burn, and made you to feel irritated in the presence of this pollutant. You might then wonder how tobacco companies have been allowed to dupe the public about the health hazards of smoking for so many decades. You might even visualize yourself feeling independent and free of the urge to smoke by simply taking a deep breath of fresh air and exhaling until the urge passes.

4 AquaDios-Med™ - MBM - PPM Copyright © 2005 – 2012 – 2013 2nd Edition
If you are a student, can you suggest to yourself that you will easily and automatically focus on the most valuable information of your studies, both in lecture and your reading? You might imagine becoming automatically proficient at recalling information during tests.
If you are an athlete, can you visualize a specific level of performance that produces the results you want, and practice this imagery on a regular basis?
If you are having bouts of sleeplessness, can you conceive of suggestions to produce deep, healthful sleep—including peaceful and relaxing dreams—with each breath you take, as you prepare to enter the state of slumber? More Powerful Than You Know
Your mind is a far more powerful tool than you have ever been allowed to believe. It truly does have dominion over your body and your physical health. Allow yourself to learn the potential of your mind and develop your ability to bring positive states of being to your life.
The Mind-Body Medicine practices featuring the spinning spiral can be your gateway to these advanced abilities. The AquaDios web site and the Mind-Body Medicine DVD both feature two practices, one guided by narration by Dr. Alfred A. Barrios, the other with classical music only, so as not to distract from your own self-suggestions. Allow yourself to experience these wonderful states of mind and be well! The AquaDios-Med™ Philosophy
• EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING!
AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race
Copyright © 2008 – 2012 – 2013 2nd Edition AquaDios-Med™ • AquaDios Corp.
All rights reserved.
Respectfully,
Dr. Alan Jensen (Alan) Founder • CEO • Creator, AquaDios-Med™ http://www.aquadios.com/ A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing Phone 310-897-5055 - Email: [email protected] - P.O. Box 2228 Malibu, Ca. 90265

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California 90265
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
310•897•5055 www.aquadios.com [email protected]
AquaDios-Med™ - MBM - PPM Copyright © 2005 – 2012 – 2013 2nd Edition
Magic of The Mind
Name: Date: Reason for Treatment: Goal: Three Favorite: Colors Places: People: Events: Tastes: Experiences: Sensations: Sounds: Smells: Situations, places, events, people, behavior, animals, etc. you hate, despise, fear - love. Three Traumatic Events in Life following Birth, age: RECALL: Three Positive Events following Birth, age: RECALL:

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
P.O. Box 2228 • Malibu • California 90265
Dr. Alan Jensen • Founder • CEO • Creator • AquaDios-Med™ •
310•897•5055 www.aquadios.com [email protected]
Magic of the Mind
AquaDios-Med™ Proactive Preventive Medicine
AquaDios-Med™ Mind Body Medicine Practice
The AquaDios-Med™ Philosophy
• EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING! • AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race
Copyright © 2008 – 2012 – 2013 2nd Edition
AquaDios-Med™ • AquaDios Corp.
All rights reserved. Respectfully,
Dr. Alan Jensen (Alan) Founder • CEO • Creator, AquaDios-Med™ http://www.aquadios.com/ A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing Phone 310-897-5055 - Email: [email protected] - P.O. Box 2228 Malibu, Ca. 90265

1
End
AquaDios-Med™ Proactive Preventive Medicine Solution to Man - Made • Healthcare Crisis
Begin Proprietary Innovations Intellectual Property
AquaDios-Med™ Created By Dr. Alan Jensen
AquaDios-Med™ Proactive Preventive Medicine
Proprietary Innovations • Deep Immersion Chambers
Other Intellectual Property • Overhead Views
• AquaDios-Med™ • Medical Prototype
Main Exercise Chamber
Deep Strider Lounge Spa Chamber
Designed • Built • By Dr. Jensen
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination. - Albert Einstein

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section XI
The Health Care Crisis
Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
Expanded Research
Proprietary Innovations • Intellectual Property AquaDios-Med™
Created By Dr. Alan Jensen AquaDios-Med™ Proactive Preventive Medicine
Section XI
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
20 Pages
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Proprietary Innovations Intellectual Property
AquaDios-Med Created
By Dr. Alan Jensen
www.AquaDios.com
P.O. Box 2228 Malibu, CA 90265
Dr. Alan Jensen
• Founder • CEO • Creator • • AquaDios-Med™ •
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM 2nd Edition All Rights Reserved

2 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
AquaDios-Med™ Medical Prototype With multiple Deep-Water Immersion Chambers
The 98 “F” Degree Lounge Spa Chamber The 80 “F” Degree Deep Strider Chamber The 68 “F” Degree Main Exercise Chamber [Cold Chamber not shown]
• AquaDios-Med™ • Multiple • Immersion • Chambers
• AquaDios-Med™ Main Exercise Chamber • Deep Strider • Lounge Spa Chamber
Main Exercise Chamber >>>
• Proprietary Multiple • Depths
• Proprietary Flat Bottom Surfaces
• Proprietary Safety Handles
• Proprietary Dam Walls
• Proprietary Easy Access
• Proprietary Immersion • Chambers

3 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Proprietary Deep Water
• Main Exercise • Chamber • Proprietary Safety Handles
• Entire • Perimeter
• Swim Gym
• Proprietary Variable Depths
• Proprietary Flat Bottom Surface
• Multiple Jacuzzi Jets • Power Massage • Safety Handles
Proprietary Deep Strider Chamber Design • People Who Cannot Exercise • Injury • Where Structured Deep Water Running Taught To All People •
• Deep Strider Chamber • • Proprietary Safety Handles • Teaching Correct Posture • Deep Water Running Teaches patients how to perform Safe daily structured deep-water running.

4 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Proprietary
Deep Strider Chamber
Multiple Jacuzzi Jets
Proprietary Power Massage
Numerous Proprietary
Safety Handles
Various Standing Locations
Ergonomic Design
Comfort Safety
Lounge Spa Chamber
Multiple Depths
Jacuzzi Jets
Power Massage
Lounge Spa
Chamber
Multiple Proprietary
Handles
• Safety • Assist
• Power Massage
• All Body Areas

5 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
AquaDios-Med™ Lounge Spa Chamber
Multiple Depths • Jacuzzi Jets • Proprietary Safety Handles Massage • Head • Neck • Shoulders • Lower Back • Thighs • Knees • Calves • Ankles • Feet
AquaDios-Med™ Lounge Spa Chamber
Patients learn how to perform Safe Power Massage
with Proprietary Safety Handles

6 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
AquaDios-Med™ Proprietary Plenums
Proprietary Plenums Absolutely Necessary To
Supply Sufficient Water Pressure Forces For
Power Massage To Numerous Jacuzzi Jets
AquaDios-Med™ Proprietary Safety Handles

7 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
AquaDios-Med™ Proprietary Safety Handles
AquaDios-Med™ Proprietary Computer Power Center Controller for
Multiple Plenums and Numerous Jacuzzi Jets
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

8 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Dr. Jensen Demonstrating Curative - Healing Yoga Poses
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

9 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
AquaDios-Med™ Pictures – Graphs
Dr. Jensen Deep-Water Running in a Wet Vest Steve Scott Deep-Water Running
In a Wet Vest Correct Posture Deep-Water Running
The AquaDios-Med™ Philosophy • EXERCISE IS MEDICINE! • THE IMPAIRED BECOME REPAIRED! • YOU DON'T STOP EXERCISING BECAUSE YOU GROW OLD; • YOU GROW OLD BECAUSE YOU STOP EXERCISING!
AquaDios-Med™ is not a panacea; it's a reality waiting to be implemented for the human race

10 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Borg’s RATING OF PERCEIVED EXERTION (RPE)
0 nothing at all
1 very, very weak
2 very weak
3 weak
4 somewhat weak
5 moderate
6 somewhat hard
7 hard
8 very hard
9 very, very hard
10 maximal (all-out effort)
AquaDios-Med - Rehabilitation Pain
RATINGS OF PERCEIVED PAIN
0 nothing at all No Pain
1 very, very weak Minimal Discomfort
2 very weak Minor Pain
3 weak Experienced Discomfort
4 somewhat weak Low Grade Pain
5 moderate Tolerable Pain
6 somewhat hard Uncomfortable Pain (Safe) 7 hard Moderate Pain (Safe-Marginal)
8 very hard Severe Pain (UNSAFE)
9 very, very hard Unmanageable Pain (DANGEROUS)
10 maximal (all-out effort) - Intractable Pain (UNSAFE-RE-INJURY)
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination. - Albert Einstein

11 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
AquaDios-Med™ Dr. Alan Jensen
TABLE 2 • AEROBIC ACTIVITIES • ADVANTAGES • DISADVANTAGES ACTIVITY ADVANTAGES DISADVANTAGES RUNNING Convenient. Extremely hard on joints, muscles bones Provides aerobic benefits in short period of time Decreases flexibility.
Causes muscle imbalance. Low skill level required
Increases speed, endurance. Most of activity performed by lower body.
SWIMMING Reduced pressure on joints 80-90% of activity-performed bones. by upper body. Eliminates neuro- Possible ear - eye infections muscular trauma. Sinus - other problems Allows extended exercise High skill level required
Increases endurance. Pool - immersion water required CROSS- Many muscles involved. High altitude. COUNTRY Provides vigorous workout Cold. SKIING Limited season. Overload principle. Limited access. Increases endurance. High skill level required DEEP WATER Nearly all muscles involved. Pool or body of deep water required RUNNING Provides vigorous workout. Overload principle. Reduced pressure on joints, bones. Eliminates neuro-muscular trauma. Allows extended exercise. Provides aerobic benefits in short
period of time. Low skill level required. Maintains or increases flexibility. Prevents muscle imbalance. Increases speed, endurance.
Exercise is a weapon against Disease
The true sign of intelligence is not knowledge but imagination - Albert Einstein

12 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Isokinetic Contraction Isotonic Contraction
Eccentric Contraction Isometric Contraction
Controlled Breathing Through BRACEDVE:
a) Breathing e) Energy
b) Relaxation f) Detachment
c) Attention g) Visual Imagery
d) Concentration h) Equilibrium-Balance-Being Centered
Deep-Water Running Nearly All Muscles Involved Deep-water running exercise uses all the upper and lower body muscles -- the safest and best
aerobic exercise for developing cardiovascular capacity – also - best safest for muscular strength -- endurance because it is isokinetic exercise. Edward Fox, in Sports Physiology … From a physiology viewpoint, isokinetic training programs are the best for improving athletic performance ... Muscles can undergo four basic types of contractions: isokinetic, isotonic, eccentric, and isometric:

13 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Isokinetic Contraction Isokinetic - - same speed contractions are positive muscle contractions -- occur when a muscle is subjected to an even amount of tension at a constant speed over the full range of motion. Isokinetic activities maintain an equal amount of tension on the muscle throughout the range of motion. A bicep curl is performed in water at a constant speed using only the resistance of the water -- the muscle receives equal amounts of tension -- the more quickly the arm moves, the more resistance it encounters. Isotonic Contraction
Isotonic -- meaning same weight -- are positive contractions -- occurs when a muscle shortens under tension such as a bicep curl. Isotonic exercises require a weight that can be moved the full range of motion because the velocity of the weight carries it through the range where the muscles are otherwise too weak.
Eccentric Contraction Eccentric contractions -- muscles lengthen under
tension is a -- negative contraction -- opposite of isotonic contractions -- occurs when you lower the dumbbell from the shoulder to the starting position in a bicep curl -- takes effort to control the weight as it is lowered.
The more slowly the weight is lowered, the more pronounced the exercise becomes. Eccentric Contraction - A 50- pound weight is lowered slowly from the shoulder to the starting position.
Isometric Contraction Isometric -- same length contraction -- muscle is subjected to tension without changing length -- contraction occurs when you attempt to lift a weight that is too heavy to lift, as illustrated – you strain with the weight for several seconds before deciding -- you cannot lift it -- this straining period -- is an isometric exercise. The muscle does not move, but it is subjected to tension. A bicep curl is attempted with more weight than the subject can lift. The muscle is subjected to tension but does not move.

14 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Necessary Deep-Water Running Equipment WetVest • AquaJoggeer
AquaJogger Buoyancy Belt
Wet Vest – Hydrotone Structured Deep Water Running AquaJogger Buoyancy Belt >>>>
Deep Water Running Wet Vest
Structured Deep Water Running AquaJogger
Buoyancy Belt <<<<<
WetVest

15 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Correct Posture • Deep-Water Running • Graphs
Deep-Water Running Examples

16 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Aquatic Exercise Examples

17 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Advanced Aquatic Exercise Equipment
Hydratone Aquatic Equipment
Advanced Athlete
In-Water Aquatic Equipment

18 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Isokinetic resistance
Isokinetic resistance is an even opposition to power ratio, it builds the most durable, elastic and strong connectivity for muscle to bone.
Sustained vigorous intense power water running is the safest way to build physical fitness and both muscle and skeletal strength. It is the only exercise possible when injured; making it the safest exercise for all walks of life. Physiologists recognize isokinetic activity as a speed – strength - power relationship
As speed of movement in the water is accelerated a certain level of strength is required and this repeated action builds Isokinetic resistance muscle power --
Exercise is a weapon against Disease The true sign of intelligence is not knowledge but imagination - Albert Einstein

19 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Equipment Needed • Deep-Water Immersion Running AquaJogger • Wet Vest • Hydrotone
ISOKENITIC PURPOSE See picture >>>
Wet vest is a lightweight, snug fitting, training aid for superior conditioning and fitness specifically designed for deep-water exercise. During immersion it's design comfortably allows total freedom of movement while keeping the head above water for easy breathing and visibility. There is no risk of injury because there is no impact trauma in deep water. Aqua-Jogger Belt – see picture>> Each movement is isokinetically opposed by water's natural soothing resistance. It takes about 3 times more energy to run in deep water compared to dry land. Superior conditioning with increased cardiovascular safety is possible because during immersion heart rate averages are around 10 to 20 beats less per minute. Waters added resistance requires more neuromuscular activation at the lower back, stomach wall, upper back and chest to maintain the correct walking-running position.
STRUCTURED DEEP WATER RESISTANCE EXERCISE
The Wet Vest or Aqua-Jogger allows body immersion up to the neck in a safe and comfortable manner. Joints and muscles can then become easily aligned. During immersion active exercise motion takes place with no pressure or distress on the body. Muscles are soothed and pain and fatigue are reduced while healthy aerobic cardiovascular strengthening and endurance are stimulated. Structured Deep Water Resistance Exercise-running Physiotherapy is safe and has virtually no disadvantages when use of the WET VEST is integrated with practical assistance, Behavior Medicine, and Applied Clinical Hypnosis for creative healing and performance imagery.
Physiologist’s rate benefits of Deep Cool water exercise Highest!
Exercise physiologists rate benefits of structured deep cool water resistance exercise while immersed to the neck highest of all physical activities because of the following facts: ***Approximately 90% of the major muscle groups are activated resulting in superior cardiovascular conditioning; ***arterial venous difference allows a greater volume of oxygen consumption; ***bone mass density strength and regeneration increases; ***lungs vital air capacity increases; ***lactic acid is higher, dissipates faster; ***at the same RPE, rate of perceived exertion, heart rates are 10 to 20 beats less per minute in water than dry land, heart muscle can grow stronger during exertion ; ***elimination of high body heat, and neuromuscular trauma to joints, ligaments, tendons, muscles; ***hemoglobin oxygen in the blood is increased; improved body tissue oxygen extraction from blood; ***water resistance increases strength, endurance, balance, coordination, and flexibility.
Exercise is a weapon against Disease

20 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Evidence Based • AquaDios-Med™, PPM Deep-Water Immersion • Preventive Medcine AquaDios-Med™, PPM is evidence based, research shows immersion to the neck in multiple
hot – cold water temperatures together with safe sustained vigorous physical activity, in cool water, natural healthy physiologic changes are generated that cannot be duplicated in any other way. These immersions to substantially increase the speed of the body’s ability to remove metabolic waste -- to improve cardiac function – to lower blood pressure – to learn pain management -- to maximize body healing and rebuilding tissues. These natural physiological changes result in the elimination of toxins that cause disease and inhibit the natural healing processes of the body. AquaDios-Med™, PPM is designed to be the safest, quickest, most complete natural detoxification procedure for complete, total rejuvenation, healthy homeostasis and a foundation to achieve peak health, wellness and balance
Recently research physiologists acknowledged cold water immersion to the neck boosts the
immune system because, in simple terms, this purposeful sudden and drastic cold water immersion temperature change represents an assault that fools the body to significantly increase white blood cell counts and several other positive factors that maximize immune system function. Cold water immersion is a designed stressor to automatically stimulate neurotransmitter’s to produce endorphins, the body’s natural analgesics or pain killers. Endorphins also create a euphoric natural high accompanied by a positive and energizing outlook on life. Simultaneously the parasympathetic nervous system, releases dopamine and serotonin, these neurotransmitters are responsible for rest and repair which further increases positive immune system function.
Current research shows hot water immersion brings a stable balance to the autonomic nervous system and the sympathetic nervous system, similar to the process of meditation and associated with a reduction in the risk of cardiovascular disease, improved memory, enhanced cognitive processes and increased concentration; this means heart rate, digestion, respiration, salivation, circulation, calm and sexual arousal are normalized
Combined Hot Cold Immersion • Positive Blood Transformation
Hot water immersion brings blood to the surface while cold immersion moves blood to your
organs; these immersion extremes effortlessly cause the heart to increase blood flow – for healing. These alternating immersions help to flush blood circulation pushing blood through all the capillaries, veins and arteries; this exfoliates skin and flush impurities from it, helping complexion and some say it stops cellulite. Evidence shows the General Adaptation Syndrome at work – the body adapts to the hot - cold immersions with repeated exposure and this improves circulation, particularly to the extremities. Researchers also found increased production of testosterone and estrogen in men and women respectively, enhancing libido in both sexes; these hormones also play an important role in fertility. Cold water immersion exercise makes the body work twice as hard to keep warm and burns more calories in the process, a benefit for weight control -- for this exercise, fat is your body’s primary source of energy and the increased work rate will increase your metabolism in the long run
Colder water immersion 64° • 68° F • Coldest water immersion 51° • 58° F •Accelerates Healing
Physiologists confirm Cool – Cold water immersion 68 to 72 degrees F triggers the body to
increase hemoglobin oxygen which improves body tissue oxygen extraction from blood, this allows more rapid – complete cell production with a high density lipoprotein increase to reduce arteriosclerosis -- the heart is stronger with better blood supply with increased stroke volume due to the effects of immersion. Further research shows Colder Water immersion 48° to 58° F accelerates hemoglobin oxygen, the blood's oxygen transportation and extracts even more oxygen from the blood.

21 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Another physiological benefit of deep-water immersion exercise is that 80-90% of the major muscles groups are used -- especially the gluts, quadriceps and hamstrings to improve posture. There is a total blood volume increase for better oxygen transport; Vital air capacity of the Lungs increases to improve longevity; Warm to Hot water immersion dilates vessels, engorges blood, and accelerates flexibility, mobility; there is No Impact Trauma; Physical movement in the water requires Isokinetic muscle contractions -- an even tension, constant speed, full range of motion – this is the strongest most durable connective tissue and helps reflexes, while quicker movement’s increases water resistance. Water running in Cool water immersion is a Full regime of cardiovascular fitness providing joint motion, flexibility, strength, balance, and coordination. Colder Water Immersion from 51° – 68° F has a powerful healing capacity, but utilized most often only by athletes.
Historical Research • Deep-Water Immersion • Temperature • Therapeutics Research on the cultural use of Deep-Water Immersion Therapy shows the evolution from
before 2000 B.C. For thousands of years Deep-Water Immersion Therapy has been a part of cultures around the world. Even in ancient times the distinctive thermodynamic properties of Water, with its markedly different therapeutic effects at different temperatures has been known and applied for healing.
Hot water is above body at temperature 100° to 103° F, is stimulating, raises the body temperature slightly, very relaxing and dispersing, especially to the muscles, joints and blood vessels. It opens the pores, induces sweating, and penetrates the skin and muscles quite deeply. Hot water can also ripen latent boils, abscesses or skin eruptions and bring them to the surface for release. Hot water draws the body's circulation outwards, opening up the pores and capillaries. Prolonged hot water immersion is not recommended.
Warm water 96° – 99° F, about body temperature or slightly cooler, is gently relaxing, stimulates appetite – digestion and activity of the digestive organs when done about an hour before eating. Warm water, particularly water that's almost lukewarm -- called tepid is best for general bathing purposes -- warm water is harmonizing and balancing.
Cool water 82° – 88° F is good for soothing heat and inflammation, and for cooling the body on
hot summer days; cool water immersion is good for bringing down fevers. Cold water immersion 72° – 74° F for short periods of time, act as a bracing, stimulating tonic;
after bathing in the hot water pools, Romans would go for a quick dip in the frigidarium, or cold water bath, to brace their skin and close back up their pores.
Sebastian Kneipp a German priest in the 1800s is recognized as the originator – promoter of
cold water therapy in the modern Western world. He was pronounced terminally ill with lung disease and his self-treatment included daily baths in the icy Danube River for just a few minutes; in a year he was cured. He developed a system of hydrotherapy with treatments of alternating hot and cold water therapies for many different health complaints. Today the Kneipp Association has a network of treatment and training centers throughout Europe and in South Africa.
Hot water 100° – 103° F relaxes, disperses, and thrusts blood circulation out to the body's
exterior -- cold water 72° – 74° F stimulates, consolidates and shunts blood circulation inwards towards the core and internal organs. Cold water constricts the blood vessels, stimulates circulation, digestion and metabolism, and awakens the appetite, having an exhilarating effect. Cold water compresses reduce swelling and inflammation. Passive Cold water immersion should only be for a maximum of about 3 to 4 minutes.
22 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved
Alternating Hot and Cold water immersions is a particularly powerful technique. The hot water draws old, stagnant blood out of the internal organs or the body’s interior, and the cold water drives fresh blood back into the internal organs and the body's core. With alternating hot and cold immersion, the circulation is powerfully increased, the affected area begins to throb and pulsate -- a sign of healing and regeneration; Hot immersion -- about 3 to 4 minutes -- followed by cold immersion of 1 to 2 minutes. Repeat this two or three time or more, but always end on a short hot or warm application to remove or neutralize any remaining chills.
Summation • AquaDios-Med™ Proactive Preventive Medicine • Design
Deep-Water Running Immersion Therapy • Mind Body Medicine
The evidenced based AquaDios-Med™, PPM is a robust design that integrates the safest, most well established, vigorous deep-water immersion exercise, known to maximize immune system function, together with the most robust deep-rooted and proven physiological self-regulation , a process that interlinks psychological, autonomic, immune, and nervous system functioning.
These physical and mental exercise programs rely on natural positive occurring human events, that of scientific physiology together with that of identified Altered State of Conscious or ASC; scientific research shows all people naturally experience ASC daily – the two activities combined produce a natural positive state of psychophysiological self-regulation.AquaDios-Med™ proactive preventive medicine design is to facilitate and produce a lasting homeostatic bio-physiology balance that eliminates the dependence on and the abuse of biopharmaceuticals, many surgeries and hospital stays.
Research shows structured deep-water exercise while immersed to the neck in water is the
safest, most well established, proven vigorous exercise because this exercise naturally produces positive physiologic changes that accelerate the removal of metabolic waste, improve cardiac function, and lower blood pressure, all of which accelerate the body in rebuilding and healing the tissues to maximize healing, rehabilitation and well-being.
• END
• Solution to Man-Made Healthcare Crisis Is
AquaDios-Med™ Proactive Preventive Medicine
Inner Mental Training • Positive Psychology • Mind Body Medicine
Psychoneuroimmunology • Clinical Hypnosis
Exercise Is Medcine The true sign of intelligence is not knowledge but imagination - Albert Einstein

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section XII
The Health Care Crisis Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
References • Expanded Research
Healthcare Crisis • Manufactured • Man-Made Deep-Water Running • Aquatic Exercise
Physiology Changes • Deep-Water Immersion Psychoneuroimmunology PNI • Mind Body Medcine MBM •
Preventive Medcine • Rehabilitation • Pain Management • Heart Disease • Obesity • Diabetes • Cancer •
• Placebo Analgesia • Gerontology • Aging • 79 Pages
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

1 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Partial List of References • XI • 79 Pages The Health Care Crisis
Is Man-Made • Manufactured The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
********************************************************************************* Partial List References: Deep-Water Running • Psychoneuroimmunology PNI • Mind Body Medcine MBM • Preventive Medcine • Rehabilitation • Pain Management • Obesity • Diabetes • Heart Disease • Cancer • Physiology during deep-water immersion • Placebo Analgesia • Gerontology-Aging; and Much More ********************************************************************************** Abraham, Edward A. Freedom From Back Pain. Emmaus, PA: Rodale Press, 1986. Abraham, A., Szezerba, J., & Jackson, M. (1994). The effects of an eleven week aqua aerobic program on relatively inactive college age women. Medicine and Science in Sports and Exercise, 26, S103 (Abstract). ACOG Exercise Programs. "American College of Obstetricians and Gynecologists Guidelines.” Los Angeles, 1984. Adverse Childhood Experiences (ACE) Study Ader, R. Psychoneuroimmunology - Academic Press, 1981 New York, Ader, R. D.L. Felten and N. Cohen, Psychoneuroimmunology - (Third Edition), Academic Press, Editors: Vol. 1, 727 pp., Vol. 2, 856 pp Ader, R. - D.L. Felten, & N. Cohen. Innervation of lymphoid tissue. In (Eds.) Psychoneuroimmunology, 2d ed. Pp. 27-69. San Diego: Academic Press Adler R. The Crystal Ball of Chaos. Nature. U) 01; 414(6863):480-481. Ader R. Behavioral conditioning and immunity. In: Fabris N, Garaci E, Hadden J, Mitchison NA, eds. Immunoregulation. New York: Plenum Press, 1983:283Ð313. Ader R, Cohen N. Behaviorally conditioned immunosuppression. *46. Andrews SE, Blumenthal TD, Flaten MA. Effects of caffeine and caffeine-associated stimuli on the human startle eye blink reflex. Pharmacol Biochem Behav 1998; 59:39Ð44. Agress, Clarence M. Energetics. New York: Gossett & Dunlap, 1978. Aikens JE, Kiolbasa TA, Sobel R. Psychological predictors of glycemic change with relaxation training in non-insulin dependent diabetes mellitus. Psychother Psychosomatic 1997; 66: 302Ð306. Aldana S. Financial impact of worksite health and quality of methodological evidence. Art of Health Promotion, 2:1Ð8.

2 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Aldana S. Financial impact of health promotion programs: A comprehensive review of the literature. Am J Health Promot 2001;15:296-320. Aldana S. Financial impact of worksite health promotion and methodological quality of the evidence. Am J Health Promot 1998;2:1Ð8. Al-Delaimy WK, Manson JE, Solomon CG, et al. Smoking and risk of coronary heart disease among women with type 2 diabetes mellitus. Arch Intern Med 2002; 162:273Ð279. Alexander CN, R.P., Orme-Johnson DW, Schneider RH, The Effects of Transcendental Meditation Compared to Other Methods of Relaxation and Meditation in Reducing Risk Factors, Morbidity, and Mortality. Homeostasis in Health and Disease. 35: p. 243-63. \ Aleccia, JoNel - Health writer, MSNBC, Patients still stuck with bill for medical errors - 11 states waive fees for worst mistakes, but most will charge you or insurer - Feb. 29, 2008 - National Quality Forum. Allen DA. Measuring rehabilitation outcomes for infants and young children. In: Fuhrer MJ, ed. Rehabilitation Outcomes: Analysis and Measurement. Baltimore: Brookes, 1987:185Ð195. Allen JK, Scott LB. Alternative models in the delivery of primary and secondary prevention programs. J Cardiovasc Nurs 2003; 18:150Ð157. Alhnannova K. Weigl E. Stress proteins: nomenclature, division and functions. Bionred Pap Medfic Utiv Palachk Olonouc Check Repub 2001; 145(2):39-47. Altan L, Bingol U, Aykac M, Koc Z, Yurtkuran M: Investigation of the effects of pool-based exercise on fibromyalgia syndrome. Rheumatol Int 2004, 24:272-277. Alternative medicine: Expanding medical horizons. A report to NIH on alternative medical systems and practices in the United States. Chantilly, VVA: Workshop on Alternative Medicine; 1992 Sept. 14-16.1992. Amanzio M, Pollo A, Maggi G, Benedetti F. Response variability to analgesics: A role for non-specific activation of endogenous opioids. Pain 2001; 90:205Ð215. Amanzio M, Benedetti F. Neuropharmacological dissection of placebo analgesia expectation-activated opioid systems versus conditioning-activated specific subsystems. J Neurosci 1999; 19:484Ð494. American Academy of Pediatrics, Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome. Clinical practice guideline: Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002;109:704Ð712. American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc 1998;30: 975–91.

3 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
American College of Sports Medicine (ACSM) (2006). ACSM’s Guidelines for Exercise Testing and Prescription, 7th edition. Baltimore MD: Lippincott Williams & Wilkins. American College of Sports Medicine. (2006). ACSM’s Guidelines for Exercise Testing and Prescription, 7th Edition. Philadelphia, PA: Lippincott Williams & Wilkins. American College of Sports Medicine: Guidelines for Exercise Testing and Prescription, Ed 5. Baltimore, Williams & Wilkins, 1995, American Journal of Preventive Medicine, the Association of Teachers of Preventive Medicine and the American College of Preventive Medicine, Elsevier Science - a forum for the communication of information, knowledge and wisdom in prevention science, education, practice and policy American Physical Therapy Association. Aquatic Physical Therapy: An APTA Fact Sheet. Alexandria, VA. American with Disabilities Act (1990). Pub.L.No. 101-336,42 U.S. Online document at: www.ada.gov American Academy of Pediatrics, Committee on Communications. Children, adolescents, and television. Pediatrics 1995; 96:786Ð797. American College of Physicians-American Society of Internal Medicine (ACP-ASIM), "Statement for the Record of the Ways and Means Health Subcommittee Hearing on the Nation’s Uninsured", April 4, 2001. (http://www.acponline.org/hpp/ways_means.htm) American Heart Association. Heart Disease and Stroke Statistics—2006 Update. Dallas, Texas: American Heart Association, 2006. Hoyert DL, Heron MP, American Heart Association. Heart Disease and Stroke Statistics Ñ2003 Update. Dallas: American Heart Association, 2003. American Journal of Preventive Medicine May 1998; 14(4): 245-258 Am J Sports Med, Vol 21, No1, 1993 Andersen RE, Crespo CJ, Bartlett SJ, Cheskin LJ, and Pratt M. Relationship of physical activity and television watching with body weight and level of fatness among children: results from the Third National Health and Nutrition Examination Survey. JAMA 1998;279:938Ð942. Anderson DA, Wadden TA. Treating the obese patient: Suggestions for primary care practice. Arch Fam Med 1999;8:156Ð167. Anderson RN. Deaths: Leading Causes for 1999. National Vital Statistics Reports, Vol 49, No. 11. Hyattsville, MD: National Center for Health Statistics, 2001. Anderson JW. Fiber and health: An overview. Am J Gastroenterol 1986; 81:892Ð897. Anderson, J.K. (1985). Hunting in the Ancient World. Berkeley, CA: University of California Press.

4 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Anderson, RA, Cheng N, Bryden NA, et al. Beneficial effects of chromium for people with diabetes. Diabetes 1997; 46: 1786Ð1791. Antman EM, Braunwald E. Acute myocardial infarction. In: Braunwald E, Zipes DP, Libby P, eds. Heart Disease. A Textbook of Cardiovascular Medicine, 6th ed. Philadelphia; WB Saunders, 2001:1115. Antonwsky A. Unraveling the Mystery Of Health. How people manage stress and stay well. San Francisco, California: Jossey-Bass; 1987. Appenseller, Otto and Atkinson, Ruth. Sports Medicine. Baltimore-Munich: Urban & Schwarzenberg, 1983. A Profile of Medicare: Chartbook 1998, U.S. Health Care Financing Administration; May 1998, p. 27. Arborelius, M., Balldin, U. I., Lilja, B., & Lundgren, C. E. G. (1972). Hemodynamic changes in man during immersion with the head above water. Aerospace Medicine, 43, 592-598. Armstrong K, Kerns KA. The assessment of parent needs following pediatric traumatic brain injury. Pediatr Rehabil 2002;5:149Ð160. Aronne LJ. Treatment of obesity in the primary care setting. In: Wadden TA, Stunkard AJ, eds. Handbook of Obesity Treatment. New York: Guilford Press, 2002:383Ð394. Asher, Anne - About.Com a part of the New York Times 2006 “Back Pain and Deep water running” Astrand, Per-Olof and Rodahl, Kaere. Textbook of Work Physiology. 3rd ed. New York: McGraw-Hill Book Co., 1986. Assis, Marcos Renato, et al. “A randomized controlled trial of deep water running: Clinical effectiveness of aquatic exercise to treat fibromyalgia.” Arthritis and Rheumatism. 55.1 (Feb. 2006): 57-65. Association of Workplace Health-Promotion Programs, U.S. Department of Health and Human Services. 1999 National Worksite Health Promotion Survey. Northbrook, IL: William M. Mercer, 2000. Astin JA. Why patients use alternative medicine: Results of a national study. JAMA 1998:279(19):1548.1553. Acad Political Soc Sci. 2002:583:2943. Astin, J.A., Mind-body therapies for the management of pain. Clin J Pain, 2004. 20(1): p. 27-32. Astin, J.A., et al., Mind-body medicine: state of the science, implications for practice. J Am Board Fam Pract, 2003. 16(2): p. 131-47. Astin, J.A., et al., Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum, 2002. 47(3): p. 291-302. Arthritis and Rheumatism. 55.1 (Feb. 2006): 66-73.

5 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Aubrey, Coult. "Jaworski: This is Dallas; I'll Play With Soreness." The Morning Call, 21 November 1985. Aus J Sci Med Sport, Vol 23, No 1, pp13- 22, 1990 Avellini, B. A., Shapiro, Y., & Pandolf, K. B. (1983). Cardio-respiratory physical training in water and on land. European Journal of Applied Physiology and Occupational Physiology, 50, 255-263. Avellini BA, Shapiro Y, Pandolf KB: Cardiorespiratory physical training in water and on land. Eur J Appl Physiol 1983; 50: 255-63. Avellini BA, Shapiro Y, Pandolf KB. Cardio-respiratory physical training in water and on land. Eur J Appl Physiol Occup Physiol 1983;50:255–63. Awbrey B. J., Dye K. K. Plunging into aquatic exercise: Walking in Water. Training Conditioning, 1996. Ayres, Stephen M. M.D.; Health Care in the United States: The Facts and the Choices. Chicago and London: American Library Association: 1996, Physicians for a National Health Plan. Ayurvedic Interventions for Diabetes Mellitus: A Systematic Review. Summary, Evidence Report/Technology Assessment: Number 41. AHRQ Publication No. 01-E039, June 2001. Agency for Healthcare Research and Quality, Rockville, MD. Online document at: www.ahrq.gov/clinic/epcsums/ayurvsum.htm. Accessed December 26, 2003. Badia X, Roset M, Montserrat S, Herdman M, and Segura A: The Spanish version of EuroQol: a description and its applications. European Quality of Life scale. Med Clin (Barc) 1999, 112(Suppl 1):79-85. Bandler R, Grinder J. Trance-formations. Mohab, Utah: Real People Press; 1981. Bandura A, Locke EA. Negative self-efficacy and goal effects revisited. J Appl Psychol 2003;88:87Ð99. Bankhead, Charles Staff Writer, MedPage Today; Published: February 22, 2008 Bandler R, Grinder J. Frogs to Princes. Mohab, Utah: Real People Press; 1979.Archives Web Forum Barber, Ph. D. Joseph - Adrian, Ph. D Cheri Psychological Approaches to the Management of Pain BRUNNERlMAZEL Bates A., Hanson N. Aquatic Exercise Therapy. Philadelphia. W. B. Saunders & Company, 1996. Baretta R., Robergs, R. Physiological Adaptations to a 14 Week Deep Water Exercise Program. Aquatic Physical Therapy Report: Vol. 3, 1995.

6 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Barnes, P.M., et al., Complementary and alternative medicine use among adults: United States, 2002. Adv Data, 2004(343): p. 1-19. Barrow, H.M. and Brown, J.P. (1988). Man and Movement: Principles of Physical Education. 4th Ed. Philadelphia Lea & Febiger. Barrows, K.A. and B.P. Jacobs, Mind-body medicine. An introduction and review of the literature. Med Clin North Am, 2002. 86(1): p. 11-31. Barlow SE, Dietz WH. Obesity evaluation and treatment: Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and Services Administration and the Department of Health and Human Services. Pediatrics 1998;102:E29. Barlow SE, Trowbridge FL, Klish WJ, Dietz WH. Treatment of child and adolescent obesity: Reports from pediatricians, pediatric nurse practitioners, and registered dietitians. Pediatrics 2002;110:229Ð235. Barnard RJ, Jung T, Inkeles SB. Diet and exercise in the treatment of NIDDM. Diabetes Care 1994; 17:1469Ð1472. Barnes, P.M., et al., Complementary and alternative medicine use among adults: United States, 2002. Adv Data, 2004(343): p. 1-19. Barrios, PhD. Alfred A. Toward Greater Freedom and Happiness, Self-Programmed Control Press, PO Box 49939 Los Angeles Ca. 90049. Batey DM, Kaufnmann PG, Raczynski JM, Hollis JF, Murphy JK, Rosner B, Corrigan SA, Rappaport NB, Danielson EM, Lasser NL, Kuhn CM. Stress management intervention for primary prevention of hypertension: Detailed results from Phase l Trials of Hypertension Prevention (TOHP-l). Ann Epidemiol 2000; 10:45Ð58. Beauregard TR. Driving a more effective health care market by putting consumers behind the wheel. Manag Care Q 2001;9:1Ð4. Beckman PJ. Providing family-centered services. In Batshaw ML, ed. Children with Disabilities, 5th ed. Baltimore: Paul H. Brookes Publishing Co., 2002:683Ð691. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561–571. Beck, A.T., Cognitive Therapy and the Emotional Disorders. 1979, New York: International Universities Press. Beck, A.T., Cognitive Therapy and the Emotional Disorders. 1979, New York: International Universities Press. Becker BE: The biologic aspects of hydrotherapy. J Back Musculoskel Rehabil 1994;4:255-64.

7 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Beecher HK. The powerful placebo. JAMA 1955; 159:1602Ð 1606 analysis. Int J Nurs Studies 1998;35:322Ð 329. Beinfield H, Korngold E. Between Heaven and Earth: A Guide to Chinese Medicine. New York, NY: Ballantine Books; 1991. Bell I, Caspi 0. Schwartz G, et al. Integrative medicine and systemic outcomes research: Issues in the emergence of a new model for primary health care. Arch Intern Med 2002:162(2):133-140. Benedetti F, Arduino C, Amanzio M. Somatotopic activation of opioid systems by target-directed expectations of analgesia. J Neurosci 1999; 19:3639Ð3648. Benedetti F, Amanzio M, Baldi S, Casadio C, Maggi G. Inducing placebo respiratory depressant responses in humans via opioid receptors. Eur J Neurosci 1999; 11:625Ð631. Benedetti F, Amanzio M, Baldi S, et al. The specific effects of prior opioid exposure on placebo analgesia and placebo respiratory depression. Pain 1998; 75:313Ð319. Benedetti F, Amanzio M. The neurobiology of placebo analgesia: From endogenous opioids to cholecystekinin. Prog Neurobiol 1997; 52:109Ð125. Benedetti F, Amanzio M, Maggi G. Potentiation of placebo analgesia by proglumide. Lancet 1995; 346:1231. Benedetti F. The opposite effects of the opiate antagonist naloxone and the cholecystokinin antagonist proglumide on placebo analgesia. Pain 1996; 64:535Ð543. Bennett RM, Clark SR, Goldberg L, Nelson D, Bonafede RP, and Porter J, et al. Aerobic fitness in patients with fibrositis: a controlled study of respiratory gas exchange and 133xenon clearance from exercising muscle. Arthritis Rheum 1989;32: 454–60. Bennett RM. Beyond fibromyalgia: ideas on etiology and treatment. J Rheumatol Suppl 1989;19:185–91. Bennett RM, Clark SR, Goldberg L, Nelson D, Bonafede RP, and Porter J, et al. Aerobic fitness in patients with fibrositis: a controlled study of respiratory gas exchange and 133xenon clearance from exercising muscle. Arthritis Rheum 1989;32: 454–60. Benson H. The relaxation response. New York: Avon Books; 1975. Benson H, Beary JF, Carol MP. The relaxation response.Psychiatry.1974;37:37-46. Bennett-Goleman, T. 2001. Emotional alchemy: How the mind can heal the heart. Nevada City, CA: Harmony Books. Benson, H. & M.Z. Klippur. 2000. The relaxation response. Rev. ed. New York: Harper Torch.

8 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Benson, H., The relaxation response: therapeutic effect. Science, 1997. 278(5344): p. 1694-5. Benzein E, Saveman BI. One step towards the understanding of hope: A concept Bergmann J-F, Chassany O, Gandiol J, et al. A randomised clinical trial of the effect of informed consent on the analgesic activity of placebo and naproxen in cancer patients. Clin Trials Metaanal 1994; 29:41Ð47. Berkman L. Social networks and health: the bonds that heal. In: Tarlov A, St. Peter R. eds. The Society and Population Health Reader. New York: The New Press: 2000.259277. 1999:180:875-882. Berton CT. What is the future of health promotion in HMOs? Am J Health Promot 1987;1:24 - 27. Berryman, J.W. (1995) Out of Many, ONE: A History of the American College of Sports Medicine. Champaign, IL: Human Kinetics. Berson, Dvera. Pain-Free Arthritis. New York: Simon & Shuster, 1978. Bilchik GS. A better place to heal. Health Forum J 2002; 7: 10Ð15.
Billings L. Schwartz I. Exciting chaos with noise: Unexpected dynamics in epidemic outbreaks. /Mat11 Bid 2002:44(1):31-48. Biosciences of institutes - department OF Physical Education - São Paulo State University - Rio Claro, frame. Bishop PA, Frazier S, Smith J, Jacobs D: Physiologic responses to treadmill and water running. Physician Sportsmed 1989; 17: 87-94. Bilkis, Michael R. MD, MSC; Kenneth A. Mark, MD, Mind-Body Medicine Practical Applications in Dermatology, 1998 Blanchard K, Carlos JP, Randolph A. The Three Keys to Empowerment. San Francisco: Berrett-Koehler Publishers, 1999. Blanche, W., Evans, W., Cureton, K. J., & Purvis, J. W. (1978). Metabolic and circulatory responses to walking and jogging in water. Research Quarterly, 49, 442-449. Blalock JE. The syntax of immune-neuroendocrine communication. Immunol Today 1994; 15:504Ð511. Blackburn GL, Copeland T, Khaodhiar L, et al. Diet and breast cancer. J Womens Health 2003; 12:183Ð192. Blaser P (1993). Characteristic of the co-ordination structure of cyclic movements when more differently psycho physical demand in swimming (CO surgery OF cyclic movements with difference velocity under psycho engine loads in swimming). German sport university Cologne: Research report

9 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Blendon, Robert J. - Kim, Minah - and John M. Benson; "The Public Versus The World Health Organization on Health System Performance"; Health Affairs; Vol. 20: No. 3; (May/June 2001); pp. 10-20. Bloom M: Pooling your efforts. Runner's World 1991: August: 41-5. Boone, Tommy. "Exercise Prescription For Cardiac Patients." Sports Medicine, 3: 157. Boonen A, van den Heuvel R, van Tubergen A, Goossens M, Severens JL, van der Heijde D, van der Linden S: Large differences in cost of illness and wellbeing between patients with fibromyalgia, chronic low back pain, or ankylosing spondylitis. Ann Rheum Dis 2005, 64:396-402. Borg GAV. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982;14:377-81. Borg G Psychophysical bases of perceived exertion. Medicine and Science in Sport and Exercise, 1982 - 14:377-381. Borg, G. (1998). Borg’s perceived exertion and pain scales. Champaign IL: Human Kinetics. Br J Sports Med, Vol32, pp44-48, 1998 Borg G: Perceived exertion: a note on "history" and methods. Med Set Sports Exercise 1973: 5: 90-3. Borg GV: Psychophysical basis of perceived exertion. Med Sci Sports Exercise 1982; 14: 377-87. Bouchard, C., and Despres, J.-P. (1995). Physical activity and health: Atherosclerotic, metabolic, and hypertensive disease. Research Quarterly for Exercise and Sport, 66, 268-275. Boule NG, Haddad E, Kenny GP, et al. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: A meta-analysis of controlled clinical trials. JAMA 2001; 286: 1218Ð1227. Boudreaux ED, O’Hea E, Chausuk R. Spiritual role in healing: An alternative way of thinking. Prim Care 2002; 29:439Ð454. Bowman SA, Gortmaker SL, Ebbeling CB, Pereira MA, Ludwig DS. Effects of fast-food consumption on energy intake and diet quality among children in a national household survey. Pediatrics 2004;113:112Ð118. Boxer GH, Bauer AM, Miller BD. Obesity-hypoventilation in childhood. J Am Acad Child Adolesc Psychiatry 1988;27: 552Ð558. Brennan, D. K. Aqua running, no pain, much gain. Master Sports. 1992. Brennan DK, Wilder RP: Aquarunning: An Instructor's Manual. Houston, TX, Houston International Running Center, 1990. Breslow L. From disease prevention to health promotion, JAMA 1999; 281 :1030Ð1033. Brewis A. Biocultural aspects of obesity in young Mexican Schoolchildren. Am J Human Biol 2003;15:446Ð460.

10 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Brocato, Robin Guest Editor, is a Health Specialist at the Head Start Bureau. The Mind-Body Connection Brody H. The placebo response. Recent research and implications for family medicine. J Family Pract 2000; 49:649Ð654. Brosse, A.L., Sheets, E.S., Lett, H.S., and Blumenthal, J.A. (2002). Exercise and the treatment of clinical depression in adults: recent findings and future directions. Sports Medicine, 32, 741-760. Brown SP, Chitwood LF, Beason KR, McLemore DR: Physiological correlates with perceived exertion during deep water running. Percept Mot Skills 1996; 83: 155-62. Brown SP, Chitwood LF, Beason KR, McLemore DR. Perceptual responses to deep water running and treadmill exercise. Percept Mot Skills 1996;83:131-9. Brown SP, Chitwood LF, Beason KR, McLemore DR. Physiological correlates with perceived exertion during deep water running. Percept Mot Skills 1996;83: 155-62. Brown SP, Chitwood LF, Beason KR and McLemore DR (1996) Perceptual responses to deep water running and treadmill exercise. Perceptual and Motor Skills. 88:131-139. Br J Sports Med, Vol 34, 2000 Brown SP, Chitwood LF, Beason KR and McLemore DR (1997) Deep water running physiologic responses: gender differences at treadmill-matched walking/running cadences. Journal of Strength and Conditioning Research. 11:107-114. Brown SP, Jordon JC, Chitwood LF, Beason KR, Alvarez JG and Honea KP (1998) Relationship of heart rate and oxygen uptake kinetics during deep water running in the adult population — ages 50 to 70 years. Journal of Aging and Physical Activity. 6:248-255. Brown KW, Ryan RM. The benefits of being present: Mindfulness and its role in psychological well-being. J Pers Soc Psychol 2003;84:822Ð848. Brown, S. P., Chitwood, L. F., Beason, K. R., & McLemore, D. R., 1997. Deep water running physiological responses: Gender differences at treadmill-matched walking/running cadences. Journal of Strength and Conditioning Research, 11, 107-114. Brownell KD, Horgen KB. Food Fight: The Inside Story of the Food Industry, America’s Obesity Crisis, and What We Can Do About It. Chicago: Contemporary Books, 2004. Bushman, B. A., Flynn, M. G., Andres, F. F., Lambert, C. P., Taylor, M. S., & Braun, W. A. (1997). Effect of 4 wk deep water run training on running performance. Medicine and Science in Sports and Exercise, 29, 694-699. Butts, N. K., Tucker, M., & Greening, C. (1991). Physiologic responses to maximal treadmill and deep water running in men and women. The American Journal of Sports Medicine, 19, 612-614.

11 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Butts, N. K., Tucker, M., & Smith, R. (1991). Maximal responses to treadmill and deep water running in high school female cross country runners. Research Quarterly for Exercise and Sport, 62, 236-239. Butts NK, Tucker M. Greening C: Physiological responses to maximal treadmill and deep water running in men and women. AM J Sports Med 1991; 19: 612-4. Butts NK, Tucker M, and Smith R: Maximal responses to treadmill and deep water running in high school female cross country runners. Res Q Exercise Sport 1991; 2: 236-9. Butts, Nancy K.; Gushiken, Thomas T. and Zarins, Bertram. The E l i t e Athlete. New York: Medical & Spectrum Publications, 1985. Butts NK, Tucker, M. and Greening C (1991) Physiologic responses to maximal treadmill and deep water running in men and women. The American Journal of Sports Medicine. 19:612-614. Buckelew SP, Murray SE, Hewett JE, Johnson J, Huyser B. Self-efficacy, pain, and physical activity among fibromyalgia subjects. Arthritis Care Res 1995;8:43–50. Bücking J, pointing churches G, pulse G (1991). The increase OF cardiac outputs by immersion in more water measured by transesophageal echocardiography. European journal OF Physiology, 419: 109-113 Budiansky, S; Carey, J.; Wellborn, S.N.; and Silberner, J. "Taking the Pain Out of Pain." U.S. News & World Report, 29 June 1987, pp 50 - 5 7. Busch A, Schachter CL, Peloso PM, Bombardier C. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst Rev 2002;3:CD003786. Burke, Edmund R. Off-Season Training for Cyclists. Boulder, CO: VeloPress, 1997. Concept 2."Rowing Technique." www.concept2.com Burckhardt CS, Clark SR, Bennett RM. The Fibromyalgia Impact Questionnaire: development and validation. J Rheumatol 1991;18:728–33. Burckhardt CS, Mannerkorpi K, Hedenberg L, Bjelle A. A randomized, controlled clinical trial of education and physical training for women with fibromyalgia. J Rheumatol 1994; 21:714–20. Burt VL, Whelton P, Rocella EJ, et al. Prevalence of hyper- tension in the U.S. adult population: Results from the Third National Health and Nutrition Examination Survey, 1988Ð 1991. Hypertension 1995; 25:305Ð313Baskaran K, Butler C, Steptoe A. Placebo responses: an experimental study of psychophysiological processes in asthmatic volunteers. Br J Clin Psychol 1986; 25:173Ð183. Burfoot, Amby. "Screen Tests." Runner's World, March 1986, pp. 48-9. Buxton, Karen - Cardiovascular Conditioning: Alternatives to Swim, Bike, and Run Part 3: Rowing Ergometers, Feb. 3, 2008

12 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Byrd RC. Positive therapeutic effects of intercessory prayer in a coronary care unit population. South Med J 1988; 81:826Ð829. Byrd R. Positive therapeutic effects of intercessary prayer in a coronary care unit population. South Med J. 1988;81:826-829. Cabot PJ, Carter L, Sch.fer M, Stein C. Methionineenkephalin dynorphin A-release from immune cells and control of inflammatory pain. Pain 2001; 93:207 -212. Cachelin FM, Rebeck RM, Chung GH, Pelayo E. Does ethnicity influence body-size preference? A comparison of body image and body size. Obes Res 2002;10:158 -166. 28. Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH. Longterm morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med 1992;327:1350Ð1355. Cafarelli E. Peripheral contributions to the perception of effort. Med Sci Sports Exerc 1982;14:382-9. Califano J. Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention. Washington, D.C.: US Department of Health, Education and Welfare, US Public Health Service, 1979: vii. Callaghan, P. (2004). Exercise: a neglected intervention in mental health care? Journal of Psychiatric and Mental Health Nursing, 11, 476-483. Calman KC. Definitions and dimensions of quality of life. In Aaronson NK, and Beckmann J, eds. The Quality of Life of Cancer Patients. New York: Raven Press, 1987:1Ð9. Camoriano JK, Loprinzi CL, Ingle JN, et al. Weight change in women treated with adjuvant therapy or observed following mastectomy for node-positive breast cancer. J Clin Oncol 1990; 8:1327Ð1334. Canyon Ranch, Staff of. The Canyon Ranch Guide to Living Younger Longer. New York: Simon & Schuster, 2001. Cantwell, John D. "Cardiac Rehabilitation in the Mid-1980's." The Physician and Sports Medicine, April 1986, p. 89. Carlson LE, Speca M, Patel KD. Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosom Med 2003; 65:571Ð581. Carlson LE, Ursuliak Z, Goodey E. The effects of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients: 6-month follow-up. Support Care Cancer 2001; 9:112Ð123. Carlson, C.R. and A.J. Nitz, Negative side effects of self-regulation training: relaxation and the role of the professional in service delivery. Biofeedback Self Regul, 1991. 16(2): p. 191-7 Carrier K. The healing revolutions impact on health promotion. Employee Benefit News 1997;11:51.

13 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Carton, Richard L. and Rhodes, Edward C. "A Critical Review of the Literature of Ratings Scales for Perceived Exertion." Sports Medicine, vol. 2, no. 3 (&y/June 1985): 198-222. , Cassady, S. L., & Nielsen, D. H. (1992). Cardiorespiratory responses of healthy subjects to calisthenics performed on land versus water. Physical Therapy, 72, 532-538. Cassel E. The Nature of suffering and the goals of medicine. NEJM. 1982:306(11):639-645. CDC 2005, http://apps.nccd.cdc.gov/PASurveillance/StateSumResultV.asp CDC 2007: http://www.cdc.gov/nccdphp/dnpa/obesity/consequences.htm Center for evidence based physiotherapy Center for the Advancement of Health; Ira R. Allen - Director of Public Affairs Carmona L, Ballina J, and Gabriel R, Laffon A: The burden of musculoskeletal diseases in the general population of Spain: results from a national survey. Ann Rheum Dis 2001, 60:1040-104 Chapman L. Consumer-driven health plans (CDHP) and health promotion. Art Health Promot Newsletter 2002;6:12. Chapman LS. Health cost management (HCM) strategies for health promotion Chapman LS, Nelson L, Sloan B, Plankenhorn R, Wright G. Primary, secondary, and tertiary prevention capabilities of selected HMOs: Findings of an employer survey. Am J Health Promot 1997;12:102Ð109. programs. Art Health Promot Newsletter 2001;5:12. Chapman LS. Affordable Employee Health Care: A Model Health Benefit Program. New York: AMACOM Press, Inc., American Management Association, 1991. Chapman LS. Integrated Prevention: Applications for Managed Care Settings. Seattle, WA: Summex Corporation, 1996. Chapman L. Proof Positive: An Analysis of the Cost-effectiveness of Wellness, 2nd ed. Seattle: Corporate Health Designs, 1995. Chapman LS, Barchet S. Consumer-driven health plans (CDHP) and health promotion. Art Health Promotion Newsletter 2002;6:12. Celebi D. The power of predictive modeling. Rules-based tools can forecast costs and health risk for an entire population or a single patient. Healthcare Inform 2003;20:56. Ceci R, Hassmén P. Self-monitored exercise at different RPE intensities in treadmill vs field running. Med Sci Sports Exerc 1991;23:732-8.

14 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Centers for Disease Control and Prevention. Physical activity levels among children aged 9 - 13 years United States, 2002. MMWR 2003:52:785Ð788. Centers for Disease Control and Prevention. National Diabetes Fact Sheet: General Information and National Estimates on Diabetes in the United States, 2000. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2002. Centers for Disease Control and Prevention. Obesity and Overweight. Obesity Trends. Online:www.cdc.gov/nccdphp/dnpa/obesity/trend/prev_char.htm - October 23, 2003. Centers for Disease Control and Prevention. At a Glance. Physical Activity and Nutrition: Essential Elements to Prevent Chronic Disease and Obesity. 2002. Centers for Disease Control and Prevention. Online document at: www.cdc.gov/nccdphp/populati.htm Center for Weight and Health, College of Natural Resources, University of California, Berkeley. Pediatric Overweight: A Review of the Literature. Online document at: www.nature. berkeley.edu January 2004. Centers for Disease Control and Prevention. Heart Disease Death Rates, 1999–2003: Adults Ages 35 Years and Older, by County. http://www.cdc.gov/dhdsp/library/maps/index.htm. Centers for Disease Control and Prevention, Health, United States, 2005 with Chartbook on Trends in the Health of Americans. Hyattsville, MD: National Center for Health Statistics, 2005. Cherkin DC, Eisenberg D, Sherman KJ, et al. Randomized trial comparing traditional Chinese medical acupuncture, therapeutic massage, and self-care education for chronic low back pain. Arch Intern Med 2001; 161:1081Ð1088. Chobanian AV, Bakris GL, Black HR, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and treatment of High Blood Pressure [JNC 7: Complete Version]. Hypertension 1993; 42:1206Ð1252. Chopra, Deepak, M.D., The Chopra Center for Wellbeing. 1987 Creating Health ISBN 0-395-75515-8; 1988 Return of the Rishi ISBN 0-395-57420-X; 1989 Quantum Healing: Exploring the Frontiers of Mind/Body Medicine ISBN 0-553-34869-8; 1991 Unconditional Life: Mastering the Forces That Shape Personal Reality;1991 Perfect Health: The Complete Mind/Body Guide ISBN 0-517-58421-2; 1993 Ageless Body, Timeless Mind : The Quantum Alternative to Growing Old ISBN 0-517-59257-6 ; 1995 The Path to Love: Spiritual Strategies for Healing 1997 The Path to Love: Renewing the Power of Spirit in Your Life ISBN 0-517-70622-9 ; 2001 The Deeper Wound: Recovering the Soul from Fear and Suffering, 100 Days of Healing; 2001 Grow Younger, Live Longer: 10 Steps to Reverse Aging ISBN 0-609-60079-6; 2004 Fire in the Heart: A Spiritual Guide for Teens ISBN 0-689-86216-4; 2006 Life After Death: The Burden of Proof ISBN 0-307-34578-5 Ciconelli RM, Ferraz MB, Santos W, Meinao I, Quaresma Marina R. Brazilian-Portuguese version of the SF-36: a reliable and valid quality of life outcome measure. Rev Bras Reumatol 1999;39:143–50. In Portuguese.

15 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Christie JL, Sheldahl LM, Tristani FE, et al: Cardiovascular regulation during head-out water immersion exercise. J Appl Physiol 1990; 69: 657-64. Clark M, Hampson SE. Implementing a psychological intervention to improve lifestyle self-management in patients with type 2 diabetes. Patient Educ Couns 2001; 42:247Ð256. Clark N, Becker M, Janz N, et al. Self-management of chronic disease by older adults: A review and questions for research. J Aging Health 1991; 3:3. Clarke WR, Woolson RF, Lauer RM. Changes in ponderosity and blood pressure in childhood: The Muscatine Study. Am J Epidemiol 1986;124:195Ð206. Coster W, Mancini M, Ludlow L. Factor structure of the School Function Assessment. Educ Psychol Measure 1999;59: 665Ð677. Cheek, David B. Ernest L. Rossi, PhD. “Mind-Body Therapy: Methods of Ideodynamic Healing in Hypnosis”, 1992 - New York: Norton
Cheek, MD, David B. Leslie M. LeCron Clinical Hypnotherapy, Prentice Hall
CHENG, MARIA AP Medical Writer January 8, 2008 Susan Jebb - Nutrition and Health Britain's Medical Research Council Chobanian AV, Bakris GL, Black HR, et al., and the National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA 2003; 289:3560Ð3572.
CLINICAL HYPNOSIS, PRINCIPLES APPLICATIONS; H. B. CRASILNECK, J. A. HALL, 1976 GRUNE & STRATTON, NEW YORK, SAN FRANCISCO, LONDON
CLINICAL EXPERIMENTAL HYPNOSIS, (1ST. & 2ND EDITIONS), W. KROGER, 1963, 1976, LIPPINCOT. PHILADELPHIA, TORONTO Coe Sebastian and Coe, Peter. Running For Fitness. London: Pavilion, 1983. Cohen K. Native American medicine. In: Jonas W. Levin J, eds. Essentials of Complementary and Alternative Medicine. Philadelphia: Lippincott Williams & Wilkis; 1999. p. 233251. Cole, Laura K. "Physiological and Perceptual Responses to Running in Water." Master's Thesis, University of Toledo, 1987. Collins J. Good to Great. New York: Harper Business, 2001. Cohen-Boulakia F, Valensi PE, Boulahdour H, et al. In vivo sequential study of skeletal muscle capillary permeability in diabetic rats: Effect of anthocyanosides. Metabolism. 2000; 49: 880Ð885.

16 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Cohen JL. Diabetes: A 21st Century Epidemic. 2nd Annual D.C. Chronic Disease Conference, The George Washington University School of Medicine, Washington, D.C., September 25, 2003. Cole, A. J., Comprehensive Aquatic Therapy (p. 123–135). Boston MA: Butterworth-Heinemann. Cole, Andrew J. MD - Becker, Bruce E. MD, MS; “Water therapy exercise program; Water therapy pain relief; December 27, 2006; Adapted from: American College of Sports Medicine. (2006). ACSM’s Guidelines for Exercise Testing and Prescription, 7th Edition. Philadelphia, PA: Lippincott Williams & Wilkins; Collins J. Good to Great. New York: Harper Business, 2001. Collins JS, Paul S, West-Frasier J. The utilization of spirituality in occupational therapy: Beliefs, practices, and perceived barriers. Occup Ther Healthcare 2001;14:73Ð92. Commission on Accreditation of Rehabilitation Facilities (CARF). Medical Rehabilitation Standards Manual. Tucson: CARF International, 2001:250. Consumer Reports. "What To Do For Your Aching Back." June 1987, pp. 379 - 383. Cook S, Weitzman M, Auinger P, Nguyen M, Dietz WH. Prevalence of a metabolic syndrome phenotype in adolescents: Findings from the third National Health and Nutrition Examination Survey, 1988Ð1994. Arch Pediatr Adolesc Med 2003;157:821Ð827. Cooper Aerobics Center, Kenneth H. Cooper, M.D., M.P.H.: Founder, President, and CEO - The Cooper Aerobics Center, Cooper, Kenneth H. The Aerobics Program For Total Well-Being. New York: M. Evans & Co., 1982. Cooper, Kenneth H. Aerobics. New York: M. Evans & Co., 1968. Coronary Drug Project Research Group. Influence of adherence to treatment and response of cholesterol on mortality in the Coronary Drug Project. N Engl J Med 1980; 303:1038Ð 1041. Costill DL, Maglischo EW, Richardson OFF (1992). Swimming. Oxford: Mayfield Publishing company Covey SR. Principle-Centered Leadership. New York: Summit Books, 1991. Covey SR. Principle-Centered Leadership. New York: Summit Books, 1991. Courneya KS, Friedenreich CM. Physical exercise and quality of life following cancer diagnosis: A literature review. Ann Behav Med 1999; 21:171Ð179. Coyle EF, Martin WH, Sinacore DR, et al (1984) Time course of loss of adaptations after stopping prolonged intense endurance exercise. Journal of Applied Physiology. 57:1857-1864.

17 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Coyle EF, Martin VM, Sinacore DR, et al: Time course of loss of adaptations after stopping prolonged intense endurance training. J Appl Physiol 1984; 57: 1857-64. Crabbe, Buster and Cilento, Raphael. Buster Crabbe's Arthritis Exercise Book. New York: Simon & Shuster, 1980. Crane, C. - Tacia, S. -Thompson, J.; and Stevenson, J.R. "A Comparison of Land and Water Exercise Programs For Older Individuals. Unpublished. Dr. John R. Stevenson, Dept. of Kinesiological Sciences, School of Health Sciences, Oakland University, Rochester, MI. Curtiss FR. Finding the truth about health care cost drivers Price versus utilization factors. J Manage Care Pharm 2003;9:274Ð275. Dalleck Lance C. and Kravitz, Len, Ph.D. - The Physiological Effects of Aquatic Exercise; University of New Mexico - 2007 Davis, P. (1998). Aromatherapy an A-Z Guide. Essex, Englqnd: C.W. Daniel Co., Davey L The oath of Hippocrates an historical review. Neurosurgery .2001; 49(3):554566. D’Acquisto, L. J., D’Acquisto, D. M., & Renne, D. (2000). Metabolic and cardiovascular responses in older women during shallow-water exercise. Davidson K and McNaughton DK (2000) Deep water running training and road running improve VO2max in untrained women. Journal of Strength and Conditioning Research. 14:191-195. Davison KK, Birch LL. Weight status, parent reaction, and self-concept in five-year-old girls. Pediatrics 2001;107:46Ð53. Daniels J. S. Obesity hypertension in children: A problem of epidemic proportions. Hypertension 2002;40:441Ð447. DeBakey, Michael and Gotto, Antonio. The Living Heart. New York: D. McKay Co., 1977. De Boer R. Perelson A, Kevrekidis I. Immune network behavior-11. From oscillations to chaos and stationary states.BullMalhBio1. 1993; 55(4):781-816. DeBusk RF, Miller NH, Superko R, et al. A case-management system from coronary risk factor modification after myocardial infarction. Ann Intern Med 1994; 120:721Ð729. de Craen AJM, Moerman DE, Heisterkamp SH, Tytgat GNJ, Tijssen J, Kleijnen J. Placebo effect in the treatment of duodenal ulcer. Br J Clin Pharmacol 1999; 48:853Ð860. DeMaere, J., Ruby, B. C., & Swan, J. (1997). Effects of deep water and treadmill running on oxygen uptake and energy expenditure in seasonally trained cross country runners. Medicine and Science in Exercise and Sport, 29 S221 (Abstract).

18 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
DeMaere JM, Ruby BC: Effects of deep water and treadmill running on oxygen uptake and energy expenditure in seasonally trained cross country runners. J Sports Med Phys Fitness 1997; 37: 175- 81. Dennison BA, Erb TA, Jenkins PL. Television viewing and television in bedroom associated with overweight risk among low-income preschool children. Pediatrics 2002;109:1028Ð 1035. deLateur BJ, Lehman JF, Stonebridge J, Warren CG: Isotonic versus isometric exercise: a double-shift transfer-of-training study. Arch Phys Med Rehabil 1972; 53: 212-7. DEEP WATER EXERCISE HEALTH & FITNESS; J.G. MCWATERS 1988 PUBLITECH EDITIONS Laguna Beach, CA. 92652A. DeFronzo R. Pharmacologic therapy for type 2 diabetes mellitus. Ann Intern Med 1999; 131:281Ð303. de la Fuente-Fern.ndez R, Schulzer M, Stoessl AJ. The placebo effect in neurological disorders. Lancet Neurol 2002; 1:85Ð91. de la Fuente-Fern.ndez R, Ruth TJ, Sossi V, Schulzer M, Calne DB, Stoessl AJ. Expectation and dopamine release: Mechanism of the placebo effect in ParkinsonÕs disease. Science 2001; 293:1164Ð1166. Demello, J. - J . Cureton, K. J.; Boineau, R.E. and Singh, M.M. "Ratings of Perceived Exertion at the Lactate Threshold in Trained and Untrained Men and Women." Medicine and Science in Sports and Exercise, vol. 19, no. 4 (August 1987), pp. 354-61. Department of Rehabilitation Medicine, Thomas Jefferson University, Philadelphia, PA 19107. Tamara D. Lauder, MD; Anthony S. Burns, MD*; Tamara D. Lauder, MD Department of Physical Medicine and Rehabilitation, Mayo Clinic, Rochester, MN 55905. DHHS National Center for Child Health & Development. Research. Research plan for the National Center for Medical Rehabilitation Research. NIH publication No. 93-3509. March 1993. Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics 1998;101:518Ð525. Dietz WH, Jr., Gross WL, Kirkpatrick JA, Jr. Blount disease (tibia vara): Another skeletal disorder associated with childhood obesity. J Pediatr 1982;101:735Ð737. DeRubeis RJ, Tang TZ, Beck AT. Cognitive therapy. In: Dobson KS, ed. Handbook of Cognitive Behavioral Therapies, 2nd ed. New York: Guilford, 2001:349Ð392. Destination Spa Vacations. Tucson, AZ: Destination Spa Group, 2004 Edition. Detterman DK, Sternberg RJ. Transfer on Trial: Intelligence, Cognition and Instruction. Norwood, NJ: Ablex, 1993. DeVierville, JP. Spa industry, culture and evolution: Time, temperature, touch and truth. Massage & Bodywork, August/ September, 2003;20Ð31.

19 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
DeVries HA, Moritani T, Nagata A, Magnussen K. The relation between critical power and neuromuscular fatigue as estimated from electromyographic data. Ergonomics 1982;25:738-91. Di Blasi Z. Harkness E, Ernst E. Georgiou A, Kleijnen J. Influence of context effects on health outcomes: a systematic review. Lancet. 2002:357(9358):757. Diehl HA. Coronary risk reduction through intensive community- based lifestyle intervention: The Coronary Health Improvement Project (CHIP) experience. Am J Cardiol 1998;82: 83TÐ87T. Diener HC. Issues in migraine trial design: A case study. The 311C Symposium Presentations given in the 311C90 Symposion of the 3rd European Headache Conference (Abstract). June 5Ð8, 1996, S Margherita die Pula 1996;10Ð11. Diener HC, Klein KB, Multinational Oral 311C90 and Sumatriptan Comparative Study Group. The first comparison of the efficacy and safety of 311C90 and sumatriptan in the treatment of migraine (Abstract). 3rd European Headache Conference. S Margherita di Pula, Italy, June 5Ð8, 1996. Diener H-C, Dowson AJ, Ferrari M, Nappi G, Tfelt-Hansen P. Unbalanced randomization influences placebo response: Scientific versus ethical issues around the use of placebo in migraine trials. Cephalalgia 1999;19:699Ð700. Dintiman, George B. Sprinting Speed. Springfield: Charles C. Thomas, Publisher, 1971. Di Prampero, P. E. (1986). The energy cost of human locomotion on land and in water. International Journal of Sports Medicine, 7, 55-72. Ditmyer MM, Price JH, Telljohann SK, Rogalski F. Pediatricians perceptions and practices regarding prevention and treatment of type 2 diabetes mellitus in children and adolescents. Arch Pediatr Adolesc Med 2003;157:913Ð918. Donald CA, Ware JE. The Quantification of Social Contacts and Resources. Santa Monica, CA. RAND Publication R-2937-HHS. Doron Y, Peleg R, Peleg A, Neumann L, Buskila D: The clinical and economic burden of fibromyalgia compared with diabetes mellitus and hypertension among Bedouin women in the Negev. Fam Pract 2004, 21:415-419. Dossey L. Samueli conference on definitions and standards in healing research: Working definitions and terms. Altern Ther 2003;9:A10ÐA12. Dossey L. Samueli Conference on Definitions and Standards in Healing Research: working definitions and terms. Altern Ther Health Med 2003;9:A10ÐA12. Dossey L. Samueli conference on definitions and standards: Working definitions and terms. Alter Health Med. 2003; 9(3): A10Al2. Dossey. Florence Nightingale: mystic, visionary, healer. Springhouse. Pa: Springhouse; 1999.

20 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Dossey L. Healing Words. San Francisco, Calif: Harper Collins Publishers; 1993. Downey M, Stern JSS. The importance of being earnest. Lancet 2003;362:42Ð43. Dowzer CN, Reilly T, Cable NT. Effects of deep and shallow water running on spinal shrinkage. Br J Sports Med 1998;32: 44–8. Dowzer CN, Reilly T, Cable Mr, Nevill A: Maximal physiological responses to deep and shallow water running. Ergonomics 1999; 42: 275-81. Dreher, H. (2005). A Look at Dr. Jon Kaiser's Complementary Approach to HIV/AIDS. Duff, John F., M.D. Youth Sports Injuries. New York: Macmillan, 1992. Dubbert, P.M. (2002). Physical activity and exercise: recent advances and current challenges. Journal of Consulting Clinical Psychology, 70, 526-536. Dunn, A.L., Trivedi, M.H., Kampert, J.B., Clark, C.G., and Chambliss, H.O. (2002). The DOSE study. A clinical trial to examine efficacy and dose response of exercise as treatment for depression. Controlled Clinical Trials, 23, 584-603 Durand MV, Crimmins DB. The Motivation Assessment Scale. Topeka, KS: Monaco & Assoc., 1992. Durkin MB. A community of caring: Patients in a rehabilitation unit experience holistic healing through a spiritual support group. Health Prog 1992;73:48Ð50, 70. Durstine, L.J., Grandjean, P.W., Cox, C.A., and Thompson, P.D. (2002). Lipids, lipoproteins, and exercise. Journal of Cardiopulmonary Rehabilitation. 22, 385-398. Dzau VJ. Theodore Cooper Lecture: Tissue angiotensin and pathobiology of vascular disease. A unifying hypothesis. Hypertension 2001;37:1047Ð1052. Eaton, S.B., Shostak, M., and Konner, M. (1988). The Paleolithic Prescription: A Program of Diet and Exercise and a Design for Living. New York: Harper and Row. Ebbeling CB, Leidig MM, Sinclair KB, Hangen JP, Ludwig DS. A reduced-glycemic load diet in the treatment of adolescent obesity. Arch Pediatr Adolesc Med 2003;157:773Ð779. Eckerson, J., & Anderson, T. (1992). Physiological response to water aerobics. Journal of Sports Medicine and Physical Fitness, 32, 255-261. Edelman G, Tononi G. A Universe of consciousness: How matter becomes imagination. New York: Basic Books: 2000. Edelson, Ed - report on a new study for the Health Day Reporter; Stephen F. Crouse, Ph.D., professor, kinesiology - internal medicine, Texas A&M, College Station; William E. Kraus, M.D., research director, Duke University Center for Living, Durham, N.C.; April 8, 2008, presentation, Experimental Biology conference, San Diego

21 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Eddy J, Fitzhugh E, Wojtpwicz CG, Wang MQ. The impact of worksite-based safety belt programs: A review of the literature. Am J Health Promot 1997;11:281Ð289. Edington D, Yen L. Is it possible to simultaneously reduce risk factors and excess health care costs? Am J Health Promot 1992;6:403Ð406, 409. Education of the Handicapped Act Amendments of 1990. Pub.L.No. 101-476, 20 U.S.C. Online document at: www. ideapractices.org Edwards, R.R., et al., Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Rheum, 2006. 55(2): p. 325-32 Edlich RF, Towler MA, Goitz RJ, Wilder RP, Buschbacher LP, Morgan RF, et al. Bioengineering principles of hydrotherapy. J Burn Care Rehabil 1987;8:580–4. Egede LE, Zheng D, Ye X, Silverstein MD. The prevalence and pattern of complementary and alternative medicine use in individuals with diabetes. Diabetes Care 2002;25:324Ð329. Edwards A, Unigwe S, Elwyn G, Hood K. Effects of communicating individual risks in screening programmes: Cochrane systematic review. BMJ 2003;327:703Ð709. Effects of aquatic plus walking exercises on weight loss and function in sedentary obese females. Medicine & Science in Sports & Exercise, 35(5), May, S136, Abstract 753. Eisenberg DM, Delbanco TL, Berkley CS, Kaptchuk TJ, Kupelnick B, Kuhl J, Chalmers TC. Cognitive behavioral techniques for hypertension: Are they effective? Ann Intern Med 1993;118:964Ð972. Eisenberg, D.M., et al., Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med, 1993. 328(4): p. 246-52. Eisenberg, D.M., et al., Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. Jama, 1998. 280(18): p.1569-75. Eisenberg ME, Neumark-Sztainer D, Story M. Associations of weight-based teasing and emotional well-being among adolescents. Arch Pediatr Adolesc Med 2003;157:733Ð738Eisen M, Ware JE Jr, Donald CA, Brook RH. Measuring components of children’s health status. Med Care 1979;17:902Ð 921. Engel, G.L., The need for a new medical model: a challenge for biomedicine. Science, 1977. 196(4286): p. 129-36. Engel, G.L., The clinical application of the biopsychosocial model. Am J Psychiatry, 1980. 137(5): p. 535-44. Enright PL, Goodwin JL, Sherrill DL, Quan JR, Quan SF. Blood pressure elevation associated with sleep-related breathing disorder in a community sample of white and Hispanic children: The Tucson Children’s Assessment of Sleep Apnea study. Arch Pediatr Adolesc Med 2003;157:901Ð904.

22 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Encarta Encyclopedia Deluxe 2004 – 2006 Microsoft Corporation: HISTORICAL BACKGROUND In the United States; physiotherapy;
Physical Therapy; Hydrotherapy; Millennium; Synergy; ANCIENT WORLD Ancient Times-History; Hydrotherapy and Healing; Medicine; Alternative Medicine; Immune System; Sports Medicine; Diagnosis and Treatment; Injury Prevention; Aerobics; Rolfing; Shiatsu; Acupuncture-Acupressure; Rehabilitation; State Federal Worker Compensation;
Enos WF, Holmes RH, Beyer J. Coronary disease among United States soldiers killed in action in Korea. JAMA 1953; 152:1090Ð1093. Engquist DE, Short-Degraff M, Gliner J, Oltjenbruns K. Occupational Therapists beliefs and practices with regard to spirituality and therapy. Am J Occup Ther 1997;51:173Ð180. Epstein LH, Myers MD, Raynor HA, Saelens BE. Treatment of pediatric obesity. Pediatrics 1998;101:554Ð570. Epstein LH, Squires S. The Stoplight Diet for Children: An Eight-Week Program for Parents and Children, 1st ed. Boston: Little, Brown, 1988. Epstein LH, Valoski A, Wing RR, McCurley J. Ten-year follow- up of behavioral, family-based treatment for obese children. JAMA 1990;264:2519Ð2523. S-240 FREEDMAN AND STERN Epstein LH, Wing RR, Koeske R, Andrasik F, Ossip DJ. Child and parent weight loss in family-based behavior modification programs. J Consult Clin Psychol 1981;49:674Ð 685. Epstein LH, Paluch RA, Gordy CC, Dorn J. Decreasing sedentary behaviors in treating pediatric obesity. Arch Pediatr Adolesc Med 2000;154:220Ð226. Erickson SJ, Robinson TN, Haydel KF, Killen JD. Are overweight children unhappy? Body mass index, depressive symptoms, and overweight concerns in elementary school children. Arch Pediatr Adolesc Med 2000;154:931Ð935. Eriksson KF, Lindgarde F. Prevention of type 2 (non-insulin dependent) diabetes mellitus by diet and physical exercise: The 6-year Malmo feasibility study. Diabetologia 1991;34:891Ð 898. Ernst E, Resch KL. Concept of true and perceived placebo effects. BMJ 1995;311:551Ð553. Essert, Mary. “Why Water Works.” Aquatic Resources Network. Jan. 13, 2003. Etelson D, Brand DA, Patrick PA, Shirali A. Childhood obesity: Do parents recognize this health risk? Obes Res 2003; 11:1362Ð1368. European Spas Association. Online document at: www. espa-ehv.com Evans, B. W. - Cureton, K . J. and Purvis, J.W. 'Metabolic and Circulatory Responses to Walking or Jogging i n Water .I1 Research Quarterly, vol. 49, no. 4 (1978), pp. 442-9. Evcik D, Kizilay B, Gokcen E. The effects of balneotherapy on fibromyalgia patients. Rheumatol Int
23 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
2002;22:56–9. Eyestone, E. D., Fellingham, G., George, J., & Fisher, A. G. (1993). Effect of water running and cycling on maximum oxygen consumption and 2-mile run performance. The American Journal of Sports Medicine, 21, 41-44. Fagard, R. H. (2001). Exercise characteristics and the blood pressure response to dynamic physical training. Medicine & Science in Sports & Exercise, 33, S484-492. Falkner NH, French SA, Jeffery RW, Neumark-Sztainer D, Sherwood NE, Morton N. Mistreatment due to weight: Prevalence and sources of perceived mistreatment in women and men. Obes Res 1999;7:572Ð576. Faith MS, Berman N, Heo M, et al. Effects of contingent television on physical activity and television viewing in obese children. Pediatrics 2001;107:1043Ð1048. Fauvel JP, MÕPio I, Quelin P, Rigaud JP, Laville M, Ducher M. Neither perceived job stress nor individual cardiovascular reactivity predict high blood pressure. Hypertension 2003;42: 1112Ð1116. Fenwick E, Byford S: A guide to cost-effectiveness acceptability curves. Br J Psychiatry 2005, 187:106-108. Faymonville, M.E., M. Boly, and S. Laureys, Functional neuroanatomy of the hypnotic state. J Physiol Paris, 2006. 99(4-6): p. 463-9. Federle S (1991). Swimming technology (Swim Technique). In Pfeifer H (OD.). Swim. Berlin: Sport publishing house, 65-94 Fibromyalgia Back Pain and Sciatica Water Exercise - Benefits of Water Exercise for Back Pain - Water Exercise and Aquatic Therapy - What is Water Exercise Aquatic Resources Network. 2003. Fletcher JM, Ewing-Cobbs L, Francis DJ, et al. Variability in outcome after traumatic brain injury in children: A developmental perspective. In: Broman SH, Michel ME, eds. Traumatic Head Injury in Children. New York: Oxford University Press, 1995:3Ð21. Flor, H., T. Fydrich, and D.C. Turk, Efficacy of multidisciplinary pain treatment centers: a meta-analytic review. Pain, 1992. 49(2): p. 221-30. Flor, H. and D.C. Turk, Chronic back pain and rheumatoid arthritis: predicting pain and disability from cognitive variables. J Behav Med, 1988. 11(3): p. 251-65. Fields JZ, Walton KG, Schneider RH, et al. Effect of a multimodality natural medicine program on carotid atherosclerosis in older subjects: A pilot trial of Maharishi Vedic Medicine. Am J Cardiol 2002;89:952Ð958. Fields HL. Naloxone dose dependently produces analgesia and hyperalgia in postoperative pain. Nature 1979;278:740Ð741.

24 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Fillmore MT, Mulvihill L E, Vogel-Sprott M. The expected drug and its expected effect interact to determine placebo responses to alcohol and caffeine. Psychopharmacology 1994; 115:383Ð388. Fillmore M, Vogel-Sprott M. Expected effect of caffeine on motor performance predicts the type of response to placebo. Psychopharmacology 1992;106:209Ð214. Finckh, A., Iversen, M. and Liang, M.H. (2003). The exercise prescription for rheumatoid arthritis: Primum non Nocere. Arthritis & Rheumatism, 48(9) September, 2393-2395. Finucane, A. and S.W. Mercer, An exploratory mixed methods study of the acceptability and effectiveness of Mindfulness-Based Cognitive Therapy for patients with active depression and anxiety in primary care. BMC Psychiatry, 2006. 6: p. 14. Fishman, S.M., et al., The case for pain medicine. Pain Med, 2004. 5(3): p. 281-6. Fitness Swimmer: Get a little eccentric during your water workouts. Summer, 1996. Fitzmaurice J, Rose J. Cutting to the chase: What physician executives need to know about HIPAA. Physician Exec May/June 2000, 42Ð49. Fixx, James F. The Complete Book of Running. New York: Random House, 1977. Flaten MA, Blumenthal TD. Caffeine-associated stimuli elicit conditioned response: An experimental model of the placebo effect. Psychopharmacology 1999;145:105Ð112. Flegel, Melinda. Sports First Aid. Rev. ed. Human Kinetics, 1997. Florey E. Ars Magnetica. Franz Anton Mesmer 1734Ð1815: Magier vom Bodensee. Konstanz: Universit.tsverlag Konstanz, 1995. Foster GD, Wadden TA, Makris AP, et al. Primary care physicians attitudes about obesity and its treatment. Obes Res 2003;11:1168Ð1177. Foot DK, Lewis RP, Pearson TA, Beller GA. Demographics and Cardiology, 1950Ð2050. J Am Coll Cardiol 2000;35:1067Ð1068. Forrester B, Weaver M, Brown K, Philips J, Hilyer J. Personal health risk predicators of occupational injury among 3,415 municipal employees. J Occup Environ Med 1996;38:515Ð521. Forbes, C.A. (1929). Greek Physical Education. New York: The Century Company. Fordyce, W., Behavioral methods for chronic pain and illness. 1976, St. Louis Mosby. Fox, K.R. (1999). The influence of physical activity on mental well-being. Public Health Nutrition. 2, 411-418. Fox, Edward L. Sports Physiology. New York: CBS College Publishing, 1984.

25 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Fox JEB. Alternative medicine in coronary disease. In: Topol EJ, ed. Califf RM, Isner J, Prsytowsky EN, Serruys P, Swain J, Thomas J, Thompson P, Young JB, assoc. eds. Textbook of Cardiovascular Medicine. New York: Lippincott Williams & Wilkins, 2001. Frank A. A multidisciplinary approach to obesity management: The physician’s role and team care alternatives. J Am Diet Assoc 1998;98(Suppl):S44ÐS48. Frank JD. Non-specific aspects of treatment: The view of a psychotherapist. In: Shepherd M, Sartorius N, eds. Non-Specific Aspects of Treatment. Bern: Huber, 1989:95Ð114. Frank JD. Persuasion and Healing: A Comparative Study of Psychotherapy. Baltimore: Johns Hopkins University Press, 1961. Frango DD, Rhodes EC: Maximal and ventilatory threshold responses to treadmill and water immersion running. Med Sci Sports Exercise 1995; 27: 1007-13. Frangolias DD, Taunton JE, Rhodes EC, McConkey JP, Moon M: Maintenance of aerobic capacity during recovery from right foot Jones fracture: a case report. Clin J Sport Med 1997: 7: 54-8. Frangolias DD, Rhodes EC, Taunton JE: Deep-water running: a low-impact approach to fitness. Your Patient & Fitness 1995; 9(4): 14-21. Frangolias DD, Rhodes EC, Belcastro AN, Coutts KD, Taunton JE, Mekjavic IB: Comparison of metabolic responses of prolonged work at Tvent during treadmill and water immersion running [abstract]. Med Sci Sports Exercise 1994; 26(suppl): SIO. Frangolias DD, Rhodes EC: Metabolic responses and mechanisms during water immersion running and exercise. Sports Med 1996; 22: 38-53. Frangolias, D. D., & Rhodes, E. C. (1995). Maximal and ventilatory threshold response to treadmill and water immersion running. Medicine and Science in Exercise and Sport, 27, 1007-1013. Frangolias, D. D., Rhodes, E. C., & Taunton, J. E. (1996). The effect of familiarity with deep water running on maximal oxygen consumption. Journal Strength Conditioning Research, 10, 215-219. Freedman DS, Dietz WH, Srinivasan SR, Berenson GS. The relation of overweight to cardiovascular risk factors among children and adolescents: The Bogalusa Heart Study. Pediatrics 1999;103:1175Ð1182. Friedlander SL, Larkin EK, Rosen CL, Palermo TM, Redline S. Decreased quality of life associated with obesity in school aged children. Arch Pediatr Adolesc Med 2003;157:1206Ð 1211. Fries JF, Koop CE, Beadle CE, Cooper PP, England MJ, Greaves RF. Reducing health care costs by reducing the need and demand for medical services. N Engl J Med 1993;329: 321Ð325. Fries J, Bloch D, Harrington H, et al. Two-year results of a randomized controlled trial of a health promotion program in a retiree population: The Bank of America Study. Am J Med 1993;94:455Ð462.

26 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Fries JF. Measuring and monitoring success in compressing morbidity. Ann Intern Med 2003;139(5 Pt 2):455Ð459. Frisch, Rose E. "Lower Cancer Rates Among Female College Athletes. " British Journal of Cancer, vol. 52 (December l985), pp. 88591. Froelicher VF. Cardiac rehabilitation. In: Willerson JT, Cohn JN, eds. Cardiovascular Medicine, 2nd ed. Philadelphia: Churchill Livingstone, 2000:893Ð911. Frost, Ph.D. Gary J. - JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE, Volume 10, 2004 titled “The Spa as a Model of an Optimal Healing Environment”. Canyon Ranch Health Resorts, Tucson, AZ 85750. FUNCTIONAL ANATOMY IN SPORTS; J. WEINECK 1986 YEAR BOOK MEDICAL PUBLISHER, CHICAGO-LONDON Fung TT, Hu FB, Pereira MA, et al. Whole-grain intake and the risk of type 2 diabetes: A prospective study in men. Am J Clin Nutr 2002;76:535Ð540. Fye WB. American Cardiology. Baltimore. Johns Hopkins University Press, 1996. Gallagher, R.M., Treatment planning in pain medicine. Integrating medical, physical, and behavioral therapies. Med Clin North Am, 1999. 83(3): p. 823-49, viii. Gaesser GA, Poole D. The slow component of oxygen uptake kinetics in humans. Exerc Sport Sci Rev 1996;24:35-70. Gallagher, R.M., Treatment planning in pain medicine. Integrating medical, physical, and behavioral therapies. Med Clin North Am, 1999. 83(3): p. 823-49, viii. Galper DI, Taylor AG, Cox DJ. Current status of mind-body interventions for vascular complications of diabetes. Fam Community Health 2003;26:34Ð40. Galuska DA, Will JC, Serdula MK, Ford ES. Are health care professionals advising obese patients to lose weight? JAMA 1999;282:1576Ð1578. Garnsey, P. (1999). Food and Society in Classical Antiquity. New York: Cambridge University Press. Garvy, Helen. The Immune System: Your Magic Doctor. Los Gatos, Calif.: Shire Press, 1992. Gaspard, G., Schmal, J., Porcari, J., Butts, N., Simpson, A., & Brice, G. (1995). Effects of a seven-week aqua step training program on aerobic capacity and body composition of college-aged women. Medicine and Science in Sports and Exercise, 27. Gauthier, Michele M. "Guidelines f o r Exercise During Pregnancy: Too Little or Too Much?" The Physician and Sports Medicine, April 1986, pp. 162-9.

27 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Gaziano JM, Manson JE, Ridker PM, et al. Primary and secondary prevention of coronary heart disease. In: Braunwald E, Zipes DP, Libby P, eds. Heart Disease. A Textbook of Cardiovascular Medicine. Philadelphia: WB Saunders, 2001: 1058 -1059. Gehring M. Keller B, Brehm B: Physiological responses to deep water running in competitive and non-competitive runners [abstract. Med Sci Sports Exercise 1992; 24(suppl): S23. Genuth S, Eastman R, Kahn R. et al. American Diabetes Association. Implications of the United Kingdom prospective diabetes study. Diabetes Care 2003;26(Suppl 1):S28ÐS32. Gerard Anderson and Peter Sotir Hussey, "Comparing Health System Performance in OECD Countries". Health Affairs; Vol. 20: No. 3 (May/June 2001) Gheorghiu VA, Netter P, Eysenck HJ, Rosenthal R, eds. Suggestion and Suggestibility: Theory and Research. Heidelberg: Springer, 1989. Gilliland SS, Perez GE, Azen SP, Carter JS. Strong in body and spirit: Lifestyle intervention for Native American adults with diabetes in New Mexico. Diabetes Care 2002;25:78Ð83. Gillman MA, Lichtigfeld FJ. Randomized double-blind trial of psychotropic analgesic nitrous oxide compared with diazepam for alcohol withdrawal state. J Subs Abuse Treat 2002;22:129Ð134. Gillman MA, Lichtigfeld FJ. Placebo and analgesic nitrous oxide for treatment of the alcohol withdrawal state. Br J Psychiatry 1991;159:672Ð675. Gillman MA, Lichtigfeld FJ. Minimal sedation required with nitrous oxide-oxygen treatment of the alcohol withdrawal state. Br J Psychiatry 1986;148:604Ð606. Glanz K. Behavioral research contributions and needs in cancer prevention and control: Dietary change. Prev Med 1997; 26:S43ÐS55. Glass, Becky, e t al. "Comparative Physiological Responses of Suspended Deep Water Running to Hard Surface Running. " Research Council Proceedings: Southern District, American Alliance of Health, Physical Education, Recreation and Dance. Auburn University, 1987. Giammattei J, Blix G, Marshak HH, Wollitzer AO, Pettit DJ. Television watching and soft drink consumption: associations with obesity in 11- to 13-year-old schoolchildren. Arch Pediatr Adolesc Med 2003;157:882Ð886. Gidding SS, Bao W, Srinivasan SR, Berenson GS. Effects of secular trends in obesity on coronary risk factors in children: The Bogalusa Heart Study. J Pediatr 1995;127:868Ð874. Gilfoyle EM. Caring: A philosophy for practice. Am J Occup Ther 1980;34:517Ð521. Gillette NP. A vision of society in the 21st century. Am J Occup Ther 2002;56:699Ð700.

28 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Gleason P, Suitor C. Children’s Diets in the Mid-1990s: Dietary Intake and its Relationship with School Meal Participation. USDA, Food and Nutrition Service, Office of Analysis, Nutrition and Evaluation. Online document at: www. fns.usda.gov/oane/menu/published/cnp/files/childiet.pdf Globus, Sheila. "The Pool of Youth.'' Women's Sports and Fitness, May 1986, p. 50. Golan M, Weizman A, Apter A, Fainaru M. Parents as the exclusive agents of change in the treatment of childhood obesity. Am J Clin Nutr 1998;67:1130Ð1135. Goetzel R. The financial impact of health promotion and disease prevention programs Why it is so hard to prove value? Am J Health Promot 2001;15:277Ð288. Goetzel R, Juday T, Ozminkowski R. What’s the ROI? A systematic review of return-on-investment studies of corporate health and productivity management initiatives. Worksite Health 1999;63:12Ð21. Goetzel RZ, Anderson DR, Whitmer RW, Ozminkowski RJ, Dunn RL, Wasserman J. The relationship between modifiable health risks and health care expenditures: An analysis of the multi-employer HERO health risk and cost database. J Occup Environ Med 1998;40:843Ð854. Gorenstein C, Andrade L. Validation of a Portuguese version of the Beck Depression Inventory and the State-Trait Anxiety Inventory in Brazilian subjects. Braz J Med Biol Res 1996;29: 453–7. Goss JR, Elmore JG, Lessler DS. Quality of health care delivered to adults in the United States. N Engl J Med 2003;349:1866Ð1868. Gollnick PD, Armstrong RB, Saubert CW fV, Piehl D, Saltin B: Enzyme activity and fiber composition in skeletal muscle of untrained and trained men. J App] Physiol 1972; 33: 312-9. Gollnick PD, Armstrong RB, Salon B, Saubert CW IV, Sembrowich WL, Shepherd RE: Effect of training on enzyme activity and fiber composition of human skeletal muscle. J Appl Physiol 1973; 34: 107-11. Gordon-Larsen P, Adair LS, Popkin BM. The relationship of ethnicity, socioeconomic factors, and overweight in US adolescents. Obes Res 2003;11:121Ð129. Gortmaker SL, Peterson K, Wiecha J, et al. Reducing obesity via a school-based interdisciplinary intervention among youth: Planet Health. Arch Pediatr Adolesc Med 1999;153: 409Ð418. Gortmaker SL, Must A, Perrin JM, Sobol AM, Dietz WH. Social and economic consequences of overweight in adolescence and young adulthood. N Engl J Med 1993;329:1008Ð 1012. Goulding A, Taylor RW, Jones IE, McAuley KA, Manning PJ, Williams SM. Overweight and obese children have low bone mass and area for their weight. Int J Obes Relat Metab Disord 2000;24:627Ð632. Gowans SE, DeHueck A, Abbey SE. Measuring exercise-induced mood changes in fibromyalgia: a comparison of several measures. Arthritis Rheum 2002;47:603–9.

29 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Gowans SE, deHueck A, Voss S, Richardson M. A randomized, controlled trial of exercise and education for individuals with fibromyalgia. Arthritis Care Res 1999;12:120–8. Gowans SE, deHueck A, Voss S, Silaj A, Abbey SE, Reynolds WJ. Effect of a randomized, controlled trial of exercise on mood and physical function in individuals with fibromyalgia. Arthritis Rheum 2001;45:519–29. Grant, M. (1991). A Short History of Classical Civilization. London: Weidenfeld and Nicolson. Grant, M. (1964). The Birth of Western Civilization: Greece and Rome. New York: McGraw-Hill. Gracely RH, Dubner R, Deeter WR, Wolskee PJ. Clinicians expectation influence placebo analgesia [letter]. Lancet 1985; i:43. Gracely RH, Dubner R, Wolskee PJ, Deeter WR. Placebo and naloxone can alter post-surgical pain by separate mechanisms. Nature 1983;306:264Ð265. Gregg EW, Gerzoff RB, Caspersen CJ, et al. Relationship of walking to mortality among U.S. adults with diabetes. Arch Intern Med 2003;163:1440Ð1447. Green S, Hassan F, Immelt J, Marks M, Meiland D. In search of global leaders. Harv Bus Rev 2003;81:38Ð45. Green, P. (1989). Classical Bearings: Interpreting Ancient History- Culture. London: Thames; Hudson. Greenland P, Knoll MD, Stamler J, Neaton JD, Dyer AR, Garside DB, Wilson PW. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA 2003;290:891–897. Grimaldi B, Bonnin A, Fillion MP, et al. Interaction of the serotonergic and the immune systems: 5HT-Moduline. In: M.ller N, ed. Psychiatry, Psychoimmunology, and Viruses. Wien/New York: Springer, 1999:45Ð54. Grimm RH Jr, Grandits GA, Cutler JA, et al. Relationships of quality-of-life measures to long-term lifestyle and drug treatment of mild hypertension study. Grossman, MD Kate fibromyalgia and water running. Aquatic Resources Network. 2003 Grundy S [chair of expert panel]. Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Final Report. US Department of Health and Human Services; Public Health Service; National Institutes of Health; National Heart, Lung, and Blood Institute. (NIH Publication No. 02-5215, September 2002.) Circulation 2002;106:3143Ð3421. Gunther V, Mur E, Kinigadner U, Miller C. Fibromyalgia: the effect of relaxation and hydrogalvanic bath therapy on the subjective pain experience. Clin Rheumatol 1994;13:573–8. Gusi N, Tomas-Carus P, Hakkinen A, Hakkinen K, Ortega-Alonso A: Exercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgia.

30 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Arthritis Rheum 2006, 55:66-73. Gusi, N., et al. “Exercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgia.” Guo SS, Roche AF, Chumlea WC, Gardner JD, Siervogel RM. The predictive value of childhood body mass index values for overweight at age 35 y. Am J Clin Nutr 1994;59:810Ð819. Gupta A, Gupta R, Lal B. Effect of Trigonella foenum-graecum (fenugreek) seeds on glycaemic control and insulin resistance in type 2 diabetes mellitus: A double blind placebo controlled study. J Assoc Physicians India 2001:49:1055Ð 1056. Gureje, O., et al., Persistent pain and well-being: a World Health Organization Study in Primary Care. Jama, 1998. 280(2): p. 147-51. Gusi N, Tomas-Carus P, Hakkinen A, Hakkinen K, Ortega-Alonso A: Exercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgia. Arthritis Rheum 2006, 55:66-73. Gusi, N., et al. “Exercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgia.” Gutin B, Cucuzzo N, Islam S, Smith C, Moffatt R, Pargman D. Physical training improves body composition of black obese 7- to 11-year-old girls. Obes Res 1995;3:305Ð312. Hadhazy, V.A., et al., Mind-body therapies for the treatment of fibromyalgia. A systematic review. J Rheumatol, 2000. 27(12): p. 2911-8. Haigh C. Using chaos theory: the implications for nursing. J Adv Nurs. 2002:37(5):462469. Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988Ð 2000. JAMA 2003;290:199Ð206. Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988Ð 2000. JAMA 2003;290:199Ð206. Hale, J. (1994). The Civilization of Europe in the Renaissance. New York: Maxwell Macmillan International. Haley S, Coster W, Faas R. A content validity study of the Pediatric Evaluation of Disability Inventory. Pediatr Phys Ther 1991;3:177Ð184. Halar EM, Bell KR: Rehabilitation's relationship to inactivity. In Krusen's Handbook of Physical Medicine and Rehabilitation, pp 11 13-33. Edited by Kottke FJ, Lehman JF. Philadelphia, WB Saunders, 1990.

31 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Hall, J., S.M. Skevington et al. "A randomized and controlled trial of hydrotherapy in rheumatoid arthritis." Arthritis Care Research, June 1996; (3):206-15. Halstead LS. The power of compassion and caring in rehabilitation healing. Arch Phys Med Rehabil 2001;82:149Ð154. Hallisdorsdottir S. Five basic models of being with another. In: Gaut DA, Leininger MM, eds. Caring: The Compassionate Healer. New York: Center for Human Caring; National League for Nursing Press, 1991:37Ð49. Hanh TN. Peace Is Every Step. New York, NY: Bantam Books; 1991. Hanna RD, Sheldahl LM, Tristani FE (1993). Effect OF enhanced preload with head out water immersion on exercise response in men with healed myocardial infarction. American journal OF Cardiology, 71: 1041-1044 Hambrecht R, Niebauer J, Marburger C, et al. Various intensities of leisure time physical activity in patients with coronary artery disease: Effects on cardiorespiratory fitness and progression of coronary atherosclerotic lesions. J Am Coll Cardiol 1993;22:468Ð477. Hammer M. Beyond Reengineering. New York: Harper Business, 1996. Health Facilities Management. Online document www. planetree.org/nws_facilities.htm Hamer PW and Morton AR (1990) Water running: Training effects and specificity of aerobic, anaerobic and muscular parameters following an eight-week training programme. The Australian Journal of Science and Medicine in Sport. 22:13-22. Hamer PW and Slocombe B (1997) The psychophysical and heart rate relationship between treadmill and deep water running. Australian Journal of Physiotherapy. 43:265-271. Hamilton, William G.. "Common Acute Problems i n Ballet Dancers." Sports Medicine Digest, vol. 8, no. 1 (January 19861, p. 1 Hamer, T., & Morton, A. (1990). Water running: Training effects and specificity of aerobic, anaerobic and muscular parameters following an eight-week interval training program. Australian Journal of Scientific Medicine in Sport, 22, 13-22. Hammell KW. Intrinsicality: Reconsidering spiritual meaning(s) and mandates. Can J Occup Ther 2001;68:186Ð194. Harris MI, Flegal KM, Cowie CC, et al. Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults. The Third National Health and Nutrition Examination Survey, 1988Ð1994. Diabetes Care 1998;21: 518Ð526. Harris WS. A randomized, controlled trial of the effects of remote, intercessory prayer on outcomes in patients admitted to the coronary care unit. Arch Intern Med 1999;159:2273Ð 2278.

32 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Harris, H.A. (1972). Sport in Greece and Rome. Ithaca, NY: Cornell University Press. Harvard Medical School Health Letter. "After Your Heart Attack (Or Before) ." 9 (March 1999), pp. 3-5. Harvard Medical School Health Letter. "Hazards of Dancing: Ballet." vol. 11, no. 4 (February l986), pp. 7-8. Haskell, W.L. (2003). Cardiovascular disease prevention and lifestyle interventions: Effectiveness and Efficacy. Journal of Cardiovascular Nursing, 18(4), 245-255. Hassmen, P. Koivula, N., and Uutela, A. (2000). Physical exercise and psychological well-being: a population study in Finland. Preventative Medicine, 30, 17-25. Haskell WL, Alderman EL, Fair JM, et al. Effects of intensive multiple risk factor reduction on coronary atherosclerosis and clinical cardiac events in men and women with coronary artery disease. The Stanford Coronary Risk Intervention Project (SCRIP). Circulation 1994;89:975Ð990. Hay, D. (1986). The Age of the Renaissance. London: Thames and Hudson. Haynes SG, Feinleib M, Kannel WB. The relationship of psychosocial factors to coronary heart disease in the Framingham Study. Am J Epidemiol 1980;111:37Ð58. Haynes SG, Feinleib M, Kannel WB. The relationship of psychosocial factors to coronary heart disease in the Framingham Study. Am J Epidemiol 1980;111:37Ð58.Arch Intern Med 1997;157: 638Ð648. Healthcare System - Leading Cause of Death in U.S. - By Gary Null PhD, Carolyn Dean MD ND, Martin Feldman MD, Debora Rasio MD, Dorothy Smith PhD Health Facilities Management. Online document at: www. planetree.org/nws_facilities.htm Health Insurance Coverage", Current Population Reports, U.S. Census Bureau, September 2000. Health Insurance Coverage", U.S. Census, Sept. 2000.16 U.S. Health and Human Services, "Preventing Infant Mortality", 2001 and 1997. Health and Fitness Journal, Vol 8, No 5, pp 5-8, 2004 Health On the Net Foundation - About.com reliable trusted health information. Health On the Net Foundation About.com - About.com is accredited by the, which promotes reliable and trusted online health information. Heaney C, Goetzel R. A review of health related outcomes of multi-component worksite health promotion programs. Am J Health Promot 1997;11:290Ð307. Heberlein, T., Perez, H., Wygand, J., & Connor, K. (1987). The metabolic cost of high impact aerobics and hydroaerobic exercise in middle-aged females. Medicine and Science in Sports and Exercise, 19, S89 (Abstract).

33 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Herdman M, Badia X, Berra S: EuroQol-5D: a simple alternative for measuring health-related quality of life in primary care. Aten Primaria 2001, 28:425-430. Heilbronn LK, Noakes M, Clifton PM. The effect of high- and low-glycemic index energy restricted diets on plasma lipid and glucose profiles in type 2 diabetic subjects with varying glycemic control. J Am Coll Nutr 2003;21:120Ð127. Heinonen, Janet . "Running For Two. "Her's World, September 1985, pp. 45-75. Henry JL, Wilson PH, Bruce DG, et al. Cognitive-behavioral stress management for patients with non-insulin dependent diabetes mellitus. Psychol Health Med 1997;2:109Ð118. Herder L, Provost-Craig M, Sestili D, Hove A, Fees M: Water running and the maintenance of maximum oxygen consumption and leg strength in runners [abstract]. Med Sci Sports Exercise 1992; 24(suppl): S23. Hered, S. L., Darby, L. A., & Yaekle, G. C. (1997). Comparison of physiological responses to comparable land and water exercises. Medicine and Science in Exercise and Sport, 29, S162 (Abstract). Hertler, L., Provost-Craig, M., Sestili, P., Hove, A., & Fees, M. (1992). Water running and the maintenance of maximum oxygen consumption and leg strength in women. Medicine and Science in Sports and Exercise, 24, S23 (Abstract). Hessler RM, Eriksson BG, Dey D, Steen G, Sundh V, Steen B. The compression of morbidity debate in aging: An empirical test using the gerontological and geriatric population studies in Goteborg, Sweden. Arch Gerontol Geriatr 2003;37:213Ð222. Hesselbein F, Goldsmith M, Beckhard R. The Organization of the Future. San Francisco: Jossey-Bass Publishers, 2001. Hewitt Associates, LLC. Health and productivity programs continue to grow in popularity as health care cost rise. More Organizations Provide Education, Incentives & Disease Management Program. Lincolnshire, IL: Hewitt; 2002. Hickson RC, Foster C and Pollick ML (1985) Reduced training intensities and loss of aerobic power endurance and cardiac growth. Journal of Applied Physiology. 58:492-499. Hill DW, Smith JC. A method to ensure the accuracy of estimates of anaerobic capacity derived using the critical power concept. J Sports Med Phys Fitness 1994;34:23-37. Hill DW. The critical power concept: a review. Sports Med 1993;16:237-54. Hill DW, Cureton KJ, Grisham SC, Collins MA. Effect of training on the rating of perceived exertion at the ventilatory threshold. Eur J Appl Physiol 1987;56:206- 11. Hill DW, Ferguson CS. A physiological description of critical velocity. Eur J Appl Physiol 1999;79:290-3.

34 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Hill JO, Wyatt H. Outpatient management of obesity: A primary care perspective. Obes Res 2002;10(Suppl 2):124SÐ130S. Himes JH, Dietz WH. Guidelines for overweight in adolescent preventive services: Recommendations from an expert committee. The Expert Committee on Clinical Guidelines for Overweight in Adolescent Preventive Services. Am J Clin Nutr 1994;59:307Ð316. Hoffmans MD, Kromhout D, de Lezenne Coulander C. The impact of body mass index of 78,612 18-year old Dutch men on 32-year mortality from all causes. J Clin Epidemiol 1988; 41:749Ð756. Hoeger, W. K., Gibson, T., Moore, J., & Hopkins, D. (1992). A comparison of selected training responses to water aerobics and low impact aerobic dance. National Aquatics Journal, Winter Ed., 13-16. Hoeger, W. K., Hopkins, D. R., Barber, D. J., & Gibson, T. (1992). Comparison of maximal VO2, HR, and RPE between treadmill running and water aerobics. Medicine and Science in Sports and Exercise, 24, S96 (Abstract). Hoeger, W.W.K and Hoeger, S.A. (1999). Principles & Labs for Fitness & Wellness (5th ed.). Englewood, CO: Morton Publishing Company. Holroyd, K.A. and D.B. Penzien, Psychosocial interventions in the management of recurrent headache disorders. 1: Overview and effectiveness. Behav Med, 1994. 20(2). Holroyd, K.A. and D.B. Penzien, Pharmacological versus non-pharmacological prophylaxis of recurrent migraine headache: a meta-analytic review of clinical trials. Pain, 1990. 42(1): p. 1-13. Holt, Mark, and Patton, Robert. "Deep Water Running: Life i n the Wet Lane." Running Through Texas, January/ February 1986, pp. 17-9. Holloszy, J.O. "Biomechanical Adaptations to Exercise: Aerobic Metabolism." Exercise and Sport Sciences Reviews, vol. 1 (l973), pp. 45-71. Holmes MD, Stampfer MJ, Colditz GA, et al. Dietary factors and the survival of women with breast carcinoma. Cancer 1999;86:826Ð835. Hoppeler, H. ; Luthi, P. ; Claassen, H. ; Weibel, E.R.; and Howald, H. "The Ultrastructure of the Noml Human Skelatal Muscle. " Plugers Archiv, vol. 344 (1973), pp. 217-32. Horwitz RI, Horwitz SM. Adherence to treatment and health outcomes. Arch Intern Med 1993;153:1863Ð1868. Hospital Engineering & Facilities Management. Online document at: www.bbriefings.com/pdf/13 hosp031_r_malkin Hospitals’ ‘Code Blue’ most deadly at night - More patients die if they go into cardiac arrest after 11 p.m., study finds; Associated Press CHICAGO February 2008.

35 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Hotteling H. (1933). Analysis OF A complex OF statistical variable into principal components. Journal OF Educational Psychology, 24: 498-520 Hughson RL, Orok CJ, Staudt LE. A high velocity treadmill running test to access endurance running potential. Int J Sports Med 1984;5:23-5. Housh TJ, Johnson GO, McDowell SL, Housh DJ, Pepper ML. The relationship between anaerobic running capacity and peak plasma lactate. J Sports Med Phys Fitness 1992;32:117-22. Hr.bjartsson A, Gotzsche PC. Is the placebo powerless? An analysis of clinical trials comparing placebo with no treatment. N Engl J Med 2001;344:1594Ð1602. Hr.bjartsson A. What are the main methodological problems in the estimation of placebo effects? J Clin Epidemiol 2002; 55:430Ð435. Hull JG, Bond CF. Social and behavioral consequences of alcohol consumption and expectancy: A meta-analysis. Psychol Bull 1986;99:347Ð360. Hu FB, Manson JE, Stampfer MJ, et al. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N Engl J Med 2001;345:790Ð797. Hu, F.B., Willett, W.C., Li, T., Stampfer, M.J., Colditz, G.A., and Manson, J.E. (2004). Adiposity as compared with physical activity in predicting mortality among women. New England Journal of Medicine. Dec 23;351(26), 2694-2703. Hyde, Margaret O., and Elizabeth H. Forsyth, M.D. The Disease Book: A Kid's Guide. New York: Walker and Company, 1997. Hydro-Tone: The New Science of Total Fitness. Unpublished manuscript. HydroTone Fitness System, Inc., Huntington Beach, CA. Hung CT (1989). Food exchange list based on 80-kilocalorie rice unit. Taiwan yi xue hui za zhi. Journal of the Formosan Medical Association, 88: 595-600. Hurt C, Rice R, McIntosh G, et al. Rhythmic auditory stimulation in gait training for patients with traumatic brain injury. J Music Ther 1998;35:228Ð241. Hyman S. LD, McCarthy S, Lange R, Bronson M, Tamborlane WV. Fat distribution and cardiovascular risk factors in obese adolescent girls: Importance of the intraabdominal fat depot. Am J Clin Nutr 1996;64:12Ð17. Hyatt JD. Future of obesity and chronic-disease management in health care: The HMO perspective. Obes Res 2002; (10 Suppl 1):79SÐ81S. HYPNOSIS, BEHAVIORAL MEDICINE; D. P. BROWN & E. FROMM 1987 ERLBAUM PUBLISHER, HILLSDALE NEW JERSEY 07642 HYPNOSIS, BEHAVIOR MODIFICATION, IMAGERY CONDITIONING; W. KROGER, W.

36 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
FEZLER, 1976, LIPPINCOT. PHILADELPHIA, TORONTO HYPNOSIS IN THE RELIEF OF PAIN; HILGARD & HILGARD, 1975 W. KAUFMANN, LOS ALTOS CA. 94022 HYPNOSIS IN THE SEVENTIES, LARS ERIC UNESTAHL, 1971-74 WELINS TRYCKERI EFTR. AB, OREBRO SWEDEN, HYPNOSIS, POSTHYPNOTIC SUGGESTION; LARS ERIC UNESTAHL, 1971-74 ENVAGEN 7,S-70221, OREBERO, SWEDEN) Ida Hellander, Physicians for a National Health Plan, and JoAnne Bailey, U.S. General Accounting Office. Emrie, David. Goodbye Backache. New York: Arco Publishing, 1983. Illhardt FJ. Plazebo und Ethik. Zeitschrift f.r Allgemeinmedizin 1988;64:279Ð283. INNOVATIONS IN PAIN MANAGEMENT, A PRACTICAL GUIDE FOR CLINICIANS, 1 & 2 EDITED, RICHARD S. WEINER 1990, P. M. DEUTSCH PRESS, ORLANDO, FLORIDA Institute of Medicine. Crossing the quality chasm A new Health system for the 21st century. Washington. DC: National Academy of Sciences Press; 2001. Integrated Benefits Institute. Linking Medical Care to Productivity, February 2001. Online document at: www.ibiweb. org/publications/download/402 Integration of behavioral and relaxation approaches into the treatment of chronic pain and insomnia. NIH Technology Assessment Panel on Integration of Behavioral and Relaxation Approaches into the Treatment of Chronic Pain and Insomnia. Jama, 1996. 276(4): p. 313-8. Isamch, Judy. "Long Swims, Strong Bones." American Health Magazine, July/August 1987, p. 42. ISPA EUROPE. Online document at: www.ispa-europe.com/definition.asp Isokinetics and Exercise Science, Vol 3, No 4, pp207-215, 1993 Jablon SL, Naliboff BD, Gilmore SL, Rosenthal MJ. Effects of relaxation training on glucose tolerance and diabetic control in type II diabetes. Appl Psychophysiol Biofeedback 1997;22:155Ð169. Jackson Y, Dietz WH, Sanders C, et al. Summary of the 2000 Surgeon Generals listening session: Toward a national action plan on overweight and obesity. Obes Res 2002;10:1299Ð1305. Jain SC, Uppal A, Bhatnagar SO, et al. A study of response pattern of non-insulin dependent diabetics to yoga therapy. Diabetes Res Clin Pract 1993;19:69Ð74. Jamison L., Ogden, D. Aquatic Therapy Using PNF Patterns. Tucson. Therapy Skill Builders, 1994. Jatoi A, Loprinzi CL. Nutritional determinants of survival among patients with breast cancer. Surg Clin

37 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
North Am 1999;79:1145Ð1156. Jayagopal V, Albertazzi P, Kilpatrick ES, et al. Beneficial effects of soy phytoestrogen intake in postmenopausal women with type 2 diabetes. Diabetes Care 2002;25:1709Ð1714. Jelalian E, Boergers J, Alday CS, Frank R. Survey of physician attitudes and practices related to pediatric obesity. Clin Pediatr (Phila) 2003;42:235Ð245. Jenkins, P. (1997). A History of the United States. New York: St. Martin's Press. Jensen, Alan, Ph.D. Published and Unpublished Documents;
HYPNOTIC TREATMENT OF DISEASE: A HOLISTIC APPROACH; VALUE OF AGE REGRESSION IN TREATMENT OF DISEASE TREATMENT STRATEGIES OF MEDICAL PSYCHOLOGIST; APPLIED ATHLETIC HYPNOSIS - MENTAL TRAINING PHYSIOLOGICAL SELF-REGULATION, ACTIVATION - IDEAL PERFORMANCE STATE; APPLIED MEDICAL HYPNOSIS COMBINED WITH BEHAVIOR MEDICINE IN TREATMENT OF DISEASE HEALTH, HAPPINESS HYPNOSIS AND REALITY; THE PSYCHOLOGICAL EDGE IN SPORTS; MIND POWER THE DIFFERENCE BETWEEN WINNING AND LOSING; APPLIED CLINICAL HYPNOSIS, BEHAVIOR/SPORTS MEDICINE, PAIN MANAGEMENT, REHABILITATION PSYCHOLOGY, HYDROLOGY CLIMATOLOGY; STRUCTURED DEEP/SHALLOW WATER RESISTANCE EXERCISE REHABILITATION FOR CHRONIC INTRACTABLE BACK PAIN, ENDURANCE AND PAIN MANAGEMENT;
AquaDios-Med SPORTS MEDICINE CONDITIONING AND REHABILITATION CENTER; UNIQUE AQUATIC HEALING & EXERCISE AquaDios-Med™ more than just a splash for cash: Physical fitness, rehabilitation, rejuvenation by
sustained deep-water immersion activities in 4 separate hot-cold chambers and multiple depths. Presented at the International Medical Hydrology Society, Istanbul, Turkey 2006. Jensen, T., Pain: From Molecules to Suffering. Nature Reviews Neuroscience, 2005.6. Jennings B. Healing the self: The moral meaning of relationships in rehabilitation. Am J Phys Med Rehabil 1993;72:401Ð 404. Jetter, Judy and Kadlec, Nancy - The Arthritis Book of Water Exercise. New York: Holt, Rinehart and Winston, 1985.

38 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Jevning, R., R.K. Wallace, and M. Beidebach, The physiology of meditation: a review. A wakeful hypometabolic integrated response. Neurosci Biobehav Rev, 1992. 16(3): p. 415-24. Johansen, J.P., H.L. Fields, and B.H. Manning, The affective component of pain in rodents: direct evidence for a contribution of the anterior cingulate cortex. Proc Natl Acad Sci U S A, 2001. 98(14): p. 8077-82. Jentoft ES, Kvalvik AG, Mengshoel AM: Effects of pool-based and land-based aerobic exercise on women with fibromyalgia/chronic widespread muscle pain. Arthritis Rheum 2001, 45:42-47. Jentoft, Eva Saltskar, et al. “Effects of pool based and land-based aerobic exercise on women with fibromyalgia/chronic widespread muscle pain.” Arthritis and Rheumatism. 45.1 (Feb. 2001) 42-47. Assis et al gia/chronic widespread muscle pain. Arthritis Rheum 2001; 45:42–7. Jin C, Watanabe, K (2003). The practice of Tai Chi Chuan in middle and elderly person and its effect to static and dynamic postural stability. Jpn J Phys Fitness Sports Med, 52: 369-80, in Japanese Johnson DA, Rivlin E, Stein DG. Paediatric rehabilitation: Improving recovery and outcome in childhood disorders [editorial]. Pediatr Rehabil 2001;4:1Ð3. Johnson AL, Cornoni JC, Cassel JC, Tyroler HA, Heyden S, Hames CG. Influence of race, sex and weight on blood pressure behavior in young adults. Am J Cardiol 1975;35:523Ð530. Johnson C. Obesity, weight management, and self-esteem. In: Wadden TA, Stunkard AJ, eds. Handbook of Obesity Treatment. New York: Guilford Press, 2002:480Ð493. Jokes K, support H, Strob U, Blaser P (2003). A synergetic approach to describe the stability and variability of behavior. In: Tscharner W, Dauwalder JP (eds.). The dynamical system approach on cognition. New jersey, London, Singapore: World Scientific, 133-144. 6 Rev Bras Med Esporte _ volume. 11, Nº Jonas WB, Chez RA, Duffy B, et al. Investigating the impact of optimal healing environments. Altern Ther Health Med 2003;9:58Ð64. Jonides L, Buschbacher V, Barlow SE. Management of child and adolescent obesity: Psychological, emotional, and behavioral assessment. Pediatrics. 2002;110:215Ð221. Jonas W. Kaptchuk T, Linde K. Critical overview of homeopathy. Ann Inten1 Med 2003:138: 395399. Jonas W, Crawford C. Healing & Intention and Energy Medicine: Science, research methods and clinical implications London: Harcourt; 2003. Jonas W. The evidence house. West J Med 2001:175:79-80. Jonas WB, Chez R, Duffy B, et al. Investigating the impact of optimal healing environments. Altern Ther Health Med 2003;9:58Ð64.

39 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Jonas WB, Chez RA, Duffy B, Strand D, et al. Investigating the impact of optimal healing environments. Altern Ther Health Med 2003;9:58Ð64. Jonds WB, Chez RA. The role and importance of definitions and standards in healing research. Altern Ther Health Med 2003;9:A5ÐA7. Jones KD, Clark SR. Individualizing the exercise prescription for persons with fibromyalgia. Rheum Dis Clin North Am 2002;28:419–36. Journal of Strength and Conditioning Research, 15(1), 12–19. Frangolias, D., Rhodes, E., & Tauton, J. (1996). J Sports Sci, Vol 21, No 12, pp 959- 972, 2003 J Appl Physiol, Vol 69, pp657- 664, 1990 JOURNAL OF SPORT & EXERCISE PSYCHOLOGY 1987, 1988, 1989 HUMAN KINETICS, CHAMPAIGN ILL 61820 Justice B. Who gets sick How - beliefs, moods and thoughts affect health. Peak Press: 2000. Kabat-Zinn, J., An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry, 1982. 4(1): p. 33-47. Kabir M, Oppert JM, Vidal H, et al. Four week low-glycemic index breakfast with a modest amount of soluble fibers in type 2 diabetic men. Metabolism 2002;51:819Ð826. Kaiser Preventive Medicine and Politics and Kaiser Daily Health Policy Report - “Prevention Efforts Can Increase Overall Health Care Costs”, April 2008 the Washington Post. Kalauokalani D, Cherkin DC, Sherman KJ, Koepsell TD, Deyo RA. Lessons from a trial of acupuncture and massage for low back pain. Spine 2001;26:1418Ð1424. Kaplan, Sheri M.D.; The History of Physical Fitness – Preventive Medicine, July 2007 Kaptchuk TJ. Powerful placebo: The dark side of the randomised controlled trial. Lancet 1998;351:1722Ð1725. Kaptchuk TJ. Intentional ignorance: A history of blind assessment and placebo controls in medicine. Bull History Med 1998;72:389Ð433. Kaptchuk T. Esenberg D. Varieties of healing. 1: Medical pluralism in the United States. Ann Intan MeA 2001;135(3):18%195. Karolides, N.J. and Karolides, M. (1993). Focus on Fitness. Santa Barbara, CA: ABC-CLIO.

40 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Karwachi I. Kennedy B, Glass R. Social capital and self-rated health: A mixed level analysis. Amer J Pup Health. 1999:89:1187-93. Katz, Jane and Bruning, Nancy P. Swimming For Total Fitness. New York: Dolphin Books/Doubleday & Co., 1981. Katz, Jane. The W. E. T. Workout. New York: Facts on File Publications, 1985. Kelly tl (1935). Essential traits OF mentally would run. Harvard Stud. in Educ. 26. Cambridge, measure.: Harvard Univ. Press Kelner M, Wellman B. Complementary and Alternative Medicine: Challenge and change. London: Gordon and Breach; 2000. Keller, A. (1971). Colonial America: A Compact History. New York: Hawthorn Books. Kennedy, J.F. (1960) The soft American. Sports Illustrated. 13:15-17. Kennedy, J.F. (1962). The vigor we need. Sports Illustrated. 17:12-15. Kennedy, J.F. (1960) The soft American. Sports Illustrated. 13:15-17. Kennedy, J.F. (1962). The vigor we need. Sports Illustrated. 17:12-15. Kempner W. Treatment of hypertensive vascular disease with rice diet. Arch Int Med 1974;133:758Ð790. Kemper KA, Sargent RG, Drane JW, Valois RF, Husseye JR. Black and white females perceptions of ideal body size and social norms. Obes Res 994;2:117Ð126. Kennelly J, Brien-Elliott K. The role of music therapy in paediatric Rehabilitation. Pediatr Rehabil 2002;4:137Ð143. Kienle GS, Kiene H. The powerful placebo effect: Fact or fiction? J Clin Epidemiol 1997;50:1311Ð1318. Kienle G, Kiene H. Placeboeffekt und Placebokonzept-eine kritische methodologische und konzeptionelle Analyse von Angaben zum Ausmass des Placeboeffekts. Forschende Komplement.rmedizin 1996;3:121Ð138. Kirsch, I. and H. Walach, [Montgomery GH, DuHamel KN, Redd WH: A meta-analysis of hypnotically induced analgesia: How effective is hypnosis? Int J Clin Exp Hypn 2000; 48: 138-153]. Forsch Komplementarmed Klass Naturheilkd, 2000. 7(5): p. 248. Kizar Ahamath B, Radha Shanmugasundarum K, et al. Antidiabetic effect of a leaf extract from Gymnema sylvestre in non-insulin dependent diabetes mellitus. J Ethnopharmacol 1990;30:295Ð300. Kleijnen J, de Craen AJM, Van Everdingen J, Krol L. Placebo effect in double-blind clinical trials: A review of interactions with medications. Lancet 1994;344:1347Ð1349.

41 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Klein S. Clinical obesity issues from an internists perspective. Obes Res 2002;10(Suppl 1):87SÐ88S. Kleinman A, Eisenberg L, Good B. Culture, illness, and care: clinical Iessons6om anthropologic and cross-cultural research Ann Intern Med.l978;88(2):251-8. Kligler, M.D., M.P.H. - Department of Family Medicine Beth Israel Medical Center - 245 Fifth Avenue, 2nd Floor, New York, NY 10016 Kopecek P, Kiecolt-Glaser J. Psychoneuroimmunology: psychological influences on immune function and health. J Consult Clinc Psychl. 2002:70(3):537-547. King SJ, Wessel J, Bhambhani Y, Sholter D, Maksymowych W. The effects of exercise and education, individually or combined, in women with fibromyalgia. J Rheumatol 2002;29: 2620–7. Kisner, C., & Colby, L.A. (2002). Therapeutic Exercise: Foundations and Techniques. Philadelphia: F.A. Davis Company. Kirsch I. Specifying nonspecifics: Psychological mechanisms of placebo effects. In: Harrington A, ed. The Placebo Effect: Interdisciplinary Explorations. Cambridge, MA: Harvard University Press, 1997:166Ð186. Kirsch I, Sapirstein G. Listening to prozac but hearing placebo: A meta-analysis of antidepressant medication. Prevention & Treatment 1998;1:2a. Online document at: journals apa org/prevention Kirsch I, Baker SL. Clinical implications of expectancy research: Activating placebo effects without deception. Contemp Hypnosis 1993;10:130Ð132. Kirsch I, Rosadino MJ. Do double-blind studies with informed consent yield externally valid results? An empirical test. Psychopharmacology 1993;110:437Ð442. Kirsch 1. How Expectancies shape experience. Washington, DC: American Psychological Assoc: 1999. Kivimaki M, Leino-Arjas P, Kaila-Kangas L, Virtanen M, Elovainio M, Puttonen S, Keltikangas-Jarvinen L, Pentti J, Vahtera J: Increased sickness absence among employees with fibromyalgia. Ann Rheum Dis 2007, 66:65-69. Krebs NF, Jacobson MS. Prevention of pediatric overweight and obesity. Pediatrics 2003;112:424Ð430. Kreutzer JS, Witol AD, Marwitz JH. Alcohol and drug use among young persons with traumatic brain injury. J Learn Disabil 1996;29:643Ð651. Kneipp, Sebastian -- "My Water Cure" (1886), Germany

42 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Kneipp, Sebastian -- 1889, “The Way You Should Live,” - The Man and His Mission - The technique aims to increase blood flow, stimulate the metabolism, temper pain, and boost
immunity; useful for high blood pressure, low blood pressure, arthritis, and rheumatism, sleep disorders, vascular diseases, cramps, pains, stress, food allergies, digestive problems, immune deficiency, and respiratory disorders.
Kneipp Therapy; known as Kneipping, Kneipp Cure, and Kneipptherapie, is a hydropathy-centered system of "natural healing" founded by Bavarian almoner and Dominican priest Sebastian Kneipp (1821-1897); author of My Water Cure; "Thus Thou Shalt Live"; promoted by the Kneipp Institute, in Germany. Herbalism is among its major components. Kobasa SC. Maddi SR, Courington S. Personality and Constitution as Mediators in the Stress-Illness Relationship. Journal of Health and Social Behavior 981;22(December):368& 378. Koenig H. McCullough M, Larson D. Handbook of Relgion and Health. Oxford: Oxford University Press; 2001. Kolkhorst FW, Mittelstadt SW, Dolgener FA. Perceived exertion and blood lactate concentration during graded treadmill running. Eur J Appl Physiol 1996;72: 272-7. Kokubun E. Speed criticism, anaerobic threshold and maximum intensity of swimming in stable phase; Swimmers – juveniles in Blood Lactate1996;10:5-20. Kohrt, W. M., Bloomfield, S. A., Little, K. D., Nelson, M. E., and Yingling, V. R. American College of Sports Medicine. (2004). American College of Sports Medicine Position Stand: Physical activity and bone health. Medicine & Science in Sports & Exercise, 36(11), 1985-1996. Koopman J, Weed D. Epigenesis theory: A mathematical model relating causal concepts of pathogenesis in individuals to disease patterns in populations. ,4111 J Epidemiology. 1990;132(2):366-390. Korel, L.E. The Properties of Water and Their Effect on Aquatic Therapy. Athletic Therapy Today. 1 (2): 1996. Kosterlitz HW, Hughes J. Peptides with morphine-like actions in the brain. Br J Psychiatry 1977;130:298Ð304. Koulil SV, Effting M, Kraaimaat FW, Lankveld WV, Helmond TV, Cats H, van Riel P, de Jong A, Haverman J, Evers A: A review of cognitive behaviour therapies and exercise programmes for fibromyalgia patients: state of the art and future directions. Ann Rheum Dis 2006. doi:10.1136/ard.2006.054692 Konlian, C., Aquatic therapy: making a wave in the treatment of low back injuries. Orthop Nurs. 1999 Jan-Feb 18(1) Krantz DS, Contrada RJ, Hill DR, Freidler E. Environmental stress and biobehavioral antecedents of coronary heart disease. J Counsel Clin Psychol 1988;56:333Ð341.

43 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Kravitz, L., & Mayo, J. (1997). The effect of familiarity with deep water running on maximal oxygen consumption. Journal of Strength and Conditioning, 10(4), 215–219. Aquatic exercise: a review. AKWA letter, October/November. Kravitz, Len, Ph.D and J.J. Mayo, Ph.D. “Training Effects of Aquatic Exercise” University of New Mexico
Kravitz, Len, Ph.D. and Jonathan N. Mike, MS, Exercise Science and Researcher at the University of New Mexico, “The 25 Most Significant Health Benefits of Physical Activity and Exercise” Kravitz, Len, Ph.D; Li, F., P. Harmer, K. J. Fisher, and E. Mcauley; a study in Medicine & Science in Sports & Exercise – “Tai Chi: Improving functional balance and predicting subsequent falls in older persons.” 2004 Kravitz, Len PhD, The 25 Most Significant Health Benefits of Physical Activity and Exercise Kraus, H. and Hirschland, R. (1954). Minimum muscular fitness tests in school children. Research Quarterly. 25:178. Kreitzer MJ, Snyder M. Healing the heart: Integrating complementary therapies and healing practices into the care of cardiovascular patients. Prog Cardiovasc Nurs 2002;17:73Ð80. Krucoff MW, Crater SW, Green CL, et al. The Monitoring and Actualization of Noetic Trainings (MANTRA) Study Project Phase II: First Look at results from a prospective, multicenter randomized trial of energy healing and prayer in patients undergoing elective coronary intervention. Presented at the American College of Cardiology Second Annual Conference on the Integration of Complementary Medicine into Cardiology. Kona HI: October 2003. Kuland, Daniel N. "Poolex For the Injured Runner. The Sports Medicine and Rehabilitation Center, 503 Faulconer Drive #3, Charlottesville, VA 22901. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC growth charts: United States. Adv Data 2000:1Ð27. Kushner RF. Barriers to providing nutrition counseling by physicians: A survey of primary care practitioners. Prev Med 1995;24:546Ð552. Kushi LH, Cunningham JE, Hebert JR, et al. The macrobiotic diet in cancer. J Nutr 2001;131:3056SÐ3064S. Kutz I, Borysenko JZ, Benson H. Meditation and psychotherapy: a rationale for the integration of dynamic psychotherapy: the relaxation response, and mindfulness training. Am J Psychiatry.1985;142:1-8. Kvaavik E, Tell GS, Klepp KI. Predictors and tracking of body mass index from adolescence into adulthood: Followup of 18 to 20 years in the Oslo Youth Study. Arch Pediatr Adolesc Med 2003;157:1212Ð1218.

44 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Lad D. Ayurvedic medicine. In: Jonas W, Levin J, eds. Essentials of Complementary and Alternative Medicine. Philadelphia: Lippincott Williams & Wilkins; 1999. p. 200215. Lamb, David R. Physiology of Exercise, Responses and Adaptations. New York: Madillan Publishing Co., 1984. Lance C. Dalleck and Len Kravitz, Ph.D. “The History of Fitness”, 2007 U, New Mexico. Lane, A.M. and Lovejoy, D.J. (2001). The effects of exercise on mood changes: the moderating effect of depressed mood. Journal of Sports Medicine and Physical Fitness, 41, 539-545. Lao L. Traditional Chinese medicine. In: Jonas W, Levin J, eds. Essentials of Complementary and Alternative Medicine. Philadelphia: Lippincott Williams & Wilkins; 1999. p. 216-232. Lappe M. The Tao of Immunology. New York Plenum; 1997. Landgraf JM, Abetz L, Ware JE. Child Health Questionnaire (CHQ): A User’s Manual. Boston: The Health Institute, New England Medical Center, 1996. Larson J: Bounce Back Ability; videotape educational production. Eugene, OR, Aquatic Networks. Last JM, Wallace RB, eds. Maxcy-Rosenau-Last, Public Health and Preventive Medicine, 13th ed. Norwalk, CT: Appleton & Lange, 1992:1Ð257. Latner JD, Stunkard AJ. Getting worse: The stigmatization of obese children. Obes Res 2003;11:452Ð456. Lawford J, Eiser C. Exploring links between the concepts of Quality of Life and resilience. Pediatr Rehabil 2001;4:209Ð216. Lawrence C, Weisz G. Greater than the Parts: Holism in biomedicine 1920-1950. Oxford: Oxford University Press; 1998. Leclerc BS, Dunnigan L, Cote H, Zunzunegui MV, Hagan L, Morin D. Callers ability to understand advice received from a telephone health-line service: Comparison of self-reported and registered data. Health Serv Res 2003;38:697 - 710. Le Chevalier JM, Vandewalle H, Thépaut-Mathieu C, Stein JF, Caplan L. Local critical power is an index of local endurance. Eur J Appl Physiol 2000;81:120-7. Lee, I.M., 2003. Physical activity and cancer prevention; data from epidemiologic studies. Medicine & Science in Sports & Exercise. 35(11), 1823-1827. Lee, I.M., Sesso, H.D., Oguma, Y, and Paffenbarger, Jr, R.S. (2004). The “Weekend Warrior” and Risk of Mortality. American Journal of Epidemiology, 160(7), 636-641. Leigh JP, Fries JF. Health habits, health care use and costs in a sample of retirees. Inquiry 1992;29:44Ð54.

45 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Leskowitz E. Complementary and Alternative Medicine in Rehabilitation. New York: Churchill Livingstone, 2003. Leslie M Lecron, Self-Hypnotism: The technique & its use in Daily Living, Signet, 1966 Leslie M. Lecron, Complete guide to Hypnosis. Prentice Hall, 1966 Leuchter AF, Cook IA, Witte EA, Morgan M, Abrams M. Changes in brain function of depressed subjects during treatment with placebo. Am J Psychiatry 2002;159:122Ð129. Levine B. Your Body Believes Every Word You Say. Lower Lake, Calif: Aslan Publishing; 1991. Levine JD, Gordon NC. Influence of the method of drug administration on analgesic response. Nature 1984;312:755Ð 756. Levine JD, Gordon NC, Smith R, Fields HL. Analgesic responses to morphine and placebo in individuals with postoperative pain. Pain 1981;10:379Ð389. Levine JD, Gordon NC, Bornstein JC, Fields HL. Role of pain in placebo analgesia. Proc Nat Acad Sci 1979;76:3528Ð3531. 50. Levine JD, Gordon NC, Levine JD, Gordon NC, Fields HL. The mechanism of placebo analgesia. Lancet 1978;ii:654Ð657. Levine JD, Gordon NC, Jones RT, Fields HL. The narcotic antagonist naloxone enhances clinical pain. Nature 1978;272: 826Ð827. Lewis C. Disease prevention and health promotion practices of primary care physicians in the United States. Am J Prev Med 1988;4(suppl):9Ð17. Lewis, S; Thompson P.; Areskog, H. ; Vodak, P. ; Marconyak, M; Debusk, R. ; Mellen, S; and Haskell, W. "Transfer Effects of Endurance Training to Exercise With Untrained Limbs." European Journal of Applied Physiology, vol. 44 (1980), pp. 2534. Libby P. Current concepts of the pathogenesis of the acute coronary syndromes. Circulation 2001;104:365Ð372. Lichtigfeld FJ, Gillman MA. Analgesic nitrous oxide for alcohol withdrawal is better than placebo. Int J Neurosci 1989;49:71Ð74. Lichtigfeld FJ, Gillman MA. Possible role of the endogenous opioid system in the placebo response in depression. Int J Neuropsychopharmacol 2002;5:107Ð108. Lienert GA. Die Bedeutung der Suggestion in pharmakopsychologischen Unterschungen. Zeitschrift f.r experimentelle und angewandte Psychologie 1955;3:418Ð438. Linden W, Lenz JW, Con AH. Individualized stress management for primary hypertension: A randomized trial. Arch Intl Med 2001;161:1071Ð1080.

46 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Linden W, Stossel C, Maruice J. Psychosocial interventions for patients with coronary artery disease: A meta-analysis. Arch Intern Med 1996;156:745Ð752. Lissau I, Overpeck MD, Ruan WJ, Due P, Holstein BE, Hediger ML. Body mass index and overweight in adolescents in 13 European countries, Israel, and the United States. Arch Pediatr Adolesc Med 2004;158:27Ð33. Li S, Chen W, Srinivasan SR, et al. Childhood cardiovascular risk factors and carotid vascular changes in adulthood: The Bogalusa Heart Study. JAMA 2003;290:2271Ð2276. Loder RT, Aronson DD, Greenfield ML. The epidemiology of bilateral slipped capital femoral epiphysis. A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141Ð1147. Lollar DJ, Simeonsson RJ, Nanda U. Measures of outcomes for children and youth. Arch Phys Med Rehabil 2002;81(suppl 2):S46ÐS52. Long, K. A., Lee, E. J., & Swank, S. A. (1996). Effects of deep water exercise on aerobic capacity in older women. Medicine and Science in Sports and Exercise, 28, S210 (Abstract). Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial. Med Care 1999;37:5Ð14. Lotti T, Hautmann G, Panconesi E. Neuropeptides in skin. J Am Acad Dermatol. 1995;33:482-496. Luthar SS, Cicchetti D, Brown B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev 2000;71:543Ð562. Lynch W. ROI bullseye: How a small measure of change can yield a big ROI. Absolute Advantage 2003;5:20Ð21. Maddox GL, Liederman V. Overweight as a social disability with medical implications. J Med Educ 1969;44:214Ð220. Maeder, Edward C. Postgrad Med, vol. 77 (1 February 1985), pp. 112-4. Maes, J. and Kravitz, L. (2004). Training clients with arthritis. IDEA Personal Trainer, 15(2), 27-31. Maestroni GJM, Conti A. Role of the pineal neurohormone melatonin in the psycho-neuroendocrine-immune network. In: Ader R, Felten DL, Cohen N, eds. Psychoneuroimmunology, 2nd ed. San Diego, CA: Academic Press, 1991:495Ð 513. Magel JR, Foglia GF, McArdle WD, Gutin B, Pechar GS, Katch FI: Specificity of swim training cn maximum oxygen uptake. J Appl Physiol 1975; 38: 151-5. Magni, G., et al., Chronic musculoskeletal pain and depressive symptoms in the National Health and Nutrition Examination. I. Epidemiologic follow-up study. Pain, 1993. 53(2): p. 163-8.

47 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Mahon AD, Gay JA, Stolen KQ. Differentiated ratings of perceived exertion at ventilatory threshold in children and adults. Eur J Appl Physiol 1998;18:115-20. Mallory GB, Jr., Fiser DH, Jackson R. Sleep-associated breathing disorders in morbidly obese children and adolescents. J Pediatr 1989;115:892Ð897. Manca A, Hawkins N, Sculpher MJ: Estimating mean QALYs in trial-based cost-effectiveness analysis: the importance of controlling for baseline utility. Health Econ 2005, 14:487-496. Manchanda SC, Narang R, Reddy KS, et al. Retardation of coronary atherosclerosis with yoga lifestyle intervention. J Assoc Physicians India 2000;48:687Ð694. Mandas, Michael, P.T.;. Einhorn, Andrew R , P.T. C.S.M.T.; Ellertson, Jon, B.S., P.T.A.; Hickling, Shawn B.S. Exercise Physiology; Kirsten Pieters, B.S., Athletic Training; Michael Quinn; Gilbert Orbeso of Los Alamitos Orthopaedic & Sports; “Physical Therapy Exercise Program as an Effective Alternative Method of Cross Training for Cross Country and Track Athlete” Mannerkorpi K, Burckhardt CS, Bjelle A. Physical performance characteristics of women with fibromyalgia. Arthritis Care Res 1994;7:123–9. Mannerkorpi K, Nyberg B, Ahlmen M, Ekdahl C. Pool exercise combined with an education program for patients with fibromyalgia syndrome: a prospective, randomized study. J Rheumatol 2000;27:2473–81. Mannerkorpi K, Ahlmen M, Ekdahl C. Six- and 24-month follow-up of pool exercise therapy and education for patients with fibromyalgia. Scand J Rheumatol 2002;31:306–10. Mannerkorpi K: Exercise in fibromyalgia. Curr Opin Rheumatol 2005, 17:190-194. Mannerkorpi K, Ahlmen M, Ekdahl C: Six- and 24-month follow-up of pool exercise therapy and education for patients with fibromyalgia. Scand J Rheumatol 2002, 31:306-310. Mannerkorpi K, Nyberg B, Ahlmen M, Ekdahl C: Pool exercise combined with an education program for patients with fibromyalgia syndrome. A prospective, randomized study. J Rheumatol 2000, 27:2473-2481. Manson JE, Spelsberg A. Primary prevention of non-insulin dependent diabetes mellitus. Am J Prev Med 1994;10: 172Ð184. Maquet, P., et al., Functional neuroanatomy of hypnotic state. Biol Psychiatry, 1999. 45(3): p. 327-33. Marcell, T.J. (2003). Sarcopenia: Causes, consequences, and preventions. Journal of Gerontology, 58A(10), 911-916. Marlatt GA, Rohsenow DJ. Cognitive processes in alcohol use: Expectancy and the balanced placebo design. In: Mello N, ed. Advances in Substance Abuse. Greenwich: JAI Press, 1980:159Ð199.

48 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Masek K, Petrovicky P, Sevcik J, Zidek Z, Frankova D. Past, present and future of psychoneuroimmunology. Toxicology 2000;142:179Ð188. MARSHALL, DEBRA A. M.D., ELAINE WALIZER, R.N., M.S.N., and MARINA N. VERNALIS, D.O.2, “Optimal Healing Environments for Chronic Cardiovascular Disease”, THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE and for Mary Ann Liebert, Martin L, Nutting A, MacIntosh BR, Edworthy SM, Butterwick D, Cook J. An exercise program in the treatment of fibromyalgia. J Rheumatol 1996;23:1050–3. Martinez-Lavin M, Hermosillo AG, Rosas M, Soto ME. Circadian studies of autonomic nervous balance in patients with fibromyalgia: a heart rate variability analysis. Arthritis Rheum 1998;41:1966–71. Massachusetts Medical Society House of Delegates Report 207, A-99 (B), cited in Physicians for a National Health Program, ibid., "How Much Does Single Payer National Health Care Cost?" Massey, Joe B. Journal of the Medical Association of Georgia, vol. 73 (July 1984), pp. 457-9. Masek K, Petrovicky P, Sevcik J, Zidek Z, Frankova D. Past, present and future of psychoneuroimmunology. Toxicology 2000;142:179Ð188. Matthews, D.O. (1969). A Historical Study of the Aims, Contents, and Methods of Swedish, Danish, and German Gymnastics. Proceedings National College Physical Education Association for Men. 72nd, January. Matthews KA, Kiefe CI, Lewis CE, Liu K, Sidney S, Yunis C. Socioeconomic trajectories and incident hypertension in a biracial cohort of young adults. Hypertension 2002;39:772Ð776. Matthews JN, Altman DG, Campbell MJ, Royston P: Analysis of serial measurements in medical research. BMJ 1990, 300:230-235. Mayberg HS, Silva JA, Brannan SK, et al. The functional neuroanatomy of the placebo effect. Am J Psychiatry 2002; 159:728Ð737. Marx, J.O., Ratamess, N.A., Nindl, B.C., Gotshalk, L.A., Volek, J.S., Dohi, K., Bush, J.A., Gomez, A.L., Mazzetti, S.A., Fleck, S.J. Hakkinen, K., Newton, R.U. and Kraemer, W.J. (2001). Low-volume circuit versus high-volume periodized resistance training in women. Medicine & Science in Sports & Exercise. 33 (4), 635-643. Maximal physiological responses to deep water running at thermoneutral temperature. Applied Human Science. 18:31-35. McArdle WD, Katch F, Katch VL (1996) Exercise Physiology (fourth edition) McCain GA, Bell DA, Mai FM, Halliday PD. A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis Rheum 1988;31:1135–41.

49 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
McAuley, E. Blissmer, B. Katula, J., Duncan, T.E., and Mihalko, S.L. (2000). Physical activity, self-esteem, and self-efficacy relationships in older adults: a randomized controlled trial. Annals of Behavioral Medicine, 22, 131-139. McCaffrey, A.M., et al., Prayer for health concerns: results of a national survey on prevalence and patterns of use. Arch Intern Med, 2004. 164(8): p. 858-62. McWaters JG: Run fast, run deep. In Deep Water Exercise for Health and Fitness, pp 106-20. Edited by McWaters JG. Laguna Beach, CA, Publitec Editions, 1993. McClung J, Tuten C, Pritschet B, McInerny J and Emmett J (1998) Cardiac output and stroke volume during deep water running and treadmill running. Medicine and Science in Sports and Exercise. 30:241-246. McArdle, W., Katch, R., & Katch, V. (1991) Exercise Physiology: Energy, Nutrition and Human Performance, 3rd edition. Philadelphia PA: Lea & Febiger. McNeal RL. Aquatic therapy for patients with rheumatic disease. Rheum Dis Clin North Am 1990;16:915–29. McGill University Health Centre Journal. Online document at: www.muhc.ca/media/ensemble/v01n14/design McGimis J. Health in America: The sum of its parts. JAMA. 2002;287:2711. McGinnis JM, Williams-Russo P, Knickman JR. The case for more active policy attention to health promotion. Health Affair 2002;21:78Ð93. McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA 1993;270:2207Ð2212. McGill University Health Centre Journal. www.muhc.ca/media/ensemble/v01n14/design McMurry RG, Fieselmann CC, Avery KE, Sheps DS (1988). Exercise hemodynamics in water and on country into patients with coronary artery disease. Journal OF Cardiopulmonary rehabilitation, 8: 69-74 McNamara JJ, Molot MA, Stremple JF, Cutting RT. Coronary artery disease in combat causalities in Vietnam. JAMA 1971; 216:1185Ð1187. Medell JL, Alexander NB (2000). A clinical measure of maximal and rapid stepping in older women. Journal of Gerontology: Medical Sciences, 55A(8): M429-33 Medicine and Science in Sports and Exercise - Peter B. Raven, B.S., M.S., Ph.D. Professor - Chairman, Department Integrative Physiology, University North Texas Health Science Center. Editor-in-Chief; Kathie Davis, B.A. Executive Director, IDEA, The Health & Fitness Source. Med Sci Sports, Vol 29, pp 649-699, 1997

50 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Med Sci Sports, Vol 28, No 8, pp1056- 1062, 1996 Med Sci Sports, Vol 16, No1, pp1-7, 1984 Med Sci Sports, Vol 27, pp1007-1013, 1995
Mehta RH, Montoye CK, Gallogly M, et al. Improving quality of care for acute myocardial infarction. The Guidelines Applied in Practice (GAP) Initiative. JAMA 2002;287:1269Ð1276. Mehling, W.E., et al., Randomized, controlled trial of breath therapy for patients with chronic low-back pain. Altern Ther Health Med, 2005. 11(4): p. 44-52. Melzack, R. and P.D. Wall, Pain mechanisms: a new theory. Science, 1965. 150(699): p. 971-9. Melzack, R., Sensory, Motivational, and Central Control Determinants of Pain, in The Skin Senses, D.R. Kenshalo, Editor. 1968, CC Thomas: Springfield. p. 423-439. Mengshoel AM, Komnaes HB, Forre O. The effects of 20 weeks of physical fitness training in female patients with fibromyalgia. Clin Exp Rheumatol 1992;10:345–9. Mengshoel AM, Vollestad NK, Forre O. Pain and fatigue induced by exercise in fibromyalgia patients and sedentary healthy subjects. Clin Exp Rheumatol 1995;13:477–82. Mercer, Ph.D. John A. - Biomechanical Comparison of Deep Water and Treadmill Running, UNLV. Mercer, J.A. & Jensen, R.L (1997). Reliability and Validity of a Deep Water Running Graded Exercise Test. Measurement in Physical Education and Exercise Science, 1(4), 213-222. Mercer, J.A. & Jensen, R.L. (1997) Heart Rates at equivalent submaximal VO2 do not differ between Deep Water Running & Treadmill Running. Journal of Strength and Conditioning Research (in press). Meusel, Heinz. British Journal of Sports Medicine, vol. 18 (March l984).. Meyer K, Bücking J (2004). Exercise in Heart failure: Should Aqua Therapy and Swimming allowed? Med Sci of sport Exerc, 36: 2017-2023 Meyer BB, Lemley KJ. Utilizing exercise to affect the symptomology of fibromyalgia: a pilot study. Med Sci Sports Exerc 2000;32:1691–7. Mercer, Ph.D. John, "Deep-Water Running: When Your Training Should Land You in Deep Water."
Michaud, T. J., Brennan, D. K., Wilder, R. P., & Sherman, N. W. (1995). Aquarunning and gains in cardiorespiratory fitness. Journal of Strength and Conditioning Research, 9, 78-84. Michaud, T. J., Rodriquez-Zayas, J., Andres, F. F., Flynn, M. G., & Lambert, C. P. (1995). Comparative exercise responses of deep-water and treadmill running. Journal of Strength and Conditioning Research, 9, 104-109.

51 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Michaud TJ, Brennan DF, Wilder RP, Sherman NW: Aquarun training and changes in treadmill running maximal oxygen consumption [abstract]. Med Sci Sports Exercise 1992; 24(suppl): 523. Michaud TJ, Brennan DF. Wilder RP, Sherman NW. Aquarunning and gains in cardiorespiratory fitness. J Strength Cond Res 1995; 9: 78-84. Micheli, Lyle J., M.D. Sportswise: An Essential Guide for Young Athletes, Parents, and Coaches. New York: Houghton Mifflin, 1990.-Web sites Michaud, T., Rodriguez-Zayas, J., Andres, F., et al. (1995). Comparative exercise responses of deep water and treadmill running. Journal of Strength and Conditioning, 9(2), 104–109. Nagle, E. F., Otto, A. D., Jakicic, J. M., et al. (2003). Miller WL, Crabtree BF, Duffy B, Epstein RM, Stange KC. Research guidelines for assessing the impact of healing relationships in clinical medicine. Altern Ther 2003;9:A80ÐA95. Miller LA, Grunwald GK, Johnson SL, Krebs NF. Disease severity at time of referral for pediatric failure to thrive and obesity: Time for a paradigm shift? J Pediatr 2002;141:121Ð 124. Mikalsen A, Bertelsen B, Flaten MA. Effects of caffeine, caffeine- associated stimuli, and caffeine-related information on physiological and psychological arousal. psychopharmacology 2001;157:373Ð380. Miller J. Going unconscious. In: Silver RB, ed. Hidden Histories of Science, London: Granta Books, 1997:1Ð35. Miller WM, Crabtree BF, Duffy B, et al. Research guidelines for assessing the impact of healing relationships in clinical medicine. Altern Ther Health Med 2003;9(3 Suppl):80AÐ95A. Miller NH, Hill M, Kottke T, Ockene IS. The multilevel compliance challenge: Recommendations for a call to action: A statement for health care professionals. Circulation 1997;95: 1085Ð1090. Ministry of Health, Labour and Welfare (2005). Dietary Reference Intakes for Japanese. Tokyo. Japan: Dai-ichi Syuppan Publishing Co. LTD. Mirkin, Gabe and Hoffman, Marshall. The Sports Medicine Book. Boston: Little, Brown, 1978. MIND BODY COMMUNICATION IN HYPNOSIS, VOL III; MILTON ERICKSON, 1986, E. ROSSI, M. O. RYAN, IRVINGTON PUB. NEW YORK MIND BODY THERAPY; D. CHEEK, E. ROSSI 1988 NORTON NEW YORK 10110 MIND SYMBOLISM-THE SOMATIC INK BLOT SERIES; W.A.CASSELL 1980, AURORA PUBLISHING, ANCHORAGE ALASKA 99501 Mirkin, Gabe and Hoffman, Marshall. The Sports Medicine Book. Boston: Little, Brown, 1978.

52 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Miyoshi T, Shirota T, Yamamoto S, Nakazawa K, Akai M (2004). Effect of the walking speed to the lower limb joint angular displacements, joint moments and ground reaction forces during walking in water. Disability and Rehabilitation, 26(12): 724-32 Mock V, Dow KH, Meares CJ, et al. Effects of exercise on fatigue, physical functioning, and emotional distress during radiation therapy for breast cancer. Oncol Nurs Forum 1997;24: 991Ð1000. Moerman DE, Jonas WB. Deconstructing the placebo effect and finding the meaning response. Ann Intern Med 2002;136: 471Ð476. Moening D, Scheidt A, Shepardson L, Davies GJ (1993). Biomechanical comparison of water running and treadmill running. Isokinetics and Exercise Science, 3(4): 207-15 Moennan D, Jonas W. Deconstructing the placebo effect and finding the meaning response. Ann Intern Med 2002:136:471476. Moerman D, Jonas W. Toward a research agenda on placebo. Adv Mind-Body Med 2000;16:3346. Moldofsky H, Scarisbrick P. Induction of neurasthenic musculoskeletal pain syndrome by selective sleep stage deprivation. Psychosom Med 1976;38:35–44. Monod H, Scherrer J. The work capacity of a synergic muscular group. Ergonomics 1965;8:329-38. Montgomery GH, Kirsch I. Classical conditioning and the placebo effect. Pain 1997;72:107Ð113. Montgomery GH, Kirsch I. Mechanisms of placebo pain reduction: An empirical investigation. Psychol Sci 1996;7:174Ð 176. Montonen J, Knekt P, Jarvinen R, et al. Whole-grain and fiber intake and the incidence of type 2 diabetes. Am J Clin Nutr 2003;77:622Ð629.
Moore LL, Lombardi DA, White MJ, Campbell JL, Oliveria SA, Ellison RC. Influence of parents physical activity levels on activity levels of young children. J Pediatr 1991;118: 215Ð219. Moore BJ. A preliminary Quick Assessment of Overweight in Children and Teens: Shape Up America! 2003. Online document at: www.shapeup.org Morone NE, W.D., Greco CM, Mindfulness meditation for the treatment of chronic low back pain in older adults: A randomized controlled pilot study Pain 8/3/06). Morone NE, G.C., Mind-Body Interventions for Chronic Pain in Older Adults: A Structured Review Pain Medicine, under review, 8/06. Morley, S., C. Eccleston, and A. Williams, Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain, 1999. 80(1-2): p. 1-13.

53 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Morrow, M., Jensen, R., & Peace, C. (1996). Physiological adaptations to deep water and land based running training programs. Medicine and Science in Exercise and Sport, 28. S210 (Abstract). Moritani T, Nagata A, DeVries HA, Muro M. Critical power as a measure of physical work capacity and anaerobic threshold. Ergonomics 1981;24:339-50. Morrison JA, Laskarzewski PM, Rauh JL, et al. Lipids, lipoproteins, and sexual maturation during adolescence: The Princeton maturation study. Metabolism 1979;28:641Ð649. Mossberg HO. 40-year follow-up of overweight children. Lancet 1989;2:491Ð493. Mougios, V., & Deligiannis, A. 1993. Effect of water temperature on performance, lactate production and heart rate at swimming of maximal and submaximal intensity. The Journal of Sports Medicine and Physical Fitness, 33 -27-33 Msall ME, DiGaudio K, Duffy LC, et al. WeeFIM: Normative sample of an instrument for tracking functional independence in children. Clin Pediatr 1994;33:431Ð438. M.ssner R, Lesch K-P. Role of serotonin in the immune system and in neuroimmune interactions. Brain Behav Immun 1998;12:249Ð271. Moore S, LoGerfo I, Inui T. Effect of a self-care book on physician visits. JAMA 1980;243:2317Ð2320. Mooradian AD. Cardiovascular disease in type 2 diabetes mellitus: Current management guidelines. Arch Intern Med 2003;163:33Ð40. Morris EL. The relationship of spirituality to coronary heart disease. Altern Ther Health Med 2001;7:96Ð98. Moyad MA. Dietary fat reduction to reduce prostate cancer risk: Controlled enthusiasm, learning a lesson from breast or other cancers, and the big picture. Urology 2002;59(suppl4A): 51Ð62. Morehouse, Laurence E. and Miller, Augustus T. Jr. Physiology of Exercise. 6th ed. rev. Baton Rouge: C.V. Mosby Co., 1971. Murphy SL, Kung H. Deaths: Final Data for 2003. National vital statistics reports; vol 54 no 13. Hyattsville, MD: National Center for Health Statistics. 2006. Murphy M, Donovan S. The Physical and Psychological effects of meditation: a review of contemporary research with a comprehensive bibliography. 1931-1996. 2 ed. Petaluma. CA: Institute of Noetic Sciences; 1997. Myers J., Kaykha A., George S., Abella J., Zaheer N., Lear S., Yamazaki T., and Froelicher V. (2004). Fitness versus physical activity patterns in predicting mortality in men. American Journal of Medicine. Dec 15;117(12), 912-918. Murray MP, Seireg A, Scholz RC (1967). Center of gravity, center of pressure, and supportive forces during human activities. J Appl Physiol, 23(6): 831-8

54 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Nash, Heyward L. Sports Activity and Arthritis: Individually Determined or Pre-Planned?" The Physician and Sports medicine, April 1986, pp. 148-56. Napoletan, J. Aquatic Therapy: Overview. Rehab and Therapy Products Review. Jan/Feb, 1995. National Association for Health Care Recruitment. NAHCR Allied Health Turnover and Vacancy Rate Survey Results. Prepared by JWT Specialized Communications, July 2002. National Center for Health Statistics. Prevalence of Overweight Among Children and Adolescents: United States, 1999Ð2000. Online document at: www.cdc.gov/nchs/products/ pubs/pubd/hestats/overwght99.htm Posted in 2000. National Institutes of Health. The Practical Guide to the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. National Institutes of Health. Online document: ww.nhlbi.nih.gov/guidelines/obesity/practgde.htm National Center for Health Statistics, National Health Interview Survey, Early Release of Selected Estimates Based on Data from the January-March 2003 National Health Interview Survey. Online document at: www.cdc.gov/nchs. Accessed on October 10, 2003. National Strength and Conditioning Association Journal, "Speed Development." January 1986, pp. 12-73. Natanishi Y, Kimura T and Yokoo Y (1999) Natanishi Y, Kimura T and Yokoo Y (1999) Maximal physiological responses to deep water running at thermoneutral temperature. Applied Human Science. 18:31-35. Neaton JD, Grimm RH Jr, Prineas RJ, et al. Treatment of mild hypertension study: Final results. JAMA 1993;270:713Ð724. Neuhaus BE. Including hope in occupational therapy practice: A pilot study. Am J Occup Ther 1997;51:228Ð234. Neiman, D.C. (2003). Exercise Testing and Prescription (5th edition). Boston, MA: McGraw-Hill. Nieman, D.C. (1990). Fitness & Sports Medicine: An Introduction. Palo Alto, CA: Bull Publishing Co. Newman, D.J. Moving Through Fluids. Biomechanics. May, 1995. Newman, Robert Bruce, “Calm Birth: New Method for Conscious Childbirth, North Atlantic Books, October 2005; Calm Healing: Methods for a New Era of Medicine North Atlantic Books, November 2006. The Emergence of Mind/Body Medicine, Sentient Times, August 1999. Nichols DS, Glenn TM. Effects of aerobic exercise on pain perception, affect, and level of disability in individuals with fibromyalgia. Phys Ther 1994;74:327–32.

55 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
NlH Consensus Development Panel on Acupuncture. Acupuncture. JAMA 1998;280:1518. NIH Videocasting. Online document at: videocast.nih.gov/ PastEvents.asp?c51 Niebauer J, Hambrecht R, Velich T, et al. Attenuated progression of coronary artery disease after six years of multifactorial risk intervention: Role of physical exercise. Circulation 1997;96:2534Ð2541. Nilsson J, Thorstensson A, Halbertsma J (1985). Changes in leg movements and muscle activity with speed of locomotion and mode of progression in humans. Acta Physiol Scand, 123: 457-75 Norris SL, Nichols PJ, Caspersen CJ, et al. Increasing diabetes self-management education in community settings: A systematic review. Am J Prev Med 2002;22:39Ð66. Norregaard J, Lykkegaard JJ, Mehlsen J, Danneskiold-Samsoe B. Exercise training in treatment of fibromyalgia. J Musculoskeletal Pain 1997;5:71–9. Nyman JA. The income transfer effect, the access value of insurance and the Rand health insurance experiment. J Health Econ 2001;20:295Ð298. O’Baugh J, Wilkes LM, Luke S, George A. Being positive: Perceptions of patients with cancer and their nurses. J Adv Nurs 2003;44:262Ð270. O’Brien E, Petrie J, Littler W, deSwiet M, Padfield PL, O’Malley K, Jamieson M, Altman D, Bland M, Atkins N. The British Hypertension Society protocol for the evaluation of automated and semi-automated blood pressure measuring devices with special reference to ambulatory systems. J Hypertens 1990;8:607Ð619. O’Brien E. Modification of blood-pressure-measuring devices and the protocol of the British Hypertension Society. Blood Pressure Monitoring 1999;4:53Ð54. O'Connor B. Personal experience, popular epistemology and CAM research. In: Callahan D, ed. The Role of Complementary and Alternative Medicine: Accommodating pluralism. Washington, DC: Georgetown University Press; 2002. O’Connor GT, Buring JE, Yusef S, et al. An overview of randomized trials of rehabilitation with exercise after myocardial infarction. Circulation 1989;80:234Ð244. O’Connor PJ, Youngstedt SD. Influence of exercise on human sleep. Exerc Sport Sci Rev 1995;23:105–34. O’Donnell, Michael M.B.A., M.P.H., Ph.D., “Health-Promotion Behaviors That Promote Self-Healing”, the JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE, and Mary Ann Liebert, Inc. 2004 O’Donnell M. Definition of Health Promotion: Part III. Expanding the definition. Am J Health Promotion 1989,3:5.

56 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
O’Donnell M. Evolution of workplace health promotion. In: O’Donnell M, ed. Health Promotion in the Workplace. Albany, NY: Delmar, 2002:xivÐxxv. O’Donnell M. Health impact of workplace health promotion programs and methodological quality of the research literature. Am J Health Promot 997;1:1Ð7. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999Ð2000. JAMA 2002;288:1728Ð1732. Oldridge NB, Guyatt GH, Fischer ME, Rimm AA. Cardiac rehabilitation after myocardial infarction. Combined experience of randomized clinical trials. JAMA 1988;260:945Ð950. Olsen JA, Richardson J, Dolan P, Menzel P. The moral relevance of personal characteristics in setting health care priorities. Soc Sci Med 2003;57:1163Ð1172. Ono K, Ito M, Kawaoka T, Kawano H, Shiba D, Seno N, Terawaki F, Nakajima M, Nishimura K, Onodera S (2005). Changes in heart rate, rectal temperature and oxygen uptake during treadmill walking in water and walking in a pool. Journal of Kawasaki Medical Welfare Society 14: 323-330. Organization for Economic Cooperation and Development (OECD) Health Data 2000: A Comparative Analysis of Twenty-nine Countries (Paris: OECD, 2000). Ornish D. Dr Dean Ornish’s program for reversing heart disease. New York: Ballantine Books; 1991. Ornish D. Scherwitz L. Billings J, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998:280(23):2001-2007. Ornish D, Scherwitz LW, Doody RS, et al. Effects of stress management training and dietary changes in treating ischemic heart disease. JAMA 1983;249:54Ð59. Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet 1990;336:129Ð133. Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA 1998; 280:2001Ð2007. Orsay EM, Turnbull TL, Dunne M, et al. Prospective study of the effect of safety belts on morbidity and health care costs in motor-vehicle accidents. JAMA 1988;260:3598Ð3603. Ostelo, R.W., et al., Behavioural treatment for chronic low-back pain. Cochrane Database Syst Rev, 2005(1): p. CD002014. Otis, Carol L. "The Female Athlete - Special Concerns." Sports Medicine Digest, October 1986. Otto von Guericke, Lutz Schega1, and Daniel Daly, MOVEMENT ANALYSIS IN Coronary Artery Disease PATIENTS, University Magdeburg, Institute of Sport Science, Germany 2K.U. Leuven, Department of Rehabilitation Sciences, Belgium; ADAPTED SWIMMING SPORTS AND REHABILITATION Rev Port Cien Desp 6(Supl.2) 351-357 356.

57 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Outside Online, Jack LaLanne is Still an Animal, February 18, 2001. http://www.outsidemag.com/magazine/1195/11f_jack.html, Overmeyer S, Taylor E. Neuroimaging in hyperkinetic children and adults: An overview. Pediatr Rehabil 2001;4:57Ð70. Oxman TE, Freeman DH, Manheimer ED. Lack of social participation or religious strength and comfort as risk factors for death after cardiac surgery in the elderly. Psychosom Med 1995;57:5Ð15. Ozminkowski, Dunn R, Goetzel R, et al. A return on investment evaluation of Citibank, N.A., health management program. Am J Health Promot 999;14:31Ð39. Padgett J, Biro FM. Different shapes in different cultures: Body dissatisfaction, overweight, and obesity in African- American and Caucasian females. J Pediatr Adolesc Gynecol 2003;16:349Ð354. Paffenbarger, Ralph, Jr. "Increased Physical Activity and Increased Longevity." New England Journal of Medicine, vol. 314 (6 March 1986), pp. 60513. Pahor M, Psaty BM, Alderman MH, et al.Therapeutic benefits of ACE inhibitors and other antihypertensive drugs in patients with type 2 diabetes. Diabetes Care 2000;23:888Ð892. Pan X-R, Li G-W, Hu Y-H, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance: The Da Qing IGT and Diabetes Study. Diabetes Care 1997;20:537Ð544. Patient Safety, WASHINGTON - Associated Press Monday February 18, 2008: New push sticks hospitals with cost of errors; Medicare leads no-pay movement; side effect may be better patient safety Patrick DL, Connell FA, Edwards TC, et al. Age-Appropriate Measures of Quality of Life and Disability Outcomes Among Children: The Youth Quality of Life Study. Atlanta: Centers for Disease Control and Prevention, 1998. Pate, R. R., & Kriska, A. (1984). Physiological basis of the sex difference in cardiorespiratory endurance. Sports Medicine, 1, 87-98. Paulus M, Braff D. Chaos and schizophrenia; Does the method fit the madness? Biol Pycl1iaty2003;53(1):3-11. Pierce JW, Wardle J. Cause and effect beliefs and self-esteem of overweight children. J Child Psychol Psychiatry 1997;38:645Ð650. Pietrobelli A, Faith MS, Allison DB, Gallagher D, Chiumello G, Heymsfield SB. Body mass index as a measure of adiposity among children and adolescents: A validation study. J Pediatr 1998;132:204Ð210. Pinhas-Hamiel O, Dolan LM, Daniels SR, Standiford D, Khoury PR, Zeitler P. Increased incidence of non-insulin-dependent diabetes mellitus among adolescents. J Pediatr 1996; 128:608Ð615. PEAK PERFORMANCE, Mental Training Techniques of Greatest Athletes, CHARLES A. GARFIELD, HAL BENNETT, 1984, WARNER BOOKS 666 FIFTH AVE. NY. NY 10103

58 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Pearsall P. The Heart’s Code. New York: Random House, Inc., 1998. Pearson TA, Bazzarre TL, Daniels SR, et al. American Heart Association guide for improving cardiovascular health at the community level: A statement for public health practitioners, healthcare providers, and health policy makers from the American Heart Association Expert Panel on Population and Prevention Science. Circulation 2003;107:645Ð651. Pechar G, McArdle W, Katch F, Magel J, DeLuca J: Specificity of cardiorespiratory adaptations to bicycle and treadmill training. J Appl Physiol 1974; 36: 753-6. 27. Tanaka H: Effects of cross-training: transfer of training effects on V02 max between cycling, running and swimming. Sports Med 1994: 18: 330-9. Pederson PK, Jorgenson K: Maximal oxygen uptake in young women with training, inactivity, and retraining. Med Sci Sports Exercise 1978; 10: 223-37. Pekka P. Influencing public nutrition for non-communicable disease prevention: from community intervention to national programmed experiences from Finland. Public Health Nutr 2002;5:245Ð251. Pelletier K. A review and analysis of the clinical and cost effectiveness studies of comprehensive health promotion and disease management programs at the worksite: 1998. 2000 update. The Science of Health Promotion. 2001. Pelletier KR, Astin JA, Haskell WL. Current trends in the integration and reimbursement of complementary and alternative medicine by managed care organizations and insurance providers: 1998 update and core analysis. Am J Health Promotion 1999;14:125Ð133. Pelletier K. Conventional and integrative medicine-evidence based? Sorting fact from fiction. Focus on Alternative and Complementary Therapies (FACT. 2003;8(1):3-6. Pelletier K. A review and analysis of the health and cost-effective outcome studies of comprehensive health promotion and disease prevention programs in the work-site: 1993Ð1995 update. Am J Health Promot 1996;10:380Ð388. Pelletier KR. A review and analysis of the health and cost-effective outcome studies of comprehensive health promotion and disease prevention programs. Am J Health Promot 1991;5:311Ð313. Pelletier K. A review and analysis of the health and cost-effective outcome studies of comprehensive health promotion and disease prevention programs at the worksite. 1991Ð1993 update. Am J Health Promot 1993;8:43Ð49. Pelletier K. A review and analysis of the clinical and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite. 1995Ð1998 update (IV). Am J Health Promot 1999;136:333Ð345. Pelletier K. A review and analysis of the clinical and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: 1998Ð2000 update. Am J Health Promot 2001;16:107Ð116.

59 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Pelletier K. A review and analysis of the health and cost effective outcomes studies of comprehensive health promotion and disease prevention programs. Am J Health Promot 1991; 5:311Ð315. Pemebaker JW. Opening up-the healing power of confiding in others. 1st ed. New York: William Morrow and Company, Inc.; 1990. Penzien, D.B. and K.A. Holroyd, Psychosocial interventions in the management of recurrent headache disorders. 2: Description of treatment techniques. Behav Med, 1994. 20(2): p. 64-73. Perloff D, Grim C, Flack J, et al. Human blood pressure determination by sphygmomanometry. Circulation 1993;88: 2460Ð2470. Personal Fitness Professional, Fitness Through the Ages, http://www.fit-pro.com/editorial2.asp?ID=49, Accessed March 1, 2001. Petrovic, P., et al., Placebo and opioid analgesia-- imaging a shared neuronal network. Science, 2002. 295(5560): p. 1737-40. Petrovic P, Kalso E, Petersson KM, Ingvar M. Placebo and opioid analgesia Imaging a shared neuronal network. Science 2002;295:1737Ð1740. Physicians for a National Health Program, "How Much Does Single Payer National Health Care Cost?" PNHP Newsletter, October 1999. (http://www.thirdworldtraveler.com/Health/HowMuchSPCost.html) PHYSICIAN & SPORT MEDICINE JOURNAL 1987, 1988, 1989 MONTHLY-MCGRAW HILL MINNEAPOLIS, MINN. 55435 PHYSIOLOGY OF EXERCISE; D.R. LAMB 1984,(2ND EDITION) MACMILLAN PUBLISHING NEW YORK, LONDON Pierce JP, Faerber S, Wright FA, et al. A randomized trial of the effect of a plant-based dietary pattern on additional breast cancer events and survival: The Women’s Healthy Eating and Living (WHEL) Study. Control Clin Trials 2002;23:728Ð756. Pierce EF, Weltman A. Seip RL, Snead D: Effects of training specificity on the lactate threshold and VO2 peak. Int J Sports Med 1990; 11: 267-72. Placebo Theory, Research, Mechanisms. New York: Guilford Press, 1985:255Ð Person Soc Psychol 1985;48:47Ð53. Pleis JR, Coles R. Summary health statistics for U.S. adults: National Health Interview Survey, 1999. National Center for Health Statistics. Vital Health Stat 2003;series 10(No. 212). Pitchot W, Reggers J, Pinto E, et al. Reduced dopaminergic activity in depressed suicides. Psychoneuroendocrinology 2001;26:331Ð335.

60 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Pollock, M.L., Franklin, B.A., Balady, G.J., Chaitman, B.L., Fleg, J.L., Fletcher, B., Limacher, M., Pina, I.L., Stein, R.A., Williams, M, and Bazarre, T. (2001). Resistance exercise in individuals with and without cardiovascular disease: Benefits, rationale, safety, and prescription. Circulation, 101, 828-833. Pollo A, Vighetti S, Rainero I, Benedetti F. Placebo analgesia and the heart. Pain 2003;102:125Ð133. Pollo A, Torre E, Lopiano L, et al. Expectation modulates the response to subthalamic nucleus stimulation in Parkinsonian patients. Neuroreport 2002;13:1383Ð1386. Pollo A, Amanzio M, Arlsanian A, Casadio C, Maggi G, Benedetti F. Response expectancies in placebo analgesia and their clinical relevance. Pain 2001;93:77Ð84. Posner J, Burke CA. The effects of naloxone on opiate and placebo analgesia in healthy volunteers. Psychopharmacology 1985;87:468Ð472. Poon C. Cardiac chaos: Implications for congestive heart failure. Congest Heart Fail 1999;5(6):2702.74. Poole DC. Letter to the editor-in-chief. Med Sci Sports Exerc 1986;26:1335-40. Pöyhönen, T., Sipliä, S., Keskinen, K. L., et al. (2002). Medicine & Science in Sports & Exercise, 24(12), 2103–2109. Price JH, Desmond SM, Krol RA, Snyder FF, O’Connell JK. Family practice physician’s beliefs, attitudes, and practices regarding obesity. Am J Prev Med 1987;3:339Ð345. Price, D.D., Placebo analgesia is accompanied by large reductions in pain-related brain activity in irritable bowel syndrome patients. Pain (in press, 8/06). Price, D.D., Psychological and neural mechanisms of the affective dimension of pain. Science, 2000. 288(5472): p. 1769-72. Price, D.D., S.W. Harkins, and C. Baker, Sensory-affective relationships among different types of clinical and experimental pain. Pain, 1987. 28(3): p. 297-307. Price, D.D., Central neural mechanisms that interrelate sensory and affective dimensions of pain. Mol Interv, 2002. 2(6): p. 392-403, 339. Prochaska JO, DiClemente CC. Stages of change in the modification of problem behaviors. Prog Behav Modif 1992;28: 183Ð218. Prochaska JO. Staging: A revolution in helping people change. Manag Care 2003;12(9 Suppl):6Ð9. Pronk NP, Boucher J. Systems approach to childhood and adolescent obesity prevention and treatment in a managed care organization. Int J Obes Relat Metab Disord 1999;23Suppl 2:S38ÐS42. Puhl R, Brownell KD. Bias, discrimination, and obesity. Obes Res 2001;9:788Ð805.

61 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Press-Ganey Satisfaction Measurement. Online document at: www.pressganey.com PSYCHOBIOLOGY OF MIND-BODY HEALING; E. ROSSI, 1986 NORTON NEW YORK 10110 Quinn JF, Smith M, Ritenbaugh C, Swanson K, Watson MJ. Research guidelines for assessing the impact of the healing relationship in clinical nursing. Altern Ther 2003;9:A65ÐA79. Quinn J. Healing: a model for an integrative health care system. Adv Prac Nurs Q. 1997;3:1-7. Quinn, T. J., Sedory, D. R., & Fisher, B. S. (1994). Physiological effects of deep water running following a land-based training program. Research Quarterly for Exercise and Sport, 65, 386-389. Quirk, Ronald. "A Special Approach to Injured Ballet Dancers." Australian Fam Physician, vol. 13 (November 1984). Raikkonen K, Matthews KA, Kuller LH. Trajectory of psychological risk and incident hypertension in middle-aged women. Hypertension 2001;38:798Ð802. Rainville, P., Brain mechanisms of pain affect and pain modulation. Curr Opin Neurobiol, 2002. 12(2): p. 195-204. Rainville, P., et al., Pain affect encoded in human anterior cingulate but not somatosensory cortex. Science, 1997. 277(5328): p. 968-71. Rashid M, Roberts EA. Nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2000;30:48Ð53. 52. Crichlow RW, Seltzer MH, Jannetta PJ. Cholecystitis in adolescents. Am J Dig Dis 1972;17:68Ð72. Rattay KT, Fulton JE, Galuska DA. Weight counseling patterns of U.S. pediatricians. Obes Res 2004;12:161Ð169. Redondo JR, Justo CM, Moraleda FV, Velayos YG, Puche JJ, Zubero JR, Hernandez TG, Ortells LC, Pareja MA: Long-term efficacy of therapy in patients with fibromyalgia: a physical exercise-based program and a cognitive-behavioral approach. Arthritis Rheum 2004, 51:184-192. Reid DT. Benefits of a virtual play rehabilitation environment for children with cerebral palsy on perceptions of self-efficacy: A pilot study. Pediatr Rehabil 2002;5:141Ð148. Reilly T, Dowzer CN, Cable NT. The physiology of deep-water running. J Sports Sci 2003;21:959-72. Res Quart Ex and Sport, Vol 65, No4, pp386-389, 1994 Sports Med, Vol 16, No6, pp374- 380, 1993 Richards SC, Scott DL. Prescribed exercise in people with fibromyalgia: parallel group randomised controlled trial. BMJ 2002;325:185–9. Richie SE and Hopkins WG (1991) The intensity of exercise in deep water running. International Journal of Sports Medicine. 12:27-29.

62 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Richie, S., & Hopkins, W. (1991). The intensity of deep water running. International Journal of Sports Medicine 12, 27–29. Richie SE and Hopkins WG (1991) The intensity of exercise in deep water running. International Journal of Sports Medicine. 12:27-29. Rice B, Kalker AJ, Schindler JV, Dixon RM. Effect of biofeedback-assisted relaxation training on foot ulcer healing. J Am Podiatr Med Assoc 2001;91:132Ð141. Rice, E.A. Hutchinson, J.L., and Lee, M. (1958). A Brief History of Physical Education. New York: The Ronald Press Co. Richie, S. E., & Hopkins, W. G. (1991). The intensity of exercise in deep-water running. International Journal of Sports Medicine, 12, 27-29. Riley DJ, Santiago TV, Edelman NH. Complications of obesity- hypoventilation syndrome in childhood. Am J Dis Child 1976;130:671Ð674. Rippe JM, McInnis KJ, Melanson KJ. Physician involvement in the management of obesity as a primary medical condition. Obes Res 2001;9(suppl 4):302SÐ311S. Rizzo-Roberts N. Gaseous discharge visualization (GDV) bioelectrography: An overview. In: Francomano CA, Jonas WB, eds. Measuring the Human Energy Field: State of the Science. Gerontology Research Center, NIA. Corona del Mar, CA: Samueli Institute, 2002:23Ð30. Robinson TN, Chang JY, Haydel KF, Killen JD. Overweight concerns and body dissatisfaction among third-grade children: The impacts of ethnicity and socioeconomic status. J Pediatr 2001;138:181Ð187. Robinson TN. Reducing children’s television viewing to prevent obesity: A randomized controlled trial. JAMA 1999; 282:1561Ð1567. Roberts BP, Blinkhorn AS, Duxbury JT. The power of children over adults when obtaining sweet snacks. Int J Paediatr Dent 2003;13:76Ð84. Robert, J. J., Jones, L., & Bobo, M. (1996). The physiologica response of exercising in the water and on land with and without the X1000 Walk ‘n Tone Exercise Belt. Research Quarterly for Exercise and Sport, 67, 310-315. Robert-McComb, J. (2007). Cancer in the elderly: Exercise intervention increases quality of life in patients with multiple myeloma. ACSM’s Certified News, 17(2), 1-3. Roberts JA, Alspaugh JW: Specificity of training effects resulting from programs of treadmill running and bicycle ergometer riding. Med Set Sports Exercise 1972; 4:6-10. Robertson RJ, Falkel JE, Drash AM, Swank AM, Metz KF, Spungen SA, et al. Effects of blood pH on peripheral and central signals of perceived exertion. Med Sci Sports Exerc 1986;18:114-22. Rock CL, Demark-Wahnefried W. Can lifestyle modification increase survival in women diagnosed with breast cancer? J Nutr 2002;132:3504SÐ3509S.

63 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Rodriguez-Moran M, Guerrero-Romero F. Oral magnesium supplementation improves insulin sensitivity and metabolic control in type 2 diabetic subjects: A randomized double-blind controlled trial. Diabetes Care 2003;26:1147Ð1152 Rodriguez MA, Winkleby MA, Ahn D, Sundquist J, Kraemer HC. Identification of population subgroups of children and adolescents with high asthma prevalence: Findings from the Third National Health and Nutrition Examination Survey. Arch Pediatr Adolesc Med 2002;156:269Ð275. Roehling M. Weight-based discrimination in employment: Psychological and legal aspects. Personnel Psychol 1999; 52:969Ð1016. Rohan TE, Hiller JE, McMichael AJ. Dietary factors and survival from breast cancer. Nutr Cancer 1993;20:167Ð177. Rosen DH. Modern medicine and the healing process. Hum Med 1989;5:18Ð23. Rosser WW. Nutritional advice in Canadian family practice. Am J Clin Nutr 2003;77:1011SÐ1015S. Rosser WW. Nutritional advice in Canadian family practice. Am J Clin Nutr 2003;77:1011SÐ1015S. Rossi Ph.D., Ernest, “Symptom Path to Enlightenment: The New Dynamics of Self-Organization in Hypnotherapy” Rossi EL. A conceptual review of the psychosocial genomics of expectancy and surprise: Neuroscience perspectives about the deep psychobiology of therapeutic hypnosis. Am J Clin Hypn 2002;45:103Ð118. Roth G. Das Gehirn und seine Wirklichkeit. Kognitive Neurobiologie und ihre philosophischen Konsequenzen. Frankfurt: Suhrkamp, 1997. Rovere, George D. ll Musculoskeletal In juries i n Theatrical Dance Students. " American Journal of Sports Medicine, vol. 11 (July/August 1983). p. 1958. Rozanski A, Blumenthal JA, Kaplan J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation 1999;99:2192Ð2217. Rucker CE, Cash TF. Body images, body-size perceptions, and eating behaviors among African-American and white college women. Int J Eat Disord 1992;12:291Ð299. Ryan, M. and R. Gevirtz, Biofeedback-based psychophysiological treatment in a primary care setting: an initial feasibility study. Appl Psychophysiol Biofeedback, 2004. 29(2): p. 79-93. Sacco, R.L., Adams, R. Greg Albers, Alberts, M.J., Benavente, O., Furie, K., Goldstein, L.B., Gorelick, P., Halperin, J., Harbaugh, R., Johnston, C., Katzan, I., Kelly-Hayes, M., Kenton, E.J., Marks, M., Schwamm, L.H. and Tomsick, T. (2006). Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke, 37: 577-617.

64 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Sanders, M., & Rippe, N. (1994). Probing the depths of water fitness research. IDEA Today. Sanders, M. E. (1993). Selected physiological training adaptations during a water fitness program called wave aerobics. Thesis, University of Nevada, Reno. Sandy L Homeostasis without reserve-the risk of health system collapse. NEJM. 2002:347:1971-1975. Sachs D, Labovitz DR. The caring occupational therapist: Scope of professional roles and boundaries. Am J Occup Ther 1994;48:997Ð1005. Sacristan JA, Oliva J, Del Llano J, Prieto L, Pinto JL: What is an efficient health technology in Spain? Gac Sanit 2002, 16:334-343. Sanders, M. (2006). Program evaluation: Determining the impact of a water-based cross-cultural exercise program for women aged 50 years and older to improve or maintain functional activities of daily living on land. Doctoral Dissertation, University of Nevada, Reno. Sanders, PhD, FACSM, Mary E. Buring the fat! University of Nevada, Reno; Health & Fitness Journal for the American College of Sports Medicine Scanlon, Kevin. "An Epidemic of Back Pain. MacLean, 7 April 1986, pp. M. Schwimmer JB, Burwinkle TM, Varni JW. Health-related quality of life of severely obese children and adolescents. JAMA 2003;289:1813Ð1819. Schauffler Helen, Rodriguez T. Availability and utilization of health promotion programs and satisfaction with health plan. Med Care 1994; 1182Ð1196. Schnall PL, Schwartz JE, Landsbergis PA, et al. A longitudinal study of job strain and ambulatory blood pressure: Results from a three-year follow up. Psychosom Med 1988;60:697Ð 706. Schneider R, Castillo Richmond A. Alexander C, et al. Behavioral treatment of hypertensive heart disease in African Americans: rationale and design of a randomized controlled t d . Behav Med 2001;27(2):83-95. Schwade S. Hospitals with the human touch. Prevention Magazine 1994;46:92Ð99. Schultz W. The primate basal ganglia and the voluntary control of behaviour. J Consciousness Stud 1999;6:31Ð45. Schuler G, Hambrecht R, Schlierf G, et al. Regular physical exercise and low-fat diet. Effects on progression of coronary artery disease. Circulation 1992;86:1Ð11. Scott T, Mannion R, Davies H, Marshall M. The quantitative measurement of organizational culture in health care: a review of the available instruments. Health Serv Res 2003;38: 923Ð945. Scratch E. (1987). University text book sport swimming (University textbook OF sport Swimming. Berlin: Sport publishing house 11. Weston CF, O´Hare JP, Evans JM, Corrall RJ. (1987).

65 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Haemodynamic CHANGE in one during immersion in water RK difference of temperatures. Clin Sci, 73: 613-616 Scully, D., Kremer, J., Meade, M.M., Graham, R., and Dudgeon, K. (1998). Physical exercise and psychological well-being: a critical review. British Journal of Sports Medicine, 32, 111-120. Sdringola S, Nakagawa K, Nakagawa Y, et al. Combined intense lifestyle and pharmacologic lipid treatment further reduces coronary events and myocardial perfusion abnormalities compared with usual-care cholesterol-lowering drugs in coronary heart disease. J Am Coll Cardiol 2003;41:263Ð272. Sebregts EH, Falger PR, Bar FW. Risk factor modification through nonpharmacological interventions in patients with coronary heart disease. J Psychosomat Res 2000;48:425Ð 441. Sevick MA, Dunn AL, Morrow MS, Marcus BH, Chen GJ, Blair SN: Cost-effectiveness of lifestyle and structured exercise interventions in sedentary adults: results of project ACTIVE. Am J Prev Med 2000, 19:1-8. Shangold, Mona and Mirkin, Gabe. The Complete Sports Medicine Book For Women. New York: Simon & Schuster, 1985. Shapiro SL. Effects of mindfulness-based stress reduction on medical and premedical students. J Behav Med 1998;21: 581Ð599. Shapiro AK, Morris LA. The placebo effect in medicine and psychological therapies. In: Garfield SL, Bergin A, eds. Handbook of Psychotherapy and Behavior Change: An Empirical Analysis, 2nd ed. New York: Wiley, 1978:369Ð410. Sharkey, Brian J. Physiology of Fitness. Champaign, IL: Human Kinetics Publishers, 1979. Sheehan, George. Dr. Sheehan on Running. New York: Bantam Books, 1978. Sherman, Carl. "School For Bad Backs." Consumers Digest, September/October 1984, pp. 58-60. Shepard, R. J. "Exercise i n Coronary Heart Disease." Sports Medicine, vol. 3. Sheslow D, Hassink S, Wallace W, DeLancey E. The relationship between self-esteem and depression in obese children. Ann NY Acad Sci 1993;699:289Ð291. Sid-Ali B, Vandewalle H, Chaïr K, Moreaux A, Monod H. Lactate steady state and distance-exhaustion time relationship in running. Arch Int Physiol Biochim 1991; 99:297-301. Sjogren T, Long N, Storay I, Smith J Physiother Res Int. 1997;2(4):212-22. SKIING, JANUARY 1991; NEW YORK, TIMES MIRROR Siegel MD. Peace, Love and Healing. New York, NY: Harper Perennial; 1990: 224-225.

66 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Sher L. The placebo effect on mood and behavior: the role of the endogenous opioid system. Med Hypotheses 1997;48: 347Ð349. Siegrist J, Peter R, Junge A, Cremer P, Seidel D. Low status of control, high effort at work and ischemic heart disease: Prospective evidence from blue-collar men. Soc Sci Med 1990; 31:1127Ð1134. Simpson, A., & Lemon, P. (1995). Effects of an eight week deep water vertical exercise training program in adult women. AKWA Newsletter. Simmons V, Hansen PD (1996). Effectiveness of water exercise on postural mobility in the well elderly: An experimental study on balance enhancement. Journal of Gerontology: Medical Sciences, 51A(5): M233-8 Sinclair R, Cassuto J, H.gstr.m S, et al. Topical anesthesia with lidocaine aerosol in the control of postoperative pain. Anesthesiology 1988;68:895Ð901. Singh RB, Rastogi SS, Verma R, et al. Randomised controlled trial of cardioprotective diet in patients with recent acute myocardial infarction: Results of one year follow up. BMJ 1992; 304:1015Ð1019. Sinha R, Fisch G, Teague B, et al. Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N Engl J Med 2002;346:802Ð810. Sinking-Silverman LR, Wing RR. Management of obesity in primary care. Obes Res 1997;5:603Ð612. Silvestri JM, Weese-Mayer DE, Bass MT, Kenny AS, Hauptman SA, Pearsall SM. Polysomnography in obese children with a history of sleep-associated breathing disorders. Pediatr Pulmonol 1993;16:124Ð129. Skinner, B., Science and human behavior. 1953, New York: McMillan Skovlund E. Should we tell trials patients that they might receive placebo? Lancet 1991;337:1041. Skovlund E, Fyllingen G, Landre H, Nesheim B-I. Comparison of postpartum pain treatments using a sequential trial design I: Paracetamol versus placebo. Eur J Clin Pharmacol 1991;40:343Ð347. Skovlund E, Fyllingen G, Landre H, Nesheim B-I. Comparison of postpartum pain treatments using a sequential trial design II: naproxen versus paracetamol. Eur J Clin Pharmacol 1991;40:539Ð542. Slater-Hamel, Arthur. "Possible Neuromuscular Mechanisms as Limiting Factor for Rate of Leg Movement in Sprinting." Research Waterly, vol. 12 (December 1941). Smarr, K.L., et al., The importance of enhancing self-efficacy in rheumatoid arthritis. Arthritis Care Res, 1997. 10(1): p. 18-26. Smith, Everett L. "Exercise and Older Women." Sports Medicine Digest, January 1985, p. 1. Smith TW, Ruiz JM. Psychosocial influences on the development and course of coronary heart disease: Current status and implications for research and practice. J Consult Clin Psychol 2002;70:548Ð568.

67 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Smyth J, Stone A. Hurewitz A, Kaell A. Effects of writing about stressful experiences on symptom reduction in patients with asthma or rheumatoid arthritis: a randomized trial .JAMA. 1999;281:13041309. Sobel, D.S., MSJAMA: mind matters, money matters: the cost-effectiveness of mind/body medicine. Jama, 2000. 284(13): p. 1705. Sobel, D.S., The cost-effectiveness of mind-body medicine interventions. Prog Brain Res, 2000. 122: p. 393-412. Sothern MS. Exercise as a modality in the treatment of childhood obesity. Pediatr Clin North Am 2001;48:995Ð1015. SOMATIC INK BLOT SERIES II ADMINISTRATION-INTERPRETATION; CASSELL 1989, SOMATIC INK BLOT CENTER ANCHORAGE ALASKA 99504 Sone H, Katagiri A, Ishibashi S, et al. Effects of lifestyle modifications on patients with type 2 diabetes: the Japan Diabetes Complications Study (JDCS) study design, baseline analysis and three year-interim report. Horm Metab Res 2002;34:509Ð515. Spiegel, D. and R. Moore, Imagery and hypnosis in the treatment of cancer patients. Oncology (Williston Park), 1997. 11(8): p. 1179-89; discussion 1189-95. SPORTS MEDICINE YEARBOOK 1988 YEAR BOOK MEDICAL PUBLISHERS, CHICAGO, LONDON Sports Medicine Digest, "Exercise During Pregnancy." vol. 7 (March 1985), p. 5. Sports Medicine Digest, "Pregnancy and Exercise. " vol. 7 (October 1985), p. 4. Stainton T. The positive impact of children with an intellectual disability on the family. J Intellect Dev Disab 1998;23: 57Ð70. Stamler J, Stamler R, Neaton JD. Low risk-factor profile and long-term cardiovascular and noncardiovascular mortality and life expectancy: Findings for 5 large cohorts of young adult and middle-aged men and women. JAMA 1999;282:2012Ð2018. Stanton BR. Does family functioning affect outcome in children with neurological disorders? Pediatr Rehabil 1999;3:193Ð 199. Starfield B, Bergner M, Ensminger M, et al. Adolescent health status measurement: Development of the Child Health and Illness Profile. Pediatrics 1993;91:430Ð435. Stefanick, M.L., Mackey, S., Sheehan, M., Ellsworth, N., Haskell, W.L., and Wood, P.D. (1998). Effects of diet and exercise in men and postmenopausal women with low levels of HDL cholesterol and high levels of LDL cholesterol. New England Journal of Medicine, July 2, 339(1), 12-20. Steinhoff JP, Smith SC. Putting prevention into daily practice. Cardiol Clin 2003;21:471Ð482.

68 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Steyn, N.P., Mann, J., Bennett, P.H., Temple, N., Zimmet, P., Tuomilehto, J., Lindstrom, J, and Louheranta, A. (2004). Diet, nutrition and the prevention of type 2 diabetes. Public Health and Nutrition. Feb;7(1A), 147-65. Stokols D, Pelletier K, and Fieldings J. 1ntegration of medical care and worksite health promotion. JAMA 1995;275: 1136 - 1142. Story MT, Neumark-Stzainer DR, Sherwood NE, et al. Management of child and adolescent obesity: Attitudes, barriers, skills, and training needs among health care professionals. Pediatrics 2002;110:210Ð214. Strauss RS. Childhood obesity and self-esteem. Pediatrics 2000;105:e15. Strauss RS, Pollack HA. Epidemic increase in childhood overweight, 1986Ð1998. JAMA 2001;286:2845Ð2848. Strauss RS, Pollack HA. Social marginalization of overweight children. Arch Pediatr Adolesc Med 2003;157:746Ð 752. Starkweather, PhD, RN Angela R. The Effects of Exercise on Perceived Stress and IL-6 Levels Among Older Adults Stromme SB, Ingjer F. Meen HD: Assessment of maximal aerobic power in specifically trained athletes. J Appl Physiol 1977; 42: 833-7. Stumvoll, M., Goldstein, B.J., and van Haeften, T.W. (2005). Type 2 diabetes: principles of pathogenesis and therapy. Lancet, 365, 1333-1346. Study Group and Research in Metabolism, Nutrition and Exercise - Physical Education and of sport center - Londrina State University - Londrina, PR. January/Fev, 2005 Stoudmire NM, Wideman L, Pass KA, McGinnes CL, Gaesser GA, Weltman A. The validity of regulating blood lactate concentration during running by ratings of perceived exertion. Med Sci Sports Exerc 1996;28:490-5. Strohman RC. Ancient genomes, wise bodies, unhealthy people: limits of a genetic paradigm in biology and medicine. Perspectives in Biology and Medicine 1993;37(1):112-145. STUDIES ON HYSTERIA (1893-1895), JOSEF BREUER, SIGMUND FREUD AND ANNA FREUD BASIC BOOKS, HARPER COLOPHON BOOKS, NEW YORK Stuler, Stu. "Run Long and Prosper." Runner's World, July 1986, pp. 77-81. Sullivan MJ. Return to Aesclepius The healer’s path. Presented at the Second Conference on the Integration of Complementary Medicine Into Cardiology. American College of Cardiology Extramural Symposium. Kona, HI: October 2003.

69 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Suomi R, Koceja DM (2000). Postural sway characteristics in women with lower extremity arthritis before and after an aquatic exercise intervention. Arch Phys Med Rehabil, 81: 780-5 Surwit RS, van Tilburg M, Zucker N, et al. Stress management improves long-term glycemic control in type 2 diabetes. Diabetes Care 2002;25:30Ð34. Svedenhag J, Seger J: Running on land and in water: comparative exercise physiology. Med Sci Sports Exercise 1992; 24: 1155-60. Svedenhag J, Seger J. Running on land and in water: comparative exercise physiology. Med Sci Sports Exerc 1992;24: 1155–60. Swain, D.P. and Franklin, B.A. (2006). Comparison of cardioprotective benefits of vigorous versus moderate intensity aerobic exercise. American Journal of Cardiology, 97: 141-147. Tabacchi MH. Spa development in the World. Paper presented to the Asian International Spa Association, April 28Ð30, 2003. Takeshima, N., Rogera, M. E., Wantanebe, E., et al. (2002). Water-based exercise improves health related aspects of fitness in older women. Medicine & Science in Sports & Exercise, 33(3), 544–551. Tarlov AR, Ware JE, Greenfield S, et al. The Medical Outcomes Study: An application of methods for monitoring the results of medical care. JAMA 1989;262:925Ð930. Taylor EM, Mitchell JE, Kenan S, Tacker R. Attitudes of occupational Therapists toward spirituality in practice. Am J Occup Ther 2000;54:421Ð426. Taylor HG, Yeates KO, Wade SL, Drotar D, Stancin T, Burant C. Bidirectional child family influences on outcomes of traumatic brain injury in children. J Int Neuropsychol Soc 2001;7:755Ð767. Taylor CB, Houston-Miller N, Haskell WL, DeBusk RF. Smoking cessation after acute myocardial infarction: The effects of exercise training. Addict Behav 1988;13:331Ð335. Teasdale, J.D., et al., Metacognitive awareness and prevention of relapse in depression: empirical evidence. J Consult Clin Psychol, 2002. 70(2): p. 275-87. Teasdale, J.D., et al., Metacognitive awareness and prevention of relapse in depression: empirical evidence. J Consult Clin Psychol, 2002. 70(2): p. 275-87. Templeton, M.S., Booth, D. L., O'Kelly, W. D. Effects of Aquatic Therapy on Joint Flexibility and Functional Ability in Subjects with Rheumatic Disease. JOSPT 23 (6): 1996. G ter Riet G, de Craen AJM, de Boer A, Kessels AGH. Is placebo analgesia mediated by endogenous opioids? A systematic review. Pain 1998;76:273Ð275. Tesch, Per A. "Exercise Performance and B-Blockade. "Sports Medicine, vol. 2, no. 6, p. 389.

70 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Tershakovec AM, Watson MH, Wenner WJ, Jr, Marx AL. Insurance reimbursement for the treatment of obesity in children. J Pediatr 1999;134:573Ð578. The International SPA Association’s 2002 Spa Industry Study. Price Waterhouse Coopers, September 2002. The Science of the Placebo: Toward an interdisciplinary research agenda. In; 2000 Nov 1921,2000; Natcher Conference Center, NIH. Bethesda, MD:2000. Available6om URL: http://placebo.nih.gov. The NHS Plan", a plan for reforming National Health Service, in part to repair the damage from years of underfunding by previous governments. The British Council, Health Insight” August 2000. (http://www.britishcouncil.org/health/themes/insight/aug00/aug.htm) "The Psychobiology of Gene Expression: Neuroscience and Neurogenesis in Hypnosis and the Healing Arts." W. W. Norton Professional Books, New York, Tel. 800-233-4830. The U.S. Health Care System: Best in the World, or Just the Most Expensive? The University of Maine System Bureau of Labor Education University of Maine Orono, Maine 2001 Thomas KB. General practice consultations: Is there any point in being positive? Br Med J 1987;294:1200Ð1202. Thomas KB. The placebo in general practice. Lancet. 1994;344(0ctober 15):1066-1067. Thompson RS, Taplin SH, McAfee TA, et al. Primary and secondary prevention services in clinical practice: Twenty years’ experience in development, implementation, and evaluation. JAMA 273:1130Ð1135. Thomas, T. R., Ziogas, G., Smith, T., Zhang, Q., & Londeree, B. R. (1995). Physiological and perceived exertion responses to six modes of submaximal exercise. Research Quarterly for Exercise and Sport, 66, 239-246. Tindle, H.A., et al., Factors associated with the use of mind body therapies among United States adults with musculoskeletal pain. Complement Ther Med, 2005. 13(3): p. 155-64. Tindle, H.A., et al., Trends in use of complementary and alternative medicine by US adults: 1997-2002. Altern Ther Health Med, 2005. 11(1): p. 42-9. Tolle, T.R., et al., Region-specific encoding of sensory and affective components of pain in the human brain: a positron emission tomography correlation analysis. Ann Neurol, 1999. 45(1): p. 40-7. Tomas-Carus P, Hakkinen A, Gusi N, Leal A, Hakkinen K, Ortega-Alonso A: Aquatic training and detraining on fitness and quality of life in fibromyalgia. Med Sci Sports Exerc 2007, 39:1044-1050. Torii H, Yan Z, Hosoi J, Granstein R. Expression of neurotrophic factors and neuropeptide receptors by Langerhans cells and the Langerhans cell-like cell line XS52: further support for a functional relationship between Langerhans cells and epidermal nerves. J Invest Dermatol.1997;109:586-591.

71 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Tovin, B. J., Wolf, S. L., Greenfield, B. H., et al. Comparison of the effects of exercise in water and on land on the rehabilitation of patients with intra-articular anterior cruciate ligament reconstructions. Phys. Ther. 74 (8): 1994. Town GP, Bradley SS: Maximal metabolic responses of deep and shallow water running in trained runners. Med Sci Sports Exercise 1991; 23: 238-41. Treise D, Weigold MF. AIDS public service announcements: Effects of fear and repetition on predictors of condom use. Health Mark Q 2001;18:39Ð61. Trento M, Passera P, Bajardi M, et al. Lifestyle intervention by group care prevents deterioration of Type II diabetes: A 4-year randomized controlled clinical trial. Diabetologia 2002; 45:1231Ð1239.
Tresolini C, Force P-FT. Health professions education and relationship-centered care. San Francisco, CA. Pew Health Professions Commission; 1994. Tretli S, Haldorsen T, Ottestad L. The effect of pre-morbid height and weight on the survival of breast cancer patients. Br J Cancer 1990;62:299Ð303. Troiano RP, Flegal KM. Overweight children and adolescents: Description, epidemiology, and demographics. Pediatrics 1998;101:497Ð504. Trowbridge FL, Sofka D, Holt K, Barlow SE. Management of child and adolescent obesity: Study design and practitioner characteristics. Pediatrics 2002;110:205Ð209. Trute B, Hiebert-Murphy D. Family adjustment to childhood developmental disability: A measure of parent appraisal of family impacts. J Pediatr Psychol 2002;27:271Ð280. Tsuda I. Toward an interpretation of dynamic neural activity in terms of chaotic dynamical systems. Behnv Brain Sri 2001;24(5):793-810. Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001;344: 1343Ð1350. Turk, D.C. and A. Okifuji, Psychological factors in chronic pain: evolution and revolution. J Consult Clin Psychol, 2002. 70(3): p. 678-90. Turk, D.C., Cognitive-behavioral approach to the treatment of chronic pain patients. Reg Anesth Pain Med, 2003. 28(6): p. 573-9. Uexk.ll TV. Biosemiotic research and not further molecular analysis is necessary to describe pathways between cells, personalities, and social systems. Adv J Mind Body Health 1995;11:24Ð27. Ulrich RS. Effects of health facility interior design on wellness: Theory and recent scientific research. J Healthcare Design 1991;3;97Ð109. USA Cycling Coaching Staff. USA Cycling Sport Coach Manual. Colorado Springs, CO: USA Cycling, Inc., 1999.

72 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
USA Today. "Office Workers Suffer More Than Physical Laborers." February 1987, pp. 11-12. USA Today. "Office Workers Suffer More Than Physical Laborers." February 1987, pp. 11-12. USA WEEKEND health expert Tedd Mitchell, M.D The Gerontologist 2006 The Gerontological Society of America; Further Resources - Wellness Program Cooper Clinic, Dallas - Texas State Board on Aging. U.S. Department of Health and Human Services. Healthy People 2010, 2nd ed. Washington, D.C.: U.S. Department of Health and Human Services, 2000. U.S. Department of Health and Human Services. The Surgeon Generals Call to Action to Prevent and Decrease Overweight and Obesity. Rockville, M.D.: U.S. Department of Health and Human Services, Public Health Service, Office of the Surgeon General, 2001. U.S. Department of Health and Human Services. Healthy People 2010: Understanding and Improving Health, 2nd ed. Washington, D.C.: U.S. Government Printing Office, November 2000. U.S. Department of Health and Human Services. A systematic approach to health, healthy people 2010 goals. Goal 2: Eliminate health disparities. Healthy People 2010, conference ed., in 2 vols. Washington, DC., U.S. Government Printing Office, 2000. US Department of Health and Human Services. Physical activity and health: A report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services. National Center for Control and Prevention; 1996. Available from URL: http://vnnv.cdc.gov/nccdphp/sgdcontents.hhnl. U.S. Preventive Services Task Force. Guide to Clinical and Preventive Services. Baltimore, MD: William & Wilkins, 1989. U.S. Preventive Services Task Force. Guide to Clinical and Preventive Services, 2nd ed. Baltimore, MD: William & Wilkins, 1996. U.S. Preventive Services Task Force. Guide to Clinical and Preventive Services, 3rd ed. www.ahcpr.gov/ clinic/gcpspu.htm October 23, 2003. US Public Health Service Office of the Surgeon General; The Surgeon General's report on nutrition and health. Nestle. M(ed): US Public Health Service, Office of the Surgeon General; 1988. http://sgreports.nlm.nih.gov/NN/B/C/4/G/segments.html Valim V, Oliveira L, Suda A, Silva L, de Assis M, Neto T, et al. Aerobic fitness effects in fibromyalgia. J Rheumatol 2003;30:1060–9. Valim V, Oliveira LM, Suda AL, Silva LE, Faro M, Neto TL, et al. Peak oxygen uptake and ventilatory anaerobic threshold in fibromyalgia. J Rheumatol 2002;29:353–7. Van Santen M, Bolwijn P, Landewe R, Verstappen F, Bakker C, Hidding A, et al. High or low intensity aerobic fitness training in fibromyalgia: does it matter? J Rheumatol 2002;29: 582–7.

73 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
van Dam RM, Rimm EB, Willett WC, et al. Dietary patterns and risk for type 2 diabetes mellitus in U.S. men. Ann Intern Med 2002;136:201Ð209. Van Denderen JC, Boersma JW, Zeinstra P, Hollander AP, van Neerbos BR. Physiological effects of exhaustive physical exercise in primary fibromyalgia syndrome (PFS): is PFS a disorder of neuroendocrine reactivity? Scand J Rheumatol 1992; 21:35–7. van den Hout WB, Tijhuis GJ, Hazes JM, Breedveld FC, Vliet Vlieland TP: Cost effectiveness and cost utility analysis of multidisciplinary care in patients with rheumatoid arthritis: a randomised comparison of clinical nurse specialist care, inpatient team care, and day patient team care. Van Santen M, Bolwijn P, Verstappen F, Bakker C, Hidding A, Houben H, et al. A randomized clinical trial comparing fitness and biofeedback training versus basic treatment in patients with fibromyalgia. J Rheumatol 2002;29:575–81. van Weert J, van Dulmen S, Bar P, Venus E. Interdisciplinary preoperative patient education in cardiac surgery. Patient Educ Couns 2003;49:105Ð114. Vase L, Riley JL, Price DD. A comparison of placebo effects in clinical analgesic trials versus studies of placebo analgesia. Pain 2002;99:443Ð452. Vase L, Robinson ME, Verne GN, Price DD. The contributions of suggestion, desire, and expectation to placebo effects in irritable bowel syndrome patients: An empirical investigation. Pain 2003;105:17Ð25. Verhagen A.P., h.c.w. de Vet et al. "Balneotherapy for rheumatoid arthritis and osteoarthritis." (Cochrane Review) In: The Cochrane Library health database, Issue 3, 2002, Oxford. Verstegen, M. Plunging into aquatic exercise: Underwater speed. Training & Conditioning, 1996. Verstappen FT, Santen-Hoeuftt HM, Bolwijn PH, van der Linden S, Kuipers H. Effect of a group activity program for fibromyalgia patients on physical fitness and well-being. J Musculoskeletal Pain 1997;5:17–28. Vickery, S. R., Cureton, K. J., & Langstaff, J. L. (1983). Heart rate and energy expenditure during aqua dynamics. Physician and Sports medicine, 11, 67-72. Vickery D, Kalmer H, Lowery D, et al. Effect of a self-care education program on medical visits. JAMA 1983;250: 2952Ð2956. Voudouris NJ, Peck CL, Coleman G. The role of conditioning and verbal expectancy in the placebo response. Pain 1990; 43:121Ð128. Voudouris NJ, Peck CL, Coleman G. Conditioned response models of placebo phenomena: Further support. Pain 1989; 38:109Ð116. Voudouris NJ, Peck CL, Coleman G. Conditioned placebo responses. J *97.

74 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Waelti P, Dickinsen A, Schultz W. Dopamine responses comply with basic assumptions of formal learning theory. Nature 2001;412:43Ð48. Walach H. Das Wirksamkeitsparadox in der Komplement .rmedizin. Forschende Komplement.rmedizin und Klassische Naturheilkunde 2001;8:193Ð195. Walach H, Sadaghiani C. Plazebo und Plazebo-Effekte: Eine Bestandsaufnahme. Psychotherapie, Psychosomatik, medizinische Psychologie 2002;52:332Ð342. Wadden TA, Anderson DA, Foster GD, Bennett A, Steinberg C, Sarwer DB. Obese women’s perceptions of their physicians weight management attitudes and practices. Arch Fam Med 2000;9:854Ð860. Wadden TA, Didie E. What’s in a name? Patient’s preferred terms for describing obesity. Obes Res 2003;11:1140Ð1146. Wells-Federman, C., P. Arnstein, and M. Caudill, Nurse-led pain management program: effect on self-efficacy, pain intensity, pain-related disability, and depressive symptoms in chronic pain patients. Pain Manag Nurs, 2002. 3(4): p. 131-40. Wickramasekera I. A conditioned response model of the placebo effect: Predictions from the model. In: White L, Tursky B, Schwartz GE, eds. Wilmore, J. H., & Costill, D. L. (1994). Physiology of Sport and Exercise. Champaign: Human Kinetics. Vedhara K, Bennett PD, Clark S, et al. Enhancement of antibody responses to influenza vaccination in the elderly following a cognitive-Behavioural stress management intervention. Psychother Psychosom 2003;72:245Ð252. Villarosa, Linda. "Water Works. " The Runner, November 1984, pp. 124-6. Villarosa, Linda. "Having It All: Running and Pregnancy." The Runner, August 1985, pp. 24-31. Vita AJ, Terry RB, Hubert HB, Fries JF. Aging, health risks, and cumulative disability. N Engl J Med 1998;338:1035Ð1041. Vogt, B.A., Pain and emotion interactions in subregions of the cingulate gyrus. Nat Rev Neurosci, 2005. 6(7): p. 533-44. Voss, D. E., Ionta, M.K., Myers, B.J. Proprioceptive neuromuscular facilitation patterns and techniques. Philadelphia, Harper and Row Publishers, 1985. Vusjan V, Sievenpiper JL, Xu Z, et al. Konjac-Mannan and American ginseng: Emerging alternative therapies for type 2 diabetes mellitus. J Am Coll Nutr 2001;20(5 Suppl):370SÐ 380S; discussion 381SÐ383S.

75 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Vuskan, V, Sievenpiper JL, Koo VY, et al. American ginseng (Panax quinquefolius L) reduces postprandial glycemia in nondiabetic subjects and subjects with type 2 diabetes mellitus. Arch Intern Med 2000:160:1009Ð1013 Wallace, K.G., Analysis of recent literature concerning relaxation and imagery interventions for cancer pain. Cancer Nurs, 1997. 20(2): p. 79-87. Wakayoshi K, Yoshida T, Udo M, Kasai T, Moritani T, Mutoh Y, et al. A simple method for determining critical speed as swimming fatigue threshold in competitive swimming. Int J Sports Med 1992;13:367-71. Wakayoshi K, Yoshida T, Udo M, Harada T, Moritani T, Mutoh Y, et al. Does critical swimming velocity represent exercise intensity at maximal lactate steadystate? Eur J Appl Physiol 1993;66:90-5. Walleczek J. Self-Organized Biological Dynamics and Nonlinear Control. Cambridge, UK: Cambridge University Press; 2000. Wallner S, Watzinger N, Lindschinger M, et al. Effects of intensified lifestyle modification on the need for further revascularization after coronary angioplasty. Eur J Clin Invest 1999; 29:372Ð379. Waliszewki P, Konarski J. Neuronal differentiation and synapse formation occur in space and time with fractal dimension. Synapse. 2002;43(4):252-258. Wang Y. Is obesity associated with early sexual maturation? A comparison of the association in American boys versus girls. Pediatrics 2002;110:903Ð910. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992;30:473–83. Wasserman K, Whipp BJ, Koyl SN, Beaver WL. Anaerobic threshold and respiratory gas exchange during exercise. J Appl Physiol 1973;35:236–43. Wasson J, Gaudette C, Whaley F, et al. Telephone care as a substitute for routine clinical follow-up. JAMA 1992;267: 1788Ð1793. Weltman A. The blood lactate response to exercise. 1st rev. ed. Champaign: Human Kinetics, 1995. Weighing and, K, wish, D, Jaehnig, W (1975). The division OF swimming of strokes into phases, based upon kinetics parameter. In Lewillie, L, Clarys, JP (eds.), Swimming II (pp. 161-166). Baltimore: University park press W. Chez R Definitions and-standards in healing research. 1st American Samueli Symposium. Altern Therap Health Med 2003;9(3 Suppl.). Welch, P.D. (1996). History of American Physical Education and Sport (2nd ed.). Springfield, IL: Charles C. Thomas.

76 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Whelton, S.P., Chin, A., Xin, X, and He, J. 2002. Effect of aerobic exercise on blood pressure: A meta-analysis of randomized, controlled trials. Annals of Internal Medicine, 136 (7), 493-503. White KP, Speechley M, Harth M, Ostbye T: The London Fibromyalgia Epidemiology Study: the prevalence of fibromyalgia syndrome in London, Ontario. J Rheumatol 1999, 26:1570-1576. White KP, Speechley M, Harth M, Ostbye T: The London Fibromyalgia Epidemiology Study: direct health care costs of fibromyalgia syndrome in London, Canada. J Rheumatol 1999, 26:885-889. Wilber, R. L., Moffatt, R. J., Scott, B. E., Lee, D. T., & Cucuzzo, N. A. (1996). Influence of water run training on the maintenance of aerobic performance. Medicine and Science in Sports and Exercise, 28, 1056-1062. Wilber RL, Moffatt RJ, Scott BE, Lee DT, Cucuzzo NA: Influence of water run training on the maintenance of aerobic performance. Med Sci Sports Exercise 1996;28:1056-62. Wilber RL, Moffatt RI, Scott BE, Lee DT, Cucuzzo NA: Influence of water-run training on running performance [abstract[. Med Sci Sports Exercise 1994; 26(suppl): S4. Wilder RP, Brennan DK, Schotte DE: A standard measure for exercise prescription for aqua running. Am J Sports Med 1993; 21: 45- 8. Wilder RP, Brennan DK: Techniques of aqua running. in Comprehensive Aquatic Therapy, pp 123-34. Edited by Becker BE, Cole ALL Boston, Butterworth-Heinemann, 1997. Wilder RP, Brennan DK: Physiologic responses to deep water running in athletes. Sports Med 1993; 16: 374-80. Wilder RP, Brennan DK. Physiological responses to deep water running in athletes Sports Med 1993;16:374-80. Wilder, R. P., & Brennan, D. K. (1997). Techniques of aqua running. In Becker, B. E., & Cole, A. J., Comprehensive Aquatic Therapy (p. 123–135). Boston MA: Butterworth-Heinemann. Wigers SH, Stiles TC, Vogel PA. Effects of aerobic exercise versus stress management treatment in fibromyalgia: a 4.5 year prospective study. Scand J Rheumatol 1996;25:77–86. Withers RT, Sherman WM, Miller JM, Costill DL: Assessment of the anaerobic power in threshold in endurance trained cyclists and runners. Eur J Appl Physiol 1981; 42: 833-7. 47: 93-104. Wilinson R. Income, quality and social cohesion. An1 /Pub Health. 1997;87. Willan AR: On the probability of cost-effectiveness using data from randomized clinical trials. BMC Med Res Methodol 2001, 1:8. White House Commission for Complementary and Alternative Medicine Policy. Final Report.2002.Available from URL: www.whccamp.hhs.gov/finalreport.html

77 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Williams RB. Psychological factors in coronary artery disease: Epidemiologic evidence. Circulation 1987;76:1117Ð1123. Williams RB, Barefoot JC, Schneiderman N. Psychosocial risk factors for cardiovascular disease. More than one culprit at work. JAMA 2003;290:2190Ð2192. Wilson M, Holman P B, Hammock A. A comprehensive review of the effects of worksite health promotion on health-related outcomes. Am J Health Promotion 1996;10:6. Winter, Lloyd C. So You Want To Be a Sprinter. San Jose: Winter Enterprises Publishers, 1973. Winzelberg AJ, Classen C, Alpers GW, et al. Evaluation of an internet support group for women with primary breast cancer. Cancer 2003;97:1164Ð1173. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the multicenter criteria committee. Arthritis Rheum 1990;33: 160–72. Wolfe F, Anderson J, Harkness D, Bennett RM, Caro XJ, Goldenberg DL, Russell IJ, Yunus MB: A prospective, longitudinal, multicenter study of service utilization and costs in fibromyalgia. Arthritis Rheum 1997, 40:1560-1570. Wolff M, Spens R, Young S, Lucey P, Cooper J, Ahmed S, Maurana C. Patient empowerment strategies for a safety net. Nurs Econ 2003;21:219Ð225. Wolsko, P.M., et al., Use of mind-body medical therapies. J Gen Intern Med, 2004. 19(1): p. 43-50. Wood MJ. Use of complementary and alternative medicine therapies in patients with cardiovascular disease. Am Heart J 2003;145:841Ð846. Woollacott M (1993). Age-related changes in posture and movement. The Journal of Gerontology, 48: 56-60 Woolhandler, Steffie M.D., M.P.H. and David U. Himmelstein, M.D., "The Deteriorating Administrative Efficiency of the U.S. Health Care System"; New England Journal of Medicine 324:1253-1258 (May 2), 1991. Woolhandler, Steffie M.D, M.P.H.. and David U. Himmelstein, M.D.; "Costs of Care and Administration at For-Profit and Other Hospitals in the United States"; New England Journal of Medicine 336:769-774 (March 13), 1997. World Health Organization, The World Health Report 2000 . Health Systems: Improving Performance (Geneva: WHO, 2000). Wuest, D.A., and Bucher, C.A. (1995). Foundations of Physical Education and Sport. St. Louis, MO: Mosby. Wyatt, F.B., s. Milam et al. "The effects of aquatic and traditional exercise programs on persons with knee osteoarthritis," Journal of Strength Conditioning Research, August 15, 2001; (3): 337-40.

78 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Yamaji Greenley M, Northey DR, Hughson RL: Oxygen uptake and heart rate responses to treadmill and water running. Can J Sports Sci 1990; 15: 96-8. 37. Ritchie SE, Hopkins WG: The intensity of exercise in deep water running. Int J Sports Med 1991; 12: 27-9. Yancy WS, Westman EC, French PA, Califf RM. Diets and clinical coronary events. The truth is out there. Circulation 2003;107:10Ð16. Yardley, Lucy PhD, Bishop, Felicity L. PhD, Beyer, Nina PhD, Hauer, Klaus PhD, Gertrudis, I. J., Kempen, M. PhD, Piot-Ziegler, Chantal PhD, Todd, Chris J. PhD, “Older People's Views of Falls-Prevention Interventions in Six European Countries”; School of Psychology, University of Southampton, Southampton, United Kingdom SO17 1BJ. Yarosh D. Why is DNA damage signaling so complicated? Chaos and molecular signaling. Environ Mol Mutagen 2001:38(2-3). Yeragani V, Rao K. Smitha M, Pohl R, Balon R, Srinivasan K. Diminished chaos of heart rate time series in patients with major depression. Biol Psychiatry. 2002:51(9). Ylvisaker M, Feeney T. Executive functions, self-regulation, and learned optimism in paediatric rehabilitation: A review and implications for intervention. Pediatr Rehabil 2002;5:51Ð70. Ylvisaker M, Jacobs H, Feeney T. Positive supports for people who experience disability following brain injury: A review. J Head Trauma Rehabil 2003;18:7Ð32. Ylvisaker M. Long-term rehabilitation after TBI in children and adolescents: A real-world balancing act. Recovery 2001;12:19Ð21. Yocum DE, Hodes R, Sundstrom WR, Cleeland CS. Use of biofeedback training in the treatment of Raynaud’s disease and phenomenon. J Rheumatol.1985;12: 90-93. Yoneda T, Muraki T, Taketomi Y (1994). Influence of aging on standing balance. Bulletin of Allied Medical Sciences, Kobe 10: 61-68. Young NL, Williams JI, Yoshida KK, Bobardier C, Wright, JG. The context of measuring disability: Does it matter whether capability of performance is measured? J Clin Epidemiol 1996;49:1097Ð1101. Young Men's Christian Association, "Arthritis Aquatic Program Official Activity Guide. " Seattle Young Men' s Christian Association, 1986. Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH. Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med 1997;337:869Ð873. Zatzick DF, Johnson FA. Alternative psychotherapeutic practice among middle class Americans: I: Case studies and follow-up. Culture Med Psychiatry 1997;21:53Ð88. Zeni, A. I., Hoffman, M. D., & Clifford, P. S. (1996). Energy expenditure with indoor exercise machines. Journal of the American Medical Association, 275, 1424-1427.

79 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Zijlstra TR, Braakman-Jansen LM, Taal E, Rasker JJ, van de Laar MA: Cost-effectiveness of Spa treatment for fibromyalgia: general health improvement is not for free. Rheumatology (Oxford) 2007, 46:1454-1459. Zinner ES, Ball JD, Stutts ML, Philput C. Grief reactions of mothers of adolescents and young adults with traumatic brain injury. Arch Clin Neuropsychol 1997;12:435Ð447. Zimmerman GL, Olsen CG, Bosworth MF. A stages of change approach to helping patients change behavior. Am Fam Physician 2000;61:1409Ð1416. Zubieta, J.K., et al., Regional mu opioid receptor regulation of sensory and affective dimensions of pain. Science, 2001. 293(5528): p. 311-5.
Partial List of References XII • 79 Pages ***
The Health Care Crisis
Is Man-Made • Manufactured
The Solution Is AquaDios-Med Proactive Preventive Medicine
By Dr. Alan Jensen
Copyright © 1985 - 2008 – 2013
AquaDiosTM / AquaDios-MedTM AquaDiosMed™
All Rights Reserved

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section XIII
The Health Care Crisis Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
References • Expanded Research
Healthcare Crisis • Manufactured • Man-Made • Includes • Clinical Hypnosis • Inner Mental Training
• Mind Body Medicine • Positive Psychology • Hypnotizability• Sport Psychology • Sport Medicine • Placebo Analgesia
• Psychoneuroimmunology • Aquatic Exercise • Deep-Water Immersion • Physiology • And much more
• 10 Pages
Evidence Based AquaDios-Med™ Proactive Preventive Medicine
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

1 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Partial List of References Section XIII • 10 Pages The Health Care Crisis
Is Man-Made • Manufactured The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
********************************************************************************** Partial List References: Clinical Hypnosis • Inner Mental Training • Mind Body Medicine • Positive Psychology •Hypnotizability • Sport Psychology • Sport Medicine • Placebo Analgesia • Psychoneuroimmunology • Deep-Water Immersion • Physiology • And much more ********************************************************************************** References
American Psychologist, 60, 410–421. American Psychologist, 61, 774–788.
Antonuncio D, Danton W, (1995) Psychotherapy versus medication for depression: Challenging the conventional wisdom with data. Professional Psychology: Research and Practice, vol 26, no 6, 574-585
Brewin, C. R., Reynolds, M., & Tata, P. (1998). Autobiographical memory processes and the course of depression. Journal of Abnormal Psychology, 108, 511-517.
Brittlebank A, Scott J, Williams J Ferrier I (1993) Autobiographical memory in depression: State or Trait marker British Journal of Psychiatry 162 118-121
C R Snyder, S J Bibliography health well-being. In C. R. & S. J. Dobbin A, Maxwell M (2005) A feasibility study to test the methods and recruitment
procedures towards a future randomized trial of self-hypnosis versus antidepressant medication for the management of depression. Report to CSO office in Scotland no CZG/2/121
Jensen, Alan, The Healthcare Problem and Solution; AquaDios-Med™, unpublished paper 2006. Available at http://www.aquadios.com/ [email protected]
Jensen, Alan - The Health Care Problem: Research of the Crisis; The Solution Is AquaDios-Med™ A Preventive Medicine Process and Workbook for Mind Body Medicine; Use of a Pendulum, Ideomotor Finger Responses; THE SEVEN KEYS; 725 pages. An unpublished research By Dr. Alan Jensen.
Kirsch I, Montgomery G, Sapirstein G (1995) Hypnosis as an adjunct to cognitive behavioural therapy Journal of Consulting and Clinical Psychology Vol 63, No 2, 214-220
Kirsch I, Moore T, Scobonia A, Nicholls S (2002) The emperor's new drugs: An analysis of antidepressant medication data submitted to the U.S. Food and Drug Administration Prevention & Treatment. Vol 5 Jul 2002, np.
Laverture N, Kumar V, Pekala R (2002) The effectiveness of a hypnotic ego strengthening procedure for improving self-esteem and depression American Journal of Clinical and Experimental Hypnosis Vol 30, no 1,2002, 1-23
Lopez (Eds.), Handbook of positive psychology (pp. 541–555). New York: Oxford University Press.
Moncrieff J, Wessely S, Hardy R (2002) Active Placebo versus antidepressants for depression. (Cochrane Review) Cochrane Library, Issue 3, 2002
Positive Psychology Interventions: A Practice-Friendly Meta-Analysis Journal of Clinical Psychology in Session Vol 65 (5) 467 – 487. Positive Mental Training Lars-Eric Uneståhl 4

2 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Ryff, C. D., & Singer, B. (2002). From social structure to biology: Integrative science in pursuit of human and well being
Schwartz, Richard (2001) Introduction to the Internal Family Systems Model Trailheads Publications Illinois.
Sheppard L, Teasdale J (2000) Dysfunctional Thinking in Major Depressive Disorder: A Deficit in Metacognitive Monitoring, Journal Abnormal psychology Volume 109(4) 768–776
Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction. American Psychologist, 55, 5–14.
Seligman, M. E. P., Steen, T. A., Park, N., & Peterson, C. (2005). Positive psychology progress: Empirical validation of interventions.
Sin N & Lyubomirsky (2009) Enhancing Well-Being and Alleviating Depressive Symptoms with Positive Psychology Interventions: A Practice-Friendly Meta-Analysis Journal of Clinical Psychology in Session Vol 65 (5) 467 – 487.
Teasdale J, Cox S (2001) Dysphoria: self-devaluative and affective components in recovered depressed patients and never depressed controls Psychological Medicine Volume 31(7) 1311-1316
Teasdale J, Moore R Hayhurst H, Pope M, Williams S, Segal, Zindel V (2002) Metacognitive Awareness and Prevention of Relapse in Depression: Empirical Evidence Journal of Abnormal Psychology, 104, 585–591
Uneståhl, L-E (1973), Hypnosis and Posthypnotic suggestions (PhD thesis Uppsala University). Örebro, Sweden: VEJE International.
Uneståhl L-E (1996), Intergraded Mental Training Forlag, Stockholm. SISU ISBN 91 87660 11 3. Uneståhl, L-E.: Hypnosis - posthypnotic suggestions, VEJE International Publ., 1973. Uneståhl, L-E.: Hypnosis in the seventies. VEJE International, Publ., 1975 Uneståhl, L-E.: Self-Control by Mental Training. VEJE International Publ., 1979 Uneståhl, L-E.: Hypnosis in Theory and Practice, VEJE International Publ., 1982 Uneståhl, L-E (Ed.) Contemporary Sport Psychology. VEJE International Publ., 1985 Uneståhl, L-E (Ed) Sport Psychology Theory - Practice; VEJE International Publ.1985 Uneståhl, L-E.: Motivation; The Core of Life. VEJE International Publ., 1990 Uneståhl, L-E.: Applied Motivation. VEJE International Publ., 1994 Uneståhl, L-E.: Integrated Mental Training. VEJE International Publ., 1998 Veenhoven, R. (2006) Health Happiness: Effects of happiness on physical health and the
consequences for preventive health care Watkins E, Teasdale J, (2001) Rumination and Over general Memory in Depression: Effects of
Self-Focus and Analytic Thinking Journal of Abnormal Psychology Volume 110(2) 353–357 Watkins E, Teasdale J (2004) Adaptive and maladaptive self-focus in depression Journal of
Affective Disorders Volume 82, Issue 1, 1-8

3 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
References • MBM • PNI • Immune System Ader R, Cohen N. Behaviorally conditioned immunosuppression.*46. Andrews SE, Aikens JE, Kiolbasa TA, Sobel R. Psychological predictors of glycemic change
with relaxation training in non-insulin dependent diabetes mellitus. Psychother Psychosomatic 1997; 66: 302Ð306.
Allen JK, Scott LB. Alternative models in the delivery of primary and secondary prevention programs. J Cardiovasc Nurs 2003; 18:150Ð157.
Alternative medicine: Expanding medical horizons. A report to NIH on alternative medical systems and practices in the United States. Chantilly, VVA: Workshop on Alternative Medicine; 1992 Sept. 14-16.1992.
Amanzio M, Pollo A, Maggi G, Benedetti F. Response variability to analgesics: A role for non-specific activation of endogenous opioids. Pain 2001; 90:205Ð215.
American Psychologist, 60, 410–421. American Psychologist, 61, 774–788. American College of Sports Medicine: Guidelines for Exercise Testing and Prescription, Ed 5.
Baltimore, Williams & Wilkins, 1995 American Journal of Preventive Medicine, the Association of Teachers of Preventive Medicine
and the American College of Preventive Medicine, Elsevier Science - a forum for the communication of information, knowledge and wisdom in prevention science, education, practice and policy.
American Heart Association. Heart Disease and Stroke Statistics—2006 Update. Dallas, Texas: American Heart Association, 2006. Hoyert DL, Heron MP,
American Heart Association. Heart Disease and Stroke Statistics Ñ2003 Update. Dallas: American Heart Association, 2003.
American Journal of Preventive Medicine May 1998; 14(4): 245-258 Am J Sports Med, Vol 21, No1, 1993 Anderson, E.L., Frischholz, E.J., & Trentalange, M.J. (1988). Hypnotic and non-hypnotic
control of ventilation. American Journal of Clinical Hypnosis, 31, 118-128. American Society of Clinical Hypnosis, (1976). Annual Meeting, Scientific Session; Panel on
Medical Hypnosis, Dabney Ewin, Bertha Roger, Eric Wright, Chicago Antonuncio D, Danton W, (1995) Psychotherapy versus medication for depression: Challenging the conventional wisdom with data. Professional Psychology: Research and Practice, vol 26, no 6, 574-585
Hemodynamic changes in man during immersion with the head above water. Aerospace Medicine, 43, 592-598.
Asher, Anne - About.Com a part of the New York Times 2006 “Back Pain and Deep water running”
Assis, Marcos Renato, et al. “A randomized controlled trial of deep water running: Clinical effectiveness of aquatic exercise to treat fibromyalgia.” Arthritis and Rheumatism. 55.1 (Feb. 2006): 57-65.
Astin JA. Why patients use alternative medicine: Results of a national study. JAMA 1998:279(19):1548.1553. Acad Political Soc Sci. 2002:583:2943.
Astin, J.A., et al., Mind-body medicine: state of the science, implications for practice. J Am Board Fam Pract, 2003. 16(2): p. 131-47.
Astin, J.A., et al., Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum, 2002. 47(3): p. 291-302.
Barnes, P.M., et al., Complementary and alternative medicine use among adults: United States, 2002. Adv Data, 2004(343): p. 1-19.

4 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Barrios, PhD. Alfred A. Toward Greater Freedom and Happiness, Self-Programmed Control Press, PO Box 49939 Los Angeles Ca. 90049.
Batey DM, Kaufnmann PG, Raczynski JM, Hollis JF, Murphy JK, Rosner B, Corrigan SA, Rappaport NB, Danielson EM, Lasser NL, Kuhn CM. Stress management
intervention for primary prevention of hypertension: Detailed results from Phase l Trials of Hypertension Prevention (TOHP-l). Ann Epidemiol 2000; 10:45Ð58.
Beck A (1967) Depression: Causes and treatment Philadelphia: University Pennsylvania Press Bell I, Caspi 0. Schwartz G, et al. Integrative medicine and systemic outcomes research: Issues
in the emergence of a new model for primary health care. Arch Intern Med 2002:162(2):133-140. Benedetti F, Amanzio M. The neurobiology of placebo analgesia: From endogenous opioids to
cholecystokinin. Prog Neurobiol 1997; 52:109Ð125. Benzein E, Saveman BI. One step towards the understanding of hope: A concept Bergmann J-F, Chassany O, Gandiol J, et al. A randomized clinical trial of the effect of
informed consent on the analgesic activity of placebo and naproxen in cancer patients. Clin Trials Metaanal 1994; 29:41Ð47.
Blalock JE. The syntax of immune-neuroendocrine communication. Immunol Today 1994; 15:504Ð511.
Blumenthal TD, Flaten MA. Effects of caffeine and caffeine-associated stimuli on the human startle eye blink reflex. Pharmacol Biochem Behav 1998; 59:39Ð44.
Borg G Psychophysical bases of perceived exertion. Medicine and Science in Sport and Exercise, 1982 - 14:377-381.
Borg, G. (1998). Borg’s perceived exertion and pain scales. Champaign IL: Human Kinetics. Br J Sports Med, Vol32, pp44-48, 1998
Brewin, C. R., Reynolds, M., & Tata, P. (1998). Autobiographical memory processes and the course of depression. Journal of Abnormal Psychology, 108, 511-517.
Brittlebank A, Scott J, Williams J Ferrier I (1993) Autobiographical memory in depression: State or Trait marker British Journal of Psychiatry 162 118-121
Bogdanich, W. (1991;1992). The great white lie. New York: TOUCHSTONE: Simon & Schuster.
Carey, B. (2005). In the hospital, a degrading shift from person to patient. New York Times, Aug 16: 1, 12
CLINICAL HYPNOSIS, PRINCIPLES APPLICATIONS; H. B. CRASILNECK, J. A. HALL, 1976 GRUNE & STRATTON, NEW YORK, SAN FRANCISCO, LONDON
CLINICAL EXPERIMENTAL HYPNOSIS, (1ST. & 2ND EDITIONS), W. KROGER, 1963, 1976, LIPPINCOT. PHILADELPHIA, TORONTO
Cohen K. Native American medicine. In: Jonas W. Levin J, eds. Essentials of Complementary
and Alternative Medicine. Philadelphia: Lippincott Williams & Wilkis; 1999. p. 233251. Cole, Andrew J. MD - Becker, Bruce E. MD, MS; “Water therapy exercise program; Water
therapy pain relief; December 27, 2006; Adapted from: American College of Sports Medicine. (2006). ACSM’s Guidelines for Exercise Testing and Prescription, 7th Edition. Philadelphia, PA: Lippincott Williams & Wilkins;
Cooper, Kenneth H. The Aerobics Program For Total Well-Being. New York: M. Evans & Co., 1982.
C R Snyder, S J Bibliography health well-being. In C. R. & S. J. DEEP WATER EXERCISE HEALTH & FITNESS; J.G. MCWATERS 1988 PUBLITECH
EDITIONS Laguna Beach, CA. 92652A.

5 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
DeFronzo R. Pharmacologic therapy for type 2 diabetes mellitus. Ann Intern Med 1999; 131:281Ð303.
Daniel, S. (1999). The healthy patient: Empowering women in their encounters with the health care system. American Journal of Clinical Hypnosis, 42(2), 108-114.
DuHamel, K.N., Difede, J., Foley, F., Greenleaf, M. (2002). Hypnotizability and trauma symptoms after burn surgery. Journal of Clinical and Experimental Hypnosis, 50(1), 33-50.
Edelman G, Tononi G. A Universe of consciousness: How matter becomes imagination. New York: Basic Books: 2000.
Dobbin A, Maxwell M (2005) A feasibility study to test methods and recruitment procedures towards a future randomized trial of self-hypnosis versus antidepressant medication for the management of depression. Report to CSO office in Scotland no CZG/2/121
Edington D, Yen L. Is it possible to simultaneously reduce risk factors and excess health care costs? Am J Health Promot 1992;6: 403Ð406, 409.
Eisenberg, D.M., et al., Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. Jama, 1998. 280(18): p.1569-75.
Ewin, D. (1999). Hypnosis in the emergency room. In Temes, R. (Ed.) Medical hypnosis: An introduction and clinical guide. p. 59-64. Philadelphia: Churchill Livingston.
Fibromyalgia Back Pain and Sciatica Water Exercise - Benefits of Water Exercise for Back Pain - Water Exercise and Aquatic Therapy - What is Water Exercise Aquatic Resources Network. 2003.
Finkelstein, S. (2003). Rapid hypnotic inductions and therapeutic suggestions in the dental setting, Journal of Clinical and Experimental Hypnosis, 51(1), 77-85.
Frischholz, E.J., Lipman, L.S., Braun, B.G., & Sachs, R.G. (1992). Psychopathology, hypnotizability and dissociation. American Journal of Psychiatry, 149, 1521-1525.
Frischholz, E.J. (1997). Medicare procedure code 90880 (medical hypnotherapy): Use the code (not the word). American Journal of Clinical Hypnosis, 40(2), 85-88.
Frischholz, E.J., Spiegel, D., Trentalange, M.J., & Spiegel, H. (1987). The hypnotic induction profile and absorption. American Journal of Clinical Hypnosis, 30, 87-93.
Frischholz, E.J., & Spiegel, D. (1983). Hypnosis is not therapy. Bulletin of the British Society of Clinical and Experimental Hypnosis, 6, 3-8.
Frischholz, E.J. & Tryon, W.W. (1980). Hypnotizability in relation to the ability to learn thermal biofeedback. American Journal of Clinical Hypnosis, 23, 53-56.
Fordyce, W., Behavioral methods for chronic pain and illness. 1976, St. Louis Mosby. Fox, K.R. (1999). The influence of physical activity on mental well-being. Public Health
Nutrition. 2, 411-418. Ginandes, C.S., Rosenthal DI (1999). Using hypnosis to accelerate the healing of bone
fractures.” Alternative Therapies in Health - Medicine, 5(2), 67-75. Ginandes, C.S., Brooks P, Sando W, Jones C, Aker J. (2003). Can medical hypnosis accelerate
post-surgical wound healing? Results of a clinical trial. American Journal of Clinical Hypnosis, 45(4):333-51.
Greenleaf, M. (1992). Clinical implications of hypnotizability: Enhancing the care of medical patients and surgical patients. Psychiatric Medicine, 10 (77), 77- 87.
Greenleaf, M., Fisher, S., Miaskowski, C., DuHamel, K. (1992). Hypnotizability and recovery from cardiac surgery. American Journal of Clinical Hypnosis, 35 (2), 119-128.
Greenleaf, M. (1994). Cancer and women: redefining the self. Gynecologic Oncology Nursing, 4(2)
Gross, J. (2005) Alone in illness, seeking a strong arm to lean on. New York Times, Aug 26, 1, 14 Hammond, D.C., Garver, R.B., Mutter, C.B., Crasilneck, H.G., Frischholz, E.J., Gravitz, M.A.,

6 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Hadhazy, V.A., et al., Mind-body therapies for the treatment of fibromyalgia. A systematic review. J Rheumatol, 2000. 27(12): p. 2911-8.
Hilgard, E.R. (1965). Hypnotic susceptibility. NY: Harcourt, Brace & World. Hilgard, E.R. (1975). Hypnosis annual review of psychology, 26, 19-44. Hilgard, J.R. (1970). Personality and hypnosis: A study of imaginative involvement. Chicago:
University of Chicago Press. Hornyak, L.M. (1999). Empowerment through giving symptoms voice. American Journal of
Clinical Hypnosis, 42(2) 132-139. Horton, J.E., Crawford, H.J., Harrington, G., & Downs, J.H. (2004). Increased anterior corpus
callosum associated positively with hypnotizability and the ability to control pain. Brain, 127, 1741-1747.
Hospitals’ ‘Code Blue’ most deadly at night - More patients die if they go into cardiac arrest after 11 p.m., study finds; Associated Press CHICAGO Feb. 2008.
HYPNOSIS, BEHAVIORAL MEDICINE; D. P. BROWN & E. FROMM 1987 ERLBAUM PUBLISHER, HILLSDALE NEW JERSEY 07642
HYPNOSIS, BEHAVIOR MODIFICATION, IMAGERY CONDITIONING; W. KROGER, W. FEZLER, 1976, LIPPINCOT. PHILADELPHIA, TORONTO
HYPNOSIS IN THE RELIEF OF PAIN; HILGARD & HILGARD, 1975 W. KAUFMANN, LOS ALTOS CA. 94022
HYPNOSIS IN THE SEVENTIES, LARS ERIC UNESTAHL, 1971-74 WELINS TRYCKERI EFTR. AB, OREBRO SWEDEN.
HYPNOSIS, POSTHYPNOTIC SUGGESTION; LARS ERIC UNESTAHL, 1971-74 ENVAGEN 7, S-70221, OREBERO, SWEDEN)
Jensen, Alan, Ph.D. Published and Unpublished Documents; The Healthcare Problem – the Solution is AquaDios™ proactive preventive medicine;
Unpublished paper, 2006; The Health Care Problem Research of the Crisis; The Solution Is AquaDios-Med A
Preventive Medicine Process; A Workbook for Mind Body Medicine - Use of a Pendulum - Ideomotor Finger Responses AND THE SEVEN KEYS By Dr. Alan Jensen, 2008
HYPNOTIC TREATMENT OF DISEASE: A HOLISTIC APPROACH; VALUE OF AGE
REGRESSION IN TREATMENT OF DISEASE TREATMENT STRATEGIES OF MEDICAL PSYCHOLOGIST; APPLIED ATHLETIC HYPNOSIS - MENTAL TRAINING
PHYSIOLOGICAL SELF-REGULATION, ACTIVATION - IDEAL PERFORMANCE STATE; APPLIED MEDICAL HYPNOSIS COMBINED WITH BEHAVIOR MEDICINE IN TREATMENT OF DISEASE HEALTH, HAPPINESS HYPNOSIS AND REALITY;
THE PSYCHOLOGICAL EDGE IN SPORTS; MIND POWER THE DIFFERENCE BETWEEN WINNING AND LOSING;
APPLIED CLINICAL HYPNOSIS, BEHAVIOR/SPORTS MEDICINE, PAIN MANAGEMENT, REHABILITATION PSYCHOLOGY, HYDROLOGY CLIMATOLOGY;
STRUCTURED DEEP/SHALLOW WATER RESISTANCE EXERCISE REHABILITATION FOR CHRONIC INTRACTABLE BACK PAIN, ENDURANCE AND PAIN MANAGEMENT;
AquaDios-Med™ SPORTS MEDICINE CONDITIONING AND REHABILITATION CENTER; UNIQUE AQUATIC HEALING & EXERCISE
AquaDios-Med™ more than just a splash for cash: Physical fitness, rehabilitation, rejuvenation by sustained deep-water immersion activities in 4 separate hot-cold chambers and multiple depths; Presented at the International Medical Hydrology Society, Istanbul, Turkey 2006.

7 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
The Eye Roll Technique - a Rapid Trance Induction for Mind-Body Communication, Pain management, Mind-Body Healing; An Experiential Workshop Presented by Dr. Alan Jensen, Malibu California, 90265 - May 2012
The eye roll "up-gaze", while closing the eyelids on signal, correlates highly with hypnotic trance and results in a rapid trance to begin hypnotic communication with the unconscious through finger signals to safely and rapidly explore symptomatology, symptom relief, symptom substitution, age regression, age progression and to establish the affect bridge to self-empowerment and will be demonstrated in the workshop.
Ideomotor Signals for Hypnotic Exploration of Symptoms Adapted from the work of my friend and colleague David Cheek, MD by Dr. Jensen; Hypnotic
communication is with simple "Yes", "No", and "I Don't Want To" answers to questions to help the therapist establish rapid symptom control, management and remission.
THE HYPNOTIC INDUCTION PROFILE [HIP] A MOST USEFUL PRACTICAL TOOL
FOR THE MEDICAL PRACTIONER; A workshop presented by Dr. Alan Jensen for the ACHE Convention May 2012
The HIP is a brief 5 minute clinical instrument that measures compatible "hypnotizability" while developing a useful “trance state’. Herbert Spiegel, MD and David Spiegel MD developed the HIP to yield an individual's hypnosis capacity to assist in treatment. The HIP is a brief, empirically validated test. -
Giving Misery the Finger - Ideo-Motor-Finger Response (IMFR); Mind-Body Communication; To assist Mind-Body Medicine (MBM); An Interactive Hypnotic Process developed by David Cheek M.D., Leslie LeCron and memorialized by Ernie Rossi, PhD; An Experiential Workshop Presented by Dr. Alan Jensen, Malibu California, 90265 April 1, 2011; This workshop involves use of Ideo-Motor-Response (IMR) with the Cheverul Pendulum and "ideomotor finger signals" and explores use of the Ideo-Motor-Response (IMR) with the Pendulum together with "ideomotor finger signals" to better understand self-help methods in Mind-Body Medicine (MBM).
Justice B. Who gets sick How - beliefs, moods and thoughts affect health. Peak Press: 2000. Kessler, R. & Dane, J. (1996). Psychological and hypnotic preparation for anesthesia and
surgery: An individual differences perspective. International Journal of Clinical and Experimental Hypnosis, 44 (3), 189-207.
Kosslyn, S.M., Thompson, W.L., Costantini-Ferrando, M.F., Alpert, N.M., & Spiegel, D. (2000). Hypnotic visual alters color processing in the brain. American Journal of Psychiatry, 157(8), 1279-1284.
Kleijnen J, de Craen AJM, Van Everdingen J, Krol L. Placebo effect in double-blind clinical trials: A review of interactions with medications. Lancet 1994; 344:1347Ð1349.
Kirsch I, Montgomery G, Sapirstein G (1995) Hypnosis as an adjunct to cognitive behavioural therapy Journal of Consulting and Clinical Psychology Vol 63, No 2, 214-220
Kirsch I, Moore T, Scobonia A, Nicholls S (2002) The emperor's new drugs: An analysis of antidepressant medication data submitted to the U.S. Food and Drug Administration Prevention & Treatment. Vol 5 Jul 2002, np.
Laverture N, Kumar V, Pekala R (2002) The effectiveness of a hypnotic ego strengthening procedure for improving self-esteem and depression American Journal of Clinical and Experimental Hypnosis Vol 30, no 1,2002, 1-23
Lang, E.V., Joyce J, Spiegel D, Hamilton D, Lee K: (1996). Self-hypnotic relaxation during interventional radiological procedures: Effects on pain perception and intravenous drug use. International Journal of Clinical and Experimental Hypnosis, 4(2):106-119.

8 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Lang, E.V., Benotsch, E.G., Flick, L.J. , Lutgendorf, S., Berbaum, K.S., Logan, H., Spiegel, D. (2000). Adjunctive non-pharmacological analgesia for invasive medical procedures: a randomized trial. Lancet 355: 1486-1490.
Leslie M Lecron, Self-Hypnotism: The technique & its use in Daily Living, Signet, 1966 Leslie M. Lecron, Complete guide to Hypnosis. Prentice Hall, 1966 Linden, J. (1999). Discussion of symposium: enhancing healing: the contributions of hypnosis
in women’s health care. American Journal of Clinical Hypnosis, 42(2) 140-144 Lynch, D.F.(1999). Empowering the patient: hypnosis in the management of cancer, surgical
disease and chronic pain. American Journal of Clinical Hypnosis, 42(2)122-130. Lopez (Eds.), Handbook of positive psychology (pp. 541–555). New York: Oxford University
Press. Maestroni GJM, Conti A. Role of the pineal neurohormone melatonin in the psycho-
neuroendocrine-immune network. In: Ader R, Felten DL, Cohen N, eds. Psychoneuroimmunology, 2nd ed. San Diego, CA: Academic Press, 1991:495Ð 513.
McWaters JG: Run fast, run deep. In Deep Water Exercise for Health and Fitness, pp 106-20 Edited by McWaters JG. Laguna Beach, CA, Publitec Editions, 1993.
Meares, Ainslie MD Relief without Drugs: How You Can Overcome Tension, Anxiety and Pain (Aug 25, 1994)
Melzack, R. and P.D. Wall, Pain mechanisms: a new theory. Science, 1965. 150(699): p. 971-9. Melzack, R., Sensory, Motivational, and Central Control Determinants of Pain, in The Skin
Senses, D.R. Kenshalo, Editor. 1968, CC Thomas-Springfield. p.423-439. MIND BODY COMMUNICATION IN HYPNOSIS, VOL III; MILTON ERICKSON, MD
Milton1986, E. ROSSI, M. O. RYAN, IRVINGTON PUB. NEW YORK NORTON NEW YORK 10110
MIND BODY THERAPY; D. CHEEK, E. ROSSI 1988 NORTON NEW YORK 10110 Moncrieff J, Wessely S, Hardy R (2002) Active Placebo versus antidepressants for depression.
(Cochrane Review) Cochrane Library, Issue 3, 2002 PEAK PERFORMANCE, Mental Training Techniques of Greatest Athletes, CHARLES A.
GARFIELD, HAL BENNETT, 1984, WARNER BOOKS 666 FIFTH AVE. NY. NY 10103 Montgomery, G.H., DuHamel, K.N., Redd, W.H. (2000). A meta-analysis of hypnotically
induced analgesia: how effective is hypnosis? International Journal of Clinical and Experimental Hypnosis, 48(2): 138-153.
Montgomery, G.H., Weltz, C.R., Seltz, M., Bovbjerg, D. (2002). Brief presurgery hypnosis reduces distress and pain in excisional breast biopsy patients. International Journal of Clinical and Experimental Hypnosis, 50(1), 17-32.
Pinnell, C. M., & Covino, N.A. (2000). Empirical findings on the use of hypnosis in medicine:
A critical review. International Journal of Clinical and Experimental Hypnosis, 48:170-194. Shapiro, A. & Shapiro, E., The powerful placebo: From ancient priest to modern physician.
Baltimore: Johns Hopkins University Press. Spiegel, D. & Classen C. (2000). Group therapy for cancer patients: A research-based
handbook of psychosocial care. New York: Basic Books Spiegel, D. 1996). Hypnosis in the treatment of posttraumatic stress disorder, In Casebook of
clinical hypnosis, p. 999-111, Eds. Lynn S., Kirsch I. & Rhue, J. Washington, DC: American Psychological Press, .

9 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Spiegel, D. (1993). Psychosocial interventions in cancer. Journal of the National Cancer
Institute, 85, 1198-1205. Spiegel, H. & Spiegel, D. (2004). Trance & treatment: Clinical uses of hypnosis. 2nd Edition,
Washington, DC: American Psychiatric Press. Spiegel, H. (1972) An eye-roll test for hypnotizability. American Journal of Clinical Hypnosis,
15: 25-28. Spiegel, H. (1974) The grade 5 syndrome: The highly hypnotizable person. International
Journal of Clinical and Experimental Hypnosis, 22: 303-319 Spiegel, H. (1977). The hypnotic induction profile (HIP): A review of its development. Annals
of the New York Academy of Sciences, 21:129-142. Spiegel, H. (1997). Nocebo: the power of suggestibility. Preventive Medicine, 26 (5) 616-621. Spiegel, H. (2000). Silver linings in the clouds of war: A five-decade retrospective. In:
Menninger Siegel MD. Peace, Love and Healing. New York, NY: Harper Perennial; 1990: 224-225. Simonton, Carl MD "Getting Well Again", Bantam Books 1978 Spiegel, D. and R. Moore, Imagery and hypnosis in the treatment of cancer patients. Oncology
(Williston Park), 1997. 11(8): p. 1179-89; discussion 1189-95. Spiegel, H (2006). The neural trance: A new look at hypnosis. Invited address: The Herbert
Spiegel Lectureship, Department of Psychiatry, Columbia University, College of Physians & Surgeons.
Spiegel, H. & Greenleaf, M. (2005-06). Commentary: Defining hypnosis. American Journal of Clinical Hypnosis, 48(2-3): 111-116.
Spiegel, H. & Spiegel, D. (1978). Trance and treatment: Clinical uses of hypnosis. New York: Basic Books, Inc.
PSYCHOBIOLOGY OF MIND-BODY HEALING; E. ROSSI, 1986 Positive Psychology Interventions: A Practice-Friendly Meta-Analysis Journal of Clinical
Psychology in Session Vol 65 (5) 467 – 487. Positive Mental Training Lars-Eric Uneståhl 4 Ryff, C. D., & Singer, B. (2002). From social structure to biology: Integrative science in pursuit
of human and well being Sher L. The placebo effect on mood and behavior: the role of the endogenous opioid system.
Med Hypotheses 1997; 48: 347Ð349. Schwartz, Richard (2001) Introduction to the Internal Family Systems Model Trailheads
Publications Illinois. Sheppard L, Teasdale J (2000) Dysfunctional Thinking in Major Depressive Disorder: A
Deficit in Metacognitive Monitoring, Journal Abnormal psychology Volume 109(4) 768–776 Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction.
American Psychologist, 55, 5–14. Seligman, M. E. P., Steen, T. A., Park, N., & Peterson, C. (2005). Positive psychology
progress: Empirical validation of interventions. Sin N & Lyubomirsky (2009) Enhancing Well-Being and Alleviating Depressive Symptoms
with Positive Psychology Interventions: A Practice-Friendly Meta-Analysis Journal of Clinical Psychology in Session Vol 65 (5) 467 – 487.
Teasdale J, Cox S (2001) Dysphoria: self-devaluative and affective components in recovered depressed patients and never depressed controls Psychological Medicine Volume 31(7) 1311-1316
Teasdale J, Moore R Hayhurst H, Pope M, Williams S, Segal, Zindel V (2002) Metacognitive Awareness and Prevention of Relapse in Depression: Empirical Evidence Journal of Abnormal Psychology, 104, 585–591

10 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Uneståhl, L-E (1973), Hypnosis and Posthypnotic suggestions (PhD thesis Uppsala University). Örebro, Sweden: VEJE International.
Veenhoven, R. (2006) Health Happiness: Effects of happiness on physical health and the consequences for preventive health care
Watkins E, Teasdale J, (2001) Rumination and Over general Memory in Depression: Effects of Self-Focus and Analytic Thinking Journal of Abnormal Psychology Volume 110(2) 353–357
Watkins E, Teasdale J (2004) Adaptive and maladaptive self-focus in depression Journal of Affective Disorders Volume 82, Issue 1, 1-8
Wood MJ. Use of complementary and alternative medicine therapies in patients with cardiovascular disease. Am Heart J 2003; 145:841Ð846.
Woolhandler, Steffie M.D., M.P.H. and David U. Himmelstein, M.D., "The Deteriorating Administrative Efficiency of the U.S. Health Care System"; New England Journal of medicine 324:1253-1258 (May 2), 1991.
Partial List of References XIII • 10 Pages ***
The Health Care Crisis •
Is Man-Made • Manufactured
The Solution Is AquaDios-Med Proactive Preventive Medicine
By Dr. Alan Jensen

A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
Part II • Section XIV
The Health Care Crisis Is Manufactured • Man-Made
The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
References • Expanded Research
Healthcare Crisis • Manufactured • Man-Made • Includes • Media • Placebo • Preventive Medicine
Aquatic Exercise Hospital • ChargeMaster Prices
Unnecessary Surgery • Adverse Events Unnecessary Hospitalization
Negligence • Hospitalized Patients Fibromyalgia & Much More • 33 Pages
Evidence Based
AquaDios-Med™ Proactive Preventive Medicine
www.AquaDios.com
P.O. Box 2228
Malibu, CA 90265
310-897-5055
Copyright © 1985 - 2008 – 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
Exercise Is Medicine

1 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Partial List of References • XIV • 33 Pages The Health Care Crisis
Is Man-Made • Manufactured The Solution Is AquaDios-Med
Proactive Preventive Medicine By Dr. Alan Jensen
********************************************************************************* Partial List References • Healthcare Crisis • Manufactured • Man-Made • Includes • Media • Placebo • Preventive Medicine • Aquatic Exercise • Hospital • ChargeMaster Prices •Unnecessary surgery • Adverse Events • Unnecessary Hospitalization • Negligence - hospitalized patients • Fibromyalgia & Much More ********************************************************************************** Almost one-third of chemotherapy used "off-label" NY (Reuters Health) February, 19 2013 By Andrew M. Seaman; SOURCE: bit.ly/W1OrcD Journal of Clinical Oncology, February 19, 2013. FOXC2 vital to epithelial-mesenchymal transition in breast cancer; Published on February 14, 2013 Source: University of Texas M. D. Anderson Cancer Center - Posted in: Medical Science News | Medical Condition News | Pharmaceutical News- MD Anderson has filed a patent application connected to this study. Source: University of Texas M. D. Anderson Cancer Center Tags: Bone, Brain, Breast Cancer, Cancer, Cell, Chemotherapy, DNA, Embryonic Development, Leukemia, Metastasis, Paclitaxel, Pathology, Protein, RNA, Stem Cell, Sunitinib, Translational Afraid to Speak Up to Medical Power By PAULINE W. CHEN, M.D. NY Times Health Science February 14, 2013 Health Insurance - Bitter Pill: Why Medical Bills Are Killing Us By Steven Brill - February 20, 2013; Time Magazine cover Story Funding of alternative treatments questioned - Some see tax dollar waste in spending by the National Center for Complementary and Alternative Medicine. The NCCAM director, though, sees a need for scientific attention. - By Trine Tsouderos, Chicago Tribune - January 23, 2012 Most All News Media Reported - Soldier with a Double-Arm Transplant Soldier with new arms determined to be independent By ALEX DOMINGUEZ - BALTIMORE (AP) Associated Press January 29, 2013 the New York - Los Angeles Times Published clinical trials shown to be misleading | Science & Society - Comparison of internal and public reports about Pfizer’s drug Neurontin reveals many discrepancies - By Rachel Ehrenberg - Web edition: January 29, 2013; Citations - S. S. Vedula, T. Li and K. Dickersin. Differences in reporting of analyses in internal company documents versus published trial reports: comparisons in industry-sponsored trials in sciencenews.orghttp: sciencenews.org/view/generic/id/347933/description/Published_clinical_trials_shown_to_be_misleading Defective Hip Implant; Attorney for Defective Hip Implant Patients Urges FDA to Increase Regulation of All Metal-on-Metal Devices - Phoenix, Arizona (PRWEB) February 12, 2013

2 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
RESOURCES: Letter from Van O’Steen to the U.S. Food and Drug Administration dated January 28, 2013; Krausky v. DePuy, BC456086, Los Angeles County Superior Court; In re DePuy Orthopedics, Inc., 10-MD-2197, U.S. District Court, Northern District of Ohio; “Maker Aware of 40% Failure in Hip Implant” by Barry Meier, The New York Times, January 22, 2013. Johnson & Johnson Confirms Inquiry Into Hip Devices - ASSOCIATED PRESS February 22, 2013 NY Times Small Employers To Receive $200 Million For Prevention Programs - May 26, 2010 What Effect Will Healthcare Reform Have on Jobs? - By John Rossheim, Monster Senior Contributing Writer Health Care - America's Most Profitable Hospitals - David Whelan, August 31, 2010, American Hospital Directory Nature's medicine offers relief for many diseases - By Reese Halter | Friday, February 8, 2013 Earth Dr. Reese Halter is a broadcaster, biologist and author of "The Incomparable Honeybee" and "Insatiable Bark Beetle. RNA Fragments May Yield Rapid, Accurate Cancer Diagnosis; A new method to noninvasively diagnose cancer and monitor its progression could eliminate the need for painful and sometimes life-threatening biopsies - By William Ferguson, January 30, 2013 Just say don't: Doctors question routine tests and treatments - Now there are 135, By Sharon Begley NEW YORK (Reuters). February 21, 2013 - Editing Jilian Mincer and Prudence Crowther) Health insurers highlight excessive out-of-network charges - By Chad Terhune, February 1, 2013 – LA Times latimes.com/business/money/la-fi-mo-medical-bills-20130201,0,3225077.story The Los Angeles Times detailed more of the outrageous prices [4] in a piece this week. Article printed from The Daily Dose February 1, 2013 http://blogs.denverpost.com/health/2013/02/01/outrageous-outofnetwork-health-charges-dinged-colorado-national-report/2595/ Outrageous out-of-network health charges dinged in new Colorado, national report By Michael Booth | The Daily Dose February 1, 2013; Denver Post.Com The Benefits of Exercising Outdoors By GRETCHEN REYNOLDS FEBRUARY 21, 2013, The New York Times 620 Eighth Avenue New York, NY 10018 Scientists infuse 'life' into inanimate compounds - February 01, 2013|By Joseph Serna, Los Angeles Times - The study was funded by the National Science Foundation, the U.S. Army Research Office and NASA. [email protected] Los Angeles Times Scientific American January 31, 2013 - A New Cancer Test: Invasive tests to diagnose cancer could soon be a thing of the past, Scientific American reports. On January 31, 2013 Scientific American reports progress on research of a new non-invasive cancer test.

3 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
RNA Fragments May Yield Rapid, Accurate Cancer Diagnosis - A new method to noninvasively diagnose cancer and monitor its progression could eliminate the need for painful and sometimes life-threatening biopsies By William Ferguson, January 30, 2013 Small surgeries, huge markups- Los Angeles Times January 31, 2013 An $87,500 bill for a 20-minute knee procedure is just an extreme example of high amounts that insurers are billed by out-of-network surgery centers, experts say. Insurers are starting to fight back. By Chad Terhune, Los Angeles Times January 31, 2013 Small surgeries, huge markups - An $87,500 bill for a 20-minute knee procedure is just an extreme example of high amounts that insurers are billed by out-of-network surgery centers, experts say. Insurers are starting to fight back. By Chad Terhune January 31, 2013 Los Angeles Times Price for a New Hip • Many Hospitals Are Stumped - By ELISABETH ROSENTHAL • NY Times Health & Science February 11, 2013 The Confusion of Hospital Pricing - By RONI CARYN RABIN • NY Times April 2012, Focus on Hospitals July Effect By NICHOLAS BAKALAR - NY Times February 2013, Leaving the Hospital Early By TARA PARKER-POPE • NY Times March 2011 The Fraying Hospital Safety Net By PAULINE W. CHEN, M.D. • NY Times September 2012 How One Small Group Sets Doctors Pay By PAULINE W. CHEN, M.D. • NY Times September 2011 New York Times October 25, 2012, Challenging Assumptions in the Push for Better Care By PAULINE W. CHEN, M.D. Why Doctors Order So Many Tests By PAULINE W. CHEN, M.D. New York Times September 29, 2011 How Doctors and Patients Do Harm By TARA PARKER-POPE The New York Times April 20, 2012, "Lobbying Spending by Sector". Center for Responsive Politics. Archived from the original According to the Center for Responsive Politics Health Lobby spent about $ 4.5 Billion in 2010 http://en.wikipedia.org/wiki/Direct_lobbying_in_the_United_States Panel on Health Care Work Force, Lacking a Budget, Is Left Waiting By ROBERT PEAR - NY Times February 24, 2013 The invisible health-care panel – By Kyle Cheney January 30, 2013 © 2013 POLITICO LLC Health Care - America's Most Profitable Hospitals David Whelan, 08.31.10, 10:00 AM ET Preventive Health Care Luminaries Form U.S. Preventive Medicine International Advisory Board Leading Researchers, Physicians and Executives Outline Bold Agenda for Advancing Prevention in Health Care

4 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
U.S. Preventive Medicine, Monday March 29, 2010, JACKSONVILLE, Fla., March 29 /PRNewswire/ Insight: Think preventive medicine will save money? It seems like a no-brainer - Think again By Sharon Begley NEW YORK (Reuters) - NEW YORK | Tue Jan 29, 2013 World's 100 richest people got $241 billion richer in 2012 - Their aggregate net worth climbs to $1.9 trillion, according to the Bloomberg Billionaires Index, a daily ranking of the world's 100 wealthiest individuals. Bloomberg News, January 3, 2013 - latimes.com Waiting for Cloud to Lift on State Cancer Institute By BECCA AARONSON Texas Tribune NY Times February 16, 2013 [email protected] High-stakes cholesterol study could lift Merck cloud - By Ransdell Pierson and Bill Berkrot Favorable results from a huge heart study could help redeem investors' faith in Merck & Co and its two biggest cholesterol drugs, Vytorin and Zetia, and potentially add billions of dollars in annual revenue; Reporting By Ransdell Pierson and Bill Berkrot in New York; Editing by Jilian Mincer and Nick Zieminski) - Friday February 15, 2013 NEW YORK (Reuters) - The Confusion of Hospital Pricing By RONI CARYN RABIN - The New York Times April 23, 2012, A Hospital Room With a View By PAULINE W. CHEN, M.D. The New York Times December 16, 2010 Challenging Assumptions in the Push for Better Care By PAULINE W. CHEN, M.D. New York Times October 25, 2012, Why Doctors Order So Many Tests By PAULINE W. CHEN, M.D. New York Times September 29, 2011 How Doctors and Patients Do Harm By TARA PARKER-POPE The New York Times April 20, 2012 The RUC survives and now our health system is worse off Brian Klepper, PhD | Policy | February 14, 2013 Why would hospitals like HCA perform unnecessary surgery? Because it pays By Sarah Kliff, Washington Post August 7, 2012 N.J. system pays $12.6 million to settle whistle-blower case by Joe Carlson ModernHealthcare.com January 26, 2013 More Unnecessary Surgery BY JONATHAN CHAIT December 21, 2010 Obama Medicare rebate plan could hurt drug companies - By Bill Berkrot and David Morgan - Feb 13, 2013 Reuters - Reporting by David Morgan in Washington and by Bill Berkrot in New York; Editing by Jilian Mincer and Leslie Gevirtz) Inappropriate heart procedures are expensive and risky. And studies show Thousands happen every year. By Sarah Kliff, Washington Post August 8, 2012

5 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Unnecessary Heart Surgery • aka • Oculostenotic Reflex Mass. Family Awarded $63M In Motrin Lawsuit By Todd Wallack, Boston Globe February 13, 2013 Focus on Hospitals - July Effect By NICHOLAS BAKALAR The New York Times February 4, 2013 Why Four Workouts a Week May Be Better Than Six By GRETCHEN REYNOLDS February 13, 2013, NY Times Unnecessary surgery exposed! Why 60% of all surgeries are medically unjustified and how surgeons exploit patients to generate profits - by Alexis Black naturalnews.com printable article - Originally published October 7 2005 Wrong patient got kidney at USC - USC University Hospital shut down its kidney transplant program last month after realizing the error. The hospital said transplants may resume as early as Friday. Missed diagnoses common in the doctor's office (Reuters) - Missed or wrong diagnoses are common in primary care and may put some patients at risk of serious complications, according to a U.S. study. Researchers whose findings appeared in JAMA Internal Medicine; February 18, 2011|By Alan Zarembo and Lisa Girion, Los Angeles Times Medicare Needs Fixing, but Not Right Now By EDUARDO PORTER - NY Times February 26, 2013 [email protected] American Heart Association. Heart Disease and Stroke Statistics—2006 Update. Dallas, Texas: American Heart Association, 2006. Hoyert DL, Heron MP, Murphy SL, Kung H. Deaths: Final Data for 2003. National vital statistics reports; vol 54 no 13. Hyattsville, MD: National Center for Health Statistics. 2006. Centers for Disease Control and Prevention. Heart Disease Death Rates, 1999–2003: Adults Ages 35 Years and Older, by County. http://www.cdc.gov/dhdsp/library/maps/index.htm. Centers for Disease Control and Prevention, Health, United States, 2005 with Chartbook on Trends in the Health of Americans. Hyattsville, MD: National Center for Health Statistics, 2005. Greenland P, Knoll MD, Stamler J, Neaton JD, Dyer AR, Garside DB, Wilson PW. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events; JAMA 2003 - 290:891–897. The Adverse Childhood Experiences (ACE) Study American Journal of Preventive Medicine May 1998; 14(4): 245-258 Healthcare System - Leading Cause of Death in U.S. - By Gary Null PhD, Carolyn Dean MD ND, Martin Feldman MD, Debora Rasio MD, Dorothy Smith PhD Good medicine or a bitter pill? Implications of health care reform for businesses in America

6 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
By Robert W. Clarke > Paul H. Keckley and Steven Kraus > illustration by JON KRAU SE Deloitte Review – Issue 7, 2010 - Endnotes 1. http://www.cbo.gov/ftpdocs/113xx/doc11379/Manager%27sAmendmenttoReconciliationProposal.pdf [page 9] 2. http://www.whitehouse.gov/recovery/anniversary/chapter1 3. U.S. implementation of ICD-10 is scheduled October 1, 2013 [http://www.ahima.org/icd10/icd-10-faqs-all.html#1] 4. http://www.healthreform.gov/ 5. http://dpc.senate.gov/healthreformbill/healthbill73.pdf 6. “Some of the changes go into effect for the first [insurance] plan year that begins on or after six months after enactment (September 23, 2010), so for calendar year plans, January 1, 2011.” http://www.dol.gov/ebsa/faqs/faq-PPACA.html 7. Ron Barlow, The Implications of Health Reform for Plan Sponsors, Deloitte Consulting LLP presentation. 8. http://www.ncsl.org/documents/health/EmployerPenalties.pdf 9. http://www.npr.org/templates/story/story.php?storyId=111967435 10. http://www.irs.gov/compliance/enforcement/article/0,,id=117524,00.html 11. http://www.deloitte.com/view/en_US/us/Insights/centers/center-for-health-solutions/health-care-reform/health-carereform-memo/6a8e7661b62f7210VgnVCM100000ba42f00aRCRD.htm 12. http://www.deloitte.com/view/en_US/us/Insights/Browse-by-Content-Type/deloitte-review/article/0c801dfbe0426210VgnVCM100000ba42f00aRCRD.htm 13. http://www.cbsnews.com/stories/2009/10/23/60minutes/main5414390.shtml Robert W. Clarke is a partner with Deloitte Financial Advisory Services LLP (Deloitte FAS), and is the Deloitte FAS National Health Sciences Leader; Paul H. Keckley is a director with Deloitte Consulting LLP, and is the Executive Director of the Deloitte Center for Health Solutions. Steven Kraus is a principal with Deloitte Consulting LLP. Unified Placebo Theory (UPT); Everything Out of Nothing or Anything You Want” The (R)evolution (With)in the (R)evolution:The Unified Placebo Theory (UPT) Rado Gorjup¹ Alfred Angel Barrios² March, 2012 Barrios A. A, & Kroger, W. S. (1976). Psychological Variables and the Immunological Response: a New Approach to the Treatment of Cancer. Journal of Holistic Health. 1:71-80. Barrios, A. A. (1961). Hypnosis as a Possible Means of Curing Cancer. Unpublished Manuscript. Barrios, A. A. (1965). An Explanation of the Behavioral and Therapeutic Effects of the Hallucinogens. International Journal of Neuropsychiatry, 1:574-592. Barrios, A. A. (1969). Towards Understanding the Effectiveness of Hypnotherapy. A Combined Clinical, Theoretical and Experimental Approach. Doctoral Dissertation, (UCLA). Barrios, A. A. (1970). Hypnotherapy: A Reappraisal. Psychotherapy: Theory, Research and Practice, 7:2-7. Barrios, A. A. (1973a) Post Hypnotic Suggestion as Higher-Order Conditioning: a Methodological and Experimental Analysis. The International Journal of Clinical and Experimental Hypnosis, 21(1):32-50.

7 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Barrios, A. A. (1973c). Self-Programmed Control: A New Approach to Learning. Proceedings of the Sixth annual Conference of the Western College Reading Association. Barrios, A. A. (1985). Towards Greater Freedom & Happiness. Los Angeles, SPC Press. Barrios, A. A. (2001). A Theory of Hypnosis Based on Principles of Conditioning and Inhibition. Contemporary Hypnosis. 18; 4:163-203. Barrios, A. A. (2002). Science in Support of Religion: From the Perspective of a Behavioral Scientist. Banning, California, Cancer Federation Press. Barrios, A. A. (2007b). Commentary on a Theory of Hypnosis Based on Principles of Conditioning and Inhibition Part II: Benefits of the Theory. Contemporary Hypnosis, 24(3): 123-138. Barrios, A.A. (2009). Understanding Hypnosis: Theory, Scope and Potential. New York, Nova Science Publishers. Benedetti, F., & Amanzio, M. (1997). The Neurobiology of Placebo Analgesia: From Endogenous Opioids to Cholecystokinin. Progresses in Neurobiology; 52 (2):109–125. Benedetti, F., & Pollo, A. (2001). The Pharmacology of Placebos. International Journal of Pain Medicine and Palliative Care, 1:42-48. Di Blasi, Z., Harkness, E., Georgiu, A., & Kleijnen, J. (2001). Influence of Context Effects on Health Outcomes. A Systematic Review. Lancet; 357:757-762. Gorjup, R. (2011a). Nothing, something or everything: The Unified Placebo Theory (UPT). Elsaeldorado, Development of New Technologies. Unpublished Manuscript. Gorjup, R. (2011b). Towards Understanding the Unified Placebo Theory (UPT) through Subjective (Physiological and Psycho Physiological) Interpretation Response in the Healing Process Supported by the Theory of Hypnosis Based on Principles of Conditioning and Inhibition. Unpublished Doctoral Dissertation. California University, Los Angeles. Kirsch, I. (1985). Response expectancy as a determinant of experience and behavior American Psychologist, 40:1189-1202. Kirsch, I. (1997). Specyfiing non specifics:Psychological mechanisms of placebo effects. In A. Harringtonn (Ed), The Placebo effect : An interdisciplinary exploration (p.p. 166-186). Cambridge MA: Harward University Press. Kirsch, I. and Wiexel, L. J. (1988). Double blind versus deceptive administration of a placebo Lipton, B.H. (2005). The Biology of Belief. ISBN 978-953-7039-55-2. Moerman, D.E., (2002). Deconstructing the Placebo Effect and Finding the Meaning Response. Annual of Internal Medicine, 136:471-476.

8 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Pavlov, I.P. (1960). Conditioned reflexes: An investigation of physiological activity of the cerebral cortex.[Re-issue of 1927edit.] New York: Dover. Shapiro, A. K., & Shapiro, E. (1997) The Powerful Placebo: From Ancient Priest to Modern Physician. Baltimore, MD: Johns Hopkins University Press. Thomas, W. I. & Thomas, D. S. (1928). The Child in America: Behavior Problems and Programs. New York: Knopf; 571-572. Creating New Consciousness in Everyday Life: The Psycho-Social Genomics of Self-Creation by Kathryn Lane Rossi, Ernest Lawrence Rossi, Lee Lawson and Bella Castle; The Creative Psychosocial Genomic Healing Experience: A New Epigenetic Psychotherapeutic Protocol; Cozzolino, M., Tagliaferri, R.1, Castiglione, S.1, Fusco, F.2, Fortino, V.1, Cicatelli, A.1, De Luca, P.3, Guarino, F.1, Napolitano, F.1, Celia, G.1,4, Iannotti, S.5, Raiconi, G.1, Rossi, K.4,5, 6 & Rossi, E. 4,5, 6; University of Salerno, (Italy) 2 IGB-ABT-CNR International Institute of Genetics and Biophysics, Naples (Italy) 3 Biogem Institute-Ariano Irpino and Zoological Station “A. DOHRN”, Naples (Italy). 4 CIPPS- International Center of Strategic Psychology and Psychotherapy, Salerno (Italy) 5 Mind Body Institute, Solopaca (Italy) 6 The Milton H. Erickson Foundation, Central California Coast Institute, USA Clinical Review: Current Concepts - Aquatic Therapy: Scientific Foundations and Clinical Rehabilitation Applications Bruce E. Becker, MD, MS, B.E.B. Washington State University; Director, National Aquatics and Sports Medicine Institute; Department of Rehabilitation Medicine, University of Washington School of Medicine Spokane WA 99224 PM&R © 2009 by the American Academy of Physical Medicine and Rehabilitation 1934-1482/09/$36.00 Vol. 1, 859-872, September 2009 FOXC2 vital to epithelial-mesenchymal transition in breast cancer Published on February 14, 2013 University of Texas M. D. Anderson Cancer Center; Posted in: Medical Science News | Medical Condition News | Pharmaceutical News Preventive-Medicine at the US National Library of Medicine Medical Subject Headings (MeSH) Primal Research Centre, London - Primal Health Research Databank Effect of In Utero and Early-Life Conditions on Adult Health and Disease, by P.D.Gluckman et al., N ENGL J MED 359; 1 Origins: How the nine months before birth shape the rest of your life, by Annie Murphy Paul, Time magazine, 176.14, 2010 Kuehlein T, Sghedoni D, Visentin G, Gérvas J, Jamoule M. Quaternary prevention: a task of the general practitioner. PrimaryCare. 2010; 10(18):350-4. Primary+Prevention at the US National Library of Medicine Medical Subject Headings (MeSH) Secondary+Prevention at the US National Library of Medicine Medical Subject Headings (MeSH) Tertiary+Prevention at the US National Library of Medicine Medical Subject Headings (MeSH) Gofrit ON, Shemer J, Leibovici D, Modan B, Shapira SC. Quaternary prevention: a new look at an old challenge. Isr Med Assoc J. 2000; 2(7):498-500.

9 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Gordon, R. (1987), ‘An operational classification of disease prevention’, in Steinberg, J. A. and Silverman, M. M. (eds.), Preventing Mental Disorders, Rockville, MD: U.S. Department of Health and Human Services, 1987. Kumpfer, K. L., and Baxley, G. B. (1997), 'Drug abuse prevention: What works?’ National Institute on Drug Abuse, Rockville. Jamie Michelle Womack (2010) "Safety and adherence: Issues that hinder childhood vaccinations" Journal of the American Academy of Physician Assistants Lars Bo Andersen et al. (June 2000). "All-cause mortality associated with physical activity during leisure time, work, sports, and cycling to work". Archives of Internal Medicine 160 (11): 1621–8. doi:10.1001/archinte.160.11.1621. PMID 10847255. "Why is it important to eat fruit?” United States Department of Agriculture; Retrieved 8 February 2012. de Oliveira JC, Martinelli M, D'Orio Nishioka SA, et al. (2009). "Efficacy of antibiotic prophylaxis prior to the implantation of pacemakers and cardioverter-defibrillators: Results of a large, prospective, randomized, double-blinded, placebo-controlled trial". Circulation: Arrhythmia and Electrophysiology 2 (1): 29–34. doi:10.1161/CIRCEP.108.795906. PMID 19808441. Qaseem A, Chou R, Humphrey LL, et al. (2011). "Venous Thromboembolism Prophylaxis in Hospitalized Patients: A Clinical Practice Guideline From the American College of Physicians". Annals of Internal Medicine 155 (9): 625–632. doi:10.1059/0003-4819-155-9-201111010-00011. PMID 22041951. Lederle FA, Zylla D, MacDonald R, et al. (2011). "Venous Thromboembolism Prophylaxis in Hospitalized Medical Patients and Those With Stroke: A Background Review for an American College of Physicians Clinical Practice Guideline". Annals of Internal Medicine 155 (9): 602–615. doi:10.1059/0003-4819-155-9-201111010-00008. PMID 22041949. Kahn SR, Lim W, Dunn AS, et al. (February 2012). "Prevention of VTE in Nonsurgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines". Chest 141 (2 suppl): e195S–e226S. doi:10.1378/chest.11-2296. PMID 22315261. Ip S, Chung M, Raman G, ChewP, Magula N, DeVine D, Litt M, Trikalinos T, Lau J. Breastfeeding and maternal and infant health outcomes in developed countries. Evidence Report/Technology Assessment Number 153. 2007 April; AHRQ Publication No. 07-E007. Ab J. Joseph Speidel, Cynthia C. Harper, and Wayne C. Shields (September 2008). "The Potential of Long-acting Reversible Contraception to Decrease Unintended Pregnancy". Contraception. Ab James Trussell, Anjana Lalla, Quan Doan, Eileen Reyes, Lionel Pinto, Joseph Gricar (2009). "Cost effectiveness of contraceptives in the United States". Contraception 79 (1): 5–14. doi:10.1016/j.contraception.2008.08.003. PMID 19041435.

10 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Monea J, Thomas A (June 2011). "Unintended pregnancy and taxpayer spending". Perspectives on Sexual and Reproductive Health 43 (2): 88–93. doi:10.1363/4308811. PMID 21651707. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ (May 2006). "Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data". Lancet 367 (9524): 1747–57. doi:10.1016/S0140-6736(06)68770-9. PMID 16731270. Jones G, Steketee R, Black R, Bhutta Z, Morris S, and the Bellagio Child Survival Study Group* (July 5, 2003 2003). "How many child deaths can we prevent this year?". Lancet 362 (9524): 1747–57. Mokdad AH, Marks JS, Stroup DF, Gerberding JL (March 2004). "Actual causes of death in the United States, 2000". JAMA 291 (10): 1238–45. doi:10.1001/jama.291.10.1238. PMID 15010446. Sackett DL. The arrogance of preventive medicine. CMAJ. 2004;167:363-4. Starfield B, Hyde J, Gérvas J, Heath I. The concept of prevention: a good idea gone astray? J Epidemiol Community Health. 2008;62(7):580-3. Gérvas J, Starfield B, Heath I. Is clinical prevention better than cure? Lancet. 2008;372:1997-9. Gérvas J, Heath I, Durán A, Gené J; Members of the Seminar of Primary Health Innovation 2008. Clinical prevention: patients' fear and the doctor's guilt. Eur J Gen Pract. 2009; 15(3):122-4. Heneghan C. Considerable uncertainty remains in the evidence for primary prevention of cardiovascular disease (editorial). The Cochrane Library 2011 (19 Jan). John R. Paul and the Definition of Preventive Medicine by Arthur J. Viseltear; Yale J Biol Med. 1982 May-Aug; 55(3-4): 167–172. PMCID: PMC2596460 John R. Paul to C.-F.A. Winslow. August 1. 1942. Winslow MSS, 1/22/565 Winslow C-FA: Preventive Medicine and Health Promotion-Ideals or Realities. Yale J Biol Med 14:443-452.1942 Paul to Winslow 111 Paul JR: A Clinician's Place in Academic Preventive Medicine: My Favorite Hobby. Bull NY Acad Med 47:1263. 1971 Miller CP: John Rodman Paul, 1S93-197l. 'trans Assoc Am Phys 85:40-43. 1972; see also NY Times obituary, May 7. 1971; Horstmann DM: Foreword. Yale 3 Biol Med 34:161-162, 1961/2 Paul JR: Clinical Epidemiology.1Clm Investig 17:539-541, 1938. See olio Paul JR: Clinical Epidemiology. Chicago. University of Chicago Pres.1955 Paul JR: Preventive Medicine at the Yale University School of Medicine. Yale J Biol Med 11:253-258, 1940

11 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Paul JR: Preventive Medicine at the Yale University School of Medicine. 1940-49. Yale 1 Riol Med 22 199 211. 1950 Yale 3 Biol Med 22:200, 1950 Paul JR: The Advancement of Scientific and Practical Medicine. Trans Assoc Am Phys 69:3, 1956. 11 See Paul JR: Epidemiology and its Teaching in Medical Schools. Yale J Biol Mcd 27:35-45, 1954: Development and Use of Scrum Surveys in Epidemiology, Serum Epidemiology. Edited by J R Paul, C White. New York, Academic Press. 1973. pp1-13. Yale 1 Riot Med 22:207-208. 1950. In the early 1940s. but not institutionalized until 1955. Dr. Paul added a fourth-year course in "External (Ens iron mental) Medicine" to the Section curriculum. Through which Section faculty and students studied in the home the diagnosis, therapy, and prognosit of diseases, such as tuberculosis. Diabetes mellitus. Mental retardation, rheumatic fever, rheumatoid arthritis, duodenal ulcer, asthma, pneumonia, anemia. Psychoneurosis, myocardial infarction, epilepsy, rubella. nephritis. and others. See Nicderman JC, Paul JR: The Home Visit as a Teaching Exercise: A Clinical Concept. 1 Med 1-duc 33:29-34. 1958 Yale 1 Btol Med 22:210-211. 1950. See also Paul JR: Account of the American Epidemiological Society: A Retrospect of Some Fifty Years. Yale J Biol Med 46:1-148, 1973. In 1941 Dr. Paul served with the Commission on Neurorropi. Virus Diseases of the Armv Epidemiology Board and. in 1943.headed a small team (including Albert Sabin and Cornelius Phillip) known as the Virus Commission of the A.E.B. The Virus Commission was dispatched to North Africa to study infecmous hepatitis. Sandfly sevCr. and polio. Paul IR I he Advancement of Scientdte and Practical Medicine brans Acsoe Am Phyc 69:5. 1956 5. Yau11R. A (main's Ptacc nt Academic Preventive Medicine. \1Fasoritc Hohhy. Hull NY Acad bled 1265-1266. 1971. Sw• aiw Francis T Jr: Epidemic Influenza: Studies in (linseal l-piJem:olog). Ann Intern Mcd 13 915-922, 1939. Opic El . McPhedran EM: f he Sprcdd of Tuber r:uloais within Families. JAMA 87:1549 155).1926. Coburn AF. Pauli RH. Studies on the Immune Response of the Rheumatic Subject acid its Relationship to.Actisity of the Rheunwti. Process. J Clin Invest 14:769 791. 935. For a contrasting viewpoint. we (Winslow C.E.A.) What arc Epidemrologisis7 Editorial Amer J Pub Health 32: 414-4 1942; Who are F. prdemiologntc° Amer I Pub Ilralth 31t:It52-K56. 1949 See Rylc IA: (Changing Disciphnc lectures on the History. Methods. and Mnhvcs or So ml Pathology. London. Oxford University Press, 1948. Professor Ryk delivered These lectures as the Centenmwl Discourse of The New York Academy of Medicine. 191'. Paul JR. A Clinician's Place in Academic Preventive Medicine: Ms Favorite Hobhr. Bull NY Aud Med 1266 1971 Bull NY Acad \W 47:1267. 19'1 Bull NY Acad Med 47:1270, 1971 Evidence-based systematic review of the effectiveness of hydrotherapy in acute and chronic medical conditions. Dr. Gordon Doig, Senior Lecturer in Intensive Care, University of Sydney; 29 July 2008

12 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA . 1998 Apr 15;279(15):1200-5. Rabin R. Caution about overuse of antibiotics. Newsday . September 18, 2003. Centers for Disease Control and Prevention, CDC antimicrobial resistance and antibiotic resistance—general information. Available at: http://www.cdc.gov/drugresistance/community/ For calculations detail, see “Unnecessary Surgery.” Sources: HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville , MD. Available at: http://www.ahrq.gov/data/hcup/hcupnet.htm . Accessed December 18, 2003 . US Congressional House Subcommittee Oversight Investigation. Cost and Quality of Health Care: Unnecessary Surgery. Washington , DC : Government Printing Office;1976. Cited in: McClelland GB, Foundation for Chiropractic Education and Research. Testimony to the Department of Veterans Affairs' Chiropractic Advisory Committee. March 25, 2003 . For calculations detail, see “Unnecessary Hospitalization.” Sources: HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville , MD. Available at: http://www.ahrq.gov/data/hcup/hcupnet.htm . Accessed December 18, 2003 . Siu AL, Sonnenberg FA, Manning WG, et al. Inappropriate use of hospitals in a randomized trial of health insurance plans. N Engl J Med . 1986 Nov 13;315(20):1259-66. Siu AL, Manning WG, Benjamin B. Patient, provider and hospital characteristics associated with inappropriate hospitalization. Am J Public Health . 1990 Oct;80(10):1253-6. Eriksen BO, Kristiansen IS, Nord E, et al. The cost of inappropriate admissions: a study of health benefits and resource utilization in a department of internal medicine. J Intern Med . 1999 Oct;246(4):379-87. U.S. National Center for Health Statistics. National Vital Statistics Report, vol. 51, no. 5, March 14, 2003 . Thomas, EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000 Mar;38(3):261-71. Thomas, EJ, Studdert DM, Newhouse JP, et al. Costs of medical injuries in Utah and Colorado . Inquiry . 1999 Fall;36(3):255-64. [Two references.] Xakellis GC, Frantz R, Lewis A. Cost of pressure ulcer prevention in long-term care. Am Geriatr Soc . 1995 May;43(5):496-501. Barczak CA, Barnett RI, Childs EJ, Bosley LM. Fourth national pressure ulcer prevalence survey. Adv Wound Care . 1997 Jul-Aug;10(4):18-26. Weinstein RA. Nosocomial Infection Update. Emerg Infect Dis . 1998 Jul-Sep;4(3):416-20. Fourth Decennial International Conference on Nosocomial and Healthcare-Associated Infections. Morbidity and Mortality Weekly Report. February 25, 2000 , Vol. 49, No. 7, p.138.

13 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Burger SG, Kayser-Jones J, Bell JP. Malnutrition and dehydration in nursing homes: key issues in prevention and treatment. National Citizens' Coalition for Nursing Home Reform. June 2000. Available at: http://www.cmwf.org/programs/elders/burger_mal_386.asp. Starfield B. Is US health really the best in the world? JAMA . 2000 Jul 26;284(4):483-5. Starfield B. Deficiencies in US medical care. JAMA . 2000 Nov 1;284(17):2184-5. HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville , MD. Available at: http://www.ahrq.gov/data/hcup/hcupnet.htm . Nationwide poll on patient safety: 100 million Americans see medical mistakes directly touching them [press release]. McLean , VA : National Patient Safety Foundation; October 9, 1997 . The Society of Actuaries Health Benefit Systems Practice Advancement Committee. The Troubled Healthcare System in the US. September 13, 2003 Leape LL. Error in medicine. JAMA . 1994 Dec 21;272(23):1851-7. a. Brennan TA, Leape LL, Laird NM , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med . 1991 Feb 7;324(6):370-6. Campbell EG, Weissman JS, Clarridge B, Yucel R, Causino N, Blumenthal D. Characteristics of medical school faculty members serving on institutional review boards: results of a national survey. Acad Med . 2003 Aug;78(8):831-6. Possible conflict of interest within medical profession. HealthDayNews. August 15, 2003. World Health Organization. Press Release Bulletin #9. December 17, 2001. Angell M. Is academic medicine for sale? N Engl J Med . 2000 May 18;342(20):1516-8. McKenzie J. Conflict of interest? Medical journal changes policy of finding independent doctors [transcript]. ABC News. June 12, 2002 . Crossen C. Tainted Truth: The Manipulation of Fact in America . New York , NY : Simon & Schuster; 1994. Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA . 1995 Jul 5;274(1):29-34. Vincent C, Stanhope N, and Crowley-Murphy M. Reasons for not reporting adverse incidents: an empirical study. J Eval Clin Pract . 1999 Feb;5(1):13-21. Wald H, Shojania KG. Incident reporting. In: Shojania KG, Duncan BW, McDonald KM, et al, eds. Making Health Care Safer: A Critical Analysis of Patient Safety Practices. Rockville , MD : Agency for Healthcare Research and Quality; 2001:chap 4. Evidence Report/Technology Assessment No. 43. AHRQ publication 01-E058. Grinfeld MJ. The debate over medical error reporting. Psychiatric Times . April 2000.

14 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
King G III, Hermodson A. Peer reporting of coworker wrongdoing: A qualitative analysis of observer attitudes in the decision to report versus not report unethical behavior. Journal of Applied Communication Research . 2000;(28), 309-29. Gilman AG, Rall TW, Nies AS , Taylor P. Goodman and Gilman's The Pharmacological Basis of Therapeutics. New York , NY : Pergamon Press; 1996. Kolata G. New York Times News Service. Who cares when our drugs fail? San Diego Union-Tribune . October 15, 1997 :E-1,5. Melmon KL, Morrelli HF, Hoffman BB, Nierenberg DW, eds. Melmon and Morrelli's Clinical Pharmacology: Basic Principles in Therapeutics . 3rd ed. New York , NY : McGraw-Hill, Inc., 1992. Moore TJ, Psaty BM, Furberg CD. Time to act on drug safety . JAMA . 1998 May 20, 279 (19):15713. Cullen DJ, Bates DW, Small SD, Cooper JB, Nemeskal AR , Leape LL. The incident reporting system does not detect adverse drug events: a problem for quality improvement. Jt Comm J Qual Improv . 1995 Oct;21(10):541-8. Bates DW. Drugs and adverse drug reactions: how worried should we be? JAMA . 1998 Apr 15;279(15):1216-7. Dickinson, JG. FDA seeks to double effort on confusing drug names. Dickinson 's FDA Review . 2000 Mar;7(3):13-4. Cohen JS. Overdose: The Case Against the Drug Companies . New York , NY : Tarcher-Putnum; 2001. Stenson J. Few residents report medical errors, survey finds. Reuters Health. February 21, 2003 Survey by Henry J. Kaiser Family Foundation, Harvard School of Public Health. Methodology: Fieldwork conducted by ICR - International Communications Research, April 11- June 11, 2002 Bond CA, Raehl CL, Franke T. Clinical pharmacy services, hospital pharmacy staffing, and medication errors in United States hospitals. Pharmacotherapy . 2002 Feb;22(2):134-47. Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Arch Intern Med . 2002 Sep 9;162(16):1897-903. LaPointe NM , Jollis JG. Medication errors in hospitalized cardiovascular patients. Arch Intern Med . 2003 Jun 23;163(12):1461-6. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med . 2003 Feb 4;138(3):161-7. Gandhi TK, Weingart SN, Borus J, et al. Adverse drug events in ambulatory care. N Engl J Med . 2003 Apr 17;348(16):1556-64. Medication side effects strike 1 in 4. Reuters. April 17, 2003 .

15 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Vastag B. Pay attention: ritalin acts much like cocaine. JAMA . 2001 Aug 22-29;286(8):905-6. Rosenthal MB, Berndt ER, Donohue JM, Frank RG, Epstein AM. Promotion of prescription drugs to consumers. N Engl J Med . 2002 Feb 14;346(7):498-505. Wolfe SM. Direct-to-consumer advertising—education or emotion promotion? N Engl J Med . 2002 Feb 14;346(7):524-6. Ibid. US General Accounting Office. Report to the Chairman, Subcommittee on Human Resources and Intergovernmental Relations, Committee on Government Operations, House of Representatives: FDA Drug Review Postapproval Risks 1976-85 . Washington , DC : US General Accounting Office; 1990:3. Drug giant accused of false claims. MSNBC News. July 11, 2003. http://msnbc.com/news/937302.asp?0sl=-42&cp1=1. Suh DC , Woodall BS, Shin SK , Hermes-De Santis ER. Clinical and economic impact of adverse drug reactions in hospitalized patients. Ann Pharmacother . 2000 Dec;34(12):1373-9. Agger WA. Antibiotic resistance: unnatural selection in the office and on the farm. Wisconsin Medical Journal . August 2002. Nash DR, Harman J, Wald ER, Kelleher KJ. Antibiotic prescribing by primary care physicians for children with upper respiratory tract infections. Arch Pediatr Adolesc Med . 2002 Nov;156(11):1114-9. Schindler C, Krappweis J, Morgenstern I, Kirch W. Prescriptions of systemic antibiotics for children in Germany aged between 0 and 6 years. Pharmacoepidemiol Drug Saf . 2003 Mar;12(2):113-20. Finkelstein JA, Stille C, Nordin J, et al. Reduction in antibiotic use among US children, 1996-2000. Pediatrics . 2003 Sep;112(3 Pt 1):620-7. Linder JA, Stafford RS. Antibiotic treatment of adults with sore throat by community primary care physicians: a national survey, 1989-1999. JAMA . 2001 Sep 12;286(10):1181-6. Drug resistance page. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/drugresistance/community/ Available at: http://www.health.state.ok.us/program/cdd/ar/. Available at: http://www.librainitiative.com/life/en/libra_initiative.html. Ohlsen K, Ternes T, Werner G, et al. Impact of antibiotics on conjugational resistance gene transfer in Staphylococcus aureus in sewage. Environ Microbiol . 2003 Aug;5(8):711-6. Pawlowski S, Ternes T, Bonerz M, et al. Combined in situ and in vitro assessment of the estrogenic activity of sewage and surface water samples. Toxicol Sci . 2003 Sep;75(1):57-65. Epub 2003 Jun 12. Ternes TA, Stuber J, Herrmann N, et al. Ozonation: a tool for removal of pharmaceuticals, contrast media and musk fragrances from wastewater? Water Res . 2003 Apr;37(8):1976-82. Ternes TA, Meisenheimer M, McDowell D, et al. Removal of pharmaceuticals during drinking water treatment. Environ Sci Technol . 2002 Sep 1;36(17):3855-63.

16 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Ternes T, Bonerz M, Schmidt T. Determination of neutral pharmaceuticals in wastewater and rivers by liquid chromatography-electrospray tandem mass spectrometry. J Chromatogr A . 2001 Dec 14;938(1-2):175-85. Golet EM, Alder AC, Hartmann A, Ternes TA, Giger W. Trace determination of fluoroquinolone antibacterial agents in urban wastewater by solid-phase extraction and liquid chromatography with fluorescence detection. Anal Chem . 2001 Aug 1;73(15):3632-8. Daughton CG, Ternes TA. Pharmaceuticals and personal care products in the environment: agents of subtle change? Environ Health Perspect . 1999 Dec;107 Suppl 6:907-38. Hirsch R, Ternes T, Haberer K, Kratz KL. Occurrence of antibiotics in the aquatic environment. Sci Total Environ . 1999 Jan 12;225(1-2):109-18. Ternes TA, Stumpf M, Mueller J, Haberer K, Wilken RD , Servos M. Behavior and occurrence of estrogens in municipal sewage treatment plants—I. Investigations in Germany , Canada and Brazil . Sci Total Environ . 1999 Jan 12;225(1-2):81-90. Hirsch R, Ternes TA, Haberer K, Mehlich A, Ballwanz F, Kratz KL. Determination of antibiotics in different water compartments via liquid chromatography-electrospray tandem mass spectrometry. J Chromatogr A . 1998 Jul 31;815(2):213-23. Coste J, Hanotin C, Leutenegger E. Prescription of non-steroidal anti-inflammatory agents and risk of iatrogenic adverse effects: a survey of 1072 French general practitioners. Therapie . 1995 May-Jun;50(3):265-70. Kouyanou K, Pither CE, Wessely S. Iatrogenic factors and chronic pain. Psychosom Med . 1997 Nov-Dec;59(6):597-604. Abel U. Chemotherapy of advanced epithelial cancer—a critical review. Biomed Pharmacother . 1992;46(10):439-52. Schulman KA, Stadtmauer EA, Reed SD , et al. Economic analysis of conventional-dose chemotherapy compared with high-dose chemotherapy plus autologous hematopoietic stem-cell transplantation for metastatic breast cancer. Bone Marrow Transplant . 2003 Feb;31(3):205-10. Kaufman, M. Drugmaker to pay FDA $500 million. Manufacturing problems found at schering-plough. The Washington Post . May 18, 2002 :A01. US Congressional House Subcommittee Oversight Investigation. Cost and Quality of Health Care: Unnecessary Surgery . Washington , DC : Government Printing Office;1976. Cited in: McClelland GB, Foundation for Chiropractic Education and Research. Testimony to the Department of Veterans Affairs' Chiropractic Advisory Committee. March 25, 2003 . Leape LL. Unnecessary surgery. Health Serv Res . 1989 Aug;24(3):351-407.

17 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
McClelland GB, Foundation for Chiropractic Education and Research. Testimony to the Department of Veterans Affairs' Chiropractic Advisory Committee. March 25, 2003 . Coile RC Jr. Internet-driven surgery. Russ Coiles Health Trends . 2003 Jun;15(8):2-4. Guarner V. Unnecessary operations in the exercise of surgery. A topic of our times with serious implications in medical ethics. Gac Med Mex . 2000 Mar-Apr;136(2):183-8. Rutkow IM. Surgical operations in the United States : 1979 to 1984. Surgery . 1987 Feb;101(2):192-200. Rutkow IM. Surgical operations in the United States . Then (1983) and now (1994). Arch Surg . 1997 Sep;132(9):983-90. Linnemann MU, Bulow HH. Infections after insertion of epidural catheters. Ugeskr Laeger . 1993 Jul 26;155(30):2350-2 Seres JL, Newman RI . Perspectives on surgical indications. Implications for controls. Clin J Pain . 1989 Jun;5(2):131-6. Chassin MR, Kosecoff J, Park RE, et al. Does inappropriate use explain geographic variations in the use of health care services? A study of three procedures. JAMA. 1987 Nov 13;258(18):2533-7. Office of Technology Assessment, US Congress. Assessing the Efficacy and Safety of Medical Technologies. Washington DC : Office of Technology Assessment, US Congress; 1978. Tunis SR, Gelband H. Health care technology in the United States . Health Policy . 1994 Oct-Dec;30(1-3):335-96. Zhan C, Miller M. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA . 2003;290:1868-1874. Injuries in hospitals pose a significant threat to patients and a substantial increase in health care charges [press release]. Rockville , MD : Agency for Healthcare Research and Quality. October 7, 2003 . http://www.ahrq.gov/news/ress/pr2003/injurypr.htm. Weingart SN, Iezzoni LI. Looking for medical injuries where the light is bright. JAMA . 2003 Oct 8 ;290(14):1917-9. MacMahon B. Prenatal x-ray exposure and childhood cancer. J Natl Cancer Inst. 1962 May;28:1173 91. Health Physics Society. Available at: http://hps.org/publicinformation/ate/q1084.html. Accessed December 17, 2003 . Gofman, JW. Radiation from Medical Procedures in the Pathogenesis of Cancer and Ischemic Heart Disease: Dose-Response Studies with Physicians per 100,000 Population. San Francisco , CA : CNR Books; 1999.
18 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Gofman J W. Preventing Breast Cancer: The Story of a Major, Proven, Preventable Cause of This Disease. 2nd ed. San Francisco , CA : CNR Books; 1996. Sarno JE. Healing Back Pain: The Mind-Body Connection. Warner Books; 1991. Siu AL, Sonnenberg FA, Manning WG, et al. Inappropriate use of hospitals in a randomized trial of health insurance plans. N Engl J Med . 1986 Nov 13;315(20):1259-66. Siu AL, Manning WG, Benjamin B. Patient, provider and hospital characteristics associated with inappropriate hospitalization. Am J Public Health . 1990 Oct;80(10):1253-6. Eriksen BO, Kristiansen IS, Nord E, et al. The cost of inappropriate admissions: a study of health benefits and resource utilization in a department of internal medicine. J Intern Med . 1999 Oct;246(4):379-87. Showalter E. Hystories: Hysterical Epidemics and Modern Media . New York , NY : Columbia University Press; 1997. Fugh-Berman A. Alternative healing. In: Smith B, Steinem G, Mink G, Navarro M, and Mankiller W, eds. The Reader's Companion to U.S. Women's History. New York , NY : Houghton Mifflin; 1998. Available at: http://college.hmco.com/history/readerscomp/women/html/wh_001200_alternativeh.htm. Thacker SB, Stroup D, Chang M. Continuous electronic heart rate monitoring for fetal assessment during labor (Cochrane Review). In: The Cochrane Library, issue 1, 2003. Oxford : Update Software. Cole C. Admission electronic fetal monitoring does not improve neonatal outcomes . J Fam Pract . 2003 Jun;52(6):443-4. Nelson HD, Humphrey LI, Nygren P, Teutsch SM, Allan JD. Postmenopausal hormone replacement therapy: scientific review. JAMA . 2002 Aug 21;288(7):872–81. Nelson HD. Assessing benefits and harms of hormone replacement therapy: clinical applications. JAMA . 2002 Aug 21;288(7):882-4 Fletcher SW, Colditz GA. Failure of estrogen plus progestin therapy for prevention. JAMA . 2002 Jul 17;288(3):366-8. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group for the Women's Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA . 2002 Jul 17; 288(3):321-33. Rutkow IM. Obstetric and gynecologic operations in the United States , 1979 to 1984. Obstet Gynecol 1986 Jun;67(6):755-9. Family Practice News . February 15, 1995 : 29.

19 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Sakala C. Medically unnecessary cesarean section births: introduction to a symposium. Soc Sci Med . 1993 Nov;37(10):1177-98. VanHam MA, van Dongen PW, Mulder J. Maternal consequences of cesarean section. A retrospective study of intra-operative and postoperative maternal complications of cesarean section during a 10-year period. Eur J Obstet Reprod Biol . 1997 Jul;74(1):1-6. Weiner J. Smoking and cancer: the cigarette papers: how the industry is trying to smoke us all . The Nation . January 1, 1996 :11-18. Tobacco.org. Tobacco timeline. Available at: http://www.tobacco.org/resources/history/tobacco_history.html. December 16, 2003 . Lasser KE, Allen PD, Woolhandler SJ, Himmelstein DU, Wolfe SM, Bor DH. 2002. Timing of new black box warnings and withdrawals for prescription medications. JAMA . 2002 May 1;287(17):2215-20. Injuryboard.com. General Accounting Office study sheds light on nursing home abuse. July 17, 2003 . Available at: http://www.injuryboard.com/view.cfm/Article=3005. Accessed December 17, 2003 . Weingart SN, McL Wilson R, Gibberd RW, Harrison B. Epidemiology of medical error. West J Med . 2000 Jun;172(6):390-3. Blendon R, Schoen C, et al. Five nation survey exposes flaws in the U.S. health care system. Health Affairs . May/June 2002. Institute of Medicine . Care Without Coverage: Too Little, Too Late . May 21, 2002 . A Shared Destiny: Community Effects of Uninsurance . March 6, 2003 . US Department of Health and Human Services and US Department of Justice. Health Care Fraud and Abuse Control Program Annual Report for FY 1998. April 1999. Health Care Fraud and Abuse Control Program Annual Report for FY 2001. April 2002. Abuse of residents is a major problem in U.S. nursing homes [transcript]. CNN television. July 30, 2001 Available at: http://www.house.gov/waxman. Accessed December 17, 2003 . Mitka M. Unacceptable nursing home deaths unautopsied. JAMA . 1998 Sep 23-30;280(12):1038-9 New data is in on North Carolina 's nursing home residents. Medical Review of North Carolina, Inc. July 21, 2003 . Weinstein RA. Nosocomial infection update. Emerg Infect Dis . 1998 Jul-Sep;4(3):416-20. Centers for Medicare & Medicaid Services. Report to Congress: Appropriateness of Minimum Nurse Staffing Ratios In Nursing Homes: Phase II Final Report . December 24, 2001 .

20 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Consumer group criticizes Thompson letter dismissing report on dangerous staffing levels in nursing homes [news release]. Washington , DC : National Citizens' Coalition for Nursing Home Reform. March 22, 2002 . Bergstrom N, Braden B, Kemp M, Champagne M, Ruby E. Multi-site study of incidence of pressure ulcers and the relationship between risk level, demographic characteristics, diagnoses and prescription of preventive interventions . J Am Geriatr Soc . 1996 Jan;44(1):22-30. Miles SH. Concealing accidental nursing home deaths. HEC Forum . 2002 Sep;14(3):224-34. Corey TS, Weakley-Jones B, Nichols GR 2nd, Theuer HH. Unnatural deaths in nursing home patients. J Forensic Sci . 1992 Jan;37(1):222-7. Lloyd-Jones DM, Martin DO, Larson MG, Levy D. Accuracy of death certificates for coding coronary heart disease as the cause of death. Ann Intern Med . 1998 Dec 15;129(12):1020-6. Thomas DR , Zdrowski CD, Wilson MM, et al. Malnutrition in subacute care. Am J Clin Nutr . 2002 Feb;75(2):308-13. Robinson BE. Death by destruction of will. Lest we forget. Arch Intern Med . 1995 Nov 13;155(20):2250-1. Capezuti E, Strumpf NE, Evans LK, Grisso JA, Maislin G. The relationship between physical restraint removal and falls and injuries among nursing home residents . J Gerontol A Biol Sci Med Sci . 1998 Jan;53(1):M47-52. Phillips CD, Hawes C, Fries BE. Reducing the use of physical restraints in nursing homes: will it increase costs? Am J Public Health . 1993 Mar;83(3):342-8. Miles SH, Irvine P. Deaths caused by physical restraints. Gerontologist . 1992 Dec;32(6):762-6. Annas GJ. The last resort—the use of physical restraints in medical emergencies. N Engl J Med . 1999 Oct 28;341(18):1408-12. Parker K, Miles SH. Deaths caused by bedrails. J Am Geriatr Soc . 1997 Jul;45(7):797-802. Miles SH. Concealing accidental nursing home deaths. HEC Forum . 2002 Sep;14(3):224-34. Katz PR, Seidel G. Nursing home autopsies. Survey of physician attitudes and practice patterns. Arch Pathol Lab Med . 1990 Feb;114(2):145-7. Overmedication of U.S. seniors. Reuters Health. May 21, 2003. Average number of prescriptions by HMOs increases. Drug Benefit Trends . 2002 Sep 12;14(8). Kaiser Family Foundation. Prescription Drug Trends . November 2001. Williams BR, Nichol MB, Lowe B, Yoon PS, McCombs JS, Margolies J. Medication use in residential care facilities for the elderly. Ann Pharmacother . 1999 Feb;33(2):149-55.

21 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
AARP. Medicare and prescription drugs. Available at: http://www.aarp.org/prescriptiondrugs. Accessed December 16, 2003. California reaches $100 million multi-state settlement with drug giant Mylan over alleged price-fixing scheme [press release]. Sacramento , CA : Office of the Attorney General, Department of Justice, State of California ; July 12, 2000. Attorney general reaches settlement with drug giant. WRAL News. March 7, 2003 . Available at: http://www.wral.com/money/2026364/detail.html Blowing the final whistle. The Observer. November 25, 2001 . Available at: http://education.guardian.co.uk/businessofresearch/comment/0,9976,606260,00.html. AARP. Are food supplements for me. Available at: http://www.aarp.org/Articles/a2003-03-07-supplements.html. Bernabei R, Gambassi G, Lapane K, et al. Management of pain in elderly patients with cancer. SAGE study group. Systematic assessment of geriatric drug use via epidemiology. JAMA . 1998 Jun 17;279(23):1877-82. Panel names estrogen as carcinogen. The Washington Post; Associated Press, December 16, 2000 :A05. Estrogen hikes ovarian cancer risk. MSNBC staff and wire reports. July 16, 2002 . Grady D. Study recommends NOT using hormone therapy for bone loss. New York Times . October 1, 2003 . Anderson GL, Judd HL, Kaunitz AM, et al. Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: the Women's Health Initiative randomized trial. JAMA . 2003 Oct 1;290(13):1739-48. Chlebowski RT, Hendrix SL, Langer RD , et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women's Health Initiative randomized trial. JAMA . 2003 Jun 25;289(24):3243-53. Wassertheil-Smoller S, Hendrix SL, Limacher M, et al . Effect of estrogen plus progestin on stroke in postmenopausal women: the Women's Health Initiative: a randomized trial. JAMA 2003 May 28;289(20):2673-84. Shumaker SA, Legault C, Rapp SR, et al. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women's Health Initiative memory study: a randomized controlled trial. JAMA 2003;289:2651-62 . Beral V; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet . 2003 Aug 9;362(9382):419-27. THE EFFECT OF AQUATIC EXERCISE ON PAIN AND POSTURAL CONTROL IN WOMEN WITH LOW BACK PAIN; Leila Zameni1. Mina Haghighi2 1. Department of Physical Education and Sport Sciences, Sari Branch, Islamic Azad University, Sari, Iran; 2. Department of Physical Education and Sport Sciences, Najafabad Branch, Islamic Azad University, Najafabad, Iran Leila Zameni,

22 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
[email protected] International Journal of Sport Studies. Vol., 1 (4), 152-156, 2011 Available online at http://www.ecisi.com ISSN 2251-7502 ©2011 ECISI Journals The Effect of Aquatic Exercise and Education on Lowering Fall Risk in Older Adults With Hip Osteoarthritis; Cathy M. Arnold and Robert A. Faulkner; Journal of Aging and Physical Activity, 2010, 18, 245-260 - © 2010 Human Kinetics, Inc. The Effect of Aquatic Exercise and Education on Lowering Fall Risk in Older Adults With Hip Osteoarthritis; Cathy M. Arnold and Robert A. Faulkner; Journal of Aging and Physical Activity, 2010, 18, 245-260 - © 2010 Human Kinetics, Inc. Comparison of the Effects of Exercise by Chronic Stroke Patients in Aquatic and Land Environments; Journal Physiotherapy Science – Vol. 23, No. 5 - 821-824, 2011 The Effects on Muscle Strength and Visual Analog Scale Pain of Aquatic Therapy for individuals with Low Back Pain; Journal Physiotherapy Science – Vol. 23, 57-60 No. 1 - 2011 The Effect of Aquatic Exercise and Education on Lowering Fall Risk in Older Adults With Hip Osteoarthritis, Cathy M. Arnold and Robert A. Faulkner, Journal of Aging and Physical Activity, 2010, 18, 245-260 - © 2010 Human Kinetics, Inc. Postural Balance of Stroke Survivors in Aquatic and Land Environments Journal of Aging and Physical Activity, 2010, 18, 245-260 - © 2010 Human Kinetics, Inc. UK Aquatic Physiotherapy Data Collection. London: Chartered Society of Physiotherapy; The University of Brighton, Brighton and Sussex University Hospitals NHS Trust, East Sussex Hospitals NHS Trust and Western Sussex Hospitals NHS Trust for staff and other expert resources. Aquatic Therapy Association Chartered Physiotherapists University Brighton; Aquatic Physiotherapy Data Collection 2009; HyDAT team: Liz Bryant, Anna Carter, Sarah Cox, Do Heath, Anne Jackson*, Ann Moore, Raija Kuisma, Jacqueline Pattman, Sarah-Jane Ryan*University of Brighton Aquatic Therapy Association of Chartered Physiotherapists Association of Chartered Physiotherapists. 2006. Guidance on Good Practice in Hydrotherapy. Chartered Society of Physiotherapy: London. Carter A, Heath D, Jackson A, Kuisma R & Ryan S-J. 2005. Report from the Southeast hydrotherapy research group: Planning a national audit. Aqualines; 17(2): 20-22. Cox S, Bryant L, Carter A, Jackson A, Kuisma R, Pattman J, Ryan S-J. 2009. HyDAT Floats! National Hydrotherapy Data Collection (HyDAT) Project - Summary and Findings. Aqualines; 21 (1) 4-7. Department of Health, News, Recent stories. 2009. Jim Easton has been appointed NHS National Director for Improvement and Efficiency, the Department of Health announced today. Department of Health: London. http://www.dh.gov.uk/en/News/Recentstories/DH_101712. Department of Health. 2009. Be active, Be healthy. Surrey: The Stationary office: London. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_094358 Department of Health. 2008. High Quality Care For All, NHS Next Stage Review Final Report. The Stationery Office: London.

23 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
http://www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/DH_085825 Hydrotherapy Association of Chartered Physiotherapists. 2006. Guidance on good practice in hydrotherapy. Chartered Society of Physiotherapy: London Jackson A. 2001. Using Measure Yourself Medical Outcome Profile (MYMOP) in hydrotherapy. Aqualines, Autumn, 8-20. Jackson A & Jackson CJ. 2003. The outcome of different combinations of physiotherapy treatment with an emphasis on combinations that include hydrotherapy. Aqualines; spring: 6-9. Jackson A, Kuisma R, Mason Z and Cox J. 2004. Older people's experience of water based exercise programmes. Aqualines 16 (2) 5-11. Mercer C, Jackson A, Hettinga D, Barlos P, Ferguson S, Greenhalgh S, Harding V, Hurley Osing D, Klaber Moffett J, Martin D, May S, Monteath J, Roberts L, Taylor N & Woby S. 2006. Clinical guidelines for the physiotherapy management of persistent low back pain. Part 1: exercise and Part 2: manual therapy. Chartered Society of Physiotherapy: London. Moore A P. 1996. The development of the mid Kent and Brighton outcome measurement tool for physiotherapy outpatient services. University of Brighton: Brighton. Moore A P. 1998. An audit of the outcome of the physiotherapy intervention for outpatients with back pain against set clinical standards. University of Brighton: Brighton. Moore A P. 1999. An audit of the outcome of physiotherapy intervention for outpatients with cervical spine pain and dysfunction. University of Brighton: Brighton. Moore A, Bryant E, Barfield J et al. 2006. Whiplash associated disorder: a one year standardized data collection project. University of Brighton: Brighton. Moore A. 2007. The power of multi-centre audit: standard data collection (SDC) (short article). Aqualines; 19(2): 18. National Institute for health and Clinical Excellence. 2009. Low back pain:48 Early management of persistent non-specific low back pain. NICE clinical guideline 88. National Institute of Health and Clinical Excellence: London. http://guidance.nice.org.uk/CG88/NiceGuidance/pdf/English Royal College of Physicians. 2008. Osteoarthritis: National clinical guideline for care and management in adults. NICE clinical guideline 59. National Institute of Health and Clinical Excellence: London. http://guidance.nice.org.uk/CG59/Guidance/pdf/English Standard Occupational Classification. 2000 National Office of Statistics. Standard Occupational Classification. 2000. National Office of Statistics: Hampshire. http://www.ons.gov.uk/about-statistics/classifications/current/SOC2000/index.html

24 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Waller B, Lambeck J, & Daly D. 2009. Therapeutic aquatic exercise in the treatment of low back pain; a systematic review. Clinical Rehabilitation 23: 3-14 World Health Organisation (WHO). 1990. International Classication of Disease (ICD) http://www.who.int/classification/icd/en/ The University of Brighton, Brighton and Sussex University Hospitals NHS Trust, East Sussex Hospitals NHS Trust and Western Sussex Hospitals NHS Trust for staff and other expert resources.
Partial List of References
The Health Care Crisis •
Is Man-Made • Manufactured
The Solution Is AquaDios-Med Proactive Preventive Medicine
By Dr. Alan Jensen
********************************************************************************* Partial List References • Healthcare Crisis • Manufactured • Man-Made • Includes • Media • Placebo • Preventive Medicine • Aquatic Exercise Hospital • ChargeMaster Prices •Unnecessary surgery • Adverse Events • Unnecessary Hospitalization • Negligence - hospitalized patients • Fibromyalgia & More **********************************************************************************

25 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
********************************************************************************** Partial List Rreferences •Deep-Water Running • Aquatics • Sports Medicine • Back Pain •Arthritis •Rheumatism • Balneotherapy • Applied Physiology • Fibromyalgia & Much More ********************************************************************************** American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc 1998;30: 975–91. American College of Sports Medicine (ACSM) (2006). ACSM’s Guidelines for Exercise Testing and Prescription, 7th edition. Baltimore MD: Lippincott Williams & Wilkins. Aquatic exercise: a review. AKWA letter, October/November. Asher, Anne - About.Com a part of the New York Times 2006 “Back Pain and Deep water running” Arthritis and Rheumatism. 55.1 (Feb. 2006): 66-73. Assis, Marcos Renato, et al. “A randomized controlled trial of deep water running: Clinical effectiveness of aquatic exercise to treat fibromyalgia.” Arthritis and Rheumatism. 55.1 (Feb. 2006): 57-65. Aus J Sci Med Sport, Vol 23, No 1, pp13- 22, 1990 Avellini BA, Shapiro Y, Pandolf KB. Cardio-respiratory physical training in water and on land. Eur J Appl Physiol Occup Physiol 1983;50:255–63. Am J Sports Med, Vol 21, No1, 1993 Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561–71. Bennett RM, Clark SR, Goldberg L, Nelson D, Bonafede RP, Porter J, et al. Aerobic fitness in patients with fibrositis: a controlled study of respiratory gas exchange and 133xenon clearance from exercising muscle. Arthritis Rheum 1989;32: 454–60. Bennett RM. Beyond fibromyalgia: ideas on etiology and treatment. J Rheumatol Suppl 1989;19:185–91. Borg, G. (1998). Borg’s perceived exertion and pain scales. Champaign IL: Human Kinetics. Borg G (1982) - Psychophysical bases of perceived exertion. Medicine and Science in Sport and Exercise. 14:377-381. Brown SP, Chitwood LF, Beason KR and McLemore DR (1996) - Perceptual responses to deep water running and treadmill exercise. Perceptual and Motor Skills. 88:131-139.

26 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Brown SP, Chitwood LF, Beason KR and McLemore DR (1997) Deep water running physiologic responses: gender differences at treadmill-matched walking/running cadences. Journal of Strength and Conditioning Research. 11:107-114. Brown SP, Jordon JC, Chitwood LF, Beason KR, Alvarez JG and Honea KP (1998) Relationship of heart rate and oxygen uptake kinetics during deep water running in the adult population — ages 50 to 70 years. Journal of Aging and Physical Activity. 6:248-255. Br J Sports Med, Vol32, pp44-48, 1998 Buckelew SP, Murray SE, Hewett JE, Johnson J, Huyser B. Self-efficacy, pain, and physical activity among fibromyalgia subjects. Arthritis Care Res 1995;8:43–50. Busch A, Schachter CL, Peloso PM, Bombardier C. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst Rev 2002;3:CD003786. Butts NK, Tucker M and Greening C (1991) Physiologic responses to maximal treadmill and deep water running in men and women. The American Journal of Sports Medicine. 19:612-614. Burke, Edmund R. Off-Season Training for Cyclists. Boulder, CO: VeloPress, 1997. Concept 2."Rowing Technique." www.concept2.com Burckhardt CS, Clark SR, Bennett RM. The Fibromyalgia Impact Questionnaire: development and validation. J Rheumatol 1991;18:728–33. Burckhardt CS, Mannerkorpi K, Hedenberg L, Bjelle A. A randomized, controlled clinical trial of education and physical training for women with fibromyalgia. J Rheumatol 1994; 21:714–20. Buxton, Karen - Cardiovascular Conditioning: Alternatives to Swim, Bike, Run Part 3: Rowing Ergometers, Feb. 3, 2008 Ciconelli RM, Ferraz MB, Santos W, Meinao I, Quaresma Marina R. Brazilian-Portuguese version of the SF-36: a reliable and valid quality of life outcome measure. Rev Bras Reumatol 1999;39:143–50. In Portuguese. Cole, A. J., Comprehensive Aquatic Therapy (p. 123–135). Boston MA: Butterworth-Heinemann. Coyle EF, Martin WH, Sinacore DR, et al (1984) Time course of loss of adaptations after stopping prolonged intense endurance exercise. Journal of Applied Physiology. 57:1857-1864. Comparative exercise responses of deep water and treadmill running. Journal of Strength and Conditioning, 9(2), 104–109. Nagle, E. F., Otto, A. D., Jakicic, J. M., et al. (2003). D’Acquisto, L. J., D’Acquisto, D. M., & Renne, D. (2000). Metabolic and cardiovascular responses in older women during shallow-water exercise.

27 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Davidson K and McNaughton DK (2000) Deep water running training and road running improve VO2max in untrained women. Journal of Strength and Conditioning Research. 14:191-195. Dowzer CN, Reilly T, Cable NT. Effects of deep and shallow water running on spinal shrinkage. Br J Sports Med 1998;32: 44–8. Edlich RF, Towler MA, Goitz RJ, Wilder RP, Buschbacher LP, Morgan RF, et al. Bioengineering principles of hydrotherapy. J Burn Care Rehabil 1987;8:580–4. Effects of aquatic plus walking exercises on weight loss and function in sedentary obese females. Medicine & Science in Sports & Exercise, 35(5), May, S136, Abstract 753. Essert, Mary. “Why Water Works.” Aquatic Resources Network. Jan. 13, 2003. Eyestone ED, Fellingham G, George J and Fisher A (1993) Effects of water running and cycling on maximum oxygen and two-mile run performance. The American Journal of Sports Medicine. 21:41-44. Evcik D, Kizilay B, Gokcen E. The effects of balneotherapy on fibromyalgia patients. Rheumatol Int 2002;22:56–9. Fibromyalgia Back Pain and Sciatica Water Exercise - Benefits of Water Exercise for Back Pain - Water Exercise and Aquatic Therapy - What is Water Exercise Aquatic Resources Network. 2003. Fibromyalgia and water running by Kate Grossman, MD Gorenstein C, Andrade L. Validation of a Portuguese version of the Beck Depression Inventory and the State-Trait Anxiety Inventory in Brazilian subjects. Braz J Med Biol Res 1996;29: 453–7. Gowans SE, DeHueck A, Abbey SE. Measuring exercise-induced mood changes in fibromyalgia: a comparison of several measures. Arthritis Rheum 2002;47:603–9. Gowans SE, deHueck A, Voss S, Richardson M. A randomized, controlled trial of exercise and education for individuals with fibromyalgia. Arthritis Care Res 1999;12:120–8. Gowans SE, deHueck A, Voss S, Silaj A, Abbey SE, Reynolds WJ. Effect of a randomized, controlled trial of exercise on mood and physical function in individuals with fibromyalgia. Arthritis Rheum 2001;45:519–29. Gunther V, Mur E, Kinigadner U, Miller C. Fibromyalgia: the effect of relaxation and hydrogalvanic bath therapy on the subjective pain experience. Clin Rheumatol 1994;13:573–8. Grossman, MD Kate fibromyalgia and water running. Aquatic Resources Network. 2003 Gusi, N., et al. “Exercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgia.”

28 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Hamer PW and Morton AR (1990) - Water running: Training effects and specificity of aerobic, anaerobic and muscular parameters following an eight-week training programme. The Australian Journal of Science and Medicine in Sport. 22:13-22. Hamer PW and Slocombe B (1997) - The psychophysical and heart rate relationship between treadmill and deep water running. Australian Journal of Physiotherapy. 43:265-271. Health and Fitness Journal, Vol 8, No 5, pp 5-8, 2004 Health On the Net Foundation - About.com reliable trusted health information. Health On the Net Foundation About.com - About.com is accredited by the, which promotes reliable and trusted online health information. Hickson RC, Foster C and Pollick ML (1985) Reduced training intensities and loss of aerobic power endurance and cardiac growth. Journal of Applied Physiology. 58:492-499. Isokinetics and Exercise Science, Vol 3, No 4, pp207-215, 1993 Jentoft, Eva Saltskar, et al. “Effects of pool based and land-based aerobic exercise on women with fibromyalgia/chronic widespread muscle pain.” Arthritis and Rheumatism. 45.1 (Feb. 2001) 42-47. Jentoft ES, Kvalvik AG, Mengshoel AM. Effects of pool-based and land-based aerobic exercise on women with fibromyal- 64 Assis et al gia/chronic widespread muscle pain. Arthritis Rheum 2001; 45:42–7. Jones KD, Clark SR. Individualizing the exercise prescription for persons with fibromyalgia. Rheum Dis Clin North Am 2002;28:419–36. Journal of Strength and Conditioning Research, 15(1), 12–19. Frangolias, D., Rhodes, E., & Tauton, J. (1996). J Sports Sci, Vol 21, No 12, pp 959- 972, 2003 J Appl Physiol, Vol 69, pp657- 664, 1990 King SJ, Wessel J, Bhambhani Y, Sholter D, Maksymowych W. The effects of exercise and education, individually or combined, in women with fibromyalgia. J Rheumatol 2002;29: 2620–7. Kisner, C., & Colby, L.A. (2002). Therapeutic Exercise: Foundations and Techniques. Philadelphia: F.A. Davis Company. Konlian, C., Aquatic therapy: making a wave in the treatment of low back injuries. Orthop Nurs. 1999 Jan-Feb 18(1) Kravitz, L., & Mayo, J. (1997). The effect of familiarity with deep water running on maximal oxygen consumption. Journal of Strength and Conditioning, 10(4), 215–219. Kravitz, L., & Mayo, J. (1997). Aquatic exercise: a review. AKWA letter, October/November.

29 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
McArdle, W., Katch, R., & Katch, V. (1991) Exercise Physiology: Energy, Nutrition and Human Performance, 3rd edition. Philadelphia PA: Lea & Febiger. Michaud, T., Rodriguez-Zayas, J., Andres, F., et al. (1995). Mannerkorpi K, Burckhardt CS, Bjelle A. Physical performance characteristics of women with fibromyalgia. Arthritis Care Res 1994;7:123–9. Mannerkorpi K, Nyberg B, Ahlmen M, Ekdahl C. Pool exercise combined with an education program for patients with fibromyalgia syndrome: a prospective, randomized study. J Rheumatol 2000;27:2473–81. Mannerkorpi K, Ahlmen M, Ekdahl C. Six- and 24-month follow-up of pool exercise therapy and education for patients with fibromyalgia. Scand J Rheumatol 2002;31:306–10. Martin L, Nutting A, MacIntosh BR, Edworthy SM, Butterwick D, Cook J. An exercise program in the treatment of fibromyalgia. J Rheumatol 1996;23:1050–3. Martinez-Lavin M, Hermosillo AG, Rosas M, Soto ME. Circadian studies of autonomic nervous balance in patients with fibromyalgia: a heart rate variability analysis. Arthritis Rheum 1998;41:1966–71. Maximal physiological responses to deep water running at thermoneutral temperature. Applied Human Science. 18:31-35. McArdle WD, Katch F, Katch VL (1996) Exercise Physiology (fourth edition) McCain GA, Bell DA, Mai FM, Halliday PD. A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis Rheum 1988;31:1135–41. McClung J, Tuten C, Pritschet B, McInerny J and Emmett J (1998) Cardiac output and stroke volume during deep water running and treadmill running. Medicine and Science in Sports and Exercise. 30:241-246. McArdle, W., Katch, R., & Katch, V. (1991) Exercise Physiology: Energy, Nutrition and Human Performance, 3rd edition. Philadelphia PA: Lea & Febiger. 17. McNeal RL. Aquatic therapy for patients with rheumatic disease. Rheum Dis Clin North Am 1990;16:915–29. Michaud, T., Rodriguez-Zayas, J., Andres, F., et al. (1995). Comparative exercise responses of deep water and treadmill running. Journal of Strength and Conditioning, 9(2), 104–109. Nagle, E. F., Otto, A. D., Jakicic, J. M., et al. (2003). Mengshoel AM, Vollestad NK, Forre O. Pain and fatigue induced by exercise in fibromyalgia patients and sedentary healthy subjects. Clin Exp Rheumatol 1995;13:477–82. Med Sci Sports, Vol 16, No1, pp1-7, 1984

30 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Med Sci Sports, Vol 27, pp1007-1013, 1995 Mercer, Ph.D. John, "Deep-Water Running: When Your Training Should Land You in Deep Water." Mercer, Ph.D. John A. - Biomechanical Comparison of Deep Water and Treadmill Running, UNLV. Mercer, J.A. & Jensen, R.L (1997). Reliability and Validity of a Deep Water Running Graded Exercise Test. Measurement in Physical Education and Exercise Science, 1(4), 213-222. Mercer, J.A. & Jensen, R.L. (1997) Heart Rates at equivalent submaximal VO2 do not differ between Deep Water Running and Treadmill Running. Journal of Strength and Conditioning Research (in press). Meyer BB, Lemley KJ. Utilizing exercise to affect the symptomology of fibromyalgia: a pilot study. Med Sci Sports Exerc 2000;32:1691–7. Mengshoel AM, Komnaes HB, Forre O. The effects of 20 weeks of physical fitness training in female patients with fibromyalgia. Clin Exp Rheumatol 1992;10:345–9. Moldofsky H, Scarisbrick P. Induction of neurasthenic musculoskeletal pain syndrome by selective sleep stage deprivation. Psychosom Med 1976;38:35–44. Natanishi Y, Kimura T and Yokoo Y (1999) Maximal physiological responses to deep water running at thermoneutral temperature. Applied Human Science. 18:31-35. Nichols DS, Glenn TM. Effects of aerobic exercise on pain perception, affect, and level of disability in individuals with fibromyalgia. Phys Ther 1994;74:327–32. Norregaard J, Lykkegaard JJ, Mehlsen J, Danneskiold-Samsoe B. Exercise training in treatment of fibromyalgia. J Musculoskeletal Pain 1997;5:71–9. Res Quart Ex and Sport, Vol 65, No4, pp386-389, 1994 Sports Med, Vol 16, No6, pp374- 380, 1993 O’Connor PJ, Youngstedt SD. Influence of exercise on human sleep. Exerc Sport Sci Rev 1995;23:105–34. Pöyhönen, T., Sipliä, S., Keskinen, K. L., et al. (2002). Medicine & Science in Sports & Exercise, 24(12), 2103–2109. Richards SC, Scott DL. Prescribed exercise in people with fibromyalgia: parallel group randomised controlled trial. BMJ 2002;325:185–9. Richie SE and Hopkins WG (1991) The intensity of exercise in deep water running. International Journal of Sports Medicine. 12:27-29.

31 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Sanders, M. (2006). Program evaluation: Determining the impact of a water-based cross-cultural exercise program for women aged 50 years and older to improve or maintain functional activities of daily living on land. Doctoral Dissertation, University of Nevada, Reno. Sanders, PhD, FACSM, Mary E. Buring the fat! University of Nevada, Reno; Health & Fitness Journal for the American College of Sports Medicine Sjogren T, Long N, Storay I, Smith J Physiother Res Int. 1997;2(4):212-22. Svedenhag J, Seger J. Running on land and in water: comparative exercise physiology. Med Sci Sports Exerc 1992;24: 1155–60. Pöyhönen, T., Sipliä, S., Keskinen, K. L., et al. (2002). Medicine & Science in Sports & Exercise, 24(12), 2103–2109. Takeshima, N., Rogera, M. E., Wantanebe, E., et al. (2002). Water-based exercise improves health related aspects of fitness in older women. Medicine & Science in Sports & Exercise, 33(3), 544–551. The effect of familiarity with deep water running on maximal oxygen consumption. Journal of Strength and Conditioning, 10(4), 215–219. USA Cycling Coaching Staff. USA Cycling Sport Coach Manual. Colorado Springs, CO: USA Cycling, Inc., 1999. Valim V, Oliveira L, Suda A, Silva L, de Assis M, Neto T, et al. Aerobic fitness effects in fibromyalgia. J Rheumatol 2003;30:1060–9. alim V, Oliveira LM, Suda AL, Silva LE, Faro M, Neto TL, et al. Peak oxygen uptake and ventilatory anaerobic threshold in fibromyalgia. J Rheumatol 2002;29:353–7. Van Santen M, Bolwijn P, Landewe R, Verstappen F, Bakker C, Hidding A, et al. High or low intensity aerobic fitness training in fibromyalgia: does it matter? J Rheumatol 2002;29: 582–7. Van Denderen JC, Boersma JW, Zeinstra P, Hollander AP, van Neerbos BR. Physiological effects of exhaustive physical exercise in primary fibromyalgia syndrome (PFS): is PFS a disorder of neuroendocrine reactivity? Scand J Rheumatol 1992; 21:35–7. Van Santen M, Bolwijn P, Verstappen F, Bakker C, Hidding A, Houben H, et al. A randomized clinical trial comparing fitness and biofeedback training versus basic treatment in patients with fibromyalgia. J Rheumatol 2002;29:575–81. Verstappen FT, Santen-Hoeuftt HM, Bolwijn PH, van der Linden S, Kuipers H. Effect of a group activity program for fibromyalgia patients on physical fitness and well being. J Musculoskeletal Pain 1997;5:17–28. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992;30:473–83.

32 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
Wasserman K, Whipp BJ, Koyl SN, Beaver WL. Anaerobic threshold and respiratory gas exchange during exercise. J Appl Physiol 1973;35:236–43. What Is Fibromyalgia?Fibromyalgia Fact SheetHow to Diagnose Fibromyalgia Wigers SH, Stiles TC, Vogel PA. Effects of aerobic exercise versus stress management treatment in fibromyalgia: a 4.5 year prospective study. Scand J Rheumatol 1996;25:77–86. Wilder, R. P., & Brennan, D. K. (1997). Techniques of aqua running. In Becker, B. E., & Cole, A. J., Comprehensive Aquatic Therapy (p. 123–135). Boston MA: Butterworth-Heinemann. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the multicenter criteria committee. Arthritis Rheum 1990;33: 160–72. Interests for study: FibromyalgiaBack Pain and SciaticaWater Exercise - Benefits of Water Exercise for Back Pa...Water Exercise and Aquatic Therapy - What is Water Exer...Exercise Water WorkoutWater Aerobic DVDs, Shoes, CDs, Aqua Exercise Barbells, Float Beltswww.waterworkout.com Aerobic Water ExerciseGet Helpful Info And Details On Aerobic Water Exercise. Check Out!Blurtit.com Disability IncomeCan't work because of Fibromyalgia? Qualify for disability income!www.Allsup.com Fibromyalgia ExerciseTotal guide to research proven natural & prescription treatmentswww.EndFatigue.com Cure Fibromyalgia PainAmazing Natural Remedy Works. Say Goodbye To Fibromyalgia Pain!www.GoodbyeFibroPain.com About.com is accredited by the Health On the Net Foundation, which promotes reliable and trusted online health information. Heart Disease BasicsCommon SymptomsTreatment OptionsReducing Your RiskWomen and Heart Disease History of FibromyalgiaWhat Causes Fibromyalgia?FM ExerciseFibromyalgia ClothesNew FM Treatment Options Cardiovascular Conditioning: Alternatives to Swim, Bike, Run (Part 3: Rowing Ergometers By Karen Buxton Posted Feb. 3, 2008 Burke, Edmund R. Off-Season Training for Cyclists. Boulder, CO: VeloPress, 1997. Concept 2."Rowing Technique." www.concept2.com

33 AquaDios-Med™ PPM Copyright © 2005 – 2012 – 2013 – 2nd Edition – All Right Reserved • AquaDios.Com
"Deep-Water Running: When Your Training Should Land You in Deep Water." http://www.pponline.co.uk/encyc/0601.htmMercer, John. "Biomechanical Comparison of Deep Water and Treadmill Running." http://www.unlv.edu/faculty/jmercer/dwr/dwr.html USA Cycling Coaching Staff. USA Cycling Sport Coach Manual. Colorado Springs, CO: USA Cycling, Inc., 1999.
Partial List of References XIV • 33 Pages
The Health Care Crisis
Is Man-Made • Manufactured
The Solution Is AquaDios-Med Proactive Preventive Medicine
By Dr. Alan Jensen
********************************************************************************** Partial List References: Partial List Rreferences •Deep-Water Running • Aquatics • Sports Medicine • Back Pain •Arthritis •Rheumatism • Balneotherapy • Applied Physiology • Fibromyalgia & Much More **********************************************************************************
A 21st Century Immersion Environment for Advanced Fitness & Accelerated Healing
AquaDios-Med™ Proactive Preventive Medicine Is The SOLUTION • To
The Manufactured • Man-Made Healthcare • Crisis
Research • Solution • Analysis • Answers
By Dr. Alan Jensen
www.AquaDios.com [email protected]
P.O. Box 2228
Malibu, CA 90265 310-897-5055
Dr. Alan Jensen • Founder • CEO • Creator •
• AquaDios-Med™ •
Copyright © 1985 • 2008 • 2012 • 2013 AquaDiosTM / AquaDios-MedTM AquaDiosMedTM All Rights Reserved
AquaDios-Med™ PPM • Healthcare Crisis • Solution