
Endothelial progenitor cells participate in nicotine-mediated angiogenesis
Upload
independentCategory
view
0download
0
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 2 December 2001726
Angiogenesis, the formation of new blood vessels fromexisting vasculature, is essential to the late stages ofcarcinogenesis, allowing tumours to grow beyond 1–2 mm in diameter, invade surrounding tissue, andmetastasise. However, more than two decades ago,angiogenesis that preceded neoplastic transformationwas seen. Indeed, it can be detected in inflammatoryand infectious diseases that increase the risk ofdeveloping cancer. Recent advances in fluorescenceendoscopy and histological assessment suggest that,for certain cancers, the degree of new blood-vesselformation may differ between the early and late stagesof carcinogenic progression. The association betweenangiogenesis and cancer occurrence, and ease ofdetection of this process in accessible tissues early incarcinogenesis, mean that angiogenesis fulfils thecriteria for a biomarker of the effectiveness ofchemopreventive intervention. There is also someevidence that biochemical assays of angiogenic growthfactors may offer similar potential as surrogatebiomarkers. Many natural and syntheticchemopreventive agents in development or in clinicaluse inhibit new vessel formation in vivo. Validation ofangiogenesis as a biomarker for the effectiveness ofchemoprevention should further the advancement ofsome chemopreventive agents. Lancet Oncol 2001; 2: 726–32
Angiogenesis, the formation of new blood vessels fromexisting vasculature (Figure 1), has been associated withneoplasia since the experiments of Greene, published in1941.1 Angiogenesis is critical to the transition ofpremalignant lesions in a hyperproliferative state to themalignant phenotype, which leads to tumour growth andmetastasis.2 The intensity of angiogenesis, as assessed bycounting of microvessels in neoplastic tissue (Figure 2), actsas a prognostic factor for many solid tumours such asbreast, prostate, and ovarian cancers,3–5 and very earlycancers of the endometrium and lung.6,7 Similarly,expression of angiogenic growth factors is associated withprognosis for lung and other cancers.8–10 Angiogenesisenables tumours to grow larger than 1–2 mm in diameter,invade surrounding tissue, and travel to distant sites in thebody (metastasise).2 In this review, we argue thatangiogenesis is not only relevant to preneoplastic stages ofcarcinogenesis, but also fulfils the criteria for a surrogatebiomarker of chemopreventive intervention in its ownright. In fact, angiogenesis is already targeted bychemopreventive agents at various stages of drugdevelopment or in clinical practice.
HistologyIncreased vascularity precedes neoplasia. In 1982, Ziche andGullino11 showed that several cell lines, including humanBALB/c fibroblasts, C57BL-MG epithelium, and Syriangolden hamster embryo cells, acquired the ability to inducenew capillary formation before neoplastic transformationoccurred. In these experiments, the cells were cultured invitro and then injected into rabbit cornea; capillaryformation was measured by slit-lamp stereomicroscopy andconfirmed by histology. Similar observations were made inhamster models of chemically induced carcinogenesis.12,13
Collectively, these data supported the idea that theacquisition of angiogenic capability by a previously non-angiogenic cell population may be associated with anincreased risk of neoplastic transformation. Around thesame time, Brem and colleagues reported that preneoplasticlesions of the human breast, when implanted onto the rabbitiris, stimulated the formation of capillaries that were ‘leaky’to fluorescein dye.14 Chodak and colleagues reported similarobservations using atypical cells from biopsies ofpremalignant human bladder lesions implanted onto rabbitirises.15 Using slit-lamp stereomicroscopy to investigate
Review Angiogenesis and chemoprevention
RAS, WPS, and KJO’B are at the Department of Oncology,University of Leicester Royal Infirmary, Leicester, UK. ALH isdirector of the Imperial Cancer Research Fund Medical OncologyUnit, Churchill Hospital, Oxford, UK. AGD is Director, Division ofOncology, Gastroenterology, Endocrinology and Metabolism, StGeorge’s Hospital Medical School, London, UK.
Correspondence: Dr Ricky Sharma, Oncology Department,University of Leicester, Leicester Royal Infirmary, Leicester, LE1 5WW, UK. Tel: + 44 (0) 116 252 5541. Fax: + 44 (0) 116 2525616. Email: [email protected]
Angiogenesis as a biomarker andtarget in cancer chemoprevention
Ricky A Sharma, Adrian L Harris, Angus G Dalgleish, William P Steward, and Kenneth J O’Byrne
Figure 1. Growing tubules immunostained with CD 31 representingimmature vessel formation.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 2 December 2001 727
normal skin, Polverini and colleagueshad already shown that new capillaryformation occurs during delayedhypersensitivity responses inguineapigs.16 Thus, before relevantgrowth factors and specific geneticabnormalities had been identified, itwas recognised that the ‘switch’ to anangiogenic phenotype involvedoverexpression of one or morepositive regulators of angiogenesis,mobilisation of proteins from theextracellular matrix, recruitment ofhost cells such as macrophages, or acombination of these processes.2
More recently, histological markersof angiogenesis have been linked todysplasia in human beings (Figure 2).Carcinoma in situ (CIS) denotes severedysplasia of epithelial tissue beforeinvasion of the basement membrane.17
In the cervix, significant increases inmicrovessel density (MVD) are seen asnormal cells progress through cervicalintraepithelial neoplasia stages I, II,and III to invasive squamous-cellcarcinoma.18 Similarly, increasedangiogenesis has been confirmedhistologically in lung metaplasia,dysplasia, and CIS,19,20 in breast ductalCIS,21 and in Barrett’s oesophagus incomparison with normal tissue.22
Recent advances in fluorescenceendoscopy have improved thesensitivity and reproducibility ofangiogenesis detection in premalignant tissue.23 Thistechnique has been used to identify abnormal areas ofbronchial epithelium in smokers who are at high risk ofdeveloping lung cancer. Immunohistochemical analysis ofthese areas shows a unique lesion, consisting of capillaryblood vessels close to, and projecting into, metaplastic ordysplastic squamous bronchial epithelium, known asangiogenic squamous dysplasia (ASD). MVD wassubstantially increased, compared with normal mucosa, inhyperplastic and metaplastic epithelium, and in ASD.Interestingly, ASD was not detected in normal, non-smokingcontrols. The presence of this lesion in high-risk smokerssuggests that unusual patterns of neovascularisation may beuseful biomarkers for the identification of early stages ofbronchial carcinogenesis.23
Unlike cervix and lung tissues, colonic epithelium doesnot undergo squamous metaplasia before the developmentof intraepithelial neoplasia, but instead becomeshyperplastic directly.17 In hyperproliferative human colonicepithelium, angiogenesis has been detected at the same timeas the earliest signs of focal dysplasia, and MVD increasesgradually through the transition from low-grade to high-grade dysplasia and cancer.24 In rats with chemically induced,multistage skin carcinogenesis, the angiogenic ‘switch’ is avery early event, occurring during focal hyperplasia.25
Other features that predispose individuals to thedevelopment of malignant disease have also been associatedwith angiogenesis. Examples include many viral infections,including human herpes virus 8 (HHV8), hepatitis C, andhuman immunodeficiency virus (HIV), and several chronicinflammatory conditions associated with the developmentof tumours, including cigarette smoking, asbestos exposure,and liver cirrhosis (Figure 2).26–33 These observations suggesta role for angiogenesis in carcinogenesis, before the onset ofmetaplasia and hyperplasia. They also imply that theprocesses resulting in chronic immune activation provide anenvironment that facilitates the development of malignantdisease.34 Interestingly, MVD in normal liver tissue canpredict tumour recurrence in patients undergoingpotentially curative resection for hepatocellular carcinoma.27
Angiogenic growth factors An alternative approach to studying angiogenesis involvesgrowth factors necessary for new blood-vessel formation. Inestablished malignant disease, angiogenic growth factors maybe released directly, by tumour cells themselves, or indirectly,via recruitment of other cells such as macrophages andendothelial cells.2 The initial release of these substances, orevidence of complex formation between angiogenic growthfactors and high-affinity receptors, can be referred to as an
ReviewAngiogenesis and chemoprevention
Figure 2. Immunohistochemical demonstration of angiogenesis in human tissues in a potentiallypreneoplastic phase or at different stages of carcinogenesis. Panels A, B, and C are sections fromcirrhotic liver, a colorectal adenoma, and a superficial bladder cancer, respectively. They are stainedwith an antibody to CD34 (QB-END/10) to show blood vessels. In Panel D, an epithelioidmesothelioma is shown stained with an antibody to CD31, which labels endothelial cells and variouscellular components of whole blood.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 2 December 2001728
angiogenic ‘switch’.2 This stage can beinduced by several processes, includinghypoxia, or may result from alterationsin the genes (mutations or changes inexpression) involved in the promotionand progression stages of car-cinogenesis, eg RAS and P53.35,36 Thecapacity of malignant cells to induceangiogenesis is associated with theproduction of these growth factors,37
and peripheral-blood concentrationsmay correlate with MVD in someprimary tumours.38
The expression of angiogenicgrowth factors may also be increasedin preneoplastic tissue (Figure 3),although interpretation of experi-mental results is complicated by theconstitutive expression of growthfactors in normal epithelia34 andinducible expression in acute disease.39
In rats with chemically inducedcancer, concentrations of vascularendothelial growth factor (VEGF) areincreased in simple hyperplasia of thebladder40 and pituitary gland;41 VEGFproduction may be a rate-limiting stepin the development of premalignantskin lesions.42 Similar evidence fromtransgenic mice with skin cancersuggests a role for matrix metal-loproteinase 9 (MMP9).43 In hamsterbuccal pouch keratinocytes, studies ofthe angiogenic growth factor,transforming growth factor �1 (TGF�1), imply that angio-inhibitoryactivity is lost at the earliest stages ofcarcinogenesis.44 High expression ofVEGF, especially under hypoxicconditions has been seen in studies ofliver cirrhosis and hepatitis B virusinfection, which both predispose individuals tohepatocarcinogenesis.27,32 Similarly, HIV and HHV 8, bothimplicated in the development of Kaposi’s sarcoma, causethe production of factors that promote angiogenesis.30,31
There is also convincing evidence in CIS of humancervix, oesophagus, and breast tissues that overexpression ofVEGF or platelet-derived endothelial-cell growth factor(PDEGF) occurs.18,22,45,46 In human bronchus, significantincreases in VEGF expression have been detected inspecimens representative of the transition from normalepithelium through moderate dysplasia to CIS.20 Highconcentrations of growth factors have been found indysplastic adenomas, which are precursors of colorectalcancer.24,34 In one study, VEGF expression was absent in mildto moderately dysplastic adenomas of the colorectum,present in the majority of CIS, and present in all colorectalcarcinomas invading the submucosa.47
Similarly, increasing levels of expression of MMPs andtissue inhibitors of MMP (TIMPs) have been described in
many lesions as they progress from dysplasia through CISand to invasive carcinoma, including those of the breast,lung, and prostate.34,47,48 Increased expression of MMP 2 andmembrane-type MMPs, which both facilitate tumourinvasion and angiogenesis, has been shown in colorectalpreneoplasia.37 This association is particularly strong foradenomas that overexpress the cyclo-oxygenase COX 2enzyme.34
COX 2 is the inducible form of the enzyme that catalysesprostaglandin and thromboxane formation fromarachidonic acid. COX 2, and its isozyme COX 1, areinvolved in the induction of angiogenesis in humanendothelial cells cultured with colon cancer cells.37
Overexpression of COX 2 has been implicated in thetumorigenesis of cancers of the colon, rectum, stomach,lung, breast, and head and neck.34 COX activity seems toconfer a survival advantage to transformed cells through theinhibition of apoptosis, enhanced cell proliferation, reducedcell-to-cell adhesion, increased adherence of cells to the
Review Angiogenesis and chemoprevention
PRO
GR
ESS
ION
PR
OM
OTI
ON
INIT
IATI
ON
Normalepithelium
Predisposingconditions
Metaplasia
Hyperplasia
Mild-moderatedysplasia
Severedysplasia
Invasivecarcinoma
Metastasis
Smoking
Viralinfection
Cirrhosis
MICROVESSEL DENSITY (MVD)
VEGF
MMPs
INC
REA
SED
EXP
RES
SIO
N
TIMPs
Intraepithelialneoplasia
Intra-mucosalcapillaryloops
Carcinomain situ
MVD
MVD
Figure 3. Multistep model of carcinogenesis (modified from 60). Whereas metaplasia andhyperplasia may be reactive and frequently regress, dysplasia is characterised by more advancedmolecular changes and persists for many years. Black arrows indicate detection at the earliest stageof the multistep model, and for some measures of angiogenesis (broken lines) increasing expressionhas been observed within or across subsequent stages (see text). VEGF, vascular endothelial growthfactor; MMPs, matrix metalloproteinases; TIMPs, tissue inhibitors of matrix metalloproteinases.
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 2 December 2001 729
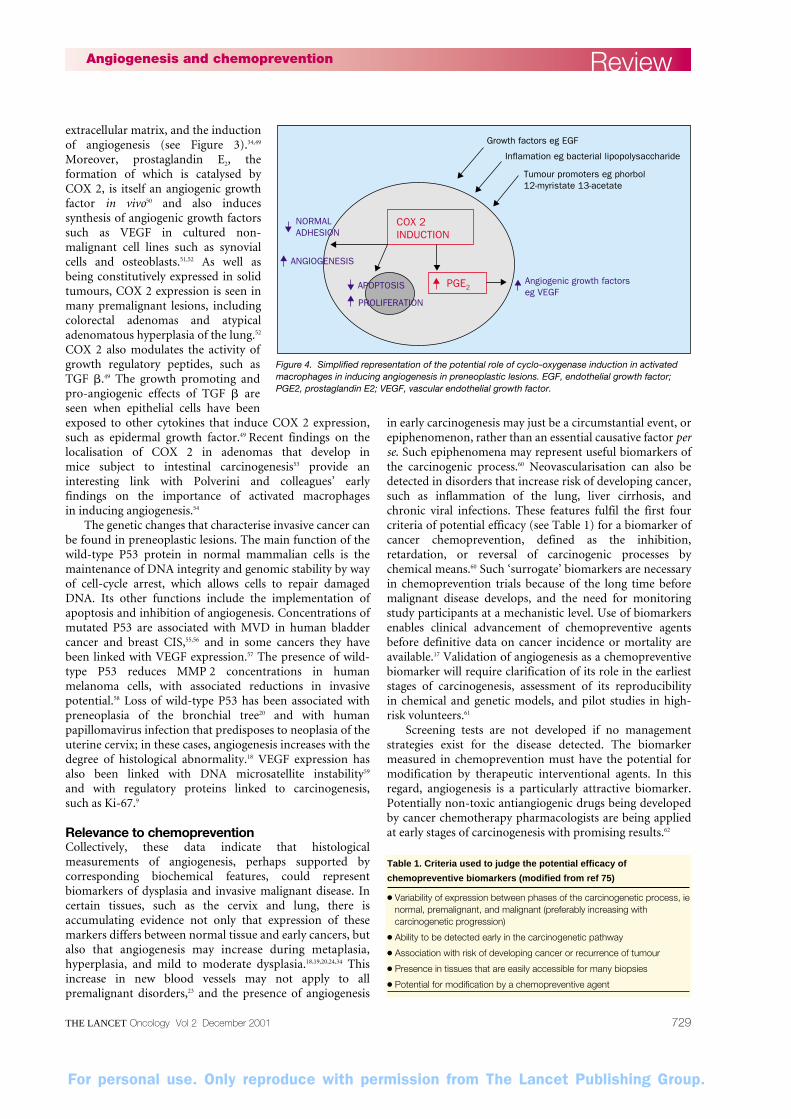
extracellular matrix, and the inductionof angiogenesis (see Figure 3).34,49
Moreover, prostaglandin E2, theformation of which is catalysed byCOX 2, is itself an angiogenic growthfactor in vivo50 and also inducessynthesis of angiogenic growth factorssuch as VEGF in cultured non-malignant cell lines such as synovialcells and osteoblasts.51,52 As well asbeing constitutively expressed in solidtumours, COX 2 expression is seen inmany premalignant lesions, includingcolorectal adenomas and atypicaladenomatous hyperplasia of the lung.52
COX 2 also modulates the activity ofgrowth regulatory peptides, such asTGF �.49 The growth promoting andpro-angiogenic effects of TGF � areseen when epithelial cells have beenexposed to other cytokines that induce COX 2 expression,such as epidermal growth factor.49 Recent findings on thelocalisation of COX 2 in adenomas that develop in mice subject to intestinal carcinogenesis53 provide aninteresting link with Polverini and colleagues’ early findings on the importance of activated macrophages in inducing angiogenesis.54
The genetic changes that characterise invasive cancer canbe found in preneoplastic lesions. The main function of thewild-type P53 protein in normal mammalian cells is themaintenance of DNA integrity and genomic stability by wayof cell-cycle arrest, which allows cells to repair damagedDNA. Its other functions include the implementation ofapoptosis and inhibition of angiogenesis. Concentrations ofmutated P53 are associated with MVD in human bladdercancer and breast CIS,55,56 and in some cancers they havebeen linked with VEGF expression.57 The presence of wild-type P53 reduces MMP 2 concentrations in humanmelanoma cells, with associated reductions in invasivepotential.58 Loss of wild-type P53 has been associated withpreneoplasia of the bronchial tree20 and with humanpapillomavirus infection that predisposes to neoplasia of theuterine cervix; in these cases, angiogenesis increases with thedegree of histological abnormality.18 VEGF expression hasalso been linked with DNA microsatellite instability59
and with regulatory proteins linked to carcinogenesis, such as Ki-67.9
Relevance to chemopreventionCollectively, these data indicate that histologicalmeasurements of angiogenesis, perhaps supported bycorresponding biochemical features, could representbiomarkers of dysplasia and invasive malignant disease. Incertain tissues, such as the cervix and lung, there isaccumulating evidence not only that expression of thesemarkers differs between normal tissue and early cancers, butalso that angiogenesis may increase during metaplasia,hyperplasia, and mild to moderate dysplasia.18,19,20,24,34 Thisincrease in new blood vessels may not apply to allpremalignant disorders,23 and the presence of angiogenesis
in early carcinogenesis may just be a circumstantial event, orepiphenomenon, rather than an essential causative factor perse. Such epiphenomena may represent useful biomarkers ofthe carcinogenic process.60 Neovascularisation can also bedetected in disorders that increase risk of developing cancer,such as inflammation of the lung, liver cirrhosis, andchronic viral infections. These features fulfil the first fourcriteria of potential efficacy (see Table 1) for a biomarker ofcancer chemoprevention, defined as the inhibition,retardation, or reversal of carcinogenic processes bychemical means.60 Such ‘surrogate’ biomarkers are necessaryin chemoprevention trials because of the long time beforemalignant disease develops, and the need for monitoringstudy participants at a mechanistic level. Use of biomarkersenables clinical advancement of chemopreventive agentsbefore definitive data on cancer incidence or mortality areavailable.17 Validation of angiogenesis as a chemopreventivebiomarker will require clarification of its role in the earlieststages of carcinogenesis, assessment of its reproducibility in chemical and genetic models, and pilot studies in high-risk volunteers.61
Screening tests are not developed if no managementstrategies exist for the disease detected. The biomarkermeasured in chemoprevention must have the potential formodification by therapeutic interventional agents. In thisregard, angiogenesis is a particularly attractive biomarker.Potentially non-toxic antiangiogenic drugs being developedby cancer chemotherapy pharmacologists are being appliedat early stages of carcinogenesis with promising results.62
ReviewAngiogenesis and chemoprevention
Table 1. Criteria used to judge the potential efficacy of
chemopreventive biomarkers (modified from ref 75)
● Variability of expression between phases of the carcinogenetic process, ienormal, premalignant, and malignant (preferably increasing withcarcinogenetic progression)
● Ability to be detected early in the carcinogenetic pathway
● Association with risk of developing cancer or recurrence of tumour
● Presence in tissues that are easily accessible for many biopsies
● Potential for modification by a chemopreventive agent
Growth factors eg EGF
Inflamation eg bacterial lipopolysaccharide
Tumour promoters eg phorbol 12-myristate 13-acetate
Angiogenic growth factorseg VEGF
NORMALADHESION
ANGIOGENESIS
APOPTOSIS
PROLIFERATION
COX 2INDUCTION
PGE2
Figure 4. Simplified representation of the potential role of cyclo-oxygenase induction in activatedmacrophages in inducing angiogenesis in preneoplastic lesions. EGF, endothelial growth factor;PGE2, prostaglandin E2; VEGF, vascular endothelial growth factor.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 2 December 2001730
Furthermore, many chemopreventive agents at variousstages of development appear to inhibit angiogenesis.Epidemiological evidence suggests that aspirin63 andcaptopril64 use is associated with a lower risk of malignantdisease. Aspirin is significantly antiangiogenic in vivo,37
although its chemopreventive effectiveness may depend oncellular factors such as P53 status.65 Captopril also hasantiangiogenic activity, via inhibition of zinc-dependentendothelial-cell gelatinase MMP activity.66 Tamoxifen andcelecoxib, which were recently licensed for certain well-defined populations of patients by the US Food and DrugAdministration for the chemoprevention of breast andcolorectal cancers, respectively,61 also have antiangiogenicproperties in xenograft models.37,67 Finally, the dietaryconstituents and potential cancer chemopreventives,selenium, N-acetyl cysteine, vitamin D3, curcumin,genistein and related flavonoids, and the tea constituentepigallocatechin-3-gallate have all been shown to inhibitangiogenesis in vivo without causing toxic effects.68–73 Thepleiotropic activity of each of these phytochemicals at morethan one level within cellular pathways61 may avoidpotentially proangiogenic consequences of selectiveinhibition of one angiogenic growth factor, as shownrecently in transgenic mice with abnormalities of MMP 7and MMP 9 production.74 Current clinical trials of naturaland synthetic agents as chemopreventives60 are not atpresent measuring biomarkers of angiogenesis.
ConclusionAngiogenesis seems to be present in many disorders thatpredispose individuals to cancer and during the stages ofcarcinogenesis that precede CIS. Improvements inendoscopic techniques, histological assessment, and assaysof angiogenic growth factors will allow further clarificationof these findings. Early indications suggest that angiogenesismay fulfil the criteria for a suitable biomarker of the efficacyof chemopreventive intervention. Most notably, itsassociation with risk of cancer occurrence or recurrence, itsdetectability in accessible tissues early in carcinogenesis, andits differential expression during various stages ofcarcinogenesis, support this idea. Furthermore, theangiogenic process may be modified by potentialchemopreventive agents such as aspirin, celecoxib,tamoxifen, and epigallocatechin-3-gallate. We suggestmonitoring angiogenesis as a biomarker in metaplastic andhyperplastic lesions in preneoplastic or premalignantconditions such as Barrett’s oesophagus, colorectaladenomas, and ASD. Validation of this biomarker may
facilitate the development of new synthetic drugs andpromising phytochemicals in cancer chemoprevention.
AcknowledgmentsWe acknowledge the support of the Imperial Cancer Research Fund,the Institute of Cancer Studies, Leicester, UK, and the UniversityHospitals of Leicester Research Funding Group. RAS would like tothank Clare Winfield for renumbering the references and Sue Spriggsfor checking their accuracy. KOB thanks Jonathan Goddard, John Edwards, and Diana Cullen for help with Figure 1.
References1 Greene HSN. Heterologous transplantation of mammalian tumors.
The transfer of human tumors to alien species. J Exp Med 1941; 73:461–86.
2 Folkman J. Clinical applications of research on angiogenesis. N EnglJ Med 1995; 333: 1757–63.
3 Fox SB, Leek RD, Weekes MP, Whitehouse RM, Gatter KC, Harris AL. Quantitation and prognostic value of breast cancerangiogenesis: comparison of microvessel density, Chalkley count,and computer image analysis. J Pathol 1995; 177: 275–83.
4 Weidner N, Carroll PR, Flax J, et al. Tumor angiogenesis correlateswith metastasis in invasive prostate carcinoma. Am J Pathol 1993;143: 401–09.
5 Brustmann H, Riss P, Naude S. The relevance of angiogenesis inbenign and malignant epithelial tumors of the ovary: a quantitativehistological study. Gynecol Oncol 1997; 67: 20–26.
6 Giatromanolaki A, Sivridis E, Koukourakis MI, et al. Intratumoralangiogenesis: a new prognostic indicator for stage I endometrialadenocarcinomas? Oncol Res 1999; 11: 205–12.
7 Chiba Y, Taniguchi T, Matsuyama K, et al. Tumor angiogenesis,apoptosis and p53 oncogene in stage I lung adenocarcinoma. Surg Today 1999; 29: 1148–53.
8 O’Byrne KJ, Koukourakis MI, Giatromanolaki A, et al. Vascularendothelial growth factor, platelet-derived endothelial cell growthfactor and angiogenesis in non-small-call lung cancer. Br J Cancer2000; 82: 1427–32.
9 Maeda K, Kang SM, Onoda N, et al. Expression of P53 and vascularendothelial growth factor associated with tumor angiogenesis andprognosis in gastric cancer. Oncology 1998; 55: 594–99.
10 van Triest B, Pinedo HM, Blaauwgeers JL, et al. Prognostic role ofthymidylate synthase, thymidine phosphorylase/platelet-derivedendothelial cell growth factor, and proliferation markers incolorectal cancer. Clin Cancer Res 2000; 6: 1063–72.
11 Ziche M, Gullino PM. Angiogenesis and neoplastic progression invitro. J Natl Cancer Inst 1982; 69: 483–87.
12 Ferguson JW, Smillie AC. Vascularization of premalignant lesionsin carcinogen-treated hamster cheek pouch. J Natl Cancer Inst 1979;63: 1383–92.
13 Polverini PJ, Solt DB. Expression of angiogenic phenotype by asubpopulation of keratinocytes derived from 7,12-dimethylbenz[a]anthracene-initiated hamster buccal pouchepithelium. Carcinogenesis 1988; 9: 117–22.
14 Brem SS, Jensen HM, Gullino PM. Angiogenesis as a marker ofpreneoplastic lesions of the human breast. Cancer 1978; 41: 239–44.
15 Chodak GW, Haudenschild CC, Gittles RF, Folkman J. Angiogenicactivity as a marker of neoplastic and preneoplastic lesions of thehuman bladder. Ann Surg 1980; 192: 762–71.
16 Polverini PJ, Cotran RS, Sholley MM. Endothelial proliferation inthe delayed hypersensitivity reaction: an autoradiographic study. J Immunol 1977; 118: 529–32.
17 Boone CW, Kelloff GJ, Steele VE. Natural history of intraepithelialneoplasia in humans with implications for cancer chemopreventionstrategy. Cancer Res 1992; 52: 1651–59.
18 Dobbs SP, Hewett PW, Johnson IR, Carmichael J, Murray JC.Angiogenesis is associated with vascular endothelial growth factorexpression in cervical intraepithelial neoplasia. Br J Cancer 1997; 76:1410–15.
19 Fisseler-Eckhoff A, Rothstein D, Muller KM. Neovascularisation inhyperplastic, metaplastic and potentially preneoplastic lesions of thebronchial mucosa. Virchows Arch 1996; 429: 95–100.
20 Fontanini G, Calcinai A, Boldrini L, et al. Modulation ofneoangiogenesis in bronchial preneoplastic lesions. Oncol Rep 1999;6: 813–17.
21 Engels K, Fox SB, Whitehouse RM, Gatter KC, Harris AL. Up-regulation of thymidine phosphorylase expression is associated witha discrete pattern of angiogenesis in ductal carcinomas in situ of thebreast. J Pathol 1997; 182: 414–20.
Review Angiogenesis and chemoprevention
Search strategy and selection criteriaPublished data for this review were identified by searchesof Web of Science and MEDLINE among papers publishedin peer-reviewed journals (English language only) from1966 to January 2001. Keywords used: angiogenesis,neovascularisation, chemoprevention, cancer, carcino-genesis, neoplasia, malignancy, premalignancy, andpreneoplasia. We have attempted to select original articlesrather than reviews or commentaries, where possible.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 2 December 2001 731
22 Couvelard A, Paraf F, Gratio V, et al. Angiogenesis in the neoplasticsequence of Barrett’s oesophagus: correlation with VEGFexpression. J Pathol 2000; 192: 14–18.
23 Keith RL, Miller YE, Gemmill RM, et al. Angiogenic squamousdysplasia in bronchi of individuals at high risk for lung cancer. ClinCancer Res 2000; 6: 1616–25.
24 Aotake T, Lu CD, Chiba Y, Muraoka R, Tanigawa N. Changes ofangiogenesis and tumor cell apoptosis during colorectalcarcinogenesis. Clin Cancer Res 1999; 5: 135–42.
25 Bolontrade MF, Stern MC, Binder RL, et al. Angiogenesis is an earlyevent in the development of chemically induced skin tumors.Carcinogenesis 1998; 19: 2107–13.
26 Mazzanti R, Messerini L, Monsacchi L, et al. Chronic viral hepatitisinduced by hepatitis C but not hepatitis B virus infection correlateswith increased liver angiogenesis. Hepatology 1997; 25: 229–34.
27 El-Assal ON, Yamanoi A, Soda Y, et al. Clinical significance ofmicrovessel density and vascular endothelial growth factorexpression in hepatocellular carcinoma and surrounding liver:possible involvement of vascular endothelial growth factor in theangiogenesis of cirrhotic liver. Hepatology 1998; 27: 1554–62.
28 Bielefeldt-Ohmann H, Jarnicki AG, Fitzpatrick DR. Molecularpathobiology and immunology of malignant mesothelioma. J Pathol 1996; 178: 369–78.
29 Shibata M, Morizane T, Uchida T, et al. Irregular regeneration ofhepatocytes and the risk of hepatocellular carcinoma in chronichepatitis and cirrhosis with hepatitis-C-virus infection. Lancet 1998;351: 1773–77.
30 Albini A, Barillari G, Benelli R, et al. Angiogenic properties ofhuman immunodeficiency virus type 1 Tat protein. Proc Natl AcadSci USA 1995; 92: 4838–42.
31 Bais C, Santomasso B, Coso O, et al. G-protein coupled receptor ofKaposi’s sarcoma-associated herpesvirus is a viral oncogene andangiogenesis activator. Nature 1998; 391: 86–89.
32 Lee SW, Lee YM, Bae SK, Murakami S, Yun Y, Kim KW. Humanhepatitis B virus X protein is a possible mediator of hypoxia-induced angiogenesis in hepatocarcinogenesis. Biochem Biophys ResCommun 2000; 268: 456–61.
33 Mayne ST, Buenconsejo J, Janerich DT. Previous lung disease andrisk of lung cancer among men and women nonsmokers. Am JEpidemiol 1999; 149: 13–20.
34 O’Byrne KJ, Dalgleish AG, Browning MJ, Steward WP, Harris AL.The relationship between angiogenesis and the immune response incarcinogenesis and the progression of malignant disease. Eur JCancer 2000; 36: 151–69.
35 Rak J, Filmus J, Finkenzeller G, Grugel S, Marme D, Kerbel RS.Oncogenes as inducers of tumor angiogenesis. Cancer MetastasisRev 1995; 14: 263–77.
36 Chiarugi V, Magnelli L, Gallo O. Cox-2, iNOS and p53 as play-makers of tumor angiogenesis. Int J Mol Med 1998; 2: 715–19.
37 Tsujii M, Kawano S, Tsuji S, Sawaoka H, Hori M, DuBois RN.Cyclooxygenase regulates angiogenesis induced by colon cancercells. Cell 1998; 93: 705–16.
38 Ito N, Kawata S, Tamura S, et al. Positive correlation of plasmatransforming growth factor-beta 1 levels with tumor vascularity inhepatocellular carcinoma. Cancer Lett 1995; 89: 45–48.
39 Akiyoshi F, Sata M, Suzuki H, et al. Serum vascular endothelialgrowth factor levels in various liver diseases. Dig Dis Sci 1998; 43:41–45.
40 Wakui S, Furusato M, Sasaki S, et al. Expression of vascularendothelial growth factor in N-butyl-N-(4-hydroxybutyl)nitrosamine-induced rat bladder carcinogenesis. Vet Pathol 1999; 26: 111–16.
41 Banerjee SK, Sarkar DK, Weston AP, De A, Campbell DR. Overexpression of vascular endothelial growth factor and its receptorduring the development of estrogen-induced rat pituitary tumorsmay mediate estrogen-initiated tumor angiogenesis. Carcinogenesis1997; 18: 1155–61.
42 Larcher F, Murillas R, Bolontrade M, Conti CJ, Jorcano JL.VEGF/VPF overexpression in skin of transgenic mice inducesangiogenesis, vascular hyperpermeability and accelerated tumordevelopment. Oncogene 1998; 17: 303–11.
43 Coussens LM, Raymond WW, Bergers G, et al. Inflammatory mastcells upregulate angiogenesis during squamous epithelialcarcinogenesis. Genes Dev 1999; 13: 1382–97.
44 Lingen MW, DiPetro LA, Solt DB, Bouck NP, Polverini PJ. Theangiogenic switch in hamster buccal pouch keratinocytes isdependent on TGF�-1 and is unaffected by ras activation.Carcinogenesis 1997; 18: 329–38.
45 Brown LF, Berse B, Jackman RW, et al. Expression of vascular
permeability factor (vascular endothelial growth factor) and itsreceptors in breast cancer. Hum Pathol 1995; 26: 86–91.
46 Dobbs SP, Brown LPJ, Ireland D, et al. Platelet-derived endothelialcell growth factor expression and angiogenesis in cervicalintraepithelial neoplasia and squamous cell carcinoma of the cervix.Ann Diagn Pathol 2000; 4: 286–92.
47 Kondo Y, Arii S, Furutani M, et al. Implication of vascularendothelial growth factor and p53 status for angiogenesis innoninvasive colorectal carcinoma. Cancer 2000; 88: 1820–27.
48 Karameris A, Panagou P, Tsilalis T, Bouros D. Association ofexpression of metalloproteinases and their inhibitors with themetastatic potential of squamous-cell lung carcinomas: a molecularand immunohistochemical study. Am J Respir Crit Care Med 1997;156: 1930–36.
49 Saha D, Datta PK, Sheng H, et al. Synergistic induction ofcyclooxygenase-2 by transforming growth factor-beta1 andepidermal growth factor inhibits apoptosis in epithelial cells.Neoplasia 1999; 1: 508–17.
50 Benefield J, Petruzzelli GJ, Fowler S, Taitz A, Kalkanis J, Young MR.Regulation of the steps of angiogenesis by human head and necksquamous cell carcinomas. Invasion Metastasis 1996; 16: 291–301.
51 Ben-Av P, Crofford LJ, Wilder RL, Hla T. Induction of vascularendothelial growth factor expression in synovial fibroblasts byprostaglandin E and interleukin-1: a potential mechanism forinflammatory angiogenesis. FEBS Lett 1995; 372: 83–87.
52 Hosomi Y, Yokose T, Hirose Y, et al. Increased cyclooxygenase 2(COX-2) expression occurs frequently in precursor lesions ofhuman adenocarcinoma of the lung. Lung Cancer 2000; 30:73–81.
53 Hull MA, Booth JK, Tisbury A, et al. Cyclooxygenase 2 isupregulated and localized to macrophages in the intestine of Minmice. Br J Cancer 1999; 79: 1399–1405.
54 Polverini PJ, Cotran RS, Gimbone MA Jr, Unanue ER. Activatedmacrophages induce vascular proliferation. Nature 1977; 269:804–06.
55 Bochner BH, Esrig D, Groshen S, et al. Relationship of tumorangiogenesis and nuclear p53 accumulation in invasive bladdercancer. Clin Cancer Res 1997; 3: 1615–22.
56 Zolota V, Gerokosta A, Melachrinou M, et al. Microvessel density,proliferating activity, p53 and bcl-2 expression in in situ ductalcarcinoma of the breast. Anticancer Res 1999; 19: 3269–74.
57 Giatromanolaki A, Koukourakis MI, Kakolyris S, et al. Vascularendothelial growth factor, wild-type p53, and angiogenesis in earlyoperable non-small cell lung cancer. Clin Cancer Res 1998; 4:3017–24.
58 Toschi E, Rota R, Antonini A, Melillo G, Capogrossi MC. Wild-typep53 gene transfer inhibits invasion and reduces matrixmetalloproteinae-2 levels in p53-mutated human melanoma cells. J Invest Dermatol 2000; 114: 1188–94.
59 Wynter CV, Simms LA, Buttenshaw RL, et al. Angiogenic factorVEGF is decreased in human colorectal neoplasms showing DNAmicrosatellite instability. J Pathol 1999; 189: 319–25.
60 Sharma RA, Manson MM, Gescher A, Steward WP. Colorectalcancer chemoprevention: biochemical targets and clinicaldevelopment of promising agents. Eur J Cancer 2001; 37: 12–22.
61 Gescher AJ, Sharma RA, Steward WP. Cancer chemoprevention bydietary constituents: a salutary tale of failure and promise. LancetOncol 2001; 2: 371–79.
62 Bergers G, Javaherian K, Lo KM, Folkman J, Hanahan D. Effects ofangiogenesis inhibitors on multistage carcinogenesis in mice.Science 1999; 284: 808–12.
63 Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Ascherio A,Willett WC. Aspirin use and the risk for colorectal cancer andadenoma in male health professionals. Ann Intern Med 1994; 121:241–46.
64 Lever AF, Hole DJ, Gillis CR, et al. Do inhibitors of angiotensin-I-converting enzyme protect against the risk of cancer? Lancet 1998;352: 179–84.
65 Shao J, Fujiwara T, Kadowaki Y, et al. Overexpression of the wild-type p53 gene inhibites NF-kappa B activity and synergizes withaspirin to induce apoptosis in human colon cancer cells. Oncogene2000; 19: 726–36.
66 Volpert OV, Ward WF, Lingen MW, et al. Captopril inhibitsangiogenesis and slows the growth of experimental tumors in rats. J Clin Invest 1996; 98: 671–79.
67 Lindner DJ, Borden EC. Effects of tamoxifen and interferon-beta orthe combination on tumor-induced angiogenesis. Int J Cancer 1997;71: 456–61.
68 Jiang C, Jiang W, Ip C, Ganther H, Lu J. Selenium-induced
ReviewAngiogenesis and chemoprevention

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 2 December 2001732
inhibition of angiogenesis in mammary cancer at chemopreventivelevels of intake. Mol Carcinog 1999; 26: 213–25.
69 Cai T, Fassina G, Morini M, et al. N-acetylcysteine inhibitsendothelial cell invasion and angiogenesis. Lab Invest 1999; 79:1151–59.
70 Iseki K, Tatsuta M, Uehara H, et al. Inhibition of angiogenesis as amechanism for inhibition by 1-alpha-hydroxyvitamin D3 and 1,25-dihydroxyvitamin D3 of colon carcinogenesis induced byazoxymethane in Wistar rats. Int J Cancer 1999; 81: 730–33.
71 Arbiser JL, Klauber N, Rohan R, et al. Curcumin is an in vivoinhibitor of angiogenesis. Mol Med 1998; 4: 376–83.
72 Barnes S, Peterson TG, Coward L. Rationale for use of genistein-
containing soy matrices in chemoprevention trials for breast andprostate cancer. J Cell Biochem 1995; 58 (suppl 22): 181–87.
73 Cao Y, Cao R. Angiogenesis inhibited by drinking tea. Nature 1999;398: 381.
74 Pozzi A, Moberg PE, Miles LA, et al. Elevated matrixmetalloprotease and angiostatin levels in integrin alfa 1 knockoutmice cause reduced tumor vascularization. Proc Natl Acad Sci 2000;97: 2202–07.
75 Einspahr JG, Alberts DS, Gapstur SM, Bostick RM, Emerson SS,Gerner EW. Surrogate end-point biomarkers as measures of coloncancer risk and their use in cancer chemoprevention trials. CancerEpidemiol Biomarkers Prev 1997; 6: 37–48.
Review Angiogenesis and chemoprevention
Copyright © 2022 FDOKUMEN




















