
Application of composites to orthopedic prostheses for effective bone healing: A review
14
Review Application of composites to orthopedic prostheses for effective bone healing: A review Hassan Mehboob, Seung-Hwan Chang ⇑ School of Mechanical Engineering, Chung-Ang University, 221, Huksuk-Dong, Dongjak-Gu, Seoul 156-756, Republic of Korea article info Article history: Available online 7 August 2014 Keywords: Composite materials Prostheses Mechano-regulation theory Bone healing Fracture fixation abstract This paper aims to provide useful and practical information on the design of composite prostheses for healing bone fractures and describes the material properties of living tissues such as cartilage, structural materials and loading conditions according to various cases, and modeling techniques for the simulation of tissue differentiation during bone healing. In addition, the present review paper provides an overview of composite materials for the design of prostheses and highlights the merits of using composites. The history and recent trends in fixation methods and types, types of materials used for prostheses, loading conditions, mechano-regulation theories, and modeling techniques for finite element analyses to estimate the healing of bone fractures are also introduced. The healing process of bone fractures is fully influenced by the biomechanical characteristics of an orthopedic prosthesis and the injured bone such as fracture configurations, prosthesis shape, material properties, and degradation rate of the material. The appropriate parameters are highlighted for the optimal design of composite prostheses to heal bone fractures successfully. Ó 2014 Elsevier Ltd. All rights reserved. Contents 1. Introduction ......................................................................................................... 329 1.1. Fixation techniques .............................................................................................. 329 1.2. Defects of conventional prostheses ................................................................................. 329 1.3. Mechano-regulation theories ...................................................................................... 329 1.4. Conditions of implants for successful healing ......................................................................... 329 1.5. Materials and designs for composite prostheses ....................................................................... 329 2. History, development, and methods of fracture fixation ...................................................................... 330 2.1. History and development of fixation devices ......................................................................... 330 2.2. Types of fixation techniques and devices ............................................................................ 332 3. MR theories correlating mechanical conditions and tissue development ......................................................... 332 3.1. History of MR theory............................................................................................. 332 3.2. Applications of MR theories ....................................................................................... 333 4. Biomechanical conditions for simulated bone fracture models................................................................. 333 4.1. Biomechanics ................................................................................................... 333 4.2. Computer models for the bone healing process ....................................................................... 333 5. Biomaterials used for prosthesis design and fabrication ...................................................................... 333 5.1. Metals ........................................................................................................ 333 5.1.1. Nondegradable metals .................................................................................... 333 5.1.2. Biodegradable metals ..................................................................................... 336 5.2. Bioceramics .................................................................................................... 336 5.3. Polymers ...................................................................................................... 336 5.4. Polymer-based composite materials ................................................................................ 336 http://dx.doi.org/10.1016/j.compstruct.2014.07.052 0263-8223/Ó 2014 Elsevier Ltd. All rights reserved. ⇑ Corresponding author. Tel.: +82 2 820 5354; fax: +82 2 814 9476. E-mail address: [email protected] (S.-H. Chang). Composite Structures 118 (2014) 328–341 Contents lists available at ScienceDirect Composite Structures journal homepage: www.elsevier.com/locate/compstruct
Transcript of Application of composites to orthopedic prostheses for effective bone healing: A review
Composite Structures 118 (2014) 328–341
Contents lists available at ScienceDirect
Composite Structures
journal homepage: www.elsevier .com/locate /compstruct
Review
Application of composites to orthopedic prostheses for effective bonehealing: A review
http://dx.doi.org/10.1016/j.compstruct.2014.07.0520263-8223/� 2014 Elsevier Ltd. All rights reserved.
⇑ Corresponding author. Tel.: +82 2 820 5354; fax: +82 2 814 9476.E-mail address: [email protected] (S.-H. Chang).
Hassan Mehboob, Seung-Hwan Chang ⇑School of Mechanical Engineering, Chung-Ang University, 221, Huksuk-Dong, Dongjak-Gu, Seoul 156-756, Republic of Korea
a r t i c l e i n f o a b s t r a c t
Article history:Available online 7 August 2014
Keywords:Composite materialsProsthesesMechano-regulation theoryBone healingFracture fixation
This paper aims to provide useful and practical information on the design of composite prostheses forhealing bone fractures and describes the material properties of living tissues such as cartilage, structuralmaterials and loading conditions according to various cases, and modeling techniques for the simulationof tissue differentiation during bone healing. In addition, the present review paper provides an overviewof composite materials for the design of prostheses and highlights the merits of using composites. Thehistory and recent trends in fixation methods and types, types of materials used for prostheses, loadingconditions, mechano-regulation theories, and modeling techniques for finite element analyses toestimate the healing of bone fractures are also introduced. The healing process of bone fractures is fullyinfluenced by the biomechanical characteristics of an orthopedic prosthesis and the injured bone such asfracture configurations, prosthesis shape, material properties, and degradation rate of the material. Theappropriate parameters are highlighted for the optimal design of composite prostheses to heal bonefractures successfully.
� 2014 Elsevier Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329
1.1. Fixation techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3291.2. Defects of conventional prostheses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3291.3. Mechano-regulation theories . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3291.4. Conditions of implants for successful healing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3291.5. Materials and designs for composite prostheses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3292. History, development, and methods of fracture fixation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 330
2.1. History and development of fixation devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3302.2. Types of fixation techniques and devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3323. MR theories correlating mechanical conditions and tissue development. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 332
3.1. History of MR theory. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3323.2. Applications of MR theories . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3334. Biomechanical conditions for simulated bone fracture models. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 333
4.1. Biomechanics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3334.2. Computer models for the bone healing process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3335. Biomaterials used for prosthesis design and fabrication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 333
5.1. Metals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3335.1.1. Nondegradable metals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3335.1.2. Biodegradable metals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
5.2. Bioceramics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3365.3. Polymers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3365.4. Polymer-based composite materials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336

H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341 329
6. FEA for the design of composite prostheses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337
6.1. Engineering design of composite orthopedic prostheses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3376.2. Optimal design and prospects of composite prostheses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3387. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 338Acknowledgment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 339References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 339
1. Introduction
Fractures occur more often in lower-limb long bones than inother bones because of their high aspect ratios and exposure toimpacts and other dangers. The extrinsic causes of these fracturesinclude trauma such as that from vehicle accidents, sportinginjuries, and falls, and sometimes the cause is intrinsic, for examplefrom muscular action or some pathology resulting in fracture [1,2].Several fracture fixation devices and techniques are used to fixbone fractures according to the severity of fractures.
1.1. Fixation techniques
Several types of fixation devices are used according to the frac-ture types as shown in Fig. 1a. Unstable diaphyseal tibial fractureshave been treated by traditional bone fixation methods such asabsolute fixation and open reduction, but high rates of complica-tions such as infection, delayed union, nonunion, and osteoporosishave been reported [3–6]. Similarly, external fixation is alsoassociated with complications due to the loosening of pins, pininfection, and malunion of fractures [7]. The internal fixation offractures, including absolute fixation and flexible fixation, has beenintroduced in recent decades. Absolute fixation does not allow rel-ative movement at the fracture site and is generally used in artic-ular fixation, whereas flexible fixation allows some relativemovement at the fracture gap and induces formation of callusesthat bridge the fractured bones and are eventually transformedinto bone under favorable conditions. Intramedullary (IM) rodsand bone plates are good choices for the treatment of diaphysealtibial fractures, but currently, the application of IM rods isrestricted due to the technical limitations of design [8]. Theminimally invasive percutaneous plate osteosynthesis (MIPPO)technique has drawn attention as a biological means to minimizesoft-tissue dissection and preserve periosteal blood supply [9–11]as shown in Fig. 1b.
1.2. Defects of conventional prostheses
Conventionally, metallic prostheses made of stainless steel andtitanium alloys, which provide stabilization of the fractured bone,have been used for the internal fixation of bone fractures, but havereportedly induced osteoporosis and bone necrosis, and delayedbone union [3]. Furthermore, metals may have adverse effects suchas corrosion, fatigue failure, release of metal ions, looseningof implant, allergic skin reactions, and artifacts on radiography[12–14]. In orthopedic surgery, a major problem is mismatch ofthe stiffness between the prosthesis and host bone. Most of the bodyweight is transferred by the high-modulus prosthesis, and insuffi-cient load is transferred to the fracture site, a phenomenon knownas ‘‘stress shielding’’ [15–17], which weakens the bones. Toovercome this critical problem, promising alternatives of flexiblefixation using low-modulus materials have been introduced.Recently, the MIPPO technique has been successfully used as a flex-ible fixation method that induces more callus formation and earlybone union. This approach is also called ‘‘biological fixation’’ [18,19].
1.3. Mechano-regulation theories
To investigate the healing process of bone fractures, many sci-entists have proposed various mechano-regulation (MR) theories,as shown in Fig. 2. Several types of mechanical and biologicalparameters were considered to investigate their effects on tissuedifferentiation qualitatively and quantitatively [20–22]. Isakssonet al. [23,24] carried out extensive research on the effect of variousbiomechanical parameters on tissue differentiation and comparedthe accuracy of various MR theories; as a result, a single-parameterMR with deviatoric strain can predict the bone healing processefficiently (see Fig. 2e).
1.4. Conditions of implants for successful healing
An ideal prosthesis should guarantee sufficient structural stabil-ity of fractured bones but allow small relative movements toinduce early bone healing and gradual body weight transfer tothe fracture site. Biocompatible, biodegradable, and bioactive pros-theses should minimize stress shielding and plate-bone interfacialcontact stresses; control the release of drugs and bioactive ions toprevent infection and enhance healing, respectively; and need tobe completely degraded within a certain period to avoid a secondsurgery. For better bone healing, flexible polymer compositeprostheses have been developed to meet these mechanical andbiological requirements.
1.5. Materials and designs for composite prostheses
Biocompatible materials, usually called biomaterials, have beendeveloped for the repair or replacement of living tissues andorgans [25–28]. Biocompatibility is the ability of a material tobehave similar to tissues and have no adverse effects whenexposed to living tissues. Biomaterials can be divided into metalsand their alloys, ceramics, polymers, and composites according tothe composed materials.
Conventional metals and pure ceramics for prostheses areincompatible with bones due to the large difference in materialproperties as discussed above. Various types of composite materi-als have been studied [25,29–36] and their performance evaluated.The mechanical properties of fiber-reinforced polymer compositescan be easily tailored by changing the stacking sequence and fibervolume fraction; therefore, the desired properties can be obtainedaccording to the application site and fracture configurations.Orthopedic prostheses made of polymer-based composites maysolve problems associated with metals as discussed earlier. Pros-theses made of completely bioresorbable composite materials areof great interest for application to weight-bearing long bones.Recently, prostheses made of completely bioresorbable materialshave been developed, and their degradation rates can be engi-neered using various techniques [37,38] according to their applica-tions. It is known that the healing process is sensitive to thedegradation rate of the material, which leads to changes in the bio-mechanical environment of the tissues surrounding of the injuredbone. To set the optimum parameters of prostheses for successful

(a)
(b)
External fixator
Complex fracture
Callus
Simple fracture
Bone plate
Screw Wedge fracture
Intramedullary rod
Screw
ScrewWires
Partial fracture
Bone fracture
Skin incision
Bone plate
Aiming handle
Bone
Screw drill guide
Screw
After a few days of surgeryCallus
Fig. 1. Bone healing methods and fixation devices; (a) types of bone fractures and prostheses used for fracture fixation, (b) minimally invasive percutaneous plateosteosynthesis (MIPPO) technique.
330 H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341
bone healing, every single parameter needs to be selectedcarefully.
This paper provides an overview of novel and recent studies onbone healing, with the scope ranging from the fixation methods toprosthesis design using optimal design schemes with new materi-als. This paper also provides valuable and in-depth information onthe simulation of the bone-healing process.
2. History, development, and methods of fracture fixation
2.1. History and development of fixation devices
Bone plates and IM rods as internal fixation prostheses havebeen used for more than 100 years. First, the metallic bone platewas introduced in 1895 by Lane [39] but eventually abandoned

(a) (b)
(c)
(d)
(e)(f)
Hyd
rost
atic
def
orm
atio
n
Shear deformation
or
Tens
ion
Com
pres
sion
Pure shear
Granulation tissue
Bone Cartilage Fibrous tissue
0% 2% 10% 15% 100%Interfragmentary strain
Fibro-cartilage Fibrous tissue
Cartilage Bone
Hydrostatic stress history
TensionCompression 0
Principal tensile strain history
Cartilage
Fibrous (connective) tissue
Immature woven bone
Mature woven bone
Resorption
Octahedral shear strain (%)11.250.04 1.0 3.750
9
3
0.8
0.032
Flui
d flo
w (µ
m/s
)
Endochondral ossification
Intramembranous ossification Hydrostatic pressure (MPa)
TensionCompression -0.15 0 0.15
15
5
Local tensile/compressive strain (%)
10052.50.050.0051
>100
Mature bone
Inter. bone
Immaturebone
Cartilage Fibrous tissue
5
500
1000
6000
0
You
ng’s
mod
ulus
of t
issu
e ph
enot
ype
(MPa
)
Gran. tissue
Deviatoric strain in tissue phenotype (%)
2000
R
E
S
O
R
P
T
I
O
N
Fig. 2. Mechano-regulation theories using various parameters; (a) theory of Pauwels [71], (b) theory of Carter et al. [21], (c) interfragmentary strain theory [72], (d) theory ofPrendergast et al. [76], (e) theory of deviatoric strain [24], (f) theory of Claes and Heigele [75].
H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341 331
due to corrosion problems. Subsequently, the metallurgicalformulation was improved and new plates with improved corro-sion resistance and tapered round ends were introduced by Lamb-otte in 1909 [40] and then Sherman in 1912 [41]; however, theseplates were also abandoned due to poor mechanical properties.The next development was made in 1948 by Eggers [42], whodeveloped a plate with two long slots to provide a sliding pathfor screw heads. This plate was also abandoned due to structuralweakness. In 1949, Danis [43] proposed a compression plate thatsuppressed interfragmentary motion, which led to the concept ofprimary bone healing for fractures and revolutionized the designof bone plates. Bagby and Janes [44] proposed a plate design withoval screw holes to provide the same mechanical function of Dan-is’s invention. In 1965, Müller et al. [45] presented a plate with atightening tensioner that allowed the interfragmentary movementof bone fractures. Müller and his group concluded that rigid platingresulted in the absence of periosteal callus formation, whereas thepresence of a callus indicates instability of the plate-bone assem-bly. In 1967, Schenk and Willenegger [46] developed a plate withoval holes similar to the design of Bagby and Janes [44]. This typeof plate was called a dynamic compression plate (DCP), whichgenerates axial compressive forces to keep the broken bones incontact. The high stiffness of DCP led to delayed union of bone
fracture, refracture after plate removal, bone loss under the plate,and absence of an external bridging callus. The first hypothesisattributed refracture to inadequate rigidity of the plate. As a conse-quence, double plating was recommended, but this approach didnot rectify the issue [47]. Perren’s group [48] hypothesized thatrefracture after removal of the bone plate was caused by excessiveplate-bone contact with high stress that led to cortical bone necro-sis. Therefore, Gautier and Perren [49] developed a limited-contactDCP (LC-DCP) to reduce the plate-bone contact by approximately50%. Few studies have investigated the biomechanical aspects ofDCP and LC-DCP. Later, Jain et al. [50] calculated the blood flowin the cortical bone beneath the bone plate and concluded thatthere was no difference between DCP and LC-DCP and thatLC-DCP was not advantageous when they measured the biome-chanical properties of recovered tibia, which discouraged furtherdevelopment of LC-DCP. Finally, clinical studies revealed the realcause of refractures as stress shielding due to a high Young’s mod-ulus of the rigid bone plates [51,52]. Fundamentally, a newapproach of flexible plates with enough structural stability neededto be sought to remedy the aforementioned complications. Good-ship and Kenwright [53] developed plates with an elastic cushioninserted between the screw and screw holes, which increasedmicromotion only in the axial direction with sufficient shear and

332 H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341
rotational rigidity. Essentially, these plates truly act as dynamiccompression at the fracture site.
Because micromovement at the fracture gap can promote bonehealing [54,55], in recent years, considerable research has been car-ried out for the development of less-stiff plates to improve fracturehealing and prevent stress shielding. Functionally graded materialswere also used for the medical applications successfully [56,57].Within the last decade, Ramakrishna et al. [25,29,30] performedfinite element analysis (FEA) of fractured bones when low-stiffnessand functionally graded plates were assembled with bone. Thebending stiffness of a plate and stresses in the plate-bone assemblywith different plate thicknesses and various Young’s moduli werecalculated. It was concluded that bone plates made of functionallygraded material (FGM) reduced stress shielding. Fujihara et al.[32–34] developed carbon/polyether ether ketone (PEEK) compos-ite bone plates and estimated the stiffness and strength when dif-ferent fibrous preforms and stacking angles were used.
Chang’s group [55] proposed bone plates made of plain-weavecarbon/epoxy fabric composite with an axial Young’s modulusranging from 18 to 70 GPa. Finite element analyses were carriedout to determine the most appropriate axial Young’s modulusand bending stiffness of a plate. A composite bone plate with sim-ilar modulus to cortical bones (18–20 GPa) generated the mostappropriate strain distributions (2–10%) at the fracture site andreduced contact stresses by 64% in contrast with a stainless steelbone plate.
An ideal implant should provide sufficient stabilization imme-diate after surgery followed by material degradation to allow grad-ual stress transfer to the bone at the fracture site and leaching ofbioactive material to enhance healing of injured tissue. Further-more, a second surgery for removal of the implant should beavoided. Therefore, completely resorbable polymers and compos-ites were developed for orthopedic applications and successfullyused for small bone fractures [58]. The strength and degradationrate of completely resorbable composites, however, was achallenge for weight-bearing long-bone fractures. Recently, Ahmedet al. [37,59–62] developed resorbable flexible bone plates made ofphosphate glass fiber-reinforced polylactic acid (PLA) compositesfor weight-bearing long-bone fractures.
2.2. Types of fixation techniques and devices
Bone fractures are categorized in several types according totheir geometrical configurations as shown in Fig. 1a. To fix thebone fractures, two types of techniques are used, internal andexternal fixations. External fixations are nonoperative techniques,and simple fractures can easily be treated by plaster casts, braces,splints, and external fixators [63]. Conventionally, external fix-ators are made of metals such as stainless steel to provide suffi-cient stabilization of fractured bones, but this leads to patientdiscomfort due to the heavy weight. To resolve this problem,external fixators currently are fabricated by carbon/epoxy com-posites that are lighter in weight and provide sufficient stiffnessto the fractured bones and no artifacts in radiographs [64,65].Unstable bone fractures, however, are treated by internal fixationdevices, which require patients to undergo a surgical procedure.For internal fixation methods, bone fractures are treated by wires,pins, screws, bone plates, and IM rods. Usually a surgeon decidesthe surgical procedure according to the fracture configuration.These implants are inserted temporarily and removed after heal-ing of bone fractures. Among the many types of prostheses, boneplates and IM rods are most frequently used to fix unstablefractures.
The stabilization of broken bones using fixation devices isassociated with both direct and indirect bone healing [53,66–68].Rigid fixation (absolute fixation) devices promote the direct bone
healing (primary healing or intramembranous ossification) processduring which tissue differentiation does not occur. Indirect bonehealing (secondary healing or endochondral ossification) occurswhen the bone fracture is assembled with a flexible device witha small gap that allows relative movement at the fracture gap. Indi-rect bone healing stabilizes the bone fracture by promoting callusformation and healing followed by a tissue differentiation process.Rigid or absolute fixation devices restrict the micromovement offractured bone and callus formation.
Biological flexible fixation devices have been more successfulfor healing bone fractures. Flexible devices effectively stimulatethe formation and development of calluses and, as a result,enhance bone healing. The development of biological fixationdevices revolutionized the surgical management of fractures. Fur-ther developments include the MIPPO technique, which minimizesthe incision (2–3 cm) and blood loss [69] and avoids an extensivesurgical procedure as the incision is made remote from the fracturesite. Currently, MIPPO is the most attractive technique for surgeonsas well as scientists, and flexible composites are strong candidatesfor designing the most efficient devices for the MIPPO technique.
3. MR theories correlating mechanical conditions and tissuedevelopment
3.1. History of MR theory
The bone healing process is related to the structural stability ofthe prosthesis-bone assembly and the local mechanical environ-ment surrounding the injured tissues. These mechanical conditionsin the soft tissue (calluses) can be described as magnitudes ofstresses or strains that stimulate tissues to develop their pheno-types as shown in Fig. 2. The initial work on MR theory was doneby Roux [70] when he explained that the tissue differentiation pro-cess is regulated by mechanical conditions. Later on, Pauwels [71]proposed that the process was associated with hydrostaticcompression and shear deformation. Hydrostatic compressionstimulates mesenchymal cells to the cartilage, which causes a vol-umetric change, and the pure shear differentiates the mesenchy-mal cells into fibrous tissue, which leads to shape deformation.The combination of hydrostatic compression and shear stimulatesthe tissue toward fibrocartilage. Perren and Cordey [72] proposed asimple tissue differentiation theory based on the interfragmentarystrain (IFS), which is determined by the displacement along theaxial movement of fractured bones divided by the total fracturegap size. This theory did not consider the strain in the radial andhoop directions and cannot predict the whole healing process,but only the initial condition for bone healing. DiGioia et al. [73]carried out a quantitative study on IFS in healing bone fracturesand concluded that IFS cannot completely describe the bone heal-ing process. Cheal et al. [74] continued DiGioia’s research by eval-uating images of a tibial cross-section of a sheep. They tried todescribe a relationship between bone resorption and stresses;unfortunately, however, such a relationship was not found, but aspatial distribution of bone resorption was found at high strainareas. Based on Pauwels’ research, Carter and co-workers [21] pos-tulated that the local stress or strain history could be used todescribe the tissue healing process. According to Carter’s theory,if a tissue had a compressive hydrostatic environment, then carti-lage would have formed, whereas a tensile strain history resultedin fibrous tissue and bone that is formed under low-stressedregions. Claes and colleagues [75] proposed an MR theory, similarto Carter’s theory, in which local tensile/compressive strains of lessthan 5% cause intramembranous ossification, whereas compressivehydrostatic pressure more than �0.15 MPa cause endochondralossification and all remaining conditions resulted in fibrocartilage.Finally, Prendergast and co-workers [76] followed the previous
H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341 333
work and formulated a different MR theory based on twobiophysical stimuli: octahedral strain or shear strain in tissue andinterstitial fluid flow at the interface of bone and prosthesis. Inthe latest models, two mechanical parameters are considered: vol-umetric measurement (fluid flow or pressure) and deviatoric load(octahedral or shear strain). Recently, the model of Prendergastet al. [76] has been further developed by Checa and Prendergast[77], who included in the MR model more biological factors suchas angiogenesis and the influence of mechanical stimuli on thearchitecture of soft tissue [78]. All the MR theories were comparedby Isaksson et al. [24], who found that a single-parameter MR the-ory with deviatoric strain provided a good estimation of tissuedevelopment. All of the models reviewed here describe how thecells sense the mechanical loading or displacement and respondaccordingly, and these quantitative relationships between tissuedevelopment and mechanical stimuli enable us to design appropri-ate and efficient prostheses.
3.2. Applications of MR theories
For the application of MR theories, three main domains arepresent:
1. Advancements have been made in clinical procedures forbone healing. Many researchers have used these theoriescombined with finite element models to investigate the tis-sue differentiation process in injured long bones under load-ing conditions [20].
2. To improve the design of prostheses such as bone plates andIM rods, a number of studies can be found in the literaturein which MR theories are being used to predict the tissuedifferentiation process of endochondral ossification in cal-luses [79,80].
3. To design bone scaffolds for bone regeneration and tissueengineering, the nutrient supplements and oxygen arerequired for a successful tissue differentiation process. Inthe literature, FEA and MR algorithms have been used toefficiently evaluate the tissue differentiation process in bonescaffolds [81,82].
4. Biomechanical conditions for simulated bone fracturemodels
4.1. Biomechanics
The bone healing process is highly sensitive to the initial load-ing conditions after surgery. Because the initial mechanical envi-ronment may have a lasting impact on the course of healing, adetailed understanding of the loading conditions in the fracturedbone and callus may lead to improved treatment of fractures. Theloading conditions are different during daily activities such asstanding, walking, running, rising from a chair, and climbingstairs [83,84]. When a fracture occurs, immediately after the sur-gical procedure, a patient is restricted from applying body weighton the injured leg and suggested to walk with the help of a pair ofcrutches. In this motion, a patient swings the injured leg whilethe other leg bears the body weight alternatively with crutches.Only the muscular forces are applied to the fractured bone, whichare difficult to determine accurately. The muscle forces duringgait cannot be measured directly, and further simulationtechniques are used to quantify the muscular forces. Electromy-ography (EMG) is most commonly used to determine musclebehavior in experimental studies of human motion, and muscleforce can be calculated using the EMG. Mathematical optimiza-tion is carried out to validate the muscular forces and EMG data
[85]. Bogey et al. [86] demonstrated an accurate procedure toencode the EMG data into the muscle moments and forces. Dur-ing the gait cycle, the leg in the swing phase bears a mean 10%of body weight by surrounding muscles such as gastrocnemiusand soleus. However, the direct measurement of forces in vivohas not been reported when the body weight is applied. There-fore, many researchers have studied in vitro implanted prosthesesinstrumented with a force transducer to measure the muscularforces with the help of telemetry [85]. These studies havereported the difference in contact forces on the medial and lateralside of the knee during gait [87]. In a computer simulation fordesigning such prostheses, imbalance forces were considered[80,88]. The maximum forces borne by the tibia measured duringa normal walking gait cycle were almost 3 times the body weight[85]. In addition, finite element analyses were carried out for asimulated fractured tibia under various types of loading condi-tions to investigate the tissue differentiation process during bonehealing [88,89]. These studies showed that loading conditionsgreatly influence the healing process. On the basis of these anal-yses, the best and most realistic loading conditions were sug-gested for a particular type of prosthesis to achieve successfulhealing bone fracture.
4.2. Computer models for the bone healing process
Experimental studies of the in vivo and in vitro bone healingprocess are complex, time consuming, expensive, associated withethical issues, and not accurate due to heterogeneity within thehuman body. Therefore, computer simulations of fractured boneshave been carried out to investigate the healing process. Finite ele-ment analyses are being performed to investigate the influence ofvarious biomechanical parameters on the healing of bone fractures[90–99]. A complete understanding of the local mechanicalenvironment is necessary to predict the healing processaccurately. However, the local mechanical environment is morecomplex and difficult to describe with one mode of motion. Byconsidering the difficulties in actual modeling, the simulated bonefracture models have been used to investigate the tissue differen-tiation process according to the variations of several controlledparameters. Additionally, the idealization of computer modelsand simplification of biophysical conditions may not accuratelyreflect real-life conditions. Table 1 gives an overview of severalconducted simulations on bone healing under different conditions[24,100–106].
5. Biomaterials used for prosthesis design and fabrication
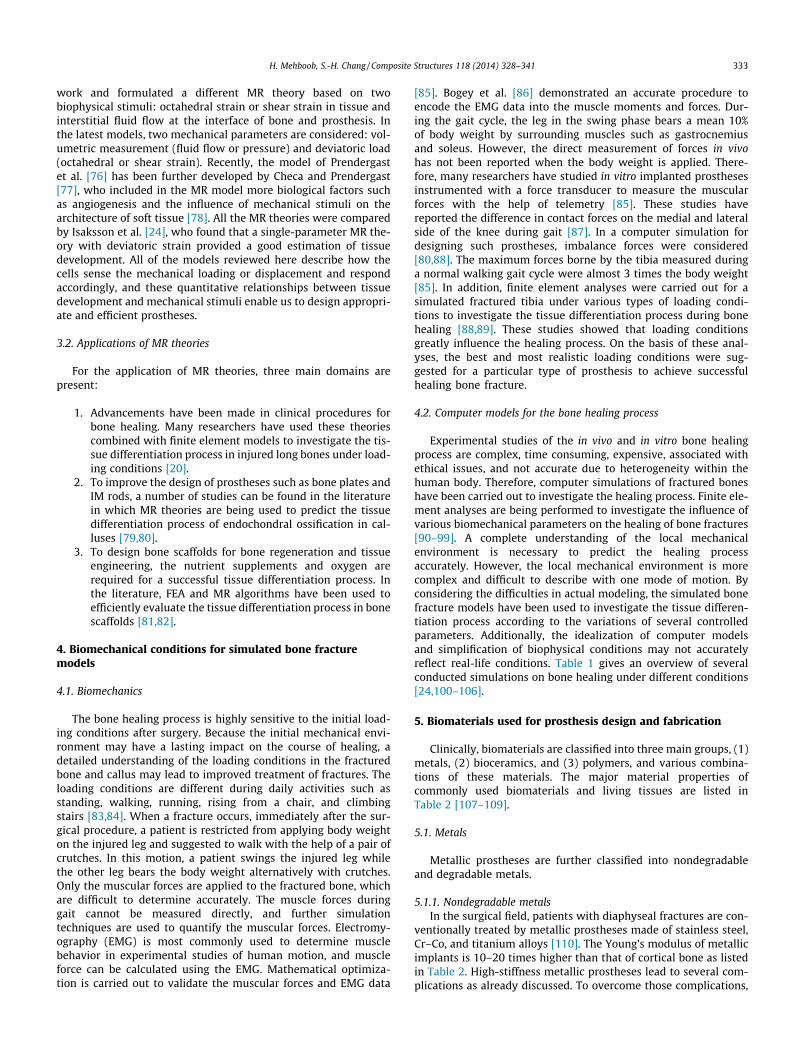
Clinically, biomaterials are classified into three main groups, (1)metals, (2) bioceramics, and (3) polymers, and various combina-tions of these materials. The major material properties ofcommonly used biomaterials and living tissues are listed inTable 2 [107–109].
5.1. Metals
Metallic prostheses are further classified into nondegradableand degradable metals.
5.1.1. Nondegradable metalsIn the surgical field, patients with diaphyseal fractures are con-
ventionally treated by metallic prostheses made of stainless steel,Cr–Co, and titanium alloys [110]. The Young’s modulus of metallicimplants is 10–20 times higher than that of cortical bone as listedin Table 2. High-stiffness metallic prostheses lead to several com-plications as already discussed. To overcome those complications,

Table 1A short history of computer models used to predict the bone healing process.
Authors Type of FEmodel
Geometry Materials and methods Biological information Results and evaluation
Materialdescription
Loading condition Mechanicalstimulus
Ament and Hofer(2000)
Sheep, 2Dquartersection
2 mm gapsize
Linear elastic Axial force = 500 N Strain energydensity
No cells but osteogenic factors Interfragmentary movement d(t)Disp. Max. = 1.3 mm
Kuiper et al.(2000)
2D halfsection
2 mm gapsize
Linearporoelastic
Axial force = 1000 N Shear stress andshear strain
- Callus formation at 20 and 40 days,Several disp. (t) Axial stiffness at 4 and 7 weeks
Lacroix et al.(2002)
Human, 2Dquartersection
1, 3 and6 mm gapsize
Linearporoelastic
Axial force = 500 N with ramp load of0.5 s
Shear strain andfluid flow
Mesenchymal stem cell Interfragmentary strain e(t), Elasticmodulus E(t)
Bailon-Plaza andMeulen(2003)
Sheep, 2Dquartersection
3 mm gapsize
Linear elasticandhyperelastic
Axial force = 360 N at 0.5 Hz Deviatoric strainand shear strain
Mesenchymal stem cell, Chondrocytes,Osteoblasts
Axial stiffness f(t),Bone mineral density f(t)
Gomez-Benitoet al. (2006)
3D half, axialsymmetric
3 mm gapsize
Linearporoelastic
Axial force = 500 N at 1.0 Hz, Axialforce = 300 N, 600 N at 1.0 Hz
Second invariant ofdeviatoric strain
Mesenchymal stem cell, Fibroblasts,Chondrocytes, Osteoblasts
Interfragmentary strain e(t), Cellconcentration C(t)
Isaksson et al.(2006)
2D quartersection
3 mm gapsize
Linearporoelastic
Axial force = 300 N, 600 N at 1.0 Hz Comparison ofvarious theories
Mesenchymal stem cell Comparison with Lacroix and Prendergastsimulation results.Interfragmentary movement d(t), Axialstiffness f(t), Elastic modulus E(t)
Andreykiv et al.(2008)
Ovine, 2Dquartersection
3 mm gapsize
Linearporoelastic
Axial force = 200 N and 500 N, Bendingmoment = 95 N.cm and 760 N cm
Shear strain andfluid flow
Mesenchymal stem cell, Fibroblasts,Chondrocytes, Osteoblasts
Interfragmentary movement d(t), Cellconcentration C(t, x), Bone fraction f(t, x)
Isaksson et al.(2008)
Sheep, 2Dquartersection
3 mm gapsize
Linearporoelastic
Cyclic axial force = 300 N, 400 N, 500 Nat 1.0 Hz
Shear strain andfluid flow
Mesenchymal stem cell, Fibroblasts,Chondrocytes, Osteoblasts
Cell concentration C(t), Elastic modulusE(t)
Geris et al.(2008)
Murinemodel, 2D
3 mm gapsize
Linearporoelastic
Several cases Fluid flow Mesenchymal stem cell, Fibroblasts,Chondrocytes, Osteoblasts, Endothelialcells
Bone fraction f(t), Bone density f(t, x)
Chang‘s group(2010–2014)
Human, 3Dfull section
1–10 mmgap sizes
Linear elastic Several cases Deviatoric strain – Bone healing f(t), Tissue differentiationf(t)
334H
.Mehboob,S.-H
.Chang/Com
positeStructures
118(2014)
328–341
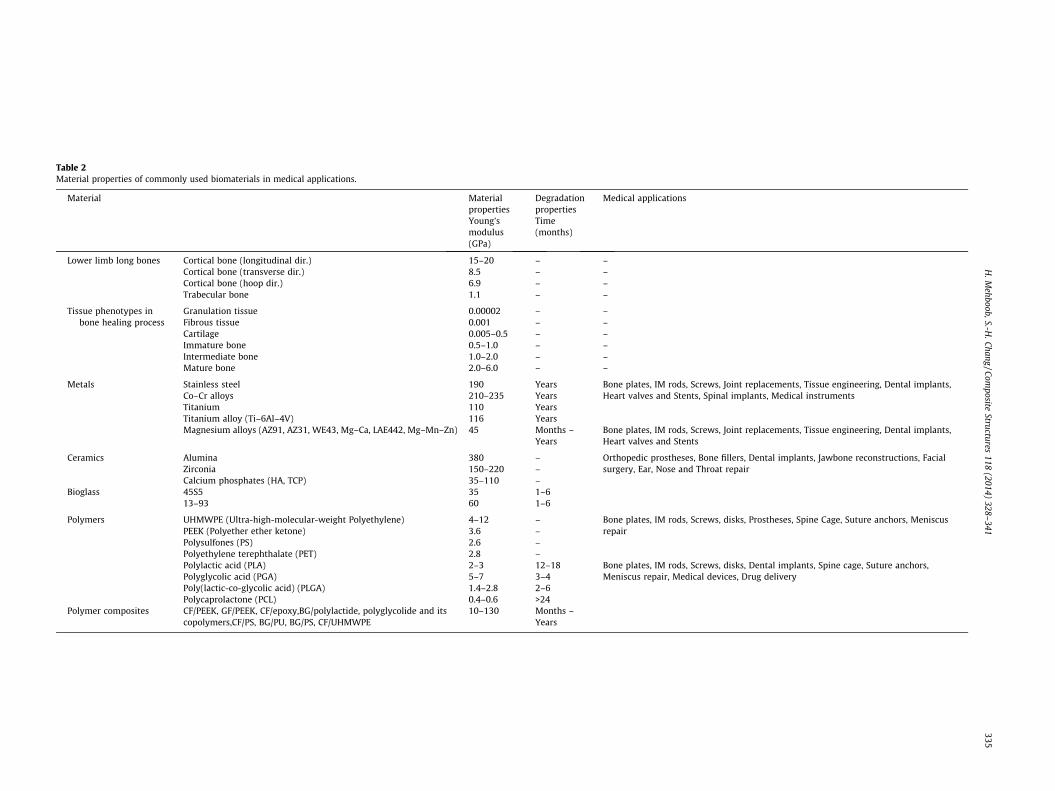
Table 2Material properties of commonly used biomaterials in medical applications.
Material Materialproperties
Degradationproperties
Medical applications
Young’smodulus(GPa)
Time(months)
Lower limb long bones Cortical bone (longitudinal dir.) 15–20 – –Cortical bone (transverse dir.) 8.5 – –Cortical bone (hoop dir.) 6.9 – –Trabecular bone 1.1 – –
Tissue phenotypes inbone healing process
Granulation tissue 0.00002 – –Fibrous tissue 0.001 – –Cartilage 0.005–0.5 – –Immature bone 0.5–1.0 – –Intermediate bone 1.0–2.0 – –Mature bone 2.0–6.0 – –
Metals Stainless steel 190 Years Bone plates, IM rods, Screws, Joint replacements, Tissue engineering, Dental implants,Heart valves and Stents, Spinal implants, Medical instrumentsCo–Cr alloys 210–235 Years
Titanium 110 YearsTitanium alloy (Ti–6Al–4V) 116 YearsMagnesium alloys (AZ91, AZ31, WE43, Mg–Ca, LAE442, Mg–Mn–Zn) 45 Months –
YearsBone plates, IM rods, Screws, Joint replacements, Tissue engineering, Dental implants,Heart valves and Stents
Ceramics Alumina 380 – Orthopedic prostheses, Bone fillers, Dental implants, Jawbone reconstructions, Facialsurgery, Ear, Nose and Throat repairZirconia 150–220 –
Calcium phosphates (HA, TCP) 35–110 –Bioglass 45S5 35 1–6
13–93 60 1–6
Polymers UHMWPE (Ultra-high-molecular-weight Polyethylene) 4–12 – Bone plates, IM rods, Screws, disks, Prostheses, Spine Cage, Suture anchors, MeniscusrepairPEEK (Polyether ether ketone) 3.6 –
Polysulfones (PS) 2.6 –Polyethylene terephthalate (PET) 2.8 –Polylactic acid (PLA) 2–3 12–18 Bone plates, IM rods, Screws, disks, Dental implants, Spine cage, Suture anchors,
Meniscus repair, Medical devices, Drug deliveryPolyglycolic acid (PGA) 5–7 3–4Poly(lactic-co-glycolic acid) (PLGA) 1.4–2.8 2–6Polycaprolactone (PCL) 0.4–0.6 >24
Polymer composites CF/PEEK, GF/PEEK, CF/epoxy,BG/polylactide, polyglycolide and itscopolymers,CF/PS, BG/PU, BG/PS, CF/UHMWPE
10–130 Months –Years
H.M
ehboob,S.-H.Chang
/Composite
Structures118
(2014)328–
341335

336 H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341
new materials are receiving more attention due to their advanta-geous nature and similar material properties to bones.
5.1.2. Biodegradable metalsMagnesium (Mg) and its alloys biodegrade when exposed to
body fluid. Originally, magnesium alloys were not designed formedical application, because they may cause diseases; for exam-ple, the AZ91 magnesium alloy may cause Alzheimer’s diseasesdue to the concentration of aluminum (Al) ions in the human body[111]. Therefore, recently, new magnesium alloys were developedfor medical applications such as Mg–Ca, Mg–Zn, and Mg–Mn[111,112]. Although their application is limited due to their fastdegradation rates and physical stimulation of gas bubbles, theystill possess some advantages:
(1) Material properties: Among conventional metal groups,magnesium-based metals have an elastic modulus close tothat of natural bones. Prostheses made of Mg alloys can pro-vide adequate strength and are expected to mitigate thestress shielding effect induced by conventional metals. Inaddition, the density of magnesium-based metals (1700–2000 kg/m3) is close to that of natural bones (1800–2100 kg/m3) [111,112].
(2) Biocompatibility: Magnesium is essential and the fourthmost abundant element in the human body. Biodegradablemagnesium can be absorbed easily by the human body andeliminated in urine [112].
5.2. Bioceramics
Ceramics are known as good biomaterials for corrosion resis-tance, biocompatibility, and bioactivity, but their drawbacksinclude brittleness, poor fracture toughness, difficulty in manufac-turing complex shapes, and an elastic modulus that is too high.Bioceramics are classified into two groups according to theresponse of the living tissue to the material: (1) bio-inert ceramicssuch as zirconia and alumina and (2) bioresorbable and bioactiveceramics such as hydroxyapatite and other calcium phosphateceramics such as b-tricalcium phosphate. The properties of themost commonly used ceramics are listed in Table 2. The fabricationof pure ceramic prostheses is not appropriate for weight-bearinglong-bone prostheses due to their poor mechanical properties;however, they are used for small bone-filling defects, makingscaffolds, and filling tooth defects in dentistry.
5.3. Polymers
Among the biodegradable materials, biodegradable polymersare one of the primary materials being considered for use bonerepairs. The polymers are more beneficial due to their biocompat-ibility and degradation rates, which can be easily controlled bychanging the composition and fabrication techniques. Based ontheir origin, they are classified as natural polymers such as starch,alginate, chitosan, collagen, and silk and synthetic polymers suchas PLA, polyglycolic acid, poly-l-lactic acid (PLLA), polylactic co-glycolic acid (PLGA), polycaprolactone (PCL), and polydioxanone(PDS). The use of pure natural and synthetic polymers is limitedto the repair of small bone fractures and soft tissues due to theirlow strength.
5.4. Polymer-based composite materials
In the early period of research, scientists developed prosthesesmade of different types of polymers. Pure polymers seldom provideadequate mechanical properties for the sufficient stabilization oflower-limb long-bone fractures, making it necessary to develop
new materials with satisfactory mechanical and biological proper-ties. Thus, reinforcements were added to polymers to improvetheir properties to meet clinical requirements. These polymer-based composite materials are grouped into nonresorbable,partially resorbable, and fully resorbable composites. The nonre-sorbable composites are further divided into thermoset and ther-moplastic polymer composites. Carbon/epoxy and glass/epoxycomposites are examples of nonresorbable thermoset composites[113,114], and carbon fiber (CF)/PP, CF/PMMA, CF/PS, CF/PEEK,and CF/PBT are examples of nonresorbable thermoplastic compos-ites [115,116]. The nonresorbable thermoset composites are notused as much in internal fixation devices due to the possible toxiceffects in the human body [117,118]. Thermoplastic polymers aregetting more attention due to their advantageous behavior suchas not having unused monomers, and during the surgery, the platescan be reshaped according to the shape of the bone by simplyapplying heat. Among other thermoplastic materials, the CF/PEEKcomposite has potential for meeting mechanical and biologicalrequirements. Prepregs of unidirectional long fibers and random/unidirectional short fibers were used to fabricate the prostheses,and the mechanical performances of CF-reinforced composite boneplates were evaluated accordingly [119,120]. Within the last dec-ade, braided and knitted fabric composites were developed to sat-isfy the mechanical and biological requirements for effective bonehealing [121]. Many researchers introduced various modelingtechniques and optimized the weaving patterns for braided andwoven composites [122–129]. The mechanical properties ofbraided composites can be changed by several parameters suchas braid angle, stacking angle, fabrication method, and fiber vol-ume fraction. Mayer [130,131] developed knitted composite boneplates using CFs and PEEK. Within the last decade, Ramakrishnaet al. [25,29,30,132] introduced a new technique to fabricate theCF/PEEK composites using microbraided yarns of carbon and PEEKthat were then knitted again into the fabrics. The bone plates weremanufactured by a compression molding process by using the fab-rics made of braided yarns. Such bone plates provided excellentmechanical properties with low mass and volume. Recently,Chang’s group [36] introduced bone plates made of plain-weavecarbon/epoxy composite and glass/polypropylene fabric compositeand carried out extensive research on the behavior of bone healingand the design of internal fixation devices such as bone plates byconsidering mechanical performance.
As the bone fracture healing progresses, a gradual increase inload is desirable at the fracture site to stimulate the healing tissuesby increasing the stress, which is possible when biodegradablematerials are used. Furthermore, by using these materials, surgery,including the cost, to remove the prosthesis after the completehealing of the fracture can be avoided. To meet this need, research-ers introduced resorbable materials for the application of internalfixation devices. Previously, completely resorbable compositeshad been used for non-weight-bearing bones, for example in oraland maxillofacial surgery, but their poor mechanical propertiesprevented their application to the weight-bearing long bones.The material properties of resorbable polymers (polylactide) andits co-polymers such as PLA, PLLA, and PLGA cause them to degradewhen exposed to body fluid. The initial material properties of com-monly used polymers are shown in Table 2 [133,134]. To improvethe material properties, many researchers used nonresorbablereinforcements such as CFs and polyamide fibers and applied thesecomposites to the design of prostheses. Such materials are calledpartially resorbable composites. One problem of the partiallyresorbable composite is that a second surgery is required toremove the nonresorbable fibers. Therefore, completely resorbableand/or bioactive ceramics were used for reinforcement. Phosphateglass fiber (PGF)/PLA, HA/PLA, and TCP/PLGA are examples ofcompletely resorbable polymer-based ceramic composites
H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341 337
[59–62,135,136]. The degradation rate of resorbable compositescan be engineered by adding, for example, coupling agents, fibertreatments, or coatings.
In 2004, Ahmed et al. [137,138] started work on the processingand characterization of PGF, a completely resorbable and bioactivematerial, for tissue engineering. They extended the research toPGF/PLA composites and investigated the in vitro chemical,mechanical, and morphological properties in an effort to developcompletely resorbable polymer-based composites for bone fracturefixation [139–142]. The biodegradation rate and the effect of bind-ing agents on the degradation rate of various types of compositeswere also studied [37]. As a result, completely resorbable boneplates, IM rods, and screws were developed with different kindsof techniques, and their properties were studied for the applicationto weight-bearing long-bone fractures [60,61,143–148]. Thesetypes of composite prostheses fulfilled almost all the modern clin-ical demands for weight-bearing long-bone fractures; that is, they
Loading condition
Compute deviatoric strains in calluses
Bod
y w
eigh
t (%
)
0.22
4.4
6.6
0 4 8 12 16Iteration number (weeks)
200
10
225250275300
Loa
d (M
Pa)
Abnormal walk
Normal walk
Walk with crutches
Fixed
Trabecular bone
Corticalbone
Bone plate
Screw hole
Screw
Screw hole in bone
CallusFracture
Load
Details
4.516
r=13.7
Side view
4.5
25
8.1
Screw
1625
119
74.5
Top view Fiber direction
25 15
41300
33
Tie between bone and screw surfaces
Interface contact condition
Load
Fixed
zr
zr
Detail view of bone-plate assemblyNote: All dimensions in mm
5
10
60
You
ng’s
mod
ulus
of t
issu
e ph
enot
ype
(MPa
)
20
FEA modelling
Update loading conditions and material properties of bone plate
Initial, FEA codeIteration = n+1Time = n+1
Iteration = 0Time = 0
Fig. 3. Iterative calculation procedure for simulating tissue differentiation by finite
provide sufficient stabilization, steady degradation of material, andrelease of bioactive materials.
6. FEA for the design of composite prostheses
6.1. Engineering design of composite orthopedic prostheses
The use of FEA ranges from simple calculations of stress ordeformation to the optimal design of internal fixation devices viaelegant estimation of healing performance. Ramakrishna et al.[25,29,30] and Fujihara et al. [31–34] developed polymer-basedcomposite bone plates and carried out FEA to check the mechanicalperformance such as bending stiffness of various types of boneplates. The contact stress at the interface of a plate-bone assemblywas also calculated at various healing stages; when a bone platemade of FGM was assembled with a bone, the generated stresswas compared with that of a conventional stainless steel bone
Mechano-regulation algorithm
Update material properties of calluses
Compute distribution ratio and average Young’s modulus of tissue phenotypes
Cartilage
Fibrous Tissue
Immature Bone
Intermediate Bone
Mature Bone
Granulation Tissue
Resorption
Iteration = 1 … … ... … Iteration = n+1Time (weeks) = 1 … … ... Time (weeks) = n+1
10052.50.050.0051
>100
Mature bone
Inter. bone
Immaturebone
Cartilage Fibrous tissue
5
00
00
00
0
Gran. tissue
Deviatoric strain in tissue phenotype (%)
00
R
E
S
O
R
P
T
I
O
N
0% 20% 40% 60% 80% 100%
0123456789
10111213141516
Distribution ratio of tissue phenotypes
Iter
atio
ns in
wee
ks
-100
400
900
1400
1900
2400
2900
3400
3900
4400
4900
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16Iterations in weeks
Phen
otyp
e av
g. m
odul
us (M
Pa)
Intermediate Bone Mature BoneImmature BoneCartilageFibrous TissueGranulation Tissue
element analysis and the mechano-regulation theory with a deviatoric strain.

338 H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341
plate case. Many other researchers carried out FEAs to investigatethe stress in bone plates and bones by changing parameters such asnumber of screws, position of screws, fracture stability, loadingconditions, and material type [90,149–151] to alleviate the gener-ated stress. Fouad [92] estimated the stress at the fracture sitewhen a gap existed between the bone and a plate by using FEA,with stainless steel, titanium alloy, and FGM used for the boneplate. As a result, stress was reduced when FGM bone plates wereused when a gap was present.
The design of prostheses made of resorbable composites is alsoof great interest to researchers. Kharazi et al. [152] used the finiteelement method to design bone plates made of partially resorbabletextile composites, estimating bending and tensile behaviors of thebone plates. Harper et al. [59] proposed a new finite element modelfor completely resorbable discontinuous fiber composite boneplates for estimating the flexural properties by varying the fiberand matrix moduli and fiber volume fraction to fulfill the mechan-ical properties for weight-bearing long-bone applications.
As discussed in previous sections, the healing of bone fracturescan be estimated using MR theories. Many researchers have usedMR theories for the design of composite scaffolds considering var-ious design parameters such as scaffold porosity, degradation rates,loading conditions, and types of materials [81,82,153] and estimat-ing the tissue differentiation process.
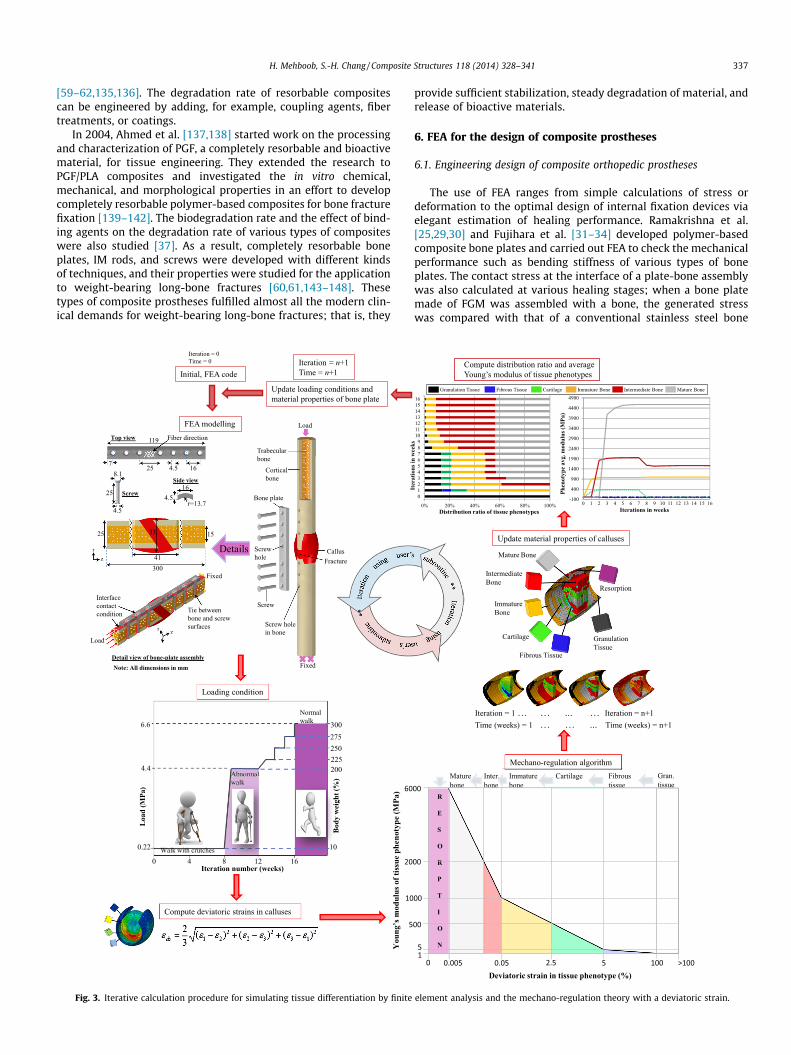
However, until now, few FEAs have combined the design ofcomposite prostheses using MR theories with consideration ofthe bone healing process. Chang’s group [55,79,80,88,89,98,99,154–156] performed FEAs extensively for composite prosthesisdesign to enhance bone healing performance in weight-bearinglong-bone fractures of the tibia and femur. Basic lower-limb bonedata including geometry and configurations of bone fractures,geometry and material properties of cortical and trabecular bonesand calluses, and material properties of various types of tissuesformed during the bone healing process were summarized todevelop three-dimensional finite element models (see Table 2and Fig. 3). In addition, the contact conditions between the boneand bone plate and screws, friction coefficients, loading conditionsduring the gait cycle, and boundary conditions were determinedto carry out the FEAs (see Fig. 3). The loading history also affectsthe prosthesis healing performance during bone healing. Theappropriate loading condition was analyzed and the best patternthat healed the bone most efficiently was suggested [88,89]. Inpreliminary studies, Chang’s group investigated the strain distri-bution in the central callus when various types of bone plate wereused [98]. It was concluded that the Young’s modulus of a boneplate is more influential in bone healing than the bendingstiffness.
To continue the research, FEA of a tibial fracture was carried outto investigate the gap strain distribution and plate-bone contactstress. The composite bone plate with an axial Young’s modulusof 18 GPa, which is similar to the modulus of cortical bone, allowed2.6 times more callus healing than stainless steel bone plates. Formore realistic simulations, the healing process of a tibia with var-ious fracture angles (15�, 25�, and 35�) was also investigated andthe design schedule of a composite bone plate got more sophisti-cated [89]. The most severe angle (35�) needed more stabilizationfor successful bone fracture healing, and therefore, a slightly higherYoung’s modulus (36 GPa) of the bone plate was needed. Further-more, an FEA was done to estimate appropriate bending stiffnessand the contact conditions of a plate-bone assembly to realizethe concept of locking compression plate (LCP) [55,99]. From theanalysis results, it was verified that the IFS varies not only withbending stiffness, but also with the contact condition of the boneplate. Moreover, the IFS theory, which is the simplest among theMR theories, was implemented to investigate callus healing, butIFS cannot accurately predict the whole healing process [157].
Therefore, iterative calculations using an MR theory with adeviatoric strain programmed in a subroutine was implemented(see Fig. 3) on the improved finite element model of a tibial bonefracture [89]. Detailed simulations were carried out to predict thehealing performances of composite bone plates when assembledwith various types of fracture configurations, and the most appro-priate Young’s modulus of the bone plate was suggested accordingto the fracture configurations [89]. Similarly, the design of a com-posite IM rod was evaluated, and according to the fracture config-urations, the best Young’s modulus among the choices wassuggested [80] and its healing performance was compared withthe composite bone plate [88]. Mehboob and Chang [155,158] car-ried out an FEA for the design of completely degradable compositebone plates and functionally graded bone plates. Various materialdegradation rates were considered in various types of fracture con-figurations, and the healing process was predicted using an MRtheory with a deviatoric strain that was programmed in asubroutine coded by Python. An iterative calculation was carriedout to evaluate 16 weeks of the healing process (see Fig. 3),and as a result, bone healing was enhanced and the most suitabledegradation rate was suggested according to the fractureconfigurations.
6.2. Optimal design and prospects of composite prostheses
Like other structures, composite prostheses need to be opti-mized [159], which represents a prospective change in the designaspect of composite internal fixation devices in the near future.For optimal prosthesis design, all mechanical and biological clinicalrequirements that could successfully induce early bone healingneed to be considered. Furthermore, it is necessary to combine inone study all the parameters of optimal design, such as completelyresorbable/biodegradable materials, FGMs, appropriate Young’smodulus of prostheses, prosthesis volume, initial loading condi-tions, bone healing rate, and bone resorption after successful bonehealing. This optimal design will maximize the bone healing per-formance and minimize the complications after surgery and duringthe bone healing period. In future, the bioactivity of bioactivematerial, drug loading, and drug release rate can open the wayfor new trends in prosthesis design.
7. Summary
Developing biomaterials for bone repairs is a challenge for med-ical science as well as from an engineering point of view for thedesign of prostheses. Conventional metallic prostheses have a longhistory but are becoming obsolete due to various disadvantages.Composite materials are getting more attention in the engineeringfield for development of high-performance implants to enhancethe healing of bone fractures, and more efficient function-orientedcomposite materials such as resorbable/biodegradable and bioac-tive composites are being developed to meet the required perfor-mance characteristics of orthopedic prostheses and implants.
The healing process can be estimated using MR theory with adeviatoric strain, which is a simple and efficient method to predicttissue differentiation and, as a result, used for the design of pros-theses and implants. Because the healing process is also influencedby fracture configurations such as fracture gap and fracture angle,the adaptive design of a prosthesis should take these fracture con-figurations into account along with other factors such as the mate-rial properties of the prosthesis, the shape of the structure, andloading conditions. Because of the excessive complexity of per-forming procedures experimentally, FEAs were alternatively usedto estimate the healing performance of bone fractures, and as aresult, composite prostheses with the appropriate modulus weredesigned.
H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341 339
Because the mechanical properties of prostheses, degradationmechanism, mechanical environment surrounding the injuredtissue, and biological behaviors at the fracture site are different,prostheses should be optimally designed to achieve targeted heal-ing of bone fractures without complications. Many researchershave tried to design efficient fixation devices using various typesof composite materials, and some have proposed successful designmethodologies and products for possibly applicable compositefixation devices. The triumph of function-oriented compositematerials for the design of orthopedic prostheses and implants liesin our ability to achieve desirable mechanical, physical, chemical,and biological properties.
Acknowledgment
This work was supported by a National Research Foundation ofKorea (NRF) grant funded by the Korean government (MSIP) (No.2013R1A2A2A05004444).
References
[1] Courtbrown CM, Mcbirnie J. The epidemiology of tibial fractures. J Bone JointSurg Br 1995;77B:417–21.
[2] Goga IE, Gongal P. Severe soccer injuries in amateurs. Br J Sports Med2003;37:498–501.
[3] Dickson K, Katzman S, Delgado E, Contreras D. Delayed unions and nonunionsof open tibial fractures – correlation with arteriography results. Clin OrthopRelat Res 1994:189–93.
[4] Claes L. The mechanical and morphological properties of bone beneathinternal-fixation plates of differing rigidity. J Orthopaed Res 1989;7:170–7.
[5] Claes L, Kinzl L, Neugebauer R. Experimental studies on the influence of platematerial on stress-relief and atrophy of the bone beneath osteosynthesisplates. Biomed Tech 1981;26:66–71.
[6] Uhthoff HK, Dubuc FL. Bone structure changes in the dog under rigid internalfixation. Clin Orthop Relat R 1971;81:165–70.
[7] Weber SC, Szabo RM. Severely comminuted distal radial fracture as anunsolved problem – complications associated with external fixation and pinsand plaster techniques. J Hand Surg-Am 1986;11A:157–65.
[8] Janssen KW, Biert J, van Kampen A. Treatment of distal tibial fractures: plateversus nail. Int Orthop 2007;31:709–14.
[9] Hazarika S, Chakravarthy J, Cooper J. Minimally invasive locking plateosteosynthesis for fractures of the distal tibia – results in 20 patients.Injury 2006;37:877–87.
[10] Zou J, Zhang W, Zhang CQ. Comparison of minimally invasive percutaneousplate osteosynthesis with open reduction and internal fixation for treatmentof extra-articular distal tibia fractures. Injury 2013;44:1102–6.
[11] Redfern DJ, Syed SU, Davies SJM. Fractures of the distal tibia: minimallyinvasive plate osteosynthesis. Injury 2004;35:615–20.
[12] Baidya KP, Ramakrishna S, Rahman M, Ritchie A. Quantitative radiographicanalysis of fiber reinforced polymer composites. J Biomater Appl2001;15:279–89.
[13] Okazaki Y, Gotoh E. Comparison of metal release from various metallicbiomaterials in vitro. Biomaterials 2005;26:11–21.
[14] Teoh SH. Fatigue of biomaterials: a review. Int J Fatigue 2000;22:825–37.[15] Moyen BJ, Lahey Jr PJ, Weinberg EH, Harris WH. Effects on intact femora of
dogs of the application and removal of metal plates. A metabolic andstructural study comparing stiffer and more flexible plates. J Bone Joint SurgAm 1978;60:940–7.
[16] Uhthoff HK, Finnegan M. The effects of metal plates on post-traumaticremodelling and bone mass. J Bone Joint Surg Br 1983;65:66–71.
[17] Moyen BJ, Lahey PJ, Weinberg EH, Rumelhart C, Harris WH. Effects ofapplication of metal plates to bone. Comparison of a rigid with a flexibleplate. Acta Orthop Belg 1980;46:806–15.
[18] Collinge C, Protzman R. Outcomes of minimally invasive plate osteosynthesisfor metaphyseal distal tibia fractures. J Orthop Trauma 2010;24:24–9.
[19] Ronga M, Longo UG, Maffulli N. Minimally invasive locked plating of distaltibia fractures is safe and effective. Clin Orthop Relat R 2010;468:975–82.
[20] Lacroix D, Prendergast PJ. A mechano-regulation model for tissuedifferentiation during fracture healing: analysis of gap size and loading. JBiomech 2002;35:1163–71.
[21] Carter DR, Beaupre GS, Giori NJ, Helms JA. Mechanobiology of skeletalregeneration. Clin Orthop Relat R 1998:S41–55.
[22] Claes LE, Heigele CA. Magnitudes of local stress and strain along bonysurfaces predict the course and type of fracture healing. J Biomech1999;32:255–66.
[23] Isaksson H. Recent advances in mechanobiological modeling of boneregeneration. Mech Res Commun 2012;42:22–31.
[24] Isaksson H, Wilson W, van Donkelaar CC, Huiskes R, Ito K. Comparison ofbiophysical stimuli for mechano-regulation of tissue differentiation duringfracture healing. J Biomech 2006;39:1507–16.
[25] Ramakrishna S, Mayer J, Wintermantel E, Leong KW. Biomedical applicationsof polymer-composite materials: a review. Compos Sci Technol2001;61:1189–224.
[26] Vieira AC, Guedes RM, Tita V. Constitutive models for biodegradablethermoplastic ropes for ligament repair. Compos Struct 2012;94:3149–59.
[27] Srinivasan S, de Andrade JR, Biggers SB, Latour RA. 3-D global local analysis ofcomposite hip prostheses – a model for multiscale structural analysis.Compos Struct 1999;45:163–70.
[28] Kulkarni SG, Gao XL, Horner SE, Zheng JQ, David NV. Ballistic helmets – theirdesign, materials, and performance against traumatic brain injury. ComposStruct 2013;101:313–31.
[29] Ramakrishna K, Sridhar I, Sivashanker S, Ganesh VK, Ghista DN. Analysis of aninternal fixation of a long bone fracture. J Mech Med Biol 2005;5:89–103.
[30] Ramakrishna S, Hull D. tensile behavior of knitted carbon-fiber–fabric/epoxylaminates. 1. Experimental. Compos Sci Technol 1994;50:237–47.
[31] Fujihara K, Huang ZM, Ramakrishna S, Satknanantham K, Hamada H.Performance study of braided carbon/PEEK composite compression boneplates. Biomaterials 2003;24:2661–7.
[32] Fujihara K, Huang ZM, Ramakrishna S, Hamada H. Influence of processingconditions on bending property of continuous carbon fiber reinforced PEEKcomposites. Compos Sci Technol 2004;64:2525–34.
[33] Fujihara K, Huang ZM, Ramakrishna S, Satknanantham K, Hamada H.Feasibility of knitted carbon/PEEK composites for orthopedic bone plates.Biomaterials 2004;25:3877–85.
[34] Fujihara K, Teo K, Gopal R, Loh PL, Ganesh VK, Ramakrishna S, et al. Fibrouscomposite materials in dentistry and orthopaedics: review and applications.Compos Sci Technol 2004;64:775–88.
[35] Huang ZM, Fujihara K. Stiffness and strength design of composite bone plates.Compos Sci Technol 2005;65:73–85.
[36] Park SW, Yoo SH, An ST, Chang SH. Material characterization of glass/polypropylene composite bone plates according to the forming. Conditionand performance evaluation under a simulated human body environment.Compos Part B-Eng 2012;43:1101–8.
[37] Ahmed I, Cronin PS, Abou Neel EA, Parsons AJ, Knowles JC, Rudd CD. Retentionof mechanical properties and cytocompatibility of a phosphate-based glassfiber/polylactic acid composite. J Biomed Mater Res B 2009;89B:18–27.
[38] Zhou H, Lawrence JG, Bhaduri SB. Fabrication aspects of PLA-CaP/PLGA-CaPcomposites for orthopedic applications: a review. Acta Biomater2012;8:1999–2016.
[39] Lane WA. Some remarks on the treatment of fractures. BMJ 1895;1:861–3.[40] Lambotte A. Technique et indication des prothèses dans le traitement des
fractures. Presse Med 1909;17:321.[41] Sherman WO. Vanadium steel bone plates and screws. Surg Gynecol Obstet
1912;14:629–34.[42] Eggers GW. Internal contact splint. J Bone Joint Surg Am 1948;30A:40–52.[43] Danis R. Théorie et pratique de ostéosynthèse. Paris: Masson; 1949.[44] Bagby GW, Janes JM. The effect of compression on the rate of fracture healing
using a special plate. Am J Surg 1958;95:761–71.[45] Müller ME, Allgöwer M, Willenegger H. Compression fixation with plates. In:
Technique of internal fixation of fractures. Berlin: Springer; 1965. p. 47–51.[46] Schenk R, Willenegger H. Morphological findings in primary fracture healing.
In: Krompecher S, Kerner E, editors. Callus formation symposium on thebiology of fracture healing. Budapest: Akadémiai Kiadó; 1967. p. 75–86.
[47] Berkin CR, Marshall DV. Three-sided plate fixation for fractures of thetibial and femoral shafts. A follow-up note. J Bone Joint Surg Am 1972;54:1105–13.
[48] Perren SM, Cordey J, Rahn BA, Gautier E, Schneider E. Early temporary porosisof bone induced by internal-fixation implants – a reaction to necrosis, not tostress protection. Clin Orthop Relat R 1988:139–51.
[49] Gautier E, Perren SM. The limited contact dynamic compression plate (Lc-Dcp) – biomechanical research as a basis for the modified plate design.Orthopade 1992;21:11–23.
[50] Jain R, Podworny N, Hupel TM, Weinberg J, Schemitsch EH. Influence of platedesign on cortical bone perfusion and fracture healing in canine segmentaltibial fractures. J Orthop Trauma 1999;13(3):178–86.
[51] Akeson WH, Woo SL, Rutherford L, Coutts RD, Gonsalves M, Amiel D. Theeffects of rigidity of internal fixation plates on long bone remodeling. Abiomechanical and quantitative histological study. Acta Orthop Scand1976;47:241–9.
[52] Slatis P, Paavolainen P, Karaharju E, Holmstrom T. Structural andbiomechanical changes in bone after rigid plate fixation. Can J Surg1980;23:247–50.
[53] Goodship AE, Kenwright J. The influence of induced micromovement uponthe healing of experimental tibial fractures. J Bone Joint Surg Br1985;67:650–5.
[54] Foux A, Yeadon AJ, Uhthoff HK. Improved fracture healing with less rigidplates – a biomechanical study in dogs. Clin Orthop Relat R 1997:232–45.
[55] Kim JH, Kim SH, Chang SH. Estimation of the movement of the inter-fragmentary gap of a fractured human femur in the presence of a compositebone plate. J Compos Mater 2011;45:1491–8.
[56] Jha DK, Kant T, Singh RK. A critical review of recent research on functionallygraded plates. Compos Struct 2013;96:833–49.
[57] Boss JN, Ganesh VK. Fabrication and properties of graded composite rods forbiomedical applications. Compos Struct 2006;74:289–93.
[58] Claes LE. Mechanical characterization of biodegradable implants. Clin Mater1992;10:41–6.
340 H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341
[59] Harper LT, Ahmed I, Felfel RM, Qian C. Finite element modelling of theflexural performance of resorbable phosphate glass fibre reinforced PLAcomposite bone plates. J Mech Behav Biomed 2012;15:13–23.
[60] Parsons AJ, Ahmed I, Haque P, Fitzpatrick B, Niazi MIK, Walker GS, et al.Phosphate glass fibre composites for bone repair. J Bionic Eng2009;6(4):318–23.
[61] Ahmed I, Jones IA, Parsons AJ, Bernard J, Farmer J, Scotchford CA, et al.Composites for bone repair: phosphate glass fibre reinforced PLA withvarying fibre architecture. J Mater Sci - Mater Med 2011;22:1825–34.
[62] Haque P, Parsons AJ, Barker IA, Ahmed I, Irvine DJ, Walker GS, et al. Interfacialproperties of phosphate glass fibres/PLA composites: effect of the endfunctionalities of oligomeric PLA coupling agents. Compos Sci Technol2010;70:1854–60.
[63] Black J. Orthopaedic biomaterials in research and practice. NewYork: Churchill Livingstone; 1988. p. 197–210.
[64] Baidya KP, Ramakrishna S, Rahman M, Ritchie A. Advanced textile compositering for Ilizarov external fixator system. Proc Inst Mech Eng H2001;215:11–23.
[65] Stiffler KS. Internal fracture fixation. Clin Tech Small Anim Pract2004;19:105–13.
[66] Perren SM. Evolution of the internal fixation of long bone fractures – thescientific basis of biological internal fixation: choosing a new balancebetween stability and biology. J Bone Joint Surg Br 2002;84B:1093–110.
[67] Baumgaertel F, Buhl M, Rahn BA. Fracture healing in biological plateosteosynthesis. Injury 1998;29:3–6.
[68] Perren SM. Physical and biological aspects of fracture healing with specialreference to internal fixation. Clin Orthop Relat R 1979:175–96.
[69] Ji F, Tong D, Tang H, Cai XB, Zhang QL, Li JF, et al. Minimally invasivepercutaneous plate osteosynthesis (MIPPO) technique applied in thetreatment of humeral shaft distal fractures through a lateral approach. IntOrthop 2009;33:543–7.
[70] Roux W. Gesammelte abhandlungen über entwicklungsmechanik derorganismen. Leipzig, Berlin: Wilhelm Engelmann; 1895.
[71] Pauwels F. Biomechanics of the locomotor apparatus. Berlin: Springer-Verlag;1980.
[72] Perren SM, Cordey J. The concept of interfragmentary strain. In: Uhthoff HK,editor. Current concepts of internal fixation of fractures. Berlin: Springer-Verlag; 1980. p. 63–77.
[73] DiGioia 3rd AM, Cheal EJ, Hayes WC. Three-dimensional strain fields in auniform osteotomy gap. J Biomech Eng 1986;108:273–80.
[74] Cheal EJ, Mansmann KA, DiGioia 3rd AM, Hayes WC, Perren SM. Role ofinterfragmentary strain in fracture healing: ovine model of a healingosteotomy. J Orthop Res 1991;9:131–42.
[75] Claes LE, Heigele CA, Neidlinger-Wilke C, Kaspar D, Seidl W, Margevicius KJ,et al. Effects of mechanical factors on the fracture healing process. ClinOrthop Relat R 1998:S132–47.
[76] Prendergast PJ, Huiskes R, Soballe K. Biophysical stimuli on cells during tissuedifferentiation at implant interfaces. J Biomech 1997;30:539–48.
[77] Checa S, Prendergast PJ. A mechanobiological model for tissue differentiationthat includes angiogenesis: a lattice-based modeling approach. Ann BiomedEng 2009;37:129–45.
[78] Nagel T, Kelly DJ. Mechano-regulation of mesenchymal stem celldifferentiation and collagen organisation during skeletal tissue repair.Biomech Model Mechan 2010;9:359–72.
[79] Kim HJ, Chang SH, Jung HJ. The simulation of tissue differentiation at afracture gap using a mechano-regulation theory dealing with deviatoricstrains in the presence of a composite bone plate. Compos Part B-Eng2012;43:978–87.
[80] Mehboob H, Son DS, Chang SH. Finite element analysis of tissuedifferentiation process of a tibia with various fracture configurations whena composite intramedullary rod was applied. Compos Sci Technol2013;80:55–65.
[81] Milan JL, Planell JA, Lacroix D. Simulation of bone tissue formation within aporous scaffold under dynamic compression. Biomech Model Mechan2010;9:583–96.
[82] Checa S, Prendergast PJ. Effect of cell seeding and mechanical loading onvascularization and tissue formation inside a scaffold: a mechano-biologicalmodel using a lattice approach to simulate cell activity. J Biomech2010;43:961–8.
[83] Zhao D, Banks SA, D’Lima DD, Colwell CW, Fregly BJ. In vivo medial and lateraltibial loads during dynamic and high flexion activities. J Orthop Res2007;25:593–602.
[84] Taylor WR, Heller MO, Bergmann G, Duda GN. Tibio-femoral loading duringhuman gait and stair climbing. J Orthop Res 2004;22:625–32.
[85] D’Lima DD, Patil S, Steklov N, Slamin JE, Colwell CW. Tibial forces measuredin vivo after total knee arthroplasty. J Arthroplasty 2006;21:255–62.
[86] Bogey RA, Perry J, Gitter AJ. An EMG-to-force processing approach fordetermining ankle muscle forces during normal human gait. IEEE TransNeural Syst Rehabil Eng 2005;13:302–10.
[87] Donahue TLH, Hull ML, Rashid MM, Jacobs CR. A finite element model of thehuman knee joint for the study of tibio-femoral contact. J Biomech Eng-TASME 2002;124:273–80.
[88] Son DS, Mehboob H, Jung HJ, Chang SH. The finite element analysis forendochondral ossification process of a fractured tibia applied with acomposite IM-rod based on a mechano-regulation theory using a deviatoricstrain. Compos Part B-Eng 2014;56:189–96.
[89] Son DS, Chang SH. The simulation of bone healing process of fractured tibiaapplied with composite bone plates according to the diaphyseal oblique angleand plate modulus. Compos Part B-Eng 2013;45:1325–35.
[90] Benli S, Aksoy S, Havitcioglu H, Kucuk M. Evaluation of bone plate withlow-stiffness material in terms of stress distribution. J Biomech 2008;41:3229–35.
[91] Fouad H. Assessment of function-graded materials as fracture fixation bone-plates under combined loading conditions using finite element modelling.Med Eng Phys 2011;33:456–63.
[92] Fouad H. Effects of the bone-plate material and the presence of a gap betweenthe fractured bone and plate on the predicted stresses at the fractured bone.Med Eng Phys 2010;32:783–9.
[93] MacLeod AR, Pankaj P, Simpson AHRW. Does screw-bone interface modellingmatter in finite element analyses? J Biomech 2012;45:1712–6.
[94] Prendergast PJ. Finite element models in tissue mechanics and orthopaedicimplant design. Clin Biomech 1997;12:343–66.
[95] Huiskes R, Chao EYS. A survey of finite-element analysis in orthopedicbiomechanics – the 1st decade. J Biomech 1983;16:385.
[96] Avery CME, Bujtar P, Simonovics J, Dezsi T, Varadi K, Sandor GKB, et al. A finiteelement analysis of bone plates available for prophylactic internal fixation ofthe radial osteocutaneous donor site using the sheep tibia model. Med EngPhys 2013;35:1421–30.
[97] Ferguson SJ, Wyss UP, Pichora DR. Finite element stress analysis of a hybridfracture fixation plate. Med Eng Phys 1996;18:241–50.
[98] Kim SH, Chang SH, Jung HJ. The finite element analysis of a fracturedtibia applied by composite bone plates considering contact conditions andtime-varying properties of curing tissues. Compos Struct 2010;92:2109–18.
[99] Kim SH, Chang SH, Son DS. Finite element analysis of the effect of bendingstiffness and contact condition of composite bone plates with simplerectangular cross-section on the bio-mechanical behaviour of fracturedlong bones. Compos Part B-Eng 2011;42:1731–8.
[100] Ament C, Hofer EP. A fuzzy logic model of fracture healing. J Biomech2000;33:961–8.
[101] Lacroix D, Prendergast PJ, Li G, Marsh D. Biomechanical model to simulatetissue differentiation and bone regeneration: application to fracture healing.Med Biol Eng Comput 2002;40:14–21.
[102] Bailon-Plaza A, van der Meulen MC. Beneficial effects of moderate, earlyloading and adverse effects of delayed or excessive loading on bone healing. JBiomech 2003;36:1069–77.
[103] Kuiper JH, Ashton BA, Richardson JB. Computer simulation of fracture callusformation and stiffness restoration. In: 12th Conference of European Societyof Biomechanics, Dublin; 2000.
[104] Gomez-Benito MJ, Garcia-Aznar JM, Kuiper JH, Doblare M. A 3Dcomputational simulation of fracture callus formation: influence of thestiffness of the external fixator. J Biomech Eng 2006;128:290–9.
[105] Andreykiv A, van Keulen F, Prendergast PJ. Simulation of fracture healingincorporating mechanoregulation of tissue differentiation and dispersal/proliferation of cells. Biomech Model Mechanobiol 2008;7:443–61.
[106] Isaksson H, van Donkelaar CC, Huiskes R, Ito K. A mechano-regulatory bone-healing model incorporating cell-phenotype specific activity. J Theor Biol2008;252:230–46.
[107] Walker J, Shadanbaz S, Woodfield TB, Staiger MP, Dias GJ. Magnesiumbiomaterials for orthopedic application: a review from a biologicalperspective. J Biomed Mater Res B Appl Biomater 2014.
[108] Sabir MI, Xu XX, Li L. A review on biodegradable polymeric materials for bonetissue engineering applications. J Mater Sci 2009;44:5713–24.
[109] Santiuste C, Rodríguez-Millán M, Giner E, Miguélez H. The influence ofanisotropy in numerical modeling of orthogonal cutting of cortical bone.Compos Struct 2014;116:423–31.
[110] Uhthoff HK, Poitras P, Backman DS. Internal plate fixation of fractures: shorthistory and recent developments. J Orthop Sci 2006;11:118–26.
[111] Tan LL, Yu XM, Wan P, Yang K. Biodegradable materials for bone repairs: areview. J Mater Sci 2013;29:503–13.
[112] Staiger MP, Pietak AM, Huadmai J, Dias G. Magnesium and its alloys asorthopedic biomaterials: a review. Biomaterials 2006;27:1728–34.
[113] Bradley JS, Hastings GW, Johnson-Nurse C. Carbon fibre reinforced epoxy as ahigh strength, low modulus material for internal fixation plates. Biomaterials1980;1:38–40.
[114] McKenna GB, Bradley GW, Dunn HK, Statton WO. Mechanical properties ofsome fibre reinforced polymer composites after implantation as fracturefixation plates. Biomaterials 1980;1:189–92.
[115] Gillett N, Brown SA, Dumbleton JH, Pool RP. The use of short carbon-fiberreinforced thermoplastic plates for fracture fixation. Biomaterials1985;6:113–21.
[116] Jockisch KA, Brown SA, Bauer TW, Merritt K. Biological response to chopped-carbon-fiber-reinforced peek. J Biomed Mater Res 1992;26:133–46.
[117] Morrison C, Macnair R, Macdonald C, Wykman A, Goldie I, Grant MH. In-vitrobiocompatibility testing of polymers for orthopedic implants using culturedfibroblasts and osteoblasts. Biomaterials 1995;16:987–92.
[118] Peluso G, Ambrosio L, Cinquegrani M, Nicolais L, Saiello S, Tajana G. Ratperitoneal immune-response to carbon-fiber reinforced epoxy compositeimplants. Biomaterials 1991;12:231–5.
[119] Ali MS, French TA, Hastings GW, Rae T, Rushton N, Ross ERS, et al. Carbon-fiber composite bone plates – development, evaluation and early clinical-experience. J Bone Joint Surg Br 1990;72:586–91.

H. Mehboob, S.-H. Chang / Composite Structures 118 (2014) 328–341 341
[120] Schambron T, Lowe A, McGregor HV. Effects of environmental ageing on thestatic and cyclic bending properties of braided carbon fibre/PEEK bone plates.Compos Part B-Eng 2008;39:1216–20.
[121] Fujihara K, Huang ZM, Ramakrishna S, Satkunanantham K, Hamada H.Development of braided carbon/peek composite bone plates. Adv ComposLett 2001;10:13–20.
[122] Ansar M, Wang XW, Zhou CW. Modeling strategies of 3D woven composites:a review. Compos Struct 2011;93:1947–63.
[123] Jiang LL, Zeng T, Yan S, Fang DN. Theoretical prediction on the mechanicalproperties of 3D braided composites using a helix geometry model. ComposStruct 2013;100:511–6.
[124] Zhang C, Xu XW. Finite element analysis of 3D braided composites based onthree unit-cells models. Compos Struct 2013;98:130–42.
[125] Stig F, Hallstrom S. A modelling framework for composites containing 3Dreinforcement. Compos Struct 2012;94:2895–901.
[126] Stig F, Hallstrom S. Spatial modelling of 3D-woven textiles. Compos Struct2012;94:1495–502.
[127] Stig F, Hallstrom S. Influence of crimp on 3D-woven fibre reinforcedcomposites. Compos Struct 2013;95:114–22.
[128] Abu Bakar IA, Kramer O, Bordas S, Rabczuk T. Optimization of elasticproperties and weaving patterns of woven composites. Compos Struct2013;100:575–91.
[129] Ferreira RTL, Rodrigues HC, Guedes JM, Hernandes JA. Hierarchicaloptimization of laminated fiber reinforced composites. Compos Struct2014;107:246–59.
[130] Mayer J. Gestricke aus kohlenstoffasern fur biokompatibleverbundwerkstoffe, dargestellt an einer homoelastischenosteosyntheseplatte [Ph.D. thesis]. ETH Zurich, Switzerland; 1994.
[131] Ayranci C, Carey J. 2D braided composites: a review for stiffness criticalapplications. Compos Struct 2008;85:43–58.
[132] Ramakrishna S, Hull D. Tensile behavior of knitted carbon-fiber–fabric/epoxylaminates. 2. Prediction of tensile properties. Compos Sci Technol1994;50:249–58.
[133] Armentano I, Dottori M, Fortunati E, Mattioli S, Kenny JM. Biodegradablepolymer matrix nanocomposites for tissue engineering: a review. PolymDegrad Stabil 2010;95:2126–46.
[134] Giannoudis PV, Dinopoulos H, Tsiridis E. Bone substitutes: an update. Injury2005;36:20–7.
[135] Jiang G, Evans ME, Jones IA, Rudd CD, Scotchford CA, Walker GS. Preparationof poly(epsilon-caprolactone)/continuous bioglass fibre composite usingmonomer transfer moulding for bone implant. Biomaterials 2005;26:2281–8.
[136] Andriano KP, Daniels AU, Heller J. Biocompatibility and mechanical-properties of a totally absorbable composite-material for orthopedicfixation devices. J Appl Biomater 1992;3:197–206.
[137] Ahmed I, Lewis M, Olsen I, Knowles JC. Phosphate glasses for tissueengineering: Part 1. Processing and characterisation of a ternary-basedP(2)O(5)-CaO-Na(2)O glass system. Biomaterials 2004;25:491–9.
[138] Ahmed I, Lewis M, Olsen I, Knowles JC. Phosphate glasses for tissueengineering: Part 2. Processing and characterisation of a ternary-basedP(2)O(5)-CaO-Na(2)O glass fibre system. Biomaterials 2004;25:501–7.
[139] Ahmed I, Parsons AJ, Palmer G, Knowles JC, Walkers GS, Rudd CD. Weightloss, ion release and initial mechanical properties of a binary calciumphosphate glass fibre/PCL composite. Acta Biomater 2008;4:1307–14.
[140] Felfel RM, Ahmed I, Parsons AJ, Haque P, Walker GS, Rudd CD. Investigation ofcrystallinity, molecular weight change, and mechanical properties of PLA/PBG bioresorbable composites as bone fracture fixation plates. J BiomaterAppl 2012;26:765–89.
[141] Cannillo V, Chiellini F, Fabbri P, Sola A. Production of Bioglass (R) 45S5-polycaprolactone composite scaffolds via salt-leaching. Compos Struct2010;92:1823–32.
[142] Gupta G, Zbib A, El-Ghannam A, Khraisheh M, Zbib H. Characterization of anovel bioactive composite using advanced X-ray computed tomography.Compos Struct 2005;71:423–8.
[143] Felfel RM, Ahmed I, Parsons AJ, Rudd CD. Bioresorbable screws reinforcedwith phosphate glass fibre: manufacturing and mechanical propertycharacterisation. J Mech Behav Biomed 2013;17:76–88.
[144] Felfel RM, Ahmed I, Parsons AJ, Rudd CD. Bioresorbable composite screwsmanufactured via forging process: pull-out, shear, flexural and degradationcharacteristics. J Mech Behav Biomed 2013;18:108–22.
[145] Felfel RM, Ahmed I, Parsons AJ, Harper LT, Rudd CD. Initial mechanicalproperties of phosphate–glass fibre-reinforced rods for use as resorbableintramedullary nails. J Mater Sci 2012;47:4884–94.
[146] Felfel RM, Ahmed I, Parsons AJ, Walker GS, Rudd CD. In vitro degradation,flexural, compressive and shear properties of fully bioresorbable compositerods. J Mech Behav Biomed 2011;4:1462–72.
[147] Hasan MS, Ahmed I, Parsons AJ, Rudd CD, Walker GS, Scotchford CA.Investigating the use of coupling agents to improve the interfacial propertiesbetween a resorbable phosphate glass and polylactic acid matrix. J BiomaterAppl 2013;28:354–66.
[148] Han N, Ahmed I, Parsons AJ, Harper L, Scotchford CA, Scammell BE, et al.Influence of screw holes and gamma sterilization on properties of phosphateglass fiber-reinforced composite bone plates. J Biomater Appl2013;27:990–1002.
[149] Moazen M, Mak JH, Etchels LW, Jin ZM, Wilcox RK, Jones AC, et al. The effectof fracture stability on the performance of locking plate fixation inperiprosthetic femoral fractures. J Arthroplasty 2013;28:1589–95.
[150] Wieding J, Souffrant R, Fritsche A, Mittelmeier W, Bader R. Finite elementanalysis of osteosynthesis screw fixation in the bone stock: an appropriatemethod for automatic screw modelling. PLoS ONE 2012:7.
[151] Gefen A. Optimizing the biomechanical compatibility of orthopedic screwsfor bone fracture fixation. Med Eng Phys 2002;24:337–47.
[152] Kharazi AZ, Fathi MH, Bahmany F. Design of a textile composite bone plateusing 3D-finite element method. Mater Des 2010;31:1468–74.
[153] Kelly DJ, Prendergast PJ. Prediction of the optimal mechanical properties for ascaffold used in osteochondral defect repair. Tissue Eng 2006;12:2509–19.
[154] Kim HJ, Kim SH, Chang SH. Bio-mechanical analysis of a fractured tibia withcomposite bone plates according to the diaphyseal oblique fracture angle.Compos Part B-Eng 2011;42:666–74.
[155] Mehboob H, Chang SH. Evaluation of the healing performance ofbiodegradable composite bone plates for fractured tibia by finite elementanalysis. Compos Struct 2014;111:193–204.
[156] Son DS, Mehboob H, Chang SH. Simulation of the bone healing process offractured long bones applied with a composite bone plate with considerationof the blood vessel growth. Compos Part B-Eng 2014;58:443–50.
[157] Kim HJ, Kim SH, Chang SH. Finite element analysis using interfragmentarystrain theory for the fracture healing process to which composite bone platesare applied. Compos Struct 2011;93:2953–62.
[158] Mehboob H, Chang SH. Evaluation of the development of tissue phenotypes:bone fracture healing using functionally graded material composite boneplates. Compos Struct 2014;117:105–13.
[159] Katayama T, Yamamoto H, Inoue N. Optimum design of artificial jointsconsidering initial fixation of prosthesis. Compos Struct 1995;32:427–33.




















