
A time-lagged momentary assessment study on daily life physical activity and affect
11
Health Psychology A Time-Lagged Momentary Assessment Study on Daily Life Physical Activity and Affect Marieke Wichers, Frenk Peeters, Bart P. F. Rutten, Nele Jacobs, Catherine Derom, Evert Thiery, Philippe Delespaul, and Jim van Os Online First Publication, October 10, 2011. doi: 10.1037/a0025688 CITATION Wichers, M., Peeters, F., Rutten, B. P. F., Jacobs, N., Derom, C., Thiery, E., Delespaul, P., & van Os, J. (2011, October 10). A Time-Lagged Momentary Assessment Study on Daily Life Physical Activity and Affect. Health Psychology. Advance online publication. doi: 10.1037/a0025688
Transcript of A time-lagged momentary assessment study on daily life physical activity and affect
Health Psychology
A Time-Lagged Momentary Assessment Study on DailyLife Physical Activity and AffectMarieke Wichers, Frenk Peeters, Bart P. F. Rutten, Nele Jacobs, Catherine Derom, EvertThiery, Philippe Delespaul, and Jim van OsOnline First Publication, October 10, 2011. doi: 10.1037/a0025688
CITATIONWichers, M., Peeters, F., Rutten, B. P. F., Jacobs, N., Derom, C., Thiery, E., Delespaul, P., &van Os, J. (2011, October 10). A Time-Lagged Momentary Assessment Study on Daily LifePhysical Activity and Affect. Health Psychology. Advance online publication. doi:10.1037/a0025688

A Time-Lagged Momentary Assessment Study on Daily Life PhysicalActivity and Affect
Marieke Wichers, Frenk Peeters, andBart P. F. RuttenMaastricht University
Nele JacobsMaastricht University and Open University of The Netherlands
Catherine DeromKatholieke Universiteit Leuven
Evert ThieryAssociation for Scientific Research in Multiple Births, Ghent,
Belgium
Philippe DelespaulMaastricht University
Jim van OsMaastricht University, King’s College London, and Institute of
Psychiatry, London, United Kingdom
Objective: Novel study designs using within-subject methodology and frequent and prospective measurementsare required to unravel direction of causality and dynamic processes of behavior over time. The current studyexamined the effects of physical activity on affective state. A primary and within-study replication sample wasderived from twin pairs. Methods: Female twins (n � 504) participated in an experience sampling methodstudy at baseline. Positive and negative affective changes were examined before and following daily lifeincreases in physical activity. Neuroticism was measured at baseline and depressive symptoms were assessedat baseline and at each of four follow-up assessments. Diagnoses, derived by Structured Clinical Interview forDiagnostic and Statistical Manual for Mental Health–IV axis I disorders, (A. P. A., 1994) were obtained atbaseline. Results: A significant increase in positive affect (PA) following the moment of increase in physicalactivity was replicated across both samples up to 180 min after physical activity. There was no effect ofphysical activity on negative affect (NA). Across the two samples, a history of fulfilling diagnostic criteria fordepression at least once moderated the effect of physical activity on PA, in that the effect was lost morerapidly. Conclusions: The study supports a causal effect of physical activity on PA. However, people withpast experience of clinical depression may benefit less from the PA-inducing effect of physical activity. Thesefindings have implications for the use of physical exercise in clinical practice.
Keywords: physical activity, positive affect, negative affect, depression, experience sampling method
Major depressive disorder (MDD) is characterized by increasednegative affect (NA) and decreased positive affect (PA; Clark &Watson, 1991). Restoration of this imbalance in affective statesrequires lowering the level of NA and/or increasing the level ofPA. Recent studies have shown that PA, apart from impactingpositively on physical health (Sugawara, Tarumi, & Tanaka, 2010;Tugade, Fredrickson, & Barrett, 2004; Zautra, Johnson, & Davis,2005), also improves mental health. Positive affect reduces stress-
sensitivity, trims down expression of genetic risk for depression,and predicts better future course of symptoms (Fredrickson &Levenson, 1998; Tugade & Fredrickson, 2004; Vazquez, Cervel-lon, Perez–Sales, Vidales, & Gaborit, 2005; Wichers et al., 2008;Wichers et al., 2007a; Wichers et al., 2010; Wichers et al., 2007b).It has been suggested that physical activity may be a source of PA(Elavsky & McAuley, 2007; Elavsky et al., 2005), backed byevidence that physical activity may be effective as a treatment for
Marieke Wichers, Frenk Peeters, Bart P. F. Rutten, and Philippe Deles-paul, Department of Psychiatry and Neuropsychology, South LimburgMental Health Research and Teaching Network, EURON, MaastrichtUniversity, Maastricht, The Netherlands; Nele Jacobs, Department of Psy-chiatry and Neuropsychology, South Limburg Mental Health Research andTeaching Network, EURON, Maastricht University, Maastricht, The Neth-erlands, Faculty of Psychology, Open University of the Netherlands, Heer-len, The Netherlands; Catherine Derom, Department of Human Genetics,University Hospital Gasthuisberg, Katholieke Universiteit Leuven, Leu-ven, Belgium; Evert Thiery, Association for Scientific Research in Multi-ple Births, Ghent, Belgium; Jim van Os, Department of Psychiatry and
Neuropsychology, South Limburg Mental Health Research and Teach-ing Network, EURON, Maastricht University, Maastricht, The Nether-lands, King’s College London, King’s Health Partners, Department ofPsychosis Studies, Institute of Psychiatry, London, United Kingdom.
Marieke Wichers was supported by the Dutch organization forscientific research (VENI grant nr 916.76.147; ZONMW grant171001002).
Correspondence concerning this article should be addressed to MariekeWichers, Department of Psychiatry and Psychology, South Limburg Men-tal Health Research and Teaching Network, EURON, Maastricht Univer-sity Medical Centre, Maastricht, The Netherlands. E-mail: [email protected]
Health Psychology © 2011 American Psychological Association2011, Vol. ●●, No. ●, 000–000 0278-6133/11/$12.00 DOI: 10.1037/a0025688
1

depression, although results of a recent meta-analysis were ambig-uous (Mead et al., 2009). Therefore, there is a need to betterunderstand the relationship between physical activity and affectivestates.
Previous experimental studies (Bartholomew, Morrison, & Cic-colo, 2005; Ekkekakis, 2003; Ekkekakis, Hall, & Petruzzello,2008) have shown positive effects of physical exercise on well-being and positively appraised mental state. Experimental studiesare well placed to examine effects of varying intensity of physicalexercise and the perceived autonomy associated with it (Ekkekakiset al., 2008; Vazou–Ekkekakis & Ekkekakis, 2009). At intensitiesthat exceeded the individual ventilatory threshold, exercise nega-tively impacts on the experience of pleasure during exercise, butnot afterward (Ekkekakis et al., 2008). Also, it was found thatreduced perception of autonomy and choice attenuated increases inenergy and levels of interest/enjoyment (Vazou–Ekkekakis & Ek-kekakis, 2009). However, placebo effects or social desirabilitymay have affected the results, given that participants were aware ofthe study goals. In addition, in experimental studies, cognitiveaspects may play a role in the effect on affect. Both the internal(the subject him/herself) and external (the investigators) recogni-tion of goal attainment may impact on affect following exercise inlab experiments. This effect is less likely to happen in natural dailylife physical activity. Some studies (Giacobbi, Hausenblas, &Frye, 2005; Ready, Marquez, & Akerstedt, 2009; Steptoe, Kim-bell, & Basford, 1998) have used repeated observations to assessthe association between physical activity and mood in the flow ofdaily life. Repetitive momentary assessments allow for the exam-ination of within-subject associations, which reduces the risk ofconfounding by subject-level factors, such as socioeconomic statusor physical health. Mood level and physical activity over the daywere measured once daily in these studies. Results showed thatday-level reports of positive mood were associated with higherlevels of physical activity on that day, and that subjects reportedhigher levels of positive mood on days that they had exercised, ascompared with nonexercise days. However, positive mood statesand physical activity may have bidirectional effects in that moodstates may also affect people’s engagement in physical activityinstead of vice versa (Hawkley, Thisted, & Cacioppo, 2009; Schw-erdtfeger, Eberhardt, Chmitorz, & Schaller, 2010), which mayexplain the observed associations. Momentary assessment tech-niques (Csikszentmihalyi & Larson, 1987; Larson & Csikszentmi-halyi, 1983) (Shiffman, Stone, & Hufford, 2008) are ideal for theprospective examination of the dynamics of observed behavior,and enable the researcher to capture the film, rather than a snapshotof daily life reality (Myin–Germeys et al., 2009; Trull & Ebner–Priemer, 2009). They allow for examination of subtle fluctuationsof behavior and affect over the course of the day, and the prospec-tive nature of the data allows for examination of the temporalassociation between physical activity and affect. Kanning andcolleagues (Kanning & Schlicht, 2010) examined the temporalassociation by letting participants (n � 13) rate their levels ofaffect following some self-selected daily life activities such aswalking or gardening. In another study, participants (n � 61) hadto fill out a small diary following signals by random beeps fourtimes per day and at some additional moments following exercise(Lepage & Crowther, 2010). Both studies showed higher levels ofpositive mood following the selected activities and physical exer-
cise, as compared with moments with lower levels of physicalactivity.
To date, only a few studies have examined the temporal asso-ciation between physical activity and affect in the flow of dailylife. There is a need for such studies in order to examine theassociation between physical exercise and affective states witheven greater precision and in larger samples. The current studyemploys momentary assessment techniques, with 10 assessmenteach day for five consecutive days in a large sample of individuals(n � 504) to examine the subtle hour-to-hour fluctuations in affectin relation to increases in physical activity in the flow of daily life.An analytic strategy was applied that made use of the time-laggedstructure of the data, allowing for the examination of changes inaffect over time before and following within-subject increases inphysical activity. In addition, a twin design was used, providingthe possibility for within-study replication of the results with twooptimally matched subsamples, both consisting of one of twomembers within a single twin pair.
Second, we wished to examine whether any effect of physicalactivity on affective states was moderated by depression (subclin-ical symptomatology and MDD) or depression risk states, forexample, high neuroticism scores. The second aim has relevance tothe question whether physical activity could be effective as treat-ment against depression because of its positive effect on affectivestates. In this context, there is an urgent need to study to whatdegree physical activity has the same beneficial properties forpeople with depression, people with subthreshold depressivesymptoms, and nonsymptomatic individuals at risk for depression.
Methods
Sample
The study sample consisted of 621 female subjects from thegeneral population, who were part of twin pairs or were sisters oftwin pairs living in Flanders (Belgium). Their ages were between18 and 46 years. Of the 621 subjects, 610 participated in thecurrent experience sampling method (ESM) study. Most twin pairsand sisters of twin pairs were recruited from the East-FlandersProspective Twin Survey, a population-based survey prospectivelyrecording all multiple births in the province of East Flanders since1964 (Derom et al., 2002; Derom et al., 2006). The project wasapproved by the Local Ethics Committee and all participants gavewritten informed consent. The sample was female only, givenevidence for qualitative differences in the type of environmentaleffects that are associated with depression in men and women(Kendler, Thornton, & Prescott, 2001). Mean age of the twins was27 years (standard deviation [SD] � 7.6 years, range 18–46).Sixty-five percent had a college or university degree, 33% com-pleted secondary education, and 2% had primary education only.The majority was currently employed (61.3% employed, 33.8%student, 2.2% unemployed, 2.3% homemaker, and 0.4% sickleave).
Experience Sampling Method
ESM is a structured diary technique to assess subjects in theirdaily living environment, validated for the study of daily lifecontextual effects on mood (Csikszentmihalyi & Larson, 1987;
2 WICHERS ET AL.

Delespaul, 1995; DeVries, 1992; Myin–Germeys, van Os,Schwartz, Stone, & Delespaul, 2001). Subjects received a digitalwristwatch and a set of ESM self-assessment forms collated in abooklet for each day. The wristwatch was programmed to emit asignal (“beep”) at an unpredictable moment in each of 10 90-mintime blocks between 7:30 and 22:30, on five consecutive days. Thestudy uses a semirandom beep design in order to prevent antici-patory behavior of participants, which is likely present when thetiming of the next beep is known. Beep intervals do not overlap,thus ensuring that the first beep on the day is always earlier in timethan the second and the second earlier than the third, and so forth.
After each beep, subjects were asked to complete the ESMself-assessment forms previously handed to them, collecting re-ports of thoughts, current context (activity, persons present, andlocation), appraisals of the current situation and affect (see below).All self-assessments were rated on 7-point Likert scales. Trainedresearch assistants with ample experience in momentary assess-ment technology explained the ESM procedure to the participantsduring an initial briefing session, and a practice form was com-pleted to confirm that subjects were able to understand the 7-pointLikert scale. Subjects could call a telephone number in case theyhad questions or problems during the ESM sampling period.Subjects were instructed to complete their reports immediatelyafter the beep, thus minimizing memory distortion, and torecord the time at which they completed the form. In order toknow whether the subjects had completed the form within 15 minof the beep, the time at which subjects indicated they completedthe report was compared to the actual time of the beep. All reportsnot filled in within 15 min after the beep were excluded from theanalysis, since previous work (Delespaul, 1995) has shown thatreports completed after this interval are less reliable and conse-quently less valid. In addition, subjects with less than 17 validreports (out of 50) were excluded from the analysis, as previouswork has shown that measures of individuals with less than 30% ofcompleted reports are less reliable (Delespaul, 1995). Complianceto the ESM protocol was evaluated in a random subsample (58subjects, 1,938 observations) of the sample used in the currentstudy using 100-cc bottles with electronic monitoring caps. Thesebottles contained participants’ saliva swabs that they needed tocollect at each beep in addition to completing the ESM self-assessment forms. Participants were told that the bottle was de-signed to keep the swabs sanitary and were unaware that the timingof their actions was monitored. Self-reported compliance, thusassessed, was very high (96.4%; Jacobs et al., 2005).
Procedure
The sample was assessed at five time points, including a base-line (T0) and four follow-up measurements (T1–T4). The averagenumber of days between T0 and T1 was 132, 91 between T1 andT2, 116 between T2 and T3, and 91 between T3 and T4. Assess-ments at T0 took place at individuals’ homes, with the interviewerpresent. At each follow-up, questionnaires were sent to the partic-ipants by mail for completion at home, after which participantsreturned them to the research team in a prepaid envelope. Allinterviews were carried out by trained research psychologists orgraduate psychological assistants. ESM (consisting of a 5-dayperiod of data collection in daily life, see below) was carried out
only at T0 (during the week before the visit of the researcher at theparticipant’s home).
Measurements
Structured Clinical Interview for Diagnostic and StatisticalManual for Mental Health (DSM)–IV axis I disorders (SCID)(First, Spitzer, Gibbon, & Williams, 1996) was administered at T0(by the interviewer at the participant’s home) and at T4 (by theinterviewer over the telephone) in order to obtain current andlifetime diagnoses of MDD. Subjects completed the SymptomChecklist (SCL-90R; Derogatis, Rickels, & Rock, 1976) in orderto obtain a continuous measure of depressive symptoms. In addi-tion, subjects completed the Neuroticism–Extraversion subscale ofthe Eysenck Personality Scale (Eysenck & Eysenck, 1991). Thelatter two questionnaires were completed at all time points.
Measures of physical activity and momentary affective stateswere collected at each beep within the ESM framework at T0.ESM physical activity was assessed with a single item askingsubjects how physically active they had been since the last beep,rated on a 7-point Likert scale. During the ESM briefing, partici-pants were instructed how to score their level of physical activity.To this end, they were given an indication of the level of activitythat corresponded to the score on the 7-point Likert scale. Anchorpoints were provided as examples, as follows: a score of 1 corre-sponds to the level of physical activity of “resting”; 2 correspondsto “sitting”; 3 to “walking”; 4 to “household chores such asvacuum cleaning”; 5 to “biking”; 6 to “playing tennis”; and 7 to“running.” These anchor points were also provided in the ESMself-assessment forms subjects completed at each beep. Thus, foreach physical activity approximately equaling the level of physicalactivity associated with vacuum cleaning, participants rated ascore of 4 on the 7-point Likert scale. Momentary affective stateswere assessed with 10 adjectives rated on 7-point Likert scales.The choice of the ESM affect items was guided in part by thePositive and Negative Affect Scale (PANAS) questionnaire (Wat-son, Clark, & Tellegen, 1988) and in part by the results of previousESM studies (selecting items with high loadings on NA and PAlatent factors and sufficient within-person variability). Factor anal-ysis identified two affect factors with Eigenvalue �1 Ratings onthe items “insecure,” “lonely,” “anxious,” “low,” “guilty,” and“suspicious”—weighted for factor loadings—were averaged toform NA (respective loadings were: 0.71, 0.60, 0.66, 0.68, 0.61,0.64) The weighted average of ratings on “cheerful,” “content,”“energetic,” and “enthusiastic” formed PA (respective loadingswere: (0.84, 0.71, 0.84, 0.83). All items loaded specifically on onlyone of the two factors. The strongest cross-loading was �0.13(loading of “content” on NA factor). Cronbach’s alpha was calcu-lated for each individual separately. Mean Cronbach’s alpha was0.53 (SD � 0.26) for NA and 0.75 (0.14) for PA. Appraisals ofcurrent activities (work, relaxation, household chores, etc.) wereassessed at each beep, in order to correct for the confounding of theassociation between physical activity and affect by pleasantness ofthe activity (which might be the case, e.g., when relaxation activ-ities are more pleasant and more active than work-related activi-ties). Participants rated to what extent statements as “I prefer doingsomething else” or “I am skilled at this activity” applied to thecurrent activity on a 7-point Likert scale from 1 not at all to 7 verymuch. Consistent with previous studies (Lardinois, Lataster, Men-
3PHYSICAL ACTIVITY AND MOMENTARY DAILY LIFE AFFECT

gelers, Van Os, & Myin–Germeys, 2011; Wichers et al., 2009) acomposite score of several appraisals (“I would rather do some-thing else,” “this activity requires effort,” and “I am skilled atdoing this activity”) was made. The first two were recoded inreverse so that high scores reflect a more positive appraisal of theactivity.
Analyses
Since ESM measurements of affect and physical activity areavailable for five days with a maximum of 10 measurements perday per person with on average 90 min in between, the data areideally suited to explore the dynamic within-subject temporalassociations between physical activity and affective states. To thisend, reactivity of negative and positive emotions, following in-creases in physical activity in daily life, was analyzed prospec-tively.
Within-subject increase in activity was defined as reporting ahigher level of physical activity (t) than at the beep before (t � 1).An advantage of this measure is that a variable of within-personchange eliminates all potential between-person differences in scor-ing tendencies on the Likert scale. Variables were created repre-senting NA/PA at beep moments before and following the increasein physical activity (t � 5, t � 4, t � 3 t � 1, t, t � 1, t � 2, t �3, t � 5). Thus, instead of examining a single time-lag only,multiple time-lags were examined in order to create a fine-grained“film” of changes in affect relating to changes in physical activityin daily life. The data were reshaped in long format with a newtime variable representing the distance in beeps from the momentof “increase in physical activity.” In that way, a multilevel regres-sion analysis could be performed, with time as the independent andaffect as the dependent variable. The time value t � 1 (one beepbefore the increase in physical activity) was taken as referencevalue.
ESM data have a hierarchical structure in which ESM observa-tions (level 1) are clustered within participants (level 2). In addi-tion, in the current data set participants (level 2) were clusteredwithin twin pairs (level 3). STATA 11.0 (StataCorp., 2009) wasused to conduct multilevel regression analyses. Analyses werecorrected for appraisal (pleasantness) of the current activity. Con-tinuous variables were standardized in order to obtain comparablestandardized effect sizes.
In order to carry out within study replication of the findings, twohighly comparable subsamples were created by splitting up thetwin pairs. In all twin pairs, the first-born was selected for the firstsubsample and her cotwin for the second; analyses were carriedout for the combined sample and separately for both subsamples.
Next, where significant associations between time of physicalactivity and PA/NA were evident, effect modification by depres-sion and depression risk states (cross-level interaction) was exam-ined in both samples. Thus, it was examined whether the (within-person) effect of physical activity on PA/NA would differ forpeople with different depression risk states. Four depression (risk)states were included: (i) neuroticism score, (ii) current SCL-90depression score, (iii) future SCL-90 depression score correctedfor baseline (effectively modeling increase in depression scoreover time), and (iv) history of MDD (defined as fulfilling DSM–IVcriteria for lifetime diagnosis of MDD). Because of the relativelysmall numbers of the MDD diagnosis group after splitting the twin
pairs in two subsamples (n1 � 31 and n2 � 42), effect size, ratherthan p value, was set as the criterion for replication in this analysis.
Results
Subject Characteristics
Of the 610 subjects who participated in the ESM study, 31 wereexcluded because they had too few (less than 30%) beeps withvalid responses. Of the 579 remaining subjects, 12 had missingdata for PA, leaving 567 subjects with NA, PA, and physicalactivity measurements. As the twin design was used specifically toobtain two separate, but matched samples, all nontwin sisters (n �45) were excluded as were all twins whose cotwin had incompleteinformation (n � 18). This resulted in a dataset of 504 subjectsconsisting of 252 complete twin pairs (155 monozygotic and 96dizygotic twin pairs and 1 twin pair with unknown zygosity). In thefinal sample, six subjects had so many missing values on the ESMmeasure of physical activity that not a single occasion of increasein physical activity was observed with respect to the beep before.Three subjects had missing data for neuroticism and four hadmissing data for SCL-90 depression score. Follow-up SCL-90scores were available in 474 subjects.
In the sample, 73 subjects (15%) fulfilled DSM–IV criteria forlifetime history of MDD at baseline. Average reported NA in thesample was 0.82 (SD � 0.20), average PA was 3.55 (SD � 0.56),and average reported physical activity was 2.88 (SD � 0.48).Average baseline neuroticism score was 0.45 (SD � 0.23). Aver-age baseline SCL-90 depression score was 1.44 (SD � 0.42).Table 1 displays details of physical activity, NA and PA in relationto the moment of increase in physical activity, stratified by ahistory of MDD. There were no significant differences betweengroups in mean increase in physical activity, or in the resultingabsolute level of physical activity at moments of activity increase,or in mean levels of PA before and at the moment of increase inphysical activity. Subjects with a past history of MDD showedincreased mean levels of NA at moments before (t-1) and at (t)activity increase, as compared with those without a history ofMDD.
Temporal Associations Between Within-SubjectIncrease in Physical Activity and Affective States
Within-subject increase in physical activity—from the beepmoment before any increase in physical activity (t � 1) to themoment where increase in physical activity was observed (t)—wasassociated with a significant increase in PA. For three consecutivemoments (t, t � 1 and t � 2; up to 180 min following the increasein activity), increase in PA was significant and replicated acrossboth subsamples (subsample 1: Bt � 0.12, p � .001, Bt�1 � 0.09,p � .001, Bt�2 � 0.06, p � .023 and subsample 2: Bt � 0.12, p �.001, Bt�1 � 0.10, p � .001, Bt�2 � 0.09, p � .001; see Figure1). In addition, in the combined sample, PA was significantlyhigher three beeps before the increase in physical activity ascompared with one beep before the increase. This effect was notreplicated across subsamples. Within-subject increase in physicalactivity was not significantly associated with NA at any moment.The absence of this effect was replicated across both subsamples.
4 WICHERS ET AL.
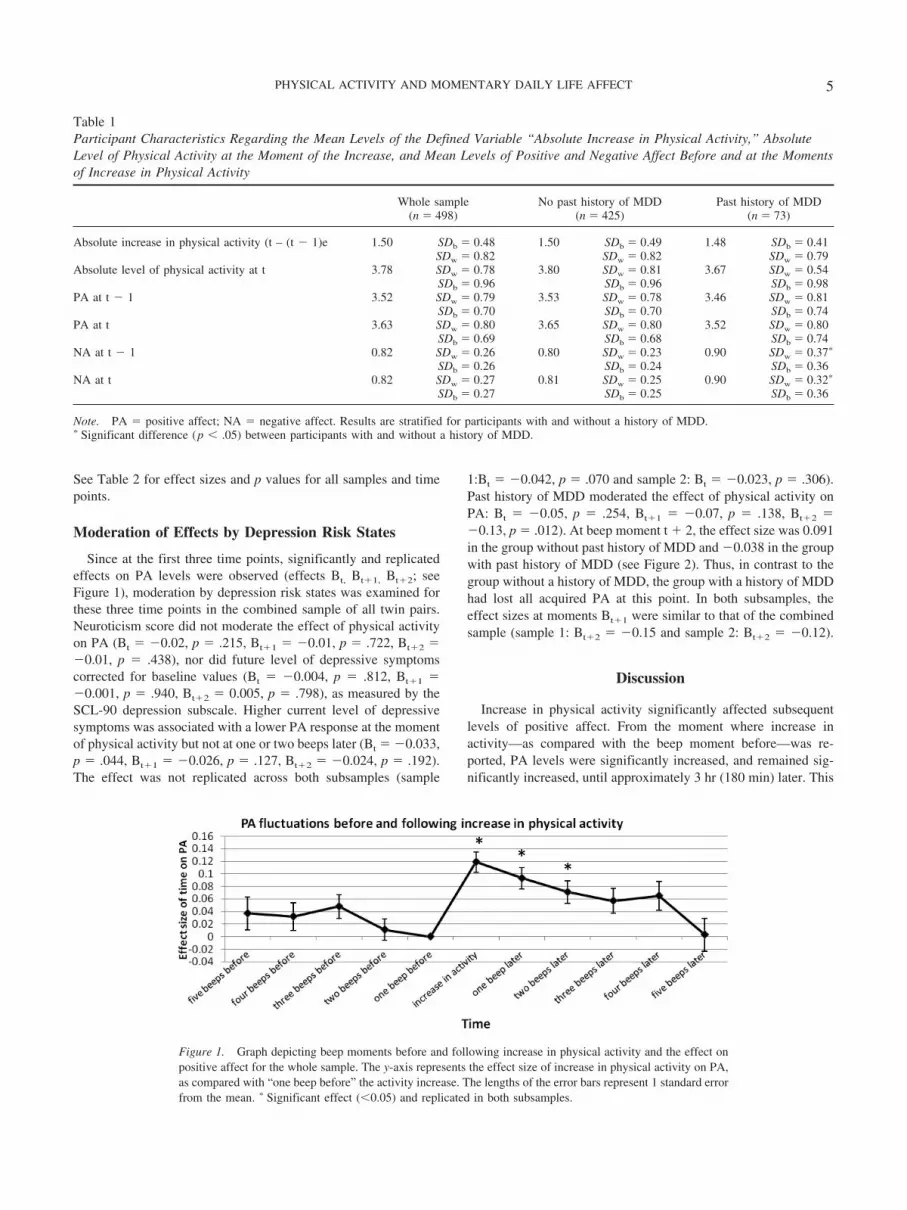
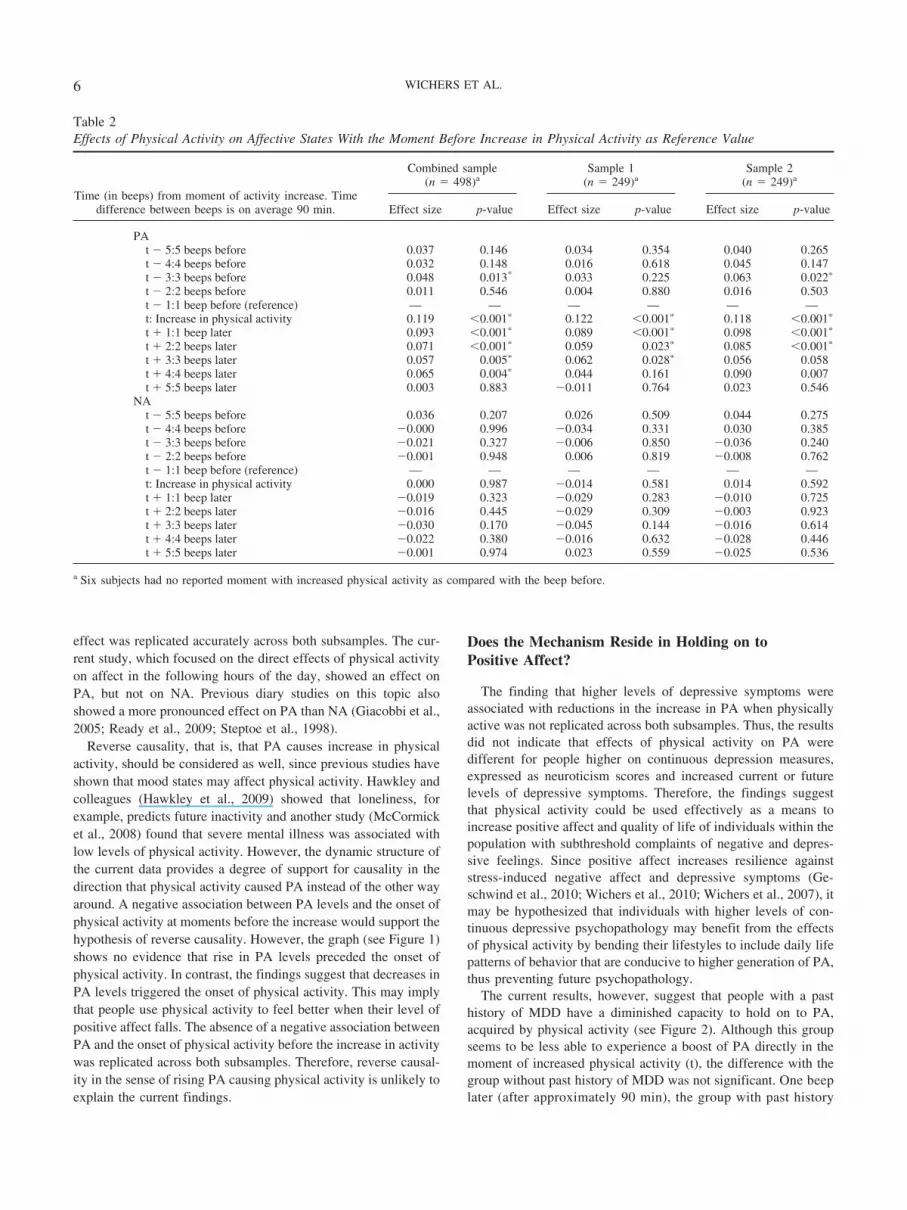
See Table 2 for effect sizes and p values for all samples and timepoints.
Moderation of Effects by Depression Risk States
Since at the first three time points, significantly and replicatedeffects on PA levels were observed (effects Bt, Bt�1, Bt�2; seeFigure 1), moderation by depression risk states was examined forthese three time points in the combined sample of all twin pairs.Neuroticism score did not moderate the effect of physical activityon PA (Bt � �0.02, p � .215, Bt�1 � �0.01, p � .722, Bt�2 ��0.01, p � .438), nor did future level of depressive symptomscorrected for baseline values (Bt � �0.004, p � .812, Bt�1 ��0.001, p � .940, Bt�2 � 0.005, p � .798), as measured by theSCL-90 depression subscale. Higher current level of depressivesymptoms was associated with a lower PA response at the momentof physical activity but not at one or two beeps later (Bt � �0.033,p � .044, Bt�1 � �0.026, p � .127, Bt�2 � �0.024, p � .192).The effect was not replicated across both subsamples (sample
1:Bt � �0.042, p � .070 and sample 2: Bt � �0.023, p � .306).Past history of MDD moderated the effect of physical activity onPA: Bt � �0.05, p � .254, Bt�1 � �0.07, p � .138, Bt�2 ��0.13, p � .012). At beep moment t � 2, the effect size was 0.091in the group without past history of MDD and �0.038 in the groupwith past history of MDD (see Figure 2). Thus, in contrast to thegroup without a history of MDD, the group with a history of MDDhad lost all acquired PA at this point. In both subsamples, theeffect sizes at moments Bt�1 were similar to that of the combinedsample (sample 1: Bt�2 � �0.15 and sample 2: Bt�2 � �0.12).
Discussion
Increase in physical activity significantly affected subsequentlevels of positive affect. From the moment where increase inactivity—as compared with the beep moment before—was re-ported, PA levels were significantly increased, and remained sig-nificantly increased, until approximately 3 hr (180 min) later. This
Table 1Participant Characteristics Regarding the Mean Levels of the Defined Variable “Absolute Increase in Physical Activity,” AbsoluteLevel of Physical Activity at the Moment of the Increase, and Mean Levels of Positive and Negative Affect Before and at the Momentsof Increase in Physical Activity
Whole sample(n � 498)
No past history of MDD(n � 425)
Past history of MDD(n � 73)
Absolute increase in physical activity (t – (t � 1)e 1.50 SDb � 0.48 1.50 SDb � 0.49 1.48 SDb � 0.41SDw � 0.82 SDw � 0.82 SDw � 0.79
Absolute level of physical activity at t 3.78 SDw � 0.78 3.80 SDw � 0.81 3.67 SDw � 0.54SDb � 0.96 SDb � 0.96 SDb � 0.98
PA at t � 1 3.52 SDw � 0.79 3.53 SDw � 0.78 3.46 SDw � 0.81SDb � 0.70 SDb � 0.70 SDb � 0.74
PA at t 3.63 SDw � 0.80 3.65 SDw � 0.80 3.52 SDw � 0.80SDb � 0.69 SDb � 0.68 SDb � 0.74
NA at t � 1 0.82 SDw � 0.26 0.80 SDw � 0.23 0.90 SDw � 0.37�
SDb � 0.26 SDb � 0.24 SDb � 0.36NA at t 0.82 SDw � 0.27 0.81 SDw � 0.25 0.90 SDw � 0.32�
SDb � 0.27 SDb � 0.25 SDb � 0.36
Note. PA � positive affect; NA � negative affect. Results are stratified for participants with and without a history of MDD.� Significant difference (p � .05) between participants with and without a history of MDD.
Figure 1. Graph depicting beep moments before and following increase in physical activity and the effect onpositive affect for the whole sample. The y-axis represents the effect size of increase in physical activity on PA,as compared with “one beep before” the activity increase. The lengths of the error bars represent 1 standard errorfrom the mean. � Significant effect (�0.05) and replicated in both subsamples.
5PHYSICAL ACTIVITY AND MOMENTARY DAILY LIFE AFFECT
effect was replicated accurately across both subsamples. The cur-rent study, which focused on the direct effects of physical activityon affect in the following hours of the day, showed an effect onPA, but not on NA. Previous diary studies on this topic alsoshowed a more pronounced effect on PA than NA (Giacobbi et al.,2005; Ready et al., 2009; Steptoe et al., 1998).
Reverse causality, that is, that PA causes increase in physicalactivity, should be considered as well, since previous studies haveshown that mood states may affect physical activity. Hawkley andcolleagues (Hawkley et al., 2009) showed that loneliness, forexample, predicts future inactivity and another study (McCormicket al., 2008) found that severe mental illness was associated withlow levels of physical activity. However, the dynamic structure ofthe current data provides a degree of support for causality in thedirection that physical activity caused PA instead of the other wayaround. A negative association between PA levels and the onset ofphysical activity at moments before the increase would support thehypothesis of reverse causality. However, the graph (see Figure 1)shows no evidence that rise in PA levels preceded the onset ofphysical activity. In contrast, the findings suggest that decreases inPA levels triggered the onset of physical activity. This may implythat people use physical activity to feel better when their level ofpositive affect falls. The absence of a negative association betweenPA and the onset of physical activity before the increase in activitywas replicated across both subsamples. Therefore, reverse causal-ity in the sense of rising PA causing physical activity is unlikely toexplain the current findings.
Does the Mechanism Reside in Holding on toPositive Affect?
The finding that higher levels of depressive symptoms wereassociated with reductions in the increase in PA when physicallyactive was not replicated across both subsamples. Thus, the resultsdid not indicate that effects of physical activity on PA weredifferent for people higher on continuous depression measures,expressed as neuroticism scores and increased current or futurelevels of depressive symptoms. Therefore, the findings suggestthat physical activity could be used effectively as a means toincrease positive affect and quality of life of individuals within thepopulation with subthreshold complaints of negative and depres-sive feelings. Since positive affect increases resilience againststress-induced negative affect and depressive symptoms (Ge-schwind et al., 2010; Wichers et al., 2010; Wichers et al., 2007), itmay be hypothesized that individuals with higher levels of con-tinuous depressive psychopathology may benefit from the effectsof physical activity by bending their lifestyles to include daily lifepatterns of behavior that are conducive to higher generation of PA,thus preventing future psychopathology.
The current results, however, suggest that people with a pasthistory of MDD have a diminished capacity to hold on to PA,acquired by physical activity (see Figure 2). Although this groupseems to be less able to experience a boost of PA directly in themoment of increased physical activity (t), the difference with thegroup without past history of MDD was not significant. One beeplater (after approximately 90 min), the group with past history
Table 2Effects of Physical Activity on Affective States With the Moment Before Increase in Physical Activity as Reference Value
Time (in beeps) from moment of activity increase. Timedifference between beeps is on average 90 min.
Combined sample(n � 498)a
Sample 1(n � 249)a
Sample 2(n � 249)a
Effect size p-value Effect size p-value Effect size p-value
PAt � 5:5 beeps before 0.037 0.146 0.034 0.354 0.040 0.265t � 4:4 beeps before 0.032 0.148 0.016 0.618 0.045 0.147t � 3:3 beeps before 0.048 0.013* 0.033 0.225 0.063 0.022�
t � 2:2 beeps before 0.011 0.546 0.004 0.880 0.016 0.503t � 1:1 beep before (reference) — — — — — —t: Increase in physical activity 0.119 �0.001� 0.122 �0.001� 0.118 �0.001�
t � 1:1 beep later 0.093 �0.001� 0.089 �0.001� 0.098 �0.001�
t � 2:2 beeps later 0.071 �0.001� 0.059 0.023� 0.085 �0.001�
t � 3:3 beeps later 0.057 0.005� 0.062 0.028� 0.056 0.058t � 4:4 beeps later 0.065 0.004� 0.044 0.161 0.090 0.007t � 5:5 beeps later 0.003 0.883 �0.011 0.764 0.023 0.546
NAt � 5:5 beeps before 0.036 0.207 0.026 0.509 0.044 0.275t � 4:4 beeps before �0.000 0.996 �0.034 0.331 0.030 0.385t � 3:3 beeps before �0.021 0.327 �0.006 0.850 �0.036 0.240t � 2:2 beeps before �0.001 0.948 0.006 0.819 �0.008 0.762t � 1:1 beep before (reference) — — — — — —t: Increase in physical activity 0.000 0.987 �0.014 0.581 0.014 0.592t � 1:1 beep later �0.019 0.323 �0.029 0.283 �0.010 0.725t � 2:2 beeps later �0.016 0.445 �0.029 0.309 �0.003 0.923t � 3:3 beeps later �0.030 0.170 �0.045 0.144 �0.016 0.614t � 4:4 beeps later �0.022 0.380 �0.016 0.632 �0.028 0.446t � 5:5 beeps later �0.001 0.974 0.023 0.559 �0.025 0.536
a Six subjects had no reported moment with increased physical activity as compared with the beep before.
6 WICHERS ET AL.

of MDD was losing the acquired PA at a quicker rate than theother group, and two beeps later the difference became signif-icant; the group with history of MDD had lost all PA at thismoment, while the group without a history of MDD still expe-rienced more than 80% of the PA acquired with the increase inphysical activity. Overall, people with past experience of de-pression, at the clinical level, seemed to benefit less fromphysical activity in terms of PA compared to others, mostlybecause the beneficial effects were lost much more rapidly. Aplausible explanation may be that the first increase in PAfollowing physical activity is caused by automatic biologicalprocesses (Neeper, Gomez–Pinilla, Choi, & Cotman, 1996),while the ability to hold on to PA over time is much moreinfluenced by emotional and cognitive processing. For example,negative cognitive schemas in the group with a history of MDDmay interfere with the transfer of positive affect from onemoment to the next. The fact that depressed patients alreadyhave very low levels of motivation, and that acquired “rewards”following exercise may fade away much faster than in otherpeople, can explain the difficulty patients face in their attemptsto participate in physical exercise interventions. A recent ex-perience sampling study (Mata et al., 2011) also examined theassociated between levels of physical activity and PA separatelyfor individuals diagnosed with MDD (n � 53) and controls (n �53). This study similarly found that physical activity precededincreases in PA in daily life and that this was true for bothindividuals with MDD and controls. This study was not infor-mative, however, regarding differences between individualswith MDD and controls in the duration (in hours) that PAremained elevated following physical activity.
Implications for Future Research and Clinical Practice
The current findings shed light on some issues relevant to futureresearch and clinical practice. First, a modification of people’sability to hold on to acquired PA would open new sources (likephysical activity, but likely also other rewarding activities) fordepressed patients to restore the imbalance between negative andpositive affect. Therefore, future research should focus on themechanisms that disrupt this process and on new ways of modi-fying this ability.
Second, the current findings may explain some of the discrep-ancies in research findings between, on the one hand, animals andhumans (Achiron & Kalron, 2008; Zheng et al., 2006), suggestingthat physical activity may be mood-enhancing and, on the other,the ambiguous findings presented in a recent meta-analysis onphysical activity as an intervention in depression (Mead et al.,2009). Previous experimental studies on the association betweenexercise and affect have shown considerable individual variabilityin affect during exercise on the one hand, but a uniformly positiveaffective response immediately following exercise on the other(Ekkekakis, 2003). This is consistent with the current results inthat all participants, including the group with a history of depres-sion, exhibited increased PA immediately following increases inphysical activity (at time t). However, the current study confirmedindividual variability in the duration (t � 1, t � 2 etc.) of thisimmediate positive response to physical activity. The fact thatpeople with a history of MDD did not benefit to the same extentfrom physical exercise as other people may have consequences forthe use of physical exercise as an intervention in clinically de-pressed patients. To the extent that positive affect following phys-
Figure 2. Graph depicting beep moments before and following increase in physical activity and the effect onpositive affect in the whole sample, stratified for people with and without DSM–IV depression diagnosis ever.The y-axis represents the effect size of increase in physical activity on PA, as compared with “one beep before”the activity increase. The lengths of the error bars represent 1 standard error from the mean. � Significant effect(�0.05) with effect size replicated in both subsamples (tests were performed only for differences in mean changein PA (with t � 1 as reference) at t, t � 1 and t � 2).
7PHYSICAL ACTIVITY AND MOMENTARY DAILY LIFE AFFECT

ical activity may be lost as quickly as it was acquired, othertreatment options may be preferable, considering the effort it takesfor depressed patients to engage in exercise interventions. How-ever, also within patients, interindividual variations in the benefi-cial effects of physical activity are likely present. Finally, thecurrent findings were not informative with regard to possibleinteractions with other treatments. For example, pharmacotherapy,cognitive–behavior therapy or mindfulness therapy may increasethe benefits depressed patients experience from physical exercise,by modifying habitual cognitive styles associated with not beingable to hold on to positive affect. Therefore, individually tailoredassessment of the potential benefit of exercise interventions seemsdesirable in the future, allowing for person-specific optimization oftreatment choice and treatment characteristics (such as the optimallevel of physical exercise). A new electronic device with touchscreen (the PsyMate)—which will replace the paper and pencilmethod in experience sampling studies—is currently being pilotedand may bring new scientific and clinical applications. This newelectronic diary allows for immediate storage of data which makesit possible to provide direct and person-tailored feedback to pa-tients, and their attending therapists, on the patient’s daily lifepattern of affect and behavior. Direct feedback on positive affectand the contexts in which they occur may provide both patientsand doctors with person-specific information regarding the useful-ness of physical activity (or other daily life behaviors) as anintervention, as well as the optimum level of physical activity.Also, it may increase insight into the cognitive and emotionalmechanisms that influence the ability to hold on to positive affect.
Statistical Significance and Clinical Relevance
Daily life increase in physical activity was statistically signifi-cantly associated with daily life PA. However, the question rises towhat extent these effects represent clinically meaningful findings.Generally, effect sizes of around 0.2 are considered relevant butlow and those around 0.8 high (Cohen, 1988). In the current study,the effect sizes vary but are generally low (around 0.1 for within-person differences and an effect size difference of the nonde-pressed with the depressed group of 0.16; see Figure 2) accordingto Cohen (Cohen, 1988). However, the results of the current studywere derived from data reflecting a daily life context of repetitiveevents (unlike effects reported in most unilevel studies). Thecurrent findings reflect the average increase in positive affect atevery moment with a positive change in a person’s physicalactivity in daily life. It thus represents a repetitive pattern of boostsin PA in response to increases in physical activity during everysingle day. Therefore, effect sizes reported in the current study,although small, cumulatively may well be clinically relevant.
Limitations
A limitation regarding the above findings on moderation of theeffect of physical activity is that they result from between-subjectsanalyses (in contrast to the first analyses regarding the main effectof physical activity on affective states). Therefore, it is possiblethat other group differences, such as lifestyle factors differentiatingbetween those with and without (risk for) depression confoundedobserved effects. Future studies should try to replicate these find-ings using a within-subject design to examine whether depression
risk state moderates the effect of physical activity on PA, prefer-ably carrying out ESM assessments before and following a firstepisode of depression or across different depression risk states(higher and lower amount of symptoms) within the same individ-ual over time. Replication of these findings will be valuable forfurther efforts to create effective and person-tailored interventionsin depression, focusing on physical activity.
In addition, the power of the interaction analyses—to detectsignificant differences between people with and without a diagno-sis of depression—was low, especially in the replication analysesin the two subsamples (total sample: 0.70; subsample 1: 0.33 andsubsample 2: 0.39). Therefore, it is possible that true effects weremissed.
Also, the data collected in this study were not entirely prospec-tive. At each beep moment, participants were asked about theirphysical activity level since the last beep. Thus, people had tojudge their behavior retrospectively. However, the retrospectivewindow was very small—on average 90 min long—and thereforelikely more reliable than retrospective windows of a whole day oreven longer. Measures of affect were measured in the moment,without any retrospective window.
New technological advances, such as the advent of actigraphy,allow for objective monitoring of physical activity in daily life.Previous studies have shown that objective assessments of physi-cal activity and subjective ratings of physical activity are onlymodestly related (Bussmann, Ebner–Priemer, & Fahrenberg,2009). Therefore, future studies should aim to replicate the currentfindings using objective assessments of physical activity.
Questions have been raised about compliance to the ESM pro-tocol in paper-and-pencil studies (Broderick, Schwartz, Shiffman,Hufford, & Stone, 2003). However, as shown earlier (Jacobs et al.,2005), compliance in this sample was very high. Although non-compliance was not an issue in the current study, it can bemonitored much more easily, and avoided in part by using elec-tronic momentary assessment devices instead of paper-and-pencilprotocols.
Furthermore, since the sample consisted of women, the findingsmay not necessarily generalize to men. In addition, the participantsin the current study were recruited from the general population.Therefore, the results should be replicated in patient samples.Since MDD diagnosed in individuals that are not necessarilyseeking help may be less severe than in help-seeking patients, thedifferential effect of physical activity on PA between nonde-pressed and depressed individuals may be even more pronouncedwhen compared to a clinical population.
In conclusion, the results suggest a temporal association be-tween the level of physical activity and subsequent levels ofpositive affect. However, the emotional benefit of physical activitymay differ between individuals as it was lower in people with ahistory of depression. Therefore, individually tailored assessmentof the potential benefit of exercise interventions may be necessary.
References
Achiron, A., & Kalron, A. (2008). [Physical activity: Positive impact onbrain plasticity]. Harefuah, 147, 252, 255, 276.
A. P. A. (1994). Diagnostic and statistical manual of mental disorders:DSM-IV; Washington, DC.
Bartholomew, J. B., Morrison, D., & Ciccolo, J. T. (2005). Effects of acute
8 WICHERS ET AL.
exercise on mood and well-being in patients with major depressivedisorder. Medicine and Science in Sports and Exercise, 37, 2032–2037.
Broderick, J. E., Schwartz, J. E., Shiffman, S., Hufford, M. R., & Stone,A. A. (2003). Signaling does not adequately improve diary compliance.Annals of Behavioral Medicine, 26, 143–148.
Bussmann, B. J., Ebner–Priemer, U. W., & Fahrenberg, J. (2009). Ambu-latory activity monitoring: Progress in measurement of activity, posture,and specific motion patterns in daily life. European Psychologist, 14,142–152.
Clark, L. A., & Watson, D. (1991). Tripartite model of anxiety anddepression: Psychometric evidence and taxonomic implications. Journalof Abnormal Psychology, 100, 316–336.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences(2nd ed.). Hillsdale, NJ: Erlbaum.
Csikszentmihalyi, M., & Larson, R. (1987). Validity and reliability of theexperience-sampling method. Journal of Nervous and Mental Disease,175, 526–536.
Delespaul, P. (1995). Assessing schizophrenia in daily life: The experiencesampling method. Maastricht, The Netherlands: University of Limburg.
Derogatis, L. R., Rickels, K., & Rock, A. F. (1976). The SCL-90 and theMMPI: A step in the validation of a new self-report scale. BritishJournal of Psychiatry, 128, 280–289.
Derom, C., Vlietinck, R., Thiery, E., Leroy, F., Fryns, J. P., & Derom, R.(2002). The East Flanders Prospective Twin Survey (EFPTS). TwinResearch, 5, 337–341.
Derom, C. A., Vlietinck, R. F., Thiery, E. W., Leroy, F. O., Fryns, J. P., &Derom, R. M. (2006). The East Flanders Prospective Twin Survey(EFPTS). Twin Research and Human Genetics, 9, 733–738.
DeVries, M. W. (Ed.). (1992). The experience of psychopathology: Inves-tigating mental disorders in their natural settings. Cambridge, U.K.:Cambridge University Press.
Ekkekakis, P. (2003). Pleasure and displeasure from the body: Perspectivesfrom exercise. Cognition and Emotion, 17, 213–239.
Ekkekakis, P., Hall, E. E., & Petruzzello, S. J. (2008). The relationshipbetween exercise intensity and affective responses demystified: To crackthe 40-year-old nut, replace the 40-year-old nutcracker! Annals of Be-havioral Medicine, 35, 136–149.
Elavsky, S., & McAuley, E. (2007). Physical activity and mental healthoutcomes during menopause: A randomized controlled trial. Annals ofBehavioral Medicine, 33, 132–142.
Elavsky, S., McAuley, E., Motl, R. W., Konopack, J. F., Marquez, D. X.,Hu, L., . . . Diener, E. (2005). Physical activity enhances long-termquality of life in older adults: Efficacy, esteem, and affective influences.Annals of Behavioral Medicine, 30, 138–145.
Eysenck, H., & Eysenck, S. (1991). Manual of the Eysenck personalityscales. London, U.K.: Hodder & Stoughton.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1996).Structured clinical interview for DSM-IV axis I disorders - PatientEdition (SCID-I/P, Version 2.0). New York: Biometrics Research De-partment.
Fredrickson, B. L., & Levenson, R. W. (1998). Positive emotions speedrecovery from the cardiovascular sequelae of negative emotions. Cog-nition and Emotion, 12, 191–220.
Geschwind, N., Peeters, F., Jacobs, N., Delespaul, P., Derom, C., Thiery,E., . . . Wichers, M. (2010). Meeting risk with resilience: High daily lifereward experience preserves mental health. Acta Psychiatrica Scandi-navica, 122, 129–138.
Giacobbi, P. R., Hausenblas, H. A., & Frye, N. (2005). A naturalistic assessmentof the relationship between personality, daily life events, leisure-time exercise,and mood. Psychology of Sport & Exercise, 6, 67–81.
Hawkley, L. C., Thisted, R. A., & Cacioppo, J. T. (2009). Lonelinesspredicts reduced physical activity: Cross-sectional & longitudinal anal-yses. Health Psychology, 28, 354–363.
Jacobs, N., Nicolson, N. A., Derom, C., Delespaul, P., van Os, J., &
Myin–Germeys, I. (2005). Electronic monitoring of salivary cortisolsampling compliance in daily life. Life Sciences, 76, 2431–2443.
Kanning, M., & Schlicht, W. (2010). Be active and become happy: Anecological momentary assessment of physical activity and mood. Jour-nal of Sport and Exercise Psychology, 32, 253–261.
Kendler, K. S., Thornton, L. M., & Prescott, C. A. (2001). Gender differences inthe rates of exposure to stressful life events and sensitivity to their depressogeniceffects. American Journal of Psychiatry, 158, 587–593.
Lardinois, M., Lataster, T., Mengelers, R., Van Os, J., & Myin–Germeys,I. (2011). Childhood trauma and increased stress sensitivity in psychosis.Acta Psychiatrica Scandinavica, 123, 28–35.
Larson, R., & Csikszentmihalyi, M. (1983). The experience samplingmethod. New directions for methodology of social and behavioral sci-ence, 15, 41–56.
Lepage, M. L., & Crowther, J. H. (2010). The effects of exercise on bodysatisfaction and affect. Body Image, 7, 124–130.
Mata, J., Thompson, R. J., Jaeggi, S. M., Buschkuehl, M., Jonides, J., &Gotlib, I. H. (2011). Walk on the bright side: Physical activity and affectin major depressive disorder. Journal of Abnormal Psychology. Advanceonline publication. http://dx.doi.org/10.1037/a0023533
McCormick, B. P., Frey, G., Lee, C. T., Chun, S., Sibthorp, J., Gajic,T., . . . Maksimovich, M. (2008). Predicting transitory mood from phys-ical activity level among people with severe mental illness in twocultures. International Journal of Social Psychiatry, 54, 527–538.
Mead, G. E., Morley, W., Campbell, P., Greig, C. A., McMurdo, M., &Lawlor, D. A. (2009). Exercise for depression. Cochrane DatabaseSystematic Reviews, 3, http://dx.doi.org/10.1002/14651858.CD14004366.pub14651854
Myin–Germeys, I., Oorschot, M., Collip, D., Lataster, J., Delespaul, P., & van Os,J. (2009). Experience sampling research in psychopathology: Opening the blackbox of daily life. Psychological Medicine, 39, 1533–1547.
Myin–Germeys, I., van Os, J., Schwartz, J. E., Stone, A. A., & Delespaul,P. A. (2001). Emotional reactivity to daily life stress in psychosis.Archives of General Psychiatry, 58, 1137–1144.
Neeper, S. A., Gomez–Pinilla, F., Choi, J., & Cotman, C. W. (1996).Physical activity increases mRNA for brain-derived neurotrophic factorand nerve growth factor in rat brain. Brain Research, 726, 49–56.
Ready, R. E., Marquez, D. X., & Akerstedt, A. (2009). Emotion in youngerand older adults: Retrospective and prospective associations with sleepand physical activity. Experimental Aging Research, 35, 348–368.
Schwerdtfeger, A., Eberhardt, R., Chmitorz, A., & Schaller, E. (2010). Momentaryaffect predicts bodily movement in daily life: An ambulatory monitoring study.Journal of Sport and Exercise Psychology, 32, 674–693.
Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momen-tary assessment. Annual Reviews in Clinical Psychology, 4, 1–32.
StataCorp. (2009). Stata statistical software, College Station, TX: StataCorp.Steptoe, A., Kimbell, J., & Basford, P. (1998). Exercise and the experience
and appraisal of daily stressors: A naturalistic study. Journal of Behav-ioral Medicine, 21, 363–374.
Sugawara, J., Tarumi, T., & Tanaka, H. (2010). Effect of mirthful laughteron vascular function. American Journal of Cardiology, 106, 856–859.
Trull, T. J., & Ebner–Priemer, U. W. (2009). Using experience samplingmethods/ecological momentary assessment (ESM/EMA) in clinical as-sessment and clinical research: Introduction to the special section. Psy-chological Assessment, 21, 457–462.
Tugade, M. M., & Fredrickson, B. L. (2004). Resilient individuals usepositive emotions to bounce back from negative emotional experiences.Journal of Personality and Social Psychology, 86, 320–333.
Tugade, M. M., Fredrickson, B. L., & Barrett, L. F. (2004). Psychologicalresilience and positive emotional granularity: Examining the benefits ofpositive emotions on coping and health. Journal of Personality, 72,1161–1190.
Vazou–Ekkekakis, S., & Ekkekakis, P. (2009). Affective consequences of
9PHYSICAL ACTIVITY AND MOMENTARY DAILY LIFE AFFECT

imposing the intensity of physical activity: Does the loss of perceivedautonomy matter? Hellenic Journal of Psychology, 6, 125–144.
Vazquez, C., Cervellon, P., Perez–Sales, P., Vidales, D., & Gaborit, M.(2005). Positive emotions in earthquake survivors in El Salvador (2001).Journal of Anxiety Disorders, 19, 313–328.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and vali-dation of brief measures of positive and negative affect: The PANASscales. Journal of Personality and Social Psychology, 54, 1063–1070.
Wichers, M., Kenis, G., Jacobs, N., Myin–Germeys, I., Schruers, K.,Mengelers, R., . . . Van Os, J. (2008). The psychology of psychiatricgenetics: Evidence that positive emotions in females moderate geneticsensitivity to social stress associated with the BDNF Val-sup-6-sup-6Met polymorphism. Journal of Abnormal Psychology, 117, 699–704.
Wichers, M., Myin–Germeys, I., Jacobs, N., Peeters, F., Kenis, G., Derom,C., & Van Os, J. (2007a). Genetic risk of depression and stress-inducednegative affect in daily life. British Journal of Psychiatry, 191, 218–223.
Wichers, M., Peeters, F., Geschwind, N., Jacobs, N., Simons, C. J., Derom,C., . . . Van Os, J. (2010). Unveiling patterns of affective responses in
daily life may improve outcome prediction in depression: A momentaryassessment study. Journal of Affective Disorders, 124, 191–195.
Wichers, M. C., Barge–Schaapveld, D. Q., Nicolson, N. A., Peeters, F., deVries, M., Mengelers, R., . . . Van Os, J. (2009). Reduced stress-sensitivity or increased reward experience: The psychological mecha-nism of response to antidepressant medication. Neuropsychopharmacol-ogy, 34, 923–931.
Wichers, M. C., Myin–Germeys, I., Jacobs, N., Peeters, F., Kenis, G.,Derom, C., . . . Van Os, J. (2007b). Evidence that moment-to-momentvariation in positive emotions buffer genetic risk for depression: Amomentary assessment twin study. Acta Psychiatrica Scandinavica,115, 451–457.
Zautra, A. J., Johnson, L. M., & Davis, M. C. (2005). Positive affect as asource of resilience for women in chronic pain. Journal of Consultingand Clinical Psychology, 73, 212–220.
Zheng, H., Liu, Y., Li, W., Yang, B., Chen, D., Wang, X., . . . Halberg, F.(2006). Beneficial effects of exercise and its molecular mechanisms ondepression in rats. Behavioural Brain Research, 168, 47–55.
10 WICHERS ET AL.




















