Above the Huron - Medicine at Michigan
12
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Above the Huron - Medicine at Michigan
6 Fall 2002
Above the Huron
N E W C H A I R F O R C E L L A N D D E V E L O P M E N TA L B I O L O G Y
J.D. (Doug) Engel, Ph.D., joinedthe U-M Medical School fac-
ulty on September 1, 2002.Engel is the school’s first G. CarlHuber Professor of Developmen-tal Biology, as well as professorand chair of the Department ofCell and Developmental Biology.
An expert on the genetics of tran-scription factors and how theycontrol the development of redblood cells, Engel comes to U-M from Northwestern University,where he was a professor of bio-chemistry, molecular biology andcell biology, and the associatedirector for basic sciences of theRobert H. Lurie ComprehensiveCancer Center. He also heldNorthwestern’s prestigious OwenL. Coon Chair in Molecular Biology.
“The Medical School is fortunateto have attracted such an out-standing scientist, mentor andleader to serve as our newestdepartment chair and first HuberProfessor,” says Allen S. Lichter,M.D., dean of the U-M MedicalSchool. “Strengthening andenhancing our reputation for sci-entific research is vital to our goalof becoming one of the top fivemedical schools in the country by2010. Doug Engel has the vision,knowledge and experience tohelp us meet that goal.”
G. Carl Huber was professor ofanatomy and histology at the U-M from 1887–1934. He wasan internationally known experton the structure of the auto-nomic and sympathetic nervoussystem. During and followingWorld War I, Huber conducted aseries of investigations on nerveregeneration, which were respon-sible for the autotransplant ofperipheral nervous tissue aftertraumatic injuries.
“The University of Michigan hasan outstanding reputation asone of the world’s premier scien-tific institutions and academicenterprises,” Engel says. “There ismore activity and excitementhere in genetics and genomics —areas of particular interest to me— than at any other institution.I’m delighted to be part of it.”
Engel uses molecular genetics tostudy how tissue-restricted tran-scription factors, which turn geneson and off, regulate mammaliandevelopment. His goal is to under-stand how these factors act togenerate the enormous variety ofpotential cell responses involved
in mammalian organ and tissueformation and function. “Whensomething goes awry in the nor-mal regulatory processes con-trolled by these transcriptionfactors, their misregulation canresult in different forms of cancer,inherited blood disorders, orimpairment and dysfunction ofseveral organ systems,” Engelsays.
As part of his responsibilities,Engel also will direct the U-MCenter for Organogenesis, aninterdisciplinary research centerdevoted to the study of how tis-sues and organs form and aremaintained during embryonicdevelopment. The Center’s goal isto use this knowledge to createartificial organs, stem cell thera-pies or organ transplantationsystems to correct genetic andacquired diseases.
“It is the most pre-eminentorganization of its kind in thecountry,” says Engel, whohopes to build the Center forOrganogenesis into a uniquenational center focusingbasic, translational and clin-ical research on multiplehuman diseases.
A native of California, DougEngel received a B.S. degreein chemistry from the Uni-versity of California-San Diegoin 1970 and a Ph.D. in chem-istry from the University ofOregon in 1975. He was aHelen Hay Whitney postdoc-toral research fellow at the
California Institute of Technologybefore joining Northwestern’s fac-ulty in 1978. Author of more than100 research articles, Engelserves on the editorial boards ofseveral prestigious scientific jour-nals. He was appointed as aDistinguished Visiting Facultymember by the Mombushyo (theJapanese version of the NationalScience Foundation) in 1997,and is a fellow of the AmericanAssociation for the Advancementof Science.
“My goal is to see the U-MDepartment of Cell and Dev-elopmental Biology become oneof the top 10 in the country,”Engel says. “Our current facultyare very high quality, but thedepartment is too small. DeanLichter has given me a green
light for new recruitment, and I’manxious to get started.”
Kim-Chew Lim, Engel’s wife, alsohas joined the Medical Schoolas an independent assistantresearch scientist. She studiesgenes involved in breast cancer.Engel has two adult children,Geoff and Katrina, who live inChicago.
—SFP
Doug Engel
Photo: Martin Vloet
“There is more activity and excitement here in genetics andgenomics — areas of particular interest to me — than at anyother institution. I’m delighted to be part of it.” –Doug Engel
Medicine at Michigan 7
Hypertension is not an equal opportunitydisease. If you are African-American,
everything about high blood pressure is moredangerous for you, says Kenneth Jamerson(M.D. 1986), an associate professor of inter-nal medicine in the University of MichiganMedical School.
“When compared to other racial and ethnicgroups in the U.S., African-Americans havemuch higher rates of high blood pressure,”says Jamerson, who serves as medical direc-tor for the U-M Health System’s Program forMulti-Cultural Health. “African-Americanstend to develop high blood pressure at anearlier age and are 18 times more likely thanwhites to develop kidney failure as a compli-cation of the disease. Blacks make up only12 percent of the U.S. population, but theyare more than one-third of the patients in anyrenal dialysis clinic.”
The good news, according to Jamerson, isthat it doesn’t have to be this way. He andanother U-M physician, Axinlolu Ojo, studied1,100 African-Americans with hypertension-induced kidney damage to determine whichtype of medication was most effective forthem. They found that, with the right medica-tion and lifestyle changes, the risk of kidneyfailure in African-Americans was no higherthan in the rest of the population.
“Until recently, most physicians believed thatdiuretics, a class of drugs that helps youeliminate more urine from your kidneys, wasthe best therapy, but we found that was notthe case,” Jamerson explains. Results fromhis study showed that blacks with high bloodpressure and kidney damage benefited mostfrom medications called angiotensin-convert-ing enzyme (ACE) inhibitors, which help pre-serve kidney function by acting on hormonesproduced by the kidney.
Hypertension andAfrican-Americans:Proper medication and lifestyle changes could eliminate racial disparities in high blood pressure rates and complications
“Scientists used to believe that blacks weregenetically predisposed to develop high bloodpressure,” Jamerson says. But a study calledthe African-American Study of Kidney Diseaseand Hypertension, conducted in part at the U-M, has so far found little evidence of agenetic basis for high blood pressure inblacks. “Interestingly, what our resultsshow is that blacks in the UnitedStates are genetically more similarto whites in the United Statesthan they are to blacks inAfrica,” Jamerson says.
“The bottom line advicefor anyone with highblood pressure is to be inregular contact with yourphysician, because if an organin your body is being damaged byhigh blood pressure, you won’t know it
until it is too late,” Jamerson adds. “If you areAfrican-American, the message is even moreurgent.”
—SFP
“Scientists used to believe that blacks were genetically predisposed to develop high blood pressure. Interestingly,what our results show is that blacks in the United States aregenetically more similar to whites in the United States thanthey are to blacks in Africa.” —Kenneth Jamerson
Kenneth JamersonPhoto: Marcia Ledford
U-M Health System’s African-AmericanCardiovascular Health Program: Learn how toprevent hypertension and what to do if you’vebeen diagnosed with high blood pressure:
www.med.umich.edu/1libr/heart/afamer01.htm
Acurious child strikes a match.A frustrated girl starts a fire to attractattention. An angry boy burns down an abandoned building.
Educators at the University of Michigan Trauma Burn Center had all ofthem in mind when they created Straight Talk, a hospital-based pro-gram for young people who are involved in fire play, fire-setting andarson. Pamela Pucci, a registered nurse, is the program’s injury pre-vention educator. She says the main goal is to prevent injuries.“Education is a critical component of prevention.”
Paul Taheri, M.D., director of the Trauma Burn Center, agrees. “Byshowing kids what can happen when they carelessly strike a match orplay with fire, we hope to drive home the importance of caution andprevention.We want to bring these children through the front door andeducate them about the dangers of fire, rather than having to treatthem after they are already injured,” he says.
Straight Talk was created in 1999 after specialists at the Trauma BurnCenter noticed a 17 percent increase in pediatric burn admissions. Todate, more than 200 chil-dren have been through the program, and less than one percent of them havereturned to their fire-settingbehavior. By comparison,the recidivism rate for non-participants is 37 percent.
“A distraught grandmotheronce called for help withher 10-year-old grandson,who had just set his 10thfire,” says Pucci. “He hadbeen to a psychiatrist. Thefire department had spo-ken to him. Nothinghelped. He and his grand-parents drove three hoursto attend one of our classes. In the two years since, he has not setone fire.”
Straight Talk places a special emphasis on the medical conse-quences of playing with fire — an aspect rarely addressed by otherprograms. “When the program was first introduced, many agencieswondered what a hospital was doing teaching fire safety,” says Pucci.“Now, those same agencies are the ones referring children to us.”
The program, sponsored by the FRIENDS of U-M Hospitals and HealthCenters, is geared toward children ages eight to 17. The juvenile courtsystem, fire departments, parents, schools and other community
Extinguishing the Desire to Play with Fire
8 Fall 2002
Pamela Pucci and Paul Taheri
Phot
o: M
artin
Vlo
et
agencies can all make referrals. Day-long sessions are held onceeach month.
Classes give high-risk youths and their parents the opportunity tointeract with medical professionals, injury prevention specialists,local firefighters and burn survivors.
Children learn about fire’s damaging effects on the body: scalds;electrical, chemical and fire injuries; the anatomy and function of theskin; the different degrees of burn and the treatment process. Theyalso hear from a burn victim, who speaks to them about the emo-tional difficulties of a burn injury and the recovery process. “Survivorsplay an extremely important role,” says Pucci. “The program givesthem the opportunity to come back and teach prevention.”
“When the programwas first introduced,
many agencies wondered what a
hospital was doingteaching fire safety.Now, those same
agencies are the onesreferring children
to us.” –Pamela Pucci

In addition to hearing first-hand medicalknowledge, children and their parentswatch “In an Instant...” — a video that pullsno punches in telling the stories of chil-dren and teens with painful burn injuries.Produced by Victor/Harder Productions,Inc., the video recently won a GoldenEagle award from CINE, a national organization that recognizes excel-lence in non-theatrical films.
Kids also learn from firefighters about fire investigation, and searchand rescue efforts. Hearing about the dangers of fighting firesreminds the program’s participants that their high-risk behavior putsothers in danger. “Firefighters have families and lives that they riskevery time they respond to a call,” says Pucci. “Many kids fail to real-ize that.”
The program concludes with a talk from a social worker. During thepresentation, children learn why and where people set fires. They alsolearn about consequences like punishment, probation and economiccosts.
At the end of the class, children and their families are given a homesafety kit. The package includes a video, smoke detector tester, emer-gency beacon light, a fire safety book and home safety magazines.Families can also obtain free fire extinguishers and smoke detectorsthrough the program. “The goal is to provide them with the suppliesthey need to have a safe home,” says Pucci.
Pucci emphasizes that Straight Talk is not a “scared straight” pro-gram. Instead, she says, the class is meant to be an educational,hands-on experience. “There are so many people who don’t under-stand the full scope of a burn injury,” she says. “Every day is a con-stant fight to teach parents and children about the dangers andlife-long consequences of playing with fire.”
—GS
To learn more about Straight Talk, visit the U-M Trauma Burn CenterWeb site at: www.traumaburn.org.
Pamela Pucci can be contacted at [email protected].
F O R M E R S U R G E R Y C H A I RN A M E D I N T E R I M E X E C U T I V EV I C E P R E S I D E N T F O RM E D I C A L A F FA I R S
Lazar J. Greenfield, M.D., professor ofsurgery at the U-M Medical School, hasbeen appointed by U-M President Mary Sue Coleman to serve as theUniversity’s interim executive vice pres-ident for medical affairs followingGilbert S. Omenn, M.D., Ph.D., whostepped down from the post at the con-clusion of his five-year term on July 31.Greenfield will serve until a new per-manent executive vice president takesoffice.
Greenfield has been a member of the U-M faculty since 1987,when he became chair of the Department of Surgery, a positionhe held until earlier this year. A leading vascular and thoracicsurgeon, he is the author of 128 book chapters, more than 360scientific articles in peer-reviewed journals, and two major text-books of surgery. Greenfield is renowned for his development ofan intracaval filter device, which bears his name, used to pre-vent pulmonary embolism. He is a member of the Institute ofMedicine of the National Academy of Sciences, has served on15 scientific editorial boards, and is a fellow of the AmericanCollege of Surgeons.
Medicine at Michigan 9
Less than one per-cent of Straight Talkparticipants havereturned to theirfire-setting behavior.By comparison, therecidivism rate fornon-participants is37 percent.
Prior to Straight Talk’s premier, volunteers from the community participated in a trial run. Here, volunteer childrenpeer into the Trauma Burn operating room.
Lazar Greenfield
10 Fall 2002
When a Stroke Strikes,Speed is EssentialHow fast you get treatment when having a stroke could be more impor-tant than who provides it, says Phillip Scott, M.D., director of the U-M’sEmergency Stroke Team and an assistant professor of emergency med-icine. Scott directed a study of 140 stroke patients treated with clot-busting drugs called tissue plasminogen activators or tPA. If treatmentwas received within the recommended three hours of the stroke’sonset, Scott found that the complication rate for patients treated byemergency room physicians was the same as for those treated by spe-cialized stroke teams. But successful treatment depends on getting tothe ER in time. “Any sudden change in speech, sensation or strength isa medical emergency,” says Scott. “Call 911 and get to the nearestemergency room as quickly as possible.”
—KG
For more details, read the complete press release at:www.med.umich.edu/opm/newspage/2002/stroke.htm
Phillip Scott
Phot
o: M
artin
Vlo
et
Men and women differ significantly in the way they describe theirsymptoms during a stroke, says Lewis Morgenstern (M.D. 1990),
director of the U-M Stroke Program. The difference can affect how andwhen women receive emergency stroke treatment.
In research published in the November 2002 issue of the Annals ofEmergency Medicine, Morgenstern described how women were 62 per-cent more likely than men to describe sensations other than the tradi-tional symptoms of sudden weakness or numbness on one side of thebody, difficulty speaking or understanding, facial drooping, dizziness orvision changes. The study, conducted with colleagues at the Universityof Texas, is the first to document significant gender differences in theperception and reporting of stroke symptoms.
Because emergency responders and emergency room physicians oftengo by patients' descriptions and the traditional symptom list when diag-nosing and treating a suspected stroke, women’s symptoms may beoverlooked during the precious hours when stroke therapies work best,says Morgenstern. Delayed treatment can mean long-term disability oreven death from a stroke.
“These gender differences are both biologically interesting and sociallyconsequential,” says Morgenstern, an associate professor of neurology,epidemiology, emergency medicine and neurosurgery in the U-MMedical School and the U-M School of Public Health. “They are impor-tant to medical education, too, because often medical students aretrained that stroke is a man’s disease, which it is not.”
Previous studies have shown that women who have a stroke are morelikely to die than men, or if they survive, more likely to have a poor out-
Stroke and Gender Differences‘ B I O L O G I C A L LY I N T E R E S T I N G…S O C I A L LY C O N S E Q U E N T I A L’
come. Researchers also have discovered that women face longerdelays than men in being evaluated for a stroke by emergency roomphysicians. Stroke is the leading cause of disability in American adults,and the third leading cause of death.
—KG
For more details on stroke prevention and warning signs, visit:www.med.umich.edu/1libr/topics/brain13.htm
Lewis Morgenstern and stroke patient Valdina WileyPh
oto:
Mar
tin V
loet

Medicine at Michigan 11
Junk DNA is the RodneyDangerfield of the genetics
world. It makes up nearly half ofall human DNA, but since it does-n’t include genes, many scientistsdismiss it as useless gibberish.New U-M research, however, sug-gests that segments of junk DNAcalled LINE-1 or L1 elementsdeserve more respect.
“L1s have helped build ourgenome and their movement con-tinues to influence its evolution,”says John V. Moran, Ph.D., anassistant professor of humangenetics and internal medicine inthe U-M Medical School, recruitedhere as part of the prestigiousBiological Scholars Training Pro-gram. Moran is one of only a fewscientists who study L1s in thehuman genome. “The more welearn about L1s, the more we’lllearn about the evolution of thehuman genome,” he says.
“Some L1 elements are transpos-able, meaning they make copiesof themselves and then move tonew locations in the genome.Although L1s make up 17 per-cent of our DNA, very little isknown about them,” Moran adds.“Until now, everyone thought theywere just intracellular DNA para-sites left over from the distantevolutionary past.”
Because L1s are so ancient andbecause they sometimes carrysegments of genes with themwhen they jump to a new loca-tion, Moran believes they haveplayed an important role inhuman evolution by increasinggenetic diversity.
In recently published research inNature Genetics and Cell, Moranand his team found that somehuman L1 elements can jump tochromosomes with broken strandsof DNA, slip into the break andrepair the damage. They also dis-covered that L1s can delete DNAwhen they jump to a new location— possibly knocking out genes orcreating devastating mutations inthe process. Jumping elementsmay have a significant influenceon the human genome.
Collaborators on the two researchstudies include Nicolas Gilbert,Ph.D., a postdoctoral fellow inhuman genetics; Sheila Lutz-Prigge, U-M research associate;and Tammy A. Morrish, a U-M grad-uate student in human genetics.
—SFP
Read the complete stories online at: www.med.umich.edu/opm/newspage/2002/junkdel.htm
www.med.umich.edu/opm/newspage/2002/junkdna.htm
To learn more about research in the Moran lab, go to:www.med.umich.edu/hg/research/faculty/Moran/moranweb.htm
John Moran
Because L1s are so ancient and sometimes carrysegments of genes with them when they jump to
a new location, Moran believes they haveplayed an important role in human evolution by
increasing genetic diversity.
D E A N ' S R I D E T O D E X T E RMedical School faculty, staff, students and their families pedaled downHuron River Drive between Ann Arbor and neighboring Dexter on Sunday,June 30, as part of Dean Lichter’s Ride to Dexter. The bikers left Ann Arborat 10 a.m., then rendezvoused for lunch at Dexter-Huron Metroparkbefore heading back to campus. The 86 participants and their familymembers each received T-shirts commemorating the first occurrence ofwhat is planned to be an annual event.
Visit www.medicineatmichigan.org/magazine to see additional pho-tos from this event.
Junk DNA Gains RespectPh
oto:
Mar
tin V
loet
Phot
o: H
orac
e Bo
mar

12 Fall 2002
2002. She also served as provost and vicepresident for academic affairs (1993-95) atthe University of New Mexico, and as vicechancellor for graduate studies and research(1992-93) and associate provost and deanof research (1990-92) for the University ofNorth Carolina at Chapel Hill. Prior to hercareer in academic administration, Colemanspent 19 years on the biochemistry facultyand as a cancer center administrator at theUniversity of Kentucky in Lexington. Herresearch focused on the immune system’sresponse to cancer, especially in leukemia.
Coleman was elected to the National Academyof Sciences’ Institute of Medicine in 1997,where she co-chairs the Institute’s Committeeon the Consequences of Uninsurance.
—SFP
To learn more about President Coleman, goto: www.umich.edu/pres
On August 1, Mary Sue Coleman, Ph.D., abiochemist and former president of the
University of Iowa, became the University ofMichigan’s 13th president and the firstwoman to hold the post.
Coleman also received tenured joint facultyappointments as a professor of biologicalchemistry in the U-M Medical School and aprofessor of chemistry in the U-M College ofLiterature, Science, and the Arts.
“I am delighted that the University ofMichigan has such a strong and dynamic aca-demic medical center,” Coleman says. “It con-tributes enormously to Michigan’s stature asa world-class research university. MedicalSchool research is generating promising col-laborations within our academic communityand with scientists across the country andaround the world. Caring for patients andtraining tomorrow’s physicians are excellentexamples of the way a great university fulfillsits public service mission.”
Before joining the U-M, Coleman was presi-dent of the University of Iowa from 1995-
A N E W L E A D E R F O R T H E U N I V E R S I T Y
“Caring for patientsand training
tomorrow’s physiciansare excellent examples
of the way a great university fulfills its
public service mission.”—U-M President Mary Sue Coleman
U - M H E A LT HS Y S T E M A G A I NM A K E S T O P 1 0The University of Michigan Health Systemonce again has been named one of the10 top hospitals in the country, accordingto U.S. News & World Report’s annualsurvey released in July. U-M came in eighththis year, maintaining its coveted spot of being among the nation’s leading health care institutions. Last year, it rankedseventh.
The magazine’s annual report not onlyranks the honor roll of “Best Hospitals,” butalso assesses hospitals in various medicalspecialties. Again this year, UMHS wasrecognized in nearly all the specialties,ranking in the top 15 in 12 of the cate-gories. Four specialties were within the top 10: cancer (9); ear, nose and throat(4); geriatrics (10); and respiratory disor-ders (10).
—CH
Phot
o: M
artin
Vlo
et
New Life for Life SciencesU-M President Mary Sue Coleman has appointed Alan R. Saltiel,Ph.D., the John Jacob Abel Collegiate Professor of the Life Sciencesand professor of internal medicine and physiology in the MedicalSchool, as the new director of the University’s Life SciencesInstitute, filling the vacancy left by the resignation of Jack E. Dixon,Ph.D. Saltiel is a leader in the field of signal transduction, the studyof how hormones, particularly insulin, send messages within cells.
Coleman also appointed six charter faculty to help define the sci-entific focus of the Institute and guide the critical faculty recruitingefforts to come. All six members have Medical School ties: David
Ginsburg, M.D.,Warner-Lambert /Parke-Davis Professor of Genetics and Internal Medicine; DanielJ. Klionsky, Ph.D., professor of molecular, cellular and developmental biology and biological chem-istry; John B. Lowe, M.D., Warner-Lambert/Parke-Davis Professor of Pathology; Rowena G.Matthews Ph.D., G. Robert Greenberg Professor of Biological Chemistry; Carol A. Fierke, Ph.D., pro-fessor of biological chemistry; and Gary D. Glick, Ph.D., professor of biological chemistry. Fierke,Glick, Klionsky and Matthews also hold appointments in the College of Literature, Science, and the Arts.
Phot
o: D
.C.G
oing
s

Medicine at Michigan 13
Tiny cells called pericytes may play a pivotal role in setting off thechain of events that leads to diabetic eye disease, according to
Donald G. Puro, M.D., Ph.D., professor of ophthalmology and visual sci-ences and of physiology in the U-M Medical School. Pericytes are tinycells which sit on the wall of capillaries throughout the body but are mostconcentrated in the retina.
Diabetes takes its toll on vision by damaging blood vessels in the retina,and Puro believes pericytes could be involved in the flow of blood in theretina. Diabetes affects some 16 million Americans, many of whom don’trealize they have the disease. About two-thirds of the patients Puro seesin Kellogg’s General Ophthalmology Clinic suffer from diabetes.
Using a technique developed by Puro’s team to isolate capillaries fromthe retina, the researchers study the functions of pericytes under con-trolled laboratory conditions. After viewing the isolated vessels withtime-lapse photography, members of the team observed an intriguingphenomenon: the pericytes contract, and this action may change theflow of the blood. According to Puro, “It’s reasonable to ask whetherpericytes are part of a control mechanism that is essential to blood flowin the retina. Perhaps diabetes causes the pericytes to malfunction, andthis is the first action in a cascading series of events leading to visionloss.”
For some reason the eye’s capillaries are extremely vulnerable to theelevated glucose that accompanies diabetes. “It’s the Holy Grail,” saysPuro. “If we can prove which feature makes the eye so vulnerable, pre-sumably we could modify it.”
Puro notes that Kellogg has the only research team studying capillarieswith the patch-clamp technique, in which fine-tipped glass tubes forma seal with the surface of a pericyte. The method essentially allowsresearchers to “listen in” on vital aspects of cellular activity. Says Puro,“We think pericytes respond to all sorts of signals about how to controlblood flow in the retina.”
In a related series of experiments, the Kellogg research lab is collectingmore clues to describe the chain of events and the pathways in diabetic
Diabetes’ Toll on VisionK E L L O G G R E S E A R C H E R S E D G E C L O S E R T O U N D E R S TA N D I N GT H E PAT H WAY S O F D I A B E T I C E Y E D I S E A S E
Photo: Richard Hackel
eye disease. This line of research reveals that pericytes operate as acommunity rather than simply as individual units. Puro and his cowork-ers recently discovered that this communication between cells withinretinal capillaries is severely disrupted soon after the onset of dia-betes, bringing the research team a step closer to understanding howdiabetes affects vision: it may disrupt the ability of capillaries to sup-ply essential oxygen and nutrients to the nerve cells of the retina.
“We are still trying to better understand what is ‘normal behavior,’” Purosays, “so that we can intervene when the cells begin the abnormalbehavior associated with diabetes. If we can understand the processearly on, we could almost certainly prevent damage down the road.”
—BN
Diabetes takes its toll on vision by damaging bloodvessels in the retina, and Puro believes pericytescould be involved in the flow of blood in theretina.
Donald G. Puro

14 Fall 2002
Research in a Land in ConflictD E S P I T E T H E H O S T I L I T I E S , L I F E — A N D I N T E R N AT I O N A LS T U DY — G O E S O N
For a Pennsylvania Catholic and an IsraeliJew, Steve Gruber and Gad Rennert have a
lot in common. They are both cancer geneti-cists with active research programs and physi-cians who treat patients with colorectalcancer. Both are married and raising youngfamilies. Steve Gruber has three children,ages 11, seven and one. Rennert has 12- and15-year-old daughters.
“Not only do our professional lives overlapcompletely, our personalities are similar, too,”says Gruber, M.D., Ph.D., the director of clini-cal cancer genetics at the U-M Compre-hensive Cancer Center and an assistantprofessor of internal medicine and epidemiol-ogy. “The only difference is that I’m not nearlyas talented as Gadi.”
Gadi is Gad Rennert, M.D., Ph.D., the chair ofcommunity medicine and epidemiology at theTechnion Faculty of Medicine and CarmelMedical Center in Haifa, Israel. Rennertdirects the National Cancer Control Center forClalit Health Services, Israel’s largest HMO.He also speaks five languages and is, accord-ing to Gruber, “one of the most amazing peopleI have ever met.”
The two scientists met about a year afterSteve Gruber joined the U-M Medical Schoolfaculty in 1997. Fresh from a fellowship atJohns Hopkins, with a medical degree fromPenn and a Ph.D. from Yale, Gruber wanted tostudy how genes, diet, exercise and other fac-tors interact to produce colon cancer.
He was looking for a research partner. Alongthe way, he found a friend and discovered thateven science is not immune to the world’stroubles.
Gruber knew that descendants of AshkenaziJews — a closely related ethnic group that for-merly lived in Eastern Europe — have unusu-ally high rates of colon cancer. He thoughtthey would be the ideal study population. Butfinding them, along with organizing and man-aging a complex field study, is expensive anda big job for a young scientist early in hisresearch career.
That’s when Dean Brenner, M.D., a professorof internal medicine and pharmacology inthe Medical School, entered the picture,Gruber recalls. “Dean said, ‘There’s no ques-tion you should do this study in Israel, and Iknow the perfect person to talk to. In fact, I’mgoing there in two weeks. Why don’t youcome with me?’ So I flew to Israel with Dean,who introduced me to Gadi, and it justclicked.”
So a new international research collabora-tion — the Molecular Epidemiology of Colo-rectal Cancer (MECC) Study — was born, andfunded in 1999 with a $4.8 million grantfrom the National Cancer Institute and addi-tional funding from the Irving WeinsteinFoundation.
Today, the study includes 4,200 people livingin northern Israel — half who have been diag-nosed with colorectal cancer and half whohaven’t. Gruber’s lab handles DNA and
molecular profiling of blood and tumor tissuesamples from people in the study. Rennertmanages 12 field researchers who visit studysubjects in their homes to take blood sam-ples and administer an 800-question surveyon diet, physical activity, medical history andother lifestyle factors.
“We understand genes aren’t the whole story,because some people with a genetic suscep-tibility develop the disease, while others donot,” says Gruber. “This is why Gadi’s fieldresearch is so important. Without it, we wouldhave no way of understanding the role of dietand other environmental factors.”
Rennert selects his study subjects withpainstaking care to eliminate sample bias.“First, we include every person in our definedgeographic area with colorectal cancer. Thenwe find a control subject without cancer whomatches each patient’s demographics asclosely as possible,” Rennert explains. “Let’s
Phot
o: P
ictu
reQu
est

Medicine at Michigan 15
say I have an 82-year-old male patient withcolon cancer who is an Ashkenazi Jew living ona certain street in Haifa. To find a matchingcontrol subject, we go to the same street andfind an 82-year-old male Ashkenazi Jew whodoes not have cancer. This is not easy to do,but it’s the only way to ensure reliable data.”
As the research developed, so did the friend-ship. Rennert and Gruber stayed in constanttouch by e-mail and telephone, and visitedeach other’s laboratories several times ayear. With their wives, they went to concertsand picnics together, and their childrenbecame trans-Atlantic pen pals.
But in September 2000, after several years ofrelative peace between the Jewish andPalestinian populations in Israel, hostilitiesbegan again. The U.S. State Departmentissued a travel advisory and, for the first time,Steve Gruber had to postpone a planned visitto Israel.
“We had to figure out new ways to keep dataflowing back and forth, but we were able tocontinue with minimal interruptions,” Grubersays. “The biggest change for me is that Iworry about him. Whenever I see in the newsthat there’s been another bombing, I pick upthe phone to see if everyone is OK. When
Gadi’s daughter had her Bat Mitzvah, I wasreally nervous for her.
“There was a bus bombing near Haifa notlong ago, so I called Gadi’s office and spoketo Ronit Almog, one of the study coordina-tors,” Gruber adds. “She was bringing sam-ples back from a hospital near the West Bankand had driven past that same intersectionjust an hour before the bombing.”
Gruber and Rennert find it ironic that conflictin the Middle East could interfere withresearch designed to benefit the entire popu-lation. “In our study, we have Arabs, we haveSephardic Jews, we have Ashkenazi Jews, wehave everybody,” Rennert says. “Our resultsdefinitely will make a major contribution tounderstanding how colorectal cancer developsand progresses in the Arabic, as well as theJewish, population.”
“What’s so wonderful about this collaborationis the fact that we can learn how genetic andenvironmental contributions differ amongethnic groups living in the same geographicarea,” Gruber says. “Colon cancer isn’t ascommon in the Arab population, but we stillneed to learn how to care for everyone whosuffers from this disease.”
Rennert is proud of the fact that not one member of his field research team has left theproject, even though travel to and from theirsite visits is much more dangerous now. “It’salready a way of life for us,” Rennert says. “Weuse public transportation less; we consider thesafest way to travel. There’s a higher level ofawareness. It’s not foolproof, but it’s how we’velearned to behave, because otherwise we’dnever go anywhere.”
Gruber still travels to Israel, but now he staysin a different hotel away from Haifa’s centralcommercial district. “The crisis does influenceevery element of daily life, but everyone refusesto have their lives dictated by conflict. Despitethe hostilities, life goes on.”
No matter what happens in the Middle East,Gruber says he and Rennert are determined tocontinue their work. In fact, Gruber has appliedfor an extension to his research funding, so thestudy can continue for several more years.
—SFP
No matter what happensin the Middle East,Gruber says he andRennert are determinedto continue their workon colorectal cancer.
Phot
o: G
rego
ry F
ox
Steve Gruber and Gad Rennert
16 Fall 2002
When fibromyalgia patients say they’re inpain, they aren’t kidding. A new brain-
scan study found that a gentle finger squeezeproduced measurable pain signals in thebrains of people diagnosed with fibromyalgia.Twice the squeezing force was required beforehealthy people felt the same levels of pain.
The study is the first to compare whatfibromyalgia patients report they feel andwhat's happening in their brains when theyfeel it. The findings were published in the May 2002 issue of Arthritis & Rheumatism,the journal of the American College ofRheumatology.
Lead authors Richard Gracely, Ph.D., professorof internal medicine and neurology in the U-M
Medical School,and Daniel Clauw(M.D. 1985), U-Mprofessor of inter-nal medicine, con-ducted the study atG e o r g e t o w nUniversity MedicalCenter and theNational Institutesof Health. They arenow continuing theirwork at the Uni-versity of MichiganHealth System. Inan accompanyingeditorial, Clauw and Leslie Crofford,M.D., an associateprofessor of inter-nal medicine in theMedical School,stressed the import-ance of researchon fibromyalgia.
Patients and many physicians say fibromyalgiais a specific, diagnosable chronic disease. Itaffects more than two percent of Americans,particularly women of childbearing age, and ischaracterized by tenderness and stiffness as
well as fatigue, headaches, gastrointestinalproblems and depression. Skeptics say fibro-myalgia is rooted more in psychological andsocial factors than in physical, biologicalones. Their argument has been bolstered bythe failure to find a clear cause, an effectivetreatment or a non-subjective way of assess-ing patients.
The new study confirms scientifically whatpatients have been telling skeptics in themedical community for years. “The brain scantechnology gave us an opportunity to look atthe neurobiology of tenderness, the hallmarkof fibromyalgia,” says Clauw. “These results,combined with work done by others, con-vinced us that some pathologic process ismaking these patients more sensitive. Forsome reason, still unknown, there’s a neuro-biological amplification of their pain signals.”
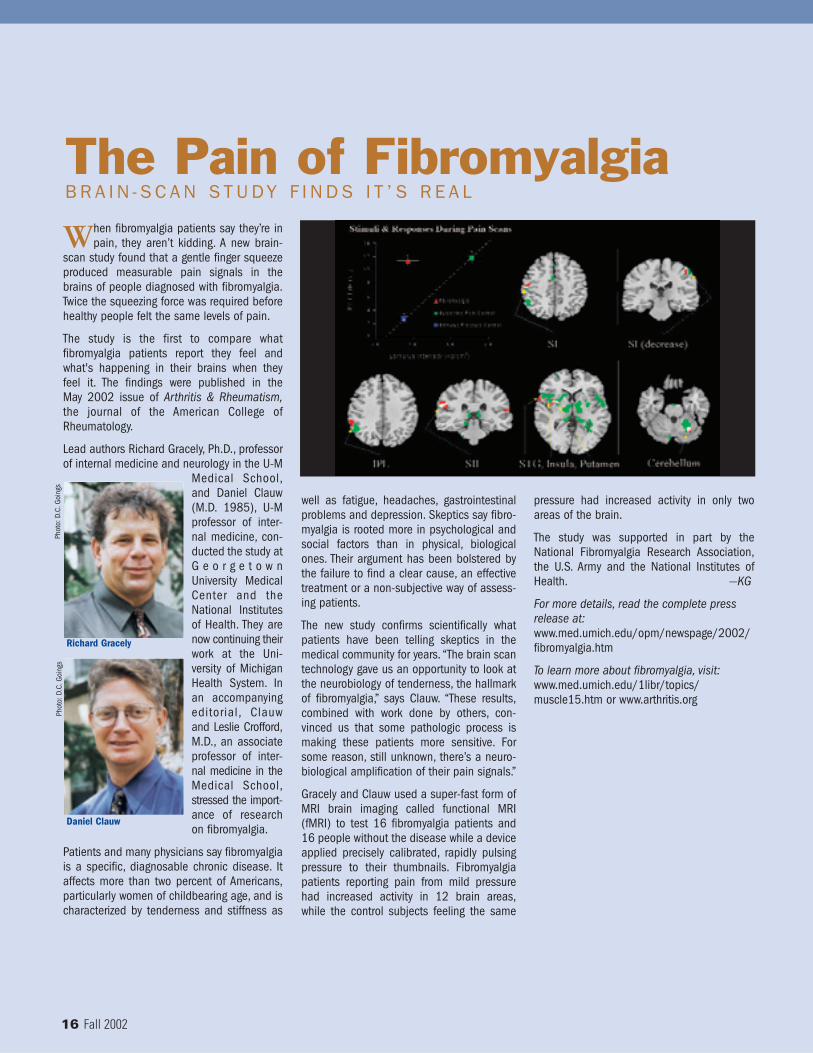
Gracely and Clauw used a super-fast form ofMRI brain imaging called functional MRI(fMRI) to test 16 fibromyalgia patients and16 people without the disease while a deviceapplied precisely calibrated, rapidly pulsingpressure to their thumbnails. Fibromyalgiapatients reporting pain from mild pressurehad increased activity in 12 brain areas,while the control subjects feeling the same
The Pain of FibromyalgiaB R A I N - S C A N S T U DY F I N D S I T ’ S R E A L
pressure had increased activity in only twoareas of the brain.
The study was supported in part by theNational Fibromyalgia Research Association,the U.S. Army and the National Institutes ofHealth. —KG
For more details, read the complete pressrelease at:www.med.umich.edu/opm/newspage/2002/fibromyalgia.htm
To learn more about fibromyalgia, visit:www.med.umich.edu/1libr/topics/muscle15.htm or www.arthritis.org
Phot
o: D
.C.G
oing
sPh
oto:
D.C
.Goi
ngs
Richard Gracely
Daniel Clauw