
AAPC DL - AWS
68
www.aapc.com May 2020 Welcome to the Industry 16 We have resources galore! 2021 E/M Changes on Primary Care 24 Prepare to implement leveling guidelines. Losing Business? 46 Maybe it’s your customer service.
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of AAPC DL - AWS

www.aapc.com May 2020 1
www.aapc.comMay 2020
Welcome to the Industry 16 We have resources galore!
2021 E/M Changes on Primary Care 24 Prepare to implement leveling guidelines.
Losing Business? 46 Maybe it’s your customer service.

AAPC DL
Up to 50% OffEverything You Need toGet Certified Through
May 29
For more details call 877-290-0440or visit aapc.com/exam-prep

www.aapc.com May 2020 3
[[contentscontents]]■ Added Edge
[continued on next page]
Healthcare Business Monthly | May 2020
■ Coder’s Voice
42 Maximize Your Stroke Dx Coding By Brett Rosenberg, MA, CPC, CCS-P, COC
16 Welcome to the Industry: We Have Resources Galore!By Michelle A. Dick, BS
64 Commit to Zero HarmBy Valerie Fernandez, PhD, MBA, RHIA, CPC, COC, CPMA, CRC, CCS
■ Coding/Billing
COVER | Coding/Billing | 30
Expert Documentation & Coding Practices in the EMRBy Lynn Handy, LPN, CPC, CPC-I, COC, CCS-P
4 Healthcare Business Monthly
Healthcare Business Monthly | May 2020 | contents
26
46
56
DEPARTMENTS7 Letter From the CEO
8 Letters to the Editor
9 I Am AAPC
10 AAPC Chapter Association
19 Career Development
38 Health Awareness
66 Minute With a Member
EDUCATION58 Newly Credentialed Members
Online Test Yourself – Earn 1 CEU www.aapc.com/resources/publications/
healthcare-business-monthly/archive.aspx Or try it on your My AAPC application.
Availability expires 1 year after publication date.
COMING UP: • Telehealth • Social Media • Code With Confidence • MDM • 2020 CV Coding
On the Cover: Lynn Handy, LPN, CPC, CPC-I, COC, CCS-P, talks about the proper use of contemporary electronic medical records. Cover design by Mahfooz Alam.
■ Coding/Billing20 2020 Radiology and Imaging CPT® Changes
By Elizabeth Hylton, CPC, CEMC
24 Calculating the Effect of the 2021 E/M Changes on Primary Care
By Bruce Pegg, MA, CPC-A
26 Anemia: ICD-10-CM Guidelines Update Clarification
By Angelica Mae Celis-Duran, RN, CPC, BCHH-C, CPMA
28 Words Are Important in Oncology Coding
By Jacolyn Bailey, LPN, CPC-A, CHONC, CRC, AAPC MACRA Proficient, CEMA
36 How Patient Prehistories Improve Health Outcomes
By Michael Warner, DO, CPC, CPMA, AAPC Fellow
■ Practice Management46 Losing Business? Maybe It’s Your Customer Service
By Joshua Caillouet, CPC, CASCC
48 How to Cultivate Healthy Care Teams and Eliminate Risk
By Sarah Prom, MA, LPC, ODCP
■ Auditing/Compliance52 Boost Password Acumen With Expert Insight
By Kristin J. Webb-Hollering
■ Hot Topic56 COVID-19: Be Informed, Take Precautions, Stay Calm, and Carry On
By Leesa A. Israel, BA, CPC, CUC, CEMC, CPPM, CMBS, AAPC MACRA Proficient
www.aapc.com May 2020 5
AAPC Workshops
E/M Guideline Changes are on the way. It’s already time to prepare. Join AAPC in our monthly workshop training. Swim into 2021 without a scratch.
AAPC 2021 E/M Guideline Changes Series
E/M Fundamentals: Steps to Prepare for the Coming Changes
E/M Guideline Changes: Primary Care
E/M Guideline Changes: Cardiology
E/M Guideline Changes: Orthopedics
E/M Guideline Changes: Obstetrics & GGynecology (OB/GYN)
E/M Guideline Changes: Otolaryngology
E/M Guideline Changes: Neurology
E/M Guideline Changes: Dermatology
E/M Guideline Changes: Gastrointestinal
E/M Guideline Changes: Hematology and Oncology
EE/M Guideline Changes: Pediatric
E/M Guideline Changes: Putting it all Together
On-Demand
On-Demand
On-Demand
April 28
May 26
June 23
JJuly 28
August 25
September 29
October 27
November 17
December 15
Ready or Not, Here They Come.
Sign Up Today!aapc.com/prepare

6 Healthcare Business Monthly
Volume 7 Number 5 May 1, 2020Healthcare Business Monthly (ISSN: 23327499) is published monthly by AAPC, 2233 South Presidents Drive, Suites F-C, Salt Lake City UT 84120-7240, for its paid members. Periodicals Postage Paid at Salt Lake City UT and at additional mailing office. POSTMASTER: Send address changes to: Healthcare Business Monthly c/o AAPC, 2233 South Presidents Drive, Suites F-C, Salt Lake City UT 84120-7240.
Head of Publishing, Editorial & TechnologyLeesa A. Israel, BA, CPC, CUC, CEMC, CPPM, CMBS
Senior Development EditorsRenee Dustman, BS, AAPC MACRA Proficient
Chris Boucher, MS, CPC
Development EditorsStacy Chaplain, MD, CPC
Lee Fifield, BS [email protected]
Rachel Dorrell, MA, MS
Graphic Design Mahfooz Alam
Advertising SalesVictoria Fuentes
Address all inquires, contributions, and change of address notices to:
Healthcare Business MonthlyPO Box 704004
Salt Lake City, UT 84170(800) 626-2633
©2020 Healthcare Business Monthly. All rights reserved. Reproduction in whole or in part, in
any form, without written permission from AAPC® is prohibited. Contributions are welcome.
Healthcare Business Monthly is a publication for members of AAPC. Statements of fact or
opinion are the responsibility of the authors alone and do not represent an opinion of AAPC,
or sponsoring organizations.
CPT® copyright 2019 American Medical Association. All rights reserved.
Fee schedules, relative value units, conversion factors and/or related components are not
assigned by the AMA, are not part of CPT®, and the AMA is not recommending their use. The
AMA does not directly or indirectly practice medicine or dispense medical services. The AMA
assumes no liability for data contained or not contained herein.
The responsibility for the content of any “National Correct Coding Policy” included in this
product is with the Centers for Medicare and Medicaid Services and no endorsement
by the AMA is intended or should be implied. The AMA disclaims responsibility for any
consequences or liability attributable to or related to any use, nonuse or interpretation of
information contained in this product.
CPT® is a registered trademark of the American Medical Association.
HEALTHCAREBUSINESS MONTHLYCoding | Billing | Auditing | Compliance | Practice Management
Go Green!Why should you sign up to receive Healthcare Business Monthly in digital format?
Here are some great reasons:
• You will save a few trees.
• You won’t have to wait for issues to come in the mail.
• You can read Healthcare Business Monthly on your computer, tablet, or other mobile device—anywhere, anytime.
• You will always know where your issues are.
• Digital issues take up a lot less room in your home or office than paper issues.
Go into your Profile on www.aapc.com and make the change!
May 2020
When you advertise in Healthcare Business Monthly, you’ll reach the largest and most engaged audience of medical coders, billers, auditors, compliance officers, and practice managers anywhere on the planet!
HBM reaches more than 180,000 AAPC members every month who read both the proprietary content in realtime and archived past issues as a valuable reference.
www.aapc.com March 2019 1
STRA
IGHTF
ORWARD MODERATE
HIGH
LOW
THINK ABOUTMDM SCORING IN THEEMERGENCY DEPARTMENTTHINK ABOUTMDM SCORING IN THEEMERGENCY DEPARTMENTTHINK ABOUT
EMERGENCY DEPARTMENT
What’s in Store for 2019 OPPS? 18
Hint: More site-of-service payment equalization
Be Specific with National Drug Codes: 38
How to report “what’s in the box”
Make Artificial Intelligence Your Friend: 51
Will the robot next to you affect your coding career?
www.aapc.comMarch 2019
HBM_Mar2019.indd 1
08/02/19 1:14 PM
Healthcare Business Monthly
To get in front of our audience, contact Victoria Fuentes at (800) 626-2633 x-298 or [email protected].
Advertiser IndexNAMAS ....................................................................................... 50 https://namas.co/2021.changes
ZHealth ....................................................................................... 45 www.zhealthpublishing.com

www.aapc.com May 2020 7
We Are in This Together
Letter From the CEO
As I write this letter, it’s March, and many of us are sequestered in our homes for an indeterminate time, while the healthcare
industry is on the frontlines in the battle against COVID-19. There is tremendous uncertainty, forcing us to make decisions to solve immediate challenges, while remaining mindful of our inability to predict the future.
As safety is a top priority, we have been monitoring the emergent situation so that we can make educated and timely decisions regard-ing all AAPC operations. With incredibly fast-moving changes in the world around us, we’ll continue to pivot quickly, and I’m hopeful the choices we make today will produce positive outcomes by the time this letter reaches you.
Tactical ManeuversIn response to the national public health emergency and in consid-eration of our customers, members, staff, and communities, we have taken the following measures:
Remote staff – We began in March to transition AAPC employees to work remotely for the protection of themselves, colleagues, and our communities. Even during this social distancing, I am confident we have been delivering the high standards of support you have come to expect from us.
Charitable works – We also realize that charities suffer greatly during times of economic uncertainty. We have partnered with the Susan G. Komen foundation to give $1 for every AAPC book sale and AAPC Coder subscription.
Virtual HEALTHCON – We converted the national conference into a virtual experience.
Local chapters – We mandated a shift of all physical meetings to virtual.
Exams – We mandated the postponement of exams until further notice (while extending expiring vouchers).
Students – We extended soon-to-be expiring 2019 and 2020 distance learning courses and awarded eight scholarships.
AAPC Coder – We’re offering an extended free trial of our coding software to new users through June 30 to help alleviate the burden of our members’ transition to remote work. AAPC Coder has been updated with the latest ICD-10-CM, CPT®, and HCPCS Level II codes and descriptions for COVID-19 diagnoses and testing.
Education – We’ve made several webinars and courses available for free to help with continuing education units and training sur-rounding COVID-19, telehealth, working from home, and related topics. And we’ve been posting federal and CPT® guidance on our Knowledge Center (www.aapc.com/blog) as quickly as it is released.
Fees/payments – We’ve waived late fees and/or ex-tended payments for those financially affected by the pandemic. All members (and friends and family) can now take AAPC’s training programs with monthly payment financing available (no interest or credit check).
Member outreach – In this time of so many people working remotely, AAPC leadership and the National Advisory Board mem-bers have been conducting weekly Facebook Live sessions to discuss coding, reimbursement, and career topics.
We Will RallyI’m hopeful that as you’re reading this letter in this May issue of Healthcare Business Monthly, the world has been able to slow or stop the spread of the disease, is in recovery, and we’re beginning to get back to our jobs and normal patterns in our lives. Thanks for maintaining infectious positivity and optimism to combat the broader and nonclinical effects of this disease. And thank you for your support, concern, friendship, contributions, and continued commitment to AAPC.
Stay well and safe!
Sincerely,
Bevan EricksonAAPC CEO
“We have partnered with the Susan G. Komen foundation to
give $1 for every AAPC book sale and AAPC Coder subscription.”
8 Healthcare Business Monthly
TCI Newsletter
Please send your letters to the editor to: [email protected] to the Editor
In the February 2020 Healthcare Business Monthly, Nikki Taylor, MBA, COC, CPC, CPMA, CRC, states in her article “CPT® 2020: Get the Inside Scoop on Code Changes” that during the AMA CPT® and RBRVS Symposium, Dr. Barkley stated that continuous EEG monitoring does not mean monitoring the patient 100 percent of the time: “If the patient is monitored for at least 80 percent of the service, you may bill continuous monitoring.” I attended the Symposium and that is not my recollection of the discussion. I believe there may be some confusion over continuous monitoring and continuous record-ing, as well as confusion over the rules from PC to TC reporting.
CPT® discusses the 80 percent rule in relation to the percentage of time that video must be captured during the diagnostic EEG to report the services as VEEG (CPT® codes 95711-95716). It does NOT relate to continuous versus intermittent monitoring for proper reporting of the TC codes. The guidelines state that the entire study is reported as EEG without video if concurrent diagnostic video occurs less than 80 percent of the entire study. Guidelines also state, “If there is a break in the real-time monitoring of the EEG recording, the study is an intermittent study.” The syllabus from the Symposium further clarifies, “Tip: Continuous, real-time monitoring is at a maximum ratio of 1 tech:4 patients; cannot be used if there is a break in the recording, such as sending patient off unit for a diagnostic test; intermittent monitoring is up to 1 tech:12 patients.”
We have advised our technologists that any break in video monitoring makes a study intermittent, as this is our understanding of the guidelines.
— Karen Hale, CPC, CPCO, CRC
Thank you for the clarification. The new long-term EEG monitoring codes related to the technical component (95705-95716) require: 1. Identification of whether the video recording was performed simulta-
neously along with the EEG service. This would mean that the service is a VEEG (95711-95716); and
2. If the technologist who monitored the service performed unmonitored, intermittent, continuous, or real-time monitoring.
To bill a continuously monitored VEEG, the technologist must meet the requirements for continuous monitoring based on the CPT® guidelines AND the recording must meet at least 80 percent of the total concurrent study. This is concurrent with the diagnostic EEG recording. For long-term VEEG studies, it is quite common to have breaks in the recording due to the patient having to use the restroom, or other reasons. Twenty percent is the threshold for the maximum time that is allowed for recording breaks; if the monitoring is interrupted, you should look to the intermittent monitoring codes. When selecting the code for the technical part of the service, you need to know whether there was video, the duration of the study, and the type of monitoring that was performed during the study. — Nikki Taylor, MBA, COC, CPC, CPMA, CRC
Confusion Over EEG Monitoring vs. Recording
Get the guidance you need for CMS coding compliance.TCI’s 25+ specialty-specific newsletters feature: Analysis of latest codes and regulatory changes
Must-have advice for day-to-day scenarios
How-to articles and archives
Reader questions with expert answers
Subscribe Now Visit www.codinginstitute.com/newsletters or call 800.508.2582 to get started
Save time, increase coding accuracy, and earn CEU opportunities!
February 2020, Vol. 22, No. 2 (Pages 9-16)
2020
Call us: 1-800-508-2582
The Coding Institute LLC, 2222 Sedwick Road, Durham, NC 27713
Urology Coding Alert
Your practical adviser for ethically optimizing coding, payment, and efficiency in urology practicesNow Also Access Your Alert Online at www.SuperCoder.com
In this issue
Surgical Focus
Are You Using These 2
Codes for Penile Repair? p11
XWatch for th
e type of
injury — and don’t
confuse it with
exploration.
Compliance
Fitness Trackers Might H
ave
More Regulations Coming p12
XLawmakers are looking
at ways to keep HIPAA
on pace with technology.
You Be the Coder
p13
XReportin
g Ureteral Stent
Placement Via Ileal Conduit
Diagnosis Coding }
Avoid the Trap of A
ssigning N39.0 for E
very
UTI Diagnosis
Hit: Check whether other anatomic sites are involved.
While a urinary
tract i
nfection (U
TI) might be one of th
e most c
ommon conditions
that a urologist t
reats, th
at doesn
’t mean
you can make as
sumptions about re
porting
the care.
Selecting the co
rrect diagnosis
code is param
ount, especia
lly when
symptoms that a
ppeared to point to
a UTI ac
tually lea
d elsewhere.
Now follow our experts
’ top tip
s for co
nfirming that t
he conditio
n is a UTI an
d
selectin
g the correc
t diagnosis.
Tip 1: Pinpoint the Associated Symptoms
Starting point: T
he first
ICD-10-CM code that p
ops up when you search
for
“infection/urinary
(tract)”
is N39.0 (U
rinary tract i
nfection, sit
e not specif
ied). But
when you dig further into the li
sting, you’ll f
ind codes for U
TIs that a
re asso
ciated
with conditions su
ch as preg
nancy or childbirth
. You’ll also fin
d entries fo
r
differen
t organs and anatomic l
ocations w
here a “u
rinary” in
fection might str
ike:
the bladder, kidneys, a
nd urethra.
Because t
here are
a number of sy
mptoms that m
ight point to UTI but ar
en’t UTIs
themselves,
you’ll want to
consider every
symptom that the physici
an documented.
Some signs an
d symptoms are co
nsistent w
ith a UTI, s
uch as:
» R30.- (Pain asso
ciated with micturitio
n)
» R33.- (Reten
tion of urine)
» R35.- (Polyuria)
» R39.1- (Other d
ifficultie
s with mictu
rition)
Documentation might al
so show that the patie
nt has a histo
ry of UTI. If
so, you’ll
want to include diagnosis
Z87.440 (Personal histo
ry of urinary (
tract) infect
ions)
on your claim
.
All of th
ese could, af
ter test
ing, result in
a defin
itive diagnosis.
But you’ll need
to
find other codes o
nce your provider p
ins down the specif
ic UTI.
Tip 2: Explore Other Sites and Names
As noted above, patie
nts might have U
TI symptoms th
at stem
from other a
natomic
sites in
stead of th
e urinary tra
ct. If y
ou learn this is
the case,
the conditio
n goes
(and more...)
Reader Questio
ns
Remember That 50948 Service
Includes 50650
p13
Select Ureteroneocystostomy
Code Based on Other
Services
p13
Add Modifier 62 for Case
Involving 2 Surgeons
p13
Ultrasound Guidance Is Not
Separate from Lith
otripsy p14
Turn to D49.59 for Pending
PSA Results
p14
Code 13160 Applies to
Scrotal Wound Dehiscence p14
February 2020, Vol. 23, No. 2 (Pages 9-16)
2020
Call us: 1-800-508-2582
The Coding Institute LLC, 2222 Sedwick Road, Durham, NC 27713
Orthopedic Coding Alert
Your practical adviser for ethically optimizing coding, reimbursement, and efficiency for orthopedic practicesNow Also Access Your Alert Online at www.SuperCoder.com
In this issue
Featured Condition: Plantar Fasciitis }
Get Off on Right Foot When Coding for
Plantar Fasciitis
Remember, surgery is a last option.
Patients reporting to the orthopedist with symptoms of plantar fasciitis could be
subject to a wide range of treatments, both to confirm the condition and to alleviate it.
There’s an order of treatment options as well, and your provider needs to follow the
hierarchy of options in the proper order, or the payer might just deny your claim.
Check out the ins and outs of coding for plantar fasciitis.
E/M Typically Tests for PF
A physician will usually diagnose plantar fasciitis during a routine evaluation and
management (E/M) service, explains Kristin Drummelsmith, medical biller at Foot
& Ankle Associates of Michigan In Shelby Township.
These E/Ms will likely take place in your practice’s office setting; so, if your
provider diagnoses plantar fasciitis during an office E/M, you’ll report a code from
the 99201 (Office or other outpatient visit for the evaluation and management of
a new patient, which requires these 3 key components: A problem focused history;
A problem focused examination; Straightforward medical decision making …)
through 99215 (Office or other outpatient visit for the evaluation and management
of an established patient, which requires at least 2 of these 3 key components: A
comprehensive history; A comprehensive examination; Medical decision making of
high complexity …) code set.
The provider would diagnose plantar fasciitis during (or after) a physical exam and
medical history review. “The location of the patient’s pain would tell the doctor if it
was plantar fasciitis or not,” Drummelsmith says.
More specifically, the provider will typically test the patient’s heel pain while
walking, especially when first getting up after sitting, says Denise Paige, CPC,
COSC, of PIH Health in Whittier, California.
Plantar fasciitis symptoms are often relieved by rest.
Once you’ve a confirmed diagnosis of plantar fasciitis, you should assign the patient
M72.2 (Plantar fascial fibromatosis) to represent the condition.
Reader Questions
Documentation Strengthens
Unlisted Procedure Claims p14
Tighten Up Loose Body in
Joint Dx
p15
Rack Up Coding Success
on Rib Repairs p15
Case Study Corner
Check Out These Emergency
Debridement Scenarios p11
X Remember to pay
attention to NCCI on
multiple debridements.
Q&AMax Out Incident-To Pay
The Right Way — While
You Still Can
p13
X Remember, the end
of 2020 might also be
the end of incident-to.
You Be the Coder
X Reporting Ankle Injury
Services
p13

www.aapc.com May 2020 9
I Am AAPC
#Ia
mA
AP
C
#IamAAPC#IamAAPCHealthcare Business Monthly wants to know why you chose to be a healthcare business professional. Explain in fewer than 400 words why you chose your healthcare career, how you got to where you are, and your future career plans. Send your story and a digital photo of yourself to [email protected].
Having a child with special needs tilts your world. For the past decade, I
have been immersed in the world of doctors, specialists, rare diseases, re-search, sleepless nights, durable medi-cal equipment, trial medicines, billing, insurance, Medicaid, heartache, and unbelievable joy.
The healthcare industry, which had always been of interest to me, now consumed my life from the patient per-spective. Only recently have I come to a comfort level with our child’s status. With my husband’s career change al-lowing him a flexible schedule, so he can help maintain our child’s needs during the day, it was time for me to pursue my passion outside of my per-sonal world.
Step 1: Choose Medical CodingI had a conversation with a friend who suggested I look into medical coding. It checked all the boxes for me. There is the aspect of continual learning, the immersion in the medical field, the black and white of some diagnoses, and the thrill of the hunt in researching the patient information that doesn’t fall into a neat little box. After dissecting the coder lifestyle, I decided it was for me.
The first step was to get AAPC certi-fied. If I were an employer, I’d want someone who is certified.
Step 2: Study for the CPC® ExamThe second step was getting over the hurdle of paying for the education; that is where I had to find a workaround. I decided I would gather all the AAPC materials I could find and study for the exam myself. If I had had the re-sources, I would have absolutely taken the AAPC online course. I didn’t, so I dedicated myself to studying anatomy,
physiology, medical terminology, ICD-10-CM, CPT®, and HCPCS Level II.
Step 3: Take the CPC® Exam and PassStep three was passing AAPC’s Certified Professional Coder (CPC®) exam. Amid an exam location two and a half hours from my home, a 3:15 a.m. tornado warning to seek shelter im-mediately, and nerves off the charts, I am happy to say I passed on the first try!
Step 4: Find a JobStep four is to find a position with my shiny, new credential. My Orlando lo-cal chapter support has been amazing!
Some people have warned me not to let it be known that I have a child with special needs because some em-ployers may have a misconception of unreliability. But having a child with special needs has made me who I am as a person: strong, reliable, tenacious, inventive, and grateful. I think those are some good qualities to bring to a team.
MONIQUE GRIFFIN, CPC-A
“With a lot of hard work and practice exams
from AAPC, I passed my Certified Professional Coder (CPC®) exam on
the first attempt.”
AAPC Members: If hard times are making it difficult for you to pay for membership dues, a certification exam, books, or other job-related items, remember the Hardship Fund. Informa-tion is available online at www.aapc.com/memberarea/chapters/scholarship.aspx.

10 Healthcare Business Monthly
■ AAPC Chapter Association Board of DirectorsBy Lee Fifield
AAPC is excited to announce the 2020-2021 AAPC Chapter Association (AAPCCA) Board of Directors (BOD) — a voting board of 16 coders and one AAPC representative. This elected board provides local chapters with the resources and support necessary to succeed.Here are your regional representatives and executive committee officers for 2020-2021.
Chapter Leaders
MEET AND WELCOME
YOUR2020-2021
shutterstock / ProStockStudio

www.aapc.com May 2020 11
1 - NortheastTreasurer Michele Stevens, CPC, CPMA, AAPC FellowClinical Coding Manager, MaineHealth
Michele Stevens has over 18 years of experience in the healthcare industry. She started out as a receptionist and was promoted to office manager. She discovered her love of ICD, CPT®, and HCPCS Level II when asked to take over the practice billing. Stevens has worked as a coder, an auditor/physician educator, and a practice manager. She is a member of NAMAS.Contact: [email protected] affiliation: Seacoast-Dover, N.H.Offices held: President, vice president, education officer, treasurer
Aileen Baldwin, CPC, CPPMClinical Revenue and Compliance Manager, Yale School of Medicine Department of PathologyAileen Baldwin has dedicated her career to the
business of healthcare for more than 30 years. Early on she worked as the director of billing and operations for a large rehabilitation practice with over 100 providers and several locations in Connecticut. In 2002, she founded and served as CEO of a multispecialty medical billing and practice management firm providing services to practices across five states. Eleven years later she successfully sold the firm and fulfilled her dream of working for Yale University. Baldwin joined Yale School of Medicine in 2012, where she spent her first few years as clinical practice manager for the Department of Radiology and Biomedical Imaging. She now works as the revenue and compliance manager in the Department of Pathology.Contact: [email protected] affiliation: New Haven, Conn.Offices held: President (2019, 2018)
2 - AtlanticVictoria Moll, CPC, CPMA, CRC, CPRC, Approved Instructor, AAPC Fellow
Professional Coding Quality Specialist, Penn State HealthVictoria Moll has more than 10 years of multispecialty experience in coding, auditing, and healthcare management, with expertise in plas-tic and reconstructive surgery. She has spoken at HEALTHCON, as well as many local chapter seminars and meetings, and is known for her infectious enthusiasm. Moll is a contributor to Healthcare Business Monthly, as well as various coding blogs and podcasts.Contact: [email protected] affiliation: Allentown, Pa.Offices held: President, vice president, education officer
Brenda Stevens, COC, CPC, CDEO, CPMA, CRC, CPC-ILead coder, MedkoderBrenda Stevens has 20 years of experience working
on the business side of medicine. She uses her medical coding skills to review billing, coding, and documentation practices to ensure compliance and reimbursement success. Stevens has a passion for teaching, and she uses her communication skills and knowledge to educate students at the community college level on accurate and ethical coding for a successful career in medical coding and billing.Contact: [email protected] affiliation: Salisbury, Md.Offices held: President, vice president,
member development officer, treasurer
3 - Mid-AtlanticSecretary Rik Salomon, CPC, CRC, CEDC, CEMA, CMCSCoder/Auditor, HIMagine Solutions Inc.
Rik Salomon has more than 25 years of health information manage-ment experience as a coder, auditor, educator, and documentation specialist. He is a frequent speaker at many local, regional, and na-tional venues. He has presented at numerous local chapter meetings/conferences on topics such as risk adjustment, emergency/critical care, mentoring, and leadership development. Contact: [email protected] affiliation: Carolina Coders, Charlotte, N.C.Offices held: President, secretary/treasurer
2020-21 AAPCCA BOD
“Serving the AAPCCA BOD as national secretary is not only an amazing experience — it has allowed me to connect with outstanding local chapter officers and to further develop our AAPC community.” – Rik Salomon, CPC, CRC, CEDC, CEMA, CMCS

12 Healthcare Business Monthly
Roslyn Jones, CPC, CPCO
Compliance Specialist, Duke University Private Diagnostic Clinic LLCRoslyn Jones is always willing to teach, motivate, and
inspire individuals interested in coding, compliance, and the revenue cycle. She has been working in healthcare since 1990 in all aspects of auditing, billing, coding, compliance, healthcare consulting, management, physician education, and revenue cycle. Contact: [email protected] affiliation: Durham, N.C.Offices held: President
4 - SoutheastChair Susan O’Loughlin, CPC, CPMA, CRC
Director of Provider Education and Professional Coding, The University of Vermont Health Network, Champlain Valley Physicians Hospital
Susan O’Loughlin has worked in the medical field for more than 35 years. Initially, she was in nursing, and then she transitioned to coding, provider education, auditing, and compliance for a large multispecialty group facility, where she was instrumental in implementing ICD-10 as an AAPC ICD-10 trainer and developing provider education for a new residency program. Among her greatest accomplishments was founding the Plattsburgh, New York, local chapter in 2003. She’s also been treasurer of the Irvine, California, local chapter. O’Loughlin loves meeting new members, encourages networking, and mentors members and staff to help them grow and achieve career goals.Contact: [email protected] affiliation: Plattsburgh, N.Y.Offices held: President, vice president, treasurer
Robin Goudy, CPC, CRCCoding Coordinator, Coders World LLCRobin Goudy began her career in healthcare 27 years ago in the clinical laboratory and has continued to
grow in many roles. She spent several years in patient access and administrative support. Goudy served as the billing and coding coordinator for mental health, as well as auditing various specialties, and is now a risk adjustment coder for Medicare and commercial insurance. In her free time, she volunteers in the community and networks to bring new and exciting things to chapter members. Upon joining her local chapter, Goudy quickly began proctoring exams. She also started what is now an annual back-to-school drive.Contact: [email protected] affiliation: Covington Cares, Covington, Ga.Offices held: Education officer
5 - SouthwestJoan Snodgrass, CPC, CRC, CPB
Coding/Billing Manager, County Obstetrics & GynecologyJoan Snodgrass has been in the medical field for over 20
years and has worked in several areas for hospitals, private physicians, and centralized business offices for physician groups. She enjoys every aspect of serving her chapter and representing AAPC, and she finds networking very gratifying. Snodgrass also enjoys planning local chapter events as a team with fellow officers and members.Contact: [email protected] affiliation: St. Louis West, Mo.Offices held: President, education officer
Vice Chair Heather Allen, LPN, COC, CPMACoding, Auditing, and Client Management, RevCycle+Heather Allen has more than 18 years of experience in coding, billing, auditing, management, and consulting
in addition to her clinical experience. She has worked for hospital inpatient, solo and group practices, and insurance defense auditing. Allen has been employed the last eight years with RevCycle+, where she oversees coding, auditing, and client management for 40-plus emergency departments and urgent care clinics.Contact: [email protected] affiliation: Jefferson City, Mo.Offices held: President, treasurer, secretary/treasurer
6 - Great LakesLetitia Patterson, MPA, RHIA, CPC, CPMA, CPC-I, CCS-PCEO, A Coder’s Resource
Letitia Patterson has been in the healthcare industry for 23 years. Throughout her career, she has refined her expertise in the areas of practice management, training, consulting, auditing, medical billing and reimbursement, and diagnostic and procedural coding. Patterson has developed educational materials for coders and healthcare profes-sionals and holds a master’s degree in public administration with a concentration in healthcare. She founded the Chicago – Southeast, Ill., local chapter.Contact: [email protected] affiliation: Chicago Southeast, Ill.Offices held: President, vice president, president-elect, education
officer, treasurer, member development officer
2020-21 AAPCCA BOD

www.aapc.com May 2020 13
Denise Garrett, CPC, CPCO, CPMA, CPPM, CSFAC, CHA Account Manager, Yeo & Yeo Medical Billing & Consulting
Denise Garrett has been in the healthcare field for over 21 years. Garrett is greatly looking forward to serving Region 6!Contact: [email protected] affiliation: Bay City Michigan, Mich.Offices held: President, secretary
7 - Mountains/PlainsTabitha Iverson, BA, CPCCompliance Manager, Essentia HealthTabitha Iverson has been in healthcare for more than 15 years. Her journey began in registration, then moved
through pre-certification, reimbursement, practice management, and coding education. In her current role in compliance, she manages internal audits and external audits response teams. Denial manage-ment and bridging the gaps between the multidisciplinary teams within healthcare are some of her greatest accomplishments. Iverson hopes to bring new flare to her local chapter.Contact: [email protected] affiliation: Red River Valley Chapter, Fargo, N.D.Offices held: Secretary, member development, president
Lynn Deaton, CPC, CPMA, CEMCProfee Coder, HIMagine Solutions, Inc.Audit and Education Specialist, Deaton ConsultingLynn Deaton began her career in the healthcare indus-
try more than 30 years ago. She has worked remotely for 10 years, auditing and coding for clients. Consulting, auditing, and educating are Deaton’s passions. Contact: [email protected] affiliation: Billings, Mont.Offices held: Vice president, president, president-elect,
secretary/treasurer, education
8 - WestCorrie Alvarez, CPC, CPMA, CEDC, CPC-IManager of Revenue Operations, Optum360Corrie Alvarez has more than 25 years of professional experience in medical billing, coding, and auditing
in various practice settings. She earned a bachelor’s degree from California State University, Northridge, and a teaching credential while teaching courses at the Los Angeles Unified School District. Alvarez is the founder of the Mission Hills, California, local chapter. She was a member of the AAPC NAB from 2009-2011.Contact: [email protected] affiliation: Mission Hills, Calif.Offices held: President, vice president, secretary, secretary/treasurer,
education officer
Meeting Coordinator Kristin Rodriguez, CPC, CEMC, CPC-I, CPMA, COC, CRCCoding Operations Lead, Alignment Healthcare
Kristin Rodriguez has more than 30 years’ experience in the industry. She has worked at private offices, consulting firms, and health plans, giving her exposure to all areas in the industry. Rodriguez has contributed to blog posts and articles regarding hierarchical condition category coding. She is still pursuing her education with possibly more credentials in her future.Contact: [email protected] affiliation: Orange-Irvine, Calif.Offices held: President (2020, 2019) and education officer (2018)
AAPC RepresentativeMarti JohnsonDirector of Local Chapter Support, AAPCSince 1994, when Marti Johnson joined AAPC, the number of chapters has grown from 30 to just under
500. Her tenure has been dedicated to establishing and supporting AAPC members and local chapters. Contact: [email protected]
“I am really looking forward to working with this board and I already appreciate their dedication to the officers.” – Marti Johnson
2020-21 AAPCCA BOD
Lee Fifield is a development editor at AAPC. She has a Bachelor of Science in communications from Ithaca College, N.Y., and has worked as a writer and editor for more than 15 years.
AAPC DL
By
No matter where you are in your career, AAPC is here to help take you to the next level.
AAPC DL
50%OFF
Certification Training
Through May 29
Visit aapc.com/training to join the game!

16 Healthcare Business Monthly
■ ADDED EDGEBy Michelle A. Dick, BS
AAPC wants members to have access to all the tools and resources they need for a successful career in the business of healthcare. We
pride ourselves on being the go-to place for every resource you may ever need to do your job, and do it well. There is a lot of information to tap into, and you may feel overwhelmed and not know where to start. Here is a comprehensive list of AAPC resources, as well as outside information, all in one convenient location.
Arm Yourself With Gold Standard Code BooksAAPC’s ICD-10-CM/PCS and HCPCS Level II code books, and the American Medical Association’s (AMA) CPT® code book, are the best in the industry:
• CPT® codes are used by clinicians to report healthcare procedures. The codes are defined by the AMA’s Editorial Panel, which updates and publishes the official CPT® code book annually. You can take the current year’s CPT® code book into the Certified Professional Coder (CPC®) exam (and into most of our certification exams) for reference.
• ICD-10-CM and ICD-10-PCS Expert code books feature diagnosis and facility procedure codes, respectively. You may take the current year’s ICD-10-CM code book into most AAPC certification exams. The ICD-10-PCS book is allowed in the Certified Inpatient Coder (CIC™) exam.
• HCPCS Level II codes capture durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS), including injectables, Medicare services, ambulance services, etc. You can bring the current year’s code book into most AAPC certification exams, as well.
These code books house codes, descriptions, guidelines, annota-tions, reference tables, colored illustrations, coding tips, and clinical examples you need in a color-coded, tabbed, spiral-bound format. They are specially designed by coders for speed and accuracy. To see all the features of these coding books, read the article “2020 Code Books Will Knock Your Socks Off” on pages 40-41 of the September 2019 issue of Healthcare Business Monthly. AAPC code books may be purchased here: www.aapc.com/medical-coding-books.
It’s also important to have a good medical dictionary such as Mosby’s Dictionary of Medicine, Nursing & Health Professions. Medical dictionaries provide a quick way to look up human anatomy and terminology, medical instruments, procedures, and diseases.
Online ResourcesIf you go to AAPC’s Medical Coding and Billing Free Tools webpage (www.aapc.com/resources/free-tools), you’ll find all sorts of free stuff, from Mentorship Program information to the E/M Utilization Tool, to the Salary Survey, RVU, and MIPS Score Calculators, to Risk Adjustment and CPT® Code Searches. Other resources include:
Welcome to the Industry: We Have Resources Galore!When it comes to medical coding resources to make your job easier, AAPC delivers.
shutterstock / ImageFlow
www.aapc.com May 2020 17
Welcome to the Industry
AAPC Coder: This is the go-to resource for quick CPT®, HCPCS Level II, and ICD-10 code lookups online. You can get a free trial at www.aapc.com/code.
Knowledge Center: The Knowledge Center (www.aapc.com/blog) is a great place to search for articles on the most current medical coding news and other pertinent information. You can also browse through past Healthcare Business Monthly articles here. Just hover your mouse over the “View More” link under “Hot Topics” in the lower right corner of the page and click on “Healthcare Business Monthly” (www.aapc.com/blog/category/healthcare-business-monthly).
Webinars: AAPC webinars provide education and continuing education units (CEUs) from experts in our industry, at a great
price. You can pay for them individually, purchase a year’s worth on demand, or purchase a multiuser subscription (www.aapc.com/medical-coding-education/webinars). From orthopedics to artificial intelligence, there’s a webinar for you.
Workshops: Workshops are held in a virtual classroom learning environment from your home or office computer. AAPC workshops (www.aapc.com/workshops) provide in-depth information on timely healthcare topics. Learn through interactive exercises and online discussions from subject matter experts and interact with presenters to discuss your challenges. Workshop recordings are available on-demand shortly after the live presentations are completed.
Job and Networking ResourcesAfter you pass an AAPC certification exam, reality sets in and you know you need to find a job in your field. The good news is that AAPC has job resources to start your employment search (www.aapc.com/medical-coding-jobs). This is just one of the perks of being a member. You also have access to local chapters, conferences, online forums, Project Xtern, and the AAPC Facebook page. Start networking today!
Local chapters and conferences: The best way to get a job is to be social and network. Attend local chapter meetings (www.aapc.com/localchapters), AAPC conferences (www.aapc.com/medical-coding-education/conferences), and other social events. Look online to find your local chapter officers, meeting times, and dates. Through local chapters and conferences, you can network with healthcare professionals, discover local job opportunities, and earn a lot of CEUs.
Project Xtern (www.aapc.com/medical-coding-jobs/project-xtern): This program helps newly certified coders qualify for a medical coding job by providing work experience that can be applied to resumes and toward the removal of an “apprentice” designation.
“Knowing where to go for authoritative healthcare guidelines and reliable
coding information is part of your job.”
18 Healthcare Business Monthly
Welcome to the Industry
Practicode (www.aapc.com/practicode): This is an online rapid proficiency testing tool that uses real, redacted medical records. You gain real-world coding experience that you can apply to a new job or to advance your career. You can also use it to help remove an apprentice designation.
AAPC Facebook page: There are medical coding and billing jobs posted on the AAPC Facebook page, and you can post that you are looking for a job. You can also ask questions about the field, events, and exams. AAPC members and moderators are quick to respond.
Forums: Our discussion boards (www.aapc.com/discuss) are a great place to post jobs and resumes, find upcoming local chapter events, and for general employment discussions with other AAPC members.
Live chat: Still can’t find what you’re looking for on the AAPC website? Start a live chat with an AAPC representative via the web-site’s Contact Us page (www.aapc.com/contactus.aspx) by clicking the “Chat Now” button.
Find Authoritative Coding GuidanceAs a professional coder, you must help your employer stay compliant with payer rules and government regulations. Part of your job is knowing where to go for authoritative healthcare guidelines and reliable coding information. Here is a list of no-cost reliable resources to aid in making correct coding decisions:
The Centers for Medicare & Medicaid Services (CMS): www.cms.gov offers information for Medicare and Medicaid claims processing forms, manuals, and other directives. Here are a few important resources on the CMS website:
• Medicare Physician Fee Schedule (MPFS): The MPFS lists CPT® and HCPCS Level II physician services and procedures reimbursed under Medicare Part B. The relative value units (RVUs) are calculated according to physician work, practice expense, and professional liability insurance. The MPFS provides payment indicators on each procedure code, such as global surgery, multiple surgery, co-surgery/assistant surgery, bilateral procedures, RVUs, etc. (www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/index).
• Internet-Only Manuals (IOMs): These provide day-to-day operating instructions, policies, and procedures based on
statutes, regulations, guidelines, models, and directives for Medicare and Medicaid providers and contractors (www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs).
• Transmittals: These communicate new or revised policies or procedures incorporated into the CMS Online Manual System (www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/index).
• National Correct Coding Initiative (NCCI) edits: These are updated quarterly according to AMA’s coding conventions, national and local policies and edits, national society coding guidelines, analysis of standard medical and surgical practices, and current coding practices. NCCI policies may be different from the CPT® code book. Use these guidelines and bundling rules to ensure proper Medicare and Medicaid billing (www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd).
• Medicare Learning Network® (MLN): MLN is a source for free educational materials, training, news, and updates for healthcare professionals on CMS programs, policies, and initiatives (www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNGenInfo).
• Medicare Administrative Contractor (MAC) resources: MAC handbooks, regulations, compliance guidance, and processing standards can be found here: www.cms.gov/Medicare/Medicare-Contracting/Medicare-Administrative-Contractors/Resources-for-MACs.
Office of Inspector General (OIG) Work Plan: The OIG as-sesses relative risks in the U.S. Department of Health and Human Services’ operations and programs to identify and target areas most in need of compliance attention. You can use the risk items on their list as an auditing tool to review your own provider billing activities and compliance plans (https://oig.hhs.gov/reports-and-publications/workplan/index.asp).
Medical societies: Do not rule out seeking guidance offered by specialties on their websites. Although specialty societies’ guidance doesn’t rank over code book authority, AMA and CMS routinely base their own guidelines on recommendations from specialty societies. For more info on medical societies, go to “Your Guide to Specialty Society Webpages” in the November 2019 issue of Healthcare Business Monthly, available in the Knowledge Center at www.aapc.com/blog/49129-your-guide-to-specialty-society-webpages.
An Information Smorgasbord Awaits YouWe’ve given you a lot of resources and tools to digest, but you chose this field because you like to research medical procedures, codes, regulations, and guidelines to ensure proper coding and reimburse-ment is carried out. Healthcare is an endless array of information — dive in and enjoy!
Michelle A. Dick, BS, is a freelance content specialist providing writing, editorial expertise, and graphic imagery to clients. Prior to becoming a free agent, she was an executive editor for AAPC, editor-in-chief at Eli Research, and editor at Element K Journals. After earning a Bachelor of Science from the State University of New York at Buffalo State, Dick entered the publishing industry as a graphic artist, ad coordinator, and web designer for White Directory Publishers Inc.

www.aapc.com May 2020 19
CAREER ADVANCEMENT ■
AAPC member Kristina Desjardins, CPC, CEDC, works as a specialty coder for a local hospital in central Maine. She has been
working in the medical arena for the last 30 years, starting as a receptionist before becoming a patient care coordinator and eventually a certified medical coder.
In addition to teaching coders to read and abstract physician of-fice notes and procedure notes to apply correct ICD-10-CM, CPT®, HCPCS Level II, and modifier coding assignments, the Certified Emergency Department Coder (CEDC™) credential gives experienced emergency department (ED) coders further skills in evaluation and management, Medicare billing, coding of surgical procedures, coding of moderation sedation, time-based coding, and medical terminology.
Desjardins’ impressive CEDC™ credential signifies her expertise in emergency medicine coding, yet she plans to soon expand her education by obtaining the Certified Professional Medical Auditor (CPMA®) credential, as well.
AAPC asked Desjardins about her experience with earning the CEDC™ credential and how it has helped her in her career.
What led you to obtain the CEDC™ credential?I began my journey with coding through employment with an urgent care/occupational health facility and enjoyed that portion of my job very much. That led me to obtain my [Certified Professional Coder] CPC® credential and find employment at a local hospital. My duties started with coding for a hospitalist, palliatist, and intensivist, eventu-ally leading to the ED. I enjoy coding for the ED very much, as there is such a wide variety of services provided. I obtained CEDC™ certifica-tion to have my credentialing correctly reflect the work I perform.
Do you have any tips for individuals preparing for the CEDC™ exam?If you have experience with ED coding, using the CEDC™ study guide will be very helpful. If you do not have ED experience, I would recommend taking AAPC’s full CEDC™ study course and practice exams to ensure you are fully prepared.
How has the CEDC™ credential helped you in your job/career?The CEDC™ credential has given me greater knowledge and confi-dence in my coding ability. AAPC credentialing also helped me obtain employment that would have otherwise been unavailable to me.
Who in the revenue integrity business do you think would most benefit from the CEDC™ credential?Anyone who reviews ED claims as part of their job. The ED treats such a wide variety of conditions — everything from a simple rash to complex traumatic injuries — making proficiency in ED coding essential.
What resources do you use most to earn your CEUs?I use local chapter meetings and conferences mostly, as well as AAPC online CEU resources.
Lee Fifield is a development editor at AAPC. She has a Bachelor of Science in communications from Ithaca College, N.Y., and has worked as a writer and editor for more than 15 years.
By Lee Fifield
Advice From a CEDC™
“The CEDC™ credential has given me greater knowledge and confidence in my coding ability.”
shutterstock / Monkey Business Images
20 Healthcare Business Monthly
By Elizabeth Hylton, CPC, CEMC
■ CODING/BILLING
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
When is imaging separately reported, and how? The relative value units (RVUs) for some codes include the provider’s use of imag-
ing to accurately visualize the specimen or problem the code is meant to address. The most notable changes with regards to radiology for 2020 can be found in the Gastrointestinal (GI) and Nuclear Medicine sections of the CPT® code book. Anatomic regions are highlighted, and codes are revised to offer greater overall consistency.
We’ll discuss these changes and offer some helpful reminders in this article.
Arm Yourself With InformationWhen imaging guidance is involved, coders may have difficulty selecting the correct procedure code due to several factors. These commonly include:
• Inadequate or unclear documentation by the provider regarding the type of imaging used;
• Misunderstanding of the extent of an imaging code’s description;
• Body region being studied within a specific imaging code set; and
• Outdated understanding of National Correct Coding Initiative (NCCI) edits and/or lack of current educational materials that specify coding updates.
As coding professionals, it is our responsibility to stay abreast of changes in our field and advance our education to include the most up-to-date information available to us. When we encounter portions of the provider’s documentation that may be unclear, or as cutting-edge medicine continues to outstrip black-and-white coding definitions, we are obligated to ask questions that will clarify our understanding of what was performed. Only then can we select the code that accurately represents the full body of work for the patient. Reimbursement is under constant scrutiny, and bulletproof coding can go a long way toward enhancing our practice’s bottom line.
Educate Providers of ChangesVariances in RVUs for procedures incorrectly billed add up over time, and the difference between profit and loss often comes down to coder knowledge. For example, let’s go back in time to the fine needle aspiration (FNA) biopsy code changes that 2019 brought us. Services were previously reported either as without imaging guidance (10021),
or with imaging guidance (10022). CPT® Assistant (April 2019) tells us that “code 10022 was reported with imaging guidance more than 75% of the time; therefore, imaging guidance should be bundled into the service.” That being said, one code was revised and five “first lesion” codes and three “additional lesion” codes were added to differentiate between the type of imaging used for FNA.
2020 Radiology and Imaging CPT® ChangesBecome a coding superhero with X-ray vision.
shutterstock / metamorworks

www.aapc.com May 2020 21
RadiologyCODING/BILLING
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
The difference in total RVUs between imaging modalities is pro-nounced, as shown in the following table.
What is the moral of the story? If your provider is still using outdated language like “FNA performed with imaging guidance” in documentation, you will need to ask what type of imaging was used. A difference of nearly 10 RVUs (on the non-facility side) between
our lowest and our highest valued code cannot be ignored. Details like this can easily become the target of an audit if an in-doubt coder should bypass the step of clarifying. On the reverse side, picking the lowest-valued code because it seems “safest” could be doing your practice’s overall revenue a serious disservice.
How to Stomach GI CodingAs a coder, I get excited when I see red circles, blue triangles, and green text in my new CPT® code book, and I often spend several evenings of my leisure time paging through my book, highlighting what’s been added, what’s been changed, and what’s been taken away.
For example, CPT® 74210 Radiologic examination, pharynx and/or cervical esophagus, including scout neck radiograph(s) and delayed image(s), when performed, contrast (eg, barium) study has been expanded to include scout radiographs and delayed images, as well as the type of contrast being used. The previous code description did not include the addition of the optional images (usually standard procedure when contrast is utilized), nor did it specify what type of contrast was being used.
While not new information, it’s important to note that this code is specific to the pharynx and cervical portion of the esophagus. As you move through the code set, and through the human anatomy it corresponds to, you’ll see this pattern repeat, with both the optional images and the type of contrast used now specified as part of the code description.
The difference in total RVUs between imaging modalities.Code Description Total Non-
Facility RVUs
Total Facility RVUs
10021 Fine needle aspiration biopsy, without imaging guidance; first lesion
2.80 1.60
10005 Fine needle aspiration biopsy, including ultrasound guidance; first lesion
3.67 2.07
10007 Fine needle aspiration biopsy, including fluoroscopic guidance; first lesion
8.43 2.69
10009 Fine needle aspiration biopsy, including CT guidance; first lesion
13.32 3.28
10011 Fine needle aspiration biopsy, including MR guidance; first lesion
0.00 0.00
“What is the moral of the story? If your provider is still using outdated language like ‘FNA performed
with imaging guidance’ in documentation, you will need to ask what type of imaging was used.”

22 Healthcare Business Monthly
RadiologyCO
DING
/BIL
LING
CPT® has also given us new code 74221 Radiologic examination, esophagus, including scout chest radiograph(s) and delayed image(s), when performed; double-contrast (eg, high-density barium and effer-vescent agent) study, which specifies the use of double-contrast mo-dality for the esophagus, as well as small intestine follow-through. This may not be reported with add-on code +74248 Radiologic small intestine follow-through study, including multiple serial images (List separately in addition to code for primary procedure for upper GI radiologic examination).
Also in this section, note the advice regarding which codes may be billed together. Consider, for example, the code pair 74220 Radiologic examination, esophagus, including scout chest radiograph(s) and delayed image(s), when performed; single-contrast (eg, barium) study and 74240 Radiologic examination, upper gastrointestinal tract, including scout abdominal radiograph(s) and delayed image(s), when performed; single-contrast (eg, barium) study. These codes may never be billed together, according to NCCI edits. The work associated with 74240 includes the entire esophagus, not just the portion 74220 describes (the cervical esophagus).
Pay attention to both the anatomy described and the modality used to perform the study for the most thorough and accurate code selection. When in doubt as to whether two codes may be billed together, utilize available resources to confirm whether the services are significant and separate enough to warrant the use of modifier 59 Distinct procedural service, or if the work described in documentation may be reported with one all-encompassing CPT® code.
Nuclear Medicine Section ChangesThe greatest concentration of new codes in this section may be found in relation to positron emission technology (PET) scans. CPT® codes 78429-78434 specify whether metabolic evaluation studies, includ-ing ventricular wall motion and/or ejection fraction measurements, were performed. Additionally, these codes specify whether computed tomography (CT) was performed at the same time.
Be careful when noting whether these metabolic studies were performed versus perfusion studies, as this will influence code
“Be careful when noting whether these metabolic studies were performed versus perfusion studies, as this will influence code selection.”
shutterstock / Gorodenkoff

www.aapc.com May 2020 23
Radiology
AAPC Audit Services
CODING/BILLINGDiscuss this article or topic in a forum at www.aapc.com
selection. Scan documentation of these studies to identify if single or multiple studies were performed, and whether stress (exercise or pharmacologic) studies were performed in addition to studies at rest.
“And/or” is especially prevalent in this section — read the code descriptor thoroughly, on the lookout for the points men-tioned, to make sure your code selection is accurate and covers all imaging modalities used. Knowing the equipment being utilized is key, as PET can be performed on a dedicated machine using only PET imaging, or it may be performed using a combination PET/CT camera. These types of studies will include reviewing anatomy in the field of view by examining the CT transmission images.
Single-photon emission computed tomography (SPECT) imag-ing has also gotten revisions to its code descriptors, as well as four new codes. The description revisions allow for greater definition of the extent of the examination as it relates to body areas. The new codes 78830-78835 describe imaging for localization of tumor, inflammatory processes, or distribution of radiopharmaceutical using SPECT imaging. These codes also include concurrent CT transmission in two cases. Again, reading imaging reports carefully to determine which region of the body is being addressed, as well as being aware of the type of technology used to perform the study, is crucial in correct code selection.
Get the Picture?In summary, read the coding advice at the beginning of each CPT® section carefully each year. Thoroughly explore the changes made to the code set, especially if it has a significant impact on the specialty you code for. Utilize any trusted specialty resources that offer fact-checked and verified information that correspond with both NCCI edits and CPT® guidelines. This will power up your coding vision and help you successfully implement each year’s new guidelines.
Elizabeth Hylton, CPC, CEMC, is a senior auditor with AAPC’s Audit Services Group (formerly Healthcity). She began her coding career by identifying claims submission errors involving ICD-9 and CPT® codes on hospital claims. Hylton has worked as a charge entry specialist for a local family medicine practice; a coding tech I at Carolinas Medical Center–Northeast; a front desk clerk/coder at Sanger Heart and Vascular Institute; an auditor/
educator for Carolinas HealthCare System; and a business office supervisor for one of the larger physician groups within Carolinas HealthCare System, where she gained experience with LEAN.
ResourcesCPT® 2020, Professional Edition, AMA.
CPT® Assistant of April 2019, Vol. 39, Issue 4.
NCCI Policy Manual for Medicare Services, effective Jan. 1, 2020.
Medicare Physician Fee Schedule, CMS, 2018, 2019, and 2020.
AUDIT SERVICES
BOOST REVENUE. reduce risk.Let us help you prepare today for annual compliance audits.
aapc.com/auditOr call us: 866-200-4157
24 Healthcare Business Monthly
■ CODING/BILLINGBy Bruce Pegg, MA, CPC-A
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Unless you’ve been hiding under a rock for the last two years, you should now be fully aware that big changes to the way you will
determine evaluation and management (E/M) office and outpatient visit levels are coming Jan. 1, 2021.
Will the pros of these changes outweigh the cons to primary care providers?
While it is still too early to know, here are our best educated guesses about how the average primary care practice will be affected by three of the big consequences of this E/M overhaul.
Streamlined Documentation and Paperwork ReductionBy now, primary care providers should be taking full advantage of the documentation changes for office and outpatient E/M visits that were introduced in the Medicare Physician Fee Schedule (MPFS) 2019 final rule and which became effective Jan. 1, 2019. These include:
• Focusing documentation “on what has changed since the last visit or on pertinent items that have not changed, rather than redocumenting a defined list of required elements such as review of a specified number of systems and family/social history.”
• Acknowledging, rather than re-documenting, that a patient’s history of present illness or chief complaint has been reviewed and verified.
• Also acknowledging, rather than re-documenting, that notations in a patient’s medical record made by residents or other members of the medical team have been reviewed
and verified. On Jan. 1, 2020, CMS extended this guideline to include notations made by physician assistants and advanced practice registered nurse preceptors, including other nonphysician practitioners such as nurse practitioners, clinical nurse specialists, and certified nurse-midwives.
• No longer documenting medical necessity for a home visit.
Pro: These efficiencies will doubtless result in savings to provider time and, by extension, to increases in primary care practice revenues.
Con: The extent of these time savings and revenue increases is yet unknown.
Simplified Leveling ProcessThe next, and most significant, development involves the way coding for office and outpatient E/M visit levels will change. Beginning Jan. 1, 2021, history and exam will no longer make up two of the three components needed in level determinations. Instead, E/M levels will be determined by medical decision making (MDM) or time only, regardless of whether more than half of the visit was comprised of counseling.
CPT® guidelines regarding time are also going to change. Per the new guidelines, in 2021:
Time for these services [will be] the total time on the date of the encounter. It [will include] both the face-to-face and non-face-to-face time personally spent by the physician and/or other qualified health care professional(s) on the day of
Calculating the Effect of the 2021 E/M Changes on Primary CareWeigh the pros and cons as the healthcare industry prepares to implement new leveling guidelines.
shutterstock / sebra

www.aapc.com May 2020 25
Primary CareCODING/BILLING
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
Discuss this article or topic in a forum at www.aapc.com
the encounter (includes time in activities that require the physician or other qualified health care professional and does not include time in activities normally performed by clinical staff).
Pro: Primary care practices should be cautiously optimistic that this change will result in some real gains.
The new rules, especially regarding time, should allow providers to get full credit for all the work they do for their patients.
Additionally, the changes should make coders’ lives somewhat easier, as they will no longer have to determine the extent of history the provider obtained or the extent of the examination the provider performed in order to calculate the appropriate level for a given office and outpatient E/M visit. And while the MDM calculation will dif-fer from the way it has previously been done, the similarity between the current Centers for Medicare & Medicaid Services (CMS) MDM table and the new CPT® 2021 table means the transition won’t be too difficult for experienced coders to handle. (See the Resources section for links to the MDM table and CPT® 2021 table.)
Con: Again, how this will play out remains to be seen. For providers, time and financial savings from this change will be minimal simply because it will not substantially alter their current practices. After all, even though history and exam won’t count toward the E/M level, medical necessity dictates that providers will still have to perform a condition-appropriate history and exam for each patient they see.
This area of the change may also result in the most significant financial costs to primary care practices.
First, there is the cost of educating all stakeholders about the chang-es, whether it be through workshops, seminars, or even just time spent away from normal work duties in understanding CMS’ revisions.
Second, there’s the cost to the practice in work hours spent reviewing old, and implementing new, office procedures to ac-commodate the new guidelines. For example, practices will need to spend time and money reviewing and removing any clinically unnecessary tasks in office history and physical exam templates or electronic medical records (EMRs), along with changing templates and EMRs to account for the change to the 2021 MDM elements.
Third, practices will have to review timekeeping procedures to make sure they capture all the time spent on the date of service for a given patient visit, whether that be changing office protocols or EMRs to record total face-to-face and non-face-to-face time spent by each provider per patient per visit.
Loss of 99201One casualty of these revisions will be 99201 Office or other outpatient visit for the evaluation and management of a new patient,
which requires these 3 key components: A problem focused history; A problem focused examination; Straightforward medical decision making, which you will not find among your CPT® 2021 codes.
That’s because removing the history and exam from office and outpatient E/M level calculations means there is nothing left to distinguish it from 99202 Office or other outpatient visit for the evaluation and management of a new patient, which requires these 3 key components: An expanded problem focused history; An expanded problem focused examination; Straightforward medical decision mak-ing. The current 99202 calls for a higher level of history and exam (expanded problem focused) than 99201, but MDM for both levels is straightforward. With the removal of history and exam from leveling calculations, that makes 99201 unnecessary.
Pro: Primary care practices will be largely unaffected by this change, as a 2016 analysis of Medicare family care practices cited by the American Academy of Family Physicians notes that 99201 makes up less than one percent of their office and outpatient E/M code distribution.
Additionally, that miniscule loss will be more than offset if Medicare’s current proposal to raise work relevant value units (RVUs) in 2021 goes through as planned. As it stands, Medicare plans to raise the work RVUs for 99203 and 99204 by 13 and 7 percent from 2020, respectively, while 99213 and 99214 are slated for hefty increases of 34 and 28 percent, respectively.
Con: Is there is a con to losing 99201?
The Bottom LineOn balance, the long-term benefits of documentation streamlining and workload reduction, both for providers and coders, will likely offset the short-term inconveniences of stakeholder education and workflow and EMR revisions surrounding the new office and outpatient E/M codes.
Bruce Pegg, MA, CPC-A, is an experienced teacher and published author. Pegg has a Bachelor of Arts degree from Loughborough University in England and a Master of Arts degree from SUNY Brockport. He specializes in E/M, pediatric, and primary care coding.
“Beginning Jan. 1, 2021, history and exam will no longer make up two of the three components needed in level determinations.”
ResourcesAmerican Academy of Family Physicians: www.aafp.org/journals/fpm/blogs/gettingpaid/entry/whats_your_coding_profile.html
2020 MPFS final rule: s3.amazonaws.com/public-inspection.federalregister.gov/2019-24086.pdf
2021 CPT® MDM table: www.ama-assn.org/system/files/2019-06/cpt-revised-mdm-grid.pdf
AMA 2021 E/M guideline changes: www.ama-assn.org/system/files/2019-06/cpt-office-prolonged-svs-code-changes.pdf

26 Healthcare Business Monthly
■ CODING/BILLINGBy Angelica Mae Celis-Duran, RN, CPC, BCHH-C, CPMA
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
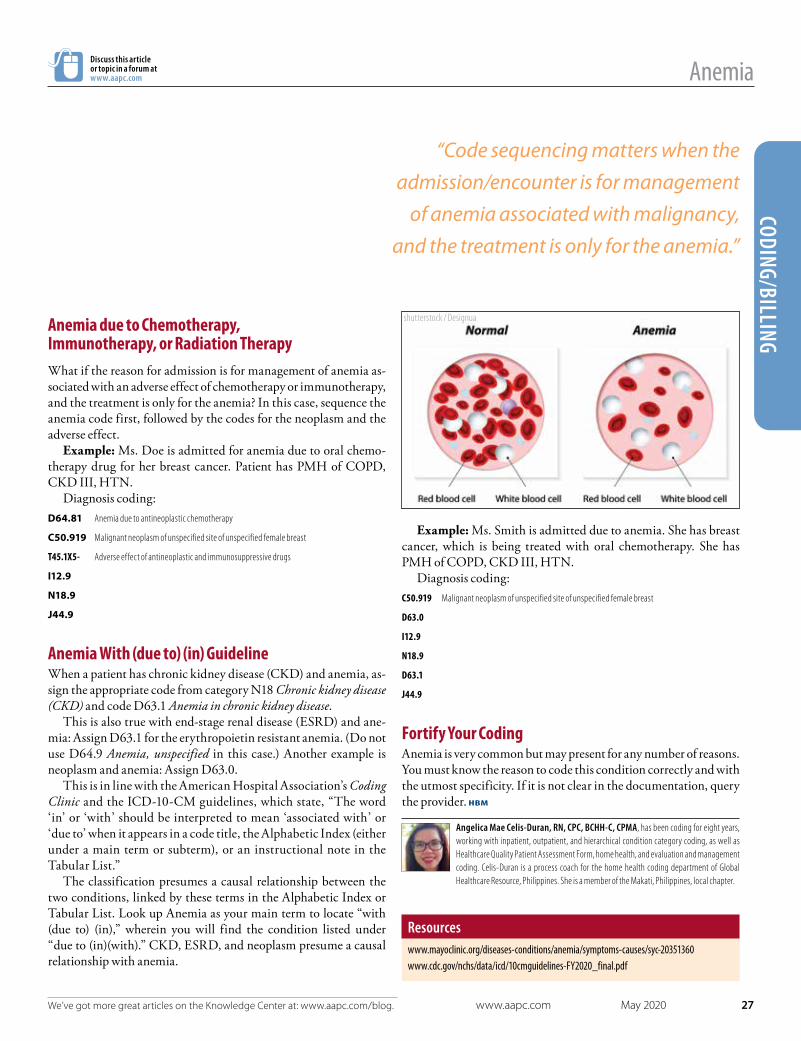
Anemia, according to Mayo Clinic, is a condition in which the body isn’t making enough healthy red blood cells to carry adequate
oxygen to the body’s tissues. That’s why common manifestations are feelings of weakness and tiredness. There are many types of anemia and many causes; it can be temporary or long-term, and with different levels of severity.
ICD-10-CM chapter-specific guidelines (Chapter 3: Diseases of Blood/Blood-Forming Organs & Disorders Involving Immune Mechanism) are currently reserved for future guideline expansion. However, you can find anemia coding guidelines in other chapters because of anemia’s overlap with other conditions.
Knowing where to look for these guidelines is key to coding properly.
Anemia Associated With Malignancy Code sequencing matters when the admission/encounter is for manage-ment of anemia associated with malignancy, and the treatment is only for the anemia. According to ICD-10-CM guidelines, the appropriate
code for the malignancy is sequenced as the principal (or first-listed) diagnosis, followed by the appropriate code for the anemia.
Example: Mr. Doe is admitted due to anemia secondary to his prostate cancer, for which he is undergoing oral chemotherapy. Patient has PMH of COPD, CKD III, HTN.
Diagnosis coding: C61 Malignant neoplasm of prostate
D63.0 Anemia in neoplastic disease
I12.9 Hypertensive chronic kidney disease with stage 1 through stage 4 chronic kidney disease, or unspecified chronic kidney disease
N18.9 Chronic kidney disease, unspecified
J44.9 Chronic obstructive pulmonary disease, unspecified
Under D63.0 is an official guideline reference that tells you where to look for the guidelines specific to this code. There is also a Code first alert stating, “Code first neoplasm (C00-D49),” followed by EXCLUDES1 and EXCLUDES2 notes.
Anemia: ICD-10-CM Guidelines Update Clarification Understand the many nuances of this blood disease to code it correctly.
shutterstock / Image Point Fr
www.aapc.com May 2020 27
AnemiaCODING/BILLING
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
Discuss this article or topic in a forum at www.aapc.com
Anemia due to Chemotherapy, Immunotherapy, or Radiation TherapyWhat if the reason for admission is for management of anemia as-sociated with an adverse effect of chemotherapy or immunotherapy, and the treatment is only for the anemia? In this case, sequence the anemia code first, followed by the codes for the neoplasm and the adverse effect.
Example: Ms. Doe is admitted for anemia due to oral chemo-therapy drug for her breast cancer. Patient has PMH of COPD, CKD III, HTN.
Diagnosis coding: D64.81 Anemia due to antineoplastic chemotherapy
C50.919 Malignant neoplasm of unspecified site of unspecified female breast
T45.1X5- Adverse effect of antineoplastic and immunosuppressive drugs
I12.9
N18.9
J44.9
Anemia With (due to) (in) GuidelineWhen a patient has chronic kidney disease (CKD) and anemia, as-sign the appropriate code from category N18 Chronic kidney disease (CKD) and code D63.1 Anemia in chronic kidney disease.
This is also true with end-stage renal disease (ESRD) and ane-mia: Assign D63.1 for the erythropoietin resistant anemia. (Do not use D64.9 Anemia, unspecified in this case.) Another example is neoplasm and anemia: Assign D63.0.
This is in line with the American Hospital Association’s Coding Clinic and the ICD-10-CM guidelines, which state, “The word ‘in’ or ‘with’ should be interpreted to mean ‘associated with’ or ‘due to’ when it appears in a code title, the Alphabetic Index (either under a main term or subterm), or an instructional note in the Tabular List.”
The classification presumes a causal relationship between the two conditions, linked by these terms in the Alphabetic Index or Tabular List. Look up Anemia as your main term to locate “with (due to) (in),” wherein you will find the condition listed under “due to (in)(with).” CKD, ESRD, and neoplasm presume a causal relationship with anemia.
Example: Ms. Smith is admitted due to anemia. She has breast cancer, which is being treated with oral chemotherapy. She has PMH of COPD, CKD III, HTN.
Diagnosis coding: C50.919 Malignant neoplasm of unspecified site of unspecified female breast
D63.0
I12.9
N18.9
D63.1
J44.9
Fortify Your CodingAnemia is very common but may present for any number of reasons. You must know the reason to code this condition correctly and with the utmost specificity. If it is not clear in the documentation, query the provider.
Angelica Mae Celis-Duran, RN, CPC, BCHH-C, CPMA, has been coding for eight years, working with inpatient, outpatient, and hierarchical condition category coding, as well as Healthcare Quality Patient Assessment Form, home health, and evaluation and management coding. Celis-Duran is a process coach for the home health coding department of Global Healthcare Resource, Philippines. She is a member of the Makati, Philippines, local chapter.
Resourceswww.mayoclinic.org/diseases-conditions/anemia/symptoms-causes/syc-20351360www.cdc.gov/nchs/data/icd/10cmguidelines-FY2020_final.pdf
“Code sequencing matters when the admission/encounter is for management
of anemia associated with malignancy, and the treatment is only for the anemia.”
shutterstock / Designua

28 Healthcare Business Monthly
■ CODING/BILLINGBy Jacolyn Bailey, LPN, CPC-A, CHONC, CRC, AAPC MACRA Proficient, CEMA
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Since the beginning of grade school, we are encouraged to expand our vocabulary, read literature, and improve our grammar. We quickly
learn that spelling words correctly and knowing their definitions is key to comprehension. This level of understanding is extremely important in coding, as well, as every aspect of ICD-10-CM coding affects the patient, physician, and payer. It’s our job as coders to understand what everyone is saying and code it as such. Let’s look at how our words affect coding oncology claims.
Active vs. History OfMany medical terms are similar, some words may have multiple mean-ings, and other words can change the ICD-10 code from “active” to “history of.” When coding for malignancy it’s important to know if the malignancy is active or if it’s a history of. Terms that will help you determine status include:
Current: Active treatment is occurring for the purpose of curing or palliating cancer. Adjuvant: Additional treatment such as hormonal therapy, radiation therapy, or chemotherapy. History: Cancer-free state with no evidence of disease and no treat-ment occurring.Debulked: Partially removed.Removed/Eradicated: Completely removed. Remission: This can be a partial or complete decrease of symptoms/signs of cancer. In partial remission, some signs and symptoms may still be occurring; while in complete remission, the signs and symp-toms are gone but the chance of having malignancy in the body is possible. Watch and wait: Closely monitoring a patient without treatment unless symptoms begin occurring.
If it’s noted in a chart that the patient has stage IV cancer with malignancy, it’s time to become an investigator and read through the chart to determine:
• Was the first malignancy removed or debulked?• Was the treatment completed, or did the patient stop and not
complete treatment?
If the patient stopped treatment, the malignancy was not removed, the mass was debulked, or the patient is receiving adjuvant treatment, then the stage IV malignancy diagnosis is current/active. If there are new secondary cancers, then this is metastasis, and these are also active.
Words Are Important in Oncology Coding
Understand what the physician is documenting to improve coding accuracy.
shutterstock / eurobanks

www.aapc.com May 2020 29
OncologyCODING/BILLING
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
Discuss this article or topic in a forum at www.aapc.com
If the patient completed all the treatments that were ordered by the physician and the malignancy was removed, then it’s coded as history of. According to Medicare guidelines, the diagnosis of history of malignancy occurs if the primary malignancy has been eradicated, no further treatment is being directed at the site, and there is no evidence of existing primary malignancy.
Coding ExamplesIf a patient has breast malignancy stage IV with metastasis to the bones, and the breast malignancy had been eradicated 15 years earlier, and no treatment had been occurring in the interim, with no new malignancy in breast, you would code:C79.51 Metastasis to bones
Z85.3 History of breast malignancy
If a patient has a right upper outer breast malignancy, and now has secondary bone malignancy, and the patient had refused radiation and adjuvant therapy for the breast malignancy some time ago, you would code:C50.411 Malignant neoplasm of upper-outer quadrant of right female breast
C79.51
If a patient had a breast cancer treatment of radiation and is now on adjuvant treatment of Tamoxifen, then the cancer is current because the hormonal medication is in addition to the other treat-ments. If a provider orders Tamoxifen for prophylactic treatment after breast cancer treatment, this is coded as a history of breast cancer — the medication is intended to prevent disease, not treat it.
Another example of active or history of is when the patient is noted to have stage IV neuroendocrine cancer of pancreas with metastasis to the liver. If the patient is in remission and doing well, with only fatigue and intermittent abdominal pain, the codes for the malignancies would be:C7A.094 Malignant carcinoid tumor of the foregut, unspecified
C7B.02 Secondary carcinoid tumors of liver
The patient still has the diseases, but they are in remission, still present in the body, but not actively treated at present.
Suspect WordsOutpatient coders need to be particularly vigilant to catch words in documentation that indicate the diagnosis is not confirmed. Words such as:
• Suspected• Questionable• Likely• Possible• Still to be ruled out
• May be• Presumed• Consistent with• Suggestive of• Compatible with
These are all uncertain words that do not qualify the diagnosis. When any of these words are used, code only the symptoms (for
outpatient coding; inpatient guidelines differ). For example, if the provider writes, “The patient’s mass is likely malignant lung cancer,” you must code a mass until a definitive diagnosis is made.
Uncertain vs. UnspecifiedNote that “mass” is not always a neoplastic growth. The physician may also use the term “lump.” These are not to be coded from the Neoplasm table unless the provider gives a more definitive diagno-sis. Usually with a mass or lump the coder is diverted to “disease.”
When coding for a mass, the mass cannot be listed as malignant, benign, uncertain behavior, or unspecified behavior:
• Uncertain behavior for neoplasms is used when the behavior of the cells is not able to be predicted by the pathologist and charted as such by the physician.
• Unspecified behavior for neoplasms is used when the information in the chart is not enough to sign a more accurate code. This could occur if the chart has the diagnosis of ovarian tumor but does not document the behavior as benign or malignant.
The use of words, in all aspects of our lives, is always important. With ICD-10-CM coding, it can mean the difference for the patient’s diagnosis on charts, reimbursement for physicians and facilities, and accuracy in our work as coders.
Jacolyn Bailey, LPN, CPC-A, CHONC, CRC, AAPC MACRA Proficient, CEMA.
ResourcesCenters for Medicare & Medicaid Services: www.cms.gov/Medicare/Coding/ICD10/Downloads/2020-Coding-Guidelines.pdf
Emily Bredehoeft, COC, CPC, AAPC Fellow. AAPC: www.aapc.com/blog/40016-clear-up-confusion-as-to-when-cancer-becomes-history-of
Sharma, Rohit, MD; Dancher, Luke, MD, et al.: https://radiopaedia.org/articles/small-cell-lung-cancer-4?lang=us
“Outpatient coders need to be particularly vigilant to catch words in documentation that indicate the
diagnosis is not confirmed.”
30 Healthcare Business Monthly
■ CODING/BILLINGBy Lynn Handy, LPN, CPC, CPC-I, COC, CCS-P
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
Heightened documentation requirements and new technology require us to see the flaws in our EMRs and correct them.
shutterstock / Milles Studio

www.aapc.com May 2020 31
EMR
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
CODING/BILLINGI’ve been working in healthcare for more than 30 years. I’ve man-aged internal medicine, family, behavioral health, and cardiology
practices. I’ve taught coding to thousands upon thousands of cod-ers, billers, physicians, and overburdened office assistants. Through all of this, I’ve witnessed the evolution of the medical record.
I remember when we had the paper chart with handwritten progress notes. Maybe you remember struggling to read the notes, too. Then, we started creating template forms to help our providers with the documentation requirements. Those proved helpful at first, but we started to see too many check boxes and less narrative stories. Next came the rise of dictation and transcribed notes, and the rise in delays in getting the transcribed notes back into the chart (not to mention the increased cost.) Finally, all of the pieces came together, and we had the emergence of a full-fledged, honest-to-goodness electronic medical record (EMR).
Implementing the EMR was a painful process that slowed pro-ductivity. After a few years of working in it, I learned its limitations. I got my sea legs just in time for the health information management team to meet with the financial team and switch to a newer, more robust system. The more things change, eh?
Another learning curve ensued, but this time I was more ready for it. And as it turns out, there are some extraordinarily useful features in these newer systems, provided they are used correctly. Which leads us to the point of this article: The proper use of contemporary EMRs.
Pros and Cons of the EMRThe current state of the EMR includes cloning, canned notes, and copy/paste capabilities. The functionality of the EMR is reported to be a burdensome process to many providers, which is akin to being upset at all of the icons that pop up when you turn on your smartphone. That is to say, the power of these EMRs can be confusing and overwhelming to providers and health information management (HIM) professionals alike.
There have been many articles and discussions about the pros and cons of the EMR. Here are just a few of them:
• EMR pros: ° The computing power enables healthcare leaders and
payers to track a huge range of metrics — from blood
pressure control to blood glucose management to cancer prevention.
° Reduces paperwork, improves efficiency, and reduces healthcare costs (theoretically, anyway). - MY OPINION: Both anecdotal experience and
empirical data support the conclusion that these goals are unlikely to be reached with present EMR systems alone. We are in for even more stops on our medical record adventure.
° More portable and accessible. Providers can access the EMR from multiple locations and finish their notes from home. - Improves communication with a shared platform
for all providers treating the patient. - Centralizes data. - Ensures legible medical records.
• EMR cons: ° EMR technology doesn’t include the end user’s
workflow in the design: - Altogether too many clicks, and cumbersome to
learn and use. - Incorrect or overuse of the EMR templates, quick
text, and smart phrases that do not produce meaningful documentation.
° EMR templates don’t consider regulatory requirements (for example, coding, meaningful use, quality measures, clinical, etc.).
° EMR updates don’t keep up with the ever-changing regulatory guidelines.
° Inadequate EMR training for providers and clinical staff.
° EMR vendors not responding to client questions. ° Downtime due to technology issues and updates to the
system.
EMR Coding and Documentation ChallengesIf you’ve been reviewing medical records and training providers on coding and documentation, you know very well there are challenges as a direct result of the EMR. The solution to most of these issues
“The solution to most of these issues requires a working partnership with your EMR vendor and,
most likely, additional end-user EMR training.”

32 Healthcare Business Monthly
CODI
NG/B
ILLI
NG
EMR
requires a working partnership with your EMR vendor and, most likely, additional end-user EMR training for the following:
• Templates: ° EMRs tend to add irrelevant information into
the clinical record through templates or default information. EMR templates may prompt providers to choose higher levels of evaluation and management (E/M) services when medical necessity may be absent. - Prepopulated templates or pre-charting:
¤ The only portion of the medical record that can be prepopulated is the review of symptoms (ROS) and past, family, and social history (PFSH). The provider must document the review and update of any information documented by ancillary staff.
- Auto-populating PFSH:¤ Same as above
- Smart phrases and quick text - Over-clicking of elements in a template
¤ How many times have you seen documentation of the “pertinent positive ROS” in the subjective portion of the note and a statement that “All other ROS was reviewed and negative except as stated in the HPI?” The question I ask the providers all the time is, “Did you review all 14 systems when you made that statement?” This is just one example of over-clicking or over-documenting in the EMR. E/M guidelines only require an extended ROS for new patient levels 99204 and 99205, and sometimes established patient level 99215, if a comprehensive exam is not performed.
¤ The exam templates are another area in which we see lots of clicks. Watch out for the “abnormal exam finding.” There must be elaboration of the abnormality in the documentation. Just clicking a box doesn’t suffice.
° Templates do not meet the coding guidelines: - When coding or auditing an
E/M visit, the provider may be able to assess the level of service better using the multisystem exam elements in the 1995 Documentation Guidelines for Evaluation and Management Services (guidelines). If the provider is using the EMR
calculator, however, the system may only look for exam elements per the 1997 guidelines and, subsequently, undervalue the service level.
- The exam template may have both body areas and organ system listed, but under the 1995 guidelines, a comprehensive exam cannot be obtained unless there are at least eight organ systems. Most Medicare carriers will not allow providers to mix body areas and organ systems, so this is misleading.
• Incorrect labeling of body areas and organ systems (for example, head, eyes, ear, nose, and throat (HEENT) only contains an eye exam or extremities contains skin, musculoskeletal, or cardiovascular).
• Copy and paste functions or cloned notes: ° The Centers for Medicare & Medicaid Services (CMS)
makes it very clear that a note that is copied without updates to the patient’s current status does not meet medical necessity standards and will not be reimbursed. We are seeing all areas of the note copied from the history of present illness (HPI) or exam and pasted into the assessment and plan. Identifying cloned notes is now the responsibility of compliance officers, coders, and auditors. This often requires us to pull up previous notes and compare the content. Some EMRs identify copied notes, which is optimal.
• Signatures: ° CMS requires all entries into the medical record to be
signed and dated by the author. ° Some EMR systems do not have the capability to
capture multiple signatures/authentication. Examples include:
shutterstock / metamorworks

www.aapc.com May 2020 33
EMRCODING/BILLING
AAPC Coder
- Non-physician practitioner (NPP) and supervising physician
- Medical student, resident, and teaching physician ° The result of not capturing the proper signature/
authentication is an unbillable service: - Medicare does allow signature attestations, but
this is very time-consuming and a costly long-term solution.
• Addendums: ° An addendum is used to provide information that
was not available at the time of the original entry. The addendum should be timely and contain the current date and reason for the addition or clarification of information being added to the medical record and be signed by the person making the addendum.
° How should addendums be done in an EMR? - Late entries, addendums, or corrections to a medical
record are legitimate occurrences in documentation of clinical services. A late entry, an addendum, or a correction to the medical record bears the current date of that entry and is signed by the person making the addition or change.
° There are several other scenarios where an addendum may be required: - Teaching physician attestations - Split/Shared services addendums - Supervising physician addendums - Scribe attestations
° An addendum is a separate entry in the medical record; the original note should not be edited. Addendums to a resident’s or NPP’s notes may be needed when their work is performed incorrectly. Most EMR systems require the resident or NPP to sign and close their note before sending it to their teaching or supervising physician. This allows the physician to perform an actual dated and signed addendum.
Tip: To learn more about the 2021 E/M changes, read “Are You Ready for the Big E/M Overhaul?” by Bruce Pegg, MA, CPC-A, in the Knowledge Center at www.aapc.com/blog/49387-are-you-ready-for-the-big-e-m-overhaul.
34 Healthcare Business Monthly
Discuss this article or topic in a forum at www.aapc.comEMR
• Audit trail: ° Most EMR systems have an audit function that allows
the coder or auditor to see who documented in the medical record and when. This is a helpful function when determining if the documentation was performed by ancillary staff, medical student, resident, fellow, NPP, or scribe. Identifying the service provider helps to determine the coding and billing rules to apply.
What Does the Future Hold for the EMR?The proposed changes to the E/M guidelines beginning in 2021 will be a very welcome relief for many of the items listed above. The changes will focus on the complexity of medical decision making or time to level the E/M service. The history and exam documentation will be what the provider determines is medically necessary. I look forward to seeing the final rule in the fall.
Here’s what’s happening now:• Paperwork reduction: In 2019, we saw changes that
allowed the ancillary staff to document the HPI, as long as the provider documented they reviewed that information.
• Voice recognition: Some providers have already embraced this new technology and find it very beneficial and timesaving. There are still some risks to consider. There is an initial investment, but it’s well worth getting a good system. You will need to do a 100 percent review of the notes in the beginning, but as your staff gets more experienced, the system’s accuracy will increase.
• Scribes: We’re seeing an increased interest in and use of scribes. This is a good option for some providers who do not have the time or computer skills needed for today’s level of required documentation. Medicare will allow the use of scribes if they are clearly identified in the medical record and the provider signs the document. Many organizations are still requiring the provider to document that they reviewed and agree with its accuracy. There is an ongoing expense when utilizing scribes and the skill level of scribes can vary greatly, but when you find a good one it can be a very effective partnership. An additional bonus may be that the scribe is tech savvy in using the features of the EMR correctly!
• Split/shared services: ° A split/shared E/M visit is defined by Medicare Part B
payment policy as a medically necessary encounter with a patient where the physician and a qualified NPP each personally perform a substantive portion of an E/M visit face-to-face with the same patient on the same date of service.
° Split/shared billing regulations limit the types of services that can be reported under this methodology, recognizing only E/M services provided in certain facility-based settings (i.e., emergency departments, outpatient hospital clinics, and inpatient hospitals). Critical care services, nursing and skilled nursing facilities, consultation services, patient homes, and domiciliary sites are excluded. There are several other requirements when reviewing a split/shared service.
° We are seeing increased use of NPPs in the hospital setting. Several of the above discussions are relevant to this topic (i.e., signatures, addendums, and the use of the audit function in the EMR to identify who is providing the service).
The Long Road AheadI set out to share some of my most common issues encountered in the EMR but fear I have merely scratched the surface. I know there are as many EMRs as there are healthcare providers, as the habits of each informs the function of the EMR. As a rule, we must prioritize the application of the coding and documentation guidelines to our electronic world. We cannot stop at reading the note. Those days have been gone for a long while, for better or worse.
EMRs are for the better! But we have to consider the workflow of the EMR and sometimes dig a little deeper in our reviews, critically thinking throughout its entire use.
Lynn Handy, LPN, CPC, CPC-I, COC, CCS-P, has more than 30 years of healthcare experience in medical office management, insurance billing and coding, and professional nursing. She is an accomplished medical practice consultant and an experienced educator in the areas of insurance billing and coding, physician E/M coding and documentation training, computerized insurance billing, and Medicare compliance. Handy is vice president of
consulting and education services at CodingAid. She is affiliated with the Orange County, Los Angeles, and Long Beach local chapters.
ResourceCMS Medicare Program Integrity Manual Pub. 100-08, Transmittal 732, July 21, 2017: www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/2017Downloads/R732PI.pdf.
Tip: For more information on split/shared services, read “Split/Shared E/M Encounters,” by Jean Acevedo, LHRM, CPC, CHC, CENTC, on the Knowledge Center at www.aapc.com/blog/28571-splitshared-em-encounters.
CODI
NG/B
ILLI
NG

AAPC Conference
For more information:
aapc.com/conferences800-626-2633
August 12-14, 2020Gaylord Rockies Resort & Convention Center
September 14-16, 2020Charleston Marriott
Sharpen your skills and learnfrom the industry's best!
12 CEUs 50+ Educational Sessions 1,000 Attendees
HEALTHCONREGIONAL 2020
DENVER CHARLESTON
HEALTHCONREGIONAL 2020 E A S THEALTHCON
REGIONAL 2020 W E S T

36 Healthcare Business Monthly
■ CODING/BILLINGBy Michael Warner, DO, CPC, CPCO, CPMA, AAPC Fellow
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
At the point of triage, patients and family members are typi-cally asked a series of medical interview/history questions. At this
juncture, however, staff members do not have the luxury of time to ask a long list of questions and enter responses into health records. Opportunity exists now for patients to answer these standardized questions before a medical encounter to ensure healthcare profession-als have a complete health history prior to making medical decisions. This proactive measure promises to make it easier for patients to be heard and providers to understand, resulting in appropriate care.
From the Front LineTypically, patients seeking healthcare can be represented by family members or caregivers, who can assist with completing the patient’s health history. Hospital protocols, however, may disallow these helpers from accompanying the patient through the triage/medical interview process — such as during a pandemic or other emergent situation.
Mary Masek, a TUC-MSMHS post graduate student and vice president for Touro’s Patient Advocacy Club, is a witness to the importance of patient-generated health data. “Medical providers have very little time to gather patient information, especially in light of COVID-19. Working as a medical scribe in a California emergency department, I see this firsthand. When patients bring med lists and other pertinent information, it really helps. The ultimate would be for patients to bring a complete history,” says Masek.
What Does the Patient History Include?The history, examination, and medical decision making (MDM) are key components of evaluation and management (E/M) services. History is structured and defined by 1995/1997 Documentation Guidelines for Evaluation and Management Services and comprised of the history of present illness (HPI), review of systems (ROS), and past, family, and social history (PFSH).
How Patient Prehistories Improve Health OutcomesEnsure providers have the information they need, before they need it.
shutterstock / Rawpixel.com

www.aapc.com May 2020 37
PreHxCODING/BILLING
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
Discuss this article or topic in a forum at www.aapc.com
The formal prehistory questionnaire (preHx) includes nearly 30 questions that ask the journalism equivalent of who, what, where, when, how, and why. A complete history can reveal telltale clues to patterns of disease.
History of Present IllnessIn addition to the chief complaint, the patient should answer in the preHx these HPI elements:
• Location: Where do you feel badly in your body?• Severity: Rate how bad your problem is on a scale 0 to 10.• Duration: How long have you had this problem?• Timing: Do you feel differently different times of the day
or night?• Context: What was going on when you started getting sick?• Modifying factors: What makes you feel better? What
makes you feel worse?• Associated signs/Symptoms: Can you think of anything
else we need to know?
HPI/Disease StatusHPI subcategory HPI/disease (status) gives the patient the opportu-nity to describe in the preHx their experience of living with chronic conditions and diseases. Limiting the HPI to only a few questions blocks the intake of information. Having the patient’s entire story enables the provider to better understand the patient’s experience and potentially uncover patterns of disease presentation. But that is a narrow view. In a much broader view, these data could potentially reveal new disease insights — for example, how the novel coronavirus reacts in patients with specific diseases and disease combinations.
Review of SymptomsROS is head-to-toe/mind-body checklist of 14 systems:
• Constitutional: How do you feel overall? What is your energy level?
• Eyes: Are they blurry? Do you have any visual loss?• Ears, nose, throat: Do you have an earache? Mouth pain?
Sore throat? Have you lost the ability to smell?• Cardiovascular: Are you experiencing any chest pain?
Palpitations or skipped beats?• Respiratory: Do you have a cough? Trouble breathing?
Shortness of breath? Can you hold your breath for 10 seconds?
• Gastrointestinal: Do you have any trouble eating? Moving your bowels? Have you had any diarrhea?
• Genitourinary: Any urination changes? Any genital sores?• Musculoskeletal: Are you experiencing any joint or muscle
pain? Stiffness?• Integumentary: Any skin color changes? Moles? Rashes?• Neurological: Any numbness? Pain? Trouble moving?• Endocrine: Any fatigue? Increased thirst?
• Psychological: Any mood changes, feelings of depression, or anxiety?
• Hematologic/Lymphatic: Any bruising or swelling?• Allergy/Immunologic: Any allergies? Changes in your
ability to fight infection?
A patient’s answers to ROS questions in the preHx should not be limited to only “Yes” or “No.” Descriptive responses are more likely to expose disease patterns, especially in cumulative data.
Past, Family, and Social HistoryPFSH can capture previous infectious diseases, all chronic condi-tions, medications, allergies, genetics, surgeries, and social habits. Having accurate medication and allergy lists is critical to good care. Medication descriptions should include: Name of the medication, dose, route, frequency, reason, prescribing provider, and pharmacy.
PreHx Templates Make Data Collection EasyPatients, family members, and caregivers can access online forms to prepare for a potential medical encounter. Nonprofit www.PatientAdvocacyInitiatives.org offers free downloadable forms on its home page that can be printed. The three-page paper PreHx is the same as is used in a JAOA PreHx clinical research publication.
A free online tool is also available at www.PreHx.com. The electronic version includes audio/video instructions and creates a document that can be printed or sent electronically to the healthcare provider. The nonprofit maintains the website and has vowed to never sell, share, or read content entered in this online tool. Research at Touro University California is exploring ways to best help patients with this tool.
Encourage and Empower Patients Eventually, all patient portals will grant individuals the oppor-tunity to tell their whole story and routinely prepare for medical encounters. For now, it’s reasonable to ask your patients to prepare for a potential medical encounter by answering all of the history questions asked of them.
Michael Warner, DO, CPC, CPCO, CPMA, AAPC Fellow, is an associate professor at Touro University California – College of Osteopathic Medicine. He is also an AAPC National Advisory Board member, AOA alternate advisor on AMA RUC, and president of Patient Advocacy Initiatives.
ResourceWarner et al, “Use of Patient-Authored Prehistory to Improve Patient Experiences and Accommodate Federal Law”, JAOA Feb 2017: https://jaoa.org/article.aspx?articleid=2599978
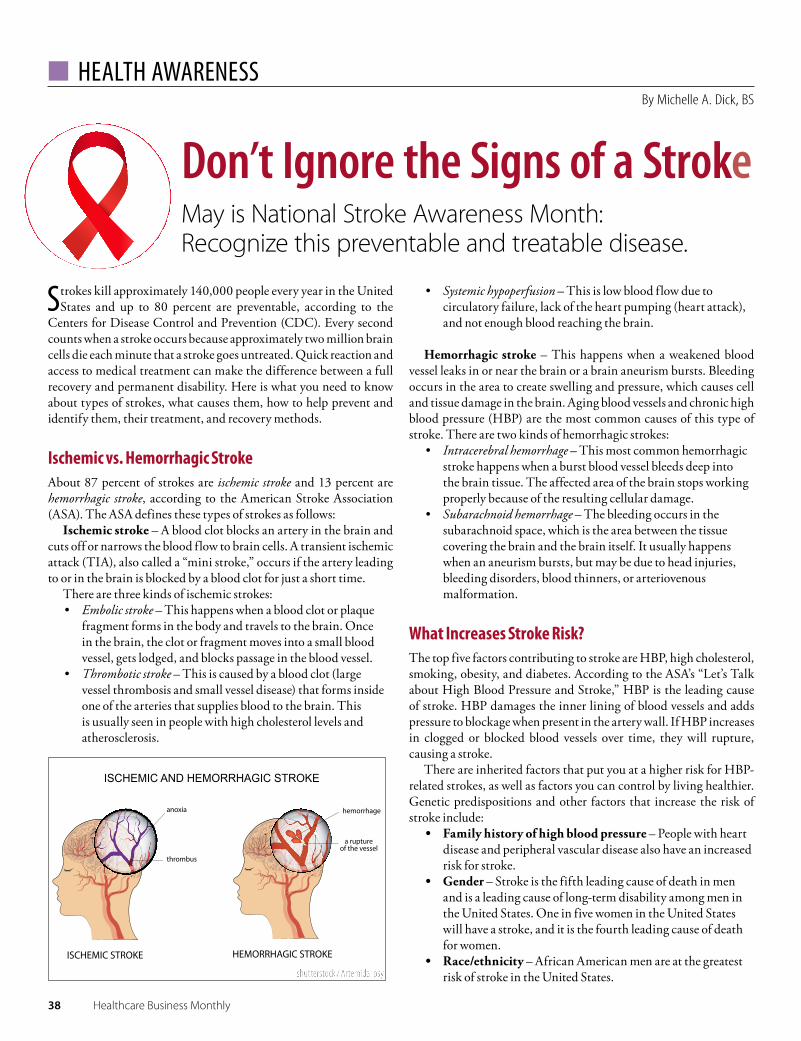
38 Healthcare Business Monthly
■ HEALTH AWARENESSBy Michelle A. Dick, BS
Strokes kill approximately 140,000 people every year in the United States and up to 80 percent are preventable, according to the
Centers for Disease Control and Prevention (CDC). Every second counts when a stroke occurs because approximately two million brain cells die each minute that a stroke goes untreated. Quick reaction and access to medical treatment can make the difference between a full recovery and permanent disability. Here is what you need to know about types of strokes, what causes them, how to help prevent and identify them, their treatment, and recovery methods.
Ischemic vs. Hemorrhagic StrokeAbout 87 percent of strokes are ischemic stroke and 13 percent are hemorrhagic stroke, according to the American Stroke Association (ASA). The ASA defines these types of strokes as follows:
Ischemic stroke – A blood clot blocks an artery in the brain and cuts off or narrows the blood flow to brain cells. A transient ischemic attack (TIA), also called a “mini stroke,” occurs if the artery leading to or in the brain is blocked by a blood clot for just a short time.
There are three kinds of ischemic strokes:• Embolic stroke – This happens when a blood clot or plaque
fragment forms in the body and travels to the brain. Once in the brain, the clot or fragment moves into a small blood vessel, gets lodged, and blocks passage in the blood vessel.
• Thrombotic stroke – This is caused by a blood clot (large vessel thrombosis and small vessel disease) that forms inside one of the arteries that supplies blood to the brain. This is usually seen in people with high cholesterol levels and atherosclerosis.
• Systemic hypoperfusion – This is low blood flow due to circulatory failure, lack of the heart pumping (heart attack), and not enough blood reaching the brain.
Hemorrhagic stroke – This happens when a weakened blood vessel leaks in or near the brain or a brain aneurism bursts. Bleeding occurs in the area to create swelling and pressure, which causes cell and tissue damage in the brain. Aging blood vessels and chronic high blood pressure (HBP) are the most common causes of this type of stroke. There are two kinds of hemorrhagic strokes:
• Intracerebral hemorrhage – This most common hemorrhagic stroke happens when a burst blood vessel bleeds deep into the brain tissue. The affected area of the brain stops working properly because of the resulting cellular damage.
• Subarachnoid hemorrhage – The bleeding occurs in the subarachnoid space, which is the area between the tissue covering the brain and the brain itself. It usually happens when an aneurism bursts, but may be due to head injuries, bleeding disorders, blood thinners, or arteriovenous malformation.
What Increases Stroke Risk?The top five factors contributing to stroke are HBP, high cholesterol, smoking, obesity, and diabetes. According to the ASA’s “Let’s Talk about High Blood Pressure and Stroke,” HBP is the leading cause of stroke. HBP damages the inner lining of blood vessels and adds pressure to blockage when present in the artery wall. If HBP increases in clogged or blocked blood vessels over time, they will rupture, causing a stroke.
There are inherited factors that put you at a higher risk for HBP-related strokes, as well as factors you can control by living healthier. Genetic predispositions and other factors that increase the risk of stroke include:
• Family history of high blood pressure – People with heart disease and peripheral vascular disease also have an increased risk for stroke.
• Gender – Stroke is the fifth leading cause of death in men and is a leading cause of long-term disability among men in the United States. One in five women in the United States will have a stroke, and it is the fourth leading cause of death for women.
• Race/ethnicity – African American men are at the greatest risk of stroke in the United States.
Don’t Ignore the Signs of a StrokeMay is National Stroke Awareness Month: Recognize this preventable and treatable disease.
shutterstock / Artemida-psy
www.aapc.com May 2020 39
Stroke
• Increasing age – The older you are, the more likely you are to have a stroke. The chance of having a stroke nearly doubles every 10 years after age 55.
• Diabetes – This disease causes pathologic changes in blood vessels, which can lead to stroke if cerebral vessels are affected. Mortality is higher and stroke outcomes are poorer with patients who have uncontrolled glucose levels.
• Sickle cell anemia – With sickle cell anemia, red blood cells become hard and sticky. When they travel through small blood vessels, they can get stuck more easily than normal cells and clog blood flow, causing stroke.
• Chronic kidney disease (CKD) – People with CKD are at increased risk of stroke, and those with end-stage renal disease are especially at risk because common vascular factors for stroke (i.e., hypertension, diabetes, atrial fibrillation) are more prevalent in patients with CKD.
• Obstructive sleep apnea (OSA) –OSA creates surges in systolic and diastolic pressure that elevate blood pressure levels during the night, causing secondary hypertension.
Social determinants of health play a role, too. Those with socio-economic hardships and inadequate access to basic living necessities, healthcare providers, and medication, and those who are unable to make healthier lifestyle changes due to these hardships, are more prone to strokes due to HBP.
How to Lower the Risks for StrokeMany risk factors can be controlled before they cause a stroke. Although some are genetic, there are lifestyle choices you can make
to help prevent stroke and heart disease while keeping your brain mentally sharp. The ASA recommends:
• Don’t smoke, avoid secondhand smoke, and limit alcohol intake.
• Lose weight, if you’re overweight. Eat a healthy diet that’s low in sodium (salt), saturated fats, and trans fats. Eat only small amounts of red meats, sweets, sugar-sweetened beverages, saturated fat, and cholesterol.
• Eat a well-balanced diet that is high in fruits, vegetables, poultry, fish, nuts, low-fat dairy products, and whole grains. Include foods rich in potassium.
• Enjoy regular physical activity. Do 150 minutes of physical activity per week (after consulting with a physician).
• Take all medicines as prescribed to control blood pressure.• Manage your blood glucose and cholesterol levels.• Sleep well and manage stress.
Don’t Dismiss Signs of StrokeSymptoms of stroke are varied and are not always recognized quickly. The ASA says the most common symptoms of a stroke are:
• Weakness or numbness of the face, arm, or leg on one side of the body
• Loss of vision or difficulty seeing in one or both eyes• Loss of speech, difficulty talking, or difficulty
understanding what others are saying• Sudden, severe headache with no known cause• Loss of balance or unstable walking, usually combined with
another symptom
Less distinctive symptoms include somnolence, nausea, or the sudden onset of headache. TIAs can cause symptoms such as numb-ness, trouble speaking, and loss of balance or coordination; it’s common for these symptoms to last for a very short time and then resolve. Although TIAs cause no permanent brain damage, they are a dangerous warning sign that should not be ignored.
HBP Can Also Affect Lung ArteriesFor information on pulmonary arterial hypertension and its effects, specifically regarding high blood pressure (HBP) in the arteries that supply the lungs, read the article “Relieve Pulmonary Hypertension Coding Pressures” on AAPC’s Knowledge Center: www.aapc.com/blog/40519-relieve-pulmonary-hypertension-coding-pressures.
“Quick reaction and access to medical treatment can make the difference between a full recovery and permanent disability.”
shutterstock / Artem Oleshko
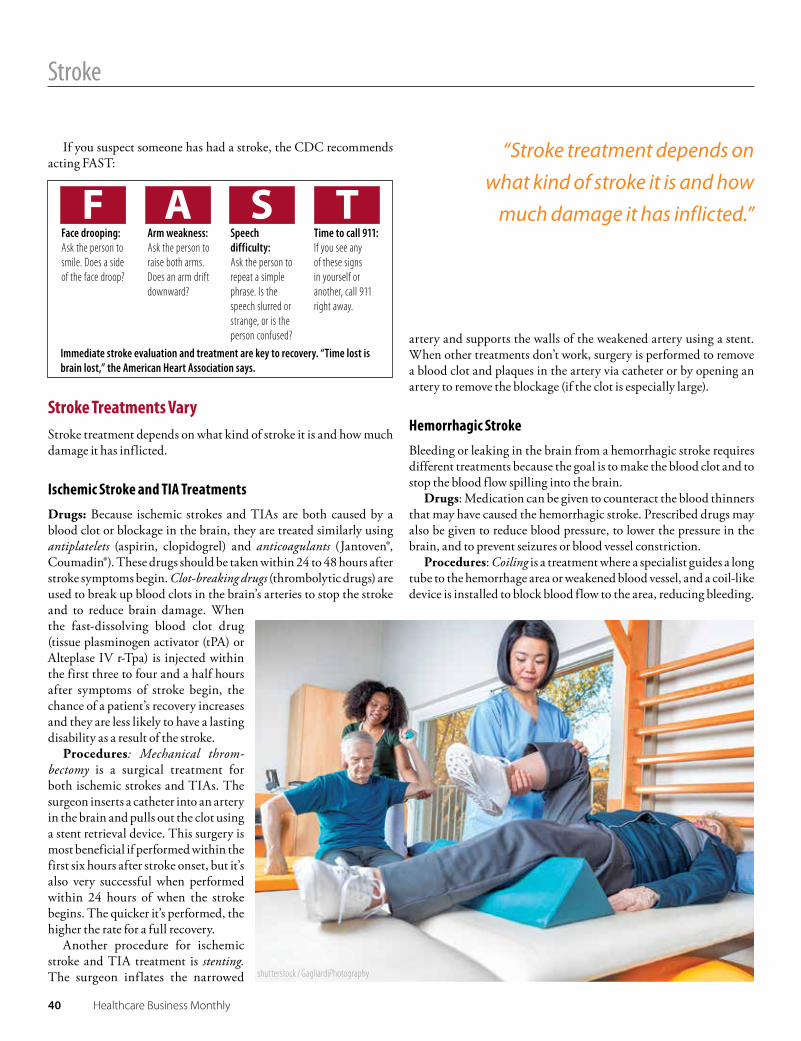
40 Healthcare Business Monthly
Stroke
If you suspect someone has had a stroke, the CDC recommends acting FAST:
Stroke Treatments VaryStroke treatment depends on what kind of stroke it is and how much damage it has inflicted.
Ischemic Stroke and TIA TreatmentsDrugs: Because ischemic strokes and TIAs are both caused by a blood clot or blockage in the brain, they are treated similarly using antiplatelets (aspirin, clopidogrel) and anticoagulants (Jantoven®, Coumadin®). These drugs should be taken within 24 to 48 hours after stroke symptoms begin. Clot-breaking drugs (thrombolytic drugs) are used to break up blood clots in the brain’s arteries to stop the stroke and to reduce brain damage. When the fast-dissolving blood clot drug (tissue plasminogen activator (tPA) or Alteplase IV r-Tpa) is injected within the first three to four and a half hours after symptoms of stroke begin, the chance of a patient’s recovery increases and they are less likely to have a lasting disability as a result of the stroke.
Procedures: Mechanical throm-bectomy is a surgical treatment for both ischemic strokes and TIAs. The surgeon inserts a catheter into an artery in the brain and pulls out the clot using a stent retrieval device. This surgery is most beneficial if performed within the first six hours after stroke onset, but it’s also very successful when performed within 24 hours of when the stroke begins. The quicker it’s performed, the higher the rate for a full recovery.
Another procedure for ischemic stroke and TIA treatment is stenting. The surgeon inflates the narrowed
artery and supports the walls of the weakened artery using a stent. When other treatments don’t work, surgery is performed to remove a blood clot and plaques in the artery via catheter or by opening an artery to remove the blockage (if the clot is especially large).
Hemorrhagic Stroke Bleeding or leaking in the brain from a hemorrhagic stroke requires different treatments because the goal is to make the blood clot and to stop the blood flow spilling into the brain.
Drugs: Medication can be given to counteract the blood thinners that may have caused the hemorrhagic stroke. Prescribed drugs may also be given to reduce blood pressure, to lower the pressure in the brain, and to prevent seizures or blood vessel constriction.
Procedures: Coiling is a treatment where a specialist guides a long tube to the hemorrhage area or weakened blood vessel, and a coil-like device is installed to block blood flow to the area, reducing bleeding.
“Stroke treatment depends on what kind of stroke it is and how
much damage it has inflicted.”Face drooping: Ask the person to smile. Does a side of the face droop?
Arm weakness: Ask the person to raise both arms. Does an arm drift downward?
Speech difficulty: Ask the person to repeat a simple phrase. Is the speech slurred or strange, or is the person confused?
Time to call 911: If you see any of these signs in yourself or another, call 911 right away.
Immediate stroke evaluation and treatment are key to recovery. “Time lost is brain lost,” the American Heart Association says.
shutterstock / GagliardiPhotography
www.aapc.com May 2020 41
Stroke
AAPC Books
NEW BOOK SMELL
GET THAT
And reduce denials with updated 2021 codes, guidelines, Quick View Flow Charts, and more.
Preorder your 2021 books today at
aapc.com/newbooks
Another procedure for hemorrhagic stroke treatment is clamping, where a specialist may discover via imaging that an aneurysm hasn’t started bleeding yet or has stopped. The surgeon may put a small clamp at the discovered aneurysm base to stop blood supply and prevent new bleeding or a broken blood vessel from occurring.
If an aneurysm has burst, the specialist may surgically clip the an-eurysm to prevent further bleeding. For a larger stroke, a craniotomy may be done to relieve brain pressure.
The goal of surgical procedures and prescribed medicines is to prevent a future stroke. Other prescribed stroke prevention drugs control high blood pressure and statins (rosuvastatin, simvastatin, atorvastatin), which lower cholesterol levels. Besides being a blood thinner, aspirin may be prescribed as a preventive medicine for those with a high risk of atherosclerotic cardiovascular disease.
Stroke Recovery Requires TherapyTo increase chances of a full recovery, rehabilitation from a stroke should start as fast as possible. Once the condition is stabilized, assessed, and factors are identified, therapy should begin immediately to rehabilitate and get back use of affected skills. Stroke recovery fo-cuses on speech therapy, cognitive therapy, relearning sensory skills, and physical therapy. Occupational therapy may also be required.
Michelle A. Dick, BS, is a freelance content specialist, providing writing, editorial expertise, and graphic imagery to clients. Prior to becoming a free agent, she was an executive editor for AAPC, editor-in-chief at Eli Research, and editor at Element K Journals. After earning a Bachelor of Science from the State University of New York at Buffalo State, Dick entered the publishing industry as a graphic artist, ad coordinator, and web designer for White Directory Publishers Inc.
ResourceAmerican Stroke Association, American Stroke Month Patient and Consumer Resources: www.stroke.org/en/about-the-american-stroke-association/american-stroke-month/community-resources-english
CDC, African-American Men and Stroke, fact sheet: www.cdc.gov/stroke/men.htm
CDC, Stroke Facts: www.cdc.gov/stroke/facts.htm
CDC, Family History and Other Characteristics That Increase Risk for Stroke: www.cdc.gov/stroke/family_history.htm
CardioSmart, American College of Cardiology, Sleep Apnea and High Blood Pressure: A Dangerous Pair: www.cardiosmart.org/news-and-events/2015/05/sleep-apnea-and-high-blood-pressure-a-dangerous-pair
Healthline, Everything You Need to Know About Stroke: www.healthline.com/health/stroke
Official Journal of the International Society of Nephrology, Kidney International, Prevention and treatment of stroke in patients with chronic kidney disease: an overview of evidence and current guidelines: www.kidney-international.org/article/S0085-2538(19)31020-8/fulltext

42 Healthcare Business Monthly
■ CODING/BILLINGBy Brett Rosenberg, MA, CPC, CCS-P, COC
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
There are a lot of variables at play when it comes to stroke diagnosis coding in a clinical office setting. That set of variables gets multi-
plied even further for those coding stroke diagnoses from radiological dictation reports. That’s because there’s a seemingly endless array of factors to consider if you want to get the coding mechanics down pat. Whether it’s understanding the lingo, discerning between old versus new cerebral infarctions, or using each component of the report to make sure you’ve got the most detailed diagnosis possible, you’ve got to be on high alert if you want to get the job done right.
Rely on this set of helpful tools, tips, and tricks of the trade to ensure you’re coding radiological stroke-related diagnoses accurately and compliantly.
Consider This Loose TimetableYour first point of order is to compare the U.S. National Center for Health Statistics (NCHS) timetable for acute and chronic diseases
with acute and chronic stroke timetables. As defined by the NCHS, a disease is to be considered chronic if its symptoms last more than three months. Formulating the series of steps from which a hyperacute stroke becomes chronic is not as straightforward — in part because no universal set of guidelines exists to help elaborate on those distinctions.
That doesn’t mean you’re left to figure it out on your own, though. When you have a generalized timetable to fall back on, subtle fluc-tuations between one provider, peer-reviewed journal, or specialty society shouldn’t matter all that much. The steps in which a stroke evolves from hyperacute to chronic (with generalized time estimates) are as follows:
• Early hyperacute: Zero to six hours• Late hyperacute stroke: Six to 24 hours• Acute stroke: 24 hours to one week• Subacute stroke: One to three weeks• Chronic stroke: Greater than three weeks
Maximize Your Stroke Dx Coding Tips to improve and streamline your stroke diagnosis coding processes.
shutterstock / peterschreiber.media

www.aapc.com May 2020 43
Stroke DxCODING/BILLING
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
While various peer-reviewed studies chronicling how a stroke manifests (both symptomatically and on imaging scans) over the course of the first few months will vary in their time estimates, cerebral infarction ICD-10-CM codes don’t distinguish between acute and chronic. The job of the coder is to translate the patient’s documented diagnostic status into the most accurate ICD-10-CM code.
Beware of Tricky Terminology There are a few scenarios to look out for to avoid making the mistake of coding a stroke when the documentation doesn’t support the diagnosis. For instance, mistaking a transient ischemic attack (TIA) to be synonymous with a stroke is a common error in a field such as diagnostic radiology. While there’s a clear-cut diagnosis (G45.9 Transient cerebral ischemic attack, unspecified) for a TIA, it’s often the surrounding speculative documentation that leads you to question the original diagnosis. While a TIA is often referred to as a “mini stroke,” from an ICD-10-CM coding perspective, it’s important to keep the two diagnoses entirely separate.
Another common indicating diagnosis that may or may not accompany a TIA diagnosis is a “stroke alert.” A stroke alert may be included as a supplementary diagnosis when the patient’s signs and symptoms are indicative of a possible stroke. However, the impres-sion of the dictation report will have final say as to whether a stroke is revealed in the imaging scan. If not, there’s a possibility that the patient’s symptoms are the result of a TIA, but without a definitive TIA diagnosis, you should code only the signs and symptoms.
Coder’s note: A TIA diagnosis, unlike a stroke diagnosis, can be coded from the indication. Preliminary TIA diagnoses are often made based on a patient’s presentation of signs and symptoms. Follow-up imaging is then ordered to determine the underlying cause of the TIA.
Consider Full Scope of Coding PossibilitiesWhile the majority of stroke diagnoses outside of the diagnostic ra-diology setting will not include enough supplementary information to code beyond I63.9 Cerebral infarction, unspecified, you should be prepared if, and when, the clinical encounter presents itself.
On an imaging scan that does include a diagnosis of a cerebral infarction (stroke), ask yourself:
• Is the stroke current?• Is there documentation to support a diagnosis beyond that
of an unspecified code?
The documentation will typically be straightforward in distin-guishing between a current and “old” stroke. In most instances, the provider will also make a clear distinction between a current and old cerebral infarction in the findings and impression of the report. What’s more, the indication should give you a better idea as to whether the underlying reason for the scan is related to a possible stroke.
Coder’s note: If you’re a seasoned diagnostic radiology coder, you know that old infarctions are a relatively common diagnostic finding and may be entirely incidental to the reason for the patient’s scan. In reporting an old, incidental cerebral infarction as a secondary diagnosis, use code Z86.73 Personal history of transient ischemic attack (TIA), and cerebral infarction without residual deficits.
Use the Indication, Findings to Your AdvantageIn the case of a current cerebral infarction, you’ll typically encounter one of two scenarios, both of which may require some due diligence on your part.
The first scenario involves the initial diagnosis of the infarction. This could yield an indication exclusively involving signs and symptoms, or it could offer a more straightforward diagnosis of stroke or stroke alert. If the indication states “stroke,” and the scan does not reveal a cerebral infarction, send the report back to the provider for an addendum.
Consider a second scenario in which you encounter a diagnosis of “infarction of the right anterior cerebral artery” in the impression. Without any additional details explaining the etiology or context surrounding the stroke, you should report code I63.9. Venturing beyond the impression, the findings may elaborate that the infarc-tion of the right anterior cerebral artery is the result of occlusion
“The job of the coder is to translate the patient’s documented diagnostic status
into the most accurate ICD-10-CM code.”
shutterstock / BlurryMe

44 Healthcare Business Monthly ■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
AAPC WebinarsGROUPSUBSCRIPTION
SINGLEE V E N T
INDIVIDUAL S U B S C R I P T I O N
Get the Latest Healthcare Updates with AAPC Webinars
EDUCATION CEUs UPDATES
See our upcoming webinars at aapc.com/webinars
Stroke DxCO
DING
/BIL
LING
Discuss this article or topic in a forum at www.aapc.com
and/or stenosis. In this case, the diagnosis would shift to I63.521 Cerebral infarction due to unspecified occlusion or stenosis of right anterior cerebral artery.
This second scenario will only occur if you’re coding an imaging study on the cerebral arteries, such as a magnetic resonance angiog-raphy (MRA) or computed tomography angiography (CTA). That’s because angiographies, or arteriograms, image the perfusion of the cerebral arteries. A traditional computed tomography (CT) scan or magnetic resonance imaging (MRI) scan evaluates the parenchyma of the brain. These scans will show the result of an occluded artery (i.e., stroke), but not the occlusion itself. This means that if you’re working on a traditional MRI or CT scan of the brain, you don’t need to be on the lookout for any underlying embolism, occlusion, stenosis, or thrombosis diagnoses.
However, you should still be on high alert for information that adds to the context of the stroke, as it may impact your diagnosis coding. For example, if the indication reads “facial droop follow-ing coronary artery bypass surgery” and the impression reveals a “cerebral infarction due to a left vertebral artery embolism,” you’ll report the following diagnosis codes:I63.112 Cerebral infarction due to embolism of left vertebral artery
I97.820 Postprocedural cerebrovascular infarction following cardiac surgery
There are many variables to consider if you want to code stroke diagnoses accurately and confidently. Your success is predicated on a thorough analysis of the dictation report and implementing all the pertinent guidelines at your disposal. If you’re ever unsure of how to code a respective report, consult with fellow coders and, if necessary, query the interpreting physician.
Brett Rosenberg, MA, CPC, CCS-P, COC, has six years of experience as a medical coder, specializing in the field of radiology. He currently serves as the editor of The Coding Institute’s (TCI’s) Radiology, Otolaryngology, and Outpatient Facility Coding Alerts. His work as a coder included excelling in the administrative ins-and-outs of medical billing, such as appealing coverage denials and negotiating insurance contracts for physicians.
ResourceICD-10-CM code book, 2020U.S. National Center for Health Statistics (NCHS)Schmid, MD, Johannes; Gaillard, Frank. Radiopaedia, “Ischemic stroke”: https://radiopaedia.org/articles/ischaemic-stroke?lang=us
ZHealth
46 Healthcare Business Monthly
By Joshua Caillouet, CPC, CASCC
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
■ PRACTICE MANAGEMENT
From time immemorial, many societies have been based around one thing: commerce. Although what we perceive as currency has
changed throughout history, our expectation to get what we paid for has not. The medical field is no exception. Ranging from the use of cutting-edge medical technology to treat the most inoperable disease to a simple bandage over a scraped knee, healthcare providers offer goods and services in the expectation that they will be paid. That’s partly why we’re in the business office — to guarantee this trade goes off without a hitch. One thing which can derail this, however, is an angry patient.
Wait, what?Yes, should a patient become dissatisfied with a provider’s service,
not only may the patient refuse to pay their bill and go elsewhere, but they also may harm your organization’s reputation. In the age of social media, the ripple effect can be astronomical.
Reviews Can Make or Break a ProviderSites like healthgrades.com and ratemds.com allow patients to express their satisfaction or dissatisfaction with their doctor and ancillary staff. Google and Yelp also have popular message boards where dissatisfied patients can vent. And there are endless other outlets, not to mention the Centers for Medicare & Medicaid Services’ (CMS’) star ratings and compare programs.
Here are two actual examples of ratings posted on Google about two hospitals in my area of Georgia:
“The majority of staff lacks common decency and people skills … I was bounced around between 7 departments to find a solution to an issue THEY created, left multiple voice messages, haven’t received a call back (2.5 weeks later), and the issue remains unresolved.”
“In my experience the on-duty MD has no compassion and horrific bedside manner … When pressed to provide a clear answer
Losing Business? Maybe It’s Your Customer Service Consider implementing these recommendations to score high with patients.
shutterstock / Tyler Olson

www.aapc.com May 2020 47
Customer Service
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
PRACTICE MANAGEM
ENTTo discuss this article or topic, go to www.aapc.com
the conversation actually devolved into a cursing match. Have you ever had a doctor call you an a-hole? This one will.”
Both hospitals have a valuable niche and are instrumental in keeping millions healthy in my city. However, those negative reports will remain forefront in people’s minds.
What Causes Patients to Be Disgruntled?In the article “The Man who Lied to His Laptop: What Machines Teach Us About Human Relationships,” co-author Clifford Nass says: “The brain handles positive and negative information in different hemispheres. Negative emotions generally involve more thinking, and the information is processed more thoroughly than positive ones.” Negative experiences leave lasting impressions.
According to an American Customer Satisfaction Index (ACSI) 2019 report, “customers aren’t happy with hospital care, which falls 5.3% to 72” from a prior score of 76 in 2018. While the chief cause of this dissatisfaction seems to be the emergency room departments, the impact can be felt in outpatient and other healthcare settings, as well. While one of the chief complaints is wait time, and provid-ers have been educating the public about emergency room visits, the other complaints ring the same: clinical staff interaction and registration, and business staff interaction.
How Can You Improve Customer Satisfaction?If you’re concerned about how your staff would measure up to a patient satisfaction review, ask yourself these questions:
Do we respect our patients and their privacy?• Post signs asking other patients to give a bit of space when
patients check in.• Place the sign-in sheet so it’s visible from your entrance.• When clinical staff calls a patient about their care, they
should be discreet about leaving voice messages.• There should be a standard protocol to follow when a
patient requires financial counseling.
Are we respectful of our patients’ time?• If you work in an office setting, make sure there is a
protocol in place for when the doctor is running late.
• The admission and discharge process should be quick and efficient, allowing for the required information to be shared without inconveniencing the patient.
Are we respectful to patients with our communication?In the article “The Impact of Rudeness on Medical Team Performance: A Randomized Trial,” the researchers surmise, “Not only does rudeness harm the diagnostic and procedural performance of practitioners, it also seems to adversely affect the very collaborative process that might otherwise allow for teams to compensate for these effects.”
If rudeness has an impact on provider care, imagine its effect on patients. All patients should be shown the same level of courtesy that you yourself would like to receive if in their shoes.
It Pays to Be NiceCustomer satisfaction plays an integral part of a practice’s or hospital’s ongoing financial stability. Patients are much more selective about where they receive treatment and they are able to share their experience globally. What’s the best insurance for getting a claim paid? Make sure your patients receive excellent customer service throughout their healthcare experience with your office or facility.
Joshua Caillouet, CPC, CASCC, has six years’ experience in the healthcare field. Starting off at a five-provider nephrology practice, his experience has focused primarily on denial management, insurance precertification, and commercial and government reimbursement. He currently works as an insurance specialist.
ResourcesYen, Corina; Clifford Nass. “The Man who Lied to His Laptop: What Machines Teach Us About Human Relationships.” Penguin Books. 2010
Riskin, Arieh; Erez, Amir; Foulk, Trevor A.; Kugelman, Amir; Gover, Ayala; Shoris, Irit; Riskin, Kinneret S.; Bamberger, Peter A. “The Impact of Rudeness on Medical Team Performance: A Randomized Trial.” Pediatrics. September 2015. 136 (3) 487-495; DOI. https://pediatrics.aappublications.org/content/136/3/487
DiMeglio, Denise. ASCI Finance, Insurance, and Health Care Report 2018-2019. Nov. 19, 2019.
“Negative experiences leave lasting impressions.”
48 Healthcare Business Monthly
By Sarah Prom, MA, LPC, ODCP
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
■ PRACTICE MANAGEMENT
Teamwork has become crucial in contemporary healthcare, and the reasons are multiple. As the Human Resources for Health Global
Resource Center explains, “Clinical care is becoming more complex and specialized, forcing medical staffs to attempt complicated health services and quickly learn new methods. Aging populations, [and] the increase of chronic diseases like diabetes, cancer, and heart disease, have forced medical staffs to take a multidisciplinary approach to healthcare. In countries like the United States, medical teams must manage patients’ suffering from multiple health problems.”
As teams of physicians, advanced practitioners, nurses, techs, and other medical professionals face these interdisciplinary challenges, it’s important they find ways to work together at an optimal level of cooperation — because failure to do so is a source of real trouble. For instance, according to a 2014 study published in Health Care Management Review, more than 70 percent of medical errors can be attributed to dysfunctional interpersonal dynamics on care teams.
A comprehensive article on medical teamwork in AAMC News un-derlines the effect of dysfunction on the team members themselves: “Numerous peer-reviewed studies show group dysfunction leads to burnout, emotional distress, depression, substance abuse, reduced productivity, and other psychosocial issues.”
Respect, Empathy, CommunicationWhat makes a medical team optimally functional: in other words, most cooperative and productively interactive?
For V. Simon Mittal, MD, a leadership and career development coach, the indispensable ingredients are two very basic positive human qualities and one very basic human skill: mutual respect and mutual empathy, and good communication.
“In a team working together optimally,” Dr. Mittal says, “there is the sense everyone is listened to in an active, responsive and thoughtful way and everyone is recognized for the value they bring to the team.” Mutual respect supports good medical decisions, since multiple perspectives are honored and considered before decisions are made, and good communication means decisions will be arrived at and carried out effectively.
Psychologist and workplace burnout expert Christine Maslach, quoted in AAMC News, notes going the extra mile in respect and empathy pays dividends. “It’s important to recognize people in a positive way when they do something good,” she says. “Rather than say, ‘Well, you did your job, big deal, so what,’ if you periodically say, ‘You really handled that patient well, nice job,’ that goes far. It’s huge. It doesn’t cost anything, but you have to be sensitive enough and willing to care about each other.”
Warning SignsIt’s not hard, then, to spot the signs of a dysfunctional team. “Limited communication; snippy, disrespectful comments; team members whose contributions aren’t valued and who then become less engaged, more detached from the processes they’re working in,” says Dr. Mittal.
How to Cultivate Healthy Care Teams and Eliminate Risk Ensure healthy working relationships to improve patient health and satisfaction.
shutterstock / Syda Productions
www.aapc.com May 2020 49
Care Teams
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
PRACTICE MANAGEM
ENT
The sources of these problems may be personal, but they may also have an institutional aspect, as Michelle O’Daniel and Alan H. Rosenstein, MD, point out in a study of team communication and collaboration. Developing interpersonal sensitivity may take considerable effort for healthcare physicians. Medical education tends to value individual excellence and error-free practice over co-operation and willingness to admit error and ask for help. Individual team members may feel a loss of autonomy working on a team, as well as “lack of confidence or trust in decisions of others; clashing perceptions; territorialism; and lack of awareness of one provider of the education, knowledge, and skills held by colleagues from other disciplines and professions,” O’Daniel and Dr. Rosenstein say.
The Patient’s-Eye-ViewEveryone involved in healthcare wants the patient to be safe, get better, and feel comfortable and confident during the process of healing. Dr. Mittal believes seeing the work of the team from the patient’s point of view can help team members understand the value of overcoming those obstacles to cooperation.
When a care team is aligned according to these three major values, he asserts, the patient immediately feels more secure. Of course, the team needs to show the patient respect, listen to their
input about care, and take them seriously. “The old model of medicine was, the doctor says, ‘do this,’ and you do it. Today it’s much more of an active collaboration between the providers and the patient,” says Dr. Mittal.
But good relationships among the team members are reassuring for the patient, too. “When care team members show respect for each other in front of the patient, and empathy, too, it shows they really care about one another as people,” Dr. Mittal says, “the patient feels if a difficult issue comes up in his or her care, the team members ‘have each other’s back’ and will work well together to solve the problem.”
Cultivating Good TeamsHow, then, can leaders promote optimal cooperation and the best relationships among care team members? Writing in Critical Care, Constantine Manthous, MD, and his colleagues underline the responsibility of the team leader.
“Team leader behavior is a well-documented contributor to team effectiveness,” they write. “How team leaders structure the team, define its purpose, remove organizational barriers, help individual members enhance their contributions to the team, and coach to help members use their collective resources to fulfill team goals all influence team success. Additionally, team leaders are influential on an interpersonal level …. Members look to leaders’ behaviors as an indicator of what is expected and accepted of their own behavior.”
Dr. Mittal says institutional leaders need to set clear standards, too — and, he insists, “They don’t have to wait for a problem to arise in order to make things better for everybody.” Even if teams are functioning well, without prompting complaints from patients
“Medical education tends to value
individual excellence and error-free practice over cooperation and
willingness to admit error and ask for help.”

50 Healthcare Business Monthly
Care TeamsPR
ACTI
CE M
ANAG
EMEN
TTo discuss this article or topic, go to www.aapc.com
NAMAS
For TheFinal Rule
The Final Stop
Your Road Map to the 2021 E&M Changesand What's Next for E&M Audiing
Tools and Resources To Help You Navigate The 2021 E&M Changes
• FREE E&M Comparison Chart• Webinars• Live E&M Training Events• 2021 Audit Tool• 5 Steps for Implementaion• Sample Audit Notes• Audit Ti• Audit Tips
https://namas.co/2021-changes
or team members, he says, leaders should see what can be improved. Can there be more expressions of respect, trust, and empathy — those qualities shown to be reassuring to patients while they ensure better care?
And, of course, leaders should be alert for even subtle signs of dysfunction. “Like the unnecessarily short, slightly rude response to a question, the verbal disagreement that shows lack of respect, the look of disengagement or demoralization on the face of a team mem-ber. Just walking around the institution and observing the teams at work can tell a leader a great deal about how healthy his or her teams are.” Team meetings are a good place to assess interpersonal dynamics, too, and Dr. Mittal thinks chief medical officers and other leaders should attend them as observers whenever they can.
“Ultimately,” he says, “leaders should think: ‘Even if we’re good, there’s always something more we can do in this area. No matter what the challenges, we choose to be an organization with healthy work relationships and healthy work teams.’”
Sarah Prom, MA, LPC, ODCP, leads the Service Delivery Team for VITAL WorkLife and serves as a senior consultant and practice lead. She has more than 15 years of counseling, coaching, and mediation experience. She has expertise in the areas of team development and facilitation; workplace stress and conflict management; and supporting relational and emotional intelligence issues. She is a licensed professional counselor, a certified transformative mediator, and she serves on the leadership team at VITAL WorkLife.
Resources“Why Is Teamwork in Health Care Important?” Human Resources for Health Global Resource Center. www.hrhresourcecenter.org/HRH_Info_Teamwork.html
Mitchell, R. and colleagues, “The ABC of Health Care Team Dynamics: Understanding Complex Affective, Behavioral, and Cognitive Dynamics in Interprofessional Teams,” Health Care Management Review, January-March, 2014. www.ncbi.nlm.nih.gov/pubmed/24304597
“Teamwork: The Heart of Health Care,” AAMC News, Sept. 27, 2016. www.aamc.org/news-insights/teamwork-heart-health-care
O’Daniel, MHA; Michelle and Rosenstein, MD, Alan H. “Professional Communication and Team Collaboration,” Patient Safety and Quality: An Evidence-Based Handbook for Nurses. www.ncbi.nlm.nih.gov/books/NBK2637
Manthous, Constantine and colleagues, “Building Effective Critical Care Teams,” Critical Care 15/4, 2011. www.ncbi.nlm.nih.gov/pmc/articles/PMC3387583
“Just walking around the institution and observing the teams at work
can tell a leader a great deal about how healthy his or her teams are.”
TCIAAPC DL
52 Healthcare Business Monthly
Hint: Don’t use the same password for your personal and o�ce devices.Boost Password Acumen With Expert Insight
■ Coding/Billing ■ Auditing/Compliance ■ Practice Management
■ AUDITING/COMPLIANCEBy Kristin J. Webb-Hollering
There’s no denying that the digital revolution has reshaped healthcare with products that boost efficiency, enhance care, and
streamline administration. In fact, your practice probably utilizes mobile devices, electronic health records, and other high-tech tools every day. Despite its plethora of benefits, technology does have a downside: It must be managed and secured against myriad threats, both internal and external.
Your information technology (IT) staff is likely on top of things as varied as logging and monitoring network activity to managing patches and installing antivirus software. But even the strongest security measures aren’t always foolproof, and that can leave both
your patients’ electronic protected health information (ePHI) and your business exposed and vulnerable. If you add heightened federal enforcement to the mix, you’ve got a recipe for disaster that can cost your practice big bucks.
Start With HIPAA Security TrainingComprehensive HIPAA security training for administrative staff and clinicians is a great place to start. A central piece of your organization’s compliance planning and overviews should include robust password protocols. It might sound simple, but strong password creation and controls are often overlooked or pushed to the wayside when accounts
shutterstock / Syda Productions
www.aapc.com May 2020 53
Hint: Don’t use the same password for your personal and o�ce devices.Boost Password Acumen With Expert Insight
PasswordAUDITING/COM
PLIANCE
We’ve got more great articles on the Knowledge Center at: www.aapc.com/blog.
are set up and logins are established — despite being a quick and easy officewide security measure.
Here’s Why Usernames Are Usually Standard Your organization’s usernames are likely straightforward, and there’s a good reason why. Formatting is essential to promote quick identification and assessment by IT staff.
“Usernames at work aren’t usually up to the individual; they’re set by the IT department and they usually follow a common stan-dard such as ‘first_initial,’‘last_name,’ but you can take steps to keep your work username more secure by using it only for work,” explains Jen Stone, MSCIS, CISSP, QSA, a security analyst with SecurityMetrics in Orem, Utah.
Adam Kehler, CISSP, principal consultant and healthcare prac-tice lead with Online Business Systems, adds, “Username formats should meet a corporate standard for consistency, but should not be considered confidential information.”
This is particularly critical when network monitoring shows unauthorized access to the practice systems. If a data security incident occurs, IT staff can quickly pinpoint the account involved
and do the necessary damage control.
Don’t Mix Business With PleasureIt’s smart business to separate your home life from your work life, which translates to using different logins for your home accounts than those you use for work. The division between work and home tech not only protects your patients — it protects your business, too.
“If you use your work email as an account name, chances are good you’ll be tempted to use your work password as well,” says Stone. “Then, when ‘Flower Sparkle Games’ is hacked, the hackers not only get access to your game, they also get access to your work account.”
HIPAA Security Factors into the Password Equation
Over the past few years, the Office for Civil Rights has really ramped up its enforcement of HIPAA security violations. The loss of devices and the lack of encryption on many of these mobile units has made password security a hot topic in healthcare. Case after case illustrates the need for stronger risk analysis, with unauthorized access a common issue among both covered entities (CEs) and their business associates (BAs).
The HIPAA Security Rule places primary importance on policies and procedures that protect and secure ePHI. Under the administrative safeguards, CEs are required to identify and analyze potential risks to ePHI as part of their security management process, the rule summary instructs. In addition, the provision mandates
the implementation of “security measures that reduce risks and vulnerabilities to a reasonable and appropriate level.” This includes the creation and maintenance of strong passwords.
7 Password Creation Steps Stop Hackers in Their TracksReview these seven password steps that Adam Kehler, CISSP, a principal consultant and healthcare practice lead with Online Business Systems, recommends for covered entities (CEs):1. Make it long. Longer passwords equal greater security — it’s just that simple. “Increase
length to 10 or 12 characters,” he suggests.
2. Don’t go over the top with complexity. An overly complicated password that must be changed weekly or monthly can be a headache and lead to password fails. “Eliminate requirements for complexity and scheduled change — only change if a password has been compromised,” instructs Kehler.
3. Register a breached password checklist. It’s never a great idea to reuse a password that’s created problems in the past. “Reject passwords that appear on a breached password list,” he says.
4. Streamline reset protocols. It’s best not to overcomplicate the reset processes for users’ passwords. “Make password resets easy by sending a temporary link to the user’s backup email account,” Kehler advises.
5. Eliminate password hints. “They actually decrease security,” Kehler warns. Hackers can easily investigate a user’s background with just a username. If you must use hints, think neutral and impersonal when creating them.
6. Use hashing functions and cryptography. Password storage that utilizes hashing or inputting random data into passwords through cryptography limits cyber thugs. “Ensure passwords are stored using a strong, nonreversible hash like Bcrypt instead of SHA256,” explains Kehler.
7. Institute user-friendly password protocols. The nuances of high-tech password policy can be confusing and impede practice controls, so provide easy-to-understand guidelines. “Increase usability with methods such as providing real-time feedback on password strength and ensuring systems are compatible with popular password safes,” Kehler says.
“Passwords alone are by and large not a great way
to authenticate individuals. Organizations should strongly
consider implementing multifactor authentication
(MFA) for all remote access or privileged access to sensitive
systems.” —Adam Kehler

54 Healthcare Business Monthly
PasswordAU
DITI
NG/C
OMPL
IANC
E
The emphasis on risk assessment and reduction is clear — and this includes the creation and maintenance of strong passwords. Whether you’re a CE operating a small practice in a rural zone or a multifaceted BA with departments that span an entire region of the country, you must put risk analysis and password protection at the top of your HIPAA compliance planning.
Use Two-Factor AuthenticationFortunately, there are strategies that you can employ to safeguard your mobile devices and workstations, as well as your patients’ ePHI, that go beyond traditional measures and bolster password controls.
“Passwords alone are by and large not a great way to authenticate individuals. Organizations should strongly consider implementing multifactor authentication (MFA) for all remote access or privileged access to sensitive systems,” Kehler stresses. “Implementing these controls can result in an incredible decrease of the number and severity of breaches.”
MFA is a handy tool that prompts you to report at least two types of evidence to authenticate your identity during login. This is also known as two-factor authentication (2FA).
Stone says to make sure 2FA is turned on for all your accounts. “It might take a few more seconds for you to log in,” Stone says, “but the increased security is absolutely worth it!”
Employ 4 Quick Tips for Better Password ManagementWhen you’re busy, you may be compelled to reuse old passwords — over and over. Hackers look specifically for these types of patterns, however, so repeatedly using the same passwords leaves your organization vulnerable to a cyberattack.Plus, if your office experiences a data breach or a HIPAA violation, one of the first inquiries in the investigation of your case will be whether you assessed, analyzed, and managed your practice risks. Lackluster password controls will likely be categorized as ignoring potential risks.One of the easiest security measures you can implement is a strong password. Think about adding these four password actions from Adam Kehler, CISSP, a principal consultant and healthcare practice lead with Online Business Systems, to your checklist:1. Strengthen security with multifactor authentication (MFA). If the sites you utilize
the most offer MFA, use it for the added protection.
2. Institute a password safe. A password vault, safe, or management system will help you both create and corral your choices. “Use a password safe that is compatible with all of your devices,” Kehler cautions.
3. Get creative. When you’re busy, it’s easy to fall into password patterns and reuse old ones. Make your passwords random and unique and add them to your password safe.
4. Dig deep for innovative hints. Some sites require users to add hints for password retrieval. You should use random words instead of meaningful ones “and store those in the password safe,” Kehler advises.
shutterstock / Irina Strelnikova
www.aapc.com May 2020 55
PasswordAUDITING/COM
PLIANCEDiscuss this article or topic in a forum at www.aapc.com
AAPC Ebooks
Ready for a change?
Try AAPC eBooks. Same books you love –just faster and easier to work with.
Preorder Now at aapc.com/change
Stay Up to Date on GuidanceThe National Institute of Standards and Technology (NIST) updated its password guidance with recommendations for improv-ing identity security. The new guidelines bemoan complicated composition rules for passwords because they create more problems.
“Research and the updated NIST SP 800-63B Digital Identity Guidelines agree that most of what we know about password strength is incorrect,” says Kehler. “Passwords change and complex-ity rules generally result in password reuse, writing down passwords, and creating predictable passwords such as ‘Password123.’”
If your practice struggles with password management, you may want to consider using a password management tool. “In my experi-ence, the best passwords come from a password manager,” says Stone. “They can be long, complex, and unique without taxing your ability to remember all the passwords to all your accounts.”
Kristin J. Webb-Hollering is the editor-in-chief of the TCI newsletters Part B Insider, Medicare Compliance and Reimbursement, and Health Information Compliance Alert.
ResourcesHIPAA Security Rule summary: www.hhs.gov/hipaa/for-professionals/security/laws-regulations/index.html
NIST guidelines: https://pages.nist.gov/800-63-3
NIST MFA guidance: www.nist.gov/itl/tig/back-basics-multi-factor-authentication
“If you use your work email as an account name, chances are good you’ll be tempted to use your work password as well. Then, when ‘Flower Sparkle Games’ is hacked, the hackers not only get access to your game, they also get access to your work account.” —Jen Stone

56 Healthcare Business Monthly
By Leesa A. Israel, BA, CPC, CUC, CEMC, CPPM, CMBS, AAPC MACRA Proficient
■ HOT TOPIC
Hours after the coronavirus was declared a global pandemic, Americans braced themselves for what was to come, without
really knowing what to expect. A lot has happened since that day. As a healthcare business professional, your contribution is to stay abreast of the coding and billing changes, and there are many.
New Codes for COVID-19The World Health Organization (WHO) established a new ICD-10-CM code:U07.1 COVID-19
This code is effective April 1, 2020. Also available are:• ICD-10-CM Official Coding Guidelines for COVID-19
April 1, 2020 - September 20, 2020• ICD-10-CM April 1, 2020 Addenda• Announcement New ICD-10-CM Code 2019 Novel
Coronavirus (COVID-19)
You can download these documents at www.cdc.gov/nchs/icd/icd10cm.htm.The Centers for Medicare & Medicaid Services (CMS) has devel-
oped two new HCPCS Level II codes for testing: U0001 CDC 2019 novel coronavirus (2019-ncov) real-time rt-pcr diagnostic panel
U0002 2019-ncov coronavirus, sars-cov-2/2019-ncov (covid-19), any technique, multiple types or subtypes (includes all targets), non-CDC
To identify and reimburse specimen collection for COVID-19 testing, CMS established two HCPCS Level II codes, effective March 1, 2020:G2023 Specimen collection for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus
disease [COVID-19]), any specimen source
G2024 Specimen collection for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), from an individual in a skilled nursing facility or by a laboratory on behalf of a home health agency, any specimen source
The new testing codes will allow Centers for Disease Control and Prevention (CDC) and non-CDC clinical labs and other providers to bill for certain coronavirus lab tests, supporting tests, and tracking of new cases. Medicare claims will be accepted starting April 1, 2020, for tests billed with these codes with dates of service on or after Feb. 4, 2020.
The American Medical Association (AMA) has approved a new CPT® code to report laboratory testing, as well:87635 Infectious agent detection by nucleic acid (DNA or RNA); severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), amplified probe technique.
The AMA published the code March 13, 2020, and the code is effective immediately.
The U.S. Congress also passed the Coronavirus Preparedness and Response Supplemental Appropriations Act, granting physicians and healthcare professionals expanded Medicare fee-for-service billing privileges for patient care delivered via telehealth during the ongoing public health emergency.
What Are the Symptoms of COVID-19?Symptoms range from a mild cough to pneumonia. Patients may experience fever; flu-like symptoms such as coughing, sore throat, and fatigue; and shortness of breath. In severe cases, there can be more serious progression including respiratory distress and fatal organ failure.
COVID-19: Be Informed, Take Precautions, Stay Calm, and Carry OnNew telemedicine rules, diagnosis and testing codes, and critical developments you should know.
Tip: Download a special edition CPT® Assistant from the AMA website at: www.ama-assn.org/system/files/2020-03/cpt-assistant-guide-coronavirus.pdf.
shutterstock / ImageFlow
www.aapc.com May 2020 57
COVID-19
How Does the Virus Spread?According to the CDC, COVID-19 spreads from person to person through respiratory droplets produced when an infected person sneezes or coughs. These droplets can transfer to those who are nearby via contact with mouth, nose, or eyes. The virus also lives on surfaces, enabling the disease to spread through surface contact. SARS-CoV-2 has been shown to survive as long as three days on some surfaces, according to a study from National Institutes of Health (NIH), CDC, and other stakeholders.
How Can We Protect Ourselves From the Illness?At this writing, there is no vaccine for COVID-19. The best way to prevent infection from the virus is to avoid being exposed to it. This can be achieved in the following ways:
• Wash your hands with soap and water (or use alcohol-based sanitizer) frequently.
• Keep your hands away from your eyes, nose, and mouth.• Keep a safe distance from people who are coughing or
sneezing.• Social distancing.• Talk to your manager about working remotely.
If you begin to experience any symptoms, stay away from others and immediately contact your healthcare provider.
The White House has released “Coronavirus Guidelines for America: 15 Days to Slow the Spread,” which you can download at: www.whitehouse.gov/wp-content/uploads/2020/03/03.16.20_coronavirus-guidance_8.5x11_315PM.pdf.
What Should Your Organization Do to Prevent an Outbreak?As per CMS, healthcare facilities should review plans for emergency preparedness, including policies and practices to prevent the spread of infection:
• Follow the CDC’s Standard, Contact, and Airborne Precautions, including the use of eye protection.
• Adhere to CDC recommendations on standard hand hygiene practices, including use of alcohol-based hand rub/hand sanitizer (ABHR/ABHS).
• Implement communal surface cleaning to help prevent the spread of germs.
• Review appropriate personal protective equipment (PPE) use and availability.
Keep in mind that the HIPAA Privacy Rule protections are not set aside during an emergency, but some leniency has been granted for:
• The requirements to obtain a patient’s agreement to speak with family members or friends involved in the patient’s care.
• The requirements to honor a request to opt out of the facility directory.
• The requirement to distribute a notice of privacy practices.• The patient’s right to request privacy restrictions.• The patient’s right to request confidential communications.
Disclaimer: Information related to COVID-19 is changing rap-idly. This information was accurate at the time of writing. Please con-tinue to check payer websites, CMS, CDC, and AAPC’s Knowledge Center for the most up-to-date information.
Leesa A. Israel, BA, CPC, CUC, CEMC, CPPM, CMBS, AAPC MACRA Proficient, head of publishing, editorial and technology at AAPC, specializes in medical coding and reimbursement for evaluation and management, urology, and general surgery, as well as billing and collections policies and strategies for physician practices. Israel is a member of the Rochester, N.Y., local chapter.
ResourcesWHO Director-General’s opening remarks at the media briefing on COVID-19, March 11, 2020: www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
CDC Coronavirus (COVID-19): www.cdc.gov/coronavirus/2019-ncov/index.html.
Coronavirus Preparedness and Response Supplemental Appropriations Act: www.congress.gov/116/bills/hr6074/BILLS-116hr6074enr.pdf.
CMS, “President Trump Expands Telehealth Benefits for Medicare Beneficiaries During COVID-19 Outbreak,” March 17, 2020: www.cms.gov/newsroom/press-releases/president-trump-expands-telehealth-benefits-medicare-beneficiaries-during-covid-19-outbreak.
NIH, “New Coronavirus Stable for Hours on Surfaces,” March 17: www.nih.gov/news-events/news-releases/new-coronavirus-stable-hours-surfaces.
Tip: For up-to-date guidance on coding telehealth services during the COVID-19 public health emergency, look to the Knowledge Center (www.aapc.com/blog).
shutterstock / kasarp studio

58 Healthcare Business Monthly
NEWLY CREDENTIALED MEMBERSNEWLY CREDENTIALED MEMBERSCan’t find your name? It takes about three months after you pass the exam before your name appears in Healthcare Business Monthly.
Magna Cum LaudeMagna Cum LaudeMagna Cum Laude
Aisha Ali, CPC-AAiswarya K P, CPC-AAlba J Schoener, CPC, COPCAli Swanson, CPC-AAlison Rangel, CPC-AAmanda Cox, CPC-AAmanda Sue Shinskie, CPC-AAmy Dellinger, CPC-AAnitt T A, CPC-AAnna R S, CPC-AAnnu Rose Sebastian, CPC-AAnupama Maheendran, CPC-AArathi M M, CPC-AArchana Nadkarni, CPC-AAysha Hemenway, CPC-A, COPCBetsy Williams, CPC-ABradley Parrish, CPC-ABrittany Rood, CPCCatherine Annette Huber, CPC,
COPCCherlyn Roberts, CPC-ACindy Frohlich, CPC-ADaniel Abraham Halevy, CPC-ADeepika Vinodraj P, CPC-AElenora Roberts, CPC-AElizabeth Cook, CPC-AElizabeth Szymanski, CPC-AEva Leony, CPC-AGonnabhaktula Pavani, CPC-AGrettel Llana, CPC-AHafiya Aboobacker, CPC-AHajun Jeong, CPC-AHannah Ferreria, CPC-AHeather Daniels, CPC-AJacqueline Joi Matthews, CPCJameela Yasseen, CPC-AJamie Gordon, CPC-AJean Morrison, CPC-AJeffrey Abulencia, CPC-AJennifer Davis, CPC-AJennifer Hartung, CPC-AJessica Gatimu, CPC-AJoanne Ryan, CPC-AKaren Cartwright, CPC-AKing Bryan Morales, CPC-ALakshmi Prasanth, CPC-ALaura Hammett, CPC-ALekshmy G M, CPC-ALisa Lumsden, CPC-ALori Foernzler, CPC-AMallory Hendrickson, CPC-AMallory Klum, CPCManal M, CPC-AMaricris Macalalag, CPC, COPCMarisa Lomanto, CPC-AMary Elizabeth Donnelly, CPC, CRCMary June Moreto, CPC-A
Matthew Otoole, CPCMelanie Capp, CPC-AMelissa Proctor, CPC-AMichelle Foster, CPC-AMichelle Rodriguez, CPC-APaul Ortquist, CPC-APayal Salve, CPC-APreya Parekh, COC, CRCRachelle Abrenica, CPC-ASamer Oweis, CIC, CPCSarah Corleto, CRCShahasina Rasheed K P, CPC-AShibla T K, CPC-ASintheya Islam, CPC-ASuvarna Khalkar, CPC-ATaushiyona White, CPC-ATaylor Ross, CPC-ATeresa Anderson, CPC-AThresa Dennis, COBGC, CPCTori Alford, CPC-ATracy Lynn Johnson, CPC-ATrella Brinkley, CPC-AVeronica Urueta, CPC-AVictoria Tuchinsky, CPC, CCCVijaya Perumalla, CPC
CPC®CPCCPCAdam Gooding, CPCAdriana Torres-Leuck, CPCAmanda Johnson, CPCAmanda Marie Gingrich, CRC, CPCAmanda Vincent, CPCAmaris Johnson, CPCAmbika Rani Gadiyaram, CPCAmie Watson, CPCAmy Learn, COCAndrea Clanton, CPCAngela Fulgham, CPCAngela Barnwell, CPCAngela Ervin, CPCAngely Marte, CRC, CPCAnn Kathrine S Cucio, CPCAnna Kelemen, CPC, COCAnnie Hannon, CPCApril Tarvin, CPCAshley Patterson, CPCAshley Perras, CPCAshley Whitney, CPCAujine Burt, CPCBetty Prescott-Paschal, CPC, CPMA,
CRC, CEMC, CGSC, COBGC, COC
Beverly Radley, CPCBianca Roman, CPCBrenda Michelle Kipferl, CPCBrenda Moncada, CPCBriann Thomas, CPCBrittney Marlin Chavarria, CPCBrynn Floyd, CPCBunny Mathre, CPC, CPMA, CRC,
COCCamille Eusebio, CPCCandice Spraggins, CPC, CRC, COC
Carol Jean Schindel, CPCCasey Smith, CPCCassandra Richmond, CPCCassie Boylan, CPCCathleen Chenel, CPCCecilia Catalina Chavez, CPCCharlet Lee, CPCChelsea Smith, CPCCheryl Lachman, CPCChiquita Hawkins, CPCChivon Pealer, CPCChristina Pencile, CPCClara Sehorn, CPC, COCClaudine A Allen, CPCContessa Washington, CPCCourtney Adriana Sims, CPCCynthia Herron, CPCD’Ondria McFadden, CPCDaena Pinchot, CPCDaisy Pereira, CPCDaljis Cardounel, CPCDavid Anderson, CPCDeana Brown, CPCDeepak Shanmugam, CPCDeshaun Mack, CPCDestiny Harvey, CPCDiane Zagorski, CPCDylan Weidlich, CPCEdilma Hayes, CPCElaine K Fiant, CPCElizabeth J Shaw, CPC, COCElizabeth Ludwig, CPC, COCEllie Alphin, CPC, COCEmily Franchini, CPCEmily Whelan, CPCEstella Borquez, CPCFatima Jorge, CPCFatmata Scott, CPCFree Hardaway, CPCGalina Roper, CPCHeather Reiter, CPCHelen Walter, CPCHongloan Nguyen, CPCJames Cotton, CPCJames Wright, CPCJamesetta Grandberry, CPCJamie Elizabeth Pitzer, CPC, CPMA,
CEMC, COCJamie Simmons, CPCJane Ross, CPCJanice Florio, CPCJasmine Ham, CPCJasmine Morales, CPCJeanine Wigfall, CPCJeff Yuettner, CPCJennifer A Tobben, CPC, COCJennifer Burianek, CPCJennifer H Im, CPCJennifer Lischinsky, CPCJennifer Wilson, CPCJessica Meece, CPCJessica Robinson, CPCJessica Valenzuela, CPCJill Holloway, CPCJill Marie Mahoney, CPCJillian Collins, CGIC, CPC
Joanna Abbott, CPCJobelle F Rosales-Tan , CPCJonna Summers, CPCJoseph Michael Brookes, CPCJudith Ann Beley, CPC, COCJulia A Divino, CPCJuliana Nolasco, CPCJulie Dubose, CPCKaren Burgess, CPCKaren Fisher-Ford, CPCKaren L Saenz, CPC, CRC, COCKasey Krabler, CPC, CPB, COCKatharina Domek, CPB, CPCKathleen M Heller, CPCKathleen Marie Duff, CPCKathy Thornton, CPCKavya Ramesh, CPCKea D Gaddis, CPCKelly L Rogers, CPC, CPMA, COCKelsey L Shiner, CPCKim Cripe, CEDC, CPCKim Sheffield, CPCKimberly Anne Dunn, CPCKira Swanson, CPC, COCKrashawna Marshall, CPCKrislynne Markey Schultz, CPCKuppusamy Subramaniyam, CPCLacey Rae Coleman, CPB, CPCLakeshia Wilson, CPCLatonia Dacanay, CPCLatoshia James, CPCLaureano Ajo Cortes, CRC, CPCLaurel Obermuller, CPC, CPMA,
CRC, COCLaurie Clancey, CPCLavonne Pettie, CPCLeeann Herman, CPCLeslie Coggsdale, CPCLillian Chotkowski, CPCLinda D Jones, CPCLinda E Montano, CPCLinda Harlan, CPCLinda M Williams, CPCLinda Vazquez Soto, CPCLisa Lopez, CPCLisa Marie Sarvis, CPCLisanne Sanchez, CPCLois Zebro, CPCLora L Oswald, CPCLoretta Ceneviva, CPCLori Bivins, CPCLutricia Brown, CPCLynette A Meyer, CPCLynnae Behrens, CPCMallorie Terry, CPCManogna Sree Ganapa, CPC, CPB,
COCMara Dukin, CPCMaria Rios, CPCMartha Ives, CPCMartha Klobucar, CPCMary M Loomis, CPC, COCMelanie Gomes, CPCMelanie Gwendoline Smith, CPCMelanie Papier, CPCMelissa Booms, CPC
Melissa Davis, CPCMichael Muerth, CPCMichele Flood, CPCMichele Pinto, CPCMichelle Thornton, CPCMichelle Vanderweele, CPCMigdalia Martinez, CEDC, CPCMitzi Degiacomo, CPCMohamed Atef, CPCMohamed Elkomy, CPCMonica E Garcia, CPCNakia Bolden, CPCNancy Williams, CPCNatalie Earnshaw, CPCNatasha Curry, CPCNikesha Yvonne McCoy, CPCOlivia Crouthamel, CPCPam Dougherty, CPCPamela Payne, CPCPamela Sue Ledoux, CPCRachel Gordon, CPCRachel Guerrero, CPCRebecca Eleftheriou, CPCRebecca Greenlaw, CPCRegina Lojpersberger, CPCRegina Park, CPC, CRC, COCSalini M, CPCSamantha Kraft, CPCSandra Gay, CPCSandy Arther, CPCSantilata Achari, CPCSara Steimel, CPCSarah Diamond, CPCSarah Elizabeth Waters, CPCSarah Kane, CPC, COCSean Gowers, CPCShakuwra Gay, CPCShanee Kinzer, CPCShanna Diane Hulsey, CPCShannon Marie Moore, CPCShaquana Lewis, CPCSharon Henstra, CPCShauna Chatman, CPCShawna L Phillips, CPC, COCSheila Purvis, CPCShelby R Rauls, CPCShelby Thomas, CPCShereen Walker, CPCSheryl Davis, CPCStacie Richey, CPB, CPCStephanie Alicia Muzzin, COC, CPCStephanie Cabral, CPCStephanie F Wilkerson, CPCSuryakala Modali, CPCSusan Ladner, CPCTalisha Dansby, CPCTamara Benefield, CPCTamara Bradford, CPCTamerria Jackson, CPB, CPCTammy Fields, CPCTammy Middleton, CPCTera Mendoza, CPCTeresa Townsend, CPCTiffany McKiddy-Reetz, CPCTina Messery, CPCTina Meyer, CPC

www.aapc.com May 2020 59
NEWLY CREDENTIALED MEMBERSNEWLY CREDENTIALED MEMBERSTina Scroggins, CPCTonya Chadwell, CPCTonya Wallace, CPCTori Cordova, CPCTrudi Holt, CPCValerie Jones, CPCVanessa Addicks, CPCVenkata Ramani Munipalle, CPCVictoria Novak, CPCVini Chawla, CPCVontresia Jackson, CPCWanda Allen, CPCYasmine Rose, CPCYokita T Gardiner, CPCYuvaraj Andamuthu, CPCYvette Lerma, CPCYvonne Hiter, CPC
ApprenticeApprenticeApprentice
April Joy L Kelly, CPC-AAaron Kane, CPC-AAbbey Dunkley, COC-AAbhijith G, CPC-AAbigail Rowe, CPC-AAbra Gilbert, CPC-AAbron Kelly, CPC-AAdarsh A, CPC-AAdinan Cholakkattil, CPC-AAdlin J J, CPC-AAdrian Ritter, CPC-AAdriana Walton, CPC-AAimee Michelle Lupo, CPC-AAiyuan Liu, CPC-AAkhila V, CPC-AAkshay Dambale, CPC-AAkshaya P, CPC-AAkula Uhasree, CPC-AAlanni Baldwin, CPC-AAlayna Eosze, CPC-AAlberto Rosario Jr, CPC-AAleena Anto, CPC-AAlena Gutierrez, CPC-AAlex Marvin Florendo, CPC-AAlfredo Ruiz, CPC-AAlgesh P R, CPC-AAlicia Oltz, CPC-AAlisha Hix, CPC-AAlison Rex, CPC-AAllison Herrmann, CPC-AAllison Westcott, CPC-AAmanda Beck, CPC-AAmanda Cooper, CPC-AAmanda Davis, CPC-AAmanda Dawn Spores, CPC-AAmanda Jose, CPC-AAmanda Kimball, COC-AAmanda Wright, CPC-AAmarnath P P, CPC-AAmber Woodliff, CPC-AAmber Dawn Lorensen, CPC-AAmber Flannery, CPC-AAmber Hammons, CPC-AAmber Henry, CPC-A
Amber Lynn Weber, CPC-AAmeena T K, CPC-AAmie Veater, CPC-AAmrutha A P, CPC-AAmrutha Surendran, CPC-AAmy Halliday, CPC-AAmy L Settle, CPC-AAmy Mossman, CPC-AAmy Tvorik, CPC-AAmy Wenzl, CPC-AAna Beatriz Criado, CPC-AAnanda Bhadra T, CPC-AAnbuselvi Arumugam, CPC-AAndrea Crouse, CPC-AAndrea Doyle, CPC-AAndrea Frew, CPC-AAndrea Glace, CPC-AAndrea Hreha, CPC-AAndrea Lassiter, CPC-AAndrea Lehman, CPC-AAneesa V, CPC-AAneeshma Rahman, CPC-AAneez Abdul, CPC-AAngela Fletcher, CPC-AAngela Goldthwaite, CPC-AAngela Hixon, CPC-AAngela Jahns, CPC-AAngela Lee, CPC-AAngela Schmidt, CPC-AAngelika L Bodie, CPC-AAngelina Chase, CPC-AAngie Dubisher, CPC-AAnita Dawn Hudson, CPC-AAnjali K V, CPC-AAnjana K M Babu, CPC-AAnju Kv, CPC-AAnn Imholte, CPC-AAnna Oliver, CPC-AAnna Warrington, CPC-AAnne Marie Haggerty, CPC-AAnnette Kramar, CPC-AAnnmaria Paul, CPC-AAnn-Marie Templeton, CPC-AAnoodha S, CPC-AAnushka Kaul, CPC-AAparna Anbu, CPC-AAparna P S, CPC-AApple Rose M Locloc, CPC-AApril Richardson, CPC-AAquila Toby, CPC-AArathi O, CPC-AArchana Kumari Kaushal, CPC-AArchana P, CPC-AArchi Carino, CPC-AArdelia Wright Johnson, CPC-AArdra P, CPC-AAron Battreall, CPC-AArunima P, CPC-AArya S, CPC-AAryalekshmi A S, CPC-AAsha Parveen Mohamed Anees,
CPC-AAshir K P, CPC-AAshitha P, CPC-AAshley Antoinette Bethea, CPC-AAshley Axon, CPB, CPC
Ashley Brown, CPC-AAshley Coury, CPC-AAshley Einsiedel, CPC-AAshley Hyde, CPC-AAshley Joseph, CPC-AAshley Mobley Doyle, CPC-AAshley Ramey, CPC-AAshley Reed, CPC-AAshley Sewing, CPC-AAshley Wilkie, CPC-AAshley Williams, CPC-AAshlyn Caputo, CPC-AAshvini Ghorpade, CPC-AAshwini Arumaikannu, CPC-AAshwini Pandit, CPC-AAslam E, CPC-AAubrianna Halley, CPC-AAutumn Myers, CPC-AAyana Santhosh, CPC-AAyesha Shaikh, CPC-ABader Issa, CPC-ABao Lee, CPC-ABarbara Michelle Perry, CPC-ABarbara Pomales, CPC-ABarrett Nakasone, CPC-ABeatrice Kearney, CPC-ABenjamin Coate, CPC-ABerdinell Tanetra Evans, CPC-ABeth Gibbs, CPC-ABeth Laper, CPC-ABeth Mims, CPC-ABetsy Pimblott, CPC-ABharathi D, CPC-ABhargavi K, CPC-ABhuvaneshwari Jagannathan, CPC-ABhuvaneshwari Mallika, CRC, CPCBincy Binoj, CPC-ABincy M J, CPC-ABlake Salyer, CPC-ABoobalan Thatchinamoorthy, CPC-ABoyini Praveen, CPC-ABrandee Casey, CPC-ABrandi Delao, CPC-ABrandie Cissell, CRC, CPCBreah Wasson, CPC-ABreanna Barker, CPC-ABreanna Bernard, CPC-ABreanna Burrough, CPC-ABrenda Kytle-Pfeifer, CPC-ABrianna Carter, CPC-ABrianna Featherly, CPC-ABrianna Young, CPC-ABrianne Hood, CPC-ABrindha Mani, CPC-ABrittany Jordan, CPC-ABrittany Paige Cress, CPC-ABrittany Salazar, CPC-ABrittany Whitehurst, CPC-ABrittany Wise, CPC-ABrooke McLoughlin, CPC-ABrunda Ramesh, CPC-ABryant Grace, CPC-ACaitlin Carden, CPC-ACandace Carswell, CPC-ACandace Cornelison, CPC-ACara Conroy, CPC-A
Carla Burgess, CPC-ACarla Joy Valencia, CPC-ACarlise Cranmer, CPC-ACarly Marie Sullivan, CPC-ACarmen Rosa Cruz, COC-ACarol Stubbs, CPC-ACarrie Walker, CPC-ACassandra Renee Foster, CPC-ACatherine Garduce, CPC-ACatherine Whitehead, CPC-ACecilia Rodgers, CPC-ACeleste Olds, CPC-AChaithanya Sivaraj, CPC-AChelsea Barbour, CPC-AChelsea Meehl, CPC-AChelsie Lee, CPC-ACheryl A Carroll, CPC-ACheryl Kurimski, CPC-ACheryll Trower, CPC-AChikkegowda H C, CPC-AChilmarie Tuca Tentativa, CPC-AChris Gilbert, CPC-AChristen Davis, CPC-AChristian Perez, CPC-AChristian Russell Russell, CPC-AChristie Bower, CPC-AChristina Chang, CPC-AChristina Bienick, CPC-AChristina Dionaldo, CPC-AChristina Waddicor, CPC-AChristina Webb, CPC-AChristine Deaton, CPC-AChristine Hrymack, CPC-AChristine Tacktill, CPC-AChristopher Grove, CPC-AChristopher Lee Serrano, CPC-AChristopher Walker, CPC-AChristy Arezzo, CPC-AChristy L Andrews, CPC-AChristy Varghese Chirayath, CPC-ACiera Golston, CPC-ACierra Lawler, CPC-ACindi Dickey, CPC-ACindy Kostner, CPC-ACindy Mendez, CPC-AClaryce Slaughter, CPC-AClaudia Pendergrass, CPC-AClintu K Tomy, CPC-AColeen Rae Juhl-Alexander, CPC-AConda Little, CPC-AConnie Muetzel, CPC-ACourtney Malpass, CPC-ACraig Helvie, CPC-ACrystal Silverira, CPC-ACynthia Simmons, CPC-ACynthia Hughes, CPC-ACynthia Jones, CPC-ACynthia Sepulveda, CPC-ADaerleth Dayoha, CPC-ADale Derby, CPC-ADana Elzie, CPC-ADana Millican, CPC-ADanielle Bloch, CPC-ADanielle Yerkey, CPC-ADaphne Kigler, CPC-ADarcey M Kotar, CPC-A
Darleen Kapana, CPC-ADavid Beebe, CPC-ADavid Johnson, CPC-ADeana Routson, CPC-ADeanna Houle, CPC-ADeanna Shae Weakland, CPC-ADebarati Mallick, CPC-ADeborah McWalters, CPC-ADeborah Padgett, CPC-ADebra Vischulis, CPC-ADelphia-Grace Anderson, CPC-ADemetrius Knight, CPC-ADena Rehkop, CPC-ADenise Crosby, CPC-ADenise Walker, CPC-ADevina Narayan, CPC-ADevon Smith, CPC-ADhananjay Panduru, CPC-ADhanu P Thampi, CPC-ADhanya S B, CPC-ADhivya Veeran, CPC-ADiamyn Rogers, CPC-ADiana Serafin-Molina, CPC-ADiana Carreno, CPC-ADiana Faye Pangilinan, CPC-ADiana Taylor, CPC-ADianne Rape, CPC-ADiany Feliz, CPC-ADipali Shekade, CPC-ADisha Bisht, CPC-ADivya Narayanan, CPC-ADominic Christopher Morse, CPC-ADonna Browning, CPC-ADonna Koziol, CPC-ADorothy Brown, CPC-A, CPB, CPMA,
CRC, COCJisha Unni A, CPC-ADwayne Malcolm, CPC-AEduina Legros, CPC-AEediga Roopa, CPC-AEkaterina Plotnikova, CPC-AElano Cunigan, CPC-AElijah Whitten, CPC-AElissa Vitagliano, CPC-AElizabeth Banks, CPC-AElizabeth Bashaw, CPC-AElizabeth Gomez Pereira, CPC-AElizabeth Margaret Lunder, CRC,
CPCElizabeth Stanley, CPC-AElleen Mae D Tirona , CPC-AElliott Good, CPPM, CPCEmery Taylor, CPC-AEmilee Coyle, CPC-AEmily Fisher, CPC-AEmily Reicholf, CPC-AEric J Washington, CPC-AErica Anne Arrighi, CPC-AErica Caldwell, CPC-AErica Hogan, CPC-AErica Mazzeo, CPC-AErica R Monsivais, CPC-AErika Goicochea, CPC-AErin Hurd, CPC-AErin Soto, CPC-AEsmeralda C Villanueva, CPC-A
60 Healthcare Business Monthly
NEWLY CREDENTIALED MEMBERSNEWLY CREDENTIALED MEMBERSEva Cortez, CPC-AEva Couto, CPC-AEvelyn Shirilla, CPC-AFabiola Goldbaum, CPC-AFarsana N, CPC-AFathima Henna, CPC-AFathima Jirsha, CPC-AFathima Sunila C, CPC-AFebie Lou Friend, CPC-AFidji Plaza, CPC-AFonya Chinn, CPC-AFrancesca Di Leo, CPC-AFrancisco Jay-P Abayari, CPC-AFredine Warnke, CPC-AFreya Brown, CPC-AGaines Carey, CPC-AGeethu Varghese, CPC-AGeorge Joseph, CPC-AGovarthani Palani, CPC-AGowri Arumugam, CPC-AGreeshma K J, CPC-AGriselis McKiernan, CPC-AGwendolyn Renee Rankins, CPC-AHaley Davis, CPC-AHallary Scheideman, CPC-AHallie Heffington, CPC-AHaneena P, CPC-AHannah Booth, CPC-AHannah Fritz, CPC-AHannah Lui, CPC-AHannah Roberts, CPC-AHannah Wyatt, CPC-AHao Nguyen, CPC-AHarini Muthu, CPC-AHariprasad Mani, CPC-AHariprasad Poojari, CPC-AHaripriya S, CPC-AHarish Kumar S R, CPC-AHazie Young, CPC-AHeather Wilborn, CPC-AHeidi Emmert, CPC-AHeidi Robertson, CPC-AHelen Beach, CPC-AHelen Langlois, CPC-AHelen Watts, CPC-AHiba Farhan Edamuttath Haris,
CPC-AHolly Shumway, CPC-AIgdaliah Chapman-Rogers, CPC-AIndya Brown, CPC-AIsrael Solorio, CPC-AIvette Velez, CPC-AIzamar Dorantes, CPC-AJaber Tocalo, CPC-AJackie Corcoran, CPC-AJaclyn Shirakata, CPB, CPCJacqueline Jackson, CPC-AJacqueline Siguenza, CPC-AJacquelyn Figueroa, CPC-AJacquline Bradley, CPC-AJahnice Taylor, CPC-AJalia Sinclair, CPC-AJamayce Yarde, CPC-AJamela Davis, CPC-AJames Willis, CPC-AJamie Farnsworth, CPC-A
Jamie Vickerman, CPC-AJamilah Rogers, CPC-AJanelle Robey, CPC-AJanice Rohlin, CPC-AJanika Bryant, CPC-AJaquelyn Sirias, CPC-AJasmine Narvaez, CPC-AJasna Saji, CPC-AJason Michael Bushell, CPC-AJasvir Sethi, CPC-AJavana Snowden, CPC-AJay Vanhuss, CPC-AJayasurya Kannan, CPC-AJayce Smith, CPC-AJazmaien Cruz, CPC-AJeevitha Gopish, CPC-AJeffrey R Sotelo , CPC-AJenalyn P Lapisac , CPC-AJenette Roxas, CPC-AJenna Einsig, CPC-AJennafer Gaventa, CPC-AJennifer Allen, CPC-AJennifer Brinkley, CPC-AJennifer Brown, CPC-AJennifer Bryant, CPC-AJennifer Fornicola, CPC-AJennifer Gladney, CPC-AJennifer Liphart, CPC-AJennifer Marlowe, CPC-AJennifer Patrick, CPC-AJennifer Silva, CPC-AJennifer Ventresca, CPC-AJenny Murphy, CPC-AJenny Unger, CPC-AJeralyn Carter, CPC-AJeremy Engebretson, CPC-AJesmy Susan Philip, CPC-AJesse Anderberg, CPC-AJessica De Jesus, CPC-AJessica Dalton, CPC-AJessica Deardeuff, CPC-AJessica Marquez, CPC-AJessica Nelson, CPC-AJessica Newsome, CPC-AJessica Priest, CPC-AJessica Reyes Corona, CPC-AJessica Riefer, CPC-AJill Howard, CPC-AJill Lavelle, CPC-AJo Sidhu, CPC-AJoann Hudson, CPC-AJoanne Marie Kissock, CPC-AJobin Chacko, CPC-AJohn Defere, CPC-AJohn Houskamp, CPC-AJohnson Ephraim Navalaperumal,
CPC-AJonathan Braceros, CPC-AJonathan Carlo Romans, CPC-AJoni Callis, CPC-AJonna Joy Torres, CPC-AJonnie Kay Anderson, CPC-AJordan Mathis, CPC-AJori Remington, CPC-AJose Quijano, CPC-AJoseph Rochet, CPC-A
Josephine Bowerman, CPC-AJuhi Das, CPC-AJulie Austin-Warthaw, CPC-AJulie Gutman, CPC-AJulie Hyde, CPC-AJulie Lund, CPC-AJulie Simpson, CPC-AJulie Word, CPC-A, COCJun Cao, CPC-AJustin Franke, CPC-AJustin Suen, CPC-AJustin Varghese, CPC-AJustine Guiliano, CPC-AKadambari Patel, CPC-AKalaiarasi V, CPC-AKandace Griffin, CPC-AKapil Bhuktar, CPC-AKara Ann Engelmore, CPC-AKaren Gabriel, CPC-AKaren Price, CPC-AKaren Stewart, CPC-AKari Byington, CPC-AKarla Nickles, CPC-AKarli Price, CPC-AKarneedi Satya Rama Chandra
Pavan, CPC-AKartik Somase, CPC-AKaruna Salunke, CPC-AKatherine Baptista, CPC-AKatherine Dalee, CPC-AKatherine Jack, CPC-AKatherine Kellum, CPC-AKatherine Mizerk, CPC-AKatherine Van Acker, CPC-AKathleen Crawford, CPC-AKathleen Lester, CPC-AKathleen Naqvi, CPC-AKathryn Godbout, CPC-AKathryn Keating, CPC-AKathy Bay, COC-AKathy Franco, CPC-AKatie Vandrew, CPC-AKatoya Winston, CPC-AKatrina Burnett, CPC-AKaustav Sanyal, CPC-AKavita Gaul, CPC-AKavitha Jayaraman, CPC-AKavya Jayanandan, CPC-AKayla B Hanshaw, CPC-AKayla Bessette, CPC-AKayla Dixon, CPC-AKayla Gruver, CPC-AKayla Thomas, CPC-AKaylee Evans, CPC-AKeerthana Muthukumar, CPC-AKelley Ann Traver, CPC-AKelli Norris, CPC-AKelly Ellis, CPC-AKelly Keith, CPC-AKelly Little, CPC-AKelly Lyons, CPC-AKelly Perron, CPC-AKelly Smith, CPC-AKelly Toter, CPC-AKenya Blake, CPC-AKerrie Grosenbeck, CRC, CPC
Keyleigh Shae Mullins, CPC-AKhaled Mohamed Mohamed Has-
sanein, CPC-AKia Jenkins, CPC-AKim C Germany, CPC-AKim Hasson, CPC-AKim Rayburn, CPC-AKimberly Romanchik, CPC-AKimberly Warp, CPC-AKineka Keyion Comeaux, CPC-AKomala N, CPC-AKonanki Dinesh, CPC-AKoreena Carpenter, CPC-AKourtney Gardner, CPC-AKourtney Sinor, CPC-AKrishnaveni Malakondiah, CPC-AKrista Weber, CPC-AKristen Armando, CPC-AKristen Kidd, CPC-AKristen Mills, CPC-AKristen Rago, CPC-AKristi Joles, CPC-AKristin Alyce Roberts, CPC-AKristin Stahel, CPC-AKwadwo Asiedu, CPC-AKyla Huchendorf, CPC-AKylee Kutcher, CPC-AKym Edelman, CPC-ALady Diana M Bulalacao, CPC-ALaissa Esquivel, CPC-ALakisha White, CPC-ALakshmi K S, CPC-ALakshmisree C S, CPC-ALana Dancy, CPC-ALarry Gambrell, CPC-ALatesha White, CPC-ALatoya Jones, CPC-ALatoya Mitchell, CPC-ALatoya Wright, CPC-ALaura Cartier, CPC-ALaura Eve Stinelli, CPC-ALaura Lane, CPC-ALaura Paquette, CPC-ALaura Reid, CPC-ALaura St Hilaire, CPC-ALaura Valeriano, CPB, CPCLauren Bethune, CPC-ALauren Bowles, CPC-ALauren Mackenzie, CPC-ALauren Sizemore, CPC-ALaurie Hocking, CPC-ALavanya Rudraraju, CPC-ALea Francisco Lusung, CPC-ALeah Cooper, CPC-ALeigha Giglio, CPC-ALelarae Murray, CPC-ALenore Reb, CPC-ALesa Bailey, CPB, CPCLeslie Hemric, CPC-ALillian Bueno, CPC-ALinda Glenn, CPC-ALinda Hallinan, CRC, CPCLinda Whitehead, CPC-ALindsey Darisse, CPC-ALindsey Jackson, CPC-ALindsey Kwasnik, CPC-A
Lindsey Meter, CPC-ALinh Lac, CPC-ALinnea A Johnson, CPC-ALisa Blevins, CPC-ALisa Dahlstrom, CPC-ALisa Hirsch, CPC-ALisa Kahl, CPC-ALisa Milanese, CPC-ALloyd K James, CPC-ALoganathan Selvaraj, CPC-ALori McDonough, CPC-ALori Renee Justice, CPC-ALorianna Roberts, CPC-ALuis Leyva, CPC-ALydia Green, CPC-ALydia Lassiter, CPC-ALyndse Downing, CPC-ALynette Dee Keith, CPC-ALynn Pense, CPC-ALynnette Annunziata, CPC-AM Carmelle Content, CPC-AMadhavi Velkuri, CPC-AMajanice Seals, CPC-AMamta Thakkar, CPC-AManda Sri Sai Srujini, CPC-AManeesh M S, CPC-AManisha Pattnaik, CPC-AManisha Tiwari, CPC-AManjima Thomas, CPC-AManjunatha S, CPC-AManojkumar Ganesan, CPC-AManuprasad S, CPC-AMari Siva Sankari N, CPC-AMaria Bennett, CPC-AMaria D Del Puerto, CPC-AMaria I Duran, CPC-AMaria Miller, CPC-AMaria Monte-O’Connor, CPC-AMaricruz Mecalco, CPC-AMarilyn Ortiz, CPC-AMarlene Camacho, CPC-AMarlo Merwin, CPC-AMarsha Williamson, CPC-AMarta Antoniuk, CPC-AMary Burkart, CPC-AMary Doss, CPC-AMary Grace M Daan , CPC-AMary Hannah Jones, CPC-AMary Masemore, CPC-AMary Young, CPC-AMaryann Lobianco, CPC-AMaryanna Harris Wilson, CPC-AMatt L Nice, CPC-AMatthew Endres, CPC-AMayra Calcanas, CPC-AMayuri Katkar, CPC-AMckenzie Doyle, CPC-AMeagan Coyle, CPC-AMegan Bownes, CPC-AMegan Burke, CPC-AMeghan Carlile, CPC-AMekha V Pillai, CPC-AMelanie Hager, CPC-AMelinda Sperandio, CPC-AMelissa Garcia, CPC-AMelissa Hansen, CPC-A
www.aapc.com May 2020 61
NEWLY CREDENTIALED MEMBERSNEWLY CREDENTIALED MEMBERSMelissa Kee, CPC-AMelissa Lopez, CPC-AMelissa Maybee, CPC-AMelissa Miller, CPC-AMelissa Pena, CPC-AMelissa Powers, CPC-AMelissa Thompson, CPC-AMelissa Zavorski, CPC-AMelody Craft, CPC-AMelyssa Ferguson, CPC-AMereena Xavier, CPC-AMiarocelle Crane, CPC-AMichael Lopez, CPC-AMichael Marsh, CPC-AMichael Worrell, CPC-AMichele Bradford, CPC-AMichelle Matkin, CPC-AMichelle Gonzalez, CPC-AMichelle Harrell, CPC-AMichelle Molen, CPC-AMichelle Perez, CPC-AMilena Bellettini, CPC-AMinah Lee, CPC-AMing Lin, CPC-AMiranda Brown, CPC-AMiryala Bhanuchandar, CPC-AMisheal Mathew, CPC-AMisty Baxter, CPC-AModesto Alejandro Carvajal Romero,
CPC-AMohamed Riaz, CPC-AMohammed Bilal T, CPC-AMohammed Mahroof A M, CPC-AMohammed Musthafa P, CPC-AMohammed Shahid, CPC-AMona Lisa Davis, CPC-AMonica Manley, CPC-AMonica Checo, CPC-AMonica Villamoran Soriano, CPC-AMonice Montague, CPC-AMonique Griffin, CPC-AMonique Rosenau, CPC-AMubarak K, CPC-AMuhammad Ravas Ck, CPC-AMuhammad Suhail N, CPC-AMuhammed Anas M S, CPC-AMuhammed Nahar, CPC-AMuhammed Rashid T A, CPC-AMuhammed Safvan V, CPC-AMuhammed Shibil T, CPC-AMuhsin Thangal K, CPC-AMundluri Haritha, CPC-AMurali S, CPC-AMusthahsina M P, CPC-AMyisha Thronson, CPC-ANadhiya Ap, CPC-ANancy Gunderman, CPC-ANancy Liebenguth, CPC-ANancy Manoj, CPC-ANancy Rivera, CPC-ANarendra Gaikwad, CPC-ANatalie Palmer, CPC-ANatasha Daniel, CPC-ANavya M, CPC-ANeeraja K, CPC-ANeeta Dhore, CPC-A
Neha Naik, CPC-ANick Mortel, CPC-ANicole Fletcher-Bell, CPC-ANicole L Ramsay, CPC-ANileshsingh Rajput, CPC-ANirmal Satheesh, CPC-ANivetha B, CPC-ANiyonnah Thompson, CPC-ANneka Williams, CPC-ANoemaris Lopez, CPC-ANora Wineland, CPC-ANurian Quintanilla, CPC-ANusrat Chaudhry, CPC-AOhini Kouanvih, CPC-AOlga Johnston, CPC-AOlivia Madorin, CPC-AOrissa Sanders, CPC-APa Kue Vang, CPC-APamela Kearney-Jones, CPC-APamela Keller, CPC-APamela Pettis, CPC-APamela Rosa, CPC-APamela Soles, CPC-AParvathy M, CPC-APatricia Branch, CPC-APatricia Brewer, CPC-APatricia Lynn Ripoll, CPC-APatrick Panetta, CPC-APatsy Poulton, CPC-APatti Burnette, CPC-APelita Gomez-Eusebio, CPC-APhilip Waters, CPC-APhuong Nguyen, CPC-APiyalee Dey, CPC-APonbalan M, CPC-APooja Gabhud, CPC-APooja Gaikwad, CPC-APooja Kale, CPC-APrachi Bansode, CPC-APradip Jangle, CPC-APrasanna B C, CPC-APrathibha Ram Sethuram, CPC-APraveena A, CPC-APrecious Braddy, CPC-APrem Sagar Sagar Fernandes,
CPC-APrinsha K P, CPC-APriscilla Head, CPC-APriscilla Rivera, CPC-APriya N, CPC-APuneeth K, CPC-AQuasheeda Tamika Mosley, CPC-ARachel Christman, CPC-ARachel Goett, CPC-ARachel Ray, CPC-ARachelle A Miller, CPC-ARachelle Stamper, CPC-ARanil Kottakkal, CPC-ARaquel Tabares, CPC-ARavina N Sharma, CPC-ARaychel Perry, CPC-AReanna Vicari, CPC-ARebecca Catherine Adams, CPC-ARebecca Duncan, CPC-ARebecca Hatton, CPC-ARebecca Honny, CPC-A
Rebecca Schultz, CPC-ARebekah M Roop, CPC-ARebekah Bush, CPC-ARebel Clarke, CPC-ARegina Selvam, CPC-ARegina Wall, CPC-ARena Emerson, CPC-ARenee Guerrero, CPC-ARenee Hoffer, CPC-AReneeta Sam, CPC-AReshma B, CPC-AReshma S, CPC-ARevanth R, CPC-ARevathi Subramanian, CPC-ARevathy Govintharaj, CPC-ARhianna Overton, CPC-ARhishikesh Kulkarni, CPC-ARhonda McConnell, CPC-ARhonda Wells, CPC-ARichard Buzon, CPC-ARichard Mezzacappa, CPC-ARiswana T N, CPC-ARiya Mariam Rajan, CPC-ARizza E Paguirigan , CPC-ARobbie Jenkins, CPC-ARobin Babu, CPC-ARobin Marie Gagne, CPC-ARocitta Paul, CPC-ARomy Mathew, CPC-ARonda Mae Lopez, CPC-ARosa Rodriguez, CPC-ARose Leroy, CPC-ARoselin Jeniffer J, CPC-ARosemary Jensen, CPC-ARubi J Gaytan, CPC-ARumshida M K, CPC-ARustamdeep Singh Baidwan,
CPC-ASabareesh M, CPC-ASabarinathan Perumal, CPC-ASabeena Sekeer, CPC-ASabrina Fields, CPC-A, COCSabrinah Baety, CPC-ASachin Jaybhaye, CPC-ASahab Raj, CPC-ASahana Venugopal, CPC-ASai Vandana, CPC-ASailaja Tippisetty, CPC-ASairaj S, CPC-ASalandra Moore, CPC-ASamah M Ali, CPC-ASamantha Schultz, CPC-ASamantha Zachmeyer, CPC-ASameera Chishti, CPC-ASandip Markad, CPC-ASandra Brown, CPC-ASandra Moore, CPC-ASangeetha Arumugam, CPC-ASangeetha Saju, CPC-ASara Jose, CPC-ASarah Carroll, CPC-ASarah Fawley, CPC-ASarah Kiselycznyk, CPC-ASarah Peduzzi, COC-ASarah Peeples, CPC-ASarah Randolph, CPC-A
Sarah Schmidt, CPC-ASaranya K, CPC-ASaraswathi Padavala, CPC-ASaravanan Manjappan, CPC-ASasikala Govindhan, CPC-ASathya S, CPC-ASeason Conrad, CPC-ASegan S, CPC-ASelina Ridge, CPC-AShabinar Kausar, CPC-AShahana A P, CPC-AShahla Labeeb, CPC-AShahla P E, CPC-AShaifil Vahora, CPC-AShaikh Mohammad Shoaib, CPC-AShaikh Shakil Shaikh Zahir Ahemad,
CPC-AShailja Pandey, CPC-AShameka Johnson, CPC-AShamini Barath, CPC-AShamnad Basheer, CPC-AShampa Rahman, CPC-A, CDEO,
CRC, COCShana Mcdaniel, CPC-AShaniece Brown, CPC-AShanise Martin, CPC-AShanna McClure, CPC-AShanna Williams, CPC-AShannalynn Campbell, CPC-AShannon Bonham, CPC-AShannon Epps, CPC-AShannon Hebert, CPC-AShannon Lucero, CPC-AShannon Rinehart, CPC-AShannon Tuise, CPC-ASharla Berry, CPC-ASharon Johnson, CPC-ASharon Mullins, CPC-ASharon Pv, CPC-ASharone Coleman, CPC-ASharri M Bauman, CPC-AShawn Meuer, CPC-AShawna Moorer, CPC-AShay Ann Paul, CPC-AShayla Havens, CPC-AShaylee Osterholt, CPC-ASheena A K, CPC-ASheena Trejo-Jimenez, CPC-ASheena Welch, CPC-ASheethal Es, CPC-ASheila Palmer, CPC-AShelby Jurewicz, CPC-AShelia Ogle, CPC-AShelley Clum-Murphy, CPC-ASherry Guevara, CPC-ASherry Lynn Belcher, CPC-AShilpa M Nair, CPC-AShourya Shekhar Sonune, CPC-AShruthi D C, CPC-AShruti Hadapad, CPC-ASidra Muntaha, CPC-ASija E K, CPC-ASilvia Lopez, CPC-ASimone Bryant, CPC-ASini Mol P V, CPC-ASkyler Nevins, CPC-A
Socorrito Claudio, CPC-ASona P, CPC-ASonali Bhople, CPC-ASonali Peiris, CPC-ASonali Suryawanshi, CPC-ASoninbayar Batbayar, CPC-ASoniya Baby, CPC-ASonumol Joseph, CPC-ASoumya Rani M, CPC-ASreejith N, CPC-ASreemol V R, CPC-ASreepadma P, CPC-ASreyamohan V, CPC-ASrinivasa Rao Piriya, CPC-ASrividhya R, CPC-ASruthi Surendran, CPC-AStacey Rhodes, CPC-AStacey Stoops, CPC-AStacie Longo, CPC-AStacy Halls, CPC-AStacy Robinson, CPC-AStefanie Fuller, CPC-ASteffi Ocon, CPC-AStephana Reid, CPC-AStephanie Groves, CPC-AStephanie Hattie, CPB, CPCStephanie Hood-Thompson, CRC,
CPCStephanie Mae Knaub, CPC-AStephanie Schauer, CPC-ASteven Otalvaro, CPC-AStormy Onken, CPC-ASuleidys Ortega Gonzalez, CRC,
CPCSunitha Katragadda, CPC-ASunitha Mallikarjuna, CPC-ASupanya Kumar, CPC-ASupriya Mondal, CPC-ASusan Crawford, CPC-ASusan Deandrea, CPC-ASusan Johnson, CPC-ASusan Kondra, CPC-ASusan Myddelton, CPC-ASusan Yancey, CPC-ASuzanne L Krug, CPC-ASwapna Buddharaju, CPC-ASwapna Jagdale, CPC-ASwati Waghmare, CPC-ASwetha Yarramsetti, CPC-ASyed Arshad, CPC-ASylvia A Hollingsworth, CPC-ATamara Palm, CPC-ATamika Climpson, CPC-ATammy Cochran, CPC-ATammy Elliott Heydari, CPC-ATara Dunn, CPC-ATara Hall, CPC-ATara Martus, CPC-ATara Williams, CPC-ATatjana Vasilic, CPC-ATaus Khan, CPC-ATaylor Clayton, CPC-ATeddi Neal, CPC-ATenisha Gachupin, CPC-ATeresa Harris, CPC-ATerina Marie Hodges, CPC-A
62 Healthcare Business Monthly
NEWLY CREDENTIALED MEMBERSNEWLY CREDENTIALED MEMBERSTessa Eckman, CPC-ATevin Jamel Lespinasse, CPC-AThaddeus Pyfrom, CPC-AThajunniza Ashraf, CPC-AThalia Morales, CPB, CPCThasleema Ukkash, CPC-AThasni Banu C, CPC-ATheresa Rogers, CPC-AThomas E Mueller, CPC-AThomas Grissom, CPC-AThouseef Mubashir C B, CPC-ATiera Gravely, CPC-ATiffani Frazier, CPC-ATiffany Johnson, CPC-ATiffany Mobilio, CPC-ATiffeny Monson, CPC-ATimios Cook, CPC-ATina Funk, CPC-ATina George C, CPC-ATobey Young, CPC-ATodd Hoffman, CPC-ATomeika Rice, CPC-ATonya Hawley, CPC-ATonya Platt, CPC-ATracey L Petzold, CPC-ATraci Pearson, CPC-ATracy Decillis, CPC-ATrevon Spikes, CPC-ATyanny Carrola, CPC-ATyesha Henry, CPC-ATyffany Wilkes, CPC-ATyler Kasper, CPC-AUfaira M A, CPC-AUma Pisal, CPC-AUmayal C, CPC-AValerie Perkins, CPC-AValorie Temples, CPC-A, CPB, COCVanessa Montoya, CPC-AVarsha Doifode, CPC-AVeena Shrivatsa, CPC-AVeronica Galvan, CPC-AVictoria Choquette, CPC-AVignesh Sivakumar, CPC-AVijaya K, CPC-AViktoriia Kozak, CPC-AVinodhini Dhanaraj, CPC-AVinodkumar Jaybhaye, CPC-AVinuja G, CPC-AViolet Tawadrous, CPC-AVirabala Patel, CPC-AVirginia Hay, CPC-AVirginia Jorden, CPC-AVishal Hake, CPC-AVishal Misal, CPC-AVishalakshmi Chakilam, CPC-AVishnu Babu, CPC-AVishwanath Mestha, CPC-AViswanathan K, CPC-AVivekananda Angadi Rudrappa,
CPC-AVrushika Khairnar, CPC-AWafa Chakkala, CPC-AWajid Bagwan, CPC-AWanda Bilello, CPC-AWendette Karlene Acreus, CPC-AWendi Young, CPC-A
Wendy Marie Walsh, CPC-AWendy Marshall, CPC-AWilliam Mosley, CPC-AWindy Truluck, CPC-AYacelin Vazquez, CPC-AYamiles Rosado, CPC-AYasmine Byrd, CPC-AYemiah Elizabeth Chandy, CPC-AYessenia L Dominguez, CPC-AYessika Reyes Estevez, CPC-AYogesh Subhash Swami, CPC-AYolanda Maldonado, CPC-AYuliya Kuibida, CPC-AYvette Perry, CPC-AZachary Robert Treweek, CPC-A
SpecialtiesSpecialtiesSpecialtiesAbelardo Abreu, CPC, CRCAdam McKnight, CPC, CEMC, CPMAAddie Kimball, CPC, CPBAdenike Busari-Salau, CPC, CPMAAjay Suryawanshi, CEDCAjay Yarra, CEDCAlena Byrd, CPC, CPMAAlexandra Martin, CRCAlexandria Nicol Rivera, CPC, CRCAlexis Zacher, CPC, CEMCAlicia A Lehman, CPC, CPPMAlisa McCullough, CPC, CPMAAlissa Lawrence, CPC, CRCAllyn M Smith, CPC, CRCAmanda Belcher, CIRCCAmanda Clifton, CPC, CRCAmanda J Lugo, CPC-A, CRCAmanda Kay Shaffer, CPC,, CUCAmar Kandesar, CEDCAmauris M Valera Sales, CRC, CPMAAmber Cragun, CPC, CPBAmber D Ruckle, CPC, CEMCAmin Mequita, CPC, CRCAmy Corkins, CPC, CRC, CPMAAndrea Arnzen, COC, CPC, CPMA,
CEDC, CEMC, CRCAndrea Brager, CPMAAndrea Devon Hicks, CPC, CRCAndrea Fleck, CPC-A, CANPCAndrea Joy Steeves, CPBAndrea Nicole Wolfe, CPC, CGSCAngela Frances Hazel, CPBAngela Karhu, CIRCCAngela Randolph, CCCAnnapoorani Srinivasan, CPBAntoinette Gutierrez, CPC-A, COPCAnuja Sabharwal, CPC, CPBArlene Valente, COC, CPC, CDEO,
CIC, CPMA, CRCAshlee Couillard, CPC-A, CFPC,
CEMCAshley Richard, CPBAshton Lange, CPC-A, CRCAudra P Swafford, CPC, CRC, CDEOAudrey Anderson, CPC, CPMAAudrey Naifeh, CPB
Barbara A Amato, CPC, CPCOBarbara A Bell, CPC, CPMA, CFPC,
CRCBarbara Ann Myers, CPC, CPB,
CGSC, CANPCBarbara Maria Shaw, CPC, CRC,
CEDCBarbara N Miles, CPC, CDEOBarbara Parsons, CPC, CPPMBeatrice Clark, CPBBeckie Jo Walden, CPC, CCC,
CCVTC, CDEOBertha Milton, CPC, CPMA, CRCBhavna Desai, CPC, CPMABianca Howard, CPC, CRCBrenda K Edwards, CPC, CDEO,
CPC-I, CEMC, CEDCBrenda Watkins, CPC, CPBBrian Hackman, CRCBriana Ickowicz, CPC, CPCOBrittany Marks, CPC-A, CRCBrittany Smith, CPBCandice Kay Mcintosh, CPC, CPBCara Kromer, CPC, CEMCCarlos Llanes Alvarez, CRC, CPMACarmelita Harley, CPC, CPMACarmella Adell Camacho, CRC,
CPMACarra Benson, CPC, CPMA, CDEOCassi Nelson, CPBCatherine Bishai, CPC, CDEO,
CRC, CPBCatherine Gray, CPC, CCCCatherine Radford, CPC, CRCCathy Spinelli, CPC, CPMACesar F Delgado, CRCChakrapani Behara, CEDCChala Riddick, CRCCharisse Greene, COC, CRC, CDEOCharity Tracey, CPC, CRC, CDEOChatoya Dudley, CPC, CGSCChengxia Zhai, CPBChereese Chao, CPC, COSCCheryl Scarbro, CPC, CPB, CPCOChristina Anne Morrell, CPC-A, CPBChristina Hunt, CPC, CPBChristina Sorem, CPC, COSCChristine Jacela, CPC, CRCChristine Jang, CPC, CEDCChristy Ly, CPC-A, CPMAColleen Moreland, CRCCoral Towers, CPC, CEDC, CRCCrystal Tompkins, CPC, CRC,
COBGC, CPMACynthia Acosta, CPC-A, CRCCynthia Blazys, CPC, CPMACynthia Ferrier, CIRCCDamaisy Diaz, CPC, CRCDavid Munoz, COC, CPC, CDEO,
CEMC, CPMADavid Zetterman, CPC-A, CPPM,
CEMC, CFPC, CPCODawn Herrington, CPC, CEMC, CRCDawnya Hostetler, CPC, CRCDeborah Bencsis, CRCDecola Knight, CPC, CRC
Delnita Cruz Kennedy, CPC-A, CRCDiana Mitchell, CPPMDiane Elizabeth Sanders, CPC, CPMADodie A Berg, CPC, CDEODominic Nemeth, CPC, CPMADominique Zapata, CPC, CPMA,
CRC, CDEODonna Herchenroeder, CPMADonna Jones, CPBDonna Marie Gonzalez, CPC, CRCDovile Lapaitiene, CEMCDylan Macalinao, CPBEbony Stinson, CPC, CPMA, CRC,
CPCOEglis Tomas Carralero, CRC, CPMAElda Linezo, CPC-A, CEMC, CPMAElizabeth Alia, CPC, CRCElizabeth Barnett, CPC-A, CPBElizabeth Larue, CPC-A, CPBElizabeth Velazquez Zaldivar, CPC-A,
CRC, CPMAElizabeth Wade Hankins, CPC,
CPMA, CPC-I, CRCEllise Harvey, CPC-A, CPMAElvia Ann Ramos, COBGCEmily Marinaro, CPC, CPB, CEMCEnrique Limon, CPBErika Currier, CPC-A, CPBErika Swigert Phelps, CPC, CHONCErin Bame, CRCErin Langenderfer, CPPMFaith Momodu, CPC, CPCOFarah Handley, CPC, CRC, CDEOFrancine Baheneka, CPC-A, CRCGamal Lawrence, CPCOGauri Mathi, CRC, CPPMGayle Riley, CPBGina Alias, CPC, CPBGina Emmenegger, CPC, CPCO,
CPMA, CPC-I, CEMC, CGSC, CHONC, CUC
Gina Leonardis, CPC-A, CRCGinger C Lamore, CPC, CRCGinger Kay Walden, CPC, CRC,
CPMAHannah Nash, CPC, CPBHaris Pervaiz, CRCHeather Roberts, CANPCHeather Thacker, CFPCHolly Cebina, CPBHolly May, COC, CPC, CIRCC, CCCIvonne Atanacio, CPC, CPB, CPMA,
CPC-I, CRCIvy Clark, CPC, CRCJacalyn Fort, CPC, CRCJacqueline Lehman, CPC, CGSCJamie Ewing, COC-A, CICJamie Smith, CPMAJammie Quimby, CPC, CPMA, CRC,
CCC, CEMC, CDEOJana Hammam, CPBJanice L Emerson, CPC, COSCJanice Willis-Gillam, CPC, CGSC,
CRCJanis Snyder, CPC, CCC, CCVTCJayraldine Ann Yuson, CPMA
Jeanne Carol Tinari, CPC, CPMAJeanne Muller, CPC, CRCJeannette Perez, CRCJeannie Marie Mosinski, CPC, CRCJeneen King, CPC, CCC, CCVTCJennifer Brown, COSCJennifer Dompier, CPC, CANPCJennifer Francis, CPC, CPBJennifer G Johannes, CRCJennifer Goodman, CPC, CRC,
CDEOJennifer Heiser, CPC, CGIC, CGSCJennifer Koppen, CPC-A, CRCJennifer L Hohensee, CPC, CPMAJennifer Latva, COC, CPC, CDEO,
CGSC, CPMAJennifer McNamara, CPC, CPC-I,
CGSC, COPC, CRCJennifer Rogers, CPC, CPMAJennifer Woodworth, CPC, COBGCJenny Elizabeth Benoit, CPC,
CEMCJenny Russett, CPC, CEMCJessica A Aspengren, CPC, CGSCJessica Erin Blake, CPBJessica Kelley, CPC, CPMA, CRC,
CPCD, CEMCJessica Oldenburg, CPPMJessica Shaw, CPC, COSCJessica Silverman, CPC, CEMCJill Castro, CPBJill Flora, CRCJohn Carlo Moreno, CPC, CPBJohn Piaskowski, CPC, CPMA,
CRC, CCC, CCVTC, CGIC, CGSC, COSC, CUC, CIRCC
John Tomas, CRCJoie McFerran, CPC-A, CRCJordan Regan White, CPC, CHONC,
COBGCJoy Otibhor Igberaese, CPC, CRC,
CPMAJudith Gay Hoeykens, COC, CPC,
CRCJudith Wade-Bradley, CPPMJulie Otten, CPC, CPMA, CPCOJulie Roberts, CPC, CPMA, CPCOJulie Sharar, COC, CPC, CRCJulio C Paque Pena, CPC, CPMA,
CRCKaren Galik, CPBKaren Morris, CPC, CRCKarina Felizola, CRCKarl Krumbach, CPC, CRCKathlean Downing, CPC, CDEO,
CEMCKathleen Hernandez, CPBKathleen Rowland, CPBKathryn Nicole Kolyer, CPC-A, CRCKathy Tringali, CPC, CPBKatrina Renee Benton, CPC-A, CPBKay Tracy, CPC, CPMAKayla Kennedy, CRCKeicia Tamara Cornwall, COC, CPC,
CPC-P, CPMA, CRC, CDEOKeith Portillo, CPMA, CPEDC
www.aapc.com May 2020 63
NEWLY CREDENTIALED MEMBERSNEWLY CREDENTIALED MEMBERSKelly Ausiello, CPC, CPMAKelly J White, CPC, CPMAKellye Torres, CPBKendra R Thomas, CPC, CPMAKenneth Rosenstock, CPC, CPMAKerry Lynnette Free, CPC, CPEDCKevin Ward, CPC, CPMAKimberly Crews Jones, CPC, CPPMKimberly M Jolivette Williams,
CPC, CPMA, CPC-I, CCC, CEMC, CANPC
Kimberly S Ingamells, CPC, CEMC, CRC
Kimberly Shaw, CPBKimberly Staten, COC, CPC, COSC,
CPBKimberly Watson, CPC, CEMC,
COSC, CPMAKimyla R Lyons, CPC, CPMAKinsey Tickell, CPCOKrista Vannostrand, CPC, CRCKristen M Jimenez, CPB, CPMAKristen Nelson, CGICKristi Williamson, CPC, COBGC,
CANPCKristin Lyles, CPBKristy O’Bryan, CIRCC, CRCKrupa Raval, CPC, CRCLachelle Richmond, CPC, CRCLaquita Evans, COC-A, CPC-A, CRCLartica W Duze, CPC, CRCLatasha L Cannon, CPC, CPC-I, CRCLatoya ThomasJones, CPBLaura Kivlehan, CPBLaura Vitelli, CPC, CPMALauren Arnold, CPC, CRCLaurie Carey, CRCLaurie Crossman, CRCLaurie Weyerstrass, CPC, CPMALeslie A Reece, CPC, CPCOLeslie Marie Pou, CPC, CPCO,
CPMA, CRC, CEMC, CFPC, CPPM
Leslie Morris, CPC, CRC, CPMALiesa Kyer, CPPMLilia Echavarria, CRCLilybeth Alattica, CPC, CRC, CPMALindsey Bernardini, COPCLisa De Jong, CPC-A, CPBLisa Erban, CPC, CRCLisa G Bishop, CPC, CRCLisa Ng, CPBLisa S Freeman, CPC, CRCLisandry Rodriguez, CPBLora Dawn Duffy, CPC, CASCCLorraine Ann Hayward, CPC, CRC,
CPPMLovina Farden, COC, CPC, CPPMLtanya Jenkins, COC, CPC, CRCLucero Aguayo, CPC, CRCLucica Larion, CPC, COPC, CPMALucy Alejandra Baldelomar, CPC,
CPMA, CPPM, CRCLuis Julio, CPC, CRCLynn Ann Hare-Felker, CPC, CPPMMadison Washington, CPC-A, CPCD
Mae Huffman-Mote, CPPMMaegan Langer, CPC, COBGCMargaret K Ucella, CPC, CIRCCMargarita Lamazares, CPC, CRCMaria Sabrina Mariano, CPC,
COBGCMarlys Boyer, CPC, CGSCMary Kreider, CPPMMary Krieger, CRHCMary McDonald, CPC, CPPMMarybeth Gatton Horne, CPC, CCC,
CPMAMary-Jo Griffith, COC, CPC, CDEO,
CPMA, CPC-I, CASCC, CCVTC, CEMC, CGIC, CGSC, COSC, CANPC
Matthew Gramlich, CPPMMatthew Schweyer, CPCOMedina Colon, CPC, CPB, CRC,
CCCMegan Herrick, CPC, CPB, CHONCMeghan Bull, COC, CEDC, CRCMelinda Bartley, CPC, CCCMelinda D Willis, CPC, CEMCMelisa R Sallad, CPC, CPCOMelissa Ann Montgomery, CPC,
CPCDMelissa Breedlove, CPBMelissa Dethlefs, CPC, COSC,
CPPMMelissa J Aponte, CPC, CPC-P,
CPMAMelissa K Hoff, CPC, CPMA, CRC,
CEMC, CASCCMelissa L Kulavic, CPC, CPMA,
CRCMelody Powers, CPC, CPMA, CCC,
CRCMelonee Lorraine Cain, CPC, CRCMessena Smude, COC, CPC,
CASCCMichele Attaway-Caputo, CCCMichele Werner, CPC, CDEOMichelle Galloway, CPC-A, CRCMichelle Irene Holt-Jarmacz, CPC,
CPC-I, CDEOMichelle Lambert, CPC, CPCOMichelle Leigh Morris, CPBMichelle Martin, CGIC, CPBMichelle Riggleman, CPC, CRCMichelle Safi, CPC, CRCMike Carson, CIRCCMisty Clark, CPC, CRCMonaf Shaban, CPPMMonica Andrews Morrow, CPC,
CEMCMonica Marthell, CPPMMor Xiong, CPC-A, CRCNancy Grandmaison, COSC,
CPEDCNancy L Healy, CPC, CPCO,
CENTC, COBGC, CASCCNancy McKissick, CRCNancy Rial, CRCNataliia Moore, COC-A, CPC-A,
CPCO, CPB, CPMA, CRC, CANPC, CCC, CHONC, CPPM
Nayla Cruz, CRCNeera Vashisht, CPC, CPCONgan-Ha Pham, CRCNicole M Dockter, CPC, CPPMNicole Mendizabal, CPC, CEMC,
CRCNora Sanders, CPC, COSCNorah Al-Hussaini, CPC, CPPM,
COBGC, CPMAOlga Del Rosario Sanchez Garcia, CRCOlivia Wyles, COC-A, CPC-A, CRC,
CPMAOwen Owens, CPB, CPCOPakita Mobley, CPC-A, CPMAPamela Clark, CPMAPamela J Girkins, CPC, CEMCPat Blevins, CPC, CPCO, CRCPatricia G Carrow, COC, CPC, CRCPatricia Paparella, CPC, CPMAPerla Lopez, CPC, CRCPetal Brusch, CPC, CPMAPradnya Bal, COC, CRC, CDEOPriyanka Kharat, CEDCQuinsana Latrell Grier, CPC, CRCRachel Holdaway, CPC, CPMARachel Maki, CPC-A, CRCRani Thomas Cholankeril, CPC-A,
CHONCRebecca A Patrick, CPC, CRCRebecca Burges, CPC, CPMARebecca Teel, CIRCCRebecca Woodhams, CPC, CPB, CRCReetuparna Dutta, CPCORegina Ann Thomas, CPC, CIRCC,
CGSC, CRCRegina King, CPC, CPMARene Maxey, CPC, CRCRhonda Brown, CPPMRichard Banez, CPBRob Jones, CEMCRobbin Lloyd, CPC, CPMARobin Carle, CPC, CPMA, CRCRobyn Anderson, CPC, CPB, CPCORonda Rene Dixon, COC, CPC,
CRC, CPMARonntriesse Cope, CPC, CRCRosemarie S Garcia, CPBRosemary Weilemann, CPC-A, CPB,
COBGCRosezella Kindall, CPC, CPMA,
CDEORossana Velasco Contreras, CPC,
CRCRoxana Izadi, CPC, CRCSamantha Hale, CPC-A, CPBSamantha Kern, CPBSandra Martin, CPC, CRCSandra Patricia Velasquez, COC,
CPC, CEMCSandra Steele, CRCSara F Diblasio, CPC, CRCSara Nebeker, CPC, CRCSarah Tran, CPCDSarita Ratanaram Chaudhary, CPC,
CEMCSattie Jugmohan, CPC, CRC
Selina Yguerabide, CPC, CEMCSerah Nganga, CPC, CRCShamell L Hambrick, COC, CGSC,
CRCShankar Swaminathan, CPC, CRC,
CPMAShannon Cutting, CPC, CPMAShannon Van Nortwick, CPBSharon A Smith, CEMCShawnna Delores Cullins, COC, CRCSheila Rodriguez, CPC, CRC, CCC,
CEMC, CPMASheri Harwood, CPC, CPMASheri Henderson, COC, CPC,
CPMA, CRCSherrene Mason, CRCSherri Marzola, CPC, CEMCSherri Wilson, CPBSherry Sroka, COC, CPC, CPMAShimaila Ahmed, CRCSmith Pulido, CPBSonia Brundige, CPC-A, CPBSonia Karth, CPC, CPMA, CDEOStacey Thomas, CPC, CPCO, CPBStaci Henry, CPC, CFPCStacy Weigandt, CANPCStephanie A White, CPC, CEDCStephanie Alfano, CPCDStephanie Lynn Jones, CPC, CGSC,
CPMASurendra Kashyap, CEDCSusan Egan, CPC, CPMA, CRC,
CEDCSusan Ellen Marr, COC, CPC,
COBGCSusan M Burgess, CPC, CFPCSusan Ouellette, CPC, CPMA,
CDEOSvetlana Kirshteyn, CRCTabitha Ramey Nesta, CPC,
CPEDCTamara Cole, CRCTamara Haeberle, CPC, CRCTanuja Devi Kodali, CPC, CPMA, CRCTasha Bell, CPC-A, CPMATasia Powers, CPPMTawanaka Torres, CPC, CEDCTeresa Ellis, CPC-A, CRCTeresa Tart Duncan, CPC, CDEO, CRCTiffaney Green, CPC, CRCToni Nicole Robinson, COC, CPC,
CDEO, CPMA, CRC, CEDC, CEMC, CPEDC, COBGC
Traci Mahaffey Horst, CPC, CPMA, CRC, CPCO
Traci R Mifsud, CPC, CPPM, CEDCTracy Rangel, CPC, CEMCVanessa Perius, CICVenus D Davis, CPBVeronica Vendetti, CPC, CEMCVictor Fernández Santiesteban,
CRC, CPMAVictoria Bolick, CPC, CPMAVivian Ruczynski, CPC, CPMAVontresa L Moses, COC, CPC,
CPMA, CPC-I, CASCC
Wanda Maxwell, CPMAWendi Gillard, CPCOWendy K Soergel, CPC-A, CPBWendy L Lacey, CPC, CDEOWilma Groover, CPC, CEDCYamile Mulet Velazquez, CRC, CPMAYarelys Rodriguez Alberto, CPC,
CRC, CPMAYoanna Aguila, CPC, CRCYolanda Harris, CRCYolanda Maye, CRCYvette Richardson, CPC, CRCZydrune Bartkute, CEMC
Current and Comprehensive
- The book
MEDicalABBREViations:
55,000Conveniences atthe Expense of
Communitication & Safety (16th Edition)
Author: Neil M Davis
The 2020 edition has 20,000 new entries
Book price includes a 1-year, single-user access to the Medabbrev.com website, a $20 value.
Discounted price to members, on
AAPC.comor order from
Medabbrev.com
Updated daily
Find the meaning of an abbreviation in milliseconds
If requested, we will search for the meaning of an abbreviation not listed

64 Healthcare Business Monthly
■ CODER’S VOICEBy Valerie Fernandez, PhD, MBA, RHIA, CPC, COC, CPMA, CRC, CCS
The Joint Commission is providing a national focus on zero harm. To that end, from a clinical perspective, The Joint Commission is
collaborating with institutions to take a path toward zero falls, zero complications, zero infections, and zero lost revenue. That is zero harm of any kind. This initiative is possible when everyone works together — not only clinicians but business staff, as well.
What can organizations do to make healthcare harm a thing of the past? The Joint Commission’s Leading the Way to Zero™ initiative advises that they:
1. Ensure leadership is committed to a goal of zero harm.2. Develop and adopt a safety culture.3. Incorporate process improvement tools and methodologies
in their work.4. Demonstrate how everyone is accountable for safety and
quality.
Healthcare business professionals have an essential role in their organization’s goal of zero harm to ensure zero lost revenue.
Set the Tone at ReceptionEnsuring that the correct demographics are captured as patients enter the health system is imperative. Reviewing insurance and updating information as needed is an important aspect of ensuring the claim is submitted to the correct carrier so revenue can be collected. Assessing service requirements related to prior authorization and notifying the insurance company of any planned procedures offers an opportunity for setting expectations with the carrier.
Making a follow-up call to alert the carrier of any change to the anticipated procedure after the final operative report is made available can expedite claim processing. If a service is not covered by the insurance carrier, educating the patient about the procedure, alternatives, and the expense related to the proposed procedure will enable the patient to make an informed decision about how to proceed.
Remember: The patient must sign an Advance Beneficiary Notice of Noncoverage (ABN) form if they choose to have a procedure that is not covered under their insurance. This form must be completed prior to rendering the service or you cannot bill the patient for the service.
Fast-Track Providers’ EnrollmentAs new providers enter the health system, ensuring prompt enrollment with the various payers enables them to bill for their services. Decisions regarding enrolling nurse practitioners, physician
assistants, and registered dieticians with insurance carriers must be made to capture all potential revenue sources.
Ensure Correct Coding for Quality DataMedical coders must ensure comprehensive documentation is avail-able and should query the provider if clarification is needed. These measures will enable coders to submit all relevant diagnosis and procedure codes at the highest level of specificity. It’s important for coders to adhere to local and national coverage determinations and the various system edits in use. Ongoing training will ensure adherence to the most up-to-date guidelines.
Commit to Zero HarmImagine a future of zero harm in healthcare. It starts here, and now.

www.aapc.com May 2020 65
Commit to Zero
Streamline Billing Processes for Timely PaymentMedical billers are instrumental in reducing the amount of patient financial responsibility and preventing surprise billing. Work queues are established for candidates for bills that have edits preventing a final claim submission. It’s important for both coders and billers to review accounts in these work queues, make necessary updates, and to release claims timely.
Educating staff for improved data entry, from registration to coding, will reduce the work queue volume. Another aspect of work queue review includes critically assessing recurring edits that may require a system build to prevent repopulating the work queue. Optimizing the electronic medical record by establishing
rules for various work queues diminishes edits that may delay claim submission.
If a claim is denied, a thorough review of the encounter, including all documentation, will ensure claim updates are made timely and appeals are submitted with supporting documentation. This is a time to determine trends and assess opportunities for improvement to reduce or minimize recurrence.
Put Customer Service FirstCustomer service is imperative at all levels of the revenue cycle. Interactions with providers and collaboration within and across teams ensures the focus is on timely reimbursement and reducing patient financial responsibility.
Take Time to ReviewQuality reviews ensure compliance with guidelines, offer an op-portunity for education, and are a venue for collaboration related to process and policy across teams.
We can all commit to zero. With an objective to protect the patient and improve interaction with our colleagues through accountability for process improvement, we can’t go wrong.
For more information about The Joint Commission’s Leading the Way to Zero™ initiative, go to www.jointcommission.org/performance-improvement/joint-commission/leading-the-way-to-zero.
Valerie Fernandez, PhD, MBA, RHIA, CPC, COC, CPMA, CRC, CCS, is an ICD-10-CM and ICD-10-PCS trainer with over 20 years of progressive healthcare management experience. She is the coding integrity manager at Duke Health and an active member of several professional societies including AAPC, AHIMA, and HFMA.
“As patients enter the health system, ensuring that the correct demographics
are captured is imperative.”
shutterstock / michaeljung
66 Healthcare Business Monthly
Minute With a Member
Sonal Patel, CPMA, CPC, CMC
Tell us a little about how you got into cod-ing, what you have done during your coding career, and where you work now.I spent the first part of my working life as an art historian, with a specialty in South Asian art history, working in museums such as the Smithsonian in Washington, D.C., and the Peabody Essex in Boston. When the market tanked in 2008, life happened, and I decided to invest in my future in a more secure profession.
I attended Kaplan University and re-ceived my medical coding certificate. From there, I got my first job in the accounts/receivables department at a large medical billing company. I had tremendous suc-cess in collecting on aging claims with my appeals and gained my own multispecialty provider accounts.
After some years passed, I wanted to experience the hospital side of coding. I got that break and learned so much about hos-pital technical systems. I mastered ICD-10, the hospital underwent a huge crossover to Epic, and I obtained two AAPC credentials.
I am now a healthcare coder and com-pliance consultant at Nexsen Pruet LLC, a multispecialty business law firm with offices in both North Carolina and South Carolina. I work remotely for the healthcare reimbursement division in Charleston and the healthcare practice group in Columbia.
My primary role is to support the health-care and litigation attorneys in their defense strategies of mitigating risk and damages for both providers and healthcare systems. My coding acumen in all medical special-ties, reimbursement knowledge for both value-based and fee-for-service programs, and strong research and exceptional writing skills allow me to develop corrective action plans, compliance plans, and educational presentations for individual providers. I have a lot of experience with fraud, waste, and abuse in whistleblower and False Claims Act cases and recovery audits that need my auditing skills to assist the attorneys on client defense.
What AAPC benefits do you like the most?What’s not to like? From the Knowledge Center to Healthcare Business Monthly to the certification classes and study guides, and all the coding books you could dream of — all of these items help keep me armed with necessary resources to perform my job with integrity.
How has your certification helped you?My AAPC credentials have allowed me to establish and maintain credibility. When I am speaking with providers of any type, of any specialty, I am confident in what I am presenting to them.
Do you have any advice for those new to coding and/or those looking for jobs in the field?I am very sorry in advance, but this is some tough-love advice: Apply to entry-level positions. Do not dishearten yourself by
applying to anything above that paygrade. Stop believing you can work remotely on your first coding job — all of those advertisements are false and keep you from getting out there and networking. Try a records department, a billing company, or a small doctor’s office answering phones and verifying benefits. These skills are critical elements to the revenue cycle and patient satisfaction. Stay humble, because it is about getting your foot in the door to gain experience. With experience, you can pivot and start applying for the next role.
What has been your biggest challenge as a coder?I did not have a mentor or wise sage helping me along my way in coding. I promised myself I would always help another when they reached out and asked for it. I have given so many students advice and guid-ance, encouragement, and ways to find success. I contribute to Healthcare Business Monthly and the Knowledge Center and I actively post on LinkedIn.
If you could do any other job, what would it be?If I dare to dream, it would be as editor of some fabulous publishing house or magazine with full travel and the ability to perform that job anywhere.
How do you spend your spare time? Tell us about your hobbies, family, etc.In just two more years, I will have a high school graduate ready to start his next stage in life — college! When my hands are not full with his sports, I am traveling to see out-of-town friends and family, attending art shows or gallery openings, reading the latest best-list books (especially mystery, murder, crime), picking up the old pastels or paintbrush, and just feeling gratitude. GOT A MINUTE?
If you are an AAPC member who strives to advance in the business of healthcare, we want to know about it! Please submit your answers to the above questions to [email protected].
AAPC Certificates
Learn more ataapc.com/newtraining
• Home Health Coding
• Skilled Nursing Facility Coding
• EMR/EHR Training
• Advanced Neurology and Neurosurgery Coding
• Physical Medicine and Rehabilitation Coding
NEWADVANCEDCERTIFICATECOURSESWITH AAPC.
AAPC B2B
Optimize your revenue cycle today.
Streamline your revenue cycle with our complete business solution platform. From customized training to audit services and everything in between, we have what you need to stay ahead.
https://www.aapc.com/business/Call today for a free consultation: 844-825-1679




















