
Administration of olive oil followed by a low volume of polyethylene glycol-electrolyte lavage...
7
ORIGINAL ARTICLE: Clinical Endoscopy Administration of olive oil followed by a low volume of polyethylene glycol-electrolyte lavage solution improves patient satisfaction with right-side colonic cleansing over administration of the conventional volume of polyethylene glycol-electrolyte lavage solution for colonoscopy preparation Evren Abut, MD, Hakan Guveli, MD, Bulent Yasar, MD, Cengiz Bolukbas, MD, Filiz Fusun Bolukbas, MD, Ali Tuzun Ince, MD, Tulin Kendir, MD, Ali Remzi Dalay, MD, Oya Ovunc Kurdas, MD Istanbul, Sanliurfa, Turkey Background: Proper bowel cleansing before colonoscopy is essential for satisfactory evaluation of the colon. The required consumption of a large volume of salty-tasting liquid, 4 L of polyethylene glycol-electrolyte lavage solution (PEG-ELS), is the primary limitation to achieving this goal. Objective: To achieve better patient satisfaction with efficient bowel cleansing, we compared the effects of the conventional volume (4 L) of PEG-ELS with those of a low volume (2 L) in combination with pretreatment using different laxatives, such as magnesium hydroxide (milk of magnesia) and olive oil. Design: Randomized, controlled study. Setting: A single research hospital. Patients: Patients undergoing elective colonoscopy. Interventions: A total of 120 patients were randomized to 1 of 3 different preparation regimens: 39 patients were prepared with a conventional volume (4 L) of PEG-ELS (Preparation [Prep] 1), and the remaining patients were prepared with a lower volume (2 L) of PEG-ELS and pretreatment with a laxative, either 15 g of magnesium hydroxide (40 patients, Prep 2) or 60 mL of olive oil (41 patients, Prep 3) 3 hours before PEG-ELS administration. Main Outcome Measurements: The primary outcome was the efficacy of colonic cleansing on the left and right sides. Secondary outcomes were patient satisfaction and side effects. Results: The olive oil regimen (Prep 3) resulted in significantly more adequate bowel cleansing of the right colon than administration of the conventional volume of PEG-ELS (Prep 1) and the magnesium hydroxide (Prep 2) regimen (97.6% vs 74.5% and 72.5%, respectively, P Z .007). However, this difference was not observed in the left colon (91.5%, 85.5%, and 91.8% for Preps 1, 2, and 3, respectively, P Z .776). When asked, 38 patients (95%) taking Prep 2, 35 patients (85.3%) taking Prep 3, and only 11 patients (28.2%) taking Prep 1 preferred the same preparation regimen if they required a future colonoscopy (P Z.006), based on ease of use and taste. The side effects were comparable in each group. Limitations: The limitations of this study include the relatively small sample size, the single-center study design, and the use of a nonvalidated symptom scoring system. Conclusion: Pretreatment with olive oil before administration of a low volume of PEG-ELS enhances both patient satisfaction and the quality of right-side colonic cleansing over the administration of the conventional volume of PEG-ELS for colonoscopy preparation. Although the magnesium hydroxide regimen (Prep 2) was the preferred regimen in this study, its colonic cleansing effectiveness was not as great as those of the other reg- imens. Based on our results, the olive oil regimen is recommended, especially for patients who are not able to consume large volumes of liquids, such as the elderly, and those who are suspected of having subtle right-side colonic lesions. (Gastrointest Endosc 2009;70:515-21.) Abbreviations: PEG-ELS, polyethylene glycol-electrolyte lavage solution; Prep, preparation; SPS, sodium phosphate solution. DISCLOSURE: All authors disclosed no financial relationships relevant to this publication. Copyright ª 2009 by the American Society for Gastrointestinal Endoscopy 0016-5107/$36.00 doi:10.1016/j.gie.2009.01.002 www.giejournal.org Volume 70, No. 3 : 2009 GASTROINTESTINAL ENDOSCOPY 515
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Administration of olive oil followed by a low volume of polyethylene glycol-electrolyte lavage...

ORIGINAL ARTICLE: Clinical Endoscopy
Administration of olive oil followed by a low volume ofpolyethylene glycol-electrolyte lavage solution improvespatient satisfaction with right-side colonic cleansing overadministration of the conventional volume of polyethyleneglycol-electrolyte lavage solution for colonoscopy preparation
Evren Abut, MD, Hakan Guveli, MD, Bulent Yasar, MD, Cengiz Bolukbas, MD, Filiz Fusun Bolukbas, MD,Ali Tuzun Ince, MD, Tulin Kendir, MD, Ali Remzi Dalay, MD, Oya Ovunc Kurdas, MD
Istanbul, Sanliurfa, Turkey
doi:
ww
Background: Proper bowel cleansing before colonoscopy is essential for satisfactory evaluation of the colon.The required consumption of a large volume of salty-tasting liquid, 4 L of polyethylene glycol-electrolyte lavagesolution (PEG-ELS), is the primary limitation to achieving this goal.
Objective: To achieve better patient satisfaction with efficient bowel cleansing, we compared the effects of theconventional volume (4 L) of PEG-ELS with those of a low volume (2 L) in combination with pretreatment usingdifferent laxatives, such as magnesium hydroxide (milk of magnesia) and olive oil.
Design: Randomized, controlled study.
Setting: A single research hospital.
Patients: Patients undergoing elective colonoscopy.
Interventions: A total of 120 patients were randomized to 1 of 3 different preparation regimens: 39 patientswere prepared with a conventional volume (4 L) of PEG-ELS (Preparation [Prep] 1), and the remaining patientswere prepared with a lower volume (2 L) of PEG-ELS and pretreatment with a laxative, either 15 g of magnesiumhydroxide (40 patients, Prep 2) or 60 mL of olive oil (41 patients, Prep 3) 3 hours before PEG-ELS administration.
Main Outcome Measurements: The primary outcome was the efficacy of colonic cleansing on the left andright sides. Secondary outcomes were patient satisfaction and side effects.
Results: The olive oil regimen (Prep 3) resulted in significantly more adequate bowel cleansing of the right colon thanadministration of the conventional volume of PEG-ELS (Prep 1) and the magnesium hydroxide (Prep 2) regimen (97.6%vs 74.5% and 72.5%, respectively, P Z .007). However, this difference was not observed in the left colon (91.5%, 85.5%,and 91.8% for Preps 1, 2, and 3, respectively, P Z .776). When asked, 38 patients (95%) taking Prep 2, 35 patients (85.3%)taking Prep 3, and only 11 patients (28.2%) taking Prep 1 preferred the same preparation regimen if they requireda future colonoscopy (P Z.006), based on ease of use and taste. The side effects were comparable in each group.
Limitations: The limitations of this study include the relatively small sample size, the single-center studydesign, and the use of a nonvalidated symptom scoring system.
Conclusion: Pretreatment with olive oil before administration of a low volume of PEG-ELS enhances bothpatient satisfaction and the quality of right-side colonic cleansing over the administration of the conventionalvolume of PEG-ELS for colonoscopy preparation. Although the magnesium hydroxide regimen (Prep 2) wasthe preferred regimen in this study, its colonic cleansing effectiveness was not as great as those of the other reg-imens. Based on our results, the olive oil regimen is recommended, especially for patients who are not able toconsume large volumes of liquids, such as the elderly, and those who are suspected of having subtle right-sidecolonic lesions. (Gastrointest Endosc 2009;70:515-21.)
Abbreviations: PEG-ELS, polyethylene glycol-electrolyte lavage solution;
Prep, preparation; SPS, sodium phosphate solution.
DISCLOSURE: All authors disclosed no financial relationships relevant to thispublication.
Copyright ª 2009 by the American Society for Gastrointestinal Endoscopy
0016-5107/$36.00
10.1016/j.gie.2009.01.002
w.giejournal.org Volume 70, No. 3 : 2009 GASTROINTESTINAL ENDOSCOPY 515

Olive oil and PEG-ELS for colonic cleansing Abut et al
Colonoscopy became the standard procedure for thediagnosis and treatment of diseases of the colon in theearly 1960s.1 Adequate bowel cleansing is a prerequisitefor proper evaluation of the entire colonic mucosa duringa colonoscopy. Poor colonic cleansing may preventdetection of clinically significant pathological lesions. Fur-thermore, it may lead to a prolonged duration or resched-uling of the colonoscopy.
In current practice, polyethylene glycol-electrolyte la-vage solution (PEG-ELS)2 and sodium phosphate solution(SPS)3 have been used since the 1980s and 1990s, respec-tively, because of their abilities to achieve rapid colonoscopypreparation, even though they have many limitations. Im-portantly, approximately 20% of patients who consumedPEG-ELS or SPS did not have adequate bowel cleansing.4
Furthermore, SPS is generally not recommended for pa-tients with renal failure, congestive heart failure, uncon-trolled hypertension, or ascites because of its potentialrisks for clinically significant alterations in serum electrolytelevels and hemodynamic stability.5-8
Numerous clinical trials have assessed prokinetic (me-toclopramide, cisapride, and tegaserod)9-13 and laxativeagents (magnesium citrate and bisacodyl)14-16 as adjunctsto standard or lower volumes of PEG-ELS. Among thesepreparations, no additive effect was demonstrated for me-toclopramide or cisapride on bowel cleansing. However,Sharma et al15 found that pretreatment with magnesiumcitrate or bisacodyl in addition to 2 L of PEG-ELS was su-perior to 4 L of PEG-ELS in terms of the preparation qual-ity and patient satisfaction. Evaluation of the effectivenessof a range of laxatives may indicate preferred laxatives withsuperior results.
To our knowledge, there is no study examining the ef-fects of other magnesium salts, such as magnesium hy-droxide, or natural laxatives, such as olive oil, for thispurpose. This study compared the quality of coloniccleansing, patient satisfaction, and side effects of a conven-tional volume (4 L) of PEG-ELS with those of a low (2 L)volume of PEG-ELS combined with pretreatment witha laxative, either magnesium hydroxide (milk of magnesia)or olive oil.
MATERIALS AND METHODS
This was a prospective, randomized, controlled study,and the study protocol was carried out in accordancewith the Declaration of Helsinki as revised in 1989. Allpatients signed approved informed consent forms beforeenrollment in the study.
Study populationPatients of either sex who were at least 18 years of age
and were scheduled for elective outpatient colonoscopywere eligible for participation in this study.
516 GASTROINTESTINAL ENDOSCOPY Volume 70, No. 3 : 2009
Capsule Summary
What is already known on this topic
d Many bowel preparations have been studied forprecolonoscopy cleansing, but none is clearly superiorto the others.
What this study adds to our knowledge
d In a randomized trial of 120 patients undergoingcolonoscopy, 60 mL of olive oil ingested before 2 L ofpolyethylene glycol-electrolyte lavage solution (PEG-ELS)resulted in superior cleaning of the right colon comparedwith 4 L of PEG-ELS or 15 g of magnesium hydroxidefollowed by 2 L of PEG-ELS.
Patients who met at least one of the following criteriawere excluded: (1) age younger than 18 years; (2) hospital-ized patients undergoing colonoscopy; (3) disturbed bowelmovements (!2 bowel movements per week or O3 bowelmovements per day in the past 3 months); (4) evidence ofacute or chronic renal failure; (5) cardiovascular diseases(including recent myocardial infarction, congestive heartfailure, unstable angina pectoris, unstable hypertension,and cardiac arrhythmias); (6) ascites; (7) electrolyte imbal-ance, including hyponatremia, hypokalemia, hyperphos-phatemia, hypocalcemia, and hypomagnesemia; (8) activeinflammatory bowel disease; (9) previous partial or subtotalcolectomy; (10) ileus and/or suspected bowel obstruction;(11) pregnancy or breast-feeding; and (12) childbearingpotential without adequate contraception.
Study designIn the screening period, the patient’s medical history,
demographic data, bowel habits (number of bowel move-ments per day), indications for colonoscopy, and bodyweight were noted. For all patients, clinical hemodynamic,hematological, and biochemical measurements, includingwhole blood count, blood sugar, blood urea nitrogen,creatinine, and serum electrolyte (sodium, potassium,chloride, phosphorus, ionized calcium and magnesium)levels were performed.
After initial evaluations, patients who met all the inclu-sion criteria and no exclusion criteria were randomized toreceive one of the following preparation (Prep) regimensaccording to a computer-generated randomization list byone physician (HG) who was blinded to the results ofprevious colonoscopies.
Prep 1 consisted of 4 L of PEG-ELS (GoLYTELY; Brain-tree Laboratories, Inc, Boston, Mass) alone, starting at4:00 PM on the day before the colonoscopy at a rate of250 mL every 15 minutes until all the solution has beenconsumed, as recommended by the manufacturer.
Prep 2 consisted of 15 g of magnesium hydroxide (Mag-nesie Calsinee; Carlo Erba, Inc, Istanbul, Turkey) mixed
www.giejournal.org

Abut et al Olive oil and PEG-ELS for colonic cleansing
with 1 glass of water (250 mL) taken 3 hours before start-ing 2 L of PEG-ELS, which was given in the same fashion asdescribed above.
Prep 3 consisted of 60 mL of olive oil mixed with 1 glassof apple juice taken 3 hours before starting 2 L of PEG-ELS, which was given in the same fashion as describedabove.
Patients in all groups were encouraged to adhere to clearliquid diets from 6:00 AM to midnight on the day before thecolonoscopy, and further oral intake was not allowed aftermidnight. Before the colonoscopy, a physical examinationand clinical hemodynamic, hematological, and biochemicalmeasurements were repeated, as described above. Patientswere asked to complete a questionnaire designed to assessthe bowel preparation’s tolerability, patient satisfaction,and symptoms that were experienced during the colono-scopy preparation. This questionnaire consisted of 18 ques-tions and was based on questionnaires used in similarprevious studies.4,17
To ensure consistency in the evaluations, colonoscopieswere performed by the same attending endoscopist (EA)from 8:00 AM to 12:00 PM without conscious sedation. Be-fore the colonoscopy, all patients were instructed not toreveal their assigned preparation regimen to the endos-copy unit staff. Therefore, all persons present in the en-doscopy unit, including the endoscopist, were blindedto the patient preparation. A Pentax EC-3840F videocolo-noscope (Asahi Optical Co., Tokyo, Japan) was used forall examinations. The duration of the complete endoscopyprocedure and the cecal intubation time were recorded.The quality of colonic cleansing was evaluated by a previ-ously validated grading system (Table 1).4 In this evalua-tion, the left colon was defined as spanning from therectum to the splenic flexure, and the right colon as theregion from the splenic flexure to the cecum.
After completion of the colonoscopy, the symptoms expe-rienced during the procedure (nausea, vomiting, abdominalpain, abdominal distention, and lethargy) were evaluatedaccording to a scoring system that was arbitrarily graded ona 4-point scale. This scale was adapted from previous similarstudies16,17 (none, 0; mild, 1; moderate, 2; severe, 3). Theoverall patient symptom score (range, 0-15) was calculatedas the sum of the individual symptom scores.
Statistical analysisStatistical analyses were performed by using commer-
cially available statistics software (SPSS for Windows10.0, SPSS Inc., Chicago, Ill). At the beginning of the study,a sample size calculation was performed, assuming a 30%difference in the rate of colonic cleansing. To detect thisdifference with a significance level (a) of .05 and a powerof 80% with a 2-tailed test, we calculated that at least 36patients were needed for each treatment group.
Continuous measures were analyzed by using an analy-sis of variance. A paired-samples t test was used tocompare the changes on clinical hemodynamic, hemato-
www.giejournal.org
logical, and biochemical measurements during the prepa-ration in the 3 groups. Categorical measures wereanalyzed with a c2 test. Ordered categorical measureswere analyzed with the Kruskal-Wallis test as estimatedby the Cochran-Mantel-Haenszel test by using row meanrank scores. The results of the quality of bowel cleansingwere also dichotomized as adequate (excellent, good,and fair results pooled) or inadequate (poor and verypoor results pooled) preparation, and pairwise compari-sons were made with a c2 test for the right colon andFisher’s exact test for the left colon.
RESULTS
A total of 224 consecutive outpatients scheduled for elec-tive colonoscopy participated in this study. Ninety-eight ofthese patients were excluded because they met one ormore exclusion criteria. Thus, 126 patients were recruitedand equally randomized to 1 of 3 different preparationregimens (42 patients in each preparation group). After ran-domization, 3 patients in the Prep 1 group, 2 patients in thePrep 2 group, and 1 patient in the Prep 3 group did not keeptheir colonoscopy appointments because of personal rea-sons. The remaining patients were compared by a per-pro-tocol analysis.
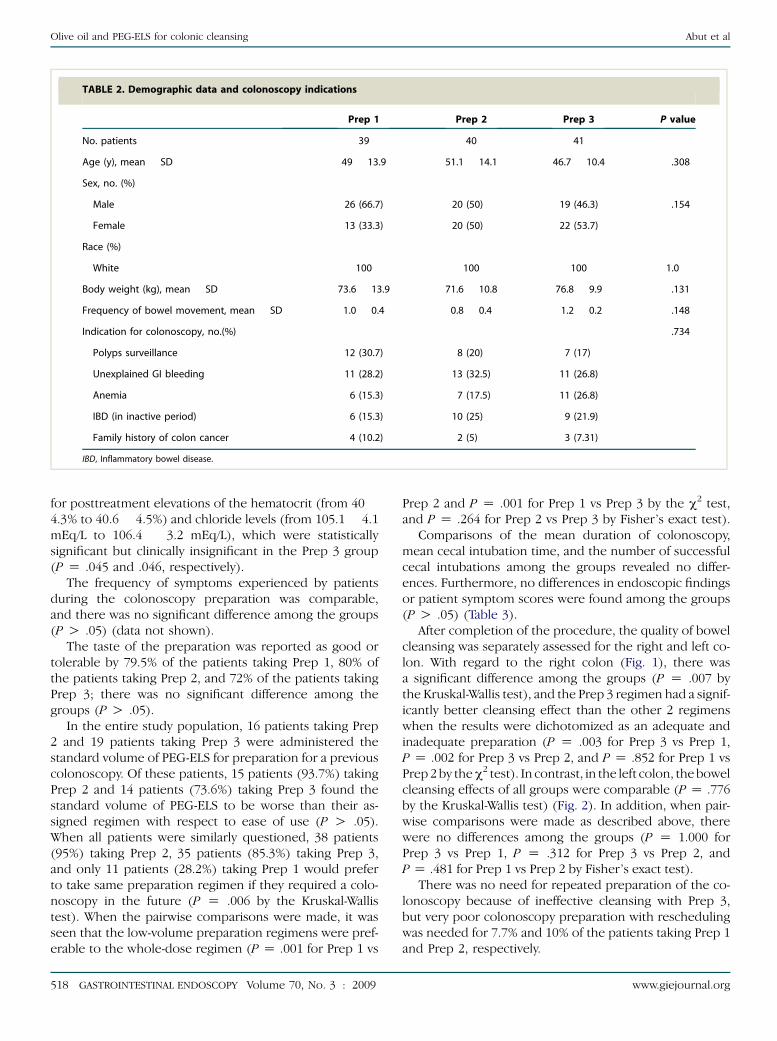
There were no significant differences among the 3preparation groups with respect to age, sex, race, bodyweight, frequency of bowel movements, or indicationsfor colonoscopy (Table 2). All patients completely con-sumed their assigned preparations.
There was no significant difference among the groupswith respect to changes in body weight (median, –1 kgin each group, P Z .555). Orthostatic hypotension wasnot reported in any patient during the pretreatment eval-uation or after the preparation. Hematological and bio-chemical changes during the colonoscopic preparationwere not different among the groups (P O .05), except
TABLE 1. Grading system for evaluation of colonoscopic
bowel cleansing
1. Excellent Small volume of clear liquid or O95%
of surface visible
2. Good Large volume of clear liquid covering
5%-25% of the surface but O90% of
the surface visible
3. Fair Some semisolid stool that could be suctioned
or washed away, but O90% of the surface
visible
4. Poor Semisolid stool that could not be suctioned
or washed away with !90% of the surface
visible
5. Very
poor
Repeated preparation needed
Volume 70, No. 3 : 2009 GASTROINTESTINAL ENDOSCOPY 517
Olive oil and PEG-ELS for colonic cleansing Abut et al
TABLE 2. Demographic data and colonoscopy indications
Prep 1 Prep 2 Prep 3 P value
No. patients 39 40 41
Age (y), mean � SD 49 � 13.9 51.1 � 14.1 46.7 � 10.4 .308
Sex, no. (%)
Male 26 (66.7) 20 (50) 19 (46.3) .154
Female 13 (33.3) 20 (50) 22 (53.7)
Race (%)
White 100 100 100 1.0
Body weight (kg), mean � SD 73.6 � 13.9 71.6 � 10.8 76.8 � 9.9 .131
Frequency of bowel movement, mean � SD 1.0 � 0.4 0.8 � 0.4 1.2 � 0.2 .148
Indication for colonoscopy, no.(%) .734
Polyps surveillance 12 (30.7) 8 (20) 7 (17)
Unexplained GI bleeding 11 (28.2) 13 (32.5) 11 (26.8)
Anemia 6 (15.3) 7 (17.5) 11 (26.8)
IBD (in inactive period) 6 (15.3) 10 (25) 9 (21.9)
Family history of colon cancer 4 (10.2) 2 (5) 3 (7.31)
IBD, Inflammatory bowel disease.
for posttreatment elevations of the hematocrit (from 40 �4.3% to 40.6 � 4.5%) and chloride levels (from 105.1 � 4.1mEq/L to 106.4 � 3.2 mEq/L), which were statisticallysignificant but clinically insignificant in the Prep 3 group(P Z .045 and .046, respectively).
The frequency of symptoms experienced by patientsduring the colonoscopy preparation was comparable,and there was no significant difference among the groups(P O .05) (data not shown).
The taste of the preparation was reported as good ortolerable by 79.5% of the patients taking Prep 1, 80% ofthe patients taking Prep 2, and 72% of the patients takingPrep 3; there was no significant difference among thegroups (P O .05).
In the entire study population, 16 patients taking Prep2 and 19 patients taking Prep 3 were administered thestandard volume of PEG-ELS for preparation for a previouscolonoscopy. Of these patients, 15 patients (93.7%) takingPrep 2 and 14 patients (73.6%) taking Prep 3 found thestandard volume of PEG-ELS to be worse than their as-signed regimen with respect to ease of use (P O .05).When all patients were similarly questioned, 38 patients(95%) taking Prep 2, 35 patients (85.3%) taking Prep 3,and only 11 patients (28.2%) taking Prep 1 would preferto take same preparation regimen if they required a colo-noscopy in the future (P Z .006 by the Kruskal-Wallistest). When the pairwise comparisons were made, it wasseen that the low-volume preparation regimens were pref-erable to the whole-dose regimen (P Z .001 for Prep 1 vs
518 GASTROINTESTINAL ENDOSCOPY Volume 70, No. 3 : 2009
Prep 2 and P Z .001 for Prep 1 vs Prep 3 by the c2 test,and P Z .264 for Prep 2 vs Prep 3 by Fisher’s exact test).
Comparisons of the mean duration of colonoscopy,mean cecal intubation time, and the number of successfulcecal intubations among the groups revealed no differ-ences. Furthermore, no differences in endoscopic findingsor patient symptom scores were found among the groups(P O .05) (Table 3).
After completion of the procedure, the quality of bowelcleansing was separately assessed for the right and left co-lon. With regard to the right colon (Fig. 1), there wasa significant difference among the groups (P Z .007 bythe Kruskal-Wallis test), and the Prep 3 regimen had a signif-icantly better cleansing effect than the other 2 regimenswhen the results were dichotomized as an adequate andinadequate preparation (P Z .003 for Prep 3 vs Prep 1,P Z .002 for Prep 3 vs Prep 2, and P Z .852 for Prep 1 vsPrep 2 by the c2 test). In contrast, in the left colon, the bowelcleansing effects of all groups were comparable (P Z .776by the Kruskal-Wallis test) (Fig. 2). In addition, when pair-wise comparisons were made as described above, therewere no differences among the groups (P Z 1.000 forPrep 3 vs Prep 1, P Z .312 for Prep 3 vs Prep 2, andP Z .481 for Prep 1 vs Prep 2 by Fisher’s exact test).
There was no need for repeated preparation of the co-lonoscopy because of ineffective cleansing with Prep 3,but very poor colonoscopy preparation with reschedulingwas needed for 7.7% and 10% of the patients taking Prep 1and Prep 2, respectively.
www.giejournal.org

Abut et al Olive oil and PEG-ELS for colonic cleansing
TABLE 3. Comparison of various parameters related to colonoscopic procedure
Prep 1 Prep 2 Prep 3 P value
Duration of colonoscopy (min), no. � SD 30.5 � 11.8 30.2 � 14.6 27.7 � 22 .711
Cecal intubation time (min), no. � SD 18.3 � 8.4 17.8 � 6.3 15.6 � 7.4 .661
Successful cecal intubation, no. (%) 37 (94.8) 38 (95) 40 (97.5) .742
Endoscopic findings, no. (%) .664
No mucosal lesions 17 (43.5) 19 (47.5) 14 (34.1)
Polyps 7 (17.9) 5 (12.5) 11 (26.8)
Diverticulosis 3 (7.6) 2 (5) 2 (4.8)
Colitis 8 (20.5) 12 (30) 8 (19.5)
Cancer 3 (7.6) 2 (5) 5 (12.1)
Others 1 (2.5) – 1 (2.4)
Patient symptom score (range, 0-15) 2.5 � 1.5 2.9 � 2 1.9 � 1.4 .129
DISCUSSION
Among the natural laxatives, olive oil is considered bysome to be the most commonly recommended, nonpre-scribed, natural medicine for chronic constipation in Euro-pean and other Mediterranean countries. In addition to itsculinary uses, it has been used for centuries as a laxative.In the medical literature, it was first recommended as a lax-ative for chronic constipation in the British Pharmaceuti-cal Codex at a dose of 15 to 30 mL/d in 1911.18
Although a detailed study of its laxative effect is not avail-able, it is generally thought that consumption of morethan 30 mL of olive oil on an empty stomach exceedsthe absorption capacity of the small intestine, which re-sults in the remainder of the oil passing to the colon.The olive oil acts as a lubricant; it coats the bowel wall
Figure 1. Endoscopic evaluation of the bowel-cleansing quality in the
right colon. Values are expressed as the percentage of patients. Prep 1,
4 L of PEG-ELS; Prep 2, 15 g of magnesium hydroxide followed by 2 L
PEG-ELS; Prep 3, 60 mL of olive oil followed by 2 L of PEG-ELS.
www.giejournal.org
and stool mass with a waterproof film that permits easierpassage through the colon and rectum. Therefore, oliveoil is predicted to enhance the bowel cleansing effect ofPEG-ELS.
In this study, we evaluated the effects of the various co-lon-cleansing regimens on the left and right colon sepa-rately instead of evaluating the colon as a whole becausewe believe that colon-cleansing difficulties are mainly ob-served on the right side of the colon. When the resultswere dichotomized as an adequate (excellent, good, andfair results pooled) or inadequate (poor and very poor re-sults pooled) preparation, the olive oil pretreatment regi-men resulted in a significantly more adequate cleansing inthe right side of the colon than the standard PEG-ELS andmagnesium hydroxide pretreatment regimens (97.6% vs74.5% and 72.5%, respectively, P Z .007). However, each
Figure 2. Endoscopic evaluation of the bowel-cleansing quality in the
left colon. Values are expressed as the percentage of patients. Prep 1, 4
L of PEG-ELS; Prep 2, 15 g of magnesium hydroxide followed by 2 L of
PEG-ELS; Prep 3, 60 mL of olive oil followed by 2 L of PEG-ELS.
Volume 70, No. 3 : 2009 GASTROINTESTINAL ENDOSCOPY 519

Olive oil and PEG-ELS for colonic cleansing Abut et al
regimen had comparable and acceptable effects on left co-lonic cleansing (91.5%, 85.5%, and 91.8% in Preps 1, 2, and3, respectively; P Z .776).
Although the split-dose PEG-ELS regimen has been shownto be superior to whole-dose PEG-ELS,19 we used the stan-dard whole-dose regimen (4 L of PEG-ELS) in our study be-cause the split-dose PEG-ELS regimen was not widelyaccepted for colonoscopy preparation when we plannedthis study. However, when the results of the regimens werecompared across studies, we observed that adequate or sat-isfactory right colonic cleansing was more frequent with theolive oil pretreatment regimen (97.5%) than with the split-dose PEG-ELS regimen (81.31%). However, a prospectivestudy is necessary to properly compare the effects of the oliveoil regimen and split dosing of PEG-ELS.
Adequate bowel cleansing, as expected, has a significantimpact on the detection of clinically significant lesions.2-4
In this study, it was shown that slightly more colonicpolyps were detected, especially in the right colon, inthe olive oil group than in the other groups, althoughthe differences were not significant. Adding olive oil toPEG-ELS may lead to more accurate diagnoses of coloniclesions and reduce the rescheduling of colonoscopies.However, this study had a relatively small sample size todefinitively consider these suggestions.
Patient acceptance and tolerability and the side effectsof the pretreatment regimens are very important factorsthat determine the optimal colon-cleansing approach.5-8
In this study, all preparation regimens were well toleratedand elicited equivalent symptom scores. The magnesiumhydroxide pretreatment regimen was the most preferredregimen with respect to taste, ease of use, nausea, andvomiting. However, because these differences did notreach statistical significance and given its less-adequatecleansing effect, we concluded that pretreatment withmagnesium hydroxide added to the low volume of PEG-ELS is not a suitable colonoscopy preparation regimen.This result is contrary to the findings of studies of magne-sium citrate. This difference can likely be attributed to theweaker laxative effect of magnesium hydroxide relative tomagnesium citrate.13,14 Importantly, the majority of pa-tients who had previously consumed the standard volumeof PEG-ELS in preparing for a previous colonoscopy fa-vored the low-volume preparations.
In summary, this study demonstrates that pretreatmentwith olive oil followed by a low volume of PEG-ELS en-hances both patient satisfaction and the quality of right-side colonic cleansing during colonoscopy preparationover the conventional volume of PEG-ELS. However, theadministration of magnesium hydroxide followed bya low volume of PEG-ELS does not produce a satisfactorycolonic cleansing. Based on our results, the olive oil regi-men is recommended, especially for patients who are notable to consume large volumes of liquids, such as the el-derly, and those who are suspected of having subtleright-side colonic lesions. Furthermore, the results of
520 GASTROINTESTINAL ENDOSCOPY Volume 70, No. 3 : 2009
this study suggest that the olive oil preparation regimenmay also be appropriate for patients who have chronicrenal failure or are hospitalized and generally havea more complicated and more difficult preparation forthe colonoscopy.
REFERENCES
1. Hirshowitz BI, Modlin IM. The history of endoscopy: the American per-
spective. In: Classen M, Tytgat GN, Lightdale CJ, editors. Gastroenter-
ological endoscopy. Stuttgart: Thieme; 2002. p. 2-16.
2. Davis GR, Santa Ana CA, Morawski SG, et al. Development of a lavage
solution associated with minimal water and electrolyte absorption or
secretion. Gastroenterology 1980;78:991-5.
3. Vanner SJ, MacDonald PH, Paterson WG, et al. A randomized pro-
spective trial comparing oral sodium phosphate with standard
polyethylene glycol-based lavage solution (Golytely) in the prepa-
ration of patients for colonoscopy. Am J Gastroenterol 1990;85:
422-7.
4. Aronchick CA, Lipshutz WH, Wright SH, et al. A novel tableted purga-
tive for colonoscopic preparation: efficacy and safety comparisons
with Colyte and Fleet Phospho-Soda. Gastrointest Endosc 2000;52:
346-52.
5. Pitcher DE, Ford RS, Nelson MT, et al. Fatal hypocalcemic, hyperphos-
phatemic, metabolic acidosis following sequential sodium phos-
phate–based enema administration. Gastrointest Endosc 1997;46:
266-8.
6. Shaoul R, Wolff R, Seligmann H, et al. Symptoms of hyperphosphate-
mia, hypocalcemia, and hypomagnesemia in an adolescent after the
oral administration of sodium phosphate in preparation for a colono-
scopy. Gastrointest Endosc 2001;53:650-2.
7. Lieberman DA, Ghormley J, Flora K. Effect of oral sodium phosphate
colon preparation on serum electrolytes in patients with normal se-
rum creatinine. Gastrointest Endosc 1996;43:467-9.
8. Barclay RL, Depew WT, Vanner SJ. Carbohydrate-electrolyte rehydra-
tion protects against intravascular volume contraction during colonic
cleansing with orally administered sodium phosphate. Gastrointest
Endosc 2002;56:633-8.
9. Brady CE 3rd, DiPalma JA, Pierson WP. Golytely lavagedis metoclopra-
mide necessary? Am J Gastroenterol 1985;80:180-4.
10. Martinek J, Hess J, Delarive J, et al. Cisapride does not improve preco-
lonoscopy bowel preparation with either sodium phosphate or
polyethylene glycol electrolyte lavage. Gastrointest Endosc 2001;54:
180-5.
11. Lazarczyk DA, Stein AD, Courval JM, et al. Controlled study of cisapr-
ide-assisted lavage preparatory to colonoscopy. Gastrointest Endosc
1998;48:44-8.
12. Reiser JR, Rosman AS, Rajendran SK, et al. The effects of cisapride on
the quality and tolerance of colonic lavage: a double-blind random-
ized study. Gastrointest Endosc 1995;41:481-4.
13. Abdul-Baki H, Hashash JG, ElHajj II, et al. A randomized, controlled,
double-blind trial of the adjunct use of tegaserod in whole-dose or
split-dose polyethylene glycol electrolyte solution for colonoscopy
preparation. Gastrointest Endosc 2008;68:294-300.
14. Sharma VK, Steinberg EN, Vasudeva R, et al. Randomized, controlled
study of pretreatment with magnesium citrate on the quality of colo-
noscopy preparation with polyethylene glycol electrolyte lavage solu-
tion. Gastrointest Endosc 1997;46:541-3.
15. Sharma VK, Chockalingham SK, Ugheoke EA, et al. Prospective,
randomized, controlled comparison of the use of polyethylene
glycol electrolyte lavage solution in four-liter versus two-liter
volumes and pretreatment with either magnesium citrate or bisa-
codyl for colonoscopy preparation. Gastrointest Endosc 1998;47:
167-71.
www.giejournal.org

Abut et al Olive oil and PEG-ELS for colonic cleansing
16. Afridi SA, Barthel JS, King PD, et al. Prospective, randomized trial com-
paring a new sodium phosphate-bisacodyl regimen with conventional
PEG-ES lavage for outpatient colonoscopy preparation. Gastrointest
Endosc 1995;41:485-9.
17. Berkelhammer C, Ekambaram A, Silva RG. Low-volume oral colono-
scopy bowel preparation: sodium phosphate and magnesium citrate.
Gastrointest Endosc 2002;56:89-94.
18. The British Pharmaceutical Codex: an imperial dispensatory for the use
of medical practitioners and pharmacists. London: The Pharmaceutical
Press; 1911.
19. El Sayed AM, Kanafani ZA, Mourad FH, et al. A randomized single-blind
trial of whole versus split-dose polyethylene glycol-electrolyte
www.giejournal.org
solution for colonoscopy preparation. Gastrointest Endosc 2003;58:
36-40.
Received July 30, 2008. Accepted January 5, 2009.
Current affiliations: Department of Gastroenterology (E.A., H.G., B.Y., A.T.I.,
T.K., A.R.D., O.O.K.), Haydarpasa Numune Training and Research Hospital,
Istanbul, Turkey, Department of Gastroenterology (C.B., F.F.B.), Faculty of
Medicine, Harran University, Sanliurfa, Turkey.
Reprint requests: Evren Abut, MD, Department of Gastroenterology,
Haydarpasa Numune Training and Research Hospital, Tibbiye Street,
34668, Selimiye/Istanbul, Turkey.
Volume 70, No. 3 : 2009 GASTROINTESTINAL ENDOSCOPY 521




















