ACUTE RENAL INSUFFICIENCY IS A CHALLENGING ...
48
LITHUANIAN UNIVERSITY OF HEALTH SCIENCE MEDICAL ACADEMY FACULTY OF NURSING DEPARTMENT OF NURSING AND CARE DILSON DAVIS ACUTE RENAL INSUFFICIENCY IS A CHALLENGING PROBLEM AFTER CARDIAC SURGERY The graduate thesis of the Master’s degree study program “Advanced Nursing Practice” (State Code 6211GX008) Tutor of graduate thesis, PhD MD, MildaŠvagždienė KAUNAS, 2019
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ACUTE RENAL INSUFFICIENCY IS A CHALLENGING ...

1
LITHUANIAN UNIVERSITY OF HEALTH SCIENCE
MEDICAL ACADEMY
FACULTY OF NURSING
DEPARTMENT OF NURSING AND CARE
DILSON DAVIS
ACUTE RENAL INSUFFICIENCY IS A CHALLENGING PROBLEM
AFTER CARDIAC SURGERY
The graduate thesis of the Master’s degree study program “Advanced Nursing Practice” (State
Code 6211GX008)
Tutor of graduate thesis,
PhD MD, MildaŠvagždienė
KAUNAS, 2019

2
TABLE OF CONTENTS
ABSTRACT.......................................................................................................3
ABBREVATIONS ..............................................................................................6
INTRODUCTION ............................................................................................. 7
1. REVIEW OF LITERATURE ............................................................................ 9
Main risk factors of renal failure after cardiac surgery .................................................. 9
Pathologic changes in renal failure after cardiac surgery .............................................. 11
Other events associated with CPB ............................................................................... 15
Strategies to reduce the risk of renal failure ................................................................. 20
2. OBJECTIVES ................................................................................................... 26
3. ORGANISATION & METHODOLOGY ......................................................... 26
4. DISCUSSION OF RESULTS ............................................................................ 27
5. CONCLUSION ................................................................................................. 37
6. PRACTICAL RECOMMENDATION .............................................................. 37
LIST OF SCIENTIFIC REPORTS PUBLICATIONS ....................................... 41
LIST OF LITERATURE RESOURCES ........................................................... 42
ANNEXS… ...................................................................................................... 46
DECLARATION OF THE AUTHOR’S CONTRIBUTION AND ACADEMIC
HONESTY

3
ABSTRACT
Dilson Davis. Acute renal insufficiency is a challenging problem after cardiac surgery. The graduate
Master’s thesis. The tutor - Dr. MildaŠvagždienėMD, Lithuanian University of Health
Sciences,Medical Academy, the Faculty of Nursing, Department of Nursing and Care. Kaunas, 2019.
48p.
Acute renal failure (ARF) refers to the abrupt loss of kidney function. There are many possible
causes of acute renal failure categorized into three major areas prerenal, intrarenal, and postrenal.
Acute kidney injury following major cardiovascular surgery has a complex and multifactorial etiology
which includes pre-operative renal insufficiency, advanced age, history of congestive heart failure,
diabetes mellitus, recent exposure to nephrotoxic agents such as contrast dye, intra-aortic balloon
pump, emergency operation, prolonged cardiopulmonary bypass (CPB) time, low urinary output during
CPB, and need for deep hypothermic circulatory arrest. The twentieth international consensus
conference of acute disease quality initiative group found that acute kidney injury is a common
perioperative complication for patients undergoing cardiovascular surgery. When renal failure after
cardiac surgery is severe enough to require renal replacement therapy, the mortality rate is close to
60%. The successful prevention and management of acute kidney injury involves identifying patients at
risk for acute kidney injury, recognizing subtle abnormalities in a timely manner, performing basic
clinical assessments and responding appropriately to the data obtained.
OBJECTIVES OF THE PRESENT STUDY:
1. To find the main risk factors of renal failure after cardiac surgery
2. To find the possibilities to reduce the risk of renal failure in the patient undergoing elective
cardiac surgery
3. Prepare a plan for reducing the risk of renal insufficiency in the patient undergoing elective
cardiac surgery.

4
MATERIALS AND METHODS:For this research, the literature search was conducted in the
PubMed, Medline updates from web sites, library data base, science direct and 30 literature sources
where reviewed. Studies published in English between 2009–2019 have been reviewed.
RESULTS:56 years old white male patient arrived for elective cardiac surgery due to coronary artery
disease. He complains for shortness of breath during physical activity. He was scheduled to elective
coronary artery bypass grafting surgery. The patient has history of chronic renal failure, chronic atrial
fibrillation. Preoperative heart ultrasound – Showed moderately reduced systolic LV function,
concentric LV hypertrophy, MV fibrocalcinosis, degenerative changes in leaflets, II-III degree MV
regurgitation, II degree TV regurgitation. Max. pressure in RV about 46 mmHg, moderately pulmonary
hypertension. Elective MV and TV reconstruction and coronary artery bypass grafting surgery was
performed under standard anesthesia.
Duration of cardiopulmonary bypass (CPB) was 172 min. Ao cross-clamping time – 99 min.
After the surgery the patient was hemodynamicallystabel and recovery of normal muscle tone
and consciousness the patient was safely extubated. Patient in sinus rhythm, breathing spontaneous
oxygen via the face mask 10–8–6 l/min, diuresis > 50–100 ml/hour. During the night period blood
gases showed respiratory acidosis due to increased pCO2 (up to 65 mmHg). Oxygen therapy was
changed to oxygen via nasal cannulas 5–6 l/min.On the second postoperative day the patient added to
his history the episodes of bronchospasms. During auscultation the wheeze was found and the
treatment was supplemented by inhalations of salbutamol. Blood gases were returning to normal
ranges, hypercapnia decreasing (48 mmHg), but there was still non lactic metabolic acidosis.
Laboratory exams revealed the increase in serum creatinine (310 mol/l) and urea . Blood pressure
remained within normal ranges, heart rate was sinus rhythm. Diuresis was adequate. The patient started
to drink clear fluids. Infusion therapy was still continued with crystalloid solutions at the rate of 150
ml/hour. On the third postoperative day the condition of the patient was gradually improving. He
started to eat solid food. He had mild respiratory failure, which was compensated by additional oxygen
via nasal cannulas (6 l/min). The blood gases remained within normal limits. The patient remained
haemodynamically stable, heart rate – normarythmic atrial fibrillation. As the patient had AF before the
surgery, the recovery of sinus rhythm was ineffective. Though diuresis was still adequate serum levels
of creatinine increased to 336mol/l. Metabolic non lactic acidosis was still persistent as well. In order to
maintain diuresis infusion therapy with crystalloids was still continued at the rate of 100 ml/hour. On
the fourth postoperative day serum creatinine levels started to decrease, ie 281mol/l, as well as

5
metabolic non lactic acidosis. And on the sixth postoperative day the patient was transferred to the
Department of Cardiac surgery for further treatment.
SUMMARY: Medical management measures like diuretic therapy, crystalloid administration, constant
monitoring and early prompt management is essential to prevent renal insufficiency after cardiac
surgery. A compassionate and knowledgeable and skilled nurse who cares for the patient after cardiac
surgery is an asset in the achievement of positive outcome for the patient and family.

6
ABBREVIATIONS
ARF : Acute renal failure
CPB : Cardio pulmonary bypass
MV : Mitral valve
TV : Tricuspid valve
RV : Right ventricle
AO : Aorta
CVP :Central venous pressure
RBC : Red blood cell corpuscles
ACEI :Angiotensin converting enzyme inhiitors
CVS : Cardiovascular surgery
RCRI : Revised cardiac risk index
ASA : American society of anesthesiologists
PACU : Post anesthesia care unit
NSAID : Non steroidalanti inflammatory drugs
ARB : Angiotensin receptor blocker
GFR : Glomerular filtration rate
VO2 : Minute volume of oxygen consumption
ATP : Adenosine triphosphate
ANP : Atrial natriuretic peptide
DA : Dopamine agonist
N-AC : N acetyl cysteine

7
INTRODUCTION
Cardiac surgery associated acute kidney injury is a common and serious postoperative
complication of cardiac surgery requiring cardiopulmonary bypass and it is the second most common
cause of acute kidney injury in intensive care unit[1]. Acute kidney injury following major
cardiovascular surgery has a complex and multifactorial etiology which includes pre-operative renal
insufficiency, advanced age, history of congestive heart failure, diabetes mellitus, recent exposure to
nephrotoxic agents such as contrast dye, intra-aortic balloon pump, emergency operation, prolonged
cardiopulmonary bypass (CPB) time, low urinary output during CPB, and need for deep hypothermic
circulatory arrest[2].
Renal perfusion is complex and highly regulated. Although 20 % of cardiac output perfuses the
kidneys, the majority of blood filtered by cortex glomeruli is shunted away from the vasa recta. This
shunt may help maintain the electrolyte and water concentration gradients in the renal medulla required
for tubule and collecting system reabsorption, but renders the renal medulla and corticomedullary
junction hypoxic relative to other tissues this may be a protective mechanism for oxidative injury but
increases susceptibility to ischemia. During surgery many factors alter renal perfusion, and tubules at
the corticomedullary junction and in the medulla are often damaged. Hence acute renal insufficiency
after cardiac surgery is a complex and frequent clinical problem[3].
The twentieth international consensus conference of acute disease quality initiative group found
that acute kidney injury is a common perioperative complication for patients undergoing cardiovascular
surgery [4].
The successful prevention and management of acute kidney injury involves identifying patients
at risk for acute kidney injury, recognizing subtle abnormalities in a timely manner, performing basic
clinical assessments and responding appropriately to the data obtained. Nurses are an important part of
the health care team. A compassionate and knowledgeable and skilled nurse who cares for the patient
after cardiac surgery is an asset in the achievement of positive outcome for the patient and family. With
the advancement of technology there is a continuous change in the diagnostic and treatment modalities.
The medical field is a dynamic field which goes under continuous research and application of those
findings in providing care. Few studies are found on the nursing care of patients undergoing cardiac

8
surgery though cardiothoracic nursing is a very important aspectnow days. It reflects the need to
investigate on the area of cardiovascular nursing to improve a patient’s outcome after cardiac surgery.
In this context the investigator would like to conduct a study to assess the main risk factors of
renal insufficiency and a perioperative plan to reduce the risk of renal insufficiency in the patient
undergoing elective cardiac surgery.
Definition of acute renal insufficiency: It is defined as the sudden loss of the ability of the kidneys to
excrete wastes, concentrates urine, conserve electrolytes and maintain fluid balance[5].
Cardiac surgery: cardiac surgery is any surgery done on the heart muscle, valves, arteries or the aorta
and other large arteries connected to the heart. In open heart surgery cardiopulmonary bypass machine
or octopus is used to take over the function of heart during surgery[5].

9
1. REVIEW OF LITERATURE
MAIN RISK FACTORS OF RENAL FAILURE AFTER CARDIAC
SURGERY
Investigator located studies from 2009-2019 and review articles from the Web of Science
databases, PubMed, Google Scholar, Medline, the Cochrane Library, Embase, and Science Citation
Index for articles written in English. RVarious perioperative risk factors for postoperative renal
dysfunction and failure have been identified. The important preoperative factors are advanced age,
anemia,history of congestive heart failure, emergency surgery, preoperative use of intra-aortic balloon
pump, preoperative renal insufficiency, elevated preoperative serum glucose and creatinine and recent
exposure to nephrotoxic agents such as contrast dye. Most important intraoperative risk factor is the
intraoperative haemodynamic instability, prolonged cardiopulmonary bypassand need for deep
hypothermic circulatory arrest. Causes of postoperative renal failure are low output syndrome, RBC
transfusion and postoperative infection [6].
A retrospective study evaluated 1056 patients undergoing cardiac surgery and identified the
major risk factors for renal failure were advanced age, postoperative use of ACEI, low left ventricular
ejection fraction, multiple organ dysfunction syndrome , reexploration and low CVP [7].
Recently published data suggest that perioperative BP lability influences both the risk of
postoperative renal dysfunction and 30-day mortality. Future studies will determine whether the use of
agents that allow improved BP control within a desirable range will reduce the incidence of
postoperative AKI in cardiac surgery patients [8].
Unusual from that impairment of renal function after cardiac surgery is uncommon without
preoperative renal impairment [9].
Studies revealed that many common factors contribute to the development of CVS‐AKI.
Hemodynamic perturbations such as exposure to cardiopulmonary bypass (CPB), cross‐clamping of the
aorta, high doses of exogenous vasopressors, and blood‐product transfusion all increase the risk
of AKI. Similarly, the mechanical factors outlined may be associated with renal perfusion injury
following episodes of ischemia, resulting in increased oxidative stress and associated inflammation as
well as embolic disease including cholesterol emboli, all of which increase the pathological burden on

10
the kidney. Other mechanisms such as neurohormonal activation are relevant, as is the generation of
free hemoglobin and the liberation of free iron perioperatively, all potentiating AKI. Associated tissue
damage is reflected in a systemic inflammatory response, and all these factors contribute to a
significant inflammatory response. Immune activation, the generation of reactive oxygen species, and
upregulation of proinflammatory transcription factors all play roles[10].
Traditionally, clinicians have referred to acute renal failure as a clinical situation that leads to a
decline in renal function such that nitrogenous waste accumulates in the circulation and manifests
as azotemia. changes in serum creatinine occur late in the development of AKI—typically 48 hours
after the initiating event (surgery in the case of cardiac surgery-associated AKI). An earlier diagnosis
would surely assist with treatment and, even in the absence of demonstrably effective therapies, would
at least permit avoidance of dehydration, excessive diuretic prescription, and other nephrotoxic
interventions.
Neutrophil Gelatinase-Associated LipocalinNGAL is a naturally occurring protein found in
tissue and circulating in very low concentrations in the plasma. In cardiac surgery-associated AKI, it
has been shown to be elevated very early after surgery (2 hours after cardiopulmonary bypass in some
reports), and both urinary and plasma assays are available [13]. The tests are available for clinical use
in Europe and will eventually also be available for use in North America. It is currently unclear which
test provides the best diagnostic performance for AKI, but there is some suggestion that the
combination of the two tests might be better than either alone. In general, urine is an attractive
proximal fluid for kidney biomarker discovery and development, because tubular proteins leaking from
damaged nephrons are concentrated, rather than diluted, as is the case in plasma. It is also probable that
plasma NGAL is a closer reflection of systemic inflammation than the extent of renal injury inflicted
[16]. It is certain that once introduced into clinical practice, observational studies of this novel test will
define its role in our diagnostic armory more clearly. In the meantime, it has great potential for use
in intervention trials as a way of enriching the study population for randomization of putative
interventions.
Kidney Injury Molecule 1 (KIM-1) is a transmembrane protein present in the renal proximal
tubule whose expression is markedly upregulated in response to acute ischemia or exposure to
nephrotoxins. Although several reports from noncardiac surgical patient populations have shown that
KIM-1 appears to be a very sensitive indicator of AKI [17], fewer cardiac surgery studies have been

11
published. In one study of 103 adult patients undergoing cardiopulmonary bypass, the KIM-1 levels
were significantly increased at both 2 and 24 hours after surgery in patients who subsequently
developed AKI [18]. In a recent review, KIM-1 was found to be a useful diagnostic assay for AKI after
cardiac surgery but was less sensitive for predicting the need for dialysis or death [19].
Cystatin C is a ―housekeeping‖ protein that is produced continuously by all nucleated cells.
Because it is freely filtered at the glomerulus, is completely reabsorbed by the proximal convoluted
tubule, and is not secreted, it has qualities that make it suitable for measuring the glomerular
filtration rate.Compared with serum creatinine, it is less affected by age, gender, and body weight. In
one prospective study, cystatin C and NGAL were measured in both the plasma and urine of 72 adults
undergoing cardiac surgery. Within the first 6 hours, neither of the plasma assays for cystatin C or
NGAL were predictive of AKI; however, the urinary values of both were elevated, suggesting that at
least for these two candidate biomarkers, the urinary testmight be superior to the plasma assay for the
early detection of AKI.
It is reported that age, emergency and high risk surgery, ischemic heart disease, congestive
heart disease, ASA physical status and RCRI score were considered risk factors for the development of
AKI, in patients needing intensive care after surgery. AKI has serious impact on PACU length of stay
and mortality. AKI was an independent risk factor for hospital mortality [11].
PATHOLOGIC CHANGES IN RENAL FAILURE AFTER CARDIAC
SURGERY
Clinically, the pathogenesis of ARF associated with CPB can be divided into preoperative,
intraoperative, and postoperative events. The sum of all of these various insults is ultimately reflected
in the development of tubular injury that when severe enough is manifested as a rise in serum
creatinine often associated with a decreased urine output.
Patients have had recent myocardial infarctions or severe valvular disease with reduced left
ventricular function and reduced renal perfusion. In the extreme, patients may be in cardiogenic shock
and require inotropic support or an intra-aortic balloon pump. This pre-existing prerenal state may be
exacerbated by the use of diuretics, nonsteroidal anti-inflammatory drugs (NSAID), angiotensin-
converting enzyme inhibitors (ACEI), or angiotensin receptor blockers (ARB), which impair the
autoregulation of renal blood flow. Furthermore, episodes of preoperative hypotension may lead to
sublethal endothelial injury, which may impair the production of vasodilatory substances such as

12
endothelial nitric oxide and promote vasoconstriction as a result of the release of endothelin,
catecholamines, and angiotensin II, promoting further tubular ischemia and injury [12]. Compounding
these factors may be a lack of renal functional reserve as a result of underlying chronic kidney disease,
including small- and large-vessel renovascular disease. These hemodynamic alterations in the
preoperative setting may increase the vulnerability of the kidney (particularly the inner stripe of the
outer medulla, where metabolic demands are high and the pO2 is between 10 and 20 mmHg) to any
further ischemic or nephrotoxic insult[13].
There may be activation of inflammatory mediators in the preoperative period that also serve to
prime the kidney for subsequent injury. Endotoxin levels have been noted to be elevated in some
patients in the preoperative period, despite no evidence of active infection, and these levels have been
correlated to postoperative myocardial dysfunction. The elevation in preoperative endotoxin levels may
reflect the effect of poor cardiac output states’ contributing to intestinal ischemia and bacterial
translocation or may be related to the preoperative care of patients (e.g., subclinical catheter infections).
Levels of TNF-α have also been shown to be elevated in patients with pre-existing congestive heart
failure and may also play a role in stimulation of the immune system[14].
Nephrotoxic medications or intravenous contrast that is given in the immediate preoperative
period may also lead to overt or occult tubular injury that can interact with other factors to lead to ARF.
These medications include vasoactive (pressor) drugs, NSAID, ACEI, ARB, and antibiotics.
Thus, the preoperative period is a critical time when events (hemodynamic, nephrotoxic, and
inflammatory) can occur and can lead to subtle renal injury that is not necessarily reflected by changes
in GFR. This subtle injury is likely substantiated by the fact that the preoperative risk scoring systems
all rely on factors that ultimately act to reduce renal perfusion, result in lack of renal functional reserve,
or set up a proinflammatory milieu[15].
Intraoperative Events
The intraoperative period is a critical time when patients are exposed to anesthesia and
cardiopulmonary bypass. These events lead to dramatic hemodynamic effects as well as activation of
both innate and adaptive immune responses that can initiate or extend renal injury.
CPB is associated with significant hemodynamic changes, and the maintenance of
cardiovascular stability during CPB requires interplay between the function of the CPB machine and
patient factors such as systemic vascular resistance, venous compliance, and autoregulatory capacity of

13
various vascular beds. The ultimate goal is to maintain regional perfusion at a level that supports
optimal cellular and organ function. Thus, any decrease in renal perfusion during CPB, depending on
its magnitude and duration, can lead to significant cellular injury.
Minute oxygen consumption (VO2) is the major determinant of blood flow requirements
normally and during CPB. Experimentally, CPB flow rates have been determined by calculating VO2 at
different perfusion rates. Perfusion is increased until VO2 reaches a plateau, after which further
increases in CPB flow rates do not lead to increases in oxygen consumption. In general, CPB flow rates
of 1.8 to 2.2 L/min per m2 are recommended on the basis of this analysis..
In addition to CPB flow rates, perfusion pressure during CPB is an important determinant of
adequate nutrient delivery to vascular beds. Perfusion pressure is determined by the interaction of
blood flow and overall arterial resistance. Resistance, in this case, is related to actual friction resistance
because of the steady, nonpulsatile nature of CPB, which negates the elastance, inertial, and reflective
components of arterial resistance during normal pulsatile flow . Friction resistance is primarily a
function of vasomotor tone and blood viscosity (which is further dependent on hematocrit and
temperature). Importantly, both variables are changing during CPB (e.g., blood viscosity increases as
hypothermia is induced and vasomotor tone is affected by anesthesia) and lead to associated changes in
perfusion pressure. In general, a mean perfusion pressure of 50 to 70 mmHg is maintained during CPB
Given hemodynamic goals of a mean perfusion pressure of 50 to 70 mmHg and CPB flow rates of 1.8
to 2.4 L/min per m2, it is not known what effect these goals have on renal perfusion and oxygen
delivery. The majority of studies on autoregulation of regional blood flow during CPB has focused on
the cerebral circulation and demonstrates preserved cerebral autoregulation with these parameters
Small studies have suggested that mean arterial pressures on CPB >70 mmHg lead to higher
intraoperative creatinine clearances but without a change in postoperative renal function as compared
with pressures between 50 and 60 mmHg. Thus, it is likely that renal perfusion and autoregulation are
also maintained as long as these hemodynamic goals are met. However, these values are likely near the
minimum blood flows that support normal organ function, and any perturbation may lead to ischemia
and cellular damage. Furthermore, the effect of these parameters in patients with impaired baseline
renal function is not known. In patients with pre-existing hypertension, the relationship between renal
blood flow and mean arterial pressure is shifted such that falls in BP that normally would not impair
renal perfusion now do so. This means that higher mean pressure may be required to maintain adequate
renal perfusion in these patients.Furthermore, if there is any degree of pre-existing acute tubular

14
necrosis, then autoregulatory capacity of the kidney may be lost and renal blood flow becomes linearly
dependent on pressure[16].
Whether alterations of these CPB flow and pressure goals would lead to improved renal
outcomes is not known. Gold et al. reported that maintenance of higher perfusion pressures in the
range of a mean perfusion pressure of 70 mmHg was associated with a reduced incidence of cardiac
and neurologic complications when compared with patients whose pressures were maintained at 50 to
60 mmHg. Renal function was not assessed in this study.
Other procedural factors that likely have an impact on renal hemodynamics include
hemodilution (oxygen delivery capacity), hypothermia (oxygen consumption), the absence of pulsatile
perfusion, and the use of crystalloid versus colloidal prime solutions. As discussed above, with the
exception of hemodilution, no deleterious effects on renal function have been found associated with
alterations in body temperature or in the absence of pulsatile flow.
In total, these hemodynamic changes may lead to regional renal ischemia and cellular injury
that could either initiate acute kidney injury (AKI) or extend pre-existing renal injury. Furthermore,
these hemodynamic changes are potentially modifiable[17].
Inflammation
CPB provokes a systemic inflammatory response syndrome, Contact of blood components with
the artificial surface of the bypass circuit, ischemia-reperfusion injury, endotoxemia, operative trauma,
nonpulsatile blood flow, and pre-existing left ventricular dysfunction all are possible causes of SIRS in
this setting. In its most severe form, a spectrum of injury that includes one or more of the following
clinical manifestations may be observed: Pulmonary, renal, gastrointestinal, central nervous system,
and myocardial dysfunction; coagulopathy; vasodilation and increased capillary permeability;
hemolysis; pyrexia; and increased susceptibility to infection[18].
Open heart surgery, as do many surgeries, induces a generalized state of inflammation during
and after surgery. Many heart surgeries require the use of a heart-lung machine, a machine that
circulates blood while surgery is performed on the heart, which compounds the inflammatory response.
Researchers at the Duke University Medical Center in a 2012 study reported evidence in an October
2012 "Heartwire" that this widespread inflammatory response can injure the kidneys, leading to kidney
failure.
During CPB, both neutrophils and vascular endothelium are activated with upregulation of
adhesion molecules such as CD11b and CD41. Platelets also undergo activation, degranulation, and

15
adherence to vascular endothelium. These events led to elaboration of cytotoxic oxygen-derived free
radicals, proteases, cytokines and chemokines. These inflammatory mediators, such as IL-6, IL-8, and
TNF-α, show a considerable rise in serum levels during CPB and generally reach peak levels 2 to 4 h
after termination of CPB[19].
CPB is also a potent activator of factor XII (Hageman factor) to factor XIIa. This process
initiates the intrinsic coagulation system, the kallikrein system, and the fibrinolytic system.
Furthermore, complement proteins are activated through both the classical and the alternative
pathways. Ultimately, this humoral response amplifies the cellular response that leads to neutrophil,
endothelial, and monocyte activation and further elaboration of proinflammatory cytokines. Finally,
diffuse end-organ ischemia likely causes endothelial cells, circulating monocytes, and tissue-fixed
macrophages to release cytokines and oxygen-derived free radicals that further drive the inflammatory
response[20].
The end result of this generalized inflammatory response induced by CPB within the kidney is
not known. It is interesting that animal models of renal ischemia-reperfusion injury have clearly
demonstrated the pathologic role of interstitial inflammation and the elaboration of proinflammatory
cytokines and reactive oxygen species in the production of tubular injury. This local inflammatory
response in experimental models is identical to that seen on a more global scale during CPB. Thus, it is
likely a safe assumption that CPB-induced inflammation has significant deleterious effects on the
kidney through similar mechanisms. Despite efforts to produce a CPB system that does not produce
contact activation of blood components, this goal has not been realized and CPB still remains a potent
proinflammatory stimulus [21].
OTHER EVENTS ASSOCIATED WITH CPB
Macroscopic and microscopic emboli, both gaseous and particulate, are often generated during
CPB. These emboli are temporally related to certain intraoperative events such as aortic cannulation
and aortic clamp placement and release. One study demonstrated a significant correlation between the
total number of Doppler-detected emboli and postoperative changes in serum creatinine[22]. This
suggests that embolic events to the renal circulation may be responsible in part for postoperative
changes in GFR.
Hypotension, or decreased blood pressure, is often seen during and after open heart surgery.
According to the Duke University Medical Center researchers, this decrease in blood pressure

16
decreases blood flow to the kidneys. Low kidney blood flow is a cause of acute renal failure and is one
of the most common causes of kidney failure after open heart surgery.
Patients undergoing open heart surgery, particularly a CABG, there is diffuse plaque buildup of
the major arteries including the aorta, the main artery supplying blood to the body. During surgery,
pieces of plaque, called emboli, can break off and travel to various organs, decreasing blood flow. A
John Hopkins University School of Medicine study published in the April 2013 issue of "Annals of
Thoracic Surgery" demonstrated that 48 percent of plaque emboli during open heart surgery lodged in
the kidneys. Such plaque emboli in the kidneys may lead to kidney failure and a need for dialysis.
Aprotinin is a serine protease inhibitor and potent antifibrinolytic agent that is used to attenuate
blood loss and transfusion requirements during CPB. Aprotinin is eliminated by glomerular filtration
and is actively reabsorbed by the proximal tubules, where it is metabolized .Aprotinin also inhibits the
production of renal kallikreins and kinins involved in vasodilatoryresponses.For these reasons, there
has been concern that the use of aprotinin may lead to renal injury. Several studies in patients who
underwent CPB, as well as liver transplantation, did not demonstrate any renal toxicity directly
attributable to aprotinin use[23].
CPB exposes blood to nonphysiologic surfaces and shear forces that lead to lysis of red blood
cells with release of free hemoglobin into the circulation. In the presence of oxidants such as hydrogen
peroxide and superoxide, free low molecular mass iron is released from the hemeinto the circulation.
This redox active iron is able to participate in organic and inorganic oxygen radical reactions, such as
stimulating lipid peroxidation and catalyzing the formation of damaging hydroxyl radicals with
subsequent tissue damage. Normally, iron-transporting proteins such as transferrin and lactoferrin
sequester this free iron and minimize its potential toxicity. In contradiction the release of free iron can
be so great as to saturate the iron-binding capacity of transferrin. At this point, all iron-binding
antioxidant capacity is lost and the serum displays pro-oxidant feature. Reperfusion injury during CPB
may exacerbate further the oxidant stress in the setting of free circulating iron[24].
Tuttle et al. could not find an association between low iron-binding capacity and the risk for
ARF after CPB. Although deferoxamine has been demonstrated to decrease the occurrence of lipid
peroxidation during CPB, no studies have investigated any protective role of iron chelation in human
kidney injury.
Postoperative Events
The postoperative events that are critical in affecting renal function are similar to traditional
causative mechanisms seen in the general intensive care setting. Thus, the use of vasoactive agents,

17
hemodynamic instability, exposure to nephrotoxic medications, volume depletion, and sepsis/SIRS all
are critical events that can lead to kidney injury. A critical factor is postoperative cardiac performance
and the need for either inotropic or mechanical support. In the presence of postoperative left ventricular
dysfunction, the risk for significant renal injury becomes very high as the vulnerable kidney is
subjected to marginal perfusion pressures[25].
The pathologic changes in the kidney of patients with ARF following OPCAB are largely assumed
to be due to acute tubular necrosis which is usually confirmed by granular casts in the urine. Hypoxia-
ischemia is the predominant cause of perioperative ARF and results from low renal blood flow due to a
reduced cardiac output; from regional factors reducing renal blood flow; or from disturbances
ofintrarenal blood flow related to inflammation, sepsis or toxin. It was demonstrated that the
transmembrane gradient for glomemlarultrafiltration was significantly diminished and there is a back-
leak of glornerularultrafiltrate across the injured epithelium. ARF begins with an early phase of
vasomotornephropathy in which there is associated alterations in vasoreactivity and renal perfusion
leading to prerenalazotaemia and eventually cellular ATP depletion26. These ultimately lead to
mitochondrial dysfunction and accumulation of intracellular sodium, calcium and reactive oxygen
species. Subsequently, multiple enzyme systems are activated and cause disruption of the cytoskeleton,
membrane damage, nucleic acid degradation and cell death. Vascular endothelial cell injury induces
vascular congestion, edema and infiltration of inflammatory cells. Furthermore, elaborations of inflam-
matory mediators lead to additional cellular injury.
An important cause of AKI in cardiac surgery is cellular ischemia, which results in tubular
epithelial and vascular endothelial injury and activation. Cardiac surgery heightens the risk of ischemic
kidney injury by several processes. Normally, kidney perfusion is autoregulated such that glomerular
filtration rate is maintained until the mean arterial blood pressure falls below 80 mm Hg. Mean arterial
blood pressure during cardiac surgery is often at the lower limits or below the limits of autoregulation,
especially during periods of hemodynamic instability. In addition, many cardiac surgery patients have
impaired autoregulation due to existing comorbidities (eg, advanced age, atherosclerosis, chronic
hypertension, or chronic kidney disease), administration of drugs that impact kidney autoregulation (eg,
nonsteroidalantiinflammatory drugs, ACE inhibitors, angiotensin receptor blockers, and radiocontrast
agents), or a proinflammatory state (see below). In patients with impaired autoregulation, kidney
function may deteriorate even when the mean arterial blood pressure is within the normal range.

18
Another process by which cardiac surgery may contribute to ischemic kidney injury is by inciting a
strong systemic inflammatory response. Proinflammatory events during cardiac surgery include
operative trauma, contact of the blood components with the artificial surface of the CPB circuit,
ischemia-reperfusion injury, and endotoxemia Inflammation plays a central role in the development of
ischemic kidney injury, and it is thought that the systemic inflammatory response caused by cardiac
surgery is similarly deleterious.
Perioperative anemia in cardiac surgery is independently associated with various adverse outcomes,
including kidney injury. Anemia may contribute to kidney injury by reducing renal oxygen delivery,
worsening oxidative stress, and impairing hemostasis.
Studies suggest that Intraoperative avoidance of the extremes of anaemia, especially during severe
hypotension and avoidance of transfusion in patients with haemoglobin levels >8 g/dL (>5 mmol/L)
may help decrease AKI in patients undergoing cardiac surgery and represent targets for future
controlled interventions [27].
All patients in both groups received similar standardized anaesthesia management with use of
propofol (1-2.5 mg/kg), remifentanil (1 mg/kg) bolus and infusion (0.4 μg/kg), and inhalational agents
during CPB.Mild or modarate hypothermia (240-340) was used in all cases. Prime solution was
contained 1100cc ringer lactate, 300cc mannitol, 100 mg unfractioned heparin, 250 mg
methylprednisolone.Non-pulsatile perfusion techniques were used and flow rates of perfusion were1.8,
2.0, 2.2 and 2.4 L/m2/min at 240C, 300C, 340C and 370C, respectively. Crystalloid and blood
cardiolegia were used for cardiac arrest. Dialysis administration criteria during CPB were based upon
the institutional protocol and experience including excessive fluid volume overload (central venous
pressure > 15 cmH2O), oliguria (urine output < 20 mL at the first hour of CPB), hyperkalemia (blood
potassium level > 5.5 meq/L) and prolonged CPB time (> 180 min).
Tissue oxygen delivery is directly related to arterial oxygen content, which is primarily dependent
on the hemoglobin concentration. Anemia would therefore decrease oxygen delivery to the kidneys,
especially to the vulnerable renal medulla, where the normal partial pressure of oxygen in the renal
tissue is very low. The adverse consequences of anemia are likely enhanced further during cardiac
surgery, during which, for reasons outlined earlier, the kidney is more prone to renal hypoperfusion.
During CPB, hemodilution is induced to decrease blood viscosity in the hope of improving regional
blood flow in the setting of hypoperfusion and hypothermia as well as limiting the need for blood

19
transfusion. The resulting increase in regional blood flow is thought to offset any risk of decreased
oxygen carrying capacity of the blood. However, two recent studies demonstrated that hemodilution
(down to hematocrits <25%) is associated with an increased risk for renal injury as measured by
changes in serum creatinine. This may be due to impairment of oxygen delivery to an already hypoxic
renal medulla or to alterations in systemic inflammatory mediators caused by regional ischemia.
Anemia may enhance renal oxidative stress, because RBCs serve important antioxidant
functions. Anemia impairs hemostasis because normal platelet function is dependent on the presence of
an adequate (but as yet undetermined) hemoglobin concentration. In cardiac surgery, during which
patients are already at increased risk for bleeding due to CPB-related hemostatic defects, the added
burden of anemia-induced platelet dysfunction may lead to excessive bleeding, which in turn may
necessitate multiple RBC transfusions and reexploration, both of which are associated with AKI.
RBC transfusion is to improve organ function by increasing tissue oxygen delivery, there is
increasing evidence that transfused RBCs may actually contribute to organ injury in susceptible
patients, likely because of changes that occur to RBCs during storage. During storage, RBCs become
less deformable, undergo ATP and 2,3-diphosphoglycerate depletion, lose their ability to generate
nitric oxide, have increased adhesiveness to vascular endothelium, release procoagulant phospholipids,
and accumulate proinflammatory molecules, as well as free iron and hemoglobin. As a result,
transfused stored RBCs may impair tissue oxygen delivery, promote a proinflammatory state,
exacerbate tissue oxidative stress, and activate leukocytes and the coagulation cascade. In susceptible
patients, such as those undergoing cardiac surgery, these changes can lead to organ dysfunction, with
the kidney seemingly at particularly high risk for injury[28].
Surgical reexploration after cardiac surgery is independently associated with various adverse
outcomes, including kidney injury. Although the mechanisms by which reexploration can cause kidney
injury have not been fully elucidated, it is likely a safe assumption that they involve exacerbation of
many of the factors outlined above, such as hemodynamic instability and operative trauma. Surgical
reexploration is also inextricably linked to both anemia and RBC transfusion, because the principal
reason for reexploration after cardiac surgery is coagulopathy (which is exacerbated by anemia), which
leads to excessive blood loss (and massive RBC transfusion).
It is evident that therapies aimed at mitigating preoperative anemia, perioperative red blood cell
transfusions, and surgical reexploration may offer protection against acute kidney injury[28].

20
Strategies to reduce the risk of renal failure in the patient undergoing elective
cardiac surgery
Variety pharmacological and non-pharmacological strategies be used to prevent AKI in patients
undergoing cardiac surgery.
PharmacologicInterventions
Prevention of postoperative renal dysfunction after OPCAB needs knowledge of identifyingthe
preoperative risk factors.The aim is to select patients who are at risk and then to adopt strategies that
would offer renal protection. Medications such as nonsteroidalantiinflammatory drugs (NSAIDs) and
other nephrotoxic agents should be discontinued.
Several studies demonstrate that withholding angiotensin‐converting enzyme inhibitors and
angiotensin receptor blockers in the preoperative period is associated with reduced incidence of AKI.
Correction of hypoalbuminemia (level of <4 g/dL) by exogenous albumin supplementation has been
shown to be renoprotective in off‐pump cardiac surgery.In contradiction it is reported that Early
postoperative use of ACEI/ARB or diuretics is associated with a lower incidence of AKI after cardiac
surgery with extracorporeal circulation in elderly patients[28].
Preventing significant hemodynarnic events which may insult the kidney and meticulous
postoperative care including optimizing ventricular function, aggressive control of serum glucose and
close monitoring of fluid and renal status, perioperative hydration and use ofhemodynamic monitoring
and inotropic is agents to optimize cardiac output are of important strategies.
Several drugs have been tried in attempting to reduce postoperative renal dysfunction with inconsistent
results. Loop diuretics increase renal cortical blood flow. Dopamine at low doses certainly interacts
with vascular dopaminergic receptors and stimulates diuresis and natriuresis. Fenoldopam, a selective
Dl receptor antagonist, has used in the prevention of contrast-induced nephropathy
Atria Natriuretic Peptide (ANP) increases natriuresis by increasing GFR as well as by
inhibiting sodium reabsorption by the medullary collecting duct.

21
N-acetylcysteine (NAC) has been shown to block oxidant stress on cardiac surgery patients and
may hold promise as aprotective measure. Although it has been used in the prevention of contrast-
induced nephropathy
The calcium channel blocker diltiazem has been evaluated as a renoprotective agent in cardiac
surgery due to its renal vasodialatory effects. Hyperglycemia is common in cardiac surgery and
increased serum glucose in pre orintraoperative period is independently known to cause ARF after
cardiac surgery. So it is important to control blood glucose levels.
Glycemic Control With Intravenous Insulin is essentialReabsorption of tubular glucose is an
active, energy-consuming process; thus, it is thought that reducing the metabolic burden in the tubules
by reducing the concentration of urinary glucose might preferentially affect intrarenal oxygen flux. A
randomized study of 1548 critically ill patients (63% of whom had undergone cardiac surgery) found a
lower incidence of renal replacement therapy and improved survival with intensive (target glucose 80–
110 mg/dL) compared with conventional (target 180–200 mg/dL) glycemic control [37].However, a
large clinical trial in Australia and New Zealand subsequently questioned the benefit of tight glycemic
control, suggesting no benefit compared with a less-aggressive glucose target.
Urinary Alkalinization has been suggested that cardiac surgery-associated AKI is in large part a
pigment nephropathy. Cold, nonpulsatile, extracorporeal circulation with passage
through suction catheters, oxygenators, bubble traps, and filters is certainly a good recipe
for hemolysis, and pink urine in the bladder catheter bag is indeed a familiar sight. Haase and
colleagues conducted a preliminary trial of urinary alkalinization in cardiac surgery patients at high risk
of AKI and showed that in patients randomized to a tonically equivalent dose of sodium
bicarbonate (compared with sodium chloride), the incidence of AKI was less in the bicarbonate group.
The urine of the bicarbonate patients was effectively alkalinized, which might have enhanced urinary
excretion of free filtered hemoglobin. However, it is also possible that avoiding a chloride load also has
beneficial effects on the kidney. A large follow-up trial is currently underway, the results of which are
eagerly awaited.
Renal Replacement TherapyRRT is generally a nephrologic business; however, in the rest of the
world, continuous RRT (eg, hemofiltration) is largely an intensive care unit treatment. This disconnect
has resulted because of nonclinical issues and represents an unfortunate development. Extracorporeal
therapywill attract an ever increasing presence in the modern intensive care unit, as the extracorporeal

22
philosophy leans more toward earlier, partial organ assist rather than later organ function replacement.
As such, all those involved in intensive care management will require a working knowledge of partial
cardiac assist, partial lung assist, partial liver assist, and partial kidney assist techniques. Although
continuous venovenous hemofiltration is a physiologically simple concept (it is just like a glomerulus),
it is important to consider the potential downside (ie, catheter placement complications, infection,
bleeding, metabolic disturbance, fluid shifts) before its initiation.However, it is important that this
technique becomes available to the wider intensive care unit community, just as ultrasonography has in
recent years. In surgical practice, especially, understanding of the benefits of a zero-weight gain
approach for perioperative medicine is increasing, and cardiac surgeons are well placed to lead the
trend toward the earlier use of continuous venovenous hemofiltration in their volume-overloaded
patients.
Research studies shows that elderly patients (above age 65) with underlying CKD
preoperatively may never regain kidney function following AKI and may require lifetime renal
replacement therapy. Identifying at-risk individuals and proactive early intervention to optimize
outcomes is extremely important. If AKI develops, proper daily modification of medication dosing and
avoidance of potentially nephrotoxic agents is mandatory. Likewise, restoration of hemodynamics
using inotropic and vasopressor agents as well as intra-aortic balloon when indicated should help
minimize the extent of AKI. Cautious volume replacement or the use of loop diuretics can be used
depending on the clinical setting. Early termination of ventilator support as well as sepsis prevention
(i.e., removing unnecessary lines, aggressive wound care) can favorably impact the course of AKI.
Proper nutrition to promote tissue repair and to secure immune competence is also an important part of
the overall treatment. Finally, timely initiation of HD or CVVHD to simultaneously correct fluid
overload and metabolic disarray should be initiated to prevent and manage acute kidney injury[14].
New pharmacologic agents currently under investigation include levosimendan, a novel calcium
sensitizer, with inotropic and vasodilatory effects that may offer protective effects in endotoxemic and
ischemia-reperfusion injury and ABT-719, a novel α-melanocyte-stimulating hormone analog (α-
MSH). A recent meta-analysis of 13 randomized trials involving 1345 patients undergoing cardiac
surgery noted that perioperative infusion of levosimendan reduced the incidence of AKI, RRT, length
of intensive care unit stay, and death. Alpha-MSH is an endogenous hormone that inhibits
inflammatory, cytotoxic, and apoptotic pathways, hence prevents renal injury caused by ischemia-

23
reperfusion-induced AKI. In addition, α-MSH has direct protective effects on the kidney, which may
result from stimulation of the melanocortin receptors in the outer renal medulla.
Non- pharmacological strategies
Perioperative.
Again, results in this area are contradictory. Intravenous contrast before surgery may increase the
incidence of AKI and has led to some recommendations for delaying surgery 24 to 72 hours after
contrast administration. Preoperative placement of an intra‐aortic balloon pump may prevent AKI and
reduce the incidence of RRT in high‐risk patients by improving perfusion and reducing endothelial
activation. Contrast media used for coronary angiography may result in a contrast-induced
nephropathy. It has been hypothesized that cardiac surgery in close succession to coronary angiography
may increase the risk of postoperative AKI. However, data from the existing literature are conflicting.
Acute kidney injury after cardiac surgery is a multifactorial event; surgery on the same day of
angiography significantly increases the risk of AKI, and limiting this practice results in a containment
of the postoperative AKI incidence[29].
Several studies suggest that cardiac surgery can be performed within 1 day of cardiovascular
catheterization and contrast administration without an increase in the incidence of postoperative AKI.
Recommendations to delay cardiac surgery for a specified period after contrast administration to reduce
the risk of postoperative AKI are premature[29].
Intraoperative.
Catheter manipulation in the thoracic and abdominal aorta may lead to renal artery
embolization, with aortic cross‐clamping proximal to the renal arteries associated with ischemia–
reperfusion injury, further aggravated by atheroemboli secondary to aortic manipulation. Aortic
clamping above bilateral renal arteries, adjunctive renal artery procedures, and left renal vein division
have been found to increase the incidence of AKI. Emboli protection devices may help preserve renal
function and prevent procedure‐related atheroembolism during endovascular renal interventions.
Transradial coronary angiography avoids catheter manipulation in the descending and abdominal aorta,
which, compounded by reduced bleeding, leads to less AKI than transfemoral angiography. Avoidance
of aortic manipulation (the ―no touch‖ technique) in OPCAB has been shown to decrease the risk of
postoperative stroke in several studies; however, its effect on AKI incidence remains controversial,
with some studies demonstrating lower incidence, but others failing to do so.

24
CSA-AKI patients had significantly longer aortic cross-clamp and cardiopulmonary bypass times.
Furthermore, CSA-AKI patients had higher hospital mortality (5.5% vs 1.5%, P<.001) and significantly
longer ICU and hospital stays. Independent risk factors for CSA-AKI were age, peripheral vascular
disease, hypertension, left ventricular ejection fraction, cardiopulmonary bypass time, and surgery on
the thoracic aorta. In conclusion, patients who develop CSA-AKI have a higher preoperative risk
profile, more complex surgery, and worse clinical outcomes[15].
One study of patients who underwent cardiac surgery found that more severe AKI was associated with
an increased risk of progression of chronic kidney disease stage. Studies in various clinical settings
found that patients with relatively small short-term changes in serum creatinine (s-Cr) levels had up to
a 4-fold increase in the long-term risk of ESRD.
In a recently published randomized, controlled trial, the risk of AKI and loss of renal function
was investigated after off-pump versus on-pump CABG. The authors found that off-pump surgery
reduced the risk of postoperative AKI but not loss of renal function at 1 year after surgery. In summary,
studies of various cohorts found an increased risk of ESRD in patients with AKI. To the best of our
knowledge, no previously reported studies investigated the relationship between AKI after CABG and
the risk of ESRD. This study used a large nationwide cohort of patients who underwent primary
isolated CABG to investigate the long-term risk of ESRD in patients who developed postoperative
AKI[17].
Moderate hypothermic circulatory arrest with antegrade cerebral perfusion during complex
aortic surgery has been embraced by an increasing number of surgical groups, with data suggesting that
this is not associated with an increased AKI risk. Conversely, hyperthermic perfusion during CPB,
defined as a cumulative time at >37°C, is associated with an increase in AKI incidence. In a study
achieving clinical equipoise through propensity score matching, duration of hyperthermic perfusion
was independently associated with severity of AKI, with a 51% increase in the incidence for every
10 minutes of hyperthermic perfusion. Cold renal perfusion has been suggested for pararenal
abdominal aorta aneurysm surgery to reduce the incidence of AKI associated with juxtarenal and
thoracoabdominal aortic operations.
Pulsatile perfusion provides surplus mechanical energy transmission to the vascular
endothelium. Its impact on clinical outcomes has been extensively studied in a variety of settings;
however, the data on renal outcomes are conflicting because of the lack of uniformity in pulsatility

25
delivery. A retrospective analysis showed pulsatile CPB conferred a renoprotective effect in higher risk
patients undergoing cardiac surgery. However, the contemporary use of implantable continuous‐flow
left ventricular assist devices challenges this concept. The improvement in the hemodynamic
environment provided by continuous‐flow left ventricular assist devices leads to better renal function in
heart failure patients, implying that the theoretical importance of pulsatility is superseded by increased
cardiac output.
Hemodilution during CPB is an independent risk factor for AKI in adult cardiac surgery, with
improved outcomes for cases in which significant hemodilution (hematocrit <24%) is avoided during
CPB Although lower hemoglobin (8.8 versus 13.1 g/dL) preoperatively and on arrival to the intensive
care unit has been associated with persistent AKI after cardiac surgery, transfusion of at least 2 U of
packed red blood cells has also been associated with higher incidence of CVS‐AKI. In 2 recent RCTs
in which patients were randomized to a liberal (Hg <9.5 g/dL) or restrictive (Hg <7.5 g/dL) transfusion
policy intraoperatively and postoperatively, there was no difference in postoperative outcomes
including AKI. Conventional ultrafiltration has been used to treat the hemodilutional effects of CPB
circuits. The risk of developing severe AKI depended on the type of cardiac surgical procedure. Thirty-
day mortality was associated with severe perioperative circulation impairment or bleeding, but overall
long-term mortality was additionally predicted by age, postoperative myocardial infarct, and
preoperative circulation status [15].
Postoperative.
Implementation of a ―KDIGO bundle of care‖—consisting of avoidance of nephrotoxic agents,
discontinuation of angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers for the
first 48 hours after surgery, close monitoring of renal function, avoidance of hyperglycemia for the first
72 hours after surgery, consideration of alternatives to radiocontrast agents, and close hemodynamic
monitoring using a prespecified algorithm—prevented CVS‐AKI in high‐risk patients defined as
biomarker positive. According KDIGO acute kidney injury is the presence of increase in serum
creatinine 0.3 mg/dL or more within 48 hours or increase in serum creatinine to 1.5 times or more than
base line data or urine volume less than 0.5 ml/kg/h for at least 6 hours[29].
Recent literature offers hope that understanding of the pathogenesis of AKI after cardiac
surgery continues to improve, new directions for the prevention and amelioration of AKI will emerge.
Approaches to the prevention of postoperative AKI include careful risk stratification of patients,

26
allowing adequate recovery following a prior AKI, consideration of less extensive surgical procedures,
avoidance of cardiopulmonary bypass, minimizing injury from radiocontrast dyes or other nephrotoxic
agents, and optimizing cardiovascular function and oxygen delivery. Early identification of AKI and
prompt, judicious application of RRT may also improve outcomes. Interest in pharmacologic
renoprotection is currently directed toward statins and sodium bicarbonate[30].
2. OBJECTIVES OF THE PRESENT STUDY :
1. To find the main risk factors of renal failure after cardiac surgery
2. To find the possibilities to reduce the risk of renal failure in the patient undergoing
elective cardiac surgery
3. Prepare a plan for reducing the risk of renal insufficiency in the patient undergoing
elective cardiac surgery.
3. ORGANISATION AND METHODOLOGY OF A RESEARCH
Qualitative research approach and case study method is used
56 years old white male patient arrived for elective cardiac surgery due to coronary artery
disease. He complains for shortness of breath during physical activity. He was scheduled to elective
coronary artery bypass grafting surgery. The patient has history of chronic renal failure, chronic atrial
fibrillation.
Preoperative heart ultrasound – Showed moderately reduced systolic LV function, concentric
LV hypertrophy, MV fibrocalcinosis, degenerative changes in leaflets, II-III degree MV regurgitation,
II degree TV regurgitation. Max. pressure in RV about 46 mmHg, moderately pulmonary hypertension.
Elective MV and TV reconstruction and coronary artery bypass grafting surgery was performed
under standard anesthesia.
Duration of cardiopulmonary bypass (CPB) was 172 min. Ao cross-clamping time – 99 min.
After the surgery the patient was hemodynamicallystable and recovery of normal muscle tone
and consciousness the patient was safely extubated. Patient in sinus rhythm, breathing spontaneous
oxygen via the face mask 10–8–6 l/min, diuresis > 50–100 ml/hour. During the night period blood
gases showed respiratory acidosis due to increased pCO2 (up to 65 mmHg). Oxygen therapy was
changed to oxygen via nasal cannulas 5–6 l/min.

27
On the second postoperative day the patient added to his history the episodes of
bronchospasms. During auscultation the wheeze was found and the treatment was supplemented by
inhalations of salbutamol. Blood gases were returning to normal ranges, hypercapnia decreasing (48
mmHg), but there was still non lactic metabolic acidosis. Laboratory exams revealed the increase in
serum creatinine (310 mol/l) and urea. Blood pressure remained within normal ranges, heart rate was
sinus rhythm. Diuresis was adequate. The patient started to drink clear fluids. Infusion therapy was still
continued with crystalloid solutions at the rate of 150 ml/hour.
On the third postoperative day the condition of the patient was gradually improving. He
started to eat solid food. He had mild respiratory failure, which was compensated by additional oxygen
via nasal cannulas (6 l/min). The blood gases remained within normal limits. The patient remained
haemodynamically stable, heart rate – normarythmic atrial fibrillation. As the patient had AF before the
surgery, the recovery of sinus rhythm was ineffective. Though diuresis was still adequate serum levels
of creatinine increased to 336mol/l. Metabolic non lactic acidosis was still persistent as well. In order to
maintain diuresis infusion therapy with crystalloids was still continued at the rate of 100 ml/hour[31].
On the fourth postoperative day serum creatinine levels started to decrease, ie 281mol/l, as
well as metabolic non lactic acidosis. And on the sixth postoperative day the patient was transferred to
the Department of Cardiac surgery for further treatment.
4. DISCUSSION OF THE RESULTS
Elective cardiac surgery is highly effective in reducing complications after cardiac surgery
especially in patients with advanced age and other co-morbidities. Acute renal insufficiency is a
challenging problem after cardiac surgery. Investigator report a case of patient arrived for elective
cardiac surgery due to coronary artery disease and also the patient has history of chronic renal failure
and diabetes mellitus. Thus it aids in high risk for surgery and prone to develop renal insufficiency after
cardiac surgery[31].
In patients who undergo cardiac surgery, identifying patients who are at high risk for ARF is
critically important. The risk of developing myocardial ischaemia and infarction has been shown to be
16 to 19 fold more in patients with renal failure than in patients without renal failure. Many clinicians
are reluctant to do coronary artery bypass grafting (CABG) in patients of CAD with CRF despite
favourable surgical results in several studies. Patients with CRF on chronic haemodialysis have several
physiologic abnormalities and pose a number of problems during and after cardiopulmonary bypass

28
(CPB) that could contribute to adverse operative outcome. These patients need special attention during
and after CPB for the ongoing problems in the balance of fluid and electrolytes, the maintenance of
adequate red cell mass, peri-operative bleeding diathesis and the timing and route of pre- and post-
operative dialysis[32].
The author present the successful management of a case of coronary artery disease with chronic
renal failure and diabetes mellitus underwent cardiac surgery. CPB procedure causes tremendous fluid
shifts in the different compartments of the body. In the absence of renal function, the ability of a patient
to tolerate CPB is markedly reduced. Thus patients with CRF undergoing CABG pose problems in the
management of fluid and electrolytes during and after CPB procedures.
Patients with CRF undergoing CPB have risk of developing intraoperative ischaemicviscus
associated with low flow state during CPB which may be exacerbated by atherosclerotic mesenteric
arteries in these patients (15). To avoid such complications in the case presented had a duration of
cardiopulmonary bypass (CPB) was 172 min. Ao cross-clamping time – 99 min.
Factors that alter renal blood flow and lead to prerenal azotemia should be identified and
corrected. Treatment of volume depletion and congestive heart failure before cardiac surgery will
increase cardiac output and renal perfusion. Perioperative hydration and the use of hemodynamic
monitoring and inotropic agents to optimize cardiac output may be necessary. It is unknown whether
intraoperative optimization of bypass flow, perfusion pressure, and oxygen delivery would affect the
subsequent development of AKI, although conceptually this would seem to be a reasonable goal.
Medications such as NSAID and other nephrotoxic agents should be discontinued. If radiographic
contrast is needed, then newer isosmolar contrast agents may be less toxicIn stable patients, cardiac
surgery should be postponed in patients with contrast-induced ARF. Avoided all the nephrotoxic agents
in the reported case.
They also have a number of chronic conditions including their inability to excrete certain
medications, bleeding diathesis secondary to coagulation defects and platelet dysfunction, and
susceptibility to infections that partly account for their increased operative morbidity and mortality.
Dialysis more than 24 hours before the CPB procedure to avoid haemodynamic instability that may
arise immediately after dialysis, whereas others recommend to have dialysis as close to the procedure

29
as possible to provide the most optimal fluid and electrolyte balance at the time of operation. Some
others advocate the use of intraoperative dialysis.
Dialysis was not performed in this case but after the surgery the patient was hemodynamically
stable and recovery of normal muscle tone and consciousness the patient was safely extubated. Patient
in sinus rhythm, breathing spontaneous oxygen via the face mask 10–8–6 l/min, diuresis > 50–100
ml/hour. During the night period blood gases showed respiratory acidosis due to increased pCO2 (up to
65 mmHg). Oxygen therapy was changed to oxygen via nasal cannulas 5–6 l/min.
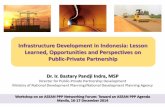
Laboratory exams revealed the increase in serum creatinine (310 mol/l) and urea. Blood
pressure remained within normal ranges, heart rate was sinus rhythm.

30
Serum Urea
25
20
15
Serum Urea
10
5
0
PRE OP POST OP
DAY 1
POST OP
DAY 2
POST OP
DAY 3
POST OP
DAY 4
POST OP
DAY 5
POST OP
DAY 6
Fig. 1: Above figure shows the trend of serum urea from preoperative to sixth postoperative day. From
the fourth postop day serum urea level decreased

31
Serum Creatinine 400
350
300
250
200
Serum Creatinine
150
100
50
0
PRE OP POST OP
DAY 1
POST OP
DAY 2
POST OP
DAY 3
POST OP
DAY 4
POST OP
DAY 5
POST OP
DAY 6
Fig. 2: Above figure shows the trend of serum creatinine from preoperative to sixth postoperative day.
From the third postop day serum creatinine level decreased
Diuresis was adequate. The patient started to drink clear fluids. Infusion therapy was still
continued with crystalloid solutions at the rate of 150 ml/hour.

32
250
200
150
100
post op day 0
POST OP DAY 1
POST OP DAY 2
50
0
Ph pco2 po2 Hco3 LACTATE
Fig. 3: Above figure shows the trend of ABG reports from Postop day zero to two postoperative day.
From the second postop day ABG values returned to normal
On the third postoperative day the condition of the patient was gradually improving. He started
to eat solid food. He had mild respiratory failure, which was compensated by additional oxygen via
nasal cannulas (6 l/min). The blood gases remained within normal limits. The patient remained
haemodynamically stable, heart rate – normarythmic atrial fibrillation. As the patient had AF before the
surgery, the recovery of sinus rhythm was ineffective. Though diuresis was still adequate serum levels
of creatinine increased to 336mol/l. Metabolic non lactic acidosis was still persistent as well. In order to
maintain diuresis infusion therapy with crystalloids was still continued at the rate of 100 ml/hour.
ABG REPORT

33
Drugs that Increase Renal Blood Flow
In low doses (3 μg/kg per min), dopamine stimulates DA-1 and DA-2 dopamine receptors,
increasing renal blood flow and inhibiting proximal tubule sodium reabsorption. Although dopamine
has been used extensively, studies have failed to show its efficacy in ARF after cardiac surgery or
associated with other conditions. Thus, there is no role for the use of dopamine in the treatment or
prevention of ARF[31].
Fenoldopam is a selective DA-1 agonist that has been used in the prevention of ARF with
variable results. In patients who had chronic kidney disease and underwent cardiac angiography,
fenoldopam failed to reduce renal dysfunction, 30-d morality, dialysis, or rehospitalization. However,
small randomized or uncontrolled studies that used fenoldopam demonstrated a reduction of renal
dysfunction in patients who underwent cardiac surgery. A potential complication is the associated
systemic hypotension that occurs after administration of fenoldopam. The beneficial effect of renal
vasodilation in this situation may be offset by systemic hypotension that results in an overall net
reduction of blood flow to the kidney. This systemic hypotensive effect may be abrogated by local
infusion of fenoldopam directly into the renal arteries using a novel vascular delivery system.
Theophylline, a nonselective adenosine antagonist, is thought to block vasoconstriction induced by A1-
adenosine receptors. In a recent clinical trial, theophylline infusion in CPB was ineffective in reducing
the incidence of ARF.
Drugs that Induce Natriuresis
Atrial natriuretic peptide (ANP) increases natriuresis by increasing GFR as well as by inhibiting
sodium reabsorption by the medullary collecting duct. In a multicenter trial, anaritide, a 25–amino acid
synthetic form of ANP was administered to critically ill patients to treat acute tubular necrosis.
Whether patients received anaritide or not, the dialysis-free survival was the same in both groups.
Although a subgroup of oliguric patients benefited from anaritide in the original study, this observation
was not confirmed in a follow-up study. Hypotension was a complicating factor in 46% of patients who
received anaritide. In a recent study, recombinant human ANP (rhANP) was used to treat ARF after
cardiac surgery in patients who required inotropic support for heart failure. In patients who received
rhANP, there was a significant reduction in the incidence of dialysis at day 21 after the start of
treatment. In this trial, ANP was infused at a lower rate (50 as opposed to 200 ng/kg per min; thus
lowering the incidence of hypotension) and for a more prolonged period than previous studies. These
changes may explain the benefit seen in this study as opposed to earlier ones[32].

34
Diuretics may reduce the severity of ARF by preventing tubule obstruction and decreasing oxygen
consumption. In a double-blind, randomized, controlled trial, furosemide treatment was found not to be
protective as the incidence of ARF was twice that of the dopamine or placebo.
Mannitol has a variety of effects, including the production of an osmotic diuresis with a
reduction of tubular obstruction, as well as the capability of scavenging free radicals. It is often added
to the prime solution during CPB, with the thought that it may help to maintain urine output during the
procedure, minimize tissue edema, and serve as a free radical scavenger. An early study in children
who underwent cardiac surgery demonstrated than prophylactic administration of mannitol (0.5 g/kg
body wt) was beneficial in the prevention of ARF. Fisher et al. demonstrated that mannitol added to
the CPB prime solution was effective at maintaining urine output at varying doses. In fact, Carcoana et
al. (147) showed an increased urinary excretion of β-2 microglobulin in patients who received mannitol
and dopamine, suggestive of increased tubular injury in this group.
Sirivella et al. randomly assigned 100 patients with postoperative oliguric or anuric renal failure
to therapy with either intermittent doses of loop diuretics or a continuous infusion of mannitol,
furosemide, and dopamine (2 mg/kg per min). Whereas 90% of patients who received the intermittent
diuretic required dialysis, only 6.7% of the patients who received the continuous mannitol, furosemide,
and dopamine infusion required dialysis. Furthermore, early therapy with this ―cocktail‖ was associated
with early restoration of renal function.
Drugs that Block Inflammation
Inflammation is well documented to occur during CPB and has a prominent role in the
pathogenesis of ARF and CPB. It thus is an attractive therapeutic target. Pentoxifylline, a
phosphodiesterase inhibitor, blocks the activation of neutrophils by TNF-α and IL-1 (149) and TNF-α
release by inflammatory cells. Pentoxifylline has been demonstrated to reduce cardiac dysfunction and
TNF-α release in ischemia-reperfusion models. However, pentoxifylline did not affect renal function in
elderly patients who underwent cardiac surgery. Dexamethasone also failed to protect against renal
dysfunction after cardiac surgery. A recent study examined the effect of blocking complement
activation in patients who underwent CPB. A single-chain antibody specific for human C5
(pexelizumab) was found to block complement activation and postoperative myocardial injury[33].
N-acetylcysteine (N-AC) has been shown to block inflammation and oxidant stress in cardiac
surgery patients and thus may hold promise as a simple, nontoxic protective measure. N-AC has not
been used in a prospective clinical trial that examines renal outcomes. N-AC has been studied most

35
extensively in the prevention of radiocontrast-induced nephropathy. In this area, the utility of N-AC has
been questioned with the publication of a meta-analysis of 16 controlled studies that demonstrated no
protective benefit.
Other Strategies
The sympathetic nervous system is activated during and after cardiac surgery and may lead to
impairment of renal function through a hemodynamic mechanism. Clonidine (an α-2 agonist) has been
used to attenuate these effects, with improvement in hemodynamic stability during CPB. In a study of
48 normal-risk patients who underwent cardiac surgery, preoperative treatment with clonidine
prevented the deterioration of renal function in this small trial, with creatinine clearances significantly
higher in the clonidine-treated group 24 h after CPB.
Diltiazem has been used in clinical trials to prevent ARF after cardiothoracic surgery. Diltiazem
has been shown to inhibit some of the inflammatory effects of CPB and is often used to prevent
vasospasm of radial grafts. Although diltiazem reduced urinary excretion of markers of tubule injury (α
glutathione s-transferase and N-acetyl-β-glucosaminidase) .its effectiveness in the prevention of renal
dysfunction was inconsistent.
In patients who were at highest risk for AKI, prophylactic hemodialysis has been attempted. In
a single study, 44 patients with a baseline serum creatinine >2.5 mg/dl were randomly assigned to
either perioperative prophylactic dialysis or dialysis only when postoperative ARF that required the
procedure was indicated (control). In the group that received prophylactic dialysis, mortality was
versus 30.4% in the control group35. Furthermore, postoperative ARF that required dialysis was
reduced from 34.8% in the control group to 4.8% in the intervention arm. These results will
have to be repeated in other randomized, controlled studies before this invasive approach can be
broadly recommended.
Treatment options for AKI have focused on attenuating ischemia, reducing intrarenal
inflammation, and supportive care. Nutrition is an important component of perioperative care and
should not be neglected. Malnourished patients with AKI have an increased risk of mortality. Goals to
provide 20–30 kcal/kg/day in patients with any stage of AKI should be met with either parenteral or
enteral feeding. If AKI is severe enough to require RRT, higher caloric intake via protein
supplementation may be necessary. Glycemic control is also indicated in patients developing AKI.
Maintaining a glucose concentration ≤ 150 mg/dl is an appropriate target, while avoiding hypoglycemia
(≤80 mg/dl).

36
In severe AKI, RRT is frequently required to treat hyperkalemia, remove excess fluid, treat
uremia, or reverse acidosis. Clinical trials of early versus late initiation of RRT in cardiac surgery
patients with severe AKI suggest early RRT may lower mortality and shorten the ICU length of stay. In
one study, early RRT was associated with lower mortality (51.5 versus 77.9 %, P = 0.001) and
decreased time on the ventilator (12.8 versus 18.9 days, P = 0.03) .Studies of dialysis dose, frequency,
and modality (continuous versus intermittent) have also failed to demonstrate a consistent benefit of
one technique versus another. The undisputed benefit of continuous versus intermittent RRT is
hemodynamic stability, but otherwise, if a patient meets dialysis criteria (i.e., electrolyte abnormality,
acidosis, uremic sequelae, or volume overload), modality does not appear to affect outcomes.
Mesenchymal stem cells (MSCs) possess anti-inflammatory and immunoregulatory characteristics that
promote cell survival and tissue repair, and therefore present an attractive potential treatment for AKI.
Bleeding and blood transfusion are central issues in cardiac surgical medicine and can account
for up to 50% of the blood products prescribed and delivered in some institutions. It is known
that anemia is a risk factor for AKI; however, so is the transfusion of stored blood [27]. Whether the
adverse effects of transfused stored blood that were reported in studies using nonleucodepleted
blood28 will be reproduced in studies using leucodepleted blood is unclear. Antifibrinolytics have been
associated with the development of AKI [29] and also with the absence of increased risk [30]. The
currently available antifibrinolytic drugs appear not to carry any extra risk of AKI.
Adequate hydration reduces the risk that a patient will develop AKI [22]. Typically, in
postoperative cardiac surgery patients, the problem is that of too much extracellular fluid rather than
too little, such that dehydration is less of a problem. Hypovolemia, however, is a different issue and
requires aggressive correction if end-organ perfusion (and thus function) is to be preserved. Although
in normal volunteers, the kidney has been shown to autoregulate its blood flow within a mean arterial
pressure range of 60 to 120 mm Hg, it is not known whether this is also the case in patients who have
recently been exposed to a period of hypothermic, nonpulsatile perfusion. However, the benefits of
maintaining a cardiac index greater than 2 l ∙ min−1 ∙ m−2 in the immediate postoperative period are
widely appreciated in cardiac surgical intensive care units [23], and uncorrected gross hypovolemia is
thus uncommon. There has recently been a suggestion that synthetic colloids based on starches might
be nephrotoxic [24]. It is important to realize, however, that that study used a second-generation starch
product in an unbalanced crystalloid carrier. Therefore, these data are not generalizable to
contemporary North American practice. It is clear that stroke volume optimization in high-risk general

37
surgery patients reduces the length of stay[25], and data have suggested this might also be the case in
heart surgery [26].
The present case is managed with infusion therapy and constant monitoring of lab values and its
corrections. It is as follows on the second postoperative day the patient added to his history the
episodes of bronchospasms. During auscultation the wheeze was found and the treatment was
supplemented by inhalations of salbutamol[34]. Blood gases were returning to normal ranges,
hypercapnia decreasing (48 mmHg), but there was still non lactic metabolic acidosis. Laboratory exams
revealed the increase in serum creatinine (310 mol/l) and urea. Blood pressure remained within normal
ranges, heart rate was sinus rhythm. Diuresis was adequate. The patient started to drink clear fluids.
Infusion therapy was still continued with crystalloid solutions at the rate of 150 ml/hour.
On the fourth postoperative day serum creatinine levels started to decrease, ie 281mol/l, as
well as metabolic non lactic acidosis. And on the sixth postoperative day the patient was transferred to
the Department of Cardiac surgery for further treatment[35].
Hence, CAD patients with CRF who was supposed to be at high risk for cardiac surgery under
CPB could be successfully managed by infusion therapy and correction abnormal lab values.
5. CONCLUSION
AKI after cardiac surgery is common, although most often mild. The development of any AKI
remains a major predictor of adverse outcomes, including progression of CKD. Effective prevention
and treatment strategies for AKI after cardiac surgery may be on the horizon, and the discovery,
validation, and adaptation of biomarkers of nephron damage may accelerate their development as well
as shorten the time for diagnosis. For now, efforts to reduce AKI following cardiac surgery and its
influence on patient morbidity are confined to hemodynamic manipulations, close attention to
intravenous resuscitation strategies including goal-directed therapy and balanced-salt fluid
administration, reduced exposure to CPB, and the identification and mitigation of modifiable risk
factors.
6. PRACTICAL RECOMMENDATIONS TO PREVENT ACUTE
KIDNEY INJURY AFTER CARDIAC SURGERY
Health care personnels has a major role in preventing and treating renal insufficiency after
cardiac surgery.

38
DOCTORS
• Identification of high-risk patients, optimization of renal perfusion and avoidance of
nephrotoxins, pharmacologic interventions to prevent AKI after cardiac surgery includes drugs
that increase renal blood flow, drugs that induce natriuresis, drugs that block inflammation and
other strategies like constant monitoring and prompt management prevents acute kidney injury
after cardiac surgery.
• When prevention fails, a prompt diagnosis of AKI is required to allow physicians to implement
the few strategies that are known to improve renal function. The diagnosis of AKI typically
includes the use of serum creatinine (SCr) concentrations and urine output. Urine output is
relatively nonspecific, and increases in SCr concentration require several days, extending the
time to diagnose AKI and initiate treatment. Measurement of urinary markers of kidney damage
may provide a more rapid diagnosis, although candidate biomarkers require further validation
before clinicians will incorporate them into routine patient care and expert groups implement
them into AKI diagnostic criteria
• Researchers believe physicians should focus extra attention on helping to prevent renal failure
for bypass patients and identifying patients at high risk for developing renal failure, as
preventing renal failure might help improve patient outcomes.
ANAESTHETIST
This includes assessing cardiac and overall health risks, identifying issues that could cause problems
during and after surgery, working with the cardiologist and cardiac surgeon to optimize medical
conditions, developing an anesthetic care plan, educating the patient regarding anesthetic care, and
alleviating patient anxiety. Intraoperative anesthetic management for cardiac surgical procedures (eg,
coronary artery bypass grafting [CABG] and cardiac valve surgery) is discussed separately.
(See "Anesthesia for coronary artery bypass grafting surgery" and "Anesthesia for cardiac valve surgery".)
GOALS OF THE PREANESTHESIA EVALUATION
During the preoperative consultation, the anesthesiologist will:
● Review the patient's history, physical examination, and available cardiac and other diagnostic
tests to assess risks for the proposed operation, and then develop an anesthetic plan to minimize
risks.

39
● Discuss opportunities to optimize the patient's preoperative condition with the cardiologist and
cardiac surgeon. As a general rule, surgery should be postponed if all of the following criteria are
met: the surgery is elective, the patient's medical condition can be significantly improved, and the
risk of postponing surgery is less than the benefit of optimizing the patient's condition.
● Explain the proposed anesthetic plan to the patient and obtain informed consent for anesthetic
care. Answer all questions related to perioperative anesthetic care.
NURSE PRACTITIONER
• This is an exciting time to be in perioperative nephrology, and showing practitioners ability to
identify an enriched at-risk population clinically and further stratify them with the use of new
biomarkers makes cardiac surgery-associated AKI a particularly attractive domain
for intervention trials.
STAFF NURSE
• Early detection of complications helps to reduce hospital admission by improving the quality of
life of the patients after cardiac surgery.
• Nurses have a major role in preventive aspects than the curative aspect. Nurses should do the
preoperative assessment of renal parameters and should remind the other health team members
regarding the risk factors that helps to adopt preventive measures for renal insufficiency before
during and after cardiac surgery.
• Preoperative management of patients with chronic kidney disease can be challenging. A number
of factors, including preoperative assessment, fluid and electrolyte issues, bleeding, and dialysis
issues, must be considered simultaneously to decrease morbidity and mortality related to
surgery.
NURSING EDUCATOR
• Nurse educator can help the student nurses to update their knowledge on preoperative and
postoperative assessment to identify renal injury as early with recent advancement and evidence
based practice.
• This study serves as a reference material for students in the library.
NURSING ADMINISTRATOR
• The nurse administrator can influences the staff nurses to incorporate various measures to
prevent renal injury after cardiac surgery.

40
• Nurse leader can preoperative risk assessment for renal injury after cardiac surgery protocol
to the hospital policy for short term teaching programme.
• Most nurses do not hold enough knowledge on early identification of AKI, therefore, there
is a need for developing and applying qualification programs with the aim of improving
competences and skills for preventing and identifying early kidney injury.
NURSING RESEARCHER
• In nursing there is scarce literature and research done on acute renal insufficiency after
cardiac surgery.
• Research should be conducted to assess the risk factors and measures to be adopted inorder
to prevent renal failure after cardiac surgery.
• Study helps to enhance the body of knowledge in nursing.
• Study serves as a reference material and good source of related literature for future
investigators.

41
LIST OF SCIENTIFIC REPORTS PUBLICATIONS
Dilson Davis, MildaŠvagždienė, acute renal insufficiency is a challenging problem after cardiac
surgery. 2019-Nurses Avoice to lead-health for all, Kaunas (Lithuania). Abstract is accepted for oral
presentation.

42
LIST OF LITERATURE SOURCES
1. Mao H, Katz N, Ariyanon W, Blanca-Martos L, Adýbelli Z, Giuliani A, Danesi TH, Kim
JC, Nayak A, Neri M, Virzi GM, Brocca A, Scalzotto E, Salvador L, Ronco C. Cardiac surgery-
associated acute kidney injury. Blood Purif. 2014;37Suppl 2:34-50. doi: 10.1159/000361062.
Epub 2014 Jul 31. Available from https://www.ncbi.nlm.nih.gov/pubmed/25196567.
2. Lewis, Heitkemper, Dirksen, O’Brien, Bucher. Medical surgical nursing.7thed. Missouri:
Mosby Elsevier publication; 2009. p. 1136-97.
3. Adabag A, Ishani A, Bloomfield H, Ngo A, Wilt T. Efficacy of N-acetylcysteine in preventing
renal injury after heart surgery: a systematic review of randomized trials. European Heart
Journal. 2009;30(15):1910-1917.
4. Kasper, Braunwald, Fauci, Hauser, Longo, Jameson. Et al. Harrisons Principles of internal
medicine. Vol II.16th ed. Combo: McGraw Hill medical publishing division; 2005. p. 1644-63.
5. Aydin SI, Seiden HS, Blaufox AD, Parnell VA, Choudhury T, Punnoose A, Schneider J, Acute
kidney injury after surgery for congenital heart disease. Annals Of Thoracic Surgery. 2012
Nov;94(5):1589-95. Available from https://www.ncbi.nlm.nih.gov/pubmed/22884599.
6. Juan Jose Olivero, Juan Jorge Olivero, Peter Tuan Nguyen, and Anna Kagan, Acute Kidney
Injury after Cardiovascular Surgery: An Overview.Methodist Debakey Cardiovasc J. 2012 Jul-
Sep; 8(3): 31–36. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3487575/
7. Che M, Li Y, Liang X, Xie B, Xue S, Qian J, Ni Z et.al. Nephron Clinical Practice
. 2011;117(4):c305-11. Available from https://www.ncbi.nlm.nih.gov/pubmed/20861652
8. Weir MR1, Aronson S, Avery EG, Pollack CV JrAcute kidney injury following cardiac surgery:
role of perioperative blood pressure control. Am J Nephrol. 2011;33(5):438-52. doi:
10.1159/000327601. Epub 2011 Apr 21. Available from :
https://www.ncbi.nlm.nih.gov/pubmed/21508632
9. Kowalik MM1, Lango R, Klajbor K, Musiał-Światkiewicz V, Kołaczkowska M, Pawlaczyk
R, Rogowski J. Incidence- and mortality-related risk factors of acute kidney injury requiring
hemofiltration treatment in patients undergoing cardiac surgery: a single-center 6-year
experience. Journal of Cardiothorac Vascular Anesthesia. 2011 Aug;25(4):619-24. Available
from : https://www.ncbi.nlm.nih.gov/pubmed/21354827

43
10. Hashemzadeh K1, Hashemzadeh S, Dehdilani M, Risk factors and outcomes of acute renal
failure after open cardiac surgery. Asian Cardiovasc Thorac Ann. 2012 Jun;20(3):275-80.
Available from .https://www.ncbi.nlm.nih.gov/pubmed/22718715
11. Ranucci M1, Ballotta A, Agnelli B, Frigiola A, Menicanti L, Castelvecchio S. Acute kidney
injury in patients undergoing cardiac surgery and coronary angiography on the same day. Ann
Thorac Surg. 2013 Feb;95(2):513-9. doi: 10.1016/j.athoracsur.2012.09.012. Epub 2012 Nov 30.
Available from .https://www.ncbi.nlm.nih.gov/pubmed/23201106
12. D'Onofrio A1, Cruz D, Bolgan I, Auriemma S, Cresce GD, Fabbri A, Ronco C. RIFLE criteria
for cardiac surgery-associated acute kidney injury: risk factors and outcomes. Congest Heart
Fail. 2010 Jul;16Suppl 1:S32-6. doi: 10.1111/j.1751-7133.2010.00170.x. Available from
.https://www.ncbi.nlm.nih.gov/pubmed/20653709
13. Haase M1, Bellomo R, Story D, Letis A, Klemz K, Matalanis G, Seevanayagam S, Dragun
D, Seeliger E, Mertens PR, Haase-Fielitz A. Effect of mean arterial pressure, haemoglobin and
blood transfusion during cardiopulmonary bypass on post-operative acute kidney injury.
Nephrol Dial Transplant. 2012 Jan;27(1):153-60. doi: 10.1093/ndt/gfr275. Epub 2011 Jun 15.
Available from : https://www.ncbi.nlm.nih.gov/pubmed/21677302
14. Coleman MD1, Shaefi S, Sladen RN. Preventing acute kidney injury after cardiac surgery. Curr
Opin Anaesthesiol. 2011 Feb;24(1):70-6. doi: 10.1097/ACO.0b013e3283422ebc. Available
from : https://www.ncbi.nlm.nih.gov/pubmed/21157303
15. Karkouti K, Wijeysundera DN, Yau TM, Callum JL, Cheng DC, Crowther M, Dupuis JY,et.al
Acute kidney injury after cardiac surgery: focus on modifiable risk factors. Circulation. 2009
Feb 3;119(4):495-502. doi: 10.1161/CIRCULATIONAHA.108.786913. Epub 2009 Jan 19.
Available from : https://www.ncbi.nlm.nih.gov/pubmed/19153273
16. Abelha FJ1, Botelho M, Fernandes V, Barros H. Determinants of postoperative acute kidney
injury. Crit Care. 2009;13(3):R79. doi: 10.1186/cc7894. Epub 2009 May 22. Available from :
https://www.ncbi.nlm.nih.gov/pubmed/19463152
17. Hu PH1, Chen YH, Liang XL, Li RZ, Li ZL, Jiang F, Shi W. Effect of early postoperative use
of ACEI/ARB or diuretics on the incidence of acute kidney injury after cardiac surgery in
elderly patients. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013 Jul;25(7):394-8. doi:
10.3760/cma.j.issn.2095-4352.2013.06.003. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/23834935

44
18. McIlroy DR, Epi MC, Argenziano M, Farkas D, Umann T. Acute kidney injury after cardiac
surgery: does the time interval from contrast administration to surgery matter?J Cardiothorac
Vasc Anesth. 2012 Oct;26(5):804-12. doi: 10.1053/j.jvca.2012.02.013. Epub 2012 Apr 21.
Available from: https://www.ncbi.nlm.nih.gov/pubmed/22521404
19. Ashita J. Tolwani. A Patient with AKI after Cardiac Surgery. CJASN August 2014, 9 (8) 1470-
1478; DOI: https://doi.org/10.2215/CJN.10461013. Available from :
https://cjasn.asnjournals.org/content/9/8/1470
20. Mitchell H. Rosner and Mark D. Okusa. Acute Kidney Injury Associated with Cardiac Surgery
CJASN January 2009, 1 (1) 19-32; Available from : https://cjasn.asnjournals.org/content/1/1/19
21. Hu Y, Li Z, Chen J, Shen C, Song Y, Zhong Q: The effect of the time interval between
coronary angiography and on-pump cardiac surgery on risk of postoperative acute kidney
injury: A meta-analysis. J CardiothoracSurg 8: 178, 2013CrossRefPubMedGoogle Scholar
22. Mehta RH, Honeycutt E, Patel UD, Lopes RD, Williams JB, Shaw LK, O’Brien SM, Califf
RM, Hughes GC, Sketch MH Jr..: Relationship of the time interval between cardiac
catheterization and elective coronary artery bypass surgery with postprocedural acute kidney
injury. Circulation 124[Suppl]: S149–S155, 2011Abstract/FREE Full TextGoogle Scholar
23. Ko B, Garcia S, Mithani S, Tholakanahalli V, Adabag S: Risk of acute kidney injury in patients
who undergo coronary angiography and cardiac surgery in close succession. Eur Heart J 33:
2065–2070, 2012Abstract/FREE Full TextGoogle Scholar
24. Prowle JR, Calzavacca P, Licari E, Ligabo EV, Echeverri JE, Haase M, Haase-Fielitz A,
Bagshaw SM, Devarajan P, Bellomo R: Pilot double-blind, randomized controlled trial of short-
term atorvastatin for prevention of acute kidney injury after cardiac surgery. Nephrology
(Carlton) 17: 215–224, 2012CrossRefPubMedGoogle Scholar
25. Mithani S, Kuskowski M, Slinin Y, Ishani A, McFalls E, Adabag S: Dose-dependent effect of
statins on the incidence of acute kidney injury after cardiac surgery. Ann ThoracSurg 91: 520–
525, 2011CrossRefPubMedGoogle Scholar
26. Layton JB, Kshirsagar AV, Simpson RJ Jr.., Pate V, Jonsson Funk M, Stürmer T, Brookhart
MA: Effect of statin use on acute kidney injury risk following coronary artery bypass grafting.
Am J Cardiol 111: 823–828, 2013CrossRefPubMedGoogle Scholar
27. Singh I, Rajagopalan S, Srinivasan A, Achuthan S, Dhamija P, Hota D, Chakrabarti A:
Preoperative statin therapy is associated with lower requirement of renal replacement therapy in

45
patients undergoing cardiac surgery: A meta-analysis of observational studies. Interact
CardiovascThoracSurg 17: 345–352, 2013Abstract/FREE Full TextGoogle Scholar
28. Billings FT, Pretorius M, Schildcrout JS, Mercaldo ND, Byrne JG, Ikizler TA, et al. Obesity
and oxidative stress predict AKI after cardiac surgery. J Am SocNephrol. 2012;23(7):1221–8.
doi: 10.1681/ASN.2011090940. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
29. Ricksten SE, Bragadottir G, Redfors B. Renal oxygenation in clinical acute kidney injury. Crit
Care. 2013;17(2):221. doi: 10.1186/cc12530. [PMC free article] [PubMed] [CrossRef] [Google
Scholar]
30. Granata A, Insalaco M, Di Pietro F, Di Rosa S, Romano G, Scuderi R. Atheroembolism renal
disease: diagnosis and etiologic factors. Clin Ter. 2012;163(4):313–22. [PubMed] [Google
Scholar]
31. Sreedharan RDP, Van Why S. Pathogenesis of acute renal failure. Pediatric Nephrology 2009.
Heidleberg: Springer-Verlag; pp. 1579–1602.
32. Fleming GA, Billings FT, Klein TM, Bichell DP, Christian KG, Pretorius M. Angiotensin-
converting enzyme inhibition alters the inflammatory and fibrinolytic response to
cardiopulmonary bypass in children. PediatrCrit Care Med. 2011;12(5):532–8. doi:
10.1097/PCC.0b013e3181fe3925
33. Meersch M, Schmidt C, Van Aken H, Martens S, Rossaint J, Singbartl K, Gorlich D, Kellum
JA, Zarbock A. Urinary TIMP‐2 and IGFBP7 as early biomarkers of acute kidney injury and
renal recovery following cardiac surgery. PLoS One. 2014; 9:e93460.
34. Murray PT, Mehta RL, Shaw A, Ronco C, Endre Z, Kellum JA, Chawla LS, Cruz D, Ince C,
Okusa MD; ADQI 10 workgroup . Potential use of biomarkers in acute kidney injury: report
and summary of recommendations from the 10th Acute Dialysis Quality Initiative consensus
conference. Kidney Int. 2014; 85:513–521.
35. Vijayan A, Faubel S, Askenazi DJ, Cerda J, Fissell WH, Heung M, Humphreys BD, Koyner JL,
Liu KD, Mour G, Nolin TD, Bihorac A; American Society of Nephrology Acute Kidney Injury
Advisory G . Clinical use of the urine biomarker [TIMP‐2] x [IGFBP7] for acute kidney injury
risk assessment. Am J Kidney Dis. 2016; 68:19–28.