
Abstract 2693: MDR1 and ERCC1 expression predict outcome in patients with locally advanced bladder...
9
MDR1 and ERCC1 Expression Predict Outcome of Patients with Locally Advanced Bladder Cancer Receiving Adjuvant Chemotherapy 1,2,3 Andreas-Claudius Hoffmann * ,†,‡ , Peter Wild § , Christina Leicht ¶ , Simone Bertz # , Kathleen D. Danenberg ‡ , Peter V. Danenberg † , Robert Stöhr # , Michael Stöckle ** , Jan Lehmann †† , Martin Schuler * and Arndt Hartmann # *Department of Medicine (Cancer Research), West German Cancer Center, University Duisburg-Essen, Essen, Germany; † Department of Biochemistry and Molecular Biology, and Norris Comprehensive Cancer Center, University of Southern California, Los Angeles, CA, USA; ‡ Response Genetics, Inc, Los Angeles, CA, USA; § ETH Zurich, Zurich, Switzerland; ¶ Department of Pathology, University Hospital Regensburg, Regensburg, Germany; # Department of Pathology, University Hospital Erlangen, Erlangen, Germany; **Department of Urology, Saarland University, Homburg, Germany; †† Urology Practice Prüner Gang, Kiel, Germany Abstract PURPOSE: The role of adjuvant chemotherapy in patients with locally advanced bladder cancer still remains to be defined. We hy- pothesized that assessing the gene expression of the chemotherapy response modifiers multidrug resistance gene 1 (MDR1) and excision repair cross-complementing 1 (ERCC1) may help identify the group of patients benefiting from cisplatin-based adjuvant chemotherapy. EXPERIMENTAL DESIGN: Formalin-fixed paraffin-embedded tumor samples from 108 patients with locally ad- vanced bladder cancer, who had been enrolled in AUO-AB 05/95, a phase 3 trial randomizing a maximum of three courses of adjuvant cisplatin and methotrexate (CM) versus methotrexate, vinblastine, epirubicin, and cisplatin (M-VEC), were included in the study. Tumor cells were retrieved by laser-captured microdissection and analyzed for MDR1 and ERCC1 expression using a quantitative real-time reverse transcription–polymerase chain reaction assay. Gene expression levels were correlated with clinical outcomes by multivariate Cox proportional hazards regression analysis. RESULTS: Expressions of MDR1 and ERCC1 were independently asso- ciated with overall progression-free survival (P = .001, relative risk = 2.9 and P = .01, relative risk = 2.24, respectively). The cor- relation of high MDR1 expression with inferior outcome was stronger in patients receiving M-VEC, whereas ERCC1 analysis performed equally in the CM and M-VEC groups. CONCLUSIONS: High MDR1 and ERCC1 gene expressions are associated with inferior outcome after cisplatin-based adjuvant chemotherapy for locally advanced bladder cancer. Prospective studies are war- ranted to define a role for MDR1 and ERCC1 analysis in individualizing multimodality treatment in locally advanced bladder cancer. Neoplasia (2010) 12, 628–636 Abbreviations: MDR1, multidrug resistance gene 1; ERCC1, excision repair cross-complementing 1; FFPE, formalin-fixed paraffin-embedded; M-VEC, methotrexate, vinblastine, epirubicin, and cisplatin; CM, methotrexate and cisplatin; Pgp, P-glycoprotein Address all correspondence to: Andreas-Claudius Hoffmann, MD, Department of Medicine (Cancer Research), Molecular Oncology Risk – Profile Evaluation, West German Cancer Center, University Hospital Essen, Hufelandstrasse 55, 45147 Essen, Germany. E-mail: [email protected] 1 Authors’ disclosures of potential conflicts of interest: Kathleen D. Danenberg, Response Genetics, Inc, leadership role (CEO), stock ownership. Peter V. Danenberg, Response Genetics, Inc, advisory role, stock ownership. Andreas-Claudius Hoffmann, Response Genetics, Inc, consultant, research funding. Peter Wild, Christina Leicht, Simone Bertz, Robert Stöhr, Michael Stöckle, Jan Lehmann, Martin Schuler, and Arndt Hartmann—none. Response Genetics, Inc, funded the gene expression analysis. A.-C.H. received research funding from “Kampf dem Krebs” eV of the German Cancer Society (Deutsche Krebsgesellschaft). 2 The results of this study were presented at the American Society of Clinical Oncology Annual Meeting 2009. 3 This is the first description of the suitability of MDR1 and ERCC1 expression to predict overall survival and progression-free survival in patients enrolled in a prospective randomized phase 3 trial of adjuvant chemotherapy for locally advanced bladder cancer. These findings represent an important step toward the development of biomarkers for individualizing adjuvant treatment decisions in bladder cancer patients. Received 11 March 2010; Revised 22 May 2010; Accepted 27 May 2010 Copyright © 2010 Neoplasia Press, Inc. All rights reserved 1522-8002/10/$25.00 DOI 10.1593/neo.10402 www.neoplasia.com Volume 12 Number 8 August 2010 pp. 628–636 628
Transcript of Abstract 2693: MDR1 and ERCC1 expression predict outcome in patients with locally advanced bladder...

Volume 12 Number 8 August 2010 pp. 628–636 628
AbbreviatiepirubicinAddress allCenter, Un1Authors’ dGenetics, IRobert Störesearch fu2The resul3This is thrandomizeindividualiReceived 1
CopyrightDOI 10.1
www.neoplasia.com
MDR1 and ERCC1 ExpressionPredict Outcome of Patientswith Locally AdvancedBladder Cancer ReceivingAdjuvant Chemotherapy1,2,3
ons: MDR1, multidrug resistance gene 1; ERCC1, excision repair cross-complemen, and cisplatin; CM, methotrexate and cisplatin; Pgp, P-glycoproteincorrespondence to: Andreas-Claudius Hoffmann, MD, Department of Medicineiversity Hospital Essen, Hufelandstrasse 55, 45147 Essen, Germany. E-mail: achisclosures of potential conflicts of interest: Kathleen D. Danenberg, Responsenc, advisory role, stock ownership. Andreas-Claudius Hoffmann, Response Gehr, Michael Stöckle, Jan Lehmann, Martin Schuler, and Arndt Hartmann—nnding from “Kampf dem Krebs” eV of the German Cancer Society (Deutschts of this study were presented at the American Society of Clinical Oncologye first description of the suitability of MDR1 and ERCC1 expression to predd phase 3 trial of adjuvant chemotherapy for locally advanced bladder cancer. Tzing adjuvant treatment decisions in bladder cancer patients.1 March 2010; Revised 22 May 2010; Accepted 27 May 2010
© 2010 Neoplasia Press, Inc. All rights reserved 1522-8002/10/$25.00593/neo.10402
Andreas-Claudius Hoffmann*,†,‡, Peter Wild§,Christina Leicht¶, Simone Bertz#,Kathleen D. Danenberg‡, Peter V. Danenberg†,Robert Stöhr#, Michael Stöckle**, Jan Lehmann††,Martin Schuler* and Arndt Hartmann#
*Department of Medicine (Cancer Research), West GermanCancer Center, University Duisburg-Essen, Essen, Germany;†Department of Biochemistry and Molecular Biology, andNorris Comprehensive Cancer Center, University of SouthernCalifornia, Los Angeles, CA, USA; ‡Response Genetics, Inc,Los Angeles, CA, USA; §ETH Zurich, Zurich, Switzerland;¶Department of Pathology, University Hospital Regensburg,Regensburg, Germany; #Department of Pathology,University Hospital Erlangen, Erlangen, Germany;**Department of Urology, Saarland University, Homburg,Germany; ††Urology Practice Prüner Gang, Kiel, Germany
AbstractPURPOSE: The role of adjuvant chemotherapy in patients with locally advanced bladder cancer still remains to be defined. We hy-pothesized that assessing the gene expression of the chemotherapy response modifiersmultidrug resistance gene 1 (MDR1) andexcision repair cross-complementing 1 (ERCC1) may help identify the group of patients benefiting from cisplatin-based adjuvantchemotherapy. EXPERIMENTAL DESIGN: Formalin-fixed paraffin-embedded tumor samples from 108 patients with locally ad-vancedbladder cancer,whohadbeenenrolled inAUO-AB05/95, a phase3 trial randomizing amaximumof three courses of adjuvantcisplatin and methotrexate (CM) versus methotrexate, vinblastine, epirubicin, and cisplatin (M-VEC), were included in the study.Tumor cells were retrieved by laser-captured microdissection and analyzed for MDR1 and ERCC1 expression using a quantitativereal-time reverse transcription–polymerase chain reaction assay. Gene expression levels were correlated with clinical outcomes bymultivariate Cox proportional hazards regression analysis. RESULTS: Expressions of MDR1 and ERCC1 were independently asso-ciated with overall progression-free survival (P = .001, relative risk = 2.9 and P = .01, relative risk = 2.24, respectively). The cor-relation of high MDR1 expression with inferior outcome was stronger in patients receiving M-VEC, whereas ERCC1 analysisperformed equally in the CM and M-VEC groups. CONCLUSIONS: High MDR1 and ERCC1 gene expressions are associated withinferior outcome after cisplatin-based adjuvant chemotherapy for locally advanced bladder cancer. Prospective studies are war-ranted to define a role forMDR1 and ERCC1 analysis in individualizing multimodality treatment in locally advanced bladder cancer.
Neoplasia (2010) 12, 628–636
ting 1; FFPE, formalin-fixed paraffin-embedded; M-VEC, methotrexate, vinblastine,
(Cancer Research), Molecular Oncology Risk – Profile Evaluation, West German [email protected], Inc, leadership role (CEO), stock ownership. Peter V. Danenberg, Responsenetics, Inc, consultant, research funding. Peter Wild, Christina Leicht, Simone Bertz,one. Response Genetics, Inc, funded the gene expression analysis. A.-C.H. receivede Krebsgesellschaft).Annual Meeting 2009.ict overall survival and progression-free survival in patients enrolled in a prospectivehese findings represent an important step toward the development of biomarkers for

Neoplasia Vol. 12, No. 8, 2010 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. 629
IntroductionThe role of adjuvant chemotherapy in locally advanced urothelial carci-noma of the bladder is still a matter of debate. Whereas some random-ized multicenter trials have demonstrated superior progression-freesurvival after treatment with three to four courses of methotrexate, vin-blastine, adriamycin or epirubicin, and cisplatin (M-VAC/M-VEC)[1–5], no benefit in overall survival has been demonstrated. In addi-tion, the M-VEC regimen is associated with significant toxicities,which may outweigh its potential benefits especially in elderly patients.Against this background, the AUO-AB 05/95 trial was designed toexplore a deescalated adjuvant chemotherapy regimen consisting of cis-platin and methotrexate (CM). In this randomized multicenter phase 3study, the anthracycline-containing M-VEC standard therapy failed tooutperform the less toxic CM regimen [6]. However, because of the lackof an observation arm, it remains unclear whether adjuvant CM isthe standard for all patients with locally advanced bladder cancer. More-over, the superior progression-free survival after adjuvant chemother-apy in locally advanced bladder cancer could result from a strongeffect in a subgroup of patients, whereas others experience no benefit.Hence, biomarkers predicting the relative risk reduction from adju-vant therapy are needed to individualize treatment strategies in bladdercancer patients.Several gene products have been described to modify the cellular
response to chemotherapeutic agents in vitro and to correlate with clin-ical outcome in vivo. Excision repair cross-complementing 1 (ERCC1)is a component of the nucleotide excision repair pathway, a major re-pair mechanism of DNA damage induced by platin compounds react-ing with DNA and forming interstrand and intrastrand cross links.The balance of DNA damage to DNA repair dictates tumor cell deathor survival after cisplatin therapy [7]. ERCC1 expression as detected byimmunohistochemistry as well as gene expression has been linked toresponse and survival in many retrospective and some prospectivestudies in non–small cell lung cancer, colorectal cancer, and bladdercancer patients treated with platin-based therapies [8–10]. The multi-drug resistance gene 1 (MDR1) encodes an integral membrane protein
denamed P-glycoprotein (Pgp) or an ATP-binding cassette subfamily B,member 1, which acts as an energy-dependent cellular efflux pump.Pgp was shown to reduce intracellular concentrations of a variety ofcytotoxic drugs, including anthracyclines, vinca alkaloids, and taxanes.Under certain conditions, such as the presence of defective folate car-rier transport proteins, methotrexate can also be a substrate of Pgp[11]. Pgp activity results in blunted chemotherapy-induced cytotoxicityin vitro and in vivo. Moreover, anticancer drugs were found to induceMDR1 gene [12]. High Pgp levels were associated with inferior treat-ment outcome in elderly patients with acute myeloid leukemia [13–15], breast cancer [16,17] sarcoma [18,19], and other entities.
Thus far, only a few chemotherapy response modifiers have beenassessed in small retrospective studies of bladder cancer, which failedto produce unequivocal results [20]. More than a decade ago, it was re-ported that M-VAC treatment of bladder cancer leads to transactiva-tion and significantly increased expression of MDR1, although thisresult was not obtained in an outcome-driven study [21]. Analyzingtumor samples from bladder cancer patients receiving uniform adju-vant chemotherapy in a large randomized multicenter trial should in-crease the ability to identify truly predictive biomarkers. To this end,we retrieved formalin-fixed paraffin-embedded (FFPE) tumor samplesfrom patients enrolled in the AUO-AB 05/95 trial [6], which com-pared adjuvant CM to M-VEC in 327 patients with locally advancedbladder cancer. Because both treatment arms were based on cisplatin,we focused on ERCC1 expression. In addition, we assessed MDR1 ex-pression because its gene product was shown to modulate the cytotoxic-ity of epirubicin, vinblastine, and possibly methotrexate.
Materials and Methods
Study Population and Tumor SamplesThe study population has been described previously (Table 1) [6].
Tumor staging was performed according to the criteria of the Inter-national Union Against Cancer [22].
Table 1. Patients’ Demographics.
Demographic
AUO-AB 05/95 Trial Group Study GroupCM (n = 163)
M-VEC (n = 164) Total (n = 327) CM (n = 56) M-VEC (n = 52) Total (n = 108)n
% n % n % n % n % n %Tumor category
pTis/pT1 pN+ 7 4.3 4 2.4 11 3.4 4 7.1 0 0.0 4 3.7 pT2 pN+ 14 8.6 29 17.7 43 13.1 7 12.5 11 21.2 18 16.7 pT3 pN0 58 35.6 61 37.2 119 36.4 17 30.4 17 32.7 34 31.5 pT3 pN+ 56 34.3 44 26.8 100 30.6 18 32.1 16 30.8 34 31.5 pT4a pN0 13 8.0 10 6.1 23 7.0 5 8.9 3 5.8 8 7.4 pT4a pN+ 15 9.2 16 9.8 31 9.5 5 8.9 5 9.6 10 9.3Nodal status
pN0 71 43.6 71 43.3 142 43.4 22 39.3 20 38.5 42 38.9 pN+ 92 56.4 93 56.7 185 56.6 34 60.7 32 61.5 66 61.1 1 lymph node 43 46.7 38 40.9 81 43.8 15 44.1 13 40.6 28 25.9 2-5 lymph nodes 37 40.2 48 51.6 85 45.9 14 41.2 17 53.1 31 28.7 >5 lymph nodes 12 13.1 7 7.5 19 10.3 5 14.7 2 6.3 7 6.5Age, years
≤50 26 16.0 24 14.6 50 15.3 5 8.9 11 21.2 16 14.8 51-60 61 37.4 61 37.2 122 37.3 25 44.6 19 36.5 44 40.7 61-70 76 46.6 79 48.2 155 47.4 26 46.4 22 42.3 48 44.4 Median 60.2 60.7 60.5 59.5 59 59Sex
Male 123 75.5 134 81.7 257 78.6 43 76.8 42 75.0 85 78.7 Female 40 24.5 30 18.3 70 21.4 13 23.2 10 17.9 23 21.3
630 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. Neoplasia Vol. 12, No. 8, 2010
FFPE tissue samples were available for expression analysis from 108of 327 study patients. The clinicopathologic characteristics of all pa-tients were reviewed by one surgical pathologist (A.H.). Representativehematoxylin and eosin–stained slides of FFPE tissue blocks obtainedat cystectomy were reviewed to estimate the tumor load per sample.For laser-captured microdissection (PALM Microlaser TechnologiesAG, Munich, Germany), slides of 10-μm thickness were obtained.All tumor slides were prepared as described previously [23].
Quantitative Real-time Polymerase Chain ReactionRNA was isolated from microdissected tumor samples following
a proprietary procedure at Response Genetics, Inc (Los Angeles, CA;US patent no. 6248,535). The resulting tumor RNA was reverse-transcribed into complementary DNA (cDNA) as described previously[23]. Expression of MDR1, ERCC1, and ACTB (β-actin, endogenousreference) was quantified by real-time fluorescence detection of ampli-fied cDNA (ABI PRISM 7900 Sequence Detection System [TaqMan];Perkin-Elmer Applied Biosystems, Foster City, CA). The reversetranscription–polymerase chain reaction (RT-PCR) assay was imple-mented as described previously [23]. All primers were selected usingthe Gene Express software (Applied Biosystems) but were adaptedto the requirements of cDNA generated from RNA, which was ex-tracted from the FFPE tissue. We used previously published sequencesof MDR1, ERCC1, and ACTB [7,18,24]. All primers were validatedfollowing a previously described protocol [25]. All genes were run onall samples in triplicates, that is, one sample was run with each genethree times on the same plate to identify potential outliers. The detec-tion of amplified cDNA results in a cycle threshold (C t) value, which isreciprocal to the amount of cDNA contained in the sample. Normalcolon, liver, and St. Universal Mix RNA (Stratagene, La Jolla, CA)were used as control calibrators on each assay plate. Gene expressionlevels were described as ratio between two absolute measurements (geneof interest/endogenous reference gene, here beta-actin) to control forintersample variation. Before statistical analysis, all ratios were logarith-mically transformed including a multiplier, which accounted the aver-age C t values obtained for each gene during the validation process. Thisprocedure facilitated the comparison samples, which were run on dif-ferent assay plates. Depending on the used genes and mutlipliers, theinterplate variation is around 5%.
Statistical AnalysesAssociations of gene expression levels and progression-free or overall
survival were tested for each gene by the Kaplan-Meier method. Sur-vival differences between the high- and low-expression group were an-alyzed by the log-rank test. To detect independent prognostic factorsassociated with overall and progression-free survival, multivariate Coxproportional hazards regression analysis with stepwise selection was ap-plied. After adjusting for potential confounders, the following param-eters were accounted for: pathologic tumor stage (pT), lymph nodeinvolvement (pN), vascular invasion (V), tumor grade (G), and thegene set. In addition, receiver operating characteristic curve analysiswas performed to test the ability of the chosen cut points to discrim-inate short survivors from long survivors [26,27].
The level of significance was set to P < .05. All P values reportedwere based on two-sided tests. All statistical analyses were performedusing the Software Packages SPSS for Windows (Version 16.0; SPSS,Inc, Chicago, IL) and JMP 7.0 software (SAS, Cary, NC).
Results
Study Group and Tumor SamplesThe AUO-AB 05/95 trial enrolled a total of 327 patients [6]. Tissue
blocks suitable for RNA extraction were retrieved from 108 patients(33%) and subjected to further analysis. This subgroup was equallybalanced for clinicopathologic parameters compared with the entirestudy population (Table 1). The Spearman coefficient of rank correla-tion of 17 staging parameters of the trial and the study group was0.987 (P = .0001, 95% confidence interval [CI] = 0.964-0.995).
Gene Expression and SurvivalKaplan-Meier analysis revealed that patients with MDR1 expression
below the 75th percentile (P = .0006, hazard ratio [HR] = 0.25, 95%CI = 0.11-0.55) had a higher chance for prolonged survival. After5 years, only 23% of patients with highMDR1 expression (>75th per-centile) were still alive, whereas 62% of patients with low MDR1 ex-pression (<75th percentile) survived 5 years. This association was stillsignificant, when each treatment arm, CM (P = .01, HR = 0.26, 95%CI = 0.09-0.74; Figure 1) and M-VEC (P = .02, HR = 0.27, 95%CI = 0.083-0.88; Figure 2) was analyzed separately. Furthermore, pa-tients with lowMDR1 expression had a lower risk for early progression(P = .002, HR = 0.28, 95% CI = 0.13-0.62). After 2 years, only 25%of patients with lowMDR1 expression experienced disease progression,whereas more than 65% of patients with high MDR1 expression hadprogressed. When evaluating progression-free survival in relation toMDR1 expression for each treatment arm, significant associations wereobtained (CM: P = .01, HR = 0.26, 95% CI = 0.09-0.76; M-VEC:P = .05, HR = 0.34, 95% CI = 0.11-1.04). Next, we built a statisticalmodel for overall survival based on MDR1 expression, pT, pN, andpV as covariates using Cox proportional hazards regression analysiswith stepwise selection (Table 2). Vascular invasion, which was appar-ent in 7% (8/107 patients) of the study group, was revealed as thestrongest independent risk factor in this model, with a relative riskof 3.09 (P = .02, 95% CI = 1.19-8.03) for reduced survival time.The relative risks for high MDR1 expression and pN2 were 2.88(P = .001, 95% CI = 1.52-5.48) and 2.87 (P = .001, 95% CI =1.52-5.43), respectively. Comparable results were obtained in a modelfor progression-free survival based on MDR1 expression, pT, pN, andpV as covariates (Table 3).
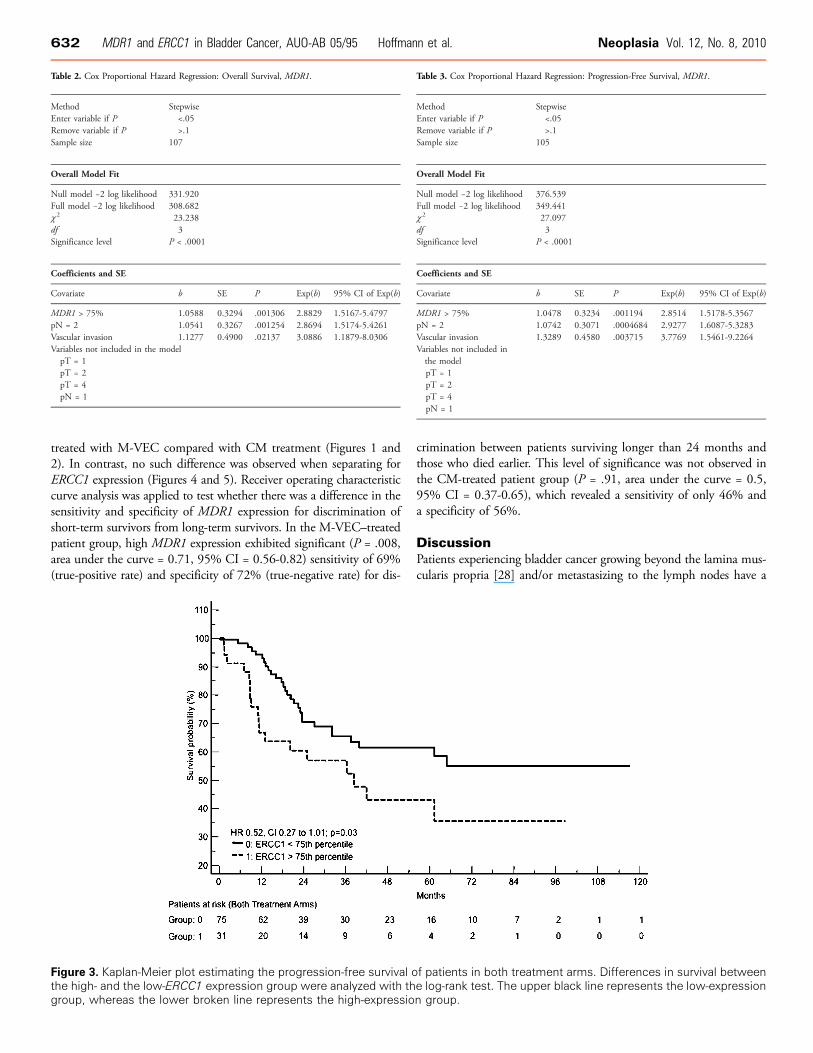
Low ERCC1 expression (<75th percentile) was also associated withprolonged progression-free survival (P = .03, HR = 0.52, 95% CI =0.27-1.01; Figure 3). Within 5 years of follow-up, only 45% of pa-tients with low ERCC1 expression had progressed, whereas almost70% of patients with high ERCC1 expression (>75th percentile) ex-perienced disease progression. Separate subgroup analyses of bothtreatment arms revealed a trend for a reduced risk of progression inpatients with low ERCC1 expression (CM: P = .21, HR = 0.54,95% CI = 0.20-1.42 [Figure 4]; M-VEC: P = .07, HR = 0.43,95% CI = 0.17-1.10 [Figure 5]). A significant association of ERCC1expression with progression-free survival (relative risk = 2.24; P = .01,95% CI = 1.23-4.08) was revealed by Cox regression analysis (Table 4).Median overall survival times were 72.4 months for the low-ERCC1 ex-pression group and 33.1 months for the high-ERCC1 expression group,which failed to reach significance at Kaplan-Meier analysis (P = .19,HR = 0.66, 95% CI = 0.35-1.24) or Cox regression analysis (relativerisk = 1.75, P = .10, 95% CI = 0.89-3.44; Table 5). Both genes weretested together in multivariate regression models for their independent

Figure 1. Kaplan-Meier plot estimating the overall survival of patients in the CM treatment arm. Differences in survival between the high-and the low-MDR1 expression group were analyzed with the log-rank test. The upper black line represents the low-expression group,whereas the lower broken line represents the high-expression group.
Neoplasia Vol. 12, No. 8, 2010 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. 631
association with both overall survival and progressions-free survival.However, when both genes were included in the above-mentionedmodel, only MDR1 remained as the most significant divisor of patientswith a longer or a shorter survival (Tables 6 and 7).
Figure 2. Kaplan-Meier plot estimating the overall survival of patientshigh- and the low-MDR1 expression group were analyzed with thegroup, whereas the lower broken line represents the high-expressio
Performance of MDR1 and ERCC1 Expression in Relation toTreatment Regimen
Kaplan-Meier plot analysis for overall survival revealed an early sep-aration of the groups with high and low MDR1 expression in patients
in the M-VEC treatment arm. Differences in survival between thelog-rank test. The upper black line represents the low-expressionn group.
632 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. Neoplasia Vol. 12, No. 8, 2010
treated with M-VEC compared with CM treatment (Figures 1 and2). In contrast, no such difference was observed when separating forERCC1 expression (Figures 4 and 5). Receiver operating characteristiccurve analysis was applied to test whether there was a difference in thesensitivity and specificity of MDR1 expression for discrimination ofshort-term survivors from long-term survivors. In the M-VEC–treatedpatient group, high MDR1 expression exhibited significant (P = .008,area under the curve = 0.71, 95% CI = 0.56-0.82) sensitivity of 69%(true-positive rate) and specificity of 72% (true-negative rate) for dis-
Figure 3. Kaplan-Meier plot estimating the progression-free survival othe high- and the low-ERCC1 expression group were analyzed with thgroup, whereas the lower broken line represents the high-expressio
crimination between patients surviving longer than 24 months andthose who died earlier. This level of significance was not observed inthe CM-treated patient group (P = .91, area under the curve = 0.5,95% CI = 0.37-0.65), which revealed a sensitivity of only 46% anda specificity of 56%.
DiscussionPatients experiencing bladder cancer growing beyond the lamina mus-cularis propria [28] and/or metastasizing to the lymph nodes have a
Table 2. Cox Proportional Hazard Regression: Overall Survival, MDR1.
Method
Stepwise Enter variable if P <.05 Remove variable if P >.1 Sample size 107Overall Model Fit
Null model −2 log likelihood
331.920 Full model −2 log likelihood 308.682 χ 2 23.238 df 3 Significance level P < .0001Coefficients and SE
Covariate
b SE P Exp(b) 95% CI of Exp(b)MDR1 > 75%
1.0588 0.3294 .001306 2.8829 1.5167-5.4797 pN = 2 1.0541 0.3267 .001254 2.8694 1.5174-5.4261 Vascular invasion 1.1277 0.4900 .02137 3.0886 1.1879-8.0306 Variables not included in the model pT = 1pT = 2pT = 4pN = 1Table 3. Cox Proportional Hazard Regression: Progression-Free Survival, MDR1.
Method
f patients in both treate log-rank test. The upn group.
Stepwise
Enter variable if P <.05 Remove variable if P >.1 Sample size 105Overall Model Fit
Null model −2 log likelihood
376.539 Full model −2 log likelihood 349.441 χ 2 27.097 df 3 Significance level P < .0001Coefficients and SE
Covariate
bment aper blac
SE
rms. Dik line r
P
fferencesepresents
Exp(b)
in survthe lo
95% CI of Exp(b)
MDR1 > 75%
1.0478 0.3234 .001194 2.8514 1.5178-5.3567 pN = 2 1.0742 0.3071 .0004684 2.9277 1.6087-5.3283 Vascular invasion 1.3289 0.4580 .003715 3.7769 1.5461-9.2264 Variables not included inthe model pT = 1pT = 2pT = 4pN = 1ival betweenw-expression
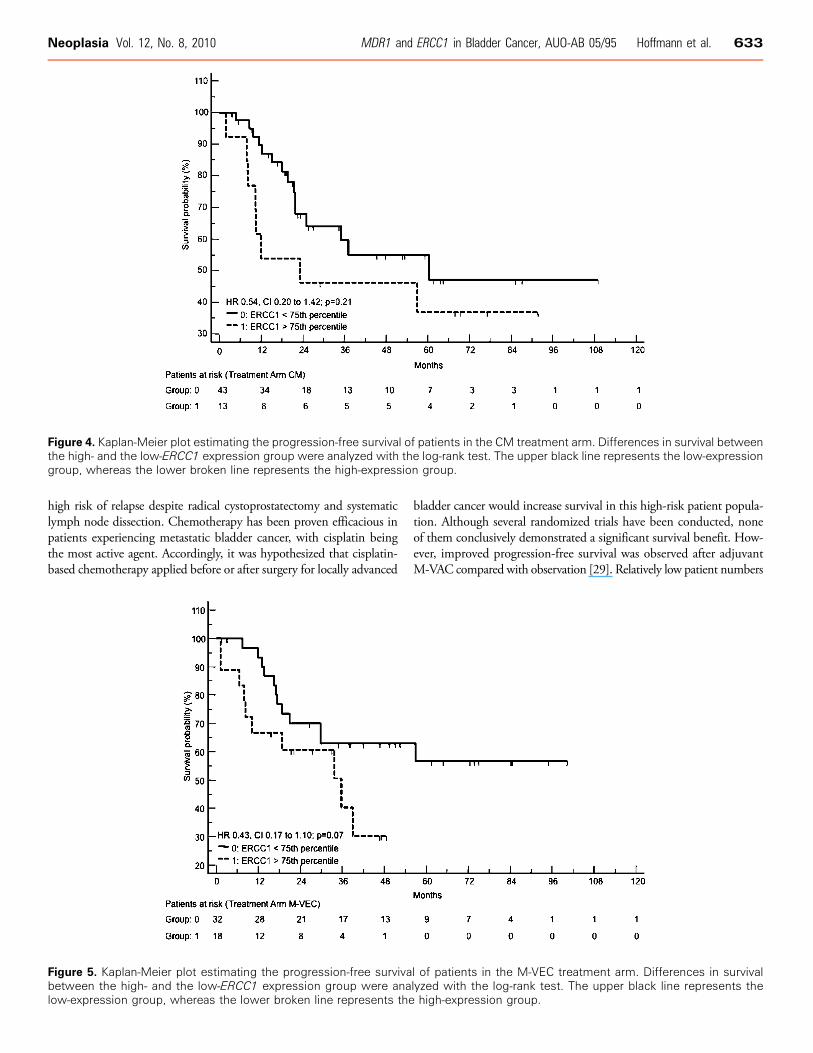
Figure 4. Kaplan-Meier plot estimating the progression-free survival of patients in the CM treatment arm. Differences in survival betweenthe high- and the low-ERCC1 expression group were analyzed with the log-rank test. The upper black line represents the low-expressiongroup, whereas the lower broken line represents the high-expression group.
Neoplasia Vol. 12, No. 8, 2010 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. 633
high risk of relapse despite radical cystoprostatectomy and systematiclymph node dissection. Chemotherapy has been proven efficacious inpatients experiencing metastatic bladder cancer, with cisplatin beingthe most active agent. Accordingly, it was hypothesized that cisplatin-based chemotherapy applied before or after surgery for locally advanced
Figure 5. Kaplan-Meier plot estimating the progression-free survivabetween the high- and the low-ERCC1 expression group were analow-expression group, whereas the lower broken line represents the
bladder cancer would increase survival in this high-risk patient popula-tion. Although several randomized trials have been conducted, noneof them conclusively demonstrated a significant survival benefit. How-ever, improved progression-free survival was observed after adjuvantM-VAC compared with observation [29]. Relatively low patient numbers
l of patients in the M-VEC treatment arm. Differences in survivallyzed with the log-rank test. The upper black line represents thehigh-expression group.

634 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. Neoplasia Vol. 12, No. 8, 2010
and brief follow-up in these studies could explain the lack of a mea-surable survival benefit from adjuvant chemotherapy. Alternatively, itis conceivable that only a subgroup of bladder cancer patients benefitsfrom adjuvant chemotherapy, whereas it is of no effect or even detri-mental for other patients. Thus, the development of biomarkers thatare able to predict the presence or the absence of a benefit from ad-juvant chemotherapy is of high importance for optimizing the care ofpatients with locally advanced bladder cancer. To this end, the presentstudy was conducted to correlate MDR1 and ERCC1 gene expressionwith the outcome of patients undergoing adjuvant chemotherapy formuscle-invasive and/or nodal-metastasized urothelial bladder cancerwithin the randomized, prospective AUO-AB 05/95 phase 3 trial
[6]. The MDR1 and ERCC1 genes were chosen for analysis becausetheir encoded gene products have been implied as modifiers of the tu-mor cell response to the anticancer agents tested in AUO-AB 05/95.
The MDR1 gene product Pgp is an energy-dependent effluxpump, which, among others, reduces intracellular concentrations ofepirubicine and vinblastine, both of which were administered in theM-VEC arm of the trial. Moreover, methotrexate seems to be a sub-strate of Pgp when cells show deficient carrier-mediated methotrexateuptake [11]. Although cisplatin is not considered a de novo substrateof Pgp, some studies have suggested an altered expression of MDR1after cisplatin administration, possibly resulting in decreased cytotoxic
Table 4. Cox Proportional Hazards Regression: Overall Survival, ERCC1.
Method
Stepwise Enter variable if P <.05 Remove variable if P >.1 Sample size 107Overall Model Fit
Null model −2 log likelihood
331.920 Full model −2 log likelihood 318.061 χ 2 13.859 df 2 Significance level P = .0010Coefficients and SE
Covariate
b SE P Exp(b) 95% CI of Exp(b)pN = 2
1.0649 0.3246 .001037 2.9006 1.5402-5.4627 Vascular invasion = 1 0.9975 0.4860 .04011 2.7115 1.0512-6.9945 Variables not included inthe model ERCC1 > 75%pT = 1pT = 2pT = 4pN = 1Table 5. Cox Proportional Hazards Regression: Progression-Free Survival, ERCC1.
Method
Stepwise Enter variable if P <.05 Remove variable if P >.1 Sample size 105Overall Model Fit
Null model −2 log likelihood
376.539 Full model −2 log likelihood 352.487 χ 2 24.052 df 3 Significance level P < .0001Coefficients and SE
Covariate
b SE P Exp(b) 95% CI of Exp(b)ERCC1 > 75%
0.8054 0.3082 .008969 2.2377 1.2268-4.0815 pN = 2 1.1446 0.3077 .0001991 3.1411 1.7240-5.7231 Vascular invasion 1.1676 0.4514 .009690 3.2142 1.3330-7.7507 Variables not included inthe model pT = 1pT = 2pT = 4pN = 1Table 6. Cox Proportional Hazards Regression: Overall Survival, MDR1 and ERCC1.
Method
Stepwise Enter variable if P <.05 Remove variable if P >.1 Sample size 107Overall Model Fit
Null model −2 log likelihood
331.920 Full model −2 log likelihood 308.682 χ 2 23.238 df 3 Significance level P < .0001Coefficients and SE
Covariate
b SE P Exp(b) 95% CI of Exp(b)pN = 2
1.0541 0.3267 .001254 2.8694 1.5174-5.4261 Vascular invasion 1.1277 0.4900 .02137 3.0886 1.1879-8.0306 MDR1 > 75% 1.0588 0.3294 .001306 2.8829 1.5167-5.4797 Variables not included inthe model pT = 1pT = 2pT = 4pN = 1ERCC1 > 75%Table 7. Cox Proportional Hazards Regression: Progression-Free Survival, MDR1 and ERCC1.
Method
Stepwise Enter variable if P <.05 Remove variable if P >.1 Sample size 105Overall Model Fit
Null model −2 log likelihood
376.539 Full model −2 log likelihood 349.441 χ 2 27.097 df 3 Significance level P < .0001Coefficients and SE
Covariate
b SE P Exp(b) 95% CI of Exp(b)pN = 2
1.0742 0.3071 .0004684 2.9277 1.6087-5.3283 Vascular invasion 1.3289 0.4580 .003715 3.7769 1.5461-9.2264 MDR1 > 75% 1.0478 0.3234 .001194 2.8514 1.5178-5.3567 Variables not included in the modelpT = 1pT = 2pT = 4pN = 1ERCC1 > 75%
Neoplasia Vol. 12, No. 8, 2010 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. 635
efficacy [30–33]. Whereas these studies might argue for a correlationbetween MDR1 expression and resistance to platin compounds, addi-tional reports failed to establish such an association [34]. Accordingly,the positive correlation between high MDR1 expression and inferiorsurvival and progression-free survival after adjuvant cisplatin-basedchemotherapy as observed in our study does not automatically implya causative role of Pgp. Moreover, it is tempting to speculate that thebulk of the prognostic or predictive value ofMDR1 expression is basedon the inclusion of patients from the M-VEC arm. This hypothesis issupported by our findings studying the biomarkers separately in bothtreatment arms. MDR1 expression performed significantly better as adiscriminator of patient outcomes in the M-VEC arm than in the CMarm. In contrast, ERCC1, which encodes a gene product primarilymodifying the cellular response to platin compounds and demonstratessignificant association with progression-free survival in the whole studygroup, showed no difference between the two platin-based treatmentarms. Because of the low patient numbers per group, these findingshave to be interpreted with caution. However, they are in line witha potential biologic explanation for the association of MDR1 expres-sion and patient outcome after adjuvant chemotherapy.As cisplatin is still regarded the main active drug in urothelial blad-
der cancer treatment, it is biologically plausible that the expression ofan established modifier of the cellular platin response correlates withtreatment efficacy. In our homogeneously defined and prospectivelycollected patient cohort, ERCC1 expression was significantly andindependently associated with progression-free survival, thus sub-stantiating its role as biomarker for chemotherapy response in blad-der cancer.Our present study has been retrospectively conducted in samples
collected from a completed clinical trial. Accordingly, the results mayhave been influenced by confounders that have occurred during thefollow-up period but were not reported and by additional bias result-ing from the fact that evaluable tissue blocks were only available fromone third of the patients. Importantly, clinicopathologic parameterswere equally balanced in the present study group and the entire trialpopulation. Because of the lack of an observation arm in AUO-AB05/95, it is impossible to decide whether expressions of MDR1 andERCC1 are prognostic or predictive markers in this high-risk bladdercancer population. Interestingly, the results obtained with the twobiomarkers applied in the present study can be corroborated by a bi-ologic hypothesis, which is different from findings revealed by unse-lected expression analysis of thousands of parallel genes. This providesa strong rationale for implementing MDR1 and ERCC1 expressionanalysis in future trials of biomarker development in bladder cancer.To this end, the adjuvant setting is particularly suitable because tissueavailability is not an issue. Because RT-PCR is a feasible method to re-trieve results even from small tissue fractions, expressions of MDR1and ERCC1 may also be used to better estimate which patients couldbenefit from neoadjuvant chemotherapy, even more because Hussainet al. [35] recently pointed out that administering chemotherapy topatients with resistant disease delays definitive local therapy whilethe disease progresses. In two large randomized trials, neoadjuvant che-motherapy with three courses of M-VAC before radical cystectomyprovided a significant survival benefit [36–38]. However, this hasnot entered clinical practice in many centers, in part because of thesubstantial toxicities of the M-VAC regimen as well as the fear of tu-mor progression because of delayed surgery. As new drugs, such asgemcitabine and taxanes, have been introduced to the managementof urothelial cancer, biomarkers in addition to MDR1 and ERCC1
may be required to provide a broader basis for the selection of treat-ment options for individualized patient care. This calls for furtherexploratory studies comparable to this one before embarking on a pro-spective biomarker trial. It will be of particular interest to our findingsto explore the prognostic value of MDR1 expression in a sufficientlypowered bladder cancer population treated without anthracyclines andvinblastine. In conclusion, we have identified MDR1 and ERCC1 ex-pressions as determined by real-time RT-PCR analysis as indepen-dent markers, which significantly correlate with overall survival andprogression-free survival in patients undergoing cisplatin-based adju-vant chemotherapy after resection of locally advanced urothelial blad-der cancer. This defines two promising and robust biomarkers to beprospectively validated toward the implementation of individualizedcare for bladder cancer patients.
AcknowledgmentsThe authors thank the patients, investigators, and pathologists ofAUO-AB 05/95 who primarily diagnosed the tumor for contributingmaterials and clinical data.
References[1] Freiha F, Reese J, and Torti FM (1996). A randomized trial of radical cystectomy
versus radical cystectomy plus cisplatin, vinblastine and methotrexate chemother-apy for muscle invasive bladder cancer. J Urol 155, 495–499; discussion 499–500.
[2] Stockle M, Meyenburg W, Wellek S, Voges GE, Rossmann M, Gertenbach U,Thuroff JW, Huber C, and Hohenfellner R (1995). Adjuvant polychemotherapyof nonorgan-confined bladder cancer after radical cystectomy revisited: long-termresults of a controlled prospective study and further clinical experience. J Urol 153,47–52.
[3] Skinner DG, Daniels JR, Russell CA, Lieskovsky G, Boyd SD, Nichols P, KernW, Sakamoto J, Krailo M, and Groshen S (1991). The role of adjuvant chemo-therapy following cystectomy for invasive bladder cancer: a prospective compar-ative trial. J Urol 145, 459–464; discussion 464–467.
[4] Sternberg CN, Yagoda A, Scher HI, Watson RC, Ahmed T, Weiselberg LR,Geller N, Hollander PS, Herr HW, Sogani PC, et al. (1985). Preliminary resultsof M-VAC (methotrexate, vinblastine, doxorubicin and cisplatin) for transitionalcell carcinoma of the urothelium. J Urol 133, 403–407.
[5] Logothetis CJ, Dexeus FH, Finn L, Sella A, Amato RJ, Ayala AG, and KilbournRG (1990). A prospective randomized trial comparing MVAC and CISCA chemo-therapy for patients with metastatic urothelial tumors. J Clin Oncol 8, 1050–1055.
[6] Lehmann J, RetzM,Wiemers C,Beck J, Thuroff J,WeiningC,Albers P, FrohnebergD, Becker T, Funke PJ, et al. (2005). Adjuvant cisplatin plus methotrexate versusmethotrexate, vinblastine, epirubicin, and cisplatin in locally advanced bladder can-cer: results of a randomized, multicenter, phase III trial (AUO-AB 05/95). J ClinOncol 23, 4963–4974.
[7] Metzger R, Leichman CG, Danenberg KD, Danenberg PV, Lenz HJ, Hayashi K,Groshen S, Salonga D, Cohen H, Laine L, et al. (1998). ERCC1 mRNA levelscomplement thymidylate synthase mRNA levels in predicting response and sur-vival for gastric cancer patients receiving combination cisplatin and fluorouracilchemotherapy. J Clin Oncol 16, 309–316.
[8] Bellmunt J, Paz-Ares L, Cuello M, Cecere FL, Albiol S, Guillem V, Gallardo E,Carles J, Mendez P, de la Cruz JJ, et al. (2007). Gene expression of ERCC1 as anovel prognostic marker in advanced bladder cancer patients receiving cisplatin-based chemotherapy. Ann Oncol 18, 522–528.
[9] Cobo M, Isla D, Massuti B, Montes A, Sanchez JM, Provencio M, Vinolas N,Paz-Ares L, Lopez-Vivanco G, Munoz MA, et al. (2007). Customizing cisplatinbased on quantitative excision repair cross-complementing 1 mRNA expression:a phase III trial in non–small-cell lung cancer. J Clin Oncol 25, 2747–2754.
[10] Simon G, Sharma A, Li X, Hazelton T, Walsh F, Williams C, Chiappori A,Haura E, Tanvetyanon T, Antonia S, et al. (2007). Feasibility and efficacy ofmolecular analysis–directed individualized therapy in advanced non–small-celllung cancer. J Clin Oncol 25, 2741–2746.
[11] de Graaf D, Sharma RC, Mechetner EB, Schimke RT, and Roninson IB (1996).P-glycoprotein confers methotrexate resistance in 3T6 cells with deficient carrier-mediated methotrexate uptake. Proc Natl Acad Sci USA 93, 1238–1242.

636 MDR1 and ERCC1 in Bladder Cancer, AUO-AB 05/95 Hoffmann et al. Neoplasia Vol. 12, No. 8, 2010
[12] Pastan I, WillinghamMC, and Gottesman M (1991). Molecular manipulations ofthe multidrug transporter: a new role for transgenic mice. FASEB J 5, 2523–2528.
[13] Walter RB,GooleyTA, van derVeldenVH,LokenMR, vanDongen JJ, FlowersDA,Bernstein ID, and Appelbaum FR (2007). CD33 expression and P-glycoprotein–mediated drug efflux inversely correlate and predict clinical outcome in patientswith acute myeloid leukemia treated with gemtuzumab ozogamicin monotherapy.Blood 109, 4168–4170.
[14] Walter RB, Raden BW, Hong TC, Flowers DA, Bernstein ID, and LinenbergerML (2003). Multidrug resistance protein attenuates gemtuzumab ozogamicin–induced cytotoxicity in acute myeloid leukemia cells. Blood 102, 1466–1473.
[15] Pallis M and Russell N (2000). P-glycoprotein plays a drug-efflux–independentrole in augmenting cell survival in acute myeloblastic leukemia and is associatedwith modulation of a sphingomyelin-ceramide apoptotic pathway. Blood 95,2897–2904.
[16] Ashariati A (2008). Polymorphism C3435T of the MDR-1 gene predict re-sponse to preoperative chemotherapy in locally advanced breast cancer withHer2/neu expression. Acta Med Indones 40, 187–191.
[17] Cizmarikova M, Wagnerova M, Schonova L, Habalova V, Kohut A, Linkova A,Sarissky M, Mojzis J, Mirossay L, and Mirossay A (2010). MDR1 (C3435T)polymorphism: relation to the risk of breast cancer and therapeutic outcome.Pharmacogenomics J 10(1), 62–69.
[18] Abolhoda A, Wilson AE, Ross H, Danenberg PV, Burt M, and Scotto KW(1999). Rapid activation of MDR1 gene expression in human metastatic sarcomaafter in vivo exposure to doxorubicin. Clin Cancer Res 5, 3352–3356.
[19] Baldini N, Scotlandi K, Barbanti-Brodano G, Manara MC, Maurici D, BacciG, Bertoni F, Picci P, Sottili S, Campanacci M, et al. (1995). Expression of P-glycoprotein in high-grade osteosarcomas in relation to clinical outcome. N Engl JMed 333, 1380–1385.
[20] Goebell PJ (2009). Outcomes and response to therapy in bladder cancer. Arebiomarkers of any help? Minerva Urol Nefrol 61, 91–107.
[21] Petrylak DP, Scher HI, Reuter V, O’Brien JP, and Cordon-Cardo C (1994).P-glycoprotein expression in primary and metastatic transitional cell carcinomaof the bladder. Ann Oncol 5, 835–840.
[22] Sobin LH and Fleming ID (1997). TNM Classification of Malignant Tumors,fifth edition (1997). Union Internationale Contre le Cancer and the AmericanJoint Committee on Cancer. Cancer 80, 1803–1804.
[23] Hoffmann AC, Danenberg KD, Taubert H, Danenberg PV, and Wuerl P (2009).A three-gene signature for outcome in soft tissue sarcoma. Clin Cancer Res 15,5191–5198.
[24] Somlo G, Chu P, Frankel P, Ye W, Groshen S, Doroshow JH, Danenberg K, andDanenberg P (2008). Molecular profiling including epidermal growth factor re-ceptor and p21 expression in high-risk breast cancer patients as indicators ofoutcome. Ann Oncol 19, 1853–1859.
[25] Hoffmann AC, Mori R, Vallbohmer D, Brabender J, Klein E, Drebber U, BaldusSE, Cooc J, Azuma M, Metzger R, et al. (2008). High expression of HIF1a is apredictor of clinical outcome in patients with pancreatic ductal adenocarcinomasand correlated to PDGFA, VEGF, and bFGF. Neoplasia 10, 674–679.
[26] Metz CE (1978). Basic principles of ROC analysis. Semin Nucl Med 8, 283–298.[27] Zweig MH and Campbell G (1993). Receiver-operating characteristic (ROC)
plots: a fundamental evaluation tool in clinical medicine. Clin Chem 39, 561–577.[28] Angulo JC, Lopez JI, Grignon DJ, and Sanchez-Chapado M (1995). Muscularis
mucosa differentiates two populations with different prognosis in stage T1 blad-der cancer. Urology 45, 47–53.
[29] Lehmann J, Franzaring L, Thuroff J, Wellek S, and Stockle M (2006). Com-plete long-term survival data from a trial of adjuvant chemotherapy vs controlafter radical cystectomy for locally advanced bladder cancer. BJU Int 97, 42–47.
[30] Demeule M, Brossard M, and Beliveau R (1999). Cisplatin induces renal expres-sion of P-glycoprotein and canalicular multispecific organic anion transporter.Am J Physiol 277, F832–F840.
[31] Takara K, Tsujimoto M, Kokufu M, Ohnishi N, and Yokoyama T (2003). Up-regulation of MDR1 function and expression by cisplatin in LLC-PK1 cells. BiolPharm Bull 26, 205–209.
[32] van den Broek GB, Wildeman M, Rasch CR, Armstrong N, Schuuring E, BeggAC, Looijenga LH, Scheper R, van der Wal JE, Menkema L, et al. (2009). Mo-lecular markers predict outcome in squamous cell carcinoma of the head and neckafter concomitant cisplatin-based chemoradiation. Int J Cancer 124, 2643–2650.
[33] Pu YS, Tsai TC, Cheng AL, Tsai CY, Tseng NF, Su IJ, Hsieh CY, and Lai MK(1996). Expression of MDR-1 gene in transitional cell carcinoma and its corre-lation with chemotherapy response. J Urol 156, 271–275.
[34] Ren L, Xiao L, and Hu J (2007). MDR1 and MDR3 genes and drug resistanceto cisplatin of ovarian cancer cells. J Huazhong Univ Sci Technolog Med Sci 27,721–724.
[35] Hussain MH, Wood DP, Bajorin DF, Bochner BH, Dreicer R, Lamm DL,O’Donnell MA, Siefker-Radtke AO, Theodorescu D, and Dinney CP (2009).Bladder cancer: narrowing the gap between evidence and practice. J Clin Oncol27, 5680–5684.
[36] Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL,deVere White RW, Sarosdy MF, Wood DP Jr, Raghavan D, et al. (2003). Neo-adjuvant chemotherapy plus cystectomy compared with cystectomy alone for lo-cally advanced bladder cancer. N Engl J Med 349, 859–866.
[37] International Collaboration of Trialists (1999). Neoadjuvant cisplatin, metho-trexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: a ran-domised controlled trial. Lancet 354, 533–540.
[38] Wallace DM, Raghavan D, Kelly KA, Sandeman TF, Conn IG, Teriana N, Dunn J,Boulas J, and Latief T (1991). Neo-adjuvant (pre-emptive) cisplatin therapy ininvasive transitional cell carcinoma of the bladder. Br J Urol 67, 608–615.




















