Activity-Oriented Antiedema Proprioceptive Therapy (TAPA ...
11
Citation: Muñoz-Alcaraz, M.N.; Jiménez-Vílchez, A.J.; Santamaría- Peláez, M.; Perola-de Torres, L.A.; Olmo-Carmona, M.V.; Muñoz-García, M.T.; Jorge-Gutiérrez, P.; Serrano- Merino, J.; Romero-Rodríguez, E.; Rodríguez-Elena, L.; et al. Activity- Oriented Antiedema Proprioceptive Therapy (TAPA) for Shoulder Mobility Improvement in Women with Upper Limb Lymphedema Secondary to Breast Cancer: A Multicenter Controlled Clinical Trial. J. Clin. Med. 2022, 11, 2234. https:// doi.org/10.3390/jcm11082234 Academic Editor: Venerando Rapisarda Received: 4 March 2022 Accepted: 12 April 2022 Published: 16 April 2022 Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affil- iations. Copyright: © 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https:// creativecommons.org/licenses/by/ 4.0/). Journal of Clinical Medicine Article Activity-Oriented Antiedema Proprioceptive Therapy (TAPA) for Shoulder Mobility Improvement in Women with Upper Limb Lymphedema Secondary to Breast Cancer: A Multicenter Controlled Clinical Trial María Nieves Muñoz-Alcaraz 1,2 , Antonio José Jiménez-Vílchez 3 , Mirian Santamaría-Peláez 4 , Luis A. Pérula-de Torres 2,5, * , María Victoria Olmo-Carmona 1 , María Teresa Muñoz-García 1 , Presentación Jorge-Gutiérrez 1 , Jesús Serrano-Merino 2,5 , Esperanza Romero-Rodríguez 2,5 , Lorena Rodríguez-Elena 6 , Raquel Refusta-Ainaga 6 , María Pilar Lahoz-Sánchez 6 , Belén Miró-Palacios 7 , Mayra Medrano-Cid 8 , Rosa Magallón-Botaya 9 , Luis A. Mínguez-Mínguez 10, *, Josefa González-Santos 4 and Jerónimo J. González-Bernal 4 1 Inter-Level Clinical Management Unit of Physical Medicine and Rehabilitation, Córdoba and Guadalquivir Health District, Reina Sofía University Hospital, Andalusia Health Service, 14011 Cordoba, Spain; [email protected] (M.N.M.-A.); [email protected] (M.V.O.-C.); [email protected] (M.T.M.-G.); [email protected] (P.J.-G.) 2 Maimonides Institute for Biomedical Research of Córdoba, Reina Sofía University Hospital, University of Córdoba, 14011 Cordoba, Spain; [email protected] (J.S.-M.); [email protected] (E.R.-R.) 3 Valle de los Pedroches Hospital, Andalusia Health Service, 14400 Pozoblanco, Spain; [email protected] 4 Department of Health Sciences, University of Burgos, 09001 Burgos, Spain; [email protected] (M.S.-P.); [email protected] (J.G.-S.); [email protected] (J.J.G.-B.) 5 Multiprofessional Teaching Unit for Family and Community Care, Córdoba and Guadalquivir Health District, 14011 Cordoba, Spain 6 San Jose Health Center, Aragonese Health Service, 50013 Zaragoza, Spain; [email protected] (L.R.-E.); [email protected] (R.R.-A.); [email protected] (M.P.L.-S.) 7 Association of People with Lymphedema in Aragon (ADPLA), 50007 Zaragoza, Spain; [email protected] 8 Lozano Blesa University Clinical Hospital, Aragonese Health Service, 50013 Zaragoza, Spain; [email protected] 9 Institute for Health Research Aragon (IIS Aragon), University of Zaragoza, 50009 Zaragoza, Spain; [email protected] 10 Department of Educational Sciences, University of Burgos, 09001 Burgos, Spain * Correspondence: [email protected] (L.A.P.-d.T.); [email protected] (L.A.M.-M.) Abstract: Background: Lymphedema, secondary to breast cancer (BCRL), is the abnormal accumula- tion of protein-rich fluid in the interstitium caused by a malfunction of the lymphatic system. It causes swelling, deficiencies in upper limb functions and structures, sensory pain and emotional alterations, which have a chronic course and affect the upper limb’s functionality. This study aims to verify the efficacy and efficiency in the upper limbs functionality of a protocolized experimental approach based on occupational therapy, TAPA (activity-oriented proprioceptive antiedema therapy), in the rehabilitation of BCRL in stages I and II, comparing it with the conservative treatment considered as the standard, complex decongestive therapy (CDT), through a multicenter randomized clinical trial. Methods: a randomized and prospective clinical trial was conducted with experimental and control groups. Women diagnosed with BCRL belonging to institutions in Córdoba and Aragon (Spain) participated. Sociodemographic variables and those related to the functionality of the affected upper limb were evaluated before and after the intervention. Results: The results showed statistically significant differences in the analysis of covariance performed for the variable joint balance of the shoulders external rotation (p = 0.045) that could be attributed to the intervention performed; how- ever, the effect size was minimal (η 2 ≤ 0.080). In the rest of the variables, no significant differences were found. Conclusions: TAPA may be an alternative to the conservative treatment of women with J. Clin. Med. 2022, 11, 2234. https://doi.org/10.3390/jcm11082234 https://www.mdpi.com/journal/jcm
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Activity-Oriented Antiedema Proprioceptive Therapy (TAPA ...

�����������������
Citation: Muñoz-Alcaraz, M.N.;
Jiménez-Vílchez, A.J.; Santamaría-
Peláez, M.; Perola-de Torres, L.A.;
Olmo-Carmona, M.V.; Muñoz-García,
M.T.; Jorge-Gutiérrez, P.; Serrano-
Merino, J.; Romero-Rodríguez, E.;
Rodríguez-Elena, L.; et al. Activity-
Oriented Antiedema Proprioceptive
Therapy (TAPA) for Shoulder
Mobility Improvement in Women
with Upper Limb Lymphedema
Secondary to Breast Cancer: A
Multicenter Controlled Clinical Trial.
J. Clin. Med. 2022, 11, 2234. https://
doi.org/10.3390/jcm11082234
Academic Editor: Venerando
Rapisarda
Received: 4 March 2022
Accepted: 12 April 2022
Published: 16 April 2022
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
Copyright: © 2022 by the authors.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
Journal of
Clinical Medicine
Article
Activity-Oriented Antiedema Proprioceptive Therapy (TAPA)for Shoulder Mobility Improvement in Women with UpperLimb Lymphedema Secondary to Breast Cancer: A MulticenterControlled Clinical TrialMaría Nieves Muñoz-Alcaraz 1,2 , Antonio José Jiménez-Vílchez 3 , Mirian Santamaría-Peláez 4 ,Luis A. Pérula-de Torres 2,5,* , María Victoria Olmo-Carmona 1, María Teresa Muñoz-García 1,Presentación Jorge-Gutiérrez 1, Jesús Serrano-Merino 2,5, Esperanza Romero-Rodríguez 2,5 ,Lorena Rodríguez-Elena 6, Raquel Refusta-Ainaga 6 , María Pilar Lahoz-Sánchez 6 , Belén Miró-Palacios 7,Mayra Medrano-Cid 8, Rosa Magallón-Botaya 9 , Luis A. Mínguez-Mínguez 10,*, Josefa González-Santos 4
and Jerónimo J. González-Bernal 4
1 Inter-Level Clinical Management Unit of Physical Medicine and Rehabilitation, Córdoba and GuadalquivirHealth District, Reina Sofía University Hospital, Andalusia Health Service, 14011 Cordoba, Spain;[email protected] (M.N.M.-A.); [email protected] (M.V.O.-C.);[email protected] (M.T.M.-G.); [email protected] (P.J.-G.)
2 Maimonides Institute for Biomedical Research of Córdoba, Reina Sofía University Hospital,University of Córdoba, 14011 Cordoba, Spain; [email protected] (J.S.-M.);[email protected] (E.R.-R.)
3 Valle de los Pedroches Hospital, Andalusia Health Service, 14400 Pozoblanco, Spain;[email protected]
4 Department of Health Sciences, University of Burgos, 09001 Burgos, Spain; [email protected] (M.S.-P.);[email protected] (J.G.-S.); [email protected] (J.J.G.-B.)
5 Multiprofessional Teaching Unit for Family and Community Care, Córdoba and Guadalquivir Health District,14011 Cordoba, Spain
6 San Jose Health Center, Aragonese Health Service, 50013 Zaragoza, Spain; [email protected] (L.R.-E.);[email protected] (R.R.-A.); [email protected] (M.P.L.-S.)
7 Association of People with Lymphedema in Aragon (ADPLA), 50007 Zaragoza, Spain;[email protected]
8 Lozano Blesa University Clinical Hospital, Aragonese Health Service, 50013 Zaragoza, Spain;[email protected]
9 Institute for Health Research Aragon (IIS Aragon), University of Zaragoza, 50009 Zaragoza, Spain;[email protected]
10 Department of Educational Sciences, University of Burgos, 09001 Burgos, Spain* Correspondence: [email protected] (L.A.P.-d.T.); [email protected] (L.A.M.-M.)
Abstract: Background: Lymphedema, secondary to breast cancer (BCRL), is the abnormal accumula-tion of protein-rich fluid in the interstitium caused by a malfunction of the lymphatic system. It causesswelling, deficiencies in upper limb functions and structures, sensory pain and emotional alterations,which have a chronic course and affect the upper limb’s functionality. This study aims to verify theefficacy and efficiency in the upper limb´s functionality of a protocolized experimental approachbased on occupational therapy, TAPA (activity-oriented proprioceptive antiedema therapy), in therehabilitation of BCRL in stages I and II, comparing it with the conservative treatment consideredas the standard, complex decongestive therapy (CDT), through a multicenter randomized clinicaltrial. Methods: a randomized and prospective clinical trial was conducted with experimental andcontrol groups. Women diagnosed with BCRL belonging to institutions in Córdoba and Aragon(Spain) participated. Sociodemographic variables and those related to the functionality of the affectedupper limb were evaluated before and after the intervention. Results: The results showed statisticallysignificant differences in the analysis of covariance performed for the variable joint balance of theshoulder´s external rotation (p = 0.045) that could be attributed to the intervention performed; how-ever, the effect size was minimal (η2 ≤ 0.080). In the rest of the variables, no significant differenceswere found. Conclusions: TAPA may be an alternative to the conservative treatment of women with
J. Clin. Med. 2022, 11, 2234. https://doi.org/10.3390/jcm11082234 https://www.mdpi.com/journal/jcm

J. Clin. Med. 2022, 11, 2234 2 of 11
BCRL. It was shown to be just as effective for volume reduction and activity performance as CDT butmore effective in improving external rotation in shoulder joint balance.
Keywords: occupational therapy; breast cancer; secondary lymphedema; upper limb; complexdecongestive therapy; multidisciplinary oncological rehabilitation; activity-oriented anti-edematherapy; manual lymphatic drainage
1. Introduction
The International Society of Lymphology (ISL) defines lymphedema as an externaland/or internal lymphatic system insufficiency manifested by a reduction in general lym-phatic transport. It produces swelling due to the accumulation of excess water, diffusedfiltered plasma proteins, extravascular and parenchymal blood cells and stromal cellsproducts in the extracellular space. The World Health Organization´s International Classifi-cation of Diseases includes this disease as a disorder of the circulatory system [1]; its courseusually becomes chronic and requires lifelong biopsychosocial treatment, whose results areoften not optimal [2].
The most frequent cause of secondary lymphedema in developed countries is sec-ondary to neoplasms, their complications and treatments being the most frequent the upperlimb BCRL [3], which is currently the most diagnosed tumor in the world, with more than2.26 million new cases in 2020 [4].
BCRL can lead to inflammatory complications that cause skin hardening that can breakand leave the area exposed to frequent infections, which worsen the BCRL. There may bean alteration of the patient’s sensitivity to touch and kinesthetics, their sexuality perception,self-image problems, decreased levels of physical activity, fatigue, psychological distress,limitations in the strength, endurance and active range of motion of the upper limbs andother sensations related to pain, swelling and heaviness, which decrease the functionalityof the affected arm [5–10].
There is no clear consensus on the diagnostic criteria for BCRL. The most commonlyused system is that of the ISL, based on a three-stage scale for the classification of alymphedematous limb, from stage 0, subclinical or latent, to stage III, that is lymphostaticelephantiasis [2].
Complex or combined decongestive physical therapy (CDT) is considered the stan-dard in the conservative treatment of lymphedema, with limited evidence [11]. It includesskin care, manual lymphatic drainage, joint mobility exercises, compression garments andmultilayer bandages. However, there is no clear optimal treatment strategy, both becauseof the variability in the protocols, as well as the lack of standardization of results and thevariability in the quality of the studies carried out [12]. A wide variety of compression gar-ments are prescribed for lymphedema [13], and the non-serious adverse effects associatedwith it are identified as skin irritation, discomfort and pain, as well as very rare but seriousadverse events, including soft tissue and nerve injuries [14]. It is also contraindicatedin arterial insufficiency, severe heart failure and untreated infections [15]. Furthermore,there is no optimal level of adherence to its use because it causes patients to experiencediscomfort, negative emotions and interference with function and social situations [16];in addition, its use does not provide a benefit or is contraindicated during the practice ofphysical activity [17].
Current evidence agrees with the need for further research in multidisciplinary oncologyrehabilitation and recommends a multidisciplinary approach in patients with BCRL, includingbut not limited to occupational therapy [18–25], health training/promotion [9,26–28] andphysical activity [29,30].
People with BCRL can present alterations of mechanosensitivity [31]. Surgery, chemother-apy and treatment with taxanes can also cause peripheral neuropathies, causing pain andsensitivity alteration in the upper limb, so it is advisable to incorporate neurodynamic

J. Clin. Med. 2022, 11, 2234 3 of 11
activity [32,33]. The literature also recommends adding patterns of proprioceptive neuro-muscular facilitation to BCRL rehabilitation [34–36]. New cohesive, adaptable bandagesystems that provide greater comfort [37,38] are being evaluated, allowing activities andparticipation in fundamental areas of life.
Based on this evidence, the proposed experimental treatment, TAPA (activity-orientedproprioceptive antiedema therapy), whose results are presented in this article, is comparedto the standard treatment, CDT.
The purpose of this study is to evaluate the effectiveness of TAPA as a safe andeffective alternative in conservative BCRL treatment to improve the functionality of theupper limb affected by lymphedema, especially in individuals who did not adapt tocontinuous compression garment use and who had no optimal results.
2. Materials and Methods2.1. Study Design
Controlled clinical trial, multicenter, randomized by stratification in two gradients,with two parallel arms and single-blind.
The protocol of this study was published in BMC Cancer [39] and was modified from aunicentric to multicenter design in order to facilitate recruitment due to the current stateof the SARS-CoV-2 (COVID-19) pandemic, which forced the interruption of activity inthe rehabilitation centers, both public and private, of the National Health System. Thetrial is registered in ClinicalTrials.gov [NCT03762044], dated 23 November 2018: https://clinicaltrials.gov/ct2/show/NCT03762044.
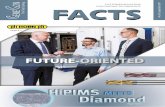
The study followed the following flowchart (Figure 1):
J. Clin. Med. 2021, 10, x FOR PEER REVIEW 5 of 14
The study followed the following flowchart (Figure 1): 170 171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
Figure 1. Flowchart. CDT: Complex descongestive physical therapy; TAPA: activity-oriented proprioceptive antiedema 197 therapy. 198
199
Assessed for eligibility (n= 64)
Excluded (n=1) Not meeting inclusion criteria
(n=1) Declined to participate (n=0)
Analysed (n=25) Excluded from analysis (incomplete data)
(n=3)
Lost to follow-up (abandonment) (n=2) Discontinued intervention (complication: cellulite) (n=1)
Allocated to CDT intervention (n=32) Received allocated intervention (n=31) Did not receive allocated intervention
(difficulties in getting to the health centre)
Lost to follow-up (doesn´t go to the review) (n=1) Discontinued intervention (inadequate treatment adherence) (n=1)
Allocated to TAPA intervention (n=31) Received allocated intervention (n=30) Did not receive allocated intervention
(surgical intervention breast reconstruction) (n=1)
Analysed (n=26) Excluded from analysis (incomplete data)
(n=2 )
Analysis
Randomized (n=63)
Enrollment
Allocation
Follow-Up
Formatted: Indent: Left: 0 cm, First line: 0 cm
Formatted: MDPI_3.1_text, Space Before: 0 pt
Figure 1. Flowchart. CDT: Complex decongestive physical therapy; TAPA: activity-oriented proprio-ceptive antiedema therapy.

J. Clin. Med. 2022, 11, 2234 4 of 11
2.2. Study Participants
The study population consisted of women operated on for breast cancer (BC) anddiagnosed with upper limb BCRL in stages I and II. They were recruited in two areas:(a) referred to the Clinical Management Unit Inter-levels of Rehabilitation of the ReinaSofía University Hospital of Córdoba and Córdoba and Guadalquivir Health District ofthe Andalusian Health Service from primary and specialized care and (b) derived from theAssociation of Aragonese Women with Genital and Breast Cancer (AMAC-GEMA) andAssociation of People with Lymphedema of Aragon (ADPLA) to the San José Health Centreand University Clinical Hospital of the Aragonese Health Service.
Inclusion criteria were women operated on for BC with BCRL in stages I and II (asdefined in the consensus document of the International Society of Lymphology 2020 [2])and those who signed the informed consent form. The study excluded patients withhealth problems, diseases or dysfunctions that prevented them from participating in theintervention or those with bilateral lymphedema.
It was determined that a reduction of 150 mL in the volume of lymphedema couldbe established as relevant (minimum detectable value), approximately 20% with respectto baseline [40]. Taking into account the data from the literature on means and standarddeviations obtained in other studies [35,41], for an alpha error of 0.05 and a statistical powerof 80%, the necessary sample size would be 29 subjects per group (calculated with EPIDAT4.2). It was assumed that the effect of the standard treatment in the control group (CG)would result in a reduction in arm volume by an average of 5%, the treatment effect in theexperimental group (EG) would cause an average reduction in arm volume of 20% and thestandard deviation would be similar in both groups, approaching 20% [42]. Considering adropout rate of 10% in each group, the estimated corrected sample size was 64 patients,randomly assigned to two groups of 32 patients each, with 16 per stage for each treatmentgroup (CG: 16 in stage I and 16 in stage II. EC: 16 in stage I and 16 in stage II).
2.3. Procedure and Randomization
Consecutive sampling was performed in which patients who met the criteria wereinvited to participate in the study as they were identified and recruited. The patientswere grouped by stratified random selection using the statistical software EPIDAT, 3.1,which stratifies patients by lymphedema stage in a 1:1 ratio using random-sized blocksof four. The assignment sequence was concealed from the evaluating researcher usingnumbered, opaque, sealed and stapled envelopes. The researchers in charge of monitoringand analyzing the data (a Specialist in Preventive Medicine and Public Health, a nurse anda Specialist in Family and Community Medicine) were also blinded to the result after theinterventions were assigned.
The degree of interobserver reliability between the different evaluators in the mea-surement of the circometry of both arms (affection and healthy) in 4 volunteer subjectswas analyzed, with 7 measurements in 7 predefined anatomical regions and with 5 cm ofdifference between them in each of them. The interobserver agreement for these measure-ments was analyzed by measuring the intraclass correlation coefficient (ICC) with Epidat4.2 software, obtaining a value of 0.60, which indicates a good degree of agreement. Forthe interpretation of the CCI, the classification obtained by Fleiss was used [43], accordingto which a CCI > 0.91 corresponded to very good concordance; 0.71–0.90, good; 0.51–0.70,moderate; 0.31–0.50, mediocre and if it was <0.30, the agreement would be bad or very bad.
2.4. Main Outcomes
The degree of lymphedema was measured by calculating the volume difference be-tween the affected upper limb and the contralateral limb as a percentage and in millilitres(mL). According to the percentage of volumetry through circometry (manual measurementof limb perimeters with measuring tape, the volume value is approximate and volumecalculation is according to Kuhnke’s formula), Vol = (C1 2 + C2 2 + . . . Cn 2)/π) [44–46]. Adistinction was made between Grade 1 or mild (difference in volume 5–20% with respect to

J. Clin. Med. 2022, 11, 2234 5 of 11
the healthy arm) and Grade 2 or moderate (difference in volume 20–40% with respect tothe healthy arm). According to volumetry expressing the volume in mL by the differencein volume as a % between both extremities, a reduction of edema of 150 mL (20%) overbaseline was required to be considered clinically relevant [47].
Shoulder joint balance for flexion (JBF), abduction (JBABD) and external rotation(JBER) was measured with a goniometer.
Upper limb function/activity performance: Measured with the Quick Disabilities ofthe Arm, Shoulder and Hand (Quick-DASH), with cross-cultural adaptation, reliability,validity and sensitivity to changes from its extended version in 2006 [48–50]. For the valueof the Quick-DASH, the result was calculated as a percentage; the higher the result obtained,the greater the disability or symptom.
2.5. Statistical Analysis
Statistical analysis was performed with the intention to treat. Quantitative variablesare described as the mean, standard deviation and limits of each distribution and qualitativevariable as absolute and relative frequencies. A bivariate analysis was performed, verify-ing that the quantitative variables follow a normal distribution, using the Shapiro–Wilktest. After that, the differential scores for all the continuous variables were calculated bysubtracting the pretest score from the post-test score; these differential scores were used inthe covariance analysis (ANCOVA) to check if statistically significant differences appearedbetween CG and EG for the variables analyzed. The pretest score of the dependent variablewas used as a covariate and the intervention group was used as a fixed factor. The effectsize was estimated using the eta square coefficient (η2) so that if 0 ≤ η2 < 0.05, there was noeffect; if 0.05 ≤ η2 < 0.26, the effect was minimal; if 0.26 ≤ η2 < 0.64, the effect was moderate;and if η2 ≥ 0.64, the effect was strong [51]. The statistical analysis was performed with thestatistical package for social sciences (SPSS v.28), establishing a statistical significance valueof p < 0.05.
2.6. Intervention
Both groups received a 3 h health education workshop on lymphedema prior to theintervention, in which basic knowledge about the pathophysiology of lymphedema, earlyidentification of symptoms, preventive skin care measures, guidance for ADL performance,including physical activity, and recommendations for exercises and anti-edema postures tobe performed at least once a day were taught.
The EG group applied the TAPA treatment to stages I and II. They received 10 sessions(2 weekly) of 30 min each, led by two occupational therapists, one from the health district ofCórdoba and Guadalquivir and another from the San José de Zaragoza Health Centre. Thistreatment consisted of myolinfokinetic therapeutic activity which reduced the volume oflymphedema and was significant for each individual. It also involved the measurement andgraduation of neurodynamic components, the proprioceptive neuromuscular facilitation ofsignificant activities and a proprioceptive cohesive anti-edema bandage, similar to a Cobantype bandage, single layer, without compression and with high cotton content. The patientand/or caregiver was instructed on its use and placement, and modifications/adaptationswere recommended for optimal performance in their activities of daily living (ADL). Afterthe 10 sessions, each patient had to perform 5 individually prescribed daily activities andwas told not to wear any compression garment.
The intervention of the CG in stage I was developed by a Physical Medicine andRehabilitation Specialist and a Family and Community Medicine Specialist, and in stage IIby two physiotherapists, one from the UGC Interleaved of Physical Medicine and rehabil-itation and the other from the University Clinical Hospital of Zaragoza and consisted ofaction collected by the Integrated Breast Cancer Care Process of the Ministry of Health [52].Stage I consisted of preventive measures, skin care, exercise and the use of compressiongarments (duration of 5 weeks). Stage II consisted of 10 60 min sessions with conservativeCDTY treatment, three times per week, as usual, with the full CDT session length, but

J. Clin. Med. 2022, 11, 2234 6 of 11
there are no protocols that defined specific guidelines for the application of the treatment,leaving it to the professional´s discretion according to the patient´s state. Stage II patientsalso received skin protection, multilayer bandages, manual lymphatic drainage and weretold to wear a compression garment.
The project was approved by the Research Ethics Committee of Córdoba in a meetingheld on November 27, 2018 (Act no. 282, ref. 4084) and the authorization of the Man-agement/Direction of the Health District of Córdoba and Guadalquivir, the Reina SofíaUniversity Hospital and the AECC Headquarters Córdoba.
The principles established in the Declaration of Helsinki of 1964, of the World MedicalAssociation and subsequent amendments and the 1996 Council of Europe Conventionon Human Rights and Biomedicine, as well as the requirements established in Spanishlegislation, were respected. The investigation complied with the rules of good clinicalpractice (art. 34 RD 223/2004; community directive 2001/20/EC), the protection of personaldata and confidentiality (European Data Protection Regulation, and in accordance withOrganic Law 3/2018 on the Protection of Personal Data and guarantee of digital rights).In the development of the study, Law 41/2002 on Patient Autonomy and Law 14/2007 onBiomedical Research were considered.
3. Results3.1. Main Characteristics of the Participants
Of the 63 women who were recruited for this study, 51 finished it, 25 belonged to theGC and 26 to the GE. There were 12 losses as a result of inadequate adherence to treatmentand data collection issues.
The mean age was 59.24 years (SD ± 9.55), and they were mainly active (n = 26; 51%)or retired (n = 19; 37%). In relation to the surgical intervention, two participants (4%)underwent breast-conserving surgery, while the rest underwent a mastectomy (n = 49; 96%).In most cases (n = 43; 84%) there were no post-surgical complications.
3.2. Volume, Joint Balance and Upper Limb Function: Differences between Groups
Table 1 show the descriptive results of the study, comparing them basally according tothe group. Only a statistically significant difference in age was observed (p = 0.026).
Table 1. Analysis of the baseline comparability of both results.
VariableType of
TreatmentReceived
n Mean SD SEM
Age Experimental 31 58.00 9.71 1.74Control 32 63.66 9.96 1.76
Body mass index Experimental 30 28.76 4.73 0.86Control 31 27.59 4.91 0.88
Number of nodes removedExperimental 29 14.00 9.73 1.80
Control 24 12.20 7.21 1.47
Pain, VAS scale 0–10Experimental 31 3.77 2.82 0.50
Control 32 3.88 3.11 0.55
Heaviness, VAS scale 0–10Experimental 31 4.87 2.79 0.50
Control 32 4.88 2.25 0.39
Tightness, VAS scale 0–10 Experimental 31 4.19 2.67 0.48Control 32 4.38 2.72 0.48
Health QuestionnaireExperimental 31 67.10 18.42 3.31
Control 30 64.83 16.47 3.00SD: Standard deviation; SEM: Standard error mean.

J. Clin. Med. 2022, 11, 2234 7 of 11
The data in Table 2 show the main results obtained from the Covariance Analysis(ANCOVA) performed for each of the continuous variables in order to determine if therewere significant statistical differences between the GC and EG after the intervention.
Table 2. Comparison between groups in continuous variables differential punctuation, controllingpretest scores. ANCOVA.
Variable SourceType IIISum ofSquare
df MS F p-Value η2
Differential Vol%Vol% pre-test 194,568,957 1 194,568,957 1,809,568 <0.001 0.974
CG/EG 82,518 1 82,518 0.767 0.385 0.016Error 5,161,072 48 107,522
Differential Vol mLVol mL pre-test 8,698,016 1 8,698,016 0.478 0.493 0.010
CG/EG 10,305,528 1 10,305,528 0.567 0.455 0.012Error 872,983,058 48 18,187,147
DifferentialQDASH
QDASH pre-test 3325 1 3.325 0.019 0.890 0.000CG/EG 94,477 1 94.477 0.545 0.464 0.011
Error 8,317,476 48 173.281
Differential JBERJBER pre-test 200,036 1 200,036 6289 0.016 0.114
CG/EG 135,014 1 135,014 4245 0.045 0.080Error 1,558,617 49 31,809
Differential JBFJBF pre-test 624,712 1 624,712 6723 0.013 0.121
CG/EG 128,549 1 128,549 1383 0.245 0.027Error 4,553,173 49 92,922
Differential JBABDJBABD pre-test 239,799 1 239,799 1171 0.284 0.023
CG/EG 477,384 1 477,384 2331 0.133 0.045Error 10,034,239 49 204,780
Vol%: degree of lymphedema according to volumetric percentage; Vol mL: degree of lymphedema accordingto the volume expressed in mL; QDASH: upper limb function; JBER: joint balance external rotation; JBF: jointbalance flexion; JBABD: joint balance abduction; MS: mean square; CG: Control Group; EG: Experimental Group.
ANCOVA showed statistically significant differences between GC and GE in the jointbalance of the external rotation of the shoulder, controlling the scores obtained in thepretest, which could be attributed to the intervention performed. This means that theJBER scored higher at the end of the EG and improved more in the group of participantswho received the TAPA treatment based on activity as a treatment method and withoutcompression in the upper limb of the affected side, compared to the group that received theconventional treatment. Despite being significant, the effect size was (η2 ≤ 0.080), and nostatistically significant differences were obtained in the other dimensions of functionalityand volume studied between the two intervention groups. However, there were verysignificant differences (p < 0.001) in the percentage of edema volume reduction and in theshoulder flexion joint balance improvement (p = 0.013) within patients who underwent theexperimental intervention with respect to their baseline situation, although this was notcorrelated with statistically significant improvements between groups for the performanceof upper limb activities evaluated with QuickDash (p = 0.464).
4. Discussion
The results of this study do not show significant differences in the volume reduction ofBCRL between the intervention groups (control and experimental) that are consistentwiththe review performed by Jeanette Ezzo et al. [53]. However, the decrease in volumereduction with the experimental treatment, TAPA, was very significant with respect to thebaseline evaluation of the patients. On the other hand, they observe contradictory resultsin the function of the range of motion, while this research shows a significant improvement

J. Clin. Med. 2022, 11, 2234 8 of 11
in the joint balance of external shoulder rotation. The experimental intervention alsoimproved significantly the shoulder flexion joint balance.
In this line of results, the meta-analysis by Flávia Belavenuto Rangon BS et al. [54]notes, like our findings, found that there were no statistically significant differences in theeffect between CDT and short-term multimodal approaches on volume reduction. Theseauthors also found no significant differences regarding upper limb physical function whencompared with TAPA.
Paolo Marchica et al. [55] reviewed the state of the art treatment of BCRL, noting thatonly bandages and intermittent pneumatic pressure showed a substantial beneficial effectin reducing lymphedema volume in the acute-intensive phase and that manual lymphaticdrainage, an essential component of CDT, was not effective for BCRL. They also pointedout that physical activity remains a milestone in BCRL as it reduces volume and improvesupper limb strength; these conclusions support TAPA’s effectiveness since it uses significantactivity and a proprioceptive bandage as treatment methods, with optimal results both involume reduction and upper limb function. TAPA facilitates therapeutic decision-making,establishing treatment doses, as it involves an intervention protocol with a specific numberof sessions and activities and with a treatment duration also defined, with five activitiesand a self-bandage that is not compressive but proprioceptive. Currently, the number ofhours and contexts in which the patient needs to use the compression garments is left tothe therapist’s discretion, as well as the frequency and need for rehabilitative treatmentand its temporalization.
One of the strengths of this study is that it stands as an effective therapeutic alternativefor people with BCRL who have contraindications to perform CDT, as well as for those whodo not wish to use compression garments while eliminating the possible adverse effects ofdifferent compressive treatments.
Another important aspect of this study is that it can help to plan the care and needsof people with BC by increasing, to a greater degree, the joint balance of the externalrotation of the shoulder compared to conventional treatments since, as observed by RoserBelmonte et al. [56], the loss of strength for external rotators and range of motion of theshoulder and health-related quality of life in the physical domains and the arm persistsat 5 years in the groups of patients operated on for BC. Similarly, Emine Baran et al. [57]described that BCRL patients have a lower active shoulder range of motion on all measuresthan unaffected people without BCRL.
The authors consider it a limitation of the study not to have evaluated the joint balanceof the elbow since it could have provided additional information of interest on the impact ofthe loss of joint range in the difficulties of carrying out activities and problems of restrictionof participation as shoulder and elbow angles are necessary to perform activities of dailyliving. Still, elbow angles are considered of greater relevance [58], which could justify thatsignificant improvements in upper limb functionality measured with QDASH were notfound in this randomized clinical trial.
This research provides information on the effect of each intervention dependingon lymphedema stages, but not on other relevant variables such as types of treatmentor surgeries; current evidence identifies clear risk factors for lymphedema secondary tobreast cancer axillary node dissection and regional radiation of axillary nodes. In addition,conservative surgery through sentinel node biopsy has shown a promising reduction inpostoperative node incidence [59]. It is also considered that further research would benecessary to describe the effects of the experimental treatment in all stages of BCRL, as wellas in BCRL in men, to continue the advance in informed therapeutic decisions.
5. Conclusions
Activity-Oriented Proprioceptive Antiedema Therapy (TAPA) may be an alternative inthe conservative treatment of women with BCRL. It is just as effective in reducing volumeand performing activities as CDT but it is more effective in improving external rotation inshoulder joint balance.

J. Clin. Med. 2022, 11, 2234 9 of 11
TAPA is an effective treatment, simpler in terms of organization, which is somethingto consider for the optimization of resources.
Author Contributions: Conceptualization, M.N.M.-A., M.V.O.-C., M.T.M.-G., P.J.-G., L.A.P.-d.T., J.S.-M., E.R.-R., A.J.J.-V., L.R.-E., R.R.-A., B.M.-P., M.M.-C. and R.M.-B.; methodology, M.N.M.-A., L.A.P.-d.T., L.A.M.-M., J.G.-S. and J.J.G.-B.; software, M.S.-P., J.G.-S. and J.J.G.-B.; validation, M.N.M.-A.,L.A.P.-d.T., M.S.-P. and J.J.G.-B.; formal analysis, M.S.-P., J.G.-S. and J.J.G.-B.; investigation, M.N.M.-A.,M.V.O.-C., M.T.M.-G., P.J.-G., L.A.P.-d.T., J.S.-M., E.R.-R., A.J.J.-V., L.R.-E., R.R.-A., B.M.-P., M.M.-C.and R.M.-B.; resources, M.N.M.-A., M.V.O.-C., M.T.M.-G., P.J.-G., L.A.P.-d.T., J.S.-M., E.R.-R., A.J.J.-V.,L.R.-E., R.R.-A., B.M.-P., M.M.-C. and R.M.-B.; data curation, M.N.M.-A., L.A.P.-d.T., M.S.-P., J.G.-S.and J.J.G.-B.; writing—original draft preparation, M.S.-P., M.N.M.-A., L.A.P.-d.T. and L.A.M.-M.;writing—review and editing, M.S.-P., M.N.M.-A., L.A.P.-d.T., L.A.M.-M., M.P.L.-S. and L.A.M.-M.;visualization, M.S.-P., M.N.M.-A., L.A.P.-d.T., L.A.M.-M.; J.G.-S. and J.J.G.-B.; supervision, M.N.M.-A., L.A.P.-d.T., L.A.M.-M. and J.J.G.-B.; project administration, M.N.M.-A., M.V.O.-C., M.T.M.-G.,P.J.-G., L.A.P.-d.T., J.S.-M., E.R.-R., A.J.J.-V., L.R.-E., R.R.-A., B.M.-P., M.M.-C. and R.M.-B.; fundingacquisition, M.N.M.-A. All authors have read and agreed to the published version of the manuscript.
Funding: The study has been financed in the call for competitive competition of research andinnovation projects in the field of Primary Care, Regional Hospitals and High Resolution HospitalCenters of the Public Health System of Andalusia for the year 2021, of the Andalusian PublicFoundation Progress and Health, according to the definitive list of funded projects, published on23 December 2021, with EXP. No.: AP-0160-2021-C2-F2, also in the call for “Grants for researchprojects in Occupational Therapy. Call 2020”, granted by the Professional Association of OccupationalTherapists of Extremadura (COPTOEX), Spain and, in 2020, received an economic contribution fromthe Research Group in Primary Health Care of Aragon (GAIAP-B21-17R group).
Institutional Review Board Statement: The study was conducted in accordance with the Declarationof Helsinki and approved by the Ethics Committee of the University of Cordoba (4084, 27 November2018).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: Not applicable.
Conflicts of Interest: The authors declare no conflict of interest.
References1. 2022 ICD-10-CM Diagnosis Code I97.2: Postmastectomy Lymphedema Syndrome. Available online: https://www.icd10data.
com/ICD10CM/Codes/I00-I99/I95-I99/I97-/I97.2 (accessed on 23 February 2022).2. Congress, I. The diagnosis and treatment of peripheral lymphedema: 2020 consensus document of the international society of
lymphology. Lymphology 2020, 53, 3–19.3. Cristina Puigdellivol Serafí; Belén Alonso Álvarez. Guía de Práctica Clínica-Orientación Diagnóstica y Terapéutica del Linfedema, 2nd
ed.; Sociedad Española de Rehabilitación y Medicina Física: Madrid, Spain, 2017; ISBN 9788469743294.4. Breast Cancer Awareness Month 2021—IARC. Available online: https://iarc.who.int/featured-news/breast-cancer-awareness-
month-2021/ (accessed on 12 December 2021).5. De Britto, L.R.P.B.; de Souza, E.C.; Ribeiro, L.T.; Schwingel, P.A.; de Melo, A.R.A.; do Nascimento, P.L.; Portela, G.J.S. The impact
of sensory alterations on upper limb function after a mastectomy. Mastology 2017, 27, 287–292. [CrossRef]6. Braveman, B.; Newman, R. Cancer and Occupational Therapy: Enabling Performance and Participation Across the Lifespan.
Available online: https://eds-s-ebscohost-com.bvsspa.idm.oclc.org/eds/ebookviewer/ebook/ZTAwMHh3d19fMjUwOTAzNV9fQU41?sid=ad4e45d6-b6dc-470f-bc26-2b570c5523b7@redis&vid=1&format=EB (accessed on 19 December 2021).
7. Viehoff, P.B.; Gielink, P.D.C.; Damstra, R.J.; Heerkens, Y.F.; Van Ravensberg, D.C.; Neumann, M.H.A. Functioning in lymphedemafrom the patients’ perspective using the International Classification of Functioning, Disability and health (ICF) as a reference.Acta Oncol. 2015, 54, 411–421. [CrossRef] [PubMed]
8. Eaton, L.H.; Narkthong, N.; Hulett, J.M. Psychosocial Issues Associated with Breast Cancer-Related Lymphedema: A LiteratureReview. Curr. Breast Cancer Rep. 2020, 12, 216–224. [CrossRef] [PubMed]
9. Loh, S.Y.; Musa, A.N. Methods to improve rehabilitation of patients following breast cancer surgery: A review of systematicreviews. Breast Cancer Targets Ther. 2015, 7, 81–98. [CrossRef]
10. Olsson Möller, U.; Beck, I.; Rydén, L.; Malmström, M. A comprehensive approach to rehabilitation interventions following breastcancer treatment—A systematic review of systematic reviews. BMC Cancer 2019, 19, 472. [CrossRef]
11. O’Donnell, T.F.; Allison, G.M.; Iafrati, M.D. A systematic review of guidelines for lymphedema and the need for contemporaryintersocietal guidelines for the management of lymphedema. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 676–684. [CrossRef]

J. Clin. Med. 2022, 11, 2234 10 of 11
12. Fish, M.L.; Grover, R.; Schwarz, G.S. Quality-of-life outcomes in surgical vs nonsurgical treatment of breast cancer-relatedlymphedema: A systematic review. JAMA Surg. 2020, 155, 513–519. [CrossRef]
13. Longhurst, E.; Dylke, E.S.; Kilbreath, S.L. Use of compression garments by women with lymphoedema secondary to breast cancertreatment. Support. Care Cancer 2018, 26, 2625–2632. [CrossRef]
14. Rabe, E.; Partsch, H.; Morrison, N.; Meissner, M.H.; Mosti, G.; Lattimer, C.R.; Carpentier, P.H.; Gaillard, S.; Jünger, M.; Urbanek,T.; et al. Risks and contraindications of medical compression treatment—A critical reappraisal. An international consensusstatement. Phlebology 2020, 35, 447–460. [CrossRef]
15. Woods, M. Using compression garments in the management of lymphoedema. Br. J. Nurs. 2019, 28, 50–52. [CrossRef] [PubMed]16. Al Onazi, M.; Dolgoy, N.; Parkinson, J.; McNeely, M.L. Exploring adherence to daytime compression in women with breast cancer
related lymphedema: A multi-methods study. Plast. Aesthetic Res. 2020, 2020, 23. [CrossRef]17. Hasenoehrl, T.; Palma, S.; Ramazanova, D.; Kölbl, H.; Dorner, T.E.; Keilani, M.; Crevenna, R. Resistance exercise and breast
cancer–related lymphedema—A systematic review update and meta-analysis. Support. Care Cancer 2020, 28, 3593–3603. [CrossRef][PubMed]
18. Taylor, S.; Keesing, S.; Wallis, A.; Russell, B.; Smith, A.; Grant, R. Occupational therapy intervention for cancer patients followinghospital discharge: How and when should we intervene? A systematic review. Aust. Occup. Ther. J. 2021, 68, 546–562. [CrossRef]
19. Hunter, E.G.; Gibson, R.W.; Arbesman, M.; D’Amico, M. Systematic Review of Occupational Therapy and Adult CancerRehabilitation: Part 2. Impact of Multidisciplinary Rehabilitation and Psychosocial, Sexuality, and Return-to-Work Interventions.Am. J. Occup. Ther. 2017, 71, 7102100040p1–7102100040p8. [CrossRef]
20. Scheiman, N.R. Comprehensive Occupational Therapy in a Breast Cancer Program; Nova Southeastern University: Davie, FL, USA,2018; p. 1.
21. Stout, N.L.; Santa Mina, D.; Lyons, K.D.; Robb, K.; Silver, J.K. A systematic review of rehabilitation and exercise recommendationsin oncology guidelines. CA Cancer J. Clin. 2021, 71, 149–175. [CrossRef]
22. Maldonado, A.A.; Ramos, E.; García-Alonso, P.; Jover, J.J.; Holguín, P.; Fernández-Cañamaque, J.L.; Cristóbal, L. Multidisciplinaryapproach in the lymphedema patient: From rehabilitation to microsurgery. Rehabilitacion 2021, in press. [CrossRef]
23. Pilot Study with Myolymphokinetic Activities in the Treatment of Lymphedema after Breast Cancer. Available online:https://www.researchgate.net/publication/283599950_Pilot_study_with_Myolymphokinetic_activities_in_the_treatment_of_lymphedema_after_breast_cancer (accessed on 24 March 2021).
24. Activities and Myolymphokinetic Exercises: Therapeutic Approach to Lymphedema—Kindle Edition by de Godoy, José MariaPereira, Hewitt, David. Professional & Technical Kindle [email protected]. Available online: https://www.amazon.com/Activities-Myolymphokinetic-Exercises-therapeutic-lymphedema-ebook/dp/B00H9K3MG8 (accessed on 25 July 2021).
25. Drenaje Linfático Global: Concepto Godoy & Godoy. Available online: https://www.researchgate.net/publication/305607823_DRENAJE_LINFATICO_GLOBAL_Concepto_Godoy_Godoy (accessed on 25 July 2021).
26. Luctkar-Flude, M.; Aiken, A.; McColl, M.A.; Tranmer, J. What do primary care providers think about implementing breast cancersurvivorship care? Curr. Oncol. 2018, 25, 196–205. [CrossRef]
27. Jones, E.N. Lymphedema Self-Management by Breast Cancer Survivors: A Focus on Psychosocial and Occupational PerformanceFactors. Ph.D. Thesis, St. Catherine University, Saint Paul, MN, USA, 2020.
28. Douglass, J.; Graves, P.; Gordon, S. Self-Care for Management of Secondary Lymphedema: A Systematic Review. PLoS Negl. Trop.Dis. 2016, 10, e0004740. [CrossRef]
29. Pollán, M.; Casla-Barrio, S.; Alfaro, J.; Esteban, C.; Segui-Palmer, M.A.; Lucia, A.; Martín, M. Exercise and cancer: A positionstatement from the Spanish Society of Medical Oncology. Clin. Transl. Oncol. 2020, 22, 1710–1729. [CrossRef]
30. Yildiz Kabak, V.; Gursen, C.; Aytar, A.; Akbayrak, T.; Duger, T. Physical activity level, exercise behavior, barriers, and preferencesof patients with breast cancer–related lymphedema. Support. Care Cancer 2020, 29, 3593–3602. [CrossRef] [PubMed]
31. Smoot, B.; Boyd, B.S.; Byl, N.; Dodd, M. Mechanosensitivity in the upper extremity following breast cancer treatment. J. HandTher. 2014, 27, 4–11. [CrossRef] [PubMed]
32. de la Rosa Díaz, I.; Torres Lacomba, M.; Cerezo Téllez, E.; Díaz del Campo Gómez-Rico, C.; Gutiérrez Ortega, C. Accessory Jointand Neural Mobilizations for Shoulder Range of Motion Restriction After Breast Cancer Surgery: A Pilot Randomized ClinicalTrial. J. Chiropr. Med. 2017, 16, 31–40. [CrossRef] [PubMed]
33. Andersen Hammond, E.; Pitz, M.; Steinfeld, K.; Lambert, P.; Shay, B. An Exploratory Randomized Trial of Physical Therapyfor the Treatment of Chemotherapy-Induced Peripheral Neuropathy. Neurorehabilit. Neural Repair 2020, 34, 235–246. [CrossRef][PubMed]
34. Jo, Y.; Lee, M.S.S. The Effects of Proprioceptive Neuromuscular Facilitation (PNF) Using Elastic Bands on Edema, Range ofMotion, and Pain in Post-Mastectomy Patients with Upper Limb. Ph.D. Thesis, Korea Proprioceptive Neuromuscular FacilitationAssociation, Busan, Korea, 2020; pp. 1–10.
35. Ha, K.J.; Lee, S.Y.; Lee, H.; Choi, S.J. Synergistic effects of proprioceptive neuromuscular facilitation and manual lymphaticdrainage in patients with mastectomy-related lymphedema. Front. Physiol. 2017, 8, 959. [CrossRef] [PubMed]
36. Hwang, W.T.; Chung, S.H.; Chung, M.S.; Lee, K.H.; Kim, T. Effect of proprioceptive neuromuscular facilitation D2 flexionand breathing exercises on lymphedema without a short stretch compression bandage. J. Phys. Ther. Sci. 2015, 27, 3341–3343.[CrossRef] [PubMed]

J. Clin. Med. 2022, 11, 2234 11 of 11
37. Borman, P.; Koyuncu, E.G.; Yaman, A.; Calp, E.; Koç, F.; Sargut, R.; Karahan, S. The Comparative Efficacy of ConventionalShort-Stretch Multilayer Bandages and Velcro Adjustable Compression Wraps in Active Treatment Phase of Patients with LowerLimb Lymphedema. Lymphat. Res. Biol. 2021, 19, 286–294. [CrossRef]
38. Yaman, A.; Borman, P.; Inanli, A.; Kul, F.; Karahan, S. The efficacy of different bandaging methods in patients with breastcancer-related lymphedema: A prospective, randomized study. Turk. J. Phys. Med. Rehabil. 2021, 67, 155–166. [CrossRef]
39. Muñoz-Alcaraz, M.N.; Pérula-de-Torres, L.Á.; Serrano-Merino, J.; Jiménez-Vílchez, A.J.; Olmo-Carmona, M.V.; Muñoz-García,M.T.; Bartolomé-Moreno, C.; Oliván-Blázquez, B.; Magallón-Botaya, R. Efficacy and efficiency of a new therapeutic approach basedon activity-oriented proprioceptive antiedema therapy (TAPA) for edema reduction and improved occupational performance inthe rehabilitation of breast cancer-related arm lymphedema in women: A controlled, randomized clinical trial. BMC Cancer 2020,20, 1074. [CrossRef]
40. Johnson, K.C.; Kennedy, A.G.; Henry, S.M. Clinical Measurements of Lymphedema. Lymphat. Res. Biol. 2014, 12, 216–221.[CrossRef]
41. Kizil, R.; Dilek, B.; Sahin, E.; Engin, O.; Soylu, A.C.; Akalin, E.; Alper, S. Is Continuous Passive Motion Effective in Patients withLymphedema? A Randomized Controlled Trial. Lymphat. Res. Biol. 2018, 16, 263–269. [CrossRef] [PubMed]
42. Martín, M.L.; Hernández, M.A.; Avendaño, C.; Rodríguez, F.; Martínez, H. Manual lymphatic drainage therapy in patients withbreast cancer related lymphoedema. BMC Cancer 2011, 11, 94. [CrossRef] [PubMed]
43. Fleiss, J.L. The Design and Analysis of Clinical Experiments. Des. Anal. Clin. Exp. 1999. [CrossRef]44. Romero Cullerés, G.; Almendáriz Juárez, A. Linfedema después de la cirugía por cáncer de mama. Estudio de la incidencia y
factores de riesgo en 113 pacientes. Rehabilitación 2004, 38, 72–77. [CrossRef]45. Cuadrado, A.; Vázquez, A. Rehabilitación del linfedema. In Actualización y Protocolo; Medicina, 72; Servicio de Medicina Física y
Rehabilitación del Servicio Gallego de Salud: Galicia, Spain, 2008; Volume 72. Available online: http://www.sld.cu/galerias/pdf/sitios/rehabilitacion/tratamiento_del_linfedema.pdf (accessed on 25 July 2021).
46. López Martín, M.; Valencia Álvarez, F.J.; González González, R.; Rodríguez Salvanés, F.J.; Crespo Cobo, P.; Hernández García,M.A. Validación de herramienta informática para el cálculo de linfedema en pacientes con afectación unilateral de extremidadsuperior. Rehabilitación 2011, 45, 127–133. [CrossRef]
47. Arias-Cuadrado, A.; Lvarez-Vzquez, M.J.; Martn-Mourelle, R.; Villarino-Daz Jimnez, C. Clnica, clasificacin y estadiaje dellinfedema. Rehabilitacion 2010, 44, 29–34. [CrossRef]
48. Forner Cordero, I.; Maldonado Garrido, D.; Muñoz Langa, J. Necesidad de información para la prevención del linfedemaposmastectomía. Rehabilitación 2003, 37, 141–144. [CrossRef]
49. Hervás, M.T.; Navarro Collado, M.J.; Peiró, S.; Rodrigo Pérez, J.L.; López Matéu, P.; Martínez Tello, I. Versión Española delcuestionario DASH. Adaptación transcultural, fiabilidad, validez y sensibilidad a los cambios. Med. Clin. 2006, 127, 441–447.[CrossRef]
50. Beaton, D.E.; Wright, J.G.; Katz, J.N.; Amadio, P.; Bombardier, C.; Cole, D.; Davis, A.; Hudak, P.; Marx, R.; Hawker, G.; et al.Development of the QuickDASH: COmparison of three item-reduction approaches. J. Bone Jt. Surg.-Ser. A 2005, 87, 1038–1046.[CrossRef]
51. Ferguson, C.J. Una cartilla de tamaño de efecto: Una guía para médicos e investigadores. Prof. Psychol. Res. Pract. 2009, 40,532–538. [CrossRef]
52. Alba Conejo, E.; Alvarez, M.; Bayo, E.; Del Río, S.; Doctor, M.; Dueñas, B.; Fernandez, R. Proceso Asistencial Integrado Cáncer deMama. 2011. ISBN 8474681375. Available online: https://www.juntadeandalucia.es/export/drupaljda/salud_5af1956e6a064_mama_deteccion_3e_nuevo.pdf (accessed on 19 December 2021).
53. Ezzo, J.; Manheimer, E.; Mcneely, M.L.; Howell, D.M.; Weiss, R.; Johansson, K.I.; Bao, T.; Bily, L.; Tuppo, C.M.; Williams, A.F.; et al.Manual lymphatic drainage for lymphedema following breast cancer treatment. Cochrane Database Syst. Rev. 2015, 5, CD003475.[CrossRef] [PubMed]
54. Rangon, F.B.; da Silva, J.; Dibai-Filho, A.V.; Guirro, R.R.d.J.; Guirro, E.C.d.O. Effects of Complex Physical Therapy and MultimodalApproaches on Lymphedema Secondary to Breast Cancer: A Systematic Review and Meta-analysis of Randomized ControlledTrials. Arch. Phys. Med. Rehabil. 2022, 103, 353–363. [CrossRef] [PubMed]
55. Marchica, P.; Darpa, S.; Magno, S.; Rossi, C.; Forcina, L.; Capizzi, V.; Oieni, S.; Amato, C.; Piazza, D.; Gebbia, V. Integratedtreatment of breast cancer-related lymphedema: A descriptive review of the state of the art. Anticancer Res. 2021, 41, 3233–3246.[CrossRef] [PubMed]
56. Belmonte, R.; Messaggi-Sartor, M.; Ferrer, M.; Pont, A.; Escalada, F. Prospective study of shoulder strength, shoulder range ofmotion, and lymphedema in breast cancer patients from pre-surgery to 5 years after ALND or SLNB. Support. Care Cancer 2018,26, 3277–3287. [CrossRef] [PubMed]
57. Baran, E.; Yildiz, T.I.; Gursen, C.; Üzelpasaci, E.; Özgül, S.; Düzgün, I.; Akbayrak, T. The association of breast cancer-relatedlymphedema after unilateral mastectomy with shoulder girdle kinematics and upper extremity function. J. Biomech. 2021, 121,110432. [CrossRef]
58. Oosterwijk, A.M.; Nieuwenhuis, M.K.; van der Schans, C.P.; Mouton, L.J. Shoulder and elbow range of motion for the performanceof activities of daily living: A systematic review. Physiother. Theory Pract. 2018, 34, 505–528. [CrossRef]
59. Gillespie, T.C.; Sayegh, H.E.; Brunelle, C.L.; Daniell, K.M.; Taghian, A.G. Breast cancer-related lymphedema: Risk factors,precautionary measures, and treatments. Gland Surg. 2018, 7, 379–403. [CrossRef]