Acute Effects of Passive Smoking on Peripheral Vascular Function
11
Guy Berkenboom and Philippe van de Borne Jean-François Argacha, Dionysios Adamopoulos, Marko Gujic, David Fontaine, Nadia Amyai, Acute Effects of Passive Smoking on Peripheral Vascular Function Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2008 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Hypertension doi: 10.1161/HYPERTENSIONAHA.107.104059 2008;51:1506-1511; originally published online April 7, 2008; Hypertension. http://hyper.ahajournals.org/content/51/6/1506 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://hyper.ahajournals.org/content/suppl/2008/04/07/HYPERTENSIONAHA.107.104059.DC1.html Data Supplement (unedited) at: http://hyper.ahajournals.org//subscriptions/ is online at: Hypertension Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer this process is available in the click Request Permissions in the middle column of the Web page under Services. Further information about Office. Once the online version of the published article for which permission is being requested is located, can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Hypertension in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on December 13, 2013 http://hyper.ahajournals.org/ Downloaded from by guest on December 13, 2013 http://hyper.ahajournals.org/ Downloaded from by guest on December 13, 2013 http://hyper.ahajournals.org/ Downloaded from by guest on December 13, 2013 http://hyper.ahajournals.org/ Downloaded from by guest on December 13, 2013 http://hyper.ahajournals.org/ Downloaded from by guest on December 13, 2013 http://hyper.ahajournals.org/ Downloaded from
Transcript of Acute Effects of Passive Smoking on Peripheral Vascular Function
Guy Berkenboom and Philippe van de BorneJean-François Argacha, Dionysios Adamopoulos, Marko Gujic, David Fontaine, Nadia Amyai,
Acute Effects of Passive Smoking on Peripheral Vascular Function
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2008 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/HYPERTENSIONAHA.107.1040592008;51:1506-1511; originally published online April 7, 2008;Hypertension.
http://hyper.ahajournals.org/content/51/6/1506World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org/content/suppl/2008/04/07/HYPERTENSIONAHA.107.104059.DC1.htmlData Supplement (unedited) at:
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from

Acute Effects of Passive Smoking on PeripheralVascular Function
Jean-Francois Argacha, Dionysios Adamopoulos, Marko Gujic, David Fontaine, Nadia Amyai,Guy Berkenboom, Philippe van de Borne
Abstract—Environmental tobacco smoke (ETS) acutely affects peripheral and coronary vascular tone. Whether ETS exertsspecific deleterious effects on aortic wave reflection through nicotine exposure, whether they persist after ETS cessation,and whether the smoke environment impairs microvascular function and increases asymmetrical dimethyl-argininelevels are not known. We tested these hypotheses in a randomized, crossover study design in 11 healthy malenonsmokers. The effects of 1 hour of exposure to ETS, as compared with a nontobacco smoke and normal air, onaugmentation index corrected for heart rate and skin microvascular hyperemia to local heating were examined.Augmentation index increased both during (P�0.01) and after (P�0.01) the ETS session but remained unchanged inthe nontobacco smoke session when compared with normal air. Nicotine levels after the exposure were related to thepeak rise in augmentation index (r�0.84; P�0.01), denoting a predominant role of nicotine in ETS vascular effects.This was confirmed in a second set of experiments (n�14), where the sublingual administration of nicotine wasassociated with an acute impairment in wave reflection as compared with placebo (P�0.001). Both ETS and nontobaccosmokes increased plasma asymmetrical dimethyl-arginine levels (P�0.001), but only ETS reduced the late rise in skinblood flow in response to heating (P�0.03). In conclusion, passive smoking specifically increases aortic wave reflectionthrough a nicotine-dependent pathway and impairs microvascular function, even after the end of the exposure. However,both tobacco and nontobacco passive smoking inhalation increase plasma asymmetrical dimethyl-arginine levels.(Hypertension. 2008;51:1506-1511.)
Key Words: passive smoking � nicotine � endothelium � wave reflection � nitric oxide
Exposure to environmental tobacco smoke (ETS) has beenrecognized recently as a strong contributor to cardiovas-
cular mortality, accounting for �50 000 deaths annually inthe United States.1 In recent years, extensive research haselucidated many aspects of the long-term ETS-related ad-verse effects on the cardiovascular system.1 However, the useof normal air inhalation as a control limits the interpretationof the physiopathological processes underlying the acutecardiovascular toxicity of ETS.2–4 Whether lung irritationand/or the stress provoked by smoke inhalation generate anonspecific cardiovascular reaction5 and whether this canexplain the effect of ETS2–4 are not known. We, therefore,decided to test the hypothesis that the vascular effects of ETScannot simply be ascribed to a nonspecific reaction to smoke.This would provide further clear-cut evidence that ETS exertsspecific deleterious cardiovascular effects beyond those ofsmoke pollution.
To further prove the specificity of the toxic effects of ETS,our second new hypothesis was that the deleterious vasculareffects of ETS would be related to the rise in plasma nicotinelevels. The above-mentioned studies2–4 did not determine
plasma nicotine. The role of nicotine in the changes in aorticwave reflection to ETS2,4 can be suspected from the estab-lished sympathoexcitatory effects of nicotine in active smok-ers6 but has not been demonstrated previously to ourknowledge.
Third, previous human studies on the acute effects ofpassive smoking have considered only the cardiovascularresponse during the acute smoke exposure.2,4,7 However, ETSexposure is an intermittent phenomenon, and it is unknownwhether the acute deleterious effects of ETS persist after thesmoke exposure. We tested the new hypothesis that thenegative effects of ETS persist during periods where subjectsagain breathe normal air. This would reveal that the toxicityof ETS exposure is underestimated when only the duration ofthe acute exposure is taken into account.
Fourth, the effects of ETS and nontobacco smoke onmicrovascular function are unknown in humans. BecauseETS exposure induces endothelial dysfunction of large con-ductance arteries,7,8 we also assessed the effects of ETS onmicrovascular function by evaluating the skin hyperemicresponse to heating.
Received October 29, 2007; first decision November 20, 2007; revision accepted March 13, 2008.From the Department of Cardiology, Erasme Hospital (J.-F.A., D.A., M.G., N.A., G.B., P.v.d.B.), and Laboratory of Pharmacology and Physiology
(D.F.), Universite Libre de Bruxelles, Brussels, Belgium.The first 2 authors contributed equally to the study.Correspondence to Jean-Francois Argacha, Department of Cardiology, Erasme Hospital, 808 Lennik St, 1070 Brussels, Belgium. E-mail [email protected]© 2008 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.107.104059
1506
Vascular Mechanisms
by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from

Finally, several in vitro studies have emphasized theadverse effects of chronic cigarette smoke exposure onendothelial NO bioavailability, particularly through a com-petitive inhibition of NO synthase by asymmetrical dimethyl-arginine (ADMA).6,9,10 Effects of nontobacco smoke onADMA levels are unknown and were compared with those ofETS in our study. We believed that this was important toprovide a broader understanding of the effects of smokeexposure on the endothelial arginine metabolism.
Materials and MethodsSubjectsTwenty-five healthy male subjects with normal physical examinationwho were on no medication were enrolled in the study. All werenonsmokers, and they were not regularly exposed to ETS. Theethical committee approved the study protocol, and informed writtenconsent was obtained from each subject.
Study Design
Passive Smoking ProtocolDuring 3 sessions at 1-week intervals, 11 healthy male subjects(mean age: 24.6�3 years; body mass index: 22.5�2.1 kg/m2) wererandomly exposed for 1 hour to sidestream tobacco smoke, side-stream nontobacco smoke, and normal air. We used a randomized,single-blinded, placebo-controlled, crossover study design with iden-tical air particle densities during ETS and nontobacco smokeexposure. All of the measurements were performed in a quiet roomwith the subject resting, but not sleeping, in the supine position undercarefully standardized conditions. All of the subjects abstained frommeals, alcohol, and coffee beverages for 12 hours before each studyperiod. Subjects were excluded from the experiment if they had usednonsteroidal antiinflammatory drugs for �3 days before each visit.
After a resting period of 20 minutes, subjects were exposed to thetested smoke or air for 1 hour. We used sidestream smoke fromcommercial cigarettes (Lucky-Strike; nicotine: 0.8 mg; tar: 10.0 mg)for tobacco smoke and herbal cigarettes (NTB, Arkopharma; nico-tine: 5.0 �g; tar: 3.0 mg) for nontobacco smoke. Standardized smokeexposure conditions were achieved by placing a hermetic Plexiglasbox of 0.1 m3 over the head of the subject. For the duration of theexperiment, the box was ventilated by a motorized system composedof 2 separate tubes (input and output) ensuring a constant airflowthrough the box. Subjects breathed through a low-resistance mouth-piece with a nose clip to ensure exclusive mouth breathing. Expiredgases were brought out of the box through a nonrebreathing valve.Eyes were protected by glasses that were delicately placed on theeyes to avoid any pressure to the ocular globes. A total of 6 cigaretteswere lit in the input tube, 1 every 10 minutes for 1 hour, to allow aprogressive infusion of the sidestream smoke inside the box. Duringthe normal air session, the same protocol was applied with asimulation of a lighting cigarette every 10 minutes.
Nicotine ProtocolTo assess the role played by nicotine in aortic wave reflectionchanges produced by passive smoking, a separate group of 14 malehealthy subjects (mean age: 24�1 years; body mass index: 24�0.5kg/m2) were randomly exposed to a 2-mg nicotine sublingual tablet(Nicorette microtab, nicotine betadex, Pfizer) or to a placebo tablet,using a randomized, double-blind crossover study design. Similarexperimental conditions than those of the passive smoke protocolwere applied.
Measures
Aortic Wave Reflection AssessmentAortic wave reflection was assessed noninvasively in all of thesubjects at baseline, at 10-minute intervals during the 60 minutes ofsmoke exposure, and 20 minutes after smoke cessation, using a fullyautomated and validated, commercially available system (Sphygmo-
Cor, Atcor Medical). This technique has been described in detailpreviously.11
The augmentation index (AIx; 100� augmentation pressure/pulsepressure) represents the pressure boost that is induced by the returnof the reflected waves to the aorta, expressed as a percentage of thepulse pressure. Higher values of AIx indicate an earlier return of thereflected wave to the aorta, either because of decreased aorticcompliance or because of increased peripheral resistance. The aorticpressure waveform depends on the ventricular ejection time, which isproportionally associated with cardiac cycle duration.12 Conse-quently, the change in AIx may be masked or overestimated whenthere are concomitant alterations in HR. This is why all of the AIxpresented in the article are corrected for HR according to the linearrelationship established by Wilkinson et al,13 namely, that for every10-bpm increase in HR, AIx decreases by 4%. Two consecutive AIxmeasurements were performed at each time interval, and their meanvalue was calculated. A third measurement was performed, accord-ing to the Task Force III recommendations for user procedures, if thefirst 2 measures differed by �3%.14 The aortic pulse transit time,defined as the time of reflection from the foot of the pressure waveto the shoulder of the first systolic peak, was also evaluated. All ofthe measurements were made by the same observer (D.A).
Assessment of Skin Blood Flow ReactivitySkin blood flow measurement was performed using a laser Dopplerflowmeter (PeriFlux PF4001 and 5000, Perimed). The blood flowresponse to local heating, normalized for beat-to-beat mean bloodpressure (BP), was measured with a specific module (PeriTempSystem, Perimed) before and after exposure to ETS. A 3-minuterecording under resting conditions preceded all of the skin bloodflow reactivity tests. The probe used for the heating test was placedon the antecubital region of the left forearm and heated to 44°C for20 minutes to allow maximal vasodilatation.
All of the subjects underwent continuous ECG recording through-out the study. Finger BP was also measured by a beat-to-beathemodynamic monitoring system (Finometer Pro, FMS). HR, fingerBP, and blood flow response to local heating were recorded onlineon a computer with a Powerlab data acquisition system (ADInstruments) for subsequent analysis.
Carboxyhemoglobin, ADMA, and Nicotine DosageCarboxyhemoglobin levels were measured at baseline and after thesmoke exposure (COoximeter IL682, Instrumentation Laboratory).Nicotine and ADMA plasma levels were assessed by an independentlaboratory (Advanced Technology Corp, University Hospital Centreof Liege), using a liquid chromatographic method coupled withtandem mass spectrometry. Because our subjects were not usuallyexposed to passive smoking, nicotine was determined only at the endof the tobacco and nontobacco sessions, whereas ADMA levels weremeasured both before and after the smoke exposure in each session.These dosages were not performed in 1 subject because of difficultvenous access.
Particulate ExposureParticulate exposure was measured in real time with a portableinstrument (MetOne Aerocet 531) placed inside the box during theexperimental session. This particulate counter provides estimates of4 usual categories of particulate matter (PM) size (PM 1.0, PM 2.5,PM 7.5, and PM 10.0).
Data AnalysisAll of the measurements were analyzed in a blinded fashion. Systolicand diastolic BP, HR, AIx corrected for HR, and transit time areexpressed as absolute unit changes from baseline values. Skin bloodflow values during the heating laser Doppler test were analyzed bythe Powerlab data acquisition system. The mean values for everyminute during the test were calculated and expressed as the percent-ages of the maximal vasodilatation observed during each session.Thereafter, the response to heating stimulation was quantified as theabsolute unit change of every minute from baseline skin blood flowvalues.
Argacha et al Acute Vascular Effects of Passive Smoking 1507
by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from
Statistical AnalysisData are expressed as means�SEMs. Baseline hemodynamic param-eters and carboxyhemoglobin levels in tobacco smoke, nontobaccosmoke, and normal air sessions were compared using a 1-wayANOVA (SPSS Windows 13.0). A 2-way repeated-measuresANOVA was used to detect significant changes in variables overtime between the experimental sessions and separately during andafter the 3 exposures, after applying a Bonferroni correction formultiple comparisons. A 2-way repeated-measures ANOVA wasalso used to detect changes in skin blood flow during the heatingprovocation test performed before and after the 3 experimentalsessions. Smoke particle concentrations and serum nicotine levelswere compared using a Student’s paired t test. Carboxyhemoglobinand ADMA changes after the smoke exposure were compared usinga 2-way repeated-measures ANOVA (time�smoke interaction). Therelation among serum nicotine levels, AIx corrected for HR, and skinblood flow heating test changes was assessed using Pearson’scorrelation coefficient. Significance was assumed at P�0.05.
Results
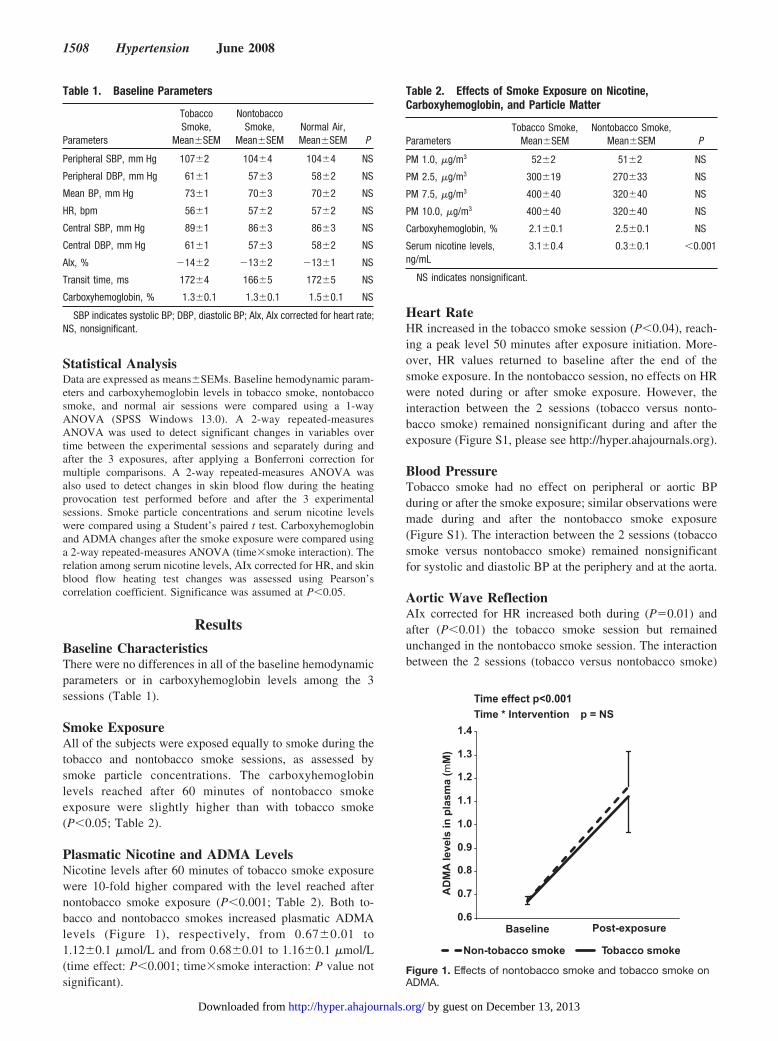
Baseline CharacteristicsThere were no differences in all of the baseline hemodynamicparameters or in carboxyhemoglobin levels among the 3sessions (Table 1).
Smoke ExposureAll of the subjects were exposed equally to smoke during thetobacco and nontobacco smoke sessions, as assessed bysmoke particle concentrations. The carboxyhemoglobinlevels reached after 60 minutes of nontobacco smokeexposure were slightly higher than with tobacco smoke(P�0.05; Table 2).
Plasmatic Nicotine and ADMA LevelsNicotine levels after 60 minutes of tobacco smoke exposurewere 10-fold higher compared with the level reached afternontobacco smoke exposure (P�0.001; Table 2). Both to-bacco and nontobacco smokes increased plasmatic ADMAlevels (Figure 1), respectively, from 0.67�0.01 to1.12�0.1 �mol/L and from 0.68�0.01 to 1.16�0.1 �mol/L(time effect: P�0.001; time�smoke interaction: P value notsignificant).
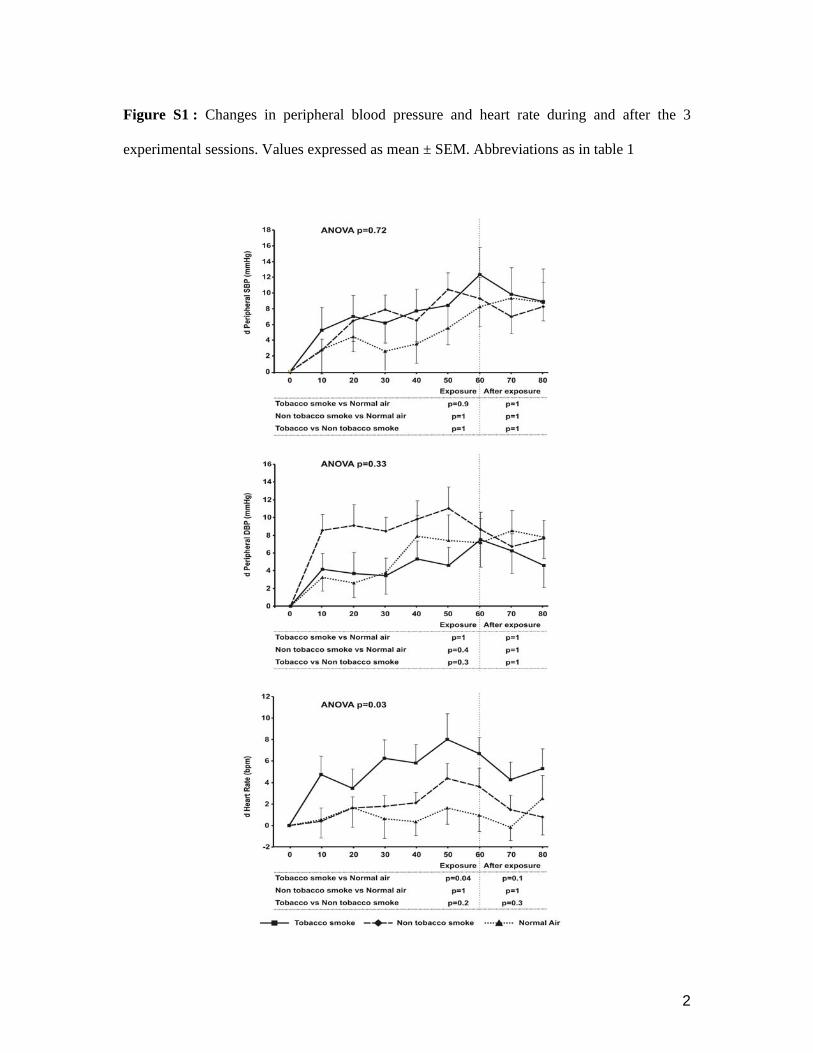
Heart RateHR increased in the tobacco smoke session (P�0.04), reach-ing a peak level 50 minutes after exposure initiation. More-over, HR values returned to baseline after the end of thesmoke exposure. In the nontobacco session, no effects on HRwere noted during or after smoke exposure. However, theinteraction between the 2 sessions (tobacco versus nonto-bacco smoke) remained nonsignificant during and after theexposure (Figure S1, please see http://hyper.ahajournals.org).
Blood PressureTobacco smoke had no effect on peripheral or aortic BPduring or after the smoke exposure; similar observations weremade during and after the nontobacco smoke exposure(Figure S1). The interaction between the 2 sessions (tobaccosmoke versus nontobacco smoke) remained nonsignificantfor systolic and diastolic BP at the periphery and at the aorta.
Aortic Wave ReflectionAIx corrected for HR increased both during (P�0.01) andafter (P�0.01) the tobacco smoke session but remainedunchanged in the nontobacco smoke session. The interactionbetween the 2 sessions (tobacco versus nontobacco smoke)
Table 1. Baseline Parameters
Parameters
TobaccoSmoke,
Mean�SEM
NontobaccoSmoke,
Mean�SEMNormal Air,Mean�SEM P
Peripheral SBP, mm Hg 107�2 104�4 104�4 NS
Peripheral DBP, mm Hg 61�1 57�3 58�2 NS
Mean BP, mm Hg 73�1 70�3 70�2 NS
HR, bpm 56�1 57�2 57�2 NS
Central SBP, mm Hg 89�1 86�3 86�3 NS
Central DBP, mm Hg 61�1 57�3 58�2 NS
AIx, % �14�2 �13�2 �13�1 NS
Transit time, ms 172�4 166�5 172�5 NS
Carboxyhemoglobin, % 1.3�0.1 1.3�0.1 1.5�0.1 NS
SBP indicates systolic BP; DBP, diastolic BP; AIx, AIx corrected for heart rate;NS, nonsignificant.
Table 2. Effects of Smoke Exposure on Nicotine,Carboxyhemoglobin, and Particle Matter
ParametersTobacco Smoke,
Mean�SEMNontobacco Smoke,
Mean�SEM P
PM 1.0, �g/m3 52�2 51�2 NS
PM 2.5, �g/m3 300�19 270�33 NS
PM 7.5, �g/m3 400�40 320�40 NS
PM 10.0, �g/m3 400�40 320�40 NS
Carboxyhemoglobin, % 2.1�0.1 2.5�0.1 NS
Serum nicotine levels,ng/mL
3.1�0.4 0.3�0.1 �0.001
NS indicates nonsignificant.
Time * Intervention p = NSTime effect p<0.001
0.6
0.7
0.8
0.9
1.0
1.1
1.2
1.3
1.4
Baseline Post-exposure
Non-tobacco smoke Tobacco smoke
AD
MA
leve
ls in
pla
sma
(mM
)
Figure 1. Effects of nontobacco smoke and tobacco smoke onADMA.
1508 Hypertension June 2008
by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from
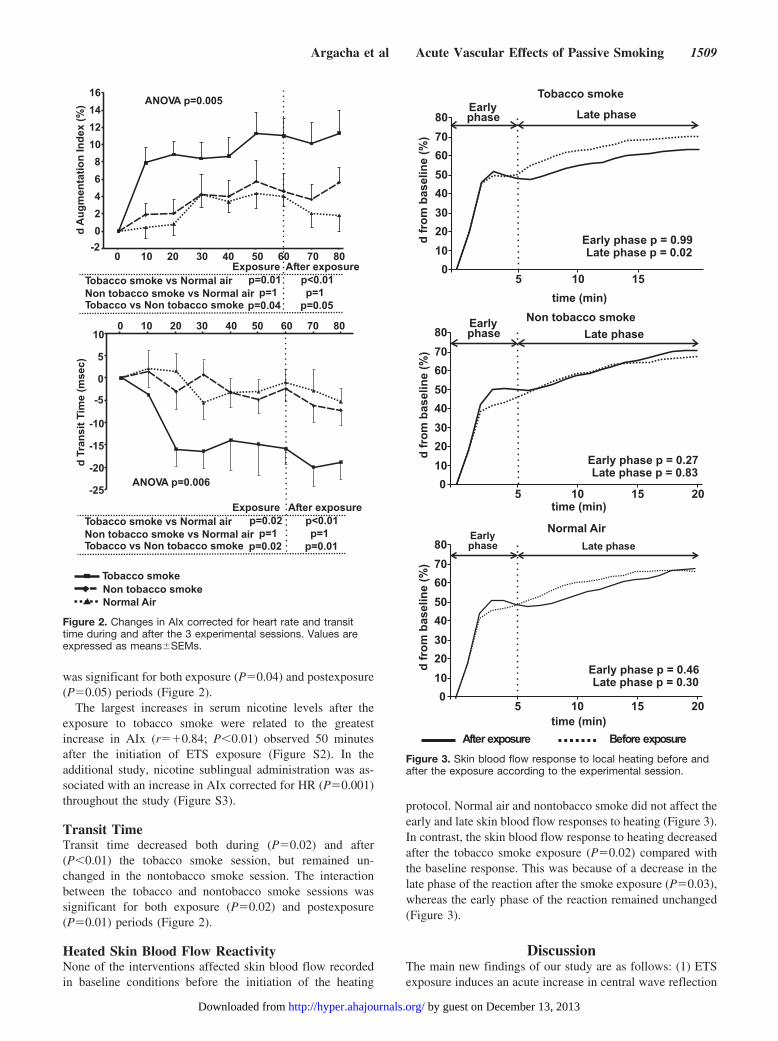
was significant for both exposure (P�0.04) and postexposure(P�0.05) periods (Figure 2).
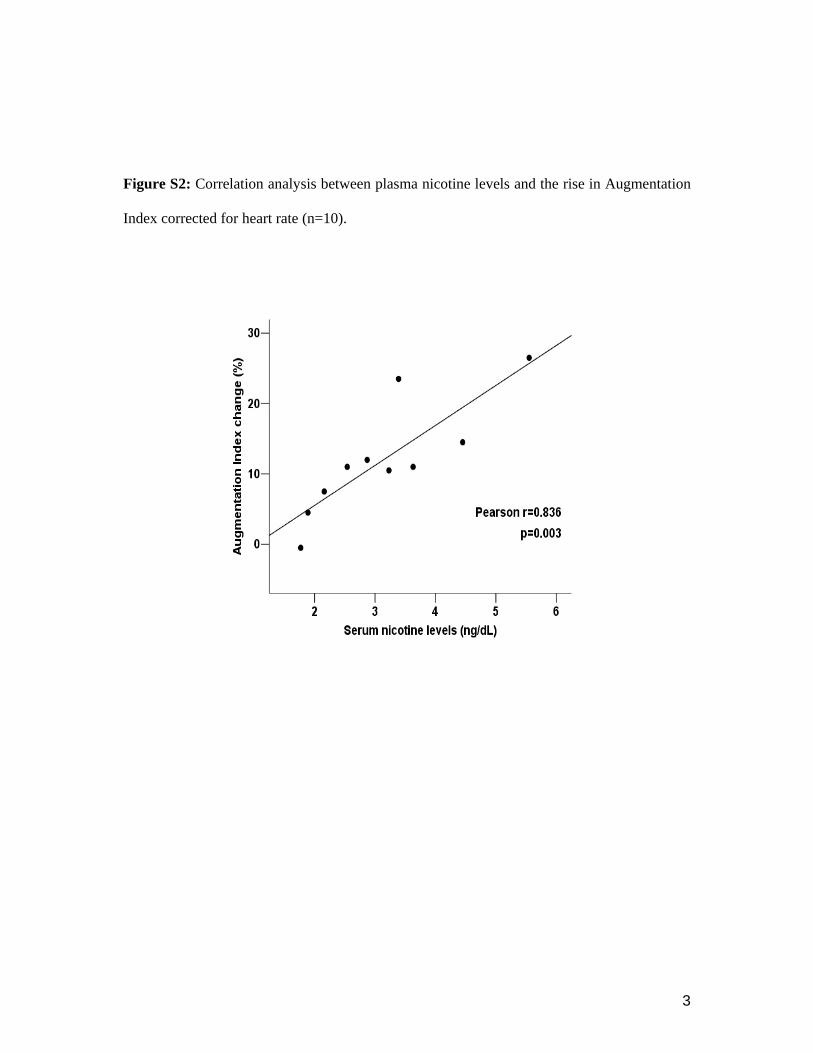
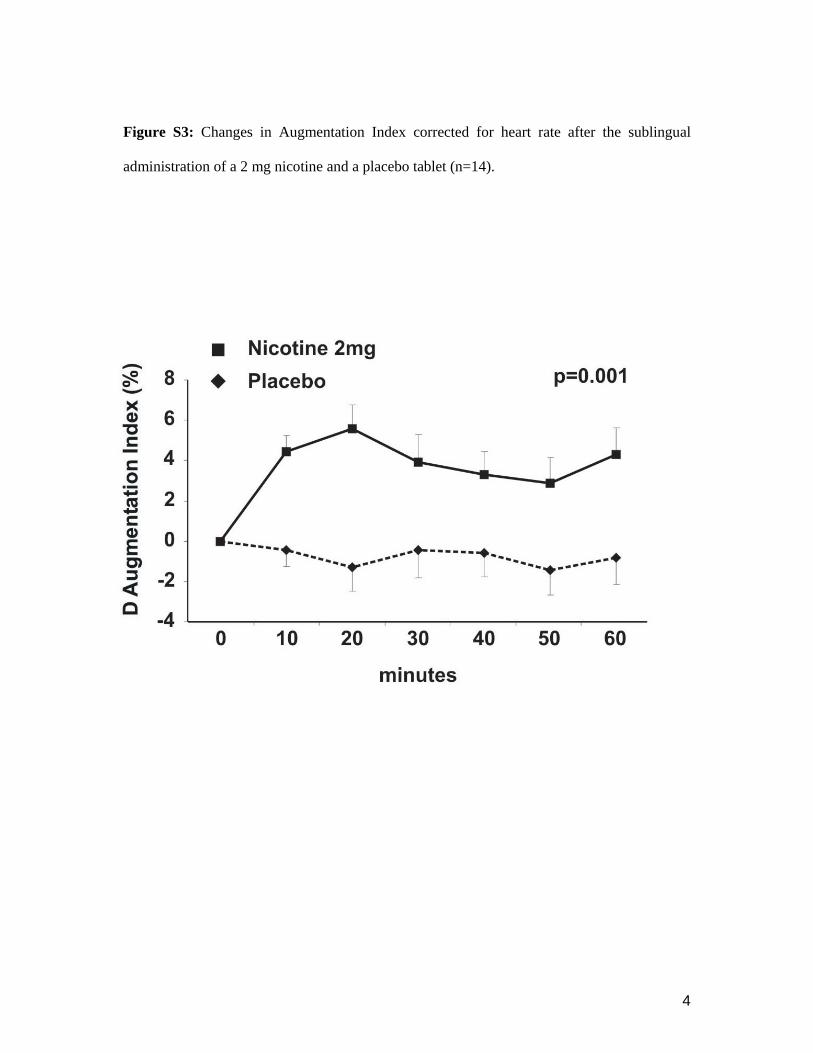
The largest increases in serum nicotine levels after theexposure to tobacco smoke were related to the greatestincrease in AIx (r��0.84; P�0.01) observed 50 minutesafter the initiation of ETS exposure (Figure S2). In theadditional study, nicotine sublingual administration was as-sociated with an increase in AIx corrected for HR (P�0.001)throughout the study (Figure S3).
Transit TimeTransit time decreased both during (P�0.02) and after(P�0.01) the tobacco smoke session, but remained un-changed in the nontobacco smoke session. The interactionbetween the tobacco and nontobacco smoke sessions wassignificant for both exposure (P�0.02) and postexposure(P�0.01) periods (Figure 2).
Heated Skin Blood Flow ReactivityNone of the interventions affected skin blood flow recordedin baseline conditions before the initiation of the heating
protocol. Normal air and nontobacco smoke did not affect theearly and late skin blood flow responses to heating (Figure 3).In contrast, the skin blood flow response to heating decreasedafter the tobacco smoke exposure (P�0.02) compared withthe baseline response. This was because of a decrease in thelate phase of the reaction after the smoke exposure (P�0.03),whereas the early phase of the reaction remained unchanged(Figure 3).
DiscussionThe main new findings of our study are as follows: (1) ETSexposure induces an acute increase in central wave reflection
-202468
10121416
0 10 20 30 40 50 60 70 80Exposure After exposure
Tobacco smoke vs Normal airNon tobacco smoke vs Normal airTobacco vs Non tobacco smoke
p=0.01p=1
p=0.04
p<0.01p=1
p=0.05
ANOVA p=0.005
d A
ugm
enta
tion
Inde
x (%
)
-25
-20
-15
-10
-5
0
5
10
Tobacco smoke vs Normal airNon tobacco smoke vs Normal airTobacco vs Non tobacco smoke
ANOVA p=0.006
Tobacco smoke
Exposurep=0.02
p=1p=0.02
After exposurep<0.01p=1
p=0.01
0 10 20 30 40 50 60 70 80
d Tr
ansi
t Tim
e (m
sec)
Non tobacco smokeNormal Air
Figure 2. Changes in AIx corrected for heart rate and transittime during and after the 3 experimental sessions. Values areexpressed as means�SEMs.
erusopxeerofeB
dfr
omba
selin
e(%
)
)nim(emit
01020304050607080
5 10 15 20
ekomsoccabotnoN
dfr
omba
selin
e(%
)
1020304050607080
Early Late phase
dfr
omba
selin
e(%
)
)nim(emit
01020304050607080
5 10 15
ekomsoccaboT
)nim(emit
05 10 15 20
lamroN riA
erusopxeretfA
phase
Early phase p = 0.99Late phase p = 0.02
Earlyphase
Earlyphase
Late phase
Late phase
Early phase p = 0.27Late phase p = 0.83
Early phase p = 0.46Late phase p = 0.30
Figure 3. Skin blood flow response to local heating before andafter the exposure according to the experimental session.
Argacha et al Acute Vascular Effects of Passive Smoking 1509
by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from

and a decrease in skin microvascular dilatation, when com-pared with nontobacco smoke; (2) increased central wavereflection is linked to the levels of nicotine achieved withETS; (3) these modifications persist �20 minutes after ETScessation; and (4) smoke inhalation, regardless to the tobaccocontent, is followed by a plasmatic increase in ADMA.Hence, large and small arterial vascular functions are alteredby acute exposure to tobacco smoke. Hemodynamic changesprovoked by ETS are the result of a primary nicotinic toxicmechanism acting on the vascular tree and are not mediatedby a sensory stimulation or a stressful reaction to the smokeitself. In addition, our study suggests that the toxicity of ETSis markedly underestimated when only the direct exposuretime is taken into account.
ETS Effects on Aortic Wave Reflection: The Roleof NicotineIn a previous study, 1 hour of ETS exposure acutely increasedAIx by 16%.2 However, this reaction could be interpreted asthe sum of 3 different effects: a placebo effect, a cardiovas-cular response secondary to sensory stimulation and stress bysmoke, and a specific effect of the tobacco smoke on vascularfunction.5,15,16 In contrast, our results demonstrate that ETSexposure produces a marked change in the aortic waveformthrough a primary toxicity induced by tobacco on the vasculartree.
Enhanced arterial wave reflection, because of a change inperipheral vascular reflection site, and/or augmented pulsewave velocity can generate an increase in AIx. Althoughpulse wave velocity was not measured directly, the aorticpulse transit time, which has been used as a surrogate markerof pulse wave velocity,17 was decreased by tobacco smoke.This finding suggests that the intensified arterial wave reflec-tion in the aorta could be explained by a reduction in vesselcompliance after ETS exposure. In patients with coronaryartery disease, invasive measurements of the aortic pressure-diameter loop have demonstrated that 4 minutes of ETSexposure were able to decrease aortic distensibility.4 Ourresults are in accordance with this finding and suggest thatchanges in the aortic waveform in response to passive smokeare favored by active stiffening of the aorta. However,concomitant changes in aortic wave reflection resulting froman increased peripheral vascular tone, as reported previouslyin active smokers,18 may also have played a role. Previously,short-term ETS exposure (15 minutes) did not interfere withforearm vascular resistance measured by plethysmography.19
However, this segmental analysis of vascular resistancecannot rule out a systemic arteriolar vasoconstriction after amore prolonged ETS exposure and larger increases in plasmanicotine. Further studies are required to characterize thepossible differential effects of impaired arterial complianceand early reflection site in the rise in AIx with ETS.
The comparison of the vascular response to passive smok-ing of a real cigarette and an herbal cigarette reveals a moretoxic effect of the tobacco smoke. At first glance, the maintoxic difference between the 2 smokes may reside in thenicotine content of tobacco smoke.6 Indeed, it is widelyaccepted that nicotine has pleiotropic actions that could affectvasomotor regulation.20 Our results reveal a significant rela-
tionship between the changes in aortic waveform and thenicotine levels reached in plasma after 1 hour of tobaccosmoke exposure (Figure S2). This relationship was confirmedin our second protocol demonstrating an acute impairment inarterial wave reflection produced by a pure nicotinic stimulus.This finding provides novel information regarding the roleplayed by nicotine in the smoke-related vascular damage.However, the exact mechanisms responsible for the nicotine-induced rise in arterial wave reflection, the effect of the aortichemodynamic changes on myocardial perfusion, and thepossibility of tolerance development after chronic exposure tonicotine require further investigation.
Effects of ADMAAn important contribution of our study also resides in thedemonstration that nontobacco smoke increases plasmaticADMA levels, a competitive inhibitor of NO synthase. Thisoccurred to a similar extent as with tobacco smoke. Usuallythe most common mechanism leading to accumulation ofADMA involves impaired metabolism by dimethylargininedimethylaminohydrolase, an enzyme extremely sensitive tooxidative stress. Thus, we hypothesized that the free radicalexposure, arising from identical particulate exposure of bothsmokes,21 produces the same inhibition of dimethylargininedimethylaminohydrolase activity and generates the samedegree of competitive inhibition of NO synthase. We believethat these results further add to the escalating evidence thatexposure to polluted air is associated with short-term adversecardiovascular effects.22 Increased ADMA levels in ourstudy, not reported previously in vivo, as well as withnontobacco smoke, provide a further indication on how airpollution may elicit cardiovascular events.
Tobacco-Free Cigarette: A Safe Smoke?Contrary to tobacco smoke, nontobacco smoke exposureproduced no significant change in arterial waveform and skinblood flow, suggesting a key role of the nicotine content ofsmoke, at least in acute conditions. Despite this “relative”safety, herbal cigarette smoke increased plasmatic ADMAlevels and exposed the subject to the same level of particlematter as ETS. Even if a previous study did not identify acutesympathetic or peripheral vascular effects of carbon monox-ide,23 carboxyhemoglobin increase from nontobacco smokeexposure has some detrimental effect on myocardial bloodflow.24 For these reasons, we believe that herbal smokecannot be considered as a safe cardiovascular smoke, espe-cially because the role of fine particle matter25 in theendothelial toxicity of cigarette smoke and air pollutants22
remains unclear.
Perspectives: Microvascular Effect of ETSETS exposure has immediate effects on endothelium-dependent vasodilatation of large arteries,7 but our study alsoreveals an impairment of vascular reactivity in small-sizevessels. Many studies have established the physiologicalsubstrate of skin thermal hyperemia.26 Local heating evokedan initial vasodilatation followed by a plateau, which is�70% mediated by NO.27 However, even if the role ofendothelium-derived NO is predominant, endothelium-
1510 Hypertension June 2008
by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from

dependent hyperpolarizing factors are also involved in thisreaction.28 Consequently, the microvascular impairment oc-curring after 1 hour of ETS exposure may be interpreted as adecrease in endothelium-dependent hyperpolarizing factorand/or endothelium-derived NO bioavailability. This willrequire further studies to better identify the mechanismsinvolved in the microvascular endothelial impairment ob-served with ETS. Moreover, only tobacco smoke impairedmicrovascular function in the presence of an increase inplasmatic ADMA. This paradox could be explained by aspecific ability of tobacco smoke to decrease endothelialproduction of endothelium-dependent hyperpolarizing factorand/or NO, because nicotine can directly impair NO synthaseexpression,6 whereas acrolein can increase endogenous reac-tive oxygen species produced by NADPH activation.29 Thisalso requires additional experiments, which will furtherunderscore the importance of achieving a complete smoke-free environment.30
AcknowledgmentWe are indebted to Pierre Abraham (Angers, France) for hisguidance on laser Doppler measurements.
Sources of FundingThis study was supported and funded by the Erasme Foundation,Astra Zeneca, Pfizer, Medtronic, Novartis, the David and Alice VanBuuren Fund, the Belgian National Fund for Research, the Lamber-tine Lacroix Prize, the Foundation Saucez-Van Poucke, and theFoundation for Cardiac Surgery.
DisclosuresNone.
References1. Barnoya J, Glantz SA. Cardiovascular effects of secondhand smoke:
nearly as large as smoking. Circulation. 2005;111:2684–2698.2. Mahmud A, Feely J. Effects of passive smoking on blood pressure and
aortic pressure waveform in healthy young adults–influence of gender.Br J Clin Pharmacol. 2004;57:37–43.
3. Otsuka R, Watanabe H, Hirata K, Tokai K, Muro T, Yoshiyama M,Takeuchi K, Yoshikawa J. Acute effects of passive smoking on thecoronary circulation in healthy young adults. JAMA. 2001;286:436–441.
4. Stefanadis C, Vlachopoulos C, Tsiamis E, Diamantopoulos L, ToutouzasK, Giatrakos N, Vaina S, Tsekoura D, Toutouzas P. Unfavorable effectsof passive smoking on aortic function in men. Ann Intern Med. 1998;128:426–434.
5. Raupach T, Schafer K, Konstantinides S, Andreas S. Secondhand smokeas an acute threat for the cardiovascular system: a change in paradigm.Eur Heart J. 2006;27:386–392.
6. Adamopoulos D, van de Borne P, Argacha J. New insights into thesympathetic, endothelial and coronary effects of nicotine. Clin ExpPharm Phys. 2008;35:458–463.
7. Kato T, Inoue T, Morooka T, Yoshimoto N, Node K. Short-term passivesmoking causes endothelial dysfunction via oxidative stress in non-smokers. Can J Physiol Pharmacol. 2006;84:523–529.
8. Hutchison SJ, Sievers RE, Zhu BQ, Sun YP, Stewart DJ, Parmley WW,Chatterjee K. Secondhand tobacco smoke impairs rabbit pulmonary arteryendothelium-dependent relaxation. Chest. 2001;120:2004–2012.
9. Imamura M, Waseda Y, Marinova GV, Ishibashi T, Obayashi S, SasakiA, Nagai A, Azuma H. Alterations of NOS, arginase and DDAH proteins
expression in the rabbit cavernous tissue following administration ofcigarette smoke extract. Am J Physiol Regul Integr Comp Physiol. 2007;293:R2081–R2089.
10. Zhang WZ, Venardos K, Chin-Dusting J, Kaye DM. Adverse effects ofcigarette smoke on NO bioavailability: role of arginine metabolism andoxidative stress. Hypertension. 2006;48:278–285.
11. Vlachopoulos C, O’Rourke M. Genesis of the normal and abnormalarterial pulse. Curr Probl Cardiol. 2000;25:303–367.
12. Braundwald E, Sarnoff SJ, Stainsby WN. Determinants of duration andmean rate of ventricular ejection. Circ Res. 1958;6:319–325.
13. Wilkinson IB, MacCallum H, Flint L, Cockcroft JR, Newby DE, WebbDJ. The influence of heart rate on augmentation index and central arterialpressure in humans. J Physiol. 2000;525(pt 1):263–270.
14. Van Bortel LM, Duprez D, Starmans-Kool MJ, Safar ME, Giannattasio C,Cockcroft J, Kaiser DR, Thuillez C. Clinical applications of arterialstiffness, Task Force III: recommendations for user procedures. Am JHypertens. 2002;15:445–452.
15. Smith CJ, Scott SM, Ryan BA. Cardiovascular effects of odors. ToxicolInd Health. 1999;15:595–601.
16. Smith CJ, Fischer TH, Sears SB. Environmental tobacco smoke, cardio-vascular disease, and the nonlinear dose-response hypothesis. Toxicol Sci.2000;54:462–472.
17. Wilkinson IB, Prasad K, Hall IR, Thomas A, MacCallum H, Webb DJ,Frenneaux MP, Cockcroft JR. Increased central pulse pressure and aug-mentation index in subjects with hypercholesterolemia. J Am CollCardiol. 2002;39:1005–1011.
18. Mahmud A, Feely J. Effect of smoking on arterial stiffness and pulsepressure amplification. Hypertension. 2003;41:183–187.
19. Hausberg M, Mark AL, Winniford MD, Brown RE, Somers VK. Sym-pathetic and vascular effects of short-term passive smoke exposure inhealthy nonsmokers. Circulation. 1997;96:282–287.
20. Hanna ST. Nicotine effect on cardiovascular system and ion channels.J Cardiovasc Pharmacol. 2006;47:348–358.
21. Barua RS, Ambrose JA, Srivastava S, DeVoe MC, Eales-Reynolds LJ.Reactive oxygen species are involved in smoking-induced dysfunction ofnitric oxide biosynthesis and upregulation of endothelial nitric oxidesynthase: an in vitro demonstration in human coronary artery endothelialcells. Circulation. 2003;107:2342–2347.
22. Mills NL, Tornqvist H, Gonzalez MC, Vink E, Robinson SD, SoderbergS, Boon NA, Donaldson K, Sandstrom T, Blomberg A, Newby DE.Ischemic and thrombotic effects of dilute diesel-exhaust inhalation in menwith coronary heart disease. N Engl J Med. 2007;357:1075–1082.
23. Hausberg M, Somers VK. Neural circulatory responses to carbonmonoxide in healthy humans. Hypertension. 1997;29:1114–1118.
24. Favory R, Lancel S, Tissier S, Mathieu D, Decoster B, Neviere R.Myocardial dysfunction and potential cardiac hypoxia in rats induced bycarbon monoxide inhalation. Am J Respir Crit Care Med. 2006;174:320–325.
25. Rundell KW, Hoffman JR, Caviston R, Bulbulian R, Hollenbach AM.Inhalation of ultrafine and fine particulate matter disrupts systemicvascular function. Inhal Toxicol. 2007;19:133–140.
26. Cracowski JL, Minson CT, Salvat-Melis M, Halliwill JR. Methodologicalissues in the assessment of skin microvascular endothelial function inhumans. Trends Pharmacol Sci. 2006;27:503–508.
27. Kellogg DL Jr. In vivo mechanisms of cutaneous vasodilation and vaso-constriction in humans during thermoregulatory challenges. J ApplPhysiol. 2006;100:1709–1718.
28. Gooding KM, Hannemann MM, Tooke JE, Clough GF, Shore AC.Maximum skin hyperaemia induced by local heating: possible mech-anisms. J Vasc Res. 2006;43:270–277.
29. Orosz Z, Csiszar A, Labinskyy N, Smith K, Kaminski PM, Ferdinandy P,Wolin MS, Rivera A, Ungvari Z. Cigarette smoke-induced proinflam-matory alterations in the endothelial phenotype: role of NAD(P)H oxidaseactivation. Am J Physiol Heart Circ Physiol. 2007;292:H130–H139.
30. Frieden TR, Bloomberg MR. How to prevent 100 million deaths fromtobacco. Lancet. 2007;369:1758–1761.
Argacha et al Acute Vascular Effects of Passive Smoking 1511
by guest on December 13, 2013http://hyper.ahajournals.org/Downloaded from

1
Acute effects of passive smoking on peripheral vascular function.
Running title: Acute vascular effects of passive smoking
Argacha Jean François, MD¹; Adamopoulos Dionysios, MD¹; Gujic Marko, MD¹;
Fontaine David, PhD2, Amai Nadia, MD1; Berkenboom Guy, MD PhD1 and van de Borne
Philippe, MD PhD¹.
1: Department of Cardiology, Erasme Hospital, Université Libre de Bruxelles, Belgium
2: Laboratory of Pharmacology and Physiology, Université Libre de Bruxelles, Belgium
Both first authors contributed equally to the study.
Address for correspondence and reprint requests:
Argacha Jean-François Department of Cardiology, Erasme Hospital, 808 Lennik Street, 1070 Brussels, Belgium E-mail: [email protected] Phone: +32-2-555.3381 Fax: +32-2-555.6713
2
Figure S1 : Changes in peripheral blood pressure and heart rate during and after the 3
experimental sessions. Values expressed as mean ± SEM. Abbreviations as in table 1
3
Figure S2: Correlation analysis between plasma nicotine levels and the rise in Augmentation
Index corrected for heart rate (n=10).
4
Figure S3: Changes in Augmentation Index corrected for heart rate after the sublingual
administration of a 2 mg nicotine and a placebo tablet (n=14).