Acquisition and analysis of cardiovascular signals on smartphones: potential, pitfalls and...
13
Review Article Corresponding author: Catherine Chronaki, HL7 Foundation, 38-40 Square de Meeûs, Brussels, Belgium, [email protected] Acquisition and analysis of cardiovascular signals on smartphones: potential, pitfalls and perspectives. Nico Bruining Erasmus Medical Center, Thoraxcenter, Rotterdam, The Netherlands, Member ESC WG on e-Cardiology Enrico Caiani Politecnico di Milano, Department of Electronics, Information and Biomedical Engineering, Milan, Italy, Secretary ESC WG on e-Cardiology Catherine Chronaki HL7 Foundation, Belgium, Member ESC WG on e-Cardiology Przemyslaw Guzik Poznan University of Medical Sciences, Poland, Member ESC WG on e-Cardiology Enno van der Velde Leiden Medical Center, department of Cardiology, Leiden, The Netherlands, Past Chair ESC WG on e-Cardiology Abstract Smartphones, mobile applications (‘apps’), social media, analytics, and the cloud are profoundly changing the practice of medicine and the way health decisions are made. With the constant progress of technology, the measurement of vital signals becomes easier, cheaper, and practically a standard approach in clinical practice. The interest in measuring vital signals goes beyond medical professionals to the general public, patients, informal caregivers, and healthy individuals, who frequently lack any formal medical training. On smartphone platforms such as iOS and android, a proliferation of health or medical ‘apps’ acquire and analyse a variety of vital signs through embedded sensors, interconnected devices or peripherals utilizing on occasion analytics and social media. Smartphone vendors compete with traditional medical device manufacturers in the grey area between health care, wellness, and fitness, as US and EU regulatory bodies are setting and revising rules for these new technologies. On the other hand, in the absence of robust validation results, clinicians are hesitant to trust measurements by apps or recommend specific apps to their patients, partly also due to lack of a cost reimbursement policy. This review focuses on the acquisition and analysis on smartphones of three important vital signs in the cardiovascular and respiratory field as well as in rehabilitation i.e. heart or pulse rate, blood pressure and blood oxygenation. The potential, pitfalls, and perspectives on mobile devices and smartphone apps for health management by patients and healthy individuals are discussed. Keywords blood pressure; health apps; heart rate; mobile health; medical devices; oximetry; pulse rate; smartphones; vital signs; ECG monitoring; ECG recording. 1. Introduction and Background Mobile devices and applications (i.e. apps) entwine in our daily activities and affect the way we conduct business, form and maintain relationships, seek relaxation and entertainment, and more recently acquire information about our health. Smartphones are continuously developing devices equipped with powerful processors, considerable memory, touch screen, built-in wireless connectivity (e-mail, Internet access), geolocalization (i.e. location, accelerometer and compass) and a variety of other sensors. With their ability to interface peripheral devices, smartphones frequently serve as a personal hubs.
-
Upload
leidenuniv -
Category
Documents
-
view
4 -
download
0
Transcript of Acquisition and analysis of cardiovascular signals on smartphones: potential, pitfalls and...

Review Article
Corresponding author:
Catherine Chronaki, HL7 Foundation, 38-40 Square de Meeûs, Brussels, Belgium, [email protected]
Acquisition and analysis of cardiovascular signals on
smartphones: potential, pitfalls and perspectives.
Nico Bruining Erasmus Medical Center, Thoraxcenter, Rotterdam, The Netherlands, Member ESC WG on e-Cardiology
Enrico Caiani Politecnico di Milano, Department of Electronics, Information and Biomedical Engineering, Milan, Italy, Secretary ESC WG on e-Cardiology
Catherine Chronaki HL7 Foundation, Belgium, Member ESC WG on e-Cardiology
Przemyslaw Guzik Poznan University of Medical Sciences, Poland, Member ESC WG on e-Cardiology
Enno van der Velde Leiden Medical Center, department of Cardiology, Leiden, The Netherlands, Past Chair ESC WG on e-Cardiology
Abstract Smartphones, mobile applications (‘apps’), social media, analytics, and the cloud are profoundly changing the practice of medicine and
the way health decisions are made. With the constant progress of technology, the measurement of vital signals becomes easier, cheaper,
and practically a standard approach in clinical practice. The interest in measuring vital signals goes beyond medical professionals to the
general public, patients, informal caregivers, and healthy individuals, who frequently lack any formal medical training. On smartphone
platforms such as iOS and android, a proliferation of health or medical ‘apps’ acquire and analyse a variety of vital signs through
embedded sensors, interconnected devices or peripherals utilizing on occasion analytics and social media. Smartphone vendors compete
with traditional medical device manufacturers in the grey area between health care, wellness, and fitness, as US and EU regulatory
bodies are setting and revising rules for these new technologies. On the other hand, in the absence of robust validation results, clinicians
are hesitant to trust measurements by apps or recommend specific apps to their patients, partly also due to lack of a cost
reimbursement policy. This review focuses on the acquisition and analysis on smartphones of three important vital signs in the
cardiovascular and respiratory field as well as in rehabilitation i.e. heart or pulse rate, blood pressure and blood oxygenation. The
potential, pitfalls, and perspectives on mobile devices and smartphone apps for health management by patients and healthy individuals
are discussed.
Keywords blood pressure; health apps; heart rate; mobile health; medical devices; oximetry; pulse rate; smartphones; vital signs; ECG monitoring;
ECG recording.
1. Introduction and Background
Mobile devices and applications (i.e. apps) entwine in our daily activities and affect the way we conduct business, form
and maintain relationships, seek relaxation and entertainment, and more recently acquire information about our health.
Smartphones are continuously developing devices equipped with powerful processors, considerable memory, touch screen,
built-in wireless connectivity (e-mail, Internet access), geolocalization (i.e. location, accelerometer and compass) and a
variety of other sensors. With their ability to interface peripheral devices, smartphones frequently serve as a personal hubs.

Bruining et al 2
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
Mobile health apps, i.e. application programs offering health information and management related services across
platforms including smartphones change the way health care is accessed, monitored, and delivered. Mobile health apps
along with social media, analytics for Big Data as well as cloud computing and storage technologies are emerging as a
critical aspect of a new health economy centred on the consumer, transparency, convenience, and prevention [1]. It is
projected that by 2017, half the 3.4 billion smartphone users worldwide will be using mobile health apps [2]. Currently,
with nearly 100,000 mobile health apps in 62 appstores and an increasing number of medical sensors and peripherals, a
future of mobile health is unavoidable [3,4].
In clinical practice, acquisition and analysis of vital signs is crucial. Heart or pulse rate, arterial blood pressure,
respiratory rate, body temperature, blood oxygen saturation, and blood glucose concentration are classic examples of signals
acquired from patients when admitted to the emergency room or to the outpatient clinic during regular follow-ups by health
professionals. Recently however, using a smartphone, patients or their caregivers can acquire these signals anytime and
anywhere, more often passively without manual input of the measured values [5, 6].
Patients that rely on their smartphone for daily activities will soon trust apps for assessing health risks or deciding
whether they need to visit a health professional. Almost half the patients or caregivers who responded to a 2014 survey
were likely or somewhat likely to have an electrocardiogram at home using a device attached to their smartphone and have
the results sent to their physician (43.6%), or have a pacemaker or defibrillator checked at home wirelessly by their
physician (42.6%). Slightly fewer would have a doctor’s appointment with a smartphone app (38.6%) or would use a
lifestyle app recommended by their doctor (34%) [1]. One of the problems is that the extent to which health apps are reliable
or safe is unclear. Extensive validation data for each app are frequently unavailable, highlighting the need for formal
validation, consumer guidance, and regulatory oversight.
The next section presents smartphone related technology solutions for the acquisition and analysis of heart or pulse rate,
ECG, blood pressure and blood oxygenation (SpO2), along with validation data, where available. The discussion reflects
at the potential, the pitfalls and the different perspectives underpinning the phenomenal innovations that disrupt healthcare
systems worldwide.
2. Acquisition and Analysis of Cardiovascular Signals on Smartphones
2.1. Heart rate or pulse rate
Several smartphone apps for non-clinical use, such as fitness or life-logging [7], are available to measure the heart or pulse
rate (see Table I). These apps acquire video images obtained by the smartphone camera and process them to derive the
pulsation of the skin capillary blood flow in the fingertips as the skin is illuminated by ambient light or by light from the
camera flash, while the camera is recording the image [8, 9]. However, several major limitations can affect this approach:
ambient light, white flash heating, frequency resolution of the camera, motion artefacts, sweating, cold fingers with
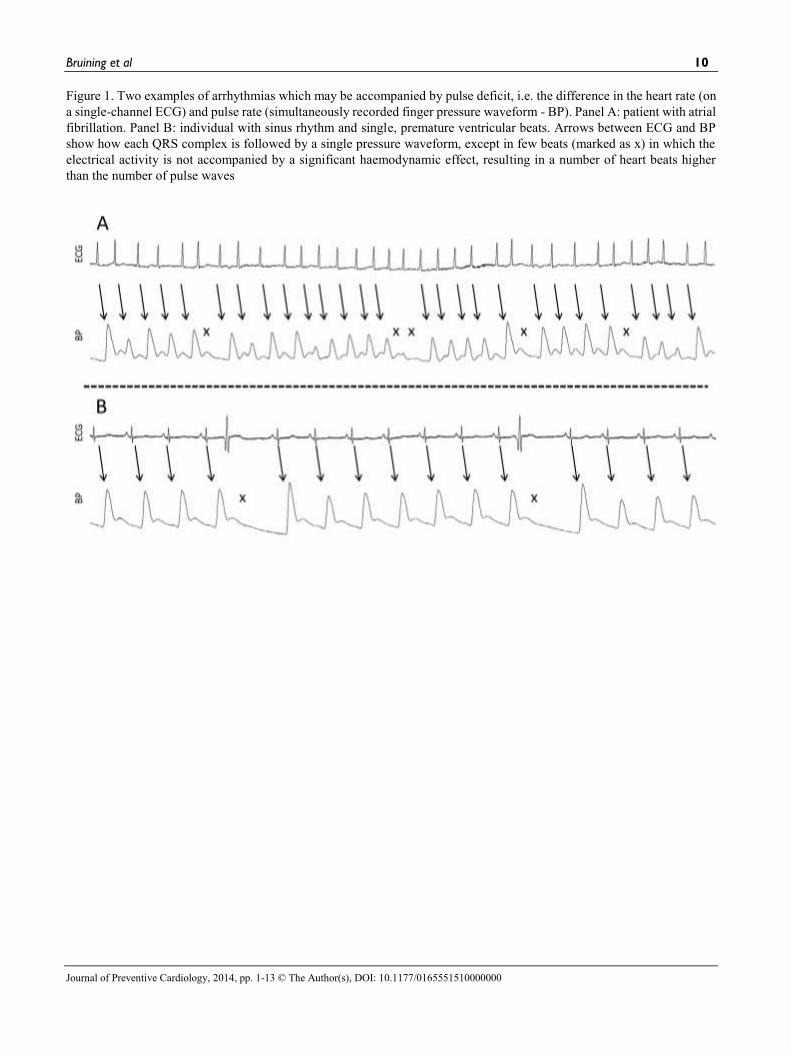
constricted capillaries, arrhythmia with low or variable stroke volume (see Figure 1) and undetectable pulse. Whereas
validation studies are relevant to specific apps and phone models, their results should not be automatically extrapolated to
other mobile devices and applications: even the same app installed on a different smartphone could show different results,
due to the different hardware specifications.
PLEASE PLACE FIGURE 1 HERE
Other limitations are reliability for different heart rate ranges and reproducibility of measurements, particularly in a real-
life (i.e., not in the laboratory) environment. Recently, a new smartphone from Samsung, i.e. Galaxy S5, has incorporated
a dedicated infrared light emitting diode to improve heart rate detection in an effort to overcome some of these limitations.
Some validation studies relevant to this kind of applications are present in literature:
(1) Losa-Inglesias et al. [10] compared the accuracy of the Heart Rate Plus app for the Samsung Galaxy Note® in 46
healthy volunteers, with both palpation of the radial artery and a low-cost portable finger pulse oximeter. Although
they demonstrated high reliability (ICC>.93) and consistency between the studied approaches with respect to heart
rate, the results were comparable but not identical.
(2) Ho Chi-Lin et al. [11] measured pulse rates at the finger/toe and earlobe in 40 small children using four free
smartphone apps on an iPhone 4S, and compared those to the baseline heart rate measured by ECG monitors. The
accuracy rates of the best performing app in the finger/toe group was significantly lower than that in the earlobe
when the heart rate was ≥120 bpm (29.4 vs 76.5%), while minor differences were found for heart rates <120 bpm
(60.9 vs 91.3%).

Bruining et al 3
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
(3) Wackel et al. [12] studied 26 paediatric patients undergoing an electrophysiology study, with heart rates measured
at baseline and during sustained ventricular tachycardia (SVT) using two apps (Instant Heart Rate and Heart Beat
Rate). At baseline, the heart rate was correctly estimated within a ±4 bpm range (r=.99). However, during SVT
(>200 bpm) performance decreased significantly, concluding that the tested apps should not be considered a
reliable tool for assessing the heart rate of children during tachycardia.
(4) McManus et al. [13] tested the hypothesis that camera pulsometry (iPhone 4S) could detect an irregular pulse from
Atrial Fibrillation (AF). However, the tests were performed under controlled conditions, in 76 patients with
persistent AF who were studied before and after cardioversion and showed an accurate discrimination (96.1%
sensitivity, 97.5% specificity) between AF and sinus rhythm, but did not allow any conclusion about more general
prospective applications.
TABLE I SHOULD BE PLACED HERE
2.2. ECG Monitoring
The use of a smartphones as ECG monitors (Class II medical device), with a special smartphone case or smartphone-
connected electrodes allows patients to acquire, display and transmit their ECG to medical professionals. This technology
can be adopted by patients with arrhythmia, palpitations, and recurrent syncope or under specific pharmacological treatment
for either diagnostic or monitoring purposes. Healthy individuals can also purchase such devices over-the-counter (OTC).
ECG readings are stored in the smartphone and on secure servers in the cloud, and analysed by a qualified expert. Most mobile ECG monitors record only single-channel ECG signal and thus their use is limited mainly to measuring
heart rate and rhythm. Their use for the diagnosis of other conditions such as myocardial ischemia or infarction is not
recommended. For such a task a 12-lead mobile ECG device should be employed [14]. Table II summarizes the main
technical characteristics of some available ECG monitor apps and devices.
TABLE II SHOULD BE PLACED HERE
The ECG Check monitor (Cardiac Designs, Park City, UT), cleared by the Food and Drug Administration (FDA) in
February 2013, attaches to the back of the iPhone and acquires a single-channel ECG signal for 30 sec using two metal
electrodes, which communicate via Bluetooth with the smartphone.
The eMotion (Mega Electronics Ltd., Kuopio FINLAND) device, is a CE marked and FDA Class II approved medical
device (Dec 2013) that continuously transmits via Bluetooth to the smartphone a single-channel ECG obtained by an
external electrode on the patient’s chest. Thirty seconds to five days of ECG recordings are uploaded to a secure server in
real-time for viewing and analysis. eMotion offers a service that sends an automatic alert with the GPS location of the
patient upon arrhythmia detection. The AliveCor (AliveCor Inc., San Francisco, CA) case, cleared by the FDA (for prescription and OTC) and CE marked,
acquires short ECG rhythm strips from 30 sec up to 10 min. Several validation studies showed that the AliveCor 1-lead
system (iPhone 4S) has the same lead I QRS morphology as the standard12-lead ECG, characterized by higher baseline
noise [15].
Smartphones applied as ECG monitor give patients the possibility of rapid cardiac monitoring from virtually anywhere
to confirm an arrhythmia e.g. AF and take immediate therapeutic actions. In 204 patients, including 48 with AF, AliveCor
lead I analysed by an embedded automated algorithm (iECG) detected AF with 98% sensitivity, 97% specificity and 97%
accuracy in comparison with a standard 12-lead ECG [16]. In July 2014, AliveCor announced that it had acquired and
reviewed 1,000,000 ECGs [17] reporting high levels of patient satisfaction [18]. The iECG algorithm was also tested in
1,000 pharmacy customers ≥65 years in whom it helped to detect new episodes of AF in 1.5% of the participants who had
the CHA2DS2-VASc score ≥2 [19]. Orchard et al. [21] studied the feasibility of using the iECG algorithm to systematically
screen patients ≥65 years for AF by nurses and receptionists prior to their general practitioner consultation.
CardioSecur Active (Personal MedSystems GmbH, Berlin, Germany) is a CE marked 4-electrode system for
personalized 12-lead ECG on the iPhone. After 10-second acquisition it provides instant feedback for ischaemic and
arrhythmia episodes based on comparison with control readings. In 148 ECGs recorded during percutaneous coronary
balloon angioplasty, CardioSecur showed 100% agreement in electrocardiographic localization of myocardial ischaemia or
infarction of ST-segment changes with simultaneously registered standard 12-lead ECG. [14]. In retrospect, ECG monitoring by smartphones allows to characterize heart rate and rhythm, and in some cases
ischaemia/infarction ST-segment changes.

Bruining et al 4
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
2.3. Blood pressure monitors with cuff
The gold standard for clinical blood pressure measurement is still the sphygmomanometer (mercury or mercury-free),
applying the Korotkoff sound technique for determining systolic and diastolic pressure [21]. However, automatic blood
pressure monitors are gaining popularity, both in the clinic and for home use. These automated devices use an oscillometric
technique, and algorithms derived empirically by each manufacturer [22]. Home BP monitoring is recommended as an
adjunct to office BP monitoring by several international guidelines for the management of hypertension, including those
by the European Society of Hypertension and the European Society of Cardiology [23].
There are reliable devices for measuring blood pressure in the home environment, for instance the BP786 (2014 Series)
Wireless Upper Arm Blood Pressure Monitor – by Omron1. This device can send the measurements to a smartphone via
Bluetooth. Omron has created a dedicated website2 where patients can synchronise all readings between the blood pressure
monitor and smartphone for storage and analysis. Reliable (and FDA certified) blood pressure monitor systems in
combination with a smartphone app are produced by a number of other vendors, for example Withings3 or iHealth.4 A
smartphone app may also control the inflation and deflation of the cuff. The smartphone version of a blood pressure monitor
is thus just as reliable as a standard stand-alone digital home monitor. For this reason, equivalence, the mobile version is
considered a medical device that complies with European medical device regulations and is given clearance from the FDA.
An important issue is the accuracy, at first use, as well as calibration on the long run. In most hospitals, the performance
of electronic blood pressure monitors is periodically checked (once every 1 or 2 years). It seems therefore logical that the
accuracy of a home blood pressure monitor should be also checked periodically. Most likely, the market for mobile blood
pressure monitors ‘for home use’ should not be considered or treated differently than the devices for clinical use. For many
years, patients have been monitoring their blood pressure at home and the advent of mHealth increases the potential use of
such monitoring in prevention and follow-up. Tthe British Hypertension Society [24] has compiled a list with hundreds of
blood pressure monitors that are validated for home use. Some of these devices have Bluetooth for communication with
smartphones.
2.4. Blood pressure monitors without cuff
Besides blood pressure monitors with an arm or wrist cuff, there are also mobile solutions that work differently: blood
pressure is measured without a cuff. At least two mobile devices, SOMNOtouch™ NIBP from Somnomedics in Germany5
and ViSi Mobile Monitoring System from Sotera Wireless in USA6, reconstruct beat-to-beat blood pressure waveforms
and measure arterial blood pressure without cuff. Both companies developed their own patented algorithms which are based
on the continuous estimation of the Pulse Transit Time or Pulse Arrival Time with the use of ECG and SpO2 signals. These
devices have been clinically tested. The SOMNOtouch™ NIBP has been validated by the European Society of
Hypertension [25]. The cuffless blood pressure monitor, ViSi Mobile Monitoring System, got FDA clearance for medical
use in 2013.
Some other cuffless mobile solutions for blood pressure measurement that can be found in appstores are not as realiable.
For example, there is a mobile app from Aura Labs Inc. which uses only the touchscreen of the smartphone7. To measure
blood pressure a thumb is placed on the screen for a few seconds. This suggests that the basic approach to measurement is
similar to that of applanation tonometry where changes in the shape of the arterial walls are directly transmitted through
surrounding tissues to the smartphone screen, which measures changes in the instant pressure acting on the screen.
However, anecdotal experience with this app marks it as very unreliable: the obtained readings are random, usually very
low in comparison with blood pressure measurements taken by brachial blood pressure monitor and they need to be adjusted
to both heart rate and gender. Others have also come to the conclusion that these apps are just for entertainment not to be
recommended for medical use[26, 27]. Similar mobile apps are neither validated nor approved by the FDA or EU.
1 http://omronhealthcare.com/products/10-series-upper-arm-blood-pressure-monitor-plus-bluetooth-smart-bp786/ 2 www.OmronWellness.com 3 http://www.withings.com 4 http://www.ihealthlabs.com/blood-pressure-monitors/wireless-blood-pressure-monitor/ 5 somnomedics.eu/products/new-somnotouch 6www.soterawireless.com 7www.instantbloodpressure.com
Bruining et al 5
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
2.5. Blood oxygen saturation
Blood oxygen saturation is measured by pulse oximetry (SpO2), a non-invasive quantification of infrared light absorption
by oxygenated or saturated and deoxygenated or unsaturated haemoglobin. A conventional pulse oximeter sensor shines
light beams of different wavelengths (red and infrared) through the blood that is circulating in the small skin blood vessels,
for example of the finger, and detects the amount of light that is passing through. Haemoglobin with oxygen absorbs more
infrared light and allows more red light to pass than haemoglobin without oxygen, which allows more infrared light to pass.
The oxygen saturation is expressed as a percentage: 100% saturation is attained when all the haemoglobin in the blood is
completely saturated with oxygen (see Figure 2). To measure pulse oximetry, a special sensor is placed on a fingertip, toe
tip, earlobe, and wrist or across the feet of an infant.
FIGURE 2 SHOULD BE PLACED HERE
There is an increasing number of pulse oximetry peripherals, which either directly connect with a smartphone or
communicate with it via Bluetooth. Such devices are made by either professional producers of medical equipment such as
Nonin8, Masimo9, and Contec10 or by companies whose main area of interest is health and wellness, for example Withings
and iHealth. Pulse oximetry can be recorded up to 24 hours in ambulatory patients frequently together with other signals
such as ECG, movements of the chest and abdomen for respiratory rate, nasal air flow and pressure, body position,
electroencephalography or other vital signals, e.g. SOMNOtouch™ RESP11 or ViSi Mobile Monitoring System12. Although
there is quite a substantial number of pulse oximeters that communicate with smartphones, published clinical studies
validating such devices are rather scarce [28, 29]. Hudson et al. [29] tested the prototype phone oximeter in high- and low-
medical resource environments (i.e., Canada and Uganda, respectively). However, the tests were mainly made for
development purposes. Garde et al. [30] tested a phone oximeter for a different purpose, i.e. diagnosing the obstructive
sleep apnea in a group of 68 children during a night’s sleep, and compared the results with polysomnography. Their
conclusion was that phone oximeters might be helpful as sleep-screening tools to identify children with significant
obstructive sleep apnea.
As already mentioned, a separate device or peripheral with red/infrared light sensors is required to measure SpO2.
However, quite recently, digiDoc Technologies (digidoctech.no), has released probably the first in the world solution that
does not need any additional equipment for oximetry. Their product measures SpO2 only with the iPhone camera. So far,
there are no clinical studies comparing the digiDoc app for SpO2 with validated pulse oximeters.
3. Potential, Pitfalls, and Perspectives
With the introduction of the iPhone in 2007 the smartphone era really took off. The ease of use and the processing power
in smartphones having continuous connection to the Internet opened dozens of new opportunities also in the health domain.
In parallel, new and improved sensor technologies have been developed to self-measure cardiovascular signals (such as
blood pressure and blood oxygen saturation) something previously possible only in the hospital or with the help of a general
practitioner.
The potential of cardiovascular signal acquisition, storage and analysis by smartphones is already recognized and very
fascinating. Recording, monitoring, and communication of heart rate, blood pressure, ECG, oxygen blood saturation and
of many other vital signals may increase the chance of survival for thousands of people who have limited access to medical
care. It can also reduce the costs of healthcare and contribute to better management of patients with chronic diseases like
heart failure, diabetes or hypertension, or of individuals at high risk of premature death like patients with long QT syndrome,
or hypertrophic cardiomyopathy. Transferring medical care from the hospital to the home environment can be crucial in
building a culture of prevention, early diagnosis, and effective rehabilitation that would help bend down the costs of care.
Technology can act as workforce multiplier as physicians make better diagnoses and treatment decisions and gain up to
30% in productivity by saving time in accessing and analysing clinical information [31]. Cardiac implant vendors offer
cardiologists medical apps that allow them to receive and review alerts from patients, together with a variety of useful
analytics [32].
8 www.nonin.com 9 www.masimo.com 10 www.contecmed.com 11 somnomedics.eu/products/new-somnotouch/somnotouch-resp 12 www.soterawireless.com

Bruining et al 6
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
Advances in technology make data collection on smartphones cheaper and more convenient allowing individuals to
quantify their biometrics and share them with their social network [8]. Medical devices are available practically over-the-
counter and at ever decreasing prices. Substantial amounts of health, lifestyle, and activities data are collected from mobile
devices such as smartphones, smart watches, glasses, tablets, patches, bracelets, and necklaces with sensors and implants.
It is estimated that in the US, 30% of healthy individuals regularly measure and monitor their heart rate, blood pressure or
SpO2 as they engage in a healthy lifestyle. Mobile apps reminders and behavioural nudges help them stay on track with
medication, exercise, and healthy living. In addition to heart rate and blood oxygenation, skin temperature, body position,
activity level, blood pressure, respiratory rate, ECG, pressure and flow in the airways, many more bio-signals can be
continuously monitored. Often the recording of such signals can last at least 24 hours or longer, sometimes up to several
weeks. The potential of such devices exceeds the possibilities of standard solutions used for decades in medicine like for
example a 24-hour Holter ECG or 24-hour ambulatory blood pressure monitor. This is an unprecedented opportunity for
clinicians to access health data before clinical symptoms occur or when early indications are barely present. Collecting data
from many individuals allows to study large cohorts with increasing statistical power, i.e. Big Data analytics, which was
impossible in the past.
Along with remarkable innovations, come several pitfalls, risks and limitations. Further research is needed to identify
the correct measurement methods for different pathologies, e.g. non-ECG based measurements of heart rate such as
pulsometry devices are not accurate for the detection of AF whereas they are sufficient for health and fitness. Moreover,
the acquisition of multiple signals at a time may compensate for transiently inaccurate measurements.
The use of smartphone sensors for the measurement of vital signs is a new area and quite often, during the development
of mobile apps, validation of essential components does not receive adequate attention. ECG recorders, blood pressure
monitors or pulse oximeters made by medical device vendors producing validated devices, have already obtained FDA
approval, can be supplemented with Bluetooth connectivity, and can work reliably with a smartphone in non-clinical
settings. New companies, in an effort to reduce costs and test novel ideas, could start producing devices, sensors, and apps
that measure vital signals without substantial validation, regulatory clearance or certifications. They forego regulatory
approval and robust validations efforts, positioning their apps and associated sensors in the area of health and wellness. The
resulting products could impose a safety risk for their users, if utilized for medical purposes.
Legal regulations for the use of mobile health apps and devices for vital signs recording, storing, transferring, analysing,
or problems related to sensitive personal data frequently neglected by app developers and vendors, may undermine
consumer confidence and trust. The FDA evaluates mobile medical apps that serve as accessories to regulated medical
devices (Class II or III) or are intended to transform a mobile platform to a medical device [33]. Recently, it issued guidance
on mobile medical apps and identified different classes of apps for which it may exercise enforcement discretion [34,35].
Regulatory scrutiny may be applied on health apps intended for individuals to collect, log, track and trend data such as
blood glucose, blood pressure, heart rate, weight or other data from a device to eventually share with a health care provider,
or upload it to an online (cloud) database, personal or electronic health record. In general, if the ‘intended use’ of the device
is diagnostic rather than informational, regulatory scrutiny is likely [36]. In the future, appstores may play a stronger role
as well, by setting a higher or lower bar as to which apps they accept to host. However, the smartphone and
telecommunications industry is concerned that excessive regulation might hinder competition, challenging the traditional
role of regulatory bodies such as the FDA [37, 38]. The limited success of early third party validation/certification ventures
like HappTique [39], a third-party health app validator/certifier, commercial spin-off of the NY hospital association,
indicates that perhaps a different paradigm embodying a dynamic “social” community approach is called for.
Another limitation is the currently poor integration of mobile health apps with EHR systems. Interoperability standards
in this area are quite nascent, but IHE and HL7 are rapidly catching up, with innovative and lean standards like HL7 FHIR
(www.HL7.org/FHIR).
There are many, so-called medical, personal health or lifestyle apps, available. An important question is in what way
these apps will improve health outcomes? They may be exciting from a technological point of view, but they can only be
truly useful if they have a positive impact on health. While the use of health apps measuring vitals on smartphones is still
in its infancy, it might be difficult to systematically evaluate the possible cost-benefits or quality of life improvements.
Early findings, however, suggest that mobile health apps can have a positive impact on health outcomes: e.g. researchers
at the Mayo Clinic found that incorporating a smartphone app into cardiac rehabilitation reduces emergency room visits
and hospital readmissions by 40% [40, 41].
An important perspective that can impact adoption is reimbursement as a recent meeting of Apple health executives with
insurance companies reveals [42]. In case that in the near future, apps and peripheral devices, such as described in this
paper, are prescribed to be used by patients, reimbursement should be clear. Some devices might be expensive and some
applied sensors could perhaps be consumables, used only once, e.g. contact lenses or bio-signal patches that are single use

Bruining et al 7
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
only. Thus, there are costs involved, whether for the patients themselves or for the health insurance companies. As the
health insurance companies are currently in contact with the smartphone companies, it might be possible that the application
of such vital signs measurements and monitoring will be realised very soon. At the time of this writing, there is high
anticipation for new technologies that will be soon released on the market from different companies, with novel sensors
on-board to monitor several different body parameters that could herald the eve of a new era for personal healthcare [43,
44].
4. Summary
Smartphones, mobile ‘apps’, social media, Big Data analytics, and the cloud are changing the practice of medicine. Rapid
technological progress in the area of biosensors and health apps allows the acquisition and analysis of vital signs with the
smartphone as a personal hub. Increasing the usability of medical technology and bringing it closer to the people has the
advantage of enabling the possibility for unprecedented patient participation and active engagement in their own medical
education and healthcare. For example, ECG monitoring using smartphones allows users to learn about and characterize
their heart rate and rhythm, and it has the potential to provide global identification of arrhythmias. Home blood pressure
measurement in combination with a smartphone app allows people to monitor and document their blood pressure over time
and show and discuss the results with their doctor and perhaps also their social network.
Some smartphone based technological solutions have gone through FDA clearance and thus can be considered reliable.
Atrial Fibrillation seems to represent one important field of application for this technology, with benefits both in community
AF screening and detection of AF recurrence.
Those that have not received regulatory approval may still be reliable, but it is uncertain whether they are acceptable for
clinical or personal use. Proper information is needed to avoid misuse of health applications not designed for medical
purposes (i.e., for fitness). This includes proper validation and knowledge of limits of operability.
The outlook of this technology for improving public awareness of health metrics and for the early diagnosis of cardiac
symptoms is quite promising. At the same time, there is hope that the use of technology in large scale by serving as a
workforce multiplier will improve access to medical expertise and contribute to the sustainability of healthcare systems
worldwide.
Acknowledgements
The ESC WG on e-Cardiology has been a driver behind this work. The authors would like to deeply thank them collectively and
individually.
Funding
Catherine Chronaki has been supported by the European Commission under contract “FP7-610756” Trillium Bridge project.
References
[1] Health Research Institute, PwC. New Health Economy Healthcare’s new entrants: Who will be the industry’s Amazon.com? April
2014. http://pwchealth.com/cgi-local/hregister.cgi/reg/pwc-hri-new-entrants.pdf
[2] Research2Guidance. Mobile Health Market Report 2013-2017. The commercialization of mHealth Apps (vol. 3), March 2013
[3] Barnes K, Connolly C, Gitlin J. Health Research Institute, PwC, Top health industry issues of 2014: A new health economy takes
shape, December 2013, http://pwchealth.com/cgi-local/hregister.cgi/reg/pwc-hri-top-healthcare-issues.pdf
[4] Economist Intelligence Unit, Emerging mHealth: Paths for growth, PwC, June 2012,
http://www.pwc.com/gx/en/healthcare/mhealth/assets/pwc-emerging-mhealth-full.pdf
[5] European Directory of Health Apps 2012-2013: A review by patient groups and empowered consumers. http://www.patient-
view.com/uploads/6/5/7/9/6579846/pv_appdirectory_final_web_300812.pdf
[6] Martínez-Pérez B, de la Torre-Díez I, López-Coronado M, Herreros-González J, Mobile Apps in Cardiology: Review, JMIR
Mhealth Uhealth. 2013 Jul-Dec; 1(2): e15. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4114428/
[7] Singer E. The Measured Life. MIT Technology Review, July/August 2011
http://www.technologyreview.com/featuredstory/424390/the-measured-life/
[8] Scully CG, Lee J, Meyer J, Gorbach AM, Granquist-Fraser D, Mendelson Y, Chon KH, Physiological Parameter Monitoring
from Optical Recordings with a Mobile Phone, IEEE Trans Biomed Eng. Feb 2012; 59(2): 303–306.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3476722/
[9] Bolkhovsky JB1, Scully CG, Chon KH. Statistical analysis of heart rate and heart rate variability monitoring through the use of
smartphone cameras. Conf Proc IEEE Eng Med Biol Soc. 2012:1610-3

Bruining et al 8
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
[10] Losa-Iglesias ME, Becerro-de-Bengoa-Vallejo R, Becerro-de-Bengoa-Losa KR. Reliability and concurrent validity of a
peripheral pulse oximeter and health-app system for the quantification of heart rate in healthy adults. Health Informatics J. 2014
Jul 18
[11] Ho CL, Fu YC, Lin MC, Chan SC, Hwang B, Jan SL. Smartphone applications (apps) for heart rate measurement in children:
comparison with electrocardiography monitor. Pediatr Cardiol. 2014 Apr;35(4):726-31. doi: 10.1007/s00246-013-0844-8.
[12] Wackel P, Beerman L, West L, Arora G. Tachycardia detection using smartphone applications in pediatric patients. J Pediatr.
2014 May;164(5):1133-5.
[13] McManus DD, Lee J, Maitas O, Esa N, Pidikiti R, Carlucci A, Harrington J, Mick E, et al. A novel application for the detection
of an irregular pulse using an iPhone 4S in patients with atrial fibrillation. Heart Rhythm, Vol. 10, Issue 3, p315–319
[14] Bonaventura K, Wellnhofer E, and Fleck E. Comparison of Standard and Derived 12-Lead Electrocardiograms Registrated by a
Simplified 3-Lead Setting with Four Electrodes for Diagnosis of Coronary Angioplasty-induced Myocardial Ischaemia.
European Cardiology Review, 2012;8(3):179-
[15] Garabelli P, Albert D, Reynolds D. Accuracy and Novelty of an Inexpensive iPhone-based Event Recorder, Heart Rhythm 2012.
http://bit.ly/Yk8npC
[16] Lau JK, Lowres N, Neubeck L, et al, Galloway CD, Albert DE, Freedman SB. iPhone ECG application for community screening
to detect silent atrial fibrillation: a novel technology to prevent stroke. Int J Cardiol. 2013 Apr 30;165(1):193-4.
[17] Diagnostic and Interventional Cardiology. One Million ECGs Recorded with AliveCor Heart Monitor. July 18, 2014
http://www.dicardiology.com/article/one-million-ecgs-recorded-alivecor-heart-monitor [last accessed August 25, 2014]
[18] Diagnostic and Interventional Cardiology. Studies Presented at Heart Rhythm 2014 Demonstrate Accuracy of AliveCor Heart
Monitor, Confirm Patient Satisfaction, May 23, 2014 http://www.dicardiology.com/article/studies-presented-heart-rhythm-2014-
demonstrate-accuracy-alivecor-heart-monitor-confirm-pati [last accessed August 25, 2014]
[19] Lowres N, Freedman SB, Redfern J, et al. Screening Education And Recognition in Community pharmacies of Atrial
Fibrillation to prevent stroke in an ambulant population aged >=65 years (SEARCH-AF stroke prevention study): a cross-
sectional study protocol. Br Med J Open 2012; 2: e0011355.
[20] Orchard J, Freedman SB, Lowres N, Peiris D, Neubeck L. iPhone ECG screening by practice nurses and receptionists for atrial
fibrillation in general practice: the GP-SEARCH qualitative pilot study. Australian Family Physician 2014;43:315-9
[21] Perloff D, Grim C, Flack J, et al. Human blood pressure determination by sphygmomanometry. Circulation 1993; 88:2460-70
[22] Pickering TG et al. Recommendations for blood pressure measurement in humans and and experimental animals. Part 1: blood
pressure measurement in humans. Hypertension 2005; 45: 142-161
[23] 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the management of Arterial
Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J
2013; 34: 2159-2219
[24] British Hypertension Society. Blood Pressure Monitors Validated for Home Use http://www.bhsoc.org/index.php?cID=246 [last
accessed August 25, 2014]
[25] Gesche H, Grosskurth D, Küchler G, Patzak A. Continuous blood pressure measurement by using the pulse transit time:
comparison to a cuff-based method. Eur J Appl Physiol. 2012; 112:309-15
somnomedics.eu/fileadmin/SOMNOmedics/Dokumente/BILO_Somnotouch_poster_ESH2014.pdf
[26] Iltifat H, Top 10 downloaded iPhone health app can cause significant patient harm, July 14, 2014,
http://www.imedicalapps.com/2014/07/iphone-health-app-patient-harm/ [last accessed August 25, 2014]
[27] Dolan B. The rise of the seemingly serious but “just for entertainment purposes” medical app Aug 7, 2014
http://mobihealthnews.com/35444/the-rise-of-the-seemingly-serious-but-just-for-entertainment-purposes-medical-app/
[28] Ansermino JM. Universal access to essential vital signs monitoring. Anesth Analg. 2013 Oct;117(4):883-90.
[29] Hudson J, Nguku SM, Sleiman J, Karlen W, Dumont GA, Petersen CL, Warriner CB, Ansermino JM. Usability testing of a
prototype Phone Oximeter with healthcare providers in high- and low-medical resource environments. Anaesthesia. 2012
Sep;67(9):957-67.
[30] Garde A, Karlen W, Dehkordi P, Wensley D, Ansermino JM, Dumont GA. Oxygen Saturation in Children with and without
Obstructive Sleep Apnea Using the Phone-Oximeter. 35th Annual International Conference of the IEEE EMBS, Osaka, Japan, 3
- 7 July, 2013.
[31] European Commission, Green Paper on mobile Health (“mHealth”) SWD (2014) 135 final, Brussels, 10.4.2014, COM (2014) 219
final. http://ec.europa.eu/information_society/newsroom/cf/dae/document.cfm?doc_id=5147
[32] Afolabi BA, Kusumoto FM. Remote Monitoring of Patients with Implanted Cardiac Devices – A Review. Eur Cardiol,
2012;8(2):88–93.
[33] FDA: Mobile Medical Apps.
http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ConnectedHealth/MobileMedicalApplications/default.htm
[34] FDASIA Health IT Report, Proposed Strategy and Recommendations for a Risk-Based Framework, April 2014
http://www.fda.gov/downloads/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacco/CDRH/CDRHReports/UCM391521.pdf
[35] Examples of Mobile Apps For Which the FDA Will Exercise Enforcement Discretion
http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ConnectedHealth/MobileMedicalApplications/ucm368744.htm

Bruining et al 9
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
[36] Tsang L, Pollard V, Kracov D, EU and US regulation of health information technology, software and mobile Apps, Multi-
jurisdictional guide 2012, Life Sciences, www.practicallaw.com/3-518-3154
[37] Cortez NG, Cohen IG, and Kesselheim AS. FDA Regulation of Mobile Health Technologies. New England Journal of Medicine
371; 4 nejm.org, July 24, 2014
[38] European Commission, Staff Working Document, Existing EU legal framework applicable to lifestyle & wellbeing apps, SWD
(2014) 135 final. http://ec.europa.eu/digital-agenda/en/news/commission-staff-working-document-existing-eu-legal-framework-
applicable-lifestyle-and
[39] Misra, S. Happtique’s recent setback shows that health app certification is a flawed proposition, January 8, 2014
http://www.imedicalapps.com/2014/01/happtiques-setback-future-app-certification/ [last accessed August 25, 2014]
[40] Widmer RJ, Allison TJ, Keane B, Dallas A, Lerman LO, Lerman A. Using an online, personalized program reduces cardiovascular
risk factor profiles in a motivated, adherent population of participants. Am Heart Journal – 2014:167(1):93-100.
[41] Widmer RJ, Report from the American College of Cardiology meeting 2014
http://newsnetwork.mayoclinic.org/discussion/cardiac-rehab-patients-who-use-smartphone-app-recover-better-mayo-clinic-
research-shows
[42] Hein B. Apple met with top health insurance providers about HealthKit partnership. Read more at
http://www.cultofmac.com/292319/apple-met-unitedhealth-talk-health-initiatives/ [last accessed August 25, 2014]
[43] Parmar A. 5 Humble Medical Devices Get an mHealth Makeover, July 2014, http://www.mddionline.com/article/5-humble-
medical-devices-get-mhealth-makeover [last accessed August 25, 2014]
[44] Lin G, Nakajima T, Rahul P, Hodge A. Seamlessly embedded heart rate monitor US 8615290 B2. Dec 2013
http://www.google.com/patents/US8615290
Bruining et al 10
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
Figure 1. Two examples of arrhythmias which may be accompanied by pulse deficit, i.e. the difference in the heart rate (on
a single-channel ECG) and pulse rate (simultaneously recorded finger pressure waveform - BP). Panel A: patient with atrial
fibrillation. Panel B: individual with sinus rhythm and single, premature ventricular beats. Arrows between ECG and BP
show how each QRS complex is followed by a single pressure waveform, except in few beats (marked as x) in which the
electrical activity is not accompanied by a significant haemodynamic effect, resulting in a number of heart beats higher
than the number of pulse waves
Bruining et al 11
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
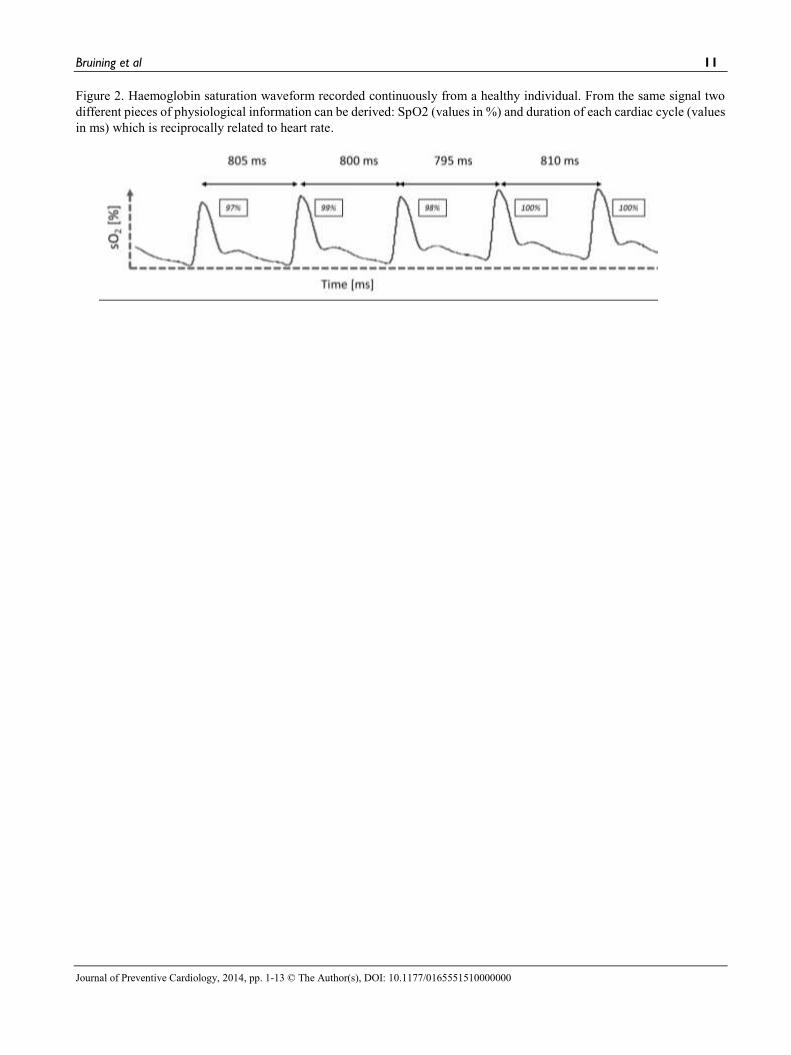
Figure 2. Haemoglobin saturation waveform recorded continuously from a healthy individual. From the same signal two
different pieces of physiological information can be derived: SpO2 (values in %) and duration of each cardiac cycle (values
in ms) which is reciprocally related to heart rate.

Bruining et al 12
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
Table 1: A non-exclusive list of smartphone apps measuring HR.
Name Platform Functionality Processing Method cost Downloads (thousands)
Rate Last update
EasyPulse (heartbeat estimate) Android, iOS HR tap your rhythm free 3.7/5 1/24/2014
Pulse calculator Android HR tap your rhythm free 1-5 3.2/5 7/9/2013
Tap the Pulse iOS, iPad HR tap your rhythm free - 12/5/2013
SKEEPER Heart Rate Android HR, real-time spectrogram
thoracic audio signal 3,44€ 0.5-1 3.9/5 12/23/2013
Thinklabs Stethoscope App iOS, iPad HR, real-time spectrogram
mic audio signal 3.59€ - 4/11/2013
Rilevatore Frequenza Cardiaco Android HR finger video free 500-1.000 3/5 7/8/2013
Heart Rate Plus Android HR finger video free 10-50 4/5 20-Jul-14
Instant Heart Rate Android, iOS HR finger video free 100-500 4.3/5 3/12/2012
Precise Heart Rate Android HR finger video free 100-500 3.8/5 7/6/2013
Acc. Heart Beat Monitor (BPM) Android HR finger video free 10-50 3.8/5 2/10/2014
Quick Heart rate check Android HR finger video free 1.000-5.000 3.5/5 12/7/2013
Heart Rate Monitor Android HR finger video free 100-500 3.6/5 6/5/2014
Heart Beat Rate Android HR finger video free 100-500 4.3/5 12/13/2013
Real Heart Rate Calc. Android HR finger video free 100-500 4.2/5 4/1/2014
Runtastic Heart Rate Android HR finger video free 1.000-5.000 4.4/5 11/29/2013
myPulse Lite - Instant Heart Rate Monitor
iOS HR finger video free - 12/16/2013
Quick Heart Rate Monitor Pro Android HR finger video 0,68€ 10_50 4/5 2/13/2014
Rapid Heart Rate Android HR finger video .73€ 10_50 5/5 4/26/2014
AF Detect Android, iOS HR and AF finger video 1.49€ 1-5 3.7/5 2/27/2014
Heart Rate Monitor BPM iOS HR finger video 0,89€ - 12/26/2013 Instant Heart Rate – Pro Android HR finger video 1,56€ 100- 500 4.4/5 1/26/2014
Heart Rate + Cardiorespiratory Coherence
iOS HR+ breathing coherence
finger video 4.99$ 4.5/5 6/22/2014
Cardiografo – Cardiograph iOS, Android HR finger video $1.99 10.000-50.000
4/4 4-Jun-14
Plus Sports’ Heart Rate Monitor iOS, iPad HR finger or facial video $1.99 3.5/4 7/9/2014
Cardio - Heart Rate Monitor, 7 minute Workout, Calories
iOS, iPad HR facial video free 4.5/5 6/2/2014
Frequenza cardiaca Cam iOS, iPad HR facial video 1,79€ - 9/5/2012

Bruining et al 13
Journal of Preventive Cardiology, 2014, pp. 1-13 © The Author(s), DOI: 10.1177/0165551510000000
Table I1: Main technical characteristics of currently available ECG monitor apps. ECG Check Cardiac
Designs AliveCor eMotion
Mega Electronics CardioSecur
Personal MedSystems GmbH
Leads 1 1 1 12
FDA approved Yes Yes Yes On-going
Over the Counter Yes Yes No Yes
Battery life 8 h 83 h 27 h (100 Hz) USB
Sampling rate 200 Hz 300 Hz Up to 1000 Hz 250 Hz
ECG recording length 30 sec 30 sec – 10 min 30 sec - 5 days 10 sec
Acquisition Method Phone case electrodes+ Bluetooth
Phone case electrodes+ mic
External electrodes+ Bluetooth
External electrodes + USB cable