Altered bile composition after liver transplantation is associated with the development of...
232
Molecular and biochemical mechanisms of bile duct injury after liver transplantation Carlijn I. Buis
Transcript of Altered bile composition after liver transplantation is associated with the development of...
Molecular and biochemical mechanisms of bile duct injury after liver transplantation
Carlijn I. Buis
This thesis is funded by: . Different parts of this thesis were funded by grants
from the Jan Kornelis de Cock Foundation and the Groningen Graduate School for Drug
Exploration GUIDE.
The financial support of the following institutions and companies in the publication of this
thesis is highly appreciated:
Buis, C.I.
Molecular and biochemical mechanisms of bile duct injury after liver transplantation.
Thesis, University of Groningen, The Netherlands
ISBN: 978-90-367-3639-8
© Copyright 2008 Carlijn I. Buis, The Netherlands
All rights reserved. No part of this book may be reproduced, stored in a retrieval system or
transmitted in any form or by any means, without prior permission of the author.
Cover: ICO-Communucations & Carlijn Buis
Lay-out: Gildeprint drukkerijen, Enschede, the Netherlands
Printed by: Gildeprint drukkerijen, Enschede, the Netherlands
Molecular and biochemical mechanisms of bile duct injury after liver transplantation
Proefschrift
ter verkrijging van het doctoraat in de
Medische Wetenschappen
aan de Rijksuniversiteit Groningen
op gezag van de
Rector Magnificus, dr. F. Zwarts,
in het openbaar te verdedigen op
maandag 8 december 2008
om 13:15 uur
door
Carlijn Ineke Buis
geboren op 29 december 1978
te Vught

Promotor: Prof. dr. R. J. Porte
Beoordelingscommissie: Prof. dr. H.J. Metselaar
Prof. dr. M.J.H. Slooff
Prof. dr. H.J. Verkade

Paranimfen: Marieke de Boer
Mark-Hugo Maathuis
The cover shows an old advertisement of ‘ossegalzeep’ by Jawson Wood, dated in
1915. This soap made from ox bile was especially used in the twentieth century to
clean clothes with fatty stains. The bile salts acts as detergents and thereby enables
fatty stains to dissolve in water by formation of micelles.
A similar pattern can be found in human bile after transplantation. Bile salts form
micelles with phospholipids in the bile. In case phospholipids are relatively reduced
compared to bile salts, in other words if there is a low biliary phospholipids-to-bile
salt ratio, bile can act as a detergent for the bile ducts by recruiting phospholipids
from the membrane. After liver transplantation the bile formation is altered and in
some patients, a detergent – toxic – bile composition, with a low phospholipids-to-
bile salt ratio, is observed. This toxic bile is found to contribute to the development of
bile duct injury after liver transplantation.
Contents
Chapter 1 Introduction and outline of this thesis 9
Chapter 2 Causes and consequences of ischemic type biliary 15
lesions after liver transplantation.
Journal of HPB surgery 2006; 13:517–24.
Part I. Non-anastomotic biliary complications after liver transplantation
Chapter 3 Non-anastomotic biliary strictures after adult liver 37
transplantation part I: radiological features and risk factors
for early versus late presentation
Liver Transpl 2007; 13:708-718.
Chapter 4 Non-anastomotic biliary strictures after adult liver 61
transplantation part 2: Management, outcome and
risk factors for disease progression
Liver Transpl 2007; 13:725-732.
Part II. Bile physiology after liver transplantation
Chapter 5 The role of bile salt toxicity in the pathogenesis of bile duct 81
injury after non heart-beating porcine liver transplantation
Transplantation 2008; 85:1625–1631.
Chapter 6
Altered bile composition after liver transplantation is associated
with the development of Nonanastomotic biliary strictures
J of Hepatol, in press.
99
Chapter 7 Polymorphisms of hepatobiliary phospholipid transporter 123
MDR-3 associated with non anastomotic strictures after
human liver transplantation
submitted
Part III. HO-1 and hepatobiliary injury after liver transplantation
Chapter 8 Expression of Heme oxygenase -1 in human livers before 139
transplantation correlates with graft injury and function
after transplantation
Am J Transplant. 2005; 5:1875–1885.
Chapter 9 Heme oxygenase-1 genotype of the donor is associated 167
with graft survival after liver transplantation.
Am J Transplant. 2008; 8:377–385.
Chapter 10 Summary, discussion and future perspectives 191
Nederlandse samenvatting 203
List of contributing authors 211
List of publications 217
Dankwoord 221
Curriculum Vitae 229
List of abbreviations
Introduction and outline of this thesis
1
Introduction and outline
10
Chapter 1
Introduction and outline of this thesis
Liver transplantation is the ultimate treatment for end-stage liver disease. Survival following
liver transplantation has improved substantially over the years due to better pre-transplant
care, improved anesthesia and surgical techniques, enhanced intensive care medicine, and
more effective immunosuppressant medications. Currently, 1-year patient survival rate is
almost 90% and 5-year patient survival rate is 75% (1).
The first attempt to transplant a liver in a human was reported by Starzl in 1963 (2). In the
Netherlands, the first liver was transplanted in Groningen in 1979 (3). Nowadays, around 120
livers are transplanted annually in the Netherlands.
In the Netherlands, around 135 patients are currently on the waiting list for liver transplantation.
Although transplantation accounts for 77% of the outflow from the waiting list, unfortunately
still 12% of the patients die whilst on the waiting list. Worldwide, around 17000 patients are on
a waiting list for liver transplantation, while the estimated number of liver transplants performed
in 2008 will be less then 14000 (4). The focus on the recruitment of organ donors therefore
remains of vital importance in order to continue and improve the success of transplantation.
Posttransplant-related complications can grossly be classified into primary graft dysfunction,
vascular complications, graft rejection, recurrent disease, and biliary complications.
Reconstruction of biliary drainage is historically considered as the technical ‘Achilles heel’ of
liver transplantation (5). Although the surgical technique of biliary reconstruction has emerged
and is now a more or less standardized technique, complications arising from the bile duct
and its reconstruction remain a serious source of morbidity. The resulting biliary complications
comprise leakage and strictures. Depending on the localization, strictures are classified as
anastomotic or non-anastomotic. Non-anastomotic strictures (NAS) are considered to be
the most troublesome biliary complication after liver transplantation. NAS are defined as any
stricture, dilatation or irregularity of the intra- or extrahepatic bile ducts detected on imaging
studies of the biliary tree after liver transplantation. Approximately one in seven patients suffers
from NAS after liver transplantation. In patients with NAS graft loss is reported in up to 50% after
2 years (6). Accepted risk factors for NAS are hepatic artery thrombosis, chronic ductopenic
rejection, and ABO blood group incompatibility. In 1991 it was first described that NAS may
Chapter 1
11
also occur in the absence of these known risk factors (7). Because of the resemblance of
intrahepatic biliary strictures occurring after hepatic artery thrombosis, NAS that appeared
despite occlusion of the hepatic artery were also called ischemic type biliary lesions (ITBL).
The two names NAS and ITBL are still both used in the literature. A relationship between
NAS and the duration of cold ischemia time was discovered soon after. Ever since, research
in this area has focussed on identifying pathophysiological mechanisms and implementing
therapeutic strategies. Nevertheless, NAS still occur in many patients and in most cases no
apparent clinical risk factor can be identified. Therefore, the aim of this thesis was to perform a
more fundamental analysis, using genetic, molecular and biochemical methods in an attempt
to identify the underlying mechanisms of these biliary complications.
This thesis is divided in three parts, focusing on I) Clinical risk factors for the development and
progression of NAS, II) The role of bile salt toxicity in the development of bile duct injury and
NAS after liver transplantation, III) The role of heme oxygenase-1 (HO-1) in the protection of
liver grafts from ischemia / reperfusion (I/R) injury.
The three parts are preceded by a general overview of the causes and consequences of non-
anastomotic biliary strictures (chapter 2).
Part I. Non-anastomotic biliary complications after liver trans-
plantation.
The specific aims of this section were to describe the various forms of NAS and the
accompanying clinical risk factors as well as to study clinical risk factors for progression of
NAS. Chapter 3 describes the non-anastomotic biliary strictures in the Groningen cohort of
liver transplant recipients. All imaging studies of the biliary tree were reviewed. Localization and
severity of NAS at first presentation were categorized using a newly developed classification.
Time interval between transplantation and the initial presentation of NAS were recorded. The
purpose of this study was to identify risk factors for the clinical and radiological presentation of
NAS, as well as for the timing of NAS after liver transplantation. Chapter 4 concerns the cohort
of patients identified with NAS in chapter 3. This chapter focuses mostly on the consequences
of NAS. We defined a number of serious complications of NAS, studied their prevalence and
risk factors, and evaluated the effects of therapeutic measures.
Introduction and outline
12
Chapter 1
Part II. Bile physiology after liver transplantation.
The specific aims of this section were to evaluate the contribution of bile composition to the
development of bile duct injury. Bile salts have potent detergent properties and may damage
cells of the biliary tract by affecting the integrity of the membranes. The detergent properties
of bile salts are normally counteracted by phospholipids. By forming mixed micelles of bile
salts, phospholipids and cholesterol, phospholipids “neutralize” bile salts thereby protecting
against cellular injury. In a previous study our group has shown that bile produced early after
transplantation has an abnormal composition characterized by a low phospholipids-to-bile
salt ratio (8). Based on these findings we hypothesized that bile salt toxicity early after liver
transplantation contributes to the formation of NAS.
NAS are a frequently encountered complication after non-heart-beating (NHB) liver
transplantation. Aim of chapter 5 was to study the role of bile salt toxicity in the pathogenesis of
bile duct injury after NHB liver transplantation. We hypothesized that NHB liver transplantation
is associated with increased bile salt toxicity early after liver transplantation depending on the
length of the warm ischemia time in the donor. To test this hypothesis we studied bile composition,
graft survival and the degree of bile duct injury in a porcine liver transplant model.
Chapter 6 describes the role of altered bile composition in the development of NAS after
human liver transplantation. In a large clinical study in 111 patients bile composition and the
development of NAS were studied in a prospective fashion. The aim was to test whether bile
composition is involved in the pathogenesis of NAS.
Chapter 7 concerns the genetic variations in hepatobiliary transporters. These transporter
proteins are responsible for bile secretion. The bile salt export pump (BSEP, official name ATP
binding cassette, subfamily B, member 11. ABCB11) mediates ATP-dependent secretion of bile
salts across the canalicular membrane of hepatocytes. Multidrug resistant protein 3 (MDR3,
official name ATP binding cassette, subfamily B, member 4. ABCB4) acts as a primary active
phospholipid flippase and translocates phosphatidylcholine from the inner to the outer leaflet
of the canalicular membrane. Multidrug resistant related protein 2 (MRP-2, official name ATP
binding cassette, subfamily C, member 2. ABCC2 is a multispecific organic anion transporter
that mediates biliary excretion of a broad spectrum of divalent organic anions, including bilirubin
and glutathione. Via the subsequent passive diffusion of water into the bile, this process is
the most significant contributor to the bile salt–independent bile flow. Aim of this study was to
assess whether genetic variations in the above described transporters, present in the donor
liver, are associated with the occurrence of NAS in the recipient after transplantation.

Chapter 1
13
Part III. HO-1 and hepatobiliary injury after liver transplantation.
HO-1 has been proposed as a graft survival gene. Upregulation of HO-1 is considered to be
one of the most critical cellular protection mechanisms during cellular stress such as ischemia
and reperfusion occurring during a transplant procedure. The specific aim of this section was
to study the role of HO-1 expression in relation to postoperative hepatobiliary injury and graft
function.
Chapter 8 concerns endogenous HO-1 expression levels in human liver transplants. We
studied changes in HO-1 expression levels during liver transplantation and correlated this
with immediate postoperative hepatobiliary injury and graft function after transplantation.
Chapter 9 describes two genetic polymorphisms in the promoter influencing the inducebility
of HO-1: a (GT)n polymorphism and a single nucleotide polymorphism (SNP), A(-413)T. We
analyzed these two functional HO-1 promoter polymorphisms in donor genomic DNA in
relation to hepatobiliary injury and outcome after human liver transplantation. Furthermore,
we studied the functional relevance of these polymorphisms by measuring hepatic messenger
ribonucleic acid (mRNA) expression.
Finally, in Chapter 10 the results as described in this thesis are summarized and future
perspectives are discussed.
Referenceswww.unos.org; www.eurotransplant.nl1.
Starzl TE, Marchioro TL, Vonkaulla KN, Hermann G, Brittain RS, Waddell WR. Homotransplantation of the liver 2.
in humans. Surg Gynecol Obstet 1963; 117:659-76.
Krom RA, Gips CH, Houthoff HJ, Newton D, van der Waaij D, Beelen J, Haagsma EB, Slooff MJ. Orthotopic 3.
liver transplantation in Groningen, The Netherlands (1979-1983). Hepatology 1984; 4:61S-65S.
O’Leary JG, Lepe R, Davis GL. Indications for liver transplantation. Gastroenterology. 2008;134:1764-76. 4.
Calne RY. A new technique for biliary drainage in orthotopic liver transplantation utilizing the gall bladder as a 5.
pedicle graft conduit between the donor and recipient common bile ducts. Ann Surg 1976; 184:605-09.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 6.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003;3:885-890.
Sanchez-Urdazpal L, Gores GJ, Ward EM, Maus TP, Wahlstrom HE, Moore SB, et al. Ischemic-type biliary 7.
complications after orthotopic liver transplantation. Hepatology 1992;16:49–53.
Geuken E, Visser D, Kuipers F, Blokzijl H, Leuvenink HG, de Jong KP, et al. Rapid increase of bile salt secretion 8.
is associated with bile duct injury after human liver transplantation. J Hepatol 2004;41:1017-25
Causes and Consequences of ischemic type biliary lesions after liver transplantation2
Jounal of HPB surgery 2006; 13:517-524
Carlijn I BuisHarm H HoekstraRobert C Verdonk
Robert J Porte
16
Causes and consequences of ITBL after liver transplantation Chapter 2
Abstract
Biliary complications are a major source of morbidity, graft loss and even mortality after liver
transplantation. The most troublesome are the so called ischemic type biliary lesions (ITBL),
with an incidence varying between 5-15%. ITBL is a radiological diagnosis, characterized
by intrahepatic strictures and dilatations on a cholangiogram in the absence of hepatic
artery thrombosis. Several risk factors of ITBL have been identified, strongly suggesting a
multifactorial origin. Main categories of risk factors for ITBL include ischemia related injury,
immunological induced injury and cytotoxic injury by bile salts. However, in many cases no
specific risk factor can be identified. Ischemia related injury comprises prolonged ischemic
times and disturbance in blood flow through the peribiliary vascular plexus. Immunological
injury is assumed as risk factor based on the relationship of ITBL with ABO incompatibility,
polymorphism in genes coding for chemokines, and pre-existing immunologically mediated
diseases as primary sclerosing cholangitis and autoimmune hepatitis. The clinical presentation
of patients with ITBL is often not specific, symptoms may include fever, abdominal complaints
and increased cholestatic liver function tests. Diagnosis is made by imaging studies of
the bile ducts. Treatment starts with relieving symptoms of cholestasis and dilatation by
endoscopic retrograde cholangiopancreaticography (ERCP) or percutaneous transhepatic
cholangiodrainage (PTCD) followed by stenting if possible. Eventually up to 50% of the patients
with ITBL will require a re-transplantation or may die. In selected cases, a re-transplantation
can be avoided or delayed by resection of the extra hepatic bile ducts and construction of a
hepatico-jejunostomy. More research on the pathogenesis of ITBL is needed before more
specific preventive or therapeutic strategies can be developed.
17
Chapter 2
Introduction
Biliary complications have since long been recognized as a major cause of morbidity and graft
failure in patients after orthotopic liver transplantation (OLT) (1-3). Bile leakage and bile duct
strictures are the most common complications. According to the localization, strictures can be
classified as anastomotic or non-anastomotic. Non-anastomotic intrahepatic strictures (NAS)
are considered to be the most troublesome biliary complication. NAS were first described
in OLT associated with hepatic artery thrombosis, where the biliary tree becomes ischemic
and eventually necrotic, resulting in a typical cholangiographic picture of biliary strictures,
dilatations and intraductal cast formation (4). However, these cholangiographic abnormalities
of strictures and dilatations can also be seen in patients who do not have an hepatic artery
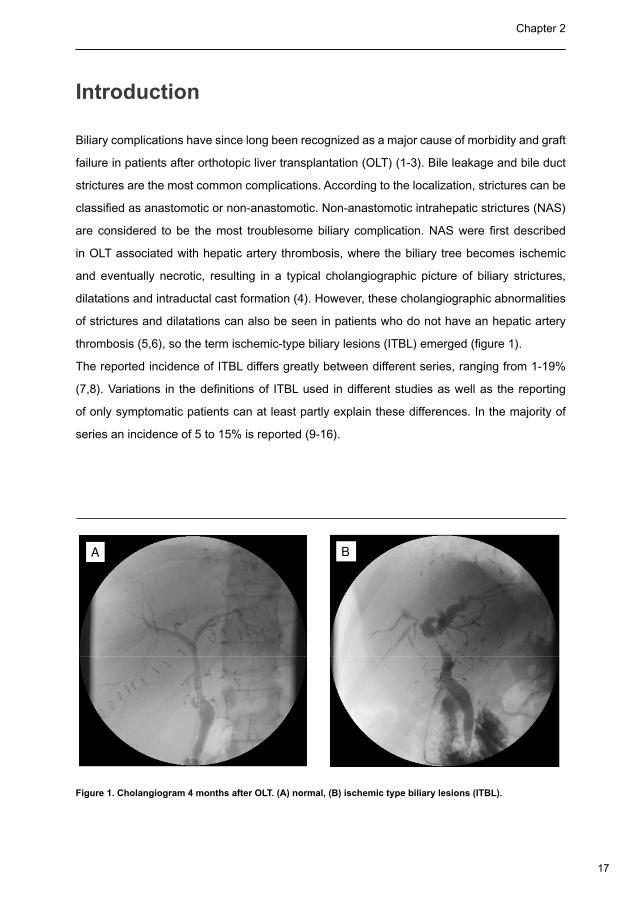
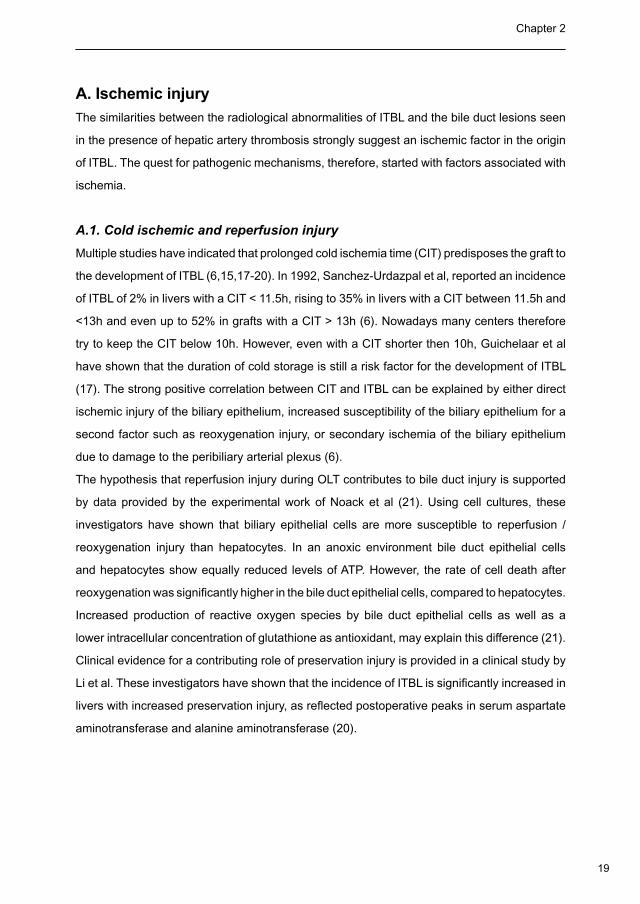
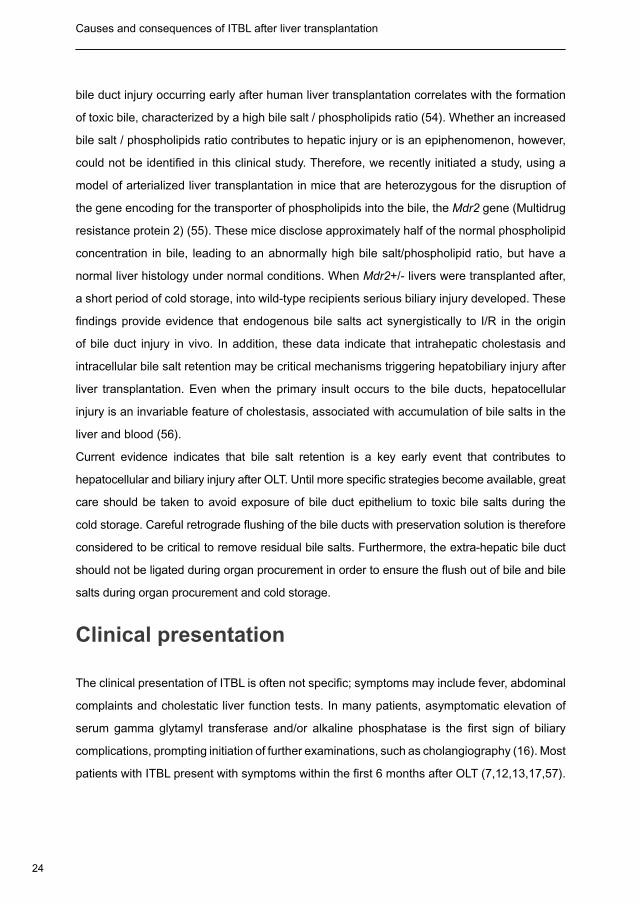
thrombosis (5,6), so the term ischemic-type biliary lesions (ITBL) emerged (figure 1).
The reported incidence of ITBL differs greatly between different series, ranging from 1-19%
(7,8). Variations in the definitions of ITBL used in different studies as well as the reporting
of only symptomatic patients can at least partly explain these differences. In the majority of
series an incidence of 5 to 15% is reported (9-16).
A B
Figure 1. Cholangiogram 4 months after OLT. (A) normal, (B) ischemic type biliary lesions (ITBL).
18
Causes and consequences of ITBL after liver transplantation Chapter 2
Etiology and risk factors
The exact pathophysiological mechanism of ITBL is still unknown. However, several risk
factors of this often cumbersome complication have been identified, strongly suggesting a
multifactorial origin (Table 1). In general, risk factors of ITBL can be divided in three different
categories: ischemia related injury to the biliary epithelium, imunologically mediated injury and
cytotoxic injury induced by bile salts. These categories may point towards different etiological
mechanisms of ITBL, as will be described below.
Table 1. Risk factors for the development of ITBL
Ischemic injury
Warm ischemia in the donor
Prolonged cold ischemia
Reperfusion injury
Warm ischemia during implantation
Disturbed blood flow in the peribiliary plexus
Immunological injury
ABO incompatibility
Pre-existing disease with auto immune component
Auto-immune hepatitis
Primary sclerosing cholangitis
Cytomegalovirus infection
Chronic rejection
Chemokine polymorphism CCR5 delta 32
Bile salt induced injury
Hydrophilic bile salts are cytoprotective
Hydrophobic bile salts are cytotoxic
19
Chapter 2
A. Ischemic injury
The similarities between the radiological abnormalities of ITBL and the bile duct lesions seen
in the presence of hepatic artery thrombosis strongly suggest an ischemic factor in the origin
of ITBL. The quest for pathogenic mechanisms, therefore, started with factors associated with
ischemia.
A.1. Cold ischemic and reperfusion injury
Multiple studies have indicated that prolonged cold ischemia time (CIT) predisposes the graft to
the development of ITBL (6,15,17-20). In 1992, Sanchez-Urdazpal et al, reported an incidence
of ITBL of 2% in livers with a CIT < 11.5h, rising to 35% in livers with a CIT between 11.5h and
<13h and even up to 52% in grafts with a CIT > 13h (6). Nowadays many centers therefore
try to keep the CIT below 10h. However, even with a CIT shorter then 10h, Guichelaar et al
have shown that the duration of cold storage is still a risk factor for the development of ITBL
(17). The strong positive correlation between CIT and ITBL can be explained by either direct
ischemic injury of the biliary epithelium, increased susceptibility of the biliary epithelium for a
second factor such as reoxygenation injury, or secondary ischemia of the biliary epithelium
due to damage to the peribiliary arterial plexus (6).
The hypothesis that reperfusion injury during OLT contributes to bile duct injury is supported
by data provided by the experimental work of Noack et al (21). Using cell cultures, these
investigators have shown that biliary epithelial cells are more susceptible to reperfusion /
reoxygenation injury than hepatocytes. In an anoxic environment bile duct epithelial cells
and hepatocytes show equally reduced levels of ATP. However, the rate of cell death after
reoxygenation was significantly higher in the bile duct epithelial cells, compared to hepatocytes.
Increased production of reactive oxygen species by bile duct epithelial cells as well as a
lower intracellular concentration of glutathione as antioxidant, may explain this difference (21).
Clinical evidence for a contributing role of preservation injury is provided in a clinical study by
Li et al. These investigators have shown that the incidence of ITBL is significantly increased in
livers with increased preservation injury, as reflected postoperative peaks in serum aspartate
aminotransferase and alanine aminotransferase (20).
20
Causes and consequences of ITBL after liver transplantation Chapter 2
A.2. Injury of the peribiliary vascular plexus
Preservation injury results in increased arterial resistance and may cause circulatory disturbances
in small capillaries, such as the biliary plexus (20). Since the blood supply to the biliary tract is
solely dependant on arterial inflow, disturbances in the blood flow through the peribiliary plexus
may result in insufficient preservation and subsequent damage of the biliary epithelium.
Several studies have indicated that the viscosity of preservation solutions may play a
role in the development of ITBL (22,23). The highly viscous University of Wisconsin (UW)
preservation solution, now routinely used in most centers, might not completely flush out the
small donor peribiliary arterial plexus. Microcirculatory disturbances in the peribiliary plexus
may lead to obstruction and subsequently result in insufficient bile duct preservation (23).
Strengthening the evidence that insufficient perfusion of the peribiliary plexus might contribute
to the development of ITBL is provided in a study by Moench et al (24). These investigators
have shown that additional flushing of the peribiliary plexus by controlled arterial back-table
pressure perfusion is associated with a considerable reduction in ITBL after preservation with
UW solution (24). Apart from this, a proper harvesting technique of the liver and the extra
hepatic bile duct is critically important to preserve the viability and vasculature of the bile duct.
Although, never studied in a clinical trial, it is accepted by every surgeon that the extra hepatic
bile duct should be left covered with as much tissue as possible. Stripping of the bile duct
should be avoided in order not to injure the microcirculatory blood supply.
A.3. Warm ischemic Injury
Two periods of warm ischemia can be distinguished during the transplant procedure. The first
warm ischemia time (WIT), during harvesting and before cold preservation, and the second
WIT during graft implantation and before complete reperfusion. The first WIT is especially
a major concern in grafts from non heart-beating (NHB) donors. Several studies have
shown that liver grafts form NHB donors are at increased risk of developing ITBL (25-27).
Concern exists that harvesting time, extending the first WIT, in addition to subsequent CIT
and ischemia-reperfusion injury may result in damage to the biliary epithelium (25). Despite
plausible reasoning, no direct clinical evidence has directly linked prolonged harvesting time
with ITBL, and the literature concerning this item is not conclusive (25-29).
To reduce the incidence of ITBL, attempts have been made to reduce the second WIT.
During revascularization of the graft the most common technique is initial reperfusion via the
21
Chapter 2
portal vein with subsequent reconstruction and reperfusion of the hepatic artery. Bile ducts,
solely dependant on the hepatic artery for their blood supply, are exposed to warm ischemia
during reperfusion via the portal vein alone. This situation has been hypothesized to increase
damage of the biliary epithelium. To overcome this potential harmful situation, Sankary et al.
(18) have studied the impact of simultaneous versus sequential reperfusion of the portal vein
and hepatic artery on the incidence of ITBL. These investigators have observed a significant
reduction of ITBL when livers were reperfused simultaneously via the portal vein and hepatic
artery (18). However, in a more recent study, we were not able to demonstrate a favorable
effect of simultaneous arterial and portal reperfusion on the incidence of ITBL (30).
In an attempt to reduce the second WIT further, some investigators have introduced retrograde
perfusion of the liver graft via the inferior vena cava, after completing its anastomosis and
during construction of the portal vein anastomosis (31). Although this technique certainly
results in an earlier reperfusion of the graft, the central venous blood it is reperfused with
has a lower oxygen pressure than the portal or arterial blood. In a randomized controlled
clinical trial, Heidenhain et al. (32) have recently observed a higher incidence of ITBL in livers
that were reperfused in a retrograde fashion, compared to antegrade reperfusion via the
portal vein. The low perfusion pressure obtained during retrograde perfusion via the caval
anastomosis may be an explanation for this. This low venous pressure may result in poor flush
out and reperfusion of the peribiliary plexus, causing more ischemic biliary injury (J. Langrehr,
personal communication, 2005).
B. Immunological injury
Several papers have provided evidence for an immunological component in the pathogenesis of
ITBL (15,17,33). ITBL has been associated with various immunologically mediated processes,
such as ABO incompatible liver transplantation, pre-existing diseases with a presumed
autoimmune component (such as primary sclerosing cholangitis (PSC) and autoimmune
hepatitis (AIH)), cytomegalovirus (CMV) infection, chronic rejection, and finally with genetic
polymorphism of chemokines.
B.1. ABO incompatibility
ABO blood type mismatched liver transplantation has since long been recognized to give
rise to multiple complications (5,34). The incidence of ITBL in ABO-incompatible OLT varies
22
Causes and consequences of ITBL after liver transplantation Chapter 2
from 20-82% (15). An explanation for this could be the fact that the antigens of the blood type
system are not only expressed on the vascular endothelium, but also on the biliary epithelial
cells, making them a target for preformed ABO blood group antibodies (5,15). Because of this
high rate of complications and reduced graft survival rates, transplantation across the ABO
border is nowadays discouraged.
B.2. Association with pre-existing disease
It has been well described in several studies that patients who are transplanted for PSC have
a higher incidence of ITBL after transplantation (13,14,17,35,36). The association between
ITBL and AIH has only been described recently (17). PSC and AIH share a similar genetic
predisposition to autoimmunity (17). All together, these findings strengthen the hypothesis that
ITBL may have an underlying (auto) immune component.
B.3. Cytomegalovirus
In patients suffering from acquired immunodeficiency syndrome (AIDS), infection with CMV has
been shown to contribute to biliary problems, like cholangitis (37). After OLT, CMV infection
has been associated with an increased incidence of anastomotic strictures and biliary leaks
(38). CMV inclusions have been demonstrated histopathologically in the extra-hepatic bile duct
specimen in a liver transplant patient developing a biliary stricture during CMV infection (38,39).
A clear association between CMV and ITBL, however, has never been demonstrated (17). In
a recent large study of 1714 liver transplant recipients, Heidenhain et al. (40) could not find a
higher incidence of ITBL in patients who had suffered from CMV infection versus those who had
not. The role for CMV infection in the pathogenesis of ITBL, therefore, remains unclear.
B.4. Chronic rejection
Chronic rejection has been implicated as a potential cause of biliary strictures (12,41,42). This
effect is thought to be modulated not via direct injury to the biliary epithelium, but rather via the
arteriopathy accompanying chronic rejection, leading to narrowing of the medium-sized arteries.
The resulting ischemia of the bile duct wall seems to play an important role in the loss of small bile
ducts (15,43,44). Although chronic rejection has been identified as a risk factor for the development
of ITBL in several series (15,20,41,45), this could not always be confirmed by others (13,46).
Therefore the role of chronic rejection in the pathogenesis of ITBL remains to be elucidated.
23
Chapter 2
B.5. Chemokines
Chemokines play a key role in the postoperative immunomodulation, especially during rejection
as well as in post-ischemic injury. Evidence for a role of chemokines in the pathogenesis of
ITBL after OLT has been provided by a genetic association study focusing on CC-chemokine
receptor 5 (CCR5). CCR5 is a receptor for CC-chemokine ligand (CCL) 3 (macrophage
inflammatory protein 1 alpha) and CCL4 (macrophage inflammatory protein 1 beta), which
are over-expressed in infiltrating leukocytes (47). Biliary epithelial cells have been shown to
produce CC-chemokines that may bind specifically to CCR5 (48). CCR5∆32 polymorphism is
a nonfunctional mutant allele of CCR5 with an internal deletion of 32 base pairs. A study on
this polymorphism showed no differences in patient survival, rejection rates, re-transplantation
rates, and survival in OLT patients with CCR5∆32 compared with patients with wild-type CCR5
(49). Interestingly however, Moench et al recently found a very strong association between
the presence of the CCR5∆32 polymorphism in recipients and the development of ITBL after
OLT (33). These findings add to the existing evidence that immunological factors play a role
in the pathogenesis of ITBL.
C. Bile salt induced injury
Another potential factor in the pathogenesis of bile duct injury after liver transplantation
is bile salt toxicity. Bile salts have potent detergent properties towards cellular
membranes of hepatocytes and biliary epithelial cells. Normally, the toxic effects of
bile salts are prevented by complex (mixed micelle) formation with phospholipids.
Evidence for a pivotal role of bile salt-mediated hepatotoxicity in the pathogenesis of I/R injury
of liver grafts, has gradually emerged during the last decade. Using experiments in pigs, Hertl
et al. (50) have shown that bile salts can seriously amplify preservation injury of the biliary
epithelium. When porcine livers are flushed at the time of procurement with saline containing
hydrophobic bile salts, intrahepatic bile ducts are more seriously injured after even short
periods of ischemia, compared to control livers which are flushed with saline (50-52). Injury
of the biliary tree can be prevented when an infusion of hydrophilic, instead of hydrophobic,
bile salts are given to the donor animals prior to liver procurement (50). Moreover, it has been
demonstrated that morphological characteristics of human common bile ducts alter significantly
when livers are perfused with UW solution mixed with gallbladder bile, compared to livers which
are preserved with normal UW solution (53). Of interest, we recently found that microscopic
24
Causes and consequences of ITBL after liver transplantation Chapter 2
bile duct injury occurring early after human liver transplantation correlates with the formation
of toxic bile, characterized by a high bile salt / phospholipids ratio (54). Whether an increased
bile salt / phospholipids ratio contributes to hepatic injury or is an epiphenomenon, however,
could not be identified in this clinical study. Therefore, we recently initiated a study, using a
model of arterialized liver transplantation in mice that are heterozygous for the disruption of
the gene encoding for the transporter of phospholipids into the bile, the Mdr2 gene (Multidrug
resistance protein 2) (55). These mice disclose approximately half of the normal phospholipid
concentration in bile, leading to an abnormally high bile salt/phospholipid ratio, but have a
normal liver histology under normal conditions. When Mdr2+/- livers were transplanted after,
a short period of cold storage, into wild-type recipients serious biliary injury developed. These
findings provide evidence that endogenous bile salts act synergistically to I/R in the origin
of bile duct injury in vivo. In addition, these data indicate that intrahepatic cholestasis and
intracellular bile salt retention may be critical mechanisms triggering hepatobiliary injury after
liver transplantation. Even when the primary insult occurs to the bile ducts, hepatocellular
injury is an invariable feature of cholestasis, associated with accumulation of bile salts in the
liver and blood (56).
Current evidence indicates that bile salt retention is a key early event that contributes to
hepatocellular and biliary injury after OLT. Until more specific strategies become available, great
care should be taken to avoid exposure of bile duct epithelium to toxic bile salts during the
cold storage. Careful retrograde flushing of the bile ducts with preservation solution is therefore
considered to be critical to remove residual bile salts. Furthermore, the extra-hepatic bile duct
should not be ligated during organ procurement in order to ensure the flush out of bile and bile
salts during organ procurement and cold storage.
Clinical presentation
The clinical presentation of ITBL is often not specific; symptoms may include fever, abdominal
complaints and cholestatic liver function tests. In many patients, asymptomatic elevation of
serum gamma glytamyl transferase and/or alkaline phosphatase is the first sign of biliary
complications, prompting initiation of further examinations, such as cholangiography (16). Most
patients with ITBL present with symptoms within the first 6 months after OLT (7,12,13,17,57).
25
Chapter 2
Diagnostic work-up
The appropriate diagnostic workup has been discussed in several recent review papers (58-
60). Direct visualization of the bile ducts by endoscopic retrograde cholangiopancreaticography
(ERCP), percutaneous transhepatic cholangiodrainage (PTCD) or drain-cholangiography
remains the gold standard for making the diagnosis ITBL (7,12,13,17,24,61). Magnetic resonance
cholangiopancreaticography (MRCP) is becoming increasingly important as a diagnostic test,
with high positive and negative predictive values (62-64). Cholangiographic imaging can show
mucosal irregularities, narrowing of the lumen, and ductal dilatations (65). A classification of ITBL
has been proposed based on the localization of the abnormalities, distinguishing type I (extra-
hepatic lesions), type II (intrahepatic lesions), and type III (intra- and extra-hepatic alterations)
(66,67). However, this classification has not been widely accepted and used. In all cases of
non-anastomotic biliary strictures, patency of the hepatic artery should be carefully studied and
confirmed before the diagnosis of ITBL can be made. The presence of ITBL can be suggested
by biliary abnormalities in a liver biopsy, such as ductular proliferation and cholestasis (13).
However, ITBL remains a macroscopic and not a microscopic entity. No studies have been
conducted correlating histological abnormalities in liver biopsies and the presence of ITBL.
Treatment
More than in any other biliary complication, treatment of ITBL has to be individualized. Direct
treatment of strictures should be attempted via endoscopy or percutaneous dilatations and
stenting. With prolonged and intensive endoscopic or radiological treatment, over 50% of
patients can be treated successfully (7,12,17,20,68,69) some centers even reporting success
in over 70% (70). In many other cases, re-transplantation may at least be postponed by using
this strategy. Success will depend mainly on the severity of strictures and their localization, with
extra-hepatic strictures responding better to therapy. In patients with successful radiological
treatment, liver tests may improve, but often remain disturbed (14,69). Many physicians will
provide medical treatment with ursodeoxycholic to their patients in order improve bile flow and
to obtain a more favorable composition of the bile (68,71,72). However, the efficacy of this
strategy in influencing the incidence or outcome of ITBL has never been properly evaluated in
a randomized controlled clinical trial.
26
Causes and consequences of ITBL after liver transplantation Chapter 2
If non-operative techniques are unsuccessful, surgery may be appropriate in selected cases.
Especially when lesions are predominantly present at the level of the bile duct bifurcation,
resection of the extrahepatic bile ducts and Roux-en-Y hepatico-jejunostomy should be
considered. Schlitt et al. (73) have reported clinical and biochemical improvement in 14 out of
16 patients with hilar ITBL, who were treated by a hepatico-jejunostomy or portoenterostomy.
If all other treatment options have failed, retransplantation may be the only therapy left.
Especially in the presence of secondary biliary cirrhosis, recurrent cholangitis, or progressive
cholestasis due to extensive intrahepatic ITBL, retransplantation is mostly unavoidable.
The presence of ITBL is associated with a marked decrease in graft survival. Ultimately, up to
50% of patients with ITBL either die or need a re-transplantation, however mortality rates differ
markedly amongst studies (12,15,17).
Conclusion
Since the introduction of liver transplantation, biliary drainage has formed the so called ‘Achilles
heel’ of this procedure. Early studies have reported disabling complications of the biliary tract in
over 30% of the patients (74). Fortunately, much has changed during the last decades. Liver
transplantation is nowadays a standard treatment for patients with end stage liver disease and
survival is excellent, with one-year patient survival rates of 80 to 90%. Multiple improvements
in patient selection, perioperative management, as well as changes in surgical technique have
contributed to the success of OLT today. Unfortunately, despite these important improvements
and enormous gain in experience, biliary complications can still be regarded as the ‘Achilles
heel’. The most incomprehensible type of biliary complications is ITBL. Although several risk
factors for ITBL have been identified in recent years, the direct cause of ITBL can often not
be identified in an individual patient. Although it is most likely that the pathogenesis of ITBL is
multifactorial, several studies have strongly suggested a critical role for ischemic injury of the
peribiliary vascular plexus. In addition, studies have provided evidence for the involvement of
immunological processes, as well as bile salt induced injury of the biliary epithelium. Despite the
important progress that has been made in the understanding of the pathogenesis of ITBL, the
actual cause remains unidentified in many patients suffering from this troublesome complication
after OLT. Therefore, more research will be needed in this area to better identify and understand
the mechanism of ITBL. Only in this way, more specific preventive and therapeutic strategies
can developed, which may further improve patient and graft survival after OLT
27
Chapter 2
Reference List
Starzl TE, Marchioro TL, Vonkaulla KN, Hermann G, Brittain RS, Waddell WR. Homotransplantation of the liver 1.
in humans. Surg Gynecol Obstet 1963; 117:659-676.
Lerut J, Gordon RD, Iwatsuki S, Esquivel CO, Todo S, Tzakis A Starzl,TE Biliary tract complications in human 2.
orthotopic liver transplantation. Transplantation 1987; 43:47-51.
Calne RY. A new technique for biliary drainage in orthotopic liver transplantation utilizing the gall bladder as a 3.
pedicle graft conduit between the donor and recipient common bile ducts. Ann Surg 1976; 184:605-609.
Zajko AB, Campbell WL, Logsdon GA, Bron KM, Tzakis A, Esquivel CO Starzl,TE. Cholangiographic findings in 4.
hepatic artery occlusion after liver transplantation. AJR Am J Roentgenol 1987; 149:485-489.
Sanchez-Urdazpal L, Sterioff S, Janes C, Schwerman L, Rosen C, Krom RA. Increased bile duct complications 5.
in ABO incompatible liver transplant recipients. Transplant Proc 1991; 23:1440-1441.
Sanchez-Urdazpal L, Gores GJ, Ward EM, Maus TP, Wahlstrom HE, Moore SB Wiesner RH, Krom RA. 6.
Ischemic-type biliary complications after orthotopic liver transplantation. Hepatology 1992; 16:49-53.
Sanchez Urdazpal L. Diagnostic features and clinical outcome of ischemic-type biliary. Hepatology 1993; 7.
17:605.
Thethy S, Thomson BN, Pleass H, Wigmore SJ, Madhavan K, Akyol M Akyol M, Forsythe JL, James Garden 8.
O. Management of biliary tract complications after orthotopic liver transplantation. Clin Transplant 2004; 18:647-
653.
Sawyer RG, Punch JD. Incidence and management of biliary complications after 291 liver transplants following 9.
the introduction of transcystic stenting. Transplantation 1998; 66:1201-1207.
Turrion VS, Alvira LG, Jimenez M, Lucena JL, Nuno J, Pereira F, Vicente E, Ardaiz J. Management of the biliary 10.
complications associated with liver transplantation: 13 years of experience. Transplant Proc 1999; 31(6):2392-
2393.
Rizk RS, McVicar JP, Emond MJ, Rohrmann CA, Jr., Kowdley KV, Perkins J, Carithers RL Jr, Kimmey MB. 11.
Endoscopic management of biliary strictures in liver transplant recipients: effect on patient and graft survival.
Gastrointest Endosc 1998; 47:128-135.
Ward EM, Kiely MJ, Maus TP, Wiesner RH, Krom RA. Hilar biliary strictures after liver transplantation: 12.
cholangiography and percutaneous treatment. Radiology 1990; 177:259-263.
Campbell WL, Sheng R, Zajko AB, Abu-Elmagd K, Demetris AJ. Intrahepatic biliary strictures after liver 13.
transplantation. Radiology 1994; 191:735-740.
Feller RB, Waugh RC, Selby WS, Dolan PM, Sheil AG, McCaughan GW. Biliary strictures after liver 14.
transplantation: clinical picture, correlates and outcomes. J Gastroenterol Hepatol 1996; 11:21-25.
28
Causes and consequences of ITBL after liver transplantation Chapter 2
Rull R, Garcia Valdecasas JC, Grande L, Fuster J, Lacy AM, Gonzalez FX, Rimola A, Navasa M, Iglesias C, 15.
Visa J. Intrahepatic biliary lesions after orthotopic liver transplantation. Transpl Int 2001; 14:129-134.
Pascher A, Neuhaus P. Bile duct complications after liver transplantation. Transpl Int 2005; 18:627-642.16.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 17.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003; 3:885-890.
Sankary HN, McChesney L, Frye E, Cohn S, Foster P, Williams J. A simple modification in operative technique 18.
can reduce the incidence of nonanastomotic biliary strictures after orthotopic liver transplantation. Hepatology
1995; 21:63-69.
Torras J, Llado L, Figueras J, Ramos E, Lama C, Fabregat, J Rafecas A, Escalante E, Dominguez J, Sancho C, 19.
Jaurrieta E. Biliary tract complications after liver transplantation: type, management, and outcome. Transplant
Proc 1999; 31:2406.
Li S, Stratta RJ, Langnas AN, Wood RP, Marujo W, Shaw BW, Jr. Diffuse biliary tract injury after orthotopic liver 20.
transplantation. Am J Surg 1992; 164:536-540.
Noack K. The greater vulnerability of bile duct cells to reoxygenation injury than to anoxia. Transplantation 21.
1993; 56:495.
Canelo R, Hakim NS, Ringe B. Experience with hystidine tryptophan ketoglutarate versus University Wisconsin 22.
preservation solutions in transplantation. Int Surg 2003; 88:145-151.
Pirenne J, Van Gelder F, Coosemans W, Aerts R, Gunson B, Koshiba T, Fourneau I, Mirza D, Van Steenbergen 23.
W, Fevery J, Nevens F, McMaster P. Type of donor aortic preservation solution and not cold ischemia time is a
major determinant of biliary strictures after liver transplantation. Liver Transpl 2001; 7:540-545.
Moench C, Moench K, Lohse AW, Thies J, Otto G. Prevention of ischemic-type biliary lesions by arterial back-24.
table pressure perfusion. Liver Transpl 2003; 9:285-289.
Abt P, Crawford M, Desai N, Markmann J, Olthoff K, Shaked A. Liver transplantation from controlled non-heart-25.
beating donors: an increased incidence of biliary complications. Transplantation 2003; 75:1659-1663.
D’alessandro AM, Hoffmann RM, Knechtle SJ, Odorico JS, Becker YT, Musat A, Pirsch JD, Sollinger HW, 26.
Kalayoglu M. Liver transplantation from controlled non-heart-beating donors. Surgery 2000; 128:579-588.
Otero A, Gomez-Gutierrez M, Suarez F, Arnal F, Fernandez-Garcia A, Aguirrezabalaga J, Garcia-Buitron J, 27.
Alvarez J, Manez R. Liver transplantation from Maastricht category 2 non-heart-beating donors. Transplantation
2005; 15:1068-1073.
Foley DP, Fernandez L, Leverson G, Chin LT, Kreiger N, Cooper JT et al. Donation After Cardiac Death: The 28.
University of Wisconsin Experience With Liver Transplantation. Ann.Surg 2005; 242:724-731.
29
Chapter 2
Manzarbeitia CY, Ortiz JA, Jeon H, Rothstein KD, Martinez O, Araya VR, Munoz SJ, Reich DJ. Long-term 29.
outcome of controlled, non-heart-beating donor liver transplantation. Transplantation 2004; 78:211-215.
Polak WG, Miyamoto S, Nemes BA, Peeters PM, de Jong KP, Porte RJ, Slooff MJH. Sequential and simultaneous 30.
revascularization in adult orthotopic piggyback liver transplantation. Liver Transpl 2005; 11:934-940.
Kniepeiss D, Iberer F, Grasser B, Schaffellner S, Stadlbauer V, Tscheliessnigg KH. A single-center experience 31.
with retrograde reperfusion in liver transplantation. Transpl Int 2005; 16 :730-735.
Heidenhain C., Heise M, Jonas S, Neuhaus P, Langrehr J. Retrograde reperfusion via the vena cava lowers the 32.
risk of initial non function but increases the risk of ischemic-type biliary lesions in human liver transplantation. A
prospective, controlled, randomised clinical trial. [abstract] Transpl.Int 2005; 18[S1], 21.
Moench C, Uhrig A, Lohse AW, Otto G. CC chemokine receptor 5delta32 polymorphism-a risk factor for 33.
ischemic-type biliary lesions following orthotopic liver transplantation. Liver Transpl 2004; 10 :434-439.
Gugenheim J, Samuel D, Reynes M, Bismuth H. Liver transplantation across ABO blood group barriers. Lancet 34.
1990; 336 :519-523.
Sankary HN, McChesney L, Hart M, Foster P, Williams J. Identification of donor and recipient risk factors 35.
associated with nonanastomotic biliary strictures in human hepatic allografts. Transplant Proc 1993; 25:1964-
1967.
Brandsaeter B, Schrumpf E, Bentdal O, Brabrand K, Smith HJ, Abildgaard A, Clausen OP, Bjoro K. Recurrent 36.
primary sclerosing cholangitis after liver transplantation: A magnetic resonance cholangiography study with
analyses of predictive factors. Liver Transpl 2005; 11:1361-1369.
Dolmatch BL, Laing FC, Ferderle MP, Jeffrey RB, Cello J. AIDS-related cholangitis: radiographic findings in nine 37.
patients. Radiology 1987; 163:313-316.
Halme L, Hockerstedt K, Lautenschlager I. Cytomegalovirus infection and development of biliary complications 38.
after liver transplantation. Transplantation 2003; 75:1853-1858.
Kowdley KV, Fawaz KA, Kaplan MM. Extrahepatic biliary stricture associated with cytomegalovirus in a liver 39.
transplant recipient. Transpl Int 1996; 9:161-163.
Heidenhain C., Heise M, Jonas S, Schmitt S., Neuhaus P, Langrehr J. Incidence and risk factors for ischemic-40.
type biliary lesions following orthotopic liver transplantation. A retrospective analysis of 1714 patients. [abstract]
Transpl.Int 2005; 18[s1]: 225-226..
Scotte M, Dousset B, Calmus Y, Conti F, Houssin D, Chapuis Y. The influence of cold ischemia time on biliary 41.
complications following liver transplantation. J Hepatol 1994; 21:340-346.
30
Causes and consequences of ITBL after liver transplantation Chapter 2
Lerut J, Demetris AJ, Stieber AC, Marsh JW, Gordon RD, Esquivel CO, Iwatsuki S, Starzl TE. Intrahepatic bile 42.
duct strictures after human orthotopic liver transplantation. Recurrence of primary sclerosing cholangitis or
unusual presentation of allograft rejection? Transpl Int 1988; 1:127-130.
Ludwig J, Wiesner RH, Batts KP, Perkins JD, Krom RA. The acute vanishing bile duct syndrome (acute 43.
irreversible rejection) after orthotopic liver transplantation. Hepatology 1987; 7:476-483.
Oguma S, Belle S, Starzl TE, Demetris AJ. A histometric analysis of chronically rejected human liver allografts: 44.
insights into the mechanisms of bile duct loss: direct immunologic and ischemic factors. Hepatology 1989;
9:204-209.
Lewis WD. Biliary strictures after liver transplantation. The Surgical clinics of North America 1994; 74:967.45.
Colonna JO, Shaked A, Gomes AS, Colquhoun SD, Jurim O, McDiarmid SV, Millis JM, Goldstein LI, Busuttil 46.
RW. Biliary strictures complicating liver transplantation. Incidence, pathogenesis, management, and outcome.
Ann Surg 1992; 216:344-350.
Moench C, Uhrig A, Wunsch A, Thies J, Otto G. Chemokines: reliable markers for diagnosis of rejection and 47.
inflammation following orthotopic liver transplantation. Transplant Proc 2001; 33:3293-3294.
Morland CM, Fear J, McNab G, Joplin R, Adams DH. Promotion of leukocyte transendothelial cell migration by 48.
chemokines derived from human biliary epithelial cells in vitro. Proc Assoc Am Physicians 1997; 109:372-382.
Schroppel B, Fischereder M, Ashkar R, Lin M, Kramer BK, Mardera B, Schiano T, Murphy B. The impact of 49.
polymorphisms in chemokine and chemokine receptors on outcomes in liver transplantation. Am J Transplant
2002; 2:640-645.
Hertl M, Harvey PR, Swanson PE, West DD, Howard TK, Shenoy S, Strasberg SM. Evidence of preservation 50.
injury to bile ducts by bile salts in the pig and. Hepatology 1995; 21:1130.
Hertl M, Hertl MC, Kluth D, Broelsch CE. Hydrophilic bile salts protect bile duct epithelium during cold. Liver 51.
transplantation 2000; 6:207.
Knoop M, Schnoy N, Keck H, Neuhaus P. Morphological changes of human common bile ducts after extended 52.
cold preservation. Transplantation 1993; 56:1572.
Doctor R, ahl R, alter K, ouassier. ATP depletion in rat cholangiocytes leads to marked internalization of 53.
membrane proteins. Hepatology 2000; 31:1045.
Geuken E, Visser D, Kuipers F, Blokzijl H, Leuvenink HG, de Jong KP, Peeters PM, Jansen PL, Slooff MJH, 54.
Gouw AS, Porte RJ. Rapid increase of bile salt secretion is associated with bile duct injury after human liver
transplantation. J Hepatol 2004; 41:1017-1025.
Hoekstra H, Porte RJ, Tian Y, Jochum W, Stieger B, Moritz W, et al. Bile salt toxicity aggravates cold ischemic 55.
injury of bile ducts after liver transplantation in Mdr2+/- mice. Hepatology 2006 20;43:1022-31.
31
Chapter 2
Palmeira CM, Rolo AP. Mitochondrially-mediated toxicity of bile acids. Toxicology 2004; 203 :1-15.56.
Sanchez-Urdazpal L, Gores GJ, Ward EM, Hay E, Buckel EG, Wiesner RH, Krom RA. Clinical outcome of 57.
ischemic-type biliary complications after liver transplantation. Transplant Proc 1993; 25 :1107-1109.
Holbert BL, Campbell WL, Skolnick ML. Evaluation of the transplanted liver and postoperative complications. 58.
Radiol Clin North Am 1995; 33:521-540.
Bowen A, Hungate RG, Kaye RD, Reyes J, Towbin RB. Imaging in liver transplantation. Radiol Clin North Am 59.
1996; 34:757-778.
Keogan MT, McDermott VG, Price SK, Low VH, Baillie J. The role of imaging in the diagnosis and management 60.
of biliary complications after liver transplantation. AJR Am J Roentgenol 1999; 173:215-219.
Kok T, Van der Sluis A, Klein JP, Van der Jagt EJ, Peeters PM, Slooff MJ, Bijleveld CM, Haagsma EB. 61.
Ultrasound and cholangiography for the diagnosis of biliary complications after orthotopic liver transplantation:
a comparative study. J Clin Ultrasound 1996; 24:103-115.
Boraschi P, Donati F, Gigoni R, Urbani L, Femia M, Cossu MC, Filipponi F, Falaschi F. Ischemic-type biliary 62.
lesions in liver transplant recipients: evaluation with magnetic resonance cholangiography. Transplant Proc
2004; 36:2744-2747.
Boraschi P, Braccini G, Gigoni R, Sartoni G, Neri E, Filipponi F, Mosca F, Bartolozzi C. Detection of biliary 63.
complications after orthotopic liver transplantation with MR cholangiography. Magn Reson Imaging 2001;
19:1097-1105.
Ward J, Sheridan MB, Guthrie JA, Davies MH, Millson CE, Lodge JP, Pollard SG, Prasad KR, Toogood GJ, 64.
Robinson PJ. Bile duct strictures after hepatobiliary surgery: assessment with MR cholangiography. Radiology
2004; 231:101-108.
Malcolm S CP-A. Biliary complications following liver transplantation. Medical care of the liver transplant patient. 65.
Massachusetts: Blackwell Science; 1997., 2005: 193-201.
Hintze RE, Adler A, Veltzke W, Abou-Rebyeh H, Felix R, Neuhaus P. Endoscopic management of biliary 66.
complications after orthotopic liver transplantation. Hepatogastroenterology 1997; 44:258-262.
Theilmann L, Kuppers B, Kadmon M, Roeren T, Notheisen H, Stiehl A, Otto G. Biliary tract strictures after 67.
orthotopic liver transplantation: diagnosis and management. Endoscopy 1994; 26:517-522.
Gopal DV, Pfau PR, Lucey MR. Endoscopic Management of Biliary Complications After Orthotopic Liver 68.
Transplantation. Curr Treat Options Gastroenterol 2003; 6:509-515.
Rerknimitr R, Sherman S, Fogel EL, Kalayci C, Lumeng L, Chalasani N, Kwo P, Lehman GA. Biliary tract 69.
complications after orthotopic liver transplantation with choledochocholedochostomy anastomosis: endoscopic
findings and results of therapy. Gastrointest Endosc 2002; 55:224-231.
32
Causes and consequences of ITBL after liver transplantation
Pfau PR, Kochman ML, Lewis JD, Long WB, Lucey MR, Olthoff K, Shaked A, Ginsberg GG. Endoscopic 70.
management of postoperative biliary complications in orthotopic liver transplantation. Gastrointest Endosc
2000; 52:55-63.
Farouk M, Branum GD, Watters CR, Cucchiaro G, Helms M, McCann R, Bollinger R, Meyers W C. Bile 71.
compositional changes and cholesterol stone formation following orthotopic liver transplantation. Transplantation
1991; 52:727-730.
Gong Y, Gluud C. Colchicine for primary biliary cirrhosis. Cochrane Database Syst Rev 2004;:CD004481.72.
Schlitt HJ, Meier PN, Nashan B, Oldhafer KJ, Boeker K, Flemming P, Raab R, Manns MP, Pichlmayr R. 73.
Reconstructive surgery for ischemic-type lesions at the bile duct bifurcation after liver transplantation. Ann Surg
1999; 229:137-145.
Calne RY. A new technique for biliary drainage in orthotopic liver transplantation utilizing the gall bladder as a 74.
pedicle graft conduit between the donor and recipient common bile ducts. Ann Surg 1976; 184:605-609.


Part I
Non-anastomotic biliary complications after liver transplantation


Non-anastomotic biliary strictures after adult liver transplantation: part I: radiological features and risk factors for early versus late presentation3
Liver Transpl 2007; 13:708-718
Carlijn I BuisRobert C Verdonk
Eric J Van der JagtChristian S van der Hilst
Maarten JH SlooffElizabeth B Haagsma
Robert J Porte
38
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
Abstract
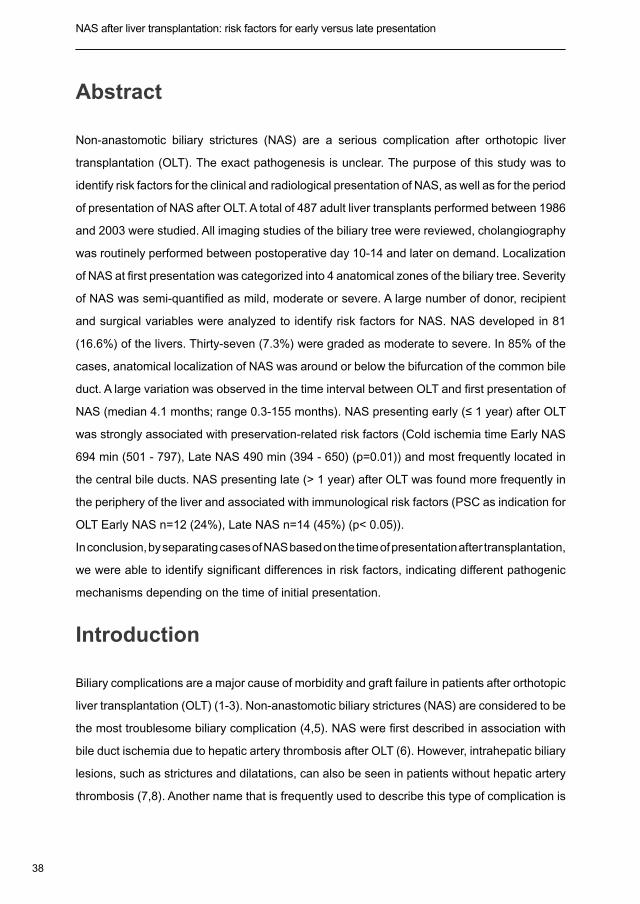
Non-anastomotic biliary strictures (NAS) are a serious complication after orthotopic liver
transplantation (OLT). The exact pathogenesis is unclear. The purpose of this study was to
identify risk factors for the clinical and radiological presentation of NAS, as well as for the period
of presentation of NAS after OLT. A total of 487 adult liver transplants performed between 1986
and 2003 were studied. All imaging studies of the biliary tree were reviewed, cholangiography
was routinely performed between postoperative day 10-14 and later on demand. Localization
of NAS at first presentation was categorized into 4 anatomical zones of the biliary tree. Severity
of NAS was semi-quantified as mild, moderate or severe. A large number of donor, recipient
and surgical variables were analyzed to identify risk factors for NAS. NAS developed in 81
(16.6%) of the livers. Thirty-seven (7.3%) were graded as moderate to severe. In 85% of the
cases, anatomical localization of NAS was around or below the bifurcation of the common bile
duct. A large variation was observed in the time interval between OLT and first presentation of
NAS (median 4.1 months; range 0.3-155 months). NAS presenting early (≤ 1 year) after OLT
was strongly associated with preservation-related risk factors (Cold ischemia time Early NAS
694 min (501 - 797), Late NAS 490 min (394 - 650) (p=0.01)) and most frequently located in
the central bile ducts. NAS presenting late (> 1 year) after OLT was found more frequently in
the periphery of the liver and associated with immunological risk factors (PSC as indication for
OLT Early NAS n=12 (24%), Late NAS n=14 (45%) (p< 0.05)).
In conclusion, by separating cases of NAS based on the time of presentation after transplantation,
we were able to identify significant differences in risk factors, indicating different pathogenic
mechanisms depending on the time of initial presentation.
Introduction
Biliary complications are a major cause of morbidity and graft failure in patients after orthotopic
liver transplantation (OLT) (1-3). Non-anastomotic biliary strictures (NAS) are considered to be
the most troublesome biliary complication (4,5). NAS were first described in association with
bile duct ischemia due to hepatic artery thrombosis after OLT (6). However, intrahepatic biliary
lesions, such as strictures and dilatations, can also be seen in patients without hepatic artery
thrombosis (7,8). Another name that is frequently used to describe this type of complication is
39
Chapter 3
‘ischemic-type biliary lesions’ based on the radiological resemblance with biliary abnormalities
that can be seen after hepatic artery occlusion (8). The reported incidence of NAS varies
greatly between different series, ranging from 1-19% (9,10). This variation can, at least partly,
be explained by differences in the definition of NAS used in different studies, as well as the
reporting of only symptomatic patients and variations in the length of follow up after OLT. In the
majority of series an incidence between 5 to 15% has been reported for NAS (11-18).
The exact pathogenic mechanisms of NAS occurring in the absence of hepatic artery
thrombosis are still unknown. However, previous studies have strongly suggested two major
groups of risk factors: a) preservation (ischemia / reperfusion) injury-related factors and b)
variables related to immunological processes (4,19-21). In addition, recent studies have
indicated that hydrophobic bile salts are involved in the pathogenesis of biliary injury after
OLT (22-25).
In most previous studies, all patients with NAS were considered as one group, independent
from the time of occurrence after OLT and the anatomical localization (8,17,19,21,26-29), In
some studies only NAS occurring within 6 months after OLT were analyzed (20). However,
the time of presentation of NAS after OLT varies widely among different patients. In addition,
the severity and anatomical localization of biliary abnormalities at initial presentation may vary
considerably. We therefore performed a analysis of the anatomical localization and the severity
of NAS at the time of initial presentation in a large group of liver transplant recipients with long-
term follow-up. By separating cases based on the time of presentation after transplantation,
we were able to identify significant differences in risk factors for NAS, suggesting different
pathogenic mechanisms depending on the time of initial presentation. Progression of the
disease after initial presentation as well as long-term outcome of NAS in the same cohort of
liver transplants are presented separately (30).
Patients and Methods
Patients
Between January 1986 and May 2003 a total number of 717 liver transplants were performed
in 639 patients at the University Medical Center Groningen. After exclusion of children (<18
years), and patients with NAS based on hepatic artery thrombosis, 487 transplants in 428
adult patients were included in this study. Follow-up was until November 1, 2005 and median

40
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
follow-up was 7.9 years (interquartile range 4.2-12.6 years). Clinical information was obtained
from a prospectively collected database. If necessary the original patient notes were reviewed
for missing information. Retrospective studies were approved by the institutional ethical
committee.
Surgical Procedure
ABO blood group identical or compatible grafts from brain-death donors with normal or near
normal liver function tests were used for all patients. Organ procurement was performed
according to standard techniques, using either university of Wisconsin (UW) preservation
fluid, histidine-tryptophane-ketoglutarate (HTK) solution, or Euro-Collins (EC) solution (before
1989) (31). On the back table, bile ducts were thoroughly flushed with preservation solution. A
standardized technique was used for implantation, as has been described previously (32,33).
In our institution a duct-to-duct bile duct anastomosis is preferred, including in patients with
primary sclerosing cholangitis (PSC) if the recipient bile duct is suitable (34). A straight, open
tip silicon drain was placed transanastomotically in the bile duct, independent from the type of
bile duct anastomosis (duct-to-duct or Roux-en-Y hepatico-jejunostomy).
Postoperative Management
Two types of immunosuppressive scheme was used during the study period. For patients
with autoimmune diseases like autoimmune hepatitis, primary biliary cirrhosis, and primary
sclerosing cholangitis a triple immunosuppressive scheme [prednisolon, azathioprine and
cyclosporine A (CyA)]. All other patients received a double immunosuppressive scheme,
consisting of prednisolon together with either tacrolimus or CyA. In patients with compromised
renal function calcineurin inhibitors were withheld until creatinine clearance was over 50 mL/
min. If postoperative renal insufficiency was anticipated, induction therapy with basiliximab
was started. Biopsy-proven acute rejection was treated, when clinically indicated, with a
bolus of methylprednisolone on three consecutive days. Steroid-resistant rejections were
treated either by conversion to tacrolimus in patients on cyclosporine A, or by giving 5 doses
of antithymocyte globulin (4 mg/kg i.v.) on alternating days. When the cytomegalovirus
(CMV) status of the donor/recipient combination was positive/negative, prophylaxis with oral
ganciclovir was started at postoperative day 10 and continued for three months.
41
Chapter 3
Doppler ultrasound was performed routinely at postoperative days 1, 3, and 7 and on demand,
to rule out vascular or biliary complications or parenchymal lesions. Cholangiography via the
bile drain was routinely performed between postoperative day 10-14 and later on demand
(i.e. for rising cholestatic parameters or dilatation of bile ducts on ultrasound). The drain was
clamped when no anastomotic leakage or biliary complications were found at cholangiography.
The timing of bile drain removal has increased during the study period from one to currently
six months after transplantation. When a biliary complication was suspected after removal
of the bile drain, the preferred method for further imaging and or treatment was endoscopic
retrograde cholangiopancreaticography (ERCP). This technique has been available in our
center since the early 1980’s. In case of a hepatico-jejunostomy, percutaneous transhepatic
cholangiographic drainage (PTCD) was used to treat biliary complications. In recent years,
magnetic resonance cholangiopancreaticography (MRCP) has been used more frequently as
a diagnostic tool.
Diagnosis and Radiological Classification of NAS
For the purpose of this study, NAS were defined as any stricture, dilatation or irregularity of the
intra- or extrahepatic bile ducts of the liver graft, either with or without biliary sludge formation,
after exclusion of hepatic artery thrombosis by either Doppler ultrasound or conventional
angiography. Isolated strictures at the bile duct anastomosis were, by definition, excluded
from this analysis and have been described elsewhere (35). The time of first presentation of
NAS was recorded for all patients.
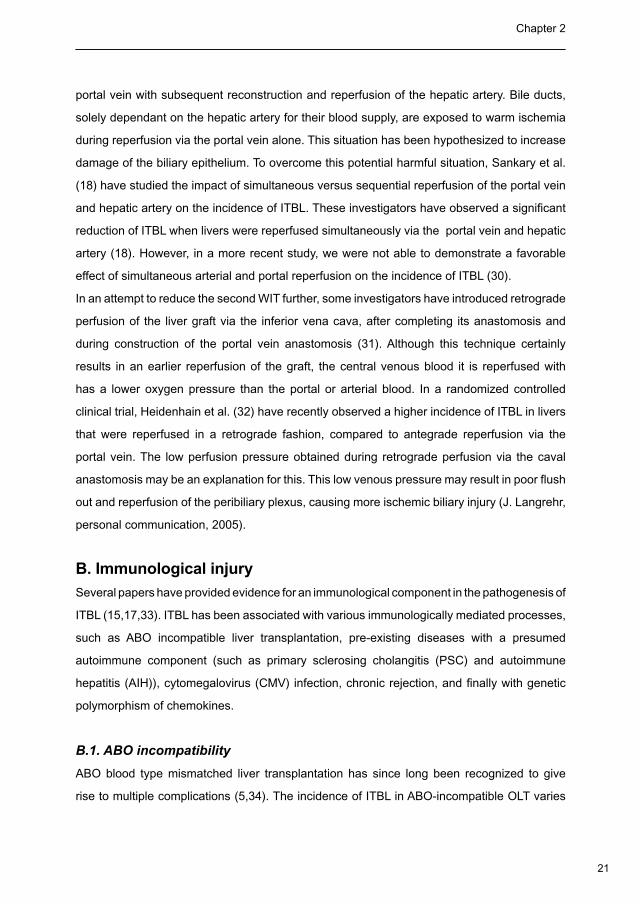
For the purpose of this study, all imaging studies of the biliary tree (cholangiography via the
biliary drain, PTCD, MRCP, or ERCP) of patients diagnosed with NAS were reviewed by a single
radiologist (EJ), who was blinded to the clinical information. The localization of biliary lesions
at the time of initial presentation was categorized according to predefined criteria, based on
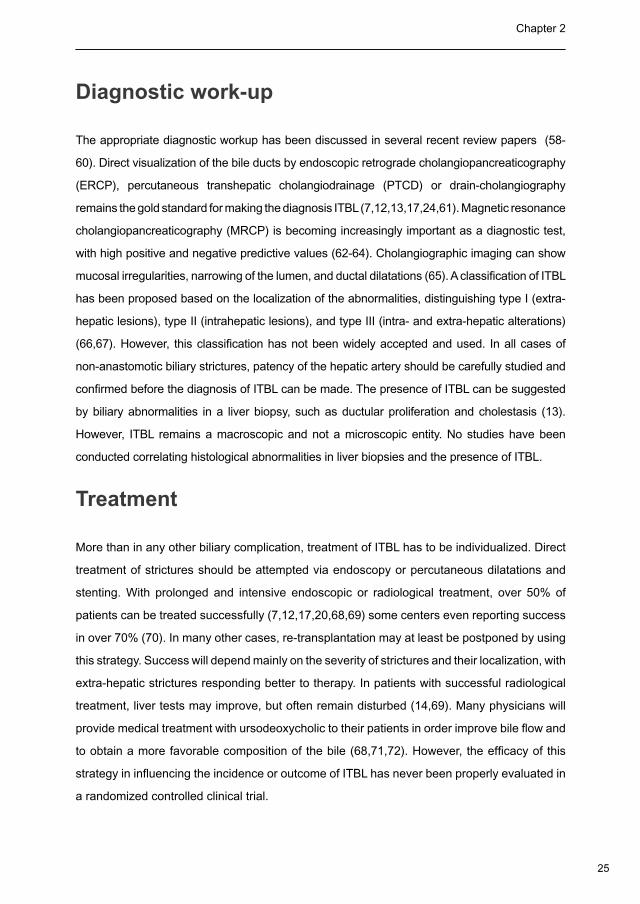
the region and side of the liver. For this purpose we developed a schematic presentation of
the biliary tree in 4 different zones: the extrahepatic common bile duct (CBD) including the
hilar bifurcation (Zone A), the bile ducts between 1st and 2nd order branches (Zone B), the
bile ducts between 2nd and 3rd order branches (Zone C), and bile ducts in the periphery of
the liver (Zone D). In addition, the location of the stricture(s) was/were categorized as left or
right-sided, or bilateral (Figure 1).
42
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
Figure 1. Schematic presentation of the anatomical zones of biliary tree used to define the localization of NAS
after liver transplantation
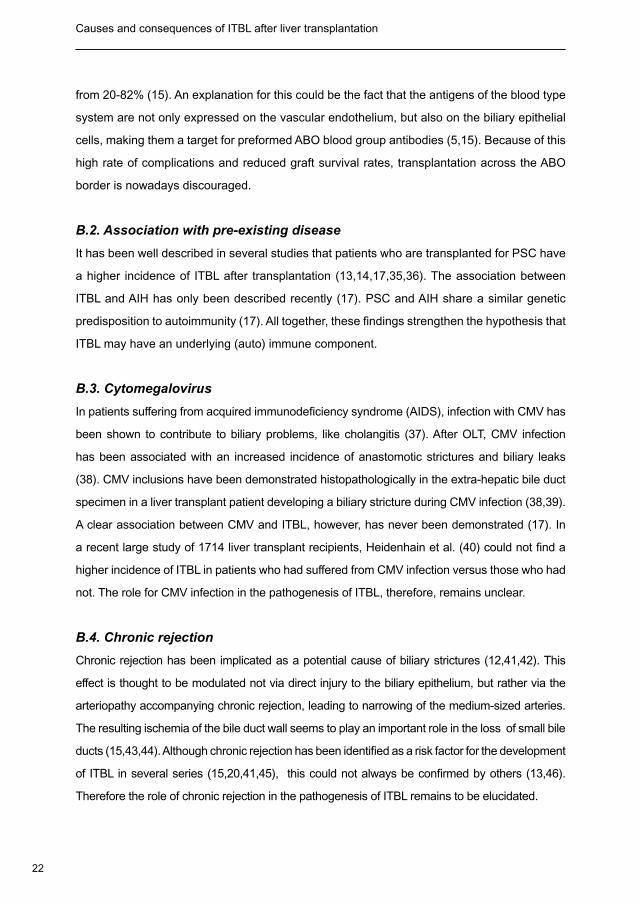
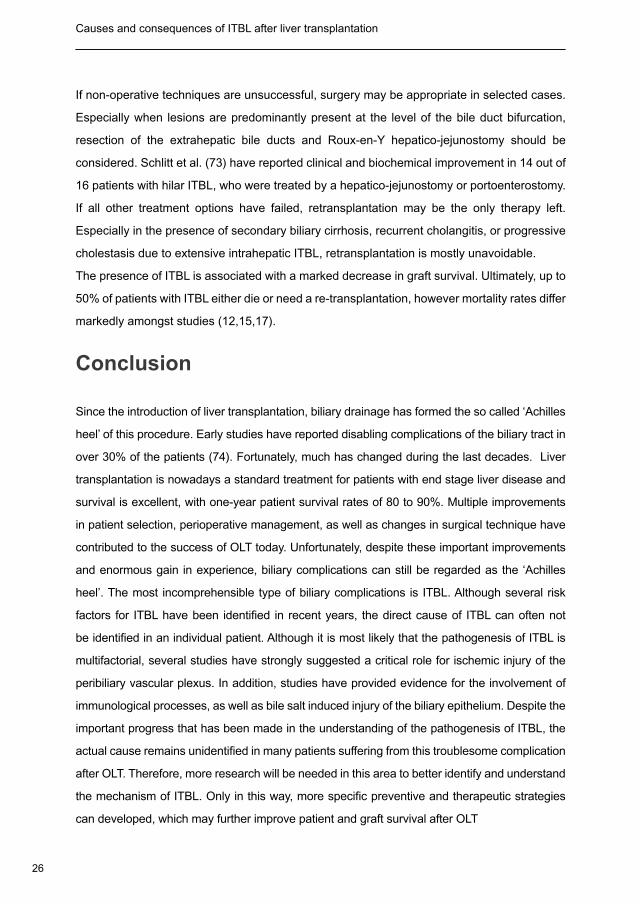
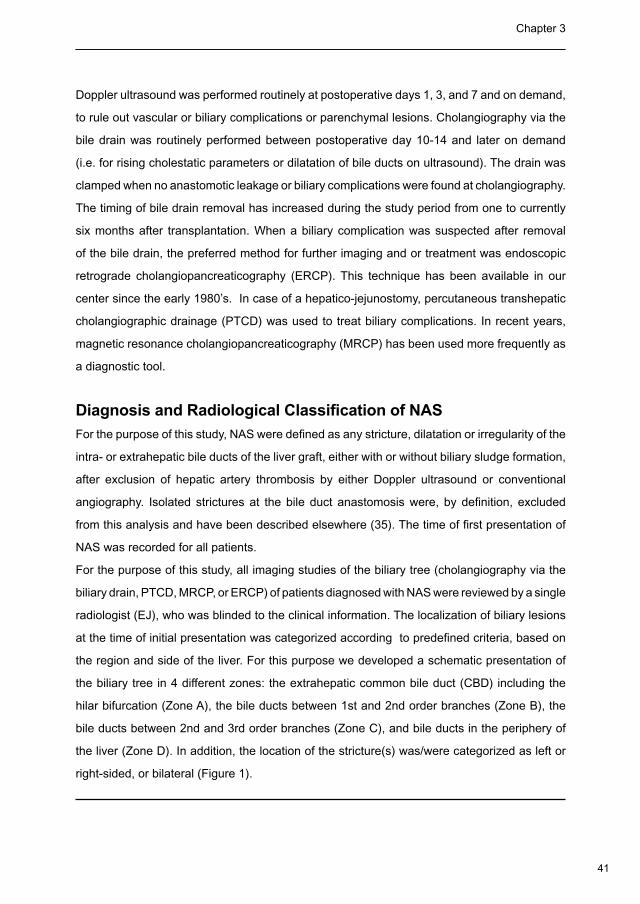
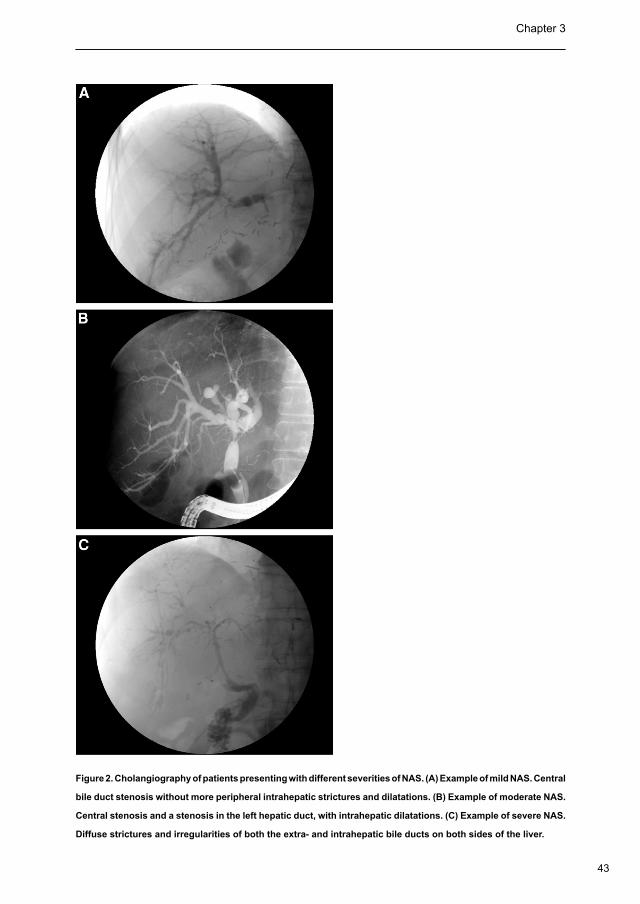
The severity of biliary strictures was categorized based on an arbitrary severity index in which
strictures were scored per area as mild, moderate or severe. Severity scoring was based on
number of strictures in total, the severity according to the degree of narrowing, pre-stenotic dila-
tation and mucosal irregularity and finally the extensiveness of the strictures per area. (fig. 2)
Risk Factors for NAS
A large number of potential risk factors for NAS were studied by comparing the group of
patients with NAS with those who did not develop NAS. In addition, patients with NAS within
the first year after transplantation were compared with those who developed NAS after the first
year. Risk factors were grouped as donor-related variables (age, gender), recipient-related
variables (age, gender, indication for transplantation and Child-Pugh score), surgical variables
(preservation solution, cold ischemia time, warm ischemia time, revacularization time, type of
graft and bile duct reconstruction) and postoperative outcome variables (anastomotic leakage,
serum aspartate amino-transferase (AST), type of immunosuppression, length of stay in ICU,
CMV infection, and acute rejection).
43
Chapter 3
Figure 2. Cholangiography of patients presenting with different severities of NAS. (A) Example of mild NAS. Central
bile duct stenosis without more peripheral intrahepatic strictures and dilatations. (B) Example of moderate NAS.
Central stenosis and a stenosis in the left hepatic duct, with intrahepatic dilatations. (C) Example of severe NAS.
Diffuse strictures and irregularities of both the extra- and intrahepatic bile ducts on both sides of the liver.
44
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
Statistical Methods
Continuous variables were presented as medians with interquartile range (IQR) and categorical
variables as numbers with percentages. Time to occurrence of NAS was calculated according
to the Kaplan-Meier method. Categorical variables were compared using Pearson’s chi-
square test or Fisher exact test where appropriate. Comparison of continuous variables was
performed using the Mann-Whitney U test. The level of significance was set at 0.05. Statistical
analysis was performed using the SPSS/PC+ Advanced Statistics Package, Version 12.0.2
(SPSS, Chicago, IL).
Results
Initial Clinical and Radiological Presentation of NAS
Clinical characteristics of donor and recipients for the entire series are presented in Table 1.
Out of the total of 487 liver grafts, NAS was found in 81 (16.6%) livers, transplanted in 77
patients. Within the group with NAS, 71 were first transplants and 10 were retransplants. Four
patients developed NAS in both a first and a second graft.
The majority of patients with NAS presented with either elevated serum liver enzymes (n=49,
60%), and/or an episode of cholangitis (n=24, 30%). In 13 (16%) cases, the diagnosis of NAS
was based on coincidental findings on routine cholangiography in an otherwise asymptomatic
patient. The radiological modality, which led to the diagnosis of NAS, was cholangiography
via ERCP in 29, bile drain cholangiography in 24, MRCP in 23, and PTCD in 5 patients.
According to the inclusion criteria, all patients had a patent hepatic artery as confirmed by
Doppler ultrasonography or angiography.
The anatomical distribution of biliary lesions at the time of presentation is shown in Table 2.
Imaging studies for radiological evaluation was present in 78 of the 81 (96%) transplants.
45
Chapter 3
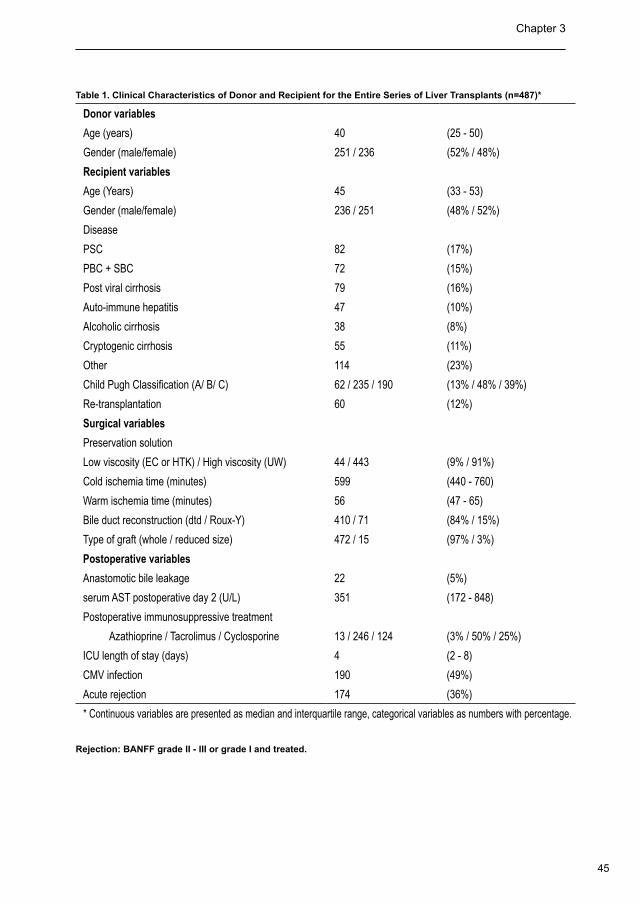
Table 1. Clinical Characteristics of Donor and Recipient for the Entire Series of Liver Transplants (n=487)*
Donor variables
Age (years) 40 (25 - 50)
Gender (male/female) 251 / 236 (52% / 48%)
Recipient variables
Age (Years) 45 (33 - 53)
Gender (male/female) 236 / 251 (48% / 52%)
Disease
PSC 82 (17%)
PBC + SBC 72 (15%)
Post viral cirrhosis 79 (16%)
Auto-immune hepatitis 47 (10%)
Alcoholic cirrhosis 38 (8%)
Cryptogenic cirrhosis 55 (11%)
Other 114 (23%)
Child Pugh Classification (A/ B/ C) 62 / 235 / 190 (13% / 48% / 39%)
Re-transplantation 60 (12%)
Surgical variables
Preservation solution
Low viscosity (EC or HTK) / High viscosity (UW) 44 / 443 (9% / 91%)
Cold ischemia time (minutes) 599 (440 - 760)
Warm ischemia time (minutes) 56 (47 - 65)
Bile duct reconstruction (dtd / Roux-Y) 410 / 71 (84% / 15%)
Type of graft (whole / reduced size) 472 / 15 (97% / 3%)
Postoperative variables
Anastomotic bile leakage 22 (5%)
serum AST postoperative day 2 (U/L) 351 (172 - 848)
Postoperative immunosuppressive treatment
Azathioprine / Tacrolimus / Cyclosporine 13 / 246 / 124 (3% / 50% / 25%)
ICU length of stay (days) 4 (2 - 8)
CMV infection 190 (49%)
Acute rejection 174 (36%)
* Continuous variables are presented as median and interquartile range, categorical variables as numbers with percentage.
Rejection: BANFF grade II - III or grade I and treated.
46
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
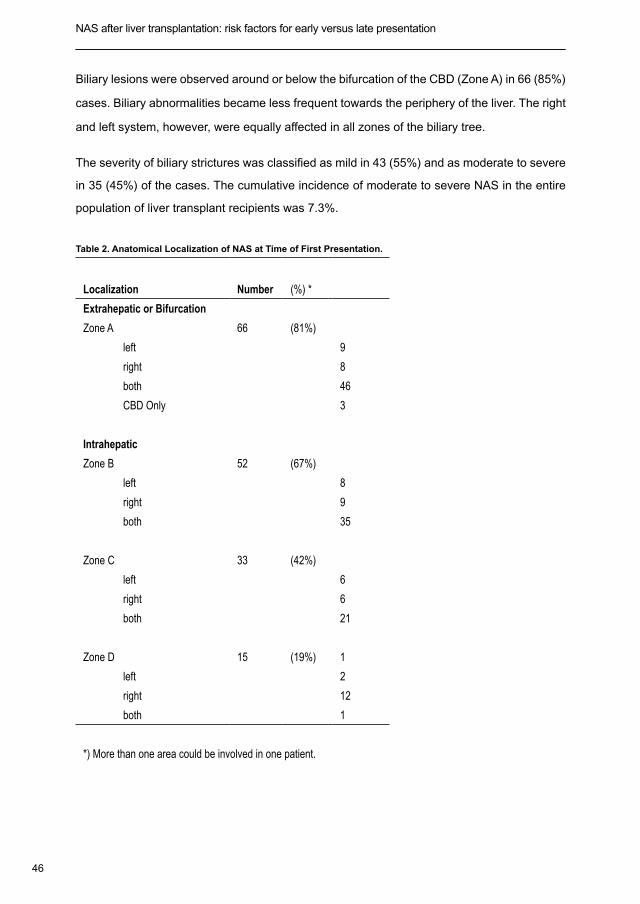
Biliary lesions were observed around or below the bifurcation of the CBD (Zone A) in 66 (85%)
cases. Biliary abnormalities became less frequent towards the periphery of the liver. The right
and left system, however, were equally affected in all zones of the biliary tree.
The severity of biliary strictures was classified as mild in 43 (55%) and as moderate to severe
in 35 (45%) of the cases. The cumulative incidence of moderate to severe NAS in the entire
population of liver transplant recipients was 7.3%.
Table 2. Anatomical Localization of NAS at Time of First Presentation.
Localization
Number (%) *
Extrahepatic or Bifurcation
Zone A 66 (81%)
left 9
right 8
both 46
CBD Only 3
Intrahepatic
Zone B 52 (67%)
left 8
right 9
both 35
Zone C 33 (42%)
left 6
right 6
both 21
Zone D 15 (19%) 1
left 2
right 12
both 1
*) More than one area could be involved in one patient.
47
Chapter 3
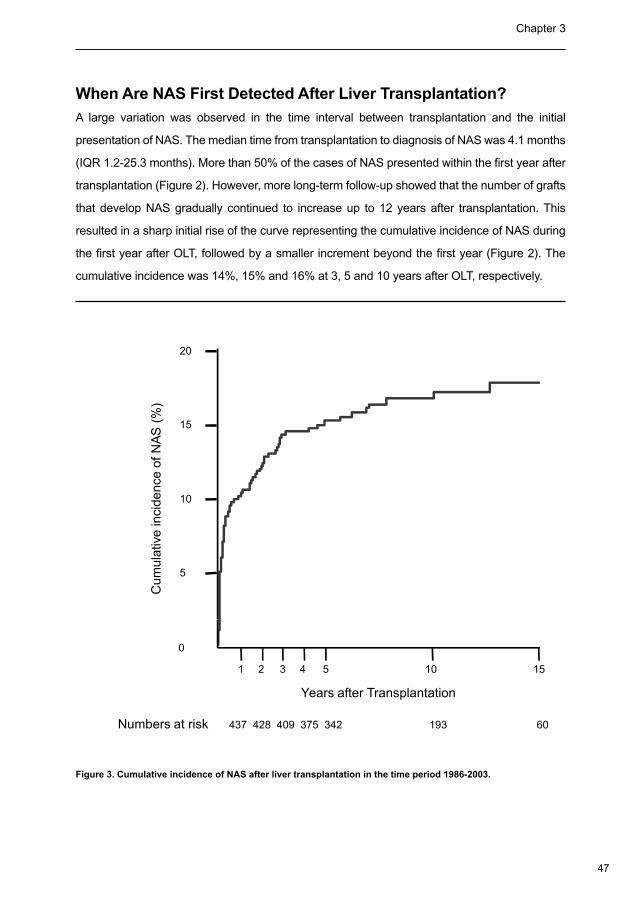
When Are NAS First Detected After Liver Transplantation?
A large variation was observed in the time interval between transplantation and the initial
presentation of NAS. The median time from transplantation to diagnosis of NAS was 4.1 months
(IQR 1.2-25.3 months). More than 50% of the cases of NAS presented within the first year after
transplantation (Figure 2). However, more long-term follow-up showed that the number of grafts
that develop NAS gradually continued to increase up to 12 years after transplantation. This
resulted in a sharp initial rise of the curve representing the cumulative incidence of NAS during
the first year after OLT, followed by a smaller increment beyond the first year (Figure 2). The
cumulative incidence was 14%, 15% and 16% at 3, 5 and 10 years after OLT, respectively.
Cum
ulat
ive
inci
denc
e of
NAS
(%)
5
10
15
20
Years after Transplantation
1 2 3 4 5 10 15
0
Numbers at risk 437 428 409 375 342 193 60
Figure 3. Cumulative incidence of NAS after liver transplantation in the time period 1986-2003.

48
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
Which Risk Factors Are Associated with NAS?
A comparison of demographic and clinical variables between grafts without NAS and the
entire group of livers that developed NAS, independent from the time of occurrence after
OLT, is presented in Table 3. The only significantly different variables between the two groups
were PSC as the indication for transplantation, type of preservation solution (high-viscosity
(UW-solution) versus low-viscosity solution (EC and HTK)), the type of bile duct reconstruction
(duct-to-duct versus Roux-Y hepatico-jejunostomy), and postoperative CMV infection.
However, standard testing whether a patient suffered from a CMV infection became only
routine clinical practice in our center around 1992, and was therefore available in only a subset
of 383 patients. In this first analysis, ischemia times did not emerge as a risk factor for NAS.
This was surprising, because cold and warm ischemia time have both been associated with
NAS in previous studies (8,20,26). However, as we have noted above, a change in the pattern
of the cumulative incidence could be observed after one year and about half of the cases of
NAS in our series were detected beyond the first year after transplantation. It is not likely that
the length of warm or cold ischemia still has an impact on the development of NAS at such
a long interval after transplantation. Therefore, we next examined radiological characteristics
and potential risk factors for early (< 1 year) versus late (> 1 year) initial presentation of NAS
after OLT.
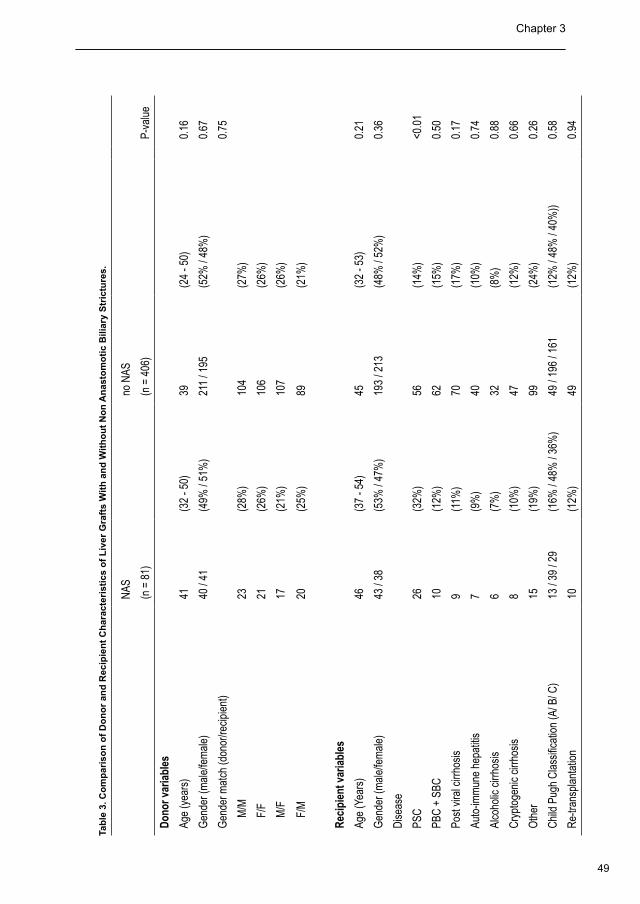
49
Chapter 3
Tab
le 3
. Co
mp
aris
on
of
Do
no
r an
d R
ecip
ien
t C
har
acte
rist
ics
of
Liv
er G
raft
s W
ith
an
d W
ith
ou
t N
on
An
asto
mo
tic
Bili
ary
Str
ictu
res.
NAS
no N
AS
(n
= 8
1)
(n =
406
)
P-
valu
e
Don
or v
aria
bles
Age
(yea
rs)
41(3
2 - 5
0)39
(24
- 50)
0.16
Gen
der (
mal
e/fe
mal
e)40
/ 41
(49%
/ 51
%)
211
/ 195
(52%
/ 48
%)
0.67
Gen
der m
atch
(don
or/re
cipi
ent)
0.75
M
/M23
(28%
)10
4(2
7%)
F
/F21
(26%
)10
6(2
6%)
M
/F17
(21%
)10
7(2
6%)
F
/M20
(25%
)89
(21%
)
Rec
ipie
nt v
aria
bles
Age
(Yea
rs)
46(3
7 - 5
4)45
(32
- 53)
0.21
Gen
der (
mal
e/fe
mal
e)43
/ 38
(53%
/ 47
%)
193
/ 213
(48%
/ 52
%)
0.36
Dis
ease
PSC
26(3
2%)
56(1
4%)
<0.0
1
PBC
+ S
BC10
(12%
)62
(15%
)0.
50
Post
vira
l cirr
hosi
s9
(11%
)70
(17%
)0.
17
Auto
-imm
une
hepa
titis
7(9
%)
40(1
0%)
0.74
Alco
holic
cirr
hosi
s6
(7%
)32
(8%
)0.
88
Cry
ptog
enic
cirr
hosi
s8
(10%
)47
(12%
)0.
66
Oth
er15
(19%
)99
(24%
)0.
26
Chi
ld P
ugh
Cla
ssifi
catio
n (A
/ B/ C
)13
/ 39
/ 29
(16%
/ 48
% /
36%
)49
/ 19
6 / 1
61(1
2% /
48%
/ 40
%))
0.58
Re-
trans
plan
tatio
n 10
(12%
)49
(12%
)0.
94
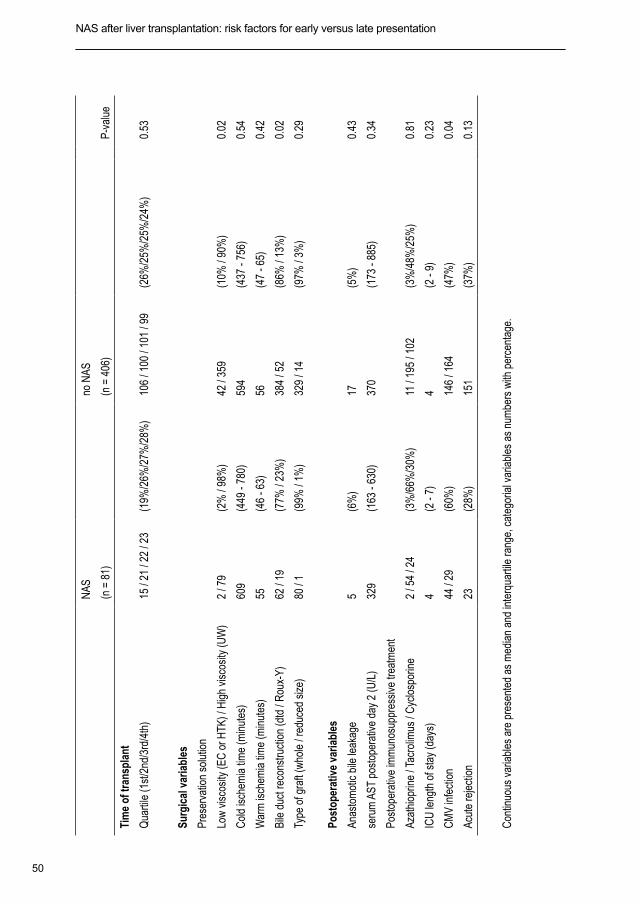
50
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
NAS
no N
AS
(n
= 8
1)
(n =
406
)
P-
valu
e
Tim
e of
tran
spla
nt
Qua
rtile
(1st
/2nd
/3rd
/4th
)15
/ 21
/ 22
/ 23
(19%
/26%
/27%
/28%
)10
6 / 1
00 /
101
/ 99
(26%
/25%
/25%
/24%
)0.
53
Surg
ical
var
iabl
es
Pres
erva
tion
solu
tion
Low
vis
cosi
ty (E
C o
r HTK
) / H
igh
visc
osity
(UW
) 2
/ 79
(2%
/ 98
%)
42 /
359
(10%
/ 90
%)
0.02
Col
d is
chem
ia ti
me
(min
utes
)60
9(4
49 -
780)
594
(437
- 75
6)0.
54
War
m is
chem
ia ti
me
(min
utes
)55
(46
- 63)
56(4
7 - 6
5)0.
42
Bile
duc
t rec
onst
ruct
ion
(dtd
/ R
oux-
Y)62
/ 19
(77%
/ 23
%)
384
/ 52
(86%
/ 13
%)
0.02
Type
of g
raft
(who
le /
redu
ced
size
)80
/ 1
(99%
/ 1%
)32
9 / 1
4(9
7% /
3%)
0.29
Post
oper
ativ
e va
riabl
es
Anas
tom
otic
bile
leak
age
5(6
%)
17(5
%)
0.43
seru
m A
ST p
osto
pera
tive
day
2 (U
/L)
329
(163
- 63
0)37
0(1
73 -
885)
0.34
Post
oper
ativ
e im
mun
osup
pres
sive
trea
tmen
t
Azat
hiop
rine
/ Tac
rolim
us /
Cyc
losp
orin
e2
/ 54
/ 24
(3%
/66%
/30%
)11
/ 19
5 / 1
02(3
%/4
8%/2
5%)
0.81
ICU
leng
th o
f sta
y (d
ays)
4(2
- 7)
4(2
- 9)
0.23
CM
V in
fect
ion
44 /
29(6
0%)
146
/ 164
(47%
)0.
04
Acut
e re
ject
ion
23(2
8%)
151
(37%
)
0.13
Con
tinuo
us v
aria
bles
are
pre
sent
ed a
s m
edia
n an
d in
terq
uarti
le ra
nge,
cat
egor
ial v
aria
bles
as
num
bers
with
per
cent
age.
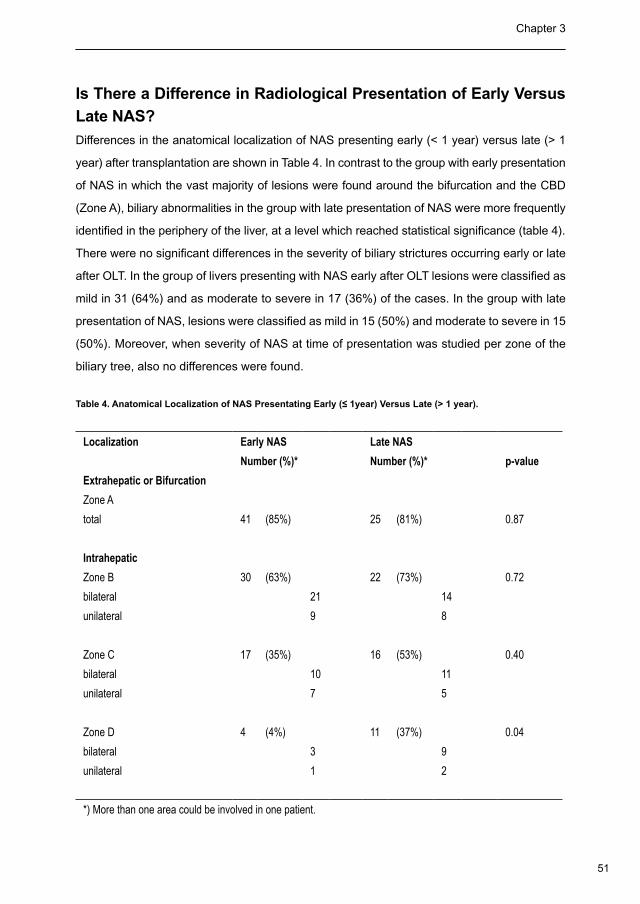
51
Chapter 3
NAS
no N
AS
(n
= 8
1)
(n =
406
)
P-
valu
e
Tim
e of
tran
spla
nt
Qua
rtile
(1st
/2nd
/3rd
/4th
)15
/ 21
/ 22
/ 23
(19%
/26%
/27%
/28%
)10
6 / 1
00 /
101
/ 99
(26%
/25%
/25%
/24%
)0.
53
Surg
ical
var
iabl
es
Pres
erva
tion
solu
tion
Low
vis
cosi
ty (E
C o
r HTK
) / H
igh
visc
osity
(UW
) 2
/ 79
(2%
/ 98
%)
42 /
359
(10%
/ 90
%)
0.02
Col
d is
chem
ia ti
me
(min
utes
)60
9(4
49 -
780)
594
(437
- 75
6)0.
54
War
m is
chem
ia ti
me
(min
utes
)55
(46
- 63)
56(4
7 - 6
5)0.
42
Bile
duc
t rec
onst
ruct
ion
(dtd
/ R
oux-
Y)62
/ 19
(77%
/ 23
%)
384
/ 52
(86%
/ 13
%)
0.02
Type
of g
raft
(who
le /
redu
ced
size
)80
/ 1
(99%
/ 1%
)32
9 / 1
4(9
7% /
3%)
0.29
Post
oper
ativ
e va
riabl
es
Anas
tom
otic
bile
leak
age
5(6
%)
17(5
%)
0.43
seru
m A
ST p
osto
pera
tive
day
2 (U
/L)
329
(163
- 63
0)37
0(1
73 -
885)
0.34
Post
oper
ativ
e im
mun
osup
pres
sive
trea
tmen
t
Azat
hiop
rine
/ Tac
rolim
us /
Cyc
losp
orin
e2
/ 54
/ 24
(3%
/66%
/30%
)11
/ 19
5 / 1
02(3
%/4
8%/2
5%)
0.81
ICU
leng
th o
f sta
y (d
ays)
4(2
- 7)
4(2
- 9)
0.23
CM
V in
fect
ion
44 /
29(6
0%)
146
/ 164
(47%
)0.
04
Acut
e re
ject
ion
23(2
8%)
151
(37%
)
0.13
Con
tinuo
us v
aria
bles
are
pre
sent
ed a
s m
edia
n an
d in
terq
uarti
le ra
nge,
cat
egor
ial v
aria
bles
as
num
bers
with
per
cent
age.
Is There a Difference in Radiological Presentation of Early Versus
Late NAS?
Differences in the anatomical localization of NAS presenting early (< 1 year) versus late (> 1
year) after transplantation are shown in Table 4. In contrast to the group with early presentation
of NAS in which the vast majority of lesions were found around the bifurcation and the CBD
(Zone A), biliary abnormalities in the group with late presentation of NAS were more frequently
identified in the periphery of the liver, at a level which reached statistical significance (table 4).
There were no significant differences in the severity of biliary strictures occurring early or late
after OLT. In the group of livers presenting with NAS early after OLT lesions were classified as
mild in 31 (64%) and as moderate to severe in 17 (36%) of the cases. In the group with late
presentation of NAS, lesions were classified as mild in 15 (50%) and moderate to severe in 15
(50%). Moreover, when severity of NAS at time of presentation was studied per zone of the
biliary tree, also no differences were found.
Table 4. Anatomical Localization of NAS Presentating Early (≤ 1year) Versus Late (> 1 year).
Localization Early NAS Late NAS
Number (%)* Number (%)* p-value
Extrahepatic or Bifurcation
Zone A
total 41 (85%) 25 (81%) 0.87
Intrahepatic
Zone B 30 (63%) 22 (73%) 0.72
bilateral 21 14
unilateral 9 8
Zone C 17 (35%) 16 (53%) 0.40
bilateral 10 11
unilateral 7 5
Zone D 4 (4%) 11 (37%) 0.04
bilateral 3 9
unilateral 1 2
*) More than one area could be involved in one patient.
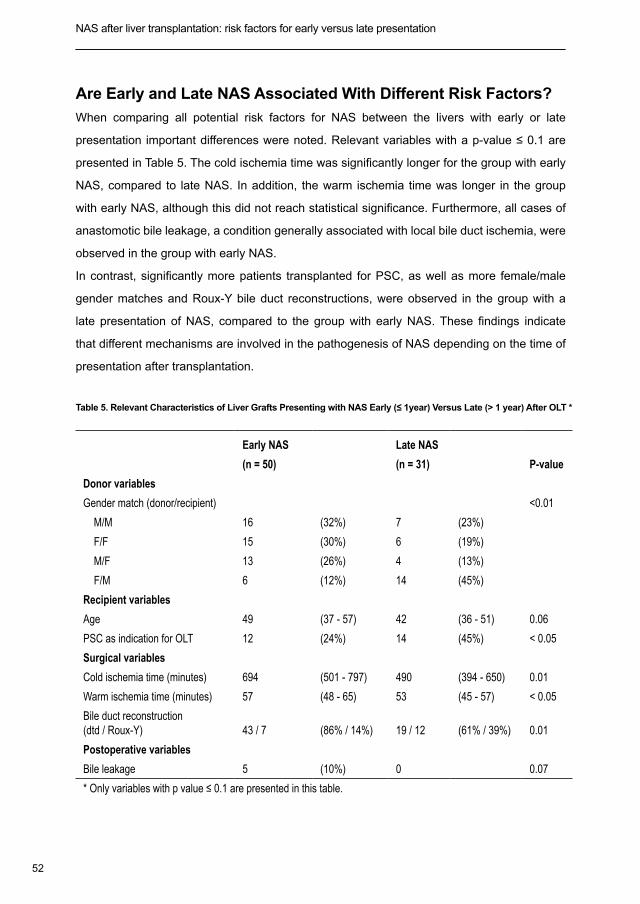
52
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
Are Early and Late NAS Associated With Different Risk Factors?
When comparing all potential risk factors for NAS between the livers with early or late
presentation important differences were noted. Relevant variables with a p-value ≤ 0.1 are
presented in Table 5. The cold ischemia time was significantly longer for the group with early
NAS, compared to late NAS. In addition, the warm ischemia time was longer in the group
with early NAS, although this did not reach statistical significance. Furthermore, all cases of
anastomotic bile leakage, a condition generally associated with local bile duct ischemia, were
observed in the group with early NAS.
In contrast, significantly more patients transplanted for PSC, as well as more female/male
gender matches and Roux-Y bile duct reconstructions, were observed in the group with a
late presentation of NAS, compared to the group with early NAS. These findings indicate
that different mechanisms are involved in the pathogenesis of NAS depending on the time of
presentation after transplantation.
Table 5. Relevant Characteristics of Liver Grafts Presenting with NAS Early (≤ 1year) Versus Late (> 1 year) After OLT *
Early NAS Late NAS
(n = 50) (n = 31) P-value
Donor variables
Gender match (donor/recipient) <0.01
M/M 16 (32%) 7 (23%)
F/F 15 (30%) 6 (19%)
M/F 13 (26%) 4 (13%)
F/M 6 (12%) 14 (45%)
Recipient variables
Age 49 (37 - 57) 42 (36 - 51) 0.06
PSC as indication for OLT 12 (24%) 14 (45%) < 0.05
Surgical variables
Cold ischemia time (minutes) 694 (501 - 797) 490 (394 - 650) 0.01
Warm ischemia time (minutes) 57 (48 - 65) 53 (45 - 57) < 0.05
Bile duct reconstruction (dtd / Roux-Y) 43 / 7 (86% / 14%) 19 / 12 (61% / 39%) 0.01
Postoperative variables
Bile leakage 5 (10%) 0 0.07
* Only variables with p value ≤ 0.1 are presented in this table.
53
Chapter 3
Discussion
Strictures of the bile ducts are a serious complication after OLT, causing increased morbidity
and graft loss (9,20). Although the exact pathogenesis of this type of biliary complication
remains unknown, both preservation-related factors and immunological processes have
been suggested to play a role (4,19,20). Results from previous clinical studies focusing on
potential risk factors of NAS, however, are not unequivocal and conflicting data have been
found (20,36,37)
In this study we were able to identify differences in the anatomical localization as well as
differences in risk factors for NAS depending on the time of first presentation after OLT. While
ischemia and preservation-related variables were most prominent in the group with early
presentation, a late presentation of NAS was more frequently associated with immunological
factors. These findings provide new insights in the pathophysiological mechanisms of NAS.
In the current series, the cumulative incidence of NAS at 15 years after transplantation
was almost 17%, and 7% of all liver grafts were radiological graded as having moderate or
severe biliary strictures. These figures are in line with most previous studies (11,15,18,20).
However, lower percentages have also been reported in some series, which may be explained
by differences in the definition and diagnostics used, as well as differences in the duration
of follow up (17,38). The routine use of a biliary drain and postoperative cholangiography
allowed us not only to carefully identify and localize all biliary abnormalities, but also to include
minor or single strictures in otherwise asymptomatic patients. Routine cholangiography has
not always been used in previous studies. These factors may largely explain the differences in
the incidence of NAS reported in different series (9-18,20). In addition, we had a long follow-
up in our series with a median of almost 8 years. However, a limitation of this retrospective
single centre study could be different imaging modalities over the years and should be kept
in mind.
When all cases with NAS were studied as one group, independent from the severity and time
of occurrence after OLT, only PSC as the indication for transplantation, the type of preservation
solution and postoperative CMV infection could be identified as risk factors for NAS. The
higher incidence of NAS in patients transplanted for PSC (15,20,21) and patients who suffered
CMV infection postoperatively are in accordance with previous studies (19,36,37,39). Also the
54
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
more frequent occurrence of NAS in patients with a Roux-Y hepatico-jejunostomy has been
reported before and this can be explained by the more frequent use of this type of bile duct
reconstruction in patients transplanted for PSC, compared to patients transplanted for other
indications (20). The lower incidence of NAS in our series in livers which were preserved with
a low viscosity preservation solution is in agreement with previous reports (40). It has been
suggested that the peribiliary vascular plexus is better flushed out and better preserved when
low viscosity fluids are used compared with high viscosity fluids. These observations, however,
have not yet been confirmed to our knowledge in randomized controlled trials (41,42).
In contrast with previous studies, we were not able to identify an association between the
lengths of warm or cold ischemia time and the development of NAS when we analyzed all
grafts with NAS as one group, regardless the time of occurrence after OLT. Most previous
studies, however, had a short postoperative follow-up of less than one year, whereas in our
series the median follow-up was 7.9 years with an interquartile range of 4.2 to 12.6 years.
Although the cumulative incidence of NAS increased sharply within the first year, almost 50%
of all cases were detected beyond the first year after transplantation. Biologically it is not
plausible that preservation-related factors are still responsible for NAS that first present more
than one year after OLT. We therefore performed a second analysis comparing patients with
early (< 1 year after OLT) versus late (> 1 year after OLT) presentation of NAS. This analysis
showed significant associations between preservation-related risk factors, such as the length
of cold ischemia time and bile duct anastomotic leakage, and the occurrence of NAS early after
OLT. Ischemia reperfusion- and preservation injury-related variables are well described risk
factors for NAS, and include prolonged cold ischemia time (> 12 hours) or warm ischemia time
(> 60 min) and variables related to the efficacy of preservation of the peribiliary plexus, such
as viscosity and perfusion pressure of the preservation fluid (20,26,40). Moreover, the higher
incidence of NAS in liver transplantation from donors after cardiac death (non-heart-beating
donors) also strongly suggests an ischemia-related factor in the pathogenesis of NAS (43-45).
For many years, it has been policy in our center to keep the cold ischemia time as short as
possible and recipient operations usually start before the donor liver has arrived and as soon
as the liver has been judged transplantable by the surgical team performing the procurement
operation. In addition, the use of the piggyback technique has allowed us to shorten the warm
ischemia time during implantation, in comparison with conventional implantation (33,46). With
this policy we were able to keep the median cold and warm ischemia time below 12 hours
55
Chapter 3
and 60 min, respectively. Nevertheless, we could still identify cold ischemia time as one of the
most important discriminators of NAS occurring early after OLT.
Risk factors for the development of NAS late (> 1 year) after transplantation were a female to
male donor/recipient match, and PSC as the indication for transplantation. These variables
are not associated with preservation injury and suggest a more immunological pathogenesis
of NAS presenting late after OLT. An immunological origin of NAS has been suggested by
other investigators based on the relationship between NAS and ABO incompatibility, the
strong association with pre-existing diseases with a presumed autoimmune component (such
as PSC and autoimmune hepatitis), CMV infection, chronic rejection, but also with genetic
polymorphism of chemokines (17,20,28). It is very likely that recurrent PSC may have been
accountable for the occurrence of biliary lesions in some of the patients presenting with
NAS late after OLT. Based on radiological evaluation, however, recurrent PSC cannot be
distinguished from a late presentation of NAS. Although some of our patients fit well within the
definition of recurrent PSC as proposed by Graziadei et al. (47), more than half of our patients
who presented with NAS late after OLT were not transplanted for PSC.
Several studies have shown a lower survival rate for grafts from female donors transplanted in
male recipients. (48-51). Although some investigators have tried to explain this by differences
in estrogen receptor expression (49), reduced outcome for the female to male donor/
recipient match has also been described after OLT in children below 10 years of age (48).
This observation makes it less likely that a sex hormone-related pathogenesis is the only
explanation for the worse outcome of female livers into male recipients and immunological
processes have been suggested to play a role as well in other transplant settings (52).
Immunologically-mediated injury of the bile ducts resulting in NAS may be a direct result of
activated proinflammatory cytokines and influx of inflammatory cells. However, it cannot be
deducted from a clinical study like this whether this type of bile duct injury is (at least partially)
also caused by relative ischemia of the biliary epithelium due to immune-mediated obliterative
arteriopathy of the peribiliary vascular plexus (8,9,19). Further research in this area seems
warranted.
Very few studies to our knowledge have focused on the anatomical localization of NAS at the
time of first presentation. In the current series, over 80% of the NAS were localized around or
below the bifurcation of the CBD and less than 20% presented in the peripheral branches of
the biliary tree. Livers presenting with NAS more than one year after OLT had more frequently

56
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
involvement of the smaller and peripheral bile ducts of the liver. These differences in the
anatomical localization between NAS presenting early or late after OLT provide additional
support for differences in the pathogenesis of NAS depending on the time of presentation after
OLT. The critical relevance of arterial blood supply for the viability of the larger and extrahepatic
bile ducts is well described (53). This part of the biliary tree depends entirely on the arterial
peribiliary plexus which is perfused via the gastroduodenal artery and the hepatic artery.
During OLT, blood supply via the pancreatic head and the gastro-duodenal artery, supplying
the peribiliary plexus, is interrupted and the bile ducts become entirely depended on arterial
blood from the hepatic artery, making them more prone to hypoperfusion and ischemia. This
may explain the central localization of NAS presenting early after OLT. In addition, previous
studies have shown a large morphological and functional heterogeneity of different sized
intrahepatic bile ducts, providing an explanation why biliary lesions predominates in specific
sized bile ducts in various types of diseases affecting the biliary tree (54). This could also
be an explanation why immunologically-mediated NAS, presenting late after OLT, is more
pronounced at the level the smaller bile ducts.
In summary, by separating cases of NAS based on the time of presentation after transplantation,
we were able to identify significant differences in risk factors, indicating different pathogenic
mechanisms depending on the time of initial presentation. NAS presenting within the first
year after transplantation is strongly correlated with ischemia related risk factors, whereas
NAS presenting late, more than one year after OLT, is more associated with immunologically
related risk factors. These finding have implications for the development of new strategies to
prevent or treat NAS.
57
Chapter 3
Reference List
Starzl TE, Marchioro TL, Vonkaulla KN, Hermann G, Brittain RS, Waddell WR. Homotransplantation of the liver 1.
in humans. Surg Gynecol Obstet 1963; 117:659-676.
Lerut J, Gordon RD, Iwatsuki S, Esquivel CO, Todo S, Tzakis A et al. Biliary tract complications in human 2.
orthotopic liver transplantation. Transplantation 1987; 43:47-51.
Calne RY. A new technique for biliary drainage in orthotopic liver transplantation utilizing the gall bladder as a 3.
pedicle graft conduit between the donor and recipient common bile ducts. Ann Surg 1976; 184:605-609.
Buis CI, Hoekstra H, Verdonk RC, Porte RJ. Causes and consequences of ischemic-type biliary lesions after 4.
liver transplantation. J Hepatobiliary Pancreat Surg 2006; 13:517-524.
Verdonk RC, Buis CI, Porte RJ, Haagsma EB. Biliary complications after liver transplantation: a review. Scand 5.
J Gastroenterol Suppl 2006;89-101.
Zajko AB, Campbell WL, Logsdon GA, Bron KM, Tzakis A, Esquivel CO et al. Cholangiographic findings in 6.
hepatic artery occlusion after liver transplantation. AJR Am J Roentgenol 1987; 149:485-489.
Sanchez-Urdazpal L, Sterioff S, Janes C, Schwerman L, Rosen C, Krom RA. Increased bile duct complications 7.
in ABO incompatible liver transplant recipients. Transplant Proc 1991; 23(1 Pt 2):1440-1441.
Sanchez-Urdazpal L, Gores GJ, Ward EM, Maus TP, Wahlstrom HE, Moore SB et al. Ischemic-type biliary 8.
complications after orthotopic liver transplantation. Hepatology 1992; 16:49-53.
Sanchez Urdazpal L, Gores GJ, Ward EM, Maus TP, Buckel EG, Steers JL et al. Diagnostic features and clinical 9.
outcome of ischemic-type biliary. Hepatology 1993; 17:605-609.
Thethy S, Thomson BN, Pleass H, Wigmore SJ, Madhavan K, Akyol M et al. Management of biliary tract 10.
complications after orthotopic liver transplantation. Clin Transplant 2004; 18:647-653.
Sawyer RG, Punch JD. Incidence and management of biliary complications after 291 liver transplants following 11.
the introduction of transcystic stenting. Transplantation 1998; 66:1201-1207.
Turrion VS, Alvira LG, Jimenez M, Lucena JL, Nuno J, Pereira F et al. Management of the biliary complications 12.
associated with liver transplantation: 13 years of experience. Transplant Proc 1999; 31:2392-2393.
Rizk RS, McVicar JP, Emond MJ, Rohrmann CA, Jr., Kowdley KV, Perkins J et al. Endoscopic management 13.
of biliary strictures in liver transplant recipients: effect on patient and graft survival. Gastrointest Endosc 1998;
47:128-135.
Ward EM, Kiely MJ, Maus TP, Wiesner RH, Krom RA. Hilar biliary strictures after liver transplantation: 14.
cholangiography and percutaneous treatment. Radiology 1990; 177:259-263.
Campbell WL, Sheng R, Zajko AB, Abu-Elmagd K, Demetris AJ. Intrahepatic biliary strictures after liver 15.
transplantation. Radiology 1994; 191:735-740.
58
NAS after liver transplantation: risk factors for early versus late presentation Chapter 3
Feller RB, Waugh RC, Selby WS, Dolan PM, Sheil AG, McCaughan GW. Biliary strictures after liver 16.
transplantation: clinical picture, correlates and outcomes. J Gastroenterol Hepatol 1996; 11:21-25.
Rull R, Garcia Valdecasas JC, Grande L, Fuster J, Lacy AM, Gonzalez FX et al. Intrahepatic biliary lesions after 17.
orthotopic liver transplantation. Transpl Int 2001; 14:129-134.
Pascher A, Neuhaus P. Bile duct complications after liver transplantation. Transpl Int 2005; 18:627-642.18.
Colonna JO, Shaked A, Gomes AS, Colquhoun SD, Jurim O, McDiarmid SV et al. Biliary strictures complicating 19.
liver transplantation. Incidence, pathogenesis, management, and outcome. Ann Surg 1992; 216:344-350.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 20.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003; 3:885-890.
Sankary HN, McChesney L, Hart M, Foster P, Williams J. Identification of donor and recipient risk factors 21.
associated with nonanastomotic biliary strictures in human hepatic allografts. Transplant Proc 1993; 25:1964-
1967.
Geuken E, Visser D, Kuipers F, Blokzijl H, Leuvenink HG, de Jong KP et al. Rapid increase of bile salt secretion 22.
is associated with bile duct injury after human liver transplantation. J Hepatol 2004; 41:1017-1025.
Hertl M, Hertl MC, Kluth D, Broelsch CE. Hydrophilic bile salts protect bile duct epithelium during cold. Liver 23.
transplantation 2000; 6:207-212.
Hertl M, Harvey PR, Swanson PE, West DD, Howard TK, Shenoy S et al. Evidence of preservation injury to 24.
bile ducts by bile salts in the pig and its prevention by infusions of hydrophilic bile salts. Hepatology 1995;
21:1130-1137.
Hoekstra H, Porte RJ, Tian Y, Jochum W, Stieger B, Moritz W et al. Bile salt toxicity aggravates cold ischemic 25.
injury of bile ducts after liver transplantation in Mdr2+/- mice. Hepatology 2006; 43:1022-1031.
Moench C, Moench K, Lohse AW, Thies J, Otto G. Prevention of ischemic-type biliary lesions by arterial back-26.
table pressure perfusion. Liver Transpl 2003; 9:285-289.
Li S, Stratta RJ, Langnas AN, Wood RP, Marujo W, Shaw BW, Jr. Diffuse biliary tract injury after orthotopic liver 27.
transplantation. Am J Surg 1992; 164:536-540.
Moench C, Uhrig A, Lohse AW, Otto G. CC chemokine receptor 5delta32 polymorphism-a risk factor for 28.
ischemic-type biliary lesions following orthotopic liver transplantation. Liver Transpl 2004; 10:434-439.
Graziadei IW, Schwaighofer H, Koch R, Nachbaur K, Koenigsrainer A, Margreiter R et al. Long-term outcome of 29.
endoscopic treatment of biliary strictures after liver transplantation. Liver Transpl 2006; 12:718-725.
Verdonk RC, Buis CI, van der Jagt EJ, Gouw ASH, Limburg AJ, Slooff MJH, Kleibeuker JH, Porte RJ, Haagsma 30.
EB. Non-anastomotic biliary strictures after adult liver transplantation part two: Management, outcome and risk
59
Chapter 3
factors for disease progression. Liver Transpl. 2007;13:725-32.
Starzl TE, Hakala TR, Shaw BW, Jr., Hardesty RL, Rosenthal TJ, Griffith BP et al. A flexible procedure for 31.
multiple cadaveric organ procurement. Surg Gynecol Obstet 1984; 158:223-230.
Miyamoto S, Polak WG, Geuken E, Peeters PM, de Jong KP, Porte RJ et al. Liver transplantation with 32.
preservation of the inferior vena cava. A comparison of conventional and piggyback techniques in adults. Clin
Transplant 2004; 18:686-693.
Polak WG, Miyamoto S, Nemes BA, Peeters PM, de Jong KP, Porte RJ et al. Sequential and simultaneous 33.
revascularization in adult orthotopic piggyback liver transplantation. Liver Transpl 2005; 11:934-940.
Feith MP, Klompmaker IJ, Maring JK, Peeters PM, van den Berg AP, de Jong KP et al. Biliary reconstruction 34.
during liver transplantation in patients with primary sclerosing cholangitis. Transplant Proc 1997; 29:560-561.
Verdonk RC, Buis CI, Porte RJ, Van der Jagt EJ, Limburg AJ, van den Berg AP et al. Anastomotic biliary 35.
strictures after liver transplantation: Causes and consequences. Liver Transpl 2006; 12:726-735.
Halme L, Hockerstedt K, Lautenschlager I. Cytomegalovirus infection and development of biliary complications 36.
after liver transplantation. Transplantation 2003; 75:1853-1858.
Kowdley KV, Fawaz KA, Kaplan MM. Extrahepatic biliary stricture associated with cytomegalovirus in a liver 37.
transplant recipient. Transpl Int 1996; 9:161-163.
Torras J, Llado L, Figueras J, Ramos E, Lama C, Fabregat J et al. Biliary tract complications after liver 38.
transplantation: type, management, and outcome. Transplant Proc 1999; 31:2406.
Dolmatch BL, Laing FC, Ferderle MP, Jeffrey RB, Cello J. AIDS-related cholangitis: radiographic findings in nine 39.
patients. Radiology 1987; 163:313-316.
Pirenne J, Van Gelder F, Coosemans W, Aerts R, Gunson B, Koshiba T et al. Type of donor aortic preservation 40.
solution and not cold ischemia time is a major determinant of biliary strictures after liver transplantation. Liver
Transpl 2001; 7:540-545.
Canelo R, Hakim NS, Ringe B. Experience with hystidine tryptophan ketoglutarate versus University Wisconsin 41.
preservation solutions in transplantation. Int Surg 2003; 88:145-151.
Cavallari A, Cillo U, Nardo B, Filipponi F, Gringeri E, Montalti R et al. A multicenter pilot prospective study 42.
comparing Celsior and University of Wisconsin preserving solutions for use in liver transplantation. Liver
Transpl 2003; 9:814-821.
Abt P, Crawford M, Desai N, Markmann J, Olthoff K, Shaked A. Liver transplantation from controlled non-heart-43.
beating donors: an increased incidence of biliary complications. Transplantation 2003; 75:1659-1663.
D’alessandro AM, Hoffmann RM, Knechtle SJ, Odorico JS, Becker YT, Musat A et al. Liver transplantation from 44.
controlled non-heart-beating donors. Surgery 2000; 128:579-588.
Otero A, Gomez-Gutierrez M, Suarez F, Arnal F, Fernandez-Garcia A, Aguirrezabalaga J et al. Liver transplantation 45.
from Maastricht category 2 non-heart-beating donors. Transplantation 15[76], 1068-1073. 2005.
Ref Type: Abstract46.
Miyamoto S, Polak WG, Geuken E, Peeters PM, de Jong KP, Porte RJ et al. Liver transplantation with 47.
preservation of the inferior vena cava. A comparison of conventional and piggyback techniques in adults. Clin
Transplant 2004; 18:686-693.
Graziadei IW, Wiesner RH, Batts KP, Marotta PJ, Larusso NF, Porayko MK et al. Recurrence of primary 48.
sclerosing cholangitis following liver transplantation. Hepatology 1999; 29:1050-1056.
Francavilla R, Hadzic N, Heaton ND, Rela M, Baker AJ, Dhawan A et al. Gender matching and outcome after 49.
pediatric liver transplantation. Transplantation 1998; 66:602-605.
Kahn D, Gavaler JS, Makowka L, van Thiel DH. Gender of donor influences outcome after orthotopic liver 50.
transplantation in adults. Dig Dis Sci 1993; 38:1485-1488.
Brooks BK, Levy MF, Jennings LW, Abbasoglu O, Vodapally M, Goldstein RM et al. Influence of donor and 51.
recipient gender on the outcome of liver transplantation. Transplantation 1996; 62:1784-1787.
Marino IR, Doyle HR, Aldrighetti L, Doria C, McMichael J, Gayowski T et al. Effect of donor age and sex on the 52.
outcome of liver transplantation. Hepatology 1995; 22:1754-1762.
Sato M, Gutierrez C, Kaneda H, Liu M, Waddell TK, Keshavjee S. The effect of gender combinations on outcome 53.
in human lung transplantation: the International Society of Heart and Lung Transplantation Registry experience.
J Heart Lung Transplant 2006; 25:634-637.
Deltenre P, Valla DC. Ischemic cholangiopathy. J Hepatol 2006; 44:806-817.54.
Marzioni M, Glaser SS, Francis H, Phinizy JL, Lesage G, Alpini G. Functional heterogeneity of cholangiocytes. 55.
Semin Liver Dis 2002; 22:227-240.
Non-anastomotic biliary strictures after liver transplantation part 2: Management, outcome and risk factors for disease progression4
Liver Transpl 2007; 13:725-732
Robert C VerdonkCarlijn I Buis
Eric J Van der JagtAnnette SH Gouw
Abraham J LimburgMaarten JH SlooffJan H Kleibeuker
Robert J PorteElizabeth B Haagsma
62
NAS after liver transplantation: risk factors for disease progression Chapter 4
Abstract
Non-anastomotic biliary strictures (NAS) after orthotopic liver transplantation (OLT) are
associated with high retransplant rates. The aim of the present study was to describe the
treatment, and identify risk factors for radiological progression of bile duct abnormalities,
recurrent cholangitis, biliary cirrhosis and retransplantation in patients with NAS. We
retrospectively studied 81 cases of NAS. Strictures were classified according to severity and
location. Management of strictures was recorded. Possible prognostic factors for bacterial
cholangitis, radiological progression of strictures, development of severe fibrosis/cirrhosis and
graft and patient survival were evaluated. Median follow up after OLT was 7.9 years. NAS
were most prevalent in the extrahepatic bile duct. Twenty-eight patients (35%) underwent
some kind of interventional treatment, leading to a significant improvement in biochemistry.
Progression of disease was noted in 68% of cases with radiological follow-up. Radiological
progression was more prevalent in patients with early NAS and one or more episodes of
bacterial cholangitis. Recurrent bacterial cholangitis (> 3 episodes) was more prevalent in
patients with a hepaticojejunostomy. Severe fibrosis or cirrhosis developed in 23 cases,
especially in cases with biliary abnormalities in the periphery of the liver. Graft but not patient
survival was influenced by the presence of NAS. Thirteen patients (16%) were re-transplanted
for NAS. In conclusion, especially patients with a hepatico-jejunostomy, those with an early
diagnosis of NAS, and those with NAS presenting at the level of the peripheral branches of
the biliary tree, are at risk for progressive disease with severe outcome.
63
Chapter 4
Introduction
Biliary complications are common after orthotopic liver transplantation (OLT). Biliary strictures
and leakage of bile are most frequently encountered. Strictures are often referred to as
anastomotic or non-anastomotic. Non-anastomotic strictures (NAS) are generally considered
to be the most troublesome type of biliary complications after liver transplantation, with a graft
loss rate of up to 46% after two years (1).
In a separate study we have analyzed the radiological characteristics of NAS at the time
of diagnosis and risk factors for the development of NAS (2). In this study, we were able to
identify significant differences in risk factors for the development of NAS depending on the
time of initial presentation. In addition, large variations in anatomical localization and severity
of NAS at the time of presentation were found, indicating that NAS is not a single disease,
but rather a group of biliary abnormalities with different pathogenesis. It is unknown whether
the different subtypes of NAS are also associated with difference in outcome and prognosis.
Previous studies concerning the treatment and outcome of NAS have not considered different
types of NAS as relevant subgroups and risk factors for radiological and clinical progression
once the diagnosis has been established have not been identified so far.
The aim of the present work was to study NAS in a large cohort of liver transplant recipients
with long-term follow up and to describe the results of treatment. In addition, we aimed to
identify risk factors for radiological progression of bile duct abnormalities, recurrent cholangitis,
biliary cirrhosis and re-transplantation.
Patients and Methods
Patients
Between January 1986 and May 2003 a total number of 717 liver transplants were performed
in 639 patients at the University Medical Center Groningen. After exclusion of children (<18
years), and patients with NAS caused by hepatic artery thrombosis, 487 transplants in 428 adult
patients were included in this study. Follow-up was until November 1st 2005, allowing a minimal
follow up time after transplantation of 2.5 years. Eighty-one grafts with NAS were identified in
77 patients as described previously (2). In short, all post-transplant radiological material of the
biliary tree was reviewed by a radiologist blinded to the clinical data (EJ). Anatomical extent
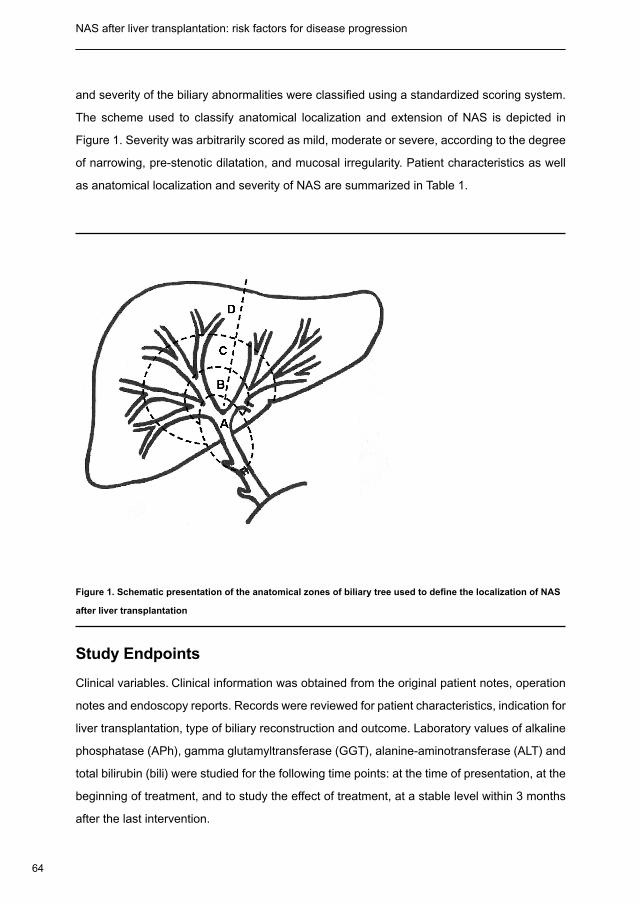
64
NAS after liver transplantation: risk factors for disease progression Chapter 4
and severity of the biliary abnormalities were classified using a standardized scoring system.
The scheme used to classify anatomical localization and extension of NAS is depicted in
Figure 1. Severity was arbitrarily scored as mild, moderate or severe, according to the degree
of narrowing, pre-stenotic dilatation, and mucosal irregularity. Patient characteristics as well
as anatomical localization and severity of NAS are summarized in Table 1.
Figure 1. Schematic presentation of the anatomical zones of biliary tree used to define the localization of NAS
after liver transplantation
Study Endpoints
Clinical variables. Clinical information was obtained from the original patient notes, operation
notes and endoscopy reports. Records were reviewed for patient characteristics, indication for
liver transplantation, type of biliary reconstruction and outcome. Laboratory values of alkaline
phosphatase (APh), gamma glutamyltransferase (GGT), alanine-aminotransferase (ALT) and
total bilirubin (bili) were studied for the following time points: at the time of presentation, at the
beginning of treatment, and to study the effect of treatment, at a stable level within 3 months
after the last intervention.
65
Chapter 4
Management of NAS. Information about interventions was obtained from the patient notes.
Endoscopic retrograde cholangiopancreaticography (ERCP), percutaneous transhepatic
cholangiodrainage (PTCD), surgery, and medical therapies (ursodeoxycholic acid, antibiotics)
were noted. When ERCP or PTCD with interventions had been performed, the number of
sessions was registered, as well as technical details of the procedure. In case of surgical
treatment, the type of surgical procedure was recorded. Complications of treatment
were registered. Radiological progression. To study radiological progression of NAS all
cholangiograms (drain cholangiography, PTCD, MRCP, ERCP) that were performed after
transplantation were reviewed by a single radiologist (EJ), blinded to clinical information,
and using the same scoring system as described above. Bacterial cholangitis. Bacterial
cholangitis episodes were noted. Bacterial cholangitis was defined as an episode of liver
test abnormalities combined with fever for which antibiotic treatment was given. Recurrent
cholangitis was defined as three or more episodes of cholangitis.
Table 1. Patient Characteristics and Possible Prognostic Factors
Characteristic N (% or range)
Age at time of transplantation (median, range)Gender (M/F)Primary liver disease: PSC / OtherBiliary reconstruction: Duct-to-duct / Roux-en-YRe-transplant graftIBD before OLTIBD after OLTEarly NAS (<1 year after OLT)Extent of NAS at presentation* Zone AZone BZone CZone DSeverity of NAS at presentation* Mild / Moderate / SevereType of immunosuppresionPrednisone / azathioprine / cyclosporinePrednisone / tacrolimusPrednisone / tacrolimus / azathioprineOther
46 (18-66)40 / 3725 (31%) / 56 (69%)62 (77%) / 19 (23%)10 (12%)13 (16%)14 (17%)50 (62%)
66 (81%)52 (67%)33 (42%)15 (19%)
43 / 28 / 7
51 (63%)8 (10%)6 (7%)16 (20%)
* Data on patients with radiological material available (n=78)

66
NAS after liver transplantation: risk factors for disease progression Chapter 4
Pathology. To see whether NAS led to biliary fibrosis of cirrhosis, the most recent available
pathology specimen of the liver of all patients was retrieved and scored by a liver pathologist
(AG) blinded to the clinical context. Liver fibrosis was scored as absent, minimal, moderate or
severe, with severe being either extensive bridging fibrosis or cirrhosis.
Survival. Graft and patient survival were analyzed by comparing patients with NAS to controls
matched for age and period of transplantation. Controls also had to be alive at the time of
diagnosis of NAS in the patients with NAS. Causes of death and graft failure were noted.
Prognostic factors. Possible prognostic factors for several outcome parameters are listed
in Table 1. The definition of inflammatory bowel disease (IBD) after liver transplantation was
an episode of abdominal pain and/or diarrhea, with inflammation seen during endoscopy,
confirmed pathologically and after exclusion of infectious causes. In addition the following
factors were included in the analysis: (type of) interventional treatment, the presence of
radiological progression, the occurrence of bacterial cholangitis, the maintenance use of
antibiotics, and the use of ursodeoxycholic acid.
Statistical Methods
Data were analyzed using SPSS 12.0 software. Comparison between groups was made using
the Chi-square test for categorical variables and the Mann-Whitney U test for continuous
variables. When indicated, a risk estimate was made calculating the relative risk (RR) and
confidence intervals using a Chi-Square test. Comparison of survival between groups
was made using Kaplan-Meier statistics with a log-rank test. A p-value of 0.05 or less was
considered to indicate statistical significance.
Ethical statement
Retrospective studies are approved by the institutional ethical committee.
Results
NAS were present in 81 grafts of 77 patients. In four patients NAS occurred in both a first and
second graft. Apart from NAS, a concomitant anastomotic stricture was diagnosed at some
point in the postoperative course in 21 patients. Median follow-up after the diagnosis of NAS
was 6.0 years (1.0-17.0). Median follow-up after OLT was 7.9 years (range 1.0-17.1). The
biliary reconstruction was duct-to-duct in 62 cases (77%), and a hepaticojejunostomy with
Roux-en-Y deviation in 19 cases (23%).
67
Chapter 4
Which Modalities Were Used for Treatment of NAS?
Interventions. Twenty eight patients (35%) were treated with ERCP, PTCD, surgery, or a
combination of these. Thirteen patients underwent one or more sessions of ERCP. Dilatation
was performed in all cases; in 12 also one or more stents were placed. Complications occurred
in 7, mostly cholangitis. No severe complications were observed. The median number of
therapeutic ERCP’s in these patients was 3 (range 1-11).
Seven patients underwent PTCD. Four patients underwent both ERCP and PTCD. In patients
treated with PTCD dilatation and stenting was performed in all cases. In two cases an
expandable metal stent was placed. The median number of therapeutic PTCD sessions in
these patients was 3 (range 1-6). A minor complication occurred in 2 cases.
In the end, eight patients underwent surgery for NAS, four after previous ERCP or PTCD. The
surgical procedure was conversion of duct-to-duct anastomosis to a hepatico-jejunostomy in
five patients, and revision of a previous hepatico-jejunostomy in three. Patients with a dilated
biliary tree were treated surgically more often than those without dilatation (20% vs. 2%,
p=0.01). All concomitant anastomotic strictures were successfully treated with success by
ERCP (n=13), PTCD (n=5), surgery (n=1) or a combination of these (n=2).
Ursodeoxycholic acid. Seventy-one patients (88%) were treated with long-term ursodeoxycholic
acid, mostly at a dose of 600 mg b.i.d.
Biochemical response to interventions. When the biochemical response within 3 months after
completion of interventional treatment was studied, significant improvements in serum ALT
(median 65 U/l vs. 36 U/l, p=0.015), bilirubin (median 46 µmol/l vs. 23 µmol/l, p<0.000) and
GGT (median 360 U/l vs. 125 U/l, p=0.014) was noted, compared to pretreatment values. No
significant improvement in APh was seen. In 8 of the 28 patients no biochemical response to
treatment was seen.
Is NAS a Progressive Disease?
Radiological progression. Material for retrospective radiological evaluation of NAS at
presentation was available in 78 of the 81 transplants (96%). In 59 cases (80%) follow-up
cholangiography was performed and available for determination of progression of the biliary
abnormalities. The median time between the diagnostic and last cholangiography was 1.7
years (range 0.1 – 11.7). Progression of the severity of biliary abnormalities was observed
in 28 (42%) of the 59 grafts with follow up cholangiography. At the time of diagnosis, the
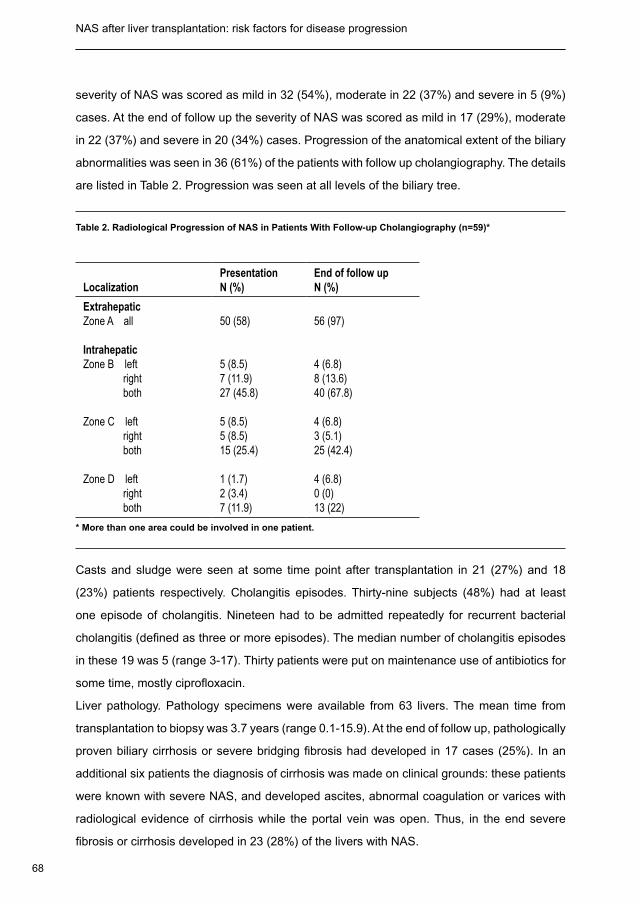
68
NAS after liver transplantation: risk factors for disease progression Chapter 4
severity of NAS was scored as mild in 32 (54%), moderate in 22 (37%) and severe in 5 (9%)
cases. At the end of follow up the severity of NAS was scored as mild in 17 (29%), moderate
in 22 (37%) and severe in 20 (34%) cases. Progression of the anatomical extent of the biliary
abnormalities was seen in 36 (61%) of the patients with follow up cholangiography. The details
are listed in Table 2. Progression was seen at all levels of the biliary tree.
Table 2. Radiological Progression of NAS in Patients With Follow-up Cholangiography (n=59)*
LocalizationPresentationN (%)
End of follow upN (%)
ExtrahepaticZone A all
IntrahepaticZone B left right both
Zone C left right both
Zone D left right both
50 (58)
5 (8.5)7 (11.9)27 (45.8)
5 (8.5)5 (8.5)15 (25.4)
1 (1.7)2 (3.4)7 (11.9)
56 (97)
4 (6.8)8 (13.6)40 (67.8)
4 (6.8)3 (5.1)25 (42.4)
4 (6.8)0 (0)13 (22)
* More than one area could be involved in one patient.
Casts and sludge were seen at some time point after transplantation in 21 (27%) and 18
(23%) patients respectively. Cholangitis episodes. Thirty-nine subjects (48%) had at least
one episode of cholangitis. Nineteen had to be admitted repeatedly for recurrent bacterial
cholangitis (defined as three or more episodes). The median number of cholangitis episodes
in these 19 was 5 (range 3-17). Thirty patients were put on maintenance use of antibiotics for
some time, mostly ciprofloxacin.
Liver pathology. Pathology specimens were available from 63 livers. The mean time from
transplantation to biopsy was 3.7 years (range 0.1-15.9). At the end of follow up, pathologically
proven biliary cirrhosis or severe bridging fibrosis had developed in 17 cases (25%). In an
additional six patients the diagnosis of cirrhosis was made on clinical grounds: these patients
were known with severe NAS, and developed ascites, abnormal coagulation or varices with
radiological evidence of cirrhosis while the portal vein was open. Thus, in the end severe
fibrosis or cirrhosis developed in 23 (28%) of the livers with NAS.
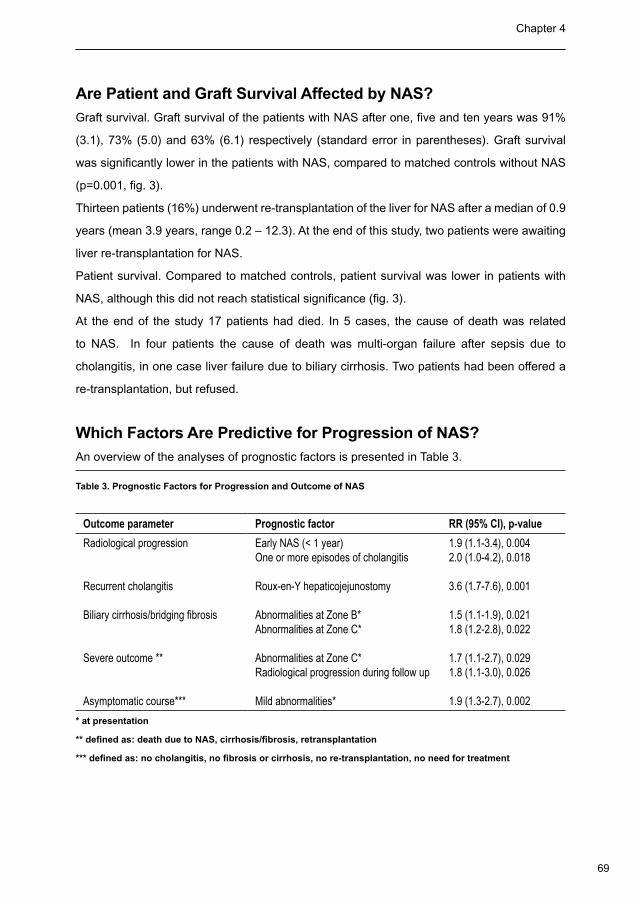
69
Chapter 4
Are Patient and Graft Survival Affected by NAS?
Graft survival. Graft survival of the patients with NAS after one, five and ten years was 91%
(3.1), 73% (5.0) and 63% (6.1) respectively (standard error in parentheses). Graft survival
was significantly lower in the patients with NAS, compared to matched controls without NAS
(p=0.001, fig. 3).
Thirteen patients (16%) underwent re-transplantation of the liver for NAS after a median of 0.9
years (mean 3.9 years, range 0.2 – 12.3). At the end of this study, two patients were awaiting
liver re-transplantation for NAS.
Patient survival. Compared to matched controls, patient survival was lower in patients with
NAS, although this did not reach statistical significance (fig. 3).
At the end of the study 17 patients had died. In 5 cases, the cause of death was related
to NAS. In four patients the cause of death was multi-organ failure after sepsis due to
cholangitis, in one case liver failure due to biliary cirrhosis. Two patients had been offered a
re-transplantation, but refused.
Which Factors Are Predictive for Progression of NAS?
An overview of the analyses of prognostic factors is presented in Table 3.
Table 3. Prognostic Factors for Progression and Outcome of NAS
Outcome parameter Prognostic factor RR (95% CI), p-value
Radiological progression
Recurrent cholangitis
Biliary cirrhosis/bridging fibrosis
Severe outcome **
Asymptomatic course***
Early NAS (< 1 year)One or more episodes of cholangitis
Roux-en-Y hepaticojejunostomy
Abnormalities at Zone B*Abnormalities at Zone C*
Abnormalities at Zone C*Radiological progression during follow up
Mild abnormalities*
1.9 (1.1-3.4), 0.0042.0 (1.0-4.2), 0.018
3.6 (1.7-7.6), 0.001
1.5 (1.1-1.9), 0.0211.8 (1.2-2.8), 0.022
1.7 (1.1-2.7), 0.0291.8 (1.1-3.0), 0.026
1.9 (1.3-2.7), 0.002
* at presentation
** defined as: death due to NAS, cirrhosis/fibrosis, retransplantation
*** defined as: no cholangitis, no fibrosis or cirrhosis, no re-transplantation, no need for treatment
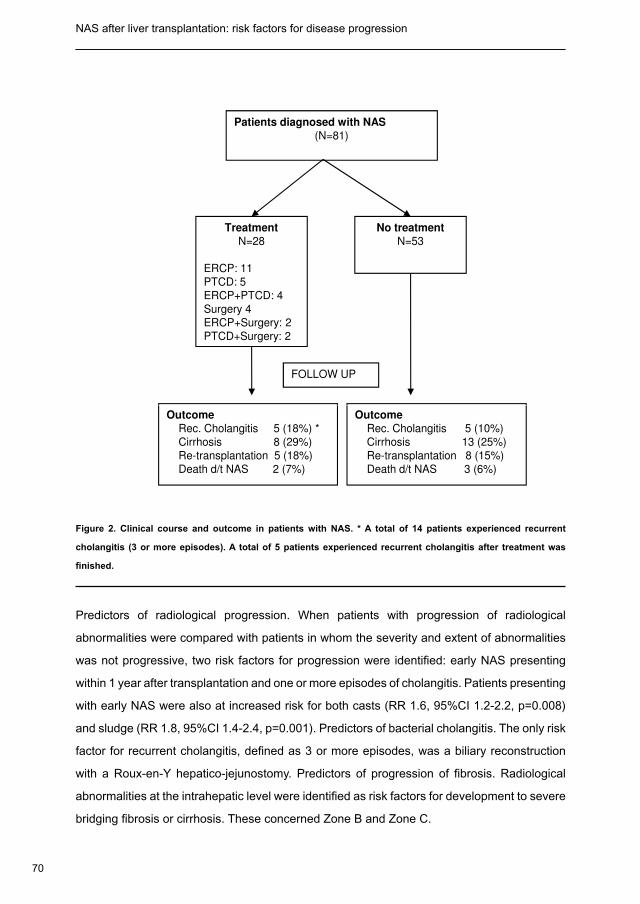
70
NAS after liver transplantation: risk factors for disease progression Chapter 4
Patients diagnosed with NAS
(N=81)
Treatment
N=28
ERCP: 11
PTCD: 5
ERCP+PTCD: 4
Surgery 4
ERCP+Surgery: 2
PTCD+Surgery: 2
No treatment
N=53
FOLLOW UP
Outcome
Rec. Cholangitis 5 (18%) *
Cirrhosis 8 (29%)
Re-transplantation 5 (18%)
Death d/t NAS 2 (7%)
Outcome
Rec. Cholangitis 5 (10%)
Cirrhosis 13 (25%)
Re-transplantation 8 (15%)
Death d/t NAS 3 (6%)
Figure 2. Clinical course and outcome in patients with NAS. * A total of 14 patients experienced recurrent
cholangitis (3 or more episodes). A total of 5 patients experienced recurrent cholangitis after treatment was
finished.
Predictors of radiological progression. When patients with progression of radiological
abnormalities were compared with patients in whom the severity and extent of abnormalities
was not progressive, two risk factors for progression were identified: early NAS presenting
within 1 year after transplantation and one or more episodes of cholangitis. Patients presenting
with early NAS were also at increased risk for both casts (RR 1.6, 95%CI 1.2-2.2, p=0.008)
and sludge (RR 1.8, 95%CI 1.4-2.4, p=0.001). Predictors of bacterial cholangitis. The only risk
factor for recurrent cholangitis, defined as 3 or more episodes, was a biliary reconstruction
with a Roux-en-Y hepatico-jejunostomy. Predictors of progression of fibrosis. Radiological
abnormalities at the intrahepatic level were identified as risk factors for development to severe
bridging fibrosis or cirrhosis. These concerned Zone B and Zone C.
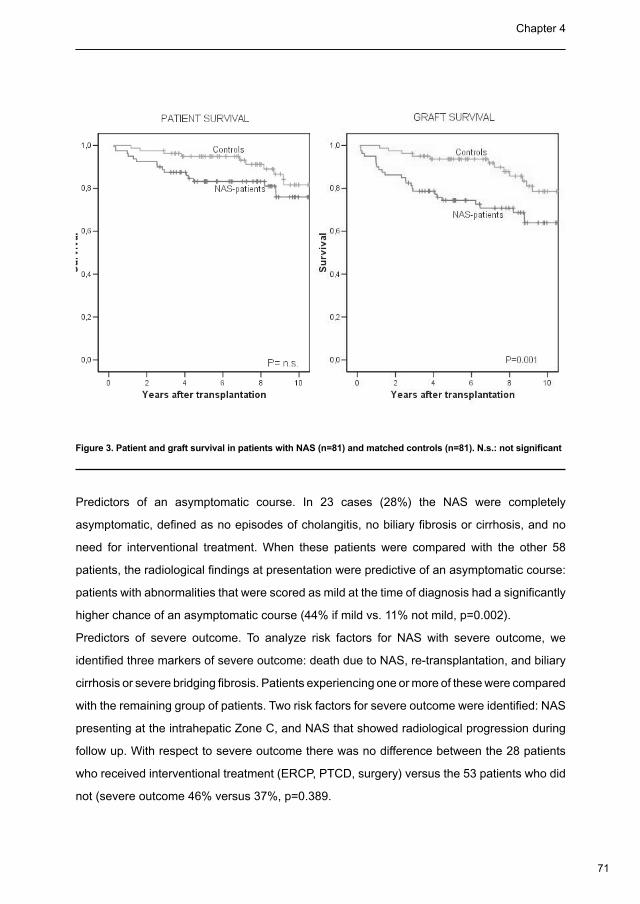
71
Chapter 4
Patients diagnosed with NAS
(N=81)
Treatment
N=28
ERCP: 11
PTCD: 5
ERCP+PTCD: 4
Surgery 4
ERCP+Surgery: 2
PTCD+Surgery: 2
No treatment
N=53
FOLLOW UP
Outcome
Rec. Cholangitis 5 (18%) *
Cirrhosis 8 (29%)
Re-transplantation 5 (18%)
Death d/t NAS 2 (7%)
Outcome
Rec. Cholangitis 5 (10%)
Cirrhosis 13 (25%)
Re-transplantation 8 (15%)
Death d/t NAS 3 (6%)
Figure 2. Clinical course and outcome in patients with NAS. * A total of 14 patients experienced recurrent
cholangitis (3 or more episodes). A total of 5 patients experienced recurrent cholangitis after treatment was
finished.
Predictors of radiological progression. When patients with progression of radiological
abnormalities were compared with patients in whom the severity and extent of abnormalities
was not progressive, two risk factors for progression were identified: early NAS presenting
within 1 year after transplantation and one or more episodes of cholangitis. Patients presenting
with early NAS were also at increased risk for both casts (RR 1.6, 95%CI 1.2-2.2, p=0.008)
and sludge (RR 1.8, 95%CI 1.4-2.4, p=0.001). Predictors of bacterial cholangitis. The only risk
factor for recurrent cholangitis, defined as 3 or more episodes, was a biliary reconstruction
with a Roux-en-Y hepatico-jejunostomy. Predictors of progression of fibrosis. Radiological
abnormalities at the intrahepatic level were identified as risk factors for development to severe
bridging fibrosis or cirrhosis. These concerned Zone B and Zone C.
Figure 3. Patient and graft survival in patients with NAS (n=81) and matched controls (n=81). N.s.: not significant
Predictors of an asymptomatic course. In 23 cases (28%) the NAS were completely
asymptomatic, defined as no episodes of cholangitis, no biliary fibrosis or cirrhosis, and no
need for interventional treatment. When these patients were compared with the other 58
patients, the radiological findings at presentation were predictive of an asymptomatic course:
patients with abnormalities that were scored as mild at the time of diagnosis had a significantly
higher chance of an asymptomatic course (44% if mild vs. 11% not mild, p=0.002).
Predictors of severe outcome. To analyze risk factors for NAS with severe outcome, we
identified three markers of severe outcome: death due to NAS, re-transplantation, and biliary
cirrhosis or severe bridging fibrosis. Patients experiencing one or more of these were compared
with the remaining group of patients. Two risk factors for severe outcome were identified: NAS
presenting at the intrahepatic Zone C, and NAS that showed radiological progression during
follow up. With respect to severe outcome there was no difference between the 28 patients
who received interventional treatment (ERCP, PTCD, surgery) versus the 53 patients who did
not (severe outcome 46% versus 37%, p=0.389.
72
NAS after liver transplantation: risk factors for disease progression Chapter 4
Discussion
NAS or intrahepatic biliary strictures are a common and often troublesome complication after
liver transplantation. Although previous studies on this subject differ markedly concerning
methodology and results, a high incidence of retransplantation has been reported almost
uniformly, as well as the need for frequent biliary interventions and admissions (3-5). In the
present study, we found a relatively high incidence of NAS compared to previous reports.
Whereas most large series report an incidence of NAS of 5-10% (6-8), we found that 17% of
patients were diagnosed with NAS at some point after OLT. Most likely, this difference is due
to the fact that we defined any type of biliary stricture other than anastomotic strictures as
NAS. In adition, postoperative cholangiography via the biliary drain has been routine practice
in our center. This allowed us to identify a large number of cases without any persisting clinical
signs of biliary disease (23 cases, 28%). This is also reflected by the rather low number of
retransplantations (16%) compared to previous reports from other centers. Another possible
explanation is the large number of patients transplanted for PSC (17%) and relatively low
number transplanted for viral disease (16%) in our center. PSC is a known risk factor for the
development of NAS (9-12).
From the present material it becomes clear that NAS after liver transplantation is not just one
disease, but a spectrum of abnormalities, ranging from slight, localized mucosal irregularity
to extensive and diffuse biliary strictures. Possibly, not all areas of non-anastomotic bile duct
narrowing are due to a fibrotic type of stricture (13). We thus aimed to identify from this diverse
group of NAS those cases that would progress to a clinically relevant or progressive disease.
We found radiological progression in 68% of our patients with cholangiographic follow-up.
Most likely, this number is lower for the entire group of patients with NAS, since those patients
without radiological follow-up probably did not have marked progression. Interestingly, NAS
presenting early after transplantation had a higher risk of progression. Previous investigators
have also mentioned a more severe course of disease in patients with NAS presenting
early after transplantation (14-16). Besides a higher risk of radiological progression, these
cases also showed a significantly higher risk for the development of casts and sludge. These
differences are probably due to a different pathogenesis of NAS presenting early or late after
transplantation, as has been described by Buis et al. earlier in this journal.
The most critical clinical consequences of NAS are recurrent cholangitis and biliary cirrhosis.
73
Chapter 4
Both may necessitate re-transplantation. We found recurrent cholangitis (arbitrarily defined as
three or more episodes) in 19 of our patients, despite treatment with maintenance therapy with
antibiotics in most patients. The only risk factor for recurrent cholangitis that was identified
was the presence of a hepaticojejunostomy instead of a duct-to-duct anastomosis. Most likely,
this type of biliary reconstruction leads to reflux of bacteria into the biliary tree, as has been
shown in animal models (17). In a patient that is immunosuppressed and has diminished flow
of bile due to NAS, it is foreseeable that this situation will lead to bacterial colonization of the
bile ducts and repeated episodes of cholangitis.
Biliary cirrhosis is the ‘end-point’ of long-standing NAS. We found biliary cirrhosis or severe fibrosis
in 23 of our cases (28%). At the end of follow up, nine of these 23 (39%) were re-transplanted.
Interestingly, the two risk factors for development of biliary cirrhosis were strictures at the level
of the segmental (Zone B) and sub-segmental (Zone C) branches. Apparently, these strictures
cause more long-term damage to the liver than more centrally located lesions. This may be due
to a number of factors. Perhaps, this type of NAS has a different pathogenesis than the more
‘proximal’ type of NAS, leading to ongoing biliary damage. Another possible explanation is that
these abnormalities are less amenable to treatment. Knowing that strictures at the site of the
segmental and sub-segmental branches are a risk factor for biliary cirrhosis, one can make an
estimate of the risk for progressive disease at the time of diagnosis.
When biliary cirrhosis, retransplantation and death due to NAS were combined to define serious
disease, strictures at the level of the subsegmental branches (Zone C) and radiological progression
of strictures were identified as significant risk factors. Thus, one can use these characteristics to
define patients with a higher risk of serious disease in the future.
Although we did see NAS-related mortality in our series, overall patient survival was not significantly
affected. This corresponds to previous studies on this subject (18-21). Graft survival however was
impaired compared to matched controls (73% vs. 94% after five years). This is not a surprising
finding. It is not possible from our results to conclude whether or not treatment for NAS prevented
re-transplantation in a number of cases. Although the number of re-transplantations was similar
in patients with and without endoscopic, percutaneous or surgical therapy; we do not know
what these numbers would have been like without treatment. Previously, others have described
successful treatment of NAS with a number of modalities (22-26).
We did not study the success of treatment in these patients, since the group of patients
treated with ERCP, PTCD or surgery is rather small (28 cases), heterogeneous concerning
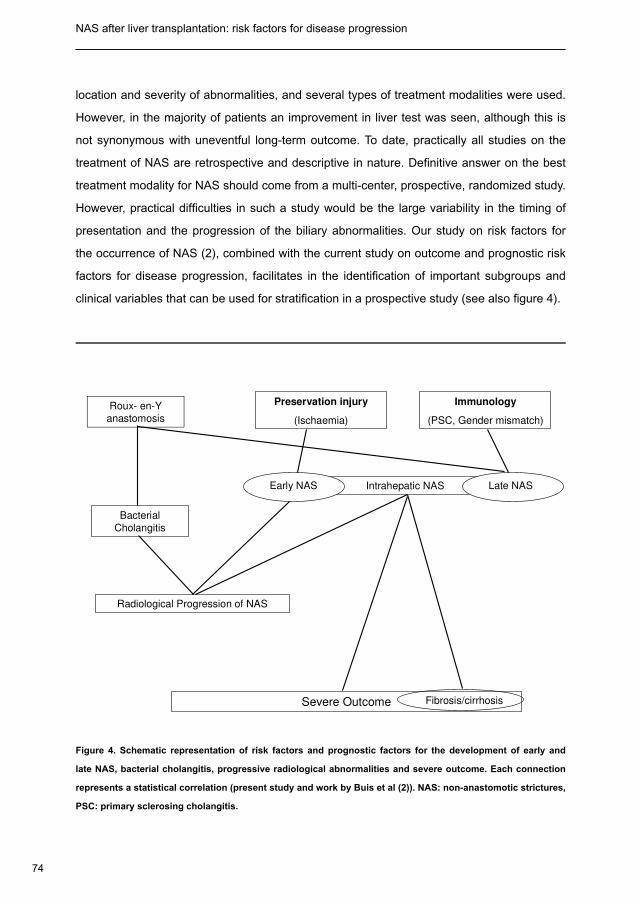
74
NAS after liver transplantation: risk factors for disease progression Chapter 4
location and severity of abnormalities, and several types of treatment modalities were used.
However, in the majority of patients an improvement in liver test was seen, although this is
not synonymous with uneventful long-term outcome. To date, practically all studies on the
treatment of NAS are retrospective and descriptive in nature. Definitive answer on the best
treatment modality for NAS should come from a multi-center, prospective, randomized study.
However, practical difficulties in such a study would be the large variability in the timing of
presentation and the progression of the biliary abnormalities. Our study on risk factors for
the occurrence of NAS (2), combined with the current study on outcome and prognostic risk
factors for disease progression, facilitates in the identification of important subgroups and
clinical variables that can be used for stratification in a prospective study (see also figure 4).
Roux- en-Y
anastomosis
Preservation injury
(Ischaemia)
Immunology
(PSC, Gender mismatch)
Intrahepatic NASEarly NAS Late NAS
Bacterial
Cholangitis
Radiological Progression of NAS
Severe Outcome Fibrosis/cirrhosis
Figure 4. Schematic representation of risk factors and prognostic factors for the development of early and
late NAS, bacterial cholangitis, progressive radiological abnormalities and severe outcome. Each connection
represents a statistical correlation (present study and work by Buis et al (2)). NAS: non-anastomotic strictures,
PSC: primary sclerosing cholangitis.

75
Chapter 4
In conclusion, non-anastomotic biliary strictures are a common complication after orthotopic
liver transplantation. The radiological and clinical picture of NAS shows a spectrum ranging
from minor abnormalities without any symptoms to severe strictures eventually leading to
re-transplantation. Graft survival is significantly reduced in patients suffering from NAS.
Especially patients with a hepatico-jejunostomy, those with an early diagnosis of NAS, and
those with NAS presenting at the level of the peripheral branches of the biliary tree, are at
risk for the development of recurrent cholangitis, radiological progression, development of
cirrhosis and eventually retransplantation.
76
NAS after liver transplantation: risk factors for disease progression Chapter 4
References
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 1.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003 Jul;3:885-90.
Buis CI, Verdonk RC, van der Jagt EJ, van der Hilst CS, Slooff MJH, Haagsma EB, Porte RJ. Non-anastomotic 2.
biliary strictures after adult liver liver transplantation part one: Radiological features and risk factors for early
versus late presentation. Liver Transpl 2007; 13:708-18.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 3.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003 Jul;3:885-90.
Hintze RE, Adler A, Veltzke W, Abou-Rebyeh H, Felix R, Neuhaus P. Endoscopic management of biliary 4.
complications after orthotopic liver transplantation. Hepatogastroenterology 1997 Jan;44:258-62.
Rull R, Garcia Valdecasas JC, Grande L, Fuster J, Lacy AM, Gonzalez FX, et al. Intrahepatic biliary lesions after 5.
orthotopic liver transplantation. Transpl Int 2001 Jun;14:129-34.
Campbell WL, Sheng R, Zajko AB, Abu-Elmagd K, Demetris AJ. Intrahepatic biliary strictures after liver 6.
transplantation. Radiology 1994 Jun;191:735-40.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 7.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003 Jul;3:885-90.
Rull R, Garcia Valdecasas JC, Grande L, Fuster J, Lacy AM, Gonzalez FX, et al. Intrahepatic biliary lesions after 8.
orthotopic liver transplantation. Transpl Int 2001 Jun;14:129-34.
Campbell WL, Sheng R, Zajko AB, Abu-Elmagd K, Demetris AJ. Intrahepatic biliary strictures after liver 9.
transplantation. Radiology 1994 Jun;191:735-40.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 10.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003 Jul;3:885-90.
Sankary HN, McChesney L, Hart M, Foster P, Williams J. Identification of donor and recipient risk factors 11.
associated with nonanastomotic biliary strictures in human hepatic allografts. Transplant Proc 1993
Apr;25:1964-7.
Sawyer RG, Punch JD. Incidence and management of biliary complications after 291 liver transplants following 12.
the introduction of transcystic stenting. Transplantation 1998 Nov 15;66:1201-7.
Campbell WL, Sheng R, Zajko AB, Abu-Elmagd K, Demetris AJ. Intrahepatic biliary strictures after liver 13.
transplantation. Radiology 1994 Jun;191:735-40.
Kuo PC, Lewis WD, Stokes K, Pleskow D, Simpson MA, Jenkins RL. A comparison of operation, endoscopic 14.
retrograde cholangiopancreatography, and percutaneous transhepatic cholangiography in biliary complications
after hepatic transplantation. J Am Coll Surg 1994 Aug;179:177-81.
77
Chapter 4
Sanchez-Urdazpal L, Gores GJ, Ward EM, Maus TP, Buckel EG, Steers JL, et al. Diagnostic features and 15.
clinical outcome of ischemic-type biliary complications after liver transplantation. Hepatology 1993 Apr;17:
605-9.
Sanchez-Urdazpal L, Gores GJ, Ward EM, Hay E, Buckel EG, Wiesner RH, et al. Clinical outcome of ischemic-16.
type biliary complications after liver transplantation. Transplant Proc 1993 Feb;25(1 Pt 2):1107-9.
Chuang JH, Chen WJ, Lee SY, Chang NK. Prompt colonization of the hepaticojejunostomy and translocation of 17.
bacteria to liver after bile duct reconstruction. J Pediatr Surg 1998 Aug;33:1215-8.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 18.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003 Jul;3:885-90.
Moench C, Uhrig A, Lohse AW, Otto G. CC chemokine receptor 5delta32 polymorphism-a risk factor for 19.
ischemic-type biliary lesions following orthotopic liver transplantation. Liver Transpl 2004 Mar;10:434-9.
Otto G, Roeren T, Golling M, Datsis K, Hofmann WJ, Herfarth C, et al. [Ischemic type lesions of the bile ducts 20.
after liver transplantation: 2 years results]. Zentralbl Chir 1995;120:450-4.
Sanchez-Urdazpal L, Gores GJ, Ward EM, Hay E, Buckel EG, Wiesner RH, et al. Clinical outcome of ischemic-21.
type biliary complications after liver transplantation. Transplant Proc 1993 Feb;25(1 Pt 2):1107-9.
Hintze RE, Adler A, Veltzke W, Abou-Rebyeh H, Felix R, Neuhaus P. Endoscopic management of biliary 22.
complications after orthotopic liver transplantation. Hepatogastroenterology 1997 Jan;44:258-62.
Schlitt HJ, Meier PN, Nashan B, Oldhafer KJ, Boeker K, Flemming P, et al. Reconstructive surgery for ischemic-23.
type lesions at the bile duct bifurcation after liver transplantation. Ann Surg 1999 Jan;229:137-45.
Sung RS, Campbell DA, Jr., Rudich SM, Punch JD, Shieck VL, Armstrong JM, et al. Long-term follow-up 24.
of percutaneous transhepatic balloon cholangioplasty in the management of biliary strictures after liver
transplantation. Transplantation 2004 Jan 15;77:110-5.
Theilmann L, Kuppers B, Kadmon M, Roeren T, Notheisen H, Stiehl A, et al. Biliary tract strictures after orthotopic 25.
liver transplantation: diagnosis and management. Endoscopy 1994 Aug;26:517-22.
Zajko AB, Sheng R, Zetti GM, Madariaga JR, Bron KM. Transhepatic balloon dilation of biliary strictures in liver 26.
transplant patients: a 10-year experience. J Vasc Interv Radiol 1995 Jan;6:79-83.

Part II
Bile physiology after
liver transplantation

The role of bile salt toxicity in the pathogenesis of bile duct injury after non heart-beating porcine liver transplantation5
Transplantation 2008; 85:1625-1631
Marit J YskaCarlijn I Buis
Diethard MonbaliuTheo A Schuurs
Annette SH GouwOlivier NH Kahman
Dorien S VisserJacques Pirenne
Robert J Porte
82
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
Abstract
Background. Intrahepatic bile duct strictures are a serious complication after non-heart-
beating (NHB) liver transplantation. Bile salt toxicity has been identified as an important factor
in the pathogenesis of bile duct injury and cholangiopathies. The role of bile salt toxicity in the
development of biliary strictures after NHB liver transplantation is unclear.
Methods. In a porcine model of NHB liver transplantation, we studied the effect of different
periods of warm ischemia in the donor on bile composition and subsequent bile duct injury
after transplantation. After induction of cardiac arrest in the donor, liver procurement was
delayed for 0 min (group A), 15 min (group B) or > 30 min (group C). Livers were subsequently
transplanted after four hours of cold preservation. In the recipients, bile flow was measured
and bile samples were collected daily to determine the bile salt / phospholipid ratio. Severity
of bile duct injury was semi-quantified by using a histological grading scale.
Results. Posttransplant survival was directly related to the duration of warm ischemia in
the donor. The bile salt / phospholipid ratio in bile produced early after transplantation was
significantly higher in group C, compared to group A and B. Histopathology showed the highest
degree of bile duct injury in group C.
Conclusion. Prolonged warm ischemia in NHB donors is associated with the formation of
toxic bile after transplantation, with a high biliary bile salt / phospholipid ratio. These data
suggest that bile salt toxicity contributes to the pathogenesis of bile duct injury after NHB liver
transplantation.
83
Chapter 5
Introduction
The success of orthotopic liver transplantation as a therapy for patients with end-stage liver
disease has resulted in an increasing demand for donor livers. In many parts of the world this
created a growing shortage of organs from brain death or deceased donors. A possible solution
to reduce shortage of donor organs is expansion of the donor pool by accepting donation after
cardiac death (DCD) or non-heart-beating (NHB) donors. Patient survival after transplantation
of livers from NHB donors has shown to be comparable to survival after transplantation of
livers from brain death donors (1-4). Graft survival after NHB liver transplantation, however,
is about 10-15% lower due to a higher rate of primary non-function and other graft-related
complications. Intrahepatic bile duct strictures, also known as non-anastomotic strictures or
ischemic-type biliary lesions, are a serious cause of morbidity and a leading cause of graft
failure after NHB liver transplantation (5-7). Although the exact pathogenesis is unknown, it is
generally believed that warm ischemia in the NHB donor due to hypotension before cardiac
arrest, as well as during the time period between cardiac and organ procurement, is a critical
factor in the pathogenesis of these biliary strictures (5-7). Although hepatocytes may recover
from the warm ischemic insult in donor, bile duct epithelial cells have a poor tolerance towards
ischemia and regeneration of cellular ATP is much slower than in hepatocytes (8-12). Apart from
this direct detrimental effect of ischemia on the bile duct epithelium (13), there is accumulating
evidence that bile salt toxicity contributes to bile duct injury after liver transplantation (14-
16). Although secretion of bile salts by hepatocytes is the main driving force of bile flow, bile
salts can act as detergents injuring cellular phospholipid membranes. Under physiological
circumstances, bile salts are therefore neutralized in bile by phospholipids after formation of
mixed micelles (17).
Experimental studies in mice as well as clinical studies in humans have indicated that bile
formation early after liver transplantation may be disturbed, resulting in the formation of more
toxic bile with a relatively high bile salt / phospholipid ratio. A high bile salt / phospholipid ratio
has been associated with more severe bile duct injury after transplantation (14-16).
The role of bile salts in the pathogenesis of bile duct injury after NHB liver transplantation has not
been studied before. We hypothesized that bile salt toxicity acts in concert with warm ischemia
injury in the pathogenesis of intrahepatic bile duct injury after NHB liver transplantation. To study
the role of bile salts in the development of bile duct injury after NHB liver transplantation, we
84
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
have used a well established model of NHB liver transplantation in pigs (18,19). The specific
aim was to study whether increasing length of warm ischemia in NHB donors is associated with
more toxic bile formation after transplantation, as indicated by the bile salt / phospholipid ratio,
and subsequently more severe injury of the intrahepatic bile ducts.
Materials and Methods
Animals and NHB Liver Transplant Model
Inbred female Landrace pigs, weighing 18 to 37 kg, were used as donors and recipients.
In donors, cardiac arrest was induced by ventricular fibrillation, followed by standardized
periods of warm ischemia before cold preservation and procurement of the liver, to mimic
NHB donation. The pigs were divided in 5 groups (n=6 each) with different periods of donor
warm ischemia time (WIT): 0 min (controls; group A), 15 min (group B), and 30, 45 or 60
minutes. Because of a low rate of survivors in the latter three subgroups (2/6, 2/6, and 0/6
at postoperative day 4, respectively) we regarded these as one group for analysis (group C,
> 30 min WIT). In general, there were no major differences in outcome parameters between
these three groups.
After the period of warm ischemia, the liver was flushed with ice cold histidine tryptophan
ketoglutarate (HTK) preservation solution. During cold perfusion, a cholecystectomy was
performed and the common bile duct was transected and flushed out with cold saline solution.
Subsequently, livers were stored at 4˚C for four hours until transplantation.
In the recipients, a midline laparotomy was performed, the native liver was removed, and the
donor liver was implanted in an orthotopic position. No veno-venous bypass was used. After
completing the anastomosis between the suprahepatic inferior vena cava of the recipient
and donor, the portal vein was reconstructed and the liver was reperfused. Subsequently, the
infrahepatic vena cava was reconstructed. Arterial recirculation was established by an end-to-
side anastomosis between the donor aorta (left in continuity with the hepatic artery) and the
recipient aorta. There were no significant differences in the duration of the anhepatic time or
the time interval between portal reperfusion and restoration of arterial blood low among the
three groups. Mean (range) duration of the anhepatic phase in group A, B and C was 23 min
(20-26 min), 25 min (20-30 min), and 24 min (18-30 min), respectively. Time interval between
portal and arterial reperfusion was 38 min (30-45 min), 42 min (28-68 min), and 37 min (20-
85
Chapter 5
68 min), respectively. Flow probes (Transonic Systems, Ithaca, NY, USA) were implanted
around the hepatic artery and portal vein and connected to a dual channel ultrasonic transit-
time volume flow meter (T206, Transonic). Blood flow was measured continuously during the
first 3 hours after reperfusion and twice daily thereafter. In addition, patency of the vascular
anastomoses was macroscopically inspected during necropsy. All hepatic artery anastomoses
were found to be patent.
Perioperatively, arterial blood pressure was monitored via an arterial line in the left common
carotid artery. Central venous pressure was monitored via a catheter in the left external jugular
vein. Infusion of intravenous fluids was individually guided by clinical signs of hypovolemia,
hemodynamic parameters, and laboratory blood analysis. Although moderate hypotension up
to a period of 30 min was well tolerated during the anhepatic phase, 500 ml of oxyplatin was
administered IV during the anhepatic phase to avoid severe hypotension (20). In general,
there were no major differences in hemodynamics among the groups.
During transplantation a catheter was inserted in the common bile duct and externalized via
the abdominal wall. Daily bile production was completely diverted into a collecting bag. To
maintain the enterohepatic circulation of bile salts, bile was readministered via a jejunostomy
catheter. Antibiotic prophylaxis was provided by IV Ceftazidime, 500 mg.
Postoperatively, animals received tacrolimus (0.05 mg/kg bid) as immunosuppressant. All
animals had free access to water and food. All surviving animals were able to feed themselves
normally as of postoperative day 2 and there were no apparent differences between the groups.
The postoperative observation period was limited to four days to minimize confounding effects
caused by sepsis and other late-onset phenomena. After four days the pigs were killed and
animals surviving less than four days were autopsied to identify the cause of death (19).
Experiments were performed in accordance with the Belgian law regarding animal welfare.
Biochemical serum analyses
Serum levels of aspartate aminotransferase (AST) and bilirubin were determined using routine
chemical methods.
Collection of Bile and Determination of Bile Composition
Bile production was measured 3 hours after reperfusion and daily thereafter to calculate bile
flow (bile production / kg body weight of the donor). Bile samples were collected daily to
86
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
examine bile composition and determination of the biliary bile salt / phospholipid ratio. Total
biliary bile salt concentration was measured spectrophotometrically using 3α-hydroxysteroid
dehydrogenase (21). Biliary phospholipid concentration was analysed using a commercially
available enzymatic method (Wako Chemicals GmbH, Neuss, Germany).
Hepatic Gene Expression of Bile Transporters
In parallel with the measurement of bile composition, we measured hepatic mRNA expression
of the bile salt transporter (bile salt export pump; BSEP or Abcb11) and the phospholipid
translocator (multidrug resistance protein; MDR3 or Abcb4). The gene sequence of porcine
MDR3 was not known and, therefore, determined for this experiment (NCBI Accession #:
EF067318).
Wedge biopsies were taken one hour after reperfusion and on postoperative day (POD) four
in surviving animals. Biopsies were snap frozen and stored at -80° C until analysis. RNA
isolation from liver biopsies was performed using TRIzol (Invitrogen Life Technologies, Breda,
The Netherlands), Chloroform (Merck, Darmstadt, Germany) and the DNAse-kit from Sigma
(Sigma-Aldrich, Zwijndrecht, The Netherlands). RNA integrity was quantified by electrophoresis
using agarose-gel (Sphaero Q, Leiden, The Netherlands) and ethidiumbromide (Sigma-
Aldrich). The enzyme M-MLV reverse transcriptase (Sigma-Aldrich) was used to convert
RNA (1µg in a final volume of 21 µl) in copy-DNA (cDNA). Taq polymerase (Invitrogen Life
Technologies, Breda, The Netherlands) and conventional PCR were used to multiply the cDNA
and make it detectable with DNA electrophoresis by an UV-transilluminator. For quantitative
real-time detection, sense, anti-sense porcine primers (Invitrogen, Paisley, Scotland) and
fluorogenic probes (Eurogentec, Herstal, Belgium) were designed for the hepatobiliary
transporters BSEP and MDR3, using Primer Express software (PE Aplied Biosystems, Foster
City, CA, USA). All probes were 5’ labeled by a 6-carboxy-fluorescein (FAM) reporter and 3’
labeled with a 6-carboxy-tetramethyl-rhodamine (TAMRA) quencher (table 1). In each PCR
reaction duplicate samples of 5 µl cDNA (25x) (2 ng RNA / µl) were used in a final volume
of 20 µl (qPCR Core Kit Eurogentec, Seraing, Belgium). Every PCR sample was duplicated
in triplo, in a real-time RT PCR 384 wells plate (Applied Biosystems). mRNA copy numbers
of transporter genes were normalized to those of porcine β-actine mRNA. The ABI PRISM
7700 sequence detector (Applied Biosystems) was used for quantitative real-time RT PCR
according to the manufacturer’s instructions.
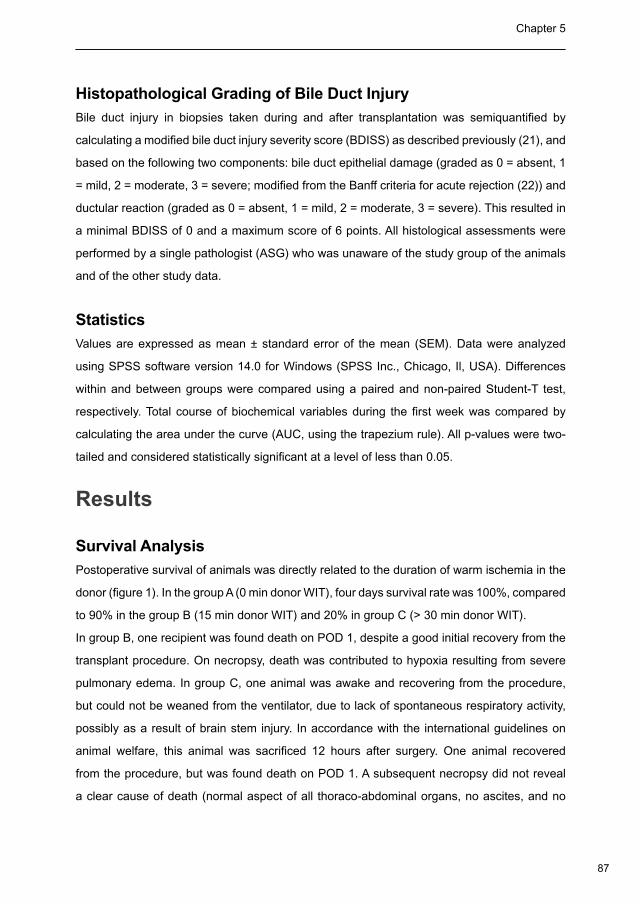
87
Chapter 5
Histopathological Grading of Bile Duct Injury
Bile duct injury in biopsies taken during and after transplantation was semiquantified by
calculating a modified bile duct injury severity score (BDISS) as described previously (21), and
based on the following two components: bile duct epithelial damage (graded as 0 = absent, 1
= mild, 2 = moderate, 3 = severe; modified from the Banff criteria for acute rejection (22)) and
ductular reaction (graded as 0 = absent, 1 = mild, 2 = moderate, 3 = severe). This resulted in
a minimal BDISS of 0 and a maximum score of 6 points. All histological assessments were
performed by a single pathologist (ASG) who was unaware of the study group of the animals
and of the other study data.
Statistics
Values are expressed as mean ± standard error of the mean (SEM). Data were analyzed
using SPSS software version 14.0 for Windows (SPSS Inc., Chicago, Il, USA). Differences
within and between groups were compared using a paired and non-paired Student-T test,
respectively. Total course of biochemical variables during the first week was compared by
calculating the area under the curve (AUC, using the trapezium rule). All p-values were two-
tailed and considered statistically significant at a level of less than 0.05.
Results
Survival Analysis
Postoperative survival of animals was directly related to the duration of warm ischemia in the
donor (figure 1). In the group A (0 min donor WIT), four days survival rate was 100%, compared
to 90% in the group B (15 min donor WIT) and 20% in group C (> 30 min donor WIT).
In group B, one recipient was found death on POD 1, despite a good initial recovery from the
transplant procedure. On necropsy, death was contributed to hypoxia resulting from severe
pulmonary edema. In group C, one animal was awake and recovering from the procedure,
but could not be weaned from the ventilator, due to lack of spontaneous respiratory activity,
possibly as a result of brain stem injury. In accordance with the international guidelines on
animal welfare, this animal was sacrificed 12 hours after surgery. One animal recovered
from the procedure, but was found death on POD 1. A subsequent necropsy did not reveal
a clear cause of death (normal aspect of all thoraco-abdominal organs, no ascites, and no
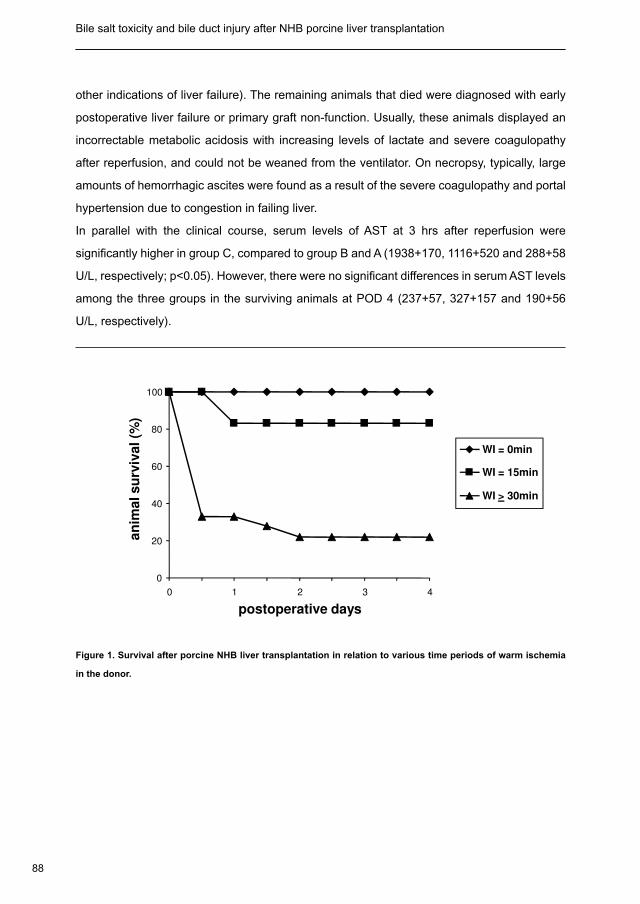
88
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
other indications of liver failure). The remaining animals that died were diagnosed with early
postoperative liver failure or primary graft non-function. Usually, these animals displayed an
incorrectable metabolic acidosis with increasing levels of lactate and severe coagulopathy
after reperfusion, and could not be weaned from the ventilator. On necropsy, typically, large
amounts of hemorrhagic ascites were found as a result of the severe coagulopathy and portal
hypertension due to congestion in failing liver.
In parallel with the clinical course, serum levels of AST at 3 hrs after reperfusion were
significantly higher in group C, compared to group B and A (1938+170, 1116+520 and 288+58
U/L, respectively; p<0.05). However, there were no significant differences in serum AST levels
among the three groups in the surviving animals at POD 4 (237+57, 327+157 and 190+56
U/L, respectively).
0
20
40
60
80
100
WI = 0min
WI = 15min
WI > 30min
an
imal su
rviv
al (%
)
30 21 4
0
0 1 2 3 4
postoperative days
Figure 1. Survival after porcine NHB liver transplantation in relation to various time periods of warm ischemia
in the donor.
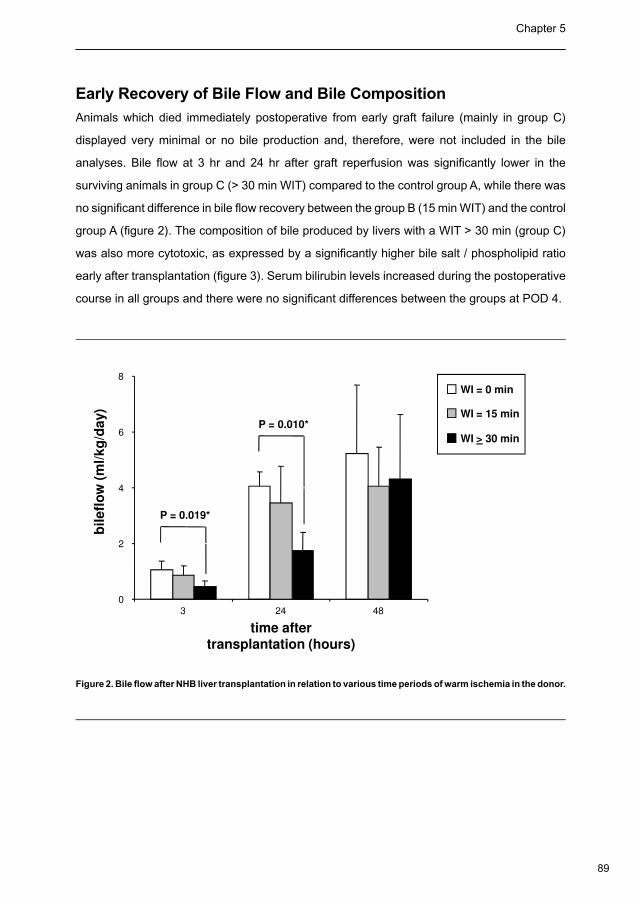
89
Chapter 5
Early Recovery of Bile Flow and Bile Composition
Animals which died immediately postoperative from early graft failure (mainly in group C)
displayed very minimal or no bile production and, therefore, were not included in the bile
analyses. Bile flow at 3 hr and 24 hr after graft reperfusion was significantly lower in the
surviving animals in group C (> 30 min WIT) compared to the control group A, while there was
no significant difference in bile flow recovery between the group B (15 min WIT) and the control
group A (figure 2). The composition of bile produced by livers with a WIT > 30 min (group C)
was also more cytotoxic, as expressed by a significantly higher bile salt / phospholipid ratio
early after transplantation (figure 3). Serum bilirubin levels increased during the postoperative
course in all groups and there were no significant differences between the groups at POD 4.
P = 0.019*
P = 0.010*
3
0
2
4
6
8
48
bil
efl
ow
(m
l/kg
/day)
24
WI = 0 min
WI = 15 min
WI > 30 min
time after
transplantation (hours)
3 4824
Figure 2. Bile flow after NHB liver transplantation in relation to various time periods of warm ischemia in the donor.
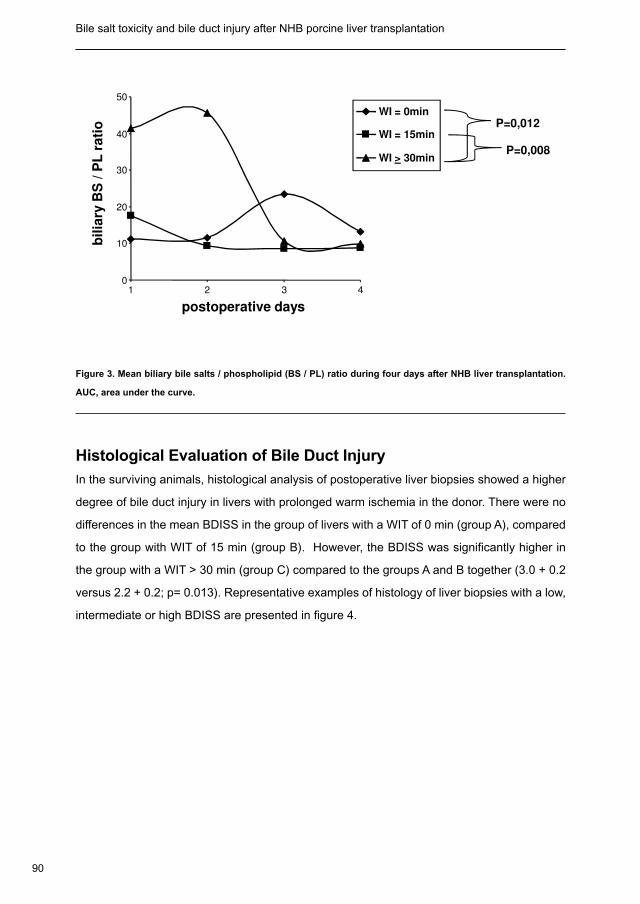
90
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
0
10
20
30
40
50
1 2 3 4
WI = 0min
WI = 15min
WI > 30minP=0,008
P=0,012
postoperative days
bil
iary
BS
/ P
L r
ati
o
Figure 3. Mean biliary bile salts / phospholipid (BS / PL) ratio during four days after NHB liver transplantation.
AUC, area under the curve.
Histological Evaluation of Bile Duct Injury
In the surviving animals, histological analysis of postoperative liver biopsies showed a higher
degree of bile duct injury in livers with prolonged warm ischemia in the donor. There were no
differences in the mean BDISS in the group of livers with a WIT of 0 min (group A), compared
to the group with WIT of 15 min (group B). However, the BDISS was significantly higher in
the group with a WIT > 30 min (group C) compared to the groups A and B together (3.0 + 0.2
versus 2.2 + 0.2; p= 0.013). Representative examples of histology of liver biopsies with a low,
intermediate or high BDISS are presented in figure 4.
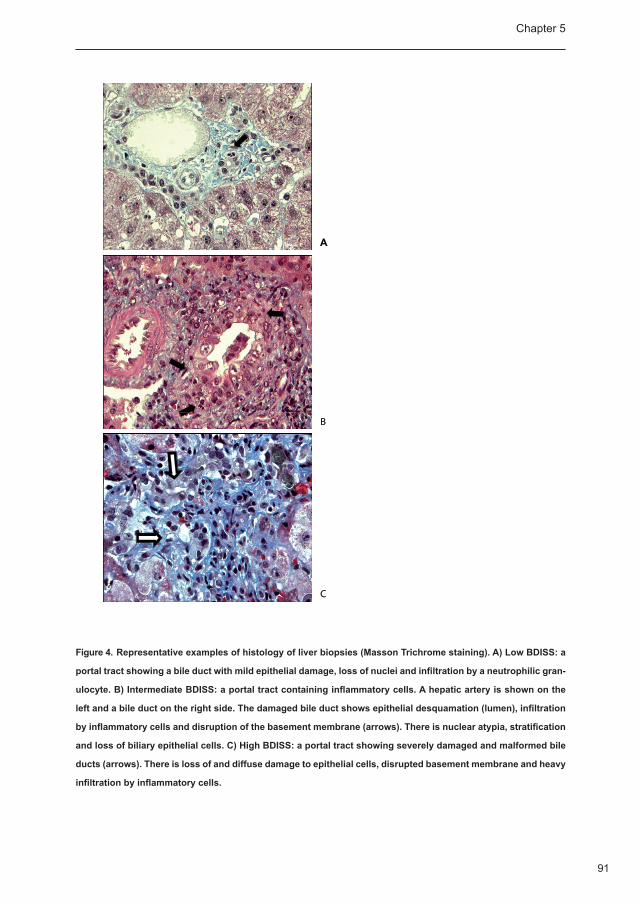
91
Chapter 5
A
C
B
Figure 4. Representative examples of histology of liver biopsies (Masson Trichrome staining). A) Low BDISS: a
portal tract showing a bile duct with mild epithelial damage, loss of nuclei and infiltration by a neutrophilic gran-
ulocyte. B) Intermediate BDISS: a portal tract containing inflammatory cells. A hepatic artery is shown on the
left and a bile duct on the right side. The damaged bile duct shows epithelial desquamation (lumen), infiltration
by inflammatory cells and disruption of the basement membrane (arrows). There is nuclear atypia, stratification
and loss of biliary epithelial cells. C) High BDISS: a portal tract showing severely damaged and malformed bile
ducts (arrows). There is loss of and diffuse damage to epithelial cells, disrupted basement membrane and heavy
infiltration by inflammatory cells.
creo
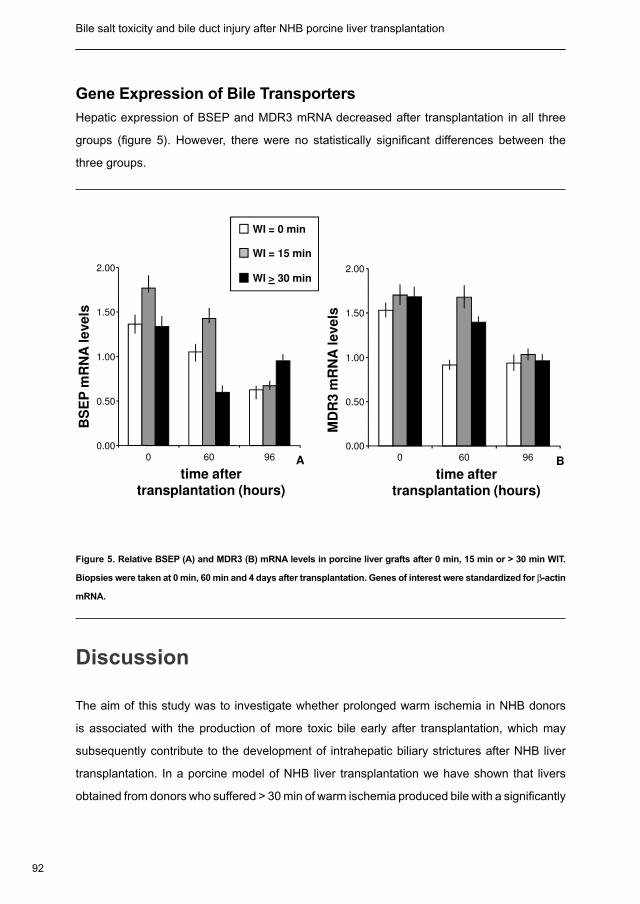
92
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
Gene Expression of Bile Transporters
Hepatic expression of BSEP and MDR3 mRNA decreased after transplantation in all three
groups (figure 5). However, there were no statistically significant differences between the
three groups.
BS
EP
mR
NA
levels
MD
R3 m
RN
A l
evels
A
0.00
0.50
1.00
1.50
2.00
WI = 0 min
WI = 15 min
WI > 30 min
0 60 96 B
0.00
0.50
1.00
1.50
2.00
60 960
time after transplantation (hours)
A
time after transplantation (hours)
B
Figure 5. Relative BSEP (A) and MDR3 (B) mRNA levels in porcine liver grafts after 0 min, 15 min or > 30 min WIT.
Biopsies were taken at 0 min, 60 min and 4 days after transplantation. Genes of interest were standardized for β-actin
mRNA.
Discussion
The aim of this study was to investigate whether prolonged warm ischemia in NHB donors
is associated with the production of more toxic bile early after transplantation, which may
subsequently contribute to the development of intrahepatic biliary strictures after NHB liver
transplantation. In a porcine model of NHB liver transplantation we have shown that livers
obtained from donors who suffered > 30 min of warm ischemia produced bile with a significantly
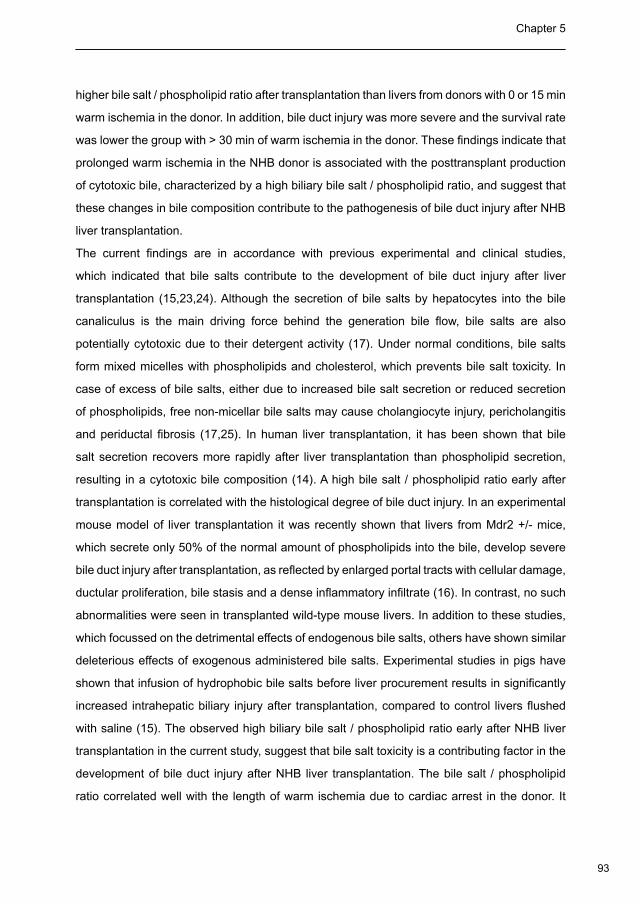
93
Chapter 5
higher bile salt / phospholipid ratio after transplantation than livers from donors with 0 or 15 min
warm ischemia in the donor. In addition, bile duct injury was more severe and the survival rate
was lower the group with > 30 min of warm ischemia in the donor. These findings indicate that
prolonged warm ischemia in the NHB donor is associated with the posttransplant production
of cytotoxic bile, characterized by a high biliary bile salt / phospholipid ratio, and suggest that
these changes in bile composition contribute to the pathogenesis of bile duct injury after NHB
liver transplantation.
The current findings are in accordance with previous experimental and clinical studies,
which indicated that bile salts contribute to the development of bile duct injury after liver
transplantation (15,23,24). Although the secretion of bile salts by hepatocytes into the bile
canaliculus is the main driving force behind the generation bile flow, bile salts are also
potentially cytotoxic due to their detergent activity (17). Under normal conditions, bile salts
form mixed micelles with phospholipids and cholesterol, which prevents bile salt toxicity. In
case of excess of bile salts, either due to increased bile salt secretion or reduced secretion
of phospholipids, free non-micellar bile salts may cause cholangiocyte injury, pericholangitis
and periductal fibrosis (17,25). In human liver transplantation, it has been shown that bile
salt secretion recovers more rapidly after liver transplantation than phospholipid secretion,
resulting in a cytotoxic bile composition (14). A high bile salt / phospholipid ratio early after
transplantation is correlated with the histological degree of bile duct injury. In an experimental
mouse model of liver transplantation it was recently shown that livers from Mdr2 +/- mice,
which secrete only 50% of the normal amount of phospholipids into the bile, develop severe
bile duct injury after transplantation, as reflected by enlarged portal tracts with cellular damage,
ductular proliferation, bile stasis and a dense inflammatory infiltrate (16). In contrast, no such
abnormalities were seen in transplanted wild-type mouse livers. In addition to these studies,
which focussed on the detrimental effects of endogenous bile salts, others have shown similar
deleterious effects of exogenous administered bile salts. Experimental studies in pigs have
shown that infusion of hydrophobic bile salts before liver procurement results in significantly
increased intrahepatic biliary injury after transplantation, compared to control livers flushed
with saline (15). The observed high biliary bile salt / phospholipid ratio early after NHB liver
transplantation in the current study, suggest that bile salt toxicity is a contributing factor in the
development of bile duct injury after NHB liver transplantation. The bile salt / phospholipid
ratio correlated well with the length of warm ischemia due to cardiac arrest in the donor. It
94
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
is likely that the ischemic insult to the biliary epithelium remains a key determinant in the
pathogenesis bile duct injury after NHB liver transplantation, however, bile salt toxicity could
aggravate the degree of injury.
Hepatobiliary secretion of bile salts and phospholipids is an active process which is determined
by the hepatic transporters BSEP and MDR3, respectively. Various molecular changes of
hepatocellular-transport systems have been described in patients with cholangiopathy or
cholestatic disorders (17), illustrating the importance of these transporter functions. Decreased
activity of the MDR3 (26-28) or BSEP (29) transporters, due to a gene mutation for example,
is associated with decreased bile formation and cholestasis. In our study we observed a
reduction in the expression of BSEP and MDR3 mRNA after transplantation. However, no
significant differences were noted between the three groups. These data are in accordance
with a recent study in human livers from heart-beating (deceased) donors where also no
differences were found in BSEP and MDR3 mRNA expression at three hours after graft
reperfusion (13). In this human study, however, a small, but significant, increase in BSEP
expression was found at one week after transplantation (14). Follow-up in our study was limited
to only four days and further studies will be needed to determine whether similar changes also
occur in this porcine model of NHB donor liver transplantation. In general, current findings
suggest that the observed differences in bile composition are caused by posttranscriptional
processes or changes in transporter activity rather than a direct effect on gene transcription.
It is increasingly recognized that changes in protein levels of BSEP and NTCP are largely
determined by the subapical storage or mobilization of these transporter proteins and to a
lesser degree by changes in gene expression (30). Unfortunately, we were unable to perform
immunohistochemistry or western blot analyses, due to the lack of adequate antibodies
against porcine BSEP and MDR3.
The accumulating evidence supporting the concept of bile salt toxicity as an important
determinant in the pathogenesis of bile duct injury after liver transplantation opens new
avenues for preventive and therapeutic measures. One obvious option would be the exogenous
administration of hydrophilic bile salts, such as ursodeoxycholic acid, which lack the detergent
properties of hydrophobic bile salts. Daily oral administration of ursodeoxycholic acid is a well
known therapy to reduce bile salt toxicity by replacement of the hydrophobic bile salts in the
bile salt pool (31,32). In addition, hydrophilic bile salts have been shown to possess more direct
cytoprotective properties which are independent from the reduction in hydrophobic bile salts,
95
Chapter 5
and involve inhibition of apoptotic pathways (15,31). Another interesting therapeutic target
could be MDR3, given the key role of biliary phospholipids in protecting bile duct epithelium
from potentially toxic, aggressive biliary content (30). Therapeutic strategies aimed at reducing
bile toxicity through stimulation of MDR3 expression and function may be an important future
therapeutic approach to prevent bile duct injury after liver transplantation. Administration of
fibrates, statins or peroxisome proliferators, have been shown to stimulate biliary phospholipid
secretion by the induction of MDR3 (or its rodent homolog mdr2), making bile less toxic (33-
35). However, more research in this area, including assessment of potential side effects of
these compounds will be needed before clinical application of these compounds to prevent
bile duct strictures can be advised.
Currently, there is not an established animal model of bile duct injury after NHB-donor liver
transplantation. Development of such a model, however, is of great relevance to facilitate
studies on the pathogenesis and development of biliary strictures in liver grafts from NHB
donors. In the current study we have focussed on injury of the small (microscopic) bile ducts
in the liver parenchyma. In clinical practice, bile duct lesions in livers from NHB donors are
typically found in the larger (macroscopic) bile ducts (9). More research using the current
porcine model with more longterm follow-up will be needed to determine whether bile salt
toxicity is also involved in the development of bilary strictures in the larger bile ducts. The ideal
model of NHB liver donation is one in which the time period of cardiac arrest results in a timely
recoverable hepatocellular injury (an thus animal and graft survival), but yet the developement
of enough biliary damage to develop biliary strictures more longterm after transplantation. In
this respect, 30 minutes of donor warm ischemia appeared to be a useful model for further
research.
In summary, we investigated the role of toxic bile composition in the pathogenesis of bile
duct injury after NHB liver transplantation, using a well established porcine model. Our data
indicate that the length of warm ischemia due to cardiac arrest in the NHB donor correlates
with the formation of toxic bile, characterized by a high biliary bile salt / phospholipid ratio, after
transplantation. These findings suggest that bile salt toxicity contributes to the pathogenesis
of bile duct injury after NHB liver transplantation.
96
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation Chapter 5
Reference List
Recommendations for nonheartbeating organ donation. A position paper by the Ethics Committee, American 1.
College of Critical Care Medicine, Society of Critical Care Medicine. Crit Care Med 2001; 29: 1826-1831.
Neuberger J. Developments in liver transplantation. Gut 2004; 53: 759-768.2.
Reddy S, Zilvetti M, Brockmann J, McLaren A, Friend P. Liver transplantation from non-heart-beating donors: 3.
current status and future prospects. Liver Transpl 2004; 10: 1223-1232.
Zawistowski CA, Devita MA. Non-heartbeating organ donation: a review. J Intensive Care Med 2003; 18: 189-4.
197.
Abt P, Crawford M, Desai N, Markmann J, Olthoff K, Shaked A. Liver transplantation from controlled non-heart-5.
beating donors: an increased incidence of biliary complications. Transplantation 2003; 75: 1659-1663.
Abt PL, Desai NM, Crawford MD et al. Survival following liver transplantation from non-heart-beating donors. 6.
Ann Surg 2004; 239: 87-92.
Garcia-Valdecasas JC, Tabet J, Valero R et al. Evaluation of ischemic injury during liver procurement from non-7.
heart-beating donors. Eur Surg Res 1999; 31: 447-456.
Lewis WD, Jenkins RL. Biliary strictures after liver transplantation. Surg Clin North Am 1994; 74: 967-978.8.
Verdonk RC, Buis CI, Porte RJ, Haagsma EB. Biliary complications after liver transplantation: a review. Scand 9.
J Gastroenterol 2006; Suppl: 89-101.
Strazzabosco M, Fabris L, Spirli C. Pathophysiology of cholangiopathies. J Clin Gastroenterol 2005; 39: 10.
S90-S102.
Cameron AM, Busuttil RW. Ischemic cholangiopathy after liver transplantation. Hepatobiliary Pancreat Dis Int 11.
2005; 4: 495-501.
Noack K, Bronk SF, Kato A, Gores GJ. The greater vulnerability of bile duct cells to reoxygenation injury than 12.
to anoxia. Implications for the pathogenesis of biliary strictures after liver transplantation. Transplantation 1993;
56: 495-500.
Lazaridis KN, Strazzabosco M, Larusso NF. The cholangiopathies: disorders of biliary epithelia. Gastroenterology 13.
2004; 127: 1565-1577.
Geuken E, Visser D, Kuipers F et al. Rapid increase of bile salt secretion is associated with bile duct injury after 14.
human liver transplantation. J Hepatol 2004; 41: 1017-1025.
Hertl M, Harvey PR, Swanson PE et al. Evidence of preservation injury to bile ducts by bile salts in the pig and 15.
its prevention by infusions of hydrophilic bile salts. Hepatology 1995; 21: 1130-1137.
Hoekstra H, Porte RJ, Tian Y et al. Bile salt toxicity aggravates cold ischemic injury of bile ducts after liver 16.
97
Chapter 5
transplantation in Mdr2+/- mice. Hepatology 2006; 43: 1022-1031.
Trauner M, Meier PJ, Boyer JL. Molecular pathogenesis of cholestasis. N Engl J Med 1998; 339: 1217-1227.17.
Monbaliu D, Crabbe T, Roskams T, Fevery J, Verwaest C, Pirenne J. Livers from non-heart-beating donors 18.
tolerate short periods of warm ischemia. Transplantation 2005; 79: 1226-1230.
Monbaliu D, van PJ, De VR et al. Primary graft nonfunction and Kupffer cell activation after liver transplantation 19.
from non-heart-beating donors in pigs. Liver Transpl 2007; 13: 239-247.
Oike F, Uryuhara K, Otsuka M et al. Simplified technique of orthotopic liver transplantation in pigs. Transplantation 20.
2001; 71: 328-331.
Turley SD, Dietschy JM. Re-evaluation of the 3 alpha-hydroxysteroid dehydrogenase assay for total bile acids 21.
in bile. J Lipid Res 1978; 19: 924-928.
Banff schema for grading liver allograft rejection: an international consensus document. Hepatology 1997; 25: 22.
658-663.
Schmucker DL, Ohta M, Kanai S, Sato Y, Kitani K. Hepatic injury induced by bile salts: correlation between 23.
biochemical and morphological events. Hepatology 1990; 12: 1216-1221.
Buis CI, Hoekstra H, Verdonk RC, Porte RJ. Causes and consequences of ischemic-type biliary lesions after 24.
liver transplantation. J Hepatobiliary Pancreat Surg 2006; 13: 517-524.
Arrese M, Trauner M. Molecular aspects of bile formation and cholestasis. Trends Mol Med 2003; 9: 558-564.25.
de Vree JM, Jacquemin E, Sturm E et al. Mutations in the MDR3 gene cause progressive familial intrahepatic 26.
cholestasis. Proc Natl Acad Sci U S A 1998; 95: 282-287.
Deleuze JF, Jacquemin E, Dubuisson C et al. Defect of multidrug-resistance 3 gene expression in a subtype of 27.
progressive familial intrahepatic cholestasis. Hepatology 1996; 23: 904-908.
Jacquemin E, de Vree JM, Cresteil D et al. The wide spectrum of multidrug resistance 3 deficiency: from 28.
neonatal cholestasis to cirrhosis of adulthood. Gastroenterology 2001; 120: 1448-1458.
Suchy FJ, Ananthanarayanan M. Bile salt excretory pump: biology and pathobiology. J Pediatr Gastroenterol 29.
Nutr 2006; 43 Suppl 1: S10-S16.
Trauner M, Boyer JL. Bile salt transporters: molecular characterization, function, and regulation. Physiol Rev 30.
2003; 83: 633-671.
Fickert P, Zollner G, Fuchsbichler A et al. Effects of ursodeoxycholic and cholic acid feeding on hepatocellular 31.
transporter expression in mouse liver. Gastroenterology 2001; 121: 170-183.
Trauner M, Fickert P, Wagner M. MDR3 (ABCB4) defects: a paradigm for the genetics of adult cholestatic 32.
syndromes. Semin Liver Dis 2007; 27: 77-98.
Miranda S, Vollrath V, Wielandt AM, Loyola G, Bronfman M, Chianale J. Overexpression of mdr2 gene by 33.
peroxisome proliferators in the mouse liver. J Hepatol 1997; 26: 1331-1339.
98
Bile salt toxicity and bile duct injury after NHB porcine liver transplantation
Hooiveld GJ, Vos TA, Scheffer GL et al. 3-Hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors (statins) 34.
induce hepatic expression of the phospholipid translocase mdr2 in rats. Gastroenterology 1999; 117: 678-687.
Chianale J, Vollrath V, Wielandt AM et al. Fibrates induce mdr2 gene expression and biliary phospholipid 35.
secretion in the mouse. Biochem J 1996; 314: 781-786.
Altered bile composition after liver transplantation is associated with the development of Nonanastomotic biliary strictures6
J of Hepatol. In Press
Carlijn I BuisErwin Geuken
Dorien S VisserFolkert Kuipers
Elizabeth B HaagsmaHenkjan J Verkade
Robert J Porte

100
Bile composition after liver transplantation and NAS Chapter 6
Abstract
Nonanastomotic biliary strictures are troublesome complications after liver transplantation.
The pathogenesis of NAS is not completely clear, but experimental studies suggest that
bile salt toxicity is involved. In 111 adult liver transplant bile samples were collected daily
posttransplantation for determination of bile composition. Expression of bile transporters was
studied perioperativly. Nonanastomotic biliary strictures were detected in 14 patients (13%)
within one year after transplantation. Patient- and donor characteristics and postoperative
serum liver enzymes were similar between patients who developed nonanastomotic biliary
strictures and those who did not. Secretions of bile salts, phospholipids and cholesterol were
significantly lower in patients who developed strictures. In parallel, biliary phospholipids/bile
salt ratio was lower in patients developing strictures, suggestive for increased bile cytotoxicity.
There were no differences in bile salt pool composition or in hepatobiliary transporter
expression.
Conclusion. Although patients who develop nonanastomotic biliary strictures are initially
clinically indiscernible from patients who do not develop nonanastomotic biliary strictures, the
biliary bile salts and phospholipids secretion, as well as biliary phospholipids/bile salt ratio in
the first week after transplantation, was significantly lower in the former group. This supports
the concept that bile cytotoxicity is involved in the pathogenesis of nonanastomotic biliary
strictures.
101
Chapter 6
Introduction
Biliary complications are a major cause of morbidity and graft failure in patients after liver
transplantation (1-3). Nonanastomotic strictures (NAS) of the larger bile ducts are considered
to represent the most troublesome biliary complication as they are frequently resistant to
therapy (4). The reported incidence of NAS is 5-15% (5-11). The occurrence of NAS can be
partly attributed to thrombosis of the hepatic artery. The pathogenesis of NAS that develop in
the absence of hepatic artery thrombosis is less clear (1,12). In general, three mechanisms
contributing to bile duct injury after liver transplantation have been postulated: preservation or
ischemia-related injury (7,13-18), immunological processes (7,19,20) and injury induced by
cytotoxicity of biliary bile salts (21-24).
Bile salts have potent detergent properties and may damage cells by affecting the integrity of
cellular membranes (22,25). In the biliary tree, the toxic effects of bile salts are usually reduced
by the formation of mixed micelles with phospholipids (26,27). Studies in mice and pigs, as well
as clinical studies in humans, have indicated that bile formation early after liver transplantation
may be disturbed, resulting in more cytotoxic bile with a relatively low phospholipids / bile salt
ratio (1,21-24,28,29). We previously showed a strong relationship between this ratio early after
liver transplantation and injury of the small bile ducts in the liver (21,24,29). The small bile ducts,
however, are lined by distinct cholangiocytes, that have different characteristics compared with
cholangiocytes in larger bile ducts, i.e. the location of NAS (30-33). It is unknown whether bile
toxicity is also involved in the pathogenesis of transplantation-related injury of the large bile
ducts, which may lead to the development of NAS.
In contrast to the cytotoxic properties of bile salts, evidence has accumulated that bile salts
may also influence cholangiocyte proliferation and survival, especially in the larger bile
ducts (31,34-36). Some bile salts, including taurocholate and taurolithocholate stimulate
cholangiocyte proliferation in vitro and in vivo, and bile salts are considered a survival factor
for cholangiocytes in the larger bile ducts (34,35). Cholangiocytes of the large bile ducts
are able to take up bile salts from bile via the apical Na+-dependent bile acid transporter
(ASBT, gene symbol SLC10A2). After basolateral secretion, bile salts are transported back
to hepatocytes and resecreted into bile, thereby contributing to bile flow via the “cholehepatic
shunt pathway” (30,37). Bile production and composition, is therefore not exclusively
determined by hepatocytes.
102
Bile composition after liver transplantation and NAS Chapter 6
It has remained unclear whether bile salts are detrimental or beneficial for cholangiocyte
function in large bile ducts after human liver transplantation, and whether or not bile production
and composition are involved in the pathogenesis of NAS. In contrast to the small bile ducts,
bile salts may not only have toxic effects but could also exert a proliferative restoration or
preservation of the biliary epithelial lining of large bile ducts after transplantation. If bile
composition is involved in the pathogenesis of NAS, one would expect that the bile composition
in the first week after liver transplantation is different in those patients who will develop NAS
as compared to patients who will not develop NAS. We tested this hypothesis by prospectively
assessing bile production and composition within one week after liver transplantation and the
subsequent development of NAS in a large cohort of adult liver transplant recipients.
Patients and Methods
Patients
Between August 2000 and December 2004 a total of 222 liver transplants were performed
at the University Medical Center Groningen. After excluding children (<18 years; n=70) and
non heart-beating donor liver transplants (n=5), 147 patients were potential candidates for
the study. Thirty six cases were excluded, because of graft loss within 90 days (n=22), initial
poor graft function (defined as in (38,39); n=12), or hepatic artery thrombosis (confirmed by
either Doppler ultrasound or angiography; n=2). This resulted in a study population of 111 liver
transplant procedures. Surgical technique and perioperative management were as previously
described by our group (5,40,41). Clinical variables and laboratory data were prospectively
collected in a computerized database. Tissue and data collection was performed according to
the guidelines of the medical ethical committee of our institution and the Dutch Federation of
Scientific Societies.
Diagnosis of NAS
NAS was defined as any stricture, dilatation, or irregularity of the intra- or extrahepatic bile ducts
of the liver graft, occurring within the first year after transplantation (Figure 1). The diagnosis
NAS was based on at least one adequate imaging study of the biliary tree, after exclusion of
hepatic artery thrombosis by either Doppler ultrasound or conventional angiography. Imaging
studies of the arterial vasculature were repeated over time if no other explanation for the
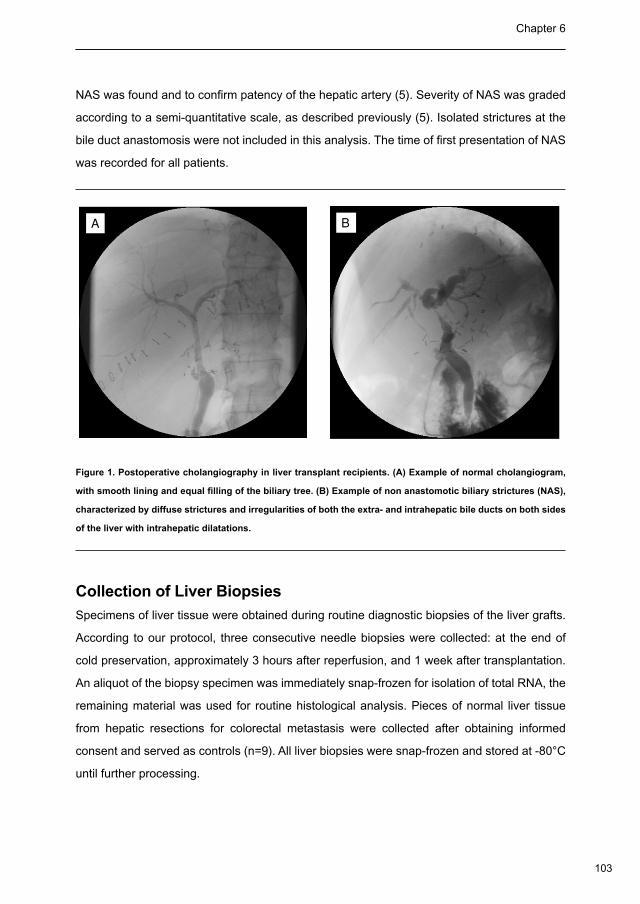
103
Chapter 6
NAS was found and to confirm patency of the hepatic artery (5). Severity of NAS was graded
according to a semi-quantitative scale, as described previously (5). Isolated strictures at the
bile duct anastomosis were not included in this analysis. The time of first presentation of NAS
was recorded for all patients.
A B
Figure 1. Postoperative cholangiography in liver transplant recipients. (A) Example of normal cholangiogram,
with smooth lining and equal filling of the biliary tree. (B) Example of non anastomotic biliary strictures (NAS),
characterized by diffuse strictures and irregularities of both the extra- and intrahepatic bile ducts on both sides
of the liver with intrahepatic dilatations.
Collection of Liver Biopsies
Specimens of liver tissue were obtained during routine diagnostic biopsies of the liver grafts.
According to our protocol, three consecutive needle biopsies were collected: at the end of
cold preservation, approximately 3 hours after reperfusion, and 1 week after transplantation.
An aliquot of the biopsy specimen was immediately snap-frozen for isolation of total RNA, the
remaining material was used for routine histological analysis. Pieces of normal liver tissue
from hepatic resections for colorectal metastasis were collected after obtaining informed
consent and served as controls (n=9). All liver biopsies were snap-frozen and stored at -80°C
until further processing.

104
Bile composition after liver transplantation and NAS Chapter 6
Collection and Analysis of Bile Samples
Before transplantation, the gallbladder was removed and the bile ducts were flushed with
preservation fluid on the backtable during preparation for implantation. During the transplantation
an open tip silicon catheter was inserted in the recipient common bile duct and placed retrograde
through the anastomosis. Via this open biliary tube, bile flow was entirely diverted outside the
patient into a collection bag that was placed below the horizontal bed level (42). Interruption
of the enterohepatic circulation in the patient was prevented by re-administration of bile via a
percutaneous feeding jejunostomy catheter. Samples of bile were collected daily in the first
postoperative week between 8:00 and 9:00 am. Bile samples were frozen and stored at -80°C
until further processing. None of the patients received a statin or ursodeoxycholic acid during the
first week after transplantation. Bile samples were analyzed for total bile salts, phospholipids,
and cholesterol contents. Total bile salt concentrations were measured with fluorescent method
using 3α-hydroxysteroid dehydrogenase (43). Phospholipid and cholesterol concentrations in bile
were assayed spectrophotometrically, using commercially available enzymatic methods (Wako
Chemicals GmbH, Neuss, Germany; and Roche Diagnostics GmbH, Mannheim, Germany;
respectively). Postoperative secretion of bile components was defined as concentration
multiplied by daily bile production per kilogram body weight of the donor. Bile salt composition
of bile samples was determined by capillary gas chromatography in a 50µL bile sample on a
Hewlett-Packard gas chromatograph (HP 5880A) equipped with a 50 m x 0.32 mm CP-Sil-19
fused silica column (Chrompack B.V., Middelburg, The Netherlands) (44). Subsequently the
hydrophobicity of the bile salt pool was determined by the Heuman index (45).
RNA Extraction and Reverse Transcription Polymerase Chain
Reaction
Isolation and reverse transcription of RNA was performed as described previously (21). Messenger
RNA levels of following hepatobiliary transporters were analyzed: the most prominent bile salt
uptake system (NTCP, Na+-dependent taurocholate cotransporting polypeptide: gene symbol
SLC10A1) and secretion system (BSEP, bile salt export pump: gene symbol ABCB11), the
phospholipid translocator (MDR3, multidrug resistance protein 3: gene symbol ABCB4) and the
main canalicular organic anion transporter and driving force of the bile salt independent bile flow
(MRP2, multidrug resistant associated protein-2: gene symbol ABCC2). Additionally, cholesterol
7α-hydroxylase (gene symbol CYP7A1) was analyzed by real-time polymerase chain reaction
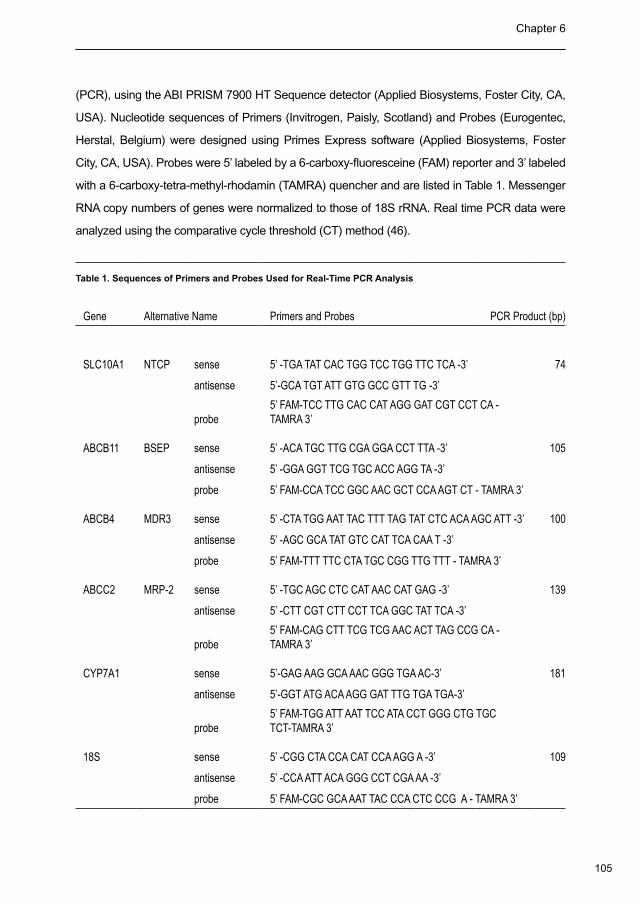
105
Chapter 6
(PCR), using the ABI PRISM 7900 HT Sequence detector (Applied Biosystems, Foster City, CA,
USA). Nucleotide sequences of Primers (Invitrogen, Paisly, Scotland) and Probes (Eurogentec,
Herstal, Belgium) were designed using Primes Express software (Applied Biosystems, Foster
City, CA, USA). Probes were 5’ labeled by a 6-carboxy-fluoresceine (FAM) reporter and 3’ labeled
with a 6-carboxy-tetra-methyl-rhodamin (TAMRA) quencher and are listed in Table 1. Messenger
RNA copy numbers of genes were normalized to those of 18S rRNA. Real time PCR data were
analyzed using the comparative cycle threshold (CT) method (46).
Table 1. Sequences of Primers and Probes Used for Real-Time PCR Analysis
Gene Alternative Name Primers and Probes PCR Product (bp)
SLC10A1 NTCP sense 5’ -TGA TAT CAC TGG TCC TGG TTC TCA -3’ 74
antisense 5’-GCA TGT ATT GTG GCC GTT TG -3’
probe5’ FAM-TCC TTG CAC CAT AGG GAT CGT CCT CA - TAMRA 3’
ABCB11 BSEP sense 5’ -ACA TGC TTG CGA GGA CCT TTA -3’ 105
antisense 5’ -GGA GGT TCG TGC ACC AGG TA -3’
probe 5’ FAM-CCA TCC GGC AAC GCT CCA AGT CT - TAMRA 3’
ABCB4 MDR3 sense 5’ -CTA TGG AAT TAC TTT TAG TAT CTC ACA AGC ATT -3’ 100
antisense 5’ -AGC GCA TAT GTC CAT TCA CAA T -3’
probe 5’ FAM-TTT TTC CTA TGC CGG TTG TTT - TAMRA 3’
ABCC2 MRP-2 sense 5’ -TGC AGC CTC CAT AAC CAT GAG -3’ 139
antisense 5’ -CTT CGT CTT CCT TCA GGC TAT TCA -3’
probe5’ FAM-CAG CTT TCG TCG AAC ACT TAG CCG CA - TAMRA 3’
CYP7A1 sense 5’-GAG AAG GCA AAC GGG TGA AC-3’ 181
antisense 5’-GGT ATG ACA AGG GAT TTG TGA TGA-3’
probe5’ FAM-TGG ATT AAT TCC ATA CCT GGG CTG TGC TCT-TAMRA 3’
18S sense 5’ -CGG CTA CCA CAT CCA AGG A -3’ 109
antisense 5’ -CCA ATT ACA GGG CCT CGA AA -3’
probe 5’ FAM-CGC GCA AAT TAC CCA CTC CCG A - TAMRA 3’
106
Bile composition after liver transplantation and NAS Chapter 6
Statistical Analysis
Collection of laboratory values from the central laboratory database was conducted as
described previously (46). Continuous variables were presented as medians with interquartile
range (IQR) or means with standard error of the mean (SEM) when appropriate. Categorical
variables were presented as numbers with percentages and compared using Pearson’s chi-
square test. Comparison of continuous variables was performed using the Mann-Whitney
U test. Area under the curve (AUC) was analyzed by the trapezium method. The level of
significance was set at 0.05. Statistical analysis was performed using SPSS 14.0 (SPSS,
Chicago, IL, USA).
Results
Development of NAS
NAS was diagnosed in 14 of the 111 liver transplant recipients (13%) at a median time interval
of 2.4 months (IQR 1.3 - 4.0 months) after transplantation. Signs of NAS were mild/moderate
in 12 patients and severe in 2 patients. There were no significant differences in donor and
recipient characteristics or surgical variables in patients who developed NAS compared to
patients who did not develop NAS (Table 2).
Serum Markers of Hepatocellular Injury and Cholestasis
Serum levels of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) in
the first week after transplantation, as markers of ischemia reperfusion injury, were similar
in patients who did or did not develop NAS (Figure 2). Similarly, gamma glutamyltransferase
(γGT) and alkaline phosphatase (ALP), markers of cholestasis, were not different between the
two groups in the first postoperative week (Figure 2).
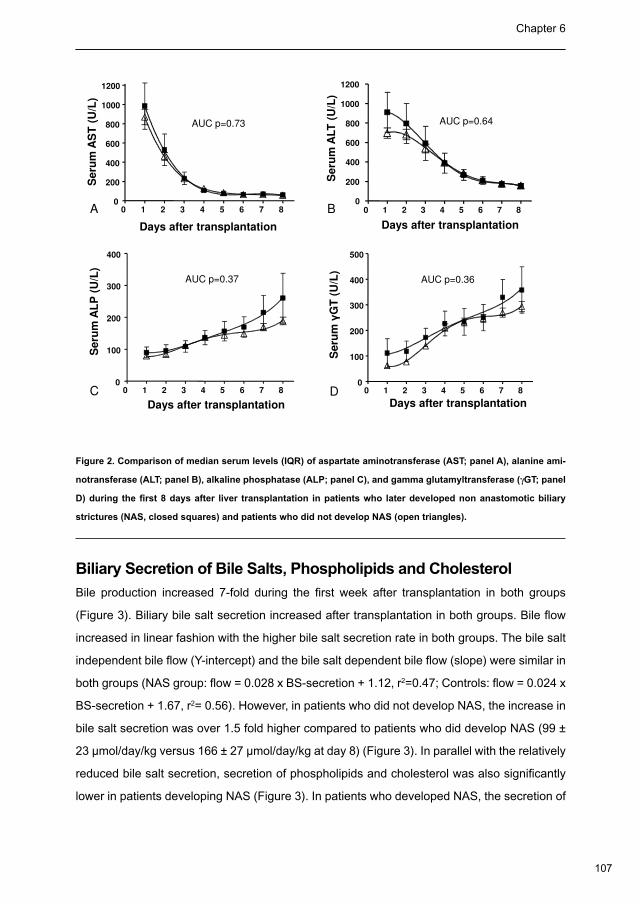
107
Chapter 6
Days after transplantation
Se
rum
AS
T (
U/L
)
AUC p=0.73
A 0 1 2 3 4 5 6 7 80
200
400
600
800
1000
1200
Se
rum
ALT
(U
/L)
AUC p=0.64
B 0 1 2 3 4 5 6 7 80
200
400
600
800
1000
1200
Days after transplantation
Se
rum
AL
P (
U/L
)
AUC p=0.37
C 0 1 2 3 4 5 6 7 80
100
200
300
400
Se
rum
G
T (
U/L
)
AUC p=0.36
D 0 1 2 3 4 5 6 7 80
100
200
300
400
500
Days after transplantation Days after transplantation
Figure 2. Comparison of median serum levels (IQR) of aspartate aminotransferase (AST; panel A), alanine ami-
notransferase (ALT; panel B), alkaline phosphatase (ALP; panel C), and gamma glutamyltransferase (γGT; panel
D) during the first 8 days after liver transplantation in patients who later developed non anastomotic biliary
strictures (NAS, closed squares) and patients who did not develop NAS (open triangles).
Biliary Secretion of Bile Salts, Phospholipids and Cholesterol
Bile production increased 7-fold during the first week after transplantation in both groups
(Figure 3). Biliary bile salt secretion increased after transplantation in both groups. Bile flow
increased in linear fashion with the higher bile salt secretion rate in both groups. The bile salt
independent bile flow (Y-intercept) and the bile salt dependent bile flow (slope) were similar in
both groups (NAS group: flow = 0.028 x BS-secretion + 1.12, r2=0.47; Controls: flow = 0.024 x
BS-secretion + 1.67, r2= 0.56). However, in patients who did not develop NAS, the increase in
bile salt secretion was over 1.5 fold higher compared to patients who did develop NAS (99 ±
23 µmol/day/kg versus 166 ± 27 µmol/day/kg at day 8) (Figure 3). In parallel with the relatively
reduced bile salt secretion, secretion of phospholipids and cholesterol was also significantly
lower in patients developing NAS (Figure 3). In patients who developed NAS, the secretion of
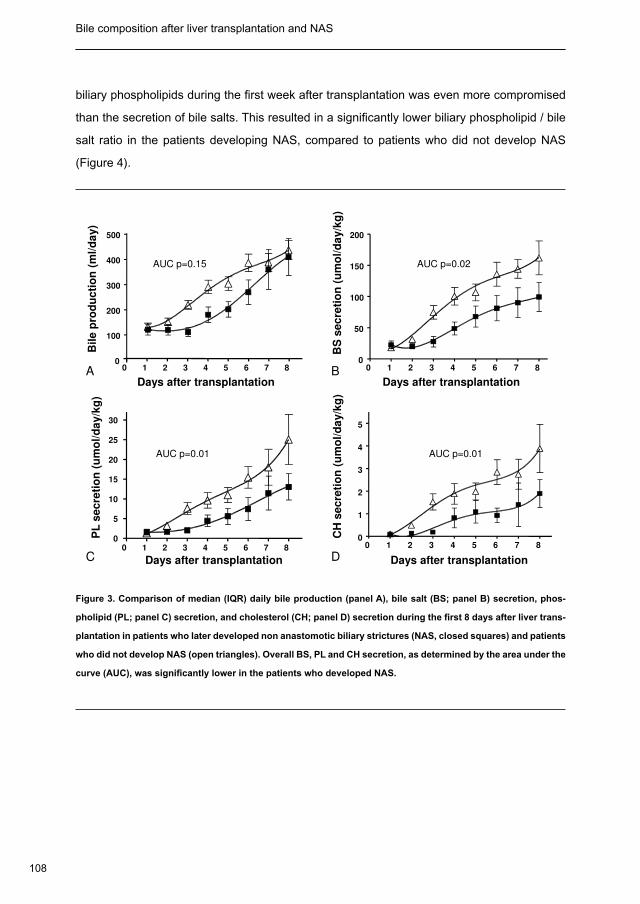
108
Bile composition after liver transplantation and NAS Chapter 6
biliary phospholipids during the first week after transplantation was even more compromised
than the secretion of bile salts. This resulted in a significantly lower biliary phospholipid / bile
salt ratio in the patients developing NAS, compared to patients who did not develop NAS
(Figure 4).
BS
se
cre
tio
n (
um
ol/
da
y/k
g)
AUC p=0.02
B 0 1 2 3 4 5 6 7 80
50
100
150
200
Bil
e p
rod
uc
tio
n (
ml/
da
y)
AUC p=0.15
A0
100
200
300
400
500
0 1 2 3 4 5 6 7 8
Days after transplantation Days after transplantation
AUC p=0.01 AUC p=0.01
PL
se
cre
tio
n (
um
ol/
da
y/k
g)
CH
se
cre
tio
n (
um
ol/
da
y/k
g)
DC0 1 2 3 4 5 6 7 8
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 80
1
2
3
4
5
Days after transplantation Days after transplantation
Days after transplantation Days after transplantation
Figure 3. Comparison of median (IQR) daily bile production (panel A), bile salt (BS; panel B) secretion, phos-
pholipid (PL; panel C) secretion, and cholesterol (CH; panel D) secretion during the first 8 days after liver trans-
plantation in patients who later developed non anastomotic biliary strictures (NAS, closed squares) and patients
who did not develop NAS (open triangles). Overall BS, PL and CH secretion, as determined by the area under the
curve (AUC), was significantly lower in the patients who developed NAS.
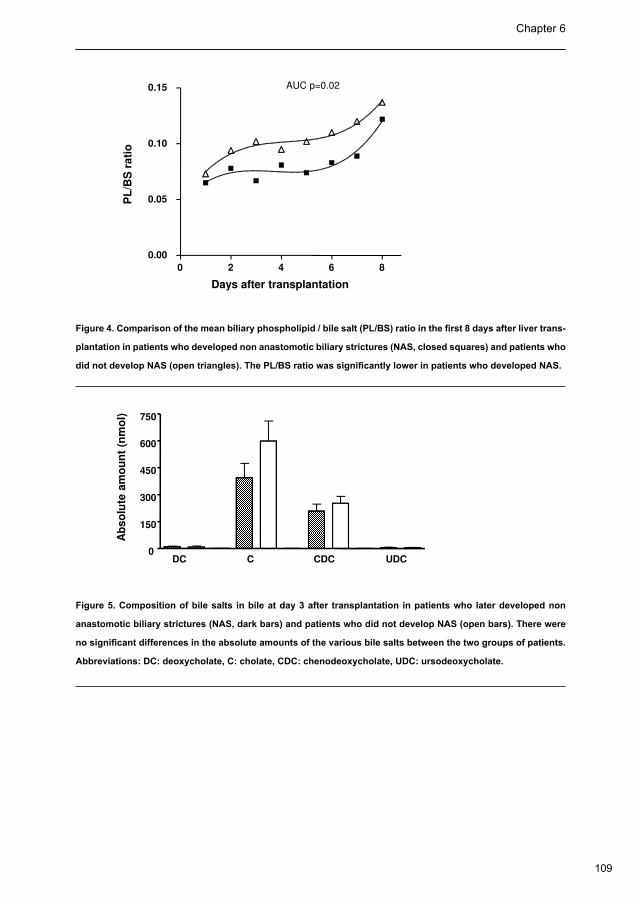
109
Chapter 6
0.05
0.10
0.15 AUC p=0.02
PL
/BS
ra
tio
0 2 4 6 8
0.00
0.05
Days after transplantation
PL
/BS
ra
tio
Figure 4. Comparison of the mean biliary phospholipid / bile salt (PL/BS) ratio in the first 8 days after liver trans-
plantation in patients who developed non anastomotic biliary strictures (NAS, closed squares) and patients who
did not develop NAS (open triangles). The PL/BS ratio was significantly lower in patients who developed NAS.
150
300
450
600
750
Ab
so
lute
am
ou
nt
(nm
ol)
DC C CDC UDC0
Ab
so
lute
am
ou
nt
(nm
ol)
Figure 5. Composition of bile salts in bile at day 3 after transplantation in patients who later developed non
anastomotic biliary strictures (NAS, dark bars) and patients who did not develop NAS (open bars). There were
no significant differences in the absolute amounts of the various bile salts between the two groups of patients.
Abbreviations: DC: deoxycholate, C: cholate, CDC: chenodeoxycholate, UDC: ursodeoxycholate.
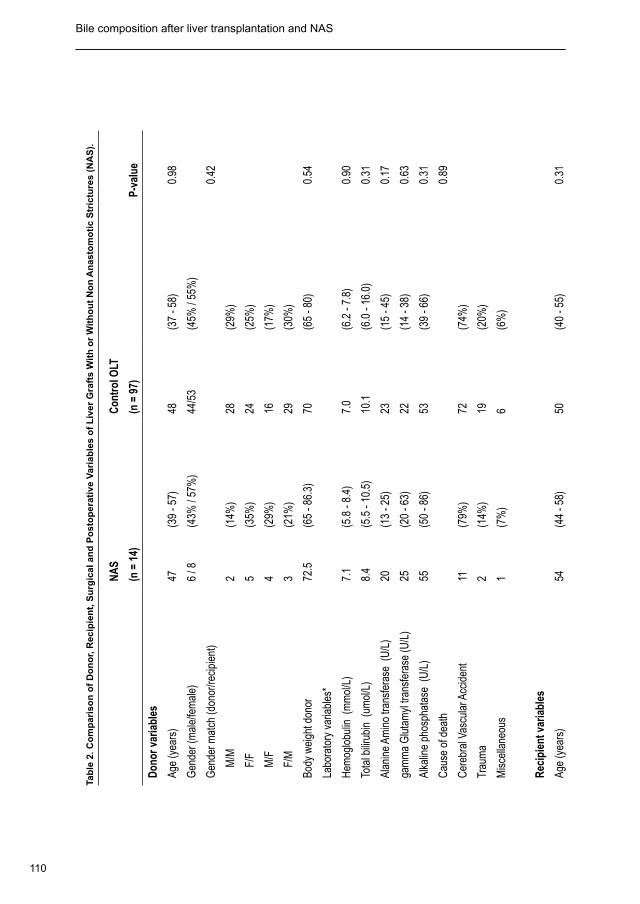
110
Bile composition after liver transplantation and NAS Chapter 6
Tab
le 2
. Co
mp
aris
on
of
Do
no
r, R
ecip
ien
t, S
urg
ical
an
d P
ost
op
erat
ive
Var
iab
les
of
Liv
er G
raft
s W
ith
or
Wit
ho
ut
No
n A
nas
tom
oti
c S
tric
ture
s (N
AS
).
NA
SC
ontr
ol O
LT
(n
= 1
4)
(n =
97)
P-
valu
e
Don
or v
aria
bles
Age
(yea
rs)
47(3
9 - 5
7)48
(37
- 58)
0.98
Gen
der (
mal
e/fe
mal
e)6
/ 8(4
3% /
57%
)44
/53
(45%
/ 55
%)
Gen
der m
atch
(don
or/re
cipi
ent)
0.42
M
/M2
(14%
)28
(29%
)
F
/F5
(35%
)24
(25%
)
M
/F4
(29%
)16
(17%
)
F
/M3
(21%
)29
(30%
)
Body
wei
ght d
onor
72.5
(65
- 86.
3)70
(65
- 80)
0.54
Labo
rato
ry v
aria
bles
*
Hem
oglo
bulin
(m
mol
/L)
7.1
(5.8
- 8.
4)7.
0(6
.2 -
7.8)
0.90
Tota
l bilir
ubin
(um
ol/L
)8.
4(5
.5 -
10.5
)10
.1(6
.0 -
16.0
)0.
31
Alan
ine
Amin
o tra
nsfe
rase
(U
/L)
20(1
3 - 2
5)23
(15
- 45)
0.17
gam
ma
Glu
tam
yl tr
ansf
eras
e (U
/L)
25(2
0 - 6
3)22
(14
- 38)
0.63
Alka
line
phos
phat
ase
(U/L
)55
(50
- 86)
53(3
9 - 6
6)0.
31
Cau
se o
f dea
th0.
89
Cer
ebra
l Vas
cula
r Acc
iden
t11
(79%
)72
(74%
)
Trau
ma
2(1
4%)
19(2
0%)
Mis
cella
neou
s1
(7%
)6
(6%
)
Rec
ipie
nt v
aria
bles
Age
(yea
rs)
54(4
4 - 5
8)50
(40
- 55)
0.31
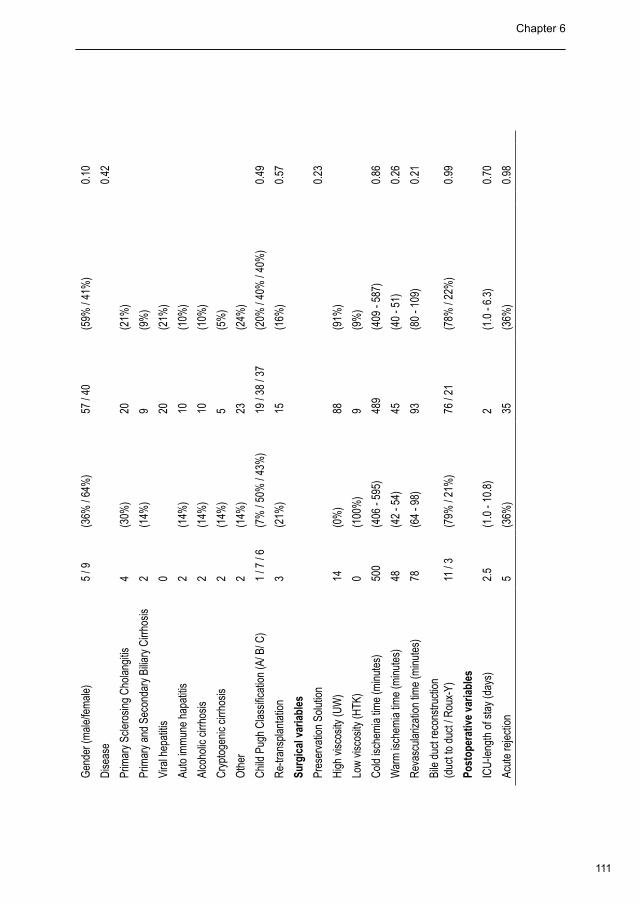
111
Chapter 6
Gen
der (
mal
e/fe
mal
e)5
/ 9(3
6% /
64%
)57
/ 40
(59%
/ 41
%)
0.10
Dis
ease
0.
42
Prim
ary
Scle
rosi
ng C
hola
ngiti
s4
(30%
)20
(21%
)
Prim
ary
and
Seco
ndar
y Bi
liary
Cirr
hosi
s2
(14%
)9
(9%
)
Vira
l hep
atiti
s0
20(2
1%)
Auto
imm
une
hapa
titis
2(1
4%)
10(1
0%)
Alco
holic
cirr
hosi
s2
(14%
)10
(10%
)
Cry
ptog
enic
cirr
hosi
s2
(14%
)5
(5%
)
Oth
er2
(14%
)23
(24%
)
Chi
ld P
ugh
Cla
ssifi
catio
n (A
/ B/ C
)1
/ 7 /
6(7
% /
50%
/ 43
%)
19 /
38 /
37(2
0% /
40%
/ 40
%)
0.49
Re-
trans
plan
tatio
n 3
(21%
)15
(16%
)0.
57
Surg
ical
var
iabl
es
Pres
erva
tion
Solu
tion
0.23
Hig
h vi
scos
ity (U
W)
14(0
%)
88(9
1%)
Low
vis
cosi
ty (H
TK)
0(1
00%
)9
(9%
)
Col
d is
chem
ia ti
me
(min
utes
)50
0(4
06 -
595)
489
(409
- 58
7)0.
86
War
m is
chem
ia ti
me
(min
utes
)48
(42
- 54)
45(4
0 - 5
1)0.
26
Rev
ascu
lariz
atio
n tim
e (m
inut
es)
78(6
4 - 9
8)93
(80
- 109
)0.
21
Bile
duc
t rec
onst
ruct
ion
(duc
t to
duct
/ R
oux-
Y)11
/ 3
(79%
/ 21
%)
76 /
21(7
8% /
22%
)0.
99
Post
oper
ativ
e va
riabl
es
ICU
-leng
th o
f sta
y (d
ays)
2.5
(1.0
- 10
.8)
2(1
.0 -
6.3)
0.70
Acut
e re
ject
ion
5(3
6%)
35(3
6%)
0.
98
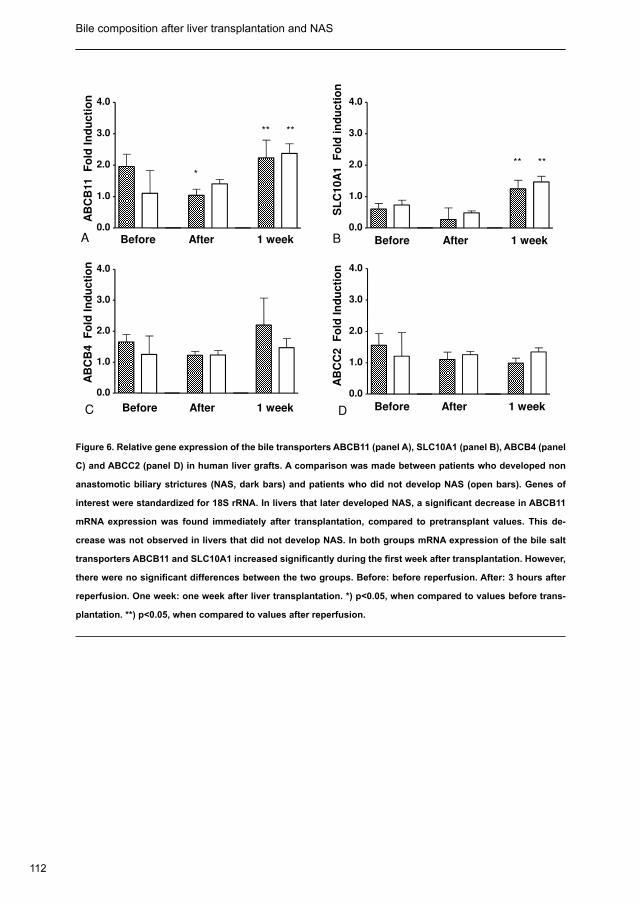
112
Bile composition after liver transplantation and NAS Chapter 6
Before After 1 week0.0
1.0
2.0
3.0
4.0
AB
CB
11
F
old
In
du
cti
on
A
*
** **
Before After 1 week
0.0
1.0
2.0
3.0
4.0
SL
C1
0A
1
Fo
ld i
nd
uc
tio
n
B
** **
Before After 1 week
0.0
1.0
2.0
3.0
4.0
AB
CC
2
Fo
ld I
nd
uc
tio
n
DBefore After 1 week
0.0
1.0
2.0
3.0
4.0
AB
CB
4
Fo
ld I
nd
uc
tio
n
C
Figure 6. Relative gene expression of the bile transporters ABCB11 (panel A), SLC10A1 (panel B), ABCB4 (panel
C) and ABCC2 (panel D) in human liver grafts. A comparison was made between patients who developed non
anastomotic biliary strictures (NAS, dark bars) and patients who did not develop NAS (open bars). Genes of
interest were standardized for 18S rRNA. In livers that later developed NAS, a significant decrease in ABCB11
mRNA expression was found immediately after transplantation, compared to pretransplant values. This de-
crease was not observed in livers that did not develop NAS. In both groups mRNA expression of the bile salt
transporters ABCB11 and SLC10A1 increased significantly during the first week after transplantation. However,
there were no significant differences between the two groups. Before: before reperfusion. After: 3 hours after
reperfusion. One week: one week after liver transplantation. *) p<0.05, when compared to values before trans-
plantation. **) p<0.05, when compared to values after reperfusion.
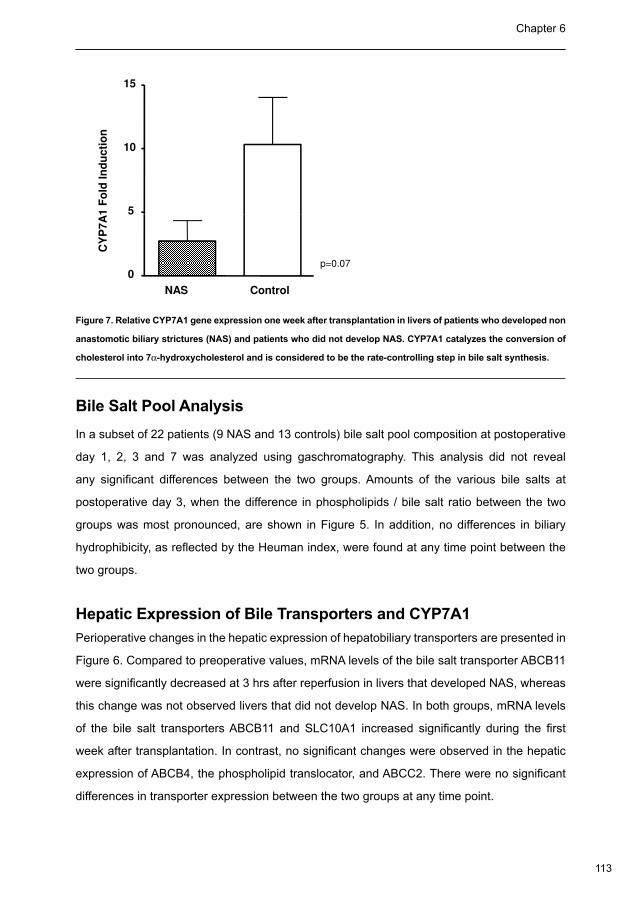
113
Chapter 6
CY
P7
A1
Fo
ld I
nd
uc
tio
n
5
10
15
p=0.07
CY
P7
A1
Fo
ld I
nd
uc
tio
n
NAS Control
0
5
Figure 7. Relative CYP7A1 gene expression one week after transplantation in livers of patients who developed non
anastomotic biliary strictures (NAS) and patients who did not develop NAS. CYP7A1 catalyzes the conversion of
cholesterol into 7α-hydroxycholesterol and is considered to be the rate-controlling step in bile salt synthesis.
Bile Salt Pool Analysis
In a subset of 22 patients (9 NAS and 13 controls) bile salt pool composition at postoperative
day 1, 2, 3 and 7 was analyzed using gaschromatography. This analysis did not reveal
any significant differences between the two groups. Amounts of the various bile salts at
postoperative day 3, when the difference in phospholipids / bile salt ratio between the two
groups was most pronounced, are shown in Figure 5. In addition, no differences in biliary
hydrophibicity, as reflected by the Heuman index, were found at any time point between the
two groups.
Hepatic Expression of Bile Transporters and CYP7A1
Perioperative changes in the hepatic expression of hepatobiliary transporters are presented in
Figure 6. Compared to preoperative values, mRNA levels of the bile salt transporter ABCB11
were significantly decreased at 3 hrs after reperfusion in livers that developed NAS, whereas
this change was not observed livers that did not develop NAS. In both groups, mRNA levels
of the bile salt transporters ABCB11 and SLC10A1 increased significantly during the first
week after transplantation. In contrast, no significant changes were observed in the hepatic
expression of ABCB4, the phospholipid translocator, and ABCC2. There were no significant
differences in transporter expression between the two groups at any time point.

114
Bile composition after liver transplantation and NAS Chapter 6
In parallel with the low bile salt secretion, expression of CYP7A1 (the rate-controlling enzyme
in de novo bile salt synthesis) at one week after transplantation was substantially lower in
patients who developed NAS, compared to those who did not (Figure 7).
Discussion
In a prospective clinical study, we evaluated the potential role of bile composition and especially
the relative contribution of bile salts and phospholipids in the development strictures of the
large bile ducts, or NAS, after otherwise successful liver transplantation. Interestingly, the
overall biliary secretion of bile salts, phospholipids and cholesterol during the first week after
transplantation was significantly lower in patients who later developed NAS, compared to
patients who did not develop NAS. The secretion of phospholipids was relatively more affected
than bile salt secretion, resulting in a lower biliary phospholipids / bile salt ratio in patients who
developed NAS. These findings indicate that the development of strictures of the large bile
ducts is preceded by abnormal bile composition early after transplantation, several weeks
before clinical symptoms of bile duct injury appear. This study supports the hypothesis that
early changes in bile composition contribute to the relatively late stricturing of the large bile
ducts, leading to the radiological diagnosis of NAS after transplantation.
In the current study the incidence of NAS up to one year after transplantation was 13%. This
rate is similar to data reported in most previous studies (6,7,10,46) but higher than reported in
some others (15,18,47). Variations in the reported incidence of NAS among different studies
can be explained by differences in study design (retrospective versus prospective) and
differences in the diagnostic criteria used.
Bile salts possess potent detergent properties and as such, are potentially cytotoxic
(48,49). In case of relative excess of bile salts, either due to increased bile salt secretion
or reduced secretion of phospholipids, micellar bile salts may cause cholangiocyte injury,
pericholangitis and periductal fibrosis (50,51). In previous studies we have shown that toxic
bile composition early after transplantation, characterized by a low biliary phospholipid / bile
salt ratio, is associated with histological signs of injury of the small bile ducts in the liver
(21,24,29). The role of bile salt toxicity in the pathogenesis of injury of the small intrahepatic
bile ducts was also demonstrated in an experimental study using a liver transplant model
in mice (24). Livers transplanted from Abcb4-/+ mice, which have only 50% expression of
115
Chapter 6
the phospholipids translocator Abcb4, into wild-type recipients developed signs of severe
injury of the small intrahepatic bile ducts within two weeks after transplantation (24). In the
current study we focused on the development of NAS, which is a disease of the large bile
ducts (5,52). Our results suggest for the first time that bile salt toxicity is also involved in the
development of large bile duct injury, leading to the clinical and radiological diagnosis of NAS.
Despite the observed low phospholipid / bile salt ratio in patients developing NAS, reflecting
bile toxicity, the overall biliary secretion of bile salts in these patients was lower than in
patients who did not develop NAS. This observation was not expected and introduces the
intriguing possibility that, apart from relative bile salt toxicity, relative bile salt deprivation could
(also) contribute to cholangiocyte injury and the development of NAS. There is substantial
evidence that bile salts are potent inducers of cholangiocyte proliferation and thus bile duct
repair (31,34-36). Uptake of bile salts by cholangiocytes is mediated by the transporter ASBT
(SLC10A2) at the ductular membrane of these cells (30,37). In contrast to cholangiocytes
of the small bile ducts, cholangiocytes in larger bile ducts do express ASBT and, therefore,
these cells can re-absorb bile salts from bile (30,37). This important difference between
cholangiocytes from small and large bile ducts may explain why a previous clinical study
focusing on posttransplant injury of the small bile ducts did not reveal a relationship between
small bile duct injury and reduced bile salt secretion. Collectively, these observations raise the
possibility that the pathogenesis of biliary injury after liver transplantation is different for small
and large bile ducts. In this respect it would have been interesting to study the expression of
ASBT (SLC10A2) in the large bile ducts in the current study. However, it is difficult to take serial
biopsies of the large bile ducts in patients and we were unable to detect ASBT (SLC10A2)
mRNA expression in liver biopsies, which mainly contain small bile ducts (data not shown).
Some bile salts have a more pronounced effect on cholangiocyte proliferation than others.
Taurocholate, for example, may enhance proliferation, while ursodeoxycholate may reduce
the proliferative effects of other bile salts (36,53). In the current study we found no differences
in the bile salt pool composition in patients who developed NAS, compared to those who did
not. Therefore, we have no evidence to suggest that differences in composition of the bile salt
pool are involved in the altered overall bile salt secretion or in the pathogenesis of NAS after
liver transplantation.
A key question that emerges from this study is: what determines the low bile salt secretion
in livers that are developing NAS? Theoretically, reduced biliary bile salt secretion can result
116
Bile composition after liver transplantation and NAS Chapter 6
from a) decreased de novo synthesis, b) impaired hepatobiliary transport at the level of the
canalicular membrane (ABCB11), and/or c) impaired intestinal bile salt re-absorption and fecal
loss of bile salts leading to reduced bile salt pool size. In the classical pathway of de novo bile
salt biosynthesis, CYP7A1 catalyzes the conversion of cholesterol into 7α-hydroxycholesterol,
which is considered to be the rate-controlling step. In humans, the classical pathway accounts
for approximately 80% of total bile salt synthesis (54,55). We observed a lower hepatic
expression of CYP7A1 in patients who later developed NAS, compared to those who did not.
It is tempting to ascribe the reduced bile salt secretion in patients who developed NAS to the
lower expression of CYP7A1. Yet, three issues should be considered in this respect: a) the
difference in CYP7A1 expression was striking, but it did not reach statistical significance, in
contrast to the difference in bile secretion; b) no information is available on the correlation
between CYP7A1 mRNA levels and actual cholate synthesis in the early post-transplant period;
and c) it can be anticipated that the amount of bile salts secreted after liver transplantation is
increasingly derived from re-absorbed (“conserved”) bile salts from the intestine.
To demonstrate or refute increased intestinal loss of bile salts as an explanation for the
differences in biliary bile salt secretion we would have needed the collection of faeces. Although
this was not performed, we have other arguments to assume that the observed differences in
bile salt secretion are not caused by differences in intestinal bile salt loss. Reduced bile salt
pool size due to impaired intestinal reabsorption would be expected to lead to an increased
rather than a decreased hepatic CYP7A1 expression. In addition, a previous study from our
centre has shown that serum bile salt concentrations increase during the first week after
transplantation, which is not compatible with increased intestinal losses (56).
Hepatobiliary secretion of bile salts is an active process which, under normal circumstances,
is mainly influenced by the sinusoidal transporter SLC10A1 and the canalicular transporter
ABCB11. Theoretically, impaired hepatobiliary transport could have resulted form a reduced
expression of these transporter proteins. Compared to pretransplant values, ABCB11 mRNA
expression was decreased immediately after transplantation in livers that later developed
NAS. Although this decrease was not observed in livers that did not develop NAS, there
were no significant differences between the two groups either before or immediately after
transplantation. In accordance with previous observations by Geuken et al. (21), we observed
an increased mRNA expression of the bile salt transporters SLC10A1 and ABCB11 in both
groups after transplantation, while mRNA levels of the phospholipid translocator ABCB4 did
117
Chapter 6
not change. These findings are compatible with the relatively low biliary phospholipid / bile salt
ratio observed early after transplantation. However, there were no significant differences in
the expression of the bile transporters between the two groups, suggesting that the observed
differences in bile salt secretion cannot be explained by differences in gene transcription.
Based on the current study, we cannot exclude that posttranscriptional processes or changes
in transporter activity are involved. Unfortunately, we were unable to perform Western blot
analyses for quantification of transporter protein levels due to the small amount of liver tissue
obtained from needle biopsies.
We also examined whether differences in bile composition between patients who developed
NAS and those who did not could be explained by differences in phospholipids secreted per
bile salt. Therefore we additionally analyzed the biliary hydrophobicity index and the bile salt
independent bile flow. There were no significant differences in the hydrophobicity index or in
the bile salt independent bile flow, indicating that these factors cannot explain the observed
differences between the two groups (57,58).
Several other factors have been shown to contribute to the development of NAS after liver
transplantation, including long cold or warm ischemia times (7,9), inadequate washout and
perfusion of the peribiliary capillary plexus (16,17), and immunological injury (19,59). In the
current study we found no differences in the duration of cold and warm ischemia in livers with
or without NAS. These data support previous suggestions that the pathogenesis of NAS is not
only related to a direct ischemic injury of the biliary epithelium (1,12).
In summary, the results of this prospective clinical study strongly support the hypothesis
that bile composition is involved in the pathogenesis of NAS after liver transplantation.
Patients who developed NAS within one year after liver transplantation were initially clinically
indiscernible from patients who did not develop NAS. However, bile composition in this early
postoperative period was different in these two groups. Patients who developed NAS were
characterized by a reduced biliary secretion of bile salts and phospholipids and a decreased
biliary phospholipid / bile salt ratio. We speculate that those early defects in bile formation,
possibly genetically based, play a role in the injury of the biliary epithelium of large bile ducts
early after transplantation, subsequently leading to the formation of biliary strictures.
118
Bile composition after liver transplantation and NAS Chapter 6
Reference List
Buis CI, Hoekstra H, Verdonk RC, Porte RJ. Causes and consequences of ischemic-type biliary lesions after 1.
liver transplantation. J Hepatobiliary Pancreat Surg 2006;13:517-524.
Calne RY. A new technique for biliary drainage in orthotopic liver transplantation utilizing the gall bladder as a 2.
pedicle graft conduit between the donor and recipient common bile ducts. Ann Surg 1976;184:605-609.
Starzl TE, Marchioro TL, Vonkualla KN, Hermann G, Brittain RS, Waddell WR. Homotransplantation of the liver 3.
in humans. Surg Gynecol Obstet 1963 ;117:659-676.
Verdonk RC, Buis CI, Porte RJ, Van der Jagt EJ, Limburg AJ, van den Berg AP, et al. Anastomotic biliary 4.
strictures after liver transplantation: Causes and consequences. Liver Transpl 2006;12:726-735.
Buis CI, Verdonk RC, Van der Jagt EJ, van der Hilst CS, Slooff MJ, Haagsma EB, et al. Nonanastomotic biliary 5.
strictures after liver transplantation, part 1: Radiological features and risk factors for early vs. late presentation.
Liver Transpl 2007;13:708-718.
Campbell WL, Sheng R, Zajko AB, Abu-Elmagd K, Demetris AJ. Intrahepatic biliary strictures after liver 6.
transplantation. Radiology 1994;191:735-740.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 7.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003;3:885-890.
Pascher A, Neuhaus P. Bile duct complications after liver transplantation. Transpl Int 2005;18:627-642.8.
Sanchez-Urdazpal L, Gores GJ, Ward EM, Maus TP, Wahlstrom HE, Moore SB, et al. Ischemic-type biliary 9.
complications after orthotopic liver transplantation. Hepatology 1992;16:49-53.
Sawyer RG, Punch JD. Incidence and management of biliary complications after 291 liver transplants following 10.
the introduction of transcystic stenting. Transplantation 1998 15;66:1201-1207.
Turrion VS, Alvira LG, Jimenez M, Lucena JL, Nuno J, Pereira F, et al. Management of the biliary complications 11.
associated with liver transplantation: 13 years of experience. Transplant Proc 1999;31:2392-233.
Verdonk RC, Buis CI, Porte RJ, Haagsma EB. Biliary complications after liver transplantation: a review. Scand 12.
J Gastroenterol Suppl 2006; 243: 89-101.
Abt P, Crawford M, Desai N, Markmann J, Olthoff K, Shaked A. Liver transplantation from controlled non-heart-13.
beating donors: an increased incidence of biliary complications. Transplantation 2003;75:1659-1663.
Foley DP, Fernandez L, Leverson G, Chin LT, Kreiger N, Cooper JT, et al. Donation After Cardiac Death: The 14.
University of Wisconsin Experience With Liver Transplantation. Ann Surg 2005; 242: 724-731.
Li S, Stratta RJ, Langnas AN, Wood RP, Marujo W, Shaw BW, Jr. Diffuse biliary tract injury after orthotopic liver 15.
transplantation. Am J Surg 1992;164:536-540.
119
Chapter 6
Moench C, Moench K, Lohse AW, Thies J, Otto G. Prevention of ischemic-type biliary lesions by arterial back-16.
table pressure perfusion. Liver Transpl 2003;9:285-289.
Pirenne J, Van Gelder F, Coosemans W, Aerts R, Gunson B, Koshiba T, et al. Type of donor aortic preservation 17.
solution and not cold ischemia time is a major determinant of biliary strictures after liver transplantation. Liver
Transpl 2001;7:540-545.
Sankary HN, McChesney L, Frye E, Cohn S, Foster P, Williams J. A simple modification in operative technique 18.
can reduce the incidence of nonanastomotic biliary strictures after orthotopic liver transplantation. Hepatology
1995;21:63-69.
Moench C, Uhrig A, Lohse AW, Otto G. CC chemokine receptor 5delta32 polymorphism-a risk factor for 19.
ischemic-type biliary lesions following orthotopic liver transplantation. Liver Transpl 2004;10:434-439.
Sanchez-Urdazpal L, Sterioff S, Janes C, Schwerman L, Rosen C, Krom RA. Increased bile duct complications 20.
in ABO incompatible liver transplant recipients. Transplant Proc 1991;23:1440-1441.
Geuken E, Visser D, Kuipers F, Blokzijl H, Leuvenink HG, de Jong KP, et al. Rapid increase of bile salt secretion 21.
is associated with bile duct injury after human liver transplantation. J Hepatol 2004;41:1017-1025.
Hertl M, Harvey PR, Swanson PE, West DD, Howard TK, Shenoy S, et al. Evidence of preservation injury to bile 22.
ducts by bile salts in the pig and its prevention by infusions of hydrophilic bile salts. Hepatology 1995;21:1130-
1137.
Hertl M, Hertl MC, Kluth D, Broelsch CE. Hydrophilic bile salts protect bile duct epithelium during cold 23.
preservation: a scanning electron microscopy study. Liver transplantation 2000;6:207-212.
Hoekstra H, Porte RJ, Tian Y, Jochum W, Stieger B, Moritz W, et al. Bile salt toxicity aggravates cold ischemic 24.
injury of bile ducts after liver transplantation in Mdr2+/- mice. Hepatology 2006 20;43:1022-1031.
Palmeira CM, Rolo AP. Mitochondrially-mediated toxicity of bile acids. Toxicology 2004 15;203:1-15.25.
De Vree JM, Jacquemin E, Sturm E, Cresteil D, Bosma PJ, Aten J, et al. Mutations in the MDR3 gene cause 26.
progressive familial intrahepatic cholestasis. Proc Natl Acad Sci U S A 1998 6;95:282-287.
Smit J, Schinkel A, Oude Elferink R, Groen A, Wagenaar E, van Deemter. Homozygous disruption of the murine 27.
mdr2 P-glycoprotein gene leads to a. Cell 1993;75:451.
Wagner M, Zollner G, Trauner M. Ischemia and cholestasis: more than (just) the bile ducts! Transplantation 28.
2008 27;85:1083-5.
Yska MJ, Buis CI, Monbaliu D, Schuurs TA, Gouw ASH, Kahmann ONH, Visser DS, Pirenne J, Porte RJ. The 29.
role of bile salt toxicity in the pathogenesis of bile duct injury after non heart-beating porcine liver transplantation.
Transplantation 2008;85:1625-31.
Alpini G, Glaser SS, Rodgers R, Phinizy JL, Robertson WE, Lasater J, et al. Functional expression of the apical Na+-30.
dependent bile acid transporter in large but not small rat cholangiocytes. Gastroenterology 1997;113:1734-1740.
120
Bile composition after liver transplantation and NAS Chapter 6
Alpini G, Glaser S, Robertson W, Phinizy JL, Rodgers RE, Caligiuri A, et al. Bile acids stimulate proliferative and 31.
secretory events in large but not small cholangiocytes. Am J Physiol 1997;273:G518-G529.
Glaser S, Francis H, Demorrow S, Lesage G, Fava G, Marzioni M, et al. Heterogeneity of the intrahepatic biliary 32.
epithelium. World J Gastroenterol 2006 14;12:3523-3536.
Ueno Y, Alpini G, Yahagi K, Kanno N, Moritoki Y, Fukushima K, et al. Evaluation of differential gene expression 33.
by microarray analysis in small and large cholangiocytes isolated from normal mice. Liver Int 2003;23:449-
459.
Alpini G, Glaser SS, Ueno Y, Rodgers R, Phinizy JL, Francis H, et al. Bile acid feeding induces cholangiocyte 34.
proliferation and secretion: evidence for bile acid-regulated ductal secretion. Gastroenterology 1999;116:179-
186.
Alpini G, Glaser S, Alvaro D, Ueno Y, Marzioni M, Francis H, et al. Bile acid depletion and repletion 35.
regulate cholangiocyte growth and secretion by a phosphatidylinositol 3-kinase-dependent pathway in rats.
Gastroenterology 2002;123:1226-1237.
Xia X, Francis H, Glaser S, Alpini G, Lesage G. Bile acid interactions with cholangiocytes. World J Gastroenterol 36.
2006 14;12:3553-3563.
Lazaridis KN, Tietz P, Wu T, Kip S, Dawson PA, Larusso NF. Alternative splicing of the rat sodium/bile acid 37.
transporter changes its cellular localization and transport properties. Proc Natl Acad Sci U S A 2000 26;97:11092-
11097.
Ploeg RJ, D’alessandro AM, Knechtle SJ, Stegall MD, Pirsch JD, Hoffmann RM, et al. Risk factors for primary 38.
dysfunction after liver transplantation--a multivariate analysis. Transplantation 1993;55:807-813.
Buis CI, van der SG, Visser DS, Nolte IM, Hepkema BG, Nijsten M, et al. Heme oxygenase-1 genotype of the 39.
donor is associated with graft survival after liver transplantation. Am J Transplant 2008;8:377-385.
Miyamoto S, Polak WG, Geuken E, Peeters PM, de Jong KP, Porte RJ, et al. Liver transplantation with 40.
preservation of the inferior vena cava. A comparison of conventional and piggyback techniques in adults. Clin
Transplant 2004;18:686-693.
Polak WG, Miyamoto S, Nemes BA, Peeters PM, de Jong KP, Porte RJ, et al. Sequential and simultaneous 41.
revascularization in adult orthotopic piggyback liver transplantation. Liver Transpl 2005;11:934-940.
Lenzen R. In liver transplantation, T tube bile represents total bile flow. Liver transplantation and surgery 42.
1999;5:8.
Turley SD, Dietschy JM. Re-evaluation of the 3 alpha-hydroxysteroid dehydrogenase assay for total bile acids 43.
in bile. J Lipid Res 1978;19:924-928.
Kok T, Hulzebos CV, Wolters H, Havinga R, Agellon LB, Stellaard F, et al. Enterohepatic circulation of bile salts 44.
in farnesoid X receptor-deficient mice: efficient intestinal bile salt absorption in the absence of ileal bile acid-
binding protein. J Biol Chem 2003;278:41930-41937.
121
Chapter 6
Heuman DM. Quantitative estimation of the hydrophilic-hydrophobic balance of mixed bile salt solutions. J Lipid 45.
Res 1989;30:719-730.
Feller RB, Waugh RC, Selby WS, Dolan PM, Sheil AG, McCaughan GW. Biliary strictures after liver 46.
transplantation: clinical picture, correlates and outcomes. J Gastroenterol Hepatol 1996;11:21-25.
Rull R, Garcia Valdecasas JC, Grande L, Fuster J, Lacy AM, Gonzalez FX, et al. Intrahepatic biliary lesions after 47.
orthotopic liver transplantation. Transpl Int 2001;14:129-134.
Galle PR, Theilmann L, Raedsch R, Otto G, Stiehl A. Ursodeoxycholate reduces hepatotoxicity of bile salts in 48.
primary human hepatocytes. Hepatology 1990;12:486-491.
Schmucker DL, Ohta M, Kanai S, Sato Y, Kitani K. Hepatic injury induced by bile salts: correlation between 49.
biochemical and morphological events. Hepatology 1990;12:1216-1221.
Trauner M, Meier PJ, Boyer JL. Molecular pathogenesis of cholestasis. N Engl J Med 1998 22;339:1217-50.
1227.
Arrese M, Trauner M. Molecular aspects of bile formation and cholestasis. Trends Mol Med 2003;9:558-564.51.
Verdonk RC, Buis CI, Van der Jagt EJ, Gouw AS, Limburg AJ, Slooff MJ, et al. Nonanastomotic biliary strictures 52.
after liver transplantation, part 2: Management, outcome, and risk factors for disease progression. Liver Transpl
2007;13:725-732.
Alvaro D, Gigliozzi A, Attili AF. Regulation and deregulation of cholangiocyte proliferation. J Hepatol 2000;33:333-53.
340.
Vlahcevic ZR, Stravitz RT, Heuman DM, Hylemon PB, Pandak WM. Quantitative estimations of the contribution 54.
of different bile acid pathways to total bile acid synthesis in the rat. Gastroenterology 1997;113:1949-1957.
Duane WC, Javitt NB. 27-hydroxycholesterol: production rates in normal human subjects. J Lipid Res 55.
1999;40:1194-1199.
Haagsma EB, Huizenga JR, Vonk RJ, Albers CJ, Grond J, Krom RA, et al. Composition of bile after orthotopic 56.
liver transplantation. Scand J Gastroenterol 1987;22:1049-1055.
Verkade HJ. Inhibition of biliary phospholipid and cholesterol secretion by organic anions affects bile canalicular 57.
membrane composition and fluidity. J Gastroenterol 2000;35:481-485.
Verkade HJ, Vonk RJ, Kuipers F. New insights into the mechanism of bile acid-induced biliary lipid secretion. 58.
Hepatology 1995;21:1174-1189.
Carrasco L. Effects of cold ischemia time on the graft after orthotopic liver. Transplantation 1996;61:393.59.


Polymorphisms of hepatobiliary phospholipid transporter MDR-3 associated with non anastomotic strictures after human liver transplantation7
Submitted
Carlijn I BuisGerrit van der Steege
Ilja M NolteDorien S VisserRobert J Porte
124
ABCB4 gene polymorphism and NAS Chapter 7
Abstract
Non-anastomotic biliary strictures (NAS) are an important and troublesome biliary
complication after liver transplantation. The pathogenesis of NAS is not completely clear,
but studies have suggested that bile salt toxicity, due to an imbalance between biliary bile
salts and phospholipids is involved. Hepatobiliary transporter proteins are responsible for bile
secretion and composition. Aim of this study was to assess whether genetic variations in these
transporters are associated with the development of NAS.
In 461 liver transplant procedures, we studied donor genotype of three of the most relevant
hepatobiliary transporters: the bile salt export pump (ABCB11), the transporter of phospholipids
(ABCB4) and the transporter of glutathione and bilirubin (ABCC2). Four to five tagging single
nucleotide polymorphisms (SNPs) with an equal physical distribution per gene were selected
using HapMap data. Haplotypes were constructed using an Expectation-Maximization
algorithm to estimate haplotype frequencies. The occurrence of NAS was determined for
livers with the various transporter genotypes.
NAS were detected in 77 patients (16.7%) after transplantation. Patients who received a donor
liver with ABCB4 haplotype AGGTA developed NAS almost twice as often as donor livers with
other haplotypes (28% versus 15%; p = 0.007). In a multivariate Cox regression analysis, the
AGGTA haplotype of the ABCB4 gene in the donor, was confirmed as an independent risk
factor for NAS (HR=2.23, 95% CI= 1.29 – 3.85; p = 0.004). Various haplotypes of the ABCB11
and the ABCC2 gene, or individual SNPs, were not associated with NAS.
Conclusion: A common haplotype in the transporter of phospholipids (ABCB4) in donor livers
is independently associated with a two-fold increased risk for NAS after liver transplantation.
Transport of phospholipids into the bile in livers with this risk haplotype might be altered after
liver transplantation, contributing to the development of NAS.
125
Chapter 7
Introduction
Biliary complications are reported in 10 to 30% of the patients after liver transplantation
representing a major cause of morbidity and mortality (1). Non-anastomotic biliary strictures
(NAS) are considered to be the most troublesome biliary complication, because they may
occur at multiple locations in the biliary tree and are frequently resistant to therapy (2,3). Graft
survival is markedly reduced in patients developing NAS; 16% of all patients with NAS need a
re-transplantation and 35% will require an interventional treatment (3).
The occurrence of NAS can partly be attributed to thrombosis of the hepatic artery. The
pathogenesis of NAS developing in the absence of hepatic artery thrombosis is less clear
(1,4). In general, three mechanisms contributing to bile duct injury after liver transplantation
have been postulated: preservation or ischemia-related injury (5-11), immunological processes
(7,12,13) and injury induced by cytotoxicity of biliary bile salts (14-17). Bile salts have potent
detergent properties and may damage cells in the absence of phospholipids by affecting the
integrity of cellular membranes (15,18). Damage to the canalicular membrane of the biliary
epithelial cells could result in progressive destruction of bile ducts (19). Normally, these toxic
effects of bile salts are prevented through neutralization by phospholipids. We have recently
shown that changes in bile formation, leading to cytotoxic bile with a relative low phospholipid-
to-bile salt ratio, are associated with bile duct injury and the development of NAS after liver
transplantation (14,17,20,21).
Bile production depends on an active process involving the transport of bile acids,
phospholipids and other osmotic compounds across a concentration gradient into the bile
canaliculus. Hepatobiliary transporter proteins play a rate-limiting role in this process. Genetic
variations in the phospholipid translocator, multiple drug resistance protein 3 (MDR3, official
name ATP binding cassette, subfamily B, member 4 or ABCB4) have been associated with
abnormal phenotypes, characterized by the production of bile with a low biliary phospholipid
content, leading to bile duct injury and intrahepatic cholestasis. A genetic variation inevitably
leading to disease is the mutation in the ABCB4 gene associated with progressive familial
intrahepatic cholestasis type III (PFIC III) (22). Characteristic clinical features of these patients
are jaundice, recurrent cholangitis and elevated serum γ-glutamyltransferase levels, reflecting
the destruction of cell membranes of the biliary epithelium. Other genetic variations of the
ABCB4 gene have a less stable phenotype and may lead to symptoms only under specific
126
ABCB4 gene polymorphism and NAS Chapter 7
circumstances. An example of this is intrahepatic cholestasis of pregnancy (ICP), which
may occur in women who were previously without symptoms, but develop jaundice during
pregnancy. (19,23-28).
SNPs in the bile salt exporter pump (BSEP, official name ABCB11) have been related with
a spectrum of clinical phenotypes such as the syndrome of benign recurrent intrahepatic
cholestasis (BRIC) (29), PFIC-2 (30), and ICP (28,31). Multidrug resistance related protein 2
(MRP-2, official name ABCC2), which is a transporter of bilirubin and glutathion (GSH) into
bile, is known from the benign human disorder Dubin Johnson, which is characterized by an
increase of conjugated bilirubin without elevation of liver enzymes (32).
It has remained unclear whether variations in these genes encoding for hepatobiliary
transporters might contribute to the pathogenesis of NAS after liver transplantation. We
hypothesized that there variations in these genes that do not result in an abnormal phenotype
under normal, physiological conditions, but that are associated with to the development of bile
duct injury under stressful conditions, such as liver transplantation. Such a mechanism would
be similar to the development of ICP in women with certain ABCB4 polymorphisms.
The aim of the present study was to determine whether genetic variations in the genes
encoding for hepatobiliary transporters are associated with the development of NAS in a large
prospective cohort of 461 adult liver transplant recipients.
Patients and Methods
Patients
Between January 1990 and January 2005, 720 liver transplantations were performed in 621
patients in our center. After exclusion of pediatric patients (n=160), 461 adult liver transplant
recipients remained. Cryopreserved splenocyts from the donors were used for the genotyping.
Recipient follow-up was until December 2007, resulting in a median follow-up of 8.2 years
(interquartile range 4.6–12.6 years). Surgical procedure and postoperative management
have been described previously (2). In short, ABO blood group-identical or compatible grafts
from brain-death donors with normal or near normal liver function tests were used for all
patients. Immunosuppressive protocols were based on a calcineurin inhibitor (tacrolimus or
cyclosporine A) either with or without azathioprine and a rapid taper of steroids. Biopsy-proven
acute rejection was treated when clinically indicated with a bolus of methylprednisolone on
127
Chapter 7
three consecutive days. Doppler ultrasound was performed routinely at postoperative days
1, 3, and 7 and later on demand to rule out vascular or biliary complications or parenchymal
lesions. Cholangiography via a biliary drain was routinely performed between postoperative
day 10 –14 and later on demand (i.e. for rising cholestatic laboratory parameters or dilatation
of bile ducts on ultrasound).
Donor data was collected from the donor forms and checked and completed with information
from the archives of the Eurotransplant Organization, Leiden, The Netherlands. Recipient
data were obtained from a prospectively collected computer database. If necessary the
original patient notes were reviewed for missing information. Tissue and data collection was
performed according to the guidelines of the medical ethical committee of our institution and
the Dutch Federation of Scientific Societies.
Diagnosis of NAS
Primary outcome parameter in this study was the development of NAS. For this study NAS
were defined as any stricture, dilatation, or irregularity of the intra- or extrahepatic bile ducts
of the liver graft, either with or without biliary sludge formation, after exclusion of hepatic artery
thrombosis by either Doppler ultrasound or conventional angiography. Isolated strictures at
the bile duct anastomosis were, by definition, excluded from this analysis and have been
described elsewhere (33).
Selection of Hepatobiliary Transporter SNPs and Genotyping
The following genes were studied: the phospholipid translocator (ABCB4), the most prominent
bile salt transporter (ABCB11), and the main canalicular organic anion transporter and driving
force of the bile salt independent bile flow (ABCC2). Genomic DNA was isolated from donor
splenocytes using a commercial kit (Gentra Systems, Minneapolis, MN, USA). SNPs were
selected based on data from the HapMap database (release #16, www.hapmap.org), using
the Haploview tagging tool. Per locus only those SNPs were selected that tagged haplotypes
with a frequency in the HapMap Caucasian dataset of more than 10% and with a minor allele
frequency around 20%. In addition, we tried to combine this selection criterion with an equal
physical distribution across the genes, preferably with exonic location. TaqMan assays were
used to genotype the ABC transporter SNPs. These were obtained from Applied Biosystems
(Foster City, CA, USA) by the assay-on-demand or the assay-by-design services. Details of
the various SNPs are given in Table 1.
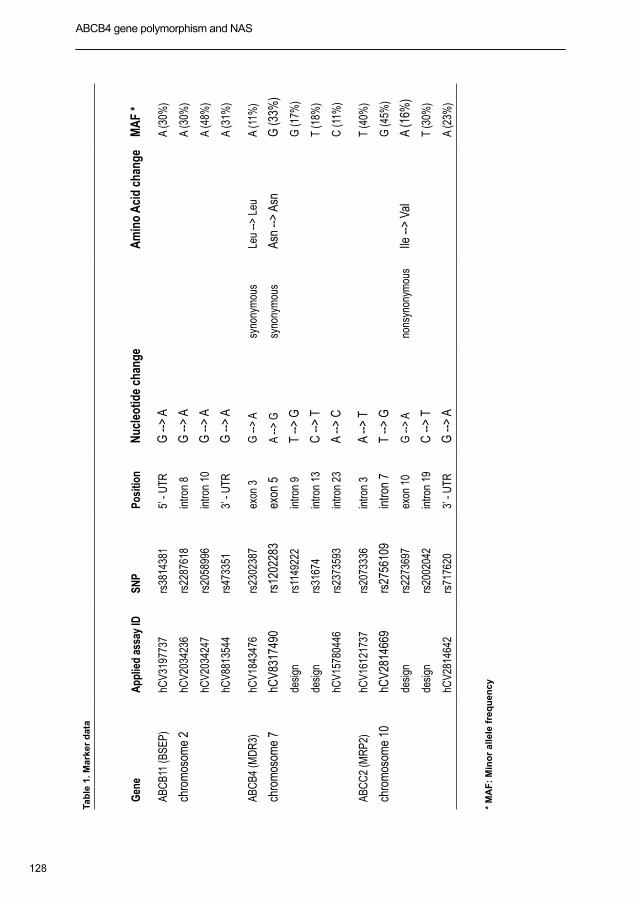
128
ABCB4 gene polymorphism and NAS Chapter 7
Tab
le 1
. Mar
ker
dat
a
Gen
eA
pplie
d as
say
IDSN
PPo
sitio
n N
ucle
otid
e ch
ange
Am
ino
Aci
d ch
ange
MA
F *
ABC
B11
(BSE
P)hC
V319
7737
rs38
1438
15’
- U
TRG
-->
AA
(30%
)
chro
mos
ome
2hC
V203
4236
rs22
8761
8in
tron
8G
-->
AA
(30%
)
hCV2
0342
47rs
2058
996
intro
n 10
G --
> A
A (4
8%)
hCV8
8135
44rs
4733
513’
- U
TRG
-->
AA
(31%
)
ABC
B4 (M
DR
3)hC
V184
3476
rs23
0238
7ex
on 3
G --
> A
syno
nym
ous
Leu
--> L
euA
(11%
)
chro
mos
ome
7hC
V831
7490
rs12
0228
3ex
on 5
A -->
Gsy
nony
mou
sAs
n -->
Asn
G (3
3%)
desi
gnrs
1149
222
intro
n 9
T -->
GG
(17%
)
desi
gnrs
3167
4in
tron
13
C --
> T
T (1
8%)
hCV1
5780
446
rs23
7359
3in
tron
23A
--> C
C (1
1%)
ABC
C2
(MR
P2)
hCV1
6121
737
rs20
7333
6in
tron
3A
--> T
T (4
0%)
chro
mos
ome
10hC
V281
4669
rs27
5610
9in
tron
7T
--> G
G (4
5%)
desi
gnrs
2273
697
exon
10
G --
> A
nons
ynon
ymou
sIle
-->
Val
A (1
6%)
desi
gnrs
2002
042
intro
n 19
C --
> T
T (3
0%)
hCV2
8146
42rs
7176
203’
- U
TRG
-->
AA
(23%
)
* M
AF
: M
ino
r al
lele
fre
qu
ency

129
Chapter 7
Statistical Analysis
Descriptive, continuous variables are reported as median and interquartile ranges (IQR) and
categorical variables are reported as numbers with percentage. The power of this study was greater
than 80% to detect an odds ratio (HR) of 1.71 or larger for SNPs with a minor allele frequency
of at least 20% at the statistical significant level of 5%. Prior to all analyses, Hardy–Weinberg
equilibrium was confirmed for all genotypes using the chi-squared test. Single SNP analysis
was performed with chi-squared test. Haplotype analysis was performed using an Expectation-
Maximization algorithm to estimate haplotype frequencies (in-house software). The frequencies
were estimated on the total group of patients and these frequencies were used to estimate the
haplotype frequencies among patients with and patients without NAS. In addition for each specific
haplotype a log-likelihood ratio test was performed to test whether the frequencies of this haplotype
differed between patients with and without NAS. Incidence rate of NAS was estimated with the
Kaplan–Meier actuarial method and compared with the log-rank test. Furthermore, if the probability
of a specific haplotype combination (using frequencies of the total group) was higher than 90%, that
combination was assumed to the true combination. In this way, being carrier of specific haplotypes
could be determined for use as a covariate in a multivariate Cox regression model.
Statistical analyses were performed using SPSS Version 14.0 for Windows (SPSS Inc., Chicago,
IL, USA). All p-values were two-tailed and considered as statistically significant at levels < 0.05.
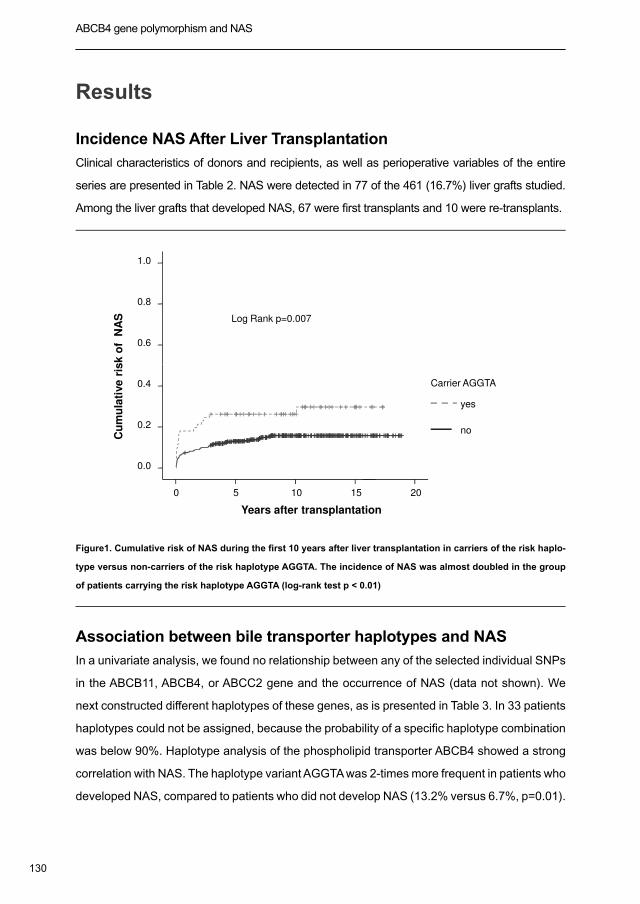
130
ABCB4 gene polymorphism and NAS Chapter 7
Results
Incidence NAS After Liver Transplantation
Clinical characteristics of donors and recipients, as well as perioperative variables of the entire
series are presented in Table 2. NAS were detected in 77 of the 461 (16.7%) liver grafts studied.
Among the liver grafts that developed NAS, 67 were first transplants and 10 were re-transplants.
1.0
0.8
0.6
Cu
mu
lati
ve
ris
k o
f N
AS Log Rank p=0.007
20151050
0.4
0.2
0.0
Years after transplantation
Cu
mu
lati
ve
ris
k o
f N
AS
yes
no
Carrier AGGTA
Figure1. Cumulative risk of NAS during the first 10 years after liver transplantation in carriers of the risk haplo-
type versus non-carriers of the risk haplotype AGGTA. The incidence of NAS was almost doubled in the group
of patients carrying the risk haplotype AGGTA (log-rank test p < 0.01)
Association between bile transporter haplotypes and NAS
In a univariate analysis, we found no relationship between any of the selected individual SNPs
in the ABCB11, ABCB4, or ABCC2 gene and the occurrence of NAS (data not shown). We
next constructed different haplotypes of these genes, as is presented in Table 3. In 33 patients
haplotypes could not be assigned, because the probability of a specific haplotype combination
was below 90%. Haplotype analysis of the phospholipid transporter ABCB4 showed a strong
correlation with NAS. The haplotype variant AGGTA was 2-times more frequent in patients who
developed NAS, compared to patients who did not develop NAS (13.2% versus 6.7%, p=0.01).
131
Chapter 7
Analyses of haplotype variations of the ABCB11 and ABCC2 genes were not associated with
the occurrence of NAS (data not shown).
As shown in figure 1, the cumulative incidence of NAS in livers with the AGGTA risk haplotype
was almost two-times higher than in livers that did not carry the AGGTA risk haplotype (28%
versus 15%; p < 0.01).
To determine whether the AGGTA haplotype of the ABCB4 gene is an independent risk factor
for NAS, we next performed a multivariate Cox regression analysis. In this analysis we included
all accepted clinical risk factors for NAS that have been described previously, including type
of perfusion solution, cold ischemia time, warm ischemia time, indication for transplantation,
gender match, as well as the risk haplotype AGGTA. In this multivariate Cox regression model,
the donor AGGTA haplotype of the ABCB4 gene was independently associated with NAS
(HR=2.23, 95% CI= 1.29 – 3.85; p=0.004).
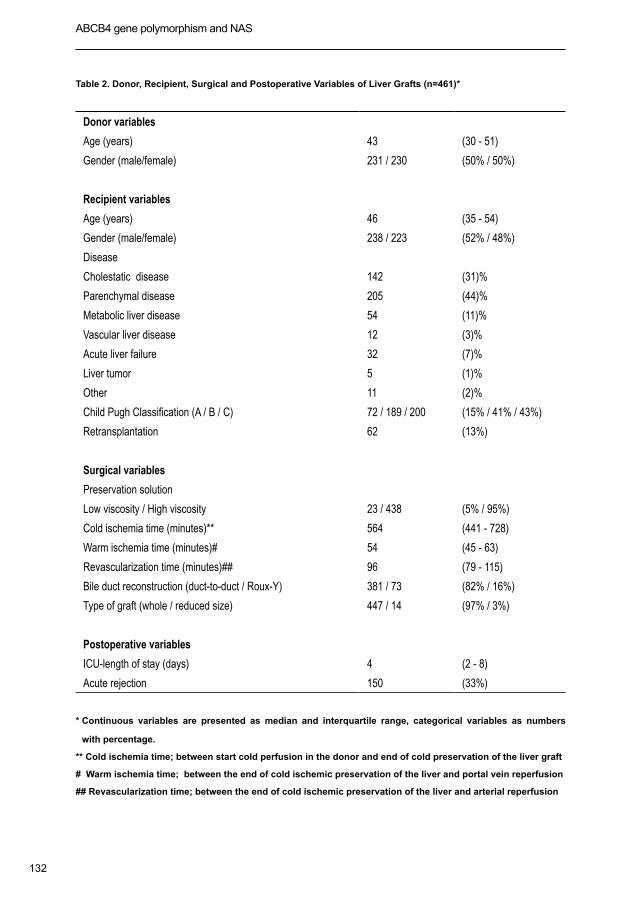
132
ABCB4 gene polymorphism and NAS Chapter 7
Table 2. Donor, Recipient, Surgical and Postoperative Variables of Liver Grafts (n=461)*
Donor variables
Age (years) 43 (30 - 51)
Gender (male/female) 231 / 230 (50% / 50%)
Recipient variables
Age (years) 46 (35 - 54)
Gender (male/female) 238 / 223 (52% / 48%)
Disease
Cholestatic disease 142 (31)%
Parenchymal disease 205 (44)%
Metabolic liver disease 54 (11)%
Vascular liver disease 12 (3)%
Acute liver failure 32 (7)%
Liver tumor 5 (1)%
Other 11 (2)%
Child Pugh Classification (A / B / C) 72 / 189 / 200 (15% / 41% / 43%)
Retransplantation 62 (13%)
Surgical variables
Preservation solution
Low viscosity / High viscosity 23 / 438 (5% / 95%)
Cold ischemia time (minutes)** 564 (441 - 728)
Warm ischemia time (minutes)# 54 (45 - 63)
Revascularization time (minutes)## 96 (79 - 115)
Bile duct reconstruction (duct-to-duct / Roux-Y) 381 / 73 (82% / 16%)
Type of graft (whole / reduced size) 447 / 14 (97% / 3%)
Postoperative variables
ICU-length of stay (days) 4 (2 - 8)
Acute rejection 150 (33%)
* Continuous variables are presented as median and interquartile range, categorical variables as numbers
with percentage.
** Cold ischemia time; between start cold perfusion in the donor and end of cold preservation of the liver graft
# Warm ischemia time; between the end of cold ischemic preservation of the liver and portal vein reperfusion
## Revascularization time; between the end of cold ischemic preservation of the liver and arterial reperfusion
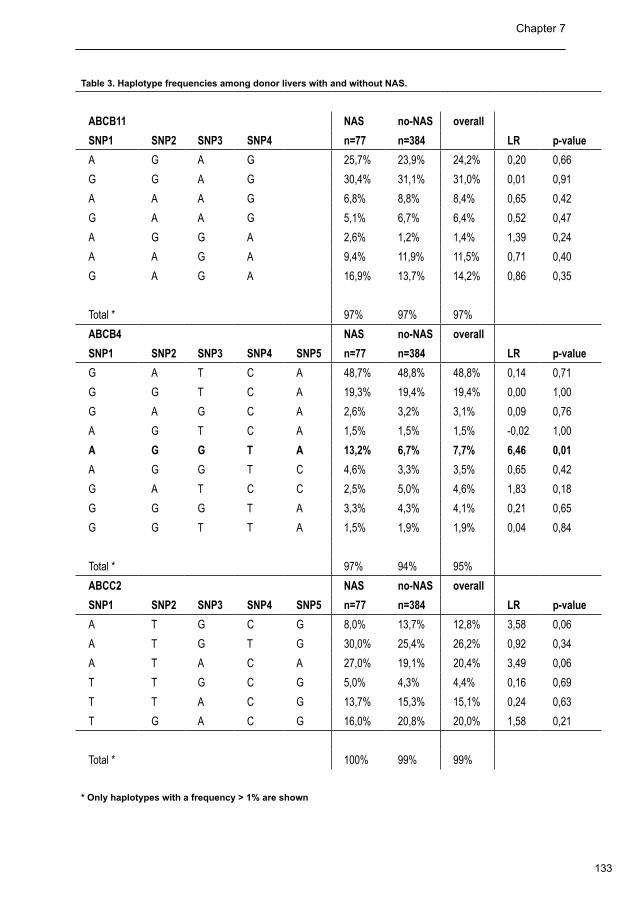
133
Chapter 7
Table 3. Haplotype frequencies among donor livers with and without NAS.
ABCB11 NAS no-NAS overall
SNP1 SNP2 SNP3 SNP4 n=77 n=384 LR p-value
A G A G 25,7% 23,9% 24,2% 0,20 0,66
G G A G 30,4% 31,1% 31,0% 0,01 0,91
A A A G 6,8% 8,8% 8,4% 0,65 0,42
G A A G 5,1% 6,7% 6,4% 0,52 0,47
A G G A 2,6% 1,2% 1,4% 1,39 0,24
A A G A 9,4% 11,9% 11,5% 0,71 0,40
G A G A 16,9% 13,7% 14,2% 0,86 0,35
Total * 97% 97% 97%
ABCB4 NAS no-NAS overall
SNP1 SNP2 SNP3 SNP4 SNP5 n=77 n=384 LR p-value
G A T C A 48,7% 48,8% 48,8% 0,14 0,71
G G T C A 19,3% 19,4% 19,4% 0,00 1,00
G A G C A 2,6% 3,2% 3,1% 0,09 0,76
A G T C A 1,5% 1,5% 1,5% -0,02 1,00
A G G T A 13,2% 6,7% 7,7% 6,46 0,01
A G G T C 4,6% 3,3% 3,5% 0,65 0,42
G A T C C 2,5% 5,0% 4,6% 1,83 0,18
G G G T A 3,3% 4,3% 4,1% 0,21 0,65
G G T T A 1,5% 1,9% 1,9% 0,04 0,84
Total * 97% 94% 95%
ABCC2 NAS no-NAS overall
SNP1 SNP2 SNP3 SNP4 SNP5 n=77 n=384 LR p-value
A T G C G 8,0% 13,7% 12,8% 3,58 0,06
A T G T G 30,0% 25,4% 26,2% 0,92 0,34
A T A C A 27,0% 19,1% 20,4% 3,49 0,06
T T G C G 5,0% 4,3% 4,4% 0,16 0,69
T T A C G 13,7% 15,3% 15,1% 0,24 0,63
T G A C G 16,0% 20,8% 20,0% 1,58 0,21
Total * 100% 99% 99%
* Only haplotypes with a frequency > 1% are shown
134
ABCB4 gene polymorphism and NAS Chapter 7
Discussion
We have tested the hypothesis that genetic variability in hepatobiliary transporters in donor
livers is associated with the development of NAS after transplantation. We have evaluated
this in a large cohort of 461 liver transplant recipients. The most important finding in this
study was a strong association between the phospholipid translocator ABCB4 genotype and
the development of NAS after liver transplantation. A common haplotype in the ABCB4 gene
was significantly more present in livers that developed NAS, compared to those that did not
develop NAS. A multivariate Cox regression analysis confirmed that the risk haplotype of
the ABCB4 gene is an independent risk factor for the development of NAS. We found no
association between haplotypes of the ABCB11 and ABCC2 gene and the occurrence of NAS
after liver transplantation.
There is accumulating evidence from both clinical and experimental studies that altered
bile composition with decreased phospholipid secretion may contribute to biliary injury and
subsequent intrahepatic biliary strictures after liver transplantation (14,17,20). Although previous
studies have suggested that changes in the expression of the phospholipids translocator ABCB4
may play a role in the reduced biliary excretion of biliary phospholipids after liver transplantation,
the impact of a genetic predisposition has not been reported before (14,21).
Although we did not perform bile analysis in this large cohort of patients, the observed
association between the AGGTA ABCB4 haplotype strongly suggests that biliary phospholipid
secretion in livers with this haplotype is reduced after liver transplantation. Reduced biliary
secretion of phospholipids results in a lower biliary phospholipids-to-bile salt ratio, which has
been associated with increased bile duct damage. Normally, the toxic effects of bile salts
are prevented by the neutralization of bile salts by phospholipids through the formation of
mixed micelles in bile. In case of relative excess of bile salts, either due to increased bile
salt secretion or reduced secretion of phospholipids, free non-micellar bile salts may cause
cholangiocyte injury, pericholangitis and periductal fibrosis (34,35). The role of diminished
biliary phospholipids secretion and increased bile salt toxicity in the pathogenesis of bile
duct injury has previously been demonstrated in an experimental study using a murine liver
transplant model (17). In this study livers from Abcb4-/+ mice, expressing only 50% of the
phospholipids translocator Abcb4, were transplanted into wild-type recipients. Although livers
and bile ducts from Abcb4-/+ mice are phenotypically normal under normal circumstances,
135
Chapter 7
these livers developed severe injury of the intrahepatic bile ducts after transplantation. This
finding indicates that, although a reduction of biliary phospholipid secretion of up to 50%
alone does not result in bile duct injury, this may result in overt bile duct injury when a second
insult is present, such as ischemia / reperfusion injury (17). This animal study suggest that
the impact of cold ischemia and reperfusion on ABCB4 function – specifically in genetically
susceptible individuals with an ABCB4 genetic variation – could contribute to bile duct injury
following liver transplantation (36).
Several genetic variations in hepatobiliary transporters have been linked to various types of
cholestatic disorders and cholangiopathies (19,36). A large number of clinicall relevant SNPs
of the ABCB4 gene have been reported in literature (22,24,26-28,37-39). For two reasons
we found it not rational to analyse these individual SNPs in the current study. First of all,
some of the reported gene variations have been linked to a known and permanent cholestatic
phenotype, such as PFIC-3, and it is unlikely that patients with such a phenotype were
selected as organ donor. Secondly, the prevelance of most of the individual SNPs reported in
the literature is low, and it is unlikely that very rare SNPs could accountable for a complication
such as NAS with an incidence of around 16%.
In conclusion, in this large series of 461 liver transplant recipients, we established a strong
association between donor ABCB4 haplotype and the development of NAS after liver
transplantation. Livers with the AGGTA haplotype of the ABCB4 gene were found to have a
two-times higher risk of developing NAS, compared to livers without this haplotype. These
data contribute to the accumulating evidence that a (relative) reduction in biliary phospholipid
secretion, resulting in the increased toxicity of bile salts, play an important role in the
development of bile duct injury and NAS after liver transplantation, and that alterations in bile
composition after transplantation may have part of its origin in the donor.
136
ABCB4 gene polymorphism and NAS Chapter 7
Reference List
Buis CI, Hoekstra H, Verdonk RC, Porte RJ. Causes and consequences of ischemic-type biliary lesions after 1.
liver transplantation. J Hepatobiliary Pancreat Surg 2006;13:517-24.
Buis CI, Verdonk RC, Van der Jagt EJ, van der Hilst CS, Slooff MJ, Haagsma EB, et al. Nonanastomotic biliary 2.
strictures after liver transplantation, part 1: Radiological features and risk factors for early vs. late presentation.
Liver Transpl 2007;13:708-18.
Verdonk RC, Buis CI, Van der Jagt EJ, Gouw AS, Limburg AJ, Slooff MJ, et al. Nonanastomotic biliary strictures 3.
after liver transplantation, part 2: Management, outcome, and risk factors for disease progression. Liver Transpl
2007;13:725-32.
Verdonk RC, Buis CI, Porte RJ, Haagsma EB. Biliary complications after liver transplantation: a review. Scand 4.
J Gastroenterol Suppl 2006;89-101.
Abt P, Crawford M, Desai N, Markmann J, Olthoff K, Shaked A. Liver transplantation from controlled non-heart-5.
beating donors: an increased incidence of biliary complications. Transplantation 2003;75:1659-63.
Foley DP, Fernandez L, Leverson G, Chin LT, Kreiger N, Cooper JT, et al. Donation After Cardiac Death: The 6.
University of Wisconsin Experience With Liver Transplantation. Ann.Surg. 242, 724-731. 2005.
Guichelaar MM, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk factors for and clinical 7.
course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003;3:885-90.
Li S, Stratta RJ, Langnas AN, Wood RP, Marujo W, Shaw BW, Jr. Diffuse biliary tract injury after orthotopic liver 8.
transplantation. Am J Surg 1992;164:536-40.
Moench C, Moench K, Lohse AW, Thies J, Otto G. Prevention of ischemic-type biliary lesions by arterial back-9.
table pressure perfusion. Liver Transpl 2003;9:285-9.
Pirenne J, Van Gelder F, Coosemans W, Aerts R, Gunson B, Koshiba T, et al. Type of donor aortic preservation 10.
solution and not cold ischemia time is a major determinant of biliary strictures after liver transplantation. Liver
Transpl 2001;7:540-5.
Sankary HN, McChesney L, Frye E, Cohn S, Foster P, Williams J. A simple modification in operative technique 11.
can reduce the incidence of nonanastomotic biliary strictures after orthotopic liver transplantation. Hepatology
1995;21:63-9.
Moench C, Uhrig A, Lohse AW, Otto G. CC chemokine receptor 5delta32 polymorphism-a risk factor for 12.
ischemic-type biliary lesions following orthotopic liver transplantation. Liver Transpl 2004;10:434-9.
Sanchez-Urdazpal L, Sterioff S, Janes C, Schwerman L, Rosen C, Krom RA. Increased bile duct complications 13.
in ABO incompatible liver transplant recipients. Transplant Proc 1991;23(1 Pt 2):1440-1.
137
Chapter 7
Geuken E, Visser D, Kuipers F, Blokzijl H, Leuvenink HG, de Jong KP, et al. Rapid increase of bile salt secretion 14.
is associated with bile duct injury after human liver transplantation. J Hepatol 2004;41:1017-25.
Hertl M, Harvey PR, Swanson PE, West DD, Howard TK, Shenoy S, et al. Evidence of preservation injury to bile 15.
ducts by bile salts in the pig and its prevention by infusions of hydrophilic bile salts. Hepatology 1995;21:1130-7.
Hertl M, Hertl MC, Kluth D, Broelsch CE. Hydrophilic bile salts protect bile duct epithelium during cold 16.
preservation: a scanning electron microscopy study. Liver transplantation 2000;6:207-12.
Hoekstra H, Porte RJ, Tian Y, Jochum W, Stieger B, Moritz W, et al. Bile salt toxicity aggravates cold ischemic 17.
injury of bile ducts after liver transplantation in Mdr2+/- mice. Hepatology 2006 20;43:1022-31.
Palmeira CM, Rolo AP. Mitochondrially-mediated toxicity of bile acids. Toxicology 2004 ;203:1-15.18.
De Vree JM, Jacquemin E, Sturm E, Cresteil D, Bosma PJ, Aten J, et al. Mutations in the MDR3 gene cause 19.
progressive familial intrahepatic cholestasis. Proc Natl Acad Sci U S A 1998 6;95:282-7.
Buis CI, Geuken E, Visser D, Kuipers F, Haagsma EB, Verkade HJ, et al. Altered bile composition after liver 20.
transplantation is associated with the development of non-anastomotic biliary strictures. J Hepatol. In press
2008.
Yska MJ, Buis CI, Monbaliu D, Schuurs TA, Gouw AS, Kahmann ON, et al. The role of bile salt toxicity in 21.
the pathogenesis of bile duct injury after non-heart-beating porcine liver transplantation. Transplantation 2008
15;85:1625-31.
Jacquemin E, De Vree JM, Cresteil D, Sokal EM, Sturm E, Dumont M, et al. The wide spectrum of multidrug 22.
resistance 3 deficiency: from neonatal cholestasis to cirrhosis of adulthood. Gastroenterology 2001;120:1448-
58.
Deleuze JF, Jacquemin E, Dubuisson C, Cresteil D, Dumont M, Erlinger S, et al. Defect of multidrug-resistance 23.
3 gene expression in a subtype of progressive familial intrahepatic cholestasis. Hepatology 1996;23:904-8.
Jacquemin E. Heterozygous non-sense mutation of the MDR3 gene in familial intrahepatic cholestasis of 24.
pregnancy. The lancet 1999;353:210-1.
Dixon PH, Weerasekera N, Linton KJ, Donaldson O, Chambers J, Egginton E, et al. Heterozygous MDR3 25.
missense mutation associated with intrahepatic cholestasis of pregnancy: evidence for a defect in protein
trafficking. Hum Mol Genet 2000 1;9:1209-17.
Gendrot C, Bacq Y, Brechot MC, Lansac J, Andres C. A second heterozygous MDR3 nonsense mutation 26.
associated with intrahepatic cholestasis of pregnancy. J Med Genet 2003;40:e32.
Lucena JF, Herrero JI, Quiroga J, Sangro B, Garcia-Foncillas J, Zabalegui N, et al. A multidrug resistance 3 27.
gene mutation causing cholelithiasis, cholestasis of pregnancy, and adulthood biliary cirrhosis. Gastroenterology
2003;124:1037-42.
138
ABCB4 gene polymorphism and NAS
Pauli-Magnus C, Lang T, Meier Y, Zodan-Marin T, Jung D, Breymann C, et al. Sequence analysis of bile salt 28.
export pump (ABCB11) and multidrug resistance p-glycoprotein 3 (ABCB4, MDR3) in patients with intrahepatic
cholestasis of pregnancy. Pharmacogenetics 2004;14:91-102.
van Mil SW, van der Woerd WL, van der Brugge G, Sturm E, Jansen PL, Bull LN, et al. Benign recurrent 29.
intrahepatic cholestasis type 2 is caused by mutations in ABCB11. Gastroenterology 2004;127:379-84.
Strautnieks SS, Bull LN, Knisely AS, Kocoshis SA, Dahl N, Arnell H, et al. A gene encoding a liver-specific ABC 30.
transporter is mutated in progressive familial intrahepatic cholestasis. Nat Genet 1998;20:233-8.
Noe J, Kullak-Ublick GA, Jochum W, Stieger B, Kerb R, Haberl M, et al. Impaired expression and function of the 31.
bile salt export pump due to three novel ABCB11 mutations in intrahepatic cholestasis. J Hepatol 2005;43:536-
43.
Toh S. Genomic structure of the canalicular multispecific organic anion-transporter gene (MRP2/cMOAT) and 32.
mutations in the ATP-binding-cassette region in Dubin-Johnson syndrome. American journal of human genetics
1999;64:739-46.
Verdonk RC, Buis CI, Porte RJ, Van der Jagt EJ, Limburg AJ, van den Berg AP, et al. Anastomotic biliary 33.
strictures after liver transplantation: Causes and consequences. Liver Transpl 2006;12:726-35.
Trauner M, Meier PJ, Boyer JL. Molecular pathogenesis of cholestasis. N Engl J Med 1998 22;339:1217-27.34.
Arrese M, Trauner M. Molecular aspects of bile formation and cholestasis. Trends Mol Med 2003;9:558-64.35.
Trauner M, Fickert P, Wagner M. MDR3 (ABCB4) defects: a paradigm for the genetics of adult cholestatic 36.
syndromes. Semin Liver Dis 2007;27:77-98.
Rosmorduc O, Hermelin B, Poupon R. MDR3 gene defect in adults with symptomatic intrahepatic and 37.
gallbladder cholesterol cholelithiasis. Gastroenterology 2001;120:1459-67.
Eloranta ML. Association of single nucleotide polymorphisms of the bile salt export pump gene with intrahepatic 38.
cholestasis of pregnancy. Scandinavian journal of gastroenterology 2003;38:648-52.
Pauli-Magnus C, Kerb R, Fattinger K, Lang T, Anwald B, Kullak-Ublick GA, et al. BSEP and MDR3 haplotype 39.
structure in healthy Caucasians, primary biliary cirrhosis and primary sclerosing cholangitis. Hepatology
2004;39:779-91.

Part III
HO-1 and hepatobiliary
injury after liver transplantation


Expression of Heme oxygenase -1 in human livers before transplantation correlates with graft injury and function after transplantation 8
Am J Transplant. 2005; 5:1875-1885
Erwin GeukenCarlijn I Buis
Dorien S VisserHans Blokzijl
Han MoshageBalazs Nemes
Henri GD LeuveninkKoert P de Jong
Paul MJG PeetersMaarten JH Slooff
Robert J Porte
144
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
Abstract
Upregulation of heme oxygenase-1 (HO-1) has been proposed as an adaptive mechanism
protecting against ischemia/reperfusion (I/R) injury. We investigated HO-1 expression
in 38 human liver transplants and correlated this with I/R injury and graft function. Before
transplantation, median HO-1 mRNA levels were 3.4-fold higher (range 0.7-9.3) than in normal
controls. Based on the median value, livers were divided into two groups: low and high HO-1
expression. These groups had similar donor characteristics, donor serum transaminases,
cold ischemia time, HSP-70 expression, and distribution of HO-1 promoter polymorphism.
After reperfusion, HO-1 expression increased significantly further in the initial low HO-1
expression group, but not in the high HO-1 group. Postoperatively, serum transaminases were
significantly lower and bile salt secretion was higher in the initial low HO-1 group, compared
to high expression group. Immunofluorescence staining identified Kupffer cells as the main
localization of HO-1.
In conclusion, human livers with initial low HO-1 expression (< 3.4 times controls) are able
to induce HO-1 further during reperfusion and this is associated with less injury and better
function than initial high HO-1 expression (> 3.4 times controls). These data suggest that
increase in HO-1 during transplantation is more protective than a high HO-1 expression before
transplantation.
145
Chapter 8
Introduction
Orthotopic liver transplantation (OLT) is an effective treatment for end-stage liver diseases (1).
However, ischemia and subsequent reperfusion of the liver remain a major cause of graft injury,
causing liver dysfunction and even failure after transplantation (2). This is particularly true for
livers from older donors and steatotic livers, which have a higher susceptibility to ischemia/
reperfusion (I/R) injury (3,4). During organ procurement and transplantation, the liver is exposed
to oxidative stress. Besides the ischemia during cold storage, hypoxia may occur before or
during procurement due to hypotension or cardiac arrest in the donor. After graft reperfusion,
several cascades are triggered leading to the formation of reactive oxygen species (ROS), which
are well-known sources of oxidative stress. Methods to protect liver grafts against I/R injury have
considerable clinical consequences and are therefore of great interest.
It is increasingly recognized that cells respond to stressful events, such as ischemia, hypoxia
and ROS, by the activation of various cytoprotective genes and pathways. Heme oxygenase-1
(HO-1) has recently been proposed as a graft survival gene (5,6). Up-regulation of HO-1 is
considered to be one of the most critical cellular protection mechanisms (7,8). It is rapidly
induced under various conditions of oxidative stress, including hypoxia, hyperoxia and ROS
(9). HO-1 catalyzes the rate-limiting step in the oxidative detoxification of excess heme, by
cleaving the α-methene bridge into equimolar amounts of free iron, biliverdin and carbon
monoxide (CO) (9). Free iron, catalyzing oxidative reactions, is bound by iron regulatory
proteins that stimulate synthesis of ferritin, thereby preventing iron-dependent oxidative
stress (10,11). Biliverdin is subsequently converted into bilirubin and both have the ability
to scavenge ROS (12-15). CO has been shown to serve as an endogenous regulator for
maintaining microvascular blood flow of the liver (16,17).
Two- to three-fold induction of HO-1 by pharmacologic agents or genetic engineering has been
shown to reduce I/R injury in rat liver grafts after extended cold ischemia time (6). Moreover,
steatotic livers from genetically obese Zucker rats are markedly protected against I/R injury
after exogenous upregulation of HO-1 (5). Based on these observations, exogenous induction
of HO-1 prior to transplantation has been proposed as a potentially powerful therapeutic option
to protect liver grafts against I/R injury (5,6). Molecules such as HO-1, however, are probably
not exclusively cytoprotective and each of the products generated by the action of heme
oxygenase (Fe2+, bilirubin and CO) can cause injury under certain circumstances (18). Indeed,
146
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
several experimental studies have shown that excessive overexpression of HO-1 is directly
related with increased injury (19-21). Recently, also a (GT)n dinucleotide repeat polymorphism
that modulates the level of HO-1 inducibility was identified in the promoter region of the human
HO-1 gene. Short GT repeats (<25) are associated with highly significant upregulation of HO-1
in response to inflammatory stimuli (22,23). Therefore, it is critically important to understand the
endogenous changes in HO-1 expression under clinical conditions, such as transplantation,
before the exogenous induction of HO-1 can be safely attempted as a possible therapeutic or
prophylactic measure to reduce I/R injury.
We have therefore studied the changes in endogenous HO-1 expression in human liver
grafts before and after transplantation and correlated these with biochemical markers of graft
injury and hepatobiliary function. This study provides important new information on the role of
endogenous HO-1 expression during human liver transplantation
Patients and Methods
Patient and Donor Data
Thirty-eight patients undergoing OLT were included. All patients received livers from brain
death, multi-organ donors. In the control group (n=5), biopsies were collected in patients
undergoing partial hepatectomy for metastatic tumors. Tissue and data collection was
performed according to the guidelines of the medical ethical committee of our institution and
the Dutch Federation of Scientific Societies.
Collection of Liver Biopsies and Bile Samples from Recipients
Three sequential needle biopsies were taken from each liver graft: at the end of cold storage,
3 hours after reperfusion and 1 week after transplantation. Biopsies were immediately divided:
one part was snap-frozen in liquid nitrogen for RNA and protein isolation and one part was
frozen in isopentane at -80°C for histology studies. During transplantation a bile drain was
routinely placed into the common bile duct, allowing collection of bile (24). To avoid interruption
of the entero-hepatic circulation bile was daily readministered via a jejunostomy catheter. After
the transplantation, bile samples were collected daily between 8 and 9 am. Liver and bile
specimens were stored at -80°C.

147
Chapter 8
RNA Isolation and Reverse-Transcriptase Polymerase Chain
Reaction
Total RNA was isolated from liver biopsies using TRIzol (Invitrogen Life Technologies, Breda, the
Netherlands) and quantified using Ribogreen (Molecular Probes, Inc., Eugene, OR). Reverse
transcription was performed on 3.36 µg RNA using random primers in a final volume of 75 µl
(Reverse Transcription System, Promega, Madison, WI). For quantitative real-time detection
RT-PCR (25,26), sense and antisense primers (Invitrogen, Paisley, Scotland) and fluorogenic
probes (Eurogentec, Herstal, Belgium) for HO-1, HSP-70 and 18S were designed using Primer
Express software (PE Applied Biosystems, Foster City, CA). For HO-1, the primers and probe used
were 5’-GACTGCGTTCCTGCTCAACAT-3’ (sense), 5’-GCTCTGGTCCTTGGTGTCATG-3’
(antisense), and 5’-TCAGCAGCTCCTGCAACTCCTCAAAGAG-3’ (probe), generating a 75
base pair PCR product. For heat shock protein-70 (HSP-70), used as a molecular stress marker,
the following primers and probe were used: 5’-TCTTCTCGCGGATCCAGTCT-3’ (sense),
5’-GGTTCCCTGCTCTCTGTCG-3’ (antisense), and 5’-CCGTTTCCAGCCCCCAATCTCAG-3’
(probe), generating a 70 base pair PCR product. For 18S, the primers and probe used were
5’-CGGCTACCACATCCAAGG-3’ (sense), 5’-CCAATTACAGGGCCTCGAAA-3’ (antisense),
and 5’-CGCGCAAATTACCCACTCCCGA-3’ (probe), generating a 109-base pair PCR
fragment. The ABI PRISM 7700 (Applied Biosystems, Foster City, CA) was used for PCR.
Protein Isolation and Western Blot Analysis
Frozen liver tissue was homogenized in buffer containing protease inhibitors. Protein
concentrations were measured using a standard Lowry assay. Fifteen µg of protein was
fractioned on a 5% SDS-PAGE gel and transferred to PVDF membranes (Pall Life Sciences,
Ann Arbor, MI). The membranes were blocked with 1% SKIM milk (Fluka BioChemica, Buchs,
Switzerland) and labeled with the anti HO-1 polyclonal antibody (dilution, 1:5000, StressGen,
Victoria, British Columbia, Canada). After washing in PBS/0.05% Tween-20 (Sigma, Malden,
The Netherlands), blots were incubated with a horseradish peroxidase-labled goat anti-rabbit
IgG (dilution, 1:2000, DAKO, Glostrup, Denmark). Finally membranes were developed with
ECL (Amersham, Chalfont St Giles, UK). Five separate cases were examined in each group.
148
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
HO-1 Genotype assessment
Genomic DNA was isolated from donor splenocytes using a commercial kit (Gentra Systems,
Minneapolis, MN). PCR and genotyping procedures were similar as described by de Jong
et al. (27). The 5’-flanking region of the HO-1 gene containing the poly (GT)n repeat was
amplified by PCR using as forward primer 5’-CAGCTTTCTGGAACCTTCTGG-3’, carrying
a 6-FAM flourescent label (Sigma, Malden, the Netherlands), and as reversed primer
5’-GAAACAAAGTCTGGCCATAGGAC-3’. Sequence analysis of the amplification products of
individuals homozygous for the 222 and 229 basepairs alleles showed correspondence with
GT numbers 26 and 29, respectively (results not shown). We divided allelic repeats into two
subclasses using a classification as previously described in transfection studies (28). Short
repeats, with less than 25 GT repeats (amplicons of 220 basepairs and less), were designated
as allele class S (short), and long repeats with 25 or more GT repeats as allele class L (long).
Recipients of class S allele liver transplants (homozygous S/S and heterozygous S/L) were
compared with recipients of non-class S allele transplants (L/L).
Immunofluorescence Microscopy
Frozen liver sections were stained for HO-1 and the Kupffer cell marker CD68, using an anti-HO-1
polyclonal antibody (dilution, 1:100, StressGen) and an anti-human CD68 monoclonal antibody
KP-1 (dilution, 1:2000, DAKO). After washing, sections were subsequently incubated with a
goat anti-rabbit IgG with a red fluorescent label (Alexa Fluor 568, Molecular Probes, Leiden, the
Netherlands), and with a goat anti-mouse IgG with a green fluorescent label (Alexa Fluor 488,
Molecular Probes). Double-positive cells were identified as those stained yellow. Percentages
of HO-1-positive Kupffer cells were calculated by dividing the number of cells stained yellow by
the number of cells stained green (29). Five different high power fields (x400) were analyzed in
an individual liver sample, and five separate cases were examined in each group. Images were
taken with a Leica DM LB fluorescence microscope (Leica, Wetzlar, Germany).
Total Bile Salt Secretion and Serum Biochemistry
Postoperatively, bile flow was expressed as daily bile production in mL per kg body weight
of the donor. Total bile salt concentration was measured spectrophotometrically with
3α-hydroxysteroid dehydrogenase (30). Serum samples were analyzed for aspartate- and
alanine aminotransferase (AST and ALT) and gamma glutamyltransferase (GGT), by routine
clinical chemistry testing.
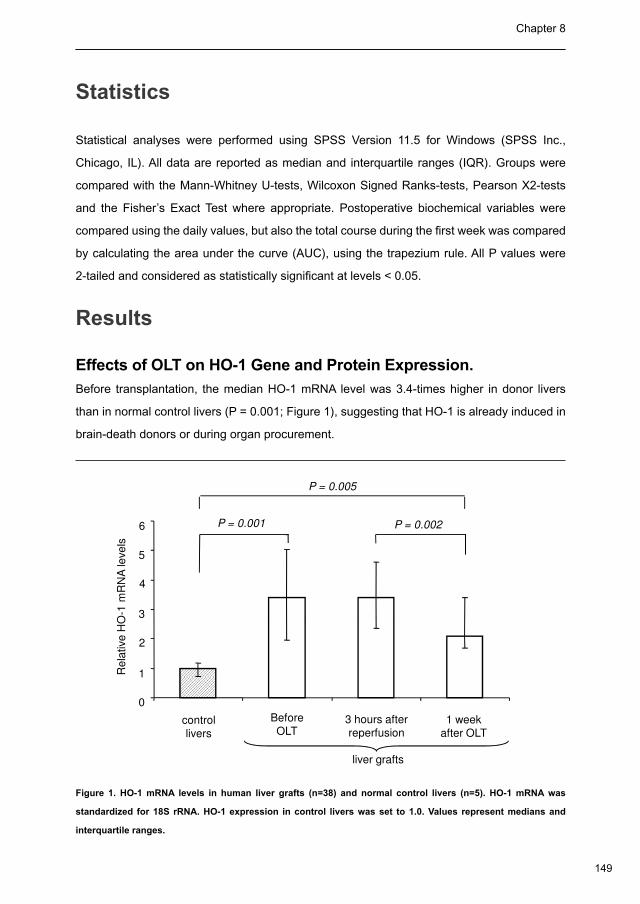
149
Chapter 8
Statistics
Statistical analyses were performed using SPSS Version 11.5 for Windows (SPSS Inc.,
Chicago, IL). All data are reported as median and interquartile ranges (IQR). Groups were
compared with the Mann-Whitney U-tests, Wilcoxon Signed Ranks-tests, Pearson X2-tests
and the Fisher’s Exact Test where appropriate. Postoperative biochemical variables were
compared using the daily values, but also the total course during the first week was compared
by calculating the area under the curve (AUC), using the trapezium rule. All P values were
2-tailed and considered as statistically significant at levels < 0.05.
Results
Effects of OLT on HO-1 Gene and Protein Expression.
Before transplantation, the median HO-1 mRNA level was 3.4-times higher in donor livers
than in normal control livers (P = 0.001; Figure 1), suggesting that HO-1 is already induced in
brain-death donors or during organ procurement.
Re
lative
HO
-1 m
RN
A le
ve
ls
P = 0.001 P = 0.002
P = 0.005
3
4
5
6
Re
lative
HO
control
livers
Before
OLT3 hours after
reperfusion1 week
after OLT
liver grafts
0
1
2
3
Figure 1. HO-1 mRNA levels in human liver grafts (n=38) and normal control livers (n=5). HO-1 mRNA was
standardized for 18S rRNA. HO-1 expression in control livers was set to 1.0. Values represent medians and
interquartile ranges.
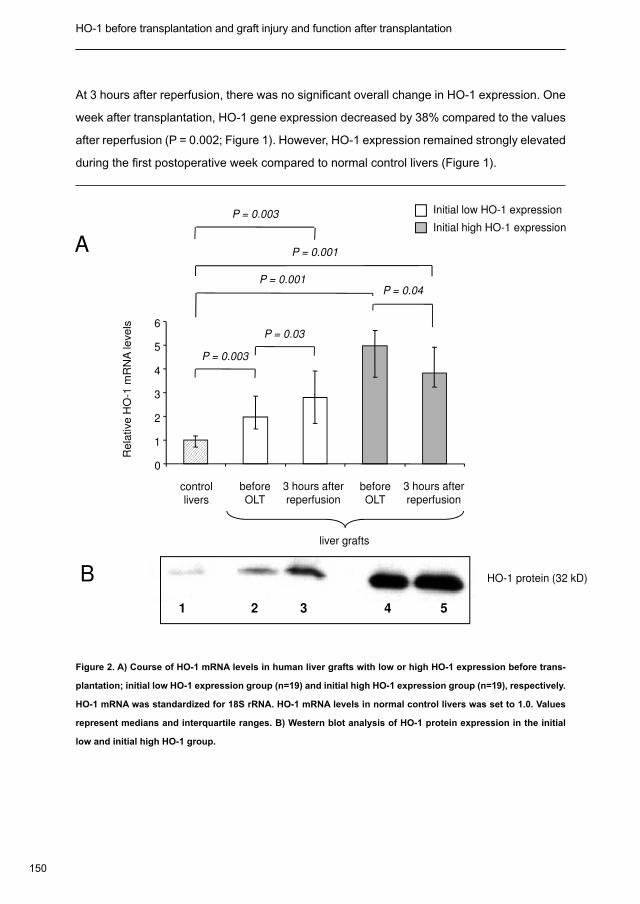
150
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
At 3 hours after reperfusion, there was no significant overall change in HO-1 expression. One
week after transplantation, HO-1 gene expression decreased by 38% compared to the values
after reperfusion (P = 0.002; Figure 1). However, HO-1 expression remained strongly elevated
during the first postoperative week compared to normal control livers (Figure 1).
Initial low HO-1 expression
Initial high HO-1 expression
3
4
5
6
P = 0.04
- 1 m
RN
A le
ve
ls
P = 0.001
P = 0.003
P = 0.03
P = 0.001
P = 0.003
A
before
OLT
3 hours after
reperfusionbefore
OLT
3 hours after
reperfusioncontrol
livers
liver grafts
0
1
2
3
Re
lative
HO
-
HO-1 protein (32 kD)B
1 2 3 4 5
Figure 2. A) Course of HO-1 mRNA levels in human liver grafts with low or high HO-1 expression before trans-
plantation; initial low HO-1 expression group (n=19) and initial high HO-1 expression group (n=19), respectively.
HO-1 mRNA was standardized for 18S rRNA. HO-1 mRNA levels in normal control livers was set to 1.0. Values
represent medians and interquartile ranges. B) Western blot analysis of HO-1 protein expression in the initial
low and initial high HO-1 group.
151
Chapter 8
At 3 hours after reperfusion, there was no significant overall change in HO-1 expression. One
week after transplantation, HO-1 gene expression decreased by 38% compared to the values
after reperfusion (P = 0.002; Figure 1). However, HO-1 expression remained strongly elevated
during the first postoperative week compared to normal control livers (Figure 1).
Initial low HO-1 expression
Initial high HO-1 expression
3
4
5
6
P = 0.04
-1 m
RN
A le
ve
ls
P = 0.001
P = 0.003
P = 0.03
P = 0.001
P = 0.003
A
before
OLT
3 hours after
reperfusionbefore
OLT
3 hours after
reperfusioncontrol
livers
liver grafts
0
1
2
3
Re
lative
HO
-
HO-1 protein (32 kD)B
1 2 3 4 5
Figure 2. A) Course of HO-1 mRNA levels in human liver grafts with low or high HO-1 expression before trans-
plantation; initial low HO-1 expression group (n=19) and initial high HO-1 expression group (n=19), respectively.
HO-1 mRNA was standardized for 18S rRNA. HO-1 mRNA levels in normal control livers was set to 1.0. Values
represent medians and interquartile ranges. B) Western blot analysis of HO-1 protein expression in the initial
low and initial high HO-1 group.
A wide variation in HO-1 gene expression was detected in liver biopsies that were collected
before transplantation, ranging from 0.7- to 9.3-times the levels in normal control livers. To
be able to identify donor variables that are associated with HO-1 induction, and to study the
possible impact of HO-1 on I/R injury and graft viability after transplantation, we decided to
divide liver grafts into two groups based on the level of HO-1 expression before transplantation.
A low HO-1 expression group (n=19) was formed by livers with an initial HO-1 mRNA level
below the median value (< 3.4-times control levels) and a high HO-1 expression group (n=19)
was formed by livers with an initial HO-1 gene expression above the median value (> 3.4-times
control levels). Median HO-1 expression in the low and high expression group was 2.0- and
5.0-times higher than in control livers (Figure 2A). Interestingly, HO-1 mRNA level increased
significantly by 43% after reperfusion in the initial low expression group, whereas HO-1
expression decreased by 23% after reperfusion in the inital high expression group (Figure
2A). In both groups, HO-1 gene expression remained significantly elevated during the first
postoperative week, compared to controls (data not shown).
Changes in HO-1 protein concentrations, as detected by Western blot analysis, were similar to
the changes in HO-1 mRNA expression. HO-1 protein concentration was low in normal control
livers, compared to the donor livers. After reperfusion, HO-1 protein expression increased further
in the initial low HO-1 expression group, but not in the initial high HO-1 group (Figure 2B).
Comparison of Donor Data for Livers with Low and High HO-1
Expression
A large number of donor characteristics and laboratory values were investigated in an attempt
to explain the differences in HO-1 gene expression before transplantation. Several events
that are known to induce HO-1 expression in animal models, such as hypotension, cardiac
arrest, blood transfusions and ischemia, may also occur in brain-death donors or during organ
procurement. In addition to this, some drugs (i.e. dopamine) have been shown to induce HO-1
expression (31). We have compared all these donor-related events and variables in the two
groups, but were unable to find statistically significant differences (Table 1).
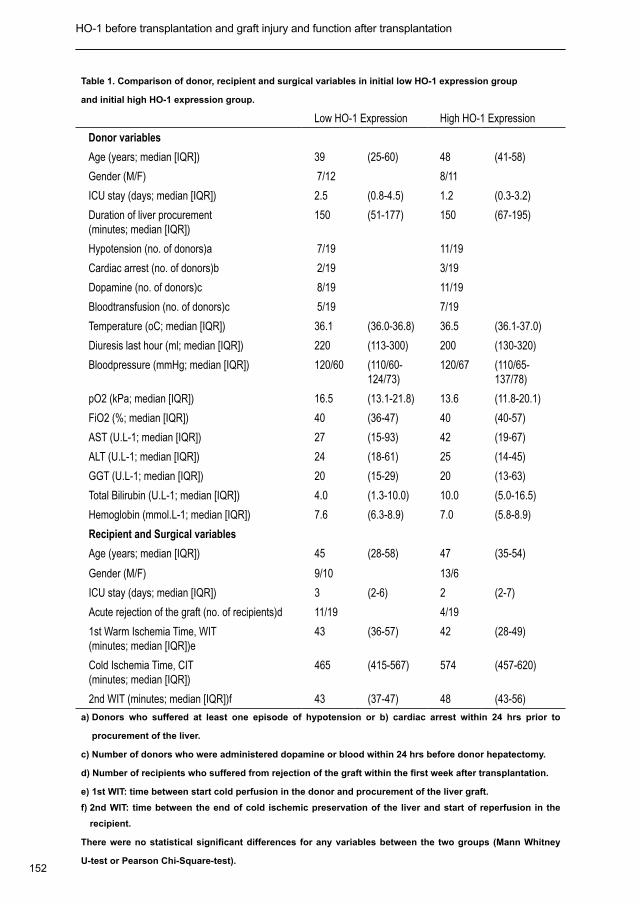
152
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
Table 1. Comparison of donor, recipient and surgical variables in initial low HO-1 expression group
and initial high HO-1 expression group.
Low HO-1 Expression High HO-1 Expression
Donor variables
Age (years; median [IQR]) 39 (25-60) 48 (41-58)
Gender (M/F) 7/12 8/11
ICU stay (days; median [IQR]) 2.5 (0.8-4.5) 1.2 (0.3-3.2)
Duration of liver procurement (minutes; median [IQR])
150 (51-177) 150 (67-195)
Hypotension (no. of donors)a 7/19 11/19
Cardiac arrest (no. of donors)b 2/19 3/19
Dopamine (no. of donors)c 8/19 11/19
Bloodtransfusion (no. of donors)c 5/19 7/19
Temperature (oC; median [IQR]) 36.1 (36.0-36.8) 36.5 (36.1-37.0)
Diuresis last hour (ml; median [IQR]) 220 (113-300) 200 (130-320)
Bloodpressure (mmHg; median [IQR]) 120/60 (110/60-124/73)
120/67 (110/65-137/78)
pO2 (kPa; median [IQR]) 16.5 (13.1-21.8) 13.6 (11.8-20.1)
FiO2 (%; median [IQR]) 40 (36-47) 40 (40-57)
AST (U.L-1; median [IQR]) 27 (15-93) 42 (19-67)
ALT (U.L-1; median [IQR]) 24 (18-61) 25 (14-45)
GGT (U.L-1; median [IQR]) 20 (15-29) 20 (13-63)
Total Bilirubin (U.L-1; median [IQR]) 4.0 (1.3-10.0) 10.0 (5.0-16.5)
Hemoglobin (mmol.L-1; median [IQR]) 7.6 (6.3-8.9) 7.0 (5.8-8.9)
Recipient and Surgical variables
Age (years; median [IQR]) 45 (28-58) 47 (35-54)
Gender (M/F) 9/10 13/6
ICU stay (days; median [IQR]) 3 (2-6) 2 (2-7)
Acute rejection of the graft (no. of recipients)d 11/19 4/19
1st Warm Ischemia Time, WIT (minutes; median [IQR])e
43 (36-57) 42 (28-49)
Cold Ischemia Time, CIT (minutes; median [IQR])
465 (415-567) 574 (457-620)
2nd WIT (minutes; median [IQR])f 43 (37-47) 48 (43-56)
a) Donors who suffered at least one episode of hypotension or b) cardiac arrest within 24 hrs prior to
procurement of the liver.
c) Number of donors who were administered dopamine or blood within 24 hrs before donor hepatectomy.
d) Number of recipients who suffered from rejection of the graft within the first week after transplantation.
e) 1st WIT: time between start cold perfusion in the donor and procurement of the liver graft.
f) 2nd WIT: time between the end of cold ischemic preservation of the liver and start of reperfusion in the
recipient.
There were no statistical significant differences for any variables between the two groups (Mann Whitney
U-test or Pearson Chi-Square-test).
153
Chapter 8
There were also no significant differences in the time between start of in situ cold perfusion
in the donor and actual hepatectomy (1st “relatively” warm ischemia) or in the duration of
cold storage (Table 1). Interestingly, there were also no differences in donor serum markers
of liver injury (AST, ALT and GGT) or liver function (bilirubin) between the two groups (Table
1). Moreover, there was no significant difference in pretransplant mRNA expression of the
stress protein HSP-70 in the low and high HO-1 group (1.18 [ IQR 0.30 – 3.76] versus 0.57
[IQR 0.22 – 2.27]; p = 0.44). These data suggest that differences in HO-1 expression in liver
grafts before transplantation cannot simply be explained by a higher number of compromised
donors in the high HO-1 expression group.
The Effect of HO-1 Donor Genotype
To examine whether the differences in initial HO-1 expression could be explained by the the
number of (GT)n repeats in the HO-1 promoter region, HO-1 donor genotypes were analyzed.
Allele class S/S was present in 8% of the donors, 35% of the donors were heterozygous for
class S alleles (S/L), and 57% of the donors were non-carriers of the class S allele (L/L).
Distribution of the numbers of (GT)n repeats was not different for donor livers in the initial low
and high HO-1 expression group (Figure 3). There were also no significant differences in the
distribution of class S allele donor livers (S/S and S/L) and non-class S donor livers (L/L) in
the two groups (Table 2).
Table 2. Distribution of HO-1 genotype in the livers with initial low or high HO-1 mRNA expression.
Initial HO-1 Expression
Genotype* Low High
p-value = 1
Short Allele (SS or SL) 8 (42%) 8 (44%)
Long Allele (LL) 11 (58%) 10 (56%)
19 (100%) 18** (100%)
a) Short allele (S) status defined as < 25 (GT) repeats in the HO-1 promoter region; Long allele (L) status
defined as > 25 (GT) repeats in the HO-1 promter region.
b) Genomic DNA for gene sequencing was not available in one donor.
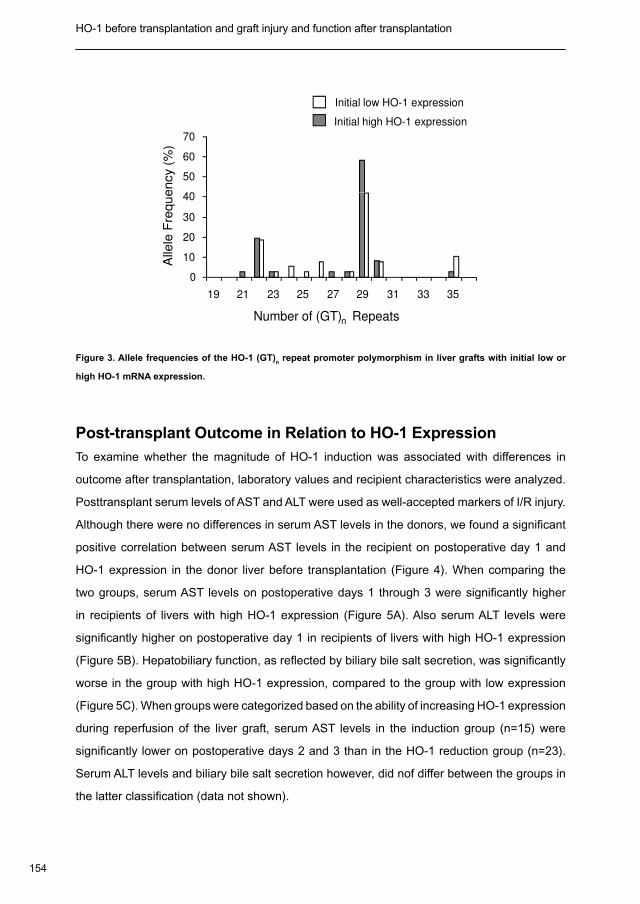
154
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
40
50
60
70
Alle
le F
req
ue
ncy (
%)
Initial high HO-1 expression
Initial low HO-1 expression
0
10
20
30
40
19 21 23 25 27 29 31 33 35
Number of (GT)n Repeats
Alle
le F
req
ue
ncy (
%)
Figure 3. Allele frequencies of the HO-1 (GT)n repeat promoter polymorphism in liver grafts with initial low or
high HO-1 mRNA expression.
Post-transplant Outcome in Relation to HO-1 Expression
To examine whether the magnitude of HO-1 induction was associated with differences in
outcome after transplantation, laboratory values and recipient characteristics were analyzed.
Posttransplant serum levels of AST and ALT were used as well-accepted markers of I/R injury.
Although there were no differences in serum AST levels in the donors, we found a significant
positive correlation between serum AST levels in the recipient on postoperative day 1 and
HO-1 expression in the donor liver before transplantation (Figure 4). When comparing the
two groups, serum AST levels on postoperative days 1 through 3 were significantly higher
in recipients of livers with high HO-1 expression (Figure 5A). Also serum ALT levels were
significantly higher on postoperative day 1 in recipients of livers with high HO-1 expression
(Figure 5B). Hepatobiliary function, as reflected by biliary bile salt secretion, was significantly
worse in the group with high HO-1 expression, compared to the group with low expression
(Figure 5C). When groups were categorized based on the ability of increasing HO-1 expression
during reperfusion of the liver graft, serum AST levels in the induction group (n=15) were
significantly lower on postoperative days 2 and 3 than in the HO-1 reduction group (n=23).
Serum ALT levels and biliary bile salt secretion however, did nof differ between the groups in
the latter classification (data not shown).
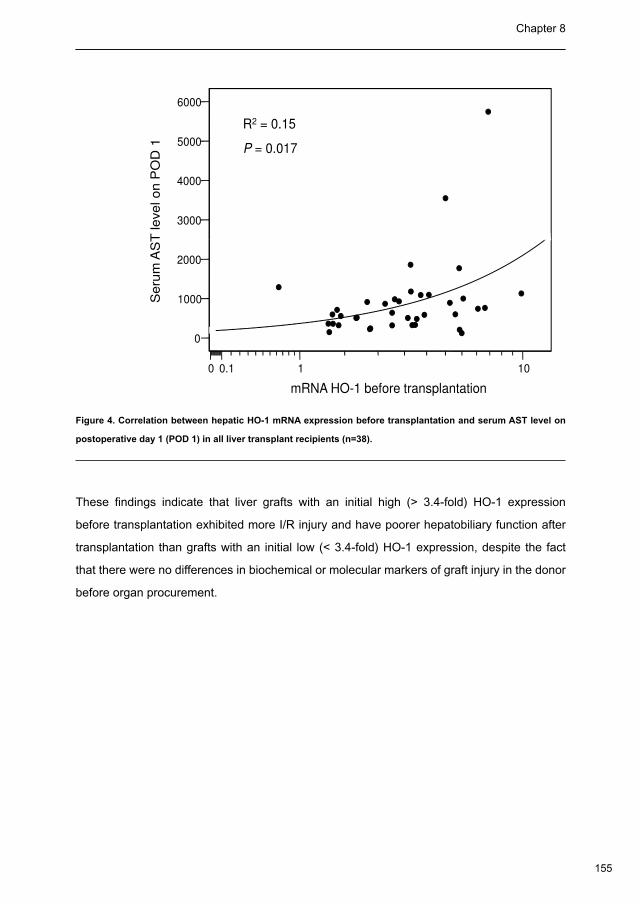
155
Chapter 8
40
50
60
70
Alle
le F
req
ue
ncy (
%)
Initial high HO-1 expression
Initial low HO-1 expression
0
10
20
30
40
19 21 23 25 27 29 31 33 35
Number of (GT)n Repeats
Alle
le F
req
ue
ncy (
%)
Figure 3. Allele frequencies of the HO-1 (GT)n repeat promoter polymorphism in liver grafts with initial low or
high HO-1 mRNA expression.
Post-transplant Outcome in Relation to HO-1 Expression
To examine whether the magnitude of HO-1 induction was associated with differences in
outcome after transplantation, laboratory values and recipient characteristics were analyzed.
Posttransplant serum levels of AST and ALT were used as well-accepted markers of I/R injury.
Although there were no differences in serum AST levels in the donors, we found a significant
positive correlation between serum AST levels in the recipient on postoperative day 1 and
HO-1 expression in the donor liver before transplantation (Figure 4). When comparing the
two groups, serum AST levels on postoperative days 1 through 3 were significantly higher
in recipients of livers with high HO-1 expression (Figure 5A). Also serum ALT levels were
significantly higher on postoperative day 1 in recipients of livers with high HO-1 expression
(Figure 5B). Hepatobiliary function, as reflected by biliary bile salt secretion, was significantly
worse in the group with high HO-1 expression, compared to the group with low expression
(Figure 5C). When groups were categorized based on the ability of increasing HO-1 expression
during reperfusion of the liver graft, serum AST levels in the induction group (n=15) were
significantly lower on postoperative days 2 and 3 than in the HO-1 reduction group (n=23).
Serum ALT levels and biliary bile salt secretion however, did nof differ between the groups in
the latter classification (data not shown).
3000
4000
5000
6000
Seru
m A
ST
level on P
OD
1
R2 = 0.15
P = 0.017
0
1000
2000
0 0.1 1 10
mRNA HO-1 before transplantation
Seru
m A
ST
level on P
OD
1
Figure 4. Correlation between hepatic HO-1 mRNA expression before transplantation and serum AST level on
postoperative day 1 (POD 1) in all liver transplant recipients (n=38).
These findings indicate that liver grafts with an initial high (> 3.4-fold) HO-1 expression
before transplantation exhibited more I/R injury and have poorer hepatobiliary function after
transplantation than grafts with an initial low (< 3.4-fold) HO-1 expression, despite the fact
that there were no differences in biochemical or molecular markers of graft injury in the donor
before organ procurement.
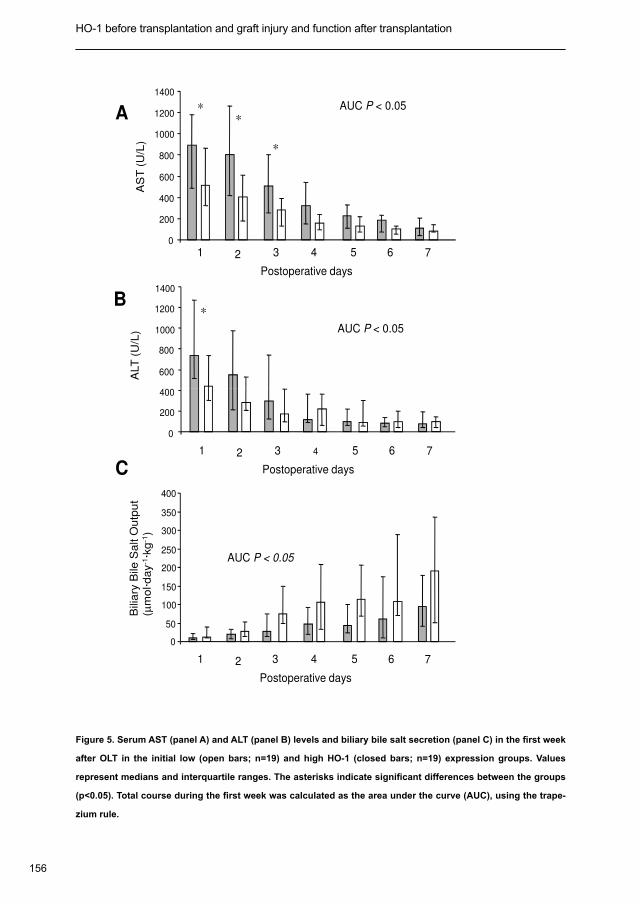
156
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
AS
T (
U/L
)
Postoperative days
1 2 3 4 5 6 7
*
*
*
0
200
400
600
800
1000
1200
1400
AUC P < 0.05
ALT
(U
/L)
400
600
800
1000
1200
1400
*
AUC P < 0.05
A
B
Postoperative days
1 2 3 4 5 6 7
0
200
400
Bili
ary
Bile
Sa
lt O
utp
ut
(µm
ol·d
ay
-1·k
g-1
)
AUC P < 0.05
Postoperative days
1 2 3 4 5 6 7
0
50
100
150
200
250
300
350
400
C
Figure 5. Serum AST (panel A) and ALT (panel B) levels and biliary bile salt secretion (panel C) in the first week
after OLT in the initial low (open bars; n=19) and high HO-1 (closed bars; n=19) expression groups. Values
represent medians and interquartile ranges. The asterisks indicate significant differences between the groups
(p<0.05). Total course during the first week was calculated as the area under the curve (AUC), using the trape-
zium rule.

157
Chapter 8
Immunofluorescence Microscopy
Specific immunostaining showed that HO-1 was predominantly localized in irregular and
star-shaped cells. These characteristics suggested that HO-1 protein is mainly expressed in
Kupffer cells, which was confirmed by double-color immunofluorescence labeling, using the
anti-HO-1 and anti-human CD68 MoAb KP-1, a marker of Kupffer cells. As shown in Figure 6,
the distribution of anti-HO-1 positive (red) cells overlapped with that of KP-1-positive (green)
cells, resulting in a yellow staining. In control livers, a considerable proportion of Kupffer cells
did not express HO-1-associated immunoreactivity and displayed mainly a green staining
(Figure 6A). In contrast with this, almost all Kupffer cells in liver grafts demonstrated positive
staining for HO-1 (Figure 6B-E). Indeed, morphometrical analysis showed significantly higher
percentages of HO-1-positive Kupffer cells in liver grafts before transplantation, compared
to normal control livers (low and high HO-1 expression group 88% and 95%, respectively,
compared to 50% in normal control livers, P < 0.02 for both groups; Table 3). After reperfusion,
HO-1 expression in Kupffer cells increased further, resulting in a positive staining of all Kupffer
cells in both groups (Table 3).
Although, after reperfusion, all Kupffer cells in both groups stained positive for HO-1, the red
staining (HO-1) per cell was far more intense in the group with high HO-1 expression than
in the low expression group (Figure 6C and E). This indicates that not only the percentage
of Kupffer cells expressing HO-1 is increased in liver grafts, but that also the HO-1 protein
expression per Kupffer cell is enhanced, where the latter seems to discriminate the group with
high HO-1 expression from the livers with low HO-1 expression. This is in line with the higher
HO-1 mRNA and protein levels after reperfusion in the group with high HO-1 expression,
compared to the low expression group.
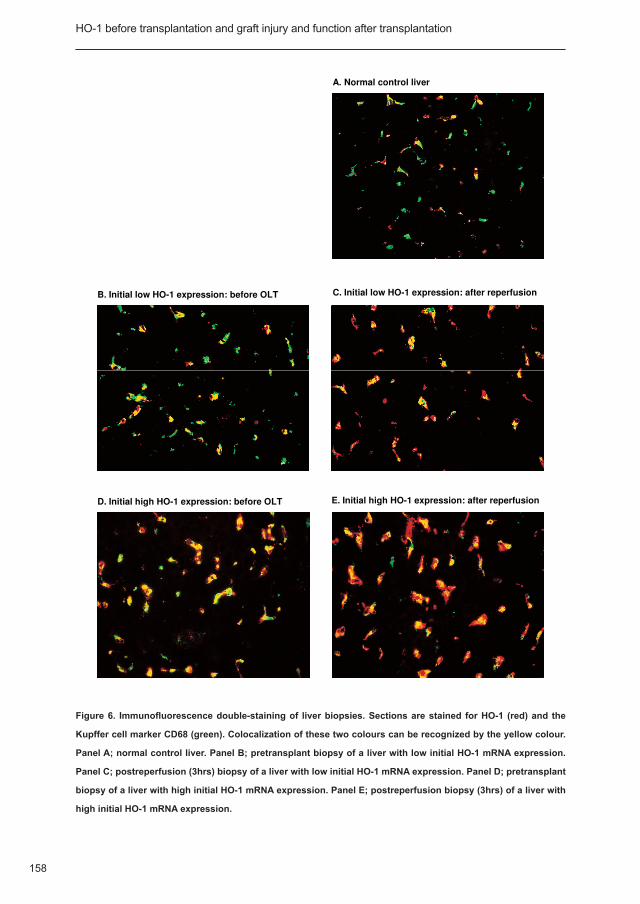
158
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
A. Normal control liver
B. Initial low HO-1 expression: before OLT C. Initial low HO-1 expression: after reperfusion
D. Initial high HO-1 expression: before OLT E. Initial high HO-1 expression: after reperfusion
Figure 6. Immunofluorescence double-staining of liver biopsies. Sections are stained for HO-1 (red) and the
Kupffer cell marker CD68 (green). Colocalization of these two colours can be recognized by the yellow colour.
Panel A; normal control liver. Panel B; pretransplant biopsy of a liver with low initial HO-1 mRNA expression.
Panel C; postreperfusion (3hrs) biopsy of a liver with low initial HO-1 mRNA expression. Panel D; pretransplant
biopsy of a liver with high initial HO-1 mRNA expression. Panel E; postreperfusion biopsy (3hrs) of a liver with
high initial HO-1 mRNA expression.
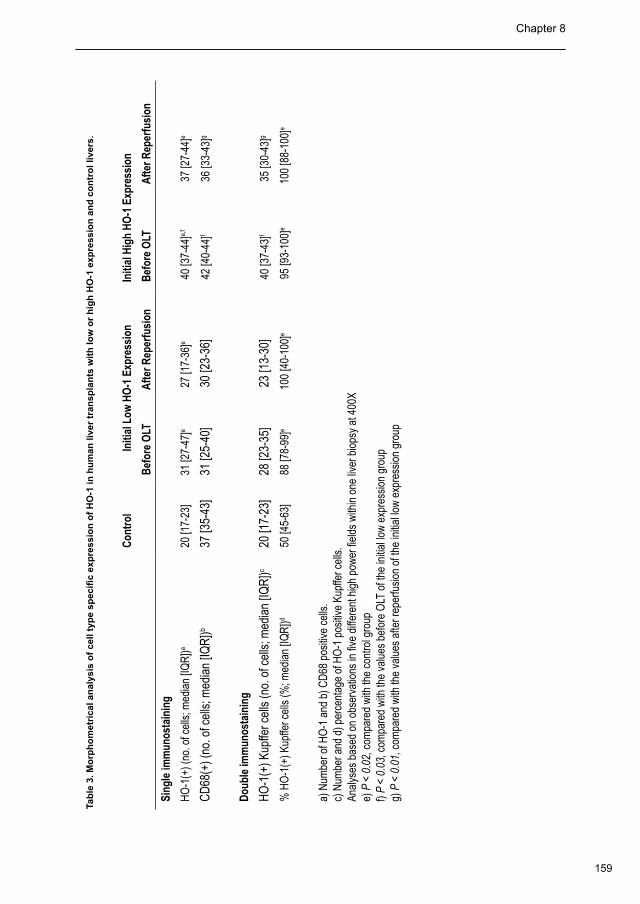
159
Chapter 8
Tab
le 3
. Mo
rph
om
etri
cal a
nal
ysis
of
cell
typ
e sp
ecifi
c ex
pre
ssio
n o
f H
O-1
in h
um
an li
ver
tran
spla
nts
wit
h lo
w o
r h
igh
HO
-1 e
xpre
ssio
n a
nd
co
ntr
ol l
iver
s.
Con
trol
In
itial
Low
HO
-1 E
xpre
ssio
n In
itial
Hig
h H
O-1
Exp
ress
ion
Bef
ore
OLT
Afte
r Rep
erfu
sion
Bef
ore
OLT
Afte
r Rep
erfu
sion
Sing
le im
mun
osta
inin
g
HO
-1(+
) (no
. of c
ells
; med
ian
[IQR
])a 20
[17-
23]
31 [2
7-47
]e 2
7 [1
7-36
]e 4
0 [3
7-44
]e,f
37
[27-
44]e
CD
68(+
) (no
. of c
ells
; med
ian
[IQR
])b37
[35-
43]
31 [2
5-40
] 3
0 [2
3-36
] 4
2 [4
0-44
]f 3
6 [3
3-43
]g
Dou
ble
imm
unos
tain
ing
HO
-1(+
) Kup
ffer c
ells
(no.
of c
ells
; med
ian
[IQR
])c20
[17-
23]
28 [2
3-35
] 2
3 [1
3-30
] 4
0 [3
7-43
]f 3
5 [3
0-43
]g
% H
O-1
(+) K
upffe
r cel
ls (%
; med
ian
[IQR
])d50
[45-
63]
88 [7
8-99
]e10
0 [4
0-10
0]e
95
[93-
100]
e10
0 [8
8-10
0]e
a) N
umbe
r of H
O-1
and
b) C
D68
pos
itive
cel
ls.
c) N
umbe
r and
d) p
erce
ntag
e of
HO
-1 p
ositi
ve K
upffe
r cel
ls.
Anal
yses
bas
ed o
n ob
serv
atio
ns in
five
diff
eren
t hig
h po
wer
fiel
ds w
ithin
one
live
r bio
psy
at 4
00X
e) P
< 0
.02,
com
pare
d w
ith th
e co
ntro
l gro
upf)
P <
0.03
, com
pare
d w
ith th
e va
lues
bef
ore
OLT
of t
he in
itial
low
exp
ress
ion
grou
pg)
P <
0.0
1, c
ompa
red
with
the
valu
es a
fter r
eper
fusi
on o
f the
initi
al lo
w e
xpre
ssio
n gr
oup
160
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
Discussion
We have investigated HO-1 expression in human liver allografts during transplantation and
correlated this with clinical signs of graft injury and hepatobiliary function. There are three
novel findings in this study. First, we have shown that, compared to normal control livers,
HO-1 gene and protein expression in human liver grafts from brain-death donors is induced
already prior to transplantation. After reperfusion, HO-1 expression increased further in livers
with relatively low initial HO-1 expression (< 3.4 times controls), but not in livers with initial
high HO-1 expression (> 3.4 times controls). Second, allografts with initial high expression of
HO-1 demonstrated significantly more I/R injury and had worse hepatobiliary function than
grafts with a low upregulation of HO-1. Finally, we were able to identify Kupffer cells as the
main site of HO-1 protein expression in human liver grafts. While about 50% of the Kupffer
cells in normal control liver expressed HO-1, positive staining for HO-1 was found in 100% of
the Kupffer cells of transplanted livers. These findings provide important new information on
the endogenous regulation of HO-1 during human liver transplantation.
There is accumulating evidence that the HO-1 system has important vasoregulatory properties
and actively maintains hepatic microperfusion and tissue oxygenation via the production of
CO (16). In addition to this, the HO-1 system has been shown to have anti-oxidant, anti-
inflammatory, anti-apoptotic and platelet aggregation-inhibiting properties and, therefore, it
has been proposed a graft survival gene. Animal studies have suggested that exogenous
induction of HO-1 before transplantation may confer cytoprotective and immune regulatory
functions (6,32-34) and could become a novel and potentially powerful strategy to protect
(marginal) liver grafts from I/R injury (5,8). Induction of HO-1 can be obtained by a variety of
methods, such as administration of HO-1 inducers (i.e. cobalt protoporphyrin) or adenoviral
HO-1 genetransfer (5,8). These methods generally lead to a 2 to 3-fold upregulation of
HO-1 activity (5). There is increasing evidence that overexpression of HO-1 higher than this
is not exclusively cytoprotective (19,21). In fibroblast cell cultures, low induction of HO-1
(less than 5-fold) was shown to be cytoprotective against hyperoxia, but excessive HO-1
activation resulted in the accumulation of free divalent iron and increased oxidative injury (19).
Moreover, it has been shown that highly increased (about eight- to nine-fold) activity of HO-1
contributes to endotoxin-induced shock in rats, due to the increased production of CO, a potent
vasorelaxant (21). Therefore, it is of paramount importance that the endogenous changes in
161
Chapter 8
HO-1 expression during transplantation, as well as the therapeutic window of protection, are
well defined before clinical application of HO-1 inducing protocols are attempted.
All donor livers in our study were obtained from brain-death multi-organ donors. The
increased HO-1 mRNA and protein expression observed in these livers before transplantation
suggests that HO-1 is induced in brain-death donors. This observation is in line with studies
in kidney allografts from brain-death donors (35). We have tried to identify variables which
could have contributed to the increased expression of HO-1 in the donor livers before
transplantation. Several factors have been shown to induce HO-1 gene expression in vivo,
including hypotension (36), hypoxia (37-39), hyperoxia (9,40), blood transfusions (41,42),
and inotropic drugs like dopamine (31). All of these factors may also occur in postmortem
organ donors. Comparison of these known inducers of HO-1 gene expression, as well as
several other donor and procurement related variables, however, did not show any statistically
significant differences between the two groups. Variations in initial HO-1 expression could
also not be explained by differences in the distribution of the (GT)n repeat polymorphism of
the HO-1 promoter. The functionally relevant short allele status (<25 repeats) was not found
more frequently in livers with initial low HO-1 expression. Further studies will be necessary to
elucidate the mechanisms of endogenous HO-1 induction in organs from brain death donors.
Although we did not find differences in biochemical (liver enzymes) or molecular (HSP-70)
markers of liver injury before transplantation between the liver grafts with low or high HO-1
expression, we did observe a significant correlation between postoperative serum AST in the
recipients and initial HO-1 expression. In parallel with this, serum AST levels were significantly
higher and biliary bile salt output significantly lower after transplantation in recipients of livers
with high HO-1 expression, compared to grafts with low HO-1 expression. Liberation of
divalent iron is one of the effects resulting from increased HO-1 activity (9). Iron is a mediator
of the generation of ROS and it has been shown to play an important role in I/R injury (43,44).
We, therefore, speculate that exaggerated HO-1 activity in liver grafts may cause increased
injury due to the liberation of iron, resulting in a pro-oxidant condition and higher susceptibility
to I/R injury. The apparent paradox of one molecule or pathway causing both cytoprotection
and cytotoxicicty has also been found in other systems, like the nitric oxide system (45). More
studies will be needed to clarify this issue.
Interestingly, a significant further increase in HO-1 expression was found after reperfusion of livers
with an initially low expression, whereas a small, but significant decrease in HO-1 expression was
162
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
observed in livers with initially high HO-1 expression. This data could imply that HO-1 mRNA
expression cannot be further upregulated upon reperfusion when levels are already high to start
with, whereas further upregulation can occur in livers with moderately elevated HO-1 expression
before reperfusion. Although we observed a better postoperative outcome in the initial low HO-1
expression group, it remains indefinite whether it is the initial low HO-1 expression or the ability
to increase HO-1 expression upon reperfusion that confers cytoprotection.
We identified Kupffer cells as the main site of HO-1 expression in human livers. Makino et al.
(29) have recently reported similar findings in human cirrhotic livers. These studies in human
liver are in contrast with data from rat livers, where considerable expression of HO-1 has also
been found in hepatocytes (46). While in our study about 50% of the Kupffer cells in the control
livers expressed HO-1, this was more than 80% in the liver grafts before transplantation and
even 100% after transplantation. These findings suggest that a subpopulation of Kupffer cells,
which does not express HO-1 under normal circumstances may induce HO-1 expression. It
has been suggested that Kupffer cells may serve as sensor cells detecting local hemodynamic
changes and mechanical forces in sinusoids (29,47). By increasing HO-1 activity and the
generation of the vasorelaxing gaseous CO, Kupffer cells are able to maintain microvascular
blood flow in the liver (29). On the other hand, it is well-known that Kuppfer cells play a
critical role in the pathogenesis of I/R injury of the cold preserved liver through the production
of ROS and cytokines, like tumor necrosis factor-α (48,49). Our data suggests that high
overexpression of HO-1 in Kupffer cells prior to transplantation contributes to the deleterious
effects of these cells in I/R injury.
Although there is a large body of evidence suggesting that exogenous up-regulation of HO-1
in transplant models in animals confers cytoprotective effects (5,32-34), our findings caution
against an uncontrolled application of non-cell specific methods to induce HO-1 expression in
human organ donors. Exogenous induction of HO-1 in postmortem organ donors could further
increase an already elevated HO-1 expression, resulting in potentially detrimental effects
instead of cytoprotection. The main difference between our study in patients undergoing
liver transplantation and studies in animal models of liver transplantation is that in the clinical
situation liver grafts are usually obtained from brain death organ donors, whereas healthy
animals are used as donors in experimental models. Moreover, cellular localization of HO-1
expression in human liver transplantation is predominantly restricted to the Kupffer cells,
whereas in stress-exposed rat livers, HO-1 is also upregulated in hepatocytes (46).

163
Chapter 8
Our data suggest a dual role for HO-1 in human liver transplants, with either cytoportection or
increased cytotoxicity, depending on the initial level of overexpression. New pharmacological
interventions should probably not focus on the induction of HO-1 prior to transplantation, but
rather aim for induction during transplantation.
164
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
Reference List
Starzl TE, Demetris AJ. Liver transplantation: a 31-year perspective. Part III. Curr Probl Surg 1990; 27: 1.
181-240.
Clavien PA, Harvey PR, Strasberg SM. Preservation and reperfusion injuries in liver allografts. An overview and 2.
synthesis of current studies. Transplantation 1992; 53: 957-978.
D’Alessandro AM, Kalayoglu M, Sollinger HW, Hoffmann RM, Reed A, Knechtle SJ et al. The predictive 3.
value of donor liver biopsies for the development of primary nonfunction after orthotopic liver transplantation.
Transplantation 1991; 51: 157-163.
Strasberg SM, Howard TK, Molmenti EP, Hertl M. Selecting the donor liver: risk factors for poor function after 4.
orthotopic liver transplantation. Hepatology 1994; 20: 829-838.
Amersi F, Buelow R, Kato H, Ke B, Coito AJ, Shen XD et al. Upregulation of heme oxygenase-1 protects 5.
genetically fat Zucker rat livers from ischemia/reperfusion injury. J Clin Invest 1999; 104: 1631-1639.
Redaelli CA, Tian YH, Schaffner T, Ledermann M, Baer HU, Dufour JF. Extended preservation of rat liver graft 6.
by induction of heme oxygenase-1. Hepatology 2002; 35: 1082-1092.
Fujita T, Toda K, Karimova A, Yan SF, Naka Y, Yet SF et al. Paradoxical rescue from ischemic lung injury by 7.
inhaled carbon monoxide driven by derepression of fibrinolysis. Nat Med 2001; 7: 598-604.
Coito AJ, Buelow R, Shen XD, Amersi F, Moore C, Volk HD et al. Heme oxygenase-1 gene transfer inhibits 8.
inducible nitric oxide synthase expression and protects genetically fat Zucker rat livers from ischemia-reperfusion
injury. Transplantation 2002; 74: 96-102.
Maines MD. The heme oxygenase system: a regulator of second messenger gases. Annu Rev Pharmacol 9.
Toxicol 1997; 37: 517-554.
Vile GF, Tyrrell RM. Oxidative stress resulting from ultraviolet A irradiation of human skin fibroblasts leads to a 10.
heme oxygenase-dependent increase in ferritin. J Biol Chem 1993; 268: 14678-14681.
DeRusso PA, Philpott CC, Iwai K, et al. Expression of a constitutive mutant of iron regulatory protein 1 abolishes 11.
iron homeostasis in mammalian cells. J Biol Chem 1995; 270: 15451-15454.
Kutty RK, Maines MD. Purification and characterization of biliverdin reductase from rat liver. J Biol Chem 1981; 12.
256: 3956-3962.
McCoubrey WK, Jr., Cooklis MA, Maines MD. The structure, organization and differential expression of the rat 13.
gene encoding biliverdin reductase. Gene 1995; 160: 235-240.
Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological 14.
importance. Science 1987; 235: 1043-1046.
165
Chapter 8
Stocker R, Glazer AN, Ames BN. Antioxidant activity of albumin-bound bilirubin. Proc Natl Acad Sci U S A 1987; 15.
84: 5918-5922.
Suematsu M, Kashiwagi S, Sano T, Goda N, Shinoda Y, Ishimura Y. Carbon monoxide as an endogenous 16.
modulator of hepatic vascular perfusion. Biochem Biophys Res Commun 1994; 205: 1333-1337.
Suematsu M, Goda N, Sano T, Kashiwagi S, Egawa T, Shinoda Y et al. Carbon monoxide: an endogenous 17.
modulator of sinusoidal tone in the perfused rat liver. J Clin Invest 1995; 96: 2431-2437.
Platt JL, Nath KA. Heme oxygenase: protective gene or Trojan horse. Nat Med 1998; 4: 1364-1365.18.
Suttner DM, Dennery PA. Reversal of HO-1 related cytoprotection with increased expression is due to reactive 19.
iron. FASEB J 1999; 13: 1800-1809.
Dennery PA, Sridhar KJ, Lee CS, Wong HE, Shokoohi V, Rodgers PA et al. Heme oxygenase-mediated 20.
resistance to oxygen toxicity in hamster fibroblasts. J Biol Chem 1997; 272: 14937-14942.
Yet SF, Pellacani A, Patterson C, Tan L, Folta SC, Foster L et al. Induction of heme oxygenase-1 expression in 21.
vascular smooth muscle cells. A link to endotoxic shock. J Biol Chem 1997; 272: 4295-4301.
Exner M, Schillinger M, Minar E, Mlekusch W, Schlerka G, Haumer M et al. Heme oxygenase-1 gene promoter 22.
microsatellite polymorphism is associated with restenosis after percutaneous transluminal angioplasty. J
Endovasc Ther 2001; 8:433-440.
Schillinger M, Exner M, Mlekusch W, Ahmadi R, Rumpold H, Mannhalter C et al. Heme oxygenase-1 genotype 23.
is a vascular anti-inflammatory factor following balloon angioplasty. J Endovasc Ther 2002;9:385-394.
Lenzen R, Bahr A, Eichstadt H, Marschall U, Bechstein WO, Neuhaus P. In liver transplantation, T tube bile 24.
represents total bile flow: physiological and scintigraphic studies on biliary secretion of organic anions. Liver
Transpl Surg 1999; 5: 8-15.
Gibson UE, Heid CA, Williams PM. A novel method for real time quantitative RT-PCR. Genome Res 1996; 25.
6: 995-1001.
Heid CA, Stevens J, Livak KJ, Williams PM. Real time quantitative PCR. Genome Res 1996; 6: 986-994.26.
De Jong MM, Nolte IM, De Vries EG, Schaapveld M, Kleibeuker JH, Oosterom E et al. The HLA class III 27.
subregion is responsible for an increased breast cancer risk. Hum Mol Gen 2003; 12: 2311-2319
Funk M, Endler G, Schillinger M, Mustafa S, Hsieh K, Exner M et al. The effect of a promoter polymorphism in 28.
the heme oxygenase-1 gene on the risk of ischemic cerbrovascular events: The influence of other vascular risk
factors. Thromb Res 2004; 113: 217-223
Makino N, Suematsu M, Sugiura Y, Morikawa H, Shiomi S, Goda N et al. Altered expression of heme oxygenase-1 29.
in the livers of patients with portal hypertensive diseases. Hepatology 2001; 33: 32-42.
Turley SD, Dietschy JM. Re-evaluation of the 3 alpha-hydroxysteroid dehydrogenase assay for total bile acids 30.
in bile. J Lipid Res 1978; 19: 924-928.
166
HO-1 before transplantation and graft injury and function after transplantation Chapter 8
Berger SP, Hunger M, Yard BA, Schnuelle P, Van der Woude FJ. Dopamine induces the expression of heme 31.
oxygenase-1 by human endothelial cells in vitro. Kidney Int 2000; 58: 2314-2319.
Maines MD, Raju VS, Panahian N. Spin trap (N-t-butyl-alpha-phenylnitrone)-mediated suprainduction of heme 32.
oxygenase-1 in kidney ischemia/reperfusion model: role of the oxygenase in protection against oxidative injury.
J Pharmacol Exp Ther 1999; 291: 911-919.
Squiers EC, Bruch D, Buelow R, Tice DG. Pretreatment of small bowel isograft donors with cobalt-protoporphyrin 33.
decreases preservation injury. Transplant Proc 1999; 31: 585-586.
Katori M, Buelow R, Ke B, Ma J, Coito AJ, Iyer S et al. Heme oxygenase-1 overexpression protects rat hearts 34.
from cold ischemia/reperfusion injury via an antiapoptotic pathway. Transplantation 2002; 73: 287-292.
Nijboer WN, Schuurs TA, Van der Hoeven JA, Fekken S, Wiersema-Buist J, Leuvenink HG et al. Effect of brain 35.
death on gene expression and tissue activation in human donor kidneys. Transplantation 2004; 78: 978-986.
Rensing H, Jaeschke H, Bauer I, Patau C, Datene V, Pannen BH et al. Differential activation pattern of redox-36.
sensitive transcription factors and stress-inducible dilator systems heme oxygenase-1 and inducible nitric oxide
synthase in hemorrhagic and endotoxic shock. Crit Care Med 2001; 29: 1962-1971.
Motterlini R, Foresti R, Bassi R, Calabrese V, Clark JE, Green CJ. Endothelial heme oxygenase-1 induction 37.
by hypoxia. Modulation by inducible nitric-oxide synthase and S-nitrosothiols. J Biol Chem 2000; 275:
13613-13620.
Morita T, Perrella MA, Lee ME, Kourembanas S. Smooth muscle cell-derived carbon monoxide is a regulator of 38.
vascular cGMP. Proc Natl Acad Sci U S A 1995; 92: 1475-1479.
Borger DR, Essig DA. Induction of HSP 32 gene in hypoxic cardiomyocytes is attenuated by treatment with 39.
N-acetyl-L-cysteine. Am J Physiol 1998; 274(3Pt2): H965-973.
Otterbein LE, Kolls JK, Mantell LL, Cook JL, Alam J, Choi AM. Exogenous administration of heme oxygenase-1 40.
by gene transfer provides protection against hyperoxia-induced lung injury. J Clin Invest 1999; 103:
1047-1054.
Abraham NG, Lavrovsky Y, Schwartzman ML, Stoltz RA, Levere RD, Gerritsen ME et al. Transfection of the 41.
human heme oxygenase gene into rabbit coronary microvessel endothelial cells: protective effect against heme
and hemoglobin toxicity. Proc Natl Acad Sci U S A 1995; 92: 6798-6802.
Jeney V, Balla J, Yachie A, Varga Z, Vercellotti GM, Eaton JW et al. Pro-oxidant and cytotoxic effects of 42.
circulating heme. Blood 2002; 100: 879-887.
Arora AS, Gores GJ. The role of metals in ischemia/reperfusion injury of the liver. Semin Liver Dis 1996; 16: 43.
31-38.
167
Chapter 8
Wyllie S, Seu P, Gao FQ, Goss JA. Deregulation of iron homeostasis and cold-preservation injury to rat liver 44.
stored in University of Wisconsin solution. Liver Transpl 2003; 9: 401-410.
Clemens MG. Nitric oxide in liver injury. Hepatology 1999; 30: 1-5.45.
Bauer I, Wanner GA, Rensing H, Alte C, Miescher EA, Wolf B et al. Expression pattern of heme oxygenase 46.
isoenzymes 1 and 2 in normal and stress-exposed rat liver. Hepatology 1998; 27: 829-838.
Schemmer P, Connor HD, Arteel GE, Raleigh JA, Bunzendahl H, Mason RR et al. Reperfusion injury in livers 47.
due to gentle in situ organ manipulation during harvest involves hypoxia and free radicals. J Pharmacol Exp
Ther 1999; 290: 235-240.
Sindram D, Porte RJ, Hoffman MR, Bentley RC, Clavien PA. Synergism between platelets and leukocytes in 48.
inducing endothelial cell apoptosis in the cold ischemic rat liver: a Kupffer cell-mediated injury. FASEB J 2001;
15: 1230-1232.
Cutrin JC, Perrelli MG, Cavalieri B, Peralta C, Rosell Catafau J, Poli G. Microvascular dysfunction induced 49.
by reperfusion injury and protective effect of ischemic preconditioning. Free Radic Biol Med 2002; 33:
1200-1208.

Heme oxygenase-1 genotype of the donor is associated with graft survival after liver transplantation9
Am J Transplant. 2008; 8:377-385
Carlijn I BuisGerrit van der Steege
Dorien S VisserIlja M Nolte
Bouke G HepkemaMaarten Nijsten
Maarten JH SlooffRobert J Porte
170
HO-1 genotype of the donor and graft survival Chapter 9
Abstract
Heme oxygenase 1 (HO-1) has been suggested as a cytoprotective gene during liver
transplantation. Inducibility of HO-1 is modulated by a (GT)n polymorphism and a single
nucleotide polymorphism (SNP) A(-413)T in the promoter. Both a short (GT)n allele and the
A-allele have been associated with increased HO-1 promoter activity.
In 308 liver transplantations, we assessed donor HO-1 genotype and correlated this with
outcome variables. For (GT)n genotype, livers were divided into two classes: short alleles
(<25 repeats; class-S) and long alleles (≥ 25 repeats; class-L). In a subset, hepatic mRNA
expression was correlated with genotypes.
Graft survival at 1 year was significantly better for A-allele genotype compared to TT-genotype
(84% versus 63%, p=0.004). Graft loss due to primary dysfunction occurred more frequently
in TT-genotype compared to A-receivers (p=0.03). Recipients of a liver with TT-genotype had
significantly higher serum transaminases after transplantation and hepatic HO-1 mRNA levels
were significantly lower compared to the A-allele livers (p=0.03). No differences were found for
any outcome variable between class S and LL-variant of the (GT)n polymorphism. Haplotype
analysis confirmed dominance of the A(-413)T SNP over the (GT)n polymorphism.
In conclusion, HO-1 genotype is associated with outcome after liver transplantation. These
findings suggest that HO-1 mediates graft survival after liver transplantation.
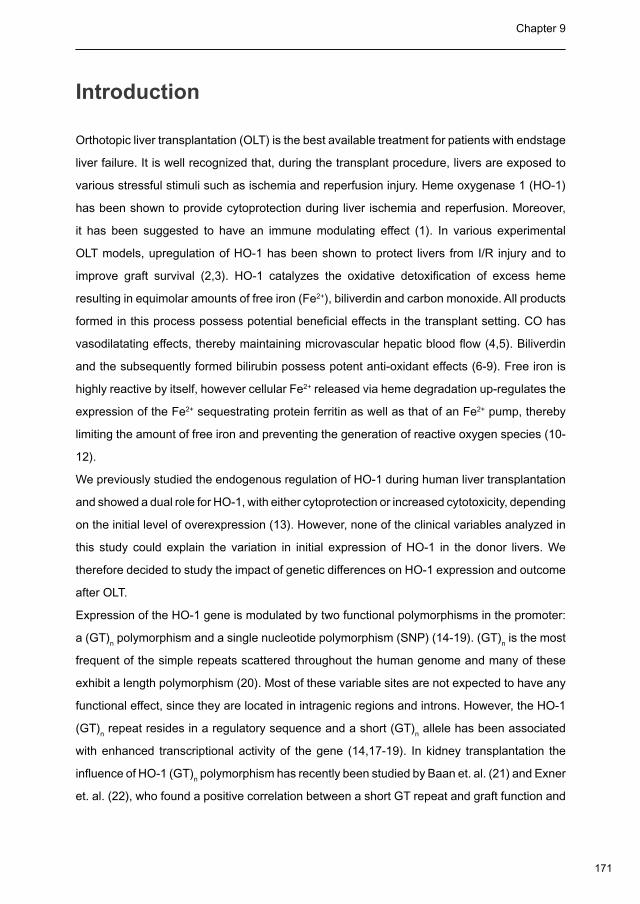
171
Chapter 9
Introduction
Orthotopic liver transplantation (OLT) is the best available treatment for patients with endstage
liver failure. It is well recognized that, during the transplant procedure, livers are exposed to
various stressful stimuli such as ischemia and reperfusion injury. Heme oxygenase 1 (HO-1)
has been shown to provide cytoprotection during liver ischemia and reperfusion. Moreover,
it has been suggested to have an immune modulating effect (1). In various experimental
OLT models, upregulation of HO-1 has been shown to protect livers from I/R injury and to
improve graft survival (2,3). HO-1 catalyzes the oxidative detoxification of excess heme
resulting in equimolar amounts of free iron (Fe2+), biliverdin and carbon monoxide. All products
formed in this process possess potential beneficial effects in the transplant setting. CO has
vasodilatating effects, thereby maintaining microvascular hepatic blood flow (4,5). Biliverdin
and the subsequently formed bilirubin possess potent anti-oxidant effects (6-9). Free iron is
highly reactive by itself, however cellular Fe2+ released via heme degradation up-regulates the
expression of the Fe2+ sequestrating protein ferritin as well as that of an Fe2+ pump, thereby
limiting the amount of free iron and preventing the generation of reactive oxygen species (10-
12).
We previously studied the endogenous regulation of HO-1 during human liver transplantation
and showed a dual role for HO-1, with either cytoprotection or increased cytotoxicity, depending
on the initial level of overexpression (13). However, none of the clinical variables analyzed in
this study could explain the variation in initial expression of HO-1 in the donor livers. We
therefore decided to study the impact of genetic differences on HO-1 expression and outcome
after OLT.
Expression of the HO-1 gene is modulated by two functional polymorphisms in the promoter:
a (GT)n polymorphism and a single nucleotide polymorphism (SNP) (14-19). (GT)
n is the most
frequent of the simple repeats scattered throughout the human genome and many of these
exhibit a length polymorphism (20). Most of these variable sites are not expected to have any
functional effect, since they are located in intragenic regions and introns. However, the HO-1
(GT)n repeat resides in a regulatory sequence and a short (GT)
n allele has been associated
with enhanced transcriptional activity of the gene (14,17-19). In kidney transplantation the
influence of HO-1 (GT)n polymorphism has recently been studied by Baan et. al. (21) and Exner
et. al. (22), who found a positive correlation between a short GT repeat and graft function and

172
HO-1 genotype of the donor and graft survival Chapter 9
survival after transplantation. In addition to the (GT)n polymorphism, the A(-413)T SNP has
been identified as a functionally relevant variation of the HO-1 gene (15,16). Using a transient
transfection assay of HO-1 promoter luciferase genes in bovine aortic endothelial cells Ono et
al have shown that the A-allele of this SNP is associated with a higher promoter activity than
the T-allele. Interestingly, the A(-413)T SNP appeared in vitro to be more important for HO-1
promoter activity than the (GT)n polymorphism (15,16). Only limited work has been conducted
evaluating the A(-413)T SNP in clinical research (15).
Based on the accumulating evidence that HO-1 is an important enzyme influencing graft survival
after transplantation, we hypothesized that these two functionally relevant polymorphisms
in the HO-1 promoter are associated with outcome after OLT. Therefore, we analyzed the
two functional HO-1 promoter polymorphisms in donor genomic DNA in relation to outcome
after human liver transplantation. Furthermore we studied the functional relevance of these
polymorphisms by measuring hepatic mRNA expression.
Patients and methods
Patients
Between January 1996 and January 2005, a total number of 465 consecutive OLT’s were
performed at the University Medical Center Groningen. After exclusion of children (<18
years), 320 transplants in 282 adult patients were included in this study. Of 308 donors (96%)
cryopreserved splenocytes were available for the HO-1 genotyping. Median follow up time for
this cohort was 4 years and 6 months (range 20-81 months).
ABO blood group-identical or compatible grafts from brain-death donors with normal or
near normal liver function tests were used for all patients. A standardized technique was
used for implantation, as has been described previously (23,24). During the study period,
immunosuppressive protocols were based on tacrolimus or cyclosporine A, either with or
without azathioprine and a rapid taper of steroids. Biopsy-proven acute rejection was treated
when clinically indicated, with a bolus of methylprednisolone on three consecutive days.
Steroid-resistant rejections were treated either by conversion to tacrolimus in patients on
cyclosporine A, or by giving 5 doses of antithymocyte globulin (4 mg/kg i.v.) on alternating days.
Doppler ultrasound was performed routinely at postoperative days 1, 3, and 7 and on demand
to rule out vascular or biliary complications or parenchymal lesions. Cholangiography via a
173
Chapter 9
biliary drain was routinely performed between postoperative day 10-14 and later on demand
(i.e. for rising cholestatic parameters or dilatation of bile ducts on ultrasound). Tissue and data
collection was performed according to the guidelines of the medical ethical committee of our
institution and the Dutch Federation of Scientific Societies.
HO-1 genotype assessment
Genomic DNA was isolated from donor splenocytes using a commercial kit (Gentra Systems,
Minneapolis, MN, USA). The 5’-flanking region of the HO-1 gene containing the (GT)n
polymorphism was amplified by polymerase chain reaction (PCR) using as forward primer
5’-CAG CTT TCT GGA ACC TTC TGG-3’ (sense), carrying a 6-FAM fluorescent label (Sigma,
Malden, the Netherlands), and as reversed primer 5’-GAA ACA AAG TCT GGC CAT AG
GAC-3’ (antisense). PCR and genotyping procedures were similar as described earlier (25).
Sequence analysis of the amplification products of individuals homozygous for the 222 and 229
base-pairs alleles showed correspondence with GT numbers 26 and 29, respectively (results
not shown). Allelic repeats were divided into two subclasses using a similar classification
based on transfection studies as described previously (26). A short allele, with less than 25 GT
repeats, were designated as class S, and long allele with 25 or more GT repeats (amplicons
of 220 base-pairs and more), as class L (26). Recipients of class S allele liver transplants
(homozygous SS and heterozygous SL) were compared with recipients of non-class S allele
transplants (LL).
The single nucleotide polymorphism A(-413)T (rs2071746) was analyzed using the ABI7900HT
TaqMan system (Applied Biosystems, Foster City, CA, USA) with a probe/primer assay
hCV15869717, developed by and purchased from Applied Biosytems (Assay-on-Demand).
Recipients of at least one A-allele liver transplants (homozygous AA and heterozygous AT)
were compared with recipients of heterozygous T-allele recipients (TT).
Collection of liver biopsies, RNA isolation and reverse-transcriptase
polymerase chain reaction
In a subset of 38 patients we collected liver biopsies at the end of cold storage to compare
HO-1 mRNA expression in the various genotype groups. RNA isolation and cDNA synthesis
were performed as described before (13). cDNA levels of HO-1 and 18S were measured
by Real Time Polymerase Chain Reaction (PCR) using the ABI PRISM 7900 HT Sequence

174
HO-1 genotype of the donor and graft survival Chapter 9
detector (Applied Biosystems). Nucleotide sequences of Primers (Invitrogen) and Probes
(Eurogentec) were designed using Primes Express software (PE Applied Biosystems). Probes
were 5’ labeled by a 6-carboxy-fluoresceine (FAM) reporter and 3’ labeled with a 6-carboxy-
tetra-methyl-rhodamin (TAMRA) quencher. Real time RT-PCR data were analyzed using the
comparative cycle threshold (CT) method. Briefly, the difference in cycle times, ∆CT, was
determined as the difference between the tested gene and the reference RNA, 18S. We then
obtained ∆∆CT by finding the difference compared to a control group of liver biopsies from
patients undergoing an hemihepatectomy for colorectal metastasis. The fold induction (FI)
was calculated as 2-∆∆CT.
Clinical Outcome parameters
Outcome parameters included serum concentrations of aspartate aminotransferase (AST) and
alanine aminotransferase (ALT), as marker for ischemia / reperfusion injury after OLT, graft
survival, incidence of acute rejection, and causes of graft loss. Recipient data were obtained
from a prospectively collected database. Donor data were extracted from the national and
hospital’s donor databases.
Acute rejection was suspected on the basis of daily liver function tests, fever and deterioration
of the clinical condition and proven by needle biopsy of the liver. The degree of acute rejection
was histologically graded according to the Banff classification (27). Only rejections within
the first three months with grade II and III, or grade I with a clinical indication for treatment,
were considered in this study. As individual causes of graft loss, five different etiologies were
identified: 1) Primary dysfunction (PDF), defined as either primary non function (PNF) or graft
loss due to initial poor function (IPF). PNF was defined as non life sustaining function of the liver
requiring retransplantation or leading to death within seven days after OLT. IPF was defined
as early graft dysfunction characterized by serum AST levels > 2000 U/l on any day between
postoperative day 2-7, and a prothrombine time (PT) >16 sec (modified according to Ploeg
et. al. (28)), which was not explained by biliary or vascular complications; 2) Hepatic artery
thrombosis, which was always confirmed by doppler ultrasonography and or angiography; 3)
Non-anastomotic biliary strictures, as detected on imaging studies of the biliary tree and in
the absence of arterial complications (29); 4) Recurrent disease, and 5) non-graft related graft
loss, including extrahepatic conditions that contributed to the loss of the donor liver, such as
postoperative sepsis and multi-organ failure.
175
Chapter 9
Statistics
All data are reported as median and interquartile ranges (IQR) or number with percentage.
Collection of laboratory values from the central hospital database was conducted as follows.
For every postoperative biochemical variable of each patient a time curve was constructed
before further analysis. In case multiple measurements of a parameter were performed on
one day, these values were averaged to a single value before further analysis. Likewise,
in case laboratory values were missing on certain days, these values were interpolated.
Extrapolations were not performed.
Groups were compared with the chi-square test or Mann Whitney U test, where appropriate.
Biochemical variables were compared using the daily values, but also the total course during
the first two post operative weeks was compared by calculating the area under the curve (AUC),
using the trapezium rule. Graft survival curves were calculated according to the Kaplan-Meier
method and compared using the log-rank test. A two-tailed p-value of < 0.05 was considered
statistically significant. Statistical analyses were performed using SPSS version 12.0.2 (SPSS
Inc., Chicago, IL, USA).
To study linkage disequilibrium between the two polymorphisms in the promoter of the HO-1
gene, the frequencies of the combined genotypes of the (GT)n polymorphism and A(-413)T
were counted. Linkage disequilibrium is the occurrence of two or more polymorphism variants
together on the chromosome more often than could be expected based on recombination
possibilities, most likely due to their close locations, but it may also arise when the combination
confers a selective advantage. A haplotype is a vector of polymorphisms. Haplotype frequencies
were estimated from the genotype counts using the expectation-maximization algorithm (own
software). Linkage disequilibrium is then determined from these haplotype frequencies by
means of D’ and the correlation coefficient R2, which both range from 0 to 1 with 1 implying the
strongest possible linkage disequilibrium and 0 as no linkage disequilibrium.
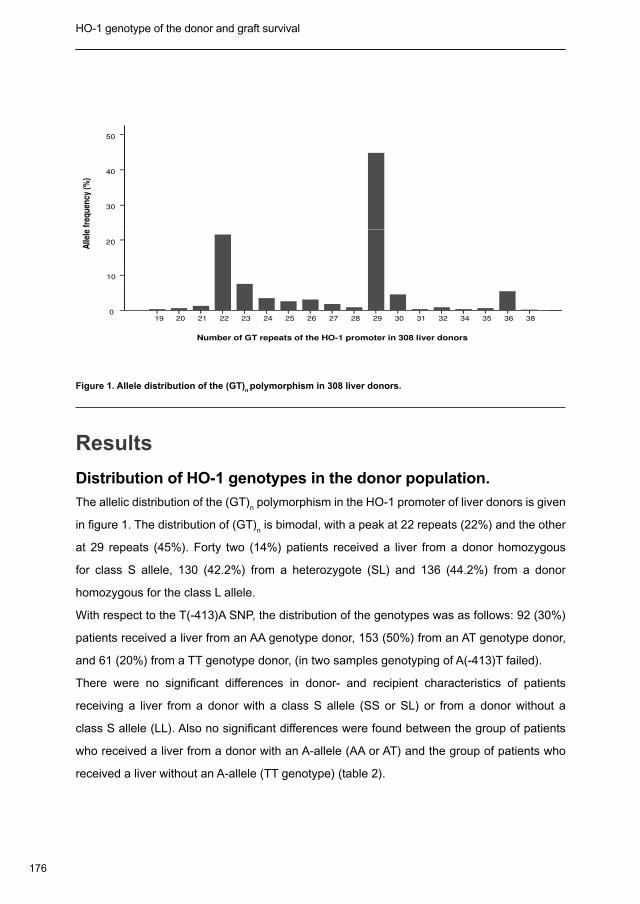
176
HO-1 genotype of the donor and graft survival Chapter 9
30
40
50
Alle
le f
req
uen
cy (
%)
19 20 21 22 23 24 25 26 27 28 29 30 31 32 34 35 36 38
Number of GT repeats of the HO-1 promoter in 308 liver donors
0
10
20
Alle
le f
req
uen
cy (
%)
Figure 1. Allele distribution of the (GT)n polymorphism in 308 liver donors.
Results
Distribution of HO-1 genotypes in the donor population.
The allelic distribution of the (GT)n polymorphism in the HO-1 promoter of liver donors is given
in figure 1. The distribution of (GT)n is bimodal, with a peak at 22 repeats (22%) and the other
at 29 repeats (45%). Forty two (14%) patients received a liver from a donor homozygous
for class S allele, 130 (42.2%) from a heterozygote (SL) and 136 (44.2%) from a donor
homozygous for the class L allele.
With respect to the T(-413)A SNP, the distribution of the genotypes was as follows: 92 (30%)
patients received a liver from an AA genotype donor, 153 (50%) from an AT genotype donor,
and 61 (20%) from a TT genotype donor, (in two samples genotyping of A(-413)T failed).
There were no significant differences in donor- and recipient characteristics of patients
receiving a liver from a donor with a class S allele (SS or SL) or from a donor without a
class S allele (LL). Also no significant differences were found between the group of patients
who received a liver from a donor with an A-allele (AA or AT) and the group of patients who
received a liver without an A-allele (TT genotype) (table 2).
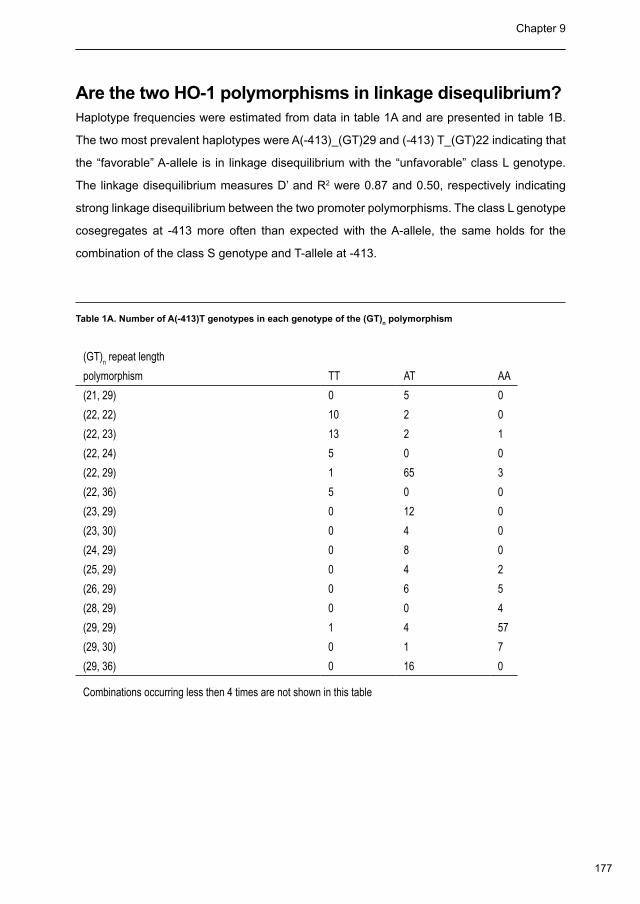
177
Chapter 9
30
40
50
Alle
le f
req
uen
cy (
%)
19 20 21 22 23 24 25 26 27 28 29 30 31 32 34 35 36 38
Number of GT repeats of the HO-1 promoter in 308 liver donors
0
10
20
Alle
le f
req
uen
cy (
%)
Figure 1. Allele distribution of the (GT)n polymorphism in 308 liver donors.
Results
Distribution of HO-1 genotypes in the donor population.
The allelic distribution of the (GT)n polymorphism in the HO-1 promoter of liver donors is given
in figure 1. The distribution of (GT)n is bimodal, with a peak at 22 repeats (22%) and the other
at 29 repeats (45%). Forty two (14%) patients received a liver from a donor homozygous
for class S allele, 130 (42.2%) from a heterozygote (SL) and 136 (44.2%) from a donor
homozygous for the class L allele.
With respect to the T(-413)A SNP, the distribution of the genotypes was as follows: 92 (30%)
patients received a liver from an AA genotype donor, 153 (50%) from an AT genotype donor,
and 61 (20%) from a TT genotype donor, (in two samples genotyping of A(-413)T failed).
There were no significant differences in donor- and recipient characteristics of patients
receiving a liver from a donor with a class S allele (SS or SL) or from a donor without a
class S allele (LL). Also no significant differences were found between the group of patients
who received a liver from a donor with an A-allele (AA or AT) and the group of patients who
received a liver without an A-allele (TT genotype) (table 2).
Are the two HO-1 polymorphisms in linkage disequlibrium?Haplotype frequencies were estimated from data in table 1A and are presented in table 1B.
The two most prevalent haplotypes were A(-413)_(GT)29 and (-413) T_(GT)22 indicating that
the “favorable” A-allele is in linkage disequilibrium with the “unfavorable” class L genotype.
The linkage disequilibrium measures D’ and R2 were 0.87 and 0.50, respectively indicating
strong linkage disequilibrium between the two promoter polymorphisms. The class L genotype
cosegregates at -413 more often than expected with the A-allele, the same holds for the
combination of the class S genotype and T-allele at -413.
Table 1A. Number of A(-413)T genotypes in each genotype of the (GT)n polymorphism
(GT)n repeat length
polymorphism TT AT AA
(21, 29) 0 5 0
(22, 22) 10 2 0
(22, 23) 13 2 1
(22, 24) 5 0 0
(22, 29) 1 65 3
(22, 36) 5 0 0
(23, 29) 0 12 0
(23, 30) 0 4 0
(24, 29) 0 8 0
(25, 29) 0 4 2
(26, 29) 0 6 5
(28, 29) 0 0 4
(29, 29) 1 4 57
(29, 30) 0 1 7
(29, 36) 0 16 0
Combinations occurring less then 4 times are not shown in this table
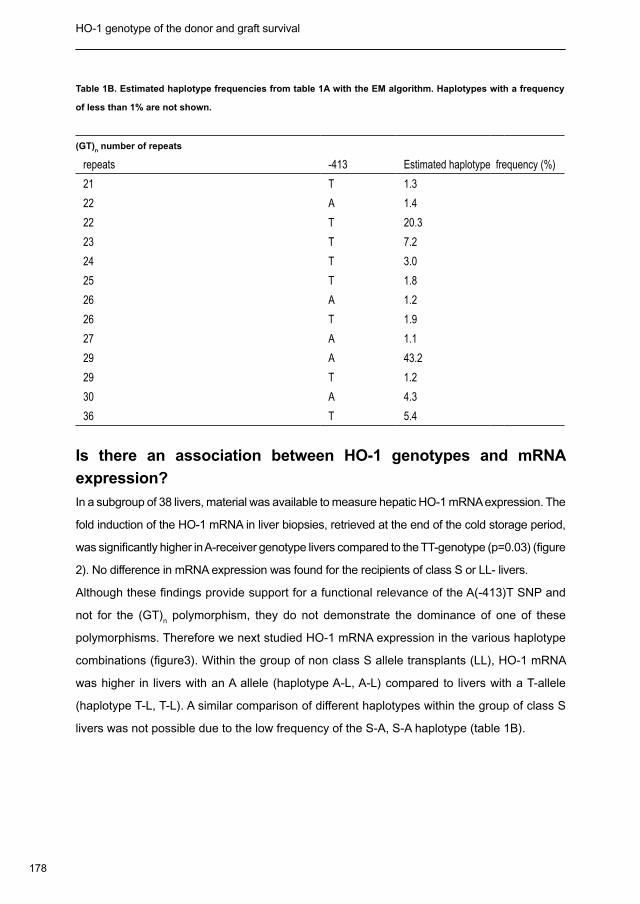
178
HO-1 genotype of the donor and graft survival Chapter 9
Table 1B. Estimated haplotype frequencies from table 1A with the EM algorithm. Haplotypes with a frequency
of less than 1% are not shown.
(GT)n number of repeats
repeats -413 Estimated haplotype frequency (%)
21 T 1.3
22 A 1.4
22 T 20.3
23 T 7.2
24 T 3.0
25 T 1.8
26 A 1.2
26 T 1.9
27 A 1.1
29 A 43.2
29 T 1.2
30 A 4.3
36 T 5.4
Is there an association between HO-1 genotypes and mRNA
expression?
In a subgroup of 38 livers, material was available to measure hepatic HO-1 mRNA expression. The
fold induction of the HO-1 mRNA in liver biopsies, retrieved at the end of the cold storage period,
was significantly higher in A-receiver genotype livers compared to the TT-genotype (p=0.03) (figure
2). No difference in mRNA expression was found for the recipients of class S or LL- livers.
Although these findings provide support for a functional relevance of the A(-413)T SNP and
not for the (GT)n polymorphism, they do not demonstrate the dominance of one of these
polymorphisms. Therefore we next studied HO-1 mRNA expression in the various haplotype
combinations (figure3). Within the group of non class S allele transplants (LL), HO-1 mRNA
was higher in livers with an A allele (haplotype A-L, A-L) compared to livers with a T-allele
(haplotype T-L, T-L). A similar comparison of different haplotypes within the group of class S
livers was not possible due to the low frequency of the S-A, S-A haplotype (table 1B).
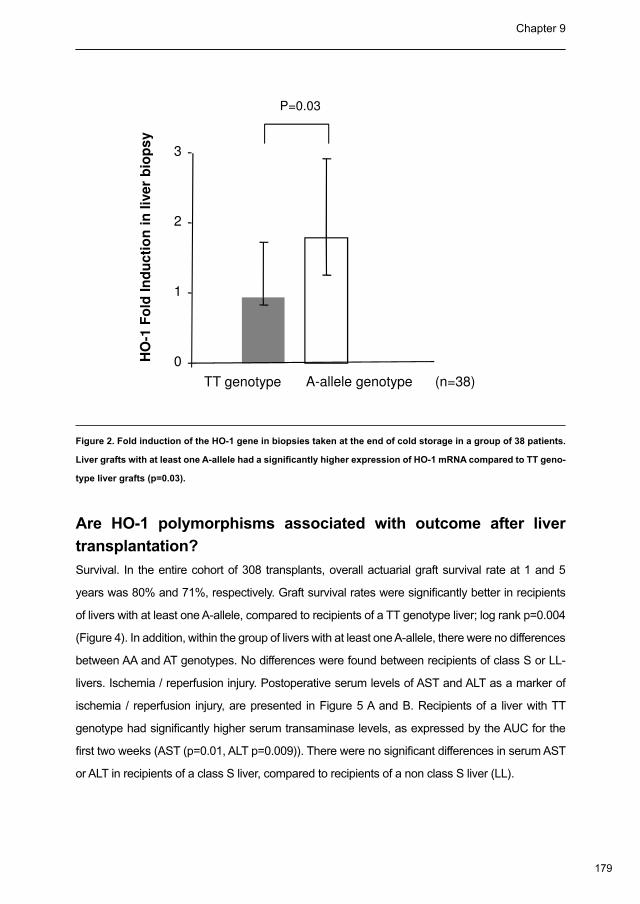
179
Chapter 9
1 F
old
In
du
cti
on
in
liv
er
bio
ps
y
2
3
P=0.03
(n=38)
HO
-1 F
old
In
du
cti
on
in
liv
er
bio
ps
y
TT genotype A-allele genotype
0
1
Figure 2. Fold induction of the HO-1 gene in biopsies taken at the end of cold storage in a group of 38 patients.
Liver grafts with at least one A-allele had a significantly higher expression of HO-1 mRNA compared to TT geno-
type liver grafts (p=0.03).
Are HO-1 polymorphisms associated with outcome after liver
transplantation?
Survival. In the entire cohort of 308 transplants, overall actuarial graft survival rate at 1 and 5
years was 80% and 71%, respectively. Graft survival rates were significantly better in recipients
of livers with at least one A-allele, compared to recipients of a TT genotype liver; log rank p=0.004
(Figure 4). In addition, within the group of livers with at least one A-allele, there were no differences
between AA and AT genotypes. No differences were found between recipients of class S or LL-
livers. Ischemia / reperfusion injury. Postoperative serum levels of AST and ALT as a marker of
ischemia / reperfusion injury, are presented in Figure 5 A and B. Recipients of a liver with TT
genotype had significantly higher serum transaminase levels, as expressed by the AUC for the
first two weeks (AST (p=0.01, ALT p=0.009)). There were no significant differences in serum AST
or ALT in recipients of a class S liver, compared to recipients of a non class S liver (LL).
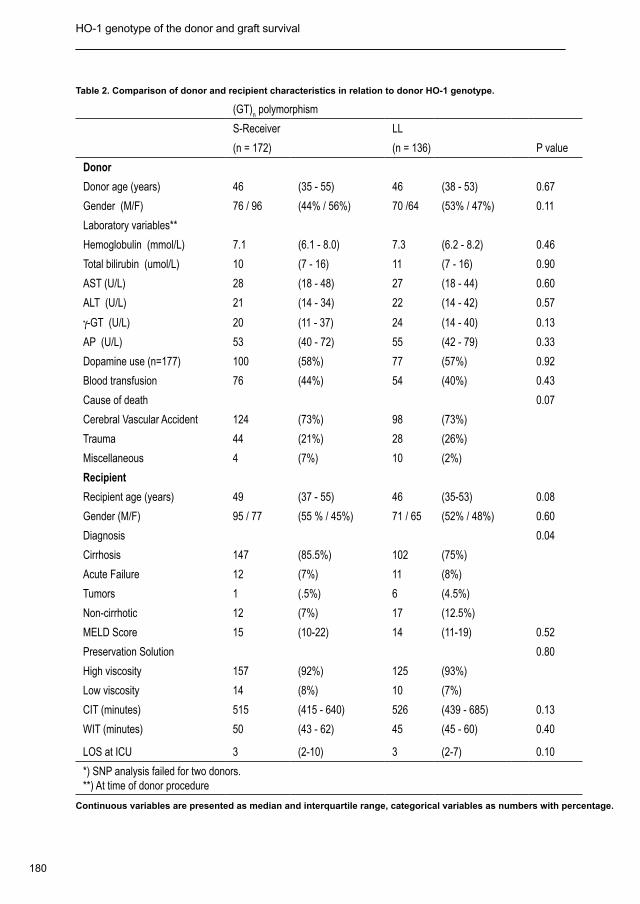
180
HO-1 genotype of the donor and graft survival Chapter 9
Table 2. Comparison of donor and recipient characteristics in relation to donor HO-1 genotype.
(GT)n polymorphism A(-413)T SNP *
S-Receiver LL A-Receiver TT
(n = 172) (n = 136) P value (n=245) (n=61) P value
Donor
Donor age (years) 46 (35 - 55) 46 (38 - 53) 0.67 45 (37 - 54) 47 (37 - 55) 0.77
Gender (M/F) 76 / 96 (44% / 56%) 70 /64 (53% / 47%) 0.11 120 / 125 (49% / 51%) 34 / 27 (43% / 57%) 0.43
Laboratory variables**
Hemoglobulin (mmol/L) 7.1 (6.1 - 8.0) 7.3 (6.2 - 8.2) 0.46 7.1 (6.2 - 8.0) 7.2 (6.0 - 8.1) 0.97
Total bilirubin (umol/L) 10 (7 - 16) 11 (7 - 16) 0.90 11 (7 - 16) 12 (7 - 14) 0.45
AST (U/L) 28 (18 - 48) 27 (18 - 44) 0.60 27 (18 - 44) 32 (20 - 54) 0.23
ALT (U/L) 21 (14 - 34) 22 (14 - 42) 0.57 21 (13 - 36) 27 (18 - 46) 0.02
γ-GT (U/L) 20 (11 - 37) 24 (14 - 40) 0.13 21 (12 - 39) 24 (15 - 37) 0.66
AP (U/L) 53 (40 - 72) 55 (42 - 79) 0.33 54 (41 - 76) 49 (36 - 68) 0.25
Dopamine use (n=177) 100 (58%) 77 (57%) 0.92 137 (56%) 40 (66%) 0.56
Blood transfusion 76 (44%) 54 (40%) 0.43 108 (44%) 22 (36%) 0.25
Cause of death 0.07 0.94
Cerebral Vascular Accident 124 (73%) 98 (73%) 177 (73%) 44 (73%)
Trauma 44 (21%) 28 (26%) 57 (23%) 15 (25%)
Miscellaneous 4 (7%) 10 (2%) 11 (10%) 2 (3%)
Recipient
Recipient age (years) 49 (37 - 55) 46 (35-53) 0.08 46 (35 - 55) 49 (38 - 54) 0.33
Gender (M/F) 95 / 77 (55 % / 45%) 71 / 65 (52% / 48%) 0.60 131 / 114 (53% / 47%) 33 / 28 (54% / 46%) 0.93
Diagnosis 0.04 0.76
Cirrhosis 147 (85.5%) 102 (75%) 196 (80%) 51 (84%)
Acute Failure 12 (7%) 11 (8%) 19 (8.5%) 4 (6.5%)
Tumors 1 (.5%) 6 (4.5%) 5 (1.5%) 2 (3%)
Non-cirrhotic 12 (7%) 17 (12.5%) 25 (10%) 4 (6.5%)
MELD Score 15 (10-22) 14 (11-19) 0.52 14 (11-20) 16 (11-24) 0.31
Preservation Solution 0.80 0.39
High viscosity 157 (92%) 125 (93%) 225 (92%) 58 (95%)
Low viscosity 14 (8%) 10 (7%) 20 (8%) 3 (5%)
CIT (minutes) 515 (415 - 640) 526 (439 - 685) 0.13 519 (434 - 643) 531 (411 - 663) 0.99
WIT (minutes) 50 (43 - 62) 45 (45 - 60) 0.40 51 (44 - 60) 50 (42 - 63) 0.83
LOS at ICU 3 (2-10) 3 (2-7) 0.10 3 (2-7) 3 (2-12) 0.54
*) SNP analysis failed for two donors. **) At time of donor procedure
Continuous variables are presented as median and interquartile range, categorical variables as numbers with percentage.
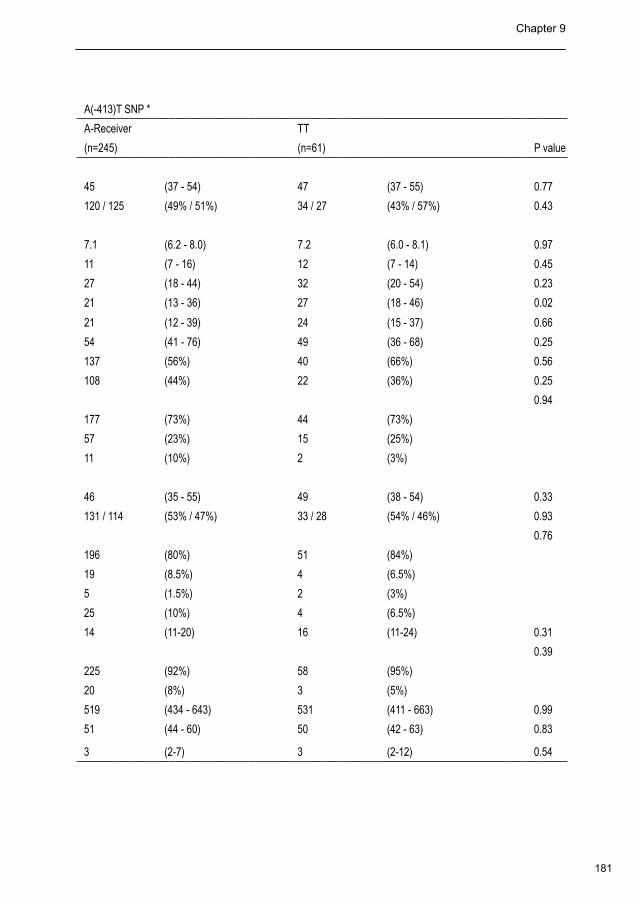
181
Chapter 9
Table 2. Comparison of donor and recipient characteristics in relation to donor HO-1 genotype.
(GT)n polymorphism A(-413)T SNP *
S-Receiver LL A-Receiver TT
(n = 172) (n = 136) P value (n=245) (n=61) P value
Donor
Donor age (years) 46 (35 - 55) 46 (38 - 53) 0.67 45 (37 - 54) 47 (37 - 55) 0.77
Gender (M/F) 76 / 96 (44% / 56%) 70 /64 (53% / 47%) 0.11 120 / 125 (49% / 51%) 34 / 27 (43% / 57%) 0.43
Laboratory variables**
Hemoglobulin (mmol/L) 7.1 (6.1 - 8.0) 7.3 (6.2 - 8.2) 0.46 7.1 (6.2 - 8.0) 7.2 (6.0 - 8.1) 0.97
Total bilirubin (umol/L) 10 (7 - 16) 11 (7 - 16) 0.90 11 (7 - 16) 12 (7 - 14) 0.45
AST (U/L) 28 (18 - 48) 27 (18 - 44) 0.60 27 (18 - 44) 32 (20 - 54) 0.23
ALT (U/L) 21 (14 - 34) 22 (14 - 42) 0.57 21 (13 - 36) 27 (18 - 46) 0.02
γ-GT (U/L) 20 (11 - 37) 24 (14 - 40) 0.13 21 (12 - 39) 24 (15 - 37) 0.66
AP (U/L) 53 (40 - 72) 55 (42 - 79) 0.33 54 (41 - 76) 49 (36 - 68) 0.25
Dopamine use (n=177) 100 (58%) 77 (57%) 0.92 137 (56%) 40 (66%) 0.56
Blood transfusion 76 (44%) 54 (40%) 0.43 108 (44%) 22 (36%) 0.25
Cause of death 0.07 0.94
Cerebral Vascular Accident 124 (73%) 98 (73%) 177 (73%) 44 (73%)
Trauma 44 (21%) 28 (26%) 57 (23%) 15 (25%)
Miscellaneous 4 (7%) 10 (2%) 11 (10%) 2 (3%)
Recipient
Recipient age (years) 49 (37 - 55) 46 (35-53) 0.08 46 (35 - 55) 49 (38 - 54) 0.33
Gender (M/F) 95 / 77 (55 % / 45%) 71 / 65 (52% / 48%) 0.60 131 / 114 (53% / 47%) 33 / 28 (54% / 46%) 0.93
Diagnosis 0.04 0.76
Cirrhosis 147 (85.5%) 102 (75%) 196 (80%) 51 (84%)
Acute Failure 12 (7%) 11 (8%) 19 (8.5%) 4 (6.5%)
Tumors 1 (.5%) 6 (4.5%) 5 (1.5%) 2 (3%)
Non-cirrhotic 12 (7%) 17 (12.5%) 25 (10%) 4 (6.5%)
MELD Score 15 (10-22) 14 (11-19) 0.52 14 (11-20) 16 (11-24) 0.31
Preservation Solution 0.80 0.39
High viscosity 157 (92%) 125 (93%) 225 (92%) 58 (95%)
Low viscosity 14 (8%) 10 (7%) 20 (8%) 3 (5%)
CIT (minutes) 515 (415 - 640) 526 (439 - 685) 0.13 519 (434 - 643) 531 (411 - 663) 0.99
WIT (minutes) 50 (43 - 62) 45 (45 - 60) 0.40 51 (44 - 60) 50 (42 - 63) 0.83
LOS at ICU 3 (2-10) 3 (2-7) 0.10 3 (2-7) 3 (2-12) 0.54
*) SNP analysis failed for two donors. **) At time of donor procedure
Continuous variables are presented as median and interquartile range, categorical variables as numbers with percentage.
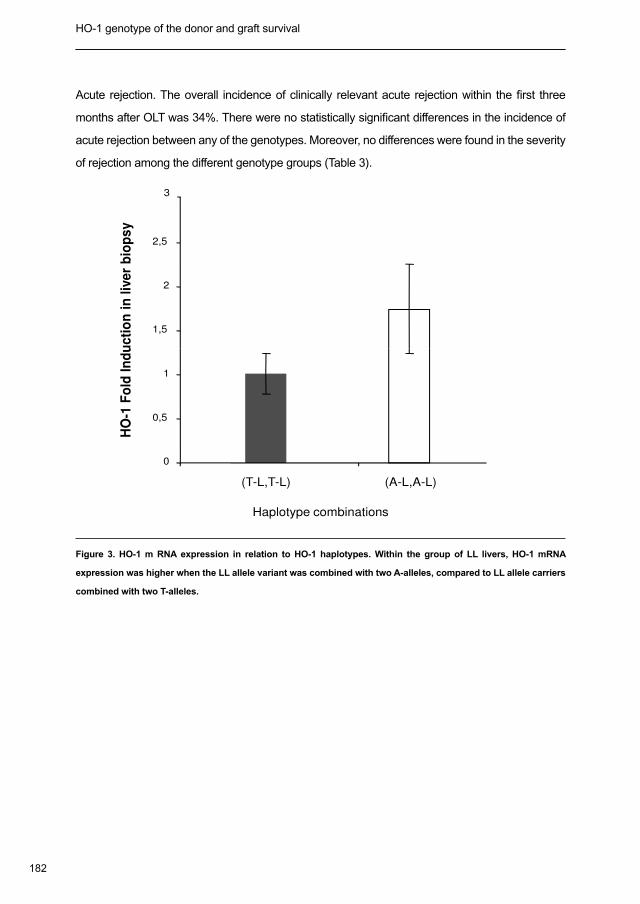
182
HO-1 genotype of the donor and graft survival Chapter 9
Acute rejection. The overall incidence of clinically relevant acute rejection within the first three
months after OLT was 34%. There were no statistically significant differences in the incidence of
acute rejection between any of the genotypes. Moreover, no differences were found in the severity
of rejection among the different genotype groups (Table 3).
1,5
2
2,5
3
1 F
old
In
du
cti
on
in
liv
er
bio
ps
y
Haplotype combinations
0
0,5
1
(T-L,T-L) (A-L,A-L)
HO
-1 F
old
In
du
cti
on
in
liv
er
bio
ps
y
Figure 3. HO-1 m RNA expression in relation to HO-1 haplotypes. Within the group of LL livers, HO-1 mRNA
expression was higher when the LL allele variant was combined with two A-alleles, compared to LL allele carriers
combined with two T-alleles.
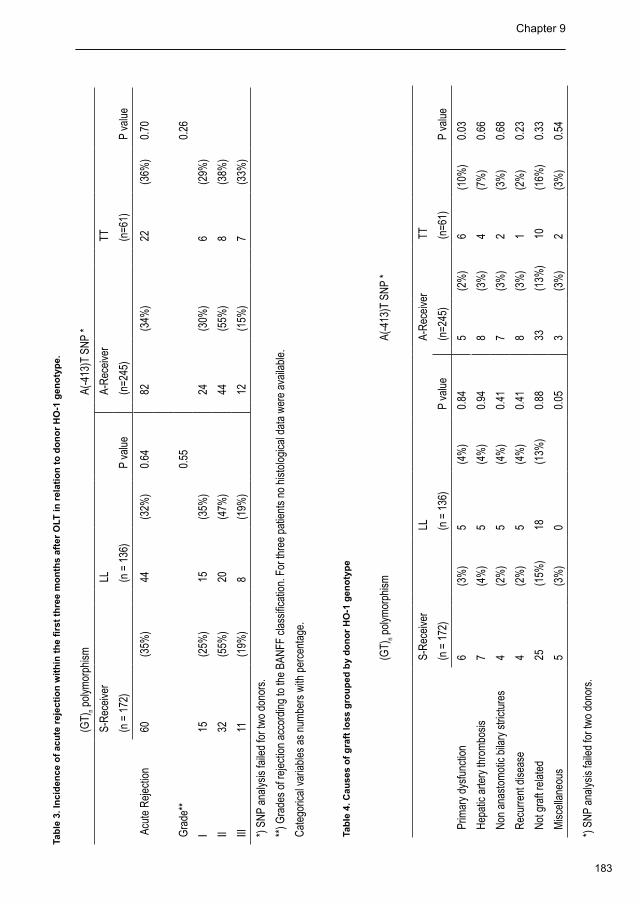
183
Chapter 9
Acute rejection. The overall incidence of clinically relevant acute rejection within the first three
months after OLT was 34%. There were no statistically significant differences in the incidence of
acute rejection between any of the genotypes. Moreover, no differences were found in the severity
of rejection among the different genotype groups (Table 3).
1,5
2
2,5
3
1 F
old
In
du
cti
on
in
liv
er
bio
ps
y
Haplotype combinations
0
0,5
1
(T-L,T-L) (A-L,A-L)
HO
-1 F
old
In
du
cti
on
in
liv
er
bio
ps
y
Figure 3. HO-1 m RNA expression in relation to HO-1 haplotypes. Within the group of LL livers, HO-1 mRNA
expression was higher when the LL allele variant was combined with two A-alleles, compared to LL allele carriers
combined with two T-alleles.
Tab
le 3
. In
cid
ence
of
acu
te r
ejec
tio
n w
ith
in t
he
firs
t th
ree
mo
nth
s af
ter
OLT
in r
elat
ion
to
do
no
r H
O-1
gen
oty
pe.
(GT)
n pol
ymor
phis
mA(
-413
)T S
NP
*
S-R
ecei
ver
LL
A-
Rec
eive
r TT
(n =
172
)
(n
= 1
36)
P
valu
e
(n=2
45)
(n=6
1)
P va
lue
Acu
te R
ejec
tion
60(3
5%)
44(3
2%)
0.64
82(3
4%)
22(3
6%)
0.70
Gra
de**
0.55
0.26
I15
(25%
)15
(35%
)
24(3
0%)
6(2
9%)
II32
(55%
)20
(47%
)
44(5
5%)
8(3
8%)
III11
(19%
)
8(1
9%)
12(1
5%)
7
(33%
)
*) S
NP
anal
ysis
faile
d fo
r tw
o do
nors
.
**) G
rade
s of
reje
ctio
n ac
cord
ing
to th
e BA
NFF
cla
ssifi
catio
n. F
or th
ree
patie
nts
no h
isto
logi
cal d
ata
wer
e av
aila
ble.
Cat
egor
ical
var
iabl
es a
s nu
mbe
rs w
ith p
erce
ntag
e.
Tab
le 4
. Cau
ses
of
gra
ft lo
ss g
rou
ped
by
do
no
r H
O-1
gen
oty
pe
(GT)
n pol
ymor
phis
mA(
-413
)T S
NP
*
S-R
ecei
ver
LL
A-R
ecei
ver
TT
(n =
172
)
(n =
136
)
P va
lue
(n=2
45)
(n
=61)
P
valu
e
Prim
ary
dysf
unct
ion
6(3
%)
5(4
%)
0.84
5(2
%)
6(1
0%)
0.03
Hep
atic
arte
ry th
rom
bosi
s7
(4%
)5
(4%
)0.
948
(3%
)4
(7%
)0.
66
Non
ana
stom
otic
bila
ry s
trict
ures
4(2
%)
5(4
%)
0.41
7(3
%)
2(3
%)
0.68
Rec
urre
nt d
isea
se4
(2%
)5
(4%
)0.
418
(3%
)1
(2%
)0.
23
Not
gra
ft re
late
d25
(15%
)18
(13%
)0.
8833
(13%
)10
(16%
)0.
33
Mis
cella
neou
s 5
(3%
)0
0.
053
(3%
)2
(3%
)0.
54
*) S
NP
anal
ysis
faile
d fo
r tw
o do
nors
.
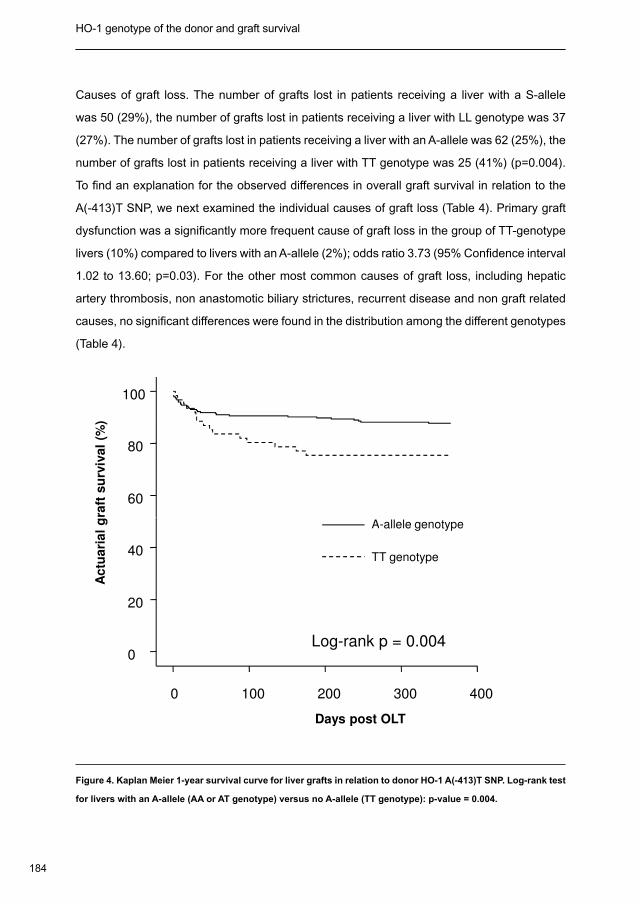
184
HO-1 genotype of the donor and graft survival Chapter 9
Causes of graft loss. The number of grafts lost in patients receiving a liver with a S-allele
was 50 (29%), the number of grafts lost in patients receiving a liver with LL genotype was 37
(27%). The number of grafts lost in patients receiving a liver with an A-allele was 62 (25%), the
number of grafts lost in patients receiving a liver with TT genotype was 25 (41%) (p=0.004).
To find an explanation for the observed differences in overall graft survival in relation to the
A(-413)T SNP, we next examined the individual causes of graft loss (Table 4). Primary graft
dysfunction was a significantly more frequent cause of graft loss in the group of TT-genotype
livers (10%) compared to livers with an A-allele (2%); odds ratio 3.73 (95% Confidence interval
1.02 to 13.60; p=0.03). For the other most common causes of graft loss, including hepatic
artery thrombosis, non anastomotic biliary strictures, recurrent disease and non graft related
causes, no significant differences were found in the distribution among the different genotypes
(Table 4).
100
80
60
Ac
tua
ria
l g
raft
su
rviv
al
(%)
A-allele genotype
4003002001000
Days post OLT
40
20
0
Ac
tua
ria
l g
raft
su
rviv
al
(%)
TT genotype
A-allele genotype
Log-rank p = 0.004
Figure 4. Kaplan Meier 1-year survival curve for liver grafts in relation to donor HO-1 A(-413)T SNP. Log-rank test
for livers with an A-allele (AA or AT genotype) versus no A-allele (TT genotype): p-value = 0.004.
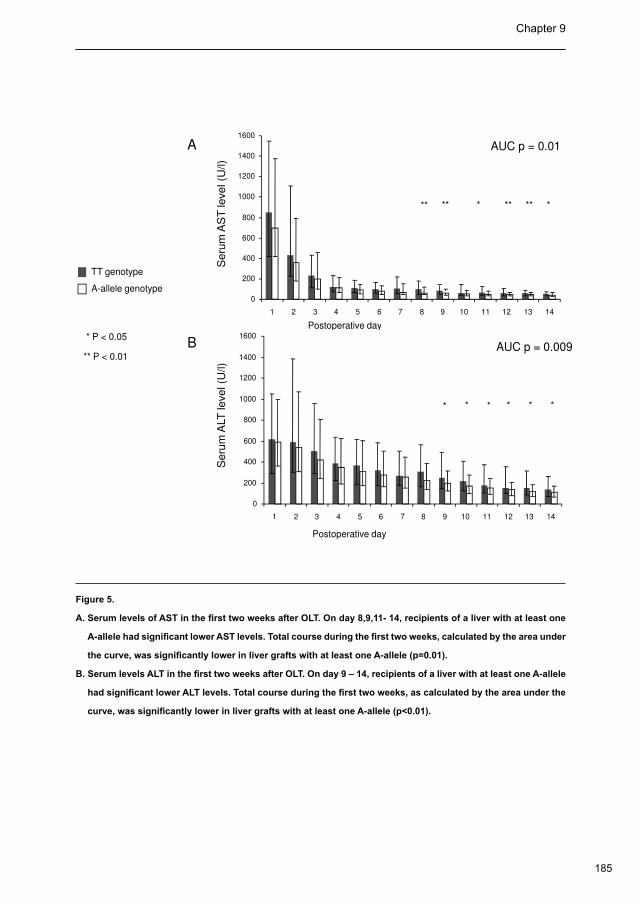
185
Chapter 9
Causes of graft loss. The number of grafts lost in patients receiving a liver with a S-allele
was 50 (29%), the number of grafts lost in patients receiving a liver with LL genotype was 37
(27%). The number of grafts lost in patients receiving a liver with an A-allele was 62 (25%), the
number of grafts lost in patients receiving a liver with TT genotype was 25 (41%) (p=0.004).
To find an explanation for the observed differences in overall graft survival in relation to the
A(-413)T SNP, we next examined the individual causes of graft loss (Table 4). Primary graft
dysfunction was a significantly more frequent cause of graft loss in the group of TT-genotype
livers (10%) compared to livers with an A-allele (2%); odds ratio 3.73 (95% Confidence interval
1.02 to 13.60; p=0.03). For the other most common causes of graft loss, including hepatic
artery thrombosis, non anastomotic biliary strictures, recurrent disease and non graft related
causes, no significant differences were found in the distribution among the different genotypes
(Table 4).
100
80
60
Ac
tua
ria
l g
raft
su
rviv
al
(%)
A-allele genotype
4003002001000
Days post OLT
40
20
0
Ac
tua
ria
l g
raft
su
rviv
al
(%)
TT genotype
A-allele genotype
Log-rank p = 0.004
Figure 4. Kaplan Meier 1-year survival curve for liver grafts in relation to donor HO-1 A(-413)T SNP. Log-rank test
for livers with an A-allele (AA or AT genotype) versus no A-allele (TT genotype): p-value = 0.004.
TT genotype
A-allele genotype
Seru
m A
ST
level (U
/l)
Postoperative day
0
200
400
600
800
1000
1200
1400
1600
1 2 3 4 5 6 7 8 9 10 11 12 13 14
** ** * ** ** *
AUC p = 0.01A
* P < 0.05
** P < 0.01
Postoperative day
Seru
m A
LT
level (U
/l)
Postoperative day
AUC p = 0.009B
0
200
400
600
800
1000
1200
1400
1600
1 2 3 4 5 6 7 8 9 10 11 12 13 14
* * * * **
Figure 5.
A. Serum levels of AST in the first two weeks after OLT. On day 8,9,11- 14, recipients of a liver with at least one
A-allele had significant lower AST levels. Total course during the first two weeks, calculated by the area under
the curve, was significantly lower in liver grafts with at least one A-allele (p=0.01).
B. Serum levels ALT in the first two weeks after OLT. On day 9 – 14, recipients of a liver with at least one A-allele
had significant lower ALT levels. Total course during the first two weeks, as calculated by the area under the
curve, was significantly lower in liver grafts with at least one A-allele (p<0.01).
186
HO-1 genotype of the donor and graft survival Chapter 9
Discussion
In this study we have examined the relationship between two functionally relevant
polymorphisms in the promoter of the HO-1 gene in the donor and postoperative outcome
in a large cohort of 308 liver transplant recipients. There are three novel findings in this
study. Firstly we observed significantly worse outcome in patients receiving a liver from a TT
genotype donor, compared to recipients from donors with at least one A allele. Secondly, we
have shown that the A(-413)T SNP and the (GT)n polymorphism are in linkage disequilibrium
with each other in this predominantly Caucasian population. Finally, we have shown, for the
fist time in a human population, the differences in functional relevance of these two HO-1
promoter polymorphisms. Our association study of the various haplotypes and actual HO-1
mRNA expression suggests that the A(-413)T SNP is of greater functional relevance than the
(GT)n polymorphism. No differences were found in any outcome parameter between the class
S and the LL-receivers of the (GT)n polymorphism. The power of this study with an overall
sample size of 308 subjects was greater than 80% to detect a difference of 13% in graft
survival at the statistical significant lever of 5%.
An association with functional polymorphisms of the HO-1 gene and clinical outcome parameters
has also been found in other pathological conditions, such as pulmonary emphysema, certain
cardiovascular diseases and malignancies (14,19,30-35). With respect to transplantation, two
groups have previously reported an association between HO-1 polymorphism in the donor
and outcome after kidney transplantation (21,22). Baan et al and Exner et al have shown
a positive correlation between the presence of a short (GT)n allele in the HO-1 promoter
and a favorable outcome after kidney transplantation (21,22). Although our data and the
two studies in kidney transplant recipients all point towards a critical role for the HO-1 / CO
pathway in maintaining graft function after solid organ transplantation, in detail the studies
are different. The two studies in kidney transplantation revealed an association between the
(GT)n polymorphism and outcome after transplantation, whereas we found an association
with the A(-413)T SNP. Unfortunately, this SNP was not tested in the two previous studies in
kidney transplant recipients. Moreover, a third large genetic association study between the
(GT)n polymorphism and outcome after kidney transplantation did not provide evidence for
a protective effect of class S alleles on kidney graft survival (36). The linkage disequilibrium
between the short (GT)n variant and the T-allele at -413 in the current study, in combination
187
Chapter 9
with the known dominant effect of the A(-413)T SNP in relation to the (GT)n polymorphism
(16), could possibly explain the inconsistent results of studies in kidney transplant recipients
focusing on the (GT)n polymorphism only. It could well be that HO-1 expression has actually
been lower in kidney grafts with a short (GT)n allele. Unfortunately, tissue levels of HO-1
mRNA, as a marker of actual HO-1 gene expression, were not measured in the three studies
in kidney transplantation.
In our study population, which mainly consisted of Caucasians, we found the A(-413)T
SNP and the (GT)n polymorphism within the promoter of the HO-1 gene to be in linkage
disequilibrium. The two most frequent haplotypes were the A-allele at -413 in combination
with a long (29) (GT)n allele (43.2%) and the T-allele at -413 in combination with a short (22)
(GT)n allele (20.3%). This finding is in accordance with results from previous studies in
Japanese populations (15,16). Theoretically, these combinations are counterproductive, as
the A-allele at -413 and a short (GT)n allele are both associated with enhanced expression
of HO-1, whereas the T-allele and a long (GT)n allele are associated with reduced HO-1
expression. Our data, however, consistently point towards a dominant effect of the A(-413)
T SNP over the (GT)n polymorphism. Not only clinical outcome parameters but also hepatic
HO-1 mRNA correlated with the A(-413)T SNP, but not with the (GT)n polymorphism. To
our knowledge this is the first study in humans suggesting an association between mRNA
expression and the various HO-1 haplotypes. Similar observations have been made by Ono et
al. who have studied the functional role of the A(-413)T SNP and the (GT)n polymorphism in an
in vitro system of bovine aortic endothelial cells, using a luciferase reporter assay (15). These
investigators suggested that, with respect to HO-1 promoter activity, the A(-413)T SNP is
dominant over the (GT)n polymorphism. In a previous study we have shown the HO-1 mRNA
expression correlates well with protein expression in human livers (13).
The exact mechanisms explaining the clinical observations in this study are incompletely
understood. Experimental studies have previously shown that upregulation of HO-1 protects
liver grafts against ischemia / reperfusion injury and improves graft survival (2,3,37-39)
Especially, steatotic livers, which are highly sensitive to ischemic injury, seem effectively
protected against this type of injury by induction of HO-1 (37,40). The inferior outcomes of livers
with the unfavorable TT genotype (associated with a reduced HO-1 promoter activity) in the
current study supports these previous findings. The effect of HO-1 genotype on graft survival
could, at least partly, be explained by a higher incidence of PDF in livers with a TT-genotype,

188
HO-1 genotype of the donor and graft survival Chapter 9
compared to livers with an A-allele (p=0.03). However, when the Kaplan Meier curves are
carefully observed, the lines started to separate from day 25 and were further divergent later
after transplantation. In accordance with this, the differences in serum transaminases became
more pronounced in the second week after transplantation. These observations suggest that
the observed differences in graft survival are not only explained by differences in ischemia
/ reperfusion injury, but also result from other mechanisms. In fact, the absolute number
of grafts lost due to PDF is relatively small, again suggesting that other factors have also
contributed to the observed differences in graft survival. Apparently, the impact HO-1 is not
limited to the early postoperative period. We speculate that other, possibly immune-mediated
processes, could explain the more late effects of HO-1 on graft survival. Several studies have
shown that HO-1 is a key enzyme in certain immune processes. Nevertheless, we observed
no differences in the incidence or severity of acute rejection between the various genotypes.
However, it would be of interest to study HO-1 mRNA expression in donor livers more long-
term after transplantation and to see if differences in HO-1 expression persist. Unfortunately,
we had no access to repeated biopsies during long term follow-up after OLT. More studies
on the mechanisms underlying the more long-term effects of HO-1 on graft survival will be
needed.
In conclusion, in this large series of 308 liver transplant recipients, we found an association
between donor HO-1 genotype and outcome after liver transplantation. Livers with at least
one A-allele of the A(-413)T SNP had significantly better graft survival rate and a lower rate of
PDF than livers with the TT genotype. In addition, our data indicate a functional dominance
of the A(-413)T SNP over the (GT)n polymorphism. These data suggest that HO-1 is critically
involved in maintaining graft function during and after liver transplantation.
189
Chapter 9
Reference List
Choi AM, Alam J. Heme oxygenase-1: function, regulation, and implication of a novel stress-inducible protein in 1.
oxidant-induced lung injury. Am J Respir Cell Mol Biol 1996;15: 9-19.
Amersi F, Buelow R, Kato H et al. Upregulation of heme oxygenase-1 protects genetically fat Zucker rat livers 2.
from ischemia/reperfusion injury. J Clin Invest 1999;104: 1631-1639.
Kato H, Amersi F, Buelow R et al. Heme oxygenase-1 overexpression protects rat livers from ischemia/3.
reperfusion injury with extended cold preservation. Am J Transplant 2001;1: 121-128.
Suematsu M, Goda N, Sano T et al. Carbon monoxide: an endogenous modulator of sinusoidal tone in the 4.
perfused rat liver. J Clin Invest 1995;96: 2431-2437.
Suematsu M, Ishimura Y. The heme oxygenase-carbon monoxide system: a regulator of hepatobiliary function. 5.
Hepatology 2000;31: 3-6.
Kutty RK, Maines MD. Purification and characterization of biliverdin reductase from rat liver. J Biol Chem 6.
1981;256: 3956-3962.
McCoubrey WK, Jr., Cooklis MA, Maines MD. The structure, organization and differential expression of the rat 7.
gene encoding biliverdin reductase. Gene 1995;160: 235-240.
Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological 8.
importance. Science 1987;235: 1043-1046.
Stocker R, Glazer AN, Ames BN. Antioxidant activity of albumin-bound bilirubin. Proc Natl Acad Sci U S A 9.
1987;84: 5918-5922.
Vile GF, Tyrrell RM. Oxidative stress resulting from ultraviolet A irradiation of human skin fibroblasts leads to a 10.
heme oxygenase-dependent increase in ferritin. J Biol Chem 1993;268: 14678-14681.
Ferris CD, Jaffrey SR, Sawa A et al. Haem oxygenase-1 prevents cell death by regulating cellular iron. Nat Cell 11.
Biol 1999;1: 152-157.
DeRusso PA, Philpott CC, Iwai K, Mostowski HS, Klausner RD, Rouault TA. Expression of a constitutive mutant 12.
of iron regulatory protein 1 abolishes iron homeostasis in mammalian cells. J Biol Chem 1995;270: 15451-
15454.
Geuken E, Buis CI, Visser DS et al. Expression of heme oxygenase-1 in human livers before transplantation 13.
correlates with graft injury and function after transplantation. Am J Transplant 2005;5: 1875-1885.
Yamada N, Yamaya M, Okinaga S et al. Microsatellite polymorphism in the heme oxygenase-1 gene promoter 14.
is associated with susceptibility to emphysema. Am J Hum Genet 2000;66: 187-195.
190
HO-1 genotype of the donor and graft survival Chapter 9
Ono K, Goto Y, Takagi S et al. A promoter variant of the heme oxygenase-1 gene may reduce the incidence of 15.
ischemic heart disease in Japanese. Atherosclerosis 2004;173: 315-319.
Ono K, Mannami T, Iwai N. Association of a promoter variant of the haeme oxygenase-1 gene with hypertension 16.
in women. J Hypertens 2003;21: 1497-1503.
Okinaga S, Takahashi K, Takeda K et al. Regulation of human heme oxygenase-1 gene expression under 17.
thermal stress. Blood 1996;87: 5074-5084.
Hirai H, Kubo H, Yamaya M et al. Microsatellite polymorphism in heme oxygenase-1 gene promoter is associated 18.
with susceptibility to oxidant-induced apoptosis in lymphoblastoid cell lines. Blood 2003;102: 1619-1621.
Chen YH, Lin SJ, Lin MW et al. Microsatellite polymorphism in promoter of heme oxygenase-1 gene is 19.
associated with susceptibility to coronary artery disease in type 2 diabetic patients. Hum Genet 2002;111: 1-8.
Naylor LH, Clark EM. d(TG)20. n.d(CA)
n sequences upstream of the rat prolactin gene form Z-DNA and inhibit gene
transcription. Nucleic Acids Res 1990;18: 1595-1601.
Baan C. Fundamental role for HO-1 in the self-protection of renal allografts. American journal of transplantation 21.
2004;4: 811-818.
Exner M. Donor heme oxygenase-1 genotype is associated with renal allograft function. Transplantation 22.
2004;77: 538-5342.
Miyamoto S, Polak WG, Geuken E et al. Liver transplantation with preservation of the inferior vena cava. A 23.
comparison of conventional and piggyback techniques in adults. Clin Transplant 2004;18: 686-693.
Polak WG, Miyamoto S, Nemes BA et al. Sequential and simultaneous revascularization in adult orthotopic 24.
piggyback liver transplantation. Liver Transpl 2005;11: 934-940.
de Jong MM, Nolte IM, de Vries EG et al. The HLA class III subregion is responsible for an increased breast 25.
cancer risk. Hum Mol Genet 2003;12: 2311-2319.
Funk M. The effect of a promoter polymorphism in the heme oxygenase-1 gene on the risk of ischaemic 26.
cerebrovascular events: the influence of other vascular risk factors. Thrombosis research 2004;113: 217-223.
Banff schema for grading liver allograft rejection: an international consensus document. Hepatology 1997;25: 27.
658-663.
Ploeg RJ, D’Alessandro AM, Knechtle SJ et al. Risk factors for primary dysfunction after liver transplantation--a 28.
multivariate analysis. Transplantation 1993;55: 807-813.
Buis CI, Verdonk RC, Van der Jagt EJ et al. Nonanastomotic biliary strictures after liver transplantation, part 1: 29.
Radiological features and risk factors for early vs. late presentation. Liver Transpl 2007;13: 708-718.
Chen YH, Chau LY, Lin MW et al. Heme oxygenase-1 gene promotor microsatellite polymorphism is associated 30.
with angiographic restenosis after coronary stenting. Eur Heart J 2004;25: 39-47.
191
Chapter 9
Exner M, Schillinger M, Minar E et al. Heme oxygenase-1 gene promoter microsatellite polymorphism is 31.
associated with restenosis after percutaneous transluminal angioplasty. J Endovasc Ther 2001;8: 433-440.
Exner M. The role of heme oxygenase-1 promoter polymorphisms in human disease. Free radical biology 32.
2004;37: 1097-1104.
Kaneda H, Ohno M, Taguchi J et al. Heme oxygenase-1 gene promoter polymorphism is associated with 33.
coronary artery disease in Japanese patients with coronary risk factors. Arterioscler Thromb Vasc Biol 2002;22:
1680-1685.
Schillinger M, Exner M, Mlekusch W et al. Heme oxygenase-1 genotype is a vascular anti-inflammatory factor 34.
following balloon angioplasty. J Endovasc Ther 2002;9: 385-394.
Lo SS, Lin SC, Wu CW et al. Heme Oxygenase-1 Gene Promoter Polymorphism is Associated with Risk of 35.
Gastric Adenocarcinoma and Lymphovascular Tumor Invasion. Ann Surg Oncol 2007;14: 2250-2256.
Courtney AE, McNamee PT, Middleton D, Heggarty S, Patterson CC, Maxwell AP. Association of functional 36.
heme oxygenase-1 gene promoter polymorphism with renal transplantation outcomes. Am J Transplant 2007;7:
908-913.
Coito AJ, Buelow R, Shen XD et al. Heme oxygenase-1 gene transfer inhibits inducible nitric oxide synthase 37.
expression and protects genetically fat Zucker rat livers from ischemia-reperfusion injury. Transplantation
2002;74: 96-102.
Lai IR, Ma MC, Chen CF, Chang KJ. The protective role of heme oxygenase-1 on the liver after hypoxic 38.
preconditioning in rats. Transplantation 2004;77: 1004-1008.
Yang Z, Tsui T, Ho D, Tang T, Fan S. Heme oxygenase-1 potentiates the survival of small-for-size liver graft. 39.
Liver transplantation 2004;10: 784.
Lehmann TG, Wheeler MD, Froh M et al. Effects of three superoxide dismutase genes delivered with an 40.
adenovirus on graft function after transplantation of fatty livers in the rat. Transplantation 2003;76: 28-37.

Summary, general discussion and future perspectives10
194
Summary, discussion and future perspectives Chapter 10
Summary
Chapter 1 provides a short introduction of the facts and figures in liver transplantation.
Furthermore, the aims of this thesis are discussed. These aims were to evaluate the molecular
and biochemical mechanisms of bile duct injury after liver transplantation.
In Chapter 2 the literature regarding the causes and consequences of non-anastomotic
strictures (NAS) is reviewed. The aim of this chapter was to describe the current knowledge
about the pathophysiological mechanisms, the clinical presentation, and the treatment of
NAS. NAS is a radiological diagnosis, characterized by intrahepatic strictures and dilatations
on a cholangiogram. NAS were first described after liver transplantation in association with
hepatic artery thrombosis (HAT). In case of early HAT after liver transplantation the biliary tree
becomes ischemic and eventually necrotic, resulting in a typical cholangiographic picture of
biliary strictures, dilatations and intraductal cast formation. However, these cholangiographic
abnormalities of strictures and dilatations can also be seen in patients who do not have a
hepatic artery thrombosis, so the term ischemic-type biliary lesions emerged. In this thesis the
term NAS was used to describe intrahepatic biliary strictures and dilatations in the confirmed
absence of HAT. The incidence of NAS varies around 15% in different series. Several risk
factors for NAS have been identified, strongly suggesting a multifactorial origin. Main categories
include ischemia related injury, immunological induced injury and cytotoxic injury by bile salts.
However, in many cases no specific risk factor can be identified. The clinical presentation of
patients with NAS is often not specific. Symptoms may include fever, abdominal complaints and
increased cholestatic liver function tests. The diagnosis is made by imaging studies of the bile
ducts. Treatment starts with relieving symptoms of cholestasis and dilatation of the stenosed
bile ducts by endoscopic retrograde cholangiopancreaticography (ERCP) or percutaneous
transhepatic cholangiodrainage (PTCD), if possible followed by stenting. Eventually up to
50% of the patients with NAS will require a re-transplantation or may die. In selected cases, a
re-transplantation can be avoided or delayed by surgical intervention.
In the clinical study described in Chapter 3 we aimed to identify clinical risk factors for the
development of NAS after liver transplantation. A total of 487 adult liver transplants with a
median follow-up of 7.9 years were studied. All imaging studies of the biliary tree were reviewed.
195
Chapter 10
Localization of NAS at first presentation was categorized into 4 anatomical zones of the biliary
tree. Severity of NAS was semiquantified as mild, moderate, or severe. NAS developed in 81
livers (16.6%). In 85% of the cases, anatomical localization of NAS was around or below the
bifurcation of the common bile duct. The severity of biliary strictures was classified as mild
in 43 (55%) and as moderate to severe in 35 (45%) of the cases. The cumulative incidence
of moderate to severe NAS in the entire population of liver transplant recipients was 7.3%.
A large variation was observed in the time interval between liver transplantation and first
presentation of NAS (median 4.1 months; range 0.3-155 months). NAS presenting early (<1
year) after liver transplantation were associated with preservation related risk factors. Cold and
warm ischemia times were significantly longer in patients with early NAS compared with NAS
presenting late (>1 year) after transplantation, and early NAS were more frequently located in
the central bile ducts. NAS presenting late after transplantation were more frequently found
in the periphery of the liver and were more frequently associated with immunological factors,
such as primary sclerosing cholangitis as the indication for liver transplantation. By separating
cases of NAS on the basis of the time of presentation after transplantation, we were able to
identify differences in risk factors, indicating different pathogenic mechanisms depending on
the time of initial presentation.
The population of patients suffering from NAS as described in Chapter 3 is further studied
in Chapter 4. The aim of this particular study was to describe the treatment, and identify risk
factors for radiological progression of bile duct abnormalities, recurrent cholangitis, biliary
cirrhosis and retransplantation in patients with NAS. Progression of disease was noted in
68% of cases in whom follow-up radiology was available. Radiological progression was more
common in patients with early NAS (≤ 1 year) and with one or more episodes of bacterial
cholangitis, and less prevalent in patients with extrahepatic biliary abnormalities. Recurrent
bacterial cholangitis (3 or more episodes) was more frequently seen in patients with a Roux-
en-Y anastomosis. Severe fibrosis or cirrhosis developed in 23 cases, especially in cases with
peripheral biliary abnormalities. Graft survival, but not patient survival, was influenced by the
presence of NAS. Thirteen patients (16%) were retransplanted for NAS. The conclusion of the
study is that especially patients with a hepatico-jejunostomy, those with an early diagnosis of
NAS, and those with NAS presenting at the level of the peripheral branches of the biliary tree,
are at risk for progressive disease with severe outcome.
196
Summary, discussion and future perspectives Chapter 10
In Chapter 5 we took a closer look at the role of bile composition in the development of bile duct
injury after liver transplantation, in a porcine model of non heart-beating liver transplantation.
After non-heart-beating (NHB) liver transplantation, the occurrence of NAS is a serious and
often encountered complication. Bile salt toxicity has been identified as an important factor
in the pathogenesis of bile duct injury and cholangiopathies in general. The role of bile salt
toxicity in the development of biliary strictures after NHB liver transplantation was, however,
unclear. In a porcine model of NHB liver transplantation, we studied the effect of different
periods of warm ischemia in the donor on bile composition and subsequent bile duct injury after
transplantation. After induction of cardiac arrest in the donor, liver procurement was delayed
for 0 min (group A), 15 min (group B), and 30 min or more (group C). Subsequently livers were
transplanted after 4 hr of cold preservation. In the recipients, bile flow was measured, and bile
samples were collected daily to determine the phospholipids-to-bile salt ratio. Severity of bile
duct injury was semi quantified by using a histological grading scale.
Survival after transplantation was directly related to the duration of warm ischemia in the
donor. The phospholipids-to-bile salt ratio in bile produced early after transplantation was
significantly higher in group C, compared with group A and B. Histopathologic examination
showed the highest degree of bile duct injury in group C. Based on these results, it was
concluded that prolonged warm ischemia in NHB donors is associated with the formation of
toxic bile after transplantation, characterized by a low biliary phospholipids-to-bile salt ratio.
These data suggest that bile salt toxicity contributes to the pathogenesis of bile duct injury
after NHB liver transplantation.
The previous chapter, as well as other studies from our group, have indicated that bile
formation early after liver transplantation may be disturbed, resulting in more cytotoxic bile
with a relatively low phospholipids-to-bile salt ratio. It was unknown whether bile toxicity is
also involved in the pathogenesis of NAS, a disease of the larger bile ducts. If bile composition
is involved in the pathogenesis of NAS, one would expect that the bile composition in the
first week after liver transplantation is different in those patients who will develop NAS than
in patients who will not develop NAS. We tested this hypothesis in a prospective clinical
study, described in Chapter 6. In this study, bile production and composition within one week
after liver transplantation were correlated with the subsequent development of NAS in a large
cohort of adult liver transplant recipients. In 111 adult liver transplants bile samples were
197
Chapter 10
collected daily after transplantation for determination of bile composition. Expression of bile
transporters was studied perioperatively. NAS were detected in 14 patients (13%) within
one year after transplantation. Patient and donor characteristics and postoperative serum
liver enzymes were similar between patients who developed NAS and those who did not.
Secretions of bile salts, phospholipids and cholesterol were significantly lower in patients
who developed NAS. In parallel, biliary phospholipids-to-bile salt ratio was lower in patients
developing NAS, suggestive for increased bile cytotoxicity. There were no differences in bile
salt pool composition or in hepatobiliary transporter mRNA expression.
Although patients who develop NAS were initially clinically indiscernible from patients who
did not develop NAS, the biliary bile salts and phospholipids secretion, as well as biliary
phospholipids-to-bile salt ratio in the first week after transplantation, was significantly lower in
the former group. This supports the concept that bile cytotoxicity is involved in the pathogenesis
of NAS.
In the previous chapter we have shown that altered bile composition, with a lower phospholipids-
to-bile salt ratio is associated with NAS after liver transplantation. Hepatobiliary transporter
proteins are responsible for the biliary secretion of phospholipids and bile salts. Aim of Chapter
7 was to assess whether variations in the genes in the donor encoding for these transporters
are associated with the occurrence of NAS in the recipient. Without transplantation, genetic
variations itself may not result in bile duct injury. However, early after transplantation, when
the graft is still recovering from I/R injury, these variations might be a critical second factor in
the sequence of events leading to bile duct injury. A similar phenomenon can be found in other
diseases, such as intrahepatic cholestasis of pregnancy (ICP), where patients with a genetic
variation in hepatobiliary transporters display an abnormal phenotype only during pregnancy.
Of 458 procedures in adults, cryopreserved splenocytes were available form the donors and
used for genotyping. The following genes were studied: bile salt export pump (ABCB11),
transporter of phospholipids (ABCB4) and transporter of glutathione and bilirubin (ABCC2).
Four to five tagging single nucleotide polymorphisms (SNPs) with an equal physical
distribution per gene were selected using HapMap data. Haplotypes were constructed using
an Expectation-Maximization algorithm to estimate haplotype frequencies. NAS was detected
in 77 patients (16%) after transplantation. Patients who received a donor liver with ABCB4
haplotype AGGTA developed NAS almost twice as often (28%) as donor livers with other
198
Summary, discussion and future perspectives Chapter 10
haplotypes (15%) (p=0.007). Analysis in a multivariate Cox regression model showed AGGTA
haplotype of ABCB4 from the donor to be an independent risk factor for NAS (p=0.004,
OR=2.23, 95% CI= 1.29 – 3.85). ABCB11 and ABCC2 haplotypes or single SNPs, were not
associated with NAS.
These data indicate that a common haplotype in the transporter of phospholipids (ABCB4)
in donor livers is independently associated with a two-fold increased risk for NAS after liver
transplantation. Transport of phospholipids into the bile in livers which are carriers of this risk
haplotype might be altered in the time period early after transplantation.
Upregulation of heme oxygenase-1 (HO-1) has been considered an adaptive and protective
mechanism against ischemia/reperfusion (I/R) injury. In Chapter 8 we studied the role of
endogenous HO-1 expression in human liver transplants in relation to early postoperative
hepatobiliary injury and dysfunction. Before transplantation, median HO-1 mRNA levels were
3.4-fold higher (range: 0.7–9.3) in donors than in normal controls. Based on the median value,
livers were divided into two groups: low and high HO-1 expression. There were no differences
in donor characteristics, donor serum transaminases or cold ischemia time between the two
groups. Postoperatively, however, serum transaminases were significantly lower and the
bile salt secretion was higher in the group with an initial low HO-1 expression, compared to
the high expression group. Immunofluorescence staining identified Kupffer cells as the main
localization of HO-1.
To study possible effects of HO-1 induction upon reperfusion, we categorized groups based
on the ability to increase HO-1 expression during reperfusion of the liver graft. In this analysis,
serum AST levels immediately after liver transplantation were significantly lower in the group
with an increase in HO-1 expression compared to livers without upregulation of HO-1 upon
reperfusion. These findings suggest that the ability to induce HO-1 expression at the time of
graft reperfusion may confer hepatobiliary protection. Further research will be necessary to
determine which is more important: a low expression of HO-1 before liver transplantation, or
the ability to induce HO-1 at the time of graft reperfusion.
In the previous chapter, the endogenous regulation of HO-1 during human liver transplantation
was studied. None of the clinical variables analyzed in this study could explain the variation in
initial expression of HO-1 in the donor livers. We therefore hypothesized that genetic variations
199
Chapter 10
may be responsible for the differences in HO-1 expression and subsequent outcome after
liver transplantation. The inducibility of HO-1 is modulated by a (GT)n polymorphism and a
single nucleotide polymorphism (SNP) A(-413)T in the promoter. Both a short (GT)n allele and
the A-allele have been associated with increased HO-1 promoter activity. In Chapter 9, a study
is described in which HO-1 genotype in the donor was tested and correlated with outcome in
308 adult patients. For (GT)n genotype, livers were divided into two classes: short alleles (<25
repeats; class-S) and long alleles (≥ 25 repeats; class-L). For the A(-413)T SNP, livers were
grouped as A-carriers (AT or AA) versus TT-genotype livers. In a subset of each group, hepatic
mRNA expression was correlated with genotypes. Graft survival at 1 year was significantly
better for A-allele genotype compared to TT-genotype (84% versus 63%, p=0.004). Graft loss
due to primary dysfunction occurred more frequently in TT-genotype compared to A-receivers
(p=0.03). No differences were found for the occurrence of NAS in both groups. Recipients of
a liver with TT-genotype had significantly higher serum transaminases after transplantation.
Hepatic HO-1 mRNA levels were significantly lower in TT genotype livers compared to the
A-allele livers (p=0.03). No differences were found for any outcome variable between class S
and LL-variant of the (GT)n polymorphism. Haplotype analysis indicated the dominance of the
A(-413)T SNP over the (GT)n polymorphism.
The main conclusion of this study was that the HO-1 promoter polymorphism A(-413)T is
associated with outcome after liver transplantation. The TT variant is linked with worse graft
survival, more primary dysfunction, increased I/R injury and reduced HO-1 mRNA levels.
Furthermore we provided evidence for a greater functional relevance of the A(-413)T SNP
over the (GT)n polymorphism.

200
Summary, discussion and future perspectives Chapter 10
General discussion and future perspectives
Part I: Non-anastomotic biliary complications after liver trans-
plantation
The specific aims of this section were to describe the various forms of NAS and the accompanying
clinical risk factors as well as to study the risk factors for progression of NAS. We found a
difference in risk factors for NAS presenting early (≤1 year) and NAS presenting late (>1 year)
after transplantation. NAS occurring early after transplantation were correlated with prolonged
ischemia times. NAS occurring late after transplantation were more strongly associated with
immunological risk factors. These data suggest that there are different subtypes of NAS that
have different etiologies. This aspect should be considered in future studies.
The following groups of patients were found to have an increased risk for disease progression:
patients with a hepaticojejunostomy, those with an early diagnosis of NAS, and those with
NAS presenting at the level of the peripheral branches of the biliary tree. In clinical practice it
is important to identify these patients for a close follow up and early intervention.
Our newly proposed classification system for NAS is a promising tool to better classify patients
with NAS. However, to become useable and successful in the currently expanding international
field of liver transplantation, our system should be validated. This would enable us to confirm
our findings on the relevance of the localization of NAS and subsequent consequences
for prognosis and management. Aligning many different international centres with different
protocols, facilities and expertise for a prospective study into this classification system might
be complex and time consuming. Therefore and second best, this validation could be achieved
by retrospectively studying other cohorts of liver transplant patients by reviewing the images
of the biliary tree and correlating the classification with risk factors and level of progression.
It is likely that recurrent PSC may have been accountable for the occurrence of late NAS in a
number of patients. On the basis of radiological evaluation, however, recurrent PSC cannot
be distinguished from a late presentation of NAS. Although some of our patients fit well within
the definition of recurrent PSC, more than half of our patients who presented with NAS late
after transplantation were not transplanted for PSC. In an attempt to reduce the occurrence of
early NAS, it remains important to focus on a further reduction of ischemic times, in particular
201
Chapter 10
the cold ischemia time. However, many centres have already put a lot of effort in this, and
it is questionable whether a substantial further reduction of cold ischemic time is feasible.
New perspectives in preservation of the liver graft might realize these assiduously sought-
after improvements of graft quality. Maintaining organ viability via (normothermic) machine
perfusion during preservation might be effective in reducing postoperative bile duct injury.
The central concept behind (normothermic) perfusion is to maintain normal function of the
liver during the whole period of preservation and enable immediate graft function and protect
the vulnerable biliary epithelial cells from I/R injury. Currently great efforts are being taken to
better understand the concepts of machine perfusion, as well as to find the ideal preservation
fluid and to create possibilities to implement machine perfusion in daily practice (1).
Part II: Bile physiology after liver transplantation
The specific aims of this second section were to evaluate the contribution of bile composition to
the development of bile duct injury. We found supporting evidence that toxic bile, characterized
by a low phospholipids-to-bile salt ratio, contributes to the development of bile duct injury, not
only at a microscopic level but also at a macroscopic level, like NAS.
The questions whether bile duct injury and toxic bile composition are not just two consequences
of the same underlying factor, has been studied previously by our group. Using mice
heterozygous for disruption of the Mdr2 gene (equivalent of human MDR3), Hoekstra et al.
confirmed that there is indeed a cause-effect relationship between toxic bile formation and bile
duct injury after liver transplantation and ruled out the possibility that toxic bile composition
and bile duct injury both result from the same underlying factor (2). In this study it was
demonstrated that endogenous bile salts act synergistically with I/R in the origin of bile duct
injury in vivo.
The question of which role toxic bile plays in bile duct injury is of great interest. What is
exactly happening on a cellular level? What is happening on epithelial level? What is the
sequence of events before the epithelial cells are damaged so severely that we can detect
it by radiological examination? Fickert et al proposed a very appealing mechanism similar to
the pathogenesis of primary sclerosing cholangitis in humans. They stated that due to a lack
of phospholipids the nonmiccellar-bound, free bile acids might damage the tight junctions and
basement membranes of the epithelial lining, leading to leakage of potentially toxic bile acids
202
Summary, discussion and future perspectives Chapter 10
into the periductal area. As a result the inflammatory response is induced, ultimately resulting
in fibrosis and narrowing of the biliary ducts (3).
Therapeutic strategies to modify intrahepatic cholestasis and to prevent bile duct injury after
OLT may include the administration of the hydrophilic bile salt ursodeoxycholic acid. Daily oral
administration of ursodeoxycholic acid is a well-known therapy to reduce bile salt toxicity by
replacement of the hydrophobic bile salts in the bile salt pool (4,5). Although the exact mechanisms
underlying its cytoprotective effect are not fully understood, it may reduce bile salt–induced injury
by replacing the toxic hydrophobic biliary bile salts. In addition, it has been shown to stimulate
cannalicular transport and biliary excretion, enhancing bile flow and reducing the exposure time
of biliary epithelium to toxic bile salts (4). The potentially beneficial effects of ursodeoxycholic
acid make this drug an interesting strategy to prevent NAS. Current experimental and clinical
research provides strong support for a prospective clinical trial focussing on the abilities of
ursodeoxycholic acid to prevent NAS early after liver transplantation.
Another interesting therapeutic target could be the MDR3 gene, given the key role of biliary
phospholipids in protecting bile duct epithelium from potentially toxic, aggressive biliary
content (5). Administration of fibrates, statins, or peroxisome proliferators in mice, have been
shown to stimulate biliary phospholipid secretion by the induction of MDR3 making bile less
toxic (7-9). Further research in this direction seems justified.
Part III: HO-1 and hepatobiliary injury after liver transplantation
The specific aim of the third section was to study the role of HO-1 in relation to postoperative
hepatobiliary injury and graft function. We showed that upregulation of HO-1 during liver
transplantation correlates with better hepatobiliary function after transplantation. Furthermore
we demonstrated that patients possessing a polymorphism that is associated with reduced
HO-1 expression on mRNA level have a worse hepatobiliary function after transplantation and
an increased risk of graft loss on the long run. The role of HO-1 as a cytoprotective protein
was confirmed by these studies.
It was noted that HO-1 is already upregulated in many livers form brain death donors. The
variations in the observed upregulation of HO-1 mRNA levels could not be explained by a
larger number of marginal donors in the group with high HO-1 expression. Moreover, factors
associated with major hemodynamic alterations in the donor and several surgical variables
203
Chapter 10
were similarly distributed amongst the donor groups with initial low expression of HO-1,
compared to the donor group with initial high expression of HO-1. To find an explanation
for these differences we studied two functional polymorphisms in the promoter region of the
gene: a (GT)n polymorphism and the single nucleotide polymorphism A(-413)T SNP.
The finding that the A(-413)T SNP exerts its effect not only in the immediate moments after
the transplant procedure, but has also consequences in the longer term (figure 4 in chapter 9),
is interesting. This could indicate that not only attenuation of I/R injury by a favourable HO-1
phenotype is beneficial but that HO-1 mediated processes may also play a role in later phases
after the transplantation.
Clinical application of interventions in the HO-1 system should be considered. However, we
should bear in mind that the beneficial effects of HO-1 may have a narrow therapeutic window
as shown in chapter 8. Highly overexpressed HO-1 displays pro-oxidant properties secondary
to iron accumulation, and may therefore be harmful instead of cytoprotective.
It would be very interesting to focus this research on the specific effect of HO-1 on biliary
epithelial cells which are especially vulnerable for I/R injury. We know from the study
described in chapter 8 that human HO-1 in the liver is mainly located in the Kupffer cells, and
not abundantly present in biliary epithelial cells. Strategies to enter HO-1 in these cells might
be of great interest to study whether HO-1 over expression could protect the bile ducts from
injury resulting from I/R injury or bile toxicity.
In summary, new insights are provided into the molecular and biochemical mechanisms of bile
duct injury after liver transplantation. We have proposed a classification system of NAS based
on the localization and severity of the biliary abnormalities. This classification system appeared
valuable in identifying different etiologies of NAS and also allowed the identification of patients
with NAS who are more at risk for complications or disease progression. Toxic bile composition,
characterized by a low phospholipids-to-bile salt ratio was discovered as a contributing
mechanism in the development of bile duct injury and NAS after liver transplantation. Further
interventional studies aimed at prevention of NAS based on the principle of this altered bile
composition are warranted. Finally, we have demonstrated a cytoprotective role of HO-1 in
liver transplantation, opening new avenues for the development of novel preventive strategies
or therapies.
204
Summary, discussion and future perspectives
References
Maathuis MH, Leuvenink HG, Ploeg RJ. Perspectives in organ preservation. Transplantation 2007 27;83:1289-1.
98.
Hoekstra H, Porte RJ, Tian Y, Jochum W, Stieger B, Moritz W, et al. Bile salt toxicity aggravates cold ischemic 2.
injury of bile ducts after liver transplantation in Mdr2+/- mice. Hepatology 2006 20;43:1022-31.
Fickert P, Fuchsbichler A, Wagner M, Zollner G, Kaser A, Tilg H et al. Regurgitation of bile acids from leaky bile 3.
ducts causes sclerosing cholangitis in Mdr2 (Abcb4) knockout mice. Gastroenterology 2004;127:261-74.
Fickert P, Zollner G, Fuchsbichler A, Stumptner C, Pojer C, Zenz R, et al. Effects of ursodeoxycholic and cholic 4.
acid feeding on hepatocellular transporter expression in mouse liver. Gastroenterology 2001;121:170-183.
Trauner M,Fickert P,Wagner M. MDR3(ABCB4) defects: Aparadigm for the genetics of adult cholestatic 5.
syndromes. Semin Liver Dis 2007; 27: 77.
Trauner M, Boyer JL. Bile salt transporters: Molecular characterization, function, and regulation. Physiol Rev 6.
2003; 83: 633.
Miranda S, Vollrath V, Wielandt AM, et al. Overexpression of mdr2 gene by peroxisome proliferators in the 7.
mouse liver. J Hepatol 1997; 26: 1331.
Hooiveld GJ, Vos TA, Scheffer GL, et al. 3-Hydroxy-3-methylglutarylcoenzymeAreductase inhibitors (statins) 8.
induce hepatic expression of the phospholipid translocase mdr2 in rats. Gastroenterology 1999; 117: 678.
Chianale J, Vollrath V, Wielandt AM, et al. Fibrates induce mdr2 gene expression and biliary phospholipid 9.
secretion in the mouse. Biochem J 1996; 314: 781.
Nederlandse samenvatting
206
Nederlandse samenvatting
Samenvatting
Levertransplantatie is de aangewezen behandeling voor patiënten met eindstadium leverfalen.
Het succespercentage van een transplantatie is groot, na 5 jaar is meer dan 75% van de
patiënten nog in leven. Er kunnen echter complicaties optreden, onder meer van de galwegen.
Complicaties van de galwegen betreffen lekkage, stricturen van de anastomose (AS) en
stricturen en verwijdingen van de galwegen in de lever, de non-anastomotische stricturen
(NAS).
In dit proefschrift zijn NAS nader onderzocht, we hebben gekeken naar moleculaire en
biochemische mechanismen van deze complicatie.
NAS is een diagnose die gesteld wordt door de radioloog op basis van afbeelding van de
galwegen, een cholangiogram. Het beeld wordt gekarakteriseerd door vernauwingen en
verwijdingen van de galwegen in de lever (intrahepatisch). NAS na levertransplantatie zijn
initieel veel beschreven in combinatie met een trombose van de arteria hepatica (HAT).
In het geval van een vroege HAT na levertransplantatie worden de galwegen ischemisch
en uiteindelijk necrotisch, hetgeen resulteert in een typisch beeld op het cholangiogram
met vernauwingen en verwijdingen. Deze typische cholangiografische afwijkingen van
vernauwingen en verwijdingen worden echter soms ook gezien in de afwezigheid van HAT,
vandaar dat de term ‘ischemic-type biliary lesions’ (ITBL) is ontstaan. In dit proefschrift is de
term NAS gebruikt om intrahepatische vernauwingen en verwijdingen te beschrijven in de
bevestigde afwezigheid van HAT. De incidentie van NAS varieert rond 15% in verschillende
onderzoeken. Er zijn meerdere risico factoren voor NAS geïdentificeerd wat sterk suggereert
dat er een multifactoriele origine is. De belangrijkste categorieën zijn ischemisch gerelateerde
schade, immunologisch geïnduceerde schade en schadelijke effecten door galzouten. In
sommige gevallen kan echter geen specifieke risicofactor worden aangewezen. De klinische
presentatie van patiënten met NAS is vaak niet specifiek. Symptomen als koorts, buikklachten
en afwijkende lever waarden in het bloed duidend op cholestase kunnen voorkomen. De
diagnose wordt gesteld met behulp van beeldvormende studies van de galwegen. De
behandeling begint met het verlichten van de klachten veroorzaakt door de cholestase en
verwijding van de eventueel gestenoseerde galwegen met behulp van ‘endoscopisch retrograde
207
cholangiopancreaticography’ (ERCP) of ‘percutanes transhepatische cholangiodrainage
(PTCD) zo mogelijk gevolgd door het achterlaten van een stent in de galwegen. Uiteindelijk
moet er bij een deel van de patiënten een re-transplantatie plaatsvinden of komen ze te
overlijden. In geselecteerde gevallen kan een re-transplantatie worden vermeden of in ieder
geval uitgesteld door chirurgische interventie.
Part I: Non-anastomotische galwegstricturen na levertransplantatie
In dit eerste gedeelte beschrijven we een tweetal studies met als doel a) de verschillende
vormen van NAS en bijbehorende klinische risico factoren te beschrijven, b) te achterhalen
welke patiënten met NAS een risico lopen op het ontwikkelen van ernstige problemen en de
behandeling daarvan.
In hoofdstuk 3 presenteren we een nieuwe classificatie van NAS. Met deze methode hebben
we alle beeldvorming van de patiënten met NAS van de afgelopen jaren in het UMCG opnieuw
beoordeeld. Verder hebben we gekeken naar risicofactoren voor het ontstaan van NAS, het
moment na de transplantatie waarop NAS zich presenteren en de progressie van de ziekte in
de loop van de jaren na de transplantatie.
In een groep van 487 volwassen transplantatie patiënten met een mediane follow-up van bijna 8
jaar waren er 81 (16.6%) patiënten die NAS ontwikkelden. We hebben aanwijzingen gevonden
dat er 2 vormen van NAS bestaan. NAS welke zich vroeg, binnen 1 jaar na de transplantatie,
presenteren en NAS welke zich na meer dan 1 jaar presenteren. Vroege NAS zijn geassocieerd
met preservatie en ischemisch gerelateerde risocofactoren, zoals een langere koude en
warme ischemie tijd. Tevens presenteren de vroege NAS zich vaker centraal in de lever. Late
NAS daarentegen zijn meer geassocieerd met immunologische risico factoren, zoals primair
scleroserende cholangitis als indicatie voor de transplantatie. Deze late vorm van NAS werd
vaker gezien in de periferie van de galwegen. We kunnen dus zeggen dat er verschillende
pathogenetische processen een rol spelen bij het ontstaan van NAS.
Als we verder kijken naar de groep patiënten met diagnose NAS, in hoofdstuk 4, konden
we de volgende risicofactoren identificeren voor radiologische progressie, wat bij bijna
70% van de patiënten optrad: vroege NAS en één of meerdere episodes van bacteriële
cholangitis. Bij patiënten met NAS bleek een galwegreconstructie met een Roux-Y hepatico-
jejunostormie een risicofactor voor het ontstaan van bacteriële cholangitis. Ernstige fibrose
208
Nederlandse samenvatting
of cirrose ontstond in 23 gevallen, vooral in gevallen waarbij de NAS perifeer in de lever
gelokaliseerd was. Transplantaatoverleving, maar niet patiëntenoverleving, werd beïnvloed
door de aanwezigheid van NAS. Dertien patiënten (16%) onderging een re-transplantatie
vanwege de NAS.
De conclusie van deze studie was dat vooral patiënten met een Roux-Y reconstructie,
patiënten met vroege NAS en patiënten met NAS in de periferie van de lever risico lopen op
voortschrijdende ziekte met ernstige uitkomsten.
Part II: Gal fysiologie na levertransplantatie
De specifieke doelen van dit tweede gedeelte waren te evalueren welke bijdrage de gal
samenstelling heeft op het ontstaan van galwegschade. Van galzouten is het bekend dat ze
een detergente, vetoplossende werking hebben (zie de titelpagina verklaring). Galzouten,
zonder beschermende fosfolipiden, hebben een schadelijke werking. Het is bekend dat
ze een rol spelen in het ontstaan van galwegschade en cholangiopathie bij vele andere
ziektebeelden. Galformatie direct na de transplantatie kan verstoord zijn hetgeen resulteert in
een dergelijke schadelijke samenstelling met een lage fosfolipiden – galzouten ratio. De rol van
schadelijke galsamenstelling in de ontwikkeling van galwegstricturen na levertransplantatie is
echter onduidelijk.
Na ‘non heart-beating’ (NHB) levertransplantatie zijn NAS een vaak voorkomende complicatie. In
hoofdstuk 5 wordt in een varkensmodel van NHB levertransplantatie het effect van verschillende
periodes van warme ischemie in de donor op galsamenstelling en daaropvolgende schade aan
de galwegen na transplantatie bestudeerd. In drie groepen werd een oplopende vertraging
voor uitname van de lever toegepast, waarna het orgaan wordt getransplanteerd na 4h koude
bewaartijd. De galflow werd gemeten en galmonsters werden dagelijks verzameld om de
fosfolipiden – galzout ratio te bepalen. De mate van schade aan de galwegen werd gescoord
door middel van een histologische scoringsschaal. De resultaten toonden dat de fosfolipiden –
galzouten ratio in de gal die vlak na de transplantatie werd geproduceerd significant lager is in
groep met de langste warme ischemietijd in de donor. In deze groep was ook de grootste mate
van galwegschade te zien. Op basis van de resultaten van deze studie werd geconcludeerd dat
langere warme ischemie in NHB donoren is geassocieerd met de vorming van schadelijke gal
na transplantatie, deze bevindingen suggereren dat schade door galzouten bijdraagt aan het
ontstaan van galwegschade na NHB levertransplantatie.
209
In het voorgaande hoofdstuk en ook andere studies uit onze groep hebben aangetoond dat
galformatie direct na de transplantatie verstoord kan zijn wat resulteert in een schadelijke
samenstelling van de gal met een lage fosfolipiden - galzouten ratio. Het was onbekend
of deze veranderde samenstelling ook en rol speelt bij de ontwikkeling van NAS, een
aandoening van de grotere galwegen. Indien veranderingen in de galsamenstelling
een rol spelen bij het ontstaan van NAS na transplantatie dan is te verwachten dat de
galsamenstelling na transplantatie anders is bij patiënten die NAS ontwikkelen ten opzichte
van patiënten die geen NAS ontwikkelen. Deze hypothese werd getest in een prospectieve
klinische studie welke beschreven is in hoofdstuk 6. In deze grote cohort studie bij
volwassen levertransplantatiepatiënten werd galproductie en samenstelling in de eerste
week na transplantatie gecorreleerd aan het ontstaan van NAS in het verdere beloop na
transplantatie. In 111 levertransplantatiepatiënten werden dagelijks galmonsters verzameld
om de samenstelling te analyseren. NAS werden gediagnosticeerd in 14 patiënten (13%)
binnen 1 jaar na transplantatie. Patiënten die uiteindelijke NAS ontwikkelden bleken minder
galzouten, fosfolipiden en cholesterol uit te scheiden in de gal. Tegelijkertijd was de biliare
fosfolipiden - galzouten ratio lager in patiënten die NAS ontwikkelden, wat duidt op mogelijk
meer schadelijke samenstelling van de gal. Deze bevindingen passen in het concept dat
galzouten betrokken is bij het ontstaan van NAS.
In het voorgaande hoofdstuk hebben we laten zien dat schadelijke gal samenstelling met
een verlaagde fosfolipiden - galzouten ratio geassocieerd is met NAS na levertransplantatie.
Hepatobiliare transporteiwitten zijn verantwoordelijk voor de secretie van fosfolipiden en
galzouten vanuit de hepatocyten naar de gal. Omdat de verschillen in de galsamenstelling
niet te verklaren waren door klinische variaties bij de donor of ontvanger was het doel van
hoofdstuk 7 om te analyseren of variaties in de genen die coderen voor deze transporters in
de donor geassocieerd zijn met het ontstaan van NAS in de ontvanger. Zonder transplantatie
leiden deze variaties op zichzelf niet tot galwegschade. Echter, direct na transplantatie, op
het moment dat de lever nog herstellende is van de schade van de ischemie en reperfusie
(I/R), kunnen deze variaties juist een belangrijke factor zijn in de serie van gebeurtenissen die
leidt tot het ontstaan van galweschade. Een vergelijkbare situatie wordt gezien bij patiënten
met intrahepatische cholestase tijdens de zwangerschap. Wanneer deze patiënten niet
zwanger zijn hebben zij geen klachten, echter op het moment dat er iets bijzonders gebeurt,
een zwangerschap vertonen ze ziekte verschijnselen. Bij 458 levertransplantatie procedures
210
Nederlandse samenvatting
konden we de verschillende hepatobiliare transport eiwitten genotyperen. Zevenenzeventig
patiënten (16%) ontwikkelden NAS na transplantatie. Patiënten die een donorlever ontvingen
met een genetische variatie in de fosfolipidentransporter ontwikkelde bijna 2 keer zo vaak
NAS (28%) als patiënten die een donorlever ontvingen zonder deze variatie (15%). Ook in een
multivariate analyse was deze variatie een onafhankelijke risicofactor voor het ontstaan van
NAS. Hoewel we dat in deze studie niet hebben onderzocht, zou het transport van fosfolipiden
naar de gal in levers welke drager zijn van het risico haplotype veranderd kunnen zijn in de
direct postoperatieve periode en op deze wijze een bijdrage kunnen leveren aan het ontstaan
van NAS.
Part III: HO-1 en hepatobiliaire schade na lever transplantatie
Het specifieke doel van het derde deel was om de rol van heme oxygenase-1 (HO-1) te
bestuderen in relatie tot hepatobiliaire schade en leverfunctie. Opregulatie van HO-1
wordt beschouwd als een belangrijk beschermingsmechanisme tegen I/R schade bij
levertransplantatie. In hoofdstuk 8 hebben we in 38 volwassen levertransplantatiepatiënten de
rol van endogene HO-1 expressie, voor tijdens en na transplantatie, bestudeerd in relatie tot
postoperatieve hepatobiliaire schade en functie direct na transplantatie. Voorafgaand aan de
operatie was de mediane HO-1 expressie reeds 3,4-keer verhoogd (spreiding 0,7 tot 9,3-keer
verhoogd). Deze spreiding was niet te verklaren door de klinische condities of behandelingen
van de donoren. We vonden dat in de groep van levers die het vermogen hadden om het
HO-1 tijdens de transplantatie verder op te reguleren, de schade aan de lever minder was dan
bij de patiënten waarbij de HO-1 expressie in de lever niet toenam. Dit suggereert dat levers
die tijdens reperfusie het HO-1 kunnen induceren beter beschermd zijn tegen I/R-schade
dan donorlevers die dit niet kunnen. Verder onderzoek zal nodig zijn om te achterhalen wat
belangrijker is: een lage HO-1 expressie voor aanvang van de transplantatie, of het vermogen
om HO-1 tijdens de reperfusie te induceren.
In het voorgaande hoofdstuk is de endogene regulatie van HO-1 tijdens levertransplantatie
onderzocht. Omdat de variatie die werd gevonden in de initiële HO-1 expressie in de donor
levers kon niet worden verklaard door klinische variabelen, werd de hypothese opgevat
dat genetische verschillen verantwoordelijke zouden kunnen zijn voor de variatie in HO-
1. De expressie van HO-1 wordt in belangrijke mate bepaald door 2 variaties in het gen,
zogenaamde polymorfismen. Eén daarvan is het ‘single nucleotide polymorfisme’ (SNP)
211
A(-413)T. Aangezien ieder mens 2 allelen heeft kunnen de volgende variaties ontstaan: AA,
AT en TT. De A-variant is geassocieerd met een verhoogde HO-1 activiteit. In hoofdstuk 9
beschrijven we een studie waarin de genetische variatie van de donor werd geanalyseerd en
gecorreleerd aan uitkomsten na transplantatie in een groep van 308 volwassen patiënten die
een levertransplantatie ondergingen. In een subgroep werd de HO-1 genexpressie in de lever
gecorreleerd aan de genotypen. Overleving van het transplantaat na 1 jaar was beter voor
A-varianten in vergelijking met de TT-genotypes. Verlies van het transplantaat als gevolg van
primaire disfunctie werd vaker waargenomen bij levers met het TT-genotype. Er werd geen
verschil gezien in de incidentie van NAS in beide groepen. Ontvangers van een TT-genotype
lever hadden meer schade aan de lever direct na transplantatie. HO-1 genexpressie in de
lever was lager in de levers met het TT-genotype, in vergelijking met levers met een A-allel.
De belangrijkste conclusie van deze studie was dat het A(-413)T polymorphisme in de HO-1
promoter geassocieerd is met uitkomsten na levertransplantatie.
Tot besluit kunnen we stellen dat onderzoek naar de moleculaire en biochemische mechanismen
van het ontstaan van galwegschade belangrijke nieuwe gezichtspunten hebben opgeleverd.
We hebben een nieuw classificatie systeem voor NAS voorgesteld, dat is gebaseerd op de
lokalisatie en ernst van de galwegafwijkingen. Dit classificatiesysteem bleek waardevol in het
identificeren van verschillende ontstaansmechanismen van NAS, tevens was het mogelijk
patiënten te identificeren die een groter risico liepen op complicaties en progressie van de
ziekte. Schadelijke samenstelling van de gal, gekarakteriseerd door een lage fosfolipiden -
galzouten ratio, werd geïdentificeerd als een belangrijk bijdragende factor aan het ontstaan
van galwegschade en NAS na levertransplantatie. Verder interventie onderzoeken gericht op
het voorkómen van NAS gebaseerd op de bevindingen van deze veranderde gal samenstelling
zijn nu het aangewezen vervolg. Tot slot hebben we een beschermende rol aangetoond voor
HO-1 in levertransplantatie, dit opent nieuwe wegen voor het ontwikkelen van preventieve
strategieën en therapieën.

List of contributing authors
214
List of Contributing Authors
List of Contributing Authors
Dr. H. Blokzijl
Department of Gastroenterology and Hepatology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. W. Geuken
Surgical Research Laboratory, Department of Surgery.
Currently Department of Pathology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. A.S.H. Gouw
Department of Pathology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. E.B. Haagsma
Department of Gastroenterology and Hepatology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. B.G. Hepkema
Department of Laboratory medicine, Transplantation Immnology
University Medical Centre Groningen
Groningen, the Netherlands
Drs. C.S. van der Hilst
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
215
Drs. H.H. Hoekstra
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
Dr. E.J. Van der Jagt
Department of Radiology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. K.P. de Jong
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
O.N.H. Kahmann
Surgical Research Laboratory
University Medical Centre Groningen
Groningen, the Netherlands
Prof. dr. H. Kleibeuker
Department of Gastroenterology and Hepatology
University Medical Centre Groningen
Groningen, the Netherlands
Prof. dr. F. Kuipers
Pediatric Gastroenterology, Department of Pediatrics
University Medical Centre Groningen
Groningen, the Netherlands
216
List of Contributing Authors
Dr. H.G.D. Leuvenink
Surgical Research Laboratory
University Medical Centre Groningen
Groningen, the Netherlands
Dr. A.J. Limburg
Department of Gastroenterology and Hepatology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. D. Monbaliu
Department of Abdominal Transplant Surgery and coordination
University Hospitals Leuven
Leuven, Belgium
Prof. H. Moshage
Department of Gastroenterology and Hepatology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. B.A. Nemes
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
Dr. M. Nijsten
Surgical Intensive Care Unit
University Medical Centre Groningen
Groningen, the Netherlands
217
Dr. I.M. Nolte
Department of Epidemiology
University Medical Centre Groningen
Groningen, the Netherlands
Dr. P. M.J.G. Peeters
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
Prof. dr. J. Pirenne
Department of Abdominal Transplant Surgery and coordination
University Hospitals Leuven
Leuven, Belgium
Prof. dr. R.J. Porte
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
Dr. T.A. Schuurs
Surgical Research Laboratory
University Medical Centre Groningen
Groningen, the Netherlands
Prof. dr. M.J.H. Slooff
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
218
List of Contributing Authors
Dr. G. van der Steege
Department of Genetics
University Medical Centre Groningen
Groningen, the Netherlands
Dr. R.C. Verdonk
Department of Gastroenterology and Hepatology
University Medical Centre Groningen
Groningen, the Netherlands
Prof. dr. H.J. Verkade
Pediatric Gastroenterology, Department of Pediatrics
University Medical Centre Groningen
Groningen, the Netherlands
Ing. D.S. Visser
Surgical Research Laboratory, Department of Surgery
University Medical Centre Groningen
Groningen, the Netherlands
Drs. M.J. Yska
Section Hepatobiliary Surgery and Liver Transplantation, Department of Surgery
Surgical Research Laboratory
University Medical Centre Groningen
Groningen, the Netherlands
List of publications
220
List of Publications
List of Publications
Buis CI, Bakker SJL. ACE- inhibitie niet effectief bij voorkómen van restenose na coronaire
stentimplantatie. Ned Tijdschr Geneeskd 2001; 145:2051. (short review paper).
Buis CI, Wijdicks EFM. Serial MR imaging in central pontine myelinolysis. Liver Transpl 2002;
8:643-5.
Buis CI, Wiesner RH, Krom RAF, Kremers WK, Wijdicks EFM. Acute confusional state following
liver transplantation for alcoholic liver disease. Neurology 2002; 59:601-5.
Geuken E, Buis CI, Visser DS, Blokzijl J, Moshage H, Nemes B, Leuvenink HGD, Jong de
KP,Peeters PMJG, Slooff MJH, Porte RJ. Expression of Heme oxygenese-1 in human livers
before transplantation correlates with graft injury and function after transplantation. Am J
Transplant 2005; 5:1875-85.
Buis CI, Porte RJ, Slooff MJH. Levertransplantatie. In: H.G. Smeenk, N.W.L. Schep, W.M.U.
van Grevenstein ed. Leidraad chirurgie. Houten: Bohn Stafleu van Loghum, 2005; 211.
Buis CI, Porte RJ, Slooff MJH. Niertransplantatie. In: H.G. Smeenk, N.W.L. Schep, W.M.U.
van Grevenstein ed. Leidraad chirurgie. Houten: Bohn Stafleu van Loghum, 2005; 219.
Verdonk RC, Buis CI, Porte RJ, Haagsma EB. Biliary complications after liver transplantation,
A review. Scand J Gastroenterol 2006; 243:89-101.
Buis CI, Hoekstra H, Verdonk RC, Porte RJ. Causes and Consequences of Ischemic Type
Biliary Lesions After Liver Transplantation. J Hepatobiliary Pancreat Surg 2006; 13:517-24.
Su Huawei, van Dam GM, Buis CI, Visser DS, Hesselink JW, Schuurs TA, Leuvenink HGD,
Contag CH, Porte RJ. Spatiotemporal Expression of heme oxygenase-1 Detected by in vivo
bioluminescence after hepatic ischemia in HO-1/Luc mice. Liver Transpl 2006; 12:1634-9.
221
Verdonk RC, Buis CI, Porte RJ, van der Jagt EJ, Limburg AJ, vd Berg AP, Slooff MJH, Peeters
PMJG, de Jong KP, Kleibeuker JH, Haagsma EB. Anastomotic biliary strictures after liver
transplantation: prevalence, presentation, management and outcome. Liver Transpl 2006;
12:726-35.
Mantel HTJ, Buis CI, Homan van der Heide JJ, van den Berg AP, Verkade HJ, Haagsma EB,
Peeters PMGJ, de Jong KP, Slooff MJH, Porte RJ. Gecombineerde lever-niertransplantaties:
Indicaties en resultaten in het UMC Groningen. Ned Tijdschr Geneeskd 2006; 150:2260-5.
Buis CI, Verdonk RC, van der Jagt EJ, van der Hilst CS, Slooff MJH, Haagsma EB, Porte
RJ. Non-anastomotic biliary strictures after adult liver transplantation part one: Radiological
features and risk factors for early versus late presentation. Liver Transpl 2007; 13:708-18.
Verdonk RC, Buis CI, van der Jagt EJ, Gouw ASH, Limburg AJ, Slooff MJH, Kleibeuker JH,
Porte RJ, Haagsma EB. Non-anastomotic biliary strictures after adult liver transplantation
part two: Management, outcome and risk factors for disease progression. Liver Transpl 2007;
13:725-32.
Buis CI, Steege vd G, Visser DS, Nolte IM, Hepkema BG, Nijsten M, Slooff MJH, Porte
RJ. Heme oxygenase-1 genotype of the donor is associated with graft survival after liver
transplantation. Am J Transplant 2008; 8:377-85.
Buis CI, Hofker HS, Nieuwenhuijs VB. Diverticulitis of the Jejunum, an uncommon diagnosis.
Dig Surg. 2008; 25:83-4.
Yska MJ, Buis CI, Monbaliu D, Schuurs TA, Gouw ASH, Kahmann ONH, Visser DS, Pirenne
J, Porte RJ. The role of bile salt toxicity in the pathogenesis of bile duct injury after non heart-
beating porcine liver transplantation. Transplantation 2008; 85:1625-31.
Buis CI, Geuken E, Visser DS, Kuipers F, Haagsma EB, Verkade HJ, Porte RJ. Altered
bile composition is associated with the development of nonanastomotic biliary strictures. J of
Hepatol, in press.
222
Buis CI, Steege vd G, Visser DS, Nolte IM, Porte RJ. Polymorphism of hepatobiliary
phospholipid transporter ABCB4 associated with nonanastomotic biliary strictures after human
liver transplantation. Submitted.
Hoekstra H, Buis CI, Verdonk RC, van der Hilst CS, van der Jagt EJ, Haagsma EB, Porte
RJ. Is Roux-Y choledochojejeunostomy an indipendant risk factor for non-anastomotic biliary
strictures after liver transplantation? Submitted.
List of Publications
Summary, discussion and future per-spectives
Dankwoord
Summary, discussion and future per-spectives

224
Dankwoord
Dankwoord
Het állerleukste van promoveren is dat je met zoveel verschillende mensen mag samenwerken
en van hen kan leren. Graag w il ik velen van hen in dit meest gelezen hoofdstuk noemen.
Professor dr. R.J. Porte, beste Robert, vanzelfsprekend ben jij de eerste, de allerbelangrijkste.
Jij hebt voor mij de mogelijkheid gecreëerd om AGIKO te worden. Jij hebt mij in staat gesteld
dit mooie (al zeg ik het zelf) proefschrift af te leveren. Het is fantastisch om met je te werken!
Je bezieling voor wetenschappelijk onderzoek is ongelooflijk groot en voortdurend aanstekelijk
omdat het is gebaseerd op een zeer scherpe en heldere analyse van de onderwerpen. Iedere
keer na overleg met jou had ik nóg meer inspiratie om aan de slag te gaan, jammer dat de
promotie nu klaar is. Gelukkig is er in ieder geval nog één artikel dat we samen verder mogen
polijsten, zodat de samenwerking op deze manier nog even door mag gaan.
Tot slot, je hebt een uitermate groot talent om een hele goede, leuke en bovenal gezellige groep
van onderzoekers om je heen te verzamelen, het is genieten om daar onderdeel van uit te
mogen maken.
Professor dr. M.J.H. Slooff, beste professor, u bent het boegbeeld van de hepatobiliare
chirurgie en levertransplantatie in Groningen. Op de achtergrond bent u voor mij heel belangrijk
geweest voor het welslagen van deze promotie. Uw wijsheid en warmte die ik heb leren kennen
voor het vak, maar zeker ook voor de ‘andere mooie dingen’ van het leven zal ik niet vergeten.
Dank voor het beoordelen van dit proefschrift.
Professor dr. H.J. Verkade, beste Henkjan, ik heb heel veel van je geleerd. Voor mij ben je
hét voorbeeld van combinatie van klinische top zorg met top wetenschappelijk onderzoek. Je
analyseert, denkt (en praat) zó snel dat het voor een gewone sterveling zoals ik vaak moeilijk
is bij te houden. Maar ik heb je altijd alle vragen mogen stellen totdat ik het begreep, dank voor
alle heldere uitleg. Dank voor het beoordelen van dit proefschrift.
Professor dr. H.J. Metselaar, beste Herold, ik heb je (en de onderzoeksgroep uit Rotterdam)
mogen ontmoeten op vele mooie plaatsten in de wereld. Dank voor het beoordelen van dit
proefschrift.
225
Professor dr. H.J. ten Duis, beste opleider, zonder uw steun was dit proefschrift nooit in deze
vorm tot stand gekomen. Graag wil ik u danken voor het vertrouwen dat u al heel vroeg in mij
heeft gesteld.
Dr. M. Eeftinck Schattenkerk, beste dr. Schattenkerk, graag wil ik ook u danken voor het
vertrouwen dat u reeds vroeg in mij gesteld heeft, dat ik mijn opleiding juist in Deventer mag
vervolgen. Nu dit proefschrift succesvol is afgerond kijk ik er erg naar uit onder uw leiding ook
mijn chirurgische vaardigheden verder te ontwikkelen.
Drs. M.T. de Boer, lieve Marieke, samen kunnen wij de wereld aan! Rio de Janiero, Milaan, San
Fransisco, Los Angeles, Amsterdam, Mumbai, (New York...?). Een voor een hoogtepunten. Kijk
uit naar (het feest van) jouw promotie. De manier waarop jij je vak bedrijft is een groot voorbeeld
voor me, ik ben apetrots dat jij mijn paranimf bent.
Dr. M.H.J. Maathuis, lieve Hugo, wat een feest was het om tegelijk met jou onderzoek te doen.
Het is fantastisch om met jou samen te werken, je bent ongelooflijk positief, organisatorisch de
beste, en een echte teamspeler, superlatieven te kort. Van het organiseren van het SEOHS heb
ik dan ook intens genoten. Ik weet zeker dat je succesvol en gelukkig zal worden in je nieuwe
functie. Ik ben waanzinnig vereerd dat je mijn paranimf bent.
Dr. W. Geuken, beste Erwin, dank voor het mede opzetten van de lijn galwegcomplicaties
na levertransplantatie in het lab. Dr. R.C. Verdonk, beste Robert, nu is het mijn beurt jou te
bedanken voor het samenwerken. Dank ook voor alle biopten waar ik een stukje van mocht
hebben. Ik kom graag op je oratie over een paar jaar! Drs. M.J. Yska, beste Marit, jij hebt als
student in het lab een uitzonderlijke prestatie geleverd! Dank voor het trekken van het ‘Leuven’
project, en veel succes in je verdere carrière.
Ing D.S. Visser, Beste Dorien, dank voor je grote hulp bij alle labbepalingen! We hebben
fantastisch samengewerkt, hetgeen ook blijkt uit het feit dat jullie zoon pas werd geboren toen al
het werk voor dit proefschrift klaar was! Veel geluk met het leven op Ameland!
Dr. G. van der Steege, beste Gerrit, jij nam alle tijd om mij in te wijden in de wereld van de
polymorfismen en haplotypes. Het was genieten om samen te puzzelen achter jouw computer.
226
Dankwoord
Hoofdstuk 9 is inmiddels heel mooi gepubliceerd, en ik weet zeker dat dit ook met Hoofdstuk 7
gaat lukken! Dr. E.J. van der Jagt, beste dr. van der Jagt, dank voor de vele uren dat u samen
met Robert Verdonk en mij alle beeldmaterieel van mogelijke NAS patiënten heeft gereviseerd
en gescoord. De uitkomsten van dit werk waren essentieel voor dit proefschrift. Professor dr.
F. Kuipers, beste Folkert, hoe fantastisch is het ergens te mogen werken waar je grootheden
als jij gewoon tegen het lijf loopt bij het koffieapparaat. Dank voor je warme betrokkenheid bij
mijn promotie onderzoek en in het bijzonder hoofdstuk 6. Dr. I.M. Nolte, beste Ilja, jouw inzicht
in statistiek is onnavolgbaar, toch slaagde je erin mij te laten begrijpen wat je deed. Dank voor
je hulp bij Hoofdstuk 7 en 9. Dr. E.B. Haagsma, beste dr. Haagsma, als begeleider van Robert
Verdonk bent u betrokken geweest bij het welslagen van Part I van mijn proefschrift, dank
daarvoor. Professor dr. J. Pirenne en dr. D. Monbaliu, beste professor, beste Diethard, dank
voor de succesvolle samenwerking en de warme ontvangst in Leuven, ook voor Marit.
De medeauteurs van de artikelen en nog niet eerder genoemd; Dr. A.S.H. Gouw, beste
Annette, dank voor uw hulp bij alle pathologische vraagstukken. Dr. B.G. Hepkema, beste
Bouke, dank voor de hulp vanuit de transplantatie immunologie bij hoofdstuk 7 en 9. Dr. M.
Nijsten, beste Maarten, dank voor de hulp bij het verkrijgen van alle labwaarden van de
levertransplantatiepatiënten. Dr. H. Blokzijl, beste Hans, alweer lang geleden heb jij mijn eerste
schreden in het lab begeleid, dank daarvoor en voor al het advies ‘along the way’. Drs. C.S. van
der Hilst, beste Christian, al mijn statistische kennis heb ik van jou! Dank voor je voortdurende
uitleg. Drs. H.H. Hoekstra, beste Harm, ik heb respect voor jouw eigen manier waarop je je
onderzoek bedrijft. Je muizen studie is mechanistisch gezien voor dit proefschrift van groot
belang geweest.
HPB en Levertransplantatie chirurgen en fellows uit Groningen dank ik voor alle uitleg en het
verzamelen van materiaal zodat er onderzoek gedaan kon worden; Dr. P.M.J.G. Peeters,
beste Paul, de precisie en toewijding waarmee jij opereert en klinische zorg verleent heb ik als
keuzeco leren kennen en zal voor altijd een voorbeeld blijven. Daarnaast heb ik de gesprekken
over zeilen, schilderen en het leven bijzonder gewaardeerd. Dr. K.P. de Jong, beste Koert, na
ons gestrande KOROCA project durfde ik bijna niet opnieuw bij de HPB club in Groningen aan
te kloppen, ik ben blij dat ik toch de stap heb genomen. Dr. I.Q. Molenaar, beste Q, hoe kan ik
jou bedanken? Het feestje had al ruim 2 jaar geleden kunnen zijn ;-) . Je bent een waanzinnig
227
groot voorbeeld van een ambitieuze chirurg met een prachtgezin! Dr. W.G. Polak, beste Wojtek,
dr. B.A. Nemes, dear Balasz, dr. S. Eguchi, dear Susumu, dr. A. Soyama, dear Aki en dr. E.
Sieders, beste Ger, thank you so much for all your explanations during the past years.
Professor dr. H. Kleibeuker, dr. A.J. Limburg, dank voor uw bijdrage aan hoofdstuk 4 van dit
proefschrift. Dr. A.P. van den Berg, beste Aad, dank voor al je uitleg en warme belangstelling
tijdens en na mijn keuzecoschap tijd.
Graag wil ik de volgende mensen danken voor hun bijdrage aan mijn proefschrift. Tina Crabbé
uit Leuven is onmisbaar geweest voor het uitvoeren van de experimenten uit Hoofdstuk 5,
zodat wij met de verkregen monsters onderzoek konden doen. Jan Bottema, dank voor het
verzamelen van gal voor Hoofdstuk 6, zodat ik ook eens een weekendje weg kon! Renze
Boverhof, dank voor het uitvoeren van de gaschromatografie van de galmonsters in hoofdstuk
6. Mariska Geuken, Fjodor van der Sluijs en Petra Suichies-Ottens, voor jullie technische
ondersteuning, en niet alleen voor hoofdstuk 8! Marcel Mulder, dank voor het uitvoeren van
de genotypering van Hoofdstuk 7 en 9. Tot slot Daniëlle Nijkamp, dank voor vele zaken, maar
ook voor de gezellige tijd in het oude archief van Eurotransplant in Leiden alwaar we alle oude
donordata hebben nagezocht!
De omgeving waar ik mijn onderzoek heb uitgevoerd is het Chirurgisch Onderzoekslaboratorium.
Vanuit de kliniek uiteraard professor dr. R.J. Ploeg, dank voor uw vele scherpe vragen tijdens
de labbesprekingen, en voor het meenemen van de jonge dokter op donor (vlucht (!) met
whisky). Dr. G.M. van Dam, je bent een waanzinnig enthousiaste wetenschapper en een super
begeleider van een jonge assistent.
Organisatorisch waren het soms roerige tijden, maar het chirurgisch lab is een fantastische
plek om te werken. Veel dank, dr. T. Lisman, beste Ton, voor je komst om te beginnen, je
wetenschappelijke inzicht en gezelligheid! Dr. H.G.D. Leuvenink, beste Henri, dank voor je
opvang van de jonge en onervaren onderzoeker in het lab die ik in het begin was! Dr. T.A
Schuurs, beste Theo, dank voor je wetenschappelijk inzicht en je begeleiding van Marit en het
totstandkomen van Hoofdstuk 5. Ing J.J Zwaagstra, beste Jacco, je weet dat ik groot respect
heb voor hoe jij het hoofdanalist-schap invult! Veel dank ook aan Ing A.van Dijk, beste Anthony,
dank voor het dierexperimentele werk, ik heb veel van je geleerd op microchirurgisch gebied,
228
Dankwoord
Ing J. Wiersema-Buist, beste Janneke, dank voor je algemene ondersteuning.
Het laboratorium kindergeneeskunde en MDL wil ik graag danken voor hun gastvrijheid en
voortdurende hulp tijdens mijn onderzoek. Beter een goede buur dan een verre vriend! Met
name dr. K.N. Faber en professor dr. A.J. Moshage. Drs. J. Mulder, beste Jaap, jammer
dat we (nog) geen artikel samen hebben geschreven, wel veel dank voor al je advies (op PCR
gebied).
Huawei Su, MD, dear Su, it was great to get to know and work with you! You published a
wonderful paper in the American Journal and I am pleased with my first citation in a Chinese
journal!
Collega onderzoekers en kamergenoten, Mijntje Nijboer (collega, we blijven elkaar zeker nog
tegenkomen!), Jayant Janandunsing (aan de andere kant van het doek), Cyril Moers (collega,
de lat is gelegd), Lyan koudstaal (succes met afronden van jouw proefschrift), Anne Margot
Roskott (dank voor de overheerlijke cappu’s!), Micheal Sutton (lang leve de galwegen), Tan
Hongtao (thank you so much for your contribution in the rapamycin project), Hugo Maathuis
(paranimf!) en Ilona Peereboom (dank voor het zijn van een hele hele leuke collega, dat dat nog
maar lang mag duren!), dank voor alle gezellige momenten en (wetenschappelijke) reflectie.
Graag wil ik ook op deze plaats de mensen bedanken die mijn eerste schreden op het
wetenschappelijke pad hebben begeleid en gestimuleerd. Professor dr. T.H. The, door mij te
selecteren voor de JSM en goede adviezen nadien. Professor dr. C.H. Gips, zoals gezegd, de
eerste basis is gelegd bij de GISH-T! Dankzij mijn succesvolle afstuderen in the Mayo Clinics
ben ik gestimuleerd door te gaan met wetenschap. Professor dr. R.A.F. Krom, icoon op het
gebied van levertransplantatie, dank voor uw begeleiding op en naast het wetenschappelijke
gebied en uw voortdurende belangstelling in mijn (helaas chirurgische) carrière. Professor dr.
E.F.M. Wijdicks, uw kunde om in een razend tempo een goed artikel te schrijven zal me altijd
bijblijven! Het was fantastisch met u samen te werken! Dr. C.B. Rosen, dear Chuck, our small
project together resulted in the first international oral presentation in my career, thanks for the
opportunities you created for me as a medical student to come to the OR and join in liver
transplant and donor procedures.
229
Het leverteam is een prachtige Groningse traditie! Dank aan alle studenten die in de loop van
de jaren hebben geholpen met het verzamelen van biopten tijdens de transplantaties! Verder wil
ik ook graag de andere studenten waar ik kort of lang mee heb mogen samenwerken bedanken:
Danka, Olivier (medeauteur H5!), Mohammed, Bakhtawar, Mickey, Henk-Jan (Mayo-collega
en auteur van CLKTx stuk), Maurits (weer terug!) en natuurlijk Fraukje en Heleen.
It has been a great honour to work with professor dr. G.J. Barrit, head of the department of
Medical Biochemistry, Flinders Medical School, Adelaide, Australia. Dear Greg and dear Yabin
Zhou, thank you for your hospitality in and outside the lab. Dr. V.B. Nieuwenhuijs, beste Vincent,
dankzij jouw contacten was het voor mij mogelijk naar Greg’s lab te gaan en een nieuw project,
dat we hier ook samen met Robert hebben geschreven, daar op te zetten. Dutchies! Marije,
Heleen, Fraukje, Claire, Meike, Claire en Judith, dank voor de ongelooflijke gezelligheid, op
het lab en daarbuiten en voor alle hele mooie tripjes die we hebben gemaakt!
Onderzoekers van het eerste uur uit het TRIADE gebouw Anne Brecht (dank voor het precedent
van een uitgebreid dankwoord), Tjeerd, Lucas, Annemarie, Kirsten, Marten, Eric, Esther en
Martin. In mijn eerste maanden werd ik meteen opgenomen in ‘de club’. Het was als jonge
onderzoeker fantastisch om ‘collegae’ te hebben!
SEOHS bestuur 2006, Hugo, Marcel, Justine (OH’s 4ever), Coralien, Hilke, Anton, Marinus
en Martin, het was een topcongres! Dank voor de heerlijk afwisseling in het wetenschappelijke
werk in de vorm van onze vele vergaderingen.
Onderzoek en congresbezoek-collegae; Quintus, Marieke, Nienke, Sander, Daantje, Christian,
Harm, Ilona, Margijske het is fantastisch met jullie de halve wereld over te vliegen!!
Collegae assistenten en chirurgen van het UMCG. Het voelde fantastisch om als jonkie
meteen opgenomen te worden in de club. Veel dank voor alle gezelligheid tijdens mijn tijd als
onderzoeker. Veel dank voor het wegwijs maken van datzelfde jonkie 2 jaar later in de kliniek
toen ik eindelijk ‘mocht’. En alvast voor de toekomst: veel dank voor alle gezelligheid en het
wegwijs blijven maken in de chirurgie!
230
Dankwoord
Ongelooflijk veel dank aan Linda, de regassen van C4 en alle andere secretaresses, voor het
bestellen van vele statussen en andere regeldingen! Veel dank ook aan de medewerkers van C4
waar ik niet alleen begon als keuzeco, maar ook nog heel vaak kwam om gal te verzamelen.
Veel mensen die niet direct bij het onderzoek betrokken zijn geweest, maar wel in mijn leven
een belangrijke rol spelen; Kickers (vanaf nu meer tijd om die ‘band voor het leven’ weer wat
meer aandacht te geven), GGGG (lieve oud-huisgenootjes: “wat wij hebben, heeft niemand!”),
Boswandeling (weekend van 22 januari 2009 staat geblokkeerd!), en alle verschillende
hockeyteams die mijn tijd in Groningen van de nodige inspanning en ontspanning hebben
voorzien. Een klein stukje gedicht voor jullie allen (naar Eric Brey):
Ik denk terug aan duizendtallen hapjes, nipjes, slokken
Maar ‘t was vooral m’n Ziel die daar zo gulzig zat te schrokken
Dat wij zo weer eens met elkaar langdurig haute-cuisine’den:
Kom, laat er altijd Eten zijn, en Drinken zijn, met Vrienden...
Lieve Pappa & Mamma en Hanne & Rikkert, Oom Wouter, dank voor alle 1001 leuke
momenten die wij met elkaar hebben! Mamma, dank voor alle wijze adviezen die ik gevraagd
en ongevraagd van je krijg op zoveel terreinen. Pappa, dank voor het inzicht dat ik van je heb
mogen leren (afkijken eigenlijk) terwijl jij alles maakte wat je bedacht (boot!). Wel spannend dat
ik straks als chirurg sta te knutselen zonder jou! Lieve Hanne, dank voor het zijn van mijn steun
en toeverlaat! Het is zo heerlijk om je te realiseren dat jullie voor altijd mijn Pappa, Mamma en
Zussie zijn!!
Mijn allerliefste Luitzen,
Je zoenen zijn zoeter dan
zoeter dan honing en ik vind je
mooier en liever, liever
en aardiger nog
dan de koning
Naar Judith Herzberg en Herman van Veen
Curriculum Vitae
232
Curriculum Vitae
Curriculum Vitae
Carlijn Buis was born on December 29th, 1978 in Vught, the Netherlands. After 6 years of
primary school at the ‘Rudolf Steiner Vrije School’ in ’s-Hertogenbosch she went to high
school (Gymnasium Beekvliet) in st. Michielsgestel where she graduated in 1997. In the
same year she started her medical study at the University of Groningen. During her study
at university Carlijn contributed as a board member to AIESEC (l’Association International
des Etudients en Science Economique et Commercial), a worldwide student organisation
focussing on international exchange. As a medical student Carlijn participated in the Junior
Scientific Master Class programme, under the guidance of professor dr. T.H. The. Carlijn
conducted her graduating scientific rotation via professor dr. C.H. Gips in Rochester, MN, USA
at the liver transplant unit in the Mayo Clinic under the guidance of professor dr. R.A.F. Krom
and professor dr. E.F.M. Wijdicks. In 2001 she passed her doctoral examination.
She followed her clinical rotations with great pleasure in the ‘Deventer Ziekenhuizen’ in
Deventer, the Netherlands. As a preparation for her MD-clinical trainee ship she conducted
her last clinical rotation at the Hepatobiliary Surgery and Liver Transplant unit at the University
Medical Center Groningen (UMCG). After graduating as a medical doctor, in January 2004,
Carlijn started her PhD at the UMCG, in the surgical research laboratory under the guidance
of professor dr. R.J. Porte. In May 2004 a MD-Clinical Research Traineeship (AGIKO) was
granted by the Netherlands Organization for Scientific Research (NWO). After conducting
2 years of research Carlijn accomplished the first year of her surgical training at the UMCG
under the guidance of professor dr. H.J. ten Duis. In 2008, a visiting research traineeship
was conducted at the Department of Medical Biochemistry and the Liver Transplant Unit at
Flinders Medical Center, Adelaide, in Australia under guidance of professor dr. G. Barritt, dr.
V.B. Nieuwenhuijs and professor R.J. Porte. Carlijn started a new project that is currently
being taken forward by various graduating students from the Netherlands. The upcoming year
Carlijn will continue her surgical training in the UMCG. In September 2009 and onwards she
will continue her surgical training in het ‘Deventer Ziekenhuis’ under guidance of dr. M Eeftinck
Schattenkerk.