
Anti oxident status in Saliva
66
PROJECT REPORT ON ANTIOXIDANT STATUS OF SALIVA Submitted to the University of Kerala in partial fulfillment for the award of B.Sc Biochemistry and Industrial Microbiology. BY GOPIKA GOPAL.V(REG.NO:24810807010) JUHI MOHAN (REG.NO:24810807011) SREEJA.S(REG.N0:24810807016) ASWATHY GOPAN(REG.NO:24810807006) SUSMI.B(REG.N:248108018) Under BIOGENIX Research Centre,Thiruvanathapuram
-
Upload
keralauniversity -
Category
Documents
-
view
2 -
download
0
Transcript of Anti oxident status in Saliva
PROJECT REPORT
ON
ANTIOXIDANT STATUS OF SALIVASubmitted to the University of Kerala in partial fulfillment for the
award of B.Sc Biochemistry and Industrial Microbiology.
BY
GOPIKA GOPAL.V(REG.NO:24810807010)
JUHI MOHAN (REG.NO:24810807011)
SREEJA.S(REG.N0:24810807016)
ASWATHY GOPAN(REG.NO:24810807006)
SUSMI.B(REG.N:248108018)
Under
BIOGENIX Research Centre,Thiruvanathapuram
DEPARTMENT OF INDUSTRIAL MICROBIOLOGYNATIONAL COLLEGE
(Affiliated to University of Kerala)Thiruvananthapuram-9PROJECT REPORT
ON
ANTIOXIDANT STATUS OF SALIVASubmitted to the University of Kerala in partial fulfillment for the
award of B.Sc Biochemistry and Industrial Microbiology.
BY
GOPIKA GOPAL.V(REG.NO:24810807010)
JUHI MOHAN (REG.NO:24810807011)
SREEJA.S(REG.N0:248108016)
ASWATHY GOPAN(REG.NO:24810807006)
SUSMI.B(REG.N0:24810807018)
Under
BIOGENIX Research Centre,Thiruvanathapuram
DEPARTMENT OF INDUSTRIAL MICROBIOLOGY NATIONAL COLLEGE
(Affiliated to University of Kerala)Thiruvananthapuram-9
NATIONAL COLLEGE
Manacaud,Thiruvananthapuram-9
(Afflilated to the University of Kerala)
DEPARTMENT OF BIOCHEMISTRY
CERTIFICATE
This is to certify that the project report entitled “Antioxidantstatus of saliva”, is submitted by GOPIKA GOPAL.V, JUHI MOHAN,SREEJA.S, SUSMI.B, ASWATHY GOPAN, Department of Biochemistry,National College, Thiruvananthapuram, towards the partialfulfilment of the requirement for the award of the Degree of B.scin Biochemistry and Industrial Microbiology of the University ofKerala during the period of 2010-2013. It is the bonafide recordof the project work done by us at Biogenix Research Centre,Thiruvananthapuram.
Miss.Smitha.S Dr.Sreelekha Prof (Major) Basheer KannuInternal guide Head of the Department Principal
External examiners: 1 )
2 )


DECLARATION

DECLARATIONWe JUHI MOHAN.S, SREEJA.S, GOPIKA GOPAL.V, ASWATHY GOPAN ANDSUSMI.B hereby declare that the dissertation entitled“ANTIOXIDANT STATUS OF SALIVA”. Submitted to the national collegein partial fulfillment of the requirements for the awards of thedegree of the Bachelor of science in Biochemistry and IndustrialMicrobiology is a record of original research work done by usduring (2010- 2013) under the supervision and guidance of Dr.Sreelekha , Department of Biochemistry, National college Manacaudand it has not formed the basis for the award of any degree/diploma/ associate ship/ fellow ship or other similar title toany candidate of any university.


ACKNOWLEDGEMENT

ACKNOWLEDGEMENT
We humbly bow our head before God Almighty, who blessed us withthe power to complete this endeavor successful.
We express our sincere thanks to Professor (Major) BasheerKannu, Principal, National college, Manacaud, for having providedthe opportunity and necessary facilities for doing the projectwork.
We here wish to record our sense of indebtedness and gratitude toDr.Sreelekha, Head of the department and Ms.Smitha, Lecturer ofbiochemistry, National college, Manacaud for their kind adviceand continuous encouragement for the successful completion of ourresearch work and providing us necessary facilities.
We render our gratitude to Mr.Rajesh.R, Director of BiogenixResearch Center, Thiruvananthapuram, Kerala, for his valuableguidance, helpful ideas,and great concern show throughout theperiod of our work and the completion of the same.
Our sincere thanks to Ms.Sruthi,co-ordinator of Biogenix ResearchCenter, Thiruvananthapuram, Kerala, for her help and enormousmoral support.
Above all, I Wish to express thanks to our parents for theirprayers, love, care, support and help in completing this projectsuccessfully.


CONTENTS
CONTENTSSL.No CONTENT PAGE.NO.
1. INTRODUCTION2. AIM AND OBJECTIVE 3. REVIEW OF LITERATURE4. MATERIALS AND
METHODS5. RESULTS6. DISCUSSION
7. CONCLUSION
8.BIBLIOGRAPHY
9. APPENDIX


ABBREVIATION
ABBREVIATIONSROS Reactive Oxygen Species
µl Micro litre
TCA Tri Chloro Aceticacid
MDA Malonaldehyde
SDS Sodium Dodecyl Sulphate
PAGE Polyacrylamide GelElectrophoresis
Nm Nanometer
OD Optical Density


INTRODUCTION
INTRODUCTION
SALIVARY ANTIOXIDANTS
The oral cavity is under constant bombardment from food anddrink, as well as substances such as alcohol, tobacco productsand nicotine, dental materials and much more. Bacteria and otherdisease-causing agents along with systemic conditions presentfurther insult. Because the oral tissues are delicate, they areespecially vulnerable to cell damage caused by free radicals andoxidative stress.
Saliva is a natural defence against bacteria and other substancesharmful to health. Research is confirming that antioxidants areamong the most important elements in saliva, and that they helpprotect against diseases including oral diseases and oral cancer.
Composition of Saliva
Saliva is the clear, viscous fluid secreted by the three pairs ofmajor salivary glands. It is 98 percent water, and the remainingtwo percent includes proteins, electrolytes, enzymes, hormones,and other substances.
One of the major functions of saliva is digestion. The liquid andthe enzymes soften food and begin the process of breaking itdown.

Saliva is also important in maintaining oral health. Itlubricates the teeth and tongue, and helps wash away particles offood. Although saliva can harbour bacteria and other microorganisms, it also has natural antibacterial compounds, includingthiocyanate, hydrogen peroxide and immunoglobulin A.
Human saliva also contains antioxidant compounds that arecritical in fighting reactive oxygen species (ROS), reactivenitrogen species (RNS) that can cause oxidative stress and DNAmutations. In addition, because saliva reflects the body’s levelsof various hormonal, immunological, toxicological and infectiousdisease markers, it is an excellent tool for monitoring oral andsystemic health.
Antioxidants in Saliva
Saliva is rich in antioxidant compounds. The primary antioxidantsinclude uric acid, albumin, ascorbic acid, glutathione andantioxidant enzymes. Antioxidants are critical to the body’sdefence system because of their ability to neutralize freeradicals—ROS and RNS—and counteract oxidative stress.
Saliva and Periodontal Disease
The antioxidants in saliva can have a mitigating effect againstperiodontitis, the inflammatory disease that often results inloss of periodontal ligament and alveolar bone.
One major cause of periodontal disease is bacteria, such asporphyromonas gingivalis. An invasion of P. gingivalis triggers therelease of chemicals that bring about inflammation, includingcytokines (e.g., interleukin 8), chemokines, prostaglandins, anddestructive enzymes such as MMPs (matrix metalloproteinases).These pro-inflammatory mediators signal for an increase in thenumber and activity of polymorphonuclear neutrophils (PMNs),i.e., white blood cells. As the PMNs attack and ingest thebacteria, they release additional cytokines and in doing socreate large quantities of ROS, leading to oxidative stress andpotential cell damage to gingival tissue, periodontal ligamentand alveolar bone.
A reduced level of salivary antioxidants is characteristic ofpatients with periodontal disease. It is not yet clear whetherthe lower level of antioxidants contributes to the cause ofperiodontitis, or whether the antioxidants are reduced as aresult of the their heightened action in neutralizing freeradicals and ROS.
PeriodontitisPeriodontitis is a set of inflammatory disease affecting theperiodontium, i.e., the tissues that surround and support theteeth. Periodontitis involves progressive loss of the alveolarbone around the teeth, and if left untreated, can lead to theloosening and subsequent loss of teeth. Periodontitis is causedby microorganisms that adhere to and grow on the tooth'ssurfaces, along with an overly aggressive immune response againstthese microorganisms. A diagnosis of periodontitis is establishedby inspecting the soft gum tissues around the teeth with a probe(i.e., a clinical examination) and by evaluating the patient's X-ray films (i.e. a radiographic examination), to determine theamount of bone loss around the teeth. Specialists in the

treatment of periodontitis are periodontists; their field isknown as "periodontology" or "periodontics".
The word "periodontitis" comes from the Greek peri, "around",odous (genitive odontos), "tooth", and the suffix -itis, in medicalterminology "inflammation". Periodontitis is an inflammation ofthe periodontium, i.e., the tissues that support the teeth. Theperiodontium consists of four tissues:
gingiva, or gum tissue, cementum, or outer layer of the roots of teeth, alveolar bone, or the bony sockets into which the teeth are
anchored, and Periodontal ligaments (PDLs), which are the connective
tissue fibers that run between the cementum and the alveolarbone.
Periodontitis occurs when inflammation or infection of the gums(gingivitis) is untreated or treatment is delayed. Infection andinflammation spreads from the gums (gingiva) to the ligaments andbone that support the teeth. Loss of support causes the teeth tobecome loose and eventually fall out. Periodontitis is theprimary cause of tooth loss in adults. This disorder is uncommonin childhood but increases during adolescence.
Plaque and tartar build up at the base of the teeth. Inflammationcauses a pocket to develop between the gums and the teeth, whichfills with plaque and tartar. Soft tissue swelling traps theplaque in the pocket. Continued inflammation leads to damage ofthe tissues and bone surrounding the tooth. Because plaquecontains bacteria, infection is likely and a tooth abscess mayalso develop, which increases the rate of bone destruction.

Classification
The 1999 classification system for periodontal diseases andconditions listed eight major categories of periodontal diseasesof which 2-6 are termed destructive periodontal disease becausethe damage is essentially irreversible. The eight categories areas follows:
1. Gingivitis2. Chronic periodontitis3. Aggressive periodontitis4. Periodontitis as a manifestation of systemic disease5. Necrotizing ulcerative gingivitis/periodontitis6. Abscesses of the periodontium7. Combined periodontic-endodontic lesions
Moreover, terminology expressing both the extent and severity ofperiodontal diseases are appended to the terms above to denotethe specific diagnosis of a particular patient or group ofpatients.
Extent
The 'extent' of disease refers to the proportion of the dentitionaffected by the disease in terms of percentage of sites. Sitesare defined as the positions at which probing measurements aretaken around each tooth and, generally, six probing sites aroundeach tooth are recorded, as follows:
1. mesiobuccal2. midbuccal3. distobuccal4. mesiolingual5. midlingual6. distolingual
If up to 30% of sites in the mouth are affected, the manifestation is classification as 'localized'; for more than 30%, the term 'generalized' is used.
Severity
The 'severity' of disease refers to the amount of periodontalligament fibers that have been lost, termed 'clinical attachmentloss'. According to the American Academy of Periodontology, theclassification of severity is as follows:[3]
Mild: 1–2 mm (0.039–0.079 in) of attachment loss Moderate: 3–4 mm (0.12–0.16 in) of attachment loss Severe: ≥ 5 mm (0.20 in) of attachment loss
Signs and symptoms
In the early stages, periodontitis has very few symptoms; and inmany individuals the disease has progressed significantly beforethey seek treatment.
Examination of the mouth and teeth by the dentist shows soft,swollen, red-purple gums. Deposits of plaque and calculus may beseen at the base of the teeth, with enlarged pockets in the gums.The gums are usually painless or mildly tender, unless a toothabscess is also present. Teeth may be loose and gums may bereceded
Symptoms may include:
Redness or bleeding of gums while brushing teeth, usingdental floss or biting into hard food (e.g. apples) (thoughthis may occur even in gingivitis, where there is noattachment loss)
Gum swelling that recurs Spitting out blood after brushing teeth Halitosis, or bad breath, and a persistent metallic taste in
the mouth

Gingival recession, resulting in apparent lengthening ofteeth. (This may also be caused by heavy-handed brushing orwith a stiff tooth brush.)
Deep pockets between the teeth and the gums (pockets aresites where the attachment has been gradually destroyed bycollagen-destroying enzymes, known as collagenases)
Loose teeth, in the later stages (though this may occur forother reasons, as well)
Patients should realize gingival inflammation and bonedestruction are largely painless. Hence, people may wronglyassume painless bleeding after teeth cleaning is insignificant,although this may be a symptom of progressing periodontitis inthat patient.
Dental x-rays reveal the loss of supporting bone and may alsoshow the presence of plaque deposits under the gums. This X-rayfilm displays two lone-standing mandibular teeth, the lower leftfirst premolar and canine, exhibiting severe bone loss of 30–50%.Widening of the periodontal ligament surrounding the premolar isdue to secondary occlusal trauma
Effects outside the mouth
Periodontitis has been linked to increased inflammation in thebody, such as indicated by raised levels of C-reactive proteinand interleukin-6. It is linked through this to increased risk ofstroke, myocardial infarction, and atherosclerosis. It alsolinked in those over 60 years of age to impairments in delayedmemory and calculation abilities. Individuals with impairedfasting glucose and diabetes mellitus have higher degrees ofperiodontal inflammation, and often have difficulties withbalancing their blood glucose level owing to the constantsystemic inflammatory state, caused by the periodontalinflammation. Although no causative connection was proved yet, arecent study revealed an epidemiological association betweenchronic periodontitis and erectile dysfunction.
Complications
Infection or abscess of the soft tissue (facial cellulitis) Infection of the jaw bones (osteomyelitis) Return of periodontitis Tooth abscess Tooth loss Tooth flaring or shifting Trench mouth
Causes
The primary etiology (cause) of gingivitis is poor or ineffectiveoral hygiene which leads to the accumulation of a mycotic andbacterial matrix at the gum line, called dental plaque. Othercontributors are poor nutrition and underlying medical issuessuch as diabetes. New finger nick tests have been approved by theFood and Drug Administration in the US, and are being used indental offices to identify and screen patients for possiblecontributory causes of gum disease, such as diabetes.
In some people, gingivitis progresses to periodontitis –- withthe destruction of the gingival fibers, the gum tissues separatefrom the tooth and deepened sulcus, called a periodontal pocket.Subgingival micro-organisms (those that exist under the gum line)colonize the periodontal pockets and cause further inflammationin the gum tissues and progressive bone loss. Examples ofsecondary etiology are those things that, by definition, causemicrobic plaque accumulation, such as restoration overhangs androot proximity.
The excess restorative material that exceeds the natural contoursof restored teeth, such as these, are termed "overhangs", andserve to trap microbic plaque, potentially leading to localizedperiodontitis.

Smoking is another factor that increases the occurrence ofperiodontitis, directly or indirectly and may interfere with oradversely affect its treatment.
Ehlers–Danlos syndrome is a periodontitis risk factor and so isthe Papillon-Lefèvre syndrome also known as palmoplantarkeratoderma.
If left undisturbed, microbial plaque calcifies to form calculus,which is commonly called tartar. Calculus above and below the gumline must be removed completely by the dental hygienist ordentist to treat gingivitis and periodontitis. Although theprimary cause of both gingivitis and periodontitis is themicrobial plaque that adheres to the tooth surfaces, there aremany other modifying factors. A very strong risk factor is one'sgenetic susceptibility. Several conditions and diseases,including Down syndrome, diabetes, and other diseases that affectone's resistance to infection, also increase susceptibility toperiodontitis.
Another factor that makes periodontitis a difficult disease tostudy is that human host response can also affect the alveolarbone resorption. Host response to the bacterial-mycotic insult ismainly determined by genetics; however, immune development mayplay some role in susceptibility.
According to some researchers periodontitis may be associatedwith higher stress.
Expectations (prognosis)
Dentists and dental hygienists measure periodontal disease usinga device called a periodontal probe. This thin "measuring stick"is gently placed into the space between the gums and the teeth,and slipped below the gumline. If the probe can slip more than3 mm (0.12 in) below the gumline, the patient is said to have agingival pocket if no migration of the epithelial attachment hasoccurred or a periodontal pocket if apical migration has

occurred. This is somewhat of a misnomer, as any depth is inessence a pocket, which in turn is defined by its depth, i.e., a2-mm pocket or a 6-mm pocket. However, pockets are generallyaccepted as self-cleansable (at home, by the patient, with atoothbrush) if they are 3 mm or less in depth. This is importantbecause if a pocket is deeper than 3 mm around the tooth, at-homecare will not be sufficient to cleanse the pocket, andprofessional care should be sought. When the pocket depths reach6 to 7 mm (0.24 to 0.28 in) in depth, the hand instruments andcavitrons used by the dental professionals may not reach deeplyenough into the pocket to clean out the microbial plaque thatcause gingival inflammation. In such a situation, the bone or thegums around that tooth should be surgically altered or it willalways have inflammation which will likely result in more boneloss around that tooth. An additional way to stop theinflammation would be for the patient to receive subgingivalantibiotics (such as minocycline) or undergo some form ofgingival surgery to access the depths of the pockets and perhapseven change the pocket depths so they become 3 mm or less indepth and can once again be properly cleaned by the patient athome with his or her toothbrush.
If patients have 7-mm or deeper pockets around their teeth, thenthey would likely risk eventual tooth loss over the years. Ifthis periodontal condition is not identified and the patientsremain unaware of the progressive nature of the disease, thenyears later, they may be surprised that some teeth will graduallybecome loose and may need to be extracted, sometimes due to asevere infection or even pain.
According to the Sri Lankan tea labourer study, in the absence ofany oral hygiene activity, approximately 10% will suffer fromsevere periodontal disease with rapid loss of attachment(>2 mm/year). About 80% will suffer from moderate loss (1–2 mm/year) and the remaining 10% will not suffer any loss.

Some people find the removal of dental plaque from inflamed gumsto be uncomfortable. Bleeding and tenderness of the gums shouldgo away within 1 or 2 weeks of treatment. (Healthy gums are pinkand firm in appearance.)
You need to follow careful oral hygiene for your entire life orthe disorder may return.
Prevention
Daily oral hygiene measures to prevent periodontal diseaseinclude:
Brushing properly on a regular basis (at least twice daily),with the patient attempting to direct the toothbrushbristles underneath the gum-line, helps disrupt thebacterial-mycotic growth and formation of subgingivalplaque.
Flossing daily and using interdental brushes (if the spacebetween teeth is large enough), as well as cleaning behindthe last tooth, the third molar, in each quarter
Using an antiseptic mouthwash: Chlorhexidine gluconate-basedmouthwash in combination with careful oral hygiene may curegingivitis, although they cannot reverse any attachment lossdue to periodontitis.
Using periodontal trays to maintain dentist-prescribedmedications at the source of the disease: The use of traysallows the medication to stay in place long enough topenetrate the biofilms where the micro-organism are found.
Regular dental check-ups and professional teeth cleaning asrequired: Dental check-ups serve to monitor the person'soral hygiene methods and levels of attachment around teeth,identify any early signs of periodontitis, and monitorresponse to treatment.
Typically, dental hygienists (or dentists) use specialinstruments to clean (debride) teeth below the gumline anddisrupt any plaque growing below the gumline. This is a standard

treatment to prevent any further progress of establishedperiodontitis. Studies show that after such a professionalcleaning (periodontal debridement), microbial plaque tends togrow back to precleaning levels after about three to four months.Nonetheless, the continued stabilization of a patient'speriodontal state depends largely, if not primarily, on thepatient's oral hygiene at home, as well as on the go. Withoutdaily oral hygiene, periodontal disease will not be overcome,especially if the patient has a history of extensive periodontaldisease.
Periodontal disease and tooth loss are associated with anincreased risk, in male patients, of cancer.
Contributing causes may be high alcohol consumption or a diet lowin antioxidants.
Management
The cornerstone of successful periodontal treatment starts withestablishing excellent oral hygiene. This includes twice-dailybrushing with daily flossing. Also, the use of an interdentalbrush is helpful if space between the teeth allows. For smallerspaces, a product called "Soft Picks" is an excellent manualcleaning device. Persons with dexterity problems, such asarthritis, may find oral hygiene to be difficult and may requiremore frequent professional care and/or the use of a powered toothbrush. Persons with periodontitis must realize it is a chronicinflammatory disease and a lifelong regimen of excellent hygieneand professional maintenance care with a dentist/hygienist orperiodontist is required to maintain affected teeth.
Initial therapy
Removal of microbial plaque and calculus is necessary toestablish periodontal health. The first step in the treatment ofperiodontitis involves nonsurgical cleaning below the gumlinewith a procedure called scaling and debridement. In the past,

root planing was used (removal of cemental layer as well ascalculus). This procedure involves use of specialized curettes tomechanically remove plaque and calculus from below the gumline,and may require multiple visits and local anesthesia toadequately complete. In addition to initial scaling and rootplaning, it may also be necessary to adjust the occlusion (bite)to prevent excessive force on teeth that have reduced bonesupport. Also, it may be necessary to complete any other dentalneeds, such as replacement of rough, plaque-retentiverestorations, closure of open contacts between teeth, and anyother requirements diagnosed at the initial evaluation.
Reevaluation
Multiple clinical studies have shown nonsurgical scaling and rootplaning are usually successful if the periodontal pockets areshallower than 4–5 mm (0.16–0.20 in). The dentist or hygienistmust perform a re-evaluation four to six weeks after the initialscaling and root planing, to determine if the patient's oralhygiene has improved and inflammation has regressed. Probingshould be avoided then, and an analysis by gingival index shoulddetermine the presence or absence of inflammation. The monthlyreevaluation of periodontal therapy should involve periodontalcharting as a better indication of the success of treatment, andto see if other courses of treatment can be identified. Pocketdepths of greater than 5–6 mm (0.20–0.24 in) which remain afterinitial therapy, with bleeding upon probing, indicate continuedactive disease and will very likely lead to further bone lossover time. This is especially true in molar tooth sites wherefurcations (areas between the roots) have been exposed.
Surgery
If nonsurgical therapy is found to have been unsuccessful inmanaging signs of disease activity, periodontal surgery may beneeded to stop progressive bone loss and regenerate lost bonewhere possible. Many surgical approaches are used in treatment ofadvanced periodontitis, including open flap debridement and

osseous surgery, as well as guided tissue regeneration and bonegrafting. The goal of periodontal surgery is access fordefinitive calculus removal and surgical management of bonyirregularities which have resulted from the disease process toreduce pockets as much as possible. Long-term studies have shown,in moderate to advanced periodontitis, surgically treated casesoften have less further breakdown over time and, when coupledwith a regular post-treatment maintenance regimen, are successfulin nearly halting tooth loss in nearly 85% of patients.
Maintenance
Once successful periodontal treatment has been completed, with orwithout surgery, an ongoing regimen of "periodontal maintenance"is required. This involves regular checkups and detailedcleanings every three months to prevent repopulation ofperiodontitis-causing microorganism, and to closely monitoraffected teeth so early treatment can be rendered if diseaserecurs. Usually, periodontal disease exists due to poor plaquecontrol, therefore if the brushing techniques are not modified, aperiodontal recurrence is probable.
Alternative treatments
Periodontitis has an inescapable relationship with subgingivalcalculus (tartar). The first step in any procedure is toeliminate calculus under the gum line, as it houses destructiveanaerobic microorganisms that consume bone, gum and cementum(connective tissue) for food.
Most alternative “at-home” gum disease treatments involveinjecting antimicrobial solutions, such as hydrogen peroxide,into periodontal pockets via slender applicators or oralirrigators. This process disrupts anaerobic micro-organismcolonies and is effective at reducing infections and inflammationwhen used daily. A number of other products, functionallyequivalent to hydrogen peroxide, are commercially available, butat substantially higher cost. However, such treatments do not
address calculus formations, and so are short-lived, as anaerobicmicrobial colonies quickly regenerate in and around calculus.
Additionally, periodontitis can be treated in a noninvasivemanner by means of Periostat, an FDA-approved, orallyadministered drug that has been shown to reduce bone loss. Itsmechanism of action in part involves inhibition of matrixmetalloproteinases (such as collagenase), which degrade theextracellular matrix under inflammatory conditions. Thisultimately can lead to reduction of aveolar bone loss in patientswith periodontal disease (as well as patients withoutperiodontitis).
Epidemiology
Periodontitis is very common, and is widely regarded as thesecond most common disease worldwide, after dental decay, and inthe United States has a prevalence of 30–50% of the population,but only about 10% have severe forms.
Chronic periodontitis effects about 750 million people or about10.8% of the population as of 2010.
Like other conditions intimately related to access to hygiene andbasic medical monitoring and care, periodontitis tends to be morecommon in economically disadvantaged populations or regions. Itsoccurrence decreases with higher standard of living. In Israelipopulation, individuals of Yemenite, North-African, South Asian,or Mediterranean origin have higher prevalence of periodontaldisease than individuals from European descent.
In other animals
Periodontal disease is the most common disease found in dogs andaffects more than 80% of dogs aged three years or older. Itsprevalence in dogs increases with age, but decreases withincreasing body weight; i.e., toy and miniature breeds are moreseverely affected. Systemic disease may develop because the gums

are very vascular (have a good blood supply). The blood streamcarries these anaerobic micro-organisms, and they are filteredout by the kidneys and liver, where they may colonize and createmicroabscesses. The micro-organisms traveling through the bloodmay also attach to the heart valves, causing vegetativeendocarditis (infected heart valves). Additional diseases thatmay result from periodontitis include chronic bronchitis andpulmonary fibrosis.

AIM AND OBJECTIVE

AIM AND OBJECTIVE

REVIEW OF LITERATURE

REVIEW OF LITERATURE
AbstractPeriodontal disease is considered an inflammatory disorder thatdamages tissue through the complex interactions betweenperiodontopathic bacteria and host defense systems. It is likelythat the role of reactive oxygen species (ROS) is common to bothbacterial- and host-mediated pathways of tissue damage. In recentyears, there has been a tremendous expansion in the medical anddental research concerned with free radicals (FR), ROS andantioxidant defense mechanisms. This review is intended toprovide a critical up-to-date summary of the field withparticular emphasis on the evidence for oxidative damage andcompromised antioxidant status in periodontal diseases.
Periodontitis, an inflammatory disease, is considered to beinitiated and perpetuated by a small group of predominantly gram-negative, anaerobic or microaerophilic bacteria that colonize thesubgingival area. Bacteria cause the observed tissue destructiondirectly by toxic products and indirectly by activating hostdefense systems (i.e. inflammation).
Plasma Antioxidant Status in PeriodontalDiseases

In periodontal literature, early studies of individualantioxidant micronutrients were unconvincing in theirassociations between dietary antioxidant intake andperiodontitis. Few studies (Nishada et al 2000, Amarasena et al2005,Chapple et al 2007 that have explored individual antioxidantscavengers in serum or plasma have shown only mildly compromisedlevels in periodontitis subjects relative to healthy controls,except where smoking is a co-factor. Sobaniec and S Lotowska (2000) reported lower serum antioxidantenzyme levels in ligature-induced periodontitis in a rat model(15).Abnormally high levels of hydroperoxide and compromised serum co-enzyme Q10 and vitamin E were observed in Papillon-Lefèvresyndrome subjects, suggesting substantial oxidative stress inthese subjects and a potential role for specified antioxidanttherapies.An inverse relationship was found between serum vitamin Cconcentrations and antibody levels to porphyromonas gingivalis(Pussinen et al 2003) (12). Panjamurthy et al 16 observed lower plasma vitamin C, vitamin Eand reduced GHS in periodontitis subjects. However, antioxidantenzyme levels were raised and the authors attributed this to aprotective response to oxidative stress.Total antioxidant capacity (TAOC) concentration was found to bereduced in serum and plasma of periodontitis patients.Tamaki et al 17 observed a positive correlation between plasmaoxidative status and clinical attachment loss in patients in themaintenance phase of periodontal treatment. They suggested that asystemic increase in oxidative stress may influence the rate ofprogression of periodontal disease.Low levels of a number of carotenoids, in particular b-cryptoxanthin and b-carotene were found to be associated with anincreased prevalence of periodontitis in the year 60-70 year oldmen.Though, these studies reveal an antioxidant compromise in theplasma of periodontitis patients, the changes in antioxidantstatus lack relevance or significance, given their low

concentrations and rates of activity, relative to the antioxidantscavengers.
Salivary Antioxidant Status in PeriodontalDiseasesMoore et al 18 who were the first to explore salivary totalantioxidant activity found no difference in TAOC levels inperiodontitis and nonperiodontitis subjects. The predominantantioxidant component of saliva was uric acid (>70% ofantioxidant activity).However, Chapple et al 19 found lower total antioxidantconcentration in the saliva of periodontitis patients whencompared to periodontally healthy controls. Similar results wereobserved in a larger cohort study20 and in small case-controlstudies (Diab Ladki and Brock). Lower TAOC was reported in womenthan men. A higher level of protein carbonyls (oxidative stress)was found in periodontitis patients than in controls.Salivary antioxidant levels (SOD, GPX, reduced GHS, ascorbicacid, a-tocopherol) were observed to be lower in periodontitispatients as well as in patients under antiepileptic therapy withgingival hyperplasia.Markers of oxidative damage such as malondialdehyde 8-hydroxy-deoxy-guanosin were found to be higher in saliva of patients withperiodontitis which decreased following initial treatmentapproaching the mean control values.Overall, the relevance of saliva as a medium for assessingsurrogate markers of reactive oxygen and antioxidant species inperiodontitis patients must be open to question. Moreover, salivacontains GCF and the contribution of GCF antioxidants to salivawill vary according to the degree of salivary stimulation.
GCF Antioxidant Status in PeriodontalDiseasesGCF is the most appropriate fluid to sample when investigatingbiomarkers of tissue events in periodontium.

Guarnieri et al 22 observed spontaneous generation of superoxidein the GCF of periodontitis subjects, with no differences inantioxidant scavenging capacity between cases and controls.However, no difference was reported in the SOD activity in GCF ofperiodontitis subjects.Reduced GSH was the most important antioxidant in GCF with levels1,000-fold higher than paired plasma samples and wassignificantly lower in periodontitis relative to matched controlsubjects.The antioxidant enzyme GPX correlated negatively with pocketdepth and attachment loss and increased post therapy (Hung et al2000). However, significantly greater levels of GPX, lactoferrin,myeloperoxidase and IL-1b in the GCF were in periodontallydiseased sites when compared to healthy sites.Studies investigating oxidative stress and antioxidant statusboth locally and peripherally (in serum, saliva and GCF) inperiodontitis patients reported higher levels of malondialdehydeand total oxidant status, which decreased following Phase Itherapy.Tsai et al 21 reported a positive correlation between GCF lipidperoxidation and periodontopathogens and a negative correlationbetween GCF GPX and periodontopathogens. They concluded that theincreased levels of lipid peroxidation with decreased level ofantioxidants provided the evidence that oxidative stress, afterthe stimulation of periodontopathogens might play a role in thepathogenesis of periodontitis.A negative correlation between serum and GCF TAOC and gingivalinflammation was reported in miniature poodle dogs (Pavlica et al2004). Similarly, TAOC in the GCF of periodontitis subjects wassignificantly lower. Based on GCF studies, it can be concludedthat local antioxidant scavenging defenses are compromised inperiodontitis, but whether this represents a predisposition todisease or result from the inflammatory lesion is not clear.
Periodontal Tissue Antioxidant Status inPeriodontal Diseases
Gingivitis subjects exhibited higher levels of GSH in gingivaltissue samples when compared to controls (Giorgi et al, 1992).Tissue levels of CAT and SOD decreased with increasing pocketdepth in periodontitis patients scheduled for extractions.On the contrary, higher levels of SOD activity were observed inthe GCF and gingival tissue samples of Periodontitis patients.Smokers with periodontitis exhibited increased levels ofmetallothionein (a radical scavenging and preventive antioxidant)in the gingival tissue indicating a protective response to theincreased inflammation in these patients. Another study insmokers observed higher levels of HO-1 antioxidant enzyme levelsin smokers with periodontitis than in nonsmoker periodontitispatients. Higher levels of thiobarbituric acid reactivesubstances (TBARS), a marker of oxidative stress was found in thegingival tissue obtained from unresolved pockets following PhaseI therapy in patients with chronic periodontitis. In a similarstudy, Panjamurthy et al 14 also observed higher levels of TBARSand enzyme antioxidants with lower levels of scavengingantioxidants in the gingival tissue of periodontitis subjectswhen compared to controls.Recently, Borges et al 23 reported increased activities ofmyeloperoxidase, GPX, glutathione-S-transferase, oxidized GSH andhigher levels of TBARS in gingival tissue of chronicperiodontitis patients when compared to controls, suggesting acorrelation between oxidative stress biomarkers and periodontaldiseases. Biopsy studies are difficult to implement for ethicaland technical reasons, but the limited data so far confirm thepresence of more significant oxidative stress in the periodontaltissues of diseased periodontium relative to control tissue andthe apparent up regulation of antioxidant enzyme systems.
MATERIALS AND METHOD

MATERIALS AND METHODESTIMATION OF HYDROPEROXIDES 500µl of saliva samples were treated with chloroform: methanol(2:1) mixture, followed by vigorous vortexing. The samples werecentrifuged at 2000 rpm for 10 minutes. The upper aqueous layerobtained was discarded along with protein layer. The lowerchloroform layer was dried under a steam of nitrogen at 45˚C .The residue obtained was treated with potassium iodide andincubated in the dark for 6-8 minutes. After incubation, aceticacid: chloroform mixture (3:2) was added and followed by 0.25 %cadmium acetate. After each step vortexing was done. The mixturewas centrifuged at 2000 rpm for 10 minutes. The upper layer wastransferred into fresh tubes. Absorbance was read at 373 nm.
ESTIMATION OF PROTEIN CARBONYLDNPH method was described by Levine et al. (1990) with slightmodifications. Transfer 300 µl of sample to two test tubes. Onetube will be the sample and other will be the control tube. Add300 µl of DNPH to the sample tube. Incubate both tubes in thedark at room temperature for 1 hour. Vortex each tubes brieflyevery 15 minutes during the incubation. Add 1ml of 10% TCA toeach tube and vortex. Centrifuge tubes at 8000 rpm for 10 mintsat 4˚ C in a micro centrifuge. Discard the supernatant andresuspend the pellet in 1 ml of ethanol: ethyl acetate (1:1)mixture. Resuspend the protein pellets in 1 ml of guanidinehydrochloride by vortexing. Centrifuge the tubes at 10000 rpm for10 mints at 4 ˚C in a micro centrifuge to remove any leftoverdebris. The supernatant samples were collected. Measure theabsorbance at 360- 385 nm .Read against HCL blank.

TOTAL PROTEIN ESTIMATION0.2 ml of saliva samples were aliquoted to test tubes followed by5 ml of alkaline copper reagent. The solution was mixed well andincubated for 10 minutes followed by addition of 0.5ml of folinsreagent. A set of blank was also maintained with distilled wateras test solution. 0.5ml of Folins Ciocalteau reagent was added toall the tubes and incubated at room temperature for 30minutes indark. A set of standards were also performed in concentration of1m/ml.
ESTIMATION OF NITRATE LEVEL
0.5ml of saliva samples were taken as test solution and 0.1ml
of sulphosalicylic acid was added then vortex for 30 minutes
at room temperature. Centrifugation was done at 5000rpm for 15
minutes. To 200µl of supernatant, 30µl of 10% NaoH was added
followed by the addition of 300 µl Tris-Hcl buffer and mixed
well, to this 530µl Griess reagent was added and incubated in
dark for 10-15 minutes. The absorbance was read at 540nm.
ESTIMATION OF LIPID PEROXIDATION
Lipid per oxidation referred as theoxidative degradation of lipids. It was the process whereby free
radicals “steal” electrons from the lipids in the cell membrane
resulting in cell damage. This process proceeded by a free
radical often affected poly unsaturated fatty acids because they
contain multiple double bonds in between which lies methylene-

CH2 groups that poses especially reactive hydrolysis.
Polyunsaturated fatty acid peroxides generate malondialdehyde
(MDA) upon decomposition, and the measurement of MDA has been
used as an indicator of lipid peroxidation.
50µl of saliva samples were taken as test solution
and add 500µl of 70% alcohol and 1ml of 1% TBA were added. Then
all the tubes were kept in boiling water bath for 20 minutes.
After cooling to room temperature and added 50 µl of acetone to
all the test tubes and read absorbance at 535 nm in
spectrophotometer and the concentration of MDH was calculated by
using the extinction coefficient of MDH (1.56 × 105).
URIC ACID TEST
Procedure
Pipette intotubes marked
Blank Standard Test
Working Reagent 1000µl 1000µl 1000µl
Distilled water 20 µl - -Standard - 20 µl -Test - - 20 µlMix and incubate for 5 mints at 37 C. Read the absorbance of thestandard and each test at 505 nm. Read against reagent blank.
SDS-PAGE
SDS-PAGE is most widely used method for qualitatively analyzingany protein mixtures, monitoring protein purity and to determinethe molecular weight. It is based on the separation of proteinsaccording to their size and then locating them by binding to adye.
Glass plates used were cleaned and were assembled withappropriate spacers (1 mm). 5 ml of 12.5% resolving gel waspoured and covered with a layer of distilled water. Afterpolymerization, distilled water was removed and 2 ml of 5%stacking gel was poured and a comb was inserted. After 10-15minutes, the comb was carefully removed and the wells were washedwith water. The assembly was transferred to the electrophoresisapparatus.
20µl of sample was mixedwith 10µl of loading buffer and boiled for 10 minutes in aboiling water bath. The Protein marker [Genei, Bangalore] wasalso boiled for 10 minutes in a boiling water bath. 20µl of thesamples were added to wells, also protein marker was added to onewell. The apparatus was connected with power supply and turnedon. After the run, stacking gel was removed and stained in Ezeeblue.
RESULTS

RESULTSHYDRO PERIOXIDES
SAMPLE OD at 470nm S.DCONTROL 1 0.04
0.0481±0.017
CONTROL2 0.030CONTROL3 0.057CONTROL4 0.074CONTROL5 0.057CONTROL6 0.031
T1 0.044
0.1082±0.102T2 0.052T3 0.29T4 0.074T5 0.081

Category 1 Category 20
0.02
0.04
0.06
0.08
0.1
0.12
Series 1Series 2
PROTEIN CARBONYL TESTSAMPLE OD VALUECONTROL1 0.166
0.076±0.038
CONTROL2 0.O81CONTROL3 0.099CONTROL4 0.018CONTROL5 0.096CONTROL6 0.091
T1 0.038
0.049±0.025
T2 0.046T3 0.088T4 0.056T5 0.018
Category 1 Category 20
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
Series 1Series 2
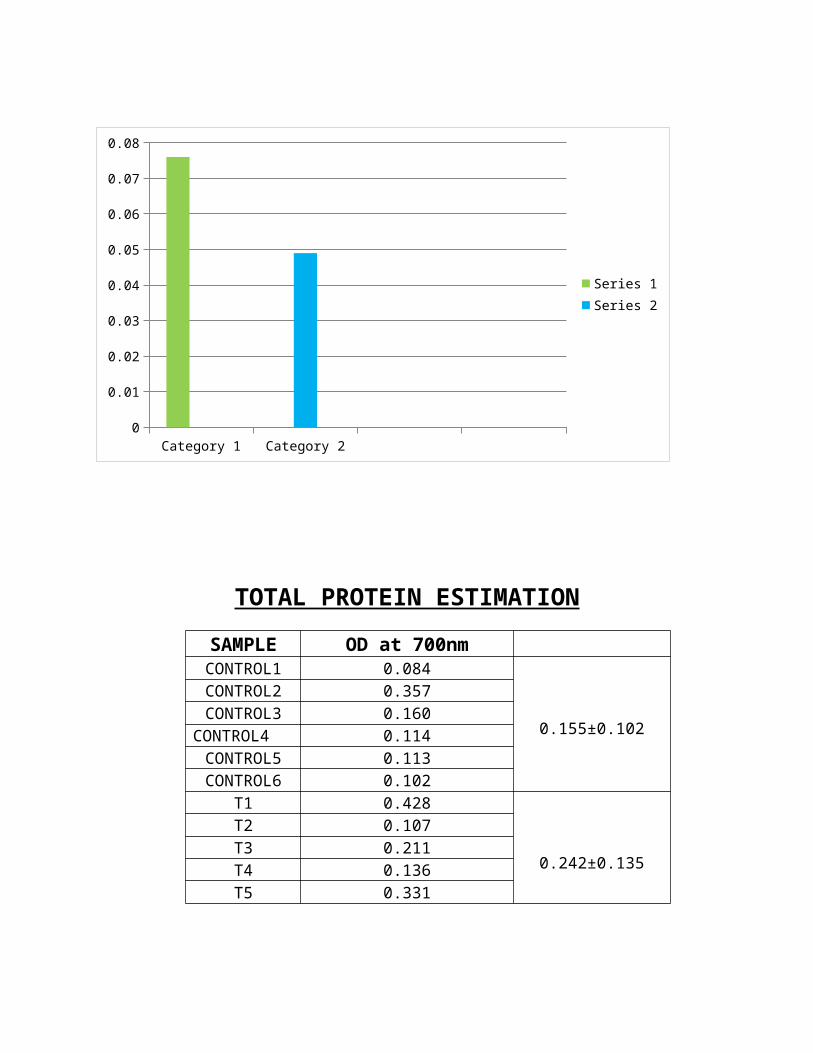
TOTAL PROTEIN ESTIMATIONSAMPLE OD at 700nmCONTROL1 0.084
0.155±0.102
CONTROL2 0.357CONTROL3 0.160
CONTROL4 0.114CONTROL5 0.113CONTROL6 0.102
T1 0.428
0.242±0.135
T2 0.107T3 0.211T4 0.136T5 0.331

Category 1 Category 20
0.2
0.4
0.6
0.8
1
1.2
Series 1Series 2
ESTIMATION OF NITRATE LEVELSAMPLE OD VALUECONTROL1 0.093
0.106±0.015
CONTROL2 0.082CONTROL3 0.121CONTROL4 0.110CONTROL5 0.112CONTROL6 0.119
T1 0.132T2
0.072
0.962±0.024T3 0.112T4 0.082T5 0.083
Category 1 Category 20
0.2
0.4
0.6
0.8
1
1.2
Series 1
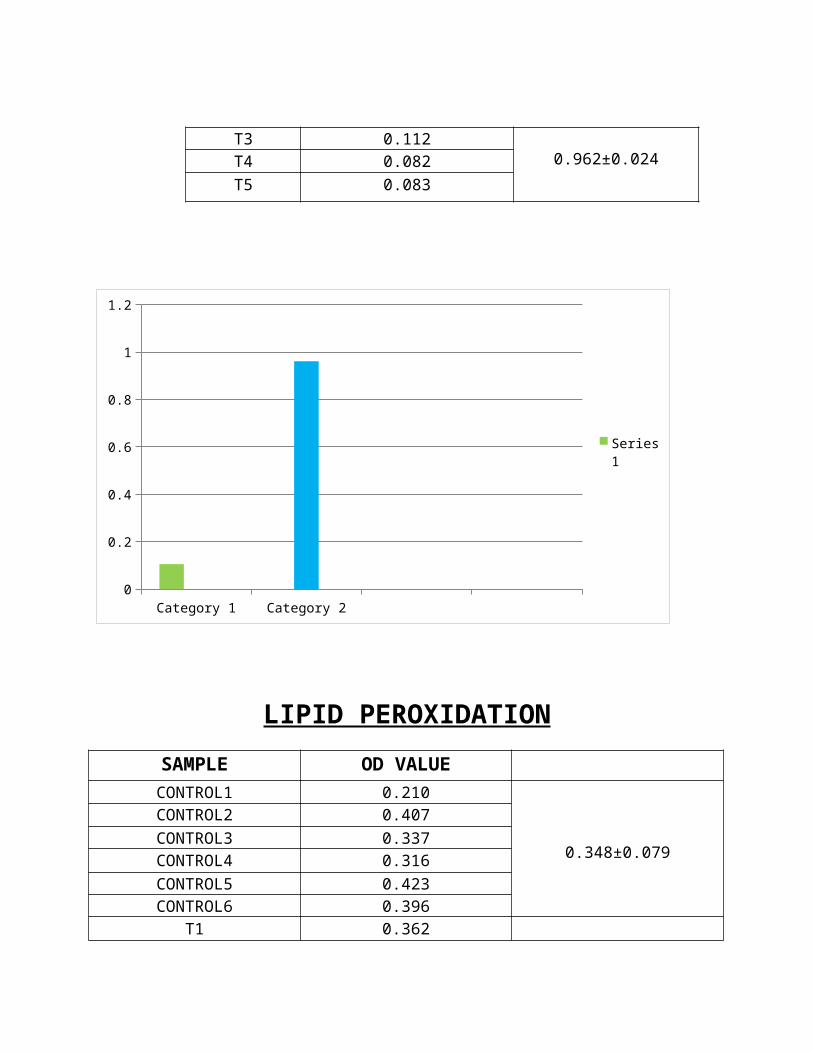
LIPID PEROXIDATIONSAMPLE OD VALUECONTROL1 0.210
0.348±0.079
CONTROL2 0.407CONTROL3 0.337CONTROL4 0.316CONTROL5 0.423CONTROL6 0.396
T1 0.362

0.349±0.029T2 0.299T3 0.355T4 0.370T5 0.362
Category 1 Category 20.3474
0.3476
0.3478
0.348
0.3482
0.3484
0.3486
0.3488
0.349
0.3492
Series 1Series 2
URIC ACID TESTSAMPLE OD VALUECONTROL1 0.263
0.258±0.161
CONTROL2 0.026CONTROL3 0.108CONTROL4 0.414CONTROL5 0.318CONTROL6 0.419
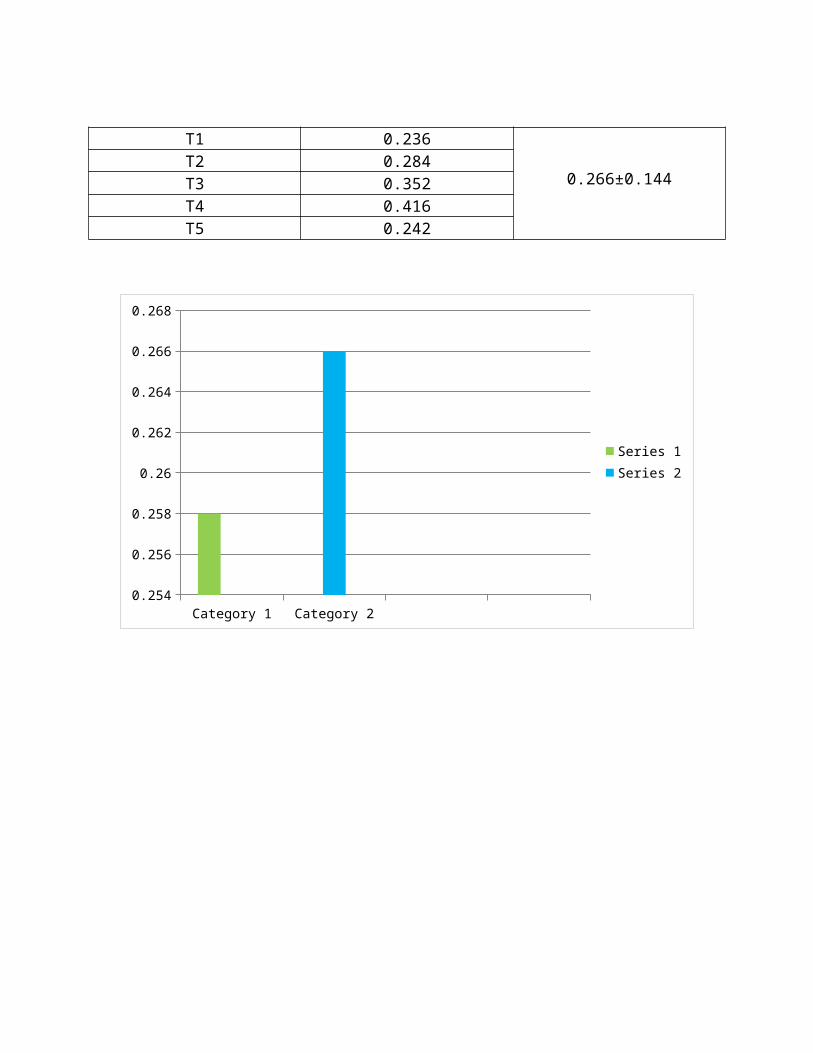
T1 0.236
0.266±0.144T2 0.284T3 0.352T4 0.416T5 0.242
Category 1 Category 20.254
0.256
0.258
0.26
0.262
0.264
0.266
0.268
Series 1Series 2

DISCUSSION
DISCUSSION


CONCLUSION

CONCLUSION

BIBLIOGRAPHY


BIBLIOGRAPHY1. Savage, Amir; Eaton, Kenneth A.; Moles, David R.; Needleman,
Ian (2009). "A systematic review of definitions ofperiodontitis and methods that have been used to identifythis disease". Journal of Clinical Periodontology 36 (6): 458–467.
2. Armitage, Gary C. (1999). "Development of a classificationsystem for periodontal diseases and conditions". Annals ofPeriodontology 4 (1). pp. 1–6..
3. D'Aiuto, Francesco; Parkar, Mohammed; Andreou, Georgios;Suvan, Hannu; Brett, Peter M.; Ready, Derren; Tonetti,Maurizio S. (2004). "Periodontitis and systemicinflammation: control of the local infection is associatedwith a reduction in serum inflammatory markers". J Dent Res 83(2): 156–160.
4. Nibali, Luigi; D'Aiuto, Francesco; Griffiths, Gareth;Patel, Kalpesh; Suvan, Jean; Tonetti, Maurizio S. (2007)."Severe periodontitis is associated with systemicinflammation and a dysmetabolic status: a case-controlstudy". Journal of Clinical Periodontology 34 (11): 931–7.
5. Paraskevas, Spiros; Huizinga, John D.; Loos, Bruno G.(2008). "A systematic review and meta-analyses on C-reactiveprotein in relation to periodontitis". Journal of ClinicalPeriodontology 35 (4): 277–290..
6. D'Aiuto, Francesco; Ready, Derren; Tonetti, Maurizio S.(2004). "Periodontal disease and C-reactive protein-associated cardiovascular risk". Journal of Periodontal Research 39(4): 236–241.
7. Pussinen PJ, Alfthan G, Jousilahti P, Paju S, Tuomilehto J(2007). "Systemic exposure to Porphyromonas gingivalispredicts incident stroke". Atherosclerosis 193 (1): 222–8.
8. Pussinen PJ, Alfthan G, Rissanen H, Reunanen A, AsikainenS, Knekt P (September 2004). "Antibodies to periodontalpathogens and stroke risk". Stroke 35 (9): 2020–3.
9. Pussinen PJ, Alfthan G, Tuomilehto J, Asikainen S,Jousilahti P (October 2004). "High serum antibody levels toPorphyromonas gingivalis predict myocardial infarction".European Journal of Cardiovascular Prevention & Rehabilitation 11 (5):408–11.
10. Ford PJ, Gemmell E, Timms P, Chan A, Preston FM,Seymour GJ (2007). "Anti-P. gingivalis response correlateswith atherosclerosis". J Dent Res 86 (1): 35–40.
11. Beck, James D.; Eke, Paul; Heiss, Gerardo; Madianos,Phoebus; Couper, David; Lin, Dongming; Moss, Kevin; Elter,John et al. (2005). "Periodontal Disease and Coronary HeartDisease : A Reappraisal of the Exposure". Circulation 112 (1):19–24.
12. Scannapieco, Frank A.; Bush, Renee B.; Paju, Susanna(2003). "Associations Between Periodontal Disease and Riskfor Atherosclerosis, Cardiovascular Disease, and Stroke. ASystematic Review". Annals of Periodontology 8 (1): 38–53.
13. Wu, Tiejian; Trevisan, Maurizio; Genco, Robert J.;Dorn, Joan P.; Falkner, Karen L.; Sempos, Christopher T.(2000). "Periodontal Disease and Risk of CerebrovascularDisease: The First National Health and Nutrition ExaminationSurvey and Its Follow-up Study". Archives of International Medicine160 (18): 2749–2755.
14. Beck, James D.; Elter, John R.; Heiss, Gerardo; Couper,David; Mauriello, Sally M.; Offenbacher, Steven (2001)."Relationship of Periodontal Disease to Carotid ArteryIntima-Media Wall Thickness : The Atherosclerosis Risk inCommunities (ARIC) Study". Arteriosclerosis, Thrombosis, and VascularBiology 21 (21): 1816–1822.

15. Chapple IL, Matthews JB. The role of reactive oxygenand antioxidant species in periodontal tissuedestruction.Periodontol 2000 2007; 43:160-232.
16. Panjamurthy K, Manoharan S, Ramachandran CR. Lipidperoxidation and antioxidant status in patients withperiodontitis. Cell Mol Biol Lett 2005; 10(2):255-64.
17.Tamaki N, Tomofuji T, Maruyama T, Ekuni D,Yamanaka R,Takeuchi N, et al. Relationship between periodontalcondition and plasma reactive oxygen metabolites in patientsin the maintenance phase of periodontal treatment. JPeriodontol 2008; 79(11):2136-42.
18.Moore S, Calder KA, Miller NJ, Rice-Evans CA. Antioxidantactivity of saliva and periodontal disease. Free Radic Res1994 ; 21(6):417-25.
19.Chapple IL, Mason GI, Garner I, Matthews JB, Thorpe GH,Maxwell SR, et al. Enhanced chemiluminescent assay formeasuring the total antioxidant capacity of serum, salivaand crevicular fluid. Ann Clin Biochem 1997; 34(Pt 4):412-21.
20.Sculley DV, Langley-Evans SC. Periodontal disease isassociated with lower antioxidant capacity in whole salivaand evidence of increased protein oxidation. Clin Sci (Lond)2003; 105(2):167-72.
21.Tsai CC, Chen HS, Ho YP, Ho KY, Wu YM, Hou GL.Periodontopathogens and oxidative stress in periodontaldiseases. Paper 0595, 81st General Session of InternationalAssociation for Dental Research June 25-28, 2003.
22. Guarnieri C, Zucchelli G, Bernardi F, Scheda M, ValentiniAF, Calandriello M. Enhanced superoxide production with nochange of the antioxidant activity in gingival fluid ofpatients with chronic adult periodontitis. Free Radic ResCommun 1991; 15(1):11-6.
23.Borges I Jr, Moreira EA, Filho DW, de Oliveira TB, da SilvaMB, Frõde TS. Proinflammatory and oxidative stress markersin patients with periodontal disease. Mediators Inflamm2007; 2007:45794.
APPENDIX
APPENDIXREAGENT PREPARATION
HYDRO PEROXIDES Cadmium Acetate (0.5%) - 3ml Chloroform : Methanol (2:1) -500µl Chloroform :Acetic acid (2:3) -1ml Pottassium Iodide (120%) -0.05ml
PROTEIN CARBONYL TEST 6M Guanidine
-1ml 10Mm DNPH dissolved in 2N HCL -300µl

1% TCA -1ml
Ethanol : Ethyle Acetate(1:1) -1ml
TOTAL PROTEIN ESTIMATION 2% Na2CO3 0.1N NAOH 1.56% CuSO4 2.37% Sodium Potassium Tartarate Folin – Ciocalteau Reagent
NITRATE LEVEL Sulphosalicyclic Acid - 0.1ml 10% NAOH - 30µl Griess Reagent - 530µl
1% Suphanilamide 2% Phosphoric Acid 0.1% Naphthyl Ethylene Diamine (NED)
Tris HCL -300µl
LIPID PEROXIDATION 70% Alcohol - 500µl Acetone - 50
µl 1% TBA - 1ml
0.25N HCL 15% TCA
1% TBA
URIC ACID Uric Acid Reagent




















