An Overview of US Health Care Delivery
15
I: I): , • 111 ,,.u ... · .,n,f flrt'n.111_11.':-- (,fc.·l:l.' t."\J until 20 15) , 111;'1''''' : 11 • . • tnd lx·ih.'fH:- 111h.kr the.• AC'/\ ..• rm111,11H •. \f,, 11 ,, 1 ~ ·, . -; ·ukl lh ti11.lll\,;lll!! undt. ·r the: AC A , 1;1:,, ,,,t \k, h,lh • fl .If t'f1••1~k , ;llh.l lhl' \( \ . • 1 • ... 1 trd 1 .1,,nl.! .ind,,:- dli..'l'IS on provider re-in,b \ 1,111,'·''·' '('( J', · · _ _ - ~1'\.,. • I f 'tl\ ,.'1\l ~l' :,,c,.'c,'0,lrl(l~ .. , Cfll # ,k, . .'h ,' 1hl ,II• t., • , (' . . . _ 111 <1 lill·h dli.x·rs ot thi.! A A /'•111J.lf\ 1,;Ut. • · • • 1 .. 1 in 110.._.timp .. ·ns..:1h:d can .· and 1..·rncrgenc y de I ,J...1.· h "'' ..... ' ' . I I P!trtrne · 1 . ,· 1111 ,w, ,rn Jwm~ hc.. ·J r, c. ·are ru ll"· I h1. \ ' I ., . "'I; Ilk.' \( \ .;\ llllf\lc.'I 1 111 1to,p1i:l' ~c:n 1 1ces I \( . 1 . 1111 ,11.:r,mt.·,,m11111n1t) health ce nt e rs f IC: I · :,. I • , - • • I \( .,. ,·l·itiv• , 111 n1111d1:-.t·r111111 w1 1 on agamst health car JIC J/ '•·'" _- Cpro· n, .... ACA ;11lll ,1/r1.·n1.1HH' rh _ cr,lflll.'S . Yiders 11H .. ' /\("A·, Ullf),lll (IU ph)~ICUHH)\\ ll t.. 'd h ospitals NC\\ «kmands 11> cft:lt\l. "I t:clm1 nu1111y benefits by nonprofit instituli M •cl ··,,·c ind he.11th 1nsur: 111cc exchanges ans ;.1 11,1gt: .... ' • . P,111k11>;11i<111 <1fC'O-OP< and Mcd, ca ,d ·' l~Os '." the e"changes P..irtn:1pa1 ion ofa1..'l '0111tWblc: .. ·art: o~gamzat, ons m Medicare, based on inn: 11 r 11 cs 1hrouih a Shared Sav111gs Progran1 Cmn nHllll f) J ·ir,1 Choice op1 11'. 11 for s1~1es 10 ~romote home- and coll ll nlllllty-ti.,,cd ,cn,,·c ., tor rcc1p 1ents ol long-renn care under Mecf . f:, ,rcnswn of Money follows the Person progrnm IClicf R cq11ircmcn r. for 11ursing homes under lhe ACA J· s1inu11 c., e1f 1 l1c unin, 11rc~I wi rh and wi1ho u1 rhe ACA llcnclit, of r hc /\CA tilr ccrt11in vu/ncrab/c g roups f'/lL..:1011 hc ,1/th 11dmi11i,1m1i vc cosrs Crn11m,cr,ic, su rro u nd ing v uluc-tn,scd paymcms adop1ed under the ACA 11,c /\C/\ 111111 co,1 eo111ni11111cnt 1'11c AC/\ and uccc~s 10 care · 111c AC/\ and qual11y of care Ro/ cs ofrhc 0111/ S and 1/1c IRS /> o/iti c a/ foc wrs cri1ic al to rhc cnac 1mcn1 ofrhe ACA fm pl c mcnt.uion of1h c AC/\ Policy implic at ions ofrhc ACA l'li c /\C/\ 's s tanding in rhc contcxr of lorccs of future change ,i kcly futur e of rhc /\CA and hcahh care reform C hapt er 1 An Overview of US Health Care Delivery l earning O bjecti ves • To undenland the basic natun: of the US health care system To outline the key functional components of a health care delivery system To get a basic o•'ffVicw of health care n:fonn and the Affordable Care Act To discuss lhc primary characteristics of the US health can: system To emphasize why it is imponan1 for health care practitioners and manasm 10 understand lhc intricacies of the health care delivery system • To get an o~icw of health care systems in selected countries To point out global health challenges and refonn efforts To introduce lhc systems model as a framework for studying the health services system in the United States .::::,...,;> -- --- The us health an cifwwr S}'S1l!lll is a behem,/lt dl1I is rJmast (111 my silllje t11fity IO moooge one/ control.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of An Overview of US Health Care Delivery
I:
I):
, • 111,,.u ... · .,n,f flrt'n.111_11.':-- (,fc.·l:l.' t."\J until 2015) , 111;'1''''' :11• . • tnd lx·ih.'fH:- 111h.kr the.• AC'/\ ..• rm111,11H •. \f,,11
,,1~ ·, . - ; ·ukl lh ti11.lll\,;lll!! undt.·r the: AC A
, 1;1:,,,,,t \k, h,lh • fl .If t'f1••1~k, ;llh.l lhl' \( \ . •
1• ... 1 trd1.1,,nl.! .ind,,:- dli..'l'IS on provider re-in,b
\ 1,111,'·''·''('( J', · · _ _ - ~1'\.,.
• I f 'tl\ ,.'1\l~l' :,,c,.'c,'0,lrl(l~ .. ,Cfll # ,k, . .'h ,'1hl ,II• t., • , ('
. . . _111<1 lill·h dli.x·rs ot thi.! A A /'•111J.lf\ 1,;Ut. • ·
• • 1 .. 1 in 110.._.timp .. ·ns..:1h:d can.· and 1..·rncrgency de I ,J...1.·h "'' ..... ' ' . I I P!trtrne ·1. ,· 1111,w, ,rn Jwm~ hc..·J r, c.·are ru ll"· I h1. \ ' I ., . "'I;
Ilk.' \( \ .;\ llllf\lc.'I 1111 1to,p1i:l' ~c:n11ces
I \( . 1. 1111,11.:r,mt.·,,m11111n1t) health centers f IC: I · :,. I • , - • •
I \( .,. ,·l·itiv• ,111 n1111d1:-.t·r111111w1 1on agamst health car JIC J/ '•·'" _- Cpro· n, .... ACA ;11lll ,1/r1.·n1.1HH' rh_cr,lflll.'S . Yiders 11H .. ' /\("A·, Ullf),lll (IU ph)~ICUHH)\\ llt..'d hospitals
NC\\ «kmands 11> cft:lt\l."I t:clm1nu1111y benefits by nonprofit instituli M •cl ··,,·c ind he.11th 1nsur:111cc exchanges ans ;.111,1gt: .... ' • .
P,111k11>;11i<111 <1fC'O-OP< and Mcd,ca ,d ·' l~Os '." the e"changes P..irtn:1pa1ion ofa1..'l'0111tWblc: .. ·art: o~gamzat,ons m Medicare, based on
inn:11r11 cs 1hrouih a Shared Sav111gs Progran1 CmnnHllllf) J·ir,1 Choice op111'.11 for s1~1es 10 ~romote home- and
collllnlllllty-ti.,,cd ,cn,,·c., tor rcc1p1ents ol long-renn care under Mecf . f:,,rcnswn of Money follows the Person progrnm IClicf Rcq11ircmcnr. for 11ursing homes under lhe ACA J·s1inu11c., e1f1l1c unin,11rc~I wirh and wi1hou1 rhe ACA llcnclit, of rhc /\CA tilr ccrt11in vu/ncrab/c groups f'/lL..:1011 hc,1/th 11dmi11i,1m1ivc cosrs Crn11m,cr,ic, surrounding vuluc-tn,scd paymcms adop1ed under the ACA 11,c /\C/\ 111111 co,1 eo111ni11111cnt 1'11c AC/\ and uccc~s 10 care
·111c AC/\ and qual11y of care Ro/cs ofrhc 0111/S and 1/1c IRS />o/itica/ focwrs cri1ical to rhc cnac1mcn1 ofrhe ACA fmplcmcnt.uion of1hc AC/\ Policy implications ofrhc ACA
l'lic /\C/\ 's standing in rhc contcxr of lorccs of future change ,ikcly future of rhc /\CA and hcahh care reform
Chapter 1
An Overview of US Health Care Delivery
learning Objectives
• To undenland the basic natun: of the US health care system To outline the key functional components of a health care delivery system
To get a basic o•'ffVicw of health care n:fonn and the Affordable Care Act
To discuss lhc primary characteristics of the US health can: system
To emphasize why it is imponan1 for health care practitioners and manasm 10 understand lhc intricacies of the health care delivery system
• To get an o~icw of health care systems in selected countries
To point out global health challenges and refonn efforts
To introduce lhc systems model as a framework for studying the health services system in the United States
~ .::::,...,;> --~ --
The us health an cifwwr S}'S1l!lll is a behem,/lt dl1I is rJmast ~ (111 my silllje t11fity IO moooge one/ control.
• ~ 0,.-,,..of US H.,,. (11e Deb.er/ (H,\Pf{F 1
1,1roduclioa h \ " un1qvc , .. ,11:m or
,~ r ur~·cl 'ii.ti., a i. .. h t1h tt.: ,klPt=r .• unhkc .in} o1111.r ca
Ji ·~ ,tre "'"rid \ioi,1 dc\cl-,~ .,1c111 in h
, d, ,unin~, ti.n..: n-111-.n,.I hwlt m..ur· I" nm,,., th..: v,,,crntn1:nl c1nd
,m,: ~r .. ~ra , . If 1,n.ir u·d thruot h fl net.ti lJ\C' \lrl'>o\l a
11/i;u, 1ft ,ulh {11,mltlc .. Jrc c:n111h:d H' 'tH'l\l.: h, .. llh C"JfC ',C(\ 11.C\ \uc.:h ,., not }C1
tht l,1\C ,n ·ti.: I rutt..:d \tau:,. "'here no1 all \rrn.r!\.,tr,., .ire ii1Uloma11call) co .. en:d b)
hl.';,lth ,nwr41n<.c Jlk: I ', tk:;1hh UIC dch,cr) ',}~tern IS
n;alh nul 4 ,~,tcm ,n 11, true 'loCO'te. c,tn ihou~h ,1 ,, ullcd a \)'<,tern "hen reference ,, nude 10 ,tc, urK,u) feature.....,. componcnb, ,'Kl 'M:f"\1c:e., llentc. n ma) be wmc'4hal m,,k.1ding io talk about the Amcncan ht.11th u 11c dehu:I')' .. c,)~U:m .. because a 1rue
,,.,,cm doc\ not eXl\t t\\'ohnr.k-) 1988) One .;.,. fc,,urc of chc L.S hc•lch care sysccm " ch,i 11 " fraamcn1cd because d11T<rcn1 P'" PI< otmi,n heahh carc 1hrough d11Tcren1 m,.,,, The S) s1em hasconunucd 10 undtrgo p<nod1c change<. mainly ,n ,nponsc IO con• ccm, rcg,rd1na co;1, access. and quahcy.
lx"SCribmg hcaflh care delivery in 1he Un11ed S1a1« can be a daunung cask. To fac1hllllC an undcrscanding of 1he Sll1'C·
1ural and conccprual basis for 1he delivery of hrahh services. chis 1ex1 is organized •ccord,ng 10 a sy,;cems framework presenced a11he end of1h1s chapcer. Also, for 1he sake ofsimplieny, 1he mechanisms of health scr• vices delivery in 1he Uniced S1a1cs arc col· fec1ivcly referred 10 as a syscem 1hroughou1 this text
The main objective of chis chap1er is 10 provide a broad understanding of how health c,ire is delivered in the United Scates. Examples of how health care is delivered in other countries are also presented. The
u" i.:rv1cw pn.:scn1cd here int,; rcadi:r to sc..,cral conccpt1 tr Odtact. ft extcn,1vcly m later chaptClli. ~ ,
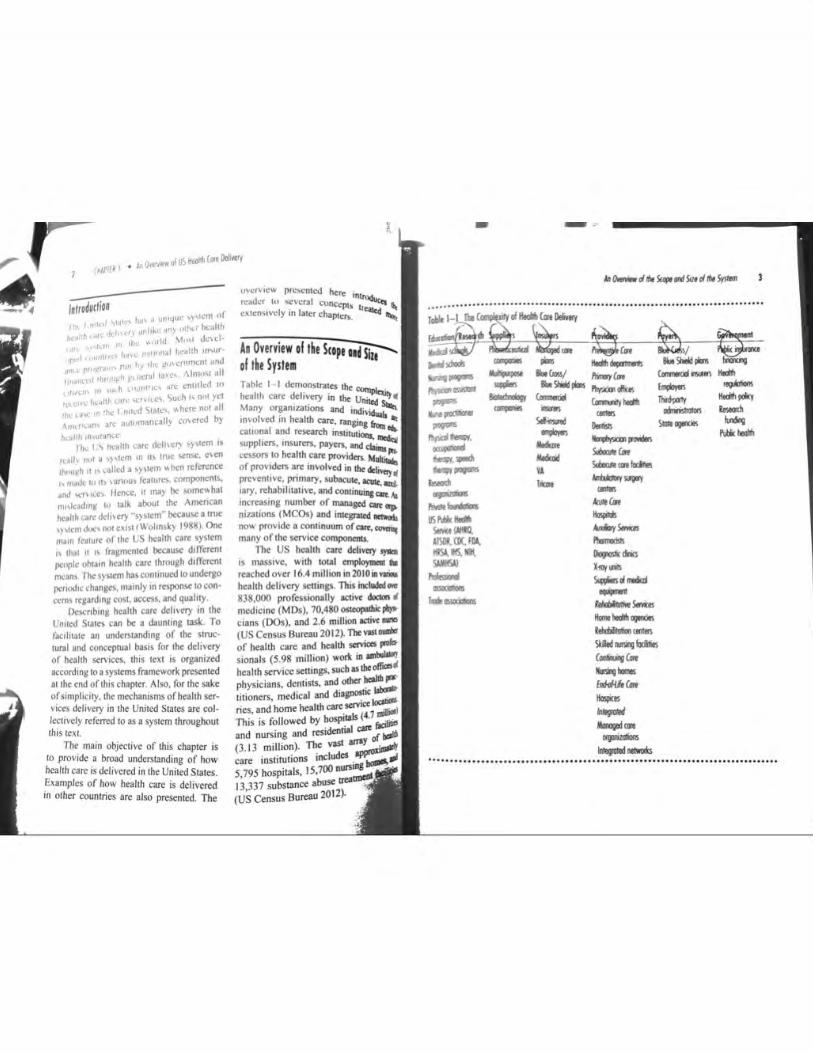
An Overview of the Scope oiislu' of t~e System Table I I demonstnices lhe . health care delivery in 1h, ~ Many organizations and individ S.... m,_ofved in hcallh care, ranging~ ., cat1onal and research in.stitu1ions_ "-suppliers. insurers. payc~. and c~ ccssors IO health care providcn, M~ of providers a~ involved in !he dd"">'c prevcnuvc: ~n~ry. subacute. lCUlt,llld. 1ary, rchab1htat1\'C, and continu.~cart.Aa mcreasing number of l!Wlag,:d ""' "'> niiacions (MCOs) and inlegrakd oen.ait, now provide a conlinuum of cart,. ~ many of 1hc service componcms.
The US health care delivery J)'llal
,s massive, wich tocal cmploymn,c a. reached over 16.4 million in 20f0ill...,. hcahh delivery scuings. This incfudod.,. 838,000 professionally active doaorl , medicine (M Ds), 70,480 ostCOpllhic" cians (00s), and 2.6 million ecti,~,... (US Census Bureau 2012). TheVOSC.,.. of heahh care and heallh saviccs pco/1> sionals (S.98 million) work in~ health service settings, such as lheofficis physicians, dentists, and other heallll I"'' ti1ioners, medical and diagnoot"::::; ries and home health ca,,, ....,ce ·.:-1
' · Is (4 7 ,,..,_ This is followed by hosp•_" · ~ and nursing and res1den~al °"" of b,111 (3.13 millio~}. The vast~
ca.re iostitunons cneludes . """"'"' 5,795 hospitals, 15,700 ours::.. : 13 33 7 substllllce abuse uea , (US Census Bureau 20ll).
- -.................................... .............................................
-AaMun Ho,jid, AdoryS-., "-'dsl,
°"""*dnu x..., ...... ~-mockd _... ~s.... .. Home ..... ogondes leldlilldioo (IN"1
SiiedlUlilglocilin (OllliuvC... W,gllon-.s &ri<AAC... lbpi<es
1///ff/1* Mooog,dm ~
lolepod oelwr.ru ................................................................................
r ~
In WI I, I, 11~ fcdcntll) quahlicd h"·ahh '"enter grantees. "1th 138.403 tullumc cmpJo)i..~' pro" 1111.'d pre, cnlt\~ and rrnnal")' c.:arc ,crvu,:c .. to uppro,m1a1cl) 10.2 mtlhnn peop .: In mM in mcd1i.."a.JI} undc-r"'C'l\00 rural aod u,llan Jrca~ (IIRSA 201 J}. \ ,inou\ t)' pt.~ of health cart: prok,~tunal.s a, '-" trained 111 I :';l) incd1cal and ostct.lJ):Uh1c ,1.:ht.l()I,. 61 d1.•ntal M.hool,. o,cr 10 "'hool) ot rl\arnlac.:y. and mon .. • 1han I .500 nur,111,g proirnm, IO\:Jlcd thrw •houl I~ i.ountr') (lJS Bureau ot l...ahc,r ~tat1st1c, 201 1 ). Mui• t1tudc!\ol go\.cmmcn1 a¥cn<'tC°' are 1n\oht'd wuh the:' firnmi:m.: of hcahh care. medical rt.:\4.!tm:h, and n:KulalOI') o,cf"l1g_h1 of the uuou\ •'fXXh of 1hc h(ahh care <lclh·cry S)'I\IClll,
A Brood Oemiption of the Syste• U). health care doh\01)' dot, not function a.s tt rn11onal und 1ntcg.rntcd network ol ,ompononh dos1an•d 10 ... or1c 1oac1hor coherently. ·r o the contrury, 11 1s a kalc1· do,copc of financing. 1nsuntnco, dch,o,y, •nd payment mc-cha111sm, that remn111 loo;ely coordinated Each ol these ba,1c func1JOnal componcnas financing. insurance, delivery, and payment rep<aenb an amala•m of public (ao\Crnm<nl) and privn1c sources. Thus, go\.tmmcnt-run programs tinanco and insure health care for select groups of people who meet each program's prcscnbe(I critena for eligibility To a lesser degree, government programs also deli,cr cenain health care servi«s d1rcc1ly 10 certain recipients, such as veterans, military personnel, American Indians( Alaska Nath·es, and some of the uninsured. However, the financing, insurance, payment, and delivery functions are l"'l!cly 1n private hands.
l he markct-oncntcd economy ,.. t.. mtcd States attracts • , ane,y or pr, Iii, cntrcprcncur:o. drl\cn by the Pf.11'5Uit of Vilt 11> obtainod b) carrymg out the key ror. uon, of health care dcli,cry ~ purcha,c health insuntnco for their employ ccs through pma1t soorec.. and • = rccel\c health care SOTV1ecs ~ b) the pmatc scc10<. The '"""""finances pub!1c msuraaec throu&h Medi. care. \1cd1ca1d. and the Ch11dr<a's Heala Jnsumnce Progmm (CHI P) f0<a11gnifteaat pon1on of the lo.,·1ncomc. elderly, dis, abled. and pcdiatnc populattons. Ho_., msunncc arranacmcn,s fo,- many ()Ubl!Cfy msurcd people are made throuah ()rl>Mt
cn1111es. sucb as health main~ or.., 11iza11ons (1 IMOs), and health care scrvictS arc n:ndcrcd by pm .. tc phyt>NOS ud hospllals. 1 he blend of pubhc and pnvaie ln\Oh·cmcnt in the <kll\tty of htallh C!IN:
has rc;ul1ed in:
• mult1plic11y or llnancitl tn'lfl&Ctnenll
that enable 1nd1>1dual110 poy for~ care scrvic:ts~ numerous 1nsur11noc agencies or MCO. that employ ,-aned mechanisms r« insuring against nsk; multiple pa)m that make their .,,... dctcrmina11ons n:aa,ding how much 10 pay for each type of service;
a large array of scnu,p "here roedical S<:rviccs arc delivered; and numerous consuluog firms olTcriae cxpcnisc in planning. cost rontainrnen~ electronic systems, quahl)', and r<StnlC' runng of resowcc:s.
There is linle sundardizatioll ~ 5;;; 1cm that is functionally fragmen tJ,el the various system components lit ioac
oc>l)-'>Secb•-..... sut,e,ei ., 0 ,-crall pl>nnmi. dif"'110n, and <00<d,.
- from • """"'111 ai,mty. l«b • thc ,.,,cmmcnL Oupheat1<111. o•nlop, i...i. cqaac>. IIICOIISHlfflCy, 111d ,.._ aua. )Odmg 10 compln,iy and 1nomc-,., du( ., 111< ...,..., ~ or l).....,,.,.ldt p1ann,.., du<et1on, and coonhna1.,.. The ,1._ ., • •bole does noi kad iudr .. ,w,dud bud~ l1X1hods or <0Stcon1n>1. b<la mdmdual and corpon,c """Y •idun • pn:dommlntly pn,-.i, ""~ l) .wm tttts IO rrmupnllle 6nanciaJ ~ U\d IO Its O*D advan~,. -wnhouc rtgard
., ,u unpoct m the 1)-SlaD u 1 • llok Hence. COSt containment remains an tl'*lt,t pl la .i.o.t. dae US bctlth ~ ddrvcry 5>>10111 IS hle • bchcmo<h or an «onom1< owpblh dial is al.- l!llpO<Slblc for •Y <onalc <RIii)' IO manage or cc,,1rot. The US CC<"*") IS dae b,p 1ft the •'Crld, IDd, compar,d IC> ocher n.11<1111, cc,,suffl()(1011 or llallh aon: scn>ea,. the Umtcd S... rrp, tttffllS • ~11tt propon,on of the CO\lntry's IOCai <C<XIOffllC OUtpul. Althoup di< l)'ll<lll
can be cttd11cd (o,- d<IMnna IIOfn< or the bell clinical a,n: ,a th< •Oftd. 11 r.,111 sllort o( dcll\Onn& oqu1table l<rYIC<S 10 C\'e!)'
Ammcan. An ocaptablc health Cit< d<lwery sy>
lffll should ha\-e 1'11'0 pnmat) oij<C11,-... (I) 11 must cru,blc ell c11iz<M 10 oba1n DO<ded health care scnica. IIICI (2) the scr, \1CCS must be cos1 effecti\'C •nd mctt cer• Q,n CSQbl1SMCI suncbrds of q,,aMy Th< US health a,n: dcli,'el')' sy•tem falls short or both ~ ideals. On the och<r hand. -foaturcs of US health can art the <flV'J of the "orld. The United States lcadslh<world • the btcsl and the bcsl in medical t<Chnol· "SY, training. and raeatth. It olTm somt or tbc inost ,opbiSIICaltd institutioos. produ«s. and proctS.SCS of health an: d<h,-ery,
Rlllcilt r...,c.,. It MC<SYI)' 10ol>ca1n health ins11t• anc:e or to pay for health care '"''"' F« """1 pnVJltly UllUred Ammclnl, health llllUrlnC< IS fflll)lo)'mm~......,, dlal IS, the fflll)lo)ffl fuw,c:e hc•hh ure 11 1 fri"&• b<nefrt. A dcpeMmi ,pousc or ch11dmi may
lltO be 00\crod by the wook1na · - ·· or ~ .. pere,u's cmplo)-er MOSI emplC>yen purmasc health 1MU1111Cc for their employ, «s duOlllh an MCO or an 111SU1111Ce
...._,. sctcc:t<d by the <mploy<r. Small emplo)ffl may or may not be 1n I po,!lllOft
10 alTord health insurance COVfflgc ror their employ«$. In publ,c prognms, the gov..,.. .,... fllectioM as the fmancier: the iMur· ance lunction may be carved out to"' HMO.
--· tnswoncc procee1S the insure,! lpUISI cal· asll'<Jl)hi< risb ... hon nccdi11& cxp<nsivc
I I I I I I I I I I I I I I I I I I I I

,,r
f
(HAPTEf I • All Ov,rview ol US Her.Ith Core 0eM<y
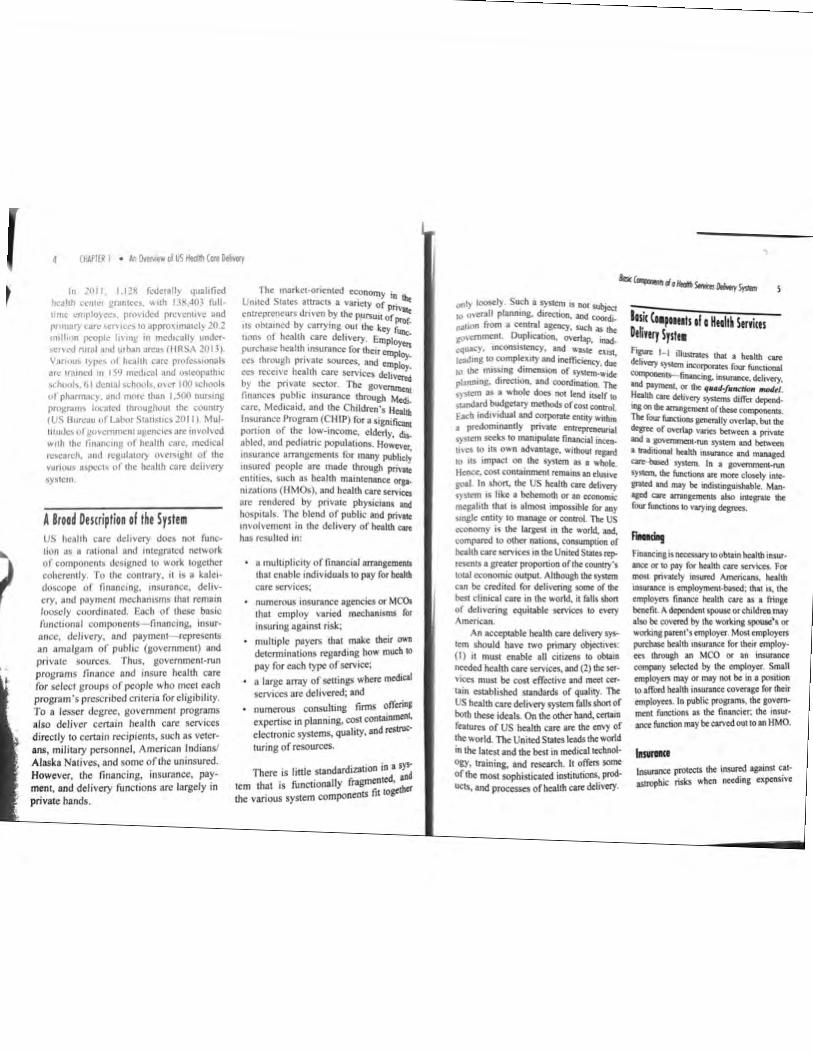
fl11ANON6 lmployer,
,-- - -- - • • -- -- • • Goverrrnenl-Medicort, Niedi<:oid
/ A : INSUllANCE DIIMIY lP'IMersJ : lllSUfon<e compo.nies Atcess Physiciom: f • · Blue Cro<l/llue llield _...,;.:;;::;..__ Hospilols : s.lf . .,,...,nc, Nurlilg homes
1 v :r.r~= ..... : c-~hiahl,-: . . . . .
@' PAYMENT ®' lnsu11WKt co,npo11ies Ulatm 81"' Ctowll"' ll,lold -al!
, 111ifd-por1y dolms procfflOll , . . i. ................ (;b ......... ..i ! ····· lnlegrotion of fuoelion! thr"'lii moq,d core (HMO., Pt'OI) I
health care servic-cs. The insurance (unction also detennines the package or health services the insured individual is entitled Lo receive. It specifies how and where health care services may be received. The MCO or insurance company also fonctions as a claims processor and manages the disbursement or funds to the health care providers.
The = "delivery" refers to the provision o(bealth care services by various providers.
The term provider refers to any entity tbal delivers health care services and can c1'l>a independently bill for those serviceso<~111
supponed. Common examples of p<O~
include physicians, dentistS. op~ and therapists in private pracuces. ~ tals and diagnostic and im>giog din( ..,
' · n""'1t C &, and suppliers of medical equ,,,. •. ~ wheelchairs, walkers, ostomY ...,.
• 111()51 r· oxygen). With few excepuons. bo • ., .. · .-.pie w .,.. viders render services 10 r- ~ health insurance. With 3 few ·~ ~ even those covered under public ,ns
-Pay-I '(be P"rn- function deal$ w11h rt.lmb.,.,. _,,, 10 pro,,·Mkrs for services delivered.
'(be - clc<ernWleS '- much is paid (or • c,cruin s,mcx. Fwids for actual di>i,oncmco• C"'1lC fiom lhe pramwns paid 10 t11e ,1COorinsunnC<cornpa,,y. Tbepa1;.,,,1 ,s u,ually r<qlllf<d, al lhe lime of ,avice, 10 pay an ou1-<>f-pocket JfflOUDl.. such ,s $25 or SJ0. io sec • phys,ci,n. The rem1111det ,s co,-cred by lhe MCO or msunnce,.,.,,. P""Y· In go,·cmment ,_ plam. such as Medl<Ot'C and Mechc,id. ,.. revenues art u,cd 10 pay """''cleB.
lamam aad Htoll~ CueRelar•
without any health 10$I.IJ'l6« (US Ccnws Bureau 2012~
fa·c:n the predominant employmentbased financing $)'5ltt'n ln the United States: bas left some anplo)·cd individuals uninsured for two main reason.1: ( 1) In many statts, employcn arc not mandated to offer hcalth insunncc to their employees~ there,. fore. some employers. due tO economic C005'ra:U'lts. do noc offer it. Some small busit\CS$e$ slmpty cannot get group insurance u. affordab4t: rates and. therefore, are not able to offer health insurance as a benefit to Lhtir cmploy,cs. (2) In many work selli~. parucipuioa 10 health i05unnoe programs is volunwy and do<, not r,qui"' employees IO J(»o. Some employed choose not to sip up, mainly because \hey cannot afford the cost or health lllSurance premiums. Employ,n nrcly P"Y 100¾ of the insurance premium; most require thclT employees to pay • po<llOO or lhc cost. called pr,mlum coJI Ute,ing. People such as those who art sclf-loycd have to obt>in heahll insurance on lheir own. 1r.d1vidual r:ues arc typically hi&het dlan aroup .. ,cs •vailab\e 10 employffl, In the Unilcd SUltes, wor1<ing people nm•na low w.1gcs have been the "'°" hkely 10 be uninsun:d because molt
In 2009. lhett"' ere 194.S mtlhoo Amonuns ,.,th P"""' health ,nsusance covfflg< (US Census Bureau 2012). The US &o•em· mm• finances health t,cncfiu for certain _ .. 1 pop,la1,ons, 1nclod1ng government <ffll)k>yecs. lhe elderty (people age 6S and 0\-eT). people with disabihties. some people w,th \Cf)' low inccrnes, and childmt from ro-.-,ncome famihes. The prog,am fnr the elderly and cauin disabled individuals ,s called M~dicor~. The prog,om for lhc md,gen~ Jointly administc,-ed by lhc fed· mJ govemmeot and SlatC govenunet>IS, is namedMuie11id. The prog121n for children from low-inoome families. anomer federaV SlalC pannership, is called the Children's Health Insurance Program (CHIP). In 2009, there were 43.4 million Medicare bcneficia· rics and 4 7 .8 million Medicaid recipients, but S0.7 million people (16.7%) remained
c,nno, ,ITord pmnium cost sharin& and ore DOI eligible for public b<nefiu.
In lhe US context, heollh core rt/orm ref en 10 the expansion of health il\Surance 10 covet the u/WISurtd-tho5.c without private or public health insurance covCfllg<. The AITordable Core Act (ACA) of 2010 is the most sweeping health care reform in recent US biscory. How the ACA became law is discussed in ChaplUS 3 and 13. One of the main objectives of the /\CA is to n:ducc the number of uninsured- This section provides a brief overview of how the /\CA plans 10 accomplish this; more complete deUlils are furnished in Chapter 6.

(!' I!!
I h: \ ( \ <A;l, rolled ()UI gr.1duall.y ,Lu1 n m 21110 ...,Ju:n rhuranc.: roropani~:. \\1.;rc m.anda11.-d lU ,1.ut co\c-nng_ children ;uld >,1t1n~ adull, klo.,.. 1hc a11,.: ol ~6 u~cr their riarcnh· h .. .slth !n\W'3m:;; plan~ \iost odt,\;J 10\UlJII'-~ pru\l\lOn, \\ COi IRIO cff«t
c,o JamW'\ I !1>14. c,,cpt lor a rnand,1h! lur cmrlt"''' tu prornk hcahh ,n,urancc. ""tuch 1., ~}\l~lll\..J un11I 2015. rhe Afi\ rcq,urc, th,11 ,Ill L \ c11111:ns and legal rc-.idenh mu,1 he: co,cr .. -d b) c11~r puli11c or pmate ,nwrafk.'.t rht.: la" al..o rel,~ed ,1,ndarJ, 10 qu.1111~ add11tonal numbers of fl(~'rk fu1 \ k d11.:a1d . .il\hough many \tatcs h,u c c.:hi""-·n nut m 1mplcmen1 1l b,a"'-"(j on the t \ ..,UJ'll"(n'IC ( oun·, ruling ,n :OJ 2 •~et ( hartl.'r \ hit dcu1hl lndP•lduah " uhout pf1\.111.' N ruti.lk: ln\Ur,mi:e lllU\I Clbtam he.ti th ,n .. uranl."\' tnim rw,t1;1rJ11ng 1n!iwancc comr'ilfll"" thn'll,l!h \\ eb-bascd. go,tmtn(nt•run c,~h.an~l .... f,11hn~ &l "'-'· the) musi pa) a ta.\ llll.• m,1n fol'lli.U,'111 ol UlC' (\\hant,~ also rd,:m.-d111,1, h,ihh in .. ur.ukX rn.MkctplaicC\. ,, 11, tiN lk1crm1ftt "'hc-lhcr an ar,phc1n1 \fUJhlf\.~ fN \kJK.t1d c,r CHIP pro,:rtms 11 .ln 1rrh..:.tn1 ooc .. nN 1.1uahl~ for I publt1.· r'(111rJm, 1hr (\Chan11c \\Ould cnablt the ,nJu 1d~I U\ ,t,m~rc hcahh plani ofTcrtd ~ rr,,11~ m,urm ind lO purthbt a su11-JMr hcJhh plan. Ftdrral sub4i1d1~ ha, t tx~n miJc ,1, :ul:ihlc to ()N)ple " 1th incomes up 1,, .ioo-. M lht ft'dt~I po,en, lc,tt 10 p:1n,3IIJ i,ffl>Ct tM c~t of heallh tnsuranC'e 'imJII <mplo~t rs c3.n also obtain health rO\ cr.tgt for th~1r tmploym through ihc t'(ch:in~-s The la,, mand:nC) insurance pl.a.M ro C'O\tr a \'IMly of SCr\iCts rtferrcd 10 as ··~noal ht-31th bt11tfils ..
A pr<d1<1i, < model de, elop,:d by Pven1c and Ftldm,n (2013) es1ima1ed 1h01 a1 b<s1 full unplemen,.uon or,1,e ACA .. ; i1 rcduc; che ~~bcr of uninsu""' by more than 20m,lhon. If achieved m 2014. ihis would be
the largci.l co,·cragc expansion in rcccot his1ory. 'le, erthcless. by ,is own design_ US AC,\ would fad to ach1e,·c uni.,t1$ol co die: "X' 1ha1 "ould enable all c,1izens and.:; resident-: to have health insurance, p~Dlt future scenanos for health care rcfonn 1ft d1~u~ m Chapu:r 14.
Role of Managed Care tndcr traditional insurance. the four basit heal1h dch, cry functions have been lilt mcnccd; that is. the financiers. inswets. pro,. \ ,den.. and pay~ ha,c oftm been difTCffll ( nUucs. with a few exceptions, During lbt 1990~. ho"'c:,cr. hcahh care delivery 10 die \..mtcd <itatc.$ underwent a fundamcmal change invoh mg a ughter mtcgnnion of the ba!1C funcuons through managed care.
Prc,iou~ly, frag~ntation or the"*-11ons meant 11 lac\: of control o,u uuliu,. uon ;nd paymenis. The quan111y o( beala care consumed refers 10 utUl:.,otion of~ ioer'\ ices. Trad1uona1ly. dctcnn1na(ion ofdlt uuhT.Auon or health S<'iviecs ond !he pnct t har&cd forcac:h ffi'\'1ce has been left up10 1hc msurcd ind1\ ,duals and the proVldets ol hcalth care. Due 10 nsong heallh can: cosa. ho~c,cr. current delivery mcchantsmsha't'e mstituted some controls over both urilizt. hon and price.
Monogtd car, ts a system of ~ care dehvery 1ha1 ( 1) seeks 10 achiev< ellicitncics by antes.rating the four fun(O~ of heallh can, dehvery discussal earl"'· (2) employs mechanisms 10 oonuol <in;,:; age) u1iliza1ion or medical . .,,.,.,ces. ,... (3) deicrmincslhc pncea1 wh1dl lhcse<' ,,ell arc purchased and, consequendy. ho"':...lhc providers gc1 paid. The P"""'.:.,....-. cocr is srill lhc employer or ohe S".:'.'.:.;:;;;,c as lhe case may be. lnsiead o( I""--
i,..llh ....,ranee lhrough • 1radi1ional insur· .,._., oompany. lhc employer COOlnCtS willt .., MCO, such a< an HMO or a pn,fmed Po'id<f orpni,a1ion (PPO). 10 offer a ,.,i..-.:t<d heallh plan 10 ilS employ«S. In 1hi$ cr,,t'. the \tCO functions like an insuranct ""1'1*'Y and promiS<S 10 provide heallh art S(f'ICCS cootraelcd under chc health ptao ,o !he enrollees o( lhc plan. The 1tnn
,,.,.JI« (mcml><t) mm 10 lhe individual co,ered uncl<t Ille plan. The con111CtUal amo£ffl1CDI bet\<ttn lhc MCO and lhc (llttlllce-mcluding Ille collcctave array or co,ettd hcal1h S<1\'IC<S lha1 lhe mrollee is caullcd U>- 1$ ~rcm:d to a.s the "'""" plan (tw "plan.- for short). The heallh plan u"" ,elttled P"" ,den from whom lhc mrollees can choose 10 rec::c,, c services.
Compared "1th hcalth scrv1ces dell,·· a) under ree-(or-S<1\ic•, managed cane • ti succasful m accomph5hing cost ooc,. lrOI 111d a,u1er u,1eira11on or heallh em dtl"..Y By ..,...,na ae«u 10 nc«kd hrahh 5Cn'tc:CS, cmpha$1zin& preveo1ive 0tff.. and ma1nta.1n1n1 a broad provuJtt nc1-•cd. efT«11,e COSl•avma measures can b< ,mpltmcnlcd by manaacd can, willt· cu comprom1s1na acce:Ss and quahty, 1hus p-o,,d,ng heallh can: budge, pr..S,clabilioy UNIIWnablc by CJlbcr kind$ or heallh Cite drh,cnes.
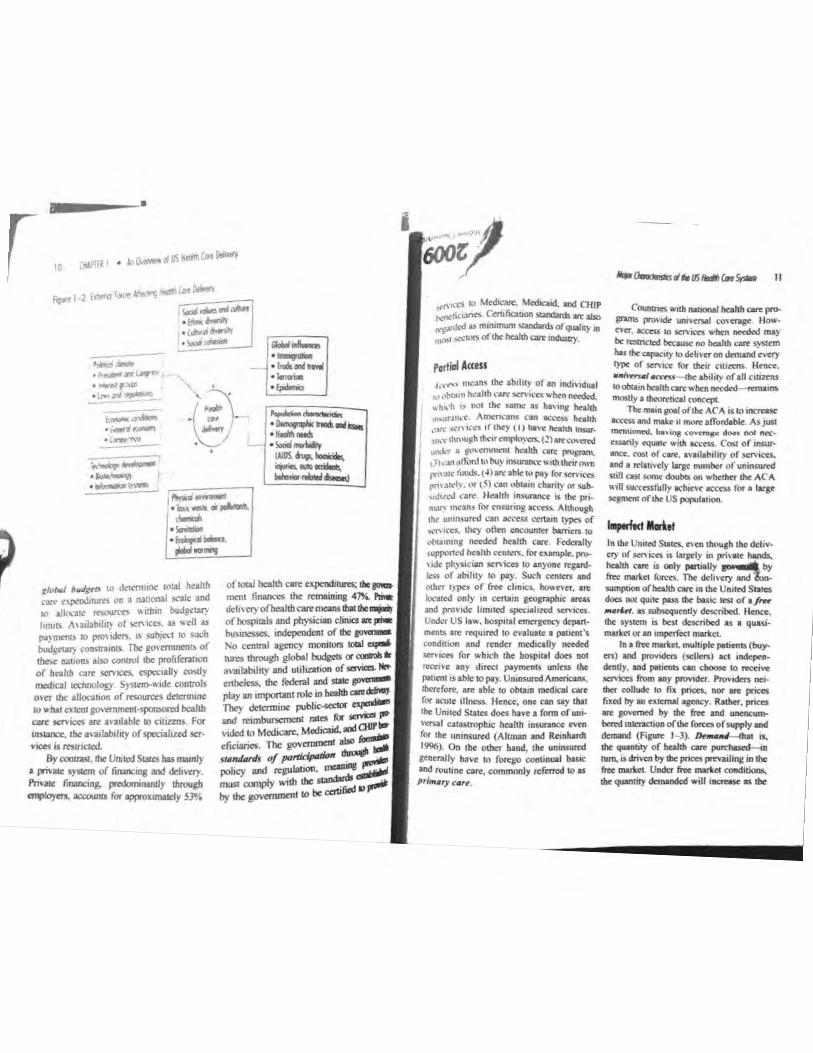
loj11 C~omteristiu ol t~e US Hult~ Care Systea 111 any country. ctrtain external influences .i..p. lhc ba$ic chon<:1cr of lhc hcallh sec.._ dcli,e,y sys1<m. These forces consist of lhe pohlical clima,, of a oatioo; eco-110mtc dc\-clopment: ""hnological progr<$S: SO<ial and culnnl values: physical mvironmrni; fXlll')latioo characteri111es. such as
demogr.,phic and hcallh m:nds; and global influences (Figure 1- 2). The combined in1enc1ion of these environmental forces inOueatts the course of~.alth care delivery.
Ten basic characteristics differentiate lhe US health care delivery system from that of most other countries:
I. No ccntraJ agency eoverns the system.
2. Access to health care serv1c.cs is selteth·cJy based on insurance coverage.
3. Health care 1s dehvc:rtd under imper· feet market oond111ons.
4. Third.party insurccs act as intttmediancs between the financing and dchvery functians.
S. The existence of multiple payers makes the ,ystem cumbersome.
6. The b.:ilancc or power amon1 variou11 players prcver11s any sinKIC entity from domimuina the system,
7. L'll•I nsk, influence prmice behav, lOf of physicians.
8 Development or new tcchnoloi)' creates an automatic demand for its use.
9. New service setting$ have evolved along 3 continuum.
10. Quahty is no longer tcccptcd as e.n unachievable goal.
No Ceatral Agettcy 1nc VS health care sys1em is not administnath•ely controlled by a depanment or an agency of the government. Most other developed nation$ have national health care programs in which every citizen is en1itled to receive a defined sci of health care services. To control costs, these systems use
r 10
•
---~"ell , _,,,
•",,_..."(~ ~ ....... ,, .... •:w<,,..~ ...... ll".)
;:..; .. .:: .~11. .. ~ ·
• \,,,., .... - ---,.,,... __ ,, lo,;i<_ ·'*"""' .... ·~ . m1,g,a1 .....
pl,,1'--.
,,., ·*" 10 J,,tnnlll< IOW h<allh ,_ ,-.p<OdiNr<S on • nonon.\l "11k and 10 allocalt rnourttS "1:h1n budgc-W} l,m,r, Au1J.a~1br,. of Stt\1CO. as Wf'II as pl\fflt1\ts lO pro,,ders. IS SUbJt'Ct IO soc-b
budgrtal} roosua,01> The go, enuncn1> of ~ nanon.,, abo contrOI lhe prohfcrallon or b .. 1111 car, =~ cspcc..U) c<)(d) medal ICClloolog) Srn•m-~ ode cootr0ls o,er dx allocauon of resources de1cnn,ne IO what CXltOI go,ernmeol•spcmoml bealtb can, ~ att 1nJl.a.bk ID catiztns. for iiwancc. lht a,-a,lab,hly of spcc1al11..al ser· VJCC< drntncttd
By cmtras1, lhe Urul<ld States bas ma,nly a privau: S}"""'1 of f,nancang and det,vny. /'t,Qlc fmonc,ng, ~ ly dvoup, ....,.,,,.,., ......,.. fo, .,,,..oximaltly 53¾
11,W ..... . ...,. - ....... ...., ·--~
II
,<t'KX' 10 M<d,can,. MedlCJOd. 111d C!UP .-ri<..ri<s C'11lfiaoon -.datdsat<abo ~ardtd as mmi,num standards or qualrty m
· ·"' "'""" oflh, hea!lb con, ~
c_,.,.. Mtl>-lw:a/thcon:Plffll P'O\'ldt un,~J to\crag,( However, ac:tts.s 10 scn·ten when .nttdod may be ralr1Cled b«ausir no health care s:ystt:m hu t1t< capacil)' 10 d,l,vtt on dem>.nd <Y"'f cyp, of """" r .. tltar Cffl«nS. lkn«:. •IV\'ff'UJI ~ l'-fbr ability of all citizens IOobcllin httlthe&rc'v.htn 1t«d<d lffll81n5
po,tiol Access
4,'<11"-' m~ans the :,b1hcy or an mdl\1duaf h11~11,~hhC'an:s,eni<ff • htn nttded., .tt~·h 1:,, not the same as M,·1ng htahh u,,urJO\(', Am<fl\-am ,~ actUs hnlth ,~rt s,("1\1,"'"1 1ftl\c'y ( I> hl\'C: ~Ahb lng-:Ull."C.' thf\\U~h thi.'1r ~'UL (1) ft 1."0\'a'rJ
,..,,.._.., a ,-.wmvn mc. hcallh C1U'C pnlg'lm.
t ll1...utalli.mt "' huy tnSUf'ln(.~Wilh the-irown J'"'-'tc hmd.<. t·Oatt ablt 10 pay forSff\ttt1 pn,.srd, . \'If t~) ... an obuin charity N' .ub,_,J111.-J 1.·•~-H~hh in>W'lf'K't ti tht pri-, """' rn<>m for """"Iii ac«ss. Al-gh 1he- unin~uttd can l«'tSS t"trta.,n cypn of
'''"=· th<) oft<n -I« buri<n to ,>beamtllJ ne<d«I h<1hh <ore. Federally i.upportcd hc1hh cnitm . for c:xamp&e. ~ ,>ck ph)Socian s,n i= to 111)'00< r<flrd· ks$ of ab,licy 10 pay. Such «111m and othff ryptl or free d1ntc:S. --C\tt. Ile
iocol«I only in c,na,n ceoa,aph,c ...... and provide hmited sp«i1hud kMN"S.
~- US law. bo<plul emeraenc:y d<partmems are requlred to evah.tacc a patient"s coodmon and r<ndc< m<dically -.led 11<r>icos for which lhe hospital dn,s not rtcc1't-c any d1tte1 paymm&s unltss dtit l*Jffll IS ll>Je lO pay. Unin-Americans. lbcrcfore, are able to obta,n medJCal ,;a,-cfor 1ane 1t!oe:ss.. Hence. one can uy tha1 I.he Uniced States dotS have a form of un1-\otnal caca.strophtc hea.rth inswa1'CC evm ror the untoswed (Altm111 and Reinhardt 1996), On 1he olher hand, the un,nsllftd ,..,.,.l ly have to forego con~! i..s.c and routine care, commonJy referred to as primo,, rore.
~·~--The main pl ofthr At A. IS to HK1ff.SC aa:cssandmatc 11 more1~ A.sjUSI mm.tioncd., hav11\g .;-ow111;11,o doet not MC'•
....,,1y cquot< ""b OCttSO. COIi of......,.. ence. C'ost or cart. ,,·111&b1lity of $C.f\'f«s. and• rtlau~ry I~ number ofun1nsurecf Sh tl <'l:st somt doubu on v.·hd.hn' lht- AC A
"111 SUC'ttSSf'ully trhl'Cv~ lt('('('S,,' l("lf • large ...-ofdl<US_lal_
1-,.m<tMntt In the United s~ccs. t"\ a, though &he d(liv,. "> of= - is llrp-ly in pri,._ hands. helllh <are is ooly ponillly _..,,.._ by
free "'""'" rcn-.s. The c1<1,...;y and i,..:. SWl1pO(lOI ofhelltl> WC lO lht Un,led States does no1 qu,1< pass lhe boste t<S1 ofafrtt
--· .. subs<qucntly det<ribcd. """"'· tht system ,s: bc-5t described as , quas1 ..
ma,t., er an '"""'*"' martta. lo• Im: matl<e~ mulliplc perients (buy•
en) and P""'Klm (Klf<n) act -dmdy. and pMicnb: cao cboose to retti-..e ~= from any provider. Provlden nc,.
ti>« collllclc 10 fix pnas. - we prices fi.ted by 11n •Alcmal •$ncy. Rather, pnces ... gov<med by lhe free and -......., - of lhe ro,,ca of "'f'l)ly and demand (Figure 1- 3). 0..--.1 n. lhe q,,IIACJI)' of - 0Me ~ 111m. is driven by lhe prices prevailing in lhe froe marl<et. Under &oe martet concbtJoos.
ID< quanril)l d<mandcd will ·-.. lhe

,-
' ,
,
17
figufl 1-3 ~,,,_,Q Bt·•;e,, Pr«. ~.,jy. onl Demond Under free-/,lnrlet (ondili~.
o,,:,ond
i
p~cc is lowered for a gi\•en product or servr~. Conversely. the quanrity demanded will decrease as the price increases.
Ar casual observation it may appear rh~t multiple patients and providers do exist. Most patients, however are no enrolled · · h • w ,n en er a private health plan or govemment•sponsorcd progra plans acr as intermediaries for:~)- :i,ese and the consolid . . patients, I• a11on of parrenrs into health
Pans has rhe effect of sh'ft' from rhc · 1 mg the power th patrenrs ro the administrators of
e plans. The result is that the health plans,
not the patients, are the real buyers io tbo health care services maricet. Private heli6 plans, in many instances, offer rheir.,.,,. ees a Ii mired choice of providen ralherdlP an open choice.
Theoretically, prices are neg04iat<d berween the payers and providers, In I"'°' tice, however, prices are detennincd !; the payers, such as MCOs, Mcdicait. Medicaid. Because prices are set by'':; cies external to the mark•~ !MY are ,J governed by the unencumbered for¢ supply and demand.
, .. for rhc hcallh catt nw!<n 10 be free.
unrcsua1ned oomptt1uon mu.st ocoa among p<O"dcrS baS<d on pnce and quahry. The consohdatioo of buymg pov.cr in lhc hands of pnvatc hallh plans, hov.-cver. ho$ bcell (Otclng pro .. idcn to fonn aJlianc:ts and ante-grated dch"cry syscems (discussed in ChaplCT 9) on lhc supply 51de. In cenain gcogr>?'ic secto<S of lhc counuy, a singk gianl medical syscem ms takm ovu as the sole pro,'lder or map health care savica. resui<Unc competition. As lhc health core sy,,tcm c:onunues to mo,·e an 1h11 dlttd.K>n, ,1 appean lhar only ,n larie me1rO!X>liran areas"' ,II lhcrc be more than one large ,ntt• grated system c<>mp<1ln& 10 ce< lhc bu,ioess of the health plans.
A fm: marl.ct rcquuu lhat patients ha, e ,nronnauoo about lhc appropriateness of "'"°"s Kn ices Such infonmtion
meet major CX.pense$ when unlikely events occur. bavtng insuraoce foe basic &nd rou-tmc health can uodcnnines the principle of ,nsunncc. Wbea you buy home insurance to protect your propert:y against lhe wthkdy C\·cn1 of a ftre. you do oot anticipate me occunmcc of a loss. The probaml-ity that you will suffer a loss by fire i, vtty small. If a fire don occur and cause major damage., insurance will cover the toss.. but io.suraoce does aot cover routine wear and cear on the house. such as chipped paint ot a leaky faucitt. Health insurance. however. generally co"m basic and routine services that are ptedactablc. Health msurancc cov• crage ror miDOf SttVl«S, , uch as colds and roughs. earaches, and so forth, amounts tO
prepaymcot for such services. Health insurance bas the effce,t or insulating patienu from the fuU ~t of beahh care. There is a MOrtd lu,:ard tblt. oocc enrollees have purchased health insurance, they will use hnhh c11c scrv1ces to a greater extent than ,f they wcte t0 poy for the"' ,crvice, OUt•Of•pockCL
At leut two additional facton limit the abihty or paucnts to make decisions. fin,t. decisions about the utilization ofheahh cart are often d«ennincd by need rather than by price-based d<rnaod. Nud has been defined
,s difficult 10 obla1n becaU$t t«:hnoiol)'· drivtn mcchcal care 1w bceomc highly soplusucatcd New d,_.,....,ic methods. 1n1C'f\cntion 1echmques. and mDR: effective drup fall in rhe domain oflhc pcofessional phys1c1an. Al'O. mcd1ctl ,ntenrentions are commonly requu~d In • stare of uriency. HeBCC. pa.ucnlS ha,c neither the !kills nor the time and resources to obtain accurate infonnauM "hen needed. Channeling all heallh care needs lhrou&b a prim>ry can: prl>'ider can reduce this infonnation gap whm the primary care pcovidcr 001s as lhc patient"sacl\ocate oragenL Conversely. th• lnlemet is becoming a prominet11 soun:e of medical information, and medical ,dvc,-
tising is having an impact on cotUumer expectations.
In a r- mall<et, patients most directly bear the cost ofservi= r,ceived. The pur· pose of insuran<:e is 10 prote<t against lhe risk of unf o,eseen c:ausuophic ..,..,,ts. Since the fundamental pwpose of illSUf&JlCt is to
as the 1mOUnt or medical care that mcdi· cal expens bclie\te , person should have t0 remain or become hcallhy (Feldstein 1993). Second, the delivery of health care can result in demand creation. This follows from seJf-u,cssed need, which, coupled with moral hazard. leads to grearcr utilization. creating an artificial demand t,eca.use prices are not lllcn into consideration. PraclittOners who have a financiil inierest in addittOnal treatments also create artifi· cial demand (Hemenway and Fallon 198S), referred to as provid,r•-induced dtm.ond, 01'

14 OOPIER I • An ()w,w:w of US Heiiln (o,e Oelivecy
sop1-.licr·i1lduc...:,d dc1nand. Functiomng as pat1cnt\i· ;,gents. physicians exert c,,ormous .ullucm.:t: on tht.: demand for hc:.thh care serv1CL'!; (Altm~u, and Wallack 1996). Demand creation cx:cur,;, \\.hen physician'\ pr~ribe 1rn:<l1cal can: hcylrnd ,,hat is climc:.1lly nee• cssary. 1 ht, l'•JU include pr:.11.:11cc!\ such as m;1h111g. more frequc.:nt follow-up ap1X>1nt• m\!nts than 111..-cc,:-,11). ,,rcs..:nbmg cxccssive mcd1cul tcs1s. or r,crfomung unnecessary surg.cry (Snnu.:rrc and Neun tt>96).
Third-Party Insurers and p ayers
In a t'n:c ma1·kc1. patients ha,c infonnn• tion on price and qu..,hty for e.ach pro, iJer. The current srtclll hos other drawbacks that obsmu.:t 111tbnnat1on•scck1ng efforts. lh:m•hascd pncing , i, une such hurdle. Surgery is a good c'<amplc to 11lustrntc item• ba:,cd pncins. also relcrrc.-d to as fee for servicC". Patients can gcnerully obtau\ the fo..:s the surgeon would charge for a par .. ticulor opcmtion. 13ut the final bill. aflcr the ,urgcry ho~ been pcrfomted. is hkely 10 ,ncludc charges for ,upplics. use of the hospiinl's focih11c>. and scmces performed by providers. such as ancsthesiolog1s1s, nurse ane.1hc1ists, and pathologists. These pro, ider>, sometimes refcm:d 10 as phan• tom providers. who func1ion in an adjunct capacity, bill for their services separately. hem billing for such additional services, which some1imes cannot be anticipated, makes it extremely difficult 10 ascertain !he total price before services have actually been rcceh ed. Package pricing can help o,ncome lhese drawbacks. but it bas made relati,el~ linlc 1,ea,t,,,ay for pricing rocdi· cal procedures- Pacug~ pricing rcfe,s to a buDdled t~ for a paclcagc of r,,lated ser,ices.. In the ~ - cxampk. this 1ll'ould mean ~ aJ.l.inclusi>·e price for tho, surg,tclll' • fees. bospital faciliti<s. supplies.. ~ ~- anesd,esia. and ~ !Oilo,o-up.
Insurance often functio diary among those wh;\ts the i' :,nd receive health care. Lnan~ .• dt~ mtcnnediary does not b The '""'- · . b ave t•-·7,.. tl"e to c the patient's ad 'l!t' •,
price or quality. At best e vocal le oa ..-..,
h . d. . ' ' mp oy-1 eir 1ssat1s,ac1ions with the .,.., ca.111
employer, who has the po pl.,. to liq · wcr to di unue the current plan and choose sea.. company. In reality, however
100lltt,
may be reluctant to change ' 1';'P"'1,,, current plan offers lower pr/. ns if lit pared to a different plan. muun,.,.
Multiple Payers A na1ionol health care system is . also referred to as a singlt-pa)= because there is one prima,y payer, i1t govcmmcnt. When delivering smicol. pro, iders send tho bill 10 an agCftC)' oflt government that subsequently sends po,ment to each provider. By coouast. Gr United Swtes has a multiplicity or heal' plans. Multiple payers oflcn rCI"'*"' 1 billing and collection nightnw< foe do providers of services, Multiple paycnmalx the system more cumbersome in ,.,.,,.
ways:
It is extremely difficult fo< pro,ickl'' keep tabs on the numerous J,callh pJIII, For example. 11 is difficult tO ~ with which services are covered .,a each plan and bOW much cad> pa,,t
pay for thoSe SC'~ . -ProviderS must birC claJOIS .""";;, to bill for~ ,md ~,,. ,. of paymesns- Billing I"- _ ,:,; ~ ,md .-:II ~ lisbeS nsO""II f(](1113L
l'o)'ffl"nlS ~ be denied f0< not precisely folloW1ng the requirements set
b)' each payer. 0c01cd cbims necessitate rebilling.
\\'heft only partial pa)inent is rcceivtd. S<JOlC tteallh plans may allow the pro,idcf 10 Nian« bill the patitnl for the ,mount the health plan did ""' pay. Other plans prohibit balance billing. E,c:n "hen the balance billing option lS a,-.ilable lO the provider, it trigg<TS
1 .,.,. cycle of billinp llld collection
dTO<IS,
11
~ cmploycn_- and the govcmmcn1. Big _ ness. labor, msurancc com-nies phv5i-
c1ans, and ..__. ~ • ' and . . ,.._,..,~ts make. up the powcfful
(>rOvldcrs must some.tunes enpge in lengthY collec,1100 effons. including v.nting col\ec.uoo \ctten.. turn1ns delio· queot accoun\S over 10 colleclk>n agencies. and finally ""'ling off as bad debt • .,,....n,s that cannot be collected. c;o--emmc:nt proar-m$ bavc complex ~ula11ons for c!tiemt1nu11 "ltctbct payment lS made for ,,,,,ices IICIU·
ally dehvcttd. Medteat<, f0< euml)lc, requires that each provtder maint>in leng!.hY documc:nlallOII on services pro\ldcd. Medtet1d ,s known for len&1hY dela)'S ,n poy1n& pn,vtden.
pohttcally aci1vt spectal intetcst groups rtpr<SCnted _before lawmakers by hiahpric,d lobbytSU. Each ''" of players has its 0 ~ econonuc intcresr.s to protect. Pbysi~.ans. for instance. want to maintain their n\Comcs and have minimum interfctence ~th the way they practice medicine~ \nstitu-uonal adminisuators seek to m.a,.imize reimbursement from private and public: insurers. Insurance companies and MCOs a.re inter· ested in maintaining tbe-lr stw.rc of the health insurance matkc.t~ large employers want to coota.tn 1hc costs they incur pto"iding health lDsuranc:c as a benefit to their employees. The eo'V(fflfflCnt tr\($ to maintain Of cnhai.\CC aisling btncfits for those CO\'eted under public insurara pnli111ms and simulw,eomly tootain the cost of providin& lhcSC benefits. The probLtm is lhat sc1f-intcrtSU of d1ffettnt pbyers are ofien at odds. For ellAfflllle, p<0viden IICCk 10 1ne,.... go..,m· ment tttn"lbuncmecu for SCf"Viccs dc1ivcfed t0 Medicare, Medicaid, &nd CIIIP benefi• c;arics. t,u1 the So"cmmcnt wants to con• tain cost increases, Employers dislike rising bcalllt rnsuran<• pn:miums, Hco.lllt plans, undct pn:ssut< from tltc employeff. may constrain f«s f0< the providers who then
ment lhCS< MS.
It is generally t,c,lie-,'td that 1hc United States spends far more on administrOlivt co,,,-<:OSIS assoc:ia1ed willt billing. collCC· bOClS, bod dcl>u. and ,nainlaining medical ~ W national t,ealth Cott sy>"
terns u1 other countries.
Power Wcacilg
lltcftagmentedSCll·ini=softhcvar•
iouS pl•yer> produ« ooun=•ili•g foroes within the sys,,,n. In'" environment tbal "rife with ~ionS to pn>l<C' conflict· ing sclf-in1"'S1S, adueving oompttltcnsh-e syotc:nt·wide reforms bas t,een next
Thr US health ..mccs sys= involves multiple playetS. not just multiple pay· .... Tbr key players ;,, d>t S)'<1t1I\ bav<: btto pb · · adminislt3t0"5 of J,talth
""ice ~ inslJnllCC ~
co unpossible, and cost coow.nmeot bas ,emained. mojor cllallat&•· ~ly. thc lfllll'-" to bealtb can: reform in thc
Uoned SQltS bas bet11 ~ as ~ "' p;cc,meal. md the focuS
16
of f\:ronn , 11 AII\I!~ ha~ been ca1nfincd 10 heJhh ins.urancc co,<n1.;c and p.t)mtnt cub 10 pro,·idef'\ rather 1han ho"' cJrc can be bell« pro, idcJ.
Litigation Risks Amcnca 1s a hug,ou~ sococl} \1otl\ated by 111<: prospects of enormou, Jury awards. AmtncanS are qu,cL to drag an alleged offender mto a courtroom al the slight· est pcrcqlllon of incurred harm. Private health car< pro,idcrs ha,e bcrome 1ocrcas-1ngl) susceptible to 111,gauon. Hence. m the UniLCd S1a1c,. the risk of malpracuce Jawsuns as a real coosidcntion m lhc praa,ce of medicine To pro1cc1 th<:mscl,cs agains1 lhe poss1bil1ty of li1igauon. ii is not uncommon for pnctlllOOCfS IO engage ,n .,ba, ,s rcfc"."1 to as d,f,nsfr, medicine by prescnb1ng add111onal diagllOsiic 1esis. scheduling mum checkup vm15, and mamwnma copious documcniauon Many of ihcse add111onal effortS may be unnecessary· bcncc. they are cosdy and 1nefTic,coL '
High T edinology The Un1ted S1a1cs has been the h01bed f research and Innovation in new rnedi~J le<hnology. Giowlh 1n scieoc,, and ~h :°'oar oft~ crca1es demand for qew m~ ices dcsp11e shrinking reSOUrccs IO finance
5'.""'•S11Ca1Cc1 catt. People generally h1gh-1eth CUC IO hin• . <quale wan, ··,1,c I b'•-(!ualny care. They
aics, and the bc$t .. especial) whffl bcahJi '~ wiU • y 1tea1mcnu Phy . pay for new
• "Clans and ICCh · wan, 10 cry lhe la1esi rnc,ans COfflp(1e 00 the btSIS aadgcu. llospualJ mode of ha-,01 lhe ,_1 capi1a~n=~':'.,:~~c1ln1cs. Once tceoupcd lhrou&h uuJ • costs mus1 be
inioon. ~pl nsh for
providers and health lans pla> a role in d,seou! . Ilic,..., 1echnology. Thus, sevc!:~ ~Of~ lhc use of costly new led,~-. dc,elopcd -"""IY<aq~ ,,
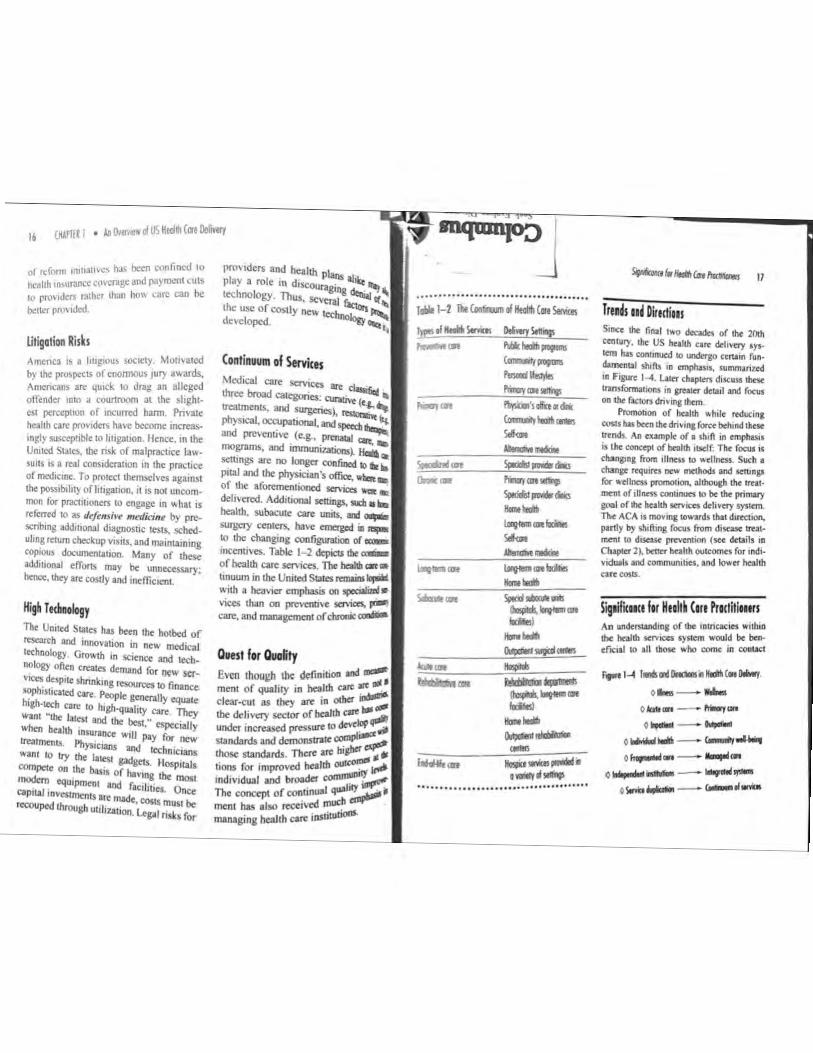
Continuum of SffVi<es Medical care ser.,ces .,.. ,1~ .
lhrce broad c:aleg(Jnes• ....... - " ITCalments. and surgeries) ·, (t.g., ...
physical, OCCUpationaJ. and·~ and ptC\CflU\'C (C.&-, P<'1Wal mo~, and immunizations~ :i. ... semngs arc no lon&cr confined ,. " "' p,ral and lhc physician's olfJCC, .._,: of the aforementioned scrvic:.s wa. delivered. Additional settings. tucl, • .: health. SUbeculC care units, 111d .... surgery cemers. have emerged in 111pa
IO the ch3n&lllg conf rgwation ol -JOCffill\'CS. Table 1-2 dcpicu Ill< -of health care seiviccs. The hcahh cat ..
tinuum in the Uniled SlalCs mnaios.,.... wnh a bca">Cr emphasis on~· vices than on preventive ~ ~ care, and managcmcnr of chr0luc rm,lilioa
Ouest for Ouolity Even thou&h t~ definition end i.mc,n1 of quahty in heallh cm ~ Id• dear-cut as they are in omcr -": 1he delivery sector of heallb cue"" qa,111 under increased pressure to rle-'<lol' ,_ Slandards and dcmonSintt c:ompbl""'~ those s1andards. There arc hijber - ., lions for impro,-ed health ou""';"" ~ md1v1dual and brolldcr ~"""""' The concepl of conunual quab~, ment has also rccei.c:d much managing beallh cate ,nSlitutioOI-
........................................ J.W. 1-2 The c-..n al Heal!li (ire Serius
0.-ca
°""?S.C.,
,_, ..... ~,-Sdnio llat ... lavlmlanilcills Sel<M ........
.......................................
Tre1ls u• Dlmtiou S,IIC'< lhc final 11,0 decodes of th< 20lh cen1ury. ohe US h .. llh care dch,cry •Y•· tem hn con11nued co uMcrgo etnam fun• dammtat ,Mts 10 emphu,s, sun,monzed 1t1 Figure 1-4. l.attt c;haptC"rs d1xuss 1hese nnsfonnauons in &JCaltr detail tind focus .., lhc r.,_ c1,,.in, 11xm.
"'°"1ol,on of hnllh while rcducma COS!$ bas been lhc drMna force behind lhe1< lrmds. Ali <umpk of I ,i,jft JO m,phaslJ IS the CIOIIC<pl of hnllh rlldf: Tho fO<UI IJ
cha.ngmg from ,Untss to wcllne-ss. Such 1
c:han~ requ1rts new mtChods and tettinga for •<IIJJ<SS ~ 1llhoup lh< ,,.... mc-n, of illnns conUnUC"S t0 be the prirrwy '°"' oflhc health SCIVJC<S d<livny Syst<m. Th< ACA is moving - •rds that dumic,,,. partly by sh11\1ng (OCUj from d,,u,c 1ttat
mcn1 co disea.st prt:vC"nt10f'I (see details in Cb'l)l<r 2). btt-.tt heallh OULCOffl<S for ind, . ,,duals and c:onwunu1a. and lo .. n health
cart cos&s.
S~1ilicme fer Heall~ Care Practitlours An undm&and.Jng of the Lntricaciei witbu, ll>c lxallh ..,,,_ 'YJl<ffl would be b<ft. cfte1aJ to 111 those who come In c:oacact
fpc l-1 i..1111~.,..""°""' o- - w .....
oi...- - -, .. 0 ..... - 0...-
0 ............. - '---"-'
o~,.. - llaapjm
0 ........ - - i.ir-.,Olonb ....... - -·-

18
• ., ~ t, ,.\SW~ In 1he1r ~fk."(u"e train • · h I h ,,..,•·•1ah, ,uch 3S n~ rro~ri.lm,. ca t pol
rh),,,i;1n,. nul"\t . cc,,:bluc,an,. lherap1sh, J ,~ull;an • and ph.aml.tel~h. a, well a~ oth+ Cf'.. ma~ und1.·r,1Jn<I th~tt O\\ n 111J1" ,dual rolci bul n:rnam ,~rwrant o l tnc: (O'"cc.~
uuhtde 1he1r profo.,1c.1" that couJJ s.1gmfi· untl) tmpkl currt:nl and future practices A,n und<r,.1and1ng ol 1h< hcahh care dc:h, ery ,y,1,m cJn anun.: hullh profe<s,on· 11b 1,1 1h~1r rd.,uon~rp \l 1lh the n:'il of the hcal1h Clll'C cnHronmcnt II can help 1hem undcr,iand chJngc, and 1hc 1mJMCt of1hl,,c ...:hangc) un tht.:ir o~n prkUCC' Adaptauon ;nd n:Jwnin1 uc <tr:alcj!ie< 1ha1 can prepare hC'ahh p1ofc(\tt'H1als to cope "11h on en\,. mnrnc,n thal "'111 ,ec ongc.nng chan~ long 11110 1hc lutun: f<ll ,-unrk:. many of lb< AC>\\ rcquirtmcnt> rresenl bo1b OJ)ponunu,c, an<l challcniic> for he.11th core pm<ll• 1,oncD. t·vr e,11mplc, bt,,~ ... ,ncrnmta the numbtrc•f the 1n\Ul'cd 1<ho 1<111 Rock 10 pro"'""' 10 ,....,civc ,,:rv1cc,, 1he ACA plnccs 11dd1110MI rc;pon>ib1fl11c\ on "'°"""" to dd1,cr 5tf\ 1cc, 1n I MOff: C'O(lf'd1natcJ mann<r" hilt 1f101mp<o,ina 1hc quafuy or care.
,n.1nagcment, reg;i,c1ics. manage a private instiru~r "hcu..t vice agency. Such d= . or a .. ,.. Ii,
-.ISl<>ns , ..... II, e,cntually, affect the em illld -. ·
f ICJcnc:y .• ~ II} o services &h,ctod. T!ic llad'lllll among lhe sys1cm's key 1~ 1he 1mphca11ons of rbose i~ lllC be "ell understood becaust ~ ...,. of health care ins1i1u1ionsarc ~ cnctd. c1~1er directly or indi stro,,gi,Wi. linuncong or heahh SCrvic..._l'OCII),, II), It ment ra1cs. insurance mcchan "" mocks, ne" s1a1utes and legaJ 1$1111, dc""'i go,emmcol regulations. op,oq,,.,.
The cnv1ronmcn1 of health -de "111 continue to rc111.1m nu,d and ""'1 The, , oab1li1y of dcli,cry lfflinp, ::;-. the succc,s of health care ""'lll&cn,:: depends on ho"' 1he ma11.1g.,.. rtact to• ))>l<m d)nam1cs. Timclinc,ss of.._ 1s often • critical factor 1hat can makt • d11Tcrcncc bc:1"ecn failure and ._ fullo"' ma are sorne more spcc,fic -"hY unckisuind,ng 1hc hcallll care doll,. try syMcm is ind1>pcnsabfe for hwdl .. mona11-crb,
Positioning tht Orgallliatiow
1 luwc:\/C:r, health core procrn1oncrs arc con«mcd IMI thang<" ,n 1hc, ACA rtfl,lrd1na hcallh..,. financ,na may afl'ec1 1hc a1a1t-1b1li1y of l<loquate and susu11nable funding as 1hcy make •dJu11menh 10 cope v.11h 1hc mOu, or rc«nll) m,urcd ronsumm "ho arc likely 10 ha,e gruatr hcallll care needs 1han 1hc general populauon.
S~1illcme I or Hull• Cue Mmgm An undcniand,og ."r 111c, hcthh can: •>•· l<'m ,.., 'l)CC1fic 1mphc11.,.,. fot hctllll \Crv,cc, m1n11gcr", whn mu,t undct'>ltand th~ macro en\11mnmcn1 ,n whN.:h lh\:"y m11kc tnlfcal dcci'IHNt11 ,n pi1nn,n, •nd ,iratctc,<.:
Managers need 10 undffttand dww.., organ11a11onal position .. 11liin tht -'"' 1ronmcn1 of tht heallh care •>Senior managers, such as ch1tf ex..,... omcers, must conJtantl) puae die..: anJ impact of 1hc fundJJncnW 1flustra1cd ,n r,gurc 1-4. Managtn C:: 10 consider which changes in dit configura11on of financing. 1ns...,...,:;. mc:n1, and ddi, cry mijhl 1/'fcct 1~-" nia1ion', lon11-tcrm 111b1hty. ~ firHl-lino m•nagers also need to tioll -" llic,r role 1n the currcn1 c:o11li1•111 ..-• 1he ,_. huw thlt role mish« change 1•
lfO" $hould ,.__ be rcal,a.d 10 clf«U\tl) l'npo,,d 10 lho<c dw,ses? For c=\amplc. thne manasers oecd 10 eutu.Jte -.hccher ccnam fUDCtions III dacu ~IS ,.,11 hl\c 10 be eliffllnal<d. mod1Ji,d, or added. Would tbc ebonies JOH-.hC furtha t.n.JnlDJ? \\,Q1 Pf'Ot'tSSC::S
an: 1,Ldy 10 cbanic aad bo"'? W~t cf<> 1hc manaacn nc,ed 10 do 10 ma.1nta1n ihe 1n1eg:nl) oftku1ASOt11UOO·smwaon.d,e
l',od"'" oftl>< p<tlllS they""'· and 1t,c quahly of care? Wdl lhough1-<>u1 and 1ppropnarrly planed d!atlae 11 hhly lo ca= ks> ,.,.,..knee ro. lb< pro,idrrs. as "tll a, the rec1p1cnu orca~.
fflfflO'nag Tltreots N4 Oppomiititt { hlftJ<S '" In) or lbe l'imc1,om of finaoc.... - pay-. and drb,fl)' cu paent nc"' &hrats or opponun1hts ,n the hc•llh catt m.1tl«• Hnld, are __,. .,. - cfl'CCll" ,f Ibey _.,,dy deal •ith &n) t.tvou to their ,nsurutaon's profit· 1b1l11y and H•bthl)'. M...., n«d 10 find ••>, eo U'Mbfonn cau,,a dweeb ao ncv. 011pon .. ,111,n
Sm;,,, manag,rs arc often mpc>nS<blc fo, .......,. pfaruuag rrprdi11& which scr· .... ces sboukl be added or disconunucd, ,.1,ICft ~ shoold b< c:omm,n,d 10
fanlil)' npansiao. o, a1la1 should be done """h t"lccss capacny Any lona•ran,e plan· IIUIJ mu.u W<r ,nco ccm1dcnul0ft lhc currmt makrup or hulm = itts deliver;. lhe cvofvmg l1<nds, and lhe po1<n11al impact of lhcKIICads
c.,rn, lltw Wets Haltb ~ ..,....,..,. .,. ,n a betlcr posi· uon to captun:: new hetihh services markers 1r lhc) undmland cmcrg1na U'Cnd, ID lhc r,.......,_ i.osunnce. paymcn~ and delivery fuoc110t1S New opponun111c:s m1.1St be c.,ploml brfon, 1111)' ....,1y C\olu11& Kl• maiu or !ht morket act overcrowded. An un<J<,rs11nd1na or lhe dynam,cs w,1h1n Ille system " cssrnt11I to r..,,., nc" matkei..,.......,..1011ay lhnd or 1hc coms><li· 1100 and often to lind1na I sen-,cc mctw.
C-,lyilf wM R.,.i.11ot, hollaling lmplcotiots Managers arc bentt able 10 enltak the 1mplical10M of bnJIII policy and new rrfum, Pf'OIJOUls "hen Ibey undcrs11nd th• rclc\-anl 1uue.s and ho~ 1uch 11osutt link 10 thrdch-.,yorha1t1,..,_.,...,nl!irtiubfuJ,...,,,. they ,,,.,,.,. n.., upan11on or hcahh 1nlura.nce CO\-etagc ul'Nkr lhe ACA bnnp more rnd1>rdualt '"'° 1llr btallh can, '>""m. cttat"'I further demand for huhh .en 1c-e1 Pla11n1ng 1:nd s:11ffina f« Ille: "ill• m11 of hcallh can, ,.v,tfotce 10
111C<t 1h11 an11cipotcd IWll< '" demand 11 trllltll.
o.tr,ety or llntlh nre ..,.,... 11 ,,.,,,.
dy rtplatrd. Hn/d, care mllllllffl muat comply .. uh go•,emmen1 rcaut111ons, such 111tandiards o-f p1,oc1p1uon 1n ao .. -emmtn1 -. he,.,.,.. Nin. and'"""'>' •nd pnvacy laws rca;ardan& paucn1 information. and mu11 opcrace "1dun dte conwa1nts or mmbuntmmc l'IIICI. The Medicare and Medicaid proarama havr, ptriochc1lly, mod• d'"""' ct,..,,.. to lhtir n,ll!lburJ,. mm1 ~ NI bl,·e lri...,.., lhe nttd fa, opc'"UOllll chanj ei 111 lhe way .. r. vicn an, 0<sm1ud and drh,cml. l'rtnk ...,......, ,uct, M !ht Jornl Commi,.,on,
I (l!AJ'TER 1 • An 0,-e,v;ew ol US Heolrb (ere 0eF.,ery
also pla} an indirect regulat~ry role, mainly m rhe monitoring of quality of services. 1 lcalth care managers ha,·e no choice but
10 play by ,he rules set by the "arious public and prhate agencies. Hence. 1t 1s pa~mount 1hat health care managers acquamt 1hemsehes wi1h 1hc rules and regulations go,emmg 1heir areas of operauon.
Following the Organizational Mission Knowledge of 1he heallh care sys1em and its dc\'clopmen1 is csscn11al for effective management of health c-arc organ1zauons. By keeping up to da1e on comrnuniry needs, 1cchnolog1cal progress. consumer demand, and economic prospcc1s. managers can be in a bcn<r posiuon 10 fulfill !heir organiza-1ional missions to enhance access. improve service quality, ond achieve efficiency in th• d<hvery of services.
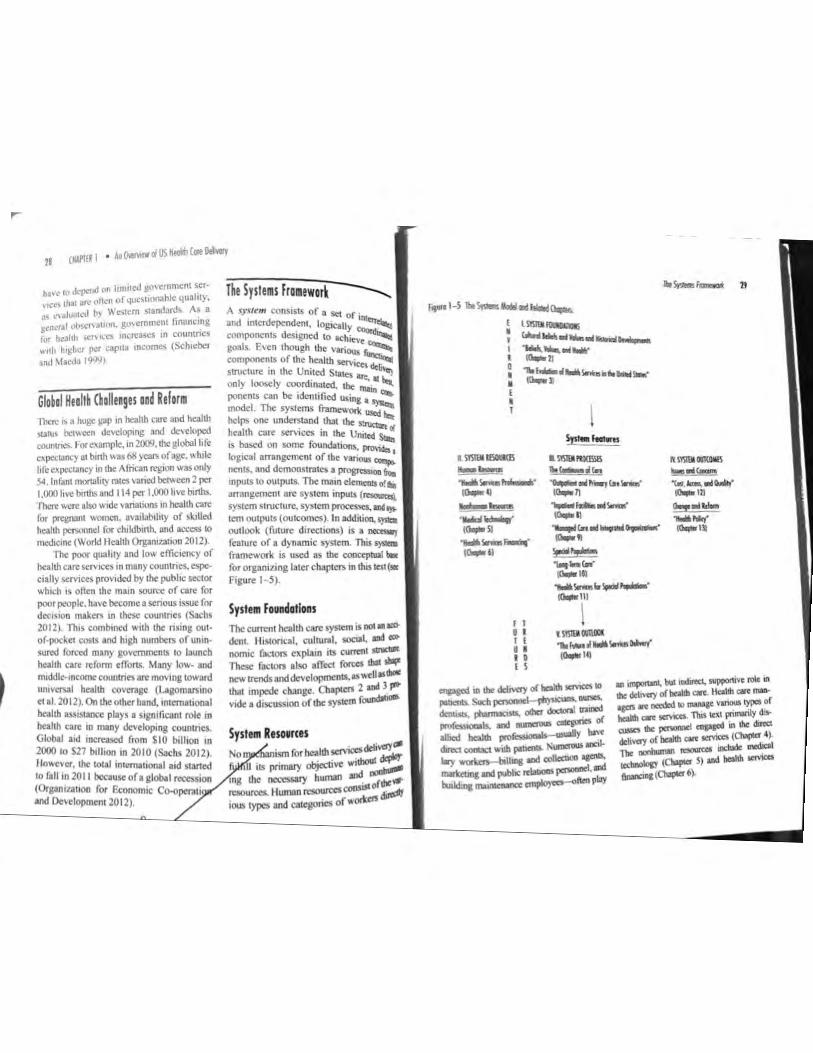
Heall~ Care Syslems of Olher (aunlries By 2012, 1hc 25 weahhiesr narions all had some form of universal coverage (Rodin and de Fcrranri 2012). Canada and Wesrcm European narions have used •!tree basic models for s1nic1uring !heir narional heallh care sysrems:
I. In a system under 11a1t'o,ra/ hea/1/, i11.<11ru11c, (NH I), such as in Canada rhe government finances heallh ca~ lhr~gh g~neral raxcs, but !he acrual care is dehvered by privare providers In the comexr of the quad-funcrio~ m":"el, Nl{I requires• righrer consolida11on of the financing, insurance, and paymeor funcr to~s coordinared by lhe government. Dehvery is characte . d by derached privare anangemen:.u
2. In a 11ati<>11a/ It. such as in Gre ••l11t .,,,,..,
31 llr;1.:. -~ o. ... to financing a ....,, in ,j.,"l program, the go:-~~ the mfras1ructure r, '""'eai ~ medical care. u~ die~ the govemmen, ~, ' medical institu:~~ care providers, suc:l, i..,.. are either govcrrim: ~ or are tighUy organ;~"' hcly managed infras ID • Ill conrext of the quad-~ It~ NHS requires a 1ighrcr ~ of all four functions. ~
3. In • socialiud health . (SHI) system, such as in .....,,.. govcmmenr-mancbted coo~ by employers and cmpl<lyea rm. heahh care. Private providcrt dii,, heahh care services. Pri-....., profir insurance 00mplllics, CIIW sickness funds, are r'CSjX)l1lil,le 1, collecring the contributions IOd Plf' ing physicians and hospitals(Snnd Neun 1996). lnasocializod~ insumncc sysrern. insurance ...Sfllt mcnt functions are c106Cly inltpW. and rhe financing function " tdl coordinared with !he ins..-- al paymenl functions !ban in !he~ S1a1es. Delivery is chataCreri!Otl 1'f indepcndenr privare arnngem<d' TI1e government exercises oiual conll'OI.
In the remainder of Ibis ~: terms "narional beahh care prograD' _,,;. "national health insurance" are used .....-111! cally and inrerchaogeably 10 refer ~ type of government-supported ~ ;, , health insurance program. Fonz,:,.;, brief discussion of heallh care
1
sc1<cu:d ~ from various pons or lhc .. -orld io dl""11l1c lbc: ll(lplicatioo of lbc: ~ models discussed and IO provide a sample of me~ of l><ahh cm: sy,iems lD the world.
A1stra_t.a In lhc pas,. Ausnba had swncbed from aw,;. ,.,..1 oational hcallh cue prog,1m io I pri-, .... 1y financed sys,,m. In 1984, ii rtiumcd ., a oauooal prog,om-allod Mcdicatefu,anc,cd by .-no W<cs and an in<ome• bo,<d Mcdican: kry. The S)'S(lem is bw~ on me phi 1o5op1iy or "''U)'OOO co,,lribuu,.
AUSUllia ·s health system. At the same time. lhc Na1io...l Heallh Reform Act 2011 CSllll>lishcs a new lrul<pcnd<n1 ttospn•I Pricing Aulhoriiy and Ille National ttcallh Peno,. mance Aulhoriiy. Thc Pricing Authority will determine and publish the national price for services provided by public 00$pitals. The Com.monwealtb Government will dttamine its c:onaibution to funding public hospitals on lhe basis or lhcse prices. The Performance Authority is to monitor. and r<por1 oo. lhc pcrfonnancc of local hospital nclWO<b. ll"blic and privaic hospilAls. primary health care organizations and other bodies or otganiutions that provide hea1th ca.re strVica. The Act providts a new sta~ IOr)' framework (or lhc AuJtn.Han Commi.ssioo on Sare,y and Qualil)' in Hcallh care (Austtalia Govemmcn1 2011 ).
Rcccn1 hcallh care rcfom, undertaken by 1hc AUSU'llian go,·cmme1n has focused mainly on lhc rollowi"i aspcclS: (l) ca1al>hs.h1n1 1 more sustainable fundin; framo'""" for ..,bhc ho1pi1Als, (2) reducin11 emc:ricncY dq,onm<nt and clcc1ive sur11cry wai1ina times, (3) improving primary cam by .,.1bl1sh11111 more primary care raellitics..,,..., the couniry. (4) 1r1nsrcrring run policy and runding ,...ponsibili1y for aacd care scrvtec:S to the AU5tralian Government. and (S) enhancing ttansparcncy and accoun1-abiti1y in Ille health system (Austtalian Oov• emmcnt 2011 ).
Canoda
., thc OOSl of hcallh c:are occonlin& ., bis or her capaaly IO pay. In addit>On 10 Mcdicar<. ljlPOXlmll<ly 43% or Aus1nbans cany pri,..,c l><allh imunnce (AUlhlian Gofflll· -- 2004) IO Q",:r gap$ in public <OVCOlgC,
,uct, .. denial S<f"ic,es and con: r<OCiY<d in plWIIC hosp11als (Willcox 2001~ Allhou&h p11'~1< hcallh msurance IS volw,rary, ii is Sll'Ongly encounacd by Ille AIISllllian govcmm<nl lhrouaJI w subsidies ror puro11ascr> and w pcnalll<S for non-pu,d,ascrs (Healy 2002). Public bo6p,lll spcachna is rundcd by lhc eo•cmn-. b<II pnvale hoopiiab OITC1' bcllcr cbol<,es. Cools 1ncun<d by p1111cnis mcciving pn,-al< medical services, wh<lhcr in or OU1 of the 1">spi1a1, an: n:imbwsed in ,.1,o1c or in part by Medicare. PriWlt policnis an: fite io choose and/or change !heir doc· IOI$. The medical profession in AU$1111ia is composed mainly or privau: pn,ctitionm. ,.1,o provide can, pn:dominantly on a rec-for· s,rv,cc basis (Hall 1999; Podgo, 1999), .
In 2011 !he Council of Ausinhan GovommeolS sign«! thc Narional Heallh Reform Agrccmenl, which selS ou1 thc an:hi=re of na1M>01l heallh reform. In panieu(ar, the Agreem<nl provides for more sustainable funding arrangcmcnlS for
Canada imptomcn~ iis na1ional hcahh insurance sysaem-<efcned 10 as Medicare-under !he Medical Care ACI of 1966, C=tly. Medicare is com~ or 13 provincial and terriiorial hcallh insurance plans, sharing basic s,andards of coverage, as defined by the Canad> Heald> Act (llcalth
22 (HAPlfR I • All Ow!IYiew of US Heolill Core Oeive,y
Canada 2013). The bulk of financing for Medicare comes from general provincial tax revc~wes; the federal government pro, 1de) a hxed amount that is 111dependent of actua_l expenditures. The health expcndinire 111 the public sector accounts for 70% of_ the total health care expenditures. The private sector expenditure is composed of household out-of-pocket expenditure, comn~cn.::ml and not-for-profit insuran<:e expend1~ure ~nd no.n~consumption expendicure (Canadian lns111u1e for Health lnfonnation 2012). Many employers offer private insurance for :.upplemcntal coverage.
. Provincial and lcrritorial departments ?1 health have the rcsponsrbility lo admin-1st.cr medical insurance plans, dctennine reimbursement for providers. and deliver ccnain ~ublic health services. Provinces arc required by law to provide reasonable :icccs, to all mcd1cally necessary services and to provide portability of benefits from 1>~ovmcc !O province. Patients arc free 10 !:'.•ct 111•ir providers (Aknho ct al. I 99S). ci~'ord1ng to ~onada's Fraser Institute, spc.3 ,~1 phys,c,nns surveyed across 12 s
c1olt1es and 10 Canadian provinces re ,i~ o total waiting 1i1nc of 18 2 k po c referral rrom · wee s between def' a general practitioner and
as private nonprofit e .. nrry boards of tru ntrbes run,._ . stees v 1 "Yea... hons: o r municipaliti • o llntary . '°' are on private pra:andtnos1~ 2013). Most provin~ec (Heaitit 'r::" and allocate set reimb use &lcoaJ ~ each hospital Phys· ~mcm ....,;.:---. · 1c1ans --:-"'Cf&it service rates, negotiated be arc Plid r..,.._ vmc1al government and ~ ·een Clcb (MaePhee I 996: Naylor ~edica) assoc.:
In 2004 the J 0-y 999
>· H I ear Plan tos.-... . ea th Care was created r, . -.._
trmcs, health human ocus,og °"..., . resources .,__ ceut1cal management. el~..-records, health innovation, ~ aad reporting, public health ~ lii ~al health. Overall, progress has been i... m these fields, but the goals h lllldt fully achieved (Health Counc~lvef"!_~ 2013). IO.._._
. A !though most Canadians aic quil<,.. rsfoed "'.ith their health caic system, boa to susuun current health caic deli"cry 1111 nnancrng remains a challenge. Spe,mc on health care has increased from lboll 7% of program spending at the provincial level 10 the 1970s 10 almost 40% today. It ii expeete~ to su':"ass SO% in every pro,ince and temtory wuhin the next few ycan.
'r ,very of treatment in 2010, an increase " om 16. 1 weeks in 2009 r . wa1 h
1 · ahems had 10
1 1 c ongcSI to undergo onhopcd' China 8ery (35 6 k ) 1c Sur-
Since the economic refonns initiated iJ •he late 1970s, health care in the people'• Republic of China has undergooc sigi,ifi. cant changes. In urban China, health io!llf· ance has evolved from a predorni0Jll11)' public insurance (either govemmentorpul> he enterprise) system 10 a multipayer syttem. Government employees arc covered under government insurance as a part of th~ir benefits. Employees for public en~· pnses are largely covered through publlC
. wee s (13orua et al. 2010) Nearly all the c d' ·
(Ontario being one excc;~~11;•~ provinces to regionalization. b . ave ~~ned tive districts . h. Y creating adm1111stra•
wJt m each · ?bjectivc of regionalization _Provance. The ,ze authority and res . . . " to decentralciently address loc r•s1b1l11y 10 moic effi-citizen panicipatio: i;~::h~nd to prom?te makrng (Church and B k caic dcc1s1on majority of Canadian ho a'. cir 1998). The
sp11a s are operated
el'ltcrprtse insurance. but the actual bt:nefilS and payments ,•ary accooling 10 the financial v.ell·being of the enterpri:ses. Employees of foreign t,usinesscs or joint .. enrures ore 1)1';.;ally well insuffll lhrough private ,nsurance anangemcnts. AIDl0$l au of tbtS< p\anS cootain costS thr<Mlgh • variety of ,neans. such as expcrience-boscd pmniums. deductibles. C()\)aymc,>ts. and bealth 1,enefi1 doll.,. (i.e., pre-allocated benefit ciollaJ$ for health care that can be con,cRed tn!O income if DO< lully used). The unemployed. self-emplo)'ed. and employees .. ortt,ng for small enterprises (public or pn,-a1<) are largely umoswed. They can put<hase individual or r.mily plans in ,he prwa1c market or pay for SCl'\'iccs out of pocket. In "'ral Chma. the New Coopcrall" Medical Sdicrnc (l'(CMS: discussed la1cr) has t,ecornc "''despread. with funds pooled from natiooal and local govern• mcnt, as ,-ell as pnva1< cmfflll. Allhoua)! the ,nsuranc< c(Mfll&• ,..., ,, hia)! (reach-
Health care delivery has undersonc $igniftca,u changes. The fonner tbfce,.ricr rcfeml system (primary. second, tertiary) has been largely abolished. Patients can DOW go to any hospital of their choice as long 1$ thty arc ins-wed or ca.n pay out of pocket. As a mull, targe (tertiary) hospitals arc typically overuti1ized. whereas srnaUcr (primary and~) ho<pitals an: underutiliztd. Use of large hospitals contributes IO medicaJ c:ost CSQlation and medical spccializatioo.
Major changes in health ios.urance and deb-.·tty havt: made accm to medical care more dif'ncu1t for the poor, uninsured. and uodcrinsured. A5 t. resu\t, wide and growing disparities m access. quality, and outcomes are becoming apparent between run.l and urban areas, and between the rich and the poor. Since the severe acute r0$pitator)I syndrome (SA RS) epidemic in 2003. tbc aovemmenl created an c1cctronic dise:asc-.reponina sy11cm at the district level. In addition. each district in China
'"' o,er 90%). the 1Ctual t,cncfits are .i\11 , Cf'f hm11ed.
S1m1lar 10 the United StalU, China has been fac,na the Vo" ma problems of a la,se uninsur<d J>Oll"lal,on and health care COS1 inll01ioo. Althollgh health care funding ns increased by 87"• in 2006 and 2001, the COWIIIY has yet 10 icfonn its heahh cm S)'Sttm in10 one \bat is efficient and ctTecu, ... Emptoymeot-based insurance in China docs no100, et clcpcndcnts, nor docs it cover m1gran1 v;O<l<C<S, leading to high out-ofpockc, COSl sharing in 10131 bcalth spending. Rutal amos in China are the most vulnerable because of a lack of true ;nsum,ce plans and the accompanying oomprchensive coverage. Health= coot inOation is also growing at a "'"' that is 7% faster than the )!JOSS domcsti<: product (GOP) gr0"'1h of I 6'/• per
now has a hospital dcdic•ted to infectious disea.,c, However, flaws still remain, par· ticularly in monitoring infcctiou.s disease in the remote localities that comprise some d,stnets (Blumcn1h•I w,d H,ino 200S).
To f,x some of its p<0blems, the Chinese government has pushed through health reform initiatives in five prominent areas: health insurance, phannaccuticals. primary eaic, public health, and public/community hospitals. For example, it created the New Coopctative Medical Scheme 10 provide rural areas wilh a government-run voluntary insurance prog,am. h prevents individuals U'ling in these areas from becoming impoverished due 10 illness or catastrophic health expenses (Yip w,d Hsiao 2008). A similar program was established in urbllll ""8S in 2008. called the Urban Resident Basic
year (Yip &lid Hsiao 2008)-
74
·h<f!IC n,c ,chem< McJ1cal h1.,ut11nc~u,:i children, cldedy. targets lhe unuo. t,an residenu; and and othec n0n"orl:1ng vr r.,rn at rhe h()t.lSC·
c11rolls d1en1 ,n10 ihe proi 1nd1\·1dual fc\•el hold 1c.,..·cl ra1her than at I fWag:i.taff cc al 2009). 10 primary CllfC,
To ,mpro,e access 11 abhstl,-d comrntunl) hca t 1 China has ~ rovldc prcH.'1lll' ·e and cenlCIS (CIK•> 1° p rrse, ,he e,<p<O· pnma,Y care .scl'\1cts 10 o ·w1s The I\( outpaucnl scf\'ICCS az hosp• ,
' ~~c i.~ nual uuh1,auon in goal ,s to re"""' ,,.,,.,, . ra ...-or of ClfCs Lhal can provide pre, en11on. tiome care. and rchab1hWU\'e $crv1ces (Yip , nd 11,100 2008: Yip and Mahal 2008). Th< enc, haw n<M b<tn "'Y popular among ,h, publ~ bccauscoflhcir pertc1, e<1 lock of qu11hty wwl rcpumuon h ren111os un~am "IM:fhcr Chin1t will resrorc us previously integrated helhh care dehvery system.
1umcd at 1el11cv1ng un,versol a~ss, or con• 11nuc ,H c:urrcnt course: or medic.a.I special· 111.uon nl'd pn"auia11on
An01hcr maio«omponcnt of the health r,f01n1 ,s 10 estabhsh en css,ntial drug system which 1ums at mh1nc1ng access 10 1111d r<duc1ng 001-of-pock<I spending for c~n,,al 1ncdic1nes The ttfonn polic1e.s s.p«ilitd a comprthtns1vc sysrem includ· ,ng sckci.on. procuremtnt, pricing, prcscrip1ion, and quali1y and safety s1andards 18.,ber <t al. 2013). As f0< public hospitals r<fonn, qualil)' and efficiency as well
as hospital governance structwt have been cmphasitcd. Several pilo1 n:fonns ha1·c been l~unch':'1 in various cities in China, bur DO na11onaJ implementation plan has been formulated (Yipe, al. 2012).
Ger11111,y
:::~:~ ;~,\;~c;!aspcbeen made mandaiory mi.anent residents in
Gcm1ony since. 2009 (Blume! 20 pointed out earlier, the Gennan he 12), ;\a sys1em is based on the SHI model •Ith c,,, uon, 1hcre is voluntary substiiut· · In ldcti. ivc P. health insurance. Aboul 85¾ of the """uon has been enrolled in a sick ~ and 10"• is covered by private incss fQIJd
There arc also special programs.,......_ tl>e rest of the population (Blume\
0 2""'~
Sickness funds ac1 as purchasing .... 0.1ti.
by ncgo1ia1ing contracts wilb h<ispbi.., Ho\l,evcr. with an aging populatio t'-1
l people ,n the workforce, and stagna:, °"" ~rowth. during rcccssio?s· paying fo;: ,ncreas,ng cost of medical care has betu challenging.
During 1he 1990s. Gem.any &dopooj legislation lO promote competition amcq sickness funds (Brown and Ametll!li 1999), To further control costs. 1he syse,,, employs global budgets for the hospilll..., ,or and places a,mual limits on spcndina for physician services. lnpa1ien1 care is paid per adnuss1on based on diagnosis-relltl<I groups (ORGs)-<liscusscd in Chaplet <>which was made obligatory in 2004 (Blumd 2012).
Great Britain Grcot Britain fo llows the national beol~ sysiem (NHS) model. The British htal~ delivery system is a lso named NHS (Na1ional Health Service), and is nowmor< than 65 years old. The NHS is founde<I OI
1he principles of primary care and bas• strong focus on community ~Ith seJYi«S. Thesys1em owns its hospitals and emplo)'SJIS hospital-based specialists and other stalf
001
salaried basis. The primary care physiciall$. referred 10 as general practitioners (GP>~ are mostly private practi1ioners. p,op~ are required to register with a Jocal G ·
11.ere were on average 6,651 pr&tienu per p<><IICC and 1,562 pa1icnis per GP in 2011
111,rnson 2012). Delivery of primary e~ is thioogh .
m:,ry care "'"'.s (PCT•) in England. ..: 1i<>l1h groups in Wales, health boatds scodand. and primary care partnenhips :
""'hem Ireland. PCTs have geognp1,,. callY assigned responsibility for conuoonity t.callh services.. in which each person Irving
1n a gi,cn geographic: area is assigned to a panicular PCT. A typical PCT is responsible ror approximately 50,000-250,000 puknts (O,,on and Robinson 2002). PCT, NIICbCla ,ndcpendcnlly of 1hc local he1l1h authonrics end are go,cme<I by• consumcr-dommlecl l,oard. A fully devclOpCd PCT has its.,,.,. budget allocat10ns. used f0< both pru1W)'
care and hospital-based services. lo dus respcel, PCT s function hke MCOs III the Un11e<I Stau:s.
About 82% of the hc>llh cxpcnd!IUre in 2009 "as 1n 1hc public sccuw (Hwruoo 2012). Priva1c cxpcnditwe ,, mo,nly for drul)S and other me<lical p<OdUCIS " .. ~11 as pnvale hospilll care. Dcspi1c M"1ftl , na11onal health care 5)"tcm, 11.5% or the Briush populotion holds pnvalc beolth 1mun.1'1CC (Dixon and Robin.son 2002). Fu1ure ··pro-markcl" refonns in the Unued Kingdom's NHS would likely shin dc:Cl$H)tl making 10 geooral pr11eti1ionen. let some hospillls become nonprofi~ and g,,-e palients more conl!Ol ovtt thelr health care.
The Health and Social Care Aa 2012 demands an cx1ensjve reorganization of the Structure of the National Health Servi«, II proposes 10 abolish the l'C'Ts and 10 uamfcr between £60 and £80 billion of health care funds to sc\'eral hundred "clinic:11 commissioning groups," partly JUD by the general praclitioncrs (GPs) in England. A new executive agency of the 0epa,,,_i of
Israel Until l99S. lsnd had.• S)'Skm of uniY-cr· Sil -<rage based oo tht German SHI modd. li!W>C<d lhrouch "' employer W< ~ lDCCJmC,.bascd contnbubom from ind,~ viduals. Wbcn 1hc Nloonal Heallb ln>Ut• Mee (NHI) Law • -cnt inao cfTCCI in 199S, ii made lDSW'1U:ICC CO\'U'I&'( lnaOl»tory for all lsndi c:tnmlS. AdultS are ieqwml to pay a health tax. Gtocral ta.'C mrcouc supplemco&s tbt health &ax tt\-cftut. -Mch lhc IO'fflllllCllt cbs'1lbula to 1hc , ....... , health plans boscd oo • ap,w,oo formula. Each )'CU the go'tl'U'DffieDt ddmn1nes bow much fnMII the g,menl WC m..,,ue should be cootnbuled to"-.rd die NHI. In 2009. pubbe funds OO<'OW11Cd for 77% or NH.I J<Venucs Tht mnal11Ull W'll:S from mdividuab' CO!llymc,,IS.supplcmcolll hnldl 1nsUl'lll<< lll>d .... of hnlth p,oduc1s (z .... .,,., lll>d Bnmmh-Or«0bers 2011),
H<alth pbns (or sJCkncss funds) olTer • p«dtfio<d bosJC pocbc• of b<ahh care SCM«S lll>d ~ pn,lliblled fnMII di,cnm1-na11n1 1i&,11nst thole wbo have pcuxlstln& mccbcal coodluons. The cap,ia11on rormub hos buih-1n mt<ftri•·es for the funds to MXtJJ1 a Iara« ollfflbu of tldcrly and chronic:llly ill membm. Rather lb2n relying oo • S1.11gle·P")'Cf syslcm. lhc reform allo•.-e<I the ex1..-c of mul1ipl< hn\111 plans (today tit<ft.,. four oompeting. nonprofit sJCkne<s fwlds) to fO<t« compe1i1ion ..-g funds .. ,lb the l$SWJlllllOO thal compeiitioo would lead to better quality of care and an u,creascd mpoosi.eaess IO potit111 needs, The plans ''"' sell private b<alth insurlftCC to suppl"""'' the basic pack.lg•. The sys,cm is bclie>-ed to provide a big)!

r· I
...
I
f !Iii ..,, •
• :i= • iZ!I "'o ,d)c::l<> ll'• '"' ria n llcal!!I :-an« 'IIO'le]<d
&."I C t,a.)Cd ~---t,Uffl. _._.,._ Tb< set(JDd
•fta ,,.,,,.-. ' .. - .. - Gen"a Ill!" n,I htallh n .mn<c pr~
300 cnll) latl< .,.1oycn " ·h"""" cmpk.-cn1h1,clhc ,.,..nkallh ~ ~ • 2.(llJ P'""' nonprofil h<allll ,~-~.....,_,for ll!l" fimu \mJII« componio c11l1er band .....,.,l"""-.d<pn>IIIC!xallhuuurance
.,, h<lona 10 • '"""'"""'·run "'""· Day - ......,., ..,,c-ullural ,.o,1..,., the .clf-<ffll'lo) ed. and mdffl ""' oil ..-, ered undrr the: 111Mnal health care proa,am '"'*' _, CllfPO><n ,,.~ roucN> 8% or thc,r Hkme, as premiums and ~1\c CO\•
mo;. h .i.o,,, 90',. of Ille rosi of medical ><Ot<CS, ,.,lh ,ome hrru111t- Oepondcnb .-.ctr>< sl,i\lltly lts1 lhan 90'• oo,erage Empl<,)en and Ille ...uoneJ ao,cmmen1 subsidize 1he oos, or pmate premiums Co,e,age 1$ coo,pdkDSI\C. 111Cludrng denLll care and p,escnpclOII drup. and pol>CDb are fro, IO ielecl !heir providers (Ahho n II 199!, &b&t.ono n al 19911) J>ro\Jd. en are paid on a fee-for,serv,cc basis w11h IJIIJecomof Cl'..,,..,,...,.._IMcClellan and Kcnl<r 1999).
Snml heald, polq ....,.. have tmerxed .. Japan '" the pul r... ycan F,roc., IIJICC 2,,,2. 1M1C """- leaden and ra_,.,, urged lhe J,pane,e p c-m-
men I'" 1,n '"ban"" m"<d pc,bhepn•aie l»}rnmli for medal ,m,,cn. "'ll'""I that pr,vale paymcnl• 4/,,,ufd he aJk,..ed for """'" n,4 c,,.lnd ily mcd1C.1J 1n.unncc
•
~-......... l _ _ ..... ._ .... ed ...... ,...-_n..._...,.. __ _ ----.... --"''""--"'~-.,cn101i,,,..tlacN11M1a 1a1a,.........._ ...Slo<S-la2011.ttbm - .. .... ~ou;s I Wlf~c:at" ..... .
"''""' •:t Tm aodd ~ ~ ..,..... ............... .-.. ...... ·--------J..c1b11<$1Dd"ld<_..(orlepl..,._, ·--·~•11ar:111 tWa,M,-., n,. J.:uo - !ft'- .. - -..,Jodaboft IS <.'q>OCIOd IO mu~ • dcc......s _o( ______ _
~·---........... S.,.,.t .......... 'IS4.o;_. .... ~ .. 'lb ~ ........ aodocal --.. .,. pro, 1dod mainly by Ibo P<lbl,c 1<e.., _. r.-1011 ...... _.. ....._ 'ilncc !hen. lhc: IIIIIOII llos dcs,a,,cd I IY$-
- booed - ..ta "' """' - lldf. ~~- .......... ....i ""'....., dvouaJ> a pol,cy dial requiru -..,. pm- _...._ i.. .... lie pcmmcnt financms. Tht p<OSrOIII. t-11 .. Med,oa,,._ aondola ""'ff'f .. u1c. IIIC- ........... ldf-aaplo)-.d. ID tiq,os,1 I pol1JOn Of ...,,,ngJ 1nl0 an 1nd1· ,..., .......... ..,.__&lploy<n_ teq,11,<d 10 ma1eh <mplo)tt contnbuoons. Tlac ••ap ca oely be • ,llldra,.·n (I) IO pl)" forhoop,cal...,,-.ocsad-sd<ctod. cxpcns,,c ph~iaan ...,,;ca or (2) 10 pur·
c:taa. • puwww.o,,oaso,cd -plan. call<d Mcd1Shield. for catasuopluc '"'-'" ad -,or) llbca. far ballc 11111 IOUbncsav,ca, p<q>iearc opffltdtol"') out of pocket. Thole ""° canno1 afford to
-r..._ ... _ ti
0n..,..c..int1
Otvrlop,oa ............ con111n1na ··&s... or Ibo """14·, populabo,\. cll,m ..,,.. 11, o( .. """''• l,aJdi apmdaaa. Y<t, UICI< COllftln<f ICCOllnl for 93% of .. _idrbwdcaof ........ ,,,. ... dn-.topma .._ of die •'Otld are £OSI AMII Md Ibo Pacilic, Europe (mainly Eas1an Earai,<) ad c...i A$II, Latia -and Ille Caribbean. lhe Middle East IDd Nardi Afnca. Soad, Asia, 111d Sub-Sahann Africa. Of lhae. lhe 1111,r...., hove die ..... l'<SCMIICtf and Ibo &JelleSI h<ahh burden. On • per .... basis, mdllllnalm,d .....,..,..
hove 1i1 hmt1 as many holpital beck IDd .... - • -y pbysiciam .. ci...-.~ ,ng CGUlltrics. PUl\11< .. ,111 pn- financial - CID fond ralOOlbly Jood heallh ~ • _, pol1S of die cin'tlo!'ma .. -or1c1. Howev<r. Ille majoril)' of lhc populaballl
I I I I
28
haH' 10 ckpcnd tln lirnllcd g(nemment ,er: \ ,c.:, 1ha1 arc ofkn ot quoOlx\ablC quah1).
15 cuJuatc.-J b~ Wesa.·m s1andar~, A\ a geru:nal ob~l"\Jl1ot'L .1u\emmcnt hnaIKmg ,
1,, ~l('alth wn ic.-c~ ini.:rea.scs m counu tcs
w11h ht~h..:r per ,ap1w in..:omes (Schieber •nd \fo«b 1'1'1'11
Global Heall~ Challenges and Reform There" o huge ~ap in heahh c,ue and hcallh ,Lln" bct"ccn dc,-.lop,ng and dc\ek>p<d oountnes. ~or example. 111 2009. lhe global hfe c,pe,;IJJ1C) It bnth wa• 61! )eal'S of age." luk hfc expeclllnCy m tloe African n:g1on was only 54. lnlant monalt1) r11es ,ancd ~een 2 per J.000 h,-c b1nhs a,,d 114 per 1.000 hvc b1nhs. lhe,c "ere al,o ",de , .. nations ,n hcallh care for prq;,w,1 "omen. avuilab1li1y of skilled hcahh pcoonnel for ch1ldb1nh. and acces, to med1<1nc (Worid Heallh Organiza1ion 2012).
The poor quah1y and Jo., cflic1e11<.y of hcahh care ~·,c-c, in many counlries, cspc· c1ally ~crv,ccs provided by 1hc pubhc sector "h1ch ts ol\cn the ma,n source of care for poor people. have become a scnous ,ssuc for d«JStoo ma.Lm ,n these countncs (Sac:h> 2012) This combined with the rtStng out· of-pocket costs and htah numbm or untn• sured forced many go,cmmenis 10 launch heahh care rtfonn efforis. Man) Jo ... and rruddlc-llt<OCDCCOWJtncsarc movin& toward um,cn;al heahh coverage (Laaomamno cul 2012) On thcodtcr band. mtcmauooal health tlSSt<lance plays a s1gmficant role u, hcallh care ,n many dc,clop,ng coon1nes. Global aid tncreascd from SIO bilhon m 2000 IO S27 btlhon 1n 2010 (Sachs 2012). However, !ho total in1oma1ional 11d sianed 10 fall ,n 20 II bcausc or a global R!C'CSStOfl
(Or&an11.ation for &onomic Co-opcr11i and Dc,elopmcni 2012).
The Systems framework A ~ysr,m consists of a Set or in: anti tnlCrdepcndent, log,ca)1) ~ c(lmponcnts designed to &chic~ goals E,cn though thc 'lric,,a ........ componen1s of the heahh servlCCS ~ s1nteturc in the Un,1cd Siatcs llt -"'l only looo:ly coordmated, thc ~ ~ ponems can be 1dcnti~ using • "mooel. The systems framcwortt ..:-: help, one understand that the ~ health care "'"ices in thc Uniled S..: ,s boscd on some foundot,ons, P'OYlclea
1 logical arrangement of the vanous ._,,. ncnlS, and demonslrntes I progresslOO .._
tnpulS to outputs. The main elC11JallsG{ .. arrnngemcn, ore sys1cm tnpulS c ........... i S},lcm struc1ure, sy,tem procascs, _..,.. tem outpu1s (ou1comes). In addition..,.... oullool (future dil'CCtlOIIS) JS • -r feature of a dynamic sys1em. This syMa frlllle\\Orlt IS used as the concq,<all a for organizing later chaptCfS 1n !his tcSl (.,
Figure I 5).
System Foundations The cun'Cnl heallh cart sys1em IS IIOI •dcnL lhstoncal. culwral. soaaL lltd 0
nom,c factors cxplnm 11S cum,nt ..,_ These faclorS also affm f(ll()CS 1h11 sbll" new 1rtnds and developments, 1s .. -en•• thal impede change OlapCCfl 2 ood 3 ~ vidc a discussion of !he system r~
~ l Sl!IUI ''Utiotl-----....... I ........... _. • io..11 0 I
• I
... _.,_lnu,~ .. -io..J1
I 1
I.S'MIIIBOl;lm
!!!-_!!m! ,...,._,...,.. «.Cl ...__ ._,,.....,.. ta.ail ,._'--!' C0..,.11
Sysl• ltt11<1s
.. _lll)(l\lll .,_.,.., ,.._ ... .....,(a,i.-'
'°"'"I) ..... f ..... lrill" io.11
..... t,,, ......... a.,,,,...,.,. lp,W ....... ,.... .. l«-111 ... __ ..,...,._. io.,m
I tS!!llll"1lllll ........ , ..... -"""l'
'°""''"
lt\lll!IOlltlillll --'tto,IIM.•~ t°""" Ill 0.,,•IM ... Mr( 10.,tll