An Ageing-in-Place Service Innovation Model by Using TRIZ Methodology
17
An Ageing-in-Place Service Innovation Model by Using TRIZ Methodology Chi-Kuang Chen, 1 An-Jin Shie, 1 Kuo-Ming Wang, 1 and Chang-Hsi Yu 2 1 Department of Industrial Engineering & Management, Yuan Ze University, Taiwan 2 Department of Business Administration, Yu Da University, Taiwan Abstract Most of the research on the concept of “ageing-in-place” has focused on surveys of the needs of senior citizens and/or the quality of the services delivered to them. Service innovation for ageing-in-place has received little research attention, however. The present study addresses this issue by proposing a service innovation model for ageing-in-place. In this model, a TRIZ methodology is used to develop the parameter correspondence table, which integrates TRIZ contradiction parameters and ageing-in- place service-quality determinants, to deal with service contradiction. A TRIZ contradiction matrix is then applied to generate inventive solutions for the innovation of the ageing-in-place service system. A case study is also conducted to demonstrate the applicability of the proposed model. C 2012 Wiley Periodicals, Inc. Keywords: Service innovation; Ageing-in-place; Home care; TRIZ; Contradiction matrix 1. INTRODUCTION Advances in medical care and public health have meant that people are living longer, which has resulted in ev- ery developed country in the world facing significant difficulties in coping with the accommodation and so- cial needs of an increasingly older population. In re- sponse to these demographic problems, various strate- gies have been suggested to facilitate independent living by senior citizens, preferably in their own homes (Birn- baum, Burke, Swearingen, & Dunlop, 1984; Fashimpar, 1983). One such strategy is the concept of “ageing-in- place,” which is a diversified care model first proposed in the 1960s to deal with the issues of an ageing pop- Correspondence to: Chi-Kuang Chen, Department of Industrial Engineering and Management, Yuan Ze University, 135 Yuan-Tung Road, Chung-Li 320, Taiwan, ROC. Phone: 886-3-4638800 ext. 2528; e-mail: [email protected] Received: 4 April 2012; revised 20 May 2012; accepted 12 September 2012 View this article online at wileyonlinelibrary.com/journal/hfm DOI: 10.1002/hfm.20536 ulation. The aim of ageing-in-place is to provide ap- propriate care for senior citizens in their local area by integrating the services of nursing homes, community- care agencies, and home-care agencies (Birnbaum et al., 1984; Kane, 1995; Wu & Chuang, 2001). In doing so, the strategy takes into account the preference of many senior citizens to maintain their independence, dignity, and quality of life by having appropriate care services delivered to their own homes or to nearby community centers and nursing homes (Cutchin, 2003; Francis & Netten, 2004; Gilleard, Hyde, & Higgs, 2007; Palley, 2003). A review of the relevant literature reveals that the ageing-in-place strategy has been implemented through three main service-delivery models: (i) institution-care services; (ii) community-care services; and (iii) home-care services (Chapin & Dobbs-Kepper, 2001; Cohen-Mansfield & Frank, 2008; Cutchin, 2003; Hawes, Phillips, Rose, Holan, & Sherman, 2003; Marek & Rantz, 2000; Stone & Reinhard, 2007; Wu & Chuang, 2001). The first of these models, the institution-care ser- vice model, provides care services for senior citizens in the context of institutions (such as hospitals and/or 166 Human Factors and Ergonomics in Manufacturing & Service Industries 25 (2) 166–182 (2015) c 2012 Wiley Periodicals, Inc.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of An Ageing-in-Place Service Innovation Model by Using TRIZ Methodology

An Ageing-in-Place Service Innovation Model by UsingTRIZ MethodologyChi-Kuang Chen,1 An-Jin Shie,1 Kuo-Ming Wang,1 and Chang-Hsi Yu2
1 Department of Industrial Engineering & Management, Yuan Ze University, Taiwan2 Department of Business Administration, Yu Da University, Taiwan
Abstract
Most of the research on the concept of “ageing-in-place” has focused on surveys of the needs of seniorcitizens and/or the quality of the services delivered to them. Service innovation for ageing-in-placehas received little research attention, however. The present study addresses this issue by proposing aservice innovation model for ageing-in-place. In this model, a TRIZ methodology is used to developthe parameter correspondence table, which integrates TRIZ contradiction parameters and ageing-in-place service-quality determinants, to deal with service contradiction. A TRIZ contradiction matrix isthen applied to generate inventive solutions for the innovation of the ageing-in-place service system.A case study is also conducted to demonstrate the applicability of the proposed model. C© 2012 WileyPeriodicals, Inc.
Keywords: Service innovation; Ageing-in-place; Home care; TRIZ; Contradiction matrix
1. INTRODUCTIONAdvances in medical care and public health have meantthat people are living longer, which has resulted in ev-ery developed country in the world facing significantdifficulties in coping with the accommodation and so-cial needs of an increasingly older population. In re-sponse to these demographic problems, various strate-gies have been suggested to facilitate independent livingby senior citizens, preferably in their own homes (Birn-baum, Burke, Swearingen, & Dunlop, 1984; Fashimpar,1983). One such strategy is the concept of “ageing-in-place,” which is a diversified care model first proposedin the 1960s to deal with the issues of an ageing pop-
Correspondence to: Chi-Kuang Chen, Department ofIndustrial Engineering and Management, Yuan Ze University,135 Yuan-Tung Road, Chung-Li 320, Taiwan, ROC. Phone:886-3-4638800 ext. 2528; e-mail: [email protected]
Received: 4 April 2012; revised 20 May 2012; accepted 12September 2012
View this article online at wileyonlinelibrary.com/journal/hfm
DOI: 10.1002/hfm.20536
ulation. The aim of ageing-in-place is to provide ap-propriate care for senior citizens in their local area byintegrating the services of nursing homes, community-care agencies, and home-care agencies (Birnbaum et al.,1984; Kane, 1995; Wu & Chuang, 2001). In doing so,the strategy takes into account the preference of manysenior citizens to maintain their independence, dignity,and quality of life by having appropriate care servicesdelivered to their own homes or to nearby communitycenters and nursing homes (Cutchin, 2003; Francis &Netten, 2004; Gilleard, Hyde, & Higgs, 2007; Palley,2003).
A review of the relevant literature reveals thatthe ageing-in-place strategy has been implementedthrough three main service-delivery models: (i)institution-care services; (ii) community-care services;and (iii) home-care services (Chapin & Dobbs-Kepper,2001; Cohen-Mansfield & Frank, 2008; Cutchin, 2003;Hawes, Phillips, Rose, Holan, & Sherman, 2003; Marek& Rantz, 2000; Stone & Reinhard, 2007; Wu & Chuang,2001). The first of these models, the institution-care ser-vice model, provides care services for senior citizens inthe context of institutions (such as hospitals and/or
166 Human Factors and Ergonomics in Manufacturing & Service Industries 25 (2) 166–182 (2015) c© 2012 Wiley Periodicals, Inc.

Chen et al. Ageing-in-Place Service Innovation Model
nursing homes). This model is suitable for senior citi-zens who are not able to live independently as a conse-quence of debilitating physical or mental illnesses thatrequire intensive treatment. However, the suitability ofservices provided by this model is typically constrainedby inflexible administrative procedures that often failto satisfy clients’ needs. Moreover, senior citizens ser-viced by the institution-care model are obviously un-able to fulfil the requirement of living in an individualliving environment in close proximity to their families(Cutchin, 2003; Gilleard et al., 2007; Raynes, Temple,Glenister, & Coulthard, 2001; Schade & Brehm, 2010;Wu & Chuang, 2001).
The second model, the community-care servicemodel, provides recreational facilities and health-careservices for senior citizens in a nearby community cen-ter. This model enables senior citizens to receive appro-priate care services in the community, while allowingthem to maintain accommodation in their own homesor with their families. This model is suitable for se-nior citizens who are relatively healthy, mobile, andself-sufficient on their own without any need for in-tensive medical care (Cohen-Mansfield & Frank, 2008;Cutchin, 2003; Jensen, Saunders, Thierer, & Friedman,2008; Stone & Reinhard, 2007; Wu & Chuang, 2001).
The third model, the home-care service model, en-ables senior citizens to access care services withoutleaving home by providing for visits from licensedhealth-care professionals. This model enables seniorcitizens who are able to live at home, but unable toaccess external professional health-care services, to re-main within their own personal living environment(Chapin & Dobbs-Kepper, 2001; Citro & Hermanson,1999; Cohen-Mansfield & Frank, 2008; Cutchin, 2003;Hawes et al., 2003; Marek & Rantz, 2000; Stone & Rein-hard, 2007; Wu & Chuang, 2001).
The strategy of ageing-in-place, delivered by one ormore of these diversified service-delivery models, hasbeen recognized by most developed countries as a desir-able endeavor in public policy. However, the efficiencyof any ageing-in-place program is often constrainedby one or more of its critical determinants (Eiriz &Figueiredo, 2005; Francis & Netten, 2004; Mitchell &Kemp, 2000; Raynes et al., 2001). These determinantsinclude service capacity, service flexibility, number ofcare providers, care service quality, facility equipment,and so on (Eiriz & Figueiredo, 2005; Francis & Net-ten, 2004; Raynes et al., 2001; Starfish, 2002). Limitedservice resources in any of these determinants havebeen shown to result in inadequate services being de-
livered to senior citizens under many ageing-in-placeprograms (Baron-Epel, Dushenat, & Friedman, 2001;Birnbaum et al., 1984; Cohen-Mansfield & Frank, 2008;Cutler, 2007; Francis & Netten, 2004; Jensen et al., 2008;Reilly, Challis, Burns, & Hughes, 2004).
Against this background, the present study proposesa systematic innovation model for the improvement ofageing-in-place programs. The proposed model, whichis based on the Theory of Inventive Problem Solving(Russian acronym: TRIZ), seeks to enhance service-system development in ageing-in-place programs. Thespecific objectives of the present study are therefore
� to establish correspondence between theservice-quality determinants of ageing-in-placeand TRIZ parameters;
� to develop an service innovation model thatcan be used by managers to provide systematicimprovements in their ageing-in-place servicesystems;
� to conduct a case study for the purpose ofdemonstrating the feasibility of the proposedmodel; and
� to identify innovative strategies for the im-provement of service systems for ageing-in-place programs.
The remainder of this article is organized as follows:The following section presents a review of the literatureon ageing-in-place service quality and TRIZ method-ology. A conceptual framework is then presented todemonstrate how the service innovation model forageing-in-place is developed. The practical efficacy ofthe proposed model is then demonstrated in a casestudy of ageing-in-place in Taiwan. The article con-cludes with a summary of the main findings, implica-tions, and suggestions for future research.
2. LITERATURE REVIEW2.1. Ageing-in-Place Service Quality
Senior citizens are increasingly expressing a preferencefor remaining in their own homes because so-calledageing-in-place offers a continuation of the privacyand flexibility to which they have become accustomedin their lives (Chapin & Dobbs-Kepper, 2001; Marek& Rantz, 2000; Wu & Chuang, 2001). Furthermore,the provision of assistance in the form of services tosupport daily living decreases the dependence of seniorcitizens on the services of institutional nursing homes
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 167

Ageing-in-Place Service Innovation Model Chen et al.
and hospitals (Chapin & Dobbs-Kepper, 2001; Marek& Rantz, 2000). A well-developed service system forageing-in-place can thus support the desire of manysenior citizens to maintain independent living in theirown homes.
The issue of service quality in the context of ageing-in-place programs has become a popular research topicin the past two decades (American Association of Re-tired Persons, 1990; Cohen-Mansfield & Frank, 2008;Francis & Netten, 2004; Yang & Hsiao, 2009). In par-ticular, the determinants of service quality to improvethe quality of life of senior citizens have been examinedin the research undertaken by several authors (Francis& Netten, 2004; Raynes et al., 2001; Rubin, Pronovost,& Diette, 2001; Salomon, Gasquet, Mesbah, & Ravaud,1999). Drawing on reviews of the literature and in-terviews with senior citizens, these researchers haveestablished that the issues of greatest concern to se-nior citizens are service reliability, service flexibility,service continuity, and the communication skills, atti-tude, and knowledge of service providers. In a similarvein, Salomon et al. (1999) found that senior citizenswere concerned about transparency of medical infor-mation, a wide selection of available services, continu-ity of service, psychological and social support, and thenumbers and attributes of staff members (caregivingskills, communication skills, attitude, trustworthiness,etc.).
Francis & Netten (2004) found six determinants ofservice quality in ageing-in-place: (i) continuity of carestaff and the development of trusting relationships be-tween staff and clients; (ii) communication skills ofcare staff and clear comprehensible service schedules;(iii) flexibility of services to meet senior citizens’ fluc-tuating needs; (iv) reliability of care staff members; (v)staff attitudes; and (vi) competence of care workers.
In addition to studying the determinants of servicequality in ageing-in-place, researchers have also ex-amined the question of the availability of resourcesfor adequate service quality. Several authors have indi-cated that demand is growing for both ageing-in-placeand assisted living facilities (Birnbaum et al., 1984;Chapin & Dobbs-Kepper, 2001; Citro & Hermanson,1999; Haight, Michel, & Hendrix, 1998; Hooyman &Kiyak, 1996; Lander, Brazill, & Ladrigan, 1997; Leon &Moyer, 1999; Mitchell & Kemp, 2000; Stone & Rein-hard, 2007). These researchers all agree that the pro-vision of high-quality service is an essential aspect ofmeeting the demand for home care for senior citizenswith supportive services in a homelike environment.
Indeed, several researchers have suggested that ageing-in-place should provide a home-care service on a 24-hour basis with a high degree of customer choice andcontrol (Chapin & Dobbs-Kepper, 2001; Zimmerman& Sloane, 1999). This will require the provision of fur-ther supportive resources if ageing-in-place is to pro-vide an appropriate level of service quality for seniorcitizens.
2.2. TRIZ Methodology
TRIZ was proposed by the Russian inventor GenrikhAltshuller in 1946 when he categorized more than200,000 worldwide engineering patents in a novel way.The aim was to define generalizable patterns in in-ventive solutions and to identify the distinguishingcharacteristics of the problems that these inventionshad overcome. Altshuller claimed that the same prob-lems were often solved repeatedly using 40 fundamen-tal principles, which he subsequently proposed as the“40 TRIZ inventive principles.” He also categorized the200,000 patents in accordance with “39 engineering pa-rameters,” some of which were noted to be mutuallycontradictory. These engineering parameters and theinventive principles were subsequently combined toproduce the “TRIZ contradiction matrix.” In this ma-trix, the 39 parameters are arranged on each side of atwo-dimensional matrix according to their contradic-tions. At each intersection, some inventive principlesare nominated as a reference to resolve the contradic-tion between these corresponding parameters.
The 40 inventive principles of TRIZ, which areclaimed to provide a complete description of inno-vative solution thinking, are applied to solve a givensituation involving a contradiction. The contradictionmatrix, which is one of the most popular tools in TRIZ,has since been used in a diversity of nontechnical fields(Chai, Zhang, & Tan, 2005; Lin & Su, 2007; Su & Lin,2008; Su, Lin, & Chiang, 2008).
An example of part of a TRIZ contradiction matrixis shown in Table 1. It shows that each of the parame-ters could be either improving or worsening comparedwith others. For example, if one of the improving pa-rameters is Reliability (Parameter 27), its correspond-ing worsening parameter is Productivity (Parameter39). The intersecting cell in the table recommends fourinventive principles as suggestions for improvement:Principle 1 (segmentation), Principle 35 (parameterchanges), Principle 29 (pneumatics and hydraulics),and Principle 38 (strong oxidants).
168 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm

Chen et al. Ageing-in-Place Service Innovation Model
TABLE 1. A Partial TRIZ Contradiction Matrix with Inventive Principles
Worsening Parameters
1 2 — 27 38 39ImprovingParameters
Weight ofMoving Object
Weight ofStationary Object — Reliability
Extent ofAutomation Productivity
1 Weight of MovingObject
+ — 1, 3 11, 27 26, 35, 18, 19 35, 3, 24, 37
2 Weight of StationaryObject
+ — 10, 28, 8, 3 2, 26, 35 1, 28, 15, 35
— — — — + — — —27 Reliability 3, 8, 10, 40 3, 10, 8, 28 — + 11, 13, 27 1, 35, 29, 3838 Extent of
Automation28, 26, 18, 35 28, 26, 35, 10 — 11, 27 32 + 5, 12, 35, 26
39 Productivity 35, 26, 24, 37 28, 27, 15, 3 — 1, 35 10, 38 5, 12, 35, 26 +Left rows and top columns are engineering parameters; bold numbers are inventive principles.
2.3. Application of TRIZ to ServiceInnovation
Although several authors have contended that success-ful service innovation to improve service quality re-quires a systematic approach, any such approach isinvariably limited by the previous experience, intu-ition, fancy, or inspiration of the person responsiblefor service development (Chai et al., 2005; Zhang, Chai,& Tan, 2005). To overcome these deficiencies in per-sonal knowledge and/or attitudes, some authors (Chaiet al., 2005; Zhang et al., 2005) have mentioned that theTRIZ methodology can be used to identify the elementsthat require improvement in a service system and themeans of achieving this. In particular, these authorshave examined how the distinctive characteristics ofservices can be aligned to the 40 inventive principles ofTRIZ for the purpose of service design. In addition, Suet al. (2008) have suggested that the 39 engineeringparameters of TRIZ should be analyzed with a viewto establishing whether analogical relationships can beestablished among the 39 engineering parameters andthe characteristic features of services.
3. MODEL DEVELOPMENTAs noted earlier in text, ageing-in-place programs haveoften faced conflicts between the needs of clients andthe delivered service quality. In seeking to resolve theseconflicts, ageing-in-place programs have lacked an ob-jective innovation approach to the task of improvingservice quality. It is the contention of the present studythat the TRIZ methodology, adapted in accordancewith the proposals of Chai et al. (2005) and Su et al.
(2008), offers a promising starting point for the devel-opment of a service-innovation model for ageing-in-place. In particular, it is contended that the conflictsthat require resolution in accordance with the TRIZapproach are those that exist between extant servicequality and the needs of senior citizens.
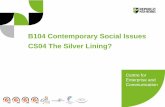
The stages in the proposed model are illustrated inFigure 1. As shown in the diagram, the model has four
Figure 1 The proposed model.
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 169

Ageing-in-Place Service Innovation Model Chen et al.
stages: (i) TRIZ model preparation; (ii) service qual-ity survey; (iii) conduct of the TRIZ process; and (iv)generation of inventive solutions. Each of the stages isdescribed in more detail next.
The purpose of the first stage is to prepare the essen-tial information that the TRIZ methodology requires.First, clients of ageing-in-place programs are identifiedand their service-quality needs are delineated by a com-bination of: (i) a review of the relevant literature and(ii) surveys of users’ needs through observation andinterview. The determinants of ageing-in-place servicequality are then mapped into the corresponding 39TRIZ engineering parameters by interviews with man-agers or staff, thus establishing the TRIZ parametercorrespondence table, which is an essential tool forestablishing the applicability and reliability of the pa-rameter mapping results.
In the second stage, the service quality of ageing-in-place is assessed by a questionnaire survey of seniorcitizens who receive the services and staff members whoprovide the services. This requires the development ofan ageing-in-place service-quality questionnaire basedon the service-quality determinants identified in thefirst stage. As a result of the survey, the worst service-quality determinants are identified.
In the third stage, the TRIZ process is conductedto analyze the problems of the service systems used inageing-in-place. First, a function-attribute analysis di-agram is constructed to detect relationships betweennegative (“harmful”) and positive (“useful”) param-eters in the service system. The TRIZ contradictionmatrix is then used to generate inventive princi-ples for improving ageing-in-place service systems.The “harmful” and “useful” parameters, as previouslydetected, are mapped individually onto the TRIZ con-tradiction matrix, following which the inventive prin-ciples that exist within the contradiction matrix aregenerated. A systematic TRIZ process is thus used to il-lustrate that the service system functions as a networkof cause-and-effect relationships between “harmful”and “useful” functions. Meanwhile, the TRIZ contra-diction matrix also provides a systematic approach togenerate inventive principles.
In the fourth stage, the inventive solutions are gen-erated and evaluated by managers of ageing-in-placeprograms, which can stimulate the managers to pro-pose further inventive solutions for improving theirservice systems. All of the proposed inventive solu-tions are then evaluated by the senior managementof the organization that is ultimately responsible for
the particular ageing-in-place program (e.g., a hospi-tal, public-sector entity, private nursing home). Finally,the inventive solutions are prioritized and the optimalsolutions are selected.
In summary, the service innovation model proposedin this study provides a systematic approach that en-ables managers to generate inventive principles to in-novate their ageing-in-place service systems.
4. CASE STUDY4.1. Background to the Case Study
As previously noted, three models (institution care,community care, and home care) have been used toprovide services in support of senior citizens in theirown homes or in nearby community centers or nursinghomes. Of these, the home-care services model offersthe greatest flexibility and convenience for senior citi-zens who are living in their own dwellings. This modelhas often been adopted by governments as part of theirlong-term care service policy (American Association ofRetired Persons, 1990; Chapin & Dobbs-Kepper, 2001;Cohen-Mansfield & Frank, 2008; Cutchin, 2003; Gil-leard et al., 2007; Rubin et al., 2001; Stone & Reinhard,2007; Wu & Chuang, 2001; Yang & Hsiao, 2009).
Nevertheless, despite the many advantages of thismodel reported in these numerous studies, it is appar-ent that the model consumes huge amounts of serviceresources in delivering care services to clients’ homes.As a consequence, there are often insufficient resourcesto meet the needs of clients, which often generatesconflicts between the level of service quality and the re-quirements of senior citizens (Baron-Epel et al., 2001;Birnbaum et al., 1984; Cohen-Mansfield & Frank, 2008;Cutler, 2007; Francis & Netten, 2004; Jensen et al., 2008;Stone & Reinhard, 2007).
To address such conflicts, the present study has pro-posed the ageing-in-place service innovation modeldescribed earlier in text. A case study of a Taiwaneseageing-in-place agency that offers home-care servicesto senior citizens was therefore conducted to demon-strate the applicability of the four-stage proposedmodel.
4.2. Application of the Model
4.2.1. Stage 1: TRIZ Model Preparation
The first step is to identify the determinants ofservice quality which concern senior citizens. The
170 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm

Chen et al. Ageing-in-Place Service Innovation Model
procedures are illustrated as follows: First, the service-quality implications that will affect senior citizen sat-isfaction were summarized from the reviews of 21studies. The appropriate determinants of service qual-ity were then given in accordance with the service-quality implications. In this step, 35 determinants ofservice quality were identified (see Table 2). For exam-ple, the ageing-in-place service agency provides extraservices for satisfying senior citizen’s needs, which isidentified as “service flexibility.” The other example,that the ageing-in-place service agency should pro-vide appropriate services for senior citizens accord-ing to their health condition, is identified as “serviceadaptability.”
The next step is to map determinants into TRIZ pa-rameters. In this step, each of the 35 service-qualitydeterminants was mapped into the corresponding 39TRIZ engineering parameters (adapted to ageing-in-place service quality). This provided the TRIZ param-eter correspondence table (see Table 3).
The third step is to conduct a reliability analysisto examine the correspondence of service-quality de-terminants and TRIZ parameters. An expert checklistbased on the correspondence table was also developedto examine the reliability of the table. Six experts wereinvited to provide the checklist. The experts are: (i) twosenior managers of an ageing-in-place service agency;(ii) two academics whose research area focuses on theageing-in-place service; and (iii) two TRIZ consultants.Each expert indicated “agreement” (with an asterisk ∗in each cell in Table 3) or “disagreement” (with a blankspace in each cell). The degree of mutual agreementwas calculated by equation 1 (below) and the reli-ability was determined by equation 2. As shown inTable 3, the degree of agreement between the re-searcher and each of the experts was 0.94, 0.94, 0.89,0.94, 0.94, and 0.94. The reliability index was 0.987.Both of these were greater than 0.70, which impliesacceptable reliability (Kolbe & Burnett, 1991; Weber,1985).
Degree of mutual agreement
= 2 × number of items completely agreed by two parties
number agreed by reseacher + number agreed by expert
[1]
Reliablity
= n × Degree of average mutual agreement
1 + [(n − 1) × Degree of average mutual agreement]
[2][n = Number of experts]
Table 3 suggests that the service-quality determi-nants could be mapped onto their corresponding TRIZparameters, which facilitated the selection of appro-priate TRIZ parameters for the innovation required inthis case study. For instance, Determinant 11 (Cost)can be said to correspond to TRIZ Parameter 22 (Lossof energy) because “cost” involves the use of resources(manpower, time, etc.), which is equivalent to “loss ofenergy” (TRIZ Parameter 22). To use another example,Determinant 24 (Service automation) corresponds toTRIZ Parameter 38 (Extent of automation). In addi-tion, the degrees of agreement for corresponding pairsbetween the service-quality determinants and TRIZparameters were examined (see the right column inTable 3). The criterion of acceptance of the correspond-ing pairs is at least three of the six experts showing theiragreement.
4.2.2. Stage 2: Service-Quality Survey
In the second stage, a 35-item questionnaire was devel-oped, based on the service-quality determinants iden-tified in Stage 1 (see Table 2). Each determinant wasscored on a 5-point Likert-type scale (1 = “very dissat-isfied”; 5 = “very satisfied”). Satisfactory service qual-ity was thus indicated with a higher score; conversely,a lower score indicated a need to improve the servicequality as currently provided.
Thirty-one home-care staff members from theageing-in-place service agencies were invited to re-spond to this questionnaire survey. The average of theresponse from 31 home-care staff members in eachitem was calculated. The results are shown in Table 4.From Table 4, it is found that two determinants (33 [ser-vice automation] and 24 [equipment maintenance])have the lowest satisfactory level. In other words, thosetwo determinants need the most improvement to im-prove the overall service quality. They indicate thatthe ageing-in-place agency lacks “service automation”for the senior citizens and that insufficient resourcesallocated to “equipment maintenance” results in themalfunction of home-care service facilities. Thus thetwo determinants will be analyzed further by conduct-ing a function attribute analysis diagram and TRIZcontradiction matrix in the next stage.
4.2.3. Stage 3: Conduct of TRIZ Process
The third stage consisted of three steps: (i) formulationof a function attribute analysis diagram; (ii) problem
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 171

Ageing-in-Place Service Innovation Model Chen et al.
TABLE 2. Summary of Ageing-in-Place Service-Quality Determinants
DeterminantNumber
Service QualityDeterminants Implications Cited References
1 Service flexibility Agencies should provide extra services not included inoriginal plans.
[2], [4], [8], [17],[19]
2 Service reliability Staff should provide trustworthy and reliable services. [4], [8], [14], [16]3 Service continuity Reliable and regulated services (such as daily food
delivery, bathing assistance, and laundry cleaning)are required.
[1], [2], [4], [9],[13], [16]
4 Symmetry ofinformation
Clear communications from doctors and caregivers arerequired to ensure clients are not waiting at homefor uncertain service deliveries.
[4], [9]
5 Service adaptability Agencies should provide appropriate services forsenior citizens according to their health conditionand needs.
[2], [9], [16], [18],[21]
6 Service accuracy Service-delivery model must satisfy needs withminimal waste (such as appropriate food quantitiesthat satisfy needs).
[14], [15]
7 Care staff members’attitude
Care staff members’ should demonstrate friendliness,respect, and understanding of senior citizens’needs.
[2], [4], [16]
8 Psychological and socialsupport
Agencies should provide psychological and socialsupport (such as counseling, social activities, andchatting with clients).
[1], [2], [7], [8], [9],[10], [11], [14],[16], [18], [19],[21]
9 Active service Doctors and care staff members should show initiativein actively taking care of senior citizens’ healthconditions.
[9]
10 Care staff members’skills and knowledge
Knowledgeable, experienced, and skillful staff arerequired to effectively handle the diverse problemsof senior citizens.
[2], [4], [5], [16],[18]
11 Cost Senior citizens should not have to spend more thanexpected in purchasing care services.
[3], [4], [13], [14],[15], [17], [18]
12 Waiting time Senior citizens should not have to wait for longperiods for delivery of services.
[4]
13 Care staff numbers Agencies should provide a sufficient number ofexperienced staff members (nurses, doctors,physiotherapists, etc.).
[1]
14 Convenience Agencies should provide services at a time convenientto senior citizens.
[1], [8], [14], [15]
15 Selectivity Agencies should provide a wide selection of services. [1], [8], [21]16 Efficiency & functionality
of serviceAgencies should use new equipment to improve
service efficiency and functionality.[6], [14], [15]
17 Customization Agencies should learn from customers’ experiences toprovide more customized services for senior citizens.
[8], [15], [21]
18 Service capacity There should be sufficient service resource capacity(including numbers of nursing and medical staff).
[18]
19 Informationtransparency
Seniors should be able to immediately obtain careservice information (including cost, purpose andprocedure for each service, information aboutmedications and side effects).
[1], [4], [8], [14],[15]
(Continued)
172 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm

Chen et al. Ageing-in-Place Service Innovation Model
TABLE 2. Continued
DeterminantNumber
Service QualityDeterminants Implications Cited References
20 Time of service delivery Travel time required for doctors and care staffmembers should ensure prompt arrival at seniorcitizens’ dwellings.
[8], [14], [15]
21 Environment comfort Agencies should offer comfortable and satisfactoryliving environments for senior citizens.
[19]
22 Safety and privacy Agencies should provide a safe and privateenvironment for senior citizens, with minimalinterference from the external environment.
[14], [15], [19], [21]
23 Staff members’ patience Doctors and care staff members should be willing topatiently answer seniors’ questions and performrepeated care services (including massage,rehabilitation, and care services).
[4]
24 Service automation Automated equipment (including electric vehicles tomeet mobility needs, electronic medicine box,automatic eating aid, etc.) should be used.
[14], [15]
25 Service compensation Agencies should provide some compensation forsenior citizens who lose time, money, and rights.For example, staff members should offer extraservices and time to compensate for such losses.
[4], [20]
26 Expertise Doctors and care staff members must be proficient inall aspects of care-service delivery.
[2], [4], [5], [16],[18]
27 Efficiency On-time service completion is required for both groupservices in a fixed time period and a single serviceon an individual basis.
[6], [14], [15], [16],[18]
28 Waste of resources Agencies should assess (and if necessary adjust)services to provide adequate service to the changingneeds of senior citizens without resource waste.
[4], [13], [18]
29 Equipment convenience Staff should be provided with easily handled andmaintained devices and equipment.
[14], [15], [19]
30 Equipment complexity Devices and equipment should not have unnecessaryand complex functions.
[14], [15]
31 Equipment accuracy All measuring equipment must accurately analyzehealth conditions, thus enabling doctors to makeaccurate diagnosis and treatment decisions.
[14], [15]
32 Equipment stability All provided medical equipment must beperformance-ready at all times.
[14], [15]
33 Equipment maintenance Devices and equipment must be maintained andupdated regularly.
[14], [15], [21]
34 Ease of operation Medical equipment operation interface must haveergonomic designs and be user-friendly for seniors.
[14]
35 Service scope Agencies must provide sufficient services to satisfytheir scope.
[11], [12], [14],[15], [17], [18],[19]
References: [1] Salomon et al. (1999); [2] Geron et al. (2000); [3] Starfish (2002); [4] Francis & Netten (2004); [5] Rayneset al. (2001); [6] Rubin et al. (2001); [7] Woodruff & Applebaum (1996); [8] Eustis et al. (1993); [9] Cohen-Mansfield &Frank (2008); [10] Cohen-Mansfield et al. (2010); [11] Cutchin (2003); [12] Schade & Brehm (2010); [13] Stone & Reinhard(2007); [14] Chae et al. (2001); [15] Sanford & Butterfield (2005); [16] Donabedian (2003); [17] Chapin & Dobbs-Kepper(2001); [18] Birnbaum et al. (1984); [19] Wu & Chuang (2001); [20] Gilliland Ii (1999); [21] Cutler (2007)The table was prepared by the authors of this research.
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 173

Ageing-in-Place Service Innovation Model Chen et al.
TABLE 3. Reliability of TRIZ Parameter Correspondence Table for Ageing-in-Place Service Quality
TRIZ Parameter Correspondence Table Agreement/Disagreement of Six Experts (1 to 6)
Service-QualityDeterminants TRIZ Parameters 1 2 3 4 5 6
Degree of Agreementfor Corresponding Pairs
1 Service flexibility 35 Adaptability orversatility
∗ ∗ ∗ ∗ ∗ ∗ 100%
2 Service reliability 27 Reliability ∗ ∗ ∗ ∗ ∗ ∗ 100%3 Service continuity 13 Stability of the
objectcomposition
∗ ∗ ∗ ∗ ∗ ∗ 100%
4 Symmetry ofinformation
24 Loss ofinformation
∗ ∗ ∗ ∗ 67.6%
5 Serviceadaptability
35 Adaptability orversatility
∗ ∗ ∗ ∗ ∗ ∗ 100%
6 Service accuracy 29 Manufacturingprecision
∗ ∗ ∗ ∗ ∗ ∗ 100%
7 Care staffmembers’attitude
17 Temperature ∗ ∗ ∗ ∗ ∗ 83.3%
8 Psychological andsocial support
17 Temperature ∗ ∗ ∗ ∗ ∗ 83.3%
9 Active service 17 Temperature ∗ ∗ ∗ 50%10 Care staff
members’ skillsandknowledge
35 Adaptability orversatility
∗ ∗ ∗ ∗ ∗ ∗ 100%
11 Cost 22 Loss of energy ∗ ∗ ∗ ∗ ∗ ∗ 100%12 Waiting time 25 Loss of time ∗ ∗ ∗ ∗ ∗ ∗ 100%13 Care staff
numbers26 Amount of
substance
∗ ∗ ∗ ∗ ∗ ∗ 100%
14 Convenience 33 Ease ofoperation
∗ ∗ ∗ ∗ ∗ ∗ 100%
15 Selectivity 35 Adaptability orversatility
∗ ∗ ∗ ∗ ∗ ∗ 100%
16 Efficiency &functionality ofservice
11 Stress or pressure ∗ ∗ ∗ ∗ ∗ 83.3%
17 Customization 35 Adaptability orversatility
∗ ∗ ∗ ∗ ∗ ∗ 100%
18 Service capacity 26 Amount ofsubstance
∗ ∗ ∗ ∗ ∗ ∗ 100%
19 Informationtransparency
24 Loss ofinformation
∗ ∗ ∗ ∗ ∗ ∗ 100%
20 Time of servicedelivery
9 Speed ∗ ∗ ∗ ∗ ∗ ∗ 100%
21 Environmentcomfort
12 Shape ∗ ∗ ∗ ∗ 67.6%
22 Safety andprivacy
30 Object affectedharmfulfactors
∗ ∗ ∗ ∗ ∗ ∗ 100%
(Continued)
174 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm

Chen et al. Ageing-in-Place Service Innovation Model
TABLE 3. Continued
TRIZ Parameter Correspondence Table Agreement/Disagreement of Six Experts (1 to 6)
Service-QualityDeterminants TRIZ Parameters 1 2 3 4 5 6
Degree of Agreementfor Corresponding Pairs
23 Staff members’patience
14 Strength ∗ ∗ ∗ ∗ ∗ ∗ 100%
24 Serviceautomation
38 Extent ofautomation
∗ ∗ ∗ ∗ ∗ ∗ 100%
25 Servicecompensation
34 Ease of repair ∗ ∗ ∗ ∗ ∗ ∗ 100%
26 Expertise 32 Ease ofmanufacture
∗ ∗ ∗ ∗ ∗ 83.3%
27 Efficiency 39 Productivity ∗ ∗ ∗ ∗ ∗ 83.3%28 Waste of
resources23 Loss of
substance
∗ ∗ ∗ ∗ ∗ ∗ 100%
29 Equipmentconvenience
33 Ease ofoperation
∗ ∗ ∗ ∗ ∗ ∗ 100%
30 Equipmentcomplexity
36 Devicecomplexity
∗ ∗ ∗ ∗ ∗ ∗ 100%
31 Equipmentaccuracy
28 Measurementaccuracy
∗ ∗ ∗ ∗ ∗ ∗ 100%
32 Equipmentstability
13 Stability of theobjectcomposition
∗ ∗ ∗ ∗ ∗ ∗ 100%
33 Equipmentmaintenance
34 Ease of repair ∗ ∗ ∗ ∗ ∗ ∗ 100%
34 Ease of operation 33 Ease ofoperation
∗ ∗ ∗ ∗ ∗ 83.3%
35 Service scope 8 Volume ofstationaryobject
∗ ∗ ∗ ∗ ∗ 83.3%
Total33 33 31 33 33 33
Degree of agreement with researcher 0.94 0.94 0.89 0.94 0.94 0.94Reliability 0.987
∗Indicates agreement; blank indicates disagreement.
formulation; and (iii) analysis of the TRIZ contradic-tion matrix.
First, in the step of formulation of a function at-tribute analysis diagram, all functions of the servicesystem were distinguished into one of two types: (i)“Harmful Function” (HF) or (ii) “Useful Function”(UF) by the researchers. In practical situations, it issuggested that the service system designer or analystplay the role. The two functions, harmful and use-ful functions in the service system, were then used toillustrate the existing network of cause-and-effect rela-tionships. This facilitated understanding of the existingproblems in the service system.
It is apparent from Table 4 that Determinant 24(Service automation) and Determinant 33 (Equipmentmaintenance) were the two determinants most in needof improvement. To illustrate the use of the proposedmodel, these two items were then used to conduct afunction attribute analysis diagram (see Figure 2). Acause-and-effect relationship between “harmful” (HF1) and “useful” functions (UF 1, UF 2, UF 3, and UF4) is presented.
In Figure 2, service system effectiveness (UF 1) isrequired to meet senior citizens’ needs (UF 2). Theanalysis suggests that the best way is to offer serviceautomation (UF 3), which enables senior citizens to
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 175

Ageing-in-Place Service Innovation Model Chen et al.
TABLE 4. Analysis of Ageing-in-Place Service-Quality Determinants
DeterminantNumber
Service-Quality Determinantsof Aging–in-Place
AverageSatisfaction
DeterminantNumber
Service-Quality Determinantsof Aging-in-Place
AverageSatisfaction
5. Service adaptability 3.94 35. Service scope 3.267. Care staff members’ attitude 3.94 1. Service flexibility 3.103. Service continuity 3.77 4. Symmetry of information 3.0026. Expertise 3.74 28. Waste of resources 3.0010. Care staff members’ skills
and knowledge3.71 12. Waiting time 2.94
9. Active service 3.65 13. Care staff numbers 2.9416. Efficiency & functionality of
service3.61 15. Selectivity 2.90
27. Efficiency 3.61 20. Time of service delivery 2.902. Service reliability 3.58 18. Service capacity 2.7422. Safety and privacy 3.58 29. Equipment convenience 2.658. Psychological and social
support3.55 19. Information transparency 2.58
23. Staff members’ patience 3.55 30. Equipment complexity 2.5517. Customization 3.52 32. Equipment stability 2.5521. Environment comfort 3.52 34. Ease of operation 2.4825. Service compensation 3.52 31. Equipment accuracy 2.426. Service accuracy 3.35 33. Equipment maintenance 1.94∗
11. Cost 3.32 24. Service automation 1.55∗
14. Convenience 3.26
access sufficient self-services (such as remote medicalsystem, smart electronic medicine boxes, and electricvehicles). However, service automation also brings theproblem of cost increases (HF 1) as a consequence ofequipment consumption costs, setup costs, and main-tenance costs. As shown in Figure 2, UF 3 (serviceautomation) and UF 4 (equipment maintenance) will
worsen HF 1 (service system cost) while enhancing theeffectiveness of the service system.
In the second step, problem formulation analyzesthe service-system conflict problems into a series ofsimple formulas, which enables systematic detectionof the conflict between harmful and useful func-tions. According to the function attribute analysis
cause
is required to
influences
Improvingservice systemeffectiveness
UF 1
is required to Quickly meetingseniors’ needs
UF 2
Service automation
UF 3
Increasing servicesystem cost
HF1
is required to
Equipment maintenance
UF 4
cause
Figure 2 Function attribute analysis diagram. Each box indicates an existing function in service systems. UF = usefulfunction; HF = harmful function; = worse function enables to affect useful function.
176 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm

Chen et al. Ageing-in-Place Service Innovation Model
diagram, which includes the home-care service sys-tem, there exists a cause-and-effect relationshipamong UF 3 (service automation), UF 4 (equip-ment maintenance), UF 1 (improving service systemeffectiveness), and HF 1 (increasing service systemcost). Two problem statements can be formulated asfollows:
� Find a way to resolve the contradiction that UF3 (service automation) should be establishedto enhance UF 2 (quickly meeting senior citi-zens’ needs) but will cause worsening of HF 1(increasing service system cost).
� Find a way to resolve the contradiction that UF4 (equipment maintenance) should be estab-lished to enhance UF 3 (service automation)but will cause worsening of HF 1 (increasingservice system cost).
The first problem statement indicates that the home-care service system generates a conflict between UF 3(service automation) and HF 1 (increasing service sys-tem cost). The conflict indicates that service automa-tion can immediately satisfy senior citizens’ demands,but will increase costs in purchasing and setting up theautomated equipment.
The second problem statement indicates that thishome-care service system generates a conflict betweenUF 4 (equipment maintenance) and HF 1 (increasingservice system cost) because home-care service agen-cies need to pay additional costs in manpower, trans-portation, and maintenance to maintain automatedservice equipment. Improvement in the effectivenessof the home-care service system thus implies assis-tance with regard to service automation and supportof equipment maintenance. It becomes necessary toimprove service automation and equipment mainte-nance, as well as to minimize cost.
In the third step, the analysis of the TRIZ con-tradiction matrix generated inventive principles. Ac-cording to the TRIZ parameter correspondence table(Table 3), improvement in equipment maintenanceand service automation are individually mapped ontothe TRIZ improvement Parameters 34 (Ease of repair)and 38 (Extent of automation). In addition, the ob-stacle for improving service system effectiveness is thecost, which is mapped onto the TRIZ worsening Pa-rameter 22 (Loss of energy). Table 5 presents the in-ventive principles in terms of the TRIZ contradictionanalysis.
TABLE 5. TRIZ Contradiction Matrix Analysis
Worsening Parameters
Improving Parameters 22 Loss of energy (cost)
34 Ease of repair (Equipmentmaintenance)
15, 1, 32, 19
38 Extent of automation(service automation)
23, 28
The boldface numbers are TRIZ inventive principles.
The intersecting cell in the table of the improvingParameter 34 and the corresponding worsening Pa-rameter 22 generated four inventive principles (15, 1,32, and 19) as suggestions for improvement. The in-tersecting cell of the improving Parameter 38 and thecorresponding worsening Parameter 22 generated twoinventive principles (23 and 28) as improvement sug-gestions.
4.2.4. Stage 4: Generation of InventiveSolutions
The six inventive principles that were generated in Stage3 (see Table 5) were then modified into inventive prin-ciples for ageing-in-place, in accordance with the sug-gestions of Chai et al. (2005).
The first inventive solution was Inventive Princi-ple 15 (Dynamics). In the context of ageing-in-place,dynamics can be interpreted as referring to dynamicsystems and/or equipment. For example, service ef-fectiveness could be enhanced by integrating existingmedical equipment through wireless networks, net-worked video equipment, and/or radio frequency iden-tification (RFID). This would enable doctors in hos-pitals to make prompt diagnoses of unwell clients vianetworked video equipment. It would also enable tech-nical staff to detect and repair faulty technical equip-ment through real-time monitoring networks. In bothinstances, time and transportation costs are minimizedby dynamic medical and technical monitoring systems.In addition, the principles of dynamics can be appliedto ergonomically designed bathroom facilities. Thesedevices enable senior citizens to use a control panelto adjust the height of a bathroom sink and/or seat tosuit their personal needs or health conditions. Such amechanism has the potential to decrease the risks offalls on wet bathroom floors (Aksoy, Erturk, & Ozturk,1977; Mclean, 2008; Schuller, 2010).
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 177

Ageing-in-Place Service Innovation Model Chen et al.
The second inventive solution was Inventive Prin-ciple 1 (Segmentation), which refers to an object orsystem being divided into independent parts. Apply-ing this to ageing-in-place, equipment maintenancecould be outsourced to equipment suppliers, and med-ical equipment could be designed as modules, whichfacilitates continuous operation without interruptionwhen individual parts of equipment are disassembledfor repair. These innovative suggestions have the po-tential to minimize the waiting time for repairing med-ical equipment. In addition, the segmentation solutioncan be applied to user interfaces of equipment (Akay,Demıray, & Kurt, 2008). For example, emergency but-tons on the control panels of equipment should beindependently segmented from the common functionbuttons to minimize the possibility of careless touch bysenior citizens.
The third inventive solution was Inventive Principle32 (Changing the color), which refers to the notion thatthe color of an object or system should be designed toenable users to identify it easily. In applying this toageing-in-place, frequently replaced parts of medicalequipment should be indicated with distinctive colors,so that users can identify and replace new parts easily. Inaddition, to avoid operational errors by senior citizens,equipment designers could use distinctive colors todesign user-friendly interfaces for medical equipment(Akay et al., 2008; Han, Kim, Yun, Hong, & Kim, 2004;Senol, Dagdeviren, Cilingir, & Kurt, 2010).
The fourth inventive solution was Inventive Princi-ple 19 (Periodic action), which refers to using periodicactions, rather than continuous action. Applying thisto ageing-in-place, agency managers could use infor-mation communication technology to ensure periodicmaintenance of the dwellings of senior citizens and tomaintain medical equipment (such as battery replace-ment in electric cars, tire mileages, and so on). Theprinciple of periodic action can also be applied to in-door lighting systems to enable the illumination levelto be decreased automatically at certain times (suchas rest times) and increased at other times (such asworking or reading times) (Akay et al., 2008). Thesesuggestions can minimize unnecessary costs associatedwith continuous services.
The fifth inventive solution was Inventive Principle23 (Feedback), which refers to feedback mechanismsto improve a process or action. Applying this principleto ageing-in-place, agencies should establish an inte-grated feedback mechanism that automatically recordsthe needs and health conditions of senior citizens, as
well as triggering response mechanisms for hospitaland ageing-in-place agencies. Such an integrated feed-back mechanism enables managers and doctors to de-liver more appropriate care services to senior citizens(Jaana, Pare, & Sicotte, 2007; Louis, Turner, Gretton,Baksh, & Cleland, 2003; Pickering, Gerin, & Holland,1999). Staff members providing services could alsorecord the opinions of clients regarding deficienciesin the services being provided. Such feedback mech-anisms would enable agencies to provide appropriatecare services and improve service effectiveness whileminimizing costs. In addition, from the seniors’ er-gonomics perspective, medical equipment should setfeedback devices to provide step-by-step guidelineswith messages, visual icons, and voice for reminding se-niors (Chabukswar, Gramopadhye, Melloy, & Grimes,2003; Kuo & Wang, 2007; Na, 2009; Park, 2011). Thiswould allow seniors to correctly use medical equipmentand avoid operational errors and hazards.
Finally, the sixth inventive solution was InventivePrinciple 28 (Replacement of mechanical system). Ap-plying this to ageing-in-place, electronic medical boxescould adopt acoustic and touch design (with music orvibration functions) to remind senior citizens of thetime for their medications. Similarly, touch designscan be incorporated into electric heaters to provideautomatic warm air when required, and bedroom lightswitches could adopt an acoustic design that respondswhen senior citizens get up and make a sound. The pro-posed suggestions, taking into account the ergonomicsof senior citizens, have the potential to minimize thepotential for falls and injuries.
4.2.5. Evaluations of Inventive Solutions
The six inventive solutions were then evaluated bysix experts (doctors, managers, and consultants ofageing-in-place service agencies). These experts wererequested to prioritize the six inventive solutions interms of three criteria: (i) innovativeness; (ii) solvingthe existing problems; and (iii) bringing benefits toimprove the service system (see Table 6). A 5-pointLikert-type scale was used for this evaluation (1 =“strong disagreement”; 5 = “strong agreement”).
The results of this evaluation are shown in Table 6.It is apparent that the order of priority of the six in-ventive solutions was: (i) dynamics; (ii) replacementof mechanical system; (iii) feedback; (iv) changingthe color; (v) periodic action; and (vi) segmentation.The top three optimal innovative solutions (dynamics,
178 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm

Chen et al. Ageing-in-Place Service Innovation Model
TABLE 6. Evaluation of the Inventive Solutions
The Generated Inventive Solution
Evaluation Criteria Dynamics SegmentationChangingthe Color
PeriodicAction Feedback
Replacement ofMechanical System
The inventive solution hasinnovativeness.
26 23 24 22 25 27
The inventive solution can solvethe existing problems.
26 21 24 23 26 25
The inventive solution can bringexpected benefits to improvethe service system.
27 23 25 24 27 26
Total 79 67 73 69 78 78Priority 1 6 4 5 2 2
replacement of mechanical system, and feedback)should be preferentially implemented to improvehome-care services by solving conflicts between ser-vice quality and seniors’ needs and satisfaction.
5. CONCLUSIONS ANDIMPLICATIONSThe previous literature on ageing-in-place has focusedprimarily on surveys of service quality; however, therehas been a conspicuous lack of studies that have exam-ined how the service systems of ageing-in-place pro-grams might be improved through service innovation.The present study has addressed this issue by propos-ing an ageing-in-place service innovation model thatprovides a systematic procedure to generate innovativesolutions for service improvement. The three advan-tages of the proposed model are as follows:
� The model integrates TRIZ parameters andageing-in-place service-quality determinants tobuild a TRIZ parameter correspondence table,which enables service developers to identify ap-propriate TRIZ parameters from the contradic-tion matrix.
� The model proposes an approach with system-atic analysis to enable service developers to in-vent effective solutions for aging-in-place ser-vice conflicts.
� The model uses scientific function attributeanalysis, problem formulation, and a TRIZ con-tradiction matrix to identify existing service-system conflict problems systematically and todevelop inventive solutions for improving ser-vice systems, rather than relying on the in-
tuition and/or personal experience of servicedevelopers.
The feasibility and advantages of using the proposedmodel have been demonstrated by a case study of anageing-in-place service agency that provides home-care services to the dwellings of senior citizens in Tai-wan. Based on TRIZ inventive principles, six inven-tive solutions for improving the services are proposed.These inventive solutions can feasibly be applied tomedical equipment designs and ageing-in-place ser-vice systems. In summary, the study has successfullyshown that the proposed service innovation model candeliver a systematic set of feasible innovation solutions.
Several managerial implications accrue from thisstudy. The case study demonstrates to managers thatthe proposed model can facilitate the systematic im-provement of their service systems by formulating ef-fective innovative solutions. In particular, the TRIZparameter correspondence table can help service de-velopers who are less experienced in using the TRIZtechnique to select appropriate TRIZ parameters andgenerate innovative solutions. Moreover, because theTRIZ technique has a powerful knowledge base anda collection of tested innovation patterns (Chai et al.,2005; J. Zhang, K. Chai, & K. Tan, 2003a; J. Zhang, K.H. Chai, & K. C. Tan, 2003b; Zhang et al., 2005), theproposed service innovation model can help servicedevelopers to design new ageing-in-place services byusing existing innovation knowledge. Managers shouldalso establish a standard operational procedure (SOP)to generate innovation solutions, thus enabling themto maintain continuous innovation in their ageing-in-place services. In addition, given that the customer-oriented approach is increasingly valued in all service
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 179

Ageing-in-Place Service Innovation Model Chen et al.
industries, ageing-in-place managers need to take ac-count of the viewpoints of multiple stakeholders (suchas senior citizens, their families, caregivers, and gov-ernment). Finally, managers of ageing-in-place ser-vice agencies should regularly conduct surveys to un-derstand the needs of their clients; this will enablemanagers to make optimal use of the proposed TRIZprocess.
Future studies could use the approach adopted hereto improve services that are delivered by other models,such as community-care services or institution-careservices. Such studies would also serve to validate thepracticability of the model proposed here. These stud-ies might develop other service-quality determinantsto improve the effectiveness of the service innovationmodel proposed here.
ACKNOWLEDGMENTSThis research is supported by the National ScienceCouncil, Taiwan (NSC-97–2221-E-155–051-MY3). Wethank Pan-Chio Tuan (Nan Kai University of Technol-ogy in Taiwan) and Ju-Lu Chen (The Methodist Churchin Taiwan) for their assistance in the research survey.
References
Akay, D., Demıray, A., & Kurt, M. (2008). Collaborativetool for solving human factors problems in the manu-facturing environment: The Theory of Inventive Prob-lem Solving Technique (TRIZ) method. InternationalJournal of Production Research, 46(11), 2913–2925.
Aksoy, O., Erturk, Z., & Ozturk, K. (1977). A study ofergonomics factors in washbasin design. Applied Er-gonomics, 8(2), 79–86.
American Association of Retired Persons. (1990). Under-standing Senior Housing for the 1990s. Washington,DC: AARP.
Baron-Epel, O., Dushenat, M., & Friedman, N. (2001).Evaluation of the consumer model: relationship be-tween patients’ expectations, perceptions and satisfac-tion with care. International Journal for Quality inHealth Care, 13(4), 317–323.
Birnbaum, H., Burke, R., Swearingen, C., & Dunlop,B. (1984). Implementing community-based long-termcare: Experience of New York’s long term home healthcare program. Gerontologist, 24(4), 380–386.
Chabukswar, S., Gramopadhye, A. K., Melloy, B. J., &Grimes, L. W. (2003). Use of aiding and feedback inimproving visual search performance for an inspection
task. Human Factors and Ergonomics in Manufactur-ing, 13(2), 115–136.
Chai, K. H., Zhang, J., & Tan, K. C. (2005). A TRIZ-based method for new service design. Journal of ServiceResearch, 8(1), 48–66.
Chapin, R., & Dobbs-Kepper, D. (2001). Aging in place inassisted living: Philosophy versus policy. Gerontologist,41(1), 43–50.
Citro, J., & Hermanson, S. (1999). Assisted Living in theUnited States. Washington, DC: American Associationof Retired Persons.
Cohen-Mansfield, J., Dakheel-Ali, M., & Frank, J. K.(2010). The impact of a naturally occurring retire-ment communities service program in Maryland, USA.Health Promotion International, 25(2), 210–220.
Cohen-Mansfield, J., & Frank, J. (2008). Relationship be-tween perceived needs and assessed needs for servicesin community-dwelling older persons. Gerontologist,48(4), 505–516.
Cutchin, M. P. (2003). The process of mediated aging-in-place: A theoretically and empirically based model.Social Science and Medicine, 57(6), 1077–1090.
Cutler, L. J. (2007). Physical environments of assistedliving: Research needs and challenges. Gerontologist,47 Spec No 3, 68–82.
Donabedian, A. (2003). An Introduction to Quality As-surance in Health Care. Oxford: Oxford UniversityPress.
Eiriz, V., & Figueiredo, J. A. (2005). Quality evaluation inhealth care services based on customer-provider rela-tionships. International Journal of Health Care QualityAssurance, 18(6), 404–412.
Eustis, N. N., Kane, R. A., & Fischer, L. R. (1993). Homecare quality and the home care worker: Beyond qualityassurance as usual. Gerontologist, 33(1), 64–73.
Fashimpar, G. A. (1983). A management tool for eval-uating the adequacy and quality of homemaker homehealth aide programs. Gerontologist, 23(2), 127–131.
Francis, J., & Netten, A. (2004). Raising the quality ofhome care: A study of service user’s views. Social Policyand Administration, 38(3), 290–305.
Geron, S. M., Smith, K., Tennstedt, S., Jette, A., Chas-sler, D., & Kasten, L. (2000). The home care satisfactionmeasure: A client-centered approach to assessing thesatisfaction of frail older adults with home care ser-vices. Journals of Gerontology – Series B PsychologicalSciences and Social Sciences, 55(5), 5259–5270.
Gilleard, C., Hyde, M., & Higgs, P. (2007). The impact ofage, place, aging in place, and attachment to place onthe well-being of the over 50s in England. Research onAging, 29(6), 590–605.
Gilliland Ii, J. C. (1999). Changing home care compen-sation. Home Health Care Management and Practice,11(6), 4–10.
180 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm

Chen et al. Ageing-in-Place Service Innovation Model
Haight, B. K., Michel, Y., & Hendrix, S. (1998). Life review:Preventing despair in newly relocated nursing home res-idents short- and long-term effects. International Jour-nal of Aging and Human Development, 47(2), 119–142.
Han, S. H., Kim, K. J., Yun, M. H., Hong, S. W., & Kim, J.(2004). Identifying mobile phone design features criti-cal to user satisfaction. Human Factors and Ergonomicsin Manufacturing, 14(1), 15–29.
Hawes, C., Phillips, C. D., Rose, M., Holan, S., & Sherman,M. (2003). A national survey of assisted living facilities.Gerontologist, 43(6), 875–882.
Hooyman, N., & Kiyak, H. A. (1996). Social Gerontology:A Multidisciplinary Perspective (Fifth ed.). Boston: Al-lyn & Bacon.
Jaana, M., Pare, G., & Sicotte, C. (2007). Hypertensionhome telemonitoring: Current evidence and recom-mendations for future studies. Disease Managementand Health Outcomes, 15(1), 19–31.
Jensen, P. M., Saunders, R. L., Thierer, T., & Friedman, B.(2008). Factors associated with oral health-related qual-ity of life in community-dwelling elderly persons withdisabilities. Journal of the American Geriatrics Society,56(4), 711–717.
Kane, R. A. (1995). Expanding the home care concept:Blurring distinctions among home care, institutionalcare, and other long-term-care services. The MilbankQuarterly, 73(2), 161–186.
Kolbe, R. H., & Burnett, M. S. (1991). Content-analysisresearch: An examination of applications with direc-tives for improving research reliability and objectivity.Journal of Consumer Research, 18, 243–250.
Kuo, C. F., & Wang, M. J. J. (2007). Interactive virtualevaluation for interface design. Human Factors and Er-gonomics in Manufacturing, 17(5), 485–495.
Lander, S. M., Brazill, A. L., & Ladrigan, P. M. (1997). In-trainstitutional relocation. Effects on residents’ behav-ior and psychosocial functioning. Journal of Geronto-logical Nursing, 23(4), 35–41.
Leon, J., & Moyer, D. (1999). Potential cost savings inresidential care for Alzheimer’s disease patients. Geron-tologist, 39(4), 440–449.
Lin, C. S., & Su, C. T. (2007). An innovative way to createnew services: Applying the TRIZ methodology. Journalof the Chinese Institute of Industrial Engineers, 24(2),142–152.
Louis, A. A., Turner, T., Gretton, M., Baksh, A., & Cleland,J. G. F. (2003). A systematic review of telemonitoringfor the management of heart failure. European Journalof Heart Failure, 5(5), 583–590.
Marek, K. D., & Rantz, M. J. (2000). Aging in place: Anew model for long-term care. Nursing AdministrationQuarterly, 24(3), 1–11.
Mclean, A. (2008). Universal bathroom makeover designideas for planning an accessible bathroom. Retrieved
May 18, 2012, from http://www.bathroomgurureview.com/universal-design/universal-bathroom-makeover-design-ideas-for-planning-an-accessible-bathroom.html
Mitchell, J. M., & Kemp, B. J. (2000). Quality of life in as-sisted living homes: A multidimensional analysis. Jour-nals of Gerontology – Series B Psychological Sciencesand Social Sciences, 55(2), P117–P127.
Na, Y. (2009). Fashion design styles recommended byconsumers’ sensibility and emotion. Human Factorsand Ergonomics in Manufacturing, 19(2), 158–167.
Palley, H. A. (2003). Long-term care policy for olderAmericans: Building a continuum of care. Journal ofHealth and Social Policy, 16(3), 7–18.
Park, M. (2011). Evaluation of earcons for portable digitalelectronic products considering perceptual user charac-teristics. Human Factors and Ergonomics in Manufac-turing & Service Industries, 21(5), 464–473.
Pickering, T. G., Gerin, W., & Holland, J. K. (1999).Home blood pressure teletransmission for better di-agnosis and treatment. Current hypertension reports,1(6), 489–494.
Raynes, N., Temple, B., Glenister, C., & Coulthard, L.(2001). Quality at Home for Older People: InvolvingService Users in Defining Home Care Specifications.York: Policy Press and Joseph Rowntree Foundation.
Reilly, S., Challis, D., Burns, A., & Hughes, J. (2004). Theuse of assessment scales in old age psychiatry servicesin England and Northern Ireland. Aging and MentalHealth, 8(3), 249–255.
Rubin, H. R., Pronovost, P., & Diette, G. B. (2001). The ad-vantages and disadvantages of process-based measuresof health care quality. International Journal for Qualityin Health Care, 13(6), 469–474.
Salomon, L., Gasquet, I., Mesbah, M., & Ravaud, P. (1999).Construction of a scale measuring inpatients’ opinionon quality of care. International Journal for Quality inHealth Care, 11(6), 507–516.
Schade, C. P., & Brehm, J. G. (2010). Improving thehome health acute-care hospitalization quality mea-sure. Health Services Research, 45(3), 712–727.
Schuller, J. (2010). Housing for Minnesota’s Aging Popu-lation: Discussion Paper. Minnesota: University of Min-nesota.
Senol, M. B., Dagdeviren, M., Cilingir, C., & Kurt, M.(2010). Display panel design of a general utility he-licopter by applying quantitative and qualitative ap-proaches. Human Factors and Ergonomics in Manu-facturing, 20(1), 73–86.
Starfish, C. (2002). The Elusive Costs of Home Care. Lon-don: Starfish Consulting.
Stone, R. I., & Reinhard, S. C. (2007). The place of assistedliving in long-term care and related service systems.Gerontologist, 47 Spec No 3, 23–32.
Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm 181

Ageing-in-Place Service Innovation Model Chen et al.
Su, C. T., & Lin, C. S. (2008). A case study on the applica-tion of fuzzy QFD in TRIZ for service quality improve-ment. Quality and Quantity, 42(5), 563–578.
Su, C. T., Lin, C. S., & Chiang, T. L. (2008). Systematicimprovement in service quality through TRIZ method-ology: An exploratory study. Total Quality Managementand Business Excellence, 19(3), 223–243.
Weber, R. P. (1985). Basic Content Analysis. London:Sage.
Woodruff, L., & Applebaum, R. (1996). Assuring thequality of in-home supportive services: A consumerperspective. Journal of Aging Studies, 10(2), 157–169.
Wu, S. C., & Chuang, K. Y. (2001). Aging in place: Thedirection of Taiwan long-term care policy in the 21stcentury. Taiwan Journal of Public Health, 20(3), 192–201.
Yang, H. L., & Hsiao, S. L. (2009). Mechanisms of de-veloping innovative IT-enabled services: A case studyof Taiwanese healthcare service. Technovation, 29(5),327–337.
Zhang, J., Chai, K., & Tan, K. (2003a). 40 Inventive prin-ciples with applications in service operations manage-ment. The TRIZ Journal, December.
Zhang, J., Chai, K. H., & Tan, K. C. (2003b). Systematicinnovation in service design through TRIZ. The TRIZJournal, September.
Zhang, J., Chai, K. H., & Tan, K. C. (2005). Applying TRIZto service conceptual design: An exploratory study. Cre-ativity and Innovation Management, 14(1), 34–42.
Zimmerman, S., & Sloane, P. (1999). Residential Care andAssisted Living in Four States: The Collaborative Studiesof Long-Term Care. San Francisco, CA: The AnnualMeeting of The Gerontological Society of America.
182 Human Factors and Ergonomics in Manufacturing & Service Industries DOI: 10.1002/hfm