
Altered neural correlates of affective processing after internet-delivered cognitive behavior...
10
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/authorsrights
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Altered neural correlates of affective processing after internet-delivered cognitive behavior...
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/authorsrights

Author's personal copy
Altered neural correlates of affective processing afterinternet-delivered cognitive behavior therapy for socialanxiety disorder
Kristoffer N.T. Månsson a,n, Per Carlbring b, Andreas Frick c, Jonas Engman c,Carl-Johan Olsson d,e, Owe Bodlund f, Tomas Furmark c, Gerhard Andersson a,g
a Department of Behavioural Sciences and Learning, Psychology, Linköping University, Linköping, Swedenb Department of Psychology, Stockholm University, Stockholm, Swedenc Department of Psychology, Uppsala University, Uppsala, Swedend Centre for Population Studies, Ageing and Living Conditions, Umeå University, Umeå, Swedene Umeå Centre for Functional Brain Imaging (UFBI), Umeå University, Umeå, Swedenf Department of Clinical Sciences, Division of Psychiatry, Umeå University, Umeå, Swedeng Department of Clinical Neuroscience, Psychiatry Section, Karolinska Institutet, Stockholm, Sweden
a r t i c l e i n f o
Article history:Received 10 April 2013Received in revised form22 August 2013Accepted 29 August 2013
Keywords:AmygdalaCognitive behavior therapydlPFCfMRImOFCvlPFC
a b s t r a c t
Randomized controlled trials have yielded promising results for internet-delivered cognitive behaviortherapy (iCBT) for patients with social anxiety disorder (SAD). The present study investigated anxiety-related neural changes after iCBT for SAD. The amygdala is a critical hub in the neural fear network,receptive to change using emotion regulation strategies and a putative target for iCBT. Twenty-twosubjects were included in pre- and post-treatment functional magnetic resonance imaging at 3Tassessing neural changes during an affective face processing task. Treatment outcome was assessedusing social anxiety self-reports and the Clinical Global Impression-Improvement (CGI-I) scale. ICBTyielded better outcome than ABM (66% vs. 25% CGI-I responders). A significant differential activation ofthe left amygdala was found with relatively decreased reactivity after iCBT. Changes in the amygdalawere related to a behavioral measure of social anxiety. Functional connectivity analysis in the iCBT groupshowed that the amygdala attenuation was associated with increased activity in the medial orbitofrontalcortex and decreased activity in the right ventrolateral and dorsolateral (dlPFC) cortices. Treatment-induced neural changes with iCBT were consistent with previously reported studies on regular CBT andemotion regulation in general.
& 2013 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Social anxiety disorder (SAD), also referred to as social phobia,is a debilitating psychiatric condition characterized by excessiveand persistent fear and concerns about embarrassment andhumiliation from others (American Psychiatric Association,2000). It is a common condition with a lifetime prevalence ofaround 13% (Fehm et al., 2005; Kessler et al., 2005). SAD oftenprecedes other complications such as depression (Beesdo et al.,2007), alcohol and drug use disorders (Grant et al., 2005), and it isassociated with considerable societal costs (François et al., 2010).Many sufferers do not seek treatment (Baldwin and Buis, 2004)
despite that effective pharmacological (Ravindran and Stein, 2010)and psychological (Acarturk et al., 2009) treatment exists.
Internet-delivered cognitive behavior therapy (iCBT) has beendemonstrated to be efficacious in at least fifteen controlled trials ofSAD (Andersson et al., 2012). Effectiveness studies conducted inclinical settings have also provided evidence for this treatmentapproach (Hedman et al., 2011a). Effect sizes over the short termhave been moderate to large (Andersson et al., 2006; Carlbringet al., 2007; Furmark et al., 2009), and treatment gains havebeen maintained at long-term follow-ups (Carlbring et al., 2009;Hedman et al., 2011b). The treatment is evidence-based, standar-dized and relatively easy to set-up, making it suitable for func-tional brain imaging research.
Moreover, there is an extensive literature on attentional biasesin emotional disorders (MacLeod et al., 1986), suggesting thataltering this bias reduces anxiety (MacLeod and Mathews, 2012).Faster response towards threat-relevant information in relation toneutral stimuli is regarded as a bias. In attention bias modification
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/psychresns
Psychiatry Research: Neuroimaging
0925-4927/$ - see front matter & 2013 Elsevier Ireland Ltd. All rights reserved.http://dx.doi.org/10.1016/j.pscychresns.2013.08.012
n Correspondence to: Linköping University, IBL, Psychology, SE-581 83 Linköping,Sweden. Tel.: þ46 70 585082; fax: þ46 13 282145.
E-mail addresses: [email protected],[email protected] (K.N.T. Månsson).
Psychiatry Research: Neuroimaging 214 (2013) 229–237
Author's personal copy
(ABM) the participant learns to redirect attention away fromthreats, such as facial expressions of fear or disgust. ABM havebeen suggested to share a therapeutic mechanism with CBT(MacLeod and Mathews, 2012). In a study by Schmidt et al.(2009), 72% of the participants in the treatment group as comparedto 11% in the control condition, no longer met the criteria for SADfollowing ABM. These results were maintained at a 4-monthfollow-up assessment. Two meta-analyses have demonstratedsmall to medium effect sizes of ABM for anxiety disorders(Hakamata et al., 2010; Hallion and Ruscio, 2011). However, thesepromising results have not yet been replicated when the sametreatment has been delivered via the internet when comparing toplacebo conditions (Boettcher et al., 2011; Carlbring et al., 2012;Neubauer et al., 2013). Therefore, in the present study, we used theinternet-delivered ABM as a control treatment.
Studying brain mechanisms and associated behavioral changesafter treatment could further enhance knowledge about themaintenance of SAD and improve the specificity of interventions.The most consistent finding in neuroimaging studies of SAD is thatthe disorder is associated with exaggerated activity in the amyg-dala (Freitas-Ferrari et al., 2010). The amygdala is part of a fearcircuit involved in detecting threat signals and coordinatingautonomic responses (LeDoux, 2000). In addition, the prefrontalcortex acts in concert with subcortical regions involved in emo-tional expressions (Barbas et al., 2003), and is crucial for emotionregulation (Hartley and Phelps, 2009; Ochsner and Gross, 2005),extinction learning (Phelps et al., 2004) and resolving emotionalconflicts (Etkin et al., 2006). Prior studies have highlighted theorbitofrontal (OFC), ventromedial (vmPFC) and rostral anteriorcingulate (rACC) cortices to be involved in regulation of emotionalresponses (Etkin et al., 2011; Hartley and Phelps, 2009; Milad et al.,2007; Milad and Rauch, 2007). Prefrontal regions may be directlyor indirectly connected to the amygdala, and are able to exertinhibitory influences. Regions within the OFC and ACC have thedensest connections to the amygdala, accounting for about half ofall the prefrontal projecting neurons (Ghashghaei et al., 2007).Hence, it is of particular interest to study if these regions areinvolved in therapeutic change by psychological interventions.
Viewing emotionally valenced faces has been shown to reliablyactivate the amygdala in patients with SAD (Lira Yoon et al., 2007;Stein et al., 2002; Straube et al., 2004), and severity of symptomspredicts the amygdala activation to negative faces (Evans et al.,2008; Goldin et al., 2009a; Phan et al., 2006). Affective faceprocessing tasks have also been used as predictors for outcomeof CBT for SAD (Doehrmann et al., 2013; Klumpp et al., 2013), andthe pharmacological treatment of anxiety (Whalen et al., 2008). Aneuroimaging study of SAD by Furmark et al. (2002) reported thatresponders to CBT delivered in group, and to selective serotoninreuptake inhibitors (SSRIs) both resulted in decreased anxiety-related reactivity in the amygdala after treatment. Phan et al.(2013) also noted reduced amygdala reactivity to fearful faces afterSSRI treatment although this was not related to social anxietysymptom improvement.
The present study aimed to investigate neural changes, mea-sured during an emotional face processing task (Hariri et al.,2002), following internet-delivered CBT for SAD in comparisonto an active control condition using ABM. We used func-tional magnetic resonance imaging (fMRI) before and after thetreatments to explore therapeutic effects on functional neuralresponses. We hypothesized that a positive treatment outcomewould be associated with attenuated amygdala reactivity. WithiniCBT we also investigated concomitant activation changes of theprefrontal cortex that might exert regulatory effects on theamygdala. We expected to find increased activity in prefrontalregions (e.g. dlPFC, mOFC, rACC, vmPFC) in relation to decreases inamygdala.
2. Materials and methods
2.1. Subjects
The study was approved by the local ethics committee. The screening andinclusion procedures were similar to our previous randomized controlled trials(RCTs) of iCBT and ABM (Andersson et al., 2012; Andersson et al., 2006; Carlbringet al., 2012; Furmark et al., 2009). Subjects were recruited via media advertise-ments and a total of 131 individuals reported interest on a webpage and answeredall self-report questionnaires for social anxiety and depression. Also, magneticresonance safety criteria were assessed. The subjects had to be at least 18 years ofage, have no neurological disorder, no other current psychological treatment, and ifon pharmacotherapy (e.g. SSRIs), the dose had to be stable during the treatment.Applicants fulfilling the initial screening criteria (n¼44) were interviewed viatelephone using the structured clinical interview for DSM-IV (SCID; First et al.,1997) for presence of SAD and major depressive disorder (MDD). This study wasregistered at clinicaltrials.gov (identifier NCT01312571).
Twenty-six subjects having SAD as primary diagnosis and no current MDD wereinitially included but twenty-four subjects completed self-report measures and clinicalassessment at post treatment, i.e. two subjects withdrew from the study. Brain imagingdata from 22 subjects were analyzed, i.e. four were excluded due to withdrawal orcorrupt fMRI data (see Fig. 1). Five iCBT subjects and four in the ABM group had ongoingSSRI treatment during the study. A majority of the subjects met the criteria for thegeneralized subtype of SAD (n¼22, 85%). All subjects were right handed by self-reportand gave written informed consent prior to participation. Demographic data arepresented in Table 1.
2.2. Clinical assessment
The Liebowitz Social Anxiety Scale – self-report version (LSAS-SR; Baker et al.,2002; Liebowitz, 1987) was the main outcome measure for SAD symptoms. LSAS-SRhas been reported to have good psychometric properties (Baker et al., 2002). TheSocial Phobia Screening Questionnaire (SPSQ; Furmark et al., 1999) is a measure usedfor diagnostic screening and was administrated prior to the SCID. In addition, theSocial Phobia Scale (SPS) and Social Interaction and Anxiety Scale (SIAS; Mattick andClarke, 1998) were used as secondary outcome measures. In screening of depressivesymptoms the Montgomery Åsberg Depression Rating Scale, self-report version(MADRS-S; Svanborg and Åsberg, 1994) was used. All self-report measures wereadministered over the internet, a procedure that has good established psychometricproperties (Hedman et al., 2010). An experienced clinical psychologist, independentand blind to the experimental conditions, estimated global improvement at posttreatment, using the Clinical Global Impression-Improvement scale (CGI-I; Zaideret al., 2003). Patient who were classified as much or very much improved on the CGI-Iwere considered to be treatment responders. In addition, the subjects verballyreported fear and distress on a continuous 0–100 (min–max) scale in conjunctionwith the fMRI task.
2.3. General procedure
During brain imaging data acquisition, an emotional face processing task wasused (Hariri et al., 2002). Two other tasks were administered but are not reportedhere. Subjects were randomized to either iCBT or ABM by a blinded externalresearcher using an independent third-party online true random-number service(www.random.org). Information regarding the assigned treatment was placed in asealed envelope, distributed to the subject after the pretreatment brain imagingsession. After treatment, clinical outcome measures were acquired prior to the lastimaging session. A second treatment phase started after this session (cross-overdesign, data not reported).
2.4. Treatments
The iCBT for SAD used in this study has been evaluated in several RCTs(Andersson et al., 2012; Andersson et al., 2006; Carlbring et al., 2007; Furmarket al., 2009). The guided internet-delivered treatment protocol contains a 9-weekintervention supported by a clinician. The treatment is based upon the model byClark and Wells (1995) and includes cognitive components, exposure instructions,and relapse prevention. Each week the therapist introduces a new modulecontaining information, work sheets and homework assignments. In total therewere nine modules. For more information about the iCBT, see Andersson et al.(2006).
The ABM was also delivered via the internet, over a period of 4 weeks, withexercises implemented twice a week, totaling eight sessions. Male and femaledisgust faces or neutral expressions and fixation crosses (“þ”) were presentedduring 500 ms on the participants´ own computer screen. Then a probe (letter E orF) replaced the neutral facial expression. The subject was instructed to respond tothe probe as fast as possible. Training sessions consisted of 160 trials. With theexception of reminders via e-mail or SMS, the research group had no other contact
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237230
Author's personal copy
with the subject during the treatment. For a more detailed description of the ABMprocedures, see Carlbring et al. (2012).
2.5. fMRI task
We used a paradigm described by Hariri et al. (2002). This emotional faceprocessing task included a standard set of pictures of faces (Ekman and Friesen, 1976)
expressing anger, fear, surprise, or neutral affect. Geometric shapes were used as acontrol condition. The paradigm consisted of eighteen pseudo-randomized blocks withsix trials in each. The stimulus onset asynchrony (SOA) was set at 4000 ms and the inter-trial interval (ITI) ranged between 2000 and 6000 ms. Stimuli were presented on ascreen, viewed through a tilted mirror attached to the head coil. Participants wereinstructed to match the stimuli of the emotional faces or geometric shapes. Correspond-ing emotional faces were identical in both valence (facial expression) and character.
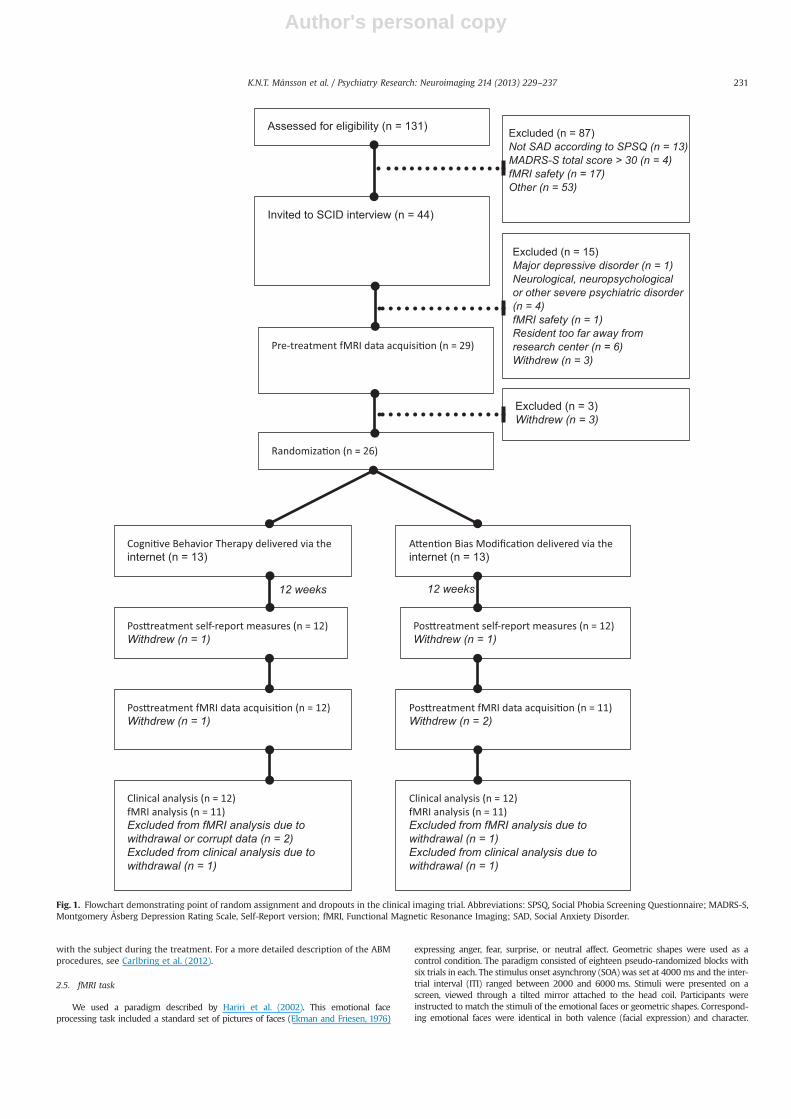
Assessed for eligibility (n = 131) Excluded (n = 87)Not SAD according to SPSQ (n = 13) MADRS-S total score > 30 (n = 4)fMRI safety (n = 17)Other (n = 53)
Invited to SCID interview (n = 44)
Excluded (n = 15)Major depressive disorder (n = 1)Neurological, neuropsychological or other severe psychiatric disorder (n = 4)fMRI safety (n = 1)Resident too far away from research center (n = 6)Withdrew (n = 3)
internet (n = 13) internet (n = 13)
Excluded (n = 3)Withdrew (n = 3)
Withdrew (n = 1) Withdrew (n = 1)
12 weeks 12 weeks
Withdrew (n = 1) Withdrew (n = 2)
Excluded from fMRI analysis due to withdrawal or corrupt data (n = 2)Excluded from clinical analysis due to withdrawal (n = 1)
Excluded from fMRI analysis due to withdrawal (n = 1)Excluded from clinical analysis due to withdrawal (n = 1)
Fig. 1. Flowchart demonstrating point of random assignment and dropouts in the clinical imaging trial. Abbreviations: SPSQ, Social Phobia Screening Questionnaire; MADRS-S,Montgomery Asberg Depression Rating Scale, Self-Report version; fMRI, Functional Magnetic Resonance Imaging; SAD, Social Anxiety Disorder.
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237 231

Author's personal copy
Three face stimuli appeared on the screen, one on the upper part, two other on thelower part. The instruction was to indicate if it was the left or right stimuli on the lowerpart that matched the upper stimuli by pressing a button response pad using the righthand (Lumitouch reply system, Lightwave Medical Industries, Canada). The responsepad was connected to a computer running E-prime (Psychology Software Tools, PA,USA). Response time was recorded as a manipulation check.
2.6. Acquisition and preprocessing of fMRI data
Blood-oxygen level-dependent (BOLD) contrast images were acquired using a GE3.0 T (T2n weighted), 32 channel head coil with the following parameters: Echo time:30 ms, repetition time: 2000 ms, flip-angle: 801, field of view: 25�25 cm2, matrix size:96�96. Thirty-seven slices with a thickness of 3.4 mm were acquired every 2000 ms.Ten dummy scans were run before the image acquisition started to avoid signalsresulting from progressive saturation. Functional scans were realigned to the meanimage of each run to correct for head movements during image acquisition, after whichslice timing correction was performed to correct for differences in acquisition time. Thefunctional scans were then normalized to the Montreal Neurological Institute (MNI152)template and, smoothed with an 8 mm Gaussian kernel. The voxel dimensions were3�3�3mm3. Structural high-resolution T1-weighted images (180 slices, 1 mm thick-ness, field of view: 250 mm, voxel size: 0.5�0.5�1mm3) were collected prior to thefunctional images.
2.7. Clinical and fMRI analyses
Clinical outcome and response time data were analyzed using repeatedunivariate and multivariate ANOVAs and independent t-test's with the α level setto po0.05. Chi-2 was used to assess nominal data. Data were computed with IBMSPSS 19 (IBM, Somer, NY, USA).
Functional brain imaging data were fitted to the general linear model andcomputed with Statistical Parametric Mapping Software 8 (SPM8; WellcomeDepartment of Cognitive Neurology, London, UK) implemented in Matlab8.0.0.783. (MathWorks, Natick, MA, USA). A priori regions of interest (ROIs) werethe bilateral amygdala defined by the Wake Forest University School of Medicine(WFU) PickAtlas (Maldjian et al., 2003) and the Automated Anatomical Labelingatlas (Tzourio-Mazoyer et al., 2002). The amygdala ROIs were examined at po0.05with family wise error (FWE) correction for multiple comparisons. Whole-brainanalyses were additionally performed at the Z43, po0.001, uncorrected level. Toincrease number of data points and statistical power, all fMRI-analyses used themean activity of all faces (anger, fear, surprise, or neutral affect) in contrast togeometrical shapes. Pretreatment differences in neural reactivity of the amygdala(mean values of peak voxel activations) were evaluated using an independent t-test. Therapeutic change in social anxiety, measured by LSAS-SR (post–pre), wasused as a covariate of interest to reveal treatment-specific effects on neural activityrelated to symptom improvement.
Analyses were performed in three steps:
(1) BOLD change scores were computed for each subject and treatment groupseparately (BOLDpost–BOLDpre) in one-sample t-test's, i.e. post–pre differencesbetween signal changes for faces in contrast to shapes
(2) Differences in anxiety-related neural changes (post–pre) between the iCBT andABM were examined, using independent t-test between-groups
(3) The left amygdala showing significant treatment-induced changes were usedin a functional connectivity analysis within the iCBT group (similar approachreported in Åhs et al. (2009)). In the first-level analyses we contrastedemotional faces against geometrical shapes, including also movement regres-sors (from the realignment preprocessing step) and mean BOLD activity(implicit in SPM) in the model. For each subject the mean beta weights inthe left amygdala were extracted using the SPM toolbox MarsBaR 0.43. Thebeta weights were subsequently entered as regressors in a one-sample t-testwithin the iCBT group using the same contrast. We implemented the regressoras a covariate of interest and explored prefrontal activations, includingBrodmann area (BA) 9, 10, 11, 12, 24, 25, 32, 33, 45, 46, and 47, that werecorrelated to the left amygdala reactivity
3. Results
3.1. Behavioral results
Pretreatment differences: there were no statistically significantdifferences between the two treatment groups with regards todemographics or pretreatment self-report measures (all p's40.15);see also Supplementary Table S1. No differences were found inpretreatment LSAS-SR scores between subjects who completed thestudy and excluded participants (n¼4; t(24)¼0.95, p40.35).
Treatment outcome: repeated measurement ANOVA of LSAS-SRdata revealed a significant main effect of time (F(2,22)¼37.33,po0.001), but no significant time � group interaction, F(2,22)¼0.84, p¼0.37 (see also Supplementary Table S1). Moderate to largewithin-group effect sizes (Cohen's d) were observed on LSAS-SR,d¼0.91 (CI 95% 0.44–1.37) for iCBT, and d¼1.08 (CI 95% 0.43–1.74)for ABM. A repeated measure MANOVA including all social anxietyself-reports (LSAS-SR, SIAS, SPS and SPSQ) revealed a significantmultivariate time � group interaction effect, Wilks's λ¼0.535, F(4,19)¼4.13, p¼0.01 (see also Supplementary Table S1), suggestinga differential treatment outcome in favor of iCBT. Also, the numberof CGI-I responders was significantly higher (χ2(1)¼4.20, p¼0.04)in the iCBT group, having eight (66%) responders as compared tothree (25%) in the ABM control group.
Response times and subjective ratings: regarding reaction timesto the emotional face processing task, there were no significantinteraction effects (time � group) for the different facial expres-sions (F(1,20)¼1.16–3.44, all p's40.08). Analyses of all facescombined revealed a trend-level interaction effect (F(1,20)¼3.82,p¼0.065) suggesting faster responses when matching faces afterABM (Mpost¼1 174.19 ms, S.D.¼219.12) compared to iCBT (Mpost¼1250.34 ms, S.D.¼208.29). We also analyzed self-reported fear anddistress during brain image acquisition and found no interaction(time� group), nor main effects (F(2,20)¼0.00–2.60, all p's40.12)before or after treatment.
3.2. fMRI results
Pretreatment effects: as expected, we found that the fMRI taskrobustly activated the amygdala in a full sample analysis beforetreatment (left amygdala xyz [–30,–4,–20], Z¼3.32, pFWE¼0.009,513 mm3; right amygdala xyz [24,–7,–14], Z¼3.39, pFWE¼0.008,837 mm3). We found no significant pretreatment differences inbilateral amygdala reactivity between iCBT and ABM; t(20)¼�0.17to 0.32, all p's40.75.
Within-group treatment effects: changes in LSAS-SR-related amyg-dala reactivity were nonsignificant at the corrected level within bothtreatment modalities. At a more lenient statistical threshold, activityin the left amygdala decreased (pre4post) with iCBT while thereverse pattern (preopost) was suggested in subjects treated withABM (Table 2). Whole-brain analyses revealed decreases in thecaudate, cerebellum, dlPFC, putamen and rACC with iCBT whereas
Table 1Demographic and clinical characteristics.
iCBT (n¼13) ABM (n¼13)
Demographic characteristicsGender: female, n (%) 11 (85) 11 (85)Ethnicity: caucasian, n (%) 10 (91) 11 (100)Age, Mean (S.D.) 32.46 (8.6) 32.08 (10.9)Range, (years) 20–47 19–57Right handedness, n (%) 13 (100) 13 (100)
Education, n (%)Completed university 4 (31) 5 (39)Current university 5 (39) 5 (39)Vocational 0 (0) 2 (15)Completed high school 4 (31) 1 (8)
Unrelated treatments, n (%)Current prescription medication (SSRIs) 5 (39) 4 (31)Previously had prescription medication 1 (8) 4 (31)Never had prescription medication 7 (54) 5 (39)
Social anxietyAge of onset, Mean (S.D.) 16.77 (6.3) 15.00 (5.8)Generalized subtype, n (%) 10 (77) 12 (92)
Abbreviations: iCBT, internet-delivered cognitive behavior therapy; ABM, attentionbias modification; SSRI, selective serotonin reuptake inhibitor;
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237232

Author's personal copy
the ABM group increased in the postcentral gyrus, putamen, supple-mentary motor area (SMA) and superior temporal lobe (Table 2).
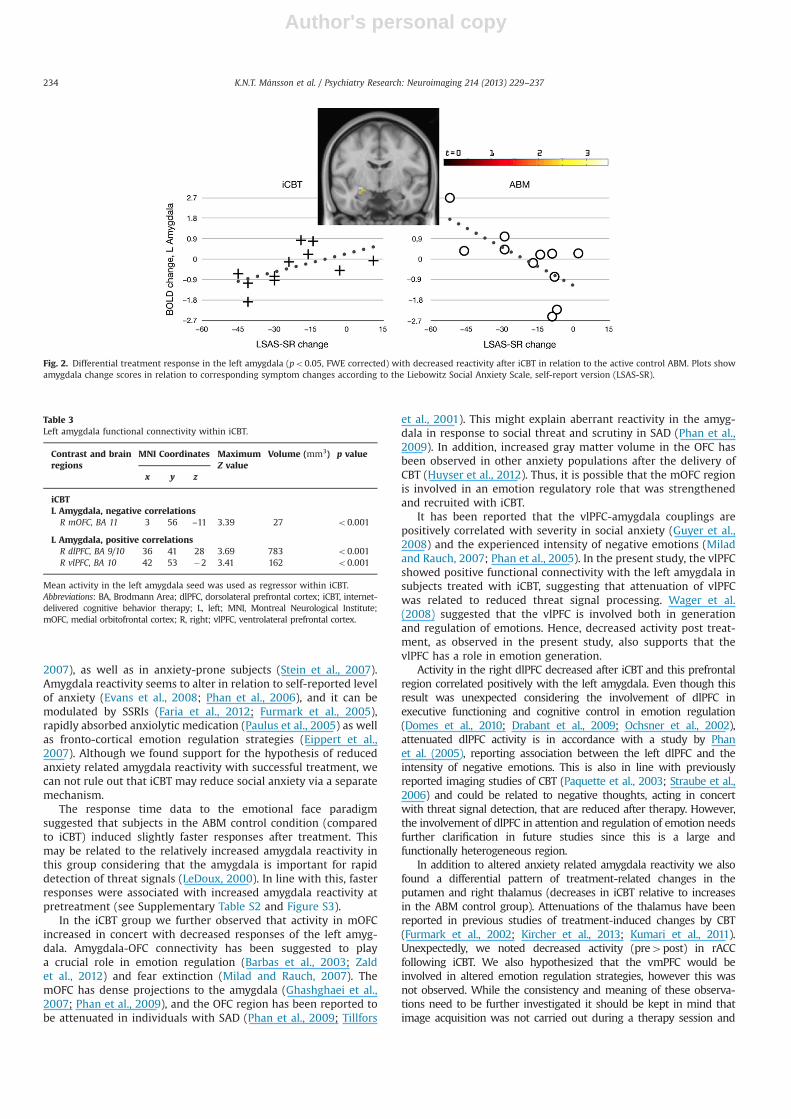
Differential treatment effects: between-group analysis indicateda significant time � group interaction, i.e. a different neuralchange (post compared to pre), in the left amygdala withdecreased reactivity in iCBT in relation to ABM subjects (Table 2,Fig. 2). Whole-brain analyses further showed that activity in thecerebellum, postcentral gyrus, putamen and thalamus decreasedwith iCBT, relative to increases with ABM, yielding significantinteraction (group by time) effects, see Table 2.
Functional connectivity: multiple regression analyses indicatedthat changes within the mOFC were significantly negativelycorrelated with left amygdala changes in the iCBT group (Supple-mentary Figure S1). Thus, increased activity in mOFC after treat-ment was linked to reduced amygdala reactivity. Activity withinthe right ventrolateral (vlPFC; Supplementary Figure S2) and dlPFCdecreased in concert with attenuated left amygdala responses, i.e.a positive correlation (Table 3).
4. Discussion
The present study investigated anxiety-related neural changesafter internet-delivered CBT in comparison to ABM for SAD. Theclinical response rate (CGI-I) was higher in iCBT relative to the
ABM control condition. The fMRI results showed a significant timeby group interaction in the amygdala, i.e. after iCBT, anxietyrelated amygdala reactivity decreased relatively more during theemotional face processing task. According to functional connec-tivity analyses, activity in mOFC increased in association withdecreases in the left amygdala following iCBT while neuralresponses in the right ventrolateral and dorsolateral prefrontalcortices decreased together with the amygdala.
There were no differences between the two groups on the LSAS-SR as main clinical outcome measure. However, superior improve-ment in favor of iCBT was found in terms of global clinical responserates and multivariate analysis. Lower response rate in ABM was inline with previous studies on internet-delivered ABM reporting nosignificant differences to a placebo condition (Boettcher et al., 2011;Carlbring et al., 2012; Neubauer et al., 2013).
In accordance with prior studies of CBT (Fu et al., 2008;Furmark et al., 2002; Goossens et al., 2007; Kircher et al., 2013)and pharmacologic treatment (Faria et al., 2012; Furmark et al.,2005) results suggested that anxiety-related amygdala reactivitydecreased following internet-delivered CBT. In this respect, thecurrent results imply that the effect of iCBT is mediated by similarbrain mechanisms as regular CBT delivered face-to-face. Theamygdala is held to be an important fear processing hub andexaggerated amygdala responses have been reported in indivi-duals with anxiety disorders including SAD (Etkin and Wager,
Table 2Anxiety-related neural changes within and between-groups.
Contrast and brain regions MNI Coordinates Maximum Z value Volume (mm3) p value
x y z
iCBT (pre4post)L Amygdala (ROI) –21 –1 –11 2.68 189 0.07#
L Caudate –18 8 19 3.25 27 0.001L Cerebellum –42 –76 –29 3.31 27 o0.001R Cerebellum 39 –64 –29 3.26 108 0.001L dlPFC, BA 9 –27 38 34 3.59 243 o0.001L Putamen –18 23 –5 5.16 513 o0.001R Putamen 18 14 –11 3.46 162 o0.001R rACC, BA 32 3 35 –2 3.11 27 0.001
iCBT (preopost)ns
ABM (pre4post)ns
ABM (preopost)L Amygdala (ROI) –27 –7 –11 2.26 216 0.13#R Amygdala (ROI) 24 –7 –14 2.23 324 0.15#R Postcentral gyrus, BA 4 45 –16 40 3.09 27 0.001L Putamen –24 –1 10 3.14 135 0.001R Putamen 24 8 10 3.84 486 o0.001L SMA, BA 6 –12 20 61 3.13 27 0.001L Temporal superior, BA 13 –54 –40 16 3.78 216 o0.001
ABM4iCBTL Amygdala (ROI) –27 –7 –11 2.98 378 0.03#R Amygdala (ROI) 27 –1 –11 2.08 351 0.20#L Cerebellum –24 –61 –47 3.41 216 o0.001R Cerebellum 45 –58 –29 3.24 27 0.001R Corpus callosum/Cingulate cortex 9 –13 28 3.29 27 0.001L Postcentral gyrus, BA 4 –42 –19 43 3.18 54 o0.001L Putamen –24 2 7 3.91 5 022 o0.001R Putamen 27 8 10 4.12 837 o0.001R Thalamus 18 –13 10 3.28 162 0.001
Abbreviations: ABM, attention bias modification; BA, Brodmann Area; dlPFC, dorsolateral prefrontal cortex; FWE, family wise errorcorrected; iCBT, internet-delivered cognitive behavior therapy; L, left; MNI, Montreal Neurological Institute; ns, non significance; R,right; rACC, rostral anterior cingulate cortex; ROI, region of interest; SMA, supplementary motor area; #, Family-wise error corrected(FWE) p-value
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237 233
Author's personal copy
2007), as well as in anxiety-prone subjects (Stein et al., 2007).Amygdala reactivity seems to alter in relation to self-reported levelof anxiety (Evans et al., 2008; Phan et al., 2006), and it can bemodulated by SSRIs (Faria et al., 2012; Furmark et al., 2005),rapidly absorbed anxiolytic medication (Paulus et al., 2005) as wellas fronto-cortical emotion regulation strategies (Eippert et al.,2007). Although we found support for the hypothesis of reducedanxiety related amygdala reactivity with successful treatment, wecan not rule out that iCBT may reduce social anxiety via a separatemechanism.
The response time data to the emotional face paradigmsuggested that subjects in the ABM control condition (comparedto iCBT) induced slightly faster responses after treatment. Thismay be related to the relatively increased amygdala reactivity inthis group considering that the amygdala is important for rapiddetection of threat signals (LeDoux, 2000). In line with this, fasterresponses were associated with increased amygdala reactivity atpretreatment (see Supplementary Table S2 and Figure S3).
In the iCBT group we further observed that activity in mOFCincreased in concert with decreased responses of the left amyg-dala. Amygdala-OFC connectivity has been suggested to playa crucial role in emotion regulation (Barbas et al., 2003; Zaldet al., 2012) and fear extinction (Milad and Rauch, 2007). ThemOFC has dense projections to the amygdala (Ghashghaei et al.,2007; Phan et al., 2009), and the OFC region has been reported tobe attenuated in individuals with SAD (Phan et al., 2009; Tillfors
et al., 2001). This might explain aberrant reactivity in the amyg-dala in response to social threat and scrutiny in SAD (Phan et al.,2009). In addition, increased gray matter volume in the OFC hasbeen observed in other anxiety populations after the delivery ofCBT (Huyser et al., 2012). Thus, it is possible that the mOFC regionis involved in an emotion regulatory role that was strengthenedand recruited with iCBT.
It has been reported that the vlPFC-amygdala couplings arepositively correlated with severity in social anxiety (Guyer et al.,2008) and the experienced intensity of negative emotions (Miladand Rauch, 2007; Phan et al., 2005). In the present study, the vlPFCshowed positive functional connectivity with the left amygdala insubjects treated with iCBT, suggesting that attenuation of vlPFCwas related to reduced threat signal processing. Wager et al.(2008) suggested that the vlPFC is involved both in generationand regulation of emotions. Hence, decreased activity post treat-ment, as observed in the present study, also supports that thevlPFC has a role in emotion generation.
Activity in the right dlPFC decreased after iCBT and this prefrontalregion correlated positively with the left amygdala. Even though thisresult was unexpected considering the involvement of dlPFC inexecutive functioning and cognitive control in emotion regulation(Domes et al., 2010; Drabant et al., 2009; Ochsner et al., 2002),attenuated dlPFC activity is in accordance with a study by Phanet al. (2005), reporting association between the left dlPFC and theintensity of negative emotions. This is also in line with previouslyreported imaging studies of CBT (Paquette et al., 2003; Straube et al.,2006) and could be related to negative thoughts, acting in concertwith threat signal detection, that are reduced after therapy. However,the involvement of dlPFC in attention and regulation of emotion needsfurther clarification in future studies since this is a large andfunctionally heterogeneous region.
In addition to altered anxiety related amygdala reactivity we alsofound a differential pattern of treatment-related changes in theputamen and right thalamus (decreases in iCBT relative to increasesin the ABM control group). Attenuations of the thalamus have beenreported in previous studies of treatment-induced changes by CBT(Furmark et al., 2002; Kircher et al., 2013; Kumari et al., 2011).Unexpectedly, we noted decreased activity (pre4post) in rACCfollowing iCBT. We also hypothesized that the vmPFC would beinvolved in altered emotion regulation strategies, however this wasnot observed. While the consistency and meaning of these observa-tions need to be further investigated it should be kept in mind thatimage acquisition was not carried out during a therapy session and
Fig. 2. Differential treatment response in the left amygdala (po0.05, FWE corrected) with decreased reactivity after iCBT in relation to the active control ABM. Plots showamygdala change scores in relation to corresponding symptom changes according to the Liebowitz Social Anxiety Scale, self-report version (LSAS-SR).
Table 3Left amygdala functional connectivity within iCBT.
Contrast and brainregions
MNI Coordinates MaximumZ value
Volume (mm3) p value
x y z
iCBTL Amygdala, negative correlations
R mOFC, BA 11 3 56 –11 3.39 27 o0.001
L Amygdala, positive correlationsR dlPFC, BA 9/10 36 41 28 3.69 783 o0.001R vlPFC, BA 10 42 53 �2 3.41 162 o0.001
Mean activity in the left amygdala seed was used as regressor within iCBT.Abbreviations: BA, Brodmann Area; dlPFC, dorsolateral prefrontal cortex; iCBT, internet-delivered cognitive behavior therapy; L, left; MNI, Montreal Neurological Institute;mOFC, medial orbitofrontal cortex; R, right; vlPFC, ventrolateral prefrontal cortex.
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237234

Author's personal copy
that relevant therapeutic or emotional regulatory effects on brainactivity thus could have remained undetected.
Among the limitations of the present study it should first bementioned that the sample size was relatively low thus reducingstatistical power. Therefore, we did not carry out subgroupanalyses of responders compared to nonresponders. In addition,subjects were mainly women (85%). However, SAD is moreprevalent in women than men (Furmark et al., 1999). We com-pared iCBT with an active control group providing adequatecontrol for time and repeated testing. However, we did not includea wait-list control group. Moreover, the treatment periods variedbetween the two groups, i.e. nine vs. four weeks, althoughposttreatment brain imaging data acquisitions were conductedwith the same time interval, 12 weeks after randomization. Also,while the present paradigm has been reported to reliably activatethe amygdala, we did not include an experimental paradigm thatwas directly designed to measure prefrontal cognitive mechanismsin emotion regulation, e.g. timing factors need to be considered(Goldin et al., 2009b; Kalisch, 2009). Also, the affective faceprocessing task imposes a considerably lower emotional load thansocial anxiety provocation paradigms like public speaking whichlimits the generalizability of the treatment effects reported here.Finally, in this study we used a contrast including all facesexpressing emotional content (disgust, fear, neutral and surprise),which generates more data points but might mask differencesbetween the emotional valence categories.
To our knowledge, this is the first study evaluating neuralchanges following internet-delivered CBT. We demonstrate thatsubjects treated with iCBT respond differently to affective facestimuli in the left amygdala, with a relative attenuation, incomparison to the ABM control group. Also, the left amygdalawas acting together with increased activation of the mOFC.Clinical ratings (CGI-I) and multivariate analysis showed thatiCBT was more efficient, which may be in concordance with theobserved neural alterations. These results are consistent withprior neuroimaging findings on CBT and emotion regulation ingeneral. This study gives additional support to iCBT as aneffective treatment for SAD and we argue that it operates largelyvia similar brain mechanisms as traditional CBT delivered face-to-face.
Acknowledgments
This study was supported by Grants to three co-authors:Gerhard Andersson (Linköping University), Tomas Furmark(Swedish Research Council) and Per Carlbring (Swedish Councilfor Working Life and Social Research, FAS 2009–0222). We aregrateful to the staff of the Umeå Functional Brain Imaging Centre(UFBI) for providing excellent research conditions. Carl-JohanUckelstam contributed as a cognitive behavior therapist. Wealso like to thank Ahmad R. Hariri for providing the experi-mental paradigm and to Mats Fredrikson for valuable commentson the manuscript.
Appendix A. Supplementary material
Supplementary data associated with this article can be found in theonline version at http://dx.doi.org/10.1016/j.pscychresns.2013.08.012.
References
Acarturk, C., Cuijpers, P., van Straten, A., de Graaf, R., 2009. Psychological treatmentof social anxiety disorder: a meta-analysis. Psychological Medicine 39,241–254.
Åhs, F., Pissiota, A., Michelgård, Å., Frans, Ö., Furmark, T., Appel, L., Fredrikson, M.,2009. Disentangling the web of fear: amygdala reactivity and functionalconnectivity in spider and snake phobia. Psychiatry Research: Neuroimaging172, 103–108.
American Psychiatric Association, 2000. Diagnostic and Statistical Manual ofMental Disorders, 4th ed. American Psychiatric Press, Washington, DC.
Andersson, G., Carlbring, P., Furmark, T., Group, S.O.F.I.E.R., 2012. Therapist experi-ence and knowledge acquisition in internet-delivered CBT for social anxietydisorder: a randomized controlled trial. PLOS ONE 7, e37411.
Andersson, G., Carlbring, P., Holmström, A., Sparthan, E., Furmark, T., Nilsson-Ihrfelt,E., Buhrman, M., Ekselius, L., 2006. Internet-based self-help with therapistfeedback and in vivo group exposure for social phobia: a randomized controlledtrial. Journal of Consulting and Clinical Psychology 74, 677–686.
Baker, S.L.S., Heinrichs, N.N., Kim, H.-J.H., Hofmann, S.S., 2002. The Liebowitz socialanxiety scale as a self-report instrument: a preliminary psychometric analysis.Behaviour Research and Therapy 40, 701–715.
Baldwin, D.S., Buis, C., 2004. Burden of social anxiety disorder. In: Bandelow, D.S., Stein, D.J. (Eds.), Social Anxiety Disorder. Marcel Dekker, New York,pp. 65–74.
Barbas, H., Saha, S., Rempel-Clower, N., Ghashghaei, T., 2003. Serial pathways fromprimate prefrontal cortex to autonomic areas may influence emotional expres-sion. BMC Neuroscience 4, 25, online publication: /http://www.biomedcentral.com/1471-2202/4/25/citationS.
Beesdo, K., Bittner, A., Pine, D.S., Stein, M.B., Höfler, M., Lieb, R., Wittchen, H.-U.,2007. Incidence of social anxiety disorder and the consistent risk for secondarydepression in the first three decades of life. Archives of General Psychiatry 64,903–912.
Boettcher, J., Berger, T., Renneberg, B., 2011. Internet-based attention training forsocial anxiety: a randomized controlled trial. Cognitive Therapy and Research36, 522–536.
Carlbring, P., Apelstrand, M., Sehlin, H., Amir, N., Rousseau, A., Hofmann, S.G.,Andersson, G., 2012. Internet-delivered attention bias modification training inindividuals with social anxiety disorder – a double blind randomized controlledtrial. BMC Psychiatry 12. (66-66).
Carlbring, P., Gunnarsdóttir, M., Hedensjö, L., Andersson, G., Ekselius, L., Furmark, T.,2007. Treatment of social phobia: randomised trial of internet-deliveredcognitive-behavioural therapy with telephone support. British Journal ofPsychiatry 190, 123–128.
Carlbring, P., Nordgren, L.B., Furmark, T., Andersson, G., 2009. Long-term outcome ofInternet-delivered cognitive–behavioural therapy for social phobia: a 30-month follow-up. Behaviour Research and Therapy 47, 848–850.
Clark, D.M., Wells, A., 1995. A cognitive model of social phobia. In: Heimberg, R., M.L., Hope, D.A., Schneier, F.R. (Eds.), Social Phobia: Diagnosis, Assessment andTreatment, (Ed.) Guilford Press, New York, pp. 69–93.
Doehrmann, O., Ghosh, S.S., Polli, F.E., Reynolds, G.O., Horn, F., Keshavan, A.,Triantafyllou, C., Saygin, Z.M., Whitfield-Gabrieli, S., Hofmann, S.G., 2013.Predicting treatment response in social anxiety disorder from functionalmagnetic resonance imaging. JAMA Psychiatry 70, 87–97.
Domes, G., Schulze, L., Böttger, M., Grossmann, A., Hauenstein, K., Wirtz, P.H., Heinrichs,M., Herpertz, S.C., 2010. The neural correlates of sex differences in emotionalreactivity and emotion regulation. Human Brain Mapping 31, 758–769.
Drabant, E.M., McRae, K., Manuck, S.B., Hariri, A.R., Gross, J.J., 2009. Individualdifferences in typical reappraisal use predict amygdala and prefrontalresponses. Biological Psychiatry 65, 367–373.
Eippert, F., Veit, R., Weiskopf, N., Erb, M., Birbaumer, N., Anders, S., 2007. Regulationof emotional responses elicited by threat-related stimuli. Human Brain Map-ping 28, 409–423.
Ekman, P., Friesen, W., 1976. Pictures of Facial Affect. Consulting Psychologists Press,Palo Alto.
Etkin, A., Egner, T., Kalisch, R., 2011. Emotional processing in anterior cingulate andmedial prefrontal cortex. Trends in Cognitive Sciences 15, 85–93.
Etkin, A., Egner, T., Peraza, D.M., Kandel, E.R., Hirsch, J., 2006. Resolving emotionalconflict: a role for the rostral anterior cingulate cortex in modulating activity inthe amygdala. Neuron 51, 871–882.
Etkin, A., Wager, T., 2007. Functional neuroimaging of anxiety: a meta-analysis ofemotional processing in PTSD, social anxiety disorder, and specific phobia.American Journal of Psychiatry 164, 1476–1488.
Evans, K.C., Wright, C.I., Wedig, M.M., Gold, A.L., Pollack, M.H., Rauch, S.L., 2008. Afunctional MRI study of amygdala responses to angry schematic faces in socialanxiety disorder. Depression and Anxiety 25, 496–505.
Faria, V., Appel, L., hs, F., Linnman, C., Pissiota, A., Frans, Ö., Bani, M., Bettica, P., Pich,E.M., Jacobsson, E., Wahlstedt, K., Fredrikson, M., Furmark, T., 2012. Amygdalasubregions tied to SSRI and placebo response in patients with social anxietydisorder. Neuropsychopharmacology 37, 2222–2232.
Fehm, L., Pelissolo, A., Furmark, T., Wittchen, H.-U., 2005. Size and burden of socialphobia in Europe. European Neuropsychopharmacology 15, 453–462.
First, M., Gibbon, M., Spitzer, R., Williams, J., 1997. Structured Clinical Interview forDSM–IV Axis I Disorders (SCID–I). American Psychiatric Press, Washington.
François, C., Despiégel, N., Maman, K., Saragoussi, D., Auquier, P., 2010. Anxietydisorders, major depressive disorder and the dynamic relationship betweenthese conditions: treatment patterns and cost analysis. Journal of MedicalEconomics 13, 99–109.
Freitas-Ferrari, M.C., Hallak, J.E.C., Trzesniak, C., Filho, A.S., Machado-De-Sousa, J.P.,Chagas, M.H.N., Nardi, A.E., Crippa, J.A.S., 2010. Neuroimaging in social anxietydisorder: a systematic review of the literature. Progress in Neuro-Psychopharmacology and Biological Psychiatry 34, 565–580.
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237 235
Author's personal copy
Fu, C.H.Y., Williams, S.C.R., Cleare, A.J., Scott, J., Mitterschiffthaler, M.T., Walsh, N.D.,Donaldson, C., Suckling, J., Andrew, C., Steiner, H., Murray, R.M., 2008. Neuralresponses to sad facial expressions in major depression following cognitivebehavioral therapy. Biological Psychiatry 64, 505–512.
Furmark, T., Appel, L., Michelgård, Å., Wahlstedt, K., Åhs, F., Zancan, S., Jacobsson, E.,Flyckt, K., Grohp, M., Bergström, M., Pich, E.M., Nilsson, L.-G., Bani, M.,Långström, B., Fredrikson, M., 2005. Cerebral blood flow changes after treat-ment of social phobia with the Neurokinin-1 antagonist GR205171, citalopram,or placebo. Biological Psychiatry 58, 132–142.
Furmark, T., Carlbring, P., Hedman, E., Sonnenstein, A., Clevberger, P., Bohman, B.,Eriksson, A., Hallen, A., Frykman, M., Holmstrom, A., Sparthan, E., Tillfors, M.,Ihrfelt, E.N., Spak, M., Eriksson, A., Ekselius, L., Andersson, G., 2009. Guided andunguided self-help for social anxiety disorder: randomised controlled trial.British Journal of Psychiatry 195, 440–447.
Furmark, T., Tillfors, M., Everz, P., Marteinsdottir, I., Gefvert, O., Fredrikson, M., 1999.Social phobia in the general population: prevalence and sociodemographicprofile. Social Psychiatry and Psychiatric Epidemiology 34, 416–424.
Furmark, T., Tillfors, M., Marteinsdottir, I., Fischer, H., Pissiota, A., Langstrom, B.,Fredrikson, M., 2002. Common changes in cerebral blood flow in patients withsocial phobia treated with citalopram or cognitive-behavioral therapy. Archivesof General Psychiatry 59, 425–433.
Ghashghaei, H.T., Hilgetag, C.C., Barbas, H., 2007. Sequence of information proces-sing for emotions based on the anatomic dialogue between prefrontal cortexand amygdala. NeuroImage 34, 905–923.
Goldin, P.R., Manber, T., Hakimi, S., Canli, T., Gross, J.J., 2009a. Neural bases of socialanxiety disorder: emotional reactivity and cognitive regulation during socialand physical threat. Archives of General Psychiatry 66, 170–180.
Goldin, P.R., Manber-Ball, T., Werner, K., Heimberg, R., Gross, J.J., 2009b. Neuralmechanisms of cognitive reappraisal of negative self-beliefs in social anxietydisorder. Biological Psychiatry 66, 1091–1099.
Goossens, L., Sunaert, S., Peeters, R., Griez, E.J.L., Schruers, K.R.J., 2007. Amygdalahyperfunction in phobic fear normalizes after exposure. Biological Psychiatry62, 1119–1125.
Grant, B.F., Hasin, D.S., Blanco, C., Stinson, F.S., Chou, S.P., Goldstein, R.B., Dawson, D.A., Smith, S., Saha, T.D., Huang, B., 2005. The epidemiology of social anxietydisorder in the United States: results from the national epidemiologic survey onalcohol and related conditions. Journal of Clinical Psychiatry 66, 1351–1361.
Guyer, A.E., Lau, J.Y.F., McClure-Tone, E.B., Parrish, J., Shiffrin, N.D., Reynolds, R.C.,Chen, G., Blair, R.J.R., Leibenluft, E., Fox, N.A., Ernst, M., Pine, D.S., Nelson, E.E.,2008. Amygdala and ventrolateral prefrontal cortex function during anticipatedpeer evaluation in pediatric social anxiety. Archives of General Psychiatry 65,1303–1312.
Hakamata, Y., Lissek, S., Bar-Haim, Y., Britton, J.C., Fox, N.A., Leibenluft, E., Ernst, M.,Pine, D.S., 2010. Attention bias modification treatment: a meta-analysis toward theestablishment of novel treatment for anxiety. Biological Psychiatry 68, 982–990.
Hallion, L.S., Ruscio, A.M., 2011. A meta-analysis of the effect of cognitive biasmodification on anxiety and depression. Psychological Bulletin 137, 940–958.
Hariri, A.R., Mattay, V.S., Tessitore, A., Kolachana, B., Fera, F., Goldman, D., Egan, M.F.,Weinberger, D.R., 2002. Serotonin transporter genetic variation and theresponse of the human amygdala. Science Signaling 297, 400–403.
Hartley, C.A., Phelps, E.A., 2009. Changing fear: the neurocircuitry of emotionregulation. Neuropsychopharmacology 35, 136–146.
Hedman, E., Andersson, G., Ljótsson, B., Andersson, E., Rück, C., Mörtberg, E.,Lindefors, N., 2011a. Internet-based cognitive behavior therapy vs. cognitivebehavioral group therapy for social anxiety disorder: a randomized controllednon-inferiority trial. PLOS ONE 6, e18001.
Hedman, E., Furmark, T., Carlbring, P., Ljótsson, B., Rück, C., Lindefors, N., Andersson,G., 2011b. A 5-year follow-up of internet-based cognitive behavior therapy forsocial anxiety disorder. Journal of Medical Internet Research 13, e39.
Hedman, E., Ljótsson, B., Rück, C., Furmark, T., Carlbring, P., Lindefors, N., Andersson,G., 2010. Internet administration of self-report measures commonly used inresearch on social anxiety disorder: a psychometric evaluation. Computers inHuman Behavior 26, 736–740.
Huyser, C., van den Heuvel, O.A., Wolters, L.H., de Haan, E., Boer, F., Veltman, D.J.,2012. Increased orbital frontal gray matter volume after cognitive behaviouraltherapy in paediatric obsessive compulsive disorder. World Journal of BiologicalPsychiatry 14, 319–331.
Kalisch, R., 2009. The functional neuroanatomy of reappraisal: time matters.Neuroscience and Biobehavioral Reviews 33, 1215–1226.
Kessler, R.C., Berglund, P., Demler, O., Jin, R., 2005. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity surveyreplication. Archives of General Psychiatry 62, 593–602.
Kircher, T., Arolt, V., Jansen, A., Pyka, M., Reinhardt, I., Kellermann, T., Konrad, C., Lueken,U., Gloster, A.T., Gerlach, A.L., Ströhle, A., Wittmann, A., Pfleiderer, B., Wittchen, H.-U.,Straube, B., 2013. Effect of cognitive-behavioral therapy on neural correlates of fearconditioning in panic disorder. Biological Psychiatry 73, 93–101.
Klumpp, H., Fitzgerald, D.A., Phan, K.L., 2013. Neural predictors and mechanismsof cognitive behavioral therapy on threat processing in social anxietydisorder. Progress in Neuro-Psychopharmacology and Biological Psychiatry45, 83–91.
Kumari, V., Fannon, D., Peters, E.R., Ffytche, D.H., Sumich, A.L., Premkumar, P.,Anilkumar, A.P., Andrew, C., Phillips, M.L., Williams, S.C.R., Kuipers, E., 2011.Neural changes following cognitive behaviour therapy for psychosis: a long-itudinal study. Brain 134, 2396–2407.
LeDoux, J., 2000. Emotion circuits in the brain. Annual Review of Neuroscience 23,155–184.
Liebowitz, M.R., 1987. Social phobia. Modern Problems of Pharmacopsychiatry 22,141–173.
Lira Yoon, K., Fitzgerald, D.A., Angstadt, M., McCarron, R.A., Phan, K.L., 2007.Amygdala reactivity to emotional faces at high and low intensity in generalizedsocial phobia: a 4-tesla functional MRI study. Psychiatry Research: Neuroima-ging 154, 93–98.
MacLeod, C., Mathews, A., 2012. Cognitive bias modification approaches to anxiety.Annual Review of Clinical Psychology 8, 189–217.
MacLeod, C., Mathews, A., Tata, P., 1986. Attentional bias in emotional disorders.Journal of Abnormal Psychology 95, 15–20.
Maldjian, J.A., Laurienti, P.J., Kraft, R.A., Burdette, J.H., 2003. An automated methodfor neuroanatomic and cytoarchitectonic atlas-based interrogation of fMRI datasets. NeuroImage 19, 1233–1239.
Mattick, R.P., Clarke, J.C., 1998. Development and validation of measures of socialphobia scrutiny fear and social interaction anxiety. Behaviour Research andTherapy 36, 455–470.
Milad, M.R., Quirk, G.J., Pitman, R.K., Orr, S.P., Fischl, B., Rauch, S.L., 2007. A role forthe human dorsal anterior cingulate cortex in fear expression. BiologicalPsychiatry 62, 1191–1194.
Milad, M.R., Rauch, S.L., 2007. The role of the orbitofrontal cortex in anxietydisorders. Annals of the New York Academy of Sciences 1121, 546–561.
Neubauer, K., von Auer, M., Murray, E., Petermann, F., Helbig-Lang, S., Gerlach, A.L.,2013. Internet-delivered attention modification training as a treatment forsocial phobia: a randomized controlled trial. Behaviour Research and Therapy51, 87–97.
Ochsner, K.N., Bunge, S.A., Gross, J.J., Gabrieli, J.D.E., 2002. Rethinking feelings: anfMRI study of the cognitive regulation of emotion. Journal of CognitiveNeuroscience 14, 1215–1229.
Ochsner, K.N., Gross, J.J., 2005. The cognitive control of emotion. Trends in CognitiveSciences 9, 242–249.
Paquette, V., Lévesque, J., Mensour, B., Leroux, J.-M., Beaudoin, G., Bourgouin, P.,Beauregard, M., 2003. “Change the mind and you change the brain”: effects ofcognitive-behavioral therapy on the neural correlates of spider phobia. Neuro-Image 18, 401–409.
Paulus, M.P., Feinstein, J.S., Castillo, G., Simmons, A.N., Stein, M.B., 2005. Dose-dependent decrease of activation in bilateral amygdala and insula by lorazepamduring emotion processing. Archives of General Psychiatry 62, 282–288.
Phan, K.L., Coccaro, E.F., Angstadt, M., Kreger, K.J., Mayberg, H.S., Liberzon, I., Stein,M.B., 2013. Corticolimbic brain reactivity to social signals of threat before andafter sertraline treatment in generalized social phobia. Biological Psychiatry 73,329–336.
Phan, K.L., Fitzgerald, D.A., Nathan, P.J., Moore, G.J., Uhde, T.W., Tancer, M.E., 2005.Neural substrates for voluntary suppression of negative affect: a functionalmagnetic resonance imaging study. Biological Psychiatry 57, 210–219.
Phan, K.L., Fitzgerald, D.A., Nathan, P.J., Tancer, M.E., 2006. Association betweenamygdala hyperactivity to harsh faces and severity of social anxiety in general-ized social phobia. Biological Psychiatry 59, 424–429.
Phan, K.L., Orlichenko, A., Boyd, E., Angstadt, M., Coccaro, E.F., Liberzon, I., Arfanakis,K., 2009. Preliminary evidence of white matter abnormality in the uncinatefasciculus in generalized social anxiety disorder. Biological Psychiatry 66,691–694.
Phelps, E.A., Delgado, M.R., Nearing, K.I., LeDoux, J.E., 2004. Extinction learning inhumans: role of the amygdala and vmPFC. Neuron 43, 897–905.
Ravindran, L.N., Stein, M.B., 2010. The pharmacologic treatment of anxiety dis-orders. Journal of Clinical Psychiatry 71, 839–854.
Schmidt, N.B., Richey, J.A., Buckner, J.D., Timpano, K.R., 2009. Attention training forgeneralized social anxiety disorder. Journal of Abnormal Psychology 118, 5–14.
Stein, M.B., Goldin, P.R., Sareen, J., Zorrilla, L., Brown, G.G., 2002. Increased amygdalaactivation to angry and contemptuous faces in generalized social phobia.Archives of General Psychiatry 59, 1027–1034.
Stein, M.B., Simmons, A.N., Feinstein, J.S., Paulus, M.P., 2007. Increased amygdalaand insula activation during emotion processing in anxiety-prone subjects.American Journal of Psychiatry 164, 318–327.
Straube, T., Glauer, M., Dilger, S., Mentzel, H.-J., Miltner, W.H.R., 2006. Effects ofcognitive-behavioral therapy on brain activation in specific phobia. NeuroImage29, 125–135.
Straube, T., Kolassa, I.-T., Glauer, M., Mentzel, H.-J., Miltner, W.H.R., 2004. Effect oftask conditions on brain responses to threatening faces in social phobics: anevent-related functional magnetic resonance imaging study. Biological Psy-chiatry 56, 921–930.
Svanborg, P., Åsberg, M., 1994. A new self-rating scale for depression and anxietystates based on the comprehensive psychopathological rating scale. ActaPsychiatrica Scandinavica 89, 21–28.
Tillfors, M., Furmark, T., Marteinsdottir, I., Fischer, H., Pissiota, A., Langstrom, B.,Fredrikson, M., 2001. Cerebral blood flow in subjects with social phobia duringstressful speaking tasks: a PET study. American Journal of Psychiatry 158,1220–1226.
Tzourio-Mazoyer, N., Landeau, B., Papathanassiou, D., Crivello, F., Etard, O., Delcroix,N., Mazoyer, B., Joliot, M., 2002. Automated anatomical labeling of activations inSPM using a macroscopic anatomical parcellation of the MNI MRI single-subjectbrain. NeuroImage 15, 273–289.
Wager, T.D., Davidson, M.L., Hughes, B.L., Lindquist, M.A., Ochsner, K.N., 2008.Prefrontal-subcortical pathways mediating successful emotion regulation.Neuron 59, 1037–1050.
Whalen, P.J., Johnstone, T., Somerville, L.H., Nitschke, J.B., Polis, S., Alexander, A.L.,Davidson, R.J., Kalin, N.H., 2008. A functional magnetic resonance imaging
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237236

Author's personal copy
predictor of treatment response to venlafaxine in generalized anxiety disorder.Biological Psychiatry 63, 858–863.
Zaider, T.I., Heimberg, R.G., Fresco, D.M., Schneier, F.R., Liebowitz, M.R., 2003.Evaluation of the clinical global impression scale among individuals with socialanxiety disorder. Psychological Medicine 33, 611–622.
Zald, D.H., McHugo, M., Ray, K.L., Glahn, D.C., Eickhoff, S.B., Laird, A.R., 2012. Meta-analytic connectivity modeling reveals differential functional connectivity ofthe medial and lateral orbitofrontal cortex. Cerebral Cortex. [e-pub ahead ofprint 4 October 2012].
K.N.T. Månsson et al. / Psychiatry Research: Neuroimaging 214 (2013) 229–237 237




















