
Slum upgrading and urban governance: Case studies in three South East Asian cities
Upload
khangminh22Category
view
4download
0
Occup. Med. Vol. 50, No. 1, pp. 64-73, 2000Copyright © 2000 Lippincott Williams & Wilkins for SOM
Printed in Great Britain. All rights reserved0962-7480/00
OCCUPATIONALMEDICINE IN THE21ST CENTURY
A South-East Asian perspectiveD. Koh, S. E. Chia and J. JeyaratnamDept of Community, Occupational & Family Medicine, National University ofSingapore, Republic of Singapore
In order to discuss the subject of occupational medicine in the next century, changes inthe present demographic profile and work activity must be considered first. Only thencan the challenges be identified, and appropriate strategies be formulated to respondto them. In the diverse countries of South-East Asia, improved health and workconditions, the advent of new technology, a redistribution of work activity, and anageing workforce can be expected. Two other factors that have specific impact in theregion are the recent financial crisis and the occurrence of an internationalenvironmental haze from forest fires. The various countries in South-East Asia, which arein different stages of development, and have different problems and priorities, willrespond differently to the demands for occupational health. It is likely that there will be ashift in the focus of current health care activities towards specific work sectors, therecognition of new hazards at work, the identification of newly emerging work relateddiseases, and an increase in health promotion in the workplace. Hopefully, there will beimproved training of health professionals to ensure that there are adequate numbersand that they are well prepared to face these changes. Responsive, appropriate andwell enforced labour legislation to protect the health of all workers, and international co-operation in occupational and environmental health are also required. As global andregional economic conditions continue to remain unstable and the impact of the crisisfurther takes its course, the final effect on occupational health in South-East Asiaremains to be seen.
Key words: 21st century; environmental health; occupational health; South-East Asia.
Occup. Med. Vol. SO, 64-73, 2000
INTRODUCTION
The 21st century offers a bright vision of better health for all.It holds the prospect not merely of longer life, but superiorquality of life, with less disability and disease. As the newmillennium approaches, the global population has never hada healthier outlook. (World Health Organization, 19981).
Throughout the world, excellence in the practice ofhealth care is characterized by its responsiveness andrelevance to the needs of society. The same is true foroccupational health (OH) practice. As a result, thereexists a global spectrum of OH activities. In develop-ing countries, the activities may primarily be thecontrol of work accidents and occupational diseases.As a country develops, a shift of focus to work-related
Correspondence to: Dr David Koh, Dept of Community, Occupational andFamily Medicine (MD3), Faculty of Medicine, National University ofSingapore, 16, Medical Drive, SINGAPORE 119260, 7597.Tel: +65 8 744988; fax: +65 7 791489; e-mail: [email protected]
disorders and concern with psychosocial issues can beseen, as in many newly developing and industrializedsocieties.
In a newly industrializing region like South-EastAsia, the pattern is no different. Priorities andemphases in occupational health have changed overthe last few decades as the countries in the region havedeveloped. There is no doubt that it will continue tochange.
The countries in South-East Asia are members of theAssociation of South-East Asian Nations (ASEAN).ASEAN was established on 8 August 1967. The fivefounder members were Indonesia, Malaysia, Philippines,Singapore and Thailand. Brunei Darussalam joined theAssociation on 8 January 1984, and Vietnam became theseventh member of ASEAN on 28 July 1995. On 23 July1997, Laos and Myanmar were admitted into ASEAN.Cambodia is expected to join the grouping in duecourse.
With a total population of about 500 million, theASEAN countries are diverse in terms of size, popula-tion, language, religious beliefs, ethnicity, type of work-force and industries (Table I).2 Many, such as the
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022

D. Koh et ai: Occupational medicine in 21st century S.E. Asia 65
Table 1. Selected statistics of ASEAN countries
BRUNEICapital: Bandar Seri BegawanPopulation: 0.3 millionLabour force: 138,000 (1996*)Government type: constitutional monarchyGDP: B$7,452.1 million (1996*)Major industries: oil and gas industry, textiles, food & beverages,
building materialsMajor exports: oil and gas, ready-made garments
CAMBODIACapital: Phnom PenhPopulation: 11.5 million (1998)Currency: Riel (US$1 =3300 Riels)Major export products: garments/textile product, sawn wood furniture
and rubberMajor industries: textiles and garments, beverage, food processing,
wood processing
INDONESIACapital: JakartaPopulation: 200 million (end 1996)Labour force: 78.3 million (in 1995 est.)Religion: Islam 87%, Christianity 10%,
others (Hinduism, Buddhism, others)Government type: RepublicGDP: US$222.5 billion (1996)Exchange rate: 1 US$ = Rp 2383 (31 December 1996)Major industries: pulp and paper, cement, basic metals and fertilizer,
power generation, telecommunication, transportMajor exports: textiles, electronic goods, footwear, oil & gas, plywood,
sawn timber
LAOSCapital: VientianePopulation: 4.8 million (1996)Labour force: 2.03 million (1996)Religion: Buddism 95%, other 5%GDP: Kip 1901 billion (1997)National currency: KipMajor exports: electricity, clothing, wood and forest products
MALAYSIACapital: Kuala LumpurPopulation: 21.6 million (1997)Labour force: 8.6 million (1997)Religion: Islam, Buddhism, Taoism, Hinduism, ChristianityGovernment type: constitutional monarchyGDP: 8.0% (RM141.13 billion, 1997)Exchange rate: US$1 = RM2.5175 (1996 average)
US$1 = RM3.4000 (24 October 1997)Major industries: electronics & electrical goods, textiles, clothing &
footwear, chemicals, petroleum, wood products, metal productsand rubber
Major exports/products: electronic & electric machinery, petroleum &LNG, textiles, clothing & footwear and palm oil, sawn timber &wood products, rubber, cocoa & cocoa products
MYANMARCapital: YangonPopulation: 45.57 million (1996/97)Labour force: 26.86 million (1996/97)Religion: Buddism 89.4%, Christianity 4%, Islam and others 6.6%Government: The State Law and Order Restoration CouncilCurrency: Kyat (K)GDP: K70.586 million (1996/97), at constant 1985-1986 price
K715,438 million (1996/97), at current priceMajor economic sectors: agriculture, trade & services, industry, miningMajor industries: agro-based industries, wood-based industries, textiles,
heavy industries, steel millsMajor exports: rice, teak, beans & pulses, rubber, coffee, minerals,
gems, marine products
Land area: 5769 sq. kmPopulation growth rate: 3.1% (1996)Language: Malay Religion: IslamExchange rate: 1 unit = US$1.4 (1996)Real GDP growth rate: 3.5% (1996*)
Land area: 181,035 sq. kmOfficial language: Khmer
Land area: 1.9 million sq. kmPopulation growth rate: 1.6% (in 1996 est.)Language: Bahasa Indonesia
Real GDP growth rate: 7.8% (1996)
Land area: 236,800 sq. kmPopulation growth rate: 2.4% (1996)Language: LaoGovernment type: People's Democratic RepublicReal GDP growth rate: 7% (1996/97)Exchange rate: Kip 920 = US$1 (1996), Kip 1170 = US$1 (July 1997)
Land area: 329,758 sq. kmPopulation growth rate: 2.3% (1997)Language: Bahasa Melayu, English, Chinese, Tamil
Currency: Malaysian Ringgit (RM)
Land area: 677,000 sq. kmPopulation growth rate: 1.84% (1996/97)Language: Myanmar
Exchange rate: K5.9104 = US$1
Real GDP growth rate: 5.8% (1996/97)
Continued
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022
66 Occup. Med. Vol. 50, 2000
Table 1 . continued
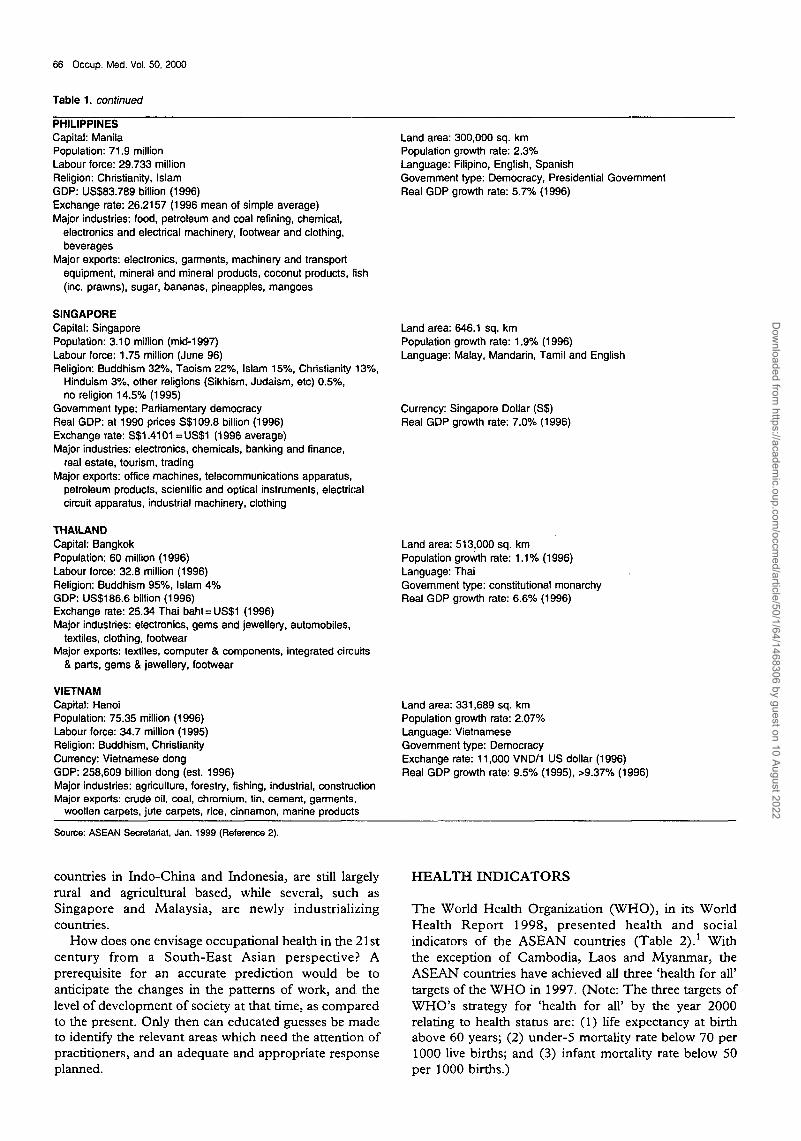
PHILIPPINESCapital: ManilaPopulation: 71.9 millionLabour force: 29.733 millionReligion: Christianity, IslamGDP: US$83,789 billion (1996)Exchange rate: 26.2157 (1996 mean of simple average)Major industries: food, petroleum and coal refining, chemical,
electronics and electrical machinery, footwear and clothing,beverages
Major exports: electronics, garments, machinery and transportequipment, mineral and mineral products, coconut products, fish(inc. prawns), sugar, bananas, pineapples, mangoes
SINGAPORECapital: SingaporePopulation: 3.10 million (mid-1997)Labour force: 1.75 million (June 96)Religion: Buddhism 32%, Taoism 22%, Islam 15%, Christianity 13%,
Hinduism 3%, other religions (Sikhism, Judaism, etc) 0.5%,no religion 14.5% (1995)
Government type: Parliamentary democracyReal GDP: at 1990 prices S$109.8 billion (1996)Exchange rate: S$1.4101 =US$1 (1996 average)Major industries: electronics, chemicals, banking and finance,
real estate, tourism, tradingMajor exports: office machines, telecommunications apparatus,
petroleum products, scientific and optical instruments, electricalcircuit apparatus, industrial machinery, clothing
THAILANDCapital: BangkokPopulation: 60 million (1996)Labour force: 32.8 million (1996)Religion: Buddhism 95%, Islam 4%GDP: US$186.6 billion (1996)Exchange rate: 25.34 Thai baht = US$1 (1996)Major industries: electronics, gems and jewellery, automobiles,
textiles, clothing, footwearMajor exports: textiles, computer & components, integrated circuits
& parts, gems & jewellery, footwear
VIETNAMCapital: HanoiPopulation: 75.35 million (1996)Labour force: 34.7 million (1995)Religion: Buddhism, ChristianityCurrency: Vietnamese dongGDP: 258,609 billion dong (est. 1996)Major industries: agriculture, forestry, fishing, industrial, constructionMajor exports: crude oil, coal, chromium, tin, cement, garments,
woollen carpets, jute carpets, rice, cinnamon, marine products
Land area: 300,000 sq. kmPopulation growth rate: 2.3%Language: Filipino, English, SpanishGovernment type: Democracy, Presidential GovernmentReal GDP growth rate: 5.7% (1996)
Land area: 646.1 sq. kmPopulation growth rate: 1.9% (1996)Language: Malay, Mandarin, Tamil and English
Currency: Singapore Dollar (S$)Real GDP growth rate: 7.0% (1996)
Land area: 513,000 sq. kmPopulation growth rate: 1.1% (1996)Language: ThaiGovernment type: constitutional monarchyReal GDP growth rate: 6.6% (1996)
Land area: 331,689 sq. kmPopulation growth rate: 2.07%Language: VietnameseGovernment type: DemocracyExchange rate: 11,000 VND/1 US dollar (1996)Real GDP growth rate: 9.5% (1995), >9.37% (1996)
Source: ASEAN Secretariat, Jan. 1999 (Reference 2).
countries in Indo-China and Indonesia, are still largelyrural and agricultural based, while several, such asSingapore and Malaysia, are newly industrializingcountries.
How does one envisage occupational health in the 21stcentury from a South-East Asian perspective? Aprerequisite for an accurate prediction would be toanticipate the changes in the patterns of work, and thelevel of development of society at that time, as comparedto the present. Only then can educated guesses be madeto identify the relevant areas which need the attention ofpractitioners, and an adequate and appropriate responseplanned.
HEALTH INDICATORS
The World Health Organization (WHO), in its WorldHealth Report 1998, presented health and socialindicators of the ASEAN countries (Table 2).1 Withthe exception of Cambodia, Laos and Myanmar, theASEAN countries have achieved all three 'health for all'targets of the WHO in 1997. (Note: The three targets ofWHO'S strategy for 'health for all' by the year 2000relating to health status are: (1) life expectancy at birthabove 60 years; (2) under-5 mortality rate below 70 per1000 live births; and (3) infant mortality rate below 50per 1000 births.)
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022

D. Koh ef a/.: Occupational medicine in 21st century S.E. Asia 67
Table 2. Life expectancy, infant mortality statistics, literacy rate, per capita GNP, and urban centre populations of ASEAN countries
Country
BruneiCambodiaIndonesiaLaosMalaysiaMyanmarPhilippinesSingaporeThailandVietnam
Life expectancyat birth (both sexes)
1997
76546553726068776967
2025
79677367777175817675
Infant mortalityrate per 1000
1997
610449871179365
3038
2025
54018397
25145
1018
Adultliteracy
rate (1995)
88.2-
83.856.683.583.194.691.193.893.7
GNP percapita
(US$, 1995)
—
270980350
3890-
105026,730
2740240
Population > 1 million inurban centres (%),
1995
008069
15100116
Table 3. Confirmed cases of occupational diseases in Singapore, by type of disease, 1990-1997
Type of disease
Noise induced hearing lossIndustrial dermatitisOccupational asthmaPoisoning/excessive absorptionSilicosisAsbestosisOthers
Total
1990
6931541171704
940
1991
842173
52682
14
1070
'1992
655164
74043
24
897
1993
560168
6124
92
31
900
1994
754161
94032
30
999
1995
1068170
979
11
17
1345
1996
1302111
76420
35
1521
1997
861126
730
11
28
1054
Source: Ministry of Manpower (previously Ministry of Labour), Singapore (Reference 4).
Adult literacy rates in most ASEAN countries arehigh, and the majority of people do not live in urbancentres of above 1 million people. The GNP per capita ishighly variable, and the whole region has been affectedby a major economic crisis in 1998, which has seen majorcurrency devaluations.
Projections for the ASEAN countries by the WHO forthe year 2025 are generally positive. Infant mortalityrates are expected to decline, and life expectancy at birthis expected to increase.
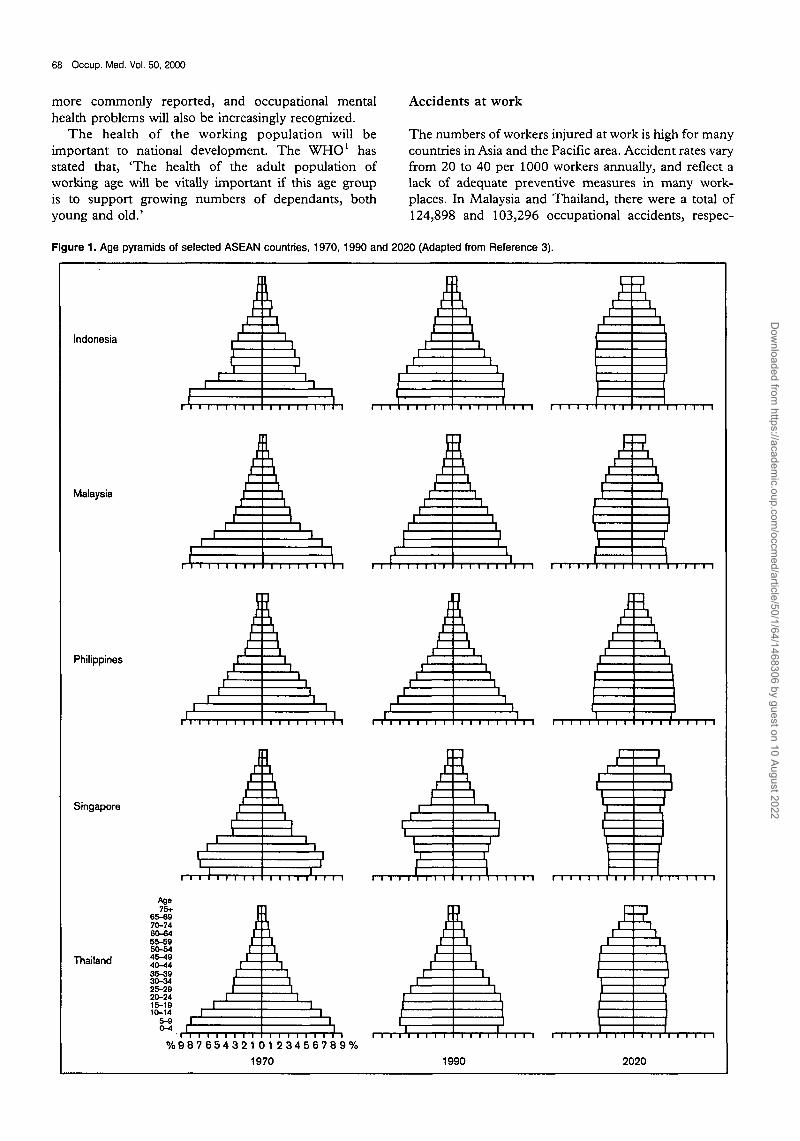
Ageing of the ASEAN population
The population in ASEAN countries will age signifi-cantly.3 The age pyramid in this region will approximatethat of developed countries, with a preponderance of olderand more experienced workers (Figure 1). Retirement ageis projected to increase. For example, in Singapore, theretirement age of 55 years was recently raised to 60 years. Itwill eventually be extended to 67 years.
Diseases in South-East Asia during the 21st century
The pattern of disease in the community will reflect theageing of the population. Life expectancy in all ASEANcountries is expected to rise. Mortality and morbidityfrom non-communicable diseases will predominate inthe more developed countries, with a significant propor-tion of the ageing workers suffering from chronic
medical conditions such as cardiovascular diseases,diabetes and other degenerative diseases. These workerswould still be expected to work productively. The cost ofhealth care will also increase, and employers willprobably have more incentive to provide preventivehealth care to employees, rather than just purely curativemedical treatment.
With improved work conditions and better preventivehealth care, the majority of the classical 'occupational'diseases, such as lead poisoning or noise induced hearingloss, should diminish. However, occupational diseasestatistics from ASEAN countries are neither readilyavailable nor accurate.
In Singapore, which arguably has one of the morecomprehensive databases for occupational diseases,about 1000 cases of occupational diseases are reportedand confirmed in Singapore by the Ministry of Labourannually.4'5 These data (Table 3) are a gross under-estimate of the true situation in industry because ofundernotification. However, the data do give some ideaof the types of occupational disease seen in the country.Data from the other more agricultural ASEAN countrieswould show other patterns of disease, such as pesticidepoisoning.
The numbers and types of occupational diseases seenin ASEAN will change in the next century. Nevertheless,traditional occupational health diseases and problemswill remain in some countries. In most countries,occupational musculoskeletal diseases are likely to be
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022
68 Occup. Med. Vol. 50, 2000
more commonly reported, and occupational mentalhealth problems will also be increasingly recognized.
The health of the working population will beimportant to national development. The WHO1 hasstated that, 'The health of the adult population ofworking age will be vitally important if this age giroupis to support growing numbers of dependants, bothyoung and old.'
Accidents at work
The numbers of workers injured at work is high for manycountries in Asia and the Pacific area. Accident rates varyfrom 20 to 40 per 1000 workers annually, and reflect alack of adequate preventive measures in many work-places. In Malaysia and Thailand, there were a total of124,898 and 103,296 occupational accidents, respec-
Flgure 1. Age pyramids of selected ASEAN countries, 1970, 1990 and 2020 (Adapted from Reference 3).
Indonesia
Malaysia
Philippines
Singapore
Thailand
I1
r
Ii
i
i ii ii i)
i ii . )
i (i {
• , • . • • i 1 . . i • I • , i • i
ii i
1i
1
i,i
PAEA
1
1I
1
f=[
Lj _
1
11
11
, , ,
kl1
1
1|
Age75+
65-6970-7460-6455-5950-5445-4940-4435-3930-3425-2920-2415-19
101I
i
/I
Ii
i
||~1
i
% 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 %
1970
I I I I 1
i
i
\|
Ii
i
|||
ii
i
[J
rIIi
i
ii
i
i
J
;i
4i 1
1
• • • / ' • • • • •
I
Li
ii
1990 2020
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022

D. Koh et a/.: Occupational medicine in 21st century S.E. Asia 69
tively, in 1991. In Singapore, there were 4835 occupa-tional accidents in 1992. The accident rates in thesecountries were 25 (Malaysia), 38 (Thailand) and 10(Singapore) per 1000 workers.6
Fatal accident rates are also high. The ILO has shownthat the annual incidence of fatal occupational accidentsis about 30 per 100,000 workers in Myanmar, Thailandand Indonesia, as compared to rates of between 5 to 10per 100,000 workers in the developed countries. Thefatality rates are much higher in some industries such asconstruction and mining.6
From this information, and noting the current rate ofdevelopment in South-East Asian countries, occupa-tional accidents and safety issues will remain a problemin many ASEAN countries in the 21st century.
SOCIAL INDICATORS
Economic activity and work style
In terms of the types of economic activity, ASEANcountries will continue to be at different stages ofdevelopment. The shift in sectoral composition of theworkforce tends to follow a pattern.7 In the countries inearly stages of development, agriculture contributesextensively to national wealth and the workforce. Withdevelopment, the role of agriculture begins to declineand the contribution of the manufacturing sector to thenational wealth and workforce becomes dominant.Finally, there comes a situation where the services sectorbecomes the largest income source, as in the higheconomy or industrialized countries.
Thus, agriculture, mining and fishing will remainimportant industries for some ASEAN countries in theforeseeable future. In others, there will be different stagesof industrialization, with small and medium scaleindustries as well as the participation of multinationalcompanies. Labour costs in several ASEAN countries arerelatively low, and labour intensive manufacturingprocesses, such as assembly-line work, may developfurther. In the more developed ASEAN nations, activitiesin the manufacturing sector will gravitate towards highvalue added manufacturing processes such as upstreamelectronics manufacture, e.g. wafer fabrication.
Some ASEAN countries will continue to developtourism, financial and business concerns. The informa-tion technology sector and its related fields shouldcontinue to observe growth in those countries withfinancial centres. An enlargement of service sectoractivities is expected, which would result in the employ-ment of a larger section of the population.
The implication here is mat OH activities, which havelargely been focused on the factory environment, mayneed to be slightly re-oriented to serve the needs of theservice sector. This is because the OH problems andneeds of the service industry are quite different.
Information technology
Another aspect to consider in the 21st century wouldrelate to the way we work. Work would be profoundly
influenced by the advent of the information superhigh-way and developments in information technology. Thegeneral public, as well as health practitioners, would haveto be computer literate. Electronically stored informationwill routinely be available on the Internet and opticalstorage media. The ASEAN countries, with their highliteracy rates and strong emphasis on education, will seestrong inroads made into information technology.
While information access is a positive development,what is needed is also further education for people to beable to sieve through and meaningfully interpret and usethe plethora of information. Another issue of concern isto ensure the training of people in the correct use ofhardware and software, thereby preventing potentialwork-related illnesses.
Teleworkers, who work from home, will be anincreasing feature of the workforce. Such a trend hasalready been noted in Singapore, where the Ministry ofManpower reported that the number of workers doingoffice work from home have increased from five to 2625since 1995.8
Other developments in ASEAN
Apart from current social and political unrest in severalASEAN countries (notably Indonesia), which will not bediscussed further, two specific issues will continue tohave an impact on the ASEAN countries in the 21stcentury. These are the regional financial crisis of the late1990s, and the problem of an environmental haze arisingfrom forest fires. Their effects will extend beyond theeconomic and social spheres into general health andenvironmental and occupational health.
The regional financial crisis. In July 1997, pressure onthe Thai baht in the foreign exchange markets resulted ina devaluation of the currency by about 40%. This led to acontagion of devaluation of other East Asian currencies,particularly Malaysia, Indonesia, the Philippines andSouth Korea. Compared to their July 1997 values, theMalaysian ringgit had fallen about 40%, the Indonesianrupiah by 80% and the peso by 30% against the USdollar. Other ASEAN countries were also affected. TheSingapore dollar devalued by 15%, the Laotion kip by70%, the Myanmar kyat by 50% and the Vietnamesedong by 15%.2 The financial crisis resulted in Thailand,and subsequently Indonesia, to resort to InternationalMonetary Fund assistance. As foreign debts increased inlocal currency terms, stock markets slumped, confidencein the financial and banking sector eroded, and output,domestic demand and investments in these economiesbegan to slow down.
Air pollution from forest fires. From the mid-1990s,forest fires in Sumatra and Borneo resulted in periodicair pollution and haze in several parts of South-East Asia,usually in the last quarter of the year. For example, inSeptember and October 1994, the atmospheric concen-tration of particulate matter less than 10 fim in aero-dynamic diameter (PM\0) was 20% higher than theprevious year in Singapore.9 Correspondingly, an
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022
70 Occup. Med. Vol. 50, 2000
increase in the emergency room attendance for acutechildhood asthma was observed in general hospitals.
From July 1997 to March 1998, the forest fires causedthe region's worst pollution to date. A conference titledThe First Regional Workshop to Strengthen the Capacity ofASEAN to Prevent and Mitigate Transboundary Atmo-spheric Pollution was held at the Asian Development Bank(ADB) in Manila on the 1 and 2 September 1998. In hisopening remarks, the Vice-president of the ADB, PeterH. Sullivan, said
In just a few months the Indonesia forest fires released aquantity of greenhouse gases equal to that emitted by all ofEurope's cars and power plants in an entire year. The 1997haze resulted in the worst pollution ever recorded in theASEAN region, and caused enormous health and safetyproblems in Indonesia, Singapore, Brunei Darussalam, andMalaysia. Environmental groups estimate the losses due tothe forest fires to be about US$4.5 billion.
THE 21ST CENTURY IN SOUTH-EAST ASIA
How then should the countries in South-East Asia respondto the changing patterns of work and developments insociety? It would have to change in terms of its activities,the training and development of OH professionals, andnational policy and legislation in OH, in order to meet theneeds of the countries involved. These changes will also beaffected by prevailing economic and social conditions.
Response to the regional financial crisis
A major fear of the economic crisis is its potential toeradicate the progress made in social and humandevelopment over the last three decades. The spectreof rising unemployment looms large as some membersface zero or negative growth in the next few years. Peoplein the lower socio-economic strata are particularlyvulnerable, with women and young school-leavers likelyto be the hardest hit.
The current financial crisis has focused attention onthe problems of employment and poverty.10 Theconclusions adopted by delegates to the ELO's TwelfthAsian Regional Meeting, held in Bangkok in December1997, called for a strong response by the ILO to minimizethe adverse social effects of the crisis by offering technicalcooperation and assistance to member states.
Among the recommendations were the following.Immediate steps should be taken for training andredeployment of displaced workers; and protectionshould be given to women, migrant workers and othergroups that may be adversely affected. Employmentshould be promoted through sound enterprise develop-ment strategies, investment in human resources and abusiness environment conducive to sustained enterprisecompetitiveness in a rapidly changing global economy.The conclusions also stressed the importance of ensuringthat additional employment, when generated, should beadequately remunerated and carry appropriate socialprotection.
The ILO meeting also suggested that efforts be made todevelop and extend mechanisms to cover workers insectors that are currently unprotected. It noted that anactive commitment to tripartite cooperation, transparentpolicy formulation and effective implementation ofpolicies to protect workers are essential not only in periodsof growth but also, especially in times of crisis, when theworkforce is expected to adjust rapidly to new situations.
As a regional grouping, ASEAN had requested thatthe G7 countries grant the region greater market accessand encourage their banks to maintain credit support forthe ASEAN economies. ASEAN also remains committedto the maintenance of an open trade and investmentenvironment, pushing on with initiatives such as theASEAN Free Trade Area (AFTA) and the ASEANInvestment Area (AIA).
Response to the environmental haze
A Regional Haze Action Plan (RHAP) was adopted byASEAN Ministers in December 1997.11 The RHAP hasthree components: prevention, mitigation, and monitor-ing the effects of forest fires and haze that are likely torecur in the region. It is based on national haze actionplans of ASEAN members that are directly or indirectlyaffected by forest fires and haze.
To ensure implementation, countries have beenassigned responsibilities: Malaysia will take the lead inprevention; Singapore in monitoring; and Indonesia inmitigation of forest fires. Fire-fighting arrangements forSumatra and Borneo will continue to be led by Malaysiaand Brunei Darussalam, respectively. Some progress hasalready been made in its implementation.2
The ASEAN secretariat has noted one positive aspectof the region's forest fire and haze problem. It has servedto unify the ASEAN countries, and has encouraged themto work together despite their differences and domesticconcerns, and the impacts that they have suffered fromthe financial crisis besetting the region.
National policy and legislation
In spite of positive developments in recent years, manyASEAN countries still face common problems, such asthe following.
• Workers are generally unaware of the hazards towhich they are exposed.
• Preventive measures are taken by large enterprises,seldom by small ones.
• The legal requirements of OSH are often notcomplied with.
• Enterprises employ few trained safety personnel, andbipartite safety committees, where they exist, arerarely active.
• Statistics on occupational accidents and diseases areinadequate.
• Labour inspectorates have limited staff and technicalexpertise.
• Training and technical advisory services by govern-ments and private institutions are insufficient.
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022
D. Koh ef a/.: Occupational medicine in 21st century S.E. Asia 71
The experience of industrialized countries shows thatoccupational accidents and diseases, even in times of rapidgrowth, can be significantly reduced. This requires a strongnational policy and legislation for occupational health.
As a crude reflection of labour standards, it can benoted that the more developed countries in the Asia-Pacific region, such as Australia, New Zealand andJapan, have ratified far more ILO conventions than thedeveloping countries in ASEAN12 (Table 4).
Some developments have occurred in South-EastAsia. For example, Malaysia enacted a comprehensiveOSH legislation in 1994, and established a NationalInstitute of Occupational Safety and Health within thelast decade. A similar National Institute of Occupationaland Environmental Health exists in Vietnam. OSHtraining has been expanded in several ASEAN countries.An example is the development of an OSH trainingcentre in Singapore, which offers training to workers,safety officers and OH personnel. The Philippines alsohas an OSH Centre that is involved in research andtraining, and provision of services and information.
However, it can be noted that, in general, for mostASEAN countries national policy on occupational healthneeds to be strengthened. Current occupational healthlegislation can be made more comprehensive (for exam-ple, Singapore has a Factories Act, which does not protectthe majority of workers in non-factory environments)reinforced and better enforced. Unfortunately, the needfor strong legislation as a driving force for employers to paymore than lip service to OH has been the experience inmany developing countries. This would most likely be thecase in South-East Asia, even in the 21st century.
Occupational health services
The ILO and WHO have recommended that everynation develop a national occupational health service andthat, as far as possible, they be integrated into thenational health care system. However, there is largevariation in the provision of such services among theASEAN nations.
Table 4. ILO conventions adopted in some East Asian countries(December 1994)
Country ILO conventions in force
AustraliaNew ZealandJapanPhilippinesSingaporeChinaMyanmarThailandVietnamIndonesiaMalaysiaCambodiaLaos
484840252017161111101054
Occupational health activities
There is some interest in occupational health in Asia.Several ASEAN countries (e.g. Indonesia, Philippines,Thailand, Malaysia, Singapore) have national associa-tions of occupational health physicians, nurses, andsafety officers. These bodies conduct various educationaland professional activities for their members. An AsianAssociation of Occupational Health exists, and hoststriennial meetings - the Asian Conference on Occupa-tional Health - which are generally well attended byseveral hundred delegates. The last meeting was held inKuala Lumpur and the next, scheduled at the end of1999, will be held in the Philippines.
In terms of workers' health, newer activity areas whichneed to be addressed would include health promotion atthe workplace, and the health of ageing and elderlyworkers. As for system specific disorders, data from thedeveloped countries suggest that work related muscu-loskeletal and mental health disorders appear to beemerging epidemics. 13
Source: Taylor, 1997 (Reference 12).
Traditional occupational health concerns willremain
Traditional OH concerns remain; for example, acutepesticide poisoning in agricultural countries, and occu-pational diseases such as silicosis. A recent report fromVietnam presented a 16% prevalence of chronic pesticidepoisoning among pesticide sprayers in rural areas, andapproximately 9000 cumulative cases of silicosis from1978 and 1997.14
Another concern, with the globalization of work, is thetransfer of hazardous industries from developed todeveloping countries. For example, a Japanese-Malay-sian company was established to extract rare-earthchlorides from monazite in Malaysia. The monazite inMalaysia contains 7% thorium, a radioactive substancewith a half-life of 14 billion years. The radiation level wasevaluated and found to be 800 times above normal. Evenafter enclosure attempts, the radioactivity level was stillfound to be 150 times above normal. After a 7-year legalbattle by residents and environmentalists against thecompany, the operations were ordered closed by a courtruling, but this was subsequently reversed by a high courtruling.15 More recently, there was a report of toxicindustrial waste dumped in Cambodia by a Taiwanesecompany. Analysis of the 3000 tonnes of waste, acompressed industrial ash, showed the mercury contentto be 675 ppm. The news of the waste sparked riots anda panicked exodus of more than 10,000 people.16
Health promotion in the workplace
As occupational diseases and work related diseases comeunder control, the movement towards health promotionin the workplace, which has begun in recent years, wouldgain momentum. Health promotion at work is animportant component of good OH practice, and theconcept of a health promoting workplace has beenestablished by the WHO.
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022

72 Occup. Med. Vol. 50, 2000
There is an urgent need for further efforts in healthpromotion, and to work hand in hand with healtheducation officers and health care facilitators. The OHapproach first aims to correct an unhealthy workenvironment, before targeting lifestyle changes of theworkers at risk. Unfortunately, some health promotionfacilitators emphasize the importance of lifestylechanges, while overlooking the need to prioritize thecontrol of an unhealthy work environment.
Another challenge in health promotion is the need forobjective and accurate evaluations of the plethora ofhealth promotion activities. While some activities, suchas smoking cessation programmes, are of unquestionablebenefit, others, such as indiscriminate multiphasicscreening, are of unsubstantiated or even questionablevalue. Unfortunately, activities such as multiphasicscreening are becoming increasingly common andoffered as corporate benefits to executives in South-EastAsia.
Mental health
Psychosocial hazards will become proportionately moreimportant in the coming years. OH professionals arelargely comfortable in assessing and managing chemical,physical and biological hazards. Much less attention hasbeen paid to the psychosocial environment, which mayhave a profound influence on the development andmanagement of work-related disease. This situationshould change in the future.
In the 21st century, assessment of the psychosocialenvironment should become a routine part of theassessment of any workplace. Improved methods ofassessment and management of psychosocial hazardswould hopefully be developed and utilized.
Training of health care professionals
Adequate numbers of occupational health personnelneed to be trained in South-East Asia in the comingyears. While statistics on the current and projectednumber of occupational health and safety personnel areunavailable, there is probably a shortage of trained andqualified personnel.
The basic and continuing training should also includetopics which are increasingly recognized as beingimportant, such as environmental health, informationtechnology and management skills, audit and qualityassessment, ageing and work, psychosocial and organiza-tional aspects of work, ethics, familiarization withmodern work practices and technology. This will equipOH professionals to face new challenges posed bychanging attitudes and values towards work, the techni-cal and organizational developments of work, and furtherenhance the close working relationship between OH andother health care professionals.
At the same time, the human aspect of health careshould remain an important feature in patient interac-tion. Several forces act to diminish empathy andcompassion in the practice of health care. Pellegrino17
identifies some of these as,
the fascination with technology, gadgets, and instruments;the inherent depersonalizing influences of our highlyinstitutionalized social structures; the replacement of careby individuals with care by the 'team'; a scientific medicaleducation that focuses on man-the-object-of-study; and,finally, a medical education, fraught with rigidities, thatdoes little to help the student develop his humanity.
On the same subject, Spencer,18 in a lecture onoccupational medicine - a desirable shift in preparationfor its practice, commented that,
Added to this negative setting is the lexicon conversion byhealth planners or health economists, or some group that mostlikely has never seen a patient in agony, of the preventive ortherapeutic relationship into an interaction between a'provider' and a 'consumer', the former concerned about costeffectiveness and the latter perplexed by the technology of thevast institution that provides tertiary care.
Quoting William Bean, he added,
Indeed, merely thinking of a physician ministering to thesick as someone providing consumables to a consumerillustrates the depersonalization which endangers our rela-tions ... cost effectiveness is not the same as care effective-
ness.18
Such forms of health care, for example, managedhealth care, have already made their appearance inSouth-East Asian countries, and their impact willincrease in the 21st century.
CONCLUSION
By taking into account the demographic and workchanges in ASEAN in the 21st century, the relevantchallenges in occupational health can be identified andpreparations made to respond to these challenges.Improved work conditions, the advent of new technol-ogy, a redistribution of work activity, an ageing work-force, and higher expectations for health care andquality of life will determine the relevant challenges wewill face.
Changes needed may include a strengthening ofnational policy and legislation in OH, a shift in the focusof health care activities, and improved training anddevelopment of OH professionals to better prepare themfor the changes.
As global and regional economic conditions continueto remain unstable and the impact of the crisis furthertakes its course, the final effect on countries in South-East Asia remains to be seen.
REFERENCES
1. The World Health Report, 1998. Life in the 21st Century. AVision for All. Geneva: World Health Organization, 1998.
2. ASEAN Secretariat. Jakarta, Indonesia, www.asean.or.id/updated Jan 1999.
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022

D. Koh et al.: Occupational medicine in 21st century S.E. Asia 73
3. Neville W. The dynamics of population ageing into the 21 stcentury: ASEAN and selected countries of Pacific Asia. In:Yeung YMj editor. Pacific Asia in the 21st Century.Geographical and Developmental Perspectives. Hong Kong:The Chinese University Press, 1993; pp. 259-283.
4. Ministry of Labour, Singapore. 1995 Singapore Yearbook ofLabour Statistics. Singapore: Ministry of Labour, 1996;p. 92.
5. Department of Industrial Health, Annual Report. Singapore:Ministry of Labour, 1997.
6. ILO East Asia Multidisciplinary Advisory Team. Preventingand Saving Lives at Work: The Emerging Challenge in Asia.Bangkok: ILO Regional Office for Asia and the Pacific,1994.
7. Jeyaratnam J, Chia KS. Occupational health issues innational development. In: Jeyaratnam J, Chia KS, editors.Occupational Health in National Development. Singapore:World Scientific Publishing Co., 1994; pp. 1 -13 .
8. Anon. More people working from home. The Straits Times(Singapore) 23 January 1999; p. 46.
9. Chew FT, Ooi BC, Hui JKS, Saharom R, Goh DYT, LeeBW. Singapore's haze and acute asthma in children. Lancet1995; 346: 1427.
10. Departmental homepage for Asia & Pacific, ILO. TheInternational Labour Organization's Regional Departmentfor Asia and the Pacific - Serve the Region URL:www.ilo.org/public/english/270asie/index.htm (updated18 December 1998).
11. ASEAN Standing Committee Annual Report 1997-1998.Jakarta, Indonesia: ASEAN Secretariat.
12. Taylor G. Workers compensation in East Asia. Interna-tional Commission on Occupational Health (ICOH);Quarterly Newsletter, 11-21 May 1997, Singapore.
13. Finnish Institute of Occupational Health. New Epidemics inOccupational Health. (People and Work Reports 1). Helsin-ki: FIOH, 1994.
14. Nguyen thi Hong Tu, Le van Trung. The occupationalhealth system in Vietnam. Asian-Pacific Newsletter onOccupational Health and Safety 1998; 5: 28 - 30.
15. Jeyaratnam J. Occupational health and developing coun-tries. In: Zena C, Dickerson OB, Horvath EP Jr, editors.Occupational Medicine, 3rd edn. St Louis: Mosby Year BookInc, 1994; pp. 1138-1144.
16. New York Times, Reuters. Extra-high mercury levels atwaste dump. The Sunday Times (Singapore). 27 December1998; p. 22.
17. Pellegrino ED. Humanism and the Physician. Knoxville, TheUniversity of Tennessee Press, 1979.
18. Spencer JF. Occupational Medicine - A Desirable Shift inPreparation for its Practice. Washington, DC: AmericanCollege of Preventive Medicine, 1981.
Dow
nloaded from https://academ
ic.oup.com/occm
ed/article/50/1/64/1468306 by guest on 10 August 2022
Copyright © 2022 FDOKUMEN




















