Aeromedical Evacuation Planning Using Geospatial Decision ...
9
MILITARY MEDICINE, 179, 2:174, 2014 Aeromedical Evacuation Planning Using Geospatial Decision-Support CPT Nathaniel D. Bastian, MS USA*†‡; Lawrence V. Fulton, PhD§ ABSTRACT In this study, we proffer an algorithmic, geospatial-based decision-support methodology that assists military decision-makers in determining which aeromedical evacuation (MEDEVAC) assets to launch after receiving an injury location, given knowledge only of terrain, aircraft location, and aircraft capabilities. The objective is for military medical planners to use this decision-support tool (1) to improve real-time situational awareness by visuali- zation of MEDEVAC coverage, showing which areas can be reached within established timelines; (2) to support medical planning by visualizing the impact of changes in the medical footprint to the MEDEVAC coverage; and (3) to support decision-making by providing a time-sorted list of MEDEVAC asset packages to select from, given the location of the patients. This same geospatial-based decision tool can be used for proper emplacement of evacuation assets such that the theater is covered within a truly representative 1-hour response time. We conclude with a discussion of applicability of this tool in medical force structure planning. INTRODUCTION The Army Health System (AHS), the U.S. Army Medical Department (AMEDD) component of the Department of Defense’s Military Health System (MHS), is focused on delivery of health care across the continuum of military operations. During combat, the AMEDD’s Health Service Support (HSS) system provides medical treatment from the patient’s point-of-injury (POI) through successive roles of health care. As a critical component of the HSS system, medical evacuation (intra- and intertheater) is the link between roles of care because it sustains the patient during transport by providing en route medical care and emergency medical intervention. Although medical evacuation occurs at the tactical, operational, and strategic levels, this study considers the tactical level (intratheater) where medical evacuation assets locate, acquire, treat, and evacuate patients from the POI to an appropriate Medical Treatment Facility (MTF)— such as a Combat Support Hospital (Role III)—where they are stabilized, prioritized, and, if required, prepared for fur- ther medical evacuation outside the battlefield. 1 The AMEDD’s medical evacuation system comprises dedicated, standardized air and ground evacuation platforms designed, staffed, and equipped to provide rapid emergency response to requests for support to efficiently move patients to an MTF. All medical evacuation platforms provide en route medical care to enhance patient survivability rates, minimize mortality, improve patient prognosis, and reduce the disability of the wounded, injured, or sick. An effective medical evacuation system serves many purposes. It is a force multiplier as it clears the battlefield, enabling the ground commander to continue the mission. It builds the morale of Soldiers by showing that care is quickly avail- able on request. It provides medical economies of force by potentially reducing the need for in-theater hospitals. Finally, an effective evacuation system provides connec- tivity of the AHS as appropriate to the MHS. 1 Overview and Purpose This article seeks to expand the current literature on aero- medical evacuation (MEDEVAC) coverage and medical planning by using geospatial analytics for decision-support. The primary objectives are (1) to improve real-time situa- tional awareness by visualization of MEDEVAC coverage, showing which areas can be reached within established timelines; (2) to support medical planning by visualizing the impact of changes in the medical footprint to the MEDEVAC coverage; and (3) to support decision-making by providing a time-sorted list of asset packages to select from, given the location of the patients. This article is structured as follows. We first review the literature to better grasp the evolution of medical evacua- tion modeling and simulation. Afterward, we introduce the application of geospatial analytics for MEDEVAC cover- age visualization and medical planning decision-support. Finally, we conclude with a discussion of applicability to force structure planning. The primary significance of this *Department of Industrial and Manufacturing Engineering, Center for Integrated Healthcare Delivery Systems, Pennsylvania State University, 355 Leonhard Building, University Park, PA 16802. †Center for AMEDD Strategic Studies, Medical Capabilities Integration Center, U.S. Army Medical Department Center and School, 1608 Stanley Road, Fort Sam Houston, TX 78234-5047. ‡U.S. Army–Baylor University, Graduate Program in Health and Busi- ness Administration, U.S. Army Medical Department Center and School, 3630 Stanley Road, Fort Sam Houston, TX 78234-6100. §Department of Computer Information Systems and Quantitative Methods, McCoy College of Business Administration, Texas State University, McCoy Hall 404, San Marcos, TX 78666-4616. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the National Science Foundation, the Pennsylvania State Univer- sity, the Texas State University, or the U.S. Army. doi: 10.7205/MILMED-D-13-00432 MILITARY MEDICINE, Vol. 179, February 2014 174 Downloaded from https://academic.oup.com/milmed/article/179/2/174/4160802 by guest on 06 February 2022
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Aeromedical Evacuation Planning Using Geospatial Decision ...

MILITARY MEDICINE, 179, 2:174, 2014
Aeromedical Evacuation Planning Using GeospatialDecision-Support
CPT Nathaniel D. Bastian, MS USA*†‡; Lawrence V. Fulton, PhD§
ABSTRACT In this study, we proffer an algorithmic, geospatial-based decision-support methodology that assistsmilitary decision-makers in determining which aeromedical evacuation (MEDEVAC) assets to launch after receivingan injury location, given knowledge only of terrain, aircraft location, and aircraft capabilities. The objective is formilitary medical planners to use this decision-support tool (1) to improve real-time situational awareness by visuali-zation of MEDEVAC coverage, showing which areas can be reached within established timelines; (2) to supportmedical planning by visualizing the impact of changes in the medical footprint to the MEDEVAC coverage; and (3) tosupport decision-making by providing a time-sorted list of MEDEVAC asset packages to select from, given thelocation of the patients. This same geospatial-based decision tool can be used for proper emplacement of evacuationassets such that the theater is covered within a truly representative 1-hour response time. We conclude with a discussionof applicability of this tool in medical force structure planning.
INTRODUCTIONThe Army Health System (AHS), the U.S. Army Medical
Department (AMEDD) component of the Department of
Defense’s Military Health System (MHS), is focused on
delivery of health care across the continuum of military
operations. During combat, the AMEDD’s Health Service
Support (HSS) system provides medical treatment from
the patient’s point-of-injury (POI) through successive roles
of health care. As a critical component of the HSS system,
medical evacuation (intra- and intertheater) is the link between
roles of care because it sustains the patient during transport
by providing en route medical care and emergency medical
intervention. Although medical evacuation occurs at the
tactical, operational, and strategic levels, this study considers
the tactical level (intratheater) where medical evacuation
assets locate, acquire, treat, and evacuate patients from the
POI to an appropriate Medical Treatment Facility (MTF)—
such as a Combat Support Hospital (Role III)—where they
are stabilized, prioritized, and, if required, prepared for fur-
ther medical evacuation outside the battlefield.1
The AMEDD’s medical evacuation system comprises
dedicated, standardized air and ground evacuation platforms
designed, staffed, and equipped to provide rapid emergency
response to requests for support to efficiently move patients
to an MTF. All medical evacuation platforms provide en
route medical care to enhance patient survivability rates,
minimize mortality, improve patient prognosis, and reduce
the disability of the wounded, injured, or sick. An effective
medical evacuation system serves many purposes. It is a
force multiplier as it clears the battlefield, enabling the
ground commander to continue the mission. It builds the
morale of Soldiers by showing that care is quickly avail-
able on request. It provides medical economies of force
by potentially reducing the need for in-theater hospitals.
Finally, an effective evacuation system provides connec-
tivity of the AHS as appropriate to the MHS.1
Overview and Purpose
This article seeks to expand the current literature on aero-
medical evacuation (MEDEVAC) coverage and medical
planning by using geospatial analytics for decision-support.
The primary objectives are (1) to improve real-time situa-
tional awareness by visualization of MEDEVAC coverage,
showing which areas can be reached within established
timelines; (2) to support medical planning by visualizing
the impact of changes in the medical footprint to the
MEDEVAC coverage; and (3) to support decision-making
by providing a time-sorted list of asset packages to select
from, given the location of the patients.
This article is structured as follows. We first review the
literature to better grasp the evolution of medical evacua-
tion modeling and simulation. Afterward, we introduce
the application of geospatial analytics for MEDEVAC cover-
age visualization and medical planning decision-support.
Finally, we conclude with a discussion of applicability to
force structure planning. The primary significance of this
*Department of Industrial and Manufacturing Engineering, Center for
Integrated Healthcare Delivery Systems, Pennsylvania State University,
355 Leonhard Building, University Park, PA 16802.
†Center for AMEDD Strategic Studies, Medical Capabilities Integration
Center, U.S. Army Medical Department Center and School, 1608 Stanley
Road, Fort Sam Houston, TX 78234-5047.
‡U.S. Army–Baylor University, Graduate Program in Health and Busi-
ness Administration, U.S. Army Medical Department Center and School,
3630 Stanley Road, Fort Sam Houston, TX 78234-6100.
§Department of Computer Information Systems and Quantitative Methods,
McCoy College of Business Administration, Texas State University, McCoy
Hall 404, San Marcos, TX 78666-4616.
Any opinions, findings, and conclusions or recommendations expressed
in this material are those of the authors and do not necessarily reflect the
views of the National Science Foundation, the Pennsylvania State Univer-
sity, the Texas State University, or the U.S. Army.
doi: 10.7205/MILMED-D-13-00432
MILITARY MEDICINE, Vol. 179, February 2014174
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022

study is that we proffer an algorithmic, geospatial-based
decision-support tool that assists decision-makers in deter-
mining which MEDEVAC assets to launch after receiving a
POI location, given knowledge only of terrain, aircraft loca-
tion, and aircraft capabilities. Further, the same decision tool
can be used for proper emplacement of evacuation assets
such that the theater is covered within a truly representative
1-hour response time.
LITERATURE REVIEWSince the United States’ initial involvement in both Opera-
tion Enduring Freedom and Operation Iraqi Freedom, mili-
tary medical planners have sought to improve the Army’s
medical evacuation system and force structure using opera-
tions research and systems analysis techniques. Before 2005,
MEDEVAC companies were independently numbered units
generally assigned to evacuation battalions. As part of a
major restructuring between AMEDD and Army Aviation,
the Army realigned the MEDEVAC company to lettered sub-
ordinate units under the General Support Aviation Battalion
(GSAB). The Army also reduced the number of organic
MEDEVAC aircraft required from 15 to 12 platforms per
company. After this transition process, the allocation of
MEDEVAC companies became a function of the required
number of GSABs, which greatly reduced the total number
of MEDEVAC airframes required for an effective HSS
system. Fulton et al2 used Monte Carlo simulation to quan-
titatively evaluate these rules of allocation and planning
factors that had an effect on MEDEVAC units. The results
of their study were used to provide decision-support for the
MEDEVAC force structure based on a Total Army Analysis
(TAA) scenario. The TAA is the Army’s method for deter-
mining and resourcing force structure requirements.
Bastian3 developed a robust, multicriteria decision analy-
sis methodology using a scenario-based, stochastic goal pro-
gramming optimization model for medical planners to use as
a strategic and tactical MEDEVAC asset-planning tool. As
part of this model, Bastian developed a three-dimensional
shortest helicopter-path algorithm to compute nearly opti-
mal helicopter flight routes with respective flight times
between an evacuation site, POI, and MTF. The goal pro-
gramming model is optimized over a set of expected sce-
narios (generated from different experimental design factors)
with stochastically determined casualty locations to emplace
the minimum number of MEDEVAC helicopters necessary
to maximize the coverage of theater-wide casualty demand
and the probability of meeting that demand (computed using
Monte Carlo simulation), while minimizing the maximal
evacuation site total vulnerability to enemy attack. This analy-
sis assumed that MEDEVAC asset evacuation sites were
colocated with MTFs, which is the optimal relationship for
minimizing travel time requirements from evacuation loca-
tion to POI to treatment facility.4
Similar to the work of Bastian,3 Fulton et al5 described
a two-stage stochastic optimization model for the relocation
of deployable military hospitals, the reallocation of hospital
beds, and the emplacement of tactical medical evacuation
assets (both air and ground ambulances) during steady-state
military combat operations. In this model, the objective func-
tion was to minimize the time traveled, weighted by patient
severity, from the evacuation site to the POI and onward to
the MTF. The optimal solution also determined the number
of air and ground ambulances and the hospital beds of each
type required at each selected site. The number, location,
and severity of casualties were stochastically generated via a
method similar to Bastian.3 In addition to this study, Fulton
et al6 also evaluated the optimal arrangement of deployable
medical capability components (intensive care units, inter-
mediate care wards, and operating room suites), given sce-
narios designed to represent stability operations through
major combat operations. These capabilities are then com-
pared to achievable medical capabilities based on certain
engineering design characteristics (e.g., bed capacity) of a
modular Combat Support Hospital proposed by AMEDD. The
study also described five stochastic optimization models pro-
vided to AMEDD decision-makers for initial hospital design.
The AMEDD continues to evaluate the medical evacua-
tion system by conducting capability-based analyses to assess
the requirements and capabilities of MEDEVAC units. As
part of a study for the future of joint force design for ver-
tical lift (Future of Vertical Lift, FVL), Bastian et al4 pro-
vided the initial assessment of the minimal MEDEVAC
aircraft capability (given doctrinal constraints) required to
ensure appropriate MEDEVAC response coverage in both
current and future combat operations. Specifically, they
investigated the required capabilities for future MEDEVAC
aircraft and developed a decision-support tool for mili-
tary medical planners in evaluating risk associated with
MEDEVAC platform capability and coverage (in terms of
aircraft ground speed and total distance traveled) within
the brigade operating space. They also determined that
colocation of MEDEVAC assets and surgical elements pro-
vides the optimum coverage for a single brigade when
casualty clusters are indeterminable or random.
In a similar study, Bastian et al7 conducted a DOTMLPF
(doctrine, organization, training, maintenance, leadership
and education, personnel, and facilities) assessment of the
MEDEVAC unit to determine gaps in the current force
structure and solutions for future force design. As part of
their mixed-methods research design, they performed quanti-
tative analysis of a Likert-scale survey (using primary data)
to identify statistically significant capability gaps associated
with the current force structure, and they conducted text
mining to analyze qualitative data (i.e., recommendations
from aviation and medical aviation leaders) to identify
themes that would provide potential solutions to those
gaps. In another part of the FVL study, Bastian et al8 use
a mixed-methods approach to provide three new, separate
analyses as part of the development of the next MEDEVAC
platform. In their analyses, they use discrete-event simulation
MILITARY MEDICINE, Vol. 179, February 2014 175
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022

based partially on qualitative assessments from the field to
determine the optimal capabilities of an FVL MEDEVAC
platform, given an Afghanistan-like scenario and parameters
associated with the treatment/ground evacuation capabilities
in that theater. Furthermore, they conduct deterministic ana-
lyses to (1) explore the MEDEVAC trade-off considerations
associated with different aircraft engines operating under
variable conditions and (2) determine how the additional
weight of weaponizing the current helicopter fleet affects
MEDEVAC range, coverage radios, and response time.
METHODS AND RESULTSDuring a combat deployment, military medical planners
and senior decision-makers will need to understand and
coordinate the lay down of all MTFs, MEDEVAC assets,
and other medical resources. The classical approach to plan-
ning MEDEVAC coverage is to draw unobstructed range
rings and ellipses around the MTFs, with the radius of these
rings based on the range that MEDEVAC assets can cover
in a specified amount of flight time. The “unobstructed”
rings do not consider altitude restrictions or other obstruc-
tions such as a Restricted Operating Zone (ROZ) that would
prohibit a helicopter from flying directly from A to B. The
helicopter could of course try to fly around the obstacle, but
that deforms the range ring, as discussed further in this
article. Figure 1 shows an example of MEDEVAC cover-
age in Afghanistan based on MEDEVAC response times
adhering to the “60-minute” standard.4
The unobstructed range rings depicted in Figure 1 do
not consider altitude restrictions nor differences in the
capabilities of the available MEDEVAC airframes. They
do, however, quickly depict what could be covered by the
lay down of MEDEVAC assets and MTFs, given perfectly
flat terrain.
Aeromedical Evacuation Response Planning Times
The radius of unobstructed range rings is based on the
MEDEVAC mission requirements, which was standardized
FIGURE 1. Example of unobstructed range rings coverage in Afghanistan.
MILITARY MEDICINE, Vol. 179, February 2014176
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022

to the “golden hour” by the U.S. Secretary of Defense.4
This 60-minute MEDEVAC response time can be broken
down into four planning times:
1. Notification to wheels-up at the helicopter landing zone
(HLZ) (<15 minutes)
2. Wheels-up at the HLZ to wheels-down at the POI
3. Casualty pickup and loading at the POI (<5 minutes)
4. Wheels-up at the POI to wheels-down at the MTF
Note that this “golden hour” standard MEDEVAC response
time does not include (1) the time between patient injury and
notification (submission and receipt of the 9-line MEDEVAC
request) and (2) the patient off-loading/transfer at the MTF.3
Despite the “golden hour” standard of MEDEVAC response
time, we emphasize rapid deployment of MEDEVAC assets
to the correct casualty location, providing immediate en route
medical treatment, and transporting the patient to the correct
MTF. We must assess those MEDEVAC missions lasting
longer than 60 minutes to identify systematic areas of con-
tinual improvement. One common method for improv-
ing MEDEVAC response time is for higher headquarters
to issue early warning to the MEDEVAC assets/crews based
on unfolding events/incidents rather than waiting for sub-
mission and receipt of the actual 9-line MEDEVAC request.
Higher headquarters normally relies heavily on instant
messaging/chat, which allows for informing multiple receivers
of unfolding events/incidents by so-called chat rooms in
which relevant notification, updates, and coordination are
achieved with very dense text messages.
Derivation of Aeromedical Evacuation Flight Timeand Range
Given certain characteristics and capabilities of each type
of MEDEVAC asset, we can derive the available flight time
(in minutes) and the range (in nautical miles [NM]); assum-
ing that notification time and patient transfer time are equal for
all platforms and not included in the 60-minute MEDEVAC
response time standard. Appendix A depicts an example
algorithm for computing MEDEVAC flight time and range
for the UH-60 Black Hawk helicopter.
The example algorithm in Appendix A is programmed
using the open-source Python 2.7.3 programming language.9
For this example, we assume the UH-60 Black Hawk flies
150 knots (nautical-miles per hour) with a maximum eleva-
tion of 1,500 m above ground level. In addition, we use a
notification to move (ntm) time of 10 minutes and a patient
load time of 5 minutes, both of which are validated times
based on recent combat deployment MEDEVAC experience.
When executed, the code in Appendix A will produce the
output: “UH-60 Black Hawk, 45 min, 112 nm @ 150 kts
and max elevation of 1500 m.”
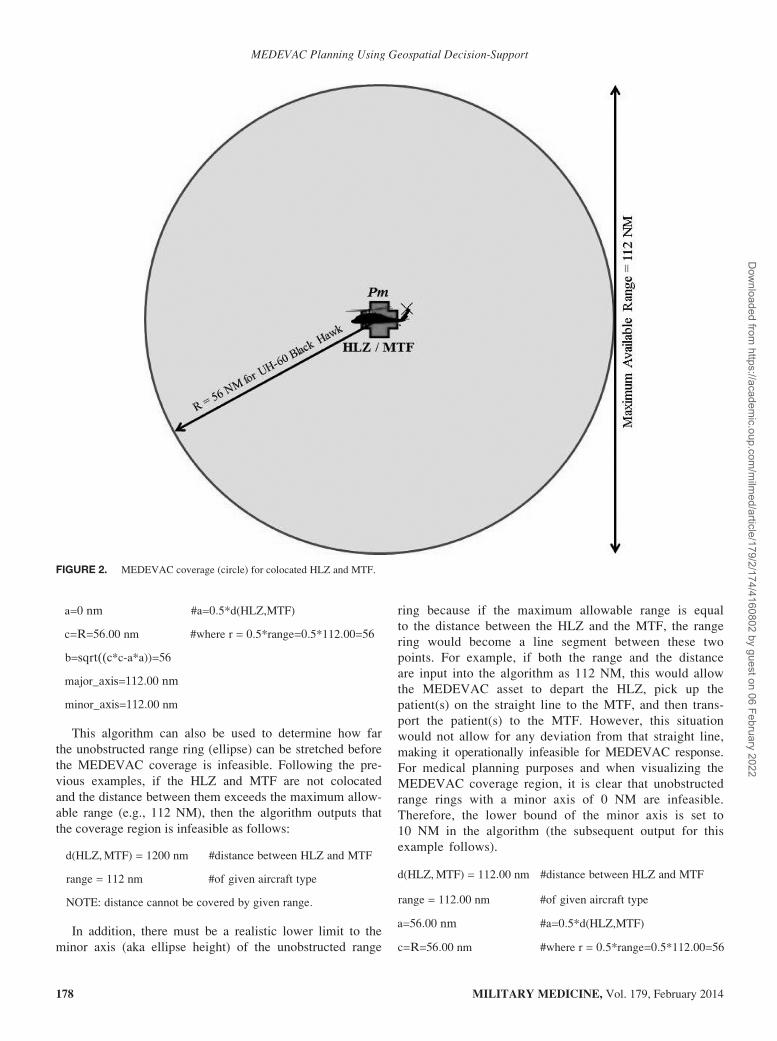
From this output, we see that the maximum available
range (measured using two-dimensional Euclidean distance)
of a UH-60 Black Hawk is 112 NM, which we can use to
draw a MEDEVAC coverage area around an MTF with a
colocated HLZ; note that colocation of MEDEVAC assets
and surgical elements was proven to be mathematically opti-
mal in the study by Bastian et al.4 This MEDEVAC coverage
circle has a midpoint (Pm) and radius (R) that is half of
the calculated range because the helicopter starts at the
colocated HLZ/MTF (at Pm), flies to any POI inside
the circle to pick up the patient(s), and then drops off the
patient(s) back at Pm (this assumes that origin and destina-
tion points are both Pm). Figure 2 shows this for the exam-
ple output above, where the MEDEVAC coverage circle
has R = 56 NM.
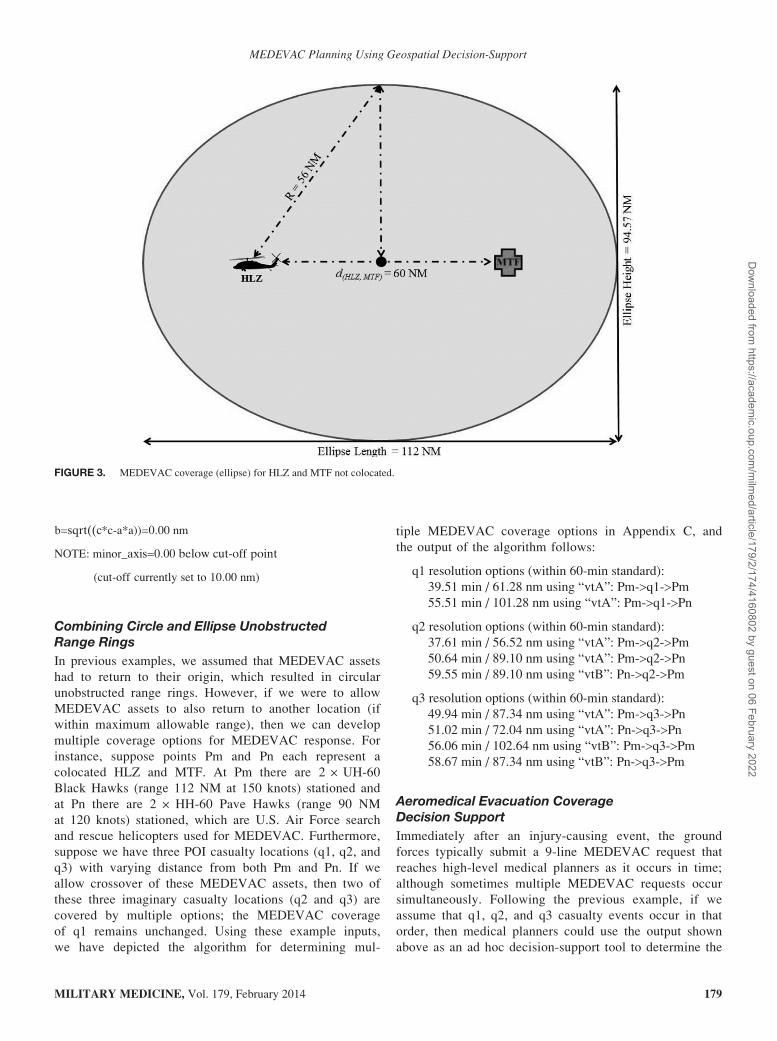
Ellipses as Unobstructed Range Rings
The example shown in Figure 2 depicts the MEDEVAC
coverage circle where the HLZ and MTF are colocated. In
the case where MEDEVAC assets are forward deployed to a
remote, geographically separated location without colocated
surgical elements (i.e., Combat Support Hospital—Role III
MTF), the MEDEVAC assets begin at the HLZ, fly to the
POI to pick up the patient(s), and then transport the
patient(s) to the MTF not colocated with the HLZ. This
case is best shown in Figure 3; the MEDEVAC crew and
assets are located at the HLZ, whereas the MTF is at
another location.
Similar to the depiction in Figure 2, Figure 3 shows
the MEDEVAC coverage region (an ellipse rather than a
circle) where casualties can be reached and evacuated with
MEDEVAC assets and then transported to the MTF within
the available flight time. In this example, the derivation of
the ellipse depends on the Euclidean distance between the
HLZ and MTF (e.g., 60 NM) and the maximum allowable
range (e.g., 112 NM at 150 knots). The algorithm to derive
this ellipse (Fig. 3) is shown in Appendix B, and this gen-
erates the following output:
d(HLZ,MTF) = 60 nm #distance between HLZ and MTF
range = 112 nm #of given aircraft type
a=30 nm #a=0:5*d(HLZ,MTF)
c=R=56:00 nm #where r = 0:5*range=0:5*112:00=56
b=sqrt((c*c-a*a))=47:29
major_axis=117 nm
minor_axis=94:57 nm
We can also use the algorithm displayed in Appendix B
to determine the unobstructed range ring (circle) when the
HLZ and MTF are colocated. In this case, the distance
between the HLZ and MTF is 0 NM, as opposed to 60 NM.
The algorithm output for the colocation scenario follows:
d(HLZ,MTF) = 0 nm #distance between HLZ and MTF
range = 112 nm #of given aircraft type
MILITARY MEDICINE, Vol. 179, February 2014 177
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022
a=0 nm #a=0:5*d(HLZ,MTF)
c=R=56:00 nm #where r = 0:5*range=0:5*112:00=56
b=sqrt((c*c-a*a))=56
major_axis=112:00 nm
minor_axis=112:00 nm
This algorithm can also be used to determine how far
the unobstructed range ring (ellipse) can be stretched before
the MEDEVAC coverage is infeasible. Following the pre-
vious examples, if the HLZ and MTF are not colocated
and the distance between them exceeds the maximum allow-
able range (e.g., 112 NM), then the algorithm outputs that
the coverage region is infeasible as follows:
d(HLZ,MTF) = 1200 nm #distance between HLZ and MTF
range = 112 nm #of given aircraft type
NOTE: distance cannot be covered by given range:
In addition, there must be a realistic lower limit to the
minor axis (aka ellipse height) of the unobstructed range
ring because if the maximum allowable range is equal
to the distance between the HLZ and the MTF, the range
ring would become a line segment between these two
points. For example, if both the range and the distance
are input into the algorithm as 112 NM, this would allow
the MEDEVAC asset to depart the HLZ, pick up the
patient(s) on the straight line to the MTF, and then trans-
port the patient(s) to the MTF. However, this situation
would not allow for any deviation from that straight line,
making it operationally infeasible for MEDEVAC response.
For medical planning purposes and when visualizing the
MEDEVAC coverage region, it is clear that unobstructed
range rings with a minor axis of 0 NM are infeasible.
Therefore, the lower bound of the minor axis is set to
10 NM in the algorithm (the subsequent output for this
example follows).
d(HLZ,MTF) = 112:00 nm #distance between HLZ and MTF
range = 112:00 nm #of given aircraft type
a=56:00 nm #a=0:5*d(HLZ,MTF)
c=R=56:00 nm #where r = 0:5*range=0:5*112:00=56
FIGURE 2. MEDEVAC coverage (circle) for colocated HLZ and MTF.
MILITARY MEDICINE, Vol. 179, February 2014178
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022
b=sqrt((c*c-a*a))=0:00 nm
NOTE: minor_axis=0:00 below cut-off point
(cut-off currently set to 10:00 nm)
Combining Circle and Ellipse UnobstructedRange Rings
In previous examples, we assumed that MEDEVAC assets
had to return to their origin, which resulted in circular
unobstructed range rings. However, if we were to allow
MEDEVAC assets to also return to another location (if
within maximum allowable range), then we can develop
multiple coverage options for MEDEVAC response. For
instance, suppose points Pm and Pn each represent a
colocated HLZ and MTF. At Pm there are 2 +UH-60Black Hawks (range 112 NM at 150 knots) stationed and
at Pn there are 2 + HH-60 Pave Hawks (range 90 NM
at 120 knots) stationed, which are U.S. Air Force search
and rescue helicopters used for MEDEVAC. Furthermore,
suppose we have three POI casualty locations (q1, q2, and
q3) with varying distance from both Pm and Pn. If we
allow crossover of these MEDEVAC assets, then two of
these three imaginary casualty locations (q2 and q3) are
covered by multiple options; the MEDEVAC coverage
of q1 remains unchanged. Using these example inputs,
we have depicted the algorithm for determining mul-
tiple MEDEVAC coverage options in Appendix C, and
the output of the algorithm follows:
q1 resolution options (within 60-min standard):
39.51 min / 61.28 nm using “vtA”: Pm->q1->Pm55.51 min / 101.28 nm using “vtA”: Pm->q1->Pn
q2 resolution options (within 60-min standard):
37.61 min / 56.52 nm using “vtA”: Pm->q2->Pm50.64 min / 89.10 nm using “vtA”: Pm->q2->Pn59.55 min / 89.10 nm using “vtB”: Pn->q2->Pm
q3 resolution options (within 60-min standard):
49.94 min / 87.34 nm using “vtA”: Pm->q3->Pn51.02 min / 72.04 nm using “vtA”: Pn->q3->Pn56.06 min / 102.64 nm using “vtB”: Pm->q3->Pm58.67 min / 87.34 nm using “vtB”: Pn->q3->Pm
Aeromedical Evacuation CoverageDecision Support
Immediately after an injury-causing event, the ground
forces typically submit a 9-line MEDEVAC request that
reaches high-level medical planners as it occurs in time;
although sometimes multiple MEDEVAC requests occur
simultaneously. Following the previous example, if we
assume that q1, q2, and q3 casualty events occur in that
order, then medical planners could use the output shown
above as an ad hoc decision-support tool to determine the
FIGURE 3. MEDEVAC coverage (ellipse) for HLZ and MTF not colocated.
MILITARY MEDICINE, Vol. 179, February 2014 179
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022

best solution for allocation of MEDEVAC assets. Follow-
ing is an example:
1. When q1 occurs, the algorithm in Appendix C could
generate the list of possible solutions shown earlier.
The medical planners could then select the best option
based on many dynamic variables, such as the patient(s)
clinical needs, availability of MTFs, equipment required,
and impact on the overall MEDEVAC coverage.
2. When q2 occurs during the execution of the q1
MEDEVAC mission, the best option for the medical
planners depends on its earlier decision (see above
point). Using the fastest option for q1, the medical
planner uses the 2 + UH-60 Black Hawks based at
Pm, making them unavailable to resolve q2 within
the “60-minute” standard. Therefore, the medical plan-
ners would have to use the 2 + HH-60 Pave Hawks
based at Pn to resolve q2 in time.
3. When q3 occurs, the best option for medical planners
is to use the 2 + UH-60 Black Hawks based at Pm
because it is the more efficient method (assuming the
MEDEVAC assets already returned to Pm after com-
pletion of the q1 mission).
As previously noted, unobstructed range rings do not
consider altitude restrictions or other obstructions such as
no-fly areas, ROZs, mountains, and other physical barriers
that prevent a helicopter from traveling from origin to des-
tination directly. Therefore, please note that these unob-
structed range rings (circles and ellipses) are nearly always
overly optimistic in representing MEDEVAC coverage.
Nevertheless, unobstructed range rings provide the neces-
sary visualization useful for medical planning and decision-
making at the strategic, operational, and tactical levels.
CONCLUSIONSThere are numerous applications that require the ability of
decision-makers to take certain actions over a geographic
region. In particular, the U.S. Army needs to allocate limited
resources (e.g., mobile hospitals, forward surgical elements,
and MEDEVAC assets) across a geographic area during
combat operations. However, allocating any resource will
cause certain effects based on the network connections
among geographic locations. Understanding what true cover-
age capabilities of evacuation assets are, given 3-dimensional
terrain considerations, is vital to in-theater evacuation analy-
sis and yet currently unavailable. The algorithms provided here
directly address this problem.
Using the algorithms provided, medical planners can
discover the optimal configuration of assets necessary to
support the medical requirements in a theater of operation.
The algorithms here can be implemented in a wide variety of
medical planning tools currently in existence, including the
Medical and Casualty Estimation tool currently maintained
by the Center for AMEDD Strategic Studies and promul-
gated through the Army Knowledge Online Web site. We
have used the algorithms presented here for several mock
and historical scenarios, and we are currently incorporating
them into simulations. Most importantly, however, future
work will validate its “in the field” utility.
In this article, we presented geospatial-based algorithms
for computing unobstructed range rings as a methodology for
MEDEVAC coverage visualization and medical planning
decision-support. The intent is for military medical plan-
ners to use these geospatial analytical methods to improve
real-time situational awareness by visualization of MEDEVAC
coverage, showing which areas can be reached within estab-
lished timelines. Furthermore, the aim of this decision-support
tool is to support medical planning by visualizing the impact
of changes in the medical footprint to the MEDEVAC cover-
age. Finally, these methods can be used to support decision-
making by providing a time-sorted list of MEDEVAC asset
packages to select from, given the location of the patients.
ACKNOWLEDGMENT
This material is based on work supported by the National Science Foun-
dation under Grant no. DGE1255832.
APPENDIX AThe algorithm below (coded in Python 2.7.2) can be used
to compute MEDEVAC flight time and range for the UH-60
Black Hawk helicopter.
## ALGORITHM FOR DERIVING MEDEVAC FLIGHT TIME
AND RANGE
# Input: characteristics of each platform type
vtA = {‘key’: ‘vtA’, ‘name’: ‘UH-60 Black Hawk’, ‘speed’: 150.0,
‘max_elev’: 1500.0, ‘ntm’: 10, ‘load_pt’: 5}
# Input: list of platform types (with their characteristics)
vehicle_types = [vtA]
# Input: Constants applicable to all platform types
max_time = 60.0
# Determine available time and range for each platform type
for vt in vehicle_types:
# Initialize flight time to the maximum time of 60 minutes
flight_time = max_time
# Further subtract platform type specifics
flight_time = flight_time - vt[‘ntm’] - vt[‘load_pt’]
vt[‘flight_time’] = flight_time
vt[‘range’] = flight_time * (vt[‘speed’] / 60.0)
# Output: show results
print ‘=’*70print ‘key: name, flight, range’
for vt in vehicle_types:
print ‘-’*70
print ‘%(key)s: %(name)s, %(flight_time)d min, %(range)d nm’
% vt
print ‘@ %(speed)d kts and max elevation of %(max_elev)d m’
% vt
MILITARY MEDICINE, Vol. 179, February 2014180
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022
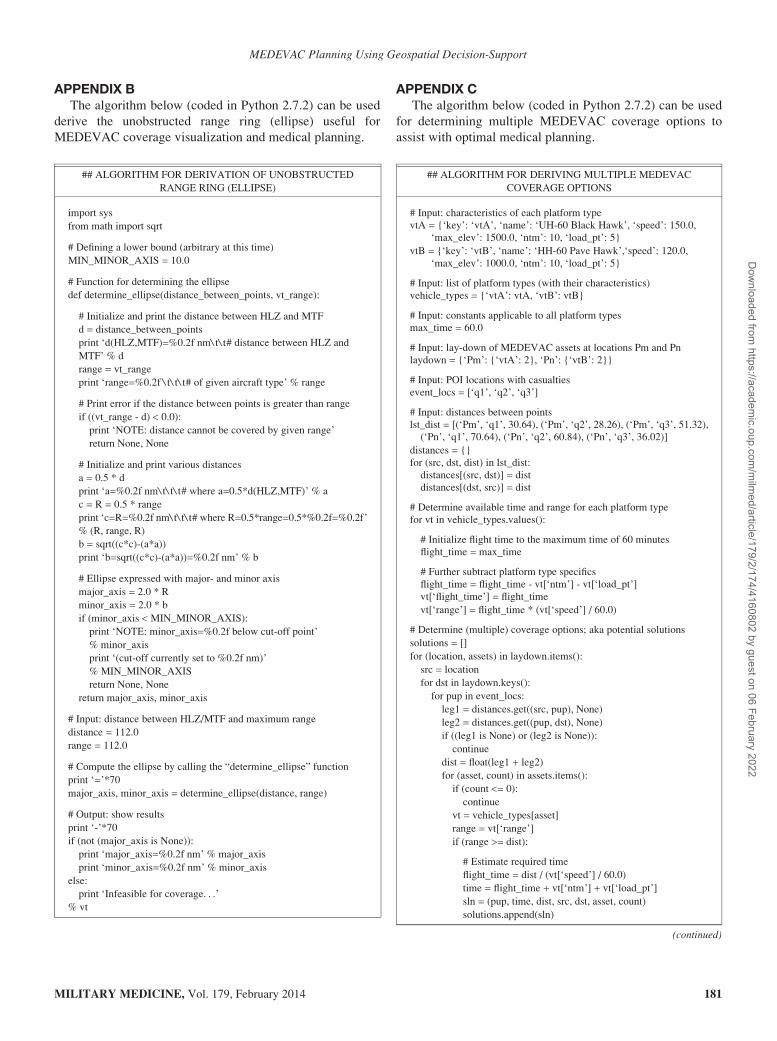
APPENDIX BThe algorithm below (coded in Python 2.7.2) can be used
derive the unobstructed range ring (ellipse) useful for
MEDEVAC coverage visualization and medical planning.
APPENDIX CThe algorithm below (coded in Python 2.7.2) can be used
for determining multiple MEDEVAC coverage options to
assist with optimal medical planning.
## ALGORITHM FOR DERIVATION OF UNOBSTRUCTED
RANGE RING (ELLIPSE)
import sys
from math import sqrt
# Defining a lower bound (arbitrary at this time)
MIN_MINOR_AXIS = 10.0
# Function for determining the ellipse
def determine_ellipse(distance_between_points, vt_range):
# Initialize and print the distance between HLZ and MTF
d = distance_between_points
print ‘d(HLZ,MTF)=%0.2f nm\ t\ t# distance between HLZ and
MTF’ % d
range = vt_range
print ‘range=%0.2f \ t\ t\ t# of given aircraft type’ % range
# Print error if the distance between points is greater than range
if ((vt_range - d) < 0.0):
print ‘NOTE: distance cannot be covered by given range’
return None, None
# Initialize and print various distances
a = 0.5 * d
print ‘a=%0.2f nm\ t\ t\ t# where a=0.5*d(HLZ,MTF)’ % a
c = R = 0.5 * range
print ‘c=R=%0.2f nm\ t\ t\ t# where R=0.5*range=0.5*%0.2f=%0.2f’
% (R, range, R)
b = sqrt((c*c)-(a*a))
print ‘b=sqrt((c*c)-(a*a))=%0.2f nm’ % b
# Ellipse expressed with major- and minor axis
major_axis = 2.0 * R
minor_axis = 2.0 * b
if (minor_axis < MIN_MINOR_AXIS):
print ‘NOTE: minor_axis=%0.2f below cut-off point’
% minor_axis
print ‘(cut-off currently set to %0.2f nm)’
% MIN_MINOR_AXIS
return None, None
return major_axis, minor_axis
# Input: distance between HLZ/MTF and maximum range
distance = 112.0
range = 112.0
# Compute the ellipse by calling the “determine_ellipse” function
print ‘=’*70major_axis, minor_axis = determine_ellipse(distance, range)
# Output: show results
print ‘-’*70
if (not (major_axis is None)):
print ‘major_axis=%0.2f nm’ % major_axis
print ‘minor_axis=%0.2f nm’ % minor_axis
else:
print ‘Infeasible for coverage. . .’
% vt
## ALGORITHM FOR DERIVING MULTIPLE MEDEVAC
COVERAGE OPTIONS
# Input: characteristics of each platform typevtA = {‘key’: ‘vtA’, ‘name’: ‘UH-60 Black Hawk’, ‘speed’: 150.0,
‘max_elev’: 1500.0, ‘ntm’: 10, ‘load_pt’: 5}
vtB = {‘key’: ‘vtB’, ‘name’: ‘HH-60 Pave Hawk’,‘speed’: 120.0,
‘max_elev’: 1000.0, ‘ntm’: 10, ‘load_pt’: 5}
# Input: list of platform types (with their characteristics)vehicle_types = {‘vtA’: vtA, ‘vtB’: vtB}
# Input: constants applicable to all platform typesmax_time = 60.0
# Input: lay-down of MEDEVAC assets at locations Pm and Pnlaydown = {‘Pm’: {‘vtA’: 2}, ‘Pn’: {‘vtB’: 2}}
# Input: POI locations with casualtiesevent_locs = [‘q1’, ‘q2’, ‘q3’]
# Input: distances between pointslst_dist = [(‘Pm’, ‘q1’, 30.64), (‘Pm’, ‘q2’, 28.26), (‘Pm’, ‘q3’, 51.32),
(‘Pn’, ‘q1’, 70.64), (‘Pn’, ‘q2’, 60.84), (‘Pn’, ‘q3’, 36.02)]
distances = {}for (src, dst, dist) in lst_dist:
distances[(src, dst)] = distdistances[(dst, src)] = dist
# Determine available time and range for each platform typefor vt in vehicle_types.values():
# Initialize flight time to the maximum time of 60 minutesflight_time = max_time
# Further subtract platform type specifics
flight_time = flight_time - vt[‘ntm’] - vt[‘load_pt’]vt[‘flight_time’] = flight_time
vt[‘range’] = flight_time * (vt[‘speed’] / 60.0)
# Determine (multiple) coverage options; aka potential solutions
solutions = []
for (location, assets) in laydown.items():
src = location
for dst in laydown.keys():
for pup in event_locs:
leg1 = distances.get((src, pup), None)
leg2 = distances.get((pup, dst), None)
if ((leg1 is None) or (leg2 is None)):
continue
dist = float(leg1 + leg2)
for (asset, count) in assets.items():
if (count <= 0):
continue
vt = vehicle_types[asset]
range = vt[‘range’]
if (range >= dist):
# Estimate required time
flight_time = dist / (vt[‘speed’] / 60.0)
time = flight_time + vt[‘ntm’] + vt[‘load_pt’]
sln = (pup, time, dist, src, dst, asset, count)
solutions.append(sln)
(continued)
MILITARY MEDICINE, Vol. 179, February 2014 181
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022

REFERENCES
1. Department of the Army. Field Manual 4-02.2—Medical Evacuation
2007: Washington, DC. Available at http://armypubs.army.mil/doctrine/
DR_pubs/dr_a/pdf/fm4_02x2.pdf; accessed September 30, 2013.
2. Fulton LV, McMurry P, Kerr B: A Monte Carlo simulation of air
ambulance requirements during major combat operations. Mil Med 2009;
174(6): 610–14.
3. Bastian ND: A robust, multi-criteria modeling approach for optimizing
aeromedical evacuation asset emplacement. J Def Model Simul 2010;
7(1): 5–23.
4. Bastian ND, Fulton LV, Mitchell R, Pollard W, Wierschem D, Wilson R:
The Future of Vertical Lift: initial insights for aircraft capability
and medical planning. Mil Med 2012; 177(7): 863–9.
5. Fulton LV, Lasdon LS, McDaniel RR, Coppola MN: Two-stage stochas-
tic optimization for the allocation of medical assets in steady-state combat
operations. J Def Model Simul 2010; 7(2): 89–102.
6. Fulton LV, Perry M, Wood S, Bewley L: Engineering the new combat
support hospital. J Def Model Simul 2010; 7(1): 25–37.
7. Bastian ND, Fulton LV, Mitchell R, Pollard W, Wilson R: Force design
analysis of the Army aeromedical evacuation company: a quantitative
approach. J Def Model Simul 2013; 10(1): 23–30.
8. Bastian ND, Brown D, Fulton LV, Mitchell R, Pollard W, Robinson M,
et al: Analyzing the future of army aeromedical evacuation units and
equipment: a mixed methods, requirements-based approach. Mil Med
2013; 178(3): 321–9.
9. Python Programming Language 2013. Available at http://www.python
.org/; accessed September 30, 2013.
## ALGORITHM FOR DERIVING MULTIPLE MEDEVAC
COVERAGE OPTIONS
# Sort the solutions found (less time needed is better)
solutions.sort()
# Output: show results
print ‘=’*70for event_loc in event_locs:
print ‘%s resolution options (within 60-min-standard):’ % event_loc
for (pup, time, dist, src, dst, asset, count) in solutions:
if (pup <> event_loc):
continue
rec = (time, dist, asset, src, pup, dst)
print ‘%8.2f min / %5.2f nm using “%s”: %s->%s->%s’ % rec
print ‘-’*70
APPENDIX C. Continued
MILITARY MEDICINE, Vol. 179, February 2014182
MEDEVAC Planning Using Geospatial Decision-Support
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/179/2/174/4160802 by guest on 06 February 2022