ABSTRACT tea
32
ABSTRACT Tea is an aromatic beverage commonly prepared by pouring hot or boiling water over cured leaves of the tea plant. All tea is produced from a plant called Camellia sinensis. The thousands of different varieties of teas available in the world only vary by the region it was grown, the time of year picked, and the processing method. There are three main varieties of tea : green, black, and oolong. Tea contains a large number of potentially bioactive chemicals, including flavinoids, amino acids, vitamins, caffeine and several polysaccharides, and a variety of health effects have been proposed and investigated. It has been suggested that green and black tea may protect against cancer, though the catechins found in green tea are thought to be more effective in preventing certain obesity-related cancers such as liver and colorectal while both green and black tea may protect against cardiovascular disease. Numerous recent epidemiological studies have been conducted to investigate the effects of green tea consumption on the incidence of human cancers. These studies suggest significant protective effects of green tea against oral, pharyngeal, esophageal, prostate, digestive, urinary tract, pancreatic, bladder, skin, lung, colon, breast, and liver cancers, and lower risk for cancer metastasis and recurrence.[34] Keywords: tea, cardiovascular disease, cancer, prostat 1
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of ABSTRACT tea

ABSTRACT
Tea is an aromatic beverage commonly prepared bypouring hot or boiling water over cured leaves of thetea plant. All tea is produced from a plant calledCamellia sinensis. The thousands of different varieties ofteas available in the world only vary by the regionit was grown, the time of year picked, and theprocessing method. There are three main varieties oftea : green, black, and oolong.
Tea contains a large number of potentially bioactivechemicals, including flavinoids, amino acids,vitamins, caffeine and several polysaccharides, and avariety of health effects have been proposed andinvestigated. It has been suggested that green andblack tea may protect against cancer, though thecatechins found in green tea are thought to be moreeffective in preventing certain obesity-relatedcancers such as liver and colorectal while both greenand black tea may protect against cardiovasculardisease.Numerous recent epidemiological studies have beenconducted to investigate the effects of green teaconsumption on the incidence of human cancers. Thesestudies suggest significant protective effects ofgreen tea against oral, pharyngeal, esophageal,prostate, digestive, urinary tract, pancreatic,bladder, skin, lung, colon, breast, and livercancers, and lower risk for cancer metastasis andrecurrence.[34]
Keywords: tea, cardiovascular disease, cancer, prostat
1

CHAPTER I
INTRODUCTION
Asthma affects 5-10% of the population or an estimated
23.4 million persons, including 7 million children. The
overall prevalence rate of exercise-induced bronchospasm is 3-
10% of the general population if persons who do not have
asthma or allergy are excluded, but the rate increases to 12-
15% of the general population if patients with underlying
asthma are included. Asthma affects an estimated 300 million
individuals worldwide. Annually, the World Health Organization
(WHO) has estimated that 15 million disability-adjusted life-
years are lost and 250,000 asthma deaths are reported
worldwide. (1)
2

The management of asthma differs according to the
classification of severity. Corticosteroids may be used from
mild to severe – persistent asthma, ranging from low dose with
alternative medicines to high dose and its combinations.
Although use of systemic corticosteroids is recommended early
in the course of acute exacerbations in patients with an
incomplete response to beta agonists, oral administration is
equivalent in efficacy to intravenous administration.
Corticosteroids speed the resolution of airway obstruction and
prevent a late-phase response. (1,2)
Diabetes is a chronic disease, which occurs when the
pancreas does not produce enough insulin, or when the body
cannot effectively use the insulin it produces. This leads to
an increased concentration of glucose in the blood
(hyperglycaemia). Type 1 diabetes (previously known as
insulin-dependent or childhood-onset diabetes) is
characterized by a lack of insulin production. Type 2 diabetes
(formerly called non-insulin-dependent or adult-onset
diabetes) is caused by the body’s ineffective use of insulin.
It often results from excess body weight and physical
inactivity. (3)
3

Rates of diabetes are increasing worldwide. The
International Diabetes Federation predicts that the number of
people living with diabetes will to rise from 366 million in
2011 to 552 million by 2030. The top 10 countries in number of
people with diabetes are currently India, China, the United
States, Indonesia, Japan, Pakistan, Russia, Brazil, Italy, and
Bangladesh. (4)
Patient with diabetes has impaired immunity which leads
to high risk from infections. In the following chapter we will
be talking about the necessity of using corticosteroids for
asthma in diabetes.
4

CHAPTER II
LITERATURE REVIEW
I. Asthma
Asthma is best described as a chronic disease that
involves inflammation of the pulmonary airways and bronchial
hyperresponsiveness that results in the clinical expression of
a lower airway obstruction that usually is reversible. Asthma
is characterised by a specific pattern of inflammation that is
largely driven via immunoglobulin (Ig)E-dependent mechanisms.
Genetic factors have an important influence on whether atopy
develops and several genes have now been identified. Most of
the genetic linkages reported for asthma are common to all
5

allergic diseases. However, environmental factors appear to be
more important in determining whether an atopic individual
develops asthma, although genetic factors may exert an
influence on how severely the disease is expressed and the
amplification of the inflammatory response. (5,6)
I. A. Etiology
Genetics
Genome-wide linkage studies and case–control studies
have identified 18 genomic regions and more than 100 genes
associated with allergy and asthma in 11 different
populations. In particular, there are consistently replicated
regions on the long arms of chromosomes 2, 5, 6, 12 and 13.
Association studies of unrelated individuals have also
identified more than 100 genes associated with allergy and
asthma, 79 of which have been replicated in at least one
further study. A recent genome-wide association
study identified a new gene, ORMDL3, that exhibited a highly
significantly association with asthma (p < 10−12) (for single
nucleotide polymorphism rs8067378, odds ratio 1.84, 95%
confidence interval 1.43–2.42) a finding that has now been
replicated in several populations. (7,8,9,10)
6

Stress
A number of animal models have suggested that prenatal
maternal stress acts through regulation of the offspring’s
hypothalamic–pituitary–adrenal axis to decrease cortisol
levels, which may affect the development of an allergic
phenotype. Although there is a correlation between caregiver
stress early in the infant’s life and higher levels of
immunoglobulin E in the infant and early wheezing, no studies
to date have shown an association with asthma. (11.12)
Obesity
A study by Cottrell et al explored the relationship
between asthma, obesity, and abnormal lipid and glucose
metabolism. The study found that community-based data linked
asthma, body mass, and metabolic variables in children.
Specifically, these findings described a statistically
significant association between asthma and abnormal lipid and
glucose metabolism beyond body mass association. Accelerated
weight gain in early infancy is associated with increased
risks of asthma symptoms according to one study of preschool
children. (1)
7

Other etiologies include environmental allergens, viral
respiratory tract infections, exercise, hyperventilation,
gastroesophageal reflux disease, chronic sinusitis or
rhinitis, aspirin or nonsteroideal anti-inflammatory drug
(NSAID) hypersensitivity, sulfite sensitivity, use of beta-
adrenergic receptor blockers, environmental pollutants,
tobacco smoke, occupational exposure, irritants and perinatal
factors. (1)
I. B. Pathophysiology
The pathophysiology of asthma can be divided into four
events: bronchoconstriction, airway edema, airway
hyperresponsiveness and airway remodeling. (13)
Bronchoconstriction
In asthma, the dominant physiological event leading to
clinical symptoms is airway narrowing and a subsequent
interference with airflow. In acute exacerbations of asthma,
bronchial smooth muscle contraction (bronchoconstriction)
occurs quickly to narrow the airways in response to exposure
to a variety of stimuli including allergens or irritants.
Allergen-induced acute bronchoconstriction results from an
IgE-dependent release of mediators from mast cells that
8

includes histamine, tryptase, leukotrienes, and prostaglandins
that directly contract airway smooth muscle. (13)
Airway edema
As the disease becomes more persistent and inflammation
more progressive, other factors further limit airflow. These
include edema, inflammation, mucus hypersecretion and the
formation of inspissated mucus plugs, as well as structural
changes including hypertrophy and hyperplasia of the airway
smooth muscle. (13)
Airway hyperresponsiveness
Airway hyperresponsiveness—an exaggerated
bronchoconstrictor response to a wide variety of stimuli—is a
major, but not necessarily unique, feature of asthma. The
degree to which airway hyperresponsiveness can be defined by
contractile responses to challenges with methacholine
correlates with the clinical severity of asthma. The
mechanisms influencing airway hyperresponsiveness are multiple
and include inflammation, dysfunctional neuroregulation, and
structural changes; inflammation appears to be a major factor
in determining the degree of airway hyperresponsiveness.
9

Treatment directed toward reducing inflammation can reduce
airway hyperresponsiveness and improve asthma control. (13)
Airway remodeling
In some persons who have asthma, airflow limitation may
be only partially reversible. Permanent structural changes can
occur in the airway; these are associated with a progressive
loss of lung function that is not prevented by or fully
reversible by current therapy. Airway remodeling involves an
activation of many of the structural cells, with consequent
permanent changes in the airway that increase airflow
obstruction and airway responsiveness and render the patient
less responsive to therapy. These structural changes can
include thickening of the sub-basement membrane, subepithelial
fibrosis, airway smooth muscle hypertrophy and hyperplasia,
blood vessel proliferation and dilation, and mucous gland
hyperplasia and hypersecretion. (13)
10

I. C. Treatment
The goal of asthma treatment is to achieve and maintain
clinical control. Medications to treat asthma can be
classified as controllers or relievers. The following will
discussed only about the role of glucocorticosteroids in
treating asthma. (14)
I. C. 1. Controllers
Inhaled glucocorticosteroids
Inhaled glucocorticosteroids are currently the most
effective anti-inflammatory medications for the treatment of
persistent asthma. Studies have demonstrated their efficacy in
reducing asthma symptoms, improving quality of life, improving11

lung function, decreasing airway hyperresponsiveness,
controlling airway inflammation, reducing frequency and
severity of exacerbations, and reducing asthma mortality.
However, they do not cure asthma, and when they are
discontinued deterioration of clinical control follows within
weeks to months in a proportion of patients. (14)
Systemic glucocorticosteroids
Long-term oral glucocorticosteroid therapy (that is, for
periods longer than two weeks as a glucocorticosteroid
“burst”) may be required for severely uncontrolled asthma, but
its use is limited by the risk of significant adverse effects.
The therapeutic index (effect/side effect) of long-term
inhaled glucocorticosteroids is always more favorable than
long-term systemic glucocorticosteroids in asthma. If oral
glucocorticosteroids have to be administered on a long-term
basis, attention must be paid to measures that minimize the
systemic side effects. Oral preparations are preferred over
parenteral (intramuscular or intravenous) for long-term
therapy because of their lower mineralocorticoid effect,
relatively short half-life, and lesser effects on striated
muscle, as well as the greater flexibility of dosing that
12

permits titration to the lowest acceptable dose that maintains
control. (14)
Other controllers are leukotriene modifiers,
theophylline, long-acting inhaled and oral β2 agonists, anti
Ig-E, allergen-specific immunotherapy and oral anti-allergic
compounds.
I. C. 2. Relievers
Systemic glucocorticosteroid
Although systemic glucocorticosteroids are not usually
thought of as reliever medications, they are important in the
treatment of severe acute exacerbations because they prevent
progression of the asthma exacerbation, reduce the need for
referral to emergency departments and hospitalization, prevent
early relapse after emergency treatment, and reduce the
morbidity of the illness. The main effects of systemic
glucocorticosteroids in acute asthma are only evident after 4
to 6 hours. Oral therapy is preferred and is as effective as
intravenous hydrocortisone. A typical short course of oral
glucocorticosterods for an exacerbation is 40-50 mg
prednisolone given daily for 5 to 10 days depending on the
severity of the exacerbation. When symptoms have subsided and
13

lung function has approached the patientʼs personal best
value, the oral glucocorticosteroids can be stopped or
tapered, provided that treatment with inhaled
glucocorticosteroids continues. Intramuscular injection of
glucocorticosteroids has no advantage over a short course of
oral glucocorticosteroids in preventing relapse. (14)
II. Diabetes
Diabetes is a chronic disease, which occurs when the
pancreas does not produce enough insulin, or when the body
cannot effectively use the insulin it produces. This leads to
an increased concentration of glucose in the blood
(hyperglycaemia). (3)
II. A. Type 1 Diabetes Mellitus
Type 1 diabetes mellitus (DM) is a multisystem disease
with both biochemical and anatomic/structural consequences. It
is a chronic disease of carbohydrate, fat, and protein
metabolism caused by the lack of insulin, which results from
the marked and progressive inability of the pancreas to
secrete insulin because of autoimmune destruction of the beta
cells. (3)
Pathophysiology
14

Type 1 diabetes usually develops as a result of
autoimmune pancreatic beta-cell destruction in genetically
susceptible individuals. Up to 90% of patients will have
autoantibodies to at least one of 3 antigens: glutamic acid
decarboxylase (GAD); insulin; and a tyrosine-phosphatase-like
molecule, islet auto-antigen-2 (IA-2). Beta-cell destruction
proceeds sub-clinically for months to years as insulitis
(inflammation of the beta cell). When 80% to 90% of beta cells
have been destroyed, hyperglycaemia develops. Insulin
resistance has no role in the pathophysiology of type 1
diabetes. However, with increasing prevalence of obesity, some
type 1 diabetic patients may be insulin resistant in addition
to being insulin deficient. (15)
II. B. Type 2 Diabetes Mellitus
Type 2 diabetes mellitus is a progressive disorder defined
by deficits in insulin secretion and action that lead to
abnormal glucose metabolism and related metabolic
derangements. Although the aetiologies of type 1 and type 2
diabetes differ dramatically, both lead to hyperglycaemic
states, and both share common macrovascular (coronary heart,
cerebrovascular, and peripheral vascular disease) and
15

microvascular (retinopathy, nephropathy, and neuropathy)
complications. Type 2 diabetes is usually diagnosed based on
screening. It is preceded by a state of pre-diabetes, which
may be clinically detected by a fasting plasma glucose of 5.6
mmol/L to 6.9 mmol/L (100 to 125 mg/dL). Diabetes diagnosis is
based on 2 confirmed values of: fasting plasma glucose >6.9
mmol/L (125 mg/dL); HbA1c of 48 mmol/mol (6.5%) or greater; or
(less commonly) abnormal glucose tolerance test results, or a
random plasma glucose of ≥200 mg/dL plus symptoms of
hyperglycaemia. (16)
Pathophysiology
The precise mechanism by which the diabetic metabolic
state leads to microvascular and macrovascular complications
is only partly understood but likely involves both
uncontrolled BP and uncontrolled glucose, increasing the risk
of microvascular complications such as retinopathy and
nephropathy. Mechanisms may involve defects in aldose
reductase and other metabolic pathways, damage to tissues from
accumulation of glycated end products, and other mechanisms.
With respect to macrovascular complications, high BP and
glucose raise risk, but so do lipid abnormalities and tobacco
16

use. One unifying theory postulates the existence of a
metabolic syndrome that includes diabetes mellitus,
hypertension, dyslipidaemias, and obesity, and predisposes to
coronary heart disease, stroke, and peripheral artery
disease. However, this theory is not universally accepted as
more clinically useful than assessing individual
cardiovascular risk factors. (16)
\
17

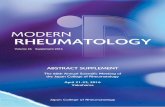
Source: Taylor SI, Olefsky JM. Diabetes mellitus: a fundamental and clinical text.3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2004.
Source: http://www.caninsulin.com/Pathophysiology-algorithm.htm
18

CHAPTER III
DISCUSSION
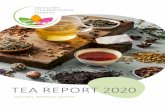
As seen in previous chapter, asthma can be determined in
any of the following ways: the underlying cause of asthma
symptoms, severity of symptoms, and the way it’s controlled.
19

20

Source: . New York State Department of Health. Clinical guideline for the
diagnosis, evaluation and management of adults and children with asthma. Available
at: http://www.nyhealth.gov. accessed on : December 1st 2012.
21

Type 1 diabetes mellitus (T1DM) is an autoimmune disease
that involves the progressive destruction of the
insulin-producing beta cells in the islets of langerhans. It
is a complex process that results from the loss of tolerance
to insulin and other beta-cell-specific antigens. Various
genetic and environmental factors have been studied so far,
but precise causation has yet to be established. Numerous
studies in rodents and human subjects have been performed in
order to elucidate the role of B and T cells, which determine
the risk of development and progression of diabetes. These
studies have demonstrated that while T1DM is fundamentally a
T-cell-mediated autoimmune response, the development of this
disease results from complex interactions between the adaptive
and innate immune systems, with numerous cell types thought to
contribute to pathogenesis. Like any complex disease, the
variation in severity and incidence of T1DM can be attributed
to a combination of genetic and environmental factors. (17)
22

Source: Ting C, Bansal V, Batal I, Mounayar M, et al. Impairment of immune
systems in diabetes. In: Diabetes: an old disease, a new insight. Ahmad
SI, editor. Texas: LANDES Bioscience; 2012.
Infectious diseases are common and serious complication
of diabetes mellitus (DM) and hyperglycemia. The increase of
infections in patients with DM is known to depend upon an
immunosuppressive condition which is brought about by impaired
innate immunity and acquired immunity. For instance, functions
of neutrophils such as phagocyte, chemotaxis and cytokine-
production are decreased in DM model mouse and hyperglycemia
and a Th2-axis shift which reduces Th1-dependent immunity are
observed in DM patients. However, the majority of results
23

concerning interaction of hyperglycemia and immune function
are controversial and relevance of hyperglycemia and/or
hyperinsulinemia to immunosuppressive mechanisms remains
unclear. (18)
High glucose levels lead to shunting through the polyol
pathway, an increase in diacylglycerol which activates protein
kinase C, an increase in the release of electrons that react
with oxygen molecules to form superoxides, and the non-
enzymatic glycosylation of proteins that result in greater
formation of advanced glycation end products. Each of these
can lead to aberrant cell signalling that affects innate
immunity for example, by activating the MAP kinase pathway or
inducing activation of transcription factors such as NF-
kappaB. This may be a common feature of several complications
including periodontal disease, atherosclerosis, nephropathy,
impaired healing and retinopathy. These complications are
frequently associated with increased expression of
inflammatory cytokines such as TNF-alpha, IL-1beta and IL-6
and enhanced generation of reactive oxygen species. (19)
24

Source: Graves DT, Kayal RA. Diabetic complications and dysregulated innate
immunity. Front Biosci 2008;13:1227-1239.
In the management of asthma, inhaled corticosteroids
(ICS) can be prescribed in low dose in mild persistent to high
dose ICS in severe persistent asthma. Whilst oral
corticosteroid is used to maintain control in severe
persistent after the initiating treatment is done. Most of the
benefit from ICS is achieved in adults at low doses,
25

equivalent to 400 ug of budenoside per day. Increasing to
higher doses provides little further benefit in terms of
asthma control but increases the risk of side effects. Current
evidence suggest that in adults, systemic effects of ICS are
not a problem at doses of 400 ug or less budesonide or
equivalent daily. In long-term high doses however, side
effects can occur such as cataract and osteoporosis. It does
not mention the correlation between ICS and blood glucose
serum. (14)
In a study by Slatore CG, et all in side effect of
inhaled corticosteroid in diabetic subjects however; there is
evidence in increasing blood glucose concentration by 1.82
mg/dL in every additional 100 ug of ICS dose. On the other
hand, oral corticosteroid has greater impact in increasing
blood glucose serum. (20)
Other study shows that moderately high dose ICS for
treatment of asthma and COPD is associated with small
disturbances in glucose control after a relatively brief
period of therapy in diabetic subjects relative to oral
montelukast therapy. The changes are detectable but smaller
than those that would be considered clinically significant,
26

therefore changing or stopping therapy is not necessary.
Careful monitoring of blood glucose is required when ICS
therapy is initiated. In diabetics use of steroids may warrant
adjusting or increasing dose of anti-diabetic therapy. (21)
The systemic side effects of long-term oral or
parenteral corticosteroid treatment include osteoporosis,
arterial hypertension, diabetes, hypothalamicpituitary-
adrenal axis suppression, obesity, cataracts, glaucoma, skin
thinning leading to cutaneous striae and easy bruising, and
muscle weakness. Patients with asthma who are on long-term
systemic glucocorticosteroids in any form should receive
preventive treatment for osteoporosis. Caution and close
medical supervision are recommended when considering the use
of systemic glucocorticosteroids in patients with asthma who
also have tuberculosis, parasitic infections, osteoporosis,
glaucoma, diabetes, severe depression, or peptic ulcers. (14)
CHAPTER IV
27

CONCLUSION
The pathophysiology of asthma involves four events:
bronchoconstriction, airway edema, airway hyperresponsiveness
and airway remodeling. Management of asthma includes
prescription of inhaled corticosteroid or oral corticosteroid,
ranging from low doses to high doses depends on the severity
of asthma. These medicines have effects in endocrine,
metabolic and immune system. Diabetes is characterized in
increased blood glucose concentration (hyperglycemia).
Diabetic patient with asthma should be monitored carefully
because the side effects of corticosteroids medicine.
In conclusion, there are some important points:
Careful monitoring of blood glucose is required
when ICS therapy is initiated.
In diabetics use of steroids may warrant adjusting
or increasing dose of anti-diabetic therapy.
Caution and close medical supervision are
recommended when considering the use of systemic
glucocorticosteroids in patients with asthma who
also have diabetes.
28

REFERENCES
1. Morris MJ. Asthma. Available at: http://emedicine.medscape.com/article/296301-overview. accessed on: December 1st 2012.
2. New York State Department of Health. Clinical guideline forthe diagnosis, evaluation and management of adults and children with asthma. Available at: http://www.nyhealth.gov. accessed on : December 1st 2012.
3. World Health Organization. Diabetes. Available at: http://www.who.int/topics/diabetes_mellitus/en/. Accessed on :December 1st 2012.
4. Khardori R. Type 2 Diabetes Mellitus. Available at: httP://emedicine.medscape.com/article/117853-overview#a0156. accessed on : December 1st 2012.
5. Fireman P. Understanding asthma pathophysiology. Allergy
Asthma Proc 2003:24;79-83.
6. Barnes PJ. Pathophysiology of asthma. Available at:
http://pneumonologia.gr/articlefiles/20060117_Pathophysiology_
of_asthma.pdf. Accessed on : December 2nd 2012.
29

7. Ober C, Hoffjan S. Asthma genetics 2006: the long and
winding road to gene discovery. Genes Immun 2006;7:95-100.
8. Moffat MF, Kabesch M, Liang L, et al. Genetic variants
regulating ORMDL3 expression contribute to the risk of
childhood asthma. Nature 2007;448:470-3.
9. Galanter J, Choudhry S, Eng C, et al. ORMDL3 gene is
associated with asthma in three ethnically diverse
populations. Am J Respir Crit Care Med 2008:177:1194-1200.
10. Tavendale R, Macgregor DF, Mukhopadhay, et al. A
polymorphism controlling ORMDL3 expression is associated with
asthma that is poorly controlled by current medications. J
Allergy Clin Immunol 2008;121:860-3.
11. Wright RJ, Finn P, Contreras JP, et al. Chronic caregiver
stress and IgE expression, allergen-induced proliferation, and
cytokine profiles in a birth cohort predisposed to atopy. J
Allergy Clin Immunol 2004;113:1051-7.
12. Lin YC, Wen HJ, Lee YL, et al. Are maternal psychological
factors associated with cord immunoglobulin E in addition to
family atopic history and mother immunoglobulin E? Clin Exp
Allergy 2004;34:548-554.
30

13. National Asthma Education and Prevention Program, Third
Expert Panel on the Diagnosis and Management of Asthma. Expert
Panel Report 3: Guidelines for the Diagnosis and Management of
Asthma. Available at:
http://www.ncbi.nlm.nih.gov/books/NBK7223/. accessed on :
December 2nd 2012.
14. Global Initiative For Asthma. Global strategy for asthma
management and prevention. Available at:
http://www.epgonline.org/documents/asthma/GINAReport2007.pdf.
accessed on : December 2nd 2012.
15. Best Practice. Type 1 diabetes. Available at:
http://bestpractice.bmj.com/best-practice/monograph/25/basics/
.html. accessed on : December 2nd 2012.
16. Best Practice. Type 2 Diabetes. Available at:
http://bestpractice.bmj.com/best-practice/monograph/24/basics.
html. accessed on : December 2nd 2012.
17. Ting C, Bansal V, Batal I, Mounayar M, et al. Impairment
of immune systems in diabetes. In: Diabetes: an old disease, a
new insight. Ahmad SI, editor. Texas: LANDES Bioscience; 2012.
18. Tanaka Y. Immunosuppresive mechanisms in diabetes
mellitus. Nihon Rinsho 2008;66:2233-7.
31

19. Graves DT, Kayal RA. Diabetic complications and
dysregulated innate immunity. Front Biosci 2008;13:1227-1239.
20. Slatore CG, Bryson CL, Au DH. The association of inhaled
corticosteroid use with serum glucose concentration in a large
cohort. Am J Med 2009;122:472-8.
21. Faul JL, Wilson SR, Chu JW, Canfield J, Kuschner WG. The
effect of an inhaled corticosteroid on glucose control in type
2 diabetes. Clin Med Res 2009;7:14-20.
32