
Am I Within My Scope? - Oregon.gov
32
OREGON BOARD OF NURSING VO.39 NO.1 FEBRUARY 2020 V [ ] OR E GO N B O A R D O F N URS IN G [ ] S ENTINEL Am I Within My Scope? Am I Within My Scope? Guidelines for Seeking Additional Nursing Education Guidelines for Seeking Additional Nursing Education
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Am I Within My Scope? - Oregon.gov
OR EG ON BOA R D OF N U R SI NG
VO.39 NO.1 FEBRUARY 2020V[ ]
OR EG ON BOA R D OF N U R SI NG
[ ]SENTINEL
Am I Within My Scope?Am I Within My Scope?
Guidelines for Seeking Additional Nursing Education
Guidelines for Seeking Additional Nursing Education
MOVINGforward
Located on the medical center campus
SkyLakes.org
The Sky Lakes Collaborative
Health Center is the future of
health care in Oregon.
By putting local primary care
in one location, our investment
enhances patient services and
supports the Oregon Health &
Science Unversity Campus for
Rural Health.
• Sky Lakes Primary Care
Clinic, top two floors
• Cascades East Family
Medicine Clinic, 1st floor
• OHSU offices, labs and
classrooms, ground floor
SENTINELCONTENTS
table of
EDITION 46
Created by Publishing Concepts, Inc.David Brown, President • 1-800-561-4686 ext.103
[email protected] Advertising info contact
Laura Wehner • [email protected]
pcipublishing.com
VO.39 NO.1 FEBRUARY 2020[ ]
Oregon State Board of Nursing17938 SW Upper Boones Ferry RoadPortland, OR 97224-7012
Phone: 971-673-0685Fax: 971-673-0684
www.oregon.gov/OSBN
Monday - Friday8:00 a.m. - 4:30 p.m.
Monday - Friday9:00 a.m. - 3:00 p.m.
Board Members:
Kathleen Chinn, RN, FNP Board President
Annette Cole, RN
Adrienne Enghouse, RN
Sheryl Oakes Caddy, JD, MSN, RN, CNE
Bobbie Turnipseed, RN
Judith Woodruff, JD
William Youngren, CNA,
Ruby Jason, MSN, RN, NEA-BCExecutive Director
Communications ManagerEditor of the Sentinel
Advertisements contained herein are not endorsed by the Oregon State Board of Nursing. The Oregon State Board of Nursing reserves the right to accept or reject advertisements in this publication. Responsibility for errors is limited to cor-rections in a subsequent issue.
TABLE OF CONTENTS
23
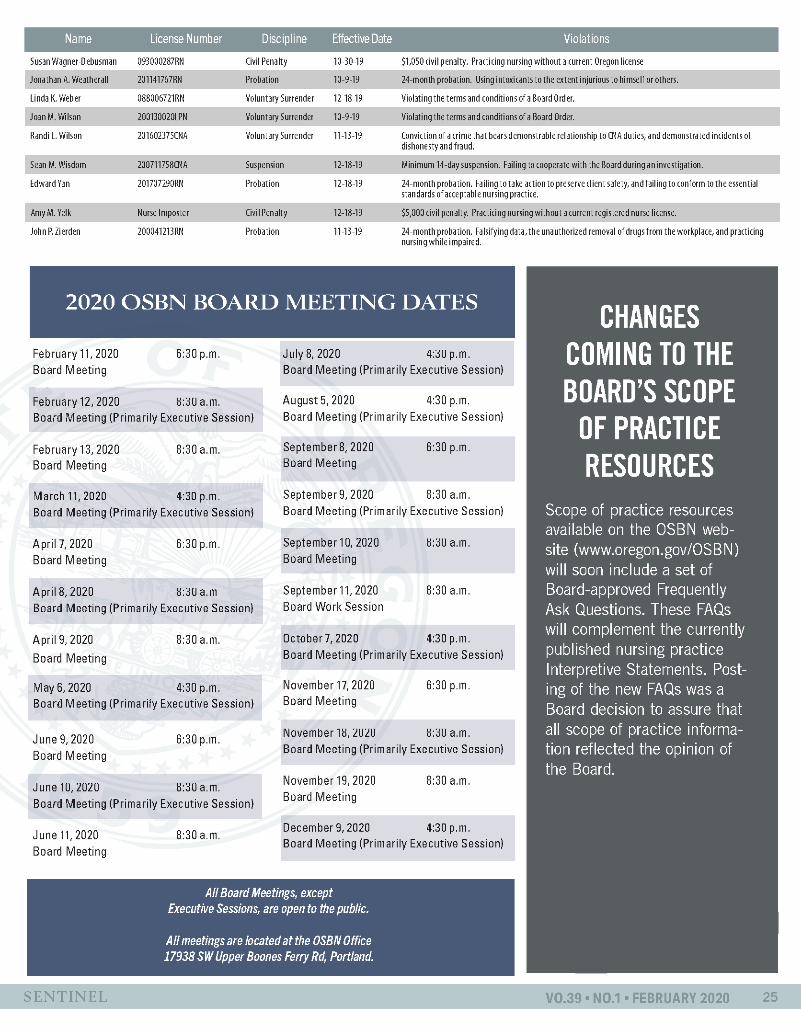
25 2020 Board Meeting Dates
27 2020 Board Members
Am I Within My Scope? . . . . . . . . . 4
Guidelines for Seeking Additional Nursing Education . . . . . . . . . . . . 10
New Interpretive Statement Clarifies Ability to Counsel Patients Regarding Marijuana . . . . . . . . . . . 13
Oregon Opioid Tapering Guidelines Coming Soon . . . . . . . . . . . . . . . . 14
National Certification and State Certification: An Oregon Difference . . . . . . . . . . . . . . . . . . 15
Oregon Office of Rural Health Activates Nurse Residenciesr . . . . . 16
Your Relationship With The Board During An Investigation . . . . . . . . 18
You Ask, We Answer . . . . . . . . . . 20
Disciplinary Case Studies: Truthfulness . . . . . . . . . . . . . . . . . 26
Meet The Team . . . . . . . . . . . . . . 28
What Does it Mean if My Application is “Assigned to Investigations”? . . . 30
All Board Meetings, except Executive Sessions, are open to the public. All
meetings are located at the OSBN Office17938 SW Upper Boones Ferry Rd, Portland.
Page 4
Page 16
Page 28
4 OREGON STATE BOARD OF NURSING
AM I WITHIN MY SCOPE?
NURSE PRACTICE
I’ll just do this first and then call Dr. Smith later, I’m sure he won’t mind… We do this all the time… I know how to do this, it’s no big deal. Have you ever said something like this? Upon further reflection, you may find that you have done this more frequently than you would have imagined. This could be the signal for you to ask yourself, “Am I exceeding my scope of practice?”
In this article, common examples seen by the Board will be presented for discussion to encourage nurses to think about their own practice. The goal is to help nurses recognize subtle actions that can lead to at-risk practice. We will review the importance of scope of practice and how to ensure you are practicing safely.
Scope of Practice HistoryIn 1903, North Carolina became
our nation’s first state to enact a nurse registration law to protect the title “nurse” and to improve the practice of nursing (Russell, 2017). Oregon’s first NPA became law on 1911 directing the formation of the Board and setting requirements for those engaging in nursing work. It is the responsibility of each state and US territory to enact
an NPA to govern the practice of nursing, providing laws and rules to protect their citizens by ensuring safe, competent, and ethical nursing care (Russel).
While the practice role of the individual RN or LPN may vary between facilities and employers, the legal requirements of nursing practice do not. These legal requirements of nursing scope of practice are outlined in each state’s NPA. According to the American Nurses Association (ANA), the method to define nursing scope of practice is a two-step process (Scope of Practice, n.d.). First, a law known as a “nurse practice act” must be passed in the state; then regulatory bodies create and implement the rules and regulations (Scope of Practice, n.d.). The Nursing Practice Act (law) and related rules define and regulate a variety of areas within in nursing, including scope of practice.
Scope of Practice in Oregon The scope of nursing practice for
the RN and for LPN in Oregon begins with Oregon Revised Statute chapter 678 and is further interpreted by the Board in chapter 851, Division 45, of Oregon Administrative Rules. The
scope of practice standards of Division 45 are succinct statements of actions that identify acceptable levels of safe practice. One of the actions required of all nurses is the responsibility to be knowledgeable of the rules governing their practice and to practice within those legal boundaries.
Division 45 also contains succinct statements of actions specific to LPN practice and actions specific to RN practice. The Board’s website provides a link to the NPA’s Division 45 standards. The Board also provides on-line resources for nurses that address questions regarding scope of practice. These resources can be accessed on the Board’s the Practice Statements and Guidance webpage in the form of interpretive statements, general policies, and information regarding nursing practice.
One of the most popular resources published is the Board’s Scope of Practice Decision Making Guidelines for the RN and the LPN. This scope of practice decision-making tool assists the licensee to determine whether a specific practice role, intervention, or activity is within the scope of practice for the licensee’s based on indicators such as level of licensure, the setting
By North Carolina Board of Nursing Investigations Director Angie Matthes, RN, MBA, MHA, CI, and Regulation Consultant Anne Hardee, RN, MSN.
Forward by OSBN Nursing Practice Policy Analyst Gretchen Koch, MSN, RN.
Forward:The term scope of practice is broadly defined as the actions one is permitted to undertake in keeping with the terms
of their license to practice. For the Oregon-licensed nurse, those actions are identified in Division 45 of Oregon’s Nurse Practice Act (NPA). This article, used with the permission of the North Carolina Board of Nursing and modified to reflect Oregon scope of practice regulations, serves to help nurses recognize behaviors that can lead to at-risk or unsafe practice.

5SENTINEL
NURSE PRACTICE
where nursing services are provided to the client, and the licensee’s individual knowledge, skills, abilities and competencies. The Board of Nursing encourages all nurses to become familiar with the Scope of Practice Decision Making Guidelines.
The Board of Nursing frequently receives complaints where a nurse is reported to have exceeded their scope of practice. Some of the reported practice situations seem obvious, while others are not. The nurse who exceeds scope of practice has typically partaken in the slippery slope activity of risk-taking decisions and behaviors.
Disciplinary actions can be imposed for exceeding scope of practice and may range from a reprimand, which is a formal notice to the nurse that OSBN standards have been violated, up to license revocation that removes a nurse’s nursing license.
“This is how we have always done it”
Frequently nurses will run into a situation where they are asked to perform a procedure that they have never performed or told that it is all right to perform a procedure or to sign an order because “this is how we have always done it.” Sometimes these situations are seen by nurses as only “bending the rules.” Regardless of patient outcomes, exceeding your scope or bending the rules could jeopardize client safety, jeopardize your employment, and jeopardize your ability to practice.
Research has shown that there are a number of reasons that nurses may bend the rules, for example, unfamiliarity with policies and regulations or believing that their professional judgement is in the best interest of
the patient (Bending the Rules, 2016). Hahtela, et al. (2017) found that unit characteristics were associated with adverse events and nurses’ perception of autonomy.
To uphold safe and legal practice, nurses are encouraged to follow their chain of command, to speak with risk management, and to utilize the Board’s website to ensure that they are practicing within their scope and not drifting beyond scope by following their unit culture.
How can I be sure I am staying within my scope?
Think about your practice. Do you bend the rules? Do you assume something is correct because it is the way it has always been done? Chastain and Burhans (2016) reported that, “If left unquestioned, the rule-bending action then tacitly becomes acceptable practice not only by that individual but may be adopted by others in the unit or facility and many times leads to what is referred to as a cultural norm.”
You are encouraged to review the following discussion questions, which are based on common Board complaints, and reflect on how they could apply to your nursing practice.
Discussion QuestionsIn the first scenario, Julia, a wound
care RN, is called by a staff nurse for a phone consultation regarding a patient’s wound because the patient does not seem to be responding favorably to the current treatment. Julia makes a recommendation based on what the staff nurse reports, without actually assessing the patient’s wound or accessing their medical record, and writes a medical order for treatment. Julia assumes that the physician will
agree because she always has. In fact, she will usually ask Julia what she suggests for wound therapy.
STOP: What is the correct action at this time?
a) Julia should not write the order until she actually speaks with the physician or office nurse communicating on behalf of the physician and receives confirmation.
b) Julia should write the order and have staff begin the new wound care with the next scheduled dressing change.
c) RN Julia should write the order but not have staff implement the order.
Discussion:Answer is (a). RN Julia should not
write a verbal or telephone order unless he/she has received the order directly from the prescriber. Additionally, no change in wound care treatment should ever be implemented until it is ordered by a health practitioner whose scope of practice includes diagnosis and prescribing.
In scenario #2, Kate RN, a nursing supervisor administers a commonly used medication to a patient after assessing the patient with respiratory distress. Katie assumes that the patient has a standing order in place which includes an order for the medication; she does not stop to check the client’s electronic health record to ascertain what current orders exist.
STOP: What is the correct action at this time?
a) Katie should go ahead and administer the medication because she is certain after assessment that the patient needs the medication.
b) Katie should check with another supervisor and make sure the medication is appropriate based on the patient assessment.
6 OREGON STATE BOARD OF NURSING6 OREGON STATE BOARD OF NURSING
NURSING PRACTICE
c) Katie should not administer the medication without speaking with the physician and obtaining an order.
Discussion: Answer is (c). Katie should not
administer any medication without a current order for the medication from the physician. The RN who assumes that an order is present without directly checking the patient’s medical record is not practicing safely.
In scenario #3, Mary, a RN working at a home health agency is preparing a recertification packet for an existing patient that has received the same care and orders for a few months. Mary has been on vacation and realizes that the patient’s recertification is overdue and the new certification period should begin today. Mary assumes the physician still wants the patient to receive home health services so she updates the orders and prepares the paperwork for the physician to sign.
STOP: What is the correct action at this time?
a) Mary should send the completed paperwork to the physician and instruct the staff assigned to the patient to continue to make visits as usual, so the patient’s services are not disrupted.
b) Mary should contact the physician directly and obtain an order to continue home health services before any additional visits are made.
c) Mary should ask the agency administrator to approve the continuation of care.
Discussion:Answer is (b). Mary should contact
the physician prior to the expiration of existing orders to obtain an order to continue services for the client. If the previous orders have expired, Mary must obtain new orders prior to staff
making any additional visits. Staff cannot continue to make visits to a patient for which no current orders exist.
In scenario #4, A Nursing Facility has an open position for Director of Nursing and is experiencing difficulty finding qualified applicants in the rural area. A day shift LPN named Robert has been employed at this facility nearly 20 years and knows everything about this facility. Robert approaches the Nursing Facility’s corporate nursing administrator stating he is willing to take the position because, after all, he has the most knowledge and seniority and would love a promotion with more money.
STOP: What should the administrator do?
a) Ask human services to prepare the Director of Nursing position description for Robert to sign.
b) Thank Robert for his previous work but explain that the functions required by the Director of Nursing position are within RN scope of practice only.
c) Allow Robert to be hired as an interim Director of Nursing until which time an RN is hired and oriented into the position.
Discussion:Answer is (b). The functions
required by the Director of Nursing position are within RN scope of practice only. The clinically directed and supervised nursing practice requirement of LPN licensure prohibits the LPN from accepting and form practicing in any independent nursing practice role such as the Director of Nursing position.
In scenario #5, Jeff, an RN working on a hospital medical telemetry unit, is
caring for a patient that has a physician’s order for Zolpidem 10mg at bedtime. When Jeff goes in to the patient’s room to administer the Zolpidem, the patient states that she will only take half of the pill. Jeff breaks the pill in half, administers half to the patient, and wastes the remaining half with the unit’s newly hired RN as a witness.
STOP: What should Jeff have done?
a) Inform the RN who witnessed the wastage that when a patient requests a different dose than what is ordered, it’s okay to accommodate the request.
b) Thank the patient for speaking up and tell her that it’s fine to give her only half.
c) Contact the physician to communicate the patient’s request and obtain an order to administer a lesser dosage to the patient.Discussion:
Answer is (c). It is not within the scope of a RN or a LPN to change the dosage of a medication unless there are existing parameters included in the order. The nurse needs to contact the prescriber and receive a new order prior to administering a different dosage.
In scenario #6, Susan, a LPN working in a long term care facility is assigned to a patient that has orders for Valium 2mg every 12 hours. The medication is scheduled to be given at 10 am and 10 pm. Susan notes that the patient is agitated around 5 am and knows the patient has Valium ordered and decides to administer the scheduled Valium early as a prn dose. Susan signs the medication out on the controlled substance form, however she does not report this to oncoming shift.
7SENTINEL
NURSING PRACTICE
STOP: What would be the appropriate action by the LPN?
a) Give the medication at 5 am because the patient was agitated and clearly needed it.
b) Give the medication at 5 am and report to oncoming nurse.
c) Contact the provider for prn order.
Discussion:Answer is (c). It is not appropriate
for the LPN to administer a regularly scheduled medication early because the patient needs it. The Valium was ordered every 12 hours in this case and the medication was not yet due. The provider should have been contacted for further orders.
In scenario #7, Thomas, an RN, works in an emergency department (ED) and is a charge nurse. Getting patients through the ED efficiently is a major quality focus of the department. Thomas enters basic lab orders indicating “based on protocol” on a patient with minor symptoms that’s been triaged. There is no protocol for routine labs in the ED. Thomas does this to make sure the patient gets moved through quickly and the ED doesn’t get backed up.
STOP: What would be the appropriate action by the RN?
a) Contact the ED provider and obtain orders for the labs.
b) Contact the ED provider when the results come back.
c) There is no need to contact the provider because the labs returned normal and now the patient can be seen and discharged more quickly.
Discussion:Answer is (a). There was no protocol
in the ED for Thomas to use. Thus, the provider had to write an order for any lab work. Thomas should have
contacted the provider and asked if any labs should be ordered.
In scenario #8, Anna, a Women’s Health Care Nurse Practitioner, is seeing a patient for an annual well check visit. The patient’s husband, who is in attendance, asks Anna if she can write him a prescription for some Adderall because he is having trouble focusing at work. He tells Anna he was on Adderall years ago, but hasn’t taken it recently.
STOP: What should the NP do?a) Write the prescription for the
patient’s husband because he seems like he is truthful.
b) Tell the patient’s husband she cannot treat him for this problem because her specialty is Women’s Health.
c) Tell the patient’s husband to make an appointment and she’ll be glad to treat his ADHD.
Discussion:Answer is (b). Anna would be
practicing outside her scope as a WHNP by prescribing Adderall for the patient’s husband.
In scenario #9, Beth comes in for her morning shift in the emergency department after a late night at a New Year’s Eve party. Because Beth has been counseled about too many absences, she goes into work really sick even though she knows she shouldn’t. Beth asks a RN coworker to start an IV and to give her some fluids and Zofran. Beth has seen other staff do this for each other and thinks it’s no big deal.
STOP: What should the RN coworker do?
a) Tell Beth that she needs to speak to ED provider and be seen if she’s that sick.
b) Take Beth to an empty room,
start an IV on here and give her some fluids along with Zofran because they need her to be able to work.
c) Tell Beth to just get some Zofran out of the Pyxis and take it.
Discussion:Answer is (a). The coworker
should not administer medication to Beth as it’s not within a nurse’s scope of practice to order IV fluids and medication or to administer such without an order.
In scenario #10, George, an ICU RN, is caring for a patient that is intubated and has an order for Fentanyl 50 mcg intravenously every 20 minutes. The patient starts to wake up and is grimacing and agitated. George removes 100 mcg of Fentanyl and begins to push the medication slowly while he monitors the patient. He administers the full 100 mcg in about 5 minutes and the patient calms downs and appears to be resting comfortably. George then documents that he gave the Fentanyl as two separate doses 20 minutes apart but tells the oncoming RN that he gave a “nursing dose” of Fentanyl to the patient and it seemed to help.
STOP: What was the correct action?
a) Report to oncoming nurse what medication was given so that nurse will have complete information on the patient’s status.
b) Contact the physician after giving the Fentanyl and tell the physician that the patient is requiring more Fentanyl than what was ordered.
c) Administer 50 mcg Fentanyl and wait 20 minutes before administering another 50 mcg.
Discussion:Answer is (c). The RN should have
followed the order as written. The RN
8 OREGON STATE BOARD OF NURSING
NURSING PRACTICE
REFERENCESChastain, K., & Burhans, L. (2016). What Could Happen: The Consequences of Practice Drift. Nursing Bulletin, pp. 7-13.
Hahtela, N., McCormack, B., Doran, D., Paavilainen, E., Helminen, M., & Suominen, T. (2017, December). Workplace Culture and Patient Outcomes: What’s the Connection. Retrieved from Nursing Management: www.nursingmanagement.com
Olin, J. (2012, January 12). Is It In Your Scope of Practice. Retrieved from RN Central: www.rncentral.com
Oregon State Board of Nursing (2019). Scope of Practice Decision Making Guidelines for the RN and the LPN.
Russell, K. A. (2017). Nurse Practice Acts Guide and Govern: Update 2017. Journal of Nursing Regulation, 18-25.
Scope of Practice. (n.d.). Retrieved from American Nurses Association: https://www.nursingworld.org
The Risks of Bending the Rules. (2016). Retrieved from HPSO: http://www.hpso.com
ADULT-GERONTOLOGY ACUTE CARE NURSE PRACTITIONER • DOCTOR OF NURSING PRACTICE
• POST-GRADUATE CERTIFICATE
Apply Now SEATTLEU.EDU/NURSING/ACUTE-CARE [email protected] | (800) 426-7123
could have contacted the physician after the first dose if the patient did not improve.
Our hope is that these scenarios have prompted you to thoughtfully self-evaluate your own nursing practice for at-risk or unsafe actions. To promote a safe practice, keep yourself informed by actively pursue formal and continuing education opportunities, know your organization’s policies, better your understanding of Division 45 scope and standards of practice, and access the Board’s scope of practice resources. Please take this opportunity to visit the OSBN web page (www.oregon.gov/osbn) for links to Oregon’s NPA and scope of practice resources.
9SENTINEL 9SENTINEL
O P E N P O S I T I O N S• Chair Biobehavioral
Health and Data Sciences Department
• Chair Rural Health and Health Equity Department
WE ARE HIRING
NURSING FACULTY
• FNP/AGPC-NP Faculty • Junior Faculty• Senior Faculty• Undergraduate
Faculty
To learn more about the positions and how to apply contact Delana Mannion at [email protected] or (505) 272-5098.
g o . u n m . e d u / n u r s i n g
emoryhealthcare.org/careers
Our Magnet®
make this the best place to work.
YOU DO.
10 OREGON STATE BOARD OF NURSING
NURSING EDUCATION
So, you’ve made the decision to earn additional nursing education, which may include an LPN-RN, RN-BSN, or some type of RN-MSN program. As if that wasn’t hard enough to decide, you are now faced with the next big decision: which program will you choose? What should you look for in evaluating the program that interests you? A frequent question asked of the Oregon State Board of Nursing (OSBN) staff is, “Does the OSBN approve of this program?”
For the sake of brevity, this article will focus primarily on out-of-state programs offered by distance education. It will also focus on regulatory information specific to Oregon rather than general advice on choosing a program based on how you learn best.
What’s the Short Answer?The short answer is that the OSBN does not approve
or disapprove of any nursing programs that are offered completely out-of-state. However, the OSBN does accept degrees awarded from out-of-state nursing programs if they are participants in the State Authorization Reciprocity Agreement (SARA). More information about what that means is discussed below.
The OSBN only has jurisdiction over pre-licensure nursing programs located in Oregon. These are referred to as “pre-licensure” because the student doesn’t yet have the new license. Pre-licensure programs are those that prepare graduates to take these examinations:
• Practical Nurse licensure examination;• Registered Nurse licensure examination; or,• Certification for Advanced Practice Registered Nurse
(APRN) licensure. You’ll notice that all of these programs culminate in a
new or additional license and a change in practice. If you are seeking an RN-BSN program, your license will not change, so the OSBN has no jurisdiction to approve or disapprove of that program, even if it is in Oregon. If you are seeking a master’s degree in leadership, healthcare administration, nursing informatics, etc., your registered nurse license requirements also stay the same, regardless of your additional education and where your program is offered since you will not be an APRN. Having said that, it’s still wise to consider the guidelines below when you select a nursing program,
even if it’s not for advanced practice.
What Should I Look For?ARTICULATION AGREEMENTS
If you want to complete your additional degree as quickly as possible, look into your initial program’s articulation agreements with universities that offer the degree you are seeking. This applies to students applying to programs in Oregon. The OSBN defines an articulation agreement as “the process of comparing or matching the coursework completed in one educational institution with the courses or requirements of another institution to assure that a student may transfer credit from one program to another without having to repeat any coursework. For the purpose of these rules, articulation specifically relates to courses completed or required within a nursing education program” (OAR 851-006-0000).
All Oregon nursing programs, whether practical nursing (PN) programs or registered nursing (RN) programs, are required by Oregon Administrative Rules to have “a signed articulation agreement for program graduates into the next level of nursing education...” (OAR 851-021-0055(7). This standard goes further to explain that every PN program must have “an agreement with an Oregon-approved program that prepares candidates for licensure as an RN” and every program leading to an associate’s degree in nursing must have “an agreement with an Oregon-approved program leading to a baccalaureate or higher degree in nursing.”
This information can be accessed on the OSBN website by clicking “Find an Oregon Nursing School” under the Education column. You can also check with your initial nursing program to see which higher education nursing program has signed an articulation agreement to partner with them. If you are applying to an out-of-state program, an articulation agreement with that program is unlikely, but some credits might still transfer.
ACCREDITATIONNursing program accreditation is different from
institutional accreditation. As of 2016, about half of all boards of nursing in the United States required nursing program accreditation (Spector, Hooper, Silvestre, & Qian, 2018). Although the OSBN strongly supports and encourages
GUIDELINES FOR SEEKING ADDITIONAL NURSING EDUCATION
By Policy Analyst for Nursing Education & Assessment Nancy Irland, DNP, RN

11SENTINEL
NURSING EDUCATION
nursing program accreditation, it remains one of the boards of nursing (BON) that does not require nursing program accreditation for undergraduate programs. This is because, unlike some states, an OSBN representative conducts nursing program surveys that are very similar in content and timing to accreditation surveys. Both the OSBN and accrediting bodies conduct surveys to confirm adherence with professional and educational standards. For accredited programs, the OSBN works collaboratively with the accrediting bodies and often conducts site surveys at the same time. The OSBN does require accreditation for master’s degree programs preparing APRNs (see Figure 2 below). Accreditation of the institution (the controlling body) that awards your degree is required of all programs (see Figure 1 and Figure 2).
The primary differences between accreditation and BON approval are that BON approval of a program is essential for National Council Licensure Examination (NCLEX) eligibility. If a program is not approved by a BON, its graduates may not sit for the licensing exam. BONs are government regulatory entities that serve the public; however, national accreditors are for-profit businesses with nursing programs as their customers. In addition, BONs have the legal authority to close substandard programs while accreditors do not.
INSTITUTIONAL ACCREDITATIONMost Pacific Northwest institutions are accredited through
the Northwest Commission on Colleges and Universities (NWCCU). When seeking an out-of-state program, ensure that the controlling body of that program is accredited by its own regional commission.
NURSING PROGRAM ACCREDITATIONThere are two primary national accrediting bodies for nursing
programs in the United States. These are the Accreditation Commission for Education in Nursing (ACEN) and the Commission on Collegiate Nursing Education (CCNE).
In Oregon, all BSN programs are accredited, even though this remains voluntary. If your associate’s degree was from a program that was not accredited, earning your BSN at an accredited program will open many doors that might not otherwise be possible. Students in accredited programs may qualify for more financial aid options. In addition, graduation from an accredited nursing program is required for initial licensure in some states, and for employment in the Veterans Health Administration hospitals and some Magnet hospitals. Graduation from an accredited program within an accredited institution is a requirement for admission to master’s degree programs.
FREQUENTLY ASKED QUESTIONS
Can I Complete Clinicals in Oregon if I’m Enrolled in an Out-of-State Program?
Yes. Many students enrolled in non-Oregon, distance education programs complete their clinical experience in Oregon. These include LPN-RN or RN-APRN courses of study. More information can be obtained from the OSBN website i by clicking on “Nursing Programs Outside Oregon.” The program is required to complete a petition to the OSBN and to confirm that faculty oversight of clinicals will be by an Oregon-licensed nurse. Ultimately, it is up to the student to confirm that their clinicals have been approved by the OSBN.
It is recommended that a student confirm the program’s process for clinical placements. Most programs have affiliation agreements with Oregon clinical sites, but some programs do not. These programs require students to find their own clinical placements. This can make completing this requirement very difficult for the student, since clinical sites are already filled with so many students from Oregon-based nursing programs they may not have room for even one more student.
How Do I Know My courses or program Will be Accepted for Licensure?
All degree-granting institutions in the U.S. must be authorized by a governmental entity to issue degrees. Since each state’s board of nursing approval is limited to that particular state, how can a state board of nursing confirm for the public that Oregon nurses who earned their education outside of Oregon have appropriate education to care for Oregon’s citizens? Enter SARA, the State Authorization Reciprocity Agreement, formed in 2013. Oregon became a SARA state in 2014. SARA is a voluntary agreement among its member states and U.S. territories that establishes comparable national standards for postsecondary distance education. Post-secondary college and university credits earned from a SARA-approved program anywhere in the country meet
Standards for Approval: Organization and Administration (1) The controlling body shall be accredited by an appropriate regional or national accrediting association or agency and meet all current standards of the accreditor.(a) Institutions offering registered nurse programs shall be approved as a degree-granting institution of higher education in Oregon, and(b) Accredited by a regional association or national agency recognized by the Council on Higher Education Accreditation (CHEA)
FIGURE 1. INSTITUTIONAL ACCREDITATION REQUIREMENTS AS STATED IN DIVISION 21851-021-0040

12 OREGON STATE BOARD OF NURSING
Oregon state licensing requirements. The SARA website indicates that as of July 2019, members of SARA include 49 states and US territories. Within these states and territories, there are around 1,993 colleges and universities (https://nc-sara.org/about-nc-sara). California is the only state not participating in SARA.
SARA makes it easier for students to take online courses and improves consumer protection. Note, however, that not all institutions in each participating state or territory are members of SARA. Each college within a SARA state must submit an application to SARA in order to participate and be
approved before their college credits will be accepted for licensure out of state. If you are considering a current or future Oregon license as an APRN, confirm the program’s SARA participation before you enroll so that your courses and program are accepted by the OSBN for licensure.
The OSBN website information (Education tab) includes a list of SARA programs that have petitioned the OSBN for clinical placements in Oregon. However, that is an evolving list, not an exclusive one. If a program you are considering is not on the list, it simply may not have previously petitioned the OSBN for clinical placements, although it may be eligible. During the petition process, the program is required to submit proof of SARA participation, BON approval, and accreditation of the controlling body.
ConclusionEducational options have grown
exponentially with the advent of distance education. Although regulating bodies and institutions are doing their best to provide accessibility for distance education, the student must also remain informed of licensing and degree-granting requirements in order to prevent expensive disappointment. Education requires the proverbial act of “jumping through hoops.” For the student seeking to enroll in distance education and/or planning a career as an APRN either now or in the future, it is essential to begin jumping those hoops by first confirming program accreditation, and then to verify that the school of your choice is a SARA participant.
REFERENCES
Spector, N., Hooper, J. I., Silvestre, J., & Qian,
H. (2018). Board of nursing approval of registered
nurse education programs. Journal of Nursing
Regulation, 8(4), p 22-31.
NURSING EDUCATION
unmhjobs .comBe a part of what makes us great.
“
Marci, RN
The training here is amazing. Everyone at UNMH is committed to learning and growth. ”
Nursing Opportunities Available!As a nurse at UNM Hospitals, you’ll be part of a collaborative team that
continually works to improve patient health and nursing practice. With our
size and scope, you can choose from a broad range of disciplines and unique
opportunities.
ED • OR • L&D • RN Case Managers
PACU • Adult & Pediatric ICU
Join a state leader in nursing, and discover a professional environment that
offers you all the tools and support you need to build a successful future.
FIGURE 2. APRN GRADUATE LICENSING REQUIREMENTS AS STATED IN DIVISION 50851-050-0002
Application for Initial Certification as a Nurse Practitioner1. An applicant for initial certification in Oregon as a nurse
practitioner shall:b. Hold a current unencumbered registered nurse license in the State of Oregon, andc. Meet the following educational requirements:
A. Master’s Degree in Nursing or a Doctorate in Nursing accredited by a national nursing organization recognized by the US Department of Education or a credentials evaluation from a Board approved or directed credentials service for graduate nursing degrees obtained outside the U.S. which demonstrates educational equivalency to U.S. graduate nursing degree accredited by a national nursing organization recognized by the US Department of Education;
13SENTINEL
The Oregon State Board of Nursing adopted the following interpretive statement during its November 2019 meeting to clarify nurses’ ability to discuss with patients how prescribed medications may interact with marijuana. The statement reads as follows:
“Oregon statutes and rules regarding the use of marijuana state that only a physician may discuss the use of marijuana for the alleviation of symptoms for specific diseases. It would be a violation of state regulation for any licensee of the Oregon State Board of Nursing to discuss or recommend the use of marijuana for the alleviation of disease symptoms or symptoms due to injury to any patient or client. This also included cannabis-derived CBD oil. This does not apply to products derived from Hemp.
OAR 851-045-0060 (5) of the Nurse Practice Act requires that nurses advocate for the client’s right to appropriate and accurate information. In the nursing function of discharge education, if the client discloses that they use recreational marijuana, the nurse must know and explain the interactions between marijuana and the client’s prescribed medication. It is incumbent of every nurse to understand the effects of marijuana and how those effects could place the client at risk, particularly if a prescription is for controlled substances. Discharge teaching regarding interaction of marijuana with prescription medications is not the same as counseling the client on the use of marijuana for alleviation of symptoms.”
A downloadable copy of the statement is available on the OSBN website.
NEW INTERPRETIVE STATEMENT CLARIFIES ABILITY TO COUNSEL
PATIENTS REGARDING MARIJUANA
NURSING PRACTICE
odocjobs.com [email protected]
- Psychiatric/Adult/Family
Registered Nurses
14 OREGON STATE BOARD OF NURSING
ADVANCED PRACTICE
Oregon has been impacted by the nationwide opioid crisis with an average of five Oregonians dying each week from an opioid overdose. These deaths result from illicit opioids such as heroin and non-pharmaceutical fentanyl and prescription opioids. Oregon has one of the highest rates of prescription opioid misuse in the U.S. and many Oregonians develop opioid use disorder (OUD) and dependency. In 2015, the Oregon Health Authority (OHA) implemented the Opioid Initiative to focus clinicians, agencies, and communities on reducing deaths, non-fatal overdoses and other harms from prescription opioids while increasing access to non-opioid pain management therapies. These efforts have led to a 52% decrease in prescription opioid related deaths since 2006 and a 29% reduction in the rate of opioid prescription fills since 2015.
As part of this multipronged approach to the crisis, the OHA has convened several task forces to address opioid management. In March 2019, the Oregon Opioid Taper Guidelines Task Force was convened. The task force was comprised of more than 20 experts with experience in pain management, addiction treatment, healthcare management, palliative care, and payers. The interprofessional members included APRNs, psychologists, MDs, LCSWs, administrators, peer supporters, and persons with lived experience.
The purpose of the task force was to develop statewide guidelines to reduce harms associated with opioid use while promoting patient-centered care. Dana Hargunani, Chief Medical Officer for OHA, and Katrina Hedberg, State Epidemiologist and Health Officer, co-led the task force, which met monthly. At each meeting, task force members considered draft language, evidence-based literature, expert opinion, and public testimony. Final guidelines “Oregon Opioid Tapering Guidelines: Recommendations for Patient-centered Care to Reduce Harms Associated with Opioid Use” were approved in October 2019.
The guidelines provide background, principles and terms, recommendations, and additional resources. Of critical importance is the guidelines are explicit about there not being a single approach to tapering and not all patients on opioids need to be tapered. Principles the task force followed while developing the guidelines included:
• care should be patient-centered, trauma informed, and evidence based;
• the overarching goals for tapering are patient safety, functional status, and quality of life;
• guidelines are meant to promote patient engagement and shared decision making;
• tapering plans should be individualized; and, • health system and payers must support an integrated
approach to tapering that ensures access to non-opioid and nonpharmacological pain therapies.
The major sections of the guidelines are: I. Assessing the Patient,
II. When to Consider Opioid Tapering, III. Approaches to Opioid Tapering, IV. Managing Withdrawal and Complicated Tapers, V. Long-term Support and Follow Up,
VI. Organization Supports, VII. Community-level Interventions, and VIII. Patient, Provider, and Community Resources.
The final guidelines will be published soon. In the meantime, the near-final draft can be viewed at https://www.oregon.gov/oha/PH/PREVENTIONWELLNESS/SUBSTANCEUSE/OPIOIDS/Documents/taskforce/tapering-taskforce/OOTG-October-2019-Meeting-Packet.pdf (starting on page 5 of the document).
By OHSU School of Nursing Assistant Professor Helen Turner, DNP, CNS
OREGON OPIOID TAPERING GUIDELINES COMING SOON
15SENTINEL
ADVANCED PRACTICE
For decades, Oregon law stated that nurse practitioners and clinical nurse specialists were state certified rather than licensed, which has caused confusion between someone’s state nursing license and any national certification they may hold. Effective January 1, 2020, Oregon advanced practice nurses are no longer ‘state certified.’ Statutory changes now refers to these practitioners as ‘licensed,’ therefore practitioners in Oregon will be state licensed and nationally certified.
Referring to an advanced practice nurse as being ‘certified’ has been in common use since the first nurse practitioner program opened in 1965 in Colorado. The program awarded a certificate rather than a degree, although Master’s Degrees where awarded later in the 1960’s by other programs. The term relates to the license the individual holds as a registered nurse (RN); the RN license is certified to practice at the advanced nursing level. State nurse practice acts also refer to the advanced practice nurse as being ‘certified.’
As advanced practice nurses gained more recognition, national certification examinations were developed to provide an entry-level examination to determine if the educational outcomes for the specific population focus or specialty had been achieved. As the NCLEX® measures entry-level competency for the licensed practical nurse and the RNs, the advanced practice national certifications measure entry-level competency for the practice of nursing at the advanced level.
To be both ‘state certified’ to practice and ‘nationally certified’ to provide evidence of entry level competency is a source for confusion for the public and for practitioners. In most states, nurse practitioners are licensed as CNP (Certified Nurse Practitioner) and then designate their population specialty by listing their national certification after their CNP license. So, for example, the signature of a NP in another state would be, “Mary Smith, CNP, FNP-BC.”
This is not the case in Oregon. Oregon nurse practitioner licenses are issued according to population specialty. That population specialty is reflected in the name of the license type. There is no CNP license type in Oregon. So, in Oregon, Mary Smith should sign her name “Mary Smith,
FNP.” In Oregon (except for grandfathered licensees), it is required that to be licensed in a population specialty, you must be nationally certified in that specialty. To write “Mary Smith, FNP-BC” illustrates the confusion in that in order to be licensed as an FNP, Mary Smith is required to be nationally certified, so there is no need to again identify herself as being certified. This mixes her state license with her national certification.
There is no mandated way to sequence your professional signature, other than you must identify yourself by your state license type. The American Nurses Association recommends the following:
Your name, then your highest obtained degree, then your license type, then any additional certifications.
Oregon does not issue an APRN license type, therefore that designation is not allowed to precede your state license type. However, once you identify yourself by your state license, there are no mandated rules about what comes after.
So Mary Smith can be “Mary Smith, DNP, FNP, AP-PNM, APRN. The signature indicates that Mary Smith earned a Doctorate of Nursing Practice, is licensed as a family nurse practitioner, has additional certification in pain management at the advanced practice level, and is an advanced practice registered nurse.
For additional information on how to sign your credentials, visit the American Nurses Credentialing Center website: https://www.nursingworld.org/~48fdf9/globalassets /certification/renewals/how-to-display-your-credentials.
NATIONAL CERTIFICATION AND STATE CERTIFICATION: AN OREGON DIFFERENCE
By OSBN Executive Director Ruby Jason, MSN, RN, NEA-BC
16 OREGON STATE BOARD OF NURSING16 OREGON STATE BOARD OF NURSING
Nurse residencies, or transition-to-practice programs, are an essential element to helping new nurse graduates and nurses moving into new settings begin practice in an efficient way. In 2010, the National Academy of Medicine released its landmark report “The Future of Nursing,” and recommended implementing more nurse residency programs. While multiple health systems and facilities across Oregon have implemented programs to help new nurses orient to their organizations, other smaller, stand-alone facilities can struggle to allocate staff and resources to onboard new colleagues in a structured way.
In 2018, the Oregon Office of Rural Health (ORH) commissioned the Oregon Center for Nursing to conduct a feasibility study on nurse mentoring/residency programs. The report highlighted the effect of nurse residency programs in the recruitment and retention of nursing staff, barriers smaller rural facilities face in onboarding new staff, evaluated different residency programs currently in existence, as well as participating Oregon critical access hospitals’ interest in and capacity to support a nurse mentoring program.
One program, the Iowa Online Nurse Residency Program (IONRP), fit the bill for ORH. IONRP is designed to help recent nursing graduates transition into professional nursing using a competency-based curriculum delivered via live webinars and interactive online modules. According to Rose Locklear, Field Services Program Manager, a standout benefit of the IONRP program is “its ability to be implemented in different ways by facilities.” Facilities can use IONRP’s
blended model to support an existing onboarding process, and facilities with more limited capacity can utilize IONRP’s online option as their transition program.
Impressed by the versatility of the IONRP program, ORH provided funding for 15 nurses from eight critical access facilities across Oregon to enroll in the program. Catholic Health Initiative St. Anthony Hospital in Pendleton, Oregon is one of those participants. Elizabeth Michael, Clinical Education Coordinator at CHI St. Anthony Hospital, said her facility started using the IONRP program in 2018 in addition to their existing in-house residency resources and has already seen results ranging from improved staff retention among program participants to staff engagement. “Program participants are coached through creating an evidence-based proposal to present to the facility’s administration,” said Michael. “It can be intimidating, but ultimately it empowers the nurses participating, and inspires the rest of the staff to see co-workers researching and recommending changes to the C-suite.”
The Oregon Office of Rural Health’s innovative approach is activating rural health workforce retention, providing an opportunity for facilities to experience the power of a structured residency program. Positive outcomes may convince participants to continue investing in these programs in the future.
For more information on the programs mentioned in this article, check out our links below.
OREGON OFFICE OF RURAL HEALTH ACTIVATES NURSE RESIDENCIES
By Oregon Center for Nursing Operations Manager Kelley ILIC

17SENTINEL 17SENTINEL 17SENTINEL
› Online and Hybrid options› Full-time or Part-time enrollment› BS Completion, Advanced Practice, Education & Leadership Concentrations Available› Integrates health, science,
and Christian faith
Ready to Take the Next Step in Your
nursing.llu.edu/BRNurseLearn more at
Nursing Career?
OSHJOBS.COM Salem
Junction City
oooossssssssiiiiibbbbbiiiiiiillllliiiiitttttiiiiieeeeesssssTwo campusseesss,,, uuuunnnnnllllliiimmmmiiiitttteeeeddddd pppppoooooCall a recruiter: 503-945-2815
ents, Get to know your patied help them get well, and
see them return to a meaningful life.
ourrrr ccccompettttttttiiiiiiitttttttiivveeeeee CCCCCChhhhhheeecck out oubbeeeeennnnnnnefitswwwwwwwwaaaaaaggggggeeeeeesssss aaaaannnnnddddd bbb !
• Nurse residency programs in Oregon: https://oregoncenterfornursing.org/explore-nursing/nurse-residency-transition-to-practice-programs/
• Oregon Office of Rural Health: https://www.ohsu.edu/oregon-office-of-rural-health
• More about the IONRP: http://www.nursing.uiowa.edu/IONRP
OCN is a nonprofit organization created by nursing leaders in 2002. OCN facilitates research and collaboration for Oregon’s nursing workforce to support informed, well-prepared, diverse and exceptional nursing professionals. Recognized by the Oregon state legislature as a state advisory for nursing workforce issues, OCN fulfills its mission through nurse workforce research, building partnerships, and promoting nursing and healthcare.
18 OREGON STATE BOARD OF NURSING
NURSING PRACTICE
The Oregon State Board of Nursing (OSBN) is one of 18 Oregon health professional regulatory boards. Investigation complaints fall under Oregon Revised Statute (ORS) 676.165, which states that when a health professional regulatory board receives a complaint about a licensee, the Board is required to conduct an investigation.
Two key components of this are worth consideration. First, the investigator will collect evidence, review documents, conduct interviews, and make an objective report to the Board. Second, the investigator shall have all investigatory powers legislatively authorized to the Board. The investigative report presented to the Board will describe the alleged event, evidence gathered, licensee and witness interviews, and any other relevant information. The investigative report also includes information about any prior Board disciplinary history.
OSBN investigators are Board staff, not Board members. The investigators do not make decisions about the outcome of the case; only the Board itself is authorized legislatively to discipline a license or certificate. Some investigators are nurses and others have backgrounds in law enforcement, legal, or other related fields. All OSBN investigators are experts in the Nurse Practice Act (NPA).
As a licensee or certificate holder, you entered into a contract with the state to keep residents of Oregon safe. That contract is the NPA. It is a 24/7 agreement. As with all contracts, you should review and become familiar with the
NPA before applying for licensure. “I didn’t know” isn’t an acceptable response.
The NPA is administrative law, not criminal law. It has a lesser burden of proof. Decisions are based on a preponderance of evidence or “more likely than not, to have occurred,” and do not require incidents to include patient harm to be considered “conduct derogatory.”
Throughout the investigative process, licensees have the right to due process, including obtaining an attorney. If you choose to have an attorney, you agree to allow your attorney to communicate with the Board on your behalf; the investigator assigned to your case will direct all subsequent communication to your attorney. To initiate this process, the investigator needs to receive a letter of representation from your attorney.
During an investigation, the investigator’s role is to gather facts and provide a report to the Board. The licensee’s role
is to answer questions and provide documents or other information as requested. The licensee’s willingness to make changes in practice, complete continuing education, accept feedback, or complete a self-assessment can demonstrate professionalism and personal accountability.
While the Board’s disciplinary decisions are probably the most frequently read pages of the Sentinel, these lists do not reveal all cases investigated. Sometimes, there isn’t enough evidence to pursue a case, or it is determined that no violation of the Nurse Practice Act occurred; these cases are dismissed by the Board without any
YOUR RELATIONSHIP WITH THE BOARD DURING AN
INVESTIGATION
By the OSBN Investigative Staff
If you find yourself the subject of a Board investigation, consider these
helpful tips:
1. Remember that an allegation is just that—it does not mean that the
allegation will be found as true.
2. Ensure the OSBN has your current contact information and that
you answer any US mail or email received from the OSBN. The NPA
requires that you maintain your contact information with the OSBN
office. All correspondence will be sent to your contact information on
record; it is your responsibility to assure that information is accurate.
3. Pay attention to any deadlines provided by your investigator and
respond in a timely manner.
4. Failure to cooperate during an investigation is a violation of the NPA.
You can disagree; just don’t disengage. The process often takes three
to six months from start to finish.
5. The initial interview is your opportunity to tell your side of the story.
Be truthful and don’t leave anything out. This includes the questions
you answer on your initial or renewal application. Failure to disclose
information and/or untruthfulness to the Board are violations of
the NPA.
6. Although the process can be stressful, professionalism by all parties
is expected.
7. Ask questions. Your investigator will be happy to provide education
and information whenever possible.
19SENTINEL 19SENTINEL
disciplinary action. An investigation is confidential unless it results in disciplinary action taken by the Board, and only about 25% of the annual total of investigated cases result in discipline. Discipline can take the form of (in order of severity) a reprimand, probation, suspension, voluntary surrender, or revocation. A voluntary surrender is an option the licensee can agree to in lieu of a revocation or suspension. Revocation is the highest level of discipline and is taken when the Board deems a licensee is a risk to the safety of the public. Both voluntary surrender and revocation are for a period of no less than three years and require significant evidence of remediation in order for the Board to consider reinstatement of the privilege to practice nursing.
For more information regarding the investigative process, please visit the OSBN website at https://www.oregon.gov/osbn / Document s / FAQ_InvestigationsProcess.pdf.
Hiring NursesAt Carolina Pines, we believe there is a better way to provide health care services. Our patient-centered teams work diligently to provide quality care while creating a meaningful and rewarding work environment. If you’re interested in becoming a part of a team like this, we encourage you to apply.
We Are Presently Hiring Nurses for the Following Areas:• Med/Surg • Emergency Department• Intensive Care • Progressive Care Unit• Surgical Services • Women’s CareBenefits and Incentives:• Competitive Salaries • Sign-On Bonus Available• New Graduate: Packages FT RN — $5,000 for days• Tuition Reimbursement with two-year commitment• Loyalty Rewards Program FT RN — $7,500 for nights• Differential Experienced Nurses (2+ Years): FT RN — $7,500 for days with two-year commitment FT RN — $10,000 for nights with two-year commitment
To schedule a facility tour, or to shadow in your area of interest, please contact Education Director, Erin Griggs,
at 843.339.4506consideration for employment without regard to race, color, religion, sex,
Come Growwith Us
For more information,please visit our
website at cprmc.com
2801 St. Anthony Way Pendleton, OR 97801 541-276-5121
We have RN and NP positions available. For more information, visit our website at: sahpendleton.org/careers
I enjoy working at St. Anthony
Hospital because of the positive work
environment. As I am new to the
nursing profession, I feel supported
and welcome in each department.
My co-workers are always open to
offering their advice and suggestions when questions arise. Coming to
work is enjoyable because of the staff
I work with are upbeat and energetic.
Kendra De Hoog, RN
20 OREGON STATE BOARD OF NURSING
NURSING PRACTICEBy OSBN RN/LPN Practice Policy Analyst Gretchen Koch, MSN, RN,
YOU ASK, WE ANSWERQ: Are nurse practitioners in
Oregon allowed to perform/provide acupuncture? If so, is there a specific certification or course(s) that is/are required?
A: No, under Oregon law only those individuals licensed by the Board of Medicine as Acupuncturists may perform/provide acupuncture in Oregon. The education that a nurse practitioner receives would not qualify them for a license as an Acupuncturist. The Veterans Health Administration does allow some NPs to do Battlefield Acupuncture, but that is limited to practice on federal property.
Q: Can a non-nurse manager supervise a RN?
A: There is nothing in the practice act that prohibits the employment management of a nurse by a non-nurse. The employing organization determines the hierarchy of their management structure and can place a non-nurse in a position that serves as an employment supervisor of the nurse.
What the non-nurse employment manager can’t do is supervise or evaluate the practice of nursing, or author policies directing the clinical practice of the nurse; these actions would constitute practicing nursing without a license. The non-nurse employment manager can write policy regarding the employment setting and enforce policies related to the appropriate standard of employment.
When it comes time to evaluate the RN’s nursing practice performance, the non-nurse employment manager can seek feedback from other licensed RNs.
These other RNs can provide written feedback on the practice performance of the RN being evaluated. The non-nurse employment manager could then incorporate the feedback data into the RN’s practice evaluation siting the source of the data.
Q: The RN at our assisted living facility has given notice that she is leaving employment in one week and is refusing to sign a transfer of delegation form. Isn’t this patient abandonment? We haven’t yet hired another RN, so how are the residents going to get their insulin injections?
A: The situation you describe is not patient abandonment. The RN who completes their assigned shift or work hours, and then notifies their employer that they are ending their employment relationship is merely ending their employment. For more information on this, please access the Board’s Interpretive Statement titled Patient Abandonment.
Now let’s discuss delegation transfer. For the situation that you describe, where there is no RN to
whom the outgoing RN can transfer the delegation, the outgoing RN’s only option is to rescind the individual care provider’s authorization to perform the specific procedure for the specific client—period.
But, let’s pretend for the sake of this article that a new RN has been hired and will start work prior to the outgoing RN leaving employment. In this situation, the outgoing RN has two options to choose from: 1) Rescind the delegation, or 2) Transfer the delegation to the other RN. Whether the outgoing RN choses option one or option two,
the RN’s decision is reached through adherence to Division 45 and Division 47 standards, standards that compel the RN to base their decision on the safety and well-being of the client.
In adherence to these standards, the outgoing RN may only transfer a delegation to an RN who possesses competencies with RN delegation process. When the new RN lacks competencies with delegation process, the prudent RN must rescind the delegation. The RN who transfers a delegation to an RN who does not understand RN delegation process is making an improper assignment of care, which is conduct derogatory to the practice of nursing.
This leads to your question, “…how are the residents going to get their insulin injections,” which is not answered the practice act. Direction, however, may be found in the rules governing your setting. Please review Oregon Department of Human Services 411-054-0045 Residential Care and Assisted Living Facilities rules on resident health services.
21SENTINEL VO.39 • NO.1 • FEBRUARY 2020 21SENTINEL VO.39 • NO. 1 • FEBRUARY 2020
Join ourNursing TeamSaint Alphonsus is a Catholic health system based in Idaho and Oregon featuring 5 hospitals, a large medical group and clinically integrated network.
BOISE | NAMPA | ONTARIO | BAKER CITY
EQ
UA
L O
PP
OR
TU
NIT
Y E
MP
LOY
ER
Opportunities Available:
• Critical Care • Emergency• Ortho/Med/Surg • Main OR
FOR MORE INFORMATIONcontact Deseria Buscher at (208) 367-7797 [email protected]
Registered Nurse
SCF Recruitment | 888-700-6966 SCFHRRecruiters@southcentralfoundation.comwww.southcentralfoundation.com/nursing-opportunities/ Alaska Native People Shaping Health Care
RN employment opportunities in Medical Detox and RN Case Management for Primary Care, Pediatrics, OB-GYN, and Nurse Family Partnership.
Sign-on Bonus | Relocation Assistance
Celebrating 25 Years of Serving Our Members and Communities!
Partnership HealthPlan of California is hiring registered nurses looking to impact the lives of our vulnerable populations while keeping a healthy work/life balance.
Seeking experienced RNs for full-time positions in the following departments:
• Care Coordination• Utilization Management• Quality Improvement
We offer excellent benefits and a sign-on bonus for selected positions.
Learn more at: www.partnershiphp.org/About/Pages/Careers.aspx
Ready to Say Goodbye to Scrubs and Long Shifts?
22 OREGON STATE BOARD OF NURSING
Blue Mountain Community College is currently accepting applications for Nursing Instructor! This is a full-time, tenure track position based in Pendleton, Oregon.
Nursing Instructors at Blue Mountain Community College (BMCC) are responsible for creating a culturally diverse learning environment that employs best practices in teaching and learning through various delivery modes in order to meet current and future educational needs of the communities served by the College. Nursing faculty bring to their classrooms and committees expertise and experience that provides a competency-based interdisciplinary curriculum, utilizes alternative pedagogies and learning technologies, promotes collaborative work skills, contributes to student success, supports the College and community, and contributes to the success of the College in achieving its mission. Responsibilities also include those listed in Oregon Revised Statutes (ORS), Chapter 678 851-021-0045.
The position is opened until filled, first review of complete applications is March 6, 2020.
For detailed information and how to apply visit https://recruiting.
paylocity.com/recruiting/jobs/Details/235748/Blue-
Mountain-Community-College/Nursing-Instructor.
Questions, contact Human Resources at 541 278-5837 or
BMCC is an EOE and Educator and participates in E-Verify.
Nursing Instructor Pendleton
Amber Zupancic-AlbinJD, BSN, RN
Licensed in Oregon andWashington
NURSING BOARDREPRESENTATION
ZUPANCIC ALBIN LAW, PCT: (505) 349-6663
As a nurse attorney, Amber is uniquely qualifiedto represent nurses before the Oregon Board of
Nursing. Call for a free consultation
Join our team at Life Care McMinnville
We are recruiting for:• NA • CNA • LPN • RN
We offer the following: • Competitive wage scale
• Shift differential• Tuition reimbursement
(for full time ) • CNA classes offered quarterly
To apply for jobs, contact us at:lifecarecareers.hcshiring.com/jobs/jRTo3F
KkkEGVDCYoHnAs6Q
23SENTINEL
Name License Number Discipline Effective Date Violations
DISCIPLINARY ACTIONSActions taken in October, November, and December 2019. Public documents for all disciplinary actions listed below are available on the OSBN website at www.oregon.gov/OSBN (click on ‘Look Up a Nurse or Nursing Assistant’).
Jennifer N. Abraham 200942108RN Reprimand 12-18-19 Failing to clinically supervise persons to whom nursing assignments have been made, and failing to conform to the essential standards of acceptable nursing practice.
Laurie A. Adams RN Applicant Application Denied 12-18-19 Failing to cooperate during the course of an investigation.
Kendra M. Balderas 200712487CNA Probation 12-18-19 24-month probation. Failing to report to the Board her misdemeanor conviction within 10 days, and using intoxicants to the extent injurious to himself or others.
Christina L. Barnes 200842581RN Voluntary Surrender 11-13-19 Violating the terms and conditions of the Health Professionals’ Services Program monitoring agreement.
Lindy J. Beers 201242466RN Revocation 11-13-19 Violating the terms and conditions of a Board Order.
Samuel J. Blackford 201394651CNA Probation 10-9-19 Six-month probation. Engaging in abusive behavior towards coworkers, and failing to answer questions truthfully.
Arianne M. Booth 200141286RN Suspension/Probation 10-9-19 One-year suspension, followed by two years of probation. Practicing while impaired, demonstrated incidents of dishonesty, and failing to conform to the essential standards of acceptable nursing practice.
Laura Boyd 201901249RN Probation 11-13-19 12-month probation. Failing to conform to the essential standards of acceptable nursing practice, and failing to answer questions truthfully.
Erik C. Brown 200530212LPN Suspension 11-13-19 30-day suspension. Inaccurate and incomplete record-keeping, and falsifying an agency record.
Heather D. Brown 201130532LPN Reprimand 10-9-19 Failing to document information pertinent to a client’s care, and failing to conform to the essential standards of acceptable nursing practice.
Eric L. Burke 200242017RN Voluntary Surrender 10-9-19 Unauthorized removal of drugs from the workplace and entering inaccurate documentation into a health record.
Veronica A. Carter 089000114RN Voluntary Surrender 11-13-19 Entering inaccurate documentation into a health record, and practicing while unable due to a mental impair-ment.
Jill M. Cates 201341790RN Probation 12-18-19 24-month probation. Convictions of crimes that bear a demonstrable relationship to the practice of nursing, and using intoxicants to the extent injurious to himself or others.
Jennifer M. Chase 200241907RN Voluntary Surrender 12-18-19 Entering falsified documentation into a health record, and failing to take action to preserve client safety.
Stephanie J. Christner 201605655RN Probation 11-13-19 24-month probation. Entering incomplete documentation into a health record, and failing to conform to the essential standards of acceptable nursing practice.
Corey J. Coffman 201706719CNA Suspension 12-18-19 Minimum 14-day suspension. Failing to cooperate with the Board during an investigation.
Carolynn Conti 201404525RN Reprimand 11-13-19 Leaving a nursing assignment without notifying appropriate personnel, and failing to conform to the essential standards of acceptable nursing practice.
Melissa K. Cook 200930601LPN Civil Penalty 12-13-19 $200 civil penalty. Practicing nursing without a current license.
Emilie M. Cranston 091003033LPN Voluntary Surrender 10-9-19 Violating the terms and conditions of a Board Order.
David S. Dam 201113082CNA Application Denied 12-18-19 Failing to answer questions truthfully.
Lauren M. Davis RN Applicant Voluntary Withdrawal 11-13-19 Willful misrepresentation in applying for a license, and using intoxicants to the extent injurious to herself or others.
Michael L. Degner 201391281CNA Revocation 12-18-19 Abuse and neglect of a person, and failing to respect the dignity and rights of a client.
Candice Dixson CNA Applicant Voluntary Withdrawal 11-13-19 Willful misrepresentation in applying for a license, and using intoxicants to the extent injurious to herself or others.
Cassandra A. Domask 201505849CNA Voluntary Surrender 10-9-19 Demonstrated incidents of reckless behavior, using intoxicants to the extent injurious to herself or others, and failing to answer questions truthfully.
Monica Ferguson 099000287RN/200650008NP
Revocation 12-18-19 Neglecting a client, violating clients' rights to privacy and confidentiality, dispensing medications to herself, and using intoxicants to the extent injurious to herself or others.
Charles H. Fike 095000312RN Reprimand 12-18-19 Failing to clinically supervise a UAP to whom a nursing procedure has been delegated, and documenting nurs-ing practice that did not occur.
Melissa S. Foote 201703605CNA Reprimand 11-13-19 Violating a person’s rights to privacy and confidentiality.
Caleb M. Gasche 201707353RN Probation 11-13-19 24-month probation. Demonstrated incidents of reckless behavior, and using intoxicants to the extent injuri-ous to himself or others.
Shirlin M. Gauthier 200540286RN/200550016NP
Voluntary Surrender 11-13-19 Using intoxicants to the extent injurious to herself and others, willful misrepresentation in applying for license
Constance S. Hagemeyer 201601266RN Voluntary Surrender 12-18-19 Failing to conform to the essential standards of acceptable nursing practice.
Wallace W. Hendrickson 200942139RN Revocation 10-9-19 Practicing while impaired, and failing to cooperate with the Board during the course of an investigation.
Sandi K. Hildebrand 201113314CNA Voluntary Surrender 12-18-19 Using intoxicants to the extent injurious to herself and others, and performing authorized duties while impaired.
Maranda M. Ingram 201807864CNA Suspension 12-18-19 Minimum 14-day suspension. Failing to cooperate with the Board during an investigation.
Name License Number Discipline Effective Date Violations
Erin Irwin RN Applicant Voluntary Withdrawal 11-13-19 Multiple arrests that bear a demonstrable relationship to the practice of nursing.
Lucille D. Judish 085075395RN Voluntary Surrender 11-13-19 Violating the terms and conditions of a Board Order.
Sara B. Kauffman 082008253RN/200150139NP/082008253N3
Voluntary Surrender 11-13-19 Failing to respect the dignity and rights of clients.
Stephanie D. Lautenbach 099000569RN Probation 12-18-19 24-month probation. Using intoxicants to the extent injurious to herself or others, and practicing nursing while impaired.
Duane A. Leichtamer 200442133RN Revocation 12-18-19 Conviction of a crime that bears a demonstrable relationship to nursing, and failing to answer questions truthfully.
Ann K. Lomax 201391613RN Revocation 10-9-19 Violating the terms and conditions of a Board Order.
Frances C. Mallory 201901428RN Voluntary Surrender 12-18-19 Failing to document client information, client neglect, and failing to answer questions truthfully.
Danielle N. McKenna 201502653LPN Suspension 12-18-19 Minimum 14-day suspension. Failing to cooperate with the Board during an investigation.
Glenda Mendoza 200612267CNA Suspension 11-13-19 Minimum 14-day suspension. Failing to cooperate with the Board during an investigation.
Jason C. Merryman 201010991CNA Voluntary Surrender 10-9-19 Failing to answer questions truthfully.
Terence L. Mitchell 200040267RN Probation 12-18-19 24-month probation. Unauthorized removal of drugs from the workplace, and using intoxicants to the extent injurious to himself or others.
Rebecca L. Moss 095003164RN Revocation 11-13-19 Violating the terms and conditions of a Board Order.
Lourie A. O’Roake 200511987CNA Reprimand 10-9-19 Demonstrated incidents of dishonesty and entering falsified documentation into an agency record.
Herma Ornes 200242299RN Reprimand 11-13-19 Performing acts beyond her authorized scope, and failing to conform to the essential standards of acceptable nursing practice.
Bradley D. Patrick 200743831RN/200760034CRNA
Revocation 11-13-19 Failing to answer questions truthfully on an application for licensure, and failing to conform to the essential standards of acceptable nursing practice.
Scott W. Pecora 200150056NP Probation 11-13-19 12-month probation. Failing to maintain professional boundaries, engaging in sexual misconduct with a client in the workplace, and failing to conform to the essential standards of acceptable nursing practice.
Meghan N. Phillips 201403431CNA Revocation 12-18-19 Abusing a person and failing to answer questions truthfully.
Clarissa L. (Rowley) Pitts 200641157RN Probation 11-13-19 24-month probation. Unauthorized removal of drugs from the workplace, and practicing while unfit due to a mental impairment.
Ryan D. Reeder 201709317CNA Suspension 11-13-19 Minimum 14-day suspension. Failing to cooperate with the Board during an investigation.
Pamela J. Reyne 000044271CNA Reprimand 11-13-19 Failing to maintain professional boundaries, and failing to conform to the essential standards of acceptable CNA duties.
River Valley Rheumatology and Infusion, Inc.
Civil Penalty 11-13-19 $3,000 civil penalty. Employing a person without a current registered nurse license.
Sharon R. Rice 090000386RN Voluntary Surrender 12-18-19 Violating the terms and conditions of a Board Order.
Molly M. Rodden 201902719NP-PP Civil Penalty 11-13-19 $2,500 civil penalty. Practicing nursing without a current license.
Tammy L. Roman 082010741RN Suspension 12-18-19 Minimum 14-day suspension. Failing to cooperate with the Board during an investigation.
Rochelle J. Russell 201391734LPN Voluntary Surrender 10-9-19 Violating the terms and conditions of a Board Order.
Tammy L. Satre 201042510RN Reprimand 11-13-19 Failing to take action to preserve client safety based on nursing assessment and judgement.
Diana K. Schweitzer 095000482RN Probation 11-13-19 12-month probation. Demonstrated incidents of neglectful behavior, and practicing while unable due to a physical impairment.
Janet E. Scurlock 201030149LPN Probation 12-18-19 24-month probation. Failing to inaccurate documentation, obtaining unauthorized medications, and using intoxicants to the extent injurious to herself or others.
Jodi L. Sharbono CNA Applicant Application Denied 12-18-19 Failing to cooperate during the course of an investigation.
Amy J. Silici 099007675RN Probation 11-13-19 24-month probation. Entering inaccurate and falsified documentation into a health record, and failing to take action to preserve client safety.
Jordan Slayton 201807805RN Revocation 12-18-19 Using intoxicants to the extent injurious to herself or others, and failing to answer questions truthfully.
Trevor A. Standfill 201606271RN Voluntary Surrender 10-9-19 Convictions of crimes that bear demonstrable relationship to nursing.
Jessica A. Stanley 201130037LPN Suspension 10-9-19 30-day suspension. Unauthorized removal of drugs from the workplace and falsifying data.
Jaime L. Stratemeyer 201607661CNA Revocation 12-18-19 Abusing and neglecting a person, and failing to answer questions truthfully.
Deborah L. Taylor 201243519RN Probation 11-13-19 12-month probation. Failing to conform to the essential standards of acceptable nursing practice.
R. Natasha Taylor 090007497RN Reprimand 12-18-19 Due to the revocation of her California RN license.
Dawn E. Teplick 090003180RN Revocation 10-9-19 Violating the terms and conditions of a Board Order.
Carolyn L. Theakston 201041771RN Reprimand 12-18-19 Failing to implement the plan of care, failing to document client care information, and failing to conform to the essential standards of acceptable nursing practice.
Veronica Villarreal 201393717RN Reprimand 11-13-19 Entering falsified documentation into an agency record,and demonstrated incidents of dishonesty.
24 OREGON STATE BOARD OF NURSING
26 OREGON STATE BOARD OF NURSING
INVESTIGATIONS
By OSBN Investigations Manager Jacy Gamble, and Investigators Nakeita West and Leslie Kilborn
DISCIPLINARY CASE STUDIES: TRUTHFULNESS
Although disciplinary action taken by the Board is a matter of public record, the identity of the nursing assistants/applicants referenced in this article will remain confidential.
Case Study #1A certified nursing assistant (CNA) submitted a renewal
application to the Board. On the application, the CNA answered “yes” to a disclosure question, which asked: “Other than a traffic ticket, since the date of your last renewal, have you been arrested, cited, or charged with an offense?” The CNA disclosed a “pending” charge involving a felony charge of delivery of a controlled substance to a minor. The CNA provided an explanation of the incident and indicated that they were innocent and would be fighting the charge in court.
The CNA was interviewed by an OSBN investigator regarding the incident. In both the interview and the CNA’s written response to the Board, the CNA minimized their culpability with regard to the criminal charges against them. The CNA also provided information that was inconsistent with the law enforcement report of the incident. The CNA was subsequently convicted of the felony charge.
At the conclusion of the investigation, the OSBN investigator offered the CNA a Stipulated Order of Reprimand as a possible resolution to present to the Board. The CNA did not sign the Stipulated Order of Reprimand. When the case was presented to the Board, it found that the CNA violated the Nurse Practice Act by engaging in conduct that adversely affects the health, safety, and welfare of the public, as well as providing inaccurate information to the Board during the course of an investigation. The Board voted to issue a Notice of Proposed Revocation of CNA Certificate. The CNA did not request a hearing within the allotted timeframe, and the Board issued a Final Order of Revocation of Nursing Assistant Certificate by Default.
Case Study #2An applicant submitted an application for CNA
certification and disclosed being arrested for “drug possession,” and added that she had been clean and sober for the last 13 years. The applicant answered “no” to the disclosure question: “Have you ever been part of an
investigation for any type of abuse or mistreatment, in any
state or jurisdiction?” A routine background check revealed
that in a five-year period, the Applicant had been arrested
22 times. Charges included, but were not limited to, Child
Neglect, Assault, Reckless Endangering, Reckless Driving,
Criminal Trespass, Theft, Supplying Contraband, Driving
While under the Influence of Intoxicants, and Parole and
Probation Violations. The Board opened an investigation
into the matter.
During an interview with an OSBN investigator, the
applicant was asked to explain each of their incidents with
Child Protective Services (CPS). The applicant disclosed
that they had involvement with CPS for leaving their
child alone in a car. At the OSBN’s request, the applicant
signed a release of information with CPS and the records
were forwarded to the Board. The records showed three
additional CPS investigations; one stated that the applicant
had admitted to using methamphetamines within the last
10 years.
In a follow-up interview, the OSBN investigator asked
the applicant why they did not disclose their entire arrest
and CPS history and to explain the discrepancy in the
applicant’s stated sobriety date. Applicant said they had
forgotten about their arrest and CPS history, and that the
CPS record regarding substance use was incorrect as they
had used cocaine, not methamphetamines.
The Board determined that the applicant violated
the Nurse Practice Act (NPA) by failing to disclose their
entire arrest, substance use, and CPS history, both on their
application to the Board and through the course of the
Board’s investigation. Additionally, the Board found that
the applicant also violated the Nurse Practice Act by abusing
and/or neglecting a person, and using controlled substances.
The Board voted to issue the applicant a Notice of Proposed
Denial of CNA certification. The CNA did not request a
hearing within the allotted timeframe, and the Board issued
a Final Order of Denial of CNA Certificate by Default.

2020 OSBN BOARD MEMBERS
27SENTINEL
MICHELLE CHAU, LPN BOARD SECRETARYTERM: 1/1/19 – 12/31/21
Ms. Chau is a Panel Manager for the Multnomah County Health Department in Portland, Ore. She completed her practical nursing program at Mt. Hood Community College in Gresham, Ore., and has a Bachelor of Science degree in Advanced Chemistry, Biology, and General Science from
Oregon State University in Corvallis, Ore. She has 10 years of nursing experience, and serves in the Licensed Practical Nurse position on the Board.
KATHLEEN CHINN, RN, FNP
BOARD PRESIDENTTERMS: 1/1/16 – 12/31/18, 1/1/19 – 12/31/21
Ms. Chinn is a Family Nurse Practitioner with the PeaceHealth Senior Health and Wellness Center in Eugene, Ore. She received her Associate Degree in Nursing from Lane Community College in Eugene, Ore., and her Bachelor of Science in Nursing and Master’s degrees from Oregon
Health Sciences University in Portland, Ore. She resides in Eugene, Ore.
ANNETTE COLE, RN PRESIDENT-ELECTTERM: 1/1/18 – 12/31/20
Ms. Cole is the Vice President of Patient Care Services and Chief Nursing Officer at Sky Lakes Medical Center in Klamath Falls and has 30 years of nursing experience. She received her Bachelors of Science in Nursing degree from the Oregon Institute of Technology in Klamath Falls,
Ore., and her Masters of Science in Nursing and Health Care Administration degree from the University of Phoenix. Ms. Cole serves in the Nurse Administrator position on the Board. She resides in Klamath Falls.
ADRIENNE ENGHOUSE, RNTERMS: 1/1/16 – 12/31/17, 1/1/18 – 12/31/20
Ms. Enghouse is a Staff Nurse at Kaiser Sunnyside Medical Center in Clackamas, Ore. She serves in one of two direct-care RN positions on the Board. She received her Associate Degree in Nursing from Mount Hood Community College in Gresham, Ore., and resides in Portland, Ore.
SHERYL OAKES CADDY, JD, MSN, RN, CNETERM: 1/1/18 – 12/31/20
Ms. Oakes-Caddy is the Dean of Nursing at Mt. Hood Community College in Gresham, Ore. She has more than 30 years of clinical nursing practice. She received her Associate of Science in Nursing from Linn-Benton Community College in Albany, Ore., her Bachelor of Science in Nursing from Oregon Health Sciences University in Portland, Ore., her Master of
Science in Nursing from Walden University, Baltimore, Md., and her Doctor of Jurisprudence from Willamette University School of Law in Salem, Ore. Ms. Oakes Caddy serves in the Nurse Educator position on the Board and resides in Lebanon, Ore.
BOBBIE TURNIPSEED, RNTERMS: 1/1/16 – 12/31/17, 1/1/18 – 12/31/20
Ms. Turnipseed is a staff nurse at St. Alphonsus Medical Center in Ontario and has more than 30 years of nursing experience. She received her Associate Degree in Nursing from Boise State University in Boise, Idaho. Ms. Turnipseed is one of two direct-patient care RNs on the Board. She resides in Ontario, Ore.
JUDITH WOODRUFF, JD PUBLIC MEMBERTERM: 1/1/20 – 12/31/22
Ms. Woodruff received her juris doctorate from the University of Oregon School of Law. During her legal career, she worked as an Assistant Attorney General with the Oregon Department of Justice and served as an Administrative Law Judge. She also worked in philanthropy and non-profit organizations, including
over a decade with the Northwest Health Foundation as the Senior Program Director, focused on healthcare workforce development. Ms. Woodruff resides in Portland, Ore.
WILLIAM YOUNGREN, CNATERMS: 6/1/16 – 12/31/18, 1/1/19 – 12/31/21
Mr. Youngren is a Unit Clerk at Legacy Emanuel Medical Center in Portland and has been a nursing assistant since 2012. He received his Bachelor’s Degree in English from Portland State University and his nursing assistant training from Portland Community College. Mr. Youngren resides in Portland, Ore.

STAFF PROFILES
MEET THE TEAM
LINDA DAWSEY, RNAlthough a native of northern Michigan, OSBN nurse
investigator Linda Dawsey, RN, is really a global citizen, having spent years working throughout Europe, the Middle East, and Africa with the military. “Once you have a diplomatic passport, it’s kind of hard to go back to a regular one!”
Her journey began after graduating high school in Whittemore, Mich., when she joined the Army as an aviation mechanic, soon working her way up to crew chief for helicopters. “As crew chief, I went up with flights. We were to step in as co-pilot if one became incapacitated during flight,” she explains. “It was wartime, so ‘incapacitated’ meant ‘shot’.” She spent most of her time stationed in Ft. Rucker, Ala., but she was also deployed to Fort Shafter in Hawaii, and Torii Station in Okinawa, Japan.
While in Alabama, she received her associate’s degree from a local community college and her BSN from the University of Southern Alabama. However, there weren’t nursing spots available in the Army, so she transferred to the Navy. “It was the nursing shortage that drew me to nursing,” she says. “But it was that transfer that truly changed my life.”
She was deployed to Europe as a medevac flight nurse, where she transported patients within the continent and to the U.S. She also spent months setting up field hospitals in Kuwait, Bahrain, Qatar, and other locations in the Middle East. Thanks to her years in aviation and what she calls, “pure luck,” she was invited to apply for a liaison position with NATO. “I was in the right place at the right time, and I absolutely loved it!”
For NATO, Dawsey taught statistical analysis and team skills to service people from several of the NATO ally countries. “I held a diplomatic passport, traveled throughout Europe, and lived in El Puerto de Santa Maria, Spain, and Gaeta, Italy. It was pretty spectacular.” She also volunteered for various humanitarian initiatives as part of NATO, such as providing immunizations in Africa, helping with a water purification project in Africa and Slovenia, and building wheelchair ramps with Habitat for Humanity International in Poland.
She transferred to the US Naval Air Station Whidbey Island in 2005 when it came time for her to retire from the military. She got her master’s degree in organizational leadership from Brandman University, and then worked for the state of Washington’s Department of Social and Health Services as an assistive living surveyor, complaint investigator, and steering committee member for nine years. “My second retirement was from the state, but I wasn’t quite done working yet,” she says with a laugh. She migrated to the Portland/Vancouver area and worked as an
The Oregon State Board of Nursing is much more than just, “that place where you get your license renewed every two years.” To achieve our mission of public protection, our team is hard at work approving educational and train-
ing programs, providing outreach presentations to employers and licensees, answering scope-of-practice questions, investigating possible violations of the Nurse Practice Act, maintaining our online systems, and, yes, issuing licenses.
In each issue of the Sentinel, we’ll introduce you to a team member who makes everything work.
MEET THE TEAMBy OSBN Communications Manager Barbara Holtry
28 OREGON STATE BOARD OF NURSING
STAFF PROFILES
29SENTINEL
executive in the private sector for a few years, before deciding she needed a change.
Dawsey joined the Board of Nursing in May 2019 as a nurse investigator. “Public service has always been a theme in my life, since I was a kid. Altruism and volunteering was very important in my family when I was growing up. And, this is a great place—I love the team I work with.” As an investigator, Dawsey works with nurses who may have committed violations of the Nurse Practice Act. “I try to make the experience as stress-free as possible,” she explains. “I’m simply here to gather information and compile a report so the Board can determine as to whether a violation occurred or not. That’s it.”
In her spare time, Dawsey enjoys spending time with her chocolate Labrador, and with her children and grandchildren in
Portland, Seattle, and Ohio. She is certified in Quality Management and has a white belt in Six Sigma, a data-driven methodology for process improvement, and is working on her Black belt. “It’s something I have a passion for—sorting out problems and finding solutions. It’s very satisfying.”
Nursing CareersFind Your Calling in Orangeburg, SC
www.trmchealth.org
• 286-bed, acute-care Hospital• TJC-accredited, Primary Stroke Center,
Level III Trauma Center• 12-hour, Day and Night Shifts • Welcoming Community
Contact: Micki Schurlknight, RNRMC CLINICAL NURSING RECRUITER
803-395-4315 | [email protected]
LICENSING
By OSBN Investigations Manager Jacy Gamble
WHAT DOES IT MEAN IF MY APPLICATION IS “ASSIGNED TO INVESTIGATIONS”?
30 OREGON STATE BOARD OF NURSING
When an applicant submits an application to the Oregon
State Board of Nursing (OSBN), there are several disclosure
questions the applicant must answer to ensure that the applicant
is safe to practice nursing. These questions include disclosures
about criminal convictions, prior investigations by OSBN or
another licensing board, use of drugs or alcohol, mental health
and physical conditions, and other issues that could make the
applicant a threat to the safety of the public and/or constitute
violations of the Nurse Practice Act (NPA). When the OSBN
learns of information either through disclosures made by the
applicant or through other investigative means, staff uses certain
criteria to determine whether an investigation needs to be
opened to obtain further information to present to the Board.
When an application is assigned to the Investigations
Department, staff opens a case and follows the established
OSBN investigative process (which is available on the OSBN
website at www.oregon.gov/OSBN/Documents/FAQ_
InvestigationsProcess.pdf). The applicant will be contacted (by
letter, email, or phone) by an investigator who will ask questions and
request certain explanations or documents, which could include
court records or police reports, etc. Once a person’s application
has been assigned to investigations, the applicant cannot simply
decide not to move forward with licensure without certain criteria
being met.
It is important to remember that the Board ultimately resolves
all investigations; investigative staff gather facts and present case
reports to the Board for review and final deliberation. It is also
important to remember that applicants have a duty to cooperate
with the Board during the course of an investigation. Refusal to
do so is a violation of the NPA and can lead to the Board issuing
a Notice of Proposed Denial to an applicant. Once issued, the
Notice will include information regarding an applicant’s due
process hearing rights. If the applicant doesn’t request a hearing
within the required timeframe, the Board will issue a Final Order
of Denial. All Notices and Final Orders of Disciplinary Action
will be public and available on the OSBN website.
Applicants who don’t wish to participate in the investigation
or move forward with their applications do have the option of
signing a Stipulated Order of Withdrawal of Application, which
is also a disciplinary action that becomes public information
on the OSBN website. These stipulations are presented to the
Board for acceptance. The applicant is free to re-apply at any
time after the issuance of a Final Order of Denial or acceptance
of a Stipulated Order of Withdrawal of Application by the Board.
For additional information regarding the OSBN investigations,
review the Investigations Process information on the OSBN
website: www.oregon.gov/OSBN.
Don’t Forget to Renew!Nursing licenses and nursing assistant certificates
expire every two years, on your birthday. This means
you need to renew—at the latest—the day before your
birthday; if you wait until your birthday to renew, it will
be too late. If you were born in an odd year, you need to
renew your license or certificate this year (if you haven’t
already). And if you were born in an even year, you
will need to renew your license next year.
You may check your license status
and expiration date using the
Board’s License Verification system: http://osbn.oregon.
gov/OSBNVerification/Default.aspx.
If your current email address is on file with the
Board office, you should receive a courtesy reminder
before your license expiration date; the board sends
out email reminders at 90, 60, and 15 days prior to an
expiration date. However, it is ultimately the licensee’s
responsibility to renew her/his license.
Don’t risk possible civil penalties by practicing
without a license—renew on time.
We have you covered — plus some.With a robust employee wellnessprogram, on-site gyms and fitness classes, community gymmemberships, healthy on-site cafeterias, and an employeeassistance program, we’re dedicated to keeping you happyand healthy.
JOIN OUR TEAM.
We’re hiring nurses for ourvarious locations throughout New Mexico.
VVisit phs.org/careers to learn more about being a nurse atPresbyterian.
AA/EEO/VET/DISABLED/NMHRA. PHS is committed to ensuring a drug-free workplace.
31SENTINEL
Oregon State Board of Nursing17938 SW Upper Boones Ferry RoadPortland, OR 97224-7012
PRESORTED STANDARD
U.S. POSTAGE
PAIDLITTLE ROCK, ARPERMIT NO. 1884
a. The f irst musical artist to perform on the moonb. The scientist who wil l someday cure cancerc . A childhood of l imitless possibi l it iesd. All of the above
W H AT D O Y O U S E E ?
If you answered “d,” you belong in our mighty brigade. CHOC’s nurses passionately preserve the magic of childhood, ensuring that
illness and injury don’t derail dreams. We support this meaningful work by promoting
an environment of collaboration, innovation, and advancement. So our nurses can be
the heroes they were meant to be. Become a defender of childhood. Visit choc.org/careers.




















