Acute effects of delayed-release hydrolyzed pine nut oil on ...
38
University of Southern Denmark Acute effects of delayed-release hydrolyzed pine nut oil on glucose tolerance, incretins, ghrelin and appetite in healthy humans Sørensen, Karina V.; Korfitzen, Svend S.; Kaspersen, Mads H.; Ulven, Elisabeth Rexen; Ekberg, Jeppe H.; Bauer-Brandl, Annette; Ulven, Trond; Højlund, Kurt Published in: Clinical Nutrition DOI: 10.1016/j.clnu.2020.09.043 Publication date: 2021 Document version: Accepted manuscript Document license: CC BY-NC-ND Citation for pulished version (APA): Sørensen, K. V., Korfitzen, S. S., Kaspersen, M. H., Ulven, E. R., Ekberg, J. H., Bauer-Brandl, A., Ulven, T., & Højlund, K. (2021). Acute effects of delayed-release hydrolyzed pine nut oil on glucose tolerance, incretins, ghrelin and appetite in healthy humans. Clinical Nutrition, 40(4), 2169-2179. https://doi.org/10.1016/j.clnu.2020.09.043 Go to publication entry in University of Southern Denmark's Research Portal Terms of use This work is brought to you by the University of Southern Denmark. Unless otherwise specified it has been shared according to the terms for self-archiving. If no other license is stated, these terms apply: • You may download this work for personal use only. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying this open access version If you believe that this document breaches copyright please contact us providing details and we will investigate your claim. Please direct all enquiries to [email protected] Download date: 14. Mar. 2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Acute effects of delayed-release hydrolyzed pine nut oil on ...

University of Southern Denmark
Acute effects of delayed-release hydrolyzed pine nut oil on glucose tolerance, incretins,ghrelin and appetite in healthy humans
Sørensen, Karina V.; Korfitzen, Svend S.; Kaspersen, Mads H.; Ulven, Elisabeth Rexen;Ekberg, Jeppe H.; Bauer-Brandl, Annette; Ulven, Trond; Højlund, Kurt
Published in:Clinical Nutrition
DOI:10.1016/j.clnu.2020.09.043
Publication date:2021
Document version:Accepted manuscript
Document license:CC BY-NC-ND
Citation for pulished version (APA):Sørensen, K. V., Korfitzen, S. S., Kaspersen, M. H., Ulven, E. R., Ekberg, J. H., Bauer-Brandl, A., Ulven, T., &Højlund, K. (2021). Acute effects of delayed-release hydrolyzed pine nut oil on glucose tolerance, incretins,ghrelin and appetite in healthy humans. Clinical Nutrition, 40(4), 2169-2179.https://doi.org/10.1016/j.clnu.2020.09.043
Go to publication entry in University of Southern Denmark's Research Portal
Terms of useThis work is brought to you by the University of Southern Denmark.Unless otherwise specified it has been shared according to the terms for self-archiving.If no other license is stated, these terms apply:
• You may download this work for personal use only. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying this open access versionIf you believe that this document breaches copyright please contact us providing details and we will investigate your claim.Please direct all enquiries to [email protected]
Download date: 14. Mar. 2022

Journal Pre-proof
Acute effects of delayed-release hydrolyzed pine nut oil on glucose tolerance,incretins, ghrelin and appetite in healthy humans
Karina V. Sørensen, Svend S. Korfitzen, Mads H. Kaspersen, Elisabeth Rexen Ulven,Jeppe H. Ekberg, Annette Bauer-Brandl, Trond Ulven, Kurt Højlund
PII: S0261-5614(20)30515-X
DOI: https://doi.org/10.1016/j.clnu.2020.09.043
Reference: YCLNU 4484
To appear in: Clinical Nutrition
Received Date: 29 November 2019
Revised Date: 22 August 2020
Accepted Date: 27 September 2020
Please cite this article as: Sørensen KV, Korfitzen SS, Kaspersen MH, Ulven ER, Ekberg JH, Bauer-Brandl A, Ulven T, Højlund K, Acute effects of delayed-release hydrolyzed pine nut oil on glucosetolerance, incretins, ghrelin and appetite in healthy humans, Clinical Nutrition, https://doi.org/10.1016/j.clnu.2020.09.043.
This is a PDF file of an article that has undergone enhancements after acceptance, such as the additionof a cover page and metadata, and formatting for readability, but it is not yet the definitive version ofrecord. This version will undergo additional copyediting, typesetting and review before it is publishedin its final form, but we are providing this version to give early visibility of the article. Please note that,during the production process, errors may be discovered which could affect the content, and all legaldisclaimers that apply to the journal pertain.
© 2020 Published by Elsevier Ltd.

1
Acute effects of delayed-release hydrolyzed pine nut oil on glucose tolerance, incretins, ghrelin and 1
appetite in healthy humans 2
Karina V. Sørensena,b, Svend S. Korfitzenb, Mads H. Kaspersenc, Elisabeth Rexen Ulvend, Jeppe H. Ekberge, 3
Annette Bauer-Brandlc, Trond Ulvenc,d, Kurt Højlunda,b 4
a Steno Diabetes Center Odense, Odense University Hospital, Denmark 5
b Department of Clinical Research, University of Southern Denmark, Odense, Denmark 6
c Department of Physics, Chemistry and Pharmacy, University of Southern Denmark, Odense, Denmark 7
d Department of Drug Design and Pharmacology, University of Copenhagen, Copenhagen, Denmark 8
e Section for Metabolic Receptology, Novo Nordisk Foundation Center for Basic Metabolic Research, University 9
of Copenhagen, Copenhagen, Denmark 10
Corresponding Author 11
Professor Kurt Højlund, e-mail: [email protected] 12
Kløvervænget 10, 5. floor, 5000 Odense, Denmark 13
Journ
al Pre-
proof

2
ABSTRACT 14
Bacground and aim Pinolenic acid, a major component (~20%) of pine nut oil, is a dual agonist of the free fatty 15
acid receptors, FFA1 and FFA4, which may regulate release of incretins and ghrelin from the gut. Here, we 16
investigated the acute effects of hydrolyzed pine nut oil (PNO-FFA), delivered to the small intestine by delayed-17
release capsules, on glucose tolerance, insulin, incretin and ghrelin secretion, and appetite. 18
Methods In two cross-over studies, we evaluated 3 g unhydrolyzed pine nut oil (PNO-TG) or 3 g PNO-FFA 19
versus no oil in eight healthy, non-obese subjects (study 1), and 3 g PNO-FFA or 6 g PNO-FFA versus no oil in 20
ten healthy, overweight/obese subjects (study 2) in both studies given in delayed-release capsules 30 min prior to 21
a 4-h-oral glucose tolerance test (OGTT). Outcomes were circulating levels of glucose, insulin, GLP-1, GIP, 22
ghrelin, appetite and gastrointestinal tolerability during OGTT. 23
Results Both 3 g PNO-FFA in study 1 and 6 g PNO-FFA in study 2 markedly increased GLP-1 levels (p<0.001) 24
and attenuated ghrelin levels (p<0.001) during the last two hours of the OGTT compared with no oil. In study 2, 25
these effects of PNO-FFA were accompanied by an increased satiety and fullness (p<0.03), and decreased 26
prospective food consumption (p<0.05). PNO-FFA caused only small reductions in glucose and insulin levels 27
during the first two hours of the OGTT. 28
Conclusions Our results provide evidence that PNO-FFA delivered to the small intestine by delayed-release 29
capsules may reduce appetite by augmenting GLP-1 release and attenuating ghrelin secretion in the late 30
postprandial state. 31
Keywords Free fatty acid receptors, pine nut oil, pinolenic acid, incretins, appetite, oral glucose tolerance test 32
Clinical Trial registry numbers: NCT03062592 and NCT03305367 33
Journ
al Pre-
proof

3
ABBRIVIATIONS 34
PNO-FFA Hydrolyzed pine nut oil 35
PNO-TG Unhydrolyzed pine nut oil 36
FFA1 Free fatty acid receptor 1 37
FFA4 Free fatty acid receptor 4 38
GLP-1 Glucagon-like Peptide-1 39
GIP Gastric inhibitory polypeptide 40
FFA Free fatty acid 41
RYGB Roux-En-Y Gastric Bypass 42
OGTT Oral glucose tolerance test 43
AUC Area under the curve 44
VAS Visual Analogue Scale 45
Journ
al Pre-
proof

4
INTRODUCTION 46
Type 2 diabetes and its serious complications remain a major health care problem (1, 2). Therefore, the 47
development of preventive and treatment strategies for type 2 diabetes is of paramount importance. Lifestyle 48
modifications focusing on physical activity and a healthy diet are recommended as first line therapies from the 49
time of diagnosis (3-5). However, long term compliance to dietary lifestyle interventions is known to be poor. 50
Moreover, there is an ongoing debate as to what constitutes a healthy diet for prevention and treatment of type 2 51
diabetes that is related to the fact that the metabolic effects of specific food items remain elusive. One of these is 52
the anti-diabetic potential of dietary fatty acids through activation of free fatty acid receptors. 53
The free fatty acid receptor 1 (FFA1) and the free fatty acid receptor 4 (FFA4), formerly known as 54
GPR40 and GPR120, respectively, have attracted considerable attention as potential targets for antidiabetic drug 55
development due to their modulatory effects on glucose metabolism and low-grade inflammation (6-10). FFA1 56
is activated by medium to long-chain fatty acids in both human and rodent cell lines and the receptor is highly 57
expressed in human and rodent pancreatic tissue, especially pancreatic beta-cells (11-14). FFA1 is also found in 58
murine enteroendocrine cells of the small intestine (14). Furthermore, activation of FFA1 by specific free fatty 59
acids (FFA) in MIN6 cells enhances glucose-stimulated insulin secretion (GSIS) (13). Insulin secretion is also 60
stimulated indirectly through the release of the incretin hormones glucagon-like-peptide-1 (GLP-1) and gastric 61
inhibitory polypeptide (GIP) from murine enteroendocrine cells (14-16). An increase in GLP-1 is known to also 62
reduce appetite and body weight (17, 18). FFA4 is also activated by medium to long-chain fatty acids and has 63
been reported to be highly expressed in enteroendocrine cells, regulating GIP and GLP-1 secretion (19, 20), 64
although its ability to promote GLP-1 release has been questioned (21, 22). Furthermore, there is evidence that 65
activation of FFA4 on gastric cells inhibits the secretion of the appetite stimulating orexigenic hormone ghrelin 66
(23-25), which could contribute to an appetite reducing effect of FFA4 agonists. Finally, FFA4 has been linked 67
to anti-inflammatory and insulin sensitizing effects in mice through its presence in adipose tissue (26-28). 68
The activity of a broad panel of dietary fatty acids was recently screened on human FFA1 and FFA4 in 69
vitro and demonstrated that the polyunsaturated fatty acid pinolenic acid is a dual FFA1/FFA4 agonist with a 70
Journ
al Pre-
proof

5
combined high potency and high efficacy on both FFA1 and FFA4 (29). This was supported by follow-up 71
experiments in mice showing that in particular purified pinolenic acid but also Siberian pine nut oil (containing 72
~20% pinolenic acid) reduced blood glucose levels during an oral glucose tolerance test (OGTT) in mice when 73
compared to maize oil (29). The more pronounced effect of purified pinolenic acid suggests that hydrolysis of 74
pine nut oil into FFAs might enhance the effect. To investigate the long term effect of hydrolyzed pine nut oil, a 75
longitudinal study of diet-induced obese mice evaluated hydrolyzed Siberian pine nut oil versus a water control 76
and found significantly lower fasting insulin and OGTT glucose levels after 21 days of supplementation 77
(Wargent, E. et al., personal communication, unpublished data in preparation). 78
As described, enteroendocrine fatty acid activation of FFA1 and FFA4 are able to regulate GLP-1 and 79
ghrelin secretion, and one important function mediated by these hormones is appetite regulation (30-33). In 80
accordance, it was shown that 3 g pine nut oil given as FFA but not as triglycerides (TG) was able to increase 81
GLP-1 and reduce feelings of prospective food consumption compared to olive oil, however no differences in 82
ghrelin was observed (34). Moreover, another study showed reduced food intake after pine nut oil given as FFA 83
but not as TG (35). Consistent with a study by Verhoef et al. reporting no effect of unhydrolyzed pine nut oil on 84
either satiety or energy intake, this provide further evidence that hydrolysis of pine nut oil may be a key element 85
(36). 86
Another possible important factor, that may enhance the effect of pine nut oil FFA mediated incretin 87
secretion through FFA1 and FFA4, is the delivery of FFA distal to the normal absorption site in the upper 88
gastrointestinal tract. This gut section is bypassed after Roux-en-Y gastric bypass (RYGB), resulting in increased 89
loads of nutrients, including FFAs, to the distal intestine, which strongly amplifies GLP-1 secretion (37). It is 90
possible that activation of FFA1 and FFA4 on the enteroendocrine L-cells contributes to this amplification, due 91
to their increased abundance in this gut section (38). In support of this, purified lauric acid, ingested as enteric-92
coated pellets, designed to release its content throughout the ileum and colon was demonstrated to reduce 93
glucose levels and enhance GLP-1 secretion compared to placebo (39). 94
Journ
al Pre-
proof

6
In the present study, we hypothesized that hydrolyzed Siberian pine nut oil (containing ~20% pinolenic 95
acid) delivered to the small intestine by delayed-release capsules, mimicking RYGB, would increase incretin 96
release and insulin secretion by activation of FFA1 and FFA4 in enteroendocrine cells and FFA1 in pancreatic 97
beta-cells resulting in improved glucose tolerance and together with an FFA4-mediated inhibition of ghrelin 98
release reduce appetite. The main objectives were to investigate the effect of hydrolyzed Siberian pine nut oil 99
(PNO-FFA) versus unhydrolyzed Siberian pine nut oil (PNO-TG) and the dose-response relationship of PNO-100
FFA compared to no oil intake on glucose tolerance, insulin, incretin and ghrelin secretion, gastrointestinal 101
tolerability and appetite in healthy humans. 102
Journ
al Pre-
proof
7
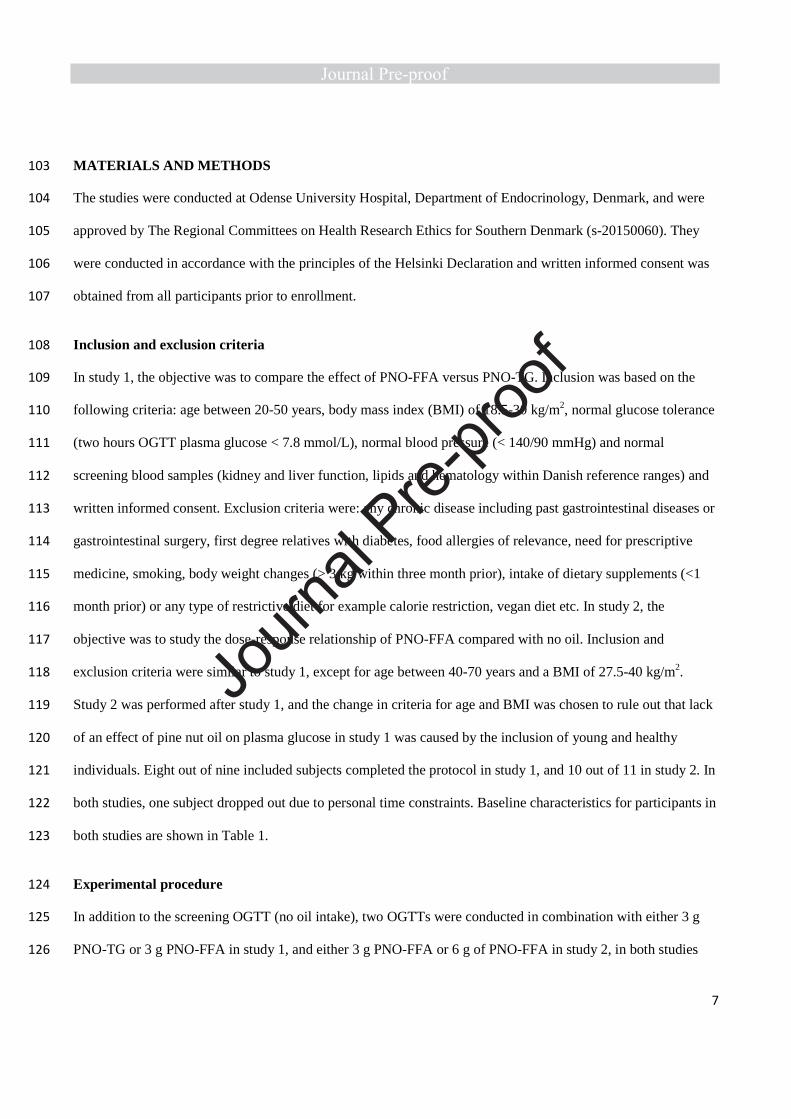
MATERIALS AND METHODS 103
The studies were conducted at Odense University Hospital, Department of Endocrinology, Denmark, and were 104
approved by The Regional Committees on Health Research Ethics for Southern Denmark (s-20150060). They 105
were conducted in accordance with the principles of the Helsinki Declaration and written informed consent was 106
obtained from all participants prior to enrollment. 107
Inclusion and exclusion criteria 108
In study 1, the objective was to compare the effect of PNO-FFA versus PNO-TG. Inclusion was based on the 109
following criteria: age between 20-50 years, body mass index (BMI) of 18.5-30 kg/m2, normal glucose tolerance 110
(two hours OGTT plasma glucose < 7.8 mmol/L), normal blood pressure (< 140/90 mmHg) and normal 111
screening blood samples (kidney and liver function, lipids and hematology within Danish reference ranges) and 112
written informed consent. Exclusion criteria were: any chronic disease including past gastrointestinal diseases or 113
gastrointestinal surgery, first degree relatives with diabetes, food allergies of relevance, need for prescriptive 114
medicine, smoking, body weight changes (> 3 kg within three month prior), intake of dietary supplements (<1 115
month prior) or any type of restrictive diet for example calorie restriction, vegan diet etc. In study 2, the 116
objective was to study the dose-response relationship of PNO-FFA compared with no oil. Inclusion and 117
exclusion criteria were similar to study 1, except for age between 40-70 years and a BMI of 27.5-40 kg/m2. 118
Study 2 was performed after study 1, and the change in criteria for age and BMI was chosen to rule out that lack 119
of an effect of pine nut oil on plasma glucose in study 1 was caused by the inclusion of young and healthy 120
individuals. Eight out of nine included subjects completed the protocol in study 1, and 10 out of 11 in study 2. In 121
both studies, one subject dropped out due to personal time constraints. Baseline characteristics for participants in 122
both studies are shown in Table 1. 123
Experimental procedure 124
In addition to the screening OGTT (no oil intake), two OGTTs were conducted in combination with either 3 g 125
PNO-TG or 3 g PNO-FFA in study 1, and either 3 g PNO-FFA or 6 g of PNO-FFA in study 2, in both studies 126
Journ
al Pre-
proof

8
using a randomized cross-over design. Supplementary Fig. 1 show a design chart of the two studies. 127
Randomization was computerized using www.randomizer.org. Prior to all experimental days, each subject was 128
instructed to consume a similar evening meal of their own preference (no calorie restriction). They showed up 129
after an overnight fast of at least ten hours; a small amount of water was allowed. Moreover, alcohol 130
consumption and physical exercise was not allowed 48 hours prior to the OGTTs. Blood was drawn using a 131
peripheral venous catheter at time points -30, -15 and 0 min prior to consumption of a 75 g glucose solution (250 132
mL), and hereafter every 30 min until 240 min of testing. The second and third OGTT were similar to the 133
screening OGTT with the exception of oil intake 30 minutes prior to the test. The oils were administered in 134
delayed-release capsules consumed with water (320 mL). Washout between tests were at least one and maximum 135
four weeks. Moreover, all subjects were instructed to maintain their habitual life style throughout the study 136
period. We measured body weight and body composition at every visit using a Tanita Body Composition 137
Analyzer (model TBF-300GS). Study 1 was conducted from February to April 2016 and study 2 from January to 138
August 2017. 139
Visual analog scale (VAS) questionnaires 140
During each OGTT a set of standard VAS questionnaires were handed out to the participants to assess 141
gastrointestinal tolerability and appetite (40, 41). In these, the degree of symptoms were indicated on a 100 mm 142
horizontal line, best feeling indicated as 0 mm and worst feeling as 100 mm. VAS on gastrointestinal symptoms 143
(flatulence, nausea/vomiting, bloating, diarrhea, constipation, and abdominal pain) were provided before (-15 144
min) and after (240 min) the OGTT. Moreover, two additional retrospective questionnaires were completed at 8 145
PM and at 8 AM after the OGTT to detect any longer-term effects. Appetite symptoms (satiety, hunger, fullness, 146
prospective food consumption and overall well-being) were assessed at minutes: -15, 15, 30, 45, 60 and every 147
half hour throughout the OGTT. 148
Fasting and OGTT derived indices of insulin sensitivity and beta-cell function 149
Journ
al Pre-
proof

9
Homeostatic model assessment of insulin resistance (HOMA-IR) was calculated as: fasting glucose mmol/L x 150
fasting insulin mU/L/22.5 (42). Indices of insulin sensitivity were: BIGTTSi, based on plasma glucose and serum 151
insulin measured at 0, 30 and 120 min, MATSUDA, based on plasma glucose and serum insulin measured at 0, 152
30, 60, 90 and 120 min, and OGIS from 0-180 min, based on plasma glucose measured at 0, 120 and 180 min 153
and serum insulin measured at 0 and 120 min (43-45). Indices of beta-cell function were: BIGTTAIR, based on 154
plasma glucose and serum insulin measured at 0, 30 and 120 min, CIR30min, based on plasma glucose and serum 155
insulin at 30 min and IGI, based on plasma glucose and serum insulin at 0 and 30 min (43, 46, 47). Finally, 156
disposition indexes, that is, beta-cell function adjusted for insulin sensitivity were: BIGTTSi x BIGTTAIR, CIR x 157
MATSUDA and IGI x MATSUDA. 158
Biochemical analyses 159
Blood glucose was measured using the ABL800 FLEX blood gas analyzer. Insulin and C-peptide were analyzed 160
using an electrochemiluminescence immunoassay (ECLIA) on Cobas e 411. The insulin intra-assay CV% was 161
1.9-2.0 and the inter-assay CV% was 2.5-2.6. For C-peptide the intra-assay CV% was 1.3-4.6 and the inter-assay 162
CV% was 1.8-5.0. Moreover, we determined GLP-1 levels using Total GLP-1 (ver. 2) Assay Kit (Meso Scale 163
Discovery). GIP and ghrelin were measured using the corresponding Human GIP (Total) or Human Ghrelin 164
(Total) ELISA Kit (Millipore). The GIP kit had an intra-assay CV% of 3.0-8.8 and an inter-assay CV% of 1.8-165
6.1 and the ghrelin kit had an intra-assay CV% of 0.90-1.91 and an inter-assay CV% of 5.18-7.81. 166
Investigational product and blinding 167
Hydrolysis of Siberian pine nut oil (The Siberian Pines Company) was conducted in the following manner: a 168
Blue Cap flask containing PNO-TG (0.16 mol, 141 g was charged with aqueous NaOH (Panreac Applichem, 169
pharmagrade 2M, 1 mmol, 480 mL.) and a magnetic stir bar. The biphasic solution was stirred at 300 rpm 170
(stirring rate is crucial to avoid emulsion) for 24 hours after which a white solid had formed. The aqueous phase 171
was decanted off and the remaining white solid was suspended in aqueous citric acid (Sigma-Aldrich, Ph. Eur. 172
grade, 2 M, 0.95 mmol, 480 mL). The suspension was stirred at 400 rpm (stirring rate is crucial to avoid 173
Journ
al Pre-
proof

10
emulsion) for 24 hours resulting in a biphasic solution. The golden oil was siphoned off and carefully washed 174
with H2O (40 mL). The biphasic solution was stirred slowly until complete separation of the two phases. The 175
golden oil was siphoned off resulting in the pure PNO-FFA. PNO-FFA was subjected to H1 NMR analysis to 176
ensure complete hydrolysis. The major fatty acid types in the Siberian pine nut oil is pinolenic acid (20.9 %), 177
linoleic acid (47.7 %) and oleic acid (21.8 %) (29). 178
To mimic the effects of RYGB, the pine nut oil (PNO-FFA and PNO-TG) was hand-filled in 179
semitransparent, acid resistant capsule shells made of hydroxypropyl methylcellulose with delayed release 180
properties (DRcaps™ from Capsugel®, size 00 batch 5332311). Doses of 3 g and 6 g amounted to five and ten 181
capsules containing a total of ~114 and 228 kJ of fat, respectively. The encapsulated oil was stored at 5 °C and 182
for a maximum of 3 months until use. Subjects in study 1 were blinded towards oil type, however differences in 183
number of capsules did not allow for blinding of subjects in study 2. DRcaps™ capsule shells were originally 184
designed for dry powder filling. To test the release profile of oils, we did a simple in vitro evaluation of capsules 185
containing mannitol (dry matter control), PNO-TG or PNO-FFA, supplemented with the dyes rhodamine B or 186
sulphorhodamine B (in the case of PNO-FFA), in triplicates. The capsules were placed in individual vials with 187
magnetic stirring containing 10 mL fasted state simulated gastric fluid without pepsin (biorelevant.com) (pH = 188
1.5, 37 °C, 400 rpm) and the release was followed by UV-measurements (550 nm). We observed a similar, yet 189
slower release profile for mannitol powder as previously described (i.e. in vivo disintegration time approx. 50 190
min, and content release completed after another 20 min)(48). For the oils, we observed a slow release over four 191
hours, where approximately half of the oil was released at 90 minutes (Supplementary Fig. 2). 192
Outcomes 193
Outcomes for both studies were treatment differences in 4-h total area under the curve (AUCtotal) of glucose, 194
insulin, C-peptide, GLP-1, GIP and ghrelin, as well as the total AUC for the first two hours (AUC0-120) and the 195
second two hours (AUC120-240). Additional outcomes were treatment differences in OGTT based indices of 196
Journ
al Pre-
proof

11
insulin sensitivity and beta-cell function and VAS scores of gastrointestinal symptoms and appetite. All AUCs 197
were calculated using the trapezoidal rule. 198
Statistics 199
All statistics were conducted using Stata/IC 14.2 package. Statistical significance was set to a p-value of < 0.05. 200
Mixed model linear regression analysis was chosen for hypothesis testing of treatment differences between oil 201
types (study 1) or oil doses (study 2). The explanatory and fixed effect variable was oil type or dose and the 202
random variable was subject ID. Non-normal data were transformed using the natural logarithm. Model 203
validation was conducted by visual assessment of q-q plots of the obtained residuals and plots of residuals versus 204
estimated values. Blood biomarkers below detection limit were imputed to the detection limit of the assay. In 205
study 2, one subject was omitted from all analyses after 3 g PNO-FFA treatment due to suspected non-206
compliance. In case of missing appetite responses (missing completely at random) these remained missing 207
during analysis and results were reported as model estimations. Treatment differences in VAS scores of 208
gastrointestinal discomfort were analyzed by the use of non-parametric Wilcoxon signed rank test adjusted for 209
multiple comparison by the Bonferroni-Holm method. 210
Journ
al Pre-
proof

12
RESULTS 211
Glucose, insulin and C-peptide 212
In study 1, neither glucose AUCtotal nor insulin AUCtotal differed significantly between treatments, whereas C-213
peptide AUCtotal tended to be increased in response to PNO-TG versus no oil (p=0.075) (Fig. 1 a-f). However, 214
glucose AUC0-120 tended to be lower in response to PNO-FFA compared to both PNO-TG (p=0.064) and no oil 215
(p=0.072), whereas no treatment differences in glucose AUC120-240 were observed (Fig. 1 a-b). Insulin AUC0-120 216
and C-peptide AUC0-120 were reduced (~10-16%) in response to PNO-FFA versus both PNO-TG and no oil (all 217
p<0.05), whereas insulin AUC120-240 and C-peptide AUC120-240 were increased (~22-35%) after intake PNO-FFA 218
compared to no oil (all p<0.05) with only a tendency to increased C-peptide AUC120-240 after PNO-TG versus no 219
oil (p=0.059) (Fig. 1 c-f). 220
In study 2, there was no significant treatment differences in glucose AUCtotal, whereas insulin AUCtotal 221
decreased (~13%; p=0.03) and C-peptide AUCtotal tended to decrease (p=0.059) after intake of 6 g PNO-FFA 222
versus no oil (Fig. 2 a-f). Glucose AUC0-120 was reduced (~9-10%) in response to 6 g PNO-FFA compared to 223
both 3 g PNO-FFA and no oil (all p<0.05), whereas glucose AUC120-240 was increased (~13%) after 6 g PNO-224
FFA versus no oil (p=0.002) and tended to be increased in response to 3 g PNO-FFA versus no oil (p=0.057). 225
Consistent with study 1, insulin AUC0-120 and C-peptide AUC0-120 were reduced (~17-22%) in response to 6 g 226
PNO-FFA compared to no oil (all p<0.05) (Fig. 2 c-f). 227
GLP-1, GIP and ghrelin 228
In study 1, GLP-1 AUCtotal was increased (~63%) in response to PNO-FFA compared to no oil (p=0.003) and 229
tended to be increased after PNO-FFA versus PNO-TG (p=0.09) (Fig. 3 a-b). These effects of PNO-FFA were 230
mainly explained by increased GLP-1 AUC120-240 (~86-156%) compared with both PNO-TG (p=0.004) and no 231
oil (p<0.001), whereas only a tendency of increased GLP-1 AUC0-120 after PNO-FFA versus no oil (p=0.079) 232
was observed. Moreover, GLP-1 AUC120-240 tended to be increased after PNO-TG versus no oil (p=0.055) (Fig. 3 233
a-b). While GIP AUCtotal was unaltered by treatment, GIP AUC0-120 decreased (~20%; p=0.021) whereas GIP 234
Journ
al Pre-
proof

13
AUC120-240 increased (~43%; p=0.011) after PNO-FFA versus no oil (Fig. 3 c-d). The orexigenic hormone 235
ghrelin showed reduced AUCtotal (~13-14%; all p<0.05) and AUC120-240 (~15-25%, all p<0.01) in response to 236
both PNO-FFA and PNO-TG compared to no oil (Fig. 3 e-f). 237
In study 2, GLP-1 AUCtotal was increased (~26%) in response to 6 g PNO-FFA compared to no oil 238
(p=0.024). Consistent with study 1, these effects of 6 g PNO-FFA were mainly explained by increased GLP-1 239
AUC120-240 (~35-52%) compared with both 3 g PNO-FFA (p=0.002) and no oil (p<0.001), whereas no treatment 240
differences were observed in the first two hours (Fig. 4 a-b). GIP AUC responses showed no differences between 241
treatments (Fig. 4 c-d). As observed in study 1, ghrelin AUCtotal were reduced (~30%) after intake of 6 g PNO-242
FFA compared to no oil (p=0.02), and ghrelin AUC120-240 decreased (~30-36%) in response to 3 g PNO-FFA 243
(p=0.013) and 6 g PNO-FFA (p<0.001) compared to no oil (Fig. 4 e-f). 244
OGTT indices 245
In study 1, insulin sensitivity estimated as BIGTTSi was slightly higher after PNO-FFA than after PNO-TG 246
(p=0.015), but there was no effect of either PNO-FFA or PNO-TG on BIGTTSi compared with no oil. Otherwise, 247
we observed no differences in insulin sensitivity measured as MATSUDA or OGIS, β-cell function measured as 248
BIGTTAIR, CIR30min or IGI, or the three estimated disposition indices between treatments. 249
In study 2, we observed no effects of 6 g PNO-FFA and 3 g PNO-FFA on any of these markers of 250
insulin sensitivity, insulin secretion and disposition indices compared with no oil. Data are presented in 251
supplementary Table 1. 252
Appetite 253
In study 1, satiety AUCtotal and AUC120-240 were increased (~17-24%) after PNO-TG versus no oil (all p<0.05), 254
whereas hunger AUCtotal and AUC120-240 were reduced (~10-11%) in response to PNO-TG versus no oil (all p 255
<0.05). Moreover, hunger AUC120-240 was also decreased (~9%) after PNO-TG versus PNO-FFA (p=0.007). 256
Lastly, fullness AUC120-240 was increased (~22%) after PNO-TG versus no oil (p=0.02), and correspondingly 257
Journ
al Pre-
proof

14
prospective food consumption AUC120-240 was reduced (~8%) after PNO-TG versus no oil (p=0.001). All other 258
symptoms did not differ between treatments (Supplementary Table 2). 259
In study 2, satiety AUCtotal and AUC120-240 were increased (~17-40%) after both 3 g PNO-FFA and 6 g 260
PNO-FFA compared with no oil (all p<0.03). Also, satiety AUC120-240 was increased (~14%) after 6 g PNO-FFA 261
versus 3 g PNO-FFA (p=0.046). Fullness AUCtotal, AUC-15-120 and AUC120-240 were increased (~22-51%) after 262
both 3g PNO-FFA and 6 g PNO-FFA versus no oil (all p<0.01). In agreement, the AUCtotal for prospective food 263
intake was reduced (~7-10%) after both 3 g PNO-FFA and 6 g PNO-FFA versus no oil (all p<0.05). After 3 g 264
PNO-FFA prospective food intake AUC-15-120 was reduced versus no oil (~11%; p=0.014), whereas prospective 265
food intake AUC120-240 was reduced after 6 g PNO-FFA versus no oil (~3%; p=0.03). Finally, overall well-being 266
AUCtotal and AUC-15-120 were increased after no oil compared to 6 g PNO-FFA (p=0.01) (Supplementary Table 267
2). 268
Gastrointestinal tolerability 269
In study 1, there were no differences in changes of the degree of gastrointestinal symptoms during the OGTT nor 270
at 8PM or at 8AM between any of the treatments (Supplementary Table 3). 271
In study 2, the degree of abdominal pain was increased after 6 g PNO-FFA versus 3 g PNO-FFA 272
(p=0.048) and no oil (p=0.02), and also after 3 g PNO-FFA versus no oil (p=0.048). Otherwise, no differences in 273
changes of the degree of gastrointestinal symptoms during the OGTT, at 8PM or at 8AM were seen between the 274
treatments (Supplementary Table 3). 275
Journ
al Pre-
proof

15
DISCUSSION 276
The major aim of the present study was to explore the effect of PNO-FFA containing ~20% of the dual 277
FFA1/FFA4 agonist pinolenic acid on metabolic outcomes relevant in obesity and type 2 diabetes, including 278
glucose tolerance, insulin response, incretin and ghrelin secretion, and appetite. We found increased GLP-1 279
secretion from 120-240 min of the OGTT after both 3 g PNO-FFA (study 1) and 6 g PNO-FFA (study 2), which 280
was accompanied by decreased circulating levels of the orexigenic hormone ghrelin versus no oil. Interestingly, 281
in study 2, these changes were accompanied by subjective appetite reducing effects. Gastrointestinal tolerability 282
was high, with only a minor increase in abdominal pain after both 3 g and 6 g PNO-FFA in study 2. 283
Unexpectedly, insulin levels were slightly decreased from 0-120 min of the OGTT after both 3 g PNO-FFA 284
(study 1) and 6 g PNO-FFA (study 2). After 6 g PNO-FFA this was accompanied by reduced glucose levels. 285
Overall, our results suggest that delayed-release PNO-FFA has an appetite reducing effect, which may be 286
mediated by increased GLP-1 secretion and reduced ghrelin levels in glucose-tolerant individuals. 287
Based on the study by Christiansen et al, demonstrating a high agonistic potency and superior efficacy of 288
pinolenic acid on FFA1 and FFA4 in vitro, as well as improved glucose tolerance in mice after intake of pine nut 289
oil given as TG and, in particular, as purified pinolenic acid [27], we hypothesized that hydrolyzed pine nut oil 290
delivered to the small intestine by delayed-release capsules would increase insulin secretion by activation of 291
FFA1/FFA4 either on enteroendocrine cells leading to increased incretin secretion or on pancreatic beta-cells 292
stimulating insulin release directly. Only a limited number of previous intervention studies have investigated the 293
effect of pine nut oil on glucose, insulin, appetite regulating hormones and subjective appetite (VAS) (34-36). 294
None of these studies used delayed-release formulation. However, in a recent study, it was reported that purified 295
lauric acid (2.35 g) administered twice in the form of enteric coated pellets for delivery to ileum and colon, in 296
combination with a mixed meal breakfast and lunch, was able to reduce postprandial breakfast and lunch AUC 297
of glucose and increase postprandial lunch AUC of GLP-1 in type 2 diabetic subjects (n=8) (39). These findings 298
partly correspond to our results, showing a pronounced increase in GLP-1 levels from 120-240 min during the 299
OGTT in both studies for the 3 g PNO-FFA (study 1) and 6 g PNO-FFA (study 2) treatment versus no oil. 300
Journ
al Pre-
proof
16
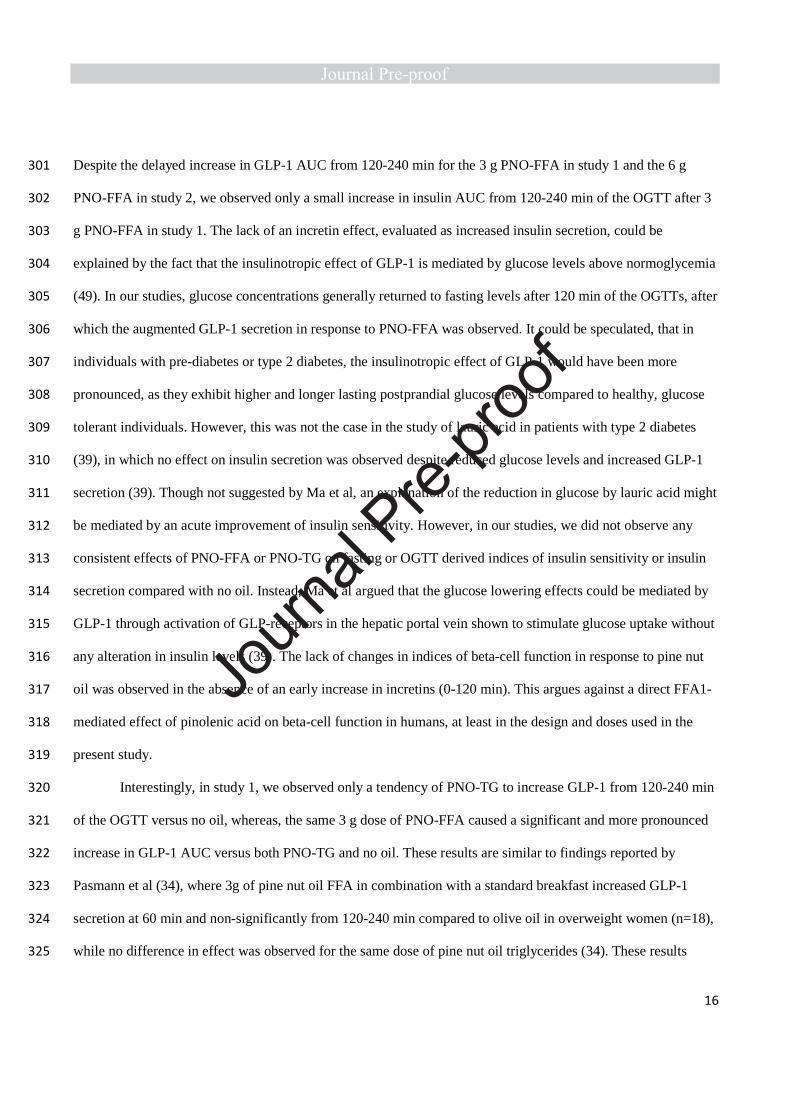
Despite the delayed increase in GLP-1 AUC from 120-240 min for the 3 g PNO-FFA in study 1 and the 6 g 301
PNO-FFA in study 2, we observed only a small increase in insulin AUC from 120-240 min of the OGTT after 3 302
g PNO-FFA in study 1. The lack of an incretin effect, evaluated as increased insulin secretion, could be 303
explained by the fact that the insulinotropic effect of GLP-1 is mediated by glucose levels above normoglycemia 304
(49). In our studies, glucose concentrations generally returned to fasting levels after 120 min of the OGTTs, after 305
which the augmented GLP-1 secretion in response to PNO-FFA was observed. It could be speculated, that in 306
individuals with pre-diabetes or type 2 diabetes, the insulinotropic effect of GLP-1 would have been more 307
pronounced, as they exhibit higher and longer lasting postprandial glucose levels compared to healthy, glucose 308
tolerant individuals. However, this was not the case in the study of lauric acid in patients with type 2 diabetes 309
(39), in which no effect on insulin secretion was observed despite reduced glucose levels and increased GLP-1 310
secretion (39). Though not suggested by Ma et al, an explanation of the reduction in glucose by lauric acid might 311
be mediated by an acute improvement of insulin sensitivity. However, in our studies, we did not observe any 312
consistent effects of PNO-FFA or PNO-TG on fasting or OGTT derived indices of insulin sensitivity or insulin 313
secretion compared with no oil. Instead, Ma et al argued that the glucose lowering effects could be mediated by 314
GLP-1 through activation of GLP-receptors in the hepatic portal vein shown to stimulate glucose uptake without 315
any alteration in insulin levels (39). The lack of changes in indices of beta-cell function in response to pine nut 316
oil was observed in the absence of an early increase in incretins (0-120 min). This argues against a direct FFA1-317
mediated effect of pinolenic acid on beta-cell function in humans, at least in the design and doses used in the 318
present study. 319
Interestingly, in study 1, we observed only a tendency of PNO-TG to increase GLP-1 from 120-240 min 320
of the OGTT versus no oil, whereas, the same 3 g dose of PNO-FFA caused a significant and more pronounced 321
increase in GLP-1 AUC versus both PNO-TG and no oil. These results are similar to findings reported by 322
Pasmann et al (34), where 3g of pine nut oil FFA in combination with a standard breakfast increased GLP-1 323
secretion at 60 min and non-significantly from 120-240 min compared to olive oil in overweight women (n=18), 324
while no difference in effect was observed for the same dose of pine nut oil triglycerides (34). These results 325
Journ
al Pre-
proof

17
provide evidence that pine nut oil given in the form of FFAs may be more powerful to stimulate GLP-1 release 326
than genuine pine nut oil (triglycerides). 327
Ghrelin is a known orexigenic hormone (50), and therefore a reduction in the postprandial release may 328
be beneficial in overweight or type 2 diabetic subjects, including a reduction in appetite and energy intake, 329
which may induce negative energy balance and over time body weight loss. Ghrelin secretion is inhibited by 330
activation of FFA4, but also other unknown mechanisms may contribute as ghrelin inhibition was reported to be 331
preserved in FFA-4 knockout models (23). Pinolenic acid may be superior in causing a FFA4-mediated 332
inhibition of ghrelin release due to its high potency on the receptor compared to other fatty acids (29). In both 333
studies, we demonstrated a decreased ghrelin AUC from 120-240 min in response to all pine nut oil interventions 334
versus no oil. These results suggest that pine nut oil given either as triglycerides or FFAs during an OGTT are 335
capable of reducing ghrelin levels more than glucose alone. As we did not include a control oil, we cannot 336
conclude that the observed ghrelin suppression is superior to other types of oil. It has been shown that ghrelin 337
inhibition is energy dependent (51) and therefore, we cannot exclude the possibility that the observed reduction 338
in ghrelin levels in response to pine nut oil could be explained by the extra energy (8-15%) consumed. However, 339
it has recently been suggested that mono and polyunsaturated fatty acids, which is the main type of fatty acids 340
contained in pine nut oil (~90%) may be superior in suppressing ghrelin secretion compared to saturated fatty 341
acids (52). Thus, it is possible that pine nut oil may be a better inhibitor of ghrelin secretion compared to other 342
oils depending on the amount of unsaturated fatty acids. The ghrelin response to pine nut oil was also evaluated 343
in the study by Pasmann et al (34). Here, none of the tested pine nut oils reduced ghrelin levels more than the 344
placebo oil (olive). Olive oil contains ~80% unsaturated fatty acids (53) and may therefore be equally effective 345
in inhibiting ghrelin release compared to pine nut oil or pinolenic acid. However, in our studies, ghrelin was 346
suppressed until 120 min and did not reach fasting levels within the 240 min of testing, while ghrelin was only 347
suppressed until 90 min and returned to fasting levels by 180 min in the study by Pasmann et al (34). Thus, 348
ghrelin was suppressed for a longer duration of time in our studies, which may be explained by enhanced FFA4 349
activation likely obtained by the delayed release formulation. Finally, in study 2, we detected no differences 350
Journ
al Pre-
proof

18
between the 3 g and 6 g PNO-FFA treatments in ghrelin suppression. This suggests that 3g PNO-FFA was 351
sufficient to cause this suppression compared to glucose alone. 352
Consistent with the study by Pasmann et al, (34), we observed an increase in satiety and fullness after 3 353
g and 6 g PNO-FFA compared to no oil in study 2. For satiety, this increase was observed for the total period of 354
testing and from 120-240 min corresponding to the observed postprandial increase in GLP-1 and decrease in 355
ghrelin secretion after intake of 6 g PNO-FFA. However, in study 2 fullness showed a significant increase in 356
both periods (-15-120 min and 120-240 min) indicating that the intake of capsules versus no oil rather than 357
changes in circulating levels of GLP-1 and ghrelin contributes to fullness also in the early phase of an OGTT. 358
Intriguingly, only 3g PNO-TG significantly increased satiety and fullness and reduced hunger in the direction of 359
appetite reduction in study 1. However, in line with our results in study 2, Hughes et al demonstrated that 2 g 360
pine nut oil FFA, but not TG, given 30 min prior to an ad libitum buffet lunch induced a significant 9% 361
reduction in food intake and tended to reduce energy intake (35). Lending further support to a superior effect of 362
pine nut oil FFAs on appetite reduction, a study by Verhoef et al. reported no effect of 3 g or 6 g pine nut oil TG 363
on subsequent ad libitum energy intake compared with 6 g milk fat (36). When considering the studies 364
investigating effects of PNO-FFA or PNO-TG on appetite as a whole, including our results, there are a number 365
of important differences between the designs including timing of oil intake, formulation, sample size and 366
metabolic state of participants. The latter is also a factor when comparing outcomes from our studies, as we 367
included older subjects with a higher BMI in study 2 compared to study 1. These differences might explain the 368
inconsistencies we observed in subjective appetite. Nonetheless, there is suggestive evidence that PNO-FFA may 369
reduce appetite, even when given in small doses in more physiological situations than during an OGTT as 370
reflected in studies using mixed meals and buffet style energy intake assessments (34, 35). However, more 371
robust, long-term studies are needed, to fully establish the potential appetite lowering effect of PNO-FFA, and to 372
what extent this effect might translate into reduced energy intake and weight loss over time. 373
Importantly, we detected no major negative effects of pine nut oil on gastrointestinal tolerability during 374
the OGTT, at 8 PM or 8 AM after. However, in study 2, we did observe a small increase in abdominal pain 375
Journ
al Pre-
proof

19
during the OGTT after 6 and 3 g PNO-FFA versus no oil, and also between doses. The mean treatment 376
difference in changes of abdominal pain was 11.8 mm between 6 g PNO-FFA and no oil, which we considered 377
small, but still of potential relevance. However, the treatment difference of 0.7 mm between 3 g PNO-FFA and 378
no oil is in our opinion not clinically relevant. In the study by Ma et al, investigating lauric acid, they did not 379
evaluate gastrointestinal symptoms; however, they reported that no adverse events occurred during the study 380
(39). As previously discussed their oil dose was 2.35 g, which almost corresponds to the 3 g PNO-FFA doses in 381
our studies. Thus, it is likely that smaller doses do not induce relevant gastrointestinal tolerability issues, but we 382
cannot exclude the possibility that giving the larger 6 g dose may pass a threshold, which may induce a few 383
adverse gastrointestinal symptoms. On the other hand, in study 2 subjects were unblinded, which may have 384
contributed to subjects being more susceptible to record a worsening in symptoms on the 6 g dose treatment. 385
Our studies have some limitations including the relatively small sample sizes, which may have 386
compromised the power of the studies to detect relevant differences. At the same time, the possibilities of type 1 387
errors were present, due to the potential influence of outlying results. Therefore, the studies should be seen as 388
explorative and hypothesis generating. While our studies demonstrated relevant effects of PNO-FFA on GLP-1, 389
ghrelin and appetite measures, there were some inconsistencies with respect to 3 g PNO-FFA in the two studies. 390
Thus, in study 2, no effect of 3 g PNO-FFA on GLP-1 (all time periods) or ghrelin (0-240 min) was observed, 391
whereas in study 1, intake of 3 g PNO-FFA showed no appetite reducing effects. Moreover, the changes in the 392
circulating levels of GLP-1 and ghreline did not match the self-reported appetite scores in several of the tested 393
conditions. Whether these differences could be explained by inclusion of older individuals with a higher BMI 394
and fat mass in study 2 as well as the large variation in the VAS-scores needs to be addressed in future studies. 395
Another potential limitation is that we did not measure the active forms of GLP-1, GIP or ghrelin. However, at 396
least for GLP-1 it has been argued that in praxis measurement of total GLP-1 is also of biological relevance (37). 397
We did not measure in vivo gastric emptying or release time of oil content from the capsules, which may be 398
important explanatory factors. Nonetheless, we believe that the manner in which ghrelin suppression differed 399
from other studies seemed plausible to depend on delayed and slow release of oil content. Lastly, we did not 400
Journ
al Pre-
proof

20
measure energy intake, thus whether the observed changes in subjective appetite would lead to a reduction in 401
energy intake is unknown. 402
In conclusion, PNO-FFA delivered to the small intestine by delayed-release capsules augmented GLP-1 403
secretion 120-240 min after glucose intake, which was accompanied by a concomitant attenuation of ghrelin 404
levels as compared with intake of glucose alone. These changes in circulating levels of GLP-1 and ghrelin could 405
explain some of the observed reductions in subjective appetite, supporting an appetite reducing effect of PNO-406
FFA. Finally, the oil interventions were well tolerated, with only the 6 g PNO-FFA dose causing minor, but 407
potentially clinically relevant changes in self-reported abdominal pain. Importantly, the suggested beneficial 408
effects of delayed-release PNO-FFA observed in our studies need to be evaluated and confirmed in long term 409
studies, preferably including patients with type 2 diabetes, in whom potential beneficial effects beyond weight 410
loss may include improved glucose tolerance, insulin sensitivity and reduced low-grade inflammation. 411
Journ
al Pre-
proof

21
FUNDING SOURCES 412
This work was supported by the Danish Research Council for Strategic Research and Innovation Fund Denmark 413
[grant number 11-116196 and 0603-00452B]. In addition, the study was supported by grants from Odense 414
University Hospital, The Region of Southern Denmark, the University of Southern Denmark and Ingemann O. 415
Bucks Fund. 416
Journ
al Pre-
proof

22
CONFLICT OF INTEREST 417
The authors declare that they have no conflict of interest. 418
Journ
al Pre-
proof

23
REFERENCES 419
1. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its 420
complications. Nature reviews Endocrinology. 2018;14(2):88-98. 421
2. Sortso C, Green A, Jensen PB, Emneus M. Societal costs of diabetes mellitus in Denmark. Diabetic 422
medicine : a journal of the British Diabetic Association. 2016;33(7):877-85. 423
3. Davies MJ, D'Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of 424
hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and 425
the European Association for the Study of Diabetes (EASD). Diabetologia. 2018;61(12):2461-98. 426
4. Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, et al. Management of 427
hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the 428
American Diabetes Association and the European Association for the Study of Diabetes. Diabetes care. 429
2015;38(1):140-9. 430
5. Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, et al. Management of 431
hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes 432
Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes care. 433
2012;35(6):1364-79. 434
6. Hara T, Ichimura A, Hirasawa A. Therapeutic role and ligands of medium- to long-chain Fatty Acid 435
receptors. Front Endocrinol (Lausanne). 2014;5:83. 436
7. Ichimura A, Hasegawa S, Kasubuchi M, Kimura I. Free fatty acid receptors as therapeutic targets for the 437
treatment of diabetes. Frontiers in pharmacology. 2014;5:236. 438
8. Watterson KR, Hudson BD, Ulven T, Milligan G. Treatment of Type 2 Diabetes by Free Fatty Acid 439
Receptor Agonists. Frontiers in Endocrinology. 2014;5. 440
Journ
al Pre-
proof

24
9. Li Z, Qiu Q, Geng X, Yang J, Huang W, Qian H. Free fatty acid receptor agonists for the treatment of type 441
2 diabetes: drugs in preclinical to phase II clinical development. Expert opinion on investigational drugs. 442
2016;25(8):871-90. 443
10. Riddy DM, Delerive P, Summers RJ, Sexton PM, Langmead CJ. G Protein-Coupled Receptors Targeting 444
Insulin Resistance, Obesity, and Type 2 Diabetes Mellitus. Pharmacological reviews. 2018;70(1):39-67. 445
11. Briscoe CP, Tadayyon M, Andrews JL, Benson WG, Chambers JK, Eilert MM, et al. The orphan G protein-446
coupled receptor GPR40 is activated by medium and long chain fatty acids. The Journal of biological chemistry. 447
2003;278(13):11303-11. 448
12. Ichimura A, Hirasawa A, Hara T, Tsujimoto G. Free fatty acid receptors act as nutrient sensors to 449
regulate energy homeostasis. Prostaglandins Other Lipid Mediat. 2009;89(3-4):82-8. 450
13. Itoh Y, Kawamata Y, Harada M, Kobayashi M, Fujii R, Fukusumi S, et al. Free fatty acids regulate insulin 451
secretion from pancreatic beta cells through GPR40. Nature. 2003;422(6928):173-6. 452
14. Edfalk S, Steneberg P, Edlund H. Gpr40 is expressed in enteroendocrine cells and mediates free fatty 453
acid stimulation of incretin secretion. Diabetes. 2008;57(9):2280-7. 454
15. Hara T, Kimura I, Inoue D, Ichimura A, Hirasawa A. Free Fatty Acid Receptors and Their Role in 455
Regulation of Energy Metabolism. In: Nilius B, Amara SG, Lill R, Offermanns S, Gudermann T, Petersen OH, et 456
al., editors. Reviews of Physiology, Biochemistry and Pharmacology. 164. Cham: Springer International 457
Publishing; 2013. p. 77-116. 458
16. Reimann F, Gribble FM. Mechanisms underlying glucose-dependent insulinotropic polypeptide and 459
glucagon-like peptide-1 secretion. Journal of diabetes investigation. 2016;7 Suppl 1:13-9. 460
17. Andersen A, Lund A, Knop FK, Vilsboll T. Glucagon-like peptide 1 in health and disease. Nature reviews 461
Endocrinology. 2018;14(7):390-403. 462
Journ
al Pre-
proof

25
18. Nauck MA, Meier JJ. Incretin hormones: Their role in health and disease. Diabetes, obesity & 463
metabolism. 2018;20 Suppl 1:5-21. 464
19. Hirasawa A, Tsumaya K, Awaji T, Katsuma S, Adachi T, Yamada M, et al. Free fatty acids regulate gut 465
incretin glucagon-like peptide-1 secretion through GPR120. Nat Med. 2005;11(1):90-4. 466
20. Iwasaki K, Harada N, Sasaki K, Yamane S, Iida K, Suzuki K, et al. Free fatty acid receptor GPR120 is highly 467
expressed in enteroendocrine K cells of the upper small intestine and has a critical role in GIP secretion after fat 468
ingestion. Endocrinology. 2015;156(3):837-46. 469
21. Paulsen SJ, Larsen LK, Hansen G, Chelur S, Larsen PJ, Vrang N. Expression of the Fatty Acid Receptor 470
GPR120 in the Gut of Diet-Induced-Obese Rats and Its Role in GLP-1 Secretion. PLoS ONE. 2014;9(2):e88227. 471
22. Ekberg JH, Hauge M, Kristensen LV, Madsen AN, Engelstoft MS, Husted AS, et al. GPR119, a Major 472
Enteroendocrine Sensor of Dietary Triglyceride Metabolites Coacting in Synergy With FFA1 (GPR40). 473
Endocrinology. 2016;157(12):4561-9. 474
23. Engelstoft MS, Park WM, Sakata I, Kristensen LV, Husted AS, Osborne-Lawrence S, et al. Seven 475
transmembrane G protein-coupled receptor repertoire of gastric ghrelin cells. Molecular metabolism. 476
2013;2(4):376-92. 477
24. Lu X, Zhao X, Feng J, Liou AP, Anthony S, Pechhold S, et al. Postprandial inhibition of gastric ghrelin 478
secretion by long-chain fatty acid through GPR120 in isolated gastric ghrelin cells and mice. American journal of 479
physiology Gastrointestinal and liver physiology. 2012;303(3):G367-76. 480
25. Gong Z, Yoshimura M, Aizawa S, Kurotani R, Zigman JM, Sakai T, et al. G protein-coupled receptor 120 481
signaling regulates ghrelin secretion in vivo and in vitro. American journal of physiology Endocrinology and 482
metabolism. 2014;306(1):E28-35. 483
26. Oh DY, Talukdar S, Bae EJ, Imamura T, Morinaga H, Fan W, et al. GPR120 is an omega-3 fatty acid 484
receptor mediating potent anti-inflammatory and insulin-sensitizing effects. Cell. 2010;142(5):687-98. 485
Journ
al Pre-
proof

26
27. Oh DY, Walenta E, Akiyama TE, Lagakos WS, Lackey D, Pessentheiner AR, et al. A Gpr120-selective 486
agonist improves insulin resistance and chronic inflammation in obese mice. Nat Med. 2014;20(8):942-7. 487
28. Azevedo CM, Watterson KR, Wargent ET, Hansen SV, Hudson BD, Kepczynska MA, et al. Non-Acidic 488
Free Fatty Acid Receptor 4 Agonists with Antidiabetic Activity. Journal of medicinal chemistry. 489
2016;59(19):8868-78. 490
29. Christiansen E, Watterson KR, Stocker CJ, Sokol E, Jenkins L, Simon K, et al. Activity of dietary fatty acids 491
on FFA1 and FFA4 and characterisation of pinolenic acid as a dual FFA1/FFA4 agonist with potential effect 492
against metabolic diseases. The British journal of nutrition. 2015;113(11):1677-88. 493
30. Flint A, Raben A, Astrup A, Holst JJ. Glucagon-like peptide 1 promotes satiety and suppresses energy 494
intake in humans. The Journal of clinical investigation. 1998;101(3):515-20. 495
31. Gutzwiller JP, Drewe J, Goke B, Schmidt H, Rohrer B, Lareida J, et al. Glucagon-like peptide-1 promotes 496
satiety and reduces food intake in patients with diabetes mellitus type 2. The American journal of physiology. 497
1999;276(5 Pt 2):R1541-4. 498
32. Verdich C, Flint A, Gutzwiller JP, Naslund E, Beglinger C, Hellstrom PM, et al. A meta-analysis of the 499
effect of glucagon-like peptide-1 (7-36) amide on ad libitum energy intake in humans. The Journal of clinical 500
endocrinology and metabolism. 2001;86(9):4382-9. 501
33. Mihalache L, Gherasim A, Nita O, Ungureanu MC, Padureanu SS, Gavril RS, et al. Effects of ghrelin in 502
energy balance and body weight homeostasis. Hormones (Athens, Greece). 2016;15(2):186-96. 503
34. Pasman WJ, Heimerikx J, Rubingh CM, van den Berg R, O'Shea M, Gambelli L, et al. The effect of Korean 504
pine nut oil on in vitro CCK release, on appetite sensations and on gut hormones in post-menopausal 505
overweight women. Lipids in health and disease. 2008;7:10. 506
Journ
al Pre-
proof

27
35. Hughes GM, Boyland EJ, Williams NJ, Mennen L, Scott C, Kirkham TC, et al. The effect of Korean pine 507
nut oil (PinnoThin) on food intake, feeding behaviour and appetite: a double-blind placebo-controlled trial. 508
Lipids in health and disease. 2008;7:6. 509
36. Verhoef SP, Westerterp KR. No effects of Korean pine nut triacylglycerol on satiety and energy intake. 510
Nutrition & metabolism. 2011;8(1):79. 511
37. Holst JJ, Madsbad S. Mechanisms of surgical control of type 2 diabetes: GLP-1 is key factor. Surg Obes 512
Relat Dis. 2016;12(6):1236-42. 513
38. Gribble FM, Diakogiannaki E, Reimann F. Gut Hormone Regulation and Secretion via FFA1 and FFA4. 514
Handbook of experimental pharmacology. 2017;236:181-203. 515
39. Ma J, Checklin HL, Wishart JM, Stevens JE, Jones KL, Horowitz M, et al. A randomised trial of enteric-516
coated nutrient pellets to stimulate gastrointestinal peptide release and lower glycaemia in type 2 diabetes. 517
Diabetologia. 2013;56(6):1236-42. 518
40. Flint A, Raben A, Blundell JE, Astrup A. Reproducibility, power and validity of visual analogue scales in 519
assessment of appetite sensations in single test meal studies. International journal of obesity and related 520
metabolic disorders : journal of the International Association for the Study of Obesity. 2000;24(1):38-48. 521
41. Kristensen M, Juul SR, Sorensen KV, Lorenzen JK, Astrup A. Supplementation with dairy calcium and/or 522
flaxseed fibers in conjunction with orlistat augments fecal fat excretion without altering ratings of 523
gastrointestinal comfort. Nutrition & metabolism. 2017;14:13. 524
42. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model 525
assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in 526
man. Diabetologia. 1985;28(7):412-9. 527
Journ
al Pre-
proof

28
43. Hansen T, Drivsholm T, Urhammer SA, Palacios RT, Volund A, Borch-Johnsen K, et al. The BIGTT test: a 528
novel test for simultaneous measurement of pancreatic beta-cell function, insulin sensitivity, and glucose 529
tolerance. Diabetes care. 2007;30(2):257-62. 530
44. Mari A, Pacini G, Murphy E, Ludvik B, Nolan JJ. A model-based method for assessing insulin sensitivity 531
from the oral glucose tolerance test. Diabetes care. 2001;24(3):539-48. 532
45. Matsuda M, DeFronzo RA. Insulin sensitivity indices obtained from oral glucose tolerance testing: 533
comparison with the euglycemic insulin clamp. Diabetes care. 1999;22(9):1462-70. 534
46. Sluiter WJ, Erkelens DW, Reitsma WD, Doorenbos H. Glucose tolerance and insulin release, a 535
mathematical approach I. Assay of the beta-cell response after oral glucose loading. Diabetes. 1976;25(4):241-536
4. 537
47. Seltzer HS, Allen EW, Herron AL, Jr., Brennan MT. Insulin secretion in response to glycemic stimulus: 538
relation of delayed initial release to carbohydrate intolerance in mild diabetes mellitus. The Journal of clinical 539
investigation. 1967;46(3):323-35. 540
48. ProductDescription_DRcaps™. A matter of timing. Ensure optimal delivery for acid-sensitive products. 541
2016 [Available from: https://s3.amazonaws.com/cpsl-web/kc/library/c1a-32029_DRCaps-A4_FIN.PDF. 542
49. Holst JJ. The physiology of glucagon-like peptide 1. Physiological reviews. 2007;87(4):1409-39. 543
50. Wren AM, Bloom SR. Gut hormones and appetite control. Gastroenterology. 2007;132(6):2116-30. 544
51. Callahan HS, Cummings DE, Pepe MS, Breen PA, Matthys CC, Weigle DS. Postprandial suppression of 545
plasma ghrelin level is proportional to ingested caloric load but does not predict intermeal interval in humans. 546
The Journal of clinical endocrinology and metabolism. 2004;89(3):1319-24. 547
52. Stevenson JL, Clevenger HC, Cooper JA. Hunger and satiety responses to high-fat meals of varying fatty 548
acid composition in women with obesity. Obesity (Silver Spring, Md). 2015;23(10):1980-6. 549
Journ
al Pre-
proof

29
53. Quintero-Florez A, Sinausia Nieva L, Sanchez-Ortiz A, Beltran G, Perona JS. The Fatty Acid Composition 550
of Virgin Olive Oil from Different Cultivars Is Determinant for Foam Cell Formation by Macrophages. Journal of 551
agricultural and food chemistry. 2015;63(30):6731-8. 552
Journ
al Pre-
proof

30
Table 1 Fasting baseline characteristics of subjects who completed study 1 and 2 553
Study 1
(n=8)
Study 2
(n=10)
Age (years) 32 ± 9 53 ± 8
Sex, m/f (%) 50 / 50 40 / 60
Height (cm) 175 ± 11 170 ± 10
Weight (kg) 77 ± 18 95 ± 13
BMI (kg/m2) 25.0 ± 3.0 31.3 ± 2.9
Fat mass (kg) 18.0 ± 6.7 34.9 ± 8.3
Fat % 23.3 ± 5.4 38.0 ± 7.8
Fat free mass (kg) 58.8 ± 13.8 57.0 ± 9.7
Systolic blood pressure (mmHg) 128 ± 20 130 ± 11
Diastolic blood pressure (mmHg) 73 ± 8 83 ± 9
Plasma glucose (mmol/L) 4.8 ± 0.6 5.3 ± 0.4
Creatinine (umol/L) 81 ± 8 79 ± 10
Triglycerides (mmol/L) 0.9 ± 0.3 1.3 ± 0.8
HDL-cholesterol (mmol/L) 1.4 ± 0.2 1.4 ± 0.6
LDL-cholesterol (mmol/L) 2.5 ± 0.4 3.4 ± 0.6
Total cholesterol (mmol/L) 4.4 ± 0.5 5.2 ± 0.7
HOMA-IR 1.2 ± 0.9 2.2 ± 0.8
Values are mean ± SD 554
Journ
al Pre-
proof

31
FIGURE LEGENDS 555
Fig. 1. Glucose (a-b), insulin (c-d) and C-peptide (e-f) levels during a 4h OGTT and corresponding AUCs 556
calculated from 0-120, 120-240 and 0-240 min in response to no oil (glucose alone) (black bars and black 557
circles), 3 g pine nut oil (PNO-TG, striped bars and grey triangles) or 3 g pine nut oil free fatty acids (PNO-558
FFA, dotted bars and white squares) in study 1. Values are mean ± SEM. *p<0.05, **p<0.01, (n = 8). 559
560
Fig. 2. Glucose (a-b), insulin (c-d) and C-peptide (e-f) levels during a 4h OGTT and corresponding AUCs 561
calculated from 0-120, 120-240 and 0-240 min in response to no oil (glucose alone) (black bars and black 562
circles), 3 g pine nut oil free fatty acids (PNO-FFA, dotted bars and white squares) or 6 g PNO FFA (checked 563
bars and grey diamonds) in study 2. Values are mean ± SEM. *p<0.05, **p<0.01, (n=10 for no oil and 6 g PNO-564
FFA treatments, and n=9 for 3g PNO-FFA, due to exclusion based on suspected non-compliance). 565
566
Fig. 3. GLP-1 (a-b), GIP (c-d) and ghrelin (e-f) levels during a 4h OGTT and corresponding AUCs calculated 567
from 0-120, 120-240 and 0-240 min in response to no oil (glucose alone) (black bars and black circles), 3 g pine 568
nut oil (PNO-TG, striped bars and grey triangles) or 3 g pine nut oil free fatty acids (PNO-FFA, dotted bars and 569
white squares) in study 1. Values are mean ± SEM. *p<0.05, **p<0.01, (n = 8). 570
571
Fig. 4 GLP-1 (a-b), GIP (c-d) and ghrelin (e-f) levels during a 4h OGTT and corresponding AUCs calculated 572
from 0-120, 120-240 and 0-240 min in response to no oil (glucose alone) (black bars and black circles), 3 g pine 573
nut oil free fatty acids (PNO-FFA, dotted bars and white squares) or 6 g PNO-FFA (checked bars and grey 574
diamonds) in study 2.Values are mean ± SEM. *p<0.05, **p<0.01, (n=10 for no oil and 6 g PNO-FFA 575
treatments, and n=9 for 3g PNO-FFA, due to exclusion based on suspected non-compliance). 576
Journ
al Pre-
proof

0
200
400
600
800
1000
1200
1400
0-120 120-240 0-240
Glu
co
se
AU
C (
mm
ol/L
*min
)
Time (min)
A
3
4
5
6
7
8
0 30 60 90 120 150 180 210 240
Glu
co
se
(m
mo
l/L
)
Time (min)
B
0
100
200
300
400
500
0 30 60 90 120 150 180 210 240
Insu
lin (
pm
ol/L
)
Time (min)
D
0
10000
20000
30000
40000
50000
60000
0-120 120-240 0-240
Insu
lin A
UC
(p
mo
l/L
*min
)
Time (min)
*
*
*
C
0
500
1000
1500
2000
2500
0 30 60 90 120 150 180 210 240
C-p
ep
tid
e (
pm
ol/L
)
Time (min)
No oil PNO-TG PNO-FFA
F
0
100000
200000
300000
400000
500000
0-120 120-240 0-240
C-p
ep
tid
e (
pm
ol/L
*min
)
Time (min)
No oil PNO-TG PNO-FFA
*
*
**
E
Journ
al Pre-
proof

Journ
al Pre-
proof

0
200
400
600
800
1000
1200
1400
1600
0-120 120-240 0-240
Glu
co
se
AU
C (
mm
ol/L
*min
)
Time (min)
*
**
*
A
3
4
5
6
7
8
9
0 30 60 90 120 150 180 210 240
Glu
co
se
(m
mo
l/L
)
Time (min)
B
0
10000
20000
30000
40000
50000
60000
70000
80000
0-120 120-240 0-240
Insu
lin A
UC
(p
mo
l/L
*min
)
Time (min)
*
*
C
0
100
200
300
400
500
600
700
0 30 60 90 120 150 180 210 240
Insu
lin (
pm
ol/L
)
Time (min)
D
0
100000
200000
300000
400000
500000
600000
700000
0-120 120-240 0-240
C-p
ep
tid
e (
pm
ol/L
*min
)
Time (min)
No oil 3g PNO-FFA 6g PNO-FFA
**
E
0
1000
2000
3000
4000
5000
0 30 60 90 120 150 180 210 240
C-p
ep
tid
e (
pm
ol/L
)
Time (min)
No oil 3g PNO-FFA 6g PNO-FFA
F
Journ
al Pre-
proof

0
1000
2000
3000
4000
5000
0-120 120-240 0-240
GL
P-1
AU
C (
pg
/mL
*min
)
Time (min)
**
**
** A
0
10
20
30
40
50
0 60 120 180 240
GL
P-1
AU
C (
pg
/mL
)
Time (min)
B
0
50
100
150
200
250
300
350
0 60 120 180 240
GIP
AU
C (
pg
/mL
)
Time(min)
D
0
10000
20000
30000
40000
50000
60000
0-120 120-240 0-240
GIP
AU
C (
pg
/mL
*min
)
Time (min)
* *
C
0
200
400
600
800
1000
1200
0 60 120 180 240
Gh
relin
(p
g/m
L)
Time (min)
No oil PNO-TG PNO-FFA
F
0
30000
60000
90000
120000
150000
180000
0-120 120-240 0-240
Gh
relin
AU
C (
pg
/mL
)
Time (min)
No oil PNO-TG PNO-FFA
* *
**
**
E
Journ
al Pre-
proof

0
1000
2000
3000
4000
5000
6000
7000
0-120 120-240 0-240
GL
P-1
AU
C (
pg
/mL
*min
)
Time (min)
**
*
**
* * A
0
5
10
15
20
25
30
35
40
45
0 60 120 180 240
GL
P-1
(p
g/m
L)
Time (min)
B
0
10000
20000
30000
40000
50000
60000
70000
0-120 120-240 0-240
GIP
AU
C (
pg
/mL
*min
)
Minutes
C
0
100
200
300
400
500
0 60 120 180 240
GIP
(p
g/m
L)
Time (min)
D
0
200
400
600
800
1000
1200
1400
0 60 120 180 240
Gh
relin
(p
g/m
L)
Time (min)
No oil 3g PNO-FFA 6g PNO-FFA
F
0
50000
100000
150000
200000
250000
0-120 120-240 0-240
Gh
relin
AU
C (
pg
/mL
*min
)
Time (min)
No oil 3g PNO-FFA 6g PNO-FFA
E
*
**
*
Journ
al Pre-
proof