Analysis of case management programs for patients with dementia: A systematic review
11
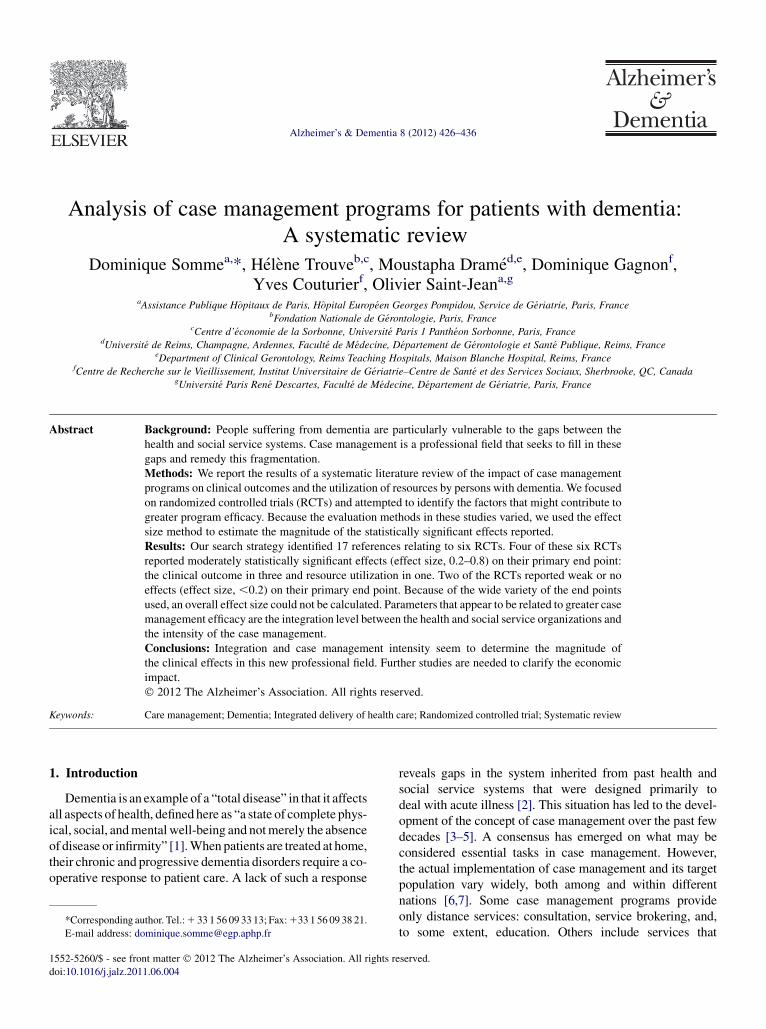
Analysis of case management programs for patients with dementia: A systematic review Dominique Somme a, *,H el ene Trouve b,c , Moustapha Dram e d,e , Dominique Gagnon f , Yves Couturier f , Olivier Saint-Jean a,g a Assistance Publique H^ opitaux de Paris, H^ opital Europ een Georges Pompidou, Service de G eriatrie, Paris, France b Fondation Nationale de G erontologie, Paris, France c Centre d’ economie de la Sorbonne, Universit e Paris 1 Panth eon Sorbonne, Paris, France d Universit e de Reims, Champagne, Ardennes, Facult e de M edecine, D epartement de G erontologie et Sant e Publique, Reims, France e Department of Clinical Gerontology, Reims Teaching Hospitals, Maison Blanche Hospital, Reims, France f Centre de Recherche sur le Vieillissement, Institut Universitaire de G eriatrie–Centre de Sant e et des Services Sociaux, Sherbrooke, QC, Canada g Universit e Paris Ren e Descartes, Facult e de M edecine, D epartement de G eriatrie, Paris, France Abstract Background: People suffering from dementia are particularly vulnerable to the gaps between the health and social service systems. Case management is a professional field that seeks to fill in these gaps and remedy this fragmentation. Methods: We report the results of a systematic literature review of the impact of case management programs on clinical outcomes and the utilization of resources by persons with dementia. We focused on randomized controlled trials (RCTs) and attempted to identify the factors that might contribute to greater program efficacy. Because the evaluation methods in these studies varied, we used the effect size method to estimate the magnitude of the statistically significant effects reported. Results: Our search strategy identified 17 references relating to six RCTs. Four of these six RCTs reported moderately statistically significant effects (effect size, 0.2–0.8) on their primary end point: the clinical outcome in three and resource utilization in one. Two of the RCTs reported weak or no effects (effect size, ,0.2) on their primary end point. Because of the wide variety of the end points used, an overall effect size could not be calculated. Parameters that appear to be related to greater case management efficacy are the integration level between the health and social service organizations and the intensity of the case management. Conclusions: Integration and case management intensity seem to determine the magnitude of the clinical effects in this new professional field. Further studies are needed to clarify the economic impact. Ó 2012 The Alzheimer’s Association. All rights reserved. Keywords: Care management; Dementia; Integrated delivery of health care; Randomized controlled trial; Systematic review 1. Introduction Dementia is an example of a “total disease” in that it affects all aspects of health, defined here as “a state of complete phys- ical, social, and mental well-being and not merely the absence of disease or infirmity” [1]. When patients are treated at home, their chronic and progressive dementia disorders require a co- operative response to patient care. A lack of such a response reveals gaps in the system inherited from past health and social service systems that were designed primarily to deal with acute illness [2]. This situation has led to the devel- opment of the concept of case management over the past few decades [3–5]. A consensus has emerged on what may be considered essential tasks in case management. However, the actual implementation of case management and its target population vary widely, both among and within different nations [6,7]. Some case management programs provide only distance services: consultation, service brokering, and, to some extent, education. Others include services that *Corresponding author. Tel.: 1 33 1 56 09 33 13; Fax: 133 1 56 09 38 21. E-mail address: [email protected] 1552-5260/$ - see front matter Ó 2012 The Alzheimer’s Association. All rights reserved. doi:10.1016/j.jalz.2011.06.004 Alzheimer’s & Dementia 8 (2012) 426–436
-
Upload
univ-reims -
Category
Documents
-
view
6 -
download
0
Transcript of Analysis of case management programs for patients with dementia: A systematic review
Alzheimer’s & Dementia 8 (2012) 426–436
Analysis of case management programs for patients with dementia:A systematic review
Dominique Sommea,*, H�el�ene Trouveb,c, Moustapha Dram�ed,e, Dominique Gagnonf,Yves Couturierf, Olivier Saint-Jeana,g
aAssistance Publique Hopitaux de Paris, Hopital Europ�een Georges Pompidou, Service de G�eriatrie, Paris, FrancebFondation Nationale de G�erontologie, Paris, France
cCentre d’�economie de la Sorbonne, Universit�e Paris 1 Panth�eon Sorbonne, Paris, FrancedUniversit�e de Reims, Champagne, Ardennes, Facult�e de M�edecine, D�epartement de G�erontologie et Sant�e Publique, Reims, France
eDepartment of Clinical Gerontology, Reims Teaching Hospitals, Maison Blanche Hospital, Reims, FrancefCentre de Recherche sur le Vieillissement, Institut Universitaire de G�eriatrie–Centre de Sant�e et des Services Sociaux, Sherbrooke, QC, Canada
gUniversit�e Paris Ren�e Descartes, Facult�e de M�edecine, D�epartement de G�eriatrie, Paris, France
Abstract Background: People suffering from dementia are particularly vulnerable to the gaps between the
*Corresponding au
E-mail address: do
1552-5260/$ - see fro
doi:10.1016/j.jalz.201
health and social service systems. Case management is a professional field that seeks to fill in thesegaps and remedy this fragmentation.Methods: We report the results of a systematic literature review of the impact of case managementprograms on clinical outcomes and the utilization of resources by persons with dementia. We focusedon randomized controlled trials (RCTs) and attempted to identify the factors that might contribute togreater program efficacy. Because the evaluation methods in these studies varied, we used the effectsize method to estimate the magnitude of the statistically significant effects reported.Results: Our search strategy identified 17 references relating to six RCTs. Four of these six RCTsreported moderately statistically significant effects (effect size, 0.2–0.8) on their primary end point:the clinical outcome in three and resource utilization in one. Two of the RCTs reported weak or noeffects (effect size, ,0.2) on their primary end point. Because of the wide variety of the end pointsused, an overall effect size could not be calculated. Parameters that appear to be related to greater casemanagement efficacy are the integration level between the health and social service organizations andthe intensity of the case management.Conclusions: Integration and case management intensity seem to determine the magnitude ofthe clinical effects in this new professional field. Further studies are needed to clarify the economicimpact.� 2012 The Alzheimer’s Association. All rights reserved.
Keywords: Care management; Dementia; Integrated delivery of health care; Randomized controlled trial; Systematic review
1. Introduction
Dementia is an example of a “total disease” in that it affectsall aspects of health, defined here as “a state of complete phys-ical, social, andmentalwell-being and notmerely the absenceof disease or infirmity” [1].When patients are treated at home,their chronic and progressive dementia disorders require a co-operative response to patient care. A lack of such a response
thor. Tel.:1 33 1 56 09 33 13; Fax:133 1 56 09 38 21.
nt matter � 2012 The Alzheimer’s Association. All rights r
1.06.004
reveals gaps in the system inherited from past health andsocial service systems that were designed primarily todeal with acute illness [2]. This situation has led to the devel-opment of the concept of case management over the past fewdecades [3–5]. A consensus has emerged on what may beconsidered essential tasks in case management. However,the actual implementation of case management and its targetpopulation vary widely, both among and within differentnations [6,7]. Some case management programs provideonly distance services: consultation, service brokering, and,to some extent, education. Others include services that
eserved.

D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436 427
require a close clinical relationship with the individual:assessment, monitoring, and setting up a service plan. It isalso possible to distinguish between team case management[8,9], where a coactive interdisciplinary group performsthe case management function, and individual casemanagement [10,11], where one professional is identified asthe person’s case manager, although this manager may stillbe part of a team. This diversity emerges in a wide variety ofcaseloads (from 7 to 300 cases per case manager). Theability of case managers to implement the service plan alsovaries greatly from one program to another [12–14]. Inaddition, the professional background of the case managercan differ greatly [6]. The common goal of these services isto deliver an individualized, simple, flexible, and adaptableresponse to people’s needs, especially when the health and/or social situation is complex. With the efficacy of case man-agement a complex end point, it is difficult tomeasure successon a single scale. We have adopted here a pragmatic strategyin which efficacy can be evaluated by how studies reporttheir primary end point: the effect size.
The questions this literature review attempts to answerare as follows:
� Has case management for persons with dementia beenproven to be effective in randomized controlled trials(RCTs)?
� Which outcomes have shown case management to beeffective in RCTs for persons with dementia?
� Which aspects of service programs (functions, team orindividual case management, caseload, professionalbackground of the case manager, case managementintensity, and target population) might explain varia-tions in their efficacy?
� Might the integration level of the system organizationexplain variations in program efficacy?
2. Methods
The systematic review presented here was undertakenvoluntarily by one of the authors and was not preregisteredas a protocol. The method used meets the criteria in the Pre-ferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for systematic reviews [15].
2.1. Definition of case management
As stated earlier, there is a general consensus that caseman-agement process includes the following tasks [6,12,13,16,17]: case identification, standardized multidimensionalassessment, individualized plan, implementation of this plan,and monitoring and reassessment of the plan.
2.2. Variations in terminology
It is often difficult to differentiate between case manage-ment, care management, and disease management programs.The purpose of the first, case management, is to cover all of
the person’s biopsychosocial dimensions, regardless of thearea of need, and to include all health and social services.The second term, care management, seems to be used synon-ymously with case management [18,19]. Finally, diseasemanagement focuses on optimal management of the chronicdisease for which there are specific guidelines (e.g., heartfailure, diabetes). However, in the case of incapacitatingdiseases, the disease manager’s function may be exactlythe same as that of the case/care manager and is usuallyreferred to as “care coordination” [18,19]. The onlydiscernable difference between case management anddisease management then lies in the eligibility criterion, i.e.,whether a specific disease is present. The Medical SubjectHeadings term “patient care management” includes both theconcept of care management and the concepts of casemanagement and disease management, which appear below“care management” in the hierarchy of keywords. Thisexplains the choice of keywords in our systematic search(see Table 1).
2.3. Search strategy and selection of articles
Our systematic search strategy focused exclusively onpublished articles referenced in databases accessible onlinein April 2009 (n5 9), summarized in Table 1, which presentsthe databases consulted in chronological order. The searchstrategy was adapted to each database on the basis of its the-saurus whenever possible. After reading the abstract, weretained only the following:
� RCTs reporting the results of longitudinal follow-up bycase management (care management, case manage-ment, or disease management involving at least thefunctions of assessment, individualized plan, and mon-itoring)
� Patients with Alzheimer’s disease and associated disor-ders (dementia)
� Patients who were not institutionalized� With the implementation of a case management pro-
gram, the only difference between control and experi-mental groups
The length of follow-up was not a selection criterion. Allstudies, regardless of the outcomes examined, were includedin the systematic review. We had planned to select only arti-cles with an English abstract, but this criterion did notexclude any study. Even when there were several articlesabout the same program, we retained all the articles relatingto the whole sample studied and pooled the results for eachRCT. Post hoc studies on part of a sample were not retained.We included all the references available in the databasessearched, regardless of the publication date.
2.4. Data collection
The datawere collected by a single reviewer with no inter-rater verification of the selection strategy and only from
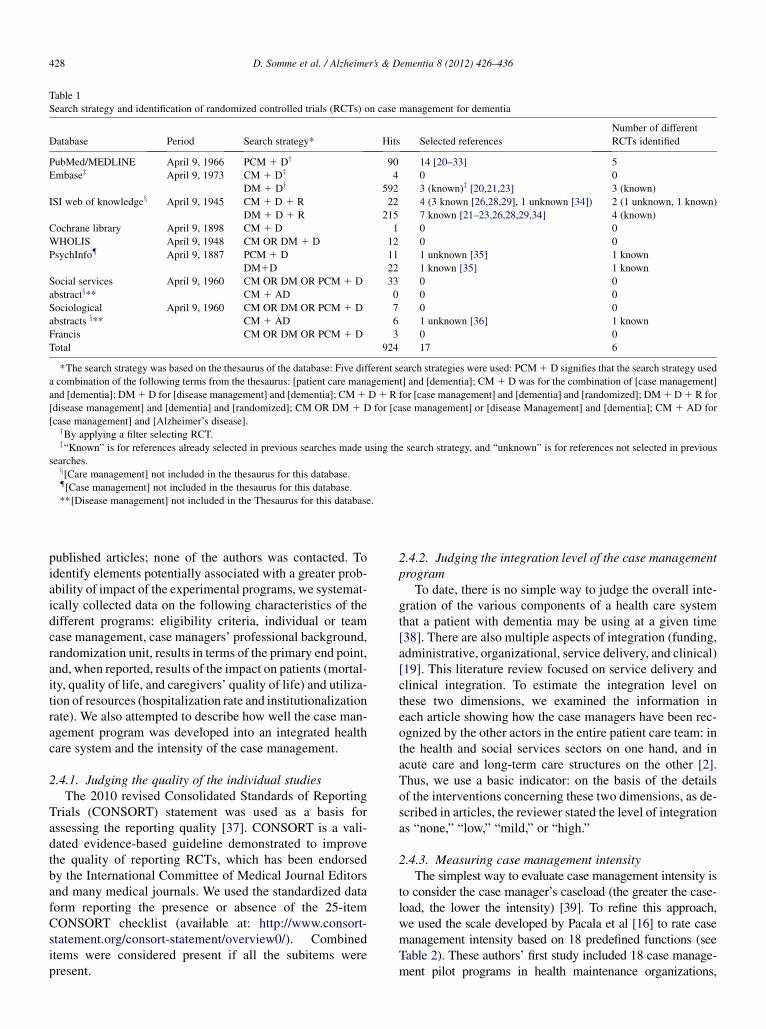
Table 1
Search strategy and identification of randomized controlled trials (RCTs) on case management for dementia
Database Period Search strategy* Hits Selected references
Number of different
RCTs identified
PubMed/MEDLINE April 9, 1966 PCM 1 Dy 90 14 [20–33] 5
Embasez April 9, 1973 CM 1 Dy 4 0 0
DM 1 Dy 592 3 (known)z [20,21,23] 3 (known)
ISI web of knowledgex April 9, 1945 CM 1 D 1 R 22 4 (3 known [26,28,29], 1 unknown [34]) 2 (1 unknown, 1 known)
DM 1 D 1 R 215 7 known [21–23,26,28,29,34] 4 (known)
Cochrane library April 9, 1898 CM 1 D 1 0 0
WHOLIS April 9, 1948 CM OR DM 1 D 12 0 0
PsychInfo{ April 9, 1887 PCM 1 D 11 1 unknown [35] 1 known
DM1D 22 1 known [35] 1 known
Social services
abstractx**April 9, 1960 CM OR DM OR PCM 1 D 33 0 0
CM 1 AD 0 0 0
Sociological
abstracts x**April 9, 1960 CM OR DM OR PCM 1 D 7 0 0
CM 1 AD 6 1 unknown [36] 1 known
Francis CM OR DM OR PCM 1 D 3 0 0
Total 924 17 6
*The search strategy was based on the thesaurus of the database: Five different search strategies were used: PCM1 D signifies that the search strategy used
a combination of the following terms from the thesaurus: [patient care management] and [dementia]; CM1 D was for the combination of [case management]
and [dementia]; DM1D for [disease management] and [dementia]; CM1D1 R for [case management] and [dementia] and [randomized]; DM1D1 R for
[disease management] and [dementia] and [randomized]; CM OR DM 1 D for [case management] or [disease Management] and [dementia]; CM 1 AD for
[case management] and [Alzheimer’s disease].yBy applying a filter selecting RCT.z“Known” is for references already selected in previous searches made using the search strategy, and “unknown” is for references not selected in previous
searches.x[Care management] not included in the thesaurus for this database.{[Case management] not included in the thesaurus for this database.
**[Disease management] not included in the Thesaurus for this database.
D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436428
published articles; none of the authors was contacted. Toidentify elements potentially associated with a greater prob-ability of impact of the experimental programs, we systemat-ically collected data on the following characteristics of thedifferent programs: eligibility criteria, individual or teamcase management, case managers’ professional background,randomization unit, results in terms of the primary end point,and, when reported, results of the impact on patients (mortal-ity, quality of life, and caregivers’ quality of life) and utiliza-tion of resources (hospitalization rate and institutionalizationrate). We also attempted to describe how well the case man-agement program was developed into an integrated healthcare system and the intensity of the case management.
2.4.1. Judging the quality of the individual studiesThe 2010 revised Consolidated Standards of Reporting
Trials (CONSORT) statement was used as a basis forassessing the reporting quality [37]. CONSORT is a vali-dated evidence-based guideline demonstrated to improvethe quality of reporting RCTs, which has been endorsedby the International Committee of Medical Journal Editorsand many medical journals. We used the standardized dataform reporting the presence or absence of the 25-itemCONSORT checklist (available at: http://www.consort-statement.org/consort-statement/overview0/). Combineditems were considered present if all the subitems werepresent.
2.4.2. Judging the integration level of the case managementprogram
To date, there is no simple way to judge the overall inte-gration of the various components of a health care systemthat a patient with dementia may be using at a given time[38]. There are also multiple aspects of integration (funding,administrative, organizational, service delivery, and clinical)[19]. This literature review focused on service delivery andclinical integration. To estimate the integration level onthese two dimensions, we examined the information ineach article showing how the case managers have been rec-ognized by the other actors in the entire patient care team: inthe health and social services sectors on one hand, and inacute care and long-term care structures on the other [2].Thus, we use a basic indicator: on the basis of the detailsof the interventions concerning these two dimensions, as de-scribed in articles, the reviewer stated the level of integrationas “none,” “low,” “mild,” or “high.”
2.4.3. Measuring case management intensityThe simplest way to evaluate case management intensity is
to consider the case manager’s caseload (the greater the case-load, the lower the intensity) [39]. To refine this approach,we used the scale developed by Pacala et al [16] to rate casemanagement intensity based on 18 predefined functions (seeTable 2). These authors’ first study included 18 case manage-ment pilot programs in health maintenance organizations,
Table 2
Analysis of the intensity of case management in the 6 randomized controlled trials (RCTs) according to the Pacala’s scale [16]
Pacala’s scale items RCT 1 RCT 2 RCT 3 RCT 4 RCT 5 RCT 6
Each case manager Intensive program Nonintensive program
1. Works with ,60 clients (caseload)
2. Spends at least 50% of his/her time face-to-
face with clients
3. Does the initial eligibility assessment him/
herself
4. Personally communicates with primary
care physician (and his/her team)
5. Organizes multidisciplinary teammeetings
6. Puts in place the services provided by the
organization that employs him/her (i.e.,
health maintenance organization: HMO)
7. Puts in place the services that the client
pays for directly
8. Puts in place the services that an
organization other than the one that
employs him/her pays for
9. Helps the client make decisions regarding
care
10. Helps the client express decisions
11. Participates in educating clients about
health problems
12. Provides advice to individuals (social
work)
13. Provides advice to families (social work)
14. Meets with the client regularly
15. Monitors the client’s situation via home
visits
16. Monitors the client’s situation by having
him/her come in for a consultation
17. Works with clients being institutionalized
18. Works with clients during hospitalization
Number of criteria (/18) 12 14 5 2 9 12 6
D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436 429
whichwere classified using an intensity scale. Ten of these pro-jects were classified as having low intensity—that is, they metbetween 3 and 11 of the scale’s criteria, whereas 8 were classi-fiedashigh intensity: theymetbetween13and16of the criteria.
2.5. Statistical analysis
The outcome criteria of the various studies were different,as were the measurement methods used. In this context andto evaluate the magnitude of the effects reported by the dif-ferent programs, we considered the results that were statisti-
cally significant in the original publication and recalculatedthem using the effect size method. The effect size was calcu-lated for the different end points in the various studies. Forthe quantitative criteria, Cohen method [40] was used tocalculate the effect size:
Effect size5jm12m2j=s
where m1 and m2 represent the means of the interventiongroup and control group, respectively, and s denotes thecommon standard deviation of the two means.

D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436430
For the qualitative criteria, the effect size was calculatedusing Cohen formula [41]:
Effect size5jPhi12Phi2j
where Phi1 5 2 ! ArcsinOP1 and Phi2 5 2 ! ArcsinOP2and P1 and P2 indicate the proportions in each group
Traditionally [40], for both the quantitative and qualita-tive criteria, an effect is considered weak if the effect sizeis below 0.20; small, if it is about 0.20; intermediate, if itis about 0.50; and large or significant, if it is close to 0.80.
3. Results
3.1. Articles selected
Our search strategy identified 924 titles, from which weretained 17 articles that met our selection criteria (Table1). Because some of the programs produced several publica-tions, these 17 articles were related to six different RCTsevaluating the impact of case management on patientswith dementia [20–36].
3.2. RCT 1
RCT 1, published in 2006, reported on a disease manage-ment program [20,21]. The family physician’s practice wasthe randomization unit in the study. The inclusion criteriawere as follows: the patient’s age, which had to be over65, and established diagnosis of Alzheimer’s disease orassociated disorders (presence of a diagnostic code onrelease from the hospital, prescription of a specific treatment,or diagnosis by the attending physician). This programused an individual case management model delivered bysocial workers. The caseload was 50 cases per casemanager. On Pacala’s scale of 18 case managementintensity criteria (see Table 1), 12 criteria were explicitlymet; hence, the program was classified as intensive. TheRCT reported an intermediate integration level. It seemsto be based on the networking of various health care orga-nizations and community agencies in one city (San Diego,CA). However, it does not appear that the case managerscould intervene in hospitals and institutions, and it is notclear whether the case managers could organize multidis-ciplinary meetings. In addition, case managers sometimesworked together with the same patient.
At 18 months, the program had an intermediate impact(effect size, 0.54) on its primary end point, which was to fol-low recommendations in good practice guides. In each of thesubdomains evaluated (assessment, treatment, education andsupport, and safety), the rate of following recommendationswas higher in the intervention group with a small to interme-diate effect size (respectively, 0.54, 0.32, 0.37, and 0.57).The results for the patients’ quality of life were significantlypositive, but the effect size was weak (0.16). The programdid not have a significant impact on the mortality or the care-givers’ quality of life. No results were reported for the utili-
zation of resources (hospitalization rate, institutionalizationrate, or cost calculation).
3.3. RCT 2
RCT 2 used a “collaborative care” model [23]. The familyphysician’s practice was the randomization unit. Inclusion inthe program was related to the probability of the diagnosis(tests revealing possible or probable disease or related codeddiagnoses). In addition, patients had to be older than 65 yearsof age. In this program, a nurse practitioner acted as the casemanager following an individual model [23]. The caseloadwas not indicated, but must have been fewer than 40 casesper case manager because a total of 84 individuals wereincluded in the case management group between 2002 and2004 for two case managers. Fourteen of Pacala’s criteria[16] (see Table 1) were explicitly met; hence, the programwas classified as intensive. Assessments were done duringvisits to the nurse’s office. No home interventions seemedto have been planned in the program. Involvement of thefamily physician and family caregivers was clearly one ofthe study’s primary objectives; this fact indicates an interme-diate integration level.
The program had a modestly statistically significantimpact (effect size, 0.24) at 18 months on its primary endpoint, the intensity of behavioral problems. Patients’ andcaregivers’ quality of life was not evaluated, but caregiverstress was significantly lower at 18 months in the interven-tion group (effect size, 0.17). The two groups had compara-ble mortality rates. There was no impact on thehospitalization rate. There was no evidence of a reductionin the institutionalization rate, but the authors pointed outthat the study’s time frame (18 months) was much shorterthan the average time between diagnosis and institutionali-zation (4 years); hence, a statistically significant differencecould not be shown.
3.4. RCT 3
RCT 3, the Medicare Alzheimer’s Disease Demonstra-tion and Evaluation (MADDE) program produced severalpublications [24–27,29,39]. The randomization unit wasthe patient. The program used a population approachincluding all those inhabitants in the area of the study whowere over 65 years of age, coming under the federalMedicare program part A and B, who had been diagnosedwith dementia.
The case managers operated individually and had variedprofessional profiles (nurse, social worker, mental healthworker, or gerontology worker). Two case managementmodels were tested: an intensive version with a caseloadof 40 cases per case manager and a less intensive versionwith a caseload of 100 cases per case manager. Only fiveof Pacala’s criteria were explicitly met in the intensivecase management program; only two, in the less intensiveprogram. Regardless of the intensity, the integration level

D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436 431
was low, with the different structures remaining independentof each other and having no formalized linkage with primarycare [39].
The main result reported by the study was a statisticallysignificant improvement in patients’ access to services [27](effect size, 0.34). It did not find any impact on the levelof informal support for patients. However, the caregiversreported 50% fewer tasks in which they required assistancein meeting clients’ activities of daily living (ADL)/instru-mental activities of daily living needs [39]. The programhad a weak statistically significant impact on caregivers’depression or feeling of burden in the caring relationship(effect size at 36 months, 0.04 and 0.03, respectively) [39].In a secondary study in Illinois, this program found a reduc-tion in the hospitalization rate of the patients’ main care-givers (effect size, 0.28) [28].
The program was not considered effective enough to beimplemented on a wider scale because it did not produceany clinically meaningful effects [27]. In addition, althoughthe study showed that the program could lead to substantialsavings in health care expenditures (mainly in acute hospi-talization), this effect was not great enough to offset the pro-gram costs [27]. Finally, as had been anticipated, theinstitutionalization rate was not affected by the program[27]. The program did not have any effect on mortality,which was the only outcome studied that was directly relatedto personal health.
3.5. RCT 4
RCT 4 took a different approach, focusing on the empow-erment of the person or family through the actions of a careconsultant [31]. The inclusion criterion was a diagnosis ofdementia in the medical record of a patient belonging toa managed care organization (Kaiser Permanente). Thecare consultants, who interacted with clients mainly byphone, were professionals with training in social work.Although carried out mostly over the phone, case manage-ment functions were included, namely, a standardizedassessment, development of an individualized plan, and per-sonalized monitoring (daily if necessary). The caseload wasnot indicated, although with 210 individuals included in thestudy, including 60% (126) in the intervention group, andthree care consultants, it is likely that the caseload, at leastinitially, was about 40 cases per care consultant. Nine ofPacala’s criteria were explicitly met; hence, the programwas classified as nonintensive. The randomization unit wasthe patient and his/her family. The integration level seemsto have been intermediate, based primarily on a partnershipbetween the local branch of the Alzheimer’s Association andthe managed care system. It was not indicated whether thecare consultants continued their intervention after hospitali-zation. The primary end point was the combined effect onthe utilization of all types of health care, for which the resultswere reported separately. The positive effects reported weremainly as follows: protection against the onset of depressive
symptoms in the caregiver, but the effect was weak (effectsize, 0.18); less use of direct community services, statisti-cally significant but with only a slight impact (effect size,0.00); and less use of information and support services otherthan those provided by the local branch of the Alzheimer’sAssociation, also of minimal impact (effect size, 0.04).The program significantly improved the satisfaction of care-givers with the information provided, the adequacy of theservices offered, and the quality of these services. However,the intensity of these effects was weak (effect size, 0.09,0.01, and 0.10, respectively). The program did not haveany impact on the utilization of hospital or emergency ser-vices or the frequency of medical visits.
3.6. RCT 5
RCT 5, a Swedish study, involved a random sample of per-sons aged65andolderwith a dementia-type disorder requiringhome help (medical certificate required to obtain this assis-tance) [34]. The patients and their caregivers also had to beable to take aneducation program twice a year, and the patientscould not have any other severe chronic diseases thatmight in-dicate imminent institutionalization. Only one case manager,a nurse by training, worked individually with these people.A caseload of less than 50 was planned, and the programmet 12 of Pacala’s criteria, making it of intermediate intensity.Theprogramdidnot seem tobebased onanymajor integrationwork and accordingly had a low integration level. The casemanager did not appear to intervene in the hospital. The pro-gram delayed institutionalization in the intervention group(effect size on institutionalization at 1 year, 0.33), but no sig-nificant difference in the institutionalization rate at 2 yearswas found, nor was the mortality rate affected. The programappeared to be more effective when targeting persons withadvanced dementia. No other outcome related to caregiversor resource utilization dimensions was reported.
3.7. RCT 6
RCT 6, published in 1993, did not refer explicitly to casemanagement but to more intensive social work after an as-sessment at a memory clinic. The description of these socialworkers’ tasks, however, matches the definition of case man-agement used in this review. The inclusion criteria for thissingle-center study were a diagnosis of dementia and thepresence of a caregiver able to join the program [33]. Threesocial workers were involved in an individual case manage-ment model. The caseload was about 65 clients per casemanager (193 clients and 3 social workers). The randomiza-tion unit was the care receiver/caregiver dyad. By applyingPacala’s classification (six criteria met), the case manage-ment was found nonintensive and was not based on any spe-cific integration work; thus, the integration level is low. Inaddition, the only follow-up was at 6 months. No linkagebetween the memory center and the hospital in its acute-care full-hospitalization sector was mentioned. The program

D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436432
did not find any evidence of a significant effect on the utili-zation of health or social service resources by the patient orcaregivers.
4. Discussion
Although case management is a well-known approach toorganize health and social services, we found only six RCTsfocused exclusively on Alzheimer’s disease and otherdementia. As expected, recent RCTs fulfilled more CON-SORT criteria than did earlier ones; therefore, part of thissystematic review is based on RCTs that did not satisfya high standard of reporting quality. Current RCTs are ad-dressing, most notably, the cost-effectiveness impact ofcase management [42].
4.1. Answers to questions 1 and 2: Has case managementfor persons with dementia been proven to be effective inRCTs? Which outcomes have shown case management tobe effective in RCTs for persons with dementia?
The studies analyzed reported a clinical impact (compli-ance with recommendations, patients’ or caregivers’ qualityof life) that is statistically significant, although only slightlyto moderately. The impact on resource utilization (e.g., pre-vention of hospitalization or institutionalization) was usu-ally not statistically significant or only very slight. Thevariability in the clinical indicators chosen to evaluate theefficacy of case management precludes calculation of anoverall effect size. Nevertheless, the magnitude of the effectsof case management on the clinical outcomes studied, esti-mated using the effect size method, was often related tothe quality of life. It is interesting to note that these effectsare on the same order of magnitude as the effect of cholines-terase inhibitors on cognitive outcomes in persons withAlzheimer’s disease (effect size, 0.01–0.39 according toRockwood [43]). In fact, to the extent that case managementmay increase the relevance of and compliance with treat-ment [21], it can be assumed that these effects could becumulative.
4.2. Answer to question 3: Which aspects of serviceprograms (functions, team or individual case management,caseload, case manager’s professional background, casemanagement intensity, and target population) mightexplain variations in their efficacy?
Because of the differences in the case management pilotprograms, assessing their efficacy requires an instrumentthat can estimate the intensity of the intervention. This reviewcompared the intensity of the programs by using Pacala’s cri-teria [16], as well as the programs’ clinical impact and theimpact on resource utilization. Table 3 shows that the twoprograms that were determined to be intensive by using Paca-la’s criteria reported at least moderate clinical effects; theonly program ofmedium intensity reported amoderate effecton resource utilization, and the three low-intensity programs
reported only slight effects (clinicallymeaningless accordingto the authors [39]). Thus, use of Pacala’s criteria enabled usto synthesize and standardize the interpretation of case man-agement programs that often differed in the functions imple-mented (see Table 2). This evaluation is more refined thanone based on the case managers’ caseload. For example,RCT 3 failed to show a variation in the results obtained basedon the caseload, but both levels would have been evaluated asnonintensive by using Pacala’s criteria [16]. However, weshould point out that all the programs had a relatively smallcaseload. Studies of populations selected using criteria otherthan dementia have shown that the efficacy of case manage-ment declined when the caseload exceeded 60 [10]. Becauseall the studies were based on individual case management, itis impossible to determine whether team case managementsuch as that used in Program of All-Inclusive Care for theElderly (PACE) programs [9] might produce results that aredifferent from those produced by the programs reportedhere. In addition, given the variability in the case managerprofessions involved in the different programs, no correlationbetween the casemanager’s professional background and theefficacy of case management could be found.
None of the programs whose results are reported here hada selection criterion related to the person’s situation for eli-gibility for case management. In their analysis, some authorsbelieve this could be an explanation for achieving no morethan moderate effects. A targeting strategy based solely ona diagnosis of Alzheimer’s disease, such as in the MADDEprogram, tends to select a heterogeneous population, a sub-stantial portion of which is not at risk of an adverse event(e.g., because the average level of depression in the care-givers was low initially, a floor effect comes into playwhen trying to reduce it) [39].
This tends to be confirmed by an RCT on the impact ofa “collaborative” care intervention (care model similar toRCT 2). The eligibility criteria were related to frailty (hospi-talization in the previous 6 months, isolation, more than fourmedications, multimorbidity, incontinence, falls, or prob-lems with ADL). These criteria, independent of the diagno-sis, were used to select an at-risk population where the flooreffect was less of a factor. The program reported a slightlystatistically significant impact on both prevention of hospi-talization (effect size, 0.11) and mortality (effect size,0.08) [44]. These effects seemed independent of the casemanagement intensity because only four of Pacala’s criteria[16] were explicitly met.
Social parameters alone are also not sufficient to targetthe appropriate population, as shown by the results ofa case management project, again using the collaborativecare model, for disadvantaged populations [45]. By usingPacala’s criteria, the intervention could be considered inten-sive because it explicitly meets 11 of the 18 criteria. Theeffects were slightly statistically significant in improvingthe quality of care and the patient’s quality of life (effectsize, 0.11 for the overall quality of life and 0.26 for the func-tional quality of life). However, the program failed to show
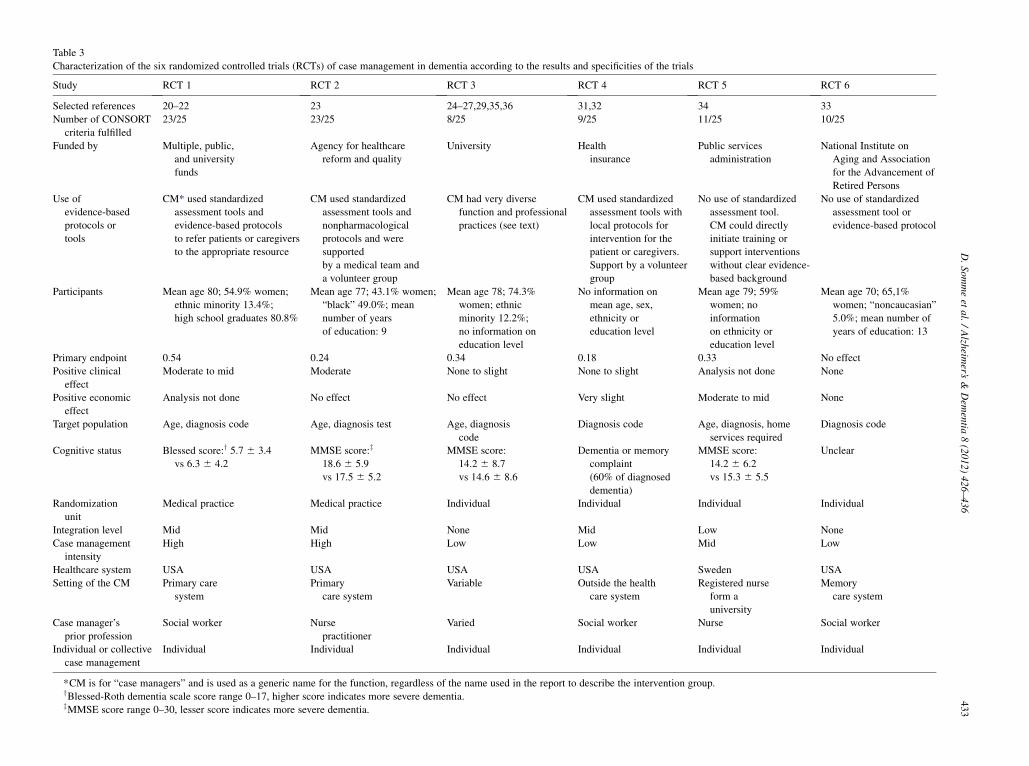
Table 3
Characterization of the six randomized controlled trials (RCTs) of case management in dementia according to the results and specificities of the trials
Study RCT 1 RCT 2 RCT 3 RCT 4 RCT 5 RCT 6
Selected references 20–22 23 24–27,29,35,36 31,32 34 33
Number of CONSORT
criteria fulfilled
23/25 23/25 8/25 9/25 11/25 10/25
Funded by Multiple, public,
and university
funds
Agency for healthcare
reform and quality
University Health
insurance
Public services
administration
National Institute on
Aging and Association
for the Advancement of
Retired Persons
Use of
evidence-based
protocols or
tools
CM* used standardized
assessment tools and
evidence-based protocols
to refer patients or caregivers
to the appropriate resource
CM used standardized
assessment tools and
nonpharmacological
protocols and were
supported
by a medical team and
a volunteer group
CM had very diverse
function and professional
practices (see text)
CM used standardized
assessment tools with
local protocols for
intervention for the
patient or caregivers.
Support by a volunteer
group
No use of standardized
assessment tool.
CM could directly
initiate training or
support interventions
without clear evidence-
based background
No use of standardized
assessment tool or
evidence-based protocol
Participants Mean age 80; 54.9% women;
ethnic minority 13.4%;
high school graduates 80.8%
Mean age 77; 43.1% women;
“black” 49.0%; mean
number of years
of education: 9
Mean age 78; 74.3%
women; ethnic
minority 12.2%;
no information on
education level
No information on
mean age, sex,
ethnicity or
education level
Mean age 79; 59%
women; no
information
on ethnicity or
education level
Mean age 70; 65,1%
women; “noncaucasian”
5.0%; mean number of
years of education: 13
Primary endpoint 0.54 0.24 0.34 0.18 0.33 No effect
Positive clinical
effect
Moderate to mid Moderate None to slight None to slight Analysis not done None
Positive economic
effect
Analysis not done No effect No effect Very slight Moderate to mid None
Target population Age, diagnosis code Age, diagnosis test Age, diagnosis
code
Diagnosis code Age, diagnosis, home
services required
Diagnosis code
Cognitive status Blessed score:y 5.7 6 3.4
vs 6.3 6 4.2
MMSE score:z
18.6 6 5.9
vs 17.5 6 5.2
MMSE score:
14.2 6 8.7
vs 14.6 6 8.6
Dementia or memory
complaint
(60% of diagnosed
dementia)
MMSE score:
14.2 6 6.2
vs 15.3 6 5.5
Unclear
Randomization
unit
Medical practice Medical practice Individual Individual Individual Individual
Integration level Mid Mid None Mid Low None
Case management
intensity
High High Low Low Mid Low
Healthcare system USA USA USA USA Sweden USA
Setting of the CM Primary care
system
Primary
care system
Variable Outside the health
care system
Registered nurse
form a
university
Memory
care system
Case manager’s
prior profession
Social worker Nurse
practitioner
Varied Social worker Nurse Social worker
Individual or collective
case management
Individual Individual Individual Individual Individual Individual
*CM is for “case managers” and is used as a generic name for the function, regardless of the name used in the report to describe the intervention group.yBlessed-Roth dementia scale score range 0–17, higher score indicates more severe dementia.zMMSE score range 0–30, lesser score indicates more severe dementia.
D.Sommeet
al./Alzh
eimer’s
&Dem
entia
8(2012)426–436
433

D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436434
that it was effective in terms of the hospitalization rate, uti-lization of emergency services, and frailty measured byADL or mortality. The authors’ explanation for this resultwas that the population targeted was too broad and not suf-ficiently at risk of an adverse event.
Thus, it seems that case management programs could op-timize their impact by implementing a targeting strategy thatconsiders not only the presence of a cognitive diagnosis butalso other parameters related to frailty, social isolation, orthe complexity of the situation.
4.3. Answer to question 4: Might integration level of thesystem organization explain variations in programefficacy?
In the studies reported here, the integration level associatedwith the programswas variable and often difficult to determineby simply reading the article. From our brief analysis of inte-gration,we can say thatRCT1, the program thatmost involvedintegration [20], also reported the strongest results in terms ofimproving quality of care as measured by following clinicalguidelines. Conversely, RCTs 3 and 6, the programs that re-ported the least impact in terms of integration, are also theones wherein the integration level appeared to be lowest[39]. The same criticismwas leveled at the Evercare program,namely, that therewas too little integration, especiallybetweenhealth and social services; the Evercare programwas tested inthe United Kingdom with populations that were not selectedon the basis of the presence of cognitive disorders [46]. In con-trast with this result, the PRISMA program tested in Quebec[47] andmore recently inFrance [48] reported solid results, es-pecially regarding client satisfaction and empowerment, aswell as prevention of frailty, and at no greater cost to the Que-bec health care system [49]. This program,whichwas not spe-cifically designed for persons with dementia, built its casemanagement program on a strong foundation of prior integra-tion work.
Methodologically, the integration level has an impact onrandomization choices. When there is an attempt to makestructural changes in the organization of the health andsocial service system, the most appropriate randomizationunit is not the patient. In such cases, the study design shouldrandomize on an “administrative or clinical” unit (medicalpractice in the articles selected here) [20,23] or shouldtake a “territory-based” population approach [47].
4.4. Analysis of biases
Because five of the six studies we report on here wereconducted in the United States, the reproducibility of the re-sults in other health care systems is questionable.
Even if the effects reported in these programs are valuable,it is not knownwhether they can be reproducedwhen the scaleof implementation is changed, for example, when a local pro-gram is implemented at the national level. The organizationalchanges required to extend these programs are highly depen-
dent on a variety of parameters, including leadership, outsidepressures, need for change, political situation, history of thesystem, and delivery method used [50]. The only nationwideprogramwhose results we report here, theMADDE program,is also the program with the smallest impact.
All systematic literature reviews involve a publicationbias because studies that have a negative effect or no effecttend to be underrepresented in the literature [15]. This biasmay apply here; however, the publication bias may be lesslikely in national programs because governments have an ob-ligation to be transparent in their public policy (as in RCT 3).This is confirmed in this review by the overrepresentation ofthis program in the references included (9 of the 17 refer-ences selected by our search strategy concern RCT 3).
The effect size method we used enabled us to compare thesize of the effect of different interventions on different out-come measures, but it does not indicate the magnitude of thechange that would be clinically relevant. It is not possible toconclude that a program that has a statistically significant butweak effect on a predetermined end point would be clini-cally ineffective. Conversely, it is not possible to determinewhether a moderate (or even large) effect of a program on anend point is in fact clinically undetectable because of the in-appropriateness of the measure. However, we believe thatthe outcomes examined in the studies reported herein couldhave a strong impact on the patients’ future.
4.5. Limitations
Wechose to analyze the evidence on casemanagement fordementia. The results presented here are not transferable toother populations for which previous reports often focusedon more robust evidence regarding the improvement in qual-ity of care [18].We found limited data in published papers oncomponents of integration other than casemanagement, suchas funding and organizational ormanagerial dimensions. Thecasemanagement setting also varied greatly between studies.Because these could both partly explain the impact of the pro-grams reported, it would be interesting to have a commonanalysis framework of integrated care [19]. Given that fewcommon clinical or economic end points were found in theRCTs included in this study, the primary end point of the pub-lished studies was used to calculate the effect size. This couldbe useful in future RCTs tomeasure the efficacy of caseman-agement (for the patient or the health care worker and toassess health resource utilization as well as the quality ofdementia care). Finally, it should be stressed that case man-agement cannot, by itself, make a system integrated and isnot a solution for all the problems of care continuity, access,and quality problems encountered by the chronically ill.
4.6. Future research
More research is needed on the precise content of the casemanagement process for Alzheimer’s disease and dementiaand especially if there are particular professional case

D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436 435
management practices with these patients. The problem ofneeds assessment using one or more standardized toolsseems particularly central. Moreover, the individualizedplanning task needs to be more clearly defined in terms ofprocess and tools. Concerning the assessment of outcomes,in addition to the need for efficacy studies already men-tioned, there is a need for cost-effectiveness studies.
5. Conclusions
Many countries reorganizing their public policy for indi-viduals with cognitive disorders are hoping that case man-agement will improve care. The scientific literaturejustifies this hope with regard to quality of care, quality oflife, and satisfaction, with the results obtained being moder-ately statistically significant. The literature is less clearabout an effect on hospitalization or the institutionalizationrates. The modulators of the results seem to be, first, theintensity of the case management intervention, for whichcaseload is an indirect and imperfect surrogate marker, andsecond, the integration level of the system in which thecase manager works. It should be stressed that the evidenceis still weak, considering the small number of RCTs pub-lished and the moderate methodological quality of most ofthese studies. Other studies are needed to identify the bestpatient-targeting strategy and determine which caregiver orcare-oriented profession would be ideal for case manage-ment with these populations and determine whether teamcase management models could be used. In addition, the sus-tainability of the practices and effects should also be exam-ined when converting pilot programs into a national policy.
Acknowledgments
This study was financially supported by the DirectionG�en�erale de la Sant�e from Ministry of Work, Employmentand Health in connection with the expertise of the AlzheimerNational Plan. The Direction G�en�erale de la Sant�e was notinvolved in any methodological issue or interpretation ofthe data. All statements reflect the ideas and opinions ofthe authors and are not necessarily those of the Ministry.
The authors thank Professor Dennis Kodner for reviewingand providing insights on the final version.
References
[1] Wolbring G. Three challenges to the Ottawa Spirit of Health promo-
tion, trends in global health, and disabled people. Can J Public Health
2006;97:405–8.
[2] Kodner DL. The quest for integrated systems of care for frail older per-
sons. Aging Clin Exp Res 2002;14:307–13.
[3] Wolff JL, Boult C. Moving beyond round pegs and square holes:
restructuring Medicare to improve chronic care. Ann Intern Med
2005;143:439–45.
[4] Reuben DB. Organizational interventions to improve health outcomes
of older persons. Med Care 2002;40:416–28.
[5] Boult C, Boult L, Pacala JT. Systems of care for older populations of
the future. J Am Geriatr Soc 1998;46:499–505.
[6] Somme D, H�ebert R, Bravo G, Blanchard F. Individualized service
plan (ISP) concept and utilization: a review of experiments on inte-
grated services for the elderly in Qu�ebec and elsewhere. In:
H�ebert R, Tourigny A, Gagnon M, eds. Integrated Service Delivery
to Ensure Persons’ Functional Autonomy. Qu�ebec, QC, Canada: EDI-
SEM; 2004. p. 271–89.
[7] MacAdamM. Frameworks of integrated care for the elderly: a system-
atic review.Ottawa,ON,Canada: Canadian PolicyResearchNetworks.
Available at: http://www.cprn.org/documents/49813_FR.pdf; 2008.
[8] Abrahams R, Capitman J, Leutz W, Macko P. Variations in care plan-
ning practice in the social/HMO: an exploratory study. Gerontologist
1989;29:725–36.
[9] Eng C, Pedulla J, Eleazer GP, McCann R, Fox N. Program of all-
inclusive care for the elderly (PACE): an innovative model of inte-
grated geriatric care and financing. J Am Geriatr Soc 1997;45:223–32.
[10] Eggert GM, Zimmer JG, Hall WJ, Friedman B. Case management:
a randomized controlled study comparing a neighborhood team and
a centralized individual model. Health Serv Res 1991;26:471–507.
[11] Foote C, Stanners C, series eds. Integrating care for older people. New
care for old- a system approach. London: Jessica Kingsley Publishers;
2002.
[12] Capitman J, Sciegaj M. A contextual approach for understanding indi-
vidual autonomy in managed community long-term care. Gerontolo-
gist 1995;35:533–40.
[13] Challis D, Darton R, Johnson L, Stone M, Traske K. An evaluation of
an alternative to long-stay hospital care for frail elderly patients: part I.
The model of care. Age Ageing 1991;20:236–44.
[14] Genrich SJ, Neatherlin JS. Case manager role. A content analysis of
published literature. Care Manag J 2001;3:14–9.
[15] Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC,
Ioannidis JP, et al. The PRISMA statement for reporting systematic
reviews and meta-analyses of studies that evaluate health care inter-
ventions: explanation and elaboration. Ann Intern Med 2009;
151:W65–94.
[16] Pacala JT, Boult C, Hepburn KW, Kane RA, Kane RL, Malone JK,
et al. Case management of older adults in health maintenance organi-
zations. J Am Geriatr Soc 1995;43:538–42.
[17] Riley PA, Fortinsky RH, Coburn AF. Developing consumer-centered
quality assurance strategies for home care: a case management model.
J Case Manag 1992;1:39–48.
[18] Hofmarcher M, Oxley H, Rusticelli E. Improved health system perfor-
mance through better care coordination. Paris: OECD. Available at:
http://www.oecd.org/dataoecd/22/9/39791610.pdf; 2007.
[19] Kodner DL. All together now: a conceptual exploration of integrated
care. Healthc Q 2009;13(Spec No):6–15.
[20] Chodosh J, Berry E, Lee M, Connor K, DeMonte R, Ganiats T, et al.
Effect of a dementia care management intervention on primary care
provider knowledge, attitudes, and perceptions of quality of care.
J Am Geriatr Soc 2006;54:311–7.
[21] Vickrey BG, Mittman BS, Connor KI, Pearson ML, Della Penna RD,
Ganiats TG, et al. The effect of a disease management intervention on
quality and outcomes of dementia care: a randomized, controlled trial.
Ann Intern Med 2006;145:713–26.
[22] Connor KI, McNeese-Smith DK, Vickrey BG, van Servellen GM,
Chang BL, Lee ML, et al. Determining care management activities
associated with mastery and relationship strain for dementia care-
givers. J Am Geriatr Soc 2008;56:891–7.
[23] Callahan CM, Boustani MA, Unverzagt FW, Austrom MG,
Damush TM, Perkins AJ, et al. Effectiveness of collaborative care
for older adults with Alzheimer disease in primary care: a randomized
controlled trial. JAMA 2006;295:2148–57.
[24] Newcomer R, Yordi C, DuNah R, Fox P, Wilkinson A. Effects of the
Medicare Alzheimer’s disease demonstration on caregiver burden
and depression. Health Serv Res 1999;34:669–89.
[25] Newcomer R, SpitalnyM, Fox P, Yordi C. Effects of theMedicare Alz-
heimer’s disease demonstration on the use of community-based ser-
vices. Health Serv Res 1999;34:645–67.

D. Somme et al. / Alzheimer’s & Dementia 8 (2012) 426–436436
[26] Newcomer R, Miller R, Clay T, Fox P. Effects of the Medicare Alz-
heimer’s disease demonstration on Medicare expenditures. Health
Care Financ Rev 1999;20:45–65.
[27] Miller R, Newcomer R, Fox P. Effects of the Medicare Alzheimer’s
disease demonstration on nursing home entry. Health Serv Res
1999;34:691–714.
[28] Shelton P, Schraeder C, Dworak D, Fraser C, Sager MA. Caregivers’
utilization of health services: results from the Medicare Alzheimer’s
disease demonstration, Illinois site. JAmGeriatr Soc 2001;49:1600–5.
[29] Yordi C, DuNah R, Bostrom A, Fox P, Wilkinson A, Newcomer R.
Caregiver supports: outcomes from the Medicare Alzheimer’s disease
demonstration. Health Care Financ Rev 1997;19:97–117.
[30] Warren PA, Dunn L, Jackson-Clark A. TheMedicare Alzheimer’s pro-
ject in Portland, Oregon. Pride Inst J Long Term Home Health Care
1991;10:20–7.
[31] Bass DM, Clark PA, LoomanWJ, McCarthy CA, Eckert S. The Cleve-
land Alzheimer’s managed care demonstration: outcomes after 12
months of implementation. Gerontologist 2003;43:73–85.
[32] Clark PA, Bass DM, Looman WJ, McCarthy CA, Eckert S. Outcomes
for patients with dementia from the Cleveland Alzheimer’s managed
care demonstration. Aging Ment Health 2004;8:40–51.
[33] Weinberger M, Gold DT, Divine GW, Cowper PA, Hodgson LG,
Schreiner PJ, et al. Social service interventions for caregivers of pa-
tients with dementia: impact on health care utilization and expendi-
tures. J Am Geriatr Soc 1993;41:153–6.
[34] Eloniemi-Sulkava U, Notkola IL, Hentinen M, Kivela SL, Sivenius J,
Sulkava R. Effects of supporting community-living demented patients
and their caregivers: a randomized trial. J Am Geriatr Soc 2001;
49:1282–7.
[35] Christenson D, Moore I. Intensive case management in Alzheimer’s
disease home care: an interim report on the Cincinnati (Ohio) Medi-
care Alzheimer’s Project. J Long Term Home Health Care 1994;
13:43–52.
[36] Arnsberger P, Fox P, Zhang X. Case manager-defined roles in the
Medicare Alzheimer’s disease demonstration: relationship to client
and caregiver outcomes. Care Manag J 1999;1:29–37.
[37] Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: up-
dated guidelines for reporting parallel group randomised trials. BMC
Med 2010;8:18.
[38] Strandberg-Larsen M, Krasnik A. Measurement of integrated health-
care delivery: a systematic review of methods and future research di-
rections. Int J Integr Care 2009;9:e01.
[39] Fox P, Newcomer R, Yordi C, Arnsberger P. Lessons learned from the
Medicare Alzheimer disease demonstration. Alzheimer Dis Assoc
Disord 2000;14:87–93.
[40] Cohen J. A power primer. Psychol Bull 1992;112:155–9.
[41] Cohen JW. Difference between proportions. In: Cohen JW, ed. Statis-
tical Power Analysis for the Behavioral Sciences. 2nd ed. Mahwah,
NJ: Lawrence Erlbaum Associates; 1988. p. 179–209.
[42] Jansen AP, van Hout HP, van Marwijk HW, Nijpels G, de Bruijne MC,
Bosmans JE, et al. (Cost)-effectiveness of case-management by district
nurses among primary informal caregivers of older adults with demen-
tia symptoms and the older adults who receive informal care: design of
a randomized controlled trial [ISCRTN83135728]. BMC Public
Health 2005;5:133.
[43] Rockwood K. Size of the treatment effect on cognition of cholinester-
ase inhibition in Alzheimer’s disease. J Neurol Neurosurg Psychiatry
2004;75:677–85.
[44] Schraeder C, Shelton P, Sager M. The effects of a collaborative model
of primary care on the mortality and hospital use of community-
dwelling older adults. J Gerontol A Biol Sci Med Sci 2001;
56:M106–12.
[45] Counsell SR, Callahan CM, Clark DO, Tu W, Buttar AB, Stump TE,
et al. Geriatric caremanagement for low-income seniors: a randomized
controlled trial. JAMA 2007;298:2623–33.
[46] Gravelle H, Dusheiko M, Sheaff R, Sargent P, Boaden R, Pickard S,
et al. Impact of case management (Evercare) on frail elderly patients:
controlled before and after analysis of quantitative outcome data. BMJ
2007;334:31.
[47] H�ebert R, Durand PJ, Dubuc N, Tourigny A. PRISMA: a newmodel of
integrated service delivery for the frail older people in Canada. Int J
Integr Care 2003;3:e08.
[48] Somme D, Trouve H, Couturier Y, Carrier S, Gagnon D, Lavallart B,
et al. [Prisma France: implementation program of an innovation in
health and services system for disabled people. Adaptation of
a case-management based integration model]. Rev Epidemiol Sante
Publique 2008;56:54–62.
[49] Hebert R, Raiche M, Dubois MF, Gueye NR, Dubuc N, Tousignant M.
Impact of PRISMA, a coordination-type integrated service delivery sys-
tem for frail older people in Quebec (Canada): a quasi-experimental
study. J Gerontol B Psychol Sci Soc Sci 2010;65B:107–18.
[50] Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffu-
sion of innovations in service organizations: systematic review and
recommendations. Milbank Q 2004;82:581–629.