Administrative Barriers to the Adoption of High-Quality Mental Health Services for Children in...
11
Abstract While the need to provide appropriate mental health services to children in foster care is well recognized, there is little information on administrative barriers to assuring that such services are provided. This article presents results from a national survey of mental health agencies to profile their awareness of currently available practice standards, the roles these standards play in guiding practice of mental health agencies, common reimbursement strategies in use for mental health services, and collaborations between mental health and child welfare agencies that enhance children’s access to appropriate mental health care. Implications and recommendations for mental health policymakers are discussed. Keywords Children Á Mental health Á Foster care Á Quality Á Child welfare Background The need to improve child and adolescent mental health services has been a policy priority for the past several decades. Following the articulation of this need by the Joint Commission on Mental Health of Children (1969), numerous reports, meetings, and initiatives have called for improved access to appropriate mental health care (Institute of Medicine, 2001; President’s Commission on Mental Health, 1978; President’s New Freedom Commission on Mental Health, 2003; U.S. Congress, 1986; U.S. Department of Health and Human Services, 2005; U.S. Department of Health and Human Services, 1999). The bulk of efforts to improve access and quality of mental health services have focused on the adoption and implementation of specific evidence-based practices at the provider level (Carpinello, Rosenberg, Stone, Schwager, & Felton, 2002; Hoagwood, Burns, Kiser, Ringeisen, & Schoen- wald, 2001; LeBel et al., 2004; Sackett, Rosenberg, Muir-Gray, Haynes, & Richardson, 1996; Tanenbaum, 2003; Torrey, Finnerty, Evans, & Wyzik, 2003). These high-quality interventions are often packaged within implementation ‘‘toolkits’’ or manuals suitable for adoption by providers (Drake et al., 2001; Ganju, 2003; NASMHPD Research Institute, 2005; Substance Abuse and Mental Health Services Administration, R. Raghavan (&) George Warren Brown School of Social Work, Department of Psychiatry, Washington University in St. Louis, Campus Box 1196, One Brookings Drive, St. Louis, MO 63130, USA e-mail: [email protected] M. Inkelas UCLA Center for Healthier Children, Families, and Communities; Department of Health Services, University of California, Los Angeles, 1100 Glendon Ave Suite 850, Los Angeles, CA 90095, USA e-mail: [email protected] T. Franke UCLA Center for Healthier Children, Families, and Communities; Department of Social Welfare, University of California, Los Angeles, 1100 Glendon Ave Suite 850, Los Angeles, CA 90095, USA e-mail: [email protected] N. Halfon UCLA Center for Healthier Children, Families, and Communities; Department of Pediatrics; Department of Public Policy; Department of Health Services, University of California, Los Angeles, 1100 Glendon Ave Suite 850, Los Angeles, CA 90095, USA e-mail: [email protected] Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201 DOI 10.1007/s10488-006-0095-6 123 ORIGINAL PAPER Administrative Barriers to the Adoption of High-Quality Mental Health Services for Children in Foster Care: A National Study Ramesh Raghavan Moira Inkelas Todd Franke Neal Halfon Published online: 9 January 2007 Ó Springer Science+Business Media, LLC 2007
Transcript of Administrative Barriers to the Adoption of High-Quality Mental Health Services for Children in...
Abstract While the need to provide appropriate
mental health services to children in foster care is well
recognized, there is little information on administrative
barriers to assuring that such services are provided.
This article presents results from a national survey of
mental health agencies to profile their awareness of
currently available practice standards, the roles these
standards play in guiding practice of mental health
agencies, common reimbursement strategies in use for
mental health services, and collaborations between
mental health and child welfare agencies that enhance
children’s access to appropriate mental health care.
Implications and recommendations for mental health
policymakers are discussed.
Keywords Children � Mental health � Foster care �Quality � Child welfare
Background
The need to improve child and adolescent mental
health services has been a policy priority for the past
several decades. Following the articulation of this need
by the Joint Commission on Mental Health of Children
(1969), numerous reports, meetings, and initiatives
have called for improved access to appropriate mental
health care (Institute of Medicine, 2001; President’s
Commission on Mental Health, 1978; President’s New
Freedom Commission on Mental Health, 2003; U.S.
Congress, 1986; U.S. Department of Health and
Human Services, 2005; U.S. Department of Health
and Human Services, 1999). The bulk of efforts to
improve access and quality of mental health services
have focused on the adoption and implementation of
specific evidence-based practices at the provider level
(Carpinello, Rosenberg, Stone, Schwager, & Felton,
2002; Hoagwood, Burns, Kiser, Ringeisen, & Schoen-
wald, 2001; LeBel et al., 2004; Sackett, Rosenberg,
Muir-Gray, Haynes, & Richardson, 1996; Tanenbaum,
2003; Torrey, Finnerty, Evans, & Wyzik, 2003). These
high-quality interventions are often packaged within
implementation ‘‘toolkits’’ or manuals suitable for
adoption by providers (Drake et al., 2001; Ganju,
2003; NASMHPD Research Institute, 2005; Substance
Abuse and Mental Health Services Administration,
R. Raghavan (&)George Warren Brown School of Social Work, Departmentof Psychiatry, Washington University in St. Louis, CampusBox 1196, One Brookings Drive, St. Louis, MO 63130, USAe-mail: [email protected]
M. InkelasUCLA Center for Healthier Children, Families, andCommunities; Department of Health Services, University ofCalifornia, Los Angeles, 1100 Glendon Ave Suite 850, LosAngeles, CA 90095, USAe-mail: [email protected]
T. FrankeUCLA Center for Healthier Children, Families, andCommunities; Department of Social Welfare, University ofCalifornia, Los Angeles, 1100 Glendon Ave Suite 850, LosAngeles, CA 90095, USAe-mail: [email protected]
N. HalfonUCLA Center for Healthier Children, Families, andCommunities; Department of Pediatrics; Department ofPublic Policy; Department of Health Services, University ofCalifornia, Los Angeles, 1100 Glendon Ave Suite 850, LosAngeles, CA 90095, USAe-mail: [email protected]
Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201
DOI 10.1007/s10488-006-0095-6
123
ORIGINAL PAPER
Administrative Barriers to the Adoption of High-Quality MentalHealth Services for Children in Foster Care: A National Study
Ramesh Raghavan Æ Moira Inkelas ÆTodd Franke Æ Neal Halfon
Published online: 9 January 2007� Springer Science+Business Media, LLC 2007
2005; Torrey et al., 2001). However, there has been less
focus on how good practices can be adopted at the
organizational level, and on the development of
procedures and policies among public child-serving
agencies that are necessary for the support of good
practices. A range of state and national studies show
that children in foster care are consuming a dispropor-
tionate share of publicly funded mental health services
given their level of need, and for these children there
is a great need to focus on the role of financial,
organizational, and administrative procedures that can
promote better access (Halfon, Berkowiz, & Klee,
1992; Halfon & Klee, 1987; Takayama, Bergman, &
Connel, 1994).
Children in foster care are a particularly vulnerable
group needing high-quality mental health interven-
tions. These children have disproportionately high
rates of emotional and behavioral problems (Clausen,
Landsverk, Ganger, Chadwick, & Litrownik, 1998;
Glisson, 1996; Halfon, Mendonca, & Berkowitz,
1995; Landsverk, Garland, & Leslie, 2002; Pilowsky,
1995; Zima et al., 2000) and mental health service use
(Halfon, Berkowiz, & Klee, 1992; Harman, Childs, &
Kelleher, 2000; Raghavan et al., 2005; Takayama,
Bergman, & Connel, 1994). Despite a high level of
need, only a quarter of children in foster care are
receiving services at any given time (Halfon, Berkowiz,
& Klee, 1992). Prior work documenting access barriers
to health services (Simms, Dubowitz, & Szilagyi, 2000)
shows that these barriers often have less to do with the
type and nature of emotional disturbances that affect
children in foster care, or with the absence of effective
treatment options, but instead derive from the unique
living situations of children in foster care, which pose
considerable challenges to the delivery, coordination,
and continuity of care. Even straightforward mental
health problems can be difficult to identify, assess, and
evaluate when placements are unstable, histories are
inadequate and incomplete, or clinicians are unable to
distinguish adaptive behaviors from underlying psy-
chopathology. Children enter foster care usually in
emergent circumstances, possess little or no health
histories at the time of their entry, and often experi-
ence multiple placements (Burns, Costello, & Angold,
1995; Halfon & Klee, 1987; Klee & Halfon, 1987;
Schor, 1981; U.S. General Accounting Office, 2003), all
of which pose considerable treatment challenges.
Therefore, assuring high-quality care for children in
foster care requires not only providing services appro-
priate to need or deploying evidence-based practices in
child settings, but also ensuring that service systems
and processes of care account for their changing
environments and relationships.
A recent national study found that by engaging in
coordinated service delivery, mental health and child
welfare systems can deliver mental health services
appropriate to need for children in child welfare
environments (Hurlburt et al., 2004). Recognizing the
challenges to delivering health interventions for such a
population, the Child Welfare League of America
(CWLA) issued standards for the provision of health
and mental health services for children in foster care
(Child Welfare League of America, 1988). Similar
standards have also been issued by the American
Academy of Pediatrics (AAP) in 1994 that were
re-affirmed in 2002 (American Academy of Pediatrics,
2002, 1994); the American Academy of Child and
Adolescent Psychiatry (AACAP) also issued compa-
rable standards (American Academy of Child and
Adolescent Psychiatry, 2001). The CWLA, AAP, and
AACAP recommendations suggest that all children
should receive a mental health screening when placed
into foster care, as well as a subsequent comprehensive
mental health assessment by a mental health profes-
sional within a month of being placed into foster care.
They also outline the need for a systematic, coordi-
nated approach to the delivery of mental health
services to meet children’s ongoing mental health
needs. The consistency and convergence of the stan-
dards from three different professional organizations,
representing purchasers and providers of care, is an
indication that there is the potential for developing
mutually agreeable service delivery pathways that
together operationalize high-quality care.
Despite their importance, the extent to which such
standards have been actually adopted within agencies
that serve children in foster care is unknown (Amer-
ican Academy of Pediatrics, 2002). While the barriers
to the deployment of specific high-quality interventions
can be examined at the provider level (Burns,
Hoagwood, & Mrazek, 1999; Weisz, Sandler, Durlak,
& Anton, 2005), identifying barriers to adopting
processes of care requires attention to organizational
and policy environments within which such delivery
occurs (Ganju, 2003; Glisson, 2002; Glisson &
Hemmelgarn, 1998; Goldman et al., 2001; Hoagwood,
2003; Rosenheck, 2001; Schoenwald & Hoagwood,
2001; Simpson, 2002; Torrey et al., 2001). Understand-
ing these environments is particularly important for
quality improvement in public mental health systems,
within which most children in foster care receive
services. However, little is known about the extent to
which the work of child-serving systems is consistent
with national standards. Consequently, the nature and
extent of administrative policies and procedures that
might support the standards for, and delivery of,
192 Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201
123
appropriate services for children in foster care is poorly
understood.
It is important to know if public mental health
agencies are aware of existing standards since aware-
ness is recognized as a necessary precursor to success-
ful adoption (Carpinello et al., 2002; Dixon et al., 2001;
Goldman, et al., 2001). Even when agencies are aware
of standards, it is unclear to what extent they have
adopted roles and responsibilities that promote ser-
vices consistent with prevailing standards. Service
delivery for children in foster care ostensibly requires
considerable coordination between mental health and
child welfare agencies, the nature and extent of which
are also largely unknown. The degree to which
Medicaid agencies align reimbursement policies to
outcomes (i.e., mandate quality through some type of
pay-for-performance mechanism) is also not well
understood in this population, though there is evi-
dence that this alignment does not always occur
(Blair-Hutchinson & Foster, 2003; Rosenbach, 2001).
This lack of knowledge about awareness of standards,
construction of roles and responsibilities that can
promote implementation of standards, and construc-
tion of fiscal mechanisms to promote their deployment
within state and county mental health and child welfare
agencies has adversely affected the ability of adminis-
trators and policymakers to design procedures and
implement processes that can adequately address the
many mental health needs of children in foster care.
To understand the extent to which public mental
health agencies are adopting roles and responsibilities
that are consistent with CWLA/AAP standards for
care, we conducted a national survey of state and
county mental health administrators on policies and
procedures relating to mental health services for
children in foster care. We first examine the extent to
which mental health agencies are aware of these
existing standards. Second, because mental health
agencies may construct systems and processes of care
in ways that approximate recommendations in these
standards even in the absence of formal knowledge
about these standards, we examine their roles in
implementing and enforcing standards of care. We
conclude with an analysis of specific barriers to mental
health service delivery to children in foster care, and
explore ways to improve service delivery for this highly
vulnerable group of children.
Methods
Administrators of mental health agencies were sur-
veyed between November 1999 and February 2000 as
part of a larger study of child welfare, child health, and
Medicaid agencies nationally. Self-administered ques-
tionnaires were sent to agency directors. Respondents
were sought from agencies in all 50 states and the
District of Columbia. In addition to state-level respon-
dents, purposive selection of respondents from mental
health agencies in counties with the largest numbers of
children in foster care was also performed. We selected
for participation the five largest counties in each of the 11
states that have county-administered child welfare
systems. We then selected an additional 10 counties
based upon size and child welfare population from the
remaining pool of counties, comprising child welfare
systems that were both state-administered and county-
administered. The overall goals of the sampling
approach were to identify mental health agencies within
counties that had large populations of children in foster
care, that were heterogeneous in terms of the level of
child welfare administration, and to identify systems and
processes at the level of service delivery (i.e., within
states for state-administered child welfare systems, and
counties for county-administered child welfare systems).
The full study targeted 204 state-level respondents and
260 county-level respondents, including 51 state and 65
county mental health agency participants.
Questionnaires were mailed out to agencies in
November 1999. Two weeks later a reminder postcard
was mailed to agencies not returning their question-
naire. A phone call was then placed two weeks later for
those agencies still not responding. Agencies were
called on a regular basis to maximize the response rate.
Mental health agency response rates were 82% for
states and 58% for counties. Further details regarding
the structure, organization, content, and design of this
survey are available elsewhere (Halfon et al., 2002).
The questionnaires included items about the provi-
sion of services representing standards of care for
children in foster care as identified by the CWLA,
AAP, and AACAP. Agencies were queried about the
provision, timing, and content of services to children in
foster care, policies and processes governing such care,
and the funding mechanisms for the provision of such
care.
Mental health agencies were first asked if they ‘‘...
directly participate in the mental, behavioral, or
developmental screening components of the initial
health screening exam...’’ at the time of entry into
foster care. They were then asked about their role in
‘‘... comprehensive health assessments... provided to
those children who will remain in out-of-home care for
a significant period of time...’’ Agencies were asked if
their agency played some role in determining who
performs the comprehensive mental health exam,
Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201 193
123

procedures that comprise this exam, tools or assess-
ment instruments used, duration of time following
removal from the home within which the exam is to be
conducted, the venue of the exam, reporting require-
ments, privacy requirements, standards for reassess-
ments, and policies governing such assessments.
Agencies were asked similar questions about policies
and procedures governing ongoing mental health ser-
vices, and transitional health services, defined as ‘‘...
those exams and treatments that occur at any transi-
tional point in out-of-home care e.g., change of place-
ment, prior to adoption, pre-termination).’’ Agencies
were also asked about their adoption of AAP/CWLA
standards, and for a description of any other standards
the agency might have adopted. Questions on policy
and procedures included the existence and benefit
structures of all contractual agreements governing
mental health care for children in foster care (including
initial health screening, comprehensive health assess-
ments, diagnostic services, transitional services, devel-
opmental services, and other services); details on a
variety of collaborative functions between mental
health and child welfare agencies (including capacity
assessment, monitoring service adequacy, utilization
review, monitoring adherence to standards, data col-
lection tools, management information systems, and
quality improvement); and a variety of mechanisms
through which such collaboration was conducted (reg-
ular meetings, interagency task forces, specific program
assistance, joint staffings, and other similar mecha-
nisms). Agencies also reported their perceptions of
current barriers to mental health service delivery.
Questions on health financing elicited details on
types of funding (Non-EPSDT Medicaid, EPSDT,
Title IV, Title V, Children’s Health Insurance Pro-
gram, other state funds, other local funds, and other
funds) used to pay for screenings and assessments.
Data were entered and analyzed using Microsoft
Excel (Microsoft Corporation, 2003).
Results
Awareness of Standards of Care
One third (33%) of mental health agencies reported
being aware of whether existing standards of care
governing services for children in the child welfare
system had been adopted in their state or county.
Roles and Responsibilities
About half of mental health agencies reported involve-
ment in determining policies and procedures at the
‘front-end’ of the service delivery pathway (Table 1).
Over half of mental health agencies (54%) play a role
in defining the procedures that are part of a compre-
hensive mental health exam as defined by the CWLA,
AAP, and AACAP standards. Somewhat fewer mental
health agencies are involved in identifying the specific
instruments used for these assessments, or in setting
standards for mental health reassessments. Few mental
health agencies report being involved with service
delivery when children transition from one placement
to another, or when they leave foster care altogether.
Most mental health agencies (71% of state agencies
and 94% of county agencies) report considerable
formal communication with child welfare agencies
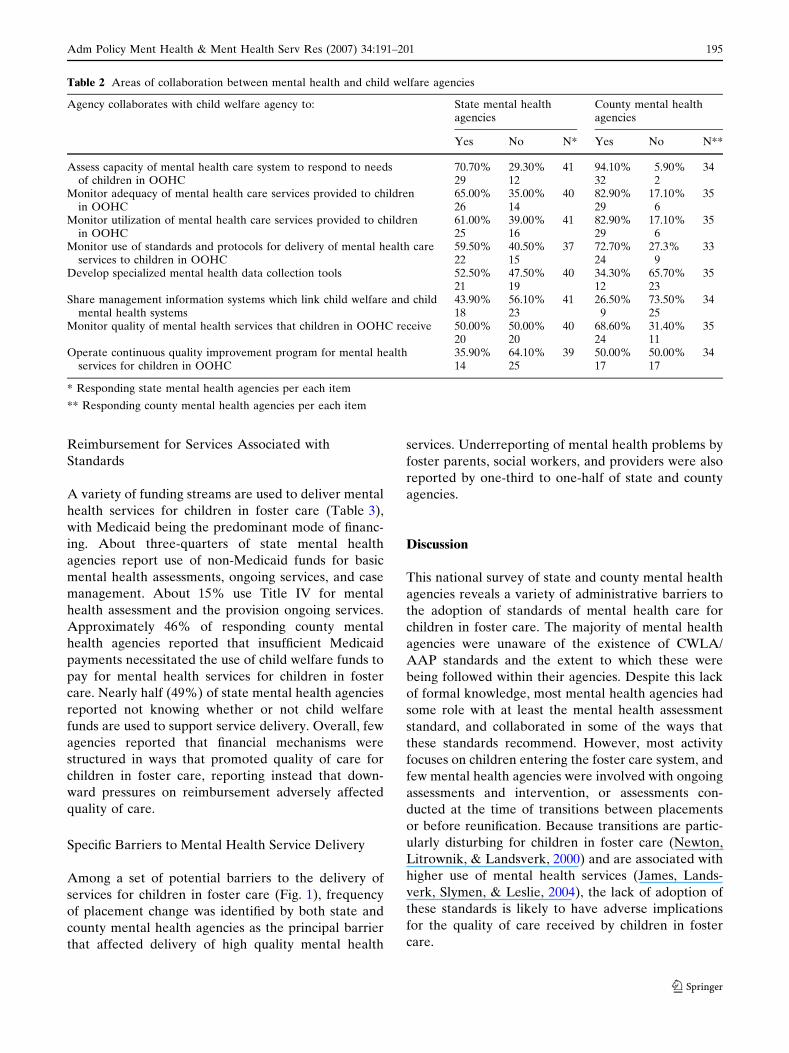
(Table 2). State and county mental health agencies
report collaborating with child welfare agencies around
capacity assessment, monitoring the adequacy and
utilization of mental health services by children in
foster care, and use of standards and protocols for
service delivery. A smaller proportion of collabora-
tions are organized around quality improvement. The
mechanisms through which this collaboration occurs
include regular meetings (72% of state and 89% of
county agencies), interagency task forces (59% and
72%, respectively), and assistance around specific
programs (31% and 56%, respectively).
Table 1 Role of child mental health agencies in determiningpolicies and procedures regarding mental health exams forchildren in foster care
Any role of mental health agency indetermining policy/procedure
Stateagencies*
Countyagencies**
Initial health screening examProcedures that comprise exam 13 8
36.10% 23.50%Comprehensive mental health examTiming of when exam is conducted 12 6
34.30% 18.20%Procedures that comprise exam 19 18
54.30% 54.50%Specific tools or assessment instruments
used for the exam16 1545.70% 45.50%
Ongoing servicesStandards for mental health reassessment 17 15
48.60% 45.50%Transitional health servicesRequiring a post-transition mental health
exam4 2
11.40% 6.10%Requiring exit-point mental health exam 5 2
14.30% 6.10%
* 35 responding state mental health agencies. 7 agencies did notrespond to this series of items
** 33 responding county mental health agencies. 4 agencies didnot respond to this series of items
194 Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201
123
Reimbursement for Services Associated with
Standards
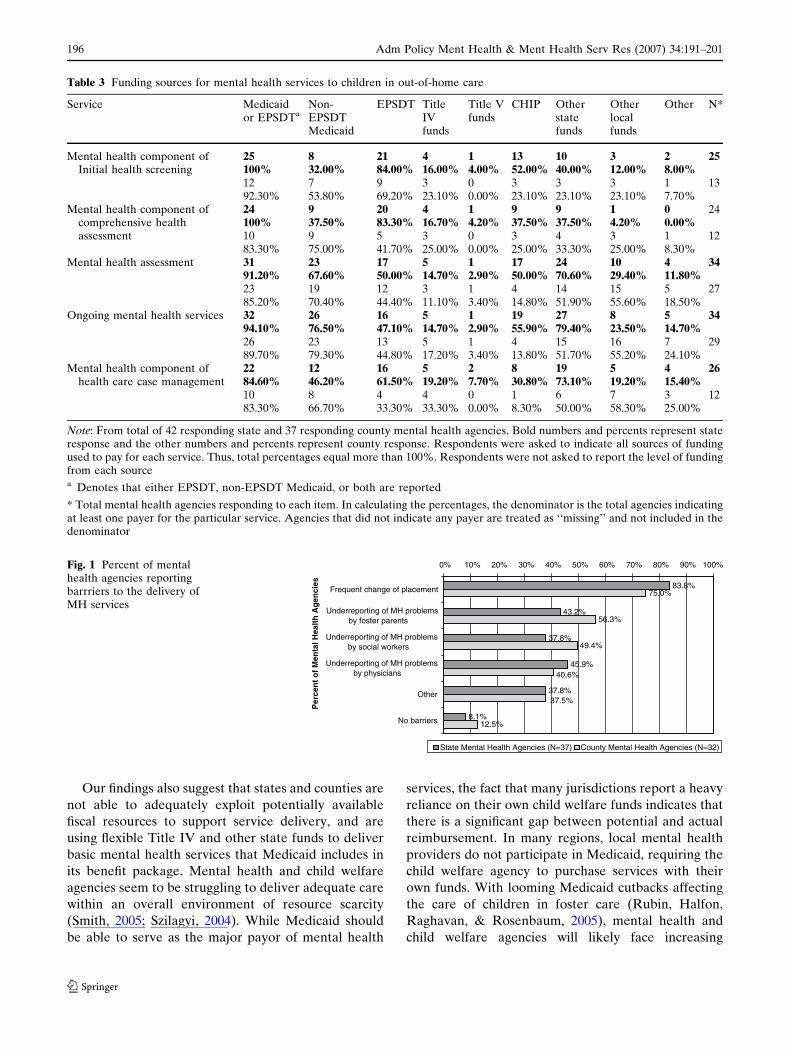
A variety of funding streams are used to deliver mental
health services for children in foster care (Table 3),
with Medicaid being the predominant mode of financ-
ing. About three-quarters of state mental health
agencies report use of non-Medicaid funds for basic
mental health assessments, ongoing services, and case
management. About 15% use Title IV for mental
health assessment and the provision ongoing services.
Approximately 46% of responding county mental
health agencies reported that insufficient Medicaid
payments necessitated the use of child welfare funds to
pay for mental health services for children in foster
care. Nearly half (49%) of state mental health agencies
reported not knowing whether or not child welfare
funds are used to support service delivery. Overall, few
agencies reported that financial mechanisms were
structured in ways that promoted quality of care for
children in foster care, reporting instead that down-
ward pressures on reimbursement adversely affected
quality of care.
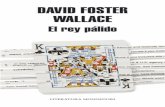
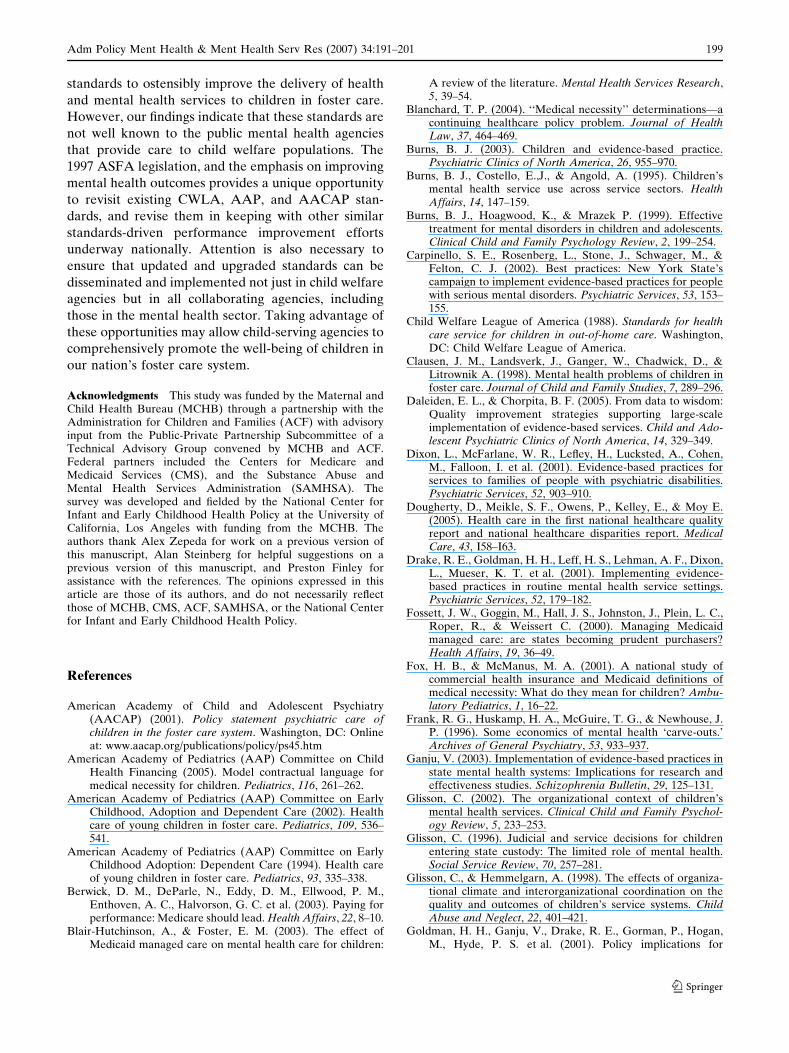
Specific Barriers to Mental Health Service Delivery
Among a set of potential barriers to the delivery of
services for children in foster care (Fig. 1), frequency
of placement change was identified by both state and
county mental health agencies as the principal barrier
that affected delivery of high quality mental health
services. Underreporting of mental health problems by
foster parents, social workers, and providers were also
reported by one-third to one-half of state and county
agencies.
Discussion
This national survey of state and county mental health
agencies reveals a variety of administrative barriers to
the adoption of standards of mental health care for
children in foster care. The majority of mental health
agencies were unaware of the existence of CWLA/
AAP standards and the extent to which these were
being followed within their agencies. Despite this lack
of formal knowledge, most mental health agencies had
some role with at least the mental health assessment
standard, and collaborated in some of the ways that
these standards recommend. However, most activity
focuses on children entering the foster care system, and
few mental health agencies were involved with ongoing
assessments and intervention, or assessments con-
ducted at the time of transitions between placements
or before reunification. Because transitions are partic-
ularly disturbing for children in foster care (Newton,
Litrownik, & Landsverk, 2000) and are associated with
higher use of mental health services (James, Lands-
verk, Slymen, & Leslie, 2004), the lack of adoption of
these standards is likely to have adverse implications
for the quality of care received by children in foster
care.
Table 2 Areas of collaboration between mental health and child welfare agencies
Agency collaborates with child welfare agency to: State mental healthagencies
County mental healthagencies
Yes No N* Yes No N**
Assess capacity of mental health care system to respond to needsof children in OOHC
70.70% 29.30% 41 94.10% 5.90% 3429 12 32 2
Monitor adequacy of mental health care services provided to childrenin OOHC
65.00% 35.00% 40 82.90% 17.10% 3526 14 29 6
Monitor utilization of mental health care services provided to childrenin OOHC
61.00% 39.00% 41 82.90% 17.10% 3525 16 29 6
Monitor use of standards and protocols for delivery of mental health careservices to children in OOHC
59.50% 40.50% 37 72.70% 27.3% 3322 15 24 9
Develop specialized mental health data collection tools 52.50% 47.50% 40 34.30% 65.70% 3521 19 12 23
Share management information systems which link child welfare and childmental health systems
43.90% 56.10% 41 26.50% 73.50% 3418 23 9 25
Monitor quality of mental health services that children in OOHC receive 50.00% 50.00% 40 68.60% 31.40% 3520 20 24 11
Operate continuous quality improvement program for mental healthservices for children in OOHC
35.90% 64.10% 39 50.00% 50.00% 3414 25 17 17
* Responding state mental health agencies per each item
** Responding county mental health agencies per each item
Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201 195
123
Our findings also suggest that states and counties are
not able to adequately exploit potentially available
fiscal resources to support service delivery, and are
using flexible Title IV and other state funds to deliver
basic mental health services that Medicaid includes in
its benefit package. Mental health and child welfare
agencies seem to be struggling to deliver adequate care
within an overall environment of resource scarcity
(Smith, 2005; Szilagyi, 2004). While Medicaid should
be able to serve as the major payor of mental health
services, the fact that many jurisdictions report a heavy
reliance on their own child welfare funds indicates that
there is a significant gap between potential and actual
reimbursement. In many regions, local mental health
providers do not participate in Medicaid, requiring the
child welfare agency to purchase services with their
own funds. With looming Medicaid cutbacks affecting
the care of children in foster care (Rubin, Halfon,
Raghavan, & Rosenbaum, 2005), mental health and
child welfare agencies will likely face increasing
83.8%
43.2%
37.8%
45.9%
37.8%
8.1%
75.0%
56.3%
49.4%
12.5%
37.5%
40.6%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Frequent change of placement
Underreporting of MH problemsby foster parents
Underreporting of MH problemsby social workers
Underreporting of MH problemsby physicians
Other
No barriers
Per
cen
t o
f M
enta
l Hea
lth
Ag
enci
es
State Mental Health Agencies (N=37) County Mental Health Agencies (N=32)
Fig. 1 Percent of mentalhealth agencies reportingbarrriers to the delivery ofMH services
Table 3 Funding sources for mental health services to children in out-of-home care
Service Medicaidor EPSDTa
Non-EPSDTMedicaid
EPSDT TitleIVfunds
Title Vfunds
CHIP Otherstatefunds
Otherlocalfunds
Other N*
Mental health component ofInitial health screening
25 8 21 4 1 13 10 3 2 25100% 32.00% 84.00% 16.00% 4.00% 52.00% 40.00% 12.00% 8.00%12 7 9 3 0 3 3 3 1 1392.30% 53.80% 69.20% 23.10% 0.00% 23.10% 23.10% 23.10% 7.70%
Mental health component ofcomprehensive healthassessment
24 9 20 4 1 9 9 1 0 24100% 37.50% 83.30% 16.70% 4.20% 37.50% 37.50% 4.20% 0.00%10 9 5 3 0 3 4 3 1 1283.30% 75.00% 41.70% 25.00% 0.00% 25.00% 33.30% 25.00% 8.30%
Mental health assessment 31 23 17 5 1 17 24 10 4 3491.20% 67.60% 50.00% 14.70% 2.90% 50.00% 70.60% 29.40% 11.80%23 19 12 3 1 4 14 15 5 2785.20% 70.40% 44.40% 11.10% 3.40% 14.80% 51.90% 55.60% 18.50%
Ongoing mental health services 32 26 16 5 1 19 27 8 5 3494.10% 76.50% 47.10% 14.70% 2.90% 55.90% 79.40% 23.50% 14.70%26 23 13 5 1 4 15 16 7 2989.70% 79.30% 44.80% 17.20% 3.40% 13.80% 51.70% 55.20% 24.10%
Mental health component ofhealth care case management
22 12 16 5 2 8 19 5 4 2684.60% 46.20% 61.50% 19.20% 7.70% 30.80% 73.10% 19.20% 15.40%10 8 4 4 0 1 6 7 3 1283.30% 66.70% 33.30% 33.30% 0.00% 8.30% 50.00% 58.30% 25.00%
Note: From total of 42 responding state and 37 responding county mental health agencies. Bold numbers and percents represent stateresponse and the other numbers and percents represent county response. Respondents were asked to indicate all sources of fundingused to pay for each service. Thus, total percentages equal more than 100%. Respondents were not asked to report the level of fundingfrom each sourcea Denotes that either EPSDT, non-EPSDT Medicaid, or both are reported
* Total mental health agencies responding to each item. In calculating the percentages, the denominator is the total agencies indicatingat least one payer for the particular service. Agencies that did not indicate any payer are treated as ‘‘missing’’ and not included in thedenominator
196 Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201
123

resource constraints to delivering the current level of
care much less an improved, more comprehensive set
of services.
The majority of agencies identified placement insta-
bility as an important barrier to service delivery. The
problem of unstable placements and its adverse con-
sequences for mental health service delivery have been
previously documented for children (James et al., 2004;
Rubin, Alessandrini, Feudtner, Localio, & Hadley,
2004; Webster, Barth, & Needell, 2000). Our findings
reveal that placement instability is a significant concern
at the agency level, and suggest the need for program-
matic and policy interventions. Support for interven-
tions that support foster families, and that provide
mental health care for the child, can improve stability
of placements. The barriers reported by these agencies
were, however, limited and largely attributed to those
factors that were external to their own policies and
procedures. Most of these identified barriers are issues
that existing health care standards address, suggesting
that adopting these standards may be a concrete first
step toward quality improvement within public mental
health agencies. And while considerable collaboration
reportedly occurs between mental health and child
welfare agencies, little of this communication seems
focused on quality improvement. However, we cannot
determine the instrumental value of this communica-
tion, and whether it results in the kinds of program-
matic, policy, and service delivery alignment and
coordination between mental health and child welfare
agencies that is necessary to deliver care to such a
cross-sector population.
Policy Implications
Repurposing Child Welfare-Mental Health
Collaborations toward Quality Improvement
Mental health and child welfare agencies may view the
CWLA/AAP standards as standards of practice. In
other words, they may represent ideal processes of
service delivery rather than practical service delivery
outcomes that agency practice and policy should
actually achieve, measure, and be held accountable
for improving. In contrast, outcomes-focused standards
such as those imposed by the Adoption and Safe
Families Act of 1997 (ASFA), when backed by federal
regulation and financial consequences for non-perfor-
mance, have been shown to have high visibility and
moderate effectiveness in changing practice among
child welfare agencies (Mitchell et al., 2005). ASFA
provisions not only focus attention on ongoing
improvement within states, but also articulate the goal
of child well-being in addition to traditional child
welfare goals of safety and permanency, and opera-
tionalize its indicators.
Attention to both process and outcome is necessary
for the adequate delivery of mental health services to
child welfare populations. Because foster care place-
ment has both secondary prevention and treatment
goals for a child, elaboration of specific processes that
are required to assure high quality care across both of
these types of services is necessary to inform child
welfare and health policymaking. Simultaneously,
adoption of indicators that can guide mental health
and child welfare agency practice toward improving
mental health outcomes for children in foster care is
also necessary. Adoption of the CWLA/AAP stan-
dards in addition to ASFA may offer a more solid
foundation for quality improvement that addresses the
essential components of prevention and treatment.
However, assuring the emotional well-being of
children in foster care requires the elaboration of
specific set of processes like the ones that are outlined
in the CWLA-AAP-guidelines that can produce
practice improvement, linkage of these steps with
outcomes monitoring, and an explicit orientation
toward achieving such performance outcomes, which
are all processes that few agencies may be currently
able to readily deploy. Mental and child welfare
agencies are each responsible for outcomes that are
influenced by the other agencies’ policy decisions.
Despite these challenges, models for quality improve-
ment initiatives exist at the state level (Daleiden &
Chorpita, 2005; Markus, Rosenbaum, Sonosky, Repa-
sch, & Mauery, 2005). The inclusion of the unique
needs of children in foster care within national quality
benchmarking efforts (Dougherty, Meikle, Owens,
Kelley, & Moy, 2005; Margolis, 2004) may further
accelerate the ‘uptake’ of standards into child welfare
and mental health agency practice.
Implementing Policy Within Programs
A policy focus on outcomes is necessary but insuffi-
cient for organizational change. Quality improvement
efforts require institutional templates, practical strate-
gies, well-defined procedures, and feasible mecha-
nisms, within which such efforts can occur; all of
these efforts need to be replicated over time and across
service settings (Burns, 2003; Carpinello, 2002; Grol,
2001; Torrey et al., 2001). Several model programs
exist that may suggest possible approaches to increas-
ing the quality of service delivery. One fiscal approach
might be the development of pay-for-performance
Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201 197
123

plans for health care delivery to children in child
welfare environments, similar to those called for in
Medicare (Berwick et al., 2003). However, Medicaid
managed care plans have posed considerable chal-
lenges to states attempting to become prudent pur-
chasers of care, and greater rate-setting ability by states
may be necessary to institute such plans (Fossett et al.,
2000). An organizational approach may be the adop-
tion of foster care carve-outs preferably with risk-
adjusted capitation rates that allow adequate resources
to finance the complex health and mental health needs
of children in foster care. Colorado currently provides
higher capitation rates for children in foster care
(McCarthy, 2003), but few states have implemented
traditional features of a carve-out (i.e., specialized
managed systems for care of a designated population
such as those created in Medicaid behavioral health
carve-outs) (Frank, Huskamp, McGuire, & Newhouse,
1996).
One provider-directed approach is the Institute for
Healthcare Improvement’s Breakthrough Series
(Homer et al., 2005; Institute for Healthcare Improve-
ment, 2003; Kilo, 1998). This methodology has been
used by the National Initiative for Children’s Health-
care Quality (www.nichq.org/nichq) to improve quality
of care for children in foster care. This initiative
attempted to support multi-agency teams from several
states to develop improvement plans and measurement
strategies designed to improve health care evaluation
content, care coordination, and follow-up in services
received. These multi-agency teams were drawn from
child welfare, child health, mental health, and Medic-
aid agencies and also required participation by parents
and providers. Quality improvement efforts under-
taken by the National Child Traumatic Stress Network
(www.NCTSN.org) also follow a similar model. The
widespread use of such practical strategies directed
explicitly toward child health quality is necessary to
improve the delivery of mental health care to children
in foster care.
Leveraging Financial Resources
While Medicaid has an expansive medical necessity
definition for children through its Early and Periodic
Screening, Diagnosis, and Treatment (EPSDT) pro-
gram, covered services vary considerably across states
(American Academy of Pediatrics, 2005; Blanchard,
2004; Fox & McManus, 2001; Lerner, Gesek, &
Adams, 2003). Nearly all children in foster care and
most services needed by children in foster care are
eligible for coverage under EPSDT. However, there
are differences across states between what EPSDT
covers and what the CWLA and AAP standards call
for (Horvath, 1997), and Medicaid benefits and pay-
ment provisions are complex and often poorly
addressed or accessed. Given the poor access to mental
health care documented in prior studies and the
relative lack of policies and procedures supporting
access that are documented in this study, Medicaid
programs should consider the establishment of disease
management programs for mental health care for
children in foster care, performance-based monitoring
of indicators of high-quality care that incorporates
existing standards, and outcomes-based reimbursement
of such care. The new provisions of the 2005 Deficit
Reduction Act (DRA) will force many states to
re-examine the scope of benefits available to children
in their state Medicaid plans, including those in foster
care, and also result in changes in how EPSDT services
can be deployed (Rubin, Halfon, Raghavan, Rosen-
baum, forthcoming).
Limitations
First, mental health and child welfare services in the
United States are organized at both the state and
county levels, with the bulk of child welfare services
organized at the state level. Hence, agencies are
heterogeneous in the extent to which they can influ-
ence specific aspects of service delivery for children in
foster care. Second, our focus was on institutional
policies and procedures governing adoption. It is not
known to what extent the existence of such agency-
level practices is associated with better child-level
outcomes, i.e., translates into implementation of high-
quality services throughout the agency and by individ-
ual providers. Third, the extent to which agencies
provided knowledgeable respondents determines the
extent to which our findings represent an accurate
assessment of administrative policies and procedure as
well as knowledge and attitudes. Although agency
heads were encouraged to solicit input from the most
knowledgeable staff, the extent to which this actually
happened is unknown. Finally, our respondents were
asked to report on highly complex and differentiated
systems, and may have been unable to adequately
capture their subtleties.
Conclusion
Mental health and child welfare agencies today face
considerable organizational and policy challenges in
their attempts to deliver care to children in foster care,
and the CWLA, AAP and AACAP have all issued
198 Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201
123
standards to ostensibly improve the delivery of health
and mental health services to children in foster care.
However, our findings indicate that these standards are
not well known to the public mental health agencies
that provide care to child welfare populations. The
1997 ASFA legislation, and the emphasis on improving
mental health outcomes provides a unique opportunity
to revisit existing CWLA, AAP, and AACAP stan-
dards, and revise them in keeping with other similar
standards-driven performance improvement efforts
underway nationally. Attention is also necessary to
ensure that updated and upgraded standards can be
disseminated and implemented not just in child welfare
agencies but in all collaborating agencies, including
those in the mental health sector. Taking advantage of
these opportunities may allow child-serving agencies to
comprehensively promote the well-being of children in
our nation’s foster care system.
Acknowledgments This study was funded by the Maternal andChild Health Bureau (MCHB) through a partnership with theAdministration for Children and Families (ACF) with advisoryinput from the Public-Private Partnership Subcommittee of aTechnical Advisory Group convened by MCHB and ACF.Federal partners included the Centers for Medicare andMedicaid Services (CMS), and the Substance Abuse andMental Health Services Administration (SAMHSA). Thesurvey was developed and fielded by the National Center forInfant and Early Childhood Health Policy at the University ofCalifornia, Los Angeles with funding from the MCHB. Theauthors thank Alex Zepeda for work on a previous version ofthis manuscript, Alan Steinberg for helpful suggestions on aprevious version of this manuscript, and Preston Finley forassistance with the references. The opinions expressed in thisarticle are those of its authors, and do not necessarily reflectthose of MCHB, CMS, ACF, SAMHSA, or the National Centerfor Infant and Early Childhood Health Policy.
References
American Academy of Child and Adolescent Psychiatry(AACAP) (2001). Policy statement psychiatric care ofchildren in the foster care system. Washington, DC: Onlineat: www.aacap.org/publications/policy/ps45.htm
American Academy of Pediatrics (AAP) Committee on ChildHealth Financing (2005). Model contractual language formedical necessity for children. Pediatrics, 116, 261–262.
American Academy of Pediatrics (AAP) Committee on EarlyChildhood, Adoption and Dependent Care (2002). Healthcare of young children in foster care. Pediatrics, 109, 536–541.
American Academy of Pediatrics (AAP) Committee on EarlyChildhood Adoption: Dependent Care (1994). Health careof young children in foster care. Pediatrics, 93, 335–338.
Berwick, D. M., DeParle, N., Eddy, D. M., Ellwood, P. M.,Enthoven, A. C., Halvorson, G. C. et al. (2003). Paying forperformance: Medicare should lead. Health Affairs, 22, 8–10.
Blair-Hutchinson, A., & Foster, E. M. (2003). The effect ofMedicaid managed care on mental health care for children:
A review of the literature. Mental Health Services Research,5, 39–54.
Blanchard, T. P. (2004). ‘‘Medical necessity’’ determinations—acontinuing healthcare policy problem. Journal of HealthLaw, 37, 464–469.
Burns, B. J. (2003). Children and evidence-based practice.Psychiatric Clinics of North America, 26, 955–970.
Burns, B. J., Costello, E.,J., & Angold, A. (1995). Children’smental health service use across service sectors. HealthAffairs, 14, 147–159.
Burns, B. J., Hoagwood, K., & Mrazek P. (1999). Effectivetreatment for mental disorders in children and adolescents.Clinical Child and Family Psychology Review, 2, 199–254.
Carpinello, S. E., Rosenberg, L., Stone, J., Schwager, M., &Felton, C. J. (2002). Best practices: New York State’scampaign to implement evidence-based practices for peoplewith serious mental disorders. Psychiatric Services, 53, 153–155.
Child Welfare League of America (1988). Standards for healthcare service for children in out-of-home care. Washington,DC: Child Welfare League of America.
Clausen, J. M., Landsverk, J., Ganger, W., Chadwick, D., &Litrownik A. (1998). Mental health problems of children infoster care. Journal of Child and Family Studies, 7, 289–296.
Daleiden, E. L., & Chorpita, B. F. (2005). From data to wisdom:Quality improvement strategies supporting large-scaleimplementation of evidence-based services. Child and Ado-lescent Psychiatric Clinics of North America, 14, 329–349.
Dixon, L., McFarlane, W. R., Lefley, H., Lucksted, A., Cohen,M., Falloon, I. et al. (2001). Evidence-based practices forservices to families of people with psychiatric disabilities.Psychiatric Services, 52, 903–910.
Dougherty, D., Meikle, S. F., Owens, P., Kelley, E., & Moy E.(2005). Health care in the first national healthcare qualityreport and national healthcare disparities report. MedicalCare, 43, I58–I63.
Drake, R. E., Goldman, H. H., Leff, H. S., Lehman, A. F., Dixon,L., Mueser, K. T. et al. (2001). Implementing evidence-based practices in routine mental health service settings.Psychiatric Services, 52, 179–182.
Fossett, J. W., Goggin, M., Hall, J. S., Johnston, J., Plein, L. C.,Roper, R., & Weissert C. (2000). Managing Medicaidmanaged care: are states becoming prudent purchasers?Health Affairs, 19, 36–49.
Fox, H. B., & McManus, M. A. (2001). A national study ofcommercial health insurance and Medicaid definitions ofmedical necessity: What do they mean for children? Ambu-latory Pediatrics, 1, 16–22.
Frank, R. G., Huskamp, H. A., McGuire, T. G., & Newhouse, J.P. (1996). Some economics of mental health ‘carve-outs.’Archives of General Psychiatry, 53, 933–937.
Ganju, V. (2003). Implementation of evidence-based practices instate mental health systems: Implications for research andeffectiveness studies. Schizophrenia Bulletin, 29, 125–131.
Glisson, C. (2002). The organizational context of children’smental health services. Clinical Child and Family Psychol-ogy Review, 5, 233–253.
Glisson, C. (1996). Judicial and service decisions for childrenentering state custody: The limited role of mental health.Social Service Review, 70, 257–281.
Glisson, C., & Hemmelgarn, A. (1998). The effects of organiza-tional climate and interorganizational coordination on thequality and outcomes of children’s service systems. ChildAbuse and Neglect, 22, 401–421.
Goldman, H. H., Ganju, V., Drake, R. E., Gorman, P., Hogan,M., Hyde, P. S. et al. (2001). Policy implications for
Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201 199
123
implementing evidence-based practices. Psychiatric Services,52, 1591–1597.
Grol, R. (2001). Successes and failures in the implementation ofevidence-based guidelines for clinical practice. MedicalCare, 39, 46–54.
Halfon, N., Berkowiz, G., & Klee, L. (1992). Mental healthservice utilization by children in foster care in California.Pediatrics, 89, 1238–1244.
Halfon, N., & Klee, L. (1987). Health services for California’sfoster children: Current practices and policy recommenda-tions. Pediatrics, 80, 183–191.
Halfon, N., Mendonca, A., & Berkowitz, G. (1995). Health statusof children in foster care: The experience of the Center forthe Vulnerable Child. Archives of Pediatrics and AdolescentMedicine, 149, 386–392.
Halfon, N., Inkelas, M., Flint, R., Shoaf, K., Zepeda, A., &Franke, T. (2002). Assessment of factors influencing theadequacy of health care services to children in foster care.Los Angeles, CA: UCLA Center for Healthier Children,Families and Communities.
Harman, J. S., Childs, G. E., & Kelleher, K. J. (2000). Mentalhealth care utilization and expenditures by children in fostercare. Archives of Pediatrics and Adolescent Medicine, 154,1114–1117.
Hoagwood, K. (2003). The policy context for child and adoles-cent mental health services: Implications for systems reformand basic science development. Annals New York Academyof Sciences, 1008, 140–148.
Hoagwood, K., Burns, B. J., Kiser, L., Ringeisen, H., &Schoenwald S. K. (2001). Evidence-based practice in childand adolescent mental health services. Psychiatric Services,52, 1179–1189.
Homer, C. J., Forbes, P., Horvitz, L., Peterson, L. E., Wypij, D.,& Heinrich, P. (2005). Impact of a quality improvementprogram on care and outcomes for children with asthma.Archives of Pediatrics and Adolescent Medicine, 159, 464–469.
Horvath, J. (1997). Improving health care for children in fostercare: Alternative delivery models. Portland, ME: NationalAcademy for State Health Policy.
Hurlburt, M. S., Leslie, L. K., Landsverk, J., Barth, R. P., Burns,B. J., Gibbons, R. D., Slymen, D. J., & Zhang, J. (2004).Contextual predictors of mental health service use amongchildren open to child welfare. Archives of General Psychi-atry, 61, 1217–1224.
Institute for Healthcare Improvement (2003). The breakthroughseries: IHI’s collaborative model for achieving breakthroughachievement. Boston, MA: Online at: http://www.ihi.org/NR/rdonlyres/3F1925B7-6C47-48ED-AA83-C85DBABB664D/0/TheBreakthroughSeriespaper.pdf
Institute of Medicine (2001). Crossing the quality chasm: A newhealth system for the 21st century. Washington, DC: NationalAcademy Press.
James, S., Landsverk, J., Slymen, D. J., & Leslie, L. K. (2004).Predictors of outpatient mental health service use-The roleof foster care placement change. Mental Health ServicesResearch, 6, 127–141.
Joint Commission on the Mental Health of Children (1969).Crisis in child mental health. Harper & Row, New York.
Kilo, C. M. (1998). A framework for collaborative improvement:Lessons from the Institute for Healthcare Improvement’sBreakthrough Series. Quality Management in Health Care,6, 1–13.
Klee, L., & Halfon, N. (1987). Mental health care for fosterchildren in California. Child Abuse and Neglect, 11, 63–74.
Landsverk, J., Garland, A. F., & Leslie, L. K. (2002). Mentalhealth services for children reported to Child ProtectiveServices. In J. E. B. Myers, L. Berliner, J. Briere, C. T.Hendrix, C. Jenny, & T. A. Reid (Eds.), APSAC handbookon child maltreatment (pp. 487–507). Thousand Oaks, CA:Sage Publications.
LeBel, J., Stromberg, N., Duckworth, K., Kerzner, J., Goldstein,R., Weeks, M. et al. (2004). Child and adolescent inpatientrestraint reduction: A state initiative to promote strength-based care. Journal of the American Academy of Child andAdolescent Psychiatry, 43, 37–45.
Lerner, J. C., Gesek, J., & Adams S. (2003). Will using evidence-based approaches to a standards development processimprove Medicaid policy making? Report on a promisingeffort. Journal of Ambulatory Care Management, 26, 322–333.
Margolis, P. A. (2004). Small steps and big leaps: Implications ofthe national survey of early childhood health for improvingthe quality of preventive and developmental care for youngchildren. Pediatrics, 113, 1988–1990.
Markus, A. R., Rosenbaum, S., Sonosky, C., Repasch, L., &Mauery, D. R. (2005). State purchasing and enforcementquality care for children in Medicaid and SCHIP managedcare. Managed Care Interface, 18, 24–30.
McCarthy, J. (2003). Child Welfare Special Analysis. Availableat http://rtckids.fmhi.usf.edu/rtcpubs/hctrking/pubs/2003_statesurvey/2003survey/17-%20CW2129–147.pdf. [ac-cessed on March 13, 2006]
Microsoft Corporation (2003). Excel 2003 for Windows Profes-sional Edition. Microsoft Corporation, Redmond WA.
Mitchell, L. B., Barth, R. P., Green, R., Wall, A., Biemer, P.,Berrick, J. D. et al. (2005). Child welfare reform in theUnited States: findings from a local agency survey. ChildWelfare, 84, 5–24.
NASMHPD Research Institute, Inc. (2005). Evidence-basedpractices. Alexandria, VA: NRI Center for Mental HealthQuality and Accountability: Online at: www.nri-inc.org/CMHQA.cfm. [accessed on March 10, 2006]
Newton, R. R., Litrownik, A. J., & Landsverk, J. A. (2000).Children and youth in foster care: Disentangling therelationship between problem behaviors and number ofreplacements. Child Abuse and Neglect, 24, 1363–1374.
Pilowsky, D. (1995). Psychopathology among children placed infamily foster care. Psychiatric Services, 46, 906–910.
President’s Commission on Mental Health (1978). Report of thesub-task panel on infants, children, and adolescents. Wash-ington, DC: President’s Commission on Mental Health.
President’s New Freedom Commission on Mental Health (2003).Achieving the promise: Transforming mental health care inAmerica. Rockville, MD: Online at: http://www.mental-healthcommission.gov/reports/FinalReport/toc.html. [ac-cessed on March 13, 2006]
Raghavan, R., Zima, B. T., Andersen, R. M., Leibowitz, A. A.,Schuster, M. A., & Landsverk, J. (2005). Psychotropicmedication use in a national probability sample of childrenin the child welfare system. Journal of Child and AdolescentPsychopharmacology, 15, 97–106.
Rosenbach, M. (2001). Children in foster care: Challenges inmeeting their health care needs through Medicaid. Mathem-atica Policy Research, Inc: Princeton, NJ.
Rosenheck, R. A. (2001). Organizational process: A missing linkbetween research and practice. Psychiatric Services, 52,1607–1612.
Rubin, D. M., Alessandrini, E. A., Feudtner, C., Localio, A. R.,& Hadley, T. (2004). Placement changes and emergency
200 Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201
123

department visits in the first year of foster care. Pediatrics,114, 354–360.
Rubin, D., Halfon, N., Raghavan, R., & Rosenbaum, S. (2005).Protecting children in foster care: Why proposed Medicaidcuts harm our nation’s most vulnerable youth. Seattle, WA:Casey Family Programs: Online at: www.casey.org/Re-sources/Publications/Medicaid.htm. [accessed on March 10,2006]
Sackett, D. L., Rosenberg, W. M. C., Muir-Gray, J. A., Haynes,R. B., & Richardson, W. S. (1996). Evidence-based medi-cine: What it is and what it isn’t. British Medical Journal,312, 71–72.
Schoenwald, S. K., & Hoagwood, K. (2001). Effectiveness,transportability, and dissemination: What matters when?Psychiatric Services, 52, 1179–1189.
Schor, E. L. (1981). Health care supervision of foster children.Child Welfare, 60, 313–319.
Simms, M. D., Dubowitz, H., & Szilagyi, M. A. (2000). Healthcare needs of children in the foster care system. Pediatrics,106, 909–918.
Simpson, D. D. (2002). A conceptual framework for transferringresearch to practice. Journal of Substance Abuse Treatment,22, 171–182.
Smith, V. K. (2005). The role of states in improving health andhealth care for young children. The Commonwealth Fund(Issue Brief), New York, NY.
Substance Abuse and Mental Health Services Administration(2005). About evidence-based practices: Shaping mentalhealth services towards recovery. Washington, DC: Onlineat: www.mentalhealth.samhsa.gov/cmhs/communitysupport/toolkits/about.asp. [accessed on March 13, 2006]
Szilagyi, P. G. (2004). Improved access and quality of care afterenrollment in the New York State Children’s HealthInsurance Program (SCHIP). Pediatrics, 113, 395–404.
Takayama, J. I., Bergman, A. B., & Connel, F. A. (1994).Children in foster care in the state of Washington: Healthcare utilization and expenditures. Journal of the AmericanMedical Association, 271, 1850–1855.
Tanenbaum, S. (2003). Evidence-based practice in mental health:Practical weaknesses meet political strengths. Journal ofEvaluation in Clinical Practice, 9, 287–301.
Torrey, W. C., Finnerty, M., Evans, A., & Wyzik P. (2003)Strategies for leading the implementation of evidence-basedpractices. Psychiatric Clinics of North America, 26, 883–897.
Torrey, W. C., Drake, R. E., Dixon, L., Burns, B. J., Flynn, L.,Rush, A. J. et al. (2001). Implementing evidence-basedpractices for persons with severe mental illness. PsychiatricServices, 52, 45–50.
U.S. Congress, Office of Technology Assessment (1986). Chil-dren’s mental health:Problems and services-a backgroundpaper. Washington, DC: U.S. Congress, Office of Technol-ogy Assessment.
U.S. Department of Health and Human Services (2005). Trans-forming mental health care in America: The federal actionagenda: First steps. Rockville, MD: U.S. Department ofHealth and Human Services, Substance Abuse and MentalHealth Services Administration, Online at: http://www.sam-hsa.gov/Federalactionagenda/NFC_TOC.aspx. [accessed onMarch 13, 2006]
U.S. Department of Health and Human Services (1999). MentalHealth: A Report of the Surgeon General. Washington, DC:U.S. Public Health Service.
U.S. General Accounting Office (2003). Child welfare andjuvenile justice: Federal agencies could play a stronger rolein helping states reduce the number of children placed solelyto obtain mental health services. Washington, DC: US GAOPub. No.GAO-03-397.
Webster, D., Barth, R. P., & Needell, B. (2000). Placementstability for children in out- of-home care: A longitudinalanalysis. Child Welfare, 79, 614–632.
Weisz, J. R., Sandler, I. N., Durlak, J. A., & Anton, B. S. (2005).Promoting and protecting youth mental health throughevidence-based prevention and treatment. American Psy-chologist, 60, 628–648.
Zima, B. T., Bussing, R., Freeman, S., Yang, X., Belin, T. R., &Forness S. R. (2000). Behavior problems, academic skilldelays and school failure among school-aged children infoster care: Their relationship to placement characteristics.Journal of Child and Family Studies, 9, 87–103.
Adm Policy Ment Health & Ment Health Serv Res (2007) 34:191–201 201
123